3 minute read
OPTICAL DISPENSING

by Prime Group

MYOPIA LENS FITTING REQUIREMENTS – PART 2
IN THE SECOND PART OF HIS SERIES ON THE DISPENSER’S ROLE IN MYOPIA MANAGEMENT, GRANT HANNAFORD COVERS THE UNIQUE FITTING DEMANDS OF NEW AND AVAILABLE SPECTACLE LENS OPTIONS.
GRANT HANNAFORD
"THERE ARE SEVERAL MAIN FAMILIES OF LENSES USED IN MYOPIA: BIFOCALS, PROGRESSIVE STYLE LENSES, AND LENSES USING RADIAL AREAS OF DEFOCUS" L ens developers are taking strong interest in spectacle lenses designed to slow myopic progression in children. Following from part one of this article, we will assess some of the fitting requirements of these treatments.
The optometrist will consider the full range of diagnostic data when selecting a lens for myopia management, from family history, risk factors, biometry and binocular function (among many others). There will be well defined reasons for a given lens selection, so even if cosmetically the lens chosen isn’t the one the patient prefers, it’s important to remember this is a treatment process, so the appearance is not a consideration, only the outcomes.
As mentioned in the previous article, there are several main families of lenses used in myopia: bifocals, progressive style lenses, and lenses using radial areas of defocus such as in the DIMS and HALT style designs. Progressive and bifocal lenses should be familiar to all practitioners in terms of fitting requirements, although there may be specific height demands placed by the optometrist for bifocals, such as segs set to lower pupil. Avoid the temptation to manipulate the fitting heights for progressive power lenses as the designs are relying on specific placement to be effective. Arbitrarily shifting heights to gain a perceived increase in distance or near vision will undo the benefits of the design.
Lenses that attempt to manipulate peripheral retinal defocus (i.e. DIMS and HALT concepts) utilise lenslets arranged on the lens surface to present the eye with areas of defocus (Figure 1, available in the online version of this article).
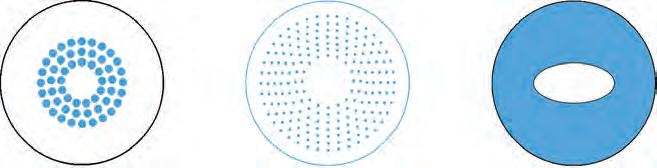
Figure 2 above shows some configurations for these lenslets or ‘dots’ of additional plus power. They provide a defocus or treatment zone as shown in blue which create areas or volumes of defocus to stimulate a response in the growth of the eye. The design on the far right does not use lenslets, instead it has a smooth treatment zone. In all cases the lenses have a central area containing the patient’s full distance prescription.
Fitting these lenses comes with their own demands. Despite being referred to as ‘highly aspheric’, the design cannot be treated as a single vision aspheric lens. The central zone of distance vision must be placed so it’s centre corresponds with direct line of sight, i.e. fit at pupil height, allowing an equal amount of the central distance section to be viewed in all directions from level gaze. Consequently, it’s desirable to have pantoscopic tilt and wrap angles minimised for these fittings to avoid oblique astigmatism and other angular aberrations. Due to production constraints, there are limitations on available lens blank sizes. Lower powers are available in large blanks (often up to 75mm) however these can shrink to 60mm blanks in higher power and cylinder combinations. Be aware of the MSU when looking at frames as this can preclude certain frame choices.
Frame selection will drive the success of the lens designs. Figure 3 shows a poorly centred eye (left), resulting in the blank size being inadequate and the treatment zone (blue dots) being cut off. Better centration (right) allows incorporation of the blank size and the entire treatment zone. Choose frames with: • Adequate depth to incorporate as much of the treatment zone as possible. • Good vertical centration to avoid vertically asymmetric treatment zones. • Minimal horizontal decentration. • Flatter fitting (tilt as low as reasonably possible and wrap close to zero).
Finally, it’s important to realise that while these lenses may help slow axial length growth and the attendant myopic progression, there is currently no mechanism for the reversal of myopia. This is important to keep in mind when discussing the prescribed treatment options with patients and their parents. Be wary of over promising results and always do the follow up to ensure compliance with the treatment protocols. n
Figure 2 – Some peripheral defocus lens designs (treatment zones in blue, distance prescription in white).
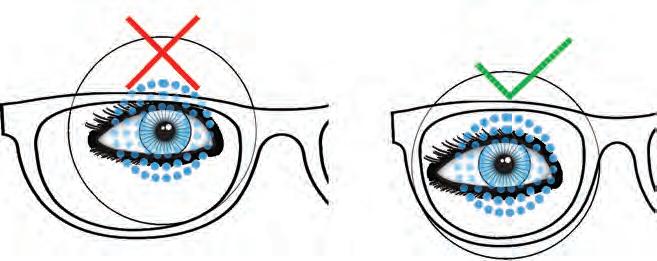
Figure 3 – Fitting requirements as dictated by the lens treatment zones.
GRANT HANNAFORD is the co-founder and director of the Academy of Advanced Ophthalmic Optics. He owns a private practice and is a senior lecturer at the UNSW SOVS. He is currently a doctoral candidate at the School of Optometry Aston University researching ocular biometry and development.




