
1 1 accountQuality 2022-2021



2 IntroductionContentsfrom the chief executive Statement of directors' responsibilities About this PrioritiesCareGovernancereportarrangementsQualityCommissionratingforqualityimprovement in 2022Statement23 relating to the quality of care Progressprovided against priorities set for 2021-22 Our patients y Infection prevention and control y Quality improvements y Patient experience and engagement y Our Patient Panel y Improving care for vulnerable patients y Learning from safety incidents y Improving medicine safety Our people y Recognising our amazing people y The national NHS staff survey y OurInclusionperformance y Performance against NHS constitutional standards y Participation in clinical audits y Achievements in information technology y Research and development Our places y Improving our estate y Environment and sustainability Statements from stakeholders Glossary of terms 9388837977756763636258535048464443383010966553
includes:strategy.ouratweorganisation,outstandingandandareworkingpacetodeliverPAHT2030This
3 3
Welcome to our quality account 202122. The year has seen us face the continued challenges of the ongoing COVID-19 pandemic and required our people to work through increased pressures, with flexibility and Theuncertainty.dedication of our people to provide high quality care for our patients, and support those who provide care, has been extraordinary. We have seen some great progress with the recovery of our services, including reducing the number of patients with cancer who are awaiting treatment; reducing the number of patients who are waiting more than two years to receive routine treatment; and steadily reducing the number of patients who are waiting longer than one year to receive their routine appointment and treatment. We also achieved the national standard of 99% of patients who require an ultrasound to receive their diagnosis within six weeks. We built on the improved patient experience that can be achieved through offering more flexibility, with virtual appointments where appropriate. By the end of March 2022, 34% of our outpatient activity was carried out virtually, above the national average (25%). There have been many proud moments across the year, from the recognition of our amazing people with a series of prestigious awards, to our ongoing work to support the health, wellbeing and development of our people, with the opening of two fantastic new facilities – the Alex Lounge staff area, and the Learning and Education Centre. These spaces enable our people to be the best they can be at work – and in turn to deliver the best care for our patients. Our vision is to become a modern, integrated
y Transforming our care: the most up-to-date and expert care designed to meet the needs of the patient, where and when they need it y Our culture: fostering and nurturing an inclusive environment that champions diversity and equality, and where our people are engaged, supported and helped to learn and grow y Digital health: Harnessing new technology and digital solutions to transform patient care and how we work y Corporate transformation: Modernising our corporate service to support our clinical teams in providing outstanding care y Our new hospital: A world-class hospital for the future, providing first-rate care for our patients and the best place to work for our people We have seen a range of exciting developments in these areas in the last year. Highlights include the board approval of our business case to move forward with a new electronic health record to benefit our patients and our people; our continued focus on partnership working to reduce inpatient stays to maximise capacity and support patient safety; and our ongoing work on the business case for a new Princess Alexandra Hospital.
The New Hospital Programme is a government-backed multi-billion pound executive
Introduction from the chief

4 programme to deliver 48 hospitals by 2030. While the timescale for completion of our new hospital has been delayed, as the New Hospital Programme team work through the benefits for staff and patients of joining up common aspects of all the new hospital builds, we are ready to progress further once we have approval from the national team. We look to the next year with our continued focus on enhancing the care we provide to our patients and the support for our people. I commend this quality account to you, and I am, as always, grateful to the many people who have contributed to its content. I confirm that, to the best of my knowledge, the information in this account is accurate. Best wishes Lance McCarthy Chief executive



We will describe to you the areas where we have reviewed our patient care in order to evaluate the quality of services
The trust directors are required under the Health Act (2009) National Health Service (Quality Accounts) Regulations (2010) and National Health Service (Quality Account) Amendment Regulation 2011 to prepare Quality Accounts for each financial year. The Department of Health has issued guidance on the form and content of annual quality accounts, which incorporates the above legal Inrequirements.preparingthe Quality Accounts, directors are required to take steps to satisfy themselves that: y The Quality Accounts present a balanced picture of the trust’s performance over the reporting period y The performance information in the Quality Account is reliable and accurate y There are proper internal controls over the collection and reporting of the measures of performance included in the Quality Accounts, and these controls are subject to review to confirm that they are working effectively in practice y The data underpinning the measures of performance reported in the Quality Accounts is robust and reliable, conforms to specified data quality standards and prescribed definitions, and is subject to appropriate scrutiny and review. The Quality Accounts have been prepared in accordance with Department of Health guidance. The directors confirm that, to the best of their knowledge and belief, they have complied with the above requirements in preparing Quality Accounts. By order of the board
5 5
Statement of Accountsrespectresponsibilitiesdirectors’inoftheQuality2021-22
About this report What is a Quality Account? Every year all NHS hospitals in England must write a report for the public about the quality of their services; this is called the annual Quality Account. The purpose of the report is to make the hospital more accountable to you and drive improvement in the quality of our Inservices.2021-22, the COVID-19 pandemic has impacted how all NHS organisations provide the best possible care and service. At The Princess Alexandra Hospital NHS Trust, we are committed to making sure that we keep our patients and our people safe. We have been working hard to respond to the fastchanging national situation through our incident management team. Our focus has been to ensure we can provide all necessary care and treatment in the safest possible way, at the right time and in the right place for our patients. Through this, we are making our pledge to you about the improvements we intend to make over the period 2022-2023.
The report will tell you how well we performed against the quality priorities and goals we set for the period of April 2021 to March 2022 and the areas we have improved through the year. It will also detail the priorities we have agreed for April 2022 to March 2023.
Theprovided.report will contain mandated information from our board, along with statements from our commissioners and partners. We will also provide a glossary of terms.
The2022.draft
6
Quality Account is planned to be presented to our Quality and Safety Committee (a subcommittee of trust board) for review on 27 May 2022. The final draft document will have delegated authority for the trust Quality and Safety Committee to approve on 24 June 2022. Quality Commission rating
implementing
Care
arrangementsGovernance Quality Account is prepared in line with the Quality Accounts toolkit guidance (2010-11). Additional information is included in line with advice received by NHS England as follows: Details of ways in which staff can speak up (including how feedback is given to those who speak up), and how the trust ensures that staff who speak up do not suffer detriment statement regarding progress in the priority clinical seven-day hospital statement that evidences an plan to reduce rota gaps for NHS doctors and dentists (Schedule 6, Paragraph 11b of the terms and conditions of service for NHS doctors and dentists in training (England) 2016) A draft of the report was shared internally with the senior management team members for peer review and with external stakeholders (clinical commissioning groups, Integrated Care Partnership, Healthwatch and the Health Overview and Scrutiny committees for both Hertfordshire and Essex) in April
y
Our
services y A
y
y
standards for
The Care Quality Commission (CQC) undertook an unannounced focused inspection over the summer of 2021, including a trust wide well led inspection. The core services inspected were Maternity care y Medicine (including elderly care) Urgent and emergency care (emergency department)
The CQC report was published on 17 November 2021 and the ratings given to the trust by the CQC were: 1: Our overall trust rating
Figure
y A
improvement

A summary of our recent CQC inspection During the 2021 inspection, the CQC identified areas where improvements have been achieved, these were: y We appointed a director of midwifery to strengthen clinical leadership y The sustainability of the obstretic rota ihad improved following the cohort of doctors that started in the summer of 2021 y Urgent and emergency care service leaders had made improvements in the governance meetings y The trust has systems and processes in place to learn from incidents, complaints and safeguarding alerts to drive improvements, utilising peer reviews and thematic deep dives All staff are committed to continually learning and improving services. They are developing a better understanding of quality improvement methods and the skills to use them. The trust is enhancing its quality improvement capacity y Despite the challenges of the pandemic, the trust continued to engage with staff, patients and their representatives and system partners in an open and transparent manner
7 7 Figure 2: Our overall ratings by service
The CQC noted outstanding practice in relation to the Patient Panel: y The trust’s Patient Panel was the only model of its kind regionally. The Patient Panel is a voluntary group whose main objective is to provide support for patients and their relatives/carers. The Patient Panel receives funding from the trust to ensure that patients' voices are heard. The panel was awarded the Queens' Award for Voluntary
y

The CQC may complete a further unannounced inspection of the emergency department in 2022 to monitor our progress against the action plan and we look forward to the opportunity to show them the improvements we have made. Our people have used the CQC inspection outcomes as the foundation upon which to critically examine our services and focus on how we plan and deliver the fundamental aspects of safe
3. The trust must devise a process to undertake a review of current and future patients' clinical risk assessments, care planning and psychological observations to ensure the level of patients’ needs are individualised, recorded and acted upon. Monthly data should be submitted of daily audits on staff compliance with the completion of patients' risk assessments and associated actions.
1. The trust must ensure there are sufficient numbers of suitably qualified, skilled competent and experienced nursing staff at all times to meet the needs of patients in the emergency department (ED). To meet this additional condition, the trust must submit weekly information detailing the planned and actual staffing figures, including skill mix. This is broken down by doctors, nurses and healthcare assistants.
4. The trust must ensure that it implements an effective system, with the aim of ensuring all patients who present to the ED have observations completed within 15 minutes of arrival and then appropriately thereafter, in line with trust policy. The trust must submit monthly audit data on staff compliance with completion of patients' psychological observations and appropriate action taken. Immediate actions were implemented following receipt of the warning notice, with further actions underway. We are confident that the actions undertaken and planned will ensure we continue to improve the safety of patients in our emergency department.
8 Services in July 2021. The report detailed 29 recommendations for the trust: y 18 must do actions y 11 should do actions
The concerns identified by the CQC from their inspection were:
given our urgent and emergency care department a rating of inadequate and issued a Section 31. This requires the trust to submit weekly and monthly data to meet the requirements of our licence.
The recommendations have been collated into individual projects and are being updated by the relevant divisional team, using our quality improvement methodology, to enable a consistent and sustained approach to the achievement of these objectives. Each project has a designated executive, a senior responsible officer (SRO) and we have appointed a quality project management team to support. We are using a quality compliance improvement plan as a dynamic document; with additional topics added over the year, as we identified areas that required further improvement. The quality improvement plan is monitored monthly through the quality compliance improvement group that reports into the trust compliance group and onto the Quality and Safety TheCommittee.CQChave
2. The trust must ensure that every patient attending the ED has an initial assessment of their condition to enable staff to identify the most clinically urgent patients and ensure they are triaged, assessed and appropriately streamlined. The trust should submit monthly information to show the outcomes of daily audits of compliance with triage, assessing and streamlining patients.
1. Digital health 2. Our new hospital care. We have taken decisive action to change everyday activities, which have led to significant improvements.
Quality
2. Continue to deliver high quality care in the right place and at the right time for our emergency and urgent care patients. This will be demonstrated through an improvement in our emergency department performance and the removal of the CQC Section 31 notice. For our patients, this will improve the quality of care and experience. Our people 3. We will improve the health and wellbeing of our people, offering a wide range of support so that every member of staff can recover from the effects of working during the pandemic, can stay well and feel they can meet the demands of their roles. y Measures of success will be improved staff health and wellbeing results in the Staff Survey, questions of 5.5 to 5.7 y Lower sickness absence rate to 3.4% 4. We will complete an annual report to review the doctors' rota gaps for staff in training roles. This will help with planning of rotas going forward. Our performance Quality improvement projects to transform services are working to modernise how we deliver care and improve timeliness of treatment and patient experience. These are three-year programmes of work and in the coming year: 5. Outpatient improvement programme: We will continue to transform outpatient services to meet the needs of our patients and to meet the NHS Long Term Plan, including use of technology and the redesign of our services to enable timely and appropriate consultations for our patients. Measures of success will include improved patient experience through patient feedback, and through reduction in do not attend appointments, reduced number of followups, improvements in timeliness of clinical treatment.
6. Theatre transformation: We will continue to ensure that all perioperative resource, including staff, is used effectively and efficiently to deliver the highest quality patient care. Measures of success include to reduce waiting times and reduce the COVID-19 related backlog. This will improve patient experience and quality of care. The measure of success will be to implement robust scheduling principles and to ensure improvements to the start and finish times of theatre lists can lead to improved theatre utilisation.
2022-2023improvementprioritiesAccountforduring
9 9
Our eight Quality Account priorities for the next year are identified in line with the quality elements of the PAHT five Ps strategy: which covers our patients, our people, our performance and our places. Our patients 1. We will maintain the trust Hospital Standardised Mortality Rate (HSMR) within expected and we will continue learning from every death. This will improve quality of care for all patients.
7. Medicines optimisation: We will continue to ensure that patients are involved in the decision-making about their medications and that they receive the correct medications at the correct time. Measures of success will include improved patient safety, reduced waste caused by unnecessary prescribing of medications and improved patient outcomes. Other measures of success will be to implement an antibiotic dashboard and for the divisions to implement a robust model for reviewing compliance with antibiotic prescribing policy including the ongoing development of the antibiotic review panels.
We own the main hospital site in Harlow, and operate outpatient and diagnostic services out of Herts and Essex Hospital, Bishop's Stortford, and St Margaret’s Hospital, Epping. The operation of these facilities forms part of the longer-term strategy of bringing patient services closer to where people live and making services, where appropriate, that are more accessible and easily available to patients. We operate over 64 different services to meet the needs of our patients (see the service portfolio in table 1, overleaf).
10 Our places 8. We will continue to work in partnership to improve our hospitals and health infrastructure for our patients. Our pounds We do not have a Quality Account priority for the coming year in respect of our pounds, however by improving the quality of care as detailed in the priorities above, this will deliver greater for money value for our patients.
Monitoring progress on our 2022-2023 quality improvements
These priorities will be monitored using our existing governance structures; this will include being monitored through our Quality and Safety Committee. Statements relating to quality of care provided PAHT is a 414 bedded hospital with a full range of general acute services, including; a 24/7 accident and emergency department (A&E), plus an intensive care unit (ICU), a maternity unit (MU) and a level II neonatal intensive care unit (NICU). During 2021-22, we opened a new building on the main site that holds the Adult Assessment Unit (AAU) and Same Day Emergency Care Unit (SDEC); both will provide an environment and new services that will improve patient experience for those patients requiring urgent care. We serve a core population of around 350,000 and are the natural hospital of choice for people living in east Hertfordshire and west Essex. In addition to the communities of Harlow and Epping, we serve the populations of Bishop's Stortford and Saffron Walden in the north, Loughton and Waltham Abbey in the south, Great Dunmow in the east, and Hoddesdon and Broxbourne in the west. The extended catchment areas incorporate a population of up to 500,000.

1111 Table 1: Directory of our services careemergencysamecareambulatoryincludingmedicineAcuteandday Dietetics radiologyInterventional Patient at home service clinicshaematologyandAnticoagulant UnitPregnancyEarly UnitAssessmentandMaternalFoetal(MAFU) careandPeri-operative,Anaesthesia,criticalmedicine Audiology Ear, nose and throat scanningUltrasoundWardPostnatalservicecounsellingPetalLaboursupportBreastfeedingBirthingWardAntenatalClinicAntenatalcomprising:MaternityUnitWard Pharmacy screeningBreast departmentEmergency surgeryMaxillofacial therapyoccupationalandPhysiotherapy Breast surgery Endocrinology oncologyMedical Radiology ationcatheterisandCardiologycardiacunit End of life care Mortuary servicesbereavementand Research developmentand
12 Chemotherapy servicesEndoscopy babyspecialincludingcriticalNeonatalcarecareunit medicineRespiratory haematologyClinical Frailty service Neurology Rheumatology oncologyClinical screeninghearingNewborn Speech therapylanguageand servicesColorectal medicineGeneral Obstetrics inpatientclinicsSurgeryandcare serviceshysteroscopyandColposcopy surgeryGeneral viabilityTissue teammidwiferyCommunity medicineGenito-urinary Oral surgery Tongue tie service neonatalCommunityteam servicesofTerminationcareAmbulatoryincludingGynaecologypregnancy departmentEmergencymedicineDiabeticcareAmbulatoryPaediatric: servicesTransfusion Day surgery unitdependencyHigh Palliative care Trauma orthopaedicsand Dermatology andpreventionInfectioncontrol Pathology Urology medicineDiabetic Intensive care unit for adults appliancesPatient servicesVascular Ophthalmology enterologyGastro The review of services and all associated data is undertaken through the trust governance structure. This includes monthly meetings reviewing information covering patient experience and engagement, patient safety, learning from deaths, vulnerable patients and the infection prevention and control committee and bi-monthly clinical effectiveness and compliance groups. All of these groups report monthly into the Quality and Safety Committee, a subcommittee of trust Reviewboard. of each services’ performance (in table 2) within the trust has been monitored through the Performance and Finance Committee, with external
(a) Specified under the contracts, agreements or arrangements under which those services are provided or (b) In the case of an NHS body providing services other than under a contract, agreement or arrangements, adopted by the provider. During 2021/22, The Princess Alexandra Hospital NHS Trust (PAHT) has provided a range of health services listed in the directory of services, table 1. Services are provided by the trust to clinical commissioning groups (CCGs) and are usually commissioned under standard form NHS contracts. However, in order to support the COVID-19 response during 21/22 operating plans and normal contractual arrangements were suspended. Instead, a national ‘adapted financial regime’ was in place. This reverted activity based contracts to be block contracts i.e. fixed levels of income. Block contracts were supplemented by ‘top up’ and COVID-19 payments. These payments were agreed with the Integrated Care System (ICS). The above arrangements will remain in place for the whole of 22/23 until we received further guidance from the national team.
1313 review undertaken by both Essex and Hertfordshire commissioners at the monthly Service Performance and Quality Review Group. Table 2: Statements of assurances from the board Prescribed information Form of statement
1. The number of different types of relevant health services provided or subcontracted by the provider during the reporting period, as determined in accordance with the categorisation of services:



1.2 The percentage that the income generated by the relevant health services reviewed by the provider, as identified under entry 1.1, represents of the total income for the provider for the reporting period under all contracts, agreements and arrangements held by the provider for the provision of or subcontracting of, relevant health services. In 2021-22, £296.2m (95%) of the total income of £312.5m was received for patient care activities for services listed in table 2. Including this reimbursement, 94% of income related to patient care. The most significant element of non-patient income (£7.8m) related to provision of education and training.
Subcontracted activity: During the year, the trust subcontracted a small number of services to private or other NHS providers. Services are generally subcontracted where there is a shortterm capacity constraint and the response to COVID-19 has required additional resources. Examples of subcontracted services were urology (day case and OPD), endoscopy surveillance, and gastroenterology and specialist clinical tests. The trust is the lead provider for musculoskeletal (MSK) services. The trust has subcontracted arrangements in place from our local mental health provider (EPUT) and Commiscio, a local GP service.
Prescribed information Form of statement
14
1.1 The number of relevant health services identified under entry one in relation to which the provider has reviewed all data available to it on the quality of care provided during the reporting period. We have reviewed all the data available on the quality of care provided by the services listed in table 1.
2.4 A list of each national clinical audit and national confidential enquiry that the provider participated in, and which data collection was completed during the reporting period, alongside the number of cases submitted to each audit, as a percentage of the number required by the terms of the audit or enquiry. The national clinical audits and national confidential enquiries that we have participated in, and for which data collection was completed during 2021-22, are listed alongside the number of cases submitted to each audit or enquiry as a percentage of the number of registered cases required by the terms of that audit or enquiry. This is detailed in table 10.
2.2 A list of the national clinical audits and national confidential enquiries identified under entry two that the provider was eligible to participate in. The national clinical audits and national confidential enquiries that the trust was eligible to participate in during 2021-22 are detailed in table 10.
2.1 The number, as a percentage, of national clinical audits and national confidential enquiries, identified under entry two, that the provider participated in during the reporting period. During that period, we have participated in 86% (37) national clinical audits and 100% of those national confidential enquiries that were relevant and which PAHT was eligible to participate in.
2. The number of national clinical audits (a) and national confidential enquiries (b) which collected data during the reporting period and which covered the relevant health services that the provider provides or subcontracts. PAHT has during 2021-22 participated in 43 national clinical audits and three national confidential enquiries covering relevant health services that are provided.
2.3 A list of the national clinical audits and national confidential enquiries, identified under entry 2.1, that the provider participated in. The national clinical audits and national confidential enquiries that we have participated in during 202122 are detailed in table 10.
1515
16
2.6 A description of the action the provider intends to take to improve the quality of healthcare following the review of reports identified under entry 2.5. During 2021-22 the local review of national clinical audits reports was impacted by COVID-19 and work is taking place to address this. The six action plans arising from national audits were discussed at the Clinical Effectiveness Group. The majority are under review to identify actions required to improve the quality of healthcare, please see page 75.
2.8 A description of the action the provider intends to take to improve the quality of healthcare following the review of reports identified under entry 2.7. y Documenting type of consultation relating to chemoprevention to review uptake (3912)) y Improving recording of results, referrals and escalation of patients diagnosed with achalasia (3925) y Improved accessibility of surgical induction pack to foundation trainees (3944) y Raise awareness on impact of inappropriate drug omissions and provide additional training on JAC prescribing system (3947) y Breast unit guidelines being updated (3954) y Please see the section on infection prevention and control where actions are detailed.
2.5 The number of national clinical audit reports published during the reporting period that were reviewed by the provider during the reporting period. The reports of six national clinical audits were reviewed by the provider in Please2021-22.see the statement detailed against point 2.6.
2.7 The number of local clinical audit (a) reports that were reviewed by the provider during the reporting period. The reports of five local clinical audits were reviewed by the trust in 202122.
1717 Prescribed information Form of statement
3. The number of patients receiving relevant health services provided or subcontracted by the provider during the reporting period that were recruited during that period to participate in research approved by a research ethics committee within the National Research Ethics Service. The number of patients receiving relevant health services provided or subcontracted by PAHT in 202122 that were recruited into research studies during the period and approved by a research ethics committee was 975.
4.1 If a proportion of the provider’s income during the reporting period was not conditional on achieving quality improvement and innovation goals through the CQUIN payment framework, the reason for this. This is unlike previous years where some aspects of the trust’s income were predicated on delivery of quality related factors e.g. CQUIN and maternity incentive, these were removed.
4.2 If a proportion of the provider’s income during the reporting period was conditional on achieving quality improvement and innovation goals through the CQUIN payment framework, where further details of the agreed goals for the reporting period and the following 12-month period can be obtained. Not applicable for 2021/22.
4. Whether or not a proportion of the provider’s income during the reporting period was conditional on achieving quality improvement and innovation goals under the Commissioning for Quality and Innovation (CQUIN) payment framework agreed between the provider and any person or body they have entered into a contract, agreement or arrangement with for the provision of relevant health services. As part of the response to COVID-19 and the adoption of an ‘adapted financial regime’, the basis of the trust’s income was derived from block contract arrangements supplemented by ‘top up’ arrangements. During the first half of the financial year the ‘top up’ arrangements ensured providers met a breakeven position and were reimbursed for costs.
Prescribed information Form of statement
5.1 If the provider is required to register with the CQC: whether at end of the reporting period the provider is: (i) registered with the CQC, with no conditions attached to (ii)registration.registered with the CQC with conditions attached to registration. If the provider’s registration with the CQC is subject to conditions, what those conditions are, and whether the CQC has taken enforcement action against the provider during the reporting period. The Care Quality Commission issued a Section 31 warning notice, requiring the trust to submit weekly and monthly data. A robust action plan has been completed and all actions are being tracked to ensure they are completed.
7. Whether or not the provider has taken part in any special reviews or investigations by the CQC under Section 48 of the Health and Social Care Act 2008 during the reporting period. PAHT has not participated in any special reviews or investigations by the CQC during the reporting period.
6. Removed from the legislation by amendments made in 2011.
7.1 If the provider has participated in a special review or investigation by CQC: (a) the subject matter of any review or investigation (b) the conclusions or requirements reported by the CQC following any review or investigation Not applicable.
18 5. Whether or not the provider is required to register with the CQC under Section 10 of the Health and Social Care Act 2008. PAHT is required to register with the Care Quality Commission.
8.1 If the provider submitted records to the secondary uses service for inclusion in the hospital episode statistics which are included in the latest published data: (a) the percentage of records relating to admitted patient care which include the (i)patient’s:ValidNHS number (ii) General Medical Practice Code (b) The percentage of records relating to outpatient care which included the patient’s: (i) Valid NHS number (ii) General Medical Practice Code (c) The percentage of records relating to accident and emergency care which included the patient’s.
The percentage of records in the published data which included the patient’s valid NHS number was: This included the patient’s valid General Medical Practice Code was: 99.9% for admitted patient 99.9%care; for outpatient care; 99.8%and for accident and emergency care.
8. Whether or not during the reporting period the provider submitted records to the secondary uses service for inclusion in the hospital episode statistics, which are included in the latest version of those statistics published prior to publication of the relevant document by the provider.
PAHT submitted records during 2021-22 to the secondary user service for inclusion in the hospital episode statistics, which are included in the latest published data.
1919 (c) the action the provider intends to take to address the conclusions or requirements reported by the CQC and (d) any progress the provider has made in taking the action identified under paragraph (e) prior to the end of the reporting period.
a) a full suite of data quality reports produced daily/weekly and circulated to operational teams for resolution of key issues b) data quality issues are monitored and addressed through the trust data quality group c) data quality updates are provided to the Performance and Finance Committee, Information Governance steering group and Elective Care Operational group d) respond in full to externally reported data quality issues from NHS Digital and our commissioners
The NHS Digital Data Quality Maturity Index score is 93.1% for December 2021; the national average is 79.1%
10.1 If the provider was subject to the payment by results clinical coding audit by the audit commission at any time during the reporting period, the error rates, as percentages, for clinical diagnosis coding and clinical treatment coding reported by the Audit Commission in any audit published in relation to the provider for the reporting period prior to publication of the relevant document by the provider. Not applicable for 2021/22.
10. Whether or not the provider was subject to the payment by results clinical coding audit at any time during the reporting period by the audit commission. PAHT was not subject to the payment by results clinical coding audit during 2021-22 by the audit commission. However, an internal clinical coding information governance audit was undertaken by an NHS Digital qualified clinical coding auditor.
11. The action taken by the provider to improve data quality. PAHT will be taking the following actions to improve data quality:
20 9. The provider’s Information Governance Assessment Report overall score for the reporting period as per the Data Security Protection Toolkit (DSPT) grading criteria. PAHT Information Governance Assessment Report via the Data Security Protection Toolkit has an overall score for 2021-22 as Standard Met.
2121 e) Conducts full user training and refresher training to support the capture and recording of good quality data, operational processes are reviewed and aligned to system protectionthequalityf)updatedregularlyuserFurthermore,functionality.systemtrainingguidesarereviewedandComplieswiththedatastandardswithindatasecurityandtoolkit 12. (a) The value and banding of the summary hospital-level mortality indicator (‘SHMI’) for the trust for the reporting period; and (b) The percentage of patient deaths with palliative care coded at either diagnosis or specialty level for the trust for the reporting period. a) SHIMI banding is within expected and is 96.8 for the period January to December 2021. For December 2021 it is 95.18 within expected. b) Palliative care coding was 4.21% at either diagnosis or speciality level. 17.16.15.14.13. Mental health trusts Ambulance trusts Ambulance trusts Ambulance trusts Mental health trusts Not applicable. 18. The trust’s patient reported reportingsurgery(iv)surgery(iii)(ii)(i)(PROMs)measuresoutcomescoresfor:groinherniasurgeryvaricoseveinsurgeryhipreplacementandkneereplacementduringtheperiod. EQ5D Index Hip replacement: 91.30% Knee replacement: 71.43% EQ-VAS Hip replacement: 83.33% Knee replacement: 57.89% EQ5DNationalIndex Hip replacement: 94.50% Knee replacement: 88.87% EQ-VAS Hip replacement: 79.10% Knee replacement: 71.42%
Total annual FFT for 2021/2022 –18.62% (introduction on text message started in quarter 2, 2021).
20. The trust’s responsiveness to the personal needs of its patients during the reporting period. The patient advice and liaison service are our first contact and point of care resolution service and in total responded to was 4236 cases this year which is a 12% increase from the previous year (3780 in 2020-21).
21. The percentage of staff employed by, or under contract to, the trust during the reporting period who would recommend the trust as a provider of care to their family or friends. The staff survey 2021 results found that 48.3% of staff would be happy with the standard of care provided by the organisation if a friend/relative needed treatment.
22 19. Monitoring of PROMs for groin hernia and varicose vein surgery was suspended nationally in 2018. The percentage of patients (i)aged:0to 14 and (ii) (ii) 15 or over Readmitted to a hospital that forms part of the trust within 28 days of being discharged from a hospital that forms part of the trust during the reporting period. It has been acknowledged that an error was made in the drafting of the regulations and that the split of patients for this indicator should be: (i) Percentage of 0 to 15 years readmitted was 7% (ii) 16 years and over readmission rate was 14.7% The regulations refer to 28-day readmissions rather than 30.
22. Friends and Family Test – patient. The data made available by the National Health Service Trust or NHS Foundation Trust by NHS Digital for all acute providers of adult NHS funded care, covering services for inpatients and patients discharged from accident and emergency (types 1 and 2). Please note: there is a not a statutory requirement to include this indicator in the Quality Account reporting, but provider organisations should consider doing so. The patient Friends and Family Test continued throughout 2021/2022, with the introduction of text messaging in July 2021. Our service users receive a link via text within 24 hours of being discharged or attending their appointment. The trust has seen an increase in responses due to this new way of collecting data.
24.
23.
25. The number and, where available, rate of patient safety incidents reported within the trust during the reporting period, and the number and percentage of such patient safety incidents that resulted in severe harm or death. April 2021 to March 2022: The total number of incidents was 12,107 with 7,446 for patients. Severe harm incidents: 25 (0.33%) Death incidents: 5 (0.06%).
26. Statement on seven-day hospital services - as a trust we are working towards the implementation of seven-day services. Due to COVID-19 priorities, there is no requirement to submit a seven-day hospital services Board Assurance Framework (BAF) return until further notice.
2323 The percentage of patients who were admitted to hospital and who were risk assessed for venous thromboembolism during the reporting period. The last data set we have for this is from the previous year for period April 2020 to December 2020. Data for the period 2021-22 has been suspended due to Covid. The rate per 100,000 bed days of cases of C.difficile infection reported within the trust amongst patients aged two or over during the reporting period. There were 17 hospital onset cases of Clostridium Difficile reported to the national surveillance database for the period April 2021 to March 2022. The rate per 100,000 bed days is 11.10 (based on our own trust data as this information has not been published for 20-21 by UK
27.1 The number of its patients who have died during the reporting period, including a quarterly breakdown of the annual figure. From 1 April 2021 to 31 March 2022, 1,116 of The Princess Alexandra Hospital NHS Trust patients died. This comprised the following number of deaths each quarter: Quarter 1: 226 Quarter 2: 283 Quarter 3: 313 Quarter 4: 294
The number of deaths included in item 27.1 which the provider has subjected to a case record review or an investigation to determine what problems (if any) there were in the care provided to the patient, including a quarterly breakdown of the annual figure. By March 2022, 315 case record reviews and nine serious incident (SI) investigations were raised in relation to 1,341 deaths (item The27.1).number of deaths in each quarter for which a case record review or a serious investigation was carried out was: Quarter 1: 44 case record reviews and three SI investigations Quarter 2: 101 case record reviews and three SI investigations Quarter 3: 94 case record reviews and one SI investigation Quarter 4: 76 case record reviews and two SI investigations
27.2
27.3 An estimate of the number of deaths during the reporting period included in item 27.2 for which a case record review or investigation has been carried out which the provider judges as a result of the review or investigation were more likely than not to have been due to problems in the care provided to the patient (including a quarterly breakdown), with an explanation of the methods used to assess this. Three cases [0.53%] of the patient deaths during the reporting period are judged more likely than not to have been due to problems in the care provided to the patients. Six incidents remain open at this Intime.relation to each quarter, this consisted of: Quarter 1: 1 - [0.07%] Quarter 2: 1- [0.07%] Quarter 3: 1 - [0.07%] Quarter 4: 0 Cases referred for a structured judgment review (or called case record review) have data captured on an electronic system called AllSMART.ofthese cases are rated with an avoidability rating of: Score 1: Definitely avoidable Score 2: Strong evidence of Scoreavoidability3:Probably avoidable (more then 50:50) Score 4: Possibly avoidable, (less than Score50:50)5:Slight evidence of avoidability Score 6: No evidence of avoidability
24
2525 There were five cases where an SJR was completed and this triggered a further investigation. All cases with an avoidability score of 1 or 2 are referred for: y A review by the trust’s learning from deaths panel y Are logged on Datix as a clinical incident and investigated y Will be reviewed by the trust’s Incident Management Group
y The investigation has identified learning and a action plan was completed and monitored by the relevant divisional team y For discussion and learning at the specialty mortality and morbidity meeting A summary of what the provider has learnt from case record reviews and investigations conducted in relation to the deaths identified in item 27.3. Learning identified from completed case record reviews and serious incident investigations includes: y The staffing model for the paediatric emergency department (ED) needs to fit the demands of the service y There needs to education on the recognition and management of sepsis in a child There continued to be a large amount of learning from COVID-19 deaths as the guidance continued to change. This learning included: y Isolation of patients at highest risk and the lack of available side rooms (this was a national issue) y The COVID-19 swabbing pathway was amended in January 2021 (above national guidance) y Contacts of COVID-19 positive patients swabbed every 48 hours (ward outbreak management) y Asymptomatic staff testing was implemented in December 2020 y 10 key actions implemented y Continued implementation of Kwickscreens between bed spaces y Face to face visiting restricted y Security personnel placed at three main entrances to reinforce hand hygiene and the wearing of facemasks
27.4
The following actions continued to be embedded during the first quarter regarding COVID-19 learning: y The ten key actions on infection prevention and control for organisations and systems were issued on patient testing and staff testing y Communications sent to all staff on the requirement to increase the overt messaging to assert expectations of behaviour regarding IPC; hands, face, space is everyone’s business y Phase 1 lateral flow testing for staff commenced on Harvey, Charnley and John Snow wards y Phase 2 lateral flow testing commenced. All adult and child inpatient areas including theatres and maternity to be led by ward and department managers y The trust to implement the 10 key actions as defined by NHS England and NHS Improvement. y Due to patient non-compliance with PPE, information leaflets were provided to all patients on admission and signage was increased y PPE champions to complete monthly hand hygiene audits in all clinical areas y Face to face restricted visiting suspended by the trust - virtual visiting only y PAHT decision: Introduction of FFP3 masks for all patient facing staff which was above
26 y Unprecedented times y Staff shortages (nationally) y Increased transmission rate of mutated virus y Ward outbreaks were difficult to manage due to high transmission rates
27.5 A description of the actions which the provider has taken in the reporting period, and proposes to take following the reporting period, in consequence of what the provider has learnt during the reporting period (see item 27.4).
2727 the national guidance. Static security commenced at the three main entrances. 1) Main entrance by ED 2) Maternity entrance 3) Entrance by hospital restaurant y Communication at ward safety huddles to include the COVID-19 watermark status of the patient, to ensure pathway compliance y COVID-19 swabbing pathway amended to increase robust routine swabbing of inpatients in compliance with national guidance y Kwickscreen installation on Lister Ward and Fleming CCU commenced. y Kwickscreens installation commenced on Nightingale and Locke Wards. 27.6 An assessment of the impact of the actions described in item 27.5, which were taken by the provider during the reporting period. The impact of the actions from SIs are as follows: y There has been 24/7 reception cover provided in paediatric ED The impact of the actions from SJRs are as follows: y Improved compliance with PPE y Reduction in nosocomial COVID-19 infections y Reduction in bed moves y Reduction in COVID-19 incidents and complaints y Improved competence in neurological infections y Improved compliance with end of life care documentation and referral to speciality palliative care team
The number of case record reviews or investigations finished in this reporting period which related to deaths during the previous reporting period but were not included in item 27.2 in the relevant document for that previous reporting period (2020/21).
Seven serious incident investigations were closed during this reporting period related to deaths.
27.8 An estimate of the number of deaths included in item 27.7 which the provider judges as a result of the review or investigation were more likely than not to have been due to problems in the care provided to the patient, with an explanation of the methods used to assess this. Four of the seven SIs investigation reports have concluded that the deaths were more likely than not due to the problems in the care provided.
27.9 A revised estimate of the number of deaths during this reporting period stated in item 27.3, and for that previous reporting period, taking account of the deaths referred to in item 27.8. Three cases detailed in 27.3 and four deaths in 27.8, making a total of seven.
27.7
28. In response to the Gosport Independent Panel Report, provide details of ways in which staff can speak up (including how feedback is given to those who speak up) and how we ensure staff who speak up do not suffer detriment. This disclosure should explain the different ways in which staff can speak up if they have concerns over quality of care, patient safety or bullying and harassment. There are a number of ways in which our people can speak up. This may be to raise concerns, about behaviours, patient or staff safety either as an individual or as a witness or to give suggestions for improvements. We have recently appointed a Lead Freedom to Speak Up Guardian, with six guardians in total, four of whom are clinical. A safe working guardian lead is in place to support medical and junior doctors. A quarterly report is submitted to the National Guardians Office and subsequent report is written and presented to the people Staffboard.can also contact a range of other people in the organisation who can signpost them to advice and support.
28
2929 These include: y The people team y Staff side y Equality, inclusion and diversity lead y Line managers y Tutors y Organisational development team y Staff health and well being y Mental health first aiders In all instances, the individuals are thanked for speaking up, are advised on both informal and formal options of how to proceed with their concern, and a way forward agreed with them in order to reach a resolution. Annual surveys including the Staff Survey and Staff Friends and Family Test enable us to identify key themes and that action plans are developed within the healthcare groups to respond to these key themes. These action plans are monitored and reviewed throughout the Pulseyear.surveys are also undertaken throughout the year to monitor the impact of changes implemented. 29. Following the terms and conditions of service for NHS Doctors and dentists in training (England) 2016 requires a consolidated annual report on rota gaps and the plans to reduce rota gaps. The trust did not complete an annual report in 2021/22, due to COVID-19 priorities.
Outcome: Achieved PAHT has shown significant improvement in its 12 monthly rolling HSMR (see figure 4 below). HSMR for the period January to December 2021 is 97.0 and “within Theexpected.”rolling-12-month HSMR has been within 98.0 and 100.5 for the past nine months. Analysis of HSMR by financial year demonstrates the improvements made over the last three years continuing in 2021/22. HSMR for the regional peer group is 102.2 and “higher-than-expected”; and as such, PAHT is performing better than the regional acute peers, please see figure 3 below. In hospital mortality has remained consistent this last year, please see figure 4 below.
30 Our 1.OurandTo1.inweagainstachievementstheprioritiessetforcompletion2021/22Ourpatientsreducemortality,improveHSMRimproveourpatients’experience.patients:Aim: to reduce the trust mortality rate (improve the Hospital Standardised Mortality Rate - HSMR), continuing with the work already started on learning from every death. This will improve quality of care for all patients.


The achievements in timeliness of treatment should be reviewed in the context of the increasing attendances to our trust.
Summary Hospital-level Mortality Indicator (SHMI) SHMI for the period January to December 2021 is 96.8 and “within expected”.
3131
The next two mortality reports will see the period with peak hospitalisations from COVID move outside the rolling periods and as such, some volatility could be expected in trends in the near future.
There are three outlying diagnosis groups: y fracture of neck of femur y sepsis; and y viral infection Fractured neck of femur continues to be reviewed with a working group looking at improving the timeframes from referral to orthopaedics to the decision for surgery and then the timeframes from diagnosis of the fracture until the operation commences. Sepsis coding continues to be reviewed for accuracy by clinicians and a sepsis identification tool is used on admission to avoid incorrect diagnosis of sepsis. There is an expectation that within the next two months, viral infection will no longer alert due to the second wave of COVID infections and hospitalisations moving outside the 12-month-rolling periods. The SMART database was implemented in July 2021 and is fully embedded at the trust. The database is used for the completion of Medical Examiner independent reviews as well as Structured Judgement Reviews. The database also produces a mortality dashboard, which can be filtered to individual specialities or divisions to review mortality over periods of time. Our patients 1. Aim: To Improve our performance for timeliness of treating patients requiring emergency and urgent care. This will improve the quality of care and experience for our patients. Outcome: This objective remains ongoing In 2020/21 the trust saw 87,984 patients in our urgent and emergency care department. During the year 2021/22 we have seen a significant and sustained increase in the number of patients attending with 122,184 coming to our Trust, an increase of 28% in year.

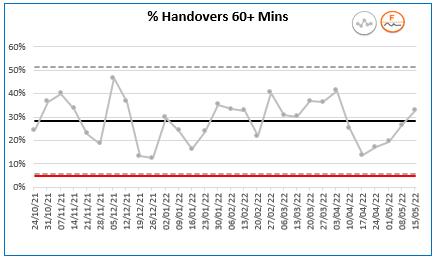
The trust is also working with our local health organisations to support opportunities to improve the speed we can take patients off ambulances. The constraints of the emergency department also include the time from the decision to admit (DTA) patients until they leave the department. This has increased from an average of 134 minutes in February 2020 to an average of 545 minutes as of February 2022. These longer waits for patients to be admitted decrease the amount of physical space in the department to see and treat new patients. PAHT has often shown significantly long waits for triage and ambulance patients to be accepted in our department, which therefore impacts on timeliness of treatment throughout the patient's journey in the emergency department.
Our triage time to exam time has been steady but still remains significantly above the national average.
How full our department is and available space to accommodate new patients plays a significant factor in being able to accept new ambulance patients. We are identified as having a much smaller initial assessment space (accommodating three trolleys), in comparison with a neighbouring trust that has 10 spaces. The size and location of our emergency department do not allow for this area to be increased in size.
32
Despite a huge improvement in performance since early December 2021, there is still work to be done to improve this further. We have developed plans to further improve arrival to triage times (figure 6 left, figure 7 and 8 below).


3333 Despite the long waits to departure, the emergency department has continued to maintain patient safety at all times. Table 3 above and 4 below shows the number of incidents in line with the number of total ED attenders. N.B: The death incident recorded in January occurred on a ward, not the emergency department. The department is working towards a number of new ways to improve ambulance handover and triage waits, these include; y Implementation of Manchester Triage Tool (in progress - staff training underway) y Revised skill mix of senior nurses within the Rapid Assessment Team (RAT). A registrar is also based in the team to expedite clinical decision making y Streaming and redirection tool in collaboration with NHS Digital (in progress) y Changes to estates to streamline pathways (in progress - business case in draft) y Developed pathways between the emergency department (ED) and Same Day Emergency Care Unit (SDEC) (in progress - local improvement network group) y Implementation of NerveCentreelectronic patient record system (July 2022) In light of the above identified areas of improvement, we remain challenged to meet all of the trust internal professional performance standards (IPPS) consistently. IPPS standards are reviewed weekly at urgent care board, and monthly within each division’s performance review meetings. The emergency department has seen a number of changes over the last 12 months and the team have adapted extremely well to these changes. Despite the ongoing challenges, significant improvement is clearly visible over the last six months, however there is still work to do. The team are focused on providing timely, safe and outstanding care to our patients.


34
Outcome: Partially met and remains ongoing The 2021/22 sickness target was to reduce sickness from 4.43% to 3.43% by March 2022. This had reduced to 3.9% therefore did not meet this target. COVID-19 has continued to have an impact on staff absence throughout the year. Whilst we have not met the target this year, the trust has undertaken a range of health and wellbeing initiatives to support our staff and help reduce the overall reduction in sickness absence, figure 9 below. In 2022/23, we would look to reach an absence target of 3.4%.
Our people 1. Aim: We will complete an annual report to review the doctors' rota gaps for staff in training roles. This will help with planning of rotas and services going forward Outcome: Not achieved The trust did not complete an annual report in 2021/22, due to lack of COVID-19 priorities. Our performance Quality improvement projects to transform services are aiming to modernise how we deliver care and improve timeliness of treatment and patient experience.
4. Aim: Outpatient improvement programme: We will improve the use of technology and redesign of our services to enable consultations to be completed to meet the needs of our patients and our services. In some instances, this will mean fewer attendances to the hospital. Measures of success will include improved patient experience, reduced numbers of face-to-face consultations and freeing up clinician time to deliver acute inpatient services.
Outcome: Achieved 10 specialities are now live with Patient Initiated Follow-Up (PIFU), with the remaining due to go live by May 2022. We went live with the first speciality (fracture) in February 2021 and over the year we have discharged a total of 1,707 patients to PIFU (21.2.22). Following a pilot in April 2021, the virtual fracture clinic went live in October 2021 for all patients referred from our emergency department or our local minor injury units. Recent data shows 42% of patients discussed in a VFC did not require a face to face appointment.
Two-way messaging is now implemented for all specialities, giving patients reminders about their appointments and accessibility to video consultations.
Our people 2. Aim: We will improve the health and wellbeing of our people, offering a wide range of support so that every member of staff can recover from the effects of working during the pandemic, can stay well and feel they can meet the demands of their roles. Measures of success will be improved staff health and wellbeing results in the Staff Survey from 5.5 to 5.7 and lower sickness absence rate by 1%, from 4.3% to 3.4%

6. Aim: Theatre transformation: We are aiming to ensure available operating resources (including staff) are used effectively and efficiently. Measures of success will include reduced additional operating sessions and reduced work being outsourced to other providers. There will be evidence of reduced waiting times for necessary operations, improving patient experience.
7. Aim: Medicines optimisation: We are aiming to ensure that patients are involved in the decision-making about their medications and that they receive the correct medications at the correct time. Measures of success will include improved patient safety, reduced waste caused by unnecessary prescribing of medications and improved patient outcomes. Outcome: Achieved Due to COVID-19, we have continued to progress the medicines management projects, but without direct interaction with patients. However, clinicians continue to discuss medicines with patients while they carry out the STOPIT reviews.
STOP IT y The STOPIT process is now embedded on Lister Ward, following a successful pilot that saw a reduction in 20% of medicines. The treating team work with patients to discuss their medication and need to stop some. There is a plan to roll this out to be embedded throughout the trust.
2. Our places Improve our clinical areas and critical 8.OurfunctionsplacesAim: We will work in partnership to improve our hospitals and health infrastructure for our patients. Outcome: Achieved During the last year, an incredible amount of progress has been achieved on the new Princess Alexandra Hospital, despite the ongoing pressures of COVID-19.
Venous thromboembolism (VTE) y Reintroduction of the VTE external submission y Ongoing development of a VTE dashboard to ensure focused QI efforts can be applied to any required changes. y Ongoing development of VTE guidelines on the microguide application y Working with the trust training and development team to implement VTE mandatory training Antibiotic stewardship y Development of an antibiotic dashboard that identifies antibiotic prescribing habits throughout the trust. The dashboard is being utilised in an antibiotic review panel working with clinicians to review and guide amending prescribing habits throughout the trust.
3535 The consultant connect service went live in October 2021, enabling GPs to have timely access to advice and guidance for speciality experts. We have secured the platform to continue to deliver virtual consultations, clinics have been reprofiled to reflect face to face and non-face to face appointments and we have achieved the national target of 25%. Our performance
Outcome: Achieved The three head and neck specialties, including ophthalmology, have undertaken root cause analysis workshops attended by clinical, operational and support colleagues. Development of a theatre utilisation dashboard to target areas for improvement is in place. Our performance
TTA workshop y Multidisciplinary workshop in October 21 to process map TTAs y Recommendations for next steps identified and to be taken forward as part of the OUT workstream
All current information about our plans and progress can be found on our new hospital website, which was launched in December. This new website replaces the previous version and is a flexible platform allowing us to update and expand content and add new functionality to facilitate engagement. PAHT staff are the faces of the new hospital website and will be a core part of our new hospital communications going forward.
The rapid progress we made in the first half of 2021 was met with a noticeable slowdown in the second. In summer 2021, the national team overseeing the New Hospital Programme announced that they would be undertaking a review to ensure the benefits of operating as a national programme are maximised going forward. This review is looking at ways to ‘join up’ common aspects of the new hospitals such as room design, procurement of contractors, and making the most of modern methods of construction. The main benefit of the review is to achieve greater value for the taxpayer; enabling the new hospitals to be built faster, better and more efficiently. On completion of the review, we will be able to continue with the development of our outline business case using the guidance and information from the national team about the way forward for the new Princess Alexandra Hospital. Communications and engagement
Stakeholder engagement Whilst we have not undertaken any proactive engagement with stakeholders, we continue to hold regular update meetings and we respond positively to requests from our communities for updates, briefings and presentations. We presented to the Epping Forest Health and Social Care Overview and Scrutiny Committee (HOSC) on 7 December 2021 and Hertfordshire HOSC on 16 March.
Staff engagement
y Outline business case is 60% drafted y Joint modelling with local stakeholders to inform the highways and transport strategy
We have briefed patient groups from East and North Herts and West Essex Clinical Commissioning Groups (CCGs) and are due to send out a detailed briefing update to senior stakeholders and partners as well as district, borough and county councillors. Public engagement
Everything is in place to get started on the detailed design phase of our new hospital, thanks to our continued close working with local authorities, health system partners and a wide range of local stakeholder and community groups: y Our demand and capacity analysis is complete and aligned to the system y Our clinical model is agreed with system partners y New ways of working are already underway y 1:200s design drawings have been signed off by our clinicians y Planning Performance Agreement is agreed with the local authority y Preparation for outline planning submission is in progress
36
We continue to enjoy strong, ongoing support for a new hospital from partners, local people, patients, clinicians and our staff. Whilst the review is underway, engagement activity is following the national guidelines set out in in the ‘Communications Playbook’ issued by Department of Health and Social Care (DHSC) in the second half of last year. Locally, we are focusing efforts on our PAHT 2030 transformation agenda as well as making preparations to push ahead with our new hospital engagement when we are given the green light to do so.
We have kept staff up to date in regular double-page spreads in the inhouse InTouch magazine. Wherever possible, weekly executive team briefings have updated on progress. Our recent staff photography campaign (see more detail below) has also been an opportunity to boost awareness and confidence in the new hospital.
3737 Artist's impressions of our new hospital


The COVID-19 pandemic has continued throughout the year. Maintaining patient safety and protecting staff and service users was an ongoing process in the trust, as well as across the NHS. Our understanding of the virus continued to develop, and a COVID-19 vaccination programme was in place in England. In mid-December 2021, the Omicron variant started replacing Delta infection at our hospital. Our respiratory physicians and critical care staff noted less severe clinical illness in our patients by the end of January 2022. The UK Health Security Agency (UKHSA) advised by the end of 2021, that the NHS should plan for a response to respiratory viruses including COVID-19, Influenza and Respiratory Syncytial virus (RSV).
38 Our Infectionpatientsprevention and control
y Hierarchy of IPC controls were applied in order - elimination; substitution, engineering controls, administration and PPE/respiratory protective equipment (RPE) y FFP3 resilience continued to be developed. Competent trained IPC associates provide fit testing that is compliant with Health and Safety Executive (HSE) guidance, and a record of the mask type is maintained y Evaluation of ventilation including alternative technologies, operational capacity, and prevalence of infection and new variants were monitored y Patients were not transferred unnecessarily between care areas unless there is a change in infectious status, clinical need, or availability of services y The IPC cell met regularly all year and reviewed reports on hand hygiene, PPE donning and doffing, IPC training, and cleaning and decontamination. Compliance with National Standards of Healthcare Cleanliness were monitored y The IPC Board Assurance Framework was kept under review
Evidence based decision making and application of national infection prevention and control (IPC) guidance continued to be central to recommendations made by the hospital IPC cell that continued to oversee all decision-making processes. Robust risk assessment with clinical and workplace risk mitigation continued. Close links between all of our teams managing the pandemic and patient care meant that our IPC messages to protect staff and patients were disseminated and shared. A variety of strategies were put in place to control COVID-19 infections across the trust including: y Point of Care (POC) testing continued to be developed throughout 2021. We have 15 functional SAMBA units (Point of Care Test), and by early 2022 purchased a further 15 to allow for rapid detection of COVID-19 infections in patients attending our emergency department (ED). This was to further assist patient triage and placement y Maternity and paediatric ED were also supported with POC testing y Plans were in place for managing increasing case numbers where they occurred, with acceleration of coordination, monitoring, and staff resource y A respiratory winter plan was developed with segregation of cases in isolation rooms or bays y Application of COVID-19 secure workplace requirements was ongoing throughout the year. This included recommendations for universal masking, COVID-19 screening of inpatients three times a week, assessments of physical distancing, bed spacing, and screens, and providing FFP3 face masks for aerosol generating procedures, and in other circumstances after risk assessment of personal or work environment
3939 Figure 10: Trust COVID-19 infection rates Figure 10 shows the number of new positive inpatients by day, and also the total cumulative number of positive patients admitted. 40% of patients who were COVID-19 positive on admission between June 2021 and February 2022 were unvaccinated. Table 5 shows the numbers of nosocomial COVID-19 at PAHT, using national definitions 01/04/21 – 30/03/22 Q1 Q2 Q3 Q4 Patients testing positive for the firsttime during days 3-7 after admission 6 17 26 90 Patients testing positive for the firsttime during days 8-14 after admission (probable nosocomial infection) 5 6 7 53 Patients positive for the first time 15 days after admission (definite nosocomial infection) 5 3 9 63

40
Notes: Infections defined as ‘indeterminate’ are where it is possible these are community acquired and not hospital associated Sequencingcases results showed patients had (almost exclusively) the more transmissible Omicron variant in Q4. As a result, nosocomial infection increased significantly despite outbreak control Mostmeasures.nosocomial infections were noted to be asymptomatic infections. An audit carried out in January 2022, showed that 42% of patients with nosocomial infection were symptomatic of COVID-19, and 58% were Otherasymptomatic.strategiesimplemented to manage COVID-19 were: y Suitable information on infections were provided to service users, their visitors and carers in a timely manner y National guidance on visiting was implemented. Visitors with respiratory symptoms were not permitted to enter a care area. Compassionate visiting (e.g. end of life) and visits from other care givers were supported y Staff testing protocols, implementation of a staff vaccination programme for COVID-19 and influenza, monitoring staff illness/absence/wellbeing, supporting pregnant, other at-risk and Black, Asian and minority ethnic (BAME) staff as required (including redeployment) were all in place, supported by staff health and wellbeing (SHaW) and our people team y Turnaround times for Polymerase Chain Reaction (PCR) testing and POC tests, recording of data, and screening for other potential infections were all monitored y Those being discharged to a care home were tested for COVID-19 (unless they had tested positive within the previous 90 days), and results were communicated y A negative PCR and three days selfisolation before elective procedures remained in place y Staff were supported in adhering to IPC policies for COVID-19 and other alert organisms y Safe spaces for staff breaks, and changing facilities were provided y Procedures were in place for identification and management of outbreaks of infection y Bank, agency, and locum staff followed the same deployment advice as permanent staff y Where possible there was reduced movement of staff and the crossover of care pathways between planned care pathways and emergency care pathways y Trust IPC and executives linked in with community colleagues and public health teams on a regular basis y Data management (COVID-19 data, mortality, and operational data), IT support and remote working continued to be facilitated y 16 COVID-19 associated outbreaks were noted in the hospital from 1 April 2021 to 31 March 2022; all were associated with clinical areas (including one staff outbreak on a ward). Regular reporting to east of England regional leads took place y Mortality reviews of all probable and definite nosocomial COVID-19 infections took place to learn lessons and implement improvements y Isolation of immunocompromised patients using a side room priority isolation list stratified by pathogen and infection risk was implemented where possible y Maintenance of microbiology laboratory capacity and diagnostics was ongoing, including participating in the UKHSA programme to detect new variants y Improvements in drug treatments was managed by the hospital clinical cell y Arrangements for antimicrobial stewardship were maintained
It has been evidenced globally that the COVID-19 pandemic has contributed to an increase in blood stream infections, not just in MRSA, but in other organisms by month
COHA infections had risen this year;
There were three hospital onset MRSA bacteraemia infections in 2021-2022 (against a trajectory of zero), and no COHA infections this year. This was an unusually high number, as the trust has previously had good MRSA bacteraemia control for many years (0-2 per year).
There was a total of 34 C. difficile patients at the trust during the year 2021-2022 (against a threshold of 23). Of these, 17 were hospital-onset, health care associated (HOHA) detected three or more days after admission, and 17 were community-onset healthcare associated (COHA), detected in the community or within two days of admissions, when the patient has been an inpatient in the trust in the previous four weeks. In 2021-2022, a number of measures were implemented, with the aim of reducing infections of C.difficile. As a result of these actions, the trust managed to reduce its HOHA incidence by 25 since 2020-2021. The initiatives included the introduction of a regular commode and dirty utility cleanliness audit (of which the results were monitored through the IPC committee), the introduction of sporicidal wipes for cleaning of commodes, continuous monitoring of antimicrobial prescribing and policy through the Antimicrobial Stewardship (AMS) meetings, huddles for staff in clinical areas on the key messages, and a review of the cleaning process in all inpatient ward areas.
MRSA Bacteraemia
there is currently a review in progress to establish whether the antibiotics prescribed in these instances were commenced in the hospital, or by GPs; at time of writing the review was ongoing and this will continue to be monitored through the AMS group. The number of community incidences (where patients have not been in the trust in the last 12 weeks, or they have been, but not in the last four weeks preceding the C.difficile diagnosis) stayed the same this year as case numbers in 2020-2021.
Table 6: C.difficile - Instances
The process remained in place for undertaking root cause analysis (RCA) investigations for all infections classed as HOHA and COHA C.difficile. This included the Appeals Panel (led by the CCG) where infections were identified as ‘unavoidable’ were reviewed; whilst these could not be removed from the national database, it did provide assurance that the correct management of infections was followed, in line with trust policy. The threshold for the coming year is not yet known. Control of C.difficile will remain a top priority for our clinical teams, the IPC Committee, and the Antimicrobial Stewardship Group in 2022-2023.
Prior to the first case in May 2021, there had not been any incidences of MRSA bacteraemia in the hospital since September 2019. Two of the infections were related to intravenous devices, and the third was likely due to IPC practices. In each of the patients, a review was undertaken and an action plan completed by the appropriate clinical teams. Infection rates were monitored through the IPC Committee and the relevant clinical areas provided an update on the actions taken.
4141 Alert Organisms Clostridiodes difficile (C.difficile)

Table 7: MRSA Bacteraemia infections in 2021-2022
Table 8: Norovirus outbreaks
MSSA Bacteraemia
Unlike with other organisms, there is no trajectory in place for MSSA bacteraemia, however, the trust has continued to closely monitor and review its infections. During 2021-2022, there was a significant increase in the number of MSSA bacteraemia, with a total of 15 HOHA and five COHA infections. Previously, the trust has had very few instances of MSSA, consistently being in the regional top quarter of hospitals with the lowest rates of infection and commended for this by the Care Quality Commission (CQC). Infection incidents and Norovirusoutbreaks
42 too. An action plan was developed to undertake a review of both MRSA and MSSA bacteraemia infections and determine what measures needed to be taken to address the situation and improve. (see below under MSSA).
Audits and surveillance Led by the IPC associate team, PPE compliance, hand hygiene and a number of other audits monitoring IPC practice continued throughout the year. Action plans were implemented by health care groups and monitored by the IPC cell/IPC Committee.
Conclusion As the year comes to an end, we continue to review lessons learned from our response to the COVID-19 virus and are following the national steer towards ‘living with COVID-19’. New IPC measures to enable this to happen are expected from 1 April 2022.
There were four outbreaks of norovirus in the trust for the latter part of 20212022. Norovirus is a common cause of diarrhoea and vomiting outbreaks in hospitals (and other close contact settings) during the winter months, however, over the last two years of the pandemic, there have not been any outbreaks in the trust. Incidences have risen at this time nationally, most likely because people are now having more contact again and reducing IPC precautions in the community. Although unpleasant, norovirus is rarely the cause of serious illness, however, operationally, it is a challenge for the trust due to the requirement to close beds (during outbreaks) in order to prevent further transmission.


Equipment: y Purchase of new modern equipment including Hydrogen Peroxide Systems to enable increased productivity measured by improvements in m2 cleaning capacity
The trust has been innovative in its approach to quality improvement in the last year and supported by our quality first team, we have developed the following improvements: Domestics and housekeeping Domestics: y Cleaning services are now provided 11 hours per day; seven days a week on each inpatient ward and ED will have 24 hours of cover y Implementation of a proactive and reactive roving team covering the hours of 7am to 8pm. This team is responsible for the maintenance and deep cleans of wards/departments as requested, including delivery of a proactive deep clean programme.
y Implementation of a comprehensive training programme for the new equipment Housekeeping: y Implementing a housekeeping workforce to cover 11 hours per ward, seven days a week y Development of training for the new housekeeping role y Housekeeper consultation completed and in place y Recruitment remains ongoing as not all posts are filled Electronic ordering: y System purchased and rolled out and commenced with auditing of cleanliness standards and portering requests. y Electronic food ordering still to be implemented to improve efficiency for catering as well as a reduction in food waste and an improvement in patient experience overall. Urgent and emergency care improvement programme In – Effectiveness of managing patients attending the department y Review of streaming and triage, including enhanced ambulance handover and effective use of clinical decision unit to reduce non-admitted breaches. y Establishment of clinical navigator role y Surgical assessment within Same Day Emergency Care y Expand the capacity within the Urgent Treatment Centre to increase our ability to increase activity and reduce ED
Theseattendanceactions have impacted positively on the time from arrival to initial assessment, with the most clinically vulnerable being seen in priority order. Improvements in expansion and increased utilisation of UTC has impacted as below: y Positive feedback from primary care and system partner colleagues in relation to direct access to clinical navigators who signpost the correct pathway for patients. Out – The effectiveness of moving patients onto the wards for ongoing care y Embedding of SAFER care bundle on four pilot wards y Tests of change developed locally with executive sponsorship and operational teams y MADE event across the local health economy in November 2021
Quality improvement
4343 As health services move closer to resume business as usual, we will need to use longstanding ways of managing COVID-19 as a respiratory illness, deploying targeted testing, and maintain resilience with ongoing surveillance and contingency measures. The consistent application of IPC measures and the booster COVID-19 vaccination programme are likely to remain our best defence mechanisms.
The ‘Improvement Partnership’ is our programme for enrolling, engaging, involving and developing our staff in quality improvement. The quality first team runs leading change and leading projects learning and development sessions, with the objective of enabling them to deliver successful quality improvement projects. When the staff member completes a quality improvement project (capturing project outcomes in poster), they become PAHT improvement partners: The improvement partnership is an enabler to address the leadership, culture and organisational development required to embed quality improvement at WePAHT.continue to develop our people with quality improvement skills, knowledge and capability, with a focus on leading change and leading projects. 422 staff members have completed leading change, with 220 completing leading projects. We now have 76 improvement partners at PAHT.
The first was to increase PALS activity (providing speedy resolution to concerns raised). This has been achieved: with an increase of 12% in year with 4,236 PALS complaints in 2021-22, increasing from 2020-21 (3780), see figure 11.
The improvement partnership
y Overall there was on average a 3% improvement in the Internal Professional Performance Standards (IPPSs) for ED
y The Adult Assessment Unit (AAU) saw more patients during MADE and reduced the average length of stay (LOS), discharging more patients y There was a very little difference in general and acute medicine bed occupancy (a slight increase) Nervecentre ED module
y There was a 4.9% increase in pathway 0 discharges before p.m. compared to the previous four weeks
y Overall there was a 3% improvement in ED performance during MADE y There was an improvement in both the number of ambulance handovers under 15 minutes and the number over 60 minutes compared to the last four weeks (overall reduction in handover times)
y Average length of stay decreased by 9.3%
y Aim to streamline methods of documenting assessments and care with a digital solution
y Enable triage with electronic solution y Improve oversight and coordination relating to patient safety in ED
44
The main findings seen as a result of the Multi-Agency Discharge Event (MADE) week are: y ED attendances decreased slightly during MADE week compared with the previous four weeks y Emergency hospital admissions increased by 1.8% during the week
Patient experience
The patient experience team set some local goals to be achieved during the period 2021-22.


The second goal was to increase the number of complaints (proving assurance our patients were effectively raising concerns to us). This has been achieved: with an increase of 46% to 263 complaints received in 2021-22 up from 179 in 20-21, in figure 12: The third goal for the team was to acknowledge 100% of complaints within three working days.
4545
Section 18 Report
The most frequently occurring themes were medical care expectations, 72, communication with 40 and attitude with 33, followed closely by delays and admission, discharge and transfer arrangements. Sub-subjects of complaints
The five most frequently occurring sub-subjects, specific issues raised within complaints about medical care, communication or attitudes for example, were as follows: y 16 complaints of a missed diagnosis, 12 of generally poor treatment provided, 10 of problems with continuing care beyond the hospital, 10 complaints which included a concern that inadequate treatment was provided, nine complaints comments about a rude approach or attitude How many were well founded? In the language of complaint services, the terminology used states whether or not the complaints are upheld. The vast majority (96%) of complaints are fully upheld or partially upheld. By this, we mean that at least one of the concerns raised by the complainant required concerted action on the part of the hospital to address the issue, 114 were partially upheld, 12 upheld and six not upheld of those closed by the end of the financial year. Actions taken Actions are taken over the year and should demonstrate a clear connection from the concern raised to the change the organisation has made. Some of these are listed below, beginning with general actions, then actions in the form of case studies, explanations of how the trust responded to specific complaints. Case number one: Patient’s mother raising concerns that PAH is not equipped, prepared or able to recognise mental health issues in children and young people due to lack of awareness, specialist training or environments suited to supporting these groups. Action plan: y To review space and cubicles across our departments within paediatrics to select a room to transform into a mental health space y To review alternative mental health provision at other units y To add information leaflets onto the ward y To work collaboratively with our mental health partners with new funded posts y Restraint training and eating disorder training to take place within department
Achieved: 100% of complaints in 202122 were acknowledged within three working days.
Every year, the trust must make a statement under the NHS Health and Social Care Act 2009 about how many complaints it has received, their subject, the issue they raise, whether or not they were well founded and any actions taken. The trust can confirm this statement is that we received 263 complaints in period 2021-22. Subjects of complaints

Case number two
Having suffered a miscarriage, there were no appropriate facilities available for a woman and her partner to go to process what they had just been told. This couple were asked to sit in the general waiting area amongst pregnant women, which they found highly insensitive. Action plan: y Lead investigator has produced a pathway that has been shared with our Early Pregnancy Unit (EPU) and the sonographers in antenatal services which sensitively supports women in this position during a clinic y The team have been given support and training, working with national charity Abigail’s Footsteps. This national charity was launched in 2010 by parents Jo and David Ward following the death of their daughter Abigail Ward, who was stillborn at 41 weeks gestation. y The trust has a dedicated quiet area called the Lily room that can be used Case number three A patient with a hearing impairment was dissatisfied with the treatment received in A&E. Action plan: y With regard to hearing impairment, ensure it is documented in the patients’ medical records that additional support may be required y Review hearing loops, access signage within ED, working with patient groups to ensure these issues are addressed adequately through the advice of those with lived experience Patient Panel Despite the pandemic, our Patient Panel were as active as ever, continuing with usual activities and taking advantage of new ways to meet using Microsoft Teams. Three new panel members joined during 2021/22, with one to represent parents whose children have additional needs, one to represent minority groups and one to support the panel's general work. Our panel member supporting parents has produced a leaflet about blood testing and is providing comfort bags for parents when their children have an unexpected stay in hospital. The panel continue to work on the new hospital project work and in year have been involved in ensuring the new trust website was ‘patient centric’ to create greater local awareness. Our Patient Panel continued to meet monthly and also participate in the complaints reference group. Panel members represent patients at many of our trust committees/meeting groups that cover topics such as inpatient falls, end of life, medicine management, patient safety and quality, research, digital senate, infection control, organ donation and nutrition.
46
The Patient Panel chair attends regular meetings with the trust chair and director of nursing, midwifery and allied health professionals, conducting ward and clinical area visits, and liaises with many external groups and organisations. Our Patient Panel vice chair represents the panel at the trust’s digital senate, which is mapping out how patient data is to be digitally captured and made accessible in both acute and primary care settings.
The Patient Panel members continue to write letters of thanks and present novelty cakes to trust teams following receiving patient compliments. Recipients this year have included the mortuary team, for their commitment at the height of the COVID-19 pandemic and for their work over the last 18 months. Our radiology team also enjoyed their skeleton themed cake, thanks to the panel.
Panel members were pleased to nominate both the chaplaincy and the estates teams for local awards for
4747 which they were both shortlisted. In year, the Patient Panel organised a cancer conference, One Step at A Time, that featured videos on living with cancer. The team were grateful to Emma Harnett from Macmillan for her support with the conference. The Patient Panel chair was honoured to meet up with Janice Bernardo, the trust’s frailty lead, who has worked tirelessly to start the trust’s Older Person's Assessment and Liaison Unit (OPAL unit) which supports acute and primary care patient referrals. At the time of the visit, over 1,300 patients took an active part in research towards a better future for all. In July 2021, our Patient Panel were presented with the Queen's Award for Voluntary Service by the Lord Lieutenant of Essex, which comprises a signed certificate from Her Majesty the Queen and a beautiful glass trophy. The panel were pleased to be joined at this celebration by many staff members with whom they have worked over the year. Lance McCarthy, chief executive, had the opportunity to present to the Harlow Hospital Radio team a certificate celebrating 50 years of service to the trust. Our thanks go to Down Hall Country House Hotel for donating their ballroom for the occasion. COVID-19 meant the volunteer’s Christmas lunch was once again sadly cancelled, but by observing Covid guidelines the Patient Panel were able to hold a thank you event at Harlow College’s lovely restaurant. A highlight of our panel's year was to meet Professor Roman in July 2021 who was credited in April 2022 with building the world’s first functioning artificial pancreas system. Our panel members are also grateful to Sir Lindsay Hoyle, Speaker of the House of Commons, who wrote about how he felt being diagnosed with type 1 diabetes and by sharing this information at our diabetes conference, they hoped it was useful to our patients with this condition. Our Patient Panel were interviewed by the Care Quality Commission (CQC) when they visited the trust in the summer of 2021, and were delighted when their report rated their important work as outstanding. This is a tremendous accolade to our group of committed volunteers.


The risk of mortality following a delirium episode in a person with dementia is more than 40%. To support our staff in the care of patients presenting or developing delirium in hospital, we now have established new pathways and guidelines. We also have a leaflet designed to be given to patients and their families or carers. There is a plan to have an electronic assessment. A recent World Delirium Day audit has been completed and findings are being analysed. Training To support our patients, we have introduced mandatory training on delirium, as well as creating simulation training, which has received excellent Thisevaluation.training complements the dementia training that already exists for staff and we are proud of our virtual dementia tour, which enables staff to experience what it may be like to have dementia, and learn how to work with people living with dementia. Namaste care Namaste care "to honour the spirit within" offers a respectful and supportive approach to care for those living with advanced dementia, integrating compassionate nursing and therapeutic activities. Working closely with St Clare’s Hospice, we have introduced Namaste care at PAHT with the support
We have made good progress on our goal to deliver the very best possible care for our patients with dementia, in line with national policy. We have in place an integrated dementia strategy, which has key performance indicators in the following areas and is monitored through our dementia and delirium steering group.
Improving care for vulnerable patientsdelirium and dementia
y Find, assess and refer pathway y Person-centred care (recording of ‘This is Me’) y Comparison of harm related incidents for patients with dementia (development of a dashboard) y WeTrainingparticipated in the national audit of dementia care in general hospitals, The Royal College of Psychiatrists (2019), and the recommendations now form part of our strategy document. An optional case note audit was completed in 2021 but there is no comparative data as less than 15% of NHS trusts took part. Music In 2019, we undertook a project to introduce singing for the brain into the hospital setting. The aims were to reduce the social isolation that patients often experience during a stay in hospital, to improve wellbeing and mobility. Music therapy is known to play a crucial role in the care of many people with or without dementia, helping to minimise apathy, anxiety, restlessness and Followingdepression.thesuccessful pilot, we provided a weekly music therapy session, which was facilitated by the clinical nurse specialist for dementia and volunteers. From 2020 to date, due to COVID-19 restrictions, the clinical nurse specialist continued to deliver this at the bedside for one to one musical therapy and activity sessions supported at times using Zoom with the help of a Hospital Radio Volunteer. The plan for the next few months is to re-establish these sessions with small groups in particular areas and work alongside therapy teams to develop a meaningful activities group. Feedback from family members and carers has been very positive; there has been a notable change in interaction, improved appetite and reduction in delirium related anxiety. Delirium Delirium (sometimes called ‘acute confusional state’) is a common clinical syndrome characterised by disturbed consciousness, cognitive function or perception, which has an acute onset and fluctuating course (NICE 2010).
48
4949 of the dementia clinical nurse specialist (Namaste champion), who will develop the role of Namaste volunteers in partnership with PAHT volunteers. A dedicated room space will need to be identified. Currently Namaste care sessions are delivered twice weekly and we are embedding a Namaste approach to delivering compassionate care in everyday nursing care. Working with our patients and their carers, we have been successful in obtaining funding through NHS Charities to recruit a carers lead, this will be a Band 6 role with a view to extension if successful. Pets as Therapy An exciting new project was developed during 2021/22 and started on 6 April 2022, supported by our voluntary services. This involves ward visits with therapy dogs, initially visiting our vulnerable patients once a week, with a view to increasing this if it is successful.

The increase in reporting is mainly related to the category of monitoring, which has increased to 1,366 (11% from 3.7%). This is due to the Datix system also being utilised to capture information required for the monitoring of deprivation of liberty, safeguarding referrals and operational issues. This category of incidents are not patient safety incidents. Top 10 patient safety incidents The top 10 categories of patient safety incidents reported in this financial year are summarised in the graph overleaf. These are reported to the National Reporting and Learning System (NRLS) to enable learning and
Figure 13: Incident reporting April 2021 – March 2022
There were 7,446 patient safety incidents (61%) reported in year, which is comparable with previous reporting. Other incident reporting categories were: y 895 staffing shortage (7.5%) y 682 staff related (6%) y 572 equipment related (5%) y 530 security (4.5%) y 546 environmental (4.5%) y 70 visitor related (0.5%)
50
Patient safety is a priority and we continuously work to ensure that incidents are managed effectively, promptly and most importantly that we learn and share the improvements from Athem.patient safety incident or adverse incident is defined as ‘any unintended or unexpected incident which could have, or did lead to harm for one or more patients receiving NHS funded care’. This includes all terms such as adverse incidents, adverse events and near misses, where an incident was recognised and averted. For the year 1 April 2021 to 31 March 2022, the trust had 12,107 incidents reported on the trust’s Datix incident management system; this is a 18% increase from the previous 12 months. This is positive, indicating that the trust has a safety culture and staff are focused on improving patient’s safety, this should be coupled with harm rates being maintained and not increased. All serious incidents generate a sharing the learning report, which is presented locally within our divisional teams and then quarterly in various trust meetings to widely share learning. This is also presented at the Quality and Safety Committee, a trust board sub group.
Learning investigationsincidents,from and changes implemented

5151 comparison with similar sized organisations across the country to occur, please see figure 13 below. Figure 14: Top 10 incident categories
Serious incidents 26 serious incidents (SIs) were reported by the trust during 1 April 2021 to 31 March 2022. In comparing this against 2020/2021, this is significantly reduced as a result of fewer nosocomial COVID-19 acquisitions, at four.
Figure 15: Serious incidents reported in year
The learning from the healthcare associated COVID-19 serious incidents has been effective, as the trust has had just one case during 2021/2022, compared to 60 during 2020/2021.


Changes implemented as part of learning from incidents y The trust has an overarching action plan to reduce falls and has implemented changes: o Enhanced care team in place to provide one to one care for patients who require constant supervision o All patients are assessed if they are at risk for falling, and if high risk are given a yellow blanket and a yellow wristband. This is a visual aid for staff to see clearly high-risk patients y The trust has put measures in place to help reduce/prevent patients getting pressure ulcers in the Intensive Care Unit (ICU). All of their patients are nursed on special pressure reducing beds from the beginning of their admission to ICU y Simplified the COVID-19 routine swabbing requirements so all wards complete swabs on every inpatient on specific days of the week to ensure a mandatory number of swabs are completed weekly y To prevent delays in ophthalmology patients receiving follow-up appointments, these are booked into a clinic rather than added to a review list for an appointment to be arranged nearer the planned timeslot y The learning disabilities team has developed a carers' contract. This is to ensure that risks are discussed and actions put in place to mitigate the risk y Maternity has set up a formal process for the review of anomaly scans to ensure that women are on the appropriate pathway y The gastrointestinal (GI) policy has been put in place, which includes the pathway for out of hours management for a patient experiencing a GI bleed. y Paediatric emergency department reception cover extended to 24 hours a day y Increase of healthcare support workers to support the children waiting for triage by completing observations within 15 minutes of arrival y Mental health trained nurses are now part of the emergency department
52
Never events The trust reported two never events in 2021/2022. The investigation has concluded on the first incident and a robust action plan was completed. A subsequent audit to confirm embedding of these actions was completed and we are assured we could not have a repeat of this incident. The second never event occurred earlier this year and the investigation remains ongoing.
2021, the trust launched our quality and patient safety strategy to support the organisation's vision to deliver outstanding healthcare to the community.
Onteam9March
The strategy recognises the biggest areas of challenge within the trust at this time. The patient safety team have identified the top five areas which PAHT needs to focus on from 2021-2023. This is to reduce avoidable harm to patients, with key priorities of: y Falls - to reduce falls with harm by 50% y Venous thromboembolism - to become an exemplar trust for venous thromboembolism in the UK y Diabetes - to run an outstanding service for all patients with diabetes, whether or not diabetes is the reason for admission y Pressure ulcers - to reduce all hospital acquired pressure ulcers that could not otherwise be avoided, and to reduce moderate and severe pressure ulcers by 50% by 2021/22, with the ambition of 0% preventable harms by 2023 y Medicines optimisation - to increase the reporting of medicine incidents, while reducing the harm

Over the last 12 months, the pharmacy team have worked collaboratively with colleagues across the whole organisation, Integrated Care Partnership (ICP) and Integrated Care System (ICS) to strengthen and improve medication safety. Medicines optimisation during year two of COVID The pharmacy department supported the trust in a number of ways during the COVID pandemic. This included the trust COVID Medicines Delivery Unit (CMDU), in providing access to new treatments for ‘high-risk’ hospitalised and nonhospitalised patients who have tested positive, the vaccination programme, maintaining and managing supplies of critical medicines, contributing to COVID clinical trials involving medication, medicine management during ward moves, and writing and validating clinical guidelines. Developing the roles of our pharmacists We have specialist pharmacists working in critical care, anticoagulation, gastroenterology, rheumatology and dermatology; these individuals provide expert advice and guidance to support patient care. We have also developed our integrated workforce within the ICP, having two joint posts with West Essex Clinical Commissioning Group (CCG), in frailty and neurology. Medicines optimisation outside of ‘normal working hours’ y Adult Assessment Unit and Charnley Ward A pharmacy team operating on a sevenday working model is now providing support to the Adult Assessment Unit 12 hours a day. This supports safe management of medication and patient flow. A pharmacist also supports Charnley Ward (short stay) six hours per day at weekends. Antimicrobial stewardship The guidelines for treatment of infection
y A big achievement for the last year was the implementation of ChemoCare, a new chemotherapy prescribing system. All oncology and haematology protocols are now prescribed, validated, prepared and administered using the new system. This has greatly improved the safety of the chemotherapy processes in the trust.
The pharmacy handover report was recognised by the CQC inspection as a valuable tool for our pharmacists to target clinical pharmacy interventions
y We continue to develop our reporting through EPMA with reports, handovers and dashboards for our clinical teams.
5353
Improving medicine safety
y The EPMA team continue to work with the clinical teams on improving and optimising the EPMA system. Examples include work with the clinical trials team on Covid-19 protocols, diabetes team on insulin prescribing, thrombosis group on venous thromboembolism (VTE) assessments, thromboprophylaxis and anticoagulant prescribing. This all contributes to safer prescribing and reduction of medication errors
have been updated in line with latest the National Institute for Health and Care Excellence (NICE) guidance and are going through the approval process. The updated guidance will be added to AlexNet and to the MicroGuide App so that they are easily available to doctors and other prescribers. This means that our patients receive the shortest effective course of antibiotics by the most appropriate route. A programme of audit, feedback, surveillance and education and review of patient safety incidents related to antimicrobial use is in place so that we can monitor our practices and ensure that our patients are receiving safe care. Electronic Prescribing and Medicines Administration (EPMA)
Medicines safety programme
54 Medication incidents
The table above also shows that the number of medication incidents involving patient harm has remained low, despite an increase in the total number reported.
Other areas where good progress has been made include: y Improved attendance by doctors at the monthly Medicines Optimisation Group meetings, enabling valuable discussion of: the results of audits relating to medicines; incident trends and patient safety alerts; medicine shortages, proposed changes to improve medication safety and approval of policies, guidelines, procedures and patient group directions y Engagement of members of the Medicines Optimisation Group with the governance requirements for patient group directions y Medication incident multi-disciplinary review meetings continue to take place on a monthly basis and are well attended by PS&Q and practice development leads and other senior nursing staff and pharmacists. This includes identification of themes and trends and actions that should be taken within each division to reduce the risk of the incidents recurring. These actions are approved by the Medicines Optimisation Group and presented to the trust Patient Safety Group to provide assurance of shared learning.
The reporting of medication incidents on the Datix incident management system fell during the busiest part of the COVID-19 pandemic, in January and February 2021; but it is generally rising again, as can be seen in figure 16 below:
y The medication safety officer is a core member of the Incident Management Group meetings, helping to ensure that all issues relating to medication safety from reported incidents are identified and addressed y The trust weekly staff bulletin continues to include a ‘medication safety tip of the week’. These are used to share the learning from medication incidents trust wide y Introduction of a new ‘Prescribing Excellence’ email to educate doctors on a particular area of prescribing y Medicines security audits by pharmacy staff continue to take place to ensure that medicines storage is appropriate and safe. These are now completed using an online platform, enabling easy generation of compliance reports and analysis of trends y A senior pharmacist now attends patient safety and quality meetings in each division, to provide advice on current priorities in relation to the safe use of medicines in the trust, including the safe storage and use of medicines and compliance with governance requirements y There is regular communication

5555 between the medication safety officer, the lead nurse for medicines safety and the EPMA team to see how JAC can be used to improve the safety of prescribing and medicines administration y Staff continue to be made aware of national medicine shortages and receive advice about alternative medicines that can be prescribed y Task and finish groups have been set up to look into reported incidents involving insulin and warfarin, respectively, and to make changes which will be effective in reducing the occurrence of these incidents Education and training The focus is still to prioritise training which will support medicines optimisation on the wards. This is the Diploma in General Pharmacy Practice and NonMedical Prescribing (for pharmacists) and the Accredited Checking Pharmacy Technician course and Certificate in Medicine Management (for pharmacy technicians).
A new Specialist Education and Training post (Band 8A) has been established (in December 2021) to provide support for junior pharmacists. Also, there is the introduction of one new hospital/ GP trainee pharmacist split placement to encourage a broader education for trainee pharmacists. The next 12-36 months
Antimicrobial stewardship y The team is being strengthened by the addition of a Band 7 pharmacist. This post is out to advert. Education and training y Plans to increase the number of split hospital/GP trainee placements to two and to consider 13-week longitudinal placements within the trainee pharmacist year to encourage more interactive working with nurses, doctors and allied health professionals (AHPs) y To ensure all new pharmacists are offered a diploma course in order to encourage recruitment and retention
Infrastructure: y Technical Services (chemotherapy production) Unit (TSU): The business case has been approved, a site has been identified and the project is now underway. We are hopeful that we will have a new chemotherapy unit in place by the autumn of 2022 y Robot: The business case for a replacement automated dispensing system (robot) is in progress and initial meetings have taken place with suppliers. However, we will need to wait until the new TSU is complete, vacating a space in pharmacy for a dispensary decant in order to progress further
hire 42 days Average
Over the last year, the group have introduced many initiatives, including a menopause policy and support App, and have health and wellbeing champions within departments across the organisation. The Alex Lounge opened in March 2022 and is a staff only area which provides a restful environment with free hot drinks and chilled filtered water for our people. This area was designed and agreed with our people through the health and wellbeing steering group.
During this time, the trust continued to recruit substantively throughout the year, ending with a final vacancy position of 6.5%. Whilst we have seen an increase in our turnover, this is a challenge that has been faced by many trusts following the previous two years. A number of retention interventions have been put in place and are being developed to improve this target, these include the launch of a recruitment and retention steering group, learning steering group and health and wellbeing steering group, attended by different divisions and staff groups. 9: target Year to
People KPI 2019-20
Time to 48
days
56 Our people In 2021-22, our people continued to face a number of ongoing challenges in response to the COVID-19 pandemic. Our people rose to the challenge of working in different ways, different services and in some cases, different roles, to support the needs of our services and keep our patients safe.
performancedate Vacancy rate 8.6% 6.5% Sickness absence 4.3% 3.9% Voluntary turnover 10.7% 15% Statutory mandatoryandtraining 92% 87% Appraisal 89% 79%
Table
Health and wellbeing In May 2021, a health and wellbeing steering group was established, with the purpose of co-ordinating health and wellbeing activities in the trust.
Alex Lounge - before

5757 Alex Lounge - after
As part of the national support for mental health, a psychological health support service called Here for you was established within the Hertfordshire and West Essex Integrated Care System (ICS). This is a mental health and wellbeing service available to any Essex or Hertfordshire health and social care worker struggling with the direct or indirect impact of the Covid-19 pandemic and wider psychological support requirements. Established in April 2021, it has supported one to one referrals and onward support with primary care, group reflective sessions and webinars on wide ranging topics linked to mental health. This service has been well received by PAHT staff and the Here for you team are allocated to the trust two days per week.
As part of the trust's commitment to support our people, we have continued to invest in training for mental health first aiders and now have a multi-disciplinary team that are able to support and signpost our people. Testimonials from our people: y “The space is lovely and open, well-lit and comfortable. We have very limited space to relax up on the wards and in our departments. This is a great space for all staff.” y “It’s really bright, airy and spacious. It’s very inviting and at the same time it's calm. The colours are lovely and calming with private spaces where you can get away and catch up with colleagues and





58
y We continued to welcome international staff into the trust, facilitating the required isolation period with designated hospital accommodation. The nursing and midwifery staff group now has a vacancy rate of 5.7% and medical staff vacancy rate of 1%. The overall trust vacancy rate is less than 6.5%
Recognising our people
y We also continue to work with integrated care system (ICS) colleagues on alternative ways of retaining staff within the ICS and are piloting rotational allied health professinal (AHP) posts across acute, mental health and community organisations
We continue to implement agile working across the organisation and have developed more agile working space both on site and at Kao Park. The allocation of laptops and digital telephone systems across the trust has supported the ability for more of our people to work in an agile way and has enabled greater productivity efficiencies though re-evaluation of current processes and systems and has enabled specific objectives and targets to be set and measured more efficiently.
y A change in the trust approach to recruit health care support workers saw 70 recruited in 2021/22, bringing the current vacancy rate to 8.72%.
At our annual Our Amazing People Awards, over 200 of our PAHT people, including our volunteers, were nominated for an award. Each nomination gave examples of how our people’s work has been driven and shaped by our values: patient at heart, everyday excellence and creative collaboration. Colleagues were invited to attend an exciting awards evening (socially-distanced), where certificates, badges and awards were presented by the executive team. This event was part of the annual three-day engagement event Event in a Tent, and was also live-streamed to enable colleagues across the organisation to attend to show support and appreciation for their colleagues. Our Long Service Awards give people the opportunity to be recognised and celebrated by their colleagues and the executive team. Over 200 colleagues with over 20 and 25 years’ of PAHT service were invited to join the 2021 event, with many able to join. Longserving colleagues received certificates, badges and those longest-serving received a special artwork gift. This event was also live streamed, with many wider colleagues joining to celebrate.
Workforce, resourcing and planning
Further collaborative work with the ICS is being undertaken to recruit into this staff group
Teams were also encouraged to celebrate their achievements in 2021 via a special ‘Teams' proudest moment event’. Colleagues were encouraged to share their moments in a creative way, with an emotive poem entry receiving the most votes from our people. All teams received prizes in recognition of their participation and valued work. The awards events, as in previous years, also paid tribute to our colleagues who passed away in the year. This was a poignant and moving way to remember and pay our shared respects to some very special people.
y The trust's monthly recruitment and retention steering group launched in 2022 and offers guidance, direction and support to areas with high vacancy or high turnover; ensuring that we implement effective methods and techniques to improve attraction and retention. This includes the use of temperature check 'stay' questionnaires.
5959 Celebrating our amazing PAHT people A huge congratulations to our people who were nominated and highly commended at our awards ceremonies. Please take a look at some of the photos of our amazing #PAHTPeople - well done to all.





















60






















6161
services
in
Other accolades for our #PAHTPeople included...
before
Mr Kar Teoh, consultant trauma and orthopaedic surgeon, won the Presidential Prize at the European Foot and Ankle Society (EFAS) Conference, held from 21-23 October 2021, in Lyon, France.
The #PAHTPeoplerecognisedcommunityourwith a special award, which was formally accepted by Lance McCarthy, chief executive, from vice chair of Harlow Council, Councillor Maggie Hulcoop, in a socially distanced presentation in May 2021.
Mr Ashraf Patel, associate specialist in breast surgery, was awarded an MBE for to funding and research for breast cancer the Queen’s Birthday Honours List 2021 (pictured the COVID-19 pandemic).



62 The National NHS Staff Survey
The annual NHS National Staff Survey (NSS) is recognised as an important tool for ensuring that the views of people working in the NHS are used to help inform local improvements. The feedback is useful in helping highlight strengths, and improvements that will make PAHT a better place to both work and be treated. A full census was held at PAHT between October and November 2021, with all of our people having the opportunity to take part. In total, 1744 (47.3%) completed their survey, which was 9.1% higher than 2020, and 1% higher than the median acute trust response rate (there are 126 acute trusts within the benchmark group).
Figure 17: Summary of the trust’s results by the key national themes, benchmarked against the 126 acute trusts
The report findings from the 2021 National Staff Survey were presented to the Strategic People Committee in March 2022. A series of workshops have been held with managers within each division to fully review the findings and commence the development of staff survey improvement plans. These plans align to four priority actions identified by the trust (continuing from those identified for 2020-21): y Priority one: improving the physical and mental health and wellbeing of our people y Priority two: improving our learning and safety culture, encouraging people to openly share feedback or concerns and ensure this is acted upon - improving psychological safety y Priority three: embedding our This is Us management practices and leadership promise in our ways of working y Priority four: ensuring our workforce plans support teams being effectively staffed to deliver high quality services These are particularly important as we continue to strive to deliver care in line with our values and our quality and patient safety strategy. Staff will be given the opportunity to attend a series of ‘Staff Survey 2021 results roadshows’, where they can share their views on the results and improvement plans. Their feedback will help to further refine these plans, ensuring positive changes within their areas, which will support better experiences for our people.

6363
Inclusion The equality, diversity and inclusion steering group meets monthly to review activities and initiatives to promote and support awareness and education of equality, diversity and inclusion (EDI) at DuePAHT.to the COVID-19 pandemic, the monthly meetings have been successfully held virtually. It has also required the steering group to review the ways it can highlight EDI activities, predominately through virtual events and a programme of planned activities continued throughout the year including LGBT+ Pride, celebrating Black History Month, International Women’s Day and International Men’s Day. Black, Asian and Minority Ethnic (BAME) staff were an identified group that is disproportionately more likely to be impacted by COVID-19. In collaboration with other trusts within the Integrated Care System (ICS), we developed a number of initiatives to support our BAME staff including: y Establishment of a BAME staff support line y Agreed consistent risk assessment and outcomes for all COVID-19 identified vulnerable groups y Research methods were explored to understand BAME staffing needs and views on the COVID-19 response y Creation of system-wide EDI network and BAME chairs' network for ongoing transformation Our performance The trust’s operational performance against national and local standards is monitored and reviewed at various trust meetings. The position is summarised as follows: Targets and national standards Delivery of all national standards has continued to be significantly impacted by ongoing waves of COVID-19 and the increased volume of emergency patients requiring care. The requirement to maintain separate urgent Covid-19 and non-Covid pathways and flows through the hospital, the change of many wards to focus on emergency care and the transfer of theatre staff to critical care significantly reduced the volume of elective activity that could be delivered. Full elective operating was significantly reduced on the PAH main site in late October 2021 due to the transfer of bed capacity to Covid facilities. Elective operating for the most critical cases was maintained with six bed capacity until February when one ward was re-opened for elective patients and a second in March 2022. This limited capacity, along with mutual aid support from the independent sector, local hospitals and London tertiary centres ensured that cancer and high priority elective operating continued over the winter.
Figure 18

Cancer and urgent diagnostics continued and despite considerable staff absence levels over the winter, the diagnostics department delivered additional activity to both the emergency department and cancer pathways. The diagnostic services have a recovery trajectory that is being exceeded and the trust is delighted to report that ultrasound reported national standard achievement of 99% in February 2022.
The trust aims to achieve the overall national standard by August 2022. The opening of the third CT machine and the replacement of the MRI equipment at St Margaret’s Hospital, Epping, will ensure resilience in diagnostics capacity into 22/23.
Diagnostic performance was also impacted by COVID-19 demand as routine appointments were paused once again during 2021-22.
The 18-week referral to treatment (RTT) standard has continued to be impacted by the restricted capacity to see and treat patients over the year. The trust continues to book patients in clinical priority order and has been successful in ensuring the highest priority patients are being booked within a month of making a decision to treat (P2s).
The trust has also reduced the number of long waiting patients, with those over 78 weeks steadily reducing over the past six months, and ensured that patients waiting two years for their treatment have been treated by 31 March 2022, (with the exception of five patients requiring a clinical recovery period due to Covid).
The trust continues to be committed to the delivery of all national cancer standards and plans are now in place to reduce the backlog from the Covid waves in 21/22. The 28-day faster diagnosis standard will be the main focus of improvement in 22/23 as the good performance in early 21/22 deteriorated over the autumn and winter.
Figure Diagnostic19 performance
64
Delivery of the national cancer standards was also impacted by COVID-19, however the trust prioritised the maintenance of cancer services by implementing new treatment pathways such as day case treatment with home post-operative nursing, using the limited bed capacity effectively and transferring activity to other trusts. A refreshed cancer recovery plan has been implemented across all specialties and this will lead to a second reduction in long waiting cancer treatments. The trust’s cancer performance was below the national average as it was more impacted by COVID-19 than other providers that had more flexible facilities to maintain elective activity during COVID-19 waves.

Urgent care and ED performance
6565 Figure 20
Figure 21
The urgent care attendances during the year have fluctuated, with reduced levels in the early part of the year due to Covid impacts, and some of the highest daily attendances in October 2021 and sustained high attendances for the rest of the year. The separate respiratory emergency department was maintained throughout the year and in November the trust created a separate area to support an expanded Urgent Treatment Centre with separate waiting areas for Covid, respiratory and other attendances. All walk-in patients went through a streaming assessment to direct them to the most appropriate emergency service which enabled the emergency department to concentrate on the most urgent cases. The ongoing waves of Covid admissions and increased pressures in the wider health and social care system has exacerbated the flow of patients through the hospital and returning to home and care settings. This also then impacted the time to admission on a ward and the ambulance handover performance. The four-hour standard to ensure patients are treated, discharged or admitted within four hours of arrival in the emergency department has been below the national standard for the year, however the trust has made some improvements over the year as a result of an intensive recovery programme and improved the trust’s ranking in the region.


66 Figure 22
We have continued to work with our system partners to further develop streamlined services that can be delivered in the most effective location and to prevent attendances and admissions to hospital. The Local Delivery Board has continued to forge close working relationships across organisations and enabled improved service provision such as increased intermediate care capacity, patient at home support for patients with existing care packages and sharing of staff. This collaboration has been essential to support the various services across the wider health and social care system, for example East of England Ambulance service, community services and receiving support for our trust. The trust has continued to focus on reducing long length of stays for patients through collaborative work with the community across the integrated care system (ICS). The trust has been part of a national support scheme to improve discharges from the trust, into the community and social care and the third visit is expected in early 2022/23.
Figure 23


6767
Participation in clinical audits We are required to participate in national audits to ensure that we are taking every opportunity to learn and improve. During the period 1 April 2021 to 31 March 2022, there were 43 national clinical audits and three national confidential enquiries that covered NHS services that we provide. During that period, the total number of national clinical audits that the trust was eligible to participate in was 43 and the trust submitted data to 37. A summary of this information can be found in table 10. There were three national confidential enquiries, which the trust was eligible to participate in; four have been paused due to COVID-19 and the trust participated in five. The summary of this information is detailed below. The national clinical audits and national confidential enquiries that we have participated in, and for which data collection was completed during 202122, are listed alongside the number of cases submitted to each audit or enquiry as a percentage of the number of registered cases required by the terms of that audit or enquiry. During 2021-22, the local review of national clinical audits reports was impacted on by COVID-19 and work is now taking place to address this.
Table Programme10 / work stream (A-Z) organisationProvider Participation Number / submitted% Case Mix ProgrammeICNARC Intensive Care National Audit & Research Centre Yes 100% Child serviceschildTransitionProgrammeReviewClinicalHealthOutcome–fromtoadulthealth National EnquiryConfidentialinto Patient Outcome and Death Yes questionnaireOrganisational submitted April 2022 and criterianotcancelledquestionnairesclinicalasdidmeetthe Chronic Kidney Disease registry The RegistryUKAssociation/TheRenalRenal Not applicable only for renal centres Cleft Registry and Audit Network Database Royal College of Surgeons - Clinical Effectiveness Unit Not applicable Elective Surgery (National PROMs) NHS Digital Yes 75%
68 Emergency Medicine ImprovementQuality a. Pain departments)inshockandb.departments)inChildrenin(careemergencySeveresepsisseptic(careemergency Royal College of Emergency Medicine a. Yes b. Project closed Audit directorynationalRemovedongoingfromaudit Falls and Fragility Fracture ProgrammeAudit a. b.LiaisonFractureNational Audit of Inpatient Falls c. DatabaseHipNationalFracture Royal College of Physicians a. Not applicable b. Yes c. Yes 100% - 6 cases 100% Inflammatory Bowel Disease Audit IBD Registry Yes 75% DisabilitiesLearning Mortality ProgrammeReview NHS England Yes 100%learningsee Maternal and Newborn Infant surveillancemortalitya.ProgrammeOutcomeClinicalReviewPerinatal b. Maternal surveillancemortality University of Oxford collaborativeMBRRACE-UK/ YesYes 100%100%
6969 Medical and Surgical a.ProgrammeOutcomeClinicalReviewCrohnsdisease c. Epilepsy study National EnquiryConfidentialinto Patient Outcome and Death YesYes Start delayed and audit is ongoing 33% Mental Health Clinical Outcome Review Programme University NCISHManchesterof/ Not applicable National Adult Diabetes Audit a. Pregnancyb.DiabetesNationalNational in Diabetes Audit c. AuditDiabetesincludingDiabetesd.AuditDiabetesNationalFootcareNationalInpatientAudit,NationalIn-patient–Harms NHS Digital a. No b. Yes c. Yes d. Yes Insufficient software 100% - see learning Data submission period still open 100% National Asthma and Chronic Obstructive a. andOrganisationalRehabilitation-d.PulmonaryObstructivec.Secondaryb.CareAsthmaPaediatricSecondaryAdultAsthmaCareChronicDiseasePulmonaryClinicalAudit Royal College of Physicians a. Yes b. No c. No d. Not applicable 13 - ongoing Due to Covid and capacity isues
70 National Audit of Breast Cancer inOlder Patients 1, 2 Royal College of Surgeons Yes 100% National Audit of Cardiac Rehabilitation University of York Not applicable National Audit DiseaseCardiovascularof NHS NetworkBenchmarking Not applicable National Audit of Care at the End of Life NHS NetworkBenchmarking Yes 40 cases equal to 100% National Audit of Dementia Royal College of Psychiatrists Yes 37 cases (25 is minimum) National Audit of HypertensionPulmonary NHS Digital Not applicable National Audit of Seizures and Epilepsies in Children and Young People (Epilepsy 12) Royal College of Paediatrics and HealthChild Yes Audit ongoing National Cardiac Arrest Audit Intensive Care National Audit and Research Centre / CouncilResuscitationUK Yes 104 / 100%
7171 National Cardiac Audit Programme a. National Audit of Cardiac DiseaseCongenitalf.Failuree.Angioplasty)(PCI)InterventionsCoronaryofd.AuditCardiacc.AuditIschaemiab.ManagementRhythmMyocardialNationalProjectNationalAdultSurgeryNationalAuditPercutaneous(CoronaryNationalHeartAuditNationalHeart a. Yes b. Yes c. Not applicable d. Not applicable e. Yes f. Not applicable 340100%cases / 100% Data openperiodcollectionremains National Child Mortality Database University of Bristol Not applicable Data comes from Child Death Overview Panels National Clinical Audit of Psychosis Royal College of Psychiatrists Not applicable National InflammatoryEarly Arthritis British Society of Rheumatology Yes 2 cases National LaparotomyEmergency Audit Royal College of Anaesthetists Yes 93 National Lung Cancer Audit Royal College of Physicians Yes 100%
72 ComparativeNational Audit of Blood a. 2021 Audit of Patient Blood b. 2021 Audit of the managementperioperative of anaemia in children undergoing elective surgery NHS Blood and Transplant a. No b. Not applicable Project remains open for data entry National Gastrointestinal Cancer a. Cancerb.CancerOesophago-gastricNationalNationalBowelAudit NHS Digital YesYes Continuous data (submittedsubmissionannually and retrospectively – 1 year behind) Continuous data (submittedsubmissionannually and retrospectively – 1 year behind) National Joint Registry Healthcare PartnershipImprovementQuality Yes 91% National Maternity and Perinatal Audit Royal College of Obstetrics Gynaecologyand Yes 100% National Neonatal Audit Programme Royal College of Paediatrics and HealthChild Yes 100% National Paediatric Diabetes Audit Royal College of Paediatrics and HealthChild Yes 135 cases National Perinatal Mortality Review Tool University of Oxford collaborativeMBRRACE-UK/ Yes 100%
7373 National Prostate Cancer Audit Royal College of Surgeons Yes 100% National Vascular Registry Royal College of Surgeons Yes 16 cases in 2021 ProgrammeNationalNeurosurgicalAudit The Society of British SurgeonsNeurological Not applicable OutcomesCardiacOut-of-HospitalArrest University of Warwick Not applicable Paediatric Intensive Care Audit University of Leeds / University of Leicester Not applicable ObservatoryPrescribing for Mental Health a. Prescribing for depression in adult mental b.serviceshealthPrescribing for substance misuse: alcohol detoxification Royal College of Psychiatrists Not applicable Respiratory Audits a. ManagementOutpatientNational of Pulmonary b.EmbolismNational Smoking Cessation 2021 Audit British SocietyThoracic YesYes 16 / 41% 100 cases
74 Sentinel Stroke National ProgrammeAudit King's College London Not applicable Serious Hazards of Transfusion Serious Hazards of Transfusion Yes 26 / 96% Society for Acute BenchmarkingMedicine Society for Acute Medicine No ResectionTransurethraland Single instillation mitomycin C Evaluation in bladder Cancer Treatment BURST Collaborative / British SurgicalResearchersUrologyinTraining No Study remains open for data submission Trauma Audit & Research Network The Trauma Audit & NetworkResearch Yes 268 cases (100%). Further cases to submit and the reporting period still open UK Cystic Fibrosis Registry Cystic Fibrosis Trust Not applicable Urology Audits a. NUAuditNephroureterectomytheb.NephrectomyRadicalCytoreductiveManagementofLowerUreterin(BAUSLowerAudit) British Association of Urological Not applicable Not applicable
During 2021/22 six national clinical audit reports were reviewed and had action plans developed against the reported recommendations, they related to: y National Paediatric Diabetes Audit o Clinical psychologist two days a week from January 2021 y Maternal Infant and Newborn clinical Outcome Review Programme Saving Lives, Improving Mothers’ Care
o Plans in place for 90% of hip fracture admissions to be transferred to the orthogeriatric ward within four hours of ED admission y National Smoking Cessation Audit
improvements from audits
o Fully implementing all recommendations y National Hip Fracture Database
o Plans in place to utilise available funding to support smoking cessation services for Ininpatientsaddition: y National Pregnancy in Diabetes Audit
7575 and
o Instigation of all Type1 DM patients to start Continuous Blood Glucose monitoring which helps improve outcomes. y Learning Disabilities Mortality Review
The information and technology (ICT) team have continued to progress the technology within the trust in a secure manner during the last year, also providing additional staff to areas as ward clerks etc. to assist in times of increased pressure. During this year ICT, together with our patient volunteers, won the Healthcare Excellence Through Technology (HETT) Unexpected Innovation Award 2021 for our virtual visiting service. The Unexpected Innovation Award celebrates the best of experimental design, creative thinking and radical innovation in healthcare from both individuals and teams. Our virtual cyber security team came highly commended in the National NHS CAN Award of Cyber Team of the Year. Five of our staff won awards in the trust's annual Our Amazing People awards. One team member completed the Edward Jenner programme and one completed the Mary Seacole programme to support their development.
Learning
o Reviews identified a number of late referrals to palliative care. PAHT have been included in a project led by St Clare’s Hospice (West Essex) which received grant funding: y Two training days have been held highlighting the issues and challenges for people with LD at the end of life y The next stage is to develop the role of end of life champions for patients with LD, this work will take place throughout 2022.
o Plans to recruit to a maternal medicine / diabetes obstetric consultant y National Diabetes Inpatient Audit
Achievements in information technology
Bidding for central funding, ICT have managed to procure during the year: y 716 iPads y 331 laptops y 103 desktops (also used for computers on wheels) y 80 new drug carts y Numerous larger monitors for staff moving from 19-inch square devices to 22-inch widescreen and where possible two screens per computer / docking station. A large percentage of these are video conferencing enabled to remove the need for webcams as
o Plans to develop hospital electronic patient record system to identify diabetes admissions y National Audit of Inpatient Falls
76 separate devices.
y New computers on wheels to increase the numbers throughout the ThetrustICT team has committed to sustainability and embraced the reduction of our environmental impact. During this period, we have moved all patient outcome letters to electronic by default (but still allowing for paper intervention where required for digital inclusivity), saving some 149 trees. The trust has moved to a recycle supplier who will (once they have destroyed hard drives) resell our old ICT equipment or donate it to schools and the community, saving the trust money and helping others. The ICT team continued to deliver in line with the previously agreed strategy and embedded the following: y Developed and embedded the desk booking system procured by the estates team and used for staff working at Kao Park to allow them to book rooms and agile working spaces across both Kao Park and the main hospital site. y Expanded the tech bar to include drop in training sessions with our ICT training team
The ICT team have continued to improve the trust security, procuring new software with the aid of a central funding bid. Within the recently released Cyber Metrics under the Model Hospital, PAHT were fourth in the country, another great accolade for our virtual team. Alongside this, ICT have managed to agree free antivirus software for all of our staff for their home PCs.
y Continued to look at applications that could be migrated to the cloud as they are reprocured or renewed (e.g. Ormis) y Connected our virtual visiting phones to our cloud telephony, allowing staff to co-ordinate and operate the system more easily y Commenced the migration of our mobile devices and iPads to Microsoft InTune to make CIP savings and improve useability for end users
y Commenced the rollout of a communications tool to allow the retirement of our non-emergency bleep system y Upgraded all desktops (RAM to 16GB) in the emergency department (ED) to aid speed and provide greater efficiency for users y Procured a new IT service management system that provides us with self-service and workflow, releasing our service desk Team to have more time to fix issues y Undertook ward refreshes of equipment for 17 areas / wards and assisted with the new Alex Agile Space and new Keats House environment y Undertaken numerous infrastructure upgrades and core application optimisations including our cloud telephony y Resilience continually improved as we procure or renew contracts to ensure downtime across the trust is minimised, including new uninterruptible power supplies not just in main computer rooms but across the trust in wards etc. y Commenced the introduction of Robotic Process Automation to reduce transactional work

7777 Research developmentand Figure 24 above and 25 below show the 13 commercial portfolio studies open throughout 2021-22, three are still open to recruitment, eight are closed to recruitment but in follow up and two were open during the year but have since been closed. We had 76 non-commercial studies open in total for 2021-22. 46 of these are still currently open to recruitment, 16 are closed to recruitment but in follow up and 14 were open during the year but have since closed.



78 Recruitment Speciality Directorate CommercialCommercial/Non Portfolio activity 4 Respiratory Medicine portfolioNon-commercial 1 Cancer Clinical servicessupport portfolioCommercial 26 Cancer Clinical servicessupport portfolioNon-commercial 39 Ophthalmology Surgery portfolioNon-commercial 21 Maternity Family women'sanddivision portfolioNon-commercial 14 Diabetes Medicine portfolioNon-commercial 120 Gastroenterology Surgery portfolioNon-commercial 26 Infection Clinical servicessupport portfolioCommercial 311 Infection Clinical servicessupport portfolioNon-commercial 45 Trauma orthopaedicsand Surgery portfolioNon-commercial 65 Critical care Surgery portfolioNon-commercial 68 R&D Corporate portfolioCommercial 99 Emergency Urgent emergencyand care portfolioNon-commercial 110 Nursing and quality Corporate portfolioNon-commercial 3 Rheumatology Medicine portfolioNon-commercial 23 Anaesthetics Surgery portfolioNon-commercial Table 11: Research recruitment per speciality
Our places
7979
To be a modern, integrated and outstanding hospital, our estate requires significant ongoing investment to enable us to provide the best services possible. During the last year, the trust invested heavily in our estate, transforming a number of key sites that have since brought significant improvements to our operations. However, this is not just about investing in spaces and places. It is about investing in our people and our patients: listening to their needs, understanding what we can do better to provide and maintain the very best environment to deliver and receive care. We have a responsibility to invest to improve the health of the planet too, and during the last year we have introduced a number of initiatives to reduce our environmental impact, in line with wider NHS green targets.
Investment summary In 2021/22, we remodelled and maintained our estate to improve the experience for everyone in our hospital by: y improving the management of buildings and engineering systems y providing excellent and sustainable facilities y ensuring safety and security at all Ourtimeshuge capital programme this year was circa £18m, this included a £4.2m investment in backlog maintenance and £14m continued investment in our patients and people. Investing in places for our patients Our patients have benefited from the following completed schemes: y Penn Ward, Saunders Ward and Winter Ward have undergone major refurbishments, allowing us to better support patient care, experience and Wetreatmenthavemade huge improvements to our Adult Assessment Unit, building a new two-storey centre that increases patient capacity as well as improves flow and care pathways. Patient feedback has included: “I would like to say a huge thank you for the care I received when I was admitted to the Adult Assessment Unit (AAU) from A&E. All of the staff that I had any dealings with were absolutely fantastic. There is not one person that I came into contact with that was not helpful. I really can’t thank you all enough.” y Our Labour Ward has been refurbished following a Care Quality Commission (CQC) inspection. The unit has had upgrades on the birthing rooms and corridor, enhancing patient experience of our CQC rated outstanding department y Our Endoscopy Unit (pictured) has been upgraded to support patient experience, care and capacity Endoscopy Unit - before

y We have invested in a new CT scanner (pictured), supporting the treatment of our patients coming through our emergency department CT scanner - before CT scanner - after
80 Endoscopy Unit - after Patient feedback has included: “I'm just writing to thank everyone involved in my endoscopy appointment this morning. I had been dreading it, as a result of the very unpleasant failed gastroscopies in the past.
"I'm particularly grateful for the sensitive way this was addressed by suggesting and allowing me to have heavy sedation. This worked, and as a result I felt little of the discomfort I experienced in the past.”



y Our children’s ward (Dolphin Ward) has been completely refurbished, to the benefit of our patients, our people and visitors. Clinical bays have been upgraded and the outside terrace has been refurbished, providing a friendly, safe and inviting environment for our paediatric patients
y The Frailty and Short Stay Assessment (OPAL Unit) has been refurbished, enhancing patient experience, care, flow and capacity OPAL Unit - before OPAL Unit - after
8181
y The mortuary department expansion and refurbishment has been completed, enhancing and supporting the dignity of our patients
y Our end of life facility, the Butterfly Unit, has been refurbished, to continue to support patients, visitors and relatives with dignity and sensitivity
y Our cancer services have been upgraded with the Williams Day Unit expansion. The unit underwent a complete refurbishment, supporting patient care and enhancing capacity with the expansion in clinical space Williams Day Unit expansion - before



The brand-new Learning and Education Centre has been built to support the professional development of our people from all disciplines. The centre offers modern training facilities, as well learning and study spaces, library and staff workspace. Feedback has included: “A fantastic, modern space which offers a vibrant environment for staff development, engagement and learning – a real opportunity for the trust to develop its people.”
82 Williams Day Unit expansion - after
Learning and Education Centre









y Fire compartmentation works to main theatres and Dolphin Ward y Fabric upgrade of the staff and seminar room to our Intensive Care Unit y Remedial works to ventilation systems site wide, supporting patient, visitors and staff safety y Statutory asbestos various remedial works have taken place sitewide The locations of the projects can be seen on this site plan: Investing in projects for a healthier planet Climate change poses a major threat to health. Tackling it will improve health and save lives. In the UK alone, air pollution is the single greatest environmental threat to human health. Reducing emissions means healthier lives, and so the NHS has committed to reaching net-zero carbon emissions by 2040. Before November’s COP26 summit, the UK government announced it will set the world’s most ambitious climate change target into law, to reduce emissions by 78% by 2035 from 1990 baseline levels. In line with this, the NHS has set the following targets: y For the emissions we control directly (the NHS Carbon Footprint), we will reach net zero by 2040, with an ambition to reach an 80% reduction by 2028 to 2032; y For the emissions we can influence (our NHS Carbon Footprint Plus), we will reach net zero by 2045, with an ambition to reach an 80% reduction by 2036 to 2039 To comply with our NHS Standard Contract requirement, we are well underway in the delivery of our three-
8383 In addition to these flagship spaces, in 2021/22 we completed a large number of projects to manage maintenance backlog and critical infrastructural risks. These include: y Replacement of obsolete electrical switchgears across the organisation y New medical records build y Cardiology common areas upgrade with new seminar room y New laundry facility and storage, supporting our domestics services team
y Electrical infrastructural upgrade, including installation of new electrical substation y Upgrade of plant rooms to include pumps; bunding; tank room floors; replacement of existing pipework; removal of redundant equipment and sealing plant room y Wireless nurse call system replacement y External security door sets y Urgent repair works have taken place on flat rooves across the trust y Insulation of ventilation ductwork in theatres

During the year, we undertook a sustainability assessment exercise with the support of a sustainability consultancy, to establish our Carbon Footprint for the 2021/22 financial year. Our carbon footprint as shown below in figure 26, is 22,000 tCO2e (the equivalent of 22,000 units of hot air balloon). This will enable us to determine our trajectory and set our targets to achieve net zero by 2045.
We developed and submitted our trust board approved three-year Green Plan to the ICS board for compilation and onward submission to our regulators, NHS England (NHSE/I). The Green Plan sets out our vision, strategy and objectives for delivering sustainable healthcare whilst considering our social and environmental impacts. Energy Energy markets have reached unprecedented highs, due to both the impacts of recovery from Covid and geopolitical/economic influencers causing demand to outstrip supply.
y The gas contract is 100% hedged for all three years. The electricity contract is 100% hedged for years one and two, whilst the third year is 50% hedged (winter 22 and summer 23); leading to cost avoidance savings over this period.
How to become a greener PAHT Baselining
84 year Green Plan. The plan has a number of bold initiatives to improve our sustainability and meet our statutory obligations.
Figure 26
y Hedging these contracts at the time we did demonstrates the trust's forward thinking and understanding of the energy markets (in conjunction with our energy broker and nationally with Crown Commercial Services), see figure 27 and 28 below.
y The savings derived from the avoided costs are the comparison of recent available gas and electricity prices in comparison to those which were attained by the trust through early hedging of our three-year flexible supply contract
Green Plan submission to the Integrated Care System (ICS) board


Energy contract The trust electricity supply is now from 100% from renewable sources and Renewable Energy Guarantee Origin scheme (REGOS) certified. This is a great achievement for the organisation.
We have started our waste compliance, audit and awareness programme with a specialist waste compliance partner. The programme will enhance our waste segregation at source and recycling agenda, as well as fulfil the waste training requirement for our domestic, pottering and clinical staff. A recycling compactor has been installed on site and a bottle bank and clothing bank will be installed in 2022/23 FY for collection of the segregated waste to avoid sending waste to landfill.
The trust completed a list of capital projects to enhance patient service provision and staff wellbeing. This led to increase in the trust square footage/ footprint. As a result, the expected reduction in carbon footprint following the installation of LED lighting across the site cannot be established without sophisticated carbon footprint calculation However,technics. despite the increase in square footage, there is minimal increase in energy related carbon footprint in 2021/22 as demonstrated in figure 29 below.
8585 Energy carbon footprint
On-site energy generation From the Solar Photovoltaic (Solar PV) system installed on site, we have generated a total of 547,484 kWh power ,leading to avoidance of 276 tonnes of CO2 emissions. This total energy generated is enough to boil water for 27,347,200 cups of tea.
Waste Re-usemanagementscheme
Re-use of walking aids: returned walking aids were taken through appropriate processes to ensure they can be re-used by other patients, thereby avoiding sending them to landfills. The trust has re-used the following in this scheme: y 165 crutches returned – 139 recycled y 80 rollator walkers returned – 70 recycled y One gutter frame returned – one recycled y Four walking frames returned – four recycled Waste recycling The trust recycled 148.65 tonnes (27%) of the total general/domestic waste it generated. In total, 96% of all waste generated by the trust does not go to landfill, it is incinerated for Energy Derived Fuel (EDF) where it cannot be recycled. Waste compliance and behavioural change

Green zone project - after Fleet vehicles
The green zone project was successfully completed in June 2021, the outputs were well received by our people and it demonstrates the trust's commitment to reducing its carbon footprint whilst supporting the welfare of our people.
Green zone project - before
Travel and Transport Green zone project – Electric vehicle charging points and cyclist facilities
The project deliverables are electric vehicle charging points, the cyclists changing facilities, cycle storage facilities and improved landscape/green outdoor Followingarea. the completion of the project, we have seen an increase in the number of electric vehicles owned by staff and establishment of a cyclist group that regularly use the on-site cycling facilities.
86
We are currently carrying out market research to enable converting our current fleet vehicles to electric. This will include the medical record delivery vans, estate vans, patient at home and the community midwives’ cars. Changing to electric vehicles will reduce both running costs and our carbon footprint.
Green travel plan (GTP) To encourage sustainable and active travel to and from the hospital sites where possible and to reduce the carbon and air quality impacts of our organisation, we are developing a green travel plan for the existing hospital site. The GTP will review the car parking facilities, amongst other actions, to


8787 support modal shift to active travel to/ from site and to reduce our travel carbon footprint. Restaurant single use plastic We have switched all of our restaurant single use plastic items to disposable alternatives such as wooden cutlery, paper cups and biodegradable ‘vegware’ soup pots. We no longer give out straws and have changed our patient single use plastic tumblers / sipping cups to re-usable washable plastic cups. We will continue to work within our integrated care system to implement our green plan and contribute to the NHSE/I goal to achieve net zero by 2045.
Conclusion We have made significant investments in our estate this year, and we will continue to ensure we maintain and develop the site to meet the needs of our patients and our people as we prepare for the new hospital and a net zero carbon future. This is, of course, a balancing act, working with the integrated care system (ICS) and trust leadership to allocate capital where needed to have the greatest impact. Our teams will continue to work tirelessly to ensure we have an as modern, integrated and outstanding physical environment as possible.
The completed schemes that have benefited our patients: y Major ward refurbishments on Saunders Ward and Winter Ward, supporting our patients care, experience and treatment y The trust has significantly invested in the Adult Assessment Unit, a twostorey new build supporting patient capacity, flow and care pathways y Our Endoscopy Unit has been upgraded y Mortuary department expansion and refurbishment has been completed, enhancing and supporting the dignity of our patients y Creation of the trust's green zone with electric vehicle charging points, supporting our sustainability objectives in reducing our carbon emissions y Our cancer services have been upgraded with the Williams Day Unit expansion and refurbishment y The frailty and short stay assessment (OPAL unit) has been refurbished, enhancing patient experience y The maternity birthing room has been refurbished y Our children’s Dolphin Ward has been refurbished, supporting the care of our paediatric patients y The trust's end of life facility (Butterfly Unit) has been refurbished, ensuring we continue to sensitively support our visitors and relatives y We have invested in a new CT scanner, supporting the treatment of our patients coming through our emergency department Completed schemes that have benefited our people: y The trust have invested in the Alex Lounge and agile working space, this will allow staff a calm space to relax as well as a modern, fresh and welcoming place to work y The Learning and Education Centre is a completely new environment, supporting the development of our people from all divisions across the trust. This area will allow modern methods of training to be delivered, as well as continued engagement and support to our people y Our clinical agile working space has been developed to allow our clinical teams a calm, comfortable and inviting space to work from
Both West Essex and East and North Hertfordshire CCGs would like to commend and thank all the staff and volunteers that work for The Princess Alexandra Hospital NHS Trust in relation to their response to the on-going Covid 19 pandemic and the complexities this brings. Staff continue to respond with professionalism, energy and adaptability. Their teamwork and tenacity have enabled the care of patients to continue during the constantly changing pandemic. The trust has identified eight priorities for 2022/23 that are fundamental elements of their five P strategy: our patients, our people, our performance, our places and our pounds. This includes continuing the work to reduce the mortality rate and to support staff affected by their experiences during the pandemic and improve well-being. Four of the priorities that have been reported as achieved in 2021/22, these remain priorities for the year ahead as they are part of on-going programmes of work. Progress against all the priorities will be monitored through the trust Quality and Safety Committee. During the last year the trust has faced continued challenges due to the Covid 19 pandemic; unwell patients, changes to ward locations due to infection, prevention and control requirements and staff sickness. All staff have had to work differently and adapt to an ever-changing position with differing requirements for the management and testing of patients. Support mechanisms for staff are in place and will continue into the next Theyear.trust has worked with partners within the local health economy, independent sector hospitals, to continue the surgical care of patients with cancer. Unfortunately, the pandemic affected the trust’s ability to achieve the requirement to treat 85% of patients with cancer within 62 days in addition to other standards for cancer care. However the trust continues to be committed to the delivery of all national cancer standards and plans are now in place to reduce the backlog from the Covid 19 waves in 21/22. The 28-day faster diagnosis standard will be the focus for the year
The trust has identified many departments and speciality teams within which improvements have been made in the last year, notably: the infection control team and their work during the pandemic to support patients and staff, the teams caring for patients with dementia, case studies in relation to learning from complaints and the wide ranging and constructive work of the Patient Panel, who were the proud recipients of the Queen's Award for Voluntary Service in July 2021.
Theahead.trust has provided a full and transparent account of the Care Quality Commission (CQC) inspections they have had in year, including the CQC issuing a Section 31 warning notice to the trust in relation to the emergency department. The elements of care that needed review and improvement are detailed in the Quality Account. The trust continues to focus on their improvement plans and regularly report progress to the trust's Quality and Safety Committee, the CCGs and the CQC.
West Essex Clinical Commissioning Group and East and North Hertfordshire Clinical Commissioning Group are responsible for the commissioning of acute health services from The Princess Alexandra Hospital NHS Trust for the citizens of west Essex and east and north Hertfordshire.
88
Statements from stakeholders Statement from West Essex Clinical Commissioning Group and East and North Hertfordshire Clinical Commissioning Group
The integrated working with staff and the high esteem with which the Patient Panel continues to be viewed, is very clear in the Quality Account. Significant learning from patient safety
The trust reported two never events in year, one investigation has been completed and there has been significant learning and changes in practice to prevent another incident of this type. The other never event remains under investigation. We confirm that the information contained within the Account has been reviewed and checked against data sources where these are available, and it is accurate in relation to the services provided. Some of the data that is required to be included for example, a comparison of the trust results to the highest and lowest scores of other organisations in England has not yet been included, we expect this will be addressed in the final version. There is no longer a national requirement for trusts to obtain external auditor assurance on the Quality WeAccount.have reviewed the content of the Account; it complies with the prescribed information as set out in legislation and by the Department of Health and Social care. We believe that the Account is a fair, representative and balanced overview of the quality of care at the trust. We will continue to collaborate with and support the trust to achieve good quality care and treatment for the people of west Essex and east and north Hertfordshire. Jane Kinniburgh Director of nursing and quality Hertfordshire and West Essex Integrated Care System May 2022
8989 incidents has been demonstrated, specifically in relation to reducing the risk of harm from falls and identifying those at highest risk, the care of people with gastrointestinal bleeding in the out of hours period, the management of women with an anomaly scan during pregnancy and the care of people with mental health issues in the emergency department.
The report details the effective use of patient safety incident report intelligence which has enabled the trust to identify the five areas of focus: falls, pressure ulcers, venous thromboembolism, diabetes and medicines optimisation. This work will benefit all patients and reduce harm.

recognise that Quality Accounts are an important way for local NHS services to report on their performance by measuring patient safety, the effectiveness of treatments that patients receive and patient experience of care. They present a useful opportunity for Healthwatch to provide a critical, but constructive, perspective on the quality of services, and we will comment where we believe we have evidence – grounded in people’s voice and lived experience –that is relevant to the quality of services delivered by The Princess Alexandra Hospital NHS Trust. In this case, we have received quality feedback about services provided by the hospital, and so offer only the following comments on the The Princess Alexandra Hospital NHS Trust Quality Account.
90
Response to The Alexandra Hospital NHS from Healthwatch Essex Healthwatch Essex is an independent organisation that works to provide a voice for the people of Essex in helping to shape and improve local health and social care. We believe that health and social care organisations should use people’s lived experience to improve services. Understanding what it is like for the patient, the service user and the carer to access services should be at the heart of transforming the NHS and social care as it meets the challenges ahead of Weit.
y It was good to see that maternity and urgent care was a primary focus during the unplanned CQC inspection. The overall rating by service table shows lots of room for improvement in maternity and urgent and emergency services y The improvements made since the previous CQC inspection are positive to see, including the improvements in the medical rota following the cohort of doctors starting in the summer of 2021 y Although a national challenge, it is concerning to see that the 18-week referral to treatment (RTT) standard has continued to be impacted upon by the restricted capacity to see and treat patients over the year and is still requiring improvement y It is great to see that the trust has systems and processes in place now to learn from incidents complaints and safeguarding alerts to drive improvements y As a local Healthwatch, it is really heartening to see that, despite the challenges of the pandemic, the trust has continued to engage with staff, patients and their representatives and system partners in an open and transparent manner y Receiving the Queen's Award for Voluntary Service for the Patient Panel is an excellent achievement y The pandemic has been practically challenging for clinical staff, so we were pleased to see that one of the priority areas for the trust is to improve the health and wellbeing of its people, offering a wide range of support so that every member of staff can recover from the effects of working during the pandemic, stay well and feel they can meet the demands of their roles. I look forward to reviewing the staff survey and staff sickness results to see the impact this has made y As an organisation, Healthwatch Essex support all forms of coproduction and patient involvement, which is why we are pleased to see that the trust will continue to ensure that patients are involved in the decision-making about their medications and that they receive the correct medications at the correct time y Moving forward, we look forward to supporting the PAHT 2030 transformation agenda as they make preparations to push ahead with the new hospital engagement when we are given the green light to do so y We look forward to seeing how the health and wellbeing steering group set up in May 2021 develops and continues to support staff. The initiatives, including a menopause policy and support App, and having health and wellbeing champions within
Princess
Trust (PAHT) Quality Account 2021-22

9191 departments across the organisation are a fantastic start Listening to the voice and lived experience of patients, service users, carers, and the wider community, is a vital component of providing good quality care and by working hard to evidence that lived experience, we hope we can continue to support the encouraging work of The Princess Alexandra Hospital NHS Trust.
Samantha Glover Chief executive officer Healthwatch Essex May 2022
Response to The Princess Alexandra Hospital NHS Trust (PAHT) Quality Account 2021-22 from Healthwatch Hertfordshire Thank you for sharing your draft Quality Account with us, which we have read with interest. As we no longer provide a full formal response, we would be pleased if you could include the following statement in the final report: Healthwatch Hertfordshire values the relationship with The Princess Alexandra Hospital NHS Trust and the opportunities to discuss matters that impact on patient experience and quality of care. We would like to commend the Patient Panel at PAHT that gained an ‘outstanding’ from CQC. In particular, for the innovative and tireless work it continues to do in partnership with the trust to ensure patient voices are part of any quality improvement work. Steve Palmer HealthwatchChair Hertfordshire May 2022




On behalf of the Chairman of Hertfordshire Health Scrutiny Committee, Dee Hart: On behalf of the Hertfordshire Health Scrutiny Committee I would like to thank The Princess Alexandra Hospital NHS Trust (PAHT) for the services it continued to deliver during the pandemic and its response in recovery. We are aware of the challenges facing the NHS and will seek to continue working constructively with the trust. Members of the committee have been appreciative of the support PAHT has provided during this challenging period. This has included, for instance regular attendance at committee meetings, providing written updates when requested. The contribution from the trust has meant the committee has maintained its overview of the health system across the integrated care system (ICS). It has enabled our health scrutiny members to hear about the impact on services and how the health system is seeking ways to address on-going needs and additional pressures. Despite the demands of the pandemic and recovery, there has been regular communication between the Health Scrutiny Committee, Scrutiny Officers and PAHT over the last 12 months. PAHT has supported the scrutiny process when approached and the committee look forward to working with the trust in the future. Yours sincerely Dee Hart HertfordshireChairman Health Scrutiny Committee
92 Quality Account 2021/2022


Antenatal – This is the care you receive from health professionals during your pregnancy. Anticoagulation - Medicines that help prevent blood clots.
Clinical Commissioning Group (CCG) - NHS organisations set up by the Health and Social Care Act 2012 to organise the delivery of NHS services in England.
Antimicrobial resistance - The ability of a bacteria to resist the effects of medication (antibiotics) that once could successfully treat the infection.
9393
Chronic obstructive pulmonary disease (COPD) - The name for a collection of lung diseases including chronic bronchitis, emphysema and chronic obstructive airways disease. Clinical audits - A process aimed to improve quality of patient care and outcomes through systematic review of care against explicit criteria and the implementation of change. Clinical coding - The process by which patient diagnosis and treatment is translated into standard, recognised codes that reflect the activity that happens to patients.
Colposcopy and hysteroscopy services - A procedure used to examine the cervix and inside of the womb (uterus).
Cardiology - The branch of medicine that deals with diseases and abnormalities of the heart.
Antimicrobial stewardship - A coordinated intervention designed to improve and measure the appropriate use of antimicrobials by promoting the selection of the optimal antimicrobial drug regimen, dose, duration of therapy, and route of administration.
Asymptomatic – a condition or person who is showing no symptoms. Audiology - The study of hearing and balance. Bacteraemia – An infection of bacteria in the blood. Cardiac arrest – Sudden loss of blood flow from failure of the heart to pump effectively. Cardiac catheter lab – Procedures of placing catheters (small tubes) into the blood stream to access the heart and blood vessels.
Care Quality Commission (CQC) - CQC is an executive non-departmental public body of the Department of Health United Kingdom. Established in 2009, it is the independent regulator of all health and social care services in England. Chemical pathology – A branch of pathology dealing with biochemical basis for disease. Chemotherapy - The treatment of disease by the use of chemical substances, especially the treatment of cancer by cytotoxic and other drugs.
Glossary of terms Allied health practitioners - Healthcare professionals working in dietetics, occupational therapy, physiotherapy, operating department assistants, radiography and speech and language therapy. This is distinct from nursing, medicine, pharmacy and healthcare scientists. Ambulatory care - Medical care provided on an outpatient basis, includes diagnosis, observation, consultation, and treatment.
CQUIN - Commissioning for Quality and
Clostridium difficile (C.difficile)Clostridium difficile, also known as C. difficile, or C. diff, is a type of bacterial infection that can affect the digestive system. Colorectal care - Treatments for patients with symptoms of the gastrointestinal tract including colorectal cancer and inflammatory bowel disease.
Delirium - Is a state of mental confusion that can happen if you become unwell. It is also known as an acute confusion.
Innovation is a system introduced in 2009 to make a proportion of healthcare providers’ income conditional on demonstrating improvements in quality and innovation in specified areas of care.
Genito-urinary - The branch of medicine relating to the genital and urinary organs. Governance - Establishment of policies, and continuous monitoring of their proper implementation, by the members of the governing body of an organisation. Gram negative blood stream infections (GNBSIs) - Type of bacterial infection and a blood stream infection.
94
Endoscopy - A procedure that allows a view the inside of a person's body. ENT clinics – An area where diagnosis and treatment are provided to conditions of the ear, nose and throat.
Dementia champions - A group of staff who have had specific training in dementia care. Their aim is to make other colleagues more understanding of why a patient may be more challenging and encourages them to tailor therapies accordingly.
Escherichia coli (E.coli) bacteraemia - Type of bacterial infection and a blood stream infection. Frailty service – Reviews frail older people using a holistic assessment of physical, mental and social needs.
Gynaecology - The branch of physiology and medicine that deals with the functions and diseases specific to women and girls, especially those affecting the reproductive system. Haematology - The branch of medicine involving the study and treatment of the blood. Healthcare associated infections (HCAI) - Infections that are acquired as a result of healthcare. The burden of healthcare-associated infections has mainly been in hospitals where more serious infections are seen.
Health Overview and Scrutiny Committee – Local authority committees that scrutinise health issues and care in their area. Healthwatch – Obtain the views of people about their health needs and experiences of having care and social services. Hospital Standardised Mortality Ratio (HSMR) - Calculation used to monitor death rates in a trust.
Endocrinology - The branch of physiology and medicine concerned with endocrine glands and hormones.
Dermatology - The branch of medicine concerned with the diagnosis and treatment of skin disorders. Diagnostics - Tools used to help identify disease and illness. Dietetics – A branch of healthcare concerned with the diet and its effects on health, especially with the practical application of a scientific understanding of nutrition.
Friends and Family Test (FFT) - Test aimed at providing a simple headline metric which, when combined with follow-up questions, is a tool to ensure transparency, celebrate success and galvanise improved patient experience. It asks “How likely are you to recommend our services to friends and family if they needed similar care or treatment?” with answers on a scale of extremely likely to extremely unlikely.
Datix - Software used in healthcare to collect patient safety incidents and for reporting adverse events.
Gastroenterology - The branch of medicine which deals with disorders of the stomach and intestines.
Hydrogen Peroxide System – a cleaning system that can cleanse a large area such as a ward.
Medicines optimisation - Is the process of ensuring patients are on the most effective and fewest medications.
Maxillofacial department – An area where diagnosis and treatment is provided to conditions of the mouth, face and adjacent structures. Medical examiner – senior medical doctors who are contracted for a number of sessions a week to undertake medical examiner duties outside of their usual clinical duties. They are trained in the legal and clinical elements of death certification processes.
9595
Methicillin-Resistant Staphylococcus Aureus (MRSA) / Methicillin-Sensitive Staphylococcus Aureus (MSSA) – A specific bacterial infection.
Intravenous – Giving fluids or drugs directly into a vein. Klebsiella bacteremia - Type of bacterial infection and a blood stream infection.
National Reporting and Learning System (NRLS) - A central database of patient safety incident reports. Neonatal (NICU) - New-born children and new-born intensive care unit. Nervecentre – electronic data base where observations are recorded. Neurology - The branch of medicine or biology that deals with the anatomy, functions, and organic disorders of nerves and the nervous system. NHS Digital – the national information and technology partners to the health and social care system.
Morbidity and mortality (M&M)Meetings established to review deaths as part of professional learning. Myocardial infarction - Commonly known as a heart attack. Myocardial ischaemia - When blood flow to your heart is reduced, preventing the heart muscle from receiving enough oxygen.
National Confidential Enquiries (NCEPOD) - National Confidential Enquiry into Patient Outcome and Death.
Norovirus - A type of viral infection that can affect the digestive system. Nosocomial – a disease originating in a hospital. Obstetrics - The branch of medicine that deals with the care of women during pregnancy, childbirth, and the recuperative period following delivery. Oesophago-gastric care – Treating patients with problems of the gullet (oesophagus) and stomach.
NHSE/I - NHS England and Improvement is responsible for overseeing trusts and NHS services, as well as independent providers that provide NHS-funded care.
Laparotomy - A surgical incision into the abdominal cavity, used for diagnosis or in preparation for major surgery.
NICE - The National Institute for Health and Care Excellence provides guidance, which supports healthcare professionals and others to make sure that the care they provide is of the best possible quality and offers the best value for money.
Inflammatory bowel disease – The name for a group of conditions that cause the digestive system to become inflamed.
Maternal and Fetal Assessment UnitOutpatient Antenatal Unit offering planned appointments for assessment of the mother and unborn baby in pregnancy.
Oncology - The study and treatment of
Integrated Care Partnership (ICP) –are alliances of NHS providers that work together to deliver care by agreeing to collaborate rather than compete.
Respiratory medicine – The branch of medicine that deals with the act of breathing. Rheumatology - The study and treatment of arthritis, autoimmune diseases, pain disorders affecting joints, and osteoporosis.
Perioperative medicine - care of patients from the time of contemplation of surgery through the operative period to full recovery. Personal protective equipment (PPE) - will protect the user against health or safety risks at work examples are FFP 2/3 face masks medical grade. Polymerase chain reaction (PCR) testing - a method widely used to look for genetic code of the COVID-19 virus, this involves taking a swab of the throat and nose. The test will confirm if a person with symptoms has the virus currently.
Pathology - The scientific study of the nature of disease and its causes, processes, development and consequences.
Paediatrics - The specialty of medical science concerned with the physical, mental and social health of children from birth to young adulthood.
Patient Advice and Liaison Service (PALS) - Offering confidential advice, support and information on health-related matters. Provides a point of contact for patients, their families and their carers.
96 cancer and tumours.
Radiology - The branch of medicine that deals with the use of radioactive substances used in diagnosis and treatment of disease. Referral to Treatment (RTT) – A constitutional standard that trusts are measured against in which a person’s waiting time starts on the day the hospital receives the referral letter from a GP to the time of first appointment or treatment.
Public Health England - A government body with the role to protect and improve the nation’s health and wellbeing and reduce health inequalities. Rapid Assessment and Treatment (RAT) - A treatment model used in emergency care to provide an early senior assessment and early treatment.
Serious Incidents (SIs) - An unexpected or unplanned event that caused harm or had the potential to cause harm to a
Palliative care - An approach that improves the quality of life of patients and their families facing the problems associated with life-threatening illness, through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems, physical, psychosocial and spiritual.
Patient Panel - A group of volunteers who represent patients, families and carers of The Princess Alexandra Hospital NHS Trust.
Point of Care Testing (POC) - such as SAMBA refers to any test that can be undertaken outside of a laboratory.
SAFER care bundle – practical tool that uses five elements of best practice. Sepsis and septicaemia - Sepsis is a serious blood stream infection. A serious complication is septicaemia, which is when inflammation occurs throughout the body, which can be life-threatening.
Ophthalmology - The study of the structure, functions, and diseases of the eye. Orthopaedic - The branch of medicine that deals with the prevention and correction of injuries or disorders of the skeletal system and associated muscles, joints, and ligaments.
Patient Safety Alerts - Issued by NHS Improvement to rapidly warn the healthcare system of risks. They provide guidance on preventing potential incidents that may lead to harm or death.
SMART – mnemonic for objectives that are Specific, Measurable, Achievable, Realistic and Timely.
Standard Operating Procedures – A set of step-by-step instructions compiled to help workers carry out complex routine work, aimed to achieve efficiency and uniformity of performance.
9797 patient, member of staff, student, visitor or contractor.
Venous thromboembolism (VTE) - A condition where a blood clot forms in a vein, most commonly in a leg where it is known as deep-vein thrombosis (DVT), a blood clot in the lungs is called a pulmonary embolism (PE).
UK Health Security Agency (UKHSA) –responsible for protecting every member of every community from the impact of infectious diseases. Urology - The study of urinary organs in females and the urinary and sex organs in males. Vascular surgery – Specialists that treat people with diseases of the circulation, which can be conditions affecting arteries, veins and where there are blockages to the flow of blood.
Stakeholders - A stakeholder is anyone with an interest in a business. Stakeholders are individuals, groups or organisations that are affected by the activity of the business. They include owners who are interested in how much profit the business makes.
VTE prophylaxis/ thromboprophylaxis - The giving of a medicine or treatment to prevent a VTEof terms.
Standardised Mortality ratio (SMR) and Summary Hospital-level Mortality Indicator (SHMI) - Ratio between the actual number of patients who die following treatment at the trust and the number that would be expected to die, based on average England figures given the characteristics of the patients treated there. Trauma Audit and Research Network (TARN) – An audit where information is collected and analysed for patients who are moderately or severely injured after an injury. Data is submitted by trusts and a comparison can be undertaken.
98 The Princess Alexandra Hospital NHS Trust, Hamstel Road, Harlow, Essex, CM20 1QX 01279 44 44 @NHSHarlowNHSHarlow55@PrincessAlexandraNHSThePrincessAlexandraHospital NHS Trust



