
21 minute read
Knowledge and Attitudes


Impact of Naloxone Education on Healthcare Professionals’ Knowledge and Attitudes
By Jacqueline Hagarty, Matthew Martin, Michael DeValve, Susan Miller
Advertisement
Abstract
Background: Naloxone, a safe opioid overdose reversal agent, is now more accessible in North Carolina through a statewide standing order. However, general awareness about naloxone is low. Previous studies identified healthcare providers’ perceived barriers to prescribing naloxone due to lack of knowledge about naloxone dosage forms for use in the community, worries about encouraging drug abuse, and concern about legal liabilities. The purpose of this study was to determine if a targeted naloxone education program increases knowledge and positive attitudes of health care professionals concerning naloxone use in the community. Methods: Educational sessions were held for healthcare professionals in one region of North Carolina. The Opioid Overdose Knowledge Scale (OOKS) and Opioid Overdose Attitudes Scale (OOAS) were administered before and after each educational session to assess for immediate changes. The mean change in overall pre- and post-test scores were analyzed and compared based on demographic information. Results: One hundred one participants completed surveys. There was a 15% increase in the average knowledge score (33 to 40 out of 45 points, p-value <0.0125), and a 9% increase (106 to 119 out of 140, p-value <0.0167) in the average attitudes scores indicating an increase in readiness and positive attitudes towards naloxone use. Limitations: This study utilized a convenience sample of healthcare professionals who attended the education sessions. Retention of knowledge and attitudes or behavioral changes following education sessions were not measured. Conclusion: Targeted naloxone education is associated with an increase in short-term knowledge and positive attitudes towards naloxone use in the community.
Background
According to the Centers for Disease Control and Prevention (CDC), the amount of opioid overdose deaths quadrupled from 1999 to 2015.1 Opioids (opioid analgesics and heroin) accounted for 28,647 fatalities in 2014, or 61% of all drug overdose deaths.2 Over 1300 of these overdose deaths occurred in North Carolina.2 The United States attempted to address the source of the problem with prescription monitoring programs and suggested daily limits of opioids. Some community organizations are focused on preventing harmful consequences of drug use, such as criminalization, incarceration, spread of HIV and hepatitis, and death from overdose.3 Naloxone is a safe opioid reversal agent; it is one harm-reduction strategy increasingly used by first responders and laypeople in the community to address overdose situations in a timely manner.3 Intranasal and injectable dosage forms of take-home naloxone are indicated for layperson use in the community.4 North Carolina joined other states in efforts to make naloxone more accessible by granting emergency responders and police departments access to naloxone in 2010, and further expanded access to patients by allowing preventative distribution with a prescription in 2015.5 In June 2016, the North Carolina State Health Director signed a statewide standing order allowing pharmacists to dispense naloxone to anyone in need.5 Prescriptions can also be dispensed to a third party, such as a friend or family member of someone at risk.5
Despite the increased access to naloxone across the country, recent evidence suggests that there are many barriers that prevent healthcare professionals from prescribing and dispensing take-home naloxone. Physicians from varying specialties across the United States (including internal medicine, family medicine, pain management, general practice, and many more),
medical students, and medical residents indicate that one of the biggest barriers to prescribing take-home naloxone is a lack of knowledge about naloxone’s role in the community.6-10 Other barriers stated in the literature include a lack of guidelines or strong evidence that identifies candidates who would benefit from take-home naloxone, perceived legal issues with dispensing naloxone, and a lack of awareness of intravenous drug users among their patient population.6,7,9,10 There are also concerns from physicians, medical residents, and students, that naloxone may encourage higher drug use, that it does not tackle the source of the opioid epidemic, and that it might offend patients, despite the evidence that says otherwise.7-9 Pharmacists and pharmacy staff identified additional barriers to dispensing naloxone, especially without a prescription. Studies of community pharmacists in West Virginia and Massachusetts indicated that a main barrier to dispensing naloxone without a prescription is a lack of training.11,12 Pharmacists who underwent naloxone training in New Mexico cited a few perceived barriers to dispensing naloxone under a statewide standing order, including reimbursement challenges, affordability for patients, and lack of patient interest.13 Evidence exists to support that naloxone education programs increase patient and family member knowledge and positive attitudes towards naloxone and managing overdose situations.14-17However, few studies evaluate naloxone education programs for healthcare professionals.
Two European studies associated naloxone education with an increase in provider knowledge and positive attitudes.18,19 One study evaluated general practice residents,18 and the other evaluated interdisciplinary healthcare workers at multiple facilities.19 These studies used the Opioid Overdose Knowledge Scale (OOKS) and the Opioid Overdose Attitudes Scale (OOAS) to assess the efficacy of education for healthcare professionals and patients on layperson administration of naloxone.20 The OOKS and OOAS were developed and validated to measure change in patient and healthcare professional knowledge and positive attitudes towards naloxone use and overdose situations in an immediate pre-post test model.20 There are no published studies that utilize these scales in the Unites States to measure the effects of naloxone education for healthcare professionals. Previously discussed studies that identify providers’ perceived barriers to prescribing of naloxone for layperson administration indicate that more education is needed.5-9 Many healthcare professionals practice in a position where they could identify patients at risk for opioid overdose, including primary care providers and emergency providers. In past studies, the take-home naloxone education was typically described as a live and active learning environment.15-19 At the time of this project proposal, there did not appear to be any published studies that assessed the efficacy of take-home naloxone education for healthcare professionals. The purpose of this study was to determine if naloxone education is associated with a change in knowledge and attitudes in healthcare professionals.
Methods
This was a single-group, pre-post quasi-experimental study. The education sessions took place from November 2016 through March 2017 within a large health system in southeastern North Carolina and assessed healthcare professionals from a medical center and affiliated clinics, a family medicine residency program, and the local public health department.
Participants – A convenience sample of 130 healthcare professionals attended one of six live education sessions. The education sessions originally targeted healthcare professionals working in an emergency department, behavioral health, an inpatient hospitalist group, and residents and faculty of a family medicine residency program. As an incentive, several of the sessions were offered with continuing education credit for physicians and nurses and advertised throughout the health system. However, these education sessions were open for any healthcare professional to attend, and they were advertised through emails and posters. Healthcare professionals who did not complete both a pre-test and post-test were excluded from the study. Individual participants’ pre-test and posttest scores were matched up by utilizing the last four digits of their social security number.
Measures – The primary endpoints of this study were the mean overall changes from pre-test to post-test scores on the OOKS and OOAS. Secondary endpoints included mean scores within each OOKS and OOAS subsection, differences in primary endpoints and pre-test scores between each demographic group, and change in the number of naloxone prescriptions at the family medicine residency program before and after education. The OOKS and OOAS measured knowledge and positive attitudes towards opioid overdose and naloxone use immediately before and after educational sessions. The OOKS (45 points total) assesses opioid overdose risks (9 points), signs (10 points), actions (11 points), and naloxone use (15 points).20 The OOAS (140 points total) assesses competence (50 points), concerns (40 points), and readiness (50 points) to manage an overdose and
use of naloxone.20 The scales were used with permission from the original author, but the wording on both scales was adapted to include the intranasal naloxone dosage form. The term “fitting” was changed to “seizures” to better align with the US medical terminology. Demographic questions were also added to the end of the post-test. The time between pre-test and post-test administration varied with the lengths of the educational sessions, but they were administered no more than one hour apart. A retrospective report generated the number of naloxone prescriptions written or electronically prescribed at the family medicine residency program before naloxone education, from June 2016 through October 2016, and after naloxone education, from December 2016 through April 2017. Naloxone prescribing habits were not tracked at any other locations where education was provided.
Education Sessions – Educational sessions were planned for varying targeted audiences and, therefore, varied slightly in content, length of time, and teaching intervention. The OOKS and OOAS pre-tests were administered on paper immediately before the educational sessions. The educational sessions generally covered the opioid epidemic, opioid pharmacology and overdose, naloxone pharmacology and dosage forms, identification of candidates for take-home naloxone, patient education, and North Carolina state laws regarding naloxone prescribing and use. All education sessions utilized a PowerPoint presentation, demonstration videos, and hands-on demonstration of various naloxone dosage forms using training devices. Immediately following the education sessions, the OOKS and OOAS post-test with added demographics was administered on paper.
Data Collection and Analysis – Before analysis, the data were sanitized so as to be fully anonymous. Descriptive statistics were used to describe naloxone prescribing at the family medicine residency clinic. Scales and subscales were examined for scalability using Cronbach’s alpha and confirmatory factor analysis. The mean change in both individual’s and overall scores, the mean change in scores within each subsection of both scales, and differences based on demographics were analyzed using paired sample t-tests. Multivariate linear regression models were constructed in order to examine the relationship of demographic variables on scale score changes.
Results
There were 130 attendees at a total of six educational sessions. Following the initial project proposal of four education sessions, two additional sessions were held for the county public health department and one hospital owned outpatient clinic. Sessions were conducted on November 8, 2016, December 2, 2016 (as shown on figure 3), January 9 and 12, 2017, February 23, 2017, and March 2, 2017. Of 130 attendees, 101 sets of scales were collected. Although the OOKS and OOAS were administered as one test, some participants only completed either the OOKS or the OOAS. Therefore, we collected 100 complete sets of OOKS and 96 complete sets of OOAS (see Table 1 for demographic information). Students were from various healthcare professions and undergraduate areas of study, including medical, pharmacy, and public health. “Others” included various healthcare professionals such as mid-level providers, physical therapists, and paramedics. Eight participants who did not provide demographic information were also classified as others.
Cronbach’s alphas for the OOAS were 0.725 for the readiness subsection, 0.877 for competence, and 0.793 for concerns. All calculated alphas were in an acceptable range (0.70 or higher in most research situations), demonstrating good internal reliability. A confirmatory factor analysis for the OOAS showed fair construct validity overall. However, several items across all three subsections had questionable validity based on our analysis. One such item may not be worded clearly enough, and could be misinterpreted. A few other items in question surveyed participants about actions taken during overdose that were shown by video, but participants did not practice these actions in any simulation settings.
A paired samples t-test was performed. The mean change in OOKS score was an increase of 6.9 points, or 15% (SD 4.3, p<0.001). The mean OOKS pre-test score was 33.6, and the mean post-test score was 40.5, out of 45 points. The distributions of pre-test and post-test OOKS scores are shown in Figure 1. The mean change in OOAS score was an increase of 12.7 points, or 9% (SD 8.4, p<0.001). The mean OOAS pre-test score was 106.4, and the mean post-test score was 119.2, out of 140 points. The distributions of pre-test and post-test OOAS scores are shown in Figure 2. The mean scores within each subsection of the OOKS and OOAS are shown in Table 2. The differences between pre-test and post-test scores within each subsection were also significant (p<0.001).
Several differences in scores based on demographic information were identified. Participants who identified as pharmacists and pharmacy technicians had lower competence subsection scores compared
to all other job title groups. The mean pre-test score was 28.11 for pharmacists and pharmacy technicians, and mean pre-test scores ranged from 32.12 to 37.40 for nurses and nursing assistants, physicians and mid-level providers, students, and other healthcare professionals. The mean post-test score in the competence subsection for pharmacists and pharmacy technicians was 38.37, in comparison to a range of 41.40 to 43.25 for all other groups. There were no differences at baseline (in pre-test scores) and no differences in change in scores between participants who had self, friend, or family members with opioid addiction, abuse or overdose and those participants who did not. However, there were a few differences between participants who had previously witnessed any overdose and those who had not. Participants who had previously witnessed an overdose had higher pre-test scores in the following subsections compared to participants who stated they had not witnessed an overdose: naloxone use (10.19 and 8.76, p<0.001), competence (37.71 and 30.55, p<0.001), and concerns (34.34 and 29.97, p<0.001).
There was no clear pattern in the number of naloxone prescriptions written or e-prescribed at the family medicine residency clinic before and after their education session. There was an overall decline in the number of monthly prescriptions from June 2016 to November 2016. Following the education session in December, the number of naloxone prescriptions increased to 7, but remained low (2 or less) for the next 4 months. The number of prescriptions each month can be found in Figure 3.
A regression model was used to look at the readiness subsection score as a dependent variable with demographics, OOKS scores, and the other two OOAS subsections as independent variables. The R square was 0.276. The adjusted R square was 0.122, the standard error of estimate was 2.988, R square change = 0.276, F change = 1.788, df1 = 13, and df2 was 61. However, only the competence and concerns scores demonstrated a significant impact on the readiness score (p=0.044 and 0.023, respectively).
Discussion
This study showed a statistically significant increase in knowledge and positive attitudes in healthcare professionals regarding naloxone and opioid overdose management immediately following education sessions. Furthermore, we found a significant increase in scores of each subsection of the OOKS and OOAS. However, the results did not reveal any overall patterns in baseline scores or change in scores based on demographic groups or educational interventions. Additionally, the clinical relevance of these changes may not be known until follow-up studies can assess behavioral changes related to the increase in knowledge and positive attitudes.
A majority of the participants had previously received “none” or only “some” training on opioid prescribing and opioid overdose. This situation indicates the need for more education about opioids in healthcare professional training programs, especially because half of the participants reported 0-5 years of practice, indicating student or recent graduate status. There may also be a need for more continuing education opportunities regarding opioid prescribing and overdose.
Pharmacists, as the medication experts, are in a position to provide education to other healthcare professionals regarding the topics of opioids, medicationassisted treatment (MAT), and naloxone. A new opioid action plan in North Carolina includes collaboration between healthcare professionals, law enforcement, the North Carolina Harm Reduction Coalition, and state governmental departments to reduce diversion, increase both awareness and naloxone access, and expand treatment programs.21 Pharmacists are called upon to aid in drug take-backs, participate in public education campaigns that includes opioid safety, dispense naloxone per the statewide standing order, and work with physicians to increase MAT for opioid use disorders. The North Carolina Association of Pharmacists (NCAP) is one organization that will provide educational resources to prepare pharmacists to educate other healthcare professionals.
Pharmacists are also in a position to provide opioid safety education to the general public. One recent news story suggests that a lack of training, awareness, and perceived importance of take-home naloxone may prevent patients from asking for it and pharmacists from prescribing it.22 Our study demonstrates that pharmacists may lack confidence to prescribe and dispense take-home naloxone. Although pharmacists may not have to respond to emergencies themselves, they should be able to counsel a patient, friend, or family member on naloxone and its use during overdose situations. Specific naloxone and overdose training for pharmacists may lead to improved patient education and awareness, but more studies are needed in this area.
The number of naloxone prescriptions was collected from the family medicine residency program
because most of the providers in the clinic were able to attend the education session. It should be noted, however, that patients in North Carolina can obtain naloxone from a pharmacy under the statewide standing order, and that this study did not track conversations where the provider recommended naloxone without creating a prescription. The number of naloxone prescriptions increased in the month following the education session compared to the previous two months. However, the total number of naloxone prescriptions in the 5 months following the education session was less than the number of naloxone prescriptions in the 6 months preceding the education session. It is possible that the education session increased immediate awareness and identification of patients eligible for take-home naloxone, but over time it became less of a priority for these physicians. These results only reflect the prescribing habits of the attendees of one education session, and it is not known if there were any changes in prescribing habits as a result of other education sessions.
Physicians and pharmacists reported lack of knowledge about naloxone’s role in the community as one of the biggest barriers to prescribing or dispensing it in previous studies.6-12 Our regression model demonstrated that participants’ readiness to use naloxone and manage an opioid overdose was significantly dependent on their attitudes (concerns and competence), but not on their increase in knowledge or demographics. Therefore, the results of this study suggest that lack of knowledge may not be the biggest barrier to prescribing naloxone. Although a significant increase in scores was found in all three subsections of the OOAS, the competence subsection had the largest increase in score. The questions in the competence subsection assessed a person’s confidence in knowing what to do during an opioid overdose. The minimal improvement in the concerns subsection may have contributed to the minimal increase in the readiness subsection. Our results suggest that an increase in confidence and decrease in concerns may be necessary to increase readiness to use naloxone to manage overdoses.
There are several limitations to this study. This study utilized a convenience sample of healthcare professionals who attended the educational sessions. Many of the participants were not required to attend. It is possible that people who attended were more willing to learn about opioid overdose and naloxone. Not all attendees turned in both the pre-test and the post-test. It is not known how their participation would have affected the results. Availability of healthcare professionals and time restrictions placed on the educational sessions may have affected the educational interventions, the participants’ knowledge and attitudes, and the amount of completed scales turned in. Finally, the scales were not designed to measure retention of knowledge, and for various logistical reasons, follow-up beyond the education sessions was not attempted in this study. Surveys were kept anonymous to encourage participation, so no contact information was collected. Contact information was not pursued because online survey response rates are generally poor. This study did not measure behavioral changes including overall naloxone dispensing or use, or other outcomes such as overdose mortality. In the one setting where prescribing habits were tracked, education did not seem to have a lasting effect on rates of naloxone prescriptions.
Conclusion
Targeted naloxone education programs may increase short-term knowledge and positive attitudes of healthcare professionals concerning opioid overdose and readiness to use naloxone. Pharmacists are in a position to provide naloxone and opioid overdose education to other members of the healthcare team. It may be of interest to assess what concerns are not adequately addressed in current naloxone education for healthcare professionals. Additionally, more studies are needed to assess behavioral changes following naloxone education in order to determine optimal educational interventions for healthcare professionals.
Authors and affiliations at the time this study was conducted: Jacqueline Hagarty PharmD1,2, Matthew Martin PhD1 , Michael DeValve PhD3 , Susan Miller PharmD1,4 1Southern Regional Area Health Education Center, Fayetteville, NC 2Cape Fear Valley Health System, Fayetteville, NC 3Fayetteville State University, Fayetteville, NC 4University of North Carolina, Chapel Hill, NC
Corresponding Author:
Jacqueline Hagarty (former PGY1 Pharmacy Practice Resident at Cape Fear/SRAHEC) jacki.chorzempa@gmail.com
Disclosures
The authors have no conflicts of interest to disclose. No financial support was required to complete this study.
References
1. Opioid Overdose. Centers for Disease Control and Prevention. https://www.cdc.gov/drugoverdose/data/statedeaths.html. Published December 16, 2016. Accessed April 21, 2017. 2. Rudd R, Aleshire N, Zibbell J, Gladden R. Increases in drug and opioid overdose deaths — United States, 2000–2014. Morb Mortal Wkly Rep [Overdose Stats]. 2016;64(51):1378-1382. 3. Hawk KF, Vaca FE, Onofrio G. Reducing fatal opioid overdose: Prevention, treatment and harm reduction strategies. Yale J Biol Med. 2015;88(3):235-245. 4. American Heart Association. Web-based integrated guidelines for cardiopulmonary resuscitation and emergency cardiovascular care - part 10: Special circumstances of resuscitation. ECCguidelines.heart.org. Updated 2015. 5. Naloxone overdose prevention laws. The Policy Surveillance Program Web site. http://lawatlas. org/query?dataset=laws-regulating-administration-of-naloxone. Published July 1, 2016. Updated 2016. Accessed September 10, 2016. 6. Beletsky L, Ruthazer R, Macalino GE, Rich JD, Tan L, Burris S. Physicians’ knowledge of and willingness to prescribe naloxone to reverse accidental opiate overdose: Challenges and opportunities. J Urban Health. 2007;84(1):126-136. 7. Binswanger IA, Koester S, Mueller SR, Gardner EM, Goddard K, Glanz JM. Overdose education and naloxone for patients prescribed opioids in primary care: A qualitative study of primary care staff. J Gen Intern Med. 2015;30(12):1837-1844. doi: 10.1007/s11606-015-3394-3. 8. Gatewood AK, Van Wert MJ, Andrada AP, Surkan PJ. Academic physicians’ and medical students’ perceived barriers toward bystander administered naloxone as an overdose prevention strategy. Addict Behav. 2016;61:40-46. doi: 10.1016/j. addbeh.2016.05.013. 9. Leece P, Orkin A, Shahin R, Steele LS. Can naloxone prescription and overdose training for opioid users work in family practice?: Perspectives of family physicians. Can Fam Physician. 2015;61(6):538-543. 10. Wilson JD, Spicyn N, Matson P, Alvanzo A, Feldman L. Internal medicine resident knowledge, attitudes, and barriers to naloxone prescription in hospital and clinic settings. Subst Abus. 2016:18. doi: 10.1080/08897077.2016.1142921. 11. Thornton JD, Lyvers E, Scott VG, Dwibedi N. Pharmacists’ readiness to provide naloxone in community pharmacies in West Virginia. J Am Pharm Assoc (2003). 2017;57(2S):S12-S18.e4. 12. Stopka TJ, Donahue A, Hutcheson M, Green TC. Nonprescription naloxone and syringe sales in the midst of opioid overdose and hepatitis C virus epidemics: Massachusetts, 2015. J Am Pharm
Assoc (2003). 2017;57(2S):S34-S44. 13. Morton KJ, Harrand B, Floyd CC, et al. Pharmacy-based statewide naloxone distribution: A novel
“top-down, bottom-up” approach. J Am Pharm
Assoc (2003). 2017;57(2S):S99-S106.e5. 14. Albert S, Brason FW,2nd, Sanford CK, Dasgupta
N, Graham J, Lovette B. Project lazarus: Community-based overdose prevention in rural north carolina. Pain Med. 2011;12 Suppl 2:S77-85. doi: 10.1111/j.1526-4637.2011.01128.x 15. Barocas JA, Baker L, Hull SJ, Stokes S, Westergaard RP. High uptake of naloxone-based overdose prevention training among previously incarcerated syringe-exchange program participants. Drug Alcohol Depend. 2015;154:283-286. doi: 10.1016/j.drugalcdep.2015.06.023 16. Walley AY, Xuan Z, Hackman HH, et al. Opioid overdose rates and implementation of overdose education and nasal naloxone distribution in massachusetts: Interrupted time series analysis.
BMJ. 2013;346:f174. doi: 10.1136/bmj.f174 17. Williams AV, Marsden J, Strang J. Training family members to manage heroin overdose and administer naloxone: Randomized trial of effects on knowledge and attitudes. Addiction. 2014;109(2):250-259. doi: 10.1111/add.12360 18. Klimas J, Egan M, Tobin H, Coleman N, Bury G.
Development and process evaluation of an educational intervention for overdose prevention and naloxone distribution by general practice trainees. BMC Med Educ. 2015;15:206-015-0487-y. 19. Madah-Amiri D, Clausen T, Lobmaier P. Utilizing a train-the-trainer model for multi-site naloxone distribution programs. Drug Alcohol
Depend. 2016;163:153-156. doi: 10.1016/j.drugalcdep.2016.04.007 20. Williams AV, Strang J, Marsden J. Development of opioid overdose knowledge (OOKS) and attitudes (OOAS) scales for take-home naloxone training evaluation. Drug Alcohol Depend. 2013;132(1-2):383-386. doi: 10.1016/j.drugalcdep.2013.02.007 21. North Carolina’s Opioid Action Plan 2017-2021.
North Carolina Department of Health and Human Services. https://www.ncdhhs.gov/opioids.
Published June 2017. Accessed October 1, 2017. 22. Gorman A. Pharmacists Slow To Dispense
Lifesaving Overdose Drug. Kaiser Health News. https://khn.org/news/pharmacists-slow-todispense-lifesaving-overdose-drug/. Published
January 2018. Accessed January 12, 2018.
Table 1: Participant Demographics
Number (%)
Job Title Physician Pharmacist/Pharmacy Technician Nurse/CNA/CMA Student Other 23 (23) 20 (20) 9 (10) 18 (18) 31 (31)
Number of Years Practicing 0-5 6-10 11-20 21-30 30+
Previously Witnessed an Overdose No Yes 48 (53) 8 (9) 15 (17) 12 (13) 7 (8)
38 (41) 36 (39) 12 (13) 7 (8)
34 (37) 32 (34) 18 (19) 9 (10)
61 (66) 32 (34)
Self/Friend/Family Opioid Dependence or Abuse No Yes 68 (73) 25 (27)
Self/Friend/Family Overdosed on Opioids No Yes 78 (84) 15 (16)
Table 2: OOKS and OOAS Subsection Scores
Pre-Test Post-Test Mean Change n (%) P-value
Median Mean Std Dev Median Mean Std Dev
OOKS
Risk 7 6.60 2.34 9 7.48 2.22 0.9 (10) <0.001 Signs 7 6.79 1.87 9 8.67 0.92 1.9 (19) <0.001 Action 10 9.62 1.08 11 10.41 0.92 0.8 (8) <0.001 Naloxone Use 11 9.21 2.18 14 12.15 1.05 2.9 (19) <0.001
OOAS
Abbreviations: Std Dev = Standard Deviation
Figure 1: Distribution of Pre-Test and Post-Test OOKS Scores

Figure 2: Distribution of Pre-Test and Post-Test OOAS Scores
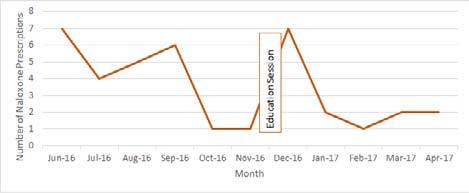
Figure 3: Number of Naloxone Prescriptions at a Family Medicine Clinic by Month

The number of naloxone prescriptions written each month at one family medicine clinic. Education was performed at this clinic on Dec 2, 2016. Naloxone prescriptions were not tracked at any other location where educations sessions were held.




