The Journal of the New York State Nurses Association, Volume 51, Number 1
THE JOURNAL
of the New York State Nurses Association
Volume 51, Number 1
n Editorial: Impressions
by Anne Bové, MSN, RN-BC, CCRN, ANP; Audrey Graham-O’Gilvie, DNP, RN, ACNS-BC, CCRN-k; Meredith King-Jensen, PhD, MSN, RN; Alsacia L. Sepulveda-Pacsi, PhD, DNS, RN, FNP, CCRN, CEN; and Coreen Simmons, PhD(c), DNP, MSN, MPH, RN
n Emergency Department Discharge With the Virus Without Return to the Hospital Within 72 hours Using Electronic Medical Records by Kenrick Cato, PhD, RN; Eugene Kim, MD; Christopher Knaplund, MPhil; Marie Romney, MD; Dana Sacco, MD; Lauren Chernick, MD; Alsacia L. Sepúlveda-Pacsi, PhD, RN; Sarah Rossetti, PhD, RN; Maxim Topaz, PhD, RN; Richard Trepp, MD; Bernard P. Chang, PhD, MD; and Katharina Schultebraucks, PhD
n A Correlational Study of the Relationship Between Nurses’ Pain Assessment and Patients’ History of Substance Use by Valerie A. Esposito Kubanick, PhD, RN, PMH-BC
n When a Medication Error Turns Into an Ethical Dilemma by Irene Auteri, PhD, RN; Bridget Maley, PhD, RN, CNE; and James A. Ferguson, MD, MPH
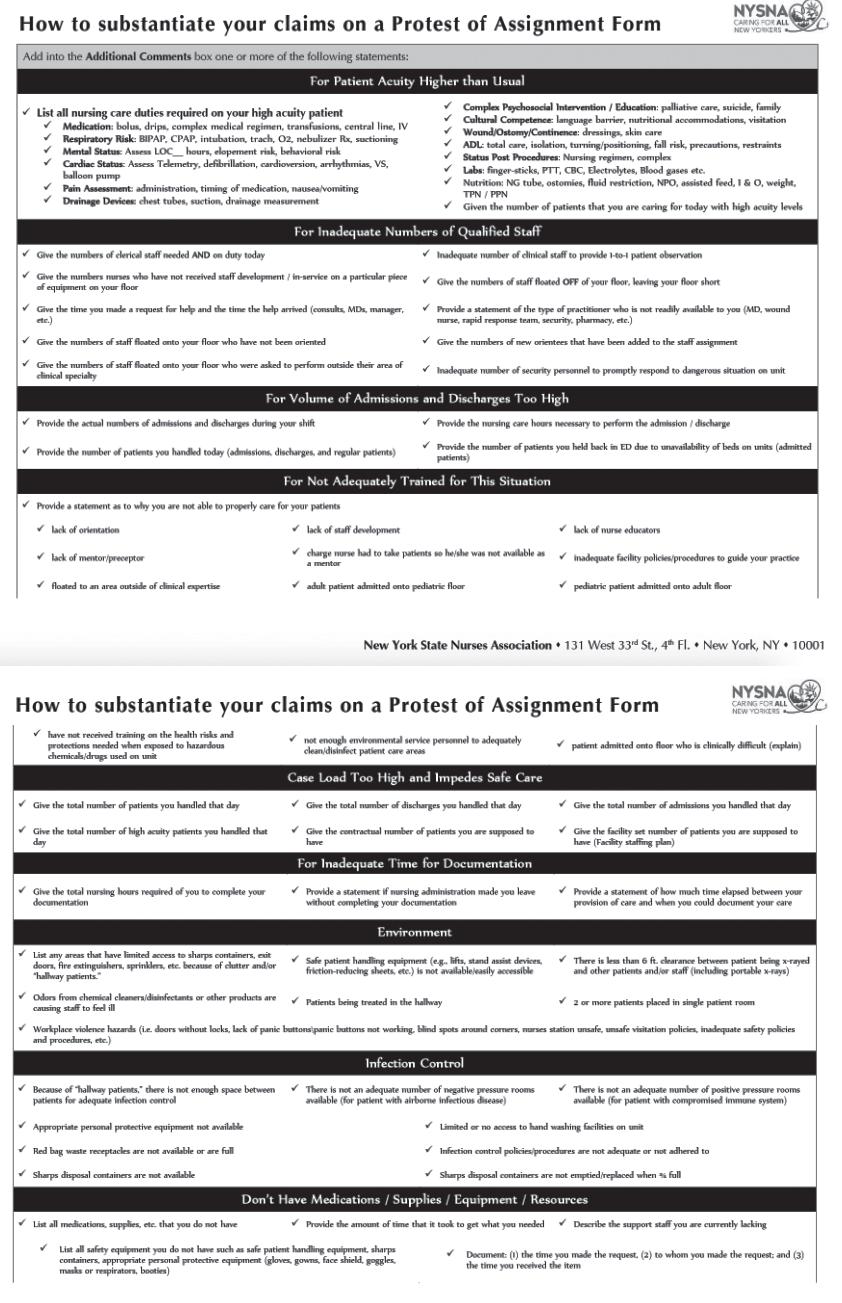
n Assignment Under Protest: A Nurse’s Rights and Responsibilities by Carol Lynn Esposito, EdD, JD, MS, RN-BC, NPD
n What's New in Healthcare Literature
n CE Activities: A Prognostic Model for COVID-19 Progression to Severe Disease: Discriminating Emergency Department Discharge With the Virus Without Return to the Hospital Within 72 Hours Using Electronic Medical Records; A Correlational Study of the Relationship of Nurses’ Pain Assessment and Patients’ History of Substance Use; Assignment Under Protest: A Nurse’s Rights and Responsibilities
THE JOURNAL
the New York State Nurses Association Volume 51, Number 1 n Editorial: Impressions
by Anne Bové, MSN, RN-BC, CCRN, ANP; Audrey Graham-O’Gilvie, DNP, RN, ACNS-BC, CCRN-k; Meredith King-Jensen, PhD, MSN, RN; Alsacia L. Sepulveda-Pacsi, PhD, DNS, RN, FNP, CCRN, CEN; and Coreen Simmons, PhD(c), DNP, MSN, MPH, RN
n A Prognostic Model for COVID-19 Progression to Severe Disease: Discriminating Emergency Department Discharge With the Virus Without Return to the Hospital Within 72 hours Using Electronic Medical Records 5 by Kenrick Cato, PhD, RN; Eugene Kim, MD; Christopher Knaplund, MPhil; Marie Romney, MD; Dana Sacco, MD; Lauren Chernick, MD; Alsacia L. Sepúlveda-Pacsi, PhD, RN; Sarah Rossetti, PhD, RN; Maxim Topaz, PhD, RN; Richard Trepp, MD; Bernard P. Chang, PhD, MD; and Katharina Schultebraucks, PhD
n A Correlational Study of the Relationship Between Nurses’ Pain Assessment and Patients’ History of Substance Use 17 by Valerie A. Esposito Kubanick, PhD, RN, PMH-BC
n When a Medication Error Turns Into an Ethical Dilemma
by Irene Auteri, PhD, RN; Bridget Maley, PhD, RN, CNE; and James A. Ferguson, MD, MPH n
Carol Lynn Esposito, EdD, JD, MS, RN-BC, NPD
n CE Activities: A Prognostic Model for COVID-19 Progression to Severe Disease: Discriminating Emergency Department Discharge With the Virus Without Return to the Hospital Within 72 Hours Using Electronic Medical Records; A Correlational Study of the Relationship of Nurses’ Pain Assessment and Patients’ History of Substance
THE JOURNAL
of the New York State Nurses Association
n The Journal of the New York State Nurses Association editorial board
Anne Bové, MSN, RN-BC, CCRN, ANP
Alsacia L. Sepulveda-Pacsi, PhD, DNS, RN, FNP, CCRN, CEN Clinical Instructor Registered Nurse III New York, NY New York-Presbyterian Adult Emergency Department New York, NY
Audrey Graham-O’Gilvie, DNP, RN, ACNS-BC, CCRN-k Coreen Simmons, PhD(c), DNP, MSN, MPH, RN Assistant Professor Professional Nursing Practice Coordinator Touro College School of Health Sciences Teaneck, NJ Hawthorne, NY
The information, views, and opinions expressed in The Journal articles are those of the authors, and do not necessarily reflect the official policy or position of the New York State Nurses Association, its Board of Directors, or any of its employees. Neither the New York State Nurses Association, the authors, the editors, nor the publisher assumes any responsibility for any errors or omissions herein contained.
The Journal of the New York State Nurses Association is peer reviewed and published biannually by the New York State Nurses Association. ISSN# 0028-7644. Editorial and general offices are located at 131 West 33rd Street, 4th Floor, New York, NY, 10001; Telephone 212-785-0157; Fax 212-785-0429; email info@nysna.org. Annual subscription: no cost for NYSNA members; $17 for nonmembers.
The Journal of the New York State Nurses Association is indexed in the Cumulative Index to Nursing, Allied Health Literature, and the International Nursing Index. It is searchable in CD-ROM and online versions of these databases available from a variety of vendors including SilverPlatter, BRS Information Services, DIALOG Services, and The National Library of Medicine’s MEDLINE system. It is available in microform from National Archive Publishing Company, Ann Arbor, Michigan.
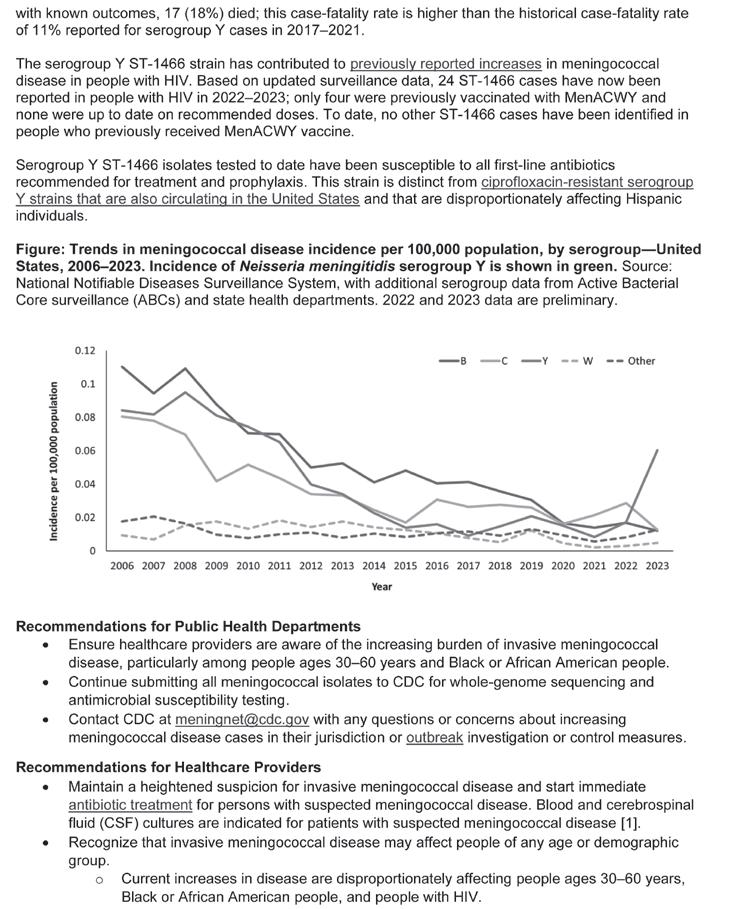
In 1961, writer and feminist Anaïs Nin wrote, “We don’t see things as they are; we see them as we are.” Authors presented in this edition of The Journal of the New York State Nurses Association are mindful of this human phenomenon and how it infuses health care with implicit biases. We naturally perceive life through our own eyes, experiences, and thoughts, but the profession of nursing entrusts us to practice in our patients’ best interests.
In “A Prognostic Model for COVID-19 Progression to Severe Disease: Discriminating Emergency Department Discharge With the Virus Without Return to the Hospital Within 72 Hours Using Electronic Medical Records,” symptom patterns lead to proper disease diagnosis and subsequent risk stratification. When providers disrupt disease patterns that are associated with implicitly biased diagnoses and care plans through electronic medical record (EMR)-patterned treatment and vaccination, resources are prudently utilized. Prognostic models enable health to be restored and lives saved.
In “A Correlational Study of the Relationship Between Nurses’ Pain Assessment and Patients’ History of Substance Use,” the author demonstrates how those who have used substances may not have access to accurate and responsible pain assessment. The author suggests “self-awareness” should be conditioned and trained in licensure programs to better help nurses astutely assess all patients without bias.
In “When a Medication Error Turns Into an Ethical Dilemma,” the authors discuss the ethical principle of veracity and how it should guide a nurse’s behaviors and subsequent actions. Adherence to this pillar of ethical nursing practice can sometimes place a nurse in an ethical dilemma. When a nurse fraudulently documents circumstances surrounding a medication error, the nurse’s lack of accountability can instigate a domino effect of adversity and biased delivery of health care when the self is prioritized over the patient.
The continuing educational offering in this issue, “Assignment Under Protest: A Nurse’s Rights and Responsibilities,” offers knowledge to nurses in providing data and evidence to protect their license and secondly, but very importantly, in being able to use the data from a completed protest form to combat and fight against bias and improve patient care in the healthcare setting.
Understanding and combating implicit biases in nursing is vital to recruiting and retaining an increasingly diverse workforce, building workplace engagement and belonging, and improving patient outcomes.
Anne Bové, MSN, RN-BC, CCRN, ANP
Audrey Graham-O’Gilvie, DNP, RN, ACNS-BC, CCRN-k
Meredith King-Jensen, PhD, MSN, RN
Alsacia L. Sepulveda-Pacsi, PhD, DNS, RN, FNP, CCRN, CEN
Coreen Simmons, PhD(c), DNP, MSN, MPH, RN
A
Prognostic model for CoVID-19 Progression to Severe Disease: Discriminating emergency Department Discharge With the Virus Without return to the Hospital Within 72 Hours using electronic medical records
Kenrick Cato, PhD, RN
Eugene Kim, MD
Christopher Knaplund, MPhil
Marie Romney, MD
Dana Sacco, MD
Lauren Chernick, MD
Alsacia L. Sepúlveda-Pacsi, PhD, RN
Sarah Rossetti, PhD, RN
Maxim Topaz, PhD, RN
Richard Trepp, MD
Bernard P. Chang, PhD, MD
Katharina Schultebraucks, PhD
n Abstract
Background: COVID-19 as a global pandemic overwhelmed healthcare and emergency service systems. Symptom progression can be heterogeneous and potentially associated with severe disease, including death. Many suspected COVID19 patients are initially evaluated in the emergency department (ED) setting. The ability of ED clinicians to reliably make informed clinical decisions based on heterogeneous acute care data is vital, but the currently available evidence to predict disease progression remains limited. The development of a prediction model aims to close this gap. We used routine clinical data from electronic health records (EHR) to classify encounters as: (1) discharged home with no return visit within 72 hours, or (2) admitted to the inpatient setting for greater than 24 hours or returned to the hospital within 72 hours of ED discharge with subsequent inpatient admission.
Methods: This retrospective observational study uses EHR data collected in the ED at one of the hotspots during the COVID-19 pandemic. We used boosted decision tree to classify deterioration and benchmarked this machine learning model using logistic regression and random forest.
Results: The data for 5,055 ED encounters from March 15 to May 5, 2020 (mean age = 54.34 ± 16.85; 44.54% female). Gradient boosted decision tree achieved high predictive accuracy to classify deterioration.
Conclusions: The clinical prognostic model successfully classified clinical course following ED evaluation based on statistical estimation of the progression of COVID-19 symptom severity. Such a model could provide frontline clinicians with robust quantitative information to support the anticipated clinical prognosis and plan acute care and disposition.
Keywords: Disease outbreaks, accurate predictions, prognostic models, treatment needs
Kenrick Cato, PhD, RN, Children’s Hospital of Philadelphia, Philadelphia, Pennsylvania; Eugene Kim, MD, Columbia University Irving Medical Center, New York, New York; Christopher Knaplund, MPhil, Sword Health, Greater New York, New York; Marie Romney, MD, NewYorkPresbyterian Hospital, New York, New York; Dana Sacco, MD, Emergency Medicine at Columbia University Medical Center, New York, New York; Lauren Chernick, MD, Emergency Medicine at Columbia University Medical Center, New York, New York; Alsacia L. Sepúlveda-Pacsi, PhD, RN, NewYork-Presbyterian Hospital, New York, New York; Sarah Rossetti, PhD, RN, Columbia University School of Nursing, New York, New York; Maxim Topaz, PhD, RN, Columbia University School of Nursing, New York, New York; Richard Trepp, MD, NewYork-Presbyterian Hospital, New York, New York; Bernard P. Chang, PhD, MD, Columbia University Irving Medical Center, New York, New York; Katharina Schultebraucks, PhD, Columbia University Data Science Institute, New York, New York
Introduction
Coronavirus disease 2019 (COVID-19) evolved into a global pandemic and a sustained international health threat. The pandemic is highly dynamic, with the risk to frequently overwhelm healthcare systems worldwide, including those of highly developed countries, and the pandemic has paralyzed economies globally. The anticipated impact of the worldwide outbreak of the severe acute respiratory syndrome coronavirus 2 (SARSCoV-2) is estimated to be similar in result to the Spanish flu of 1918, which was the deadliest influenza pandemic in human history (Morens et al., 2020). The respiratory syndrome caused by SARS-CoV-2 can lead to symptoms ranging from mild to very severe and may result in intensive care unit (ICU) admission or death. Mortality rates of COVID-19 vary dramatically by country and healthcare system, with case-fatality ratios at the time of writing of more than 10% (e.g., in the UK, France, Italy, and Belgium) and below 5% (e.g., in the USA and Germany) (Johns Hopkins University & Medicine, 2020). The mean hospital mortality rate reported in a systematic review is as high as 45% (range 5–72%, N = 83,619) across all severity levels (Aziz et al., 2020).
The ED represents a critical first point of entry in assessing and evaluating suspected COVID-19 patients. A significant proportion of suspected COVID-19 patients are first evaluated in acute care settings such as the ED. In the ED at Columbia University Irving Medical Center (CUIMC), the first confirmed COVID-19 case was March 1, 2020. Since SARS-CoV-2 is a novel virus with no safe and effective cure for COVID-19, ED staff need to rapidly learn and adapt management strategies as our understanding of the care of COVID-19 patients evolves. The need for the efficient utilization of intensive medical resources further increases when the rate of COVID-19 admissions accelerates quickly, resulting in cumulative cases exceeding ED and hospital capacities, as happened during several surges in multiple areas across the United States and worldwide.
In the initial phase of the local outbreak in New York City, the CUIMC ED maintained the standard of care that was in place before the COVID-19 epidemic. As the cases increased rapidly, including the number of severe cases, surge procedures were employed. Because of limited hospital resources, a vital component of the ED surge procedures was to send home patients with suspected cases of COVID and follow-up with telehealth (Greenwald et al., 2020). One approach to increase surge capacity is to minimize resource consumption by admitted patients, which depends on the accurate prediction of treatment needs and disease severity. Given the limited acute care capacities, acute care providers are frequently tasked to carry out risk stratification and to prognosticate disease severity to assess the future need of intensive medical care or inpatient admission. This prognostication depends on the timely identification of patients at low and high risk of approaching severe COVID-19, the latter being associated with a significantly higher mortality rate than mild disease (Gong et al., 2020).
However, given the heterogeneity in the early symptoms of COVID-19 during ED visits and the heterogeneity in symptom progression after early ED evaluation, the accurate prognosis of COVID-19 severity is a demanding, yet routine, task for the assessment of suspected COVID-19 patients. In improving resource utilization and maximizing patient care while avoiding the overloading of healthcare systems, inpatient admission decisions play a central role.
Admitting too many patients with less-severe disease progression is unfavorable, as it blocks resources for more severe cases. In contrast,
discharging patients who then develop severe symptoms is equally adverse and often worse. It leads to readmission later and wasted time that could have been important for adequate care and treatment. The prognosis of symptom severity thus plays an essential role during clinical evaluation at ED admission. Better information is needed to support the prospective assessment of COVID-19 severity using routinely available information at the time of clinical evaluation during ED admission. The discrimination between low and high risk for COVID-19 severity is crucial. It facilitates the evidence-based planning of acute care for COVID-19 while accounting for the limited availability of hospital beds and critical supplies in acute care facilities.
Early identification of risk for severe symptom progression could enormously benefit from the support of an accurate clinical prognostic model that runs directly on electronic health records (EHRs) of patients presenting in the ED with suspected COVID-19. A variety of generic prognostic models of patient deterioration exist for clinical use based on EHR. For example, Epic Systems Corporation has developed a Deterioration Index model predictive of a composite score of ICU-level care, mechanical ventilation, or death. While a large-scale evaluation of this predictive model in the setting of COVID-19 is still awaiting peer-review publication (Singh et al., 2021), such models that are developed on large datasets provide an informative benchmark for clinical prognostic models developed explicitly for COVID-19.
A recent systematic review of 145 prognostic models for COVID-19 (Wynants et al., 2020) identified eight predictive models, of which three are directly relevant for the present study (Zhu et al., 2020) and point to potential predictors for progression to severe disease. Despite this promising research to identify predictors of COVID-19 severity (Gallo Marin et al., 2021), no predictive model is currently recommended for the application in clinical practice (Wynants et al., 2020). However, given the pressing need to manage COVID-19 in a timely and resource-efficient way in the acute care setting, there is a clear indication to develop an accurate multivariable prognostic model to assist ED clinicians with prognosticating COVID-19 severity in clinical practice.
Our predictive modeling differs from traditional approaches. Currently, most predictive analytics attempts to understand characteristics of the patient that can be leveraged to realize their clinical course (Covino et al., 2020; Fu et al., 2020; Gidari et al., 2020; Myrstad et al., 2020). Our work utilizes patient elements like vital signs, but focuses more on modeling patterns of optional clinician behaviors that are proxies for expert clinician judgment (Rossetti, et al., 2019, 2021). We have found that well-performing models can be built by using expert signals contained in EHR interaction data (Rossetti et al., 2019). For example, we use variables like variation in clinician orders and timing and frequency of nursing observations, which are strong signals for expert clinical concern for patient deterioration (Rossetti et al., 2019).
The goal of the current development of a clinical prognostic model is to support the ED acute care for patients with suspected COVID-19 with a reliable predictive model to prospectively predict the risk of COVID-19 patients of returning with worsened symptoms after ED discharge and to differentiate such patients from subjects with low risk of readmission. We aimed to develop a clinical prognostic model using Machine Learning (ML) methodology (Kuhn & Johnson, 2013) to leverage EHR for clinical decision support, focusing on routinely available data from EHR and the
A Prognostic Model for COVID-19 Progression to Severe Disease: Discriminating Emergency Department Discharge
interaction of the ED clinicians with the EHR as candidate prognostic factors. The classification task for the present clinical prognostic model is to identify COVID-19 patients admitted to the ED with low predicted risk of severe progression who can be discharged safely without returning to the ED within 72 hours and to discriminate between these patients and COVID-19 patients with high risk of a more severe disease progression. Our modeling goal is to facilitate more effective evidence-based decision-making established on objective data.
methods
We performed a retrospective observational cohort study using EHR data from across two campuses of the single hospital system ED in Northern Manhattan, New York City, United States, serving a predominantly Hispanic and low-income urban population, with over 100,000 visits per year. For this system, the first confirmed COVID-19 case was March 1, 2020.
We collected data concerning COVID-19 care and routinely collected EHR data up to the time of admission. Routine data used included electronic data from nurses and physicians (including frequency, timing and values of vital signs taken, and physician orders written. Also, social determinants of health (SDOH) patient ZIP code–based data from the U.S. Census Bureau American Community Survey 2018, with five-year estimates, was used (i.e., mean household income, population density per square mile, and the number of households per square mile).
Inclusion and exclusion Criteria
The total study sample included 5,055 ED encounters of adults (age ≥ 18) between March 15 and May 5, 2020. During this period, our hospital experienced the first surge in COVID-related admissions (Figure 1). The study sample was limited to individuals who had at least one of the ICD-10 codes shown in Table 1, suggestive of possible COVID-19 infection based on CDC criteria for COVID-19 testing/guidelines, in addition to a review by an expert panel of 10 acute care clinicians. The rationale of including patients in the study sample is that clinical uncertainty would prevail about the outcome status (severe vs. mild COVID-19) in patients presenting with symptoms listed in Table 1. We excluded patients with do-not-resuscitate (DNR) orders or on hospice in the ED and patients who died during their ED visit. Since patients younger than 18 years of age are not admitted to one of the two campuses, but a separate ED not included in this study, the sample only includes adult patients. All ED clinical data after the individual patient disposition event was also excluded from our analysis.
ethics
Prior to the beginning of this study, approval from the Columbia University Institution Review Board was obtained, with informed consent waived.
Data Sources used for model Development and Validation
We randomly split the total available data into an 85% dataset for model discovery (training set) and a separate dataset of 15% for model validation on data not used to build the models (validation set) (Figure 2). Table 2 shows the distribution of predictor variables and the outcome for
both the training and validation set. We used five-fold cross-validation on the training set to assess the bias-variance trade-off (i.e., to examine “over” or “underfitting” of the models) (Cawley & Talbot, 2010).
outcome measures
The classification task for the clinical prognostic model is to discriminate between two clinically distinct populations of suspected COVID-19 patients: (1) patients who can be safely discharged home without returning to the ED within 72 hours, as opposed to (2) patients who return to hospital within 72 hours of ED discharge or patients who are transferred to the inpatient setting and remain there for 24 hours or longer.
Data Preprocessing
Categorical variables (e.g., gender, race, and ethnicity) were transformed into numeric labels and transformed into one-hot encoded numeric arrays using the OneHotEncoder function in scikit-learn v. 0.24 (Pedregosa et al., 2011) using Python v. 3.8. Continuous variables were standardized using the function StandardScaler in scikit-learn v. 0.24. Some continuous values (e.g., vital signs within range, age) were recoded to categorical based on previous work where we detected more signals in a categorical outcome than linear changes (Rossetti et al., 2019).
Clinical observations were used to calculate a modified MEWS20 score without the level of consciousness that we call a “vital sign score.” For categorical features, missing data may contain a signal; therefore, we did maintain those records. Finally, based on our previous work, we created new time-related continuous features to detect clinician workflow features and heightened clinical concern associated with patterns of increased surveillance (Kilaru et al., 2020; Rossetti et al., 2021). For example, the number of consult orders, number of vital signs and flow sheet comments, and shortest time between observations were used in modeling. Since there were five missing continuous values, we excluded one entire patient visit when that occurred.
Feature Selection
We retrieved available data from the health system EHR data warehouse at the time of visit to create data features, including demographic, historical visits, and encounter-related data. We also included visit-specific information, including timing, orders, medications administration, clinical notes metadata, laboratory results, vital signs, chief complaints, and discharge diagnoses. Features were selected based on previous research (Cecconi et al., 2020; Gallo Marin et al., 2021; Wynants, 2020) and clinical expertise, clinical relevance, and their availability in the EHR at our two sites. Prior studies frequently examined comorbidities, age, sex, lymphocyte count, C-reactive protein, body temperature, and creatinine as predictive factors (Wynants et al., 2020), which were thus included in the present study.
To select the features used in the model-building, we entered all features into random forest classifier (Breiman, 2001). We used mean accuracy loss among trees in the forest for every feature to identify which ones would enter into the model-building (Chandrashekar & Sahin, 2014). During this process, the number of features reduced from 52 to 33 (see Table 2).
n A Prognostic Model for COVID-19 Progression to Severe Disease: Discriminating Emergency Department Discharge
model Development
The aforementioned features, along with patient age at admission and gender, were applied to two tree-based learning algorithms XGBoost, random forest classifier, and also a logistic regression algorithm. Models were generated using scikit-learn package v. 0.23.2 in Python v. 2.0 and compared model performance by using a paired t-test implemented in the mlxtend v. 0.18.0 package. The validation set was not used in the model. Hyperparameters were chosen using grid search based on the training loss. The hyperparameters that were investigated in training were as follows: max_depth: [15, 30], child_weight: [5, 15], learning_rate: [0, 0.7]. After training with cross validation, we chose the following hyperparameters: max_depth: 30, min_child_weight: 15, learning_rate: 0.7, colsample_ bytree: 0.7, objective: binary: logistic subsample: 1, eta: 0.7.
model evaluation
Performance was assessed in terms of discriminatory accuracy using precision, recall, confusion matrix, and area under the ROC curve (AUC), as well as calibration using calibration plots. Bootstrapping was used to determine the 95% confidence interval for AUC. (Chandrashekar & Sahin, 2014). To compare the performance of our predictive model, we benchmarked the performance with different approaches. First, we compared the predictions of our model with a noninformative model that always assumes the worst for each patient. Second, we compared the prediction of our model with a population baseline (mean symptom severity as the predicted outcome of each patient), and, third, a personal baseline (individual baseline score of each person as the predicted outcome of each patient). We performed DeLong’s significance test to evaluate whether our model was significantly better than these benchmarks (DeLong et al., 1988).
results
We included 5,055 ED encounters of patients presenting with clinical problems as shown in Table 1 and the sample demographics are presented in Table 3. Shown in Table 4, the XGBoost decision tree achieved high predictive accuracy to classify (1) discharge vs. (2) readmission to the hospital within 72 hours (AUC of 0.90 (95% CI, 0.89–0.91), weighted averaged precision = 0.83, weighted averaged recall = 0.83, weighted averaged f1-score = 0.83). It outperformed the random forest (AUC = 0.88 [0.86, 0.89], weighted averaged precision = 0.82, weighted averaged recall = 0.82, weighted averaged f1-score = 0.82) and logistic regression benchmark models (AUC = 0.88 [0.79, 0.81], weighted averaged precision = 0.81, weighted averaged recall = 0.81, weighted averaged f1-score = 0.81).
model Calibration
We performed a graphical assessment of the predictive accuracy of the XGBoost model using a calibration curve (Van Calster & Vickers, 2015). In Figure 3, the calibration plot compares the model’s predicted and actual classification. Based on this plot, the XGBoost model performs well on predicting which patients suspected of COVID should be discharged home and which sent to the inpatient hospital setting.
order of Feature Importance for Prediction Value
Figure 4 provides clinicians with an indication of which of the variables influenced the XGBoost model classification most. This figure used feature importance and a SHAP summary plot to depict the 20 most influential features in the prognostic model (Lundberg & Lee, 2017). Panel A shows the mean most import features based on mean F1 score. Panel B depicts the features SHAP values’ importance and direction in the prognostic model. The most important features in order of importance to the model were vital sign score, number of nursing orders, number of temperature observations, age of 60 and older, time to an emergency room disposition (i.e., where the patient will go from the ED: usually home, admitted to the hospital, or to another healthcare setting), and Medicare insurance.
Discussion
Our study sought to create a machine-learning-based clinical prognostic model for suspected COVID-19 cases seen in the acute care setting. In the ED, clinicians need to make quick decisions on what action to take for an individual patient. In times of COVID-19 or other situations of overcrowding, this decision must be made in a short time and with the use of few available resources. We aimed to promote ED clinicians’ evidence-based decision-making and, therefore, the focus of the prognostic model was on transparency. The model highlights individual risk factors to clinicians and communicates uncertainties about the predictions (AUC of 0.90 (95% CI, 0.89–0.91). Our results also highlight that routinely collectible data from EHR and the interaction of the clinician with the EHR are predictive for the deterioration of COVID-19 patients (see Table 4).
Clinical Implications
The proposed clinical prognostic model will inform acute care and hospital guidelines based on the robust statistical estimation of the severity of COVID-19 symptom progression. This will provide clinicians with better quantitative information about disease progression. The proposed prognostic model leverages routinely collected clinical data from EHR to classify (1) discharge home with no return within 72 hours or (2) transferred to inpatient setting and still there within 24 hours of ED discharge or returned to the hospital after ED discharge and transferred to inpatient within 72 hours of ED discharge. This is of crucial importance to provide those patients with acute help that will need it most urgently.
As many frontline clinicians need to make high-quality decisions quickly, clinical decision rules can support clinicians in making empirically informed decisions and meeting stringent time constraints. These rules can also be
As many frontline clinicians need to make high-quality decisions quickly, clinical decision rules can support clinicians in making empirically informed decisions and meeting stringent time constraints.
A Prognostic Model for COVID-19 Progression to Severe Disease: Discriminating Emergency Department Discharge n
used to perform a risk-based approach to acute care, where potential COVID19 cases with low risk of “severe” disease course are identified early on. This approach can also provide important opportunities to take measures to avoid low-risk COVID-19 cases competing for resources that must remain reserved for COVID-19 patients with a high risk for a severe disease course. Such a risk-based approach can improve the overall efficiency and also the quality of care for individual patients. The proposed prognostic model is of high clinical importance since the global pandemic will continue to give rise to situations where the available resources become scarce and must be distributed as efficiently as possible. Empirically informed guidelines may ease the burden of frontline clinicians and improve the standard of care for patients with COVID-19.
limitations
Our study is not without limitations. First, the study is subject to the usual issues when using observational data, such as potential cofounders/ covariates not accounted for in our modeling. Second, we recognize that there could have been a loss to follow-up based on patients who deteriorated post ED discharge but could have returned to another hospital outside our health system. Other COVID-19 research in our ED that investigated loss to follow-up during the same period more closely indicates that most patients remained in the health system (Steel et al., 2021). Therefore, we are confident that most patients who returned to the hospital were identified. Finally, this one institution study should be replicated in other EDs to increase generalizability.
Conclusion
Our study in an emergency department, which was a hotspot of the COVID-19 pandemic, shows that it is possible to predict the symptom progression of COVID-19 patients only by using data directly in the ED. This is of high importance for resource allocation and to guiding early treatment.
Author Contribution
All authors contributed to study conception and design and critical revision of the manuscript for important intellectual content. KC and CK accessed and verified the underlying data. KC, KS, and CK performed model development and assessment. KC and KS drafted the manuscript. All authors contributed to analysis and interpretation of data.
Competing Interests
The authors have no competing interests to declare.
Data Statement
Datasets used in this study included the U.S. Census Data (https:// www.census.gov/programssurveys/surveyhelp/about-household-surveys. html). The electronic medical records were obtained from our institution’s data warehouse and contains personally identifiable information and cannot be shared with the public.
Distribution of Emergency Department Patients Admitted With Positive COVID Test
Figure 1
n A Prognostic Model for COVID-19 Progression to Severe Disease: Discriminating Emergency Department Discharge
Figure 2
Modeling Steps Adult
Figure 3
Calibration Plot of the XGBoost
4
XGBoost Summary Plots
Note. Panel A depicts the variable importance in the gradient-boosted model. The 20 most influential variables are ranked from top to bottom. Panel B depicts how the Shapley plot shows the relative odds of the same variables and how the distribution of Shapley values across all predictions are plotted. The magnitude of the Shapley value is displayed on the horizontal axis, while the value of the feature itself is represented by color.
Table 1
List of ICD-10 Diagnoses and Symptoms in EHR Used as Inclusion Criteria
Description of Features Used in Model Building
Sample Demographics for 5,055 Emergency Department Encounters
n A Prognostic Model for COVID-19 Progression to Severe Disease: Discriminating Emergency Department Discharge
Table 4
Classificatory Performance of Different Algorithms on the Training and Validation Dataset in Terms of Discriminatory Accuracy
Aziz, S., Arabi, Y. M., Alhazzani, W., Evans, L., Citerio, G., Fischkoff, K., Salluh, J., Meyfroidt, G., Alshamsi, F., Oczkowski, S., Aoulay, E., Price, A., Burry, L., Dzierba, A., Benintende, A., Morgan, J., Grasselli, G., Rhodes, A., Møller, M. H., … & Christian, M. D. (2020). Managing ICU surge during the COVID-19 crisis: Rapid guidelines. Intensive Care Medicine, 46(7), 1303–1325. https://doi.org/10.1007/s00134020-06092-5
Breiman, L. (2001). Random Forests. Machine Learning, 45(1), 5–32. https://doi.org/10.1023/A:1010933404324
Cawley, G. C., & Talbot, N. L. C. (2010). On over-fitting in model selection and subsequent selection bias in performance evaluation. Journal of Machine Learning Research, 11, 2079–2107.
Cecconi, M., Piovani, D., Brunetta, E., Aghemo, A., Greco, M., Ciccarelli, M., Angelini, C., Voza, A., Omodei, P., Vespa, E., Pugliese, N., Parigi, T. L., Folci, M., Danese, S., & Bonovas, S. (2020). Early predictors of clinical deterioration in a cohort of 239 patients hospitalized for COVID-19 infection in Lombardy, Italy. Journal of Clinical Medicine, 9(5), 1548. https://doi.org/10.3390/jcm9051548
Chandrashekar, G., & Sahin, F. (2014). A survey on feature selection methods. Computers & Electrical Engineering, 40 (1), 16–28. https:// doi.org/10.1016/j.compeleceng.2013.11.024
Covino, M., Sandroni, C., Santoro, M., Sabia, L., Simeoni, B., Bocci, M. G., Ojetti, V., Candelli, M., Antonelli, M., Gasbarrini, A., & Franceschi, F. (2020). Predicting intensive care unit admission and death for COVID-19 patients in the emergency department using early warning scores. Resuscitation, 156, 84–91. https://doi.org/10.1016/j. resuscitation.2020.08.124
DeLong, E. R., DeLong, D. M., & Clarke-Pearson, D. L. (1988). Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics, 44 (3), 837–845. https://doi.org/10.2307/2531595
Fu, L.-H., Schwartz, J., Moy, A., Knaplund, C., Kang, M.-J., Schnock, K. O., Garcia, J. P., Jia H., Dykes, P. C., Cato, K., Albers, D., & Rossetti, S. C. (2020). Development and validation of early warning score system: A systematic literature review. Journal of Biomedical Informatics, 105, 103410. https://doi.org/10.1016/j.jbi.2020.103410
Gallo Marin, B., Aghagoli, G., Lavine, K., Yang, L., Siff, E. J., Chiang, S. S., Salazar-Mather, T. P., Dumenco, L., Savaria, M. C., Aung, S. N., Flanigan, T., & Michelow, I. C. (2021). Predictors of COVID-19 severity: A literature review. Reviews in Medical Virology, 31, 1–10. https://doi.org/10.1002/rmv.2146. Epub 2020 e2146
Gidari, A., De Socio, G., Sabbatini, S., & Francisci, D. (2020). Predictive value of National Early Warning Score 2 (NEWS2) for intensive care unit admission in patients with SARS-CoV-2 infection. Infectious Diseases, 52, 698–704. https://doi.org/10.1080/23744235.2020.1784457
Gong, J., Ou, J., Qiu, X., Jie, Y., Chen, Y., Yuan, L., Cao, J., Tan, M., Xu, W., Zheng, F., Shi, Y., & Hu, B. (2020). A tool for early prediction of severe coronavirus disease 2019 (COVID-19): A multicenter study using the risk nomogram in Wuhan and Guangdong, China. Clinical Infectious Diseases, 71(15), 833–840.
Greenwald, P. W., the Telehealth Working Group, Olsen, E., Kessler, D., Fenster, D. B., Heravian, A., Leyden, D., Sharma, R., Lame, M., & Kim, J. (2020). 203 Telemedicine response to COVID-19 surge in New York City: How emergency department telemedicine changed with the curve. Annals of Emergency Medicine, 76, S78–S79. https://doi. org/10.1016/j.annemergmed.2020.09.216
Johns Hopkins University & Medicine. (2020). Mortality analyses: Mortality in the most affected countries. https://coronavirus.jhu. edu/data/mortality
Kilaru, A. S., Lee, K., Snider, C. K., Meisel, Z. F., Asch, D. A., Mitra, N., & Delgado, M. K. (2020). Return hospital admissions among 1,419 COVID-19 patients discharged from five U.S. emergency departments. Academic Emergency Medicine, 27(10), 1039–1042. https://doi. org/10.1111/acem.14117
Kuhn, M., & Johnson, K. (2013). Applied predictive modeling (Vol. 26). Springer.
Lundberg, S., & Lee, S.-I. (2017). A unified approach to interpreting model predictions [Preprint]. arXiv:1705.07874. https://doi.org/10.48550/ arXiv.1705.07874
Morens, D. M., Daszak, P., & Taubenberger, J. K. (2020). Escaping Pandora’s box–another novel coronavirus. New England Journal of Medicine, 382(14), 1293–1295.
Myrstad, M., Ihle-Hansen, H., Tveita, A. A., Andersen, E. L., Nygård, S., Tveit, A., & Berge, T. (2020). National Early Warning Score 2 (NEWS2) on admission predicts severe disease and in-hospital mortality from COVID-19—a prospective cohort study. Scandinavian Journal of Trauma, Resuscitation, and Emergency Medicine, 28 (1), 66. https:// doi.org/10.1186/s13049-020-00764-3
Pedregosa, F., Varoquaux, G., Gramfort, A., Michel, V., Thirion, B., Grisel, O., Blondel, M., Müller, A., Nothman, J., Louppe, G., Prettenhofer, P., Weiss, R., Dubourg, V., Vanderplas, J., Passos, A., Cournapeau, D., Brucher, M., Perrot, M., & Duchesnay, É. (2011). Scikit-learn: Machine learning in Python. Journal of Machine Learning Research, 12, 28252830. https://arxiv.org/pdf/1201.0490.pdf
Rossetti, S. C., Knaplund, C. Albers, D., Tariq, A., Tang, K., Vawdrey, D., Yip, N. H., Dykes, P. C., Klann, J. G., Kang, M. J., Garcia, J., Fu, L. H., Schnock, K., & Cato, K. (2019). Leveraging clinical expertise as a feature not an outcome of predictive models: Evaluation of an early warning system use case. (2019) AMIA ... Annual Symposium proceedings. AMIA Symposium, 323–332.
Rossetti, S. C.,Knaplund, C. Albers, D., Dykes, P. C., Kang, M. J., Korach, T. Z., Zhou, L., Schnock, K., Garcia, J., Schwartz, J., Fu, L.-H., Klann, J. G., Lowenthal, G., Cato, K. (2021). Healthcare process modeling to phenotype clinician behaviors for exploiting the signal gain of clinical expertise (HPM-ExpertSignals): Development and evaluation of a conceptual framework. Journal of the American Medical Informatics Association, 28, 1242–1251. https://doi.org/10.1093/jamia/ocab006
n
Correlational
Singh, K., Valley, T. S., Tang, S., Li, B. Y., Kamran, F., Sjoding, M. W., Wiens, J., Otles, E., Donnelly, J. P., Wei, M. Y., McBride, J. P., Cao, J., Penoza, C., Ayanian, J. Z., & Nallamothu, B. K. (2021). Evaluating a widely implemented deterioration index model among hospitalized COVID-19 patients. Annals of the American Thoracic Society, 18(7), 1129–1137. https://doi.org/10.1513/AnnalsATS.202006-698OC
Steel, P. A. D., Siegal, J., Zhang, Y., Cato, K., Greenwald, P., Melville, L. D., Gogia, K., Smith, Z., Sharma, R., & Romney, M. (2021). Telehealth follow up in emergency department patients discharged with COVIDlike illness and exertional hypoxia. The American Journal of Emergency Medicine, 49, 426–430. https://doi.org/10.1016/j.ajem.2021.02.052
Subbe, C. P., Kruger, M., Rutherford, P., & Gemmel, L. (2001). Validation of a modified Early Warning Score in medical admissions. QJM: An International Journal of Medicine, 94(10), 521–526. https://doi. org/10.1093/qjmed/94.10.521
Van Calster, B., & Vickers, A. J. (2015). Calibration of risk prediction models: Impact on decision-analytic performance. Medical Decision Making, 35(2), 162–169. https://doi.org/ 10.1177/0272989X14547233
Wynants, L., Van Calster, B., Collins, G. S., Riley, R. D., Heinze, G., Schuit, E., Albu, E., Arshi, B., Bellou, V., Bonten, M. M. J., Dahly, D. L., Damen, J. A., Debray, T. P. A., De Jong, V. M. T., De Vos, M., Dhiman, P., Ensor, J., Gao, S., Haller, M. C., ... van Smeden, M. (2020). Prediction models for diagnosis and prognosis of COVID-19: Systematic review and critical appraisal. BMJ, 369, m1328. https://doi. org/10.1136/bmj.m1328
Zhu, Z., Cai, T., Fan, L., Lou, K., Hua, X., Huang, Z., & Gao, G. (2020). Clinical value of immune-inflammatory parameters to assess the severity of coronavirus disease 2019. International Journal of Infectious Diseases, 95, 332–339. https://doi.org/10.1016/j.ijid.2020.04.041
A Correlational Study of the relationship of Nurses’ Pain Assessment and Patients’ History of Substance Abuse
Valerie A. Esposito Kubanick, PhD, RN, PMH-BC
n Abstract
The American Nurses Association Statement Position (2018) recognizes the fundamental ethical responsibility of nurses to treat and manage pain and any accompanying suffering. This study explored nurses’ perceptions about drugs, empathy, and environmental work factors as possible predictors of pain assessment in the drug use patient population. Nurses treating patients’ pain must responsibly establish therapeutic communication with their patients, advocate for their patients, and work toward positive patient outcomes all while self-reflecting and assessing their own perception of pain and remaining nonjudgmental (Gross, 2018).
According to the National Institutes of Health (NIH) (2021) pain is defined as an unpleasant sensory and emotional experience that is associated with actual or potential tissue damage and is always subjective. This research focused on the physical pain experienced by patients who have a current or past history of substance use and the appropriate pain assessment of nurses. The American Nurses Association Statement Position (2018) recognizes the fundamental ethical responsibility of nurses to treat and manage pain and any accompanying suffering. This study explored nurses’ perceptions about drugs, empathy, and environmental work factors as possible predictors of pain assessment in the drug use patient population. Nurses treating patients’ pain must responsibly establish therapeutic communication with their patients, advocate for their patients, and work toward positive patient outcomes, all while self-reflecting and assessing their own perception of pain and remaining nonjudgmental (Gross, 2018). This is extremely important for appropriate patient care to be rendered in a nonjudgmental manner. Additionally, a nurse’s self-awareness is key in performing pain assessment in the drug use patient population.
research Question
This research explores nurses’ assessment of pain with patients who have a history of substance use. The research question for this study was: Is pain assessment influenced by the nurse’s perception of a patient’s current
Valerie A. Esposito Kubanick, PhD, RN, PMH-BC York College CUNY, Jamaica, New York
and/or past use of drugs and alcohol—and does the nurse’s empathy toward the patient: environmental factors, such as the competence of the nurse; the culture of the hospital/unit; and other work environment factors—impact on the assessment or care of the patient?
Significance
According to the NIH (2021) the U.S. Department of Health and Human Services (HHS), and the Institute of Medicine (IOM), pain is recognized as a substantial health problem. The United States budget for healthcare systems is financially affected by patients’ pain through increased spending in hospital visits and length of stays. Pain is subjective to the patient who is experiencing it. No other person, not even a nurse, can decide the level of pain that another person is experiencing. However, the subjectivity of nurses’ responses to patients’ pain is possibly compelled by multiple factors, such as nurse empathy, experience, personal and professional biases, and hospital culture. These variables are concomitant with pain assessment and require investigation in order to enhance quality nursing practice and positive patient outcomes.
While current information demonstrates the delicate and problematic position of treating patient pain and the continued increase of the opioid crisis, there remains the core reality that patients require quality pain assessment and treatment. This is paramount in the nursing profession so that safe and adequate pain assessment and treatment can be carried out
in the drug use patient population. Nurses will have varying experiences treating the multitude of patients. And because pain is so prevalent across patient diagnosis and nurses’ experiences differ, there have been studies to assess nurses’ experiences treating pain. However, there are many qualitative studies that seek to find themes in nurses’ experiences when treating patient pain, with a lesser amount of quantitative data available.
literature review
Pain management has been part of humanity since ancient times. The first people to cultivate poppy (opium) were the Sumerians in Mesopotamia around 3400 BC and its use expanded throughout the globe to treat pain and any other ailments (Rosenblum, 2008). In the United States, treatment for patient pain began to emerge in the form of morphine used for injured Civil War soldiers (Hawk, 2021). Attempts were made to produce opium-like drugs to reduce the detrimental effects of opium and its addiction potential (Norn et al., 2005). The opioid Oxycodone is a medication used to treat moderate to severe pain (Gross, 2018). Opioids remain the gold standard in treating severe or acute pain, either malignant or nonmalignant, in all patients, which led to a less restrictive policy and an increase in prescribing opioids to treat patient pain (Gross, 2019).
Inpatient and outpatient Pain Assessment and measurement Tools
Nursing is considered the most trusted profession (Milton, 2018). Pain is an individual experience for each patient and acceptable pain management begins with competent pain assessment (Mallick-Searle et al., 2018). Pain scales are designed as a tool for the nurse to use in addition to questioning the patient and obtaining a history to document the patient’s physical experience and reevaluate effectiveness of medication provided for pain relief (Gregory, 2019). An example of a commonly used pain scale is the Numeric Pain Rating Scale (NPRS), which rates pain on a scale of zero through ten, with zero representing no pain and ten representing the worst pain. Picture scales are used for nonverbal patients or cognitively impaired patients. Also, the Verbal Descriptor Scale (VDS) uses words such as, “no pain,” “mild,” or “severe” to describe patient pain experience. Different types of scales are accepted to assess pain and are chosen by the provider or institution depending on the patient’s needs and ability to function (Gregory, 2019). Sometimes, reliability of tools may also be a factor. Fadayevatan et al. (2019) used a quantitative method to study the Faces Pain Scale (FPS) with an older Iranian population of patients over a one-week period. Using descriptive statistics, it was observed that
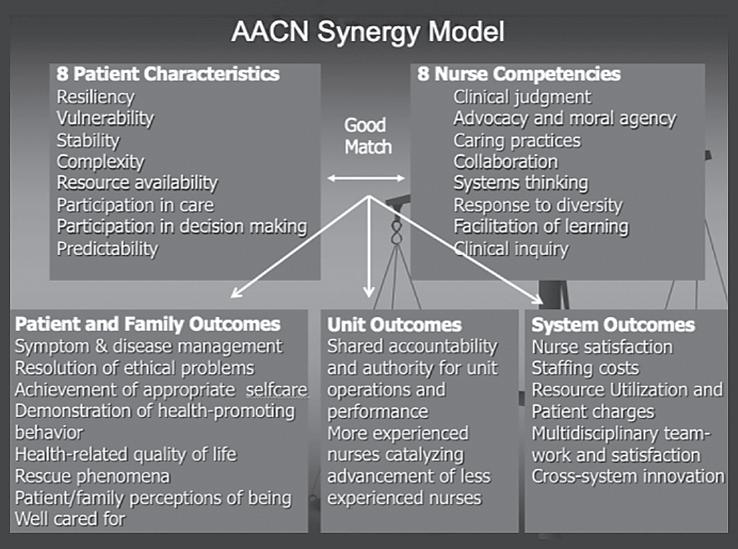
Note: From “Patient-Nurse Synergy: Optimizing Patient Outcomes” by M. A. Curley, 1998, American Journal of Critical Care 7 (https://nursology.net/nurse-theories/the-synergymodel/). Copyright 2018 Jacqueline Fawcett.
Figure 1 AACN Synergy Model
only 72% of patients agreed that the faces on the pain scale represented their level of pain.
Wadenstein et al., (2011) performed a quantitative explorative study of the prevalence of pain and pain assessment among inpatients (N = 494) in a university hospital. Using the NRS provided by the nurses, patients were asked to self-assess their pain. Sixty-five percent of the 494 inpatients reported feeling pain. Using the NRS of 1– 10 pain intensity, 81% of those who reported pain rated their pain at > 3, and 42.1% rated their pain at > 7. In summary, more than half of hospitalized patients have pain, and more than one-third of those in pain have severe pain.
Post-operative pain is expected with surgical patients. Research has shown that 80% of patients experience pain post-operatively in moderate to extreme levels. Post-operative pain is categorized as nociceptive pain, that is pain that occurs as a response to actual tissue damage and generates an unwanted sensory experience. An essential aspect for successful pain management is the use of an appropriate validated pain assessment tool (Lapkin, 2021).
A cross-sectional design study that explored nurses’ attitudes, experiences, and knowledge regarding pain management by AbuBaker et al. (2019) in Dubai, United Arab Emerates, used a convenience sample of 200 nurses working in government hospitals. The nurses were surveyed using the Knowledge and Attitudes Survey Regarding Pain (KASRP). The mean years of experience for the participants was 11.88+-6.28. Of the nurses surveyed, 62.5% reported having pain management education. The authors reported no statistically significant difference between the nurses’ overall knowledge. Both countries’ nurses said that they wanted additional education in pain, 95.7% (n = 421). It was also revealed that nurses with > 10 years of experience had a poorer perception of pain management than nurses with 5–10 years of experience. This finding indicates that as nurses’ experiences with pain increase over time, their pain management scores on the survey decreased. Limitations of this study noted that the sample was heterogenous, and no effect sizes were reported.
opioid Crisis
According to Azar (2021) the HHS has declared the opioid crisis a top concern of the current administration. Since 2017, more than 1,312 Americans lose their lives daily to opioid overdoses—an increase from 2016 data. The crisis also places a financial hardship on society in the form of an estimated $504 billion a year, which devastates communities and families. In 2016, guidelines were established by the Centers for Disease Control and Prevention (CDC) recommending practices for safe opioid prescribing for clinicians as a way to decrease opioid deaths and combat rising drug addictions. Unfortunately, an inadvertent repercussion of the guidelines led to inadequate treatment and a reduction of opioid prescriptions regardless of the patient’s presentation of symptoms or pathology (CDC, 2016). Related to opioid deaths in the United States, surgeons and healthcare providers have taken a position of responsibility to help decrease patient risk for addictions by complying with a decrease in prescribing pain medications (Theisen, 2018). Some clinicians believe that patients were undertreated and this may have led to an opioid crisis (Collier, 2018).
Theoretical model
This study used the middle range theory of the American Association of Critical-Care Nurses (AACN) Synergy Model, first developed in 1996
(Curley, 1998), and it represents the importance of aligning nurses’ competencies and patients’ needs to achieve more favorable outcomes for the patients and satisfaction for nurses. These concepts are related and there is synergistic relationship between the nurse and the patient that, when matched, delivers a positive outcome. In this study, the nurse competencies were represented by the measurement tool of nurses’ empathy, drug perceptions, work culture and environment, and demographics. Patient characteristics were represented by the three differences in the patient pain scenario. Collectively, these characteristics and competencies play a role in the successful management of patients’ pain (see Figure 1).
methodology
This is a descriptive correlational design study. A quantitative approach was used to analyze the relationships among the independent variables of empathy, personal and professional biases, and hospital culture to the dependent variable of perceived patients’ pain.
Hypotheses
Ha1: There is a significant difference in Interpersonal Reactivity Index (IRI) scores among the three patient scenarios.
Ha2: There is a significant difference in Drug and Drug Problems Perception Questionnaire (DDPPQ) scores among the three patient scenarios.
Ha3: There is a significant difference in Practice Environment Scale of the Nursing Work Index (PES-NWI) scores among the three patient scenarios.
Ha4: There is a significant difference in Numeric Pain Rating Score (NPRS) scores among the three patient scenarios.
Ha5: There is a significant difference in Comfort Behavioral Scale (CBS) scores among the three patient scenarios.
Ha6: The NPRS scores for the “frequent use…opioids” (scenarios 2 and 3) patient scenarios are significantly different from the “no drug history” (scenario 1), while controlling for IRI, DDPPQ. and PES-NWI scores.
Ha7: The CBS scores for the “frequent use…opioids” (scenarios 2 and 3) patient scenarios are significantly related to IRI, DDPPQ, and PES-NWI scores.
Sample
The participant population consisted of professional nurses in the United States caring for patients with a variety of types of diagnoses and etiologies of pain. The study was approved by the Institutional Review Board (IRB). The participants were protected by collecting data anonymously via email solicitation. No personal identifiers were used in the survey collection tools. The participants were recruited through Data Axle, which is a proprietary company that provides email addresses of people in specific industries; Gmass and TxtFlo were used to distribute the surveys. Nurses were solicited to complete the measurement tools anonymously using Qualtrics XM, a proprietary survey platform. They were solicited to participate voluntarily and do not have a relationship with the researcher. Data were then transferred from Qualtrics reports to Microsoft Excel. The sample size was estimated using G*Power 3.1 (Faul et al., 2009)
Table 1
Alphas for the 4 Multi-Item
Table 2
Response Rate and Missing Data
with power = 0.80, α = 0.05, EF = medium, using analysis of covariance (ANCOVA) with two groups and four covariates and determined that 196 participants were needed.
Standardized measures
Five standardized measurement tools were used in this study. Three were used as independent variables (DDPPQ, PES-NWI, and IRI) and two were used as dependent variables (NPRS and CBS). Two scales were employed as dependent variables to measure the subjects’ assessments of the perceived pain described in the scenario that they received as accurately as possible, given that the tools were designed to be used with an actual patient (not a description of one).
To measure the unit culture the DDPPQ (Watson et al., 2007) was used with a Cronbach’s alpha coefficient of 0.87. To determine the quality of nurses’ practice environment, the PES-NWI (Lake, 2002) measurement tool was used with the Cronbach’s alphas for three of the subscales at 0.80, 0.80, and 0.86. The participants’ cognitive and emotional aspects of empathy were measured using the IRI (Davis, 1980), with the Cronbach’s alpha reported as 0.83.
A variable of assessed pain severity based on the description in the scenarios provided to subjects (developed by the author of this dissertation) utilized the NPRS. The NPRS is an 11-point Likert-type scale with one item (Alghadir et al., 2018). This item consists of choices from the numbers 0 through 10, with a range of 0 representing “no pain” and 10 representing the “most severe pain.” The NPRS has been shown to be valid and reliable instrument with good to excellent test-retest reliability. Convergent validity was studied between the NPRS and correlated with the VRS. The NPRS was consistent in supporting pain measurement and was found to be strongly correlated with the VRS (r = 0.94). The dependent variable of patient pain was again measured; this time using the CBS (van Dijk, 2015). CBS is a measurement tool that has been validated in several languages and is used to assess sedation, distress, and pain. The six-item scale consists of the following score categories: Alertness, Calmness/Agitation, Respiratory Response, Physical Movement, Muscle Tone, and Facial Tension. Each item was found to have inter-rater reliability with the following testretest Pearson coefficients: Alertness (0.71), Calmness/Agitation (0.81), Respiratory Response (0.35), Physical Movement (0.69), Muscle Tone (0.75), Facial Tension (0.80). The rater uses a 5-point Likert-type scale with 1 representing “the least” and 5 representing “the most.” The CBS has a Cronbach’s alpha for the overall score reported as 0.87 (Suprawoto et al., 2020). This study used questions one, two, three, four, and six of the CBS. Question five refers to respiratory response and is not relevant
Table 3
Descriptive Variables Significantly Related to Standardized
to the patient scenario. A modified version of the Clinical Nurse Specialist (CNS) Demographic Questionnaire (Mayo et al., 2001) was used to obtain demographic information about the participants (see Table 1).
Setting/Patient Scenario
The patient is a 54-year-old individual who was admitted to the hospital via the emergency room two days prior for complaints of severe abdominal pain. The patient has had prior surgery for the treatment of this disease. Since the surgery, the patient has managed their disease with nonsteroidal anti-inflammatory drugs (NSAIDS), occasional courses of antibiotics, and lifestyle changes. The patient was most recently admitted to the hospital in acute pain. The patient is currently complaining of pain, has facial grimacing, is bent over in the bed, and is asking for pain medication.
Each of the following statements will be added to the Patient Scenario to create three differing versions that will be randomly assigned to study subjects.
1) The patient does not have a history of alcohol, marijuana, or opioid use.
2) The patient has a past history of alcohol, marijuana, or opioid use.
3) The patient is currently frequently using alcohol, marijuana, or opioids.
results/Analysis
The following results were derived from analyzing the data. The data was first examined for response rate, initiated respondents, partially completed and fully completed surveys, and eliminated participants who did not answer questions or only provided demographic data. Qualtrics XM reported 296 respondents to the surveys, with 223 (75.0%) of participants having initiated the surveys. Out of the 223 initiated, 130 (43.9%) of the participants fully completed the surveys and 93 (31.4%) of the participants partially completed the surveys (see Table 2).
The adjusted mean standardized scores (Z scores) for empathy, work environment, comfort behavior, and drug perceptions (the standardize measures excluding the NPRS) were then compared to each of the descriptive statistics using one-way ANOVAs. Ten (10) significant relationships were found among two (2) of the four (4) standardized measures, the comfort behavior and empathy, using an alpha level of 10% (α = 0.10). This revealed that the two measurement tools were able to identify that empathy in nurses affected comfort behavior pain assessment for patients with a past history or current use of alcohol, marijuana, or opioids (see Table 3).
Although seven hypotheses were used in this research, this article will address the outcomes of hypothesis number seven. This was found to have the most significant results. The other six hypotheses will be addressed in future articles. Hypothesis 7: The CBS scores for the “frequent use… opioids” (scenarios 2 and 3) patient scenarios are significantly related to IRI, DDPPQ, and PES-NWI scores and significant descriptive statistics, showed the following results using multiple linear regression analysis with four models to test the differences in the dependent variable (adjusted CBS) among the three groups (scenarios), while controlling for IRI, DDPPQ, and PES-NWI and significant descriptive statistics. In model 1, groups 2 and 3 were compared to group 1 while controlling for adjusted IRI, DDPPQ, and PES-NWI (R 2 = 0.16). In model 2, the variables of race, age, gender, and ethnicity (R 2 = 0.21) were added to the regression. In model 3, the descriptive variables of degree and certification (R 2 = 0.26) were added. In model 4, specialty, who nurses report to, and hospital size were added (R 2 = 0.40).
Models 1, 2, 3, and 4 were statistically significant with p < 0.01: (model 1 = < .001), (model 2 = .002), (model 3 = < .001), and (model 4 = < .001). The percentage of explained variance increased in each model, resulting to a total of 40% (model 4). Scenarios 2 and 3 were observed to be statistically different from scenario 1 with respect to adjusted CBS (p < 0.001), and the unstandardized betas indicated inverse relationships (B group2 = -0.87. B group3 = -0.72), suggesting lower adjust CBS scores in scenarios 2 and 3, compared to scenario 1. Like the results in hypothesis 6 related to NPRS scores, these results suggest lower projected pain assessment scores for individuals with either past or current histories of substance abuse. However, unlike the results of hypothesis 6, age, gender, certification, and specialty (cardiovascular compared to post-op nurses) were significantly related to CBS scores in the final regression model ( p < 0.05). This revealed that nurses scored patients lower for pain if a
patient had a past history or was currently using of alcohol, marijuana, or opioids (see Table 4).
Discussion of Clinical relevance
This study used five of the questions on the CBS. The items that were addressed were alertness, calmness/agitation, physical movement, muscle tone, and facial tension. Group 1 has a higher pain score (mean = 4.1, SD = 0.1), groups 2 and 3 have lower scores (mean = 3.7, SD = 0.1, 3.8, SD = 0.1) respectively. Groups 2 and 3 (past history and current history of drug/alcohol use) are very similar in score and lower than group 1 (no history of drug/alcohol use). The clinical implications of the CBS assessment result that the nurses performed on the scenarios may suggest that the lower scores indicate that nurses are highly cautious of using opioids to treat patients’ pain. Additionally, the lower the patient pain score (< 5) the use of nonopioids are recommended (see Table 5).
The Numerical Pain Rating Scale is an 11-point Likert-type scale with one item. This item consists of choices from the numbers 0 through 10 with a range of 0 representing “no pain” and 10 representing “the most severe pain.” Group 1 (mean = 2.7, SD = 0.1), group 2 (mean = 2.4, SD = 0.1), and group 3 (mean = 2.6, SD = 0.1). Group 1 (no history of drug/alcohol use) and groups 2 and 3 (past history and current history of drug/alcohol use) have lower pain scores. Again, lower pain scores (< 5) indicate clinically that no opioids would be used as pain management. These results illustrate that the lower pain scores of both measurement tools would influence the nurses’ treatment of pain management. Thus, the likelihood of administering opioids is extremely low. Both tables A and B represent the clinical decisions and both measurement tools performed well in predicting pain scores (see Table 6).
Conclusions
Using the Synergy Model, the relationship between nurses’ empathy, drug perceptions, work environment, and patient pain scoring were not significant. However, nurses designated a lower pain score in patients with a history of, or current use of alcohol, marijuana, or opioids. There were significantly lower CBS and NPRS scores for both patient scenarios with patients with active drug use or a history of drug use than compared to patients without a history of, or who were not actively using of drugs. The CBS is a validated measurement tool and performed as expected in this study. The NPRS, a one question measurement tool, without the ability to confirm reliability, was able to be validated in this study. Additionally, the demographics: age, gender, specialty nurse, and certified nurse, showed significant differences in how nurses scored pain for patients with a history of or who were currently using of alcohol, marijuana, or opioids; those patient scenarios were scored lower for pain than the patient scenario with
With continued research and nursing education, there may be more awareness and practice of positive pain treatments with more favorable outcomes in the drug addicted population.
Table of Multiple Linear Regression Analyses of Adjusted CBS Score
Table 4
Table of Multiple Linear Regression Analyses of Adjusted CBS Score (continued)
no history of drug use. The explained variances of past history of drug use (-0.32) and current history of drug use (-0.40) are medium range effect sizes.
Both pain measurement tools were reliable in this study and uncovered in this study that, indeed, patients with a past history of or who were currently using alcohol, marijuana or opioids were scored lower for pain, indicating nonopioid pain management from the nurse.
recommendations
Nurses treating patients’ pain must responsibly establish therapeutic communication with their patients, advocate for their patients, and work toward positive patient outcomes, all while self-reflecting and assessing their own perception of pain and remaining nonjudgmental (Gross, 2018). Literature shows some data on nurses treating patients’ pain in a variety of perspectives. However, nursing education and treating pain in patients that have a current or past drug history should be explored in relation to specialty, certified nurses, nurses’ gender, and age. Also, nursing education should include more self-examination by nurses and nursing students while treating patients with drug histories. Self-awareness is a nurse competency that interacts with patients with characteristics of drug history. Peplau (1952) stated that the central feature of nursing practice is the nurse-patient relationship and stressed the importance of the nurses’ ability to be selfaware in order to assist patients in their perceived difficulties. Teaching and practicing self-awareness in prelicensure programs and continuing education for licensed nurses may increase the appropriate response by nurses to patients’ pain. The future of nursing will continue to include patients in pain. Some of those patients will have a history of drug use, and it is not acceptable for nurses to not treat or mislabel patients’ pain. However, with continued research and nursing education, there may be more awareness and practice of positive pain treatments with more favorable outcomes in the drug addicted population.
limitations
A recognized limitation of this study was the use of fictitious patient scenarios in place of actual clinical situations. This may have implications for the participant that does not include a complete picture of the patient or the severity of the situation. Nursing assessment may differ when a real patient is presented in person, rather than in a scenario. Using scenarios does not consider the emotional complexities of the nurse-patient interactions. Another item that may have posed a limitation in this study was the lower Cronbach’s alpha score for the IRI measurement tool that was used. Although the score (0.60) is within the 0.00 and +1.00 range, it is considered a lower-accepted score (Polit & Beck, 2017). There may have been some bias in empathy that was not captured due to less reliability of the IRI in this study. Also, the descriptive statistics of ethnicity, setting, and specialty in relation to the IRI showed lower p values. It is also important to note the use of several measurement tools and the length of the survey, which included many questions. Response fatigue may have been the cause of partial answers by the respondents leading to incomplete surveys. Other conceivable limitations were the use of the CBS scale’s five questions. The CBS scale consists of six items, however for this study, one item was eliminated and five of the remaining questions were used. The question that was not used reflected respiratory rate regarding a ventilator-dependent patient. This study’s scenarios presented with a spontaneously breathing patient. Lastly, this study used correlational research as opposed to experimental research. Correlational design is an observational approach to examine relationships and correlations between independent and dependent variables. This is done without manipulation or experimentation, of the independent variables. Correlational design is not as strong in supporting casual inferences. However correlational studies are noted for their strength in authenticity (Polit et al., 2017).
n references
AbuBaker N. A., Salim N. A., Joshua, R., & Jose A. (2019). Registered nurses’ perception about pain management of hospitalized patients in one of the governmental hospitals in Dubai, UAE: A crosssectional study. Dubai Med Journal, 2, 102–106. https://www.doi. org/10.1159/000502175
Alghadir, A. H., Anwer, S., Iqbal, A., Iqbal, Z. A. (2018). Test-retest reliability, validity, and minimum detectable change of visual analog, numerical rating, and verbal rating scales for measurement of osteoarthritic knee pain. Journal of Pain Research, 26(11), 851–856. https://doi.org10.2147/JPR.S158847
American Association of Critical-Care Nurses (1996). The AACN Synergy Model for Patient Care. https://www.aacn.org/nursing-excellence/ aacn-standards/synergy-model
American Nurses Association (2018). The ethical responsibility to managing pain and the suffering it causes. Silver Spring, MD: Nursesbooks.org
Azar, A. (2021). Facing addiction in America: The surgeon general’s spotlight on opioids. https://addiction.surgeongeneral.gov/sites/ default/files/OC_SpotlightOnOpioids.pdf
Collier, R. (2018). A short history of pain management. CMAJ 190 (1), E26–E27; https://doi.org/10.1503/cmaj.109-5523
Curley, M. A. (1998). Patient-nurse synergy: Optimizing patient outcomes. American Journal of Critical Care, 7, 64–72.
Davis, M. H. (1980). A multidimensional approach to individual differences in empathy. JSAS Catalog of Selected Documents in Psychology, 10, 85.
Fadayevatan, R., Alizadeh-Khoei, M., Hessami-Azar, S., Sharifi, F., Haghi, M., & Kaboudi, B. (2019). Validity and reliability of 11-face faces pain scale in the Iranian elderly community with chronic pain. Indian Journal of Palliative Care, 25(1), 45–51.
Faul, F., Erdfelder, E., Buchner, A., & Lang, A.-G. (2009). Statistical power analyses using GPower 3.1: Tests for correlation and regression analyses. Behavior Research Methods, 41(4), 1149–1160. https://doi. org/10.3758/BRM.41.4.1149
Gregory, J. (2019). Use of pain scales and observational pain assessment tools in hospital settings. Nursing Standard, 34(9), 70–74. https:// doi.org/10.7748/ns.2019.e11308 https://doi.org/10.7748/ns.2019.e11308
Gross, J., & Gordon, D. B. (2019). The strengths and weaknesses of current U.S. policy to address pain. American Journal of Public Health, 109(1), 66–72. https://doi.org/10.2105/AJPH.2108.304746
Hawk, A. J. (2021). ArtiFacts: Built for speed—Robert Liston’s surgical technique. Clinical Orthopaedics and Related Research. 479 (4), 679–680. https://doi.org/10.1097/CORR.0000000000001712
Kmetec, S., Stiglic, G., Lorber, M., Mikkonen, I., McCormack, B., Pajnkihar, M., & Fekonja, Z. (2020). Nurses’ perceptions of early person-centered palliative care: A cross-sectional descriptive study. Scandinavian Journal of Caring Sciences, 34, 157–166.
Lake, E. T. (2002). Development of the practice environment scale of the nursing work index. Research in Nursing & Health, 25,176–188.
Lapkin, S., Ellwood, L., Diwan, A., & Fernandez, R. (2021). Reliability, validity, and responsiveness of multidimensional pain assessment tools used in postoperative adult patients: A systemic review of measurement properties. JBI Evidence Synthesis 19(2), 284–307.
Malia, R., Morrell-Scott, N., & Maine, N. (2019). A review of compliance with pain assessments within a UK ICU. British Journal of Nursing, 28(6), 382–386.
Mallick-Searle, T. & Chang H. (2018). The importance of nurse monitoring for potential opioid abuse in their patients. Journal of Applied Behavioral Research, 23, 1–12.
Mayo, A. M., Omery, A., Agocs-Scott, L., Khaghani, F., Meckes, P., Moti, N., Redeemer, J., Voorhees, M., Arguerite, M., Gravell, C., Cuenca, E. (2001). Clinical nurse specialist practice patterns. Clinical Nurse Specialist 24(2), 60–68. https://doi.org/10.1097/ NUR.0b013e3181cf5520
Milton, C. L. (2018). Will nursing continue as the most trusted profession? An ethical overview. Nursing Science Quarterly, 31(1), 15–16. https://doi.org/10.1177/0894318417741099
National Institutes of Health. Pain. https://www.ninds.nih.gov/healthinformation/disorders/pain
Norn, S., Kruse, P. R., & Kruse, E. (2005). History of opium poppy and morphine. Dansk Medicin Historik Arbog, 33, 171–184.
Peplau, H. (1952). Interpersonal Relations in Nursing. New York: G. P. Putnam’s Sons.
Polit, D. F., & Beck, C. T. (2017). Nursing research: Generating and assessing evidence for nursing practice (10th ed.) Wolters Kluwer.
Rosenblum, A., Marsch, L. A., Joseph, H., & Portnoy, R. K. (2008). Opioids and the treatment of chronic pain: Controversies, current status, and future directions. Experimental and Clinical Psychopharmacology, 16(5), 405–416.
Theisen, K., Jacobs, B., Macleod, L., & Davies, B. (2018). The United States opioid epidemic: A review of the surgeon’s contribution to it and health policy initiatives. BJU International 122, 754–759.
van Dijk, M., Jacqueline, F. M., Kappen, T. H., Schuurmans, M. J., & van Wijck, A. J. M. (2015). The relations between patients’ NPRS pain scores and their desire for additional opioids after surgery. Pain Practice, 15(7), 604–609. https://doi.org/10.1111/papr.12217
Wadenstein, B., Frojd, C., Swenne, C. L., Gordh, T., & Gunningberg, L. (2011). Why is pain still not being assessed adequately? Results of a pain study in university hospital in Sweden. Journal of Clinical Nursing, 20 (5–6), 624–634.
Watson, H., Maclaren, W., & Kerr, S. (2007). Staff attitudes towards working with drug users: Development of the drug problems perceptions questionnaire. Addiction (Abingdon, England), 102(2), 206–215. https://doi.org/10.1111/j.1360-0443.2006.01686.x
When a medication error Turns Into an ethical Dilemma
Irene Auteri, PhD, RN
Bridget Maley, PhD, RN, CNE
James
A. Ferguson, MD, MPH
n Abstract
The Code of Ethics for Nurses states that nurses should provide ethical care to the individuals they are caring for (ANA, 2015). Medication administration is one of the many responsibilities of a nurse. Nurses’ ability to safely administer medication is crucial to patient safety. When a nurse does not take this responsibility, serious injury to patients due to medication administration error can occur. When nurses fails to adhere to the Code of Ethics in their actions before or after an incident, they lose the trust of the community and individuals they are providing care for—and potentially set off a series of problems ethical, medical, and legal.
Nurses continue to garner the highest ethics rating from Americans among a diverse list of professions, a distinction they have held for more than two decades (Gallop, 2023). The Code of Ethics for Nurses states that nurses should provide ethical care to the individuals they are caring for (ANA, 2015). If nurses veer away from this ethical platform and lose the trust of the community or individuals they are providing care for, the healthcare system will be in a shamble. Medication administration is one of the many responsibilities of a nurse. Nurses’ ability to safely administer medication is crucial to patient safety. Nurses need to understand what medication they are administering and what is a safe dose of that medication. If a nurse is unsure of the safe dose or has never administered a medication, they are responsible to look up the medication prior to administration. When a nurse does not take this responsibility, serious injury to patients due to medication administration error can occur.
ethics in Nursing
The American Nurses Association (ANA) Code of Ethics for Nurses articulates the ethical obligations and responsibilities of the nurse to the patients they are providing care. The ANA Code of Ethics remains a guideline of everyday practice in nursing.
Provision I of the ANA Code of Ethics states:
The nurse practices with compassion and respect for the inherent dignity, worth, and the unique attributes of every person.
Provision 3 specifically states:
The nurse promotes, advocates for, and protects the rights and safety of the patient.
Provision 5 specifically states:
The nurse owes the same duties to self as to others, including the responsibility to promote health and safety, preserve wholeness of character and integrity, maintain competence, and continue personal and professional growth.
Provision 6 specifically states:
The nurse through individual and collective effort, establishes, maintains, and improves the ethical environment of the work setting and condition of employment that are conducive to safe quality health care.
Nurses are patients’ advocates and last line of defense in preventing harm to patients. The ethical principles that nurses must adhere to include autonomy, beneficence, nonmaleficence, and justice. The ANA Code of Ethics is taught in every beginning nursing program. These codes shape professional behavior and self-regulation, serving as guidelines for professional nursing care. The ethical principle of nonmaleficence is
Irene Auteri, PhD, RN, Adelphi University College of Nursing and Public Health, Garden City, New York; Bridget Maley, PhD, RN, Adelphi University College of Nursing and Public Health, Garden City, New York; James A. Ferguson, MD, MPH, Hofstra University Zucker School of Medicine, Hempstead, New York
borrowed from the Hippocratic oath of “Do no harm.” Nurses must do no harm intentionally. In addition to the ANA’s ethical principles of autonomy, beneficence, nonmaleficence, and justice to guide their practice, fidelity and accountability play a large role in nursing care.
The Following Case Study Is an example of a medication error
Franes, A 72-year-old female with past medical history of coronary artery disease with CABG x 3 (triple coronary bypass graft) presented to the emergency department (ED) with complaint of chest pain. Patient reports that she was watching television and developed a sudden substernal chest pain. She reports some pain radiating from her chest down her left arm. She reports that pain was a 6 out of 10 on the pain scale. She reported some nausea, denies abdominal pain or diarrhea. She called EMS and was given nitroglycerin while in the ambulance and she received a second dose in the ED, where she also received a dose of 1 mg Dilaudid (hydromorphone) and her pain decreased to a 2 out of 10 after the second dose. Electrocardiogram (EKG) showed a left bundle branch block, similar to prior EKGs, and no ST changes. Chest X-ray was unremarkable with no acute findings. Blood tests showed an unremarkable complete blood count (CBC), electrolytes within normal range, and high-sensitivity serum troponin 7 (normal level < 15), and repeat troponin 2 hours later was also 7. Attending hospitalist was paged and visited patient, then agreed to admit the patient to inpatient telemetry unit for monitoring.
The attending physician added admission orders and floor orders, including continuous cardiac telemetry monitoring, and oral Tylenol as needed for mild pain. Oxycodone as needed for severe pain and 0.5 mg Dilaudid IV for breakthrough pain. It should be noted that this week the hospital switched to a new electronic medical record (EMR) system. The nurse reviewed the existing inpatient orders and ED orders and mistakenly gave the completed ED order for 1 mg Dilaudid IV for pain. The nurse realized the mistake when the nurse went to the EMR to mark the dose as given. In a panic, the nurse then paged the attending hospitalist, asking for a one-time 1 mg Dilaudid order to cover the additional dose she just gave. The attending hospitalist physician refused and requested the nurse to notify the nursing manager on duty regarding the next step in reporting a medication error.
Dilaudid (Hydromorphone) Toxicity
Dilaudid is an opioid used in pain management and is approximately eight times stronger than morphine. Dilaudid is a highly potent opioid analgesic. The effects of Dilaudid toxicity and overdose include bluishcolored fingernails and lips, shallow and labored respirations, and cold, clammy skin leading to coma. A severe overdose of hydromorphone can cause death.
medication errors Impact on Safe Care
Globally, medication errors are the leading cause of avoidable injury to patients costing approximately $42 billion (WHO, 2017). Each year, in the United States alone, 7,000 to 9,000 people die as a result of a medication error (Tariq, 2023). In addition to the total cost of looking after patients with medication-associated errors, the cost exceeds $40 billion each year.
Additionally, patients experience psychological and physical ailments related to the error. According to the seminal 1999 landmark Institute of Medicine (IOM) To Err Is Human report, an estimated 44,000 to 98,000 Americans die every year due to preventable adverse events. Patients, on average, experience at least one medication error per day (IOM, 2007). More recently, a review found the median medication administration error rate of 20.7% for all medication routes and 53.3% for IV medication administration (Fair et al., 2023).
Medication administration performed by nurses and midwives include a specified process known as the rights of medication administration. The 10 rights include specifically right patient, right medication, right dose, right time, and right route. There are many things that could distract a nurse from performing the rights of medication administration such as simultaneous demands and interruptions, procedural omissions, and lack of clinical experience (Smith, et al., 2022; Wolf, 1989).
It is the nurse’s responsibility to provide safe and effective care for the patients in their care. This includes medication administration. Nursing is considered the most trusted profession in the United States and has been for many years (Gallup, 2023). To maintain that trust, nurses must follow the rights of medication administration and report errors when they happen to ensure the safety of their patients.
The ANA guidelines must be maintained, or the profession will lose the ability to provide good quality care. Did the nurse acknowledge her mistake and report it? The nurse tried to cover up her error and ultimately shifted the blame to the covering hospitalist. The nurse was not accountable for her actions and did not follow up any risk management protocols her facility has in place to handle such incidents. When a nurse tries to cover up an error or fraudulently documents the error, the error retains a domino effect of adversity. Nurses need to be accountable for their actions. Nursing ethics remain the heart of all patient care.
Provision 3 goes hand in hand with the importance of safe medication administration and the responsibility of the nurse to follow the rights of medication administration. The nurse in the above case study gave the incorrect dose of the medication and, instead of contacting the hospitalist to report this mistake and help the patient, the nurse tried to cover up the mistake. Safety for the patient, integrity in self, and competence all fall in line with the responsibilities of medication administration, as studies have shown that there is a detrimental effect on the nurse as well as the patient when a nurse makes a medication error (Mahat et al., 2022).
The nurse did not intentionally give an additional dose to the patient. What was alarming was that the nurse asked the hospitalist on call to write for an additional order for Dilaudid to cover for the mistake, indicating fraudulent charting. There was also an error of omission in not completing an occurrence report. Both the nurse’s actions and inactions allow the nurse to look dishonest and untrustworthy. The nurse did not uphold an important ethical principle, as the nurse asked the provider to change the order to cover up the mistake. Asking the provider to write an additional order puts the provider in a very vulnerable position. By creating a just culture for medication errors, it is possible this nurse would have felt more comfortable disclosing the error.
This nurse failed to uphold many of ethical practices. One example is nonmaleficence: Do no harm; the patient was sent to the ICU after this medication error. Fidelity: loyalty, fairness, truthfulness, advocacy, and
The need for additional strategies to improve health care and help prevent medication administration errors are needed. Formal strategies for identification of errors and analyzing these errors to determine systematic problems in health care are also warranted.
dedication; although there is no evidence that the nurse wasn’t providing good care to the patient, being truthful was not evident. Veracity: truth telling; the nurse failed to comply with this ethical principle by asking the provider to change the order. The nurse failed to tell the truth about the mistake. The conduct of the nurse violated the trust that patients have in the nursing profession.
Discussion
The nurse’s conduct was a violation of the ANA Code of Ethics. Destroying the trust of patients through the act committed by one nurse is a destruction of trust in all nurses. Globally, medication errors are the leading cause of avoidable injury to patients, costing approximately $42 billion. Each year in the United States alone, 7,000 to 9,000 people die as a result of a preventable medication error. These errors not only cost loss of life and financial issues for the facilities in which care is being provided, it
can also cause emotional trauma to the nurse who made the error, creating something known as the “second victim.”
As presented in this case study, one can see the importance of ethical behaviors by nurses, the ANA Code of Ethics, and the principles of safe medication administration. If it was not for the quick action of the hospitalist transferring the patient to the ICU in this case study, our patient could have had a much different outcome. A different outcome would have also meant something different for the nurse providing care. Making this experience a learning exercise may be beneficial to the nursing staff providing care.
Conclusion
Understanding of professional and bioethical context is fundamental in the nursing profession. Professional nursing care requires the application of all the principles of bioethics. The violation of the ethical principles that nurses abide by in everyday practice illustrate acts of malpractice and negligence. The need for additional strategies to improve health care and help prevent medication administration errors are needed. Formal strategies for identification of errors and analyzing these errors to determine systematic problems in health care are also warranted. At a national level, it is clear nurses must recognize healthcare dilemmas and make good judgments and decisions based on their values, while keeping within the laws that govern them (Haddad and Geiger, 2023). Nurses need to hold self-accountability to themselves and their profession.
American Nurses Association. (2015). Code of ethics for nurses. American Nurses Publishing.
Cohen M. R. (2007). The Institute of Medicine Report; Preventing Medication Errors: Another Good Day. American Journal of HealthSystem Pharmacy, 64(14 Suppl 9), S1–S2. https://doi.org/10.2146/ ajhp070189
Fair, L., Burns, C., Lindsley, J. (2023, July) Improving Medication Safety in an ICU. American Journal of Nursing, 123(7) 39–45. https://doi. org/10.1097/01.NAJ.0000944924.15137.c8
Gallup (2023, January 10). Nurses Retain Top Ethics Rating in U.S., but Below 2020 High. https://news.gallup.com/poll/467804/nurses-retaintop-ethics-rating-below-2020-high.aspx
Haddad, L. M., & Geiger, R. A. (2023). Nursing Ethical Considerations. In StatPearls. StatPearls Publishing.
Institute of Medicine (U.S.) Committee on Quality of Health Care in America, Kohn, L. T., Corrigan, J. M., Donaldson, M. S. (Eds.). (2000). To err is human: Building a safer health system. National Academies Press.
Mahat, S., Rafferty, A. M., Vehviläinen-Julkunen, K., Härkänen, M (2022). Negative emotions experienced by healthcare staff following medication administration errors: A descriptive study using textmining and content analysis of incident data. BMC Health Serv Res, 22, 1474. https://doi.org/10.1186/s12913-022-08818-1
Smith, L. C., Watson, H., Fair, L., Carter, G., Mackay, P., Lykens, K., Bradstock, J., Arnold, K., & Whalen, M. (2022). Evidence-based practices in developing and maintaining clinical nurse preceptors: An integrative review. Nurse Education Today, 117, 105468. https:// doi.org/10.1016/j.nedt.2022.105468
Tariq, R. A., Vashisht, R., Sinha, A., & Scherbak, Y. (2023). Medication dispensing errors and prevention. In StatPearls. StatPearls Publishing. Wolf, Z. R. (1989). Medication errors and nursing responsibility. Holistic Nursing Practice, 4 (1), 8–17. https://doi.org/10.1097/00004650198911000-00005
World Health Organization. (2017, March 29). WHO launches global effort to halve medication-related errors in 5 years. https://www. who.int/news/item/29-03-2017-who-launches-global-effort-to-halvemedication-related-errors-in-5-years
Assignment under Protest: A Nurse’s rights and responsibilities
Carol Lynn Esposito, EdD, JD, MS, RN-BC, NPD
n Abstract
A registered nurse (RN) receiving an assignment that in their professional judgment places the patient(s) at risk has an obligation under law and ethics to take action. In acting in the interest of the patient, the nurse is required to notify the administrator on duty to whom they are reporting and who has the authority to make staffing decisions.
State Nurse Practice Acts, the Code of Ethics for Nurses, and the mandates under the state Board of Nursing Rules related to nursing practice and unprofessional conduct hold the nurse responsible and accountable to their patients for the quality of the nursing care provided. However, the responsibility and accountability for the overall level of care ultimately resides with the hospital/agency, including all hospital and nursing administration staff.
Learning Outcome
Restate the importance of filing a Protest of Assignment (POA) as a way for the nurse, through individual and collective effort, to establish, maintain, and improve the ethical environment of the work setting and conditions of employment that are conducive to safe, quality health care.
Purpose Statement
Registered Nurses—based on their legal, professional and ethical responsibilities—have the right to accept, reject or object in writing to any patient assignment that puts patients or themselves at serious risk for harm. While Registered Nurses have the professional obligation to raise concerns regarding any patient assignment that puts patients or themselves at risk for harm, refusing a patient assignment carries legal and employment risks. This program is intended for nurses working in specialty care units who want to know the legal basis for the right to object to an assignment and how to professionally document their practice concerns on a Protest of Assignment form.
Course Objectives
At the completion of this learning activity, the learner will be able to:
Identify the data needed to successfully provide notice to the hospital/nursing home of staffing and patient safety issues.
Identify how to most effectively fill out a POA.
Restate how the POA data can be used to facilitate concerted activity and patient advocacy.
Use critical thinking and the POA process to solve case scenarios
Keywords: assignment under protest, protest of assignment, civil tort law, workplace safety and health, vicarious liability
Introduction
Assignment under protest (AUP) or protest of assignment (POA) forms (hereinafter POAs) are used when nurses are expected to assume responsibilities and accountabilities that exceed their experience and
Carol Lynn Esposito, EdD, JD, MS, RN-BC, NPD
New York State Nurses Association, New York, New York
educational preparation and/or the volume of care is more than the nurse can in their professional judgment safely administer. POA forms are also used when the nurse has been given an assignment that is beyond the legal scope of nursing practice under the State Nurse Practice Act.
For any single situation, multiple forms may be completed if there are multiple nurses who feel care is compromised. More frequently, however, due to time constraints, multiple nurses will file one form objecting to the conditions under which the nurse(s) must practice. This singular form, then, represents multiple nurses’ levels of analysis of the patient care situation.
Purpose of the Protest of Assignment Form
POA forms generally serve to notify management of potentially inadequate or absent efforts to:
Protect the public per the requirements of state statutory and regulatory law. For example, NYS Public Health Law Article 28 and state regulations, including Title 10 Part 405 of the New York Codes, Rules and Regulations (NYCRR), “Hospitals – Minimum Standards” requires:
Management to provide every patient in the hospital care that meets generally acceptable standards of professional practice 10 NYCRR 405.2(f)(1);
Personnel numbers sufficient to meet every patient need 10 NYCRR 405.2(f)(7);
A staffing plan that determines the types and numbers of nursing personnel and staff necessary to provide nursing care to all areas of the hospital 10 NYCRR 405.5(a)(1); and
Sufficient staff for each department or nursing unit to ensure, when needed, in accordance with generally accepted standards of nursing practice, the immediate availability of an RN for bedside care of any patient 10 NYCRR 405.5(a)(2).
Follow Code of Federal Regulations related to the Centers for Medicare and Medicaid reimbursement Conditions of Participation;
Follow standards of care as indicated by facility policy and procedures; individual competencies; certification expectations; evidence-based research in the areas of retention and turnover in ICU/ CCU/PICU/ NICU, pediatrics, medical/surgical units, psychiatric units, telemetry/ stepdown units, maternal/child units, labor and delivery units, and emergency departments where specialized orientation programs are utilized;
Follow Joint Commission standards for leadership;
Support the staffing guidelines developed in accordance with standards of practice and Joint Commission reports, and provide minimum staffing levels required to safely care for the volume and acuity of the patients.
In addition to the duty to care and advocate for their patients, nurses must assume many other collective responsibilities. These include advocating for themselves, improved nursing standards, a safe work environment that is conducive to the delivery of quality patient care, a work environment that facilitates and supports the standards of nursing practice and the nurse practice act, and community and national healthcare needs (Ketter, 1997).
understanding the legal basis for the Filing of the Protest of Assignment Form
The complexity of the delivery of nursing care is such that only professional nurses with appropriate education and experience can provide nursing care. The right of the patient to receive safe, professional nursing care at an acceptable level of quality is at the core of every RN’s decision to file a POA. The healthcare law outlines the expectations of the RN staff to deliver no less than minimum-standard nursing care once an assignment has been accepted; to be prepared mentally, physically, and educationally to deliver safe care; to delegate care appropriately; and to adequately supervise those to whom care has been delegated.
When an RN accepts employment in a healthcare facility, the nurse enters into an implied contractual agreement with that facility that they will provide nursing services in a collaborative practice environment. Under civil tort law, each party to the contractual relationship has responsibilities and is accountable to the other party for the following:
The Nurse’s Responsibility
Provide competent nursing care to the patient.
Communicate concerns regarding needed resources and/or the work environment that may potentially impede the delivery of quality patient care.
This includes utilizing the chain of command, as well as use of available documentation tools such as incident reports, quality assurance memos, and POA forms to inform healthcare leaders of issues of concern.
Exercise informed judgment and use individual competence and qualifications as criteria in giving, accepting, or rejecting an assignment.
Nurses have individual accountability for the care of each patient.
Clarify assignments, assess personal capabilities, and identify options for alternative patient care assignments when they do not feel personally competent or adequately prepared to carry out a specific function.
The nurse may be held legally and ethically responsible for judgments exercised and actions taken in the course of nursing practice.
The nurse has the right to refuse an assignment that they do not feel prepared to assume, but must also consciously decide to accept the possible consequence of this decision (being dismissed for insubordination).
Management’s Responsibility
Ensure competent nursing care is provided to the patient.
Evaluate the nurse’s ability to provide specialized patient care and provide appropriate orientation and training to a new or changing clinical setting and/or patient population.
Discuss nursing competencies at the time of employment and update as competencies change, clearly identifying clinical areas in which the nurse is competent to serve.
Provide and organize nursing resources to ensure that patients receive safe, effective, and appropriate nursing care.
Communicate in written policies and procedures the process to make consistent and appropriate assignments and reassignment decisions.
Collaborate with staff to clarify assignments, assess personal capabilities, and jointly identify options for patient care assignments when the nurse does not feel personally competent, adequately prepared, or appropriately resourced to carry out a specific function.
Recognize that working frequent long hours and adjusting to shift changes may interfere with a nurse’s physical and mental health and impair performance of clinical activities and judgments.
Recognize that a nurse floated to a charge position requires a substantial amount of clinical experience and a high level of clinical judgment and skill in that area as they are responsible for providing consultation and direction to other nursing staff.
Recognize that the use of agency nurses and/or floating an RN to another unit creates a substantial amount of stress, worry, and unhappiness on all RNs, and facilitates nurse burnout, negative RN satisfaction scores, and facility turnover.
Recognize that consistent understaffing of patient units contributes to poor patient outcomes and increased readmission within 30 days of discharge.
Ensure the presence and ongoing enhancement of a care environment conducive to the delivery of quality patient care.
Plan and budget for appropriate resources based on patient requirements and priorities for care, recognizing individual patient safety takes precedence over facility profits, needs, and priorities.
Ensure competent nursing care is provided to the patient.
Provide education to staff and management in the decision-making process regarding patient care assignments and reassignments, including patient placement and allocation of resources.
Recognize staffing decisions must be made by nurses with appropriate education and experience.
Provide a clearly defined mechanism for immediate internal review of proposed assignments. This should include participation of staff involved and the documentation and review of incidents in which the appropriateness of assignment is in question.
When, in the RN’s professional judgment, one of these responsibilities has been breached, the RN should file a POA form.
The Protest of Assignment Form Objective
The POA is a legal document that provides notice to your employer that, in your professional judgment, your assignment is unsafe and places both you and your patient(s) at risk of a negative outcome and potential
serious injury. This notice is extremely important if the RN wants to transfer accountability and liability for any subsequent patient damages to the hospital. Let’s review why this document is necessary to transfer the liability to the hospital and its management team.
Vicarious liability is a legal doctrine that assigns liability for an injury to a person who did not cause the injury, but who has a particular legal relationship to the person who did act negligently. It is also referred to as imputed liability.
The diagram in Figure 1 (using a New York State Nurses Association [NYSNA] Protest of Assignment Form as an example) shows the theory graphically. When the plaintiff sues the RN for malpractice, the RN can transfer the accountability and responsibility for the injury, and ultimately the liability for the injury, to other parties whom the RN has a special relationship with.
The special relationship between the RN and the medical doctor (MD) is that of the “captain of the ship” theory. When the RN calls the MD with a change or potential change in a patient’s condition, the MD becomes liable for the patient care decision-making regarding the medical regimen.
The special relationship between the RN and the managerial staff, chief nursing officer (CNO), and hospital is that of an employer-employee or a supervisor-employee relationship. When the RN calls the manager and files a POA with the manager and human resources department, the RN is giving notice to these parties of an actual or potential existing dangerous circumstance. Accountability, responsibility, and, ultimately, liability then transfer to those parties for the nursing regimen and patient care decisionmaking.
Think of the vicarious liability theory like the game of hot potato. The RN who is holding the hot potato by remaining silent about their
Figure 1
Vicarious Liability Theory
Figure
2 A Protest of Assignment Form Passes Along the Liability
assignment is holding on to the liability. But, if the RN passes the hot potato to another party by making a phone call and filing a POA, then the RN has mitigated their liability (see Figure 2).
Initiating the Transfer of Liability:
Giving
the First Notice to the Hospital
To initiate the transfer of liability, the RN who determines that their assignment is unsafe must give immediate notice to their supervisor. The best evidence of notice should be person-to-person by way of a telephone call with a witness. When making a call, the reporting RN should tell the supervisor that the call is being made in the presence of a witness, and should tell the supervisor the name of the witness. The RN should tell the supervisor their reasons for filing a POA, and then delineate each of the reasons about which notice of a dangerous situation is being given in the POA.
The call should sound like this:
“Hello Supervisor Jane, this is Ima Nurse on 5W med/surg. I am calling you in the presence of Anita Witness and I am giving you notice that in my professional judgment, patients are at risk today because we have only four RNs on staff and the unit has three 1:1 patients on the floor because they are on respirators and are receiving multiple IV drips and antibiotics. We have five patients who need safe patient handling equipment and who need turning and positioning every two hours and we do not have any SPH equipment on the floor.
“Our CNA was floated to another floor and we have 25 patients on the unit today, 15 of whom need moderate to total patient care assistance for all activities of daily living. We will be having five discharges and four admissions on the day shift, and we have two families who are constantly in the patient’s room and have started verbal arguments with the RNs assigned to the patient for the past three days. We are demanding that you immediately come to assess the floor and make arrangements for another two RNs and one CNA. And we are respectfully requesting that if you float RNs to our unit, that they have med/surg experience and have had recent orientation to, and are familiar with, our unit and the acuity and medical conditions of our patients.”
Passing Along the Liability: Filling Out the Protest of Assignment Form
It doesn’t matter that only one RN on the floor has been assigned a patient population that might be in jeopardy. The entire unit is disrupted if any RN has a dangerous assignment. It does not matter what time you fill out the POA form, as long as you immediately give verbal notice to your manager and note the time of the verbal notice on the POA form.
EVERY RN on the unit should sign the POA. This not only shows support for one another, it protects all RNs from liability for any untoward events resulting on that day. Remember, you are not an island. You do not work in isolation. You are a union and must work as a team. Start filling out the POA by noting on the top of the form the following items (see Figure 3):
1. Your facility name
2. The date
3. The name of your nursing unit (Don’t just write down 5W, write 5W med/surg.)
4. The name of your witness next to the unit identifier
5. Your name
6. The time you actually gave verbal notice, even if you are filling out the POA at a later time
7. The name of the supervisor you called
Next, fill out the middle section of the form as follows (see Figure 4):
1. Fill in the circle that corresponds to your unit. Also circle the unit type. For example, if you filled in the CCU/ICU/NICU circle, also circle “CCU” if that is your unit. If you work in MICU, write MICU in the spaces provided under the word “Other.” Follow this procedure for all other circles denoted on the form.
2. If the name of your unit does not appear on the form, such as “oncology,” then provide that name on the “Other” line.
3. Next, fill out the boxes under “Normal or Core Staff.” On the RN, LPN, and ancillary line, put the number of RNs that should be on your unit according to your contract or according to your hospital’s staffing plan that is submitted to JC and/or CMS. If you do not have contractual numbers and/or if you do not know what your hospital’s staffing plan numbers are, place in the box the number of nurses that you believe are the core or usual numbers your unit should be staffed at and put on the schedule. If you don’t know any of these numbers, use the Protecting Our Patient staffing book numbers. To use this book, look in the index, find your specialty unit, go to that page, and refer to the numbers recommended by the specialty nursing organizations. Please write in on top of the line “Normal” which numbers you are reporting. Write in “Contract” for contractual ratios, “Hospital” for the hospital plan, or “Core” for the usual scheduled numbers for your unit, or “Book” if you are using the Protecting Our Patients references for staffing numbers that are documented by the specialty nursing organizations.
4. For the section on “Number on duty today,” place in the appropriate boxes the numbers of RNs, LPNs, and ancillary who are on the unit that day. Please note that the “Regular” numbers includes all FT, PT, and PD staff on the unit that day. Do the same for the numbers
Figure 3
Filling Out the Top of the Protest of Assignment Form
1. Your facility name
2. The date
3. The name of your nursing unit. Don’t just write it down 5W, write 5W med/surg.
4. The name of your witness next to the unit identifier
5. Your name.
6. The time you actually gave notice, even if you are filling out the POA at a later time.
7. The name of the supervisor you called.
Figure 4
Filling Out the Middle Section of the Protest of Assignment Form
1. Fill in the circle of your unit. Circle the type of unit you are on.
2. If your unit type does not appear on the form, write it in the “Other” line.
3. Fill in the contractual, hospital staffing plan, or usually scheduled numbers of staffing the “Core staff” boxes. Use the Protecting Our Patients book as reference.
4. Fill in the total numbers of FT, PT, PD staff that are on the unit today for all regular, float, and agency staff.
5. Fill in the total ADDITIONAL numbers of staff you need for today.
6. Fill in the total numbers of beds on your unit.
7. Fill in the total number of patients on the unit today, including hallway and admission patients.
Figure 5
Filling Out the Reason for Filing the “Protest of Assignment” Section
For what reasons are you protesting this assignment? (shade all that apply)
0 patient acuity higher than usual
0 inadequate number of qualified staff
0 volume of admissions and discharges
0 not adequately trained for this situation
0 don’t have resources I need to supplies, equipment, or medications
0 case load too high and impedes safe care
0 inadequate time for documentation
0 mandatory overtime
0 other
of RNs, LPNs and ancillary staff that have been floated onto or out of your unit. Place the word “into” or “out” above the float line to denote whether the staff member has been floated onto the unit, or removed from the unit. Repeat the process for the numbers of agency staff on the unit that day.
5. For the “What you needed?” boxes, place the additional number of RNs, LPNs, or ancillary staff you believe you needed that day to meet all patient’s needs for all of the patients on the unit that day.
6. For the “Bed Capacity” boxes, place the number of beds you have on your unit.
7. For the “Census” boxes, place the total number of patients on your unit that day. This number should include all hallway patients and all patients that have been admitted to the unit on that day.
The next section to fill out is the “Reasons you are protesting” section. Fill in ALL CIRCLES that apply to your situation today. Your choices are: patient acuity higher than usual; inadequate number of qualified staff; volume of admissions and discharges; not adequately trained for this situation; don’t have the supplies I need such as supplies, equipment, or medications; case load too high and impedes safe care; inadequate time for documentation; mandatory overtime; and other (see Figure 5). Refer to the NYSNA ASSURE and WWAAA palm card when filling in the circles (see Figure 6). All WWAAA reasons should be written on the “Other” line.
Under Objection Section
The legal basis for the “reason” section on the POA form is civil tort (aka malpractice) law. Under tort law, the hospital employer has corporate responsibilities both to the patient and to its employees. Failure to meet its responsibilities can be the basis of a corporate negligence lawsuit. Only injured patients can file a corporate negligence lawsuit against the hospital.
Injured RN employees are barred by the NYS Workers’ Compensation Law from bringing such a lawsuit. Nevertheless, both injured RNs and those who anticipate being injured, can file a POA, along with filing an OSHA, Joint Commission, the State Department of Health, PESH, and/or the State Department of Labor complaint.
The NYSNA ASSURE and WWAAA palm card was developed for NYSNA RNs to assist them in identifying the responsibilities or duties owed by the hospital corporate owner to its patients and employees. The palm card can be worn behind the ID tag and referred to whenever necessary.
The tort law corporate responsibilities are arranged with the acronyms ASSURE and WWAAA as follows (see Figure 6):
Adequate staffing to meet the immediate needs of the patient
Staff development, orientation
Safe environment
Updated policies and procedures in accord with current standards of practice
R eadily available resources (human, material, equipment)
Evaluation of employees (competent hires, retain only competent practitioners)
Workplace rules, policies, and practices that conform to NYS scope of practice for RNs
Workplace rules, policies, and practices that conform to standards of practice in nursing
A facility that complies with all healthcare laws (safe patient handling, no mandatory overtime, protection against violence in the workplace, safe and healthy workplace)
A facility that complies with all labor laws (right to organize, to speak out without fear of employer retaliation or reprisal, right to bargain terms and conditions of employment, right to fair and nondisparate treatment, right to engage in concerted activities, etc.)
A facility that abides by all contractual provisions
Passing Along the Liability: Filling Out the “Other Comments” Section on the Protest of Assignment Form
Deciding which “reason” circle to fill in and what to write in the “additional comments” section on the POA form requires critical thinking and reasoning. Refer to the “How to substantiate your claims” document (see Figures 8, 9) to help you fill in the additional comments section. This document gives you some ideas on how to elaborate on the situation according to the circle you have chosen on the “Reason you are filing a POA” section. Remember, this section substantiates your claim that a dangerous situation exists on your unit that day (see Figure 7).
In this section, be sure to tell the story of what your staffing and the patient population looks like on your unit that day. Describe the situation so that anyone reading the information would be able to conclude that it would be both physically and mathematically impossible to meet all patient needs.
Describe how many 1:1 are on the unit, how many multiple drips need to be checked every hour, how many patients need turning
and positioning every two hours, how many vital sign checks every 15 minutes need to be done, etc.
Describe if staff have been floated in or out of the unit. If staff have been floated, it is important for all of the nurses on the corresponding unit to which the staff was floated onto and from file their own POAs as well.
Describe if the staff are novice staff, on orientation, or are not specialists in the type of nursing needed for your unit. For example, if a med/surg nurse is floated onto an ICU unit, denote that the hospital has provided you with an RN that does not have adequate orientation and training for the patient population.
Figure 6
NYSNA Protest of Assignment Palm Card
Figure 7 Additional Comments
Also describe if your patients are obese, fully or partially dependent, need safe patient handling equipment, and whether you have the equipment available to you. Describe any violence on the unit. Denote any equipment that is faulty or missing on your unit.
Also be sure to fill in the number of RNs that are signing the form in the box provided next to the additional comments section on the POA form. This number should correspond to the number of actual signatures placed on the bottom of the POA form. Analyzers of the POA form should use this number (along with the concomitant numbers of actual signatures) as the true number of protests that were filed on the unit, on that day, and for the reasons circled.
Figure 8
Deciding Which Reason to Use on the Protest of Assignment Form
Figure 9
The Signature and Manager Comment Section on the Protest of Assignment Form
The New York State Nurses Association has developed a “cheat sheet” to help RNs in this critical thinking process (see Figure 8).
The last sections on the POA form are the signature, date, and management comments sections (see Figure 9).
EVERY RN on the unit should sign the POA. Sign your name clearly and legibly. If you sign your name illegibly, you may be waiving the imputing of the liability because the plaintiff’s attorney might argue you never signed the POA.
Place in the date boxes the date you filled out the POA. Try to ensure that you deliver the POA to the manager on the same day you filled out the POA.
Don’t worry if the manager doesn’t come down to assess the unit or doesn’t write anything in the management comments section.
If the manager doesn’t respond, it DOES NOT NEGATE THE VALIDITY OF YOUR POA AND NOTICE.
If the manager doesn’t respond, you can write in the management comments section “Manager did not assess the unit.” If the manager calls you and tells you what they tried to correct the situation, only document negative comments the manager makes, such as, “There is no one available to send to you,” or “Just make do for today.” Remember, you are passing along the liability, so you don’t want to document any comment that might pass the liability back to you.
Best Practices for the Filing and Storage of a Protest of Assignment
Every hospital has its own process for the filing and distribution of the POA form to necessary parties. You should make sure you are aware of the process in your hospital. Despite individual hospital procedures, best practices for the filing and storage of the POA form are as follows:
Give one copy of the POA to your union representative, if applicable.
If you have a POA captain in your facility or a POA delegate on your unit, give a copy to that person as well.
Give one copy of the POA to the manager you first gave verbal notice to.
One copy should be filed with the human resources department in your facility.
Keep one copy for yourself.
Do not store your POA copies in your locker or desk at the hospital. These are hospital-owned areas. The hospital has a right to search and confiscate items from these areas.
Store your POAs for a minimum of 10 years. This is the maximum time frame for a patient to sue you for malpractice in New York State.
Store your POA copies in both paper in a file drawer at home and as a scanned copy onto your home computer. Make sure you keep an external hard-drive copy of the scanned documents as well.
Barriers to Filing a Protest of Assignment
Many nurses have indicated that they do not fill out a POA for the following reasons:
Fear of retaliation
Their manager said the policy doesn’t allow them to file a POA
The manager said the situation doesn’t warrant a POA
Their peers are not supportive of the filing of a POA
Their peers will not co-sign the POA form
Don’t let your manager bully you. You have an ethical, professional, legal, and, most likely, a contractual right to file a POA. All state nurses associations have implemented POA forms in their state’s hospitals. National and international nurses organizations support the right of the nurse to file a protest. The ANA has made the following statement with regard to protesting an assignment:
The American Nurses Association (ANA) believes that registered nurses—based on their professional judgment and ethical responsibilities—have the right to reject, accept, or object in writing to any patient assignment that potentially puts patients or themselves at serious risk for harm. The professional obligations of the registered nurse to safeguard patients are grounded in the Code of Ethics for Nurses with Interpretive Statements (ANA, 2001a), Nursing: Scope and Standards of Practice (ANA, 2005), and state regulations governing nursing practice.
If your manager retaliates against you for filing a POA, you should do the following:
Tell your manager that you are filing another POA, a grievance, and a labor board complaint for their interference with your contractual, ethical, professional, and legal right to file a POA.
If your contract has a provision about the filing of POAs, contact your NYSNA representative and ask them to file a grievance.
Contact your union representative and ask them to file a complaint with the Labor Board because your manager retaliated against you for taking a legal concerted action on behalf of your patient.
You can file a complaint with the Equal Employment Opportunity Commission because your manager has created a hostile work environment. Hostile work environment includes sexual, racial, and gender-related harassment.
Build a team spirit on your unit. Colleagues who do not want to sign the POA place themselves at risk. Explain to your colleagues how the vicarious liability theory works. Also talk about the concept that when you do nothing, then nothing changes. If after several attempts you fail to get your colleagues on board with signing a POA, contact your union representative and ask them to have a conversation with your colleagues and schedule a POA workshop at your facility.
Engaging in Concerted Activity
Federal law (the National Labor Relations Act in the private sector and the Taylor Law in the public sector) protects a nurse’s right to engage in union activity. These laws protect your right to band together with coworkers to improve your lives at work. Improvements can include demands for increased staffing, ancillary staff, safe patient handling equipment, safe work environment, policies to address workplace violence, etc.
In short, you have the right to act with coworkers to address workrelated issues in many ways. Some other examples include: talking with one or more coworkers about your wages and benefits or other working conditions; circulating a petition asking for better hours; participating in a concerted refusal to work in unsafe conditions (the POA); and joining with coworkers to talk directly to your employer, to a government agency, or to your legislators about problems in your workplace. Your employer cannot discharge, discipline, threaten you for, or coercively question you about this “protected concerted” activity. However, you can lose protection by saying things about your employer that are egregiously offensive or knowingly and maliciously false, or by publicly disparaging your employer’s reputation or services without relating your complaints to a labor controversy.
Concerted Activities Related to the Protest of Assignment
Examples of concerted activities nurses can engage in concerning their POA forms can include:
1. Filling out POA forms collectively or individually.
2. Collecting and saving a copy of all POA forms filled out on your unit. Reviewing them and making an action plan on how you will use the data on the forms to support the reason for your concerted activity.
3. Presenting the POA forms that were filled out over the past month (or the period of time that is most effective) at your next unit meeting to address the issues that have been emphasized on the POA forms.
4. Circulating a petition asking for better staffing and including copies of all of the POAs that have been filed in a particular time frame, and giving the petition to management with a copy of all of the POAs pertaining to that issue.
5. Working with colleagues to determine further concerted activities that are effective in protecting your license and the boundaries of your right to engage in concerted activity.
CASE SCENARIO: Unfamiliar Drug
Nurse Ima Nu has been asked to administer an experimental chemotherapeutic agent to one of her pediatric patients. Ima is a novice nurse who has just come off of orientation. She has no knowledge or experience with the drug. How should Ima respond?
Ima is being asked to do something that is beyond her personal knowledge, skill set, and experience. Answer the following questions about Ima’s ethical, legal, and professional rights and responsibilities by circling the best answer.
1. Does Ima have the legal right to notify her manager that she does not feel she is competent to administer the drug?
a. Yes, the right is rooted in healthcare law.
b. No, the right is only rooted in ethics, not in law.
2. Does Ima have the legal right to ask her manager to give the patient to another RN who has knowledge of the drug?
a. Yes, Ima can self-assess that the demands of her current patient assignment precludes her from safely administering the drug.
b. No, Ima already accepted the assignment and asking another RN to take over would constitute abandonment of her patient.
3. Does Ima have the legal right to ask her manager to assist another RN who has knowledge of the drug?
a, Yes, she has the legal right to determine she is not qualified to monitor the patient because she is not familiar with the potentially serious side effects of the drug.
b. No, the research protocol, unit policies and procedures, and the pharmacy are available to her and she has an obligation to render herself competent to administer the drug.
Colleagues who do not want to sign the PoA place themselves at risk. explain to your colleagues how the vicarious liability theory works. Also talk about the concept that when you do nothing, then nothing changes.
Facility code
Date / /
PROTEST OF ASSIGNMENT
Print in block letters!
Facility name
M M D D Y Y Y Y
Name of individual submitting report
Time Management notified (12 hr clock) : AM PM
What type of nursing unit is this? (shade the type that best applies)
CCU/ICU/NICU
Med/Surg
ER
Maternity/GYN
Peds/NICU/PICU
Psychiatry
Ambulatory Surgery
Other
Home Care/Public Health
School
Correctional Facility
Ambulatory Care/Clinic
OR/Anesth/Recovery
Stepdown/Telemetry
Nursing Home/Rehab
Name of nursing unit
Manager's Name Bed Capacity Census RN
What was your staffing like today? *Regular is sum of (write numbers in the boxes) FT/PT/PD
Number On duty today
Normal or Regular* Float Agency What you Core staff needed Staffing
For what reasons are you protesting this assignment? (shade all that apply) patient acuity higher than usual inadequate number of qualified staff volume of admissions and discharges not adequately trained for this situation don't have resources I need such as supplies, equipment, or medications case load too high and impedes safe care inadequate time for documentation mandatory Overtime
Other
Additional Comments
Print in Block letters!
Number of RNs signing this form 34425
Under the laws of this state, as a registered professional nurse, I am responsible and accountable to my clients. Therefore, this is to confirm that I notified you that, in my professional judgement, today's assignment is unsafe and places my clients at risk. As a result, the Hospital/Agency and you share responsibility for any adverse effects on patient care.
I will, under protest, attempt to carry out the assignment to the best of my professional ability.
Signature
Management Comments
Management Signature
Time management responded (12 hr clock) : AM PM
Date / /
Date / /
Use the sheet on the next page to practice filling out the POA for this case scenario.
This scenario is rooted in both law and ethics. The answers relevant to the nurse’s actions under NYS law should be guided by the following. Please refer to your own state’s law to guide your actions:
The Code of Ethics for Nurses (Provision 4) states, “The nurse is responsible and accountable for individual nursing practice and determines the appropriate delegation of tasks consistent with the nurse’s obligation to provide optimum patient care.”
The New York State Health Code 10 NYCRR 405.5 (a) (1),(4) states the hospital shall provide RNs who are qualified by training and experience for the job and shall have a written evaluation of the performance, credentials, and competence of registered professional nurses and ancillary nursing personnel shall be conducted on at least a biennial basis.
The Joint Commission Competency (HR.01.01.01 and HR.01.06.01) requirement states that the hospital must have the necessary staff to support the care, treatment, or services it provides, and that staff must be competent to perform their responsibilities. Competency is defined as a combination of observable and measurable knowledge, skills, abilities, and personal attributes that constitute an employee’s performance. The ultimate goal should be that the employee can demonstrate the required attributes to deliver safe, quality care.
The New York State Education Law (130 Education Law 6509) and the Board of Regents Rules, Part 29.2 states that it is professional misconduct and unprofessional conduct to practice nursing with negligence or incompetence.
CASE SCENARIO: Floating to another Unit
Nurse Ima Nu has been asked to float out of her pediatric unit onto an adult medical unit to fill a shortage of RNs due to sick calls. What actions can Ima take?
If Ima cannot come to an agreement with the management team about any of her requests, then she must:
Accept the assignment documenting carefully on the POA form her concerns related to patient safety using the process outlined in this program.
Keep a personal copy of this documentation, provide a copy to the immediate supervisor, send a copy to the union representative, and another to Human Resources.
Ask the other RNs on the unit to co-sign the POA.
Or…
Refuse the assignment and accept the possibility of disciplinary action, up to and including termination.
Document carefully her concern for patient safety and the process she used to inform the manager of her concerns.
Keep a personal copy of this documentation, provide a copy to the immediate supervisor, and send a copy to the NYSNA representative.
Once again, Ima is being asked to do something that is beyond her personal knowledge, skill set, and experience. Answer the following questions about Ima’s ethical, legal, and professional rights and responsibilities by circling the best answer.
1. Does Ima have the legal right to notify her manager that she does not feel she is competent to float?
a. Yes, Ima has never been oriented to the adult medical units by the facility.
b. No, there are no specialty RN licenses. An RN can be assigned to any unit.
2. Does Ima have the legal right to ask her manager to ask another RN who has knowledge of the medical patient float?
a. Yes, Ima can self-assess that these patients require specialty knowledge and skills that she does not possess and cannot, therefore, deliver safe nursing care.
b. No, Ima has taken and passes the NCLEX and has, therefore, minimally acceptable knowledge in medical nursing.
3. Does Ima have the legal right to ask the manager on the medical floor to assign her to another RN who can assist her with her patient assignment?
a. Yes, Ima has the legal right to determine she is not qualified to monitor the medical patient because she is not qualified or experienced in the adult patient and is not familiar with the procedures and/or medications she will be expected to administer.
b. No, Ima has access to the unit policies and procedures, and the pharmacy and Lippincott online is available to her for reference. In addition, Ima has a legal and ethical obligation to render herself competent. In addition, Ima has passed every hospital competency assessment.
4. Does Ima have the right to ask the manager on the medical floor to limit her patient assignment?
a. Yes, Ima can self-assess that she is not skilled in the nursing care of complex procedures and medications of the adult medical patient with comorbidities.
b. No, under ethics, assurance of competency is the responsibility of the individual nurse, and Ima is aware that pediatric nurses are frequently asked to float to the medical units. Answers to scenario
Use the sheet on the previous page to practice filling out a POA for this case scenario.
This scenario is rooted in both law and ethics. The answers relevant to the nurse’s actions under NYS law should be guided by the following. Please refer to your own state’s law to guide your actions:
The Code of Ethics for Nurses (Provision 4) states, “The nurse is responsible and accountable for individual nursing practice and
determines the appropriate delegation of tasks consistent with the nurse’s obligation to provide optimum patient care.”
The American Nurses Association (ANA) states that “Assurance of competence is the responsibility of the profession, individual nurses, professional organizations, credentialing and certification entities, regulatory agencies, employers, and other key stakeholders.”
New York State RN licenses carries with it certain expectations and responsibilities. It represents both basic qualifications and the commitment to maintaining competency and rendering quality services throughout the career. A licensee may legally perform services that are in the definition of the scope of practice but licensees must also be competent to deliver those services.
The literature denotes that core competencies in nursing include: keen observation and judgment, efficiency, skillfulness, responsibility, accountability, communication and collaboration, management, self-development, innovation and research, stress-adjustment, critical thinking skills, and the ability to integrate problem-based and evidence-based learning approaches into practice.
The New York State Health Code 10 NYCRR 405.5 (a) (1),(4) states the hospital shall provide RNs who are qualified by training and experience for the job and shall have a written evaluation of the performance, credentials, and competence of registered professional nurses and ancillary nursing personnel shall be conducted on at least a biennial basis.
The Joint Commission Competency (HR.01.01.01 and HR.01.06.01) requirement states that the hospital must have the necessary staff to support the care, treatment, or services it provides, and that staff must be competent to perform their responsibilities. Competency is defined as a combination of observable and measurable knowledge, skills, abilities and personal attributes that constitute an employee’s performance. The ultimate goal should be that the employee can demonstrate the required attributes to deliver safe, quality care.
The New York State Education Law (130 Education Law 6509) and the Board of Regents Rules, Part 29.2 state that it is professional misconduct and unprofessional conduct to practice nursing with negligence or incompetence.
If Ima cannot come to an agreement with the management team about any of her requests, then she must:
Accept the assignment documenting carefully on the POA form her concerns related to patient safety using the process outlined in this program.
Keep a personal copy of this documentation, provide a copy to the immediate supervisor, send a copy to the union representative, and another to Human Resources.
Ask the other RNs on the unit to co-sign the POA.
Or…
Refuse the assignment and accept the possibility of disciplinary action, up to and including termination.
Document carefully her concern for patient safety and the process she used to inform the manager of her concerns.
Keep a personal copy of this documentation, provide a copy to the immediate supervisor, and send a copy to the NYSNA representative.
Conclusion
This program describes some of the current ethical and legal issues surrounding the nurse’s legal and ethical rights and responsibilities regarding the POA. When an assignment is within a nurse’s scope of practice but not within their realm of experience or training, law, and ethics allow the nurse to make a self-determined judgment that they are not individually possessed of the necessary skills, knowledge, or experience to deliver safe nursing care. Nevertheless, an outright refusal to do the assignment carries the risk of discipline for insubordination. It’s crucial to speak up when a nurse, using their independent judgment and self-analysis, deems themself not competent to deliver safe and quality nursing care. Try to negotiate instead. Tell your supervisor you’re perfectly willing to help provide care for patients in the ICU, for instance, but that you have never worked with the new ventilator and monitoring equipment and have very limited experience caring for critically ill patients and should neither be left in charge nor given a full patient assignment.
If that tactic fails and you have little recourse other than to take on the assignment, submit a POA form. Describe the task or assignment you don’t feel equipped to handle, the reason for your feelings, and the training you would need to be more confident and better prepared.
In addition to this resource, nurses are encouraged to turn to other resources, such as the Code of Ethics for Nurses, nursing colleagues, ethics committees, management, facility policies, and nurses associations, in supporting the nurse’s ethical and legal commitment and obligations to their patient’s right to quality patient care.
Assignment Under Protest: A Nurse’s Rights and Responsibilities n
n references
American Nurses Association. (2015). Code of ethics for nurses. American Nurses Publishing.
Boehning, A. P., Haddad, L. M. (2024) Nursing Practice Act. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK559012/
Ketter, J. (1997) Nurses and strikes: A perspective from the United States. Nursing Ethics, 4 (4), 323–329. http://www/doi. org/10.1177/096973309700400408
n WHAT’S NeW IN HEALTHCARE LITERATURE
n Anaphylaxis Clinical Practice Guidelines: Findings From the Allergy Immunology Joint Task Force on Practice Parameters (JTFPP)
n Mustafa, S. S., & Kaliner, M. A. (Ed.) (2024 February 27). https://emedicine.medscape.com/article/135065
Guidelines for anaphylaxis were updated in February 2024, by the Allergy Immunology Joint Task Force on Practice Parameters (JTFPP) and published in the Annals of Allergy, Asthma & Immunology
Diagnosis
For diagnosis, clinicians are advised to obtain a baseline serum tryptase (bST) level in patients presenting with a history of recurrent, idiopathic, or severe anaphylaxis, particularly those presenting with hypotension.
Anaphylaxis in Infants and Toddlers
Because there are no criteria specific to this age group, clinicians should use current National Institute of Allergy and Infectious Disease and Food Allergy and Anaphylaxis Network (NIAID/FAAN) or World Allergy Organization (WAO) anaphylaxis criteria to assist in their diagnosis of anaphylaxis. It is suggested that clinicians prescribe either the 0.1-mg or the 0.15-mg epinephrine autoinjector (EAI) dose for infants/toddlers weighing less than 15 kg.
Beta Blocker and Angiotensin-Converting Enzyme Inhibitors
JTFPP recommends prescribing venom immunotherapy (VIT) for patients with a history of insect sting anaphylaxis who are treated with beta blocker (BB) or angiotensin-converting enzyme inhibitor (ACEI) medication. Routine prescription of epinephrine autoinjectors (EAIs) continues to be advised for patients at higher risk of anaphylaxis. Specific counseling and training of patients and caregivers is required for optimal prescribing and use of EAIs.
Mast Cell Disorders and Anaphylaxis
When there is high suspicion for systemic mastocytosis, it is recommended that clinicians order a bone marrow biopsy with staining for tryptase, CD25 immunohistochemistry and flow cytometry, and the KIT D816V mutation. Clinicians should not rely on serum tryptase levels alone for diagnostic assessment of the likelihood that a patient does or does not have a clonal mast cell disorder. Clinicians should measure bST in patients with severe insect sting anaphylaxis, in all cases of recurrent unexplained anaphylaxis, and in patients with suspected mastocytosis.
Above are some of the highlights of the guidelines without analysis or commentary. For more information, go directly to the guidelines.
n Polycystic ovary Syndrome Clinical Practice Guidelines
n International PCOS Network. (2023, December 5). https://reference.medscape.com/viewarticle/998889
Clinical practice guidelines on the diagnosis and management of polycystic ovary syndrome (PCOS) from the International PCOS Network were published in October 2023 in Fertility and Sterility.
Two of the following three criteria are observed to make the diagnosis of PCOS: (1) clinical and/or biochemical evidence of hyperandrogenism, (2) ovulatory dysfunction, and (3) polycystic ovaries as indicated by ultrasound examination or anti-Müllerian hormone (AMH) level in adults. Neither ultrasound examination nor serum AMH measurement is recommended in adolescents because of poor specificity in this age group. In patients who have both irregular menstrual cycles and hyperandrogenism, PCOS may be diagnosed. In such patients, neither an ovarian ultrasound scan nor an AMH level is required for the diagnosis.
Testing for biochemical hyperandrogenism includes measurement of total and free testosterone levels. The calculated free androgen index can be used to estimate the free testosterone level. Combined oral contraceptive pills are the first-line pharmacologic option for management of PCOS-induced irregular menstrual cycles and/or hirsutism. No specific oral contraceptive is recommended; however, preparations with a lower dose of ethinyl estradiol and fewer adverse effects are preferred.
The use of metformin is recommended for adults who have a body mass index of 25 kg/m2 or higher mainly to manage the metabolic features of PCOS, such as insulin resistance and glucose and lipid levels. Metformin is preferred over inositol, which has limited effects on hirsutism, weight, and ovulation in patients with PCOS.
n Clinical Practice Guidelines on Heart Failure-related Cardiogenic Shock
n International Society for Heart and Lung Transplantation. (2024, February 28). https://reference.medscape.com/viewarticle/1000216
The International Society for Heart and Lung Transplantation published new consensus statements for heart failure-related cardiogenic shock in the Journal of Heart and Lung Transplantation
There is a range of cardiogenic shock (CS) care. Levels of care capability can be determined by the treatment goals in each clinical setting. Advanced treatments including heart transplants and durable ventricular assist devices may only be available at a level 1 center.
To treat patients with heart-failure cardiogenic shock, it is important to focus on necessary roles rather than disciplines. Roles that must be performed include having a clinician able to provide critical care, a clinician to place temporary mechanical circulatory support (MCS) devices and perform cardiothoracic surgical procedures, a heart failure practitioner, a nursing/allied health professional, and potentially a device specialist (perfusionist, mechanical circulatory support coordinator), palliative care, and pharmacy services.
It is necessary to assess biventricular filling pressures and cardiac output, as well as serial assessment if the patient has a pulmonary artery
catheter (PAC) in place. Hemodynamic data should be correlated with clinical and laboratory perfusion indices, with close monitoring for trends.
When discussing patients with etiologies unconnected to acute coronary syndrome, the term HF-CS (heart failure cardiogenic shock) is preferred. Additional information to include when referring a patient to a higher level of care is how chronic the patient’s illness is (acute or acute on chronic), and the type (left, right, or biventricular failure).
The intensity of the initial support approach should match the cardiogenic shock patient’s severity and clinical trajectory. There is no specific numerical flow target for the management of cardiogenic shock in patients with HF-CS (heart failure cardiogenic shock). Rather, establishing and maintaining end organ perfusion is vital. Clinical improvement varies across organ systems, keeping in mind that some organ systems may improve more slowly than others. With little robust data to inform clinical decisions, the risks of thrombus (including where it might embolize) should be matched to the risk of anticoagulation type and intensity that is selected during treatment of cardiogenic shock.
For the latest suggestions for treating heart failure cardiogenic shock, go directly to the guidelines by clicking the link in the reference.
n lipid management Clinical Practice Guidelines
n College of Family Physicians of Canada. (2023, December 1). https://reference.medscape.com/viewarticle/998891
Guidelines for lipid management in the prevention of cardiovascular disease (CVD) for primary care were published in October 2023 by the College of Family Physicians of Canada (CFPC) in Canadian Family Physician.
Screening and Testing
Lipid testing as part of global cardiovascular disease (CVD) risk estimation is suggested in men age ≥ 40 years and women age ≥ 50 years. When reassessing CVD risk in patients not taking lipid-lowering therapy, clinicians should reassess lipids no more than every 5 years and preferably 10 years, unless risk factors change. Fasting for lipid testing is not recommended.
Interventions
Patients should be encouraged to participate in physical activity and adhere to a Mediterranean diet. Clinicians should discuss the initiation of high-intensity statins for primary prevention in patients with a 10-year CVD risk of ≥ 20%. Clinicians should discuss the initiation of moderate-intensity statins for primary prevention in patients with a 10-year CVD risk of 10% to 19%. Clinicians should retest lipid levels in 5 years at the earliest and preferably in 10 years for primary prevention in patients with a 10-year CVD risk of < 10%.
Patients Older Than 75 Years
Lipid testing and routine initiation of statin therapy for primary prevention are not recommended in patients older than 75 years.
Notice From NYS DoH
Notice From NYS DoH
Notice From NYS DoH,
Notice From NYS DoH,
Notice From NYS DoH,
Notice From NYS DoH,
Notice From NYS DoH,
Notice From NYS DoH,
Notice From NYS DoH,
n Ce Activity: A Prognostic model for CoVID-19 Progression to Severe Disease:
Discriminating emergency
Department Discharge
With the Virus Without return to the Hospital Within 72 Hours using electronic medical records
Thank you for your participation in “A Prognostic Model for COVID19 Progression to Severe Disease: Discriminating Emergency Department Discharge With the Virus Without Return to the Hospital Within 72 Hours Using Electronic Medical Records,” a new continuing education (CE) activity offered by NYSNA. NYSNA members and nonmembers are invited to take part in this activity, and you do not need to be a resident of New York State.
INSTRUCTIONS
In order to receive contact hours for this educational activity, participants are to read the article presented in this issue of The Journal, complete and return the post-test, evaluation form, and earn 80% or better on the post-test.
This activity is free to NYSNA members and $10 for nonmembers. Participants can pay by check (made payable to NYSNA) or credit card. The completed answer sheet and evaluation form may be mailed or faxed back to NYSNA; see the evaluation form for more information.
The New York State Nurses Association is accredited as a provider of nursing continuing professional development by the American Nurses Credentialing Center’s Commission on Accreditation.
This program has been awarded 1.0 contact hour (CH) through the New York State Nurses Association Accredited Provider Unit.
The New York State Nurses Association is accredited by the International Accreditors for Continuing Education and Training (IACET) and offers IACET CEUs for its learning events that comply with the ANSI/ IACET Continuing Education and Training Standard. IACET is recognized internationally as a standard development organization and accrediting body that promotes quality of continuing education and training. The New York State Nurses Association is authorized by IACET to offer 0.1 CEU for this program.
In order to receive CHs and CEUs, participants must read the entire article, fill out the evaluation, and get 80% or higher on the post-test.
NYSNA wishes to disclose that no commercial support was received for this educational activity.
NYSNA Program Planners, Presenters, and Content Experts declare that they have no financial relationship with an ineligible company.
Declaration of vested interest: None.
INTRODUCTION
With limited tools to predict disease progression, it is difficult for emergency department physicians to make reliably informed decisions as whether to discharge or admit patients diagnosed with COVID-19. Patients with COVID-19 may return within 72 hours or experience preventable clinical deterioration. Little data exists to support clinical prognostic models
to accurately classify a patient’s risk for developing severe symptoms from COVID-19. Participants will gain knowledge of a clinical prognostic model (XGBoost) to support the anticipated clinical prognosis and plan acute care and disposition. This will enable patients with COVID-19 to have more safe dispositions. Secondarily, this will permit better resource allocation of health systems.
LEARNING OUTCOME
Participants will distinguish characteristics of patients who can be safely discharged home without returning to the emergency department within 72 hours and those who may require an inpatient stay of 24 hours or longer.
OBJECTIVES
By completion of the article, the reader will be able to:
1. Identify rationale for distinguishing patient risk between a severe or mild course of COVID-19 disease.
2. Identify sources of predictive data in the progression of COVID-19 infection.
Please answer either True or False to the questions below. Remember to complete the answer sheet by putting the letter of your corresponding answer next to the question number. Each question has only one correct answer.
The 1.0 CH and 0.1 CEU for this program will be offered until June 30, 2027.
1) Data from electronic health records can indicate risk for COVID-19 disease progression.
a. True
b. False
2) Clinician behaviors, such as the number of physician orders entered and the number of times a temperature is taken, can indicate how severely ill a patient is.
a. True
b. False
3) Age greater than 60 was identified by the authors as a risk factor for clinical deterioration from suspected COVID-19.
a. True
b. False
4) Given limited inpatient resources during COVID-19 surge, it is best to admit patients at high risk for severe disease progression.
a. True
b. False
5) The XGBoost classification model most successfully predicted which patients suspected of COVID-19 could be either safely discharged home or who would benefit from inpatient care.
a. True
b. False
6) Vitals sign scores taken in the emergency department are the most important factor in determining an individual patient’s risk for deterioration.
a. True
b. False
7) Patients with Medicare had a lower risk for deterioration than patients with private insurance.
a. True
b. False
8) Patients presenting to the emergency department with hypoxia experienced a more severe clinical course than patients who were not hypoxic.
a. True
b. False
9) Authors found that patients with pneumonia due to COVID-19 were nearly 10 times more likely to experience severe symptoms of COVID-19 than those without pneumonia.
a. True
b. False
10) Longer emergency department length of stays were associated with greater risk for symptom deterioration among patients suspected of having COVID-19.
a. True
b. False
Answer Sheet
A Prognostic model for CoVID-19 Progression to Severe Disease: Discriminating emergency Department Discharge With the Virus Without return to the Hospital Within 72 Hours using electronic medical records
Note: The 1.0 CH and 0.1 CEU for this program will be offered until June 30, 2027.
Please print your answers in the spaces provided below. There is only one answer for each question.
Please print legibly and verify that all information is correct.
First Name: MI:
Name: Street Address: City: State:
Code: Daytime Phone Number (Include area code):
Email:
Profession: Currently Licensed in NY State? Y / N (Circle one)
NYSNA Member # (if applicable): License #:
ACTIVITY FEE: Free for NYSNA members/$10 nonmembers
PAYMENT METHOD
Check—payable to New York State Nurses Association (please include “Journal CE” on your check).
Credit Card: Mastercard Visa Discover American Express
Card Number:
Expiration Date: / CVV#
Name: Signature: Date: / /
Please complete the answer sheet above and course evaluation form on reverse. Submit both the answer sheet and course evaluation form along with the activity fee for processing. Email to: journal@nysna.org Or mail to: NYSNA, attn. Nursing Education and Practice Dept. 131 West 33rd Street, 4th Floor, New York, NY 10001 Or fax to: 212-785-0429
learning Activity evaluation
A Prognostic model for CoVID-19 Progression to Severe Disease: Discriminating emergency Department Discharge With the Virus Without return to the Hospital Within 72 Hours using electronic medical records
Please use the following scale to rate statements 1–7 below:
1. The content fulfills the overall purpose of the CE Activity.
2. The content fulfills each of the CE Activity objectives.
3. The CE Activity subject matter is current and accurate.
4. The material presented is clear and understandable.
5. The teaching/learning method is effective.
6. The test is clear and the answers are appropriately covered in the CE Activity.
7. How would you rate this CE Activity overall?
8. Time to complete the entire CE Activity and the test? ____ Hours (enter 0–99) _____ Minutes (enter 0–59)
9. Was this course fair, balanced, and free of commercial bias? Yes / No (Circle one)
10. Comments:
11. Do you have any suggestions about how we can improve this CE Activity?
n Ce Activity: A Correlational Study of the relationship of Nurses’ Pain Assessment and Patients’ History of Substance use
Thank you for your participation in a new continuing education (CE) activity offered by NYSNA. NYSNA members and nonmembers are invited to take part in this activity, and you do not need to be a resident of New York State.
INSTRUCTIONS
In order to receive contact hours for this educational activity, participants are to read the article presented in this issue of The Journal, complete and return the post-test, evaluation form, and earn 80% or better on the post-test.
This activity is free to NYSNA members and $10 for nonmembers. Participants can pay by check (made payable to NYSNA) or credit card. The completed answer sheet and evaluation form may be mailed or faxed back to NYSNA; see the evaluation form for more information.
The New York State Nurses Association is accredited as a provider of nursing continuing professional development by the American Nurses Credentialing Center’s Commission on Accreditation.
This program has been awarded 1.0 contact hour (CH) through the New York State Nurses Association Accredited Provider Unit.
The New York State Nurses Association is accredited by the International Accreditors for Continuing Education and Training (IACET) and offers IACET CEUs for its learning events that comply with the ANSI/ IACET Continuing Education and Training Standard. IACET is recognized internationally as a standard development organization and accrediting body that promotes quality of continuing education and training.
The New York State Nurses Association is authorized by IACET to offer 0.1 CEU for this program.
In order to receive CHs and CEUs, participants must read the entire article, fill out the evaluation, and get 80% or higher on the post-test.
NYSNA wishes to disclose that no commercial support was received for this educational activity.
NYSNA Program Planners, Presenters, and Content Experts declare that they have no financial relationship with an ineligible company.
Declaration of vested interest: None
INTRODUCTION
Pain has been recognized as a substantial health problem by the National Institutes of Health, the U.S. Department of Health and Human Services, and the Institute of Medicine. Use of appropriate, validated pain scales is essential for pain assessment and intervention. The ongoing opioid crisis complicates pain assessment and treatment. Nurses’ assessment of pain may be influenced by personal factors such as their perception of a patient’s current and/or past use of drugs and alcohol. A nurse’s empathy toward a patient and numerous other factors may impact the assessment or care of the patient. Nurses are not always aware of how personal characteristics interact with patient characteristics of substance use history. These characteristics may lead nurses to underrate pain scores
and ineffectively treat patients’ pain. Through participation in this CE module, nurses will gain awareness of the complex factors influencing their practices of pain assessment and treatment. When cognizant of their ethical and professional obligation to address patients’ pain, nurses can better objectively assess and treat patients, enhancing quality nursing practice and fostering positive patient outcomes for patients with histories of drug use.
LEARNING OUTCOME
Participants will identify the complex factors influencing their practices of pain assessment and treatment, particularly for the substance-use patient population.
OBJECTIVES
By completion of the article, the reader will be able to:
1. Identify the significance of pain as a health problem.
2. Recognize how pain assessment can be influenced by various factors.
3. Identify results of the descriptive correlational study related to pain assessment and management of patients with a history of drug and/ or alcohol use.
Please answer either True or False to the questions below. Remember to complete the answer sheet by putting the letter of your corresponding answer next to the question number. Each question has only one correct answer.
The 1.0 CH and 0.1 CEU for this program will be offered until June 30, 2027.
1) The experience of pain does not include an emotional component.
a. True
b. False
2) Nociceptive pain is a response to perceived tissue damage and the level of pain cannot be determined by a validated pain assessment tool.
a. True
b. False
3) The author found that when patients had a previous history of opioid, marijuana, or alcohol use, nurses scored the patients higher than patients who had no history.
a. True
b. False
4) Establishing therapeutic communication with a patient is essential for treating a patient’s pain responsibly.
a. True
b. False
5) The author implies that nurses’ perception of a patient’s pain may differ between a patient scenario and an actual patient.
a. True
b. False
6) Low COMFORT behavioral scale scores indicated nurses were not cautious of using opioids to treat patients’ pain.
a. True
b. False
7) The COMFORT behavioral scale assesses sedation, distress, and pain.
a. True
b. False
8) Authors suggest that improving nurses’ self-awareness while in nursing school would allow them to more accurately respond to patients’ pain. A nurse’s competency includes self-awareness.
a. True
b. False
9) An accurate patient history, exam, questioning, and correct use of pain scales are required for competent pain assessment.
a. True
b. False
10) The healthcare system’s response to the opioid crises has led to adequate treatment of patients’ pain.
a. True
b. False
Answer Sheet
A
Correlational Study of the relationship of Nurses’ Pain Assessment and Patients’ History of Substance use
Note: 1.0 CH and 0.1 CEU for this program will be offered until June 30, 2027.
Please print legibly and verify that all information is correct.
First Name: MI: Last Name:
Street Address: City:
Code: Daytime Phone Number (Include area code):
NYSNA Member # (if applicable): License #:
ACTIVITY FEE: Free for NYSNA members/$10 nonmembers PAYMENT METHOD
Check—payable to New York State Nurses Association (please include “Journal CE”on your check).
Credit Card: Mastercard Visa Discover American Express
Card Number: Expiration Date: / CVV#
Name: Signature: Date: / /
Please print your answers in the spaces provided below. There is only one answer for each question.
Please complete the answer sheet above and course evaluation form on reverse. Submit both the answer sheet and course evaluation form along with the activity fee for processing. Email to: journal@nysna.org
Or mail to: NYSNA, attn. Nursing Education and Practice Dept. 131 West 33rd Street, 4th Floor, New York, NY 10001 Or fax to: 212-785-0429
A Correlational Study of the relationship of Nurses’ Pain Assessment and Patients’ History of Substance use
Please use the following scale to rate statements 1–7 below:
1. The content fulfills the overall purpose of the CE Activity.
2. The content fulfills each of the CE Activity objectives.
3. The CE Activity subject matter is current and accurate.
4. The material presented is clear and understandable.
5. The teaching/learning method is effective.
6. The test is clear and the answers are appropriately covered in the CE Activity.
7. How would you rate this CE Activity overall?
8. Time to complete the entire CE Activity and the test? ____ Hours (enter 0–99) _____ Minutes (enter 0–59)
9. Was this course fair, balanced, and free of commercial bias? Yes / No (Circle one)
10. Comments:
11. Do you have any suggestions about how we can improve this CE Activity?
n Ce Activity: Assignment under Protest: A Nurse’s rights and responsibilities
Thank you for your participation in “Assignment Under Protest: A Nurse’s Rights and Responsibilities,” a new continuing education (CE) activity offered by NYSNA. NYSNA members and nonmembers are invited to take part in this activity, and you do not need to be a resident of New York State.
INSTRUCTIONS
In order to receive contact hours for this educational activity, participants are to read the article presented in this issue of The Journal, complete and return the post-test, evaluation form, and earn 80% or better on the post-test.
This activity is free to NYSNA members and $10 for nonmembers. Participants can pay by check (made payable to NYSNA) or credit card. The completed answer sheet and evaluation form may be mailed or faxed back to NYSNA; see the evaluation form for more information.
The New York State Nurses Association is accredited as a provider of nursing continuing professional development by the American Nurses Credentialing Center’s Commission on Accreditation.
This program has been awarded 1.0 contact hour (CH) through the New York State Nurses Association Accredited Provider Unit.
The New York State Nurses Association is accredited by the International Accreditors for Continuing Education and Training (IACET) and offers IACET CEUs for its learning events that comply with the ANSI/ IACET Continuing Education and Training Standard. IACET is recognized internationally as a standard development organization and accrediting body that promotes quality of continuing education and training.
The New York State Nurses Association is authorized by IACET to offer 0.1 CEU for this program.
In order to receive CHs and CEUs, participants must read the entire article, fill out the evaluation, and get 80% or higher on the post-test.
NYSNA wishes to disclose that no commercial support was received for this educational activity.
NYSNA Program Planners, Presenters, and Content Experts declare that they have no financial relationship with an ineligible company.
Declaration of vested interest: None.
INTRODUCTION
Registered nurses (RNs)—based on their legal, professional, and ethical responsibilities—have the right to accept, reject, or object in writing to any patient assignment that puts patients or themselves at serious risk for harm. While RNs have the professional obligation to raise concerns regarding any patient assignment that puts patients or themselves at risk for harm, refusing a patient assignment carries legal and employment risks. This program is intended for nurses working in specialty care units who want to know the legal basis for the right to object to an assignment and how to professionally document their practice concerns on a Protest of Assignment (POA) form.
Learning Outcome
Restate the importance of filing POAs as a way for nurses, through individual and collective effort, to establish, maintain, and improve the ethical environment of the work setting and conditions of employment that are conducive to safe and quality health care.
OBJECTIVES
By completion of the article, the reader will be able to:
1. Identify the data needed to successfully provide notice to the hospital or nursing home of staffing and patient safety issues.
2. Identify how to most effectively fill out a POA.
3. Restate how the POA data can be used to facilitate concerted activity and patient advocacy.
4. Use critical thinking and the POA process to solve case scenarios. Please answer either True or False to the questions below. Remember to complete the answer sheet by putting the letter of your corresponding answer next to the question number. Each question has only one correct answer.
The 1.0 CH and 0.1 CEU for this program will be offered until June 30, 2027.
1) All members of the healthcare team, from staff nurses to administration, share a joint responsibility to ensure that safe, effective, and appropriate nursing care is provided to patients.
a. True
b. False
2) Registered nurses do not have the right and responsibility to make informed decisions about their personal skill set, knowledge base, and experience level.
a. True
b. False
3) The nurse’s decision regarding accepting or rejecting assignments is based solely on their professional and personal value system.
a. True
b. False
4) The nurse always assumes individual accountability for their nursing judgment and actions.
a. True
b. False
5) Nursing staff, management, and administration may differ in their interpretation of the ethical and legal principles and rights of nurses to accept or reject their assignment. These differences may create conflict and can lead to disciplinary action.
a. True
b. False
6) The objective of a POA is to provide notice to the employer of a potentially unsafe situation and to impute liability onto the management team and hospital. The nurse still remains liable to a degree for any untoward patient outcomes.
a. True
b. False
7) The purpose of the POA is to constructively notify the management team of the laws, regulations, and contractual terms they may be in violation of.
a. True
b. False
8) The nurse should not hesitate to fill out a POA form when they do not have the requisite knowledge and performance skills to care for the assigned patient population. Courts have held that if an average, prudent nurse would not have accepted a particular assignment, the nurse who does accept the assignment will be held to a strict professional standard of a competent nurse in that specialty practice area.
a. True
b. False
9) Nurses who refuse a patient assignment will not risk disciplinary action from their employer if they file a POA and cite the law.
a. True
b. False
10) Filling out and delivering a copy of a POA form to an immediate supervisor does not impute liability and does not protect the nurse from any action taken against the nurse’s license.
a. True
b. False
Answer Sheet
Assignment under Protest: A Nurse’s rights and responsibilities
Note: 1.0 CH and 0.1 CEU for this program will be offered until June 30, 2027.
Please print legibly and verify that all information is correct.
First
Daytime Phone Number (Include area code): Email:
NYSNA Member # (if applicable):
PAYMENT METHOD
ACTIVITY FEE: Free for NYSNA members/$10 nonmembers
Check—payable to New York State Nurses Association (please include “Journal CE”on your check).
Credit Card: Mastercard Visa Discover American Express
Please complete the answer sheet above and course evaluation form on reverse. Submit both the answer sheet and course evaluation form along with the activity fee for processing. Email to: journal@nysna.org Or mail to: NYSNA, attn. Nursing Education and Practice Dept. 131 West 33rd Street, 4th Floor, New York, NY 10001 Or fax to: 212-785-0429
learning Activity evaluation
Assignment under Protest: A Nurse’s rights and responsibilities
Please use the following scale to rate statements 1–7 below:
1. The content fulfills the overall purpose of the CE Activity.
2. The content fulfills each of the CE Activity objectives.
3. The CE Activity subject matter is current and accurate.
4. The material presented is clear and understandable.
5. The teaching/learning method is effective.
6. The test is clear and the answers are appropriately covered in the CE Activity.
7. How would you rate this CE Activity overall?
8. Time to complete the entire CE Activity and the test? ____ Hours (enter 0–99) _____ Minutes (enter 0–59)
9. Was this course fair, balanced, and free of commercial bias? Yes / No (Circle one)
10. Comments:
11. Do you have any suggestions about how we can improve this CE Activity?
THE JOURNAL
of the New York State Nurses Association
Call for Papers
The Journal of the New York State Nurses Association is currently seeking papers.
Authors are invited to submit scholarly papers, research studies, brief reports on clinical or educational innovations, and articles of opinion on subjects important to registered nurses. Of particular interest are papers addressing direct care issues. New authors and student authors are encouraged to submit manuscripts for publication.
Information for Authors
For author’s guidelines and submission deadlines, go to the publications area of www.nysna.org or write to journal@nysna.org
Call for editorial board members
Help Promote Nursing research
The Journal of the New York State Nurses Association is currently seeking candidates interested in becoming members of the publication’s Editorial Board.
Members of the Editorial Board are appointed by the NYSNA Board of Directors and serve one 6-year term. They are responsible for guiding the overall editorial direction of The Journal and assuring that the published manuscripts meet appropriate standards through blinded peer review.
Prospective Editorial Board members should be previously published and hold an advanced nursing degree; candidates must also be current members of NYSNA. For more information or to request a nomination form, write to journal@nysna.org