147 minute read
NEWS THIS MONTH

from INSIGHT April 2022
by Prime Group

PRIVATE HOSPITALS MUST ‘PICK UP THE SLACK’ AMID OPHTHALMOLOGY WAITLIST BLOW OUT
The Australian Private Hospitals Association (APHA) believes private hospitals should play an essential role in clearing the backlog of public elective surgeries. It comes as fresh data shows wait times for ophthalmic procedures increased by 6.5 weeks in 2020-21 compared to pre-pandemic levels and have more than doubled to 172 days for cataract surgery.
The comments from the country’s peak industry body for the private hospital and day surgery sector follows the release of Australian Institute of Health and Welfare (AIHW) public elective surgery data on 25 January.
The overall trend saw more patients being treated from public hospital wait lists in 2020–21 compared to the year prior as hospitals worked to clear a backlog left by COVID-19 suspensions introduced in March 2020. However, the data does not account for additional widespread restrictions after June 30 2021, meaning waiting times for surgery are likely even longer now.
The average waiting time – or “days waited at the 50th percentile” – was 118 days for all ophthalmology procedures. This was the highest wait time among all medical specialties in 2020-21 and is significantly higher than 82 days the previous year for ophthalmology and an average of 73 days pre-pandemic.
NSW patients had the longest ophthalmology wait time, with 50% admitted within 269 days, Victoria 64 days, Queensland 77, Western Australia 68, South Australia 112, Tasmania 142, ACT 83 and Northern Territory 94.
A further breakdown of the data showed wait times for cataract surgery were now 172 days on average across Australia. This is up from 98 in 2019-20 and more than double 84 days pre-pandemic 2018-19.
After general surgery (154,677 surgeries), urological surgery (114,820) and orthopaedic surgery (108,361), ophthalmology had the fourth highest number of admissions at 100,653 for 2020-21. This was 17.8% more than 2019-20 – which featured the March 2020 surgery shutdown – and on par with pre pandemic 2018-19.
Although overall median wait time for all elective surgery increased by a week, from 41 days pre-COVID (2018-19) to 48 days in 2020-21, APHA CEO Mr Michael Roff said this represented “a very big increase in waiting times”.
“When you look at surgeries by category, the increases in median wait time are even more significant. Those waiting for head and neck surgery now wait 112 days, up from 84 pre-COVID, while ophthalmology patients wait 118 days rather than 73, an increase of six and a half weeks,” he said.
“This data illustrates the essential role private hospitals will need to play in helping Australians get the vital surgery they need. Just as private hospitals have helped the public system with the pandemic response, they will be essential to clearing the surgical backlog post-pandemic.
“Without private hospitals picking up the slack, Australians will be waiting a great deal longer to have their surgery – often important for quality of life, like cataract surgery to correct impaired vision or joint replacements to remove pain and improve mobility.”
Roff said restrictions on necessary elective surgery should not last one day longer than they need to.
“With signs the Omicron wave is plateauing in several states, health departments need to consult with private hospitals about easing restrictions in a safe way, so hospitals are ready to increase surgical capacity to provide much-needed treatment to those Australians who have had surgery deferred,” he said.
“When restrictions ease, public hospitals should not be taking in a single privately insured patient until all of their public patients have been treated. It is time to stop them treating public patients as second-class citizens.
“It would be morally reprehensible if public hospitals were to bring in a large number of privately insured patients to take advantage of the even longer wait times Australians have had to deal with, while those who need the public system languish on ever lengthening waiting lists.” n
There were 73,071 cataracts performed in 2020-21.
NOTE: Turn to page 62 for Dr Anton van Heerden’s Soapbox article on elective surgery shutdowns.
IN BRIEF
n ALCON FINANCIALS
Alcon reported its financial results for Q4 and full year ended December 31, 2021. For Q4 2021, worldwide sales were $2.1 billion (AU$2.8 b), an increase of 13% on a constant currency basis, while the company’s full year revenue was $8.2 billion (AU$11 b). Q4 surgical net sales were $1.3 billion (AU$1.7 b), increasing 14%, compared to Q4 2020, with adoption of advanced intraocular lenses, led by the launch of Vivity, driving growth. Vision Care net sales of $900 million (AU$1.2 b) increased 12% on a constant currency basis, compared Q4 2020. Contact lens sales benefited from growth in silicone hydrogel contact lenses, including Precision1, Precision1 for Astigmatism and Dailies Total1. Growth in ocular health was led by Systane artificial tear products, and the addition of Simbrinza glaucoma eye drops.
n THÉLIOS CEO
Luxury eyewear maker Thélios has named Mr Alessandro Zanardo as its new CEO. The company was previously a joint venture between French luxury goods company LVMH and Marcolin, but LVMH took full control of the entity in December 2021. Zanardo started his career at Ferrari in 2002. He then joined Roland Berger Strategy Consultants in 2007. Between 2010 and 2021, he held a series of positions at Luxottica Group, such as business and development director in Russia, country manager in South Africa and, most recently, general manager in Brazil.
n MYOPIA LAUNCH
Johnson & Johnson Vision has announced the launch of ACUVUE Abiliti in Singapore for myopia management. Singapore is the first Asia Pacific market to launch the Abiliti overnight therapeutic lenses – an orthokeratology lens with a CE mark for myopia control. Launch in the rest of the region will soon follow. Abiliti overnight lenses have been prescribed for controlling myopia progression in children as young as six years old. A recent J&J survey found a proportion of Singaporean parents reported that at least 75.9% of them had children who were diagnosed with myopia before they were nine years old. Yet, many were unaware of the implications myopia can have on their children’s long-term eye health and abilities.
GLAUCOMA SUSPECTS: MORE FREQUENT REVIEWS COST AUSTRALIAN HEALTH SYSTEM LESS
A new paper by Australian and US investigators examining glaucoma suspects has found more frequent six-monthly reviews actually cost the health system less and result in a higher number of diagnoses compared with annual reviews.
Additionally, it revealed Australian optometrists were less costly for reviewing these patients, at approximately $400 per diagnosis, compared with ophthalmologists at $600 per diagnosis, if only Australian Medicare was charged.
Recently published in Translational Vision Science & Technology, Centre for Eye Health (CFEH) and UNSW School of Optometry and Vision Science academics Dr Jack Phu, Professor Michael Kalloniatis and colleagues describe their findings as “seemingly counterintuitive”, but say they ultimately make sense from a financial and clinical perspective.
In the paper, the researchers stated that a common “clinical conundrum” for glaucoma suspect patients – in the ‘suspect’ part of their journey – is the optimal frequency of review.
While some patients are eventually diagnosed with glaucoma, many more are continually monitored as glaucoma suspects, and thus, constitute a large part of clinical service and clinical cost. This motivated the researchers to compare the cost-effectiveness of differing review periods.
Dr Jack Phu (left) and Professor Michael Kalloniatis from the Centre for Eye Health.
In the retrospective, cross-sectional review of patient records from the CFEH clinic in Sydney, open angle glaucoma suspects were allocated as “high risk” or “non high risk”, and thus reviewed six-monthly or 12 monthly, respectively. Risk allocation was based on two criteria: a less stringent criterion requiring the patient to have only one risk factor for glaucoma was compared against a more stringent criterion which required at least three risk factors. Thus, using a less stringent criterion was more likely to review in more “high risk” allocations compared to a more stringent criterion.
“Ultimately, we found that if clinics review glaucoma suspect patients with at least one risk factor on a six-monthly basis, the overall number of diagnoses is more than if 12-monthly reviews were used,” Phu said.
“We also found it surprising more frequent reviews appeared to lead to lower
“LESS FREQUENT REVIEWS MAY INTRODUCE MORE UNCERTAINTY, REQUIRING MORE REVIEWS LATER IN THE CLINICAL COURSE”
STUDY AUTHORS cost per diagnosis. We initially thought more frequent visits would equal more costs, but it also makes sense clinically, as more frequent visits are probably more likely to lead to greater clinical confidence in the diagnosis.”
In the paper, the researchers stated that the relative lower costs related to more frequent visits, based on their model, was due to the sooner exit of patients from the glaucoma suspect pathway, shifting the cost away from this specific pathway.
They wrote: “Although seemingly counterintuitive, the less stringent/more frequent criterion resulted in fewer overall clinical visits, as patient reviews quickly diminished over time due to the patients reaching the exit points sooner. In essence, more frequent reviews (and therefore testing) may potentially improve the initial clinical confidence of stability or provide means for a more conclusive diagnosis."
“In contrast, less frequent reviews may introduce more uncertainty, requiring more reviews later in the clinical course before a more conclusive diagnosis can be made.”
In terms of how community-based optometrists could interpret the findings for real world use, Phu said it demonstrated glaucoma suspect patients with risk factors can be reviewed in six-monthly intervals in the initial monitoring period, especially within the first 2.5 years. ■
from RMIT, a Master of Business Administration (MBA) from Monash University, and as a Graduate of the Australian Institute of Company Directors (GAICD), Frances is qualified and well equipped to understand the clinical and business pressures on optometric practice.”
Mirabelli is said to be looking forward to a diverse range of new challenges in the CEO role, and is particularly keen to learn from ProVision optometrists about the profession and the optical industry.
Under Johnston’s leadership, the ProVision network expanded from 366 practices when he started to 467 just prior to the pandemic; a net gain of more than 100 practices. Purchases through preferred supplier partners had also grown from $46 million to $83 million last year. ■
PROVISION ANNOUNCES NEW CHIEF EXECUTIVE APPOINTMENT
The ProVision Board has appointed Ms Frances Mirabelli as its next CEO, who commenced on 14 February. She takes over from Mr Steven Johnston who left the organisation on 27 January after 10 years.
Mirabelli is described as an experienced, results-focused executive with extensive knowledge of not-for-profit and membership associations.
According to ProVision chair Mr Ian Bluntish, she is comfortable at the forefront of healthcare advocacy and well-versed in responding to aligned social issues. She is also a leader of people, companies and communities and has a demonstrated record in strategic leadership, risk governance, policy development, change, operational and performance management, and achieving business and financial KPIs.
Prior to this role, Mirabelli held several senior roles in aged care, an industry with numerous multi-dimensional challenges delivering sustainable quality care against changing community expectations. She also has experience in health practitioner membership-based organisations – providing a foundation for the challenges and opportunities faced by ProVision.
“The board believes that over the last 10 years, ProVision has developed a highly experienced and effective leadership team skilled in the functional areas necessary to support our members, and Frances will bring new skills and understanding to this team as the chief executive,” Bluntish said.
“Further with a Bachelor of Applied Science in Medical Laboratory Science
Frances Mirabelli, ProVision.
‘OPTOMETRY SCRIPT’ FUGITIVE GRAHAM POTTER ARRESTED IN QUEENSLAND AFTER 12-YEAR MANHUNT
An Australian fugitive wanted so desperately by police they released his prescription and a $100,000 reward in the hope an optometrist would lead to his capture has been arrested in Far North Queensland after 12 years on the run.
Graham Gene Potter – dubbed as one of Australia’s most-wanted men – was last seen in Tully, Queensland, in 2010 when he ordered and paid for a pair of glasses that he never collected.
Police launched a manhunt after he failed to appear on bail at Melbourne Magistrates Court on 1 February 2010 over charges of conspiracy to murder two people.
According to The Age, at the time he went into hiding, Potter was accused of being hired to kill a man at Melbourne underworld figure Mick Gatto’s son’s wedding in 2008.
Last year, Victorian police said an Australian eyecare professional could hold the key to locating Potter – believed to be myopic – and released his script which they asked optometrists to check against their databases for a match, or near match.
A $100,000 reward was also floated for information leading to his capture.
Queensland Police released a video of Potter’s arrest on 21 February 2022 which took place in Ravenshoe in Far North Queensland.
Acting on a tip from the public, Tablelands detectives, uniformed police and the Cairns Dog Squad attended an Ascham Street residence where the 64-year-old was taken into custody.
Police had previous information regarding sightings of Potter in the Tablelands area, where it is alleged he evaded police in Tully in 2010.
Multiple law enforcement bodies
Graham Gene Potter and his optical prescription from 2010. throughout Australia have been attempting to locate him for the last 12 years.
Victorian Police Acting Assistant Commissioner Mr Mick Frewen said Potter was also wanted for allegedly trafficking a commercial quantity of drugs, namely 25,000 ecstasy pills.
“It puts to end a long and protracted hunt for a very high-end fugitive that is wanted for very serious criminal charges,” he said.
“From Victorian police’s perspective, it’s an outstanding result. While the trail has gone cold, the resolve to locate Graham right across Australia has not wavered, in collaboration with Queensland police, we have been able to locate him.”
Detectives from Victoria travelled to the Far North, to seek Potter’s extradition. As he was ushered through Cairns airport he told reporters he had been “living life” and “avoiding being killed” during the past 12 years.
He appeared in Melbourne Magistrates Court where his lawyer did not apply for bail, but did request his suitability for being placed into protective custody be assessed. He will reappear on 18 May. ■
FDA BREAKTHROUGH FOR AUSTRALIAN-MADE BIONIC EYE
Australia’s world-first Bionic Eye System has been granted designation as a Breakthrough Device by the Food and Drug Administration (FDA) in the US.
Developed by Bionic Vision Technologies (BVT), the Centre for Eye Research Australia, the Bionics Institute, CSIRO’s Data61 and the University of Melbourne, the groundbreaking technology aims to give functional vision to millions of people who have lost their sight due to retinitis pigmentosa (RP).
The late-stage RP market is estimated to be worth more than US$3.5 billion (AU$4.9 b).
The FDA’s Breakthrough Devices Program speeds up the review and assessment of medical devices which provide “more effective treatment” than any alternatives currently available.
“This is a significant achievement and a key milestone for BVT,” CEO Dr Ash Attia said.
“The life-changing bionic eye can be brought more quickly to the people who need it the most.”
According to BVT, the technology features tiny cameras that are embedded within a pair of glasses that send electrical signals to a wearable processor. The processor transmits to an implant behind the retina, delivering visual information to the blind person, giving them functional vision.
A recently published peer-reviewed twoyear study focused on four Australians using the bionic eye. They reported being able to recognise their loved ones in a cafe, identify vacant chairs, arrange their washing, and identify surroundings such as traffic lights,
Dr Ash Attia, Bionic Vision Technologies. cars, people, trees and street poles.
Meanwhile, the University of Melbourne has been awarded a $1.14m grant from the National Health and Medical Research Council (NHMRC) to work with BVT on the next generation bionic eye.
The funds will be used to develop and test a retinal implant with closed loop multichannel stimulation to further improve what patients can see and do.
In 2023, BVT will conduct a global pivotal study as the next step towards the commercialisation of its device.
“RP is a debilitating disease, and the impacts are just devastating,” Attia said.
“We are all proud to be part of BVT and our entire team is excited by leading the world in a project to restore functional vision to those who have lost their precious sight.” ■
NEW PRACTICE ACQUISITIONS AS EYEQ UNVEILS 'STRATEGIC CHANGE'
Two Sydney optometry practices – along with three former EyeQ franchise practices – have been acquired by EyeQ Optometrists.
Late last year, EyeQ announced “changes Ray Fortescue, EyeQ Optometrists. to its strategic direction” with the cessation of its Franchise Associate model, which was originally designed for clinically-focused optometrists and dispensers wanting to continue owning their business, without the back-office struggle.
Three existing EyeQ Franchise practices have now been acquired by EyeQ, with the remaining franchises exiting the group by the end of February. Of these, all except one have elected to become members of Optical Growth Partners, described as a buying group and managed services offering for all independent optometry practices, regardless of their ownership model.
Explaining the decision, EyeQ Optometrists executive chairman Mr Ray Fortescue said it had allowed EyeQ to focus on its core business and concentrate on growth of the group through acquisition.
“Independent optometry practices that share our values and are similar operationally and professionally to the existing EyeQ network are being assessed for suitability,” he said.
The first two practices acquired by EyeQ under the new model were owned by Mr Peter Kazacos and located in Maroubra and Eastgardens, in the eastern Sydney.
The practices are described as wellestablished and respected in their local communities. Kazacos and staff from both practices will transition to being EyeQ employees as part of the ownership transfer.
“There will be minimal change in the practices in the first few months as the EyeQ operations team undertakes training and an operational review,” EyeQ stated.
“The practices have been operating for over 30 years and just like the current EyeQ network, are experiencing a busy time particularly as they are inundated with eyecare appointments that were delayed during COVID restrictions in 2021.” ■
ELLEX/QUANTEL MEDICAL UNVEILS NEW IPL SYSTEM
The C.STIM IPL system. Ellex/Quantel Medical has presented a new intense pulsed light (IPL) system for dry eye disease to the Australian market.
On 9 February the company, which is part of Lumibird Medical group, announced the launch of the C.STIM IPL system. It is being described as the new generation of IPL designed by Quantel Medical to treat dry eye disease.
“Drawing on Quantel Medical’s years of experience in intense pulsed light in dermatology, we have now developed a new IPL device exclusively for use in ophthalmology, designed and manufactured by the Lumibird Medical group,” Mr Jean-Marc Gendre, CEO of Lumibird Medical, stated.
“We are convinced that this new premium product of our dry eye range will bring an innovative therapeutic solution to ophthalmologists confronted with the daily challenge of dry eye treatment.”
With dry eye affecting more than 700 million people globally, the company stated it is one of the most common pathologies in ophthalmic visits. Dry eye treatment is also a key consideration in many specialties such as glaucoma, refractive and cataract surgeries, and contact lenses, among others.
The Quantel Medical system has been designed in-house, and aims to treat the root causes of dry eye, including meibomian gland dysfunction, inflammation and demodex.
“Thanks to the unique Stim-ULI technology (Uniform Light Intensity), C.STIM offers the best combination of clinical efficacy and patient comfort,” Ms Delphine Southon, Quantel Medical’s dry eye product manager, said.
C.STIM has been designed to combine cutting-edge technology with a sleek, robust and ergonomic design. The device integrates technological features to provide efficacy, safety, ergonomics and to offer a “plug and play” product that is easily delegable, Quantel Medical stated.
Delegates attending The 52nd RANZCO Virtual Meeting (26 February – 1 March 2022), first viewed the C.STIM IPL System on the Ellex/Quantel Medical - Lumibird Medical virtual booth. ■
SUNGLASS COLLECTIVE CLAIMS TOP CUSTOMER SERVICE AWARD
Melbourne-based distributor Sunglass Collective has been lauded for its outstanding customer service, winning the 2021 Australian Achiever Award in the Optical Services and Supplies business category.
Established in 2020 by siblings Mark and Lisa Wymond, Sunglass Collective is an Australian optical wholesale business, providing a range of quality and affordable sunglass eyewear to businesses throughout Australia and New Zealand.
Ms Lisa Wymond said the company was thrilled to receive the award.
“We take pride in providing excellent product and customer service. We are absolutely delighted that our lovely customers have recognised us in this way,” she said.
The Wymonds also own eyewear businesses Eyes Right Optical and Modstyle.
Modstyle was crowned national winner

Lisa and Mark Wymond (from left) with head of sales Paul Harrison, Sunglass Collective.
in customer service in the Optical Services and Supplies business category in the 2020 Australian Achiever Awards.
Now in its 24th year, the Australian Achiever Awards are an independent award system based on assessment ratings from a business’s own customers
Sunglass Collective achieved a 98% overall score for customer service and relations, topping all other Optical Services and Supplies business applicants to become the national winner. ■
$300K GRANT FOR AUSTRALIAN FIRM TO COMMERCIALISE TEST FOR ASSESSING GLAUCOMA RISK
A pioneering solution for assessing glaucoma risk in clinical settings is closer to commercialisation with the support of a $304,000 state government seed grant.
South Australian company Seonix Bio is advancing the new polygenic risk score (PRS) test developed by a world-leading research team comprising experts from Flinders University, the QIMR Berghofer Medical Research Institute, the SA Local Health Network within SA Health, and University of Tasmania.
Flinders University ophthalmologist Professor Jamie Craig, co-author of several scientific articles outlining the research results, including in international journal Nature Genetics, said the PRS is the first test able to estimate glaucoma risk sufficiently accurately for clinical use.
“Our world-leading research represents a step change in the clinical assessment of glaucoma risk. A patient with a high risk (top decile) PRS is 15 times more likely to develop glaucoma than a patient at low risk (bottom decile),” Craig, who continues to work on the project with colleague Associate Professor Owen Siggs and others, said.
“Moreover, a glaucoma patient with a high risk PRS is significantly more likely to develop severe vision loss. Optometrists and ophthalmologists have been lacking tools to assess glaucoma risk, and our PRS

Using blood or saliva, the PRS test can be used to quantify a patient’s genetic risk of glaucoma.
has a significant role to play.”
The Government of SA Seed-Start grant will enable Seonix Bio to attain National Association of Testing Authorities (NATA) accreditation and deploy the PRS in clinics.
According to Flinders University, detecting early-stage glaucoma is challenging using current technology, as is predicting which glaucoma patients will progress to severe vision loss. Some patients whose sight could have been saved are treated too late, while other patients who will never develop severe glaucoma are unnecessarily investigated, monitored and treated.
It is believed the Seonix Bio PRS test will enable health professionals to identify individuals at greatest risk of glaucoma, such that they can be prioritised in
“OPTOMETRISTS AND OPHTHALMOLOGISTS HAVE BEEN LACKING TOOLS TO ASSESS GLAUCOMA RISK, AND OUR PRS HAS A SIGNIFICANT ROLE TO PLAY”
JAMIE CRAIG, FLINDERS UNIVERSITY ophthalmology waiting lists and receive informed clinical care sooner.
Using a blood or saliva sample taken from a patient, the PRS test can be used to assess thousands of different genetic locations, known as single nucleotide polymorphisms, to quantify a patient’s genetic risk of glaucoma.
Seonix Bio CEO Mr Nick Haan said the PRS has the potential to improve management and treatment of glaucoma patients and those at risk of glaucoma, while reducing health system costs.
“This Seed-Start grant will crucially allow us to start offering the PRS in the clinic so that clinicians and their patients can better understand glaucoma risk,” he said.
SA Minister for Innovation and Skills Mr David Pisoni said the government was pleased to support the clinical rollout of world-leading research through its SeedStart program.
“The Marshall Government is committed to supporting the growth of local early-stage ventures, particularly those like Seonix Bio with a strong foundation in research and with the potential to solve pressing health challenges,” Pisoni said.
“Seonix Bio’s technology has the potential to improve patient care while increasing the number of high-value technology jobs for South Australians.” ■
HOPE FOR TACTILE RATs FOR VISION IMPAIRED IN FUTURE
Vision 2020 Australia is working closely with its members to inform the Federal Government that Rapid Antigen Tests (RATs) are inaccessible to people who are blind or vision impaired and is proposing potential solutions.
“These tests are inaccessible to people who are blind or have vision loss, because the test results are presented visually, the processes are often complex, and the instructions are only provided in print,” the organisation said.
Vision Australia has also separately called on the government to implement further measures to ensure the vision impaired community can get access to results in a timely manner, ABC News reported.
Vision 2020 Australia acknowledged federal and state governments have this year been transitioning toward RATs to screen for COVID-19, in order to minimise pressure on PCR testing sights.
“We appreciate steps already taken, such as the provision of free tests to holders of concession cards, and the recently introduced capacity for NDIS participants to purchase tests using their plan funding,” Vision 2020 said.
In terms of potential solutions, the organisation said services such as Aira and Be My Eyes – apps that connect blind and low-vision people with sighted people who can visually interpret the surroundings – may be helpful for some.
“Both offer free assistance in completing Rapid Antigen Tests. However, these services rely on smartphones, internet, and technical literacy, so are not a solution for
RAT results are presented visually. all people,” Vision 2020 said.
Aira is offering 30 minutes free COVID-19related assistance, including reading out RAT instructions and results.
In the interim, Vision 2020 Australia is calling for increased national access to PCR tests at home, similar to the 'Call-to-test' system currently available in Victoria, as well as a mailout system to provide free RATs for people with disabilities, including vision loss.
Longer term, Vision 2020 believes the solution is innovation.
“The Royal National Institute of Blind People [in the UK] recently released a prototype pregnancy test which delivers results in tactile rather than visual form. This proves it is possible to design accessible Rapid Antigen Tests, and we hope to see these widely available in the future.” ■
VISION SECTOR JOINS ‘ASSISTIVE TECHNOLOGY FOR ALL’ CAMPAIGN
Vision 2020 Australia and Vision Australia are among 60 organisations to sign a joint statement calling on the Federal Government to establish equal access to assistive technology.
The organisations, which represent and support millions of Australians with disability plus their families and carers, believe a harmonised and nationally consistent program is needed, in response to the Royal Commission into Aged Care Quality and Safety.
The commission states that by 1 July 2024, every person receiving aged care who is living with disability, regardless of when acquired, should receive through the aged care program daily living supports and outcomes (including assistive technologies, aids and equipment) equivalent to those that would be available under the National Disability Insurance Scheme (NDIS) to a person under the age of 65 years with the same or substantially similar conditions.
“We have joined forces because we believe that urgent change is needed to ensure people with disability who are excluded from the NDIS can access the assistive technology they need,” their joint statement released in January said.
“While NDIS participants are eligible to receive fully funded assistive technology, people with disability who are excluded from the scheme continue to fall through the cracks. They are frequently forced to wait more than 12 months to access funding for assistive technology, part or fully fund it themselves or simply go without.”
The joint statement signatories have also highlighted other problems with the current system. ■

CANBERRA NAMED BEST IN THE WORLD FOR EYE HEALTH
Canberra is the best city in the world for eye health, partly owing to low levels of air, noise and light pollution, according to a new study.
Feel Good Contacts, a London-based contact lenses supplier, analysed 100 capital cities in the world to discover which cities are the best and worst for eyesight.
The data looked at several factors including noise, light and air pollution, the prevalence of vision loss in each city – which was taken from the International Agency for the Prevention of Blindness (IAPB) – and each city's national health care index scores to indicate which are the healthiest and most at-risk for maintaining good eye health.
Canberra is the best city for eyesight according to the study, with an overall eye health score of 9.47 out of 10.
The Australian capital boasts some of the lowest levels of air, noise and light pollution, meaning eyes are less irritated and benefit from more restorative sleep.
New Zealand capital, Wellington, reported the lowest levels of air pollution in the study, with a score of 4.24 out of 100. This very low rating makes it a suitable place for healthy eyesight, as well as helping those with respiratory conditions such as asthma.
Both The Netherlands and Canada reported the lowest prevalence of vision loss out of 100 capital cities, with Amsterdam and Ottawa reporting only 3.4% of the populations suffering from vision loss.
The worst city in the world for eyesight is Dhaka in Bangladesh, with the capital scoring only 2.92 out of 10 for overall eye health.
The Mongolian capital Ulaanbaatar has the highest levels of pollution (93.14 out of 100), the Peruvian capital Lima has the highest levels of noise and light pollution (73.45 out of 100), and Nepal, capital of Kathmandu, has the highest prevalence of vision loss at 27.2%. ■

Canberra scored an overall eye health score of 9.47 out of 10.
Ocuzo is approved for ocular bacterial infections.
AFT LAUNCHES PRESERVATIVE-FREE ANTIBACTERIAL EYE DROP
AFT Pharmaceuticals has opened a new front in its eye drop portfolio, with the introduction of a preservative-free product called Ocuzo for bacterial eye infections.
The antibiotic eye drop – with the active ingredient chloramphenicol 5mg/mL – is available in a 10mL multidose bottle and is a Pharmacist Only Medicine (S3) therapy.
It is approved for the treatment of ocular bacterial infections caused by organisms susceptible to chloramphenicol.
AFT – whose entire ophthalmic portfolio comprises preservativefree products – stated there is a comparative product already available, but it’s not preservative-free, indicating a significant unmet need for patients.
It said preserving agents can have negative effects, including changes to the composition of the tear film, allergies and ultimately worsening symptoms.
“Infected eyes need relief, so minimise the risk of further irritation by recommending a treatment that is preservative-free,” the company stated.
“Ocuzo may be a better choice for patients who have pre-existing ocular surface conditions, to minimise the potential risk of irritation from preservatives.”
The Ocuzo bottle design also includes a one-way valve and a silicone plug which protect the product from microbial contamination. ■
COMBINATION THERAPY DEMONSTRATES POTENTIAL TO TREAT AMD SUBTYPE
Data from patients with a subtype of AMD enrolled in Opthea’s Phase 2b clinical trial of OPT302 in combination with ranibizumab Dr Megan Baldwin, (Lucentis), compared Opthea. to ranibizumab alone, have been presented virtually at a conference in Miami.
Professor Gemmy Cheung, head and senior consultant, Medical Retina Department, Singapore National Eye Center, Singapore Eye Research Institute, presented the data at Bascom Palmer Eye Institute’s 19th annual Angiogenesis, Exudation, and Degeneration 2022 Conference.
The data demonstrated +6.7 letters comparative superiority of 2 mg OPT302 combination therapy in patients with Polypoidal Choroidal Vasculopathy (PCV) – a subtype of AMD prevalent among Asian populations with high unmet medical need.
Opthea CEO Dr Megan Baldwin said the company is proud to share the findings which build on its previous work to demonstrate the far-reaching potential of OPT-302.
The Melbourne-based clinical stage biopharmaceutical company is developing novel therapies to treat highly prevalent and progressive retinal diseases, with a goal of building out a substantial presence in the United States.
“Polypoidal Choroidal Vasculopathy (PCV) is a subtype of AMD that is particularly prevalent among Asian populations and demonstrates variable response to anti VEGF-A therapy,” Baldwin said.
“As one of the most common forms of wet AMD globally, we are excited by the results in PCV patients that further demonstrate the potential of OPT-302 to be a truly differentiated treatment option that, when used in combination, may offer patients improved vision outcomes over standard of care anti-VEGF-A monotherapy.”
Additional data on PCV lesions will be obtained from Opthea’s ongoing Phase 3 ShORe and COAST trials, which are also expected to enrol a number of treatment naive patients with PCV. n
NOVA EYE TOUTS NEW ITRACK TECH IN LATEST FINANCIALS
Despite modest sales growth during in the first half of the current financial year, ASX-listed Nova Eye Medical believes it’s poised for stronger returns from its glaucoma portfolio with a revamped canaloplasty device making the technology more accessible to a broader base of ophthalmologists.
On 17 February, the company released its half-year financial results for the six months ended 31 December 2021.
Glaucoma surgical devices – comprising its iTrack minimally invasive glaucoma surgery (MIGS) system and Molteno3 glaucoma drainage device platform – accounted for almost all sales revenue, $6.54 million.
This represented a 1.6% increase in glaucoma surgical device revenue in constant currency terms, compared with the prior comparative period (pcp).
Despite what it described as “modest sales growth”, Nova Eye stated it was confident progress on its next generation canaloplasty device, iTrack Advance, including the commencement of pre-launch activities in Europe, provided a stronger outlook in terms of sales.
The new iTrack Advance leverages the proprietary features of the original iTrack device but is said to incorporate a new

The iTrack Advance has a new handheld injector design.
handheld injector design, which improves the overall surgical efficiency. The company hopes this improved ease of use will drive procedural adoption by a new, larger demographic of surgeons.
“Following its successful introduction into key territories in Europe over the coming months, a major priority for the business in 2022 will be the US market launch of the iTrack Advance,” Mr Tom Spurling, managing director of Nova Eye Medical, said.
“This device takes the established effectiveness, accuracy and reliability of the original iTrack and combines it with an ergonomic, easy-to-use handheld injector that’s optimised for all ophthalmic surgery and specialist settings. As a result of its improved ease of use, we expect uptake by comprehensive surgeons to be strong. This will facilitate greater patient access to canaloplasty during the earlier stages of the disease process.” n
SAFILO GROUP INCREASES STAKE IN PRIVÉ REVAUX EYEWEAR COMPANY
Italian eyewear company Safilo Group’s controlling stake in high-end fashion label Privé Revaux has increased from 64.2% to 81.9% following the resignation of CEO and board member Mr David Schottenstein.
Schottenstein, who founded Privé Revaux, resigned from the company in January.
According to a Safilo, Privé Revaux was established to disrupt the eyewear with premium, quality eyewear products, co-branded through celebrity collaborations.
Safilo acquired a majority stake in Privé Revaux in 2020.
The equity interest held by Schottenstein has been transferred to Safilo in accordance with the original contractual terms of the acquisition.
Following Schottenstein’s resignation, Privé Revaux has promoted Mr George Schmidt to the new role of general manager. Schmidt has been president of the brand since November 2021.
In addition, Maureen Cavanaugh has been promoted to chief operating officer. Cavanagh joined Privé Revaux in April 2021 as senior vice president of global sales. n

Safilo’s stake in the eyewear brand has increased significantly.
REPORT REVEALS OPHTHALMOLOGISTS ARE LESS DEPRESSED THAN MEDICAL PEERS
Ophthalmologists report lower rates of clinical depression and burnout than their peers in other specialities, according to the 'Medscape Ophthalmologist Lifestyle, Happiness, and Burnout Report 2022'.
The report was compiled by online clinician website Medscape from an online survey in 2021 that included more than 13,000 physicians from 29 specialties, of which 2% of respondents were ophthalmologists.
One in four ophthalmologists (40%) said they were burnt-out, less than in the general physician pool (47%).
More than half of female ophthalmologists (52%) reported being burnt-out, compared to 35% of their male peers. The volume of bureaucratic tasks (57%) and government regulations (43%) were the top contributors to burnout, according to respondents.
Insufficient pay (36%), lack of control in life (32%), and lack of respect from colleagues (27%) were also contributing factors. More than half of ophthalmologists (56%) reported feeling more burnt-out now than during the initial phases of the COVID-19 pandemic.
Reducing work hours, making workflow or staff changes to ease workload, and participating in meditation or other stress-reduction techniques were the most common techniques used by respondents to alleviate burnout.
According to the survey, ophthalmologists also sold their practice or put their practice up for sale at five times the rate of physicians across all specialties (16% versus 3%).
One in 10 ophthalmologists reported being clinically depressed, less than half of the proportion in the general physician pool (24%). More than half of ophthalmologists (54%) said depression did not affect interactions with patients, while more than a quarter (27%) said
One in 10 ophthalmologists reported being clinically depressed. they became easily exasperated with patients.
Female ophthalmologists reported feeling conflicted about balancing work and parenthood at more than twice the rate of their male peers (44% versus 17%).
The percentage of ophthalmologists who said they were currently ‘very happy’ or ‘somewhat happy’ outside of work (65%) was slightly higher than for physicians across all specialties (59%
Ophthalmologists ranked sixth among specialists regarding marital happiness, at 89%.
Ophthalmologists participated in non–work-related hobbies, exercised, and spent time with family and friends to promote their well-being. Getting enough sleep and eating healthy were also common strategies, while only 5% of respondents said therapy helped maintain their happiness and mental health outside of work. n
B.I.G. NORM™

SEE BETTER WITH THE POWER OF AI
NEW EVIDENCE DISPELS COMMON MYTHS ABOUT FITTING SOFT CONTACT LENSES
A new peer-reviewed paper published in an Australian journal examining the top 10 myths about fitting soft contact lenses offers evidence to dispel common misconceptions held by eyecare practitioners.
Researchers at the Centre for Ocular Research & Education (CORE) at the University of Waterloo are seeking to shift persistent views about contact lenses that are no longer accurate based on current evidence.
‘Addressing common myths and misconceptions in soft contact lens practice’, co-authored by CORE’s director Professor Lyndon Jones and colleagues Ms Karen Walsh and Dr Kurt Moody, has been published in Clinical and Experimental Optometry, the official journal of Optometry Australia.
Jones reflected on several common myths and mistruths around the fitting and wearing of contact lenses that Australian Emeritus Professor Nathan Efron explored in 1992.
“Remarkably, three decades later, more than half of the current misconceptions we’ve identified were also acknowledged in those original papers,” he said.
“While there has been extraordinary technological and clinical progress over that same time, it has proven more difficult to shake off some long-held incorrect views and established clinical practices.”
The authors grouped the top 10 presentday myths into three broad categories – contact lenses and care systems, patientrelated concerns, and business focused barriers – then reviewed each with clear evidence-based data and practical guidance. Some misconceptions included: • Increasing oxygen transmissibility improves lens comfort, • Hydrogels should no longer be fitted, • Patients will be more successful wearing contact lens materials that demonstrate low levels of deposition, • When a patient reports discomfort, the first – and most appropriate – option is to change the lens. ■
Prof Lyndon Jones, CORE.

EXERCISE SHOWN TO PROVIDE DRY EYE RELIEF
An international research group has discovered a significant increase in tear secretion and tear film stability after participating in aerobic exercise can be another remedy for relieving dry eyes.
In a recent study published in Experimental Eye Research, a team led by researchers from the University of Waterloo divided 52 participants into two groups – athlete and non-athlete – to participate in an exercise session.
Participants in the athlete group exercised at least five times per week, while non-athlete participants exercised no more than once per week. Researchers, which also included experts from the University of Cape Coast in Ghana, performed visual examinations before and five minutes after each exercise session, where tear secretion and tear break-up time were assessed.
While participants in the athlete group showed the largest increase, Mr Heinz Otchere, a PhD candidate in vision science at Waterloo, said all participants experienced a meaningful boost in tear quantity and tear film stability after the exercise session.
“It can be challenging for people to regularly exercise when the demand is there to work increasingly longer hours in front of screens,” he said.
“However, our findings show physical activity can be really important for not just our overall well-being, but for our ocular health too.”
The researchers stated that a healthy tear film comprises three layers; oil, water, and mucin, which work together to hydrate the ocular surface and protect against infection-causing irritants like dust or dirt.
When any part of the tear film becomes unstable, the ocular surface can develop dry spots, causing eye symptoms like itchiness or stinging and burning sensations.
“With so much of our activity tied to screen usage, dry eye symptoms are becoming increasingly common,” Otchere said. "Instead of having to use eye drops or other alternative treatments, our study aimed to determine if remaining physically active can be an effective preventative measure against dryness.” ■

The findings show physical activity can be important for eye health.
The study is being conducted at UNSW.
HOPE FOR ‘BETTER’ CONTACT LENS WEARERS IN NEW TRIAL
Common issues associated with contact lens wear will be the focus of a new study by UNSW researchers.
Associate Professor Nicole Carnt and her research team are conducting a randomised controlled trial with the overall aim of reducing the contact lens dropout rate, boosting wearer satisfaction, improving hygiene compliance and helping new contact lens wearers along the complex wearing journey.
Recruitment for the UNSW trial is under way and practitioners are being asked to distribute flyers to their current contact lens wearers, both full time and part time.
Contact lens wearers can then enrol themselves online by scanning a QR code, with the study consisting of three sets of questionnaires running over six months.
The researchers said the trial would be ideal for new lens wearers at risk of dropout, as well as existing wearers who may need a lens hygiene refresher.
To support PhD candidate Mr Adam Samuels by recruiting contact lens wearers for the trial, contact 0404 658 330 or a.samuels@unsw. edu.au to receive a free recruitment package (50 printed flyers and a poster for each practice). ■
A three-way partnership in Dallas, Texas, has jointly filed a patent for medical imaging technology that uses automated software and a video game to provide standardised and precise identification of ocular diseases including age-related macular degeneration (AMD).
Media technology company Balanced in partnership with the Retina Foundation of the Southwest and Southern Methodist University (SMU) also signed a 10year exclusive license, development, and commercialisation agreement for Balanced to bring the medical imaging technology to the US$35 billion (A$48 b) AI healthcare market.
Balanced created and crowd-sourced an original video game, Eye in the Sky: Defender, which uses optical coherence tomography (OCT) retinal images embedded in the game’s environment to create human-computational image segmentation.
As players predict the path of the alien force in the game, they unknowingly learn to trace lines used to perform diagnostic

OCT scans are taken as the patient plays a video game. Image: Balanced Media.
measurements of OCT retinal scans and create new datasets.
Experts at the Retina Foundation of the Southwest and researchers at SMU used these new datasets to provide the information needed to train a machine learning algorithm to analyse OCT images more accurately.
Retina Foundation of the Southwest CEO Dr Karl Csaky said the technology could be a game-changer for researchers and drug manufacturers in the data analysation of disease progression, drug trials, and treatment efficacy for age-related macular degeneration, among other diseases.
“With this technology we are seeing substantial improvements to image analysis, decreasing our time and cost, and seeing a significant increase in the number of images processed and associated accuracy and precision of image processing," he said.
Csaky, a member of the American Academy of Ophthalmology, the Association for Research in Vision and Ophthalmology, and the American Society of Retinal Specialists, recently joined Balanced as an advisor, assisting the company as it prepares to bring its medical imaging technology to market.
Supported by a US$2.5 million (A$3.5 m) grant, Retina Foundation of the Southwest and SMU’s School of Engineering partnered in a collaborative venture six years ago to rapidly prototype new diagnostic and clinical treatment approaches, focusing on the specific needs of patients who are losing their vision to AMD. ■


As he calls it a day, CHARLES HORNOR recounts the moment he and Peter Larsen sent an email to Specsavers, triggering a wave of momentum that continues 16 years on. O ne of the founding partners of Specsavers in Australia and New Zealand, Mr Charles Hornor, is leaving after 16 years – in search of downtime and new challenges. CURTAIN COMES DOWN ON ‘INCREDIBLE’Specsavers career
The long-time communications director for Specsavers ANZ was jointly responsible for bringing the UK optometry brand to Australasia with optometrist Mr Peter Larsen in 2006 and has been an ever-present figure as the network has grown to more than 425 stores across the region.
“Looking back to day one, the cornerstones of Specsavers' success were a clear vision of how to meet unmet patient and customer demand, gaining the investment to build unstoppable momentum, and the right people to deliver it all,” he recalls.
“With Doug and Mary Perkins’ extraordinary investment the market changed dramatically, with new technology, eyewear ranges and unheard-of prices helping to double the size of the market in just three years – and within the profession we took the chance to tell the story as it happened.”
While people often remember that many were against Specsavers, Hornor says the reality was many more were convinced of its approach.
“And they joined in their droves, enabling us to continue to build and build. Even now we see more than 40% of graduate optometrists joining Specsavers practices. They join knowing they will have access to fantastic professional development, in-clinic support, advanced equipment used with every patient and benchmark reports helping to compare and contrast against their peers.”
Hornor recalls the letter he wrote with Larsen in 2006 that would trigger Specsavers’ rapid Australian entrance. Co-founder Mr Doug Perkins – who Larsen previously worked for in one of the inaugural UK stores – was the recipient, and the pair mulled it over in their drafts folder.
At the time, Hornor and Larsen were operating the Optovision buying group, which they founded and launched in 2004 with more than 250 independents Charles Hornor, jointly responsible for bringing Specsavers to Australia and New Zealand. joining in the first six months. It had only been in operation for two years when the duo wrote to Perkins to explain the market opportunity. centre was set up in Port Melbourne which was operational by March 2007. Hornor says they highlighted the timing was right for an optometry-led group, to short-circuit "over-priced supply chains", and deliver better prices And with positive feedback only three months later at Sydney’s ODMA Fair, practice owners were asking about the Specsavers branded franchise. to customers and better margins to optometrists. By setting up a supply “Eight months later, the store network launched in February 2008 with agreement with Specsavers, they predicted it would give participating the famous 100 stores in 100 days rollout. The first 70 were [Optovision] optometrists a chance to go toe-to-toe with the big players and provide more independents who converted to Specsavers branding under a franchise affordable care. agreement and another 30 practices were purchased. All were refitted at
“We sat on that email for hours because we knew what would happen if we no cost through an incredible display of generosity from Doug and Mary, pressed the send button,” Hornor recalls. and the keys handed over to ongoing owners and new franchise partners,”
“It led to us meeting with the senior Specsavers team in Hong Kong to look Hornor says. at the supply chain for this part of the world. The discussion led to opening a “The vast majority of stores since then have been greenfield under the JVP supply chain into Australia that would morph into the full-blown Specsavers model which pairs an optometry partner with a dispensing partner in their retail franchise if successful.” own standalone business. Fast-forward to 2022 and Specsavers now has
For Perkins, this would be his third attempt at entering Australia, after being around 425 stores across ANZ.” “gazumped” in the early 2000s in two separate deals to buy Laubman & Pank As Hornor departs Specsavers, he leaves knowing they made the right and Precision Eyecare. decision to send that 2006 letter. He says the effect was to catalyse a new
“But we presented an opportunity that couldn’t be thwarted, a way of getting optometry market in Australia and New Zealand that is now four times larger the supply in, letting optometrists and their customers try it for themselves and in total sales volume than in 2007, not to mention far more regular return enable individual practice owners to make their own decisions about teaming rates for eye examinations. up with Specsavers,” Hornor says. He isn’t sure what bodes next but knows it’s time for a change.
The supply agreement was signed, with subscribed independents agreeing “Nothing goes on forever and sometimes you look at yourself and realise you to buy a percentage of their goods from Specsavers. A glazing and distribution need a fresh challenge – but even more importantly, you need a good break.” ■

At the completion of this CPD activity, optometrists will have developed their knowledge of axial length measurement in myopia management. Including:
• Understand the role of axial length as a predictor for myopic pathology • Understand how the rate of axial length growth differs between emmetropes and myopes • Discern the rationale for the use of axial length growth charts to determine the potential risk of myopia in paediatric patients • Be acquainted with the main axial length measurement methods
AXIAL LENGTH MATTERS IN MYOPIA MANAGEMENT
Measuring axial length has not traditionally been commonplace in mainstream optometry. But as KIMBERLEY NGU and DR KATE GIFFORD point out, there are good reasons why it may soon become an indispensable part of effective myopia management.
Myopia management has come a long way in recent times. More practitioners are now aware that simply prescribing single-vision distance spectacles is insufficient management and strive to do more for their patients. The treatment options available for myopia management include orthokeratology, myopia control contact lenses, spectacle myopia control lenses and low-dose atropine.1 As interest in myopia management grows, so does the interest in monitoring axial length in primary eyecare practitioners.
Axial length (AXL) has been well established as an important measurement for myopia control outcomes in research2 and is now gaining momentum in clinical use. Average AXL at birth is 16.5 mm3 and increases to approximately 23.5 mm in adulthood.4 As the long-term eye health consequences of myopia have been revealed by research, AXL has been found to correlate more closely with future risk of vision impairment due to myopia pathology, than does myopic refraction.5
The ‘line in the sand’ for a notable increase in risk for pathology is around 26 mm – an AXL more than 26 mm is associated with a one in four chance of visual impairment by age 75 years, and in those with an AXL of 30 mm or more, 90% suffer uncorrectable vision impairment by age 75.5
Typically, an AXL of 26 mm equates to approximately 5D of myopia.5 While the correlation between AXL and refractive error is strong, refractive error accounts for only 70% of variation in AXL.5 If we consider refractive error as the sum of power of the optical system, the power of the cornea and lens can influence the overall refractive error of an eye – meaning that a low-to-moderate myope could potentially have a long AXL masked by a low-powered cornea or lens. Hence, AXL is the strongest predictor for myopic pathology and can be several times more sensitive in measuring myopic progression than refraction.2
AXIAL LENGTH GROWTH IN EMMETROPES AND MYOPES The US-based Collaborative Longitudinal Evaluation of Ethnicity and Refractive Error (CLEERE) study which studied emmetropic
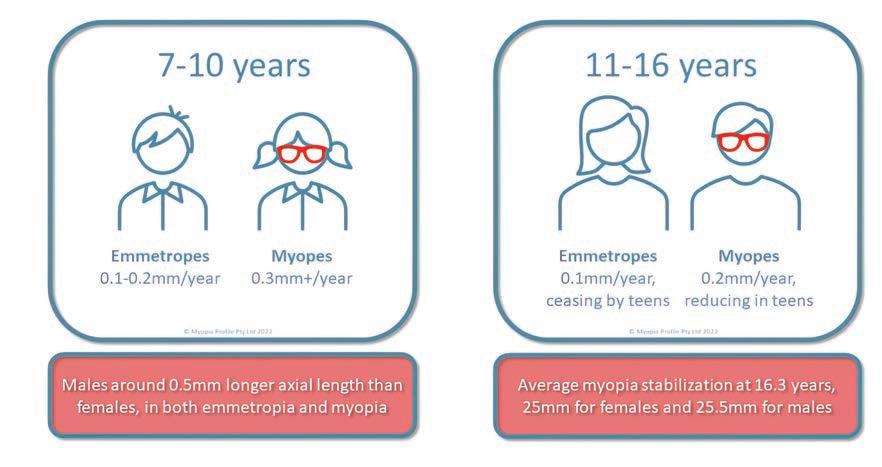
Figure 1: Axial length growth rates in emmetropes and myopes based on age. From the article 'How much axial length growth is normal?'. © Myopia Profile Pty Ltd 2022, used under limited license. ABOUT THE AUTHORS:
Kimberley Ngu
B Optom Clinical optometrist - Private practice Senior optometrist - Royal Perth Hospital Clinical educator - Myopia Profile Pty Ltd
Dr Kate Gifford
PhD BAppSc(Optom)Hons, GradCertOcTher, FBCLA, FIACLE, FCCLSA, FAAO Optometrist, professional educator and clinician-scientist Co-founder and lead educator - Myopia Profile Pty Ltd Visiting Research Fellow - Queensland University of Technology
children of various ethnicities between 6 and 14 years old found that AXL growth was on average 0.10 mm/year.6 Specifically, the AXL growth in 6 to 9-year-olds, 9 to 12-year-olds and 11 to 14-year-olds was at a rate of 0.16 mm, 0.08 mm and 0.02 mm per year, respectively. This was corroborated by European data observing emmetropic AXL growth at a rate of 0.10 mm/year until 13 years of age, with AXL growth thereafter “minute and without practical implications”.7
A study of Asian 8-year-old emmetropes noted a growth rate of 0.12 mm ± 0.24 mm a year;8 while another European cohort of 9-year-old emmetropes observed 0.19 mm ± 0.05 mm per year growth in AXL.9 In a study of 12,780 children of various ethnicities, Chinese children were found to have a longer AXL compared to that of European children,10 but these differences only emerged after 9 years of age. Overall, the rule of thumb appears to be that 0.10 mm per year of AXL growth is to be

Figure 2: Axial length growth charts for European children based on gender. (Tideman et al)9
expected in pre-teenage emmetropes.
In contrast, myopes experience greater rates of AXL growth. CLEERE showed that the fastest AXL growth occurred in the year just prior to myopia onset, whereby these future myopes had an annual growth of 0.33 mm, and then went on to progress at a rate of 0.20 to 0.27 mm/year without myopia control interventions.6
Another study in an ethnically-diverse population indicated average myopic growth of 0.30 mm annually, with 13 to 16-year-old progressing myopes increasing AXL at a rate of 0.17 mm/year.11 Tideman et al9 showed similar figures with 0.34 mm/year growth in 9-year-old European myopes, and Rozema et al8 showed annual growth of 0.30 mm/year in 7 to 9-yearold Asian myopes, slowing to 0.20 mm a year in the 12 to 13-year-old cohort. An analysis of the CLEERE data suggests AXL growth of 0.22 mm/ year will identify fast myopic progressors, and guide more proactive treatment strategies.12
Whether emmetropes or myopes, data indicates that males have, on average, 0.5 mm longer AXL than females of the same age, with the gender difference emerging around age five and persisting thereafter.7,8 When it comes to myopia stabilisation, the average age whereby myopic eyes ceased growing has been found to be 16.3 years, independent of ethnicity, gender and family history of myopia. The average AXL measurement at stabilisation is 25 mm for females and 25.5 mm for males.11
Figure 1 provides a summary of this data on axial length growth in emmetropes and myopes, based on their age, for clinical reference. AXIAL LENGTH GROWTH CHARTS While averages are useful, not every child presenting in practice fits an average. In such instances, percentile growth charts are useful to determine a child’s specific risk compared to their peers and can help monitor the outcomes of myopia management interventions. Growth charts are commonly used in paediatric healthcare, and parents are well-acquainted with their use in plotting a child’s height, weight, and head circumference for example. Hence, they are an easy visual tool. Growth charts for AXL are useful in identifying both the risk of future myopia in adulthood as well as the risk of progression to high myopia.5
The literature, informed by predominantly two studies, currently suggests AXL growth charts to be differentiated by gender and ethnicity. A European chart set has been developed from combining three studies of Dutch and UK data of almost 13,000 individuals9 and an Asian chart set has been developed from a similar volume of data from Chinese children.10
In both cases, separate charts exist for males and females. In comparing the two studies, the ethnicity differences appear to emerge from around age 9.
Figure 2 from the open-access paper of Tideman et al 20189 shows the European data, with the central dark line indicating the 50th percentile, and risk rates overlayed on the right side of each chart showing the risk of myopia and high myopia by adulthood for each AXL centile line provided.
Growth charts for AXL can be used to indicate risk of myopia or high myopia, as described above, as well as directing treatment strategies and gauging treatment outcomes. The Dutch research group who developed the European charts report now using these to identify proactivity of treatment. Children on the 75th percentile, who are at risk of high myopia, are prescribed 0.5% atropine treatment (along with photochromic, progressive addition spectacles with a +3.00 Add to manage side effects) while children with lower centiles are prescribed treatments with a lower side effect profile, such as optical or low-concentration atropine interventions. Treatment was deemed successful when the AXL percentile reduced over time.13
MYOPIA CONTROL STUDIES AND AXIAL LENGTH Reporting axial length outcomes in studies of myopia control interventions is considered the gold standard, as measurement by optical interferometry instruments is up to seven times more sensitive to change than cycloplegic refraction.2 Axial length outcomes also provide an accurate gauge of outcomes in orthokeratology and atropine myopia control studies, where refraction is intentionally altered and influenced by the treatment.14
A large-scale analysis of all myopia control interventions published up until 2020 indicated that orthokeratology and soft multifocal contact lenses reduced axial progression by around 0.2 mm in the first year of treatment and around 0.3 mm total after two years of treatment.14 The newest myopia controlling spectacles
appear to follow these same trends,15,16 as does one study on 0.05% atropine17 and another on 0.02% atropine.18 This has led to the conclusion that “no single method of treatment shows clear superiority with the best of orthokeratology, soft multifocal contact lenses, spectacles and atropine showing similar effect”.14 This simplifies both treatment selection and expected average outcomes in myopia management, encouraging eyecare practitioners to commence treatment based on additional considerations such as “their own skill set, preferences of parents and children, ability of the child to adapt to the treatment, as well as availability of product and regulatory considerations”.14
METHODS OF AXIAL LENGTH MEASUREMENT There are various instruments available to measure AXL and these can be divided into three main categories according to the measurement method: interferometry (or optical biometry), ultrasound, and OCT measurement.
Interferometry
Interferometry is a non-contact, optical biometry measure. This technology is routinely used by ophthalmologists to measure cornea curvature and axial length to enable intraocular lens power calculations for cataract surgery. It is the gold standard technique for axial length measurement in myopia control research2 and is now gaining momentum for use in myopia management by primary eyecare practitioners.
Instruments are now being released specifically for myopia management including additional functionality such as autorefraction, keratometry, corneal topography and/or pupillometry within the single instrument, plus software interfaces to chart outcomes. Optical biometry measurement is fast, non-contact, has a high repeatability and reliability, and is easy to perform which is an advantage for use in children.2
A-scan ultrasound
An older method to measure AXL is A-scan ultrasound. This involves anaesthetising the eye and applanating a probe onto the cornea. Its accuracy is more user-dependent and has a steeper learning curve in getting consistent applanations for repeatable AXL measures. It can also be intimidating for some children to have probe contact with the eye. In the context of myopia, when compared to interferometry, ultrasound gives a resolution of 0.30D while the former can measure up to 0.03D resolution, making ultrasound AXL measurement not any more accurate to track myopia progression than cycloplegic refraction.2
Some new instruments use optical coherence tomography (OCT) to measure AXL. The advantage of using OCT-based systems is that the whole eye can be visualised while

Optical biometry is up to seven times more sensitive to change than cycloplegic refraction.2
doing measurements. From the standpoint of repeatability and accuracy, it is equivalent to interferometry instruments and the differences between the two systems have been reported as clinically insignificant.19
USING AXIAL LENGTH MEASURES IN CLINICAL PRACTICE Measuring AXL in children can provide indication of risk of myopia and high myopia, supporting clinical decision-making and communication. Understanding a myopic patient’s AXL as a single measure provides an indication of their ocular disease risk across their lifetime. Even in myopic adults, knowing their AXL can help to direct frequency of ocular health review, where ‘high myopia’ defined by AXL (≥ 26mm) rather than refraction indicates necessity for annual retinal examination through dilated pupils.1
As a repeated measure, AXL provides a sensitive gauge of myopia progression, helping to track outcomes in line with both averages in research studies as well as outcomes specific to that individual. While a lack of access to axial length measurement should not be a barrier to eyecare practitioners commencing myopia management,1 it is likely to become an increasingly valuable measure and accepted standard over time. ■
REFERENCES 1. Gi fford KL, Richdale K, Kang P, Aller TA, Lam CS, Liu
YM, Michaud L, Mulder J, Orr JB, Rose KA, Saunders
KJ, Seidel D, Tideman JWL, Sankaridurg P. IMI - Clinical
Management Guidelines Report. Invest Ophthalmol Vis
Sci. 2019 Feb 28; 60 (3): M184-M203. 2. Wolffsohn JS, Kollbaum PS, Berntsen DA, Atchison DA,
Benavente A, Bradley A, Buckhurst H, Collins M, Fujikado
T, Hiraoka T, Hirota M, Jones D, Logan NS, Lundström L,
Torii H, Read SA, Naidoo K. IMI - Clinical Myopia Control
Trials and Instrumentation Report. Invest Ophthalmol Vis
Sci. 2019 Feb 28; 60 (3): M132-M160. 3. Axer-Siegel R, Herscovici Z, Davidson S, Linder N, Sherf
I, Snir M. Early Structural Status of the Eyes of Healthy
Term Neonates Conceived by In Vitro Fertilization or
Conceived Naturally. Invest Ophthalmol Vis Sci. 2007; 48 (12): 5454-5458. 4. Meng W, Butterworth J, Malecaze F, Calvas P. Axial length of myopia: a review of current research. Ophthalmologica. 2011; 225 (3): 127-34. 5. Tideman JW, Snabel MC, Tedja MS, van Rijn GA, Wong
KT, Kuijpers RW, Vingerling JR, Hofman A, Buitendijk GH,
Keunen JE, Boon CJ, Geerards AJ, Luyten GP, Verhoeven
VJ, Klaver CC. Association of Axial Length With Risk of
Uncorrectable Visual Impairment for Europeans With
Myopia. JAMA Ophthalmol. 2016 Dec 1; 134 (12): 13551363. 6. Mutti DO, Hayes JR, Mitchell GL, Jones LA, Moeschberger
ML, Cotter SA, Kleinstein RN, Manny RE, Twelker JD,
Zadnik K; CLEERE Study Group. Refractive error, axial length, and relative peripheral refractive error before and after the onset of myopia. Invest Ophthalmol Vis Sci. 2007
Jun; 48 (6): 2510-9. 7. Fledelius HC, Christensen AS, Fledelius C. Juvenile eye growth, when completed? An evaluation based on IOL-
Master axial length data, cross-sectional and longitudinal.
Acta Ophthalmol. 2014 May; 92 (3): 259-64. 8. Rozema J, Dankert S, Iribarren R, Lanca C, Saw SM.
Axial Growth and Lens Power Loss at Myopia Onset in
Singaporean Children. Invest Ophthalmol Vis Sci. 2019 Jul 1 ;60 (8): 3091-3099. 9. Tideman JWL, Polling JR, Vingerling JR, Jaddoe VWV,
Williams C, Guggenheim JA, Klaver CCW. Axial length growth and the risk of developing myopia in European children. Acta Ophthalmol. 2018 May; 96 (3): 301-309. 10. Sanz Diez P, Yang LH, Lu MX, Wahl S, Ohlendorf
A. Growth curves of myopia-related parameters to clinically monitor the refractive development in Chinese schoolchildren. Graefes Arch Clin Exp Ophthalmol. 2019
May; 257 (5): 1045-1053. 11. Hou W, Norton TT, Hyman L, Gwiazda J; COMET Group.
Axial Elongation in Myopic Children and its Association
With Myopia Progression in the Correction of Myopia
Evaluation Trial. Eye Contact Lens. 2018 Jul;44(4):248259. 12. Hernández, J., Sinnott, L., Brennan, N., Cheng, X.,
Zadnik, K., & Mutti, D. Analysis of CLEERE data to test the feasibility of identifying future fast myopic progressors.
Invest Ophthalmol Vis Sci. 2018; 59: E-abstract 3388. 13. Klaver C, Polling JR; Erasmus Myopia Research Group.
Myopia management in the Netherlands. Ophthalmic
Physiol Opt. 2020 Mar; 40 (2): 230-240 14. Brennan NA, Toubouti YM, Cheng X, Bullimore MA.
Efficacy in myopia control. Prog Retin Eye Res. 2021 Jul; 83: 100923. 15. Lam CSY, Tang WC, Tse DY, Lee RPK, Chun RKM,
Hasegawa K, Qi H, Hatanaka T, To CH. Defocus
Incorporated Multiple Segments (DIMS) spectacle lenses slow myopia progression: a 2-year randomised clinical trial. Br J Ophthalmol. 2020 Mar; 104 (3):3 63-368. doi: 10.1136/bjophthalmol-2018-313739. 16. Bao J, Yang A, Huang Y, Li X, Pan Y, Ding C, Lim EW,
Zheng J, Spiegel DP, Drobe B, Lu F, Chen H. Oneyear myopia control efficacy of spectacle lenses with aspherical lenslets. Br J Ophthalmol. 2021: 318367. 17. Yam JC, Jiang Y, Tang SM, Law AKP, Chan JJ, Wong
E, Ko ST, Young AL, Tham CC, Chen LJ, Pang CP.
Low-Concentration Atropine for Myopia Progression (LAMP) Study: A Randomized, Double-Blinded, Placebo-
Controlled Trial of 0.05%, 0.025%, and 0.01% Atropine Eye
Drops in Myopia Control. Ophthalmology. 2019 Jan; 126 (1): 113-124. 18. Cui C, Li X, Lyu Y, Wei L, Zhao B, Yu S, Rong J, Bai Y, Fu
A. Safety and efficacy of 0.02% and 0.01% atropine on controlling myopia progression: a 2-year clinical trial. Sci
Rep. 2021 Nov 15; 11 (1): 22267. 19. Wyl gała A, Bolek B, Mazur R, Wyl gała E. Repeatability, reproducibility, and comparison of ocular biometry using a new optical coherence tomography-based system and another device. Sci Rep. 2020 Sep 2; 10 (1): 14440.
NOTE: Optometry Australia members can scan the QR code or visit the online version of this article at insightnews.com.au/cpd/ to enter their details to have their CPD hours automatically updated to their Learning Plan. Event ID: 90004084, Session ID: 10391.
At the completion of this CPD activity, optometrists will have developed their knowledge of atropine as a treatment for myopia management. Including:
• Understand the clinical rationale for the use of lowconcentration atropine in the treatment of myopia • Understand the clinical safety and efficacy profiles of atropine • Explain to parents and patients the value of atropine intervention • Understand the clinical treatment protocols of atropine
ATROPINE FOR MYOPIA CONTROL: SCIENCE AND PRACTICE
In the second part of an educational feature on myopia management, CASSANDRA HAINES and DR KATE GIFFORD summarise atropine’s clinical efficacy and delve into data surrounding optimal concentrations.
When considering atropine for myopia management, it’s important to start with the fundamentals.
Known to eyecare practitioners for its mydriatic and cycloplegic effects, atropine is also a systemic medication used in cardiovascular management.1 Originally derived from Belladonna,2 the antimuscarinic agent (or muscarinic antagonist) inhibits postganglionic muscarinic receptors. When used systemically, this affects the autonomic nervous system, and increases cardiac output.1
Scientists are still unravelling the full mechanism for the myopia-controlling effect of atropine. However, it is known that acetylcholine, a neurotransmitter, is involved in retinal growth and signalling. Atropine blocks the action of acetylcholine at the muscarinic receptors, which may present a mechanism for slowing eye growth.
Atropine’s action as a mydriatic with associated relaxed accommodation tone may also play a role; it was previously thought myopia growth was due to excessive accommodation tone, but this has recently been refuted in animal models.3
HISTORY OF ATROPINE EVIDENCE Atropine has been a possible contender on the myopia-management scene for longer than most may realise, with published literature as early as 1979 and 1984 reporting the effects of 1.0% atropine on fast myopia progressors.4,5 In 2006, the landmark paper ‘Atropine for the Treatment of Childhood Myopia (ATOM)’ was published, which evaluated 1% atropine against a placebo, demonstrating for the first time in a large-scale, randomised controlled trial that atropine could become a key player in myopia management.6
Despite its effectiveness, with 1% atropine demonstrating an almost halt (100% control effect) to axial length growth, the considerable side effects made it an unappealing treatment option,6 and the race began to find the ideal lower concentration of atropine, to achieve efficacy with minimal side effects. TWIST The ATOM2 study in 2012 investigated 0.5%, 0.1% and 0.01% (as the intended placebo) for two years and found a concentrationdependent response in myopia control efficacy.7 From here, the scientific twist in the story occurred. These same participants then underwent a 12-month washout period before fast progressors (more than 0.50D myopia progression over the year) were resumed on 0.01% atropine treatment for another two years. While there was a concentration-dependent response in the first part of the study, there was also a concentration-dependent rebound effect noted in the washout year. At the conclusion of the five years, children treated with the 0.01% atropine for two years, discontinued for a year, then recommenced for another two years had the lowest final level of myopic refraction compared to children who had commenced on a higher concentration and then been shifted to 0.01% atropine.7
Given its low rate of side effects, minimal rebound and overall appearance of effective myopia-control, 0.01% atropine then rapidly gained popularity in the myopia-management landscape. The 2016 World Health Organisation (WHO) landmark myopia paper entitled: 'The Impact of Myopia and High Myopia' listed atropine 0.01% as a key treatment option for progressing myopes.8 This spurred further clinical trials such as the CHAMP study in the UK and the PEDIG group in America.9
TWIST (AGAIN) The next scientific twist away from 0.01% atropine occurred only recently, as researchers highlighted in 2018 that the ATOM2 study did not have a placebo control group, and that a historical control group comparison showed the actual impact on axial length control was minimal.10 This was affirmed with the 2019 publication of the ‘Low-concentration Atropine for Myopia Progression (LAMP)’ study, comparing 0.01%, 0.025% and 0.05% atropine directly to a placebo.
ABOUT THE AUTHORS:
Cassandra Haines
B Vis Sci M Optom CO Associate lecturer – Flinders University Clinical educator – Myopia Profile Pty Ltd Policy and advocacy advisor – Optometry Australia
Dr Kate Gifford
PhD BAppSc(Optom)Hons, GradCertOcTher, FBCLA, FIACLE, FCCLSA, FAAO Optometrist, professional educator and clinician-scientist Co-founder and lead educator – Myopia Profile Pty Ltd Visiting Research Fellow - Queensland University of Technology
After 12 months, it was found that there was a statistically-significant slowing of eye growth in the 0.025% and 0.05% group, both in axial length and refractive change, however, there was a limited effect in the 0.01% group. The overall effect of 0.05% was almost double that of the 0.01%; leading to the conclusion that there is a concentrationdependent response to atropine and 0.01% may simply not be enough. This is the case for both regular and fast progressors, further backed by studies since.11,12
SIDE EFFECTS AND SAFETY Side effect profiles reflect that higher concentrations (<0.1%) suffer higher rates of adverse effects;7,12 low-concentration atropine is reported to have very few side effects.13,14 Only 2.2% of the LAMP participants needed progressive glasses and 5% reported photophobia, with no differences noted between the various concentration and
Figure 1: Flowchart for atropine prescribing based on treatment selection and concentration. Image © Myopia Profile Pty Ltd 2022, from the online course 'Atropine for Myopia Management', used under limited license.

placebo groups. Patient preference, however, saw around one-third of the study participants prescribed photochromic glasses, including in the placebo group.13 Since these were offered at the study outset to parents concerned about side effects or pupil dilation, the authors suggested that this may have been taken up for protection against potential instead of realised side effects.15
COMPOUNDING Almost all published atropine studies use compounded atropine, made from diluted 1% atropine drops with little reference to the method of compounding, stability of end product, or independent testing of concentration to ensure accuracy.
Complex compounding, required to produce sterile eye drop formulations, is a complicated process requiring specialist pharmacy skills and in some countries, may suffer reports of contamination, error and adverse outcomes.16
This doesn’t appear to be as much the case in Australia, where strong regulation on complex compounding is in place.17 Compounded atropine is frequently preserved with benzalkonium chloride (BAK), which is a known ocular surface irritant and hence not ideal for long-term use in children. Atropine itself does not appear to be a significant ocular irritant, with low rates of allergic conjunctivitis in studies being consistent across all participants, indicating BAK as the more likely culprit.13 COMMERCIALLY-PREPARED FORMULATIONS Studies on commercially-prepared, nonpreserved solutions are currently under way, which may provide some answers on how the formulation of atropine influences efficacy and side effects and also may potentially lead to another scientific shift back towards 0.01% if it proves effective.
SAFETY AND CONTRAINDICATIONS Atropine safety and tolerance as a topical ocular preparation appears to be high, but there have been isolated case reports of fatality in a child18 and poisoning in an adult19 from oral ingestion of 1% atropine eye drops. Systemic absorption through topical application, (to avoid anticholinergic side effects such as mouth and eye dryness, delirium or restlessness, tachycardia and flushed skin and face) and risks of allergy can be minimised through punctal occlusion.20 The majority of reported systemic complications from ocular use of atropine have occurred from children or young adults with pre-existing heart conditions, such a congenital rubella syndrome and developmental delays.18,21
This means that topical atropine may be contraindicated in children with heart conditions, and caution must be exercised in congenital syndromes, history of asthma or other anticholinergic medicine use.2,18,21 In these cases, communication and comanagement with the patient’s healthcare team, especially paediatric ophthalmology, is essential to discuss risks and benefits – strict instruction and close supervision of patients in a risk category is a must.21
CHOOSING THE IDEAL PATIENT For parents who may cite concerns with cost or logistics of myopia management spectacles or contact lenses, atropine can potentially provide a lower-cost alternative, with simple night-time dosing. However, atropine doesn’t correct refractive error, which places it at significant disadvantage to spectacle or contact lens myopia management strategies.
Parents must understand that this treatment will not reduce myopia, nor correct it, and spectacles or contact lenses will still be required. Providing children with progressive addition spectacle lenses will resolve any difficulties with near vision, if they arise. Encouraging children to wear sunglasses or recommending photochromic lenses will reduce any symptoms of photophobia and protect children from any potentially increased risk of UV exposure due to dilated pupils.
Children as young as four with documented myopia progression have been included in major landmark atropine trials such as the LAMP study,15 with the majority of studies including children from six years of age.6,9,22 This does not preclude the treatment from being effective on older populations; extrapolation that atropine is still effective in progressing teenagers is reasonable.
With all parents, ensuring informed consent is essential, including a discussion of the
CASSANDRA HAINES & DR KATE GIFFORD
evidence for treating each individual child. In very young children, referral or co-management with ophthalmology may be prudent, especially when the degree of myopia exceeds the years of age, indicating high potential for systemic associations alongside the high myopia.23
Despite the fact that extended treatment with 1% atropine for amblyopia penalisation does not result in long-term side effects, and that the short-term cycloplegic effects of atropine are demonstrated to return to pre-treatment levels, there must still be consideration to potential long-term effects of atropine treatment.24
Before commencing any treatment, it is important to take thorough pupil and binocular vision measurements to help monitor for side effects, and to have a discussion with parents regarding the current evidence and likely longterm treatment protocol of atropine.
The LAMP study found that 0.05% was the most effective concentration for controlling axial length growth, achieving a balance of effectively slowing myopia progression with minimal side effects.15
Recent analysis of the ATOM2 data10 showed that 0.1% and 0.5% likely didn’t have a stronger impact on controlling axial elongation than the 0.05% outcomes in the LAMP study, although a direct comparison has not yet been undertaken. Furthermore, a 2020 analysis of all myopia control studies published to that date concluded that: “No single method of treatment shows clear superiority with the best of orthokeratology, soft multifocal contact lenses (SMCLs), spectacles and atropine showing similar effect.”25
Considering the dual correction-andcontrol benefits of spectacle or contact lens interventions, it makes clinical sense to prescribe these as first line treatments, and consider atropine a first line treatment where the ideal optical intervention is not suitable to that patient or available in your practice.
Figure 1 presents a flow chart for the prescription of atropine based on current evidence. COMBINATION TREATMENTS Atropine 0.01% combined with orthokeratology has been shown to have an additive myopia control effect over orthokeratology alone. Two randomised clinical trials have shown that the increased efficacy was evident only in 1-4D myopes, and only for the first six to 12 months of combination treatment.26,27 A study on combining 0.01% atropine with centre-distance +2.50 Add multifocal contact lenses is under way, with outcomes expected to be reported in 2022.28 There are no other investigations of combining atropine with optical interventions.
TAPERING AND CESSATION OF TREATMENT The question of tapering is yet to be fully addressed, given the rebound effects noted with 0.5% and 0.1% in the ATOM2 study7 and the current lack of investigation of rebound in lower concentrations.
The WHO recommendations from 2015 suggest a taper, however provide no instructions on reducing concentration or lowering dose frequency as the ideal approach.29 Zhu et al published a study in 2020 where a single monthly dose of atropine 1.0% for two years was reduced to every second month for a further year and then ceased, with no further myopia management intervention and no reported ‘rebound’ effects;30
Join Eyecare Plus and benefit from the support and knowledge of experienced members.
Looking to buy, sell or join contact Philip Rose 0416 807 546 or philip.rose@eyecareplus.com.au
but the side effect profile of 1.0% in this novel dosing approach raises questions regarding the best prescribing practices.
It has been demonstrated that half of myopic children stop progressing by 16 years of age, but this leaves 50% of children still with escalating myopia, so long-term treatment throughout the teenage years should be discussed with families.31 The 2015 WHO Myopia report8 suggested only two years of 0.01% atropine treatment based on the current evidence at that time. It would appear that if atropine is to be used as a primary myopia management strategy throughout childhood, treatment would likely need to continue for longer than this. While efficacy and safety appears robust with low-concentration topical atropine, longer-term treatment data beyond five years is not yet available.

PRESCRIBING ATROPINE IN PRACTICE Axial length control data in atropine studies has helped to reveal the true story of the ideal concentration, and will continue to be the key outcome measure for research trials.32 In the clinical setting, while axial length measurement is likely the ideal way to monitor for treatment efficacy, lack of access to such instrumentation should not be a barrier to practitioners offering myopia control treatment to their young patients.33
If you do wish to include this data in your practice consider working with your colleagues or interprofessional referral for axial length measurement. Co-management can also be important in providing the best possible treatments and outcomes for all patients.
In Australia, the only commercially-available topical atropine concentration is 1%, with any lower concentrations requiring compounding. The tide is shifting however, with the Therapeutic Goods Administration recently listing Eikance, a preservative-free, single use formulation of 0.01%, as an ‘extended use’ of atropine for children 4 to 14 years of age who have experienced a progression in myopia of -1.00D or more per year.34
Multiple clinical trials are under way in the United States and Europe, investigating commercially-prepared, preservative free lowconcentration formulations – 2022 may see yet another exciting twist in the scientific story of atropine for myopia management. ■
NOTE: Optometry Australia members can scan the QR code or visit the online version of this article at insightnews.com.au/cpd/ to enter their details to have their CPD hours automatically updated to their Learning Plan. Event ID: 90004083, Session ID: 10390. The optimum atropine concentration for myopia has been the focus of studies that have offered several twists.
REFERENCES 1. McLendon K, Preuss CV. Atropine. [Updated 2021
Sep 12]. In: StatPearls [Internet]. Treasure Island (FL):
StatPearls Publishing; 2022 Jan-. Available from: https:// www.ncbi.nlm.nih.gov/books/NBK470551/ 2. Drugs and Lactation Database (LactMed) [Internet].
Bethesda (MD): National Library of Medicine (US); 2006-.
Belladonna. [Updated 2021 May 17]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK501860/ 3. McBrien NA, Stell WK, Carr B. How does atropine exert its anti-myopia effects? Ophthalmic Physiol Opt. 2013 May; 33 (3): 373-8. 4. Bedrossian RH. The effect of atropine on myopia. Ann
Ophthalmol. 1971 Aug; 3 (8): 891-7. 5. Brodstein RS, Brodstein DE, Olson RJ, Hunt SC, Williams
RR. The treatment of myopia with atropine and bifocals. A long-term prospective study. Ophthalmology. 1984 Nov; 91 (11): 1373-9. 6. Chua WH, Balakrishnan V, Chan YH, Tong L, Ling Y, Quah
BL, Tan D. Atropine for the treatment of childhood myopia.
Ophthalmology. 2006 Dec; 113 (12): 2285-91. 7. Chia A, Lu QS, Tan D. Five-Year Clinical Trial on Atropine for the Treatment of Myopia 2: Myopia Control with
Atropine 0.01% Eyedrops. Ophthalmology. 2016 Feb; 123 (2): 391-399. 8. WHO. The Impact of Myopia and High Myopia. Sydney,
Australia: World Health Organisation with the University of
New South Wales; 2015. 9. Azuara-Blanco A, Logan N, Strang N, Saunders K, Allen
PM, Weir R, Doherty P, Adams C, Gardner E, Hogg R,
McFarland M, Preston J, Verghis R, Loughman JJ, Flitcroft
I, Mackey DA, Lee SS, Hammond C, Congdon N, Clarke
M. Low-dose (0.01%) atropine eye-drops to reduce progression of myopia in children: a multicentre placebocontrolled randomised trial in the UK (CHAMP-UK)-study protocol. Br J Ophthalmol. 2020 Jul; 104 (7): 950-955. 10. Bullimore MA, Berntsen DA. Low-Dose Atropine for Myopia
Control: Considering All the Data. JAMA Ophthalmol. 2018
Mar 1; 136 (3): 303. 11. Fu A, Stapleton F, Wei L, Wang W, Zhao B, Watt K, Ji N,
Lyu Y. Effect of low-dose atropine on myopia progression, pupil diameter and accommodative amplitude: low-dose atropine and myopia progression. Br J Ophthalmol. 2020
Nov; 104 (11): 1535-1541. 12. Moon JS, Shin SY. The diluted atropine for inhibition of myopia progression in Korean children. Int J Ophthalmol. 2018 Oct 18; 11 (10): 1657-1662. 13. Yam JC, Li FF, Zhang X, Tang SM, Yip BHK, Kam KW,
Ko ST, Young AL, Tham CC, Chen LJ, Pang CP. Two-
Year Clinical Trial of the Low-Concentration Atropine for
Myopia Progression (LAMP) Study: Phase 2 Report.
Ophthalmology. 2020 Jul; 127 (7): 910-919. 14. Cooper J, Eisenberg N, Schulman E, Wang FM. Maximum atropine dose without clinical signs or symptoms. Optom
Vis Sci. 2013 Dec; 90 (12): 1467-72. 15. Yam JC, Jiang Y, Tang SM, Law AKP, Chan JJ, Wong
E, Ko ST, Young AL, Tham CC, Chen LJ, Pang CP.
Low-Concentration Atropine for Myopia Progression (LAMP) Study: A Randomized, Double-Blinded, Placebo-
Controlled Trial of 0.05%, 0.025%, and 0.01% Atropine Eye
Drops in Myopia Control. Ophthalmology. 2019 Jan; 126 (1): 113-124. 16. FDA. Compounding and the FDA: Questions and Answers.
Guidance, Compliance, & Regulatory Information 2018. 17. Pharmacy Board of Australia. Frequently asked questions for pharmacists on the compounding of medications, 2020. 18. North RV, Kelly ME. A review of the uses and adverse effects of topical administration of atropine. Ophthalmic
Physiol Opt. 1987; 7 (2): 109-14. 19. Stellpflug SJ, Cole JB, Isaacson BA, Lintner CP, Bilden EF.
Massive atropine eye drop ingestion treated with highdose physostigmine to avoid intubation. West J Emerg
Med. 2012 Feb; 13 (1): 77-9. 20. Kothari M, Jain R, Khadse N, Rathod V, Mutha S.
Allergic reactions to atropine eye drops for retardation of progressive myopia in children. Indian J Ophthalmol. 2018
Oct; 66 (10): 1446-1450. 21. Hirsbein D, Genevois O, Proust N, Calenda E. Are eye drops of atropine completely safe for heart? BJA: British
Journal of Anaesthesia. 2006; 97 (eLetters Supplement). 22. McCrann S, Flitcroft I, Strang NC, Saunders KJ, Logan
NS, Lee SS, Mackey DA, Butler JS, Loughman J. Myopia
Outcome Study of Atropine in Children (MOSAIC): an investigator-led, double-masked, placebo-controlled, randomised clinical trial protocol. HRB Open Res. 2019
Jul 23; 2:15. 23. Marr JE, Halliwell-Ewen J, Fisher B, Soler L, Ainsworth JR.
Associations of high myopia in childhood. Eye (Lond). 2001 Feb; 15 (Pt 1): 70-4. 24. Tong L, Huang XL, Koh AL, Zhang X, Tan DT, Chua WH.
Atropine for the treatment of childhood myopia: effect on myopia progression after cessation of atropine.
Ophthalmology. 2009 Mar; 116 (3): 572-9. 25. Brennan NA, Toubouti YM, Cheng X, Bullimore MA.
Efficacy in myopia control. Prog Retin Eye Res. 2021 Jul; 83: 100923. 26. Tan Q, Ng AL, Choy BN, Cheng GP, Woo VC, Cho P. Oneyear results of 0.01% atropine with orthokeratology (AOK) study: a randomised clinical trial. Ophthalmic Physiol Opt. 2020 Sep; 40 (5): 557-566. 27. Kinoshita N, Konno Y, Hamada N, Kanda Y, Shimmura-
Tomita M, Kaburaki T, Kakehashi A. Efficacy of combined orthokeratology and 0.01% atropine solution for slowing axial elongation in children with myopia: a 2-year randomised trial. Sci Rep. 2020 Jul 29; 10 (1): 12750. 28. Huang J, Mutti DO, Jones-Jordan LA, Walline JJ. Bifocal & Atropine in Myopia Study: Baseline Data and Methods.
Optom Vis Sci. 2019 May; 96 (5): 335-344. 29. Holden BA, Fricke TR, Wilson DA, Jong M, Naidoo KS,
Sankaridurg P, Wong TY, Naduvilath TJ, Resnikoff S. Global
Prevalence of Myopia and High Myopia and Temporal
Trends from 2000 through 2050. Ophthalmology. 2016
May; 123 (5): 1036-42. 30. Zhu Q, Tang Y, Guo L, Tighe S, Zhou Y, Zhang X, Zhang
J, Zhu Y, Hu M. Efficacy and Safety of 1% Atropine on
Retardation of Moderate Myopia Progression in Chinese
School Children. Int J Med Sci. 2020 Jan 1; 17(2):176-181. 31. COMET Group. Myopia stabilization and associated factors among participants in the Correction of Myopia
Evaluation Trial (COMET). Invest Ophthalmol Vis Sci. 2013
Dec 3; 54 (13): 7871-84. 32. Wolffsohn JS, Kollbaum PS, Berntsen DA, Atchison DA,
Benavente A, Bradley A, Buckhurst H, Collins M, Fujikado
T, Hiraoka T, Hirota M, Jones D, Logan NS, Lundström L,
Torii H, Read SA, Naidoo K. IMI - Clinical Myopia Control
Trials and Instrumentation Report. Invest Ophthalmol Vis
Sci. 2019 Feb 28; 60 (3): M132-M160. 33. Gifford KL, Richdale K, Kang P, Aller TA, Lam CS, Liu
YM, Michaud L, Mulder J, Orr JB, Rose KA, Saunders
KJ, Seidel D, Tideman JWL, Sankaridurg P. IMI - Clinical
Management Guidelines Report. Invest Ophthalmol Vis
Sci. 2019 Feb 28; 60 (3): M184-M203. 34. The Therapeutic Goods Administration. Prescription medicines: new or extended uses, or new combinations of registered medicines. https://www.tga.gov.au/ prescription-medicines-new-or-extended-uses-registeredmedicines. Accessed 30.01.2022, 2022.
AP



PLY


THE


BRAKES

TO SLOW DOWN
MYOPIA IN CHILDREN
WITH THE FIRST REGISTERED LOW-DOSE ATROPINE EYE DROPS*1,2
*EIKANCE 0.01% eye drops (atropine sulfate monohydrate 0.01%) is indicated as a treatment to slow the progression of myopia in children aged from 4 to 14 years. Atropine treatment may be initiated in children when myopia progresses ≥ –1.0 diopter (D) per year.1



PBS information: this product is not listed on the PBS Before prescribing please review full Product Information available via www.aspenpharma.com.au/products or call 1300 659 646
This medicinal product is subject to additional monitoring in Australia. This will allow quick identification of new safety information. Healthcare professionals are asked to report any suspected adverse events at https://www.tga.gov.au/reporting-problems.
EIKANCE 0.01% EYE DROPS (atropine sulfate monohydrate 0.01%). Indication: To slow the progression of myopia in children aged 4 to 14 years. May be initiated in children when myopia progresses ≥-1.0 D per year. Contraindications: Presence of angle closure glaucoma or where angle closure glaucoma is suspected. In glaucoma susceptible patients, an estimation of the depth of the angle of the anterior chamber should be performed prior to the initiation of therapy. Known hypersensitivity to any ingredient of the product. Precautions: Risk-benefit should be considered when the following medical problems exist: Keratoconus - atropine may produce fixed dilated pupils, Synechiae - atropine may increase the risk of adherence of the iris to lens. Use in Children: atropine sulfate monohydrate should not be used in children who have previously had severe systemic reaction to atropine. Use with great caution in children with Down’s syndrome, spastic paralysis, or brain damage. Limited clinical evidence is available for the long-term safety in children and adolescents. Regular eye health clinical reviews recommended during long-term treatment, including the monitoring of anterior segment development, intraocular pressure, retinal health and myopia progression. Consider careful monitoring of anterior segment development with prolonged use in very young children. EIKANCE 0.01% eye drops should not be used in children less than 4 years of age. If children experience photophobia or glare, they may be offered polychromatic glasses or sunglasses. If children experience poor visual acuity, consider progressive glasses. Discontinuation may lead to a rebound in myopia. EIKANCE 0.01% eye drops are not indicated for use in the elderly. Possible effect on the ability to drive or use machinery due to poor visual acuity should be evaluated, particularly at the commencement of treatment. Pregnancy: Category A. Lactation: distributed into breast milk in very small amounts. Interactions: systemic absorption of ophthalmic atropine may potentiate anticholinergic effects of concomitant anticholinergics. If significant systemic absorption of ophthalmic atropine occurs, interactions may occur with antimyasthenics, potassium citrate, potassium supplements, CNS depressants, such as antiemetic agents, phenothiazines, or barbiturates. Concurrent use may interfere with anti-glaucoma agents, echothiophate, carbachol, physostigmine, pilocarpine. Adverse Effects: photophobia, blurred vision, poor visual acuity, allergy, local irritation, headache, fatigue. See full PI for other ophthalmic and systemic AEs. Dosage and administration: Treatment should be supervised by a paediatric ophthalmologist. Instil one drop into the eye as required for treatment. Minimise the risk of systemic absorption, by applying gentle pressure to the tear duct for one minute after application. Should be administered as one drop to each eye at night. The maximum benefit of treatment may not be achieved with less than a 2 year continued administration period. The duration of administration should be based on regular clinical assessment. Each container is for single use, discard after administration of dose. (Based on PI dated 25 November 2021) References: 1. Approved EIKANCE Product Information, 125 November 2021. 2. Australian Register of Therapeutic Goods. Accessed 10-Dec-2021.

Myopia products
HISTORIC 7-YEAR INTERNATIONAL STUDY YIELDS VALUABLE CLINICAL INSIGHTS

MiSight 1 day from CooperVision remains the only contact lens with US FDA approval for slowing the progression of childhood myopia. A critical reason for this was the safety and efficacy data obtained from a three-year randomised controlled trial undertaken in four countries with 8-12 year olds which showed MiSight 1 day slowed both dioptric progression and axial elongation by over 50%, comparing favourably with other treatments.
Safety and efficacy demonstrated, the trial continued for a further three years with all children wearing MiSight 1 day to understand treatment efficacy when fitting older children. Encouragingly, CooperVision says this showed an effect on the rate of progression similar to that of the children fitted from the outset. The seventh and final year of the study saw all children refitted into single-vision lenses to evaluate any post-treatment rebound effect. No rebound was observed.
“This extraordinary study, which also confirmed the overwhelming preference children have for contact lenses, gives optometrists the evidence to support their decision-making and parental conversations,” CooperVision says.
DEFOCUS SPECTACLE LENS CONTINUES TO MAKE IN-ROADS
Trials have concluded children wearing Hoya’s MiYOSMART defocus spectacle lens had 60% less myopia progression compared with single-vision wearers as measured by the axial elongation, and a 59% reduction in spherical equivalent refraction.1
Launched in Australia in October 2020, the company says the innovation has prompted more optometrists to offer myopia management. Optometrists are reportedly seeing the value in prescribing the lens for young children that have either not had any myopia treatment yet or less effective spectacle lenses. Others have found it an ideal option for kids not ready for contact lenses, or those that don’t want to continue with a contact lens approach.
According to Hoya, more recent data has shown the lens continued to slow myopia progression after three years, while patients who switched from single vision had a significant slowdown in their condition, showing the benefits of starting treatment at any time.
(References available upon request).

START OFFERING GOLD STANDARD MYOPIA CARE
Eyecare professionals can introduce or expand their myopia control capabilities with precise measurements of The Lenstar Myopia. Whether it’s for early detection of disease onset or offering state-of-the-art management, this instrument utilises Automated Positioning Technology for fully automated measurement capture process, combined with the latest graphical data from Erasmus University to detect and track progression and communicate treatment pathways effectively with patients and parents. Derived from the ophthalmology-facing Lenstar for cataract planning, the Lenstar Myopia is said to be highly accurate and repeatable, averaging multiple individual measurements for axial length measurement, enabling practitioners to identify true progression from deviation. Networkable with existing practice IT ecosystems, and chair and stand compatible, it enables easy practice integration even for those who are space conscious. The device is distributed by Device Technologies in Australia.

MASTERING MYOPIA MANAGEMENT WITH MANAGEMENT WITH CONFIDENCE
The OCULUS Myopia Master measures three key parameters to help make myopia three key parameters to help make myopia detection and management easier and detection and management easier and more reliable.
“Measurement of refraction, axial length and “Measurement of refraction, axial length and keratometry in a stylish unit, delivered keratometry in a stylish unit, delivered with a comprehensive myopia software suite, helps provide clarity software suite, helps provide clarity of diagnoses,” distributor Designs of diagnoses,” distributor Designs For Vision (DFV) says.
“Myopia Master is the only device to incorporate the latest Brien Holden Vision Institute (BHVI) data for estimating future myopia progression, enabling personalised reports detailing a child’s current myopia status and their likely outcome in adulthood.”
Professor Padmaja Sankaridurg, head of BHVI’s Myopia Program added: ”In collaboration with our research partners across the globe, the team at BHVI is continually engaged in expanding the state of knowledge as well as bringing solutions to reverse the rising myopia epidemic.”
BHVI’s data sets, with diverse strata of age, gender and ethnicity, improve modelling in a wider patient cohort and enhance parent counselling – giving practitioners confidence without compromise, DFV says.
MYOPIA INDICATION FOR LOW-DOSE ATROPINE

In February 2022, Aspen Australia launched Eikance 0.01%, the first pharmacotherapy registered on the Australian Register of Therapeutic Goods to slow the progression of myopia in Pack image Children aged 4 – 14 years1#. not to scale. Atropine treatment may be initiated in children when myopia progresses ≥-1.0 D per year.1
EIKANCE 0.01% single-use ampoules are sealed in foil pouches and are available in packs of 30 x 0.3 mL ampoules. The ophthalmic solution is sterile and preservative-free. EIKANCE 0.01% is a private, prescription only medicine available at community pharmacies across Australia.
For the Minimum Product Information and PBS status, turn to page 35.
References: 1.Eikance Approved Product Information #Australian Registered of Therapeutic Goods. Accessed 10 Dec 2021. Aspen Australia, St Leonards NSW 2065. Prepared: Feb 2022 ASP 2696 AF 06355
Myopia products
ESSILOR LENSES TARGETED AT MYOPIA CONTROL
Essilor has studied myopia control for more than 25 years. Working with myopia scientists from around the world, including in Australia, its research has led to the release of Myopilux Plus and Myopilux Max in the Australian and New Zealand market. • Myopilux Plus – is targeted for esophoric, myopes who are progressing and have a lag of accommodation greater than 0.50D. In a three-year study this short, progressive reduced progression by up to 0.45D, Essilor reports. • Myopilux Max – is for any myope progressing at more than 1.00D per year. This executive bifocal includes three prism dioptres base for each, which compensates for the exophoric shift induced by the near add. In a threeyear Canadian study, myopia progression was reduced by up to 0.85D.
“Both lenses use a +2.00D addition, this is the power used in studies where spectacle lenses slowed myopia progression,” Essilor says.

COMBATING THE MYOPIA CRISIS PLUS MORE

The Topcon MYAH is said to offer all the technologies required to support myopia management: optical biometry, corneal topography and pupillometry. In addition, it’s an all-in-one device offering an evolving platform to add or grow dry eye management.
A fully featured onboard software system allows users to review, diagnose, track and treat a variety of ocular conditions, from complex contact lens fitting applications, to the latest in minimally invasive dry eye diagnostic analysis.
Additionally, the myopia module combines highly accurate and repeatable axial length measurement facilities with detail and repeatable axial length measurement facilities with detail reporting, and growth curve reporting, and growth curve software tools to professionally software tools to professionally manage myopia, as well as manage myopia, as well as communicate effectively communicate effectively with patients and parents. with patients and parents. Networkable, and chair Networkable, and chair and stand compatibility and stand compatibility also enables easy also enables easy practice integration, and practice integration, and large colour touch screen large colour touch screen allows easy measurement allows easy measurement capture process. Device capture process. Device Technologies is the Australian Technologies is the Australian supplier of MYAH. supplier of MYAH. always be the most cooperative patients, thereby delivering real benefits to a busy practice.
The device’s keratometry practices, as it is a standthe need for a computer, allowing it to fit where some accurate measurements NIDEK AL-Scan delivers,”
SIX METRICS MEASURED IN 10 SECONDS
The NIDEK AL-Scan measures keratometry, optical biometry (axial length), pupil size, horizontal visible iris diameter (HVID), central corneal thickness (CCT) and anterior chamber depth (ACD). According to its distributor Designs For Vision, the 3D autoalignment and auto-capture makes the process fast and easy; an advantage when measuring young myopes who may not be always be the most cooperative patients, thereby delivering real benefits to a busy practice.
The device’s keratometry is said to be “extremely precise” because the AL-Scan measures 720 data points on two circles of 2.4mm and 3.3mm diameters. AL-Scan is also ideal for “space challenged” practices, as it is a standalone device without the need for a computer, allowing it to fit where some devices wouldn’t.
“When you need fast, accurate measurements in a small footprint, the NIDEK AL-Scan delivers,” DFV says.


CHANGE AGENTS Educating parents about myopia
Research estimates myopia will affect 50% of the world's population by 2050, and recent COVID lockdowns appear to have only worsened the situation. As more patients – and their parents – seek effective interventions, practitioners should prepare to meet this oncoming public health demand.
Communicating with parents of paediatric patients can be challenging. Perhaps none more so than with parents whose children have been, or are at risk of being, diagnosed with myopia.
What communication methods do optometrists adopt to educate parents about the importance of long-term interventions, as opposed to only vision corrective measures?
Academics, industry experts and clinicians with a special interest in myopia contribute to the conversation with Insight, sharing their unique perspectives on what can misconstrue parents’ understanding of myopia, how to broach conversations about the safety and efficacy of treatment, the potential cost of several years’ treatment, and overcoming aversion to contact lenses.
PLANO IS NOT NECESSARILY NORMAL Multilingual optometrists Mr Griffin Ngo and Ms Wendy Yeung initially opened greenfield practice, Rhodes Optometry, in Sydney’s inner west as a contact lens clinic – then quickly realised the pressing need for a dedicated myopia clinic, and established Sydney Myopia Clinic at Rhodes Optometry in August last year.
“Our patient base is typically young, professional, educated, with a strong Chinese ethnicity. Parents have often heard of orthokeratology (ortho-k), but it is often harder to explain concepts behind other interventions like atropine, and defocus spectacle lenses,” Yeung says.
She says having parents witness their child struggle with their vision during assessment is often the most effective way to convince parents that intervention is needed. But telling parents that intervention is recommended for a child who is pre-myopic is a much harder task.
“It can be hard to explain to a parent that being plano, or zero dioptres, as an eight-year-old is not a good thing. While it seemingly appears ‘normal’ to parents for their child to be zero dioptres, it’s on the verge of becoming myopic, as the normal refractive error for a child of that age is actually around +0.75. It’s hard for parents to understand this because their child’s vision currently appears as perfection.”
In this type of scenario, the challenge increases as Yeung and Ngo need to communicate the importance of preventing myopia from developing, when the parent believes nothing is ‘wrong’ with their child’s eye health.
“If we can intervene to prevent or delay the onset, we’ve met our goal – but it’s challenging to demonstrate that it’s the absence of myopia that shows intervention is working.”
To help guide parents through myopia assessment, diagnosis, prevention and treatment, Ngo and Yeung have created a brochure explaining why myopia control matters and outline potential treatment options.
They also refer to a manufacturer’s brochure, which features a graph that plots average childhood myopia progression over time if there is no intervention, versus myopia control. Parents are also




An example of software on the Lenstar Myopia providing easy-to-read graphs that can show aspects like axial length growth over time.
directed to www.mykidsvision.org, an information tool developed by Australian optometrists Drs Paul and Kate Gifford.
“There is a lot of information for parents to take in, in one consultation,” Yeung says. “Giving parents a brochure as well as a link to a website like ‘My Kids Vision’ gives them something to take home, to refer to again and again.”
Ngo and Yeung also discuss the cost of treatment with parents.
“Explaining to parents that their child will require myopia treatment throughout their adolescence and potentially adulthood is a shock for some,” Ngo says.
“Whether or not it is ortho-k or spectacles that is the best option in terms of treatment, we discuss how many pairs of lenses their child is likely to need over the course of their treatment, and the probable cost. Gaining parents’ consent and commitment to come back is vital.”
Another hurdle is discussing the safety of various treatments.
“A lot of parents are concerned about safety issues associated with certain treatments. When we’re discussing orthokeratology, for example, we explain the precautions we’re taking in prescribing ortho-k, we explain how the lens material is designed to be safe, and how children wearing lenses overnight when they are at home with their parents means that if their child wakes with a red eye, they can seek treatment immediately,” Ngo says.
“A lot of parents also feel their child is not ready for contact lenses. If that is the case, we do one of two things; we try a spectacle lens option and complete a three-to-six-month review. If, upon review, their prescription has increased, we advise moving into contact lenses. This way, both the patient and parent are pre-warned. Alternatively, if a parent feels their child is not ready for contact lenses, we demonstrate to them the process of inserting and removing them using trial lenses. Often, the parent realises their child is more mature than they thought.”
THE INFLUENCE OF CULTURE AND ENVIRONMENT Most of Professor Ian Morgan’s work focuses on myopia prevention. A Visiting Fellow at Australian National University (ANU), the biochemist and pharmacologist became interested in myopia almost by accident 30 years ago, when he was researching the effects of dopamine on the retina, axial elongation, and growth control. “It was the 1990s and an epidemic of myopia was emerging in East Asia and Singapore. My perspective on the role of parents in the prevalence of myopia derives from that time. Since then, we’ve witnessed the rise of the ‘Tiger Mum’, and parents pushing their children to achieve academic excellence,” he says. That cultural tendency to place high expectations on excellence has come at a cost – the health of children’s vision. Morgan, a member of the ARC Centre for Excellence in Vision Science at ANU, is chair of the International Myopia Institute’s Environmental Risk Factors in Myopia Taskforce. They produced a white paper, published last year, outlining the latest scientific evidence on causal risk factors for myopia. “Education and time outdoors – these are the two major risk factors for school-aged myopia,” Morgan says.
“In regard to education, parents – particularly in East Asia – need to be made aware of the potential consequences of placing too much burden on young children to perform academically, early in their schooling.
“However, the Chinese government is taking major steps to reform education to shift the burden or pressure away from preschool to senior high school, more like in the general Western population.”
He says research has demonstrated children in East Asia have certain patterns of behaviour when it comes to their education – and are correspondingly more myopic – and migrants to Australia carry those cultural attitudes to education with them.
“Shifting competitive pressures may help alleviate the pressure parents in East Asia place on their children to gain entry into the most desirable primary schools,” he says.
The second major driver to prevent myopia is time outdoors: “The evidence is overwhelming. The more time children spend outdoors, the more they are protecting from myopia.”
A randomised controlled trial (RCT) carried out in China showed that more time outdoors in schools would slow the onset of myopia (He et al 2015).
“Two papers reported an association between myopia and time outdoors in 2007-8. Singapore adopted a policy promoting outdoor activities in 2008, but as a parental responsibility. Taiwan first implemented it in schools from 2010, but the first RCT was small in 2013, followed by a larger trial in 2015. The excellent recent paper is a subset of the work going on in Taiwan,” Morgan says.
He is referring to a recent survey in Taiwan, undertaken before and
WENDY YEUNG RHODES OPTOMETRY


again during the coronavirus pandemic, on the prevalence of myopia after implementing a policy promoting outdoor activities in preschoolers.
A total of 21,761 pre-schoolers, aged five to six from seven schoolyear cohorts (2014 to 2020), were included in the analysis.
Since August 2014, in Taiwan, myopia prevention strategies, such as increasing outdoor activities (two hours per weekday), have been promoted in all kindergartens, and countywide schoolbased eye examinations, including cycloplegic autorefraction, and caregiver-administered questionnaires have been carried out annually for participants.
The survey results, published by the American Academy of Ophthalmology, showed the prevalence of myopia continuously decreased for two years after implementing these strategies.
“This study in Taiwan demonstrated time spent outdoors can counteract the effects of studying. How much time is spent outdoors is in the control of parents and it plays a huge role in prevention. That is a major lesson for parents; get your children outside as much as possible, two hours a day minimum,” Morgan says.
“The introduction of time outdoors, two hours per weekday, in the Taiwanese school system reduced the rate of myopia for the first time in 40 years. If they start earlier, at the beginning of pre-school, and continue through primary school, it can have a massive impact on progression.”
CHANGE AGENTS Professor Padmaja Sankaridurg is head of the myopia program at the Brien Holden Vision Institute (BHVI) and Conjoint Professor at the School of Optometry and Vision Science at the UNSW. She’s also a member of the International Myopia Institute’s Advisory Board.
Sankaridurg has been managing the myopia program at BHVI since its inception in 2003, accumulating nearly two decades of ‘intel’ into myopia and the role parents play in their child’s treatment outcome.
“With a childhood onset condition such as myopia, parents/carers are the change agents with respect to adopting and promoting new behaviour strategies and myopia treatments,” Sankaridurg says.
She believes communication methods need to be tailored to specific populations taking into account socio-economic status, cultural and social beliefs, and attitudes to change.
“As an example, in countries with high pollution levels or high density living or attitudes to sun exposure and skin colour, a message to send children outside each day may not resonate with the population. Taking into account the circumstances on the ground and providing

GRIFFIN NGO RHODES OPTOMETRY




PROF IAN MORGAN ANU
further information on when and how to achieve the required time outdoors may help engage them,” Sankaridurg says.
Additionally, communication methods need to consider the awareness level of parents.
“For example, in countries where the prevalence is already high or parents that have myopia are possibly well informed and aware of the problem, parents might be more interested in treatments or recommendations to reduce risk. In this situation, even passive websites offering information on newer treatment methods is likely to help parents make an informed choice,” she says.
“On the other hand, there may be parents/carers who are unaware of the problem, and they need to be targeted more actively to raise their level of awareness and draw their focus to the eye health of their child.”
CooperVision’s ‘Global Myopia Attitudes and Awareness Study’, released last year, revealed 54% of eyecare practitioners believe parents don’t understand the risks of significant eye health issues associated with myopia.
Delving further into this, Sankaridurg explains that the eye health issues related to higher levels of myopia mostly occur at a much later age and therefore, even if parents have experienced myopia within their close circle, they are unlikely to know the real impact.
“Educating parents and the patient (if they are old enough) is the key. Indeed, the same study indicated that 87% of parents are willing to learn about myopia management solutions. Facts should be presented in simple, uncomplicated terms and should include available options to mitigate the risk,” she says.
“Available calculators and percentile charts can demonstrate a ‘what if’ scenario that can be used to educate parents. It’s also critical to establish a rapport with the parent and child so parents feel comfortable and confident with any decision making.”
CooperVision’s survey also found 58% of eyecare practitioners said parents don’t want to put their children in contact lenses – and for parents who would consider contact lenses, they preferred their children to start at 12 years of age.
This statistic illustrates a familiar conundrum for Sankaridurg.
“The two main areas of concern for contact lens wear in children are the risk of complications and ability of the child in handling lens wear. With respect to the latter, there is substantial data that demonstrates that children as young as six to seven years of age can independently care for their lenses,” she says.
“With regards to complications, the risk of adverse events in children is no more than that observed with adult contact lens wear – and with daily disposable lens wear the risk of serious infections is quite low. Despite this data, there is a general reluctance to introduce young children to contact lenses and is likely related to negative publicity around complications and the lack of information on the positive outcomes.” GLOBAL PERSPECTIVE An optometry graduate from the University of Melbourne who completed postdoctoral research at the University of Toronto, Dr Monica Jong worked with the late Professor Brien Holden as part of the grassroots myopia control research and advocacy at BHVI, and went on to become executive director of the International Myopia Institute for six years.
Jong is now global director of professional education in myopia at Johnson & Johnson (J&J) Vision and a Visiting Fellow of the School of Optometry and Vision Science, UNSW Australia.
“My perspective on parents and myopia is global, working with experts and speaking with optometrists worldwide. Practitioners across the world no matter where they are, experience similar challenges in navigating a lack of awareness in parents about myopia as a serious ocular health issue – it’s a huge challenge,” she says.
“Optometrists have been correcting myopia for years – and doing it well. So well, in terms of visual function, that the parent and child don’t recognise that myopia is not a normal state of the eye. There isn’t enough public awareness that myopia is a problem. We need to change perceptions and behaviours.”
Jong says, generally speaking, the public is accustomed to the (misguided) idea that when a child develops myopia, they are inevitably going to wear (single vision) glasses, their myopia will likely progress over time and there is no available treatment.
“But they don’t realise myopia is associated with other sightthreatening complications, and may increase risk of glaucoma, myopic macular degeneration, retinal detachment, and permanent vision loss,”1,2 she says.
“Today there are evidence-based treatment options that have been reported in the literature to both correct myopia and slow its increase in children.3 But the challenge is to convey this in an easy-tounderstand manner. We don’t want to scare parents with statements about vision loss or overwhelm them by throwing lots of statistics at them. It’s a matter of gauging their level of initial understanding and providing a balance between communicating the urgency to manage myopia without scaring them.”
Jong says practitioner-facing websites are excellent in guiding myopia management but more patient-facing websites, like Myopia Profile’s ‘My Kids Vision’, are needed to send a positive message that detecting myopia early and treating it is the best way to reduce the risk of related complications.
“Today most parents are turning to Google first and so having a high-quality evidence-based website is really helpful to get the conversation started with patients and to build a myopia management practice. Having simple, easy to understand practitioner materials ready in your practice, and prepared answers to frequently asked questions is useful for practitioners and their staff,” Jong says.

PROF PADMAJA SANKARIDURG BHVI
“Using simple messages with the public is key, for example, spending time outdoors, reducing near work and taking regular breaks such as the 20-20-20 rule, proposed by Professor Caroline Klaver.” (Klaver proposes after 20 minutes of close work, children should gaze at objects 20 feet away for at least 20 seconds, and they should be outside intermittently for at least two hours daily).
A growing level of sophistication in myopia instrumentation is also advancing the conversation to better educate parents.
“Industry has realised the need for improved instrumentation to support practitioners in myopia management, such as ocular biometry to monitor axial length. These have been used in clinical trials as the primary measure of eye growth and increasingly being adopted in clinical practice,” Jong says.
“But you can still do myopia management without it. Some of the ocular biometers have axial growth curves in their software which displays to parents where their child’s eye growth is compared to the average for their age and ethnicity and helps demonstrate the effect of a treatment. "Several groups have developed online myopia calculators, so a child’s refraction measurements can also be plotted against an average guide, with and without treatment. There are fantastic tools available and new monitoring devices being trialled that measure time outdoors and near work exposure, to help support treatment.”
Stepping into a global education role at J&J Vision is giving her the opportunity to do more.
“Myopia management is about understanding the patient holistically, in terms of their risk factors, age, refraction, lifestyle and
TAKE ANOTHER LOOK AT PREDNEFRIN FORTE

Available now across Australia Indicated for non-infectious ocular infl ammation1 and back in stock

DR MONICA JONG J&J VISION
preference to recommend the most appropriate treatment. Having a conversation with parents and child, taking a good history and integrating that with clinical findings are part of the process," Jong says.
“Ultimately, for parents, communication is critical to build awareness. As clinicians, we need to strike a balance in what we communicate. We don’t want to scare parents but it’s imperative they understand that today there are bonafide treatments backed by scientific evidence available. It is now possible to slow the increase in myopia in children and correct vision at the same time.” ■
Disclaimer: Monica Jong is an employee of J&J Vision but this is not a J&J Vision-sponsored article. The views expressed are from her professional opinion. References available in the online version of this article.


Reference: 1. Prednefrin Forte Product Information.
PBS Information: PREDNEFRIN FORTE® is listed on the PBS for severe eye infl ammation, corneal grafts and uveitis.







Sooner or later?






THE SEQUENTIAL BILATERAL CATARACT SURGERY DEBATE
Sequential bilateral cataract surgery has been in the spotlight in recent months, prompting discussion around the risks and benefits of immediate versus delayed surgery. Insight explores both sides of the argument.
Same-day bilateral cataract surgery is not often performed in Australia; ophthalmologists are generally concerned about rare but serious complications, as well as sub-optimal refractive outcomes for people relying on the procedure to improve their vision and quality of life.
A retrospective study in the US using data from a registry of nearly two million bilateral cataract surgery patients, published in JAMA Ophthalmology last July, found immediate sequential bilateral cataract surgery (ISBCS) was associated with worse refractive outcomes than delayed sequential bilateral cataract surgery (DSBCS), although – the authors acknowledged – the small but statistically significant differences may not be clinically relevant.
The study results piqued the interest of the ophthalmology profession, locally. University of Sydney’s Associate Professor Chameen Samarawickrama discussed the study and the efficacy of same-day bilateral cataract surgery as a guest on ABC’s Radio National Health Report with Dr Norman Swan last July.
Samarawickrama told listeners the vast majority of ophthalmologists in Australia prefer delayed surgery, with most operating on the second eye within two weeks of surgery on the first eye. He delved further into the study and its implications in the Soapbox column in Insight’s December issue.
In August, about a month after the US study was published (although the timing was not intentional), the Australian Commission on Safety and Quality in Health Care (ACSQHC) released the nation’s first Cataract Clinical Care Standard, which included a quality statement relating to second-eye surgery.
“Options for a patient with bilateral cataract are discussed when the decision about first-eye surgery is being made,” the standard says. “Second-eye surgery is offered using similar criteria as for the first eye, but the potential benefits and harms of a delay in second-eye surgery are also considered, leading to a shared decision about second-eye surgery and its timing.”
In most cases, the commission says this may result in a decision to schedule second-eye surgery some weeks after the first operation, which may avoid unnecessary delays for patients, particularly those for whom refractive differences may be considerable after the first eye surgery. In others, it may be the patient’s decision to wait and see.
The standard states “there is limited evidence to support second-eye surgery on the same or next day”, however there are circumstances when this is appropriate, with appropriate precautions and informed patient consent.
In light of these developments, Insight spoke with leading surgeons about their views on same-day surgery, and what lessons can be learned from the past.
RANZCO’S POSITION Associate Professor Andrew Chang is vitreoretinal surgeon and ophthalmologist at the Sydney Eye Hospital.
In his capacity as director on the RANZCO Board, Chang spoke with Insight about RANZCO’s position on immediate sequential bilateral cataract surgery (ISBCS) versus delayed sequential bilateral cataract surgery (DSBCS).


A/PROF ANDREW CHANG
“Sequential bilateral cataract surgery, or bilateral sequential sameday surgery, is not the standard of care for the majority of patients,” Chang says.
“It is unlikely to be recommended by most RANZCO Fellows due to the advantages of sequential bilateral cataract surgery on separate days. This is evidenced in the survey results from RANZCO Fellows.”
The survey he is referring to was conducted by prominent Sydney cataract surgeon Professor Gerard Sutton and Dr Christopher Hodge who quizzed Australian ophthalmologists on their views about simultaneous bilateral cataract surgery (SBCS), which appears to have a limited local uptake.
Although it remains contentious, Sutton and Hodge point out it has become more prevalent in northern Europe with government compensation for day surgeries.
“Proponents may argue that the incidence of bilateral endophthalmitis is minimal, however it remains a primary concern for many,” they wrote in RANZCO’s Eye2Eye magazine (Q1, 2021), where the survey results were published.
“SBCS is undertaken in Australia, however our survey suggests it has minimal penetration at present with only 4.1% of respondents offering the service to patients. Furthermore, 95.4% of surgeons did not believe SBCS should be made mandatory as an alternate to routine practice of surgery on separate days. Of note, of those who complete SBCS, most surgeons (69%) only offered it to 5-10% of their patients, highlighting the current niche role in the patient/surgery discussion,” they wrote.
Chang says, in Australia and New Zealand, most surgeons and their patients chose timing of surgery on separate days. He says surgeons do this with consideration to best safety and outcomes for the individual.
“Cataract surgery is major intraocular surgery with defined risks. Although unlikely, unexpected complications and adverse outcomes may occur in preoperative preparation, during the surgery itself or in the postoperative course,” he says.
“Often this relates to the individual patient and their eye pathology. Surgeons will use this important information to learn, manage and avoid these patient eye-related issues when performing surgery on the second eye. This ensures safety and optimal outcomes for patients.”
Chang says operating on one eye at a time necessarily reduces the surgical and anaesthetic risk to both eyes and body.
“Further, depending on the regional anaesthetic block, having both eyes done at once would result in the patient being unable to see for up to six hours after the surgery,” he says.
Timing of surgery on the second eye is in part driven by the results of the first operation.
“The surgical and optical result from cataract surgery in the first eye is used to guide the patient and surgeon for any changes required when the second eye is done,” Chang says.
“The focus point for reading or distance in the first eye can be assessed for appropriateness and desirability allowing the power of the intraocular lens to be altered to match the focus in the first eye or to achieve monovision with blended vision.
“Uncommonly, the calculated power of the intraocular lens preoperatively does not give the predicted focal point once implanted in the patient (known as refractive surprise). Separate day surgery will allow this undesired situation to be detected and managed.”
Even for a highly myopic patient, bilateral sequential same-day surgery would not be necessary, in Chang’s opinion.
“In this example, if the patient were to have one eye rendered focused in the far distance (emmetropia) this would pose issues with seeing with both eyes together (binocularity) until the second eye undergoes surgery to match the first eye. In this situation, most surgeons and patients would choose to have surgery timed close together, when safe to do so,” he says.
Chang acknowledges that in certain circumstances SBCS may be an option – for example, those requiring general anaesthetic, such as the very young, very elderly, or patients with dementia.
“Patients do have a right to choose. This is reflected in the consumer section of the [Cataract Clinical Care] Standard,” he says.
However, RANZCO has “strongly disagreed” with the need to routinely discuss same or following day second-eye surgery, which some have interpreted as a recommendation in the Standard.
“Due to the low rates of bilateral sequential same-day surgery and the very particular set of circumstances that may cause a patient to require it, there should be no need to make discussions about bilateral sequential same-day surgery routine,” Chang says.
“The vast majority of surgeons and their patients chose timing of surgery on separate days. A small minority of surgeons perform bilateral sequential same-day surgery in selected patients. This would include medical or logistical issues of access and travel.”
FINANCIAL DISINCENTIVES Dr Michael Lawless from the Vision Eye Institute is one of Australia’s most experienced eye surgeons, having performed more than 30,000 surgical procedures. He is a Clinical Associate Professor at Sydney Medical School (University of Sydney) and is recognised as a global authority on laser eye surgery.
Lawless is also a contributing author in a new textbook Immediately Sequential Bilateral Cataract Surgery (ISBCS): Global History and
Methodology, due for publication this year. Working with chief author and editor, Dr Steve Arshinoff, he has penned a chapter on the Australian perspective.
From an ophthalmologist’s point of view, Lawless says the prevalence of ISBCS depends on where you are in the world, and whether your peers see it as a sensible proposition.
“In some Scandinavian countries, such as Finland, approximately 50% have same-day cataract surgery but in Australia, it has very low uptake. But both are in the right – there are no absolutes on this,” he says.
“There are definite benefits to same-day cataract surgery. There are clear benefits to society in terms of cost and efficiency; patients, who tend to be over 60 and sometimes need help getting to and from surgery, only need to come in once, and there are fewer post-op visits. There are clearly efficiencies in day surgery, requiring only one visit, and one aesthetic. Why wouldn’t you do it more commonly?”
Lawless says the fear of potential rare bilateral clinical complications is keeping same-day cataract surgery at bay among Australian ophthalmologists.
However, reliable data analysis from the University of Toronto’s Dr Steve Arshinoff – who Lawless describes as “the person who has thought about and published the most on ISBCS in 25 years” – shows a low rate of infection in both eyes in same-day surgery.
“If you’ve got the right protocols in place in theatre, the risk of infection in the second eye is almost immeasurably low. So, why don’t we do sameday? Partly because it’s not the norm – our peers aren’t doing it – but the main barrier is financial,” Lawless says.
“As Paul Keating said, back self-interest every time,” Lawless quips. [Paul Keating often quoted his long-time mentor former NSW Premier Jack Lang: “In the race of life, always back self-interest – at least you know it’s trying”].
Under the current system, Lawless says there are financial disincentives for the surgeon and the day surgery or facility to perform same-day surgery. Simply put, in order for same-day cataract surgery to be more commonplace in Australia, the financial incentives need to be sensible.
“In the US, for example, when a surgeon removes a lens for refractive purposes – not because of cataract – the patient pays the total cost of surgery. This means the patient has a financial incentive to have both eyes operated on the same day and so the uptake is higher. In the US, bilateral same-day cataract surgery is low but bilateral same-day lens extraction is significantly higher. That’s a reflection of financial incentives,” Lawless says.
“Another thing to consider is the Indigenous population, especially in remote areas. Patients commonly find it difficult to get to a clinic and
DR MICHAEL LAWLESS



A first choice for glaucoma management1

If clinically necessary for the treatment of your patient,
prescribe by brand and disallow brand substitution2
PBS Information: Xalatan (latanoprost 0.005% eye drops, 2.5 mL) is listed on the PBS as antiglaucoma preparations and miotics.
Before prescribing please review Product Information available via www.aspenpharma.com.au/products or call 1300 659 646.
Minimum Product Information: XALATAN® (Latanoprost 50 μg/mL) Eye Drops. Indication: Reduction of intraocular pressure (IOP) in patients with open-angle glaucoma or ocular hypertension. Contraindications: Hypersensitivity to ingredients. Precautions: Change in eye colour due to increased iris pigmentation, heterochromia; eyelid skin darkening; eyelash and vellus hair changes; aphakia; pseudophakia; macular oedema; other types of glaucoma; contact lenses; severe or brittle asthma; herpetic keratitis; driving or using machines; elderly; children; lactation. Pregnancy: Category (B3) Interactions: other prostaglandins, thiomersal. See PI for details. Adverse Effects: Iris hyperpigmentation; eye irritation (burning, grittiness, itching, stinging and foreign body sensation); eyelash and vellus hair changes (increased length, thickness, pigmentation and number of eyelashes); mild to moderate ocular hyperaemia; punctate keratitis; punctate epithelial erosions; blepharitis; eye pain; excessive tearing; conjunctivitis; blurred vision; eyelid oedema, localised skin reaction on eyelids; myalgia, arthralgia; dizziness; headache; skin rash; eczema; bronchitis; upper respiratory tract infection; abnormal liver function. Uncommon: Iritis, uveitis; keratitis; macular oedema; photophobia; chest pain; asthma; dyspnoea. Rare: periorbital and lid changes resulting in deepening of the eyelid sulcus; corneal calcification. See PI for details and other AEs. Dosage and Administration: One eye drop in the affected eye(s) once daily. Other eye drops should be administered at least 5 minutes apart. (Based on PI dated 2 March 2021) References: 1. NHMRC Guidelines for the screening, prognosis, diagnosis, management and prevention of glaucoma 2010 2. Australian Commission on Safety and Quality in Healthcare Active Ingredient Prescribing Guide - list of medicines for brand consideration December 2020 Aspen Australia includes Aspen Pharmacare Australia Pty Ltd (ABN 51 096 236 985) and Aspen Pharma Pty Ltd (ABN 88 004 118 594). All sales and marketing requests to: Aspen Pharmacare Pty Ltd, 34-36 Chandos Street, St Leonards NSW 2065. Tel: +61 2 8436 8300 Email: aspen@aspenpharmacare.com.au Web: www.aspenpharma. com.au Trademarks are owned by or licensed to the Aspen group of companies. © 2021 Aspen group of companies or its licensor. All rights reserved. Prepared: June 2021 AF05768 ASP2528
don’t come back for the second eye and my understanding is that in Western Australia, they are increasingly doing bilateral same day surgery for that reason.”
Dr Angus Turner, from the Lions Eye Institute in WA, confirmed this to Insight. He started offering same-day surgery to select patients in 2013.
“I started doing this with a policy for hospitals accepting it and writing out a document that essentially said it was a separate operation,” Turner says.
At the time, he cited an article in Ophthalmology Management for reference, titled ‘Doubling Down on Cataract Surgery’, by Jerry Helzner, senior editor. Since then, several ISBCS reviews and meta-analysis have been published in international peer-reviewed journals.
“I don’t routinely do bilateral surgery however, when patients have high refractive error and outreach surgery visits are infrequent, then I do offer it. Also, if patients have large logistical or geographical barriers to care, I will discuss same-day surgery with the patient,” Turner says.
Geographic and financial motivations aside, Lawless points out that while refractive outcomes used to be a reasonable argument against sameday cataract surgery, that is no longer the case because lens selection and surgical precision are of such excellence, surgeons can achieve the desired refractive outcomes in immediate sequential operations.
“If the argument against ISBCS is the refractive outcome then surgery should be scheduled six weeks apart, which is not commonly done, and so this argument is clearly nonsense,” he says.
In his own practice, Lawless routinely schedules bilateral cataract surgery one week apart.
“Occasionally I do one day apart. I don’t have a conversation with patients about doing same-day – and I won’t have that conversation until the authorities and the regulatory framework are supportive. Otherwise, you leave yourself open or vulnerable to criticism for being outside the mainstream.”
CUSTOMISATION OPPORTUNITY Associate Professor Chandra Bala is managing director at personalEYES, comprising 10 clinics in NSW and ACT, and subspecialises in cataract, cornea, glaucoma and refractive surgery.
On the balance of risk, Bala is “not a big fan” of same-day bilateral cataract surgery and would perform it only in extenuating circumstances.
He says usually cataract surgery is uncomplicated but there are patients who develop corneal edema as part of removing their dense cataract.
“They would need to recover from the first eye before one could commit them to the second,” Bala says.
“Then there are known risks associated with cataract surgery. You can execute a perfect operation but have an adverse outcome, including endophthalmitis or toxic anterior segment syndrome or refractive surprises. Adverse outcomes only occur in a very small number of cases, but they still exist, it’s not a figment of imagination. To have this happen to both eyes would be terrible for the patient,” Bala says.


DR ANGUS TURNER
There are also unknown or unexpected risks. Health systems are not immune to catastrophic failure; these can – and do – still happen. To illustrate his point, Bala recalls more than one significant health system failure resulting in cataract patients losing sight.
“It happens in Australia from time to time. The last time it happened was in 1999. Several patients had their vision affected in one eye following cataract surgery at Dubbo Base Hospital. The case went to the NSW Health Care Complaints Commission (HCCC),” he says.
According to the HCCC’s report, 12 out of 19 patients who underwent cataract surgery at Dubbo Base Hospital on 8 February 1999 experienced significant permanent damage to their corneas and visual impairment.
The report stated that it appeared supplies of the usual irrigating and intraocular agent (a balanced salt solution) were low due to errors in ordering and/or delivery and that an alternative solution was used as a substitute. On the evidence available, the substitute solution may have been responsible for the adverse outcomes on the basis that it contained a preservative, benzalkonium chloride, which is not present in the usual solution.
Another negative outcome Bala recalls involved 11 eyes of six patients from six different institutions in the US.
In 2015, the American Academy of Ophthalmology published a retrospective study on postoperative hemorrhagic occlusive retinal vasculitis (HORV) that developed in six patients who underwent otherwise uncomplicated cataract surgery, receiving prophylactic intracameral vancomycin during the procedure.
Despite good initial vision on post-operative day one, between one to 14 days after surgery, all eyes demonstrated painless vision loss resulting from HORV, a rare and devastating condition linked to the use of intraocular vancomycin.
“Five of those six patients went bilaterally blind. They walked in through the surgery doors seeing, but within two weeks were bilaterally blind,” Bala says.
“You are not offering a better outcome by doing same-day cataract surgery.”
Bala usually delays second-eye cataract surgery two weeks after the first eye, but he does offer bilateral same-day LASIK surgery, a 10-minute operation, and bilateral same-day ICL surgery (implantable collamer lens).
“I believe in technology – I’m a technophile – but I don’t trust it. In cataract surgery, I verify my outcome at week one. Rarely, I’ll operate after a two-day gap provided the vision is where I expect it to be. I haven’t had a patient with an infection in 15 years but I always worry about it,” he explains.
“Delaying surgery on the second-eye allows a ‘customisation opportunity’, to recalibrate based on the outcome of the first eye.” ■


LENS COATING TECHNOLOGY'Life-proof'


First developed 30 years ago, Crizal lenses have set the standard of anti-reflection coatings. Essilor has now improved the portfolio with new technologies that, among other features, have improved the resistance of its lenses.
Essilor Group’s origins are bedded in a unique human, industrial and business venture, starting in 1849 as a Parisian artisanal spectacle maker before evolving into an optical industry powerhouse.
With a 173-year history, the global ophthalmic lens manufacturer considers itself at the core of technological advances propelling the industry forward, notwithstanding innovations like the world’s first progressive lens (Varilux) in 1959 and other breakthroughs like the 1.5 index plastic spectacle lenses and an automatic edging machine.
The fact half of the group’s revenue today comes from products designed less than five years ago perhaps speaks volumes of its emphasis on R&D, which now amounts to more than €350 million (AU$550 m) annually.
During the past four years, the company’s Crizal lens coatings – first launched in 1992 – have been a major priority of its R&D program.
Specifically, Essilor has aimed to develop new technologies that continue to deliver anti-reflection properties, in addition to improved scratch and thermal resistance, and anti-smudge and UV protection benefits. The focus has been on producing “life-proof” lenses. As a result, the new Crizal portfolio is now protected by up to 10 patents.
While already available in some markets, Australian eyecare professionals and their patients will have access to the updated Crizal coatings from this month.
In short, the new Crizal Sapphire HR will replace Essilor’s flagship coating Crizal Sapphire UV. Crizal Rock will replace Crizal UV. Crizal Easy Pro will replace Crizal Easy, while Crizal Sun XProtect will replace Crizal Sun UV.
Ms Tara McCabe, Essilor's Sydney-based director of marketing and business partnership, says since Crizal coatings were first developed the company has been working to “redefine the standard of anti-reflection coatings for all wearers”.
More than 825 million Crizal lenses have been sold – equating to a pair sold every second worldwide – and Essilor is now seeking to build on this with its upgraded portfolio.

Essilor ANZ CEO Pierre Longerna.
“Our flagship product, Crizal Sapphire UV, has been the most popular and fastest growing coating in the Crizal range,” McCabe explains.
“With its unique anti-reflection benefits from not just the front but also the back and sides – the lens is almost invisible. Vision is virtually free from disturbing reflections, light sheen, ghost images and back and side reflections. This feature is in addition to the outstanding anti-scratch, anti-smudge, ease of cleaning and UV protection benefits that Crizal Sapphire HR now provides.”
Explaining the technology further, McCabe says Crizal Sapphire HR is the portfolio’s best anti-reflection coating overall.2 Compared to previous generations, it has a 70% improvement in scratch resistance and 20% increase in thermal resistance. It’s also easy to clean with superior smudge and water resistance. Additionally, Crizal Sapphire HR is said to offer “best in class transparency”, matching the anti-reflection efficiency of Crizal Sapphire UV.
According to Essilor, there are three innovations underpinning the coating. The first is Multi-angular Technology that reduces front, lateral and back reflections. The second element is High Resistance Technology, a combination
of four specific oxides known for their resistance against scratches and temperature (one oxide is used in the aerospace industry). The third feature is High Surface Density Process; this produces a super hydrophobic and ultrasmooth topcoat for smudge resistance and a superior ability to repel dirt and water, Essilor states.
McCabe says the second lens coating in the portfolio, Crizal Rock, offers Essilor’s best combination of scratch and smudge resistance4, whilst maintaining reduced reflections, UV protection, plus water and dust repellence.
Like Crizal Sapphire HR, it also features High-Resistance Technology. Crizal Rock is also bolstered by High Surface Density Process technology in the topcoat for ease of cleaning.
Next up, Crizal Easy Pro, is described as an easy to clean and maintain anti-reflection coating featuring High Surface Density Process in the topcoat to resist smudges and repel water.
Additionally, all three – Crizal Sapphire HR, Crizal Rock and Crizal Easy Pro – offer UV protection of E-SPF 35.5 High level UV protection is offered with all lens materials (clear CR39 is slightly lower giving ESPF 10), blocking 100% of transmitted UV, while the coating’s special UV layer cuts rays reflected from the back lens surface.
Finally, Essilor has developed Crizal Sun XProtect exclusively for its Xperio tinted and polarised sun lenses. Its Ionic Shield Technology is applied by vacuum deposition, a patent pending formulation reinforcing the front surface of the sun lens for best-in-class scratch resistance, while fluorinated molecules add superior smudge protection, keeping Xperio sun lenses looking newer for longer.9 Crizal Sun XProtect offers UV protection of E-SPF 5012 and has a subtle gold lustre on the front surface for a fashionable, premium finish.
A CHANCE TO ADD VALUE While Crizal coatings add features that enhance the performance of Essilor lenses, McCabe says it also offers a unique opportunity for Australian practitioners to increase customer satisfaction.
“It allows the practice to offer higher value vision solutions and differentiate themselves from practices offering lower value and lower performing coatings. This contributes to added value and profitability to the optical business,” she explains.
“We’ve seen the pandemic further reinforce the importance of good vision and eye health. With the increased use of screens, it’s even more important to reduce reflections, increase light transmission and improve contrast. With the frequent use of video calls, reflections from a wearer’s glasses can be distracting and unappealing for viewers. Providing optical lenses protected by an anti-reflection coating are key.”
Additionally, McCabe says UV protection remains critical for eyes and surrounding skin. While patients are aware of the harmful effects of UV headon, many are less aware of the potential impact when sunlight is reflected off the back lens surface from behind.
“Lenses with Crizal coatings combined with hi-index plastic lens materials*, reduce UV impacting the eye from both the front surface transmission but also from back surface reflection,” she says.
“We are also the only manufacturer that uses the E-SPF rating system giving patients a simple way to understand the UV protection level of their lens coating.”
TRIED AND TESTED To put its new Crizal technology to the test, Essilor has developed a protocol of technical and consumer trials to verify in-life performance and assess a lens’ resistance to scratches, smudges, and daily wear and tear.
The most notable of these is a new Sand Resistance Test, providing a more controlled and repeatable test with greater capacity to discriminate between high-scratch resistant coatings than the historical Bayer test. In this test, lenses were subjected to 300 shake-cycles in a sand filled tray; Crizal Rock and Crizal Sapphire HR showed a 70% increase in scratch resistance versus Crizal UV.
A separate extensive Cleaning Test – conducted by an external lab – replicated daily cleaning over the lens’ life. It involved 20,000 wipes with ink splattered on the lens every 5,000 wipes. Crizal was shown to be the easiest to clean lens.6
Essilor has also conducted consumer tests, including an 18-month trial in which its R&D experts evaluated the difference in abrasion level between Crizal Rock vs Crizal UV, worn in parallel. In this, Crizal Rock had superior scratch resistance over the previous generation of Crizal.8
And to push Crizal lenses to their limit – a Unique Torture Test was conducted on Crizal Rock. After a battery of wipes, rubs, shakes, drops and hits before a panel of observers, an independent third party certified the “lenses are in new condition, without any scratches or dents”.
Finally, third party testing, simulating up to two years’ real-life usage, validated Xperio sun lenses with Crizal Sun XProtect can withstand everyday wear and tear and last longer than Crizal Sun UV. Performance was more than two times better against scratches10 and the same for smudge resistance.11
INNOVATION IN THE BLOOD With this in mind, Essilor ANZ CEO Mr Pierre Longerna says it’s clear R&D sits at the core of the group. While many innovations propelled the company in the second half of the 20th century, it’s from the 1990s that the biggest changes have occurred, including the Crizal coatings portfolio.
“As computing power grew so did Essilor’s R&D capabilities. Lens designs, coatings and even materials are all dependent on data and calculations and with more computer power the bigger the calculations that can be performed,” he explains.
“There are a number of Essilor R&D facilities scattered around the world dealing with everything from lens design to materials and processes; fundamental optical science to myopia and wearer perception. I think there is some sort of Essilor R&D conducted on just about every continent on the globe – we’ve even done a wearer test in Antarctica.”
While most will recall the first progressive invented by the late Dr Bernard Martinez in 1959, he says fewer people recognise Essilor was also the first to bring other important innovations to market.
“These include the 1.5 index plastic spectacle lenses in 1963; the first automatic edging machine; the first extended focus lens in 1988; the first low power full-field aspheric single vision lenses in 1989; the first anti-fatigue lens in 2004 and even the first hard multi-coat on plastic lenses,” he says.
“Most of these products have been the mainstays of the development of the industry in the last 35 years or more.” n *Used with all materials except clear 1.5 index Crizal coatings offer ESPF 35.

Crizal lenses have been a leader in anti-reflection coating technology.
Zeiss’ Tonsley site (picutred) will move to 100% renewable solar power this year.
UPHOLDING THEcommon good Corporate responsibility has been anchored in the Zeiss business mindset since its foundation. Insight examines how its historic principles are living up to its commitments to Australasian employees and the environment in 2022.

Whether it’s electric vehicles, smartphones, diagnostic devices, surgical microscopes or vision-correcting optics, there are few areas of the modern-day human existence that Zeiss doesn’t influence.
The German headquartered group – which has been operating in Australia for more than 60 years – aims to position itself as the innovation leader in every industry it operates, creating a rich company culture that places diversity-of-thought, inclusivity, and sustainability at its core.
Most Australian eyecare professionals would be familiar with Zeiss through its OCT machines, gold standard perimeters and biometers, ophthalmic lenses, intraocular lenses and surgical microscopes, but the company is also enacting change in many other sectors.
“In all fields of our business we make products and services that help people, or help people to help people, and that’s very rewarding,” Mr Rene Hessling, who has a 20-year career with the company and was appointed managing director of Zeiss Australia and New Zealand last October, says.
“For example, we develop analytical instruments used in cancer research or drug discovery and are also integral to advancing the electronics market with our semi-conductor technology. Through our metrology solutions we’re involved in the transformation of the automotive industry to electric vehicles and additive manufacturing which require completely different quality control processes. Our equipment helps medical professionals provide better diagnoses or treatment and in every family there’s someone who’s required a lens for their glasses or to replace their cataract.
“It’s such an interesting place to work because of the positive impact we have in so many areas.”
Today, the Zeiss business is divided into four segments: semiconductor manufacturing technology (SMT), industrial quality and research (IQR), medical technology (ophthalmic devices and microsurgery) and consumer markets (vision care/ophthalmic lenses).
How it competes in various high-tech sectors is largely down to its emphasis on R&D. It aims to lead technological advancements by investing 13% of the group revenue annually in this area. In the most recent fiscal year 2020/21, Zeiss achieved the highest revenue in its long history at €7.5 billion ($AU11.8 b), seeing almost €1 billion (AU$1.58 b) devoted to R&D activities.
As a result, it creates around 450 patents a year, or in other words, 1.2 inventions a day.
“The innovation drive within the company is strong and that in itself makes it exciting. Zeiss is in this interesting position with a strong history dating back 175 years, while at the same time, having to be agile and quick to respond to shape markets with cutting-edge innovations, and that creates a lot of positive momentum within the organisation,” Hessling adds.
PHYSICIST … AND A SOCIAL REFORMER The rich history Hessling alludes to can be traced to its founding fathers. While Carl Zeiss started the company in 1846, he famously brought on the physicist Ernst Abbe in 1866 to base production and quality of its products on reproducible scientific principles. Abbe later proved pivotal in creating the Carl Zeiss Foundation as owner of the company to ensure its longevity.
While Abbe was revered for his theoretic groundwork in optical science, he was also known for implementing progressive labour policies for the era. These included an eight-hour workday at a time when most people worked 14, paid sick leave, pension fund – and a discharge compensation fund.
“He was more than a famous physicist and driver of innovation; he was a social reformer. He realised the long-term success of the company depended on the wellbeing of employees,” Hessling explains.
Equality was another principle the progressive Abbe introduced,
which meant success of an employee was based solely on their ability and performance, not on their origin, religion, or political views.
“Today, it’s not just about equality, but also diversity. When I think of what takes the company forward, it’s diversity of thought. Zeiss has many employees that have a long tenure within the organisation, which means we have experience in many areas, but we also need people to come in and provide new and different perspectives,” Hessling says.
“And that is why we have a strong emphasis on finding people from different backgrounds and experiences, while providing career progression opportunities by exposing them to other markets, cultures and ways of doing things.”
Ms Elvina D’Cruze is one employee who personifies this approach. Seven years ago, at the age of 33, she joined Zeiss ANZ in Sydney as a senior accountant. Within weeks, she was promoted to finance manager overseeing nine staff. Two years later, she joined the senior leadership team as head of finance, of the ANZ business.
“To have someone who only knew me for a matter of weeks believe in my ability, that was something that stood out,” she says, noting she was initially struck by the long service of many employees.
“As a young manger I felt part of a team and the learnings I took in two years as finance manager, you can’t get that anywhere else because you’re constantly dealing with new projects and systems, while receiving clear direction about where we are heading as a group. Even though there are people with a lot more experience, my ideas are never shut down, you are always encouraged to offer your thoughts.”
Ms Gail Giordani, another long-serving Zeiss employee of 23 years, began her career in her homeland at Zeiss South Africa in 1999 as a member of the microscopy division. In 2014, she was appointed managing director of South Africa, and last year moved to Adelaide to head the ANZ Vision Care business.
“I come from a country with great diversity, but if there is no inclusivity then you don’t harness the aspects of having a diverse team,” she explains.
“We don’t employ people for a job, we employ for a career and that is why you see many people who have stayed for over 20 years. There are so many ways to advance your career, and opportunities aren’t limited to one area of the business, we look at talent across the many business units where people can broaden their experience.”
SOCIAL RESPONSIBILITY Another key driver of the Zeiss business in 2022 is sustainability. Most notably, these include ambitious goals of carbon-neutral energy sourcing by the end of this year and reaching CO2-neutrality in all activities globally by 2025.
“Globally, Zeiss has been able to set such ambitious targets because we started specific programs on energy consumption, waste and the circular economy more than 10 years ago,” Hessling says, noting that one of its foundation principles is operating in a sustainable manner.
These initiatives are well under way in Australia where Zeiss’s stateof-the art Tonsley site in Adelaide will shortly go from 60% to 100% renewable solar power. This is in addition to other initiatives that see reductions in water consumption through dry edging of lenses, the removal of single use plastic from packaging, and 100% recyclable packaging. End-to-end electronic ordering, and integration with
Zeiss ANZ managing director Rene Hessling (from left), ANZ Vision Care head Gail Giordani, head of ANZ medical technology Dane Moloney and ANZ head of finance Elvina D’Cruze.
optometry practice management systems, has also reduced paper use.
In Sydney, Zeiss has upgraded its ANZ headquarters, moving to a new site last September in Macquarie Park that will source 100% renewable energy. The company is also making use of hybrid working models brought about by COVID, reducing travel, and has reduced paper and printer toner usage, among other initiatives.
The new Sydney premises also has a Customer Centre where clients can test new instruments, seeing how they fit into their workflow. A training lab has been established where people can learn to operate microscopes or perform surgery. Large screens have been installed so local engineers can connect with overseas factory experts for technical training.
“We are taking it a step further with our scientific equipment like electron microscopes by moving into virtual reality (VR)-based training, so our engineers can learn to dismantle this highly complex equipment in a 3D virtual world without having the equipment on site or needing to travel overseas for weeks at a time,” Hessling adds.
Elsewhere in the Australasian business, Zeiss has been focusing on sustainability in another way: the eye health of underprivileged communities. It’s Back-to-Bush initiative, first established in 2005 provides local and visiting ANZ clinicians and surgeons access to functional, state-of-the-art diagnostic and surgical technologies.
This philanthropic work is broken into three areas. The first provides recent model reconditioned Zeiss ophthalmic and ENT equipment to needy centres in outback Australia and Oceania, acquired via trade-in from private and public hospitals against new purchases.
The second element provides ANZ surgeons with access to a portable surgical microscope for on-loan use during good will surgical visits. And thirdly, it donates reconditioned and some new diagnostic devices for charitable services, with the most notable of these being the Lions Outback Vision’s Northwest Hub in Broome.
Through Back-to-Bush, Zeiss has shipped over 100 ophthalmic and ENT surgical microscopes and ophthalmic diagnostic instruments throughout the region, including Cambodia, Vietnam, Solomon Islands, East Timor, PNG, Fiji, Kenya, Philippines, Laos, Sri Lanka and Myanmar.
Zeiss ANZ head of medical technology Mr Dane Moloney says equipment used in outreach programs can be antiquated, so providing refurbished systems allows people in those areas to receive quality care, while encouraging the visiting surgeons to continue their admirable efforts.
“Sometimes these surgeons also train local doctors while they are there to ensure a more sustainable service. The Back-to-Bush program’s focus is patient care in local regions and training local doctors, whilst supporting ANZ doctors and their ambition to give back to those communities,” he adds. n



Making EVERY CLICK COUNT Many independent optometry practices struggle to convert web browsing consumers into fully fledged customers because their websites are neither optimised for patient acquisition, nor are they regularly updated. But a new strategic alliance is working to overcome that in Australia.



Holdfastbay Optometry has always considered its website a vital cog in its marketing strategy. Relatively speaking, it served its function but with the emergence of new digital marketing techniques, there was potential to achieve more return from its key digital asset. In need of a redesign, attention turned to how the new website could be built and professionally managed amid the daily demands of running the business.
“The work we had undertaken positioning our practice and offering, both from a clinical and retail perspective, had moved during the five years since our previous revamp and wasn’t reflected in the style of the graphics, so a major overhaul was needed,” Ms Joanne Thomas, optometrist at the ProVision-aligned Adelaide practice, says.
“Our previous website was a mixture of new content added over the years, and original content from an initial site. Like extending old houses, sometimes the better option is to start with a clean slate and no restrictions to get the outcome you need.”
This was the position Holdfastbay Optometry was in when approached to join a pilot program stemming from a new strategic partnership between ProVision and EyeCarePro, an international digital marketing company solely focused on optometry businesses.
The pilot has involved a cross-section of 14 single and multi-site practices – regional and city based – as well as clinical interest destinations versus general optometry. Since the trial, Holdfastbay Optometry reported an almost immediate increase in bookings, particularly from the “becoming presbyopic” demographic helping balance its patient base. In fact, it reported a couple of record months. And the new website quickly began outperforming the previous one, with Google rankings showing it is now 89% optimised for mobile devices and has a site score of 100/100 for SEO.
Encouraging data from other ProVision independents who have had their websites revamped and managed as part of the pilot shows for every dollar spent on their site, $10 to $50 in revenue has been generated. And every new patient was acquired from as low as $5 to an average of $20.
How these practices have been able to achieve such stark and rapid results lies in the complex and evolving world of digital marketing services. This involves terms like search engine optimisation (SEO), mobile-first websites, search advertising and Google’s Analytics and My Business platforms. These are vital for modern optometry practices, but have become too difficult for time-poor optometrists to manage alone.
As part of the initiative, optometrists gain access to EyeCarePro’s team of over 80 staff comprising web designers, SEO strategists and marketing experts, who also take care of ongoing website and system improvements.
After the website is built, practices then receive local support with ProVision’s digital marketing specialist Mr Euan McDonald-Madden who has had extensive training with EyeCarePro to understand its system, gain insights from results and drive future growth strategies. He is now training other colleagues to provide members with monthly monitoring meetings to tweak their strategies, as well as plan monthly campaigns around areas of special interest, eyewear, eyecare, and seasonal opportunities from a large portfolio of digital campaign options.
OUTSOURCING THE EXPERTISE When it comes to the quality of independent optometry websites in Australia, ProVision marketing manager Sarah O’Connor says the spectrum is broad. At one end there are those with powerful sites that rank well on Google to capture local search traffic. In the middle sit underperforming sites typically due to poor user experience and technical responsiveness, basic content, and no SEO strategy. Then there are those with a non-existent digital footprint.
“Websites are often ‘set and forget’ for many practices due to limited resources and know-how when it comes to regular content updates,” she explains.
“SEO and search advertising needs to be outsourced due to the expertise required, however, knowing who to trust, what to spend and having a clear view of the ROI can be challenging for practices. Any website designer can create a great looking site, but this does not mean it’s going to effectively attract, engage, and convert new patients.”
O’Connor says “content is king” but this is often the number one sticking point for practices. As optometrists and most web designers are not search engine marketing experts, the content isn’t always written to capture local eye health queries and showcase expertise in areas like dry eye, myopia, Ortho-K and contact lenses.
“This optimising of content and many other technical aspects that influence a site’s visibility in Google, will often be absent, and can result in an underperforming digital asset for a practice that may have invested in it considerably. In many circumstances, we notice that Google Analytics are either not in place or set up correctly and reviewed to understand how it’s performing, which is totally understandable as it’s not their expertise,” O’Connor says.
Recent ProVision consumer research (EY Sweeney, ProVision Consumer Purchasing Behaviour Quantitative Report, Dec 2020) identified the importance of a digital presence to influence store visitation and purchase. Six in 10 consumers indicated they would conduct research online before visiting an optometrist, with 70% of these likely to purchase from an optometrist they researched online.
In terms of what constitutes “a high functioning website”, O’Connor believes it ranks near the top of Google search results in targeted catchments that convert web browsers into customers. It loads quickly, is mobile-first in design, has relevant content refreshed regularly and is engaging people with a great user experience and clear ‘calls to action’.
“Having a website that captures this search quickly and displays your ‘why choose us’ – which should include your expertise, philosophy around care, as well as state-of-the-art technology and the latest eyewear solutions – essentially how you help patients to achieve great vision and eye health, is critical,” she adds.
TAKING CARE OF THE TECHNICAL SEO is perhaps a good example of the value EyeCarePro can bring to independents. In its simplest form, SEO provides signals and information that are vital for search engines to find a website and display it prominently.
Since the company’s inception in 2005 – during the “wild west” of SEO and websites – it has kept abreast of the latest developments to ensure its nearly 1,800 global optometry clients aren’t left behind.
“Since 2012, Google has been utilising semantic search instead of keywords. That means it is super important to use natural language on your website with content that your prospective patients are searching for,” founder and CEO Mr Daniel Rostenne explains.
“For example, prospective patients may not know to search for dry eye, but they are searching for symptoms like ‘watery itchy eyes’. Having the symptoms optimised on the website will signal to Google and other search engines that you are an appropriate website to show in search results.”
During the website build, Rostenne says onboarding specialists ensure the “WEBSITES ARE OFTEN ‘SET AND FORGET’ FOR MANY PRACTICES DUE TO LIMITED RESOURCES AND KNOW-HOW WHEN IT COMES TO REGULAR CONTENT UPDATES.”

SARAH O’CONNNOR PROVISION
practice chooses a design appropriate for the business, and its products and services are well represented. The SEO team checks the current site’s SEO scores so it can compare the old site’s performance with the new.
“If it isn’t broken, we don’t fix it. Our builders take stock of all your websites old pages and make sure to add your unique content to the new website. Most importantly, all of your old links will redirect to the new corresponding website pages so the SEO value of the old pages are preserved, and no links in search engines are broken,” he explains.
Optometrists had complained it was difficult to make website changes, so EyeCarePro created its own platform, GetSetPro, which features simple apps that allow the practice to easily make website changes.
Practices are charged a monthly subscription, rather than an upfront capital cost, and there are varying levels of membership. For example, ODSpecialty will attract high revenue specialty patients. The most popular and versatile program, ODEssentials, gives practices the basics to be found in local search with the addition of scheduled social media content. With two SEO-optimised blog posts a month and a monthly meeting with a digital marketing professional, the program is considered an ideal foundation for practice growth.
Rostenne says one of its most impactful services is called GetSetCampaigns, which features more than 700 complete marketing campaigns, including landing pages, blogs and social posts, to publicise elements of eyecare that are important to the practice.
O’Connor agrees this “incredible amount of content” to be localised for Australia drives major value for practices. The campaigns can be added to over time and scheduled months in advance – “an ‘always-on’ marketing approach”. At the touch of a button, a new landing page of content can be added, and Facebook and Google My Business posts automatically scheduled.
ProVision has also been impressed with the transparency, which sees all web traffic, appointments, and analytics fed into a dashboard where practices can see the ROI – based on EyeCarePro’s proprietary algorithm – at the end of each month.
“There’s also opportunity for future development of services – right now we are collaboratively investigating some plug-and-play patientcommerce functionality to further enhance the offering, particularly in the contact lens servicing space,” O’Connor adds.
PAYING DIVIDENDS In the case of Holdfastbay Optometry, which opted for ODEssentials, Ms Thomas says the initiative has ultimately provided “maximum outcome for minimal input on our part”.
With small businesses unable to compete with the massive corporate budgets for external marketing, she says a professional-looking and user-friendly web presence is vital.
“For most practices the ongoing cost of having a ‘wow’ website is more than offset by the business it brings in,” Ms Thomas says.
“Whilst we had been comfortable with our previous web design team, the opportunity to work with an organisation that has at its core a strong understanding of the nature of optometry seemed like a logical step to trial with very much less work required on our part. "Very few practices are large enough to have dedicated staffing and resources to undertake all that is required for a successful marketing program. For most of us it’s another – albeit important – task which often gets pushed back when the day-to-day needs of the business take precedence, so for Holdfastbay Optometry it immediately made the whole process manageable and with a much-improved timeframe.”
Optometrist Ms Leah Meulendijks, of Kay Street Eyecare in the regional Victorian town of Traralgon, also found the daily upkeep her business’ website difficult.
“We are now subscribed to the ODEssential package. The value we see is that any updates to the site and other digital listings, whether that be in content or adjusting the site structure to keep Google happy, is all done by the experts at EyeCarePro. We also, with the help of ProVision, look at the stats behind the site so there is transparency around how it’s performing,” she explains.
“To have someone else look after the digital content has meant our staff can focus on customer service. One surprise has been how much digital traffic is driven by our Google My Business listing. EyeCarePro manage this listing for us and to know they are ensuring all the information is 100% correct and the listing is optimised will no doubt keep our business up in search when local people need to find an eyecare professional."
Meulendijks says a high functioning website is critical for any business, but this is especially the case for an optometry practice.


Daniel Rostenne, EyeCarePro CEO (left), and Joanne Thomas, of Holdfastbay Optometry.
"The website performs some major functions for the practice. Firstly, it shows that we are professional and if anyone needs information about eye health or eyecare, it's there on the site," she explains. "Secondly it breaks down barriers to what you do, you can show eye tests and what happens in the practice and allay any fears people have about the unknown. Thirdly it can show people who you are and what you do and this makes people a lot more comfortable to book an appointment and relaxed when they come in." ■