

BONES. ARTERIES . .
The nllmbered d4lts sh<,w sure points for the ;l.rteries. Compare numben in text.
_ - Occipital. -" ........." Temporal.

Seventh Cervical I
Vertebra. Collar Bone (clavicle)- f.
Breast Bone t _ (sternum) I
Arm Bone (humerus)
«th Lumbar
Vertebra
Haunch Bone (pe.lvis)
_ Brachial (Digital or Tourniquet).
ort •• B chial Note the posiHon of th.se Bones when the forearm is turned. (F e' ion ---/ / - nf
knee Cap __ (patella)
Commencement of Popliteal. Popliteal Flexion). -ibial.
Shin __ (tlbiG)
Brooch Bone __ (fibula)
Tarsus
M"t.taMlull Phalanges- -

"A J. AS COMPANIONS TO THIS BOOKCATECHISM
OF FIRST AID."
BY M. CARVELL, M.R.C.S., L.S.A.( R EV IS ED 1919.)
Price 6d.; by Post, 7d.
"PROBLEMS
IN FIRST AlD."
BY THE LATE L. M. FRANK CHRISTIAN ANI) M.B ., W. R. EDWARDS, O.B.E.
Price 10d ; by Post, 11

FIRST AID TO THE IN]Ul<ED
ARRANGED ACCORDING TO THE REVISED SYLLABUS OF THE FIRST AID COURSE OF THE
ST. ]CHIN AMBULANCE ASSOCIXTION.
BY
COLONEL SIR JAMES CANTLIE, K.B.E ., :\I.A., F.R.C.S.,
KlIi'ilzt of G,'ace of the Order of St. John. HOl/ora,.y Life l1/ember 0/, and Lecturer and Examiller to. the .rlssoctntion.
\\·ith-(a). An Extract from the Home Office Official Pamphlet • F,rst Aid and Ambulance at Factories and \V orkshops."
(b). 1 nstructions on "Stretcher Transport," revised from those MIglnally written hy the late S ir JOHN FURLEY. C. H .• C.B of Jus tice of the Order of St. 10hll. in accordance with the Army Stretcher ExercIses.
(c). A CHAPTER (being the Sixth Lecture for Females only). by E. ;\lAC])OWEL COSGRAVE. M.D .• F.R.C.P.I KlIight of Grace oj the Order of C:it. fohll. HOllortlYJI Life I1Jc1I11>",· of, mId Lectll,'e r and E.'t:all7iner to. the .-1 SSOClal/oll .
I'HIRTY-SEVENTR EDITION.REVH:lED 1919 BYA SUB - COMMITTEE Fourth issue 1,878 ,00) to 1,927.000.
Pr ice 1$. 6d. net; by post, Is . 8hl.
LONDON: THE ST. JOH;\I A:\IBULANCE ASSOCIATI001, ST. JOHN 'S GATE. CLERKENWELL. E . C. 1. \Y. H. & LC.

FIRST AID AND AMBULANCE AT FACTORIES AND WORKSHOPS.
At the request of the Factory Department of the Home Office, and to assist in making known several very important First Aid Orders lssued by the H orne Office under the "Police Factories, &c. (Miscellaneous Provisions) Act' 1916," the following slightly condensed from the official pamphlet, "First Aid and Am bulance at Factories and Workshops," is preto the Association's text book for the First Aid course of instruction. ORGANIZATION.
If the full benefits of First Aid and Ambulance are to be obtained, their organization must be carried out in such a manner as to ensure the co-operation of the workers. There is no side of industrial life where the interests of employers and are more closely identified, and where combtned efforts towards improvement vvork more for mutual benefit.
Supervision is essential, and some person or persons must be made responsible for the smooth and satisfactory working of the organization throughout the factory, and as First Aid is so 3
closely allied with safety, it would seem appropriate to delegate to members of any jSafety Committee established at the works, the responsibility for the efficient carrying out of First Aid and Ambulance arrangements. To this Committee would fall the duties of considering suggestions regarding the adequacy of the provision made. It would also undertake arrangements for the trainingof persons in First Aid and the appointment of an appropriate number of them to be responsible for the First Aid Boxes.
The benefits of an effective First Aid and Ambulance service may be summarised as follows :-
Suffering is allevi a ted.
workman who has met with a slight accident enabled to r e t.urn to work almost immediately 10 comfort and with a sense of security. prevented from developing IOtO serious Injuries as a result of septic infection or blood poiwning. Experience shows that it is not always a severe accident that in the end proves the most serious.
The loss of a limb or even of life has ensued from an apparently trivial, but neg lected, injury.
Th e recovery of the workman and his return to work after a severe ac c ident may be materially
2
!?e H ome O ffice has statutory power to make Orders r equ IrIng the provision of Ambuiance and First Aid arrangements at any specified wOl'ks or class of work , a n d seve r al Orders for different classes of work are a lr eady in force, These Orde r s differ somewhat according to b u t are based on one general scheme co m prIsmg :-
1. First Aid Boxes .
(a) For the treatment of minor injuries.
(b) For preliminary treatment of more serious cases, e.g., hremor r hage, fractures, unconsciousness, etc., before medical help is available.
2 . Ce.ntral Ambulance Room under the charge of a qualified nurse or other person trained in First Aid . This will be the main centre of treatment in the works, serving in particular fo r the preliminary treatment of the more ser ious cases and also for any subsequent treatment that may be required in cases dealt w ith at the First Aid Boxes.
FIRST AID BOXES.
Number and Position of F irst Aid Box e s .-lt is essential that F irst Aid to be successful shall be rendered and First Aid Boxes should thel-efore be provided In s u ch numbers and posit ions as to be within easy reach o f every worker. The Home Office Orders prescr i be a m inimum number, which is one box to every 150 persons. T he best positio n for a First Aid Box is in the work room itself.
of F irst Aid Boxes.-T he equipment of the First Aid Boxes as specified in the Orders varies to the of the injuries likely to occur In the parttcular industry or process, but,

sgene r ally speaking, it consists of a supply of sterilised finger, hand and large size dressings, iodine solution, a bottle of eye drops and sterilised cotton wool , together with a copy of the First Aid leaflet iss u ed by the Factory Department, which gives suggestions [or the treatment of minor injuries. it is best that the equipment of a First Aid Box should in most cases be limited to the articles above specified / cases have been brought to the notice of the Factory Department where boxes have been supplied with equipment o[ a quite unnecessarily elaborate character \ Vhere, however, no ambulance room is provided, it is desirable to provide in one or more of the boxes or in a small cupboard in a central position the following addit ional appliances: scissors, safety pins, sal-volatile and measure glass, a tourniquet, splints, slings, roller bandages, an additional supply of wool and a roll of plaster (1 inch wide), and also, in places where burns are likely to occur, a supply of sterilised burn dressings. A tretcher is also advisable.
Protection and Use o f D ress in g s.-Dressings must be sterilised (subjected to heat to destroy any germs, and not merely impregnated with an antiseptic) but must also be kept sterile. Each dressing should therefore be in a separate packet carefully sealed, complete in itself, and so packed that it will not matter whethel' or not the hands of the worker who applies it are dirty, All that is necessary is to avoid touching that part of th e dressing which is to be placed upon the wound.
Waterp roo f Pl aster. - \Vaterproof to cover dressings is required in Dyeing and Tanning \Vorks where so lutions of bichromate of potassium are used, in order to pre\'ent the solution in which the worker's hands are im mer eel from saturating the dressings and attacking the
4
wound.. To be successful the plaster must be applied so that It overlaps the edges of the dressing underneath to an appreciable extent.
Washing of Wounds should not be done but iodine solution should be applied by using sterilisea Th ese should be used once only and thrown away.
. Burns:-The immediate application of a dressing is Important 10 the case of a burn, as the immediate exclusion of air allevia tes pain. The sterilised wool in the box can b.e purpose, but special burn dressings conSIStlOg of hnt Impregnated with picric acid, are included in the outfit in cases where burns are likely to occur. The use of oil and grease should be avoided . \Vhen the burn is caused by a strong acid or caustic, the burn should be thoroughly flooded wilh water before using the sterilised dressing.
Injuries to the Eye.-Two kinds of injury have to be provided for.
(a) The presence of a foreign body.
Th e only First Aid permissible for this is to brush the eye gently with a brush carrying a little of the No.1 solution mentioned in the First Aid leaflet, so that pain is relieved and the foreign body if possible brushed from the eye. Any further treat ment must be given by a doctor, and no attempt should be made to remove the foreign body by any other means.
(b) A burn caused by splashes of acids or caustics ..
In this case the eye must be thoroughly washed out with sterilised water, after which some drops ot No. 2 solution mentioned in the First Aid leaflet should be dropped into it.
No injury to the eye should be neglected, whether it appears serious or not.

7
AMBULANCE ROOl\I.
The provision of an Ambulance Room is required undel' the Orders where 500 or more persons are employed. The accommodation, site, general construction, equipment and the provision for transport to hospital will depend upon the number of persons it is required to serve.
The Ambulance Room must be a separate room used only for the pUI'pose of treatment and rest, wilh a floor space of not less than 100 square feet, smooth, hard and impervious walls and floor, and with ample means of natural and artificial lighting. It must contain at least-a glazed sink with hot and cold water always available; a table with a smooth top; means for sterilising instruments; a supply of suitable dressings, bandages and splints; a couch, and a stretcher.
A very complete illustrated brochure on the whole subject, fl'om which the above abridged extracts have been taken, should be obtained by all to whom Section 7 (1) of the Police, Factories, &c. (Miscellaneous Provisions) Act applies. It can be obtained from His Majesty's Stationery Office or from St. John Ambulance Association, price 6d. net; by post, nd .
For list of First A id Boxes to meet the 1'equirements of t1ze Factories and TVorkshops Welfare Order, see price list at end of bo ok , page 11.
6
REFERENCE Ko. 58

SYLLABUS OF INST R UCTIO N -ADULT CO UR S E.
FmST LECTURE .
A . Oul1ine and Principles of .First Aid-Very important.
B . A brief Description of the Human Skeleton and of the Muscle .
C. Fractures-Causes, varieties, signs and sy mptoms.
D . Treatment of Fractures-General Rules.
E. T he T r iangula r Bandage-Its application to the Head, Chest, Back, Shoulder, Elbow, Hand, Hip, Knee and Foot.
Arm Sling (L arge, Small and St. JOhn) .
SECOND
LECTURE.
A. Individual Fractures-Details of treatment :- The Skull, Lowe r Jaw, Shou lder-blade, Collar Bone, Arm , Forearm, Hand, Thigh, Leg, Knee-cap, Foot, Ribs, Pelvis and Spine.
B . Dislo cations, Sprains, Strains- Signs, symptoms and t r eatment.
C . Practice-Treatment of Fractures.
T HIRD LECTURE.
A. General descript ion of the Hea r t and Blood Ve els.
B. The Ci rculati on of the Blood .
C . Vali e ties of Hremorrhage .
D . \ Vounds accompanied by Arterial Hremorrhage.
E . T he situation o f the main a rteries-P r essure points.
F . Comp ression of arteries by Digital and Instrumental pressure .
G . Veno us Hremorrhage and Va ricose Veins.
II . Practice - Compression of arteries.
9
FOURTH L ECTURE.
A. ·Wounds accompanied by Venous or Capillary Hremorrhage .
B . Poisoned ·Woun ds .
C . I nterna l H remo rr hage. .
D. Hremo rr hage fr om I ' n SI-I ' n
E. Burns, Scalds , Frost-bite, tlilgS, rlS. , Embedded Needle.
F Foreian bodies in the Eye, ose or Ea r.
G: Practice-- T reatment of Fractures and Hremorrhage (as in Lectures I I. and Il L ) .
FIFTH LECTURE .
A. T he Nervous System. . .
B . T he Organs and Mechanism of Resp IratIOn.
C . Insensibility . .
D. P ractice - Artificial RespiratIOn.
SIXTH LECTURE ( for Males only).
A. Poisoning . h . k h d f II'ftl'ng and carr)'ing t e SIC - or
B. Improvised met 0 s 0 injured.
C. Hand Seats.
D . Stretcher exercise .
SIXTH LECTURE (for Females only) .
A. Poisoning. "
B. Hand Seats - Lifting and patients.
C. Preparation for the receptlOn 0 aCCI ent cases.
D. Preparation of the bed.
E. Removing clothes .
F. Preparation for surgeon.
19
T 7·
NOTE I.-The subject of poisons should be treated in a general manner; the common poisons classified, and only their general symptoms, effects and treatment taught.
NOTE H.-The latter part of each lecture should be devoted to practical work, such as the application o f bandages and spli nts, lifting and carrying wounded on stretchers.
NOTE HI.-Male classes must passin that system of stretcher exercise most suitable for the locality.
OTE IV.-\Vhen possible a skeleton should be used. Too much time should not, however, be spent on in truction in anatomical and physiological details. Lecturers and Examiners are particularly requested to remem ber that it is " First Aid" that has to be taught and tested, and not anatomy and physiology.
lJfixed classes of ,"elt and women are on 110 aaoullt permitted.

SUMl\IARY OF CONTENTS.
CHAPTER 1.
Outline of First Aid-Very important
Questions on Chapter
CHAPTER II.
The Human Skeleton. .Bones and Joints
Muscles. Voluntary and Involuntary
Fractures and their treatment
Dislocations
Sprains ... ...
Sprains and Ruptured Muscles .. .
Questions on Chapter
CHAPTER III.
Circulation of the Blood ...
Wounds and Hremorrhage
Bites of Animals (Poisoned Wounds)
Internal Hremorrhage ...
Hremorrhage from the Nose
Hremorrhage from the Mouth
Bruises
Questions on Chapter
CHAPTER IV.
Miscellaneous Injuries. and scalds; stings of plants and animals; frost bIte; under the skin; fish hook embedded III the skill : foreign body in the eye, ear passage and. und in the front wall of the abdomen; the organs within the abdomen and pelYIS; rupture ... ...
Questions on Chapter
10
I I
..
...
.
Page 17 28 29 39 40 68 70 71 72 76 80 102 ro4 ro5 106 ro7 ro8 II 1 121 ,
CH APTE R V.
The Nervous System. Cerebro-spinal, sympathetic '" 1 2 3 The Respiratory System 1 2 4
I nsensi bility .. . I 27
in all Cases 1 28 Asphyxia 13 0
When Breathing is present and there are no Convulsions 141
Chapter 15 0
CHAPTER VI.
Poisoning. Gooeral rules for t rea tment; special poisons I5 2

The Sixth Lecture (for Females only ). Preparation fo r r eceptio n of accident cases, choice and preparation of a room, lifting and ca rryin g, preparation of bed, rem o'Vin g the clothes, preparations for curgeon.. 200
on Chapter
Skeleton showing pos iti on of main a rt e ri es
The Ambulance Cross
Skull and verteb ral column
Vertebra
Bones of the left upper limb
Bones of the ri ght lower limb
Shoulde r Joint
Ankle ...
Rectus Muscle
Triangular bandage spread out and folded
Large arm sling
Small arm sl ing
Reef knot
Granny knot ...
Loop knot...
Bandage for fracture of lower Jaw.
Bandages for simple fracture of nbs
St. John sling
Bandage for fracture of shoulde r blade
Treatment of fracture of arm
Angular splint
Treatment of fracture of forearm
Treatment of crushed hand... . ..
Treatment of fracture of thigh bone
Treatment of fracture of thigh bo ne (woma n)
Fracture of knee cap ... ...
Treatment of fracture of knee cap
Treatment of fracture of leg (man and woman)
Treatment of crushed foot... :.. . ..
Diagram of the and au passage s
Diagram of the cIrCUlatIOn of the blood ...
12
Page
Treatment
Fits I47 Questions on
The
CHA
Questions on Chapter 159 CH A PT ER VII.
Triangular Bandage 160
PTER VIII. Methods of Carrying 16 5 CHAPTER IX.
ApP ENDIX
13 LIST OF ILLUSTRATIONS.
Questions
208
The Roller Bandage 2 IO
... .. . ...
... ... ... ...
... .... .. .
.. .
... ... .. .
...
.. ,
Pag-e .frontispiece 23 3 1 3 1 34 36 38 38 39 45 46 46 47 47 50 51 54 57 58 59 60 61 61 63 64 64 65 67 68 77 79
14

St. John Tourrliquet
Digital pressure on carotid artery .. .
Digital pressnre on facial artery .. .
Digital pressure on temporal artery
Digital pressure on occipital artery
Pad and bandage to arrest hremorrhage from temple
Ring pad
Digital pressure on subclavian artery
Pad and bandages to apply pressure on axillary artery ...
Digital pressure on brachial artery (two methods)
Flexion at el bow
Digital pressure on radial and ulnar arteries
Pad and bandage to arrest hremorrhage from palm
Digital pressure on femoral artery ...
Tourniquet on femoral artery
Flexion at knee
Organs of the chest and abdomen ...
The lungs and bronchial tubes
Schafer's method of artificial respiration ...
Vertical section of head
Silvester's method of artificial respiration
Triangular bandage for the head ...
Triangular bandage for the shoulder
Triangular bandage for the hip
Triangular bandage for the hand
Triangular bandage for the foot
Triangular bandage for the chest
Triangular bandage for t-he knee
Triangular bandage for the elbow ...
Lifting by two-handed seal. ..
Grip for two-handed seat .. .
Carrying by two-handecl seat
Grip for human stretcher
Carrying by human stretcher
Grip for three-handed seat ...
Grip for four-handed seat .. .
Supporting patient ... .. .
Fore and aft method of carrying
Carrying on improvised seat
Improvised stretcher ...
Furley stretchers
Stretcher exercise, No. I. "Stand to Stretcher"
Ditto, No. I. "Col!ect 'Vounded"
DillO, No. 1. "Lower Stretcher"
Ditto, ready to lift patient ...
Ditto, lifting patient ...
Ditto, placing stretcher .
Dillo, preparing to lower pal1cnt .. .
Ditto, " March"
Ditto, changing numbers
Ditto, No. II. Ready to lift patient
Ditto, patient lifted ...
Ditto, changing numbers
Ditto, No. III. First position
Ditt o , second position
B ed cradl es ...
R oller bandage machine
Finger bandage ...
Spica fo r ball of thumb
R e verse spiral for the forearm
Spica for right groin
Spica for both groins
Knee bandage
Figure of 8 bandage for the leg
Many- Tail bandage ...
PaJ;c 82 88 88 89 89 90 9 1 9 1 92 93 94 94 96 97 99 II9 126 136 13 8 139 160 16r 161 162 162 163 164 164 16 5 166 167 168 16 9 17 0 15
... .. . .. .
.. . .. .
Pfil,g-e 17 1 173 174 175 175 177 179 179 179 181 182 18 3 184 I 5 18 7 18 9 190 19 2 194 195 205 & 206 210 21 3 214 21 5 216 21 7 217 218 Z19
PREFACE.
AT the request of the Ambulance Committee of the Order of St. John, we have undertaken the revision of the Official First Aid Hand-Book of the St. John Ambulance Association, written by Colonel Sir James Cantlie, K.B .E., F.R.C .S., in 19 01 , and subseque n tly revised by him .
Our aim has throughout been to simplify the study of First Aid. With this object in view we have <extended the principle adopted by Sir James Cantlie of imparting info r mation in the form of general rules for givi n g treatment correct i n character and sufficient in extent, pending the arrival of professional help, without the complete investigation necessary to be made by a medical practitioner before he takes all the steps required in each individual case .
A short appendix on the use of the roller bandage, with typical illustrations, is included for the first time .
\iVILLIAM R . EDWARDS (Chairman ).
WILLIAM E . AUDLAND , M. R.C .S.
J . l\L\CLEAN CARVELL, M. R.C.S.
CHARLES COTTON, F. R.c .P.Edin.
R OBERT B. DUNCAN, M.D.
GEORGE S. ELLISTON, M. R. C.S.
I SAAC G . MODLIN, M.D.
A ugust, I 9 I 7.

17 CHAPTER I.
OUTL I NE OF FIRST A I D.- VERY I MPORTANT.
The St. John Ambulance Association has n.ow completed forty years of its existence, and dunng that period over a million men and women have been taught at its classes, il: all parts of the world, how to help their injured neIghbours.
\ VH,\T FIRST Am IS.
First Aid to the Inj ured is a special branch of practical medicine and surgery, by a of which trained persons are enabled to afford .skllled assistance in cases of accident and sudden Illness. The instruction begins and ends with First Aid, and the subject is taught simply, but thoroughly exhaustively. The duty of the ambulance pupIl ends where the doctor's begins, and there ought to be no overlapping or clashing of .duty or
In First Aid to the Injured three thll1gs are essential :- . .
(a) To determine the natu.re of the case attention, so far as IS necessary for ll1telbgent and efficient treatment. other words, to make a sufficient diagnOSIs for the

purposes falling within the province of the First Aid student.
(b) To decide on the character and extent of the treatment to be given.
(c) Lastly, .to apply the treatment most suited to until professional help IS avaIlable. that has any bearing on the case should be consIdered as follows :-
1. The Pat.ient Patients. -Difference in the sex. necessItate dIfferent lines of treatment. The posItIOn assu.med by the patient, either voluntarily or by force o f cIrcumstances, should not escape attentio t.han. one patient may need assistance, will be necessary to ensure that the most needs of each receive prompt attention . I, S,l,gns, Symptoms and H i sto r y - By Slgl:S. are meant any differences from the of the patient, such as pallor conaestion s,:'ellIng, dislocation, etc., which can be 'notel by dIrect use of the senses-sight touch smell h ,.- and t t ( Th '" eallng, as e sens.e of taste should very seldom) if ever, be .used for thIs purpose.) ") Symptoms)) "are the sensatIons of the patient such as paI'n nu b" 'dd' , m ness gl ll:ess r etc ., which he can, if conscious' descrIbe; "history," which may be obtained from the patIent or from witnesses, means the circumstances such as a collision, fall, being subject to a 19
particular disease, etc., attending the accident or sudden illness . Symptoms are less reliable than signs, as one patient will try to make light of a yery severe injury while another will make the most of a trifle, and history must be considered trustworthy in proportion to the reliability of the source whe-nce it is obtained . Symptoms taken alone are not of mnch value for diagnosis, but though as a rule unpleasant, they haye their uses, as yyarnings of something wrong, as guides to the seat of mischief and, il1 many cases, by their abatement or increased severity, as indications whether the treatment given is right or wrong . Symptoms when considered in conjunction with the history of the case, are distinctly enhanced in diagnostic value.
'When to the above there is added information gained by the observation of definite signs, the diagnosis rests upon a solid basis.
3. The Cause or Causes. -When a cause is known, a conclusion, more or less accurate, may be drawn as to its probable effects. But it must be remem bered :-
(a) That a cause may have more than one effect. For example, two or more injuries may result from one accident.
(b) That the effect or effects may be direct or indirect. For example, a blood-yessel may
18
in the head, causing insensibility (dJrect effect ). The patient will fall and a further injury may occur as the result of the fall , that is to say, indirectly as the result of the bursting o f the blood-vessel.
(c) That the cause may be still active . For exam pIe, a foreign body in the throat will conti.nue to impede breathing as long as it remams there.
4· Surroundings.- These will exercise a most important on first aid to be given, and therefore reqUIre careful consideration on the following :-
(a) of danger . - Fire, movmg machll1ery, electric wires, poisonous gases, a r e stive horse, slippery objects, etc., be present and necessitate the protectIon not only of the patient but also of th e first aid e r and of third parties.
(b) Possible clues to diagnosis .-A br o k e n ladder, stains of blood, escapina a a s etc b b' . , may afford suggestions . Objects suspected of havll1g some connection with the or illness should, compatibly wIth the pressll1g ne e ds of the emer ge ncy, be exammed and p erhaps preserved for future reference.
(c) The help available depends in the first
(d)

21
place on the presence or .nearness of persons capable of helping, and 111 second pl a ce upon the dIscrimination, and tact with which their efforts are ... !3y the exercise of these qualities an 111qUIsItlVe crowd may be so controlled and as to be of vital assistance to the patient. The importance of satisfa ctory provision fo r professional cannot be too strongly insisted on. For thIS r eas.on, if in doubt early enquiry as to the practIcability of obtaining such assistance .should be made . Discr e tion must be ex e rCIsed as to sending fo r the doctor or taking the patient to him . The appliances available. -Appl.iances may be at hand in plenty, means. of Improvisin g may be ad e quf1.te, or. nothll1 g but the actual resources of the patIent and may be availabl e . Th e directions and trations which are given throughout thIS book are intend e d as a standard of treatment. It will frequ e ntly be impossibl e , fo r lack o f appliances, to out the treatm e nt exactly in the manner ll1dIcated. In such cases It will be necessary to comply 'with the principles of treatment in best manner consistent with the actual circumstances.
20

(
e) The shelter. - This word m u st be understood as including an extra wrap, or an um brella, etc., as a temporary protection against the inclemency of the weath er or fierce rays of the sun, as wel l as a shed, a private house, or a hospital. If the patient is to be taken to his home, a tactful message thereto might enable suitable preparation to be made, and in any case would be an act of kindness to those concerned.
(f) Means of transpo rt av ailable .-Considerations of the best means of transport to shelter involves questions of appliances, length of journey, the nature of the ground to be traversed, and the best disposal of the help available for carrying the patient and making arrangements for proper after care.
NECESSARY QUALIFICATIONS OF A FIRST AIDER.
In order to render the skilled assistance required the first aider should be-
(a) Observant, that he may note the causes and signs of injury.
(b) Tac t fu l, that he may without thoughtless questions learn the symptoms and history of the case, and secure the confidence of the patient and bystanders.
(c ) Resourceful, that he may use to the best
22
23
FIG. I .-THE EIGHT-POINTED AMBULANCE CROSS.
advantage whatever is at hand to prevent fur ther damage and to assist Nature's efforts to repair the mischief already done.
(d) t.hat h e 111ay h a ndle a patient wIth.out causmg unnecessary pain, and use efficie ntly a nd neatly.
(e ) Exphclt, that he may give clear instructions to the patient or the bystanders hew best t o assist him.
(/) Discriminating, that he may decide which of several injuri es presses most for treatment by himself, what can best be l eft for the patient or the bystanders to do, and what should be left to the medical man.
(
g ) Persevering, that he may continue his efforts, though not at first successful.
(lz ) Sympathetic, that he may give real comfort and encourJ.gement to th e suffering.
PRINCI PLES OF FIRST Am.
.1. is not to be assumed because sIgns of lIfe are absent.-I t frequently happ ens that even a is un able to say positively a patIent lS alIve or dead ; far less can the Fnst AId student form a decision It is much better to tr.eat a dead body than to allow a livin a person to dIe for want of First Aid.

2. Remove the cause of injury o r danger whenever possible.
3. Severe ha:morrhage must receive the first attention, no matter what are the other inju ries. .,. .
4. Air. - The patient must be m a posltIOn m which breathing is possi ble; th e air passages must be free from obstruction; if breathing has ceased prompt measures must be taken to restore it.
5. Rest. -- A r estful ?f the body will assist the yi tal functions . The POSI tlon assumed by the patient should not be thoughtlessly altered. Supp ort of the injured part will help to prevent further damage. The use of pillows in this connection 15 much to be commended.
6. Warmth. -After every accident keep the patient warm, so as to prevent the hll of belov,' the normal point (98'4 degrees FahrenheIt).
7. When the skin is broken the wound shoul d be promptly covered \\'ith a . clean absorbe nt dressing. Should the wound be pOlsOl:ed, it is most important immediately to prevent th e pOlson permeati n g the system.
8. Poisons swallo\\'ed should be got rid of, 01 when that i·s inexpedient, neutralised .
9. The best means of transport must be studied, and provision made for proper care wh en the patient is brought to shelter.
24
25
IO . Removal of Clothing. -Clothes should not be taken off unnecessarily, but when it is needful t rem?ve . the rules will be found serVIce 111 senous cases :_
Remove from the sound side first, and If neces.sa:y, slit up the seam of the sleeve on the 111Jured side.
SHIRT AI D VEST: Slit down the front and remove as the coat .
TROUSERS: Slit up the outer seam.
BOOT: Stea.dy the ankle and undo the la.ces.
SOCK: Cut off.
II. is incorrect to suppose that alcohol IS the only form of stimulant and far t frequent of spirits is made to re;tore a after an accIden.t, often with serious results: the safest therefOl:e, IS to deff!l' the administration of alcohol un,til the arn val of a doctor. ' Vhen the patien t is able to swallow, strong tea or coffee, or milk as hot as can be dr u nk, or a tea-spoonful of sal volatile in a tumb ler of water may be given. Smelling sa.lts may be held to the nose. Sprinkling the face wItb cold and bot water alternately, warmth applied to the pIt ,the stomach and over the heart, and fnctIOn of the limbs upwards bave a stIrn ulat111g effect.
12, Throughout his work the First Aid Student must on no account take upon

hi mself the duties and responsibilities of a D octor. -At times an apparently slight injury is accompanied by grave danger and may actually cause loss o f lite . When sending for a doctor , state the nature of the case, the whereabouts of the patient, and, if it is intended to move him at once, the destination and the route to be followed. Written particulars are safer tha n a verbal message.
ANATOMY AND PHYSIOLOGY.
It is necessar y that something should be known of the structure of the body (anatomy), and of the function s of some of the more important organs and systems (physiology). A short description of the necessar y anatomical and physiological points is therefore given as the several subjects are discussed . No matter what is the actual position of a person, for purposes of description the body is supposed to be erect , with the arms hanging by the side and the palms of the hands directed forwards. The" middle line " of the body runs vertically from the top of the head to a point between the feet.
26
QUEST I ONS ON CHAPTER 1.
The nU1Ilerals indicate tile pages where the answers 71. ay be found.
What is First Aid to the injured?.. . ... 17
\\ hat are the three essentials of First Aid? ... ... 17, 18
How may .the treatment differ according to the pati e nt o r patIents? ......... 18
Explain signs, symptoms and history .. . IS
,Yhat is their value, separately or together? ... ... 19
\Vhat must you bear in mind in drawing conclusions from a known cause?
.. 19, 20
State fully how the surroundings of the patient may influence First Aid ..
20-22
,Vhat qualifications should a First Aider possess? ... 22, 24Is absence of signs of life proof of the presence o f death? 24
\Vhat is often the first thing to do in an accident? ... 25
"That result of injury must receive the first attention? ... 25
\Vh at three things are generally necessary fo r an injured person?
,Yhat should be done when the skin is broken? . .
How should poisoning be treated?
\Yhat steps must be taken beyond the actual treatment of injuries?
H ow you remove clothing when necessary from 25 25 an Injured person?
Explain the use and abuse of stimulants ..
,Vhat must the First Aider never do ? are anatomy and physiology?
'When describing the budy how is it supposed to be placed?
If a person raises his ann above his head which is considered to be the upper part of fhat lim b ?
(Answer: The shoulde r)
What is the middle line of the body?

CHAPTER II.
THE SKELETON.
The human body is moulded upon a bony framework (the skeleton) which serves-
I.-To give shape and firmness to the body .
2.-To afford attachment to the muscles.
3 . - To protect important organs, as in the skull, chest, and abdomen.
THE SKULL.
The Bones of the Skull are arranged in t\\'o groups, those of the brain case or cranium, and thos e of the face.
The Boundaries of the Cranium are the "ault or dome, the rounded portion forming the top of the head; the front or brow; the back of the head, where the greatest extent of brain exists, and wh e re therefore the cranium is widest and deepest; the sides or temples . The base of the skull is hidden from view by the bones of the face and of the vertebral column; in it are numerous perforations for the' passage of blood vessels and nerves; through the lar gest opening the brain and spinal cord are contin uous.
The Bones of the Face with the exception of
28
PAGE
... ... ... .
. ... .., ... . ..
... .. . .., ... ... ... .,.
...
... ... ... . ..
... ... ... ... ... 26 26 ... 26, 27 2 7
.
... ...
... ... . . . '" '" ... . ..
27
30
the lower jaw are firmly jointed together, so that movement betw ee n them is impossible. The cavities of the nose and of the eye sockets (orbits) are formed by the bones of the crani urn and of the face conjointly. The mouth cavity is formed betw ee n the upper and lower ja\Ys, the palate being the bony roof of the mouth which separates it from the nasal cavity above.
The Lower Jaw consists of:-
(a) A horizontal portion in which are the sockets for the te et h.
(b) Vertical portions terminating on either side at the joint between the lower jaw and the base of the skull situated immediately in fr o nt of the ear.
The angle of the jaw indicates the junction o f the horizontal and the vertical portions .
THE BACK-BO E, SPINE, OR VERTEBRAL COLUMN.
The Vertebral Column (Fig. 2A) is composed of bones called vertebrre, each of which consists of-
r.-A body or bony mass in front.
2.-Processes projecting backwards, which en. close a canal for the spinal cord-the spinal canal.
3.-Two transverse processes.
3 1

FIG.2A.
Co. 4
SKULL AND VERTE BRA L COLUlIlN.
Showing left ribs and portion of breast bone. The right ribs are removed.
SPINOUS PROCESS. TRANSVERsa PR OCESSES
CANAL FOR SPINAL CORD.
DODY OF \'ERTEil R A.
FIG. 2 D.
SURFACES SUPPORTING
HEADS OF RIBS.
FIG. 2C.
TRAN SVERSE PROCESS.
SPIKOUS PROCESS.
C 7

4. - A spinous process. The spmous processes of the vertebrre can be felt beneath the skin for the whole length of the back (Figs. 2B and 2C).
. 33 in all, are grouped into regIOns, 111 each of which they are known by numbers counting downwards :- '
I.- I n the neck 7 Cervical vertebrre. The first vertebra, tIle atlas, forms a joint \yith the base of the skull, at which tlte noddina movement of the head takes place; second, tlze axis, by the joint between it and the atlas, allows of the side-to-side movements of the head.
2.-1n the back 12 Dorsal vertebrre to which the ribs are attached . '
3·-1n the loin 5 Lumbar vertebrre.
4 · - Th e rump-bone, or Sacrum, consists of 5 Sacral vertebrce united in adults as a solid mass.
5·-The ta.il-.bone, or Coccyx, consists of 4 ver · tebrre together to form a single group. Between the bo.dles of the vertebrce, in the upper three are mterposed thick pieces of cartilage (gnstle), whIch, ",hile they bind the bones allow of free movement to the column as a whole: and. help to bre<l:k the shock of any sudden force applied to the spll1e (for example) when falling from
a heigh t on the feet) . The whole spine is strapped togethe r by ligaments r eaching its entire length.
THE RIBS AND BREAST-BONE •
T he Ribs consist of twelve pairs of curved bones extending from the dorsal vertebrre to the front of the body, and are known by numbers-first, second, etc., commencing from above . The ribs are not bony throughout their entire length, but at a short distance from the front the bony materia l ends, and cartilage (gristle) takes its place. The upper seven pairs, called the true ribs, are attached by their cartilages to the Breast-bone (sternum), a dagger-shaped bone with the point downwards, just above the pit of the stomach. The lower five pairs of ribs are called "false." Of these the upper three pairs are attached by cartilage to the ribs immediately above them. The last two pairs are unattached in front and are called "floating." The r ibs enclose the chest and serve to protect the lungs, heart, liver, stomach, spleen, etc.
THE UPPER Lll\IBS.
The Shoulder-bones are the Collar-bone (clavicle) and the Shoulder-blade (scapula) .
T he JCollar-bone can be felt on either side beneath the skin at the lower and front part of the neck as a narrow curved rod about the thickness of a finger. I ts inner end rests on the upper part of the C
32
33
PART OF COLLAR BONE
SHOULDER BLADE ( SCAPULA)
AR \! BONE (HUMKRUS) ••.... r

BONES {UI.NA OF
FOREARM RADIUS --H-i':-\
RADIUS _ ULNA
FIG . 3A.
BONES OF THE LEFT UPPER L IMB.
FIG. 3D.
SHOWING THE POSITION OF THE RADIUS Al\D ULNA WHEN THE THUMB IS TUR ED I NWARDS. Compare Fig. 3A, in which the thumb is turned out· wards .
35
breast-bone, and its outer end joins with t he shoulderblade .
The Shoulder-blade lies at the upper and outer part of the back of the chest, and forms joints \\'ith the collar-bone and the bone of the arm .
The bone of the Arm (lmmertts) reaches from the shoulder to the elbo\\'.
In the Forearm are two bones, the Radius 011 the outer, or thumb side, and the Ulna on the inner, or little finger side . Both bones reach from the elbow to the wrist, and they change their relative position with every turn of the hand (Figs. 3A and 3B).
The Ha nd is composed of-
r.-The bones of the wrist, or carpus, eight in number, arranged in two rows of four.
2.-The metacarpus (the framework of the palm) ; five bones which form the knuckles and support the bones of the finge rs.
3.-The phalanges, or finger-bones, three in each finger, and two in the thumb.
THl!: PELVIS AND LOWER LIMBS .
The Pelvis. - The lar ge basin-like mass of bone attached to the lower part of the spine is composed of the two haunch-bones and the sacrum. The haunchbones meet in front (at the pubes) in the middle line, only a small piece of cartilage intervening, but behind, the sacrum is placed between them. The pelvis
34
TIIIGH BONE (FEMUR ) ,
F IG. 4. BONES OF THE R I G H T LOWER LIMB, SHOW, I NG JOINT WITH THE PELVIS AT T H E HIP .

37 supports the abdomen and its contents, and provides the deep sockets for the thigh -bones- the hip joints .
The Thigh-bone (femur) reaches from the hip to the knee join t. I ts shaft is stout, rounded, and arched forwar d s ; the u pper end presents a rou n ded head, supported on a neck which projects inwards, to fit into the socket of the hip joint.
The Knee-cap (patella) is a triangular bone lying with its base upwards in front of the knee joint immediately beneath the skin.
The bones of the Leg are the Shin-bone (tibia ) and the Brooch-bone (fibula). The Shin-bone extends from the knee to the ankle, in both of which joints it plays an important part; its sharp edge, the sitin, can be felt immediately beneath the skin of the front of the leg . The Brooch-bone lies on the outer side of the tibia. I t does not enter into the formation of the knee joint, but its lower end forms the outer boundary of the ankle join t.
The Foot is compos e d of-
I,- The tarsus, a group of seven irregular bones at the instep. The largest is the heel-bone , and t h e uppermost (the ankle-bone) forms the lower part of the ankle joint.
:2. -The metatarsus, the five lo ng bones in front of the tarsus which support the toes .
3 . - The or toe-bones, two in the big toe , and three in each of the other toes.
_ •• • •••
HAUNCH BONE.
_t.-.7 "'-- KNEE CAP (PATELLA), BROOCH l30NE ( FIBULA).
JOINTS.
A Joint IS formed at the junction of two or more bones . In moveable joints such as the hip, knee, elbow, etc., the surfaces of the bones are covered by cartilage, which lessens friction and the shock of a

FIG. 6.
LEFT ANKLE.
F Compare Fig. 4, Pa(!e 36. IG. 5. fall. The capsule of the joint consists of bands of strong tissue surroundina the J'oint braced with b , I stronger bands called liaaments and holding the two b . 0' o?es. m po.sition while allowing of free movement.
I t IS Imed synovial m embrane, whose function is called s)'novial fluid, which IS 8 hyays ll1slde the JOInt and acts as a lubricant.
To explain the varieties of moyeable joints, the
following exam pIes are given :-
1\ RTERY YEIN
Museul AR TISSUE
TENDON OR OF PATELLA
FIG. 7·
DrAGRA::--f SHOWING RECTUS OF THWH, WITH ARTERY, AND NERVE.
The Should e r, a balland-socket joint, consists of ashallowsocketon the outer angle of the shoulder-blade, and of the head of the armbone (Fig. 5). 0" ing to the shallowness of the socket, which is necessary for free mo\' ement, the arm-bone is very prone to escape from its socket (dislocate).
The Ankle , a hinge joint, is formed at the junction of three bon es, the shin-bone above and on the inner side, the broochbone on the outer side, and the ankle-bone below (Fig. 6).
THE MUSCLES.
The M u scl es (red flesh) of the body are classified into two g roups-volulltary and z"1lvolzt7l tar)'.
39
TENDON
PATELLA

T r.. e Voluntary Muscles are met with in the li mbs , t he head and neck, and the surface of the tr u nk . T heir ends are attached to different bones, and as they pass from one to ano t her they cross a j oint, a n d, being e n dowed with the power of contraction a n d relaxation, cause the movements of the body. As a muscle crosses a joint, it as a rule b ecomes a fibrous cord or tendon . Blood-yessels traverse and supply the muscles, and the nerves en teri ng them br ing them under the direct control of the brain and spinal cord .
The Involuntary Muscles are met with in the walls of the stomach and intestines, in the air passages, and in most of the internal organs and blood-vessels, also, in a special form, in the heart. T hey are n ot u nder the influence of the will, but continue t heir work during the hours of sleep; their functions are regulated by a separate set of nen-es ( see Sympathetic System, page 124) .
FRACT U RES AND THE I R TREATMENT.
Whe n a bone breaks a Fracture is said to occur.
CAUSES OF FRACTURE .
I. Direct Violence. -\Vhen from a severe blow, impact of a bullet, crush of a ",heel, etc ., a bone breaks at the spot where the force is applied, t he f racture is te r med direct. --4 1
2 . Indirect Violence .-\Yhen the bone at some distance from the spot. where th: fO.rce IS applied, the fracture is indIrect. Ahght111g on the feet and fracturing the thIgh - hone or the of the leg, or falling on the hand breakll1g the radius or the collar-bone, are examp"es .
3. Muscular Acti o n . - The knee-cap and the arm-bone are occasionally broken by a violent contraction of the muscles attached to them .
VARIETIES OF FRACTURES.
Fractures are classified according to the condi t ion of the tissu e s adjacent to the bone as follo\\'s :- .,
I. S i mple. -The bone is broken WIth but slight injury to the parts: T'
2. Compound. -1 he bone IS broken th.e Sk111 and tissues are punctured or torn, thus allo\y111g dlseaseproducing germs to obtain entrance to the seat of fracture . The fractured ends may protrud: through the skin, or (for example, ",hen a bone IS broken by a bullet) the wound may lead dO\:'n to the fractur.e.
3 . Com plicated . - The bone .IS broken and 111 addition there is an injury to some 111ternal organ (fO! example, the brain, spinal cord, lung, etc. ) or to some important blood-vessel or nerve.
A fracture may be compound or complicated as the immediate result of the injury; or a fracture,
40
'Originany simple, may be converted into a compound Dr complicated fracture-
(a) By careless movement on the part of the patient.
(b) By carelessness or ignore. nc e on the part of one rendering first aid.
• ,Fractures are also . classified according to the InjUry to the bone Itself. The following varieties should be noted:-
I. Comminuted.-T he bone is broken into several pieces, and therefore requires special care in handlina-.
2. Green-stick. -In children, o\\'ina- to the of the tissues, a bone may bbend and crack wIthout breakmg completely across.
3· Impacted.- The broken ends of the bone are driven one into the other.
GENERAL SIGNS A D SYMPTOMS WHICH MAY BE PRESENT.
(A fracture of the bone of the thigh or arm, or both bones of the forearm or leg, affords the most complete example.)
I. Pain at or near the seat of fracture.
2. Loss of power in the li m b .
3· Swelling about the seat of fracture. Swellinafrequently renders it difficult to perceive other of and care must therefore be taken not to mIstake a fr.acture for less seriom; injury.
4· Deformltyof the lImb.-The limb assumes an

unnatural position, and is mis-shapen at the seat of fracture. The contracting muscles may cause the broken ends of the bone to over.ride, thereby producing shortening. .
5. Irregularity of the bone. -If the IS close to the skin the fracture may be felt, and If compound it may be seen.
6. Unnatural Mobility.-},I ovement may be made out at the seat of fracture.
7. Crepitus, or bony grating, may be felt or heard when the broken ends move one upon the other. Tlte last two Sterns slzoltld only be by a doctor. Several of the ;bove signs are absent in green-stick and impacted fractures. . In addition to the signs and symptoms the patIent or the bystanders may '-be able to the of the injury, and marks on the clothmg or skm should be noted, as they may serve to locate the fracture. The snap of the bone may have been heard or felt.
ApPARATUS FOR OF FRACTURES.
Splints and bandages haye to be used in the treatment of fractures, and It \\,111 often be found necessary to improvise them. .,
A Splint may be improvised from a walkl11g stl.ck, umbrella, billiard cue, broom or brush handle, poltceman's truncheon, rifl e, folded coat, piece of wood, cardboard, paper firmly folded, a rolled-up map, or, m fact, anything that £s firm and long e:lOuglz to keep
the joints immediately above and be/ow tlte fractured bone at rest. \Vhen the above appliances are not available, the upper limb, if fractured, may be tied to the trunk, and in all cases a fractured lower limb should be bandaged to its fellow .
Ba n dages may be improvised from handkerchiefs, belts, straps, braces, neckties, OT any piece of linen, calico, string or cord that comes to hand.
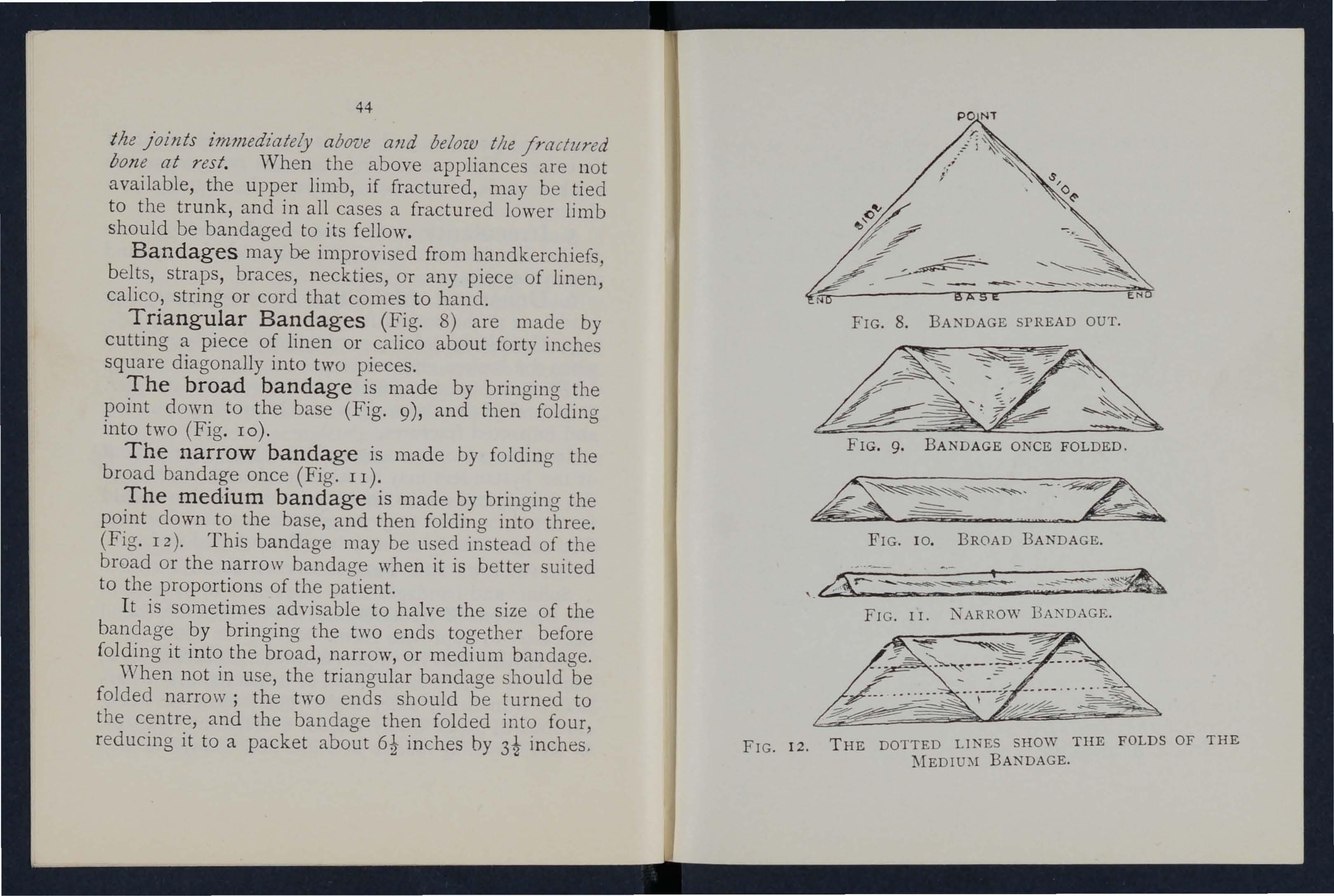
Tr iangular Bandag es (Fig. 8) are made by cutting a piece of linen or calico about forty inches square diagonally into two pieces.
The broad bandage is made by bringing the point down to the base (Fig. 9), and then folding into two (Fig. 10).
The narrow bandag e is made by folding the broad bandage once (Fig. II).
The medium banda g e is made by bringing the point down to the base, and then folding into three. (Fig. 12). This bandage may be used instead of the broad or the narrow bandage when it is better suited to the proportions of the patient.
It is sometimes advisable to halve the size of the bandage by bringing the two ends togeth e r before folding it into the broad, narrow, or medium bandage. When not in use, the triangular bandage should be folded narrow; the two ends should be turned to the centre, and the bandage then folded into four, reducing it to a packet about inches by 3i inches . FIG. 12.
44
FIG . 9. BANDAGE ONCE FOLDED .
-_ ---." -en ..
FIG. 10. BROAD BANDAGE.
FI G . I I NARROW lJA:'\DAGE.
THE DOTTED LINES SHOW THE FOLDS OF THE BANDAGE.
Large arm -slin g (pig. I3).-Spread out a triangular bandage, put one end o\'er the shoulder on the sound side, pass it round the neck so that it appears over the shoulder of the injured side, and let the other end hang dO\m in front of the chest; carry the point behind the elbow of the injured limb, and bend the

FIG. 13.
forearm over the middle of the bandage; then carry the second end up to the first and tie them; bring the point forward, and secure with two pins to the front of the bandage .
Small arm -sling (Fig. 14).-Place one end of a
47
broad bandage over the shoulder, on the sound sider pass it round the neck so that It appears the shoulder of the injured sIde; place the WrIst over the middle of the bandage; then br,mg s,econd el:d up to the first, and tie them. ThIS slm,g IS used 111 cases of fractured humerus, and occaSIOnally \\'hen the larere sling would be too conSpICU?US.
Slings may be improvised in many SImple ways, such
as pinning the sleeve to the turning up the tail of the coat, passing the hand l11sIde the button e d coat or waistcoat, etc.
Re e f Knots (Fi g , IS) are to be used. Avoid granny knots (Fig. 16 ) .
46
FlG. J 5,-REEF KNOT. FIG. 16 .- GRANNY

G ENERAL RULES FOR TREATMENT OF FRACTURES.
The object of First Aid Treatment of Fractures is to guard against further mischief, and especially to prevent a simple fracture from becom ing compound or complicated . To attain this end : _
I. Attend to the fracture on the spot. No how crowded the thoroughfare, or how short the dIstance to a more convenient or comfortable no a,ttempt must be made to move the patient untIl the 11mb has been rendered as immovable as practicable by splints o r other means of restraint.
2. When hcemorrhage accompanies a fracture it mus t be attended to first, and the wou n d covered by a clean dressing (see pages 84 and 85) .
3· Steady and support the injured limb so that its furthe r movement on the part of either the patient or the bystanders is prevented .
4· Cover the patient to keep him warm, and so lessen t he effects of shock.
With care and without using force p,Iace the In nc:ttural a position as possIble, a n d, If shortel1lng IS observed in the case of a fracture of a bo n e of the lower limb, pull upon the foot until the limb regains a more normal length . When the limb is straightened, on no account let go until it issecu. re d in positio n by sp lints,otherwise there is great dalwer of the fract ur e becoming compound or 49
Do not attempt extension in the case of a compound fracture when the bone protrudes .
6. Apply splints (when practicable ) and banda g es as follows :.-
(a) The splints be. firm, a,nd long enough to keep the jOll1ts lInmedlately above and below the fractured bone at rest. They should, if practicable, be to fit accurately to the limb ,and .be over the clothing. Ample WIdth IS very desIrable in a splint.
(b) The bandages must be applied not so ti g htly as to constnct the cIrcu,latIO,n of blood in the limb . 'Whe n the patIent IS in the recumbent position double the bandage over a splint to pass it under the trunk or lower limb. As a general rule:-
For tlze trunk the broad bandage should be Pass it once round the trunk and fasten It by tying the ends (or two or three safety pins) on the side OppOSIte to the if to secure a splInt for a broken thIgh, tI e or fasten the ends over the splint.
For tlze arm or forearm the narrow bandage should be used. Pass it twice round limb, ann tie the ends over the outer
F or tl;.e thigh or leg the narrow or medIum bandage may be used . I t is frequently
48
convenient to double the bandaO'e at the centre, pass it under the limb, the loop over the limb, pass both ends banda.ge through it in opposite directions, and tIe them over the outer splint (Fig. 17).
I n applyi ng bandages near a fracture the upper one should be secured first.

f"· r ." FIG. 17.
7. Make no attempt to remove a patient suffering from a fracture of the spine , pelv is, or thigh, except in a recumbent posit ion.
8. In all doubtful ca s es, treat as a fracture.
SPECIAL FRACTURES.
Fracture of t he Cranium .-A fracture of the upper part is usually caused by direct violence-for example, a blow on the head. A fracture of the base is caused by indirect violence, through a fall on the
51
head, a fall on the feet or lo\\-er part of the spme , or a seYere blow on the 10\\ er jaw_ If the upper part £s /ractll7ed, the siglJS are swelling, irregulanty, and frequently insensibility, either immediate or coming on gradually. II tile base £s /mdltnd insensibihty may come on immediately, blood or a clear fluid may issue from the ear channel, blood may escape from the nose, or it may pass down to the stomach, \\ hence it may be yomited ; the fracture may im-olve the orhit, causing a blood-shot eye.
TREATl\IENT.
Injury to the brain is the great danger attending a fracture of the
FIG. 18. cranium . For treatment see "Concussion and
Compression of the Brain," pages 142 to 1-1- 6 .
Fracture of the Lower Jaw .-Pain, loss of power (inability to speak and to mo,-e the jaw freely), irregularity of the teeth, crepitus and bleeding from the gum are the usual signs and symptoms.
50
TREA flIIENT.
I.-Place th e. palm of hand below the injured bone and press It gently agamst the upper jaw.
2.-.Apply the centre of a narrow bandage under the chm, carry one end over the head cross the ends at of the jaw, carry the long end across the chm, and tIe the ends on the side (Fig. 18).
Fracture of the Spine.-Th e vertebral column may be broken either by direct or indirect violence. fall of a weight upon the back, and fctlhng from a heIght on the back across a bar or upon an uneven surface are examples of direct and a fall on the head, causing a broken neck, IS an example of indirect violence. 'What is commonly regarded as a broken back consists of a fracture of one or more of the vertebrre \\'ith displacement of whereby the spinal cord and the nerves ISSUIng from it may be torn causin a complete or paralysis of the parts below fracture. Pam IS present at the seat of injury.
TR EATMENT.
I.-Prev ent all movement on the part of the patient.
2.-Cover th e patient warmly.
3·-T o remove the patient, place him on a stretcher o r shutter as follows ;-
(a) Turn up the collar of his coat; roll up a stIck or umhrella in each side of the coat

53
so that the ends are level with the top of his head; pass a broad bandage or handkerchief under the head and secure it to the sticks. If no coat is worn, or doubt as to its strength and length exists, pass a number of bandages under the patient to serve instead of, or in addition to, the coat.
(b) A bearer on each side grasps the rolled coat with his hands well apart; a third grasps the clothing on both sides on a level with the hips; a fourth bearer takes of the legs.
(C) On the word being given, all lift together and carry the patient by short side paces over the stretcher and carefully lower him on to it. If a fifth bearer is available the stretcher should be passed under the patient instead of carrying him over it.
4.-0n arrival at shelter nothing further is to be attempted until the arrival of a doctor, except to give the patient water, tea, etc., if he is conscious.
Fractured Ribs.-The
ribs usually fractur ed are the sixth, seventh, eighth, or ninth, and generally the fra ctu r e is midway between the breast-bone and the spine, The fracture may be caused by indirect violence, driving the fractured ends of the bone outwards, or by direct violence, driving the fractured ends of the bone inwards and sometimes injuring the
lungs or other internal organ. If the lower ribs on the right side are broken, the liver may be injured, and a fracture of the lower left ribs may wound the spleen. Evidence of the fracture is afforded by pain, especially on attempting to take a deep breath, and by shortand shallow breathing. If the lungs are injured blood, frothy and bright red, may be coughed up and expectorated. If the liver or spleen is wounded internal btemorrhage may occur (see page 104).
TREATMENT.
(a) TFlzm tlze fracture is ?lot complz'cated by an £Jljury to an t'nternal organ :-
I. - Apply two broad bandages round FIG. 19. the chest sufficiently firmly to afford comfort, with the centre of the first immediately above and that of the second immediately below the fracture. The lower bandage should overlap the upper to half its

55
extent. The knots are to be tied rather to the front on the opposite side of the body. Another good plan is to apply a strong towel, folded about eight inches wide, t ightly round the chest, securing it with three or four safety pins.
2.-Place the arm on the injured side 111 a large sling. (Fig . 19) .
TVllen an internal organ t's z'njured-
1. - Do not apply bandages round the chest.
2.-Lay the patient down, inclined a little towards the injured side.
3. - L oosen the clothing, give ice to suck, and place an ice bag over the seat of injury. Trea t as for internal hremorrhage (see page 104) .
4.-Place the arm on the injured side in a large sling.
Fracture of the Breast-bone (sternum).-
'Vhen this fracture can be felt o r is suspected undo all tight clothi ng, and keep the patient quiet in an easy positio n until the arrival of a doctor.
Fracture of the Collar-bone (clavide).-This fract ur e is freq uently caused by a fall on the hand or shoulder.-The arm on the injured side is partially helpless, a n d the patient usually supports it at the elbow with his hand, and inclines his head towards the injured side . The fractured ends can generally
54
be felt to overlap, the outer fragment being the lower. The genera l signs and symptoms of fracture are mostly present.
TR EATMENT.
I.-Remove the coat (see page 26), and as much more of the clothing as is expedient. Unfasten a man's brace on the injured side.
2.-Place a pad about two inches thick and four inches across in the armpit.
3·-Gently bend the forearm well up, keeping the shoulder as far back as practicable, and support it in a "St. John" sling, made as follows :-
(a) Lay an unfolded bandage across the chest over the injured limb with one end on the uninjured shoulder and the point beyond the elbow on the injured side. (Fi g. 20).
(b) 'Vhil e steadying the injured limb pass the lower end of the bandage und er it, across the back, and tie the ends somewhat lo osely in the hollow in front 0/ the sound shoulder.
(c) Fold the point over the elbow of tlle injur e d limb and secure it by one or two pins (Figs. 2 I and 22).
4.-Tightly secure the injured limb to the side by a broad bandage passed round the elbow and trunk, so as to lever out the shoulder, the pad forming the fuIcrum (Fig. 2 I). See that the pulse is present at

FI G. 20.
FIG. 22. (Body baudage omitted to show details of Sling.)
56
57
the wrist; if it is not, relax the bandage around the body .
S.-Now ti ghte n the sling.
Fracture of the Shoulder-blade (s capula).-
Apply the ce ntr e of a broa d ba nda ge in the armpit of the injured side, cross the ends over the uninjured sh oulder and tie them under the armpit (F ig . 23). Support the injured limb in a St. John sling.
Fracture of the Arm (humerus). - The bone may be brok e n :-(a) Close up to the shoulder; (b) n ear the middle of th e shaft; (c) close FIG. 23· to the elbow.
All the genera l signs and symptoms of fracture are usually present.
TREATMENT.
TVht'JZ the Fracture is close to the Sizouider-
I.-Apply a broad bandage with its centre above the middle o f the arm round the limb and body, t y in g it on the opposite side.
2 .--Support th e fo rearm by a small arm sling.
TVlten the Fracture is near th e lI1i.ddle of t ile Sita/t-
I.-Bend the forearm at a right angle to the arm.
2.-Apply splints, reaching from the shoulder to

59
the elbo\\; 0 1 the outer and inn er sides of th e arm, and, if enough can he procured, to the front and back also . Note carefully that non e of the splints press upon th e bloodvessels in th e armpit or e lb ow joint.
3.-.'ecure the sp lints by b8ndages aboye and below the fracture. If splints arc not avaibble, s('curc the arm to the siJe by t\\'o broad bandages.
4 . - 'llpport the forearm at the wrist by a small arm sling . (Fig. 24).
Fractures in volving the elbow joint, "hether of the arm or forearm, are attended \\ itl1 so much s\\elling, and it is so difficult to ascertain the exact nature of the injury, that when the accIdent o ccurs indoors the limb should be laid upon a pillow in the most comfortable position. I ce or cold FIG. 24. water dre sings sho uld be applied to the injured part, but no further
58
t reatment shou ld be attempted pending the arrival of a doctor.
the acciden t ouurs out of doors-
I.-Take two pieces of thin flat wood, one long enough to reach from the armpit to below the elbow, the other long enough to reach from beyond theel bow to the finger tips; tie -- them together to form
- arightangle.(Fig.2S)·
2.-Apply the angular splint so made on tbe side of the F flexedlimbtbatshows IG. 25. the least injury .
3.-Secure by bandages round the arm, the forearm and the band.
4.- Support the limb by a large arm sling.
5.- 0n arrival at home remove the splint, and treat the injury as if it had occurred indoors.
Fracture of the Forearm. -"When both bones (the Radius and Ulna) are broken, the general signs and symptoms of fracture are usually present. When one of the bones only is broken the signs and symp-
6r
toms are as a rule pain, loss of po\\·er, s\\"elling, and irregularity. An impacted fracture of the Radius just above the wrist is a common result of a fall on the hand .
TREATl\IENT.
This is the same, whether the fracture is of one bone or of hoth .
1 - Bend the forearm at right angles to the arm,

FIG. 26. FIG. 27. keeping the th u mb upwards, and the palm of the hand towards the body .
2.-Apply broad splints on the inner and outer sides from the elbow to the fingers .
3 . - A pply bandages, embracing both splints, imme d iately above and below the fracture and round the ha n d ( Fig. 26 ).
4 .-Applya la r ge arm-sli n g .
Crushed Hand (fracture o f th e bo nes of the carp u s, metacarpus, o r fingers) .
TREAT:\IENT
I.-Apply a carefully padded splin t t o t he f ront of
60
__
the hand, reaching from well above the wrist to beyond the ti ps of the fingers.
2.-To secure the splint apply a narrow bandage crossed in the manner of the figure 8 to the wrist and hand (Fig. 27).
3.-Apply a large arm-sling.
Fracture of the Pelvis. -\Vhen, after a severe injury in the neighbourhood of the haunch-bone, there is no sign of damage to the lower limbs, but the patient is unable to stand or even to move the lower limbs without great difficulty and pain, a fracture of the pelvis may be assumed to have occurred . The blood-vessels and organs, especially the bladder, within the pelvis are in danger of being wounded.
TREATMENT.
I.-Lay the patient in whatever position is found to give the greatest ease, and flex or straighten the lower limbs as the patient desires.
2.-Apply a broad bandage round the hips tight enough to support the parts, but not so tight as to press the broken bone further inwards.
3.-To remove the patient place him on a stretcher, acting on the same principle as that described under " Fracture of the Spine" (see pages 52 and 53) .
Fracture of the Thigh-bone (fimur).-The thigh-bone may be broken at its neck, anywhere in the shaft, or close to the knee . A fracture at the
is to occur in old people from very slight Injury, and IS often difficult to distinguish from a severe bruise of the hip, but it may be assumed that when, after an injury near the hip joint, the patient cannot, ,,,hen lying on the back, raise the heel from the ground, the bone is broken . All the aeneral signs and symptoms of fracture are usually present and a prominent sign IS the position of the foot,

28.
which, as a rule, lies on its outer side. Shortening may vary from one-half to three inches.
TREATME T.
I.-Steady the limb by holding the ankle and foot.
2.-Gently draw down the foot and bring it into line with its fellow. When two or three assistants are at hand, it is one person's duty to hold the foot in position until the splints are secured.
3.-Apply a splint on the outer side from the armpit to beyond the foot.
FIG.4·-A pply a splint on the inner side from the top of the thigh (the fork) to just above the knee.
S.-Secure the splints by bandages as follows:(a) Round the chest just below the armpits, (b) round the pe lvis on a level \"ith the hip joints, (c) above the , fracture, (d) below the fracture, (e) round the leg, (f) round both ankles and feet, and tied below the feet, (g) a broad bandage round both knees (Fig. 28).

FIG. 29.
'Vhen single-handed, or when the patient is a woman, it IS expedient, after extension of the limb, to tie the feet together, dispense with the inner splint, and pass the bandages round both limbs in the order shown by numbers in Fig. 29.
Fracture of the Knee-cap
FIG. 30. (patella).-The knee-cap may be broken by direct violence, but more frequently it is broken by muscular action, as follows:-
When the foot slips, in the attempt to prevent a fall the muscles in the front of the thigh act with such force as to snap the knee-cap in two (Fig. 30).
Pain, loss of power (the limb will be quite helpless), and irregularity (a gap may be felt between the broken fragments of bone) accompany this injury.
TREATiIlE. T.
I.-Lay the patient on his back, raise well and
FIG. 31.
support the head and shoulders, straighten and raIse the limb.
2.-Apply a splint along the back of the limb reaching from the buttock to the heel. '
. 3·-A pply a narrow bandage with its centre immedIately aboye the knee-cap, cross the ends behind
6-1
2 3 1 &7
D
over the splint, pass them again to the front of the limb just below the knee -ca p and tie them. To ensure firmness apply a second bandage in a similar way, but commenced below and tied above the broken bone.
4.-Further secure the splint by ba'ldages rOllnd the thigh and leg.
5.- Su pport the foot well off the ground by a pillow, roll of clothing, two bricks, etc. (Fig. 3 r).
6.-Apply cold (ice or cold \yater) dressings oyer the fracture to lessen effusion of blood.
Fracture of the Leg (tibz'a a?zd fib7lZa).-One or both of the bones may be broken. When both bones are broken all the general signs of fracture are usually present, but when one bone only is broken deformity is not always noticeable. A fracture of the fibula three or four inches abO\-e its lower end IS frequ ent ly mistaken for a sprain and sometimes for a dislocation of the ankle.
TREATl\LENT.
I.-Steady the limb by holding the ankle and foot.
2.-Draw the foot into its natural position , and do not let go until the splints have been fix e d.
3.- A pply splints on the outer and inner sid es of the leg, reaching from abm"e the knee to beyond the
f oot. If only one splint is available place it on the outer side .
4.-Secure the splints by bandages (a) above, (b) below the fracture, (c) immediately above the knee,

FIG. 32 .
FIG. 33.
(d) round both ankles, (e) a broad bandage round both knees (Fig. 32).
\\Then single-banded, or when the patient is a woman )
66
after extending the limb tie both feet too-ether di pense b , wIth the splint, and pass the bandages round both limbs 111 the order shown by numbers on Fig. 33.
'Wben no splint is' available t)' ino- the leo-s ankles o b ) , and knees together is of great service.
Crushed Foot (fracture of the tarsus, metatarsus and toes).-This accident is commonly caused by the passag:e of a heavy weight over the foot, and may be recogl1lsed by pain, swelling, and loss of power.
TREATl\IENT.
I .-Remove the boot (see page 25) .
2 .-A pply a wellpadded splint to the sole of the foot, reaching from the heel to the toes.
3.-The centre of the bandage being placed over the instep, apply it Frr.. 34· crossed after the manner . .of the figure 8 (Fig . 34).
4·-Su pport the foot 111 a slight ly rais ed position.
. DISLOCATIONS.
A dIslocation is the displacement of one or more o f th e bones at a joint.
The joints most frequently dislocated are those of the shoulde r, elbow, thumb, fingers, and lower jaw.
69
SIG:-IS AXD SY:\IPTOMS.
1. - Pain of a severe sickening character at or near the joint.
2.-Loss of power in the limb.
3. - Numbness of the parts belo\V the seat of dislocation.
4.-Swelling about the joint.
5. - Fixity of the joint.-The limb cannot be moYeu at the joint by either the patient or others .
6. - Deformity of the limb .-Tbe limb assumes an unnatural position, and is mis-shapen at the joint.

No attempt should be made by anyone except a doctor to reduce a dislocation. Pending his arrival;-
(a) Tf'lWl tlte a{ddellt own's out of doors'upport the limb in "batever position gives most ease to the patient, bearing in mind the necessity of lessening the effects of jolting dunng transport.
(b) TT?lC1l tlte tait'wi t's illdoorsI.-Remove the clothing from the limb . 2.-Place the patient on a couch or bed.
3.- Rest the limb on pillows in the most comfortable position.
4.- A pply cold (icc or cold water) dressings to the joint.
5. " - 'When cold ceases to give comfort apply
68
warmth (flannels or towels wrun a out of hot \-yater). 0
6 . - Tr eat shock (see pages 141 to Lt4).
SPRAINS.
W h e n , by a s u dden or twist, the ligaments and parts around a JOll1t are stretched and torn the is said to be sprained . " Going over" the ankle IS a common example .
SIGNS AND SY]\[PTOMS.
1.- Pain at the joint after a twist or wrench .
2.- I nability to use the jOIl1t.
" .-Swelling and discoloration .
TREATl\1ENT OF SPRAINED ANKLE.
Wizen out of doors -
a bandage tightly over boot, placing centre on the sole at the Il1step, crossing I.t on the front of the ankle, and carrying It round al:d round the ankle, where it is to be firmly tied .
2.-\Vet the bandage after a.pp l ication j it is thereby tightened.
After reading shelter-
I .-Remove the. boot .and stocking (see page 26).
2.-Plac.e. the 11m b Il1 the most comfortable pOSitIOn (usually well raised).

7 1
3 . - A pply cold (ice or cold water) dressings t o the joint as long as they relieve pain .
4.- 'When cold fails to give comfort, apply hot fomentations.
'When other joints are sprained, treat them as if dislocated .
When in doubt as to the nature of the injury, treat as a fracture .
STRAINS AND RUPTURED MUSe LES.
'When, during severe exertion, muscles or tendons are over-stretched they are said to be strained, if they are actually torn they are described as ruptured .
SIGNS AND SYi\lPTmIS
I .-A sudden sharp pain .
2.-When the muscles of a limb are strained they may swell and cause severe cramp .
3.- Further exertion is difficult or impossible; for example, if the strain has occurred in the back the patient may be unable to stand upright.
TREAT lENT.
I .-Place the patient in the most comfortable position, and afford support to the injured part.
2.-Apply hot water bottles or fomentations when the pain is very severe.
A so-called strain in the groin (hernia) is an injury of a totally different nature (see page 12 I).
70

QUESTIONS ON CHAPTER II.
The 1lumerals illdl'cate the pages where tlte answers may be .found.
'Vhat is the skeleton, and what purposes are server] by it?
How are the bones of the skull arranged?
\Vhat are the boundaries of the cranium?
Describe the bones of the face
Describe the lower jaw . 29, 30
What is the angle of the jaw?
\Vhat ot her names has the back-bone?
Descri be a verte bra
H ow many verte brre are there in the spine?
'V hat are the regions of the spine, and how many '-erte brre are there in each? __ .
How is the spine endowed with free movement?
What is a rib?
How many pairs of ribs are there and how are they named?
What is the breast-bone? ...
'What are the bones of the upper limbs?
"What is the pel vis? .. _
What is the hip joint?
'What are the bones of the lower limbs?
What is a join t ?
Describ e a moveable joint
Describ e the shoulder joint
D esc ribe the ankle joint
How are muscles classified?
De sc ribe voluntary mu sc les
" That are involuntary muscles and where are they found?
What is a fracture?
i2
PAGE 29 29 29
...
...
... 30 30 30 }O-3 2 3 2 3 2 3 2 33 ...... •D 33 33-35 35 37 37 38 38 39 39 39 40 40 40
are the causes of fractur e? .. 40, 41 73 'Where does a bone break when direct violence is the cause of fracture? Where does a bone break when indirect violence is the PAGH 40 cause o f fracture? 41 How maya fracture be caused by action? 41 In what lWO ways may fractures be classIfied?... ...4 1, 41. 'Vhat is a simple fracture ?... 4 1 vVhat is a compound fracture? 41 '''hat is a complicated fracture? 4 1 \\That is a comminuted fracture? 4 2 What is a green-stick fracture? 4 2 \Vhat is an impacted fracture? 42 State the general signs and symptoms that may be present in a case of fracture ... ._... 42, 43 What fractures afford the most complete example of the signs and sym ptoms? ... .. . _. _.. ... 42 43 In making up YOLlr mind whether a had occ_urred or not, what points should you take Into consIderation beyond the signs and symptoms? ... ... \Vhat apparatus may be necessary for the treatment of fractures? . _ 43, 4-1How may splints be improvised? .-. 43 lIow may bandages be improvised? 44 Describe the triangular bandage... ... ... .._ 44 In what ways may the triangular bandage be folded for use? 44 How many kinds of ann-slings are there, and what are they called? .. , ... _.. '''_ ... --.4 6, \Vhat knot is to be tied, and what knot avoIded? 56 47 48 What is the object of first aid treatment of fractures? Give the general rules tor the treatment of fractures ... How should splints be applied? ... lIow should bandages be applied? \Vhat may cause a fracture of the upper part of the cranium? 48-5 0 49 49 50
vVhat
What may cause a fracture o f the base of the cranium?
\Vhat are. the signs of fracture of the upper part of the cranIUm?
What are the of 'of of th·e cranium? ... ... ..
What is the treatment for fracture o'f the ...
\Vhat are the signs and symptoms of fracture of the lower jaw? ... ... ... ...
Hrow maya fracture of the spine be caused? ::: .. .
\\ hat is commonly regarded as a broken back? ... .. .
\Vhat are signs and symptoms of a fractured spine? ..
How may nbs be fractured?
How may fractur e of ri bs be ? '" :::
State SIgns and symptoms of a simple and of a c omplIcaled fracture of the ri bs
What is a frequent cause of ...
vVhat are the signs and symptoms of fractured
At what points may the bone of the arm be broken? ...
Are the signs and symptoms of a fracture always present In a broken forearm? ... ... ... ...60, 6r
State the cause of a common fracture of the radius 6r
How w-:)uld you recognise a fracture of the pelvis? 62
At what points may the thigh-bone be broken? '" 62
vVhat ale the signs and symptoms of fraclure of the thigh-bone?
What are the causes of fracture of the ... 64, 65
What are the signs and symptoms of fracture of the kneecap?
Are the general signs and symptoms always present fractur e of the leg?
What mistake may easily be made when the fibula is broken near its lowe r end?
is a dislocation?

What is a sprain?
are the signs and symptoms of a sprain? State the treatment of a sprained ankle
tate the treatment of other sprains
·When not sure whether the injury is a sprain or fracture how would you treat it?
llow may muscles be strained or ruptured?
tate the signs and symptoms of strains ... tate the treatment of st rains
First Aid Students should practise improvising material, folding bandages, tying knots, making slings, and the treatment of the foll owing injl1ries.
Knot for applying splint to lower limb
Fractures-Lower jaw, 52. Spine, 52, 53. Ribs (simple and complicated fractures), 53 to 55· Breast-bone, 5S. Collar-bone, 55 to Arm, close to shoulder, 58. Arm, near middle of shaft, 58,59, Arm or forearm when the elbow is involved, 59, 60. Forearm, 60, 61. Crushed hand, 60, 61. Pel vi , 62. Thigh (man), 02-64. Thigh (woman, or man when single-handed), Knee· cap, 64 - 66. Leg (man), 66, 67. Leg (woman, or man when single-handed), 67, 68. Crushed foot, 68.
·49,
Dislocations-Out of doors and indoor ... 68, 70
of
74
PAGt': 50 51 5r 5 r 5 1 52 52 52 53 53 5-155 55 58
... ... ...
... ... ... ... ... ...
What
66 66 68 69 75 PAGE State
.. . ... 69, 70
State the signs and
the treatment of dislocation
... ... ... ...
... . .. 70,
. . . ... .. .
\Vhat
7° 7° 7 1 7'1 71 71 71 71 I mproyising splints ... 43 Impr ovis ing bandages 44 Folding bandages 44 Large arm sling 46 Small arm sling ... 4 6 , 47 Reef knots 47
..
50
Sprained ankle 70 Strains and ruptured muscles 71
CHAPTER III.
TRE CIRCULATION OF THE BLOOD.
THE organs concerned in the circulation of the blood ar e the Heart, the Arteries, the Veins, and the Capillaries.
The Heart is a muscular organ wllich acts like a pump. It is situated in the chest behind the br east-bone and rib cartilages, betwe en the lungs and immediately above the diaphragm; it lies obliquely with a quarter of its bulk to the ri gh t, and the remaining three-quarters to the left of th e middle line of the body . Its beat may be felt just below and to the inner side of the left nipple. The heart has four cavities, two on either side of a central partition. Th e two upper cavities are named the right and left auricles, the two l owe r the right and left ventricles.
Arteries are vessels which convey blood from the heart. Veins carry blood to the heart. Capillaries connect the arteries and veins.
In the general (systemic) circulation arterial blood is driven from the left ventricle of the heart into the aorta (the main artery of the body). From th e aorta branch arteries are give n off to all parts of the body. These divide and sub-divide, and bp.come so small as to assume microscopic 'wh en they are t ermed capillaries.

FIG. 35 ·
L Larynx (voice box); T. Trachea (wind-pipe); Luna; L.L. Left Lung (the lungs are d:awn exbose theOheart and hlood vessels); R.A. RIght
L j.. Left Auricle' R.V. Right Ventricle; L. V. Left
P.A. PUlmo'nary Artery; Ao. Aorta; S.V.C. vena cava (the la r ge vein carrying from the upp(ehr t he body to the heart); LV.C. InferIor vena cava t e a rge . 'ng blood from the lower part of the body to the ve m carry! . b h 'n the heart). The four pulmonary vems cannot e sown ! diagram .
In the capillaries an interchange of gases and fluids takes place, whereby the nourishment and maintenance -of the tissues and organs of the body are provided for, and the blood becomes dark and impure (yenous b lood) .
Venous blood passes from the capillaries to the veins, which convey it towards the heart aettina , b b larger and larger as they proceed by being join e d by neighbouring veins until they finally, as two large vessels, reach the right auricle of the heart. The veins, especially in the limbs, are provided with valves at frequent intervals, which prevent the bacbyard flow of the blood.
The pulmonary system of blood vessels is concerned in carrying the blood through the lungs. From the right auricle the blood passes to the ri ;-ht and is thence carried by the to the lungs,. where it is purified in the capillanes by contact with air, and becomes scarlet in colour; it is then conveyed by the pulmonary veins to the left auricle of the heart and passes into the left ventricle, thus completing the circulation.
The heart contracts in adults at an average rate of seventy-two times a minute, but the rate varies . . , as the position is changed from the lying the Slttll1g or to the standing position; hence the lInportance of adjusting the patient's position in cases of hremorrhage. At every contraction of the left
79
ventncle DIood is forc e d into the arteries, causing the pulse, which may be felt wherever the finger can be

Explanativn.-In the middle of the diagram is the heart with its four chamb e rs. Above the i heart is shown the lung (pulmonary) circulation. The lower part represents the general (systemic) circulation. Vessels containing impure (venous) blood are shown black, while those containing pure (arterial) blood are shown white. The connecting vessels represent the capillaries. The arrows show the direction of the flow of blood.
FIG. 36.
placed on an artery as it lies oyer a bone. In the no pulse is to be found.
78
DIAGRAM OF THE CIRCULATION OF THE BLOOD.
WO UNDS AND HrEMORRHAGE.
In a ll cases the object of First Aid is two-fold ;_
I. - To stop the bleeding.
2.-To protect the wound against ge,rms . H remorrhage, or bleeding, is of three kinds :_
1. Arte r ial. 2. Venous. 3 . Capillary.
ARTERIAL H1E:'IORRHAGE.
I. "- Blood from an artery is scarlet.
2. - If the wound e d art e r y is near the skin the spurts out in jets corresponding to the pulsatIOn of the heart.
3 ·-The pressure point (see be low) is on the heart side of the wound.
GENERAL RULES FOR TREATMENT OF A W'OUKD ACCOMPANIED BY ARTERIAL H1E:\WRRHAGE.
I . . patient in a sui t able posi t ion, beanng In mmd that b lood escapes wi t h less fo r ce when the patient sits , and is still more checked \\ hen h e lies down .
2. Except in the case of a fractured lim b elevate the ble e ding part, as thereby less blood finds its \vay i nto it.
3 · Expose the wound, removing whatever clothi n g may be necessary.
4· Immediately apply pressure w ith the thumb . or direc tl y on the b lee di ng spot (d Ir ec t d IgIta l pressure). When making digital

pressure a,"oid crooking the thurn b or fingers and digging the tips into the part. Direct pressure must not be made over a fracture or foreign body"
If the wound is large, or if it contains a foreign hod y or is associated \yith a fracture, apply i ndi re c t dig ital pressure, i.e., with the thulTI b or fingers on the pressure point (see numbered dots on Frontispiece) ne:--t to the wound on the heart side. The n ea rest pressure point is chosen in order to avoid cutting off the circulation from as much of the part as possible, bu t someti m es it is necessary to a ppl y press u re sti [I nearer to the heart.
S. Main t ain indire ct pressu r e by a tourniq uet, pad and bandage, or flexion on the pressu re point( see Rule 4) while the wound is being examined and protected.
To improvise and apply a tourniquet :-
(a) Apply a firm pad on the pressure point.
(b) Encircle the limb by a narrow bandage, strap or cord \\ ith its centre over the pad, and tie the ends in a half knot on the OppOSIte side.
(c) Lay a short stick, pencil, stem of a pipe or other similar thmg on the half knot, and over it tie a reef knot.
(d) T\\"ist the slick to tighten the bandage, thereby pressmg the pad upon the artery, and arrestIng the flow of blood .
(f) Lock the stick III positIon by the ends of
80
81
The plac ed
the banda ge already applied, or by another bandage passed round the stick and limb. pad of the tourniqu.et must be accurately upon the pressure pomt so as completely to

FIG. 37.
compress the artery; otherwise arterial blood will be allowed to pass along the limb , and the veins, being c ompressed by the tourni que t, will not allow the
blood to return through them to the heart, and the l.;sult will be dangerous swelling and congestion. Should a suitable pad not be at hand, a knot may be made in the centre of the bandage, and when available, a stone, cork, etc., enclosed in it to give it firmness and bulk. See that the bulging and not the flat side of the knot is next the skin .
The St. John tourniq uet (Fig . 37) consists of a piece of webbing two inches wide ( B), provided with a buckle ( D ), pad (A) and twister (C ) over the pad. First place the pad on the pressure point, pass the band round the limb and buckle firmly; then, after noting that the pad is in correct position, apply sufficient pressure with the twister to arrest hremorrhage, keeping the twister as near the centre of the pad as possible . Finally secure the twister by the string ( E ) passing through it, which should be t ie d to the D of the buckle, or may be temporarily secured by passing it bet\yeen the strap and the part of the buckle on which the spikes rest.
The use of elastic bandages, except when part of a limb is cut or torn off, is to be rigorously avoided, as it stops the return flow of blood through the veins.
Flexion consists of the application of a pad on the pressure point at the knee or elbow joint, flexing the limb t o make pressure, and securing the limb in the flexed positio n by a bandage cr ossed like the fig ur e 8 .
82
C
6. Avoid contamination of the wound by t he int r oduction o f mi n ute living organisms called germs, whic h are p r ese n t in the air, in water, and on all surroun di ng ob jects, su ch as the hands, clothes, etc . I t is very easy to introduce germs into a wound :-
(a) By touching it, unless the hands are perfectly clean and have been rendered stenle by painting them \yith the mild tincture of iodine (as supplied to members of the St. John Ambulance Brigade in ampoules, which are convenient to carry and prevent the evapo r ation of the spirit in which the iodine is dissolved) or rubbing them with spi r it ( methy la t ed or otherwise) .
(b) By washing it with water which has not been previously sterilised, that is, boiled and allowed to cool.
7. Remove foreign bodies , such as broken glass, bits of clothing, hair, etc ., seen 111 the wound; do not search for foreign bodies you cannot see.
8. If the wound is obviously dirty , and surgical aid cannot be procured at once, wash away as much of the dirt as possible by pouring stenllsed ,vater ove r it freel y, notwithstanding the fac t that wound" heal best If kept dry. Never wash the surrounding parts towards a wound .
9. Apply the m il d tincture of iodine all ove r the wound and the surrounding skin, and

85
cover with a clean , dry, soft dressing, such as sterile gauze o r lm.t , boraCIC, lint, a perfectly clean handkerchief or o f llllen. Clean un printed paper, such as the 1l1sIde of an envelope, may be used in emergency..
10. Place a pad over the dressmg unless :-
(a ) Foreign bodies, of a character to do further damage if pressed upon, are suspected to be left in the wound.
(b) There is danger of causing injury to a fra.cture.
To form a pad, take a handkerchief and fold th.e four corners to the centre and continue folding untIl the desired object is attained . The smooth surface is placed on the dressing, and to prevent pad from unfolding the puckered surface may be stitched or fixed by a safety pin. J, hard subs t ance, such as a stone, may be enclosed in the centre of the pad.
II . Apply a bandag e fi r mly. over the pad .
12. When in acco r dance WIth Rul e 10, a pa d has been applied, relax indirect pressure, not direct pressure, and note whethe r has be en stopped by the direct method. It it has indirect pressure is not to be renewe?, but the tourn/quet should be left in duect pressure has been unsuccessful contmue m dtrect , but be very apprehensive of c.ongestlOn m
Ii m b, which \yill be the case if mdlrect IS maintained too long . Prompt steps to Obt:lIli medical
help are therefore extremely necessary . If it is not obtainabl e within half an hour, at the end of that time , or sooner if the tourniquet is causing much pain, again relax indirect pressure and note whether bleeding recurs. If necessary, re-apply indirect pressure, and repeat these steps at intervals of half an hour until medical help is obtained.
13 · Afford support to the injured part .
14· Do not disturb a clot of blood formed over a wound. A blood clot serves the double purpose of keeping blood in and germs out.
IS· Do not apply sticking plaster o r o i ntment to a recent wound.
\Vhen part of a limb has been torn off or the wound is lacerated (for example, by the claw of an animal or by machinery), hremorrhage frequently does not come on at once, but, as there is a danger of severe hremorrhage later, a tourniquet should be applied to the limb, but not tightened unless necessity arises.
Students practising arrest of arterial hremorrhage in the limbs or neck should feel the pulse of the radial, posterior tibial, or temporal artery, as the case may be, to note when the flow of blood in the artery stops, and should then immediately relax the pressure made on the artery. In this way the importance of the accurate application of pressure will be realised, and the amount of force necessary will be ascertained.

THE (:OURSE OF THE MAIN ARTERIES, AND THE ARREST OF HJEM0RRHAGE.
(The numbers of the pressure points refer to those on the Frontispiece.)
'THE LARGE ARTERIES \VITHIN THE CHEST AND ABDQ:\LEK.
The Aorta is the central or trunk artery of the body. Commencing at the left Yentricle, it forms an arch behind the upper part of the breast-bone. From the arch are given off the large branches which carry the blood to either side of the head and neck and to the upper limbs. The Aorta passes down on the left of the spi ne to just below the navel, where it divides into two great branches (the iliacs) which convey the blood to the organs in the pelvis and to the lower limbs.
\Vounds of these arteries are one cause of internal hremorrhage (see page 10-1)'
ARTERIES OF THE HEAD AND NECK.
The Car o tid Arteries (right and left) leave the upper part of the chest and pass up on either side of the windpipe and, just below the level of the angle of the lower jaw, divide the Internal E'l:ternal Carotid Artenes. The Internal CarotId Artery ascends deeply in the neck, and enters the cranium to ::;upply the bram WIth blood. The External Carotid Artery gives off a number of branches; to
86
the front the artery of the tongue (Lingual), the artery to the face (Facial); to the back the Occipital; the artery itself is continued upwards in front of the ear, where it changes its name to the Temporal, and supplies the scalp in the neighbourl:ood of the temples .
W hc:n a Carotid Artery is wound e d, as in the case of a cut throat, apply the thum b of one
a10ngside of the carotid artery and is usually wounded at the same time; (b) To check the flow of blood frum the upper end of the carotid artery itself, which is often considerable owing to communication between the branches of this artery and of its fellow. Digital pressure must be maintained, by

Rhand on the artery at pressure point I, pressing backwards agall1st the backbone and takin a care to aVOId the wll1dpipe. It may also be to apply pressure with the other thumb above the wound for tw o reasons: (a) To arrest the flow of blood from the mai n (j u gular) vem in the neck, whlch runs
relays of assistants if necessary, until the doctor arrives (Fig . 38) .
The Facial Artery crosses the lower jaw m a slight hollow two fingers' breadth in front of the angle, and sends branches to the chin, lips, cheek, and outside of the nose. I-hemorrhage from wounds of the face below the level of the eye is to be arrested by :(a) Digital pressure on pressure point 2 (Fig. 39) '
88
FIG. 38. FIG . 39.
FIG. 40. FIG . 41.
9°
(b) Grasping the lips or cheek on both sIdes of the wound by the finger inside and the thumb outsIde the mouth or vice versa .
(c ) Applying a pad a n d bandage l ike that described for fracture of the lower Jaw, and tied over pressure point 2 (see FIg. 18, page 51).
The TemporalArte r I may be felt pulsating front of the upper part of the ear. Hcemorrhage from the region of the temple may be arrested by pressure applied at pressure point 3 (Fig . 40) .
The Occipital Artery supplies branches to the region of the scalp from behind the ear to the back of the head . Hcemorrhage from this region may be arrested by digita l pressure on press ur e poin t 4 , fo ur
FIG. 4 2 . breadth be h in d the ear (Fig . 4 I) . This point IS dIffic u lt to fi n d, and it is u sually sufficient to apply pressure immediately below the wound. from the For e head or anywhere 1n the Scalp may be arrested by applying a
9 1
small firm pad on the bleeding point and sec u ring it by a narrow bandage with its centre laid on the pad, the en ds carried round the head in the direction most convenient , and tied tightly over the pad ( Fig. 42). f
'
Vhen a wound of the forehead or scalp is associated with a fracture, the best plan is to apply a ring pad around the seat of injury. To make a ring pad, pass one end of a narrow bandage round your

fingers ; pass the other end of the bandage thro u gh the ring thus formed and continue to pass it through and through until the whole of the bandage is and a ring as shown in Fig. 43 is formed .
ARTERIES OF THE UPPER LI.\IBS.
The Subclavian Artery passes from a point behind the inner end of the collar-bone across the first rib to the a r mpit.
FIC. 43. FIG. 44.To apply digital pressure :-
I.-Bare the n eck and upper part of the chest.
2.-Place the patient's arm against the body so as to depress the shoulder, and cause him to incline his head towards the injured side.
3. -T ake your stand opposite the shoulder.
4.-- the left hand for the right artery, and vue versa ,grasp the neck low down, placing the fin ge rs beh ind the shoulder and the thumb immediately above the centre of the collar- bone in the hollow between th e muscles attached to the bone (pressure FIG. 45· point 5).
S. -P ress the thumb deeply downwards and bacbyards against the first rib, which is the collar-bone at this spot (Fig . 44) .
The AX1llary Artery , which is a continuation of the keeps close to th e shoulder joint.

93
and can be felt pu \sating when the fingers are deeply pr essed into the armpit . Digital pressure is difficult to apply to this artery .
To apply a pad and bandage:-
I. Place a hard pad the size of a billiard ball in the armpit (pressure point 6).
2.-Apply the centre of a narrow bandage on the pad; cross the bandage on the shoulder; pull the ends tight and tie them under the , opposite arm pit, taking ca r e that the pad does not slip.
3·-Flex the fore.arm alld tie the limb tightly to th,e with a br oad bandage: applied on a level with the elbow (Fig .. 15).
92
The Brachial Artery is a continuation of the Axillary, and runs dovm the arm on th e inn er side of the biceps muscle, gradually passing forward until it reaches th e middle of the front of the elbow . The inner of the coat above the elbo w roughly indicates Its co ur se.

FIG. 48. FIG. 49.
Digital or instrumental pressure may be applied at or n ea r pressure point 7.
To apply digital pressure extend the limb at right angles to the body, palm of the hand upwards. Stand behind the lim b, and pass the fingers under the back of the a rm o ve r the seam of the coat or the groove on the i ns ide of the biceps muscle. Press the pulps
95
(not t he tips) on the artery (Fig. 46). S o me prefer to pass the hand over the front of the muscle (Fig . 47)· A slight turn of the hand outwards as it grasps the arm will better ensure compression of the artery.
The Brachial artery may be compressed at th e elbow (pressure point 8) by flexion . The pad may be a folded handkerchief with a small stone or a cork wrapped up in it, but when no pad is the coat sleeve rolled or gathe red up will serve instead (Fig . 48).
Just below the elbow the Brachial artery divides into the Radial and Ulnar arteries, which run along the front of the forearm on the outer and inner sides respectively. Th e pressure points (9 and 10) are about one inch above the wrist and about half an inch from the outer and inner sides of the forearm, where the arteries maybe felt pulsating. Branches of these arteries join to form the Palmar Arches in the hanel. The arteries run along on either side of the fingers to the tip.
Pressure may be applied to the Radial and Ulnar arteries at pressure points 9 and 10, by tbe thumbs (Fig . 49) or as follows :-
1. -Cut the cork of a quart or pint bottle in two lengthwise.
2.-Lay the rounded side of one balf on the Radial, and of the other half on the Ulna.r artery.
3. - Secure them by a tight bandage.
94
To arrest from the palm of the hand :-
I.-Apply a firm pad, and make the patient grasp it firmly.
2.-Spread out a triangular bandage, turn up the base about four inches, lay the back of the patient ' s hand on the centre of the bandage, fold the point over the knuckles and wrist, pass the two ends round the wrist, make the patient pull on the point of the bandage, cross the ends over the fingers twice and tie them as firmly as possible. Bring the point (A) down to the knuckles and fasten with a pin at J3 (Fig. 50).
3 ,-Elevate the forearm and support it with a "St. John II sling (see page 56).
Arterial from the fingers may be arrested by applying a small pad on the wound, and securing it firmly with a stri p of tape, linen or plaster.
AR TER lES OF THE LOWER LnlBs.
The Femoral Artery
, a continuation of the iliac, enters the thigh in the FIG. 50. centre of the fold of the grom, where it may be felt pulsating immediately below the skin . The cours e of the artery may be

97
indicated by a line drawn from the centre of the groin to the inner side of the back part of the knee. After traversing two-thirds of this line, the Femoral artery passes behind thE. thigh bone to the back of the knee joint as the Popliteal artery.
Digital pressure may be applied to the Femoral artery at the groin (pressure point I r) as fol1o\\'s :-
I.-Lay the patient on his ba c k.
2.-Kneel beside the patient, facing his feet.
3.- To find the groin, raise the foot high so as to flex the thigh; the fold in the clothing at the top of the thigh will indicate the groin.
4.-Place ,the thumbs one on the other upon the pressure point, grasping the thigh with the hands (Fig. 5 I).
5.-Press firmly against the brim of the pelvis. As there is immediate danger of death it is important not to waste time in removing the trousers.
'Vh e ll the Femoral artery is wounded in the upper third of its course, pressure must be maintained at the groin. No really satisfactory tourniquet has been F devised for compression at IG . 5I. this point, and relays of R
96
52 .
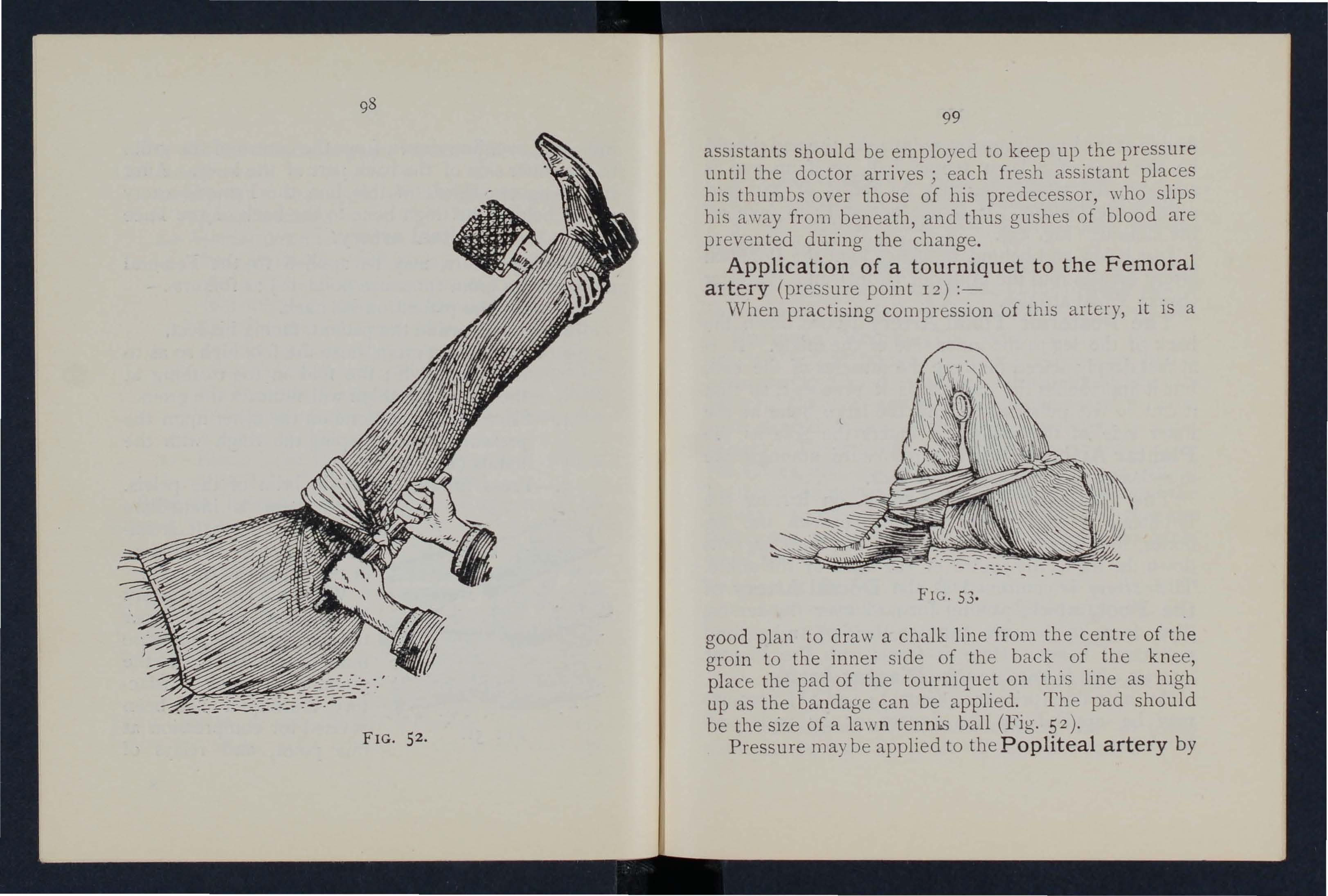
assIstants should be employed to keep up the pressure until the doctor arr ives; each fresh assistant places his thumbs over those of his predecessor, who slips bis away from beneath, and thus gushes of blood are prevented during the change .
Application of a tourniquet to the Femoral a rtery (pressure point 12) :-
"When practising compression of this artery, it is a
FIG. 53 .
goo d plan to draw a chalk line from the centre of the groin to the inner side of the back of the knee, p lace the pad of the tourniquet on this line as high up as the bandage can be applied . The pad should be the size of a law n ten n is ball (Fig. 52).
Pressure may be applied to the Popliteal artery by
98
99
FIG.
TOO
fl ex ion at knee (p re ss ur e point 13); tbe pad should be the sIze of a lawn tennis ball , or if no pad is avai labl e the trouser leg may be rolled or gathered up t o serve instead . It is not n ecessa ry to take off th e cl othing (Fig. 53) . Ju st behind the knee joi nt the Popliteal artery dIvIdes mto the Anterior (front) and Posterior (back) Tibial arteries.
The Posterior Tibial Artery passes down the back of the leg to the inner side of the ankle . I t is at first deeply placed betwee n the muscles of the calf ?ut it approaches the surface as it proceeds, so thaf 1t can be felt pulsating behind the larae bone at the inner side of the ankle . It enters the sole as the Plantar Arteries, which ru n fo[\yard amOt1O"st the o m U'scles to supply the foot and toes.
The Anterior Tibial Artery , on leavin a the Popliteal, at once passes forward betwp.en leg bones, and, deeply placed amongst the muscles, runs dow n the leg to the centre of the front of the ankle. This artery is as the Dorsal Artery of the Foot, wI-nell, pass1I1g forward over the tarsus dips down to the sole between the first and second metatarsal bones. Here it forms \\ ith the Plantar arteries what is kno\\"n as th e Plantar Arch.
At the ankle (pressure points 14 and 15) pressure may be applied by th e fingers or by pads and bandages.

101 VE OUS H£flIORRHAGE.
I. - Blood from a vein is dark red.
2 .--It flows in a slow continuous stream.
3. - 1t issues from the side of the wound further from the heart.
4. - In the case of a wound of a varicose vein it fl ows also from the side of the wound nearer to the heart, e specially if the patient is kept standing .
Varicose Veins .-The veins o f the lea are specially apt t o become varicose. A varicose ,::'ein is permanen tl y dilated, winding, and with bead-like projections along its course. A y ein becomes yaricose from several causes, such as long standing or tight garters. The first effect is to throw extra work upon the val ves , and the bead-like pro jections are ca used by the blood accumulating in the pockets behind the valves . In time the yein becomes so di lated lbClt the valves can no longer span it, thus allowing th e back\Yard flow of blood.
GENER.\L RULES FOR TREATMENT OF A \V OUND ACCOflIPANIED BY VENOUS H£MORRHAGE.
I.-Adopt the cours e laid down in Rul es 1-3 on page 80.
2. - Apply direct digital pressure (except ove r a fracture or foreign body).
3. - Remove any constrictions, such as collar and garters , from the heart side of the \vound.
4.- A pply a firm bandage near the wound on the side away from the heart. In the case of a wound of a varicose yein it is also advisable to apply a firm bandage immediately above the wound, especially if the limb cannot be maintained in an elevated position.
5.-Adopt the course laid down in Rules 6-I5 on pages 84 to 86.
CAPILLARY Ht'Er.[QRRHAGE.
I. - The blood is red.
2.-It flows briskly in a continuous stream or may merely ooze from the wound .
3. - It wells up from all parts of the wou n d .
GENERAL RULES FOR TREATMENT OF A 'WOUND ACCOMPANIED BY CAPILLARY Ht'Er.lORRHAGE.
A small amount of direct pressure will suffice to arrest capillary hcemorrhage. It must not, however, be supposed that a wound requires less protection because the bleeding is not severe; in fact, the reverse is the case, as a considerable flow of blood tellds to cleanse the wound from the inside outwards.
B I TES O F SNAKES AND RABID ANIMALS, AND 'W O UNDS BY POIS O NED ·WEAPONS.
Hydrophobia is caused by the bite of an animal, such as a dog, cat, fox, wolf, or deer suffering from rabies . The special poisons introduced into bites by venomous snakes and wounds by poisoned weapons cause danger to life.

TREATl\lENT.
I .- I m mediate ly p la c e a con str ict io n be tween th e wound and the hea rt so as to preyent the venous blood from carrying the poison through the body. If, for example, a finger is bitten, it should be encircled on tile side of the wound ne:lrest to the heart, with the finger and thumb, and as soon as possible a ligature (a string, piece of lape, or strip of handkerchief) should be placed tightly round the root of the finger. Compression with the ililger and thumb must not he relaxed until the ligature has been applied. Additional ligatures may, with advantage, be applied at intervals up the limb.
2. - Encourage bleed ing for a time, to wash the wound from within outwards:-
(a) By bathing the wound with warm water.
(b) By keeping the injured limb low; the upper limb should be allowed to hang down, and in the case of the lower limb the patient should be seated with the foot on the ground.
3. - Cauterise the wound, if it is quite impossible to obtain the services of a doc t or. This is best done by burning with afluid caustic, such as pure carbolic acid or nitric acid, or if these are not at hand, with a red-hot wire or a fusee. To ensure the caustic reaching the bottom of the wound, it
102
103

N. IJ.- The ((/T()WII mark the points at which pres!;w'e is to be made w (arterial) at any part of the limb belolc them.
should be applied on a piece of wood, such as a match cut to a point. ,Vh e n the caustic bas been thoroughly applied, but not till tben, the li gatures may be removed.
4. - In the case of a bite by a venomou s snake in addition scratch the skin round the wound , and rub in powdered permanganate of potash.
5. - Cover the wound, after a while, with a clean dressing .
6. - Afford support to the injured par t.
7. - Treat shock (see page Lp) .
I
NTERNAL HlEMORRHAGE.
,Vounds of the bl€lod vessels within th e trunk cause hremorrhage into the cavity of the chest or of the abdomen .
SIGNS AND SYMPTOMS OF HiEJ\IORRIL\GE .
I.-Rapid loss of strength, giddiness and faintness, especially when the upright position is assumed.
2.-Pallor of the face and lips, and cold clammy skin .
3.-The pulse fails, and may altogether disappear at the wrist.
4 .--Breathing hurried a n d labour ed , and accompan ied by yawning and sighing .
s .-The patient throws his arms about, tugs at the dothi n g roun d the neck, and calls fo r air (ai r hunger).

6.-Finally the patient may become totally unconSCIOUS.
TREAT1>1E! T.
I.-Keep the patient in a recumbent position, with head low and turned on one side.
2.-Undo all tight clothing about the neck.
3.-Provide for free circulation of air; fan t he patient.
4.-Spri nkle cold water on the face; hold smelling salts to the nostrils; ayoid other forms of stimulants, at all eve nts until the hremorrhage has been controlled.
5.- G i ve ice to suck or cold water to drink; if the seat of the hremorrhage is known, apply an ice bag over the region .
6.- hould the patient be reduced to a state of collapse, raise the feet and bandage the limbs firmly from the toes to the hi ps and from the fingers to the shoulders.
FROM THE NO E ( OSTRILS) .
I.-Plac e the patient in a sitting position In a current of air before an open window, with the head thrown slightly back and the hands rai sed above the head.
2.- U ndo all tight clothIng aroun d the neck and chest.
104
w5
3.-Apply cold (ice, a cold sponge or bunch of keys) over the nose and also the spine at the level of the collar; place the feet in hot water.
4.-.Cause the patient to keep the mouth open, and so aVOId breathing throu gh the nose.
HlEMORRHAGE FROM THE MOUTH.
Blood issuing from the Mouth may come from the tongue, the gums, the socket of a tooth after extraction, the throat, the nose, the lungs, or the stomach.
HiEMORRHAGE FROM THE TONGUE THE GUMS , , THE SOCKET OF A TOOTH, OR THE THROAT.
I.-Give ice to suck or cold water to hold in the mouth. If this is not successful, give water as hot as can be borne to hold in the mouth.
.
2 .-If .bleeding from the front part of the tongue IS excessive, compress the part by a piece of clean lint held between the finger and thumb.
3.-If the bleeding... is from the socket of a tooth plug the socket with a piece of clean lint or wool j over this place a small cork or other substance of suitable size, and instruct the patient to bite on it.
HiEMORRHAGE FROM THE LUNGS.
Blood from the lungs is coughed up and is scarlet and frothy in appearance. '
Treat as for Internal (see page 104.)

HiEJ\lORRHAGE FROJ\l THE STOMACH.
Blood from the stomach is vomited; it is of a dark colour and has the appearance of coffee grounds; it may be mixed \\'ith food.
Treat as for Internal H<.el11orrhage (see page 104), except that nothing is to be givell by the mouth.
lIiEMORRHAGE FROM THE EAR CHANNEL.
Blood issuing from the Ear Channel, which generally indicates a fracture of the base of the skull, must be wiped away as it issues j no attempt is to be made to plug the ear.
BRUI ES.
A blow anywhere on the surface of the body may cause extensive beneath the skin; without breaking it-a" black eye" is an instance. The injury is accompanied by discoloration and swelling.
TREATMENT.
Apply a piece of lint soaked in spint and water, or ice or cold water dressings.
106
QUESTIONS ON CHAPTER III.
The 11ltlllerals £ndicate the pag'es 7.vlure tile answers lIIay be foul/d.
\Vhat organs are concerned 111 the circulation of the blood? '"
Describe the heart ,,'
Descri be the circulation of t he blood
How many times a minute does the heart contract un the average?
vVhat is the effect of the patient's position on the rate at which the heart contracts?
What is the pulse? ",
What is the object of First Aid in connection with
wounds and hremorrhage?
How many kinds of hremorrhage are there? .. , 80, 104-I07
How would you know a case of arterial hremorrhage? ". 80
State general rules for treatment of a wound accompanied by arterial hremorrhage
Would you always elevate a bleeding limb?
How should pressure be first applied?
What is direct pressure and when should it be applied?
\Yhen should direct pressure not be applied?
What is indirect plleSSUre and when should it be applied?
How should indirect pressure be maintained? ...
What is a tourniquet?
How wou'Jd you improvise and apply a tourniquet?
\Vhy is accuracy necessary in placing the pad of a tourniquet?
Describe a St. John tourniquct
\\'hen mayan elastic bandage be used instead of (j tourniquet?
What is flexion?

Ilow would you avoid c
would you do to an obviously dirty wound?
110w would youdl'essa wound? ..... , ... 84,85
What would guide you in plac!ng, a pad over a 85 lIow long would you mal,nlal,n p,ressule, and what would guide you 111 dlscont1l1Ulng It? .. ' .. ,85, 86
Should a blood clot be disturbed? Give reasOl: 86
Should sticking p!:\ister o r ointment be applIed to a recen t wound?... ..'
If part of a limb had been torn off, or the w?und was lacerated, hut there was not much bleed1l1g, how would you act?", . , \\There would you feel the pulse when practlsHlg arrest of arterial hremorrhage?
is the aorta?
Describe the arteries of the head and neck .
86
Why is it sometimes neces ary to compress the carol1d a.rtery both below and the wound? ... 88, 89 What is a ring pad, and what I S lls .,' 9 1
Describe tl-je arteries of the upper limbs ,.. . .. 9 1-95 Describe the arteries of the lower limbs ,.. ... .. ,96- 100 How would you know a case of venous hremorrhage? 10 1 \Vhat is a \'aricose vein? 101 lIow maya vein become varicose? '" '" 101
State the general rules for treatment of a wound accompanied by venous hremorrhage .... ... 101, 102 lI ow would you know a case of capillary hremorrhage ? 102 lIo'''' would you stop capillary hrem orrhage ? 102
State the aeneral rules for treatment of wounds caused by poisonous bites or. weapOl:s 10 3, 104
What special treatment IS requued for the bite of a venomous snake? 104
lOS
PAGE 73 79
80
80-86 80 80 80 81 81 81 Sr 81- 3 3 82 83 8" .) 3 109 PAGE 84
o
?, Should
invariably
fo reIgn tr0111 a 84 wound? .. , ... ... ... ... .., \Vhat
84
o ntaminati
n. of a
you
re1110\'e
\Vhat
... .., .. ,
,,,
86
'What is internal hremorrhage ? ... . .. ... 104
vVhat would lead you to suspect internal hremorrh;Jge? 104, 105
State the treatment for internal bremorrhage... 105
How would you from the nose? 105. lOb
vVhere may blood IssUIng from the mouth come from?.. 106
How would you tr eat bleeding fr o m the gums or throat? r06
What else would you do if the tvngue were bleeding?. . 106
And if the bleeding were from the socket of th e t o oth? 106
How would y o u distinguish between bleeding from the lungs and from the stomach ?.. ... ... r06, 107
And what would be the difference in the treatment? 106 107
Of what is bleeding from the ear channel generally a sign? ' 107
What is a bruise? . . . 107
How would you treat a uruise ? ......... 107
The .Student should. l?ractise placing supposed patient s 10 a proper positIOn for the arrest of hotmorrhage (see 80, etc.), foldin g firm pads, tying hard knots In to form a t o urniquet (81), and appltcatlO?- of pressure at all the pres sur e P0111ts shown 111 the fronti spiece, at vari o us po int s on the forehead and scalp, and on the palm o f th e hand. P,essure should be digital, by patl and bandage, or flexion, as directed in the text.
Pressure points-Carotid artery, 88. Facial, 89 and 90. Temporal, 90. Occipital , 90. Subclavian, 91.
Axillary, Brachial (by pad and bandag e , pressure belllg made against the hum e rus and by flexion at the el bow), 94, 95. Radial and Ulnar, 95. Femoral.at the groin, 97. Femoral in the thigh, 99· 98, 99. Anterior and posterior Ti bial artenes, 1 00.
Hremorrhage from the forehead or scalp... 9 T
Hremorrhage from the palm of the hand ... ... 96
Venous hremorrhage from a valicose or other vein lOT

CHAPTER IV.
BURNS AND SCALDS.
A bu r n is ca u s e d -
(a) By dry heat, such as fire or a piece of hot iron.
(b) By a rail , wire or dynamo charged with a high pressure electric current, or by lightning.. . .
(c) By a corrosive acid, such as oil of vItnol.
(d) By a corrosive alkali, such as caustic soda, am monia, or quicklime.
(e) By friction, caused, for example, by contact with a revolving wheel. (Brush burn .)
A scald is caused by moist heat, such as boiling water, hd't oil or tar.
The effect may be a mere reddening of the ,skin ; blisters may be formed; or even the deeper tIss u es of the body may be charred and blackened . The clothing may adhere to the burnt skin, and its removal is impossible without further detriment to the injur e d part. The great dangers are Shock and the entry of ha r mful germs .
TREATMENT
.
I. - Carefully remove the clothin g from injured part unless it sticks to the skin. Whe n possible , place th e inj u red part in water at th e
P.'GI'.
rIO
III
lIZ
temperature of the body (98 degrees) until suitable dressings can be prepared. A dessert-spoonful of baking soda to a pint of the warm water WIll make a soothing lotion, and serve to soak off any adherent ci?thing, which may be previously cut around with SCISSorS
2. - Do not break blisters.
3 ·-Immediately excl u de a i r by coveLing the part with cotton wool. If boracic ointment is at hand, It may be spread thickly on narrow strips of lint, which should be applied to the wound and the part enveloped in cotton \\'001 and lightly bandaged . Strips are advisable as they fit better on the part, and during subsequent dressings one strip can be removed at a time and fresh dressings applied before the adjacent stri p is taken off. The shock to the system is thereby less than if the whole of the bun1t surface were laid bare to the air by the removal of all the dressings at one time .
'When the face is burnt, instead of applying the strips cut a mask out of cotton wool , lint or linen, leavll1g holes for the eyes, nose and mouth .
As it is important not to leave the part exposed to the air, it is the duty of the bystanders to prepare the dressings while the clothing is being removed. Treat Shock. -This is particularly necessary in th?-.:ase of every burn or scald of any considerable extent (see page 14z) . Be very apprehensive of

danger m the case of even slight burns of the neck.
5. - If the burn is caused by a corrosive acid, bathe the part with a weak alkaline lotion, such as washing soda or baking soda in warm water before applying the dressings.
6.- If the burn is caused by a corros ive alkali, bathe the part with a weak a cid lot i on , such as lemon juice or vinegar diluted with an equal quantity of water. Cautiorl.-Before using water brush off any lime that remains on the part.
7. - When a woman ' s dress catches fire -
(a) Lay the woman flat on the floor at once, so that the flames are uppermost; tbat is to sa y, if the front of th e dress is on fi re lay her on her back, and if the back of the dress is burning, place her face downwards. The reason for this is that flames ascend, so that if the upright position is assumed, the flames will quickly reach and burn the body, neck, and face; or if the woman lies with the flames undermost, they will, if unextinguished, pass over and burn the lim bs, and set fire to the rest of the dress.
(b) As soon as the woman is laid flat, smother the flames with anything at hand, such as a rug, coat, blanket, or table cover; if made wet so much the better. •
113
(c) A woman rendering assistance should hold a rug or blanket in front of herself when approaching the flames .
(d) If a woman's dress catches fire when nobody is by, she should lie flat, flames uppermost, smother the flames ,vith anything handy, and call for assistance; on no account should she rush into the open air. The use of fire guards would preyent many calamities.
ST I NGS OF PLANTS A ND ANIMALS.
These give rise to serious inconvenience, and 111 some cases gr ave symptoms develop.
TREATMENT.
I. - Mop the part freely with dilute ammonia or spirits. A paste of bicarbonate of soda and sal volatile is an efficient application. A solution of washing soda or potash or the application of the blue bag will relieve pain .
2.- Extract the sting if left in .
3. - Apply oil or vaseline.
4. - Treat shock if it occurs (see page 142).
FROST BITE.
During exposure to severe cold, parts of the body, usually the feet, fingers, nose, or ears, lose sensation

I I 5
and become first waxy \\ hite and afterwards congested and of a purple appearance. As sensation is lost in the part, it is often only by the remarks of bystanders that the frost-bitten person is made a ware of his condi tion.
TREATMENT.
I.-Do no t brin g t he pat ient into a wa rm r<?o m until, by friction of the hand or by rubbing wlth soft sno\y or cold water, sensation and circulation in the affected parts are restored . J eglect of this precaution may lead to death of the tissues of the frost-bitten part.
circulation is restored, keep the patJent lJ1 a room at a temperature of 60 degrees.
NEEDLE EMBEDDED UNDER THE SKI1
'Vhen a needle breaks off after penetratin a the skin and disappears, take the patient and the broken piece of needle to a doctor at once. If the wound is near a joint, keep the limb at rest on a splint.
FISH-HOOK EMBEDDED I N THE SKIN.
Do not attempt to withdraw the fish-hook by the way it went in, bnt cut off the dressin a of the hook , so that only the metal is left, and then force the point onwards through the skin until the hook can be pulled out. Afterwards apply a hot boracic fomenta-
tio n (pin k lin t soak ed ill hot water).
F O RE I GN BODY I N THE EYE.
I. - Prevent the patient rubbing the eye, tvin a down a child ' s hands if necessary.;:,
2. - Pull down the lower eyelid, when, if the foreign body is seen, it can readily be removed with a camel's hai r brush, or with the corner of a handkerchief twirled up and wetted.
3. - When the foreign body is beneath the upper eyelid l ift the lid forward , push up the lower lid beneath it and let go. The hair of the lower lid brushes the inner surface of the upper one, and may dislodge the body. Should the first attempt be unsuccess fu l, repeat it several times if necessary. If the fureign body is not dislodged call the services of a doctor as soon as possible . When, however, skilled help cannot be had, proceed as follo\\'s :-
(a) Seat the patient so as to face the light, and stand behind him, steadying his head against your chest .
(b ) Place a knitting-needle, match or bodkin on the upper eyelid, half-an-inch above the edge, pressing it backwards as far as possible. Pull the upper eye-lashes upwards over it, and thereby evert the eyelid.
(c) Remove the foreign body.

II?
4. - When a foreign body is embedded in the eyeball do not attempt to remove it, but a little olive or castor oil on the eyeball after pullll1g down the lower eyelid, close the lids, apply a soft pad of cotton \\'001, and secure it by a bandage tled sufficiently firmly to keep the eye,hall steady; take the patient to a doctor.
s. - When quick-lime is in the e ye bru.sh away as much of it as possible; bathe the eye \\',lth vinegar and warm water, and treat as for a forelgn body embedded in the eyeball.
FOREIGN BODY IN THE EAR PASSAGE.
, , 1
As a rule make no attempt to treat a patlent \\'It,1 a foreian body in the ear if the services of a doctor can b f ' possibly be had; any attempts to remove the body may lead to ratal consequences. If a child cannot be induced to keep the fingers from the ear, tie his hands down or cover up the ear. If an insect is in the ear-passage, fill the ear with olive oil, when the insect will float and may be removed . Ne\'er syringe or probe the ear.
FOREIGN BOVY IN THE NOSE.
I nduce sneezina by pepper or snuff. Cause the patient to blow nose violently after closing the unaffected nostril. If this is ineffectual, take the patient to a doctor.
11 6
THE ABDOMEN.
The abdomen is bounded above by the diaphragm: below by [he pelvis; behind by the lumbar vertebrce; and in front and at the sides by muscular walls. (Fig. 54.)
THE OF THE ABDmlE .
The Stomach lies just below the breast-bone, towards the left side.
The Liver lies in the upper part of the abdomen, \\ here it is mostly covered by the right lower ribs.
The Spleen lies beneath the ribs at the upper part of the left side of the abdomen.
The Pancreas lies behind the stomach.
The Intestines occupy the greater part of the c;Lvity of the abdomen .
The Kidneys lie at the back, one at each side, in the region of the loin.
The lies to the front in the pelvis.
IN THE FRONT 'VALL OF THE ABDOi\LEN.
HIhen the z'ntestz'nes or other organs protrude through the wo und, \Nhether vertical or transverse, bend the knees, raise the shoulders, and apply lint, a to\\ el, or cotton \\'001 wrapped in soft linen, wrung out of boiling water every two or three minutes, so as not to be allowed to get cold, and keep the patient warm u n tll the doctor arrives. 'Vh en there is no protrusion

FIG. 54.
o f organs, zf the wOlt17d is vertical: lay the. flat on the back with the lower limbs straIght; tj the wound is tralZSverse, bend the kn ees and raise the shoulders. In each case treat as an ordinary wouna.
lI8
J 19 \ LIVER -} -'
INJURIES TO T H E ORGANS WITHIN THE ABDOMEN AND PELVIS.
Injuries of the Stomach are by extreme colla pse, and sometimes by vomillng of dark blood like coffee-grounds . For treatm ent see " Hremorrhage from the Stomach" (page 10 7).
Injuries of the Liver, Spleen, Pancreas or Intestines may be caused by a blow , a stab or a bullet; the liver or spleen may be injured by a fracture of the lower ribs . The Signs and Symptoms are those of internal hremorrhage accompanied by pain an.d swelling at the seat of injury, and the treatment 15 as for that condition (see page 104)
The Kidneys may be injured by a fracture of the el eve n th or twelfth ribs, also by a crush, blow, stab or bullet. Blood may escape with the urine, and there may be pain and swelling over the injured kidney. I
The Bladder may be injured by a fl:actur? of pelvis . The signs and symptoms are. ll1abl1.1ty to pass water, or if a little is passed Jt IS tll1ged 'nth blood.
TREATMENT OF INJURY TO THE KIDNEYS OR BLA.DDER.
1. - Keep the pat ient quiet unti l the doctor arrives. 1
2 .- Apply cold (ice or cold water) dressings over the painful or injured part.
RUPTURE.
Rupture (hernia) consists of a protrusion of an internal organ, usually the bowel, through the muscular wall of the abdomen, most frequently at the aroin. Should a sudden s\\"elling accompanied by b " pain and sickness take place 111 that r eglonI.-Send fo r a doctor instantl y.
2.-Lay the patient down WIth a pillow under the knees.
3. -Apply ice or cold water dr es sings to th e affected part.

QUESTIONS CHAP fER I V.
The 1lumerals illdicate the -pages Wlt i re th e allswers ilia), be found
How maya burn be
How is a scald caused? ...
'What are the gr eat dangers of a burn or scald? ... II r Slate the general treatment fo r burns and scalds . II I -I q
How would you treat a burn cau sed by a corroSIve acid? ...
How would y o u t r eat a burn cau-eo by a corrosive alkali? I I3
120
21
flAGE
I I I
11 I
I r 3
\\'hat steps should be laken when a woman's dress catches fire? 113, 114
How would you treat a sting? 114
State the signs, symptoms al'ld treatment of frost- bite II 4, II 5
\Vould you attempt to remove a needle embedded under the skin?
How would you extract a tish hook em bedded in the lIS skin? ." .. , ... '" ... ... lIS, II6
State the general rules for removing a foreign body from the eye '"
\Vhat would you do if a foreign body were embedded in the eye ball ?
And when quick-lime is in the eye?
How would you try to remove an insect fr0111 the ear passage ?.. .
Would you tty to remove any other form of foreign body from the ear passage?... '" ... ... ...
How would you remove a foreign body from the nose?
State the boundaries of the abdomen and its contents ...
State the treatment for wounds of the abdomen.. . 118, I 19
How may injuries to the liver, spleen, pancreas or intestines be caused? ... 120
What is the difference between treatment of injuries to the stomach and of injuries to the liver, spleen, '-' pancreas and i ntestines?
Slate the treatment of injuries to the kidneys or bladder ...
State the t r eatment of hernia

Two systems of nerv e s, th e Cerebro-spinal and the Sympathetic, regulate the rno\-ernents and functions of the body.
THE CEREBRO-SPINAL SVSTDJ.
The Cerebro -spinal ystern is rnade up of the Brain, the Spinal Cord and Motor and ensory Nerves; through its agency sensations are received, and the will causes the action of the voluntary muscles. For example, when a part is injured a sensation of pain is conveyed to the brain by a sensory nerve, thus affording an indication of the seat of injury, or a warning of a possible danger of further damage. On attention being directed to the injury, motor nerves convey a message to the muscles, and an attempt is instantly made to ease the pain or to move the injured part from danger.
The Brain , situated within the cranium, is the seat of intellect, the emotions, and the will; it is the organ where impressions brough t by sensory nerves are receIved, and from which orders are given through the motor nerves.
The Spinal Cord, which is a continuation of the hrain, consists of nervous matter lying within the
122 PAGIl
Il6 I 17 117 117 117 1 I 7 II8
120
12 3 CHAPTKR V.
120, 121 121
THE I ER VOUS YSTE 1.
spinal canal (see Vertebral Column, page 29). I t leaves the brain through an opening in the base of the sk ull, and extends to the second lumbar vertebra.
The Nerves proceed from the brain and spinal cord in pairs as pearly-white trunks, and their branches can be traced throughout the tissues of the body . ·When a nerve is torn through there is paralysis in the region in which its branches arE distributed.
THE SV:\lPATHETIC SVSTEIIr.
The Sympathetic System consists of a string of small bodies of nervous tissue called ganglia, connected by nerves extending on each side of the front of the spina l column along its entire length, and sends branches to all the organs of the chest and abdomen to control the involuntary muscles, and thereby regulate the vital functions. This system is not under the control of the will, and acts alike during sleep and activity.
THE RESP I RATORY SY STEM.
Air is conveyed by the nostrils (or mouth) to the back of the throat, whence it enters the wind-pipe by an opening guarded by a flap (the epiglottis) against the entry of solids or fluids. During insensibility, however, the flap may fail to act, so that, should solids or fluids be given by the mouth , they may enter the wind·pipe and cause choking. Another danger is that the

12 5
tongue of an irlsensible person is very apt to fall back on the flap, and so obstruct the wind-pipe. (Fig. 59, page I38.) The wind-pipe extends to two inches below the top of the breast-bone, where it divides into the right and left bronchus. Each bronchus enters a lung and divides into small and still smaller bronchial tubes, until tIle ultimate recesses of the lung-the air cells or air spaces-are reached.
The Lungs , Right and Left, occupy the greater part of the chest; they lie immediately within the ribs, and practically wherever a rib is felt, whether front, back or sides, there is lung beneath. Each lung is enveloped in a fine membrane (the pleura), which allows it to move within the chest freely during breathing.
Resp ir ati o n, or breathing, consists of two actsInspiration, an enlargement of the chest cavity, during which air is drawn into the lungs, and Expiration, a diminution of the chest, during which air is driven out of the lungs . A pause follO\"\'s the act of expiration. In health fifteen to eighteen breaths are taken per minute, and at each inspiration about twenty to thirty cubic inches of air enter the lungs, and a similar quantity is expelled at each expiration.
The enlargement and diminution of the chest cavity are effected partly by the muscles of respiration attach'ed to the ribs, but chiefly by the Diaphragm, t he large arched musc u lar pa r tition which sep'l-rates
124

1 2 7
the chest from the abdomen. In inspiration, which is chiefly a muscular act, the ribs are raised, and the arch of the diaphragm fa]]s and becomes flattened, thus increasing the capacity of the chest, tending to produce a vacuum and causing air to enter. In expiration, an act performed without muscular effort, the nbs fall and the arch of the diaphragm rises j this lessens the capacity of the chest anu forces air ouL The mechanism of respiration is somewhat like that of ordinary household bellows; the ribs may be compared to the boards of the bellows, while the diaph ragm corresponds to the leather, the aIr passages being eq uivalent to the nozzle.
As the blood depends upon air for its purification and the oxygen necessary to maintain life, interference \\"ith breathing very soon may produce a dangerous state called asphyxia, examples of which are afforded by drowning, suffocation, choking, etc.
INSENSIBILITY.
Insensibility, apart from natural sleep, is of two degrees, namely, Stupor and Coma. The pa tient ca n be aroused with so me difficulty from the first, but only with great difficulty, if at all, from the second.
Broadly speaking, the pupils of the eyes (the black part surrounded by the coloured iris) respond to light -that is, contract in a bright light and expand or dilate when the light is reduced-in stupor, but not
i.Z6
.
FIG. 55. THE LUNGS AND BRONCHIAL TUBES.
A. Trachea, or Wind-pipe. R Left Bronchus. C. Right lBlOD Chus. D. Smaller BroDchial Tubes.
12 8
in coma. Also the patient wi ll objec t to th e e ye balls
b ein a t o u c he d in th e forme r but no t in t he la tt er t> s tat e .
The objects of treatment are :-
(a ) To e n sure th e actio n of the heart a n d lun.gs .
(b) If poss i b le , to p r event s t upor from deepemng in to coma .
The rules for treatment fa ll un de r fo ur heads ;-
I.-Tho se wh ich a pply in all cases. .
2.-Th o se wh ic h app ly when breathing is absent- Asphyxia. ..
3.-Those whi c h ap ply when breathln.g IS present and there are no
4. - Th ose wh ic h app ly when cCmvulslOns are present- Fits.
I. TR EAT ME NT IN ALL CA S E S.
I.-Undo all tight clothing about the neck, chest and waist. .
2.-Ensure an abundance of pure air. O pe n win d ow s a nd do o r s;; k ee p b ack a c ro wd; remov e fr o m h a rmful gases o r impur e a tm osp h e re .
3.-Arrest apparent; att e nding to m in o r In Jun es IS less Impor t-a nt than tr e2.. tin g th e u nco n sc iou s s t a t e .
4.-0btain a doctor's help as soon as possible.

12 9
5·-
Carefully examine:-
(a) The patient for signs of injury .. Depend entirely on your powers of observatIon, as, If insensibility is complete, the patient can gi\-e no information; and if insensibility is incomplete, information given by the patient is apt to be confused and therefore unreliable .
(b) The surroundings for any possible clues .
6. - G ive no food or fluids wha t ever by the mouth while the pat ient is i ns e nsible.
7.- Do not assume that a pers o n is insensible as the result of dri n k merely because the b reath or mouth smells of alcohol. Frequently when peop le are feeling ill they take or arc given alcoholic stimulants, after which they mJ.Y become insensible not from the drink, but from the cause , f . that induced them to take it; for eX8.mple, allllness coming on, effects of poisoning, etc. EYen if drink .is the actu::l1 Cluse of insensibility, it must be borne 111 mind that the patient is therefore in a very dangerous state and must be treated accordingly.
8. -' Unless unavoidable, never lea v e the patient until you have placed him in charge of a resDonsible person.
9. - Sh·ould the spine or an important bone of the upper or the lower limb be fractured, it must be stead ied and maintained at rest as soon as possible. Sbou ld the inse n sibi li ty be f
13°
prolonged, the patient may be r emoved in a recumbent position to shelter, provided that the broken bone is adequately supported .
lo.-On return to consciousness water may be given to drink. If the pulse is feeble give warm tea or coffee, provided hremorrhage, either internal or external, is not apparent or suspected. A desire to sleep should be encouraged, except in cases of narcotic poisoning, a condition that may geJlerally be recognised by the history of the case, and also by the pupils of the eyes being minutely cont racted (pin point p upi ls).
II. WHEN BREATHING I S AB SENTASPHYXIA.
I. - Do not assume death is present because signs of life are absent. Persons whose breathing has been suspended for even ten or fifteen min utes, owing to complete immersion in water or to other causes, have been restored by artificial means.
2.-Afford the treatment applicable to all cases of insensibility.
3.-Ensure that breathing is possible, i.e., that the ai r passages are not obstructed, that pressure does not prevent th e necessary expansion of the che -t, and that there is abundance of pure air. A conunuous want of pure air produces a conditio n

13 1
known as asphyxia, and may be brought about as follows :-
1. Obstruction of the air passages. ( a) ry DROWNING.
(/1) 1 Y PRESSURE FROl\I OUTSIDE: Stranguiation) hanging, smothering .
(() By A FOREIGN BOVY (e.g., a piece of meat, false teeth, etc) IN THE THROAT: Choking.
(d) By SWELLrNG OF THE TI SSUES OF THE THROAT: Inflammation, scald of the throat, poisoning by a c o rrosive, or stings of insects.
II. Inhaling poisonous gases. By coal gas (as used in the house), producer gas, smoke, fumes from a. charcoal or coke fire, sewer gas, lime-kiln gas, carbOl11C acid gas.
HI. Pressure on the chest, as wh e n crushed by sand or debris, or by a cr o wd.
IV. Nervous affections, as the result of narcotic and certain other pois o ns, collapse, electric shock, or stroke by lightning.
To ensure the possibility of breathing, act as follows :-
STRANGULATION.
Cut and remove the band constricting the throat .. HANGI G.
Do not wait for a policeman: grasp the lower limbs and raise the body to take the tension off the rope; cut the rope, and free the neck.
13 2 CHOKING.
To dislodge the obstruction thump the back hard between the shoulder-blades. If this is unsuc cessful open the mouth, forcibly if need be; pass two fingers along the tongue righ t to the back of the thro at and try to .pull up th,e forei g n body. If this is impossible push back 1I1t o the gulle t. If vomiting ImmedIately turn the head on one side.
SWELLING OF THE TISSUES OF THE THROAT.
If possi,ble, lay the patient before the fire. Apply a spon ge , pIece of flannel or other cloth, wrung out of very h ot wa ter, to the front of the neck, from the chin to the top of the breast-bone. If breathin a has not or has been give to or failing Ice, c,old to drInk. Also gIVe oil (not lamp or machme oIl), a dessert-spoonful at a time.
SUFFOCATION BY SMOKE OR GASES.
Remove the pati ent into the fresh air. Before entering a building full of smoke tie a handkerchief wet if possible, over the nos e and mouth. Keep low' or even nawl, whilst in a room full of smoke or that rises. Some gases, such as th e fumes of petrol are heavier than air, and consequently keep near resclli,:g a pati e nt from heavy gas, move, 111 an pOSItIOn. Opportunities of learning whether pOisonous gases used in one's neighhourhood

133
are lighter or heavier than air should be souaht and seized: 'Whatever the natme of the gas is, endeavour to let 111 fresh air by o p e ning doors and windows. In the case of producer gas, inhalation of oxvgen from a cylinder will be necessary. .I
ELECTRIC SHOCK.
Electric current is conveyed by a cable wire rai'l .; "t \ir bar, called the "Positive," a nd r eturns . t o th esource of supply by another cable, wire, rail, or bar. called the " N egative, " o r through the earth. In the case of an electric railway, th e current is generally cO,nveyed by an insulated rail called the third (or live) raIl, and returns through th e runnin a rails or an insulated rail called the fourth rail, which is between the two running rails; and in the case of a n electric tramway it is frequently conveyed by an overhead conductor or trolley ",ire, and r eturned throuah the b runnll1g rails.
Through contact with a "positiye " the shock may be so severe as to cause insensibility, and th e sufferer will be unable to extricate himself and must be liberated with all possib le speed. As it is ae nerallv impossible or inexpedient to switch off the °c urr ent, some other method must usually be adopted; but precautions must be taken, or else th e person rendering assistance will himself receive a dan gero us, or even fatal shock.
T o lib e ra t e the su fferer f rom con t act :-
(
a) Insulate yourself from the earth by st a n di n g o n an " in s ul a t o r" or "no n -condu cto r," t ha t is, a body \vh ich resists the cu rrent. Amo n gst such bodies are indiaru bber , linoleum , dry glass, dry bricks, dry silk, dry cloth, dry wood and dry hay or straw.
(
b) Protect your hands from contact with the sufferer and the electric medium b y cove r ing them with an insulator. Although indiarubber is probab ly the best insulator, do not \Va te time in running for indiarub ber gloves , bu t use dry articles of cl othing; an indiarubber tobacco pouch, or cap, or fo lded newspaper, wou l d serve to p r otect the hands in an emergency . If no means of insulating the hands are at hand, an attempt may be made to drag the sufferer away by means of a loop of dry rope o r a crooked stick ; an umbrella is not safe beca u se the metal ribs would act as (ond uctors of electricity, and it is not infreq u ently the case that the "stick" of the u mbrella is a metal [Ube .
(c) Pull the sufferer away from contact. Ca re should be taken to avoid touching with n aked hands the sufferer's hands, wet clothing, or boots if the soles are nailed .

135
The armpits sbould be avoided, as perspiration usually makes the clothing damp the r e .
4. - Immediately breathing is possible , whatever the cause of cessation of breathing has been, do artificial respiration by Schafer 's method as follows:-
(a) Lay the patient in a prone position (i .e., upwards) , wi th his head turned to one SIde, so as to keep his nose and mouth away from the ground . TO pad is to be placed under the patient, nor need the tongue be drawn out, as it will fall naturally.
To turn the patient to the prone position proceed as follo\\s :-If at the side of the patient, cross hIS left lea over hIS riaht leu' see that both arms are do\\ n at b b' his sides; place your left hand at the SIde of the patient's right cheek, and v,ith your right hand grasp the clothing at the left hip joint · pull smartly over.. .
(b) K n ee l at one side of or across the patIent, facing his head , and place the palms of your hands on his lowest ribs, one at each side, the thumbs parallel to each other , about two inches apart, in the small of the back. Keeping your arms quite straight and leaning your body forward, slowly apply firm but not ,-iolent pressure straight do\\'n-
134
\vards upon the back and lo\\·er part of the chest, thus driving air out and producing

13 7
expiration (Fig. 5(j) . This movement sho u ld occupy three seconds. Draw back your body somewhat more rapidly and relax the pressure, but do not remove your hands; this produces inspiration (Fig . 57). This movement should occupy two seconds .
(c) Alternate these movements by a rhythmic s\\"aying backwards and forwards of your body from the knee joints, t\\·elye times a minute, persevering until respiration is resto red, or a doctor pronounces life to be extinct .
Should an y signs of congestion be seen in the patient's face, immediately change the method of artificial r espiration to Sib;ester's , as follows:- '
I. - Adjust the patient 's position .-1Vithout wasting a moment, place the patient on his back on a fiat surface, inclined if possible from the feet upwards . Remove all tight clothlllg from about the neck and chest, and bare the front of the body as far as the pit of the stomach; unfasten the braces and the top button of trousers in men, and the corsets in women . Raise and support the sho u lders on a small, firm cllshion or folded article of dress placed under the shoulder-blades.
2. - Maintain a free entrance of air into the w ind -pipe .-An assistant must draw forward the patient's tongue as far as possible, and secure it in
I J6
FIG. 57.
that positIon . In the absence of forceps a tie (or other) clip may answer the purpos€!. If this is not done there is great danger of obstruction of the wind-pipe (compare Figs. 58 and 59) .
3·- Imi tate the movements of breathing.
Induce Inspiration.-Kneel at a convenient distance behi nd the patient 's head, a n d, grasping his

FIG. 58. F IG . 59. A. GULLE1 B . \ YINDPIPE.
forearms just below the elbow, draw the arms upwards, o ut wards, and towards you, with a sweeping movement, making the elbows touch the ground (Fig. 60). The cavity of the chest is thus enlarged, and air is drawn into the lu ngs.
Induce expiratioll.-Bring the patie nt' s flexet.l arms
6r. EXPIRATION.
FIG. 60. INSPIRATIOK . FIG.slowly forward, downwards and inw a rds, press lhe arms and elbO\ys firmly on the chest on each side of the breast-bone (Fig. 6 I). By this means air is expelled from the lungs.
Repeat these movements alternately, deliberately, and perseveringly about fifteen times a minute.
Continue this method for ten minutes, then revert to Schafer's, which may be continued until congestion IS again noticed, upon which Silvester's method should be resumed for another ten minutes.
When from any cause the above methods cannot be carried out, Laborde's method of artificial re spiration should be tried. It is especially us e ful in suffocated children, or when the ribs are broken.
The patient is placed on his back or side; th e cleared; the tongue is seized-using a handkerchIef or something to prevent it slipping from the fingers-the lower jaw depressed; the tongue is pulled forward and held for two seconds in that position, then allowed to recede into the mouth. These movements should be repeated about fifteen times a minute.
Artificial respiration by either method must be done perseveringly. Success may result even after tw o hours. \Vhen natural breathing begins, regulate the artificial respiration to correspond with it.
Excite respiration.-\Vhilst artifical respirat ion IS being done, other useful steps may be employed,

such as applying smelling salts or snuff to the nostrils.
Promote circulation and warmth after natural breathi ng has been restored. \Vrap the patient in dry bla nkets or other covering, and rub the limb s energetically towards the heart. Promote warmth by flannels, hot-water bottles or hot bricks (wrapped in flannel) applied to the feet, to the limbs and body. \Vhen the pOlyer of swallowing has r eturned give hot tea, coffee, or meat extract. The patient should be kept in bed and encouraged to go to sleep . L1.rge poultices or fomentations applied to the front and back of the chest will serve to breathing.
Watch the patient carefully for some time to see that the breathing does not fail; if it does, at once begin artifi.cial respiration again .
III. \VHEN BREATHING IS PRE ENT AND THERE ARE NO CONVULSIONS.
I. - Prevent from falling a patient about to lose cons ciousness, and lay him gently on the ground.
2. - Afford the treatment applicable to all cases of insensibility.
3. - IF THE FACE IS PALE, lay the patient on his back with his head low and turned on one side. The head must be on a level with, or lower than, the body. Raise the feet;
140
this is b es t do n e when t he patien t is in bed by raisi ng the foot of the bedstead. A pale face is a sian of an insufficien t supply of blood to the head a b con _ dition that may arise as follows :- '
(a) Concussion of the brain (stunning ).
The patie nt may be stunned by a blow or fall on the head, or by a fall on the feet or lower part of the spine. He may be in a state of stupor for a short time only, and quickly regain consciousness, or stupor may be prolonged and may deepen into coma.
I n both instances there is a grave risk that a stru c t ure within the cranium has been injured, and tha t a most s erious state of insensibility may develop la t e r . ( See Fracture of the Cranium, page 50.)
A c a u tion should t herefore be given to a patient wh o ha s lost consciousness even for only a moment after an inj ury t o the head, not to resume physical r mental activity without the consent of a doctor. Rest in bed for some hours is a very wise precaution.
(b) Shock, faint ing (syncope ) and collapse.
T hese c onditions practically differ from each ot her only in degree . The causes are ;in t he region of the abdomen)
ex t ensIve wounds and burns, fract ur es, lacerated wounds, severe crush or hcemorrhage.
Mental.-F right, anticipation of injury, and sudden bad n ews, or sometirr.es sudden r emoval of fea r and anxiety after p rol o n ged su spense.

143
Constitutional.-Heart weakness, which may be aggravated by tight clothing, fatigue, want of food or being in a close or crowded room. '
!oz"sonz'ng.-Alcohol, and many other forms of pOIsons.
SPECIAL TREATMENT.
Attend to injuries; ensure that there is no pressure upon the heart due directly to tight clothing about the chest or indirectly to tight clothing about the abdomen; remove from a close or crowded room ' 1 use encouragll1g words.
An attendant danger of the condition of collapse is the liability to sudden r elapse after a temporary improvement, and the utmost care and watchfulness must be exercised to maintain the heat of the body and to guard against failure of the heart and lungs. Cover the patient with extra clothing, rugs or blankets, and get him to bed in a well-ventilated room as soon as possible . Apply warmth to the feet and to the pit of the stomach by hot-\\ ater bottles or hot flannels. Test tbe heat of these with the bare elbow before applying them. U the patient can swallow, and there is no fear of uncontrollable hcemorrhage, hot drinks, such as milk, tea or coffee, to either of which sugar should be added, as it aids in promoting warmth, or a teaspoo.nful ?f volatile in half a tum bIer of water, may be g1Ven In SIpS; but first test ability to swallow by
14 2
I..j4
introducing a teaspoonful of cold water at a time between the gums and the cheek . Smelling salts may be hel d to the n ose . Sprinkling the face with hot an d co ld water al terna tely, warmth applied to the pit of the stomach and over the heart and viaorous friction of the limbs u p\vards have' a effect.
b
If fainting has been caused by hremorrhage it h as, by r ed uci ng the force of the heart ' s beat, proba'bly a fforded a chance of saving the patient 's life . It ou ght to be r emembe r ed t hat a wo u nd however seve r e , wi ll not b leed to any ma r ked extent while the act io n of the hear t is feeble , and it is therefore not su fficien t sa t isfy o n esel f that there is no blee d ing act u ally gomg on, but the proper remedies m us t be app l ied t o prevent bleeding, which may come on as the patIent. begms to consc!ousness . The proper cou r se m such cases IS to examme the wound to see if blood is still flowing from it ; if so, at once arrest th e If blood is not flowing, at once a tt e mpt to s t.llTI u late the heart by smelling-salts held to the . n os tn ls , w:a r.m th the heart , and tightly bandag m g the u n mJ ur ed lImbs . If these r emedies pro ve succe ssfu l, as wou l d be shown by return of col ou r to the lips and face, at once prevent further loss o f b lood fro l1l the wound . , If wan t of nourishmen t has been the cause of fai nting or collapse , give foo d sparing ly at firs t.

4. - WHEN THE FACE IS CONGESTED (red, blue or dusky ) the patient is probably suffering from Apoplexy (disease of the brain ) , Compression (injury to the brain) or Heatstroke or Sunstroke.
Apoplexy usually occurs in elderly peop l e, and no signs of injury are necessarily present.
Compression o f th e brain may result from the same causes as produce Concllssion ; in fact, Compression is frequently preceded by Concussion . 'igns of injury are u sually present.
In both conditions there is congestion in the brain; the face is flushed; t he breathing ste r torous ; one side of the body is more limp than the other, and the pupil of one eye is larger than that of the other; the temperature of the body is generally raised.
SPECIAL TREATrlIl£NT FOR ApOPLEXY Ai\'D
CO.\IPRES 10 OF THE
(a) Lay the patient on his back, raise the head and shoulders, turn the head on one side.
(b) Promote warmth in the lower part of the body by applying h ot-wate r b ottles to t h e abdomen and lower l imbs . As the pa ti e n t is insensitive to pain, care must be t aken lest h e be burnt by the bottles; they shou ld be wrapped in flannel, and their heat tested with the bare elbow after allowing time for the h ea t to come through the flannel.
(c) Apply ice or cold water to the head continuously. Me r e ly sp r in k l ing the h ead with co ld water acts as a stimu la nt to the circ ul atio n in t he head , an d does more harm th a n goo d.
(d) Afford complete rest. Un less a bsol ut ely necessary , do n o t move the patien t from where he feU .
Su STROKE OR HEATSTROKE.
Sunstroke or Heatstroke may be caused by exposure to t h e rays of t he sun during a march in ve r y weather when heavily burdened, or to grea t heat, as ll1 the of a especially in the tropics. pa ti ent . develops sickness, faintm,s s, giddiness , th ir st, and d ifficulty in breathing . The skin becomes a n d bu rn ing, the face very fl ushed, a n d the p u lse qUick and bounding . A very high temperature stertorous (snori n g) breathing and insensib ility (eithe: stupor or c oma) may ensue . I n Sunstroke or Heatstroke congestion extends not only to the brain but to the whole of the nervous chain along the e n tire le n gth o f the sp ina l column, consequently the a r ea to be r eliev e d i s greater , and d ifferent treatme nt is nec essar y.
SPECIAL TREATME T .
(a) Remove the to a cool, shady spot, and stnp hlm to the waist.
(b) Lay him down with the head and shoulders well raised.

[47
(c) Fan him vigorously.
(d ) Apply ice bags or cold t? the head , neck and spine, and ma1l1181l1 until the symptoms subside.
IV . 'WHEN CONVULS I ONS ARE FRESE T. -
F I TS .
Convulsions are involuntary contractions of the muscles of the body ; they may be limited to limbs on one side of the body or may be genelal . They may be due to-
( a) Constitutional hysteria, teethina and 1l1test1l1al irrItatIOn (stomach b troubles ). . .,
(b) Poisoning: By strychn1l1e , prussIc aCId , fungI or berries.
I. - Afford the treatment appl icable to all cases of insensibility.
2. - If breathing is seen . be .fapin g , do artificial respiration wilhout w;:l.ll1l1g unlIl It actually ceases .
3. - Endeavour to asc e rtain the c a use of the convulsions.
(a) Epilepsy may occur 111 persons of age, but usually occurs in young The patIent falls to the ground, sometinles WIth and passes into a state of convulsion, throw1l1g hiS lImbs about.
SPECIAL TREATMENT
1. SupP.ort the patient's head, and after wrapping a pIece of wood, or any other hard material, In a handkerchief, hold it in his mouth to prevent biting the tongue . ,1. Do not forcibly restra;n the patient 's limbs; prevent him from hurting himself by pullinO' him away from a source of danger, snch machinery, a wall or fireplace. Light pieces offurniture shou Id be pushed out of the way.
(b) If the patient is resting on his hee l s and head with the back arched, strychnine poisoning is the cause. Give an emetic between the fits and do artificial respiration. .
(c) If the history points to stomach troub le as caused by fungi or berries, give a tablespoonful of castor oil between the fits, and keep the patient warm in bed with hot-water bottles.
(d) Infantile convulsions will be indicated by the age of the patient . Spasm of the muscles of the limbs and trunk, blueness of the face, insensibility, more or less complete, and occasionally squinting suspended respiration and froth at the mouth the prominent signs.
TREATMENT.
I Support the child in a warm bat:1 slightly above the temperature of the body (9 8 degrees), so that the water reaches to the

149
middle of the trunk , for fifteen to t"Yenty minutes .
11. Keep a sponge frequently dipped in cold water on the top of the h ead as long as the child is in the bath.
(e) In Hys t erical Fits ( Hysteria ) t he patient, usually a young girl, in consequence of mental excitement, suddenly loses command of her feelings and actions . She subsides o n a couch or in some comfortable position, thro\\'s herself about, grinding her teeth , clenching her fists, shaking her hai r loose; she clutches at anyone or anything near her, kicks, cries and laughs alternately. The eyeballs may be turned upwards, and the eyelids opened and shut rapidly. At times froth appears at the lips, and other irregular symptoms may develop. Complete insensi· bility is not present.
i. Avoid sympathy with the patient, and speak firmly to her.
11. Threaten her with a cold water d ouche, an d if she persists i n her "fit," sprinkle her with cold water.
111. Apply a mustard leaf at t he back of the nec k . Medical treatment is n ecessary to cure the condition of mind and body which gives rise to hysterical attacks .
4. - Encourage sleep, but carefully watch th e breathing.
QUESTIONS ON CHAPTER V.
The numerals £ndicate the pages where tlte allswers lItay be found .
How are the movements and functions of the body regulated? .
Of what is the cere bro-spinal system made up ?
What is the brain? " ... ... . ..
\Yhat is the spinal cord?
\Yhat are nerves?
Explain the sympathetic system
Explain the respiratory system
Explain the acts of respiration
lI ow are the enlargement and diminution of the chest effected?
What are the degrep.s of insensibility?..... 12 7
Do the pupIls of the eyes respond to lightinall degrees? 127,128
What are the objects of treatment of insensibility? 128
Under what heads do the rul es for treatmeut fall? 12 8
State the rules which apply in all cases of in sens ihility 128 - 130
State shortly the rules which apply when brt'athing is absent
lIow may asphyxia be brought about?

13 1
\Yhat special steps must be taken in strangulation, hanging, choking, swe lling of the tissues of the throat and suffocation by smoke or gases? 13 [-133
How would you liberate a sufferer from contact with an electric positive?
\Vhat would y ou do when the sufferer was removed fr o m contact?
three systems of artificial r espiration
Describe them
What steps should be tal,en during and after doing artificial re _piration?
140, 14 [
\Vhat is the principal sign to notice 111 an !I1senslble when breathing is present and there are no convubion s? ... qI, 145
In what position should the patient be when the face is pale?
lIow may insensiLilily with a pale face be caused? \\'h at is concussion o f the brain? ... 14 2 , '43 14 2
\Yhat caution should be given to a patient who lost consciousne s, e\'en for a moment, after an !I1Jury to the h ead ? 14 2
State causes of shock, fainting and collapse Lt2, J43
State t he special treatment of these cOll.d !t ions.
State an attendant danger o f the condlllOn of collapse, and the provisions that should be made to guard aoainst it
143 , 14-+
What you do if hoemorrhage had been the cause o f fainting?
In what position should a patIent be when th e face is cong e teo?
\Vh at conditions caued the face to become congested?
State the special treatment [or apoplexy and compressi on of the br:J.'n ... .., ... ... ... Lt5. q6
State signs, symptoms and treatment of sunstroke or heatstroke 14 6 , 147
\Vha t are convulsions? 147
!low may convulsions be caused? .. I47
Slale general rules fo r of fils . 147, 14
State the treatment fo r Il1fanlile cOnntlSlOns 148 , 14 9
State the treatment [or hysLerical fits 1-+9
... 1 2 3, PAGE 12 3 12 4 12 3 I ?'l -oJ 124 124 12 5 1 2 5
... ... ...... 12 5 - 12 7
... ... ...
... ... 130-
'"
1 35
...
. . J34 135
... ... ... 135 140
PAGE
...
135- 1 40
... ..,
... .., ... ...
.. ,
...
... ... .. ...
...
.
.. . .. . .. .
CHAPTER VI. POISONING.
Poisons taken by the mouth may be classified according to their treatment under two main heads :-
I.-THOSE WHICH DO NOT STAIN
THE LIPS AND MOUTH, and in the treatment of which an EMETIC is to be given. These may be :-
Narcotics: -
1. Opium and its jneparaHolls, Morphia, Laudanum, Pare gor ic, Chloroclyne, Syrup of Poppies and various soothing drinks and cordials. These cause a tendency to go to sleep, which continues until sleep becomes deep and breathing stertorous; the pupils of the eyes become minutely contracted (pinpoint pupils).
11. Otlz er Narrotics are Chloral, Veronal, Sulphonal, Trional, Chloroform, Alcohol (including Methylated Spirit). Tbe signs are pr ofound sleep and muttering delirium, with a tendency to blueness of the face.
(b) Convulsants. -Stryc hnine, Prussic Acid, Cyanide of Potassium, Belladonna (deadly nigbtshade plant), and several otber varieties of plants, such as laburnum seeds, etc.

153
Th ese give rise to convulsIons, delirium, failure of respiration and collapse. .
(c) Irritants -Arsenic, Phosphorus (con tamed in rat poison and lucifer matches), Emetic, Corrosive Sublimate. and Iodine, which cau e a metallic taste In the mouth and a burning pain in the mouth, throat and stomach.
Decomposing mea t, fish or fruit, and poisonous fungi (often for mushrooms) . uspicion of these pOisons should be directed to cases \y here several persons who have partaken of the sal1le food similar signs and symptoms, such as yom Itin lY colicky pains and diarrhcea.
Ir.-THOSE WHICH BURN OR
THE LIPS AND and m. the treatment of which NO emeti c IS to be given.
Tbese may be :- .. .
(a) Corro s ive Acids, as .Acld (Aqua fortis), SulphUriC . (011 ?f Vitriol), Hydrochlonc, or l\Iunatl.c, (Spirits of Salt), .stro n g. Ca.rbollc i'-".Cle! (Phenol), Oxalic ACld, \\·h1ch IS con tamed in oxalate of potash, salts of sorrel , salts of lemon and some polishing pastes.
(b) Corrosive Alkalies, such as Caustic Potash, Caustic oda and Ammonia.
GENERAL RULES FOR THE TREATMENT OF POISONING .
1. - Send for a doctor at once statino- what has occurred, and if possible the name ' of the
2 : - EXCEPT when the lips and mouth are stamed or. burned by an acid or alkali, pr<?mptly a .n . EMETIC -that is, make the patIent vomIt, by gIvmg either :_
(a) lI.lustard-a table-spoonful in a tumblerful a-pint) of lukewarm water and repeated until vomiting occurs, or '
(b ) two table-spoonfuls in a tumblerful . lukewarm water, and repeated until V 01111 tll1 0- occurs.
If vomiting is putting the two fino-ers to the back of the may sometimes hasten
3 · - If hps and mouth are stained or burned gl v e NO e me t ic, but -
(a) If an is kno:vn to be the poison, at once gIve an AlkalI, such as lime-water, or a - spoonful of whitening, chalk, or wall plaster in a tumblerful (2-pmt) of water.
(b) If an A.lkali is known to be the poison at once gIve a A'd h ' . ' . n Cl, suc as vinegar or lemon JUlce diluted with an equal quantity of water.

4. - In all cases when the patient is not insensibl e , give Milk, Raw Eggs beaten up with milk or water, Cream and Flour beaten up together, Animal or Vegetable Oil (except in Phosphorus poisoning) , and Tea.
Olive, Salad, and Cod-Ii,'er Oil, or oil such as that in which sardines are preserved, may be giyen; mineral oils such as ordinary paraffin are unsuitable. Oil is soothing, and is therefore especially useful in poisoning by Acids, Alkalies and such substances as Arsenic and CorrosiYe 'ublimate . Demulcent drinks, such as barley water or thin gruel, act in the same manner, and are frG'e from danger in cases of Phosphorus poisoning.
These may be given either before or after the emetic if the poison calls for one .
Strong Tea acts as a neutraliser of many poisons, and is always safe. A handful of tea should be thrown into a kettle and boiled .
s.-When a pe rso n has swallowed p o iso n an d threaten s t o g o t o sleep , keep h i m a wake by walking him about and slapping his face, neck and chest with a wet to\\ el. trong black coffee may b·.; given to drink . ::3IaPUing the soles of the feet may also be tried . \Vhen the poison taken is known to be Opium or one of its preparations, give ten grains of perm::l.l1gc1.nate of p-c>tash in a pint of water, and repeat in half-an-hour; or three table -spoonsful of Condy's
154
I55
fluid in a pint of water, and repeat the dose in llalf. an-hour.
6.-1£ the throat is so swollen as to threater. to the air passage, apply hot o.r poultIces to the front of the neck, and give frequent SIpS of cold drinks.
7. - A pply .artificial respiration if breathing cannot be dIscerned or is failing.
8.-Treat shock and collapse.
9· - Preserve any vomited matter food or. other substance suspected of the pOlson. Do not wash vessels which may have contained the poison, but carefully guard them.
Certain poisons require special treatment, and a few of th e commoner of these are mention ed below \\'ith their treatment.
CARBOLIC ACID.
of the breath will aid in the detection of thIS pOlson; the lips and mouth are usually stained several nervous symptoms come on .
I.-GIve milk, to a pint of which half an ounce of Epsom Salts has been added .
2.-Treat according to the general rules.
PRU SS IC ACID AND CYANIDE OF POTA SS IUl\r.
.Th.e action of . is extremely rapid. Glddmess, staggenng, msensil) llity accompanied by

157
panting respiration, profound. collapse convulsions are the ge n era l sIgns, and Il1 additIOn a smell of bitter almonds is often prese nt.
I.-If the patient ca n sW:lllow, give alcoholic stimulants freely .
2.-Apply artificial resp iration, even if breathing has not ceased.
3 . - D ash cold \\'Uter all the head and spine continuously.
4 . - As patient sho ws signs of recovering, treat shock and collapse .
POISO,\/OUS
11 EAT, FISH AND Fu NGl.
The signs and symptoms are vomiting and (diarrhce a), colic, beadache, g reat \v ea kn ess, rais ed temperature and a quick pulse.
J .-Give an emetic .
2.- \V hen the emetic h:ls acted , give castor oil.
3. -Treat collapse.
STR YCH NINE (CONTAINED IN S01\1E RAT POI ONS).
'The signs and symptoms are a feeling of. suffocation, livid featur es, and convulsions . The patient rests on his head and feet, and the body is arched.
f. -Give an emetic if the patient can ·w:lllow.
.L- Apply artifici:ll re:,piration if possible, wh ethe r breathing has ceased or not.
156
ALCOHOL.
I.- an emetic if th e patient can swallow.
z .-Irea t co llapse by keeping the patient w::nn1, etc .
CORROSIVE SUBLIMATE ( P ERCHLORIDE OF MERCURY).
1:-. Give white of eggs mixed with water, 111 unlml1ted quantities .
2.-Ge n eral Rul es . I ODINE.
I.-Give starch an d water freely.
z.-Genera l Rul es .

QUESTION -- ON CHAPTER VI.
The 1lum erals illd/cate the pages where the a1lswers may be fOltlld.
Under what two main h eads are poisons classified?
State the sub -divisions of narcotics, together with names of the poi sons falling under each
Enumerate the c on vul sants and state their signs and symptoms
Enumerate the irritants and state their signs and symptoms
Enumerate the c orro ive acids
you give for poisoning by a corrosive
State the signs, symptoms and treatment of carbolic acid poisoning
State the signs, symptoms and treatment of poisoning by Prussic acid or cyanide of potassium... t56 , lSi
State the signs, symptoms and treatment of pOl onmg by p oiso n ous meat, fish or fungi ...
State t he signs, sy m ptoms and treatment of poisoning uy strychnine
What would you do in the case of alcoholic poisoning? y"hat would you do in the case of poisoning by corrosive sublimate?
would you do in the C:1.se
poisoning by iouine?
159
PAGEt 15 2 , 153 the
15 2 ,
Enumerate the corrosive alkal ies 15 2 153 I .., ).) 153 153 State shortly the general rul es fur the treatment of poisoning 154- 1 56 How would you make a patient vomit ? ... 154 What would you
son
o
acid? 154 What
154
give for poi
ing by a c
rrosive
would
alkali?
... ... ... ... ... . ..
What
157 15 1 15 8 15 8 158
of
16r
CHAPTER VII . BANDAGING .
The Triangular Bandage been described. in Chapter II. It may be apphed to keep a dressmg on a ,"\·ound, burn or scald of any part of the body, or for an injury of a 1 For the Sc a lp (FIg. 62). Fold a hem about I z inches deep along the base of a bandage; place the bandage on the head so that the h e m lies on th e fOl'ehead close down to the eyebro w s , and the point hangs down at the back ; carry the two ends round the heB.d a bove the ears and tie them on the forehead; steady the head \yjth one hand and with the other draw the point of the bandage downwards; FIG. 62. then turn it up and pin it on to the bandage on the top of the head . F or the Forehead, Side of th e Head , Cheek and for any part of the body that I S round '(as the arm or thigh, etc.), the narrow bandage
shou Id be used, its centre being placed over the dressing, and the ends being carried round the head or limb, as the case may be, and tied over the wound. For t he Should e r (Fig. 63). Place the centre of a bandage on the shoulder, with the point running

FIG . 63 .
up the side of the n ec k; fold a hem along the base r carry the ends round the middle of the arm and tie them, Place one end of a broad bandage over the sound shoulde r and sling the arm by carrying the other end over the point of the first bandage and G
160
162
tying the ends at the side of the neck; turn down the point of the first bandage, draw it tight and pin it.
For the Hip (Fig. 64). Tie a narrow bandage round the body above the haunch bones, with the knot on the injured side. Fold a hem according to the size of the patient along the base of a second bandage; place its centre over the dressing, carry the ends round the thigh and tie them; then carry the point up under the

. 66.
FIG. 65· first bandage, turn it down over the knot and pin it.
For the Hand when the fingers are extended (Fig . 65) . i401d a hem a long the base of a bandage; place the wrist on the hem with the fingers towards the point ; then bring the point the wrist, pass t he ends round the wrist, cross and tie them .;
163
bring the point over the knot and pm it to the bandage on the hand .
For the Foot (Fig. 66). Place the foot on the centre of the ban.dage with the toes towards the point; draw up the pomt over the instep, bring the ends forward and cross them.i pass the ends round the
67a.
6 7 b. and tie them. Draw the point forward and pm It to the bandage on the instep .
For the Front of t h e Chest (Figs. 67a and 67b). Place the middle of the banda rrc over the d.ressing with the point over the shoulder the same sIde; carry the ends round the waist t.ie them;
FIG; .I. " ' 1 ;, J
FIG.
FIG.
then draw the point over the shoulder and t ie it to one of the e n ds. A he m along the base of the bandage is often useful.
F or the Back. The bandage is applied as the foregoing, except that it is begun at the back.
For the Knee. Fold a narrow hem along the bas e of a bandage; lay the point on the thigh and the middle of the base just below the knee-cap; cross the ends first behind the knee, then over the thigh and tie them (Fig. 68). Bring the point down and pin it to the base.
FIC. 68. For the Elbow . Fold a narrow hem along the base of a bandage; lay the point on the back of the arm and the middle of the base on the back of the forearm; cross the ends first in front of the elbow, then over the arm and tie them (Fig. 69).
For the Fingers o r Toes wrap a strip of calJco or Imen round and round the part; split the free end, and secure it round the WrIst or ankle.

CHAPTER V II I.
I\lETHODS OF CARRYING.
THE T\yo-HANDED SEAT .
This seat may be used to carry a helpless patient.
FIG. 70.
T.-Two bearers face each other and stoop, one on each side of the patient. Each bearer pa es his forearm n earest to the patient's h ead under his back just
164
FI C. 69.
below the should e rs, and, if possible, takes hold of his clothing. They slightly raise the patient's back, and then pass their other forearms under the middle of his thighs (Fig . 70), and clasp their hands, the bearer on the left of the patient \\"ith his palm upwards, and holding a folded handkerchief to prevent hurting by the finger nails; the bearer on the right of the patient with his palm downwards, as shown in Fig. 71.

FrG. 71.
2.-The bearers rise together and step off, the right-hand bearer with the right foot, and the left-hand bearer with the left foot (Fig. 72 1.
THE HUMAN STRETCHER.
This is a modification of the two-handed seat, which is useful for lifting and carrying a patient in the recumbent or semi-recumbent position.
L- Two bearers face each other and stoop, one on each side of the patient. They clasp their left hands beneath the patient's hips in the manner of shaking hands (Fig. 73) .
2.- The bearer on the patienes left passes his right hand and forearm under the patient's head, neck and shoulders.
FIG. 72.
r66
167
3·-The bearer on the right passes his right hand and forearm under the patient's legs.
4·-Th e bearers rise together and carry the patient, feet foremost, by short side paces (Fig. 74).

FIG. 73.
THE THRl!.E-HA DED SEAT.
This seat is useful for carrying a patient and supporting either of his lower limbs, ",hen he is able to use his upper limbs.
I.-Two bearers face each other behind the patient. For supporting the left limb the bearer to the patient's right grasps his own left forearm ,,·ith his right hand, and the other bearer's right forearm with his left hand. The bearer to the left grasps the first bearer's ri ght wrist with his right hand (Fig. 75). This leaves his left hand free to support the patient's left leg. For
FI G. 74.
rE8
169
the patient's right lower limb follow the SatTle directions, substitutin a " right" for" left" and "left" for " . h " Th bb ng t. e earers stoop down.
2.-The patient places one arm round the neck of each bearer and sits on their hands.
3·-The bearers rise togeth e r and step off, the FIG. 75.
right-hand bearer with the right foot, and the lefthand bearer with the left foot.
THE FOUR-HANDED SEAT.
This seat is used when tne patient can assist tbe bearers and use his arms.
17 1
I.-Two bearers face each other behind the patient and grasp their left 'wrists with their right hands and eac h other's right wris;ts 'with their left hands (Fig. 76), and stoop down. ,
2.-The patient sits on the hands and places one arm round the neck of each bearer.
3.-The bearers rise together and step off, the

76.
bearer on the right hand side of the patient with the right foot, and the left-hand bearer with the left foot.
THE FIREl\fAN'S LIFT.
(To be attempted only by a strong man.)
Turn the pati ent face down wards; place yourself at his head, stoop down, slightly rai e his heau and
FIG.shoulders and take hold of him close under his armpits, locking your hands on his back. Raise his budy and rest it on your le ft knee; shift your arms and, taking him round his waist, lift him until his h ea d rests on your left shoulder. Throw his left arm over your head, stoop down and place your left arm between his thigh s, le tting his body fall across your shoulders. Rise to an upri gh t j hold th e patient's left wrist with your left hand and lea ve your right hand fre e .
SUPPORT BY A SINGLE HELP ER.
A single helper can give support. Put your arm round the injured person's waist, grasping his hip and placing his arm round your n ec k, holdin g his hand with yours (Fig. 77).
TIl e plan of carrying tIl e patient by tlte arms and legs wdlz th e .face downwards, commonly called the ".frogs' march," must never be used, as death may ensue .from thz's treatmeltt.
THE FORE AND AFT METHOD.
This plan of carrying is us eful when space does n o t permit of a hand seat (See Fig . 7 8).
IMPROVI SED
STRETCH ERS
.
A stretcher may be improvised as follo\\'s :_
1.- Turn the sleeves of a coat inside out; pass two strong poles through th em ; button th e coat. The

FIG. 77.
173

FIG. 78. patient sits on the back of the coat <J.nd r ests against the b3.ck of the front bearer (Fig. 79). If a lon ge r stretcher is required, two or three coats must be treated in the same manner. The poles may be kept FIG. 80.
176
apart by strips of wood lashed to the poles at both ends of the bed formed by the coats (Fig. 80).
2.-Make holes in the bottom corners of one or two sacks and pass stout poles through them.
3.-Spread out a rug, piece of sacking, tarpaulin, or a strong blanket, and roll two stout poles up in the -sides. Two bearers stand on each side and grasp the middle of the pole with one hand, and near the end with the other. They walk sideways.
4.-A hurdle, broad piece of wood, or shutter may be used as a stretcher; some straw, hay, or clothing should be placed on it, and covered with a piece of stout cloth or sacking; the latter is useful in taking the patient off the stretcher.
Always test an improvised stretcher before us e.
'fHE "FURLEY" STRETCHERS.
The "Fudey /I Stretchers (Model 1899) are of three patterns, viz.," Ordinary,"" Telescopic-handled," and "Police." In general principle they are alike, the component parts being designated the pol es , handles, jointed traverses, runners, bed, pillow sack and slings.
The Ordinary Stretcher (Fig. 8 I) is 7 feet 9 inch es in length, and I foot 10 inches wide. The bed is 6 feet in length, and the handles IO! inches. The height is St inches. The weight is 2 I to 22 lbs. At the head of the stretcher is a canvas overlay (the 177
pillow sack), which can be filled ,yith straw, hay, clothin g, etc., to form a pillow. The pillow sack opens towards the head, and its contents can therefore b e adjusted without undue disturbance of the patient. The traverses are provided with joints, for opening or closin CT the stretcher. The Telescopic-handl ed 1:> pattern (Fig. 82) is very simi Jar, but the l:andles can be slid umlerneath the poles, thus redu clt1g the

Sr.-ORDINARY STRETCHER-CLOSED.
lenoth to 6 feet. This arrangement is of great value b h . when working in confined spaces, or w en a patIent has to be taken up or down a narrow staircase with sharp turns. The Police stretcher is similar to the Ordinary pattern, but is more strongly made, and has, in addition, straps for securing a refractory pati e nt.
'When closed, the poles of the stretcher lie close
FIG. FIG. 82. -TELESCOPIC · HANDLED STRETCHER- OPEl\'.together, the traverse bars being bent inwards, the canvas bed neatly folded on the top of the poles and held in position by the slings which are laid along the canvas, and secured by a strap, placed transversely at the end of each sling, being passed through the large loop of the other, and round the poles and b ed.
CARRIAGE OF STRETCHERS.
As a general rule carry the patient feet foremost. The exceptions are:-
(a) \ Vhen going up hill with a patient whose lo\ver limbs are not injured .
(b) \ Vhen going down hill with a patient whose lower limbs are injured .
STRETCHER EXERCISES.
Originally drawn up by Sir John Furley, revised in 1917 to accord with the drills adopted by the Royal Army Medical Corps:-
EXERC I SE No . 1. FOR FOUR BEARERS .
I.-The In str u ctor selects the bearers and numbers them -1,2, 3,4 at his discretion . Should one man be taller and stronger than the o t hers, he shoul d be NO · 3, as he will have to bear the heavier part of the burden. All orders will b e give n b y NO . 4 .
2. - "Stand to Stretcher. "- ;0 1 on the left of the stretcher, with his toes 111 w.lth the front end of the poles j NO.3 with his heels 111 11l1e with the rear end of the poles; NO.2 places hi.mself midway between Nos . I and 3; NO.4 one pace 111 the rear of NO.3 (Fig . 83)·

FIG . 83. FTG. 84. FIG. 85 ·
3 --" Lift Stretcher. "-Nos . I and 3 stoop, grasp both handles of the poles firmly with t he right hand ,
178
179
fOOT OJ ill 00 ! rn HEAD ill [] . . \ . . \ \ L._.1 , !.. . \- - -, i Qj rip ..' t..; . , [1J ./ . , " I I I . , , , , , ,
rise together, holding the stretcher at full extent of the arm, runners to the right.
4· -" Collect Wounded. " - The squad will double by the shortest route to the patient, and halt when one pace from the head of the patient (Fig. 84) .
5·- " Lower Stretcher - Prepare Stretcher. " --Nos . 2 and 4 proceed to the patient and render treatment; Nos. I and 3 turn to the right, kneel on the left knee, unbuckle the transverse straps and place the slings on the ground beside them, separate the poles and straighten the traverses; then each takes up a sling, doubles it on itself, slips the loop thus formed on the near handle, and places the free ends over the opposite handle, buckle uppermost. They then rise and turn to the left together. If reg uired to assist Nos.2 and 4, they \yill proceed to the patient (Fig. 85).
6. - " Load Stre t cher."-\\'hen the patient is ready for removal on the stretcher, NO . 4 \\ill gi"e the command "Load - St re t c h e r ," when the bearers unless otherwise directed by o. 4, will place selves as follo\\'s :-Nos. I, 2 and 3 on the left of the p3.tient, NO.4 on the right; o. I at the knees, No.2 at the hips, NO . 3 at the shoulders, NO.4 opposite o. 2. The whole, turning inwards together and kneeling on the left knee, will pass their hands beneath the patient . No . I supports the legs, Nos. 2 and4 the thighs and hips, No. 3 the upper part of the trunk, passmg his left hand across the patient's chest and
under the right shoulder , and his right hand beneath the left shoulder (Fig. 86).
7. - " Lift. " - The patient will be care f ully lifted on to t he knees of Nos. I, 2 and 3 (Fig . 87) . NO . 4 will

FIG. 86.
disengage, rise, turn to his left, double to the stretcher, take hold of it, left hand across, resting the near pole on his left hip, return to the patient and place the stretcher directly beneath him (Fig. 88), then stand up
180
r8I
a nd return to his former position, kneel on his left knee, join hands with No.2, and assist in lo we ring the patient.

FIG. 87 .
8.-" Lower." -The patient is lowered s10wly and gently on to the centre of the canvas, special care being taken of the injured part (Fig. 89) . The bearers then
disengage, rise, Nos. I, 2 and 3 turn to the left, No. 4to the right, and stand to stretcher; thus No. I with t?es line with front handles, TO . 3 with heels in line with rear handles, No.2 midway between os. I and 3. NO·4 on the right hand side of the stretcher in line with No. r.
FIr.. 88 .
9·- " Lift Stretcher." - On the word
Stretcher
N os . I and 3 stoop, grasp the doubled sling between the poles with the right hand and sweep rt off the handles, rise, holding it at full length of the arm, buckle to the front. They then take a side-pace between the handle s a n d place the sling over the
1(52
10. - " Adjust Slin g s. "-No. 2 will turn about (al \Va ys t u rn from a loaded stretcher--to a closed stretcher), step forward one pace and adjust tl:e sling of NO . 3. No. 4 will turn to the left and ad J.ust the sling of No. I . Having done this, No . 2. wIll turn about and step forward on e pace; NO.4 \Y111 turn to the right.
11. - " March ."-The bearers move off : Nos. I, 2 and 4 stepping off with the left foot, and NO.3 with the right (Fig. 90) . The step should be a short one

FIG. 90.
of twenty inches, and taken \\'ith the kn ees bent and without spring from the fore part of the foot.
12. -" Halt."-The bearers remain steady .
13.- " Lower Stretcher. "-Nos. I and 3 slowly stoop and place the stretcher gently on the groUl:d (No. 3 conforming to the movements of No. r), shp the loops from th e handles and stand up. They remove the slings from the sho ul de rs, hold them as described in Order 9, take a side-pace to the l ?ft, and stand to stretcher. They then place the slll1gs on the handles (as in Order 5) and rise together. . 14.-" U nload \\"Ill place themselves as described load1l1g Order 6. The patient is lifted as descnbed for loadlllg. NO . 4 grasps the stretcher as describe.d fO.r loading, and, lifting it clear of the patient, carnes It three paces clear of the patient's feet: .He then re]ol.ns the squad, kneels on his left knee, ]OI11S .hands mth No . 2, and assists in 10"'ering the patIent to the ground . The bearers rise and turn towards th e stretcher, the whole step off to their places at the stretcher.
15. - " Close Stretcher. "- I and 3. turn to the right, kneel on the left knee, remove the and pla ce them on the ground beside push 111 the traverses, rai se the calwas, and approxImate the poles; they then rise, lifting the stretcher, and face on.e another; place the handles of the poles between theIr thighs, runn ers to the right, fold the canvas to right, lightly on the poles. Each takes up a and passes the buckle end to the other, and hold1l1g
18 7
the buckle end in the left hand, threads the transverse strap through the loop of the other sling, and buckles it tightly close to the runners, keeping the sling on top . Then grasping both handles in the ri ght hand, back of hand to the right, they turn to the ri g ht in a slightly stooping position, ri se and turn to the left together.
CHANGI ' G NUMBERS.

FIC. 9I.
FTC. 92.
U Change Numbers. "-No. 4 will turn about j the whole will step off together, No. I wheeling round by the front of the stretcher and taking up the position of NO . 4 (Fig. 9 r). Each man halts in the position of the bearer whose place he has taken. The new NO.4 will turn about.
N . B.-The figures in dotted squares (Fig. 92) show the new positions of the old numbers.
186
EXERCISE No. II.
FOR THREE BEARERS.
I.-The Instructor selects the bearers and numbers them-I, 2, 3-at his discretion. Should one man be taller and stronger than the others, he should be NO.3, as he \'lill have to bear the heavier part of the burden. All orders will be given by No.2.
2.-" Stand to Stretcher."-No. I places himself on the left of the stretcher, with his toes in line with the front end of the poles; No. 3 with his heels 111 line with the rear end of the poles; No. 2 places himself midway between Nos. I and 3.
3. -" Lift Stretcher. "-N os. I and 3 stOOPt grasp both handles of the poles firmly with the right hand, rise together, holding the stretcher at full extent of the arm, runn ers to the right.
4.-" Collect Wounded . " - Th e squad will aouble by the shortest route to the patient, and halt when one pace from the head of the patient.
5.-" Lower Stretcher-Prepare Stretcher."
2 procee ds to the patient and renders treatment; Nos. I and 3 turn to the right, kneel on the left knee, unbuckle the transverse straps and place he slings on the ground beside them, separate the pole s, and straighten the traverses; then each takes up a sling, doubles it on itself, slips the loop thus formed on the near handle, and places tht free ends ..
over the opposite handle, buckle uppermost. They then rise and turn to the left together. If required to assist No.2 they will proceed to the patient.
6.-" Load Stretcher."--Wh en the patient is ready for removal on the stretcher, No. 2 gi\'e the command "Load Stretcher, " 't'lhen the bearers,

Fro
93.
unless otherwise directed by No.2, will place themselves as follows: No. I on the left side of the patient in a line with his knees, NO.2 on the right side just below the patient's shoulders, and No. 3 at the left side, bcing NO.2. All kne e l on the left knee. No. I
188
; ,/ 11/, ; , I_ .,r_-- ..-
.
his hands, well apart, underneath the lowe r lImbs, always taking care, i n case of a fracture to have one hand on each side of the seat of Nos. 2 a nd 3 grasp each other's hands under the shoulders and hips of the patient. (Fig. 93.) 3

7.- '.' bearers. together, keeping th e patIent 111 a honzontal POSItlOl1. (Fig . 94 .)
8.-" .March." -All take short side-paces, carrying patIent over the stretcher until his head is nnmedlately above the pillow.
9. - " Halt. "-The bearers remain steady.
10. -" Lower. "--The bearers stoop down, gently place the patient on the stretcher, disengage their hands, and then stand up. Nos. I and 3 turn to the left, No. 2 to the right, and stand to stretcher; th us No. I with toes in line with front handles, NO.3 with heels in lin e with rear handles, No. 2 in the centre on the right-hand side of the stretcher.
II. -" Lift Stretcher. "-On the\yord Stretcher, Nos . I and 3 stoop, grasp the doubled sling midway beween the poles with the right hand and S\\'eep it off the handles, rise, holding it at full length of the arm, buckle to the front. They then take a side-pace between the handl es and place the sling over the shoulders, dividing it equally, buckle to the right. The sling should lie well below the collar of the coat behind and in the hollow of the shoulders in front. They stoop, slip the loops over the handles, commencing with the left, and grasp both handles firmly. They then rise slowly together lifting the stretcher, No. 3 conforming closely to the movements of No. I. (No.2 will now adjust the slings, if required.)
12.-" March."-The bearers move off: Nos. I and 2 stepping off with the left foot, NO.3 with the right. The step should be a short one of twenty inches, and taken with the knees bent and no spring from the fore part of the foot.
190
1 9 1
13.- " Halt. "-The oeJ.rers remain steady.
14. -" Lowe r Stretcher. "-Nos. rand 3 slowly stoop and place the stretcher gently on the ground (No.3 conforming to the movements of No. r), slip the loops from the handles, and stand up. RemO\' e the slings from the shoulders, hold them (as describ e d In Order r r), take a side-pace to the left, and stand
CHANGING NU:\IBERS.

FIG. 95 . FIG. 9 6 . to stretcher. Then place the slings on tbe handles (as in Order 5) and rise together.
15. -" Unload Stretch e r ."-The beare:s will place themselves and lift and carry the patIent by short side-paces (as in Orders 6 and 7) clear of the stretcher, to the bed, or other place to which it has been arranged to convey him.
16 . -" Close Stretcher. "-As in Exercise No .1. CHANGI:\'G NUMBERS.
"Change Numbers. "-No. 2 will turn abo u t; the whole will step off together, No. r wheeling round by the front of the stretcher and taking up the position of 10. 2 (Fig. 95) . Each man halts in the position of the bearer whose place he has taken. The new No. 2 will turn about.
N .B.-The figures in dotted squares (Fig. 96) show the new positions of the old numbers.
EXERCISE No. III.
FOR USE IN lINES AND NARROW CUTTINGS WHERE Two MEN ONLY CAN BE ENGAGED .
Nos. I and 2 will carefully place the stretcher in a line with the injured man's body, the foot of the stretcher being, if possible, * close to his head.
No. r straddles across the patient's legs, placing his right foot, with the toe turned outwards, a little below the patient's knees, and with the toe of the left foot close to the heel of No.2; he then stoops down, passes the left hand under the patient's thighs and
* It is not ad\·jsable to be loa particula.r as to the head or fo ol of a stretcher in a mine, as it would probably be quite impossible to reverse it.
//
I
I I
193
H
the right hand under the calves. No. 2 places his feet" one on each sIde of the patient between his body and arms, the toe of each foot as n ea r th e a rmpit s as possible. He then stoops down and passes his hands between the sides of the chest and the arms under ne Llth the shoulders, and locks

FI G. 97.
the fingers (Fig. 97). If the patient's arms ar e uninjur ed he may put them round the neck of o. 2, and by this means greatly assist him in lifting.
\Vh e n both are r eady, No. I \\'ill give the order " Lift and move forward." The patient is then to 195
be slowly lifted, just sufficient to allow his body 1:0 clear the stretcher. Both bearers will slowly and gradually move the patient forward, NO.2 by very short steps, No. I by bending his body fon\'ard as much as he .can without 17l0Vill O' Ius feet (Fig . 98). No. I . now gIves the order " Halt" whereupon 2 remams steady, and TO . I adva'n ces his right foot to his left, and
FrG. 98 .
again advanc es his left foot till the touches the heel of NO.2. J O. I then gIves the order " Advance," when the patient will again be forward. These mo \' em e nts are to be repeated untIl the patient is over the stretcher, when he is to be gent ly lowered.
194
To LOAD AN ArvIBULA CEo
The stretcher will be lowered with the head one pace from the end of the ambulance.
Nos. I and 3 turn to the right, kneel on the left knee, pass the loop of the buckle end of the sling over the near handle, buckle downwards; carry the slin a under and round the opposite handle close up to canvas, back to the near handle, round which two or three turns are made; pass the transverse strap round the pole between the runners and traverse, and fast e n the buckle outside the sling between the poles. The bearers then rise and stand to stretcher.
The bearers \yill now take up their positions as f?llows :-Nos. I and 3 on the left, 2 and 4 on the nght. No. 2 opposi te to NO.3, at the head.
" L oad . "-The bearers turn imYards, stoop, grasp the handles of the stretcher, hands wide apart, palms uppermost; they rise slowly, liftin a the stretcher holding it at the full extent of the arms. Th e; then take a SIde pace to the ambulance, lift on to a level with its floor , pbce the runners on it Nos. I and 4 slightly raisin g the foot. The stretche; is then gently pushed into its place, Nos. 2 and 3 making way for the stretcher to pass between thenl.
Many ambulances are proVIded with upper and lower berths. In such cases the upper berths should be loaded first, beginning on the off side.

197
To UNLOAD AN AMBULANCE.
N OS. I and 4 will take hold of the handles at the foot and gently withdraw the stretcher. As it is withdrawn, N os . 2 and 3 will take hold of the handles at the h ead , and taking the weight, 100yer it to the full extent of the arms, then by side paces march clear of the ambulance; lower the stretcher to the ground.
To CROSS A DITCH.
The stretcher should be lower e d with its foot one pace from the edge of th e ditch. Nos. I and 4 bearers then descend. The stretcher is now advanced, No s . I and 4 in the ditch supporting the front end while the other end r ests on the edge of the ground above. Nos. 2 and 3 now descend. All the bear e rs now carry the stretcher to th e opposite side, and the f oot of the stretcher is made to r est on the edge of t he ground, while the head is supported by Nos. 2 and 3 in the ditch. Nos. I and 4 climb out. The stretcher is lift ed forward on the ground above, and rests there while Nos. 2 and 3 climb up.
To CROSS A 'VALL.
The stretcher is lower ed with the foot about one pace from the wall; the bearers then stand to N os. I and 3 on th e left , Nos. 4 and 2 on the right. They turn inwards, stoop down, grasp the poles with both hands; they rise slowly, liftin g the stretcher , holding it level at the full extent of th e arms. The
196
by side paces ad,'ance to the wall, raise the stret her and lift it on to the \vall, so that the front runners are just over the wall. No. I then crosses the wall and takes hold of the front handles j NO.4-then crosses the wall, they grasp the poles, lift the foot of the stretcher; all the bearers then advance and lift the rear runners over the wall, resting the rear handles on the wall; NO.3 then crosses the wall and takes hold of the left pole, No. 2 then crosses the wall and takes hold of the right pole. The bearers then advance until the stretcher is clear of the wall. The stretcher is then lowered to the ground.
LIFTING INTO BED.
Place the stretcher at the side of the bed . The bearers to take positions as in Stretcher Exercise No. 1., Nos. I, 2 and 3 being on the side furthest from the bed. The patient to be unloaded on to the knees of Nos. 1,2 and 3, as in Exercise No. I. No. 4 will disengage, remove the stretcher (this can be done by pushing it under the bed). NO,4 then joins hands with NO.2. All the bearers rise to a standing position, supporting the patient on their forearms. NO.4 disengages and goes to the patient's head. All bearers then step forward and gently place the patient on the bed.
Or, if the bed is narrow, and there IS room, the stretcher may be placed on the floor with the head

199
close to the toot of the bed. The injured person may then be lifted over the foot and placed on the bed.
The first method is preferable.
CARRVING UPSTAIRS.
In carrying a stretcher upstairs, the head shou.Id go first j an extra helper should assist at the lower end, so as to raise it and keep the stretcher nearly horizontal.
198
-
CHAPTER IX.
(Being the Sixtlt Lectllre .for Females only, z"ll accordance wz'tlz Syllabus 58.)
BY E. :\IACDOWEL COSGRAVE, l\I.D., F.R.C.P.I.PREPARATION FOR RECEPTIO OF ACCIDENT CASES.
\VHEN news of an accident comes, preparations should at once be made so as to have everything 1 eady before the injured person is brought in. Of course the preparations needful will vary according to the nature and extent of the injury, but the following are the chief things which may have to be done.
CHOICE AND PREPARATION OF ROOl\I.
A room must be chosen. In a bad case this should be one easily reached, as it is difficult to carry an injured person through narrow passages and up -stairs. Unless there is some such reason against it, the injured person's own room is best.
The way to the room must be cleared, projecting furnitur e and loose mats in the hall or in lobbies should be removed. If the injured person is carried on a door, shutter, or stretcher, two strong chair should be placed ready to support it wherever the bearers would be likely to require rest.
Useless furniture should be removed from the bedroom. The bed should be drawn out from the wall

20 1
so that both sides can be approached, and the clothes turned back to one side to their full length. A hot bottle should be got ready. If there is much several hot bottles and hot blankets may be requIred; cover the hot bottles with fl annel.
If the injury is very severe, if 111 ud-stained clothes ha\'e to be removed, or if extensiye dressings have to be applied, it may be necessary to have another bed, a couch or a table placed near the bed to lay tbe sufferer on in the first instance. This should be so arranged that soiling may do no harm; old sheets, waterproof materiaJs, thin oilel.oths, or even newspaper, may be used as a protectIOn.
LIFTING AND
If present at the place where the oc.curred, it will be necessary to see that the patIent IS carefully Jifted after proper "FIrst Aid" has been rendered.
The followin a rules should be remembered :-Select the proper nur:ber-of persons to assist, and do not let them lift the patient until they thoroughly understand how they are to do it.
For ordinary cases, where the injured person has to be lifted a very short distance, three are sufficient. Two (who should be as far as of equal height) are to bear the weight, the t.e support and take charge of the injured part. [hIS IS
200
best done by a persoll who has been through a " First Aid" course . If the injured person is insen ible, another belper should suppert his head .
The lifters, one at each side, should kneel on one knee, and pass their hands under the patient's back at the lower part of the shoulder-hlades, and under the hips, clasping each his right hand in the other's left. The injured patient should, if practicable, place his arms round the necks of the bearers .
The third helper should attend to the seat of injury; if this is a fractured limb, he should support it by placing the palms of his hands under the limb, one above and one belo\\' the seat of the injury, grasplt1g it firmly but avoiding unnecessary pressure.
The helpers should remain thus until the ordel " Lift" is given, and then they should ali lift slo\\'ly and steadily, avoiding jars, attempts to change position of hands, etc .
H the injured person is to be placed on a stretcher or shutter, this should be previously placed with the bottom end at his head ; the bearers should then move, one at each side of it , until the patient is over it. c The word" Lower" should then be given, and the i nj ured person should then be slowly lowered. A pillow o r folded-up coat should be ready, and as the sufferer is lowe r ed this should be placed under his head.*
* Full directions are given in Chapte r VIII.

203
MEANS OF CARRYING.
Besides a stretcher, and substitutes such as a gate, a shutter, or a door, other means of carrying can be impro\'ised . . . .
In slight injuries, \\ here the ll1Jure.d person IS to walk t,,'o bearers can carry hIm by forming a , II band s -=at or "Human tretcher.
The two-handed seat is made as described on pages 165 and 166. . .
The Human Stretcher IS made as descnbed on pages 166 to 168.
A three-handed seat is made as described on pages 168 and 17 0 •
A four-handed seat is formed as descri bed on pages 170 and 17 1.. .'
A single helper can 11ft by supportll1g \\'lth one arm the t\\'o knees and \\ ith the other the back . The arms must be \yell under before commencing. to
A sinale helper can gi\'e support by putting nIS "'rm the waist graSI)inO' tbe hip and placing the L' ,b hId' injured person's arm round his. own neck, 0 Ing the band \yith his own h 'll1d . (FIg. 77, page 173) '
A capital stretcher can be improvised out of a stronO' sheet and two broom bandIes or other short Each side of the sheet is wound up on a handle until there is just room for a person to he between. Tbis requires four t\\'o at each side, to prevent the sheet slipping .
202

CARRYI l G UP STAIRS
.
In carrying a stretcher 11 p stairs the head should go first, and an extra helper should assist at the 10\Ver end, so as to raise i t and keep the stretcher nearly horizontal.
The two, three, or four-handed seat may be used for carrying up stairs; or a strong chair, the pati e nt being carried up backwards. In the latter case one helper should walk after the chair and help to support it, and to prevent the injured person slipping out.
LIFTING INTO BED.
Follow the instructions on page 198.
PREPARATION OF BED.
A firm mattres s, not a feather bed, should be selected. If there is much injury, or if dressings have to be applied, a draw-sheet ought to be placed on the bed . I t should be of four or more thicknes se s, extend across the bed, and r e ach from the middl e of the patient's back to the knees. A piece of wat e rproof sheeting or of thin oil-cloth should be pla ce d under the di"aw-sheet. As the draw -s he e t becomes soiled, the soiled portion should be rolled and a clean part drawn smoothly under the patient.
In fractJ.re of the leg or thigh, sprained ankle and some other cases, a "cradle" (Fig. 99) should be improvised. The use of a " cradle" is to support the bed-clothes and keep them [rom pressing on the Ii t11 b.
A band -box (Fig. roo), three-legged stool (Fig. lor), or hoop sawn across and the two halves secured
204
20 5
----... .......
FIG. 100.
FIG. 101.
together (Fig. 102), 1T1a), be used. A corkscrew passed through the bed-clothes, with its point guarded by a cork, and tied by string to the bed or a nail in the wall, will relieve the pressure of the bed-clothes effectually.
REMOVING THE
In taking clothes off an injured person a few rules should be borne in mind.
In serious cases it is much better to sacrifice the clothes than to run any risk of increasing the injury.

FIG. 102.
In removing a coat, etc., in a case of fractured arm the uninjured arm should be drawn out first.
In putting on a coat or shirt the injured arm should be put iii first.
In burns and scalds nothing should eyer be dragged off A sharp pair of scissors should be used, and
20 7
e"erything not adhering should be cut away. If anything adheres it should be left until medical aid can be obtained. Tbe clothing adhering may, with advantage, be soaked off. To remove the trousers from a severely injured limb, the olllsz'de seam sllould be ripped up.
PREPARATTOXS FOR SURGEON.
As soon as the irijured person has been attended to, preparation should be made for the surgeon's visit.
The preparations needful ",ill depend upon the nature of the case . The following hints may be of use :-
A fire in the room helps ven6lation, even in summer. There should be plenty of \Yater, hot, cold, and also boiling, also several basins, plenty of clean towels and soap. There should be something to empty water into; a foot-bath does well. The basins should be placed on a table, covered with a clean white clotb; a large to\\'el makes a suitable cloth; the to\\ els, folded up, should be placed on the same table, and the hot and cold water should be within easy reach. The foot-bath should be under the table or close at hand.
In the case of a burn, absorbent cotton wool, soft cloths. old linen, boracic ointment, and baking soda should be ready, and materials should be torn up for bandages.
In the case of hremorrhage, plenty of water shou ld be boiled and allowed to cool, and pads of absorbent
206
cotton wool should be baked in a tin box in the oven, and at least two basins should be ready.
In the case of a person rescued from dro\Vning, the sheets should be taken off the bed, plenty of blankets should be heated before the fire, and several hot bottles should be ready.
If poultices are likely to be required, boiling water, linseed meal, mustard, a loaf of stale bread, a small basin, a large spoon, sweet oil, and tow, fb.nneJ or handkerchiefs may be required.
For fomentation, have boiling water, flannel, a kitchen roller, and two sticks, or a large towel.
'Vhen summoning a medical man to all accident, always let him know by a written message what kind of case he is required to treat, so that he may bring whatever is needful. By this meallS valuable time may be saved.
QUESTIONS ON CHAPTER IX.
The 11umerals illdica,le the pages 'Where the ans'Wers !/lay be found.
What would you con iderwhen choosing a sick room ? . .
How would you prepare the way to the sick room?
How would you place and arrange the bed?
lIow would you prepare hot bottles? "
'What is often necessary to lay the sufferer on in the

hand seats a?d explaIn theIr uses...
203
200 200, 20r
first instance? 20r 20r 209 PAGE How would you see to the proper lifting and carrying of d n ? . 20 r, 202 an Injure perso. . .. ... ... .. \Vhat substitutes for a regular you suggest? 20 3 Demonstrate
110 '" can a sino-Ie helper lift? ... n ;:, hI' t? 203 How can a sin<7le e per give suppor . How would improvise a . 203 How shou 1<1 a stretch e r be u p.staus ? .. :? . . . 204 IIow would you carry a patient upstaus on a chair. .. , 204 IIow would you lift a patient from a to a bed? 204 How shouid a bed be prepared for an Injured person? ... 204 H o w should a draw s heet be made and used? ... 204 'What is the use of a "cradle " ? ... . "? ... In
: .. lIo\\" would
206
.. , . In
patient.? .. . 206 207 How wo uld you remove trousers In a senous case? ... 20 7 \\'bat preparations would you make for the surge o n? .,. 207 \Yhat w o uld you get ready in the case of a burn? .. . And what
? . . . . . . . 20 7, .. 0 And what
208 \\'hat
ready
... 208 8 . ? 20 And for
.. , .. . ... "') 8 What sort of
send to a. doc to: . 20
what ways maya cradle be ImproVIsed.
you remove or put on a coat or shut In the
case of a fractured arm?
the case of a bad burn, what would you do with clothing that adhered to the.
in the case of hc:emorrhage
in the case of a per on drownIng?
would you get
for makl11g poultices?
fomentatIOn
a message would you
ApPENDIX
THE RO L LER BA DACE AID ITS
(iVot £nciuded in the Syllabus of .Illstruction.)
THE ROLLER BAKDAGE
.Roller ba.ndages be made by tearing appropnate matenal Into strtpS of the desired width . These strips should be tightly rolled and the loose threads at the edges removed, or they may be bouaht ready made . A variety of materials, such as \\ oven cottO?, open woven cotton, gauze, domette, flannel, stoclcll1ette, etc., may be used, each having its special advantages for special purposes. They may be rolled

Flc;. J03. by hand or. by means of a machine (Fig . r03). \ Vllen a bandage IS partly unrolled the roll is called the head a n d the u nr olled part the free end. '
21 I
GENERAL RULES FOR ApPLICATION.
I. See that the bandage is tightly anu evenly rolled before attempting to use it.
2. Apply the outer side of the free end to tbe skin.
3. Never allow more than a few inches of the bandage to be unrolled at a time.
4. Bandage from below upwards.
5. As a rule, to \\"hich the figure of 8 bandage for a limb is an exception, each layer of tbe bandage should cover two-thirds of the preceding one .
6 . Apply the bandage firmly and e\'enly, but not tigbtly enough to stop the circulation. If, on running the hand down it, the edges turn up, the bandage is too loose . If, after the bandage is taken off, red lines are seen, it has not been evenly applied.
7. \Vhen the bandage is finished, fix it securely by pinning or stitching.
USES OF THE ROLLER BA DAGE.
Roller bandages are used ;-
I. To retain splints or dressings in position.
2. To afford support to a part, for a sprained or dislocated joint, ora limb with varicose veins.
3 . To make pressure on a part, for example, to l"educe or prevent swelling; or,
4-. To drive the blood from a part of the body handaged, as in the case of extreme collapse from h.:emorrhage.
210
METHODS OF ApPLICATION.
There are three principal methods of applying the roller bandage :-
I . The simple spiral, which is made by encircling the part with the bandage several times . This method should only be adopted when the part to be bandaged is of uniform thickness, as, for instance, a man's chest, the finger, the \uist and a short po rtion of the forearm above it.
2. The reverse spiral.
This is used in bandaging parts of the limbs where owing to their varying thickness it is impossible to make a simple piral li e properly. (See Fig. 107.)
3. The fi g ur e of 8.
The figure of 8 bandage consists of a series of double loops, and is so named from its resemblance to the figure 8 . It is used for bandaging at or in the neighbourhood of a joint-the thumb, the breast, groin, and other parts. It may also be used inst ea d of a reverse spiral for a limb . Certain bandages applied by the figure of 8 are called spicas.
The few bandages illustrated and described in the following pages are to be regarded only as typical of the art of roller bandaging. \Vhen the principle by which parts are covered is understood, no difficulty should arise in applying any bandage . The points to which attention should be directed are even n ess an d fir m n ess of application rather tha n making a com-
21 3
pleted bandage correspond exactly wit!1 the illustration of it-it will, in fact, be found that dIfferently shaped limbs require s l ight modifications of the bandage .
TYPICAL BANDAGES DESCRIBED.
I n the description the patient is supposed to standina with his upper limbs hangmg by hiS side the thumbs turned outwards. This, however,' will not necessarily be the position in which he is placed to be bandaged.

F IG. 1 0 4
Fo r the Fmge1's.- Wi d th oj balldag-e, i or I inch. to inner side o f front of Wrist, a sutliclent lengLh being left for. tying; across back of hand to inner Side of finger to be first bandaged (bandage the fingers in order from the little finger side), by one spira l to ro ot of fin.ger nail j round finger by simple (or If necessary. reverse) spirals; thence to root of hale finaer and round wrist. Tie to free end left fo r the purpose, or continu e to the next finger. (Fig. 104 .. '
212
Spica for the Ball of the Thumb. - Width 0.1 bandage , I inch. front of wr ist; between thumb and finger; sim ple turn round thumu; diagonally across
fr ont of thumb j ac ross back of hand to wrist; acros!' pa lm and r ound thumb, and continue until the ball of the thum b is covered. Finish b y a turn r ound wlist and secu re. (Fi gs 105 and 106.) 21 5
105.

FI G. 106
Reverse Spiral for the Forearm.- of 2 o r inches. Cow' se.-From inner to oute r side of fr ont of w ris t; ac ross back of hand to first joint of little finge r; across front of fingers; \0 inner then outer side of wrist. Repeat once.
fF1G. I ol:L
T wo o r three simple spirals r o und wrist. Re\'erse spirals on fo rearm . (Figs. 107 and 108.) The figure of 8 bandage, as for the leg, may be applied instead of the spi ral.
214
FIG.
Spica for (right) Groin.- lVidth of bandage, 3 inches. Course.-Fork to crest of right hip; across loins to left hip; thence to oute r side of and behind right thigh. Repeat until the groin is sufficiently covered. (Figs. 109 and 11 0 .)

FIG. le 9.
FIG. 110.
Spica for both Groins.- Width of bandage, 3 inches. Coun e.-(I.) Fork to crest of right hip; across loins (0 a little above hIp;. thence to side of and behind right thigh. (2.) To nght hlp; across loms to overlap the lower two-thirds
of previous layer; to inner side of and behind l eft thigh; thence to right hip. Repeat (I) and (2) alternately until the groins are sufficiently co\·erecl. (Fig s . III and 112.)
FIG. 1[3·
Figure of 8 Bandage for the Knee . - Width of ba ndage , 3 inches. CourseRound knee and then alternately above and below. (Fig. 113 ·)
216
217
-.
-
FIG. 111.
FIG. 112.
2 1 8
Figure of 8 Band ag e for the Leg. -Wiath of ballda ut 3 inches . Cou1'J-e. - From inner side of ankle to ouler side bot fool, rounel foo,t ; round ; again rounel foot and ankle; and thence up the 11mb by ascendll1g figures of 8, each layer covering the preVI?U5 one by one-half. (Figs . 1 14 and J [ 5 . 1 The reverse sPJral, as fo r the f(dfearm, may be applieu instead.

2 1 9
The r e a r e many othe r fo rms of the Many-Tail Bandag e s p ecially adapted fo r different pa r ts of th e body, fo r example,
116
114 .
the back, front of chest, right o r left shoulder, etc. In thes e bandages a "back piece" of appropriate shape i made to serve as the foundation for t he tails. T he chief advantage o f
FIG 1 15.
Many -Tail Bandage.-To make t lu bandage, f eather-stitch together six strips of calico 3 inches wide, and in length about one and a half times as much ac; the circumference of the l imb . (Fig. J 16 . ) App.y as Fig . I 17. secu ring the upper tails with a safety pin.
11 7.
th is form of bandaae is that a wound can be examined o r a d r essing changed without undue disturbance of the patie n t.
FIG...
FIG.
Flc.
IN DEX .

Abdomen
Accident case, preparation for 200
Acids, poisoning by 153, 154
Air, always necessary... 25
Alcohol, poisoning by 129, 15 2 , 15 8
Alkalies, poisoningby 153, 154
Ambulance, to load or unload... 196, 197
Ammonia, poisoning by 153
Anatomy". 2 7
Ankle 39 " sprained
Anterior tibial artery
Aort"l.
Apoplexy
Apparently drowned, to restore 130 , Arm, hone of " fracture of Arm-slings
Arsenic, poisoning by Arterial hremorrhage
Arteries ... " course of main ...
Artery, axillary ... " " brachial. .. carotid .. . dorsal of foot •. facial
Artery, femoral ...
iliac
lingual
occi
plantar
popliteal
radial
subclavian " tibial " temporal " ulnar
Artificial respiration 13 0 , Asphyxia Atlas
Auricles .. . Axillary artery Axis
Back, bandage fo r BackLone Bandage, to apply
Bladder
Blood, circulation of Brachial artery .. .
Brain ... . " Page II8, 120 76 94 12 3 " compression of 145 " concussion of 142
Breast- bone 33 " fracture of 55
Br oad bandage ... 44
Broken bones, see Fracture. Bronchial tubes... 125
Brooch-Lone 37 Bruises
Circulation of the blooel, to induce ... 14 I
Clavicle ... 33, 55, 56
ClotRes, removal of 25, 206
Coccyx ... .. . :12
Collapse ... ... £42
Collar-bone ... 33. 55, 56
Comminuted fracture ... 4
Capillaries
Capillary hremorrhage 1102
Capsule...
Carbolic acid, poisoning by...
Carotid arteries
Carpus 35, 61
Carrying, means of 165, 203
upstair5 r 99, 204
Cartilage 32
Cause 20, 24
Cerebro-spinal system
Cervical verte brze .. 123 32 89
Cheek, bleeding from Chest, bandage for Chlorodyne, poisoning by Choking .. , ... ... Circulation of.. the blood 16 3 15 2 13 2 76
Convulsions, infantile £48 Corrosive Sublimate, poisoning by ... Cradle, bed Cranium ... " fracture of Crepitl\.S .. . Crushed hand " foot
220
f>age 118
70 100 87 145 135 35 58 46 153 80 76 87 92 94 87 100 89
•,
"
.,
t,
"
...
pi tal
...
"
"
"
Page 96 87 88 90 100 97,99 95 9 1 100 90 95 135, 140 13 0 , 135 32 76 92 32 " to improvise ... 164 30 49 44 44
roller
triangular
. .. ., preparation of
poisoning by
of rabid animals ... 210 210 160 19 8 204 15 2 102
co fold
Bandaging 160, Bandaging
"
... Bed, lifting into
Belladonna,
Bites
221
Burns 107 1 I 1
...
76
... ...
38
.. ...
156
...
87
"
Page
145 Concussion
142 Conductor 133 C o
152
Digital
Direct
stretche
197
100
Complicated fracture 41 Compound fracture 41 Compression of the brain
of the brain
nvulsants
Convulsions 147
Cyanide of Potassium, poisoning by 43 61 68 Diaphragm .. 125
pressure ... 80
violenct' . . , 40 Dislocation 08 Ditch, to cross wi t h
r
Dorsal artery of foot
Dorsal verte brre ...
Dress, woman's. on fire ...
Drowning

f
Ear·channel, blood ISSUing from foreign body
In Elbow, handage for " joint, fracture involving
Electric shock
Emetic
Epiglottis
Epilepsy ...
Expiration
External carotid artery .. ,
Eye, bandage for " foreign body in Page 3 2 113 13° ra7 59
Face, bones of
Facial artery
Fainting .. ,
Femoral artery
Femur 29,3 0 89
Fibula
Fingers, bandage for " fracture of 142 96 37, 62 37, 66 164 , 21 3 61 " hremorrhage fro111
Fireman's lift 96 17 1
First Aid, meaning o f .. ,
" " princIples o f ...
First Aider, qualifications o f 17 24 22
Fish-hook, embedded 115
Fits J 47
Flexion ... 83
" at elbow 95
" at knee... 99
Food, poisoning by 157
Foot, bandage for 163
" bones of .. , 37
" crushed 68
Fore and aft method of carrying
Forearm, bandage for " bones of 35
" fracture of 60
Forehead, bandage for. .. 160
" h ::emorrhage from 90
Foreign body in the earpassage .. , II 7
" "in the eye 116
" "i nth e 11 ose I I 7
Four-handed seat J70
Fracture, apparatus for
treatment of '" 43 causes of 40 general rules for treatment 48 involving el bow joint of arm .. , of br east- bone of carpus of collar -bone 59 58 56 61 , 55, 56 of cranium so
Fracture of finger ., "
" " " " of forearm of knee-cap of leg ... of lower jaw .. , of metacarpus of of pelvis of ribs ... of s h 0 u Ide rolade of spine of tarsus of thigh-bone .. , of toes .. , signs and symptoms of " varieties of Frost-bite Fungi, poisoning by
General circulation 76
Green-stick fracture 4 2 , 43
Groin, bandage fo r 216,217
Gums, hoemorrhage from 106
from stomach "
" " " " from throat from tongue from tooth socket ... from upper
Hand, bandage for 162 " bones of .. , 35
Hanging, , , 131
Haunch-bones ... 35
Head, bandage or [bo " m jury to , 1.,p
" side of, bandage fl)r 160
Heart 76 " rate of contracti on of 78
Heat-stroke I45, 146
Hernia 121
Hip, bandage for 162
History, meaning of 18
Human st retcher .. 166
Humerus... 35, 58
Hydrophobia 102
Hysteria .. , 149
I liac arteries
Impacted fracture
IIxl1l0rrhage, arterial '" " capillary .. , " " " " from ea r channel from fingers from gums from head and neck 80 102 ra7 96 106 223 PaOTe Hremorrhage from lungs 106 " from nose 105 0
InJirect \'iolence
133 154 124 147 12
87
5
1 60 JI6
222 Page
" " " " " " "
II
" " " " "
P'Zge 61 60 64 66 51 61 68 62 53 58 52
42 41 11 4
"
"
68 62 6'
157
of
106 106
1
'
"
limbs internal kinds
ra7 ra6
9
10-l bO " venous" 10 [
Page
Insensibility 127
In sensi bility, rules for treatment 128
In spiration 125
Instep 37
Insulator... 134
Internal carotid artery... 87
Internal hremorrhage ... 104
Intestines 118, J 20
Involuntary muscles 40
Iodine, poisoning by 158
Irritants ... 153
Jaw, angle of 30 " lower 30 " "fracture of 5 I
J oint, definition of 38
Jugular vein 88
Kidneys ... . ..
Knee, bandage for
Knee-cap ... " fracture of 1 IS, 120 164. 21 7 37 64
Knot for bandage of lower limb
Knots, reef and granny
Laborde's method of arti50 47 ficial respiration .. . 140
Laburnum seeds, poisoning by... 152
Lacerated wound 86
Laudanum, poisoning by 152
Leg, bandage for 218
Leg, bones of
and carrying
into
lower
upper
Lime in the eye ...
Lips, bleeding from Liver 118, Lower limbs
bar verte bra!

from
Many-tail bandage
Medium bandage
Metacarpus Metatarsus l\fiddle line of body
Mouth, blood from
Muscles ... " ruptured
Muscular action
arrow bandage 44
Needle, embedded II5
Nervous syste m ... 123
Occi pital artery... 90
Opium, poisoning by 15'2
Pad, ring... 9 1 II to fold 85
Palm, h::emorrhage from 96 Palmar arches ... 95
Pancreas... II 8, 120
Paregoric, poisoning by 152
Patella 37, 64
Peh·is 35 " fracture of 62 of Mercury, poisoning oy ...
Phalanges of fODt " of hand
Ph o phorus, poisonIng by
Phy iology
Plantar arch 153,
Plants, various, poisoning by ... Pleura
Nose, foreign body in ... I I 7 ,,' hremorrhage from 101) Pag ,·
Poplit eal artery ...
Poi son e d w e a po n s, 15 8 37 35 155 27 100 wounds by Poisoning 102 15 2 97,99
Posterior tibial artery
Potash, caustic, poisoning by .. Pressure, digital. .. " point ... Principles of First aid ... Prussic acid, poisoning by 100 153 80 81 24 156
"
of RespiratIOn " artificial 13 0 , II to excite
Respiratory system
Rest, necessity for Ribs " fracture of ... Rupture (hernia)
Sacrum ... St. John Tourniquet Scalds
Scalp, bandage for " hremorrhage
Scapula ...
II fracture of. .. Lifting
"
bed ... Ligaments ... .. 37 66 201 198 38 Lightning, effects of I I 1, Limbs,
13 1 35 33 II7 89 120 "
Lum
Lungs
II hremorrhage
35 3 2 12 5 106
. .
27 105 39
...
. 21 9 44 35, 61 37, 68
71 41 Narcotics 152 N
Pulmonary circulation... 78 Pulse 79
Questions on Chapter 1. 28 72 lOS 121 150 J59 208 " " II. " " II III. " IV. " " V. I, " " VI. " IX. Rabid
of.
Radial artery I02 95 3S 60 Radius
Pubes 35
Pupils of eyes 130, 15 2
animals, bites
. .
fracture
135, 140 141 124
53 121 32 83 III 160 from 90 33, 58 I
12 5
25 33
Page
Schafer's method of artificial respiration 135
Seat, four-handed 17 0
"three-handed 168
" two-handed 165
Shin-bone 37
Shock 142
» electric 133
Shoulder, bandage for ... 161
" blade ... 33, 35
" " fracture of 58
» joint... 39
Sick room, choice and preparation of... 200
Sians, meaning uf ... 18
Silvester's method of arti· ficial respiration 137
Simple fracture... ... 41
Single helper, support by 17 2
Skeleton... 29
Skull
» fracture of
Slings, arm
Smothering
Snake bites
Soda, caustic, poisoning 29 13 1 102 by
Spleen 153 118, 120
Spinal canal
" c o rd 30 ,
Spine ... . .. " fracture of
Spirits of salt, poisoning by 30 12 3 3 0 52 153
Splint, angular ...
Splints, rules for applying " to improvise
Sprains Page I}o 49 43 70
Sternum ...
Stimulants
Stings 33 55 26 114
Stomach... 118,120
" h:::emorrhage from 107
Strains 7 I
Strangulation
Stretcher exercise, 13 1
" No. I. 178
" "
" No. II. 188 o. III. 193 176 " Human 166
Stretcher, to carry 178 " to im provise 17 2
Strychnine, poisoning Ly J 57 tunning 14 2
Subclavian artery 9 1
uffocation . . 13 2 unstroke 145, 146
Surgeon's preparation for 207
Surroundings 2.0
Syllabus of instrucllon ... 8
Sympat hetic system .. , 124
Symptoms, meaning of. . . Ig
Syncope ...
Synovial fluid .. ,
Systemic circulation

Tarsus
Temporal artery .. _
Thigh-bone Page 37, 68 90 37 63 » fracture of ...
Three-handed seat
Throat, hremorrhage from " swell i ng of tis· 168 106 sues of '"
Thumb, bandage for Tibia
Toes, bandage for 13 2 21 4 37, 66 164
Tongue, hremorrhage from 106
Tooth socket, hremorrhage fr0111
Tourniquet
Tran verse wound abdomen
Triangular bandage
Two-handed seat
Ulna " fracture of. ..
Ulnar artery
Unconsciousness
Upper limbs Varicose veins of IIS, 119 44 16 5 35 60 95 1 2 7 101 227 Veins
"
\Vagon, to load or unload
Wall, to stretcher 196, J97 cross with \Varmth, necessity for ... " to promote 141, Wind-pipe \Voman's dress on fire ... \Vounds ... \ Vounds by poisoned weapons " accompanied by arterial hremorrhage ... Wounds accompanied by
Pngc
76, 101
columr! Vertical wound of abdo78 101 76 3 2 30 men 11 8, II9 Vitriol, burn by... 111-113 V 01 un tary muscles 40
Venous blood
h:::emorrhage Ventricle!> Vertebrre ... Vertebral
venous h:::emorrhage !97 25 143 12 5 I J 3 80 102 80 101 86 \Vounds, lacerated Wrist 35, 61
2
\tbe St. 301)1l Bnlbulance Bssociation.
ABRIDGED PRICE LIST.
A c?mplete and Ambulance Equipment is an actual necessIty, and expenence has proved that employers of labour and others interested in the district readily subscribe for the purchase of such appliances. Complete Illustrated Price List and all information regarding the work of the Association can be obtained upon application to the Head Office, St. John's Gate, Cle r kenwell, London, E . C .
All orde rs val ue 40/. o r over will be sent carriage paid to any pa r t of the United Kingdom. Returns from classes of instruction may be sent carriage forward . If carriage is pre· paid it will be allowed .
I n order to save delay, it is requested that an amount sufficient to cove r postage or ca rriage may be kindtly added to the remittance sent in payment of orders of less value. Any amount sent in excess will be returned.
Owing to fluctuations in market prices it is impossible to guarantee that the quotations herein can be adhered to .
Orders and correspondence should be addressed to the St . John Ambulance Association, St. John's Gate, Clerkenwell, London, E. C.
should be made payable to the St . John Ambula nce ASSOCIatIOn , and crossed" London County \ Ve3tminster and Parrs' Bank Ltd . , Clerken well Branch . "
Money Orders and Postal Orders may be made payable at the Clerkenwell G reen Post Office.

Carri age Pai d on all Orders value 40/- or over In the United Kingdom
LITTERS.
Each Litte r consists of a two-wheeled under-carriage fitted Nith elliptical springs, and eithe r. the" Furley" with a cover so arranged on a JOInted frame that It can be folded up inside the stretcher, or with a hood and apron (as shown below). The" Clemetson " stretcher can be used instead of the" Furley " pattern.
THE U ASHFORD."
The under ·carriage, having a cranked axle, the pass bet ween the wheels with the stretcher, and thus a VOId lIf.tJJ1g i t over them. \Vhen travelling, the legs of a re raised and thus form the handles by whIch t o propel It·
Should it be necessary to pass over rough g r ound, two bearers can easily lift the litter and patient.
3
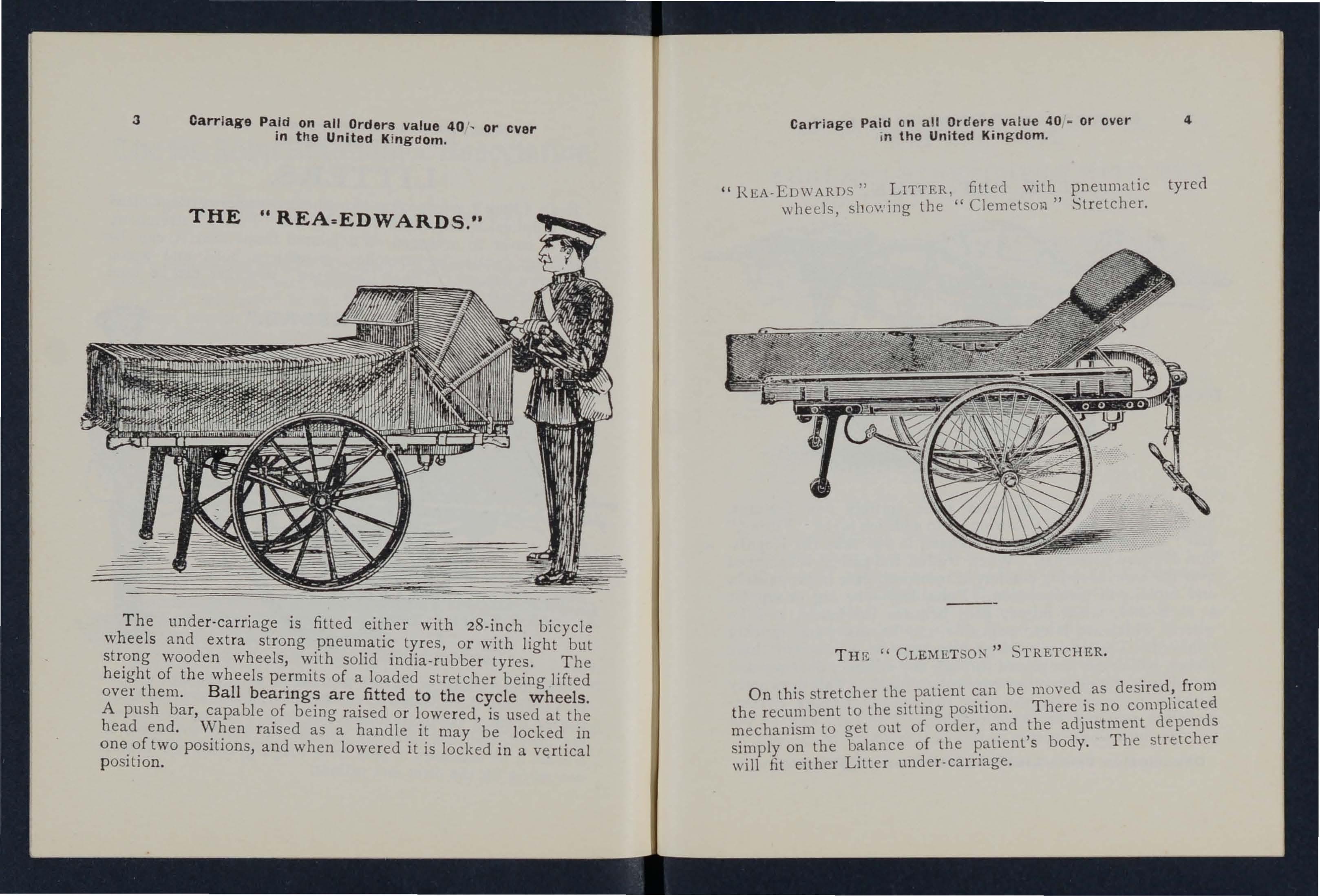
CarrIage Paid on all Orders value 40 , or ever in t he United Kingdom
THE "REA =EDW ARDS ."
Carriage Pai d on all valu e 40,. or ove r in the United Kin g dom 4
"H,EA -EDWARDS" filled with" pneum atic tyr e d \\ heels, showing the Stretcher.
T he unde r- carriage is fitted either with 28-inch bicycle wheel s and extra strong pneumatic ty r es, or with light but strong wooden wheels, with solid india-rubber tyres. The height of t h e wheels pe r mits of a loaded stretcher being lifted over them . Ball beari ngs are fi tt ed to the cycl e wh e els .
A push ba r, capable of b e ing raised or lowe r ed, is used at the head end . \-Vhen rais e d as a handle it may be locked in one of two positions, and when lowered it is locked in a vertical po sition.
On this stretcher the patient be moved, as the recu,mbe nt to the sitt}ng depends mechamsm to get out 0 f e 't' t's body Th e st retch e r simply on the 0 t le ,p:t len . will fit either LIller under-calrlage.
THll: STRETCHER.Carriage Paid on all Orders value 40 _ or ovein the United Kingdom
THE U ST. JOHN."

T h e p r esent s some enti r ely new features, amongst whIch a r e the following :-I n addition to the" Furley," a.nd pattern stretche r s, it will take the Regula· tIO n l\I1lItary Stretc.he r. loaded the patient is ualanced ove r the. comfort In lranspo r t, ease in propulsion, and rap Idity In mampu.lation. Portability-the leg or suppo r t at each end, when ra Ised, goes beneath lhe frame and lhe whee ls , which a r e i ntercha!lgeab le, can be easi ly and quickl y . T he un der-ca rnage may t h us be taken into lhree p Ie c es , .whlch can be passed t h rough any ordina ry doorway and s t? r ed In a o r ot h e r place . This does away wIt h necessIty fo r prov Iding the special accommodatIO n r equ! r ed fo r patterns. The parts can be put togethe r by a sIngle pe rson In lWo o r th r ee minutes .
Descriptive Price List of' Litters on application.
STRETCHERS
TELESCOPIC-lIA;\DLED
ORDI ARY STRETCHER - CLOSED
The s e stretchers are Yery strong, ri gid, light, and fold cl osely, and can ue confidently recomm ended as thoroughly eflicient in eve ry way. The paltern is more particularly designed fo r Inyalid Transport purposes and fo r working in confined spaces, such as mines; the "Ordinary )) pattern for general and St. J ohn Amuulance Dligade use. Either can lJe u . eel with the "Ashford," "Rea Edwards," or "St. T()hn" Litters. Should it be nec essa ry to reduce the" iclth o f a I()aded stretcher in ord e r, for example, t o carry it int o a ra.illmy carriage, this can be .Ione, either when it is r est ing on lhe ground or snpported by the bearers, with out trouble and with o ut the slightest jar to the patient.
Pr ic e s on ap pi=cat i on.
" Lo w moor Jacket/ ' [or use in mines, a!3d
Ca rr y in g S h eet, [or invali(ls. See pge r'S.
6
Ca rri age Paid on all Orders value 40 ' - or over in the U ni t ed Kin g dom 6 " FURLEY
"
WITH THE LATEST IMPROVEMENTS.
7 Carriage Paid on all Orders yalue 40 / - or oyer in the United Kingdom_
FIRST AID OUTFITS.
No- I.-LARGE HAMPER.
\ Vil h waterp roof cover and strap, suitable for ambulance stations.

For con lcnls see next page.
2 Sets of Splints.
I Set of Splint St ra ps.
I St. John Tourniquet.
lb. Cotton Wool } In Tin
! lb. Lint... ... Cases.
I Roll Adhesiv e Plaster.
36 Roller Bandages, assorted.
12 Triangular Bandages.
I piece Tape.
12 Stetilised Finger Dressings.
6 ditto H and and Foot Dres· sings.
6 ditto Large Dre ss ings.
4 mall Burn "
3 Large II II
3 Extra Large Burn Dr essin gs.
4 oz. Tincture Iodine.
1 Box Amp oules Tinclur e Iodine.
CONTAINS
4 oz. Sal Volatile.
4 oz. Powdered Boric Acid
4 oz. Bicarbonate of Soda.
I Dredger for Boric Acid.
2 pairs Dressing Forceps.
I pair Scissors.
I packet each Safety and Plain Pins.
I reel Sewing Thr ea d.
r Dressing B:lsin.
I Stopper Loosener.
I 4 oz. Graduated Glas:: ::'.Ieasure.
I cake 20 per cent. Carbolic Soap_
I Nail Brush.
3 Empty 8 oz. Bottles . " 4 oz. "
I Saucer.
2 Camel Hair Brushes.
12 I odi ne
Size: Length 24 in. Width I I in. Depth 10 in. (approx.}.
Price, £7.
Carriage Paid on a!1 Orders yalue 4()/· or oyer in the United Kingdom. 8
THE IlJ\;llPI£R
9

Carriag e P ai d on a ll 0 rd ers vnlu e 40 · or over In the Uni ted K i ng dom.
No. 2.-SMALL AMBULANCE HAMPE R .
With waterproof c o ver and strap, suitable (or collierie , small ambulance station s , also (or parochial and domestic use .
Carriage Paid on all 0 r fler s v lue 40· or i n the U ni t ed IOng.:l om .
No . 3 . FI R S T A ID BOX FOR USE IN MINES
CONTAINING
Se t of S plint s , Set of Splint Straps, St. John Tourniq!let, 1 oz. of Tincture
o f I od'ne, t oz . Sal Volatile, 6 Roller Bandages (wide and narrow),
6 Triangular Bandages, Bori c Lint, Boric Wool (two latte r in tin ca<;es).
2 Sterilised Finger Dressings, 2 ditto Hand and Foot Dressings, I dillO
Large Dr e ssing, I Small Burn Dre ss ing, I Large Burn Dressing, .1 Ext ra Large Burn Dressing, Spool of Adhesivt! Plaster, Scissors, 6 Iodine Mops, Thread, Tape, Needles and Pins.
W e igh t comp l ete, 6} Ibs . L en gth , I ft 6 in D epth. 5 in. Width, 7 in. (a pprox. ). Pri ce '£3.
CON1ENTS.
Set of Im prove d \Vooden Splints; Set of Splin t Straps; SI. J ohn Tourni. quet ; COli on W ool; Lint; 6 Compressed Rollcr as,ortedi 6
Triangular Bandages in waxed paper; ;\11 as'<0.rtment of tenltscd Dressmgs and Burn Dressings; Adhesi\'e Plaster.; Palr SClssors; sure; '2 oz. Sal Volatile; 4 oz. Boraclc Powder; 4 oz TlI1ct. Box Ampoules Tincture I odine; Dredger; Saucers; 6 I od ln e l\Iops; Pms: Safet y Pins. Price, £3 55.
1 0
1 1 Carriage Paid on a ll \'alue 40 1- or over in the United Kingdom.
No.4.-FIRST AID FACTORY BOX. to comply with the Factories {3 W orKshopsWelfare Order. 1917.

T his OU lfil is specially tiLten to meet the req uir emenls o f !ill classes of Fac tories and \Vo r ksho ps un de r the above Ord e r.
Pric e from £ t las. to £ 2 9 '5 .
Carriage P aid on all Or ders value 40/ _ or over in the United Kin g dom.
No. 5. - SMALL FIRST AID OUTFIT.
Suitable for use in Schoo's, In stit u tio n s, etc. When closed can be carrieJ by a Strap-handle.
CONTENTS: 3 l:andages. T St. John Tourniquet, 8 Spli l.1t Straps (for secUi ing Splints ,in lieu uf Wool, Lint. 6 Roller hanciages, 2 Stenltsed Finger DresSings, I ditto Hand or Foot Dressing, 1 dltlo Large DresSing, 1 Lar ge Burn Dressing J Small Burn Dres sing. [ Bottle Sal Volatile, t Tincture Iod ine, I3.P.C., t Pair of Scissor. r 2 ·OZ i\leasure Glass, China Saucer, and 2 lotline l\!ops. by by inches (approx.).
1 ice : \Y oode n Box, £ 1 55. Slout Cardboard Box. Clolh Cove r ed, r7s.
13

Carriage Paid on all Or ders value 40 - or over in the United Kingdom.
No. 6.-SURGICAL HAVERSAC.
for St. John Ambulance Brigade units.
I-Illed WLlh a lIn, so arranged thaL a ny article can be take n out with ollt disturbing the re st of th e contents.
Carriage Paid on all Orders value 40 /- or over in the Unitbd Kin g dom .
NURSES' HA VERSAC.
Bandages an I Dr ess i ngs c()111pressed.
CONTENTS: I Set o f S plints, I Set of Splint Straps, 3 Tri angular 6 R o ller Bandages (wi de and narr o w), Cotton \Vool, .Bon c I Roll Adhesive Plaster, I Pair Scissors, 2 oz. !Il1Cl. I od Ine,. I B ox Ampoules Ti nct. I odine, 2 oz. Sal VolatIle, 2 oz . BOrIC Acid Powder, I Dredger, I Graduated
Glass Measure, I St. J ohn T ourn iquet , Pins, I Saucer, 6 I od ine Mops. Price £2 lOS.
2 Compressed T rinngular Pandnges, 6 C o m· pr essed Roller Bandages (assorted sizes), I B)Ltle Sal V olatile , 6 Am poules Tinctur e I oJ in e, 2 P ackets Compressed Boric Lin t,
2 Packets Comp r essed Cotton \V ool, I Empire Plast e r, 2 S[eri· li sed Finger Dr ess in gs, 2 Sterilised ringer Ti p Dressings,
2 Sterilised Ha nd and Foot Dressings, I Sterilised Large Burn
Dr ess in g , I Sterili sed Small Burn Dressing, I Pair Scissors, I Pair Dr essing Forceps, I 2 oz. M ed icine Tum b le r, Safety Pins.
Pri ce I8 s.
14
15

Oarriage Paid on all Ord er!'! va lue It Oj . or over i n the Un i ted Kin g dom.
THE " ATTACHE " OUTFIT.
Comisting of an ordinary 14 in leather attache case (stock size), and a.tin lining holding the" First Aid" equipment, thus for the case l e mg used for ordinary purposes or as a" First Aid " outfit as de ired . The tin lining and cements can be supplied sep:uately.
Carria <Y e Pa i d en a ll O, d ers value 40 . or over in the Un ;t ed K i n g d om ,
No. 8.-" REA : EDWARDS" LITTER FIRST AID BOX.
18
• Se t of Splints, I Set of Spiil1t S!r;lPS for securing Splints in lieu of Ban. dages, 3 Triangular Bandflges , 6 Roller Bandages sizes), 4 F irst Aid Dressings, 6 Small Packets Absorbent Cotton 'Wool, 6 Small Packet Boric Lint, I S I. John Tournique t, I 2·0Z Medicine Tumbler, I Spool
Adhesive Plaster, I Packet Boric Lint Patches , I Packet Pins and Safety
Pins, I Pair Scissors , I Pair For ceps, 2 oz Sal Volatile, 2 oz. Collodion, 2 oz . Boric Acid Powder, 6 Ampoules Tincture I odin..:, I Dred. ger, 4 Sterili,ed Finger Dressings, 4 Sterilised Hand and Foot Dre,sings, I Large Burn Dressing, 2 Small B urn Dressings, 2 Camel.Ha ir Price complete , 1st quality £3 2nd quality £3. Tin and contents only £2.
For carrying below the axle,Jrom i t is easily de.tachable. Length, 18 in. Wtdth. 14 tn. Depth, 8 tn.
CONTENTS
I Set of I Set of Splint Straps for Splints in lieu of Ban. dag es, 6 .Ban.dages, 6 ! l : lb. packet. Cotton \ Vool and Bonc LInt, Adhestve Plaster.. Pair oJ S':I. sors. 6 Sterdtsed Finger Dressings, 6 ditto Hand or FOOL Dresstngs, 6 Lar!?:e Dres. sings for other part', 2 Extra Large .Burn Dres:tngs , 2 Large Bl!rn D ressings , 2 Small Burn 2 oz. of I odtne, 2 oz . Sal Velatde, 2 oz. Boric Acid Powder, J Dredger for ditto, I Graduated l'vJ easure, I St. J ohn Tourniquet, Pins, Safely Pins, 2 Saucers, 6 Iodtne Mo ps Price £3 75.
17

Carriage Paid on all value 40 / . or over in the United Kingdom
FOR THE POCKET - FIRST AID COMPANION.
CO);,T E NTS.
I S t er i lise d Finge r Dressing ,
t S t erilised Finger Tip Dres.
sing, I S t erili,ed Hand a nd
Foot Dressing , I
S mall Burn Dress ing, 2 Co m.
pr ess ed Roll e r
2 A mpoules Tinc t ur e I odille,
I Packet Boric Lin t Patches
1 P a cket Pins, I Roll Adhesive Plaster .
Le ngt h , in . Width , 31 in . D ep th, Ii in.
P rice 2 S
POCKET FIRST AID CASE.
CONTENl S.
6 Ampoules Tincture I odine,
7 S t erili sed Finger Dressin s,
t Sterilised FingerTip Dressing
I Sterilised Hand and Foo;
Dressing, I Sterilised Small
Burn Dress ing, Roll Adhesive
Pbster, Packet Pins, I Packet
Boric Lint Patches, 1 Pair
Small Sciss J rs , I Knife, 1 Pair
Splinter Forceps
Length d - in. Width , 3! in.
Depth, Ii in .
Price 9S
Carriage Paid on all 0 rders value 40 - or over in the Uni t ed Kingoom.
"LOWMOOR JACKET."
18
Fo r use in mines, hips' holds, etc., to secure a on a stretche r (see illustrat ion), which can then be placed In an upright position . ("When state patt e rn of S tretche r in use, i.e . , TelescopIc or OrdlDary pattern.)
Price on application.
CARRYING SHEET.
For carrying patients up and down stairs or otherwise about a house. The sheet is fitted with rope handles and detachable bamboo poles, and. may be. on a stretcher wIthout dU:lurblDg the IJatient. £ 1 17s .
ROLLER BANDAGE MACHINE.
Designed by Dr. A. C. Tunstall .
Price 4S .
19

Carriage Paid on all Orders value 40 - or over in the United Kin g dom.
BANDAGES. SURGICAL DRESSINGS , AND PLASTER.
Roller Bandages, 6 yards long, fr om I to 6 inches wide, white or grey, open wove or grey calico. In assortment, packed in neat cartons. Recommended for class practice-one I in . , two in ., two 3 in., 6 yards longgrey calico or thick white open wove.
Cotton Wool, absorbent white-in I, 2, 4, 8 or 16 oz. packets. i\Iedicated, Boracic, in 4 and 16 oz. p.'l.ckets.
Lint, plain white and Yfedicated, Boracic, in I, 2, 4, 8 and 16 oz. packets .
Gauzes, in 6 yd. lengths, about 36 in. wide, plain or medicated.
Plaster, l{ubb e r adhesive (Antiseptic), widths in. to 2 in., 5 and 10 yard spoo ls. Prices of the abov e on application.
Triangular Band a.ges-Plain, each 5cl.; per doz. 4S. 6d . Illustrated, showing 25 applications of the Triangular Bandage with printed instructions, each 9d.; per doz. 9 5•
NURSING INSTRUMENTS.
Forceps, dressing, large or small, IS. 3d., 2S . 3d ; Artery, 3S.
Scissors, dressing, r Ollnd points, I S. 9el., 2S . 9d., 3s. 6cl. ; sharp points, large, 3 ; . 9d.; small, for delicate work, 2s. 6d .
Knife , 2 blades , I s. 3d.
Spatula, I s. Probe, 6d . D irector, with Ear Scoop, 25.
CLINICAL THERMOMETERS.
Round.-N o I, ordinary, 2S. 6d; No . 2, minute, 2S. 9d . ; NO·3, half-minute, 3s .
With Broad Index, will not roll,- No. 7, ordina ry, 2S. 9d . ; N o.8, minute, 35.; NO . 9, half-minute, 3s. 3d . I n ordering it only necessary to quote the re gisterod number of the Thermometer required.
N.B.-Minute and half-minute instruments will only regi . t er in the time s tate d under favourable circ umstan ces .
Carriage Paid on all Orders value 40/ - or over in the Un:ted Kingdom.
SUNDRIES.
Dressing Basin , kidney shapeJ, of enamelled
St. John Tourniquet , with directions
Greatly improved Wooden Splints, with grooved joints and angle piece, strongly recOlUmended...
20 d.
Splint Straps, for securing Splints in lieu ?f Band· ages, consisting of strong 2 in. \yebblng, and suitable Buckles. Per set of eight as ' orted, sufficient for a fractured thigh 2 9
Buckles only, Is. 3d. per doz. Web1Jing only, 25. 6d. pe r doz. yards. . . It is unnecessary to sew the buckles on, Simply pass the spikes through one end of the keeping the end uppermost.
Flags. -Association-5 ft. by 3 ft., 2IS. ; 12 ft. by 6 ft., £2 2S. Briaade (New Design)-6 ft. by -+ ft., £1 IS;. 6d.; 9 ft. by 6 ft., "'£3. Brigade Pennon-3 ft. 3 in. by 7 ft. 6 in., £2 4s. 6d. ; 5 ft. 4 in. by 12 ft., £4 2S.
Electrotypes for printing the official stationery of A, The St. John Ambulance Association, and B, The .'t. John Ambulance Brigade. A or B - Badge only. All or BHBadge and Beading. N o. I for Pust Cards, NO.2 for Note Paper, NO.3 for Quarto and Foolscap paper-.-\. or B, 3s. 9d.; All or BlI, 35. 9d. NO.4 for mall Posters, A or 3s. 9d. ; o . 5 for Large Posters, 3S. 9d. No. I Dl:>tnct, S.J. A.13. Nos . 1 t) 3 each, 3s . 9d .
Safety Pins (All fasten or unfasten on either side). Empire, No. I, No.2, 3l1. ; No. 3, per doz. Box of 3 doz. assorted, 9d.
Blanket Pins, large, IS. 3d. ; small, IS. per doz.
iron... 2 0 The
0 9 Splints,
3 3
Wooden, jointed, per set
6 6
21

Carriage Paid en all Order8 value 40/ . or over in the United I<ingdom.
TEXT BOOKS, i3c.
" First Aid to the Injured." By Sir James Canllie, K.B.E., (Revised by a Committee, 1919.) The authonsed T ext Book for the First Aid Course. I S. 6d. By post , Is.
" A Preliminary Course of First Aid to the Injured." Adapted by a Committee from the authorised T ext Book Aid to the I njured," specially for those under sIxteen years of age . 6d . By post, 7d.
"First Aid in Coal Mines." A supplement to " First Aid to the In jured . " 6d. By post 7d.
"A Catechism of First Aid." Compiled from Sir James Cantlie's Manual. By J. M. Carvell, 1\1. R.C.S., L.S.A. (Revised 1919 . ) 6d. By post, 7d.
" Problems in First Aid. " A c ompanion to the authorised Text Book of the St. John Ambulance Association" First Aid to the Injured." By the late L. 1\1. F . Christian, 1\1. B., C.:\L, Ed. , and W. R. Edwards, A . C.A. rod. Bypost, I Home by a Committee principally from ongmal. manuscnpt, written at the request of the ASSOCIatIOn by Mlldrecl IIeather·Bigg, R. R. C. , Matron of Charing Cross II ospita l, and Lady of Grace of the Order of St. John of Jerusalem in England . Th e author ised Text Book fo r the ursing Course . IS. 6d. By post, I S. Bcl.
" A Catechism of Home Nursing" (based on the authorised Text Book) . By J. 1\1. Carvell, :\I.R.C.S., L .S . A. 9d. By post,
"Domestic and Personal Hygien e." By John C. Thresh, 1\1. D., D . Sc., &c. Illustrated. The authorised Text Book for the II ome lIygiene Cou rse . 2S. 6rl. By post, 2S.
Carriage Paid on all Orders value 40 . or over in the linited Kingdom
TEXT BOOKS, i3c. -( continued.) 22
" A Catechism of Domestic and Personal Hygiene." Compiled from the authorised T ext Book. By \V. R. Ed wards, O.B.E., 9d . By post,
" Notes on Military Sanitation." By Lieut.·Col. II. P . G, Elkington, R. A. M. C . 9d. By post,
"Elementary Bandaging and Surgical Dressing. " By Walter Pye, F.R.C.S. 3s.6d. By post, 3s. 8d.
"To Restore the Apparently Drowned ." Printed in large Type with two diagrams. 4d. By post,
" Manual of Drill and Camping for the St. ] ohn Ambulance Brigade. " IS. By post, I S. 2d.
"First Aid Principles." Cards of concise directions for waistcoat pocket, each; 4(1. per doz . By post 6d. Special quotations for brge quantities.
"Specimen Examination Papers, First Aid, Nu rsing and Hygiene Courses." 3d . By P03t, 41d .
Small Anatomical Diagram. Showing the human 5keleton, main arteries, and points where pr ess ure should be applied to arrest bleeding. zu. By post, Post Card [or pocket, Id. By post, 2d.
Directions as to the Restoration of Persons suffe ring from Electric Shock. Large print, poste r size. 3d. each. By post,
General Notes on First Aid to be Rendered in Cases of Poisoning. By Milnes Hey, :\1.A., i\I.R.C.. , L.R.C.P., 2d . By post, 31d .
23

Carriage paid on all Orders value 40, - or over in the UnitEd King-clom
TEXT BOOKS, &c.- (colltiuucd) .
"Order of the Hospital of St. John of Jerusalem and its Grand Priory of England ." By H. W. Fincham, assisted by W. R. Ed wa rds. 100 pp., crown 4to., on antique laid paper, with 23 Plates on Art Paper. Bound cloth boards, gilt leltered, price 6s. (packed for post 6s. 6d . ). Cheaper Edition, paper covers, price 2S. (packed for post 2S. 3d.).
General Regulations for the St. John Ambulance Brigade, 1913. 9d. By post . I rd.
Rules for Corps and Divisions, St. John Ambulance Brigade. 2d. By post,
Registers. Cl as s Attendance, 4S. 6d. By post, 4S. rod. Certificates, 4S. 9d. By post, 5s. 9d . Case Report, I S. 4d. By post, IS. 7d.
St. John Ambulance Brigade Cash Book, Minute Book and Occurrence Book. Set of three, I3 s. By post, 14S. od. Receipt Book, IS. By post. IS.
Large Physiological Diagrams (New Series) . For L ectu rers' use. The Human Skeleton, showing the main arte ri es and pressure points. Th e General Anatomy of the Body. The Systemic and Pulmonary Ci r culation of the Blood. .S ectio n Thr ough Middle Line of Head and I eck, shovnng th e T ongue in two positions in relation to the Trachea, and method of Artificial Respiration (Expiration a nd In spira tion) . Dislocations. Price, per set of five £2 2s. Th ese may be' hired for a course of " First Aid" lect u res, given under the ausp ices of the Association, for a fee o f 7s. 6d. ' or with the addition of Sp li nts, T ourn iqu et, and 30 plal11 Tri angular Bandages, for a fee of I7 S. 6d.
Stationery for the use of Class Secretaries and ot h ers connected with the Association. Packet of 24 sheets of hig h -cl ass pap e r, suitably headed, and 24 envelopes bearing the the device of the Association. IS. 3d . By post, IS. 7d.
Carriage Paid on all Orders value 40 j. or over in the United Kingdom. BADGES. N os. 3 and 6. (Actual size.)
and 8
Badges, with the device, und.er th e authority of the Central Executive COm111lttee, havmg been first at;>pro ved by H. R. II. the G rand Prio r . the sole and recognised Badge of the AssociatIOn and Bngade. N . 8.- TIL is des!:;ft is protecte i.
SERIES A.- For the use of individual certificatel pupilsN
t In Nickel Silver, Large Size
Ditto, Small Size .... ..
3. Ditto, Small Size for hole ,,0
4. In Electro Plate, Slze 2"
5. Ditto, Small Size ...... Ii
6. Ditto, Small Size fo r button hole ,. 0
7. In Enamel for button hole ,, 0
8. Ditto, as brooch I t. 3
9. In C lot h and Silk I
ro. In Cloth and Sil ver
I r. In Cloth and Cotton
12 . Small Celluloid Badge, fo r button hole 1 or brooch !!" "
13. White Satin Armlet, with woven Badge 2± " N.B.-Th ese a r e not t o be worn as decoratiofts.
24
1
s.
0
d
2 in. dia. 0 2.
I i"
6
6
t 3
0
" I
0
t"
9
a
0 6
2 ,. 3
r ii "
o
r 2 6
26

Carria g e P ai d on a ll Orde r s va lu e 40/ · or over in the Un ited Kin g dom. BADGES.
Nos. 15 to 18 (Reduced) N o . 19 (Actual Size).
SERIES B.- For members of the St. John Ambulance Brigade, not wearing uniform, having the name of the Corps or Division annexed on a label, only issued in quantities-
No. 15. In Nickel Silver, 2ins. in diam . , first doz., £1 4s.; subsequent dozs . , 13s.
" 16. In Electro Plate, 2 " " first doz., £1 r6s. ; subsequent dozs. , £1 45.
" 17. In Cloth and Silk, 2" "per d oz ., .£ I ;
" 18. In Cloth and Silver, 2" "per doz., .£3
" 19 . The "Brigade" button hole badge, each IS.; bro o ch pin, each 1/3 with
N B -These badges are not to be worn as decorations.
26
UNIFORM DEPARTMENT .
ST. JOHN AMBULANCE BRIGADE REGULATION UNI
F ORM .
The above department has been organised in order that Ambulance Members of all ranks may be able to obtain the r e gulation uniform. thoroughly reliable in quality. at the lowest possible price. The prices quoted are current at date of publ ication. market reductions reflect automatically in favour of the purchaser.
All quotations are strictly net and for cash with order.
Carriage or postage extra.
Measurement form s may be obtained free on application to the Director of tores.
For Corp s and Di vis io nal Surgeo n s, D istr i ct , Co rp s and D iv is i o n al O ffi cers , and Sergean t-Maj or .
Jacket and Trousers. including collar badges-badg es of rank extra
Cap. including bad ge . Divi sio nal Officer
(Corps Surgeon. District and Corps Officers. same price. plus cust of embroidering peak and difference in price of badge.)
Sam Browne Belt and Br ilce. black leather
Re .-Iu lat io n ecktie
Great Coat. grey. army beaver cl o th Melton. beaver finish
Including collar badges-badges of rank extra.
N . C.Os .. Rank and File.
Jacket. inc luding collar extra
Trousers. white piped ..
Great Coat. grey Yorkshire frieze. including arm badgetitlt.s extra
Cap and Badge
Belt. Staff Sergeant. black leather ..
Belt and Pouch. brown leather
Chevrons-Silver lace. per bar
Aluminium lace will not klrnish. per bar
\Vorsted lace. per bar
\Vhit e Havresac
Waterbottle and brown leather C a rrier
\Vhite Cotton Glo\'es
Leggings 3s. 6d.
s d . 85 0 16 6 17 6 4 0 180 0 90 0 20 0 17 6 34 6 5 9 3 9 10 9 1 3 o 1! o 4 2 3 4 6 2 0 7 6
27
UNIFORM DEPARTMENT - (continued).
ALTERNATIVE UNIFORM. - Brigade Overseas only.
NOTE.-it is to be undel'slood that the dis inctive wu/orm oJ the Brigade '-S black, which is to be worn whelLf''l'er tossib!e, (llld that the alternati'l'e ulH/onn is authorized J(lr W f' ar in hot climates only,
For Corps and Divisional Surgeons, District . Corps and Divisional Officers , and Serge ;mt-Major.
J aclc et , kh ak i cloth o r linen drilf, \ Vhipcord Barathl'a. Linen Drill. bl a ck colla r and cuffs, including collar badges-badges of rank extra S4 0
Trousers, khaki cloth or linen driB. piped bl3Ck
Cap. khaki, piped black. including badge (Divisional Officer) ..
(Corps Surgeons, Di trict and Corps Officers at the same price. plus cost of embroidering p eak and difference in price of badge)
Field Service Cap. including badge 7 6
Over coat, khaki cloth, including collar badges-badges of rank ext r a 126 0
N . C.Os .. Rank and F il e.
Jacket, khaki cloth or linen driB. black collar and cuffs. includ ing collar badges ..
T r ouse r s. khaki cLlth or linen drill. piped bla t It
Great Coat, khaki, Army, new (stoc:k sizes). including arm badge
Cap. khaki, piped black, including o adge
Chev r ons, Belts, White Havresac, Gloves, etc . as per pag-e 26.

PATTER'S AND PR I CES POST FREE. Tele/;holles5320. 5321. & 6297. ETC., FOR THE ST. J OHN A?\1BU LANCE BRIGADE, I\IAY BE OBTAINED AT E . & R.
To H.:\!. \\'AR OFFICE. Il.l\L bOlA OFFICE. COLo:-:rAL OFFICE. EGYPTIAN GOVERNMENT. LONDON COU 'TV COUl\"CIL, THE PRINCIPAL HOSPITALS. ETC. AN I LLUSTH.ATED PRICE LIS T ST. ISO of the various articles required by the JOHN AMBULANCE BRIGADE ON APP LI CATI O N. to r62 , Edgware Road, LONDON, W . 2 . .. GARROULD-EDGF;' LO S IJON
50 0
84 0
15
33 6 33 6
0
16 0
1st qual. 2nd Qual. 23 6 22 6 20 0 18 6 31 0 20 0 11 6 5 9
THE UNIFORMS,
CLOAKS
GARROULD,
28
BONNETS APRONS,
, DRESSES,

29 5T. JO HN 11fv\B U L11 NCE BRI 0 11D E. UNIFORMS FOR
UNITS. Comp
COA T (O u tdoo r) (Ta il o r -?lla d e) DRE S S (Gr e y C otto n) HAT CA P COLLARS CUFFS A PR ON T hese Goo ds ma y be o btai ned fr o m M ESSRS G AR R OULD wh o a l e al so pr e pared to su pply t h ose unit s who p r efe r the C loak and Bo nn e l a s o ri gi na lly w o rn . I LLU STRATED PRICE LI ST CONTAINING FULL PARTICULA RS POST FRE E ON A p PLICATIO N. E. & R. GARROULD, ISO t o 162, EDGWARE ROAD , LONDON, W . 2. T ple:/>ftolles5320 , 532 1 & 62 9 7, P ADD! NGTOX. T eleg ,-om s.. G ARROU LD-EOGEL ON DON. " INDEX TO PRICE LIST. For General Index see page 220. Ambulance Hampers ... Badges, &c. Bandages Bandage Winder Basin, Dressing Books .,. Carrying Sheet Cash Book Clinical Thermometers Cotton'Vool ... Diagrams, Large ., Small PAGK 7 to 9 .•. 24, 25 19 18 20 21 to 23 6, 18 23 19 19 21 22 20 20 Dressing Basin ElectrOl ypes ... Fir"t Aid Boxes .•• 10 II. 12,J6 " Pocket Ca es 17 " " Attache Ol1lfit 15 Flags Hampers (Ambulance) Haversacs Instruments Lint Littel's ... 20 19 1 to 9 13, '4 19 ]9 to 5 Lowmoor Jacket I1finute Book ... Nursing Instruments Occurrence Book Plasters Receipt Book Registers Roller Bandages Roller Bandage Machine Rules for Corps or Divisions St. John Ambulance Brigade Safety Pins Scissors ... Splint Straps Splints Stationery Stretchers PAGE 6, 18 23 19 23 19 23 23 ]9 18 23 20 19 20 20 23 6 19 19 20 Surgical Dressings Text Books Thermometers Tourniquet (St. John) Triangular Bandages Uniforms '9 26 to 29 W00! (Cotton) ... ]9
NURSING
r ising:


· · , f t ! ! t · · t t 1 , i ( [ , I , i f ( , f \ { ! f · I t 1 s t I ! t i I t } t ! i t I I t 1 r ! l' " ! ) j I 1 I ; f \ , t \ i 1 i I t 'l ,\ '.' \ ,<