

BONES.

vertebra! - ---. -.
COllar} Bon& (clavicle)
Bone Breast} (sternum) Arm Bone (humerus)
4th Lumbar. Vertebra HaUnCh} Bone (pelvis)
Ulna
Metacarpus - - \
phalanges __
Thigh Bone (femur)
Knee Cap (patella) Shin Bone (tibia)
Brooch Bone tfibula)
• • OCC'IPlt I•
• •• - Tempor F al.
Carot. II. S bc;lavian.
Axill.ry.
hlollDlgltal r Tourniquet)
o tao - - Bra hlal (HaXlor". - Ilta(.. Radial or (Digit e55 reI oral 'quet)
enceme, t of Popliteal.
>opllteal lex Ion).
terlor blal. terlor Iblal.
Tarsus
Miltatarsus
Phal a nges ___ _
"A
AS COMPANIONS TO THIS BOOK-
CATECHISM ON FIRST AlD."
BY 1. M. CARVELL, M.R.C.S., L.S.A.Price 6d., post free.
"PROBLEMS
IN FIRST AlD."
BY L. M. FRANK CHRISTIAN, M.B., ANDw. R. EDWARDS, A.C.A.
Price 6d., post free.

FIRsrr AID TO THE INJURED
ARRANGED ACCORDING TO THE REVISED SYLLABUS OF THE FIRST AID COURSE OF THE ST. JOHN AMBULANCE
ASSOCIATION.
BY JAMES CANTLIE,M.A., M.B., F.R.C.S., Knight of Grace of the Order of St. John. HOllora1'Y Life Member of, and Lecturer and Examiner to. the Association.
\ Vith a CHAPTER on .. Stretcher Transport." revised from that originally written by Sir JOHN FUR LEY. C. B., KlLight ofJustice of the Order of St. JohlL. in accordance with the Army Stretcher Exercises. Also a CHAPTER (being the Fifth Lecture 1M Females only), by E. MACDoWEL COSGRAVE, M.D F.R.C.P.I Knigltt of Grace of the Order of St.John, HOlLorary Life Member of, and Lecturer alLd Examiner to. the AssociatiolL.
EDITIO:'-l', 1,39J,000 to 1 ,440,003
(This edit/on is similar to the eighteenth, in which editiolt many of tl,. illustrations re-drawlL; otherwise it differs bitt little from th eleventh to the seventeenth editions.)
Price in Cloth, is. post free.
LONDON:
THE ST. JOHN AMBULANC E ASSOCIATION, ST. JOHN'S GATE. CLERKENWELL, E.C.
W. H. & L.C. SO,()()I) 1?! IO fS.
Ul)e U;ranb or ttbe of tbe 'lbo5pital of St. S-ol)l\ or S-erusalem in JEnolanb.
SOVEREIGN HEAD AND PATRON: HIS MOST GRACIOUS MAJESTY THE KING.
GRANDPRIOR: H.R.H. THE DUKE OF CONNAUGHT, K.G.
SUB-PRIOR: (Vacant).
BAILIFF OF COLONEL SIR HERBERT C. PERROTT, EXECUTIVE OFFICERS: [Bt., C.B.
PRELATE.-The Archbishop ef York.
CHANCELLOR.-CoL Sir Herbert Jekyll, K.C.M.G.
RECElvER-GENERAJ,--Edwin Freshfietd, LI-D.
DIRECTOa OF THE A)llBULANCE DEPARTMENT.-The Earl of Plymouth, P.C., C.B.
CHAIRMAN OF THE BRITISH OPHTHALMIC HOSPITAL, J)':RUSALEM.-Col. Sir Charles lVI. \Vatson, K.C.M.G., C.B.
ALMON ER.-Sir Dyce Duckworth, Bt., M.D., F.R.C.P., LL.D.
LIBRARIAN.-A. Edmund Fraser.
REGISTRAR.-The Earl of Ranfurly, P.C., G.C.M.G.
GENEALOGlST.-Sir Alfred Scott Scott-Gatty, K.C. v.o. (Garter).
DIRECTOR OF CEREMONIES.-Sir A!.fred Scott Scott-Gatty, K. c. v. o. (Garter).
ASSISTANT EXECuTIVE OFFICERS:
ASSISTANT RECEIVER-GENERAL.-Edwin H. Freshfield.
ASSISTANT DIRECTOR OF THE AMBULANCE DEPARTMENT.Lieut.-Col. Sir Richard C. Temple, Bt., ' C.I.E.
HONORARY SECRETARY OF THE BRITISH OPHTHALMI C HOSPITAL, JERUSAl:EM.-Col. Thomas H. Hendley, C.I.E., M.R.C.S.
ASSISTANT HONORARY SECRETARY (FOR SCOTLAND) OF THE BRITISH OPHTHALMIC HOSPITAL, JERUSALEM.-John Horne Stevenson (Unicorn Pursuivp.nt).
SECRETARY AND ACCOUNTANT.-\Villiam R. Edwar<1s, A.C.A.
ASSISTANT SECRETARY.-Duncan G. Monteith.
ASSISTANT ACOOUNTANT: Ivor C. Albury.

THE CHAPTER-GENERAL:
n. Chapter-General consists of the Grand Prior. the Sub-Prior, the Bailiff of Egie, the other Knights of Justice, the Prelate and the SubPrelates. dl' J'ttre; the Executive Office rs; the Offi ciating Chaplains; all members of the Council; not more than ten Kni ghts of Grace and Dot more than six E"qllires appointed by the GranJ Prior.
I'::NlGHT,; OF JUSTICE:
HIS MOST GRACIO US MAJESTY TIlE (Sovereign Head and Patron).
FIELD-MARSH AL n R H. THE DUKE OF CONNAUGIIT, K.G., K.T., K . P., P.C., Etc. (Grand Prior).
GRNERAL H.R.H. PRINCE CHRISTIAN OF SCHLESWIG-HoLSTEIN, K,G., P.C., G.C.v.O.
H.H. PRINCR ALflFRT OF SCHLESWIG-HoLSTEIN, G.C.B., a .CoV.o.
COLONEL H.H. THE DUKR OF TECK, G.C.B., G.C.V.D-, C.M.G.
ADMIRAL H.S.H, PRINCE LOUIS OF BATTENBERG, G.C.B., a,c.V.o., K,C.M.G., R.N.
H,M. HA ,\KON VII., KING OF NORWAY. K.O., G.C.B., G.C.V.O.
LIEUT.-COL. H.S H. PRINCE ALEXANDER OF TECK, G,C.B., G.e.V.O., D.S.D. MAJOR II.R.Il. PRINCE ARTHliR OF CONNAUGHT, K.G., K.T., P,C., G,C.V,O. , C.B.
H .H PRINCE ALEXANJ1ER OF BATTENBERG, G,C V.O.
Sir John Furley, C.B. (Honorary Bailiff).
Sir T. N. Dick-Lauder, Bt.
:'Ilaj. Sir A. Lamb, Bt.
Col. Sir H. C. Perrott, Bt., c. B.
Col. Sir J. Gildea, K.C.V,O., C.B. H. J. Loftus.
Col. B. M. Dawes.
Gen. G.C.M.G.. K.C.B., R.E, Maj.-G=. J. C. Dalton.
Sir A. G.if[HunterWeston of IInnterston, K.C.B., D.S.O.
Col. The Lord William Cecil. C.V.o. E. Freshfield. LL.D. (Honorary Bailiff).
The Earl Brassey, G.C. B. The Viscount TernpletowD. R. M. MacLean.
A. F. G, Leveoon Gower,
Col. F, A. H. Lam bert.
Col. Sir C. W. Murray, C.B.
The Earl of Ranfurly, P.e., (: C.M.G
Tb. Lord Sandhurst, P.C.. I",C.S.\., G.C.I.R.
Sir H. A. Blake. G.C.M,G.
The Earl o f ;\Ieath, K.P., P.C. A. E. Fraser. The Lord Mostyn.
The Marquess of Breadalbane, K.O p,c.
The Duke of Portland, K.G., P.C. R. B. Carter, F,R.C.S. (Honorary Comma nderl.
Col. C. "V. B. Bowdler, C.B. (Honorary Commander).
Lieut.-Col. A. C. Yate. Maj.-Gen. A. F. Terry.
The Earl of Plymouth, P.C., C.B. The Earl of Sandwich. K.C.V.O. E. H. Freshfield.
Lieut.-Col. The Earl of Ellesmere, M.V,O.
Field-Marshal The Earl Kitchener , of K'C:;J K.P., Etc.
Lieut.-Col. S,r R. C. lemple, Bt., C.I.E.
Sir A. S. Scott-Gatty, K C.V.O.
Col. Sir H. Jekyll, K.C.M,O.
The Lord Islington, P.C., G C.M.G., D,S.O.
KNIGHTS OF ]USTICE.-continued.
Col. Sir J. R. A. Clark, Bt., C.B., F.R.C.S .E
Sir R. Harvey. Co!. The Lord Sydenham, G.C.S.I., G.C.M.G., G.C.I.E. Lieut.-Col. ]. \V. \Vray. Sir \Y. \\T. Portal. Bt. The Duke of Somerset.

Sir n. nuckworth, Bt.. M.D. Capt. II. E. lloullon. C.v.O.
The Viscount Esher, G.C. B., G.C. V.O. Cnl. Sir C. 1\1. C.B. [G.C.B. field-l\Iarshal The Lord Nicholson. Lieut.-Col. The Lord IIerbert Scott, John Horne Stevenson. [o.s.o. Francis vVilliam Pixley.
PRELATE:
The Archbishop of York.
SUR-l'RELATES:
The B;"hop Ormqby. I The Bishop of Gibraltu.
The Prill1<1te of New Zealand. The Bishop of Peterborough. The Bi"hop 01 SOllthwark.
OFFICIATING CHAPLAINS:
The Rev. Canon E. Sheppard, I The Venerable Ernest E. Holmes, K.C.V.O., D.O. B.D. (AI·chdeacon of La don).
KNIGHTS OF GRACE APPOINTED BY THE GRAND PRIOR:
Col. Sir J: \V. Ottley, K.C.I.E., R.E'I J.. II. c. V.O., F.R C.S.
]. A. ]am.:::s. 1II.V.0. SIr \\. [I. St. J. lI ope. LITT.D.
]. S. Griffithq. lII.R.C.S. F. 1I. Cook. C.I.E. Lt.-Col. George E. Twiss, F.R.C.S.I. The Lord Norreys. R. A. Gibbons, 1\1.0. E,·elyn Cecil, M.P. ESQUIRES APPOINTED BY TilE GRAND PRIOR: B. Hamilton, C.lII.G. I Col: \V. G. Carler. E. Dawes. Major M. D. l\Iurray. C.V.O_. C.B.
THE COUNCI
L :
The Council consists of the Sub-Prior, Colonel Sir Herbert C. Perrott, Bt., C.B . (Bailiff of Egle), lhe Titular Priors of Priories, lhe Commanders of existing COl11manderies. the Executive Officers. and not more lhan fifteen members of lhe Grades o! Knight of Juslice. Chaplain. Knight of Grace <lnd Esquire appointed by the Grand Prior. 1\IEMBERS APPOINTE!)
Sir J. Furley, C.B.
1Iajor-Gen. J. C. Dalton.
Colonel The Lord 'William Cecil, C.\'.o
Sir Henry Arthur Blake, G.C.M .G. E. H. Freshfield.
BY TilE GRAND PRIOR: Lieut.-Col. Sir H. C. Temple, Bt., C.I.E.
The Bishop of Southwark. inspector-General B. Ninnis.c.v.o., M.D.• R.N. The Lord CI;llIu Ilamilton, M .P. CoL T. II. I Jentlley, C.I.B.,M.R.C.•
m)e (Bran() jprior2 of UI)e of tbe 'U)ospttal of St. Jol)1l of Jerusalem ill JEnglan().
AMBULANCE DEPARTMENT.
'U1)e St. 50()1\ :E\mbnlance E\ssociatlOll.
PATRON:
HIS l\IAJ ESTY THE KI G, Sovereign Head and Palron of the Order.
PRE IDENT:
ILR.H. THE DUKE OF CON, AlJGHT, K.G., Grand Prior of the Order.
CENTRAL EXECUTIVE CO;\Il\llTTEE: Consisting exclusively of Members and lIonorary Associales of the Order.
DIRECTOR OF THE AMBULANCE DEPARTMENT AND CflAIlUIA N OF COMl\IITTEE.-The Earl of Plymouth, P. c., C. B.
ASSISTANT DIRECTOR AND DEPUTY CH.\IRi\IAN.-Lieul.-Col.
Sir Richard C. Temple, Bt., C. 1. E.
DEPUTY CHAIRl\IAN.-Sir John Furley, C.B., Life i\Iember of the Committee, HOlloris Causa..
1\IEpIBERS:
1\hl.i.-Gen. J. C. Dallon.
The Lord Islington, G.C.I\!.G., n.s.o.
Col. Sir J. R. A. Clark, l:H C.B.• F R.C.S.E. Col. The Lord Sydenham, G.C I., G.C.M.G., G.C. I. g.
Capt. H. E. Boullon, C.V.O. Lieut.-Col. The Lord I [erber t Scott, D.S.O.
The Rev. T. C. Elsdon.
Inspector-General ll. Ninnis, C.V.O., ;11.0., R.N.
Maj. G. n . Darwin, M.D.
Col. G. S. Elliston, C.B., PI.R.C.S.
Col. C. J. Trimble, C.M.G.,' L.R.C.P.B.
The Lord Claud Hamilton, M.P.
Sir J. L. Langnnn, Bt.
S. \V. 1\Jalkin.
C. Cotton, F.R.C.P.B., IIt.R.C.S.
CENTRAL EXECUTIVE COilL\lITTEE-continued.
C. B. Palmer.
Lieut.-Col. G. E. F.R.C.S.l.
Col. T. H. Hendley. C.I.II: •• M.R.C.S.
J. H. ]\forgan. C.V.O.• F.R.C.S.
Col. Sir Trevredyn R. K.C.S.l., K.C.I.K.
Major E. H. T. Parsons.
Brig.-Gen. H. R. Mends.
Lieut.-Col. A. D. Acland.
Y.QJ; •• Col. E. D. Brown-Synge-Hutchinson.
J. A. BIoxam. F.R.C.S.
Lieut.-Col. Sir R. \V. Inglis.
Surg.-Gen. H. R. Whitehead. C.B., W.K.C.S.
The Viscount Acheson.
T. H. Woolston.
Col. C. R. Tyrrell. M.R.C.S.
Col. The Lord Bolton.
Surg.-Gen. Sir A. W. May, K.C.B., P.R.C.S., K.N.P., R.H.
F. N. Ellis.
W. E. Audland. M.R.C.S.
A. H. Johnston. M.R.C.S.
E. A. Richards.
EX-OFFICIO MEMBRRS OP CoMMITTEE:
Col. Sir H. C. Perrott, Bt.• C B. (Bailiff of Ellie).
The Secretary-General of the Order
The Receiver-General of the Order.'
The Chairman. British Ophthalmic Hospital.
CHIEF SECRETARY: Major W. O. Prichard.
ACCOUNTANT: \V. R. Edwards, A.C.A.
DIRECTOR OF STORES: \iV. H. Morgan.
ASSISTANT SECRETARY: D. G. Monteith.
TERRITORIAL BRANCH.
CONTROLLER-IN-CHIEF :
Lieut.-Col. Sir R. C. Temple, Bt., C.I.&.
SECRETARY: P. G. Darvil-Smith.
HEAD OFFICES:
Tohn's Gate. Clerkenwell. London. E.C.
REVISED 1908.

REFERENCE No. 58-. 1908•
FIRST AID TO THE INJURED.
SYLLABUS OF INSTRUCTION .
FIRST LECTURE.
A. Principles of First Aid.
B. A brief Description of the Human Skeleton and of the Muscles.
C. Fractures-Causes, varieties, signs and symptoms.
D. Treatment of Fractures-General Rules.
E. The Triangular Bandage and its application. SECOND LECTURE.
A. Treatment of Fractures (continued). Details of treatment.
B. Dislocations, Sprains, Strains-Signs, symptoms and treatment.
C. The Heart and Blood Vessels. The Circulation Qf the Blood.
D. IIremorrhage and wounds. General for treatment.
E. The Triangular Bandage and its apphcatlOn.
THIRD LECTURE.
A. Ilaemorrhage and wounds (continued). Details of treatment.
H. Internal Haemorrhage-Signs, symptoms and arrest.
C. ITaemorrhage from Special Regions.-S·igns, symptoms and arrest.
D. Bruises, Burns and Scalds, Bites and Stings, Frost-bite.
E. Foreign bodies in the Eye, Nose and Ear.
F. The Triangular Bandage and its application.
FOURTH LECTURE.
A. The Nervous System.
B. The Organs and Mechanism of Respiration-Artificial Respiration.
C. Insensibil i ty
D. l'oi,oning.
FIFTH LECTURE (for Males only).
A. Improvised methods of lifting and carrying the sick or injured.
B. Methods of lifting and carrying the sick or injured on stl;etchers.
C. The conveyance of such by rail or in country carts.
FIFTH LI!CTlTRE (for Females only).
A. Preparation fur reception of accident cases.
B. :Means of lifting and carrying.
C. Preparation of bed.
D. Removing the clothes.
E . Preparations for surgeon.

9
NOTE I.-The subject of poisons should be treated in'i. ge neral manner; the common poisons classified, and only their ge n eral symptoms, 'effects and treatment taught.
Non: 11. - T he last half-hou r of each l ecture should be devoted to practical work, such as the "ppiication of bandagei and splints, lifting and carrying wounded on stretchers .
NOTE IlL-There should be an interval of a week betweer, each lecture. A candidate for examination must attend -dt least fuu r out of the five lectures.
NOTE IV .-Male classes must pass in that system of stretcher exercise most suitable for the locality_
NOTE V .-As litt le time as possible is to be spent on iilstruction in anatomical and physiological details. Lecturels and examiners a re particularly requested to remember that It [5 " First Aid" that has to be taught and lested, and not anatomy and physiology. jJfixed classes Of men and WOme Jl are on n o account ,-t>ermitted.
PUPILS UNDER SI;,:-rEEN YEARS OF AGE CAN ONLY ATTENrD THE" JUNIOR" CuURSE (SECT,ON A, SYLLABUS 40 ).
Lecturers instructing a First Aid class, and Local Secret.rie., can obtain further particulars on application to the ChiCl'f Secretary for "Paper Reference No. 80 ."
N o Lecturer may examin e his own Class for Certijit'ates
SU Ml\l ARY OF CO NTENTS.

CH APTE R I.
Principles of First Aid
Explanatory
Questions on Chapter
CHAPTER II .
The Human Skeleton. Skull, spine, ribs and breastbone, upper limbs (co llar-bone, shoulder-blade, armbone bones of t he forearm, carpus, metaca rpus, pelvis, lowe r limbs (thigh-bone , kneecap, tarsus, metatarsus, phalanges ) ... ..,
Joints .. ,
Ml'scles. Voluntary and involuntary
Fractures . Cause5, vari eties, sign s and £ymptoms
Apparatus for treatment o f F r a ctures ...
General Rules to be observed in the treatment of Fractures
Special Fractures. Cranium, lowe r jaw, spine, ribs, br east-bo ne, colla r -bone, shoulder-blade, arm-bone or bones close to the elbow j oint, forearm, crushed ha nd, pelvis, thigh -bone, knee-cap, leg, crushed foot
Dislocations
Sprains
Spr-ains and Ruptured Muscles .. ,
Questions on Chapter
CHAPTER III.
Circulation of the Blood. Organ s ; general (systemic) and pulmona ry circulations
Hcemorrhage or Bleeding. Arterial, venous, capillary
Arterial Hcemorrhage. Plincipl es of arrest
Wounds with Arterial Hcemorrhage ...
Course of the Main Art eries and Pressure Points.
A orta, arteries of the head and neck, of the upp e r limbs, of the lower Iimus
Venous Hcemorrhage and Varicose Veins
Wounds with V e nous Hcemorrhage
Capillary Hcemorrhage
Internal Hcemorrhage
Hcemorrhage from Special R egions
Questions on Chapter
C HAPTER I V.
Miscellaneous Injuries . Bruises, burns and scalds, bites of snakes and rauid animals and wounds by poisoned weapons, stings of plants a nd animals, frost bite, needle embedded unde r the skin, fish hook embedded in the skin, injuries to joints, foreign body in the eye, ear passage and nose, wound in the front wall of the abdomen, injuries to the organs within the abdomen and pelvis
Questions on Chapter . . . . . .
CHAPTER V.
The Nervous System. Cerebra-spinal, sympathetic ...
The Respiratory System
Artificial Respiration. Schiifer's, Silvester's, Howa rd's combined with Sil veste r's, L abo rde's a nd Ma rshall IIa ll's methods ...
10
Page 17 20 21 22 3 1 3 2 33 36 4 1 43 62 64 65 66
t
I
Page 70 73 74 76 79 93 94 95 95 96 99 ' 102 II 5 II 7 I I 8 12 T
12
Insensibility. Causes, general rules for treatmeIl't, concussion of the brain, compression of the brain, apoplexy, epilepsy, hysteria, shock, fainting and collapse, sunstroke and heat-stroke, convulsions in children, asphyxia
Electric Shock and Effects of Lightning
Questions on Cha ?ter
CHAPTER VI.
Poisoning. General rules for treatment, special poisons
Questions on Chapter
CHAPTER VII.
Bandaging. Bandages for the scalp, forehead, etc., shoulder, hip, hand, foot, chest, back, knee, elbow, fingers and toes ...
CHAPTER VIII.
Methods of Carrying. Four, two, and three-handed seats, fireman's lift, fore and aft method, improvised stretchers, to cross a ditch or wall, to load or unload a wagon
CHAPTER IX.
Stretcher Transport. Stretchers, stretcher litters
CHAPTER X' .
The Fifth Lecture (for Females only ). Preparation for reception of accident cas=s, choice and preparation of a room, lifting and carrying, preparation of bed, removing the clothes, preparation for surgeon
Questions on Chapter

Skeleton showing position of main arteries
Skull and vertebral column
Vertebra
Bones of the left upper limb
Bones of the right lower limb
Shoulder Joint
Ankle...
Rectus Muscle
Triangular bandage spread out and folded
Large arm sling
Small arm sling
Reef knot
Granny knot
Loop knot...
Bandage for fracture of lower jaw
Bandages for simple fracture of ribs
St. J ohl1 sling
Band ,)ges for fracture of bot h collar bones
Bandage for fracture of shoulder blade
Treatment of fracture of arm
Angular splint '"
Treatment of fracture of forearm
Treatment of crushed hand...
Treatment of fracture of thigh bone
Treatment of fracture of thigh bone (woman)
Fracture of knee cap
Treatment of fracture of knee cap
Treatment of fracture of leg (man and wvl11an)
Treatment of crushed foot
Diagram of the heart, lungs and air pa sages
..
...
Page 128 142 145 14'3 154 ISS r60 197 206 13
OF
LIST
ILLUSTRATION'S.
... ... ... ... ...
... ... ... ... . ..
... ... ... ...
.. .
... ... ... .. .
... ... .. .
. . .
... ... ... ...
...
... .. .
.. .
. . . . ..
...
... ... . ..
Pag-e frontispiece. 2.t., 24 27 29 3[ 3[ 32 38 39 39 40 4D 43 44 47 50 5[ 52 53 54 5S 55 57 5g 58 59 6[ 62 7r.
Dlagr:;.m of the of the blood
Digital pressure on car?tld artery .. .
Digital pressure on facIal artery .. .
Digital pressure on artery
Digital pres-ure on OccIpital artery ... ..,
Pad and banuage to arrest hremorrhage from temple
Ring pad .. . ... :
Digital pressure on subclavian artery .... ...
Pall and bandages to apply pressure on aXillary artery .. .
Digital press me on brachial artery (two methods) .. .
Flexion at elbow ...
Digilal pressure on radial and ulnar arteries ...
l)ad and bandage to arrest hremorrhage from palm
Digital pressure on femoral artery ...
Tourniquet on femoral artery
Flexion at knee
Organs of the chest and abdomen .. .
The lungs and bronchial tubes .. .
Schafer's method of artificial respiration ...
Silvester's method of artificial respiration
Silvester's and Howard's methods of artifici.LI respiration combined
Bandage for the head
Bandage for the shoulder
Bandage for the hip ...
Bandage for the hand
Bandage for the foot
Bandage for the chest
Bandage for the knee
Bandage for the elbow
Grip for four-handed seat ...
Lifting by two-handed seat. ..
Grips for two-handed seats ...
Carrying by two-handed seat

Grip for three-banded seat ...
Supporting patient ... IS
Fore and aft method of carrying
Carrying on improvised seat
Improvi.sed stretcher
Furley stretchers ...
Stretcher exercise, No. I. ., Fall in"
Ditto, ready to lift patient
Ditto, lifting patient. ..
Ditto, placing stretcher '" . . .
Ditto, preparing to lower JJalient .. .
Ditto, " Lower" ... ... .. .
Ditto, No. II. Ready to lift patient
Ditto, patient lifted... ... . ..
Ditto, No. IV. First position
Ditto, second position .. . ... .
Diagrams illustrating Army stretcher drill
Ditto... ... '" ... ... . ..
Bed cradle... ...
Jmprovised bed cradles
..
.. .
. ..
. . ..
..
73 8r 81 82 82 83 84 85 86 87 87 S9 go 9 1 9 2 lIZ 119 122 124 125 155 156 156 157 15i' 158 159 159 160 161 162 163
20",), Pa r t! 164J6s 167 168 168 17 2 175 176 177 178 179 I 0 182 183 IllS 189 19 1 194 203 204

PREFA CE.
AT the request of the Central Executive C omm ittee 1 have revised the manual written by myself in 1901 , as the official handbook of the St . John Ambulance Association.
Throughout the revision an endeavour has been made to simplify the study of Flrst Aid to the Injured by drawing up a number of general rules for the tueatment of accidents and sudden ill ness, and by the Gmission of all detail \yhich is not absolutely necessary to enable the student to acquire an intelligent kno'vvledge of the sub ject.
I wish to express my thanks to Professor E. A . . chafer for furnishing instructions for performing a method of artificial respiration, to Dr. L. M. F . Christian for many valuable suggestions, and to the Medical Members of the Central Executive Committee, especially Surgeon-Major G. H . Darwin, M.D., and Dr. F. R. Cassidi, for perusing the proof sheets and for a number of useful additions to the \york .
I cannot omit also to offer my best acknowledgiI1ents to Mr. , V. R. Edwards, the Accountant and Storekeeper of the S.J .A.A., for his invaluable JAMES CANTLIE.
FIRST AID TO THE INJURED.
CHAPTER 1.
The St John A mbulance Associatio n h as n.ow completed thirty years of its existe n ce, and d u nng that period hun dreds thousands .of men and women have been taught at ltS classes, In all parts of the wo rld how to help th eir injured neighbours . Aid to the Injured is a special branch of practical medicine and surgery, by a of which trained persons are enabled to afford assistanc e in cases of accident and sudden Illness . The instruction begins and e nds with First Aid, and the subject is taught simply bu t tho roughly exhaustively . The duty of the ambulance pupIls ends where the doctor 's commences, and there ought to be no overlapping or clashing of duty or interests .
PR I NCIPLES OF F I RST AID.
I. The First Aid student should be(a ) Observant, that he may n ote the causes and signs* of injury.
(b) Tactful, that h e may wi thout questions learn the symptoms I a n d h1st oryt of t he case.
* Si 6ns are what may be perceived . t Symptoms are what the patient can te.n you. . t History means the circumstances attendmg th e ac cident or sudden illness.
(c) Resourceful, that he ma use t advantage whatever is at Yh d 0 the best further damaO"e and t . aNn to prevent t . • b 0 aSSIst ature's ef[: t
(d) EO rep.a]: the mischief already done or s , XpltClt, that he may i 1'· tions to th t' g ve c ear lnstruce pa lent or the byst d best to assist him an ers how
(e) Discrimina:ting' that h ' of several ' ,,' e may decIde which In Junes press ment by himself d' eSh most for treatI ,an w at can b t b 2 R eft for the patient or the bystanders d e emove the cause f" o. whenever possible. 0 ll1Jury or danger
3· Severe hremorrh attention no m mhust receive the Injuries. ' a er w at are the other
4· Air.- The patl'e t ' h"1 b ' L 11 must be lt1 ", W Ie 1 reath,ng is possible' th' a pOsltlOn 111 free from obstruction' 'f' b ,J au passages must be J I reat ll10" has cea d meSasuRres ItllUSt be taken to restor: it. se prompt , es -A restful 'f f the vital will assist help to prevent fu;the 0 t e lnJured part will the case of fractures ofrl' abmage, and IS essential in 6 W 1m s.
.. armth.-After ever 'd patIent warm so as to y accl ent keep the below ,the normal poinrevent the faU of temperature
7· When the skin is broken the wound

should be promptly covered with a clean absorbent dressing. Should the wound be poisoned, it is most important immediately to prevent the poison Dermeating the system.
8. Poisons swallowed should be got rid of; or \\" hen that is inexpedient, ' neutralised.
9. The best means of transport must be studied, and provision made for proper care when the patient is brought to shelter.
10. Removal of Clothing.-Clothes should not be taken off unnecessarily, but when it is needful to remove them, the following rules will be found of service in serious cases:-
: Remove from the sound side first, and, if necessary slit up the seam of the sleeve 0n the injured side.
SJIIRT AND VEST: Slit down the front and remove as the coat.
TROUSERS: Slit up the outer seam.
BOOT: Slit the back seam and undo the laces.
SOCK: Cut off,
II. Stimulants.-It is incorrect to suppose that alcohol is the only form of stimlliant, and far too frequent use of spirits is made to restore a patient after an accident, often with serious results; the safest rule, therefore, is to defer the administration of alcohol until the arrival of a doctor. "When the patient is able to s\\'a11o\\', strong tea or coffee, or milk, as hot can
18
be drunk, or a small quantity of sal volatile in water may be give n. Smelling salts may be held to the nose. Sprinkling the face with cold and hot water alternately, warmth app li ed to the pit of the stomach and over the heart, and vigorous friction of the limbs up wards have a stimulating effect.
I2. Throughout his work the First Aid student must on no account take upon himself the duties and responsibilities of a Medical man. At times an apparently slight injury is accompanied by grave danger and may actually cause loss of life. \Vhen sending for a doctor, state the nature of the case, and remember that \vrilten particulars are safer than a verbal message.
It is necessary that something should be known of the structure of the body (elementary anatomy), and o f the functions of some of the more important organs and systems (elementary physiology). A short description of the ne ces sary anatomical ana pl1ysiological points is therefore given as the several subjects are discussed. For purposes of description the human body is supposed to be erect, with the arms hanging by the side and the palms of the hC',nds directed forwards. The (( middle line" of the body runs vertically from the top of the head to a point between the feet.
QUESTIONS ON CHAPTER I.
TIlt llullw'als indicate the pages where the answe1'S may be found.
What i s First Aid to the injured ?.. .., "', qualities should the First Aid student possess.
"'hat are signs ?
at are symptoms?
What is the history of a case?
What is often the first thing to ?O In an acclden\: ,'"
\Vhat result of injury mu st reCel\'e the first alten
\\'hat three things are absolutely necessary to an InJUTec
I Tow must poisoni ng be treated?
What steps must be taken beyond the actua of injuries?
Should clothing always Le

1 treatment
llow woulg you remove clothw!5 when necessar) . Explain lhe use and abuse of stJll1ulants ...
What must the First Aid student not do
purposes of descriptIOn
to be placed?
20
2T
.. . .. . .. . ...
.. , ...
\\'h
.:. ... . , PAGII' 17 17, 18 17 17 17 IS 18
"i
18 person? ... .., .... .... ·... n' .. · ." 18 19 \Vhat must be done when the skl!1 I S broke . ..., 19
.. , ...
... .., ... .., .. ,
.. , .... ,
..,
What is elementary anatomy? ... 19 19 19 .., 19, 20 20 20 '20
physiology?
body F'1r
ow
supposed
... \\ hat is
"' " 20 2 )
?
\\'hat is elementary
. . h s the human
1
the middle line of the body?
CHAPTER II.
fRACTURES, DISLOCATIONS, SPRAIN AND STRAINS.
THE SKELETON.
The human body is I?oulded upon a bony framework (the skeleton) whIch serves-
I.-To give shape and firmness to the body.
2.- To afford attachment to the muscles.
3·-To protect important organs, as in the skull, chest, and abdomen.
THE
SKULL.
The Bones of the. Skull are arranged in two groups, those of the bram case or crolnium and those of the face. '
The Boundaries of the Cranium are the yault or dome, the rounded portion forming the top of the head; the front or brow; the back of the head "vhere the greatest extent of brain exists and therefore thE' cranium is widest and deepes't; the sides temples. The base of the cranium is hidden from VIew by th.e of the face and of the yertebral column; III It are numerous perforations for the of vessels nerves; through the largest openmg the bram and spmal cord are continuous.
The Bones of the Face with the exception of

the lower jaw are firmly jointed together, so that movement between them is impossible. The cavities of the nose and of the eye sockets (orbits) are formed by the bones of the crani um and of the face conjointly. The mouth cavity is formed between the up.per and lower jaws, the palate being the bony roof of the mouth which separates it from the nasal cavity above.
The Lower Jaw consists of:-
(a) A horizontal portion in which are the sockets for the teeth.
(b) Vertical portions terminating on either side at the joint between the lower jaw and the base of the cranium, situated immediately in front of the ear.
The angle of the jaw indicates the junction of the horizontal and the vertical portions.
THE BACK-BONE OR VERTEBRAL COLU:\lN.
The Vertebral Column (Fig. r) is composed of bones called vertebrre, each of which consists ofI.-A body or bony mass in front.
2.-Processes projecting backwards, which enclose a canal for the spinal cord- the spinal canal.
3.-Two transverse processes, twelve pans of which support the ribs.
22
BODY OF VERTEBRA.
FIG. 2A. .4f . ----
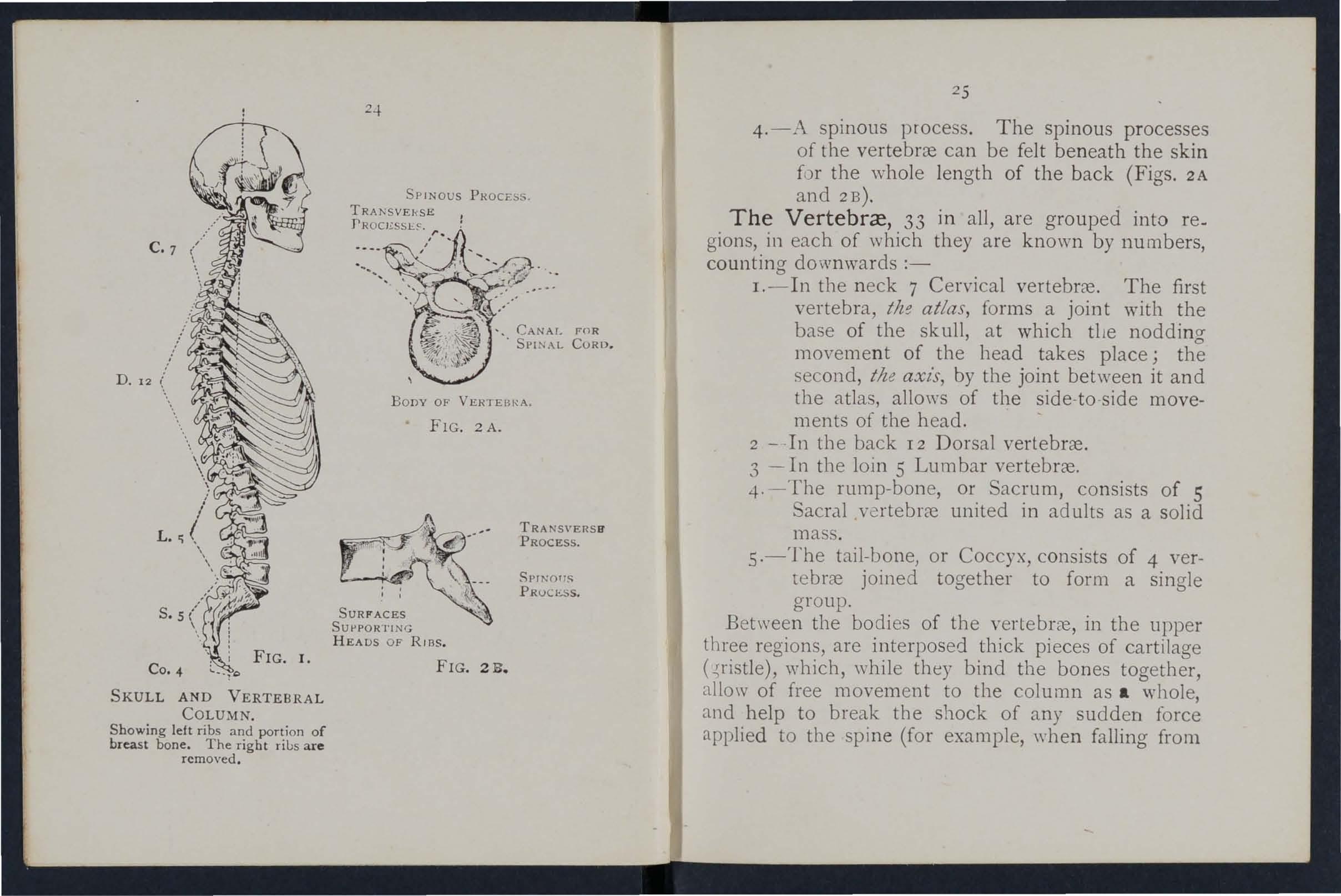
SKULL AND VERTEBRAL COLUMN.
Showing left ribs and portion of breast bone. The right rius are removed.
SUPPORTING HEADS OF RIBS.
FIG. 2B.
TRANSVERsa PROCESS.
SPINOI1S PROCESS.
4.-:\ spinous process. The spinous processes of the vertebrce can be felt beneath the skin for the whole length of the back (Figs. 2A and 2B).
The 33 in all, are grouped into gions, in each of which they are known by numbers, counting downwards :-
I.-In the n eck 7 Cervical vertebrce. The first vertebra, atlas, forms a joint with the base of the skull, at which tlte nodding movement of the head takes place; the second, th e axzs, by the joint between it and the atlas, allows of the side-to -side movements of the head.
2 - -In the back 12 Dorsal vertebrce.
3 - I n the loin 5 Lumbar vertebrce.
4· -The rump-bone, or Sacrum, consists of 5 Sacral vertebrce united in ad ults as a solid mass.
5·-The tail-bone, or Coccyx, consists of 4 vertebrce joined together to form a single group.
Between the bodies of the vertebrce, in the upper three regions, are interposed thick pieces of cartilage ( .;ristle), which, while they bind the bones together, allow of free movement to the column as a whole, and help to break the shock of any sudden force applied to the spine (for example, when falling from
: -
' . \. --:: ), '\
a height on the feet). The whole spine is strapped together by ligaments reaching its entire length.
THE RIBS AND BREAST-BONE.
The Ribs consist of bvelve pairs of curved bones extending from the dorsal vertebrre to the front of the body, and 'are known by numbers-first, second, etc., commencing from above. The ribs are not bony throughout their entire length, but at a short distance from the front the bony material ends, and cartilage takes its place. The upper seven pairs, named the true ribs, are attached by their cartilages to the Breast-bone (sterllum), a dagger -shaped bone with the point downwards, just over the pit of the stomach. The lower five pairs are termed the false ribs, as their cartilages fall short of the middle line. The eleventh and twelfth pairs are termed the floating ribs, as their ends are free in front. The ribs enclose the chest and serve to protect the lungs, heart, liver, stomach, spleen, etc.
THE UPPER LIMBS.
The Shoulder-bones are the Collar-bone (lavtde) and the Shoulder-blade (scapula).
The Collar-bone can be felt on either side beneath the skin at the lower and front part of the neck as a narrow curved rod about the thickness of a finger. Its inner end rests on the upper part of the
(SCAPUL ,\ ) B ON ES JUl.NA OF (

SIlOWING TIlE POSITIO'N OF TIlE RADIUS AND ULNA
"\'VHEN THE TUUMB IS TURKED INWARDS
Compare Fig. 3A, in which the thumb is turned out. wards.
26
BO
SHOULD
PART OF C OLl.AR
NE
E R BLADE
RAlJIUS ---\+-11,;.\
FIG. 3A.
27 RADIUS
BONES OF TIlE LEFT UPPER LIMB.
FIG. 3B.
breast-bone, and its outer end joins with the shoulderblade .
The Shoulder-blade lies at the upper and outer part of the back of the chest, and forms joints \\ ith the collar-bone and the bone of the arm.
The bone of the Arm (llZtmerlls) reaches from the shoulder to the elbo\\".
In -the Forearm are two bones, the Radius on the outer, or thumb side, and the Ulna on the inner, or little finger side. Both bones reach from the elbow to the wrist, and they change their rel at ive position with every turn of the hand (Figs. 3 A and 3 B ).
The Hand is composed of-
I.-The bones of the wrist, or Cal jllS, eight in number, arranged in two rows of four.
2.-The metacarpus (the framework of the palm) ; five bones which form the knuckles and support the bones of the fingers.
3.-The plzalallges, or finger-bones, three in each finger, and two in the thumb
T HE PELVIS A JD LOWER LIMBS.
The Pelvis.- The large basin-Lke mass of bone attached to the lower part of the spine is composed of the two haunch-bones and the sacrum. The haunchbones meet in front (at the pubes) in the middle line, only a small piece of cartilage intervening, but behind, the sacru m -is placed between them . The pelvis

THE RIGHT LOWER LIl\IB, SHOW· ING JOINT WITH TIrE PELVIS AT THE HIP.
28
FIG. 4.
OF
- PELVIS
t "'---'"
TIIIGH BONE (FEMUR).
K NEE CAP (PATELLA).
30 supports the abdomen and its contents, and provides the deep sockets for the thigh-bones-the hip joints.
The Thigh-bone (fmmr) reaches from the hip to the knee joint. Its shaft is stout, rounded, and arched forwards; the upper end presents a rounded head, supported on a neck which projects inwards, to fit into the socket of the hip joint.
The Knee-cap (patella) is a triangular bone lying with its base upwards in front of the knee joint immediately beneath the skin.
The bones of the Leg are the Shin-bone (tibia) and the Brooch-bone (jibula). The extends from the knee to the ankle, in both of which joints it plays an important part; its sharp edge, the sizin, can be felt immediately beneath the skin of the front of the leg. The Brooch-bone lies on the outer side of the tibia. It does not enter into the formation of the knee joint, but its lower end forms the outer boundary of the ankle joint.
The Foot is composed of-
1.- The tarsus, a group of seven irregular bones at the instep. The largest is the heel-bone, and the uppermost (the ankle-bone) forms the lower part of the ankle joint.
2.-The metatarsus, the five long bones in front of the tarsus which support the toes.
3.--The plzalanges, or toe-bones, two in the big toe, and three in each of the other toes.

JOINTS.
A Joint is formed at the junction vf two or more bones. In moveable joints such as the hip, knee, etc., t.he surfaces of the bones are covered by cartIlage, WhICh lessens friction and the shock of a
FIG. 5. Compare Fig. 4, Page 29.
joint is clear, rather sticky flUId, the Jomt 011, or sy"ovza, enclosed within a capsule. Tying the bones together, but allowing of movement, a number of bands or ligaments .
.To explam the formation of limb joints, the
FIG. 6. LEFT ANKLE.MUSCULAR TISSUE

PATELLA
TENDON OR LIGAMENT OF PATELLA
32
following exam iJles are given :-
The Sh oulder, a balland-socket joint, consists of a shallow socket on the outer angle of the shoulder-blade, and of the head of the arm-bone (Fig. 5). 0\\ ing to the shallowness of the sock et the arm-bone is very prone to escape from its socket (dislocate). ViI
The Ankle , a hinge join t, is formed at the junc tion of three bones, the shin-bone above and or' the inner side, the broochbone on the outer side, and the ankle-bone below (Fig. 6).
THE MUSCLES.
FIG. 7. The Musd es of the DIAGRAM SHOWING RECTUS body are classi[led into two MUSCLE OF THIGH, WITH groups-volunta 1'Y and ARTERY, VEIN AND NERVE. z"-nvolul1tary.
33
The Voluntary muscles are met with in the limbs , the head and neck, and the surface of the trunk. Their ends are attached to different bones, and as they pass from one to another they cross a joint, and, being endowed with the power of contraction and relaxation,' cause the movements of the body. As a muscle crosses a joint, it as a rule becomes a fibrous cord or tendon. Blood-vessels traverse and supply the muscles, and the nerves entering them bring them under the direct control of the brain and spinal cor d.
The Involuntary muscles are met with in the walls of the stomach and intestines, in the air passages, and in most of the internal organs and blood -vessels, also, in a special form, in the heart. They are not under the influence of the will, but continue their work during the hours of sleep; their functions a1'e regu'ated by a separate set of nen'es (see Sympathetic System, page II8).
FRACTURES AND THEI R TREATMENT.
When a bone breaks a Fracture is said to occur.
CAUSES OF FRACTURE.
I . Direct Violence. -When from a severe blow, impact of a bullet, crush of a wheel, etc., a bone breaks at the spot where the force is applied the J fracture is termed direct.
c
TENDON NEIIVI': ARTERY VEIN
2. Indirect Violence.- \Vhen the bone breaks at s?me distance from the spot ""here the force is applied the fracture is termed indirect. Alighting on the feet and fracturing the thigh-bone or the bones of the leg, or falling on the hand and breaking the radius or the collar-bone, are examples. '
3. Muscular Action. - The knee-cap and the are occasionally broken by a violent contractIon of the muscles attached to them.
VARIETIES OF FRACTURES.
Fractures are classified accordin a to the condition of the tissues adjacent to the bone follo\\ S :-
1. Simple.-The bone is broken with but sliaht . . b ll1Jury to the surrounding parts.
2. Compound.-The bone is broken and the skin and tissues are punctured or torn thus aUo\\"ina disease-producing germs to obtain to seat of The fractured ends may protrude through the skm, or (for example, when a bone is broken by a bullet) the wound may lead down to the fracture.
3. Complicated. - The bone is broken and in addition there is an injury to some internal organ (for the brain, spinal cord, lung, etc.) or to some Important blood-vessel or nerve.
A. may be compound or complicated as the Immediate result of the injury; or a fracture,

35
originally simple, may be converted into a compound or complicated fracture-
(a) By careless movement on the part of the patient.
(b) By carelessness Qr ignorance on the part of one rendering first aid.
Special varieties of fractures may be classified according to the injury to the bone itself as follows ;-
1. Comminuted. - The bone is broken 111 to several pieces.
2. Green-stick. -In children, owing to the softer state of the bony tissues, a bone may bend and crack without breaking completely across.
3. Impacted. - The broken ends of the bone are dnven one into the other.
GEJ. ERAL SIGXS AND SV:\IPTOi\IS WHICH ;'II AY DE PRESE;\'T.
(A fracture of thp. femur, or both bones of the forearm or leg, affords the most com plete example.)
1. Pain at or near the seat of fracture.
2. Loss of power in the limb.
3. Swelling about the seat of fracture. ,\Vellinofrequently renders it difficult to perceive other of fracture, and care 111 ust therefore be taken not to mistake a fracture for a less serious injury.
4. Deformity of the limb.-The limb assumes an
34
unnatural position, and is mis-shapen at the seat of fracture. The contracting muscles may cause the broken ends of the bone to override, thereby produ cing shorteni ng .
5. Irregularity of the bone.-If the bone is close t o the skin the fracture may be felt, and if compound it may be seen .
6. Unnatural Mobility. - fovement may be made out at the seat of fracture .
7. Crepitus, or bony gl aling, may be felt or heard whe n the broken ends move one upon the other.
Tlze last two sz"gns shollid OIl!.Y be sougllt by a doctor. Several of the above signs are absent in green-stick and impacted fractures.
In addition to the signs and symptoms the patient or the bystanders may be able to give the history of the injury, and marks on the clothing or skin should be noted, as they may serve to locate the fracture. The snap of the bone may have been heard or felt .
ApPARATUS FOR TREAT?lIENT OF FRACTURES.
Splints and bandap"es for First Aid frequently have to be improvised.
A Sp li n t may be lmprovised from a walkillg stick, l1m brella, billiard cue, broom or brush handle, police man's trunch eo n, rifle, folded coat, piece of \\"ood, catdboard, paper firmly foldeJ, a rolled -up map, or, in fact, allyl/dllg that is firm and long enOl/gil to k eep

37
the Joints immedz"atcljl above and below the fractur ed bone at rest. "When the al'ove appliances are not available, the upper limb, if fractured, may be to the trunk, and in all cases' a fractured lower lanb should be bandaged to its fellow. .
Bandages may be improvised from handkerchiefs, belts, straps, braces, neckties, or any piece of linen, calico strin a or cord that comes to hand.
Triangular Bandages
(Fig. 8) are made by cutting a piece of linen or calico about forty inches sq U,He diagonally into two pieces.
The broad bandage is made by bringing the point down to the base (Fig. 9), and then folding into two (Fig . 10).
The narrow bandage is made by folding the broad bandage once (Fig. I]).
The medium bandage is made by bringing the point down to the base, and then folding into three. (Fig. 12). This bandage may be instead of .the broad or the narrow bandage when It IS better SUIted to tIle proportions of the patient.
It is sometimes advisable to halve the size of ti1e bandage by bringing the two ends before folding it into the broad, narrow, or medIUm bandage.
Whet: not in use, the triangular bandage should be fOlded narrow; the two ends should be turned to the centre, and the bandage then folded into four, reducing it to a packet about 6t inches by 3! lDches.
FIG. 10. BROAD BANDAGE.
FIe;. 12. THE !JOTTED SHOW THE FOLDS OF THE l\lEDIUJI[ BANDAGE. 39
Large arm-sling (Fi g . I3).-Spread ou t a bandage, put oae end over the shoulder on the sound side, pass it round the neck so that ii: appears over the sho ulder of the injured and let the other end hang dO'v\'n in front of the chest; carry the point behind the elbow of the injured limb, and bend the forearm

FIG. I I. NARROW BANDAGR.
FIG. 13. FIG. 14. over the middle of the bandage; then carry the second end up to the first and tie them ; bring the point for\Vard, and secure with two pins to the front of the bandage.
Small arm-sling (Fig. 14,).-Place one end of a
b road band age over the shoulder o n the sound side, pass it round the neck so tha t it appears over the shoulder of the injured side; place the forearm over th e middle of the bandage; then bring the second end up to the first, and tie them. This sling is used in cases of fractured humerus , and occasionally .vhen the large sling would be too conspicu?us.
Slings may be improvised in many slmple ways, such

as pinning the sleeve to the clothing, turning up th e tail of the coat, passing the hand inside the buttoned coat or waistcoat, etc.
Reef K n ots (Fig . IS) are to be used. Avoid granny knots (Fig. 16).
GENERAL R ULES TO BE OBSERVED IN THE TREATMENT OF FRACTUREi
The object of First Aid Treatment of rractures is t o g uard against furth e r mischief, and especially to p r eve n t a simple fracture from becoming compound or complicated . To attain this end :-
I. Attend to the fracture on the spot. No matter how crowded the thoroughfare, or how short the distance to a more convenient or comfortable place, no attempt must be made to move the patient until the limb has been rendered as immovable as possible by spl ints or other restraining apparatus .
2. Steady and support the injured limb at once, so that its further movement on the part of either the patient or the bysLlI1der is prevented.
3. Straighten the limb with great care, and if hortening is obse rved in the case of a fracture of a bone of the lower limb, pull up :m the foot unti l the limb regains a more normal length. When the shape of the limb is improved, on no account let go until it is secured in position by splints, otherwise there is g rea t da nger of the fracture beco:l1ing compound or complicated.
4. Apply splints (when practicab le) and bandages as follows :-
(a) The splints must be firm, and long enough t G keep the joints immediately above and
40
FI G. 15.-REEF KNOT. FIG. 16.- GRAN:--'Y KNOT.
4 2
belo\\' the fra ' tured bOlle at re ·t. Th y hould, if practicable, b padded to fit accurately to tbe linlb and be applied ovcr the clothing.
(/7) The ban?ages must be applied firmly, but not so tIghtly a to constrict the circulation ?f blood in the limb. \Vhcn the pati nt is 111 the recumbent position double the bandage oYer a pEnt to pass it under the trunk or lower limb . A a general rule :-
For ti'e th e broad bandage should he us e d. Pass It on e round the trunk .mci fasten it tying the ends, or with two or three safety Pll1S on the side opposite to the fracture , but If to secure a plint for a brokcn th ily /1 over the splint.
b ,
For the arm or forearm the narrow bandage should be u ed. Pass it twice round the limb, tie the ends over the outer splint.
F or tlte Ihtglz or 'q;- the narrow or medium may be used. It is frequentl} convel1lent double the bandage at the centre, pas,s It under the limb, bring the loop over the hmb, pass both ends of the banda.ge through it in opposite directions, and them over the outer splint (Fig. 17),
In applymg bandages near a fracture the upper one should be secured first.
5· .When accompanies a fracture It must he atknded t') fil'it , anrl the wou nd covered by a dean dress l11 g.

F IG . 17.
6. No attempt must be made to remove a pafient suffering from a fracture of the spine, pelvis, or thigh, except in a recumbent position, preferably up on a stretcher.
7. In every case of fracture it is necessary to cover the patient to keep him warm, and so lessen th e e ffects of the S H OCK of the accident.
In all doubtful cases, tr eat as a fracture.
FRACTURES.
Fracture of the Cranium. -A fracture of the upp er part is usually caused hy direct violence-for exa mpl e, a blow on th e head. A fracture of the base is caused by indirect violence, through a fall on the
43
44
head, a fall on the feet or lower part of the spine, or a severe blow on the lower jaw. If the upper part is fractured, the signs are swelling, irregularity, and frequently insensibility, either immediate or coming on gradually. If the base z's fractured insensibility may come on immediately, blood or a clear fluid may issue from the ear channel, blood may escape from the nose, or it may pass down to the stomach, whence it may be vomited; the fracture may involve the orbit, causing a blood-shot eye.
TREATl\lENT.
Injury to the brain is the great danger attendFI G. 18. ing a fracture of the cranium. For treatment see "Concussion and Compression of the Brain," pages 13 1 , 13 2
Fracture of the Lower J aw.-Pain, loss of power (inability to speak and move tbe ja:v freely), irregularity of the teetb, crepItus and bleedmg from the gum are the usual signs and symptoms.

45
TREATMENT.
I.-Place tht palm of the hand below the injured bone and press it gently against the upper jaw.
2.-Apply the centre of a narrow bandage under the chin, carry one end over the head, cross the ends at the angle of the jaw, carry the long end across the chin, and tie the ends on the side (FIg. 18).
Fracture of the Spine.-The vertebral column may be broken either by direct or indirect violence. Falling from a height on the back across a bar or upon an uneven surface is an example of direct fracture, and a fall on the head, causing a broken neck, is an example of indirect violence. 'Vhat is commonly regarded as a broken back consists of a fracture of one or more of the vertebrre with displacement of the fragments, whereby the spinal cord and the nerves issuing from it may be torn, causing com plete or partial paralysis of the parts below the fracture. Pain is present at the seat of injury.
TREATl\lENT.
I.-Prevent all movement on the part of the patient.
2.-Cover the patient warmly.
3.-To remove the patient, place him on a stretcher or shutter as follows :-
(a) Turn up the collar of his coat; roll up a stick or umbrella in each side of the coat
46
s o that the ends are level with the top or his h ead ; pass a broad band age or handkerchief under the head and secure it to the sticks . If no coat is worn, or doubt as to its strength and length exists, pass a number of bandages under the patient to serve instead of, or in addition to, the coat.
(b) A bearer on each side grasps the rolled coat with his hands well apart; a third grasps the clothing on both sides on a level with the hips; 'a fourth bearer takes charge of the legs.
(t) On the word being given, ::tIl lift together and carry the patient by short side paces over the stretcher and carefully lower him on to it. If a fifth bearer is available the stretcher should be passed unJer the patient instead of carrying him over it.
4.-0n arrival at sheller nothing further is to be attempted until the arrival of a doctor, except to give the patient \Yater, tea, etc., if he is conscious.
Fractured Ribs. -The ribs usually fractured are the sixth, seyenth, eighth, and ninth, and generally the fracture is midway betlVeen the breast bone and the spine. The fracture may be caused by indirect violence, driving the fractured ends of the bone outwards, or by direct violence, driving the fractured ends of the bone inwards and sometimes injuring the

47
lun gs or other internal organ . If the lo wer ribs on the ri ght side are broken, the liver may be injured, and a fracture of the 10\\ er left ribs may wound the spleen. Evidence of the fracture is afforded by pain, especially on attempting to take a deep breath, and by short and shallow breathing. If the lungs are injured blood, frothy and brighl red, may be coughed up and expectorated. If the liver or spleen is wounded internal hremorrhage page 95) may occur.
TREATMENT.
( a) TT 'lzen tlu fracture is not complicated by an z"njzl7Y to 'an internal or..g an :r .-Apply two broad bandages rOLlnd the chest sufficiently firmly to
FIG. T9. afford comfort, with the centre of the first immediately above and that of the second immediately below the fracture, The lo\\"er bandage should overlap the upper to half its
48
extent. The knots are to be tied rather to the front on the opposite side of the body. Another good plan is to apply a strong to\\"el. folded about eight inches wide, tightly roune' the chest, securing it with three or fOUl safety pins.
2.-Place the arm on the injured side in a large sling. (Fig. 19).
(0) TVhen all z'nternal organ lS itljured-
1. - Do not apply bandages round the chest.
2. - Lay the patient down, inclined a little towards the injured side.
3·-Loosen the clothing, give ice to suck, and place an ice bag over the seat of injury. Treat as for internal hremorrhage (see page 95).
4· -Place the arm on the injured side in a large sling.
Fracture of the Breast-bone (sternum).-
\Vhen this fracture can be felt or is suspected undo all tIght clothing, and keep the patient quiet in an easy position until the arrival of a doctor.
FRACTURE 0F THE BONES OF THE UPPER LIMB.
Fracture of the Collar-bone (clavzCle).- This fracture is frequently caused by a fall on the hand or shoulder.-The arm on the injured side is partially

49
helpless, and the patient usually supports it at the elbow with his hand, and inclines his head towards the injured side. The fractured ends can generally be felt to overlap, the outer fragment being the lower. The general signs and symptoms of fracture are mostly present.
TREATMENT.
I.-Remove the coat (see page 19), and as much more of the clothing as is expedient.
2.-Place a pad about two inches thick and four inches across in the armpit.
3.-Gently bend the forearm well up, keeping the shoulder as far back as practicable, and support it in a "St. John" sling, made as follows :-
(a) Lay an unfolded bandage across the chest over the injured limb with one end on the uninjured shoulder and the point beyond the elbow on the injured side. (Fig. 20).
(b) Pass the lower end of the bandage under the injured limb, across the back, and tie the ends somewhat loosely in the hollow in front of the sound shoulder.
(c) Fold the point over the elbow of the injured limb and secure it by one or two pins (Figs. 2 I and 22).
4.-Tightly secure the injured limb to the side by a broad bandage passed round the elbow and trunk, so as to lever out the shoulder) the pad forming the fulcrum.
S·-Now tighten the sling.
\Vhen both collar-bones are bmken keep the

shoulders back by narrow bandages tied round each arm, close to the shoulder, passed across the back, over the opposite arm and tied together in front. The forearms should be raised and supported by the bandages. (Figs. 23A and 23B).
Fracture of the Shoulder-blade (scapN /a).Apply the centre of a broad bandage in the armpit of
50
51
FIG. 23A. FIG. 23B.
52
the injured side, cross the ends over the uninjured shoulder and tie them under the armpit. Support the limb in a St. John sling (Fig. 24).
Fracture of the Arm (/zumerw). - The bone may be broken :-(a) Close up to the shoulder; (b) near the middle of the shaft; (c) close FIG. 24· to the elbow.
All the general signs and symptoms of fracture are usually present.
TREATMENT.
When the Fracture z's close to the Shoulder-
I.-Apply a broad bandage with its centre abo\'e the middle of the arm round the limb and body, tying it on the opposite side.
2.--Support the forearm by a small arm sling.
TVlzen tlze Fracture is mar the .klddle of tl,e Slzajt-
I.-Pend the forearm at a right angle to the arm.
2.-Apply splints, reaching from the shoulder to the elbow on the outer and inner sides of the arm, and, if enough can be procured, to the front and back also. The front splint

53
must on no account be so long as to press upon the blood-vessels at the elbow joint.
3.-":ecure the splints by bandages above and below the fracture. If splints are not available, secure the arm to the side by two broad bandages.
4.-Snpport the forearm by a small arm sling. (Fig. 25).
Fractures in volving the elbow joint, whether of the arm or forearm, are attend ed with so much swelling, and it is so difficult to ascertain the exact nature of the injury, that when the acci· dent occurs indoors the limb should be laid upon a pillow in the most comfort-
FIG. 25· a bl e position; ice or cold wa ter dr essings should be applied to the injured par.t, but no treatment should be att empt ed pendmg the arrn'al of a doctor
54
TVhen the accident occurs out of doors-
I.-Take two pieces of thin flat wood, one long eJlough to reach from the armpit to below I lUll the elbow, the other , M I long enough to reach from above the elbow to the finger tips; tie "1 them together to form a right angle. (Fig. 26).
2.-Apply the angular splint so made FIG. 26 on the inner side of the flexed limb.
3·-Secure by bandages above and below the fracture.
4·- Support the limb by a large arm sling.
5·-On arrival at home remove the splint, and treat the injury as if it had occurred indoors.
Fracture of the Forearm.-Wh en both bones (the Radius and Ulna) are broken, the general signs and symptoms of fracture ,?ore usually present. \Vhell one of the bones only is broken the signs and symptoms are as a rule pain, loss of power, s\\"elling, and irregularity. An impacted fractureof the Radius
55
just above the "vrist is a common result of a lail on the hand.
TREATMENT.
This is the same, whether the fracture is ot one bone or of both.
1.- Bend the forearm at right angles to the arm,

FIG. 27. FIG. 28. keeping the thumb upwards, and the palm of the hand towards the body.
2.-Apply broad splints on the inner and outer sides from the elbo\\ s to the fingers. ..
3.-Apply bandages, embracing both splmts, Immediately above and below the fracture and round the hand (Fig. 27).
4.-Apply a large arm-sling.
Crushed Hand (fracture of the bones of the carpus, metacarpus, or fingers).
TREATMENT.
I.-Apply a carefully padded splint to the ot the hand, reaching from well above the WrIst to beyond the tips of the fingers.
56
2.--To secure the splint apply a narrow bandage crossed in the manner of the figure 8 to the wrist and hand (Fig. 28).
3.-Applya large arm-sling.
Fracture of the Pelvis.- 'When, after a severe injury in the neighbourhood of the haunch-bone there is no sign of damage to the lower limbs the patient is unable to stand or even to move lower limbs without great difficulty and pain, a fracture of the pelvis may be assumed to have occurred. The organs, especially the bladder, wlthll1 the pelvIs are in d anger of being wounded.
TREATMENT.
I.-Lay the patient in whatever position is found to give. the greatest ease, and flex or straighten the lower lImbs as the patient desires.
2.-Apply a broad bandage round the hips tight enough to support the parts, but not so tight as to p ress the broken bone further inwards.
To remove the patient place him on a stretcher, ac tmg on the same principle as that described under " F racture of the Spine" (see page 45).
FRA CTURE OF THE BONES OF THE LOWER LIMB .
.Fracture of the Thigh-bone (jemur). - The dugh-bone may be broken at its neck, anywhere in the shaft, or close to th e kn ee. A fracture at the
57
neck is likely to occur in old people from very slight injury, and is often difficult to dIstinguish from a severe bruise of the hip, but it may be assumed that when, after an injury near the hip joint, the patien t cannot, when lying on the back, raise the heel from the ground, the bone is broken . All the general signs and symptoms of fracture are usually present and a prominent sign is the position of the foot,

29 .
which, as a rule, lies on its outer side. Shortening may vary from one-half to three inches.
TREATMENT.
I.-Steady the limb by holding the ankle and foot.
2.-GentIy draw down the foot and bring it into line with its fellow. When two or three assistants are at hand, it is one person's duty to hold the foot in Dosition until the splints are secured .
3.-A pply a splint on the outer side from the armpit to beyond the foot.
f
FIG.
58
4·- A pplya splint on the inner side from the top of the thigh (the fork ) to the knee.
S.-Secure t he splints by bandages as .(a ) Roun d the chest just below the armpits, (b) round the pelvis on a level with the hip joints, (c) above the fracture, (d) below the fracture, (e) round the leg, (.f) round both ankles and feet, and bed below the feet, (g) a broad bandage round both knees (Fig. 29).

FIG. 30.
'When single-handed, or when the patient is a woman, it is expedient, after extension of the limb, to tie the feet together, dispense with the inner splint, and pass the bandages round both limbs (Fig. 30).
Fracture of the Knee-cap (patellll).-The knee-cap may be
FIG. 31. broken by falling on the knee ( direct violence), but more frequently it is broken by muscular action , as follows :-
59
\Vhen the foot slips in the attempt to prevent a fall the muscles in the front of the thigh act with such force as to snap the knee-cap in two (Fig. 3 I).
Pain, loss of power (the limb will be quite helpless), and irregularity (a gap may be felt between the broken fragments of bone) accompany this injury.
TREAT:\lENT.
I.-Lay the patient on his back, raise well and
FIG. 32.
support the head and shoulders, straightell and raise the limb .
2.-Apply a splint along the back of the limb, reaching from the buttock to ,the heel. ,
3.-Apply a narro,,- bandage WIth Its centre Immc-
diately above the knee-cap, cross the ends behind over the splint, and tie in front below the broken bone. fo ensure firmness apply a second bandage in a sImilar way, but commenced below and tied above the broken bone.
4.-Further secure the splint by bandages round the thigh and leg.
5.-Support the foot well off the ground by a pillow, roll of clothing, etc., or if none of these are at hand by resting it on its fellow (Fig. 32).
6.-Apply an ice bag or a cold water dressing over the fracture.
Fracture of the Leg (tz'bia and IibuZa).-One or both of the bones may be broken. 'Vhen both bones are broken all the general signs of fracture are usually present, but when one bone only is broken deformity is not always noticeable. A fiacture of the fibula three or four inches above its lower end :s frequently mistaken for a sprain and sometimes for a dislocation of the ankle.
TREAT}'lE l T.
I.-Steady the limb by holding the ankle and foot.
2.-Draw the foot into its natural position, and do not let go until the splints have been fixed.
3.-Apply splints on the outer and inner sides of the leg, reaching from above the knee to beyond the
6r
foot. If only one splint is available place it on the outer side.
4·-Secure the splints by bandages (a) above, (b) below the fracture, (c) immediately above the knee,

33.
34.
round both ankles, (e) a broad bandage round both knees (P"",;. 33).
'VJ-:. singl e-hand ed, or \\ hen the patient is a
60
FIG.
FIG.
62 woman, after extending the limb tie both feet together, dispense with the inner splint, and pass the bandages round both lilnbs (Fig. 34). 'Vhen no splint is available tying the legs, ankles, and knees together is of lSTeat service.
Crushed Foot (fracture of the tarsus, metatarsus and toes).-This accident is commonly caused by the passage of a heavy weight over the foot, and may be recognised by pain, swelling, and loss of power.
TREATMENT.
I.-Remove the boot (see page 19).
2.-Apply a wellpadded splint to the ole of the foot, reaching from the heel to the toes
3.-Applya bandage FIG. 35. crossed after the manner of the figure 8 (Fig. 35).
4.-SUpPor.t the foot in a slightly raised position.
DISLOCATIONS.
A dislocation is the displacement of one or more of the bones at a joint .
The joints most frequently dislocated are those of the shoulder, elbow, thumb, fingers, and lower jaw.

SIGNS AND SYMPTOMS OF D ISLOCATION.
I. - Pain of a severe sickeni ng character at o r n ear the joint.
2. - Loss of power in the limb.
3. - Numbness of the parts below the seat of dis location.
4. - Swelling about and below the joint.
S.-Fixity of the joint.-The limb cannot be moved at the joint by either the patient or others.
6.-Deformity of the limb.-The limb assumes an unnatural position, and is mis-shapen at the joint.
TREATME TT.
No attempt should be made by anyone except a doctor to reduce a dislocation. Pending his arrival :-
(a) TVhen the acczdent occurs out o.f doorsSupport the limb in whatever position gives most ease to the patient, bearing in mind the necessity of lessening the effects of jolting during transport.
(b) TVhen the patient z's £1Zdoors-
I.-Remove the clothing from the limb.
z.-Place the patient on a couch or bed.
3.-Rest the limb on pillows in the most com· fortable position.
4.-Apply.cold (ice or cold water) dressings to the ]omt.
5.- When cold ceases to give comfort apply
64
warmth (flannels or towels wrung out of hot \\ ater).
6.- Treat shock (see page 135)' SPRAINS.
'Yhen, by a sudden wrench or twist, the ligaments and the parts around a joint are stretched and torn the joint is said to be sprained. " Going over" the ankle is a common example.
SIGNS AND
I.- Pain at the joint after a twist or wrench.
2.-Inability to use the joint.
3.-Swelling and discoloration.
TREATMENT OF SPRAINED ANKLE.
TVhen out of doors-
I.-Apply a bandage tightly over the boot, beginning on the sole at the instep, crossing it on the front of the ankle, and carrying it round and round the ankle, where it is to be firmly tied.
2.-'Vet the bandage after applic:"tion; it is thereby tightened.
After reaching shelter-
r.-Remove the boot and stocking (see page 19)
2.-Place the limb in the most comfortable position; usually that is well raised.

65
3.-Apply ice or cold water dressings to the joint as long as they relieve pain.
-t. -- When cold fails to give comfort, apply hot fomentations.
'Vhen other joints are sprained, treat them as if dislocated.
When in doubt as to the nature of the injury, treat as a fracture.
STRA I 1'iS AND RUPTURED MUSCLE '.
'Yhen, during severe exertion, muscles or tendons are over-stretched they are said to be strained, if they are actually torn they are described as ruptured.
SIGNS A;;\D SYMPTOMS.
I.-A sudden sharp pain .
2. - When the muscles of a limb are strained they may swell and cause severe cramp.
3.- exertion is difficult or impossible; for example, If the strain has occurred in the back the patient may be unable to stand upright.
TREADIENT.
r.-Place the patient in the most comfortable position, and afford SUpPO!-t to the injured part.
2.-Apply hot water bottles or hot fomentations when the pain is very severe.
A so-called strain in the groin (hernia) is an injury of a totally different nature (see page 114). .
D
QUESTIONS ON CHAPT E R II .
jO<4nti.
\Vhat is t he skeleton, and what purp oses are served by it?
How are th _ bones of the skull .... rranged ?
\-VILlt are the boundal ies o f the cral,ium ?
Describe the bOlles of tile face
Desc ribe the lower jaw
'Vhat is I he angl e: of the jaw? ...
What other names has the back- bune ?
What is a vertebra ?..
H ow many vertebne a re there in the spine?
W.hat are the regions or tl1e spine and how many '--: verte bne are there in each? ...
IT ow is the spine endowed with free m O\'eme nt ?"
What is a rib?
H o w many l 'airs of ;ibs are"t'here?" ... ...
Wha ' is the breast ·bone?..
'Vhat are the bones of the upper limbs?
What is the pelvis? ...
What is the hip joint?
\\'hat are the bones of the lowe. limlJS?
What is a j oint? ... .
D sc ibe a moveable j oint ...
Describe the shoulder joint
D es cribe the ankle joint ...
}! ow are muscles classifi, d ?
D esc ribe vuluntary muscl es
Desc ribe invo 'untary musc les
\\-hat is a frac ture? ... ...
\Yhat are the causes of fracture?

Where does a bone break when direct viol e nc e is the cause of fracture?
\Vhere rloes a bone break when indi rect vio lence is the cause of fractur e ?
How maya fracture be caused by muscula r act ion?
In what two ways may fractur es be classified?
What is a sim ple fracture ? ..
What is a compound fracture?
vVh8.t is a complicated fractur e?
\\That is a comminuted fracture? \Vhat is a green-stick fractur e ? \Vhat
in
fractures afford the most complete example of the signs and symptoms?
In making up your mind whether a fracture had occurred or not, w h at points should you take into consideiation
In what ways may the t riangula r bandage be folded for use?
lIow many k inds o f a rm-slings a re there, and what are they call
is the object of fi rst a iel treatment of fractures?
the ge n e ral r ules for the treatment of fractures
n ow shou ld splints be appli ed?
Il ow should bandages be What
cause a fra c tnre of the upper part of
OC>
PAGE
TJu nume r als andicat,- th o paJ[t:S w h e r " llu Q1 L\ werJ ".,.)' b,
... ... . ..
... ... ...
22 22 22 22, 23 23 23 23 23 25
.
..
..
.
... ...
... . ..
..
25 25 26 26 26 26 10 28 28 30 30 :n 3 1 3 2 32 32 33 33 33 . .. 3';, 3 4
is an impactec1. fracture? PAGIl 33 34 34 34, 35 34 34 34 35 35 35 State the gene ral signs and symptoms that may be
fracture 35, 36 \Vhat
..
present
a case of
,
signs
35 What apparatus may
of fractures? 36 lT ow may splints
? ... .. . 36 , 37
..
37
38
beyond the
and symptoms?
be necessary for the treatment
be improyised
IIow may bandages be imp royised? .17 Describe Esmarch's t rmngu lar bandage
,
,
(Fig . 8)
37
eel ? 39, 4C 49 What knot is to be tied, and what knot avoided? 40 41 41
What
'" Give
.
4I, 42
...
..
... 4 2 , 4 3 the 43 D 2
may
clanium?
What may cause a fracture of the base of the craniurn? 43, 44
\Vh at are the signs of fracture of the upper part of the cranium? .,. ... ... ... ... ... 44
\Vhat are the signs of fracture of the base of the cranium? ... ... ... 44
What is the treatment for fracture of the cranium? 44-
What are the signs of fracture of the lower jaw? 44
How maya fractured spine be caused? ... ... 45
\Vhat is commonly regarded as a broken back? ... 45
\Vhat are the symptoms of a fractured spine? 45
How may ribs be fractured? ... ... 46
How maya fracture of ribs be complicated? .. . 47
State the signs and symptoms of a simple and of a complicated fracture of tits ... ... ... 47
What is a frequent cause of.fractured collar·bone? ... 48
What are the signs and symptoms of fractured colla;'bone? ... ... :.:- < '" 48,
At what points may the bone ohhe arm be broken? ... 52
Are the general signs and symptoms of a fracture always present in a broken forearm?
. 54
State the cause of a common fracture of the rarli llS 5 S
How would you recognise a f;acture of the pelvis? 56
At what points may the thigh-bone be broken? ... 57
vVhat are the signs and symptoms of fracture of the thigh-bone?
vVhat are the causes of fracture of the knee-cap? ... 58, 59
What are the signs and symptoms of fracture of the knee· cap?
'" 59
Are

sure whether the injury is
First Aid Students should practise improvising material, folding bandages, tying knots, making slings, and the treatment of the following injuries.
for applying splint to lower limb Frac , ures-Lower jaw. 44. Spine, 45, 46. Ribs (simple and complicated fractures), 46 to 48. Breastbone, 48. Collar·bone, 48 to 51. Both collarbones, 5 r. Arm, close up to shoulder, 52. Arm, near middle of shaft, 52. Arm or forearm wben the elbow is in\'olved, 53. Forearm,55· Crushed hand, 5 -, 56. Pelvis, 56. Tlligh (man), 57, 58. Thigb (wo;llan, or man when single-handed), 58. Kneecap, 59, 60. Leg (man), 60, 61. Leg (woman, or man when single-handed), 62. Crushed foot, 62.
of doors and indoors ... 63. 64
68 PAGE
... . .. . .. ..
... . .. ...
57
...
.. . . . . . . . ... ... 60 What
60 What
. . . 62 the
PAGE State the treatment of dislocation... 63 What is a sprain? 64 \Vhat are the signs and symptoms of a sprain? 64 S late the treatment of a sprained ankle .,. 64 State
...
65 State the signs
symptoms
.. , 65 Slate the treatment @f s! rains 65
Illlprodsing splints ... Improvising bandages Folding bandages ... 36 , 37 37 Large arm sling Small arm sling Reef and granny knots 37 39 ... 39,40 40 42 Knot
Diblocations-Out
SiJrained ankle 64 Strai1s and ruptured muscles 65
the general signs and symptoms always present in a fracture of the leg?
mistake may easily be made when the fibula is broken near its lower end?
is it dislocation?
sign's and syn'ptoms of dislocation 63
the treatment of other sprains
63, 65 When not
a sprain or fracture bow would you treat it? 65 How may muscles be strained or ruptured?
and
of s:rains
CHAPTER II I.
TdE ORGANS OF CIR CULATION .
THE organs concerned in the circulation of the blood are the Heart, the Arteries, the Veins, and the Capillaries.
The He3.r t is situated in the chest behind the breast-bone and rib cartilages, between the lun gs and im .neJiateiy ab Jve the diaphragm ; it lies obliquely with a quarter of its bulk to th e ri ght and the remaining three-quarters to the le ft of the middle line of the body. Its beat may b e felt just be low and to the inner sid e of the left nip,)le . The heart hJ.s four cclvities, two on either side of a central partiLion. The two upper cavities are named the right and left auricl es, the two lowe r the right and left ventricles.
Arteries Ilre vessels which convey blood from the heart. V eins carry blood to the he a rt. Capill a ri es connect the arteries and veins . In the general (systemic) circulation arterial blood is driven from the left ventricle of th e hea rt into the aorta (the main artery of the body). From the aorta branch arteries are given off to all of the body. These divide and sub-divide, and becom e so small as to assume microscopic dimensions, when they are termed capillaries.

L. Larynx (voice hox); T. Tra chea (wind-pipe) ; R.L. RighI Lung; L.L L eft Lung (t he lun gs are drawn uack to expoc;e the heart and blood vessels); R.A. Right 0 uri cle ; L.A. Lerl Auricle; R.V . Right V entricle; LV Lert Ventricle; P A. Pulmonary Artery; Ao. A orta; S.V.C. Superior yena cava (lhe large \'ein ca rryin g blood from the upper part of the body to the heart); LV.C. Infe rior vena cava (the la rge ve in ca rrying blood fro m the lowe r pa rt of the body to th e heart). Th e four pulmonary veins cann ot be shown in the diagram
70
FIG. 36.
In the capillaries an interchange of gases and fluids takes place, whereby the nourishment and mainte nance of the tissues and organs of the body are provided for, and the blood becomes dark and impure.
Venous blood pass es from the capillaries to the veins, which convey it towards the heart, getti ng larger and larger as they proceed by being joined by neigh bouring veins until they finally, as two large vessels, reach the ri ght auricle of the heart. The veins, especially in the limbs, are provided with valves at frequent intervals, which prevent the backward flow of the blood.
The pulmonary system of blood vessels is concerned in ca rrying the blood through the lungs. From the right auricle the blood pass :;s to the right ventricle, and is thence carried to the lungs, where it is purified by contact with air, and becomes scarlet in colour; it is then conveyed to the left auricle of the heart an::!. passes into the left ventricle, thus completing the circulation.
The heart contracts in adults at an average rate of seventy-two times a minute, but the rate varies, increasing. as the position is changed from the lying to the sitting or to the standing position; hence the importance of adjusting the patient's position in cases of hcemorrhage. At every contraction of the left ventricle blood is forced into the arteries, causing the pulse. which may be felt wherever the finger can be

Ex/lla1latiolt. - In tIcc middle of the di::; 'T!";lC the heart with its four chambers. Above the '\ heart is shown the lung (pulmonary) circulation. The lower part represents the general (systemic) circulation. Vessels containing impure (venous) blood are shown black, while those containing pure (arterial) blood are shown white. The connecting vessels represent the The arrows show :lireclion of the flow of blood.
3i.
placed on an artery as it passes over a bone. In the veins no pulse is to be found.
HiEMORR:1:AG E.
Hcemorrhage, or bleeding, is of three k.inds :1. Arterial. 2. Venous. 3. CapIllary.
72
73
FIG.
DIAGRAM G::;' THE CIRCULATION OF THE BLOOD.
ARTERIAL H}E\lORRHA GE.
I. - BI .:. od from an artery is scarlet.
2. - If the wcunded artery is near th e skin the blood spurts out in je ts correspond ina- to the pulsation of the heart.
0
3 - The pressure point (see below) is on the he :1 rt side of the wound.
ARREST OF ...-\RTERIAL H}E:\lORRHAGE.
Arterial hrem orrh age is, when practicable, to be by pressure, position of the body, and ele\'atlOn of the bleeding part.
Pressure may be :-
I .- Digital - that is, applied with the thumb or fingers, and may be (a) on the wound; (0) at a sput th e pressure point. The pressure points a re indicated by nUI1l bered dots on the frontispiece.
2. - - By a p a d an d ba :1dage (tourniquet) (a ) o n the wound; (tl) on the pressure p o int.
3 - By flex ion.

T o apply a pad and banda cre to the wou nd place a piece of lint or linen oc;. a clean chief folded into a hard pad, on the bleeding point, and . It bv a !XlI1d ,lge tightly tied round the ll1Jured part. To fold the handkerchief orinathe four corners to. th e centre, and repeat the untJl a hard pad IS formed. The smooth surface is 75
plac ed on the woun:l, and, to prevent the pad from unfolding, the puckered surface may be stitched or by a s::tfety pin. A h::trd substance, such as a stO:1e, may be enclosed in the centre of the pad.
A Tou rn iquet may consist of a pai to be placed on the p :essu re point, a strap, cord, or bandage to encircle the limb and p.ld, and a tlghtening arrangem ent, such as a stick or other means of twisting the band to tighten it.
To improvise an d apply a tourniquet.:-
I.-.-\pp ly a firm p:td on the pressure pomt. .
2.-Encircle by a narrow b.:mdage wIth its centre over the p.ld.
3.-Tie the en js of the bandage in a half knot on the opposite side to the pad.
4.- Lay the twisting stick on the half knot, and over it tie a reef knot.
5. -Twist the stick to tigbten the bandage, thereby pressing the pad upon the artery, and arresting the flow of blood.
6.-Lock the stick in position by the ends ot the bandaa-e alre tdy applied, or by another bandage round the stick and limb.
The pad of the tourniquet must be ac::urately placed upon the pressure point so as compl to compress the artery; otherwise arterial blood will be allowed to pass along the limb, and the veins, being compressed by the tourniquet, will not allow the
76
blood to return through them to the heart, and the result will be dangerous swelling and congesft o n
Should a suitable pad not be at hand) a kn o t may be made in the centre of the bandage, and \\ hen available, a stone, cork, etc, enclosed in it to give it £rmness and bulk. See that the bulging and no t the ftlt side of the knot is ne'{t the skin.
An elastic bandage passed tightly round the limb, im :nediately above the seat of arterial h::emorrhage, will arrest bleeding. The simplest prepared form of this bandage is a strip of elastic we bbing, twenty-five to thirty inches long and t·",o inc hes wide, with a p iece of tape sewn at each end. An elastic belt or brace will serve the same purpose, Except when part of a limb is torn off) ir is not advisable to use an elastic cord or bandage if other apparatus can be had, as it cuts off all c irculation in the lirTib.
Flexion co nsists of the application of a pad on the pressure point at the knee or elbow joint, fl e xing the limb to make pressure, and sel uring the limb in the position by a bandage crossed like the figure 8.
GENERAL RULES
F v R TREATMENT OF A 'VOU"D ACCOMPANIED BY ARTERIAL HJEMORRHA C[!; ,
1. Stop bleeding.
II. Prevent injurious germs from getting into the wound.

77
To attain these ends: -
1. P lace the patient in a suita ble position, be.1ring ill mind that the blood escapes with less force wh e n the patient sits, and is still more checked when he lies down .
2 . k. levate the bleeding part, as thereby less blo od finds its \\Oay into it.
3. Expose the w ound, removing whatever clothing is necessary. Rule 8, a.)
4. Apply digital pressure.
(0 ) If the wound is small on the bleeding spot:
(b) If the wound is large on the pressure pomt next to the wound on the heart side. The nearest pressure point is chosen in o :o der to avoid cutting off the circulation from as much of the part as possible, but sometimes it is necessary to apply pressure still nearer to the heart.
5. Remmre foreign bodies, such as broken g1as3, bits of clothing, hair, etc, seen in the wound j Je. not search for foreign bodies you cannot see.
6. Cover the wound with a clean and firm absorbent dressing. A hard dry pad of boracic gauLe or lint is to be preferred, but, absorber:t wool lint or g iUze, or a cl ean pIece of limon wIli answ'er the purpose. Should any doubt be entertain c J as to the cleanliness of the dressing, a clean pi ece of unprinted p.1per, such as the inside of an
78 envelope , should be placed next the wound before applying the pad. (Compare pages 75 and 76 .)
7. Bandage tightly over the pad unless :-
(a ) Foreign bodies are suspected to be left unseen in the wound.
(") There is danger of causing injury to a fracture. In these c ases a light dressing only shoull be applied.
8. Apply a pad and bandage or flexion on the pressure point (see Rule 4, b ), but only in the following cases : -
(a ) As a temporary measure while the wounJ is being exposed, examined and covered .
(b) As a more permanent measure \\'hen bleeding cannot be stopped by the pad anJ bandage on the wound, or when, in accordance with Rule 7, the tight bandage has not been applied.
9. Afford support to the injured part. When part of a limb has been torn off or the wound is lacerated (for example by the claw of an animal or by machi nery) hremorrhage freq u ently does not come o n at once, b u t as there is a danger of severe hremorrhage later, means for its arrest should be applied to th e limb, but not tightened unless r:ecessary. Do not disturb a clot of blood formed over a wound.
. No attempt shou ld be mace to cl ea nse a wound e xcept with sterilised water (that is previously boiled

79 and allowed to coo]), and experience, especially in recent wars, has shown that those wounds which we re provis ionally treated .vith a dry dressing and subsequently dressed by a surgeon with proper appliances did hest.
Students p(actising arrest of a r terial hremorrhage should feel the pulse to see when the current of blood in the artery has been stopped, and should then immediately relax th e pressure made on the artery. In this way the importance 0f the accurate application of pressure will be realised, and the amount of force ne cessary wi 11 be ascertained.
THE COURSE OF THE MAIN ARTI<2RIES, AND THE ARREST OF HJE;\IORRHAGE.
(The numbers of the pressure points refer to those on the Frontispi ece .)
THE LARG E ARTERIES WITHIN THE CHEST AND
The A orta is the central or trunk artery of the b ody . Commencing at the lett ventricle it forms an arch behind the upper part of the breast-bone. tbe arch ,He given off the large branches \\'h1 ch carry the bl ood to either side of the bead and neck and to the upper limbs . The Aorta passes down on the left of the spine to just below the navel where it divides into two great branches (th e iliacs)
80 which convey the blood to the organs III the pelvis and to the lower lim bs.
'Wou n ds of these arteries are one cause of internal hremorrhage (see page 96).
ARTERIES OF THE HEAD AND NECK.
The Carotid Arteries (right and left) leave the up per part of the chest and pass up on either side of the windpipe and, just below the level of the ana-Ie of the lower jaw, divide into the Internal and E\ternal Carotid The Internal Carotid Artery ascends deeply 111 the neck, and enters the cranium to supply the brain with blood. The External Carotid Artery gives off anum ber of branches; to the front the of the tongue (Lingual), the artery to the .face to the back the Occipital; the artery Itself IS contll1ued upwards in front of the ear it changes name to the Temporal, and supplies the scalp 111 the neighbourhood of the temples.
When a Carotid Artery is wounded, as in the case of a cut throat, apply th e thumb of one hand on the .art ery at pressure point I, pressing backwards aga\l1st the backbone and takina- care to avoid the windpipe . It may also be to apply pressure \\lth the other thumb above the wound for two reasons: (a) To arrest the flow of blood from the main (jugular) vein in the neck, which rLll1S
81
alongside of the carotid artery and is usually \vounded at the same time; (b) To check the flow of blood from the upper end of the carotid artery itself, \yhich is often considerable owing to communication between the branches of this artery and those of its

fellow. Digital pressure must be maintained, hy relays of assistants if necessary, until the doctor arrives (Fig. .')8).
The Facial Artery crosses the lower jaw in a slight hoPow t\\"o fingers' breadth in front of the angle, and sends branches to the chin, lips, cheek, and
FIG. 38. FIG. 39·outside of the nose. Hcemorrhage from wounds of the face below the leve l of the eye is to be arrested b :_
(a) p ressure on pressure poi n t 2 ( Fig. Y 39),
(b) Grasping th e lips or cheek o n both sides of the wound . by the finge r inside and the thumb outSIde the mouth or vic ' ver.ra.

. The Temp ::; ral Artery may be felt pulsating JI1 front of upper part of the ear. Hremorrhage from the of the temple may be arrested by pressure apP!le.d at pressure point 3 (Fig. 40).
The OcclP1tal Artery supplies branches to the
region of the scalp from behind the ear to the back of the head. Hremorrhage from this rEgion may be arrested by digital pressure on pressure point 4, four fingers' breadth behind the ear (Fig. 41). This point is difficult to find, and it is usually sufficient to apply pressure immediately below the wound.
Hcemorrhage
f10m
Forehead or anywhere in the Scalp may be arrested by applying a small firm pad on the bleeding point and securing it by a narrow bandage with its centre laid on the pad, the ends carried round the head in the direction most convenient, and tied tightly over the pad ( Fig. 42) .
\Vhen a wound of the forehead or scalp is associated with a fracture, the FIG. 42. best pla n is to apply a ring pad around the seat of injury. To make a ring pad, pass one end of a narrow bandage round your fingers; pass the other end of the bandage through the rillg thus formed and continue to pass it through and through until the whole of the bandage is used and a ring as shown in Fig. 43 is formed.
82
ARTERIES OF THE UPPER LIMBS
. The passes from a point beh.md the Inner end of the collar·bone across the first rIb to the armpit.

FIG. 43· FIG. 44 .
To apply digital pressure:-
I.-Bare the upper of the chest.
2,-Place the patIent s arm agal11st the .body so to dep,ress the sboulder, and cause him to l11cll11e hIS head towarJs the injured side.
3·- your stand opposite the shoulder.
4·- the left hand for the right artery, and Vlce versa, grasp ,the neck low down, placing the fingers behl11d the shoulder and the thumb above the centre of the colbr-bone 111 the hollow between the 111 usc1es attached to the bone (pressure pomt 5). f5
5.- Press the thumb deeply downwards and backwards agaillst the first rib, which is beneath the colla r bone at this spot (Fig. 44).
The Axillary Artery, which is a continuation of the subclavian, keeps close to the shoulder jo' nt, and can be felt pu lsating when the fingers are deeply pressed into the armpit. Digital pressure is difficult to apply to this artery.
To apply a pad and bandage :-
J.·-Place a hard pad the size of a billiard ball in the armpit (pressure point 6).
2. - A P ply t rre centre of a narrow band · age on the -: pad; cross the FiG. 45. . - oan':lage on the shoulder; 1- ull the ends tight and tie them under the opposite arnipit, taking care that the pad does not slip.
3. - Flex the forearm and tie the Emb tigh.tly to the trunk with a broad bandage, applIed on a level with the elbow (Fig. 45).
8.t
The Brachial Artery is a continuation of the Axillary, and runs down the arm on the inner side of the biceps muscle, gradually passing forward until it reaches the middle of the front of the elbow. The of the coat sleeve above the elbow roughly mdlcates Its course.
Digital or. instrumental pressure may be applied at or near pressure point 7.

FIG. 47.
To apply digital pressure extend the limb at right angles to the body, palm of the hand upwards. Stand behind the limb, and pass the fingers under the back
of the arm ove r the seam of the coat or the groO\'e on the inside of the biceps muscle. Press the pulps (not the tips) on th e artery (Fig. 46). Some prefer to pass the hanJ over the front of the muscle (Fig . 47) A slight turn of the hand as it grasps the arm will better ensure compressIon of the artery .
The Brachial artery may be compressed at the
FIG. 49.
elbow (pressure point $) by flexion . The pad may be a folded handkel chief 'v\'ith a small stone or a cork wrapped up in it, but when no pad is rtvailable the coat sleeve rolled or gathered up \\ ill serve insteaJ (Fig. 48).
86
Just below the elbow the Brachial artery divides into the Radial and Ulnar arteries, which run along the front of the forearm on the outer and inner sides respectively. The pressure points (9 ' and 10) a re one inch above the wrist and about half an inch fro!-:-: the outer and inner sides of the forearm, where the may be felt pulsating. Branches of these arteries join to form the Palmar Arches in the hand. The arteries run along on (,,;ther side of the fingers to tte tip.
Pressure may be applied to the Radial and Ulnar arteries at pressure points 9 and 10, by the thumbs (Fig . 49) or as follo\\'s :-
I. -Cut the cOlk of a quart or pint bottle in two length'v\ ise.
2.-Lay the rounded side of one half on the Radial, and of the other half on the Ulnar artery.
3· - Secure them by a tight bandage.
To arrest hremorrhage from the palm of the hand: -
I.-Apply a firm pad, and make the patient grasp it firmly.
2.-Spread out a triangular bandage, t urn up the base about four inches, lay the back of the patient's hand on the centre of the bandage, fold the point over the knuckles and wrist, pass the two ends round the wrist, make the

patient pull on the pornt of the the ends over the fingers twice and ,tIe them as firmly as possible. Bring the (A) down to , the knuckles and fasten WIth a pin at B (FIg. So). . .
3.-Elevate the forearm and support It wlth a " St. John" sling (see page 49).
Arterial hremorrhage from the fingers may be by apply ing a small pad on the and it firmly WIth a strIP of tape, linen or plaster.
ARTERIES OF THE LO YER LIJ\rEs.
The Femoral Arterj, a continuation of the iliac, Fl",. su. enters the thigh in centre of the fold of the groi n, where it may be felt pulsating immediately below the skin. The course of the artery may l e indicated by a line drawn from the centre of the groin to the inner side of the back part of the knee. After traversing two-thirds of this line, the femoral :lrtery passes behind the thigh bone to the back of tIle knee joint as the Popliteal artery. .
Digital pressure may be applIed to the F emoral artery at the groin (pressure P01l1t I I) as follow s :-
I. -Lay the patient on his back.
88

go
2.-Kneel beside the patient.
3.-To find the groin, raise the foot hi gh so as to fl ex the thigh; the fold in the clothin g at the top of the thi g h will indicate the groin
4. - Place the thumbs one on the other upon the pressure point, grasping the thigh with the hJ nds (FIg. 5I).
c. - Press firmly against the brim of the pelvis.
As there is immediate danger of death it is impor tant not to '.yaste time 111 removing the trous ers. When the Femoral artery is wounded in the upper . hird of its course, pressure must be maintained at the groin. No really s:1tisfactory tourniquet has b ee n
51. devis ed for compression ?.t this point, a n d relays of assisr-.!lts should be emp loyed to keep up the pressure until the doctor arrives .; each fr esh assistant places his thum bs over those of his predecessor, who slips his away from ben eath, and thus gush es of blood are prevented during the ch a nge.
Application of a tourniquet to the Femoral artery (pre")sure point 12 ):\Vhen prJ.cti sing compressi on of this artery, it is a 1· IG. 52.
92
good plan to dra\V a chalk line from the centre of th e groin to the inner side of the back of the knee; place the pad of the tourniquet on this line.. as high up as the bandage can be applied. Th e pad should b e the size of a law n tennis ball (Fig. 52 ). Pressure may be applied to the Popliteal artery by flexion at the knee (pressure point 13); the pad

FI e . 53 .
should be the size of a lawn tennis ball, or if no pad is available the trouser leg may be roll ed or gathered u p to serve instead. It is n o t necessal y to .take off the clothi ng ( Fig . 53).
Just below a nd 'behind the knee joi nt th e P opliteal artery divides into the Anterior (front) a nd Posterior (back) Tibial arteries.
The Posterior Tibial p asses down the
93
back of the leg to the innAr side o f the ankle . I t is at first deeply placed between the In uscles t f the c8.1 f, ' but it arproaches the surL1Ce as it proceeds, ,0 that it can be felt pulsating behind the la rge bone at the inner side of the ankle. It enters the sole as the Plantar Arteries, which run forward alllong t the mus Ie.; to supply the foot nnd toes.
Th:! Anterior Tibial Artery , on leavin g the PO,)litel1, at once p:lsses forward between the leg hones, and, deeply placed amon,;st the muscl es, runs down th€ leg to the centre of the front of th e ankle. This artery is continued as the Dorsal Artery of the Foot, which, pas s ing fOl'lmrd over the tarsLls, dips clown to the sole between the first and second metatarsal bones . H e re it forms ,dth the Plantar arteries what is kno \\' n as the Plantar Arch. At the ankle (pressure pJints J 4 and 15) pressure may be by the lingers or hy pads and bandages .
VENOUS HJE\lORRHAGE.
I.- Blood f.- om a vein is dark red .
2. - It flows in a slow continuous stream.
3· - It issues from the side of the wound further from the heart.
4. - In case of a wound of a varicose vein it tbws a lso from the side of the wound to the heart, espec ially if the pltient is kept standing.
Varicose Veins.-The veins of the leg are specially apt to become varicose. A varicose vein is dJlated, winding, and with bead-like (varicose) projections along its course. A vein becomes varicose from several c aus es , such as long standing or tight garters. The first effect is to throw extra work upon the valves, and the bead-like projections are caused by the blood accumulating in the pockets behind the valves. In tim e the vein becomes so dIlated that the valves can no lo nger span it.
GENERAL RUL ES FOR TREATMENT OF A \VOUND ACCOMPANIED BY VENOUS H1EMORRHAGE.
1 -Place the patient in a suitable position, bearing in mind that the blood escapes with less for ce when the patient sits and is still more checked as he lies down.
2.-Elevate the part, as thereby 1( ss blood finds its way into it.
3. - Expose the wound, removing whatever is necessary.
4. - Remove any constrictions, such as the collar or garters, from the heart side of the wound.
S.-Apply digital pressure on the wound until you can apply a pad and tight bandage. If that does not stop the bleeding, make pressure near the wound on the side away from the heart. In the case of a wound of a varicose vein may also be necessary to
95
apply a pad a nd bandage to th e vein immediately .the :" o und, especially if th e limb cannot be malJ1tall1ed 111 an elevated position.
6. - Treat the wound as directed by Rules 5, 6 and 7, stated on pages 77 a nd 78.
7. - Afford support t o the injured parl.
CA PILLARY H1E;\!ORRHAGE.
1. - The blood is red.
2. - It flows briskly in a continuous strea:n, or may merely ooze from the wound.
3. -.It wells up fr:,m all parts of the wound. slIght amoun t of pressure ",ill suffice to arres t capdlary hcemorrhaf5e.
I NTERNAL H1E.\lORRHAGE.
' Vounus of the blood vessels within the trunk cause hcemorrhage into the cavity of the chest or of the abdo:11en.
SlG:;'S AND SY:\lPTOMS OF I NTER)lAL HIE.\lORR H.\GE.
l.-:-Rapid loss of strength, giddiness and espeCIally when the uprI ght jJosition is assumed .
2. -'- Pallor of the face and lips.
3: --Breathing hurried a n d Jabour ed, and accom· panIed by ya\\'ning and sighing .
4. - pulse fails, and may altogether dlsap'Jear at the WrISt. 1
94
S. - The patient throws his a rms tugs at th e cl othina round the neck , and calls fo r au.
6.-FinallY the patient may become tota ll y unconsci ous.
TREATMENT.
I.-Keep the pa tient in a recumbent position.
2.- Und o all tight clothing about the neck.
3.-Provide for free circulation of air; fan the pati e nt. .
4. - Spri nkle cold wat.er on the face; smellll1g salts to the nostrils; a vOId other forms of stlm ulants,-at all ev ents u ntil the hcemorrhage has been c.ontro! led .
S.-·Give ice to suck or .cold water to dnnk;. If the seat of the hcem orrbage IS known, app ly an Ice bag ov €r the region .
6. - Should the patient be reduced to. a state of collaps€ raise the feet and bandage the lImbs firmly fro .n toes to the hips and from the fingers to the shoulders.
• HJEMORRdAGE FRO?Il THE NOSE (NOSfRILS).
I.-Place the patient in a sitting position in a current of air before an open window, .witb the head thrown slightly back and the hands raIsed above the head.
2.-Undo all tight clothing around the neck and chest .
3.- A p ply c old (ice, a cold sponge or b un c h of

keys) over the nose a nd also the spine at the level of the collar; place the feet in hot water.
4
.-Cause the patient to keep the mouth open, and so avoid breathing through the nose.
Blood issuing from the mouth may come from the tongue, the gums, th e socket of a tooth after extract ion , the throat, the lungs, or the stomach .
HJE:\IORRHAGE FROM THE T ONGU E , THE GUMS, THE SOCKET OF A TOOTH, OR THE THROAT.
I. - Give iGe to suck or cold water to hold in the mouth. If this is not successful give water as hot as can be borne to hold in the mouth.
2. - If n ecess .uy make press ure on the carotid art eri es.
3. -If bl eeding from the front part of the ton gue is excessive compress the part by a pi ece of clean lint h el d bet \\ een the finger and thumb.
4.-If the bleeding is from the socket of a tooth , plug th e socket with a p iece of c: ean lint or cotto n \\'0 0 1; o ver this place a s mall cork or other of suitable si :e, and instru c t the patient to bite on it.
FROM THE LUN GS .
Blood from th e lungs is (:() ughe d up, and is scarlet and frothy in a j peara nce.
Treat as for Internal Hremorrhage (s ee page 95).
E
96
97
HlEMORRHAGE FROM THE STOMACH.
Blood from the stomach is vomited; it is of a dark colour and has the appearance of coffee grounds; it may be mixed with food.
Treat as for Internal Hremorrhage (see page 95), except that nothing is to be given by the mouth.
Blood issuing from the Ear Channel, which generally indicates a fracture of the base of the cranium, must be wiped away as it issues; no attempt is to be made to plug the ear. .
QUESTIONS ON CHAPTER III.
The numerals indicate tlt e jag'es whe1'e the allSwers may be fou l/d.
'Yhat organs a"'e concerned in the circulation of the
blood?

the
and
How many times a minute does the heart contract on the average? ... '.'
'Vhat is the effect of the patient's position on the rate at which the heart contracLs ?
What is the pulse?
'" :::
IIow many kinds of hremorrhage are there?
How would you kn')w a case of arterial hremorrhage? . ..
In what way should arterial hremorrhage be controlled?
'Vhat is meant by " pressure point" ? ...
IIow may pressure be applied?
'Yhat is a tourniquet?
'Vhy is accuracy necessary in placing the pad of a tourniquet?
When mayan elastic bandage be used of a tourniquet?
What is flexion?
general rules for treatment of a wound accom-
panied uy arterial hremorrhage ... ... ... 77, 78
If part of a lim b had been torn off, uut there was not much bleeding, how would you act? 78 blood clots be. disturbed ?.. ...
It It wIse for an unskJ11t:d person to attempt to cleanse a ?
99
PAGE
... the heart ... . .. the
70 70
lungs ... .. . ... . .. 70 to 72
circulation of the blood t
b od';
...
...
.. . .. .
... . ..
... ...
...
... . ..
... ... ... ... . ..
... ... ... ... . ..
72 72 73 74 74 74 74 75 75
SLate
... ... 78
... ... ... ... ... .., ...
e
. ..
78, 79 What IS t
aorta?
79
Describe the arteries of the head and neck 80
\Vhy is it sometimes necessary to compress the carotid artery both below and above the wound? '" 80, 81
What is a ring pad, and wbat is its use? ... 84
Describe the arteries of the upper limbs... 84 to 89
Descri be the arteries of the luwer limbs... 89 to 93
How would you know a case of venous hremorrhage? 93
\Vhat is a varicose vein? 94
How maya vein become varicose? 94
State the general rules for treatment of a wound acc ompanied by venous hremorrhage? ... ... . .. 94, 95
How would you know a case of capillary hremorrhage ? 95
How would you stop capillary hremorrhage ? 95
\Vhat is internal hremorrhage ? ... ... ." ... 95
\Vhat would lead you to suspect internal hremorrhage? 95, 96
State the treatment for internal hremorrhage? ... 96
How would_you arrest hremorrhage from the nose? .. . 96, 97
\Vhere may blood issuing [rom Lhe mouth come from ?.. 97
How would you treat bleeding from the gums or thr oa t ? 97
\Vhat else would you do if the tongue were bleeding? .. 9-7
And if rhe bleeding were from the socket of the tooth? 9J
How would YOti distinguish between bleeding from Lhe lungs and 'from the stomach? ... ...... 97
And what would be the difference in the treatment? 97
Of what is bleeding from the ear channel generally a ign? 98
The Student should practise placing supposed patients in a proper position for the arrest of hremorrhage (see pages 72, '77 and 9-4), folding firm pads (74 and 75), tying hard knots in bandages to form a tourniquet (76), and the application of pressure at all the pressure points shawn in the frontispiece, at various points on the fOTehead and scalp, and on the palm of the hand. Pressure should be digital, by pad and bandage, or flexion, as directed in the text.
101
Pressure points - Carotid artery, 80. Facial, 82. T emporal, S2. Occipital , 83. Sub-cJavian, 84. A xillary, 85. Brachial (by pad and bandage, pre ssure being made against the humerus and by flexi on at the elbow), 86. Radial and Ulnar, 87. Fem oral at th.e groin, 90. Femoral in the tbigh, 92. Popliteal, 92. Anterial and posterioI Tibial art eries, 93.
Hremorrhage [mm the forehead or scalp ...
H <e morrhage from the palm 'of the hand ...
Ven ous hre morrhage from a varicose or other vein

84 87 to 89 ... 93. 94
100 PAGE
PAG8
C H AP T E R IV.
B RUI SE S.
A b low a nxwhere on the surfac e of th e body ma y
ca us e h zemorrhage beneath the skin withbre,akmg It-a" black eye " is an instance.' T h e Injury IS acco m pa nied by discoloration and swelling.
TREATMENT.
ice or col d water dressings . A piece of lint soaked In extract of witch hazel may be placed on t h e affected part.
BURNS AND SCALD S,
A bu rn is caused-
(a) By dry such as fire or a piece of hot iron .
(b) By a rail, WIre or dynJ.:l1o charged with a hiO'h press ure electric current. 0
(c) By a corrosive acid, such as oil of vitriol
(
d) By a corrosive alkali, such as caustic a mmonia, or qu icklime. '
, (e) By ca used, for example, by contact WIth a revo,lvmg wheel. (Brush burn.)
A scald IS, caused by moist heat) such as boiling water, hot oIl or tar.
.The effect may be a mere reddening of the skin; blIsters may be formed; or even the deeper tissues

of th e bod y m ::1.y be charred a nd black en ed. T he clothing may adhe re to th e burnt ski n , a nd its re moval is im possible wit hout furthe r d et ri me nt to th e injured pa rt . The g rea t d anger is Sh ock. '
TREA1 MENT.
. remove the clothing over the Injured part. If stuck to the sk in, the adherent clothing must be cut around with scissors, soaked with oil, and left to come away subsequently.
2 . - Do not break blisters.
3. - Immediately cover up the part. Soak or smea: pieces of lint or linen with oil, or vaseline, hnolme, or cold cream; a small quantity of boracic powder added to these \\'ill be of benefit. The inside of a raw potato scraped out and spread on l int- makes a soothin g applieation . 'When the injured ::; urface is exten sive do not cover it with one larO'e sheet of lint, but \\'ith str ips ab J ut the hreadth of hand; this. is advisable as th ey fi t h e. tt er on the part, and durmg subseq ue nt dr essings one strip can be removed at a time, and a fr es h dr essin g applied before the ad, jacent strip is tak e n off. The Sllock to the system is thereby less than if the whole of the burnt surface were laid bare to the air by the removal of all the dressings at one time . When covered by the oily dressing envelop the part in cotton wool or a piece of flannel a n d apply a ba n dage.
I U2
103
r04
'Vhen the face is burnt, cut a mask o ut of lint or lULn, leaving holes for the eyes, nose and mouth. Dip this in oil or smear it with vaseline and apply it to the face and cover it with cotto n wool, leaving openings to correspond with the holes in the mask.
'Vh en possible place the injured part in water at the of the body (98 degrees) until suitable dressll1gs can be prepared. A dessert spoonful of .baking soda added to a basinful of the warm water will make a soothing lotion .
As it is important not to leave the part exposed to the air? it is the duty of the bystanders to prepare the dressl11gs while the clothing is being removed. . 4.- Treat Shock. - This is particularly necessary 111 the case of every burn or -scald of any considerable extent (see page I35). Be very apprehensive of danger in the case of even slight b urns of the neck.
S· - If the burn is caused by a corrosive aCld, bathe the part with a weak alkaline lotion, such as washing soda, baking soda (bicarbol1flte of soda), magnesia, or slaked lime in warm water before applying the dressings.
6.- If the burn is caused by a corrosive alkali, bathe the part with a weak acid lotion such lemon juice or vinegar diluted with an equai quantlty of water. Cautz"on.-Before usino- water brush off any lime that remains on the part.

7.-When a woman's dress catches fire-
(a) Lay the woman flat on the floor at once, so that the flames are uppermost; that is to say, if the front of the dress is on fire lay h er on her back, and if the back of the dress is burning, place her face downwards. The reason for this is that flames ascend, so that if the upright position is assumed, the fl.ames will quickly reach and burn the body, neck, a nd face; or if the woman lies with the flames under most, they will, if unextinguished, pass over and burn the limbs an d set fire to the rest of the dress.
(b) As soon as the woman is laid flat, smother the flames with anything at hand, such as a rug, coat, blanket, or table coyer; if made wet so much the better.
(c) A woman rendp.ring assistance should hold a rug or blanket in front of herself " 'hen approaching the fiJmes.
(d) If a woman's dress catches fire when nobody is by, she should lie fl .tt, flames uppermost, smother the flames with anything handy, and call for assistance, or crawl to the bell-pull and ring; on no account should she rush into the open air.
The use of fire guards would prevent many calamities.
105
BITES OF SNAKES AND RABID ANIMALS AND WOUNDS BY POISONED WEAPONS.
'
Hydrophobia is caused by the bite of an animal, as a dog, cat, fox, wolf, or deer suffering from rabies The special poisons introduced into wounds by snakes and poisoned weapons ca use Immediate danger to life.
TREATMENT.
I. - Immediately place a con strict ion between the wound and the heart so as to prevent the ven ou s blood from carrying the poison through the body. If, for example, a finger is bitten it should be on the side of the wound to the heart, the fi nge r and thumb, and as soon as possible a (a string, piece of tap e, or strip of handk erchief) should be placed tightly round the root of the finger. Compression with the finger and thumb m LIst not relax:ed until the I iga ture has been applied. ligatures may, with advantage, be applied at mtervals up the limb.
2 - Encourage bleeding for a time :-
(a) By bathing the wound with warm water.
(b) keeping the injured limb low; the upper should be allowed to hang down, and 111 the case of the lower limb the patient .,hould be seated with the foot on the g rou n d .

107
3.-Cauterise the wound , if it is Quite impossible to obtain the services of a doctor. This is best done by burning with a fluid caustic, such as caustic potash, pure carbolic acid, or nitric acid, or if these are not at hand, with a red-hot wire or a fusee . The usual solid caustic is insufficient, as it does not reach the bottom of the wound, where the poison is.
To ensure the caustic reaching the bottom of the wound, it should be applied on a piece of wood, such as a match cut to a pnint. \ Vhen the caustic has been thoroughly applied, but not till then, the ligatures may be removed.
4. - Cover the wound, a while, with a clean dressing.
5.--Afford support to the injured part.
6. - Treat shock if it occurs (see page 135).
7.-ln the case of a bite by a venomous snake, rub in powdered permanganate of potash and inject under the skin in the neighbourhood of the wound a solution of permanganate of potash.
STINGS OF PLANTS AND ANIMALS.
These give r ise to se rio us inco n ve n ience, and in some cases grave symptoms develop .
TREA T MENT •
I . - Extract the sting if left in.
2 . - Mop the part freely with dilute ammonia
106
or spiri.ts. A paste of bicarbonate of soda and sal IS an efficien t appli cation . A solution c:f washll1g or potash or the application () [ the blue bag \\ III r el Ieve pn in .
3·- Treat collapse if it occurs (see page 135).
FRO ST fITE.
Durin,:; -exposure to se ,'er e co ld, parts of the body, usually the foet , fin gers, n o se, or ears, lose sensa ti on and become first wa xy white and after wards cong ested and of a purple appearance. As sensation is lost in the it is oft e n on ly by the remarks of the frost-bitte n perso n is made aware of h iS condl tlOl1.
TR EAT.MENT .
I .- Do . not the pat ient lnto a warm r<?om ynt Il , by fnet.JOn of tl:e ha n d or by ru bbing wIth soft snow , se nsatIon an a cIrcu lation in the a ffected parts are restcneci . of this pTecaution may leau to deat h of tl-ss u.es of. the fr ost-bitten pa rt. arculatlOn 1S r.estored, k ee p the patIent Il1 a r00111 at a temperature of 60 degre ES.
NEEDLE EMBEDDED UNDER ., THE SKIN.
a n eedle break s off aft e r pen etrating 'th e skin and di sappea rs, take the patiel'lt to a doctor at I f th d . , . o nce. ,e woun IS near a JOl11t, ke ep the l imb at rest a spIll1 t. on
FISH-HO OK EMBEDDED I N THB SKIN
.
D o not attempt to withdraw the fish-hook by the way it went in, but cut off the dressing of th e- hook, so th a t 0nly the metal is left, and then force th e point onwards throu gh th e skin until the hook can be pulled out.
I NJURIES TO JO I NTS.
\Vh e n a joint is injured b y a bul1 et, sta b, or other
G l l1Se-
1. - Wrap the pad in cotton wo ol.
2. - Afford rest and support to the injured limb ; if the upp e r limb, in a fl ex ed posili o n by a slin g ; if th e lo wer limb, in a strai ght po sition by a splint.
FOREIG . BODY IN THE EYE.
I. - Prevent the patient rubbing the eye, t yin ..; do wn a child' s h a nd s if n ecessa ry.
2 . - Pull d ')wn th e lower eyelid, when, if the LJreis n h ody is see n, it ca n rea dily be removed with a hair brush , o r with th e corner of a handkerchi e f t\\irl ed up a nd we tt e d.
3. - When the foreign body is heaea:th the upper eyelid lift the lid fo r ward, push up the lower lid be neath it and let go . Th e h a ir of the lo wer lid br us h es the inn er surface o f th e upp e r o ne, and may disl odge the Lo dy. 'h o u ld th e fir st attempt b e un successful, r ep eat it seve ral tim es if n ec essary. If
108
the fureign body is not dislodged call the services of a doctor as soon as possible. When, however skilled help cannot be had, proceed as
(a) Seat the patient so as to face the light, and stand behind him, steadying his head against your chest.
(b) Place a small rod, such as a match or bodkin, on the upper eyelid, half-an-inch above the edge, pressing it backwards as far as possible.
(c) Pull the upper eye-lashes upwards over the rod, and therehy evert the eyelid.
(d) Remove the foreign body.
4·-When a piece of steel is embedded in the eyeball drop a little olive or castor oil on the eyeball after pulling down the lower eyelid, close the lids, apply a soft pad of cotton wool and secure it by a bandage tied sufficiently firmly to keep the eyeball steady; take the patient to a doctor.
5·-When Quick-loime is in the eye brush away as much of it as possible; bathe the eye \\ith vinegar and warm water, and treat as for a piece or steel embeJded in the eyeball.
FOREIGN BODY IN THE EAR PASSAGE.
As a rule make no attempt to treat a patient ,yith a foreign body in the ear if the services of a doctor can possibly be had; any attempts to remove the foreign body· may lead to fatal consequences. If a child

III
cannot be induced to keep the fingers from ear, tie his hands down or cover up the ear. . If a? Jl1sect is in the ear-passage, fill the ear with olive oIl, when the insect will float and may be removed. Never syringe or probe the ear.
FOREIG N BODY IN THE NOSE.
Induce snee ing by pepper or snuff. the patient to blow his nose violently. after .cloSJl1g the unaffected nostril. There is no ImmedIate danger fram a foreign body in the nose.
THE ABDOMEN.
The abdomen is bounded above by the diaphragm; below by the pelvis ; bebind by thelumbarvertebr:;e; in front and at the sides by muscular walls. (FIg. 54·)
THE ORGANS OF THE ABDOMEN.
The Stomach lies immediately below the "pit of the stomach" just below the breast-bone.
The Liver lies in the upper part of the ab?omen, where it is mostly covered by the right lower nbs.
The Spleen lies beneath the nbs at the upper part of the left side of the abdomen.
The Intestines occupy the greater part of the cavity of the abdomen . . .
The Kidneys lie at the back, 111 the regIOn of the loin.
The Bladder lies in the pelvis.
110
Fw 54.
W OUND IN TH E F RONT ' VA LL OF THE A BD OMEN.
When the intestines or other organs protrude through t he wo u nd , 'whether vertical or transverse bend the k n ees, raise t he shou lders, a n d apply lin t, towel, or c otton wool wr apped in soft lin e n, anJ keep the

II3
pati e nt warm until the doct or arri,·es. ' Vhen the re is no protr usion of organs, if the wound is ve1 ,tical, Jay the patie n t fi at on the back \\ ith the lovv e r limbs straight ; if the zCIOzmd z's transverse, bend the knees and raise t h e shoulders.
IN .1 URIES TO THE ORGANS WITHIN THE ARDC"MEN AND PELV]S.
Injuries of the Stomach are attended by extreme collapse and sometimes by vomiting of dark blood like For treatm ent see " Hremorrhage from the Stomach" (page 98 ).
Injuries of the Liver, Spleen and Intestines may be caused by a blow, a stab or a bu ll et; the liver or spleen may be injured by a fracture of th e lower ribs . The Sign s and Symptoms are those of internal hremorrhag e accompa nied by pain and swelling at the sea t of injury, and the treatment is as for that condition (se e page 95).
The Kidneys may be injured by a fracture of the eleventh or tw elfth ribs, also by a crush, blow, stab or bullet. Bloe d may escape witH the urin e, and there may be pain and swelling oYer the injure d kidney.
The Bladder may be inju red by a fracture of th e pelvis . The signs and symptoms are either inabi lity to water, or if a little is passed it is tinged with blood .
1I2
T REATMENT OF I NJURY TO THE KIDNEYS OR BLADDER.
Keep the patient quiet until the doctor arnves.
hot fomentations over the painful o r Injured part.
. Rupture (hernia) consists of a protrusion of an Internal organ, usually the bowel, through the muswall of the abdomen, most frequently at the Sh.ould a sudden swelling accompanied by pam and Sickness takie place in that region
I.-Send for a ?octor instantly.
2.-Lay the. patient down with the buttocks raised.
3 · - A pply Ice or cold water dressings to the affected part.

QUESTIONS ON CHAPTER IV
114
lIS
. The numera ls ind.-ca!e the pages where the answers may be fJrt 11 d. PAGE What 1S a bruise? 102 How would you trea t a bruise? 10 2 H uw maya burn be caused? 102 How is a scald caused? 10 2 What is the great danger of a burn or scald? 103 State the general treatment for burns and scalds 103, 104 H ow would you treat a burn caused by a corrosive acid? 104 How would you \.feat a burn caused by a corrosive alkali? 10 4 What steps should be taken when a woman's dress catches fire? lOS:, State the general rules for treatment of wounds caused by poisonous bites or weapons 106, 10 7What special treatment is required for the bite of a venomous snake? 107 How would you treat a sting? 107, 10& State the signs, symptoms and treatment of frost-bite ... 10 8 Would you attempt to remove a needle embedded under the skin? ' . 108 H ow would you extract a fish hook in the skin? 10 9 State the treatment for injuries to joints .. , 10 9 State the general rules for removing a foreign body from the eye... 10 9, Il O What would you do if a piece of steel were embedded in the eye ball? 11 0 And when quick-lime is in the eye? Il O
would you try to remove an insect
ear passage? . . . I II
How
from the
\V uuld you t ry to romove any other f0rm of f0reign body from the ear passage? .. . . . . ... ... lIO II r
HoW"would -you a foreign body from the nose? 'I I [
State the boundanes of the a bdomen and its c ontents I I r
State t he nt for wo.unds of the abdomen ... I 12, I 13
How may InJunes to the spleen and intestines caused?
'" 1[3
What is the difference of !-he sl?mach and of InJunes to the liver, spleen and mtestmes?

II 3
State the treatment of injuries to the kidneys 1[4
State the trea i ment of hernia I q.
CI-L\PTER V , T HE NERVOUS SYSTEM.
Two systems of nerves, the C erebro-spinal and the Sympathetic, regulate the movements and functions of the body.
The Cerebro-spinal System is made up of the Brain, the Spinal Cord and Nerves, and through its agency sensations are recei ved and the will 'causes the action of the voluntary muscles.. For el(ampl.e, when a part is injured a sensation of pain is conveyed to the brain by the nerve, thus affording an indication of the seat of inju ry, or a warning of a possible danger of further damage. On attenticn being directed to the injury, an attempt is instantJr made to ease the pain or to move the injured part from da nger.
The Brain is situated within tIle cranium, and is divided in the middle bne, so that, with the exception of some 'connecting hands , the right an<!l left sides are separate .
The S,pinal Cord is the long cord of nervou s matter lying within the spinal canal (see Vertebral Column, page 23) · It leaves the brain through an opening in the base of the cranium and extends to the upper lumbar vertebrre.
JI6
...
...
... ...
...
...

The Nerves proceed from the brain and spinal cord in pairs as pearly-white trunks, and their branches can be traced throughout the tissu es of the body. Wh e n a nerve is torn through ther e is p of moti on and sensation in the region in which its branches are distributed.
The Sympathetic System extends as a nerv o us . chain on each side of the front of th e spinal column along its entire length, and sends bran ches to all th e organs of the chest and abdomen to control th e involuntary mus les, and thereby regulate th e vit a l functions. This syste 'n is not under the control of the will, and acts alike during sleep and activity.
THE RESPIRATORY SYSTEM.
The air r eaches the lungs by way of the nostril s ·(or mouth), the throat, the wind -pipe, and th e bronchial tubes. The nostrils convey it to the bac k -of the throat, whence it enters the winci -pipe by an opening guarded by a s ort o r trap door or valve , so that in health air, but not solids or ft.uids, may enter. During insensibility, however, the valve fails to act, so that should solids or fluids be given by the mouth, they may enter the wind ·pipe and cause :l.sphyxia . The wind -pipe extends to two inches below the top o f the breast-bone, where it divides into the ri ght and le ft bronchial tube. Each bronchial tub e enters a lung and divides into small and still smaller tubes, until
lI8
,
119
FIG. 55. TH E LUN GS AND TUBES.
A. Trachea, or Win d-pi pe. B. L eft Bronc hus. C. Bronchus. D. Smaller Bronchlal Tubes.
the ultimate recesses of the lung - the air cells or air spaces - are reached .
The Lungs, Right and Left, occupy the greater p.art of the they lie i .l1mediately within the nbs, and practIcally wherever a rib is felt , whether front, bac k or sides, there is lung beneath. Each is enveloped in a fine (the pleura) whIch allows It to move \Ylthm chest during b reathi ng without friction.
Respiration, or breathing, consists of two acts an .expansion of the chest, duri . g which aIr IS drawn Into the lungs, and Expiration a co n traction of the ches t, during which air the A pause follows the act of expiration. I n. health fifteen to. breaths are taken per at each InSpIratIon about 20 to 30 cubic mchcs of aIr enter the lungs, and a similar quantity is expelled at each expiration.
The expansion and contraction of the chest are effected partly by the muscles of respiration attached to the ribs, but the :Diaphragm, the large arched muscular partltlOH whIch separates the chest from the abdomen. In inspiration, which is chiefly a muscular act, the ribs are raised, and the arch of the diaphragm falls and becomes flattened thus increasing the capacity of the chest and the air to enter. In expiration, an act performed almost without effort, the ribs fall and the arch of the

diaphragm rises; this lessens the capacity of th e chest and forces air out. The mechanism of respiration is somewhat like that of ordinary household bellows but without a valve; the ribs may be to the boards of the bellows, \Vh.ile the diaphragm corresponds to the leather, the aIr passaaes being equivalent to the nozzle .
D As the blood depends upon the air its purification and the oxygen necessary to maintain life, interference with breathing very soon may Rrod uce a danaerolls state called asphyxia, examples of which are by drmvning, suffocation, choking, etc.
ARTIFI CIAL RESPIRATION.
PROFESSOR SCHAFER'S METHOD.
I .- Make no attempt to loose n or remm'e cl ot h ing. . . . .
2. - Lay the patient m a prone (l e , back upwards) with his head turned_ to one SIde, so as to keep his nose and mouth away the ground. No pad is to be placed under the patIent, nor ne e d the tonaue be drawn out, as it will fall naturally .
3. - Kneel at one side facing the patient's head, and place the palms of your hands on loins one at each side, the thumbs nearly touchmg one in the small of the back, and the fingers extend:ng over the lo\yest ribs . Leaning your body fo[\yard , Itt its weight press straigh t do\ynwards upon the
120
2 1
1

loins and part of the back, thus compressing the abdomen the ground and driving air out 'of the chest. ThIS produces expiration (Fig 56). Draw back 123
your body somewhat more rapidly and relax the pressure, but do not remove your h CU1ds; this produces inspiration (Fi g. 57)·
4 - Alternate these movements, by a rhythmic swaying backwards and forwards of your body, twelve to fifteen a minute, persevering until respiration is restored, or a doctor pronounces life to be extipct .
DR. SILVESTER'S METH OD .
1 . - Adjust the patient's position. -Witho ut wasting a moment place the patient on his back on a fl.l.t surface, inclined if possible from the feet upwards. Remove all tight clothIng fr0111 about the neck and chest, and bare the front of the body as far as the pit of the stomach; unf..lsten the braces and the top button of trousers in men, anJ the corsets in women. Raise and support the shoulders on a small, firm cushi on or folded article of dress placed under the shoulder-blades.
2 - Maintain a free entrance of air into windpipe -Cleanse the lips and n os trils; open and wipe the mouth; an assistant must draw forward the patient's tongue as far as possible, and keep it in that position.
3.-Imitate the movements of breathing. Induce Inspiration. - Kneel at a convenient distance behind the patient's head, and grasping his forearms just below the elbo ·.v, draw the arms
122
FIG. 58. INSPiRATION

FIG. 59. EXPIRATlD:-I. ·
12 5 . " upwaTds, outwards, and towards you, with a s\\'eeping movement, making the elbows touch the ground
FIG. 61. EXI'IRATIO:\.
(Fig. 58). The cavity of the chest is thus enlarsed, and air is drawn jnto the lungs.
124
induce expiration.- Bring the pCltient's flexed arms slowly forward, downwards and inwards, press the arms and elbows firmly on the chest on either side of the breast-bone (Fig 59)' By this means air is from the lungs.
Repeat these move llents a1ternately, deliberately, and perseveringly about fifteen times a minute. a sufficient number of assistants are present, HowJ.rJ's 1l1 3thod may be co:nbined with Silvester's, as f01l0\vs : -
T :1 additional assi:-;tant kneels astride the patient's hips b::t1ls of the thumbs resting on either side of the pit of th e sto:nach, and the fingers gr.lsping the adjacent parts of the chest. Using his kn 3es as a pivot, he presses forward on his hands. Then suddenly, with a final push, he springs back and remains erect on his knees \,"hile h e slowly counts I, 2, 3. Thes e motions are to be repeated to correspond with those b eing performed by Silvester's method, pressure on the chest being made simultan eously by thos e performing the two methods (Figs . 60 and 61).
METHOD .
When from any cause the above methods cannot be carried out, L'lbordc's metfwd of artificial respirati J n should be tried. It is especially useful in suffocated chi:drcn, and when the ribs are broken.
127
The patient is placed on his back or side; the mouth cleared; the tongue is seized-using a handkerchief or something to prevent it slipping from the fingers-the .lower jaw depressed; the tongue is pulled forward and held for two seconds in that position, then allowed to recede into the mouth. These movements should be repeated about fifteen times a minute.
Artificial r espi ration must Le continued until breathing is established, or until a doct or arrives. When natura l breathing commences, r egu late the artificial respiration to correspond \\ ith it. Success may result even after two hours' time.
Excite respiration.
- 'Whilst artifical respiration is being app lied, other useful steps may be employed, su ch as applying smelling salts or snuff to the nostrils, and flicking the chest with a damp towel.
Induce circulation and warmth after natural breathing has been resto red. vVr,.p the patient in dry blankets or other covering, and rub the linl bs energetically towards the heart. Promote warmth by hot flannels, hot-water bottles, or hot bricks (wrapped in , flannel) applied to the feet, to the limbs and body.
\Vhen the power of swallowing has r eturne d give hot tea or coffee, or meat extract. The patient should be kept in bed and encouraged to go to sleep. Large poultices or fomentations applied to the
126
front and back of the chest will serve to assist b reathing. . Watch the patient carefully for some to s e that the breathing does not fail; should Slgns of failure appear, at once begin artificial reSpIratIOn.
I NSENSIBILITY.
Unconsciousness or Insensib ility may arise 'as fo11o\\'s :-
Injury to the H ead. -Concussion and Compression of the brain.
. Dis ease of the Brain. -Apoplexy, EpIlepsy, Hysteria . . .
Various Causes. -Shock, FaIntlllg (Syncope), Collapse; Alcoholic and other po.isoning, Sun.stroke and Heat-stroke, ConvulsIOns, AsphyxIa.
GENERAL RULES FOR TREATMENT OF
I.- If a person appears t o lose scio.usness, prevent him from failmg, and lay hInl gently do\yn.
2. - A r rest H c;emQrrhage when apparent; attending to minor injuries is less important than treating the unconscious state. .., .
3. - Lay the patient in the 1':1 whlch breathing is most easY-':lsually thIS wIll be on the back, or inclined to one side. As a general rule

129
rais '= the head amI shoulders sliglztly when th e fa ce is flu::iheJ, and keep t.he head 10\\: wnen the face is pale.
4·- Undo all tIght clothmg round 1 he neck chest and walst, un.fastening the braces and button of the trousers In men, and the corsets in the object being to relieve pressure on the all' lXlssages, heart and abdominal organs . Be sure that there IS no t? the air p.lssages by the or by a foreign body 111 the throat. The po of false teeth obstructing breathmg mus t be con"Hlered.
for a sufficien cy of fresh air by openll1g doors ami wll1do\\ s, and by keepino- back a crowd. 0
6- - Wh.en . breath ing c a nno t be discerned apply artIfiCIal respiration .
. 7·- Obtain a doc t er's he lp as soon as pos- Si ble.
8 .. unavo idable, never leav e the unbl,You have placed him in charge 0 1 a responSible person.
9.Give . no food 0: . whate ver by the m outh whlle the pabent IS msensible.
IO. - Should the spine or an import ant Done the upper of the lower limb be fractured It. be steadIed and maintained a t rest as soon Should the unconsciousness be prolonged , til\.. p:1tIent may be removed 111 a recumbent position
F
to shelter, provided that the broken bone is adequately supporteJ.
lI. - When the patient is in a stat e of convulsion , support his bead, and a piece of wood or any uther hard mat ena l m ,handkerchief hold it in his mouth to prevent bltmg of the tona'ue . Do not forcibly restrain his limbs; prevent him from hurtin'J hims elf by pulling him away from a source of dang;r, such as machinery, a wall, or fireplace ; light pieces of furniture should be pushed out of the way. .
12.- On retur ll to consclOusness water may be given to drink. If the pulse is \\'arm tea or coffee, provided heemorrhage, either mternal or external, is n ot prese nt. A desire t? sleep, sho,uld be encouraged, except in cases of pOlsonmg, a condition that may generally be by the history of the case, and also by the pupils of the eyes (the black openings in the grey, blue bro\\'n iris) bei n a minutely contracted (pm-head pupils).
13,- It must not be assumed thCl;t a person is insensible as the result of drink me ely because the breath smells of alcohol ; frequ e,ntly wh en people a re feeling ill tl:ey take or are given alco h o lic stimu lants, afte r which they may become not from the d rink, but from the cause tha t in dll r ed them to take it, for example , insenSIbil ity c om in g on, eff.:;cts of p:)isoning, etc. Even if

13 I
drink is believed to be the actual cause of insensibility, it 111 ust be borne in mi n d that the patient is in a very dangerous state, and he must be treated for Collapse by being covered up and kept \\'arm.
Th e above general rules will en able first aid to be rend er ed efficiently in most cases of insensibility, although the exact (orm from which the patient is suffering is unknown.
CONCUS ' ION OF THE BRAIN.
Tb e may be stunned by a blow or fall on bead, or by a on the feet or lower part of tbe sp111e. He may qUi ckly reO'ain consciousness or insensibility, more or less may be proionged.
TRE\TME TT.
I. - Apply the ge ::. eral rules for the treatment of In se nsibility .
2. - Be apprehens ive of danger in all cases of injury to the head. The patient may be stunned, and after a short interval may recover some d eg ree of consciousness, or even tbe brain may bave escaped injury; yet in both in stances IS a grave risk that a structure within the um been injured, and that a serious state of lI1s ens" brl'ty may develop later. (See Fracture of the Cral11um, page 43 ) ' A caution should therefore be gi\"en to a patient who has lost consciousness e\"e n
130
13 2 for only a moment after an injury to the head not to resume physical or mental activity without the consent of a doctor .
OF THE BRAIN, APOPLI::XY
.
Compression of the Brain may frolll the same causes as produce ConCUSSIOn; 111 fact, Compression is frequently preceded by Concussion. Apoplexy usually in elderly people, and no sians of injury are necessarIly present. both conditions the face is flushed; the breathing stertoro us; one side of the may be more limp than the other, and the pupIl of one eye rnay be larger than that of the other; the temperature of the body is generdly raised.
TREATMENT.
I. - Apply the general rules for treatment of Insensibility.
2. - Promote warmth in the lower part of the body by the application of hot water bottles to the abdomen and lower limbs. Care must be taken not to burn the patient with the bottles, which shou ld be wrapped in flannel, and their heat test ed with the elbow.
EPILEPSY.
Epilepsy may occur in persons of any age, but usually occurs in young adults. The patient falls to

the gro und, sometimes with a scream, and passes into a state of convulsion, throwing his limbs about. treatmellt is according to th e General Rules, e:,peclaHy Rule 11.
HYSTERICAL FITS (HYSTERIA).
SIGNS AND SYMPTOMS.
The patient, usually a young girl, in consequence of mental excitement, suddenly loses command of her feelings and acLions. She subsides on a couch or in some comfortable position, thro\\s herself about, grinding her teeth, clenching her fists, shaking her hair loose; she clutches at anyone or anything near her, kicks, cries and laughs alternately. The ey.eballs may be turned upwards, and the eyelids opened and shut rapidly. At times froth appears at the lips, and other irregular symptoms may develop.
TRl£ATMb.NT.
I.-Avoid syalpathy \\'ith the patiellt, and speak firmly to her.
2.-Threaten her with a cold water douche, and if she persists in her "fit," sprinkle her ith cold water.
3 ·-Ar,ply a mustard leaf at the back of the neck . Medical treatment is necessary to cure the co ndition of mimi and body which gives rise to hysterical attacks.
133
J3-t
SHOCK, FAINTH\G CYr COPE), COLLAPSE.
C.-\USES.
I. - Injury in the region of the abdomen, extensive wounds and burns, fractures, lacerated wounds, and severe crush ale some of the more frequent physical causes of shock.
2.-Fright, anticipation of injury, and sudden bad news, or sometimes sudden removal of fear and anxiety after prol onged suspense, produce or fainting.
3.-Some poisons cause shock, while others, such as alcohol, so d epress the nervous system that c ollapse ensues.
4.-Hcemorrhage or heart weakness, a close or crowded room, tight clothing, fati gue, or ,,"ant of fo od may bring on fainting or collapse.
SIGNS AND SYMPTOIll S.
The general condition of shock may be recognised by extreme pallor, a feeling of cold, clammy skin, feeble pulse, and shallow breathing accompanied, if hcemorrhage has been severe, by yawning and sighing. The t erm "collapse" signifies a yery serious condition in which the life of the patient is in the greatest danger; the temperature of the body falls below the normal, and one great object of treatment to prevent it si , king to a point at which life is impossible. An attendant danger of the condition of

135
collapse is the liability to sudden relapse after a temporary improvem ent, and the utmost care and watchfulness must therefore be exercised to maintain the h =at of the body and to guard against fail ure of the heart and lun gs.
TREATMENT.
I. - Remove the cause by 8nesting hcemor:hage, to injuries, loosening all tight clothltlg especlally about the chest and abdomen, removing from a close or cro\\ded room, usin g encouraging words, etc.
2. - Lay the pcttient on the back, with the head low. Raise the lower limbs; when the patient is in bed this is best done by raising the foot of the bedstead.
3. - Provide for a free circulation of fresh air.
4. - If hcemorrhage has been severe and the patient is collapsed, firmly bandage the limbs from the toes to the hi ps, and from the fingers to the armpits.
5. -:-- To stimulate the action of the heart, sal volatlle and water may be given if the patient C:1n swallow, or smelling salts may be h eld to the nostrils.
6. - It is of the utmost importance to use every means of preventing a fall of temperature below the normal point. To accomplish this cover the pati ent with ext ra clothing, or by pbcing
TUgS or blankets over him; get him to bed in a warm but well ·ventllated room as soon as possi ble. i\ pply warmth to the feet and to the pit of the stol1lDch by hot water bottles or hot flannels. (Test the heat of these with the elbow before applying them.) If the patient can swallow, give hot drinks, such as milk, tea or coffee. It is well to add sugar, as it aids in raising the temperature of the body.
7.-If breathing cannot be discerned, apply artificial respiration.
S.-If want of nourishment has been the cause of fainting or collapse, give food sparingly at first.
SUNSTROKE AND HEAT-STROKE.
When exposed to great heat, as in the stoke-hole of a steamer, especially in the tropics, or to the rays of the sun during a march in very hot weath er wh en heavily burdened, persons may develop sickness, faintness, giddiness, and difficulty in breathing. The patient co !nplains of thirst, the skin becomes dry and burning, the face very flushed, the pulse quick and bounding. A very high temperature, stertorous (snoring) breathing, and ins ensibility may ensue.
TREATMENT.
I. - Undo all tight clothing.
2.-Remove the patient to a cool, sharly spot.

137
3· Stri p the patient to the waist.
4-.La y the patient down, with the head and trunk well ralsed.
. 5·-Procure as a as possible of fresh aIr, and fan the patIent vlgorously.
6. Apply ice bags or cold water freely to the head n ec k, and spine, and maintain this treatment untii the symptoms subside.
7·-0n returIl: to consciousness, the patient may have ,yater to dnnk.
CONVULSIONS IN CHILDREN.
Teething or stomach troubles are the commonest causes of this ailment.
SIGNS.
Spasm of the muscles of the limbs and trunk blueness of the fa€e, insensibility, more or less com: and occasionally squinting, suspended respiration, and froth at the mouth are the prominent signs.
TREATMENT.
1. - Support the child in a warm bath siightly above the temperature of the body (98 degrees) so that the water reaches to the middle of the trunk. '
2.-Place a sponge Jipped in cold water on the top of the head.
138 AS P f-IYXIA.
\Vhen owincr to want of air, the bIo.od is, not supplied' wi h the patient ?e.comes and is said to be asphyxiated. 1 hIS condltlUn may be brought about as follows :
1. Obstruction of the a1r passages.
(a) By DRO XNING. , .
(b) By PRESSUR 8:. FRO,:'.! OUTSIDE: StrangulatIOn, hanging, smothenng, ,
(c) By A FORElGN BODY IN THE THROAT: Chokmg:
(d) By SWELUNG OF THE TISSUES OF THE TH ROAT: Infb.111 mation, scald of the throat, poisoning by a corro ive .
II. Inhaling poisonous gases. By coal gas (as used in the house), producer, or water, gas, sm?ke, fumes from a charcoal or coke fire, se\\ er gas, lImekiln gas carbonic acid gas
Ill. 'Pressure e n the chest, as when crushed by sand or debris, or hy crowd. .
IV. Nervous affectlOns, as the result narcotic and certain other poiSJn::, collapse, electnc shock, or str oke by lightning.
GENERAL TREATMENT.
In all cases of Asphyxia attem; ts must made to remove the C;allse, or to remove the patient. fr? " the cause, \ Vhen this hJ.s been done artifiClal

respiration must be applied, taking care that th e air passages are not obstructed, and that there is abundance of fresh air.
DRO WN I TG.
Persons completely immersed in water for even ten or fifteen minutes have been restored by artificial means. Therefore, if the body is recovered within a reasonable time, absence of signs of life is not to deter immediate attempts to restore animation.
Th e first thing to d o when the body is recovered is to get rid of the water and froth obstructing the air passages, and th e n anificially t o restore breathing. This is bes t accomplished e ith e r by proceeding at once to perfo rm artificial res piration by meth od, or as follows:-
1. - As quick 1)' as l)}ssible loosen the clothing, and clear the mouth and the back of the throat.
2. - Turn th e patient face dmvn\\'ards, with a p1d b e low t he chest, and \\' ith the forehead upon the ri t, ht f rearm.
3· - \rhilst in this position apply pressure by the hands to the pati ent's back over the lower ribs, and keep the pressure up for three seconds.
4·-Turn the patient on the right side, maintaining that position also for three seconds.
5. - Repeat these m ovements alternately as long as frot!l and water issu e frol11 the mouth.
139
These operations (Marshan Hall's method) in themselves tend to promote respiration, but th,e air passages are clear of and water SIlvester s metnod of artificial respIratIon may be used by itself or \\ ith Howard's method in conjunction.
'Vhil e performing these operations send someone to the nearest house to procure blankets and dry clothing, hot water bottles, etc., and to fetch a doctor.
STRANGUL<\TION.
Cut and remove the band constricting the throat. Apply artificial respiration.
HANGING.
no not wait for a policeman: grasp the lower limbs and raise the body to take the off rope; cut the rope, free the nock. Apply artIf1clai respnatlOn.
SMOTHERING.
Remove whatever is smotherin.g the patient. Apply arti ficial respi ration.
CHOKING.
Open the mouth, forcIbly if need be; pass the forefinger right a:> the back of tl?e and attempt to dlslodge the foreign body; If vomltmg results, so much the better. If unsuccessful, thump the .back hard whil'3t the head is bent forward. Apply artIfiCIal respiration.

SWELLING OF THE TISSUES OF THE THROAT.
\Vhether the swelling is caused by inflammation by swallowing very hot water: as not infrequently happens to children attempting to drink from the spout of a kettle, or by the effect of a corrosive poison, the treatnU'llt is as follows :--
I.-A pply a sponge, piece of flannel or other cloth, wrung out of very hot water, to the front of the neck, from the chin to the top of the breast-bone.
2.-Set the patient before the fire.
3·-Give ice to suck if it can be had; if not, gi ve cold water to drink.
4·-Gi ve animal or vegetable oil, a dessertspoonful at a time, to soothe the scalded throat and ease the pain.
5·-If breathing has ceased apply artificial respiration.
SUFFOCATION BY SMOKE OR GASES.
I.-Remove the patient into the fresh air. Before entering a building full of smoke tie a handkerchief, wet if possible round the head so as to cover the n l se and mouth. It is well to move slowly, keeping low, or even cra\\'ling, whtlst in a room full of smoke in search ot a suffocated person. Every opportunity of letting in fresh air by opening doors or windows should be seized.
2.-Apply artificial respiration.
3. -In the case of p rod ucer or wat er gas, inhalation of oxygen will a lso be necessary.
ELECTRIC SHOCK.
Electric current is conveyed by a cable, wire, rail, or bar, called the "Positive," anj r et urns to the source of s u pply by another cab le, wire, rail, or bar, called the" Negative," or thr vugh the e:Hth. In the case of an electric railway, the current is generally conveyed by an insuLtted rail called the third rail, ang return s throu.sh the running rails or an insulated rail called the fourth rail, and in th e case of an e lectric; tramway it is frequently conveyed by an overhead conductor or trolley \Vi re, and returned throu gh the runnin g rails.
Through contact with a " positive" the shock may be so severe as to cause insensibility, and the suffe rer will be to extricate hi mself, and 111 ust be liberated with all possible speed As it is generally impossible or inexpedient to switch off the current some other meth od must usually b e adopted; but precautions must b e taken or else the person rendering assistance will him self receive a shock.
To liberate the sufferer from contact-
I. - Insulate yourself from the earth by stand · in lY on an " insulator" or " non-conductor, " that is, a b:dy which resists the current. Amongst su ch bodies

I43
are indiarubber, dry g lass , dry bricks, dry silk, dry cloth, dry wood and dry hay or straw.
2. - Protect your hands from contact with the sufferer or the electric medium by covering them with an insubtor. Although indiarubber is prohably the best insulator, do not waste time in runnin g for indiarubber gloves but use dry articles of clothing; an indiarubb er tobacco pouch or cap, or folded newspap er, would serve to protect the hands in an emerge ncy. 1f no means of insulating the hanrl s are at hand an attempt may be made to drag tbe sufferer away by means of a loop of d ry rope or a crooked stick; an umbrella is not safe because the metal ribs would act as conductors* of electricity, and it is not infrel uelltly the case that the" stick" of the u lTlh rella is a metal tube.
3. - Pull the suff': rer away from contact. Care should be taken to avoid touching with n aked hand s the sufferer's hands, wet clothing, or boots if the soles are nailed. The armpits should be avoided as perspiration usually makes the clothing damp there.
' Vhen the sufferer is remov ed from contact-
I.-Apply the general treatment for insen·
* A conductor is a body through which electricity readily passes. Amongst such boJies are cllpper, brass, iron, moist ure and one's own hocly.
J44
sibility (loosen clothmg, procure free circulation of air and place in a recumbent . .
2.·-Dip a towel in cold water and attempt to arouse him by sharply fli cki ng the face and chesL
3. - Commence artificial respiration if other methods fail to restore animation. " Laborde's " method (see page 126 ) has been found to be very successful.
4.-Treat burns if there are any (see pages 103, 1 0 4).
EFFECTS
OF LIGHTNING.
A person str uck by lightning is usually more or less deprived of consciousness. The treatment is the same as that for electric shock, except, of course, that the instructions for removing the patient from contact with the electric medium do n ot apply.
J45
QUESTIONS ON CHAPTER V.
The numerals indicate the pages wlure the answers may be .fou1ld.
What are the two systems of nerves?
or what is the cerebro·spinal system made up?
What is the spinal cord?
What are nerves like?
the sympatheti.:: system
In what system of artificial respirati
back upwards?
In what systems is he laid on his back?
is the patient
In what system is he laid on hi back or side ":
In what system is he rolled alternately on hIS SIde and face
Would you examine the patient to see if any
'Wha t wrong opinion may be formed when the patient smell s of
from drink a serious condition?
. ..
...
...
PACI!: 117 117 117 II8 lI8 Explain
Explain the respiratory system Explain the acts of respiration 118 to 120 120 llow are the €xpansion and contraction of the chest eftected? ... ... 120 to 121
laid 12J 123, 126 1 2 7
... ... ...
on
downwards? ". ... 139, 140 now long should artificial be persevered with? 1 2 7 What is exciting respirati on ? 127 What is inducing circulation? ...... 1 2 7, 128 'Why is it necessary to watch the patient? 128 How may insensiiJility arise? ". 128 State the various forms of insensibility 128 State the general rules for treatment of inse nsibility 128 to 13 1
bones were broken? .. , ... .., 1 2 9
drink? ... 130 Is collapse
13 [ 'What is concussion of the brain? ... 13[ State the rules for treatment of concussion 13 1 ,13 2
"Vhac danger accompanies injury to the head?
\ Vhat caution sho uld be given to a patient who has lost consciou<;ness, even for a moment, afte r an injury to the head?
\ Vhat a re the causes of compre sion of the brain?
In what agtd people docs apoplexy usually occu r?
\Vh at a re the signs and symptom.;; of compression and ap oplexy?
State the:rules for treatment of these conditions .. .
\Vh.it dang!'r is there in applying hot water hottles to insensible persons, and what precautions should be taken?

13 2
Describ e a Case of epilepsy . 133
\Vhat special care must be taken in treatina- a case of epi lepsy? ... b 130, 132 a hysterical fit ...
H ow would you treat a hysterical fit?
133
\Vh at are the comm nest physical causes of shock? 134
\Vhat may produce shock or fainling? ... ... 134
\Vh at condili?ns do certa!n poisons brin'g about? 134
What may bnng about famtmg or col apse?
134
HTow would yuu recognise the general condition of shock? 134
\\ hat special precaution must be taken in the case of collapse?
State the t reatment for shock, fainting
135, 136 135
'What IS the effect of sugar on the tempe rature of the borlyi'
"Vhat are the causes of sunstroke and heat·stroke ?
State the treatment for sun st roke and heat-stroke
"Vhat are the causes of convulsions in children?
\Vh at are the signs of convulsions in children? .. .
State the treatment for convulsions in children ..
State fully the causes of asphyxia ..
What two things have to be d one in all cases of a phyxia?
\Vhat two things must be seen to before It IS possIble for a rti ficial respirat ion to do any good? .
139 I s art ifi cial respi ration likely to. do good If the aIr passages are obstructed, or If there IS not abundance of fre sh air?
\Vh It is th e first thina- to cl o in a case of drowning?..
By what metho? maYar lific.ial respiration be performed without
taken before proceedlDg
... ... .. . '" . .. . ..
... ... ... ... .. .
PAGE 13 1 132 13 2 13 2 132 13 2
... ... ... ... ... ...
... 133
...
...
...
... ... ... . ..
... ... ... ... ...
...
... ... ... . ..
'"
.
. 136 136 136, 137 137 137 137 138 147 PAGE
... ...
...
':' . .... 13 8 , 139
... .. . ... 139
.... 139 Wh
th Silvester's metho(l? 139 \Vhat sho uld be done while artificial r espiration is being performed? . . . . . . . . .. 14° State the treatment for strangulati on 140 State the treatment for hanging 140 State the treatment for smol hering 14° State the treatment for ch oking 14° How may
of the throat
caused? . . . .. . ... ... ... 141 State th! treatment for swelling of the tissues of the throat... ... 141 State the treatment·for suffocation by smo1..::: or gases 14 1 , I4 2 lIow is electrici ty conveyed? ... ... ....... 142 lI ow would you Ii berate
suffe rer from contact Wit h an electric medium? ... . .. ... ... 14 2 • 143 \Vh
contact? ... ... ... ... ... 143 What would you do in
case of a lightning stroke? 1-t4
.
13 9
takll1g any steps?
at steps must be
wi
a swe llin g of the tis ues
be
a
at would you do when the suffe r er was removed from
the
CHA PTE R VI.
Poisons may be classified according (0 their treatmenl under two heads:-
1. - Those which do not stain the mouth and in the treatment of which an emetic is be give I. Amongst these are :_
(IT) Arsenic, (contained in rat poison and lucIfer matches), Tartar emetic and Corrosive Sublimate, which cause a metallic taste in the mouth and a burning pain in the mouth, throat and stomach.
Strychnine, Prussic Acid, BelJadonna (deadly mghtshade plant) and several other varieties of as laburnum seeds, etc. ; these gIve flse to convulsions, delirium of respiration and collapse. '
( l ) POIsonous meat, fish and fungi (often mistaken for mushrooms). Suspicion of these poisons should be directed to Ci1ses where several persons who have partaken of the same food develop similar SIgns and symptoms.
(d) Alcohol, which may cause collapse.
( e) OpiLHil amI its preparations, Morphia "
149
Laud anum, Paregoric, Syrup of Poppies and various sooth m g drinks and cordJals; cause a to to sleep, which continues untIl sleep deep and stertorous; the pupils .of the eyes become minutely contracte<..l ( plllhead pupils). h th
2 - Those which burn or stain t e , and in the treatment of which no emetlc 1S to be iven. Th ese are of two :.
g (n) Acids, such as. 1 ACId .(Aqua Sulphuric ACId OIl o.f VItr.lol), chlori c, or l\IuriatIc, ACld (Spmts Salt), stron a Carbolic Acid (Phenol), Oxal1c ACId, is contained in oxalate of potash, salts of sorrel, salts of lemon and some polishing pastes.. .
(iJ) Alkalies, su ch as .Caustlc Potash, CaustIc Soda and Ammoma.
RY OF SI \lPLE DIR F:CTIO:\fS FOR THE TREATl\JE:\fT OF POlSO:\fING
1. - Send for a doctor once, stating what has occurred and if posslble the name of the
l' d outh are
2. - Except when the lpS m or burned by an aCld or alkali,

15 )
prom.ptly give an emetic - that . k h t IS, rna e t e pa lent vomit as follows: -
(a) Tickle t lze back of the tllroa t with the finfTer or with a feather . 0
(b) Mustard - a dessert-spoonfu l in a tum blerful of lu ke-warm water.
(c) Salt-a table-s poonful 111 a tumblerful of luke-warm water.
Cd) Ipecacuanha rVim-for a you ng child, a teaspoonful repeated at intervals of fifteen minutes.
all cases when the patient is not ingive Milk, Raw Eggs beaten up wlth mtlk or water, Cream and Flour beaten together, Animal or Vegetable Oil (e:xcept m poisoning), and Tea.
_ Ollv,e, Salad, ani Cod-liver oil, or oil such as that 111, whIch are prese r ved, may be given; oils and paraffin are unsuitable. Ol! IS ,soothmg, and is therefore especi.dly useful in P01SOI:1I1g by Acids, Alkalies and such suhstances as ArsenIC a n d Corrosive Sublimate, Demulcent drinks such as barley water or thin gruel, act in the manner, a!1d free from danger in cases of phosphorus pOlsomng.
may be given either before or after the emetic If the poison calls for one.
Strong Tea acts as a of ma n y poisons l S I
and is always A handful of tea should be thrown into a kettle and boiled. .
4 - If the lips and mouth are stamed or burned give no emetic, but. .
(a) If an acid is kno\\'n, to be the pOlson gIve an Alkali at once. FlfSt \\ ash the mouth out freely with lime water or other . mixture, such as soda, chalk, whltll1g, or ma<rnesia or w..tll plaster in water, and afterwa:Js let the patient sip a little of it. Soda and potJsh are not to be giyen in th e case of poisoning by oxalic ac id . .
(b) If a strong Alkali is kn own to be the p Olson give an acid at once. First wash the l,nouth out freely \"itb lemon juice or vmegar diluted with an equal quantity of water, al:d afterwards let the patient sip a little of It.
In both cases give oil (Rule 3) ·
5. - When a person has poison and threatens to go to sleep, keep hlm awake b y walking him ab o ut a n d slapping his face, neck and chest with a wet towel. Stro ng black co ffee may be g ive n t o Sla p p ing th e soles of th e feet may also be t n ed ,
6. - 1£ the throat is so swollen as to threaten obstruction to the air passage, apply hot flannels or poultices to the front of the neck and give frequent sips of cold drinks.
7· - Apply artificial respiration if breathing cannot be discerned.
8. - Treat shock and collapse.
9·-Preserve any vomited matter, food , or .other subs tance, suspected of being the pOlson. Do not wash vessels which may bave contained the poison) and carefully guard them.
Certain poisons require special treatment, and a few of the commoner of these are mentioned below with their treatment.
C,\RDOLlC Acro.
The odour of breath ' will aid in the detection ,of. this j the lips and mouth are usu:-tlly stamed whlte, and several nervous symptoms come on.
I.-Give milk, to a pint of which half an ounce of Epsom Salts has been added.
2.-Treat according to the general rules.
PRUSSIC ACID.
The action of this poison is extremely rapid . Giddiness, staggering, insensibility accompanied by panting respiration, profound collapse and possibly convulsions are the general signs, and in addItion a smell of bitter almonds is often present.
TREATMENT.
I.-Place the patient in the open air.

1;3
2. - Dash cold water on the head and spine continuously.
3.-Apply artificial respiration.
4.-Hold smelling salts to the nostrils.
S.- Treat shock and collapse. (See page 13S )
POISONOUS MEAT, FISH AND FUNGI.
The signs and symptoms are vomiting and (diarrhrea.), colic, headache, great weakness, raIsed temp erature and a quick pulse.
J .- Give an emetic.
2.-' \Vhen the emetic has acted, give castor oil.
3.-Treat collapse. (See page 135 ·)
STRYCH;\fINE.
The signs and symptoms are a feeling of. suffocation, livid features, and convulsions. The patient rests on his head and feet, and the body is arched.
I.-Give an emetic.
?.-Apply artificial respiration.
ALCOHOL.
1.- Give an emetic jf the patient can swallow.
2.-Treat collapse by keeping the patient warm, etc . (See page 135 )
QUEST I ONS ON C H AP TE R VI.
The numerals i1ld/cate the pager where the a n swe1'S 111 ")' be fou n d.
Under what two head may poisons be clas ifled ?
\ Vhat are the symptoms of plli oning by Arsenic?

PAGE 148, 149 148
\ Vhat other poisons gi\'e rise to the same symptoms? ...
\ Vhat poisons give ri e to cO'lVulsions, Jcliriull1, failure of respiration and collapse? ...
14 8
If several people who had partaken of the same food developed similar signs and symptoms, by what would you suspect they had been poisoned? 148
\ Vhal condition may result fr ,J1l) poisoning by alcoho l ? 148
\\That a re the effects of such po isons as opium ?... 148, 149
\ Vhat two classes (,f p.)ison burn or stain the moulh ? ... 149
\ Vould you give an emetic for such poisons? 149
Name some of the pr incipal acids .. . 149
Name some of the principal alkalis 149
State the general rules fvr the treatment of poisoning ..
. 149 lo 152
State the best methods of making a person vomit 150
H ow would you treat a case of acid poisoning? ... ... 15 1
How would yon treat a case of poisoning by an alkali? 151
State the signs, symptoms and treatment of ca r bolic acid poisoning ...
State the signs, symptoms and lr<'atment of poisoning by 15 2 Prussic Acicl 15 2,1 53
State the sIgns, symptoms and treatment f poisoning by poisonous food...
... 153
State the signs, sympto ms and treatment of poisoning by Strychnine
W hat would you do in the case of alcohol ic poisoning? 153 153
155 C HAPTER V II.
BA N DAG I G.
Esmarch's Tr ia ngu la r Bandage has been d esc ribed in Chapter II . It may be applied to keep a d ressing o n a wo u nd, b u rn or scald of any part of th e body, or for a n inj ury of a joint.
For the Scalp ( Fig. 62). Fold a hem abo u t r ! F IG. 62. inches deep along the base of a bandage; place the banda;c on the head so that the hem lies on the forehead close down to the eyebrows, a nd the point hangs down at the back ; carry t he two ends round the head above the ears and tie them on the foreheJ.d ; draw the point first do\\'nwards, and the n turn it I P emd pin it on to the b:mda,;e on the top of the head .
For the Forehead, Side of the Head, Eye,
Cheek and for any part of the body that is round '(as t h e ar,TI or thigh , etc ), the narrow ba ndage should be u sed , its cen tre bei ng placed over the
154
. ..
. ...
..
... ...
... ...
...
... ... ... .. .
... ... ... ... ... ...
dressing, and the ends being carried round the head or limb, as the case may be, and tied over the wound.
For the Shoulder (Fig. 63)· Place the of a bandage on the shoulder, with the point running

FIG. 64.
up the side of the neck; fold a hem along the base; carr y the ends round the m iddle of the arm and tie
t hem . Place one end of a broad bandage over the point of the first bandage and sling the arm by carryi ng the other end over th e sound shoulder and ty ing t he ends at the side of the neck; tum down the poi n t of the first bandage, draw it tight and pin it.
For i he Hip (Fig 64) . Tie a narrow handage round the body above the haunch bones, with the knot o n the injured side . Fold a hem according to
FIG. 65. the size of the patient alcmg the base o f a second bandage; place its centre over the dressing, carry the enrs round the thigh and tie them ; then carry the point up under the
66.
first bandage, tum it down over the knot an d pin it.
For the Hand when the fingers are extended (Fig. 65). Fold a hem along the base of a bandage; place the wrist on the hem with the fingers towards the point; then bring th e point over the wrist, pass the ends round the wrist, c r oss and tie them; bring the point over the knot and pi n it to the bandage on the hand .
I5
6
FIG.
For the Foot (Fig. 66). Place the foot on the c entre of the bandage with the toes towards the point; draw up the point over the instep, pass the ends round the ankle and cross them in front; now pass t he ends [JLl nd the instep and tie them. Draw the

FI e. 67a. FIG. 67b. point forward and pm it to the bandage on the instep.
For the Front of the Chest (Fi 3s. 67a and 6 7b). Place the middle of the bandage over the dressing with the point over the shoulder on the same side; carry the ends round the waist and tie them;
15 9 then dra ',v the point over shoulder and tie it t J on e of the ends.
F or the Back . The bandage is applied as the foregoi n6, exce pt that it is begun at the back.
For the Knee. Fold a narrow hem along the base of a bandage ; lay the point on the thigh and th e mldJle of the base just below the knee-o p; cross the ends first behind the knee, then over the thi gh and tie them. Bring the point down an:i pin it to the base (Fig. 6 3) .
FIG. 68. For the Fold a narrow hem along the base of a bandage; lay the point on the back of the arm and tL e middle of the base on the back of the forearm; cross the first in front of the elbow, then over the arm and tie them in front (Fig. 69).
For the Fingers and Toes \\Tap a strip of calico or linen round and roun d the part; spIrt the freeend , md secure it round t he wrist or a n k le.
CHAPTER VIII.
METHODS OF CARRYING.
THE FOUR-HANDED SEAT.
This seat is used when the patient can assist the bearers and use his arms.
I.-Two bearers face each other behind the patit:nt and grasp their left forearm with their right hands and

70.
each other's right forearm with their left hands (Fig, 70), and stoop down.
2,- The patient sits on the hands and places one arm round the neck of each bearer.
161
3.- The bearers rise together and step off, che bearer on the right han:! sjde of the patient with the right foot, and the left han:! bearer with the left foot.
THE T\\ O-HANDED SEAT.
This seat may be used to carry a helpless patient.
71.
1.-Two bearers face each other an J stoop, one on each side of the patient. Each bearer passes his forearm nearest to the patient's head under his back just G
FIG. FIG.below the shoulders, and, if possible, takes hold of his clothing. They slightly raise the patient's back, and then pass their other forearms under the mid d le of b1S thighs (Fig. ]I), and clasp their hands by one of the methods sho\\'n in Figs. 72 and 73. A handkerchi ef should be held in the hands if the first grip is used.

7:.
2. - The bearers rise t06et her and step off, the right-hand bearer with the right foot, and the left-hand bearer with the left fo.)t (Fig. 74'.
THE THRJ.<.E-HANDED SEAT.
This seat is us eful fol' carrying a plti e nt and supporting either of his 10IVer li:nbs, when h e is able to use his upper limhs.
1.-Two bearers face each other behind the patient. For supporting the left limb the be1.rer to the patient's right his own left wrist \"ith his ri g h: hand, and the otb e r bearer's right wrist with his left hand. The bearer to the left grasps the first bearer's right wrist with h!s right hand (FIg. 75). Thi') leav es his
FIG..03

left hand free to support the patient's left leg. For the patient's right lower limb follow the same directions, substituting" right" for" left" and" left " for "right." The bearers stoop down.
2.-The patient places one arm round the neck of each bearer and sits on their hands.
3. - The bearers rise together and step off; the FIG. 75. right-hand bearer with the right foot, and the lefthand bearer with the left foot.
THE FIREMAN'S LIFT.
(To be attempted only by a strong man).
Turn the patient face down ,\'ards; place yourself at his he8d, stoop down, slightly raise his heau and
shoulders and take hold of him close under his armpIts, locking your hands on his back. Raise his body and rest it on your left knee; shift your arms and, taking him round his waist, lift him until bis head rests on your left shoulder. Throw his left arm over your head, stoop dO..,YI1 and place your left arm between his thighs, letting his body fall across your shoulders. Rise to an upright p osition j hold the patient's le ft l\rist \\ ith your left hand and leave your right hand free.
Assistance may be given to an injured person by supporting him in the manner show n in Fig_ 76
The plan of carrying tile patient Iry tlt e arms and legs wz'tlz tlze face dowJlwards, commonly called tlze "frog's marcil," 'must never be used, as death may ellsue from this treatment.
IMPROVI SED STRETCHERS.
A stretcher may be improvised as follows :_
1. - Turn the sleeves of a coa.t inside out; pass strong poles through them; butto, the coat. The patient sits on the back of the coat and rests against the back of the front bearer ( Fig. 78). If:1 lo nger stretcher is required tll'O or three coats tll 11st be treated in the same manner. The potes may be kept apart by strips of wood lasherl to the poles at both ends of the bed formed by the coats (Fig. 79).

THE FORE AND AFT METH OD.
This plan of carrying is useful wilen si-'d.ce does n0t permit of a hand seat.
166
FIG. 77.

2.-Make holes in the bJtt:)t1l corners of one or tw:) sacks and pass stout poles through them.
3·- Spread out a larg" piece of sacking, t :l.rpaulin, or a strong blanket, and roll tiro stout po les lip in the sides . TWJ bearers stand on each side and grasp the midd e of the pole \\ ith one hand, and n e:u the end with the other. They walk sideways.
4·-A. hurdle, broad piece of woo d, or shutter may be used as a stretcher; sO:l1e strclW, hay, or clothing sh ::mld be placed on it, and coYered \\ ith 3. piece of stout cl ot h or sacking; the latter is useful in taking th e patie nt off the stretcher.
Always test an improvised stretcher before use.
Stretchers must be carried, and the patient placed on the '11, as laid doyvn in the" Stretcher Exercises."
As a general rule carry the patient feet foremost. The exceptions are: -
( r1) 'Vhen going up hill with a patient whose lower limbs are not injured.
(b) When going down hill with a patient whose lower limbs are injured .
A\'oid lifting the stretcher over ditches or walls, but where these cannot be avoided the stretcher must carried in the following ways: -
To CROSS A DITCH.
In crossing a ditch, the stretcher sho u ld be lower with its foot one pace from the edge of the d itc h
169
Nos. I and 2* bearers then dtscend. The stretcher with the patient upon it, is afterwards advanced' No.s. and 2 in the ditch supporting the front end whIle Its other end r sts on the edge of the ground ahove. No. 3 now dEscends. All the Nos. now carry the stretcher to the opposite side, alld l be foot of tho:: stretcher is mad e to rest on the edae of the while the head is supported by 3 in the dItch. No. I climbs out, No. 2 remainin a in the ditch to assist NO.3. The stretcher is lifted i::>forward on the ground above, and rests there while TOS. 2 and 3 climb up.
To CROSS A "'VALL.
The stretcher is lowered \\ ith the foot about one pace from the wall. Nos. 1 and 2 bearers then take hold of the of .the stretcher, and NO.3 of the head; the stretcher IS ral sed till the foot is placed on the wall. No. I then clim bs over the wall and takes hold of the foot of the stretcher, while Nos. 2 and 3 support ' Lue head; the stretcber is then carried forward till the bead rests on the wall, No. J supporting the foot. Nos. 2 and 3 then climb over the w.dl and take hold the bead of the stretcllfr, which is then slowly hfted the wall on to the ground, and tbe bearers take theIr usual places.
* These numbels are expJain . d later in the de tailed " Stre ' cher Exercists."

To LOAD A "r AGON •
The stretcher is lowered with the foot one pace fl a m the end of the wagon. N os. I .and 2 take hold Gf the foot of the stretcher, No. 3 the head. The stretcher is then raised and carried fOr\yard till the front :vheels .rest on the fioor of the wagon. No. I then Jumps 111tO the \"agon, \\hile Ko. 2 goes to the ?ead of the ,stretcher an? helps NO.3. The stretcher IS ther. pus'l1ed slowly 111tO the wagon. If the tailboard cannot be sh ut, the stretcher must be lashed fimlly to the sides of the wagon.
To UNLOAD A ",VAGON.
Nos. :; and 3 take hold of the head of the stretcher while No. I gets into the wagon; the stretcher then gradually dra\\'n out till the foot-wheels rest on the edge of the wa gon. No. I jumps out of the wagon, and with TO. 2 takes hold of the foot of the stretcher, NO.3 supporting the head. The stretcher is nc;>".; gently dra\\l1 a\\ay one pace and lowered.
With four bearers Nos. I and 2 \\'ould lift the foot of the stretcher, \\hile Nos. 3 and 4 lift the head. This applies to crossing a ditch or ",all as well as to loading and unloading a \vagon. '
170
) -., 1-
CHAPTER IX.
STRETCHER TRANSPORT.
The "Furley II Stretcbers p fodel J 899) are cf three patterns, viz .," Ordinary,lI" Telescopic·handled " and" Police. II In general principle tbey are tbe component parts being designated the poleS:

FIG 80.-0RDINARY STRETCHER-CLOSED.
FIG. Sr. -TELESCOPIC·HANDLED STRETCHER- OI'E)<.
trayerse bars, foot \dleels, ued, pillow sack and s11l ,gs .
. Tbe Ordinary Stretcher (Fig. 80) is 7 feet 9 inches 111 length, and I foot 10 inches \\ ide. The lxd is 6 in. and the handles inches . Tbe helgbt IS 5'4 mcbes. At the bead of tbe stretcher is a overlay (the pillo\\' sack) \\ bich can be filled with bay, clothing, etc., to form a pillo\\'.
The ]omted traverse bars are proviced with joiLts, 173
for opening or closing the stretcher. The Telescopichandled pattern (Fig. 81) is very similar, but the handles can be slid underneath the poles, thus reducing the ll'ngth to 6 feet. This arrangement is of great value when working in confined spaces, or wben a patient bas to be taken up or down a narrow staircase with sharp turns. The Police stret, 'her is similar to the Ordinary pattern, but is more strongly made, and has, in addition, straps for securing a refractory patient.
\Vhen closed, the poles of the stretcher lie close together, the traverse bars being bent inwards, the canvas bed neatly folded on the top of the poles and h elel in positiDn by the slings which are laid along the canvas, and secure d by a strap, placed transversely at the end of e.1ch sling, being passed through the large loop of the other, and round the poles and bed.
In closing a stretcher care should be taken to raise the centre of the canvas wh en pushing in the traverse bar, as it is other\\'ise liable to get caught. .
To prepare, or open a stretcher, unbuckle the trans verse straps of each sling; remove the slings from the stretcher; separate the poles; take hold of each traverse bar anJ draw it forward . The slings will then be fulded to half their length, one being hid neatly over the handles at each end of the stretcher.
As a general rule, the stretcher will be prepared by :-\ (l s. I and 3 hearers in Exercises I, n., and Ill. ;
and by No. 2 in Exercise IV. These bearers will, however, if required, assist the other bearers in attendll1g to the pDtient's injuries.
Note.-The various movements detailed in the following Exercises should be carried out steadi ly, the bearers working in unison, hurrying being carefully avoided and every attention being paid to the bearer who gives the words of command .
Exr RCISES,
Original ly drawn up by Sir John Furley, and revised in 1904 to accord with the drills adopted by the Royal Army Medical Corps :-
EXERC[SE No. r.
FOR FOUR BEARERS.
1.-The Instru ctor selects the bearers and numbers them - r , 2, 3, 4 at his discretion. Should one man be taller J.nd stron;er than the others, he should be styled No. 3, as he \\'illlnve to bear the heavier part of the burJen.* All orders will be given by NO.4.
2. - " Fall in."-Nos. I, 2, and 3 take position on the left side of and tlcing the patient. No. I places himself the patient's kllees, No. 2 at the hips, NO.3 at the patient's sholllders. At the same
* Gearers should, however, he taught to take any of the positions named in the following exercises, whether that of NOT, 2, 3, or 4 bea reT.
175
ti me No. 4 places the prepared on the ground by the right side of the pati e nt about two

l'le. 82.
paces away from him, an? then takes position opposite to and facing NO.2. (Fig. 82).
17-+
3· - " Ready. "--The bearers kneel down on the knee and take hold of the patient, No. I passing hIS hand.s and fore-arms benea th tbe patient's legs, hands wlde apart. Nos . 2 and 4 pass th eir hands

F I G. and forearms be neath the patient's hips and loill!', and grasp each other 's hand s. N O.3 passes his left hand ac ross the patient's chest and under the riaht sho ulder, a n d his right hand beneath the left shoulder (Fig. 83)
177
, 4.-" L ift."-On the "ord "Lift'" the b earers raise the pa tient gently and rest him on the knees of N os . I, 2, and 3 b earers (Fi g. 84) ; as soon as he
FIG. : -1-. is e : urely rEsted, NO.4 disengages hands \\ ith 1\0. 2, runs round by the head of the stretcher and places It under the patient, close to the other bearers' fee::,
176
178
being careful that the pillow is immediately und er the patient.'s bead (Fi g. 85); he then kneels do\\"n and locks his hands with those of No.2 (Fi g. 86).
5. - " Lower."-The bearers place the patient on the stretcher (Fig. 87), disengage their hands, and .then stand up. FIG. 85.
6.-" Stand to Stretcher. "-No. I goes to the foot of the stretcher, with his back to the p3tient; NO·3 to the head wIth his face to the patient; Nos. 2 and 4 remain on each side of the stretcher .
7.-" I and 3 place the slings (if used) over theIr shoulders, stoop down, and slip the
179
loops of the slings on to the handles of the stretcher, which they then grasp.
As soon as all is ri gh t the word is given:-
8. - "Lift Stretcher."-Nos. I <:.nd 3 bearers raise the stretcher steadily together and stand up .
Note.-Nos. 2 and 4 will now adjust the slings on the shoulders of N os. I and 3, taking care that each is well below the level of the collar and lies accurately in the hollow of the shoulder in front. They will also lengthen or shorten the slings, having regard to the patient's injuries and the relative heights of the bearers.

l' IG. 86.
9.-" March." - The bearers move off :-Nos. I, 2, and 4 steppIng off \\ ith their left foot, and No 3
180
with h is right foot (Fig. 87). The step should be a short one of twenty inches, an::! taken with bent knees a nd no spring from the fore part of the foot.
10. - " Halt."- The bearers remain steady.

FIG. 87.
II. - " Lower Stretcher. "-The bearers place
t he genLly on the ground, slip the loops of t he sl.mgs off th e handles of the stretcher, remO\'e t he slIngs from the shoulders, and then stand up.
181
I2. - " Unload Stretcher - Ready. " - The bearers prepare to take the patient off the stretcher, as at Orders 2 and 3·
13. - " Lift."- The bearers raise the patient as at Order 4 (Fig. 86); o. 4, in this case, disengages hands from No.2, removes the stretcher (Fig. 85), and resumes his former position . If necessary, the bearers WJll then steadily rise together, and cJrefuJly carry the patient to the bed, or other place to which it has been arranged to convey him .
I 4.-" Lower. "-The patient is carefu ll y lowered.
EXERCISE No
. II . FOR THREE BEARERS.
I. the bearers I, 2,3.
All orders will be gi ven by No . 2, who will 10 J k after the injured part of the patient's body or limbs, to see that no bandages or splints become displaced, and also that No. I bearer, in hfting or carrying the stretcher, does not touch the patient 's feet.
2 .- " Place the Streteher."-No. 3 places the stretcher in a line with the pJtient's the foot of the stretcher being close to his head .
3. - " Fall In. "-No. 1 places h imse lf on th e :crt side of the patient in a line with his knees, No.2 on the left side just below the patient's anJ N O.3 at the right sid ?, and fa.ces NO . 2.
4·-" Re.:dy." - All kn eel on the left kne e . N o. I places his hands, well apart, underneath the low e r limbs, always taking care, in case of a fra cture, to have one hand on each side of the seat of injury. Nos. 2 and .3 grasp each other's han ds under the sh o uld ers and thighs of th e patient (Fi g . 88).

5· -" Lift." -Th e bea . e rs rise together, ke.'ping the pa ti ent in a hori zonta l position (Fig. 39) .
6. " March."--All tlke short side-paces, carrying the patient over the stretcher until his head is immedi ately above the pillow . 183
7.-" Halt. - The hearers remain steady.
8. - " Lower."- The bearers stoop down, ge ntly place th e patient on th e stretc he r, disengage thelr hands, and then stand up.
9 . - " Fall In." - N o. [ places hims elf the foot of th e stretcher with his bac k to th e patl ent , No.2 places himself at the left side of the and NO.3 at the head, wit h his face towards the patient.
10. -" Ready." -Nos. I and 3 place the slings (if used) over , their shoulders, stoop down, and slip the loops of the slings on to the handles of the stretcher, which they then grasp.
As soon as all is right the \\'ord is givenn. -" Lift Stretcher."-N os. I and 3 b earers raise the stretcher steadily together and stand up.
No. 2 wi I n ow adju st the on the sh ould e r s o f Nos. I and 3, laking car e that each is well belo w t h e level of the collar, and li es accura te ly in the h oll uw of th e shoulder in front. H e will al so le ngt h e n or shorten the sling;;, having regard to the pat ie n t's injuries and the rela tive h eights of th e bear e rs.
12. -" March."-Nos. I and 2 step off with the left foot, and NO.3 with the ri.;ht. The step sh o ul 1 be a short one of 20 inches, and taken \\·ith be nt knees, and no spring fro 11 th e fore part of th e f oo t.
13. -" Halt."-The bearers re main ste l dy.
14·-" Lower Stretcher. "- The beare rs pla ce the stretcher gently on the ground, s.lip lh e lo o ps of the slings off the handles of the stretcher, re mov e the slings fro:n the shoulders, and then stand up.
IS - " Unload Stretcher - Ready." - Th e bearers prepare to take the patient off the stretch e r, as at Orders 3 and 4 (Fig . 88).
16.-" Lift."-T he bearers raise the patient, as a t O rder S, and carry him by short side st eps, cl ear of the stretcher, to th e bed, or other place to which it has been arra "ged to convey him (Fig . 89).

18 5
17. -" Lower."- The patient is carefully lowe red.
EXERCISE No. III.
'\'HEN ONLY THREE BEARERS ARE AVAILADLE AKD THE STRETCHER DE PLACED AS IN EXERCISE II.
I.-The Instructor numbers the bearers-I, 2, 3. All orders \\'ill be given by NO.2.
2.-" Place the Stretcher. "-':'No. I taking the foot of the stretcher, and NO.3 the head, place it on the ground by the side of the patient, and as cl ose to him as practicable.
3. '-" Fall In," - The three bearers take the same positions on one side of the patient, as laid do\\'n in Exercise No. 1.
4.-" Ready."-Nos. 1 , 2, and 3 kneel d ow n on the left knee, placing as close to the patient as they conveniently can, and then take hold of hi m as directed in Exer.cise No. I.
5. -" Lift."-Nos. 1,2, and 3 raise the pati ent as directed in Exercise No. I, and then move in a kneeling position up to the stretcher.
6.-" Lower."- The bearers bend forward, carefully lower the patient on to the stretcher, and disengage hands.
184
7·- " Stand to Stretcher. "-All the bearers stand up ; No. I goes to the foot , No.2 remains in position at the side, and No. 3 goes to the head of t he stre tcher .
8. - " Ready. "-Nos. I an d 3 place the slings (if used) over their shoulders, stoop do .\"n, and slip the loops of the sli ngs on to the handles of the stretcher, which they then grasp .
9. -" Lift Stretcher. "-Nos. I and 3 bearers raise the stretcher steadily together a n d stand up.
No. 2 will now adjust the sling, on the shoulders of Nos. I and 3, taking care that each is well beluw the level of the col ar, and lies accurattly in the hollow of the shoulder in front . IIe wi ll a lso lengthen or shorten the slings, having regard to the patient's injuries and th E relative h _ights of I he bearers
10. - " March. "-Nos. I and 2 step off \\ ith the left foot, and NO.3 with the right. The step should be a short one of 20 inches, and taken with bent knees, and no spring from the fore part of the foot.
II. - " Halt. "-The bearers remain steady.
12 . - " Lower Stre tcher. " - The bearers place the stretcher gently on the ground, slip the loops of t he slings off thl::! handles of the stretcher, remove the slings from the shoulders, and then stand U IJ.
13.- " Unl o ad Stretcher - Ready."-No. places himself on the left side of the patient, and in a line with his knees, No. 2 on the left side just belJ\\' the patient's shoulJers, and NO,3 at the right

side, and faces Jo. 2. All kneel on the left knee. No. I places his hands, well apart, underneath the lower I1mbs, ahvays taking care, in case of a fracture, to have one hand on each side of the seat of Nos. 2 and 3 grasp each other's hands under the sho u lders and thighs of the patient.
14·- " Lift" The bearers rise together to their f ee t, keepll1g the patient in a horizontal position, and carry him by short side steps, c1e;:;r of the stretcher, to the bed, or other pbce to which it has been arranged to convey hil11.
15·-" Lower."-The patient is carefully lowered.
EXERCISE No. IV
. FOR USE IN MINES A;\D NARRo',r CUTTIXGS Y. HERE
T :. o MEN ONLY CAN BE EXGAGED .
Nos I and 2 will carerull), place the stretcher in a 1ll1 e with the injured man's body, the foot of the stretcher being, If possible,"'< close to hiS head.
No . I straddles across the patient's legs, placing his right foot, with the toe turned outwards, a little below the patient's knees, and with the toe of the left foot close to the heel of No . 2; he then stoops down, p1sses the Jeft hand und er the patient's thIghs and
It is not advisable to he too particular as to the head or foo t of a stretcher in a mine, as it would probably be quite impossihlc to reverse It.
the right hand across and under the patient's cal yes. NO.2 places his feet one on each side of the patIent between his body and arms, the toe of each foot as near the armpits as possible. He then stoops down and passes bis bands between the sides of the chest and the ar rlS u '1cle: n 'J.th the shoulders, and locks

the fingers (Fig. 90). If the patient 's arms are uninjured he may put them round the neck of No.2, and by this means greatly as§ist bim in lifting.
''''hen both are readv, No. I \\ ill give the ord er " L ift and move forward. " The patient is then to be slowly lifterl, just sutncient to allow his body to clear the stretcher.. Both bearers will slowly and gLldually move the patIent forward, NO.2 by very short steps, No. r by bending his body forward as much as he can wit/Witt moving ht's \'Fig. 91) . No. I no\\' gives the order " Halt," \\'hL reupon Xo. 2 remains steady, .:llld )lo. I advances his right foot to his left, and
FIG. Dr.
again advances his left foot till the toe touches the h eel of NO . 2. No. I then gi ves the order (( Advance, " when the patient will again be moved for\\'ard . These moremellts are to be repeated until
I8S
189
190
the patiellt is over the stretcher, when be is to be gently lowered.
The follo\\'ing Stretcher Exercise is adapted by permission from the Royal Army Medical Corps Manual, 1908.
All orders will be given by NO·4·
1. " Fall i n. " -. ix bearers fall 111 behind each other.
2. " Nu m b e r . "-The bearers number from front t o rear,
3 . "No.3 B e are r, right (or left ) turn-- supply stret c h er- qu ick march."-N o. 3 bearer will march to the stretcher, stoop, lay hold of it and place it on his right shoulder at the slope, holding it by the lower fool wheels, wheels to the front. As soon as the bearer is provided with a stretcher, he will turn about and rejoin his squad in quick time, halting as be arrives in his place. He turns to the front, and, passing the lower end forward , p laces the stretcher on the ground to the right of the squad, wheels to the right, fro n t end of the poles in line with the toes of No. I an d rises.
4. " Stand to Stretcher. "-No. I places himself with his toes in line with the fron t ends of the poles. NO.3 with his heels in line with the rear ends of the poks , close to and touching the stretcher with

92. m rn FiG. 93.
[]
191 /mJ 5 [§J fZ1 ,\ \' " I .' .. I I' ,"'0 I .'. \, \ I I 1; -,' , '---' Ii \ w i '.0[J \ \. \ '\ '. ,---. /'. l.?J Ii : L __ I " I FiG . 95 rn I I. 3 / / I ;I ' · ; I I . . ." ....... r" - ,' , , z '4- : ; 7, ._i' Il' : ,. , ' 1 , 6 :- -, / , , L \ ·5 :/ ' ' _.--. I -[]l /1 :',f' ,'/ --_/ J ](";.
Fit; 96
[1] E1 0 IT] m 0 G Fig.
94.
19 2 his right foot. N os . 4, 5 and ? tak.e up th eir positions one pace ?ehll1d and coverJl1g off the bearer in front of them (FIg. 9 2 ) .
5. "Lift Stretcher."-Nos . I 3 stoop, gra.sp both handles of the poles with the rIght hand, tocrether holding the stretcher at the full extent of arm,' wheel to the right. "
6. "Collect Wounded - Advance - .The squad doubles by the shortest route to the patIent, and halts without further word of one from the head of and in a line with the patient (FIg. 93)·
7. "Lowe' Stretcher." - Nos. I and 3 place the stretcher quietly on the ground, and nse smarlly together. '
8. "Prepare Stretcher."-Nos. I and 3 turn to the ricrht kneel on the left kn ee, unbu ckle the and place the slings on t.he g roun d beside them, separate the po les, and straIghten the tr<1Yerses .
Two. On the word t\\'o e;lch takes a sling, doubles it on itself, slips the lo op thus formed on the handle, and places the free ends over Opp)s!te handle, buckle uppermost. They then nse and turn to their left together.
\Vhile the stretcher is being prepared by Nos. T and 3, the disengaged bearers. will advance r ender to the patient such assIstance as may e r equi red (Fig.

193
The necessary assistance having been rendered, NO.4 will give the command-
9· "Load Stretche!'." - The bearers place themselves as follows :-Nos. I, 2 and 3 on the left, Nos. 4, 5 and 6 on the right of the patient; Nos. I and 4 at the knees, 2 and 5 at the hips, 3 and 6 at the shoulders, the whole kneeling on the left knee.
N os. I and -1- pass their hands beneath the patient's knees, 2 and 5 beneath the hips, 3 and 6 beneath the shoulders, care being taken of the injured part, one of the bearers being detailed for this purpose (Fig. 95).
10. "Lift."-The ",hole will carefully lift the patient on to the knees of Nos. I, 2 and 3.
Two. Nos. 4, 5 and 6 will then disengage, rise; Nos. 4 and 6 step back one pace. No. 5 turns to his left, dOLlbles to the stretcher, takes hold of and raises it, left hand across, the near pole resting on the left hip; carrying the stretcher, he returns to his place between 4 and 6, and places it beneath the patient.
Tltre e. Nos. 4 and 6 step forward one pace, and together \\ith No S kneel down on the left knee, and prepare to assist in lowering the patient (Fig. 9()).
II. " Lower -The patient is low ered slo\\'ly and gently on to the centre of the canvas (special care being taken of the injured part).
TW :J . The bearers disengage, rise; N os. I, 2, 3 and 6 turn to the left; Nos. -1- and 5 to the rIght; H
No. 4 places three paces in fl:ont of the stretcher. No . 6, having collected the kIt and arms of the patient , places three in rear of the stretcher, Nos . 2 and 5 OpposIte the of the stretcher The whole are now ready to lift stretcher and move off (Fig. 97).

m195
12. "Lift Stretcher."-Nos. I and 3 stoop: grasp the doubled sling midway between the poles with the forefinger and thumb of the right hand, sweep it off the handles, rise, holding the sling at the full extent of the arm, buckle to the front, take a side pace to the front between the handles, and place the sling over the shoulders dividing it equally, buckle to the right. The slings should be placed so that they lie well below the collar of the coat behind and in the hollow of the shoulders in front. In the event of the slings requiring to be adjusted, as regards length or for the greater comfort of the bearers, NO.4 will detail a bearer to carry this out, the leI:Jgth of the slings being adjusted, \yhen necessary, by means of the buckles.
Two. Nos. I and 3 stoop, slip the loops over the handles, commencing with the left, and grasp the handles firmly.
Tlzree. Nos. T and 3 rise slowly together, No. 3 conforming closely to the movements of No. I.
13· " Advance." -Nos. I, 2, 4, 5 and 6 step off with the left foot, NO.3 with the right, stepping short, knees bent, feet raised as little as possible .
14. " Halt. "-The whole halt.
IS. " Unload Stretcher. "-The bearers ?lace themselves in the same position. at the stretcher as described for Loading (Order 9).
16. " L ift. "-As described for Loading (Order 10), H2
194
il III . @] t] "
1\ , FIG .
FIG. 97.
98.
196 except that the stretcher is carried forward three paces clear of the patient's feet.
17 . " Lower."-The is gen.tly lowered to the ground. The bearers disengage, rise; I, 2 and .., turn to the left, 4, 5 and 6 to the nght, and the step off to their places at the stretcher, as at Order " Stand to Stretcher" (Fig. 98).
T he Ashford Litter is made up of either of the Furley stretchers mentioned on pages 171. and 173, a wheeled under-carriage and a hood and aoron, or, if preferred, a light wet-reslst1l1g canvas c0.ver. stretcher is kept in position on the by the foot-wheels, which fit into slots 111 the sIdes of the under-carriage, and it can be removed at pleasure. The under·carriaae is fItted with a cranked axle, which allows the bbearers to pass with the stretcher between the wheels instead of lifting it over them. At both ends are two legs which may be turne:i up as bandIes when wheeling the litter. The hood and apl:on fit into sockets screwed to the stretcher. In wheelmg the litter care should be taken to keep the patient in a position. Should it be .necessarYl two bearers can easily lift the litter and patIent.
The Rea-Edwards Litter, introduced in 1.9°.4 is used in a similar manner, and one model of It IS fitted with pneumatic tyres, which add to the comfort of the patient and to the ease ofproDulS10n.

197 CHAPTER X.
(Being the AJtlz for Females only, z'n accordance 'Wltlz S'yllabus 58.)
BY E. l\IACDOWELL COSGRAVE, M.D., F.R.C.P.I.PREPARATION FOR RECEPTIO:\T OF ACClDENT CA ES.
\VHEN news of an accident comes, preparations should at be made so. as to have everything J eady before person IS . brought in. Of course the prepalatlOns needful will vary accordin o· to the nature an? ext.ent of the injury, but the fcllowing are the chIef thll1gs which may have to be done.
CHOICE
AND PREPARATION OF ROO?lI.
A room be chosen. In a bad case this should ?e. one eaSIly reached, as it is difficult to carry an Injured p erson .through narrow passages and up-stairs. there ,Is some such reason against it, the 111 Jured person s own room is best.
way to the room ll:USt be cleared, projecting furniture and loose mats 111 the hall or in . lobbies should be removed. If the injured person is carried a door, shutter, or stretcher, tW? strong chairs ,:,hould be placed ready to support It IVherever the bearers would be likely to require rest.
Useless furniture should be removed from the bedroom. The bed should be drawn out from the wall

so that both sides can be approached, and the clothes turned back to one side to their full length. A hot bottle should be got ready. If there is much several hot bottles and hot blankets may be reqUIred; cover the hot bottles with flannel. ,
If the injury is very severe, clothes have to be removed, or if extensIve dreSSIngs have to be applied, it may be n2cessary to have another bed, a couch or a table placed near the bed to lay the sufferer on in the fi!'st instance. This should be so arranaed that soiling may do no harm; old sheets, watel1>roof materials, thin oilcl.oths, or even newspaper, may be used as a protectlOn.
LIFTING AND CARRYING.
If present at the place where the oC,curred, it will be necessary to see that the IS carefully lifted after proper "FIrst AId has been rendered.
The following rules should be :-Select the proper number of persons to aSSIst, and do not let them lift the patient until they thoroughly understand how they are to do it. , .
For ordinary cases, where the Injured person has to be lifted a very short distance, three are sufficient. Two (who should be as far as of equal height) are to bear the weight, the thIrd t,o support and take charge of the injured part. ThIS IS 199
best done by a person who has been through a " First Aid" course. If the injured person is insensible, another helper should support his head.
The lifters, one at each side, should kneel O.n one knee, and pass their hands under the patient's back at the lower part of the shoulder blades, and under tIle hips, clasping each his right hand in the other" left. The injured patient should, if practicable, place his arms round the necks of the bearers.
The third helper should attend to the seat of injury; if this is a fractured limb, he should support it by placing the palms of his hands under the limb, one above and one below the seat of the injury, grasping it firmly but avoiding unnecessary pressure.
The helpers should remain thus until tIle order " Lift" is given, and then they should all lift slowly and steadily, avoiding jars, attempts to change position .of hands, etc.
If the injured person is to be placed on a stretcher or shutter, this should be previously placed with the bottom end at his head; the bearers should then move, one at each side of it, until the patient is over it. The word" Lower" should then be given, and the injured person should then be slowly lowered. A pillow or folded-up coat should be ready, and as the sufferer is lowered this should be placed under his head.*
* Full directions are given in Chapter IX.
198
201
MEANS OF CARRYING.
Besides a stretcher, and substitutes as a gate, a shutter, or a door, othe r means of carrYll1g can be improvised. . . . bl
In slight injuries, where the IS una to walk, two bearers can carry him by formll1g a fourhanded, three-handed, or two-banded seat. .
A four-handed seat is formed as descrt bed on page 160. . d
A three-handed seat IS made as describe on page 162. . b d
The two-handed seat IS made as descri e on page 161.
1 .
A single helper can lift by supportmg WIt lone a;m the t\\"O knees, and with the other the back. 1. he arms must be passed well under before commenCll1g to lift. . h'
A single helper can suppo.rt by IS ann round the waist, graspll1g the hlp and injured person 's arm round I:is own neck, hoI mg the hand with his own hand 76, 16 5).
A capital stretcher can be Improvised out of a stronO" sheet and two broom handles or other short Each side of is up ?n a brool:1 handle until there IS Just room for a person to he between. This requires four bearers, two at each side, to prevent the sheet slipping.

CARRYING UP STAIRS.
In carrying a stretcher up stairs t!:e head should go first, and an extra helper should assist at the lo\\"er end , so as to raise it and keep the stretcher nearly horizontal.
The two, three, or four -handed seat may be used for carrying up stairs; or a strong chair the patient being carried up backwards . In the lat'ter case one ?elper should walk .the chair and help to support It, and to prevent the ll1Jured person slipping out.
LIFTING INTO BED,
If the bed is narrow and there is room the stretcher should be placed on the floor with the head close to the foot of the bed. The injured person should then be lifted over the foot and placed on the bed. If the bed is too wide to admit of this, the stretc her should be placed beside it, and two helpers should stand at the far side of the stretcher. One heJoer passes one arm beneath the shoulders and one the middle of the back, the other helper placing his under the lower part of the back and under the knees. The injured person is then lifted, another helper pulls away the stretcher, and after a sin rrle step forward the burden is placed on the b ed . .... /:)
2CO
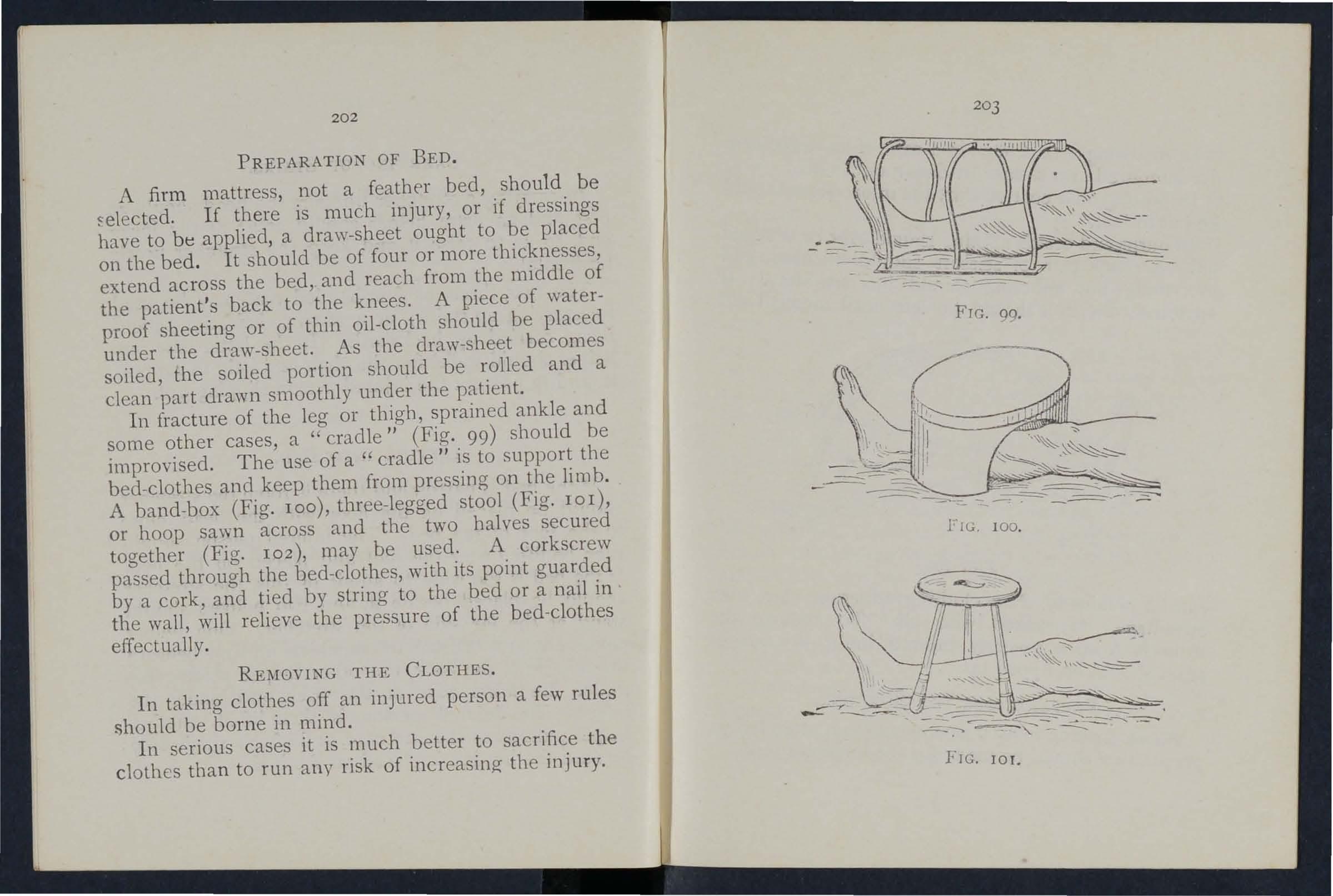
PREPARATION OF BED.
A firm mattress, not a feathf'r bed, should be If there is much injury, or if dressings have to be applied, a draw-sheet ought to be placed on the bed. It should be of four or more thicknesses, extend acroSS the bed, and reach from the middle of the patient's back to the knees. A giece of waterproof sheeting or of thin oil-cloth should be placed under the draw-sheet. As the draw-sheet becomes soiled, the soiled portion should be rolled and a clean part drawn smoothly under the patient.
In fracture of the leg or thigh, sprained ankle and some other cases, a "cradle" (Fig. 99) should be improvised. The use of a " cradle" is to support the bed-clothes and keep them from pressing on the Ii mb.
A band-box (Fig. 100), three-legged stool (Fig. lor), or hoop sawn across and the two halves secured together (Fig. 102), may be used. A corkscrew passed through the bed-clothes, with its point guarded by a cork, and tied by string to the bed or a nail in the wall, will relieve the pressure of the bed-clothes effectually.
REMOVING THE CLOTHES.
In taking clothes off an injured person a few rules !)hould be borne in mind.
In serious cases it is much better to sacrifice the clothes than to run any risk of increasing the injury.
202
203
FTG. 99.
FIG 100
20.+
, in a case of fractured ann I n removmg a coat, etc . ' t fi st 1 ld be dm \\'n ou r. the uninjured arm s 10U 1 ' t injured arm should In putting on a coat or s 1Ir
be put in first. - 'should ever be dragged In burns and scalds h ld be used and , f SCIssors s OU 'If off. A slzarp palr 0, h ld be cut away. everything not s until medical nid anything adheres It shou

FIG. 102.
, The clothin cr adhering may, with can be obtamed. '1 To remove the b soaked WIt 1 OJ. 'ct advantage, e < 1 inJ'ured limb, the outSl e trousers from a ,severe Y seam should be npped up.
PREPARATIONS FOR SURGEON .
h ' . ed person has been attended to, A oon as t e m Jur , " t s s d b de for the suraeon S VISI preparation shoul e rna :::>
205
The preparations needful \\'ill depend upon the nature of the case . The following hints may be of use :_
A fire in the room helps ventilation, even in summer. There should be plenty of water, hot, cold, and also boiling, also several basins, plenty of clean towels and soap, There shoul d be someth ing to em pty water into; a foot-bath does well. The basins should be placed on a table, covered with a clean white cloth; a large towel makes a suitable cloth; the towels, folded up, should be placed on the same table, and the hot and cold water should be within easy reach. The foot-bath should be under the table or close at band.
In the case of a burn, absorbent cotton wool, soft cloths, old linen, oil, and baking soda, should be ready, and materials should be torn up for bandages.
In the case of b::emorrhage, plenty of water should be boiled and allowed to cool, and pads of absorbent cotton wool should be baked in a tin box in the oven, and at least two basi n5 should be ready.
In the case of a person rescued from drowning the sheets should be taken off the bed, plenty of blankets should be heated before the fire, and several hot bottles should be ready,
If poultices are likely to be required, boIling water, linseed meal, mustard, a loaf of stale bread, a small basin, a large spoon, sweet oil, and tow, flannel or handkerchiefs may be required.
2cb
For fomentation, have boiling \Yater, flannel, a kitchen roller, and two sticks, or a large tm.yel. .
'When summoning a medical man to an al ways let him know by a written message \\ hat kl.nd of case he is reqUlred to treat, so that he may whatever is needful. By this means valuable tlme may be saved.
QUESTIONS 0 CHAPTER X.
The 11ltlllerals illd/tale tile ja/;-es whe1'e the answt1' S J//ay be foulld.
\Vhat points would you consider when choosing a sick room?...
?"
How would you clear the way to the slck l'?om .. PAGE 197 197
,
\ \' hat means of resting would you provlde fOl those carrying a patient on a stretcher?

197
How would you place ami arrange a bed for an accldent 8 case?
197, 19
Are hot bottles necessary, and how would you prepare them?..
\Vhat is often necessary to lay the sufferer on lD the first instance?
198
198
How would you protect this frorn soiled? . 198
How would you see to the proper Mung and canymg of an injured person?
00. 198, 199
\Vhat substitutes for a regular stretcher can you suggest? 200
How is the four-hand ed seat made? 160, 161
For what cases is this seat useful ?... 16 6 0
How is the three-handed seat made? 162, 1 4
207
F or what cases is this seaol: useful? .. .
How is the two-handed seat made?
For what cases is this seat useful ?.. .
How can a single helper lift? .. . PAGE 162 161, 162 161
lIow can a single helper give support? ... ...
lIow would you improvise a stretcher? ... . ..
How many bearers are required for this stretcher?
How should a stretcher be carried upstairs? ...
How would you carry a patient upstairs on a chair? ..
How would you lift a patient from a stretcher to a bed?
How should a bed be prepared for an injured person? ...
How should a draw sheet be made? ... '"
\Vhat would you place under the draw sheet? ...
What should be done wit h the soiled part of a draw sheet?
vV hat is the use of a " cradle"?
In what ways maya cradle be improvised?
How would you remove a coat or shirL in the case of a fractured arm?
!low would you put on a coat or shirt if "the arm were injured?
'"
In the case of a bad burn, what would you do with clothing that adhered to the patient? ... . ..
How would you remove trousers from a severely injured limb?...
\Vhat preparations would you make for the surgeon's visit?
vVhat would you get ready in the case of a burn? .. .
And what in the case of hoemorrhage ? ... '" .. .
And what in the case ofa person rescued from drowning?
vVhat would you get ready for making poultices?
And for fomentations?
\Vhat sort of a message would you send to summon a ' dector?
... ... .......
..
.......
...
... ... ... ... ... ...
... ... 00'
... ... ... ... ...
... ..,
...
... ... '" ... ...
.
...
..
... ...
...
... ... ...
... ... ...
... ... ... ... .. . '"
... ... ... ... ... ... . ..
. . . . . . . . . . ..
... 200 165 200 200 201 201 201 202 202 202 202 202 202 204 204 205 205 205 20 5 20 5 206 206
208 INDEX.

Abdomen
P..l.ge III 112 wound of
Accident case, preparation for 197
Acids, poisoning by 149 , 151
Air always necessary ... 18 caution as to smell of 1:)0
Alcohol, poisoning by 134,153
Alkalis, poisoning by 149, 151
Ammonia, poisoning by 149
Anatomy (elementary) 20
Ankle 30 ,3 2 " sprained... 64
Anterior tibial artery 93
Aorta 79
Apoplexy 13 2
Apparently drowned, to restore ...
Arm, bone of " fracture of Ann-slings ... 139 28 52 39,49 14;)
Arsenic, poisoning by Arterial hremorrhage, arrest of 74 " " practising arrest of sign, of Arteries .,. course of main .. , axillary ' -' 79 74 70 79 85
Artery, brachial. .. carotid ... dorsal of foot facial fernoral ... " " iliac occipital plantar ... popliteal radial subclavian tibial " temporal " ulnar
ArLificial respiration 121, 129, Asphyxia Atlas
Auricles ... -Axillary arlery Axis
Back, bandage for 159
Backbone 23
Bandage, to apply 42 to fold 37 " tc improvise... 37
Bandaging ... 155
Bed, lifting into... 20[ " preparation of .. , 202
Belladonna, poisoning by 148
209 Pa/:e
Bites of rabid animals 106
Bladder 111,113
Brachial artery ... 86 Brain 117 compression of 13 2 " concllssion of 13 1
Breast-bone 26 " fracture of 4 8
Broad bandage 37
Broken bones, see Fracture.
Bronchial tubes... 118
Brooch-Lone 30
Bruises 102 Burns 102
CapIllaries 70, 72
Capillary hremorrhage 95 Cap ule... ... ... 31 Carbolic acid, poioning by
Carrying, means of 160, 200 " upstairs Cartilage
Cerebro-spinal system Cervical velte bn:e Cheek, bleeding from Chest, bandage for ... Chlorodyne, poisoning by Choking ...
P(,ge 86 80 93 81 89 79 82 93 92 88 84 93 82 88 136, 138 138 25 7° 85 2$
... 15 2 Carotid arteries ... 80 hremorrhage fr om" 80 Carpus 28
Page Circulation
70
Clayicle 26 " fracture of 48 Clothes, removal
Coccyx ... 25 Collapse... 134 Collar-bone 26 " fracture of ... 48 Comminuted fracture 35 Complicated fracture 34 Compound fracture ... 34 Compre sion of the brain 132 Concussion of the brain 131 Conductor ... ... 143 Convulsions
children 137 Cradle,
Cranium ... " fracture of Crepitus
Crushed hand foot 202 22 43 36 55 62 Diaphragm 120 Digital pressure... 74 Direct violence... 33
Dorsal
vertebr,-e
.., ... 201
of the blood, organs of . .. .. .
Circulation of the blood, to induce .. , ... 127
of 19, 202
in
hed
...
Dislocation 62 Ditch, to cross with stretcher ... J 69
artery of f'Jo t 9.3
... 25

Page
Dress, woman's, on fire ... 105
Drowning 139
Ear· channel, blood issuing from
Ear-passage, foreign body in
Elbow, bandage for joint, fracture involving 98 rIO 159 53 1{2
Electric shock
EmeLie ...
Esmarch's 148, 149, ISO 13 2 bandage
Expiration triangular
External carotid artery ...
Eye, bandage for foreign body in
Face, bones of
Facial arteq
Fainting ...
Femoral arterv " "digital pressure at groin ...
Femoral artery, tourniquet for
Femur " of
Fibula " fracture of Fingers, bandage for fracture of 37 120 80 )55 109 22 01 134 89 89 90 30 56 30 60 159 55 no
Fireman's lift .F irst aid, meaning ot " student
Fish-hook, embedded
Flexion ... at elbow " at knee ...
Food, poisoning by
Foot, bandage for bones of '"
" crushed ...
Forearm, bones of " fracture of ...
Forehead, bandage for. .. " hremorrhage from
Foreign body in the earpassage ... in the eye " "in the nose
Four-handed seat '"
Fracture, apparatus for treatment of '" causes of definition of ... general rules for treatmenL involving elbow joint of arm ... of brea t-bone of carpus of collar - bone of cranium of finger
Pagl:
Flacture of forearm 54 of knee·cap 5g of leg... 60 of lower jaw.:. 44 of metacarpus 55 of metatar"us... 62 of pelvis 56 of Ii bs... 46 of spine 45 of tarsu 62 of thigh-bone... 56 of toes.. 62 signs and symptoms of 35 " yarieties of 34 Frost-bite r08
Fungi, poisoning by J 53 General circulation 70 Granny knot 40 Green-stick fracture 36 Gum, hremorrhage from 97
Hremorrhage, arterial ... 74 capillary... 95 from gums 97 from head 2I1 and neck 80 from lower limbs '" 89 from lungs 97 from nose 96 from stomach 98
Page
Hremon-hage from throat 97 from tongue 97 from tooth sockeL ... 97 from upper limbs 84 internal 95 kinds of 73 " venous 93 IJand, bandage for 157 " bones of ... 28 IIanging ... 140 Haunch-bones ... 28 11 ead and neck, arterie:; of 80 IIead bandage fOJ 155 injury to 128, 131 " side of, bandage for 155 Heart 70 " rate of contraction of 72 Heat-stroke 136 Hernia 114
Hip, bandage for 157
Histoq, meaning of 17
Howard's method of artificial respiration 126 IIumerus 28 " fracture of 52
Hydrophol)ia 106
Hysterical fits 133
Iliac arteries
Impacted fracture Indirect violence Insensibility 79 35, 36 34 ... 128
IIO 109 I II r60 36 33 33 41
Pa c e
Insensibility, general rules b for treatment 12'3
Inspiration 120
Instep 30
In sulator... ... 142
Internal carotid artery 80
Internal hcemorrhage 95
Intestines, injury of 113
Involuntary muscles 33
Jaw, angle o f 23 low e r 23
" "fracture of 44
J oint, definition of 31
" injuries to ... I09
Jugular veia 80
Kidneys .. . ... 11 I " injury of
Knee, bandage fo r .. . 113 159
Knee-cap . fracture o f
Knot fo r bandage of lower limb
Kn ots, reef and granny
Laborde's method of ar i· ficial respiration
Laburnum seeds, p oisoning uy ...
Lacerated wound
Large arm- sling ...
Laudanum, poisoning
Leg, bones of . ..
Leg, fracture of ... Lifting and cal Tying " into beel
Marshall Hall 's method o f artificial respirati o n Medium bandage
Metacarpus fracture of ... " fracture of
l\Jiddle line of body l\J ou th, blood from !\I uscles
ruptured Musc ular action
Nervo us system ...
N ose, foreign body in h ce mo rrhage from
Occ·ipital artery ...
Opium, p oisoning by
Pad, ring ... t o fold hcemorrhage from Palmar arche
'arego ri c, p'oisoning Ly
ate lla
of fr acture of of foot " of hand
Phosphoru , poisoning by 148,
Phy iology (elementary)
Plantar arch " artery
Plants, \'<uious, poi::;oning by ...
Pleura
P oisoned we a p 0 n s, wounds Ly
Poisoning
Popliteal arte ry ...
Posterior tibial artery Potash, caustic, poi !:ionby ...
Pressure, digita l. .. " point ...
Principles of F irst aiel
Pm sic ac id, poisoni·.lg by Pubes
Pulmonary circu lat i on ...
Pulse
Pupils of eyes
animals, Lites 01. Radial arte ry
Room, choice and preuarali on 0: :;)'7
58 42 40
Pa !{c
30
126 30
Lightning, effects o f
r 60 ... 198 ... 201 26, 31 " upper Lime in
... Lips,
ing from Litters Live r " injury of Lower limb 144 28 26 110 82 196 III 113 28 Lum bar velte brce Lungs 25 120 h ce m o rrhage rrom 97
... Ligam e nt s
Limbs, lowe
the eye
bleed
Narrow
a
1
embedded Nerves 140 37 28 55 30 62 20 97 3 2 65 3+ 37 108 IllS
.. .
"
...
b
ndage
eedle,
1
P
fracture
213 82 74 88 88
30
28 56 3 0 28 150 20 93 93 14 8 120 J06 14 8 9 2 9 1 _-
14')
58
Questions on Chapter I. II. III. IV. V. VI. X. Rabid
fracture of knot Respiration artificial P ag-e 74 74 17 15 2 28 ;2 72 130 21 66 99 11 5 145 154 206 106 88 '.8 5-14C 120 Id
6 , 138 " to exc ite 12 7 Respiratory
IIS
necessity
IS
"
Radius
, 129, 13
sy tem
Rest,
for
Ribs 26
fracture of ... 46
Rupture (hernia) 114
Ruptured muscles 65
Sacral velte brre ...
Sacrum ...
Scalds
Scalp, bandage [or " hremorrhage fro111
Scapula ... " fracture of Schafer's method of artificial respiration
Seat, four-handed three-handed
" two-handed
Shin-bone
Shock
" electric
Shoulder, bandage [or ... blade ...
" fracture of bones ... " joint. ..
Sick room, choice and preparalion of. ..
Signs, meaning of Silvester's method of artificial respiration
Simple fraclure ."
Skeleton ... Skull
" fracture of

I 2 3 34 22 22
Slings, arm 43 39,4 0 ,49
Small ann sling ... Smothering
Snake bites
Soda, caustic, poisoning by Spleen
" injury of. ..
Spinal canal cord 23 23, II 7
» [raclure of
Spirits uf salt, poisoning by angular
Splints, rules [or applying to improvise
Spr;,'ins
'Lernum ...
" fracture of Stimulants
Stings of plants and animals
Stomach ... hremorrhage from " injury of ...
Strains
Slrangulation
Stretcher exercise, Army No. 1. No. n. No. III. " ., No. IV.
Furley
Stretchers, to carry " to im provise
Strychnine, poisoning- uy
Subclavian artery .
Suffocation ...
Sunstroke ... . ..
Surgeon's visit, preparatif)l1 for ... .. .
Syllabus of instruction .. .
Sympathelic system .. .
Symptoms, meaning of .. .
Syncope ...
Synovia
Systemic circulation
Tarsus
Temporal artery .._
Thigh-bone ... " fracture of ... Three-handed seat
Throat, hremorrhage fr0111
" swelling of tissues of ... Tibia
" fracture of Toes, bandage for Tongue, hremorrhage from
Tooth socket, hremol'-
rhage from 97 Tourniquet 75
Transverse wo,und of abdomen
Two-handed 5ea't II3 161
Ulna .. , " fracture of.. .
Ulnar artery .. .
Unconsciousness
Upper limbs
Varicose veins
Veins
Venous blood " hremorrhage
Ventricles '"
Vertebra ...
Vertebrre... . ..
Vertebral column
Vertical wOlJnd of men ...
Vitriol, burn by '"
Voluntary muscles
\\'agon, to load or unload
'Vall, to cross with stretcher ... 'Yannlh, necessity for " to promote
Wind-pipe .. , 'Yoman's dress on fire
Wounds by poisoned weapons " . accompanied by artenal hremorrhage ... 'Younds accompanied by venous hremorrhage
\Vounds, hcerated 'Yri t
214 Fa!!e
102 1'55 83 26 51 121 Jbo 162 161 30 134 142 156 28 51 26 32 197 J7
Page 39 140 106 149 III 113
Stretchers,
23 45 149 54 10 7 III 98 113 65 I40 190 174 181 185 187 17 2 21 5
Pa!!e 169 166 153 ?)4 141 136 204 7 II/:) 17 134 3 1 70 30 82 30 56 162 97 30 60 159 97
Pa!!£! 28 54 88 128 26 94 70 72 93 70 23 25 23 II3 102 33 170 18 12 7 II8 10 5 106 76 94 78 28
Oarrlage Paid on all Orders In the United Klngd..... I .. ASHFORD" LITTER.
ttbe St. 30bn Blllbulance Bssociation.
GENERAL PRICE LIST.
A complete and reliable Ambulance Equipment is an actual necessity, and experience has proved that employers of labour and others interesteJ in the district readily subscribe for the purchase of such appliances. Collecting cards, stating the purposes for which subscriptions are requir ed , will be supplied to approved persons gratuitously on application to the Head Offi ce of the Association, where also any information with r egard to its work can be obtained.
All stores will be se nt carriage paid to any part of the United Kingdom. Returns may be sent carriage forward. If carriage is prepaid it will be allowed .
ewing t o flu ctuations in market prices it is impossible to guarantee that the qu otatio n s herein can be adher ed to.
Quotations will be furnished for Ambulance Carriages and other articles relating to Ambulance, Nursing and Hygiene, not mentioned in this list.
Orders and corre spond ence should be addre ssed to the St. John Ambulance Ass ociation, St. John's Gate, Clerkenwell, London, E . C.
Remiltances ShOlllJ be made payable to the St. John Ambulance Association, and crossed "London County and 'Vest. minster Bank , Lothbury."
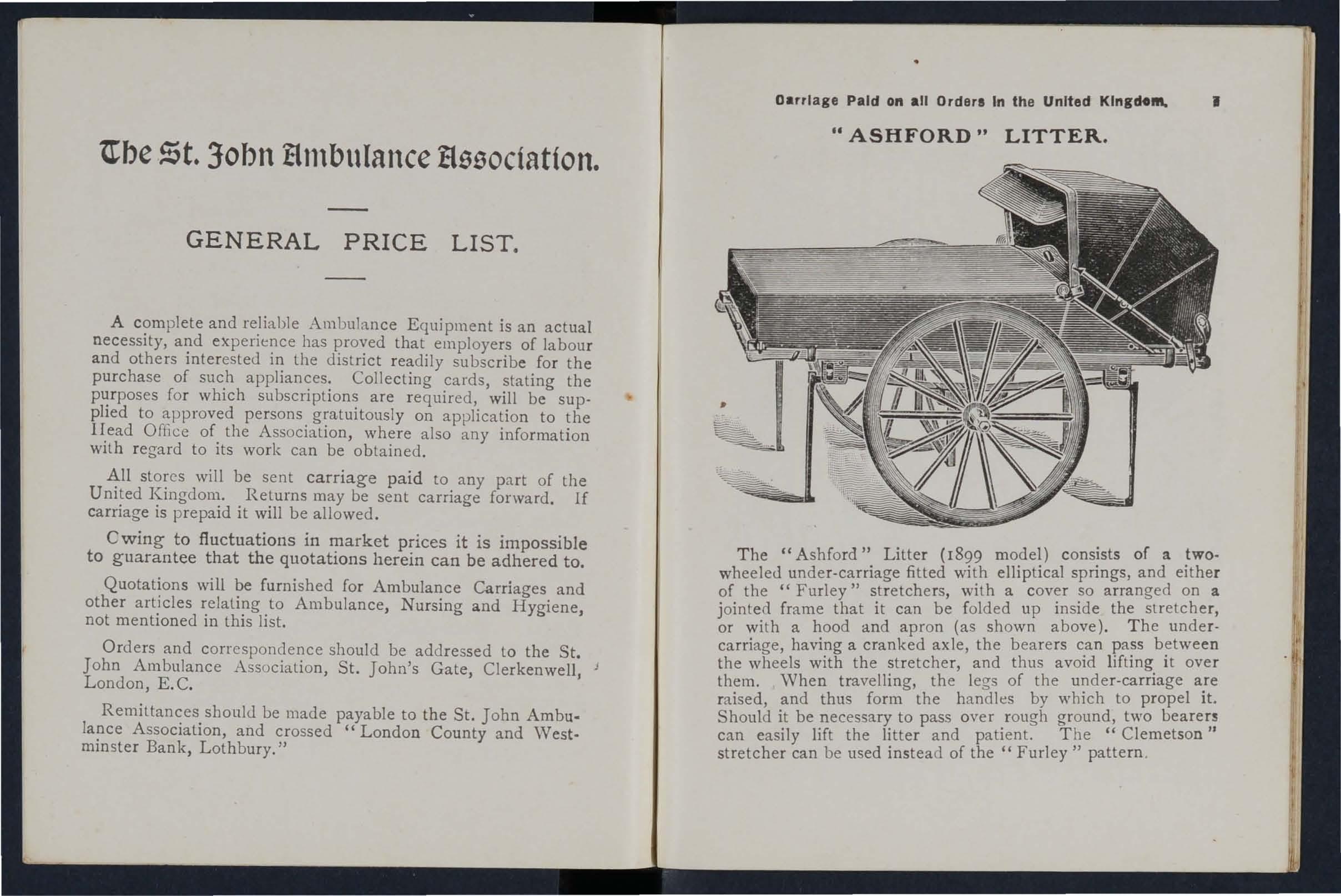
T he "Ashford" Litter (1899 model) consists of a two· wheeled under-carriage fitted with elliptical springs, and either of the "Furley" stretchers, with a cover so arranged on a jointed frame that it can be folded up inside the stretcher, or wi t h a hood and apron (as shown above) . T he undercarriage, having a cranked axle, the bearers c.an the wheels with the stretcher, and thus aVOId lIftmg It over them. When travelling, the legs of the unde r-carriage are raised, and thus form the handles by which to propel it. Should it be necessary to pass over rough ground, two bearers can easily lift the litter and patient. The" Clemetson " stretcher can be used instead of the" Furley " pattern .

PRICES OF THE IMPROVED ASHFORD LITTER, 1899 MODEL
With Iron Tyres to Wheels. IWith India RubberTyres to Wheels
-1-V\T;th--I- -Wit-h-1 With Hood and Cover. Hxod and Hood and Cover. Apron, as 3, ---------1 Apron. pron. Apron. illustrated.
Under-carriage (no Stretcher)
Litler complete with Ordinary Stretcher*
Dittowitb Telescopic handled Stretchert
DiLlo with Police Stretchert
with " Clemetson"
• Prices quoted for Litter with Ordinary Stretcher include \Vide Webbing Slings but no Chest
Strap. Leather, instead of Webbing Slings, 8s.extra : Chest Strap, IS. 6d. extra. If supplied :l without any Slings, 45. allowed. ;:;:
t Prices quoted for Litter with Telescopic-handled Stretcher include Wide 'Webbing Slings and Cbt!st Strap. Leather. instead of Webbing Slings, 8s. extra. If supplied without any Slings, ;:0:: 4S. allowed ; a nd if without Chest Strap, rs. 6d. allowed ;'
t Prices quoted for Litter with Police Stretcher include \Vide Webbing Slings and Leather tIQ Straps for securing a refractory patient. Leather, instead of Webbing Slings, 8s. extra. go Hood and Apron, cornplete (" Furley " pattern Stretcher) £2 10 0 3 Do. do. do. (" Clemetson" Stretcher) ...
Waterproof Sheet (washable) to be laid on the stretcher bed...
Cra! es (ret urnahle) ch rged 4S. 6cl. for each Liller.
[, s. d, [, s. d, ;:, s. d. [, s. d. l s. d. [, s d. "CI III
8 10 o 9 5 01 II 0 0111 15 0 112 10 0114 5 o c.:
II 2 6112 17 6 14 7 6116 2 o 6 :l II 10 011 3 5 o 14 15 0116 10 o 0 Q. 12 5 0114 0 o 15 10 01 1 7 5 o 5'
... 14 8 o 017 13 0 :;t - CD
Do.
Slretcher
c:
2 15 0
0 12 6
n n -. = !'!'.-it" >-l l'! ·"'n ..... ". .. '" _. "''' '" n 0 it n ..,,"_" • ,..-[g E;:ii'E; .. g. " ". ,, - n n -" n l'! -" --" ." ..... : = ". n --". " __ ,_, n "'go '" 9 t:l g 0- (")"- n ::E it "- g'';l _';j g '" " .. S "" Z ".. 0 '" t:l "- ::';;", - 11> c n- ••• '" : , 0 "Ogg. -"I'-g t' - '" :» n" __ .... oj S "'-- "iL ° oj 1: ° < • '" V" - 0 "-it" ,;j0ii' l'! • _0'." _ n __ O. . t! it g. "-11 • 2_ i;' • s·& ... @ 0· 8""
l::J 10 '0 _"""a. rr a. _. ri a. g, :: D c:r' n lit
0'
Carriage Paid on all Orders In the United Kingdom.

" REA-EDWARDS" LITTER, fitted with" tyred wheels, showing the "Clemetson Stretc er.
d t h h Is both cycle pattern Ball bearings are fiUe to e w ee I d th t the and wooden, and the d hflbs disturbwheels can be remove rom f' 1 made to raise ing
as an es, wId t the foot end whIle a or rollers arcl , p with a anrl comumed leg and lan e . d t the head
't' nd when lowere It IS of two POSI IOns, a I' d for this arrangevertical . The manipulation and ment are sImpllclty, ease an rap! 1
Carriage Paid on all Orders in the United Kingdom.
the facility afforded by the two fixed legs for raising the litter, if necessary, on to the pavement. The question of balance has been carefully studied, and the stretcher is shifted forward so that the middle of it is several inches in front of the axle, a perfect balance when the stretcher is loaded and in a horizontal position being thus obtained, and consequently there is no weight on the hands of the person propelling the litter.
Jfhe pneumatic tyred wheels are strongly recommended in cases where the small amount of care necessary to keep them inflated can be given, as the comfort to the patient and ease in propulsion are increased beyond all comparison with any litter yet produced. It will be noted that the prices are considerably lower than those of the "Ashford" Litter, and the following are given as examples, but owing to the vast number of combinations that can be made with the different stretchers and coverings, it is impossible within reasonable limits to set out quotations for the whole of them, but these may be calculated by adding together the prices of the under-carriage, stretcher selected, and hood and apron or cover, see pages 4 to 10.
SPECIMEN PRICES.
Under-carriage only, either with pneumatic tyred cycle wheels or solid rubber tyred wooden wheels, £10.
Litter complete with ordinary stretcher (no slings or chest strap) and hood and apron, as illustrated, £14 3s. 6d.
Ditto with Telescopic Handled Stretcher (with chest strap) and hood and apron, £14 115.
Ditto with " Clemetson " Stretcher and ventilated hood and af,ron, £15 I8s.
If with iron tyred wheels prices are £2 less.
Hand brake, which acts automatically when the litter is at rest, extra £1 las.
'''hen ordering please state which wheels are required.
carriage Paid on an Orders in the United Kingdom .

THE" CLEMETSON" STRETCHER.
STRETCHER, W ith back raised, also showing If CLEMETSON " extending legs.
On this stretcher the patient can be moved. as from 'be recumbent to the sitting position. There is no comphcated mechanism to get out of order, and the adjustment depends 'imply on the balance of the patient's body. The ",ill fit either the" Ashford" or the" Rea-Edwards UnderCarria2:e. Price £3 3s. ; with extending legs, £4 3s.
Hood and Apron, Ventilated, £2 I5s.
Carriage Paid on all Orelers in the Un i ted I(ingdom .
ADJUSTABLE LEGS FOR STRETCHERS.
Primarily these legs, which are ind ependent of and additional to the ordinary foot wheels, are intended to facilitate the carriage of a stretch er in a railway compartment, in which case two on one side would be lowered and adjusted by a tele scopic arrangement to the proper height, so that the foot wheels on one side would rest on the seat, and the adjustable legs on the other side would rest on the Boor. The four legs may be used to raise the stretcher as required. \Vhen not in use they are folded up immediately under the poles of the stretcher.
Price per set of [our, £1.
FIRST AID BOX.
To be carried below the axle of the" Rea-Edwards" Litter, from which it is easily detachable.
Contents :-Set of Splints, 12 Triangular Bandages, 12 Roller Bandages, 2 i lb. packets each Cotton \Vool and Boric Lint, Adhesive Plaster, Pair of Scissors, Knife, 2 oz. each Olive Oil, (. Tinct. Iodine B.P.C., Sal Volatile, and Spirits Ether Comp., Graduated Measure Glass, Kidneyshaped Dressing Basin, 6 Tampons for washing wounds, Tourniquet Pins, Safety Pins, Needles, Thread and Tape.
Price £2.
carriage paId on all Order s in the United K ing do m.
(I FURLEY " STRETCHERS WITH THE LATEST IMPROVEMENTS, 1899 MODELS .

TELESCOPIC HANDLED STRETCHER-OPEN.
ORDINARY STRETCHER- CLOSED.
The improvements in all patterns of the "Furley" Stretcher, 1899 Model, are numerous. The comfort to the patient is increased; the stretcher is stronger, more rigid, and lighter, it folds up more closely, and its handles are more comfortable to hold and afford greater protection to the hands of the bearers in passing through narrow doorways or passages. Should it be necessary to reduce the width of a loaded stretcher in order, for example, to carry it into a railway carriage, this can be done, either when it is resting on the ground or supported by the bearers, without trouble and without the slightest jar to the patient. Th e price of the stretchers is lowered. All minor points have heen most carefully considered, and the stretchers are confidently recommended as tho roughly efficient in eyery way.These stretchers are adapted for us e alone or as part of the " Ashford" or " Rea-Edwards" Litte r, and th e cover, hood anu apron, army rug, and waterproof sheet d escribed in this list are suilable [or us e with them.
Carriage Paid on all Orders in the United Kingdom.
"LOWMOOR. JACKET."
For use in mines, ships' holds, etc., to secure a patient on a stretcher (see illustration), which can then be placed in an gpright position. Price £1 5s.

'VATER BOTTLE.
Carriage Paid on all Orders in the United Kingdom. 12
Dressing Basin . kidney shaped, made of enamelled iron.
Price 2 s. 3d. LAMP.
Thi s is fitted with a socket, by which to fix it to a Litter, o r it can be conveniently carried hy hand, or attache d to a belt or the clothing.
Price complete, 58. 6d.
Copper tinned, with carrying strap.
Price 12S. bd.
Ambulance Station Plate. Enamelled hnn, 3s. 6d. each. Stretcher Depot Plate, Ellamelled Iron, 3s. 6d. each.
Carrying Sheet for carrying patients up and down stairs or otherwise ahout a honse. Des igned by the late J. C. Derham, ES1., Blackpool, and Mrs. Alfred Paine, Bedford. -r'he sheet is fitted with rope halldles and detachable bamboo poles, and may be placed on a stretcher without disturbing the patient. Price complete, 15s.
1I! C&I",lage Paid on all Orders in the United Kingdom.
REGULATION POUCH FITTINGS
for the St. John Ambulance Brigade, consisting of:-
I Triangular Bandage, sealed up in waxed paper.
2 Grey Calico R')ller Bandages (2 in. and I in.).
I Packet of Surgeon's Lint.
I Packet of Absorbent Cotton Wool.
I Pair Scissors.
6 Safety Pins.
I Box of 3 Phials" Vaporole JJ Iodine Tincture
I Piece of Strong Cane, for tightening improvised Tourniquets.
List Price, 2S. 8d. each; 6 doz. or more, 2S. 7d. each.
Box of 3 Phials" Vaporole JJ Iodine Tincture, packed for post, each lod.; per doz., 8s. 6d.
SAFETY PINS.
All fasten or unfasten on either side. s. d.

Pocket Cork Line and Drag, with 80 feet of line, in case; for recov ering a drowning person from the water. Pric e complete, with instructions for use, 6s. cd.
Pocket Reel and Ice Line for use in ice accidents, with 80 feet of line in case. Price complete, with instructions for lise, 6s. 6d.
Carriage Paid on all Orders in the Un ited l<ingdoN.
LARGE HAMPER FOR AMBULANCE
STATION AND RAILWAY PURPOSES.
F or contents see nex t page.
per 3 doz. 0 6 " "S 603 ... ,,0 8 Duchess Duplex, NO.2... per doz. 0 2 " " Assorted 0 3 Special Blanket Safety Pins, 3 in. 0 " " " in. 6
Facile No. S 600 or S 602
Carriage Paid on all Orders in the United Kingdom. THE IIAi\[PER CONTAlNS
I Set of Cane Splints.
I St. John Tourniquet.
Ih. Carbolic )
lb. Boric Lint
COttOIl Wool ... l In Tin ... J Cases.
I Ron Adhesive Plaster.
20 Roller Bandages, assorted.
I doz. Triangular Bandages.
3 pieces Tape.
4 oz. Sal Volatile.
4 oz. Bicarbonate of Soda.
I Dredger for Borio:: .Acid.
lb. Powdered Boric Acid .
8 oz. Tincture Iodine.
I pair Pean's Forceps.
I pai r Scissors.
1 Knife.
12 Surgeon's Needles.

I packet each Safety and Plain Pins.
-1 oz. Carbolised Chinese T"ist.
oz. Silkworm Gut.
I reel each Black and vvni te Sewing Thread.
I Kidney-shaped Basin.
I Stopper Loosener.
1 Graduated Measure.
r cake 20 per cent. Car bolic Soap.
I 1\ail Brush.
2 Empty 8 oz. Bottles.
2 4 oz. "
3 Saucers for applying Tinclure of Iodine.
3 Came l Hair Brushes apply ing Tincture Iodine. for of Price complete, £4
".rrlage Paid on all Orders in th e United Kingdom 16 SMALL AMBULANCE HAMPER.
With waterproof cover and strap, for use in faclories, collieries, stations, and large works, as well as for parochial and domes tic use.
CCNTAL'ING
S et Splin ts. I St. John Tourniquet. 1 Tampons, washing wounds. 2 Packets Lint. 4 Roller Ba ndages (Wide and narrow). 4 Tri angular Bandages.
Cotton \\'001 ... ... I In Tin Ca.ses. Bori c Wool... ... r Spool of Adhesive Plaster. . Knife, Sc issors. Thread, Tape, N eedles, and Pms. \\'eiO'ht complete, Ibs.
Length, 1ft. 6 in. Depth, 5 in. Width, 7 in. Price £r IlS. 6d.
Carriage Paid on all Orders In the United Kingdom.
SURGICAL HAVERSAC.

811n1a•• Pa14 .. all Ordere In tIN Unltell Klllidotft. II
!\{PROVED PATTERN, fitted with a tin, so arranged that any article can be taken out without disturbing the rest f)f th e contents.
Contents: I Set of Splints, 6 Triangular Bandages, 6 Roller Bandages (wide and narrow), Cotton "\vool, Boric Lint, in tin cases, I Roll Adhesive Plaster, I Pair Scissors, I Knife, 2 oz. Boric Acid Powder, 2 oz. Tinct. Iodine, 2 oz. Sal Volatile, I Dredger for Boric Acid, I Graduated Glass Measure, I St. John Tourniquet, Pins, Needles, Thread, 3 Saucers and 3 Camel Hair Brushes (for applying Tincture of Iodine).
Price £1 I IS. 6d. " White Ration Haversacs , 2S. each.
FIRST AID COMPRESSED KIT.
The box is made of wood covered with damp -r uJltin, material, and is fitted with a lock and key. It contain. a number of praotical ambulance appliances arranged so tbl.l any article can be withdrawn or replaced without disturbi ng th e remainder. Being fitted with a handle it is portable, and the lid, when let down, can be used as a table. All bandages and dressings are compressed. Size-LeT'gth, 16i in. ; width, d ill.J beight, 8 in., without handle.
Contents: Triangular Bandages, 6 Roller Bandages, Flnt AId Dressings, 6 Small Packets of Cotton Wool, 6 Small Packets of Borio LintL
I St. John I .Measure I tin Lox con taining a Roll ot Plaster, Boric Lint Patches, Scissors and Pins, I tray containing 3 Bottles (Sal Volatile, Tincture of Iodine and Boric Acid Powder), and a Dredge: for Boric Acid, I set of imI,>roved Splints, with angle piece, 8 Splint Straps (sufficient for a fractured thigh), 2 Sa ucers and 3 Camel Hair Bru..n'!s (10! applying Tincture of Iodine).
Price £1 I IS. 6d.
Carriage Paid on all Orders in lh o Pn-led King-r'r m

FIRST RID eeJMPRNION.
m.RESSINGS AND BANDAGES COMPRESSED).
st jOIJll Hsscclilllon, !Jrice Is. 6d.
SL jo/}n's 6i11e, I 0d - fondon. C.C. By Post s. () .
SIze, by 3a by Ii inches. Suitable for the pocket.
CONTENTS.
1. Triangular Bandage . 2. First Aid Dressing. 3. Cotton Wool. 4. Two Splint Straps. 5. Adhesive Plaster. 6. Permanganate of Potash . 7. Lan()line. 8. Boric Linl Patches. 9. Safety and Plain Pins.
Price , each IS. 6d. Packed for Post Is. 8d. Per doz . 17s. 6j.
SEP ARA TE ARTICLES.
No. No.
I 4d. each or 3/9 pe r doz. 6 ld. per b ox or lOd. per doz.
2 2d. " 2/0 7 1 per tin or I/4 ..
3 Jd. " Jod. ,,8 Id_ pe r packet or lOd. -,.,.-
4 2d. per strap or 1/9" " 9 Id." " lod."
5 Id. per box or IOd. " "
Not less than one dozen supplied at dozen pri ces.
CarrlC'ge Paid on all Orders in the United Kingdom.
FIRST AID BOX FOR USE IN MINES.
CONTENTS.
Set of Improved \Vooden Splints; Jou.} l'ourniquet ; ("'"non Wool; Lint J 12 R.)ller BanJao:e-, ... ; 6 Triangu lar ll'!lldages in waxed paper; Adhesive Plaster; Pair Scis<ors; Spatula , Graduated J\1easure; 2 oz. Sal Volatile; 8 oz. Boric Acid Powder; 8 oz. Tincl. Iodine; Pins; Safety Pins; Dredger for Boric Acid Powder; 3 ",weers an I 3 Camel Hair Brushes (for applying Tinct. 0 1 Iodine). PRICE COMPLETIt, £2 lOS.
This First Aid Equipment is also very suitable for use in factories and other large works , and can be fitted for carrying on the" Ashford " Litter.
••
Carriage Paid on all Orders In the United Kingdom.
SMALL FI RS T AI D OUTFIT.
'When closed can be carried by a Strap-handle. by 7£ by inches.

CoNTENTS: 2 Triangular Bandages, I St. John Tourniquet. 8 Splint
Straps (for securing Splints in lieu of Bandages), 2 OL Cotton Wool, I PAir of Scissors, 4 I-in. Roller Bandages, 2 2-in. Roller Bandages, I S-o%. Bottle Sal Volatile, I 2'OZ. Bottle Tincture Iodine, B.P.c.. 2 oz. PlaiD Lint, I S-OZ. Measure Glass, 2 China Saucers, and 2 Camel Hair Brushes to be 1ISCd when applying Tincture of Iodine.
Price:
Wooden Box, covered with Damp Resisting Material, ISS.
Stout Cardboard Box, Cloth Covered, lOS. 6d.
Darrlqe Paid on all Ordere In the United Kingdom.
The St. John Tourniquet, as supplied to the Admiralty, with directions for use ... ...
(Special quotations for large quantities.)
Splints, 'Wooden, per 2/6 ; Cane .. , ... per set
Greatly improved Wooden Splints, with grooved joints and angle piece, sLrongly recommended ...
Tow, for splint padding ... . .. per lb.
First Field Dressing (Army Pattern)
J aconette, 44 inches wiJe per yard
Tow, Carbolized or Styptic ... per lb.
First Aid Dressing, consisting of a small compressed packet of boric lint, a compressed roller bandage, and a safety pin
Dredger, containing boric acid powder
Knife with strong blade ... each IS. ; per doz. 105. 6d.
Pair of Scissors ... each IS. ; per doz. IDS. 6d.
Small Bottles strong Smelling Salts, per doz., 55. 6d.
Splint Straps, Webbing, and suitable Buckles. Per set of 12 yards of strong 2-inch 'Webbing and IS Buckles, 3s.
These make very compact Straps for in the Pouch.
The Webbing should be cut to meet local reqUlrements.
Buckles only, IS. 3d. per dozen.
Webbing only, IS. 9d. per dozen yards.
It is unnecessary to sew the Buckles. The spikes should. be passed through the webhing, and the short end of the webbing should lie outwards.
Measure
So d. o 9 7 6 4 6 o 6 o 9 2 3 o 9 o 2 4 o 5
Glass ...
23 Carriage Paid on all Orders in the UAiled Kingdom.
PLASTERS.
Leicester Adhesive Plaster on CamLric, in tins of i yard, 6 inches wide 6d.
The Leicester Adhesive
RiLbons, in tin boxes, 6 yards long.

National Rubber Adhesive Plaster (Antiseptic) on spools.
5 yds. 10 yds. inch wide 9d. IS. ad. IS. ad. IS. 6d.
2 " " IS. 9d. 2S. 3d . ! inch wide 1 inch wide
Ditto in card box, in. wide, i yd5. long ... tin I" it II " " i it 2 5 5
COURT PLASTER, TRICOLOR.
La.rge Size, 9d. ; Medium, 5d. ; Small, 3d.
Carriage Paid <>n all Orders in the United Kingdom. 24
NURSES' WALLETS.
ORDINARY PADLOCK SHAPE.
"Without instruments, 4S. 61.
Fitted complete, conta1l1ing Spring
Dressing Forceps, Spatula, Probe, 2 pairs Scissors (round and sbarp pointed), Clinical Thennometer, and Knife.
Price 12S. 6c1.
ST. JOHN'S PATTERN, as illustrated, but improved hy the addition of Oaps to protect the instruments.
\Vithout instruments, 8s. 6d.
Fitted complete, containing Spring
Dressing Forceps, Artery Forceps (also useful for dressing), Spatula, Probe, Director with Ear Scoop, 2 pairs Scissor, (round and sharp pointed), Clinical Thermometer (minute, round), Knife, Pencil, and Safety Pins.
Price £1 35
6d.
Id. 3d• 3d• 6d. 9Ci
8d.
Car r iage Paid on all Orders in the United Kingdom.
ROLLER BANDAGES.
(6 yards long. )
Grey Superior Bes t qual ity, Superior
Grey Open W hite White, wit h Calico. ·Wove. Ope n Woven White Ope n Wove Per \Vove. Edges . Compressed. doz.

ROLLER BANDAGES in Assortment.
Packed in neat Cardboard Box.
R ECOMMENDED FOR CLASS PRACTICE.
Two 3 in . ; t wo in . ; one I in.; each 6 ya rd s long .
Grey Cali co " " fast edges
Best quali ty wh ite , with woven edges
Plain Trian gu la r Bandages, eac h (S pec ial qu otations for large q uantities.)
Ditto Compressed (thinn e r q uali ty), ea ch 4d. ; per doz. 3s. 9d .
Illustrated Tria ngular Ba nd ages (afte r E sma rch ) show in g
25 applic ations of the Triang ular Bandage, wit h printed ins truct ions ... each " pe r doz. s. d.
Carriage Paid on all Orders In the United Kingdom.
ROLLER BANDAGE MACHINE.
Designed by
D r. A. C. T unstall.
Pdce 2S. 6d .
Forceps, d ressing , full size or small as desired, IS. 6d. ; Pean's Artery, 5 in., 4S. 6d. '. '
Scissors round- point ed blades, I S. ; small round -pointe d b lad es,' or 5 in., IS. 6d .; curved blades, I S. 6d . ; sharp - poi nted blades, for delIcate work, 3s. curved blad es, 3s.
Spatula, 9d . Probe, 6d. Director, with Ear Scoop, IS. 9d. Knife, very thin , i vory handle, two b lades, I e;. 9d.; single blade , IS.
Nursing Chart, d esigned by M iss Inderwick, each .
Temperature Chart, i'd. each.
CLINICAL THERMOMETERS.
Round.-Ordinary, IS.; minu te , Is. 3d. ; half-minute, IS. 6d .
Flat.-S t rongly recomm enrl ed, as they .will not roll nary IS. 6d.· minu te 2S. 3d .; half-mmu te, 3s. ; (SpeCia lly and 'reserved' for the A ssociation ), with very ope n scale.
d. d. d
d.
s. 5. 5. d
in. I 0 0 9 0 2 3 3 5 3 2 9 6 2 in. 9 3 6 3 3 9 3 g 0 3 9 2 3 3 in . 2 9 2 0 2 6 4 9 2 9 4 in. 3 6 3 6 6 0 3 9
in. S 3
6
.
5.
. I
6
4
s. d. I 0 I 6 6
4 6
o 6
Carriage Paid on all Orders in the United Kingdom.
CLINICAL THERMOMETERS-(ctmtinmd}.
With Magnifying Lens. Price, ordinary, IS. 6d.; minute, IS. 9d. ; balf-minute, 25. 3d.
N .B_.-Minute and half-minute instruments will only register in the time stated under favourable circumstance s. No liability is taken for breakage oj Thermometers in tramit.
BATH THERMOMETERS.
1'0 Dr. Forbes' specification. Japanned with zinc scale, 2S. 3d. ; Clinical Thermometer size, in case, IS. 6d.
No liability is taken for breakage of Thermometers in transit.
COTTON WOOL.
Plain, I oz., 2d. ; 2 ·oz., 3d. ; 4 oz., 4d. ; lb., 7d.; I lb., IS.;
IImall packet (Compressed), Id.
Medicated, Boracic, ! lb., 6d.; I lb., IS. 6d.; Carbolic, per lb., IS. 8d.; per lb., IS. 6d.; Double Cyanide, per lb., 2S. 6d.
LINT.
Plain, I oz., 2c1. ; 2 oz., 3d. ; 4 oz., 6d. ; ! lb., Iod. ; I lb. IS. 6d.
Boracic, 4 oz" 6d. ; I lb., IS. 6d. ; square ff"lot packet, 2d. I small packet (Compressed), Id.
GAUZES.
These are supplied in 6 yard lengths, width about 36 inches.
Unmedicated white Alembroth Double Cyanide
Boracic
Packets of Cyanide doz.,2s. 8d. Cauze (I yd.
GAUZE TISSUE.
Carriage Paid on all Orders in the United Kingdom.
TEXT BOOKS. 13c.
"First Aid to the Injured." By James Cantlie, M.B., F. R. C S. The authori ed Text Book of the First Aid Course. IS.
,. A Catechism of First Aid." Compiled from Dr. Cantlie's Manual. By J. M. Carvell, 1\1. R .C S., L.S.A. 6d.
•• Problems in First A companion to the Text Book of the St. John Ambulance Association "First Aid to the Injured." By L. \1. F. Christian, M.B., C :'1., Ed., and \Y. R. Edwards, A.CA. 6J.
"Hints and Helps for Home Nursing and Hygie .... -·" By E. MacDowell Cosgrave, :fILD., illustrated, with chat r on th e application of the roller bandage, by Sir R. J. Colile, D. 'The authorised Text Book for the Nursing Course. IS.
I< A Catechism of Home Nursing" (based on Dr. Cosgrave's Text Book). By the late J. Brown, L. R.C.P., L.R.C.S., :lIlcl J. M. Carvell, :fILR.C.S., L.S.A. 6d.
"Home Hygiene." By John F. J. Sykes, D.Sc. (Public Ilealth), M.D., &c. Illustrated. The authorised Text Book for the Home Hygiene Course.. IS.

per
s. d. per length 0 10 a compressed),
A layer of absorbent cotton wool belween two sheets of £"auze, good quality, per lb., IS. 6d.
"A Catechism of Home Hygiene" (based on Dr. Sykes' Text Book). By J. :fit Can'ell, ..H.I<. C S., L.S.A. 6d.
" Questions and Answers upon Ambulance Work." By John ",V. Martin, M.D., and John Martin, F.R.C.S. , Ed. IS.
"Questions and Answers upon Nursing." By John ",V. M. D. IS. 6d. .
.. First Aid to the Injured" (Six Ambulance Lectures). By Professor Fre ,lerich Esnurch. Tr3.nslated f[GHu the Gernun by ILR.H. Princess Christian. 2S. -
B3.ndaging and Surgical Dressing." By Walter Pye, F.R.C.S. 2S.
2 2
lanlaal Paid 011 all Order.... till United Klllllfl"
TEXT BOOKS.
·'To · Restore the Apparently Drowned," printed in large Type with two Diagrams. 2d.
Dr. G: .H. Darwin's" Aids," being a card to hang.p glvlOg treatment of vanous accidents. 2d.; packed for post, 4d.
If Manual of Drill and Camping for the St. John Ambulance Brigade." Sd.
"Manual for St. John Voluntary Aid Detachments." By Lieut.-Col. G. E. Twiss, R.A.M.C. (Retired Pay). 6d.
I. How to Act when Clothing takes Fire." By J. E. H. Mackinlay, M.R.C.S. 2d.
If First Aid Principles." Cards of concise directions for waistcoat pocket, each; 4d. per doz. Special quotationsfor large quantities.
., Specimen Examination Papers, First Aid, Nursing and Hygiene Courses." 3d.
Smal.l Anat?mical Showing the human skeleton, mam artenes, and pOInts where pressure should be applied to arrest bleeding. 2d.
Directions as. to the Restoration of Persons suffering : :Crom Electnc Shock. Large print, poster size. 3d. each; or 2S. 6d. per dozen.
General Notes on First Aid to be Rendered in Cases of Poisoning. By Milnes Hey, M.A., M.R.C.S., L.R.C.P. 2d.
Notes on Military Sanitation. By Lieut.-Col. II. P. G. Elkington, R.A.M.C. 6d.
II Eme:gepcy B.ook," for instantaneons reference, gIvmg conCIse instructIOns; to hang on wall. Size about one foot square. 2S. 6d. ; packed for pos t, 2S. 8d.

.arrlage Paid 0" all Orders In the United Kingdom. TEXT BOOKS ,
Aids to Memory for First Aid Students. Revised to date. Additional Illustrations. By L. M. Frank Christian, M.B., C.M., Edin. 6d.
General ' Regulations for the St. John Ambulance Brigade, 1913. 3d .
Rules for Corps and Divisions, St. John Ambulance Brigade. 2d.
Registers. Class Attendance, 2S. 6d. Certificates, 4S. 6<1. Case Report, IS.
St. John Ambulance Brigade Cash Book, Minute Boole and Occurrence Book. Set of three, 7s. 6d. Receipt Book, 6d.
Large Physiological Diagrams (New Series). For Lecturers' use. The Human Skeleton, showing the main arteries and pressure points. The General Anatomy of the Body. The Systemic and Pulmonary Circulati on of the Blood. Section Through Middle Line of Head and Neck, showing the T ongue in two positions in relation to the Trachea, and Schafer's method of Artificial Respiration (Expiration and Inspiration). Dislocations. Price, per set of five 15s. These may be hired for a course of "First Aid" lectures, given under the au spices of the Association, for a fee of 5s., or with the addition of Splints, Tourniquet, and 30 plain Triangular Bandages, for a fee of lOS.
90xe!-of Stationery for the use of Class Secrecaries and others connected with the Association, containing twelve sheets of high -class pape r, suitably headed, and twelve envelopes b earing the d evice of the A socia tion. 6d. Twice that qua ntity, IS.
carriage Paid on all Orders in the United Kingdom.

Arm Badges, with the device, iss ued under the authority of the Central Executive Committee, having he en fir t approved by II. R.IL the Granel Prior as the sole orficial and recognised Badge of the Associalion and Brigade . N. B. T/tis des !!!,,, is prolected.
SERIES A.-For the use of individual certificated pupilsNo.
I. In German Silver,
3.
4.
7.
9. In Cloth
10. In Cl ()th
11. In C lolh and Cotton
12. Small Celluloid Badge, for bulton h ole or brooch
13. White Satin Armlet, with woven Badge 21" 0 N.B.-These Badges are I/ot to I'e won, as de co rations .
SERIES B.-For members o f the St. J oh n Ambulance Brigade, not wearing uniform , having nam.e of th e .C;orps or Division annexed on a label, only Issued 10 quantlLlesNo. 15 . In German Silver, 2 ins. in diameter, firs.t doz., £1; su bsequen t d ozs., 1 2S.
16. In Electro PlaLe, 2" firsl doz., £ 1 125. ; su bseql1ent dozs., £ 1 45.
17. In Clothanel Silk, 2 per doz., 12S.
18. InClothandSilver,2 " per doz ., £1 I?S.
19. The Brigade Bullon Badge, eac h, u.; WIth Brooch Pin, each 1/3 H.B.-These a Je not to h wor,. as de coratil1fU.
3 1
s. d.
Large Size 2 in. dia. 0 7 :'Illall Size dilLO Ii 0 6
Small Size for bulton hole 0 6
In Electro Plate , Large Size 2 0
Small Size ditto 11 0 9
Small Size for butlon hole 0 9
5·
6.
button
0
brooch 3
In Enamel for
hole
8. "
Silk It 0 9
ancl
Sil ver 2 2 0
anJ
1'1 0 6
0 2
3J Carriage Paid on all Orders In the United Kingdom.
S.J.A.B. UNIFORM BADGES, etc.
Ambulance Divisions. Black Khaki Jniform. Uniform.
Officers.
Cap Badge (Reg. No. lOI) ..•
Collar Badges ( " 103) per pair
Pouch Badge ( " 3,657) ... Sergeants, Corporals and Privates.
Cap Badge (Reg. No. 102)
Collar Badges ( 104) per pair
Overcoat Badge ( " 1,582) ...
, Shoulder Titles, S.J.A.B., with numeral, per pair
Shoulder Slraps, filted with title and numeral ... per pair
Bugler's Badge ... 45. Bugler 's Cord Div. Secretary and Sergeant's Badge .. .
Drumm Badge ...
Hon. Surgeon's Crosses (pattern B) per pair
Medallion Badge (pallern D) ... ...
Nursing Badge (pattern E)
Reserve Badge (all ran ks) ... per pair
Signaller's Badge Signaller, IS. ; Instructor
Superintendent's Slars (pattern A) per pair
Belt Furniture ... per set
Bandsman's Wings per pair
Whistle and Chain . ..
White per packet yds.,enough for 3 paIrS of trousers (pkts. can not be broken)
Lace, per yard, Silver, lOS. ; Black
ButtOi1S{ NO. I (large) ... per doz. (White No.2 (medium) ...
MetaJ\ NO.3 (small, for caps)
DItto . 4 (large)...
(Elec tro 5 (medium)
Plate) LNo. 6 (small, for cap , )

.5.
Women's Detachments.
s. d.
d. o 8
8 I 3 0 2 6
0
... .. .
...
. ... . ..
..
0 6 0 lOl 0 6 0 8 I 5 3 0 0 5 0 0 '5 o I o 3 o 3 3 0 o 6 I 6 2 6 2 0 2 0 0 6 0 4 0 3 3 0 6 6 0 8 0 o 10 7 0 8 o 8 I 10 0 9 0 6 0 4l Carriage
Lady Officers. . s. d. s. d. Lady District Supt., Arm, 4S. 9d. ; Cloak 5 6 Lady Corps Supt., Arm, 4S. 3d. ; Cloak 5 0 Ltdy Divisional Supt., Arm,3s. 9<1.; Cloak 4 6 Nursing Officer, Arm, 3s. 3d. ; Cloak... 4 0 White Box Clolh Backs, for Badges per pair 0 3 Nursing Sisters. Ann Badge (Reg. NO.3,522) 2 0 " Cloak Badge ( " 3,521) 2 3 District Numeral for Nursing Divisions single 0 3 double 0 5 Black Silk Armlet for Arm Badge, for all ranks 0 4 Hat Badge (Reg. No. 20) I 0 Sh')uld er Titles with Numeral per pair 0 8 Pin Cushion Badge 0 3 Buttons, per doz., large, IS.; Small... 0 9
John
Cap Badge 0 6 0 8 Officer3' Stars per pair 4 0 8 Belt Furniture .. , per set 6 I 10 Buttons {NO. 7 (Iacgei per doz. 0 6 0 9 (White No. 8 (medium) 0 4 0 6 Metal) No. 9 (small, for caps) " 0 3 0 Ditto {NO, lO (large) 3 0 ( Electro No. I I (medium ) " 6 Plate) No. 12 (small, for caps) 6
Cloak Badge (Commandant) ... 2 6 " ,,(Other Rank s) ... 0 6 Hat " (Reg. No. 14) .. . [ 0 Shoulder Titles ... per pair 0 6 Buttons, per doz., large, IS.; Small 0
Paid on all Orders In the United Kingdom. 34 Nursing Divisions.
St.
Voluntary Aid Detachments. Men's Detachments.
II ......... _ aH OrdeTl tn the United Kingdom. ELBCTROTYPES. 8 No. I A. No. 2 A. No. 3 A. 8
Ube Grftntl of «me 41rOer of tbe 1)osptral of St. Sobn of 3erusalem In .EnglanD.
0 ."..,U1ft. tf'EPART'tUNY
Ube30bn Beeo.clntton. St. l\m()\Ilnllce No. I AH.

Ube Granb I)rtor\1 of trbe iSlrber of tbe 1I;)091>Itai of St. Sobn of 3erusalem In EnglanD.
DEPARTMENT Ube Sf. Job" Bmbulance 18rigai)c. No. I BIT.
Paid on all Orders In the United Kingdom·
Cards, TickeLs, &c.
For Note Paper, Small Circulars, &c.
For QuarLo and Fools· cap Letter·paper,
PrinLs of the above ElecLrotypes (I to 3) Series A and B, aml (1) Series All and BE, appear on page 35· '0. 4A is shown on page 31. The diameter of SA al1Ll SB is inches.
No. I B. No.2 B. N O. 3 B. 8
N o 1. 2. 3· 4· 5· Carriage
ELECTROTYPES
AMBULANCE DEVICE. For A sociation use. For Brigade use. Ser ies Series Series Series A. AH.. ll. llH . s. d . s. d. 5. d. s. d.
3 3 I 3 I 3
-. 3 -. I 3 .) .)
Cir-
&c. 3 7 3 I 7 ... For Small PosLers 6 For Large Posters 9 9 CompleLe Series 6 0 3 9 4 9 3 9
AMBULANce
OF THE ST. JOHN
For
culars,
£ s. d. Flags bearing Association cleyice-12 feet by 6 feet 7 6 6 5 feet by 3 feet o 12 " " " Brigade I) o 12 6 " " "
]7 aanla,1 Paid 0.. all Order. In the United Kingdom.
SW AGGER STICKS
for the use of Officers and Members of the St. John Ambulance Brigade.
Ebonised Canes, German Silver Mount. bearina the Brigade Device.
PRICK IS. EACH.
Officers' Special Canes, with SilveJ Mounts.
PRICE 75. EACH.

(For General Index see pages 208'215).
Aml»lllance Hampers " Station Plate
Bandage Rolling Machine Bandages
Basin, Dressing Bearer'. Dressing Belt and Pouch Books... ... Bottles (Water) Button5 Carrying
(Rea·Edwards) Lowmoor Jack et l\'l easure Glass... l\Iinute Book ... Nurses' \Vallets
Nursing Charts
Occurrence Book Pillow ... Plasters.. ... Pouch Fittings
Receipt Book Registers ... ... Roller Bandage Machine
(Stretcher)
BEARER'S DRESSING CASE.
PRICR 125. 6d. All Orders tor the foregoing Stores should be rlvea te til. Local Secretary, or sent direct to
n. St. John Ambulance Association, St. John's Gate, Clerkenwell, London, S.a.
12 Drowning Tackle 13 Ii: lectrotypes ... ... 35, 36 I<:mergency Book 29 Fir,t Aid Box .. . ... 8,20,21 " Compan ion .. 1q " "Compressed Kit ]8 First Field Dressings... 22 /Iag<; 36 [to rceps 26 (;auze5 ... 27 Gauze Tissue... ... 27 liampers (Ambulance) 14 t o 16 I J a versacs
17
J lood and Apron for Litler ... 3 Instrum ents (various) 26 ] aconelte... 22 Knife 22, 26
Lace for caps, &c. 33 Lamp
27
(Ashford) 3
." ... 7 lo 10 .. Adjustable for Swagger Stick ... Temperature Chart Text Books ... Thermometers ... Tourniquet ... Tow (carbol ized) " (plain)
Unirorm Sundries
Unirorms .. . \Vater Bottles W aterproof Sheet
and Chain
INDEX TO PRICE LIST.
••• ••. ...
... ...
Sheet Cash Book ... PAGR I{ to ]6 12 31 to 34 26 25 13 37 33 28 to 30 31 12 Cotton Wool... . . ." 30 29 Cove r for Stre tch er 01 J illa Diagrams, Large 30
Sma ll... 29 Dredger (B ol ic Acid) Dressing Basin
..
"
...
...
Li nt ... ...
Litter
Litter
!'AGK 4 to 6 30 TO
••
29 13 22, 26
Splint
"
.. . Splints... ... .. . Stationery... Stretcher
t Plate ]0 2' 22 22 30
Rug
Rules for Corps or Divisions St. John Ambulance Brigade Safety Pins
Scissors .., Slings
Smelling Salts ...
Padding
Straps
Depo
Stretchers
37 26 28 to 30 26, 27 22 33 ..·39,4" II 3 33 33 21
Whistle
Whit" Piping ... W oo l (Cotton) ...
39

Contractors ' L ist. Carriage out of London Extra.
PRICE LIST.
UNIFORMS FOR AMBU LANCE UNITS OF T H E S
.J.A .B .
These may be obtained from HAZEL & Co. (sole prop rie tor, D. Hazel; for many years associated with the late firm of Hebbert & Co., Ltd., as Director), Clothing and Equipment
Manufacturers, 65. East Road, City Road, London, E. C. ; and at 6, York Place, Leeds; 69, Piccadilly, Manchester; and 84, Miller Street, Glasgow. Telephone: 5678 London Wall.
Telegrams: "Hazelism, London." vVhere two pric!!s are given for an article they are for first and second qualities.
A 11 Badges, and carriagt outside London area, extra. Measurtments to be suppbed free of charge.
CORPS SURGEON AND DIVISIONAL SURGEON.
Tunic, Superfine Black Cloth ...
Trousers, Superfine Black Doeskin (if Silver Lace Stripe, extra) ...
Cross Belt and Pouch, Plain, 20/-; Silver
Embroidered
Great Coat, Grey Cloth, ..
Cap-Corps Surgeon : " Divisional Surgeon
DISTRICT SUPERIN 'llCNDENTS
AND CORPS OFFICERS,
Tunic, Superfine Black Clolh ' ..
Patrol Jack el , Black Cloth
Trousers, Superfine Black Doeskin
Cross Belt and Pouch
Gloves, 4/6; Leggings, 8/6
Great Coat, Grey Cloth
Cap-District Superintendent
Corps Officer
Oontractors ' List. Carriage Paid on all Drapery Coods.
DIVISIONAL SUPERINTENDENTS AND AMBULANCE OFFICERS.
Patrol Jacket, Superfine Black Cloth
Trousers, Superfine Black Doeskin
Cross Belt and Pouch ...
Gloves, 4/6; Leggings, 8/6
Great Coat, Grey Cloth '"
Fatigue Jacket, Black Vicuna Serge ... " Trousers, Black Vicuna Serge
Cap-Divisional Superintendent £1 4 0 and Ambulance Officer 0 15 6
FIRST CLASS SERGEANTS.
Patrol Jacket, Superfine Black Cloth ...
Chenons, Four Bars, Silver ...
Trouse rs, Superfine Black Doeskin
Cross Belt and Pouch '" ... ... ... '"
Cap, 2/9 ; Gloves, Buckskin, 4/6; Gloves, Cotton, 8d.
Leggings, I3la ck or Brown Leather ... ... ...
'Water Boltle and Carrier
Haversack, White Duck ...
Great Coat, Dark Grey Melton
SERGEANTS, CORPORALS AND PRIVATES.
Patrol Jacket, Black Tartan
Chevrons, Silver, ..
Trousers, Black Tartan ... ...
Waist Belt and Pouch. Brown Leather
Cap, 2/9; Gloves, Cotton, 8d.
Leggings, Rlack Leather ... ... ,.. ...
Water Bottle and Carrier, 3/9; Haversack, White Duck
Great Coat, Dark Grey Melton ... 16/- and
DRAB SERGE UNIFORMS.
Jacket, Drab Mixture Serge
Trousers" "
Cap " "
Great Coat, Drab Melton 16/6 and
. . Gloves £, s. d. 3 15 0 2 6 3 7 6 046 3 7 6
£ r 17 6 anJ 6 0
I 9 0 a 17 0
3 15 a 2 10 a 126 o 13 6
...
,
..
£1 12 6 and I 10 0 tJ 3 7 I o 18 6 a o
...
per Bar
£, s, d, 266 2 6 o 13 6 3 7 6 I 15 0 o 16 0 o 14 0 0 9 0 18 6 0 3 4 o 19 6 o 10 6 0 4 3 0 3 9 a I 6 0 16 0 OIl 0 o 0 10 096 066 043 016 o 14 0 09 9 08 0 02 0 o 19 6

ST. JOHN Rf\B ULRNCE BRIORD E.
UNIFORMS FOR NURSING UNITS.
THESE GOODS MAY BE OBfAINED FR.O )lMessrs. E. & R. GARROULD,
ISO to 162, EDGW ARE RD., LONDON, W.
CLOAK (Badg e extra) 19/ 1I, 25 / 6, 29/ 6
B {Nursing Sister's 9/6 ONNET " Officer's 10/6
D {Nursing Sister's Dress Length 3/7 RESS " Officer's" ,,3/1 I
{ 2! in., 5id. each; 5/6 doz. COLLARS in., 61d." 6/ 6 "
C { ... 4 in., 6t d." 6/6 " UFFS ..." 7i d." 7/6 "
C {Nursing Sister's & 1/- each AP " Officer's... 1/4"
APRON I' 1 1 & 2/6 "
" also in Pure Irish Linen 3/6 "
ILLUSTRATED PRICE LIST FREE.
r.16;Jwnes5320. 5321 , & 6297. TelegranuP ADDINGTON. "GARROULD, LoNDON."
THE UNIFORMS, CLOAKS, BONNETS, APRONS, DRESSES
ETC., FOR TIlE
ST. JOHN AMBULANCE BRIGADE, lIlAY HE OHTAI::\ ED AT E. & R. GARROULD .
To H.;\I. \VAR OFF ICE, 11.1\1. INDIA OFFIC E, COLO:\'IAL O FFICE , LONDO:\' CO UNTY COl NCIL, E TC. A i
ILLUSTRATED PRICE LI ' '1' of the vari ous a rticles required by th e
ST. JOHN AMBULANCE BRI G,\[) E. ON
, WINTER COAT, 23/6 SUMMER COAT, 27 /6
ISO to 162, Edgware Road, LONDON, W.

