

BONES.

seventh} Cervical Vertebra
COllar} Bon6 (claviole)
Bone Breast} (sternum)
Arm Bone __ (humerus)
4th Lumbar _ Vertebra
HaUnCh} : Bone (pelvis)
Metacerpus \
phalanges _ Bone (femur)
Knee Cap (patella)
Shin Bone (tibia)
Brooch Bone (fibula)
Tarsus Metatarsus
Phalanges
ARTERIES. Th Occipital. r mpQr'll. F i I. C rot! s.
Subclevlan. Ax II roy. - - Broe I 101 IFI II 011). lila. t of Popliteal.
__ _
,__ __
#
"A
AS COMPANIONS TO THIS BOOK-
CATECHISM ON FIRST AlD."
BY ]. M. CARVELL. !V1. R.C.S., L.S.A.
Price 6d., post free.
"PROBLEMS
IN FIRST AlD."
HYL. M. FRANK CHRISTIAN, M.B., AND \V. R. ED\V ARDS, A.C.A.
Price 6d., post free.

FIRST AID TO THE INJU I{ED
ARRANGED ACCORDING TO THE REVISED SYLLABUS OF THE FIRST AID COURSE OF THE
ST. JOHN AM BULANCE
BY
JAMES CANTLIE,M.A., M.B., F.R.C.S ., KlI(<rht of Grace of the Order of St. /071/. HOllorary Life Jl1emher of, al/d Lectltl-er and E.-t·amil/"" to. the Association.
\Vith a CHAPTER on .. Stretcher Transport," revised from that originally written by Sir JOH N FURLEY, C.B., Kllight of Justice of the Ordel- of St. John, in accordance with the Army Stretcher Exercises. Al 0 a CI{.\PTER (being the Fifth Lecture for Females only), by E. J.\.1AcDoWEL COSGRAVE, F.R.C.P.I., KnightofGraceo./the Ordero./St.Johll, HOllo/'aryLde IIfelJlber of, and Lecturer and to, the Associatioll.
TWENTY -EIGHTH EDITION, 1,340,000 to 1 ,39:>,000
edition IS similar to the eip;hteenth, lit which editiol/ 1II!lllyof the illllstratiolls 1vere /'e-dra7vll; otherwise it differs bitt little ./rom the eleventh to the seventeenth editiol/s.)
Price in Cloth, 1s. post free.
LONDON:
THE ST. AMBULANCE
ST. JOllN 'S GATE, CLERKENWELL, E.C.
\Y. n . & L.C. 50.000 10 '191;:;
Ube <Sranb !prior}? or ttbe ®rbel' of tbe 'lbospital of st. Jobn of Jel'Usalel1l in JEnglanb.
SOVEREIGN HEAD AND PATRON: HIS l\IOST GRACIOUS MAJESTY THE KING.
GRANDPRIOR: H.R.H. THE DUKE OF CONNAUGHT, K.G.
SUB-PRIOR: (Vacant).
BAILIFF OF EGLE: COLONEL SIR HERBERT C. PERROTT,
EXECUTIVE OFFICERS: [Bt., c. B.
PRELATE.-The Archbishop of York.
CHANCELLOR.-Col. Sir Herbert Jekyll, K.C.M.G.
SECRETARY-GENERAL.-(Vacant).
RECEI"·ER-GENERAL.-Edwin Freshfield, LL.D.
DIRECTOR OF THE AMBULANCE DEPARTMENT.-The Earl of Plymouth, P. C., C. B.
CHAIRMAN OF THE BRITISH OPHTHALMIC HOSPITAL, JERUS.\LEM.-Col. Sir Charles M. 'Vatson, K.C.M.G., C.B.
ALMONER.-Sir Dy ce Duckworlh, Bt., 1\1. D., F. R. C. P., LL. D.
LIBRARIAN.-A. Edmund Fraser.
REGISTRAR.-The Ead of Ranflldy, P.C., G.C.M.G.
GENEALOGIST. -Sir Alfl'ed Scott Scott-Gatty, K. c. V. o. (Garter).
DIRECTOR OF CEREMO , IEs.-Sir Alfred Scott Scott-Gatty, K.C.V.O. (Garter ).
ASSISTANT EXECL:TIVE OFFICERS:
ASSISTANT RECEIVER-GENERAL.-Edwin H. Freshfield.
ASSISTANT DIRECTOR OF THE AMBULANCE DEPARTMENT.Lieut.-Col. Sir Richard C. Temple, BL, C.LE.
HONORARY SECRETARY OF THE BRITISH OPHTHALMI C HOSPITAL, JERUSALEM.-Col. Thomas H. Hendley, C.LE., M.R.C.S.
ASSISTANT HONORARY SECRETARY (FOR SCOTLAND) OF THE BRITISH OPHTHALMIC Ho PI TAL, JERUSALEM.-John Horne Stevenson (Unicorn Pursilivanl).
SECRE1'ARY AND ACCOUNTANT.-V"illiam R. Edwards, A.C.A.
ASSISTANT SECRETARY.-DlIncan G. Monteith.
ASSISTANT ACCOUNTANT: Ivor C. Albury.
THE CHAPTER-GENERAL:
The Chapter-General consists of the Grand Prior. the Sub-Prio r. the Bailiff of Egle. the other Knights of Justice. the and the Prelates. de iure; the Executive the OlhclatJng Chapiallis ; all members of the Council; not more than ten Knights of Grace and nvt more than six Esquires appointed by the Grand Prior.
K;o;IGlI rs OF JUS'IIC":
IllS :'.lOST GRACIOUS MAJESTY TUE (Sovereign Head and Patron).
FIELD-:'.lARSIlAL TLR.II. TilE DUKE OF COW,AUGIIT. K.G K.T .• K.P .. P.C .. Etc. (Grand PI·ior).
GENERAL H.R.H. PRINCE CHRISTIAN OF SCIILES\\,IG-HOLSTEI;o;, ICG., P.C.. G.C. \'.0.
B.II. PRINCE ALBERT OF SCHLESWIG-HOLSTEIN, G.C.B., G.C. \'.0.
COLONEL H.H. TilE DUKE OF TECK. G.C.B., G.C. \'.0 C.M.G.
AD)JlRAL II.S.II. PRIXCE LOUIS OF BATTENBERG. G.C.B., G.C. \'.0 .• K.C.ilLG R.N.
lJ.i\J. HAAKON VII.. KING OF NORWAV. K.G., G.C.B., G.C.\·.O. LIEUT.-COL. II.S.n. PRINCE ALEXANDER OF TECK, G.C.B .. G.c.v.a., f).S.u. :\IAJOR II.R.Il. PRINCE ARfllUR OF CONNAUGHT, K.G., K.T.• P.C., G.C.V.O., C.B.
II.H. PRINCE ALEXA:-IDL'.R OF BATTENBERG. G.C.V.O.
Sir John Furley, C.B. (Honorary Sir II. A. Blake. Bailiff). The Earl of i\leath. K.P., p.e. ir T. N. Dick-Lauder, Bt. ,\ . E. Fraser.
:'Ilaj. ir A. Lamb, Bt. The Lonl i\lostyn.
Col. Sir It C. Perrott, Bt.. C.B. The i\larquess of Breadalbane, Col. Sir J. Gildea, [{.c. V.O., C. B. ICG .. P.C. H. J. Loftus. The Duke of Portland, K.G P.C. Col. B. i\J. Dawes. R. B. Carter. F.R.C.S. (Honorary Gen. Sir C. 'Varren, G.C.ilLG., K.C. B., Commanded. R.E. Col. C. 'V. B. BO\\'dler, C.B. :'IIaj.-Gen. J. C. Dalton. ( Honorary Commander).
:'.laj.-Gcn. Sir A. G.;r:\IIunter- Lieut.-Col. A. C. Yate. 'Veslon of Uunterston, K.C.B., l\laj.-Gen. A. F. Terr)'. n.s.o. The Earl of Plymouth. P.C.• C.B. Col. The Lord 'Villiam Cecil. c. V.o. The Earl of Sandwich, ICC. v.o. E. Freshfield. LL.D. (Honorary E. II. Freshfield. Bailiff). Lieut.-Col. The Earl of Ellesmere.
The Earl Brassey. G.C.B. M.V.O.
The Viscount Templetown. Field-Marshal The Earl Kitchener R. 1\1. MacLean. of Khartoum, K.G .• K.P., Etc.
A. F. G. Leveson Gower. Lieut.-Col. Sir R . C. Temple, Bt.•
Col. F. A. H. Lambert. C.LE.
Col. Sir C. "V. Murray. C.B. Sir A. S. Scott-Galty, K.C. \'.0.
The Earl ofRanfurly, P.C., G.C.M.O. Col. Sir H. J ekyll. K.C.M.G.
The Lord Sandhurst. P.C.• G.C.S.I.. The Lord Islington. P.C., G.e.M.G .. G.C.I.E. D.S.O.
KNIGII rs or J USTlcE.-conLinlled.
Col. S ir J. R. A. Clad<, 13t., C.B., F.R C S.E. ir R . Han·ey.
Col. The Lord Sydenhal11, G.C.S.I., . G.c.:lI.G., G.C.I.E .
J: .,ellt.-Col. J. \V. \Vray. ;;.,r \V . 'V. Portal. Ut. 1 he Duke of Somerset.

Sir n. DuckworLh. HI M.D.
Capt H. E. HOlllLon C v 0
The Viscollnt Esher G' C 'B . G' C v Cnl. Sir C. i\1. l{ oycis.' C'. B'.' t; The Lord L,ellt.-Col.The Lord Herbert SCOLt' ?tevenson. [o.s.O: FrancIs 'VI lham Pixlcy.
PRELATE:
The Archbishop of York.
SUH-I'REl.ATES:
J.he P' " l1i1te of New Zealand . f: ,e H.ishop (IF Gibraltar. 1 he H, h o p ot Sou Lllll'ari< . le BIshop of Peterborough.
Orm!;hy.
TI H OFl'lCIATING CIL\PLAINS :
Ie e\· Canon E. Sheppard I Th Y K.C. \'.0., D.O. ,c cnerablc Ernest , E. Holm L·s. ]' B.D. C\rchdeacon of La :don).
\.NIGHTS OF GRACE APPOIN" - G
Clli. Sir J. \V Ottl lEO BY THE .RAND PRIOR: J . 1\. James. K.C.I.E., R.E·I J .. II. C.\·.O.. F.R.C.S . .I. S . Griffiths. II. St. J. HopI.!. LIlT./).
Lt.-Col. George E Twi 1. Cook. C.U:. H A G'bb . ss, F.R.C.S.1. fhe Lord Norreys • • on". E\'elyn Cecil, M.P
. ESQUIRES APPOINTED BY Til E GRAND PRIOR'
C. B. Hamilton. C 1\1 G I cr ' E. Dawes. 01: " G. CarLeI'. Major [\1. D. MlIrray. C.V.O., C.B.
THE COUNCIL:
The COllncil consists of the Sub-P' C I . C.B. (Bailiff of Egle) the .0 one}
C. Perrott Bt. o( existing CommanJeries. the Offinones. Lhe fitteenll1el11bers (It Lhe Grades ot KnighL of not ':'lore L.han of Grace and Esquire appo inted by the K'lIghl
. i\IEMBERS APPOINTED BY THE GRAND PRIO .
S,r J. Furley, C.B. Lieut -C R • , Major-Gen. J. C. Dalton. S,r R. C. femple, BL..
Colonel The Lord 'V illiam Cecil, The Bishop or SOllthwark . C.\'.O. Inspector-Gcneral U. Ninnis.c.v.o
S,r Henry Arlhur Blake. G.C.:\i.G. 1\1.0., R.:>:. .• E. H. Freshfield lht ,Lord Clalld I familton 1\I P . o. f. II. Il clldl ey. C. I. E.•
nl)e G;tRnb lPtiOt\2 of nbe ®tbet of tbe '1I)06pital of St. 3-obn of 3- erusa lem in JEnglanb.
AMBULANCE DEPARTMENT.
Uhe St. 50hn :E\mbulunce :E\ssociation.
PATRON:
HIS MAJESTY THE KING, SoveI'eign Head and Patron of the Ord e r.
PRESIDEl\T:
Il.R.H. THE DUKE OF Cm.NAUGHT, K.G , Grand Prior of the Order.
CENTRAL EXECUTIVE COl\1l\I1TTEE:
Consisting exclusive l y of Members and lIon o rary Associates of the Order.
DIRECTOR OF THE Al\IBULANCE DEPART;\IENT AND CII:\IIOIAN OF COMi\IITTEE.-The Earl of Plymouth, P.C., C.B.
ASSISTANT DIRECTOR AND DEPUTY CHAlRMAN.-Li e ut.-Col. Sir Richard C. Temple, Bt., C.LE.
DEPUTY CHAlR;\IAN.- iI- John Furiey, C.B., Lire of the Committee, Honoris Cansa . :i\IE;\IBER
;\Iaj.-Gen. J. C. DalLon.
The Lord Islington. G.C.;\I.G., n s.O.
Col. Sir J. R j\. Clark. HL C.B F.R C S E. Col. The Lord Sydenham. G.C.S.I., G.C.M.G., G.C.I. I(
Capt. H. E. Boulton. C.V.O. Lieut.-Col. The Lord I [erbert Scott. D.S.O.
The Rev. T. C. Elsdon.
Inspector-General B. Ninnis, C.V.O ;\1. D., R N •
Maj. G. H. n arwin, I.D.
Col. G. S. Ellislon. C.B., i\I.R.C.S.
Col. C. J. Trimble. C.M.G., L.R,C.P.E.
The Lord Clallcl H amilton. i\I.P.
Sir J. L. Langm')l1. Bt.
S. \V. :\Ialkin. C. CoLLon, F.R .C.P.li .. :l1.R.C,S.
CENTRAL EXECUTIVE COMMITTEE-continued.
C. B. Palmer.
Lieut.-Col. G. E. Twis F.R.C.S.1.
Col. T. H. Hendley. C.I.E .. M. R.C.S.
J. H. l\forgan. C.V.O .. F.R.C.S.
Col. Sir Trevredyn R. \Vynne, K.C.S.I., K.C.l.R. l\fajor E. H. T. Parsons.
Brig.-Gen. H. K Mends. Lieut.-Col. A. D. Acland.
V.QL., Col. E. D. Brown-Synge-Hutchinson.
J. A. Bloxam. F.R.C.S.
Lieut.-Col. Sir R. \V. Tnglis .
Surg.-Gen. II. R. \Vhitehead, C.B., F.R.C.S.
The Viscount Acheson.
T. H. \Voolston.
Col. C. R. Tyrrell. M.R.C.S.
Col. The Lord Bolton.
Surg.-Gen. Sir A. W. May, K.C.B., F.R .C.S., I< . H . P., R . N".
F. N. Ellis.
\V. E. Audland, M.R.C.S.
A. H. Johnston, M.R.C.S.
5. A. Richards.
EX-OFFICIO MEMBERS OF COMMITTEE:
Col. Sir H. C. Perrott, Bt., C.B. (Bailiff of Egle) .
'J he Secre tary-General of the Order.
1 he Recei, er-General of the Order.
The Chairman, British Ophthalmic Hospital.
CHIEF SECRETARY: l\Iajor W. O. Prichard.
ACCOUNTANT: \V. R. Edwards, A.C.A.
DIRECTOR OF STORES: \V. H. Morgan.
ASSISTANT SECRETARY: D. G. Monteith.
TERRITORIAL BRANCH.
CONTROLLER-IN-CHIEF:
Lieut.-Col. Sir R. C. Temple, Bt., C.I.E.
SECRETARY: P. G. Darvil-Smith.
HEAD OFFICES:
St. John's Gate, Clerkenwell, London, E. C.
REVISED 1908.

FIRST AID TO THE INJURED . SYLLABUS OF INSTRUCTION .
FIRST LECTURE.
A. Principles of Fir ' t Aid.
B. A brief Description of the IIuman Skeleton a nd of the M us cles.
C. Fractures-Causes, varietie , signs and sympt oms.
D. Treatment of Fractures - G e nera l Rul es .
E. The Triangular Bandage and its application.
SECO:-lD LECT URE.
A. Treatment of Fractures (c ontinued). Details of treatm e nt.
B. Dislocations, Sprains, Strains-Signs, symp to m:; and tr ea tment.
C. The IIeart and Blood Vessels. Tile Circula t io n of the Blood.
D. Hremorrhage and wounds. G.eneral for tr ea t ment.
E. The Triangular Bandage and ItS npphcatlOl1.
R EFEREI'CE N o. 58-. 1903
THIRD LECTURE.
A. Hremorrhage and wounds (continued). Details of treatment.
B. Internal H ce morrhage-S igns. symptoms and arrest.
C. Hremorrhage from Special Regions.-Signs, symptoms and arrest. .
I? Bruis.es, Scalds, Bites and Stings, Frost-bite.
1<.,. Foreign bodIes In the Eye, Nose and Ear.
F. The Triangular Bandage and its application.
FOURTH LECTURE.
A. The Nervous System.
B .. Organs and Mechanism of Respiration-Artificial H. espiratlOn.
C . I nse nsi bility
D. Poisoning .
FIFTH LECTURE (for Males only).
.
.A . Improvised methods of lifting and carrying the sick or Injured.
B. Methods of lifting and carrying the sick or in]' ured on sll.etchers .
C. The conveyance of such by rail or in country carts.
FIFTH LECTITRE (for Females only).
A. Preparation for reception of accident cas es.
B. 1\1 eans of lifting and carrying.
C. Preparation of ued.
D. Removing the clothes.
E. Preparations for surgeon.

NOTE 1.-Th e suhject of poisons should be ueated in a general manner; the coml11on poisons classified, and only their gene ral symptoms, ·effftcts and treatment taught.
N GT E 11.-Th e last half-hour of eac h le cture should be devoted to practical work, such as the "pplication o f bandages and sp lints, lifting and carrying wounded on stretche rs.
1 OTE IlL-There should be an interval of a w eek between each lecture. A candidate for examination must attend at least fuur out of the five lectures.
NOTE IV.-Male classes must passin that system of stretcher exercise most suitable for the locality.
N OTE V.-As little time as poss ible is to be spent on in· struction in anatomical and physiological details. Lecturels and examiners are particularly requested to remem be r that it i., " First Aid" that has to be taught and tested, and not anatomJ and physiology.
111ixed classes Of men alld women are Oil ?to a cco llnf ,1Jermitted.
PUPILS UNDER Sr;aEEN YEARS OF AGE CAN O:-lLY ATTEND THE" JUNIOR " OvURSE (SECTiO:'-l A, SYLl.ABUS 40).
Lecturers instructing a First Aid class, and Local Secretaries, can obtain further particulars on application to the Chief Secretary for "Paper Rderence No . 80."
No Lecturer may examine his own Class for Certifi cates .
9
SUMMARY OF

CHAPTER 1.
Principles of First Aid
Explanatory
Questions on Chapter
CHAPTER II.
The Human Skeleton. Skull, spine, ribs and breastbone, upper limbs (colla r-bone, shoulder-blade, arlllbone, bones of the forearm, carpus, metacarpus, phalanges), pelvis, lower limhs (thigh--bone , kneecap, tarsus, metatarsus, phalanges)
Joints ..
Mt·scles. Voluntary and involuntary
Fractures. Causes, yarieties, signs and Apparatus for treatment of Fractures ...
General Rules to be observed in the treatment of Fractures
Special Fractures. Cranium, low er jaw, spine, rib", breast-bone, colh r -bone, should er-blade, arm-bone or bones close to the elbow j <)int, forearm, crushed hand, pelvis, thigh-bone, knee-cap, leg, crushed fool
Dislocations
Sprains
Sprains and Ruptured
".
CHAPTER III.
Circulation of the Blood . Org.ans; general (systemic) and pulmonary circulations
Hcemorrhage or Bleeding. Arterial, yenous, capillary
Arterial Hcemorrhage. Principles of arrest
Wounds with Arterial Hcemorrhage ...
Course of the Main Arteries and Pressure Points.
Aorta, arteries of the head and neck, of the upper limbs, of the lower limus
Venous Hcemorrhage and Varicose Veins
Wounds with Venous Hcemorrhage
Capillary Hcemorrhage
Internar Hcemorrhage
Hcemorrhage from Special Regions
Questions on Chapter
CHAPTER IV.
Miscellaneous Injuries. Bruises, bu rns and scalds, hites of snakes and rabid animals and wounds by poisoned weapons, stings of plants and anima ls, frost bite , need le emb edded unda the skin, fish hook embedded in the skin, injuries to joints, foreign body in th e eye, ear passage a nd nose , wound in the front wall of the abdomen, injuries to the organs within the abdomen and pelvis ".
Questions on Chapter
CHAPTER V.
The Nervous System. Cerebro-spinal, sympathetic ."
The Respiratory System
Artificial Respiration. chafer's, Silvester's. Howard's combined with Silvester's, L abo rd e's and Hall 's meth ods".
10
Muscles
Questions on Chapter 17 20 21 21 4I 43 62 6-+ 65 66 II
Page 70 73 74 76 79 93 94 95 95 96 99 102 I IS II7 lIS 12 I
Insensibility. Causes, general rules for treatment, concussion of the brain, compression of the brain, apoplexy, epi lepsy, hysteria, shock, fainting and col1apse, sunstroke and heat-stroke, convulsions in children, asphyxia
Electric Shock and Effects of Lightning
Questions on Cha?ter
CHAPTER VI.
Poisoning. Gene ral rules for treatment, special·poisons
Questions on Chapter
CHAPTER V II.
Bandaging. Bandages for the scalp, forehead, etc ., shoulder, hip, hand, foot, chest, back, knee, elbow, fingers and toes ...
CHAPTER VIII.
Methods of Carrying. Four, two, and three-handed seats, fireman's lift, fore and aft method, improvised stretchers, to cross a ditch or wall, to load or unload a wagon .,
CHAPTER IX.
Stretcher Transport. Stretchers, stretche r exerc ises, litters
CHAPTER X.
The Fifth Lecture (for Females only ). Preparation for reception of accident cas';!s, choice and preparation of a room, lifting and carrying, preparation of bed, removing the clothes, preparation for surgeon .. .
Questions on Chapter

Skeleton showing position of main arteries
Skull and vertebral column
Vertebra
Bones of the left upper limb
Bones of the right lower limb
Shoulder Joint
Ankle .. ,
Rectus Muscle
Triangular bandage spread out and folded
Large arm sling
Smal1 arm sling
Reef knot
Granny knot
knot
Bandage for fracture of lower jaw
Bandages for simple fracture of rib;
St. Joh n sling
Bandages for fracture of bot h cOl1ar hones
Bandage for fracture of shoulder blade
Treatment of fracture of arm
Angular splint
Treatment of fracture of forearm
Treatment of crushed hand
Treatment of fracture of thigh bone
Treatment of fracture of thigh bone (woman)
Fracture of knee cap
Treatment of fracture of knee cap
Treatment of fracture of leg (man and W0man)
Treatment of em hed foot ..
Diagram of the heart, lungs and air pa sages
12
Page 128 142 145 155 160 197 206 13 LIST OF ILLUSTRATIO TS.
. . . ... . . . . ..
...
... Loop
...
... . .. . ..
... . ..
...
.
Page frontispz·ece. 2-+. 24 • 27 29 3 1 3 1 3 2 38 39 39 40 4 0 ' 43 44 47 50 51 52 53 54 55 55 57 58 58 59 61 62 7I
DIagram of the circulation of the blood
Digital pressure on carotid arlt!ry ...
Digital on facial artery
Digital pressure on temporal artery
Digital pres ure on occipital artery
Pad and bandage to arrest hremorrhage from temple l{ing p.1d
Digital pressure on subclavian artery
Pad ann bandages to apply pressure on axillary artery ...
Digital pressure on brachial artery (two methods)
Flexion at elbow
Digital pressu(e on radial and ulnar arteries
Pad and bandage to arrest hremorrhage from palm
Digital pressure on femoral artery... ... ...
Tourniquet on femoral artery
Flexion at knee.
Organs of the chest and abdomen .. .
The lungs and bronchial tubes
Schafer's method of artificial respiration ...
Silvester's method of artificial respiration .. .
Silvester's and Howard's methods of arlifici d respiration combined
Bandage for the head
Bandage for the shoulder
Bandage for the hip ...
Bandage for the hand
Bandage for the foot
Bandage for the chest
Bandage for the knee
Bandage for the elbow
Grip for four-handed seat ..
Lifting by two-handed seal..
Grips for hovo-handed seats ..
Carrying by two-handecl seat

Grip for three-handed seat .. .
Supporting patient... .. .
Fore and aft method of carrying
Carrying on improvised seat
Improvised stretcher
Furley stretchers
Stretcher exercise, No. 1. .. Fall in"
Ditto, ready to lift patient
Ditto, lifting patient. ..
Ditto, placing stretcher
Ditto, preparing to lower patient ...
Ditto "Lower"
Ditto; No. II. Ready to lift Fatient
DillO, patient lifted ...
Dilto, No. IV. First position
Ditto, second position ... ... ...
Diagrams illustrating Army stretcher drill
Ditto .. ,
Bed cradle
l mpro\'ised bed cradles
Page 73 8r 81 82 82 83 485 86 87 87 89 90 9 1 92 1I2 JI9 122 124 12 5 155 156 156 1 157 151) 159 159 160 I6r 162 163 IS
Pa · e 16l 165 167 168 168 17 2 175 17 6 177 178 179 180 182 183 188 189 19 1 194 203 203, 204
PREFACE.
T the request of the Central Executive Committee
I have revised the manual written by myself in 19°1, as the official handbook of the St. John Ambulance Association.
Throu ghout the revision an endeavour has bee n made to simplify the study of FIrst Aid to the Injur ed by d ra wing up a n umber of general rules for th e treatment of accidents and sudden illness, and by th e omission of all detail \\"hich is not absolutely necessary to enable the student to acquire an intelligent kno\\·ledge of the subject.
I wish to express my thanks to Professor E. A. Schafer for furnishing instructions for performing a method of artificial respiration, to Dr. L. M. F. Christian for many valuable suggestions, and to the Medical :Members of the Central Executive Committee, especially Surgeon-Major G. H. Darwin, M.D., and Dr. F. R. Cassidi, for perusing the proof sheets and for a Dum ber of useful additions to the \York.
I cannot omit also to offer my best acknowled gments to 1\1r. 'V. R. Edwards, the Accountant and Storekeeper of the S.J.A.A., for his invaluable co-operation.
JAMES CANTLIE.
FI RST AID TO THE INJURED.
CHAPTER 1.
The St. John Ambulance Association has n.ow c ompleted thirty years of its existence, and dunng that period hundreds of thousands of men and women have been taught at its classes, in all parts of the world how to help the ir injured neighbours.
Fi;st Aid to the Injured is a special branch of practical medicine and surgery, by a of which trained persons are enabled to afford assistance in cases of accident and sudden lllness. The instruction begins and ends with First Aid, and the subject is taught simply but thoroughly ar:d e xhaustively. The duty of the ambulance pupils ends where the doctor's commences, and there ought to be no overlapping or clashing of duty or interests.
PRINCIPLE ' OF FIRST AID.
1. The First Aid student should be-
(a) Observant, that he may note the causes and signs* of injury.
(b) Tactful, that he may without questions learn the symptoms t and hlStoryt of the case.
* Si TI1S are what may be perceived.
t are whaL I he paLient can te.n you. .
::: History means the circumstances attendmg the accldent or sudden illness.
(c) Resourceful, that he may use to the best ad vantage whatever is at hand to prevent fur t her d amage and to as sist Nature's efforts to repair the mischief already done .
(d) Explicit, that he may give clear instructions to the patient or the bystanders how best to assist him .
(e) Discriminating, that he may decide which of several injuries presses most for treatment by himself, and what can best be left for the patient or the bystanders to do.
2 Remove the cause of injury or dancrer \\ hene\'er possible. b
3· Severe hc:emorrhage must r ece ive t h e fi rs t a ttention , no mat ter wha t are the oth e r inj u ri es.
4· A ir.- The patient must be in a position in whi ch breathing is possible j the air pas ages must be free from obstruction j if breathing has ceased prompt measures l1Iust be taken to restore it.
5· Rest .-A restful position of the body will assist the vital functions; Support of the injured part will help to prevent further damage, and is essential in the case of fract ures of limbs.
Warmth. -After every accident keep the patient warm so as to prevent the fall of temperature below the normal point . .
7· When t he skin is broken the wound

19
should b e promptly covered with?- clean .orbent dressing. Should the wound be pOIsoned, IS most important immediately to prevent the pOison oer11le,ating the system. .
8. P oi sons swallowed should. be got nd of: or \\" hen that is inexpedient, ' neutralIsed.
9 . T he best means of transpo rt must be studied. and provision made for proper care when the patient is brought to shelter.
1 0. Removal of Clothing. -Clothes should not be taken off unnecessarily, but when it is needful to remove them, the following rules will be found of service in serioLls cases:-
COAT: Remove from the sOLlnd side first, and, if necessary, sli t up the seam of the slee\'e 0n the injured side .
SHIRT A TD VEST: Slit down the front and remove as the coat.
TROUSERS: Slit up the outer seam.
BOOT: lit the back seam and undo the laces.
SOCK: Cut off.
II. Stimulants. - I t is incorrect to suppose that alcohol is the only form of stimulant, and far .too frequent use of spirits is, to restore a patient after an accident, often Wlth senous results; the safest ru le therefore is to defer the administratio n of alcohol unti'[ the of a doctor. ,\Vhen the patient is able to swallow, strong tea or coffee, or milk, as hot as can
18
be drunk, or a small quantity of sal volatile in wat e r may be give n. Smelling salts may be held to the nose. Sprinkling the face with cold and hot water alternately, war mth applied to the pit of the stomach and over the heart, and vigorous friction of the limbs upwards hav e a stimulating effect. .
12. Throughout his work the First Aid student must on no account take upon himself the duties and responsibilities of a Medical man . At times an apparently slight injury is accompanied by grave danger and may a.ctually cause loss of life. ' Vhen sending for a doctor, state the nature of the case, and remem ber that written particulars are safer than a verbal message .
It is necessary that something should be known of the structure of the body (elementary anatomy), and of the functions of some of the more important organs and systems (elementary physiology). A short description of the necessary anatomical ana physiological points is therefore given as the several subjects are discussed. For purposes of description the human body is supposed to be erect, with the arms hanging by the side and the palms of the h?nds directed forwards. The" middle line" of the body runs vertically from the top of the head to a poi n t between the feet.
QUESTIONS ON CHAPTER 1.
Tile 11l111le1'als

the first
clothing always be re moyed? 1low would you remove when necessary?
the
and abuse of stll11ulants
20
indicate tlte pages wltel e the allswers . may be fOUl/d. What
ed?.. .. , ... What qualities
First
stude nt pos ess ? -\Vhat are signs? '''hat are symptoms? .. , Wb at is the history of a case? . PACK 17 17, 18 17 17 17 18 18 What is
to
.. ,
... 'Vhat three things are absolutely
to an lDJured person? .. , ", ... . ": .. , ", 18 'Vhat must be done wh e n th e skll1 IS broken? ... 18 , 19 How must poisoning be treat ed? ... ." 19 What steps must be taken beyond the actual treatment of injuries? ", ", .. ,
Explain the use
.. . . ..
? \Vhat is elementary anatomy? 19 19 19 ." 19, 20 20 20 10 What is elementary physiology? F0r purposes of description ho w is the human body supposed to be placed? ... 20 W hat is the middle line of the body? 2,
is First Aid to the injur
should the
Aid
often the first thing
do lD an accIdent?
What result of injury must receive
necessary
Should
What must
Fir t Aid student not do
CHAPTER II.
fRACTURES , D I SLOCATI ONS, SPRAT 1 AND STRAINS. THE
The human body is moulded upon a bony framework (the skeleton) which serves-
I.-To give shape and firmness to the body.
2.-To afford attachment to the muscl es .
3.-To protect important organs, as in the skull, chest, and abdomen . THE SKULL.
The Bones of the Skull are arrang ed in two groups, those of the brain case or cranium and those of the face.
The Boundaries of the Cranium are the vault or dome, the rou n ded portion forming the top of the head ; the front or brow ; the back of the head, where the greatest extent of brain exists, and where therefore thp cranium is widest and deepest; the sides or temples . The base of the cra ni um is hidden from view by the bones of the face and of the vertebra l column ; in it are numerous perforation for the passage of blood vessels and nerves; through the iaraest opening the brain and spinal cord are contin uous. 0
The Bones of the Face with the exception of

23
the lower jaw are firmly jointed together, so movement between them is impossible. The cavItIes of the nose and of the eye sockets (orbits) are formed by the bones of the crani,um, and of the face conjointly, The mouth cavity IS between the up.per and lower jaws, the bemg the bony of the mouth which separates It from the nasal cavIty above.
The Lower Jaw consists of:-
(a) A horizontal portion in which are the sockets for the teeth.
«(J) Vertical portions terminating on either side at the joint between the lower jaw the base of the cranium, situated immediate ly in front of the ear.
Th e anO'le of the jaw indi cates the junction of the horizon tat' and the vertical portions .
THE BACK-BO:\E, 'PIXE , OR YERTEBRAL COLU;'l:\,.
The Vertebral Column (Fig . r) is composed of bones called vertebrce, each of which consists of-
I.-A body or bony Illass in front.
2.-Processes projecting backwards, which enclose a canal for the spinal cord- the spinal canal.
3.-T'wo transverse proc,esses, twelve pairs of which support tile nbs,
SPINOUS PROCE SS
TRAK S VEJ, SC: '. CANA L F (lR SPI N AL C O RD.
BO DY OF VERTEl lI< A.
FIG. 2 A.

SKULL AND VERTEBRAL COLUMN.
Showing left ribs and portion of breast bone. The right rius are removed.
SURFACES SUPPORTING HE VS O F RIBS.
FIG. 2B .
TRA N SVEnSI!" PROCESS
SPIN O US PROCESS.
4.---\. spino LIS process. The spinous processe of the vertebrre can be felt beneath the skin for the whole length of the back (Figs. 2A and 2B).
T he Vertebrce, 33 in all, are grouped into regions, in each of which they are k'no\vn by numbers, counting downwards :-
I. - In the neck 7 Cen'ical vertebrre. The first vertebra, the atlas, forms a joint with the base of the skull, at which tIle nodding movement of the head takes place; the second, the axis, by the joint between it and the atlas, allows of the side·to·side movements of the head.
2 - ·In the back 12 Dorsal vertebrre .
3 - In the loin 5 Lumbar vertebrre.
4. - The rump-bone, or Sacrum, consists of 5 Sacral vertebrce united in adults as a solid mass.
5.-The tail-bone, or Coccyx, consists of 4 vertebrre joined together to form a single group.
Between the bodies of the vertebrre, in the upper three regions, are interposed thick pieces of cartilage which, while they bind the bones together, allow of free movement to the column as a whole, and help to break the shock of any sudden force applied to the spine (for example, when falling from
2-+
a height on the feet). The whole spine is strapped together by ligaments reaching its entire length.
THE RIBS AND BREAST-BONE.
The Ribs consist of twelve pairs of curved bones extending from the dorsal vertebrre to the front of the body, and are known by numbers-first, second, etc., commencing from above. The ribs are not bony throughout their entire length, but at a short distance from the front the bony material ends, and cartilage takes its place. The upper seven pail s, named the true ribs , are attached by their cartilages to the Breast-bone (sternum), a dagger-shaped bone with the point downwards, just over the pit of the stomach. The lower five pairs are termed the false ribs, as their cartilages fall short of the middle line. The eleventh and twelfth pairs are termed the floating ribs, as their ends are free in front. The ribs enclose the chest and serve to protect the lungs, heart, liver, stomach, spleen, etc .
THE UPPER LIi\lBS.
The Shoulder-bones are the Collar-bone (lavtc!e) and the Shoulder-blade (scapula).
The Collar-bone can be felt on either side Leneath the skin at the lower and front part of the neck as a na rr ow curved rod about the thickness of a finger. Its inner end rests on the upper part of the
PART OF C OLL-AR BONE SHOULDER BLAUE (SCAPUL :\ ) BONE -

BOI'ES JULNA OF l RAIJIUS
WRIST (CARPUS)
l\IETACARPUS
PHALA:--IGES
FIG. 3A.
BONRS OF TIlE LEFT UPPER LIMB.
3r..
SHOWING THE POSTTrON OF THE RADIUS AND ULNA WHEN TIrE THUMB IS TURKrm TKWARDS
Compare Fig. 3A, in whIch lhe thumb is turned outwards.
... .
RADIUS
FIG.
breast-bo n e, and its outer end joins with the shoulcl.e rblade.
The Shoulder-blade lies at the upper and outer part of the back of the chest, and forms joints \\ ith the collar-bone and the bone of the arm.
The bone of the Arm (llltme?'us) reaches from the shoulder to the elbow.
In the Forearm are two bones, the Radius on the outer, or thumb side, and the Ulna on the inner, or little finger side. Both bones reach from the elbow to the wrist, and they change their relatiye position with every turn of the hand (Figs. 3 A and 3B).
The Hand is composed of-
r.-The bones of the wrist, or ca1jus, eight in num ber, arranged in two rows of four.
2 .-The metacarpus (the framework of the palm) ; fi ve bones which form the knuckles and support the bones of the fingers.
3.- The plzalanges, or finger-bones, three in each finger, and two in the thumb
T HE PELVIS AND LOWER LIMBS.
The Pelvis . - The large basin-Lke mass of bone attached to the lower part of the spine is composed of the two haunch-bones and the sacrum . The haunchbones meet in front (at the pubes) in the middle line, only a small piece of cartilage intervening, but behind, the sacrum - IS placed between them The pelvis

4.
lIO:'-ES OF THE lUGllT LOWER LIMB, SIlOW· IK G JOINT WITH TIlE PELVIS AT THE IIIr.
FIG._ •...•..- tHIGH BONE
. K
r--·····nROOCH
___ SH
(FEMU R).
NEE CAP
(PATELLA).
BONE (FIBULA).
IN BONE (TIBIA)\
30 supports the abdomen and its contents, and provides the deep sockets for the thigh-bones-the hip joints.
The Thigh-bone (femur) reaches from the hip to the knee joint. Its shaft is stout, rounded, and arched forwards; the upper end presents a rounded head, supported on a neck which projects im\"a rds, to fit into the so cket of the hip joint.
The Knee-cap (patella) is a triangular bone lying with its base upwards in front of the knee joint immediately beneath the skin.
The bones of th e L eg are the Shin-bone (tibia) the Brooch-bone (jibula). The S hin-b o ne extends from the knee to the ankle, in both of which joints it plays an important part; its sharp edge, the slli n, can be felt immediately beneath the skin of the front of the leg. The Brooch-bone lies on the outer side of the tibia. It does not enter into the formation of the knee joint, but its lower end forms the outer boundary of the ankle joint. The Foot is com posed of-
I.- The tarsus, a group of seven irregular bones at the instep. The largest is the heel-bone, and the uppermost (the ankle-bone) forms the lower part of the ankle joint.
2.-The metatarsus, the five long bones in front of the tarsus which support the toes.
3·--The phalanges, or toe-bones, t\\'o in the big toe, and three in each of the other toes.
31 JOINTS.
A Joint is formed at the junction vf two . or more bones. In moveable joints such as the hlP, knee, elbow etc. the surfaces of the bones are covered by ",:hich lessens friction and the shock of a

Compare Fig. 4, Page 29.
5.
fall. Lubricating the joint is a clear, rather. st.icky fluid, the "joint oil," or sYllovia, enclo ed capsule. Tying the bones together, allowmg of movement are a number of bands or lwaments. To expiain the formation of limb joints) the
FIG. 6. LEFT ANKLE. FIG.MUSCULAR TISSUE

PATELLA
TENDO)! OR LIGAMENT OF PATELLA
32 following examples are given :-
The Shoulder, a balland-socket joint, consists of a shallow socket on the outer angle of the shoulder-blade, and of the head of the arm-bone (Fig. 5). Ov\ ing to the shallo'vvness of the sod el the arm-bone is very prone to escape from its socket ( dislocate).
The Ankle , a hinge joint, is formed at the junction of three bones, the shin-bone above and on the inner side, the broochbone on the outer side, and the ankle-bone below (Fig. 6) .
THE MUSCLES.
FIG. 7· The Mus d es of the DIAGRAM SHOWING RECTUS body are classif.ed into two MUSCLE OF THIGH, WITH groups-voluntary and ARTERY, VEIN AND NERVE. z'flvoluntary.
33
The Voluntary muscles are met with in the limbs, the head and neck, and the surface of the trunk . Their ends are attached to different bones, and as they pass from one to another they cross a joint, and, being endowed with the power of contraction and relaxation, cause the movements of the body. As a muscle crosses a joint, it as a rule becomes a fibrous cord or tendon. Blood-vessels traverse and supply the muscles, and the nerves entering them bring them under the direct control of the brain and spinal cord.
The Involuntary muscles are met with in the walls of the stomach and intestines, in the air passages, and ill most of the internal organs and blood-vessels, also, in a special form, in the heart. They are not under the influence of the will, but continue their work during the hours of sleep; their functions are regu 'ated by a separate set of nerves (see Sympathetic System, page II8).
FRAC TU RES AND THE IR TREATMENT.
When a bone breaks a Fracture is said to occur.
CAUSES OF FRACTURE.
I. Direct Violence. - When from a severe blow, impact of a bullet, crush of a wheel, etc., a bone breaks at the spot where the force is applied the fracture is termed direct.
c
TENDON ARTEHY VEIN
2. Indirect Violence.- '''hen the bone breaks at some distance from the spot v, here the force is applied the fracture is termed indirect. Alighting on the feet and fracturing the thigh-bone or the bones of the leg, or falling on the hand and breaking th e radius or the collar-bone, are examples.
3. Muscular Action. - The knee-cap and the arm-bone are occasionally broken by a violent contraction of the muscles attached to them.
VARIETIES OF FRACTURES.
Fractures are classified according to the condition of the tissues adjacent to the bone as follows :-
1. Simple.-The bone is broken with but slight injury to the surrounding parts.
2. Compound. - The bone is broken and the skin and tissues are punctured or torn, thus allowing disease-producing germs to obtain entrance to the seat of fracture. The fractured ends may protrude through the skin, or (for example, when a bone is broken by a bullet) the viound may lead down to the fracture.
3- Complicated . - The bone is broken and in addition there is an injury to some internal organ (for example, the brain, spinal cord, lung, etc.) or to some important blood-vessel @r nerve.
A fracture may be compound or complicated as the immediate result of the injury; or a fracture,
originally simple, may be converted into a compound or complicated fracture-
(a) By careless movement on the part of the patient.
(b) By carelessness Qr ignorance on the part of one rendering first aid.
Special varieties of fracture may be classified accord'ng to the injury to the bone itself as follows :-
I. Comminuted. - The bone is broken 1l1to several pieces.
2. Green-stick. -In children, owing to the softer state of the bony tissues, a bone may bend and crack without breaking completely across.
3. Impacted. - The broken ends of the bone are driven one into the other.
GENERAL SIGNS AND SYMPTOMS WHICH l\L\ Y BE PRESENT.
(A fracture of the femur, humerm, or both bones of the forearm or leg, affords the most complete example.)
1. Pain at or near the seat of fracture.
2. Loss of power in the limb.
3. Swelling about the seat of fracture. welling frequently renders it difficult to perceive other signs of fracture, and care must therefore be taken not to mistake a fracture for a less serious injury.
4. Deformity of the limb.-The limb assumes an
34
35
36 unnatural position, and is mis-shapen at the seat of fracture. The contracting muscles may cause the ends of the bone to override, thereby producmg shortening.
5. Irregularity of the bone.-If the bone is close the skin the fracture may be felt, and if compound It may be seen.
6. Unnatural Mobility.-Movement may be made out at the seat of fracture.
7. Crepitus, or bony grating, may be felt or heard when the broken ends move one upon the other.
The last two signs should only be sought by a doctor.
Several of the above signs are absent in green-stick and impacted fractures.
In addition to the signs and symptoms the patient or bystanders may be able to give the history of the Injury, and marks on the clothing or skin should be noted, as they may serve to locate the fracture. The snap of the bone may have been heard or felt.
ApPARATUS FOR TREATMENT OF FRACTURES.
Splints and bandap"es for First Aid frequently have to be improvised.
A Splint may be improvised from a walkillO" stick u m b,rella, billiard cu.e, broom or brush handle, bpolice' man s truncheon, nfle, folded coat, piece of wood, paper firmly folded, a rolled-up map, or, In fact, anytfzing that £s firm and long enough to keep

37
the Joints immediately above and below the fractured bone at rest. 'Vhen the above appliances are not available, the upper limb, if fractured, may be tied to the trunk, and in all cases a fractured lower limb should be bandaged to its fellow.
Bandages may be improvised from handkerchiefs, belts, straps, braces, neckties, or any piece of linen, calico, string or cord that comes to hand.
Esmarch's Triangular Bandages (Fig. 8) are made by cutting a piece of linen or calico about forty inches square diagonally into two pieces.
The broad bandage is made by bringing the point down to the base (Fig. 9), and then folding into two (Fig. 10).
The narrow bandage is made by folding the broad bandage once (Fig. 11).
The medium bandage is made by bringing the point down to the base, and then folding into three. (Fig. 12). This bandage nlay be used instead of the broad or the narrow bandage when it is better suited to the proportions of the patient.
It is sometimes advisable to halve the size of the bandage by bringing the two ends together before folding it into the broad, narrow, or medium bandage.
Wher. not in use, the triangular bandage should be foided narrow; the two ends should be turned to the centre, and the bandage then folded into four, reducing it to a packet about inches by 3i inches.
FIG. 8. BANDAGE SPREAD OUT.

FI6. 12.
FIG. 10 BROAD BANDAGb:. ..
FIG. 11. NARROW BANDAGE.
THE DOTTED LINES SHOW THE FOLDS OF THE MEDIUM BANDAGE.
39
Large arm-sling (Fig. I3).-Spread out a bandage, put one end over the shoulder on the sound side, pass it round the neck so that it appears over the shoulder of the injured side, and let the other end hang down in front of the chest; carry the point behind t he elbow of the injured limb, and bend the forearm
FIG. 13. FIG. 14· over the middle of the bandage; then carry the second end up to the first and tie them; bring the point forward, and secure with two pins to the front of the bandage.
Small arm-sling (Fig. I4).-Place one end of a
40
broad band age over the shoulder on the so u nd side, pass it rou n d the nec k so t hat it appears ove r the shoulder of the injured side; place the forearm over the middle of the ba n dage ; then b ring the seco n d end up to the first, and tie them. This s]in.g is used in cases of fractured humerus, a n d occasIOnally when the large sling would be too conspicu?us.
Slings may be improvised in man y sImple ways, such

as pinning the sleeve to the clothing, turniHg up the tail of the coat, passing the hand inside the buttoned coat or waistcoat, etc.
Reef Knots ( Fig. IS) are to be used . Avoi d granny knots (Fig. 16).
GENERAL RULES TO BE OBSERVED IN THE TREATMENT OF FRACTURES.
T he object of First Aid Treatment o f Pract ures is to guard against furth er mischief, and especially to prevent a sinlple fracture from becomll1g compound or complicated. To attain this end :-
1. Attend to the fracture on the spot . No matter how crowded the thoroughfare, or how short the dis'ance to a more convenient or comfortable place, no attempt must be made to the p:Jtient until the limb has been rendered as llnmovable as po sible by splints or other restraining apparatus.
2 . Steady and support the injured limb at once, so that its further movement on the part of eit her the patient or the bystander is prevented.
3. Straighten the limb with great care , and jf shorten ina is observed in the case of a fracture of a bone of lower limb, pull up ,:m the foot until the limb regall1s a more normal length. When the shape of the limb is improved, on no account let p;o until it is secured in position by splints, otherWIse there is great da nger of tlle fracture beco:l1ing compound or complicated.
4. Apply splints (when practicable ) a n d bandages as follow." :-
(a) The splints must be firm, and long enough tG> keep the joints immediately above and
FIG. I 5 .-REEF KNOT. FIG. J6.-GRANNY KNOT.belo\V the fractured bone at rest. They should, if practicable, be padded to fit accurately to tbe limb and be applied over the clothing.
(b) The must be applied firmly, but not so tIghtly as to constrict the circulation of blood in the limb. " 'he n the patient m the recumbent position double the bandage over a splint to pass it under the trunk or lower limb. As a general rule :-
For the tru1lk the broad bandage should be used. Pass it once round the trunk and fasten it tying the ends, or with two or three safety pms on the side opposite to the fracture, but If to a splint for a broken thigh, over the splInt.
For the arm or .forearm the narrow bandage sho uld be used. Pass it twice round the limb, tie the ends over the outer splint.
For the thtglt or leg the narrow or medium may be used. It is frequently convenIe nt double the bandage at the cent re, pass It under the limb, bring the loop over the limb, pass both ends of the band· a.ge through it in opposite directions, and them over the outer splint (Fig. 17).
In applymg bandages near a fracture the upper one should be secured first.
5. When hcemorrhage accompanies a fracture it must be attended to fil st, and the wound covered by a clean d"ressing.

FIG. 17.
6: No attempt must be made to remove a patient suffering from a of the spine, pelvis, or thigh, except 1n a recumbent position, preferably upon a stretcher. . .
7. In every case of fracture 1t necessary to cover the patient to keep him w.arm, and so lessen the effects of the SHOCK of tbe aClident.
In all doubtful cases, treat as a fracture.
SPECIAL FRACTURES.
Fracture of the Cranium. ·-A fracture of the upper part is usually callS d by direct violence-for example, a blow on the head. A fracture of the is caused by indirect violence, through a fall on the
43
head, a fall on the feet or lower part of the spine, or a blow on lower jay\'. If the upper part tS fractured, are irregularity, and. frequently msensIbIhty, eIther immediate or cOlTImg on gradually. If the base z's fractured insensibility may come on immediately, blood or a clear fluid may issue from the ear channel, blood may escape from the nose, or it may pass down t? the stomach, v"hence It may be vomited; the fracture may involve the orbit, causing a blood-shot ey e.
TREATMENT.
Injury to the brain is the great danger attendFI C. 18. ing a fracture of the cranium. For treatment see "Concussion and Compression of the Brain, " pages 131, 13 2 • of the Lower Jaw. - Pain , loss of pO\yer (u:abIlIty to speak and to move the jaw freely), lrregulanty of the teeth, crepitus and bleeding from the gum are the usual signs and symptoms.

TREATl\IENT.
I.-Place thc palm of the hand below the injured bone and press it gently against the upper jaw.
2.-Apply the centre of a narrow bandage under the chin, carry one end over the head, cross the ends at the angle of the jaw, carry tbe lon g end across the chin, and ti.e the ends on the side (Fig. 18).
Fracture of the Spine.-The vertebral column may be broken either by direct or indirect violence. Falling from a hei ght on the back across a bar or upon an uneven surface is an example of direct fracture, and a fall on the head, causing a broken neck, is an example of indirect violence. \Vhat is commonly regarded as a broken back consists of a fracture of one or more of the with displacement of the fragments, whereby tbe spinal cord and the nerves issuing from it may be torn, causing complete or partial paralysis of the parts below the fracture. Pain is present at the seat of injury.
TREATl\IENT.
I.-Prevent all movement on the part of the patient.
2.-Cover tbe patient warmly.
3.-To remove the patient, place him on a stretcber or sh utter as follows :-
(a) Turn up the collar of his coat; roll up a stick or umbrella in each side of the coat
44
s<? that ,the ends are level wIth the top ot hIS pass a broad bandage or handkerchIef under the head and secure it tv the stick . If no coat is worn, or doubt as to its strength and length exists, pass a of bandages under the patient to s:rve Instead of, or in addition to, the coat.
(b) A. bearer on each side grasps the rolled coat \-nth hi. hands well apart; a third grasps the clothIng on both SIdes on a level with the hips; a fourth bearer takes charge of t1le leg"i.
(() On the word beiI:g given, .:ill lift together and carr)' the patIent by short side paces over t.he stretcher and carefully 10\\ er him on to It. If a fifth bearer is available the stretcher should. be p.assed unJer the patient IIlstead of carrymg h1111 oyer it.
4.- 0 n at sheller nothing further is to be the arrival of a doctor, except to g'l\'e the patIent \\'ater, tea, etc., if he is cOllscious Fr.actured Ribs.-The ribs usually fractured are the sIxth, eighth, and ninth, and generally the r 1,5 midway between the breast bone and tl:e sp111e . .1 he fract Lne may be caused by indirect Violence, drrnng the fractured ends of the bone out\\'ard. , or by violence, driving the fractured .ends of tbe bone 111wards and sometimes injuring the

lungs or other internal organ . . If the lo\\er .ri?s on the riaht side are broken, the lIver may be Injured, and a b fracture of the lower left ribs may wound the spleen. Evidence the fracture is afforded by pain, especially on attemptmg to take a deep breath, and by shortand shallow breathing. If the lungs are injured blood, frothy and bright red, may be coughed up and expectorated. If the liver or spleen is wounded internal hremorrhage (see page 95) may occur.
TREATMENT.
(a) TT'lzen tlzejrae/llre /s not complicated by all injury to an interllal on:all :-
I.-Apply t\\'o broad handages round the chest suffiFTC;. T9. ciently firmly to afford comfort, \\ ith the centre of the fiLt immediately above and that of the seconJ immediately below the fracture. The 10\\ er band8ge should ove 'lap the upper to half its
48 extent. The knots a re to be tied rather to the front on the opposite side of the body. Another good plan is to apply a strong to\vel. folded about eight inches wide, tightly rounc the chest, securi ng it with three or fOUl safe ty pins .
2. -Place the arm on the injured side in a large sling. (Fig. 19).
(0 ) Tf/hell all z'nternal orgau is £Iljured-
1. - Do not apply bandages round the che6t.
2.-Lay the patient down, inclined a little towards the injured side.
3·--Loosen the clothing, give ice to suck, and place an ice bag over the seat of injury. Treat as for internal hremorrhage (see page 95).
4· -Place the arm on the injured side in a large sling.
Fracture of the Breast-bone (st ernum).-
\Vhen this fracture can be felt or is suspected undo all tlght clothing, and kee p the patient quiet in an easy position until the arrival of a doctor .
FR·ACTURE OF THE BONES OF THE UP PER LIMB. of the Collar-bone (clavz'cle) .- This fracture IS frequently caused by a fall on the hand or shoulder. - The arm on the injured side is partially

4 9
helpless, and the patient usually supports it at the el bow with his hand, and inclines his head towards the injured side. The fractured ends can generally be felt to overlap, th e outer fragment being the lower. The general signs and symptoms of fracture are mostly present.
TREATMENT.
I.-Remove the coat (see page 19), and as much more of the clothing as is expedient.
2.-Place a pad about two inches thick and four inches across in the armpit.
3.-Gently bend the 10rearm \\'ell up, keeping the shoulder as far back as practicable, and support it in a " St. J oh n" sling, made as follows :-
(a) Lay an unfold ed bandage across the chest over the injured limb with one end on the uninjured shoulder and the point beyond the elbow on the injured side. (Fig. 20).
(b) Pass the lower end of the bandage under the injured limb, across the back, and tie the ends somewhat loosely in the hollow in front of the sound shoulder.
(c) Fold the point over the elbow of the inj ured limb and secure it by one or two pins (Figs. 2 1 and 22).
2T. \ fl' FTC;. (Boo), handage omitted tG s h o w details o f .' ling. )
51
4·- Tightly secure the inj ur ed limb to the siue br a broad bandage passed round the elbow and trunk, so as to le\'er out the shoulder , the pad forming the fulcrum . '
5·-No\\' tighten the sling.
'When both collar-bones are bwken keep the

shouluers back by narrol\' ba nd a:ges tied round each arm, close to the shoulder, passed across the back, oyer the opposite arm and tied together in front. The forearms should be raised and s u pported by the bandages. (Figs . 23A and 23B).
Fracture of the Shoulder-blade
( icafl( l a) . -
A pply the centre of a broad ba n dage in th e arm pit of
50
FIG
FI G 23A.
FIG. 23B.
t he injured side, cross the ends over the uninjured shoulder and tie them und er the armpit. Support the limb in a St. John sling ,Fig. 24).
Fracture of the
Arm (humerus). - The bone may be broken :-(a) Close up to the shoulder; (b) near the middle of the shaft ; (c) clos e FIG , 24· to the elbow.
All the general signs and symptoms of fracture are usuall y present.
TREATMENT.
TVlzen the Fracture z's close to the Shoulder-
I.-Apply a broad bandage with its centre abO\'e the middle of the arm round the limb and body, tying it on the opposite side.
2.--Support the forearm by a small arm sling.
IVlten tlze Fracture is mar tlze Middle of tIle Slzajt-
1.- Eend the forearm at a right angle to the arm.
2.-Apply splints, reaching from the shoulder to the el bow on the outer and inner sides of the arm, and, if enough can be procured, to the front and back also. The front splint

53
must on no account be so long as to p ress upo n the blood-vessels at the elbow joint.
3 .-.'ecure the splints by bandages above and below the fracture . If splints are no t available, secure the arm to the side by two broad bandages. FIG. 25.
4.-Stipport the f orearm by a small arm sling. (Fig. 25).
Fractures in volv ing the elbow joint, whether of the arm or forearm, are attend ed with so nlUch swelling, and it is so diffic ult to ascertain the exact nature of the injury, that wh en the accident occurs indoors the limb should be laid upon a pillow in the most comfortable position; ice or (:old wat er dr essings should be applied to the inju re d part, but no further treatmen t sho uld be att e m pt e d pending t he arrival of a doctor.
52
TT"lzeJl t h e acddent ocCltrs out of doors-
I.-Take two pieces of thin. flat woo<..1, one long enough to reach from the armpit to below the elbow, the other long enough to reach from above the elbow to tb e finger ti ps ; tie them together to form a right angle. (Fig. 26).
FIG. 26

2.-Apply the angular splint so made on the inner side of the flexed limb.
3.-Secure by bandages above and below the fracture.
4.- Support the limb by a large arm .. ling.
s.- On arrival at home remove the splint, and treat the injury as if it had occurred indoors.
Fracture of the Forearm. - \Vhen both bones (the Radius and Ulna) are broken, the general signs <lnd symptoms of fracture .?re usually present. When one of the bo n es only is broken the signs and symptoms are as a rule pain, loss of power, swelling, and irregularity. An impacted fractureof the Radius
5)
just above the wrist is a com111on result of a rall on the hand.
TREATl\lENT.
This is the same, whether the fracture is ot one bone or of both.
1.- Bend tne forearm at right angles to the arm, . I I , _--
FIG. 27. FIG. 28. keeping the thumb upwards, and the palm of the hand towards the body.
2.-Apply broad splints on the inner and outer sides from the elbo\\ s to the fingers.
3.-Apply bandages, embracing both splints, immediately above and belo\\' the fracture and round the hand (Fig. 27 ).
4.-Apply a large arm-sling.
Crushed Hand (fracture of the bones of the carpus, metacarpus, or fingers) .
TREATMENT
I .-Apply a carefully padded splint to the front 01 the hand, reaching from well above the wrist to beyond the tips of the fingers.
54
.
.; \ -
I
2.--To secure the splint apply a narrow bandage crossed in the manner of the figure 8 to the wrist and hand (Fig. 28).
3.-Apply a large arm-sling.
Fracture of the Pelvis .-'When, after a se,-ere injury in the neighbourhood of the haunch-bone, there is no sign of damage to the lower limbs, but the patient is unable to stand or even to move the low er limbs without great difficulty and pain, a fracture of the pelvis may be assumed to have occurred. The blood-vessels and organs, especially the bladder, within the pelvis are in danger of being wounded.
TREATMENT.
I.-Lay the patient in whatever position is found to give the greatest ease, and flex or straighten the lower limbs as the patient desires.
2.- Apply a broad bandage round the hips tight enough to support the parts, but not so tight as to press the broken bone further inwards.
3 . - To remove the patient place him on a stretcJler, acting on the same principle as that described und e r " Fracture of the Spine" (see page 45).
FRACTURE OF THE OF THE Lo\\ER LDIB.
Fracture of the Th igh-bone (lemur). - The th igh-bone may be broken at its neck, anywhere in th e sbaft, or close to the knee. A fracture at the
neck is likely to occur in old people from very slight injury, and is often difficult to distinguish from a severe bruise of the hip, but it may be assumed that when, after an injury near the hip joint, the patient cannot, when lying on the back, raise the heel from the ground, the bone is broken. All the general signs and symptoms of fracture are usually present and a prominent sign is the position of the foot,

FIG. 29.
which, as a rule, lies on its outer side. Shortening may vary from one-half to three inches.
TREATMENT.
I.-Steady the limb by holding the ankle and foot.
2.-Gently draw down the foot and bri n g it into line with its fellow. When two or three assistants are at hand, it is one person's duty to hold the foot in Dosition until the splints are secured .
3.-Apply a splint on the outer side from the armpit to beyond the foot.
57
S8
4.-Apply a splint on the inner side from the top of the thigh (the fork) to the knee.
s.-Secure the splints by bandages as follow,::> .( a ) Round the chest just below the armpits, (b) round the pelvis on a level with the hip joints, (c1 above t he fracture, (d) below the fracture, (e) round the leg, (/) round both ankles and feet, and tied below the feet, (g) a broad bandage round both kn ees ( Fig. 29).

FIG. 30.
vVhen single-handed, or when the patient is a woman, it is expedient, alt er extension of the lim b, to tie the feet together, dispense with the inner splint, and pass the bandages round both limbs (Fig. 30).
Fracture of the Knee-cap (patella) .-The knee-cap may be FIG. 3 I. broken by falling on the knee (direct violence), but more frequently it is broken by muscular action, as follows:-
'Vhen the foot slips in the attempt to prevent a fall the muscles in the front of the thigh act with such force as to snap the knee-cap in two (Fig. 31 ).
Pain, loss of power (the limb will be quite helpless), and irregularity (a gap may be ielt the broken fragments of bone) accompany thls lUJury.
I.-Lay the pati e nt on his back, raise \VeIl and
FIG. 32 •
support the head and shoulders, straighten and rais e the limb.
2.-Apply a splint along the back of the limb, reachinO' from the butto ck to beyond the heel.
3.-ApplY a narrow bandage with its centre imme-
59
diately above the knee-cap, cross the ends behind over the splint, and tie in front below the broken bone. fo ensure firmness apply a second bandage in a slmilar way, but commenced below and tied above the broken bone.
4.-Further secure the splint by bandages round the thigh and leg.
5.-Su pport the foot well off the ground by a pillow, roll of clothing, etc., or if none of these are at hand by resting it on its fellow (Fig. 3 2 ).
6.-Apply an ice bag or a cold water dressing over the fracture.
Fracture of the Leg (tibia and fibula).-One or both of the bones may be broken. \Vhen both bones are broken all the general signs of fracture are usually present, but when one bone only is broken deformity is not always noticeable. A fracture of the fibula three or four inches above its lower end is frequently mistaken for a sprain and sometimes for a dislocation of the ankle.
TREATMENT.
I.-Steady the limb by holding the ankle and foot.
2.-Draw the foot into its natural position, and do not let go until the splints have been fixed.
3.- Apply splints on the outer and inner sides of the leg, reaching from above the knee to beyond the
6r
foot. If only one splint is available place it on the outer side.
4.-Secure the splints by bandages (a) above, (b) below the fracture, (c) immediately above the knee,

FIG. 33. .'''-=-'''''....
FIG. 34.
d) round both ankles, (e) a broad bandage round both knees (Fig. 33).
When single-handed, or when the patient is a
60
D
62
woman, after extending the limb tie both feet together, dispense with the inner splint, and pass the bandages round both limbs (Fig. 34). 'W hen no splint is available tying the legs, ankles, and knees together is of great service.
Crushed Foot (fracture of the tarsus, metatarsus and toes).-This accident is commonly caused by the passage of a heavy weight over the foot, and may be recognised by pain, swelling, and loss of power.
TREAnrENT.
I.-Remove the boot (see page 19).
'2.-Apply a wellpadded splint to the sole of the foot, reachingfrom the heel to the toes,
3·-Apply a bandage FIG. 35· crossed after the manner of the figure 8 (Fig. 35).
4·-Su pport the foot in a slightly raised position.
DISLOCATIONS.
A dislocation is the displacement of one or more of the bones at a joint.
The joints most frequently dislocat ed are those of the shoulder, elbow, thumb, fingers, and lower jaw.

SIGNS AND Sv IPTOMS OF DISLOCATION.
1.- Pain of a severe sickening character at or near the joint.
2. - Loss of power in the limb.
3.- Numbness of the parts below the seat of dislocation.
4.-Swelling about and below joint.
5. - Fixity of the joint.-The, 11mb cannot be moved at the joint by either the patIent or others.
6.-Deformity of the limb.-The limb an unnatural position, and is mis-shapen at the JOll1t.
TREATMENT.
No attempt should be made by anyone except a doctor to reduce a dislocation. Pending his arrival :-
(a) T17hen the accz'dent occu'!'s out oj . Support the limb ll1 whatever pOSItIOn gIves most ease to the patient, bearing in mind the necessity of lessening the effects of jolting dtlring transport.
(b) f¥hen the patiellt is i7tdoors-
I.-Remove the clothing from the limb.
2.-Place the patient on a couch or bed.
3.-Rest the limb on pillows in the most fortable position.
4.-Apply cold (ice or cold water) dressings to the joint.
5.-When cold ceases to give comfort apply
warmth (flannels or towels wrung out of hot ater).
6.- Treat shock (see page 135)'
SPRAINS.
'Vhen, by a sudden wrench or twist, the ligaments and the parts around a joint are stretched and torn the is said to be sprained. " Going over" the ankle IS a common example.
SIGNS AND SYMPTOMS.
1.- Pain at the joint after a twist or wrench.
2.-Inability to use the joint.
3.-Swelling and discoloration.
TREATMENT OF SPRAINED ANKLE.
When out of doors-
I.-Apply a bandage tightly over the boot, beginning on the sole at the instep, crossing on the front of the ankle, and carrying It round and round the ankle, where it is to be firmly tied.
2.- vVet the bandage after applic?tion; it is thereby tightened.
Aftc:r reaching she/ter-
I.-Remove the boot and stocking (see page 19)
2.-Place the limb in the most comfortable position; usually that is well raised.
3.-Apply ice or cold water dressings to the joint as long as they relieve pain.
-f'- When cold fails to give comfort, apply hot fomentations.
"Then other joints are sprained, treat them as if dislocated.
When in doubt as to the nature of the injury, treat as a fracture.
STRAIi'TS
AND RUPTURED MUSe LE ' .
When, during severe exertion, muscles or tendons are over-stretched they are said to be strained, if they are actually torn they are described as ruptured.
SIGNS
A:-\D SY.YIProMS.
I.-A sudden sharp pain.
2. - When the muscles of a limb are strained they may swell and cause severe cramp.
3.- Further exertion is difficult or impossible; for example, if the strain has occurred in the back the patient may be unable to stand upright.
T1tEATME TT.
I.-Place the patient in the most comfortable position, and afford suppon to the injured part.
2.-Apply hot .vater bottles or hot fomentations when the pain is very severe .
A so-called strain in the groin (hernia) is an injury of a totally different nature (see page 114)'
64
65
D
QUESTIONS ON C HAPTER II.
What skeleton, and what purposes are served by ll, .. ,
How are th; bones of the skull Jed'?'
Wh3t ,are the boundal ies of the ?
Descllbe the bones uf ttlt face
Descri,be the lower jaw '" '" '"
\Vhat IS the anglt of the jaw?
What other names has the ?
What is a vene bra? '
How many in tiJ'e
What are the regions or t11e spine how " vertt: br;:e are there in each?
I I ow the ,spine endowed with' ?"
What 15 a 1'1 b ? ,,' '
Ilow many fJairs of ribs are"t'here;"
Wha ' is the breast,bone ? '
What .are the bones of the i;;nb,,?
What the pelvis? '" ... ..'
What IS the hip joint? '"
What are the bones uf the lower liml),> ? ' "
What is a joint? '" '" a moveable joint ,,' the shoulder joint
DeSCrIbe the ankle joint .. , flow are muscles classifi"d ? mu. cIes
Descnbe Invo'untary muscles
What is a fracture? .. , '"
\\' hat are the causes of fraGture ?

Where does a bone break when direct violence is the
cause of fracture? " ,"
\\There cloes a bone break when indirect violence is the
cause of fracture? ", ",
How maya fracture be caused by muscular action?
In what two ways may fractures be classified? "
\Vhat is a si mple fracture?" ,
\Vhat is a compound fracture?
Wh8.t is a complicated fracture?
\Vhat is a comminuted fracture?
\Vhat
the general signs and symptoms t hat
\Vhat fractures afforclthe most complete example of the signs and symptoms? '" .. ..' .. ' .. ,
In making up your 111i nd whether a fractur,e had e cc,urred or not, what points should you take 1I1to conslde,ation beyond the signs and ,ymptoms? .. , .. ' 35
\Vhat apparatus may be necessar} for the treatment of fractures?
lIow may splints be impro\'ised ? ", .. , 36 , 37
How may bandages be impro\'isecl? .. :)7
Describe Esmarch's tri::tngular bandage .. , 37: 38 (FIg, 8)
In what ways may the triangular handage be folded fur use? 37
lIow many kinds of arm-slings are there, and ""hat are they called?.. . ... ..' .. , .. , 39, 4 C : 49
\\' hat knot is to be tied, and what knot avoided? 4 0
What is the object of first aid treatment of fractures? 41
Give the (Teneral rules for the I reatment of fractures .. , 41
lIow sho;;lcl splints be applied? ... 41, 42
How should bandage be appliecl ? .. , 42, 43
What may cause a fraclnre of the upper part of the claniul11 ? 43
06
TJu nume
p a;;e s wh e r" f lu an.l we/'I
found.
r als ", aun t' fhe
Tn"'),
l'AGE 22 22 22
.. , '"
22, 23 23 23 23 23 25
many
25 25 26 26 26
26 to 28 28 30 30 :n 3 1 3 2 3 2 32 33 33 33 '" 3";, 34 PAGB:
33
34 34
green-stick fracture? \Vhat is an impactcrl fracture? .. , 34, 35 34 34 34 35 35 35 State
may be present
of fracture
." 35. 36
is a
in a case
", .. ,
3 6
'\That may c9.use a fracture of the base of the 43, 44
\\'hat are the signs of frac t ure of the upper part of [hI:! cranium?
\Vhat are the signs of fracture of the base of [he cranium?
\Vhat is the treatment for fracture of the cranium?
\V hat are the signs cf frac t ure of the lower jaw?
II ow maya fractured pine he caused?
" That is commonly regarded as a broken back? . ..
\VI- at are the symptoms of a fractured spine?
How may ri bs be fractured?
IIow maya fracture of ribs be complicated?
State the signs and symptoms of a sirnple and of a complicated fracture of ribs
\Vh at i-s a frequent cause of fractured collar-b one? ...
\Vh at are the signs and symptoms of fractur e d c olla: -
bone? .. 48, 49
At what points may the bone of the arm be broken? 52
Are the gene ral signs and symptom:> of a fracture al \\'ay s present in a broken forearm? ...
State the cause of a common fracture of the radius
IIow would you recognise a f::3.cture of the pelvi s?
At what points may the thigh-bone be broken? ...
\Yhat are the !;igns and symptoms of fracture uf [he
thigh-bone?
\Yhat are the causes of fracture of the knee-cap? ... 58, 59
\Vhat are the signs and symptoms of fracture of the kneecap?
Are the general signs and symptoms always present in a fracture of the leg?
What mistake may easily be made when th e fibula is broken near its lower end?
What is a dislocation?
.btate the signs and SY:l'pt0111.,; of

First Aid Students should pl'.lctise improvising mat erial, foldi ng bandages, tying kno.ls, slings, and the treatment of the followll1g lI1Jnnes.
bandages
Folding bandages
Large arm sling
Knot for applying splint lo lower lin;b
Fract ures-Lower jaw. 44. Spme, 45. 46 . Ribs (si,nple and complicated fractures). 46 to 48. Breastbone, 48. Collar· bone, 48 to 51. Both collarbones, 5 (, Ann, close up to shoulder, 52. Arm, near middle of shaft, 52. Arm or forearm when the elbow is involved, 53. Forearm,55· Crushed ha?d, 5:,5 6 . Pelvis, 56. (man), 57, 58. (wo:11an, o r man when Sll1gle-handed), 58. Kneecap, 59, 60. Leg (man), 60, 61. Leg (woman, or man when single-banded), Crushed foot , 62 .
Dil ocat ions-Out of doors and l11do or .. , 63, 64
ankle
PAG:d:
44 44 -t4 45 -+5
54 5') 56 57
57
d;slocali
59 60 60 62 PAGE State the treatment of dislocation... 63 Wha t is 3. sprain?... ... .., ... 6 + \\,h:lt are the signs and symptoms of a sprain? 6-+ S ' ate the treatment of a sp rained ankle .. , 6+ Slate the treatment of other sprains ... ... . .. 63, 65 \Vh en not sure whether th e injury is a sprain o r fracture huw would you treal it? .. , ... 65 HoI\' may muscl es be strained or ruptured? 65 Stale the 5icins and of s' rams .. , 65 Stat e the treatment of S"ralnS .. . .., 65
')J1
Il1lpro
splints .. , Improvising
ising
Small
sling r Reef and granny knots ., . .: . ... 36 37 37 37 39 ... 39, 40 40 42
arm
Sprained
... ...
Slrai IS
6-4-
and ruplured 65
CHAPTER III .
TH E O RGANS OF C I RCULAT I ON.
THE organs concerned in the circulation of the blood are the Heart, the Arteries, the Veins, and the Capillari es.
The Heart is situated in the chest behind the breast-bone and rib cartilages, between the lungs and im.neliate1y ab:)ve the diaphr.13m; it lies obliquely \\'Ith a quarter of its bulk to the right and the remaining three-quarters to the left of the ll,iddle line of the body. Its beat may be felt just below and to the inner s ide of the left n·Pi)le. The heart has four cJ.vities, t \\ O on either side of a central partilion. The two upper cavities are named the right and left auricl ( s , the two lower the right and left ventricles.
Arteries nre vessels \\'hich convey blood from the heart. Veins carry blood to the heart. Capillaries connect the arteries and veins.
In the general (syst emic) circulation arlerial blood is driven from the left ventricle of the heart into the aorta (the main artery of the body). From the aorta branch arteries are given off to all p ,rts of the body. These divide and sub-divide, and become so small as to assume microscopic dimensions, when they are termed cGtpillaries.
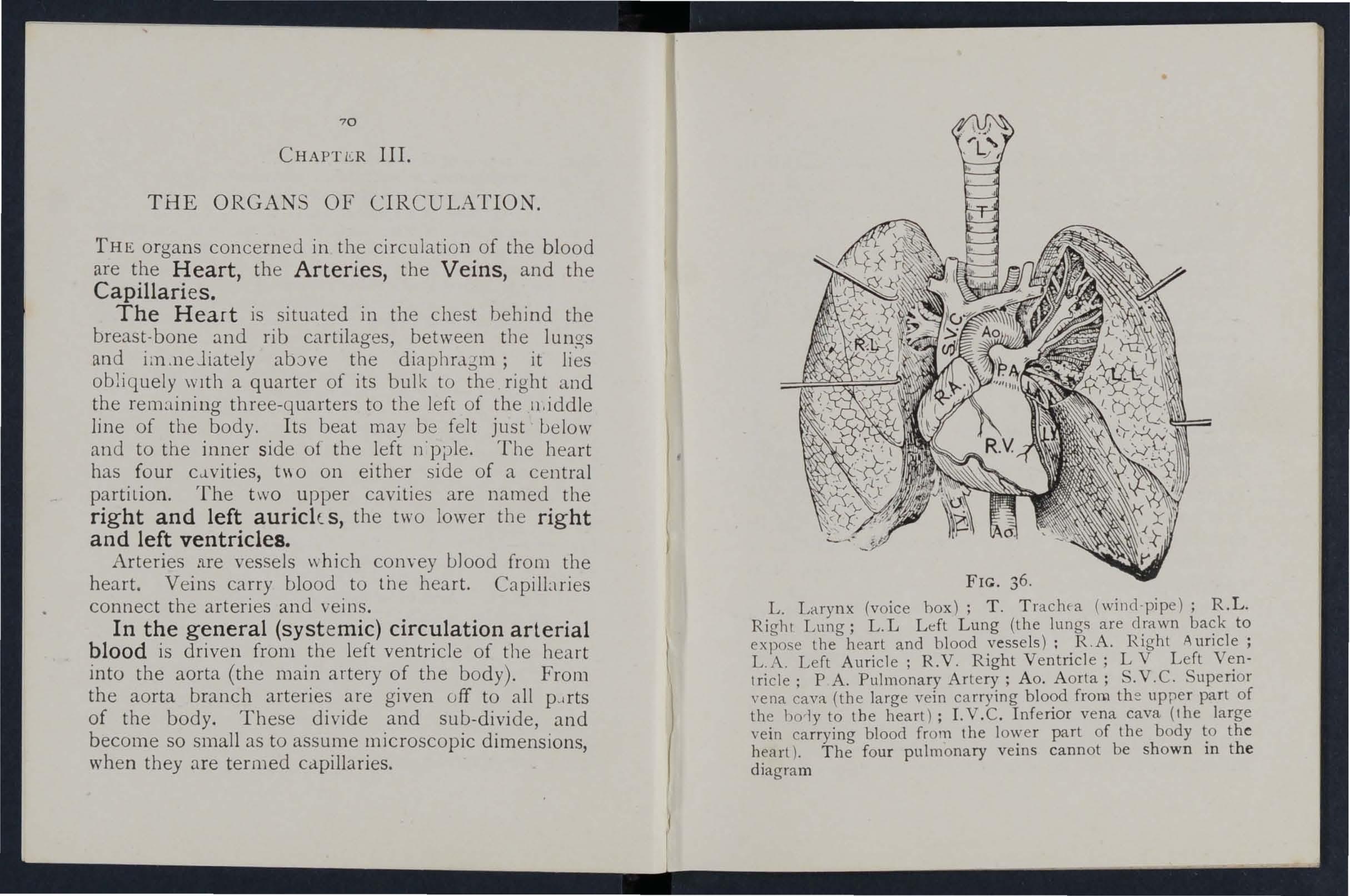
IL. Larynx (voice hox); T. Trachfa (wind-pipe); R.L. Right Lung; L.L Left Lung (the lungs are drawn back to expose lhe heart and blood vessels): R .A. H.ight Auricle; L.A. Left Auricle; R.V. Right Ventricle; L V Left Vent ric1e; P A. Pulmonary Artery; Ao . Aorta; S. V. C. Superior Yena cava (the large vein carrying blood fron.1 th e upper part of the bo 'lyto the heart); LV.C. Inferior vena cava (the large vein carryina blood from the lower part of the body to the heart). Th; four pulmonary veins cannot be shown in the diagram
In the capillaries an interchange of gases and fluids takes place, whereby the nourishment and maintenlnce of the tissues and organs of the body are provided fur, and the blood becomes dark and impure.
blood pass es fr0111 the capillaries to the vems, whIch convey it to\yards the heart, getting larger. and they. proceed by being joined by nelghbounng vellls untIl they finally, as two large vessels, reach the right auricle of the heart. The veins, especially in the limbs, are provided with vah'es at frequent intervals, which prevent the backward flow of the blood.
The pulmonary system of blood vessels is concerned i.n the blood through the lungs. From. the auncle the blood pass .: s to the right ventncle, and IS thence carr:ed to the lunO's where it is purifled by contact with air, and scarlet in colour; it is then c ,)lwey ed to the left auricle of the heart anJ pa sse s into the left ventricle, th us completing the circulation.
The he::1.rt contracts in adults at an average rate of seventy-two times a minute, but the rate varies as the position is changed from the lying to the slttmg or to the standing position; hence the importance of adjusting the patient's position in C::lSCS of heemorrhage. At every contraction of the lpft ventricle is forced into the Clrteries, causing the pulse. which may be felt where\'er the finger C-l.n be

Explallatioll. In the middle of the diagram is the heart with '> its four chambers. .A bove the heart is shown the lung (pu lmonary) circulation. The lower part represents the general (systemic) circulation. Vessels containing impure (venous) blood are shown black, while those
contain ing pure (arterial) blood are shown white. The connecting vessels represent the ca:)i.laries. The arrows show jirection of the flow of blood.
FIG. 37·
DIAGRAM THE CIRCULATION OF THE BLOOD.
placed on an artery as it passes over a bone. In the veins no pulse is to be found.
B£MORRlfAGE.
Hremorrhage, or bleeding, is of three kinds :1. Arterial. 2. Venous. 3. Capillary.
72
73
ARTERIAL
I. - BLod from an artery is scarlet.
2. - If the wcunded artery is near th e skin the blood spurts out in jets co rres ponding t v tne puisation of the h eart.
3 - The pressure point (se e below) is on the he.lrt side of the wound.
ARREST OF ..:\RTERfAL
Arteria l h<:em orrhag e is, wh en practicabl e, to be arrested by pressure, positi on of the bo d y, a nd e levation of the bleeding part.
- Pressure may be :-
I. - Digital - that is, applied with the thumb or fingers, and may be (a) on the wound; (b) at a sput call ;: d th e press ur e po int. The pressure po ints are indicat e d uy nUll1 be red dots on the frontispi ece.
2. -- Bya pad and bandage (t o urniqu e t) (a ) o n the wound; (b) on th e press ur e p o int.
3·'- By flexion.
To apply a pad and bandage to the woun d, place a piece of lint or lin e n or a clean h a nd ke rc h ief fo lJed into a hard pad, on the bleeding point, a n d secure it bv a b:;lIldage ti g htly tied round the injured part. To fold the handkerchi e f, bri ng the four corners to the centre, a nd repeat th e pro cess u nti l a hard pad tS formed . The smooth surfa ce is

75
place i on the woun], and, to prevent the pad from unfolding, the pu ck e red surface may be stitched or fix by a s1.fety pin. A h3.rd substance, such as a may b e encl osed in cen tre of the pad.
A T01J :- niquet may consIst of a pai to be placed on th e p p oint, a strap, or. bandag tJ to encir cle the limb and p1.d, and a tlglztmzng . a:rangement, s uch as a s tick or other means of tWIstIng the band to tighten it. .
To im'Jrovise an::l apply a tourmquet.:-
I.-A.ppl y a firm p1.d oa the pressure pOInt. .
2. -Encircle lim ') by a n::trrow bandage wIth its centre over the PJd.
3. - Tie the ends of the bandage in a half knot on the opposite side to the pad.
4 . - Lay the twisting stick on the half knot, and over it tie a reef knot.
5. -Twist the stick to tighten the bandage, thereby pressing the pad upon the artery, and arrestin cr the flow of blood.
6. -Lock the stic k in position by the ends Of the banda cre alre tdy applied, or by ano th er ban dage r ou nd t he stick a n d lim b. Th e pad of the t o urnique t must be ac:urately p\::i ce d u pon the pressure so com pi to com press the ; otherWis e arterIal \\'111 _ be allowed to pass a lon g the .limb, an.d the ve1l1S, be l11g c o mpressed by the tournIquet, will not allow t h e
i 6 blood to return through lhem to the heart, the resu l t will be dangerous swelling and congesflUn
Should a s ui table pad not be at hand, a knot I11JY be made in t he cent re of the bandage, and \\ llen avai lable, a stone, cork, etc, enclosed in it to give it firmness ani bulk . See that the bulging and not the fLtt side of the knot is ne'\t the skin .
An elastic bandage tightly round Lhe limb, im.l1ediately abO\'e the seat of arterial hcernorr hage, will arrest b leeding. The simplest prepared for m of this bandlge is a strip of elastic \\'ebbing, t wenty-five to thirty inches long and tIro wide, with a piece of tape se,,'n at each end. .An elastic belt or brace wi ll serve the same purpose, E'\ce)Jt when part of a l imb is torn off, it is not to use an elastic cord or bandage if other apparatus can be had, as it Guts off aU c'rculation in the lilT.b, Flexion co nsists of the application of a pad on the pressure point at the knee or elbo\\' joint, flexing the limb to make pressure, and se uring the limb in the position by a bandage crossed like the figure 8.
GE, ERAL RULES FvR TREADIENT OF A 'VOU:\D ACCO:\IPANIED BY A I-!'l'ERIAL HJE:\IORRHACE,
1. Stop bleeding .
II. Prevent injurious germs from getting into the wound .

77
To atlain these ends: -
1. Place the patient in a suitable position, bearing ill mind that the blood escapes with less force when the patient sits, and is still more checked when he lies down.
2 . lilevate the bleeding part, as thereby less blood finds its \\'ay into it.
3. Expose the wound , removing whatever clothing is necessary , (See Rule 8, a.)
4. Apply digital pressure. (a) If the wound is small on the bleeding spot, (b) If the wound is large on the pressure point next to the \r ound on the heart side. The nearest pressure point is chosen in o :'der to avoid cutting off the circulation from as much of the part as possible, but sometimes it is necesslry to apply pressure still nearer to the hearl.
S. Remmre foreign bodies, such as broken gl as.)) bits of clothing, hair, e tc, seen in the wound; Lie, not search for foreig n bodies you cannot see.
6. Cover the wound with a clean and firm absorbent dressing. A hard dry pad of boraci c gaule or lint is to be preferred, but absorbent cotton wool, lint, o r gl u ze, or a clean piece of linfn will al:swer the Should any doubt be entertallleJ as to the cleanliness of the dressing, a clean piece of unprinted p:lper, such as the inside of an
envelope, should be placed next the w,- und before applying the pad. (Compare pages 75 and 76 .)
7. Bandage tightly over the pad unless :-
(a) Foreign bodies are suspected to be left unseen in the wound.
(II) There is danger of causing injury to a fra lure. In these cas es a light dressing only shoull be applied.
8. Apply a pad and bandage or flex :o n on the pressure point ,se e Rule 4, b ), but o n1,/ in t he following cases :-
(a) As a temporary measure while the wo unJ is being exposed, examined and covered.
(b) As a more permanent measure \\ hen uleeding CJ.nnot be stopped by the lXld and bandage on the wound, or when, in accordance with Rule 7, the tight bandage has not been applied.
9. Afford support to the injured part . vVhen part of a limb has been torn off or the \, uund is lacerated (for example by the claw of an anillJ:J.l or by machinery) hremorrhage frequently does not come on at once, but as there is a danger of severe hremorrhage later, means for its arrest should be applied to the limb, but not tightened unleSS
Do not disturb a clot of blood formed OVLr a wound. No attempt should be mace to cleanse a wound except with sterilised \\ ater (that is previously boiled

79 and allowed to coo!), and experience, especially in recent wars, has shown that those wounds which were provisionally tre1ted with a dry dressing and subdresse'i by a surgeon with proper appliances dId hest.
Students p7"actising arrest of arterial hremorrhage should feel the pulse to -see when the current of blood the artery has been stopped, and should then Imm e.diate ly rel.ax th e press ure made on the artery. In thIS way th.e Ilnp o rta.nce () f the accurate application of pressure wIll be realIsed, and the amount of force necessary will be ascertained.
TH1<: COURSF: OF THE MAIN ARTKRlES, AND THE ARRE ST OF H.IE:'IIORRHAGE.
(T ;)e numbers of the pr essure points refer lo those on the Frontispiece.)
THE LARGE ARTER1F.S \V , THIN THE CHE T AND ABDOMEN.
The Aorta is the central or trunk artery of the b ody . Commencing at the lett ventricle it forms an arch behind the upper part of th e breast-bone. the arch are given off the large branches W lC 1 carry the bl ood to either side of the head and neck and to the upper limbs. The Aorta passes down on the left of the spine to just below the navel wher e it divides into two great branches (th ':' iliacs)
which convey the blood to tbe organs 111 the pelvis and to the lower limbs.
'Wounds of these arteries are one cause of internal hcemorrbage (see page 96).
ARTERIES OF THE HEAD AND NFCK.
The Ca rotid Arteries (right and left) leave the upper part of the chest amI pass up on either side of the \\'indpipe and: just below the level of tl1e ancrle of the lower jaw, divide into the Internal and E\ternal Carotid Arteries. The Internal Carotid Art ery. ascends deeply ll1 the neck, and enters the cranium to supply the brain with blood. The External Carotid Art ery gives off a number of brancbes; to the front the artery of the tongue (Lingual), the artery to the face (Facial); to the back the Occipital; the arte r y itself is continued upwards in front of the ear it changes its name to the Temporal, and su pphes scalp in the of the temples .
When a Carotid Artery is wounded , 8S in the case of a cut throat, apply t he thumb of one hand on the .artery at pressure point I, pressing backwards 8gamst the and takin a care to avoid the windpipe. It may alsa be to apply p r essure \\itb the otber thumb above the \\ound for two reasons : (a) To arrest the flo\\' of b lood fro 11 the main (jugular) vein in t:1e neck, runs
81
alongside of the carotid artery and is usually wounded at the same time; (b) To check the flow of blood from the upper end of the carotid artery itself, which is often considerahle owing to communication betlyeen the br':1I1ches of this artery and those of its

FIG. 38. FIG. 39·
fellow. Digital pressure must be maintaineci, hy relays of assistants if necessary, until tbe arrives (Fig. 38).
T he Facial Artery crOSSeS the lower j:l\\, in a slight hol!olv t\\"o in front of the anJ senJs branches to tlle chin, li: s, and
80
outsid e of the nose. Hcemorrhage from wounds of the face below the level of the eye is to be arrested by :-
(a) Digital pressure on pressure point 2 (Fi g . 39) , or
(b) Grasping the lips or cheek on both sides of the wound by the finger in si de and the thumb outSide the mouth or v/c versa.

. The Temp ::; ral Artery may be felt pulsat ing ]11 front of upper part of the ear. Hcemorrhage from the of the temple may be arrested by pressure at pressure point 3 (Fig. 40).
The OccIpital Artery sllpplips branches to the
region of the scalp from behind the ear to the of the head. Hcemorrhage from this rtgion may be arrested by digital pressure on pressure point 4, Lur fingers' breadth behind the ear (Fig. 41). This point is difficult to find, and it is usually sufficient to ap?l y pressure immediately below the \yound.
Hcemorrhage f. om the Forehead or anywhere in the Scalp may be arrested by applying a sma ll firm pad on the bleeding point and securing it by a narrow bandage with its centre laid on the pad, the ends carried round the head in the direction most convenient, and tied tightly over the pad (Fig. 42).
\Vhen ,a \\'ound of the forehead or scalp is associa ted with a fracture, the best plan is to apply a ring pad around the seat of injury. To make a ring pad, pass one end of a narrow bandage round your finge:s; pass the other end of the bandage th rough the rlllg thus formed and continue to pass it through and through until the whole of the bandage is used and a ring as shown in Fig. 43 is formed.
FIG. 42.
82
ARTERIES OF THE UPPER
The Subclavian Art _ry passes from a point behind the inner L:n :::l of the col'ar-bone across the first rib to the armpit.

FIG. 43· FIG. 44 .
To apply digital pressure :-
J
.-Bare the neck and upper part of the chest.
2.-Place the patient's arm against the body so as to depress the shoulder, and cause him to inclIne his head towards the injured side.
3·- Take your stand opposite the shoulder.
4·-Using the left hand for the right artery, and vice versa, grasp the neck low down, placing the fingers behind the shoulder and the thumb immediately above the centre of the collar-bone ]n the hollow between the 111 uscles attached to the bone (pres sure point 5)'
5·- Press the t1mmb deeply do\\ nwar ds and bacb\ ards agaillst the first rib, which is beneath the olla r bone at this spot (Fig. 4 4).
The Axillary Artery , which is a contilJuation of the subclavian, keeps close to the shoulder jo ' nt, and can be felt lJU Isating when the fingers are deeply pressed into tee armpit. Digital pressure is difficult to apply to this artery.
To apply a pad and bJ.ndage: -
J
.·-Place a hard p::td the size of a billiard ball in the armpit (pressLlie point 6).
2. - Apply the centre of a n :. rw\\' banu age on tb e pad; era s the FiG. 45. b::tn lage on tbe ulder; p1l1 tile ends tight :l nd tie them under the opposite armpit, taking (are that the pad uues llot slip .
3. Flex the forearm alld tie the limb tightly to the trunk with a broad bandnge, a[plied on a leve l with t: .e llbow (Fig. 45).
The Brachial Artery is a con tin uation of the Axillary, and runs down the arm on the inner side of the biceps muscle, gradually passing forward until it reaches the middle of the front of the elbow. The of the coat sleeve above the elbow roughly mdlcates Its course.
Digital or instrurr:tental pressure m3Y be applied at or near pressure POInt 7.

FIG. 47.
To apply digital pressure extend the limb at right angles to the body, palm of the hand upwards. Stand behind the lim b, and pass the fingers under the back
87
of the arm over the seam of the coat or the grouve on the ins.ide of the biceps muscle. Press the pulps (not the tips) on the artery (Fig. 46). Some prefer to pass the hand over the front of the muscle (Fig. 47) A slight turn of the hand out\\'ards as it grasps the arm will better ensure compression of the artery.
The Brachial artery may be compressed at the
FIG. 49.
FIG. elbow (pressure point 8) by flexion. The pad may be a folded handkel chief with a small stone or a cork wrapped up in it, but when no pad is the coot sleeve rolled or gathered up \\ ill serve instead (Fig. 48).
86
Just below the elbow the Br.achial .artery divides into the Radial and Ulnar arterIes, whIch run along the front of the forearm on the outer and inner sides respectively. The pressure points (9 and 10) are about one inch above the wrist and about half an inch from the outer and inner sides of the forearm, where the arteries may be felt pulsating. of these arteries join to form the Palmar 111 the hand. The arteries run along on f"ther sIde of the fingers to tr.e tip.
may b e applied to the Radial and Ulnar arteries at pressure points 9 and 10, by the thumbs (Fig. 49) or as folloy\ s :- . .
I. - Cut the cork of a quart or pmt bottle 111 two lengthwise.
2.-Lay the rounded side of one half on the Radial, and of the other half on the Ulnar artery.
3. - Secure them by a tight bandage.
To arrest hremorrhage from the palm of the hand: -
I.-Apply a firm pad, and make the patient grasp it firmly.
2.-Spread out a triangular bandage, I urn up the base about four inches, lay the back of the patient's hand on the centre of the bandage, fold the point over the knuckles and \-vrist r pass the two ends round the wrist, make the

patient pull on the point of the the ends over the fingers twice and tIe them as firmly as possibl e. Bring the point (A) down to the knuckles and fasten with a pin at B (Fig. 50).
3·-Elevate the forearm and support it \\'ith a "St. John" sling (see page 49).
Arterial hremorrhage from the fingers may be arrested hy :lpplying a small pad on the wound, and securing it firmly with a st rip of tape, linen or p1::\sl er. j \ RT E R II S 0 F THE Lo ' E R Ln! BS.
The Femoral Artery, a cont inuation of the iliac, l- Iv. su. enters the thigh in th= centre of the fold of the groin, where it may be felt pulsating il1lmediJlely below the skin. The course of the artery may re indicated by a line drawn from the centre of the groin to the inner side of the back part of the knee. Arter traversing two-thirds of this line, the femoral artery passes behind the thigh bone to the back of the knee joint as the Popliteal artery.
Digital pressure may be applied to the Femoral artery at the groin (pressure point I I ) as follows :I. -Lay the patient o n hi. back.
88
go
2. -Kneel beside the patient.
3.-To find the groin, raise the foot high so as to fl ex the thigh; the fold in the clothing at the top of the thigh will indicate the groin
4. -Pb.ce the thumbs one on the other upon the pressure point, grasping the thigh with the hands (Fig. 51).
t:; . - Press firmly agai n st the brim of the pelvis.
As there is immediate da nger of death it is important not to waste time I n removing the trousers.
Wh e n the Femoral artery 's wounded in the upper :lird of its course, pressure IIlUSt be maintained at the groin. No really sJtisfac o tory tourniquet has been FIG 51. de vised for compression at this point, and relays of assi c oLlts should be employed to keep up the pressure until the d octor arrives; each fresh assistant places his thumbs over those of his predecessor, who slips his away from beneath, and thus gushes of blood are prevented dur ing the change.
Application of a tourniquet to the Femoral artery (pre o;sure point 12) :W hen practising comp ressi on of this artery, it is a

52.
9t
IIG.
gOJd plan to dral\' a chalk line fr0111 the ce n tre of the groin to the in ne r side of the back of the knee; place the pad of the to u rniquet on this line as high u p as the ba n dage can be applied, The pad should be the size of a la\\'n tennis ball (Fig. 52).
Pressure may be applied to the Popliteal artery by flexion at the knee (pressure point 13 ) ; the pad

FIC · 53,
should be the size of a law n te n nis ba ll , or if n o pad is available t h e t r o u ser leg 111ay be roll ed or gathered u p to serve in s tead . I t is n ot n ecessa l y to t ake off the clothi ng ( F ig. 5 3).
Just below and b eh in d t h e k n ee jo in t t he P opliteal artery divides in to the Anterior (fro n t) a n d Posterior (back) Tibial arte r ies .
The Posterior Tibial Artery p asses dow n the
93
back of t h e leg to the inn ::- r side o f the ankle . .It is .1t fir,s t deep ly placed bet\\'een the 111 uscles <.. f the calf, It approaches the surface as it proceeds, '0 that I,t can b,e felt pulsating behind the large bone at the lO ner SIde of the ank le. I t enters t he sole as the Plantar Arteries, which run fonrard amongst the I1iUS Ie;; to supply the foot and toes.
Anterior Tibial Arter y, on leaving the rO,)lite11, at once passes forward between the leg hones, and, deeply placed al110ngst the lllLlscles, runs do\\'n the leg to the centre of the front of the ankle. This artery is continued as the Dorsal Artery of the Foot, which, passing forward oyer the L1rsLls, dips down to the sole between the first and se cond metata rsal bones . Here it fJrms \\'jth the Plantar arteries what is kno\\' n as the Plantar Arch . At the (pressure p8ints 14 and J 5) pressure may be applted by the fing e rs or by pClds and bandages.
VE:\,OUS
I. - Blood f om a vein is dark red ,
2. - It flows in a slow continuous stre am 3·-It issues from the side of the w o un'd further ftom the heart. the case of a wound of a va ricose v e m It tlJw.s also from the side of the wound nearer to the heart, especially if the p Hient is kept sL1I1ding.
92
Varicose Veins.-The veins of the leg are specially apt to become .varicose.. A va:icose vein is dJiated, winding, and with bead-lIke (vancose). projections along its course. A vein becomes vancose from several causes, such as long standing or tight garters. The first effect is to throw extra work upon the valves and the bead-like projections are caused by the blo'od accumulating in the pockets behind the valves. In time the vein becomes so dIlated that the valves can no longer span it.
GENERAL RULES FOR TREATMENT OF A WOUND ACCOMPANIED BY VENOUS HlEMORRHAGR.
I -Place the patient in a suitable position, bearing in mind that the blood escapes with less forl'e when the patient sits and is still more checked as he lies down.
2. - Elevate the part, as thereby Ie ss blood finds its way into it.
3. -Expose the wound, removin g whatever clothi::g is necessary,
4. - Remove any constrictions, such as the collar or garters, from the heart side of the wound.
S. - Apply digital pressure on the woun d until you can apply a pad and tight bandage. If that doe s not stop the bleeding, make pressure near the wound on the side away from the heart. In the case of a wound. of a varicose vein it may also be necessary to

apply a pad and bandage to the vein immediately above the wound, especially if the limb cannot be maintained in an elevated position.
6.-Treat the wound as directed by Rules 5,6 and 7, stated on pages 77 and 78.
7. - Afford support to the injured part.
CAPILLARY HlE:\WRRHAGE.
1.- The blood is red.
2.-It flows briskly in a continuous strea:::, or may merely ooze from the wound .
3.-It wells up fr all parts of the wOWld. A slight amount of pressure will suffice to arrest capillary hremorrhage.
INTERNAL HlEMORRHAGE.
,\Vounus of the blood vessels within the trunk cause hremorrhage into the cavity of the chest or of the abdomen.
AND SYlI1PTOnIS OF HJE:\lORRH.-\GE.
I.-Rapid loss of strength, giduiness anu especially wh e n the upright position is assumed.
2.--- Pallor of the face and lips.
3. - - Breathing hurried ami boour ed, anu accompanied by yawning anu sighing.
4-- The pulse fails, alld may altogether disappear at the wrist.
94
95
s. -The patienL throws his arms tugs at the clothing round the neck , and calls for aIr.
6.-Finally the patient may become totally unconscious.
TREATMENT
.
I.-Keep the patient in a recumbent position.
2.- Undo all tiaht clothing about the neck.
3. -Provide fo; free circulation of air; fan the patient. ' .
4. - Sprinkle cold ",at.er on the face; smellIng salts to the nostrils; a vOId other forms of stlln ulants, at all events until the hremorrhage has been c.ontro!led.
S.-.Give ice to suck or.cold water to drInk;. If the seat of the hremJrrhage IS kno\\'l1, apply an Ice bag over the region.
6.-Should the patient be reduced to. a state of collaps€, raise the feet an? band8ge the lImbs fro n the toes to the hIps and from the fingels to the
• FRO:.\I THE NOSE (Nos I R'ILS).
I.-Place the patient in a .sitting in a current of air before an Op 211 wmdo\\', .wIth the head thrown slightly back and tbe hands raised above the head.
2.- Undo all tight clothing around the neck and chest.
3.- A pply cold (ice, a cold sponge or bunch of

keys) over the nose and also the spine at the level of the collar; place the feet in hot water.
4.-Cause the patient to keep the mouth open, and so avoid breathing through the nose.
Bl ood is s uing from t he mou th may come from the tongue, the gums, the socket of a tooth after extraction, the throat, the lungs, or the stomach.
HlE:'lORRHAGE FR0J\I THE TO.1\GUE, THE GUM, THE SOCKET OF A rrom:H, OR THE THROAT.
1.- Give ice to suck or cold water to bold in the mouth. If this is not successful give water as hot as can be borne to hold in the mouth.
2.-If necessary make pressure on the carotid arteries.
3·- If bleeding from the front part of the tongue is excessive compress the part by a piece of clean lint held bet\\ een the finger and thumb.
4.- If the bleeding is from the socket of a tooth, plug the socket with a piece of clean lint or cotton \\'001; over tbis place a small cork or other subs :ance of suitable si Le, and instruct the patient to bite on it.
HlEMORRHAGE FROM THE LUNGS.
Blood from the lungs is .:oughed up, and is scarlet and frothy in appearance.
Treat as for Internal Hremorrhage (see page 95).
E
97

HlE.YIORRHAGE FROM THE STOMACH.
Blood from the stomach is vomited; it is of a colour and has the appearance of coffee grounds j It may be mixed wi t h food. ) as fur Internal Hrel1:orrhage (see page 9S , except that nothing is to be given by the mouth
Blood issuing from the Ear Channe ;, which aeneLllly indicates a fracture the base of the must be wiped ct\\ay as It Issues; no attempt is to be made to pi ug the ear.
.
99 QUE 'TIONS CHAPTER III. T li ,: II/tll/uals i'ldirate th e Pa.t:"fS where the answe"s may he fou l/ d. \Yhat organs concerned in the circulation of the PAG E blo od? ... 70 D '::,clibe the heart .. . 70 Trace the circulation of the blood through the b dy and lungs 70 to 72 How many times a minute does the heart contract on the average? 72 "That is the effect of the patient's position on the rate at which the heart contrac lS ? 72 What is the p ul se? ... 72 How many kinds of hzcmorrhage are there? 73 How would you know a case of arte rial h<emorrhage ? .. . 74 In what way should arterial hzcmorrhage be controlled? 74 \\'hat is meant by " pressure point" ? 74 How may pressure be applied? 74 " That is a tourniquet? 75 \Vhy is accuracy necessary in placing I he pad of a tourniquet? ... ... 75 \ Vhen mayan clastic l>andage be used instead of a tourniquet? 76 \Yhat is flexion? ... ...... ...... 76 Stale th e genera
ru les for treat:nen
by arlerial hzcmo rr hage ... . .. . .. 77 , 78 If
bleeding, how would
78 Should blood clots be di turbed ?.. ... ,.. ... 78 It it \\
for an unskilled pe
on to attempt to cleanse a wouncl ? 78 79 \ \'hat j l' e :l. ) r' a ? 79
l
t of a wound accompanied
part of a limb had been lorn off, but there was not much
you act?
ise
r
roo

D escribe the arteries of the head and neck
80
\Vhy is it sometimes necessary to compress the carutid artery both below and above the wound? ... 30, OJ
What is a ring pad, and what is its use? ... 84
Describe the arteries of the upper limbs... 84 to 89
Describe the arteries of the luwer limbs ... 89 to 93
lIow would you -know a case of venous hremorrha6c? 93
\Vhat is a Yaric5se vein? ... ... ... ... 94-
lIow maya vdn become varicose? 9t
S ,ate the general rules for treatmel1t: of a wound accompanied by VetlOUS hremorrhage? ... ... 94, 95
How w'ould you know a .case of capillary hremorrhage? 95
How would you stop cap1llary hremorrhage ? ... .., 95
\Vhat is internal hremcrrhage? ... ... .., ... 95
\Vhat would lead you to suspect internal hremorrhage? 95, 96
State the treatment for internal hremorrhage? ... 96
How would you arrest h::emorrhage from the nose? ... 96, 97
\Vhere may blood issuing from the mouth come from ? .. 97
1low would you treat bleeding from the gums or th10at? 97
What else would you do if the tongue were bleeding?.. 97
Anti if the bleeding were froal th e socket of the tooth? 97
lI ow would you di:;linguish between bleeding fr om the lungs and from the stol1lach? .. , ... ... ... 97
And what would be the di ffe rence ill the treatment?.. 97 or what is bleeding fmll1 the ·ear channel generally a sign? 98
'l'he SlHdent should practise placing supposed patient,; in a proper po,;ition for the arrest of h::em orrhage (see page.:; 72, 77 and 94), folding firm pads (74 and 75), tying hard knots in banclagesto form a tourniqud (76 ), anclthe application of pressure at all the pressure points shown in the frontispiec e, at arious poin ts on the foreheau and scalp, and on the palm of the hand. Pressure should be digital, by pad and or fie}.ion, as directed in the text.
101
Pre ssure points--Carotid artery, 80. Facial, 82. S2. Occipital , 83. Subclavian, 84. AxlllalY, 8.5. BrachIal (by pad and bandage bemg made against the hum e rus and b; fl eXIOn at the elba",:,)' 86. Radial and Ulnar, 8y.
Femoral the gram, 90.. Femoral in the thigh, 9 2 • PoplIteal, 92, Antenal and posterior Ti bial artenes, 93.
I-L:emorrhage hom the forehead or scalp... .. . from the palm 'of the hand ... .. . \ enous hremorrhage from a val'icose or other vein
84 87 to B9 ... 93, 94
PAGE
PAG !J
CHAPTER IV. BRUISES.
A blow anywhere on the surface of the body may cause extensive hremorrhage beneath the skin, without breaking it-a" black eye" is an instance. The injury is accompanied by discoloration anJ swelling . TREATMENT.
Apply ice or cold water dressings. A piece of lint soaked in extract of witch hazel may be placed on the affected part.
BURNS AND SCALDS.
A burn is caused-
(a) By dry heat, such as fire or a piece of hot iron.
(b; By a wire or dynJ.l11o charged with a high pressure electrIc current.
(c) By a corrosive acid, such as oil of vitriol.
(d) By a corrosive alkali, such as caustic so da, ammonia, or quicklime.
(e) By friction, caused, for example, by contact with a revolving wheel. (Brush burn.)
A scald is. caused by moist heat) such as boiling water, hot 011 or tar.
The effect may be a mere reddening of the skin; blisters may be formed; or even the deeper tissues

103
of the body m1.y be charr;; d and blackened. The clothing may adhere to the burnt skll1, and its removal is impossible without further detnment to the injure d part. The great danger is Shock.
TR EA 1 !I[ENT.
I.-Carefully remove the clothing over the injured part. If stuck to the skin, the adherent clot\ling must be cut around with scissors, soaked with oil, and left to come away subsequently.
2. - Do not break blisters.
3. - Immediately cover up the part. Soak or smear pieces of lint or linen with oil, or vaseline, lanoline, or cold cream; a small quantity of boraCIC powder added to these will be of benefit. The inside of a raw potato scraped out and spread on lint makes a soothing applieation. 'When the ...ill 'face is exten"ive do not cover it \\'ith one large sheet of lint, but with strips ab::>ut the breadth of the hand; this is advisable as they fi t c r on the part, and during subs eq uent dr <:' ssings one strip can be removed at a time, and a fr es h dressing applied before the ad· jacent strip is taken off. The shock to the system is thereby less than if the whole of the burnt surface were laid bare to the air by the removal of all the clres,ings at one time. 'When covered by the oily drf'ss incr envelop tl:e part in cotton \\ 001 or a piece of flannel a nd a pply a b;ndage.
lu2
'When the face is burnt, cut a mask out of lint or linen, leaving holes for the eyes, nose and mouth. Dip this in oil or smear it with vaseline and apply it to the face and cover it with cotton woo], leaving openings to correspond with the holes in the mask.
'Vh en possible place the injured part in water at the temperature of the body (98 degrees) until suitable dressings can be prepared. A dessert spoonful of baking soda added to a basinful of the warm water will make a soothing lotion
As it is important not to leave the part exposed to the air, it is the duty of the bystanders to prepare the dressings while the clothing is being removed.
4.-Treat Shock.- This is particularly necessary in the case of every burn or scald of any considerable extent (see page 135). Be yery apprehensive of danger in the case of even slight burns of the neck.
S. - If the burn is caused by a corroshe acid, bathe the part with a weak alkaline lotion, such as w<1shing soda, baking soda (bicarbonate of soda), magnesia, or slaked lime in warm water before applying the dressings.
6. - If the burn is caused by a corrosive alkali, bathe the part with a weak acid lotion, as lemon juice or vinegar diluted with an equal quantity of water. Cazttt'on.-Before using water brush off any lime that remains on the part.

105
7.-When a woman's dress catches fire-
(a) Lay the woman flat on the floor at once, so that the flames are uppermost; that is to say, if the front of the dress is on fire lay her on her back, and if the back of the dress is burning, place her face downwards. The reason for this is that flames ascend, so that if the upright position is assumed, the flames will quickly reach and burn the body, neck, and face; or if the woman lies with the flames undermost, they will, if unextinguished, pass over and burn the limbs and set fire to the rest of the dress.
(b) As soon as the woman is laid flat, smother the flames with anything at hand, such as a rug, coat, blanket, or table cover; if made wet so much the better.
(c) A woman rendering assistance should hold a rug or blanket in front of herself ",hen approaching the flames.
(d) If a woman's dress catches fire when nobody is by, she should lie fiat, flames uppermost, smother the flames with anything handy, and call for assistance, or crawl to the bell-pull and ring; on no account should she rush into the open air.
The use of fire guards would prevent many calamities.
104
B I TES O F SNAKES Ai\D RABID ANli\IALS , AND WO UNDS BY POISONED WEAPONS .
Hydrophobia is caused by the bite of an aI, such as a dog, cat, fox, wolf, or deer suffering from rabies . The special poisons introduced into \\ oll l1 ds caused by venomous sn akes and poisoned weapons ca use imme d iat e danger to life .
I. - Immediately place a con 3triction between the wound and the heart so as to prevent the ve n o u s b lood fr om carrying the poison through the body . If, fo r examp le, a finger is bitten it should be enc ir cled on the side of the wound ne <uest to the heart, with the fi n ger and thum b, and as soon as possible a ligature (a string. piece of tap e, or of band k e.rchief ) should be placed tightly round the root of the finger. Compression with the finger and thumb must not be relaxed u ntil the ligature has been appli' d . Additional ligatures may, with adYantage, be apJ:.!li e d at intervals up the limn.
2.- Encourage bleeding for a time :-
(a) By bathing the wound with war m water.
(b) By keeping the injured limb low; the upper l imb should lJe allowed to hang do\\ n, and in the case of the lower limb the patient "h o ul d be seated with the foot on the gro und.

.
3. - C.auterise the wound, if it is quite to obtain the services of a doctor. I hIs IS done by burning with a fluid ca u stic, such as ca ustIc potash, pure carbolic acid, or nitric acid, or if are not at hand, with a red-hot wire or a fusee. 1 he usual solid caustic is insufficient, as it does not reach the bottom of the wound, where the poison is.
To ensu:e the caustic reaching the bottom of the \\ound, It should be applied on a piece of wood such as a match cut to a point. \ Vhen the has been thoroughly applied, but not till then, the lIgatures may be removed.
4. -:- Cover the wound, afte i' a while, with a clean dressll1g.
5.--Afford the injured part.
6. - Treat shock If It (see page 135).
7. - In case of a bIte by a venomous rub 111 permanganate of potash and lllJect under sk111 111 the neighbourhood of the wound a solutlon of permanganate of potash.
STINGS OF PLANTS AND AN
I
MALS.
These give r ise t o se rious in co n ve n ie n ce and 111 some cases grave s ymptoms develop . ' TREATMENT.
I. - Extract the sting if left in .
2. - Mop the part freely wi t h dilute ammonia
106
107
108 or spirits. A paste of b icarbo n ate of soda and sa l volati le is an effi cien t applicatio n . A solution of washing so d a or potash o r the applica t ion of t he blue bag \\ ill relieve pr in .
3. - Treat collapse if it occurs (see page 135) .
FROST B I TE.
Duri n,; exposure to se vere colu, parts of the body, usually the fingers, n O'le, or ears, lose sensation anu become first waxy ",hite Rnd afterwards congested and of a purp le appeara n ce. As sensation is I )st in t he part, it is often on:y by t he r emarks of bystanders that the frost-oil te n perso n is made a\\ are of his condi t ion .
TREAT:'IIE ' T .
I. - Do not bring the pat ient into a warm room until, by fJ iction of the h:md or by rubbil ' g \yith soft snow, sensation a n I circuhtion in the a ffected parts are restored . Neglect of this precaution may 1 aJ to dea th 'o f the tisslles of the fr ost Gitten part.
2 .-When circulation is restored , keep the pat.i t nt in a room at a tempera t ure of 60 degree s.
NEEDLE EMBED D ED UNDE R THE
'Vhen a needle break: df after pelletrating the skin and take the patient to a doctor at once, If the \\'ound is near a joint) ktep the lin .b at rest on a 'plint.

FISH-HOOK THE SK I N.
Do not attempt to \\ithdraw the fish-hook the \\'ay it went in, bt!t cut off the dressing of the hook, so that only the metal is left, and then force th e point onwards through the skin until the hook can b e pulled out.
I KJURIE TO
"When a joint is injured by a buliet, stab, or other cause -
1. - Wrap the part in cotton wool.
. 2. - Afford rest and support to the injured 11mb ; If the upper limb, in a flexed position by a sling; if the lower limb, in a st raight position by a. splint.
BODY IN THE EYE.
I. - Prevent the patient rubbing the eye, tyinJ d o wn a child 's hands if necessary.
2. - Pull dJwn the lower eyelid , \\hen, if the f J reign body is seen, it can readily be removed with a camel 'S hair brush, or \\'ith the corner of a handkerchief t\\irled up and welted.
3. - When the foreign body is beaeath the upper eyelid l ift the lid forward, push up the lo\yer lid beneath it and let go. The hair of the lower lid brushes the inner SUI face of the upper one, and may dislodge the body . 'hould the til t attempt b e unsuccessful, r e peat it se \'eral times if necessary. If
the fureign body is not dislodged call the servic es of a doctor as soon as possible. When, however, skilled help cannot be had , proceed as follo\\ S :-
(a) Seat the patient so as to face the light, and stand behind him, steadying his head against your chest.
(b) Place a small rod, such as a match or bodk in, on the upper eyelid, half-an-inch above the edge, pressing it backwards as far as possible.
(c) Pull the upper eye-lashes upwards over the rod, and therehy evert the eyelid.
(d) Remove the foreign body .
4.-When a piece of steel is embedde d in the eyeball drop a little olive or castor oil on the eyeball after pulling down the lower eyelid, close the lids, apply a soft pad of cott o n wool and secure it by a bandage tied sufficiently firmly to keep the eyeball steady; take the patient to a doctor.
s. - When quick-rime is in the eye brush away as much of it as possible; bathe the eye \\ ith vinega r and warm water, and treat as for a piece or steel embeJded in the eyebal l.
FOREI G N BODY IN THE EAR P ASSAG E.
As a ru le make no atte :11pt to treat a patient with a foreign b ody in th e ear if the services of a doctor can possib ly be had; any attempts to remove the foreign body' may lead to fata l consequences. If a child

III
can n ot be induced to keep the fingers from the ear, tie his hands down or cover UP the ear. If an insect is in the ear-passage, fill the ear with olive oil, when th e ins ec t will float and rnay be removed. Never syringe or probe the ear.
FOREIGN BODY IN THE NOSE.
Indu ce snee ing by pepper or snuff. Cause the patient to hlow his nose vi olently after closing the unaffec ted nostril. There is no immediate danger from a foreign body in the nose.
THE ABDOMEN.
The abdomen is bounded above by the diaphragm; below bythepelvis; behind bythelumbarvertebrce; and. in fr o nt and at the sides by muscular walls. (Fig. 54·)
THE ORGANS OF THE ABDOMEN.
The Stomach lies immediately below the "pit of the stomach" just below the breast-bone.
The Liver lies in the upper part of the abdomen, where it is mostly covered by the right lower ribs.
The Spleen lies beneath the ribs at the upper part of the left side of the abdomen .
The Intestines occupy the greater part of the cavity of the abdomen .
T h e Kidneys lie at the back, in the region of the loin
T he Bladder li es in the pelvis.
110
FIG 54.
\VOUND IN THE FRONT "VALL OF THE ABDOMEN.
H 'hen the intestines or other organs protrude through the wound, whether vertical or transver se, bend the knees, raise th e shoulders, and apply lint, a towel, or cotton \\'001 wrapped in soft linen, an 1 keep the

II3
patient warm until the doctor arrives . "Vhen there is no of organs, if Ille 'Wou.nd is vertical, lay the pat Ient fl at on the back \\ ith the lower limbs straight ; if the ,teJ01tnd tmJZSverse, bend the knees and raise the shoulders.
INJURIES TO THE ORG.\:\' WITHIN THE ABDO:\.IEN AXD PI!:.LVIS.
Injuries of t he Stomach are attended by extreme collapse and sometimes by vomiting of dark blood like coffee-grounds. For treatment see " from tl:e tomach 1/ (page 98).
InJunes of the LIver, Spleen and Intestines may be caused by a blow, a stab or a bull et· the liver or spleen may be injured by a fracture ;f the !o\yer ribs. The Signs and Symptoms are those of hcemorrhage accompanied by pain and swellmg at the of injury, and the treatment is as for that condition (see page 95).
The Kidneys may be injured by a fracture of the eleventh or twelfth ribs, also by a crush, blow, stab or bullet. Blood may escape \\ irh the urine, al?d there may be pain and swelling oyer the injured kldney .
The Bladder may be inju ' ed by a fracture of the pelvis. The signs and symptoms are either inability to ra"s water, or if a littl e is passed it is tinacd with blOod . ::>
112
TREATMENT OF INJURY TO THE KIDNEYS OR BLADDER.
I. - Keep the patient quiet until the doctor 3.lTlyes.
2.-App :y hot fomentations over the painful or injured part.
Rupture (hernia) consists of a protrusion of an internal organ, usually the bowel, through the muscular wall of the abdomen, most frequently at the groin . Should a sudden swelling accompanied by pain and sickness take place in that region
1. -Send for a doctor instantly.
2. - Lay the patient down with the buttocks rai se d .
3.-Apply ice or cold water dressings to the affected part

What 1s a bruise?
114
. 115 QUESTIONS
V, Tile rWlllera ls ind:ta le the pages where
allswers may
ON CHAPTER I
the
be f,)Itnd.
How would .you treat a bruise? How maya burn be caused? ( \.-' P IGE 102 102 102 lIow is a scald caused? '" 102 \Vhat is the great danger of a burn or scald? 103 State th e general treatment for burns and scalds 103, 10 4 ] l ow would you treat a burn caused by a corrosive acid? lIow would you \feat a burn caused by a corrosive alkali? What steps should be taken when a woman's dress catches fire? ........... . 10 4 104 105 State the general I ules for treatment of wounds caused by poisonous bites or weapons 106, 107 What special treatment is required for the bite of a venomous snake? 107 lIow would you treat a sting? ...... 107,108 State the signs, symptoms and treatment of frost-bite ... 108 Would you attempt to remove a needle embedded under the skin? " 108 H ow would you extract a fish hook em in the skin? .. . State the tr eatment for injuries to joints ... ... State the gene ral r ules for removing a foreign body from the eye... 109, 11 0 What would you
?
How would you try to remove an insect from the ear passage? .. 1 10 11 0 I II
do if a piece of steel were embedded in the eye baJJ
And when quick-lime is in the eye?
PACE:
\Vvuld·you try to olher form of foreign bod)' from the ear passage? .,' I [0, I I I
IIow would you remove a foreign body from lhe nose? I I [ Slate the boundaries of the abdomen and its conlenLs I I I State the treatm nl for wounds of the abdomen .. , I 12, 11] now may injuries to the liver, spleen and intestines be caused? .. , IT 3
\YI at is the difference between treatment of injuri es to the stomach and of injuries to the liver, spleen and intestines?
113 the treatment of injuries to tbe k idneys or bladdc:r I q State the lrea'ment of hernia II -l

CHAPTER V .
THE NERVOUS S YSTEM.
Two systems of nerves, the Cerebra-spinal and theregulate the mo \'ements and functions uf the body.
The Cerebro-spinal System is made up of the Brain, the Spinal Cord and N erves, and through its 3ge ncy sensations are received and the will causes the action of the voluntary muscles . For e'\.ampleJ
\\';lien a part is injured a sens3.tiol1 of pain is con"eyed to the brain by the n e rve, thus affording an indicatio n of the seat of injury, or a \yarnin g of a poss ible danger of furth er damage. On attenticn bei ng directed t.o the injury, an attempt is instantly made to ease the pain or to move the injured from danger.
The Brain is situated within the cranium, and isdiv ided in the middle lin e, so th:1t, with the ' exception of some conn ect ing bands, the right and left sides are separat.:: .
The Spinal Cord is the lo ng coru of nervous matter lying within the spi nal canal (see V ertebra l Column, page 2 3) It kayes the Grain through an ope ning in the has e of the cranium and extends to the upper lumbar nrtebr;:e.
JI6

lIS
The Nerves proceed from the brain and spinal cord in pairs as pearly-white trunks, and their branches can be traced throughout the tiSSU eS of the body. When a nerve is torn through ther e is p ralysis of motion and sensation in the region in which its branches are distributed.
The Sympathetic System extends as a nerv ous ch::1in on each side of the front of the spinal column along its entire length, and sends branches to all the organs of the chest and abdomen to control the involuntary mus les, and thereby regulate tIL vital' functions. This systen is not under the control of the will, and acts alike during sleep and activity .
THE RESPIRATORY SY'TEM.
The air r eac hes the lungs by way of the nost rils (or mouth), the throat, the wind -pipe, and the br ,mchial tubes. The nostrils convey it to the back of the throat, whence it enters the wind-pipe by an opening guarded by a sort or trap door or valve, s that in health air, but not solids or fluids, may enter . During insensibility, however, the valve fails to act, so that should solids or fluids be given by the moutb, they may enter the wind -pipe and cause :Lsphyxia. Th e wind -pipe extends to two inches belo l\' the top of the breast-bone, wher e it divides into the ri ght and left bronchial tube. Each bronchial enters a lung and divides into small and still smaller tubes, until
) 119
FIG. 55. Tm: LUNGS AND BROKCHIAL
A. Trach ea, or Wind-pipe. B. Left Bronchus. C. ; .. Bl'OJ1chus. D. Smaller Bronchial Tubes.

the ultimate recesses of the lung- the air cells or air spaces - are reached.
The Lungs, Ri ght and Left, occupy the greater ' pc.ut of th e chest; they lie immediately wit hin the ribs, a nd practically vvherever a rib is felt, whether front, back or sides, there is lung beneath. Each lung is enveloped in a fine membrane (the pleura) which allows it to move within the chest during breathing "ithout friction.
Respiration, or breathing, consists of two aCls, Inspiration, an expansion of the chest, duri . g which air is drawn into the lungs, and Expiration, a contrac tion of the chest, during which air leaves the lungs. A pause follows the act of expiration. In hea lth fifteen to eighteen breaths are taken per minute, and at each inspiration about 20 to 30 cubic inches o( air enter the lungs, and a similar quantity is expelled at each expi ration.
The expansion and contraction of the chest are effected partly by the muscles of respiration attached to the ribs, but chiefly by the Diaphragm, the large arched muscular partition which separates the chtst from the abdomen. In inspiration, which is chiefly a m usc ul ar act, the ribs are raised, and the arch of th e diaphragm falls and becomes flattened, thus increasing the capacity of the chest and ca using the air to enter. In expiration, an act performed almost 'without effort, the ribs fall and the arch of the
diaphragm rises; . this lessens the capacity of the c.hest .and forces all' ?ut. The mechanism of respiratIon IS lIke that of ordinary household bellows, but WIthout a \'alve; the ribs may be compared to the boards of the bellmys \\ hile the diaphragm corresponds to the leather, the air passages being equivalent t o th e nozzle.
. As the blood depends upon the air fOIl' its purificatIOn and the oxygen necessary to maintain life. interference with breathing yery soon may Rrod uce a dangerous state called asphyxia, examples of which are afforded by drowning, suffocation, choking, etc.
ARTIFICIAL RESPIRATION.
PROFESSOR SCHAFER's METHOD.
I.-Make no attempt to loosen or remm'e cloth·ng.
2. - Lay the patient in a prone position (i.e., back \\'ith his head turned to one side, so as to keep hIS n ose and away from the ground. No pad is to be placed under th e patient, nor need the tongue be drawn oul, as it will fall naturally. at one side facing the pat ient' s head, and place the palms of your hands on his loins, one at each side, the thumbs nearly touchincJ' One another in the small of the back, and the finaer b extending over the 10\\ est ribs. L eani ng your y . forward,l ·t its weight press straight do\\ ll\\"ard . upon the
120
121
loins and lower part of the back, compressi,ng the abd ') men against the ground and dnvm.g aIr out of the che:;t. This produces expiration (Fig 56) . D raw back

57 . bSPIRATrON.
12 3 your body somewhat more rapidly and relax the pressure, but do n ot remove your h .l. nds; this produces inspiration (Fig. 57).
4 - Alternate these movements, by a rhythmic s\\'aying back\\ards and forwards of your body, t\\ dve to fifteen times a minute, persevering until respiration is restored, or a doctor pronounces life to be extiect.
DR. SlLVESTER'S l'IfETHOD.
I - Adjust t he patient's position .-With o ut wasting a moment place the patient on his back on a flat surface, inclined if possible from the feet upwards . Remove all tight clothing from about the neck and chest, and bare the front of the body as far as the pit of the stomach; unfJs te n the bra ces and the top button of trousers in me n, and the co rsets in women. Raise and support the shoulders on a small, firm cushion or folded article of dress placed under the shoulder-blades.
2 .- Maintain a free entrance of air into t :1 e w i ndpipe -Cleanse the lips and nostrils; open and wipe the mOllth; an assistant must drLlW forwarJ the patient's tongue as far as poss ible, and keep it in that posit :on.
3 .- Imitate the movements of breathing. Induce I1lsjiratioJl. - Kneel at a convenient distance behind the patient's heau, and grasping his forearms just below the elbo 'x, draw the arms
122
FIG.
Flc. INSPIRATIC N.

FIG. 59.
12 5
upwards, outwards, and towards you, with a s .\ eeping movement, making the elbo\\"s touch the ground
Co. l:\ SPlRA TION.
FIC. 61. LX1'Il{.·l,'llO:\.
(Fig. 58). The em'it), of the chest is thu el1brsed , and air is drawn into the lungs.
Flc.
induce expiratiolt. - Bring the pfltient's flexed arm slowly forward, downwards and inwards, press the arms and elbows firmly on the chest on either side of the breast-bone 59)' By this means is expell from the lungs.
Repeat these move l1ents alternately, deliberately, and about fifteen times a minute. a sufficient number of assistants are present, HOW LHU' , n1.1Y be combined with Silvester's, as fo1 ,\' s: -
T, ' assistant kneels astride the patient's hips \\ ,'. th e balls of the thumbs resting on either siJe of the pit of th e sto :11acb, and the fingers grasping the parts of the chest. 1!sing his kn 'es as a pivot, he presses forward on his hands. Th e n mddenly, with a final push, he spi'ings back and remains erect on his knees whil e h = counts r, 2, 3. These motions are to be repeated to correspond with those being performed by Silvester's method, pressure on the chest being made simultan eously by thos e performing the two m etho d s (1' igs 60 and 6r).
L.<\BORD .. 'S METHOD
When from any cau e the above methods cannot be carried out, Lab ord/s metfwd of :Htificial respirati m should be tried. It is especia lly useful in childr-2n, and when the ribs a re broken. 1 2 7
The patient is placeu on his back or side; the mouth cleared; the tongue is seized-using a handkerchief or something to prevent it slipping from the fingers-the lower jaw depressed; the tongue is pulled forward and h e ld for two seconds in that position, then alluweu to recede into the mouth. These moyements should be repeated about fifteen times a min ute.
Artificial r espi ra ti o n must t e continued until breathing is established, or until a doctor arrives. When natural breathing commences, regulate the artificial r es piration to correspond \\ ith it. Success may result e ven after two hours ' time.
Excite respiration.- \Vhilst artiflcal r espira tion is being appl1ed, other useful steps may be en,ployed, su c h as applying smelling salts or snuff to the nostrils, and flicking the chest with a dam) towel.
Induee circulation and warmth after natural breathing has been r estored. Wrap the patient in dry blankets or other covering, and rub the limbs energetically towards the heart. Promote warmth by hot flannels, hot-water bottles, or hot bricks (wrapped in flannel) applied to the feet, to the limbs and body.
\Vben the power of swallowing has returned give hot tea or coffee, or meat extract. The patient should be kept in bed and encouraged to go to sleep. Large poultices or fomentations applieu to the

1 28
front and back of the chest wi ll serve to assist breathi ng.
Watch the patient ca refully fo r so me ti me to see that th e br ea thing d oes not fail ; should any signs of failure appe ar, at once begi n artifici al respi ra ti on.
I NSE N SI BILI T Y.
Uncon9Ciousness or Insensibility may ar ise as follows :-
Injury to the Head. -Co ncussion a nd Compression of the brai n.
Disease of the Brain. - Apoplexy , E pilepsy, H ysteria . Various Causes. -Shoc k , Faint ing (Sync ope) , Collapse, Alcoh oli c a nd other pois oni ng, Sun stroke and Heat-s troke, In fa nt ile Conv ul sio ns, Asph yxia .
G ENE RAL RUL ES FOR TR E ATMENT OF IN SENSI BILI T Y.
I. - If a person appears about to lose oonsciousness, preve nt h im from and lay him ge n tly do\\ n.
2.- Arrest Hcemorrhage wh en a ppa ren t ; a ttending to min or injuri es is less im p<Drt a nt than treating th e un co nscious sta te.
3. - Lay the patient in the position in which breathing is most easy- usu ally this will be on th e i:>ac k, or inch ne d to one side. As a gen eral rule J 29
rais '2 the he.1d and sho ulders slightly when th e fa ce is and keep the head low when the face is pale.
4. - Undo all tight clothing round the neck, chest and waist, u nfastening t he braces and top button of trouse rs in meo, a nd the corsets in women, the obje ct bei ng to reli eve p ressure on the air pass:lges , lungs, hear t and abdomi nal organs. Be sure that there is n:) obst r uction to the air p:lssages by the tongue or by a foreign body in th e throat. The possibility of false teeth obs tructing breathing must be considered .
5. - Provide for a sufficiency of fresh air by open ing doors amI windo\\ s, and by keep ing bac k a cro wd .
- When breathing cannot be discerned apply artificial respiration.
7. - Obtain a docter 's help as soon as possible.
8. - Unless unavo idable, never leav e the patient until you have placed him in charge of a responsible person.
9. - Give no food or fluids what e ver by the mouth while the patient is insensible.
10.- Should the spine or an important bone of the upper or of the lower limb be fractured , it must be steadied a nd maintai ned at rest as soon as possible. Should the u nconsciousness be prolonged, the patient may be removed in a rec u mbent position
F
to shelter, p rovided that tLe broken bone is adequatel y supported.
11. - When the patient is in a state of convulsion , support his head, and after wrapping a piece of wood or any uther hard material in a handkerchief, hold it in llis mouth to prevent biting of the tongue. Do not forcibly restrain his limLs; prevent him from hurting himself by pulling him a\ray from a source of danger, such as machinery, a wall, or fireplace ; light pieces of furniture should be pushed out of the way.
12.- On retur n to consciousness \\:a ter may be given to drink. If the pulse is feeble give \\ arm tea or coffee, provided hremorrhage, either internal ur external, is not present. A desire to sleep should be encouraged, except in cases of opium poisoning, a condition that may f;enerally be recognised by the history of the G,se, and also by the pupils of the eyes (the black openings in the grey, blue or bro\\n iris) being minutely contracted (pin-head pupils).
13·-lt must not be assumed that a per on is insensible as the result of drink me ely because the breath smells of alcohol ; frequ " ntly when people are feeling ill they take or are giYen alcoholic stimulants, after which they may become insensible, not from the drink, but from the cause that inullreu them to take it, for example, insC'nsibdity coming on, effects of pJisoning, etc. Even if

13 1
drink is believed to be the actual cause of insensibility, it must be borne in mind that the patient is in a very dangerous state, and he must be treated for Collapse by being covered up and kept \yarm.
The above general rules will enable first aid to be rendered efficiently in most cases of insensibility, although the exact form from which the patient is suffering is unknown.
CONCUSSION OF THE BRAIN.
The pmient may be stunned by a blow or fall on the head, or by a fall on the feet or lower part of the spine. He may quickly regain consciousness, or insensibility, more or less complete, may be prolonged.
TREAT.\1ENT.
1. - Apply the ge eral rules for the treatment of Insensibility.
2 . - Be very apprehensive of danger in all cases of injury to the head. The patient may be stunneci, and after a short interval may recover some degree of consciousness, or even the brain may apparently have escaped injury; yet in both instances there is a grave risk that a structure \\'ithin the cranium has been injured, and that a serious state of insensibility may develop later. (See Fracture of the Cranium, page 43)' A caution should therefore be gi ven to a patient \\'ho has lost consciousness even F 2
130
for only a moment after an inj ury to the head not to resume physical or mental activity without the consent of a doctor.
COYIPRESSION OF THE BRAIN, APOPLEXY.
Compression of the Brain may result from the same. as produce Concussion; in fact, CompreSSIOn lS frequently preceded by Concussion.
Apoplexy usually occurs in elderly people, and no signs of injury are necessarily present.
In both conditions the face is flushed; the breathi?g stertoro us ; one side of the body may be more hmp than the other, and the pu.pil of one eye may be larger than that of the other; the temperature of the body is generally raised.
TREATMENT.
I. - Apply the general rules for treatment of Insensibility.
2. - Promote warmth in the lower part of the body by the application of hot water bottles to the abdomen and lower limbs. Care must be taken not t o burn the patient with the bottles, which shoul d be wrapped in flannel, and their heat tested \\"ith the elbow.
EPILEPSY.
Epilepsy may occur in persons of any age, but usually occurs in young adults. The patient falls to

the gTou nd, sometimes with a scream, and passes into a state of convulsion, throwing his limbs about. The treatment is according to the General Rules, especially Rule II.
HYSTERICAL FITS (HYSTERIA).
SIGNS AND SYMPTOMS.
The patient, usually a young girl, in consequence of mental excitement, suddenly loses command of her feelings and actions. She subsides on a couch or in some comfortable position, thro\\"s herself about, grinding her teetb, clenching her fists, shaking her hair loose; she clutches at anyone or anything near her, kicks, cries and laughs alternately. The ey.eballs may be turned upwards, and the eyelids opened and shut rapidly. At times froth appears at the lips, and other irregular symptoms may de\"elop.
TRE.AT;\I U'iT.
I.-A\"oid sympathy with the patient, and speak firmly to her.
2 . - Threaten ber with a cold water douche, and if she persists in her "fit," sprinkle her with cold water.
3.-A rply a mustard leaf at the back of the neck .
Medical treatment is necessary to cure the condition of mind and body which gives rise to hysterical attacks.
133
SHOCK, F AI NT I:\ G ( .)YNCOPE), COLLAPSE.
CAUSES .
I.- I njury in the region of the abdomen, extensive \vounds and burns, fractures, lacerated wounds, and severe crush a l e some of the more frequent physica l causes of shock .
2.- F righ t , anticipatio n of injury , and sudden bad n ews, or sometimes sudden removal of fear and anxiety afte r pro lo nged su spense, prod u ce shock or fainting .
3.-Some poisons ca u se shock, whi le others, suc h as alcohol, so d epr ess t h e n er vo u s system th a t c ollapse e nsu es.
4 . - Hremo rr hage o r heart weakness, a close o r croweled room, t igh t clothing, fatigue, or \,"ant of food may bri ng o n fainting or collapse.
SIG NS AND SYMPTOMS .
T he general co nd it io n of shock may be recognised by extreme pallo r, a fee ling of cold, clammy skin, feeble pu lse, a nd sha ll ow breathing accompanied, if hcemo rr hage h a s been severe, by yawning ;. nd sigh ing. The t er m "collapse" signifies a yery serious condition in which the life of the patient is in t he greatest danger; the tem perature of the bod)' falls below the n orma l, and one great object of treatment itS t o prevent it si king to a point at which lif2 is impossible. An attendant danger of the condition of

135
collapse is the liability to sudden relapse after a temporary improvernent, and the utm?st care a?d watchiulness must therefore be exercIsed to mall1tain the h ;'at of the body and to guard against failure of the heart and lungs .
TREATlIIENT
I .- Remove the cause by arlesting hremorrhage, attending to injuries, loosening all tight clothing especially about the chest and a?dOmell, rem?ving from a close or CrG\\ ded room, usmg encouragmg worJs, etc .
2.- Lay the pcttient on the back, with the head low . lZaise the lower limbs; when the patient is in bed this is best done by raising the foot of the bedstead.
3.- Provide for a free circulation of fresh air.
4. - If hcemorrhage has been seyere and the pati ent is collapsed, firmly bandage the limbs from, the toes to the hips, and from the fingers to the armpIts,
5. - To stimulate the act ion of th '.! heart, sal volatile and water llIay be given if the patient o n swallow , or smelling salts may be held to the nostrils.
6. - It is of the utmost importance to use every means of preventing a fall of temperature below the normal point. To accomplish this cover the patient with txtra clothi ng, or by phcing
134
13 6
rugs or blankets over him; get him to bed in a \rarm but well ventilated room as soon as possible. Apply warmth to the feet and to the pit of the by hot \'yater bottles or hot rl.:.ll1nels. (Test the heat of these with the elbow before applying them.) If the patient can swallow, give hot drinks, such as milk, tea or coffee. It is well to add sugar, as it aids in raising the telT.:ierature of the body.
7.-If breathing cannot be discer ned , apply artificial respiration.
S. - If want of no urishment has b een the cause of fdinting or collapse, gi\'e food sparing ly at first.
SUNSTROKE AND HEAT-STROKE.
,\Vhen exposed to grc.'at heat, as in the stoke-hole of a steamer, especially in the tropics, or to the rays of the sun during a march in very hot weath e r when heavily burdened , persons may develop sickness, faint ness, giddiness, and difficulty in breathing . The patient CO :l1plains of thirst, the skin b ecomes dry and burning, face very flushed, the pulse quick and bounding. A very high temperature, stertorous (snoring) breathing, and ins ensibility may ens ue.
TREABIEKT.
1.- Undo all tight clothing.
2.-Rernove the patient t') a cool, shari)' spot.

137
3.-- trip the patient to the waist.
4 -Lay the patient do\\ n, with the head and trunk well raised.
5. - Procure as free a circulation as possible of fr esh air, and fan the patient vigorously.
6.- ·Apply ice bags or cold water freely to the head, neck, and spine, and maintain this -treatment until the symptoms subside.
7.-0n return to consciousness, the patient may ba\'e \\at er to drink.
IN CHILDREN.
Teething or stomach troubles are the commonest causes of this ailment.
SIGNS.
pasm of the muscles of the limbs and trunk, blueness of the fa€e, insensibility, more or les compl ete, and occasionally squinting, suspended respiration, and froth at the mouth are the prominent signs.
TREATMENT.
I. - Support the child in a warm bath slightly above the temperature of the body (98 degrees), so that the \yater reaches to the middle of the trunk.
2.- Place a sponge clipped in cold water on the top of the head.

ASPf-IYX I A .
·When, owing to want of air, the blood is not supplied wi h oxygen the patient becomes insensible, and is said to be asphyxiated. This conditiun nl:ly be brought about as follows:-
I. Obstruction of the air passages.
(a) By DRO
(/I) By PRE SURE FRO:\I Strangulation, hanging, smothering .
(c) By A FOREIGN BODY THE THRO_\T: Choking.
(d) By SWl£LLING OF THE TLSUE OF THE THRO.-\T: Infia :l1matinn, scalu of the throat, poisoning by a corro ive.
II . Inhaling poisonous gases . By coal gas (as used in the house), producer, ()r water, gas, sm?ke , fumes from a charcoal or coke fire, se\\ er gas, Innekiln gas, carbonic acid gas.
I II . Pressure c. n the chest, as when crushed by sand or debris, or hy a crowd.
IV. Nervous affections , as the result 0: narcotic and certa:n other pois :) n::, collapse, electric shock , or stroke by lightning.
GENERAL TREATMENT:
In al: cases of Asphyxia attem ts must be made to remove the cause or to remove the patient fro 11 t h e cause. When h:lS been done a rt ificial 139
must be app li ed, taking care that the all' passages are n o t and that there is abundance of fresh air.
DRO NING.
Per:::,ons completely immersed in water for even ten or fifteen minutes have been restored by artificial means. Therefore, if the body is recovered within a time, absence of signs of life is not to deter Immediate attempts to restore animation.
The first thing to do when the body is recovered is to get rid of the water and froth obstructing the air passag:es, and then artificially to restore breathing. ThIS IS best accomplished either by proceeding at once to per form artificial respiration by Schiifer's method, or as follows:-
1. --As quickly as possible loosen the clothing, and clear t he mouth and the back of the throat.
Z.- Turn the patient face down\yards, with a p d below the chest, and \': ith the forehead upon thE: riuht f rearln.
I:>
3· - Whilst in this p r)sition apply pressure by the hands to the patient's back over the lower ribs and keep the pressure up for three seconds. '
4·-Turn the patient on the right side, maintaininathat position also for three seconds. I:>
S· -Repeat these movements alternately as long as and water issu e from the mouth.
fhese operations (Marshall Hall's method) in themselves tend to promote respiration, but when the air passage s are clear of froth and \rate r Sih"ester 's method of artificial respiration may be used by itself o r with Ho\\"a rd's method in conjunction.
"While performing these operations send someone to the nearest house to procure bbnkets and dry clothing, hot water bottles, etc, and to fdch a doctor.
STRANGUL .\ TION .
Cut and remove the band constricting the throat . Apply artificial respiration.
HANGING.
Do not \\ ai t for a policeman: grasp the lower lim bs and raise the body to take the tension off the rope; cut the rope, free the nock. A pply artificial respiration.
SMOTHERIKG.
Remove whatever is smothering the patient. Apply artificial respiration. _
CHOKING.
Open the mouth, forcibly if need be; pass the forefinger right to back of tl:e and attempt to dislodge the foreIgn body; If vomltll1g results, so much the better. If unsuccessful, thump the back hard whil<3t the head is bent forward. Apply artificial r vspiration.

S\\'.ELLING OF THE TIS SUES OF THE THROAT.
'Whether. the swelling is caused by inflammation by swallowmg very hot water: as not infrequently happens to children attempting to drink from the spout of a kett.le, or by the effect of a corrosi,-e poison, th e treatllll'lu' IS as foll GWS :--
I.-Apply a sponge, piece of flannel or other cloth, wrung out of very hot water, to the front of the n eck [rom the chin to the top of the breast-bone. ' the patient before the fire.
3·-Gi ve ice to suck if it can be had' if not aive cold \yater to drink. " b
4·-: Give animal or veg e table oil, a dessertspoonful at a tIme, to soothe the scalded throat and ease the pa in.
. S·-If breathing has ceased apply artificial resp :ratIOn.
SUFFOCATION BY SMOKE OR GASES.
the patient into the fresh air. Before cntenng a building full of smoke tie a handkerchief wet if possible, round the head so as to cover n l)se and mouth. .It is to move slowly, keeping !ow, or e ve n cra\\ lmg, whIlst in a room full of smoke
In sear.ch o.f a person: Every opportunity of lettIng m fresh aIr by openm a doors or windows shoulu be seized . b

2. -Apply artific ial respiration. .,
3. - I n the case of producer or water gas, mhalatlOn of oxygen wi ll also be necessary .
ELECTRIC SHOCK.
Electric current is conve) ed by a cable, \vire, rail, or tar called the and ret urns to the source' of supply by another cable, \\ ire, rail, or bar, called the" Negative," or thr ) ugh the In the case of an electric railway, the current IS generLdly conveyed by an insulated the t?ird rail, an1 returns throuCTh the funnmg rads or an msulated rLul called the rail, and in the case of 8n electric.; tramway it is freq uen lly conveyed by an overhe:ld conductor or t rolley \\"ire, and returned through the running rails.
Thro ugh contact with a " positive ". the shock may be so severe as to cau e insensibility, and the sufferer will be unable to extricate himself, and mUSl be liberated with all possible speed As it is gene· a ll y impossible or inexpedient to switch off the current some other method m u st usually be adoptec1; but pr ecautions must be. or the person renderinCT assistance will hImself receIve a shock.
To th e sufferer from contact-
I. - Insulate yourself from the earth by ing on an " insulator " or " non-conductor," that a \\ hich resists the current. Amongst such bodIes 143
are in r:lJarubber, dry glass, dry bricks, dry silk, d r y cloth, drv wood and dry hay or straw your hands from contact with the sufferer or the electric medium by them with an insubtor. Although indiarubber is pro')ably the best insulator, do not waste time in runnin,; for indiarubber gloves but use dry articles of clothing; an indiarubber tobacco pouch or cap, or foldeJ ne \\"spaper, would serve to protect the hands in an e ;11ergency. If no means of insulating the han is are at hand an altempt may be made to drag the sufferer away by means of a loop of d y rope or a crooked stick; an umbrella is not safe because the metal ribs would act as conductors* of electricity, and it is not infrequently the case that the" stick" of the umhrella is a metal tube.
3.- Pull the away from contact . Car e should be taken to avoid touching with naked hands the sufferer's hands, wet clothing, or boots if the soles are nailed. The armpits should be avoided as perspiration usually makes the clothing damp there.
'When the sufferer is removed from contact-
I. - Apply the general treatment for insen -
* A conductor is a body through which electricity readily pas<; c<; . Amongst such bot.lie are cvpper, brass, ir on, moisture an (1 vile's own hudy.
]44 sibility (loosen clothmg, procure free circulation of air and place in a r ecumbent p :: sition) .
2. -- Dip a towel in cold water and attempt to arouse him by sharply flicking the face and chest.
3. - Commence artificial respiration if other methods fail to restore animation. " Laborde's" method (see page I 26) has been found to be very successful.
4.- Treat burns if there are any (see pages 10 3, 10 4).
EFFECTS OF LlGHT:>lmG.
A person struck by lightning is usually more or less deprived of consciousness. The treatment is the same as that for electric shock, e....;cept, of course, that the instructions for removing the patient from contact with the electric medium do not apply . 145
QUESTIONS ON CHAPTER Y.
The 1l1flllel'als indicate the pages where the an s welS may be fOlll/d.
\\'hal are the two systems of nerves? ...
Of what is the cere bro -spi 'al system ll.lflde up?
What is the spinal cord?
"'hat are nen'es like? ...
the system
tbe respiratory system
the acts of respiration
I row are the exp::tnsion and contraction of the
eftected?
In what system of artificial respiration is the patient laid back IIp\\'arcls ?
In what systems is he laid on
In what system is he lain on hi back 01' side?
In what system is he rolled alternately on his side and face downwards?

State the general rules for treatment of insensibility
\Vould you the patient to see if any bones were broken?
'''hat wrong opinion may be formed when the patient smells of drink?
Is collapse from drink a seriou condition?
I'ACE 117 II7 1I7 !IS !I8 Explain
Explain
I r8 to 120 120
Explain
che t
... ... ... ... .. . 120tOl21
... ... ... ... ... ... [21
... 123, 126
hi . back?..
... 127
... ... ... ... 139, 140 Itow long Should artificial reS{liration be perseverell with? 127 What is exciting re piration ? ... ... ... .. . 1 2 7 What is inducing circulation? 127, 128 \Vhy is it necessary to watch the patient? 128 J low may insensiiJility arise? ... 128 State the \-ariOlls forms of insensi bili y 128
128
13
[0
1
...
...
What is concLlssion of the ? ... 129 130 13[ r3 1 State the rules for treatment of concussion [3 r. 13 2
,\Vhac danger accompan ies injury to the head?
\Vhat caution should be given to a patient who has lost consciou<,ness, even for a moment, after an injury to the head?
,\Vhat are the causes of com pre sion of the brain?
In what ag d people dots apoplexy usually occur?
What are the signs and symptoms of compression and apoplexy?
State the:rules for treatment of thtse conditions . . .
Wh.l.t dang.,r is there in applying hot water hottles to insensible persons, and what precautions should be
Describe a case of epilepsy 13 2 , 133
\Yhat special care must be taken in treating a case of epilepsy?
Ddcribe a hysterical fit
!low would you treaL a hysterical fit?
\Vhat are the comm nest physical causes of shock?
\Vhat may produce shock or fainting?
What conditions do certain poisons bring about?
What may bring about fainting or col'apse?
How wou'd yuu recognise the general condition of sh ck?
\Vhat special precaution must be taken in the case of
collapse?
State the treatment for shock, faintll1g (syncope) ar d collapse
135, 136
What is the effect of sugar on the temperature of the 136
body!...
,\Vhat are the causes of sunstroke and heat-stroke?
State I he treatment [or sunstroke and heat-stroke
What are the causes of convulsions in children?
,\Vhat are the signs of convulsions in children? ...
State the treatment for convulsions in children
State fully the causes of asphyxia ...

What two things have to b e d one in all cases of PAGE asphyxia.? .
What t:vo.thlllgs be seen to before it is possible for .to do any good? ... ..• 139
Is artifiCial respiratIOn lIkely to do any good if the air passages a r e obstructed, or if the re is not abundance of fresh air?
\vhlt is the first thir;g to a o(d·rown;;;g? '"
By wh.at may ar lficJaI respnatlOll be performed r WIthout taking any previou ' tep ?
\\ steps must be taken before proceeding \\ ilh Silvester's meth or! ?
What should be done while artificial respiration is performed?
State the treatment for strangulation
State the treatment for hanging ...
State the treatment for smotherincr
State the treatment for choking . .
lIow may a swelling of the tissues of the throat be caused?
or
How would you liberate a sufferer from contact wiill an 142 electric mediulll ?
\Vhat would you do when the sufferer wa fr om -, contact?
What would you do in the case of a lightning ? '.::
PAGE 13 1 13 2 13 2 13 2 132 13 2 taken? ... 13 2
13°,
13 2 133 133 134 134 134 134 134 135
...
.. . ... ... ... .. . ...
136
.. . .. . ... ... ...
136 , 137 137 137 137 138
.. . .. . . .
. .. . .. 138, 139
... .. . . ..
... ... ... . ..
. . . . . . . ..
... ... ... ... ... . .. 139 139 139 139 141 State the treatment for swellincr of the tissues of the throat ... "'......... 141 State
'" ... . ..
.. . . .. ...
143
the treatment for uffocation by smoke
crase 141, 142 lIow is electricity conycyed ?
14?
... ... '" ...
143
It4
CHAPTER VI. POISONING.
Poisons may be c1as ' ified 2.ccording to their treatment under two heads:-
I. - Those which do not stain the mouth , and in treatment of which an emetic is t o be give :1 . Among:>t these are :-
(a) Arsenic, Phosphorus (contained in rat poison and lucifer matches), Tartar emetic and Corrosive Sublimate, \\'hich cause a metalli c taste in the mouth and a burning pain in . the mouth, throat and stomach.
(it) trychnine, Prussic Acid, Belladonna (deadly nightshade plant) and several other varieties of plants, such as laburnum seeds, etc. j these give rise to conv'Jlsions, delirium, failure of respiration and collapse.
(c) Poisonous meat, fish and fungi (often mistaken for mushrooms). Suspicion of tllese poisons should b e directed to C:lses wh e re several persons who have partaken of the same food develop similar signs and symptoms.
«(1) Alcoho l , which may cause collapse.
(e) Opimi.l and its preparations, MorpIli 1,

149
L a u danum, Paregoric, Chloro dy ne, Syrup of Poppies and various soothing drinks a n d cordIals; these cause a tenden cy to go to sleep, which continues until sleep becomes deep and breathing stertorous; the pupils of the eyes become minutely contracted (pinhead pupils).
2 .-Those which burn or sta in the mouth , and in the treatment of which no e m et ic is to b e g iven . TI1 :::s ':; are of two clas.=;es : -
(0) Acids, sllch as Nitric Acid (Aqua fortis), Sulph uric Acid \ Oil of Vitriol), Hydrochloric, or Muriati c , Acid (Spirits of Salt), stron6 Carb olic Acid (Phenol), Oxali c A rid, \\'hich is contained in oxalate o f potash, S3-lts of sorrel, salts of lem o n and some polishing pastes .
(b) Alkalies, such as Caustic Potash, Cau stic Soda anJ Ammonia.
SU.\DL\RY OF SDIPLE FOR THE TREAT:\[E:--IT OF POISOXlt\G.
1. - Send for a doctor at once, stating what has occurred and if possible the name of the
2. - Except when the lips and mouth are t3ined or burned by an acid or alkali,
15 )
promptly give an emetic - that is, mak e t he patient vomit as follows:,
(a) Tickle the bCkk of the tllroat wIth the fin 6er or with a feather.
(b) )V/ustard -a dessert-spoonful in a tumblerful of luke-warm water.
(c) Salt-a table-spoonful in a tumblerful of luke-warm water.
(d) Ipecacuanlla TVine-for a young child , a t ,' aspoonful repeated at intervals of fift een minutes .
3. - In all cases when the patient is not in , sensible, give Milk, Raw Eggs beaten up with milk or water, Cream and Flour bea : en up together, Animal or Vegetable Oil (except i n phosphorus poisoning), and Tea .
Olive, Salad, an1 CoJ-liver oil, or oil such as that in which sardines are preserved, may be given; mineral machine oils an::l paraffin are unsuitable . Oil is soothing, and is therefore especially useful in poisoning by Acids, Alkalies and such as Arsenic and Corrosive Sublimate. Demulcent drinks, such as barley water or thin gruel, act in the manner, and are free from danger in cases of phcsphorus poisoning. may be given either before or after th: emetic if the poison calls for one.
Stro;l'; Tea acts as a of many poisons
and is always sJfe. A handful of tea should be thrown into a kettle and boiled.
4
- If the lips and mouth are s ta ined or bu rned give no emetic , but -
(a) If an acid is kno \Y\1 to be the poison give an Alkali at once. First wash the mouth out fre e ly with lime water or other alkaline mixture, su c h as soda, chalk, whiting, or magn esia or wall plaster in water, and afterwarJs let the patient sip a little of it Soda and potJsh are not to be given in the case of poisoning by oxalic acid.
(b) If a strong Alkali is kn own to be the p o ison give an acid at once . First wash the mouth out freely \\'ith lemon juice or vinegar diluted with an e qual quantity of \\ater, and afterwards let the patient sip a little of it.
In both cases give oil (Rule 3) .
5. - When a person has swallowe j poison and threatens to go to sleep , keep him awake by walki ng him abo u t and slapping his face, neck and chest wit h a wet to\Vel. Stro ng b lack coffee may be given to d rink. Slapping the so les of the feet may also be trie d ,
6. - !f the throat is so swollen as to threaten obstruction to the air passage , apply hot flannels or poultices to the front of the neck and give frequent sips of cold drinks .
J 5I
7. - Apply artificial respiration if breathing cannot be discerned.
8. - Treat shock and collapse.
9. - Preserve any vomited matter, food ) or other substance, suspected of being the poison . Do not wash vessels which may have contained the poison, and car efully guard them.
Certain poisons require special treatment, and a fe w of the commoner of these are mentioned b elow with their treatment.
CARDOLIC ACID.
Th e odour of the breath will aid in the detection of this poison; the lips and mouth are us uall y stained white, and several nervous symptoms come on.
TREATi\!f::.NT.
I.-Give milk, to a pint of which half an ounce o f Eps ::> m Salts has been added .
2. - Treat according to the general rules.
PRUSSIC ACID.
The action of this poison is extremely rapid. Gitldiness, staggering, insensibility accompanied by pantin g respiration, profound collapse and possibly convulsions are the gen e ral signs, and in addition a sm e ll o f bitt e r almonds is often present.
TREAT.\IENT.
I. - r Jace the patient in th e open air.

1: 3
2. - Dash cold \\'ater on th h d 1 e ea a ne s p ine c ontilluously.
3·- A pply artificial respiration.
4·-Hold smelling salts to the nostrils.
5·-Treat shock and collapse. (See page 135 )
MEAT, FISH FUNCL
u.The signs and symptoms are vomitincr and pur cr incr ( Jarrhce:t), colic, headac he, great raised and a quick pulse. '
I.-Give an emetic.
2.-;Vben the emeL c has acted, give ca stor o il.
3·- rreat collapse . (See page 135.)
STRYCHNINE
. !he signs and symptoms are a feeling of suffo c ati o n features, an.d convulsions. The pati e nt res ts hIS head and feet, and the body i. arched.
TRE<\TMENT.
I.-Give an emetic.
?.-Apply artificial respiration.
ALCOHOL.
I.-Give an emetic if the patient can swallow.
2. - Treat colla.pse by keeping the patient warm etc . (S ee page 135 ) ,
QUESTIONS ON CHAPTER VI.
Tlu 1lUIlIerals iud/cate the pa.ger wltere tlte answers may be found.
Under what two heads may poisons be classified?
\Vhat are the symptoms of poisoning by Arsenic?

148, 149 148 14 8
\Vhat other poisons gi\'e rise to the, same ",
\Vh::tt p oisons give rise tl) co:wulslOns, Jehnul11, fallure of respirati on a.nd cullap e? ,"
If several people who had partaken of the same fo od developed similar sians and symptom, by what would you suspect had Geen poisoned? ,.' 148
\Vhat condition may result frJm poiso ning by alcohol? 148
\\' hal are the effects 'of such poisons as opium ?., 148 , 149
" ' hat two classes uf p )ison burn or stain the mouth? .,. 149
\"ould you give an emetic for such poisons? 149
Nam e some of the principal acids J49
Nam e some of the principal alkalis 149
State the general rules f J r the treatment of poisoning .,.
... ... 149 to 15 2
Stale the best melhods of making a person vomit 150 II ow would you treat a case of acid pJisoning? .. , ... 15 I
H ow would you lreat a case of poisoning by an alkali.? IS [
Slate the signs, symptoms and treatment of carbohc acid poisoning ."
Slate the signs, symptoms and treatment of pOl omng by Prussic Acid ." ... 15 2 , 153
Slate the sIgn, symptoms and treatment , f poisoning by poisonoLls food
State the signs, symptoms and treatment of pOlsolllng by 153
WhatStrychnine would you do in the case of alcoholic poisoning?
155 CHAPTER VII. BANDAGING.
. Esmarch's Triangular Bandage has been described In II. It may be :' 1plied to keep a dressing on a \\ burn or scald of nny part of the bod or for an Injury of a joint. y,
For the Scal p (Fig. 62). Fold a hem about I!. inches deep along the of a bandage ; place the bandage e n the head so that the he m lies on the forehead cl o se down to eyebrows, and the PCll1t hangs down at the back ; cnrry the two ends round the head above the ears and tie them on the forehe ad ; draw the point first do\ynwards, and then turn \ P and pin it 011 to F IG. 62. the b.; on the of the head.
For the Forehead, Side of the Head Eye
Cheek , and for any part of the body that r ound (as the ariTI. or thIgh, etc ), the narrow bandacye should be used, Its centre being pJaced over the
154
PAGE
. . . . ., . .
.
... .
. .
... ...
...
..
.., ... ... , .,. . . ..
...
15 6
and the ends being carried round the head or 8S the case may be, and tied over the wound. F or the Shoulder (Fig. 63)· Place the of a handage on the shou ld e r, with the point running

FI G FIG. 64·
up the side of the neck ; a hem along the ; carry the ends round the mIddle of the arm and tle them. Place one end of a broad bandage over the point of the first bandage and sling the arm by carrying the other end over the s0U11d shoulder and tying the ends at the side of the ; turn d.ow.n the point of the first bandagE', draw It tIght and pm It.
157
For the Hip (Fig . 64). Tie a narrow bandage round the body above the haunch bones. with the knot on the injured side. Fold a hem accordina to the size of the patient [:lion.s the base of a second bandage; place its centre over the dres ing, carry the encs round Lle thigh and tie them; then carry point up under the
FIG. 65 . FIG. 66. first bandage, tum it down oyer the knot a nd pin it.
For
the Hand wh en the fingers are exte nded (Fig. 65). F?ld a hem along the base of :l bandage; place the WrIst on the hem with the finaers towards the point; then bring point over thOe wrist, pass the ends round the WrIst, cross and tie them' bring the point over the knot and pin it to bandage on the hand .
8
For the Foot (Fig. 66) . the foot on th::. centre of the bandage with the toes towards the point ; era \V up the point over the instep, pass the ends round th e a nkl e and cross th em in front; no\\" pass the ends round the instep and tie them. Dra\\" the

FIG. 67 a .
FIG. 67 b.
forward and pin it to th e bandage on the inst ep.
. the Back. The ban IS applIed as the e\ c: pt that it is hegun at the
For the Knee. Fo! I a
n arrow hem along the bas e cf a bandage; lay l'le point on thigh and the 111ldJle of the L_lse ju st below the knee -op; cross the ends first behind the kn ee, tben over the thigh and tie t:lem. Bring the point down an i pin it to the base (Fig. 6 3).
FIG. 68. For the E :bow. FoLl a narrow hem along the bm:e of a IJan?age;. hy th e point on the back of the arm and t..e 111lddle of the base on the back of the forearm; cross the first in front of the elbow over the arm and tie them in fr ont ' (FIg. 69).
Fingers and Toes \Hap a
s inp of ca lIco or linen round and round the part; splIt the fr ee end md secure it round the \vrist or ankle.
For the Front of the Chest (Fig,s . 67 a and 67 b ). Place the middle of the b a ndage over the dressing with the point over the shoulder on the same sid e; carry the ends rounl the waist and tie them; 159 then elr::-. :,· the point over the sh oulder and tie it t .J on e of the ends.
15
CH.\PTER VIII.
OF CARRYING.
THE FOUR-HANDED SEAT.
This seat is used when the patient can assist the bearers and use his arms.
1.-Two bearers face each other behind the patient and grasp their left forearm with their right hands and

FIG. 70
each other's right forelnn with their left hands (Fig. 70 ), and stoop down.
2.-The patient sits on the hands and places one arm round the neck of each bearer.
161
3·-The rise together and ste [he on the fight hand side of the patien£ with the a oot, anj the left hand bearer with the left foot.
THE T ,\ a-HANDED SEAT.
This seat may be used t h o carry a elpless patient.
FIG. 71.
I.-,Two bearers face each other and stoo each sIde of the patient Each b p, ?ne on . earer passes hIS fore arm nearest to the patient's head under his back jus;
G
I60
below the shoulders, and, if possib1e, takes hold of his clothing. They slightly raise the patient' s back, and then pass their other forearms under the middle of his thighs t Fig. 7 I), and clasp their hands by on e of the methods sho\\"n in Figs. 72 and 73· A handkerchi ef be h e ld in the hands if th e first grip is used.

G. 73.
2. - The bearers rise to.;ether and st e p off, the right-han d bearer with the right foot, and th e le ft -hand bearer with the left fo.)t (Fig. 74'·
THE THRb.E-HANDED SEAT.
This seat is fo: carrying a plti e nt and supporting eith e r of his lo .vcr li .11'Js, when h -= is able t ') US3 his upp e r limhs.
1. -Two beMers face each other b =hind the patient. For supporting the Iefe limb the bener to the pati e nt's right gr<1!"ps bis own left \\ rist \\ ith his righ: band, and the othe r bearer's right wrist with his left hand. The b earer to the left grasps the first bearer's right wri t ,,: ith h!s ri J ht ha!1d (Fig. 7 J)' Tl:ic; Is:w cs hs
= -f, I, 1 .' -:- .-. II ' ., .1, t ." - - • FI
, "" 3

left hand free to support the patient's left leg. For the patient's right lower limb follow the same directions, substituting" right" for " left" and" left" for "right." The bearers stoop down.
2.-The patient places one ann round the neck of each bearer and sits on their hands.
3. - The bearers rise toge ther and step off) the FIG. 75.
right-hand bearer with the right foot, and the lefthand bearer with the left foot.
THE FIREMAN'S LIFT.
(To be attempted only by a strong man).
Turn the patient face down wards; place yourself at his head, stoop do\\'n, slightly raise his heau and FIG. 76.
shoulders and take hold of him close under his arm· pIts, locking your hands on his back. Raise his body and rest it on your left knee; shift your arms and , taking him round his waist, lift him until his head rests on your left shou ld er. Throw his left arm over your head, stoop down and place your left arm bet\\'een his thighs, letting his body fall across your shoulders. Rise to an upright position; hold the patiel1['s L:: ft \\ rist \\ith your left hand and leaye your right hanJ free.
Assistance may be given to an injured person by supporting him in the manner show n in Fig. 76
Tlze plan of canyillg tlte patient hy tlze arms and legs 'Zm"/Il tile face downwards, commonly called tile "frog's marc/I, " must never be lIsed, as deallz may ensue from Ilzis treatment.
IMPR OVISED STRETCHERS.
A stretcher may be improvised as follo\\'s :-
I. Turn the sleeves of a coat inside out; pass two strong po les through them; butto \ the coat. The patient sits on the back of the coat and rests against the back of the front bearer ( Fig. 78). If a longer stretcher is required t\\'O or three coats must be treated in th e same manner. The poles may be kept apart by strips of wood lashed to the poles at both ends of the bed formed by the coats (Fig. 79).
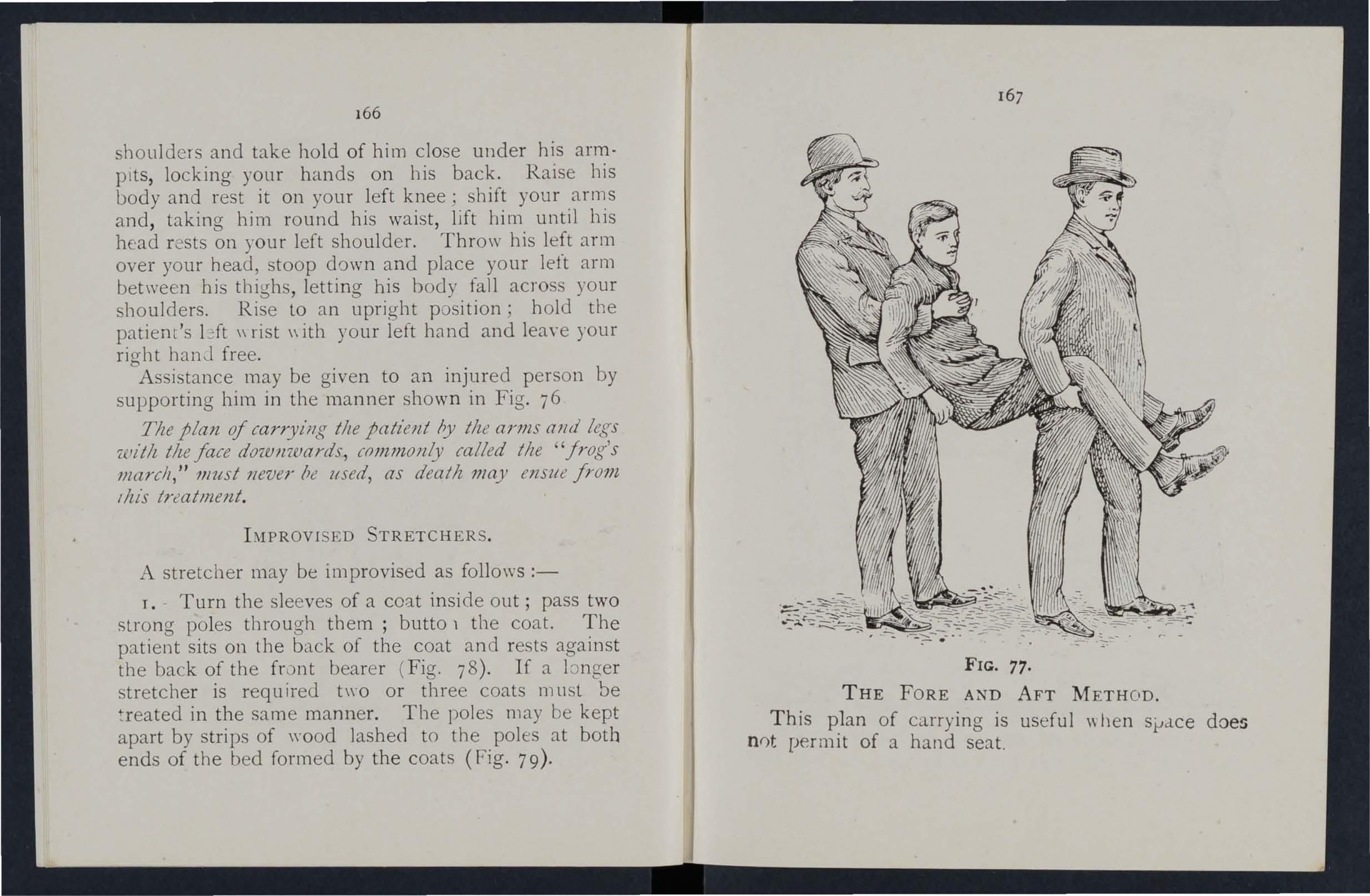
77.
THE FORE AND AFT METH OD .
This p1an of carrying is useful \\'hen sl-'d.ce does n0t permit of a hand seat.
166
FIG.

2.-2\Iake holes in the bJttom corners of one or two sacks and pass stout poles through them.
3·- Sp read out a piece of caqLt, sacking, tarpaulin, or a st rong blanket, and ' ro ll t\\"o stout poles up in the sides . T wo bearers stand on each side and grasp the midd'e of the pole \\ith one hand, and near the end with the other. They walk sideways.
-t . -:\. hurdle, broad piece of wood, or shutter may be used as a stretcher; some strclW, hay, or clothing s;lould be placed on it, and covered with a piece of stout cloth or sacking; the latter is useful in taking the patient off the stretcher.
Always test an improyised stretcher before use. Stretchers must be carried, and the palient placed on the;11, as laid down in the c: Stretcher Exercises,"
1S a general rule cury the lntient feet foremost. The exceptions are: -
(7) ",Vhen going up hill with a patient whose lOwer limbs are not injured.
(b) ",Vhen going down hill with a patient whose lower limbs are injured .
Ayoid lifting the stretcher over ditches or walls, but where these cannol be ayoided the stretcher must b:; carried in the following ways: -
To CROSS A DITCH .
In crossing a ditch, the stretcher should be lower with its fo::>t one pace from the edge of the ditch
169
Nos. I and 2* bearers th n descend. The stretcher, with the patient upon it, is afterwards advanced, Nos. I and 2 in the ditch supporting the front end while its other end rests on the edge of the ground 3.bove. No. 3 now d Escends. All the Nos. now carry the stretcher to the opposite side, alld tbe foot of the stretcher is made to rest on the edge of the ground, while the head is supported by 3 .in the ditch. No. I climbs out, No. 2 remaInIng In the ditch to assist NO.3. The stretcher is lifted forward on the ground above, and rests there while Nos. 2 and 3 climb up.
To CROSS A \VALL.
The stretcher is lowered with the foot about one pace from the wall. Nos. I and 2 bearers then take hold of the foot of the stretcher, and NO.3 (Jf the he8d ; the stretcher is raised till the foot is placed on the \\'all. No. I then clim bs over the wall and takes hold of the foot of the stretcher, while lOS . 2 and 3 support the head; the stretcller is then carried forward till the head rests on the wall, No. J supporting the foot. Nos. 2 and 3 then clil1lb over the w.lll and take hold of the head of the stretchfr, which is then slow ly lifted off the wall on to the g round, and the bearers take their usual places.
* Th e!'e numbers are explain d later in the detailed Exercises."

171
To LOAD A \\'AGON.
The stretcher is lowered with the foot one pace f1 '-' 111 the end of the wagon. N os. I and 2 take hold cf the foot of the stretcher, No. 3 the head. The stretcher is then raised and carried forward till the front wheels rest on the floor of the wagon. No. I then jumps into the wagon, \\ hi Ie No.2 goes to the head of the stretcher and helps NO.3. The stretcher is then pushed slowly into the wagon. If the tailboard cannot be shut, the stretcher must be lashed firmly to the sides of the wagon.
To UNLOAD A \V AGON.
Nos. 2 and 3 take hold of the head of the stretcher, while No. I gets into the wagon; the stretcher is then gradually drawn out till the foot-wheels rest on the edge of the wagon. No. I jumps out of the wagon, and with NO.2 takes hold of the foot of the . stretcher, NO.3 supporting the head. The stretcher is now gently dra\\ n away one pace and lowered. \Vith four bearers Nos. I and 2 would lift the foot of the stretcher, \\hile Nos. 3 and 4 lift the head. 'fhi:; applies to crossing a ditch or wall, as well as to loading and unloading a wagon.
170
CHAPTER IX.
STRETCHER PORT.
The "Furley" Stretcbers (Model ] 899) are of three patterns, viz," Ordinary,"" Telescopic-handled," and "Police." In general principle they are alike, the component parts being designated the poles,

FIG . 80.-0RDINARY STRETCHER-CLOSED.
handles, jointed traverse bars, foot \\ heels, bed, pillo\\' and slings
The Ordinary Stretcher (Fig. 80) is 7 feet 9 incbes in lengtb, and I foot 10 incbes \yide. The bed is 6 feet in length, and tbe handles inches The h@.ight is si inches. At the bead of tbe stretcher is a canvas overlay (the pillow sack) \yhich can be filled with straw, hay, clothing, etc., to form a pillow. The jointed traverse bars are proviced \\'ith joints,
173
for opening or closing the stretcher. The Telescopichandled pattern (Fig. 81) is very similar, but 'the handles can be sl id un Jerneath the poles, th us reducing tbe le ngth to 6 feet. This arrangement is of great value when working in confined spaces, or " ,. hen a patient has to be taken up or down a narrow staircase \\ ith sharp turns . The Police stret • . her is similar to the Ordinary pattern, but is more strongly made, and has, in addition, straps for securing a refractory patient.
\Vhen closed, the p ::> les of the stretcher lie close together, the traverse bars being bent inwards, the canvas bed neatly fo!ded on the top of the poles and htlJ in position by the slings which are laid along the calwas, and secured by a strap, placed transversely at the end of e.1ch sling, being passed through the large loop of the other, and round the poles and bed.
In closing a stretcher care should be taken to raise the centre of th e canvas ",h : n pushing in the traverse bar, as it is ( thel'lyise liable to get caught.
To prepare, or open a stretcher, u!1buckle the trans verse straps of each sling; remove the slings from the stretcher; separate the pules; take hold of each traverse bar and draw it forward. The slings will then be folded to balf their length, one being laid neatly over tbe handles at each end of the stretcher.
As a general rule, the stretcher will be prepared by :.; o s. T and 3 bearers in Exercises I, 11., and III.;
172
FIG. 8 r.-TE LESCOPIC·HANDLED STRETCHER- Ol'E:-i'.
17-t
and by No. 2 in Exercise IV. These bearers will, however, if required, assist the other bearers in attend1l1g to the injuries.
Jllote. -The various movements detailed in the fol1owing Exercises should be carried out steadily, the bearers working in unis ') n, hurrying b e ing carefully avoided and every attention being paid to the bearer wbo gives the words of command.
STR I TCl-IER Exf. RCISES,
Originally drawn up by Sir J oh n Furley, and revised in I904 to accord with the drills adopted by the Royal Army Medical Corps :-
EXERCISE No. r.
FOR FOUR BF:ARERS.
T.- The Instructor selects the bearers and num bers them - J, 2, 3, 4 at his discretion. Should one man be tal1er :l.nd stronJer than the o thers, he should be styled NO.3 as he \\ ill have to bear the heavier part of th e burJen.* All o rders \\il1 be given by NO.4.
2. - " Fall in ."- Nos . I, 2, and 3 t:lke position on the left side of and f.lcing the patient. No. I places himself at the patient's kllees, No. 2 at the hips, NO.3 at the p:ltienl 's sho·dders. At the same
* Pearers should, h oweve r, be taught to take any of the po"itions named in the foll ow ing exercises, whether Ihat of No T, 2, 3, or 4 bearer.

175
time No. 4 places the prepared stretcher on the ground by the right side of the pati nt about two l' .l;, 82.
paces away from him, and then takes position opposite to and facing NO . 2. (Fig. 82).
3· - " REa d y ."--The bearers kneel do\\"n on the le.ft knee and take hold of the patient, No. I passing hlS hands and fore-arms beneath the patient's less, hands wide apart. Nos. 2 and 4 pass their han Lls and forearn,s beneath the patielll's hips and loins, and grasp each other 's hands. NO.3 passes his left hand across the patient's chest and under the ri ght shoulde r, anJ his right hand ben eath the left shoulder (Fig. 83)
4·- "Lift. "-On the \\ ord c ' Lift," the bearers raise the patient gently and rest him on the knees of J, 2, r..nc1 .1 bearers 84) ; as so on a.s he

is e ' urely reste I, NO.4 disengages hands \\ ith 2, runs rouncl by the head of the stretcher and places it uncleI' the patient, c lose to the other bearers' feet)
176
Ii7
178
bein a ca reful that the pillow is immediately under the head (Fig. 85); he then do\yn and lock s his hands with those of No.2 (FIg. 86) .. " _" Lower." -The bearers place the patIent on the'" stretche r (Fig. 87), disengage their hands, and then stand up.

FIG . 85·
6. - " Stand to Stretcher."- No. I goes the foot of the stretcher \\'ith his back to the p8tlent; NO.3 to the head \\ his face to the patient; Nos. 2 and 4 remain on each side of the stretcher.
7.-" Ready. "--Nos. I and 3 place the (if used) over their shoulders, stoop do\\ n, and slIp the
179
loops of the slings on to the handles of the stretcher,. which they then grasp.
As soon as all is right the word is given:-
8. - "Lift Stretcher."-Nos. I <:.nd 3 bearers raise the stretcher steadily together and stand up .
Note.-Nos. 2 and 4 will no,,": adjust the slings on the shoulders of Nos. I and 3, takmg care that each is well below the level of the collar and li es accurately in the hollow of the shoulder in front. They will also the slings, having regard to the patlent S lnjunes and the relative heights of the.. bearers. l' JG. 86.
9·-" March." - The bear ers move off :-Nos. I, 2, and 4 stepping off with th e ir left foot, and No 3
\vith his r;ght foot (Fig. 87). The step shou.ld be a short one of twe n ty inches, and taken wIth bent Knees and no spring from the fore of the foot . ro. - " Halt. "-The bear ers remall1 steady.

F I G. 87.
II . - "Lower Stretcher." -The. bearers place the stretcher gently on the grou n d , slI p the loops t he slings off th e ha n dles of the stretcher, remm e the slino-s from the shoulders, and then stand u p.
12. - " Unload Stretcher - Ready." - The bearers prepare to take the patic.nt off the stretcher r as at Orders 2 and 3.
13·- " Lift. "-The bearers raise the patient as at Order 4 (Fig. 86); NO.4, in this case, disengages hands from No.2, removes the stretcher (Fig. 85), and resumes his former position. If necessary, the bearels will then steadily rise together, and cJrefully carry the patient to the bed, or other place to which it has been arranged to convey him .
14·- " Lower."-Tbe pat ient is carefully lowered..
EXERCISE
No . II . FOR THREE BEARERS.
I. -Number the bearers I, 2, 3.
All orders will be given by No . 2, who will look. after the injured part of the patient's body or limbs, to see that n o bandages or splints become displaced, and also that No . I bearer, in lifting or carrying the stretcher, does not to uch the patient 's feet.
2. - " Place the Stretcher. "-No . 3 places tbe stretche r in a li ne with t he pa ti ent 's body, the foot of the str etcher be ing close to his h ead .
3·- " Fall In."- N o . I places himself on the left side of the patie n t in a line wi th his k n ees , No.2 Oll the left side jus t be low t he pa ti eI}t's shou lders, an.! NO . 3 at the right side , and faces NO . 2.
180
.::> 18 1
4.-" Re_.dy."-All kneel on the left knee. No. I places his hands, well apart, underneath the lower limbs, always taking care, in case of a fracture, to have one hand on each side of the seat of injury. Nos . 2 and grasp each other's hands under the shoulders and thighs of the patient (Fig. 88).

s. - " Lift." - The bea! ers rise together, kec ' ping the patient in a horizontal (Fig. 89) · 6.-" March."-All tJke short side-paces, carrying the p atient over the stretcher until his head is immediate ly above lhe pillow.
7.-" Halt.- The hearers remain steady 8 "L "Th • . - - e bearers stoop down, gently place the patlent on the stretcher, disenga ae theIr hands, and then stand up. 0
f 9 i-" Fall In."-No. T places hin1self at the foot o t 1e with his back to the patient N places hlnlself at the left side of the pat' ' t o. NO·3 at the h ,:ad, \' ith his face towards the
10. -" Ready." -Nos. I and 3 place the slit.1gs (if used) over their shoulders, stoop down, and sltp the loops of th e slings on to the handles of the stretcher, which they then grasp.
As soon as all is right the word is given-
1I.-" Lift Stretcher."-N os . I and 3 bearers raise the stretcher steadily together and stand up.
No. 2 will now adjust the slings on the sh oulde r s of Nos. I and 3, taking care that each is well below the level of the collar, and lies accurately in the hollow (If the sho ulder in front. He will also lengt hen or shorten the slings, having rega rd to the patient' injuries and the relative heights of the bearers.
12 -" March."-N os. I and 2 step o ff with th e left and NO.3 with the right. The shoulll be a short one of 20 inches, and taken \\"tth bent knees, and no sp r ing fro:11 th e fore of th e foot.
13.-" Halt." -The bearers remall1 steady.
14.-" Lower Stretcher."- The place the stretcher gently on the ground, sltp the loops. of the slings off the handles of the stretcher, remove the slinas fro:11 the shoulders, and then stand up.
IS Unload Stretcher - Ready." - The bearers prepare to take the patient off the stretcher, .as at Orders 3 an d 4 (Fig. 88) .
16.-" Lift." -The bearers raise the patient, as at O rder S, and carry him by short side steps, the stre tcher, to the bed, or other place to WhICh lt has been arra'lged to convey him (Fig. 89)·

I7· -" Lower." - The is carefully lo\Vered .
EXERCI 'E No.
III.
ONLY THREE BEARERS ARE: AVAILADLU: THE STRETCHER CANXOT DE PLACED AS lN EXERCISE II.
I.-The Instru c to r numbers the 2, 3. All orders will be given by NO.2.
2.-" Place the Stretcher."-No. I taking the foot of the and No. 3 the head, place tt on ground by the SIde of th e patient, and as cl ose to Ln1 as praclicable.
3. ' - " Fall In. "- The three b ea rers take the same pos itions on one side of the patient, as laid dOvt,:n in Exercise No. I.
4· -" Ready." -Nos. I, 2, and 3 kneel down on the. left knee, placing (1S close to the as cOl.lVeniently can, a nd thcll take hold of hIm as dIrected 111 Exercise No. I.
5 "LOft" N . . .. 1 0 - ?s. 1,2, and 3 raIse the patient (1S dlrect.ed 111 . No. I, and then move in a kneelmg pOSItIOn up to the stretcher.
6.-" Lower."- The beare rs bend forw ard, ca refully lower the patient on to the stretcher, and dise ngage hands.
185
7. -" Stand to Stretcher. "-All the st.md up; NO . 1 goes to the foot, NO.2 remall1S 111 position at the side, and NO.3 goes to the head of the stretcher.
. .
8. - " Ready."-N os . I and 3 place the (If used) over their shoulders , stoop do., n, and slIp the loops of the slings on to the handles of the Stl etcher, which they then grasp.
9. -" Lift Stretcher. "-Nos. I and 3 bearers raise the stretcher steadi ly together and stand up.
No 2 will now adjust the sling:; on the shoulders of Nos. ; and 3, taking care thaL each is :vell beluw the level of the col ar and lies accuraltly 111 the hollow of the shoulder front. He will also ?r .shorten the slings, having regard to the patienl s l11Jltrlt!S and thv relative h . ights of the hearers .
10. - " March. "-Nos. I and 2 step off \\'Ith the left foot and NO.3 with the ri.sh t. The step should be a sh'ort one of 20 inches, and taken Wlth bent knees, and no spring from the fore of the foot.
II -" Halt."-The bearers remall1 steady.
12' -" Lower Stret : her. " - The bearers place the ;tretcher gently on the ground, slip the loops of the slings off handles of the stretcher, the slings from the shoulders, and then UI ·
13.-" Unl o ad -No . . 1
IJlacE s himself on the left side of the and. 111 a line with his knees, No. 2 on the left side )llSL be' )\V the patient's shoulJers, and NO·3 at the right

137
side, and faces NO.2. All kneel on the left knee. No. 1 places his hands, \Yell ap :Ht, underneath the lower limbs, always taking care, in case of a fracture, to h:lVe one hand on each side of the seat of Nos. 2 and 3 grasp each other's hands under the shoulders and thighs of the patient.
I 4·-" Lift " The bearers rIse together to their feet, keepll1g the patient in a horizontal posit ion , and c.:trry him by short side steps, clear of the stret cher, to the bed, or other pLtce to which it has en arrang ed to convey hIm.
15.- 11 Lower ."-The patient is carefully lowerLll.
EXERCISE No. IV.
FOR USE IN :\IINES NARRO ',\, CUTTI;\GS " T 0 MEN ONLY CAN BE ENGAGED.
Nos rand 2 will carefu'l / pbce the stret c her in a lm e \\,lth the injured man's body, the foot of the stretcher being, If pos Ible, close to hIS head.
No. I straddles across the patient's legs, placing his nght foot, with the to,- turned outwards, a little below the patiem's knees, and with the toe of the left foot close to the heel of No.2; he then stoops down, p:l.sses the Jeft hand und e r the patient's thighs and
• It is not advisable to ue too particular as to the head (l r foo r of a stretcher in a mine, as it would probably be quite imp )ssi!Jle ro reverse It.
186
I8S
th e right across and und er pati e n t's
N o.2 places his feet one on each side of the patlen: between bis body and arms, the toe of each foot a;:, nea r the armp its as possible. He stoops down and passes bis h a nds between tbe sIdes of the chest and t1e Clr.1\S ll'1de n "'ath the shoulders, and locks c.

tbe fin gers (Fig. 90). If the patient's arms are uninjured he may put them of No.2, and by this means great ly assIst him m l1ftmg.
IS9
'Vh e n both are reaJy, o. I will gi\'e the order " Lift and move forward. " The patient i::, then to be slow ly lifte d , just suffiCient to allow his boJy to clear the stretche r. Both bea re rs will slowly anJ gradua lly move the patient forward, NO.2 by yery short steps, No. I by bending his body forward as much as he can 'iOt'tiw/(/ moving h/s fe-;/ \Fig . 9T) . -0. I now gives the order I' Halt, " \\ he reupOll No.2 remains teady , alld o . I advances his right foot to his !eft; and
FIG. Si r.
again advances his left fo ot till the to e touches the heel of NO.2. No. I then gives the order "Advance," when the patient will again be forward. These morem ellts are to be rep eat ed until

19°
the patient is over the stretcher, when be is to be gently lowered.
The following Stretcher Exercise is adapted by permission from the Royal Army Medical Corps Manual, 1908.
All orders will be give n by NO·4·
I. " Fall in. " -Six bearers fall m behind each other.
2. " Number. " -The bearers number from front t o rear.
3. "No.3 Bearer, right (or left ) turn- supply stretcher- quick march." - o. 3 bearer will march to the stretch er, stoop, lay ho ld of it and place it on his right shou lde r at the slope, holding it by the lower foo l wheels, wheels to the front. As soon as the beare r is provided with a stretcher, he will turn about and r ejoin his squad in quick time, halting as h e arrives in his place . He t u rn s to the fron t, and , passing the lower en d forward , p laces the stretch er on the ground to the r ight of the squad , wheels t o the right, fro n t end of the poles in lin e with the toes of No. I and rises .
4. (( Stand to Stretcher. "-N o . 1 places himself with his toes in line wi th the fr ont ends of the poles. NO.3 with his hee ls in line with the rear ends of the poles, close to and touching the stretcher with °1 [J m 13 rn @]
Fig. 92., : .'. '," , I , ,'. \ \ '\ '. ,.... ,I '. 1.?J ': I I I I I I' • T I I. . , , r -. " , , I / ' I , :• • • , 1/ , 5 ; / ' ,.... I :.... /
FiC; . 93.
hi s right foot. Nos. 2, 5 and 6 take up their positi ons one pace behind and covc:ring off the bear e r in front o f them (1' ig. 92).
S. " Lift Stretcher. "-Nos . I and 3 stoop, grasp both handle s of the poles with the right hand, together, holdi n g the stretcher at the full extent of th e a r m, wheel to the right.
6. " Collect Wounded - Advance ." - Th e sq uad doubles by the shortest route to the patient, and halts \yithout further word of command one pa c from the head of and in a line with the patient (Fig. 93).
7. " Lowe ' Stretche r."- Nos. I and 3 stoop, phce the stretcher quietly on the ground, and ris e together.
8 . " Prepare Stretche r."-No s. I and 3 turn t o the right, kne e l on th e left knee, unbu ck le th e transYerse stra ps, and place th e slings on the g ro un d beside then" separate the poles, and straighten th e t ra yerses .
T'i.lIo. On th e word two eilc h tak e s a sling, doubles it on itself, slips the lo op thu s formed on the n ear handle, and places th e fre e e nd s over th e opPJsite h and le, buckle upp ermo st. Th ey th e n rise and turn to their left toge th e r.
\V hile th e stretcher is being prepared by No s. r and 3, the disengaged bearers will advance and r ender to the pati ent such assistance as may be required ( Fig. 94)·

193
The necessary assistance havinO' been rendered, NO.4 will give the coml11and- 0
9· "Load Stretcher." - The bearers place themselves as follows I, 2 and 3 on the left, Nos. 4, 5 and 6 on the rlgbt of the patient ; Nos. I and 4 at the knees, 2 and 5 at the hips, 3 and 6 al the shoulders, the whole kneeling on the left knee.
I and pass their hands beneath the patient's Knees, 2 and 5 ben.eath the hips, 3 and 6 beneath the shoulders, care taken of the injured part, one of . the bearers bemg detailed for this purpose (FIg. 95).
"Lift."- The \\ hole will carefully lift the patIent on to the knees of lOS. I, 2 and 3.
Two. Nos. 4, 5 and 6 will then disengage, rise; 1 and 6 step back one pace. NO.5 turns to doubles to the stretcher, takes hold of and Luses. It, left h.and across, the near pole resting on the left hlp; carrYll1g the stretcher, he returns to his place between 4 and 6, and places it beneath the patient.
Three. .Nos. 4 and 6 step forward one pace, and together \\ Ith No S kneel down on the left knee and prepare to assist in 10werinO' the patient (FiO' 9(1)' "L 0 o · .
II. ower -The patient is lowered slo;\ ly and on to the centre of the canvas (special care bell1g trrken of the injured pal t).
Tun. Th e bearers disengage, rise; N os. I, :2, and 6 turn to the left ; lOS. 4 and 5 to the H
No. 4 places him:..elf three paces in f1:ont of the stretcher. No.6, having collected the lut and arms of the patient , places himself three in rear of the stretcher, Nos. 2 and 5 Opposlte the of the stretcher The \yhole are now ready to 11ft stretcher and moye off (Fig. 97) ·

FIG . 91 · FIG, 98 .
195
12. "Lift Stretcher. "-Nos. I and 3 stoop: grasp the doubled sling midway between the poles with the forefinger and thumb of the right hand, sweep it off the handles, rise, holding the sling at the full extent of the arm, buckle to the front; take a side pace to the front between the handles, and place the sling oyer the shoulders di\'idll1g it equally, buckle to the right. The slings should be placed so that they lie well below the collar of the coat behind and in the hollow of the shoulders in front. In the event of the slings requiring to be adjusted, eit-her as regards length or for the greater comfort of the bearers, NO.4 will detail a bearer to carry this out, the length of the slings being adjusted, when necessary, by mea ns of the b uckles.
Two. Nos . I and 3 stoop, slip the loops over the handles , commencing with the left, and gra p the ha n dles firm ly.
Three. Nos. T and 3 rise slowly together, Ko . 3 confo r ming closely to the moveme n ts of No . J.
13. "Advance." - N os . I, 2, 4 , 5 and 6 step off wi th the left foot, NO .3 with th e right, steppiflg short, knees ben t, fee t raised as litt le as possible .
14. "Halt."-The who le halt.
IS. "Unload Stretcher."-The bearers themselves in the same position at the stretcher as descri b ed for L oading (O r d er 9).
16. "Lift."- As d es cr ibed for Loading (OrJer 10), H2
194
except that the stretcher is carried forward three paces cl ear of the patient 's feet . 17. "Lower."-The is gen.tly lowered to th e ground. The bearers dIsengage, nse; I, 2 and 3 turn to the left, 4, 5 and 6 to the right, and the whole step off to their places at the stretcher, 8S at Order" Stand to Stretcher " (Fig. 98).
The Ashford Litter is made up of either of the FurJey stretchers l1lentioned on pages 171. and I73, a wheeled under-carriage and a waterproof hood and apron, or, if preferred, a light wet-resisting canvas co.ver. The stretcher is kept in position on the by the foot-wheels, which fit into slots in the sldes of the under-carriage, and it can be removed at pleasure. The under -carriacre is fitted with a cranked axle, which allows the bbearers to pass with the stretcher between the wheels instead of lifting it oyer them. At both ends are two legs which may be turned up as handles when wheeling the litter . The hood and apl:on fit into sockets screwed to the stretcher. In vvheeJlt1g the litter, care should be taken to keep the patient in a horizontal position. Should it be necessary, two bearers can easily lift the litter and patient.
The Rea-Edwa rds Litter introduced in I9 0 4 is used in a similar manner, and one model of it is fitted with pneumatic tyres, which add to the comfort a f the patient and to the ease of prol?u 1SlO11.

197 CHAPTER X.
(Being the Fzfth Lect,!re .for Females only, z'n accordance 2mtlt Syllabus 58.)
BY E. l\IACDO\rELL COSGRAVE, ?l1.D., F.R.C.P.r.PREPARATION FOR RECEPTJO:\T OF ACClDENT C ,\ - ES .
'IVHEN news .of an accident comes, preparations should at be made so. as to have everything leady be fo re the lI?Jured person lS. brought in. Of course the pr eparatIOns needful WlIl vary according to the tand t t fl' . ,na Lll e < • ex .en 0 t le Injury, but the following are the chlef thlt1gs which may have to be done.
CHOICE AND PREPARATION OF ROOM.
A room n:ust be chosen. In a bad case this should ?e. one easily reached, as it is difficult to carry an 111 Jured p erson .through narrow passag es and u posta irs. there IS some such reason atfainst it the 111 Jured person's own room is best. b ,
T?e way to the room must be cleared projectil1O" furniture and loose mats in the hall or' in should be removed. If the injured person is c3.rried on a door, shutter, or stretcher, t\yO stron O" chairs be placed .ready to support it the earers would be lIkely to require rest.
Usele;s furniture should be removed from the bedroom. fhe bed should be drawn out from the wall
I96
so that both sides can be approached, 'lnd the clothes turned back to one side to their full length. A hot bottle should be got ready. If there is much several hot bottles and hot blankets may be reqUlred ; cover the hot bottles with flann el.
If the injury is very severe, clothes have to be removed, or if extensive dressmgs have to be applied, it may be to have another bed, a couch or a table placed near the bed to lay the sufferer on in the first instance. This should be so arranged that soiling may do no harm; old sheets, waterproof materials, thin oilcl.oths, or even newspaper, may be used as a protectIOn.
LIFTL G AND CARRYING.
If present at the place where the accide,nt oc:urred, it will be necessary to see that the patient IS carefully lifted after proper "First Aid" has been rendered.
The following rules should be remembered :-Select the proper number of persons to assist, and do not let them lift the patient until they thoroughly understand how they are to do it.
For ordinary cases, where the injured person has to be lifted a very short distance, three are sufficient. Two (who should be as far as of eq ual height) are to bear the weight, the third t.o support and take charge of the injured part. ThiS IS

best done by a person who has been through a ;. First Aid" course. If the injured person is another help::r should support his head.
The lifters, one at each side, should kneel 011 one knee, and pass their hands under the patient's back at the lower part of the shoulder blades, and under the hips, clasping each his right hand in the other's left. The injured patient should, if practicable, place his arms round the necks of the bearers.
The third helper should attend to the seat of injury; if this is a fractured limb, he should support it by placing the palms of his hands under the limb. one above and one below the seat of the injury, gra ping it firmly but avoiding unnecessary pressure.
The helpers should remain thus until the order " Lift" is given, and then they should all lift slowly and steadily, avoiding jars, attempts to change position of hands, etc.
H the injured person is to be placed on a stretcher or shutter, this should be previously placed with the bottom end at his head; the bearers should then move, one at each side of it, until the patient is oyer it. The word" Lower ') should then be given, and the injured person should then be slowly lower ed . A pillow or folded-up coat should be ready, and as the sufferer is lowered this should be placed under his beo.d.*
* Full directions are given in Chapter IX .
198
199
l\ I EANS OF CARRYING.
Besides a st retcher, and substitutes such as a gate , a shutter, or a door, other means of carrying can be improvised.
In slight injuries, where the injured person is unable to walk, two bearers can carry him by forming a fourhanded, three-handed, or two-banded seat.
A four.handed seat is formed as described on p:lge r60.
A three-handed seat is made as described on page r62.
The two-handed seat is made as described on page r61.
A single helper can lift by supporting with one arm the two knees, and with the other the back. The arms must be passed well under before commencing to lift.
A single helper can give support by putting his arm round the waist, grasping the hip and placing the injured person 's arm rou n d his o\\'n neck , holding hand with his own hand (Fig. 76, page r65) .
A capital stretche r can be improv ised o u t of a strong sheet and two broom hand les or other short poles. Each side of the sheet is wound u p o n a broom h:tndle until there is just room for a person to lie between. This req uires four bearers, t\\'o at each side, to prevent the sheet slipping.

201 CARRYING UP STAIRS
.
In carrying a stretcher up stairs head should go first, and an should assist at the lower end., so as to raIse It and keep the stretcher nearl honzontal. y
The three,. or four -handed seat may be used fOl: up staIrs; or a strong chair, the patient beIng earned up backwards. In the latter case one !1elper should walk .the chair and help to support It, and to prevent the Injured person slipping out.
LIFTING INTO BED.
If the bed is narrow and there is room the stretcher should be placed on the floor with the head close to the fo?t of the bed. The injured person should then be over. the foot and placed on the bed. If the bed IS too WIde to admit of thi the stretcher should be placed beside it, and two l;elpers shou ld . stand at the far side of the stretcher. One helper passes. one arm beneath the shoulders and one beneath the mIddle of t h e back, the other helper placing his under the lower part of the back and under the knees. The injured person is then lifted, another helper pulls away the stretcher, and after a single step forward the burden is placed on the bed .
2CO

PREPARATION OF BED.
A firm mattress, not a feather bed, should be . elected. If there is much injury, or if dressings have to be applied, a draw-sheet ought to be placed on the bed. It should be of four or more thicknesses, extend across the bed, and reach from the middle of the patient's back to the knees. A piece of waterproof sheeting or of thin oil-cloth should be placed under the draw"-sheet. As the draw-sheet becomes soiled, the soiled portion should be rolled and a clean part drawn smoothly under the patient.
In fracture of the leg or thigh, sprained ankle and some other cases, a "cradle" (Fig. 99) should be improvised. The use of a " cradle" is to support the bed-clothes and keep them from pressing on the limb.
A band-box (Fig. 100), three-legged stool (Fig. 101), or hoop sawn across and the two halves secured together (Fig. 102), may be used. A corkscrew passed through the bed-clothes, with its point guarded by a cork, and tied by string to the bed or a nail in the wall, will relieve the pressure of the bed-clothes effectually.
REMOVING THE CLOTHES.
In taking clothes off an injured person a few rules should be borne in mind . " In serious cases it is much better to sacrifice the clothes than to run any risk of increasing the injury.
202
203
In removing a coat, etc, in a case of fractured arm the uninjured arm should be drawn out first.
In putting on a coat or shirt the injured arm should oe put in first.
In burns and scalds nothing should ever be dragged off. A sharp pair of scissors should be used, and everythin<Y not should be cut away. If anything it be left until medical aid

FIG. 102.
can be obtained . clothing adhering may, with advantage, be soaked with oil. To remove the trousers from a severely injured limb, the outside seam should be ripped up.
PREPARATIONS FOR SURGEON.
As soon as the injured person has been attended to, preparation should be made for the surgeon's visit 205
The preparations needful \\'ill depend upon the nature of the case. The following hints may be of use :-
A fire in the room helps ventilation, e\'en in summer. There should be plenty of water, hot ,.. cold, and also boiling, also several basins, plenty of clean towels and soap. There should be something to empty water into; a foot-bath does well. The basins should be placed on a table, covered with a clean white cloth; a large towel makes a suitable cloth; the towels, folded up, should be placed on the same table, and the hot and cold water shol1lu be within easy reach. The foot-bath should be under the table or close at hand.
In the case of a burn, absorbent cotton wool, soft cloths, old linen, oil, and baking soda, should be ready, and materials should be torn up for bandages.
In the case of hremorrhage, plenty of water shall Id be boiled and allo\\'ed to cool, and pads of absorbent cotton wool should be baked in a tin box in the o\'en, and at least two basins should be ready.
In the case of a person rescued from drowning the sheets should be taken off the bed, plenty of blankets should be heated before the fire, and several hot bottles should be ready.
If poultices are likely to be required, boding water, 1inseed meal, mustard, a loaf of stale bread, a small basin, a large spoon, sweet oil, and tow, flannel or handkerchiefs may be required.
20-+
2c6
For fomentation, have boiling \Yater, flannel, a kitchen roller and two sticks, or a large towel.
'When sum'moning a medical man to all al\yays let him know by a \Hitten message what of case he is required to treat, so that he may whatever is needful. By tbis means valuable tIme may be saved.
QDESTIONS ON CHAPTER X.
The lIum erals il/dl(a.'e the ./'l1!,'"(!s where the aJlswen //lay be foul/d.
\Yhat points would you consider \, hen choosing a room? ... 197
I [ow would you clear the way to lhc sick room ? 197
What means of resting would ynu proyide [or those carrying a patient on £I. stretcher? ... ....... 197
lIow would you place and arrange a bed for an accIdent case? 197, 198
Are hot bottles necessary, and how would you prepare them?.. ... ... ... 198
\Yhat is often necessary to lay the sufferer on in the first instance? 198
lIow would you protect this from geLLing soiled? 198
How would you see to the proper lifling and carrying of an injured person? ... ... ... ... 198, 199
\Yhat substitutes for a regular stretcher can you suggest? 200
lIow is the four-handed seat made? 160, 16t
For what cases is this seat usdul ?.. 160
How is the three-handed seat made? 162, 164

207
For what cases is this sea{ useful ? ..
How is the two-handed seat made?
For what cases is this seat useful? .. .
lIow can a single helper lift? .. .
How can a single helper give support?
lIow would you improyise a stretcher? ... ...
lIow many bearers are required [or this stretcher?
How should a stretcher be carried upstairs? ...
lIow would you carry a patient upstairs on a chair? ..
lIow would you lift a patient from a stretcher to a bed?
lIow should a bed be prepared for an in jured person? .. .
ITow should a draw sheet be made? ... ... .. .
\Vhat would you place under the draw sheet? .. .
\Vhat should be done with the soiled part of a draw sheet? . .. ... ... ... ...
\Vhat is the use of a C, cradle"? .. . . ..
In what ways maya cradle be improvised?
lIow would you remove a coat or shirt in the case of a fractured arm? ...
lIow would you put on a coat or shirt if the arm were injured? ... ... '" ... '"
In the case of a bad burn, what would you do wilh clolhing that adhered to the patient? ... . ..
lIow would you remove trousers from a severely injured limb?...
... ... '" ... '"
\\' hat preparations would you make for the Slll'aeon's visit? ... ... ... ... ... '" '" ...
\Vhat would you get ready in the case of a burn? .. ,
And what in the case of hremorrhage ? ... ... . ..
And what in the case of a person rescued from dro\n1ing?
\\' hat would you get ready for making poultices?
And for fomentations? '" ... ... . ..
What sort of a message would you send to summon a . dector? ...
PAGE
PA GE 162 161, 162 161
...
200 165 200 200 201 20I 20I 202 202 202 202 202 202 204 204 204 205 205 20 5 205 20 5 206 206
Abdomen wound of
IN DEX.
Accident case, preparaPd-ge III 112 tion for 197
A cids, poisoning by 149, 151
Air, always ... 18
Alcohol, cautIOn as to smell of 13 0
Alc ohol, poi oning by 134,153
Alkalis, poisoning by 149, 151
Ammonia, poisoning 1.>y 149
Anatomy (elementary) ... 20
Ankle 30 ,3 2 " sprained 64
Anterior tibial artery 93
A orta 79
Apoplexy 13 2
Apparently drowned, to restore. . . 139
Ann, bone of ... 28 fracture of
A;';ll -slings .. ,
Arsenic, poisoning by Arterial hremorrhage, a rr est of 74 " "
Arteries ... pracLi sing arrest of 79 sign; of 74 course of main ... axillary . .. 70 79 85
Artery, brachial. .. " carotid dorsal of fooL facial femoral ... iliac occipital plantar .. , p opliteal radial subclavian tibial temporal " ulnar
ArLificial respiration 121, 129 , Asphyxia Alias
Auricles ...
Axillary artery Axis
Back, bandage for 159 23
Bandage, to apply 42 to fold 37 " tc improvise... 37
Bandaging ISS
Bed, lifLing into... 201 " preparation of 202

Biles of rabid animals 106
Bladder I I I, 113
Brachial artery ... 86
Ihain 1 I 7
c ompr ession of 132 " concussion of 13 I
Breast -bone 26 " fracture of 48
Broad bandage 37
Broken bones, see Fractlfre.
Bronchial Lu bes ... II 8
Brooch-bone 30
Bruises 102 Burns 102
CapIJlaries '" 70, 72 hremorrhage 95
Capsule... '" '" 3 1
Carbolic acid, poisoning by '" 15 2
Carotid a r teries ... 80 from" hremorrhagc
Carpus... . .. 80 28
Carrying, means of laO, 200 " upstairs
CarLilage ...
Ce rebro-spinal system
Cervical verte brre
Cheek, bleeding from .. .
Chest, bandage for .. .
Chlorodyne, poisoning by Chok ing ... 201
Belladonna, poisoning by 148 l'age
Circulation of the blood, organs of ... ... 70
Circulation of the blood, to induce Cla\'ic1e " fracture of Clothes, removal of 19, 202 Coccyx '" 25
Collapse ... 134
Collar-bone 26 " fracture of ... 48
Comminuted fracLure ... 35 Complicated fracture ... 34Compound fracture ... 34
Compression of the brain I3 2
Concussion of the brain 13 I
ConducLor ... ... 143
Convulsions in children 137
Cradle, bed
Cran ium ... " fracture of Crepitus ... Crushed hand foot
Diaphragm .. . DigiLal pressure .. . Direct violence .. . Dislocation Ditch, to cross wilh SLreLche r ... D orsal artery of foot
208
Pt<ge 86 80 93 81 89 79 82 93 02 88 84 93 82 88 136, 138 138 25 70 85 2S
J-'age
\'e rt e
202 22 43 36 55 62 120 74 33 62
. ..
210 Page
Dress, woman's, on fire ... 105
Drowning 139
Ear· channel, blood issuing from ... . ..

Fireman's lift
First aid, meaning at " student
Fish-hook, embedded
Flexion ... at elbow " at knee ".
Eleclric shock
Ear-passage, foreign body in Elbow, bandage [or joint, fracture involving 98 JIO 159 53 I..j.2
Emetic ...
Esmarch's 148 I..j.9, ISO ... 13 2 triangular bandage
Ex piration . . . . ..
External carotid artery ...
Eye, bandage for " foreign body in
Face, bones of Facial artery
Fainting ...
Femoral artery " "digital pressure at groin ...
Femoral artery, tourniquet for Femur of " fracture of Fingers, bandage [or " fracture of
Food, poisoning by Foot, bandage for bones of ... " crushed
Forearm, bones of » fracture of
Forehead, bandage for. .. " hremorrhage from
Foreign body in the ea rpassage ... in the eye » "in the nose
Four-handed seat
Fracture, apparatus for treatment of ". causes of definition of ... general rules for treatment invoh'ing elbow joint of arm ... of breast- bone of carpus of collar - bone of cranium of finger
Flacture of forearm of knee·cap of leg ." of lower jaw ... (f metacarpus o f metatarsus ... of peh'is tf ri bs ... ()f spine (f tarsus dthigh-bone ... (If toes .. !'igns and symp-
62 toms of 35 "arieties of 34 Fr05t-lJite 108 Fungi. poisoning uy 153 General ci rculation 70 Granny knot 40 Green-stick fracture 36 G Ull1S, hClt110rrhage from 97 IIremorrhage, arterial 74 capillary... 95 from gums 97 from head and neck 80 from lower limbs... 89 from lungs 97 from nose 96 from stomach 98
II remorr hage from throat 97 from tongue 97 from tooth socket ". 97 from upper limbs 84 internal 95 kinds of 73 venous 93
of 17
120 80 155 109
89
56
37
22 81 134
90 30
30 60 r59 55
110 109 III 160 36 33 33 41 52 52 48 55 48 43 55
54 53 60 44 55 62 56 46 45
bones of ."
Hanging ...
0 Haunch-bones
28 T1
Head,
155 injury
128,
Heart
Heat-stroke
Hernia
Hydrophobia
Insensibility
62 56
211
Hand, bandage for 157 "
2
14
".
ead and neck, arterie::. of 80
bandage fOl
to
131 " side of, bandage for 155
70 " rate of contraction of 72
136
114 IIip, bandage for 157 History, meaning
Howard's method of artificial respiration 126 Humerus 28 " fracture of 52
106 Hysterical fits 133 Iliac arteries Impacted fracture Indirect violence
79 35, 36 :)4 ... 128
Paue
Insensibility, general rules " for treatment .,. ... 12<3
Inspiration 120
Instep 30
Insulat':>l" ... 142
Internal carotid artery 80
Internal hremorrhage 95
Intestines, injury of 1[3
Involuntary muscles 33
Jaw, angle of 23 lower ::!3
" "fracture of 44
Joint, definition of 3 1 "injuriesto... 109
Jugular veiv 80
Kidneys .. III " injury of
Knee, bandage for ... 113 159
Knee-cap ... " fracture of
Knot for bandage of lower limb
Knots, reef and granny
Laborde's method of ar ificial respiration 126
Laburnum seeds, poisoning uy ... 148
Lacerated wound 78
Large arm-sling... 39
Laudanum, p oisoning by 149
L eg, bones of 30
Leg, fracture of ...
Lifting and canying " inlo bed
Ligaments
Lightning, effects of Lim bs, lower " upper Lime in the eye
Lips, bleeding from LitleI'
" injury of Lower limbs Lum bar verte br::e Lungs hremorrhage from 97
Hall's method of artificial respiration bandage " fracture of ...
Metatarsus
" fracture of iddle line of body
i-I Olllh, blood issuing from i-Iu sc les " ruptured j\r uscu lar action ... I arrow bandage eeelle, embeddeu 01

Nervous system ...
Nose, foreign body in h::emorrhage [rom
Ocoipital artery ...
Opium, poisoning by Pa.d, ring ... " to fold 74
Palm, hrem orrhage [rom 88
Palmar arches ... 88
Paregoric, poisoning by 149
Patella fracture of
" fracture of Phalanges of foot
" of hand
Phosphorus, poisoning by 148,
Physiology (elementary)
Plantar arch
" artery
Plants, various, poi!:ioning by ...
Pleura Poi so n e d w
n s, wound s by Poisoning
arte ry
ti bial artery
caustic,
Room, choice and prenaration OJ; :')7
.
..
. . . Pa.e-e ... 60 ... 198 . .. 201 26, 3 I
Liver 144 28 26 110 82 196 I I I 113 28 25 120
...
eryes 140 37 28 55 30 62 20 97 32 65 3+ 37 108 118
e a
0
Popliteal
... Posterior
. .. Potash,
.. 30 58 28 56 30 28 ISO 20 93 93 '48 120 106 148 92 9 l :!IJ
Pa;:e
point
aid Prussic acid, poisoni·.lg by Pubes 7474 17 15 2 28 72 72 Pulmonary circulation ... Pul e Pupils of eyes 130 Questions on Chapter I. 21 II. 66 III. 99 1\' . !I5 Y. 145 VI. 154 X. 206 " Rabid animals, bites or. .. 106 Radial artery 88 Radiu '.8 " fracture of 5+ Reef knot 4C Respiration 120 artificial Ill, 129, 136, 138 " to excite 127
tem 1[8
18
26
p
'n!; by... '"
Pressure, digita1.
"
... Principles of First
Respiratory sy
l{est, necessity for
Ribs
" fracture of... 46
2I..J.

Page
Rupture (hernia)
lZuptured muscles
Sacral \'erte brre .. , , 'acrum .. ,
Scalds .. , .. , :-'calp, bandage for hremorrhage
Tage Il4 6S .. , 25 25, 28 102 ISS fro111 83 26 51 .,. .., fracture of . ,c..;chKfer's metho.cl of artl121
Dcial respiratIOn 160
Scat, four-handed 162 "three-handed 161 two-handed
Sl;j'n-bone 30
Shock 134 . 142 " electnc .. , .... I
Shoulder, IJandage fOl. ;8 blade .. , .. , " fracture of 51 llones... 26 " joint.., 3 2
Sick" room, choice and preparatio!l of... 197
Signs, meamng of .':. 17
Sih'ester's m.eth?d of all!ficial respll'atlOn 1 2 3
:imple fracture .. ,
Skeleton... 22
Skull ....., 43 " fracture of
Slings, arm 39, 40 , 49
Small ann sling, . .
Smothering
Snake bites. 39 140 106
Soda, caustic, poisoning by 149 I I I
Spleen.:.. .. . Injury of .. . S pil;al canal " cord
Spine .. , ." 113 23 23, J I 7 23 45 fracture of . Sl;lrits of sail, 1..\-9 by.....· 54
Splint, angular. ,_ Splints, rules fOl appl) " ing . to Sprains
Sternum ... .., " fracture of
Stimulants ancl
Stings of plan ts animals
Stomach ." .. , .. , 8 • hremorrhage from 9 " f 113 " injury 0 65 ·'Lrains 140
Strangulation :.. . ...
Stretcher exerCise, Al my 19) · No. 1. 174
No. n. 181
No. HI. 1 85
No. IV· 187 " ., I 17 2
Stretchers, Fur cy
Stretchers, to carry " to improvise
Stry chnine, poisoning- by Subclavian artery
Suffocation
Sunstroke
Surgeon's yisit, preparation for
Syllabus of instruction ...
Sympathetic system
Symptoms, meaning of .. , 'y ncope .. , Synovia ...
Systemic circulation
Tarsus
Temporal artery ...
Thigh-bone " fracture of ... Three-handed seat
Throat, hremorrhage from " swell ing of tissues of ... Tibia " fracture of Toes, bandage for Tongue, hremorrhage fro 111
Tooth socket, hremorrhage from Tourniquet
21 5
Transver e \\,owld uf Page
Two-handed ,e aL
Ulna " fract ure of...
Ulnar artery
U nconsciousn ess
Upper limbs
"Varicose vein
Veins
Venous blood " hremorrhage
\' entricles
Vertebra , ..
Vertebrre ...
Vertebral coluIlln
Vertical wounel of abdomen \ -itriol, burn by ...
Voluntary mucJes
"'agon, to load or unload
"'all, to cross with stretcher
'Warmth, ncces ity for " Lo promote \Yind-pipe
\Yoman's dre s on {ire
\Younds by poisoned weapons " accompanied by arterial hremorrhage ... \Younds accompanied by venous hremorrhage \ \'ounds, hccrated
rist
169 166 153 141 13 6 204 7 lIS 17 134 31 70 30 82 30 56 162 97 141 30 60 159 97 97 75 abdomen
113 16r
\\"
Pat'" 2 54 :)' 128 26 94 70 72 9.> 70 23 25 23 II3 102 170 18 12 7 118 105 106
Caniage Paid on all Orders in the Un ited I<in gtic m . .. ASHFORD" LITTER.
ttbe St. 30hn Bmbulance Bssociation.
GENERAL PRICE LIST.
A complete and reliable Ambulance Equipment is an actual necessity, and experitnce has proved that employers of labour and others interested in the district readily subscribe for -the purchase of such appliances. Collecting cards, stating the purposes for which subscriptions are required, will be supplied to approved persons gratuitously on application to the Head Office of the Association, where also any information with regard to its work can be obtained.
All stores will be sent carriage paid to any part of the United Kingdom. Returns may be sent carriage forward. If carriage is prepaid it will be allowed.
Owing to fluctuations in market prices it is impossible to guarantee that the quotations herein can be adhered to.
Quotations will be furnished for Ambulance Carriages and other articles relating to Ambulance, Nursing and Hygiene, not mentioned in this list.
Orders and correspondence should be addressed to the St. John Ambulance Association, St. John's Gate, Clerkenwell, London, E.C.
Remittances should be made payable to the St. John Ambulance Association, and crossed "London County and \Vest· minster Bank, Lothbury."

The "Ashford" Lilter (r899 model) consists o r a twowheeled under-carriage filled with elliptical springs and either of the "Furley" stretchers, with a cover so on a jointe.d frame that it can be folded up inside the or ';YIlh a and 2"pron (as shown above). Th e undercarnage, haVl?g a cranked axle, the bearers can pass between the wheels WIth the strelcher, and thus avoid lifting it over When travelling, the legs of the under-carriage are .and thus form the handles by which to propel it. Shoulcll.t be ,necessary to pass o\'er rough g-round, tl\'O oearer:; can easIly hft the litter and patient. The" Clemetson " stretcher can be used instead of the" Fttrley" pallern
With Hood and Apron.
PRICES OF THE IMPROVED ASHFORD LITTER, 1899 MODEL. With Iron Tyres to Wheels. Without Cover or \ With Hood and Cover. Apron.
With IndiaRubberTyresto Wheels Without

(no
Lilter complete with Ordinary Stretcher* Dittowith T elescopic handled Stretchef"r Ditto with Police
• Prices quoted for Litter with Ordinary Stretcher include Wide Webbing Slings but no
Strap . Leather, instead of Webbing Slings, 8s.extra; Chest Strap, IS. 6d . extra. If supphed ::s without any Slings, 4S' allowed. ;:
t Prices quoted for Litter with Telescopic.handled Stretcher inclune Wide Webbing Slings and c. Chest Strap. Leather, instead of \Vebbing Slings, 8s. extra. If supplied without any Slings, :;;.:: allowed; and if without Chest Strap, 's. 6d. allowed. S'
t Prices quoted for Litter with Police Stretcber include Wide Webbing Slings and Leather IJQ Straps for securing a refractory patient. Leather, in stead of \VebbilTg Slings, 85 extra Hood and Apron, complete (" Furley" pattern Stretcher) £2 10 0 3 Do. do. do. (" Clemetson " Stretcher) 2 15 0
Waterproof Sheet (washable) lo be laid on lhestretcherbed... 0 12 6 Crates (returnable) chHged 45. 6cl. for each Liller. ;. -< ;. o
f, s. d I;:' s d.
;:, s. d.
a s 3,
: ;:, s. d. £, s. d. ;:, s. d. (!) 'tJ II) Under-carriage
Stretcher) ... ... I 8 [Q 019 5 01 II 0 O III 15 0 112 10 0114 5 0 c:
II 2 II 10 61 12 17 01 13 5 6 14 7 o 14 IS o 15 10 6116 2 0116 10 0 117 5 6 o o 0 o Strelchert·.. ...\ \-- -\ -Do. with
S' Slretcher... 14 8 0 I \ 117 13 0 12 0114 0
-I-With (') Cover or With Hood and III Hood and Cover. Apron,
Apron. illustrated.
"Clemetson"
c:
· :=: ri r; (D t-i 0..-<" :: ciQ" 5. ==to c ::r'-' : ....., g.::r- ::;:l n o rtQ t>J a ;;:- 0" 3 :;,.'" n'!" (J<n (1) g Ul"::1 (b g <n g CfQ So ; _. 0!" <n(1) <no.. 0' g.;; t;; ;; 2. p g:3 [g ...... g, ,....,. (b en 0 "g.n;- '" ..'" g r. g. Vi' (1) (1)rJQ t'"-1 0 en ff !""' ;!- a0· '" ;:l
0
III ....., ::l fJQ :: 37.) ::r';l> a , p..t'l:j a t:! 2 :d rJQ :: t'"-1 !" ;::J a l'l I" ;:::.' p.;::rrl-;:l p..::r' (1) a (1) I"cn :s: e' .., n ::J: tzl tzl tzl t:3 > 011 CD "CI PI c: o ::s o S' t:3 ; (J) (I) c: :!, t"4 [ :::i .., tzl 0 ?' .3 •
n
M"'C:) '" (II ::r' ;1 .., (II ,....,. - Cl 0 0 0 P"o
Carriage Paid on all Orders In the United Kingdom.
over them, and the cranked axle has, therefo re, been replace d by a slraight one constructed of tubular sl e el.

" REA-EDWARDS " LITTER, filled with pneumatic ty red wheels, showing the" Clemetson" Stretcher.
Ball bearings are fitted to the wheels, both cycle pattern and wooden, and the hubs are so arra!1ged the wheels can be removed from the axle wIthout ing the bearings. In place o f the four legs to raIse as handles, tw o fixed legs filted with small wheels or r oll ers are placed at the foot end, whIle a combined leg and handle fitted a crossbar an(1 capable of being raised or lowered IS used at tht; head end . When raised as a h andle it may he locked 111. one uf two positions, and when it is loc.ked .. 111 n. vertical posit ion. The ad vantages. for .thls ment are simp li city, ease ancl rapIdIty of mampulatlon and
Carriage PaId on all Orders in the United Kingdom.
fac.ility afforded by the two fixed legs for raising the lItter, if necessary, on to the pavement. The question of bal an ce has been carefully studied, and th e stretcher is shifted forward so that the middle of it is several inches in fr ont of the axle, a perfect balance when the str etche r is loaded and in a horizontal position b eing thus obtained and consequently there is no weight on the hands of the person propelling the litter.
JIhe pneumatic tyred wheels are strongly recommended in where the amount of care necessary to keep th em be as the comfort to the patient and ease propul slOn are ll1crease d _beyond all comparison with a ny lItt er yet produced. It WIll be n ote d that the prices are considerably lower than those of the "Ashford" Litter and the following are as examples, but owing to vast number of cOmbl11atlOns that can be made with the different and coverings, it is impossible within reasonable lImIts to set out quotations for the whole of them, but these may be calcula ted by adding together the prices of the under-carriage, str et cher selected, and hood and apron or cover, see pages 4 to 10.
SPECIMEN PRICES.
Un der- carriage only, eithe r with pneumatic tyred cycle wheels or solid rubber tyred wooden wheels, £10.
Litter complete wi t h ordinary stretcher (no slings or chest and. hood and as illustrat ed, £14 3s. 6d.
DItto WIth T e lescopIc Handled Stretcher (with chest strap ) a nd hood and apron, £14 I IS.
Ditto with" Clemetson " Stretcher and ventilated hood an d a l,ron, £15 18s.
If with iron tyred wheels prices a re £2 less.
Jland brake, which acts automatically when the litter is at fe st, ex tra £1 lOS.
\.\'ben ordering please state which wheels are required .
Carriage PaId on all OrderS in the United Kingdom

THE" CLEMETSON" STRETCHER.
STRETCHER, wl'th back raised, al so showing II CLEMETSON " extending legs.
On this stretcher the patient can be moved as desired: from the recumbent to the sitting position. There is no comphcated mechanism to get out of order, and the adjustment !imply on the balance of the patient's body. The ",.i11 fit either the" Ashford" or the "Rea-Edwards UnderCuriage. Price £3 35. ; with extending legs, £4 35 •
Hoorl and Apron, Ventilated. £2 155.
Car! iage Paid on all Orders in the United Kingdom.
ADJUSTABLE LEGS FOR STRETCHERS.
Primarily these legs, which are independent of and addi. tional to the ordinary foot wheels, are intended to facilitate the carriage of a stretcher in a railway compartment, in which case two on one side would be lowered and adjusted by a telescopic arrangement to the proper height, 50 that the foot wheels on one side would rest on the seat, and the adjustable legs on the other side would rest on the floor. The four legs may be used to raise the stretcher as required, \Yhen not in use they are folded up immediately under the poles of the stretcher.
Price per set of four, £1.
FIRST AID BOX.
To be c a rried below the axle of the" Rea-Edwards lJ Litter, from which it is easily detachable.
Contents :-Set of Splints, 12 Triangular Bandages, I2 Roller Bandages, 2 lIb. packets each Cotton Wool and BoricLint, Adhesive Plaster, Pair of Scissors, Knife, 2 oz. eacn Olive Oil, Tinct. Iodine B.P.C., Sal Volatile, and Spirits Ether Camp., Graduated Measure Glass, Kidney. Dres sing Basin, 6 Tampons for wounds, Tourniquet Pin, Sufety Pins, Needles, Thread and Tape.
Pri ce £2.
carriage paid on all Orders in the Un ited Kin g dom .
"FURLEY" STRETCHERS WITH · THE LATEST IMPROVEMENTS, 1899 MODELS .

TELESCOPIC HANDLED STRETCHER-OPEN.
ORDINARY STRETC IIER-CLO Sl<.:D
The improvements in all patterns of the "Fur ley » Stretcher, 1899 Model, are numerous. The comfort to the patient is increased; the stretcher is stronger, mor e rigid, and lighter, it folds up more closely, and its handles are more comfortable to h old and afford greater protection to the hands of the bearers in passing through narrow doorways or passages. Sh ould it be necessary to reduce the width of a loaded stretcher in order, fo r example, to carry it into a railway carr iage , this can be done, either when it is resting on the ground o r supported by the bearers, without trouble and without the slightest jar to the patient. The price of the strelchers is lowe r ed. A ll minor points hav e been most carefully considered , and the :st r etchers a r e confidently recommended as thorough ly efficient in eve ry way . These stretchers are adapted for use al on e or as part of the " .-\shfon.1 " or " Rea-Edwards" Lilte r , and th e cover, hood anu apron, a rmy rug, and wate rproof shee t de sc ribed in this list a re suitahle fo r use with them.
carriage Paid on all Orders in the United Kingdom . 10 o o .-0 0 0000 lrI ... co t't ........ ... ... 00 0 000
Carriage Paid on all Orders In th e United Kingdom "LO)YMOOR
JACKET."
.l<'o r u"e in mines, sh ips ' h olds, et c., to secure a pauent on a stretch er (se e illuslra nuu), " hich ca n t hen b e placed in an position. b ic e £1 S,, ·

WATER BOTTLE.
Carriage Paid on ail Orders in the United Kingdom .
LAMP
. T his is fiLted wiLh a sockeL, b y whi ch to fi x it to a Litter, or it ca n be conyenienLlr carried by hand, or attached to a belt or the clothing .
Price complete, 5<:. 6l.
Coppel tinn ed , lth carryi ng
stra p.
Pr ice 12s . ba.
Dressing Bas in , kidney shnped, made of enamelled iron.
Price 2 s. 3d.
Ambulance Station Plate , Enamel led Iron, 3s. Gd. e;lch.
Stretcher Depot Plate , E namelled I ron, 3s. 6cl . each.
Carrying Sheet for ca rry in g pat ients up and down tair., or ot h erw ise about a hOllse . Designed hy the late J . C. De rh am, Esq., Blac k poo l, and Alfred Pain e , Bedford.
'Th e sheet is fitted wit h rope hau d les and detachable bamboo po les, and may be placed on a st retche r without disturhing the patient. Price complete, IS S.
'I rlaga Paid on all Ordare In the Unitpn Klngrt
REGULATION POUCH FITTINGS
for the St. John Am bulance Brigade, consisting of:-
t Triangula r Ba'1dage. "caled up in waxed paper.
2 Grey Calico R )Her Ba,dages (l in. and I in.).
I Packet of Surgeon s Lint .
I P .lcket of Absorbent W
I PaIr SC1SS ,rs.
6 Safety Pins.
I Box of 3 Phials" Vap:lrole" lo:iine Tincture
I Ptece of Strong Cane, for tightemng imprcwlsed rniquets .
List Pnce, 25. 8ci. each: 6 doz. or more, 2S. 7d. eactl. of 3 Phials" Vapuro!e " Iodine Tincture, packed for post. each lOd.; per doz., 6d.
SAFETY PI NS.
All fasten or un fastell un ell her <;ide. !> i.
Facile No. S 600 or S 602 pt'r 3 doz. 0 t: ., "S 603 ... ,,0 Duchess Duplex, No.2... IWT doz. 0 " "Assoned 0 Spec ial Blanket Safety Pin!, 3 in. C in. 6
Pocket Cork Line a:-!d Drag. with 80 feet of line. it: case; for recovering a drownin15 (mm the water. complete, with ins! ructions for u!;e. 6s. 6d.
Pocket Reel and Ice Lme lor In ice accidents, with feet of line in ca"e. Price cumpk rc. wit h instructions for U"e 0" 6d

Carriage Paid on all Orders in the Un ;ted l(ingdont1
LARGE HAMPER FOR AMBULANCE STATION AND RAILWAY PURPOSES. F or c ont ent s see n e xt r age .
[5 Carriage Paid on all Ordels in th e Un i ted Kingdom.

Set of Cane Splints.
I t. John T ourniquet.
Ill. Carbo li c Cotton 'Wool
Ib. Boric Lint
1 Roll Adhesil'e I f n Tin ::: ICases . Plaster.
20 Roller Banuag-es, assorted.
[ dol. Triangula r Ballrhgl:s.
3 pieces Tape .
4 oz. Sal Volatile.
4 oz. Bicarbonate of Soda.
I Dredge r for Bori(; Acid . 11) . Powdered Eoric Acid.
8 uz . 'lIl1cture I odi ne.
I pair Pean's Forceps.
I pair Scisso rs.
1 l"ni fe.
12
I packet each Safety and Plain Pins.
oz. CarlXlliscd Chinese Tlli-;L
-1 oz. Silkwornl G UL.
I reel each Black ami \\,hi te
Sell ing- Thread.
I Kidney-shaped Basin.
1 Stopper Loosener.
I Graduated :\leasure.
ca,ke 20 per cent. Ca rb olic Soap.
I K ai l Brush.
2 Empty 8 oz. BotLles.
2 4 oz.
3 S aucers fo r applying Ti ncture:: of Iodine.
3 Camel I fair Brushes for applying Tincture of I od ine.
Pli ce complete , £4
Carriage Paid on all Orders in th e Un ited Kingdom
SMALL AMBULANCE HAMPER .
\-yit? cover and strap, for use in factories , col iJ en es , alld la rge w o rk s , as well a s for parochial and domestIC use . CC.' TArNI N"
S et Splints . I St. J ohn T ourniqu et . 1 Ta mpons, for washin g wounds. 2 Packets Lint. 4 Roller Bandages (wide and narrow) . 4 Tri a llgular Bandages .
Cotton W ool.. . .. . 1 I T' C l'oric W ool ... r n In ase".
Spool o f Adhesi ve Plaster. Knife , Sci sso rs, Thread , Tap e, 1 eedles, and Pins.
W eight complete, lbs.
Le ngt h, 1ft. 6 in, Depth, s in. Wi dth, 7 in. Price £1 I 6c1.
17

Carriage Paid on all Orders In the United Kingdom.
SURGICAL HAVERSAC.
Oarrlage PaId o. a" Order. In the United Kingdom , II
I,1PROVED PATTERN, fitted with a.tin, arranged that any !U can be taken out withollt clIsturbmg the rest of the contents. . B d 6 R lIer
Contents: I Set of Splints, 6 Tnangular an :0. Banda es (wide and narrow), Cotton \Vool, Bonc m tm cases Roll Adhesive Plaster, I Pai r I KnIfe, 2.oZ. Borid Acid Powder, 2 oz. Tinct. Iodine, 2 oz. Sal Volatlle, I Dred er for Boric Acid, I Graduated Glass Measure, I St. John fourniquet, Pins, Needles, 3 Sance.rs and Camel Hair Brushes (for applyl.ng TlOclnre of Iodine). ,3 £ 6d' White Rahon Haversacs , 2S. each. Pnce I I IS. .
FIRST AID COMPRESSED KIT.
The box is made of wood covered with damp·resisting material, and is fitted with a lock and key. It contains a nUI11 ber of practical ambulance appliances arranged so that any article can be withdrawn or replaced without disturbing the remainder. B e ing filted with a handle it is portable, and the lid, when let down, can be used as a table. All bandages and dressings are compressed. Size-Lenl:{th, I6! in.; width, in.; height, 8 in., without handle .
Contents: 4 Triangular Bandages, 6 Roller Bandages, t First Aid Dressings, 6 Small Packets of Cotton \Vool, 6 Small Packets 0 Borio Lint, I St. John Tourniquet, I l\Ieasure Glass, I tin looX containing a Roll oC Plaster, Boric Lint Patches. Scissors ami Pins, I tray containing 3 Bottles (Sal Volatile, Tincture of Iodine and Boric Acid Powder/ anci a Dredger for Boric Acid, I set of improved Splints, with angle piece, 8 Splint Straps (sufficient for a fractured thigh), 2 S:lucers and 3 Camel H a ir Brushes (101 "'I applying Tincture of Iodine).
Price £r r 1.. 6d.
Carriage Paid on all Orders in the United Kil'e-r'cm

FIRST RID et')MPRNleJN.
(1)RESSINGS AND BANDAGES COMPRESSED).
SI. .1olm Rmbulan(t Rssc(liJllon, l'rice Is. 6d.
SI• .:JO/Jd'$ Gille, I 8 . rondon. e.'. By Post S. d.
SIze, by 3! by 1;1 inches. Suitable for the pocket. CONTENTS.
I. Tliangular Bandage. 2. First Aid Dressing. 3. Colton ¥lool. 4. Two Splint Slraps. 5. Adhesive Plasler. 6. Permanganate of Potash. 7. Lanoline. 8. Boric Lint Patches.
9. Safety and Plain Pins.
Price, each IS. 6d. Packed for Post IS. 8ci. Per doz. 175. 61.
SEPARATE ARTICLES.
TU No.
I 4d. each or 3/9 per doz.
2 2d. ,,2/0
3 rd. " " rod. "
4 2<1. per str:1.p or 1/9 "
5 Id. per box or lOd. " "
6 Id. per box or lOd. per doz.
7 1 per tin or 1/4 "
8 ld. per packet or lOd.
9 Id. lad .
Not less than one dozen supplied at dozen prices.
Carri<'g e Paid on all Orders in the United Kingdom.
FIRST AID BOX FOR USE IN MINES.
Set of 1m roved W . J2 St. John l ourtllquf>t; Cotton W->O'· Lint · paper; Adhesive Plaster' p"';t; 6 Triangular Bandages in' waxed
2 oz. Sal. Volatile; 8 oz Boric Acid Graduated. Meas\lre; Safety PII1S; Dred.e;er for Boric Acid Powder.' 8 oz. TlI1ct. Iodine; (for Tinct. of Iodine). an 13 Ca£mel HalT ThIS FIrst AId EqUIpment also ve' 2 ros. other large works. and can be fitted r ry for use In factocie< and lor carrYing on the" Ashford' Littl!r.
[9
\
20
·1 carriage Paid on all Orders in the United KlngdOrrf.
SMALL FIRST AID OUTFIT
When closed can be carried by a Strap-handle.
Dimensions-91 by 7! by inches.

rs: 2 Triane;ular I St. John Tourniqcuet, 8 . S lints In heu of Bandages), 2 oz. otton 00, Stra us (C{0'c:; p in Roll e, Bandages, 2 2.in. Roller Bandages,
1 P r 80 1 2'OZ. Bottle Tincture Iodine, B. P.C., 2 PI;,; :"'Unt: t : :II'OZ. Glass, ; . China and 2 Cam el Hal' 1il ",a"'. l'-' ..Je used when ap plying Tinct ure of Iod ine .
Price:
W fWO,CLJ Box, covered with Damp Resisting Material , 15 s.
:-.tout Card boa rd Bo x, Cloth Covered, lOS. 6d.
Carriage Paid on all Orders In the United kingdom. 22
The St. John Tourniquet, as supplied to the Admiralty with directions for use ...
(Special quotations for large quantities.)
Splints, 'Vooden , per set , 2/6; Cane ... . . .per set
Greatly improved Wooden Splints, with grooved j oints and angle piece, strongly recommended ...
Tow, for splint padding ... . .. per lb.
First Field Dressing (Army Pattern)
Jaconette, 44 inches wide
Tow, Carbolized or Styptic ... per yard ...per l b.
First Aid Dressing, consisting of a small compress ed packet of boric lint, a compressed rolle r bandage, and a safety pin
Dredger, containin g boric acid powder
Measure Glass ...
Knife with strong blade each IS. ; per doz. lOS. 6d.
Pair of Scissors each IS ; per doz. lOS. 6d.
Small Bottles strong Smelling Salts, pe r doz., 55. 6d.
Splint Straps, Webbing, and suitable Buckles. Per set of 12 yards of strong 2-inch Webbing and 15 Buck les , 3s.
These make very compa ct Straps for ca rryin g in the Pouch.
The 'vVebbing should be cut to meet local requir ement s.
Buckles only, IS. 3d. p er dozen.
\Vebbin g only, IS . 9d. per dozen yards.
It is unnecessary to sew the Buckles. T he spikes be passed through the webhing, and th e sh ort end of the shou ld lie outwards .
s, d. o 9 7 6 4 Ci o 6 o 9 2 3 o 9 o 2 4 o 5
e.- Carriage Paid on all Order. In the UnUld Klngdo",PLASTERS.
Leicester Adhesive Plaster nn Cambric. in tins of yard, 6 inches wide 6d.
The Leicester Adhesive
Ribbons, in tin boxes, 6 yards long.
inch wide 6d.
I inch wide 8d.

Na tional Rubber Adhesive Plaster (Antiseptic) on spools.
S yds. 10 yds. inch wid e 9d . IS. ad.
I " IS. oel. IS. 6d.
2 " IS. 9d . 2S. 3d.
Ditto in card box, i in. wide, ytls. long -. Id. 3d • 3d . 6d. lin I 4 . 2 COURT PLASTER, TRICOLOR.
Large Size, 9(1. ; Medium, Sd. ; Sl11:1.11, 3d . 9d .
Carriage Paid 0)" all Orders In thl! United Kingdom
NURSES' WALLETS.
ORDINARY PADLOCK SHAPE.
\Vithout instruments, 4S. 6d.
Filled complete, con taming Spring Dressing Forceps, Spatula, Probe, 2 pairs Scissors (rounel and sharp pointed), Clinical Thermometer, and Knife.
Price 12S. 6d.
ST. JOHN'S PATTERN, as illus. trated, but improved by the addition of flaps to protect the instruments.
\\'ithout instruments, 85. 6d.
Fitted complete, containing Spring Dressing Forceps, Artery Forceps (also useful for dressing), Spalula, Probe, Director with Ear Scoop, 2 pairs Scissors (round and sharp pointed), Clinical Therm ometer round), Knife, Pencil, and Safety Pins.
Price '£1 3s
25

Carriage Paid on all Orders in the United Kingdom .
ROLLER
BANDAGES.
(6 yards long. )
Grey Superior Best quality, Superior Grey Open White \Vhite. with White Open Open Woven Calico \ Vove. Wove Per \Vove. Edges. Compressed.
I
ROLLER BANDAGES in Assortment.
Pack.ed in neat Cardboard Box.
RECOMMENDED FOR CLASS PRACTICE
Two 3 in. ; two in. ; one I in.; each 6 yards long. s . d.
Grey Calico
" fast edges
B est quality white, with woven edges 6
Pl ain Triangular Bandages, each (Special quotations for large quantities .)
Di tto Compressed (Lhinner quality), each 4d. ; per doz. 3s. 9d.
Ill ustrated Triangular Bandages (after Esmarch) showing 25 applications of the Triangular Bandage, with printed instructions .. . each per doz . s. d. o 6 4 6
Carriage Paid on all Orders in the United Kingdom
ROLLER BANDAGE MACHINE.
Forceps, sprin£; dressing, full size or small as desired, IS. 6d. ; Pean's Artery, Sin., 4S. 6d.
Scissors, round-pointed blades, IS.; small round -pointed 1)lades, or S in., IS. 6d.; ronnd ·pointed curved blades, IS. 6d.; sharp - pointed blades, for delicate work, 3s. curved blades, 35.
Spatula, 9d. Prob e, 6d. Director, with Ear Scoop, IS. 9d .
Knife, very thin, ivory handle, two blades, IS. 9d.; single blade, IS .
Nursing Chart, designed by Miss Inderwick, each.
Temperature Chart, id. each .
CLINICAL THERMOMETERS.
Round. -Ordinary, IS.; minute, IS. 3d. ; half-minute, IS. 6d.
Flat.-Strongly recommenrled, as they will not roll Ordi· nary, IS. 6d.; minute, 25 3d.; half-minute, 3s.; (Specially selected and r eserved for the A socialion), with very open scale.
doz s. d.
d. s. d. s. d.
d
in. 0
9 0 2 3 3 in. S 3 2 9 6 2 in. 9 3 6 3 9 in. 3 0 3 9 2 3 3 in. 9 2 0 6 4 9 2 9 4 in. 3 6 ... 3 6 6 0 3 9 6 in. 5 3 4 6
0
I 0 "
I 6
Designed by
Dr. A. C. Tunstall.
Price 2S. 6d.
carriage Paid on all OrderS in the United Kingdom.
CLINICAL THERMOMETERS-
(conti1uwJ}.
With Magnifying Lens. Price, ordinary, IS. 6d.; minute , IS. 9d. ; half-minute, 2S .. 3d . . . .
N .B.-Minute and half-m1l1ute Instruments wlll only reglster in the time stated under favourable circumstance s: . No liabilit), is taken j01-b,-eakage of Thermometers 111 frallszt.
BATH THERMOMETERS.
To Dr. Forbes' specification. Japanned with zinc scale, 2S. 3d . ; Clinical Thermometer size, in case, IS. . No liability is taken for b1-eakage of The1-moJllelen m t1 ·allszt.
COTTON WOOL.
Plain, I oz., 2d.; 2 oz., 3d.; 4 oz., 4d. ; lb., 7d.; I lb., IS.; small packet (Compressed), Id. .
Medicated, Boracic, i lb., 6d . ; I lb., IS. 6d.; Ca rb olIc, yer lb., IS. 8d.; Alembroth, per lb., IS. 6d.; Double Cyamde, per lb., 2S. 6d. LINT.
Plain, I oz., 2d . ; 2 oz., 3d.; 4 oz., 6d.; lb., lod ; I lb.
Ie:;.6d. k d
Boracic, 4 oz., 6d. ; I lb., IS. 6d. ; square foot pac 'et, 2 .; small packet (Compressed), rd.
GAUZES.
These are supplied in 6 yard lengths, width about 36 inches. s. d.
Unmedicated white Alembroth
Double Cya ni de Boracic
Packets of Cyanide doz.• 2S. 8d. Cauze yd.
GAUZE TISSUE.
compre ss ed) ,

A layer of absorbent cotton wool between two sheets of £,auze, good quality, per lb., IS. 6d .
Carriage Paid on all Orders in the United Kingdom .
TEXT BOOKS,
&c.
"First Aid to the Injured." By James Cantlie, l\1.B., F. R. C. S. Th e a uth o ri se d TexL Book of the First Aid C O LlI' e. IS.
" A Catechism of First Aid. " Compiled from Dr. Cantli e 's :'IIanua l. By J. l\I. Carvell, M.R .C.S., L.S.A. 6d.
., Problems in First Aid. " A companion to the authori -ed T e xt Boo k of the St. John Ambulance Association "First Aid to the Injured." By L. :'1. F. Christian, l\I.B., c.:'II., Ed., and W . R. Edwards, A.C.A. 6d.
" Hints and Helps for Home Nursing and By E. :'IIac Dowell Cosgrave, M. D., illustrated, with chat- r o n the l'lpplication of the roller bandage, by Sir R. J. Collie, M. D. . The authorised Text Book for the Nursing Course. I S.
" A Catechism of Home Nursing" (based on Dr. Cosgrave 's Text Book) . By the late J. Brown, L. R . C.P., L.R . C.S., :ll1d J. :'II. Carvell, l\I.R.C.S., L.S.A. 6d .
"Home Hygiene. " By John F. J. Sykes, D.Sc. (Public Ilealth), M.D., &c. Illuslrated. The aulhorised Text Book for the Home Hygiene Course. IS.
"A Catechism of Home Hygiene" (based on Dr. Syk es ' Texl Book). By J. M. Carvell, J1.R.C. S., L.S.A. 6d.
" Questions and Answers upon Ambulance Work." By John W. l\Iarlin, M.D., and John Martin, F.R.C.S ., Ed. IS.
"Questions and Answers upon Nursing." By John 'V. Martin, M.D. IS. 6d.
"First Aid to the Injured" (Six Ambctlance Lectures). By Professor Frederich Esmarch . Tr3.l1s1ated frolU the Gernun by ILR.H. Princess Christian. 25.
Bandaging and Surgical Dressing." By Waller pYc, F. R.C . S. 2S.
length 0 10 I 0
2 2
per
per
29 Carrlajitl Paid on all Order. In the United Klnldo",.
TEXT BOOKS. &c.-( cont i nued}.
II To Restore the Apparently Drowned," printed in large Type with two Diag ra ms. 2d.
Dr. G. H. Darwin 's" First Aids," b ei ng a card to hang lip givi ng tr eatment of various acci d ents. 2d. ; pa ck ed for post, 4d.
If Manual of Drill and Camping for the St. John Ambulance Brigade." 5d.
.. Manual for St. John Voluntary Aid Detachmen ts. " By Lie ut.- Col. G. E . T wiss , R. A . l'1.C . (Retired Pay ). 6d.
.. How to Act when Clothing takes Fire." By J. E. II. Mac kin lay, M .R . C.S. 2d .
If First Aid Principles." Card s of concise d ir ections fo r wa ist coat pocket, eac h; 4d. pe r d oz. Spe cial qu otations for lar ge quami ties.
It Specimen Examination Papers, First A id, Nursing and Hyg ien e C ourses. " 3d.
Small Anatomical Diagram. Showing the human skeleton, main arteries, and po ints whe re pressure should be a pplied to a rrest bleed ing. 2d.
Directions as to the Restoration of Persons suffering : from Electric Shock. Large print, posler size. 3e1. each ; or 2S. 6d . per dozen .
General Notes on First Aid to be R endered in Cases of Poisoning. By Milnes lI ey, M.A., M. R . C S ., L.R.C.P. 2d .
Notes on Military Sanitation. By L ieut. -Col. II. "P. G . E lkington , R . A . M. C. 6d .
II Emergency Book," for instantaneons refe renc e , giVing c oncise inslructions ; to hang on wall. Size about one four square. 2S. 6d. ; packed fo r post, 25. 8d .

Carriage Paid on all Orders In the United Kingdom )0
TEXT BOOKS, &c. -(cont i nued)
Aids t o Memory for First Aid Students. Re\-ised to date. Add itiona l Illustrations. By L. M . Frank l\I.B., C.M ., Ed in. 6d .
General 'Regulations for the St. John Ambulance Brigade, 1913. 3d .
Rules for Corps Brigade . 2d. and Divisions, S t. J ohn Ambulan ce
R eg isters. Class Attendan ce , 25. 6d. Cer tificates , 4S. 6d • Case Report, I S.
St. John Ambulance Brigade Cash Book, Minute Book and Occurrence Book. Set of three , 7S. 6d. Receipt Book, 6d.
Large Physiological Diagrams (New S eries ). Fo r Leclurers' use . T he IIuman Skelelon, show ing th e main a r teries and pressure points. T he General Anatom y of the Body. T h e Systemic and Pulmona ry Circulal ion of th e Blood . Sectio n Through Middle Line of Head and Neck, showing the Tongue in two positions in relati on to the Trachea, and Schafer's method of Artificial Respiration (Expiration and Inspiration). Dislocations . Pr ice, pe r set o f five ISS . These may be hired for a course of "First A id" lectures, given the auspices of the A ssociation , fo r a fee of 5s. , or "'!l,h the addition of Sp li nts, Tourniquet, and 30 plain Tnangu lar Bandages, [or a fee of lOS.
Soxes- of Stationery for the use of Class Secrt[aries and olhers connected with the Association, containing twelve sheets of papcr, suitably headed, and twelve envelopes beanng the device of the Association. 6d. Twice that quantily, IS.
Arm Badges, wilh the device, issued under the authorilY of the Central Executi\'e Commiltee, having been flrst approved by H. R.II. the Grand Prior as the sole official and recognised Badge of the A socialion and Brigade. H. 8.- lItis des/g'?1 is jrotected.
SERIES A.-For the use of individual certificated pupils-
X. In German Silver, Large
3.
4. In Electro Plate , Large
5. Small Size ditLo
o. Small Size for bullon hole
7. In Enamel for bUlton hole
8. " brooch
9. In Cloth and Silk
10. In Cloth and Silver
I!. In Cloth and Cotton
12. Small Celluloid Badge, for button hole or brooch
13. \Vhite Satin Armlet, with woven Badge H.B.-These Badges are /lot

SERIES members of the St. John Ambulance not weanng uniform, having name of the Corps or DIVISIon annexed on a label, only Issued in quanLilies-
No. 15. In German Silver, 2 ins. in diameler, first doz., £r ; subsequent dozs., 12S.
16. . In Electro Plate, 2 first doz., £1 12S. ; su bsequent dozs., £1 4s.
17. In Cloth and Silk, 2 "per doz., J2
18. In Cloth and Silver 2" ,. per doz., £1 lOS.
19. The Brigade BUL;on Hole Badge, eaclJ, IS.; wiLh Brooc h Pin, each 1/3
JV.B.- Tltese a e 110& 10 be as decorations.
s.
d.
Size 2 in. dia. 0 7 :,mall Size dillO I} 0 6
Small Size for button hole 0 6
Size 2 0
I i 11 2 Ii 2t
be worn as dc c01'fltioll s . 0 9 0 9 0 3 0 9 2 0 0 6 0 2 0 Carriage
all
in the United Kingdom. 3 2
to
Paid on
Orders
33
Carriage Paid on all Orders in the United Kingdom, S.J.A.B. UNIFORM BADGES, etc. Ambulance Divisions. Officers.
Cap Badge (Reg. No. 101) ..• .
Collar Badges ( " 103) per pair
Pouch Badge ( " 3,657) ...
Sergeants, Corporals and Privates.
Cap Bange (Reg. No. 102)
Collar Badges ( ., 1?4) per paH
Overcoat Badge( " 1.582) ...
Shoulder Titles, S.J.A.B., with numeral,
Shoulder Straps, fitted with per pair title and numeral per pair
Bugler's Badge ... 4S. Bugler 's Cord Div. Secretary and Sergeant's Badge ...
Drumm:r's Badge
Hon. Surgeon's Crosses (pattern B) per pair
Medallion Badge (pattern D) ... . ..
Nursing Badge (pallern E)
Reserve Badge (all ran ks)
Signa.ler·s Badge Signaller, IS. ; Superintendent's Stars (paLtern A)
Belt Furniture ...
Bandsman's Wings
Whistle and Chain per pair Instructor per pair per set per pair
White Piping, per packet yds.,enough for 3 pairs of trousers (pkts. cannot be broken)
Lace, per yard, Silver, lOS. ; Black ButtonS{N o. I (large) per doz. (White No.2 (medium)
Meta 1\ NO.3 (small, for caps)
D.tto o. 4 (large)
(Electro 5 (mediulll) .Plate) LNo. 6 (small, f')r C1pl)

Carriage Paid on all Orders in the United Kingdom. 34 Nursing Divisions. Lady Officers.
Officer, Arm, 3s.
Voluntary Aid Detachments. Men's Detachments.
Women's Detachments.
Black Khaki
UniflUm. s. d. s. d. o S 0 S 3 2 6 0 6 0 10 1 0 6 0 8 5 3 0 I 0 0 0 0 0 I 0 3 o 3 3 0 o 6 I 6 2 6 2 0 [ 0 o 6 o 4 o 3 o 6 G 0 0 S 0 o 10 7 0 g o 8 I 10 o 9 o 6 o 4
Cloak 5 6
Cloak 5 0
6
3d.; Cloak... 4 0 White Box Cloth Backs, for Badges per pair 0 3 Nursing Sisters. Arm Badge (Reg. NO.3,522) 2 0 " Cloak Badge ( " 3,521) 2 3 District Numeral for Nursing Divisions single 0 3 double 0 5 Black Silk Armlet for Arm Badge, for all ranks 0 4 Hat Badge (Reg. No. 20) ... ... ... I 0 Titles with Numeral per pair 0 8 Pin Cushion Badge ...... 0 31 Buttons, per doz., Jarge, IS.; Small... 0 9
Cap Badge 0 6 0 8 Officers' Stars per pair I 4 0 8 Belt Furniture ... per set 6 I 10 Botton, {NO, 7 (large) per doz. 0 6 0 9 (White No. 8 (medium) 0 4 0 6 Metal) No. 9 (sm all, for caps) 0 3 0 41 Ditto {NO, IO (large) 3 0 (Electro No. II (medium) 6 Plate) No. 12 (small, for caps) 6
Cloak Badge (Commandant) . .. 2 6 Hat' " (Other Ranks) ... 0 6 " (Reg. No. 14) ... I 0 Shoulder Titles ... ... ... per pair 0 6 Buttons, per doz., large, IS. ; Small 0 9
Jnif0rm.
Lady District Supt., Arm, 4s. ge1. ;
Lady Corp.:; Supt., Arm, 4S. 3d. ;
Lady Divisional Supt., Arm, 3s. 9(1.; Cloak 4
Nursing
St. John
IS PaId 011 all Order. In the United Kingdom ELECTROTYPES.

No. t A. No.2 A. Xo. 3 A .
trbe GranD fln or\? of !tOe of tbe tlos plfal of St. Jobn of J erus al em In JISIl glan!).
I !12PA..Rnn:NT
Ube St: 301m t\mbllllll1ce BS50cillt( on
No. I All.
No . I B. No.2 n. N O.3 B.
tIb( (lIranb flrlor \? of trbc «>rOer of Ibe lbospUal of $1 . Jobn of Jerusalem In lEn glan!).
\!be St. Jobll BmblllllllCC lBrtilai)c. No . I BTL
Carri age Pa i d on all Or de r s in the United Kingdom -
E L E C TROTYPES OF THE ST. JOHN AMBULANCE DEVICE.
3 · Fur Cards, Tickets, &c.
For Note Paper, Small Circulars, &c.
For Quarto and Foolcap Letter -pape r, Circulars, &c . ... 4. For Small Pas leI's 5· For Large Poslers
Complete Se ries
Prints of the above Electrotypes (r to 3) Series A and JJ, and ( I ) Series All and BII, appear on page 35. Ku . 4A is shOll n on page 3 1. The diailleler of 5A and 5B is inches .
Fl ag s beanng Associalion dc\'ice-
t\ o.
1.
use. Series Series A. AH s. d. !S. d . 3 3 6 9 6 0 3 3 7 3 9 For Brigade llse Seri.::s Secie.; 13. 13H . s d. s. d. 3 3 3 3 9 4 9 3 7 3 9
For Association
£ s . rI.
2 feet by 6 feet 7 6 5 feet by 3 feet 0 12 6 I3rigad " 0 12 6
I
37

Banlage Paid on all OrderS in the United Kingdom.
SWAGGER STICKS
for the use of Officers and Members of the St. John Ambulance Brigade.
Ebonised Canes, German Silver Mounts bearing the Brigade Device.
PRICK IS. KACH.
Officers' Special Canes, with Sterlinl: Silver Mounts.
PRICE 7s. EACH.
(For General Index see pages 2 08'2 15) .
Ambulance Hampers ... " Station Plate
Badges .•. '"
Banuage Rolling Machin e Handagp.s ... ...
Basin, Dressing
Hea rer's Case
Belt and P ouch
Books ... ...
Bottles (Water)
Buttons ...
Ca rrying Sheet
Cash Book ... Cotton Wool... ... Cover for Stretche r or Litter
Diagrams, Large 30 " Small... 2')
Dredger (Boric Acid) 22
BEARER'S DRESSING CASE.
PRICE I2S. 6d.
All Orders tor the foregoing Stores should be given t. tho Local Secretary, or sent direct to Tho St. John Ambulance Association, St. John's Gate, Clerkenwell, London, E .C.
uze Tissue
IND
EX T O PRICE LIST.
['AGIl: 14 to r6 12 3 1
34 26 25 r3 37 33 28 to 30
to
3
......
... .. ..
for Caps, &c. 33 Lam p Lin t ... ... 27 Litter (Ashford) >!, 3 Litter (Rea ·Ed ward.) Lowllloor Jacket J\[ easure Glass .. . !.\Iinute Book .. . Nur<es' \Vallets Nursing Charts Occurren ce Book Pillow ... Plasters.. ... Pouch Fittings Book ... I, eglsters ... ... PAGIl: .. 4 to 6 11 22 3 010 Roller BanJage l\Iachine Rug ... ... .. ... for Corps or Divisions :-;t. J ohn A muulance Brigade 29 Safety Pins ... ... ... 13 Scissors 22, 26 Slings (Stretcher) Smelling Salts ... Splint PadJing 10 22 " Straps .. . 22 Splints .. . 22 Stationery 30 Stretcher Depot Plate 12 Stretchers ... ... 7 l0 to "
Swagger
Temperature
Text Hooks ... Thermometers ...
... Uniform Sundries Uniforms Water \Vaterproo(
Whistle anJ Chain Whi'e Pipmg ... Wool (Cotton) 37 26 28 to 30 ... 26, 27 33 .., 39, 40 II 3 33 13 27
Dressing Basin r 2 Drowning Tackle 13 Electroty pes 35. 36 I': mergency Book 29 Aid Box 8, 20, 2 [ " Companion.. 19 " "Colllpresseu Kit 18 First Field Dressings ... 22
36 Forceps 26 ... 27 (;a
27 [Iamper, (Ambul ance) I.J to 16 I laversacs
'7 I food and Apron for Litt er [nstrum ents (various) 26 Jaconette K.nife..... ... 22, 26 I ,ace
Adjustable for
Sti ck
Ch:lrt
Tourniquet ... Tow (carholizeJ) " (plain)
Sheet
39 C"n....actors· List. Carriage out of London Extra
PRICE LIST.
UNIFORMS FOR AMBULANCE UNITS
OF THE S.J.A.B.
These may be ohtained from HAZEL & Co. (sole proprietor, D. Hazel, for many years as!;ociated with the late firm 01 Hebhert &. Co., Ltd., as Dirpctor), Clothing and EquipmpDr :'If<ll1ufacturers, 6S. Road, City Road, London, E.C. ; and at h, York Place, Leprjs; 00 , Piccadilly, Manchester; anJ 84, Millpr SI reet, Glasgow. Telephone: Ln\1<hn Wall. Telpgram!;: "Hazelism, London." \Vherp two pnces are given for an article they are for first and ,tcUlld qualities.
All Badf!!s, and carn'rzf[" outside London arl'fl. I'xt ra. ,1Ieasureme1l{s fO bl' sUf/'/uod jrr!e 0/ clln, «e.
CORPS SURGEo.N AND DIVISIo.NAL
Tunic, Superfine Black Cloth ...
Trousers, Superfine Black Dneskin (if Silver Lace
Stripe, extra) ...
Cross' Belt and Pouch, Plain, 20.'- ; Sih'er
Embroidered
Gloves
Great Coat, Grey Clolh ...
Cap-Corps Surgeon Divisional Surgeon
DTSTRICT C:UPRRINTKNnJ1:NTS
AND CORPS OfF[CltR<;.
Superfine mack Clvth
Patrol Jacket, Black Cloth
Tronsers, Superfine Black Doeskin
Cross Belt and Pouch
G Iovec::, 4/6 ; Leggings, S:6
Great Coat, Grey Cloth
Cap-Dist rict Superintendent

Con:ractors L:st. Carnage Paw on ail Ol'antlry COQU5. DlVIS10NAL A:>.u l-' ... nol JaLKet, Black Cloth
Black Due!;klll
Cross Belt and Pouch
Gloves, 4/6; 'is/o :::
Great Coat, Grey Cloth '"
Fatigue Jacket, Black Vicuna Serge ...
Black Vicuna Serge
Cap-Divisional Superintendent
FIRST CLASS SERGKANTS.
Patrol Jacket, Superfine Black Cloth .. .
Chevrons, Four Bars, Silyer... .. .
Trousers, Superfine Black Doesh.in
Cross l1elt and Pouch
Cap, ; 4/6': Sd.
LeggIngs, Black or Brown LeatiJe, Water Bottle and Carrier .. ..
Haversar.k, \Vhite Duck '"
Great Coal, Dark Grey
SKRGRANTS, COl<.PORALS ASU PRI\'ATES.
Patrol Jach.et, lliack Tartan
Chevrons, Silver... . ..
Trousers, Black Tartan
Waist Belt and Pouch. Brown
Cap, 2/9; Gloves, Cotton Sd
Leggings, Black Leather" ...
Water Bottle and Carrier, 3/9; Great Coat, Dark Grey Melton ... 16/- and
VI<.AH 's111,,,h, U:>.I FO/< 'IS.
Jacket, Drab Mixture Selge Trousers '.
,. "
Coal, IJlab Meltun
£,
,) IS 0.
s. d.
2
Tunic,
. .. 3 (J 3 7 /.,1 '7 b lliid I 6 I 9 0 0 17
.. . 3 IS 2 10 I 2 o 13
... " Corps Officer £1 12 6 and I 10 0 3 I o IS (, 6 6 6 o 0. o o 6 6 o
AAl1,ULA:'>Cf< I -'-' s. d 6 6 r 2 6 o 13 6
"
£ I 4 0
Ambulance Officer 0 15 6
and
per Hal
Cap
3 7 I IS a 16 o 14 o 9 I liS 0 3 o 19 a 10 0 4 0 3 0 1 c 16 0 II b o o o a b 4 6 6 3 9 6 0 0 0 o 10 0 9 0. 6 a 4 o I a 14 a o 9 8 a 2 a 19 6 6 3 6 a 9 a o 6
Great
ST. J 0 H N 11 fv\ B U L 11 NeE BRIO 11 0 E.
UNIFORMS FOR NURSING UNITS.
THESE GOODS !\fAY DE OB rAINED F Messrs. E. & R. GARROULD ,
150 to 162, EDGWARE RD., LONDON, W .
CLOAK (BadJe ext ra) 19/0 , 25 /6, 29 6
BONNET {Nursing 9/ 6 " Officer s 10/6
DRESS {Nursing Dress Length 3/7 " Officers" ,,3/11
C { 21 in., ea ch; 5/6 doz. OLLARS in., 61d." 6/6 "
CUFFS { 4 in., 6/6 " ..." hd." 7/6 "
C {Nursing Sister's 8,d. & 1/- each AP "Officer's... 1/4 ..
APRON 1/11 & 2/6 also in Pure Irish Linen 3/6"
ILLUSTRATED PR ICE LIST FREE. Telegrams-5321. & 6297, PADDINGTON. "GARROULD, LoNDON."
THE UNIFORMS, CLOAKS, BONNETS, APRONS, DRESSES,

WfNTfi:R COAT, 23 / 6
SU\l COAT, 27/6 ETC., FOR TilE ST. JOHN BRIGADE, ;\fAY BE OBTA IN ED AT E. & R. GARROULD. To OFFICI':
A:\f TLLU ' TRATED PRICE LI 'T of the \'a riou$ articles reqlli red by the ST. JOHN A;\IBULANCE BRIGAD I': , ON APPLICATI ON.
ISO to 162, Edgware Road, CONDON, W.
OFFI CI(. COLO:-li
O FFICE.
COl NT\' COl' NeIL,
11. 1\I. INDIA
\L
LON nON
ETC.

