Thank you to the following businesses who support the Oklahoma Dental Association by advertising in the Journal:
Alliant Insurance Services
Endodontic Associates OKC
Endodontic Practice Associates
Hopkins Dental Implant Institute
National Dentex Labs
Suction Solutions
The Uniform Shoppe
EDITORIAL
07 Legislature Allocates ARPA Funds for 2025 Oklahoma Mission of Mercy ASSOCIATION
Executive Director Report
Senior Signing Day Photos
STORY
Meet Your New Association President
THE OKLAHOMA DENTAL ASSOCIATION JOURNAL (ISSN 0164-9442) is the official publication of the Oklahoma Dental Association and is published bimonthly by the Oklahoma Dental Association, 317 NE 13th Street, Oklahoma City, OK 73104, Phone: (405) 848-8873; (800) 876-8890. Fax: (405) 848-8875. Email: information@ okda.org. Annual subscription rate of $39 for ODA members is included in their annual membership dues.
POSTMASTER: Send address changes to OKLAHOMA DENTAL ASSOCIATION, 317 NE 13th Street Oklahoma City, OK 73104
Periodical postage paid at Oklahoma City, OK and additional mailing offices.
Subscriptions: Rates for non-members are $56. Single copy rate is $18, payable in advance.
Reprints: of the Journal are available by contacting the ODA at (405) 848-8873, (800) 876-8890, editor@okda.org.
Opinions and statements expressed in the OKLAHOMA DENTAL ASSOCIATION JOURNAL are those of the author and are not necessarily those of the Oklahoma Dental Association. Neither the Editors nor the Oklahoma Dental Association are in any way responsible for the articles or views published in the OKLAHOMA DENTAL ASSOCIATION JOURNAL.
21 A 3-year follow-up for the conservative management of hypomineralization on deciduous and permanent dentition
CLASSIFIEDS
26 Classifed Ads
Would you like to submit a case study, scientific article, or editorial for publication in
Email editor@okda.org with story ideas.
Is Your Information Correct?
Help the ODA keep you informed about legislative actions, educational opportunities, events, and other important member-only news.
Contact Ansley Jinkins at ajinkins@okda.org or 800.876.8890 to provide ODA with your current contact information.
ODA JOURNAL STAFF
EDITOR
Mary Hamburg, DDS, MS
ASSOCIATE EDITOR
Roberta A. Wright, DMD, MDSc, FACP
EDITORIAL BOARD MEMBERS
M. Edmund Braly, DDS, FACS, FAACS
Daryn Lu, DDS
Phoebe Vaughan, DDS
Meredith Turbeville, DDS
Divesh Sardana, BDS, MDS, MBA, MPH, PhD
ODA OFFICERS 2024-2025
PRESIDENT
Daryn Lu, DDS president@okda.org
PRESIDENT-ELECT
Twana Duncan, DDS presidentelect@okda.org
VICE PRESIDENT
Nicole Nellis, DDS vicepresident@okda.org
SECRETARY/TREASURER
Sydney Rogers, DDS treasurer@okda.org
SPEAKER OF THE HOUSE
Mitch Kramer, DDS speaker@okda.org
IMMEDIATE PAST PRESIDENT
Paul Wood, DDS pastpresident@okda.org
ADMINISTRATIVE STAFF
EXECUTIVE DIRECTOR
F. Lynn Means
DIRECTOR OF GOVERNANCE & FINANCE
Shelly Frantz
DIRECTOR OF MEMBERSHIP
Ansley Jinkins
DIRECTOR OF COMMUNICATIONS & EDUCATION
Jill Johnson
DIRECTOR OF MEETINGS & EVENTS
Lindsay Dennis Stay connected with the ODA!
CALENDAR
May Mental Health Awareness Month
May Women's Health Month
May 5
Hand Hygiene Day
May 6-10
Root Canal Awareness Week
May 31 No Tobacco Day
May 13 - June 13 National Smile Month
May 3
Senior Signing Day ODA Offices Oklahoma City
May 6
Senior Signing Day OU Dentistry
Tulsa Dental Clinic
May 10
ODA Rewards Committee Meeting
June
Oral Health Month
June Dental Diversity Month
June
Men's Health Month
June
Migraine and Headache Awareness Month
June 14
Relief & Disaster Grant Program Committee Meeting
June 18
Council on Membership Services Meeting 5:30pm via Zoom
June 21
ODA Strategic Planning Session ODA Offices
June 28 Annual Meeting Planning Committee Meeting 8:00am via Zoom
July 4-5
ODA Offices Closed
Go Digital and Save Time for You and Your Patient
NDX Digital Dentures utilize an efficient workflow that may eliminate up to three appointments to help save time in your practice, making it more convenient for you and your patients.
“We now have the ability to reduce the amount of time before a patient can have their dentures. Because we are able to take digital impressions and couple it with photos, the printed try-ins are almost always spot on. That means we do not need multiple try-in appointments that add stress and cost.”
Dr. Luis Mariusso Knoxville, Tennessee
Oklahoma Legislature Allocates $300,000 in ARPA Funds for 2025 Oklahoma Mission of Mercy
John Wilgess Executive Director Oklahoma Dental Foundation
In a heartening move that underscores the importance of healthcare access for all Oklahomans, the Oklahoma Legislature has approved the allocation of $300,000 in American Rescue Plan Act (ARPA) funds to support the 2025 Oklahoma Mission of Mercy (OkMOM). This annual event, scheduled for February 7-8, 2025, in Tulsa, will bring essential dental care to some of the state’s most vulnerable residents.
Since its inception in 2010, the Oklahoma Mission of Mercy has been a beacon of hope, providing free dental care to those who are uninsured, underinsured, living in poverty, or experiencing homelessness. The event, organized by the Oklahoma Dental Foundation (ODF) and the Oklahoma Dental Association (ODA) in partnership with the Oklahoma State Department of Health, has served over 19,000 patients and delivered more than $16.4 million in donated care.
The significance of this event extends beyond the immediate dental care
provided. It represents a collaborative effort involving hundreds of dental professionals—dentists, hygienists, and assistants—alongside nearly a thousand community volunteers. These individuals come together each year at OkMOM to ensure that patients receive the highest standard of care, addressing urgent dental needs, and often uncovering other underlying health issues.
The $300,000 in ARPA funds will be instrumental in covering essential expenses for the 2025 event, such as dental supplies, equipment rental, venue costs, and provisions for volunteers and patients. The commitment to providing these funds highlights the Legislature's recognition of the critical role that oral health plays in overall well-being and its impact on an individual's quality of life and opportunities.
Each Mission of Mercy event is a logistical marvel, requiring meticulous planning and coordination. The committee and volunteers begin preparations 18 months in advance, ensuring that the event runs smoothly and that as many patients as possible receive care. Patients often travel long distances, some for over an hour, to attend the event, underscoring the high demand and critical need for accessible dental services.
The benefits of the Oklahoma Mission of Mercy are profound. Patients receive an average of six procedures, including oral surgery, root canals, extractions, restorations, pediatric care, and regular hygiene cleanings. Some even receive dentures, partials, and flippers, which can significantly enhance their quality of life and their self-esteem.
This is particularly important for young adults seeking employment, as dental health can influence their confidence and job prospects.
Moreover, the event places a strong emphasis on education, teaching patients about proper oral hygiene, the symptoms of oral cancer, and the importance of regular dental checkups. This educational component helps to instill long-term habits that can prevent future dental issues.
The allocation of these funds is not just an investment in a two-day event; it is an investment in the health and future of thousands of Oklahomans. It is a testament to the dedication of the Oklahoma Dental Foundation, the Oklahoma Dental Association, and the many volunteers who make this event possible each year.
As we look forward to the 2025 Oklahoma Mission of Mercy, the support from the Legislature is a powerful reminder of what can be achieved when communities and lawmakers come together for a common cause. The funding ensures that this vital event will continue to provide life-changing dental care to those who need it most, maintaining the dignity and health of our fellow citizens and neighbors.
On behalf of all those who will benefit from this event and the dedicated professionals who donate their time and skills, we extend our deepest gratitude to the Oklahoma Legislature for their unwavering support. The 2025 Oklahoma Mission of Mercy promises to be another resounding success, thanks to this generous allocation of ARPA funds.
n Serving the OKC Metro for 43 years - since 1977
n Your patient’s experience is top priority
n 3D CBCT scanning for improved diagnosis
n Complex endodontic cases welcomed
n Complex and “heroic” teeth salvage
n Build-up and post & core placement available
n Cutting edge instrumentation and disinfection
n Zeiss microscopes used on every case
n Specializing in finding 4+ canals in molars
n Surgical and nonsurgical retreatment
n General anesthesia and oral sedation
We pride ourselves in a trusted referral pattern that ensures your patient returns to you holding you in high regard - regardless of the reason for referral. We speak highly of you to your patient and reassure them they are in good hands in your care.
We value communication between you and our office. Give us a call to talk about anything. We are even happy to help you navigate through a difficult case in your chair.
Dr. Spencer Hinckley and Dr. Percy Bolen
STATE ASSOCIATION NEWS
Executive Director Report
Good afternoon, ODA Delegates and Officers! I want to extend a very special welcome to our ADA guests – Drs. Allen Reavis and Raymond Cohlmia – thank you again for being with us today!
And Delegates, THANK YOU for taking time from your families and practices to represent your Component today. But I’d like to ask for one more BIG favor: PLEASE attend your Annual Meeting. If you aren’t planning to stick around for the meeting this weekend, please reconsider. With 44 hours of quality CE at the deeply discounted price you get as a benefit of your membership, it is a deal you shouldn’t pass up! Onsite registration opens in the Exhibit Hall downstairs at 7:30 in the morning. PLEASE support your ODA by attending the Annual Meeting this weekend.
Speaking of the Annual Meeting: pre-registration was down again this year – a little over 7% from last year – 45% from 10 years ago – and 57% from 15 years ago. Oklahoma is not alone in this. Every state is facing the
same challenges with their meetings, as well as the ADA. Major changes need to be made as soon as possible – and with that in mind – we have already decided to move next year’s meeting in Tulsa out of the convention center downtown to the Marriott Southern Hills. I know Dr. Lu is already thinking hard on this and working on his Annual Meeting Planning Committee appointments. We’ll also be discussing the Annual Meeting in depth during the ODA’s Strategic Planning session in June. We’d love to hear your ideas of ways we can modify our meeting. Shoot me an email any time!
As Dr. Nellis just reported, reserve funds currently represent over 125% of the proposed 2024 operating budget. I want to commend the Budget and Finance Council for making some tough decisions when building this year’s budget, as well your Investments Committee for closely watching your investments and making some strategic decisions that keep your Association on firm footing. I recently made the tough decision to reduce the staff again –going from six and a half to five and a half FTE. I know many of you have faced this same challenge in your own offices, and just like you, we feel the burden of that hard decision, having to do more with less and stretching an already stretched team. Again, I appreciate the Council’s guidance, careful consideration, and confidence as we continue to work together to keep the ODA both relevant and sound.
Let’s shift to membership: We gained 95 new members in 2023, 69 of which were new graduates,
10 graduate students, and 16 who came back to us after lapsed memberships. We finished 2023 with an 80% market share of the almost 2,000 total licensed dentists in Oklahoma. That’s up one percentage point from 2022, which may not sound significant, but every percentage point represents a lot of hard work. Every member we are successful in retaining should be celebrated and I am enormously proud of the staff for the small increase. Our membership team, alongside the ADA’s membership team, works hard all year executing numerous recruitment and retention campaigns: emails, direct mail, texts, and personal phone calls. We NEVER stop recruiting. But it is getting increasingly difficult to appeal to younger dentists, especially those working in large group practices where the value of membership is more difficult to demonstrate. I make this plea every year, but WE NEED YOUR HELP. The list of 2023 non-renews is attached to my written report. As leaders in your Component, please reach out to these colleagues and encourage them to come back this year.
Member-to-member outreach is BY FAR our BEST offense in building and maintaining a healthy market share, and to add incentive, the ADA is running a member recruitment contest: for every member you recruit you’ll be entered in to a quarterly drawing for a chance to win $1000 in prizes, and for every five members you recruit, you receive a chance to win a seven-day (continued on next page)
Transcript of Executive Director Lynn Means' oral report to the ODA House of Delegates on April 11, 2024 Oklahoma City Convention Center, Oklahoma City, OK
Lynn Means Executive Director Oklahoma Dental Association
STATE ASSOCIATION NEWS
Executive Director Report, continued
interisland Hawaiian cruise for two. Find contest rules in your HOD packet – and THANK YOU in advance for your help with our recruitment and retention efforts.
Great news regarding the OkMOM Legacy Fund: We were successful in reaching the goal to match Dr. Tim and Pamela Fagan’s generous gift before the deadline last June! Their incredible generosity continues to inspire gifts to the Fund, and we hope you have been inspired today after hearing Dr. Wood’s report on how well the mission went in Lawton!
Since 2010, Oklahoma dentistry has come together to provide $16.5 million in donated dental care to more than 19,000 patients in need through the Oklahoma Mission of Mercy. While the treatment is donated, there is still a substantial cost of about $250,000 to operate the event each year. If you haven’t yet joined the OkMOM Legacy, please help us continue the life-changing work done every year by making your gift today.
Find a flyer in your packet with an easy QR code. And THANK YOU to those who have already given! Together, we will ensure essential dental care continues to be provided during the Oklahoma Mission of Mercy! Mark your calendar now for OkMOM 2025, February 7-10, in Tulsa! And thank you to Drs. Lindsay Smith and Rieger Wood for spearheading next year’s mission!
I also want to thank the Oklahoma Dental Foundation for continuing to serve as the ODA’s true partner in all things OkMOM! We could not do it without them, and we are very grateful!
So, I have reported on several of ODA’s assets: a healthy reserve, increased membership over last year, and great news regarding the OkMOM Legacy Fund. But I would argue that our greatest asset is engaged volunteers – a shrinking but extremely valuable commodity – and one with which we need to be even more intentional. One way to do that is to continue to evaluate all ODA volunteer opportunities, taking an even closer look at each to consider things like redundancy, relevance and the staff time devoted to each. Some programs have already been sunset, and more may be in the future. This DOES NOT mean that those areas are not important. But we must ensure that our volunteers’ time and energy is meaningful and constructive, benefiting both the ODA and the volunteer. For example, if the only business conducted during a Council meeting is hearing reports from staff, those Council members will stop showing up (and have). So, let us continue to work together to redistribute the creativity and leadership of those willing volunteers to more productive areas of the Association.
The ODA had several legislative priorities this session. The first was HB 3383, the ODA’s non-covered services clean-up bill. A little history: the ODA passed SB 2051 in 2010 making it illegal for third-party payers to dictate what a dentist can charge for services the insurance company did not cover. In 2013, the insurance industry asked for an Attorney General’s opinion of the new law and his opinion created a loophole in our 2010 bill that made patient contractual limitations such as his/her maximum or frequency limitations exempt from
our non-covered services law. Our bill this year would have changed the definition of non-covered services from services consistent with contractual limitations to all services that are reimbursable notwithstanding, or without regard to, the contractual limitations. Our bill passed the House committee unanimously, but ultimately, the House leadership would not bring the bill to a full House vote before the deadline, so it died.
Another top priority for us at the Capitol this year was a second attempt at getting a dental loss ratio defined and enforced in Oklahoma. Dental loss ratio is the dental insurance premium revenue that is spent on patient care instead of operating costs like marketing and executive salaries. We ran two separate bills addressing this issue, the first, to establish the definition of dental loss ratio and transparency, requiring insurance companies to start reporting their loss ratios annually. The other bill included the definition, the transparency, AND a rebate to premium payers if the required annual loss ratios were not met. We figured at least getting the definition of dental loss ratio codified in Oklahoma was a big step if we couldn’t get the whole enchilada. Again, a little history: last year, Rep. Marcus McEntire was successful in passing our bill off the House floor with a vote of 77-0, but as the bill transitioned to the Senate, it met resistance and failed on a 5-5 tie vote in the Senate Insurance Committee. The tie vote in the Senate Insurance Committee in 2023 was considered “final action” which then triggered the application of certain rules within the Senate that you cannot run a bill that has the same effect and covers the same
STATE ASSOCIATION NEWS
Executive Director Report, continued
specific subject matter two years in a row. Our Senate author, Paul Rosino, had multiple conversations with Senate staff and leadership and even though we had made substantial changes to our 2023 bill language, Senate leadership still took the position to not allow our bills to move this session.
While the Senate rule is certainly a frustrating reality, the conversations our members and lobby team have had with legislators have been very positive. The ODA continues to gain ground on this issue, and the motivation to protect patients by ensuring dental insurance premiums are directed toward actual care is an endeavor worthy of pursuit even if it takes another year. Though the outcome is disappointing for all of us, I want to make sure you know how much we accomplished. Your outreach to lawmakers propelled this effort and laid the groundwork on which we will build next year. We will begin this campaign with more allies, better-educated lawmakers, and the momentum from another incredible effort this year. I want to THANK YOU for all the calls and emails to your legislators on behalf of your patients! Setting a dental loss ratio is simply good policy for Oklahomans so we are going to come back next year and continue to fight for that, as well as fully restoring non-covered services.
And before we leave the topic of advocacy, I must mention that it is extremely important that you contribute to DENPAC every year. DENPAC is the way we MAKE and KEEP friends in the Legislature. Your personal investment each year goes a long way in helping the ODA protect your profession. If you haven’t done your part by giving this
year, please visit the DENPAC table to make your contribution today!
Also, if you are not receiving the ODA legislative alerts either by email or text, that means we do not have your cell number or an up-to-date email address (one that YOU actually see and read – not an INFO AT email address that goes to your office manager). Please help us communicate with you by updating your information. We need every ODA member engaging in our legislative efforts to protect your profession and that is not possible if we can’t effectively communicate with you.
YOU are the key to our legislative success. Grassroots lobbying is THE MOST effective way to get legislators to act on our behalf! While our bills are dead this year, our efforts are not. We ask that you continue to foster strong relationships with your legislators during the interim as we will be coming back next year to ensure necessary policies are addressed and the voices of the profession are heard!
I would like to add my congratulations to our 2024 ODA Leadership Academy’s graduates! The staff and I are excited to work alongside you! The next class will kick off in the fall of 2025. If you are an ODA Leadership Academy graduate, please stand so we can recognize you.
The ODA Rewards program offers member-only discounts on products and services you use every day in your practice and even at home, while providing the ODA nondues revenue generated by member use. Did you know that if you took advantage of every discount offered by our Rewards Partners,
you would save an average of over $15,000 in just one year? That is TWENTY-SEVEN times your ODA dues! In 2023, the ODA received over $135,000 in royalties from our Rewards Partners – and that saved you $101.00 EACH in membership dues this year! Please find a list of ODA Rewards Partners in your packet. If you are buying from other companies, you are absolutely paying too much!
To the ODA Board of Trustees – thank you for your leadership, flexibility, and support over the past year – especially Dr. Wood and the other members of the Executive Committee. Thank you for responding so quickly to my ONE MILLION emails, calls, and texts, and especially, for your friendship.
I have thanked a lot of people today, but the most gratitude will always go to the ODA staff … Shelly, Jill, and Ansley! FOUR women executed the Annual Meeting this year. We may be small, but we are mighty! These women are flexible, resourceful, creative, generous, patient and SO, SO damn smart. This team inspires and challenges me every day. I’m continuously awe-struck by what they are able to accomplish. If you didn’t hear anything else I said today, at least leave knowing that your ODA is in outstanding hands!
As I begin my 19th year with the ODA, I am still so grateful to be inspired and to experience growth and joy every day. When I count my many blessings, the ODA is always among them. THANK YOU for the opportunity to continue to serve as your Executive Director.
NEW DENTIST FEATURE
Dr. Taylor Russell
Osiyo! I am Dr. Taylor Russell and I am honored to share about my experience as a general dentist at the Cherokee Nation Outpatient Health Center in Tahlequah, OK. We offer comprehensive restorative care with referral options for specialties including endodontics, pediatrics, and oral surgery.
As a Cherokee citizen, it has been my longtime dream to work for the Cherokee Nation. A recruiter for the clinic reached out to me on the National Health Service Corps page during my final year of Dental School, and I was immediately interested.
The clinic is a Federally Qualified Health Center, and it meets a variety of needs for tribal citizens. In addition to dentistry, services like optometry, radiology, audiology, physical rehabiliation, behavioral health, lab, and pharmacy are available, and many primary care doctors office in the center, as well. The facilities are world class and equipped with state-of-the-art technology.
There are several clinics like this one located throughout the Cherokee Nation, offering reasonable travel distances for treatment to all patients who qualify for service.
We have a terrific team of dentists, hygienists, and assistants at our location here in Tahlequah, creating a collaborative environment where individual treatment plans can be created based on the experiences of many.
As a new dentist, I am grateful to the coworkers who have embraced me and offered their insights to continue my skill development.
One of the many reasons I chose dentistry was to make a positive impact in my community. I participated in multiple local and global mission opportunities before dental school and fell in love with the service aspect of dentistry.
Our dental clinic here is a popular place, often exceeding 100 patients in a day. I look forward to going to work every day at the Cherokee Nation and love seeing the smiles transformed and pain relieved from the patients that walk through the door.
The Cherokee Nation operates the largest tribal health system in the U.S. with more than 1.3 million patient visits each year, and this facility is the largest tribal outpatient facility in the country. It features more than 240 exam rooms, two MRI machines, an ambulatory surgery center, 34 dental chairs, and full service optometry and specialty health services.
Taylor Russell, DDS graduated from the dental school at University of Texas San Antonio. Prior to dental school, she earned her Bachelor of Science degree at McMurry University.
The 469,000-square-foot outpatient Cherokee Nation Healthcare Services building in Tahlequah, OK where Dr. Russell practices general dentistry. The $200 million health center opened in November 2019.
Introducing Your New Association President
Dr. Daryn Lu will lead the ODA Board until April 2025
Born on the West Coast and raised on the East Coast, Dr. Daryn Lu has called Oklahoma his home since 1999. As a 2015 graduate from the OU College of Dentistry, he has developed relationships within the dental community and across the state, believing that progress happens when groups of individuals work together to make positive change and achieve their shared goals.
However, Dr. Lu’s passion for the dental profession started long before he was even accepted into dental school. He founded and served as the president of the Pre-Dental Society at the University of Central Oklahoma, interned at the Oklahoma Dental Foundation, worked on mobile dental clinics across the state, and attended an American Student Dental Association annual meeting all prior to 2011.
"I remember the first time I met Lynn Means and the Oklahoma Dental Association team while working with
Oklahoma Dental Foundation. I learned so much about organized dentistry, and watched amazing leaders share their talents and show so much compassion. They really cared about their patients and the communities they served. I respect that so much, and it inspired me to follow their pathways" said Dr. Lu.
From being an eager predental member of the American Student Dental Association (ASDA) to then becoming its chapter president, district trustee, and national vice president, Dr. Lu's experiences throughout dental school solidified his choices.
"I have core memories of standing in front of my class in dental school, running for office, getting involved with ASDA, and I knew this was my home. This is the community I love and want to serve," said Dr. Lu.
Encouragement from incredible mentors have also shaped him as a dental professional and lifelong learner.
ODA President Dr. Daryn Lu (left) with his wife and business partner, Dr. Edith Quiñonez Lu (back row) and their LoFi Dental clinical team.
COVER STORY
"My mentors and other leaders I have been privileged to work with showed me how challenging our profession can be, but also how rewarding it can be," said Dr. Lu.
After spending two and a half years with a Dental Service Organization, Dr. Lu worked in private practice in multiple associateships, community dentistry with the ODF's Mobile Smiles program, and in dental education as an associate clinical professor in the OU College of Dentistry's Division of Comprehensive Care. He continues to speak at many conferences and conventions, and he writes guest blogs to continue educating others.
Since graduation, Dr. Lu has been nominated for the ADA 10 Under 10 award, received his Fellowship in the American College of Dentists, and was recognized
as the 2019 OU College of Dentistry's Young Dental Alumnus of the Year. He was honored as one of the 2020 Academy of General Dentistry 10 Dentists to Watch and as the winner of the 2021 Oklahoma Dental Association's Young Dentist of the Year award presented to him at their Annual Meeting.
Dr. Lu worked as a general dentist in Shawnee, Lawton, and in Oklahoma City before starting a practice in Edmond with his wife, Dr. Edith Quiñonez Lu, in 2022.
Inspired by lo-fi music that has helped him find calm in the chaos of building a practice from the ground up, their concept is called LoFi Dental. They hope to create a relaxed, comfortable experience for their patients and to soothe any anxiety or intimidation they might feel prior to or during their visit.
However, Dr. Lu is not shy about being open about the stresses of practicing dentistry.
"It can be very physically draining, mentally taxing, and difficult to serve patients who constantly tell you how much they don't want to be next to you," Dr. Lu said during his ODA presidential induction speech at the 2024 Annual Meeting.
"Our profession is challenging, and the work can take a toll on you. So mental health and wellness is one of the most important things I want to advocate for during this next year serving as president of the ODA."
Some of his roles within organized dentistry include: program chairman of the Oklahoma County Dental
Dr. Lu speaking to recent graduates of the OU College of Dentistry at the ODA's Senior Signing Day event in May 2024.
Dr. Edith Quiñonez Lu and Dr. Daryn Lu, DDS at the groundbreaking for their new office in 2022.
Edith Quiñonez Lu, DDS (left) and Daryn Lu, DDS (right) with Kois Center Director John C. Kois, DMD, MSD (center), during their time learning at the Kois Center program for advanced dentistry.
S101 ACCESS
SAFEGUARDING DENTAL PROVIDERS
• Tired of countless documents being sent over by Insur ance companies? Need a resource to help decipher them? Need to know if it is truly an issue of credentialing or contracting?
• Understand the implications of the credentialing process. Know when to enter or avoid a contracting situation to impactfully retain revenue. Stop letting market changes reduce your income.
(RE) CREDENTIALING
• Be prepared and equipped to fully understand how a network arrangement will impact your practice. Know if it is the right financial move to stay in or opt-out.
REVENUE RETENTION
• Have a quick question? Sign up for a one on one session with a market expert to confidently tackle your issue.
• Be informed! Industry leading news and speaking events at your fingertips.
Gain the upper hand over dental insurance with S101ACCESS! In today’s dental landscape, practices struggle to manage patient plans while seeking clarity. Partnering with Solutions101 puts you in control, empowering you to effectively communicate about dental benefit plans and decode Explanation of Benefits (EOBs) without relying on insurance companies. Remove the uncertainty and seize control of your practice’s financial security. Say hello to profitability and goodbye to carrier dependency with S101ACCESS!
Society, chair of the 2020 ODA Annual Meeting, member of the ODA Membership and Membership Services council, member of the ODA Journal Editorial Board, member of the J. Dean Robertson Board of Trustees, member of the Oklahoma Academy of General Dentistry, a 12th District Representative on the ADA New Dentist Committee, member of the ADA Committee on Annual Meetings, and serving as the first host of ADA's inaugural SmileCon event. Dr. Lu also volunteers his time at the Oklahoma Mission of Mercy events each year.
In a recent speech to graduating dental students, Dr. Lu discussed the importance of mentorship and community support, and how being involved with organized dentistry is how they can stay connected and influence policymaking.
"My biggest ask is to remain a member of this community, no matter what your practice setting is. Learn what organized dentistry does, take advantage of its resources and connections, and learn about the legislation that impacts how we practice and how we care for our patients," Dr. Lu said.
Dr. Lu's vision for the year ahead is centered on amplifying the value of ODA membership and
"I promise to be your largest advocate-your biggest champion-for dentistry within the state of Oklahoma."
highlighting the compassionate spirit that defines dentistry in our state.
"The people who are giving their time and dedicating resources to the future -- it means the world. There is so much change coming to our profession with technology – salivary diagnostics, AI, 3-D printing.. It's here now, and we need to have a unified voice now more than ever," Dr. Lu said. “Be a part of something bigger than you, but better because of you.”
Dr. Daryn Lu speaking to the House of Delegates at the 2024 ODA Annual Meeting on April 11 where he was inducted as president of the organization's Board of Trustees.
Dr. Lu with the incoming ODA executive committee for governance year 2024-2025.
Dr. Lu and his family during construction of the LoFi Dental office.
EVENT PHOTOS
Senior Signing Day, May 3 & 6
ODA Offices in Oklahoma City, OK and OU Dentistry Tulsa Dental Clinic in Tulsa, OK
CASE STUDY
A 3-year follow-up for conservative management of hypomineralization on deciduous
and permanent dentition
INTRODUCTION
Hypomineralization of enamel is defined as a qualitative enamel defect caused by a disturbance during initial calcification and/or maturation. The estimated global prevalence reported for Molar Incisor Hypomineralization (MIH) is around 13%.1 The etiology is multifactorial and is thought to be the result of systemic environmental factors during the first three years of life, that affect enamel development during the pre-, peri- or early post-natal phases of life.2,3,4 Despite numerous studies, the understanding of MIH factors remains inconclusive.5
Clinically, MIH presents as demarcated enamel opacities that can manifest as white, cream, yellow or brown defects and are sharply demarcated against normal enamel.6,7 Histologically, these affected areas have less distinct prism sheets and a lack of arrangement of the enamel crystals. The enamel shears off under masticatory force and can result in post-eruptive breakdown (PEB). Because of that, these affected teeth are more prone to enamel breakdown and the development of carious lesions, hypersensitivity and, consequently, an earlier and more frequent need for dental treatment.3
The great variability of clinical findings related to extension, coloration of enamel, and symptoms make diagnosis and definition of the treatment plan challenging. The most common diagnostic finding is the presence of affected molars by age 6 years, but primary and permanent second molars can also be affected alone or together, as well as primary and permanent incisors. The latter presents slightly different characteristics, without predisposition to enamel fractures and hypersensitivity when compared to molars.7 The purpose of this case report is to describe the comprehensive management and follow-up of a 3-year-old child with severe Deciduous Hypomineralization followed-up for three years until the eruption of the permanent molars which were also affected by hypomineralization.
CASE REPORT
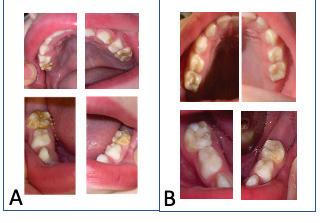
The present case report is submitted in accordance with CARE guidelines for case reports (supplemental file).8 A 3-year-old male presented to the clinic with all 4-second primary molars and 1 primary canine (tooth # H) affected by severe hypomineralization with enamel breakdown and moderate to high hypersensitivity according to WongBaker faces pain scale (WBFS). Primary incisors showed no signs of hypomineralization or other developmental
defects. No decay was observed, and the patient reported hypersensitivity on the occlusal of molars as the main chief complaint. The patient’s medical history showed a healthy patient and a healthy mother, with no MIH family history and no abnormalities or illnesses presented during pregnancy, during delivery (C-section) or after delivery. A panoramic radiograph was taken showing no structural or developmental abnormalities of the dentition and a (continued on next page)
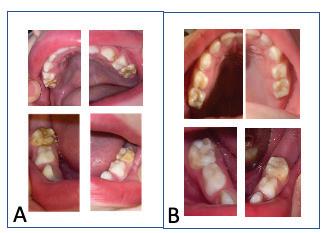
FIGURE 1
by Fernanda Pitta Ritto, DDS, MS, PhD
Divesh Sardana, MDS, MBA, MPH, PhD
Timothy Fagan, DDS, MS, and David Ciesla, DDS, MS, MAS
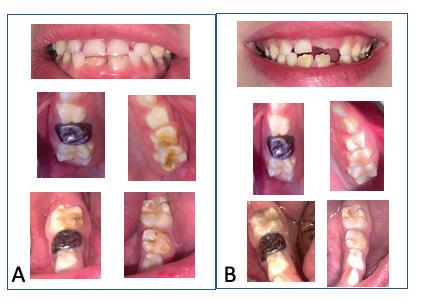
FIGURE 2
CASE STUDY
caries risk assessment was performed using the American Academy of Pediatric Dentistry caries risk assessment tool,9 where the patient was at moderate risk due to a high sugar diet. Thus, after reviewing the patient's medical history to rule out acquired, environmental or genetic causes, and after a clinical and radiographic examination, the differential diagnosis of hypomineralization, fluorosis, hypoplasia and amelogenesis imperfecta was made. The clinical aspect of the lesion showed demarcated opacities white, yellow, and brown with sharp and irregular margins on the fractured enamel, signaling a type of fracture that happens after eruption and therefore characterized as an enamel qualitative defect, with the final diagnosis being hypomineralization.
The treatment plan was divided into two phases:
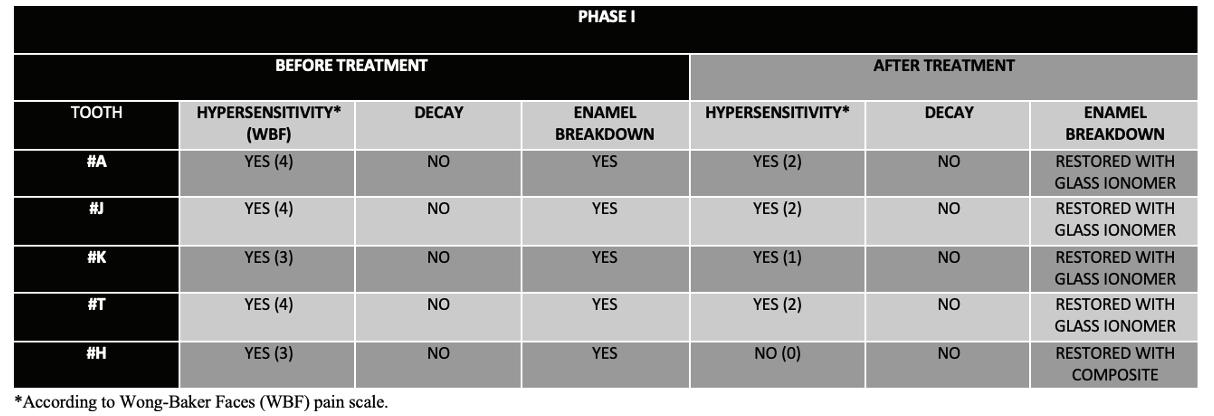
Phase I: (Figure 1) The aim of this phase was to treat pain and prevent decay. The patient’s diet diary was created with the aim of evaluating and modifying habits, reducing sugar intake, and avoiding sticky and very hard foods that could accelerate the enamel degradation process.
Treatment was started by applying (Figure 1) 5% Sodium fluoride varnish (Duraphat®, Colgate, USA) on the first 2 visits with a 4-week interval. After that, restorations, or sealants with glass ionomer (VitrebondTM and KetacTM Cem Easy mix – 3M ESPE, USA) were performed on the second molars and the canine was restored with composite as shown in Table 1. After this first approach, sensitivity was reduced from a score of 4 to 2 according to WBFS. The patient was monitored every month for the first 3 months and every 3 months thereafter.
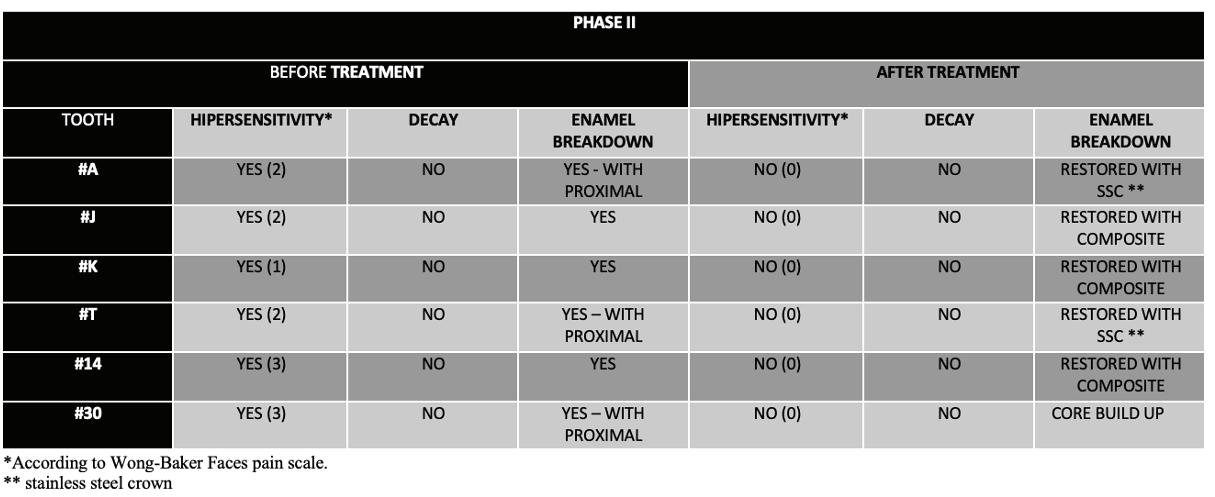
In the second phase, the pain was controlled and there was absence of decay, but the enamel loss was progressing rapidly. At this stage, the patient was 5 to 6 years old and all first permanent molars were erupted and diagnosed with
hypomineralization. Enamel breakdown was observed on the occlusal surfaces of teeth #J, #14 and #30 in different severities and #A and #T had loss of enamel on the proximal surfaces. Although the hypersensitivity had decreased compared to the beginning of the treatment, it was still present. Teeth #24 and #25 erupted presenting MIH with no enamel breakdown or hypersensitivity. Treatment at this stage began with restorations and was called Phase II treatment. (Figure 2) Before proceeding with restorations, occlusal glass ionomer sealants were placed on all erupted permanent first molars immediately after occlusal areas were exposed in the oral cavity. In addition, an at-home toothpaste protocol was implemented to reduce tooth hypersensitivity, prevent cavities, and promote remineralization. Two different toothpastes, one containing casein phosphopeptide amorphous calcium phosphate fluoride (CPP-ACFP - GC MI Paste plusTM, GC, USA) and the other containing 5000 ppm Fluoride (Clinpro®, 3M, USA) were prescribed twice a week each on alternate days for each paste. After implementing the toothpaste home protocol for a month, the sensitivity level dropped to 0 according to WBFS, and no signs of decay were observed. Restorations with stainless steel crowns (SSC) on #A and # T, and composite restorations on #J, #K and #14 were placed as shown in Table 2. A core build-up was performed on #30 due to severe enamel loss for possible indirect restoration in the future as the tooth was still erupting. Subsequently, the patient was monitored every 3 months and is currently under our routine care.
From the patient’s perspective, both the mother and the child were very satisfied with the results, pointing out that all the effort related to coming to the consultations and the involvement with the self-care part of the treatment was worth it. The parent stated that when hypersensitivity was controlled, his son was more cooperative and happier to go to appointments to receive treatment.
CASE STUDY
DISCUSSION
The conservative approach is the first choice of treatment for Molar-Incisor Hypomineralization according to the current literature, since the affected teeth are often not completely erupted yet, have wide pulp chambers, and high pulp horns.6,10,11 Nevertheless, treatment of MIH can be very challenging, and clinicians must be able to find the delicate balance between traditional conservative treatment, and more invasive options due to the fast course that this condition may present.6
The presence of hypomineralization in the primary dentition should sound an alarm signal to the patient regarding MIH in the permanent dentition. The literature states that this condition in primary second molars is a predictor that permanent dentition may be affected in some way. The fact is that permanent first molars and central incisors develop during a similar period as primary second molars, with comparable possible risk factors for hypomineralization.12 In a recent meta-analysis, it was shown that children with hypomineralized second primary molars are 5 times more likely to also develop MIH.13
In the present case, the very young age of the patient can be a challenge, and compliance plays an important role in the choice of therapy.14 In addition, hypersensitivity can be a concern in hypomineralization as it can affect the child’s behavior during treatment. Fortunately, the patient in question had a score of 4 (definitely positive) on the Frankl behavioral scale and was able to comply with the entire preestablished treatment plan.
The treatment plan began with the prevention of decay, treatment of hypersensitivity and enamel loss monitoring.
Remineralization agents were applied to the tooth structure with enamel breakdown to decrease hypersensitivity and increase the quality of the enamel for the bonding process on restorations. Combined with this, sealants and restorations with glass ionomer were preferred.
Glass ionomer sealants have the advantage of releasing and recharging fluoride, in addition to a less sensitive technique. Authors stated that sealed molars presented 77% less chance of caries than unsealed ones. Some authors also stated that remineralization protocols before sealant placement can increase retention.15,16 Regarding hypersensitivity decrease, almost all materials (CPP-ACP, CPP-ACFP, and Fluoride) showed good results17,18 and the association of protocols can demonstrate even better outcomes 6,19-22 Also, concerning decay prevention, authors agreed that 5% Sodium Fluoride varnish, CPP-ACP, and CPP-ACFP demonstrated excellent performance especially in creamy-white defects.3,23-25 This was the basis for our decision to establish an at-home toothpaste protocol for desensitization, remineralization, and decay prevention. The frequent recall intervals of 3 to 6 months and enhanced preventive measures to closely monitor MIH teeth have been suggested and were performed on the present case. 11,26
Current literature evaluating prefabricated stainless-steel crowns (SSC) has suggested that SSC can be an alternative approach for severe cases or temporary treatment in extensively destroyed teeth.27-29 For the present case, the use of the prefabricated stainless-steel crowns was indicated on primary teeth when loss of enamel on proximal surfaces would affect the loss of space in the arch.
(continued on next page)
TABLE 2
CASE STUDY
Adhesion to enamel is a challenge for MIH-affected teeth and most studies showed low bond strength values.30 Some studies31 demonstrated that when a 5th generation prime/ bond adhesive agent was used with resin sealants and composite restorations, retention was substantially increased in MIH-affected teeth. Therefore, in the present study, direct restorations with composite were performed following the bonding protocol with 5th generation adhesive.
The present case has the advantage of a long follow-up period, making it possible to present the evolution of the disease from the primary to the permanent dentition and compare the severity and evolution of enamel breakdown, hypersensitivity, and caries.
Furthermore, this conservative approach teaches professionals to combine the principles of disease prevention and control and treat caries, hypersensitivity, and loss of structure at the same time, and in a minimally invasive way, achieving a very good result. However, case reports are studies restricted to a very small sample and new randomized clinical trials are needed to validate new protocols for MIH.
CONCLUSIONS
Related to findings:
On the present case report:
1 - Each tooth can be affected differently, showing different degrees of sensitivity and different characteristics of the enamel on the same patient.
2 - The degree of severity that affected the deciduous teeth did not determine the degree of severity of the permanent teeth that erupted on the same quadrant.
3 - Yellow-brown defects showed a poor prognosis with faster enamel breakdown.
Related to treatment:
On the present case report:
1 - An early association of remineralization protocols with desensitizers and placement of sealants showed good results in controlling painful symptoms and decay.
2 - The home tooth paste protocol proved to be an important adjuvant in treating hypersensitivity and preventing decay.
3 - Close monitoring has shown to be very important to obtain early treatment decisions and success on results.
4 - The development of additional protocols for management of MIH is necessary.
RESOURCES
1. Lopes LB, Machado V, Mascarenhas P, Mendes JJ, Botelho J. The prevalence of molar-incisor hypomineralization: a systematic review and meta-analysis. Sci Rep 2021;11(1):22405.
2. Weerheijm KL, Jalevik B, Alaluusua S. Molar-incisor hypomineralisation. Caries Res 2001;35(5):390-1.
3. Weerheijm KL, Duggal M, Mejare I, et al. Judgement criteria for molar incisor hypomineralisation (MIH) in epidemiologic studies: a summary of the European meeting on MIH held in Athens, 2003. Eur J Paediatr Dent 2003;4(3):110-3.
4. Somani C, Taylor GD, Garot E, et al. An update of treatment modalities in children and adolescents with teeth affected by molar incisor hypomineralisation (MIH): a systematic review. Eur Arch Paediatr Dent 2022;23(1):39-64.
5. da Cunha Coelho ASE, Mata PCM, Lino CA, et al. Dental hypomineralization treatment: A systematic review. J Esthet Restor Dent 2019;31(1):26-39.
6. Ritto FP, Tiwana K, Dacus ZL et al. A qualitative analysis of treatment patterns for mild and severe Molar Hypomineralization – A Systematic Review. Pediatr Dent,2023;45(4) TBD.
7. Hubbard MJ. Molar hypomineralization: What is the US experience? J Am Dent Assoc 2018;149(5):329-30.
8. CARE case report guidelines. http:/www.care-statement.org.
10. Dhareula A, Goyal A, Gauba K, et al. A clinical and radiographic investigation comparing the efficacy of cast metal and indirect resin onlays in rehabilitation of permanent first molars affected with severe molar incisor hypomineralisation (MIH): a 36-month randomised controlled clinical trial. Eur Arch Paediatr Dent 2019;20(5):489-500.
11. Lygidakis NA, Garot E, Somani C, et al. Best clinical practice guidance for clinicians dealing with children presenting with molar-incisor-hypomineralisation (MIH): an updated European Academy of Paediatric Dentistry policy document. Eur Arch Paediatr Dent 2022;23(1):3-21.
12. Elfrink M, Cate J, Jaddoe V et al.Deciduous molar hypomineralization and molar incisor hypomineralization. J Dent Res 91(6):551-555, 2012.
13. Garot E, Denis A, Delbos Y,et al. Are hypomineralizad lesions on second primary molars (HSPM) a predictive sign of molar incisor hypomineralization (MIH)? A systematic review and meta-analysis. J Dent 2018:72:8-13.
CASE STUDY
14. Bekes K. Hypomineralized primary molars ( Chapter 17). In Molar Incisor Hypomineralization. 1st ed.Berlin, Germany: Quintessence Publishing Co ;2002: 172-180.
15. de Souza JF, Fragelli CB, Jeremias F, et al. Eighteen-month clinical performance of composite resin restorations with two different adhesive systems for molars affected by molar incisor hypomineralization. Clin Oral Investig 2017;21(5):1725-33.
16. Fragelli CMB, Souza JF, Bussaneli DG, et al. Survival of sealants in molars affected by molar-incisor hypomineralization: 18-month follow-up. Braz Oral Res 2017;31:e30.
17. Cardoso-Martins I, Pessanha S, Coelho A. et al. Evaluation of the efficacy of CPP-ACP remineralizing mousse in MolarIncisor Hypomineralized Teeth Using Polarized Raman and Scanning Electron Microscopy—An In Vitro Study. Biomed 2022;10,1-11.
18. Sezer B and Kargul B. Effect of remineralization agents on Molar-Incisor hypomineralization – Affected incisors: a randomized controlled clinical trial. J Clin Pediatr Dent 2022. 46(3),192-198.
19. Muniz RSC, Carvalho CN, Aranha ACC, Dias F, Ferreira MC. Efficacy of low-level laser therapy associated with fluoride therapy for the desensitisation of molar-incisor hypomineralisation: randomised clinical trial. Int J Paediatr Dent 2020;30(3):323-33.
20. Rolim TZC, da Costa TRF, Wambier LM, et al. Adhesive restoration of molars affected by molar incisor hypomineralization: a randomized clinical trial. Clin Oral Investig 2021;25(3):1513-24.
21. Ballikaya E, Unverdi GE, Cehreli ZC. Management of initial carious lesions of hypomineralized molars (MIH) with silver diamine fluoride or silver-modified atraumatic restorative treatment (SMART): 1-year results of a prospective, randomized clinical trial. Clin Oral Investig 2022;26(2):2197205.
22. Bekes K, Heinzelmann K, Lettner S, Schaller HG. Efficacy of desensitizing products containing 8% arginine and calcium carbonate for hypersensitivity relief in MIH-affected molars: an 8-week clinical study. Clin Oral Investig 2017;21(7):231117.
23. Olgen IC, Sonmez H, Bezgin T. Effects of different remineralization agents on MIH defects: a randomized clinical study. Clin Oral Investig 2022;26(3):3227-38.
24. Jalevik B, Noren JG. Enamel hypomineralization of permanent first molars: a morphological study and survey of possible aetiological factors. Int J Paediatr Dent 2000;10(4):278-89.
25. Neves AB, Americano GCA, Soares DV, Soviero VM. Breakdown of demarcated opacities related to molar-incisor hypomineralization: a longitudinal study. Clin Oral Investig 2019;23(2):611-15.
26. Nogueira VKC, Mendes Soares IP, Fragelli CMB, et al. Structural integrity of MIH-affected teeth after treatment with fluoride varnish or resin infiltration: An 18-Month randomized clinical trial. J Dent 2021;105:103570.
27. Kotsanos N, Kaklamanos EG, Arapostathis K. Treatment management of first permanent molars in children with Molar-Incisor Hypomineralisation. Eur J Paediatr Dent 2005;6(4):179-84.
28. Koleventi A, Sakellari D, Arapostathis KN, Kotsanos N. Periodontal Impact of Preformed Metal Crowns on Permanent Molars of Children and Adolescents: A Pilot Study. Pediatr Dent 2018;40(2):117-21.
29. Oh N NS, Lee J, Kim H. Retrospective Study on the survival rate of preformed metal crowns in permanent first molars. Journal of the Korean Academy of Pediatric Dentistry 2020;47 (2):140-47.
30. Lagarde M, Vennat E, Attal JP, Dursun E. Strategies to optimize bonding of adhesive materials to molar-incisor hypomineralization-affected enamel: A systematic review. Int J Paediatr Dent 2020;30(4):405-20.
31. Lygidakis NA, Dimou G, Stamataki E. Retention of fissure sealants using two different methods of application in teeth with hypomineralised molars (MIH): a 4 year clinical study. Eur Arch Paediatr Dent 2009;10(4):223-6.
AUTHORS
Fernanda Pitta Ritto, DDS, MS, PhD
Clinical Assistant Professor
Division of Operative Dentistry
Department of Restorative Sciences
University of Oklahoma College of Dentistry
Divesh Sardana, MDS, MBA, MPH, PhD
Clinical Assistant Professor
Division of Pediatric Dentistry
Department of Developmental Sciences
University of Oklahoma College of Dentistry
Timothy Fagan, DDS, MS
Division Head
Division of Pediatric Dentistry
Department of Developmental Sciences
University of Oklahoma College of Dentistry
David Ciesla, DDS, MS, MAS
Clinical Assistant Professor
Division of Pediatric Dentistry
Department of Developmental Sciences
University of Oklahoma College of Dentistry
Awesome FFS Practice for Sale in North Texas - 15 min from the OK Border
If you don't want to deal with insurance, have the skillset to keep some specialty procedures in house, and want the autonomy to do things your own way, this is the practice for you. It's located about two hours north of DFW. We’re a completely OON office. Our staff is a great close-knit group of people. Wonderful patient base. We do a little bit of everything from bread-and-butter crowns and fillings, to root canals, implants, and AOX and cosmetic/full mouth rehab stuff.
We got in on scanning, milling, and printing pretty early and have an amazing workflow that lets us do a lot of our own custom lab work for a more aesthetic and personal touch. This includes 3D printing our own dentures, partials, and nightguards, as well as milling our own crowns and AOX prostheses. We have a lab grade 5-axis mill, 3D printer, IO scanner, CBCT machine, intraoral cameras, digital X-rays, etc. All brand new in 2022. 4 ops, one full time hygienist and one part time. Last year we did 1.2 million in collections and are on track to beat that this year. The practice is also newly remodeled.
I would be willing to consider an immediate purchase or an associate with the option to buy me out after a smooth transition. If interested, please call/text Chandler at (801) 895-0514.
JOB OPENING
Dental Hygienist, Alva, OK
W Hometown Dentist is a small business in Alva, Oklahoma, renamed under the corporation our previous provider had treated dental patients since 1984. We are professional, fast-paced, fun to be around and supportive. This opportunity offers competitive pay, sizable sign-on/relocation bonus, PTO, matching 401K, health and dental benefits, CE, and office trips. Negotiations are allowed to ensure both provider and hygienist needs are met.
The dental hygienist joining our team will be expected to provide exceptional patient care. The ideal candidate will have a background in dental hygiene, be able to work independently and as part of a team and have excellent communication skills. The successful candidate will perform routine dental cleanings, take X-rays, educate patients on proper oral hygiene, and provide other preventative services.
Responsibilities:
• Clean and polish teeth.
• Educate patients on proper oral hygiene techniques.
• Assess patients’ oral health and provide preventive care.
• Perform x-rays and other diagnostic tests.
• Keep detailed records of patient visits.
• Provide fluoride treatments and sealants.
• Remove plaque and calculus from teeth.
• Perform dental prophylaxis.
• Perform scaling and root planning therapy.
• Provide necessary anesthesia.
Contact: Hannah McOsker
(580) 327-4522
htdentistalva@gmail.com
JOB OPENING
Associate Dentist, Stigler, OK
Private practice located in Stigler, OK seeking associate with possible buyout in future. Very well established office that has been in business for 45 years with a loyal patient base. Only private practice in Haskell County, located between Eufaula Lake and Kerr Lake. Office is in prime location right on the main highway across from Choctaw Travel Plaza. Building is 2000 sq ft, has 3 DR operatories, 1 hygiene operatory, break room has capabilities to be another operatory if needed. Equipment is older but fully functional. Office is open Tuesday - Thursday 8 to 5, and Saturday 8 to 3 (only hygiene patients are seen on Saturdays currently). Office has Dentrix software. Currently providers for 4 insurance companies including Medicaid and have FFS patients as well. Practice offers preventive, restorative, crown/bridge, denture/partials, some oral surgery, and some implants. Definite growth potential since the office currently refers for orthodontics, endodontics, periodontics, and some oral surgery and implants. Email lyndiejoan@gmail.com or call (918) 448-0181.
See more classified ads online at okda.org
To place a classified ad, email advertising@okda.org or visit okda.org/classifieds
CLASSIFIEDS
JOB OPENING
Oral and Maxillofacial Surgeon, Tulsa/Stillwater, OK
Are you a talented Oral Surgeon with a passion for transforming smiles and changing lives? Are you ready to take your career to the next level in a modern and patient-focused oral surgery environment?
Central Oklahoma Oral & Maxillofacial Surgery Associates is the place for you! If you’re looking for unlimited earnings potential, great benefits, and future ownership opportunities, please reach out! Our mission is simple. We strive to improve the lives of everyone we meet, not just the ones we treat.
Benefits / Compensation: You deserve to be rewarded for your hard work!
• Daily guarantee OR percentage of Collections (whichever is greater)!
• 401k after one year of employment • Unlimited earning potential
• Stable and consistent full-time schedule
• Steady new patient flow with a very busy hygiene schedule – allowing you to build your practice with confidence
• No weekends! Monday-Friday, alternating time between Stillwater, OK and Tulsa, OK.
What you should know about Dr. Miller and his team:
• Dr. Miller has owned the practice since 2000 and is a fellow of the American Association of Oral and Maxillofacial Surgeons and of the International Association of Oral and Maxillofacial Surgeons. Dr. Miller specializes in All-On-4 treatment, individual dental implants, wisdom teeth extractions, facial cosmetic treatments, and facial trauma.
• Currently, our practice involves two full-time oral surgeons and one part-time oral surgeon. Our state of the art technology allows us to provide the best results and create a productive work environment focusing our time and energy on our ultimate goal of improving our patients’ quality of life.
OKC General Dental Practice for sale near Tinker AFB & Boeing, and I-240. 1500 Sq Ft, room for 4 operatories, build out 5 years old, includes Dexis, Softdent, Vatech CBCT, better than new.
Contact:
Call or text (405) 650-0945.
PRACTICE FOR SALE
Tulsa area, OK
Practice and building (approx. 2000 sq/ft), 4 Ops, Collected $680,000 on 3 days/wk. Dr. takes 4-5 wks of vacation/yr. 25 years at current location, Computerized/ Dentrix, Most specialty wk. referred out, Hyg. is booked out 6 months with 5-6 days/wk. Experienced staff.
Contact: Cathy (539) 333-0430.
PRACTICE FOR SALE
South Central Oklahoma
General Practice for Sale
2600 sq ft, 5 ops, great visible location, 4 days per week, 8 days hygiene, softdent, cerec, laser, intraoral cameras, digital radiography, super staff, collections $1.1 million.
Contact: Call or text (580) 221-4767.
JOB OPENING
Associate Dentist, Enid, OK
Formerly a two-doctor practice of 30 years, but recently lost my associate. I’ve built a new building with all new equipment. 3 full-time hygienists booked for months. A future buy-in is possible for the right person. I’d love to mentor a young dentist or bring in an experienced dentist. We do a wide variety of procedures including implants, grafting, root canals, extractions, etc. Candidate must be honest, ethical, and hard working! Our practice is called TLC Dental.
Contact:
Dr. Jared Lack (580) 478-6652
OFFICE FOR LEASE
Stillwater, OK
Fully Equipped Dental Office for Lease
• Self-contained unit
• 2339 sq. ft.
• Four fully-equipped operatories
• Equipped sterilization room and lab
• Digital Radiography with optional Cone Beam Technology
Contact: Darrell Daugherty (405) 377-4848
JOB OPENING
Guthrie, OK
Seeking a Hygienist for IMMEDIATE start!
Proud Dental is searching for a Registered Dental Hygienist to join our dedicated team of dental professionals. Our ideal candidate is passionate about oral health and will strive to deliver outstanding patient care to our guests. We are committed to staying current with the latest technology and techniques, making appointments a breeze for both our Hygienists and our patients. Whether you are a seasoned RDH seeking a new opportunity or a recent graduate eager to begin your career, submit your application today!
** $2,000 Sign-on bonus! **
Compensation and Perks
• Competitive pay
• Medical, dental, vision, and life insurance
• PTO and paid holidays
• Traditional and Roth 401(k) options
• Weekends off
Qualifications
• A valid Hygienist license is required
• Must be certified to administer local anesthesia
Contact: Morgan (817) 733-6201 mphillips@mb2dental.com