
8 minute read
Implementation of a Sustainable Naloxone Service in Community Pharmacy Coordinated Through the Medium of Pharmacy Students Trained in Advanced Opioid Stewardship


By: Bethany Volkmar, PharmD Candidate
Introduction
According to the North Carolina Office of The Chief Medical Examiner, suspected overdose deaths in North Carolina reached 4,243 in 2022, up from 3,961 deaths in 2021.1 Between October 2021 and September 2022, fentanyl-positive overdose deaths reached 2,539, emphasizing the need for opioid harm reduction strategies to be implemented into the healthcare system2 With pharmacists being one of the most accessible healthcare providers, especially in rural North Carolina communities, counseling and dispensing of naloxone in community pharmacies has the potential to make a significant impact on reversing the increasing number of opioid overdose death trends we have seen over the last few years.
In North Carolina, any pharmacist practicing in the state and licensed with the NC Board of Pharmacy can dispense naloxone to persons under the State’s Standing Order 3 This includes persons who may need it for themselves, those who need it for family members or friends, or those who may need it to assist another person at risk of experiencing an opioid overdose. A list of approved products for dispensing under the standing order includes naloxone nasal spray, intranasal syringes, injectable vials/syringes, and prefilled injectors.4
While several barriers exist to increasing naloxone distribution in the pharmacy setting, identifying patients at the highest risk and in need of naloxone is often considered by pharmacists as one of the biggest obstacles. The validated screening tools considered most favorable among pharmacists in streamlining the assessment of high-risk patients include the North Carolina Controlled Substances Reporting System’s Overdose Risk Score (ORS) and the Risk Index for Overdose or Serious Opioid-Induced Respiratory Depression (RIOSORD) screening tool.
The Overdose Risk Score (ORS) available in the North Carolina Controlled Substances Reporting System (NC CSRS) stratifies a patient’s risk of overdose based on the number of prescribers, number of pharmacies, morphine equivalent dose, and overlapping prescriptions in a patient’s controlled substance fill history.5 Scores range from 0-999, with higher numbers indicating an increased risk of unintentional overdose. Most importantly, pharmacists can access the CSRS to view an ORS score within seconds. Any score above 450 indicates an elevated risk of unintentional overdose and a need for naloxone.5
The Risk Index for Overdose or Serious Opioid-induced Respiratory Depression (RIOSORD) is a 17-item validated screen pharmacists can use independently or as a complement to the CSRS when the ORS score falls below 450.6 Unlike the ORS, the RIOSORD accounts for other relevant factors contributing to overdoses, such as conditions known to compromise pulmonary function, other mental health conditions, and concomitant use of medications known to cause drug accumulation and toxicity resulting from impaired opioid metabolism or clearance.6 Beyond the efficiency, the appeal of this tool is that pharmacy staff can glean most of the information required in this screen simply by reviewing the patient’s medication history. Scores totaling 25 or more points represent the greatest opportunity for pharmacists to counsel and convey the benefits of carrying naloxone to their patients should they experience an opioid emergency.
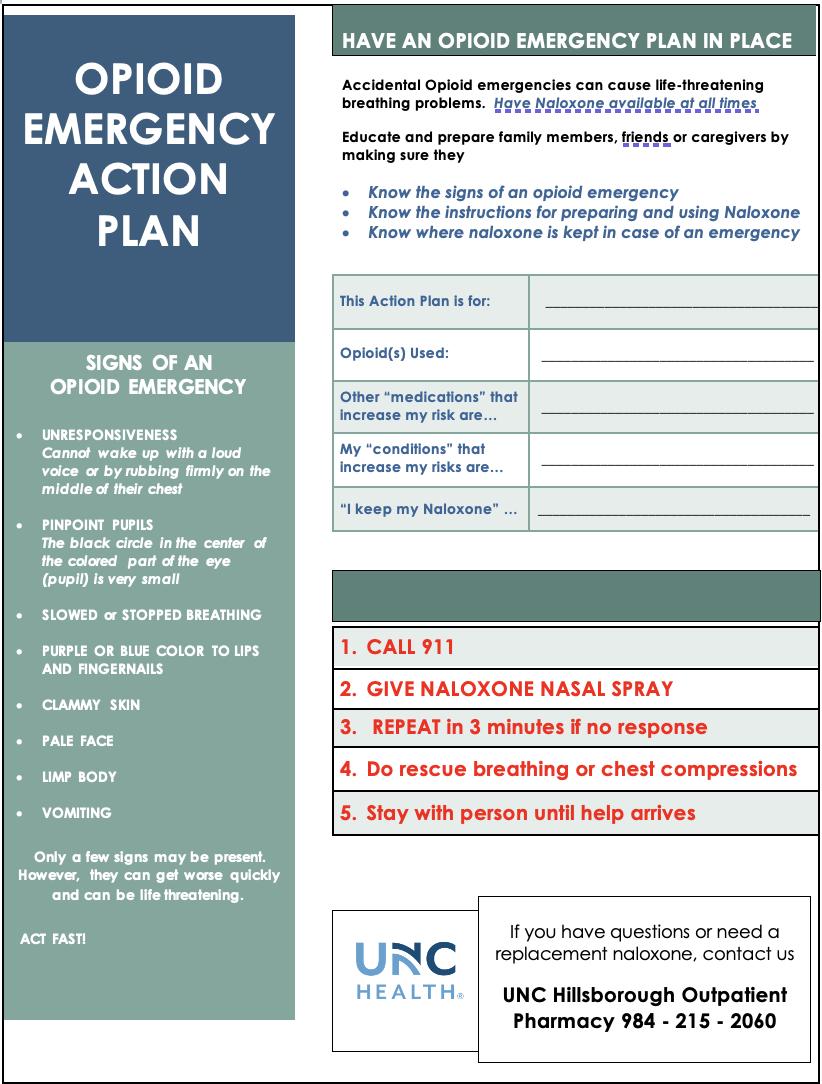
Finally, the emergency action plan is an excellent tool for pharmacists to convey necessary counseling in a strategic and time-efficient manner.7 Similar to an Asthma Action Plan, the Opioid Action Plan, as seen in Figure 1, provides a place for pharmacists to list a patient’s risk factors that could predispose them to an opioid emergency. It covers essential counseling tips, such as signs of an opioid emergency, and instructions regarding the actions and administration steps for giving naloxone. In addition, since pharmacists can provide it to patients to take home, it is an excellent resource to reinforce the counseling a patient receives at the pharmacy and helps patients train others should they become unconscious and need assistance. For access to the abovementioned tools and more information on the use of naloxone, visit the North Carolina Association of Pharmacists Naloxone to the Rescue Toolkit 7 a naloxone service model incorporating the use of these tools to identify patients at high risk that could benefit from receiving naloxone.
Methods
The service model development employing the CSRS Overdose Risk Score (ORS), the RIOSORD, and the Opioid Emergency Action Plan occurred at the Pharmacy between October 17th-26th, 2022, after an initial two weeks of shadowing, training, and workflow development. To collect additional data and test the service model’s functionality across multiple sites, a day to monitor the service at a secondary pharmacy location was also scheduled due to their high volume of opioid dispensing.
In October of 2022, a fourth-year PharmD candidate from UNC Eshelman School of Pharmacy completed an NCAP Opioid Stewardship APPE Elective partnering with a pharmacy site to develop
During the first week of the rotation, the student pharmacist worked to understand better the patient population, staff, and their roles to gauge how a new naloxone service might fit into the pharmacy’s existing workflow. The patient population for this outpatient pharmacy was primarily those with post-operative needs and, upon further inspection, in most cases, were opioid naïve. Early shadowing identified pharmacists as the point persons for the initial receipt and order entry of opioid prescriptions, with a process already in place for checking the CSRS. Providing education on the CSRS (ORS) tool and assimilating its use into the established process proved easy, ultimately saving pharmacists time in their CSRS review. During the filling process, the student pharmacist observed that technicians have quick access to the patient’s medication list, which proved a suitable place for using the RIOSORD if warranted. Based on observational findings, the remainder of the week was dedicated to creating a workflow the staff could try to test the efficiency of the naloxone service model, from performing the risk assessment to counseling and processing of naloxone for eligible candidates. In week two, the primary focus centered around training staff on the appropriate use and interpretation of the ORS and RIOSORD screening tools and capturing metrics to evaluate the number of patients screened, those deemed high-risk, and whether those at risk received naloxone. The pharmacists also reviewed the Opioid Emergency Action Plan and discussed best practices for counseling at patient pick-up.
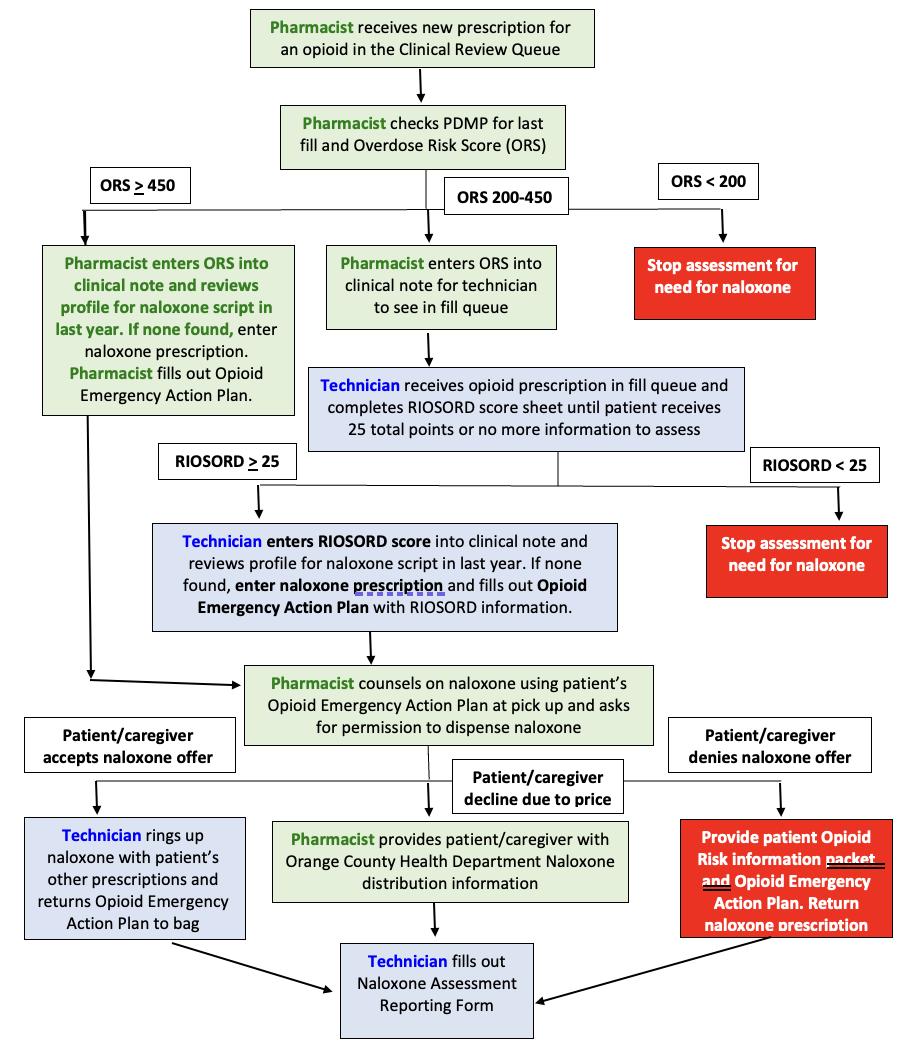
In week three, the student pharmacist worked with the staff in implementing a soft launch of the service to test the workflow, guiding the pharmacy team throughout the process. See workflow algorithm Figure 2.
In the initial verification process, the pharmacist receives the opioid prescription and verifies the patient’s risk of overdose based on the CSRS’s Opioid Risk Score (ORS). Patients with scores at or below 200 are considered low risk for unintentional overdose death and, thus, require no further assessment. For scores at or above 450, the pharmacist enters the score into the clinical note and automatically processes a prescription for naloxone per the NC Standing Order if the patient has no record of receiving naloxone in the last year. The pharmacist also fills out the patient’s Opioid Emergency Action Plan and counsels the patient at pickup, hoping the patient will be amenable to accepting the naloxone post-counseling. ORS Scores between 200 and 449 represent a gray area where the risk of overdose and need for naloxone may be less noticeable. For patients with scores in this range, the pharmacists will enter the ORS into the clinical note prompting the technician to employ the RIOSORD tool further to confirm risks and the need for naloxone. Any RIOSORD scores reportedly at or above 25, correlating with a 14% higher risk of opioid-induced respiratory depression, the technician will enter the score to the clinical note, again prompting the pharmacist to enter a naloxone prescription in the system, complete the patient’s emergency action plan and provide counseling at patient pick-up. Any naloxone prescription refused by the patient after counseling is returned to stock.
In week four, the student pharmacist discussed workflow efficiency and the results of data collected during the test implementation period with the pharmacy staff. Metrics used to analyze the value of the service included a review of the pharmacy’s dispensing report for a comparison of both opioid and naloxone dispensing. The results of the ORS and RIOSORD screens were manually tallied during the rotation. In addition, the pharmacy staff manually recorded the outcomes of each counseling attempt to capture a patient’s acceptance or refusal of naloxone. By week’s end, a sustainable service model, complete with workflow and a standardized operating procedure, was made available to the pharmacy staff.
The one day spent at the secondary pharmacy location went similarly, except the student pharmacist worked independently with the order entry pharmacists in carrying out the service at this location to test the efficiency of the workflow at this site.
Results
At the primary pharmacy location, 114 opioid prescriptions and three naloxone prescriptions were recorded and dispensed during implementation. See Table 1. One patient accepted the naloxone prescription and was counseled using the Opioid Emergency Action Plan.
During the one day spent at the secondary site, 30 opioids and four naloxone prescriptions were dispensed. Two naloxone prescriptions were co-prescribed alongside buprenorphine and naloxone (Suboxone) in patients treated for Opioid Use Disorder. Therefore, they were omitted in the analysis and Table 2 since they were not assessed for risk using the pharmacy’s service model. One patient declined naloxone at pick up during the collection period, with no data regarding the acceptance or decline of the other three naloxone prescriptions dispensed as patient pickup had not occurred before the conclusion of the student’s time at this site.
Discussion
Although results showed few patients were “high risk” at the primary pharmacy location, the service model and its screening tools still fashioned an efficient means for pharmacists to quickly assess and identify those needing naloxone, circumventing a known barrier to enhancing naloxone access in the pharmacy community. These validated screening tools were also skillfully embedded within pharmacy workflow. More patients were identified as highrisk at the secondary site, where prescription volume was much higher, allowing for appropriate intervention at prescription pickup.
Comments from host sites were positive, with pharmacy technicians expressing pride in helping identify patients at risk for harm. Administration, staff pharmacist, and technicians confirmed their desire to continue the service model and supported the expansion of the model system-wide. The next step would be to evaluate whether the screening tools can be embedded within the electronic health record to assess overdose risk electronically rather than initiating screenings manually to improve efficiency and expand interventions.
Barriers to patients accepting naloxone included cost, especially in those uninsured or with a high copay, the stigma around naloxone, and the information asymmetry on the dangers of opioids even when taken as prescribed. While the ORS and RIOSORD aided in identifying high-risk patients, the Opioid
Emergency Action Plan proved valuable in improving patient knowledge about the signs of an overdose and the use of a naloxone product. It is crucial for pharmacists to counsel patients in a non-judgmental way and to articulate that everyone is at risk of having a breathing emergency to reduce stigma. This tool helped pharmacists carry out patient-centered counseling in a time-efficient manner and through conversation that fostered a non-stigmatizing, judgment-free environment.
There were limitations to data collection. The collection period was short. With 30 days in the rotation period and the time to fully operationalize the service, data was only collected for ten days. It was concluded that medications excluded from the ORS and RIOSORD, such as muscle relaxers, gabapentin, and other sedatives, could potentially omit a population of high-risk patients. The addition of other screening assessments could help identify outliers. Still, implementation in the community pharmacy must be quick to ensure the service’s sustainability.
The study did lay the groundwork for implementing harm-re- duction screening tools in community pharmacies to reduce the increasing number of unintentional opioid overdoses in the state. A longer data collection period would allow for more robust data and potentially identify naloxone distribution effects on clinical outcomes in this setting.
References
1. OCME Suspected Overdose Deaths Report. NCDHHS. 2023. https:// injuryfreenc.dph.ncdhhs.gov/DataSurveillance/StatewideOverdoseSurveillanceReports/OpioidOverdoseEDVisitsMonthlyReports/ OCMEMonthlySuspectedOD_Report-Dec22.pdf
2. OCME Fentanyl-Positive Deaths. NCDHHS. 2023. https://injuryfreenc. dph.ncdhhs.gov/DataSurveillance/ StatewideOverdoseSurveillanceReports/OpioidOverdoseEDVisitsMonthlyReports/OCMEFentanylReport_dec22.pdf
3. North Carolina State Health Director’s Naloxone Standing Order for Pharmacists. NCDHHS. 2022. https://www.dph.ncdhhs.gov/ docs/NCNaloxoneStandingOrderforPharmacistsMarch2022.pdf
4. List of Approved Naloxone Products for Pharmacist Dispensing. NCDHHS. 2022. https://www.dph.ncdhhs. gov/docs/NaloxoneProductsforPharmacistDispensing.pdf
5. NC Controlled Substances Reporting System. NC DHHS. https:// www.ncdhhs.gov/divisions/ mental-health-developmental-disabilities-and-substance-abuse/ north-carolina-drug-control-unit/ nc-controlled-substances-reporting-system.
6. Zedler B, Xie L, Wang L, et al. Development of a Risk Index for Serious Prescription Opioid-Induced Respiratory Depression or Overdose in Veterans’ Health Administration Patients. Pain Med. 2015;16(8):15661579. doi:10.1111/pme.12777
7. Naloxone To the Rescue Toolkit. NCAP. 2022. https://ncap. memberclicks.net/naloxone-service-rp
* Patients received a Narcan prescription in the last 12 months.









