
5 minute read
Vet Forum


By Stuart Williamson BVSC MRCVS
Carpal sheath issues in focus
structure on the back of the foreleg that extends from the lower forearm region to the mid-cannon. This sheath wraps around the superficial digital flexor tendon (SDFT) and the deep digital flexor tendon (DDFT) as they run over the back aspect of the knee. Synovial fluid produced by the sheath lubricates the tendons and therefore reduces friction. In the normal horse, the carpal sheath contains only a small amount of synovial fluid and therefore cannot be palpated.
Carpal sheath issues can range from mild inflammation (tenosynovitis) and distension of the carpal sheath, without lameness, to non-weight-bearing lameness associated with significant damage to one or more of the soft tissue or bony structures enclosed within the sheath. We will take a look at some of these issues, in addition to how they may be diagnosed and some of the management options available.
DISTAL RADIAL OSTEOCHONDROMA
An osteochondroma is an overgrowth of bone with a cartilage cap that occurs near the growth plate at the end of a long bone. In the horse, they are most frequently identified above the level of the growth plate at the back of the radius in the lower forearm. Osteochondromata can cause damage to the muscular portion of the DDFT as it runs over this abnormal bony protuberance. This can result in inflammation and haemorrhage within the carpal sheath and lameness of varying severity. Some ostechondromata can however remain asymptomatic.
The diagnosis of an osteochondroma is made by radiography. Ultrasound examination can then aid in evaluating the soft tissue structures within the carpal sheath that may be damaged by the osteochondroma, in addition to evaluating the character of any carpal sheath fluid. Keyhole (tenoscopic) surgery under general anaesthesia may be required to remove the osteochondroma in addition to evaluating the remainder of the carpal sheath to identify any concurrent injury. If this condition is addressed promptly, and there is no concurrent significant National Hunt horses are more at risk of sustaining accessory carpal
The carpal sheath is a synovial
bone fractures DDFT damage, the prognosis for a return to full athletic function is ››

Figure 1 A comminuted accessory carpal bone fracture (red arrow). This was a career-ending injury
›› generally considered good. Affected horses will generally have a lengthy rehabilitation period and whilst timings will vary according to the extent of injury, most will not return to cantering exercise for approximately three months following surgery.
DISTAL RADIAL PHYSEAL EXOSTOSIS
This is very similar to a distal radial osteochondroma. In this condition the bony protuberance is located at the level of the distal radial growth plate (physis), rather than above it. Presentation, diagnosis and management are generally the same.
INJURY OF THE SDFT, DDFT OR ACCESSORY LIGAMENT OF THE SDFT
Both the SDFT and the DDFT (the flexor tendons) or the accessory ligament of the SDFT (also known as the check ligament) can suffer a primary injury, without the presence of either an osteochondroma or an exostosis. As with all tendinous and ligamentous structures, they can fail following repetitive strain cycles and therefore injury associated with these is more frequently, but not exclusively, seen in the older racing population.
Injury to one of the soft tissue structures is frequently associated with marked effusion within the carpal sheath and a sudden onset of lameness. A definitive diagnosis cannot always be reached even after a thorough ultrasound examination and keyhole (tenoscopic) examination may be required under general anaesthesia. Any necessary debridement of torn
RACING EQUIPMENT Treehouse sporting colours Silks, Paddock Equipment and Safety Wear
www.treehouseonline.co.uk Tel: 01299 851625
tendon or ligament fibres is carried out at the same time. This debridement can reduce adhesion formation, provide better resolution of the injury and reduce the required rehabilitation period. Some cases may respond to rest with anti-inflammatory therapy.
ASEPTIC IDIOPATHIC TENOSYNOVITIS
A non-infectious inflammation of the carpal sheath of unknown origin. The soft tissue structures and bony structures appear normal upon diagnostic imaging, yet there is a marked carpal sheath effusion, often associated with lameness. A period of time out of exercise is required in addition to cold therapy and antiinflammatory therapy. The sheath may be drained and medicated with low dose anti-inflammatory corticosteroids to aid resolution.
SEPTIC TENOSYNOVITIS
Involvement of the carpal sheath must be considered in any full thickness wounds at the back of the lower forearm, the knee or the top of the cannon. Diagnostic imaging including radiography and ultrasonography can be employed to evaluate the soft tissue and bony structures surrounding the wound, and if carpal sheath involvement is suspected, a sample of the synovial fluid can be obtained and analysed for evidence of infection.
ACCESSORY CARPAL BONE FRACTURE
The accessory carpal bone sits at the back of the knee. Injury to this bone is more commonly documented in National Hunt horses where it is
EQUESTRIAN PROPERTY
Jh Jh t John Johnstone MRICS
Chartered Surveyor
RICS Valuations, Leases, Sales
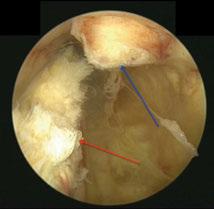
124 High Street, Newmarket, Suffolk, CB8 8JP Tel: 01638 667 118 Mob: 07802 501 548 Email: john@keylocks.com Web: www.keylocks.com Figure 2 A surgeon’s view of the carpal sheath. The red arrow points to the DDFT whilst the blue arrow is a fractured portion of the accessory carpal bone that has displaced into the carpal sheath and traumatised the DDFT
associated with a fall. These horses are often markedly lame. There are many different fracture configurations, which often result in carpal sheath involvement and possible impingement onto the DDFT. Diagnostic imaging will determine the best course of action. Some cases will be treated conservatively with prolonged rest whilst others will require surgical intervention to remove fragments displaced within the carpal sheath. These fractures can be careerending injuries.
The carpal sheath is a complicated synovial structure involving many soft tissue and bony components. A thorough and early investigation of any carpal sheath issues will avoid unnecessary further damage and identify the most appropriate management regime.





