


Our Journal Edition four Spring/summer 2023
Written by our clinical people, for our clinical people
2 2 Contents Welcome Patients - Quality - Productivity Programme - helping deliver PAHT2030 Introducing our mental health strategy Patient at home service start first patient on innovative medication pump Anaesthetic trainee focuses on the connection between humans and animals Radiology referrals achievements Medical education team share the latest learning and updates Team who are committed to enhancing cancer care services featured in national publication Consultant and library manager put pen to paper with new book Latest research supports early diagnosis of breast cancer Showcase your work in the next edition of Our Journal Research study: Pain management for older adults with a hip fracture Article and publications - our #PAHTPeople... 3 4 6 7 8 9 11 13 14 16 16 17 19
Welcome
We are pleased to share the fourth edition of Our Journal - a publication written by our clinical people, for our clinical people, at PAHT.
We are proud that Our Journal has been shortlisted in the category of Best Publication at the Chartered Institute of Public Relations (CIPR) Excellence Awards 2023. This marks a fantastic end to the first full production cycle (Our Journal is published four times a year).
Our Journal includes the below, with reference to the articles in this edition:
y Focus features on clinical issues/improvements and the impact on patient care: the patient at home service starting their first patient on an innovative medication pump; and a feature on radiology referrals achievements
y PAHT 2030: The Patients - Quality - Productivity programme - helping deliver our PAHT2030 strategy; and introducing our mental health strategy
y Research updates: an anaesthetic trainee focuses on the connection between humans and animals; a consultant and library manager have put pen to paper with a new book; how the latest research supports early diagnosis of breast cancer; and pain management for older adults with a hip fracture
y Conference and event reviews/updates: the medical education team share the latest learning and updates
y Input from external contributors: an exploration of a team who are committed to enhancing cancer care services being featured in a national publication
y Summary of research contributions and papers published by PAHT clinicians
y Clinical transformation updates
y Quality and safety agenda
y Awards/clinical recognition
y Clinical leadership successes
y Clinical audit projects
Our Journal provides an amazing opportunity for us to showcase the wonderful work we do – please share it widely and let the communications team know which developments we can profile in the next edition of Our Journal at paht.communications@nhs.net.
Best wishes
Dr Fay Gilder Medical director

 Sharon McNally Chief nurse and deputy chief executive
Sharon McNally Chief nurse and deputy chief executive
3 3
Dr Fay Gilder
Sharon McNally
Patients - Quality - Productivity programme -
helping deliver PAHT2030

Putting our patients at heart – make it count
By
Dr
Bob Ghosh,
divisional director for medicine and urgent and emergency care
You may have heard of, or been a part of, our PatientsQuality - Productivity (PQP) programme, which is helping to deliver our PAHT2030 strategy. If you haven’t been involved yet, it is very likely you will be. The aim of the programme is to ensure the highest outcomes for our patients through effective ways of working, and spending money as if it were our own.

Background
You will be aware that postCOVID, we are experiencing challenges in meeting demand from our community, both in waiting times for urgent and emergency care and for planned care, such as outpatient appointments and surgery. We are also in a
financially challenging position, anticipating approximately a £24m underlying deficit for 2022/23. We have seen a decrease in productivity of 20% since the end of 2019/20, meaning we are seeing and treating less patients, which impacts on waiting lists.
Some of the reasons for our overall operational and financial position include the impact of COVID-19, increased demand for our services, and changes in the income we receive.
Research
I would like to share two very good articles which embrace the PQP way of thinking.
y Engagement Value Outcome case study, Gloucestershire Health and Care NHS Foundation Trust >
y Correlation between hospital finances and quality and safety of patient care >
I would encourage you all to take a look at these, with a key abstract of an important piece from academics in the United States detailed overleaf. We particularly need to focus on the below findings:
y Hospitals which deliver
good care usually deliver good finances; it is not a question of choosing to provide quality or choosing to spend wisely – it will be both
y Spending wisely leads to good, effective care
y Good, effective care leads to wise, effective spending
Your involvement
We all need to be a part of this. We would like ideas on effectiveness, productivity and spending to come from those of us who deliver clinical care.
Please contact your line manager if you would like to be involved. If you are approached by a colleague, please be part of the conversation, and consider being part of the PQP team - thank you. The Project Management Office (PMO) team will work with you to support you to develop and implement your ideas – they can be contacted at paht.pmo@nhs.net. You can read more about the PQP programme on AlexNet Please look out for more updates on the Patients
– Quality – Productivity programme coming soon.
4 4
Correlation between hospital finances and quality and safety of patient care,
by Dean D. Akinleye, Louise-Anne McNutt, and Victoria Lazariu (from the United States)
Background
Hospitals under financial pressure may struggle to maintain quality and patient safety and have worse patient outcomes relative to well-resourced hospitals. Poor predictive validity may explain why previous studies on the association between finances and quality/safety have been equivocal. This manuscript employs principal component analysis to produce robust measures of both financial status and quality/safety of care, to assess our a priori hypothesis: hospital financial performance is associated with the provision of quality care, as measured by quality and safety processes, patient outcomes, and patient-centred care.
Methods
This 2014 cross-sectional study investigated hospital financial condition and hospital quality and safety at acute care hospitals. The hospital financial data from the Centers for Medicare and Medicaid Services (CMS) cost report were used to develop a composite financial performance score using principal component analysis. Hospital quality and patient safety were measured with a composite quality/safety performance score derived from principal component analysis, utilising a range of established quality and safety indicators including: risk-standardised inpatient mortality, 30-day mortality, 30-day readmissions for select conditions, patient safety indicators from inpatient admissions, process of care chart reviews, CMS value-based purchasing total performance score and patient experience of care surveys. The correlation between the composite financial performance score and the composite quality/safety performance score was calculated using linear regression adjusting for hospital characteristics.
Results
Among the 108 New York State acute care facilities for which data were available, there is a clear relationship between hospital financial performance and hospital quality/ safety performance score (standardised correlation coefficient 0.34, p<0.001). The composite financial performance score is also positively associated with the CMS Value Based Purchasing Total Performance Score (standardised correlation coefficient 0.277, p = 0.002); while it is negatively associated with 30 day readmission for all outcomes (standardised correlation coefficient -0.236, p = 0.013), 30-day readmission for congestive heart failure (standardised correlation coefficient -0.23, p = 0.018), 30 day readmission for pneumonia (standardised correlation coefficient -0.209, p = 0.033), and a decrease in 30-day mortality for acute myocardial infarction (standardised correlation coefficient -0.211, p = 0.027). Used alone, operating margin and total margin are poor predictors of quality and safety outcomes.
Conclusions
Strong financial performance is associated with improved patient reported experience of care, the strongest component distinguishing quality and safety. These findings suggest that financially stable hospitals are better able to maintain highly reliable systems and provide ongoing resources for quality improvement. Read more here >
5 5
Introducing our mental health strategy
 By Sharon McNally, chief nurse and deputy chief executive
By Sharon McNally, chief nurse and deputy chief executive
There is no health without mental health. That is the key focus of our five-year mental health strategy
I am proud of our commitment to making a difference to the way in which we support the mental health needs of our patients and their loved ones.
The strategy was approved by the Board in January 2023. I welcome the introduction of this strategy, which marks an important milestone in our work towards transforming our care, as part of our PAHT2030 strategic priorities.
We aim to provide the most up-to-date and expert care designed to meet the individual needs of our patients, where and when they need it.
One in four adults and one in ten children will experience mental illness (as shown in NHS England data) and our local population that we serve will have mental health needs whilst they are under our care.
That’s why we have developed an ambitious mental health strategy that sets out how we will improve mental health care for our patients, alongside providing services for their physical needs.
The plans within the strategy reflect what matters most to people who use our services, the people who care for them, our organisation’s partners and community providers.
To deliver our strategy, our focus is to:
y Improve the quality of care that we deliver to our patients who have mental health needs
y Support our patients with long-term physical health conditions to identify and manage their mental health needs
y Ensure that our people have the right skills and approach to care for patients with mental health needs
y Ensure that our people are confident and knowledgeable to recognise individual mental health needs and provide early intervention where required
y Engage with voluntary services to further support our patients with mental health needs
y Work collaboratively, working with local system partners to enhance care and pathways
y Ensure that our environments are quiet, clean, safe, and fit for purpose to reassure our patients with mental health needs
y Enable our mental health partners to access our electronic documents and to ensure we have a joined-up approach to the care of our patients
y Enable people to embrace conversations about mental health and wellbeing
To refer a patient to the mental health urgent care services, please complete the referral form via this link >
You can read the full strategy here >
Thank you for your support of our patients.
6 6
Patient at home service start first patient on innovative medication pump
By Thilo Pillay, senior pharmacist/ clinical specialty
support - patient at home
In the patient at home service, we have begun an area of practice that has many benefits for our patients and our people. We started our
first patient, David Fegan, from Hunsdon in Ware (pictured, right), on a Baxter Elastomeric Infuser, which is a nonelectronic medication pump that is designed to deliver intravenous antibiotics to the patient, before he returned home.

This is an innovative new practice that has only been introduced in a few trusts around the country. Medication
is pumped gently through to the delivery tube
and into the patient’s catheter/ port and is changed once a day.
Our team can administer a range of antibiotics over 24 hours. The infuser enables the patient to be cared for in the comfort of their own home, rather than staying in hospital, and to receive their medication whilst carrying out their
7 7
everyday activities.
This also supports us to enhance patient flow and create capacity within our ward areas to provide care for other patients. Thank you to everyone involved. For more information, please contact me at thiloshini.pillay1@nhs.net.
Note: The patient at home team transitioned from PAHT
to being managed by Essex Partnership University Trust (EPUT), who play a key role in delivering the Virtual Hospital service and work closely with the Care Coordination Centre, on 3 April.
To refer a patient who lives in Hertfordshire or West Essex:
y Refer via the Virtual Hospital form available on AlexNet >
y Refer via the dedicated hotline for professionals: 07581 013636 (between 8am-8pm, seven days a week)
y Refer via email at: epunft. virtualhospital@nhs.net
You can read more on AlexNet >
Anaesthetics trainee focuses on the connection between humans and animals
 By Rakhi Ghosh, CT2 anaesthetics trainee
By Rakhi Ghosh, CT2 anaesthetics trainee
The Humanimal Trust is an organisation that promotes the collaboration between medical and veterinary practice and research - a concept termed ‘One Medicine’.
I became involved with the charity after looking for an organisation that would allow me to explore my fascination about the links between these two fields and enable me to promote better care for our patients.
I hope to spread the message, particularly amongst medical professionals, about how integrated research and knowledge-sharing can be beneficial for humans and animals. I would also like to encourage the next generation of doctors and vets to consider
how their practice affects the planet and how they can be advocates for a more sustainable healthcare system.
My key areas of interest are collaboration of research into surgical and anaesthetic procedures and the impact of healthcare processes on the environment.
The Humanimal Trust have recently released the latest series of their podcast, called ‘The Humanimal Connection’. I was invited to be a guest on the second episode in which we discussed the concepts of One Medicine, and I spoke about the relevance of this in anaesthesia.
The podcast covers other interesting themes including the history of the humananimal relationship. I hope to continue my work with the charity by getting involved in their research sector, as well
as promoting their message through activities in schools and universities.
For more information, please visit www.humanimaltrust. org.uk. You can also contact me at rakhi.ghosh@nhs.net.
8 8
Radiology referrals achievements
By Stephen Townrow,
imaging systems manager and diagnostic radiographer, and Jack Oakes, PACS manager and diagnostic radiographer
Last November (2022), our radiology team implemented an application called MedCurrent Clinical Decisions Support (CDS) iRefer.
The application supports the decision-making for all diagnostic referrals sent to us from primary and secondary care settings.
The system recommends the most appropriate test that is required for the patient, based on the data that the clinician has entered into the system.
Background
Against the backdrop of the Covid-19 pandemic, our radiology department needed to clear a backlog of diagnostic tests, alongside increased pressure on the workforce. In order to achieve this goal, we required a dynamic and digital solution to:
y Reduce inappropriate diagnostic test requests
y Ensure that the correct
test is carried out to avoid unnecessary ionising radiation exposure to patients
y Enable a safe and quick vetting process
y Increase reporting capacity
y Be more cost-effective
y Standardise care in line with national guidelines to reduce clinical variance
The solution PAHT is one of five trusts in the East of England Imaging Network 2 and the first to implement MedCurrent CDS iRefer. We received funding from the Digital Diagnostics Capability Programme and were supported by the network’s digital lead to successfully implement the system.

The application is based on existing iRefer guidelines that have been produced and approved by the Royal College of Radiologists. The application also supports decision-making
by recommending the modality and the test that is required.
The existing test requesting system, called ICE from Clinisys, fully integrates with MedCurrent CDS iRefer without needing to open a separate programme.
When an imaging request is created, MedCurrent CDS iRefer launches automatically and presents the requested procedure, a recommended procedure and other options, with a clinical justification for each option.
The clinical detail that has been collected and whether the recommendation was accepted or not, is saved and continues through the remainder of the workflow in ICE. At the vetting stage, the radiologist can view all of the details.
9 9
The challenges
We are the first hospital trust in the region to implement the solution. As a result, the team received a high number of queries prior to the implementation.
Following the implementation, a few minor concerns were raised and this feedback helped to shape improvements within the system for users, including:
y Disabling CDS for appendicular and chest X-rays. This improvement was justified as these requests do not require radiologist vetting and are relatively low-dose/low complexity procedures
y Clinisys produced a script to enable the solution for large requesting groups on ICE. Completing this manually in ICE created a large strain on the database and therefore not all users had access initially
y The engagement with GP colleagues has grown over time through early contact and a dynamic array of communications with practice managers, select lead GPs and transformation managers
y Additional training, explanation sessions, discussions and further use of the system has reduced concerns raised by clinicians and the majority are now using the system confidently
y They were unable to find a newly created patient on test ICE (which was created in an electronic patient record test). The supplier resolved this issue by undertaking a configuration update
The results
Encouraging results were visible after using the system for three weeks, including:
Primary care
y 8.4% of tests (313 exams) requested by GPs were withdrawn based on the advice of CDS iRefer
y 12.6% (468 exams) started with one test, but based on the recommendations they left with another test/ imaging modality
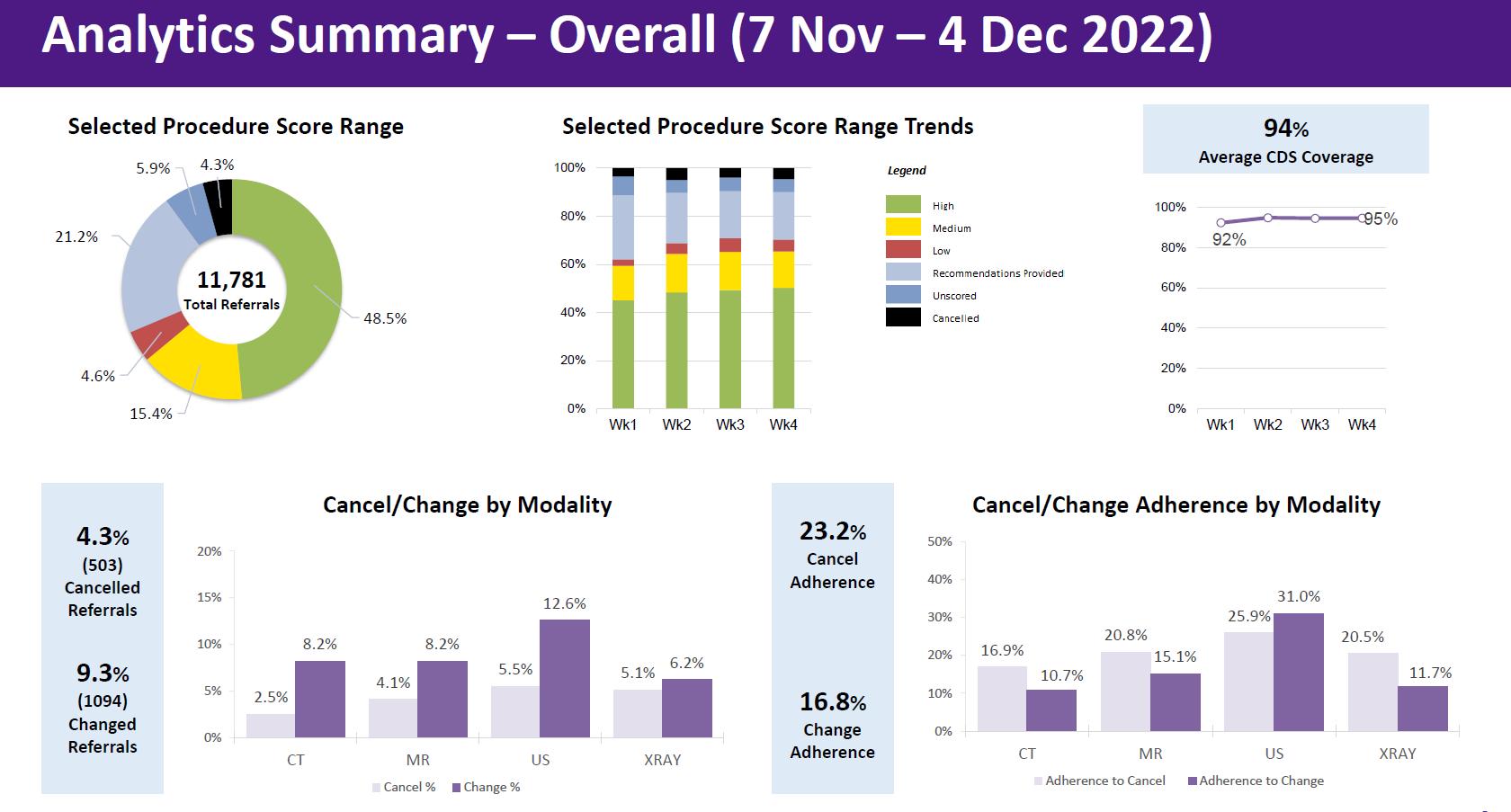
Secondary care
y 2.4% (190 exams) cancelled and 7.8% (626 exams) changed to a different imaging test
y The results show a 25-30% reduction in inappropriate requests that needed to be rejected by consultants. Moving forward, rejected requests will be reviewed regularly to see if any improvements can be made to the system to further reduce this number
Pictured below: Key analytics.
10 10
Sharing the learning
Since implementing the solution, our team has learnt and identified the following to share with the East of England Regional Radiology Network digital workstream teams and other hospital trusts.
Roles within ICE
We have focused on ensuring that all the roles within ICE are shown within the extract, detailing what users can and cannot request. MedCurrent utilises this information to ensure that the system does not recommend a test that a requester is not authorised to request. There is a high level of complexity when producing this
By Dr Preethi
Gopinath, director of medical education
Our medical education team has hosted a wide range of events since the last edition of Our Journal, including:
• Between January –March, each division has participated in an Active Bystander Training event. This is an innovative and award-winning training session which gives colleagues the skills to challenge unacceptable behaviours, which may have become normalised over time
• We hosted a Becoming More Assertive one day event for Specialty and
extract, therefore it can be time consuming to complete.
Team work
The collaborative working and commitment from the whole radiology team has contributed to the successful implementation of the solution. It is important that radiologists are supportive of the project, as their knowledge of vetting, multi-disciplinary teams and clinical pathways is imperative to enhance and improve the system.
Next steps and sustainability
y Continue to improve and enhance the system, including protocols in line
with the trust guidelines, with the support of subspecialty radiologists and MedCurrent
y Utilise the MedCurrent analytics programme to identify request trends
y Continue to discuss and review protocols
y Contact individuals that require guidance
If you have any questions or to find out more, please email me at stownrow@nhs. net. You can also contact Jack Oakes, PACS manager, at jackoakes@nhs.net and Dr James Diss, consultant radiologist, at james.diss@ nhs.net. Well done and thank you to all involved.
Associate Specialist (SAS) and Locally Employed Doctors (LED) in the Learning and Education Centre on 6 February. The objectives of this course were to build insight into assertiveness and negotiation models, to build skills in applying these models to professional practice and to be able to apply these skills to the doctors' own real-world challenges
• We held a Human Factors Training Day for Specialty and Associate Specialist (SAS) and Locally Employed Doctors (LED) in the Learning and Education Centre on 2 March. This one day course aimed to build on existing human
factors knowledge specific
to working at PAHT
Other events have included:
• Breaking Bad News Workshop - multidisciplinary (doctors/ student nurses/ occupational therapists) on 30 January
• Trauma and Orthopaedic Regional Foundation Hub on 19 January (pictured overleaf, right)
• Histopathology Regional Foundation Hub on 27 January (pictured overleaf, far right)
• Dr Andrew Ashford, GP Specialty Training (GPST) programme director, delivered in-house clinical supervisors' training on
11 11
Medical education team share the latest learning and updates
how to support trainees on hospital placements, portfolio requirements and navigation on 24 January
• International histopathology course from 20 February – 9 March
• Schwartz Round, "An act of kindness I will never forget" facilitation - 31 January
• Ongoing Freedom to Speak Up listening events
We are now looking ahead to the Planning for Emotional Intelligence EQ-i 2.0 and EQ 360 certification course on 23 May. This leading emotional intelligence assessment provides an in-depth understanding of an individual’s emotional functioning, enabling us to support our colleagues with these tools in-house.
We have weekly drop-in clinics for trainers and junior doctors at the Learning and Education Centre, please contact judith.butcher@nhs.net for more information.
We are also holding a thank you dinner and dance open to all junior doctors, physician associates and medical educators on 9 June at Harlow Rugby Club, which includes an awards ceremony.
General Medical Council (GMC) Enhanced Monitoring Programme update
In collaboration with the Junior Doctors' Committee, our junior doctors are actively contributing to the GMC Enhanced Monitoring Programme by feeding back improvements and ongoing issues with their training via a variety of platforms such as the Junior Doctors' Committee, the Medical Education Committee, the GMC Enhanced Monitoring monthly meetings, listening events with the Quality First team and the Freedom to Speak Up Guardians. This work forms part of the response to the 2022 GMC Survey and The National Education and Training Survey (NETS).
There is ongoing work towards addressing the British Medical Assocation (BMA’s) eight high impact actions for junior doctors, for example the ‘Too Tired to Drive’ policy, which is now in place. Other projects in progress are:
• Tackling work pressure
• Better engagement between trainees and the Board
• Improved access to food and drink 24/7
• Rotas that promote work/ life balance
• Clearer communication between trainees and managers
• Rewarding excellence
• Wellbeing, mentoring and support
• With the support of IT, the junior doctors completed a spot audit on computer start up times across the hospital which has helped to drive improvements in IT infrastructure
• A Clinical Escalation Standard Operating Procedure (SOP) is now in place for medicine as a result of the junior doctors' contribution to this project. Work on SOPs is progressing for the other specialties
• There is an ongoing project with the Junior Doctor Champions to improve departmental induction
• Former trainees, Mr Anoop Prasad and Dr David Ensor, have developed the ARCTERA 360 video simulation platform for clinicians to practice and develop their clinical reasoning skills in a riskfree environment, available to undergraduate and postgraduate doctors >
Read more on AlexNet >

12 12
Team who are committed to enhancing cancer care services featured in national publication
By Emma Harnett,
Macmillan cancer education lead nurse for Hertfordshire and West Essex Integrated Care Board
One Step at a Time (OSAAT) started with a conversation over a cup of tea with Ann Nutt, chair of the Patient Panel at PAHT, sharing my experience of cancer, and the need to keep information simple, in language that everyone understands. A further meeting with Shahid Sardar, associate director of patient engagement and experience at PAHT, was pivotal. Together we created our first video, which detailed my own experience as a nurse, and how cancer can affect anyone, at any time.
It doesn’t matter who you are, or what you do, nothing can prepare you for being diagnosed with cancer. The key to getting through a diagnosis is the support you receive.
Soon, more people joined the initiative to share their lived experiences. We are a group of like-minded people, but from
very different backgrounds, with a vision to amplify the patient voice. Our mission statement is simply, ‘cancer information produced by patients, for patients'.
In October 2022, we were proud to win the Team of the Year category at The Royal College of Nursing (RCN) Awards, in recognition of our work to promote the patient voice (pictured, from left to right, me, Ann Nutt and Shahid Sardar).

We have now been featured in the Nursing Standardcharting my own cancer journey and our drive as a team to improve the experience of those affected by cancer and their loved ones. This was a fantastic opportunity for us to be a part of and I would encourage everyone to take a look.
We also held a cancer conference at Harlow Rugby Club on 9 March, which was well attended and extremely well received. Topics covered included receiving a cancer diagnosis, caring for someone with cancer, and finding local support.
Our website now features a variety of patients sharing their stories, with information from family members on what it feels like when a loved one
is diagnosed with cancer. We are helping to address health inequalities in our health system, with better representation of our wider community.
Working in conjunction with the Cancer Alliance, we have had the original video translated into five additional languages, those most widely spoken after English within West Essex: Romanian, Urdu, Polish, Italian and Punjabi.
We believe the key to our success is working collaboratively and for everyone’s voice to be heard.
You can read the full article in the Nursing Standard here >
For more information, please refer to our website > You can also contact me at e.harnett@nhs.net
13 13
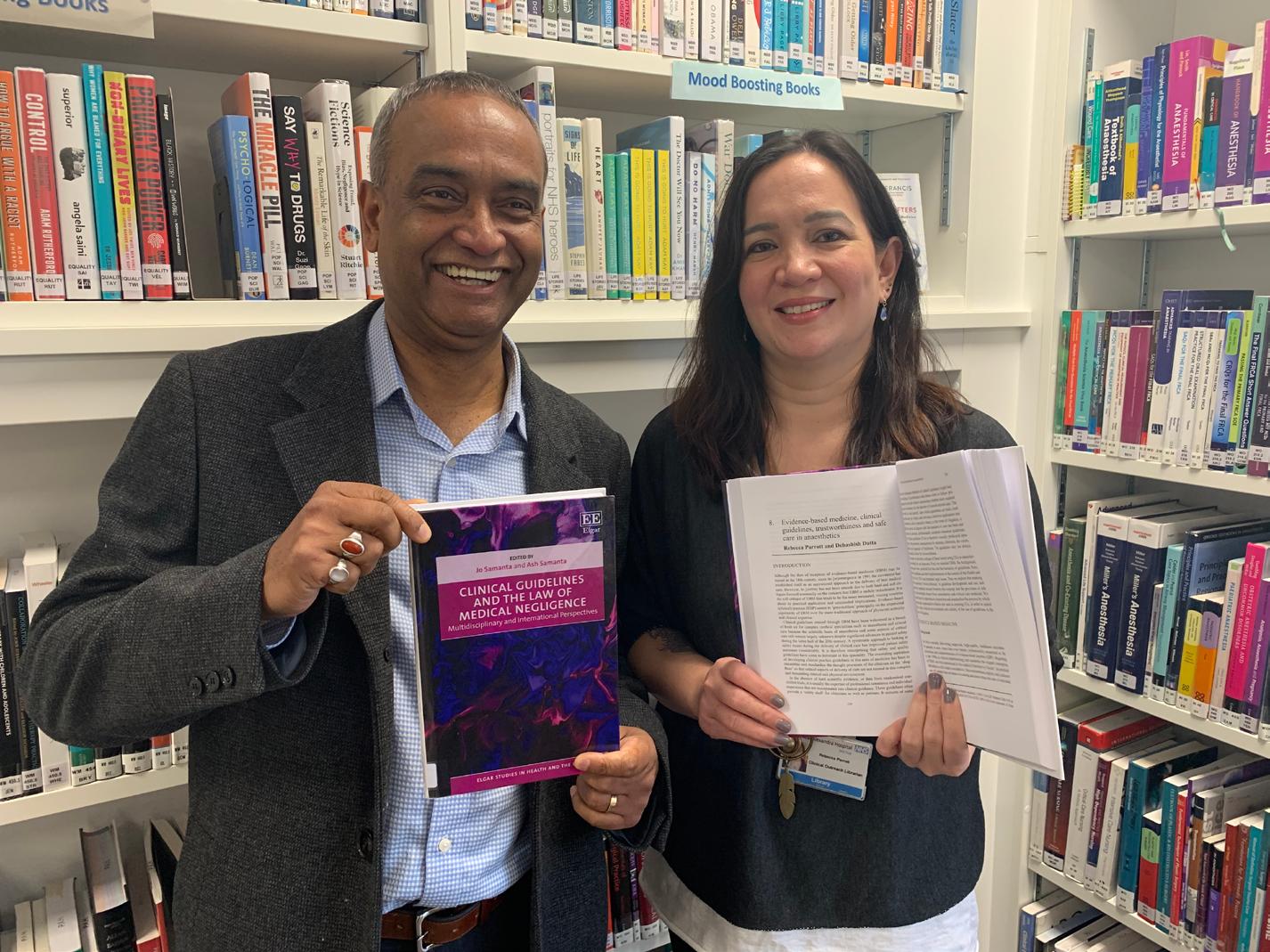
Consultant and library manager put pen to paper with new book
By Dr Dev Dutta, consultant
anaesthetist, and Becca Parrott, knowledge and library services lead
We are pleased to have put pen to paper and contributed to a newly published book.
The book, called Clinical Guidelines and the Law of Medical Negligence, is a detailed overview of the national and local clinical guidelines available for clinicians.
Edited by Jo Samanta, Emeritus Professor, Law School, De Montfort University,
this book chapter came after a time of working with Dr Dutta in our Intensive Care Unit (ICU), in the capacity of supporting evidence-based practice.
academic research around evidence-based medicine, methodologies and bias, the trustworthiness of publications, and the implementation of guidelines.
Leicester,
and
Ash
Samanta, Emeritus Consultant Physician and Rheumatologist,
University Hospitals of Leicester and Lecturer in Medical Law, Law School, also at De Montfort University, the book is an important resource for clinicians. We wrote the eighth chapter in the book, which focuses on evidence-based medicine, clinical guidelines, trustworthiness and safe care in anaesthetics.
Becca's experience
The opportunity to contribute to
I had just completed a Masters dissertation on the related topic of clinical librarianship, and how this role helps to bridge the gap between papers to patient: sourcing and applying evidence to enhance patient care. When Dr Dutta told me about a chapter he was writing for this new book, and asked if I would like to contribute; it was clear the topic was pertinent to our work together and also my own professional interests.
It was a timely opportunity that was too good to miss, as the chapter content was so relevant to my work:
Rather than sit down to write the chapter together, we each contributed sections that we wrote individually. These topics linked together, and drew on each of our interests and areas of knowledge or experience.
We initially discussed the topics we wanted to write about, and how these could flow together.
This gave us a good foundation for structuring our chapter and deciding which of us would cover particular sections. We also worked on the schedule and timings for the submission to our editors, and we had
14 14 4
regular check-in meetings to discuss progress and ensure we were on track.
I have no immediate plans to write for publication at the moment, but my experience with writing this chapter has shown me that collaborations like this are valuable and achievable. As colleagues with shared professional interests, we all make up a body of information and experiences that can be utilised to share best practice and keep topics fresh and updated.
It was a pleasure to contribute to this excellent piece of work, and a welcome opportunity to encapsulate the collective outcomes of my professional practice as a healthcare librarian.
Dr Dutta's experience I first came into contact with Professor Jo Samanta while I was doing my law degree in Leicester. She was my supervisor and guided me in learning law and its applications. Professor Samanta had also signposted my journey through the dissertation I had to complete and had invited me to a couple of national debates after I completed my law degree.
One of the debates was regarding (a) available treatment options and funding procurement for neurological rehabilitation in patients with brain damage in the UK. The other national debate she invited me to was a joint conference with various medical experts of different
clinical specialities, lawyers and barristers in London. This joint conference of national debate was based on any publication of clinical guidelines and the possible impact of those guidelines if applied in a court of law. It is after that debate that Professor Samanta approached me to write a chapter in the book she was planning to publish. I then approached and requested Becca to join me in writing the chapter. Becca and I decided to structure and include how the materials of medical evidence are explored and added to the guidelines. We also decided to include the source of the guidelines to be considered before embracing the clinical practice.
The blurb reads: “This book critically considers the dynamic relationship between clinical guidelines and medical negligence litigation, arguing that a balance must be struck between blinkered reliance on guidelines and casual disregard. It explores connections between academic law and professional practice, bringing together an array of perspectives which reveal that although guidelines may not be dispositive, they nonetheless play an important role in medical negligence law.
“The chapters provide compelling insights from academics, lawyers, barristers, doctors and healthcare professionals into the use of guidelines in determining the legal standard for breach of duty, thereby contributing
to a holistic understanding of guideline usage in this area of law. Sociological considerations along with empirical findings are used to underpin these concepts.
“While focusing on the UK, contributors draw upon international law, including that from the United States, South Africa, the Netherlands and other countries. Based on this analysis, the conclusion offers a theoretical framework for practical application illustrated by a case-based discourse. This book makes a significant contribution to the knowledge base in the subject area. It is an essential read for legal academics and lawyers working in medical and health law, as well as for doctors and other healthcare professionals. It will be a key reference point for medical regulators, health organisation policymakers and clinical governance teams.”
You can find out more about the book here >
You can also contact us at dev. dutta@nhs.net and rebecca. parrott@nhs.net.
15 15
Latest research supports early diagnosis of breast cancer
By Chris Cook, head of
research, development and innovation
The University of Cambridge, together with Cancer Research UK, have developed a study called EMBED, which stands for early markers for breast cancer detection.
EMBED is a prospective cohort study of women at an increased lifetime risk of developing breast cancer and to look for blood-markers that would enable an earlier diagnosis of the disease.
This study is taking place in the family history clinic, based in the Breast Unit at St Margaret’s Hospital and is being run by our research, development and innovation team and with Dr Ashraf Patel, associate specialist in breast surgery, as the principal investigator (pictured, right).

A blood test has been developed that could provide an earlier diagnosis of breast cancer. Circulating tumour DNA (ctDNA) is an important blood marker in detecting breast cancer. Therefore, being able to detect small amounts of ctDNA in the blood could be an important step for an earlier diagnosis of the disease in the future.
Once the participant has consented, they will have a blood sample taken. By providing a blood sample, tests can be refined in readiness for a large study, in which blood samples will be collected from women who have a strong family history of breast cancer.
Participants will not benefit personally from this study as we are not testing samples for a diagnosis of breast cancer, but participants could be helping generations of women in the future to get earlier diagnosis and treatment for the
disease. We currently have 15 patients at PAHT who are participating in the trial and we are one of 20 centres in the UK to recruit to this particular study.
Thank you to everyone involved in this vital research. For more information, please contact me at chris.cook6@nhs.net.
Showcase your work in the next edition of Our Journal
Thank you to everyone who has taken part in the first four editions of Our Journal. It has been excellent to showcase your work, with a broad range of articles written by our clinical people, for our clinical people.
Please contact us at paht.communications@nhs.net to feature in the next edition - publishing July 2023.
16 16
Research study: Pain management for older adults with a hip fracture
By Darryl De Souza, deputy therapy manager, and research fellow at the National

Institute of
Health
Research (NIHR)
2020 - April 2021, showed only 49% of patients with a neck of femur fracture had their pain assessed within 15 minutes of arrival, 15% had appropriate analgesia within the first 15 minutes, and only 3% had a reevaluation within 30 minutes of the first dose of analgesia.
In addition, older adults with a hip fracture wait longer for analgesia, are treated with lower doses, and are less likely to receive opioids compared to younger adults. Outcomes in this group of patients are poorer with prolonged hospital stays, and higher rates of anxiety and delirium.
older adults
Pain is a significant feature of a hip fracture and good clinical outcomes are dependent on early diagnosis, surgery and effective pain control.
Pre-hospital services (GP and ambulance) and emergency departments (ED) are usually the first points of contact to provide analgesia and play an important role in the patient's pain journey.
However, despite pain being the most common cause of attendance in ED (accounting for 75% of patients), acute pain is often under-treated, resulting in 'oligoanalgesia'.
A national audit of 159 emergency departments, undertaken between October
Why is this happening?
It is known that barriers to effective pain relief exist in healthcare, but this has not been wellresearched within the NHS. Evidence suggests staff and organisational priorities, patient characteristics, and variations in staff knowledge are involved. However, a deeper understanding of such issues is an important step in improving outcomes and equality in hip fracture care.
Aims of my study
The aims of my study were:
(1) to determine if older adults receive suboptimal pain management and if this is impacted by certain patient characteristics (age, gender and cognition).
(2) to see if a disparity in pain
knowledge exists among staff groups and work areas (ED and Tye Green Ward).
(3) to evaluate if staff perceive any barriers to effective pain management.
I used a mixed methodological approach, involving:
1. A retrospective analysis of patient data (April 2021 –March 2022)
Using data from the National Hip Fracture database (n=199) and patient records (n=38), I compared the analgesic management in younger (<75 years) and older adults (>90 years). This included the analgesia given in ED and dosage, if a nerve block was given, and if pain was assessed at defined points of the inpatient journey.
17 17
“Breaking bones and barriers” –The challenges of analgesic management in
2. A questionnaire to assess staff knowledge of pain
Staff knowledge of pain was assessed using a standardised questionnaire: Knowledge and Attitude Regarding Pain (KASRP).
3. Interviews with staff Semi-structured interviews with staff working in ED (n=5) and Tye Green Ward (n=3) to discuss their experience and barriers to pain relief. Staff included nurses, an advanced clinical practitioner (ACP) and consultants.
Main findings
1. Older adults received suboptimal pain management
y Fewer older adults received a nerve block compared to younger adults, (28% vs. 47%, respectively, p<0.01)
y Age was as an “acceptable” predictor for receiving a nerve block (ROC: AUC 0.665)
y Older adults stayed longer in hospital by 4.9 days (p<0.01)
y Only 45.8% of older adults (n=24) were assessed for pain compared to 32.9% of younger adults (n=14)
2. Staff knowledge did not differ between doctors, nurses and an ACP working in ED/Tye Green Ward
y No significant differences were found in KASRP scores between staff groups (p=0.710) and work areas (p=0.862)
y Staff achieved 61% correct answers, rating their performance as “fair”
Themes of barriers - Fig. 1
3. From the staff interviews, four broad themes of barriers emerged: self, environment, patient and organisation (see Fig. 1)

Conclusions
This study’s findings found inequalities in hip fracture care exists among older adults (90+ years) compared to younger adults (<75 years).
y Older adults are 19% less likely to receive a nerve block compared to younger adults
y Less than 50% of older adults received a pain assessment during their inpatient stay
y Hospital stays were five days longer in older adults
The reasons for this inequality of care are multifaceted, but barriers such as low staffing, emergency department (ED) crowding, staff knowledge, and availability of staff to administer nerve blocks are likely to play a significant part.
Furthermore, staff unintentionally prioritised patients who vocalised their
pain, often these were younger patients.
Key recommendations:
1. Update/re-circulate the hip fracture policy.
2. Regular pain education for staff.
3. Nerve block box/trolley to centralise equipment and appointed staff to maintain contents.
4. Increase volume of nurse prescribers and expand competence to administer nerve blocks.
5. Staff focus groups to support retention. There is already a recruitment and retention steering group and there are some retention initiatives currently being reviewed.
This study was funded by the NIHR and sponsored by PAHT. Special thanks to Dr Robert Ghosh, divisional director of medicine and urgent and emergency care; Katie Silk, head of therapies; and Chris Cook, head of research, development and innovation, for all their support and encouragement. For more information, please contact me at darryl.desouza@nhs. net,
18 18
Articles and publications - our #PAHTPeople...
Take a look at some examples of the range of articles published and publications contributed to by our people since the last edition of Our Journal - a fantastic achievement. Full information of authors and articles are available from the library team: paht.lib.desk@nhs.net.
y Abeysuriya V., et al., "Combination of cycle threshold time, absolute lymphocyte count and neutrophil:lymphocyte ratio is predictive of hypoxia in patients with SARS-CoV-2 infection." Trans. R. Soc. Trop. Med. Hyg. 2022;116(7):628635. PAHT author: R.S. Wijesinha. The Princess Alexandra Hospital NHS Trust, Harlow, Essex, UK.
y Alajlan A., et al., "JointPreserving Surgery in Varus Ankle Osteoarthritis." J. Clin. Med. 2022;11(8). PAHT
author: Kar Teoh. The Princess Alexandra Hospital NHS Trust, Harlow, Essex, UK.
y Al-Janabi MM, et al., "Early mobilization following elective ankle lateral collateral ligament reconstruction in adults." FOOT. . 202355doi:10.1016/j. foot.2023.101988, 10.1016/j. foot.2023.101988. PAHT
author: Al-Janabi, Mina
Mazin. The Princess Alexandra Hospital NHS Trust, Harlow, Essex, UK.
y Awasthi A., et al., "Enhanced Neoplasia Detection in Chronic ulcerative colitis: results of the ENDCaP-C Diagnostic accuracy study." medRxiv 2022.
PAHT author: Deb Ghosh. The Princess Alexandra Hospital NHS Trust, Harlow, Essex, UK.
y Carbone M., Sharp S.J., Flack S., et al., "The UK-PBC risk scores: Derivation and validation of a scoring system for long-term prediction of end-stage liver disease in primary biliary cholangitis." Hepatology 2016;63(3):930-950. There are no PAHT authors on this paper, but our research nurses are listed as members of the UK-PBC Consortium (253 people are listed as part of this). They are Ervin Shpuza, (no longer at PAHT) and Nikki White. The Princess Alexandra Hospital NHS Trust, Harlow, Essex, UK.
y Chapman R., et al., "Nanopore-Based Metagenomic Sequencing in Respiratory Tract Infection: A Developing Diagnostic Platform." Lung 2023; no pagination. PAHT authors: (Lead) Robert Chapman, Ahmed Suliman and Muhammad Anwar. The Princess Alexandra Hospital NHS Trust, Harlow, Essex, UK.
y Habashy D, et al., "Evaluation of Outcomes following Focal Ablative Therapy for Treatment of Localised Clinically
Significant Prostate Cancer in Patients >70 Years: A Multi-institute, Multi-energy 15-year Experience." J Urol. . 2023. PAHT author: Jaspal Virdi. The Princess Alexandra Hospital NHS Trust, Harlow, Essex, UK.
y Rashid, MS, et al., "Validation of three classification systems for posterior malleolus fractures of the ankle." Eur. j. orthop. surg. traumatol.. 2023. PAHT authors: Raisa Islam, Kar Teoh. The Princess Alexandra Hospital NHS Trust, Harlow, Essex, UK.
y Rehman U., Freer, et al., "Non-surgical facial aesthetics: Should this be incorporated into medical education?" Adv. Oral Maxillofac. Surg. 2022; 8.
PAHT author: F Freer. The Princess Alexandra Hospital NHS Trust, Harlow, Essex, UK.
y Thottarath S., et al., "Study protocol on prevalence of non-exudative macular neovascularisation and its contribution to prediction of exudation in fellow eyes with unilateral exudative AMD (EYE-NEON)." Eye 2023. PAHT author: P Prakash. The Princess Alexandra Hospital NHS Trust, Harlow, Essex, UK.
19 19





20 20 The Princess Alexandra Hospital NHS Trust, Hamstel Road, Harlow, Essex, CM20 1QX 01279 44 44 55 NHSHarlow @NHSHarlow @PrincessAlexandraNHS The Princess Alexandra Hospital NHS Trust











