

BO NES.

nl}
CEIlVICAL
VEl! l'E IlRA
COil AI!} BO},;I': (clavicle) , 1 RII}!; ••
BONE • (huII,erlls)
"I"H VEN I" I! Il I! A i (pelvis) 5 UISA
H Al)IUS • PHAI. (;(,I£S - •• ,
THIGH B<>Nto: (fel1llll)
KNRg CA" (patella)
SHi:-r ;ijPNE (til)iaf ,
Ill!oOCI! BONE (fibula)
T AKSUS •• '
METAT RSUS ••••
]'IIALAN G ES ····
.numher rI sht)w ' Sure for. the arteries l He IIUlubers III text •
FACIAl. CAROTlnS. SUHCl.AVIAN.
AXIl.LARY.
BUACHIAL (DigilRI Or Tourniquel).
AORTA. ._. •• BRACHIAl , (FI..-xion)
ILIAC. RADIAl.. FI MORAl. (DigilRI pressure).
• C lMMl':NCEMRNT OF POPLITEAl.•
POPlITEAl (Flexion).
• ANTKRIOI! l'JI!JAL.
POSTERlOI! TIBIAl..
•
ARTERIES.
• OCCIII ••- - •• - TSMPORAL

FIRsrr AID TO THE INJURED
ARRANGED ACCORDING TO THE REVISED SYLLABUS OF THE FIRST AID COURSE OF THE
ST. JOIIN ASSOCIATION.
BY JAMES CANTLIE,1\!.A., F.R.C.S.,
KlIl:r: At of Grace of the Ordel' of St. fohn. IIOllorar), Life J11(,/Ilber of. alld Lecturer awl Exa III iller to, the A ssocirrtioll.
\Vith a CHAPTER ()n "SLretcher Transport," revised from that originally written by Sir i<URLEY, C. B .. Kllight (d Justice of the Order of St . John, in accordance wiLh the Army Strt'lchcr Exercises. Also a CHAPTER (being the i<ifth LecLlII'e lor Females ()nlyl, by E. l\IAcDowEL COSGRAVE, M.D F.R.C.P.!., J(I/I:«ht of Grace of the Order of St. JO/III. fJOllorary L£fe JIIIembel'oJ, allfl Lecturer and Examiller to, the Associatioll.
TWENTY-SIXTH F:DITION,l,240,OOO to 1 ,2 90,000.
(This edition is similar to the ill 7vlzich editioll //Iallyof Ihe illustratiolls 'were re-dra7vll; otherwise it diifel's but little from the ele,'elltlt 10 the se7'ellteellth editiolls. )
Price in Cloth, 1s. post free.
LONDON:
THE ST. JOlIN Al\IBULANCE
ST. JOHN'S GATE. CLERKENWELL, E.C.
W. H. & L.C. 50.000/3/1915.
Ube (l;ranl) IPrior)2 of {tbe of tbe 'fbospttal of St. 50bn of 5entsalem in JCnglanl).
SOVEREIGN HEAD AND PATRON: HIS l\IOST GRACIOUS MAJESTY THE KING.
GRAND PRIOR: H.R. H. THE DUKE OF CONNAUGHT, K.G.
SUB-PRIOR:
BAILIFF OF EGLE: H.R.H. THE DUKE OF CONNAUGHT, K.G.
EXECUTIVE OFFICERS:
PRELATE.-The Archbishop of York.
CHANCELLOR.-Col. Sir Herbert Jek yll, K. C.M. G.
SECRETARy-GENERAL.-Col. Sir Herbert C. Perrott, Bt., C.B.
RECEIvER-GENERAL.-Edwin Freshfield, LL. D.
DIRECTOR OF THE Al\IBULANCE DEPARTMENT.-The Earl of Plymouth, P.C., C.B.
CHAIRMAN OF THE BRITISH OPHTHALMIC HOSPITAL, JERUSALE:\L-CO!. Sir Charles M. \V atson, K.C.l\1.G., C.B.
ALlII0NER.-Sir Dyce Duckworth, St., l\I.D., F.R.C.P., LL.D.
LrBRARIAN.-A. Edmund Fraser.
REGISTRAR.-The Earl or Ranfurly, P.C., G.C.l\I.G.
GENEALOGIST.-Sir Alfred Scott Scott-Gatty, K.C. V.o. (Garter).
AssrsTA T EXECUTIVE OFFICERS:
ASSISTANT RECEIVER-GENER .\L. -Edwin H. Freshfield.
ASSISTANT DIRECTOR OF THE AMBULANCE DEPARTi\IENT.Lieut.-Co!. Sir Richard C. Temple, Bt., C.I.E.
HONORARY SECRETARY OF THE BRITISH OPHTHAurIC HOSPITAL, JERUSALEM.-CO!. Thomas H. Hendley, . C.l. E., M.R.C.S.
ASSISTANT HONORARY SECRETARY (FOR SCOTLAND) OF THE BRITISH OPHTHALMIC HOSPITAL, JERUSALEM.-John Horne Stevenson (Unicont PttrSllivant).
ASSISTANT LIBRARIAN.-
SECRETARY.-\Villiam R. Edwards, A.C.A.
ASSISTANT SECRETARY.-Duncan G. Monteith.

'THE CHAPTER-GENERAL:
The Chapler-General consists of the Grand Prior, the Sub-Prior, the other Knights of J 11 tice, the Prelate and the Sub-Prelates, de iure; the Officiating Chaplains; all members of the Council; not more than ten Knights of Grace and not more than six Esquires app-Jinted by tl1e Grand Prior,
KNIGHTS OF JUSTICE:
IIIS l\IOST GRACIOUS l\IAJE TY TIlE KL',G (SO\'ereign Head and Palron).
FIELD-;\IARSHAL H.R.H . THE DUKE OF CONNAUGIIT, K.G., K.T., K.P P.C., Etc. (Grand Prior)
GENt':RAL H.R.H. PRINCE CHRISTIAN OF SCIlLE wIG-IIou; n:IX, K.G., P.C., G.C. \'.0.
n.II. PRINCE ALBERT OF SCHLESWIG-HOLSTEDI, G.C.B., G.C. \'.0
COLONEL 1l.H. Til E DUKE OF TECK, G.C.B., G.C.\·.O., II.S.H. PRINCE LOUIS OF BATTENllERG, G.C.ll .• G.C.\·.O.• R.N.
II.i\f. IIAAKON VII.. KI:-Iu OF :\'ORWAY, [(.G .• G.C.B .• G.C. \ '.0. l\IAJOR II.S.II. PRI:-lCE OF TECK, G.C.B., G.C.\·.O., D.S.O. l\IAJOR II.R.II. PRINCE ARTHUR OFCONNAUGHT, K.G . . I{'T .. p.e., G.C.\'.O. II.II. PRI)lCE ALEXANDER OF BATTENBERG, G.C.\'. O.
Sir John Furley, C.B. (Honorary Sir II. A. Blake, Bailiff). The Earl or i\leath. K .P.• P.C. Sir T. N. Dick-Lauder, Bt. A. E. Fraser.
l\laj. Sir A. Lamb. Bt. The Lord ",rostyn.
Col. Sir II. C. Perrott, Bt., C.B. The l\Iarque s of BreaJalban<!. Col. Sir J. Gildea, [{.c. V.O., C. B. K.G., P.C. II. J. Loftus. The Duke of Porlland, K.G .• P.C. Col. B. i\I. Dawcs. R. B. Carter. F.R.C.S. (UonL)rary Gen. SirC.\Varren, G.C.M.G., K.C.B., Commander).
R.E. Col. C. \V. B. Bowdl e r. C.B. l\Iaj.-Gen. J. C. Dalton. (Honorary Commantier).
l\laj.-Gen. A. G. IIunter-\Veston Lieut.-Col. A. C. Yate. ofIIunlerstol1, C.B .. n.s.o .• R.E. l\laj.-Gen . A. F. Terry.
Col. The Lord \Villi am Cecil, c. v.O. The Earl of Plymouth, P.C.. C.ll, E • . Freshfielcl, LL.D. (Honorary The Earl of Sandwich, K.C.\'.O. Bailiff). E. II. Freshfield.
The Earl Brassey. G.C.B. The Earl of Ellesmere, 1\I.V O. The Viscount Templelowll. Field-l\Iarshal The Earl Kilchcner
R. M. MacLcan. of Khartoum, K.P Etc., Etc. A. F. G. Leveson Gower. Lieut.-Col. Sir R. C. Temple. lH .•
Col. F. A. H. Lambert. C.l.E.
Col. Sir C. \V. Murray, C.B. ir A. S. Scott-Gatty. I{'C. v.o.
The Earl of Ranfllrly, P.C., G.C.M.O. Col. Sir II. leltyll, K.C.M.G.
The Lord Salldhurst. P.C., G.C.S.I.. The Lon! Islington, P.C., G.C.M.O., Q,C.I.II. D.S.O.
KNIGHTS OF J USTICE.-Contiuued.
Col. Sir J . R. A. Clark, Bt., C.B., The Duke of Somerset.
. F.R.C.S.E. Sir D. Duckworth. Bt., M.D.
Sir R. H arvev. Capt. H. E. Boulton. C.V. O.
Col. The Lord Sydenham, G.C.S.I., The Viscount Esher, G.C.B., G.C. V.O.
. G.C.I.E. Col. Sir C. l\1. C.B. [G.C.B. L!ellt.-Col. J. "V. \V ray. Field-l\Iarshal The Lord Nicholson, SIr W. \V. Portal, Bt. Lieut.-Col The Lord Herbert Scott, PR IOLATE: O.S.O.
The Archbishop of Yo rk .
SU B-PR ELATES:
!he OI·!11sby I The Bishop of Southwark 1 he Pnmate of New Zealand. The Bishop of Gibraltar.
OFFICIATING CH APLAINS:
The Rev. Canon E. Sheppard, IThe Rev. T. C. Elsd on. K.C.V.O., D.O.
KNIGHTS OF GRACE APPOINTED BY THE GR AND PRIOR:
Major. G. E. ';Y. l\Ialet. I R. A. M.D.
Col. J. \ V. Ottley, K.C.I.E., R.IO. I Lt.-Col. F. \ V. Pixley. F.S.A.
The " Is cou nt Alverstone, Sir \V H. St. J. II ()pe, LlTT.n .1 . A Jam es, M.V.O. F. H. Cook, C.I.E
]. S. Griffiths, M.R.C.S . I
ESQUIRES APPOI 'TED BY TilE GRAND PRIOR: B. Hamilton, C.M.G. I Col. \V . G. Carter. E . Dawes. K. \V. l\Iurray (Portcullis Pursuivant).
THE COUNCIL:
Th e Council c,onsists of the Grand Prio r, the Sub-Priol', the Executi"e Officers of the Order, the COl11manders of existing Commanderies, and not mo!,e than. fifteen members of the 9rades of Knight of J usLice, Ch.aplaln, KllIght of Grace and EsqUire appointed by the Grand Pnor.
l\IEMBERS APPOINTED BY Tllg GRAND PRIOR:
Sir J. Fudey, C.B. ln spedor-G eneral B. Ninnis.c. v.O., Major-G en. J. C. Dalton. R.N.
E. H. Freshfield. Sir D. Powell, Bt., ICC.V.O.. Liput.-Col. Sir R. C . Temple, St.. M.D.
, C.I.E. E. Owe n. F.R.C.S., LL.D.
Tne Bi shop of SOllthwark. The Lord Claud Hamilton, I nspector-General Sir J. N. Dick. Col. T. II. II endley. C.I.E.,M.R.C.S. K.C.B., R.N.

Ube a5rantl lPrtot}2 of Ube of tbe 1bospttal of St. lobn of lerusalem tn JEnglantl . AMBULANCE DEPARTMENT.
Ube St. 10l)n :ambulance :association.
PATRON: HIS MAJESTY THE KING, Sovereign Head and Patron of the Order.
PRESIDENT:
II.R.H. THE DUKE OF CONNAUGHT, K.G., Grand Prior of the Order.
CENTRAL EXECUTIVE COMMITTEE:
Consisting excl u sively of Members and lIonorary Associates of the Order.
DIRECTOR OF THE AMBULANCE D EPARTMENT AND CHAIRMAN OF COi\lMITTEE.-The Ead of Plymouth, P.C . , C. B.
ASSISTANT DIRECTOR AND DEPUTY CHAIRMAN.-Li e ut.-Col. Sir Ri chard C. Temple, Bt., C.LE.
D EPUTY CHAIRMAN.-Sir John Fudey, C.B., Life Member of the Committee, Honoris Causti..
MEMBERS:
l\laj.-Gen. J. C. Dalton.
Col. Sir J. R. A. Clark, Bt., C.B., F.R.C.S.E.
Col. The Lord Sydenham, G.C.S.I., G.C.r.I.G ., G.C.I.E.
Capt. II. E. Boulton, C V.O.
Lieut.-Col. The Lord Herbert Scott, D.S.O.
The Rev. T. C. Elsdon.
Inspector-Gen eral B. Ninnis, C.V.O., M.D., R.N.
Maj. G. H. Darwin, M.D
Col. G. S. Ellisto n, C.B., M.R.C.S.
Col. C. J. Trimble, C.M.G., L.R.C.I'.E.
Capt. Sir J. "V. Nott-Bower, c. v.o
E. Owen, F.R.C.S., LL.D.
The Lord Claud Hamilton, M.P.
Sir J. L. Langman, Bt.
S. \ V l\Ialkin.
C. Colton, F.R.C.P.R., M.R.C.S.
CENTRAL EXECUTIVE COMMITTEE-continued.
Surg.-Gen Sir B. Franklin, K.C.I.R., K.H.P, C. B. Palmer.
Lieut.-Col. G. E. Twiss, F.R.C.S.r.
Col. T. II. Hendley. C.l.E., M.R.C.S.
J. H. i\Iorgan, c. V.O .• F. R.C.S.
Col. Sir Trevredyn R. 'Vynn e, ICC.S.I., K.C.I.It.
Brig.-Gen. H. R. Mends.
Liellt.-Col. A. D. Acl a nd.
Y.41., Co!. 1':. D. Broll'n-Synge-Hutchinso n
Surg -Gen. Sir J. Porter, ICC.B., M.D., LL.D., K.H.P., R.N.
J. A. BJoxam. F.R.C.S.
Lieut.-Co!. Sir H. \V. Inglis.
i\Iaj. P. G. helVel!.
The Viscount Acheson.
T. H. \Voolston.
F. N. Ellis.
\V. E. Audland, M.R.C.S.
A. H. Johnston, l\I.R.C.S.
EX-OFFICIO J\IEMflERS OF COMMITTEE.
The Secl'elary-General of lhe Order.
The Recei\'er-General of the Order.
The Chairman, Brilish Ophthalmic Hospilal.
CHIEF SECRETARY:
Col. Sir II. C. PelTott, Bt., c. B. (Secretary-General of the Order).
DIRECTOR OF STORES AND ACCOUNTANT: \\'. R. Edwal'ds, A.C.A. (Secretary of the Order).
STOREKEEPER:
"', H. l\Iorgan (Superintendent, Invalid Transport Corps).
A.SSiSTANT SECRETARY:
D. G. Monteith (Assistant Secretary of the Order).
TERRITORIAL BRA CH. CONTROLLER-iN-CHIEF:
Lieut.-Col. Sir R. C. Temple, Bt., C.I.E.
LADY COMl\IANDANT-IN-CHIEF OF ST. JOHN 'VOMEN'S
V.A. DETACHMENTS: Lady Perrott.
SECRETARY:
P. G. Darvil-Smith.
REVISED 1908.

R EFER:':NCF. Xo. ss.. ----1908 .
FIRST AID TO THE INJURED.
SYLLABUS
OF INSTRUCTION.
FIRST LECTURE.
A. Principles of Aid. IIuman Skeleton and of the B. A brief DescnptlOn of the \luscles. .. . _ d symptoms. C Fractures-Causes, YUilel1es, SIgn" an D'. Treatment of Ru!es ..
E. The Triangula.r Rll1Jage and Its a pp!Jcal1on.
SECOND LECTURE.
A. Treatment of Fractures (continued). Details of treatm en !. . Strains-.'ie:ns, symptoms and B. Dislocations, SpraJl1s, treatment.
T I The Circulation I)f the C. The J teart and Blood \ es e s.
Blood. 1 General rules for treatment. D. Hxmorrhage an" woun c s.. ..
E. The Triangular Bandage and IlS applIca(wn.
A. Hremorrhage and d ( . treatment. woun s continued). Details of symptoms and arrest and age rom Special Regions.-Signs, symptoms
Scalds, Bites and Stings Frost-bite. :. Laches 1I1 the Eye, ose and Ear'. '
F. The Tllangular Bandage and its application.
FOURTH LECTURE.
A. The Nen'ous System .
I , B .. T0 e Organs and Mechanism of Respiration-Artinc' 1 \'esplratlOn. lit
C. Insensibility
D.

FIFTIf LEC-r'URE ((or Males only).
A. Impro\-ised meth d f rr' . injured. 0 0 1 tll1g and carrYll1g the sick or
B. Meth ods of lifling and c arrying the sick ." d Sir-etchers. 01 lnJure on
C. The conveyance n[ such by rail or in country carts.
A .
B.
C.
D. FIFTH LrCTI1RE (for Females only).
reception of ac cident cases. l\1 eans 0: Mung ar.d carrying. PreparatlUn of l>ed. H.emoving the clothes.
E . IJrep,lrations for surgeon.
NOTE 1.-The subject of poisons shoul,i be treated in a general manner; the common poisons classitied, and only their general symptums, 'effects and treatment taught.
NOTE II.- The last half-hour of each lecture should be devoted to practical work, such as the " pp ication of bandages and splints, lifting and carrying wounded on stretchers
NOTE IlL-There should be an interv.ll of a week between each lecture. A candidate for examination must at tend at least four out of the five lectures .
NOTE IV.-Male cIa ses must pa s in that system of stretcher exercise most suitable for the locality-
NOTE V . -As little time as po sible is to be spent on instruction in anatomical and physiological details. Lecl urel s and examiners are particularly requested to remember that it is " First Aiel" that has to be taught and tested, and not anatomy and physiology.
i llixed classes oJ !ltell and WJ!ltell are on no accoltlz ! l'ermitleJ.
PUPILS Ul\'DER Sl:':'TEEN YEARS OF ACE CAN ONLY ATTEND THE ,. JUNIOR" OuURSE (SECT.O"" A, SYLLABUS 4°)·
Lecturers instructing a First Aid class, and Local Secretaries , can obtain further particulars on application to the Chid Secretary for .. Paper Reference No. 80."
No Lecturer may examine Ilis own Class (or Certiji,·ates.
r se of the Maln A
and Press ure Points .

The Human Skeleton. Sku ll, sp ine, ri bs a nd breastbon e, upper lim bs (co ll ar -bone, should er- blade, armb on e, bon es of th e forea r m, ca r pus, metaca rpus , pha langes), pe lvis , lowe r li mhs (th igh-bone, k neecap, tarsus, metata rsus, phalanges)
Special Fractures. Cran ium , lowe r jaw, spine, ribs, breast -bo ne, co ll a r -bo ne, shoulder -blade, arm-bone or bo nes c lose to th e el bow j oi nt, forea rm, cru shed ha nd, pelvis, thig h-b one , k nee-cap, leg, crushed foo
iscellaneous Injuries. Bruist!s, bu rns and sca lds, bites of snakes anu rabid anima ls and wo unds by poisoned weapons, stings of plants and .anin:als , frost bite, needle embec1deu unchr t he sInn, fi h hook embedde d in the
i njuries to joints, fo reign body in t he eye, ear pa sage and nose, wound in the front
10 SUM1IAR
CH APTE R T. P,zgr: of First Aid 17 Explanatory 20 Questions on Chapter 2 I CH
.
Y OF CONTENTS.
APTE R II
2 2 Joints ... 31 Mt'sc1es. Voluntary and involuntary 32 Fractures. Causes, mrieties, signs and £ymptoms 33 Apparatus for treatment of Fractures ... 36 General Rules to be observed in the treatment of Fractures 4 I
t 43 Dislocations 62 Sprains 64 Sprains and Ruptured lVI usc1es ... 65 Questions on Chapter 66 II C H APTE R III. Circulation of the Blood. O rgans; genera l (syste mic) and pulmona ry circulat ions 70 H.emorrhage or Bleeding. A rte rial, venous, capi ll ary 73 Arterial H.emorrhage. Principles of arrest 74 Wounds with A r terial H.emorrhage . .. 76 Cou
te
Aorta, arteries of the heau and neck, of the upper limbs, of the lower limbs 79 Venous H.emorrhage and Varicose Vein s 93 Wounds w ith Venous H.emorrhage 94 CapiJlary H.emorrhage 95 Internal H.emorrhage 95 H.emorrhage from Special Regio n s 96 Questions on Chapter 99 C HAPTER
M
wall of t he abdomen, inju ries to th e orga ns within th e abu ome n a nd pe lvis 102 Questions on Chapter I I 5 C HAPTE
V. The ervous System. Cereb ro-spi
sympathetic. .. Il7 The Respiratory System 118 Artificial Respiration.
co mbin ed wi th S ilvest er's
H a ll's met h ods. . . 12
r
ries
I V.
skin,
R
nal,
chafe r' s, Silveste r's , H oward' s
, L abo rd e's and Marshall
Insensibility. Causes, general rules for treatmerrt, concussion of the brain, compression of the brain, apoplexy, epilepsy, hysteria, shock, fainting and collapse, sunstroke and heat-stroke, convulsions in children, asphyxia
Electric Shock and Effects of Lightning
Questions on Chapter
CHAPTER VI.
Poisoning. General rules for treatment, special poisons
Questions on Chapter
CHAPTER VII.
Bandaging. Bandages for the scalp, forehead, etc., shoulder, hip, hand, foot, chest, back, knee, elbow, fingers and toes ...
CHAPTER VIII.
Methods of Carrying. Four, two, and three-handed seats, fireman's lift, fore and aft method, improvised stretchers, to cross a ditch or wall, to load or unload a wagon ..
CHAPTER IX.
Stretcher Transport. Stretch e rs, stretcher exercises, litters
CHAPTER X.
The Fifth Lecture (for Females only ). Preparation for reception of accident cas<:s, choice and preparation of a room, lifting and carrying, preparation of bed, removing the clothes, preparation for surgeon .. .
Questions on Chapter

Skeleton showing position of main arteries
Skull and vertebral column
Vertebra ...
Bones of the left upper limb
Bones of the right lower limb
Shoulder Joint
Ankle ...
Rectus ?\1 uscle ...
Triangular bandage spread out and folded
Large arm sling
Small arm sling
Reef knot
Granny knot ...
Loop knot...
Bandage for fracture of lower Jaw....
Bandages for simple fracture of nb5
St. John sling
Band Iges for fracture of both collar bunes
Bandage for fracture of shoulder blade
Treatment of fracture of arm ...
Angular splint ... ...
Treatment of fracture of forearm
Treatm{nt of crushed hand... ..,
Treatment of fracture of thigh bone' . ..
Treatment of fracture of thigh bone (woman)
Fracture of knee cap
Treatment of fracture of knee cap ...
Treatment of fracture of leg (man and w0man)
Treatment of crushed foot ...
Diagram of the heart, lungs and air pa<sages
12
128 142 145 155 160 197 206 LIST OF ILLUSTRATIONS.
... .... . ..
... ... ... . . .
Paffe frontisplcce. 24 27 29 3 1 3 1 32 38 39 39 4° 4°' 43 44 47 50 5 L 5z 53 54 5S 55 S7 S8 58 59 61 62 71
Diagram of the circulation of the blood
Digital pressure on carotid artery .. .
Digital pre,sure on facial artery .. .
Digital pressure on temporal artery
Digital pres·ure on occipital artery
Pad and bandage to arrest hremorrhage from temple
Ring pad
Digital pressure on subcJayian artery
Pad and bandages to apply pressure on axillary artery ...
Digital pressu re on brachial artery (two meth ods)
Flexion at el bow
Digital pressure on radial and ulnar arteries
Pad and bandage to arrest hremorrhage from palm
Digital pressure on femoral artery ...
Tourniquet on femoral artery
Flexion at knee
Organs of the chest and abdomen ...
The lungs and bronchial tubes
Schafer's method of artificial respiration ...
Silvester's method of artificial respiration ...
Silvester's and Howard 's methods of artifici.J respiration combined
Bandage for the head
Bandage for the shoulder
Bandage for the hip ...
Bandage for the hand
Bandage for the foot
Bandage for the chest
Bandage for the knee
Bandage for the elbow
Grip for four-handed SC3.t
Lifting by two-handed seat .. .
Grips for two -handed seats .. .
Carrying by two-handed seat

Grip for three-handed seat .. .
Supporting patient ... .. .
Fore and aft method of carrying
Carrying on improvised seat
Improvised stretcher
Furley stretchers
Stretc h er exercise, No . 1. "Fall in "
Ditto, ready to lift patient
Ditto, lifting patient ...
Ditto, placing stretcher
Ditto, preparing to low er patient ...
Ditto "Lower"
Ditto: No. II. Ready to lift ratient
Ditto, patient lifted ...
Ditto, No. IV. First p osition
Ditto, second position ... ... ...
Diagrams illustrating Army stretchcr drill
Dilto ...
liee! cradle
}mprovised bed cradles
14
Page 73 8r 81 82 82 83 4 1)4 85 86 87 87 g9 90 9 1 92 112 119 122 124 12 5 155 15 6 15 6 157 15 7 15 8 159 159 160 161 162 163 IS
Pa , e 164 16 5 167 168 168 17 2 175 17 6 177 178 179 180 182 183 188 189 19 1 194 203 203, 204
PREFA CE.
AT the request of the Central Executive Committee
I have revised the manual written by myself in 1 9 01 , as the official handbook of the St. John Ambulance Associati 0 n.
Throughout the revision an endeavour has been ITlade to simplify the study of First Aid to tbe Injured by drawing up a number of general rules for the of accidents and sudden illness, and by the 0l111SSlOn of all detail \\ hich is not arsolutely necessary to enable the student to acquire an intelligent knowledge of the subject.
I wish to express my thanks to Professor E. A. Schafer for furnishing instructions for performing a method of artificial respiration, to Dr. L. J. F. for many valuable suggestions, and to the Members of the Central Executive Committee, especially Surgeon-Major G. H . Darwin, M.D., and Dr. F . R. Cassidi, for perusing the proof sheets and for anum ber of userul additions to the \\·ork.
I cannot omit also to offer my best acknO\dede-ments to Mr. 'V. R . Edwards, tIle Accountant Storekeeper of the S.J.A.A., for his invaluable co-operatio n.
JAMRS CANTLIE.
F IRST A ID TO THE I NJURED.
CHAPTER I.
The St John has n.ow completed thirty years of Its eXistence, and d unng that period hundreds of thousands of men and women have been taught at its classes, in parts of the \Yorld how to help their inj ured neIghbours.
Aid to the Injured is a special branch practical medicine and surgery, by a ot which trained persons are enabled to affol d assistance in cases of accident and .Illness. The instruction begins and ends with FHSt AId, and the subject is taught simply but thoroughly e xhaustively. The duty of the a ,n bulance puplls ends where the doctor 's comme:1ces, and there ought to be no overlapping or clashing of duty or interests.
PRIl CIPLE' OF FIRST AID.
1. The First Aiel student should be(a ) Observa nt, that he may note the causes and signs* of inj ury . (b) Tactful, that he may without questions learn the symptoms t and hlStory t of the case.
* Si TI1S are what may he perceived. are whal the paLient can te.ll you. . I1istory means the circumslan ces attendmg the ac cldent or sudden illness.
(c) Resourceful, th at he lllay us e to the b est advantage whatever is at h and to prevent furth er d amage and to assist N ature 's efforts to the mi schie f already done.
(d) that he may give cl ear instructIOns to the patient or the bystanders how best to assist him.
(e) Discriminating, that he may decide which of several injuries presses most for treatment by himself, and what can best be l eft for the patient or the bystanders to do,
2 Remove the cause of injury or danger whenever possible,
3., Severt=: hcemorrhage must receive the .attentlOn, no matter what are the other lnJunes.
4· patient must be in a position in whi ch breathing 1S, possible; the ai r passages muSl be free from obs tru ctIOn; if breathi ng has ceased prom pt measures I11USt be taken to resto re it.
5, restful position of the body will assis t the vltal funct IOns ; s upport of the injured part will help to prevent further damage, and is essential in the case of fra c tures of lim bs.
Warmth.-After every accident kee p the pat1ent warm so as to prevent the fall of temperat ure below th e normal point.
7· When the skin is broken the wound

19
should be promptly covered with ,a clean d ' Should the wound be pOlson ed , It IS most ressmg, , Important immediately to prevent the pOIson Dermcating the system . ,
8. Poisons swallowed shou ld, be got nd of; or \\ hen that is inexpedient, neutralIsed. b
9. The best of transport m e studied, and provlslOn made for proper care \\ hen the patient is brouU'ht to helter.
Removal
Clothing.-Clothes should not be off unnecessarily, but when, it is needful to remove them, th e follo\\'ing rules \\'Ill be found of service in serious cases:- ,
COAT: Remove from the sound Side fll st, and, if necessary, slit up the seam of the sleeye 0n the injured side .
SHIRT AND V EST: Slit down the front and remove as the coat.
TROUSERS: Slit up the outer seam.
BOOT: Slit the back scam and undo the laces.
SOCK: Cut off, II Stimulants. - I t is incorrect to suppose that alcoho l is the only form of stimula nt , and far ,too frequent u se of spirits is made to restore a patient afte r an accident, often with the safest rule, therefore, is to defe r the adm mlstra tIOll, of until the arrival of a doctor, ,\Vh en t,he patIent IS able to swa11o\\, strong tea or coffee, o r milk, as bot as Gill
18
be drunk, or a small quantity of sal volatile in water may be given. Smelling salts may be held to the nose. Sprinkling the face with cold and hot water alternately, warmth applied to the pit of the stomach and over the heart, and vigorous friction of the limbs upwards have a stimulating effect.
12 . Throughout his work the First Aid student must on no account take upon himself the duties and responsibilities of a Medical man. At times an apparently slight injury is accomp;:lI1ied by grave danger anj may actually cause loss of life. When sending for a doctor, state the nature of the case, and remem ber that written particulars are safer than a verbal message.
It is nec essary that something should be known of th e structure of the body (elementary a natom y), and of the functions of some of the more important organs and systems (elementary physiology). A short description of the necessary anatomical ana physiological points is therefore given as the several subjects are discussed. For purposes of description the human body is supposed to be erect, with the arms hanging by the side and the palms of the h?nds directed forwards. The "middle line" of the body runs vertically from the top of the head to a point between the feet.
QUESTIONS
The llumerals indial/e
ON CHAPTER

purp oses of description how IS the human body supposed .to be .placed
the
lme of the body?
20
II
tlte J:ages whel e tile allswers may be foulld. PAGIf 17 \Yhat is First Aid to the injur ed ?:.. .., "';> qualities should the First AId student possess. ",Y hat are sign? . " . . . .., What are symptoms? ... What is the history of a ? .:' ... . ''';> 17, 18 17 17 17 IB 18 What is often the first thIng to do m an accIdent: ;>'" \\'hat re sult of injury must rec eive the first ... i What three things are absolutely necessary to an 18 done ski n' ." ... 18, I IIow must poisoning be treated? .. ' ". I What steps must be taken beyond the actual treatme nt 19 of injur.i.es ? " . .., ?'" 19 Should c loth ing always be ... " ,';> 19 Il ow would you r emove c1othJl1!S when necessar) . Explain the use and abuse of tlmulants ... . .. \Vhat must the First Aid student not do ? What is elementary anatomy? ... 19,20 20 20 20 What is elementary phy siology? . F0r
".
is
1.
?
What
middle
C IUPTER II.
ERACTU R ES , D I SLOCAT I ONS, SF Rl lI NS AND STR1\ INS.
THE
T he human body is moulded upon a bony framework (the skeleton) which sef\'es-
I.-To give shape and firmness to the body.
2.- To afford attachment to the muscles.
3 · - To protect important organs, as in the skull, chest, and abdomen . THE SKULL.
The Bones of the Skull are arranged in two groups, those of the brain case or cLlnium, and those of the face .
The Boundaries of the Cranium are the vault or dome, the rou n ded portion forming the top of the head ; the fro n t or brow ; the back of the head, where the greatest extent of brai n exists, and where therefore th p cranium is wides t and deepest; the sides or temp les . T he base of the cra ni um is hidden from view by t he bones o f t he face and of the vertebra l column ; in it are numerous perforations for the passage of blood vessels and nerves; through the largest opening the brain and spinal cord ar e contin u ous .
The Bones o f the Face with the exception of

the lower jaw are firmly jointed. t ogether, so movement between them is impossible.. The caVities of the nose and of the eye sockets (orbits) are formed by the bones of the cranium and of the face co n..
tl The mouth cavilY is formed between the Jom y. . h b f up.per and lower jaws, the bemg t e ony of the mouth which separates It from the nasal cavity above.
The L ower Jaw consist.s
(a) A horizontal portion 111 which are the sockets for the teeth . .'
(/7) Vertical portions terminating on. either side at the joint between the lo\\'er J.aw an? the base ot the ranium, situated Immed18.tely in front of the ear.
Tbe angle of the jaw. indicate.s the junction of the horizontal and the vertIcal portIOns .
THE BACK-BONE, SPI:\"E, OR YERTEBRAL
T he Ve rt e bra l Col u mn (Fig . :r) is composed of bones caJled vertebrce, each of which consists ofI.-A body or bony mass in front.
2.-Processes projecting which enclose a canal for the spmal cord- the spinal canal.
3.-Two transverse processes, twelve pairs of which support the ribs.
22
23
SK:JLi. AND VERTEBRAL
C C LUMN.
Showing left n bs portion of breast bone. The right ribs are removed .
SPINOUS PROCESS.
TRAI"SVERSE PROCESSES.

BODY OF VE RTEBRA.
FIG. 2A.
FIG. 2B.
4.-A spinous plocess. The spinous processes of the vertebrre can be felt beneath the skin for the whole length of the back (Figs. 2A and 2B).
The Vertebrce, 33 in all, are grouped into reo gions, in each of which they are kno\\'n by numbers, counting dO I\ nwarcls :-
I.-In the n eck 7 Cervical vertebne. The first vertebra, atlas, forms a joint with the base of the skull, at which tI le nodding movement of the head takes place; the second, til e by the joint bet\\'een it and the atlas, allows of the side,to side movements of the head.
2 - In the back 12 Dorsal vertebrce.
3 - In the loi n 5 Lu i1l bar vertebrce.
4.-The rump-b o ne, or Sacrum, consists of 5 Sacral vc: rtebrrc united in ad ults as a solid mass
s.-The tail-bone) or Coccyx, consists of 4 vert e brre joined to,jether to form a sin g le group
Between the bodi es of the vertebrre, in the upp e r three regions, are interpos ed thick pieces of cartilage which, while tbey bind the bones together, a llow of free mo\'em e nt to the column as a whole, and help to reak the of any sudden force applied to the sp :ne (for example, when falling from
TRA NSI' ERSff PROCES S SI Il\'OI s : : SURFACES SUPPO RTI NG H 1' 5 \.i F RIBS
25
.
.
2b a height on the feet). The whole spine is strapped together by ligaments reaching its entire length.
THE RIBS AND BREA ST-BONE.
The Ribs consist of twelve pairs of curved bones extending from the dorsal vertebrre to the front o f the body, and are kn own bV num be rs -first, second, etc., comm e ncing from above. The ri i.s are not bony throu gho ut their entire length , but at a short distance from th e front the b ony material e nds, and cartilage takes its place. Th e upp er seven pails, named the true ribs, are attached by their cartilages to the Breast-bone (sternum), a da gger . shaped bo ne with the point downwards, just over the pit of the stomach. The lower five pairs are termed the false ribs, as th e ir cartilages fall short of the middle lin e . The eleventh and twelfth pairs are termed the fl oating ribs, as their ends are free in front. The ribs enclose the chest and serve to protect the lungs, heart, liver, stomach, spleen, etc.
THE UPPER LIMBS .
The Shoulder-bones are the Collar- bo ne (lavtde) and the Shoulder-blade (scapula).
The Collar-bone ' can be felt on either side Leneath the skm at the lower and front part of the neck as a narrow curved rod about the thickness of a finge r. I ts inner end rests on the upper part of the
PART OF C OLLAR BONE
SHOULI'ER
BL-\DE (SCAPUL\) :\.R .'1 nONE .•

RADIUS ULNA.
nO:-':ES JULNA OF )
FOREAR.,I RAIIIUS ---H-\ \
WRIST ( CARPUS) PHALANGES
FIG. 3A.
BONf':S OF THE LEI'T UPPER LIMB.
FIG. 3D. THE POSITIO'N OF TUE RADIUS AND ULNA WHEN TIIE TH UlII13 IS TUR)l"lm I)l"\,'ARDS
Compare Fig. 3A, in which the thu mb is turned outwa rds.
breast-bone, and its outer end joins with the shoulrlerblade.
The Shoulder-blade lies at the upper and outer part of the back of the chest, and forms joints \\ ith the collar-bone and the bone of the arm.
The bone of the Arm (ltumerus) reaches from the shoulder to the elbow.
In the Forearm are two bones, the Rad ius on the outer, or thumb side, and the Ulna on the inner, or little finger side. Both bones reach from the elbow to the wrist, and they change their relative position with every turn of the hand (Figs. 3A and 3B).
The Hand is composed of-
r.- The bones of the \vrist, or Ca1jJltS, eight in number, arranged in two rows of four.
z. - The metacarpus (the framework of the palm) ; five bones which form the knuck:es and support the bones of the fingers.
3.-The plzalallges, or finger-bones, thre e in each finger, and two in the thumb
THE PELVIS AND LOWER L,IMBS.
The Pelv is. - The large basin-Lke mass of bone attached to the lower part of the spine is composed of the two haun:h-bones anJ the sacrum. The haunchbones meet in front (at the pubes) in the middle line, only a small piece of cartilage intervening, but behind, the sacrum is placed between them. The pelvis

BO"ES OF TIlE RIGHT LOWER LD!B, SIIOW Il\'G JOIl\'T WITH THE PELVIS AT THE HI P.
28
FIG. 4.
...• PELVIS.
•. "'--"'-'- TIIIGH BONE (FEM UR).
'1 ---"' -'-
BROOCH DONE (FIB ULA). ----<;IIIN BONE (T IBIA).
/:'I ICT.ATARSUS_
30 supports the abdomen and its contents, and provides the deep sockets for the thigh-bones-the hip joints.
The Thigh-bone (femur) reaches from the hip to the knee joint. Its shaft is stout, rounded, and arched forwards; the upper end presents a rounded head, supported on a neck which projects inwards, to fit into the socket of the hip joint.
The Knee-cap (patella) is a trian gular bone lying with its base upwards in front of the knee joint immediately beneath the skin.
The bones of the Leg are the Shin-bone (tibia) and the Brooch-bone (fibula). The Shin-bone extends from the knee to the ankle, in both of which joints it plays an important part; its sharp edge, tlte sllin, can be felt immediately beneath the skin of the front of the leg. The Brooch-bone li es on th e outer side of the tibia. It does not enter into the formation of the knee joint, but its lower end forms the outer boundary of the ankle joint.
The Foot is composed of-
1.- The tarsus, a group of seven irregular bones at the instep. The largest is the heel-bone, and the uppermost (the ankle-bone) forms the lower part of the ankle joint.
z.-The metatarsus, the five long bones in front of the tarsus which support the toes.
3.--The phalanges, or toe-bones, t\\'o in the big toe, and three in each of the other toes.
31 JOINTS.
A Joint is formed at the junction vf two or more bones. In moveable joints such as the hip knee etc., t.he smfaces of the bones are b; cartJlage, whlch lessens friction and the shock of a

5. Compare Fig. 4, Page 29.
joint is a clear, rather sticky
c: ,the }Oll1t 011, or sYllovia, enclosed within a apSltle. Tymg the bones together but allowing of a number of bands ;r lig r ments.
o explall1 the formatIOn of lim b joints,
FIG. 6. LEFT ANKLE. FIG.32
follow ing examples are given :-
The Should e r, a balland-socket joint, consists of a shallow socket on t he outer angle of th e shoulder-blade, and of the head of the arm-bone (Fig. 5). 0\\ ing to the shallowness of the sod et the arm-bone is very prone to escape from its socket ( dislocate).
The Ankl e, a hin ge joint, is formed at the junction of three bones, the shin-bone above and on the inner side, the broochbone on the outer side, and the ankle-bone below (Fig. 6).
THE MUSCLES.
FIG 7. The Muscl e s of the DIAGRAM SHOWING RECTUS body are classified into two ::\fUSCLE OF T HIGH , WITH groups-voluntary and ARTERY, VEIN AND NERVE . involuntary .

33
The Voluntary muscles are met with in the limbs t he head and neck, and the surface of the trun k. Their ends are attacheJ to different bones, and as they pass from one to another they cross a joint, and, being endowed with the power of contraction and relaxation, cause the movements of the body. As a muscle crosses a joint, it as a rule becomes a fibrous cord or tendon . Blood-vessels traverse and supply the muscle:;, and the nerves entering them bring them und e r the direct cOlltrol of the brain and spinal cord.
The Invo lu nta ry mus cle s are met with in th e walls of the stomach and intestines, in the air passflges, and ill most of the internal orgcl11s and blood vessels, also, in a special form, in the heart. They are n o t und e r the influence of the will, but continue their work durillg the hours of sleep; their functions are regu ated by a separate set of nerves (s ee Sympathetic System, page 118).
FRACTURES AND THEIR TREAT lENT.
When a bone br",;.ks a Fracture is said to occur.
CAUSES OF FRACTURE.
I. Di rec t V io le n ce. - When from a severe blow, impact of a bullet, crush of a wheel, etc ., a bone breaks at the spot where the force is applied the fracture is termed direct . c
TENDON NERVE ARTER Y VEIN
TISSUE PATELLA
PATELLA
MUSCULAR
rENDON OR )F

2. Indirect Violence. - \ \'he n the bone breaks at some distance from the spot \\ herE: the force is applied t he fracture is termed indirect . Alighting on the feet and fractu ring the thigh - hone or the bones of the leg, or falling on the hand and breaking the radius or the collar-bone, are examples.
3. Muscular Act ion. - The knee-cap and the arm-bone are occasionally broken by a violent contraction of the muscles attached to them .
VARIETIES OF FRACTURES.
Fractures are classified according to the condition of the tiss u es adjacent to the bone as fo11o\\s :-
1. Simple. - The bone is broken with but slight injury to the surrounding parts .
2. Compound. - The bone is broken and the and tissues are punctured or torn, thus allo\ymg disease-producing germs to obtain entrance to the seat of fracture. The fractured ends may protrude through the skin, or (for example, ",hen a bone is broken by a bullet ) the wound may lead d')\\'n to the fracture .
3. Compl icated . - The bone is broken and in addition there is an injury to some internal organ (for example, the brain, spinal cord, lung, etc. ) or to some important blood-vessel or nerve.
A fracture may be compound or complicated as the immediate result of the injury; or a fracture, 35
orig inally simple, may be converted into a compound or complicated fracture-
(el) By careless movement on the part of the patient.
(b) By carelessness Ql' ignorance on the part of one rendering first aid.
Special varieties of fractures may be classified accorcling to the injury to the bone itself as follows:-
1. Com mi nu t e d . - The bone is broken ll1to seyeral pieces.
2. Gre e n-st ick. -In chilclren, o\\'ing to the softer state of the bony tissues, a bone I1'lay bend and crack \\ ithout breaking completely across.
3. Impacted. - The broken ends of the bone are Jnven one into the other.
GENERAL SIGXS AND SY..\IPT0:.\IS WHICH :"IL-\ Y BE PRESENT.
(A fracture of felnur, or both bones of the forearm or leg, affords the most complete example .)
I. Pa in at or near the seat of fracture.
2. Lo ss o f power in the limb.
3. Sw e ll ing about the seat of fracture . Swelling fre'-l u ent ly renders it difficult to perceive other signs of fracture, and care must therefore be taken not to mistake a fractu!'e for a 1 ss serious in jury.
4. Deformity of the limb . - The limb assumes an
34
unna tura l position, and is mis-shapen a t the seat of fracture . T he co n tracting muscles may cause th e broke n end s of th e bone to override, thereby produ ci ng sho r te ning.
5. Irregularity of t h e bone.-If the bone is close t o the sk in the fractme may be felt, and if compound it may be see n.
6. Unnatural Mobi lity.-Movement may be made o ut at the seat of frJ.cture.
7. Crepitus , or bony gJa ing, may be felt or heard whe n the broken e n ds move one upon the other.
The last two signs SllOlIld be SOltl!'1zt a dodor.
Severa l of the above signs are absent in green -stick a n d impacted fractures .
In addition to the signs and symptoms the patient or the bystanders may b e able to gire the history of the injury, and mark.:; on the clothing or skin should be n oted, as they may serve to locate the fr;)cturp. The snap of the bone may haye been heard or felt.
ApPARATUS FOR OF FRACTURES .
S·plin ts and handages for First Aid frequently have to be improvised .
A Splint may be improvised from a walkillg stick, um brella, billiard cue, br om or brush handle, police man 's truncheon, rifle, fo lded coat, piece of wood, cat-dboard, p:lper firmly folded, a rolled-up map, or, in fact, allythillg Ilzat z's /inn and /011g eno?lglz to keep

37
the Joints immed iately above and below t he fractured bone a t rest. 'Whe n the above appliances are not available, t he u pper limb, if fractured, may be to the t ru nk, a n d in all cases a fractured lower ll1TIb should be bandaged to its fellow .
Bandages may be improyised from h:ll1dkerchiefs, b elts, straps, braces, neck ties, or any piece of linen, calico, strin a or cord that comes to hand.
Esmarch's Triangular Bandages (Fig . 8) are made by cutting a piece of linen or calico about forty inches squ:lre diagonally into two pieces.
The broad bandage is nude by bringing the point down to the base 9), and t hen folding into two (Fig. 10) .
The narrow bandage is made by folding the broad bandage once (Fig. I J).
The medium bandage is made by bringing the point down to the base, and then folding into three. (Fig. 12). This bandage 111ay be llsed instead of the broad or the narrow bandage when it is better suited to the proportions of the patient.
It is sometimes advisable to halre the size of the bandClge by bringing the t\\ 0 ends toge ther before folding it into the broad, narrow, or medium bandage .
When not in use, the triangular bandage should be lulded narro\\' ; the two ends should be turned to the centre, and the bandage then folJed into four, reducing it to a packet about 61 inches by 31 irlvhes.
36
ID BROAD

}< ,G. I2. THE DOTTED LINES SUOW THE FOLDS OF MEDlU;'.! BANDAGE.
39
Large arm-sling (Fig. I3).-Spread out a bandage, put one end oyer th e shoulder on the sound side, pass it round the neck so that it appears over the sho ulder of the injured side, and let the other end hang dO\\l1 in front of the chest; carry the point behind the elbow of the injured limb, and bend the forearm
FIG. 13. FIG. 14. over the middle of the bandage; then carry the second end up to the first and tie them; bring the point fo rward, ann secure with two pins to the front of the ba ndage.
Small arm-sling (Fig. I4)·-Place one end of a
PO NT
FIG.
THE
broad bandage over the shoulder on the sound side pass it round the neck so that it appears over shoulder of the injur ed side; place the forearm over the middle of the bandage; then bring the second end up to the first, and tie them. This sling is used in cases of fractured humerus, and occasionally when the large sling would be too conspicuous.
Slings may be improvised in many simple ways, such

as pinning the sleeve to the clothing, turning up the tail of the coat, passing the hand inside the buttoned coat or waistcoat, etc.
Reef Knots (Fig. IS) are to be used. Avoid granny knots (Fig. 16).
GENERAl', RULES TO BE OBSERVED IN THE TREATMENT OF FRACTURES.
The object of First Aid Treatment of Fractures is to guard against furth e r mischief, and especially to prevent a simple fracture from becoming compo und or complicated. To attain this end :-
I. Attend to the fracture on the spot. No matter how crowded th e thoroughfare, or how short the dis tance to a more c onveni e nt or comfortable place, no attempt must be made to move the patient until th e limb has been r e nd ered as iI1lll1O\'able as possible by or other restraining apparatus.
2. Steady and support the injured limb at once, so that its further 1110Vement on the part of eithe r the patient or the byst :llld er is prevented.
3. Straighten the limb with great care, and if sho rt e ning is observed in the case of a fracture of a bone of th e lowe r limb, pull up :m the foot until the limb regall1s a mor", n or mal length. Wben the shape of the limb is improved, on no account let go until it is secure ll in p osi tion by splints, otherwise there is great danger of the fracture beco:,ning compound or complicated.
4. Apply splints (when practicable) and bandages as follows :-
(a) The splints must be firm, and long enough to keep the joints immediately above and
40
FIG. I5 .-REEF KNOT. FIG. 16.- GRAN''iY KNOT.
42
beloyv the fractured bone at rest. They shou ld, if practicable, be padded to fiL acc urately to the limb a n d be applied over the clo t hing .
(b) The bandages m ust be applied firmly, but not so t ightly as to cons trict the circulation of b lood in the limb. 'When the patient is in the rec u mbe n t position double the bandage over a splint to pass it under the trunk or lower limb. As a general r u le :-
For the trunk t h e b road b andage should be used. Pass it once round the trunk and fasten it by tying the en ds, or with two or three safety p ins o n the side opposite to the fracture, but if to sec u re a splint for a broken thigh, over the splint.
For tIle arm or forearm t he narrow bandage should be used. Pass it twice round the limb, ann tie the ends over the outer splint.
For tlte thiglz or leg the narrow or medium bandage may be used . It is frequently convenient to doub le the bandage at the centre, pass it un der the limb, bring the loop over the limb, pass both ends of the bandage thro ugh it in opposite directions, and tie them over the o ute r sp li nt (Fig. 17).
In applying ban dages near a fracture the upper one should be sec ur ed first.
5. When h cemor rhag e accompanies a fra c dtu re it must LJe atl·..:nded to fiIst, and the woun c ov ered by a clean dressing.

6. No attempt mus t be made to remov e a patient suffering fr om a of the s pine, pelvis, or thigh, except in a recumbent position, preferably upon a stretche r.. .
7. In every case of fracture 1t necessary to cover the patient to keep hlm w.arm, and so lessen the effects of the SHOCK of the aCCIdent. F. In all doubtful cases, trea t as a fracture.
SPEC I AL FRACTURES .
Fracture of the Cranium. ---:-A of the upper part is usually caused by direc t vlOlence-for examp le, a bl ow on the .head . A fracture of t he base is caused by in dir ect Violence , thro u gh a fall on the
43
F IC . I 'J.
44
heaa, a fall on the feet or lower part of the :::pine, or a blow on 10\\ er jaw. .1j the upper part lS fractllred, slgn.s. are irregularity, and. frequently msenSlblbty, eIther immediate or commg on gradually. .l.f the base Z5 fractllred insensibility may corne on immediately, blood or a clear fluid may issue from the ear channel blood may escape fron; the nose, or it may pass down to the stomach 1 · , \\" 1ence It may be vomitthe fracture may Involve the orbit causing a blood-shot
TREATl\IE 'T .
Injury to the brain is great danger attendFIG. I8. mg a fracture of the cranium. For treatment r' see " Concussion and .ompresslon of the Brain," pages 13IJ 13 2 . of t he Lowe r Jaw.-Pain, loss of power (ll:abll lty to speak and move the jaw freely), Irr eg ulanty of the teeth, crepItus and bleeding from the gum are the usual signs and symptoms.

-45
TREATi\lENT.
T.-Place the palm of the hand below injured bone and press it gently against the upper Jaw.
2.-Apply the centre of a narrow bandage under the chin, carry one end over the head, cross the ends at the angle of the jaw, carry tl:e long end across the chi n and tie the ends on the sIde (FIg. I8). of the Spine . -'J he yertebral column may be broken either by direct or indirect violence. F[llling from a height on back across a ba.r. or upon an uneven surface IS an example of dll E.c t fracture and a fall on the head, causmg a broke.n neck id an example of indirect violence. 'What IS regarded as a broken back consis.ts of. a fracture of one or more of the vertebrre \\"Ith dISplacement of the fragments, whereby the spinal c?rd and the nerves issuing from it may be torn, causmg com plete or partial paralysis of the below the fracture. Pain is present at the seat of Injury.
TREATl\IE ' T.
I. - Prevent al1 movement on th e part of the patient.
2.- Cover the pJtient warmly . .
3.- To remove the patient, place hm1 on a stretch er or sh utter as follows :-
(a) Turn up the collar. of his c?at; roll up a stick or umbrella m each Side of the coat
4'0
'S <:> that ,the ends are level with the top ot h IS pass a broad bandage or handkerchIef under the head and secure it to the sticks . If no coat is worn or doubt as to its strength and length pass a of bandages under the patient to serve Instead of, or in addiLion to, the coat.
(b) A. on each side grasps the rolled coat \\'lth hIS .hands well apart; a third grasps the clothIng on both sides on a level with the hips; a fourth bearer takes charae of the legs.
0
(c) On the word beil:g given, all lift together and carry the patlCnt by short side paces over t.he stretcher and carefully lower him on to It. If a fifth bearer is available the should be passed under the patient Instead of carrying him over it.
4 · - 0n at shelter nothing further is to be the arrival of. a doctor, except to gn"e the patIent water, tea, etc., If he is conscious.
Fr.actured Ribs. -The ribs usually fractured are the SIxth, seyenth, eighth, and ninth, and aenerallv the is midway between the breast bOone tl:e spIne. fracture may be caused by indirect VIolence, drIVIng the fractured ends of the bone outwards, or by violence, driving the fractured ends of the bone Inwards and sometimes injuring the

47
lungs or other internal organ. . If the lo\\"er .ri?s" on the right SIde are broken, the ll\·.e r may be 1l1]Uled, and a fracture of the 10\\ er lefL nbs may wound t!1e spleen. Evidence of the fracture is afforded by pam, especially on atlempting to take a deep breath, and by sho rt and shallow breathing. If the lungs are injured blood, frothy and red, may be coughed up and .expectorated. If the liver or spleen is wounded internal hremorrhage p:J.ge 95) may occur.
TREATMENT.
( a) Tl !lell tlz" fractllre is not c07lljl/catt'd by all z"lljll7Y to an illterllal or.;an :--
r .-Apply t\\"o broad balld<1ges round the chest suffiFie 19. ciently firmly to afford comfort, with the centre of the iirst immediately above and that of the second immediately below tbe fracture. The lower bandnge should overlap the upper to half its
48 extent. The knots are to be tied rather to the front on the opposite side of the body. Another good plan is to apply a strong to\ye! folded about eight inches wide, tightly roune the chest, securing it with three or fOUl safety pins.
2.-Place the arm on the injured side in a large sling. (Fig. 19).
(b) TV/len an internal organ z's illjured-
J. - Do not apply bJ.ndages round the chest.
2.-Lay the patient do wn, incl ined a little towards the injured si .je.
3· -Loosen clothing, ice to suck, alJd place an Ice over t:le sen t of injury. freat as for lt1ternal h::emorrhage (se e page 95).
4· -Place the ann on the injured side 111 a large sling.
of the Breast-bone (sternum).-
\V hen tOlS fra.cture can be felt or is suspected undo all tIght. and keep the patient quiet in an easy pOSItIOn until the arrival of a doctor.
FR ACTURE 0F THE BONES OF THE UPPER LIMB.
of the Collar-bone (clavicle) .- This fra c ture IS freq uently ca.used hy a fall on the hand or shoulder._ The arm on the injured side is partially

4 )
helpless, and the patient it at the elbow with his hand, and 111chnes hIS head towards the injured side. Tne fractured e nds generally be felt to overlap, the outer fragment bell1g the low er. The general signs and symptoms of frJ.cture are mostl) present.
TREA ' \l\1E [ T.
1. -Remove the coat (see page 19), and as much more of the clothing as is expedient.
2.-Place a pad about two inches thick and four inches across in the armpit.
3.-Gently bend the forearm \yell up, keeping. tl:e shoulde r as far back as practicable, and support It 111 a " St. John" sling, made as follows :-
(a) L'lY an unfold :: d bandage across the chest oyer the injured limb with one end on the uninjured shoulder and the point beyond the elbo'w on the injured side. (FIg. 20).
(b) Pass the lower end of the bandage under the injured limb, across tIle b3.ck, and tie the ends somewhat loosely in the hollow in front of the sound shoulder.
(c) Fold the point m'er the elbow of the injured limb and secure it by one or two pins (Figs. 21 and 22).
4.- Tightly secure the injured limb to the side by a broad bandage passed round the elbow and trunk, so as to lever out the shoulder, the pad forming the fulcrum.
S.-No\\" tighten the sling.
'When both collar-bones are keef,l the

FIG . 2jA.
FIG. 23B.
shoulders back by narrow bandages tied round each arm, close to the shoulder, passed across the back, over the opposite arm and tied together in front. The forearrns should be raised and supported by the bandages. (Figs. 23A and 23 B).
Fracture of the Shoulder-blade (scaplIla).-
Apply the centre of a broad bandage in the armpit of
51
the injured side, cross the ends over the uninjured shoulder and tie them under the armpit. Support the lim b in a St. John sling (Fig. 24).
Fracture of the Arm (Ilulnuus). - The bone may be broken :-(a) Close up to the shoulder; (b) near the FIG middle of the shaft; (c) close 24· to the elbow.
All the general signs and symptoms of fracture are usually present.
TREABIENT.
lVhm the Fracture zs close to the Shoulder-
I.-Apply a broad bandage with its centre abo\'e the middle of the arm round the lim band body, tying it on the opposite side.
2.--Support the forearm by a small arm sling.
TV/len tlte Fradllre is mar the JI.ftdd,e (f tile Shaft-
1.- rend the forearm at a righ t angle to the ann.
2.-Apply splinrs, reaching from the shoulder to the elbow on the outer and inner sides of the arm, and, if enough can be procured, to the front and back also. The front splint

53
111 ust on no account be so long as to press upon the blood-vessels at the elbow joint.
3.- ecure the splints by bandages above and below the fracture. If splints . are not available, Secure th'3 arm to the side by two broad bandages.
4.-Sl1pport the forearm by a small arm sling. (Fi9"' 25)·
Fractures Involving the elbow joint, whether of the arm or forearm, are attended with so much swelling, and it is so difficult to ascertain the exact nature of the injury, that when the accident occurs indoors the limb should be laid upon a pillow in the most comfortFIG. 25· able position; ice or cold water dressings 1 Id be applied to the injured par.t, but rio should be attempted pend1l1g the arnval of a doctor.
52
54
TJlhen the auidmt ocmrs out of doors-
I.-Take t\\"o pieces of thin flat wood, one long ellough to reClch from FIG. 26 the armpit to below the elbow, the other long enough to reach from above the elbow to the finger t'ips ; tie them together to form a right angle. (Fig. 26).
2.-Apply the al1gular splint so made on the inner side of the flexed limb.
3·-Sec ure by bandages above and below the fracture .
4·- Support the limb by a large arm sling.
s ·-On arrival a,t .home ren:ove the splint, and treat the I!1Jury as If it had occurred indoors .
Fracture of the Forearm.' \Then both bones (the Radi us and Ulna) are broken, the ge n eral signs a n d symp t oms of fracture ?re usually present. '\\Then one of the bo n es only is. broken the signs and symptoms. are as. a rule pam , loss of power, s\\'elling, and IrregularIty . An lt1tpacted fractureof the Radius
55
just above the wrist is a common result of a raIl on the hand.
TREATMENT
.
This is the same, whether the fracture is ot one bone or of both .
I.- Bend the forearm at right angles to the arm,

FIG. 27. FIG. 28. keeping the thumb upwards, and the palm of the hand towards the boc y.
2.-Apply broad splints on the inner and outer sides from the elbo\\ s to the fingers.
3.- A pply bandages, embracing both splints, immediately above and belo\\' the fracture and round the hand (Fig. 27).
...J. .-Apply a large arm-sling . Cru s he d Hand (fracture of the bones of the carpus, metacarpus, or fingers).
TREATTllENT.
I.-Apply a carefully padded splint to the front of the band, reaching from well above the \\'rist to beyond the tips of the fingers .
2.--To secure the spli n t apply a narrow bandage crossed in the manner of the figure 8 to the wrist and hand (Fig. 28).
3·- A pply a large arm-sling .
Fracture of the Pelvis .- \Vhen, after a severe injury in the neighbourhood of the haunch-bone, there is no sign of damage to the lower limbs, but the patient is unable to stand or even to move the lower limbs without great difficulty and pain, a fracture of the pelvis may be assumed to have occurred. The and organs, especially the bladder, Wlthm the pelvis are in danger of being wounded.
TREATMENT .
I.-Lay the patient in whatever position is found to give. the greatest ease, and fl ex or straighten the lo\\er lImbs as the patient desires.
2. - Apply a broad bandage round the hips tight enough to support the partf'1, but not so tight as to press the broken bone further inwards.
3·- To remove the patient place him on a stretcher, acting on the same principle as that descrit ed under " Fracture of the Spine" (see p:.1ge 45).
FRACTURE OF THE BONES OF THE Lo·." ER LIMB.
. .Fracture of t he Thigh - bone (femur). - The (hIgh-bone may be broken at its neck, anY\\' here in Ibe shaft, or close to the knee. A fractul e at the 57
neck is likely to occur in old people very slight injury, and is often difficult. to dlstmgulsh from a severe bruise of the hip, but It may be assumed when after an injury near the hip joint, the patient when lying on the back, raise the heel from the around the bone is broken . All the general b , 11 signs and symptoms. of fracture ar.e. usua y present and a prominent sIgn is the posltlOn of the foot,

FIG. 29 .
which, as a rule, lies on its side. Shortening may vary from one-half to three mches.
TREATMENT.
I.-Steady the lim b by holding the f?ot. 2.-Gently draw down the foot and bn,ng It mto line with its fellow. When two or three assIstants are at hand, it is one person 's duty to hold the foot in Dosition until the splints are secured .
3.- A pply a splint on the outer side from the armpit to beyond the foot.
4.-Applya splint on the inner side from the top of the thigh (the fork) to the knee.
5·-Secure the splints by bandages as follow'::> .(a) Round the cbest just below the armpits, (b) round the pelvis on a le vel \\'ith th e hip joints, ( c) above the fracture, (d) below the fracture, (e) round the leg, (.f) round both ankles and feet, and tied below tbe feet, (g) a broad bandage round both knees ( Fig. 29).

FIG. 30.
"When single-handed, or ",b e n the patient is a woman, it is expedient, ::ltter extension of the limb, to tie the fe et together, dispense with the inner splint, and pass the bandaO'es rOllnd b :) th limbs (Fig. 3 0 ) . b
Fracture of the Knee -ca p (patellll) -The knee -cap may be
FIG. 3 [. br\)ken by fa ll ing o n the knee ( Girect violence), b u t more frequently it is broken by musc ular action , as follows :-
\Vhen tbe foot slips in the attempt to prevent a fall the muscles in the front of the thigh act with such force as to snap tbe knee-cap in two ( Fig. 3 I).
Pain, loss of power (the limb will be quite h elples s), and irregularity (a gap may be felt bet\\"een the broken fragments of bone) accompany this injury.
I.-Lay the patient on bis back, rais e \yell and
FIG 32.
support tbe head and shoulders, straightell and raise th e lirnb.
2.-Apply a splint al o ng tbe back of tbe limb, reacbin O' from the butto ck to beyond the heel.
3.-1\pply a n8rrow bandage with its centre imm.:=!-
59
diately above the knee-cap, c ross t he ends behi n d over the sp l int, and tie in fron t below the broken bone. fo ens u re firm n ess app ly a second bandage in a sImilar way, but comme n ced below and tied above the broken bone.
4·-Further secure the splint b y bandages round the thigh and leg.
5·-Su pport the foot well off the ground by a pillow, roll of clothing, etc ., or if none of these are at hand by resting it on its fellow (Fig. 3 2 ).
6. -Apply an ice' bag or a CJld water dressing over the fract ure .
Fracture of the Leg (tibia and libltla).-One or both of the bones may be broken . When both bones are broken all the general signs of fracture are usually present, but when one bone only is broken deformity is not always noticeable. A fracture of the fibula three or four inches above its lower end :s frequently mistaken for a sprain and sometimes [or a dislocation of the ankle.
TREATMENT
I. -Steady the limb by holding the ankle and foot.
2.-Draw the foot into its natural position, and do not let go until the splints have been fixed.
3·-Apply splints on the outer and inner sides of the leg, reaching from above the knee to beyond the

6 1
foot. If only one splint is available place it on t he outer side. () b 1 (b) - tcure the splints by bandages a a 0\ e, beGw the fracture , (c) immediately above the knee, - -
d) round b oth ankles, (e) a broad bandage round both knees (F i,3". 33).
single-handeel, or when the patient is a
60
WOlllan, after extenJing the lilllb tie both feet together, cli::;pense with the inner splint, and pass tbe bandages round both limbs (Fig. 34) . " Then no splint is available tying the legs, ankles, and knees together is g-reat service.
Crushed Foot (fracture of the tarsus, metatarsus and toes).-This accident is commonly caused by the passage of a hem'), \\eight over the foot, and may be recognised by pain, swelling, ,md loss of power.
TREAT:'\IEl T.
I . -Remove the boot (see page 19).
'2.-Apply a weIIpadded splint to the sole of the foot, reaching from the heel to the toes.
3· -Apply a bandage FIG. 35· crossed after the manner of the figure 8 (Fig. 35).
4·-S uPport the foot in a slight ly raised position.
DI S LO CAT I ONS.
A dislocation is the d isplacement of one or more of th e bones at a joi n t.
The joi n ts most frequen tl y dislocated are those of the shoulde r, elbow, thumb , fingers, and lower jaw.

SIGNS AND SVMPTO:J1S OF Dl LOCATION .
I .- Pain of a severe sickening character at or near the joint. .
2 - Loss of power in the 11mb.
3: - Numbness of the parts belo\\' the seat of dislocation. . .
4. - Swelling about and below the jomt.
s .-Fi x ity of the )oint.-The. lImb cannot be 111m'ed at the joint by eIther .the patIent 0: others .
6.- Defo r mity of the The 11mb an unnatural position, and IS mls-shapen at the jomt.
TR EATl'IIENT.
No attempt should be .made by .anyo?e a doctor to reduce a disJocatlOn. Pendll1g hiS arrnal .-
(a) TT'Iwz tile aeaden! OC(l{1'S out oj doors-:-. . Support the limb in \\:hatever p'osltl?n most ease to the patient, bearIng 111 mmd the necessity of lessening the effects of joltina during transport.
(b) TVlten fa tie II t is .
I.-Remove the clothmg from the hmb.
2.-Place the patient on a or bed.
".-Rest the limb on pillows m the most (:om- .) .. fortable pOSitIOn. .
4 . - A pply cold (ice or cold water) dressmgs to the joint.
s .' Yhen cold ceases to give comfort apply
63
64
warmth (fl a nnels or tow els wrung out of h ot wat er).
6.- Treat shock (see page 135).
SPRAINS.
When, by a s u dden wre n ch o r tw ist, t he ligaments and the par ts around a join t ar e stretched and torn the joint is said to s,'rai n ed . " Going over" the ankle is a common example .
SIGNS AND SY.\IPTOl\IS .
1. - Pain a t t he joint after a twist or wrench.
2. - I nability to use the joint.
3.-S\\'e ll in g and disco loration .
T REATMENT OF SPRAll E D ANKLE
JJ ?zen out of doors -
I.-Apply a bandage tightly over the boot, beon the sole at the instep, crossing on the front of the ankle, amI carrying It round a n d round the an k le, where it is to b e fi r mly t ied .
2.--vVe t the bandage after application; it is thereby tighte n ed.
Alter reaching shelte r-
r.- R emove t he boot a n d stocki ng (see page 19)
2.- Place the limb in the m ost comfortable position ; us ua lly t ha t is well raised .

65
3.- A pply ice or cold sings to the joint as loner as they relIeve pam .
4 .' Nhen "cold fails to give comfort, apply hot f ome ntations . ._ ' Vh e n other joints are sprained, treat them as It dislocated. . .
When in doubt as to the nature of tIle injury, treat as a fracture.
STRAINS AND RUPTURED CLES.
·When, during severe exertion, muscles. or -e over-stretched they are said to be strall1ed, If they at 'b d d are actually torn they are descn e as rupture .
SlG:-lS AND SY:}IPTO.\lS .
I. - A sudden sharp pain . .
2. - When the muscles of a limb are stramed they may swell and cause '._
3.- Further exert.ion IS dIfficult or. ImpossIble ., f01 example, if the stram has occurred the back the patient may be unable to stand upnght.
TREAT:\lENT .
I.-rlace the patient in tIle most comfortable position, and afford support to the injured part. .
2.-Apply hot \Yater bottles or hot fomentaLlons when tIle pain is very severe.. ., ..
A so-called strain in the grom (herl1la) IS an mJury of a totally differ ent nature (see page I q).
D
,
QUESTIONS ON C HAPTER II.
The n u me r als in di cate tlu p age S wh ere the may be fo u nd. am w ers
Whabt ske leton, and \\ hat purlx,sCS , y It r '" '" arc sen'cd
ar: bones of skull arranged"?'
• h'lt .are the boundanes of the cranium) the bones of the face '
Descnbe the lower jaw
is the angle of the ja;; '? ,.,
\",hat names has the uack·uone")
\\ hat IS a Yerte ura ?,., '
vcrtelJr«; are in the spine?
lat .the regIOns. ar ll1e sl)ine anJ 11 0'\'\:
te bl<e are there 111 each? ... mall}'
IV10hw the .spine endowed \\ ith free
at 1:> a flU? '
}J,OW I,airs of ;i'bs are' 'l'here ?"
\\ IS the breast· uone ?
What the uones of the '1;;111h?
What IS the peh' is ? ...
What is the hip joint? ...
bones of the lower l' .. . \\hatlsaJOlnt?.. lI11bs? .. .
DLSCI jbe a moveable joint:: : be the shoulder joint
Descflbe the ankle joint . ..
I low are muscles classified ")
Descljbe muscles'
Descn,be mvo'untary muscles
'W hat IS a fracture ;>
What are the frac't'l; re ?

\Yhere does a bonc break \\ hen direct violence is the cause of fracture? .. ...
,\\ here does a bone break whell indirect \"iulence j,;
cause of fracture? ...
ITU\\ maya fracture !)e cau-;ed 1>)' muscular aClion ?
III \\ hat twO ways may fracture"> be classified? ."
'\"hat is a simple fracture ? ..
\\ hat is a compound fracture?
\Yhl\l is a complicatel! fractlllc ?
\Yhat is a comminuted fracture:
\\'hat is a green-slick fractnrl'?
\\-ha t is an impaCle(l fracture?
the gencral and ,>yl1lpLums that n1:1)' be pre enL in a case o f fraclme ,..... 35, 36
\\' hal fractures affurd the musl complete e.'-.alllple of the signs antI S) mpto\l1 s? ... ..
In making up your mind wheth e r a fractur.e hal! ucc.urred or not, whal p oints sho uld )'llU take 111tO COlbldeia· tion heyoml the sign,> and
\Yhat apparatu;, may I)c necessary fur the treatment of fractures? .. 3 6
Ho\\' may splint' be imprll' i"ed ? , , 36 , 37
lIo\\' may bandages be , " :'7
Describe E march's tri'l.ngular bandage... 37.3') (hg. d
1n \\hat ways may the triangular handage I)e folded fur llSL' 37
110w many kinds of ann·slings arc there, amI \\ hat art: they cal\t:cl?.. . .., ... .., ... 39, -I- e , -1-9
\ \ ' hat knot is to he lic(!' ::tnd \\ hat kn o t a"oidet\? 40
Whal is the object o[ first aicltrcatmcnt of fractures? ·tI
Civc the general rules [or the t reatmenl of fractures -+1
llow should splints be appli e d? ., 4 1 ,4 2
l l ow should bandages be appli 2d? ... 4 2 ,43
\\ hat may cause a fractnre of the upper part of the claniuJl1 ? 43 II 1
66
I'AGE
22
?-.. 22 22, 23 23 23 23 ? -J 25
25 :!o 2() .!&
26 to 28 28 30 30 31 3 1 3:! 3 2 32 33 33 33 ... 33, 34
tit.:
PAGE: 33 34 3434, 3S 3-+ 3-+ 3-+ 35 35 35
... .., ...
35
' Vha may C:3.U'ie a fracture of the base of the 43. 44
What are the of fracture of the upper part of the cranium? 44
What are the signs lIf fracture of the base uf the cranium? 44
'\'hat is the treatment fur fracture of the cranium? 44
\\'hat are the signs (j f fracture of the lower jaw? 44
lI ow maya fractured spine be caused? 45
\ \ 'hat is commonly regard ed a: a broken back? .. . 45
\ \'hat are the symptoms of a fractured spine? 45
H o w may ribs be fractur ed? 46
Irow maya fracture of riiJs be c o mplicat ed ? 47
State the signs and symptoms of a simple and of a complicated fracture o f ribs 47
" 'ha t is a frequent cau e of fractured collar·bone ? 48
'Yhat are the igns and sy mptoms of fractur ed colla:'bone?
'" .. . .. 48, 49
At what points may the bone of the arm be broken? .. . 52
Are the general signs and symptoms of a frac t ure alway present in a broken forearm? ... 54
Stale the caus e of a common fracture of the radius 5 S lIow would you recognis e a fracture of the p e h·i. ? 56
A t what points may the thigh-bone be broken? ... 57
\Vhat are the .c; igns and symptoms of fractur e of the thigh-bone? 57
"'hat are the causes of fracture of the knee-cap? ... 58, 59
\ \'hal are the signs and sym ptoms of fracture of the kn ceca p?

59
Are the general signs and symptoms always present in a fracture of the leg? 60
What mistake may ea:;ily be made when the fibula is broken ncar it. low e r end?
What is a dislocation?
60
62
'tate the signs and of dislocation 6.1
What is a sprain? .. : ..... 'f s \Vhat are the signs and 0 . P 6+
Slate the treatment of a an e... . . ...63 , 65
Stale the treatment othhcr a or fracture
\Vhen not sure whctler t. e?1I1Ju ........ . h o w would you treat It. ... d?
-I w ma muscles be straincd or rupture . thl signs and of s,rall1s ... State the treat ment o f s·
. ld racti:;e improvising malerial, Firsl Ald Students shou . p I-nots makin a slings, and ld ' b laaes tyll1g b fo wg am t lthe following injqries.
arm
l-:'eef and granny .. , i:'1 b . . ... ,p
Knot for applying lowe r . '45, 46 . Rib s
Fr'lc'ures-Lower JUw, 44· ) 46lo 48 Breast< (simple and complicated frac 8 lu:'es 5' I Bo;h collarb 8 Collar-bone, 4 0 A one, 4 . I up to shoulder, 52. rm, bone s, .5 (, Arm, c Arm or forearm when the near mIddl e of shaft, - 1:' . 55 Crushed hand, .' I 'eel 53 'o rCall11, . I' 1 elbowlsll1Vo: ' ·Thih(man), 57,5 S. -r: 1Jg 1 5 5, 56 . I) elvls, 56,' Ie- hand ed) , 58. h .nce(wo ,nu n , o r man "(11en ) to 6r Le CT (woman, or 59 60 L ea man, " b d f t 6? cap, , '.' I b h lded) 62. Crushe 00 , _. 6 6 man wh c n slI1 g e- al '. d . ... 3, 4 . . Out of cloors and 111 oms...... 6-t
DlslocatlOllS- ... . .,. _ S rained ankle .. , .. , ... 6)
Srrains and ruptured musc les
58 - PACE
... ...
...
...
69 P \ ,F. 6.> State the treatment
dislocation... 64
of
,
the treatmen () ... 36 . .> 7 11l1pro\i sing splints... 37 Improvising bandages 37 Folding 3l)
39.
Small
, ... ...
raws ..
.,.
Large
sl:ng
-to
arm s11l1g ..
4'
CH.\PTER III.
TME ORGANS OF CIRCl.:LATION.
THE concerned in the circulation of the blood are the Heart, the Arteries, the Veins , and the Ca pillaries.
The Heart is situated in the chest behind the breast-bone and rib cartilages, between the lungs :1nd the diaphragm; it lies obliquely with a q of its bulk to the right and the remaini ng three-quar ters to the left of t h e midd le line of the body, Its beat may be fe lt just be low :1nd to the inner siJe of the left nipp le. The heart has four cavities, two on either side of a central partition. The t\\·o upper cavities are named the righ t and left auricl e s, the two lower the righ t an d left ventricles.
Arteries :l.re ,-essels \\ hich cOl1yey blood. from the heart. Veins c"'<1.rry blood to the heart. Capillaries connect the arteries and yeins.
I n the general (systemic) circulation arterial blo od is drivell fro111 the left ventricle of the heart lllto the aorta (the main artery of the body). From the aorta branch arteries are given off to all pClrts of the body. These di\'ide and sub-divide, and become so small as to assume microscopic dimension " when they are termed ci.lpillaries.

T 1,\1' 'nx (voice hox); T, Trach a (wind·pipe); R.. L. )." L") (T' I 1 Left Lung (Lhe lungs are c1 ra wn to J'lght uno, ,. J I) l' A 1"(Thl expose lhe hearL and blood :esseVs ; . .' I 'Zr Left Ven: L.A. Left Auricle; R.V. Right entnc. e: SV C Sl1 erior Iricle ' P A. Pulmonary ; Ao. " ., P of ,ena (the large yein carrymg flom the the bony t,"-> the hearl); I.Y .c. to the \'ein carrying blood from lhe er pa b 1 ) in the hearl). The four pulmonary veJl1S cannot e Slown diagram
70
FIG , 36
In the capillaries an interchange of gases and fluids takes place, ,vhereby the nourishment and maintenance of the tissues and organs of the body are provided fnr, and the blood becomes dark and impure.
Venous blood passes from the capilLuies to the veins, which convey it towards the heart, getting large r and larger as they proceed by being joined by neighbouring ,-eins until they finally, as two large Yessels, reach the right auricle of the heart. The Yeins, especially in the lim bs, are provided with valves at frequent intervals, which prevent the back\\ard fbw of the tJlo od.
The pulmonary system of blood vessels is concerned in carrying the blood through the lungs. From the right auricle the blood passes to the right ventricle, and is thence carried to the I ungs, where it is purified by contact with air, and becomes scarlet in colour; it is then com-eyed to the left auricle of the heart and passes into the left ventricle, t11 us completing the circulation.
The heart contracts in adulls at an average rate of seventy-two times a min ute, but the rate varies, increasing as the position is changed [rom the lyin g to the sitting or to the standing position; hence the importance of adjusting the patient's positiO/: in C:lSCS of hcemorrhage. At every contraction of the left ventricle blood is forced into the :lrteries, causing the' pulse. which may be felt where\'er the finger CLl,n be

Ex/>lallatioll. In the of diagram is the heart its four chambers, Above t I heart is shown the lung (pucirculation. The lower Part represents the gen eral (sys, ' J t' Vessels con- temlc) CI!'CU a IOn. ) blood taining Impure (venou,s those shown black, \\ hlle pure (arterial) ar-:: shown white, The con,nect,lI1g vessels represent the The arrowS show the direction of .f the flow of blood, t
FIG. 37·
Dr.H;Ri\M OF THE CIReuLA'IION OF TIlE BLOOD. _. bone. In the d n arlery as It passes 0\ er a place on a <, be found. veins no pulse IS to E. , bl d' cr is of three kmds :011' ". Capillary. I, Artcna. 2. ,)
72
73
ARTI:<:RIAL HfEJIORRH,\CE.
1. '- IBlood from an artery is scarlet
2 - f the d d ' the' bI d wcun e is near the ski 00 spurts out m Jets .. . n pulsation of the heart. cOllesp on dll1g to tile
TS1·hde Pfrethssure point (see below) is on th e eo e wound.
ARRFST OF t\. - ,.," "RfERUL II.E\IORRI-L\CE
..:\.1 tenal hcemorrhaq-e is \ -I " ' . arrested b . v " ,\ len practIcable Lo be . y ptessure, positIon of tl !. d' ele\'atlOn of the bleecll' le uo)" and P ng part ressure may be'- . I,- Dio-ital tl" , Ii b _ - lat IS, applIed \\ith the thumb or ngel:;, and may be (a) (Ii) at a sp0t called the ' on the. \\' OllIHl; pressure points a' ,gressure POIilt. The dots on the f' . <, Ie, lt1 Icated by numbereu ? lontlsplece.
-By a pad and band ( , the wound' (0) 0 -tl age . tourl1l.quct) (a) on
3 By fl . ) n le 1)1 essure l)Oll1t - exton '
To apply a pad band 0place a piece of lint 'J'. aoe to the wound h' f [ 01 J,len or a cJea I ell ' C Ie olded into a hard )ad < ( n. 1an (erand secure It by I-.. I d' 011 t,he bleedll1g point . , a ;Jcill ,we twbtl t' J ' the lI1jureu part To fi ld {' 0)' lec round the four corners to tl 0 t le handkerchief, orino. 1e centre and re t h b until a hard pad is forn d ' c, , pea t e process 1e. I he smooth surface is

75
Vlaccd on the woun], and, to prevent the pad fro m uniolding, the puckered surface may be stitched or ft \: e u by a sJ.fet y pi n. A h:ud substance, suc h as a stone, may be enclosed in the centre of the p(ld.
A Tourniquet may consist of a pa1 to be placed
0 ,1 the p 'essure point, a strap, cord, or bandage to encircle the limb and p:l.d, and a tiglttc'lling arrangeJIlL'llt, sLlch as a stick or other means of twisting the b.ll1d to tighten it.
To improvise and apply a tourniquet :-
I . -Apply a firm pad on the pressure point.
:! .- Encircle th e lim':> by a narrow bandage with its centre o\'er the pad,
3.- Tie the ends of the bandage in a half knot on the opposite side to the pad,
-t.-L::ty the L\\isting stick on the half knot, and over it tie a reef knot.
5.-Twist the stick to tighten the bandage, thereby pressing the pad upon the artery, and arresting the flow of blood.
6 . -Lock the stick in position by the ends ot the bandage alreldy applied, or by another bandage passed rOllnd the stick and limb,
The pad of the tourniquet must be accurately placed upon the pressure pvint so as completely to com press the anery j otherwise arterial blood \\ ill be allowed to pass alont; the limb, a n d the veins, being compressed by the tourniquet, will not allow the
74

b loo d re tu rn through them to the heart, and the resu lt \\'tl l be da ngerous swelling and conge!-.fl o n,
Sh o ul d suitable pad not be at hand, a knol l1uy be ,made 111 the centre of the bandage, and \\ he;, ava ilable, a stone, cO I:k, etc, enclosed, ill it to gi\'e it and bu l k . .See that the hulgll1g and not [he fllt SIde of the knot IS next the skin.
. An. elast,ic bandage p:1ss r; d tightly round the limb, Itnl:1edlately above the seat of arterial hremor\\' 111, arrest simplest prepared fOlm of tIllS bandage IS a stnp of elastic webbil)CT to thirty inches long and t\ro incl1es wit h a piece of tape sewn at each end . An elDstic b,elt or se,lTe the sa I?le, purpose. E'\cept "hen part a 11mb IS torn off, It IS not ;ld\'isable to use an e las,tlc cord or bandage if other apparatus can be had, It cuts off all circulation in the limb.
FleXiOn co ? sists of the application of a pad on the p:ess ur e POJl1t at the knee or e lbo\\' joint, flexing the lllnb to pressure, and SCI. uring the limb in tbe fl exed pos Ition by a banclnge crossed like th e figure 8.
GENERAL RULES FuR OF' A \ Vou:-m
ACCOMPANIED BY ARTERIAL H£:\JORRH.\Cr-:.
I. Stop bleed ing .
II. Prevent injurious germs from getting into t he wound. 77
To attain these ends: -
I . Place the patient in a suitable posit jon, bearing ill mind that the blood escapes with less. force when the patient sits, and is still more checked \vhen he lies do\\'I1 .
2 . R.levate the bleeding part, a!'> thereby less blood finds its \\'ay into it.
3. Expose the wound , removing whatevei.· clothing is necessary. (See Rule 8, (7 .)
4. Apply d igital pressure. . (a) If the wound is small on the bleeding spot., (/I) If the wound is large on the pressure POll1t next to the wound on the heart side. The nearest pressu re point is cbosen in 01 der to avoid cutting off the circulation from as much of the part as possible, but sometimes it is necessary to apply pre!'>sure still nearer to the heart.
S. Remove forei g n bodies, such a broken glas3, bits of clothing, hair, etc, seen in the wound; Jc, not search for foreign bodies YOll cannot see.
6. Cover the wound with a clean and . firm absorbent dressing. A hard dry pad of boracic gau;.:e or lint is to be preferr e d, but , \\"001, lint, or g ,Ute, or a cl ea n pIece of l1mn \Ylll answer the purpos p , Should allY doubt be entertaillcJ as to the cleanliness of the dressing, a clean piece of unprinted paper, such as the inside of an
envelope, shou ld be placed next the wound before applyi ng the pad. (Compare pages 75 and 76 .)
7. Bandage tightly over the pad unless :-
(a ) Foreign bodies are s uspected to be left unseen in the wound.
(1-) There is danger of causing injury to a fracture.
I n these cases a light dressing only should be app lied .
8. Apply a pad and bandage or flexion on the pressure point (see Rule 4, b ), but only in the following cases: -
(
a ) A s a temporary llleasure while the wo u nd is being exposed, examined and coyered.
(b ) A s:J. mo r e permanent measure \\ hen bleeding Ca n no t be stopped by the pad a n d bandage on the wound, or when, in accordance with Rule 7, the tigh t bandage has not been applied.
9. Afford support to the injured part.
W hen par t of a limb has been torn off or the wound is lacerated (for example oy the claw of an animal or by machinery) hcemorrhage frequently docs not come on a t once, but as there is a danger of severe hce m orrhage later, means for its arrest should be app lied to the limb, but not tightened unless Do not disturb a clot of blood formed over a wound.

Students practising arrest of arterial hcemorrhagc should feel the pulse to see when the current of blood in the artery has been stopped, and should then immediately relax the pressure made on the I n this way the importance of the accurate applicatIOn of pressure will be and the amount of force necessary wi 11 be ascerta1l1ed.
Till<: COURS1': OF 1'111': 1\1.\lN ARTERIES, .\ND THE ..:\RRE. T OF HJE'\IORRHAGE.
(The num bers of the pr.:ssure points refer to those o n the Frontispiece.)
TlIe L\RGE .\RTERIES "\ViTHI l THE CHI·:S T A?-iD
No attempt should be made to cleanse a wound e'l:cep t with sterilised \\ ater (that is preyiously ooiled 'i9 and allowed to cool), all, I experience, especially in recent wars. has shown that those \younds which were proYisional1)' tre:1ted with a dl} dressing subs.eauentlv dresse.l by a surgeon \Ylth proper appllance. did best:
The is the central or trunk artery of the body. Commencing at the lett ventricle it forms an arch behind the upper part of the breast- b on e. From the ar ch are given off the large branch es which carry the blood to either side of the head and neck and to the upper limbs . The Aorta passes do wn on the left of the spi n e to just below the whe re it diyideS into two great branches (the Jbacs)
80 which convey the blood to the organs III the pelvis and to the lower limbs.
Wounds of these arteries are one cause of inkrnal hremorrhage (see page 96).
ARTERIES OF THE HE.\'D AND
NFCK.
The Caro t id Ar te ries (right and left) leave the upper part of the chest and pass LIp on either side of the \\'indpipe and, just below the level of the ,:llwle of the lo\\'er jav,r, divide into the Internal and E\ternal Carotid Arteries. The I nt er nal Car o tid Artery ascends deeply In the neck, and enters the cranium to supply the brain with blood. T he E x ter nal Carotid Art e ry gives off anum ber of branches; to the front the of the tongue (Lingual), the artery to the ,face \FaClal); to the back the Occipital; the artery Itself IS contll1l1ed up\\ards in front of the e:1r it changes its name to the Temporal, nl1d supplIes the scalp in the neighboL,rhood of the temples.
When a Carot id A rtery is wounde d as i 11 the case of a cut throat, apply the thumb one hand 01: the ,artery at pressure point I, pressing hackwards agamst the backbone and takin(T cnre to avoid the windpipe. It may also be to apply pressure \\Ith the other thumb above the \\ound for two reasons : (a) To arrest the flo\\' of blood from the main (jugular) vein in the neck, which runs
8 1
alongside of the carotid artery and is usually wounded at the same time ; (b) To check the flow of blood from the upper end of the carotid artery itself, which is often considerable owing to communication between the branches of this artery and those of its

fellow. Digital pr essure mllst be maintninecl, by relayS of assistnnts if necessary, lloti l the nrrives (Fig. ,')8) .
The Facial A rte ry crosses the lower jaw in a slight hollow two fingers' breadth in front of the angle, and sends branches to the chin, lips, cheek, and
FIG, 38. FIG, 39·s..!
outside of the n ose. H,-cl11orrhage from \you nels of the Llce below t he level of the eye is to be arrested by ;-
(rr) D igital pressure on pressure point 2 ( Fig. 39), or
(b) Grasping the lips or clleek on both sides of the ,,-ound by the finger in:ide and tht..: thumb outside the mouth or 'l'i(J versa.

. The Temp oral A rtery lllay be fe lt pUlsatin g 111 front of the upper part of the ear. Hremorrhagc from the region of the temple may be arrested by pressure applied at pressure point.) (Fig. -+0) . The Occipital Artery s.1ppllC:s branc.hes to tht..:
of the scalp from beh ind the ear to the back of the head. Hremorrhage from this rEgion may be arrested by digital pressure on pressure point 4, four fingers' breadth behind the ear (Fig. 41) . This point i.., difficult to find, and it is usually sufficient to ap:?ly pressure immediately below the \\ ound.
Hcemorrhage fJ om
t he Forehead or anyw here in the Scalp may be arrested by applying a sl1lall firm pad on the bleeuing point anu securing it by a nalTO\\ bandage \\ ith its centre laiJ on the pad, the ends carried round the head in the direction most convenient. and tied tightl)· o\\:"'r the pad (Fig. 42).
'When a \\ ound of the furehead or sca.lp is asso(iated wi th a fracture, the plan is to apply a ring pad around the seal of id{jury. To make a rillg p::ld, pass one end of a narrow bandage round your fingers; pass the other end of the bandage through the ling thus fo rmed and continue to pass it through :lnJ through until the whole of the bandage is used and a ring as shown in Fig. -+3 is formed.
FIG. 42.
ARTERIES OF THE UPPER LDIBS
The Subclavian Art : ry passes from a point behind the inner end of the col'ar-bone across the first rib to the armpit.

FIG. 43· FIG. 44.
To apply digital pressure:-
r
.-Bare the n eck and upper part of the chest.
2.-P lace the patient's arm against the body so as to depress the shoulder, and cause him to inclll1e his head towards the injured side.
3·-Take your stand opposite the shoulder.
4·-Using the left hand for the right artery, and vt'ce vena , g rasp th e neck Imv down, placing the fingers b eh ind the shoulder and the thumb immediately above the centre of the collar-bone jn the hollow bet\\een the muscles attached to the bone ( pre::,sure pomt 5).
.J' Pr e::s the thumb deeply dO\\'D\vards and bacb\ards agaillst the first r ib, which is be n eath the coliar IJo ne at this spot (Fig. 4-1)'
The Axillary Artery. \\ hich is a continuation of the s ubclavian , k eeps close to the shoulder jo :nt, amI can be fe lt pu Isating when the fi n gers are deeply pressed into t he armpit. Digital pressure is difficult to apply to this a r tery .
Tn apply a pad and lXlllda 0 e: -
J. Pbce a bard p:td the size of a billiard ball in th e armpit (pressu re point 6).
2. - Apply th e centre o f a nnrro\\' bandage o n th e pad; cross the b:mdage o n Fic. 45. the shoulder; pull tbe ends tight and tie them under the opposite armpit, taking care t hat the pad does not slip.
3. - Flex the for ea rm and tie the limb ti g htly to the trunk with a broad bandage, applied on a le\'el with the elbow (Fig. 45)·
The Brach ial A rt ery is a continuation of the Axillary, and runs dO\yn tbe arm on the inner side of the biceps muscle, gradually passing forward until it reaches the middle of the front of the elbow. The 1I1ner seam of the coat sleeve above the elbo\\ roughly indicates its course.
Digital or ilrtrumental pressure 111'l)' he applied at or near pressure point 7.
of the arm over the seam of the coat or the groo\"e on tbe inside of the biceps l11U. cleo Press the pulps (not the tips) on the artery (fig . ..J.6). Some prefer to pass the hand over the front of the muscle (Fig..n). A slight turn of the band out\\ards as It brasps the arm will better enSLlre compressioll of tne arkr)'.
The Brachial altery may be compressed at the

FIG. 47.
To app ly digital pressure extend the limb at ,right angles to the body, palm of the hand IIp\\arcls. behind the limb, and pass the fingers under the back
elbo\\" (prtssure point 8) by flexion. The pad may be a fulded bandkelchief \\ ith a small stone or cork wrapped up in it, but \\·hen no pad is nvailable the coat slee\"e rolled or gathered up \\ ill sene insttad (Fig. -1-8).
86
FIC.49·
FIG. 48.
Just below the elbow the Brachial artery divides into the Radial and Ulnar arteries, which run along the front of the forearm on the outer and inner sides respectively. The pressure points (9 and IO) are about one inch above the wrist and about half an inch from the outer and inner sides of the forearm, where the arteries may be felt pulsating. Branches of these arteries join to form the Palmar Arches in the hanel. The arteries run along on si l1e of the fingers to the tip.
Pressure may be applied to the Rad ia l and Ulnar a1 teries at pressure points 9 and 10, lIy the thumLs (Fig. 49) or as (0110\\ S :- .
1. -Cut the cork of a quart or pint bottle in t\ro length \\ ise.
2.-Lc,y the rounded side of one half on tLe Radial, and of the other half on the Ulnar artery.
3.- Secure them by a light bandage.
To arrest hremonhage from the palm of the hand: -
I.-Apply a firm pad, and make the patient grasp it firmly.
2.-Spread out a triangular LanJage, I urn up the base about four inche., lay the back of the patient's hand on the centre of the bandage, fold the point over the knuckles and wrist, pass the two ends round the wrist, make the

patient pull on the point of the bandage, ciOSS the ends over the fingers twice and tie them as firmly as possible. Bring the point (A) down to the knuckles and fasten with a pin at B (Fig. So).
3.-Elevate the forearm and support it with a c. t. John" sling (see page 49).
Arterial hremorrhage from the fingers may be arrested by applying a small pad on the wound, and securing it firmly with a strip of tape, linen or plaster.
,\RTERlES OF THt: LO - ER LIl\IDS.
The Femoral Artery, a continuation of the iliac, FIt... 50. enters the thigh m {he centre of the fold of the groin, where it may be felt pulsating immediately below the skin. The course of the artery may be by line drawn from the centre of the groin to the mner SIde of the back part of the knee. After traversing two-thirds of this line, the fetTlOral artery passes behind the thigh bone to the back of the knee joint as the Popliteal artery.
Digital pressure may be applied to the Femoral artery at the groin (pressure point I J) as follo\\'s :-
1. -Lay the patient on his back.
88

2.-Kneel beside the patient.
3 . - To find the groin, raise the foot high so as to flex the thigh ; the fold in the clothing at the top of the thigh v,-ill indicate the groin
4.-Place the thumbs o ne on the other up on the pressure point, grasping the thigh with the hands (Fig. 5 I).
5.- Press firmly against the brim of the peh-is.
As there is immediate danger of death it is important n ot to \ms te time In removing the tron sers. When the Femoral artery is wounded in the upper thi rd of its course, pressure must be maintain ed at the g roin . No r ea ll y s::ttisfacto ry tourniqu et has been l'IG S1. devised for compression :::t this point, and rel ays of assist:-.nts shoulu be employed to ke e p up the pressure unt il the doctor arrives; each fr esh assistant places his thumbs over those of his pr e decessor, \\-ho slips his away from beneath, and thus gushes of blood are prevented dur ing th e change .
Application of a t ourniquet to the F e m or a l artery (pre,sure point] 2) :-
-When compressi o n of this artery, it is a
90
9 2
go od pla n to d raw a c h alk li ne from the centre of the gro in t o th e inn e r side of the back of the knee' place the pad of th e on t his line as u p as the ba n dage can be applJ ed. T he pad shoulu be the size of a law n tennis ball (Fig . 52). may be applied to the Popliteal artery by flexIOn at the knee (pressure point 13); the pad

FIG 53.
be the size of a lawn tennis ball, or if no pad IS avaIlable the trouser leg may be rolled or gathered up to serve instE.ad . I t is not necessary to take off the clothing ( Fig. 53) .
J ust behind the k n ee joint the Poplit6!al artery d lvides m to the Anterior (front ) and Posterior (back) Tibial arteries.
The Posterior Tibial Art e ry passes down the
93
back of the leg to the inner side o f the ankle. I t is at first deeply placed bet\\'een the musc les cf the ca lf, bu t it approaches the surface as it proceeds, so that it can be felt pulsating behind the large bone at the in ner side of the ankle. It enters the sole as the Plantar Arteries, which run forward amongst the mus les to supply the foot and toes.
The Anterior Tibial Artery , on leaving the Popliteqj, at once passes fo[\\'ard between the leg bones, and, deeply placed amongst the muscles, ru ns down the leg to the centre of the front of the ank le. This artery is continued as the Dorsal Artery of the Foot, which, passing forward over the tarsus, clips <..1owl1 to the sole between the first a n d second metatarsal bones. Here it forms with the Plantar arteries what is kno\\"n as the Plantar Arch. At the ankle (pressure point. I4 and IS) p ressure may be applied by the fingers or by pads and bandages.
VEXOUS II.£\IORRH.\GE .
1. - Blood f rom a vein is dark red .
2 .- It flows in a slow continuous stream.
3· - It issues from the side of the wound further from the heart.
4. - In the case of a wound of a varicose vein it flows also from the side of t h e \\'ound nearer to the heart, especially if the p:1tient is kept standing.
9+
Varicose Veins .-T he veins of the leg are specially apt t o become yaricose. A varicose vein is dIlated, winding, and with bead-like (varicose) projecti ons along it s course . A vein becomes varicose from several causes, sllch a long standing or tight garters. The first effect is to thro\\ extra work upon the valves, and the bead-like pro jections are caused by the blood accumulating in the pockets behind the \'alves. In time the \'ein becomes so dIlated that lhe \'alves can no longer span it.
GENERAL RUL ES FOR TREAT\fEXT OF A "'UUXD ACCOMPANIKD BY HllDlORRHACE.
I -Place the patient in a suitable position, bearing in mind that the blood escapes with force when the patient sits and is still more checked as he lies d ow n.
2.-Elevate the part, as thereby k ss bloo 1 finds its way into it.
3.-Expose the wound, re moving \\,hate\'er clothi::g is necessary .
4.- Remove any constrictions, such as the collar or garters, from th e heart side of tIl e wound.
5.- Apply digital pressure on the wo und unt il you can apply a pad and tight bandage . If that d oes not stop the bleeding, m ake pressure near the wounJ on the side away fr om the heart. In th e case of a wound of a varicose vein it may also be nece ssary to

95
apply a pad and bandage to th e vein immediate ly above the wound, especially if the limb cannot be maintained in an elevated position.
6.-Treat the wound as directed hy Rules 5,6 and 7, stated on palres 77 and 78.
7.-Afford support to the injured parl.
C.\PILL,\R \' I LE\[OR RH
I.- The blood is red.
2. - It flows briskly in a continuous stream, or may merely ooze from the wound .
3·-It wells up from all parts of the wound.
.\ slight amount of pressure \\-ill suffice to arrest c,lpillLlry b,emorrha!5e.
I:\,Tt.R(\_\L I-L 'E.\wRR I-BCE.
\Vllunus of the bloou \'esseis within the trunk CHise hxmorrhage into the easily of the chest or of the abdomen.
S\''\[l'TO.\lS 01' 1'\ 1 b.R:;',\L ILE.\lORRIL\GE.
I.-:-Rapid loss of strength, giduillCSS and faintness, espeCIally when the upright position is assumed.
2.- Pallor of the face and lips.
3·--Breathing hUlried and laboured and aceom. p:J.nied by ya\\-ning and sighing. '
4.-T1:e pube tilils, alld l1lay altogether disappear at the \\ rISt.
5· -The patient throws his arms ahout, tugs at the clothing round the neck, and calls for air.
6. -Finally the patient may become totally unconscious.
TREAT:'lENT.
I.-K ee p th e patient in a recumbent position.
2.- Undo all ti gh t clothing about the neck.
3· -Provide for free circulation of air; fan the patient.
4. - Sprinkle cold water on the face; hold smelling salts to the nostrils j a \'oid other forms of sti 111 ulants, at all eVents until the hcemorrhage has been controlled.
5.-·Giye ice to suck or cold water to drink; if the seat of the hcem orrhage is knO\\'n, apply an ice bag over the region.
6.-Should the paf.ient be reduced to a state of collapse, raise th e feet and bandage L11e limbs firmly fro 11 the toes to the bips and from the fing ers to the shou:der:: .
H/E>\IORRdAGE FRO1\! THE NOSE ( OS1 RILS).
I.-Place the patient in a sitting p os ition in a current of air before an open windo\\', wilh the head thrown slightly back and the hands raised above the h ea d.
2 - Undo all tight clothing around the neck and chest.
3·-Apply cold (ice, a cold sponge or bunch of

keys) over the nose and also the spine at the level of the collar; place the feet in hot water.
4.-Cause the patient to keep the mouth open, and so avoid breathing through the nose.
Blood issuing from the mouth may come from the tongue, the gums, the socket of a tooth after extraction, the throat, the lungs, or the stomach.
HlE:'JORRHAGE FRG:.r THE TOXGUE, THE GU;,I S, THE SOCKET OF A TOO1H, OR THE THROAT.
1.- Give ice to suck or cold water to hold in the mouth. If tbis is not successful give water as hot as can be borne to hold in the mouth.
2.-If necessary make pressure on the carotid arteries.
3.-If bleeding from the front part of the tongue is excessive compress the part by a piece of clean lint held beh\een the finger and thumb.
_ 4.-If the bleeding is from the socket of a tooth, plug the socket with a piece of clean lint or cotton \\'001; over this place a small cork or other substance of suitable size, and instruct the patient to bite on it.
HlE:'lORRHAGE FRG:.r THE LUNGS.
Blood from the lungs is coughed up, and is scarlet and frotby in appearance.
Treat as for Internal Hremorrhage (see page 95).
E
96
97
HlEMORRHAGE FROM THE STOMACH.
Blood from the stomach is vomited; it is of a dark colour and has the appearance of coffee grounds; it may be i11ixed wi th food.
Treat as for Internal Hremorrbage (see page 95), except that nothing is to be given by the mouth.
B lood issu ing from the Ear Cha nne l, which generally indicates a fracture of the base of the cranium, must be "viped away as it issues; no attempt is to be made to plug the ear.

99
QUESTIO;\l ON CHAPTER III.
Tile J1ltlllerals indit"ale Ille 'Where tile Illa)1 lie found.
\\'hat organs are concerned in the circulation of the PAGE blood? ...
Describe the h ea rt
Trn.ce the circulation of the blood through th e Gc. .)y
and lungs
1Io\\ many times a minute does the heart contract on the average?
\Yhat is the effect of the patient's posilion on the ra tl! at which the heart contracts?
What is the pulse?
IIow many kinds of hremorrhacre are there?
. lI ow would you know a c.ase of arterial ? :::
In what way should artenal h::emorrhacre be controlled?
\Yhat is meant by " pr e sure point" ? <:> •
I [ow may pressure be applied?
What is a tourniquet?
\Yhy is necessary in placing the pad of a lOUrl1JCj uet ?
'Yhen an elastic bandage be used instead of a tourniquet?
What is flexion?
State the general for of; '\' und aCCOlll-
Gy. arterial hxmorrhage ... ' " .. 77, 78
If 1lal t of a lImb had been torn off, but there was not , much bleeding, how would you act? ... . ..
Should blood clots be disturbed ?... ...
It it \\ ise for an person to attempt to wound? . .. . ..
What is the aorta? ... . .. 7 ,
70 70
......... 70
2
'07
... ... ... ...
..
.
... ... ... ... .., ...
... ... ... ., ..
... ... . ... 72 72 73 74 74 74 74 75 75
... ... ... ... 76
76
bescribe the arteri es of the head and neck 80
\Vhy is it sometimes necessary to compress the carotid artery both below and above the wound? ... 80, 81
What is a ring pad, and what is its use? ... 84
Describe the arteries of the upper limbs... 84 to 89
Describe the arteries of the lower limbs ... ... 89 to 93
How would you know a case of venous hremorrhaae? 93
\Vhat is a varicose vein? ... ... ... ..."" 94
How maya vein become varicose? ... . .. ... 94
State the general rules for treatment of a wound accompanied by venous hremorrhage? .. . 94, 95
How would you know a case of capillary hremorrhage? 95
How would you stop capillary ha!morrhage ? ... ... 95
\Vhat is internal hemorrhage? ... ... ." ... 95
\Vhat would lead you to. suspect internal hremorrhage? 95,96
State the treatment for lllternal hremorrhage? ... 96
How would you arrest hremorrhage from the nose? ... 96, 97
\Vhere may blood issuing from the mouth come from?... 97
How would you treat bleeding from the gums or throat? 97
\Vhat else would you do if the tongue were bleeding? .. 97
And if the bleeding were from the socket of the tooth? 97
How would you distinguish between bleeding fr0111 the lungs and from the stomach? ... ... ... ... 97
And what would be the difference in the treatment? ... 97
Of what is bleeding from the ear channel generally a sign? 98
The Student should practise placing supposed patients in a proper p <fsition for the arrest of hremorrhage (see pages 72, 77 and 94), folding firm pads (74 and 75 ), tying hard knots in bandages to form a tourniquet (76), and the application of pressure at all the pressure points shown in the frontispiece, at various points on the forehead and scalp, and on the palm of the hand. Pressure should be digital, by pad and bandage, or flexion, as directed in the text.
101
Pressure poin ts - Carotid artery, 80. Facial, 82. Temporal, S2. Occipital , 83. Subclavian, 84.
Axillary, 8.5. Brachial. (by pad and bandage, bemg made agamst the humerus and by flexIOn at the elbow), 86. Radial and Ulnar, 87.
Femoral the groin, 90.. Femoral in the thigh, 92.. PoplIteal, 92. Antenal and posterior Tibial artenes, 93.
IIremorrhage frolD the forehead or scalp .. .
II::emorrhage from the palm 'of the hand ... ...
Venous hremorrhage from a varicose or other vein

84
87 to 89 ... 93,94
100 PAGE
IUZ
CHAPTER IV. BRUISES.
A blow anywhere on the surface of the body may cause extensive hremorrhage beneath the skin, without breaking it-a" black eye)J is an instance. The injury is accompanied by discoloration and swellmg.
TREATMENT.
Apply ice or cold water dressings. A piece of lint soaked in extract of witch hazel may be placed on the affected part.
BURNS AND SCALDS.
A burn is caused-
(a) By dry heat, such as fire or a piece o.f hot ir?n.
(b) By a rail, wire or dynamo charged wIth a hIgh pressure electric c.urrent: .. .
(c) By a aCId, such as oJ! of (d) By a corrOSl\;e alkal1, such as caustic sod3., ammonia, or quicklime.
(e) By friction, caused, for example, by contact with a revolving wheel. (Brush burn.) .. .\ scald is caused by moist heat, such as boIlll1g water, hot oil or tar.
The effect may be a mere reddening of the .skin ; blisters may be formed; or even the deeper tIssues

103
of the body m::ty be charred and blackened. The clothing may adhere to the burnt skll1, and its removal is lmpossible WIthout further detriment to the injured part. The great dan ger is Shock.
TREA 1
I.-Carefully remove the clothing over the injured part. If stuck to the skin, the adherent clothing must be cut around with scissors, soaked with oil, and left to come away subsequently.
2. - Do not break blisters.
3. - Immediately cover up the part. Soak or smear pieces of lint or linen with oil, or Yaseline, hnoline, or cold cream; a small quantity of boraCIC powder added to these \\ III be of benefit. The inside of a ra\\" potato scraped out and spread on lint makes a soothing- application . 'Vhen the injured :-- LHface is extensive do not cover It \\ith one large sheet of lint, but with strips about the breadth of the hand; this is ach-isable ::IS they fit better on the part, and during subsequent c1ressmgs one strip can be removed at a time, and a fresh dressing :Jpplled before the adjacent strip is taken off. The shock to the system is theTeby less than if the whole of the burnt surface \\ ere laid bare to the air by the removal of all the at one 6me. 'Vhen covered by the oIly dre .. ing erwelop tl,e part in cotton \\ 001 or a piece of flannel and npply a bandage.
' Vhen the face is burnt, cut a mask out of lint or linen, leaving holes for the eyes, nose and mouth. Dip this in oil or smear it with vaseline and apply it to the face and cover it with cotton wool, leaving openings to correspond with the holes in the mask.
'Vhen possible place the injured p:1rt in water at the temperature of the body (98 degrees) until suitable dressings can be prepared . A dessert spoonful of baking soda added to a basinful of the warm water will make a soothing lotion
As it is important not to leave the part exposed to the air, it is the duty of the bystanders to prepare the dressings while the clothing is being removed.
. 4. - Treat Shock. - This is particularly necessary 1I1 the case of every burn or scald of any considerable extent (see page 135). Be very apprehensive of danger in the case of even slight burns of the neck.
5.- If the burn is caused by a corrosive a cid, bathe the part with a weak alkaline lotion , such as washing soda, b:1king soda of soda), magnesia, or slaked lime in warm water before applying the dressings.
6.- If the burn is caused by a corrosive alkali, bathe the part with a weak acid lotion such as lemon juice or vinegar diluted with an equal quan t ity of water. Cazt t t'on .-Before using water brush off any lime that remains on the part.

7.-When a woman 's dress catches fire -
(a) L ay the woman fl at on the fl oor at once, so that the fl ames are uppe r most ; that is to say, if the fro nt of the dress is on fire lay h er on her back, a n d if the back of the d ress is burning, place her face downwards. The reason for this is that flames ascend, so that if the upright position is assumed, the flames will quickly reach and burn the body, neck, an d face ; or if the woman lies with the flames un dermost, they will, if unextinguished, pass over and burn the limbs and set fire to the rest of the dress.
(
b) As soon as the woman is laid flat, smother the flames with anything at hand, such as a r u g, coat, blanket, or table cover; if made \\ et so much the better.
(c) A woman rendf;ring assistance should hold a rug or blanket in front of herself when approaching the fbmes.
(d) If a woman's dress catches fire when nobody is by, she should lie flat, flames uppermost, smother the flames with anything handy, and call for assistance, or crawl to the bell-pull and ring; on no account should she rush into the open air.
The use of fire guards wo u ld prevent many calamities.
104
105
BITES OF SNAKES A 'D RABID ANIMALS AND WOUNDS BY POISONED 'YEAPONS.
'
Hydrophobia is caused by the bite of an animal, as a dog, cat, fox, wolf, or deer suffering from rabIes . The special poisons introduced into \\'ou nels caused by venomous snakes and poisoned weapons ca use immediate danger to life.
TREATiiIENT.
1.- Immediately place a constriction between the wound and the heart so as to prevent the venous blood from carrying the poison through the body. If, for example, a finger is bitten it should be encircle d on the side of the wound nearest to the heart, with the finger and tb um b, and as soon as possible a ligature (a string, piece of or strip of handkerchief) should be placed tightly roun d the root of the finger. Compression with the finger and thumb not relax:ed until the ligature has been applied. Ad.dltlonal li gatu res. may, with advantage, be applied at 111 tenals up the lImb.
2.- Encourage bleeding for a time :-
(a) By bathing the wound with warm water.
(b) By keeping the injured limb low; the upper should be allowed to hang down, and 111 the case of the lower limb the patient should be seated with the foot on the ground.

I07
3. - Cauterise the wound, if it is quit e impossible to obtain the services of a doctor. ThIS is best done by burning with a £luiel ca usti c, such as caustic potash, pure carbolic acid, or nitri c acid, or if these a.re not at hand, \\ ith a red-hot \\ ire or a fusee. The usual solid caustic is insufficient, as it does not reach the bottom of the ,youncl, where the poison is.
To ensure the caustic reaching the boltom of the \\ ound, it should be applied on a piece of ",;ood, such as a match cut to a point. 'Vh en the caustic has been thorou ghly applied, but not till then, the lIgatures may be removed.
4. - Cover the wound, after a ,,,hile, with a clean
5. --Afford support to the injured part.
6.- Treat shock if it occurs (see page 135)·
7.- In the case of a bite by a venomo us snake, rub in po\\"dereel permanganate of potash and inject under the skin in the neighbourhooel of the wound a solUlion of permanganate of potash .
ST ING S OF PLANTS ANIMALS.
These give r ise to serious inconvenience, and 111 some cases grave symptoms develop .
TREATi\1E T.
I. - Extract the sting if le ft in.
2. - Mop the part freely with dilute ammonia
106
1G8 or spirits. A paste of bicarbonate of soda and sal volatile is an effi cient application. A solution of washing soda or potash or the application of the blue bag \yill relieve pain . .
3. - Treat collapse if it occurs (see pnge 135).
FROST BI TE.
Durin,:; exposure to severe cold, parts of the body, usually the feet, fingers, n ose, or ears, lose sensation and become first waxy white and afterwards conaested and of a purple appearance . As sensation is Lst in the it is often only by the remarks of bystanders that the frost-bitten person is made a ware of his condition .
TREATl\fE ; T .
I .- Do not bring the patient into a warm room until, by friction of the hand or by rubbing with soft snow, sensation and circulation in tIle affected parts are restored . Neglect of this precaution may lead to dea th of the tissues of the frost -bitten part.
2.- When circulation is restored, keep the patie n t in a r oom at a temperature o f 60 degrees.
NEED LE EMBEDDED UNDE R . THE SK I N.
' Vhen a needle breaks off after penetrating 'the skin and disappea rs, take the patient to a doctor at once. If the wo u nd is near a joint, ke ep t he l imb at rest on a splin t.

109
FISH-HOOK EMBEDOED I N THE SKI N.
Do not attempt to withdraw the fish-hook by the way it went in, but cut off the dressing of the hook, so that only the metal is left, and then force the point onwards through the skin until the hook can be pulled out.
I.i JUR I ES TO JOINTS.
'Vhen a joint is injured by a bullet, stab, or other cause-
1.- Wrap the part in cotton wool.
2.-· Afford rest and support to the injured limb' if the upper limb, in a flexed position by a sling; if the 'lower Ii mb, in a straight posi tion by a splint.
BODY IN THE EYE.
I .- Prevent the patient rubbing the e ye, tyin rr down a child's hands if necessary.
d own the lower eyelid , when, if the foreign body is seen, it can readily be removed with a camel's hair brush, or wi th the corner of a handkerchief t\\irled up and wetted.
3.-When the foreign body is befleath th e upper eyelid lift the lid forward, push up the lower lid beneath it and let go . The hair of the lower lid brushes the inner surface of the upper one, and may dislodge the body . Should the fir st attempt be unsuccessful, repeat it seyeral times if necessary. If
lI O
the fureign b od y is n ot d islodged call th e se rvices of a doctor as soon as possible. When however s killed help cannot be had , proceed follo\\ S
(a) Seat the patient so as to face the light, and stand behind him, steadying his head against your chest.
(b) Place a small rod, such as a match or bodkin, on the upper eyeliu, half-an-inch above the edge, pressing it backwards as far as possible.
(c) Pull the upper eye-lashes upwards over the rod, and thereby evert the eyelid.
(d) Remove the foreign body.
4.- When a piece of steel is embedded i n th e eyeball drop a little olive or castor oil on the eyeball after pulling down the lower eyelid, close the lids, apply a soft pad of cotton wool and secure it by a bandage tied sufficiently firmly to keep the eyeball steady; take the patient to a doctor.
5.-When quick-i"ime is in the eye brush a\\ay as much of it as possible; bathe the eye \\ith VI negar and warm water, and treat as for a piece of teel embedded in the eyeball.
FOREIG N BODY IN THE EAR P ASSAG E.
As a rule make n o attempt to treat a patient with a foreign body in t he ear if the services of a doc tor can possibly be had j any attemp t s to remove the foreign body· may lead to fata l consequences. If a child

II I
can n ot be induced to keep the fingers from the ear. tie his hands down or cover UP the ear. If an insect is in the ear-passage, fill the ear with olive oil, \\ hen the insect will float and may be ret;rJoved . Never syringe or probe the ear.
FOREIG J: BODY I N THE NOSE.
Induce snee , ing by pepper or snuff. Cause the patient to blow his nose violently afLer closing the unaffected nostril. There is no immediate danger from a foreign body in the nose.
THE ABDOMEN .
The abdomen is bounded above by the diaphragm; below bythepelvis; behind bythelumbarverlebrre; anti. in front and at the sides by muscular walls. (Fig. 54.)
THE ORG.\NS OF THE ABDOl\IE
The Stomach lies immediately below the "pit of the stomach I) just below the breast-bone.
The Liver lies in the upper part of the abdomen, \\ here it is mostly covered by the right lower ribs.
The Spleen lies beneath ·the nbs at the upp er part of the left side of the abdomen .
The Intestines occupy the greater part of the cnvlty of the abdomen .
The Kidneys lie at the back, in the region of the loin.
The Bladder lies in the pelvis.
!IG 54.
\VOUND IN THE FRONT "TALL OF TIlE ABDOMEN.
T[,hen the lntestines or other organs protrude through the wound, whether vertical or transverse, bend the knees, raise the shoulders, and apply lint, a towel, or cotton wool wrapped in soft linen, anJ keep the

IIJ
patient warm until the doctor arrives. "Then there is no protrusion of organs, if tlze wound is 7)ertical, lay the patient flat on the back \\'ith the lower limbs straight; if the 'Wollnd z's transverse, bend the knees and raise the shoulders.
IN JURIES TO THE ORGANS \VITHIN THE ABDO?lIEN AND PELVIS.
Injuries of the Stomach are attended by extreme collapse and sometimes by Yomiting of dark blood like coffee-grounds. For treatment see " Hremorrhage from the tomach" (page 98).
Injuries of the Liver, Spleen and Intestines may be caused by a blow, a stab or a bullet; the liver or spleen may be injured by a fracture of the lo\\'er ribs. The Signs and Symptoms are those of internal hremorrhage accompanied by pain and swelling at the se;:1t of injury, and the treatment is as for that condition (see page 95).
The Kidneys may be injured by a fracture of the eleventh or twelfth ribs, also by a crush, blow, . tab or bullet. Blood may escape with the urine, and there may be pain and swelling oYer the injured kidney. .
The Bladder may be inju"ed by a fracture of the pelvis. The signs and symptoms are either inability to rass water, or if a little is passed it is tinged ,vith bloJd.
1I2
TREAT:\IE:\,T OF TO THE KlDl'.'EYS OR BLADDER.
Keep the patient qu i et until the doctor arrives.
2. - App ly ho t fomentations o\'er the p:1inful or injured part.
Rupture (hernia) consists of a protrusion of an internal organ, usually the bowel, through th e muswall of I he abdomen, most freg uently at the Sh,ould a sudden s\yelling accomp::1.I1ied by paIn and Sickness take place in that region
r.-$end for a doctor instantly .
2.-Lay the patient down with the buttocks raised.
3·-A pply ice or cold water dressings to the affected part.
IIS QUESTIONS ON CHAPTE R IV.
The 1ZwJlera is z'nd;ra 'e the pages wilen the answers may be found.

If ow would you {reat a burn caused by a corrosive al kali
when quick.lime is in the eye?
lI ow \\> ou ld you try to remove an insect from the ear passage
PAGE 'Vh at js a bruise? 102 How would you treat a bruise? I02 II ow maya burn be caused? I02 lIow is a scald caused? 102 ' VIm! is the great danger of a burn or scald? ... 103 Stare the general tr eatment for burns and scalds 103, 104 How would you treat a burn caused by a corrosive acid? 10 4
? I04 \Vhat
catches fire? I05 State the general rules for treatment of wounds caused by poisonous bites or weapons .,. ... 106, 107 'Yhat special treatment is required
bite of
\,enomous snake? 107 IIow would you treat a sting? 107,108 State the signs, symptoms
of frost,bite ... 108 \ Vould you attempt to remove a needle em bedded under the skin? 108
ow would you extract a fish hook em bedded in the skin? 109 Stat e the treatment fllr injuri es to joints ' .. 109 Stat e the general rules for removing
body from the eye... .. . .. . ... ... ... 109, 110 \
110
110
?.. . I I I
steps should be taken when a woman's dress
for the
a
and treatment
H
a foreign
Yh at would you do if a piece of steel were embedded in the eyeball?
And
\V vuld you try to remove any olher form of foreign bod)' from the ear passage? ... ... .., .,' 1 10, I I [
How would you remove a foreign body from the nose? II [
State the boundaries of the abdomen and its contems II [
State the nt for wO,unds of the abdomen", 112, 1 I3
How may 1I1Junes to the lIver, spleen and intestines bl.! caused? , ., '" .,' ", ". ... 113
\Yhat is the difference between treatment of injuries t o the stomach and of injuries to the liver spleen and intestines? .,. ...
.. . ' .. , ... II]
Stale the treatment of injuries to the kidneys or bladder J 14
State the treatment of ht:rnia I I 4-

CHAPTER Vo
TIlE NERVOUS SYSTEM.
Two systems of nelTes, the Cerebro-spinal and the Sympathetic, regulate the movements and functions of the body.
T he Ce re br o-sp inal Sys tem is made up of the Drain, the Spinal Cord and Nen'es, and through its agency sensations are received and the will causes the action of the voluntary muscles. For e'{ample, when a part is injured a sensation of pain is con"eyed to the brain by the nen'e, thus affording an indication of the seat of injury, or a warning of a possible danger of further damage. On attention being directed 1.0 the injury, an attempt is instantly made to ease the pain or to mO\'e the injured part from danger.
The Bra in is situated within the cranium, and is divided in the middle line, so that, with the exception of some connecting bands, the right and left sides are separate.
The Spinal Co rd is the long cord of nervous matter lying within the spinal canal (see Vertebral Column, page 23). It leaves the brain through an orening in the base of the cranium and extends to the upper lumbar vertebrre.
1I6 PAGE
..,

II8
The Nerves proceed from the brain and spinal cord in pairs as pearly-white trunks, and their branches can be traced throughout the tiSSUeS of the body. When a nerve is torn through there is p ualysis of motion and sensation in the region in which its branches are distributed.
The Sympathetic System extends as a nelTOUS chain on each side of the front of the spinal columll along its entire length, and sends branches to all the organs of the chest and abdomen to control the involuntary m us les, and thereby regulate the "ital functions. This system is not under the control of the will, and acts alike during sleep and activity.
THE RESPIRATORY SYSTEM.
The air reaches the lungs by way of the nostrils (or mouth), the throat, the wind-pipe, and the bronchial tubes. The nostrils convey it to the back of the throat, whence it enters the wind -pipe by an opening guarded by a sort of trap door or valve, so that in health air, but not solids or fluids, may enter. During insensibility, however, the valve fails to act, so that should solids or fluids be given by the mouth, they may enter the wind-pipe and cause a.sphyxia . The wind-pipe extends to two inches below the top of the breast-bone, where it divides into the right and left bronchial tube. Each bronchial tube enter:) a lung and divides into small and still smaller tUDes, until
119
FIG. 55. THE LUNGS A!\D DRO:\CHIAL TUBES.
A. Tra.chea, or Wino-pipe. D. Left Bronchus C. Right Bronchus. D. Smaller Bronchial Tubes.
the u ltimate recesses of the lung- the air cells or air spaces - are reached.
The Lungs, Right and Left, occupy the greater p.art of the they lie immediately within the nbs, a n d practIcally wherever a rib is felt whether fro n t, back or sides, there is lung beneati1. Each is enveloped in a fine membrane (the pleura) which allows It to move within chest during breathing without friction.
Respiration, or breathing, consists of two acts Inspiration, an expansion of the chest duri . which air i? drawn into the and E x p'i ration: a contractIon of the chest, dUTlng which air leaves the l u ngs . A pause follows the act of expiration. In. health fifteen to. breaths are taken per mInute, and at each InSpIratIOn about 20 to "0 cubic inches· of air enter the lungs, and a similar q is expelled at each expiration.
The expansion and contraction of the chest are effected partly by the muscles of respiration attached to the ribs , but the p iaphrag m , the large arc h ed muscular partItIOn whIch separates the ChEst fro m the abdomen. inspirat.ion, which is chiefly a muscular act, the nbs are raIsed and the arch of the diaphragm falls and becomes flattened thus inc::easing the capacity the chest and the aIr to enter. In expIratIOn, an act performed almost without effort, the nbs fall and the arch of the

d iaphragm rises; this lessens the capacity of the chest and forces air out . The mechanism of respiration is somewhat like that of ordinary household bellows but 'without a valve; the ribs may be to the boards of the bellows, while the diaphragm corresponds to the leather, the air passaaes bein a equivalent to the nozzle.
l:> As the blood depends upon the air for its purification and the oxygen necessary to maintain life, interfe r ence with breathing very soon may Rrod uce a dan rrerous state called asphyxia, examples of which are by drowning, suffocation, choking, etc.
ARTIFICIAL RESPIRATIO I
.
PROFESSOR SCH;\FER'S :l'IIETHOD.
I. - Make n o attempt to loose n or remoye cloth'ng.
. . . .
2.- Lay the pat ient m a prone (t.e., back upwards) \\'ith bis head turned to one Side, so as to keep his nose and mouth away the ground. No pad is to be placed under the patIent, nor ne ed the tonaue be drawn out, as it will fall naturally
3.- Kneel at one side facing the patient'.s head , and place the palms of your hands on loins, one at each side, the thumbs nearly touchIng one another in the small of the back, and the fingers extending over the lowest ribs. Leaning your body fonyard, let its weight press straight dO\\'ll\\'ards upon the
120
1 2 1
.

loins and part of the back, thus compressing the abdomen the ground and driving air out 'of the chest. Thls produces expiration (Fig 56) . Draw back 1 2 3 your body somewhat more rapidly and relax the pressure, but do not remove your hands; this produces inspiration (Fig . 57).
4 .- A1ternat e these movements, by a rhythmic s\\'aying backwards and forwards of your body, twelve to fifteen times a minute, p-:fsevering until respiration is restored, or a doctor prono.'nces life to be extiect.
DR. SILVESTER'S 1.i:ETHOD.
I.- Adjust the patient's position. -Without wasting a moment place the patient on his back on a flat surface, inclined if possible from the feet llpwards . Remove all tight clothing from about the neck and chest, and bare the front of the body as far as the pit of the stomach; unLtsten the braces and the top button of trollsers in men, and the corsets in women . Raise and support the shoulders on a small, firm cushion or folded article of dress placed under the shoulder-blades
2 . - Maintain a free entrance of air into t h e windpipe -Cleanse the lips and nostrils; open and wipe the mouth; an assistant must draw forward the patient's tongue as far as possible, and keep it in that position
3 .- Imitate t he movements of breathing . Induce IJlspiratioJl . - Kneel at a convenient distance behind the patient's head, and grasping his . forearms just below the elbo\\', draw the arms
12 2
.
.
FIG. 58. INSPIRATION.
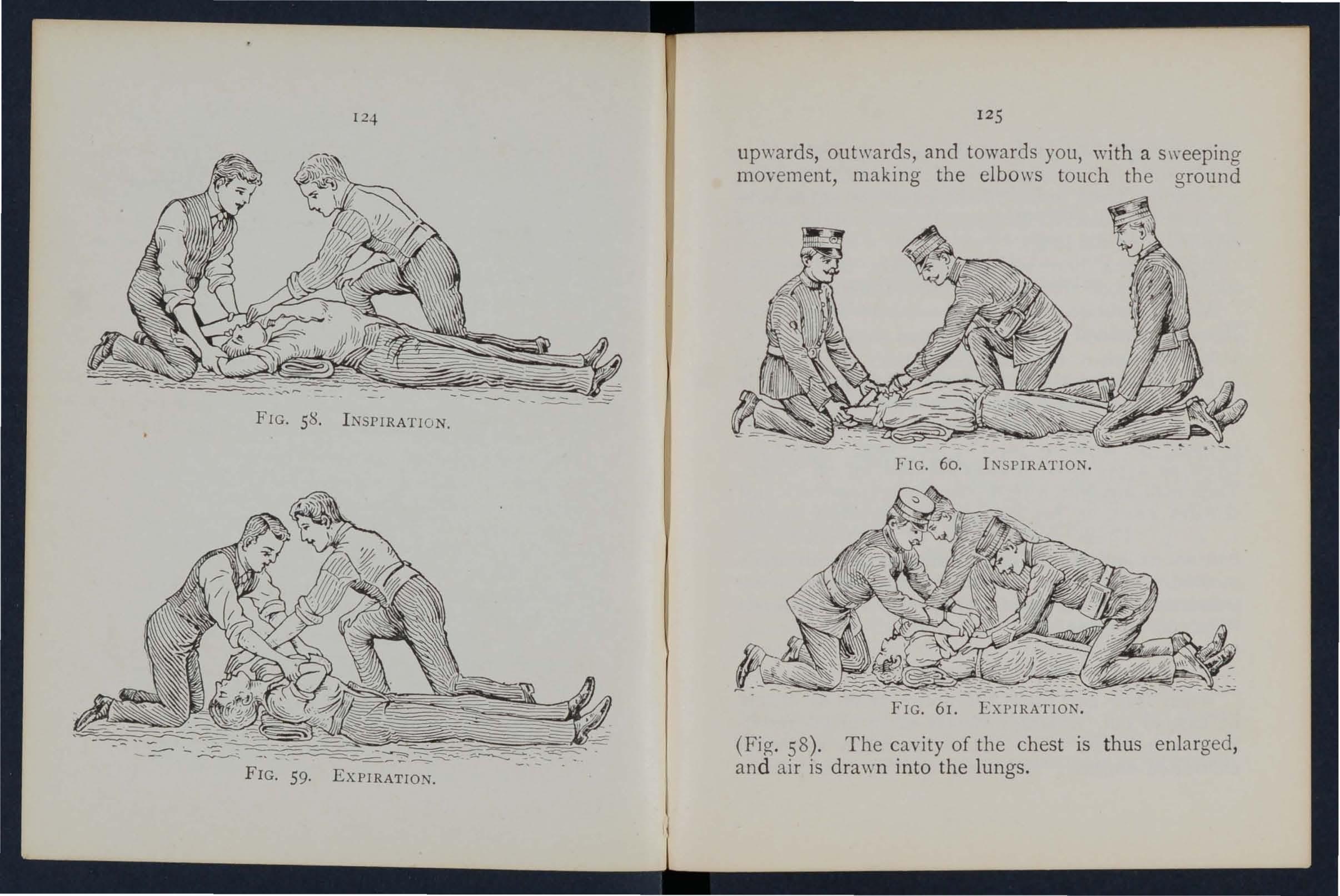
FIG. 59. EXPIRATION.
12 5
upwards, and towards you, with a sweeping movement, makmg the elbows tOllch the ground
FIG. 60. INSPIRATION.
FIG. 61. EXPIRATION.
(Fig. 58). The cavity of the chest is thus enlarged, and air is drawn into the lungs.
inductJ expiratz'o7Z.- Bring the pMient's flexed arms slowly forward, downwJrds and inwards, press the arms and elbows firmly on the chest on either side of the breast-bone (Fig 59). By this means air is expelled from the lungs.
Repeat move nents alternately, deliberately, and persevenngly about fifteen ti mes a minute.
\Vhen a sufficient number of assistants are present, Howcud's method may be combined with Silvester's, as follows: -
. The. additional assistant kneels astride the patient's h.lps wIth the balls of the thumbs resting on either SIde of the pit of the stomach, and the fino'ers grasping the adjacent parts of the chest. Usingbhis knees as a pivot, he presses forward on his hands. Then suddenly, with a final pusb, be springs back and remains erect on his knees \"hile h e slowly counts r, 2, 3. These motions are to be repeated to correspond with those being performed by Silvester's method, pressure on the chest being made simultaneously by those performing the two methods (Figs. 60 and 6r).
LABORDE'S METHOD.
When from any cause the above methods cannot carried out, Laborde's method of artificial respiratIOn should be tried. It is especially useful in suffocated children, and when the ribs are broken.

12 7
The patient is placed on his back or side; the mouth cleared; the tongue is seized-using a handkerchief or something to prevent it slipping from the fingers-the lower jaw depressed; the tongue is pulled forward and held for two seconds in that position, then allowed to recede into the mouth. These movements should be repeated about fjfteen times a minute.
.Artificial re spiration must be continued until breathing is established, or until a doctor arrives . When natural breathing commences, regulate the artificial respiration to correspond \\ ith it. Success may result even after two hours' time.
Excite respiration.-
\Vhilst artifical respiration is b e ing applIed, other useful steps may be employed, such as applying smelling salts or snuff to the nostrils. and flicking the chest with a damp towel.
Induce circulation and warmth after natural breathing has been restored. ·Wrap the patient in dry blankets or other covering, and rub the linl bs energetically towards the heart. Promote warmth by hot flannels, hot-water bottles, or hot bricks (wrapped in . flannel) applied to the feet, to the limbs and body. \Vhen the power of swallowing has returned give bot tea or coffee, or meat extract. Tbe patient should be kept in bed and encouraged to go to sleep. Large poultices or fomentations applied to the
126
front an d back of the chest will serve to assist breathing.
Watch the patient carefully for some time to see that the breathing does not fail; should any signs of failure appear, at once begin artificial respiration.
INSENSIBILITY.
Unconsciousness or Insens ibil ity may arise as follows :-
Injury to t he H ead. -Concussion and Compression of the brain .
Dis e ase of the Brain. -Apoplexy, Epilep sy, Hysteria .
Various Causes. -Shock, Fainting (Syncope), Collapse, Alcoholic and other poisoning, Sunstroke and Heat-stroke, Infantile Convulsions, Asphyxia.
GENERAL RULES FOR TREATMENT OF INSENSIBILITY.
I
.- If a person appears about to lose c onsciousness, prevent him from falling , and lay him gently down .
2.-Arrest Hcemorrhage when apparenl; attending to minor injuries is less important than treating the unconscious state .
3·-L ay the patient in the position in which breathing is most easy-us ually this will be on the back, or inclined to one side. As a general rule

raise the head and shoulders sliglttly when the face is flushed, and keep the head low when the face is pal e.
4.- Undo all tight clothing round t he nec k, chest and waist, unfastening the braces and tup button of tile trousers in men, and the corsets in women, the object being to relieve pressure on the air passages, lungs, heart and abdominal organs. Be sure that there is no obstruction to the air p3.ssages by the tongue or by a foreign body in the throat. The possibility of false teeth obstructing breathing mu:::.t be considered.
s.-Provide for a sufficiency of fresh ai r by open ing doors ant.! windo\\"s, and by keeping back a crowd.
- When breathing cannot be discerne d apply artificial respiration.
7. - 0btain a doctor's help as soon as possible.
8. - Unless unavoidable, never leav e t he patient until you have placed him in charg e of a responsible person.
9. - Give no food or fluids whatever by the mouth while the patient is insensible.
IO. - Should the spine or an important bone of the upper or of the lower limb be fractured , it must be steadied a nd maintai ned at rest as soon as possible . Sho uld the unconsciousness be prolonged, the pati ent may be remove d in a rec u mbent position F
1 28
1 2 9
IJO
to shelter, provided that tLe broken bone is adequately su],ported.
n.-When the patient is in a state o f co na vu]sion, support his head, and after wrapping a piece of \\"Ood or any uther hard mate rial in a handkerchief. hold it in his mouth to prevent biting of the tongue. Do not forcibly restrain his limbs; pre,"ent him from hurting himself by pulling him away from a source of danger, such as machinery, a wall, or fireplace ; light pieces of furniture should be pushed out of the way.
I2.-0n re tur n t o c ons ciousness ,,:ater may be giYen to drink . If the pulse is feeble gIve warm lea or coffee, provided hremorrhage, either internal or external, is not present. A desire to sleep should be e ncouraged, except in cases of opium poisoning, a condition that may generally be recognised by the history of the case, and also by the pupils of the eyes (the black openings in the grey, blue or bro\\ n iris) being minutely contracted (pin-head pupils) .
13·-It must not be assumed that a person is ins e nsible as the result of drink me rely beca use the breath smells of alcohol ; frequently when people are feeling ill they take or are given alcoholic stimulants, after which they may become insensible, not from the drink, but from the cause that indllred them to take it, for example, insensibdlty coming on, effects of poisoning, etc . Even if

13 I
drink is believed to be the .ac tual cause of. bIllty it must be borne in Jl1md that the patlent IS lId1 , d he must be treate a very dangerous state, an . for Colbpse by being covered, up and \\ bp
The above general rules \\111 enable ald. t?, r e ndered efficiently in most cases of althOlwh the exact form from which the patient IS o suffering is unknown.
CONCUSSION OF THE BRAI
The atient may be stunned by a blow or LlI_I on the head, or by a fall on the or part ot , He mav quickly r eo-a m conSCIOusness, or 111 sp1l1e. J 0 I be prolon'cd. sensibility, more or less comp ete, may d
I.-Apply the general rules for the treatment of Insensibility. . 11 2 - Be very apprehensive of 1ll a cas'es of injury to the The be stunned, and after a short ll1terYal nla) l,eCO\ er some deo-ree of consciousnes , or even the may o d ' ;, .,. yet in both ll1st ances apparently have escape Il1 J Ul) , . '1 . I is a grave risk that a structure \V.lt 1111 ,t Ie cran ium has been injured, and that a senOU:3 sLate f < I (:::; Fracture 0 of insensibility may develop ater. ee ld L 1 f the Cranium, page 43)' A caution sho.u t len: be aiven to a patient who has lost conSCIOusness e,en t'> F 2
13 2
or only a moment after an injury to the head not to resume physical or mental activity without the consent of a doctor .
COMPRESSION OF THE BRAIN APOPLEXY.
'
Compression of the Brain may result from the same. as produce Concussion; in fact, CompressIOn IS frequently preceded by Concussion . . usually occurs in elderly people, and no SIgns of Il1Jury are necessarily present.
In .both conditions the face is flush ed; the breathl.ng stertorous; one side of the body may be more lImp than the other, and the pupil of one eye may be larger than that of the other; the temperature of the body is generally raised.
TREATMENT.
I. - Apply the general rules for treatment of In se nsibility.
2.-Promote warmth in the lower part of the body by the application of hot water bottles to the abdomen and lower limbs. Care must be taken not to burn the patient with the bottles, which should be wrapped in flannel, and their heat tested \\'ith the elbow.
EPILEPSY.
Epilepsy may occur in persons of any age, but usually occurs in young adults. The patient falls to

133
the ground, sometimes with a scream, and passes into a state of convulsion, throwing his limbs about.
The treatment is according to the General Rules, especially Rule 11.
HYSTERICAL FITS (HYSTERIA).
SIGNS AND SY:\lPTOl\lS.
The patient, u sually a young girl, in consequenc e of mental exciteme:1t, suddenly loses command of her feelings and ac tions. She subsides on a couch or in some comfortable position, thro\\ s herself about, grinding her teeth, clenching her fists, shaking her hair loose; she clutches at anyone or anything near her, kicks, cries and laughs alternately. Th e ey.eballs may be turned upwards, and the eyelids opened and shut rapidly. At times froth appears a t the lips, and other irregular symptoms may develop.
TREATMENT.
I.-Avoid sympatby with the patient, and speak firmly to her.
2.-Threaten her with a cold water douche, and if she persists in her "fit," sprinkle her with colel water.
3.-A pply a mustard leaf at the back of the neck. Medical treatment is necessary to cure the condition of mind and body which gives rise to hysterical att ack s.
SHOC K , FAINTING (SYNCOPE), COLLAPSE.
CAU SES .
I.-Injury in the region of the abdomen, extensive wounds and burns, fractures, lacerated wounds, and se\'ere crush are some of the more frequent physical causes of shock.
2.-Fright, of injury , and sudden bad news, or sometImes sudden removal of fea r and anxiety after prolo nged ,s uspense, produce shock or fainting .
3·-Some pOIsons ca use shock, while others, such as alcohol, so d epress the ner vous system th at c ollapse ens ues.
4·-Hcemorrhage or heart weakness a close or crowded room,' tight clothing fatigue' or \\ant of fuod may bring on fainting or c611apse . '
SIGNS AND SYMPTOM S.
The general condition of shock Illay be reco cr nised by extreme pa ll or, a feeling of cold, -clammy b skin, pulse , and shallow breathing accompanied, has been severe, by yawning and ," collaps,e " signifies a yery senous condItIon 111 wblch the lIfe of the patient is in the greatest danger ; the temperature of the body falls ?elow the non:nal, and one great object of treatment
!,'S to prevent It si:lking to a point at which life is Imrosslble . An attendant danger of the conditio n of

135
collapse is the li ability to sudllen r elapse after a temporary improvem ent, and the utm?st care al.ld watchfulness must th e refore be exercIsed to maIntain the of the body and to guard against failure of the heart and lun gs .
TREAnIENT
I. - Remove the cause by arresting rhage, attending to 1l1junes, loosening all tight clothing especIally about the chest and rem?\'ing fro111 a close or cro\\'ded r00111, USll1 6 encouraglllg words, etc.
2. - Lay the pcttient on the back, with the head low. Rai se the lo\\'er limbs; ,,·ben the patient IS in bell this is best done by raisin g t he foot of the bedstead.
3. - Provide for a free circulation of fresh air.
4.-If has been seyere ,and the patient is collapsed, firmly bandage the limbs from, the toes to the hips, and from the fingers to the armpIts.
5. - To stimulate the action of the heart , sal volatile and wate r may be gi\'en if the patIent em swallow, or smelling salts may be held to th e nostril'.
6. - It is of the utmost importance to use every means of preventi,ng a fall of ture be low the normal POIl1t. To accomplIsh thIS cover the patient with extra clothing, or by placing
134
T30
rugs or blankets over him; get him to bed in a warm but well ventilated room as soon as possible. Apply warmth to the feet and to the pit of the stomach by hot \,yater bottles or hot fb,nnels. (T est the heat of these with the elbow befor e applying them.) If the patient can swallow, give hot drinks, such as milk, tea or coffee. It is well to add su.gar, as it aids in raising the temperature of the body.
7·- If breathing cannot be discerned, apply artIficial respiration.
8.-If want of nourishment has been the cause of binting or collapse, give food sparingly at first.
SUNSTROKE AND HEAT-STROKE.
When exposed to great heat, as in the stoke-hole of a steamer, especially in the tropics, or to the rays of the sun during a march in very hot weather when heavily burd ened, persons may develop sickness, faintness , giddiness , and difficulty in breathing. The r)8tient cO 'l1plains of thirst, the skin becomes dry and burning, th e face very flushed, the pulse quick and bo unding. A very high temperature, stertorous (snoring) breathing, and ins en si bility may ens ue .
TREAT:VIENT.
1.- Undo all ti ght clothing.
2.-Remove the patient to a -coo l, shady spo t.

137
3.--Slrip the patient to the ,:'aist.
4 .-Lay the patient down, wIth the head and tru nk well raised.
5.-Procure as fl:ee a as possible of fresh air, and fan the patIent vIgorously .
6.--Apply ice bags or \:-ater rreely to the neck, and spine, and mall1tam thIS treatment untIl the symptoms subside. . ,
7.-0i1 return to conSCIOusness, the patIent may have \\'ater to drink.
COl VULSIONS IN CHILDREN.
Teething or stomach troubles are the commonest causes of this ailment.
SlG:\'s.
Spasm of the or .t!le limbs and trunk, blueness of the msensibilIty, more or less plete, a n d occasionally squinting, suspend,ed respiration , and froth at the mouth are the promment sIgns.
TREATMENT.
1.- Support the child in a warm bath slightly above the temperature of the body (9 8 degrees), so that the water reaches to the mi ddl e of the trunk.
2.-Place a sponge dipped in cold water on the top of the head.

ASPI-1YXIA.
?wing to want of air, the blood is not supphed WIt h oxygen the patient becomes insensibl e and is said to be asphyxiated. This conditiun ma): be brought about as follows:-
1. Obs t r u ction of the air p as s ages.
(a) By DRO\\NI I G.
(/I) By E FRmr OUTSIDE: Stranguiation, hangll1g, smothering.
(c) By A FOREIGN BODY THE THROAT: ChokinO'
(d) By SWELLING OF THE TISSUES OF
TH.ROA.T : Inftam mation, scald of the throat, pOlsonmg by a corro.-ive .
II . Inhaling poisono u s gases. By coal gas (as used in the house), producer, or water, gas, smoke, from a charcoal or coke fire, se\\ er gas, limekIln gas, carbonic acid gas. -
III. Pressure on the chest, as whe n crushed by sand or debris, or by a crowd.
IV. Nervous affections , as the result of narcotic and certain other poisons, collapse , electric shock, or stroke by lightning.
TREATMENT.
In all cases of Asphyxia attem I ts must be made to remove the cause, or to remove the patient from the cause. \ Vhen this hlS been done artificia l )39
res pi r at ion m ust be ap plied , taking care that the air passages are not and that there is abundance of fresh alL ])RO \ KING.
Pers o ns completely immers ed in water for even ten or fifteen minutes h;we been restored by artificial means. Therefor e, if the body is recovered within a reasonable time, absence of signs of life is not to deter immediate atLempts to restore animation.
The first thing to do when the body is recovered is to get rid of the water and froth obstructing the air passages, and th e n artificially to restore breathing. This is best accomplished ei th er by proceeding at once to per (or in artificial by Sch:i.fer's method, or as follo\\'s:-
I.-As quickly as p)ssible loosen tile clothing, and clear the mouth and the back of the throat.
2.-Turn the patient face dowri\\arcls, \\ itb a PJd helow the chest, and with the forehead upon the right fOlearm .
3
. - Whilst in this position apply pressure by the hands to the pati e nt 's back over the lower ribs, and keep the pressure up for three seconds.
4.-Turn the patient on the right side, maintaining that position also for thr ee seconds.
5.- Re peat these movements alternately as long as froth and water issue from the mouth.
138
These operations (Marshall Hall's method) 1n themselves tend to promote respira ti on, but when the air pas sa ges are clear of froth and ,Yate r Silvester 's method of artificial respiration may be used by itself or \\"ith How ard's m ethod in conjun c tion.
'While performing tb es e op e rations se nd someone to the nearest house to procure blankets and dry clothing, hot water bottles, etc ., and to fetch a doctor.
STRANGUL&. TION.
Cut and remov e the band constri ctin g th e throat. Appl y artificial respiration.
HANGING.
no not ,,"ait for a poli ce ma n: grasp th e lower limbs and raise the body to t a ke th e tensi on off th e rop e ; c ut the rope, free the neck. A pply artificial respiration.
SMOTHERIKG.
Remove whatever is smotherin.g the pa ti e nt. Apply artificial respiration . CHOKING.
Open the m outh, forcibly if need be; pass the forefin ger right to the ba ck of the throat and attempt to dislodge the foreign body; if vomiting r esults, so much the better. If unsuccessful, thump the back hard whd')t the head is bent forward. Apply artificial respiration.

SWELLING OF THE TIS SUES OF THE THROAT.
'Whether the swellin g is caused by inflammation by swallowing ve ry h ot wat e r: as not infrequently happens to childr en att e mp ting to drink from th e spout of a kettl e, or by th e e ffec t of a c orrosi\'e p oison, the treatmmt is as foll uws ;--
I.-Apply a sp o nge, pi ec e of flannel or oth er c loth, wrung out of very h ot water, to the front of th e n eck, from the chin to th e top of th e breast-bone.
2.- et the patient b efore the fire.
3.-Give ice to suck if it can be had; if not, give cold \Yater to drink.
4.- Gi\'e animal or veg e table oil, a dessertspoonful at a time, to soothe the scalded throat and ease the pain.
S.-If breathing has ceased apply artificial resp iration .
SUFFOCATION BY SMOKE OR GASES.
L-Remo\'e the patient into the fresh air. Before entering a building full of smoke tie a handkerchief, wet if possible, round the head so as to cover the n ose and mouth. I t is well to move slowly, k eeping low, or even crawling, whilst in a room full of smoke in search of a suffocated person . Ever y opportunity of letting in fresh a ir by open in g d oors or windows should be seized.
2.-Apply artificial respiration.
3.-1n the case of producer or water gas, inhalation of oxygen will also be necessary.
ELECTRIC SHOCK.
Electric current is conveyed by a cable, wire, rail or bar, called the and returns to source of supply by another wire, rail or bar
11 d I "N . " " ca e t 1e egatlve, or through the earth. In the case of an elec.tric railway., the current is 'generally conveyed by an ll1sulated raIl called the third rail, and returns through the running rails or an insu bted raii called the fourth rail, and in the case of an electric tram way it is frequently conveyed by an overhead conductor or trolley \\ ire, and returned through the running rails.
Through contact with a "positive" the shock may be so severe as to cause insensibility, and the sufferer \yllt be unable to extricate hi mself, and must be with .all poss.ible speed . . As it is generally Impossible or ll1eXpedlent to sWitch off the current some method must usually be adopted; but ust be. or else the person renderIng assistance Will h1l11self receive a shock.
To liberate the sufferer from contact. from the earth by stand· mg on an msulator or" non-conductor" that is a body which resists the current. Amongst bodies

are indiarubber, dry glass, dry bricks, dry silk, dry cloth, dry wood and dry hay or straw ,
2.-Protect your hands from contact with the sufferer or the electric medium by covering them with an insulator. Although indiarubber is probably th e b est insulator, do not wate time in running for indiarubber glm'es, but use dry articles of clothing; an indiarubber tobacco pouch or cap, or - folded ne\\ spa per, serve to protect the hands in an emerge ncy. If no means of insulating the hands are at hand an attempt may be made to drag the sufferer away by means of a loop of d,y rope or a crooked stick; an umbrella is not safe because the metal ribs would act as conductors* of electricity, and it is not 1l1frequently the case that the" stick" of the umbrella is a metal tube.
3.-Pull the sufferer away from contact. Care should be taken to avoid touching \yith naked hands the sufferer's hands, wet clothing, or boots if the soles arc nailed. The armpits should be avoided as perspiration usually makes the clothing damp there.
'When the sufferer is removed from contact-
I. -A pp ly t he g en eral tr e atm en t fo r insen -
¥ A conductor is a body through which electricity readily Amongst such bOllies are copper, brass, iron, moi lure and one's own body.
144
sibility (loose n cloth mg, procure free circulation o f air an d place in a rec u mbent posit ion) .
2. · - Dip a towel in cold water and attempt to arouse him by sharp ly fli cki ng the face and chest.
3.-Commence artificial respiration if other methods fail to restore animation. " Laborde's" method (see page I 26 ) has been found to be very successfu l.
. 4.- Treat burns if there are any (see pages 103, 10 4).
EFFECTS OF LIGHTNIKG.
A person struck by lightning is usually more or less deprived of consciousness. The treatment is the same as that for electric shock, e'\cept, of that the instructions for removing the patIent from contact with the electric medium do not apply.

QUEST I ONS O N CHAPTER V.
The lI ltlllerals i n dicati! the pages 'wltere Ihe allswe)s may be fOlll/ d .
\\' hat are the two systems of nerv es ? ... .. .
Of what is the cere bro·spinal system made up? .. .
What is the spinal cord?
\\'hR t are nerves like?
Explain the sympatheti.: system
Explain the respiratory system
Explain the acts of respiration
[0,,, are the exp:tnsion and contractIOn of the chest eftected?
to 121
In what system of artificial respiration is the pallent laId back ?
In what systems IS he J::lcl on back?
In what system i;; he laId on hIS back or SIde .
In what system is he rolled alternately on hiS Side and fa ce downwards?
ow long should artificial r es piration be perseyered with?
7 What is exciting respiration?
I28
hy is it necessary to watch the paLIent?
ility
State the various forms of 1I1senslbllIty .. , ., .
State the gene ral rules for treatment of.insenslbllIty I28 to 13 1
\ Vould you examine the patient to see If any bones were broken? .. ,
\Yhat wrong opinion may be formed when the pati e nt smells of drink? ...
Is collapse from c\ri n k a seriou. condition?
\ Vh3.t is concLlss ion of the b 'a1l1 ? ... ...
State the rul es fo r l r eatment of concussion
PAGE II7 II7 II7 IIS lI8
... . II8 to I}O 120 I
.. , ... ... ...
..,'
.... ... . ...
. 121 123, 1 26 127
... .., ... .., 139, 140
127 What
.. , . ... 1
7,
128
IT
12
is inducing circulation?
2
\\'
IIow may insensi 'u
. ' ; ' . J 28
128
1
... ...
2 9
130 13 1 [3 1 132
\Vha( danger accompanies injury to the head? 13 1
\Vhat caution should be giyen to a patient who has lost consciou.:;ness, eVen for a moment, after an injury to the head? 13 2
\\'hat are the causes of com pre sitJ11 of the brain? 13 2
In what aged people dOfs apoplexy usually occur? I3 2
\Vhat are the signs and symptom., of compression anu apoplexy? ... ... 13 2
State the:rules for treatment of these conaitions... 13 2
\Yhat d:mgf'r is there in applying hot waler hottles to insensible persons, and what precautions should be taken? ... 13 2
Describe a case of epilepsy I32, 133
\\'hat special care must be taken in treating a case of epilepsy? I3 0 , 13 2
Describe a hysterical lit 133
lIow would you treat a hysterical fit? ... 133
\Vhat are the comm mest physical causes of shock? 134
\Vhat may produce shock or fainting? ... 134
\Vhat conditions do certain poisons bring abOllt? 134
\Vhat may bring about fainting or coPapse? . . . ... 134
How would you recognise the general condition of shod? 134
\Vhat special precaution must be taken in the case of collapse?
.. 135
State the t r eatment for shock, faintll1g (syncope) and collapse... ...
... ... 135, 136
'What is the effect of sugar on the temperature of the body;-...
... '" ... 136
\Vhat are the causes of sunstroke and heat-stroke? 136
State the treatment for sunstroke and heat-stroke 136, 137
\Vhat are the causes of convulsions in chiidren ? 137
\Vhat are the signs of convulsions in children? '" 1 37
State the treatment for convulsions in children 137
State fully the causes of asphyxia ... 13 8

\Vhat two .things have to be done in all cases 8 asphyxIa?
. ... .... 3 , 139
\Vhat' two things must be seen to before it is possIble for artificial respiration to do any good? . .
Is artificial respiration likely to. do good If the au passages are obstructed, or If there IS not abundance of fresh air? ....
\\'Int is the first thmg. to do In a cas.e drownmg.
By what metho? may arlific.ial resplfatlOll be performed without tabng any prevIOus step ?
What . teps must be taken before pwceedJl1g WIth Silvester's method?
What should be done while artificial re piration is being pelformed?
the treatment for strangulatIOn
State the treatment for hanging
State t he treatment for mothering
State the treatment for choking ....
IIow may a swelling of the l1!)sues of the throat be caused?
State the treatment for swelling of the tIssues of the
throat
the treatment for suffocation by smoke or gases 14
How is electricity cunyeyed?..
lIow would you liberate a sulferer fro111 contact with an electric medium?
14 2 , Lf3
\Vhat would YOll do when the sufferer was remoyed from contact?
What would you do in the case of a hghtlllng stroke? ...
PAGE
... ... ...
...
...
... ...
...
PAGE
... .
...
.
.... ... .. . :.. ') ...
... .... ....
... . ..
... ... .
...
... ... ... ... ....... ...
139 139 139 139 139 I-tr
... ... ... ... ... ...
, .,.
... ... .......
State
1
1+2
... ... ... ...
... ... .... ..: ... . ..
CHAPTER VI.
POISONING.
Poisons may be classified according to their treatment und er two heads:.
Those which do not stain the mouth, and t oe treatment of which an emetic is to be given. Am o ngst these are :_
(a) Arsenic, (contained in rat poison and lucIfer matches), Tartar emetic and Sublimate, \\'hich cause a metallic taste 111 the mouth and a burning pain ill th e mouth, throat and stomach .
(t ) Str1chnine, Prussic Acid, Belladonna (deadly l11ghtshade plant) and several othe r varieties of as laburnum seeds, etc . th.ese gIve rIse to co nv'jl sions deliri um of respiration and collapse. '
(c) POIsonous meat, fish and fungi (often O1isfor mushrooms). Suspicion of these pOIsons should be direc ted to c ases where several persons \yho have partaken of the same food develop similar signs and symptoms.
(d) whi ch cause collapse.
(e) 0pIurn and Ils preparations, Morpbi ;l.,

149
Laud a num, Paregoric, Chlorodyne, Syrup of P oppies and various soothi ng drinks a nd cordials; these cause a tendency to go t o sleep, which co n tinues until sleep deep and bre1.lhing stertorous; the puplls of the become minutely contracted (pinhead pupils).
2. - Those which burn or stain the mouth, and in the treatment of which no emetic is to be given. These are of tW? :.
(a) Acids, such as NItnC ACId (Aqua fortIS), Sulphuric Acid ( Oil of Vitriol), Hydrochloric, or Muriatic, Acid (Spirits of Salt), strong Carboli c Acid (Phenol), Oxalic Acid, which is contained in oxalate of potash, salts of sorrel, salts of lemon and some polishing pastes.
(b) Alkalies, such as Caustic Potash, Caustic Soda and Ammonia.
SU:V11\IARY OF SIMPLE DIRECTIONS FOR THE TREATMENT OF POISONING.
I. - Send for a doctor at once, stating what has occurred and if possible the name of the
2.- Except when the lips mouth stained or burned by an aCld or alkah,
I SO prom. ptly give an em e tic - tha t . k h t IS, ma e t e pa lent vomit as foll ow s:-
(a) t he back o.f tlze tltroat with the finITer or with a feather. b
(b) lVfltstard-a dessert-spoonful ill a tUlliblerful of luke-warm water.
(c) Salt-a table-spoonful in a tumbl erfu l of luke-warm water.
(d) IpuamCllllla lVille-for a young child, a teaspoonful repeated at intervals of fifteen minutes.
all cas es when the p atient is no t ingive M il k, Raw Eggs beat e n up w Ith mIlk or wate r, Cr ea m a n d Flou r be ate n together, An imal or V egetable Oil (exc ep " m p h osphorus po ison in g ), a nd Tea. l.
. OIlv.e, Salad,. anJ Cod-Ii ,·er oil, or oil such as that 1l1. whIch are preserved, may be (riYe n· oils and paraffin are IS .soothll1g, . and is therefo re especially us efu l in by ACIds, Alkalies and such substances as and_ Corrosive Subli?1ate . Demulcent drinks, such as barley water or thm grueJ, act in th e same manner, free from danger in cases of phosphorus pOlsonmg.
may be given either be fore or nfttr the emetIc If the poison ca ll s for one.
Strong Tea acts as a neutraliser of many poisons

IS [
and i always safe. A handful of tea should be thr u\yO into a kettle and boiled.
4.- If th e li ps a n d mou t h are s t ained or b u rne d give no e m e t ic, but(17) If an acid is kno\\ 11 to be the poison give an at once . First \\ ash the mouth out freely with lime wat e r or other alkaline mixture, such as soda, chalk, whiting, or magnesia or wall pIaster in water, and 8fterwards le t the patient sip a little of it. Soda and potash are not to be given in the case of poisoning by oxalic acid.
(I)) If a stro n g Alkali is known to be the poison give an acid at once . First wash the mouth out free ly \\"ith lemon juice or vi n egar d iluted with an equal quantity of water, and afterwa r ds let the patient sip a little of it .
I n both cases give oil (Rule 3) ·
5. - When a person has swallowed poison and threatens to go to sleep, keep him awake b y walk ing h im abo ut a nd slappi n g his face, neck and c h est wi th a wet towel. S tr o ng b lack co ffee may be g iven to drink . Sla p pi ng the so les of t he fee t m ay a lso be t ri e d.
6. - If the throat is so swollen as to threaten obstruction to the air passage, apply hot flannels or poultices to the front of the neck and give frequent sips of cold drinks.
7· - Apply artificial respiration if breathing cannot be discerned.
8. - Treat shock and collapse.
9· - Preserve any vomited matter, food, or other substance, suspected of being the poison. Do not wash vessels which. may ha\'e con. tained the poison, and carefully guard them.
Certain poisons require special treatment, and a few of the commoner of these are mentioned below with their treatment.
CARnoLIC Acro.
The odour of the breath will aid in the detection of this poison; the lips ani mouth are usually stained white, and several nervous symptoms come 011.
TREATMENT.
I.-Give milk, to a pint of which half an ounce uf Epsom Salts has been added.
2.-Treat according to the general rules.
PRU SSIC ACID .
The action of this poison is extremely rapid. Giddiness, staggering, insensibility accompanied by panting respiration, profound collapse and possibly convulsions are the general signs, and in addition a smell of bitter almonds is often present .
TREATMENT.
I.-Place the patient in the open air. 1': 3
2. - D as h cold water on the head and spine
c )ntill uously.
3 - Apply artificial respiration. .
4.-Hold smelling salts to the nostrIls.
5.-Tre.1t shock and collapse. (See page 135 )
PO:SONOUS 1EAT, FISH AND FUNGI.
The signs and symptoms are vomiting and (J iarrhce.l), colic, headache, great weakness, raIsed temperature and a quick pulse.
TREAT;\IENT.
r .-Give an emetic . .
? - "When the emetic has acted, give castor OIl.
;:-Treat collapse . (See page 135·)
STRYCHNI E.
The signs and symptoms are a feeling of. suffocation, livid features, and convulsions .. The patIent rests on his head and feet, and the body IS arched.
TRE-\T:-IENT.
I.-Give an e m etic .
?.-App ly artificial respiration.
ALCOHOL.
1.- Gi \'e an emetic if patient can
2.- Treat collapse by keeping the patIent w:um, etc. (See page 135 ")
QUESTIONS ON CHAPTER VI.
Under what two heacls may poisons be classified?
\\'hat are the symptoms of poisoning by ,\rsen ic ?
Tlte numerals illdicafe the fag-er wizen the a I1 S"LfJc'rs may be found . PM;r;; I..J.S, I..J.9 qH
\ \'hat other poisons gi,'c ri<;c to the same s),mptom" ? .
\Vhat poisons give rise to cOi1Yulsions, delirium, failure I..J.8 of respi rati on and collapse? ... qS
If several people who had par aken of the same foud developed similar signs and sympto ms, by \\ hat would you su pect they had been poisoned? I..J.S
\Vh at condition may result from poisoning by alcohol? L-I-S
\" hat are the effects of such poisons as opium ?... 148, I..J.9
\V hat two cia. ses of pJison burn or stain the mouth? .. . 149
\Vould you give an emetic for such poisons? 149
Name some of the principal acid 149
Name some of the principal alkalis 149
State the general rules for the treatment of poisoning ... 149 to 152
State the best methods of making a per. on vomit ISO
lI ow would you treat a case of acid p oisoning? ... 15 I
How would you treat a case of poisoning by an alkali? 151
State the signs, symptoms and treatment of carbolic acid poisoning .. . ..
State the signs . symptoms and treatme nt of poiso ning hy Prussic Acid 152, 153
State the sIgns, symptoms and treatment f poisoning by poisonous food ...
State the signs , symptoms an d treatment of p oiso ning 1)), Strychnine
\Yhat would you do in the case of alcoholic poisoning? 153 153 153

I55 CHAPTER VII.
BANDAGING.
Esmarcb's Triangular Bandage has been in Chapter II. It may be applied to keep a dressmg o n a \\'ound, burn or scald of any part of the body, or for an injury of a joint. 1.
For the Scalp (Fig. 62) . Fold a hem about 1.2 inches deep along tbe base of a bandage ; place the bandage on the head so that the hem lies on the for ehead close down to the eyebrows, and t be point hangs do\\-n at the back ; carry the two ends round the bead above the ears and tie them on t.he forehead ; draw the pomt first downwards, and then turn it l P and pin it on to the bandage on the lOp of FIG. 62. the head.
For the Forehead, Side of the Head,
Cheek and for any part of the body that IS round '(as th e arlll or thigb, etc ).' the narrow bandage should be used, its centre bem,g placed over the
154
and the ends being carried round the head or lImb, as the case may be, and tied over the wound. For the Shoulder (Fig. 63). Place the centr:: of a bandage on the shoulder, with the point running l) :

FIG. 63· --==::...-=- FIG. 64.
up the side of the neck; fold a hem alon a the base' carry the ends round t11e middle of the :rm and Place one end of a broad bandage over the pOll1t. of the first bandage and sling the arm by ca.rrymg the other end over the sound shoulder and tYl?g the ends at the side of the neck; turn down the POll1t of the first bandage, draw it tight and pin it.
157
For th e Hip (Fig. 64). Tie a narrow bandage round the body above the haunch bones, the knot on the injured side. Fold a hem accordll1g to the size of the patient along the base of a second bandage; place its centre over the dressing, carry the e;lcs round the thigh and tie them; then carry the point up under the
FIG. 65 . FIG. 66. first bandage, tum it do\\ n over th e knot and pin it.
For the Hand \"h en the fing ers are extended (Fig. 65). Fold a hem along base of a bandage; place the wrist on. the hem \\'.lth the fingers the point; then bnng the pomt over the v: nst , pass the ends round the wrist, cross and tie them; bring the point over the knot and pin it to the b::l.l1dage on the hand.
For the Foot (Fig. 66) . Place the foot on the centre of the bandage with the toes towards th e point; draw up the point over the instep, pass t h e ends round the ankle and cross them in front; n o\\' pass the ends round the instep and tie them. Draw the

FI C 67a.
point forward and pin it to the bandage ()n the instep.
Fo r the Fron t o f the Chest (Fi gs. 67a and 67 0). Place the middle of the bandage oy er the dressing with the point over the shoulder on th e same side; carry the ends round the waist and tie them;
FIG. 68 .
15 9
th e n draw the point over the. sh o uld er and ti e it to on e of the ends.
F or t h e B ac k. The bandag8 is a ppli e d as th e fore goin g , e xc ept that it is be a un at th e back.
Fo r Kn ee. Fold a narrow hem alon g the bas e of a bandag e ; lay the point on the thigh and th e l111dJle of the base just bel ow the ; cross the ends first behmd the kn ee, then over the thigh and tie tl:en:. Bring the point dO\\' n and pm It t o the base (Fig . 68) .
For the Fold a narrow hem along the base of a bandaae ' lay the point on the back of the arm and the b of the base on the ?ack of the forearm; cross the en ds first in ot the elbow, then over the arm a n d tie them m front
(Fig. 69) · •
For the Fingers ana Toes wrap a strip of cali c o or line n round a nd ro u n d the pa rt; split th e fr eeend, secure it ro und the '\'fist or a n kle .
158
\ \ \
CHAPTER VIII.
METHODS OF CARRYING.
THE FOUR-HANDED SEAT.
This seat is used when the patient can assist the bearers and use his arms.
I.-Two bearers face each other behind the patient and grasp their left forearm with their right hands and

FIG. 70.
each other's right foreJ.rm with their left hand s (Fig. 70), and stoop down.
2.-The patient sits on the hands and places one arm round the neck of each bearer.
3.-The bearers rise together and .step the bearer on the right hand side of the patIent WIth the right foot, and the left hand bearer with the left foot.
THE T\\"o-HANDED SEAT.
This seat may be used to carry a helpless patient.
FIG. 71.
1.-Two bearers face each other and stoop, ?ne on each side of th e patient. Each bearer hIS f?rearm nearest to the patient's head under hIS back Just G
160
161
below the shoulders, and, if possible, takes hold of his clothing. They slightly raise the patient's back, and then pass their other forearms und er the mid d le of his thi ghs (Fig . 7 I), and clasp their hands by one of th e methods shQ\n1 in Figs. 72 and 73. A handk e rchi ef should be held in the hands if the first grip is used.

73.
2.- The bearers rise toge th er and step off, the right-hand bearer with the right foot, and the left-hand bear er with the left foot (Fig. 74).
THE THREE-HANDED SEAT.
This seat is useful for carrying a patient and supporting either of his lo\Ver limbs, when he is able to use his upper iimbs.
I.-Two bearers face each other behind the patient. For suppo rting the left limb the bearer to the patient's right grasps his own left wrist with his right hand, a nd the other bearer's right wrist \vith his left hand. The bearer to the left grasps the first bearer's right ,,,rist with his right hand (Fig . 75). This leaves his
162
FIG.
FIG. 74. G2
left hand free to support the patient's left leg. For the patient's right lower limb follow the same directions, substituting" right" for" left" and" left" for "right." The bearers stoop down.
2.-The patient places one arm round the n eck of each bearer and sits on their hands.
3·- The bearers rise together and st ep off) th e

FIG. 75. right-hand bearer with the right foot, and the lefthand bearer with the left foot.
THE FIREMAN'S LIFT.
(To be attempted only by a strong man).
Turn the patient face down \,'ards; place yours elf at his head, stoop down, slightly raise his head and
164
166 shoulders and take hold of him close under his armpits, locking your hands on his back. Rais e his body and rest it on your left knee; shift your arms and, taking him round his waist, lift him until his head rests on your left shoulder. Throw his left arm over your head, stoop down and place your left arm betwe en his thighs, letting his body fall across your shoulders. Rise La an upright position; hold the patient's left \\ rist with your left hand and leave your right hand free.
Assistance may be given to an injured person by supporting him in the manner shown in Fi g. 76 .
TIle plan oj carryz'J7g tIle patient by til e arms and legs witll the face dowJlwards, commonly called tlte "frog's march," 1Ilust llever be used, as death may ensue from flu's tNatment.
blPROVI SED STRETCHERS.
A stretcher may be improvised as fol1ows :-
I. - Turn the sleeves of a coat inside out; pass two strong poles through them; button the coat. The patient sits on the back of the coat and r ests against the back of the front bearer ( Fig. 78). If a lon ger stretcher is required t\\'o or three coats must be treated in the same manner. The poles may be kept apart by strips of \\'ood lashed to the poles at both ends of the bed formed by the coats (Fig. 79).

THE FORE AND AFT METHOD.
This plan of carrying is useful \\ hen sp,lce does not permit of a hand seat.
FIG. 77.
2.-l\fake holes in the bJttom corners of one or two sacks and pass stout poles through them.
3.-Spread out a larg", piece of carpet, sacking, t:upaulin, or a strong blanket, and roll two stout poles up in the sides. Two bearers stand on each side and grasp the midd'e of the pole \yith one hand, and near the end with the other. They walk sideways.
4·-A hurdle, broad piece of wood, or shutter may be used as a stretcher j some straw, hay, or clothing should be placed on it, and covered with::t piece of stout cloth or s:1cking; the latter i::i useful in taking the patient off the stretcher.
Alwa.ys test an improvised stretch er before use.
Stretchers must be carried, and the p:uient placed on the :11, as bid down in the c. Stretcher Exercises."
As a general rule c;1rry the pltient feet foremost.
The exceptions are:-
(a) 'VhE:n going up hill with a patient whose lower limbs are not injured.
(b) When going down hill with a patient whose . lower limbs are injured.
Avoid lifting the stretcher over ditches or walls, but "here these cannot be avoided the stretcher must be carried in the following ways: -
To CROSS A DITCH
.
In crossing a ditch, the stretcher should be lower with its fOJt one pace from the edge of the ditch
168
169
l' lG.
1\os. I and 2* bearers then descend. The stretcher \\ ith the patient upon it, is afterwards advanced; No . I and 2 in the ditch supporting the front el.ld while its other end rests em the edge of the ground aboye. o. 3 now descends. All the T os. now carry the stretcher to the opposite side, alld the foot of the stretcher is made to rest on the edO"e of tbe ..l • b grounu, whIle the head is supported by NO.3 in the No: I climbs out, No. 2 remaining in the ditch to aSSIst NO.3. The stretcher is lifted forward on the ground above, and rests there \"hile Nos. 2 and 3 climb up.
To CROSS A 'VALL.
The stretcher is lowered \\ ith the foot about one pace from the wall. Nos. I and 2 bearers then take hold of the foot of the stretcher, and NO.3 of the head; the stretcher is raised till the foot is placed on the wall. No. I then climbs over the wall and takes hold of the foot of the stretcher, \\'hile Nos. 2 and 3 s L1pport the head; the stretcher is then carried forward till the head rests on the wall, No.' I supporting the foot. Nos. 2 and 3 then climb over the wall and take hold of the head of the stretcher, which is then slowly lifted off the wall on to the ground and the bearers take their usual places. '
------------------------
"The:e numbers are explained later in the detailed " 'trc chef Exerci!:>es."

To LOAD A "·AGON,
The stretcher is lowered with the foot one pace flom the end of the wagon. Jos. I and 2 take hold of the foot of the stretcher, No. 3 the head. The stretcher is then raised and carried forward till the front \\ heels rest on the floor of the \\'agon. TO. I then jumps into the wagon, \\hile 1\0. 2 goes to the head of the stretcher and helps TO. 3. The stretcher is then pushed slowly into the wagon. If the tailboard cannot be shut, the stretcher must be lashed firmly to the sides of the wagon.
To UNLOAD A 'VAGON.
Nos. 2 and 3 take hold of the head of the stretcher, \vhile No. I gets into the wagon; the stretcher is then gradually dra\\'n out till the foot-wheels rest on the edge of the wagon. No. I jumps out of the wagon, and with No.2 takes hold of the foot of the stretcher, NO.3 supporting the head. The stretcher is now gently dra\\n a\\ay one pace and lowered. 'Vith four bearers Nos. I and 2 \\'ould lift the foot of the stretcher, \\hile Nos. 3 and 4 lift the head. This applies to crossing a ditch or wall, as well as to loading and unloading a wagon.
170
CHAPTER IX.
STRETCHER TRAN PORT.
The "Furley" Stretchers (Model J 899) are of three patterns, viz .," Ordinary,"" Telescopic-handled," and" Police ." In general principle they are alike, the component parts being designated the poles,

FIG . 80.-0RDINARY STRETCHER-CLOSED.
FIG. 8I.-TELESCOPIC HANDLED STRETCHER- OPEN.
handles, jointed traverse bars, foot wheels, bed, pillow sack and slings .
The Ordinary Stretcher (Fig. .80) is 7 feet 9 inches in length, and I foot 10 inches wide. The bed is 6 feet in length, and the handles inches. The height is 51- inches. At the head of the stretcher is a canvas overlay (the pillow sack) which can be filled with straw, hay, clothing, etc., to form a pillow, The jointed traverse bars are provided with joints.
173
for opening or closing the stretcher. The Telescopichandled pattern (Fig. 81) i) very similar, but the handles can be slid underneath the poles, thus reducing the length to 6 feet. This arrangement is of great value when working in confined spaces, or when a patient has to be taken up or down a narrow staircase \\ ith sharp turns. The Police stretcher is similar to the Ordinary pattern, but is more strongly made, and has, in addition, straps for securing a refractory pati e nt.
'Vhen closed, the IDles of the stretcher lie close together, the traverse bars being bent inwards, the canvas bed neatly fo!ued on the top of the poles and held in posi tion by the slings which are laid along the canvas, and secured by a strap, placed transversely at the end of e lch sling, being passed through the large loop of the other, and round the poles and bed. .
In closing a stretcher care should be taken to raise the centre of the canvas wh en pushing in the traverse bar, as it is cther\\'ise liable to get caught.
To prepare, or open a stretcher, unbuckle the trans · verse straps of each sling; remove the slings from the stretcher; separate the poles; take hold of each traverse bar and draw it forward. The slings will then be folded to half their length, one being laid neatly over the handles at each end of the stretcher .
As a general rule, the stretcher will be prepared by Nos . I and 3 bearers in Exercises I, II., and III. ;
and by No. 2 in Exercise IV. These bearers will, however, if required, assist the other bearers in attending to the patient's injuries.
l\Tote.- The various movements detailed in the following Exercises should be carried out steadily, the bearers working in unison, hurrying being carefully avoided and every attention being paid to the bearer ",ho giYes the words of command.
STR ETCHER EXERCISES,
Originally drawn up by Sir John Furley, and revised in I904 to accord with the drills adopted by the Royal Army Medical Corps :-
EXERCISE No. r.
FOR FOUR BEARERS.
I.- The Instru ctor selects the bearers and numbers them-I, 2, 3,4 at his discretion. Should one man be taller and stronger than the others, he should be styled No. 3, as he ",ill have to bear the heavier part of the burden.* All orders will be given by NO.4.
2. -" Fall in."-Nos . I, 2, and 3 take position on the left side of and facing the patient. No. I places himself at the patient's knees, No. 2 at the hips, NO.3 at the patient's shoulders. At the same
* Bearers should, however, be taught lo take any of the po it ions named in the following exercises, whether that of No. I, 2, 3, or 4 bearer.

time No. 4 pbres tlF' prepareu stretcher on the ground by the right siue of the patient about tv,o
FIG. b2.
paces away from him, and then takes position opposite to and facing NO.2. (Fig. 82).
174
3· - "R,,: ady."--The bearers kneel down on the le,rt knee and take hold of tIle patient, No. I pas ing hIS hand.s and fore-arms beneath the patient's legs, hands wIde apart. Nos. 2 and 4 pass their hands

FIC. 8::. and forearms beneath the patient's hips and loins, and grasp each other's hands. NO.3 passes his left hand across the patient's chest and under the right shoulder, and his right hand beneath the left shoulder 83)
J77
. 4.-"Lift."-On the \\ ord "Lift," the bearers rai se the patient gently and rest him on the knees of I, 2, and 3 bearers (Fig. 84) ; as soon as he
is : e ' urely rested, NO.4 disengages hands with NO.2, run s round by the head of the stretcher and places it und er the patient, close to the other bearers' feet,
176
I78
being careful that the pillo\y is immediately un der the patient's head Fig. 85) ; he then kneels: dO\\l1 and locks his hands with those of .l. o. 2 (Fi g. 86).
5. - " Lower. "-The bearers place the patient on the stretcher (Fig. 87), disengage their hands, and then stand up.

FIG. 85.
6. - " Stand to Stretcher."- No. I goes to the of the stretcher, \\ ith _ his back to tbe patient; No. 3 to head \\Ith hIS face to the patient; Nos. 2 and 4 renlam o n each side of the stretcher.
7·-" I and 3 place the slings (if used) ov er theIr shoulders, stoop down, and slip the
179
loops of the slings on to the handles of the stretcher, \\'hich they then grasp .
As soon as all is right the \yord is given :-
8. -"Lift Stretcher."-Nos. I r..nd 3 bearers raise the stretcher steadily together and stand up .
No/e.- IOS. 2 and 4 \\ill now adjust the slings on the shoulders of Nos. I and 3, taking care that each is well below the level of the collar and lies accurately in the hollow of the shoulder in front. They will also lengthen or shorten the lings, haying regard to the patient's injuries and the relative heights of the bearers. l' IG. 86.
9.-" March."- The bearers move off :-Nos. I, 2, and -t- stepping off with their left foot, and NO·3
his right foot (Fig. 87). The step should be a sort one of inches, and taken with ben<t no from the fore of th e foot.
O. Halt. -The bearers rem am steady.

I I - " Lo e St t h " . w r re c er. -The bearers lace ge ntly on the grou nd, slip the loo Ss of t e sl,mgs off the handles of the stretcher remove the shngs from the shoulders, and then stand up. •
181
12. - " Unload Stretcher - Ready." - The bearers prepare to take the patient o ff the stretcher, as at Orders 2 and 3·
13.-" Lift." - The bearers raise the patient as at Order 4 (Fig. 86); o. 4, in this case, disengages hands from No.2, removes the stretcher (Fig. 85), and resumes his former position. If necessary, the bearers will then steadily rise together, and Guefully carry the patient to the bed, or other place to which it has been arranged to convey him.
14.-" Lower." - Th e patient is carefully lowered.
EXERCISE No. II.
FOR THREE BEARERS.
r.-N umber the beare rs I, 2, 3·
All orders will be give n by No.2, who will lo ok after the injured part of the patient's body or limbs, to see that no b:ll1dages or splints become displaced, and also that No. I bearer, in lifting or carryi ng the stretcher, does not touch th e patient's feet.
2. -" Place the Stretcher." -No. 3 places the stretcher in a line with th e patient's body, the foot of th e stretcher being close to his head.
3. -" Fall In. "-No. I places himself on the left side of the patient in a line with his knees, No.2 on the left side just below the patient's shoulders, and NO . 3 at the ri ght side, and faces NO.2.
180
4. - " Ready." -All kneel on the left knee'. No. j places his hanus, ",d l :lparl, underneath the lo\\'er limbs, always laking care, in case of a fractur , to have one haud on each side of the seat uf injury. os. and 3 grasp 'ac h other's hands LInder thl2 shoulders and thighs of the patient (Fig. SS).

5. - " Lift." - The bearers ri s!"' together, keeping th e patient in a horizontal po sitio n (Fi g . 89).
March."--All take shorl side-paces, carrying the patIe nt oyer the stretcher until his head is immediately above the pillow
1 83
7. "Halt.-Tbe bearcrs remain steaely. 1
8. " Lower."-The bcarc rs stoop do\\n, gent y place tIll' patll'nt on t11C' stretcher, disengage thclr hand s, and then stanu up.
9. -" Fall In." - No. 1 places himself th e foot of the stretch er with hi s back to the patIent, No.2 pIa es himself at th e left side of th e and NO.3 at the h ead, \\ ith hi s face towards the patIent.
• J ',2
, :-, .,.-=. _c rT ",-
.
10. -" Ready." -Nos. I and 3 place the slings (if used) over their shoulders, stoop do\Yn, and slip the loops of the slings on to the handles of the stretcher, which they then grasp.
As soon as all is right the word is given-
11.-" Lift Stretcher."-N os . I and 3 bearers raise the stretcher steadily together and stand up.
No. 2 will now adjust the slings on the shoulders of Nos. I and 3, taking care that each is well below the level of the collar, and lies accurately in the hollow of the shoulder in front. He will also lengthen or shorten the slings, having regard to the patient's injuri es and the relative heights of the bearers.
12.-" March."-N os. I and 2 step off with the left foot, and NO.3 with the right. The step shou ld be a short one of 20 inches, and taken \\ ith bent knees, and no spring from the fore part of the foot.
13.-" Halt."- The bearers remain steady.
14·-" Lower Stretcher."- The bearers place the stretcher gently on the ground, slip the loops of the slings off the handles of the stretcher. remove the slings fro !TI the shoulders, and then stand up.
15 -" Unload Stretcher - Ready." - The bearers prepare to take the patient off the stretcher, as at Ord ers 3 and 4 (Fig. 88) .
16.-" Lift."- Tbe bearers raise the patient, as at Order 5, and carry him by short side ste ps, clear of the stretcher, to the bed, or other place to which it has been arra'lged to convey him (Fig. 89).

18s
17. _cc Lower."- The patient is carefully lowered.
EXERCISE No. III.
" 'HIm ONLY THREE BEARERS ARE AVAILABLE AL\'D THE STR ETC H ER CAN:\'"OT [;E PLACED IN EXERClSE II.
T.-The Ins tructo r numbers the hearers-I, 2, 3. All orders \\ ill be gi ven by NO.2.
2.-" Place the Stretcher."-No. I taking the foot of the stretcher, and NO,3 the head, place it on the ground by the side of the patient, and as close to him as practicable.
3. '-" Fall In."- The three bearers take the same positions on one side of the patiellt, as laid down in Exercise o. I.
4.-" Ready." -Nos. 1 ,2, and 3 kneel down on th e left knee, placing as close to the pati ent as they conveniently can, and th en take hold of him as directed in Exercise No.!.
5. - " Lift."-Nos. I, 2, and 3 raise the patient as directed in Exercise N o. I, and then move in a kneeling position up to the st retcher.
6.-" Lower."- The bearers bend forward, carefull y lower the patient on to the stretcher, and disengage hands.
184
7. - " Stand to Stretcher."-All the bearers stc.lnd up; Jo. I goes to the foot , No.2 remains in po. ition at the side, and No . 3 goes to the head of the stretcher.
8. - " Ready. "-Nos. I and 3 place the slings (if used) over their shoulders, stoop do .\,11, and slip the loops of the slings on to the handles of the stretcher, ",hIch they then grasp .
9. -" L ift Stretcher. "-Nos. I and 3 bearers raise the stretcher steadIly together :lnd stand up.
No . 2 will now adju t the sling, on the shoulders of Nos. I and 3, taking care that each is well below the level of the col ar, and lies accurately in the hollow of the shoulder in front . He will also lengthen or shorten the slings, having regard to the patient's injuries and th e:: relative h , ights of t he hearers
10. - " March. "-Nos. I and 2 step off \\'ith the left foot, and NO , 3 with the right. The step should be a short one of 20 inches, and taken with bent knees, and no spring from the fore part of tbe foot.
II. - " Halt. "-The bearers remain steady.
12 . - " Lower Stretcher." - The bearers place the stretcher gently on the ground , slip the loops of the slings o ff th ,= handles of the stretcher, remove the slings from the shoulders , and then stand up.
13. - " Unload Stretcher-Ready. "-No . places himself on the left si d e o f the pa tient, and in a li ne wit h his k nees , N o. 2 on the left side just below the patien t' s sh ou lders, a n d NO. 3 at the right

187
side, and faces NO.2 . All kneel on the left k nee. N' o. I places his hands, well apart, underneath the lower lImbs, ahvays taking care, in case of a fracture, to have one hand on each side of the seat of injury.
os. 2 and 3 grasp each other's hands under the shoulders and thighs of the patient.
14.-" Lift "- The bearers rIse together to their f eet, keepmg 'the patIent in a horizontal position, and cJ.rry him by short side steps, clear of the stretcher, to the bed, or other place to which it has been arranged to convey hIm.
15.- " Lower ."-The patient is carefully lowered.
EXERCISE No. I V.
FOR USE IN I\II),TES A),TD NARROW CUTTINGS
T\\ 0 O),TLY CAN BE ENGAGED .
Nos I and 2 \\,111 carefully place the stretcher in a lme \\,lth the injured man's body, the foot of the stretcher being, If possIble,*' close to hIS head .
No. I straddles across the patient's legs, placing his rIght foot, with the toe turned outwards, a litt le below the patient's knees, and with the toe of the left foot close to the heel of NO . 2; he then stoops down, plsses the left hand under the patient's thighs and
• I t is not advisable to be too particular as to the head or ! oot a stretcher in a mine, as it would probably be quite to reverse It.
186
the right hand across and under patient's No.2 places his feet one on each sIde of the patIent between his body and arms, the toe of each foot as near the armpits as possible. He then stoops down and passes his hands between the sides of the chest and the arms undel n eath the shoulders, and locks

i·I(;. s.o.
the fingers (Fig. 90). If the patient's arms are uninjured he may put them round the neck of No.2, and by this means greatly assist him in lifting.
18 9
'\Th en both are ready, No. I will give the ord e r " Lift and move forward." The patient is then to be slowly lifted, just sufficient to allow his body to clear the stretcher. Both bearers will slowly and gradually mm'e the patient forward, NO.2 by very short steps, No. I by bending his body forward as much as he can wdltOltf moving ht"s .feet Fig. 9 r). 1 O. I now gives the order r ( Halt," " 'hereupo n o. 2 remains steady, anJ No. I ad,'a nces his right foot to his left, and
FIG. 9I.
again advances his left foot till the toe touches tbe heel of NO.2. No. I then gives the order "Advance," when the patient will again be moved forward. These movements are to be repeated until
188

the patiellt is over the stretcher, \yhen he is t o be gently lowered .
The fo llowing Stretche r Exercise is adapted by permission from the Royal Army :Medical Corps Manual, 1908 .
All orders will be gi ,"en by NO·4.
1. {( Fall in. " -Six bearers bll 111 behind each other.
2. " N u mber. "-The bearers number from front t o rear.
3. "No.3 Bearer, right (or left) turn - sup p ly stretcher-quick march. " -No . 3 bearer will 1112.rch to the stretcher, stoop, lay hold of it and place it on ' his right shoulder at the slope, holding it by the lower fooL wheels, wheels to the front. As soon as the bearer is provided with a stretcher, he will turn about and rejoin his squad in quick time, halting as he arrives in his place. He t urns to the front, and, passing the lower end forward , places the stretch er 011 the ground to the r ight of the squad, wh eels t o the right , front en d of the poles in li n e with the t oes of No. 1 a n d rises
4. "Stand to Stretcher." - No . 1 places himself with his toes in line with the fron t ends of the poles . NO . 3 with his hee ls in line with the rear ends of the p o les , cl ose t o and touching the stretcher with
I90
.
@] L!1
Fig. 92.
\ 1 ... FlG. 95 F IG. 96.
FiC. 9 3.
his righ t foo t. Nos . 2, 4, 5 a n d 6 take up their positio n s o n e pace beh ind and covtring off the bearer in fro n t of them (Fig. 92).
5. " Lift Stretcher."-Nos . I and 3 stoop, grasp both hand les of the po les with the right hand, rise together, h oldi ng the stretcher at the full extent of the arm , wheel to the right .
6. "Collect Wounded - Advance ." - The sq uad doubles by the shortest route to the patient, and halts without further word of command one pace from the head of and i n a line with the patient (Fig . 93).
7· "Lower Stretcher."- Nos . I and 3 stoop, place the stretcher q u ietly o n the gro u nd, amI rise smart ly togethe r.
8. "Prepare Stretcher."-Nos . I and 3 turn to the right, kneel on the left knee, unbuckle the transverse straps, and place the slings on the ground beside them , separate the po les, and straighten the traverses.
T wo. O n the word two each takes a sling, doubles it on itself, slips the loop thus formed on the near handle, places the free ends over the opposite handle, b u ck le uppermost. They then rise and turn to their left toge t her .
'While the stretcher is being prepared by T os . T and 3, the disengaged bearers will advance and rende r to t he patient such assistance as may be required ( Fig. 94) .

193
The necessary assistance having been rendered, NO.4 will giyc the command-
9 . (t Lo a d Stretch e r . " - The bearers place themselves as follows :-Nos. I, 2 and 3 on the left, Nos. 4, 5 and 6 on the right of the patient; os. I and 4 at the knees, 2 and 5 at the hips, 3 a.nd 6 at the shoulders the whole kneeling on the lett knee. , . , Nos. I and -+ PJ.ss th ei r ll'1nd3 b:;ne::tth the patient s knees, 2 and 5 beneath the hips, 3 al:d. 6 beneath the shoulders, care being taken of the IllJured part, one of the bearers being detailed for this purpose (Fig. 95)'
10. " Lift: '-Tbe whole will carefully lift the patient on to the knees I, 2 3· .
Two. Nos. 4, 5 and 6 w1l1 then dIsengage, nse; Nos. 4 and 6 step back one pace. No . 5 tu to his left doubles to the stretcher, takes hold ot and r<lises it left hand acros . , the near pole resting on the left hip; carrying the he returns to hi.s place between 4 and 6, and places it beneath the patient.
Tltree. Nos . 4 and 6 step forward one pace, and together \\ ith NO.5 kneel down on. the knee, and prepare to assist in lowering the patient (FIg. 9(1).
II. "Lower." -The patient is lowered slowly and gently on to the centre of the canvas (sp ec ial care being taken of the injured pal t).
Tun. The bearers disengage, rise; Nos. I, 2, 3 and 6 turn to the left ; Nos. 4 and 5 to the right; H
No. 4 places himuelf thre . stretcher. No. 6 1m fl.ont of the of tl . ,C b ec e t 1e kIt and le patJent, places himself tl . arms tIle stretcher Nos 2 d 1ree ll1 rear of of the stretcher 'i'h 1 5 opposIte the centre . I e \\ 10 e are no\" re d 1'[ stJ etner and move off (Fig. 97). \ a y to I t

FIG. 97.
195
12. "Lift Stretcher. "-Nos . I and 3 stoop: grasp the doubled sling lllic1\\ay between the poles with the forefinger and thumb of the right band, s\yeep it off the handles, ris,=, holding the sling at the full extent of the arm buckle to the front, take a side pace to the front between the handles, and place the sling over the shoulders dividing it equally, buckle to the right. The slings should be placed so that they lie well below the collar of the coat behind and in the hollow of the shouluers in front. In the event of the slings requiring to be adjusted, either as regards length or for the greater comfort of the bearers, NO.4 will detail a bearer to carry this out, the length of the slings being adjusted, when necessary, by means of the buckles.
Two . Nos . I and 3 stoop, slip the loops oyer the handles, commencing with the left, and grasp the handles firmly.
Tltree. Nos . T and 3 rise slowly together, No. 3 conforming closely to the movements of No. I.
13. " Advance." -Nos . I, 2, 4, 5 and 6 step off with the left foot, NO . 3 with the right, stepping short, knees bent, feet raised as little as possible.
14. "Halt."-The whole halt.
IS. "Unload Stretc h er. "-The bearers themselves in the same position at the stretcher as described for Loading (Order 9) ·
16. "Lift."-As described for Loading (Order 10), H2
194
excep t that the stretcher is carried forward three paces clear of the patient's feet.
I7· "Lower."-Tbe pati er t is gently lowered to th e ground . The Learers clisen':age, r :se ; Nos. I, 2 and 3 turn to the left, 4, sand 6 to the right, and the whole step off to their places at the stretcher, as at Order" Stand to Stretcher" (Fig. 98).
The Ashford Litter is made up of either of the Furley stretchers mentioned on pages 172 and 173, a wh 2e led under-carriage and a waterproof hood and or, if preferred, a light \\'et-resisting canvas cover. fbe stretcher is kept in position on the under·carriage by the foot -wheels, which fit into slots in the sides of the under-carriage, and it can be removed at pleasure. Th e under carriage is l1tt ed with a cranked axle which allows the bearers to pass with the stretche; between the \\'heels instead of lifting it over them. At both ends are two legs wbich may be turne 1 up as when wheeling the litter. The hood and apron fit mto sockets screwed to the stretcher. In wheelin<T tbe litter, care should be taken to keep the patient a horizontal position. Should it be necessary, two bearers can easily lift the litter and patient.
. The. Litter, introduced in 1904 IS used 111 a SImilar manner, and one model of it is fitted with tyres, which add immensely to the comfort of the patient and to the ease of propulsion,

197
CHAPTER X.
(B eiJzer til e Fiftlz Lecture for Females ollly, z'n accordaJlce b wdlz Syllabus 58.)
BY E. ;\IACDO.\ ELL COSGRAVE, ;\J.D., F . R.C.P.I.PREPARATlON FOR OF ACCJDE:/\T C.\SL.
news of an accident conl.es, shoyld at once be made so as to have everythlll.g l eady before the injured person is brought in. course th e preparation s needful will vary accordll1f,!; to . the nature and extent of the injury, but the followll1g are the chief things which may have to be done.
CHOICE A 'D PREPARATlON OF RomI.
A room must be chosen. In a bad case this should be one easily r eac hed, as it is difficult to carry, an injured p erson through narrow passages an,d Unless there is some such reason agall1st It, the injured person's own room is best. . .
The way to the room must be cleared, furniture and loose nlats in the hall or m lobbies should be removed. If the injured person is carried on a door, shutter, or stretcher, two strong chairs should be placed ready to support it wherever the bearers would be likely to require rest.
Useless furniture should be remoyed from the bedroom. The bed should be drawn out from the wall
196
198
so that both sides be approached, and the clothes turn:d back to one side to their full length. A hot bott ..; should be got ready. If there is much collapse several hot bottles and hot biankets may be required' cover the hot bottles with flannel. '
If the injury is very severe, if mud-stained clothes have to, be r,emm'ed, or if extensive dressings have to be applIed, It may be necessary to have another bed a couch or ,a table placed near the bed to lay sufferer on \l1 the first instance. This should be arranged that do no harm; old sheets, waterproof materials, tl1ll1 oilcloths, or even nel\'spaper, may be used as a protection.
LIFTING AND CARRYING. , present at the place where the accident occurred It will ,be necessary to see that the patient is fully l! fted after proper "Flrst Aid" has b rendered. een
The following rules should be remembered :-Select the proper number of persons to assist, and do not let them hft the patient until they thoroughly understand how' they are to do it. -
For ?rdinary cases, where the injured person has to he, hfted a very short distance, three helpers are suffiCIent: Two (who should be as far as possible of eq ual heIght) are to bear the weight, the third is to su pport and take charge of the injured part. This is

199
best done by a person who has been a .. Aid /I course. If the injured person IS another should support his head.
The lifters one at each side, should kneel on one knee, and their hands under the patient's back at the lower part of the shoulder blades, and under the hips, clasping each his right in , the other's The injured patient should, If practicable, pla ce hiS arms round the necks of the bearers. , '
The third helper should attend to th e eat of ll1}ury; if this is a fractured limb, he should support It by placing the palms of his hands limb, above and one below the seat of the 1l1Jury, grasp1l1g it firmly but avoiding pressure.
The helpers should remain thus until ord e r " Lift /I is given, and then they should all btt slo\\ ly and steadily, avoiding jars, attempts to change POSItion of hands, etc.
If the injured person is to placed on a st: e tcher or shutter, this should be preVIOusly placed WIth the bottom end at his head; the bearers should then move one at each side of it, until the patient is oyer it. The word" Lower" should then be given, the injured person should then be slowly lowered. A pillow or folded up coat should be ready, and as the sufferer is lo\vered this should be placed under his head.*'
* Full directions are gjven in Chapter IX.
::(0

J\h:ANS OF CARRYING.
a. stretcher, and substitutes such as a gate, shutt.el, Ot a door, other means of carrying can be ImprovIsed.
In slight injuries, \\'here the injured person is unable to walk, two bearers can carry bim by forming a fourbanded, three-handed, or two-handed seat.
A four-handed seat is formed as described on p3.ge 160.
A three-handed seat is made as described on p.1ge 162.
The two-handed seat is made as described on page 161.
. \ single helper can lift by supporting with one arm the two knees, and witb the other the back. The arm.s must be passed well under before commencing to 1J ft.
A single felpel: can suppo,rt by putting his round tne WaIst, graspll1g the hlp and placing the ltlJured person's arm round his own neck holdingth':'! band .with his own hand (Fig. 76, page 16 5). '-
A capItal stretcher can be im provised out of a strong sheet and two broom handles or other short poles. side of sheet is wound up on a broom h :ll1dle untIl t?ere IS .Just room for a person to lie b,etween. ThIS r eq mres four bearers, t\\'o at each SIde, to prevent the sheet slipping.
20I CARRYING UP STAIRS.
In carrying a stretch er 11 p stairs the. head should go first, and an extra helper should assist at the lower end, so as to raise it anu keep the stretcher nearly horizontal.
The (WO, three, or four-handed seat .may be u.sed for carrying up stairs; or a strong chaIr, the patIent being carried up backwards. the latter case one helper should walk .the chaIr and to support it, and to prevent the 1t1Jured person sllpp1l1g out.
LIFTING INTO BED •
If the bed is narrow and there is room the stretcher should be placed on the r floor. ':'ith the head close to the foot of the bed. The 1l1Jured person should then be lifted over the foot al!d on the bed. If the bed is too wide to admit of thIS, the stretcher should be placed beside it, and two helpers should stand at the far side of the stretcher. One hel per passes one arm beneath the shoulders and one the middle of the back, the other helper placll1g hiS under the lower part of the. back under the knees. The injured person IS then another helper pulls away the stretcher, and after a sll1g1e step forward the burden is placed on the bed.

PREPARATION OF BED.
A firm mattress, not a feathf'r bed, should be c;elected. If there is much injury, or if dressings have to be applied, a draw-sheet ought to be placed on the bed. It should be of four or more thicknesses, extend across the bed, and reach from the middle of the patient's back to the knees. A piece of waterproof sheeting or of thin oil-cloth should be placed under the draw-sheet. As the draw-sheet becomes soiled, the soiled portion should be roll ed and a clean part drawn smoothly under the patient.
In fracture of the leg or thigh, sprained ankle and some other cases, a "cradle II (Fig. 99) should be improvised. The use of a " cradle II is to support the bed-clothes and keep them [rom pressing on the Ii 111 b.
A band-box (Fig. 100), three-legged stool (Fig. lor), or hoop sa\\:n across and the two halves secured together (Fig. 102), may be used. A corkscrew passed through the bed-clothes, with its point guarded by a cork, and ti ed by string to the bed or a nail in the wall, will relieve the pressure of the bed -clothes effectually.
REMOVING THE CLOTHES.
In taking clothes off an injured person a few rules should be borne in mind.
In serious cases it is much better to sacrifice the clothes than to run any risk of incr easi ng- the injury.
202
203 Fir; OQ. 100. F1G. WI.
20 4
In removing a coat, etc, in a case of fractured arm the uninjured arm should be drawn out first. -
In putting on a coat or shirt the injured arm should be put in first.
In burns and nothing should ever be dragged off. A. sharp pall' of scissors should be used, and everyt.hmg not adl1ering should be cut away. If anythmg adheres it should be left until medical aid

FIG. I02.
can be obtained. The adhering may, with advantage, be soaked wIth ot!. To remove the trousers from a .severely injured limb, the outside seam should be ripped up.
PR EPARATIO S FOR SURGEON.
As so?n as the injured person has been attended to, preparatIOn should be made for the surgeon's visit
20 5
The preparations needf.ul depend upon the nature of the case. The followll1g hll1ts may be of use :-.
A fire in the room helps ventilation, even Jl1 summer. There should be plenty of water, hot, cold, and also boiling, also several basins, plenty of clean towels 'a nd soap . There should be something to empty water into; a foot-bath does well. The basins should be placed on a table, covered with a clean white cloth; a large towel makes a suitable cloth; the towels, folded up, should be placed on the same table, and the hot and cold water should be within easy reach. The foot-bath should be under the table or close at hand.
In the case of a burn, absorbent cotton wool, soft cloths, old linen, oil, and baking soda, should be ready, and materials should be torn up for bandages .
In the case of plenty of water should be boiled and allo\\'ed to cool, and pads of absorbent cotton wool should be baked in a tin box in the O\'en, and at least two bas ins should be ready.
In the case of a person rescued from drowning the s11eets should be taken off the bed, plenty of blankets should be heated before the fire, and several hot bottles should be ready.
If poultices are likely to be required, boiling water, linseed meal, mustard, a loaf of stale bread, a small basin, a large spoon, sweet oil, and tow, flannel or handkercl1iefs may be rcq uired.
20b
. For fomentation, have boiling \Yater, flannel, a kItchen roller, and two sticks, or a large tm,\'el.
'Vhen sur:nmoning a medical man to all accident always let hl111 know by a written message what kind of case is required to treat, so that he may brin g ,yhate ver IS ne e dful. By this means valuable may be saved.
QUESTION CHAPTER X.
Tile numerals t'lIdlta:e tile pag'Cs where the allswers lIIay be foulld .
\Yhal points wou ld you con5ic1er when choosing a sick PAGE roo m?
IIow would to lil'e I 9 7 I 9 7
What of would you proyide for th ose ca n ymg a patIent on e. stretcher;>
How would you pl ace ant.! arrange a 'bed' an case ?
Are how w ou ld you 19 8 lem. ... is often to the' in"t'h nl'St mstance? e
lI ow would you ;oiled'?'
How you see t o the proper lifting and carryin rr of
an mJured pe rson ? . . . b 8 .su bstitutes for a regu lar
ow IS the four-handed seat made?
For cases is this seat ustful ?..
How IS the three-handed scat mad e ;>

207
For wh at cases is this sea{ useful 7. ..
II ow is the two-handed seat made?
For what cases is this seat useful? ..
lI o w can a single h e lp e r lift 7
IIow can a sing le helper give supporL ?
How would you improvise a stretcher?
lIow many bearers are required for this stretcher?
II ow should a stretcher be carried upstairs?
How would you carry a patient upstairs on a chair?
IIow would you li ft a pal ient from a stretcher to a bed?
lIow should a bed be prepared for an injured person? ...
IIow should a draw s heet be made?
\Yha t would you place under the draw sheet? ...
'Yhat should be done wit 11 the soilell part of a draw sheet?
'Vh at is the use of a "cradle" 7 ."
In what ways maya cradle be improvised?
How would you remove a coat or shirt in the case of a fractured arm? ...
H ow would you put on a coat or shi r.t if the arm were injured? .. ,
In the case of a bad burn, wbat would you do with clothing that adhe red to the patient?
IIow would you rem ove trousers from a severely injured limb?.. . .. , ... .., ...
'Vhat preparations would you make for the surgeon' s visit?
'Vhat w ould you get ready in the case of a burn?
And what in the case of h;:emorrhage ?
And what in the case of a person re sc ued from dro wning?
'Vhat would you get r eady for making poultices?
And for fomentations?
'Vhat sort of a message wo uld you send to a d e ctor? ...
I98 198
I;>9 ,
'6 6
I 0,
6 6
I 2,
.
I 4
PAGE I62 16I , 162 161
200 165 200 200 201 20r 201 202 202 202 202 202 202 204 204 204 204 2 0 5 205 20 5 2 0 5 20 5 206 206
208
IN DEX.
Ahdomen Pl gc I I I wound of 112
Accident case, preparation for 19 7
Acids, poisoning by 149, 151
Air, a lways necessary 18
Alcohol, caution as to smell of 130
Alcohol, pois :m ing by 134, 153
Alkalis, poi.,oning by 149, 151
Ammonia, poisoning by 149
Anatomy (e lementa ry ) 20
Ank le 30, 32 " prained... 64
Anterio r tibia l artery 93
Aorta 79
Apoplexy 132 Apparently drowned, to restore ...
Ann, bone of " fracture of Arm-slings

Biles of rab id animal ... 106 20:.l
Bladder ... 1 II, 113
Brachial a rt ery ... b6
Brain ... II 7 compression of 13 2 " concussion of 13 [ Brea t-bone 26 , fracture of 48
Broad bandage ... 37
Broken bones, see Fracture.
Bronchial tubes... . .. II8 30
102
102
Arsenic, p oiso ning by Arterial ha!morrhag e, 139 28 52 39,49 148 arrest of 74 " Arteries practising arrest of 79 sign; o f 74 " course of main 70 79 85
Artery, axillary . .. A rL ery, brachial. .. carotid .. , do rsal of foot facial femoral ... i ' iac occipital I, plantar ... popliteal radial subclavian t i t..ia l temporal " ulnar
Asphyxia Atlas 121, 129 , I36 , 138 138 25
Auricl es ...
Axillary artery Axis
Back, bandage for 159 Back bone 23 Ba ndage, to apply 42 " t o fold 37 " to improvi se... 37
Bandaging ... . .. 155
Bed, lifting into ... 201 " preparati on o f ... 202
Belladonna, p oiso ning by 148
ri es ...
hremorrhage Cap:;ule .. , Carbolic acid, poisoning by Carotid a r te ri es .. .
Artificial
rat ion P(,ge 86 80 93 89 79 82 93 92 88 84 93 82 88
r espi
rrrce
fr om" ha!morrhage 3 I 15 2 80 80 28 Carpus... ... Carrying, m ean s of 160, 200 " upstairs Cartilage Ce rebro-spinal sys tem C ervical vertebra! C heek
ing
Chest, bandage
Chlorodyne, poisoning
C hoking ... f'a..re CirCLtlati
blood, ., urgan" of ... ... 7 0 Circulation of the blood, Lu ir.duce 127 Cla\-icle ... 26 " fracture of 43 lothes, remoyal of 19, 202 Coccyx 25 Collapse ... J 34 l'ollar-bone 26 , fracture of... 4 8 Comminuted fracture 35 Complicated fracture . .. 34 Compounc\ fracture 34 Compression of the brain I3 2 Concussion of the brain 13 1 Conductor 143 Convulsions in chi ldren ]37 Cradle, bed 2J2 Cranium ... 22 " fracture of 43 Crepitus... 36 C ru shed hand 55 foot 62 Diaphragm 120 Digital pres ure... 74 Direct yi olence ... 33 Di slocat ion 62 Ditch, to cross wi th stretcher ) 69 D orsal art e ry of f'Jot 93 vertebr.:e... 25
Bruises
Burns
Capilla
Capillary
, ble ed
from
for
by
In of the
Pa.ge
Dress, woman's, on fire ... 105
Drowning 139
Ear·channel, blood issuing from
Ear-passage, foreign body in
Elbow, bandage for joint, fracture involving
Electric shock
Emetic
Epilepsy .. ,
Esmarch's bandage
Expiration triangular
External carotid artery ...
Eye, bandage for foreign body in
Face, bones of
Facial artery
Fainting ...
Femoral ",rtery
" " digital pressure at groin '"
Femoral artery, tourniquet for
Femur " fracture of Fibula
" fracture of
Fingers, bandage for fracture of

Fireman's lift
First aid, ot " student
Fish-hook, embedded
Flexion '" at elbow ,. at knee ..
Fo od, poisoning by
Foot, bandage for bones of '" " crushed '"
Forearm, bones of " fracture of '"
Forehead, bandage for. ..
" hremorrhage from Foreign body in the ealpassage ," in the eye " "in the nose
Four-handed seat
Fractll1'e, apparatus for treatment of , causes of .. , definition of '" general rules for treatment involving el bow joint of arm... '" of breast-bone of carpus of collar - bone of cranium of finger
Flacture of forearm of knee·cap of leg ... of lower jaw ,., of metacarpus of metatarsus ... of peh'is of ribs ... of spine of tarsus ofthigh·bone ... of toes ., signs and symptoms of \'arieties of Frost-l>ite
Fungi, poisoning I»),
General circulation 70 (;ranny knot 40 Green-stick fracl nre 5, 36 G UIllS, from 97
II::emorrhage from throat 97 from tongue 97 from tooth socket... 97 from upper limbs 84 internal 95 kinds of 73 " venous 93
IIand, bandage for 157 " bones of .. , 2 IJanging ... 140 IIaunch-bones 28
1 rcad-and neck, arterie:; of 80
Head bandage for ISS injury to... 128, 13 1 " side of, bandage for ISS Heart 70 " rate of contraction of 72
Heat -st roke 13 6
Hernia 114
Hip, bandage for 157 History, meaning of 17
II::emorrhage, arterial... 74 capillary... 95 from gums 97 from head and neck 80 from lower limbs... 89 from lungs 97 from nose 9 6 from stomach 98 Page
Howard's method of artificial respiration 126 Humerus 28 " fracture of H ydropho bia 106
Hysterical fits 133
Iliac arteries
Impacted fracture Indirect violence Insensibility 79 35, 36 J4 .. ' 128
IIO 159 53 I ,,, 37 120 80 ISS 109 90 30 56 30 60 159 55 210
110 109 III 160 3 6 33 33 41 2I1 Page
54 58 60 44 55 62 56 46 45 62 56 62 35 34 108 153
212 Page
In ensibility, general rules for treatment 123
In spi rati on 120
Instep 30
In sulat')r ... 14 2
Internal carotid artery 80
Intemal hremorrhage 95
Intestines, injury of J 13
Involuntary muscles 33
Jaw, angle o f 23 lower 23 " "fracture of 44
Joint, definition of 31 " injuries to... I09
Jugular vein 80
Kidneys... I I I " injury of I J 3
Knee, bandage for 159
Knee-cap 30 fracture of 5:3
Knot for bandage of lower lim b 42
Kn ots, reef and granny 40
. Laborde's method of ar i· ficial respiration
Laburnum seeds, pois oning 11y ...
'Lacerated wound
Large arm-sling ...
Laudanum, poisoning
L eg, l)ones of ... 126 30
Leg, fracture of ...
Lifting and carrying " into bed ...
Ligaments
Lightning, effects of Limbs, lower " upper Lime in the eye ...
Lips, bleeding fr o m
Litters
Liver " injury of Lower limbs
Lumbar vertebrre Lungs
Hall's met hud of artificial respira liJll bandage :YIetacarpus fractur e of .. " fracture of ...
l\liclclle line of body
l\IOlllh, blood i5 sui ng from Mu scles " ruptured :Yluscular action ...
Narrow bandage eedle, embedded erves

Nervous system ... foreign body in hremorrhage from
Occ·ipital artery ...
Opium, poisoning by Pad, ring .. . " to fol d Palm, kemorrhage [rom Palmar arches ... Pag-
Pressure, cl i,:;i tal. .. " point ... Principles of First aid ... Pru sic acid, poisoning by Pubes ... ... .
Pulmonary
fracture of Phalange of foot
of hand
Ph osphorus, p oisoning by 148,
Physi ology (elem e ntary) Plantar arch
" artery
Plants, various, poisoning by ... Pleura
Poi son e d we a p 0 n s, wounds by ...
Poisoning
Popliteal artery
. PosLerior tibial artery '" Potash, caustic, poisoning by...
excite 127
Respiratory system 118
Rest, necessity for 18
Ribs 26 " fracLure of ... 46
Room, choice and preo( :97
Page 60 ... 198 201 3 [ ... 144 28 26 .. 110 82 196 1 II 113 28 25 120 frum 97
140 37 28 55 62 20 97 3 2 65 3+ 37 ]0<) 11<5
.: 117 II [ 96 83 74 88 88
149 Pa te
... 30 58 28 fracture
"
...
Parego ric, poisoning 11y
lla
of
"
... . ..
..
.
...
.
.. .
..
...
. 56 30 28 20 93 93 120 113
..
circulation ... Pulse Pupils of eyes Page 7474 17 15 2 28 72 72 130 Questions on Chapter 1. 21 II. 66 III. 99 IV. !I5 V. 145 VI. J 54 X. 206 Rahid animals, bites of. .. 106· Radial artery 88 Radius 8
54
" fracLure of
Reef knot 4C Respiration 120 arLificial 121, 129, 136, 138 " to
Rupture (hernia)
Ruptured muscles
Sacral \'erte bn:e ...
Sacrum ...
Scalds 25 25, 28 102
Scalp, bandage for " ha:morrhage fr o m
Scapula ... ...
" fracture of ...
Schafer's method of artificial respiration
Seat, four-handed three-handed " two -handed
Shin-bone
Shock
" electric ... . ..
SJlOul<.1er, Landage for ... blade ...
" fracture of hones .. . " joint .. .
Sick room, choice and preparation of... .. .
Signs, meaning of .. .
Silvester's method of artificial respiration
Simple fracture ...

Small arm sling .. , Smothering
Snake bites
Soda, caustic, poisoning by Spleen " injury of
21 5
Pflg-e
Stretchers, to carry 169 " to impro\'ise 166
Strychnine, poisoning by 153
Subclavian artery 1:l4
Suffocation J4 1
Sunstroke 136
16r
134 142 156 28 51 26 32 197 ]7 12 3 34 22 22
Skeleton ... Skull ISS
" fracture of
Slings, arm 43 39, 40 , 49
Spinal canal cord 23 23, II 7
" fracture of ... Spirits of salt, poisoning by ...
Splint, angular.. '"
Splints, rules for applying to improvise
Sternum '"
" fracture of Stimulants
Stings of plants and animals
Stomach ... " hremorrhage from
injury of
Strains
Strangulation...
Stretcher exercise, Army
n.
Furley
Surgeon's visit, preparation for 204 of in structi o n... 7 system ... I I meaning of ... 17
Syncope ... 134 3 [
Systemic circulation 70 Tarsus 30
artery .._ 82
30 " fracture of... 56
Three-handed seat 162
Throat, hremorrhage from 97 " swell ing of tissue of... 141
Tibia 30 " fracture of 60
Toes, bandage for 159
Tongue, h::el11orrhage from 97
Tooth socket, h::emorrhage from 97 Tourniquet 75
Transverse 'vound uf abdomen 113
Two-handed seat 161
wOllnd uf abdo-
'Wagon, to load or unload 171 \\"all, to cross with stretcher 170 \Yarmth, necessily for ) 8 " to promote 127 \\' iud-pipe 118 \Yoman's clress on nre 105 'W ounds by poi ' oned weapons .. , 106 " accompanied by arterial hremorrhage ... 76 \Younds by \"enous hremorrhage 94 \\"ounds, lacerated 7 Wrist 28
51 121 160 162
83 26
30
214
... 39 140 I06 149 III II3
. ..
.. .
.. .
"
. ..
No.
No.
" "No. IV. Stretchers,
23 45 149 54 10 7 III 98 II3 65 140 19:> 174 181 18 5 187 172
No. I.
III.
Temporal
Thigh-bone
Pag-.: Ulna 28
fracl
54
InaI' artery 88 Unconsciousness 128 Upper lim bs
Varicose
\" eins 70 \" enous bloocl 72 "h::emorrhage 93 Ventricles 70 VerteIJra...
Vertel>r::e... 25 Vertebral column
men II 3 Vitriol, burn by... 102 \' olun tary muscles 33
"
nre of...
U
26
veins 94
23
23 VerLical
Carriage Paid on all Orders in the Un;ted Kingdom. " ASHFORD"
LITTER.
St. 30bn tl1l1bn[ance BBsocifltion.
GENERAL PRICE LIST.
A complete and reliable Ambulance Equipment is an actual necessity, and experitnce has proved that empl oyers of labour and others interested in the district readily subscribe for the purchase of such appliances. Collecting ca rds , stating the purposes for which subscriptions are required, will be supplied to approved persons gratuitously on application to the Head Office of the Association, where also any information with regard to its work can be obtained.
All stores will be sent carriage paid to any part of the United Kingdom. Returns l11ay be sent carriage forward. If carriage is prepaid it will be allowed.
ewing to fluctuations in market prices it is impossible to guarantee that the quotations herein can be adhered to.
Quotations will be furnished for Ambulance Carriages and other articles relating to Ambulance, Nursing and Ilygiene, not mentioned in this list.
Orders and correspondence should be addressed to th e StJohn Ambulance Association, St. John's Ga te, Clerkenwell , London, E.C.
Remittances should be made payable to the St. John Ambulance Association, and crossed "London County and \Vestminster Bank, Lo thbury ."

The "Ashford" Litter (1899 mod el) consists o r a twowheeled under -c arriage fitted with elliplical springs, and either of the "Furley" stretchers, with a cover so arranged on a jointed frame that it can be folded up inside the stretcher, or wilh a hood and apron (as shown above). The under carriage, having a cranked axle, the b ea rers c.an the wheels with the stretcher, and thus aVOId lIftmg It over them. When travelling, the legs of the under-carriage are raised, and thus form the handlt:s by which to propel it. Should it be necessary to pass over r ough ground, two bea rers can easily lift the litt er and patient. T he" Clemetson " stretcher can be used instead of the" Furley " pattern

• Prices quoted for Litter with Ordinary Stretcher include Wide Webbing Slings but no Chest c Strap. Leather, instead of Webbing Slings, 8s.extra; Chest Strap, IS. 6d. extra If supl-'lied :;, without any Slings, 4S. allowed. ;:;:
t Prices quoted for Litter with Telescopic.handled Stretcher include Wide Webbing Slings and Chest Strap. Leather, instead of Webbing Sling-s, 8s. extra. If supplied without any Slings, ;:0:: 4S allowed; and if without Chest Strap, 1S. 6d. allowed. - '
l Prices quoted for Litter with Police Stretcher include Wide Webbing Slings and Leather Straps for securing a refractory patient. Leather, in stead of \Vehbing Slings, 8,. extra. ;; Hood and Apron, c omplete (" Furley" pattern Stretcher) £2 10 0 3 Do. do. do. (" Clemetson II Stretcher) 2 15 0
Waterproof Sheet (washable) to be laid on the stretcher bed - 0 12 6 Crates (returnable) charged 4S. 6d. for each Litter.
PRICES OF
IMPROVED
1899
With Iron
to
Wheels vynnour I I With 0 Without
Cover or I With Hood
Cover.
With Hood and Apron. £ s. d. Cover or With Hood and 1>1 Hood and Cover. Apron, as 3. Apron. illustrated. 1>1 £ 75."CL Stretcher) 8 10 0 9 SOl I 0 Litter complete with I OIII IS 0112 10 "0 0114· S 0 Ordinary Stretcher- I I 2 6 1 12 17 Dittowith Telescopic handled Stretchert II 10 0 13 6 S o 14 7 6116 2 14 IS 0116 10 6 g o 0 Ditto with Police I Stretchert... 12 S 0 14 0 01 lIS 10 0 1 1 1 7 S 0 Do. with 'Clemetson' I :;. Stretcher 14 8 0 17
THE
ASHFORD LITTER,
MODEL.
Tyres
Wheels.
Under-carriage (no
and
Apron.
;. -< ;:;: £:? ;. '" 5'!:'l UQ' 8. M- '"zj ::-. <11 Ilq:: , :T _. :,:. t:r' t:: t:: 3 """'P;l::: (b n ::!..-...t:' (1) g,8 ..... p> ';' 0, :,:. 0' ....... _. 8 <11 n 0.. M- :: 0<11 _.0',< ::l <11 !!.. (3 2.;; 0 5' en =' en <11 a I7Q : :» p> t"-4 Vi' g en g2.. Eo ;:J <11 IlQ <11 ,.... !!.. en.., Pl U);r :: -. (b 0 t:tJ p> en 0.. 9g =' 0" 5' 0.. ::- g- ;::-:Uq =' --g g. 5.: ;.. 0 M- ::n;:;.."'gt"-40"2;;: ;;=' (t) C"O (l)CIQ u 0..::: 0.. 0.. _. M- .... " t"-4 ::r' :,:.'g en 0" ri c. g 0- $U en 0"8 8 p- §. p> M- '0 Vi' P:T 0 0 . ""' n tJ: t'!j CD ::c "0 1>1 t'!j C. 0 :l t'!j 0 0 ;. It> m ::c S' 0 CJ) c: r c. ""' ;0: :;' ""' II!! C. t'!j 0 r' .3
Carr iage Pai d on all Orders In t he Un l te li Ki n g d om. over them, and the cranked axle has, therefore, been r eplaced by a straight one constructed of tubular s. c el.

" REA-EDWARDS" LITT ER, fitted with pneum atic tyred wh eels, showing the" Clernetson" :::>tretcher.
B all b earings are fitted to the wheels, b o th cycle pattern and woo den, and the h ub s are s o an-a!lged the w h eels can be rem oved fr o m the ax le with o ut in g t h e b ea rings. In place the legs :0, raise as handles, two fixed legs iltted wllh small wheels or r a il en; are placell at the fGot end, \\ hlle a comuined leg and handle filled a crossbar and capable o f being ra ised o r IS used at head end. \Vhen raised as a h and le It may, he, locked 111, on e uf two p ositions , and wh en lowered It IS loc,keel 111 a \'ertical position, The advantages, for ,thiS ment are simpl icity, ease and rapidity uf mal11pulatlOn and
Ca rr iage Paid on all Orde rs i n th e Un i ted K i ngdom ,
the facility afforded by the two fixed legs fo r raising the litter, if necessary, on to the pavement. The question of balance has been care fully studied, and the stretcher shifted forward so that the middle of it is several inches in front of the axle, a perfect balance when the stretcher is loaded and in a horizontal posit io n being thus obtained, and consequently there is no weight on the hands of the person propelling the litter.
Jfhe pneumatic tyred wheels are strongly rec omme nded in cases where the small amount of care necessary to keep them inflated can be given, a, the comfort to the patient and eas e in propul ion are increased b eyo nd all comparison with any litt e r yet produced, It will be noted that the prices are considerably lower than those of the "Ashford" Liller, and the following are given as examples, but owing to the vast number of combinations that can be made with the different stretchers and coverings, it is impossible within reasonable limits to set out quotations for the whole of them, but these may be calculated by adding together the prices of the under-carriage, stretcher selected, and hood and apron or cover, see pages 4 to 10,
SP E CIM E N P R ICES.
Under-carriage only, either with pneumatic tyred cycle wheels or solid rul>ber tyred wooden wheels, £IO.
Litter complete with ordinary stretcher (no slings or chest strap) and hood and apron, as illustrated, £14 3s, 6d.
Ditto with Telescopic Handled Stretcher (with chest strap) and hood and apron, £14 lIS ,
Ditto with" Clemetson " Slretcher and ventilated hood a nd apron, £15 I8s.
If with iron ty red wheels prices are £2 less.
lIand brake, which acts automatically when the litter is at rest, extra £ 1 lOS, \o\'hen ordering please stat e which wheels are req uired
Carriage Paid on all Orders in the United Kingd(jm.
THE" CLEMETSON"
STRETCHER.
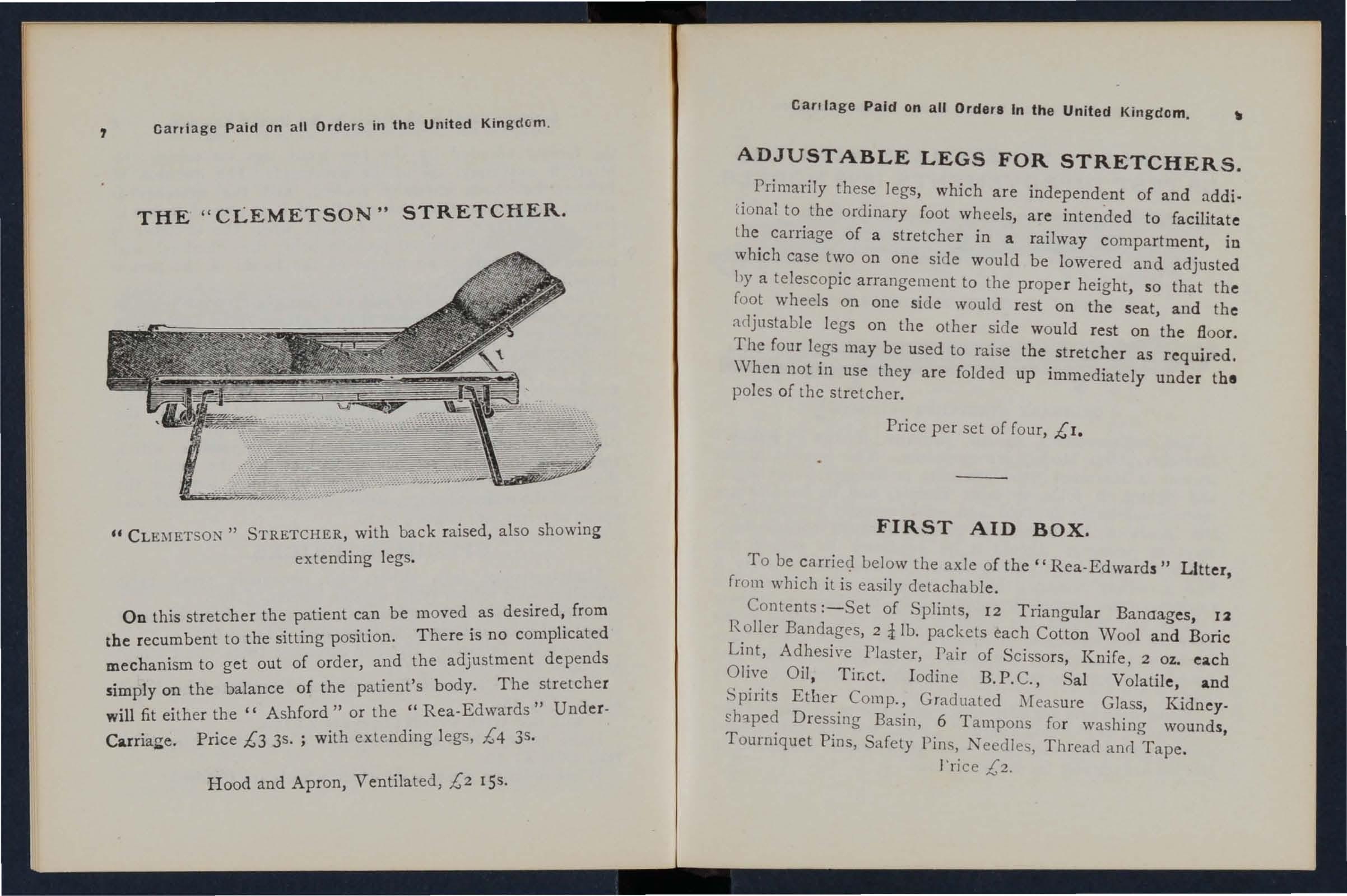
u STRETCHER, with back raised, also showing extending legs.
On this stretcher the patient can be moved as from d . . . . Th e is no comphcate the recumbent to the slttmg pOSlllon. er mechanism to get out of order, and the adjustment depends
. 1 on the balance of the patient's body. The stretcher slmp y d " U d r will fit either the" Ashford" or the" Rea-Edwar s n e -
C · Prl'ce £3 3s . with extending legs, £4 3s. . ,
Hood and Apron, Ventilated, £2 ISS.
Cart lage Paid on all Ordera In the United Kingdom. _
ADJUSTABLE LEGS FOR STRETCHERS.
Primarily these legs, which are independent of and additional to the ordinary foot wheels, are intended to facilitate the carriage of a stretcher in a railway compartment, in which case two on one side would be lowered and adjusted hy a telescopic arrangement to the proper height, so that the foot wheels on oue side would rest on the seat, and the adjustabl e legs on the other side would rest on the floor. The four legs may be used to raise the stretcher as required. When not in use they are folded up immediately under the poles of the stretcher.
Price per set of four, £1.
FIRST AID BOX.
To be carri e<:l Lelow the axle of the" Rea-Edwards" Litter, from which it is eas ily detachable.
Contents :-Set of Splints, 12 Tliangular Banaages, 12 Roller Bandages, 2 i lb. packets each Cotton Wool and Boric Lint, Adhesi\'e Plaster, Pair of Scissors, Knife, 2 oz. each Olive Oil, Tir,ct. I od ine B.P. C., Sal Volatile, and Spi rits Etber Comp., Graduated Measure Glass, Kidney£haped Dres sing Basin, 6 T ampons for washing wounds, T ourniqu et Pins, Safety Pins, Needles, T h read and T ape . I' ri ce £2.
carriage Paid on all Orders in the United Kingdom.
" FURLEY" STRETCHERS WITH THE LATEST IMPROVEMENTS, 1899 MODELS.

TELESCOPIC IIA:\DLED STRETCllER-OPEN.
ORDINARY STRETCHER--CLOSED.
The improvements in all patterns of the "Furley" Stretcher, 1899 Model, are numerous. The comfort to the patient is increased; the stretcher is stronger, more rigid, :Ion d lighter, it folds up more closely, and its handles are more comfortable to hold and afford greater protection to the hands of the bearers in passing through narrow doorways or passages. Should it be necessary to reduce the width of a loaded slretcher in order, for example, to carry it into a railway carriage, this can be done, either when it is resting on the ground or supporled by the bearers, wilhout trouble and without the slightest jar to the patient. The price of the stretchers is lowered. All minor points have been most carefully considered, and the stretchers are c onfidently recommended as thoroughly effici'Y't in every way.
These stretchers are adapted for use alone or as part of the "Ashford" or " Rea-Edwards" Litter, and lhe cover, hood and apron, army rug, and waterproof sheet described in this list are suitable fer use with them. Carnage Paid
all Orders in the United Kingdom 10 o o .-0 °0 000 .,.".. :;O@"@ 0..0.. IlJ IlJ 0..0.. .,,-< :0 e :c:j '0.. 000000 .... I!) > o U i t
on
Carriage Paid on all Orders in the United Kingdom, " LOWMOOR JACKET."
For use in mines, sh!ps' h olds, etc ., to secure a patient on a stretche r (see illustration) , which can then b e placed in an upright position. Price £1 5s.

WATER BOTTLE.
Carriage Paid on all Orders In the United KIngdom.
Dressing Basin . kidney shaped, made of enamelled iron.
Price IS. 3d. LAMP.
Thi s is filled with a sockel, by which to fix it to a Litter, or it can be conveniently carried by hand, or attached to a belt or the clothing.
Price complete, 5". 6d.
Copper tinned, with carrying strap.
Price 12s 6d .
A m bulance Station Plate, Enamelled Iron, 3S. 6d. each . Stretcher Depot Plate, Enamelled Iron, 3s. 6d. each.
Carrying Sheet for carrying patients up and down stairs or otherwise about a hou se. Designed by the late J. C. Derham, ES 'h Blackpool, and Mrs. Alfred Paine, Bedford . The sheet is fitted with r ope halldl es and detachable bamboo poles, and may be placed o n a stretcher without disturbing the patient. l'ric e complete, T5s.
IJ Carriage Paid on all Order. In the United Kingdom.
REGULATION POUCH FITTINGS
for the St. John Ambulance Brigade, consisting of:-
I TrIan gular Bandage, sealed up in waxed paper.
2 Grey Calico Bandages (2 in. and I in.).
I Packet of Surgeon's Lint.
I P dcket of Absorbent Cotton Wool.
I Pair Sciss::>rs.
6 Safety Pins.
I Box of 3 Phials" Vaporole" Iodine Tincture
I Piece of Strong Cane, for tightening improvised
List Price, 2S. 8d. each; 6 doz. or more, 2S. 7d. each.
Box of 3 Phials" Vaporole" Iodine Tincture, packed for post, each lod.; per doz., 8s. 6d.
SAFETY PINS.
All fasten or unfasten on either side. s. d.
Facile No. S 600 or S 602 per 3 doz.
" "S 603 ... " Duplex, No.2... per doz.
" "Assorted ...
Specia' Blank et Safety Pins, 3 in.

Pocket Cork Line and Drag, with 80 feet of line, il! case; for recovering a drowning person from the water. Price complete, with instructions for use, 6s. cd.
Pocket Reel and Ice Line for use in ice accidents, with 80 feet of line in case. Price c omplete, with instructions for use, 6s 6d.
Carriage Paid on all Order. In the United Kingdom r4
LARGE HAMPER FOR AMBULANCE STATION AND RAILWAY PURPOSES.
JJ JJ in. 0 6 0 8 0 2 0 3 0 6
F or cont ent s see ne xt pa
ge.
[S Carriage Paid on all Orders in the United Kingdcm. THE IIAi\[PER CONTAINS
I Set of Cane Splints.
I St. John Tourniquet.
! lb. Carbolic } Cotton \Vool ... In Tin Cases.
! lb. Boric Lint ...
J Roll Adhesive Plaster.
20 Roller Bandages, assorted.
I doz. Triangular Bandages.
3 pieces Tape.
4 oz. Sal Volatile.
4 oz. Bicarbonate of Soda.
4 oz. of Olive Oil.
4 oz. Spirit Ether Compo
i lb. Tin Powdered Botic Acid.
4 oz. Tincture Iodine.
I pair Pean's Forceps.
I pair Scissors.

I Knife.
12 Surgeon's Needles.
r packet each Safety and Plain Pins.
oz. Carbolised Chinese Twist.
! oz. Silkworm Gut.
I reel each Black and ""nite
. Sewing Thread .
1 Kidney-shaped Basin.
I Stopper Loosener.
I Graduated Measure.
r cake 20 per cent. Carbolic Soap.
I Nail Brush.
3 Empty 8 oz. Bottles.
3 Saucers.
3 Camel Hair Brushes.
Price complete, £4
Carriage Paid on all Orders In the United Kingdom. SMALL AMBULANCE HAMPER.
"Vith waterproof cover and strap, for use in factories, colli eries, stations, and large works, as well as for parochial and domestic use.
CONTAINING
Set Splints . 1 St. J ohn Tourniquet. 3 T ampons, washing wounds. 2 Packets Lint. 4 Roller Band ages (wiele and narrow). 4 Tri angu lar Bandages.
Wool... ... } In Tin Cases. Bone \Vool ... .,.
Spool of Adhesive PlasLer. . Knife, Scissors . ThTead, Tape, Needles, and Pms.
Weight complete, lhs.
Length, rft. 6in. Depth, Sin. Width,7in. Price£r 6d.
CarrIage PaId on all Orders In the United KIngdom.
SURGICAL HAVERSAC.

hlP ROVED PATTERN, fitted with a tin, so arranged that any article can be taken out with oll t disturbing the rest of the con tents.
Contents: I Set of Splints, 6 Triangular Bandages, 6 Roller Bandages (wi de and narrow), Cotton Wool, Boric Lint, in tin cases, I Roll Adhesive Plaster, I Pai r Scissors, I Knife, 2 oz. Olive Oil, 2 oz. Tinct. I od in e, 2 oz. Sal Volatile, 2 oz. Spirit Ether Comp., I Graduated Glass Measure, I St. John T ou rniquet, Pins, Needles and Thread, 3 Saucers, 3 Camel Hair Brushes. Price £1 I IS. 6d. White Ration Haversacs , 2 5. each.
Carri;? ge Paid on all Orders in the Un i ted Kingdom
FIRST AID COMPRESSED KIT.
box is. made of. wood co\'ered with damp· resisting mate flal, and IS fitted wIth a lock and key. It contains a be r of practic.al ambulance app:iances arranged so that any a rtIcle can be wIthdrawn or replaced with out disturbino- the r.emainder . Being fitted with a handle it is portable, and the lId, when let d own , can be used as a t3.hle. All bandacres and dressings are compressed. Size-Lenglh, I6i in. ; width: in .; height, 8 in., without handle.
4 Triangular Bandages, 0 Roller Bandages, 4 First Aid Dressll1gs, 6 S mall Packets of Cotton \Vool 6 Small Packets of Boric Lint 1 St. J ohn Tou:niquet, I Glas< I tin Lox containing a Roll of Plaster, -':I!lt Patches, sors tray containing 3 Bottles (S,!l Volatde,. Tincture of .and Olive Od) and a Dredger of Boric ACid, I of Improved Sphnts, with angle piece g Splint Straps (suffi cie nt for a fractured lhigll), 2 Saucers, 3 Camel Hair B'rushes. .
Price £1 lIs. 6d.
"
Carriage Paid on all Orders in the United Kingdom.
(DRESSINCS AND BAl\:7JAGES COMPRESSED).
f.i .TO/J11 }1mbIJI.3ti(t ;:-6",'a(loll, Price Is. 6d. $(. J"Dbl!'S 6ille, Uy Post Is. 8d. cem!,,". €.,.
Size, 4! by 31 by Ii inches. Su itable for the pocket.
CONTENTS.
1. Triangular Bandage. 2. First Aid Dressing. 3. Cotton Wool. 4. Two Splint Straps. 5. Adhesive Plaster. 6. Permanganate of Po tash . 7. Lanoline. 8. Boric Lint Patches. 9. Safety and Plain Pins.
Price, each IS. 6d. Packed [or Post IS. 8d. Per doz . 17s. 6J.
SEP ARATE ARTICLES.
No. No.
I 4d. each or 3/9 per doz.
2 2d. ,,2/0
3 rd. " "Jod. " 6 rd. per box or rod. per doz.
7 r per tin or r/4 "
8 rd. per packet or rod.
4 2d. per strap or 1/9" " 9 rd. " rod. "
5 Id. per box or rod. " "
Not less than one dozen supplied at dozen plices.
Carri<'ge Paid on all Orders in the Un [ted Kingdom.
FIRST AID BOX FOR USE
IN MINES.
CONTENTS. ::10
Set of Improved Wooden Splints; St. John Tourniquet; Cotton Woo,; Lint; 12 Compressed Roller Bandae;es, as'or ted ; 6 Triangular Bandages in wa.xed paper; Adhesive Plaster; Pair Scissors; Spatula; Graduated Measure j
:I oz. Sal Volatile; ::I oz. Spirit Ethe r Com p.; 8 oz. Boracic Vaseline j 8 oz. Tinct. Iodine; 3 Saucers; 3 Camel Hair Brushes Pins; Safety Pins. PRrCE COMPLETE, £2 ros.
This First Aid Equipment is also very suitable fo r use in factories and other large works, and can be fitted for carrying on the" Ashford " Litter.
:II Car.-[ age Paid on all O ders n he United KIngdom.
SMALL FIRST AID OUTFIT.
\Vhen closed can be carried by a Strap-handle. by 71 by 6k inches.

CONTENTS: 2 Triangular Bandages, I St. John Tourniquet, 8 Splint
Straps (for securing Splints in lieu of Bandages), 2 oz. Cotton \Vool, I Pair of Scissors, I-in. Roller Bandages, 2 2-in. Roller Bandages, I 2·0Z. Bottle Sal Volatile, I 2-0Z. Buttle Tincture Iodine, B.P.C., 2 oz. Plain Lint, I :I-OZ. Measure Glas'i, 2 China Saucers, and :I Camel Hair Brushes to be used when applying Tincture of Iodine.
Price:
Wooden Box, cov ered with Damp Resisting Material, ISS.
Stout Cardboard Box, Cloth Covered, lOS. 6d.
Carriage Paid on all Orders In the United Kingdom.
The St. John Tourniquet , as supplied to the Admiralty with directions for use ... ... ...
(Special quotations for large quantities.)
Splints, Wooden, per set, 2/6; Cane ... ...per set
Greatly improved Wooden Splints, with grooved joints and angle piece, strongly recommended
Tow, for splint padding ... .. .per lb.
First Field Dressing (Army Pat tern)
jaconette, 44 inches wide
Tow, Carbolized or Styptic per yard ... per lb.
First Aid Dressing, consisting of a small compressed packet of boric lint, a compressed roller bandage, and a safety pin
Dredger, containing boric acid powder
Measure Glass ...
Knife with strong blade each IS_ ; per doz. lOS. 6J.
Pair of Scissors each IS. ; per doz. lOS. 6(1.
Small Bottles strong Smelling Salts, per doz., 5s. 6d.
Splint Straps, Webbing, and suitable Buckles. Per set of I z yards of strong 2-inch 'Webbing and IS Buckles, 3s.
These make very compact Straps for carrying in the Pouch. The 'Vebbing should be cut to meet local requirements.
Buckles only, IS. 3d. per dozen.
\Yebbing only, IS. 9el. per dozen yards.
It is unnecessary to sew the Buckles. The spikes should be passed t!1l'ough the webhing, and the short end of the webbing should lIe out warcls.
s. u. o 9 7 6 4 6 o 6 o 9 2 3 o 9 o 2 4 o 5
. ; Carriage Paid on all Orders in the United Kingdom PLASTERS.
Leicester Adhesive Plasler on Cambric in tins of! yard
6 inches wide . .. ... ... ' ... ... ... ' 6d.
The Leicester Adhesive
Ribbons, in tin boxes, 6 yards long.
! inch wide 6d.
I inch wide

National Rubber Adhesive Plaster (Antiseplic) on spools.
S yds. 10 yds . inch wide gel. IS. ad.
t IS . ad. IS . 6d.
2 " rs. 9el . 2S. 3d .
Dillo in carel box, in. wide, yds. long ... tin I i 2 +, S S COURT PLASTER, TRICOLOR.
Large Size, scl. ; J\lccliu11l, Sci .. Small, 3d. 8d. rd. 3d . 3d . 6d. 9d .
Car riage Paid an all Orders in thp. United King dom.
NURSES' WALLETS.
ORDINARY PADLOCK
\Vithout inslruments, 4s. 3d.
Fitted complete, containing Spring
Dressing Forceps, Spalula, Probe, 2 pairs Scissors (round and sharp pointed), Clinical Therm omete r, and Knife.
Price lOS.
ST. JOHN'S PATTERN, as illustrated, but improved by lhe addition of flaps to protect the instruments.
'Wilhout inslrumenls, 7s. 9d .
Fitted complete, conlaining Spring
Dressing Forceps, Arlery Forc eps (also useful for dressing), Spatula, Probe, Director with Ear Scoop, 2 pairs Scissors (round and sharp point ed) , Clinical ThermomeLer (minutp., round) , Knife, Pencil, and Safely Pins.
Price I8s_
24
25

Carriage Paid on all Orders in the Un :ted Kingdom.
ROLLER BANDAGES. (6 yard . long.)
Grey Superior Re<;t quality, Superior
Grey Open White White, with White OpeD
Ca li co . Wove. O pe n \Vo ven \Vove Per \Vove. E dges. Compressed. doz. s. d. d <; U. s. d s. d. tin. I
ROLLER BANDAGES in Assortment.
PacKed in neat Cardboard Box.
RECOMMENDED FOR CLASS PRACTICE.
Two 3 in. ; two in. ; one I in.; each 6 yards long.
Grey Calico
Plain Triangula r Bandages, each (Special quotations for large quantities.)
Ditto Compressed (thinner quality) , each 4d. ; per doz. 3s. 9d •
Illustrated Banciages. (after E 5march) showing s. d. 25 appl.lcatlOns of the Tnangular Bandage, with pnnted Instructions ... each 0 6 per doz. 4 6
Car rfage Pa id (n all 01 tiers In the United k,.1gdom. 26 ROLLER BANDAGE MACHINE.
Designed by Dr. A. C. Tunstall.
Price 2S. 6d.
Forceps, dressing, full size or small as desired, IS.; Pean's Artery, 5 in., IS.3d.
Scissors, round - pointed blades, IS.; small round - pointed blades, or 5 in., IS. 6d.; round-pointed curved hlades, Is. 6d .; sharp-pointed blades, for delicate work, IS. 3d .; curved blades, IS. 9d.
Spatula, 9d. Probe,6d. Director, with Ear Scoop, IS. 9a.
Knife, very thin, i vory handle? two blades, IS. 9d .
Nursing Chart, designed by Miss Inderwick, each.
Temperature Chart, id. each.
CLINICAL THERMOMETERS.
Round.-Ordinary, IS.; minute, Is. 3d. ; half-minute, IS. 6d.
Flat.-S trongl y recommencied, as they will not roll. Ordinary, IS. 6d.; rapid (specially selected and reserved for the Association), with very open scale, 3s.
in. a a 9 a 2 3 3 Ii in. S 3 2 6 6 2 in. 9 3 6 3 3 I 9 in. 2 3 g 2 a 3 9 2 3 3 in. 2 9 2 a 2 6 4 9 2 9 4 in. 3 6 3 6 6 0 3 9 6 in. S 3
6
4
s. d. I 0
Carriage Paid on all Orders in the United Kingdom .
CLINICAL THERMOMETERS-(continued}.
With Magnifying Lens. Price, ordinary, IS. 6d.; minute, IS. gd.; half-minute, 2S. 3d. and half-minute instruments will only register in the time stated under favourable circumstances. No liability is taken/or breakage of Tlzermomete1's in tral/sit.
BATH THERMOMETERS.
To Dr. Forbes' specification. Japanned with zinc scale, 2S. 3d. ; Clinical Therm ome ter size, in case, IS. . No liability is taken for b1'eakage 0/ Tizerlllollleters m t1'aJlszt.
COTTON WOOL.
Plain, I oz., 2d. ; 2 oz., 3d. ; 4 oz., 4d. ; lb., 7d.; I lb., IS.; small packet (Compressed), Id. .
Medicated, Boracic, lib., 6c1.; I lb., IS. 6c1.; CarbolIc, per lb., IS. 8d.; Alembroth, per lb., IS. 6d.; Double Cyanide, per lb., 2S. 6d.
LINT.
Plain, I oz., 2d. ; 2 oz., 3d. ; 4 oz., 6d. ; 1- lb., lad. ; I lb. IS. 6d.
Boracic, 4 oz., 6d. ; I lb., IS. 6d. ; square foot packet, 2cl . ; small packet (Compressed), Id.
GAUZES.
The se are supplied in 6 yard lengths, width about 36 inches.
Unmedicated white
Alembroth
Double Cyanide
Boracic

yd. compressed),
Carriage Paid on all Orders in the United Kingdom.
TEXT BOOKS. &c.
"First Aid to the Injured." By James Cantlie, M. B., F. R. C. S. The authOlised Text Book of the First Aid Course. IS.
" A Catechism of First Aid." Compiled from Dr. Cantlie's Manual. By J. M. Carvell, M.R.C.S., L.S.A. 6d.
" Problems in First Aid." A companion to the authorised Text Book of the St. John Ambulance Association "First Aid to the Injured." By L. ;"1. F. Christian, M.B., C. M., Ed., and W. R. Edwards, A.C.A. 6d.
"Hints and Helps for Home Nursing and Hygiene." By E. MacDowell Cosgrave, M.D., illustrated, with chapter on the application of the roller bandage, by Sir R. J. Collie, M.D. The authorised Text Book for the Nursing Course. IS.
" A Catechism of Home Nursing" (based on Dr. Cosgrave's Text Book). By J. Brown, L.R.C.P., L.R.C.S., and J. M. Carvell , M.R.C.S., L.S.A. 6d.
"Home Hygiene." By John F. J. Sykes, D.Sc. (Public Health), M.D., &c. Illustrated. The authorised Text Book for the Home Hygiene Course. IS.
"A Catechism of Home Hygiene" (based on Dr. Sykes' Text Book). By J. M. Carvell, M.R.C.S., L.S.A. 6d.
"Questions and Answers upon Ambulance Work." By John W. Martin, M.D., and John Martin, F.R.C.S., Ed. IS.
"Questions and Answers upon Nursing." By John \V. Martin, M.D. IS. 6d.
GAUZE TISSUE.
per
Packets of Cyanide doz., 25. 8d. Gauze ( I s. d . per length a 10
A layer of absorbent cotton wool between two sheets of gauze, good quality, per lb., I S. 6d.
"First Aid to the Injured" (Six Ambulance Lectures). By Professor Frederich Esmarch. Translated from the German by H. R. H. Princess Christian. 2S.
"Elementary Bandaging and Surgical Dressing. " By Walter Pye, F.R.C.S. 2S.
27
o
2 2

Carriage Paid on all Orders In the United Kingdom.
TEXT BOOKS,
.. To Restore the Apparently Drowned," printed in large Type with two Diagrams. 2d.
Dr. G. H. Darwin's" First Aids," being a card to hang up giving treatment of various accidents. 2d.; packed for post, 4d.
" Manual of Drill and Camping for the St. John Ambulance Brigade." 5d.
I' Manual for St. John Voluntary Aid Detachments." By Lieut.-Col. G. E. T wiss , R.A.M.e. (Retired Pay). 6d.
" How to Act when Clothing takes Fire." By J. E. II. Mac\,inlay, M.R .C.S. 2d.
"First Aid Principles." Cards of concise directions ror waistcoat pocke t, each; 4d. per doz. Special quotati ons for large quantities.
" Specimen Examination Papers, First Aid, Nursing and Hygiene Courses." 3d.
Small Anatomical Diagram. Showing the human skeleton, main arteries, and points where pre.:;sure should be app:ied to arrest bleeding. 2d.
Directions as. to the Restoration of Persons suffering from Electnc Shock. Large print, poster size. 3d. each; or 25. 6d. per dozen .
General Notes on First Aid to be Rendered in Cases of Poisoning. By Milnes Hey, M.A., M. R . C.S.,L.R.C.P. 2.1.
Notes on Military Sanitation. By Lieut.-Col. II. P. G. Elkington , R .A. M.C . 6d.
"Emergency Book," for illstantaneons reference, giving concise instructions; to hang on wall. about one foot square. 2S. 6d. ; packed for post, 25. Sel.
Carriage Paid on all Orders In the United Kingdom. ]0
TEXT BOOKS,
Aids to Memory for First Aid Students. Revised to date. Additional Illustrations. By L. M . Frank Christian, M . B., C. M ., Edin. 6d.
General Regulations for the St. John Ambulance Brigade, 1913. 3d .
Rules for Corps and Divisions, St. John Ambulance Brigade. 2d.
Registers . Class Allendance, 2S. 6d. Certificates, 4S. 6d. Case Report, IS.
st. John Ambulance Brigade Cash Book, Minute Book and Occurrence Book. Set of three, 7s. 6d. Receipt Book, 6d.
Large Physiological Diag rams (New Series). For Lectur ers' use . The Human Skeleton, showing the main arteries and pressure points. The General Anatomy of the Body. The Systemic and Pulmonary Circulation of the Blood . Section Through Middle Line of Head and N eck, showing the Tongue in two poitions in r elation to the Trachea, and Scharer's method of Artificial Respiration (Expiration and Inspiration). Dislocations. Price, per set of five ISS. These may be hired for a course of "First Aid" lectures, given under the auspices of the Association, for a fee of 5s., or with the addition of Splints, T ou rniquet, and 30 plain Triangular Bandages, for a fee of lOS .
Boxes" of Stationery for the use of Class Secremries and others connected with the Association, containing twel\'e sheets of high·class paper, suitably headed, and tweh'e envelopes bearing the device of the Association. 6d. Twice that quantity, IS.
51 BADGES

Arm Badges, with the device, issu-ed under the authority of the Central Executive Committee, having been first approved by H. R.H. the Grand Prior as the sole official and recognised Badge of the Association and Brigade. N.B.-Tltis deszin is protected.
SERIES A -For the use of individual certificated pupilsNo.
12. Small Celluloid Badge, for button hole or brooch
13· \Vhite Satin Armlet, with woven Badge 2t"
Badges
Carrtage Paid on all Orders in the United Kingdom. J.
SERIES B.- For members of the St. John Ambulance Brigade, not wea ring uniform , having tl:e of the. C:orps or Division annexed on a label, only Issued In quantltlesNo , 15 In German Silver, '2 ins, in diameter, first doz., £1 J subsequent dozs, , I2S.
16, In Electro Plate, 2 first doz" £1 I 2S. ; subseque nt dozs" £1 4s.
17. In Cloth and Silk, 2 per doz., 1 2S.
18. In Cloth and Silver, 2 I, "per doz., £1 lOS. T9, The Brigade Button Hole Badge, each, IS.; with Brooch Pin, each 1/3 ,v. B -Tllese baf(,' t!s a'e Jlot to be wor as decorations,
s. d.
Silver, Large Siz e 2 in. el ia. 0
Small Size ditto ... .. . Ii 0 6 3· Small Size for button hole ... 0 6 4· In Electro Plate, Large Size 2 0 5· Small Size ditto ... '" It 0 9 6. Small Size for button hole I 0 <?
Enamel for button hole 0
r !
In
2 I!. In Cloth and Cotton . .. '" .. . I 3 o 9 2 0 () 6
I. In German
2.
7· In
8. " brooch 9· In Cloth and Silk
10.
Cloth and Silver
.. . ... .. . .. . 0 2
0 N,B,-
worn
Tilese
are 1I0t to be
as de corations

U Carriage Paid on all Orders in the United Kingdom. BRIGADE
UNIFORM BADGES,
etc.
i)fficc rs.
Cap Badge (Reg. No. lor) ...
Collar Badges ( " 103) per pair
Pouch Badge ( , . 3,657) ...
Sergeants, Corporals and Private s.
Cap Badge (Reg. No . I02)
Collar Badges ( " 104-) per pair
Overcoat Badge( " 1, 582 )
Shoulder Tilles, S.J.A.B., with numeral, perpHir
Shoulder Straps, filled wilh title and numeral .. . ... ... per pall'
Reserve Badge for all ranks .. . per pair
Lady Officers of Nursing Divisions.
Lady Di s trict Supt., Arm, 4S. 9d. ; Cl oak
Lady Corps Supt., Arm, 4S. 3d. ; Cloak
Lady Divi sional Supt., Arm. 3s. 9 r1.; Cloak
Nursing Officer, Arm, 3s 3d.; Cloak '"
White Box Cloth Backs, for Badges per pair
Nursing Sisters. Arm Badge (Reg. NO.3 , 522)
. ." Cloak Badge ( " 3,52 I)
Dlstnct Numeral for Nursing Divi sions single double
Bla.<;k Silk Armlet for A rm Badge, for all
Honorary Surgeon's Crosses (patlern B) per pair
Superin"c:ndent's Stars (pattern A) pe r pair
Medallion Badge (pallern D)
Nursing Badge (pattern E)
Satin Badge for Nursing Sister's Fin Cushion
Bu g ler's Badge 4S. Bugler' s Cord
Signaller's Badge Signaller, IS ; Drummer's Badge In
D iv. Secretary and Sergeant's Bad ge .. .
Whistle and Chain
White Pipin g, per packet of yards, enough for 3 pairs of trousers (packets can not
broken)...
Lace, per yard, Silver, l OS. ; Black ...
St . John Voluntary Aid Detachments
UNIFORM BUTTONS.
I ssue d only for the use of Officers and Members prescribed uniform. wearing the
St. John Ambulance Brigade.
Whi te M eta l, No. I (large) per d oz.
No. 2 (medium ) ... " NO.3 (sma ll, for caps)
Electro Plate, NO.4 (large )
NO.5 (medium) ...
No.6 (sm all, for caps)
St. John Voluntary Aid Detachments.
German Silve r, Nt). 7 (large) No.8 (medium) ...
(small)
rank s
.. .
..... .
Black Khaki Uniform. Uniform. s. d. s. d. o 0 I 3 0 2 6 0 6 0 0 6 0 6 I 3 0 3 5 6 5 0 4 6 4 0 0 3 2 0 2 3 0 3 0 5 0 4 0 6 0 6 0 I 0 3 0 3 0 0 1) 0 0 8 5 0 8 0 8 0 4 Paid on
OrderS in the United Ki ngdom. 34 Black Khakl Belt Furn iture . ..
Unifo n1. Unifolm . s. d. s. d . I 6 I 10 per pai r 2 6
structo r 3 0
all
Bandsman's Wings
5 0 o 2 0 be
2
0
. Cap Badge .. . ... ... ... ... 0 6 0 8 Officers' titars ... per pair 4 0 8 B elt Furniture .. . 6 I 10 Cloak B adge (Commandant ) ... 2 6 (Other Ranks) ... 0 6
N O.9
per doz. o 6 o 4 o 3 3 0 6 6 o 6 o 4 o 3 o 9 o 6 o o 9 o 6 o
JS Carriage Paid on all Orders in the Un ited Kingdom. ELECTROTYPES. No . I A . No.2 A . NO . 3 A. . , .,.o,"Y
trbe Grant! f) n or p of
U6e <SIrtler of tbe f>ospt ra( of Sr. 30b n of 3cr uoalem In lElIg l all/:)
tiEPARTMILNT
\th e $t. 301m Bmbllllll1ce t\s so.c ill tio n.
N o. I A ll.

o. I B . No.2 B . N O.3 B.
ttbe Granb f)rI Orl? of ' Ube of tbe bosillfa! of St. 30bn of 3erusal,m In lEnglan/:).
Ube $t. 30bn Rmblllllnce lSrigal>e. N o. I BI-I.
Carriage Paid on all Or ders In the United Kingdom. 36 ELECTROTYPES OF THE ST. JOHN
2 For Not e Paper, Small Circulars, &c .
3· Fo r Quarto and Foolscap Letter-paper, Circulars, &c. ...
Prints of the above Electrotypes (1 to 3) Series A and B, and (1 ) Se ries AlI and BH, appear on page 3S . No. 4A is shown on page 3 I. The diameter of SA and SB is 2 inches. Flags bearing Association device- I 2 feet by 6 feet S
N
AM B ULANCE
F or Association use. For Brigade Series Series Series S eries A. AH. B . BH . N o. s d . s d s. d. s. d . I. For Cards , T
3 3 3 3
3 3 3 3
3 7 3 7 4 · Fo r Small Posters 6 5· For Large Posters 9 9 Complete Se ries 6 0 3 9 4 9 3 9
DEVICE.
ickets, &c .
feet Brigade 4 ft. 11in. by 3 ft. £ s. d. 7 6 o 12 6 o 12 0
feel by 3
Carrlai" Paid on all Orders In thJ United Kingdom.
SWAGGER STICKS
for the use of Officers and Members of t he St. ] ohn Ambulance Brigade.
Ebon is ed Canes, German Silve r l\Iounls beari ng lhe Brigade Device .
PRICE IS . EACH .
Offi cers' Spe cial Canes , with Sterling Silver l\Iounls.
PRICE 7s. EACH.

BEARER'S DRESSING C ASE.
PRICE I2s. 6d.
A iJ Or ders for the forego in g Stor es sho ul d b e given t o t he Local Secretary, or se nt di r ect t o
The St. John Ambulan ce Ass oci ation, St. John's G a te, Clerkenwe ll , London, E C.
Contractors' List. Carriage out of London Extra.
UNIFORMS FOR AMBULANCE UNITS OF THE S.J.A.B.
These may be obtained from HAZEL & Co. (sole proprietor, D . Hazel, for many yea rs associated with the lale firm of Hebbert & Co., Ltd., as Director), Clolhing and Equipment l\Ianufacturers, 65. East R oad , Cily Road, Lo ndon, E. C. ; and al 6, York Place, Leeds; 69, Piccadilly, Manchester; and 84, Miller Street, Glasgow. Telephone : 5678 London \Vall. T elegrams: "Hazelisl11, London." \Vhe re two prices are given for an arlicle lhey are fo r first and se cond qualities.
All Badges, and carriage outside Londolt a r ea, extra. IlIeasurements to be supplied free of charge.
CORPS SURGEON AND DIV ISIO NA L S URGEON.
Tunic, Sup erfine Black Clolh ...
Trousers, Superfine Black Doeskin (if Silver Lace
Stripe, extra) ...
Cross Belt and Pouch, Plain, 20/- ; Silyer
Embroidere d ... Gloves
Greal Coat, Gre y Cloth ...
Cap-Corps S urgeon
Divisional S urgeon
D I STRICT SUP ERIN T ENDENTS
AN D CORPS OFFICERS.
Tunic, S up erfine Black Cloth ...
Palrol Jacke t , S uperfine Black Cloth .. .
Trousers, Supe rfine Black Doeskin
Cross Belt and P ouch
Gloves, 4/6 ; Leggings, 8/6
Great Coat , G rey Clot h
Cap-District Sup eri ntend ent ... " Corps Officer
PRICE LIST.
6 and £, s . d. 3 IS 0 2 6 3 7 6 04 6 3 7 6 6 0
I 9 0" 0 17 0
£1 1 2 6 and I 10 0 " 3 IS 0 J 10 0 2 6 o 13 6 3 7 6 I 0 o 18 0

,39 Contractors' List. Carriage Paid on all Drapery Goods.
DIVISIONAL SUPERINTE 'DENTS AND
Patrol Jacket, Superfine Black Cloth
Trousers, Superfine Black Doeskin
Cross Belt and Pouch ...
Gloves, 4/ 6; Leggings, 8/6
Great Coat, Grey Cloth
Fatigue Jacket, Black Vicuna Serge
" Trousers, Black Vicuna Serge
Cap-Divisional Supelintendent £1
Officer 0 15
FIRST CLASS SERGEANTS.
Patrol Jacket, Superfine Black Cloth ...
Chevrons, Four Bars, Silver
Trousers, Superfine Black Doeskin
Cross and Pouch ...
Cap, 2/9 ; Gloves, Buckskin, 4/6; Gloves, Cotton, 8d.
Leggings, Black or Brown Leather
'Valer Boltle a:nd Carrier
Haversack, White Duck
Great Coat, Dark Grey Melton
SERGEANTS, CORPORALS PRIVATES.
P a trol Jacket, Black Tartan
Chevrons, Silver ...
Trousers, Black Tartan
vVaist Belt and Pouch. Brown Leather
Cap, 2/9; Gloves, Cott on , 8d.
L eggings, Black Leath er ...
'Va Ler Bottle and Carrier, 319; Haversack, White Duck
Great Coat, Dark Grey Melton 16/- and 0 14
DRAB SERGE
Jacket, Drab Mixture Serge Trousers
Cap " "
Great Coat, Drab Melton 16/ 6 and
OFF'ICERS. £, s. d. 2 6 6 I 2 6 o 13 6
3 7 6 I 15 a o 16 a
4 0 an d 0 14 a Ambulance
0 9 a
6
per Bar I 18 6 o 3 4 o 19 6 a 10 6 043 039 a I 6 a 16 a a II a o a 10 09 6 066
.. . ... ... 0
4 3
0
I 6
0
080 020 a 19 6 ST. JOHN flMBULflNCE BRIGflOE.
UNITS. GOODS n1AY BE OBTAINED FR O:-'!Messrs. E. & R. GARROULD, ISO
EDGW ARE RD.,
CL
extra)
19/ 1 [ B {N ursing Si ,t er's 9/6 ON;\ ET " O ffi cer's 10/6 D {Nursing SiSler's Dress L ength 3 ' 7 RESS " Officer's" " 3 I [ COL LARS { 2i 5t d . each; 5/ 6 dOl. w., 64d. 6/ 6 "
in.,
6
UFFS
ILLUSTR.\.TED PRICE LIST FREE. T rle />h oJl c s5320, 532 1, & 620 7. P AD ll l:-."fO :-; TeZeg
G.\R ROU LD LONDON."
099
UNIFORMS FOR NURSING
to 162,
LONDO.\I, W.
OAK (Badg e
from
4
6/
" ,,7!d. 7/6 " C
{ Nursing Sist er' s 8td. & 1/- each CAP Officer's 1/4 I, A PRON 1/11&2/ 6 also iii Pure Irish Lin en 3/6
rams-
THE UNIFORMS, CLOAKS

Ambulance Hampers ... Station Plate
Bandage Rolling Machine Bandag..s
Ba,in, Bearer 's DreSSing Case Belt and Pou c h Books
(Water)
for Stretcher or l
TO PRICE LIST. (for General 1ndex 20>\'2T s).
... .. .
...
BONNETS, APRONS, DRESSES, ETC. • FOR THE ST. JOHN AMBULANCE BRIGADE, l\IAY BE OBTAINED AT E. & R. GARROULD . To 11.:'.!. \VAR OFFICE, H.l\!. INDIA OFFICE, COLO:-/L\L OFFICE, LONDON COUNTY COUNCIL, ETC. I LLUSTRATED P RICE LIST of the yarious articles required by the ST. JOHN A:'.IBULANCE BRIGADE , ON APPLICATION. I SO to 162 , Edgware Road, LONDON, W .
... ... Bottles
Cotton Wool... .., PAG!': 14 to 16 31 to 34 26 25 13 37 ... 33 28 to 30 12 34 Cover
i
lectrotypes 35 , 36 I':mergenry Book 20 First Aid Box 8, 20 21 " "Compan ion.. Ie) " "Compressed Kit 18 Fir,t Fi eld Dressings... 22 Flags 36 Forceps 26 Gauzes ... 27 (;:lllze Tissue...... 27 l1:lmper< (Ambulance) '4 to 16 Haversacs ... .. ... 17 Hood and Apl'On for Litter .. , 3 Instrlllnents (various) 26 Jacollette 22 Knife 22 , 26 Lace for &c. 33 Lamp.. 12 I.illt I.itter Litter !Rea·Ed Lowm(lor Jacket Measure Glass ... Minute Hook ... Turses' \Vall ets Nursing Charts Occurrence Book Pillow ... Pia ters ... Pouch Fittings Receipt Book '" Registers ... ... PAI;P •.. 4 to 6 22 30 2 26 30 10 Roller Bandage Machine Rug .. ... .. ... Rules for Corps or Divisions 23 13 30 30 26 St. John Ambulance Brigade Safety Pins 29 13 ...22, 26 Scissors ... ... Slings (Stretcher) Smelling Salts .. Splin t Padding 10 22 " Straps ... 22 Splints... .., 22 Stationery 30 Stretcher Depot Plate 12 Stretchers .., 7 10) 10 " Adjustable Legs (or Swagger Stick Temperature Chart Text Books .. . Thermometers .. . Tourniquet .. . Tow (carbolized) " (plain) Uniform Sundries Uniforms ... \Vater Bottles ... \Vaterproof Sheet Whistle and Chain Piping ... W ool (Cotton) ... 37 26 28 10 .. :!fl 2 7 3 33 ,3 27
Buttons ... Carrying Sheet Cash Book
tIt-r Diagrams , Large " Small .. , Dredger (Horic Acid) Dressi ng Basin 12 Drow ning Tackle 13 t;:

