The Benefits of a Permanent Observatory
Any astronomer familiar with setting up an equatorial telescope will realize the time required to level, polar align, and prepare an instrument for an observing session. In the case of a non-computerized system, the tasks involved with centering Polaris with its required off-set for the North Celestial Pole is daunting enough night after night. Even with a computer-assisted “scope,” set-up time still involves the usual lugging of equipment out-of-doors from either residence or vehicle (although polar alignment is greatly reduced with computer alignment hardware). Final assembly can still stretch patience with the attachment of battery, dew heaters, and a myriad of wires connecting all the apparatus. Additional to all of this, many observers still have to carry out and assemble an observing table complete with sky charts, red light, lens case, camera and film. After completing this Herculean effort, particularly in northern latitudes, an astronomer usually begins to feel cold and exhausted while a degree of anxiety increases to finally use the instrument. This is often the prelude to damaging equipment or injury through acting too hastily with impatience. Repetition of such set-up experiences eventually discourages most observers who eventually reduce the frequency of their observing sessions, or trade the heavy equipment for lighter instruments with less aperture. The “lightening up” process works opposite to the usual “aperture-fever” affliction that burdens most astronomers with greater diameter lenses and mirrors and their subsequent weight increase. Under normal circumstances, amateur astronomers also find themselves observing out in the wind, in the cold, and eventually using an instrument that is covered with dew. In order to eliminate the majority of these unwanted effects, one really needs a permanent observatory. Simple forms of observatories are available, but almost of them also require a set-up time, offer little weather protection, and are not quite as “portable” as advertised. The primary decision involved with observatory design rests between choosing either a domed-type or a roll-off roof type structure. Both have distinct advantages however, depending on your personal observing needs—including the requirement for an all-sky view, protection from the environment, and degree of privacy. There are other design options for simple observatories such as the “clam shell roof,” the new cylindrical domes, and various types of shelters or housings that roll away to expose the telescope. Although these may be simpler to construct, they most often expose the observer to the elements, and are more difficult to weather-seal when not in use.
3 © Springer-Verlag New York 2016
J.S. Hicks, Building a Roll-Off Roof or Dome Observatory, The Patrick Moore Practical Astronomy Series, DOI 10.1007/978-1-4939-3011-1_1
1 The Benefits of a Permanent
Pros and Cons: The Dome Versus the Roll-Off Roof
Many owners of the roll-off roof type prefer an all-sky view, and are willing to tolerate the residual effects of wind, cold, and less control over light pollution (without the benefit of being able to select specific sky segments as with the dome slot). They also may be interested in hosting large groups, which of course demands the more spacious accommodation offered by the roll-off model. The person demanding a high degree of privacy in his viewing may appreciate the canopy provided by the dome, although the side walls of a roll-off type observatory still afford a reasonable degree of privacy. It is hard to concentrate on solar viewing for example when a host of neighbors watch you set up and enjoy your fumbles. Solitude is important for concentration and speculation. Admittedly, the roll-off roof offers a substantial improvement over just an open observing site, while the domed observatory may further reduce most annoyances, achieving a completely sheltered structure. The crucial decision to make in selecting either is one of sky view. If you want to see the whole sky dome at once, the roll-off is the better choice (Fig. 1.1).
In addition, the roll-off roof type quickly cools down to ambient temperature with the entire roof rolled off and the instrument(s) entirely exposed to the open sky. Fast cool down is not as easily attained with a dome-type structure.
However, on the other hand one need only step outside to see the heavens, and concentrate on a portion of it inside. Cost factors and degree of skill enter into the equation also. The roll-off will be simpler to build (wood construction and no curved sections) and less expensive in parts and labor. But in terms of durability, the all-metal dome will outlast it.
Fig. 1.1 The advantage of a completely open observatory—the glorious night sky dome (Courtesy of Jeff Pettitt)
Observatory
Roll-Off Roof Variations: The Sky Is the Limit
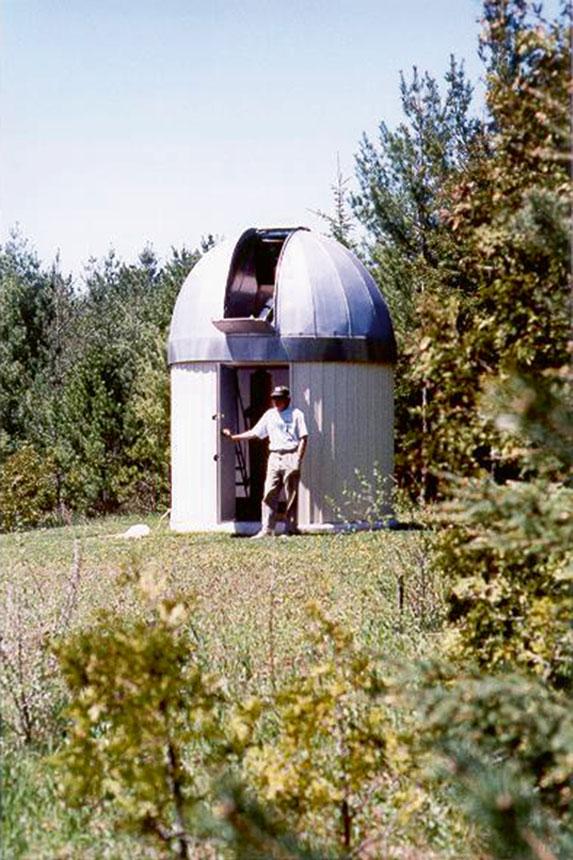
Fig. 1.2 The author’s domed observatory—while the sky is largely obscured except through the observing slot, its advantages are largely shelter from the wind and to some degree, the sun (Photo by John Hicks)
Identification of the dome as the “symbolic” structure used by astronomers may also be an asset to someone who wants to advertise to the community that their hobby is astronomy (Fig. 1.2).
On the other hand, one may want to maintain a lower profile in high crime areas, preferring to “hide” the facility as a garden shed. In essence, the choice is dependent on many factors, including site constraints and budget, along with the particular objectives and skills of the observer.
Roll-Off Roof Variations: The Sky Is the Limit
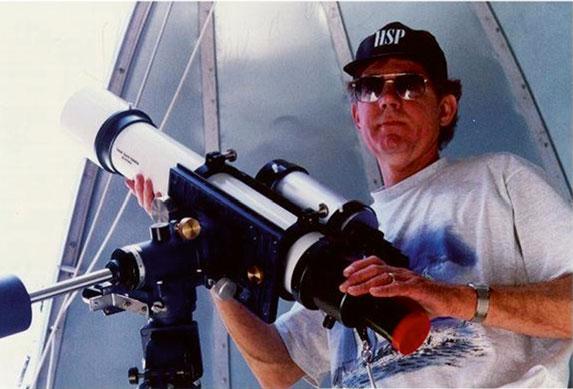
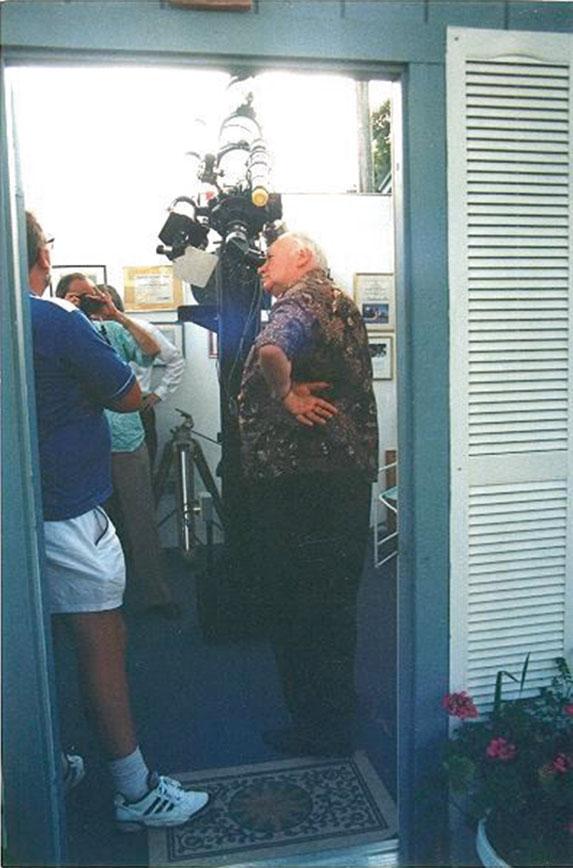
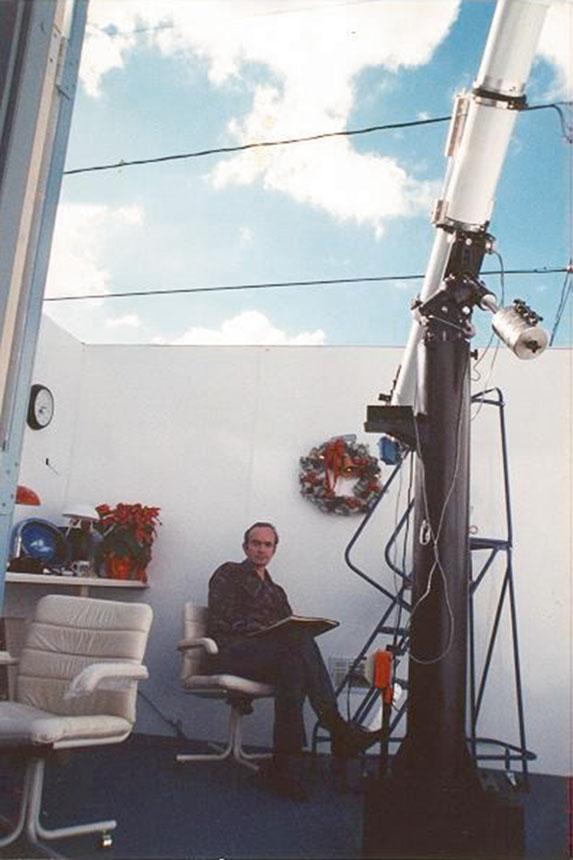
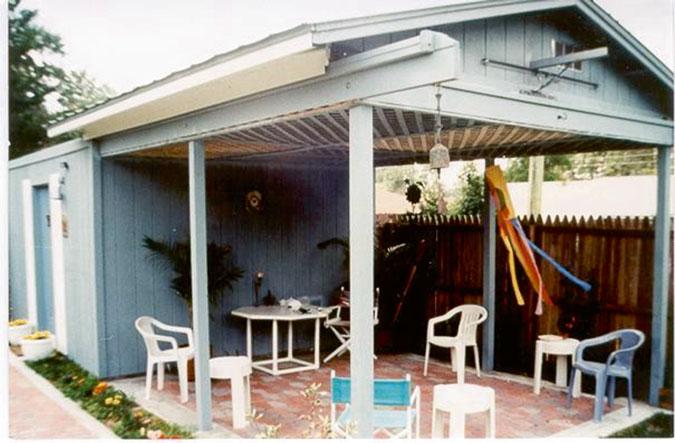
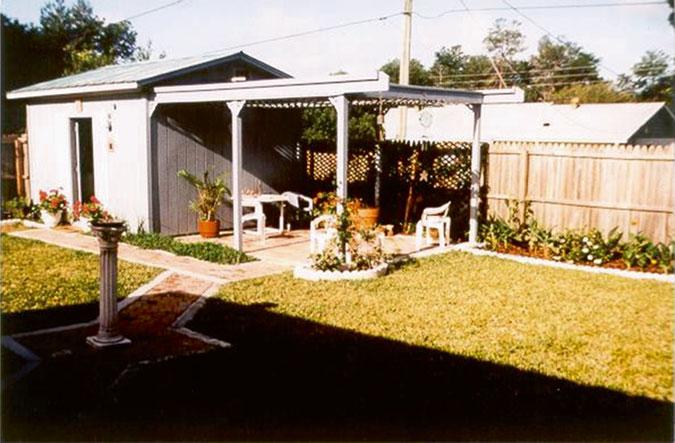
The observatory I designed for Don Trombino in Florida, fulfills both astronomical and landscape functions. With its exquisitely finished interior, and practical outdoor patio under the gantry, this observatory stands out prominently.
The owner, the late Don Trombino, was so proud of his achievement, that he spent almost all his waking hours either inside it or under the patio. He further extended the observatory feature out into the garden with a stone paver walkway leading across the yard terminating with a sundial monument. The floor under the roof gantry was also set in stone pavers and the underside of the gantry “ceiling” covered in a prefab wooden lattice. When not solar observing, Don spent many hours on the patio, examining the results of his photography, or writing. He dedicated the structure “The Davis Memorial Observatory” and symbolized the dedication with various artifacts and historical items placed in the garden and on walls of the structure (Figs. 1.3 and 1.4).
Once and a while certain observatories stand out as truly professional structures, finished to the point excellence. Such a model is Mike Hood’s observatory, complete with outside porch under the gantry, featuring a door on the gable end. Mike has put extra effort into tapering the hip roof back from the gable ends, adding a small “cottage look” to his observatory. Very tastefully finished, it has an interior just as spectacular. His structure is long enough to hold a complete control room with desks, cupboards, an air-conditioning unit, and a window. Overall the control room has the appearance of a high-tech whiteroom, temperature-controlled and very well designed. Apparently the observatory was from an original model by “Backyard Observatories” (Figs. 1.5 and 1.6).
1 The Benefits of a Permanent Observatory
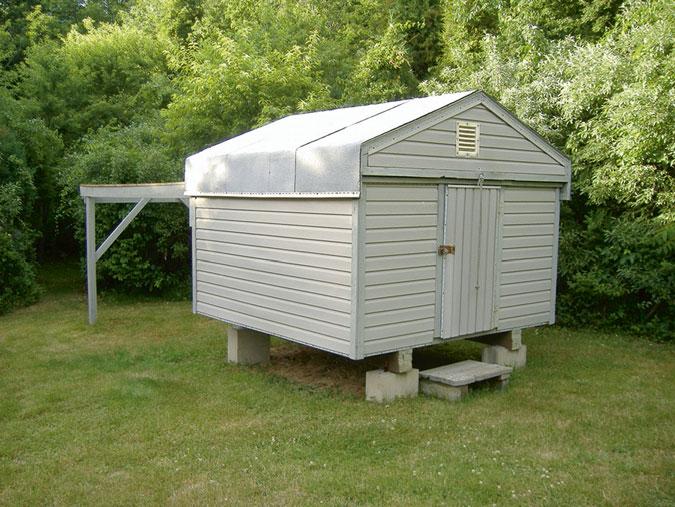
Gerald Dyck’s roll-off roof observatory in Massachusetts presents a compact, attractive addition to his yard. The roof line is particularly well-designed with a skirt that extends down over the walls to keep out insects, and the elements. Note the use of an exhaust fan on the gable (Fig. 1.7).
Fig. 1.3 Close-up “Davis Memorial Observatory” with its patio garden under the gantry (Photo from the collection of John Hicks)
Fig. 1.4 “Davis Memorial Observatory” with walkways, sundial, and landscaping (Photo from the collection of John Hicks)
1.5 “Mike Hood Observatory”—a truly well-finished roll-off observatory (Courtesy of Mike Hood)
Fig.
Fig. 1.6 Mike Hood’s Control Room complete with desks, cabinets and air conditioning (Courtesy of Mike Hood)
1 The Benefits of a Permanent Observatory
The wall height is also kept lower, presumably due to the roof skirt which replaces a portion of it below the normal soffit level. This allows for more accessible horizon-level viewing as the photo below illustrates. The telescope shown can reach lower elevations than most, swinging even further down than the position shown. The Dyck’s prefer to utilize telescopes on tripods rather than on a fixed pier. Although quite suitable for alt-azimuth mounts such as a Dobsonian cradle (shown), their future plans will most certainly involve a fixed pier with an equatorial mount (Fig. 1.8).
Although the entry door is lower than a full height door, it is made more accessible by the fact that the observatory is raised off the ground considerably. Such an arrangement allows the operator to step up into the structure rather than stoop to get into it at more normal foundation levels. I used this technique myself on my first observatory which had only 4 ft high walls. The increased height of the floor off the ground also prevents skunks, squirrels, possums and groundhogs from seeking refuge permanently under it. There is little protection from wind or the elements with so high a crawl space underneath. It also allows alterations in wiring underneath or the addition of insulation under the floor. In crawl spaces like this, it is wise to line the ground surface with landscape fabric (two layers minimum), covering the entire area underneath with 4 in. of 3/4″ crushed gravel. This treatment prevents weeds, and discourages animals with its sharp edges of gravel. It also has an attractive, clean look underneath which prevents excess moisture, moss etc., from accumulating in the shaded environment (Fig. 1.9).
Dave Petherick of Ontario, Canada has built a well-landscaped observatory on a typical sub-urban lot. He has incorporated a beautiful deck complete with trellis as an integral part of his observatory design. In fact, the deck is an extension of the observatory which allows for a large area for entertaining, barbequing etc. The trellis appears to be an extension of the gantry which transforms it into a “landscape feature” thereby creating a dual function for the observatory—both astronomy and gardening. It also serves to “hide” the true function of the gantry which would lessen the footprint area of the structure, the gantry portion appearing more like a garden trellis. Complete with shutters on
Fig. 1.7 Gerald Dyck’s Compact Observatory, well-protected from the elements (Courtesy of Gerald Dyck)
Another random document with no related content on Scribd:
Psammoma of Dorsal Cord, 38 of Table (after Charcot).
PROGNOSIS.—The prognosis of spinal tumors is generally very unfavorable. Syphilitic cases are of course the most hopeful, but even in these cases it is only when they are recognized early that much can be expected. A gumma that has grown to any dimensions will have so compressed the cord that even when the tumor is melted away by specific treatment its effects will remain.
DURATION AND TERMINATION.—Most cases of spinal tumor last from about six months to three years. Occasionally death may result, as from a rapidly-developing sarcoma, in less than six months, and somewhat more frequently in slowly-developing tumors, or in those which are held more or less in abeyance by treatment the sufferings of the patient are prolonged to four or five years or more. Hemorrhages into or around the growths sometimes take place, and are the cause of death, or more frequently of a sudden aggravation and multiplication of severe symptoms. Death sometimes takes place from the complete exhaustion which results from the disease and its accompanying secondary disorders, such as bed-sores, pyelitis, etc. Occasionally death results from intercurrent diseases, such as pneumonia, infectious fevers, etc., whose violence the weakened patient cannot well withstand. Sometimes the symptoms of a rapidly-ascending paralysis appear, probably due to an ascending myelitis or meningo-myelitis.
COMPLICATIONS AND SEQUELÆ.—Spinal tumors are sometimes complicated with other similar growths in the brain or the evidences of the same constitutional infection in other parts of the body In one case of cysticercus of the cord sclerosis of the posterior columns was also present.
TREATMENT.—The treatment of spinal tumors can be compressed into very small compass. In cases with syphilitic history, or when such history is suspected, although not admitted, antisyphilitic remedies should be applied with great vigor. It should be borne in mind, however, that even in syphilitic cases after destruction of the cord by compression or softening specific remedies will be of no avail. In tubercular cases and in those in which the system is much run down tonics and nutritives are indicated. Bramwell11 advises an operation in any case in which the symptoms are urgent, in which the diagnosis clearly indicates the presence of a tumor, when there is no evidence of malignant disease, when the exact position of the growth can be determined, and when a vigorous antisyphilitic treatment has failed to produce beneficial results. As some meningitis, meningomyelitis, or myelitis is usually present in cases of spinal tumor,
treatment for the complication will assist in relieving the torments of the patient. Anodynes, particularly opium and its preparations, should be used freely in the later stages of the affection. Bromides and chloral are of little value except in association with opiates. Operation offers even less hope than in brain tumor, but in very rare cases should be taken into consideration.
11 Diseases of the Spinal Cord, Edinburgh, 1884.
No. Sex and
Age.
TABLE OF FIFTY CASES OF SPINAL TUMOR.
Clinical History
1M. 33.Paresis of forearms, left worse. Paraplegia, then paralysis of all limbs; paralysis of intercostals. Contractures of hands, then of feet. Pain and stiffness of neck on motion. Wasting of interossei. Diplegic contractions of legs. Only partial paralysis of sphincters. Sensation perfect. Bedsores. Duration, thirteen months.
Path. Anat. and Location. Remarks.
Glioma; syringo-myelus. Dilated lymphatics.
T. Whipham, Trans. Path. Soc. London, 1881, xxxii. 8-12.
Entire length of cord, and involving medulla oblongata. Upper four inches of cord greatly enlarged.
2 F —.Constricting pains about abdomen. Paresis of legs. Persistent subsultus. Temporary improvement after labor General paralysis. Scoliosis.
Glio-myxoma. In gray columns from medulla oblongata to cauda equina.
Schueppel, Arch. d. Heilk., viii. Bd., 1867 (quoted by Rosenthal).
3M. 15.Paresis of left arm. Pain back of neck. Later, paralysis of left arm, and wasting of arm, shoulder, and neck muscles. Slight paresis of Gelatinous tumor left side of cord, and involving in S. Wilks, Lectures on Dis. of Nervous
right arm. Prolonged vomiting. Constriction of neck; dysphagia; paralysis of chest. some parts the gray matter
From medulla to sixth cervical vertebra. System, p. 266.
4M. 18.Paresis of left leg, increasing; some atrophy
Weakness in left arm. Later, numbness in both legs. Contracture of fingers. Some mental confusion. Left hand and leg livid and cold. Hyperæsthesia of left leg; anæsthesia of right leg, perineum, penis, scrotum, rectum, and inguinal region, and of left arm. Right arm normal. Islands of heat and cold in leg, and of cold in arms. Left ankle clonus. Left pupil contracted. Vomiting. Dysphagia. Occipito-cervical pain and contracture of cervical muscles. Leg contractures and tremor. Later, hyperæsthesia disappeared. Incontinence of urine. Patellar and skin reflexes increased. Facial spasm. Amblyopia, optic neuritis, diplopia, deafness, paralysis of left abducens; pupils contracted. Sacral bed-sores. Thick speech.
Round-celled sarcoma or glio-sarcoma, growing from ependyma of central canal, causing hydromyelia, softening, and secondary degeneration. Dura mater thickened. Brown exudate in cord and base of brain.
Schultze (F.), Arch. f. Psychiat., Berlin, 1878, viii. 367-393, 1 pl.
From medulla oblongata to dorsal cord.
5 F. 48.Pain in abdomen and down legs, worse on left side. Tonic spasm in flexors and adductors of thighs. No anæsthesia. Two months before death paralysis of sphincters. Great emaciation. Tumor (psammoma), growing from dura mater on right side in cervical region.
J. Hutchinson, Jr., Tr Path. Soc. Lond., 1881-82, xxxiii. 23, 24.
Upper part of cervical region.
6 Pain in arms. Contracture of fingers of right, then left side. Numbness in right foot, then upward, Sarcoma of left post. aspect of E. Long Fox, Bris. Med.-
then left foot. Girdle feeling. Priapism and dysuria. Complete anæsthesia, later, up to third rib, with paralysis of legs and paresis of fingers. Respiration diaphragmatic. Legs very jerky. Later, arms paralyzed.
cord; adjacent cord compressed and soft. Belt of yellow substance enveloped cord to cauda equina. Between cervical bulb and second cervical vertebra.
7 F 31.Pain, stiffness in neck; pain radiating, aggravated by jarring. Sudden paralysis of both arms; next day paralysis of legs, incomplete. Partial anæsthesia. Marked skin reflexes in legs. Patellar reflexes retained, weaker on right than left.
Dyspnœa. Profuse perspiration. Cardiac irregularity. Day before death temperature in right axilla 100°; left, 102.2°.
Gumma of dura mater two inches long, with intercurrent hemorrhage; flattening and softening of cord, with secondary sclerosis.
Chir Journ., 1883, i. 100106, 2 pl.
Charles K. Mills, Philada. Med. Times, Nov 8, 1879, p. 58.
From first to fifth cervical vertebra.
8M. 34.Pain in back of neck, with stiffness and torticollis. Paresis of arms; later, of legs. Anæsthesia of arms, then of legs; also paræsthesia of legs. Late symptoms: shortening and great rigidity of neck, with choking sensation (girdle sensation at neck).
Dimness of vision. Atrophy of arms and less of legs. Complete paralysis of arms, almost complete of legs. Electro-contractility preserved.
Gumma of dura mater; caries, probably syphilitic, of vertebræ. Abscess. Total (almost) transverse
Charles K. Mills, Philada. Med. Times, Nov 8, 1879, p. 58.
Violent skin reflexes in legs. Involuntary evacuations and incomplete priapism. Severe pains in knees and ankles. No acute bed-sores. Paroxysms of dyspnœa. Average temp. for two weeks before death, M. 97.9°, E. 98.3°. sclerosis of cord. Secondary degeneration. Some softening above and below tumor Cervical nerves compressed and atrophied.
From second to fifth cervical vertebra; most in front.
9M. 43.Pain between shoulders. Numbness in right hand and arm, with weakness and swelling. Numbness in left arm, which spread over chest and abdomen. Unable at first to lie down. Felt as though encased in armor Pain in back of neck. Tongue protruded to right. Exaggerated reflexes in legs. Right arm and leg weaker than left. Vertigo. Dysphagia. Sense of constriction about neck. Breathing impaired.
At third cervical vertebra, to right of front of cord. Destruction of opposite vertebra. E. H. Clark, Bost. Med. and Surg. Journal, 1859-60, lxi. 209-212.
10 No record of symptoms especially referable to the cysticercus. Symptoms of tabes dorsalis. Cysticercus in substance of cord. Lesions of tabes dorsalis. On level with third cervical nerve. Geo. L. Walton, ibid., vol. cv. p. 511.
11M. 25.Pain in back of neck; stiffness. Numbness of left hand. Gradual loss of power of left arm. Jerking of arm. Paresis of left leg. Constriction of upper chest. Right limbs involved, and eventual complete paralysis of trunk and extremities. Fibro-sarcoma at level of fourth cervical nerves. Cord compressed. H. A. Lediard, Tr. Path. Soc. Lond., 188182, xxxiii. 2527.
Severe headache. Last three days absolute anæsthesia of arms and legs. No ophthalmoscopic changes. Constipation and dysuria.
12 F 25.Œdema of ankles; pain in legs; afterward numbness, formication, and stiffness of legs. Painful contractures in upper extremities. Slight left scoliosis. Abdominal pains. Paresis of arms. Fingers flexed. Fever. Respiration became involved, and bowels and bladder paralyzed. Mind clear Died in attack of suffocation Duration, two years and three months.
Fibroma, size hazelnut, under pia mater
Bernhuber, Deutsch. Klin., Berlin, 1853, v. 406.
Between fourth and fifth cervical vertebræ.
13M. 16.Restlessness. Cramps in pharynx on swallowing. Excitability Delirium. Hallucination. Pain in the neck. On touching neck general cramps. Grimaces. Salivation. In three days complete paraplegia. No fever. Sudden change. Pulse 120. Pupils alternating. Blepharospasm. Irregular respiration. Pulmonary œdema. Suspicion of hydrophobia, because patient had been with hydrophobic dog; when offered coffee had symptoms simulating rabies. Sarcoma.
Extending from fifth to seventh cervical nerve on anterolateral face of cord, compressing left half and penetrating into right half, so that anterior longitudinal fissure described arc of circle around it.
14 F. Paresis and partial anæsthesia in all limbs for many months, most marked on left side. Brain and special senses unaffected. Had a tumor at bottom of right side of neck. Extensive bed-sore. Carcinoma.
Adamkiewicz, Arch. de Neurol., Paris, 1882, iv. 323-336, 1 pl.
Tumor caused partial absorption of sixth cervical vertebra. Cord compressed J. W. Ogle, Tr. Path. Soc. Lond., 1885, 6, vii. 40, 41.
and twisted. Right lateral aspect especially affected. Cord atrophied. At level of sixth cervical vertebra.
15 F 34.Pain in right foot, and paresis increasing to paraplegia. Paresis of arms. Contractures of legs. Hyperæsthesia in both legs up to crest of ilia. Later, great pain; paralysis of sphincters. Bedsores. Sarcoma, growing from dura mater; nerves passing through and over tumor Cord congested and pushed to one side. Thin, but not softened. Growth resembled psammoma.
T Whipham, Tr. Path. Soc. Lond., 1873, xxiv. 15-19.
Between sixth and seventh cervical nerves of left side.
16M. 57.Pain in right arm. Numbness in hand, and paresis. Paresis and coldness of left leg. Some anæsthesia and wasting of right leg. Later, paraplegia. Diminished reflexes. Contractures. Constriction sense about legs and abdomen. Triceps, deltoid, and serratus magnus of right side paralyzed. Incontinence of urine, difficult defecation, decubitus, fever Abdominal muscles Myxoma from arachnoid. Cord compressed and softened on right postero-lateral side.
Secondary Pel (P. K.), Berlin. Klin. Wochensch., 1876, xiii. 461-463.
paralyzed. Later, other muscles of arms paralyzed. Complete anæsthesia of legs. Dyspnœa, œdema of lungs. degeneration. Some œdema of brain.
At sixth and seventh cervical vertebra on postero-lateral surface of cord.
17 F 35.First, pain in right arm, weakness in right hand. Then paralysis almost complete in arms, and impaired sensation. In legs paralysis complete, sensation impaired. Alternate incontinence and dysuria. Ankle clonus and increased knee-jerks and plantar reflex. Tapping biceps causes reflex in little and ring fingers. No atrophy or bed-sores. Cold on one side, hot on other. Pain and little swelling over sixth cervical vertebra. No eye symptoms. Brain clear Inability to turn head. Before death respiratory paralysis and bed-sores. Duration, fifteen months. Spindle-cell sarcoma, springing from arachnoid and destroying cord by pressure, except posterior columns. Cord below tumor soft.
At sixth cervical vertebra.
18M. 50.Paresis in right arm. Stiffness in neck and back. Paralysis of all extremities gradually developed. Glioma in right half of cord. Old hemorrhages in adjacent parts and in medulla oblongata. A more recent hemorrhage in dorsal cord.
E. Long Fox, Bris. Med.Chir. Journ., 1883, i. 100106, 2 pl.
In lower cervical region. Schueppel, Arch. d. Heilk., viii. Bd., 1867 (quoted by Rosenthal).
19 Coldness, numbness, violent pains, first in left arm, later in both legs. Paralysis of all limbs and Tubercle, large as hazelnut. Chvostek, Med. Press,
muscles of trunk. Atrophy Reactions of degeneration. Violent leg reflexes.
Consecutive myelitis of adjacent parts and left anterior horn. In lower cervical region.
20M. 45.Interscapular pain. Chest-pressure and dyspnœa. Paræsthesia and pain in legs. Spastic paralysis. Difficulty in stools; bloody urine and dysuria. Œdema of legs. Bed-sores. Kypho-scoliosis. Pain on pressure over spine. Paralysis of left leg, paresis of right, some anæsthesia of both.
Broncho-pneumonia, fever
Phlegmon of dura mater, compressing cord. Some infiltration of tissues of throat and mediastinal space.
33-39, 1873 (quoted by Rosenthal).
Mankopff (E.), Berl. Klin. Wochensch., 1864, i. 3346, 58, 65, 78.
From seventh cervical to second dorsal vertebra.
21M. 22.Pain in back and side of neck and in limbs. Marked pain in sternal region on coughing. Pressure and jarring cause pain. Rapid loss of power in both arms Feeble and slow movements of thighs, legs, and feet. Right deltoid and flexors of fingers much wasted. No paralysis of face. Knee-jerks exaggerated. Later, complete paralysis, including bladder and rectum.
Tumor of membrane. Cord beneath compressed and degenerated. Lower cervical and upper dorsal region.
H. C. Wood, “Proceedings of Philadelphia Neurological Society,” Medical News, vol. xlviii. No. 9, Feb. 27, 1886.
22 F 50.Pain in neck, shoulders, and chest. Stiffness of neck, back, and arms. Chest fixed; breathing diaphragmatic. No paralysis or altered sensation. Secondary cancer of vertebræ. Cervical region. Gull, by Wilks, in Lect. on Dis. of Nerv System
23 F 40.Severe pain in back. At height complete paralysis in legs, some paresis in arms. Variable anæsthesia. Girdle sensation and mammary pain. Lively and distressing reflexes. Contractures in legs. Bed-sores and paralysis of sphincter of bladder. Toward close rigors (pyæmia?).
Fibro-cyst on right side, between cord and dura, and between anterior and posterior nerves.
Risdon Bennett, Tr Path. Soc. Lond., 185556, vii. 41-45.
Top of dorsal region.
24M. 30.Cough, dyspnœa, wasting, simulating phthisis. Pain in back of neck and shoulders. Pain in joints; paresis of legs and bladder Pain in chest. Paresis of arms. Later, increased paralysis, bedsores, sweating.
Tumor, size of hazelnut, inner anterior surface of dura mater Flattening and softening of cord.
Gull, in Guy's Hosp. Rep., (quoted by Wilks in Lectures on Dis. Nerv. Syst., p. 264).
Top of dorsal region.
25 F. 43.Pain in shoulders, chest, and sides. Contractures of legs; heels to nates. No anæsthesia. Later, retention of urine and bed-sores. Incessant pain in back and abdomen.
Fibro-nucleated tumor from inner surface of dura mater Opposite third dorsal vertebra.
26 F 43.Pain in chest and shoulder, then in legs. Paresis of legs. Contractures and jerking of legs. Spasm of abdominal muscles. No anæsthesia. Paresis of bladder and rectum. Wasting and bed-sores. Finally, paresis increased, but never complete paralysis. Duration, nine months.
Fibro-nucleated tumor, size of a bean, from dura mater Cord compressed backward, and softened.
Gull, by Wilks, ibid
Wilks, Trans. Path. Soc. Lond., 185556, vii. 37-40.
Opposite third dorsal vertebra.
27M. 24.Paraplegia. Depressed reflexes; girdle symptom. Partial anæsthesia. Dysuria. Vomiting. Pulse weak and intermittent. Partial recovery from paralysis, and anæsthesia in left leg, and reflexes in right foot regained. Later, complete paraplegia, anæsthesia, and bed-sores. Duration, five months.
28 F 44.Paresis in legs. Spine hypersensitive and inflexible; least attempt at bending causes great cervico-brachial pain. Paræsthesia; sense of falling out of abdominal viscera through abdominal walls. Pains in extremities increasing, and involving right shoulder, intercostals on both sides, and lumbar region. Paralysis of right arm (first); complete paralysis of leg. Excessive spinal tenderness. Loss of sensation (partial) in legs, body, and right arm. Later, dyspnœa, then dysuria, then complete inability to empty bowels or bladder. Great tympanites. Girdle sense above umbilicus, and finally complete paralysis and anæsthesia below this band. Sense of twisting of legs and feet, so that latter seemed close to face. Œdema. Later, paresis of left arm. One small bed-sore.
29 F 42.Projection of seventh, eighth, ninth, tenth, and eleventh dorsal vertebræ. Numbness below ankles, and early girdle sensation. Peronei and anterior tibial muscles first involved; then all legmuscles, then sphincters, then arms. Died in a fit.
Probable gumma.
Middle dorsal region.
B. G. McDowell, M.D., Dubl. Q. J. Med. Sci., 1861, xxxii. 299303.
Alveolar sarcoma.
Eighth and ninth dorsal vertebræ.
G. W H. Kemper, Journ. Nerv. and Ment. Dis., xii. No. 1, Jan., 1885.
Round-celled sarcoma. The anterior columns soft opposite tumor. Bodies of seventh, eighth, ninth, and tenth vertebræ soft.
Opposite
E. Long Fox, Brit. Med. Journ., 1871, p. 566.
seventh, eighth, ninth, and tenth dorsal vertebræ.
30 F —.Ill-defined hemiplegia; later, paraplegia, with contractures and rigidity Gumma and syringo-myelus. Small cavities in anterior cornua. At ninth dorsal vertebra anterior aspect. Taylor, Lancet, 1883, p. 685.
31 M. 7.Paraplegia, except adductors and rotators of thigh. Reflex contractures; most intense from irritation of penis and scrotum. Rigidity of legs. Complete anæsthesia of lower half of body. Later, anuria, incontinence of feces. Anal sphincter reflex; figured stools. Cystitis. Pain on percussion in dorsal region. Pain in back. Complete paraplegia. Very late, brain symptoms. Duration, nine months.
32 F 46.Fixed pain in left iliac region. Paresis in left leg, increasing to paraplegia. Formication. Girdle sensation. Incomplete, increasing to complete, anæsthesia of legs. Spontaneous twitchings. Bladder and sphincter ani paralyzed. Bed-sores. Duration, one year
Tubercle (?).
Cord soft for two inches. Tenth dorsal vertebra. Geoghegan, Dublin Med. Press, 1848, xix. 148-151.
Fibroma (?) from inner surface of dura. Cord hollowed out and softened. Interval between tenth and eleventh dorsal vertebræ. William Cayley, Tr Path. Soc. Lond., 186465, vol. xvi. 21-23.
33M. 30.Hyperæsthesia; later, anæsthesia in legs; then complete paraplegia.
Tubercle size of pea. Adjacent myelitis. In Chvostek, Med. Presse, 33-39, 1873
lower dorsal region. (quoted by Rosenthal).
34M. 31.Ataxia; stiffness of legs and cramps in abdomen and legs. Slight nystagmus. Difficulty in forming words. Ataxia of arms. Slight wasting of legs, especially of left. Lumbar pains; abdominal cramps. Dysuria. Impotence. Later, increased spastic state of legs. Mind depressed and emotional; attempts at suicide. Anuria. Bed-sores. Urine albuminous. Duration, one year
35 F. 50.Pains in limbs (thought to be rheumatic). Paresis in legs. Hyperæsthesia in right leg; burning pains alternating with sense or coldness.
Myxoma of dura mater 3 inches long. Dura mater of brain contained fluid and lymph. Dorsal region, left side.
Cancer of vertebræ (sarcoma?).
Shearman, Lond. Lancet, vol. ii. 1877, p. 161.
Dorsal region. Gull, by Wilks, Dis. Nerv. Syst.
36 F. 35.Paresis of left leg; soon of right leg. Pain in back and left side. Tonic spasms of legs. Darting pains in knees. Partial anæsthesia. Exalted plantar reflexes. Dysuria. Later, complete paraplegia and anæsthesia; violent reflexes; severe pain in back. Bed-sores. Duration, seven and a half years.
Tumor, osseous or fibrous, three-fourths of an inch long, growing from dura mater.
Cord flattened, and softened below tumor. Lower part of dorsal cord.
37 F. 28.Weakness in legs. Aching and shooting pains in legs. Numbness and formication. Slight spasm in legs. “Felt as if ground was some distance below feet.” Œdema of ankles. Later, numbness extended to abdomen. Paralysis of bladder Hyperæsthesia in right leg. Obstinate constipation. Bed-sores. Some paralysis of respiratory muscles. Duration, fourteen months.
H. Ewen, Tr. Path. Soc. Lond., 184850, i. 179.
Tubercle the size of cherry, which had almost obliterated cord. Tubercles in lungs, bowels, and uterus. BedS. O. Habershon, M.D., Guy's Hosp. Rep., London, 1872, 3d S., xvii. 428-436.
sore had opened spinal canal.
Lower part of dorsal cord.
38M. 63.Progressive paresis of left leg for five years. Right leg then paretic. Paralysis then in left leg. Rigidity on extension of right leg. Paroxysms of clonic spasms in right leg. Joint pains, sciatic pains. In left leg, hyperæsthesia, in right leg, anæsthesia. Plantar reflex retained; other reflexes exaggerated. Diplegic contractions in right leg from irritation in left. Late symptoms: purulent urine, with retention; chest and lumbar pains like bone pain; extension changed to flexion; swelling of legs and ecchymosis; sacral and other eschars.
Psammoma adherent to dura mater. Cord softened. Ascending degeneration in posterior columns, and descending degeneration of lateral columns.
Charcot, Arch. de Physiol., Paris, 1869, ii. 291-296.
In dorsal region just above lumbar enlargement, anterior left side.
39M. 20.Paralysis of lower extremities; tremor; exaggerated reflexes, hyperæsthesia of trunk; bed-sores. Œdema of feet. Fever. Pus in urine.
Organized blood-clot exterior to dura mater Cord compressed and softened.
C. B. Nancrede, Am. Journ. Med. Sci., O. S., lxi. 156.
Opposite lower dorsal and upper lumbar
40 F. 38.Pain around abdomen, in back, and legs. Paraplegia. Anæsthesia and tingling of feet and legs. Paralysis of bladder
Hydatid cysts of vertebræ (?) and spin. canal. S. Wilks, Dis. Nerv Syst., p. 265.
Lower part of spinal canal (probably lumbar region).
41 F 23.Bronzing of skin for two years; then headache, giddiness, fever Choreic movements in left arm, then in leg, then general. Bronzing increased. Vomiting after meals. Duration, two years and two months. Tumor, consisting of granular matter, with a few nerve-fibres and cells, springing from centre of cord backward to posterior fissure. Cord slightly widened. Suprarenal capsules large and nodulated. Lumbar enlargement.
42 10 ms. Twitching and convulsive movements of right leg. After removal of exterior tumor the movements ceased. Child died of peritonitis.
Tumor outside of sacrum, and also protruding through sacral opening. Reported to have been behind and pressing upon cord (?). Fatty growth within membranes.
W H. Broadbent, Trans. Path. Soc. Lond., 1861-62, viii. 246.
Arthur Johnson, ibid., 185657, viii. 28, 29.
43 F 54.Paresis, first of left arm and leg; then paralysis ofHydatid cyst.H. S. Wood,
these and of right arm and leg. Pain in back and hips early; then, suddenly, darting pains and incontinence of urine. Paræsthesia of left arm and leg; no anæsthesia. Coma.
Cyst also in liver Fluid beneath membranes of cord and brain. At first and second left sacral foramen, opposite last lumbar and upper three sacral vertebræ.
44M. 46.Fibrillary twitching. Increased patellar reflexes. Paræsthesia and hyperæsthesia in legs, disappearing. Constriction of chest (?). Headache. Dysuria for two years. Straining at stool. Indigestion. Bloody vomiting. Cardiac palpitation; intracardial murmurs; slow pulse. Swollen inguinal glands. Variations in temperature. Bed-sores.
45M. 38.Pain in legs. Œdema. After two years could not lie down: rested on hands and knees. Paralyzed in legs; pain in seat. Anæsthesia in legs, not complete in right. Paræsthesia in left. Dysuria and constipation. Before death had incontinence with hæmaturia, and was able to lie down.
Australian Med. Journ., 1879, N. S. i. 222.
Glioma. At filum terminale, upper part. Lachman, Arch. f. Psychiat., Berl., 1882, xiii. 50-62, 1 pl.
A lobulated tumor from pia mater at lower end of spinal canal, surrounded by nerves of cauda equina. Structure not made out. At cauda equina. W W Fisher, Tr Prov M. and S. Ass., 1882, x. 203208.
46 This case had symptoms of posterior spinal sclerosis, which possibly had no relation to Myo-lipoma attached to W R. Gowers, Tr
growth, according to reporter conus medullaris. Crescentic, clasping cord from anterior to posterior fissure. Nerveroots of cauda equina imbedded in it. Contained striated muscular fibres.
47 Und. 1 yr Spina bifida (?); hydrocephalus; convulsions, bloody stools; partial paraplegia. (Above symptoms came on after closing of sacral opening by surgical operation.)
Congenital sacral neuroma amyilinicum.
Path. Soc. Lond., 187576, xxvii. 1922.
48M. 30.Pain in back; abdominal girdle sensation. Pain in legs; paraplegia; nearly complete anæsthesia; paralysis of bladder; bed-sores.
Aneurism, eroding vert. and compressing cord. Location not given.
49M. 54.Paralysis of both legs, of sphincter ani, and of bladder; urine alkaline, with pus and blood. Partial anæsthesia. Pyonephritis.
Gumma from inner layer of dura mater and involving pia mater. Location not given.
W F Jenks, M.D., Trans. Path. Soc. Philada. (1871-73), 1874, iv 190192.
Wilks, Dis. Nerv. Syst.
Delafield, N. Y Med. Rec., 1875, x. 131.
50 Stillborn.
Tumor, size of head of child two years old, projected between legs Virchow, Monatschr. f. Geburtsk., Berl., 1857, ix. 259-262.
from spinal column. Nerves of cauda equina over anterior part. Some bone in tumor (dermoid cyst?).