




Panacea Healthcare Solutions is the leader in the continuum of healthcare pricing and revenue integrity. We offer a range of technology and consulting services specializing in areas such as chargemaster, coding, and compliance utilized by 500+ healthcare providers. Our clients include hospitals, health systems, physician practices, ambulatory surgery centers, and ancillary care providers.
Led by a seasoned team of revenue cycle, clinical coding, and financial experts, Panacea’s mission is to support healthcare providers in overcoming the challenges they face in the mid-revenue cycle, ultimately improving the financial health of the organizations they serve.





We are experts in the entire continuum of healthcare pricing.

We provide our software and technologyenabled services to a wide array of providers
We deliver our solutions in whole or in part to create a customized approach to meet our clients’ specific needs
We Help Your Organization Achieve:
• Accurate and complete charges and associated codes
• Strategic and defensible prices associated with each code

• Compliant price transparency and out-ofpocket estimates
suscipiantur vim in, ne postea debitis eleifend ius.
• Integrity of coding and revenue
• Compliance with all federal regulations









Question: Are Consumers and Patients Benefiting from Hospital Price Transparency?
Response: 404 not found
▪ Effective January 1st, 2026
▪ Passed the House on 12/11/23, up next in the Senate
▪ Directionally aligns and codifies the Hospital Price Transparency Rule (e.g., Standard Method and Uniform Method for MRF and CD)
▪ Implications for Providers
o No acceptable substitutes for Consumer Display (e.g., patient estimation system)
o Stricter Enforcement – Up to $10M in fines versus $2M
o Extends same requirements to clinical laboratories, imaging service providers, and ambulatory surgical centers that participate in Medicare
o TiC Rule – payers must produce files in an appropriate size, plain instructions for use, etc.


✓ Mirrors the HPT Requirements
✓ Monitored and enforced by the State
Passed Legislation
✓ Effective Jan 1st. 2025
✓ Expands to freestanding surgery centers, medical, dental, rad, lab, etc. with revenue >$50M

HB 7089
✓ Effective 7/1/2024, yet deferred
✓ Mirrors NSA Requirements (AEOB)
✓ Provider to disclose if cost-sharing > self-pay amount
90% of hospitals have an MRF on their website
65% of hospitals are compliant with the .txt file requirement
60% of hospitals have an MRF passing the CMS Validator
20% of hospitals have an MRF with 1/1/25 data requirements
*Study conducted by Panacea in Q3 of 2024, based on +1,000 randomly selected hospitals across the nation in 15 different states
Will you be ready by Jan 1st, 2025, to implement all the required changes?
a. Yes, we are ready!
b. Yes, but having trouble with estimated allowed amount
c. Possibly, we have a plan in place
d. Not yet implemented and may need assistance
January 1st, 2024 - Hospitals must include a .txt file in the root folder with direct link to their MRF on their public website
• The .txt file must include a standardized set of fields such as;
• the hospital location name that corresponds to the MRF
• the source page URL that hosts the MRF
• a direct link to the MRF (the MRF URL)
• hospital point of contact information
• Additionally, hospitals must include a link in the footer of their website (i.e., homepage) that links to their HPT page
• The link should be labeled ”Price Transparency" and links directly to the webpage that hosts the link to the MRF
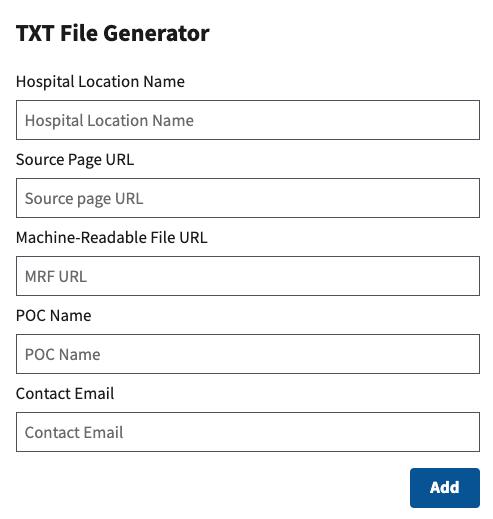
*TXT file instructions and generator tool can be found here: https://cmsgov.github.io/hpt-tool/txt-generator/
1.Generate a TXT file based on the schema or via the TXT File Generator
2.If the MRF contains standard charge information for more than one location, create a separate entry for each of the inpatient locations and standalone emergency hospitals in the TXT file (i.e., repeat the five attributes required in the TXT file with other location names).
3.Name the file “cms-hpt.txt”.
4.Place the TXT file on the root of the domain of the public website your hospital has selected to host its machine-readable file (MRF), without regard to page structure.
Health System w/ Two Locations & Separate Standard Charges
location-name: Example Hospital East
source-page-url: https://example.com/price-transparency
mrf-url: https://example.com/price-transparency/123456789_ExampleHospital-East_standardcharges.csv
contact-name: Jon Snow
contact-email: jsnow@example.com
location-name: Example Hospital West
source-page-url: https://example.com/price-transparency
mrf-url: https://example.com/price-transparency/987654321_ExampleHospital-West_standardcharges.json
contact-name: Jane Doe
contact-email: jdoe@example2.com
Health System w/ Two Locations & Same Standard Charges
location-name: Sample Hospital
source-page-url: https://vendor.com/hospital-price-transparencyfiles/links/samplehospital.aspx
mrf-url: https://vendor.com/hospital-price-transparency-files/links /101010101_Sample_standardcharges.csv
contact-name: MRF Department
contact-email: MRFteam@sample.com
location-name: Sample Standalone Emergency Department
source-page-url: https://vendor.com/hospital-price-transparencyfiles/links/samplehospital.aspx
mrf-url: https://vendor.com/hospital-price-transparency-files/links /101010101_Sample_standardcharges.csv
contact-name: MRF Department
contact-email: MRFteam@sample.com
If your hospital website is www.hospitalname.org, then type in www.hospitalname.org/cms-hpt.txt

Please note: Leveraging the Validator helps ensure adherence to CMS form and manner requirements (45 CFR 180.50(c)(2)), but it does not certify that your MRF fully complies with all HPT requirements at 45 CFR 180.50.
At 45 CFR § 180.20 we defined “estimated allowed amount” as the average dollar amount that the hospital has historically received from a third-party payer for an item or service. Beginning on January 1, 2025, hospitals are required to encode a dollar value for the “estimated allowed amount” data element, when a payer-specific negotiated charge can only be expressed as an algorithm or percentage. This includes: hybrid scenarios where the standard charge dollar is a base rate and there is an algorithm that accounts for additional individualized charges; where the standard charge is a percent that cannot be calculated as a dollar figure; and where the standard charge is an algorithm (88 FR 82100).
In the interest of reducing burden, to determine the best data source for calculating the estimated allowed amount, we declined at the time to be prescriptive, but indicated that using information from the EDI 835 electronic remittance advice (ERA) transaction, the electronic transaction that provides claim payment information, including any adjustments made to the claim, such as denials, reductions, or increases in payment, would appear to meet this requirement as the data in the 835 form is used by hospitals to track and analyze their claims and reimbursement patterns (88 FR 82101). rulemaking.
Variability in Billed Charges for Colonoscopy (N = 900 claims)

▪ Panacea Approach: Analyze 837 claims data to calculate ‘average’ billed charges by DRG or soft-coded CPT, by patient type. Exclude outliers and Medicare claims, as applicable. Apply the Standard Charge Negotiated Percent derived from the payer contract to calculate the Estimated Allowed Amount, when applicable.
▪ Note: Claims and/or Payment data should only be used when payer-specific negotiated charges *cannot* be expressed as an exact dollar figure (e.g., first two-line items). Source of all other standard payer negotiated rates should come from 3rd party health plan payer contracts or fee schedules.

• For 7/1/24, Panacea populated the ‘standard_charge | negotiated algorithm’ with descriptive language, when applicable, when payment may vary due to claims exceeding stop loss / outlier thresholds, lesser-of clauses, multi-procedure discounting, etc.
• For 1/1/25 – Panacea will leverage payment data (i.e., 835’s) to calculate the average payment amount for each applicable line item, at the payer and plan level, where stop loss / outlier provisions, multi-procedure discounting, etc. may apply and populate the Estimated Allowed Amount. Panacea recommends removing denials due to billing or payer issues and separating the analysis for peds versus adults. If insufficient 835s exist for a given health plan due to limited claims experience, then encode 999999999.
Definition:
The unit value that corresponds to the established standard charge for drugs.
The measurement type that corresponds to the established standard charge for drugs.
Naming Convention:
drug_unit_of_measurement
drug_type_of_measurement
Valid Values:
Positive Numbers (unit type)
GR – Gram, ME- Milligram, ML – Milliliter, and UN – Unit (measurement type)
CSV
Instructions:
Enter the unit value, or amount, of the drug for that particular standard charge. If the description is “aspirin 81mg chewable tablet – each” then the drug unit value is “1” and the type of measurement is “UN” since the standard charge is established per tablet.
7/1/24 Requirements
OTHER CARDIOTHORACIC PROCEDURES WITHOUT MCC
Have you leveraged the publicly negotiated rate data for contract modeling and payer negotiations?
a. Yes, we have had some success
b. Yes, used results for contract proposals and modeling
c. Not yet, need support in acquiring and cleansing data
d. No, still not confident about the accuracy of the data
Do you now feel more confident that price transparency data can be used for comparative rate analysis?
a. Yes, feeling better now!
b. Possibly, need to learn more
c. No, still not confident, sorry Panacea!
▪ Upcoming CMS Webinar - Register Now!
• CMS Hospital Price Transparency Machine-Readable File January 1, 2025, Requirements and Tips for Implementation
• https://cms.zoomgov.com/webinar/register/WN_LqZfybX7RAePe8DAPEyx3w#/registration
• Monday, October 21st at 1:00PM – 2:30PM EST
▪ CY2024 OPPS/ASC Final Rule Federal Register Page
• https://www.federalregister.gov/public-inspection/2023-14768/medicare-program-hospital-outpatient-prospectivepayment-and-ambulatory-surgical-center-payment
▪ CMS Resources Page (e.g., FAQs)
• https://www.cms.gov/priorities/key-initiatives/hospital-price-transparency/resources
▪ CMS Validator Tool to Confirm MRF Alignment with CMS Voluntary Sample Format
• https://cmsgov.github.io/hpt-validator-tool/







