

BONES.

Arm Bone (humerus)
4th Lumbar. Vertebra HaUnCh} Bone (pelvis)
Ubla
Radius _
Metacarpus • \
phalanges ,
Thigh Bontl Knee Cal> (patella) Shin BOlle (tibia)
Brooch Bone (fibula)
ARTERIES.
The .n.Jntbered dots show pres. sure pOints for the arteries. Com. r'tre numbers In text.
-.Occlpital.
Temporal.
Facial
Carotids. Subclavian.
Brachial (Digital OJ' Tourniquet)
Aorta. - - - - Brachial (Flexion).
Iliac. , Radial.
• __ --. -' -, - .Commencement of Popl ileal.
Popliteal (Flexion).
Anterior' Tibial. ,Postel'lor Tibial.
M-etatarsus. ___ _
Phalanges ,__
"A J. AS COMPANIONS TO THIS BOOKCATECHISM ON FIRST AlD."BY M. CARVELL, M.R.C.S., L.S.A.
Price 6d., post free.
"PROBLEMS IN FIRST AlD."
BY L. M. FRANK CHRISTIAN, M.B. , AND W. R. EDWARDS, A.C.A.Price 6d., post free.

PI AID TO THE IN] UI<'ED
ARRANGED ACC OR D I NG TO THE REVISED SYLl.At;LS OF T il E F I RST AID COL: RSE OF THE
ST.
)0 1IN A\ 1
BU r, \ BY JA;\IES CANTLIE, :\I.A., ,\LB., F.R.C.S., of Grace 0./ the Ord"v 0./ St. Jol/i/. !!ollorary Life 1I1emher of, and Lpctlll'cr alld Examill e ,- to, the A ssocialioll.
'Vith a CHAPTER on "Stretcher T,'ansport," re \'ised from that originally written by Sir JOHN FUJU,EY. C,B., Klli(fht ofJustice 0./ the Ordel' 0./ St. lohll, ,n accordance with the Army Stretcher Exercises. Also a CH -\PTER (beIng the F ,fth Lecture for Females only). by E. MAcDo\\, EL COSGR-\\'E. M.D F. R.C.P.I.. Klll:r:},t of Gra ce of flip Orr/PI' 0./ St, lohll. Honor,I/'Y Li./e It/ell/hl' '- 0./. alld Lecturer alld Exalllill!'r to, the Association.
THIRTY-FIRST EDITION, 1,490,000 lO 1,532,000
(This edit 011 is sillLi/ar to the eLlchteelltlt. in 7v/u'clz editiOIL 1Il<ll/y 0./ the illllstl'allOlls .,'ere l'e-drawlI; otlzerwiSf! it d lffevs bitt little /1'01/1 the Ple"Pllth to the seventeel/tll editiOlls.)
Price in Cloth, Is. post free, LONDO!';:
THE ST. ST. JOn, 'S G \ TE. E.C.
W. II. & L.C. 42.000/8/1916
alJe <Bran() !prior.2 or {We ®rt'er or tlJe ·ff)ospital of St. 50tm of 5el'll5alem III
SOVEREIGN HEAD AND PATRON:
HIS 1\IOST GRACIOUS MAJESTY THE KING.
GRAND PRIOR: B.R. H. THE DUKE OF CONNAUGHT, K.G.
SUI:l-PRIOR: THE EARL OF PLYMOUTH, C.B.
BAILIFF OF EGLE: COLONEL SIR HERBERT C. PERROTT,
EXECUTIVE OFFICERS:
PRELATE.-The Archbishop of York.
CHANCELLOR.-Col. Sir Hel·bel·t Jekyll, K.C.M.G.
SECRETARY-GENERAL.-Evelyn Cecil, M.P.
RECEIVER-GENERAL.-Edwin Freshfield, LL.D. [Bt., C.B.
DIRECTOR OF THE DEPARHIENT.-The Earl of Ranfuriy, G.C.M.G.
CHAIRMAN OF THE BRITISH OPHTHALMIC HOSPI L\L, JER USA LE1\!. -( Vacant.)
J\UIONER.-Sir Dyce Duckworth, Bt., M.D., F. R.C. P., LL. D.
LIBRARIAN.-Edmund fraser.
REGISTRAR.-The Lord Claud Hamilton, M.P.
G EN EALOGIST. -Sir Alfred Scott Scott-Gatty, Ie C. V. O. (Garter).
DIRECTOR OF CEREl\lONIES.-Sir Alfred Scott Scott-Gattv, I{. c. V. o. (Garter).
ASSISTANT EXECUTIVE OFFICERS:
ASSISTANT RECEIVER-GENERAL.-Edwin H. Freshfield.
HO:--lORARY SECRETARY OF THE BRITISH OPHTHALl\IIC HOSPITAL, J ERUSALEl\1.-Col. Thomas H. Hendley, c.!. E., 1\1. R.C.S.
ASSISTANT HONORARY SECRETARY (FOR SCOTLAND) OF THE BRITISH OPHTHALMIC HOSPITAL, JERL·SALEM.-John Home
Stevenson (Ullicorn P/trsltivant).
SECRETARY.-\Villiam R. Edwal'ds, A.C.A.
ASSISTANT SECRETARY.-Duncan G. l\Ionteith.
AUDITORs.-Price, Waterhouse & Co.
BANKERs.-.The London County & \Vestminster Bank, Ltd., Lothbury, London, E.C.
CHA.·CERY: St. John's Gate, Clerkenwell, London, E.C.
Telegraphic Address: Firstaid, London." Telephone: Cefltral903.

THE CHAPTER-GENERAL:
The consists of the Grand Prior. the Sub-Prior the other of the Prelate and the Sub-Prelates, de the Chaplains; all members of the Council; not than and not more than six Esquires appointed by
KNIGHTS OF JUSTICE:
IllS MOST GRACIOUS MAJESTY THE lU:\'G (Sovereign II ead and Patron).
f'IElD-;\IARSHAL THF.< DUKE OF Cm'.NAUGHT, KG., K .T.. KI .. I .Coo Etc. (Grand Pnor).
GENERAL II.R.II. PRI:--ICE OF SCHL ESWIG- TT OLSTEI:--I. K.G., P.C., G.C.Y.O.
I-LIT. PRINCE OF G.C.R., G.C.\'.O. n.n. fill! ])UJ(E OF TECK, G.C.B .. G.C.\·.O" C.M.G.
ADMIRAL n.S.H. PRINCE LOUIS OF BATTEXBERG, G.C.S .. G.C.V.O., K.C.i\I.G .. R.N.
'. 1I.i\T. IT ','KON vn., KING OF NORWAY, ICG G.C.B G.C.v.O. LIU T.·COL. II..:-> .H. PRINCE ALEXANDER OF TECK, (;.C.B., G.C.V.O .. I1.S.0. :\].'JOR ILR II. PRINCE ARTHUR OF K.G 1C1'.: P.C.,
. I-I.IT. PRINCE rTENSF.RG, G.C. v.O.
S,r Furl e\', C.B. (Honorary The Earl of lUe;lth, 1(,1>.. P.C. BaIliff).. A. E. Praser.
S,r T. DIck-Lauder, Bt. The Lord lUostyn HA. CLampb Bt. The :\/arquess of Breadalhane o. IT . . errott, Bt., C. B. I;:.G.. I> C ' r- I Egle). The Duk'e 'of Portland. K.G., P.C.• o. Ir . t1dea, K.C,V.O .. C.R. G C V 0 n. J. Loftus P H' C· t (II
\l'l. 13: i\T. Dawes. [R.I!, ,. on0rary s,,·C.'Varren. G.C.M.G .. K.C.H., Col. C. ,,' . H. Howd ler, C.H. Gen. J. ])alton. ( Honorary Commander>.
Lleut.;Gen. S,r 1\. G. Hunter- Lieut.-Col. A. C. \';lLe. "estOIl of HuntersLon , ICC. B.. ;\raj.-Gen. A. F. Terry. I);s.o. The Earl of Plymouth p C ol. 1 he Lord Vlilliam Ceci l. c. v.o. (S"h-Prinr). ,.C., C.B. E. LL.D. (Honor;lry E. II. Freshfield.
1'1 Lieut.-Cl)1. ThL' 1':"1'1 of 1'11: ras T :5e y , G.C.B. (Commander. lc ISCOllllt empletown. Commandel v). k i\I. :\IacLean. Lieut.-Col. Sir C. Temple Ht F. G. Leveson Gower. ('.B., C.LE.
l,o). F: A. II., L;lmbert. Sir ,\. S. S('ott-G;tttl' K c\'o ),ItJrra y , C.R. (Gart pr Princip;ll Ki,;g' 'of .'(' '.ar 0 ,anlurly, P.C.. C.C.M.G. .·\rlll!;). .
1 he- .Lord Sandhurst, P.C.. G.C.V.O, C,1. S ,r II. Jekyll. ".C.M.G.
S . (l'rC's., .. G.C.I.E. The L,)rd Isl ington. P.C., G.C.M G ,Ir . ;\. Blake. G.C.M.G . D.S.O. . .,

rs OF JUSTICfo. -L,.,Ilti llued.
Sir J. R .. \. Clark. Ut .. C.B.. JOlill rIorne StC\'C IlS\.lll (l'nj\.'l'fl1 .. F R.C.S.le. Pursui\·ant).
Sir Ilal\ er. Francis \Villialll Pixley. Cc)1. The Lord Sydell ham of Combe, Inspector-Gen. Belgra\'e l'\innis, (:.C.S.I., G.C.;II.(; .. G.C.I.E. C.\'.O., M.D., R.N. Li eut.-Cnl. J. \ V. \Vray. Charles Granville Kekewich. Sir \Y. \Y. Portal. Ut. II is Excellency 1 he Lord Ch el msTh e Duke of Somerset. [LL.D. ford. G C.M.G. Sir I), Duckworth. Bt M.D., F.R.C P., Evelyn Cecil. M.P. Capt II. E. Houlton. C.\'.O. Arthur E. G. Rhodes. The Viscount Esher. G.C.B .. (:.C. v.o. The Earl (If D e rby, K .G. fidJ,;\Ianshal The Lord 'i<:holson, Sir Owen C. Philipps, G.C.B. The Lord ClauJ lJ a milton , Lieut.-Col. The Lord Herbert Scott, Lt.-Col. A. Dyke .'\ c1anLI.
D.S.O. Th e lIon. A. Stanley, C.B., 1\1. \'.0., j'REUTE: The Archbishop ot Vork.
SUB-PREI.ATES:
The Rishop Ormsby ! I The Bishop of Southwark. Tlt e Bishop of Dun ed in (Primate :rhe B.islwp or Gihraltar. of New Zealand). The Bishop Carr Glyn.
OFFICIATING CIIAPLAINS :
Tlte Re\·. Canon E. ShepparJ, I The Venerable Ernest E. IIL,lll1e!>, ICC. \ '.0 ., D.D. B.D. (Archdeact.ln of Lond on).
KNIG!lTS OF GRACE APPOI:\'TED BY 1'111' GRAND PRIOR:
Col. Sir J. \ V. OtLley, K.C. I.E., R'!::'I t H. C.\'.O., F.R.C.S.
J. A. James, 1\1.\'.0. Sir \V. H. St. J ll.,pe. Llt r.D., J. S. GriHiths, D.C.L.
Lt.-Col. George E. TlViss, F R.C.S.1. F. H. Conic C.I.E.
R. A . Gibbons, i'I.D. The Lord Norreys. ESQUIRES APPOINTED BY TilE GRAND PRIOR:
C: . B. Hamilton. I Lieut -Col. Sir 1\1. D. Murray E. Da\\ es. K.C.V.O.,C.B. Col. \Y. G. Carter.
THE COUNCIL:
The Council consists of the Grand Prinr, the Su b- l'rior, the Executive Officers of the Order, the Commanders of existing Command e ries, and not more than fifteen members of the Gra Jes 01 Knight of Justice, Chaplain, Knight of Grace and Esquire appointed by lhe Grand Prior.
;\1 EMBERS APPOINTED
Sir J. Furley, C.B. 1\lajor-Gen. J. C. Dalton. [c \'.0.
Colonel The LbrJ \ Villiam Cecd, Sir Henry Arlhur Blake, G.C.M.G. E. II. Freshfield. [C.B., C.I,Io:. Lieut.-Col. Sir R. C. Temple, Ht ..
Col. Sir Jam es R. A. Clark, Bt. C,B., F.R.C.S.E. Francis \\1. Pixley.
BY TilE GRAND PRIOR: lnspeclol'-Gen. Belgrave Ninnis, c. V.O. M.D., R.N.
The Lord Clalld Hamilton, M.P.
The Bishop 01 Southwarlc . Sir \Villiam H. Bennett, K.C.\'.O., F.R.C.S.
Cnl. T. IT. H e ndl e v. C.I.F S ir Macke nz ie D. (',<';.1.
{tb e U; r ll lll> IPr lo n ? of ITi)C @rll c r of tb e 'n) osplt a l of St. 3- 01)11 of 3-er1l5a l em ill JEll g la lll> .
Al\IBl:LANCE DEPARTIIIENT.
TIfJe St. Jo()n Bmbulance Bs socia ti on.
PATRON:
Il lS I\ I A,J ESTY TH.E KING, SOH> I'e ign H eacl and Patl'oll of the Order.
PR I;;S IOENT:
F'''LD-I\L\R JlAL H. 1\. II. TilE Dt;I{E OF CONN.,\L'GHT, K.G., Grand l'I'i or of the Order.
CENTRAL EXECl :T1VE CO,\Il\lJTTEE: Consisting exclusively of Members and As oci<ttes of the Order.
CITAIRM. \ N,-The Earl of Ranfurly, P.C,(1.), G.C,M.G, ( Dire cto r of the Depal' tment).
[)EPUTY CHAIRMAN.-Sir John Furley, C. B., Life i\Iember of the Committee, Honoris Causa.
EX-OFFICIO MEMBERS:
Col. Sir I I. C. Perrott, Bt., C.B. (Bailiff of Egle).
Th e Secretary-General of the Order.
The Receiver-General of the Order.
The Chai rman of the British Ophlhalmic
MEMBERS:
Maj.-Gen. J. C. Dal lon.
The Lord I slington. G.C.M.G., n.s.o.
Col. Sir]' R. A. Clark, Bl" C.B., C.M.a F.R.C.S.I!, Col. The Lord Sydenham. G.C.S.I" G.C.M.G .. G.C. \.I!.
Capt. H. E. Boulton, C.Y.O.
Lieut. -Col. The Lord Herbert Scott, C.M.G.. n.s .o
Inspector-General B. Ninnis , c.v.o., M.D R.N
The Lord Claud Hamilton, "I.P.
The Rev. T. C. Elsdon.
?lI"j. G. I I. Darwin, M D
Col. G. S. Elliston, C B
Co l. C. J. Trimble. C.M.G., L.R.C.P. I!.
Sir J. L. Langnnn , Bt.
_. \Y. I\ l alkin, Esq.
C. COlton. F.R.C.P.P.., l\1.R.C.S,
CEl'TRAL EXECUTIVE COMMITTEE-continued.
C. B. Palmer
Lieut.-Col. G. E. Twiss. F.R . C.S . I.
Col. T. H . H endley. C.I.E M.R.C.S.
J . H. Morgan. C.V.O F.R.C.S.
Col. Sir Trc\'red\'ll H. \V )' l1l1 e. K.C.S.I K C.I.E
l\lajol' E. H. T.
Brig.-Gen. H. H . i\I c nds . C.R.
L ieut.-Col. A. D Acland.
Y·I!f ., Col. E. n. Brown-Sy nge-Hutchinson, C.B.
]. A. Bloxam, F.R.C.S.
Li e ul.-Col. Sir H . \V . Inglis.
Surg.-Gen. H. R. vVhitehead, C.B., F.R.C.S.
The Viscount Ach esol1.
T. H. \Voolston.
Col. C. R. Tyrrell. M. R.C.S.
Col. The Lord Boltol1.
SlIrg.-Gen. Sir A. \\'. i\Iay, K.C.B .. F .R.C.S .• K.II.P.• R " F. N . Ellis.
\V E. Alldland M.R.C.i:
A II lohnston M .R C.S.
E. A. Richards.
J. M. Carv, II. M.R.C .S
CHIEF SECRETARY: Major W. O. Prich ard
ACCOl ' NTANT: \\'. R. Edwards, A.C.A.
DIRECTOR OF STORES: 'vV. H. M Ol-ga il .
ASS ISTANT SE CRETARY : D. G. Mont ei th
TERRITORIAL BRANCH.
CONTROLLER-IN-CHIEF :- VacRn l.
SECRETARY: P. G. Darvil-Snlllli.
HE AD OfFICES:
St. John's Ga te, Cl e rkenwell, L ondon, E.
BANKERS:
Lonnon County and \Ve stminster Bank, Limited, Lothbury, E. C.
HFFERE'ICF. No . 58. 1908-:--
FIRST AID TO THE INJURED.
SYLLABUS OF INSTRUCTION
.

FIRST LECTURE.
.\ Principle of First Aiel.
B. -\ brief Description of the II uman Skeleton a nd o f the
L. Fractures-Causes, varieties, sign'> and symp toms.
I). Treatment of Fractures-General Rules.
E. The Triangular Bandage and its app lication . SECO:\ f) L ECTURE.
.-\ . Treatment of Fractures (continued). Details of treat· m'll!,
B . Dislocations, Sprains, St rain s-S igns, sympto ms and treatment.
C. The Heart a nd Blood Yes els . The Circu lati on "f the Plood.
D . Hremorrhage an I wounds. General rules for treatment.
£. The Tria ngu la r Bandage and ils application.
THIRO LECTI ' RE.
A. Hremorrhage and wounds (continued). Details of treatment.
B. Internal symptoms and arrest.
Cd' llcemorrhage from Regions. - Si ,'ns S)'lTIptoms an arrest. .:> ,
D. Burns and Scalds, Bitt s and Stings Frost-bite.
E. Forelgn bodies in the Eye , Nuse and Ea;. '
F. The Triangular Bandage anu ils application.
FOURTH LECTURE.
A. The Nervous System.
B. The Organs and Mechanism of Respiration-Artificial Respiration.
C. Insensibili'y
D. Poi,oning.
F1FTH LECTURE (for Maies only).
..A. Improvised methods of lifting and carrying the sick or lnJured.
B. ethod s of lifting and c rr)Tinrr the sick or .. d str.etchers . b lDJure on
C. The conveyance ,,( such by rail or in country cart.
FIFTH (for Females 0nly).
A. f<lr reception of accident cases.
B. 1\1 eans of hfung and tarrying.
C Preparatiun of Led.
• D. Rem oving the clothes.
E. Prep.tra lions for surgeon.

9
NOTE 1.-The subject of poisons should be treated in a general manner; the common poison'" classified, and only their general symptoms, 'effects and treatment taught.
NOTE 1I.-The last half-hour of each lectur e should be devoted to practical work, such as the h pplication of bandages and splints, lifting and carrying wound ed on
1I1.-There shoukl b e an interv,ll of a w ee k b e tween eac h lecture. A candidate for examinatio n at t e n d at le a s t fuur out of the Jive lecture s .
NOTE I\' .-:\Iale classes must pas in that system o f st retcher e xercise most suitable for the locality r orE V.-As little time as possible is t o lJ e sp e nt on instruction in anatomical and phy siological detaii s . L e cturers and examiners are panicLtiarly r equested to rem e m be r that it is " First Aid" that has to b e and tesled, an d nut anatomy and physiology.
J./ixe d d a sse:> 01 /II elt all d W I I/te ll are on n o ll t-',- oun ;fc rlJl ule i.
Lecturers instructing a First Aid class, and Local Secretaries, can obtain further particulurs on application to the Chief Secretary f"r ,. Paper Rt:ference No 80."
No Lecturer may ex a/llille Il is OWIl Class for Certiji( a les .
A G E CAN O:--il.Y AI'T[:\D
A,
4 0
PUPILS
U;-JDER SlXrIiE:-< YEARS OF
TilE ,. JUNIOR ' J C0 U RSE (::'ECT,ON
Sn.LABuS
) .
SUMMARY OF CONTENTS.
CHAPTER T.
Principles of First Aid
Explanatory
Questions on Chapter
CHAPTER II .
The Human S kull, spin e, ribs and-b reastbone, upper Ilm us (co lla r-bone, s hould e r-b lade , a rmbone, b ones of . t he forear m, car pus, metaca rp u:;, pha langes), pe lvls, lowe r li mhs (thigh-bo ne, kneecap, tars us, metatarsus, p ha langes) ... ...
Joints ...
lVIuscles. Vo lun ta ry and invo lu ntary Fractures. \'ar ieti es, signs and
Apparatus for treatment of Fractures
General Rules to be observed in Fractures
Special Fractures. C ra ni um, ri bs, breast-bone, coll a r- bon e, shoulde r ·bl a de, arm -bor.e or bo nes close to t he el bo w join t forea rm crus hed hand, pelv is, t hig h -bone, kn ee- cap, l eg, foot

or Bleeding. Arterial, venons,
. Aorta,
the
CHAPTER I V.
Miscellaneous Injuries. Bruises, bu rn s and scalds, hites of snakes and rabid animals and wound" by poisoned weapons, stings of plants a nd animals, frost bite, needle embedded under the skin, fish hook embedded in t he skin, injuries to joints, foreign body in the eye, ear passage and nose, wound in the front wall of the abdomen, injuries to the orga ns withi n the abdomen and pel\'i;
V . T h::! Nervous System. Ce reb ro-spinal, sympathetic.. .
Respiratory System I J S
A rti!1 cial Respiration. Schafe r's, Silveste r's , H oward's combined with Silvester's, L abo rde's and Ma rshall Hall 's methods...
10
... ...
Sprains
Questions on Chapter 1.7 20 2 1 2 2 31 3 2 33 36 43 62 64 65 66 1 1 CHAPTER III . Pag e C i:-culation of the Blood. Organs; ge n eral (system ic) and pulmona ry circ ulations 70 H
capillary 73 Arterial Hcemorrhage. Principles of arrest 74 Wounds with Arterial Hcemorrhage . .. 76 C
Points
arteries
upper limbs, of
lower
79 V enous Hcemorrhage an':' Varicose Vein s 93 W ou nds w ith Venous 94 C a pill ary Hcemorrhage 9 5 Internal Hcemorrhage 95 Hcemorrhage from S pecial R egions 96 Q l1p.stions on Chapter 99
Dislocations
Sprains Md Ruptured Muscles
cemorrhage
ourse of the Main Arterie s and Pressure
of the head and neck, of the
limbs
10 2 Questions on Chapter . . . . . . I 15
CHAPTER
II7 Th e
12
12
Insensibility. Causes, general rul es for treatmerrt, con. cussion of the brain, compression of th e brain, apoplexy, epilepsy, hysteria, shock, fainting and collapse, sunstroke and heat-stroke , convulsion,; in children, asphyxia
Electric Shock and Effects of Lightning
Questions on Cha.?ter
CHAPTER VI.
Poisoning. Gene ral rules for treatIl1 P :1t, special poisons
Questions on Chapter
CHAPTER YII.
Bandaging. Bandages for the scalp, forehead, etc., shoulder, hip, hand, foot, chest, back, knee, elbow, fingers and toes ...
CHAPTER VIII.
Methods of Carrying. Four, two, and three- h an d ed seats, fireman's lift, fore and aft method, improvised stretchers, to cross a ditch o r wall, to load or unload a wagon ..
CHAPTER IX.
Stretcher Transport. Stretchers, stretche r exercises, litters
CHAPTER X.
The Fifth Lecture (for Females only ). Preparation for r eceptio n of accident cases, choice and prepara(ion of a room, lifting and carrying, prepara tion of bed, removing the clot hes, preparation for surgeon ...
Questions on Chapter

Skeleton showing position of main ar teries
Skull and vertebral column
Vertebra
Bone s of the left upper limb
Bones of the right lower limiJ
Shoulde r Joint
Ankle
Rectus Muscle
Triangular bandage spr ead oul and folded
Large arm sling
Small arm sling
Reef knot
Gra.nny knot ...
Loop knot...
Bandage for of luwer Jaw.
Bandages for sImpl e fracLure uf n u,
St. J ohn sling
Band Iges for fracture of both co ll ar bones
Bandage for frac ture of shoulder blade
Treatment of fracture of a rm
Angular splint
Treat ment of fracture of forearm
Treatm : nt of crushed hand
Treatment of fracture of Lhigh bone
Tr eatment of fracture of thigh bone (woman)
F racture of knee cap
Trea tmen t of fracture of knee cap
Tre a tment of fr a clure of leg (man and W0I1lL-lIl)
Treatm ent of crushed foot
Diagram of the heart, lungs and air pacsages
Pag! 128 142 145 155 160 197 206 13 LIST OF ILLUSTRATIONS .
... ...
. ..
... .., ... ...
... .. ..
... ... .., ...
...
.. . . ..
.. .
...
...
... .., .. .
PaC'l frontisp iece. 24 27 29 3 1 3 1 3 2 38 39 39 40 4c 4J 44 47 51) 5l 52 53 54 55 55 57 58 58 59 61 62 71
Diagram of the circulation of the blood
Digital pressure on carotid artery ...
Digital on facial artery
Digital pressure on temporal artery
Digital pres ure on occipital artery
Pad and bandage to arrest hremorrhage from temple
Ring pad
I )igilal pressure on suuclavian artery
Pad and bandages to apply pressure on axillary <,rtery ...
Digital pressure on brachial artery (two method,;)
Flexion at elbow
Digital pressure on radial and ulnar arteries '"
Pad and bandage to arrest hremorrhage from palill
Digital pressure on femoral artery ...
Tourniqu e t on femoral artery
Flexion at knee
Organs of the chest and abJo:l1en ...
The lungs and bronchialtuues
Schafer's method of artificial respirati on . ..
Silvester's method of artificial respiration
Silvester's and Howard's methods of artifici.il re spiration combined
Bandage for the head
Bandage for the shoulder
Bandage for the hip . ..
Bandage for the hand
Bandage for the fo ot
Bandage for the chest
Bandage for the knee
Bandage for the eluow
Grip for four-handed seat
Lifting by two-handed seat. ..
Grips for two-handed sealS ...
Can)'ing by two-handed seat

Grip for three-handed seat .. .
' upporting patient .. , ....
Fore and aft method of carrYll1g
Carrying on improyised seat
I mprovised stretcher ...
Furley stretchers . !' ,1, 1 in"
Stretcher exercise. o. 1. -
Ditto, ready to lift patient
Ditto, lifting patient ...
Ditto, placing stretcher _
Ditto, to lower patIent .. .
Ditto "Lower ... ... ..,
Ditto: No. II. Ready to lift patient
Ditto, patient ... ..
Ditto, No. IV. FIrst p osllI on Ditto, second position ... . . . . ...
Diagrams illustrating Army stretcher drdl
Ditto ...
Bed cradle
Jmprovised bed cradles
12 5 ISS 156 156 157 157 lSI.) 159 159 r60 16r 162 103 15
Pate 16-l 105 ,67 r68 17 2 '75 l ib '77 '78 179 I 0 , 82 183 pg 189 19 1 194 203 20 3, 204
PREFACE.
AT the request of the Central Executive Committee I haye revised the manual written by myself in I9 0I as handbook of the St. John AssocIatIOn.
Throughout the revision an endeavour has been made to simplify the study of FIrst Aid to the Injured by dra\YlI1g up a number of ae neral rules for the of accidents a.nd illness, and by the ormSSIOn of all detail whIch is not abso lutely necessary to enable the student to acquire an intellige nt k?owledge of the subject.
I .. "'lsh to express my thanks to Professor E. A. Schafer for furnishing instructions for performing a met?o.d of artificial respiration, to Dr. L. M. F . for many valuable suggestions, and to the M.edlcal Members of the Central Executive CommIttee, especially G. H. Darwin, M.D., and Dr. F. R. Cassldl, for perusing the proof sheets and for anum ber of useful additions to the \york.
I cannot omit also to offer my best acknowled!!ments to Mr. ,V. R. Edwards, the Accountant and of the ..J. A. A. , for his invaluable co-operatIon.
JAMES
FIRST AID TO THE INJURED.
CHAPTER I.
The St John Ambulance Association has now completed thirty years of its existe n ce, and durin g that period hundreds of thousands of men and 'Nome n have been taught at its classes, in all parts of the world, how to help their injured neighbours.
First Aid to the Injured is a special branch of practical m ed icine and surgery, by a knowledge of which trained persons are enabled to afford skilled assistance in cases of accident and sudden illness. The instruction begins a nd ends with First Aid, and the subject is taught simply but thoroughly and exhaustively. The duty of the ambulance purils where the doctor's commences, and there ought to be no overlapping or clashing of duty or int erests.
PRINCIPLES OF FIRST AID.
I. Th e First Aid student sh o uld be-
(a) Observant, that he may note the causes and signs* of injury.
(b) Tactful, that he may without thoughtless questions learn the symptoms t and historyt of the case.
-----
i:· Si£;ns are what may be perc ei\·ed.
i'Svmpt o1l1s a re what the patient can tell YOll.
=:: HisLory means the circumstances alLending the accident cr sudden illn cs'>.
(c) Resourceful, that he may use to the best advantage whatever is at hand to prevent further damage and to assist Nature's efforts to rep.ai: the mischief already done.
(d) that he may give cleaF instructIOns to the patient or the bystanders how best to assist him.
(e) Discriminating, that he may decide which of several injuries presses most for treatment by himself, and what can best be left for the patient or the bystand ers to do-.
2 Remove the cause of injury or danaer whenever possible . b
3· Severe hcemorrhage must receive the .attention, no matter what a.re the other InJunes.
4· Air.-The. patient must be in a position in \VhI h breathll1g IS. poss!ble; air passages must be free from obstructIOn; If breathmg has ceased prompt measures must be taken to restore it.
S· restful position of the body will assist the VItal functlUns j support of the injured part will help to prevent further damage, and is essential in the case of fractures of limbs.
Warmth. -After every accident keep the patIent warm so as to prevent the fall of temperature below the normal point.
7· the skin is broken the wound

19
should be promptly covered with a clean absorbent dressing. Should the wound be poisoned, it is most important immediately to prevent the poison permeating the system.
8. Poisons swallowed should be got rid of; or ,,·hen that is inexpedient, neutralised.
9. The best means of transport must be studied, and provision made for proper care when the patient is brought to shelter.
10. Removal of Clothing.-Clothes should not be taken off unnecessarily, but when it is needful to remove them, the following rules will be found of service in serious cases :-
COAT: Remove froin the sound side £1ISt , and, jf necessary, slit up the seam of the sleeve 0n the injured side.
SHIRT AND VEST: Slit down the front and remove as the coat.
TROUSERS: Slit up the outer seam.
BOOT: Slit the back scam and undo the lac es.
SOCK: Cut off.
II. Stimulants. -It is incorrect to suppose that alcohol is the only form of stimulant, far too frequent use of spirits is made to restore a Datient after an accident, often with serious results; tile sa fest rule, therefore, is to defer the administration of alcohol until the arrival of a doctor. \Vhen the patient is able to swallow, strong tea or coffee, or milk, as hot as (.,n
18
be drunk, or a small quantity of sal \-olatile in water may be given. ,'melling salts may be held to the nose, Sprinkling the bee with cold anu hot water alternately, warmth applied to the pit of the stomach and over the heart, and vigorous friction of the limbs upwards have a stimulating 12 . Throughout h is worl ;: t he F i rs t Aid student must on no account t ake u ::o n h imsel f the duties a r. d responsi bi lit ies o f a lVl ed ical man. At times an apparently slight injury is accompanied by grave danger anJ may :Jctu<'!,lly cau, e loss of life. When sending for a doct.]r, state the nature of the case, a n d remel1lber that \\Tltten particulars are safer than a verbal mess:1gc:.
It is necessary that somethi ng should be known of the structure of the bouy (elementa ry anatomy), and of the functions of some of the more important organs and systems (elementary physiology). A short descriptio n of the necessary an<l tomical and physiological poi n ts is therefore given as the several subjects are d isc u ssed . For purposes of description the h u ma n body is supposed to be e r ect, \\ ilh the arms hanging by the siue and the palms of the hands directed forwards. The" midJle lin::: " of the body runs vertica l ly from top of the l1ead to a poi n t between the feet.

QUESTIONS ON CHAPTER 1.
The 1111l1l(,l'a/s /ltd/cale the pages 7uhel e tile answers
JIIay be found .
Wh:tt is First .Aid to the injured ?, ..
What qualities should the First Aid student ?
What are signs?
\Yhat are ympLol11s?
What is the history of a case? ." ". "
\Yhat is often the first thing to do in an accidellt ...
What result of injury must receive the first altentl.Ol:? '"
What three things are absolutely necessary to an ll1JLUed
person? ." ". '" ". ".
What must I l: done when the skin is broken? 1I0w
What steps ml;S: he taken beyond the actual treatment ofinjuri.es? '" .. . '"
Should cluthing ahays be removed?
Ilow would you remove clothing when necessary?
Explain the use and abuse of stimulants ...
\Yhat must the First Aid student not do ?
"'hat is elcmcntC1ry anatomy?
What is elementary physiology?
For purposes uf descliption how is the human body suppo ed to be placed? ...
20
21
PAGE 17 17, IS 17 17 17 J :8 IS
puisoning be treated? ... '" 18. 19 -9
What is the middle line of the body? 19 19 19 19,20 20 20 20 20 20

CHAPTER II.
FRACTURES, DI LOCATIONS, SPRAINS AND STRAINS.
THI!: SKELETO;,-[ .
The human body is moulded upon a bony framework (the skeleton) which serves-
I.-To give sllape and firmness to the body.
2.- To afford attachment to the muscles.
3.-To protect important organs, as in the skull, chest, and abdomen.
THE SKULL.
The Bones of the Skull are arranged in two groups, those of the brain case or cr lnium, and thos e of the face .
The Boundaries of the Cranium are the vault or dome, the rounded portion forming tIle top of th e head; the front or brow; the back of the head , where the greatest extent of brain exists, and where therefore thp cranium is widest and deepest; the sides or temples. The base of the cranium is hidden from "iew by the bones of the face and of the vertebral column; in it are numerous perforations for the passage of blood vessels and nen'es; through the largest orening the brain and spinal cord are continuous.
The Bo ne s o f the F a c e witb the exception of 7' -.}
the lower jaw are firmly jointed t ogether, so that movement between them is impossible. The cavities of the nose and of the eye sockets (orbits) are formed by the t)ones of the cranium and of the face conjointly. The mouth cavity is formed between the up.per and lower jaws, the palate being the bony roof of the mouth which separates it from the nasal cavity above.
Th e L o wer Jaw consists of:-
w) A horizontal portion in which are the sockets for the teeth.
(b) Vertical portions terminating on either side at the joint between the lower jaw and the base of the cranium, situated Immediately in front of the ear.
The angle of the jaw indicates the jUllction of the horizontal and the vertical portions.
THE BACK-BONE, SPINE, OR V J:.RTEBRAL COLUl\L.
T he Vertebral Column (Fig. I) is composed of bones called vertebrce, each of which consists of-
I.-A body or bony mass in front.
2.-Processes projecting backwards, which enclose a canal for the spinal cord- the spinal canal.
3.-Two transverse processes, twelve pairs of which support the ribs .
SKULL AND VERTEBRAL CCLUMN".
Showing left ribs al'c1 portion of breast bone. The right ribs are remo\'ed. SPINOUS PIWCESS. TRAN S VERSE CANAL FO R SPINAL CURD, BODY OF \ 'ERTEIIRA. FIG. 2 A.
FIG. 2B.
TRANSVERSI?

4.-A spinous process. The spinous processes of the vertebrce can be felt be neath the skin for the \yhole length of the back (Figs . 2 A and 2B).
T he V er te br ce , 33 in all, are grouped int8 regions, in each of \\'hich they are known by nu ,nbers, counting do\, nwards :-
I. - In the neck 7 Cervical vertebrre. The first ve rt eb ra, tiz 'J atlas, forms a joint with the base of the skull, at which tIle nodding movement of the head tak es place j the second, tlu axis, by the joint between it and the atlas, allows of the side to side movements of the head.
2 -111 the back I2 Dorsal vertebrce .
3 -In the loin 5 Lumbar vertebrce.
4. - The rump-bonE', or Sacrum, consists of 5 Sacral vertebrce united in ad ults as a solid ma...
S.-The tail-bone, or Coccyx, consists of 4 vertebrce joined together to form a single group.
Betwe'e n the bodies of the vertebrce, in the upper three regions, are interposed thick pieces of cartilage (gristle), which, while they bind the bones together, allow of free movement to the column as a whole, and help to break the shock of any sudden force applied to the spine (for example, when falling from
PROCESS 25
PROCESS.
a height on the feet) . The whole spine is strapped together by ligaments reaching its enti r e length.
THI!: RIBS Al'W BREAST-BONE.
The Ribs consist of t\Velve pairs of curved bones extending from the dorsal vertebrce to the front of the body, and are known by numbers-first, second, etc., commencing from above. The ri ·. s are not bon y throughout their entire length, but at a short distan ce from the front the bony material ends, and cartilage takes its place . The upper seven pai·s, nam ed the true ribs, are attached by their cartibges to the Breas t- bone (sternum), a dagger -shaped bone \\ lth the point do\Vnwards, just over the pit of th e stomach. The lower five pairs are termed the fal se rib s, as their cartilages fall short of the middle lin e. The eleventh and twelfth pairs are termed the floa ting ribs, as their ends are free in front. The ri bs t 11 close the chest and serve to protect the lungs, heart, liver, stomach, spleen, et . THE UPPER Ll:\lBS.
The Should e r-bo ne s me the Collar-bon e U!l7.)/ae) and the (scatula).
The Collar-bo ne can be felt on either side L 'neath the skm at the lower and front part of th e ne(' k as a m.rrow curved rod about the thickness of a finger. Its inner end rests on the upper part of th e
P ART OF COLLAR

B01\ES {UL:-I.,. OF F OREARM RAlJIU.3
WRIST ( CARPU S)
PHALA I'GES
FIG . 3A. Bo 'ES OF THE LEFT UPPER LIMB.
FIG. 3B.
SHO\vING THE POSITION OF TilE RADIUS AND UL:-iA \'V !I EX' THE THUMB 13 TURNED INWARDS
Compare Fig. 3A, in willch the thumb is turned outwards .
26
BONE
S HOUL1)ER BL AUE (SCAP ULA)
ARM BONE
METACARPUS
27
RADIUS
breast-bone, and its outer end joills ",ith the shoulderblade .
The Shoulder -blade lies at the upper and patt of the back of the chest, and fornls joints \\"ith the collar-bone and the bone of the arm.
The bone of the Arm (illtmerlls) reaches from the shoulder to the elba\\' .
In the Forearm are two bones, the Radius on the oute r, or thumb side, and the Ulna on the inner, or little finger .side. Both bones reach from th e elbow to the wrist, and they change their relativ e position with every turn of the hand (Figs . 3A and 3B ).
The Hand is composed of-
r.- The bones of the wrist, or cal jus, eight in number, arranged in two rows of four.
2.-The 17letacarpus(the framework of the palm); five bones which form the knuckles and support the bones of the fingers.
3.-The plza/anges, or finger-bones, tbree in each finger, and two in the thum b.
PELVIS AND LOWER LIMBS.
The Pelvis. - The larQ'e basin-like mass of bone attached to the lower part the spine is com posed of the two haunch-bones and the sacrum. The haunchbones meet in front (at the pubes) in the middle line, only a small piece of cartilage intervening, but behind, the sacrum is placed between them. The pelvis

4.
BOl'\ES OF TilE RIGHT OWER LIMB, SHOWING JOINT WITH THE PELVIS AT THE IIIP.
FIG. _ - TIIIGH I30l\E (F'EMUR). KNEE CAP (PATELLA). (FIBULA). .----'iIlIN BONE (TIBIA).30 supports the abdomen and its contents, and provid es the deep sockets for the thigh-bones--the hip joints.
The Thigh-bone (femur) reaches from the hi p to the knee joint. Its shaft is stout rounded an d arched forwards; the upper end a rou'nde d head, supported on a neck which projects invvards, to fit into the socket of the hip joint.
The Knee-cap (patella) is a triangular bone lyin g with its base upwards in front of the knee joint immediately beneath the skin.
The bones of the Leg are the Shin-hone (tibia) the Brooch-bone (fibula). The Shin-bone extends from the knee to the ankle, in both of whic h joints it plays an important part; its sharp edge, tlu sllin, can be felt immediately beneath the skin of th e front of the leg. The Brooch-bone lies on th e outer side of the tibia. It does not enter into th e formation of the knee joint, but its lower end form s thE' outer boundary of the ankle joint.
The Foot is composed of-
I.- The tarsus, a group of seven irregular bo ne s at the instep. The largest is the h eel-bone, and the uppermost (the ankle-bone) LJrm s the lower part of the ankle ioint.
The metatarsus, the five long bones in front of the tarsllS which support the toes.
3.-The plzalanges, or toe-bones, two in the bi g toe, and three each of the other toes.
3 1
JOINTS.
1\. J oLi.t is formed at the junction vf two or more bones. In moveable joints such as the hip, knee, elbow, etc., lhe s' rfaces of the bones are covered by cartib.ge, which lessens friction and the shock of a

FIG. 5.
FIG. 6.
LEFT ANKLE.
Compare Fig. 4, Page 29.
fall. Lubricating the joint is a clear, rather sticky fluid the « joint oil," or sYNovia, enclosed within a capsule. Tying the bones together, but allo\\ Ing of o\'ement, are a number of bands or ligaments. To explain the formation of lim b joints, the
TENI 'O",

NERVE
ARTIi:RY
,\IUSCULAI< TISSUE
PATELl.A
TENDON OR OF
following examples <:;.1'2 given: -
The Sh oul de r a balland-socket joint,' consists of a shallow socket on the outer ::ulo·le of the shoulder-blade, and of th e head of the arm-bone (Fig. 5). 0\\ ing to th e shallowness uf the socket the arm-bone is very pron e to escape from its socket (dislocate ).
The A n k !"', a hino·e joint, is formed at the ti o n of thre e bones, the shin-bone :1bo\'e and on the inner side, the broochbone 011 the outer side and the ankle-bone belo\: (Fig. 6,'.
FIG . 7· The Muscles of the DIAGRAM SHOWING RECTUS body are classifled into t\\O
MUSCLE OF THIGH, WITH grouPS-'ll 0 /1111 fa r y and ARTERY, VEIN AN]) NER\"E. z'nvoluJlfa(.1. 33
The Voluntary muscles are me t with in the limbs t he head a n d neck, and the su rface of the trunk . Their ends are attached to different bones, and as th<::y pass from one to another they cross a joint, and, being e n dowed with the power of contraction and relaxatio n , cause the movements of the body. As a muscle crosses a joi n t, it as a rule becomes a fibrous cord or tendon. Blood-vessels traverse and supply the muscles, and the nerves entering them bring them und e r the direct control of the brain and spinal co r d .
The Involuntary muscles are met with in the walls of the and intestines, in the air passages, and ill most of the internal org.:lI1s and blood vessels, also, in a special form, in the heart. They are not under influ e nce of the Will, but cominue their work during the hours of sleep; their functions are regu 'ated by a separate set of nerves (see Sympathetic System, page lIS) .
FRAC TU RES AND THEI R TRE ..-\.TMENT.
When a bone breaks a Fracture is said to occur.
CAUSES OF FRACTURE.
I. Direct Violence. - ·When from a severe blow, impact of a builet, crush of a wheel, etc ., a bone breaks at the spot where the force is applied the fracture is tern-J ed direct. c
THE
35

2. Indirect Violence.- 'When the bone breaks at some distance from the spot \\ here the force is applied the fracture is termed indirect. Alighting on the feet and frac,turing the thigh-hone or the bones of the . leg, or fallmg on the hand and breaking the radl us or the collar-bone, are examples ..
3. Muscular Action. - The knee -cap and th e arm-bone are OCC:1Si011ally broken by a violent con , traction of the muscles attached to them.
VARI ETIES OF FRACTURES.
Fractures are class ifi ed accordin fJ to the c onditi o n of the tis s ues adjacent to the bone follo\\ S :. .1. Simple.-The b one is broken with but slight ll1Jury to the surround ing parts.
2. Compound. - The bone is broken and th e skin a nd tissues are punctured or torn, thus allo\Yin a disease-prod ucing germs to obtain e ntrance to seat of fractur e. The fractur ed ends may protrude throu g h the skin, or (for exa mple, wh en a bone is broken by a bullet) the wound may lead down to th e fractur e.
3. Complicated . - Th e bone is broken and in addition there is an injury to some internal orga n (for example, the brain, spinal cord, lung, etc.) or to some important blood-vessel or nerve.
A fracture may be compound or complicated as the immediate resu lt of the injury; or a fractur e,
originally simple, may be converted into a compound or complicated fr::tc ture-
(a) By careles5 movement on the part of the patient.
(b) By carelessn ess or ignorance o n the part of one rendering first aid.
Special yarieties of fractur es may be classified accord· in.; to the injury to the bone itself as follows :-
1. Comminuted . - The bone is broken 1l1to several pieces .
2. Green-stick. -In children, o\ying to the softer state of the bony tissues, a bone may bend and crack . \\ithout breaking completely across .
3. Impacted. - Th e brvken ends of tbe Gone are drIve n o ne into the other.
GE!\ER_\L SIG TS AND SYi\lPTOMS WHICH Y BE PR ESENT .
(A fracture of the femur, humerm, or both bones of the forearm or leg, affords the most complete example.)
I. Pain at or n ear the seat of fr acture.
2. Loss of power in the limb.
3. Swelling abo ut the seat of fracture. Swelling freq uently renders it difficult to perceive oth er signs of fracture , and care must therefor e be tak en not to mistakE: a fr act u,e for a less serious injury.
4. Deformity of the l1mb.-The limb assumes an
34
unnatural position, and is mis-shapen at the seat of fracture. The contracting muscles may cause the broken ends of the bone to override, thereby producing shortening.
5. Irregularity of the bone.-If the ?one IS close to the skin the fracture may be felt, and If compound it may be seen.
6. Unnatural Mobility -:Hovement may be made out at the seat of fracture.
7. Crepitus, or bony gra'ing, may be felt or heard when the broken ends move one upon the other.
The last two signs slzo1tld onl.J' be souglzt by a Several of the above signs are absent in green-stIck and impacted fractures.
.
In addition to the signs and symptoms the patIent or the bystanders may b e able to give the history of the injury, and marks on the clothing or skin should be noted, as they may serve to locate the fracture. The snap of the bone may have been heard or felt.
ApPARATUS FOR TREATMENT OF FRACTURES.
Splints and banda9'es for First Aid frequently have to be improvised. '
A Splint may be improvised from a walkillg stick, umbrella, billiard cue, br oom or brush handle, police man's truncheon, rifle, folded coat, piece of \\ood, paper firmly folded, a rolled-up map, or, In fact, anytlting that is firm and long enough to keep

37
the Joints im,medz'ately above and below the fractured bone at rest. 'When the above appliances are not avai lable, the upper limb, if fractured, may be to the trunk, and in all cases a fractured lower 11mb should be bandaged to its fellow.
Bandages may be improvised from handkerchiefs, belts, straps, braces, neckties, or any piece of linen, calico, string or cord that comes to hand.
Esmarch's Triangular Bandages (Fig. 8) are made by cutting a piece of lin en or calico about forty inches square diagonally into two pieces.
The broad bandage is made by bringing the point down to the base (Fig. 9), and then folding into two (Fig. 10).
The narrow bandage is made by folding the broad bandage once (Fig. II).
The medium bandage is made by bringing the point down to the base, and then folding into three. (Fig. 12). This bandage n1ay be used i!1stead of the broad or the narrow bandage when it is suited. to the proportions of the patierL
It is sometimes advisable to halve the size of the bandage by bringing the two ends together before folding it into the broad, narrow, or medium bandage.
When not in use, the triangular bandage should be folded narrow; the two ends should be turned to the centre, and the bandage then folded into four, reducing it to a packet about 6k by 31 inches.
36
.
9. BA ,\])Al;E ONCE FOLDED
FIG. 10 BROAD 15ANIJAGE.

FIG. II. NARROW BANDAGE.
12. THE DOTTED LINES SHOW THE FOLDS OF TH& MEDIUM BANDAGE.
39
Large arm-sling (Fig. 13).-Spread out a bandage , put one end over the shoulder on the sound side, pass it round the neck so that appears over the shoulder of the injure 1 and let the other end han g do\\'n in front of th e chest; carry the point behind the elbo\\' of the injured limb, and bend the forearm over the middle of the bandage; then carry the second end up to the first and tie them; bring the point forward, and secure with two pins to the front of the bandage .
Small arm-sling (Fig. q).-Place one end of a
PU NT
FIG.
broad bandage over the shoulder on the sound side pass it round the neck so that it appears over shoulder of the injured side; place the forearm over th e middle of the bandage; then bring the second end up to the first, and tie them. This sling is used in c ases of fractured humerus, and occasionallY when the large sling would be too conspicuous. J Slings may be improvised in many simple ways, such

as. pinning the sleeve to the c lothing, turning up the taJ! of the coat, passing the band inside the buttoned coat or waistcoat, etc.
- Reef Knots (Fi g. IS) are to be used. Avoid granny knots (Fig. 16).
GENERAL RULES TO BE OBSERV ED IN THE TREATMENT OF FRACTURES.
The object of First Aid Treatment of Fractures is to guard against furth e r mischief and especially to prevent a simple fracture from bec;m:nCT compound or complicated . To attain this end:- <:>
I. Attend to the fracture on the spot. No matter how crmv;ded the thoroughfare, or how short the dis'ance to a more convenient or comfortable no must be made to move the patient untIl the 11mb has been rendered as immovable as possible by splints or othe r restraining apparatus.
2. Steady and support the injured limb at o.nce, so its further movement on the part of either the patient or the bystander is prevented.
. 3. the 11mb with great care, and If shortenmg IS observed in the case of a fracture of a bone of the lower limb, pull up :m the foot until the limb regaIns a mor2 normal length. When the shape. the limb on no .account let go untIl l.t IS secured In posltlOn by splInts, otherwise there IS great danger of the fracture beco:11ing c ompound or complicated.
4. Apply splints (when practicable) and bandages as follows :-
(a) The splints must be firm, and long enouCTh to keep the joints immediately above <:> and
FIG. IS.-REEF KNOT. FIG. 16.- GRAN:I/Y KNOT.below the fractured bone at rest. They should, if practicable, be padded to fit accurately to the limb and be applied over the clothing.
(b) The bandages must be applied firmly, but not so tightly as to constrict the circulation of blood in the limb. ·When the patient is in the recumbent position double the bandage over a splint to pass it under the trunk or lower limb. As a general rule :-
For the tn/uk the broad bandage should be us ed. Pass it once round the trunk cll1d fasten it by tying the enJs, or with two or three safety pins on the side opposite to the fracture, but if to secure a splint for a broken thigh, over the splint.
For tlxe arm (11' forearm the narrow banda::;e should be used. Pass it twice round the Ji ·nb, anci tie the ends over the outer splint.
For Ihiglz or It'g the narrow or m edium b.md.1ge may be used. It is frequently convenient to double the bandage at the ce ntre, p::tss it under the limb, bring the loop over the limb, pass both ends of the b::tnd· age through it in opposite directions, and tie them over the outer splint (Fig. 17).
In applying bandages near a fracture the upper one should be secured first.
4j
5 · .When accompanies a frae ture It must be <lttended to filSt, and the wound covered by a clean clressmg.

FIG. 11.
6. No attempt be made to remove a pafient suffering from a fracture of the spine, pelvis, or thigh, except in a recumbent position, preferably upon a stretche r.
7. In every case of fracture it is necess ·· ary to cover the patient to keep him warm, anJ so lessen the effects of the SHOCK of the accidenL
$--. In all doubtful cases, treat as a fracture.
SPECIAL FRACTURES.
Fracture of the Cranium. ·-A fra cture of the upper pent is USUJ.Jly caused by direct vi ole nce-fur examp le, a blow on the head. A fracture of the base IS caused by indirect vjn 1p nce, throu gh a bll on the
44
head, a fall on the feet or lO'v\'er part of the spine, or a hlow on lower jaw. If the upper p ,zrt zs fractured, slgns. are swelling, irregularity, and. frequently lDsenslblhty, either immediate or comIng on gradually. If tlte base Z5 fractured insensibility may come on immediately, blood or a clear fluid may issue from the ear channel, blood may escape from the nose, or it may pass d o wn to the stomach, \\'hence it may be vomited; the fracture may involve the orbit, causing a blood-shot eye.
TREATM ENT.
Injury to the brain is the great danger attendFlG. 18. ing a fracture of the cranium . For treatment see "Concussion and Compr ess ion of the Drain," pages I3I, 132.
Fracture of the Lower Jaw.-Pain . loss of power (ir:abi lit y to speak and to l110ye the jaw freely), IrregularIty of the teeth, crepitus and bleeding from the gum are the usual signs and symptoms.

45
TREAT:\IENT.
!.-Place the palm of the hand below the injured Done and press it gently against the upper jaw.
2.-Apply the centre of a narrow bandage under the chin, carry one end over the head, cross the ends at th e angle of the jaw, carry the long end across the chin, and tie the ends on the side (Fig. 18).
Fracture of the Spine.-The vertebral column may be broken either by direct or indirect violence. from a height on the back across a bar or upon an uneven surface is an example of direct fracture, and a fall on the head, causing a broken neck, is an examp le of indirect violence. 'Vh at is co mmonly regarded as a broken back consists of a fracture of one or more of the vertebrre \\"ith displacement of the fragments, whereby the spinal cord and the nerves issuing from it may be torn, causing com plete or partial paralysis of the parts below the fracture. Pain is present at the seat of injury.
TREATMENT.
I.-Prevent all movement on the part of the patient.
2.- Cover the patient warmly.
3.- To remove the patient, place him on a stretcher or shutter as follows :-
( a) Turn up the collar of his coat; roll up a stick or umbrella in each side of the coat
(

so that the ends are level with the top of 'his head; pass a broad bandage or handkerchief under the head and secure it tJ the sticks. If no coat is worn, or doubt as to its strength and length exists, pass a number of bandages under the patient to serve instead of, or in addition to, the coat.
b) A bearer on each side grasps the rolled coat ',\'ith his hands well apart; a third grasps the clothing on both sides on a level with the hips; a fourth bearer takes charge of the legs ,
(c) On the word being given, lift together and carry tIle patient by short side pacts over the stretcher and carefully lov\'er him on to it. If a fifth bearer is available the stretcher should be passed under the patient instead of carrying him over it.
4.-0n arrival at shelter nothing further is to be attempted until the arrival of a doctor, except to give the patient water, tea, etc ., if he is conscious.
Fractured Ribs.-
The ribs usually fractured are the sixth, seventh, eighth, and ninth, and generally the fracture is midway between the breast-bone and the spine. The fract L1fe may be by indirect violence, driving the fractured end s of tl:e bone outwards, or by direct violence, driving the frcicmred ends of the bone inwards and sGmetillJes injuring the
lung.:; o r other internal organ. If the 10\\ er ri bs on the rjlfht SIde are broken, the liver may be injured, and aOfractl,lre of the lo\\'er left ribs may wound the spleen. Evidence of the fracture is afforded by pain, especially on attempting to take a deep breath, and by short and shallow breathing. If the lungs are injured blood, frothy and bright red, may be coughed up and expectorated. If the liver or spleen is \\'ounded internal hremorrbage (see page 95) may occur.
TREATi\lENT.
(a) JJ lzell tlz pfracture ;s not comphtatt'd by all z"lljllry to all internal or ., an :-
r .-Apply t\\'Obroad bandages round the cbest sufficiently firmly to
FIG. Ig. afford comfort, with the centre of the first immediately above and tbat of the second immediately below the fracture. The lower bandage should onrlap the upper to balf its
46
47
extent. The knots are to be tied rather to the front on the opposite side of the body. Another good plan is to apply a strong towel, fo lded about eight inches wide, tightly round the chest , securing it with three or four safety pins.
2. -Place the arm on the injured side m a large sling. (Fig. 19).
(b) TV/zen an inte r nal organ is injured-
]. - Do not apply bandages round the chest.
2.-Lay the patient down, inclined a little tmyards the injured side.
3·-Loosen the clothing, give ice to suck, and place an ice bag over t he seat of injury. Treat as for internal hcemorrhage (see page 95) .
4· -Place the arm on the injured side in a large sling.
of the Breast-bone (sternltm) . -
' Vhen thIS fracture can be felt or is suspected undo all tIght clothing, and keep the patient quiet in an easy position unti l the ani val of a doc tor.
FRACTURE OF THE BONES OF THE UPPER LIMB.
Fracture of the Collar-bone (clav£cle) . - This fracture is freq uently caused by a fall on the hand or shoulder.-The arm on the injured side is partially

4)
helpless, anj the patient usually suppJrts it at the elbow with his hand, and inclines his head towards the injured side . The fractured ends can generally be felt to overlap, the outer fragment being the lower. The general signs and symptoms of fracture are mostly present.
TREATMENT.
I.-Remove the coat (see page 19) , and as much more of the clothing as is expedient.
2.-Place a pad about two inches thick and four inches across in the armpit.
3·-Gently bend the torearm we ll up, keeping the sho ulder as far back as practicable, and support it in a " St. John" sling, made as follows :-
(a) L:1.Y an across the chest over the injured limb with one end on the uninjured shoulder and the point beyond elbow on the injured side. (Fig. 20).
(b) Pass the lower end of the bandage und er the injured limb, across the back, and tie the ends somewhat loosely in the hollow in front of the so u nd shoulder.
(c) Fold the point over the elbow of the injured limb and sec ur e it by one or two pins (Figs. 21 a n d 22) .
48
Tightly secure the injured limb to the side by a broad bandage passed round the elbow and trunk, s') as to lever out the shoulder, the pad formin g the fulcrum.
S·-Now tighten the slin g.
'When both collar-bones are br:>ken keep the

Flc. 23A . FIG. 23B.
shou lders, back by narrow bandages tied round each arm, close to the shoulder, passed across the back, over the opposite arm and tied together in front. The forearms should be raised and supported by the bandages. (Figs. 23A and 2 3B ' .
Fracture of the Shoulder-blade (scapu la)-
App1y the centre of a broad ban dage in the armpit of
50
the injured side, cross the ends over the uninjured shoulder and tie them und er the armpit. Support the limb in a St. John sling (Fig 24)·
Fracture of the Arm (humerus). - The bone may be broken :-(a) Close up to the shoulder; (b) near the middle of the shaft; (c) close FIG 24· to the elbow.
All the general signs and symptoms of fracture are usually present.
TREATMENT.
When the Fracture £s close to the Shoulder-
I.-Apply a broad bandage with its centre above the middle of the arm round the limb and body, tying it on the opposite side.
2.--Support the forearm by a small arm sling.
IVhen the Fradure £s near the M£ddle of tilt: Slzajt-
I.-fend th e forearm at a right angle to the arm .
2.-Apply splints, reaching from the shoulder to the elbow on the outer and inner sides of the arm, and, if enough can be procured, to' the front and back also. The front splint

53
must on no account be so long as to press upon the blood-vessels at the elbow joint.
3·-Sec ur e the splints by bandages above and below the fracture. If splints are not available, secure the arm to the side by two broad bandages.
4.-S11pport the forearm by a small arm sling. (Fig. 25).
Fractures in volving the elbow joint, whether of the arm o r forearm, are attended with so much swelling, and it is so difficult to ascertain the exact nature of the injury, that wh e n the accident occurs indoors the limb should be laid upon a pillow in the m ost comfortable position; ice or cold \\'at e r dressings should be applied to the injured part, but no further treatment should be attempted pending the arri"al of a doctor.
FIG. 25.
52
TVhen the accident occurs out of doors-
1.-Tak e two pieces of thin flat wood, one long enough to reach from the armpit to below the elbow, the other long enough to reach from above the elbow . to the finger tips; tle them together to form ! a right angle. (Fig. 26).
2.-Apply the an" ular splint so made FIG. the inner side of the flexed limb.
3.-Secure by bandages above and below the fracture.
4.- Support the limb by a large arm
5.- On arrival at home remove the splint, and treat the injury as if it had occurred indoors.
Fracture of the Forearm.-Wh en both (the Radius and Ulna) are broken, the general signs lnd symptoms of fracture ?re usually l?resent. When one of the bones only is broken the SIgns and symptoms are as a rule pain, loss of power, a.nd irregularity. An impacted fractureof the RadIUS 55
just above the wrist is a common result of a fall on the hand.
TREATMENT.
This is the same, whether the fracture is ot one bone or of both.
1.- Bend the forearm at right angles to the arm,

FIG. 27. FIG. 28. keeping the thumb upwards, and the palm of the hand towards the body.
2.-Apply broad splints on the inner and outer sides from the elbo\\ s to the fingers.
3·-A pply bandages, embracing both splints, immediately above and below the fracture and round the hand (Fig. 27).
a large arm-sling.
Crushed Hand (fracture of the bones of the carpus, metacarpus, or fingers).
TREATMENT.
I.-Apply a carefully padded splint to the front of the hand, reaching from well above the wrist to beyond the tips of the fingers.
54
2.--To secure the splint apply a narrow crossed in the manner of the figure 8 to the WrIst and hand (Fig. 28).
3.-Applya large arm-sling .
F ract ur e of t he Pelvis. -When, after a severe injury in the neighbourhood of the haun,ch-bone, there is no sign of damage to the lower lrmbs, but the patient is unable to stand or even to the lower limbs without great difficulty and pam, a fracture of the pelvis m:lY be assumed to have occurred . TI"le blood-vessels and o;'O-:J.ns, especially the bladder, \\ ithin the pelvis are in danger of being wounded.

I. - Lay dle pati e nt in what e\-er is found to give the greatest c,ase, an? fl ex or straIghten the lower limbs as the p.1tlent deSires.
2.- Apply a broad bandage round the ,hips tight enouO'h to support t he but not so tight as to pressbthe broken bone further
3.-'1'0 remove the patient place hl1n on ,a stretcher, acting on the same principle as that descnbed under " Fracture of the Spine" (see page 45) .
FRACTURE OF THE BONES OF TH E Lo ',\ ER LIMB.
Fracture of the Th igh-bone (felllur).thigh-bone may be broken at its neck, anywhere III the shaft, or close to the knee. A fracture at the
neck is likely to occur in old people from very slight injury, and is often difficult to distinguish from a severe bruise of the hip, but it may ' be assumed that when, after an injury near the hip joint, the patient cannot, when lying on the back, raise the heel from the ground, the bone is broken. All the general signs and symptoms of fracture are usually present and a prominent sign is the position of the foot,
FIG , 29,
which, as a rule, lies on its outer side. Shortening may vary from one-half to three inches.
TREATMENT
.
I.-Steady the limb by holding the ankle and foot .
2.-Gently draw down the foot and br ing it into line with its fellow. When two or three assistants are at hand, it is one person 's duty to hold the foot in position until the splints are secured.
3·-A pply a splint on the outer side from the ar mpit to beyond the f00t.
56
57
4.-Applya splint on the inner side from the top of the thigh (th e fork) to th e knee.
s.-Secure th e splints hy bandages ( a) Round the chest below (b) round the p.:lvis on a level wIth th e h lp ]omts, (c) above the fracture, (d) below the fracture, (e) r ounJ the leg, (f) round both ankles and feet, and tied below the feet ( 0" ) a broad round both knees ( Fig. 29). , ('") b

FIG. 30.
'Vhen si n gle-handed, or \\hen the ' patient is a woman, it is expedient, :lIter extension of the limb, to tie the feet together, dispense with the inner splilv, a ni pass the round b ot h limbs (Fig. 30).
Fracture of the Knee-cap (patellll) -The knee-cap may be FIG . .3I. broken by falling on th e knee (direc t violence), b ut more frequently it is broken by muscular actio n, as follows:-
When the foot slips in the attempt to prevent a hll the muscles in the front of the thigh ac t with suc h force as to snap the knee-ca p in two (Fi g. 3 I).
Pain, loss of power (the limb will be qu ite helpless), and irregularity (a gap may be felt .be.t\\:een the broken fragments of bone) accompany thIS mJury.
TREAHI'IENT.
I.-Lay the patient on his back, raise weU and
FIG. 32.
support the head a n d shou lders, straighLell and raise the limb .
2.-Apply a splint along the back ')f the limb, reach in a from the buttock to beyond the h eel.
. 3.-Apply a norrow bandage with its centre
59
diately above the knee-cap, cross the ends behind over the splint, and tie in front below the broken bone. fo ensure firmness apply a second bandage in a sImilar way, but commenced below and tied above the broken bone.
4·-F urther secure the splint by bandages round the thigh and leg.
5·-Su pport the foot well off the ground by a pillow, roll of clothing, etc., or if none of these are at hand by resting it on its fellow (Fig. 3 2 )
{S.-Apply an ice bag or a cold water dressing over the fracture.
Fracture of the Leg (tz'bia and fibztla).-On e or both of the b ::mes may be broken. When both bones are broken all the general signs of fracture are USUJlly present, but when one bone only is broken deformity is not always noticeable. A fracture of the fibula three or four inches above its lower end :s frequently mistaken for a sprain and sometimes for a dislocation of the ankle.
TREATMENT-.
I.-Steady the limb by holding the ankle and foot.
2.-Draw the foot into its natural position, and do not let go until the splints have been fixed.
3·-Apply splints on the outer and inner sides of the leg, reaching from above the knee to beyond the 61
foot. If only one splint is available place it on the outer side.
4.-Secure the splints by bandages (a) above, (b) below the fracture, (c) immediately above the knee,

FIG. 34.
round ankles, (e) a broad bandage round both knees 33).
Wr. cn single-hand ed , or when the patient is a
'- -=0, ,.--. --=-=- -. - -

woman, after extending the liI11b tie both feet together, dispense with the inner splint, and pass the bandages round both limbs (Fig. 34). 'Vhen no splint is available tying the legs, ankles, and knees tog e ther is of !STeat service .
C rushed Foo t (fracture of the tarsus, metatarsus anJ toes).-This accident is commonly caused by th e p3ssage of a b ea "y " ·eight over the foot, and may be rec ognised by pain, swelling, and loss of power.
TREAT:\IE;-;T.
I.-Remove the boot (see page 19).
z . -Apply a wellpadded splint to the sole of the foot, reachingfrol1l tbe h eel to the toes
3.-Applya bandage
FIG. 35· crossed after tbe manner of the figure 8 (Fig. 35).
4·-Support the foot in a slightly raised position.
D ISLOCATIONS
.
A dislocation is the displacement of one or more of the bones at a joint.
The joints m os t frequently dislocated are those of the shoulder, elbow, thumb, fingers , nnd lower jaw.
SIGN S AND SYMPTOMS OF DISLOCATION
.
I.- Pain of a severe sickening characte r at or near the joint.
2.- Loss of power in the limb.
3.- Numbness of the parts below the seat (,f dis location .
4.-Swelling about a n d below the joint.
5.- Fixity of the joint.-The limb cannot be moyed at the joint by either the patient or others.
6.- Deformity of the limb.-The limb assumes an unnatural position, and is mis-shap en at the joint.
TREATMENT.
No attempt should be made by anyone except a docto r to reduce a dis location. Pending his arrival:-
(a) TVhen tlze acczdent occurs out 0/ doorsSupport the limb in whatever position giv es most ease to the patient, bearing in mind the necessity of lessening the effects of jolting during transport.
(b) J,Vlzen the patimt is indoors-
I.-Remove the clothing from the limb.
2.-P lace the patient on a couch or bed .
3.-Rest the limb on pillows in the most comfortable position.
4.-Apply cold (ice or cold water) to the join t.
s . - vVhen co ld ceases to give comfort apply
62
warmth (flannels or towels wrung out of hot \\ atet}
6.- Treat shock (see page 135)'
SPRAINS.
\Vhen, by a sudden wrench or twist, the ligaments and the parts around a joint are stretched and torn the joint is said to 1.Je sprained. "Going over" the ankle is a common exam pIe.
SIG'NS AND SYMPTOMS.
r,- Pain at the joint after a twist or wrench.
2.- Ina bility to use the joint.
3.-Swelling and discoloration.
TREATMENT OF SPRAINED A(\KLE.
TV/zen out oj doors-
I.-Apply a bandage tightly ove.r the boot, ginning on the sole at the mstep, it on the front of the ankle, and. carrymg it round and round the ankle, where it is to be firmly tied.
2. ·-Wet the bandage after applir::"tion; it is thereby tightened.
Alter 1'eaclzing shelter-
I.-Remove the boot and stocking (see page 19)
2.-Place the limb in the most comfortable position; usually that is well raised.

65
3·-A pply ice or cold water dressings to the joint as long as they relieve pain.
..J..- When cold fails to give comfort, apply hot fomentations.
'When other joints are sprained, treat them as if dislocated.
When in doubt as to the nature of the injury, treat as a fracture.
STRAIl'TS AND RUPTURED MUSCLE.
vVhen, during severe exertion, muscles or tendons are over-stretched they are said to be strained, if they are actually torn they are described as ruptured.
SIGNS AND SYMPTOMS.
I.-A sudden sharp pain.
2.- When the muscles of a limb are strained they may swell and cause severe cramp .
3·-Furth er exertion is difficult or impossible j for example, if the strain has occurred in the back the patient may be unable to stand upright.
TREATMENT.
I.-Place the patient in the most comfortable position, and afford support to the injured part.
2.-Apply hot water bottles or hot fomentations when the pain is very severe.
A so-called strain in the groin (hernia) is an injurv of a totally different nature (see page 114).
64
D
QUES T IONS ON CHAPT E R II .
T h. ,.um er aJs i n dica t e t h e page s w here t he may ;e jo"nd ,
'''haL is the skeleton, and what purposes are sen'ed by it?
ITO\\ are bones of the skull ;.l.rranged?
\Vh lt are the boundaries of the cranium?
Describe the bones of the face
Descril)e the lower jaw
What is the angle of the ja\\ ? ...
\\'hat other names has the back-bonl ?
\\' hat is a vertebra?..
110w many verte bra: are there in th.e spine?
\Yhat are the regions cr the spll1e and how mally verte brGe are t h ere in each? ...
How is the spine endowed with free movement?
WhaL is a rib?
lIow many pairs of ribs are there?
Wha' is the breast bone? ...
"'nat are the bones of the upper limbs?
What i" the pelvi ? ..
'Vhat is the hip joint?
'Vhat are the bones of the lowel limbs? ...
' ''hat is a j ,)int ?
D , sc ibe a moveable joint ...
Describe the shoulder joint
Describe the ankle joint
IIow are J11u,;cles c lassified?
Descrihe vuluntary muscles
Describe invo'untal)' muscles
"'hat i a fracture? ...
'''hat are the causes of fracture? ...

Where does a bone hreak when c1irect violence is the cause of fract ure ? ... ... ... . ..
Where does a bone break when indirect violence is the ca use of fracture?
TIow maya fracture be caused by muscular action?
In what two ways may fractures be classified? .,.
What is a simple fracture ? ..
'''hat is a compound fracture?
\Vhat is a complicated fractmc )
\Vhat is a comminuted fractul"l ?
\\That is a green-stick fractL.-L·?
\Vhat is an impactecl fraclun:?
"That fractures a ffo rcl the most complete example of the signs and symptom.' ?
In making up your mind whet her a fracture haJ uccurrerl or not, what points should you take inlo considelation beyone! the and symptoms?
apparatus may be necc%ar) for the treatment (If fractures?
may splints be
may l:anclages be improyised?
Describe ESl1larch' triq,ngular bandage .. 37. 38 (Fig. 'S)
In what ways may thetriangularhandage be folded for use? 37
IIow many kinds of arm,slings are there, and whal are thL y called?
' \'hal knot is to be tied, and what knot avoided?
What is the object of first aiel treatment uf fractures? -I I
the general rules for the treatment of fractures
should spli'nts b@ applied?
\\'hat may cause a flactnre of the upper parl of the clanium?
6 6
PAGE
... .,. ... ... . ..
. . . 22 22 22 22, 23 23 23 23 23 25
25 25 26 26 26 26 to 28 28 30 30 3 I 3 I 3 2 32 32 33 33 33 3j, 34
. .. . . . ... . ..
... . .. State
111:1)'
PAGR 33 3434 3-!-, 35 3434 34 35 35 35 present in a case of fracture ... ... .. 35. 36
the general igns and symptoms that
be
... .. ... ... . ..
... . .. 15 \"hat
.. . .. . .. . 36 IIow
. ..
IJow
... .., ... 17
36,37
.. . ...
... ...
'"
39. -!-c -!-9
..
, -!-o
... 4 1
...
Give
41 !Iow
.4 2 How should bandage be appiidl ?
4:!. 43
43
What may cause a fracture of the base of the 43, 44
\\'hat are the signs of fracture of the upper part of the cranium? ... 44
\Yhat are the signs of fracture of the base of the cranium? 44
\Vhat is the treatment for fracture of the cranium? 44
\Vhat are the signs of fracture of the lower jaw? 44
II ow maya fractured spine be caused? 45
\Vhat is commonly regarded as a broken back? ... 45
\Vhat are the symptoms of a fractured spine? 45
H ow may ribs be fractured? 46
How maya fracture of ribs be complicated? 47
State the signs and symptoms of a simple and of a complicated fracture of ribs 47
V,Th at is a frequent cause of fractured collar-bone? 48
\\'h at are the signs and symptoms of fractured collarbone? .. , .. , .. , ." .. , ... .. 48 , 49
At what points may the bone of the arm be broken? ... 52
Are the gene ral signs and symptoms of a frac ture always present in a broken forearm? ... ... ... 54
State the cause of a common fracture of the radius 55
H ow would you rec ognise a f.-actur e of the pelvis? 56
At wh at points may the thigh-bone be broken? .. , 57
\Vhat are the signs and symptoms of fracture of the thigh-bone? 57
\Yhat are the causes of fracture of the knee-cap? ... 58, 59
\Vba t are the signs and symptoms of fracture of the knee· cap? 59
Ar e the general signs and symptoms always present in a fracture of the leg?
What mistake may easily be made when the fibula is broken near its lower end?
What is a dislocation?

60
60
62
State the signs and sym ptom s of dislocation 63
State the treatment of el i location... PAGE
What is 3. sprain? ... ... 63
What are the signs and sympt oms a ?
Stale the treatment of a sp rained ankle ... ;-
Slate the treatment of othe r .sprains ... ... . .. 63, \Vhen not su re whether the lI1jury is a sprain or fraclure 5 how would you treat it? '" .. .
J:I0w may ':l1uscles be strained or ruptur ed?
State the an d symptoms of ...
State the treatment of s> Jains
First Students shoul? practise improvising material, foldll1g bandages, tyll1g knots making slinas ant.! the treatme nt of the following injoll'ics. b
Impro , ising splints ...
Improvising bandages
and granny knots
Knot for applying splint to lower limb ... .. .
FracLu.res-Lower 44· Spine, 45, 46. (sImple and fractures), 46 to 48. Breastbone, 48. Collar·bone, 48 to 5 I Both collarbones, .5 r. A rm, close up to shoulder, 52. Arm, near 1l:ld.dle of shaft, 52. Arm or forearl1l when the elbow IS mvol:red , 53. Forearm, 55 . Crus hed hand, 55, 56. PelVIS, 56. Thigh (man), 57, 58. Thigh (woma n, or man when single-handed), 58. Kneer lP, 59, 60. Leg (man), 60, 61. Leg (woman or
. when single-handed), 62. Cru shed foot, 6;. of doors al1( 1 inu uo rs 6 1 6
SpralOed ankle ... ... ... .). 64
Strains and ruptured muscles 61
68 PAGE
Folding
Large arm sling .. . 36 , 37 37 37 39 Small
.. . Reef
... . .. ...
bandages
arm sling
39,40
40 42
CHAPTER III.
Ti-IE OF CIRCULATION.
TH L OToans concerned in the circulation of the bl ood are the Heart, the Arteries, the Veins, and the Capillaries.
The Heart is situated in the chest behind the breast-bone and rib cartilages, between the an 1 im 'nejiateiy above the diaphragm; it lies obliquely \vith a quarter of its bulk t o the right and the r ema ining three-quarters to the left of the middle line of the body, Its beat may be felt ju st below amI to the inner s ide of the left nip;)Ie. T he heart has four, cavities, tw o on either side of a central partition, Th e t wo upper cavities are named the right and left auricl es, the two lower the right and left ventricles.
4\rt e ries nre vessels \\ hich convey blood from the h eart. Veins carry blood to the heart. Capillaries connect the arteries and veins.
In the general (systemic) circulation arterial blood is driven from the left ventricle of the heart into the aorta (the main artery of the body). From the aorta branch arteries are given off to all parts of ti1e body . These divide and sub-divide, and b ecome so small as to assume microscopic dimensions, whe n they ::Ire termed capillaries.

.L. Larynx (voice box); T. Tracl11a (\rind'pipe : r"L. RIghi Lung; L.T.., Left Lung (the lungs are drawn kl.CI, to expose the hca,rt and blood ,vessels); R ,A. Right 'uricle ; L:A, Left AUrJcle ; R.V, RIght Ventricle; L V Left \ t'nt,l'lcle j P A. Pulmonary ArterJ: ; Ao. Aorta; S. V,C. Superior \ ena cava (the large ve1l1 carryIng blo?d from the upper part of body t.o the heart) ; 1. V . C. Infenor vena cava (the large veIn, carrying blood from the 100:er part of the body to the The four pulmonary veIns cannot be shown in the dIagram
70
FIG . 36.
In the capillaries an interchange of gases and fluids takes place, whereby th e nourishment and mainten::mce of the tissues and organs of the body are provided for, and the blood becomes dark and impure.
Venous blood pass es from the capillaries to the veins, which convey it towards the heart, getting larger and larger as they proceed by being joined by n eighbouring yeins until they finally, as two large vess els, reach the right auricle of the heart. The vein, especially in the limbs, are provided with valves at fre q uent intervals, which prevent the backward fl J W of the blood.
The pulmonary system of blood vessels is concerned in carrying the blood through the lungs. From the right auricle the blood pass es to the right ventricle, and is thence carried to the lungs, where it is purified by contact with air, and becomes scarlet in colour; it is then conveyed to the left auricle of the heart anJ passes into the left ventricle, thus completing the circulation.
The heart contracts in adults at an average rate of seventy-two times a minute, but the rate varies, incr easing as the position is changed from the lying to the sitting or to the standing position; hence the importance of adjusting the patient's position in cases of hremorrhage. At every contraction Df the left ventricle blood is forced into the arteries, causing the pulse. which may be felt wherever the finger can be

Explanation. - In the middle of th e diagram is the heart with , its four chambers. .A bove the l- heart is shown the lung (pulmonary) circulation. The lower part represents the general (systemic) circulation. Vessels containing impure (venous) blood are shown black, while those containing pure (arterial) blood are shown white. The connecting vessels represent the ca:J;;laries. The arrows show th.:! Jirection of the flow of blood.
placed on an artery as it passes over a bone. In the veins no pulse is to be found.
H.tEMORRHAGE.
Hremorrhage, or bleeding, is of three kinds :1. Arterial. 2. Venous. 3. Capillary.
73
FIG. 37.
DIAGRAM 0:" THE CIRCULATION OF THE BLOOD.
ARTERIAL HtE:llORRHAGE.
I.·- Bbod from an artery is scarlet.
2. - If the wcunded artery is near the skin the blood spurts out in jets corresponding to the pulsation of the heart.
3 -The pressure point (see below) is on the heart side of the wound.
ARREST OF ARTl!:RL\L HJE,lORRHAGE.
Arterial hcemorrh:lge is, "..hen pmcticable, to be by pressure, position of the body, and ele\'ation of the bleeding
Pressure may be :-
I.-Digital-that i':i, applied with the thumb or fingers, and may be (a) on the \,"ound; (b) at a sput call.;d the pressure point. The pressure points are indIcated by nutnbered dots on the frontispiece.
2. --By a pad and bandage (tOUl niquet) (a) on the wOllnd; (b) on the pressure point.
3 - By flexion.
To apply a pad and bandage to the wound, place a piece of lint or linen or a clean handkerchief folued into a hard pad, on the bleeding point, amI secure it bv a bJ.nc1age tightly tied round the injured part. To fold the handkerchief, bring the four corners to the centre, and repeat the process until a hard pad is formed. The smooth surface is
75
placeJ on the wound, and, to prevent the pad from unfolJing, the puckered surface may be stitched or fixeJ by a safety pin. A hard substance, such as a stone, may be enclosed in the centre of the pad.
A Tourniquet may consist of a pad to be placed on the pressure point, a strap, or. bandage t'J encircle the limb and pad, and a tlglztelltlZg arrange ment, such as a stick or other means of t\\:isting the band to tighten it. .
To improvise and apply a tournlquet. :-
I.-Apply a firm pad on the pressure pomt. .
2.-Encircle the limb by a narrow bandage wIth its centre over the pad.
3.-Tie the ends of the bandage in a half knot on the opposite side to the pad.
4.-Lay the t\\"isting stick on the half knot, and over it tie a reef knot.
S. -1'\\ ist the stick to tighten the bandage, thereby pressing the pad upon the artery, and arresti ng the flow of blood.
6.-Lock the stick in position by the ends ot the bandaae already applied, or by another ban lage rounu the stick anu limb.
The paJ of the tourniquet must be accurately pbced upon the pressure so to compress the artery; othennse artf:"rl8.1.bloo.d \\' 111 • be allowed to along the limh, and the Yems, beIng compressed by the tourniquet, will not allow the
t'>lood to return through them to t he heart, and the result wlll be dangerous swelling and conge tion
Sho ul d a suitable pad not be at hand, a knot may b e made in the centre of the bandage, and when available, a ston e, cork, etc, enclosed in it to give it firmness and bulk . See that the bulging and not the fl It side of the knot is next the skin .
An elastic banda g e passed tightly round thf limb, immediately above the seat of arterial hremorrhage, will arrest bleeding . The simplest prepared form of this bandage is a strip of elastic webbing, twenty-fiv e to thirty inches long a n d two inches wide, with a piece of tape sew n at each end . An elastic belt o r brace will serve the same purpose. Except when part of a limb is torn off, it is not advisable to use an elastic cord or bandage if other apparatus can be had, as it c u ts off all circulation in the limb.
Flexion co nsists of the application of a pad on the pressure point at the knee or elbolV joint, fl exing the limb to make pressure, and securing the limb in t he fl exed position by a bandage crossed like the figure 8.
GENERAL RULES FOR TR EATMENT OF A ACCOMPANIED BY Al<TERIAL HJEi\IORRHAGE .
1. Stop bleeding.
U. Prevent injurious germs fr om getting into the wo u nd.

77
To attain these e n ds :- . .'
1. Place the patient in a suitable POSlt1Olf, bearin a in mind that the blood esca pes With less force when fhe pati e nt sits, and is still more checked \\"hen he lies down.
2. Iilevate the bleeding part , as thereby less blood finds its \\ ay into it.
3. Expose the wound, removing whatever cloth ina is n ecessary. (See Rule 8, a.)
4. Apply digital pressure . , (a) If the wound is small o n the bleed1l1g spot., (b) If the wound is large on the P01l1t nex t to the wound on the heart Side. The nearest pressure point is .choser: in order to avoid cutting off the CIrculatIOn fron: as much of the part as possible, but S?metlmes it is necessary to apply pressure still nearer to the heart.
S. Remove foreign bodies , as broken gJasJI bits of cl othing, hair, etc, see n 111 the wound j Ur.. not search for foreian bodies you can n ot see .
6. Cover the with a clean and fir!? absorbent dressing. A hard dry pad of boraCIC gaute or lint is to be preferred, but , wool, lint, or g lu ze, or a clean piece of 11l1fn wIll answer the purpos e . Should allY be entertai n ed as to the cleanliness of the dress1l1g, a clean piece of unprinted paper, such as the inside of an
76
78
em el?pe, be placed next the wound befure applying the pad. (Compare pages 75 and i6.)
7. ,Bandage tightly over the pad unless :-
a) ForeJgn bodJes are s uspec ted to Oe left unseen In the wound.
(I) There is danger of causing injury to a fract ur e. these cases a light dressing only should be applIed.
8. Apply a pad and bandage or flexion on the pressure point (see Rule 4 b ) but only in the following cases: - " .
(a ) A:; a temporary measure while the wound is being exposed, exami n ed and covered.
(b) As a more permanent measure \yhen bleed ina cannot be stopped by the pad a n ll on the wound, or \vh en, in accordance with Rule 7, the tizht bandage has not been app li ed .
9., Afford support to the injured part.
. \\ hen part of a limb has been torn off or the \\"ound IS lacerated (for example by the claw of an animal or b) 111.1chinery) ht:el11orrhage frequently does n ot come on at once, out as there is a d ange r of severe hren:orrbage later, meallS for its arrest should be applJed to limb, but not tightened unless necessary. not llJsturb a clut of blood form ed over a \y ound.
. 0 should be made to cleanse a wound e:,cept \\ Ith sterilised \Yater (that is previously boiled

and allowed to coo1), a nJ eX[1erience, especially in recent wars, has shown that those \\'ounds \\ h ich were prO\'isio nally treated with a dry dressing and subsequently dress.ed by a s ur geon with proper appliances did best.
Students p,actising arrest of arterial ht:emorrhage should feel the pulse to see ",hen the current of blood in the arte ry has been stopped, and should then Immediately relax the pressure made on the artery In this way th e importance 'lf the accurate application of pressure will be realised, and the amount of force necessary will be ascertained.
THE COURSE OF THE ARTERIF:S, TH ARREST OF H1E:\IORRHAGE.
(The numbers of the pressure points refer to those on the Frontispiece.)
THE LARGE ARTERlE \V ITHIN THE CHE T A:\,D ABDO;\fE T
The Aorta is the central or trunk artery of the body . Commencing at the lett ventricle it forms an arch behind the upper p:ut of the breast-bone. From the arch are given off the large branches which carry the blood to either side of the head and neck and to the upper limbs. The Aorta passes down 011 the left of the spine to just below the navel, \\ he re it divides into two g reat branches (the iliacs)
79
which convey the blood to the organs III the pelvis and to th e low er limbs
vVounds of these arteries are one cause of internal h remorrhage (see page 96).
ARTERIES OF THE HEAD AND NFCK.
The Carotid Arteries (right and left) leave the up per part of the chest and pass up on either side of t he windpipe and, just below th e level of the angle of th e lower jaw, divide into the Internal and E,ternal Carotid Art eri es . The Internal Carotid Artery
asc ends deeply III the neck, and en te rs the cranium to supply the brain with blood. The External Carotid g ives off a number of branches; to the front the artery of the ton gue (Lingual), the artery to the face (Facial); to the back the Occipital; th e artery itself is continued upwards in front o f the ear , where it changes its name to th e Temporal, and supplies th e scalp in the neighb ourhood of the temples .
When a Carotid Artery is wounded, as in th e case of a cut tbroat, app ly the thum b of one hand on the artery at pressure point I, pressing backwards against th e and taking care to avoid the wind pipe . It may also be necessary to apply pressure "ith the other thumb above the wound for two reasons: (a) To arrest the flow of blood from the main (jugular) vein in the neck, which runs 81
alongside of the carotid artery and is usually wounded at the same time; (b) T o check the fl ow of blood from the upper end of the carotid artery itself, which is often considerab le owing to communication between the branches of this artery a nd those of its

fellow. Di gital pressure must be maintained, by relays of assistants if n ecessa ry, until the doctor arrives (Fig. 38) . The Facial Artery crosses the lower jaw in a slight hollow two fingers' breadth in fr o nt of the angle, and sends branches to the chin, lips, cheek, and
80
FIG. 38.
FIG. 39.
outsid e of the n ose. H cemorrhage from wo un ds of the below the level of th e eye is to be arrested by :-
(a) Digita l pressure on pressure poi nt 2 (Fi g . 39), or
(b) Grasping tIle lips or cheek on both sides of th e wound by the finger inside and th e tIlumb outs id e the mouth or vz"c.: vena.

4 1 ,
The Temp:Jral Artery may be fe lt pUlsating in front of th e upper part of the ear. H cemorrb age from the region of the temple may be arrested by pressure applied at pressure point 3 (Fig. 4 0 ).
The Occipital Artery supplies branches to the
region of the scalp from behind the ear to the back ot I he head. ,Hrel11orrhage from this region may be by dJ(fltal pressure on pressure point 4 four r. I b 0 , J reaclth behllld, tl:e ear (Fig. 4 I ). This point IS dlfficul,t to find, and It IS usually sufficient to apply pressure Imm ediately below the \\·ound.
Ha:!morrhage f: om the Forehead or anywhere in the Scalp may be arrested by applying a small firm pad on the point and securing It by a narro\\' bandage with its centre bid on the pad, the e n ds carried round the head in the direction most convenient, and tied ti ghtly ove r the pad (Fig. 42)
'When a ,\'ound of the forehead or scalp is associa ted with a fracture, the best plan is to apply a ring
4 2.
pad around the seat of injury, To make a rinO' pad, pass one end of a bandage round finge:s; pass the other e n cl o f the bandage through the rlilg thus and continue to pass it through and throu gh untIl the whole of the bandage is used and a rmg as shown in 1< ig. 43 is formed.
82
FIG.
FIG.
ARTERIES OF THE UPPER LIMBS.
The Subclavian Art .: ry passes from a point behind the inner end of the coUar-bone across the first rib to the armpit.
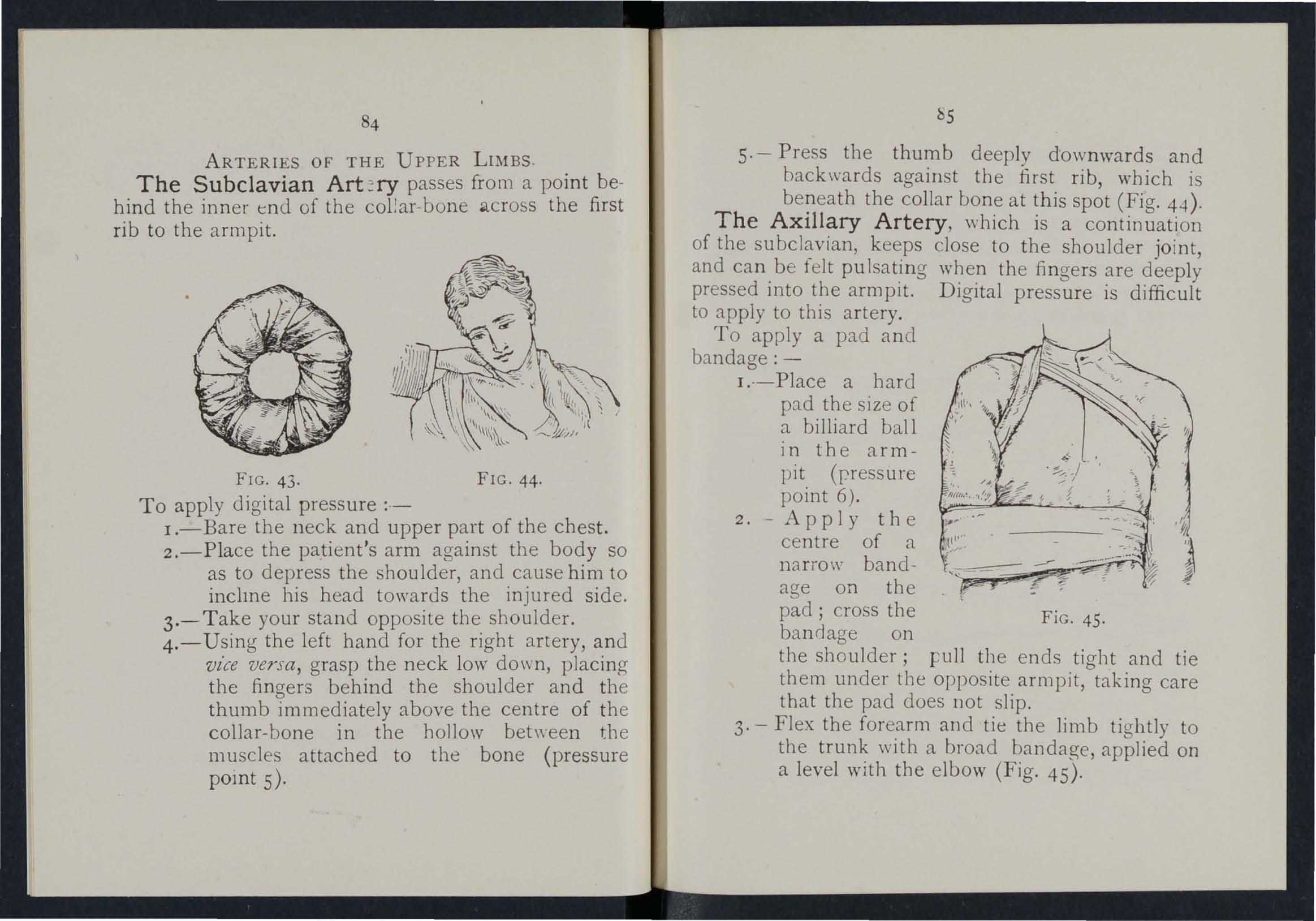
FIG. 43.
To apply digital pressure ;.-
FIG. 44·
I.-Bare the neck and upper part of the chest.
2.-P lace the patient's arm against the body so as to depress the shoulder, and cause him to inclll1e his head towards the injured side.
3.- T ake your stand opposite the shoulder.
4 . - Using the left hand for the right artery, and vz'ce versa, grasp the neck low do\Vn, placing the fingers behind the shoulder and thumb immediately above the centre of the collar-bone in the hollow between the muscles attached to the bone ( pressure POll1 t S)·
s· - Press the thumb deeply dow n wards and back\Vards against the first r ib, which is be?eath the collar at spot (Fig. 44).
The AXillary Artery , whIch IS a continuation of the keeps close to the shoulder joint, and can. be telt pu the fingers are deeply pressed ll1to t?e armpIt. DIgItal pressure is difficult to apply to thIs artery.
To apply a pad and bandage: -
J. ·-Place a hard p::td the size of a billiard ball in the armpit (rressure point 6).
2. - Apply the centre of a narrow bandage on the pad; cross the bandage on FiG. 45. the shoulder; Full the ends tiO'ht and tie them under tlle opposite armpit,btaking care that the pad does not slip .
3· - Flex the fore.arm and tie the limb tightly to the wIth a broad bandage, applied on a level wIth the elbow (Fig. 4S).
Th e Brac hi a l Artery is a continuation of the Axillary, and runs down the arm on the inner side of the biceps muscle, gradually passing forward until it reaches the middle of the front of the elbow. The inner seam of the coat sleeve above the elbow roughly indicates its course.
Digital or instrumental pressure may be applied at or near pressure point 7.
of the a.rm. over tbe seam of the CO.lt or the groove on th e mS.lde of the bictps muscle. Press the pulps (not the tips) 011 the artery (Fig . ..j.6). ome prefer to pass the han J over the front of the 111 uscle (Fig. 47) A slight turn of tbe hand out\\"ards as it grasps the arm \Yill better enStlre compression of the artery.
The Brachial artery may be compressed at the

FIG. 47,
To apply digital pressure extend the limb at right angles to the body, palm of the hand upwards. Stand behind the limb, and pass the fingers under the back
elbow (press ure point 8). by The pad may be a folded handkerchlef \\ Ith a small stone or a cork wrapped up in it, but when no pad is (wailable coat sleeye rolled or gathered up \\ ill serve instead (Fig. 4 8).
86
87
FIG 4:;1. lI G· 4 b.
Just below the elbow the Br.achial .artery divides into the Radial and Ulnar artenes, whIch. run al.ong the front of the forearm on the outer and mner sIdes respectively. The pressure (9 and 10) are about one inch above the wnst and about half an inch from the outer and inner sides of the forearm , where the arteries may be felt pulsating. Branch?s of these arteries join to form the Palmar 111 the hand. The arteries run along on f"ther sId e of the fingers to the tip.
.
Pressure may be applied to the Radial and Ulnar arteries at pressure points 9 and 10, by the thumb s (Fig. 49) or as follows :- . .
I. -Cut the cork of a quart or pll1t bottle m tw o length \-, ise.
2.-Lay the rounded side of one half on the Radial, and of the other half on the Ulnar artery.
3.- Secure them by a tight bandage.
To arrest hremorrhage from the palm of the hand :-
I.-Apply a firm pad, and make the patient grasp it firmly.
2.-Spread out a triangular bandage, I urn up the base about four inches, lay the back of the patient's hand on the centre of the fold the point over the knuckl es and wnst, pass the two ends round the wrist, make the

89
oatient pull on the point of the bandage, cross the ends over the fingers twice and tie them as firmly as possible. Bring the point (A) down to the knuckles and fasten with a pin at B (Fig. 50). . .
3.-Elevate the forearm and It w!th a "St. John II sling (see page 49).
Arterial hremorrhage from the fingers may be arrested by applying a small pad on the wound, and securing it firmly with a strip of tape, lin en or plaster.
.l..RTERIES
OF THE Lo YER LIJ\IBS.
The Femoral Artery, a con tin uation of the iliac, YI". Suo enters the thigh in the centre of the fold of the groi n, where it may be felt pulsatin g immediately below the ' skin . The course of the artery may be indicated by a line drawn from the centre of the groin to the inner side of the back part of the knee. After traversing two-thirds of this line, the femoral artery passes behind the thigh bon e to the back of the knee joint as the Popliteal artery.
Digital pressure may be applied to the Femoral artery at the groin (pressure point I I) as follows :-
I. -Lay the patient on his back.
88

2.-Kneel beside the patient.
3.-To fi'1d the groin, raise the foot high so as to flex the thigh; the fold in the clothing at the top of the thigh will indicate the groin
4.-Place the thumbs one on the other upon th e pressure point, grasping the thigh \\'ith th e hands (FIg. 5 I).
::.-Press firmly against the brim of the pelvi s. ) ,
As there is immediate danger of death it is important n ot to \\ aste tim e 111 removing the trousers.
When the Femoral artery is wounded in the upper third of its course, pressure must be maintain ed at the groin. No really satisfac· tory tourniquet has b een devised for compression ?t this point, an I relays of assistr.tlts should be employed to ke ep up the pressure until the doctor arrives; each fresh assistant plnces his thumbs over those of his predecessor, \\ho slips his away from beneath, and thus gushes of blood are prevented during the change.
Application of a tourniquet to the Femoral artery (pressure point 12) :-
\Vhen practi si ng compressi on of this artery, it 15 a llG. 52.
90
good plan to dra\V a chalk line from the centre of the groin to the inner side of the back of the knee' place the pad of the tourniquet on this line as high up as bandage can be applied. The pad should be the SIze of a lawn tennis ball (Fig . 52).
may be applied to the Popliteal arte ry by flexIon at the knee (pressure point 13); the pad

FIG 53.
be the size of a lawn tennis ball, or if no pad IS avaIlable trouser leg may be rolled or gathered up to ll1stE.ad. It is not necessary to take off the clothll1g ( Fig. 53) .
Just behind the knee joint the Popliteal artery ll1to the Anterior (front) and Posterior (back) Tibial arteries.
The Posterior Tibial Art e ry passes down the 93
back of the leg to the inn er side of the ankle. It is at first deeply placed between the muscles of the calf but it approaches the surface as it proceeds, so that it can be felt pulsating behind the large bone at the inner side of the It enters the sole as the Plantar Arteries, which run forward amongst the muscles to supply the foot and toes.
The Anterior Tibial Artery , on leaving the at once IXlsses forward between the leg bones, and, deeply placed amongst the muscles, runs dow n the leg to the centre of the flont of the ankle. This artery is continued as the Dorsal Artery of the Foot, which, passing forward over the tarsus dips down to the sole between the first and second metatarsal bones. Here it forms with the Plantar arteries what is known as the Plantar Arch.
At the ankle (pressure points 14 and IS) pressure may be applied by the fingers or by pads and bandages .
YENOUS HJE\rORRHAGE.
I. - Blood from a vein is dark red.
2. - It flows in a slow continuous stream.
3.- It issues from the side of the wound fu rther from the heart.
4. - In the case of a wound of a varicose ve in it fl ow.s also from the side of the wound nearer to the heart, especially if the p:.1tient is kept standing.
92

Varicose Veins. - The vems of the leg are specially apt t o become varicose. A varicose vein is dilated, wi nding, and with bead-like (varicose) projections along its course. A vein becomes varicose from several causes, such as long standing or tight garters. The first effect is to throlV extra work up on the valves, and the bead-like projections are c aused by the blood accumulating in the pockets behi nd the valves . In time the vein becomes so dIlated that the valves can no longer span it.
G ENERAL RULES FOR TREATMENT OF A WOUND ACCOMPANIED BY VENOUS HiEMORRHAGP:.
I -Place the patient in a suitable positio n, bearing in mind that the blood escapes with less force when th e patient sits and is sti:l more checked as he lies down.
2.-Elevate the part, as thereby Iess bloocl finds its way into it.
3· - Ex pose the wound, re movi ng \\ hatev er is necessary.
4· - Remove any constrictions, such as th e c ollar or garters, from th e heart side of the wound.
5· - Apply digital pressure on the wound un til you can apply a pad a nd bandage. If that doe s n ot stop the bleeding, mak.e pressure near the wound on the side away from the heart. In the case of a wound of a varicose vein it may also be necessary to 95
apply a pad and bandage to the vein immediately above the wound, especially if the limb cannot be maintained in an eleyated position.
6.-Treat the wound as directed by Rules 5,6 and 7, stated on pages 77 and 78.
7.-Afford support to the injured parl.
C.\PILLAR y IIiE\[oR RHAGE.
1.- The blood is red.
2.-It flows briskly in a continuous stream, or may merely ooze from the wound.
3.-It wells up fr um all parts of the wound.
.\ slight amount of pressure \\'ill suffice to arrest c.pillary hremorrhage.
I.\"TILR l AL HiE \lORRH,\G!L
Wounus of the blood vessels the trunk cause hremorrhage into the cavity of the chest or of the abdomen .
A.\"D SY1\IPTOi\IS OF I.\"TKR •.-\L
I.-Rapid loss of strength, giddiness and fain tn ess, espec ially whe n the upright position is assumed .
2.-- Pallor of the face and lips.
3.--Breathing bmried anu laboured, and accompan.ied by yawning and sighing.
4. -The pulse fails, and may altogether disappear at the wrist.
94

5.-The patient throws his arms tugs at the clothino- round the neck, and calls for au.
6.-Finally the patient may become totally unCOl1scious.
TREATMENT.
I.-Keep the patient in a recumbent position.
2.- Undo all tight clothing about the neck.
3. -Provide for free circulation of air; fan the patient. .
4. - Sprinkle cold water on the face; smell1l1g salts to the nostrils; avoid other forms of stlm ulants, at all events until the hcemorrhage has been controlled.
5.- Give ice to suck or .cold water to drink;. if the seat of the hcemorrhage IS known, apply an Ice bag over the region.
6.-Should the patient be reduced to a state of collapse, raise the feet and bandage the limbs firmly from the toes to the hips and from the fingers to the
HJE:\lORRdAGE FROM THE NOSE (NOSTRILS).
I.-Place the patient in a sitting position in a current of air before an open window, with the head thrown slightly back and the hands raised above the h ead .
2.-Undo all tight clothing around the neck and chest.
3.- Apply cold (ice, a cold sponge or bunch of
keys) over the nose and also the spine at the level of the collar; place the feet in hot \ovater.
4.-Cause the patient to keep the mouth open, and so avoid breathing lhrough the nose.
Blood issuing from the mouth may come from the tongue, the gums, the socket of a tooth after extract on, the throat, the lungs, or the stomach .
HiEi\IORRHAGE FRo:\r THE TONGUE, THE GUMS, THE SOCKET OF A TOOTH, OR THE THROAT.
1.- Give ice to suck or cold water to bold in the mouth. If tllis IS not successful give water as hot as can be borne to holJ in the mouth.
2.-If necessary make pressure on the carotid arteries.
3.-lf bleeding from the front part of the tongue is excessive compress the part by a piece of clean lint held bet" een the finger and thumb.
4.-If the bleeding is from the s06ktt of a tooth. plug the socket with a piece of c:ean lint or cotton \\'001; over this place a small cork or other subs.ance of suitable size, and insLruct the patient to bite on it.
HiEi\lORRHAGE FROM THE LU!-:Gs.
Blood from the lungs is coughed up, and is sc.lfie t and frothy in ar Jpearance.
Treat as for Internal Hcemorrhage (see page 95). E
96
97
HlE.\IORRH .GE FRO.\-I THE STOl\IACH.
Blood from the stomach is vomiled; it is of a colour and has the appearance of coffee grounds; It may be mixed with food. . a
Treat as fur Internal H<el11orrbage pabe 95), except that notbing is to be giyen by the mouth,
Blood issuing from the Ear Channel, which generZllly indicates a fracture <:>f. the base of tb e , t be \"1' ped [l\\'av as It Issues; no attempt cral1lull1, mus, ') . 's to be made to plus the C.IL

Tile 1Il/lli ends il/dimle the /,a;:':s wlh're the <lllswe's 11117)' be fellI/d .
\Yhat organs ae concerned in the circulation of the blood?
Descllbe the h<..Mt
Trilce the circulation of the blood through the b dy and lungs
How many limes a minult: does the h larL contract on the a\'crnge ?
Wbal is the elfu:L of the patient's posi ' ion on the rate at \\ hich the heart contrac lS ?
Wbat is the pulse? ,.. "
lIow many kinds of hremorrhage are lhere?
lIow would you know a case of arterial hrcmorrhage ? ...
In \\ hat way shou ld arterial be controlled ?
What is meant by " pressure puinl " ?
I {()\v may pressure be applied?
What is a tourniquet?
Why is accuracy necessary in placing the pad of a lourniquet ? .. , , ..
\\'he n mayan elastic IJ;l.l1 clage he used instead of a tourniqud?
\Yhat is fltxioll ?.. ..... ... ..
State general rules for treatment of a woulld accum·
panied by arterial h.:emorrhage .. 77, 78
If part of a limb had been lorn niT, but there \\a'i nut much bleeding, how would you act?
Should blood clots be disturbed ?.. ... ... '" it ",ise for an unskilled person to attempt to cleanse a \-vounel ? ... .., 78, 79
What is tl e aorl a? . . 79
99 O. CH ,\P fER III.
...
PAGB 70 70
;-0 to 72
72 72 73 74 7..J. 7<1 7..J. 75 75
D e"cr ibe the arteries of the head and neck 80
\V n)' is it sometimes necessary to compress the carotid ar,tery ?oth below and above the wound? .. , 80, 81
\\ haL IS a nng pad, and what is its use? ' ., 84 the arter!es of the upper limbs .. ' 84 to 89
D esc nbe the artenes of the lower limbs ... .., 89 to 93
H ,) w would you know a case of venous hreill orrh arre ? 93
vVhat is a varicose vein? ... ... ... . ..'" 94 maya vein beC0me varicose? ... ... .., 94
Slate the general rules.for treatment of a wound accompanied by hrem orrhage? .. , '" ... 94, 95
H ow would you know a case of capillary hremorrhage ? 95
Il ow you stop capillary ha!morrhage ? .. , ... 95 IS lllternal hremc.rrhage? ,., ". ., 95
\vh at would lead you lO. suspect in ternal hremorrhage? 95,9 6
Sta.te the treatment for Internal hremorrhage? ". 96
IITow would you ar:'est, hre1110rrhage from the nose? .. , 96, 97
\\ here may blood Issuing fr,om the mouLh come from?.. 97
HTow would you treat from the gums or throat? 97
\, hat else would you do If the tongue were bleeding?, 97
And if the bleeding: ,from the socket of lhe tooth? 97
How would you dl::;l1nglllsh between bleeding from lhe lungs and from the sLomach ? ... ... ... ... 97
And what would be the difference in the treatment?... 97
Of is bleeding from ear channel generally a sign? 98
Th e should. pracl1se placing supposed patients 111 a prope r posItIOn for the arrest of hremorrhage 72, 77 ancl.94), folding finn pacls (74 and 75), tyIng hard knots In bandages to form cttourniquet and the appl ication of pressure at all the pressure pOInts shown 1I1 the frontispiece, at various points on the forehead and scalp, and on the palm of the hand. Pres ure should be digital, by pad and bandage, or flexion, as directed in the text.

101
Pressure points - Carotid artery, 80. Facial, 82. T emporal, 22. Occipital , 83. Subclavian, 84. Axillary, 85 . Brachial (by pad and bandan-e , pressure being made against the humerus and "hy flexion at the elbow), 86. Radial and Ulnar, 87.
Femoral the groin, 90., Femoral in the thigh, 92. . PoplIteal, 92. Antenal and posterior Tibial artenes, 93.
IIremorrhage from the forehead or scalp",
Ilcemorrhage from the palm 'of the hand... . ..
Venous hremonhage from a varicose or other vein ... 93, 94
PAGE
100
:rAGS
1u2

CHAPTER IV. BRUISES.
A blow an) ",,-here on the surface of the body may caus e extensive h,-emorrhage beneath the skin, witho ut breaking it-a" black eye" is an instance . The injury is accompanied by discolor::1tion anJ swellll1g.
TREATME T.
A pply ice or cold water dressings . A piece of li nt soaked in extract of witch hazel may be placed on the affected part .
A i 0 SCALDS.
A burn is caused-
(a) By dry heat, such as fire or a piece o.f hot ir?l1.
(b, By a rail, wire or dynamo charged wIth a hIgh press ure electric c.unen t: .. .
({) By a corrosIve aCId, such as OIl of vltnol.
(d) By a corrosive alkali, such as caustic soda, ammonia, or qu icklime .
(e) By friction, caused, for example, by contact with a revolvin<T wh ee l. (Brush burn.)
A scald is c;used by moist heat, such as boiling hot oil or tar.
The effect l11::ty be a mere reddening of the skin blisters may be formed; or even the deeper tiss ues I 03
of th e body m:1y be charred and blackened. Th e clothing may ::tdhere to the burnt skl11, and its removal is impossible without further detnment to the injured pa rt. The great danger is Shock.
TR E.n 'I[V\' l'.
I.-Carefully remove the cJothing over the inj ured part. If stuck to the skin, the adherent cloth ing must be cut around with scissors, c;oakLd with oil, and left to come away subsequently .
2. - Do not break blisters.
3. - Immediately cover up the part. Soak or smear piec es of lint or linen ", ilh oil, or vaseline, I'mo lin e, or colc1 rream; a small quant ity of boraCIC po\v der added to these \\ III be of benefit.'" The inside of a raw potato scraped out and spread on lint mClkes a soothing aprhcation. 'When the injured ,-; urbce is exten<;l\'e do not cover It \\ ith one large sheet of lint, but \\ ith strips ab::>ut the breadth of the hand; this is ad\'is<lble they fit better on the p::trt, :md during subsequent dressings one strip can be re1110\'ed at a time, and a fr esh dressing applIed before the ad· jacent strip is taken off. The shock to the system is thereby less than if the whole of tIle burnt surface \\ ere laid bare to the air py the remoyal of all the dress ings at o ne time. ' Vhe n covered hy the OIly envelop the part 1I1 cotton \\ 001 or a plece of flanne l a nd a pply a bandage .
104
When the face is burnt, cut a mask out of lint or lillen, leaving holes for the eyes, nose and mouth. Dip this in oi l or smear it with vaseline and apply it to the face and cover it with cotton wool, leaving openings to correspond with the holes in th e mask.
Wh e n possible place the injured part in water at the temperature of the body (98 degrees) until sui ''lble dressings can be prepared. A d essert spoonfd of baking soda added to a pint of the warm water will make a soothing lotion.
As it is imp ortant not to leave the part exposed to the air, it is the duty of the bystanders to prepare the dres sings while the clothing is being removed.
4. - Treat Shock.- This is particularly necessary in the case of every burn or scald of any considerable extent (see page 135). Be very apprehensive of danger in the case of even slight burns of the nec k.
5. - If the burn is caused by a corrosive acid, bathe the part with a weak alkaline lotion, such as washing soda, baking soda (bicarbonate of soda), magnesia, or slaked lime in warm water before ' applying the dressings.
.s.-If the burn is caused by a corrosive alkali, bathe the part with a weak acid lotion, such as le mon juice or vinegar diluted with an equal quantity of water. Cautz"on.-Before using wat er brush off any lim e that remains on th e part.

105
7.-When a woman's dress catches fire -
(a) L ay the woman flat on the floor at once, so that the fl ames are uppermost; that is to say, if the front of the dress is on fire lay h er on her back, and if the' back of the dress is burning, place her face downwards. Th e reason for this is that flames ascend, so th at if the upright position is assumed, the fl ames will quickly reach and burn the body, neck, and face; or if the woman li es with the fl ames under most, they will, if unextinguished, pass over and burn the limbs and set fire to the rest of the dress.
(b) As soon as the woman is laid flat, smother the fl ames with anything at hand, such as a ru g, coat, blanket, or table cover; if made wet so much the better.
(c) A woman rendering assistance should hold a rug or blanket in front of herself when approaching the flames.
(d) If a woman 's dress catches fire when nobody is by, she should li e flat, flames uppermost, smother the flames with anything handy, and call for assistance, or crawl to the bell-pu ll and ring; on no account should she rush into the open air.
,T he u se of fire guards \\"ould prevent many calamiti es.

BITES O F SNAKE A:\ID RABID ANIMA L S, :\:\1 D WO UND BY PO I:::; Ol ED \\' EAPONS.
Hydrophobia is cJ.u"ed by the bite of animal, such as a dog, ut , fox, wo lf, or deer from r:1.1)les . The ' special poisons introd u c.ed ll1to \\ ounds caused by venomous snakes and pOIsoned we,lpons cause immediate danger to Me . place a con stric ti on be t w ee n the wound and t he heart so as to prevent the ve n ous blood from carr) ing the poison .through the body. If, for example, a finger is bitten It should encircled on the side of the wJund ne::uest to the with the finger and thumb, and as as possible a ligature (a string. piece of. tap::, or stnp of, band kerchief should be placed tight ly round the IOot of the finger. Compression with the finger and thumb not be relaxed unlll the ligature has been Additional l igatures may, with adYantage, be appltcd at intervals up the limb. .
2 - Encourage bleeding f<?r a time :-
(a) By ba thll1g the wound wIth warm \\'ater
(b) By keeping the in jured lim b low; the upper li m b shou ld be allowe d to hang do\\ n, and in t he case of the lower limb the patient sh o u ld be seated wi th the foot on the gr o und .
3.- Cauterise the wound, if it is qu it e impossible to obtain the services of a doc tor. This is best done by burning with a flUid caustic, such as caustic potash, pure carbolic acid, or nitric acid, or lf these are not at hand, \\ ith a red-hot \\ ire or a fusee.
The usual solid caustic is insufficient, as it docs not reach the bottom of the wound, wbere the poison is.
To ensure the caustic reaching the bottom of the \'.ouncl, it sbould be applieJ on a piece of wood, such as a match cut to a point. \Vhen the caustic h:1.s been thoroughly applierl, but not lill then, the ligatures may be removed.
4. - Cover the wound, after a wbile, with a cle;1O uressing.
S· Afford support to the injured pa rt.
6. - Treat shock if it occurs (see page 135\.
7. - 1n the case of a bite by a venomous s nake, rub in po\\'dereu permanganate of potash and inject under the skin in the neighbourhood of the wound a solutio n of pe r manganate of potash .
ST I i GS O F P L ANTS .AND A:-.J Il\ IALS,
These give r ise t o serious inconvenie n ce, and In some C:1.ses grave sy mptoms develop .
T REATMEWf .
I. - Extract the sting if left in .
2. - Mop the part freely with dilute ammo-nia
101)
l OS or spirits. A paste of bicarbonate of soda and sal volatile is an effi ie nt application . A solution of washing soda or potash or the application of tbe blue bag \\·ill re lieve p;::in.
3. - Treat coll a ps e if it occurs (see p8ge 135)·
FRO ST T ITE.
Dur in exposure to sc" e r 0 cold, parts of the body, uS 11all y the f<::et fin ge rs, n os e, or ears, IJse sensation and b ecome first w:n:y \\ hite and aft enrards congested and of a pur ple appear:mce. As sensation is l ost in the part, it is oft e n only by the remarks of bystanders that the frost· bitten perso n is made a\\'are of his condition . TR ;;: AT;\-IENT.
I .- Do not brin g t he pa t ient into a warm roo m until, by fri e t io 1 of t he band or by rubbing witb soft snow, se nsatio n ani circulation in tbe affected are rest o red . Neglect of tbis precaution may lea I to death of the tissues of the fr ost bitten part.
2. - When circulation is r esto r ed , keep the pal ie nt in a room at a temp e ra ture of 60 degrees.
NEEDLE El\IBEDDED U DER THE SKIN.
'"Ty"i1en a needle breaks o ff after penetrat ing the skin and take the patient to a doctor at once. If the "'ound is near a joint, keep the limb at rest on a splint.

109
FI::3H-HOuK E:\IBED OED L THE SKIN
.
Do not attempt to withdraw the fish-hook the \\ ay :t went in, but cut off the dressing of th t' hook, so that only the metal is left, and then force the point onwards through the skin until the hook can be pulled out.
INJURIES TO JOINTS.
\Vhen a joint is injured by a bullet, stab, or other cause-
I
.- Wrap the part in cotton wo ol.
2. - Afford -rest and support to th e injured li mb; if the upper limb, in a flexed po sition by a sling ; if the lower limb, in a straight positi on by a splint.
FOREIGN BODY IN THE EYE.
I
.- Prevent the patient rubb ing t he e ye, tyin g down a child's hands if n e cessary .
2. - Pull d J wn the lower eyelid , \yhen, if the foreign l')ody is seen, it can readily be removed with a camel's hair brush, or \\lth the corner of a handkerchief tv\ irled up and welted .
3. - When the foreign body is beneath the upper eyelid lift the lid fo rward, push up the lcwer lid beneath it and let go. The hair of the lower lid brushes the inner surface of the upper one, and may dislodge the body . 'hould the fil st atternpt be unsuccessful, re peat it se\'eral times if necessary. If
lIO
the fureig n body is not dislodged call the services of a doctor as soon as possible. When howeve r skilled help cannot be had, proceed follows
(a) eat the patient so as to face the light, and stand behind him, steadying his head against your chest .
(b) Place a small rod, such as a match or bodkin on the upper eyelid, half-an-inch above edge, pressing it backwards as far as possible.
(1-) Pull the upper -eye-lashes upwarus over the rod, and therehy evert the eyelid_
(d) Remove the foreign body. _
4.- When a piec e of steel is embedded in the eyeball drop a little olive or castor oil on the eyeball after pulling down the lower eyelid, close the lids, apply a soft pad of cotton \\"OJI and secure it by a bandage tied suffi ciently firmly to keep the eyeball steady; take the patient to a doctor.
s.-When quick-rime is in the eye brush a:,ay as much of it as possible; batbe the eye \\ith vInegar and warm water, and treat as for a piece c r steel embeJded in the eyeball.
FOREIGN BODY IN THE EAR PASSAGE.
As a rule make no -attempt to treat a patient ",ith a foreign body in the ear if the services of a doctor can possibly be had j any attempts to remove the foreign boely may lead to fatal If a child

III
can'not be induced to keep the fingers from the tie his bands down or cover UP tbe ear. If an ins, ct is in the ear-passage, fill the ear with oliye oil, \\ hen the insect will float and may be removed . Te':er syringe or probe tbe ear.
FOREIGN BODY IN THE NOSE.
Induce snee ing by pepper or snufL Cause the patient to blow bis nose yiolently after closing the unaffccteu nostril. Tllere is no immediate danger from a foreign bocty in the nose.
THE ABDOMEN .
The abdomen is bou n ded above by tbe diaphragm; below bythepelvis; Lehind bythelumbarvertebrce; ami in front and at the sides by muscular walls. (Fig. 54·)
THE OF THE
The Stomac h lies immediately below the" pit of the stomach" ju t below the breast-bone.
The Liv er lies in the upper part of the ab d omen, \\ here it is mostly covered by the right lower nbs.
The Spleen lies. beneath the rIbs at th e upper part of the left side of the ahdomen.
Th e Intestin e s occupy the greater part of the of the abdomen .
The Kidneys lie at the back, in the region of the loin.
The Bladder lies in the pelvis.
FIG 54.
WOUND IN THE WALL OF THE ABDOMEN.
When the z'ntestines or other organs protrude through the wound, whether vertical or transverse, bend the knees, raise th e shoulders, and apply lint, a towel, or cotton wool wrapped in soft lin en, anJ keep the

1I3
patient warm until the doctor arrives. " Then there is no protrusion of organs, if tlu wound is 'L'eniral, lay the patient flat on the back \\ ith the lower limbs straight ; if the wound z's tralZsverse, bend the knees and raise the shou Iders.
INJURIES TO THE ORG ANS WITHIN THE ABDnl\IEN AND PELVIS.
Injuries of the Stomach are attended by extreme and sometimes by vomiting of dark blood lIke coffee-grounds . For treatment see " H Gei1lorrhage from tbe Stomach " (page 98).
Injuries of the Liver, Spleen and Intestines may be caused by a blow, a stab or a bullet; the liver or spleen may be injured by a fracture of the lower ribs. The Signs and Symptoms are those of internal hGemorrhage accompanied by pain and swelling at tbe of injury, and the treatment is as for that condition (see page 95).
The Kidneys may be injured by a of the eleventh or twelfth ribs, also by a crusb, blow, stab or bullet. Blood may escaRe with the urine, al:d there may be pain and swelling over the injured kIdney. •
The Bladder may be inju··ed by a fracture of the pelvis . The sign.s and symptoms are eitber inability to pass water, or If a little is passed it is tinged with blood.
112
OF INlURY TO THE KIDNEYS OR BLADDER.
Keep the patient quiet until the doctor arrives.
2.-Apply h'ot fomentations over the painful or injured
Rupture (hernia) co nsists of a protrusion of an internal organ, usually the bowel, throu gh the m uscular wall of the abdomen, most frequently at the groin. Should a sudden swelling accompanied by pain and sickness take place in that regi on
I.-Send for a doctor instantly.
2.- Lay the patient down with the butto cks raised.
3·-A pply ice or cold water to the affected part.
QUESTIONS ON CHAPTER IV.
llUlIlera!s ind.-ca 'e tile pages wltere tlte an swers ?lta)' b,; fJUl/d.

How would you treat a burn caused by a corrosIve acid?
How would you, reat a burn caused by a corrosive alkali?
-hat steps be taken \,
a
the general I ules [or treatment of wounds caused by poisonous bites or
special treatment IS reqUlred for the bile of a yenomous snake?
\Y uuld you attempt to remove a needle em bedded under the
How would you extract a fish hook em beJded in the skin?
fur injuries Lo joints..
the general rules for r emoving a foreign body from
What would you do if a piece of stee l were embedded 111 the eye ball?
And when quick-lime is in the eye?
How would you try to remove an Insect from the ear passage?
114
lIS
Tile
P .\G K What i" a IJruise ? 102 IIow WLluld yuu treat a bruise? 102 How maya burn be caused? 102 How is a scald caused? ... 102 \Vhal is the great danger of a burn or scald? ... 103 State th u g ene ral treatment for burns and scalds . 103, 104
. .. ... ... . ..
"
hen
woma n's
catches fire? .,. . . . 104 104
..:
... 107
... ... ... .
108
. ... ... ... 108
dress
Slate
...
106, 107 \Vhat
IIow would you treat a sting?
1 07, 108 State the signs, symptoms and treatment of frost-bIte
skin?
... State
. ., ...
109 109
eye... .. , ... ... ... ...
the treatment
State
the
.109, 110
... ... . ..
..,
.
.. 110 1 IO III
,Vvuld you try to remove any other form of foreIgn body from the ear passage? ... ... ... I 10, I I I
How would you remove a foreign body from the nose? I I I
S tate the boundaries of the abdomen and its conten ts I II
State the treatm 11t for wounds of the abdomen... II2, II3
How may injuries to the liver, spleen and intestines be caused? .. . II3
\Vbat is the difference between treatment of injuries to the stomach and of injuries to the liver, spleen and intestines? .. , II3
State the treatment of injuries to the kidneys or bladder 114
State the trea .ment of ht:rnia II4

CHAPTER V .
TH E NERVOU.S SYSTBM.
Two systems (,f nen'es, the C \... reb ro-spinal and the Sympathetic, regulate the movements and functions of the body.
The System is made up of the Brain, the Spinal Cord and Nen' cs, and through its agency sensations are received and the will causes the action of the voluntary muscl es . For e ;a mple, when a part is injured a of pain is con"eyed to the brain by tile nc-rye, thus affording an indication of the se:1t of injury, or a warning of a possible danger of further dam:lge. On attention being directed t.o the injury, an attempt is instantly made to ease the pain or to mo\' e the injured part from danger.
The Brain is situated \\'itbin the cranium, and is di\'ided in the midule lin e, so that, with the exception of some connecting bands, the right and left sides are sep::1ratc.
The Spinal Cord is the long cord of nervous m8tter lying with in the spinal canal (see V e rtebral Column, page 23) It leaves the brain through an opening in the bJ.se of the crani um and extends to the upp e r lumbar vcrtebrre.
II6 PAGE
H']

IIS
The Ne rves proceed from the brain and spinal cord in pairs as pearly-white trunks, aml their branches can be traced throughout the tissu es of the body. Wh e n a nerve is torn through ther e is plralysis of motion and sensation in the rEgion in which its branches are distributed.
The S ympathetic S ystem extends as a nervous chain on each side of the front of the spinal column along its entire length, and sends branches to all the organs of the chest and ahdomen to control the involuntary mus les, and thereby regulate tho; vital functions. This sysleil1 is not under th e control of the will, and acts alike during sleep and a.cliyity.
THE RESPIR,\ TORY SYSTE:\I.
The air reaches the lungs by way of the nostrils (or mouth), the throat, th2 wind-pipe, and the bronchial tubes. The nostrils convey it to the back of the throat, whence it enters the wind -p ipe by an opening guarded by a of trap door or valve, so that in health nir, but not solids or fiLlids, Illay enter. During insensibility, howe,-c r, the valve fails to act, so that should solids or fluids be given by the mouth, they may enter the \\ ind -pipe and cause lsph)'J\ia. The \\ ind-pipe extends to t\\ 0 inches belo\\' the top of the breast-bone, where it divides into the right and left bronchial tube . Each bronchial tube enters a lung and divides into small and still s!11aller tubes, until
II9
FIG. 55. THE LUNGS AXD DIU:->CHIAL TUBES.
A. Trachea, or \\'ind-pipe. B. Lefl Bronc.hus Bronchus. D. Smaller Bronchial Tubes. c. Right
121

the ultimate recesses of the lung - the air cells or air spaces - are reached.
The Lungs, Right and Left, occupy the greater part of the chest; they lie immediately within the ribs, and practically wherever a rib is felt, whether front, back or sides, there is lung beneath. Each lu ng is enveloped in a fine membrane (the pleura) which allows it to move within the chest during breathi n g \\ ithout friction.
Re s piration, or breathing, consists of two acts, Inspiration, an expansion of the chest, duri g which air is drawn into the lungs, and Expiratio n, a contraction of the chest, during which air leaves the lungs . A pause follows the act of expiration. In health fifteen to eighteen breaths are taken per minute, and at each inspirJ.tion about 20 to 30 cubic inches of air enter the lungs, and a similar quantity is expelled at each expiration.
T he expansion and contraction of the chest are e ffected partly by the muscles of r espiration attached t o t he ribs, but chiefly by the Diaphragm, the large arch ed musc ul ar partition which separates the chest fro m the abdomen. I n inspiration, which is chiefly a muscular act, the ribs are raised, and the arch of t h e diaphragm falls and becomes flattened, thus increasing the capacity of the chest and causing the ai r to enter. In expiration, an act performed almost withou t effo r t , the ribs Ltll and the arch of the
diaphragm rises; this lessens the capacity of the chest and forces air out. The mechanism of respiration is somewhat like that of ordinary household bellows, but without a valve; the ribs may be compared to the boards of the bellows, \\'hile the diaphragm corresponds to the leather, the air passages being equivalent to the nozzle.
As the blood depends upon the air for its purification and the oxygen necessary to maintain life, interference with breathing very soon may Rrod uce a dangerous state called asphyxia, examples of which 3re afforded by drm,Yning, suffocation, choking, etc.
ARTIFICIAL RESPIRATION .
PROFESSOR SCHAFER's METHOD.
I.- Make no attempt to loo sen or remove cloth·ng.
2. - L ay the patient in a p r one pos it ion (i.e., back upwards) with his head turned to one side, so as to keep his nose and mouth away from the ground. No pad is to be placed under the patient, nor need the tongue be drawn out, as it will fall naturally.
3. - Kneel at one side facin g the patient's he ad , and place the palms of your hands on his loins, one at each side, the thumbs nearly touching One another in the small of the back, and the fingers extending over the lowest ribs. Leaning your body forward, let its weight press straight dO\\"ll\\'ards upon the
120
loins a n d lower part of the back, compressi,ng the a b domen against the ground and dnv In g aIr out of the ch est. This produces expiratio n (Fig 56). Draw back

FIG. 56. EXPIRATION.
FIG . 57. r:\'SPIRATION.
12 3 your body somewhat ll'lOre rapidly and relax the pressure, but do not remove your h::l.l1ds; this produces inspiration (Fig . 57).
4 - Al t ernate t he se m oveme nts , by a rhythmic s\\ aying backwards and forwards of your body, twelve to fifteen times a minute, per:,evering until respiration is restored, or a doctor pronounces life to be extiect.
DR . SILVES rER's
I - Adjust t he pa t ient's p osition .-vVithout wasting a momt'nt place the patient on his back on a fl.Lt surface, inclined if possible from the feet upwards . ' Remove all tight clothl11g from about the neck and chest, and bare the front of the body as far as the pit of the s 0 nach; unf lsten the braces and the top button of trousers in me n, and the corsets in women. Ra'se and support the shoulders on a small, finn cus'.l ion or folded article of dress placed under the shoulder-blades.
2 - Ma i ntain a free entra n c e of ai r in t o w in dp ipe -Cleanse the bps and nostrils' open and wipe tile mouth; an assistant must draw forward the patient 's tongue as far as possible, and keep it in that posil:on .
3 ·-Imitate t he movem e nts of bre at hing . Indllce I11Spiratioll . - Kneel at a convenient distance behind the patient's head, anJ grasping his forearms just below the elbo \, draw the arms
122
upwards, outwards, and to\\'ards you, with a S.I eeping movement, making the elbows touch the ground

LXl'IRATIO:-':.
(Fig. 58). The cavity of tIle chest is thu s enlarged, an d air is drawn into the lungs.
124
FIG. Sl5. INSPIRATI O N.
125
induce expiratz'on.- Bring the p8tient's flexed arms slowly forward, downwards and inwards, press the arms and elbo\\s firmly on the chest on either side of the breast-bone (Fig 59). By this means air is expelled from the lungs.
Repeat these move (,ents alternately, deliberately) and perseveringly about fifteen times a minute.
"\Vhen a sufficient number of assistants are present, HOWcl.rcl's method nny be CO:11 bined \\ith Silvester's, as follo\\ s : -
Th, J.dditional assistant kneels astride the patient's hips wIth the balls of the thumbs resting on either side of the pit of the stomach, and the fingers grasping the adjacent parts of the chest. Using his as a pivut, he presses forward on bis hands. Then suddenly, with a final pusb, he springs hack and remains erect on his knees \\ hile counts I, 2, 3. These motions are to be repeated to correspond with those being performed by "'11vester's method, pressure on the chest being made simultaneously by those performing the hYJ methc ds (Figs. 60 and 6 T).
METHOD.
'Vhen from any cause the above methods cannot be carried out, Laborde's method of artificial respiration should be tried. It is especially useful in suffocated children, and when the ribs are broken.

12 7
The patient is placed on his back or side; the moutl: cleared; the tongue is seized-using a handkerchIef or something to prevent it slipping from the fingers-the lower jaw depressed; the tongue is pulled forward and held for two seconds in that position, then allowed to recede inlo the mouth. These movements should be repeated about fifteen times a minute.
Artificial respiration must he continued until breathing is established, or until a doctor arriYes. When natural breathing commences, reaulate the artificial respiration to correspond \\ ith it Success may result even after two hours' time.
Excite respiration.- "\Vhilst artifical respiration is being other useful steps may be empluyed, such as applymg smellmg salts or snuff to the nostrils, and flicking the (hest with a damp towel.
Induce circulation anJ warmth after natural breathing has been restored. \Vr<.,]) the patient in dry blankets or other covering, and rub the linl bs energetically towarJs the hearL. Promote \\ armth by hot flannels, hot-water bottles, or ho bricks (wrapped in flannel) applied to the feet, to the limbs and body. When the power of swallowil1g has returned give hot tea or coffee, or meat extract. The patient should be kept in beel and encouraged to go to sleep. Large poultices or fomentations applied to the
front and back of the chest will serve to assist breathi ng. . Watch the patient carefully for some to see that the breathing does not fail j sho uld sIgns of failure appear, at once begin artificial respIratIOn.
INSENSIBILITY.
Unconsciousness or Insensib ility arise as follows :-
Injury to the H I- ad. -Concussion and Compression of the brain.
Disease of the Brain. - Ap oplexy, Epilepsy, Hysteria. . .
Various Causes. -Shock, Fal11tl11g (Syncope), Coll apse, Alcoholic and other po.isonin g, Sun.stroke and Heat-stroke, Infantile ConvulsIOns, Asphyxla.
GENERAL RULES FOR TREATMENT OF INSENSIBILITY.
I. - If a person appears about to lose sciousness, prevent him from falling, and lay hi m gently down.
2.- Arrest Hcemorrhage when apparent; attending to minor injuries is less important than treating the unconscious state. ... .
3. - Lay the patient in the poslti<?n lI.1 whic h breathing is most easy-usually thIS wIll be on t he L'ack, or inclined to one side. As a general rule

129
raise the head and shoulders slightly when the face is flushed, and keep the head low when the face is pale.
4·-Undo all tight clothing round the neck chest and waist, unfastenin g the braces and top button of the trousers in men, and th e corsets in women, the objec t being to relieve pressure on the air passages, lun gs , heart and abdominal organs. Be sure that there is no obstruction to the air pa'ssages by the tongue or by a foreign body in the throat. The possibility of false teeth obstructing breathin a must be considered .
0
S·-Provide for a sufficiency of fresh air by open ing doors and wind o\\'s, and by keeping bac k a crowd .
- When breathing cannot be discerned apply artificial respiration.
7.-0btain a docter's help as soon as poss ible.
S.-Unless unavoidable, never leave the patient until you have placed him in charge of a responsible person.
9.-Give no food or fluids whatever by the mouth while the patient is insensible.
rO.-Should the spine or an important bone of the upper or of the lower limb be fractured it must be steadied and maintained at rest as soon Should the unconsciousness be prolonged. tne patIent may be removed in a rec umb ent position
F
to shelter, provided that the broken bone is adeq u ately supported .
II.-When the patient is in a state of co nvulsion , su pport his head, and after wrapping a piece of wood or any uther hard material in .handkerchief, ho ld it in his mouth to prevent bItmg of the tongue . Do not forcibly restrain hi.s lim?s j prevent him from hurting himself by pullmg hIm away from a source of danger, such as machinery, a wall, or fireplace ; light pieces of furniture should be pushed out of the way.
12. - 0n return to consciousness may be given to drink. If the p u lse is warm tea or coffee, provided hremorrh age, eIther mternal or external, is not present. A desire to sleep. sho.uld be encouraged, except in cases of opiurr: pOlsonmg, a condition thn.t may generally be by the history of the case, and also by the pupIls of the eyes (the black openings in the b l ue brown iris) being min utely contracted (pm-head pupIls).
13.- It must not be assumed a perso n is insensible as the result of dnnk me -el y because the breath smells of alcohol ; frequently when people are feeling ill they take or are given alcoholic stim u lants, afte r which they may become insensible not from the drink, but from the cause that them to take it, for example, insensibdity coming on, effects of poisoning, etc. Even if

13 1
drink is bel ieved to be the actual cause of insensibility, it must be borne in mi n d that the patient is in a very dangerous state, and he must be treated for Collapse by being covered up and kept ,,,arm.
The above general rules will en able first aid to be rendered efficiently in most cases of insensibility, although the exact form from which the patient is suffering is unknown.
CONCUSS I ON OF THE BRAIN.
The patient may be stunned by a blow' or fall on the head, or by a fall on the feet or lower part of the spine. He may quick ly regain consciousness, or insensibility, more or less complete, may be prolonged.
TREATMENT .
I.- Apply the gen eral rules for the treatment of Insensibility.
2. - Be very apprehensive of dange r in a ll cases of injury to the head. The patient may be stunned, and after a short interval may recover some degree of consciousness, or even the brain may apparently have escaped injury; yet in both instances there is a grave risk that a structure within the cranium has been injured, and that a serious state of insensibility may develop later. (See Fracture of the Cranium, page 43). A caution should therefore be giYen to a patient who has lost consciousness even "' . ?
130
13 2
for only a moment after an inj ury to the head not to resume physical or mental activity without the consent of a doctor.
COMPRESSION OF THE BRAIN, APOPLEXY.
Compression of the Brain may result from the same causes as produce Concussion; in fact, Compression is frequently preceded by Concussion.
Apoplexy usually occurs in elderly people, and no signs of injury are necessarily present.
In both c Jnditions the face is flushed; the breathing stertorous; one side of the body may be more limp than the other, and the pupil of one eye may be larger than that of the other; the temperature of the body is generally raised.
TREATMENT.
I. - Apply the general rules for treatment of Insensibility.
2.-Promote warmth in the lower part of the body by the application of hot water bottles to the abdomen and lower limbs. Care must be taken not to burn the patient with the bottles, which should be wrapped in flannel, and their heat tested with the elbow . EPILEPSY.
Epilepsy may occur in persons of any age, but usuallY:>Gcurs in young adults. The patient falls to

133
the ground, sometimes \\'ith a scream, and passes into a state of convulsion, throwing his limbs about.
The treatment is according to the G eneral Rules, especially Rule II.
HYSTERICAL FITS (HYSTER IA).
SIGNS AND SV1IPTOl\IS.
The patient, usually a young girl, in consequence of mental excileme,1t, suddenly loses command of her feelings and actions. She subsides on a couch or in some comfortable position, thro\\ s herself about, grinding her teeth, clenching her fists, shaking her hair loose; she clutches at anyone or anything near her, kicks, cries and laughs alternately. The ey.eballs may be turned up\\'ards, and the eyelids opened and shut rapidly. At times froth appears at the lips, and other irregubr symptoms may develop.
TREA EKT.
I.-Avoid sympathy \\ith the patient, and speak firmly to her.
2.-Threaten her with a cold water douche, and If she persists in her "fit," sprinkle her \yith cold water.
3.- A rply a mustard leaf at the back of the neck.
Medical treatment is necessary to cure the condition of mind and body which gives rise to hysterical attack s.
SHOCK, FAINTING (SYNCOPE), COLLAPSE.
CAUSES. '
I.-Injury in the regio n of the abdomen, extensive wounds and burns, fractur es, lacerated wounds, and severe crush are some o f th e more frequent physical causes of shock.
2.-Fright, anticipation of injury, and sudden bad new s, or sometimes sudden removal of fear and anxiety after prolonged suspense, produce shock OT fai ntin g.
3.-Some poisons cause shock, while others, such as alcohol, so depress the nervous system that coll apse ensu es.
4.-Hcemorrhage or heart weakness, a close or crowded room, tight clothing, fati g ue, or want of fo od may bring on fainting or collapse.
SIGNS AND SYMPTOMS .
The general condition of shock may be reco gnised by extreme pallor, a feeling of cold, clammy skin, fe eble pulse, and shallow breathing accompanied, if h remonhage has been severe, by yawning and si ghing. The t erm "collapse /I s ignifies a very serious condition in which the life of the patient is in the greatest danger; the tempe ra ture of the body falls below the normal, and one grea t object of treatment to prevent it sinking to a point at which life is impossible. An a tt endant danger o f the condition of
135
collapse is the liability to sudden relapse after a temporary improvement, and the utmost care and watchfulness m ust therefore be exercised to maintain the h eat of the body and to gua rd against failure of the heart and lun gs.

,
the . by arresting hremor:hage, to 1l1Jun es, 100. ening all tight clothmg especIally about the chest and abdomen removing from a close or crowded room using words, e tc.
'u 0
2. - Lay the pcttient on the back with the low. ,Ra,ise the lower limbs; the patient IS m bed th IS IS best done by raisin a the foo t of the bepstead.
0
3.- Provide for a free circulation of fresh ai r.
4.-!f hcemorrhage has been severe and the patient is collapsed, firmly bandage the limbs from the toes to the hips, and from the fingers to the armpits.
5. - To stimulate the action of the heart sal volatile and may be given if the patient' can swallow , or smellmg salts may be held to the nostrils.
6. - 1t is of the utmost importance to use every means of a fall of temperature below pomt. To accomplish this cover the patle nt WIth extra clothing, or by placi ng
134
rugs or blankets over him; get him to bed in a warm b ut '.veIl -ventilated room as soon as possi ble. Apply warmth to the feet and to the pit of the stomach by hot .yater bottles or hot flannels. (Test the heat of these with the elbow before applying them .) If the pa tient can swallow, give hot drinks, such as milk, tea or coffee. It is well to add sugar, as it aids in raising the temperature of the body.
7. - If breathing cannot be discern e d, apply ar tificial respiration.
8. - If want of nourishment has b ee n th e cause of fainting or collapse, give food sparingly at first.
AND HEAT-STROKE.
When exposed to great heat, as in the stoke-hole of a steamer, especially in the tropics, or to the rays of t he sun during a march in very hot weather when heavily burdened, persons may develop sickness, faint ness, giddiness, and difficulty in breathing. The patient complains of thirst, the skin becomes dry and burning, the face very fl ushed, the pulse quick and bounding. A very high tern pera t ure, stertoro us (snoring) breat h ing, and insensibility may ens u e.
TREATMENT
.
I.-Undo all tight clothing.
2.-Remove the patient to a cool, shady spot.

3.-Strip the patient to the waist. .
4.-Lay the patient down, with the head and trunk well raised .
5.-Procure as free a circulation as possible of fresh air, and fan the patient vigorously.
6.-Apply ice bags or cold water freely to the head, neck, and spine, and maintain this treatment until the symptoms subside.
7.-0n return to consciousness) the patient may have water to drink.
CONVULSIONS IN CHILDREN.
Teething or stomach troubles are the commonest causes of this ailment.
SIGNS.
Spasm of the muscles of the limbs and trunk, blueness of the face, insensibility, more or less plete, and occasionally squinting, suspended respiration, and froth at the mouth are the prominent signs.
TREAD'lENT.
I.-Support the child in a warm bath slightly above the temperature of the body (98 degrees), so that the water reaches to the middle of the trunk.
2.-Place a sponge dipped in cold water on the top of the head.
136
!37
ASPHYXIA.
Wl:en, ?wing to want of air, the blood is not supplIed WI h oxygen the patient becomes insensible and is said to be asphyxiated. This condition may be brought about as follows:-
1. Obstruction of the air passages.
(a) By DROWNING.
(0) By PRESSUR E FROM OUTSIDE : Strangulation hanging, smothering. '
(c) By A FOREIGN BODY IN THE THROAT: Choking.
(d) By SWELLING OF THE TISSUES OF THE THROAT: Inflammation, scald of the throat poisoning by a corrosive. '
II. Inhaling poisonous gases. By coal gas (as used in the house), producer, or water, gas, smoke, from a charcoal or coke fire, sewer gas, limeklln gas, ca rbonic acid gas . -
II 1. Pressure on the chest as 'whe n crushed by sand or debris, or by a crowd. '
IV. Nervous affections, as the result of narcoti c and certain other pois ons, collapse) electric shock or stroke by lightning, '
GENERAL TR E.-\TMEN T.
In all cases of Asphyxia attem I ts must be made to remove the cause, or to remove the patient from the cause. 'Vhen th is h::ts been don e artificial

139
respiration must be applied, taking care that the air passages are not obstructed, and that there is abundance of fresh air.
DRO ,VN Il G,
Persons completely immersed in water for eve,n or fifteen minutes have been restored by artificIal means. Therefore, if the body is recovered within a reasonable time, absence of signs of life is not to deter immediate attempts to restore animation.
The first thing to do when the body is recovered is to get rid of the water and froth obstructing the, air passarres and then artificially to restore breathmg. This is 'best accomplished either by proceeding at once to perform artificial respiration by Schiifer 's method, or as follows :-
I.-As quickly as possible loose n the clothing, and clear the mouth and the back of the throat.
2 . - Turn the patient face downwards, with a 'pld below the chest, and \\'ith the forehead upon the rIght forearm.
3,- Whilst in this position apply pressure, by the hands to the patient's back over the lower nbs, and keep the pressure up for three seco? ds. , "
4.-Turn the patient on the right sIde, mamtammg that position also for three seconds.
s .-R epeat these movements alternately as lorlg as froth and water issue from the mouth.
These operations (Marshall Hall's method) in themselves tend to promote respiration, but when the air passages are clear of froth and water Silvester's metnod of artificial respiration may be used by itself or with Howard's method in conjunction.
'While performing these operations send someone to the nearest house to procure blankets and dry clothing, hot water bottles, etc, and to fetch a doctor.
STRANGULATION.
Cut and remove the band constricting th e throat. Apply artificial respiration.
HANGING.
Do not \yait for a policeman: grasp tbe lowe r limbs and raise the body to take the tensi on off the rope; cut the rope, free the nock. Apply artificial respiration.
SMOTHERING.
Remove whatever is smothering the patient. Apply artificial respiration.
CHOKING.
Open the mouth, forcibly if need be; pass the forefinger right to the back of the throat and attempt to dislodge the foreign body; if vomiting results, so much the better. If unsuccessful, thump the back hard whil st the head is bent forward. Apply artificial respiration.

SWELLING OF THE TIS SUES OF THE THROAT.
'Whether the s'welling is caused by il:flammation by swallowing very hot water, as not mfrequently happens to children attempting to drink. from . the spout of a kettle, or by the effect of a corrOSIve pOlson, the trea tme nt is as follows:--
I.-A pply a sponge, piece of flannel or other cloth, wrung out of very hot water, to the front of the neck, from the chin to the top of the breast-bone.
2 the patient before tbe fire.
3.- Give ice to suck if it can be had; if not, give cold water to drink.
4.- Gi ,·e animal or vegetable oil, a dessertspoonful at a time, to soothe the scalded throat and ease the pain.
5.- If breathing has ceased apply artlfiClal respiration.
SUFFOCATION BY SMOKE OR GASES.
I.-Remove the patient into the fresh air. Before enteri ng a building full of smoke tie a handkerchief, wet if possible, round the head so a.s to cover nose and mouth. It is well to move slowly, keepmg low, or even crawling, whilst in a room full of in search of a suffocated person. Every opportul1lty of letting in fresh air by opening doors or windows should be seized.
.. .
2.-Apply artificial respiration.
3·-In case of prod ucer or water gas, inhalation of oxygen wIll also be necessary.
ELECTRIC SHOCK.
Electric cur rent is conveyed by a cable wire rail or bar, called the "Positive," and ret u;ns
So u rce of supply by another cable, wire rail or bar called the " or through the I n case of an elec.tnc raIlway, the current is generally conveyed by an Insulated rail called the third rail and returns through the .running rails or an inSUlated ra ii called rail, and in the case of an e lectric tramway It IS conveyed by an overhead .o r trolley \\"Ir e, and returned throu a h the runnIng rails. b
Through contact with a " positive " the shock rn a so severe as to cause insensibility, and the be to extricate himself, and must b e WIth .all poss.ible speed As it is generally ImpossIble or InexpedIent to swi t ch o ff th e current some method must usually be adopted; but be. or else the person reqdenng aSSIstanc e WIll hIms elf receive a shock
To liberate the sufferer from contact- . . from the earth by stand. Ing on an . Insulator or" non-conductor II th"t J b d h ' h ' , <l s, a o y W IC reSIsts the current. Amongst such bodies

143
are indiarubber, dry glass, dry bricks, dry silk, dry cloth, dry wood and dry hay or straw , 2. - Protect your hands from contact with the sufferer or the electric medium by covering them with an insulator. Although indiarubber is probably the best insulator, do not waste time in running for indiarubber gloves, bu t use dry articles of clothing; an indiarubber tobacco pouch or cap, or folded newspaper, would serve to protect the hands in an emer gency. If no means of insulating the hands are at hand an attempt may be made to drag the sufferer away by means of a loop of d ry rope or a crooked stick; an umbrella is not safe because the metal ribs would act as conductors* of electricity, and it is not infrequently the case that the" stick" of the umbrella is a metal tube.
3.-Pull the sufferer away from contact. Care should be taken to avoid touching with naked hands the sufferer's hands, wet clothing, or boots if th e soles are nailed. The armpits should be avoided as perspiration usually makes the clothing damp the re.
'When the sufferer is removed from contact-
I.-Apply the general treatment for insen-
'If A conductor is a body through which electricity readily passes, Amongst such bodies are copper, brass, jron. moisture and one's own body.
14 2
-sibility (loosen clothIng, procure free circuiJtion of air and place in a recumbent P J sition).
2.-- Dip a towel in cold water and attempt to arouse him by sharply flick ing the face and chest.
3·- Commence artificial respiration if other methods fail to restore animation. " Laborde's" method (see page 126) has been found to be very successful.
4·- Treat burns if there are any (see pages I03, 104).
EFFECTS OF LIGHTNING.
A person struck by lightning is usually more or less deprived of consciousness. The treatm ent IS the same as that for electric shock, except, of course, that the instructions for removing the patient from contact with the electric medium do -llot apply.

145
QUESTIONS ON CHAPTER V.
The 1lumerals indicate the pages where tlu answers may be found.
\Vhat are the two systems of nerve s? ... ...
Of what is the cerebro-spi r.al s¥stem made up? "_
What is the spinal cord?
In what system of artificial respiration is the patient laid back upwards?... ... .
In what systems is he laid on back? . 123, 126
In what system is he laid on hiS back or side? 1 2 7
In what system is he rolled alternately on hiS side and face downwards?
.139. 140
How lon a should artificial respiration be persevered with? 127 What is ;xciting respiration? 1 What is inducing circulation? 12 7, 128
Why is it .to w::-tch the patient?
How may insenslOllity . ..... ... 128
State the various forms of InsenSI bIill y ... .:." ,
State the general ru les fo r treatment of insensibilIty 128 to 131
Would you examine the patient to see if any bones were broken? ...
\Vhat wrong opinion may be formed when the pati e nt 129 smells of drink? ... ... .. '?'
Is collapse from drink a conditIOn.
\Vhat is concussion of the braIn? ... .
State the rules fo r treatment of concussIOn
144
\Vhat are nerves like? PAGE Il7 Il7 117 IIS 118 Explain the sympatheti system Explain the respiratory 11 to 120 Explain the acts of reSpiratIOn ... . How are the expansion
co ntract IOn of the chest 120 eftected? ... ... ... ... ....
and
to 121
... ...
r21
... ... ... ...
.. . ... ... . ...
130 [3 1 13 1
, 13:!
What danger accompanies injury to the head?
\Vhat caution should be given to a patient who has lost consciousness, even for a moment, after an injury to the head?
What are the causes of com pre sion of the brain?
In what agrd people does apoplexy usually occur?
'Vhat are the signs and symptom.:; of compression and apoplexy?
State the:rules for trealment of these conditions... . ..
\Vhat dangf'r is there in applying hot water bottles to insensible persons, and what precautions should be taken?
Describe a case of epilepsy 132, 133
\Vhat special care must be taken in treating a case of epilepsy? ... 130, 13 2
D<:!scribe a hyst erical fit

133
How would you treat a hysterical fit? ... '" 133
";hat are the comm mest physical causes of shock? 134
\Ii hat may p:oduce shock or fainting?
'What condltlons do certain poisons bring a bout? . 134
What may bring about fainting or collapse? ... '" 1 34
How would you recognise the general condition of shock? 134
\Vhat special precaution must be taken in the case of collapse?
State the treatment for shock, faintlllg'(sync;pe)
135, 136
\Vhat IS the effect of sugar on the temperature of the bodyl...
'"
vVhat are the causes of sunstroke and heat·stroke ?
State the treatment for sunstroke and heat·stroke
What are the causes of convulsions in children?
vVhat are the signs of convulsions in children? .. .
State the treatment for convulsions in children .. .
State fully the causes of asphyxia
vVhat two things have to be done in all cases of asphyxia?
138, 139
\Vhat two things must be seen to before it is possible for artificial respiration to do any good? 139
Is artificial respiration likely to do any good ·if the air passages are obst ructed. or if there is not abundance of fresh air?
What is the first thing to do in a case of drowning? ... 139 By what method may artificial respiration be performed without taking any previou steps? ... ... ... 139
\\'hat steps must be taken before proceeding with Silvester's method?
139 \Vhat should be done while artificial respiration is being performed?
may a swelling of the tissues of the throat be
State the treatment fur swelling of the tissues of the throat
141 State the treatment for suffocation by moke or gases 14 I, 142 How is electricity conveyed?
How woulJ you liberate a sufferer from contact with an electric medium?
142, 143
\Vhat would you do when the suffere r ",as removecl from contact?
143
What would you do in the case of a lightning stroke?... IH
... ... ... ... ... ...
... ... ... ... ... Pl'.GE 13 1 13 2 13 2 13 2 13 2 13 2
... ...
13 2
... ... ...
...
... ...
134
... ... . ..
... ... '" ... ...
135
...
... ... . ..
... 136 136 136, 137 137 137 137 138 147 PAGE
... ... ... ... ...
............
139
... ... ... ... ...
... ... ...
State
140 State the treatment for hanging ... 140 State the treatment for smolhering 140 State the treatment for choking ... 140
? ... ...
... ... ... ...
... ... ... ...
140
the treatment for strangulation
How
causeJ
141
142
... ... ... ...
..............
CHA PTER VI.
POISONING.
Poisons may be classified according to their treatment under two heads:-
I.-:- Those which do not. stain the mouth, and the treatment of which an emetic is to be gIVe:1. Am ongs t these are :-
(a) Arsenic, (contained in rat poison and lu cI fer matches), Tartar emetic and Corrosive Sublimate, which cause a metallic taste in the mouth and a burning pain in the mouth, throat a n d stomach.
U) Strychni n e, Prussic Acid, Belladonna (deadly l11ghtshade plant) and several other varieties of as laburnum seeds, etc. j these gIve rIse to convulsions delirium of respiratio n and collapse. '
(c) POIsonous meat, fish a nd fungi (often misfor mushrooms). Suspicion of these pOIsons should be di re cted to cases where several persons who have partaken of the same food deve lop similar sIgns and symptoms.
(d ) which I:n ay cause collapse.
(e ) O pIUm and Its preparations, Morphia .,

149
Laudanum, Paregoric, Chlorodyne, Syrup of Poppies a n d various soothing drinks a nd cordlals; these ca us e a tendency to go to sleep, wbich continues until sleep becomes deep and bre:ttbing stertorous; the pupils of tbe eyes become minutely contracted (pinbead pupils).
2. - Those which burn or stain the mouth, and in the treatment of which no emetic is to be given. These are of two classes: -
(a) Acids, sucb as Nitric Acid (Aqua fortis), Sulph uric Acid (Oil of Vitriol), Hydrochloric, or Muriatic, Acid (Spirits of Salt), strong Carbolic Acid (Phenol), Oxalic Acid, wbicb is contained in oxalate of potasb, salts of sorrel, salts of lemon and some polisbing pastes.
(0) Alkalies, such as Caustic Potash, Caustic Soda and Am monia.
'3UlVD1ARY OF SIMPLE DIRECTIONS FOR THE TREATME:\,T OF POISONING.
I.-Send for a doctor at once, stating what has occurred and if possible the name of the poison.
2.-Except when the lips and mouth are stained or burned by an acid or alkali ,
140
promptly give an emetic-that is, make the patient vomit as follows:-
(a) Tickle the back 0./ the tlzroat with the finger or with a feather.
(b) Mustard -a dessert-spoonful in a tum blerf ul of I uk e-warm water.
(c) Salt-a table-spoonful in a tumblerful of luke-warm water.
Cd) Ipecacuanlza TVine-for a young child, a teaspoonful repeated at intervals of fifteen minutes.
3.-In all cases when the patient is not insensible, give Milk, Raw Eggs beaten up with milk or water, Cream and Flour beaten up together, Animal or Vegetable Oil (except in phosphorus poisoning) , and Tea.
Olive, Salad, and Cod-liver oil, or oil such as that in which sardines are preserved, may be given; mineral machine oils and paraffin are unsuitable. Oil is soothing, and is therefore especially useful in poisoning by Acids, Alkalies and such substances as Arsenic and Corrosive Sublimate. Demulcent drinks, such as barley water or thin gruel, act in the same manner, and are free from danger in cases of phosphorus poisoning.
These may be given either before or after the emetic if the poison calls for one.
Strong Tea acts as a neutraliser of many poisons

I5 I
and is always safe. A handful of tea should be thrown into a kettle and boiled.
4·-If the lips and mouth are stained or burned give no emetic, but -
(a) If an acid is kno\\'n to be' the poison give an Alkali at once. First \\ash the mouth out freely with lime water or other alkaline mixture, such as soda, chalk, whiting, or magnesia or wall plaster in water, and afterwards let the patient sip a little of it. Soda and potash are not to be given in the case of poisoning by oxalic acid.
(b) If a strong Alkali is known to be the poison give an acid at once. First wash the mouth out freely \\"ith lemon juice or vinegar diluted with an equal quantity of water, and afterwards let the patient sip a little of it.
In both cases give oil (Rule 3).
5.-When a person has swallowed poison and threatens to go to sleep, keep him a wake by walking him about and slapping his face, neck and che st with a wet towel. Strong black coffee may be given to drink. Slapping the soles of the feet may a lso be tried,
6. - If the throat is so swollen as to threaten obstruction to the air passage, apply hot flannels or poultices to the front of the neck and give frequent sips of cold drinks.
7- - Apply artificial respirat ion if breathin g cannot be discerned .
8. - Treat shock and collapse .
9. - Preserve any vomited matter foo d or .other substance , suspected of pOlson . Do not wash vessels which may have contained the poison, and carefully guard them.
Certain poisons require speci::tl tr ea tment, and a few of the commoner of these are mentioned below with their treatment.
CARDOLIC Acm.
The odour of the breath will aid in the detection of this poison; the lips and mouth are usually stained white, and several nervous symptoms come on.
TREATMENT.
I.-Give milk, to a pint of which half an ounce of Epsom Salts h:lS been added.
2.- Treat according to the general rules.
PRUSSIC ACID.
.Th.e action of . this poison is extremely rapid . insensibility accompanied by pantmg. respIratIon, profound collapse and possibly are the signs, and in addition a smell of bItter almonds IS often present.
TREAT;\lENT.
I.-Place the patient in the open air.

2. - Dash cold water on the head and spine c ::mtinuously.
3 -Apply artificial respiration.
4.-Hold smelling salts to the nostrils.
5.-Treat shock and collapse. (See page 135 )
POISONOUS MEAT, FISH A D FUNGI.
.The signs an.d symptoms are vomiting and purgmg (dlarrhce:t), colic, headache: great weakness, raised te mperature and a quick pulse.
TREAT;\IENT.
T .-Give an emetic.
2.- \Vhen the emetic has acted, give castor oil.
3.-Treat collapse. (ee page 135·)
STR YCH NINE.
The signs ana symptoms are a feeling of suffocation, livid features, and convulsions. The patient rests on his head and feet, and the body is arched.
TREATMENT .
1.-Give an emetic.
? .-Apply artificial respiration.
ALCOHOL.
1.- Give an emetic if the patient can swallow.
2.- Treat collapse by keep ing the patient warm, etc. (See page 135 ')
15
2
153
QUESTI ONS ON CHAPTER VI.
Tlze numerals illdt'cate the pages where the answe?'s may be found.
Under what two heads may poisons be classified?
\Vhat are the symptoms of poisoning by Arsenic?
vVhat other poisons give rise to the same sympLoms? ,,'
PAGE 148, 149 148 14 8
'What poisons give rise to convulsions, delirium, failure:: of respiration and '" 148
If several people who had, partaken of the same fo od developed similar signs and symptoms, by what would you suspect they had been poisoned? q8
\Vhat condition may result from poisoning by alcohol? 148
"Thar are the effects of such poisons as opium?", 148, 149
\Vhat two classes of p)ison burn or stain the mout h? '" 149
\Vould you give an emetic for such poisons? 149
Name some of the principal acids J49
Name some of the principal alkalis ", 149
State the general rules for the treatment of poisun- ing
State the best method s of making a person vomit
How would you treat a case of acid poisoning? ".
How would you treat a case of poisoning by an alkali?
State the signs, symptoms and treatment of carbolic acid poisoning '" 149 to 152 ISO 151 151
State the signs, symptoms and treatment of poisoning by Prussic Acid 15 2 , 153
State the signs, symptoms and treatment, f poisoning by poisonous food '"

ISS CHAPTER VII.
Esmarch's Triangular Bandage has been m Chapter II. It may be applied to keep a dressmg on a ,,'o und, burn or scald of any part of the body, or for an injury of a joint. 1. F or the Scalp (Fig. 62). Fold a hem abo u t I inches deep along the base of a bandage ; place the bandage on the head so that the hem lies on the forehead close down to the eyebrows, and the point hangs down at the back ; carry the two ends round the head above the ears and tie them on the forehead ; draw the pom t first downwards, and then turn it lp and pin it on to the bar:dage on .the top of FIG. 62. the head,
State the signs, symptoms and treatment of p oisoning by Strychnine J 53
vVhat would you do in the case of alcoholic poisoning? 153 153
For the Forehead, Side of the Head
, Cheek and for any part of the body that IS round '(as the arm or thigh, etc,), the narrow bandage should be used, It centre being placed over the
154
156 and the ends being carried round the head or 11mb, as the case may be, a n d tied over the wound . For the Shoulder (Fig. 63). Place the centr= of a bandage on the shou lder, with the point running

FIG. 63· --::..-=- F IG. 64. up the side of the n eck; fo ld a hem alo na the base' carry t h e ends round the midd le of the ;rm and Place one end of a broad bandage over the pOll1t. o f the fi rst bandage an d sling the arm by ca.rrymg th e ot her end over th e sound shoulder and the e n ds at the side of the neck; turn down the POll1t of t h e first bandage, draw it tight and pi n it.
157
For the Hip (Fig . 64). Tie a narrow bandage round the body above the haunch bones, with the knot on the injured side. Fold a hem according to the size of the patient alo ng the base of a sec o nd bandage; place its c entre over the dressin g, carry the en ds round the thigh and tie them; then carry th e po int up under the
FIG 65·
FIG. 66. first bandage , tum it dO\\'n oyer th e knot and pin it.
For the Hand wh en th e fin ge rs are extended (Fig. 65). Fold a hem al ong the base of a bandage; place the wrist on the hem with th e fingers towards the point; then bring the point over the wrist, pass the ends round the wrist, cross and ti e them j bring the point 0"er the knot and pin it to the bandage on the h a nd .
, I J I I ·r l
__ '
\,: 1,
158
For the Foot (Fig. 66). P1ace the foot on the centre of the with the toes towards the point; Elraw up the POInt over the instep, pass the ends round the ankle and cross them in front; now pass the ends round the instep and tie them. Dra'v" the

FIG. 67a. FIG. 67b.
point forward and pin it to the bandage on the instep.
For the Front of the Chest (Figs. 67a and 67 b). Place the mjddle of the bandage over the dressing with the point over the shoulder on the same side; carry the ends round the waist and tie them;
159
th en draw the point over shoulder and tie it t -J one of the ends.
F or the Back. The bandagE:: is applied as the foregoing, except that it is begun at the back.
For the Knee. Fold a narrow hem along the base of a bandage; lay the point on the thigh and the middle of the base just below the knee-cap; cross the ends first behind the knee, then over the thigh and tie t0 en:. I Bring the point down and pIn It \ to the base (Fig. 68).
FIG. 68. For the Elbow. Fold a narrow hem along the base of a bandage; lay the point on the back of the arm and the middle of the base on the back of the forearm; cross the ends first in front of the elbow, then over the arm and tie them in front (Fig. 69).
For the Fingers and Toes wrap a strip of calico or linen "" IJ} ,. ,-.c::;:. '/jJi round and round > . part; spl1t the freeend, '\., . d - ' d ,,''- 1; \ , 1n secure It roun "",,, . z the wrist or ank le, FIG. 69.
CHAPTER VIII.
METHODS OF CARRYING.
THE FOUR-HANDED SEAT.
This seat is used when the patient can assist the bearers and use his arms.
1.-Two bearers face each othe r behind the patient and grasp their left forearm with their right hands and

FIG. 70.
each other's right forearm with their left hands (Fig. 70), and stoop down.
2.-The patient sits on the hands and places one arm round the neck of each bearer.
3.-The bearers rise together and step off, the bearer on the right hand side of the patient with the right foot, and the left hand bearer with the left foot.
THE T\\"o-HANDED SEAT.
This seat may be used to carry a helpless patient.
FIG. 7r.
1.-Two bearers face each other and stoop, one on each side of the patient. Each bearer passes his forearm nearest to the patient's head under his back just G
160
161
below the shoulders, and, if possible, takes hold of his clothing. They slightly raise the patient's back, and then pass their other forearms under the middle of his thighs (Fig. 7 I), and clasp their hands by one of the methods shown in Figs. 72 and 73. A handkerchief should be held in the hands if the first grip is used.

FIG. 73.
2.- The bearers rise together and step off, the rie:;ht-hand bearer with the right foot, and the left-hand bearer with the left foot (Fig. 74).
THE THRh.E-HANDED SEAT.
This seat is useful for carrying a patient and supporting either of his lower limbs, when he is able to use his upper iimbs. .;,.
1.-Two bearers face each other behind the patient. For supporting the left limb the bearer to the patient's right grasps his own left wrist \\"ith his right hand, and the other bearer's right wrist with his left hand. The bearer to the left grasps the first bearer's right wrist with his right hand (Fig. 75). This leaves his
162

left hand free to support the patient's left leg. For the patient's right lower limb follow the same directions, substituting" right" for" left" and" left" for II right." The bearers stoop down.
2.-The patient places one arm round the neck of each bearer and sits on their hands.
3.- The bearers rise together and step off) the FIG. 75.
right-hand bearer with the right foot, and the left· hand bearer with th e left foot.
THE FIREMAN'S LIFT.
(To be attempted only by a strong man).
Turn the patient face downwards; place yourself at his head, stoop down, slightly raise his head and
shoulders and take hold of him close under his arm· pits, locking your hands on his back. Rais e his body and rest it on your left knee j shift your arms and, taking him round his waist, lift him until his head r ests on your left shoulder. Throw his left arm over your head, stoop down and place your left arm between his thighs, letting his body fall across your shoulders. Rise to an upright position j hold the patient's left wrist with yo ur left hand and leav e your ri ght hand free.
Assistance may be given to an injured person by supporting him in the manner shown in Fig. 76.
Th e plan of carrying tlze padent by tlte arms and legs witlz tlze face downwards, commonly called tlze "frog's marciz," 'IIlust n eve?' be used, as death may ensue fr O'J7Z this treatment.
IMPROVI SED STRETCHERS.
A stretcher may be improvised as follows :-
1. -- Turn the sleeves of a coat inside out; pass two strong poles throu gh them ; buttol1 the coat. The patient sits on the back of the coat and rests against the back of the front bearer (Fig. 78). If a lon ger stretcher is required two or three coats must be treated in the same manner. The poles may be kept apart by strips of \,"ood lashect to the poles at both ends of the bed formed by the coats (Fig. 79).

77.
THE FORE AND AFT METHOD.
This plan of carrying ' is us eful when space does not permit of a hand seat.
166
FIG.

2.-Make holes in the bottom corners of one or two sacks and pass stout poles through them.
3.-Spread out a large piece of carpet, sacking, tarpaulin, or a strong blanket, and roll two stout poles up in the sides . Two bearers stand on each side and grasp the middle of the pole with one hand, and near the end with the other. They walk sideways.
4.-A hurdle, broad piece of wood, or shutter may be used as a stretcher j some straw, hay, or clothing should be placed on it, and covered with a piece of stout cloth or sacking; the latter is useful in taking the patient off the stretcher.
Always test an improvised stretcher before use. Stretchers must be carried, and the patient placed on them, as bid down in the" Stretcher Exercises.])
As a general rule carry the patient feet foremost. The exceptions are:-
(a) "When going up hill with a patient whose lower limbs are not injured.
(b) When going down hill with a patient whose lower limbs are injured.
Avoid lifting the stretcher over ditches or walls, but where these cannot be avoided the stretcher must be carried in the following ways: -
To CROSS A DITCH.
In crossing a ditch, the stretcher should be lower with its foot one pace from the edge of the ditch
79.
169
17 0
Nos. I and 2* bearers then descend. The stretcher, with the patient upon it, is afterwards adYanced, N os. I and 2 in the ditch supporting the front end while its other end rests on the edge of the ground above. No. 3 now descends. All the Nos. now carry the stretcher to the opposite side, and the foot of the stretcher is made to rest on the edge of the ground, while the head is supported by 3 ,i n the ditch. No. I climbs out, No. 2 rema111111g 111 the ditch to assist No, 3, The stretcher is lifted forward on the ground above, and rests there while Nos. 2 and 3 climb up.
To CROSS A 'V ALL.
The stretcher is lowered with the foot about one pace from the wall. Nos. 1 and 2 bearers then take hold of the foot of the stretcher, and NO.3 of the head; the stretcher is raised till the foot is placed on the wall. No. I then clim bs over the wall and takes hold of the foot of the stretcher, while Nos. 2 and 3 support the head; the stretcher is th e n carried forward till the head rests on the wall, No. I supporting the foot. Nos. 2 and 3 then climb over the wall and take hold of the head of the stretcher, which is then slowly lifted off the wall on to the ground, and the bearers take their usual places.
* Tbei'e numbers are explaintd later in the detailed "Stretcher Exercises."
171
To LOAD A 'WAGON.
The stretcher is lowered with the foot one pace from the end of the wagon. N os. I and 2 take hold of the foot of the stretcher, No. 3 the head. The stretcher is then raised and carried forward till the front wheels rest on the floor of the wagon. No . I then jumps into the \>yagon, while No.2 goes to the head of the stretcher and helps No. 3. The is ther- pushed slowly into the wagon. If the tallboard cannot be shut, the stretcher must be lashed firmly to the sides of the "\\'agon·.
To UNLOAD A 'VAGON.
Nos. 2 and 3 take hold of the head of the stretche:, while No. I gets into the wagon; the stretcher IS then gradually drawn out till the foot-wheels rest on the edge of the ,Yagon. No. I jqn:W!i ou.t. Qf the wagon, and with No. Z ,takes hold of the foot of the stretcher, NO .3 supportmg the head. The stretcher is now gently drawn away one pace lowered. With four bearers Nos. I and z would lIft the foot of the stretcher, while Nos. 3 and 4 lift the head. This applies to crossing a ditch or wall, as well as to loading and unloading a wagon.
CHAPTER IX.
STRETCHER TRANSPORT.
The "Furley" Stretchers (Model J 899) are of Ordinary,"" Telescopic-handled," and PolIce. In general principle they are alike, the component parts being designated the poles,

8I.-TErLESCOPIC·HANDLED STRETCHER- OPEN.
handles, traverse bars, fDot wheels, bed, pilloy" sack and slIngs,
. The Ordimtry Stretcher (Fig. 80) is 7 feet 9 inches In len,gth, and 1 foot 10 inches wide. The bed is 6 In, length, and the handles inches. The heIght IS 51 inches. At the head of the stretcher is a overlay (the pillow sack) which can be filled wIth hay, clothing, etc., to form a pillow. Tht; JOInted traverse bars are provided with joints,
173
for opening or closing the stretcher. The Telescopichandled pattern (Fig. 81) is very similar, but the handles can be slid underneath the poles, thus reducing the length to 6 feet. This arrangement is of great val ue when working in confined spaces , or when a patient has to be taken up or down a narrow staircase with sharp turns. The Police stretcher is similar to the Ordinary pattern, but is more strongly made, and has, in addition, straps for securing a refractory patient.
'When closed, the poles of the stretcher lie close together, the traverse bars being bent inwards, the canvas bed neatly folded on the top of the poles and held in position by the slings which are laid along the canvas, and secured by a strap, placed transversely at the end of e::tch sling, being passed through the large loop of the other, and round the poles and bed.
In closing a stretcher care should be taken to raise the centre of the canvas when pushing in the traverse bar, as it is otherwise liable to get caught.
To prepare, or open a stretcher, unbuckle the trans verse ,straps of each sling; remove the slings from the stretcher; separate the poles; take hold of each traverse bar and draw it forward. The slings will then be folded to half their length, one being laid neatly over the handles at each end of the stretcher.
As a general rule, the stretcher will be prepared by Nos. I and 3 bearers in Exercises I, II., and III. ;
FIG 80.-0RDINARY STRETCHER-CLOSED. FIG.and by No . 2 in Exercise IV. These bearers will, however, if required, assist the other bearers in attending to the patient's injuries .
./Ilote.- The various movements detailed in the following Exercises should be carried out steadily, the bearers working in unison, hurrying being carefully avoided and every attention being paid to the bearer who gives the words of command.
STRE.TCHER EXERCISES,
Originally drawn up by Sir John Furley, and revised in I904 to accord with the drills adopted by the Royal Army Medical Corps :-
EXERCISE No. I.
FOR FOUR BEARERS.
I.-The Instructor selects the bearers and numbers them - I, 2, 3, 4 at his discretion. Should one man be taller and stronger than the others, he should be styled NO.3. as he will have to bear the heavier part of the burden.* All orders 'will be given by NO.4.
2 .- " Fall in ."-Nos. I, 2, and 3 take pqsition on the left side of and facing the patient. No. I places himself at the patient's knees, No. 2 at the hips, NO.3 at the patient's shoulders. At the same
* Bearers should, however, be taught to take any of lhe positions named in the following exercises, whether that of No. I, 2, 3, or 4 bearer. T75
ti me No. 4 places the prepared on the ground by the right side of the patIent about two

b2.
paces away from him, then takes position opposite to and facing No.2. (FIg. 82).
174
FIG.
3· " Rea dy . "-The bearers kneel down on the knee and take hold of the pabent, No. I passing h1s hand.s and fore-arms beneath the patient's legs, hands w1de apart. Nos. 2 and 4 pass their hands

FIG. and forearms beneath the patient's hips and loins and grasp each other's hands. No. 3 passes his hand across the patient's chest and under the riaht shoulder, and his right hand beneath the left shoulder (Fig. 83)
4. - "Lift."-On the word "Lift," the bearers raise the patient gently and rest him on the knees of N os. I, 2, and 3 bearers (Fig. 84) ; as soon as he
is rested, NO . 4 disengag es hands \\"ith No. '<'i runs round by the head of the stretcher and places It under the patient, close to the uther bearers' feet )
176
177
178
being careful that the pillow is immediately under the patient's head (Fi g. 85); he then kneels down and locks his hands with thos e of No.2 (Fig. 86).
5. -" Lower. "-The bearers place the patient on the stretcher (Fig. 87), disengage their hands, and then stand up.

FIG. 85.
6.-" Stand to Stretcher."-No. I goes to the foot of the stretcher, with his back to the patient; NO·3 to the head with his face to the patient; Nos. 2 and 4 remain on each side of the stretcher.
7.-" 1 and 3 place the slings (if used) over theIr shoulders, stoop down, and slip the
179
loops of the slings on to the handles of the stretcher, which they then grasp.
As soon as all is right the word is given :-
8.-"Lift Stretcher."-Nos. I G:.nd 3 bearers raise the stretcher steadily together and stand up.
Note.-Nos. 2 and 4 will now adjust the slings on the shoulders of Nos. I and 3, taking care that each is well below the level of the collar and lies accurately in the hollow of the shoulder in front. They will also lengthen or sho rt en the slings, having regard to the patient's injuries and the relative heights of the bearers.
rIG. 86.
9.-" March."-The bearers move off :-Nos. I, 2, and 4 stepp1l1g off with their left foot, and No. 3
with his r ig ht foot (Fig . 8 7). T h e step shou ld be a short one of t wenty inches, a n d taken with bent knees and no spring from the fo re part of the foot.
10. - " Halt."-The bearers remain steady.

II. - " Lower S 'w.:-etcher. "-The bear.ers place
t he stretcher gently , )11 the ground, slip the loops of t he sli ngs off t h e h<.lndles of the str etcher, remove t he slings from the shoulders, and then stand up.
18 1
12.-" Unload Stretcher - Ready. " - The bearers prepare to take the patient off the stretcher, as at Orders 2 and 3.
13. - " Lift. "-The bearers raise the as at Order 4 (Fig. 86); NO.4, in this case, dise:1gages hands from N O. 2, removes the stretcher (Fig. 85), and resumes his former position. If the bearers will then steadily rise together, and c .refully carry the patient to the bed, or other plac e to which it has been arranged to convey him.
14. - " Lower. "-The patient is carefuqy l:nvered.
EXERC I SE
No.
II.
FOR THREE BEARERS
I.-Number the bearers I, 2, 3.
All orders will be gi ven by No.2, will look after the injured part of the patient's body or limbs, to that no bandages or splints become displaced, and also that No . I bearer, in lifting or carrying the stretcher, does not touch the patient's feet.
2. - " Place the Stretcher. "-No. 3 places the stretcher in a line with the patient's body, the foot of the stretche r being close to his head.
3.- " Fall In. "-No. I places himself o n the left side of the patient in a line with his knee s, No. 2 on the left side just below the patient's ShOUld rs, and NO.3 at the right side, and faces NO . 2.
180
4.-" Ready."-All kneel on the left knee. No. I places his hands, well apart, underneath the lower limbs, always taking care, in case of a to have one hand on each side of the seat of Injury. Nos. 2 and 3 grasp each other's hands under the shoulders and thighs of the patient (Fig. 88).

5. -" Lift." -The bearers rise together, keeping the patient in a horizontal position (Fig. 89).
6.-" March."-All take short side-paces, carrying t he patient over the stretcher until his head is immediately above the pillow. 183
7.-" Halt.- The bearers remain steady. 8.-" Lower."- The bearers stooP. down, gently place the patient on the stretcher, dIsengage theIr hands, and then stand up.
FIG. 89.
9.-" Fall In."-No. I places himself the foot of the stretcher with his back to the patIent, NO.2 places himself at the left side of the and NO.3 at the head, with his face towards the patIent. Q.
182
184
r o.-" Ready."-Nos. I and 3 place the slings (if used) over their shoulders, stoop down, and slip the loops of the slings on to the handles of the stretcher, whicll they then grasp.
.-\s soon as all is right the word is given-
II.-" Lift S t retch e r ."-Nos. I and 3 bearers raise the stretcher steadily together and stand up.
No. 2 will now adjust the slings on the shoulders of Nos. I and 3, taking care that each is well below the leyel of the collar, and lies accurately in the h ollow of the shoulder in front. He will also lengthen or shorten the slings, having regard to the patient's i:lj uries and the relative heights of the bearers.
12. --, " March. "-Nos. I and 2 step off with the left foot, and NO.3 with the right. The step should be a sbort one of 20 inches. and taken with bent knees, and no spring from the fore part of the foot.
13. -" H alt."-The bearers remain steady.
14.- ,1Lower Stretcher."- The bearers place the stretcher gently on the ground, slip the loops of the slll1gs off the handles of the stretcher, remove the slin,;s from the shoulders, and then stand up.
IS _d Unload Stretcher - Ready ." - The bearers prepare to take the patient off the stretcher, as at O rders 3 and 4 (Fig . 88) .
16. -" Lift."-Tbe bearers raise the patient, as at Order 5, and carry him by short side steps, clear of the stretcher, to the bed, or other place to which it has arranged to convey him (Fig. 89).

17. -" Lower."- The patient is carefully lowered.
EXERCISE No. III.
'''HEN ONLY THREE BEARERS ARE AVAILABLE AND THE STRETCHER CANNOT PLACED AS IN EXERCISE II.
I.-The Instructor numbers the bearers-I, 2, 3. All orders will be given by NO.2.
2.-" Place t h e S tre t cher."-No. I taking the foot of the stretcher, and NO , 3 the head, place it on the ground by the side of the patient, and as close to him as practicable.
3.--" Fall I n."-The three bearers take the same positions on one side of the patient, as laid down in Exercise No. I.
4.-" Ready."-Nos. I, 2, and 3 kneel down on the left knee, placing themselves as close to the patient as they conveniently can, and then take hold of him as directed in Exercise No.1.
S. - " Lift. "-Nos. I, 2, and 3 raise the patient as directed in Exercise No. I, and then move in a kneeling position up to the stretcher.
6.- " Lower."- The bearers bend forward, carefully lower the patient on to the stretcher, and disengage hands.
185
7. - " Stand to Stretcher. "-All the bearers stand up; No. I goes to the foot, No.2 remains in position at the side, and No . 3 goes to the head of the stretcher.
8. - " Ready:"- Nos . I and 3 place the (if used) over their shoulders, stoop doxn, and slip the loops of the slings on to the handles of the stretcher, which they then grasp .
9.-" Lift Stretcher. "-Nos. I and 3 bearers raise the stretcher steadily together and stand up.
No .2 will now adjust the slings on the shoulders of Nos. I and 3, taking care that each is ,:vell below the level of the collar, and lies accurately m the hollow of the shoulder in front. He will also lengthen or shorten the slings, having regard to the patient's injuries and the:: relative heights of the hearers.
10. -" March ."-Nos. I and 2 step off with the left foot, and NO.3 with the right. The step should be a short one of 20 inches, and taken wIth bent knees, and no spring from the fore of the foot.
n.-" Halt."-The bearers remam steady.
1 2. -- " Lower Stretc her."- The bearers place the stretcher gent ly on the ground, slip the loops of the slings off handles of the st retcher, remove the slings from the shoulders, and then stand up .
13.-" Unload . places himself on the left side of the and. m a line with his knees, No. 2 on the left SIde Just below the patient's shoulders, and NO.3 at the right
187
side, and faces NO.2. All kneel on the left knee. No. I places his hands, well apart, underneath the lower limbs, always taking care, in case of a fracture, to have one hand on each side of the seat of Il1jury. Nos. 2 and 3 grasp each other's hands under the shoulders and thighs of the patient.
14·-" L ift ." - The bearers rIse together to their feet, keepmg the patient in a hOrizontal position, and carry him by short side steps, clear of the stretcher, to the bed, or other place to which it has been arranged to convey hIm.
15·-(( Lower ."-The patient is carefully lowered.
EXERCISE No. IV.
'FOR USE IN Mr ES AND NARROW '\'HERE T\\ a MEN ONLY CAN BE ENGAGED.
Nos I and 2 Will carefully place the stretcher in a lme wIth the injured man's body, the foot of the stretcher being, If possible,';;' close to hIS head.
No. I straddles across the patient's legs, placing his nght foot, with the toe turned outwards, a little below the patient's knees, and with the toe of the left foot close to the heel of NO.2; he then stoops down, passes the Jeft hand under the patient's thIghs and -----------------------------
.. It is not advisable to be too particular as to the head or foot of a stretcher in a mine, as it would probably be quit e impossible to reverse It.
186
188
the right hand across and under the patient's calves. No.2 places his feet one on each side of the patient between his body and arms, the toe of each foot as near the armpits as possible. He then stoops down and passes his hands between the sides of the chest and the arms underneath the shoulders, and locks

FIG. So.
the fingers (Fig. 90). If the patient's arms are uninjured he may put them round the neck of No.2, and by this means greatly assist him in lifting.
189
When both are ready, No I \\"ill give the order (( Lift and move forward." T.he patient is then to be slowly lifted, just sufficient to allow his body to clear the stretcher. Both bearers will slowly and gradually move the patient forward, NO.2 by very short steps, No. I by bending his body forward as much as he can 'wz't/ZOltt moving h is leet (Fig. 9 I ). No. I now gives the order" Halt," whc:-reupon No.2 remains steady, and No. I advances his right foot to his left, and
FIG. 9L
again advances his left foot till the toe touches the heel of NO.2. No. I then gives the order "Advance," when the patient will again be moved forward. These movements are to be repeated until
the patient is over the stretcher, when be is to be gently lowered.
Tbe following Stretcber Exercise is adapted by permission from the Royal Army Medical Corps Manual, 1908.
All orders will be given by NO·4·
1. " . Fall in." -Six bearers fall m behi nd each other.
2. "Number."-The bearers number from front to rear.
3.." NO.3 Bearer, right (or left) turn-supply stretcher-quick march."-No. 3 bearer will march to the stretcher, stoop, lay hold of it and place it on his right shoulder at the slope, holding it by the lower foot wheels, wheels to the front. As soon as the bearer is provided with a stretcher, he will turn about and rejoin his squad in quick time, halting as he arrives in his place. He turns to the front, and, passing the lower end forward, places the stretcher on the ground to the right of the squad, wheels to the right, front end of the poles in line with the toes of No. I and rises.
4. "Stand to I places himself with his toes in line with the front ends of the poles. No. 3 with his heels in line with the rear ends of the poles, close to and touching the stretcher with

. 93 .
190
rn
Fig. 92.
1 I '\ I .- \ \ \ , 1 I ' \' 1 \ rt"Iu '\ \ '\ '. •.... ,I '. ': : / I lit o I'. ;, " . , r-'"" I , '4 ' '7 I I' " I , :---, / ' ·5:,1 I..... I 01. /1 rif' ,';1 .... .;.'
FIG
FIG
';) 4. , , ,
FIG. 96.
his right foot. Nos. 2, 4, 5 and 6 take up their positions one pace behind and covering off the bearer in fro nt of them (Fig. 92).
S. "Lift Stretcher."-Nos. I and 3 stoop , grasp both handles of the poles with the right hand, rise together, holdin g the stretcher at the full extent of the arm, wheel to the right.
6. "Collect Wounded - Advance ." - Th e squad doubles by the shortest route to the patient, and halts wi thout further word of command one pace from the head of and in a line with the patient (Fig. 93).
7. "Lowe' Stretcher."-N os . I a nd 3 stoop, place the stretch er quietly on the ground, and rise smartly together.
8. "Prepare Stretcher. "-Nos . I and 3 turn to the right, kneel on the left knee, unbuckle the transverse straps, and place the slings on the g round beside them, separate the po les, and straighten the traverses.
T wo. On the word two each takes a sling, doubles it on itself, slips the loop thus formed on the near handle, and places the free ends over the opposite handle, buckle uppermost. They then rise and turn to their left together.
'While the stretcher is being prepared by Nos. T and 3, the disengaged beareFs will advance and rend er to the patient such assistance as may be required (Fig. 94) '

193
The necessary assistance having been rendered, NO.4 will give the command-
9· "Load Stretche:-." - The be3.rers pbce themselves as follows: -N as . I, 2 and 3 on the left, Nos. -j., 5 and. 6 on the right of the patient; Nos. r and 4 at the knees, 2 and 5 at the hips, 3 and 6 at the shoulders, the wh ole kneeling on the left knee.
N as. I and 4 p::tss lh ei r h'1nds beneath the patient's knees, 2 and 5 beneath the hips, 3 and 6 beneath the shoulders, care being taken of the injured part, one of the bearers being detailed for this purpose (Fig. 95) .
10.• , Lift." - The \\ hole will carefully lift the patient on to the knees of Nos. I, 2 and 3.
Two. Nos. 4, 5 and 6 will then disengage, rise; Nos. 4 and 6 step back one pace. NO.5 turns to his leCt, doubles to the stretcher, takes hold of and raises it, left hand across, the near pole resting on the left hip; carrying the s.retcher, he returns to his pbce between -j. and 6, and places it beneath the patient.
Tilree. Nos. 4 and b step forward one pace, and together \\ ith No S kneel down on the left knee, and prepare to assist in the patient (Fig. 9(\) .
II. " Lower -The p:u ient is lowered slo\\'1v and on to the centre of the cam'as care bei ng t:tken of the injured 1X11 t).
Tw). The bearers disengage, rise; Nos. I, 2, 3 and 6 turn to the lefl; Nos. 4 and 5 to the right j II
19+
80. 4 places hirrJ..,elf three paces in flont of the stretcher. No, 6, basing collected the kIt and of the patient, places himsdf three paces in rear of the stretcher, Nos. 2 and 5 OpposIte the centre of the stretcher The whole are no\\' ready to btt stretcher and move off (Fig . 97),

97, FIG, 9',
195
12. "Lift Stretcher. "-Nos. I and 3 grasjJ the doubled sling l11icl\\ay bet\\'een the poles the forefinger and thumb of the right hand, s\\'eep it off the handles, hold ing the sling at the full extent of the arm, buckle to the front. take a side pace to the front between the handles: and place the sling over the shoulders dividing it equally, huckle to the right. The slings should be placed so that they lie \-vell below the collar of the coat behind and in the hollow of the shoulders in front. In the event of the slings re ' l uiring to be adjusted, either as regards length or for the greater comfort of the bearers, .t: o. 4 will detail a bearer to carry this out, the length of the slings being adjusted, when necessary, by means of the buckles.
Two . Nos. I and 3 stoop, sIi p the loops over the handles, commenci n3 with the left, and grasp the han lies firmly,
7/tree . Nos . T and 3 rise slowly together, No. 3 conforming closely to the movements of No. J.
13. "Advance." -Nos. I, 2, 4, 5 and 6 step off with the left foot, NO.3 \\'ith the right, steppirlg short, knees bent, feet raised as little as possible .
14. "Halt."- The whole halt.
IS. "Unload Stretcher." -Tbe bearers ?lace themselves in the same position at the stretcher as described for Loading (Order 9).
16. "Lift."-As descrIbed for Loading (Order 10), H2
(:mo
196 except that the stretcher is carried forward three paces clear of the patient'::; fe et. 17 . " Lower."- The pati e r.t is gently lowered to th e ground . The l,earers disenq:age, r;se; I, 2 and ') turn to the left, -.t, 5 and 6 to the nght, and the ,,:hole step off to th eir places at the stretcher, as at Order" Stand to Stretcher " (Fig. 98).
The As h fo r d Li tter is made up of either of the f luley stretchers lllentioned on pages I 7 L and 173, a wh2eled under-carriage and a waterproof bood anj or if preferred a li rrht \yet-resisting cam'as cover. is kept' in position on the under-ca rriage by the foot-wheels, which fit into slots in the sHies of the under-carria CTe and it can be rel110\'ed at pleasure. The under is fitt ed with a cranked axle, which allows the °bearers to pass with the stretcher between the wheels instead of liftin g it oyer them. At Goth ends are two legs wbich may be turneJ up as handles when wheeling the litter. The hood and apron fit into sockets screwed to the stretcher. In wheeling the litter, care should be taken to keep the patient in a horizontal position . Should it be two bearers can easily lift the litter and patient.
Th e R ea- Ed wards L itt erl introduced in 19 0 4 is used in a similar manner, and one model of it is fitted with pneumatic tyres, which add immensely to the comfort of the patient and to the ease of propulsion.

197 CHAPTER X .
(Being tIle FzJlll Lecture fur Females only, z'n accord,l lh-e wdh Syllabus 58.)
BY E. :U.\CDO"\ ELL COSGRAVE, M.D., F.R.C . P.I.PREPAR"\TIOX FOR RECEPT!O:\' OF ACClDEXT
\VHE:\T news of an accident c0111es, preparations should at be made so. as to have everything l eady bef ) re the It:Jured person IS. brought in. Of course the preparatlOl1s needful \\'111 yary according to the nature an? extent of .the injury, but the following are the chIef thlllgs whIch may have to be done.
CHOICE Al\D PREPARATION OF Romr.
.\. r oom must be chosen. In a bad case this shoul<.1 ?e. one easIly reache d, as it is difficult to carry an ll1Jured p ers on .through narrow passages and up- tairs. Yl:less there ,Is some such reason against it, the Injured person s own room is best.
\\ay to the r00111 be cleared, projecting furnIture and loose mats 111 the hall or in lobbies should be removed . If the injured person is carried on a door, shutter, or stretcher, two strong chairs should be placed ready to support it wherever the bearers would be likely to require rest .
Use less furniture should be remO\'ed from the bedroom . The bed should he drawn out from the walJ
so that both sides can be approached, and the clothes turned back to one side to their full le ngth. A hot bottle should be got ready. If there is much collapse several hot bottles and hot blankets may be r equired; .:::::>ver the hot bottles \\ ith flann el.
If the injury is very severe, if mud-stained clothes have to be removed, or if extensive dressings have to be applied, it may be to have another bed, a c ouch or a table placed near the bed to lay the sufferer on in the first instance. This should be so arranged that soiling may do no harm; old sheets, waterproof materi a ls, thin oilcloths, or even n e\\·s pap er, may be used as a protection.
LIFTING AND
If present at the place where the accident occurred, it will be necec:sary to see that the patient is carefully lifted after proper "First Aid" has been rendered.
The following rules should be remem bered :-Select the proper number of persons to assist, and do not let them lift the patient until they thoroughly understand ho\\! they are to do it.
For ordinary cases, where the injured person has to be lifted a very short distance, three helpers are sufficient. Two (who should be as far as possible of eq ual height) are to bear the weight, the third is to support and take charge of the injured part. This is

199
by a person has been through a " Fir:.t Ald course . If the Injured person is insensible, :1:1 )ther help r shoulu support his head.
The lifters, one at each side, should kneel on one knee, and pass their hands under the patient's back at I lower part of the shoulder blades, and under tIle :',IPS, each his right hand in the other's ldt. I he ll1Jured patient should, if practicable, place his arms round the necks of the bearers.
. Tl:: helper sh0':lld attend to the seat of injury; If IS a fractured he should support it by placll1g the palms of hIS hands under the limb , one and one the seat of the injury, grasping It but aVOldll1g unnecessary pressure.
1 be helpers should remain thus until the ord er '. Lift" is th.en they should all lift slo\\ ly a.nd steadlly, avoldIllg prs, attempts to change positI ,)J1 of hands, etc.
H the injured person is to be placed on a stretrher or shutter, this should be preyiously placed with the bottom end at his head; the bearers should then one at each side of it, until the patient is oyer :t.. The word" Lower II should then be given, and the I11Jured person should then be slowly lower ed. A pillow ?r folded up .coat should be ready, and as the sufferer lS lowered thIS should be placed under his head.*
* Full directions are given in Chapter IX.
198
2(0
:MEANS OF CARRYING.
Besides a stretcher, and substitutes such as a gate, a shutter, or a door, other I11t'ans of carrying can be improvised.
In slight injuries, where the injured person is unable to wJ.lk, t\\'o bearers can carry him by forming a fourh::m.ied, three-handed, or t\\ o-banded seaL
A four-handed seat is formed as described on lnge [60.
A three-handed seat is made as descril)ed on page 162.
The two-handed seat is made as described on page 161.
A single helper can lift by supporting \\'ith one arm the t\\O knees, anu \\·itb the other the back. Til arms must be pJ.ssed \yell under before commencing to 11ft.
A single helper can give support by putting his arrn round the waist, grasping the hip and placing t'he injured person's arm round his o\\'n neck, holding the lund ",ith his o\\'n hand (Fig. 76, page 16 5).
A capital stretcher can be improvised out of a stron; sheet and two broom handles or other short poles. Each side of the sheet is wound up on a brool1l Inndle until there is just room for a person to lie
This req four bearers,. two at each side, to prevent the sheet slipping.
201

CARRY]);,G UP STAIRS.
In carr) ing a stretcher up stairs head should go first, and an extra helper should assIst at the lower end, so as to raise it and keep the stretcher nearly horizontal.
The three,. or four-handed seat may be used up stairs; or a strong chair, the patient bell1g carned up backwards. In the latter case one ?elper should walk .the chair and help to support 1t, and to prevent the ll1Jured person slipping out.
LIFTING INTO BED.
If the bed is narrow and there is room the stretcher should be placed on the floor with the head close to the foot of the bed . The injured person should then be over. the foot and placed on the bed.
I[ the bed IS too wIde. to admit of this, the stretcher should be placed .beslde it, and two helpers should stand at the far SIde of the stretcher. One heloer passes one arm beneath the shoulders and one the middle of the back, tbe other helper placing hiS under the lower part of the back and under the knees. The injured person is then lifted, another helper pulls away the stretcher, and after a single step forward the burden is pbcp.d on the b2d. '

PREPARATION OF BED.
A firm mattress, not a bed, should be (el ' cted. If there is much injury, or if dressings have to be applied, a draw-sheet ought to be placed on the bed. It should be of four or more thicknesses. extend across the bed, and reach from the middle of the ratient 's back to the knees. A piece of \\ aterproof sheeting or of thin oil-cloth should be placed under the draw-sheet. As the draw-sheet becomes soiled, the soiled portion should be rolled and a clean rart drawn smoothly under the ratient.
In fracture of the leg or thigh, sprained ankle and some other cases, a "cradle" (Fip. 99) should be lmprov-ised. The use of a " cradle" is to support the bed-clothes and keep them from pressing on the lim b. A band-box (Fig. 100), three-legged stool (Fig. lor), or hoop sa\':n across and the two halves secured to gether (Fig. 102), may be used. A corkscrew passed through the bed-clothes, with its point guarded by a cork, and tied by string to the bed or a nail in the wall, will relieve the pressure of the bed-clothes effectually
REMOVIKG THE CLOTHES.
In taking clothes off an injured person a few rules !1hould be borne in mind.
In serious cases it is much better to sacrifice the c10thes than to run any risk of increasing the injury.
.
FTC;.
--.;: -..,..:::=::... .-;--r_ ' -= . "'-''_ _ ;;-'__ .
09.
FIG. lOT.
In removing a coat, etc, in a case of fractured arm the uninjured arm should b e drawn out first.
In putting on a coat or shirt the injured arm should be put in first.
In burns and scalds nothing should ever be off. A slzarp pair of scissors should be used, and everything not adl1ering should be cut away. If anything adheres it should be left until medical aid FIG 102.
can be obtained. The clothing adhering may, with advantage, be soaked ""ith oil. 'To remove the trousers from a severely inj ured limb, the outside seam should be ripped up.
PR EPARATIONS FOR SURGEON.
As soon as the injured person has been attended to, preparation should be made for the surgeon's visit

The preparations needful \yill depend upon the nature of the case. The following hints may be of use :-
A fire in the room helps Yentilation, even 111 summer. There should be plenty of water, hot, cold, and also boiling, also several basins, plenty of clean to\\'els and soap. There should be something to empty \\'a ter into; a foot-bath does well.
The basins should be placed on a table, covered with a clean white cloth; a large to\\'el makes 2suitable cloth; the towels, folded up, should be placed on the same tabl e, and the bot and cold water should he within easy reach. The foot -bath should b e under the table or close at hand.
In the case of a burn, absorb e nt cotton \," 001, soft cloths, old linen, oil. and baking soda, should be re ::l dy, and materials should be torn up for bandages.
In the case of hremorrhage, plenty of water should be boiled and allowed to cool, and pads of absorbent cotton wool should be baked in a tin box in the and at least two bas'l1s should be ready.
In the case of a person rescued from drowning the sheets should be taken off the bed, plenty of blankets should he heated before the fire, and several hot bottles should be ready.
If poultices are likely to be required, boIling water, 1inseed meal, mustard, a loaf of stale bread, a small basin, a large spoon, sweet oil, and tow, flannel or handkerchiefs may be required.
2cb
For fomentation, have boiling water, flannel, a kitchen roller, and two sticks, or a large to·weI.
'When summoning a medical man to an accident always let him know by a \yritten message \\ hat kind of case he is required to treat, so that he may bring whatever is needful. By this means valuable time may be saved .
QUESTIONS ON CHAPTER X.
Tile numerals indlca/e tile pagr:s wile1'e tile aIlSW"I'S lIlay be found.
What points would you consider when choosing a sick
room? I97
How would you clear the way to the sick room? I97
What means of resting would you provide for those carrying a patient on El stretcher? I97
How would you place and arrange a bed for an accident case? 197, 198
Are hot bottles necessary, and how would you prepare them?
. .. ... ' " ... ... ... .. 198
'What is often necessary to lay the sufferer on in the first instance?
... '" ... 198
How would you protect this from getting soiled? . .. I98
How would you see to the proper lifting and carrying of an injured person?
.. . 198, r99
\Vhat substitutes fOl" a regular stretcher can you suggesl ? 200
How is the four-handed seat made? 160, r6r
For what cases is this seat useful ?.. 160
How is the three-handed seat made? r62, If4

207
For what cases is this sea{ useful ?...
IIow is the two-handed seat made?
For what cases is this seat useful ? ..
lIow can a single helper lift?
llow can a single helper give support?
How would you improvise a stretcher?
I low many bearers are required for this stretcher?
lIow should a strelcher be carried upstairs?
lIow would you carry a patient upstairs on a chair?
lIow would you lift a patient from a stretcher to a bed?
lIow should a bed be prepared for an injured person? . ..
How should a draw sh eet be made?
'Whal would you place under the draw sheet? .. .
\Vhat should be done wit h the soiled part of a draw sheet?
\\' nat is the use of a " cradle"? ...
In what ways maya cradle be improvised?
lIow \\ould you remoye a coal or shirt in the case of a fractured arm? ...
lIow would you put on a coat or shin if the arm were injured? .. .
In the case of a bad burn, what would you do with ciothing that adhered to the patient ?
lIow would you remoye trousers from a severely injured limb?
\Vhat preparations wou1d you make for the surgeon's visit?
\Vhat would you get ready in the case of a burn?
And what in the case of
And what in lhe case of a per on rescued from drowning?
\Yhat would you get ready for making poultices?
And for fomentations?
\\"lJat sort of a message would you send to a dLctor? ...
PAGE
PAGE 162 r6r, 162 I6r
200 r65 200 200 20I 20I 20r 202 202 202 202 202 202 204 204 204 205 205 205 205 20 5 206 206
208 INDEX.

Abdomen " wound of
A.ccident case, preparaI II 112 tion for 197
Acids, poisoning by 149, 151
Air, always necessary... 18
Alcohol, caution as to smell of 130
Alcohol, pois)ning by 134,153
Alkalis, poisoning by 149, 151
Ammonia, poisoning by 149
Anatomy (elementary) 20
Ankle 30, 3 2 " sprained... 64
Anteri or tibial artery 93
Aorta 79
Apoplexy 13 2
pparenLly drowned, to restore ...
Arm, bone of 139 28 " fracture of
Arm-slings
Arsenic, poisoning by
Arterial hremorrhage, arrest of 74 practising ar;est of 79 sign; of 74 .. , ., '. 7° ., course of mam 79
" .- ry, axillary . . . :5 5
A rLery, brachial... " . carotid ... dorsal of fool facial femoral ... i liac occipital plantar ... popliteal radial subclavian tibial temporal " ulnar
Artificial respiration 121, 129, Asphyxia ALIa
Auricl es ... Axillary artery ... Axis
Back, bandage for 159
Backbone 23
Rll1dage, to apply 42 to fold 37 " tc improvise... 37
Bandaging I S5
Bed, lifting into... 20r " preparation of 202
Bites of rabid animals 106
Bladder III, II3
Brachial artery ... 86
Brain 117 c ompression of 132 " concussion of 131
Breast-bone 26 " fracture of 48
Broad bandage ... 37
Broken bones, see .F·rae/llre.
Bronchial Lubes ... 118
Brooch-uone 30
Bruises 102
Burns 102
Caplilaries
Belladonna, poisoning by 14 Page
means of 160, 200 " upstairs
Cerebro-spinal system Cervical vertebr<.-e Cheek, bleeding from
Pr.ge 86 80 93 81 89 79 82 93 9 2 88 84 93 82 8E 136, 13 8 138 25 7° 85
Capsule ... 70, 72 95 Carbolic acid, poisoning by Carotid arteries ... from" Carpus hremurrhage 3 1 152 ;)0 So 28 Carrying,
Cartilage
Choking ... ... . .. 201 :LO} Circulat ion of the blood, organs of ... 70 Circulation of the blood,
induce Cla\'icle " fracture of Clolhes, removal of Coccyx COllapse ... Collar-bone 127 26 48 19, 202 25 J3-126 " fracture of ... Comminuted fracture C0111 plicated fracture Compound fracture Compression of the brain 132 Concussion of the brain 131 Conductor 143 Convulsions in children 137 48 35 3-134 Cradle, hed Cranium ... fracture of Crepitus ... Crushed hand foot 2'>2 22 43 36 55 62 Diaphragm r 20 Digital pressure... 74 Direct violence ... 33 Dislocation 62 Ditch, to cross with stretcher r 69 Dorsal artery of foot 93 verte 25
Capillary hremorrhage
Chest, bandage for Chlorodyne, poisoning by
to
210
Pa,E{e
Dress, woman's, on fire ... 105
Drowning ... J 39
Ear· channel, blood issuing from Ear-passage, foreign body in Elbow, bandage for joint, fracture involving PO I59 53
Electric shock
Emetic
Epilepsy ...
Esmarch's I..J.2 148, 149, IS0 13 2 triangular bandage
Expiration
External carotid artery ...
Eye, bandage for " foreign body in
Face, bones of
Facial artery
Fainting ...
Femoral artery " "digital pressure at groi n ...
Femoral artery, tourniquet for Femur , of Fibula " fracture of Fingers, bandage for " fracture of
Fireman's lift
First aid, meaning ot " student
Fish-hook, embedded
Flexion ... at elbow " at knee ...
Food, poisoning by
Foot, bandage for bones of ... " crushed
Forearm, bones of " fracture of
Forehead, bandage for. .. " hremorrhage from
Foreign body in the ea lpassage .,. in the eye " "in the nose
Four-handed seat
Fractme, apparatus for treatmeLt of causes of definition of general rules for treatment involving el bow joint of arm ... of brea t-bone of carpus of collar - bone of cranium of finger

Fracture " " of forearm of knec:-cap of leg ... of lower jaw ... of metacarpus of metatar<.us ... of peh'is of ribs ... of spine of tarSllS ofthigh-bnne ... of toes signs and s)'IlIp-
toms ()f 35 " varieties of Frrost-bite 108 Fungi, poisoning by 153
General circulation 70 Granny knot 40 Green-stick fracture 15, 36 Gums, ha:1l10rrhage from 97
Hremorrhage, arterial ... 74 capillary... 05 " " from gum<; 97 from hl:<ld and neck 80 from lower limbs... 89 from lungs 97 from nose 96 from stomach 98
Hremorrhage from throa ( 97 ), from tongue 97 from tooth socket... 97 from upper limbs 84 int ernal 95 kinds of 73 " venous 93
Hand, bandage for 157 " bones of ... 28 Hangin.g ... 140 rlaunch-bonps 28
Headand neck, arteries of 80 Head bandage for ... 155 injury to... 128, 13 1 " side of, bandage for ISS Heart 70 " rate of contraction of 72 Heat-stroke 136 Hernia 114 Hip, bandage for 157 History, meaning of 17 Howard's method of artificial respiration Humerus " fracture of Hydrophobia Hysterical fits Iliac arteries Impacterl fracture Indirect violen ce Insensibility 126 23
37 120 80 '55 109 90 30 56 30 60 159 55
IIO 109 III 16:) 36 ?3 33
54 58 60 44 55 62 21 I 56 46 45 62 56 62
T06
J) 79
36
52
1
35.
:H .. , 12S
Page
Imen sibility, general rules for treatment 128
Inspiration 120
Instep 30
In sulat ')r . , . 14 2
Internal carotid artery 80
Internal h::emorrhage 95
Int estines, injury of 113
Involunta ry muscles 33
Jaw, angle of 23 lower 23 " ,,[racture of 44
Joint, definition of 3 1 " injuries tn. J09
Jugular veiv 80
Kidneys 1 I I ., injury of. 113
Knee, bandage fur 159
Knee·cap 30 fracture of 58
Knot for bandage of lower lim L 42
Knots, reef and granny 40
Laborde's method uf ar i· ficial respiration ... 126
Laburnum seeds, poisoning l)y ...
Lacerated wound
Large arm-sling ...
Laudanum, poisoning
Leg, bones of 30
Leg, fracture of ... Lifting and carrying " into bed ...
Ligaments
Lightning, effects of Limbs, lower " upper Lime in the eye ...
Lips, bleeding from
Litters
Liver " injury of Lower limbs
Lum bar verte br::e
Lungs h::emorrhage
Marshall IJall's method of artificial re spiration 140 bandage 37 28 " fracture of .. , 55 r.letatarsus 30 " fracture of 62 :\liddle line of body 20 Mouth, hlood from 97 3 2 "ruptured 65
Muscular action... 3+ N arrow bandage 37
Needle, embeddecl Nerves J
Pag-c
N en'ous system... I I 7
Nu"e, bud)' ill .. . I I I h::emorrhagc frum 96
Occipital artery ...
Opium, poisuning by
Pau, ring ... " tu fuld
Palm, h::emorrhage frum
Palmar arches ...
Paregoric, pOlsuning by Patella... . .. fracture of Pel'\:is .. " fracture of Phalanges of foot .. ., of 11-1 11 d ,
Phosphorus, pJisonill"; }J;' . J..j.S, PhYSIOlogy (elcl1lcl1Lary)
Plantar arch " artery
Plants, "ariou" poisoning by... '
Pleura
Poi son w e' POll' wounds by
Poisoning . . .
Popliteal artery ...
Posterior tibial artery ... caustic, poisonmg by... 83 74 88 88 149 30 28 15 0 20 93 93 '4 8 120 J06 148 92 92 21 3
Pressure, digital. .. " point '"
Principles of First aid ...
Prussic acid, poisonin
Puues

Rabid animals, bites 0:... I06 S0 b artery ... . .. .. . fracture of 1\ecf knot
Respi ration artificial I < I, 129, ,. to excite 1\ espiratory systelll 1{est, necessity for Ribs ... " fracture of::: l\oom, choice and paration of
Pae-e .. 60 ... 198 201 26, 3 1 144 28 26 110 82 196 III I13 28 25 120 from 97
uy
0 '" Pulse ... .. Pupils of eyes Page 74 74I7 I5 2 2b /2 130 Questions on Chapltr I. ')T II. 66 III. 9 l\'. lIS \'. L+) \'[. r 5-+ 200
rr
13 6 , pre5-t 40 120 13 12 7 lIS 18 26 46 197
214 /'afe
Rupture (henlla) 114
Ruptured muscles (J5

Sl1lall arm ...
Smothering
Snake LiLes
Sacral verte bne ... .:acrum ...
Scalp, bandage for " h<emorrhage
Scapula ... . .. " fracture of method of artificial respiraliun 5 25. 2g 102 ISS from 83 26 51 121 IUO 1 62 161
Suda, caustic, puisoning by
Spleen
Seat, fuur-handed three-handed two·hanned
Shill-hone
Shuck electric
Shu 1lder, IJandage for .,. blade ... " fracture of bones .. . " juint .. .
Sick r oom , choice and preparaLion of. ..
Signs, meaning of Sil vester's method of artificial respiration
Simple fracture .. , Skeleton ...
Skuli
" fracture of Slings, arm
of.
Spine ...
" fracture of
Spirits of salt, poisoning by Splint, angular .. Splints, rules for applying to impro\'i e
SLernum ... " fracLure of
Stimulants
Stings of plants and 23 45 149 54 19 animals 107
Stomach.. . I I I hremorrhage frum 98 ,. injury of... ... 113
Strains 65
Strangul::tion 140
Stretcher exercise, Army 190 No. I. 174 No. n. 181 No. III. 185 Nu.1\', 187 17 2 21 5
Stretchers, to carry " to improvise 'Jl ry chnine, poisoning- by Subclavian artery . Suffocation
Sunstroke ... . tlOn for Syllabus of :::
Sympathetic system .. .
Symptoms, meaning of .. .
Syncope '"
Synovia ... ...
Systemic circulation
T arsus '"
Temporal artery ..
Thigh-bone ... " fracture of ... Three-handed seat
Throat, hremorrhage " swell ing of tisPage 169 166 153 1)4 14 1 136 20-17 17 134 3 1 70 30 82 30 56 162 97 sues of... 141
Tibia 30 " fracture of" 60
Toes, bandage for 1 59
Tongue, hremorrhage from 97
T ooth <;ocker hremorrhage from ' 97
T ourniq uet 75
Ulna " fi'act of Ulnar artery .
U nconsciou'illes"
Upper limb:;
Varicose veins
Veins ... Venous blood " h::emorrha6l!
Ventricles '"
Vertebra ...
Vertebr::e... ' "
Vertebral column
Vertical wound of abdomen... ...
Vitriol, burn by . Vol u:ltary muscles
Two-handed ,eat
Trans\'erse wound of abdomen II3 ... 16 1
'Wagon, to load or unload \'Tall, to cro:;s \\ ilh stretcher ,\Yarmth, necessi'['): for " to promote Wind-pipe ... ,Yoman' dress on lire \Vounds by poi"oned weapons " . accom pan ied by artenal hremorrbage ... ,\Vounds accompanied Ly venous h::emorrhacre ,,'-Tounds, hcerated t> '\Yri:;t
22 22
30 J )4 q2 15 6 28 51 26 32 197 17 1 2 3 34
43 39, 4 0 , 49
" injury
.. 39 140 w6 149 IiI 113 23 S pi:lal canal " cord II 7
Pnge 28 54 :5S 128 26 94 70 72 93 70 23 25 23 113 102 33 I7l 106 94 7' 2'
"(the St. 3(1)11 thnbn{allce tloooctatton.
GENERAL PRICE LIST.
A complete and reliable .\.m bulance Equipment is an actual necessity, and ex perience has proved that empl9yers of labour and oLhers in the Jist rict readily subsc ribe for th e PU,I'I\;\se of such appl iances. All informat ion r egarding the work of the A<;sociation can be obtained upon application to the Head Office, St. J ohn's Gate, Clerkenwell, Lond on, E. C.
All stores will be sent carriage paid to any part of Lhe Uni ted Kingdorn. I,eturns may be sent carriage forwaru. If carriage is I repaiu it will be allowed .
C wing to fluctuations in market prices it is impossible to guarantee that th e qUJtations herein can be adhered to.
Quota tions will be furn ished [o r Ambulance Carriages, moto r or horse·drawn, and u h er articles rel ating to Aml.)U, lan ce, Nursing and llygiene, not mentioned in this list.
Orders and correspondence shoulu be addressed to the St. John Ambulan ce Association, St. J ohn'5 Gate. Clerken well, Lonuon, E,C.
should be lllaJe pa,yable to the Sl. John t\.mlmlance Assuciati on, and crossed "Lol1(lon County and \V est1l1in-,ter Ballk, Lothllllry,"
Carriage Paid Oft all Order. In the Un i ted Kingdom.
THE .. ASHFORD" LITTER.

The "Ashford" Litter (1899 model) consisls of a twofilled elliptical springs, and either ?f, the Furley s,tretchers, \\ Ith a cover so arranged on a Jomted fram e that It can be folued up inside the stretcher or a anu apron (as shown aGove) , The unde/ carnage, a cranked axle, th e bearers can pass beLween the wheel? wnh the and thus a\'oid lifting iL over \\ hen th e legs of the under-carriage are ra ised, .and thus form the handles by which to propel it.
Should I,t be to pass o\"cr rough ground, two bearers can eaSily 11ft the litl er and The" Clemetson " str,etcher can be u-;eu instea I 0: the" l' urley "pattern For r nc es, see p, 7,
Ollrriage Paid on all Orders In the United Kingdom
THE
If REA=EDW ARDS" LITTER,

The und er-carriage or wheeled portion of this Li tte r is of an entirely new design, and is adapted to carry either of th e" Furley" or "Clemetson" Pattern Stretchers in prec-isely the same manner as the "Ashfurd" Litter. . It is fiued eit her wilh bicycle wheels and extra strong pneumatlc lyres. or with li rr ht but strong wooden wheels, either with solid indiarn bbe r "'or iron tyres. Owing to the reduction in the h eig ht of tIle wheels it is easy to lift a loaded stretcher over them, and
Can-Iage PaId on all Oraere In the United Kingdoll'l.
the cranked axle has, therefo r e . been replaced by a sr raigh ; nne. Ball bearings are fitted to the wheels, both cycle pattern
"RRA -Eo WAROS" LITTER, fitled with pneumatic ty red wheels, showing the "Clemetson" :;tretcher.
and wooden, and the hubs are so arranged that the wheels can be removed from the axle without disturbing the bearings. A push bar, capable of b eing raised or lowerea, IS lIsed at the head end. \Vhen raised as a handle it may be lucked in one or two positions, and when lowered it is lock ed in a vertical position. The pneumatic tyred wheels are strongly recommended in cases where the small amou nt of care necessary to keep them inflated can be given, as the comfort to the patient and ease in propulsion are increased beyond all comparision with any litter yet produced. ' F or I rices, see p. 7·
Carriage Paid 011 al\ Order. 1ft th.e Unit•• KI.. • •
THE " ST. JOHN" LITTER.

The ulld(>r-carriage of this Li tte r presents snme entirely np", features, and has ueen specially designed to carry the r egulallnr military stret cher, a matter uf some importance, at the present time . It will also carry either "Furley" or "Cl emetson" St r etchers. \Yhen 10ade J. the patient is halanced ove r the a.xle, thus ensuring I he grealest c o mFort to the patient, ease i n propulsion, and rapidity in manipulati0n . \Vhen using a military stretcher , the balance is obta.ined by adj ust ing the stretcher when load ing. The e xact positi nn ca n be as certained ill s'.alltly; but when using e ither u( t h(> ,)t h(>[ three stretchers, the balance i<; antomatic.
The \;nde"-carriage i-s fitted with a leg or 'hlppo rt at eHh en d , which i 3 rai<ec1 or !c.wcr('cl hy a new but very
Carriage P a id on all Orde rs in th 3 Un i ted l {ingLcm.
!evice. \Vh en they go IJeneath the frame of the under· carriage.
Tile question of storage, uften a 111atter of d i fficulty and e'pellse, has been carefully considered. As a rul e, a shed (J[ do l11ul'e . ,r less permanent nature is required, lJll t as the wheels of thiS litter can be easily and quickly rem oved and replaced_ and are il1l erchangealJ'e, it allows them t o he tak e n off and th e under-carriage, which can tllen be pas eel any ordinary Joorway. storeo wheJc convenient, the s,;ace rertuirecl being comparatively small. When wanted, one man can ea,ily put the parts together, a:Jd have the li !: ler ready for u.e 111 two or three minute. For prices, see p. ,.
THE" CLEMETSON" STRETCHER.
(S ee pag..: 4.)
On thiS stretcher the patient can be moved as desired, from the r eCUl11Uenl LO the sitl1ng Th e re i" no complicated mechanism w get out of urder, anJ the adjustment simply uJl the balance uf tlte patient's body . The stretchel will fit either the ., Ashford." ,. Rea-Edwards," or the " Sl. Julm "Under-Carriage. l'rice £3 35.; \\'it11 legs, £-+ 3",
FIRST AID BOX.
T o be CfllrieJ IJelow the axle of the" Rea-Edwards" Litter, from which it is casily detachable.
CUl1lenls of Splints, 12 Triangular lhnda6 es, 12 Roller Balldag('s, 2 i lb. packets eHch Cotton \\' ou l and Boric Lint, AJhesive Plaster, l'air of Scisso rs, Knife. 2 oz. earlI Tinct. I odine B.P.C., Sal Volatile, and Bor,c Acid l'oweleJ, Dredger, Graduated :-Ieasure Glass, KielneY- fh'i ped Dressinci Basin, Sl. Jllhn TOLlrnic;uet, Pins, Safety Pins, ?\ eedles, Thr ead, Tal-le, 2 Saucers, ancl 2 Camel lIair Brushes. I 'rice £2.
PRICES OF THE " ASHFORD," " REA EDWARDS," AND "ST. JOHN" LITTERS.
.C ASHFORD" and .C ST. JOHN"
LITTEI{S
Under-carriage (no Stretcher) ...
Litter complete with Ordinary StretcherDittowith Telescopic handl ed Stretchert
Ditto with Police Stretchert ...
Do. with "Clemetson" Stretcher ...
With Iron Tyres to Wheel s With IndiaRubberTyrestr Wit hollt Wit h Without Cover or With Cover or With
H ood a nd Cover. Hood a nd Hood ann Cover. AI Ap ron. Apron. A pron. illl

The prloes of the "Rea I:d ards" Litter are, with iron tyree, 10s. Od. , and with India rubber or pneumatio tyres , £1 158. Od. le88 in each instanoe.
• Prices quoted for Litter with Ordinary Stretcher include Wi de Webbing Slings but no Che't ,:; Strap. Leather, instead of Webbing Slings, lIS. 6d. extra ; Chest Stra p , IS. 6d. ex tra. I f 5' supplied without any Slings, 4S. allowed.
t Prices quoted for Litter with Telescopic-handled Stretc her in clude W ide W ebbin g Slings ann Chest Strap. Lea ther, instead of W ebbing Slings, II S 6d ex tra. If supplied without a ny Sl ings. ;j 4S. allowed; and if without Ch est Stra p, rs 6d. a ll owed
! P rices q uoled for Litter with P oli ce S tretcher incl ude \ Vide W ebbing S lings and Leathr -I raps for a refractory patient. T.e<1ther. in<tead of S lin gs, 6d. ex tra.
8' $ g- 0' :: :: <no r- ;j () 9 p..
H
£,
£, s. d. £, s . £, s. d £, s d. 7: 8 10 0 9 5 o II 5 o I I IS 01 2 10 014 - I I 2 6 13 2 6 - 14 7 616 - I I 10 o 13 10 0 - 14 I S 0 16 - 12 8 o 14 8 0 - 15 13 017 - - 14 13 0 - - 17 )d a nd on, as lra ted. JO 0 7 6 15 0 1 3 o IS o
S d.
(') j;i' I1Q " III c: o :I o C/l 5' ; c: :I : Q.
;:J g >-:l :r o-- ..(l) ro 0 (b'2,::r () g CJ 5' (1) Pol Vi" n; C' (') 8 n; ;; : :;: 2 .., >-:l <: 5" 0 5-t-., P- (b g I'1i C g. ro p.. 2' :: -< en g §, ;; : 8 c 8 B & crq (') CD s. (J) en 9 g 2 p.. ;.;" g 5: 5 :;.
::r g.!'l D p..:::: .. ,...,. -. ::r ,..... Vi' :; P: i: a '0 ;: g- !'l ;:;'C()
g J." o :>:l o Z ;p 7-' >< Ul ..., :>:l t=1 :>:l I () r' t=l ...; t=l r' t=l Ul () o '" Q ;; z o r' t=l o Ul ...; ;:j :J:: t=l 7-' I o ", t=l :.;: C t"1 t'" t'!l '"" t'!l (J) '"" (J) .., 1-4 t'!l '"" Ci o t'!l t'!l a:: (J) t'!l Z M '"" '"" = '"" ['!1 M u "0 III c: o o en = c: c. ,:; :i' GQ n :3
p..Uci
15 g ;; 0' -ti
PRI CE S OF T H E " FURL E Y" S T RETCHERS, WITH THE LATEST IMPRO V EMENTS.
r\. n -The prices of the Standard 1lodels are shown in hea vy type. Without W,th Wide With Wide Slings or Webbing Webbing Chest Slings Strap (no Chest and Che,l Strap). Strap.
Leather Slings Strap).

Ordinary Stretcher, for General
and Brigade
Telescopic -handled Stretcher fur workillgincunfined spaces
Police Stretche r, A sh Poles, Leather Straps, and Webbing Slings Slings (per pair), Wide Webbing, 4S 6d. Leather
Chest Strap, Wide Weuuing I load and Apron, " Furley" Stretcher (see i/lustrai£on, page 2) Du. do " Clemetson" Stretcher
Awning Cover for" Furley" Stretcher (when ordering please state pattern of Stretcher) .,. ' "
and Studs for fitting Ilood and Apron or A \\ !ling Cover, per
for Stretcher
f, ". tI j, s. tl f, s. d.
use I 13 6 1 17 6 I 19 0
I 19 6 2 3 6 2 5 0 With
f, s d 2 9 0 2 150 With Lea t her Slings a nd Webbing ChestSlrap £ s d 2 10 6 2 16 6 C) iii III 'tI III c.: o :s o
£, s d . ;; 3 3 0 s· o 15 6 ;
o I G 2 1 5 0 =. 3 00 ;: II.
o o 15
set 0 I 6 8 6 g- Spare Bed
Army Rug to cover Patient on Stretcher .. . Pillow for Stretcher, horsehair " 0 o 12 6 0 7 6 \\'aterproof
to be laid on the stretcher ueQ o 12 6 V> r:: frI Ir: 0 """': en C') '"0 t1> III a __ . d r ::- uf] 0 <.. ...-- r- Q. 0 '-a g- ;S. 1i' 7' :s ::i u ::-- :;- 02. =< 0 (j (l> :;- (J) ::= (Il g. g: ;n [Jq () () s· • ,., P> > ... >-:J _. "£ ;:J 0 (') ; g. 5 l-; ;: (J) c: ,- 0 :r n . 8 "'"2 g. t"1 ;:::; ::l.. ;:J 3 B 5' ;:J g, \l)
Sheet (wasllaule)
Carriage Paid on all Orders in the United Kingdom.

LAMP.
This is fitled wiLh ;1. sockel,
l,y \I hich to fix it to a Liller, or it can be conveniently carrieJ uy hand.
Price complete, od.
Can':! \;e Paid on all 0 rdsrl In the United Kil\gdom.
REGULATION POUCH FITTINGS
fOl the St. John Ambulance Brigade, consisting of;-
I Triangular Bandage, sealed up in waxed paper.
2 Grey Calico Roller Bandages (2 in. and I in.).
I Packet of Surgeon's Lint.
I Packet of Absorbent Cotton Wool
I Pair Scissors.
6 Safety Pins.
I Box of 3 Ampoules of Iodine
I Piece of Strong Cane, for tightening improvised Tourniquets.
List Price, 2S. 6d . each; 6 dol. or more, 2S. 5d . each .
B ox of 3 Amp oules Iodin e Tincture, packed for each 6d.; per doz., 5s. 9d .
SAFETY PINS.
All fasten or unfasten on either side.
Facile No. S 600 or S 602
Dressing Basi'1. kidney shaped. Il1Lt Ie of enal1lelled ir,>l1.
Price IS. 6d.
b 1 Station Plate, Enamelled Iron, 35 6 1.
Am u_ance Ellamelled Iron, 3s. 6d. eac . . Stretcher Depot Plate, 'ng palienls up and down sLam; Carrying Sheet fur canT . Des ig ned by the late J. C. or olhen\ ise about a d 1\1' Alfred Paine, Betlford. Derham. Esq .. BlackpoOI, an h J: and detachable bamuoo
Th e sheel is fitled Wllh 'drope :u stretcher withonl di!:turbillg I I may be place on 6d po alll . Price complele, 225. . t he patient.
Pocket Cork Line and Drag, with 80 feet of line, III
• cast' : for recovering a drowning person from the water. Price cUlllplete, with instructions for use, 6s. 6d.
Pocket Reel and Ice Line for use in ice accidents, with bO fet:t of line in Price complete, with instructions for . use, 6s 6<1.
s. d.
per 3 doz. 0 6 " " S 603 ... " 0 8 Duchess Duplex, No.2 ... per doz. 0 2 " " Ass orled " 0 3 Special Blanket Safety
3 in. " I 0 " " " " in. " I 6
Pins,
13 Carriage Paid on all Orders In the United Kingdom.
The St. John Tourniquet, as supplied to the Admiralty, with directions fo r use
(Specia l quotations for large quant iti es .)
Splints, \V ooden, per set, 2/6; Cane .. . . .. per set
Greatly improved Wooden Splints, with grooved joints and angle piece, strongly recommended ... Tow, for splin t padding... ...pe r lb.
First Field Dressing (Army Pattern)
Jaconette, ab out 42 inches wide Tow, Carbolized or Styptic ... per yard . .. pe r lb.
First Aid Dressing, consisting of a small compressed packet of b ori c lint, a compressed roller bandage,
and a safety pin
Dredger, containing boric a cid powder I

3
and I 4 Measure Glass ...
Small Bottles strong Smelling
Splint Straps, \V ebbing, and suitable Buckles. P e r set of 12 yards of strong 2-inch Webbing an d 15 Buckl es 4 3
These make very compact Straps fo r carrying in the Pouch. The Webbing should be c ut to meet loc al requiremen ts.
Buckles only, I S. 3d. per dozen. " -ebbin g only, 3s. c d. per dozen yards.
It is unnecessary to sew the Buckles. The spikes should be passed through the webbin g, and the short end of the webbing sh ould lie outwa rds.
Carriage Paid on all Orders In the United i<ingdom x LARGE HAMPER FOR AMBULANCE STATION AND RAILWAY PURPOSES.
For c ')ntents see next oage.
s. u. o 6 4 6 o o Q 2 3 o
0
5
... each
S.
per doz. 10 6
each IS. ; per doz. 10 6
... per doz. 5 6
s.
0
Knife with strong blade
I
;
Pair of Scissors...
Salts
Ca:rrlage Paid on all Orders in the United Kingdom, THE HAMPER CONTAINS
I Set of Cane
I St. John Tourniquet.
lb. Cotton Wool l tn Tin
! lb. Lint... ... i Cases.
I Roll Adhesive Plaster.
20 Roller Bandages, assorted.
I doz. Triangular Bandages.
3 pieces Tape.
4 oz. Tincture Iotli ne .
I Box Ampoules Ti ncture Iodine.
4 oz. Sal Voratile.
t lb. Puwdered Botic Acid.
4 oz. Bicarbonate of Soda.
I Dredger for Boric i\cid.
[ pair Artery Forceps.
I pair Scissors.

I Knife.
12 Surgeon's Needles.
1 packet each .Hld Plain Pins.
Carbolised Silk Silkworm GUl.
I reel each Black and \\ tllte Sewing Thread.
I Kidney-shaped Basin.
Stopper Loosenel.
I Graduated Measure.
1 cake 20 per cent. Soap.
I l\ail Brush.
3 Empty 8 oz. Bottles. 4 oz.
2 Saucers.
2 Camel Hair Brushes.
SiLe; Length 24 in. \Yid th r [in. Depth 10 in. (appt v lC.).
[·nr.e co mpl ete , £..J.
Carriage Paid on all Orders in the United Kingdom. 16
SMALL AMBULANCE HAMPER.
With waterproof cover and sl rap, for use in factories, co llieries, stations, and large works, as well as for parochial a nd domestic use.
C()'IJ'TAfNTNr;
Set Splints . 1 St. John T lJllrniquet. Box Ampoules of Tincture of Iodine. 2 Packets Lint. 4 Roller Bandages (wide and narrow). 4 Tri angular Bandages, Cotton \V 001, Bo ric \Vool (two latter in tin cases), Spool of Adhesive Plaster, Knife, Scissors. Thread, T ape, Needles, and Pins.
Weight complete, Ibs.
Ll"nglh, r flo 6 in. Dep! h, 5 in. Width, 7 in. (approx.) . I' nee £1 lIS f) I.
..,

Carri ag e Paid on all Orders In tile United Kln5dom . SURGICAL HAVERSAC.
Carri cgc i'aiJ on all Orde .s in the Un ited KlngC:om .
IMPR OVIW PATTER:'-I, with a.un. article ca n be taken out wlthul1t dlstur1>lng the lest 0, tht c ontents.
Contents: I Set o f Splints, 6 Tri angula r 6 Roller Bandages (wide and narro\\:l, CCllto n _\:-001, Bo n c. Lint, I R()l1 Adhesive Plaster, 1 Pair SCissors, I h.ll1fe, 07,.. Tlnct.
I Box Ampoules Ti nct. Iodine, 2 oz. Sal V olat de, 2 oz . BOl:I C Acid Powd e r, I Dredge r , I Grad uated Glass i-[ easure, I St. ] ohn Tourniquet, Pins, N eedles Thr ead . 2 Saucers, 2 C:Jnlcl Ilair Brushes. IJl1ce £1 lI S. 6d. White Ration Haversacs , 2 . each.
l'IRST AID COMPRESSED KIT.
The box is made of wood covered with damp·rcsi-;tin,,;material, and is fitted with a loc ', and key. It contains a number of practical amlmlance appliances arranged so that any article can ue wiLhdrawn or replaced without disturbing the rcmainder. Being fitted with a handle it is portable, and the lid. wh en let down, can be used as a table_ All bandages and dressings are compressed. Size-Length, in.; width, in.; height, in. (approx.), without handle.
Conlents: 4 Triangular Bandages, 6 Roller Bandages, 4 First Aid Dressings, 6 Small Packets of Cotton Wool, 6 Small Packels of Boric Lint, I St. John Tourniquet, I 1\1 easure I tin uox containing a Roll of Plaster, Bonc Lint Patches, Scissors and Pins, I tray 3 Bottles (Sal Volatile, Tincture of Iodine and Boric Acid Powder) anci a Dredger, I set of improved Splints, with angle piece, 8 Splint Straps (sufficient for a fractured thigh), 2 Saucers, 2 Camel Hair Brushes.
Plice .£1 lIS. 6d.
Canlailil P.ud 011 all Orders in lbe Umted

1RST RID eetMPRNION.
COMPRESSED).
Price Is. 6d.
€.c. By Post Is. 8d.
Size, by 3! by Ii inches (approx.). Suitable for the pocket.
CONTENTS.
1. Triangular Bandage. 2 First Aid Dressing. 3. Cotton Wool. 4. Two Splint Straps. 5. Adhesive Plaster. 6. Ampoule of Tinctur t! of Iodine. 7. Boric Lint Patches.
8. Safety and Plain Pins.
Price, each Is. 6u. Packed fur Post IS. 8u. Per doz . 17S. 6d.
SEPARATE ARTICLES.
No. No.
I each or 4/3 per dOZ'IS rd. per box or rod. per dul..
2 3d. 2/9"" 6 zd . each or r/9 "
3 " " 1/3 " " 7 rd. per packet or rod.
4- 3u. ].ler strap or 2/9 " " 8 I d." " rod . Not less than one uozen supplied at dozen
carric-ge Paid (In all Orde rS in th e United Kingdom.
FIRST AID BOX FOR USE IN MINES.
CONTENTS.
Set of Improved Wooden Splints; :; 1. Johl) Tourniquet; Cotton W ooi; Lint; 12 Compressed Roller Bandages, as<;orted ; 6 Triangular Bandages in waxed paper; Adhesive Plaster; Pair Scissors; Graduated Measure; 2 oz. Sal Volatile; 8 oz. Boracic Powder; 8 oz. Tinct. Iodine; Box Ampoules Tincture Iodine; Dredger; 2 Saucers; 2 Camel Hair Brushes; Pins; Safety Pins. PRICE COMPLETE, £2 lOS.
This First Aid Equipmert is also very suitable for in factories an' other large WOI and can be fitted for carrying on the "A hford . Lilter-.
'arrlage Paid on all Orders In the United Kingdom.
SMALL FIRST AID OUTFIT.
When closed can be carried by a Strap-hanclle.
Dimensio ns-9i by 7£ by inche s (approx.).

CONTENTS: 2 Triangular Bandages, r St. J ohn T-ourniquet , B Spl int Strapa (for securing Splints in li e u of Bandages) , 2 oz. Cotton \Vool, • oz. Plain Lint, 4 I-in. and 2 2·in. Roller Bandages, I 2 -0Z. Bottle Sal Volati le, ( >-oz. Bottle Tincture I odine, B.P.C , 1 P air of Scissors, 1 2-0%. Measure Gl ass, 2 China Saucers, and 2 Camel Hair Brushes to be used when ap plying Tln clUre of Iodine.
([ Price:
Wooden Box, covered with Damp Resisting Material, [5 5.
S tout Cardboard Box, Cloth Coverecl, IOS. 61
Carriage PaId on all Orders in the Un i ted Kingdom.
ROLLER BANDAGES.
BANDAGES in AssortDlent. Packed in neat Cardboard Box.
RECOMMENDED FO R CLASS PRACTICE
Two 3 in. two 21 in. ; one I in. each 6 yards long.
Grey Calico
ROLLER BANDAGE MACHINE.
.
Price 25. 6d .
·1
Per dOl. I In 2 in. 3 in. 4 in . 6 in
Grey CaliLo_ s . d. o (6 yards long. ) Grey Open Wo'-e. o ,j 9 Superior White Open \\'o\ e. d. o 5 3 93 6 2 3 2 0 2 9 2 0 2 6 3 6 3 6 5 3 4 6 S uperio r White ( 'pe n Wov e Compressed. s. d. 2 2 3 3 4 8 o 8 2 6 4 ROLLER
Designed
s. d. o D r. A. C
by
Tun
23

Carriage Paid on all Orders in the United Kingdom.
TRIANGULAR BANDAGES.
PI.dn, each (Special quotations for large quantlLies.)
Dittu Cumpressed (thinner quality), each ; per JUl. 4'> . 3d.
[lJustrated, sh ow ing 25 applications of the Triangular ,. d.
Bandage, with printed instru c lilln s .. . each a 6 per doz. 4 6
COTTON WOOL.
Plain. 1 oz., 2d.; 2 oz., 3d.; 4 oz., 4d.; lb., 7d.; I lb., IS. ld. : sma ll packet (Compressed), qd.
Medicated, Boracic, i lb., 6d.; I lb., IS. 6d.; Carbolic, per (b., 2S.; Alembroth, per lb., 25. 6d.; Double Cyanide, per lb., 2S. 6d.
LINT.
Plain, I oz., 2d.; 2 oz., 4d.; 4 oz., 7d.; lb., Is. Id.; fib., 2S. [d.
Boracic, 4 oz., 6d. ; I lb., IS. 9d. ; square foot packet, 3d. ; ... mall paCket (Compressed),
GAUZES.
Th e"e are supplic:d in 6 yard lengths, width about 36 inches.
U nmedicated white
Alembroth
Double Cyanide
Boracic
Pac kets of Cyanide rlo z., 2". Sd. Gauze (I s. d per length a 10 yd. compressed ), 1 a 2 2 per
GAUZE TISSUE.
CLINICAL THERMOMETERS.
Round.-No. I, ordinary, IS. 6d.; No.2, minu t e, IS. 9d.; NO.3, half-minute, 2s. a d.
With Magnifying Lens.-No. 4. ordinary,2s. od.; No·5, minute, 2S. 3d. ; No.6, half-minute, 2S. 9d.
\,Vith Broad Index , will not roll.-No. 7, ordinary, 2s. od. ; No.8, minute, 2S. 3d.; NO.9. half-minute, 2S. 6d.
In ordering it is only to quote th e registered number of the Thermometer requir"d.
N B.-Minute and half-minute instruments will only III the time stated under favourable circumstances.
BATH THERMOMETERS.
To Dr. Forbes' specification. Japanned with zinc scale, 2<;. 3d. ; Clinical Thenn o meter size, in case, IS. 6d. No liahility is taken .lor breakage of Thermomders in transt'l.
NURSING INSTRUMENTS.
Forceps, spring dressin g, full size o r small as desired, IS. 6d.; Artery, 5 in., 4S. 6d.
Scissors, round-pointed blades . small roun d-poi.nted blades, or 5 in., 2s.: sharp pOInted blades. for dehcate work, 2S. 3d.; curved blades. 2S. 6d.
Spatula, IS. Probe,6d. Director, with Ear Scoop, Js. 9d.
Knife, very thin, ivory handle, two blad s, Is. 9d.; single blade, IS.
Nursing Chart, designed by i\1iss Inci erwick, each.
Temperature Chart, each.
A layer of absorb ent cotton wuol betwc:en two sheets of gau ze, good quali ty, pe r lb., IS. 6d. Carriage Paid on all Or(fers In the United KlngdeM. It
-7 Carriage Paid en all Orders In the United Kingdom.
TEXT BOOKS. &c.
,. First Aid to the Injured." By James Cantlie, :'.LB., F.R.C.S. The authorised Text Book of the First Aid Course. IS.
.. A Catechism of First Aid." Compiled from Dr. Cantlie's Manual. By J. M. Carvell, M.R.C.S., L.S.A. 6d.
rt Problems in First Aid." A companion to the authorised Text Book of the St. John Ambulance Association" Fir t Aid to the Injured." By L. M. F. Christian, ilLB., C.M., Ed., and W. R. Edwards, A.C.A. 6d .
"Hints and Helps for Home Nursing and Hygiene." By E. MacDowell Cosgrave, M.D., illustrated, with chapter on the application of the roller bandage, by Sir R. J. Collie, M.D. The authorised Text Book for the Nursing Course. IS.
H A Catechism of Home Nursing" (bas ed on Dr. Cosgrave's Text Book). By the late J. Brown, L.l-Cc.P., L.R.C.S., and J. M. Carvell, M.R.C.S., L.S.A. 6d.
.. Home Hygiene." By John F. J. Sykes, D.Sc . {rl1blic IIealth), M.D., &c. Illustrated. The authorised Text Book for the Home Hygiene Course. Is.
"A Catechism of Home Hygiene" (based on Dr. Sykes' Text Book). By J. M. Carvell, M.R.C.S.• L.S.A. 6d.
.. Questions and Answers upon Ambulance Work." By John W. Martin, M.D., and John Martin, F.R. C.S., Ed. I S.
t< Questions and Answers upon Nursing." By J ohn \V. Martin, M.D. IS. 6d.
•• Elementary Bandaging and Surgical Dressing." By Walte r Pye, F.R .C.S. 2S.
•• To Restore the Apparently Drowned," printed in large T ype with two Diagrams. 2d.

Carrla,1 Paid on all Orders In the United Kingdom . Al TEXT BOOKS, &c.-{cont i1lued}.
Dr. G. H. Darwin 's "First Aids," being a card to hang up giving treaunent of vari ous ac cidents. 2d.; packeJ fur post, 5d.
"Manual of Drill and Camping for the St. John Ambulance Brigade." 5d.
"Manual for St. John Voluntary Aid Detachments." By Lieut.-Col. G. E. Twiss, R .A .M.C. (Retired Pay). 6J.
" H ow to Act w hen Cloth!ng takes Fire." By J. .E. H. l\1ackinlay, l\1.R.C.S. 2d.
"First Aid Principles." Cards . of concise directions f o r waistcoal pucket, each ; 4d. per doz. Special quotati un for large quantities.
" Specimen Examination Papers, First Aid, Nursing .lI l! Hygielle Courses." 3d.
Small Anatomical Diagram. Showing the human skel e ton, main anenes, and points where pressure should be aPl' ileJ to arre"t bleeding. 2d. Post card size for 'pocket, rd
Directioils as to the Restoration of Persons suffering from c'.lectric Shock. Large print, poster size. 3d. each; or 2S. 6d. per do:t.en.
General Notes on First Aid to be Rendered in Cases of Poisoning. By Milnes Hey, M.A., l\ l.R. C .S . , L.1<..C.P. 2d.
Notes on Military Sanitation. By Lieut.-Col. II. P . G. ElkingLon, R.A.M.C. 6d.
"Emergency Book," for instal1laneons reference, instructions; to hang on wall. Size about one r Ud • square. .as. 6d. ; packed for post, 2S. Sd.
Aids to Memory for F irst Aid Students. Revi ed to dal e . Addi tional Ill u I By the late L. :'1. Frank ChristlJ.u, M.B., C.M., E Ll in. 6J.
Oarrlage Paid on all Order. In the United Klnrdom.
TEXT BOOKS,
l!Jc.-(continued).
"Order of the Hospital of St. John of Jerusalem and its Grand Priory of England. " By H. W. Fincham, a.ssisted by W. R. Edwards. 100 pp., crown 4to., on antique laid paper, with 23 Plates on Art Paper. Bound cloth boards, gil t lettered, price 6s. (packed for post 65. 6d.). Cheaper EdiLion, paper covers, price 25. (packed for post 2s. 4d.).
General Regulations for the St. John Ambulance Brigade, 19 1 3. 3d.
Rules for Corps and Divisions, St. John Ambulance Brigade. 2d.
Registers . Class Attendance, 2S. 6d. Certificates, 45. 6d. Case Report, IS.
St. John Ambulance Brigade Cash Book, Minute Book and Occurrence Book. Set of three, 7s. 6d. Receipt Book, 6d.
Large Physiological Diagrams (New Series). For Locturers' use. The Human Skeleton, showing the main arteries and pressure points. The General Analomy of the Body. The Systemic and Pulmonary CirculaLion of the Blood. Section Th rough Middle Line of Head and Neck, showing the Ton gue in two positions in relation to the Trachea, and Schafer's method of Artificial Respiration (Expiration and Inspiration). Dislocations. Price, per set of five ISS. These may be hired for a course of "First Aid" lectures, given under the auspices of the Association, for a fee of 5s., or with the addition of Splints, Tourniquet, and 30 plain Triangular Bandages, for a fee of lOS. .-
Boxes of Stationery for the use of Class Secretaries and otbers connected with the Association, containing twelve sheets of high-class paper, suitabl y headed, and twelve envelopes bearing the device of the AssociaLion. 6d. Twice that quantiLy, IS.
Carriage Paid on all Order. In the United Kingdom. ELECTROTYPES.

Ube GranO of tr6c of tbe tlosplca t of St. Jobn of Jerusalem In £nglano.
Ar-tB\ LAN(E ibe St. 30"11 ambulllnce RS60.cilltion. No. I All.
Ubi: Gran!> f'rl orll of (1)rOer of tbe lboSpl!al of St. Jobn of lerusalem In It.nglRnl'
AWBU LANCIt DEPIIRTMEN T trbc St. 30fm Bmbulance NCl. ] DU.
No. I A. ]\'0. 2 A. NO.3 A. No. lB. 1\0. 2 n. No. 31131 Carriage Paid on all Orders ,'n tne United Kingdom.
ELECTROTYPES OF THE ST. JOHN AMBULANCE DEVICE.
For J\'sociation use. For Brigade use.
For Cards, Tick ets, &c. I
For Note Pape r. Small Circulars, &c. q 9 9 9
For Qun.rto and F oolscap Leu er-pape r, Circular , . ltc . ...
Small Posters
Large Posters
plete Series
I'rints of the above Electrotypes (1 to 3) Series A and B, an d (I) Series AH and BH, appear on page 30. T he diameter oj SA and SB i" inches.
FLAGS.

B r1gade Flag,
ui:rtiage Paid on all Ortie,S in the Umted Kmgdcm 32 BADGES.
Kos. 3 and 6. N os. 7 and 8. (Ac tual size.)
Badges, with the dev ice , issued under th e of tl e Central ExecuLi\'e Committee, having !Jeen lust apprm t'll by II.R.H. the Grand Prior as th e so le official and r ecognised Badge of the Associa.tion and Bligade. 11'. fl. This desi/!II IS protected.
SERIES A.- For the use of individ ual certificated pllpilsKo
In Ni ckel Silver, Large Size
Ditto. Small Size
Ditt o , Small Siz.e fur button hole
In Electro Plate , Large Size
Ditto, Small Size
Ditt(), Smal l Size for hIli I "11 h ole
In Enamel for butLul1 h'Jil;
Ditto, as brooch
In C loth and Silk
In Cloth and Sil n:'r
In C loth and Coltun
Small Cellu loid Hauge, for !JuLlon hole or brooch
'\,hite Satin Armlet. \\ ith wo\'en Badge
These Ballg,·,- are 1/(1/
No. I. 2. 3·
5·
4·
Se ries Series Series A. AH. B. BH s. d. s. d. s. d. s. d.
9 1 9 9 1 9
9
2
9 2 2
2
For
1 1 0 For
4 2 4 ('om
:-, 0 5 3 7 0 3
£ s. ri. Ass ociation Flag -I2 ft. by 6 ft. 7 6 5 f1. by 3 f t. o 12 6
new d
6 ft. by 4 ft. 1 10 0 9 ft. by 6 fr. 2 17 0 Pennon, 3 ft 3 in by 7 ft. 6 in. 2 0 0 5 ft. 4 in. by 12ft oj J J 0
esign.
1. 2. 3· 4· 5· 6. 7· 8. 9· 10 . [I. 12. [ 3· U.
2 in.
(, ia. 0
I i
t" be as deco,-a/ions_ 0 0 0 b [ 0 0 9 0 9 0 3 0 q 2 () 0 6 0 2 0 8 \
.u Carriage Paia on all Ordera in the United Kin&dorn.
BADGES.

•No.,. 15 Lo Ig (Reduced ). No. 19 (Actual Size).
SERIES B.- For meml)ers of the St. John Ambula nce not wearing uniform, having of the. C;orps or Divisi on annexed on a label, only Issued III quantlllesNo. 15 . I n Nickel Silver, 2 ins. in diameter, first doz., £1 ; subsequent dozs., 12S.
16. In Electro Plate, 2 subseq uentd ozs., £145.
17. In Cloth and Silk, 2
18. I n Cloth and Silver, 2 first doz ., £ I I 2s. " per doz. , 12S. per doz ., £1 lOS.
" 19. The "Brigade" button hole badge, each, I S. ; with brooch pin, each 1/3
N.B.-Tluse are >'l ot to be wont as decorations.
Carriage Paid on all Orders In the United Kingdom . 34
UNIFORM BADGES, BUTTONS, Etc.
St. John Ambulance Brigade.
Ambulance Divisions.
Officers.
Cap (N o. lOl)
Collar Badges (" 103 )
Pouch Badge ( " 3,657)
Rank, St. John 41)
pe r p<ir
Surgeon (Crosses IJ ::\0. 33) per pair
,. Superintendent (Stars A 3 2 ) per rair
Prince of Wales' Plume Badge (No. 44 ) pair
Reserve Badge (for all ranks) 34) pair
Lace, p er yard. Silver , lOS. ; Blacl, \Vhistle and Chain
Warrant Officers Badges (No. 35) per pair
Buttons, NO.4 (large) per doz. NO.5 (medium)
" No.6 (small. for cap)
Sergeants, Corporals and Privates.
Cap Badge (Nu. 102) ...
Collar Badges (,J 104) per pair
Overcoat Badge ( ,. 1. 582)
Tilles, S.J.A.B., 1 to 12 per pilir
Shoulder Straps, filted with titles and num erals ... per pair per bar
CI { Silver ... 1evrons, \ \'orcLcd
Div. Sec. anrl SergeanL's Badge ( 25)
Med;'lli on ('f) (\ 0. ;6)
Nursing Badge (L o. 2i)
Silver '\,"orsted
s. d. cI. o S 0 3 o 2 6 0 () o s 0 G o S 0 G o ::! 6 0 3 0 2 0 3 6 3 0 0 I 6 0 S 6 0 6\ 0 6 0 " 0) 0 0 0 6 0 8 0 10 I 5 7 0 10 0 4 r 0 0 8 0 0 3 o 4
Carriage Paid on all Orders In the Un i ted Sergeants, CO'porals and Privates. - cont inued.
. , {Instructor (No. 28)
SIgnaller s Badge Signalle r 29)
Bugler's Badge (No. 30)
Drummer'!, Badge (N J. 3I)
Bugler's Cord
Ba ndsman 's 'Wings
Belt Furniture per paIr
White Piping, per packet of 71 yards, enough for 3 pairs of trousers (packets
No. I (large) per
2 (med iu m)
NO·3 (small, for caps) 0 0
St. John Voluntary Aid Detachments. Officers. Men's Detachments.
Collar (N0. 21)
Cap Badge (N,). 23) .
Badges of Rank (Slars A N' u. 3!)
Buttons, No. 10 (large)
No. II (medium)
No. J 2 (small, for R 3.l1 k and File.
Colla r l3adges (No. 22)
Cap Badge (No. 24)
Shoulder Til les, S.J.A.A. ...
Ch { Silver ... evrons \\' orsted
Belt Furniture
BUltons NO. 7 (large)
No.8 (medium) ...
N0. 9 (small, for cap)

Carr iag e Paid on all Orders In the United Kingdom . St. John Ambulance Brigade. Officers. Nursing Divisions.
Lady Dist. Supt., Cloak (No. 3,658. 3 Stars, A)
" .. Arm (No . 3,659' 3 Stars A) ...
Lady Corps Supt., Cloak (No. 3. 6 58. 7 Stars
Arm (No. 3,659. 2 Stars A) ...
SUpl., Cloak piu. 3,658. I Star .-\)
Arm (No. 3,659. [ A)
Cloak (No·3 65))
" " Arm (Nc.. 3 ,65 1 )
Prince of Wales' Pll111le Badge (N'o. 44)... each
District Xumber, all ranks, single, 3d.; double
White Box Cloth Backs ... per pair
Badges of Rank (Stars A, No. ... each
Black Silk Armlet for Arm Badge, all ranks ...
Pin Cushion Badl:;e, all ranks (No. 37)
I JaL Badge, all ranks (No. 20) ...
Bl1ltom, all ranh , N( [3 (Ia.ge) ...
No. I4 (small) ...
Nursing Sisters- Cloak Badge (No. 3,5 21 ) .. : 3
Ann Badge (No. 3.522) ... .
Shoulder Titl es . S.J . A. B., I [0 12 per paIr
Pri"ce of \Vales' Plume Badge ( o. 45) ... each I
St. John Voluntary Aid Detachments. Officers. Women's Detachments.
IIat Bange, all ranks (No. 14) ...
Cloak Badge, Commandant (No. 42)
" " all other ranks (N o . I I )... . ..
Arm Badge, Commandant (No. 38 )
" ., Lady Superintendent, QuartermaSler and I h:umacisl ( o. 3q)
CenerFl l Sen'ice Ridge ( II. -+3 )
Trained Badge d
Black Khaki Uniform. Untform. s. d. s. d. 3 0 o 4 0 5 0 3 0 2 6 I 6 1 10 cannot be broken) 2 Buttons,
doz. 0 6 0 No.
0 41 0 8
per pai r f.lt"r pair per d oz. p ir pA r pair per bar per set per doz . 5. d. J 3 1 0 0 6 .' 0 0 6 o 10J o 6 a 8 0 ,0 0 I 6 0 6 0 41 0 s. n. I 0 0 0 8 0 la! 0 8 0 6 l J 0 o 8 o ro 1 10 0 0 8 0 6l
"
per doz. 36 s. d. 5 6 4 9 5 0 4 3 4 6 3 9 4 0 3 3 3 0 5 0 3 0 8 a 4a 3 a o 9
2 0
0
S
0
3 2 6 o 6 2 o o 2
\ ,J . 40 I
17

Carriage Paid on all Orders In the United Kingdom.
Officers- co nti Iwed .
Black Silk Armlet (all officers)
Ha.dge s of Rank (Slars A . 36)
Buttons, all ranks, No. 15 (large) .. "No. 16 (small) each per doz .
Other Ranks -Shoulder Tilles, S.J.A.A., per pair
SWAGGER STICKS
9
8
INDEX TO PRICE LIST.
(For General Index see pages 208-215 ).
PAGR
Ambulance Hampers... 14 to 16 " Station Plate. .. II
Awning Cover for Stretcher 9
Badges, &c.... ... 32 to 37
Bandage Rolling t.Iachinc 22
Bandagp.s... 22, 23
Basin, Dressing... J 1
Bearer's Dressing Case 37
for the use of Officers and Members 0; the St. Jahn Ambulance Brigade.
Ebonised Canes, Ge rman Silver illounts bearing the Brigade D e\·ice.
PRICE IS.
Officers' Special Canes, v"ilh Sterling Silver illounts.
PRICE 75. EACH.
BEARER'S DRESSING CASE.
PRICE I2s. 6d.
All Orders for the foregoing Stores should be g iven to the Local Secretary, or sent direct to The St. John Ambulance Association, St. John's Gate, Clerkenwell, London, E.C.
Belt Furniture 35
Books .. . ... 27 to 29
I30ttles (Water) 10
Buttons ...... 34 to 37
Carrying Sheet
Cash Book 29
Cotton Wool ... 23
Diagrams, Large 29 " Small... 28
Dredger (Boric Acid) 13
Dressing Basin I
Drowning Tackle
Electrotypes ... 30 3 Y
Emergency Book 28 Aid ilox 6, 20, 21 " Companion.. T9 " " Compressed Kit 18 First Field Dressings... T3
Flags 31 24
Gauzes 23
Gauze Tissue
Hampers (Ambulance) J4 to ,6
Haversacs 17
Hood and Apron for Litter 2,3, 7, 9 rnstruments (various) 24
Jaconette 13 Knife... .., .. , 13, 24
Lace for Caps, &c. 34 Lamp Lint 23 Litter (Ashford)... 2, 7 (Rea-Ed w.1rds) .. ·3, 4, 7
Litter (St. John)
Lowmoor
s. d. o 5 o 8 I 0 o
o
Jacket l\'[easure Glass... Minute Book ... Nurses' Wallets Nursing Charts Occurrence Book Pillow, Stretcbers Plasters.. Pouch Fittings Receipt Book Registers Roller Bandages PAGl!: ·5,6, 7 '3 29 25 Roller Bandage Machine Rug (Army)... ... ... Rules
22
Safety
Scissors
24 Slings
Splint Padding " Straps Splints... Stationery ... ... 13 13 13 ' 3 2Q Stretcher Depot Plate 11 Stretchers. 4. 6, 8, 9 Swagger Stick..... . 37 Temperature Chart ... Text Books Thermometers Tourniquet
t
ohn) Tow (carbolized) " (plain) ... Uniform Sundries Uniforms Water Bottle ... Waterproof Sheet Whistle and Chain White Piping Wool (Cotton) .•. 24 27 to 29 2413 13 13 34 to 37 ... 39,40 10 9 34 35 I]
for Corps or Divisions
St. John Ambulance Brigade
Pins
J3,
(Stretcher) Q Smelling Salts ...
(S
. J
39

Contractors ' List. tarriage out of L" • Extra.
PRICE LIST.
U NIFORMS FOR AM BULANCE UNITS OF TH E S ..J.A.B.
The e may be obtained fro111 HAZEL & Co. (sole proprielor, D. IIazel, for many years associated with the late tirm of llebbert & Co., Ltd., as Director), Clothing and Equipment
;\Ianufacturers, 65, East Road, City Road, London, E.C. ; and at 6, York Place, Leeds; 69, Piccadilly, Manchester; and 84, Miller Street, Glasgow. Telephone: 5678 London \Vall.
Telegrams : "Hazelism, London." 'Vhere two price.:; are gi\'l:n for an article they are for first and second qualilies.
A II Badges, and carriage outside London area, extra. ilfeasu1'ements to be supplied free of charge.
CORPS SURGEON AND DIVISIONAL SURGEON.
Tunic, Superfine Black Cloth ...
Trousers, Superfine Black Doeskin (if Silver Lace
Stripe, extra) .. .
Cross Belt and Pouch, Plain, 20/- ; Silver
Embroidered
Gloves
Great Coat, Grey Cloth
DISTRICT SUPERINTENDENTS AND CORPS
Tunic, Superfine Black Cloth ... OFFICERS .
Patrol Jacket, Superfine Black Cloth ...
Trousers, Superfine Black Doeskin
Cross Belt and Pouch
Gloves, 4/6; Leggings, 8/6
Great Coat, Grey Cloth
Patrol Jacket, Superfine Black Cloth
Superfine Black Doeskin
Cross Belt and Pouch ...
Gloves, 4/ 6; Leggings, 8/6
Greal Coat, Grey Cloth
Fatigue Jacket, Black Vicuna Serge
Patrol Jacket, Superfine Black Cloth
Chevrons, Four Bar>;, Silver
Trousers, Superfine Black Doeskin
Cross Belt and Pouch
Cap, 2/9 ; Gloves, Buckskin, 4/ 6; Gloves, Cotlon , 8d.
Leggings, Black or Brown Leather
'VaLeI' Bottle and Carrier
Haversack, White Duck
Great Coat, Dark Grey Melton
SERGEANTS, CORPORALS A:\D PRIVATES.
Patrol Jacket, Black Tartan
Chevrons, Silver ... Trousers, Black Tarlan
'Waist Belt and Pouch, Brown Leather
Cap, 2/9; Gloves, Cotton, 8d.
Leggings, Black Leather
Water Bottle and Carrier, 319; IIaversack, \Vhite Du ck
Great Coat, Dark Grey Melton 16/- and 0 14
DRAB SERGE
Jacket, Drab Mixture Serge
Trousers
Cap " " Creat Coat, Drab l\Icll on 16/6 and
;£ s. d. 3 15 0
...
Surgeon ,G I 17 6 Divisional Surgeon I 9 0 and 2 3 7 0 4 3 7 6 0 17
Cap-Corps
..
Corps Officer 6 and I 10 o 3 15 2 10 I 2 0 13 3 7 I o 18 6 6 6 6 c 0 0 0 6 6 6 o o Con t r actors Car r :a ge Paid on a ll Drapery Goods. DIVISIONAL
OFFICld{S.
Cap-Distlict Superintendent
,
SUll<:RINTE TDENTS AND
" Trousers, illack Vicuna Serge ;£ s. 2 6 1 2 0 13 .3 7 r 5 o 16
Superintendent £1 4 0 and 0 Lt Ambulan ce Onicer 0 15 6 0 9 FIRST CLASS
Cap-Divisional
SERGEANTS.
...
I IS o 3 o 19 o 10 o 4 o 3 o 1 o 16 o II U. l> 6 6 6 o o o o 6 -t 6 b 3 Y 6 o o
per nar o o o o 10 9 l> 6 6
0 4
0 I
o o 9 8 o 2 o 19 .3 6 o 9 o o b
ST. JOHN f\fv\B U Lf\NCE BRIGf\ OE.
UNIFORMS
FOR NURSIN G UNITS.
THESE GOODS MAY BE (\BTAINED FaOMMessrs. E . & R. G ARR O ULD,
ISO to 162, E D GTVV ARE RD., L ONDO N, V.
CLOAK (Badge extra) 25/ 6 , 29,'6
BONNET {Nursing 9/6 " Officer s 10/6
DRESS {NUrSingSister'spressLength 3/ 11 " Officer s" " 4/3
C ., { 2! in" Std. each; 5/6 <loz. OLLARS in., 61d." 6/6 "
C F S ,f ... 4 in., \. " 6/6 " U Fl... ,I 7id." 7/6 "
C {NUrsing Sister's & 1/- Lach AP "Officer's... 1/4 ., Ap RON Ii I I & 2/6 . also in Pure Irish Linen 3/1 I "
ILLUSTRATED PRICE LIST FREE.
Teleplzonps5320. 5321. & 6297, P \I)I>IX" ro:o< G \RROlJLD LONDON."

'l'HE
UNIFORMS,
'CLOAKS, BONNETS, APRONS,
DRESSES, FOR THE ETC•• .. , ST . J O HN AMBULANCE BRIGADE, MAY BE OBTAI "RD AT k J ,\ E & R. GARROULD. Ill,., To H.' f. W= Omc" .,. H.i\I. INDIA OFFICE. COLO:-lIAL OFF I CE. LONDON COl'NT\' COUNCIL, ETC. 1 1Jj ( I \' AN I LLUSTRATED PRICE L I T of the yarious articles required by the ST. JOHN BRIGADE ON APP L ICAT I ON. '
WINTER COAT (as illustration) SUMMER C(\AT 25/6 3 1 / 6
ISO to 162, Edgware Road, LONDON, W .

