Infection Control & Risk Management Guidelines for Pets as Therapy
Version: V3
Ratified by: Infection Prevention Group
Date ratified: 20/07/2022
Job Title of author: Specialist Infection Prevention Nurse
Reviewed by Committee or Expert Group Infection Prevention Group
Related procedural documents

IPPOL01 Management of MRSA in Hospital Wards and Community Settings
IPPOL03 Hand Hygiene Policy
IPPOL21 Standard Principles for Infection Prevention
IPGUI02 – Infection Prevention Guidelines
HSPOL08 – Health & Safety at Work Policy
Review date: 20/07/2025

It is the responsibility of users to ensure that you are using the most up to date document template – i.e. obtained via the intranet
In developing/reviewing these guidelines Provide Community has had regard to the principles of the NHS Constitution
Version Control Sheet
Version Date
v1 March 2015 Head of Infection Prevention
v2 October 2018 Specialist Infection Prevention Nurse
v3 May 2022 Specialist Infection Prevention Nurse
1. Introduction and Purpose
These guidelines have been produced in order to address concerns about the potential health risks of implementing therapeutic visits using ‘Pets as Therapy’ (PAT) dogs and cats in health and social care settings.
These guidelines include minimising risk for animals/pets kept in the care environment and supported living environment
Theseguidelines include Pets as Therapy’s policies in relation to assessing and minimising risk with its visiting volunteer teams and also information and input from other leading animal care and welfare, veterinary and human medical/nursing authorities.
Pets As Therapy (PAT ) believe that the potential benefits to recipients of its service far outweigh the possible risks, as long as standard selection procedures are followed and basic sensible guidelines which minimise, or eliminate risk are adhered to.
Pets as Therapy acknowledges that there are potential risks from the presence of companion animals in health and social care settings. Whilst there is now a huge amount of published research available on the benefits of interacting with companion animals, in contrast, there is little scientific evidence investigating or quantifying the risks.
However, the evidence that does exist points to the fact that, in well-managed programmes, using animals which are appropriately screened for health, temperament and behaviour, the risks are minimal and are far outweighed by the benefits (Khan and Farrag 2000; Guay 2001; Brodie et. al. 2002; DiSalvo et. al. 2005)
2. Animal Assisted Activities & Animal Assisted Therapy
There are two main types of therapeutic interaction with companion animals. The first of these is described as animal-assisted activities (AAA) and covers the majority of the work of Pets as Therapy’s registered volunteers. Animal-assisted activities are also referred to as “meet and greet” activities, the animal’s main function being to act as a social lubricant, initiating social interaction and promoting responsiveness, tactile contact and comfort.
In animal-assisted therapy (AAT), a companion animal is involved in a goal-directed programme for an individual. Animal-assisted therapy is always conducted under the supervision of a healthcare professional, using their own companion animal, or involving an animal and handler/volunteer team. Examples of animal-assisted therapy which Pets as Therapy volunteer teams are currently involved in include: rehabilitation of stroke patients, using a range of activities with the PAT dog or cat to improve mobility, motivation and posture and desensitisation exposure sessions for children and adults with dog phobia. Animal-assisted therapy offers huge potential to the healthcare profession in a range of disciplines and, in the UK at least, is greatly under-utilised. Alongside AAA and AAT companion animals, there are Assistance dogs. Assistance Dogs are specially trained dogs working with an individual person to support them in a number of ways. These include:
• Guide Dogs: supporting people with visual impairment or sight loss with guiding.
• Hearing Dogs: supporting people with hearing loss or impairment.
• Assistance Dogs: aiding mobility and support daily living such as undressing and picking dropped items up off the floor, opening and closing doors etc.
• Medical Alert Dogs: trained to constantly monitor their partner’s health condition and alert to impending episodes where their health would acutely deteriorate.
The alert allows the person to take preventative action to avoid/limit the episode, or to make themselves safe, thus reducing the risk of injury during the episode. For example: Type 1 diabetes, Addison’s disease, Postural Orthostatic Tachycardia Syndrome (POTs), seizures, and severe allergies.
• Autism Assistance Dogs: supporting people with autism.
• Dogs supporting people who have mental health issues. By and large, assistance dogs are with their owners 24 hours a day and play a number of different, but important roles in their life including practical support, companionship and help in dealing with anxieties.
The Equality Act 2010 makes it unlawful to refuse access to a disabled person accompanied by an assistance dog except in the most exceptional circumstances. Assistance dogs may be trained by charities that specialise in this work or by the owners themselves. Health care establishments should satisfy themselves that the dog meets the criteria to be classed as a bona fide assistance dog.
3. What are the Benefits?
Companion animals have been used to benefit the mental and physical health and wellbeing of humans for hundreds of years. In 9th Century Germany, animals were used in the treatment plans of disabled people living in a small community and in 1792, at the York Retreat in England, interactions with small animals were used to teach psychiatric patients self-control and nurturing and also as an alternative to chemical and physical restraint. Florence Nightingale was the one of the first to recognise the potential benefits of companion animals within the nursing field, when she advocated in her “Notes on Nursing” that “small companion animals can make excellent companions, especially for the chronically sick.” Psychotherapist Dr Boris Levinson was the first mental health professional to incorporate the use of his dog Jingles in treatment plans for his child clients and he published his findings in the Journal of Mental Hygiene in 1962. Since then, companion animals have been entering many different sorts of establishments, including: hospitals; nursing and residential care homes; mainstream and special needs schools, amongst others. Companion animals provide opportunities for nurturing, companionship and tactile contact. They bring comfort in distressing situations, not only to patients, clients and their families, but also to staff working in these establishments.
Since its inception in 1983, Pets as Therapy has grown to become the largest visiting companion animal service in Europe. The scheme currently has over 4,800 registered PAT dogs and 108 PAT cats which make regular visits to over 9,000 different establishments.
4. Pets as Therapy Animal & Volunteer Selection Procedure
The Application Procedure
The application procedure requires the owner to produce evidence of the animal’s health and vaccination status. In addition, all potential PAT dogs and cats must undertake a standard temperament assessment, which is carried out by one of the Charity’s trained assessors. Pets as Therapy only registers vaccinated, healthy and disease-free dogs and cats with a sound temperament appropriate for visiting.
Volunteer Selection
With their application form, all prospective volunteers are required to produce 2 character references from people who have known them for 5 years. Establishments may elect to undertake additional checks of their own, for example, Disclosure Barring Service checks.
Temperament Assessment
• The temperament test measures the animal’s ability to cope with and enjoy the demands placed upon it by the clients/Patients and the environments in which they visit.
• Assessors are also now receiving training in animal behaviour and welfare issues, including identifying behavioural signs of stress in the animals they are assessing. This helps to further reduce risk by enhancing our animal selection procedures.
Furthermore, the Charity now also asks its volunteers whether their pet has achieved any level of obedience training e.g. Canine Good Citizens, as this helps us to select more accurately, the most appropriate animals, in particular for our animal assisted therapy programmes, such as the stroke rehabilitation and phobia desensitisation sessions.
Full details of the Pets as Therapy temperament assessments can be requested from Pets as Therapy.
Identification of Pets as Therapy Registered Teams
Each PAT dog or cat has a photo ID tag on its collar and many of them also wear a distinctive yellow coat. The owner has a photo ID badge which is worn for security.
Please refer to appendix 3: Information for Pets as Therapy Dog (PAT) onto wards which gives clear advice for volunteers, patients, visitors, contractors and staff.
5. Pets as Therapy Public Liability Statement
Pets as Therapy carry public liability insurance with an indemnity limit of £5,000,000. For any further queries regarding the insurance policy, please contact Provide Head of Safety & Resilience.
6. What are the risks?
There are risks associated with any type of animal-related activity. However, these risks are very small in well-managed programmes, using appropriately selected, healthy and behaviourally suitable animals. It is important to consider the potential risks associated with animal-assisted activities and therapy, as companion animals used in this context are often brought into close contact with some of society’s most vulnerable members, for example, older people, children and those suffering from mental or physical ill-health. Such populations may have lowered immunity and therefore be potentially more likely to contract diseases.
The main risks associated with animal-assisted activities or animal-assisted therapy is: -
• Animal-related injuries e.g. bites and scratches
• Fears, phobias and allergies
• Transmission of zoonotic diseases
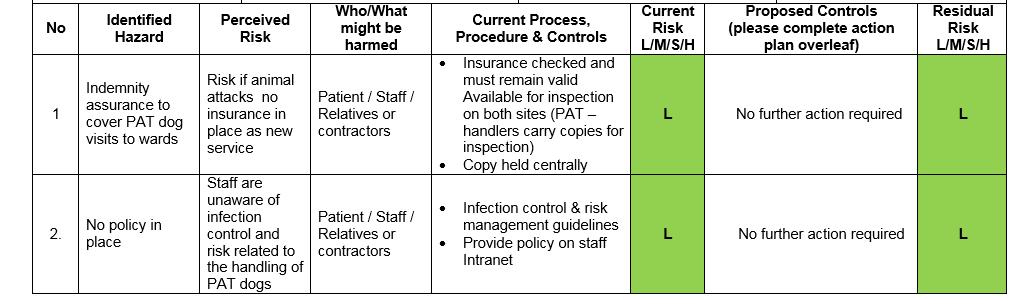
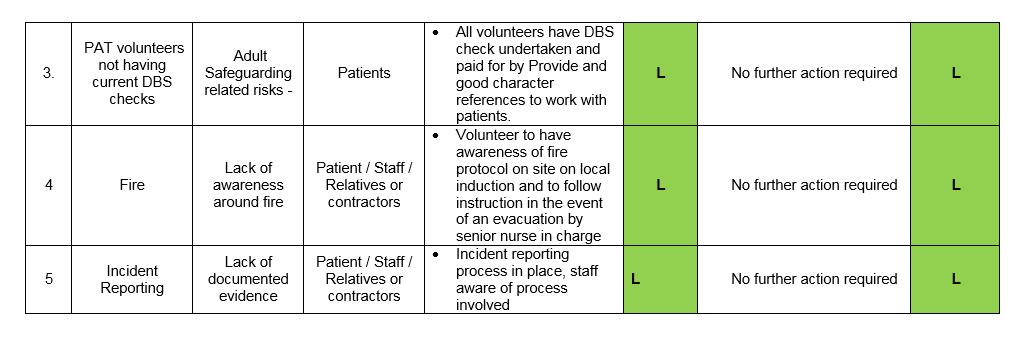
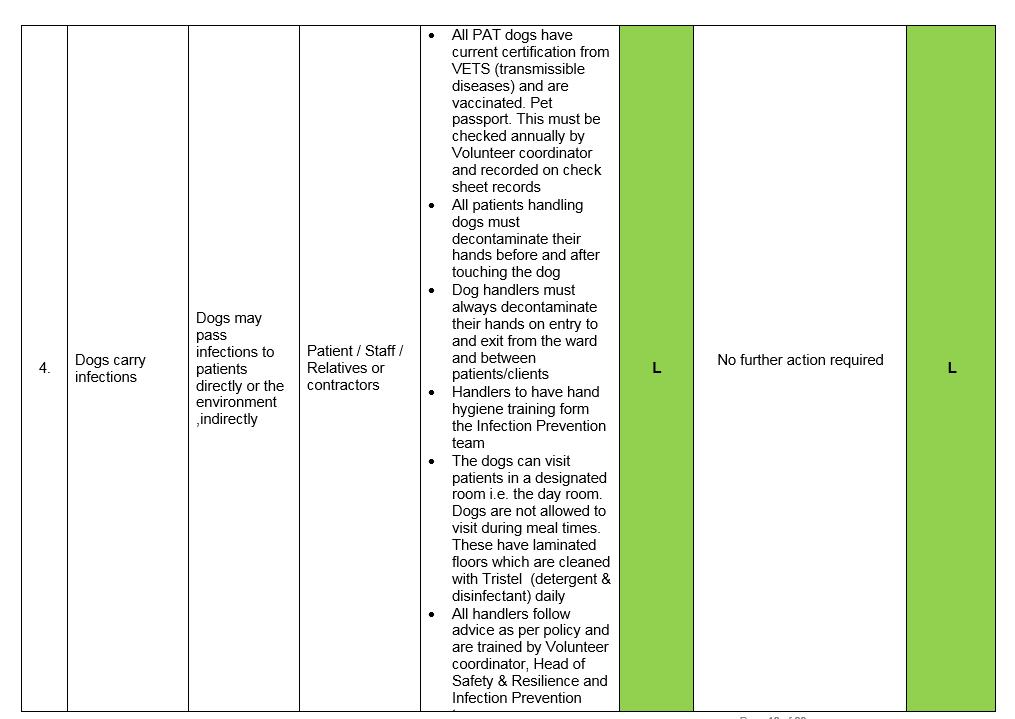
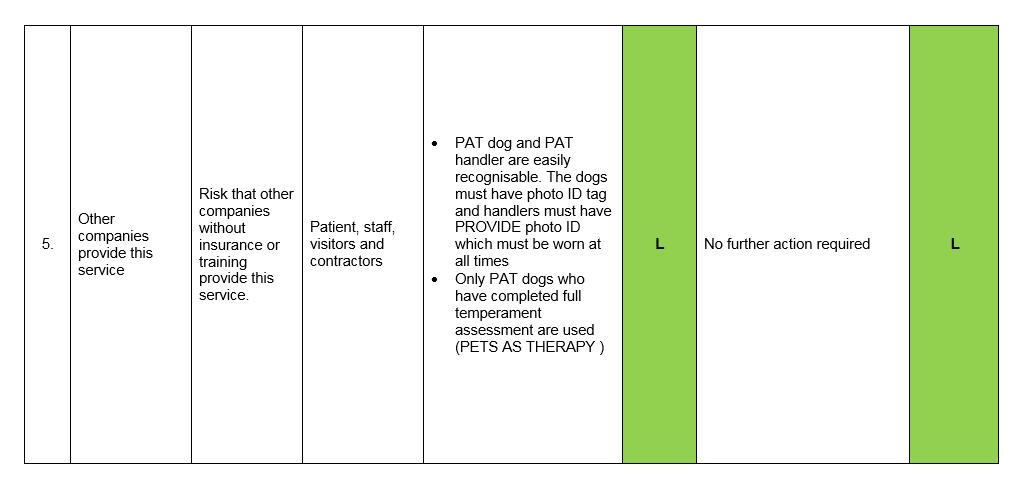
Pets As Therapy believe that with careful selection and management policies, the large majority of these risks can be minimised or even in some cases eliminated. Please see appendix 1 for a sample risk assessment
Animal Related Injuries
Therapeutic work is both socially and physically demanding for animals. An animal that does not possess an appropriate temperament for therapeutic work is more likely to bite or scratch a patient, resident or client during an interaction, through fear, stress or anxiety. The Pets as Therapy temperament assessment evaluates the animal’s suitability for therapeutic work.
Fears, Phobias & Allergies
Not everyone enjoys interacting with companion animals and Pets as Therapy respects the rights of patients, residents and clients and their representatives, staff and members of the public whom may dislike animals but may come into contact with Pets As Therapy visiting teams.
It is also a valid concern that staff, patients, residents or clients and their representatives may have fears, phobias or allergies to specific animals. Pets as Therapy would advise the establishment to survey their staff and patients/residents prior to any planned programme, to identify if this is the case for any individual. Programmes can then be tailored accordingly. There should be an appropriate point of contact (e.g. Senior Nurse/Manager) available on each Pet as Therapy visit to identify if any potential issues have arisen that need consideration, for example: locum staff on duty that have a fear, phobia or allergy.
Allergic reactions occur to animal dander (old skin scales), saliva, hair, urine and other secretions. The animal species most often implicated in allergic reactions are cats, followed by horses and guinea pigs. However, dogs and pet birds can also cause allergic reactions. Therefore, by choosing the most appropriate species and obtaining good patient/resident and staff histories of allergies, risk of exposure can be minimised. Pets as Therapy’s volunteers are advised to wash and groom their pet before each visit.
Action Point 1:
Survey your staff prior to starting any visiting companion animal programme to check if anyone has any fears, phobias or allergies to dogs or cats. Remember there may also be cultural/religious reasons why an individual doesn’t wish to interact with a companion animal. Be mindful of any changes that might occur prior to each scheduled Pets as Therapy visit too.
Action Point 2:
Choosing the most appropriate species and obtaining good patient/resident and staff histories of allergies minimises the risks of exposure.
Pet Health Council Advice on Managing Animal Allergies
Whilst it has been commonly believed that if you suffer from an allergy pet ownership is not a good idea, recent scientific evidence suggests that the opposite may in fact be true.
Research has demonstrated that children who live with a cat or dog in their early years can be protected from developing allergies (including to non-pet allergens, such as dust mites, grasses and pollen).
For people who are allergic to animals, some breeds of cat or dog with particular types of fur are less likely to provoke an allergic reaction (unfortunately, this does not generally apply to asthma sufferers). Poodles, Bichon Frisé or Labradoodles are generally less allergenic than other breeds of dog as their coat is more like wool than fur. Similarly, furless Rex cats seem to be better for some sufferers.
As a general guide, pets which moult less fur are less likely to cause a reaction. However, every individual reacts differently and there are no hard and fast rules.
Given the many benefits that pets can bring, both in terms of companionship and health benefits, the good news is that in a majority of cases, mild allergies to pets can be minimized and symptoms controlled by careful management. Please see appendix 2 for the Pet Health Council’s full guidance on minimising allergies.
7. Transmission of Zoonotic Disease
A zoonotic disease is one that can be transmitted from (vertebrate) animals to man. A zoonotic disease normally exists in animals, but has the potential to infect humans. Animals may also be carriers of a range of germs without showing any clinical signs of disease, just as humans can. A zoonotic disease can be spread following direct or indirect contact with an infected animal. Direct disease transmission can occur via bites and scratches or contact with hair and fur, or indirectly through contact with faeces, urine, saliva, blood, aerosols or environments which have been contaminated.
Zoonotic Diseases of Significance
There are several hundred zoonotic diseases which have been identified in companion animals, including dogs, cats, horses, birds, small rodents and birds. The majority of these diseases are rare, most are preventable and the large majority are treatable once detected. The diseases with particular significance to humans and occurring in cats and dogs include: campylobacter; cryptosporidiosis, salmonellosis, E. coli, ringworm, hydatids (a tapeworm), leptospirosis (Weil’s disease), toxoplasmosis and toxocariasis. Both cats and dogs have also been known to carry MRSA, which can be an issue in health and social care settings.
Relative Risk Factors
As with animals generally, potentially anyone who comes into contact with companion animals is at risk of exposure to zoonotic diseases. However, people with weakened immune systems, such as those suffering from illness, young children and pregnant women may be at particular risk.
Action Point 3:
Knowledge of susceptible populations of clients, Patients or residents should be used to guide in-house policies and guidelines identifying those individuals who may benefit most from contact with companion animals and limiting, where necessary, those who should have minimal or no contact with companion animals.
It is also important to note the relative risk of contracting a disease even if you were to come into contact with an infected animal, either directly or indirectly. For example, in
order to contract toxocariasis (an infection caught from ingesting the larvae of parasitic worms released into a cat or dog’s faeces), you would have to ingest the faeces of an infected dog or cat and the faeces would have to be 2-3 weeks old.
8. Pets as Therapy Vaccination Policy
The main zoonotic disease of concern against which animals can be protected by modern vaccinations is Leptospirosis, or Weil’s disease. This is a bacterial disease, which is contracted by allowing water contaminated by the urine of an infected animal to come into contact with broken skin. Luckily, in the developed world and due to animal vaccinations, this disease is now very rare.
Pets as Therapy operates under a strict rule from most health authorities, schools, hospices, nursing/residential homes and other long-term establishments. There must be NO risk to patients/residents of transmissible diseases from visiting animals from Leptospirosis icterohaemorrhagiae (Weil’s disease).
Regardless of the type of vaccination that the volunteer chooses for their dog, the dog must be protected against Leptospirosis.
Full details of the Charity’s vaccination policy can be requested from Pets as Therapy by contacting Reception reception@petsastherapy.org.
9. Specific Micro-Organisms of Concern (MRSA)
Many establishments have procedures in place to minimise the risk of MRSA and the majority of specific concerns received by the Charity relate to the potential cross-infection of MRSA between visiting PAT dogs or cats and Patients/residents. It is important to note however that this concern arises in part due to media reporting on the significance of this micro-organism.
MRSA stands for Methicillin Resistant Staphylococcus aureus. It is a member of the Staphylococcus aureus family of bacteria, which are capable of causing a number of infections, some of which are potentially very serious for Patients. The reason that MRSA is a concern in hospitals and care homes – and why it has become known as a “superbug” – is that it is resistant to the most common antibiotics previously used to treat infections caused by sensitive S. aureus. Therefore, an infection with MRSA can be more challenging to treat with antibiotics should it occur.
Reference: Department of Health website www.doh.gov.uk
Difference between Colonisation and Infection
An animal or human may be colonised or infected with bacteria such as S.aureus. Colonisation occurs when the organism lives on or in one or more body sites with no signs or symptoms of disease or illness. These body sites include: the nose or throat, armpits, perineum, the bowel or on the skin, usually the hands. Being colonised with MRSA is not the same as having an active infection
Infection occurs when a disease-causing organism is able to enter the body through a wound of some kind. This might include: skin ulcers that will not heal or through surgical
incision sites. The invading bacteria multiply causing the body to recognise the presence of this micro-organism, which cause the signs and symptoms of the disease.
MRSA in Companion Animals - Extent and Significance
MRSA is important to consider in the context of visiting companion animals as it is known and accepted that companion animals can be carriers of MRSA and therefore colonised just as humans can be.
MRSA was first reported to have been isolated from animals in 1972 and has since been found in several species of companion animals, including cats, dogs, horses and rabbits.
There are many factors which are still unknown about MRSA. For example, it is not known what the overall prevalence of MRSA is in companion animals in the UK and whether this is increasing or decreasing; nor is it known to what extent animals can act as a reservoir for the organism.
MRSA strains found in humans and animals are particularly adapted to colonising and/or infecting their preferred host species and therefore are usually different. For example, the staphylococci that commonly infect and colonise dogs are usually from the Staphylococcus intermedius species, which has different characteristics from Staphylococcus aureus. However, whilst different strains of the disease have preferred hosts, they may still opportunistically infect other species in some circumstances.
Reference: Defra website www.defra.gov.uk
Transmission of MRSA between Humans & Animals
How is MRSA contracted?
MRSA is usually spread by direct contact or via the air/environment through skin scale dissemination. It can be passed between people, between people and animals and between the environment and either animals or people. It is possible for pets to become colonised due to the close physical contact they have with owners and vice versa. Animals may also contract MRSA from veterinary staff who have failed to wash their hands properly after handling a colonised animal.
In the majority of cases, pets become colonised from staff in veterinary surgeries and hospitals. However, questions still remain about the direction of transmission of the organism between humans and animals and Defra is currently undertaking research investigating aspects of this.
What is the view of the Public Health England?
MRSA is an important micro-organism, associated with healthcare-associated infections (HCAI’s). The bacterium is most commonly found in hospitals, although it can occur in other residential and care settings and some nursing homes have experienced problems with MRSA. It also particularly affects the most vulnerable or debilitated Patients, for example those in intensive care and those on surgical or orthopaedic wards.
Public Health England’s view is that: -
• “MRSA does not pose a risk to hospital staff (unless they are suffering from a debilitating disease) or family members of an affected patient or their close social or work contacts.”
Their advice: -
• MRSA can be spread through direct contact by hands so hand hygiene is the most important preventative method to stop its spread.
It is particularly important that carers and healthcare workers undertake hand hygiene between caring for patients/residents. This can involve either hand washing with soap and water, or the use of alcohol hand gels.
Always undertake hand hygiene
• Before contact with client/patient
• Between contact with client/patients
• After using the toilet
• Before eating/preparing food
• After handling soiled linen/bedding/nappies
• After touching animals
• When hands appear dirty
• Healthcare workers may use an alcohol hand-rub to assist in ensuring their hands are properly clean
Public Health England further advises that no special environmental cleaning methods or products are required and that good general cleanliness is more important in helping to prevent the spread of infection. At home, clothing and bedding do not generally need to be washed separately or differently.
Reference: Public Health England: Health Protection
Action Point 4:
Pets as Therapy asks the establishments to provide appropriate facilities for Pets as Therapy volunteers and patients to wash their hands following contact with companion animals. Pets as Therapy also advises its volunteers to follow simple hand-washing procedures before, during and after visits.
What are the Public Health Implications of MRSA in Companion Animals?
Although colonised or infected companion animals may act as another potential source of MRSA infection, the risks are thought to be small. Defra believes that the Public Health England’s advice on colonised and infected people can be equally applied to infected or colonised companion animals: that is, “MRSA does not pose a risk to hospital staff (unless they are suffering from a debilitating disease) or family members of an affected patient or their close social or work contacts.”
The current view of both Defra and the Department of Health is that animals are more likely to be infected as the result of contact with colonised or infected humans, not vice-versa.
It is important to note that cases of active MRSA infections in companion animals transmitted by any route are very rare and that pet deaths from MRSA extremely uncommon. On the currently available evidence, Pets as Therapy would like to reassure
its volunteers and those that benefit from Pets as Therapy visits, that the benefits to be gained for the patients/clients, staff, volunteer and the pet far outweigh the risks.
10. Precautions against Transmission of Zoonotic Diseases
There are several simple precautions that everyone can follow to minimise the risk of contracting a zoonotic disease. Infectious diseases can be transmitted directly via animals or, indirectly, from inanimate objects in the environment, such as food bowls.
Hand Hygiene
Hand hygiene is advocated by both veterinary and medical/nursing organisations as the key method of reducing or minimising the spread of infectious diseases.
Action Point 5:
Routine and simple hand hygiene procedures remain one of the most important ways to minimise the risk of disease spread for anyone coming into contact with companion animals “To reduce the likelihood of spreading infection, you should always wash your hands or use an antibacterial hand rub after you have had any physical contact with a patient – whether the patient has a wound or not. Remember that healthcare workers can be carriers of the bacteria even if they are not infected themselves”
Source: Department of Health website www.doh.gov.uk
11. Advice to Pets as Therapy Volunteers to Reduce Risk on Visits
Prior to any Pets as Therapy Visit: -
• Only visit with healthy, disease and illness-free pets by establishing a close association with your vetto ensure that the animal is clinically healthy, appropriately vaccinated and that you are following a comprehensive parasite control programme
• Do not visit if you or your pet is or has recently been unwell with diarrhoea and vomiting or have had diarrhoea and vomiting in the last 48 hours. This also applies to respiratory symptoms such as a cough and cold.
• It is advisable to check with your vet following any period of illness in your dog or cat, to check that they are fit to return to visiting
• Wash and groom your pet before each visit
• Make sure your pet has been given the chance to go to the toilet before each visit
• Make sure you immediately clean up any faeces or urine
During Pets as Therapy Visits: -
• Always seek the advice of the nurse/manager in charge at the start of each visit and do not visit patients or residents in isolation or those with potential or known infections present
• The volunteer must be aware of the fire evacuation plan and where the fire assembly point is situated.
• Wash your hands between patients and also advise patients to do the same (some volunteers carry hand-wipes with them and these can be offered to patients with the establishment’s permission – these do not have to be alcohol hand-wipes –wet-wipes are sufficient)
• Remain vigilant for dropped medication and alert a nurse if any medication is found
• It is better to take your own treats for the patients/residents to feed to your dog.
And do not: -
• Make visits to patients who have open or uncovered sores or wounds. This would generally include: surgical wards, ITUs and burns units, but please be aware that patients on any type of ward, (including medical wards), may have open sores or wounds. Any open sores or wounds should be covered by a dressing and if they are not, it may not be appropriate for you to visit that patient
• The dog should not be allowed to lick anyone. They should not be allowed to sit fully on the bed and, in particular, not near a person’s face.
• If the dog is putting their feet on a bed then a protective pad (e.g. incontinence pad) should be put under their paws and discarded after each individual visit to avoid contamination from one patient to the next.
• Enter any areas of food preparation or any other areas restricted by the establishment
• Touch your mouth with your hands, or lick your fingers
• Eat during a visit or eat any food intended for animals
• Wipe hands on clothing, if avoidable
Only eat or drink in designated areas and not in any areas where animal contact occurs. If an establishment does not have separate visitor eating areas, visitors should be advised that hands should be thoroughly washed with soap and running water after touching animals and before eating.
12. What Can Establishments Do to Minimise Risk?
• Involve everyone in the planning stages before any animal is introduced. Establish whether there are any fears, anxieties, allergies or phobias and define strategies for dealing with these issues when they arise
• The volunteers coordination service to arrange support for PAT handlers visits, and where possible, the PAT handler to be accompanied by a Provide volunteer
• It is the nurse in charges responsibility to ensure the PAT volunteer is familiar with the wards fire evacuation procedures, fire exits and where the fire assembly point is situated.
• Make sure that there is an agreed process for escorting volunteer and pet off the site if the fire alarm is sounded. (i.e. volunteer to take responsibility for taking pet off the premise)
• Inform and involve patients and patient representatives/PAL’s of the intention to introduce a pet-visiting programme
• Involve and inform other staff, including the Infection Prevention and Control Team and Public Health England of the intention to introduce a pet-visiting programme
• Ensure you have written policies in place in your own facility, which define the benefits of having a companion animal programme and a consideration of how the potential risks may be reduced or eliminated
• Develop your own policies regarding animal visits, including restricted areas, etc.
• Knowledge of susceptible populations of clients/patients should be used to guide in-house policies and guidelines limiting who should have contact with companion animals
• Only consider using animals from a known source and which have been assessed in terms of their health, behaviour and temperament to be suitable for visiting in health and social care environments
When receiving Pets as Therapy Visits: -
• Ensure the volunteer has a regular point of contact before and during their visit.
• Inform any visiting pet-volunteer team in advance of the outbreak of infection and cancel the visit as necessary
• Develop and adhere to simple hygiene measures, such as a hand hygiene policy following contact with companion animals. Do not allow any animal to lick faces or hands
• Advise your staff, patients and clients to always wash their hands and other exposed body parts with soap and running water, particularly after touching animals, since any part of the animal or its surroundings can be contaminated with faeces or urine
• Being licked by an animal (NB: excessive licking would preclude an animal from being registered as a Pets As Therapy visiting PAT dog or cat)
• Having contact with soil or faeces - Staff should supervise patients who are interacting with animals by using the precautions outlined above. It is recommended that staff do not handle the animals
• Hand-washing of the patients should be closely supervised immediately following any contact with a companion animal, ensuring that hand-washed patients do not become re-contaminated by being in contact with other patients who have not washed their hands
13. Advice for animals/pets kept on the premises in the care and supported living environment
The presence of animals/pets in the care and supported living environment can enhance the quality of life for service users. Disease, however can be acquired through contact with animals/pets, especially if the service user has reduced immunity through age, illness or therapy
High risk pets
• Stray animals
• Wild animals/birds
• Sick animals/birds
• Exotic and tropical pets, includes caged birds and reptiles.
Factors for consideration;
• Who will hold responsibility for the animal/pet.
• Is the animal/pet suitable for the environment and its restrictions.
• Feeding.
• Grooming arrangements, their coats should be cleaned regularly, claws kept trimmed.
• Can the animal/pet be kept out of the kitchen/food areas.
• Veterinary arrangements.
• Who will be responsible for animals/pets records of vaccinations, worming treatment and flea treatment.
• Cleaning and disposing of excrement arrangements, including litter trays.
• Equipment – purchasing and cleaning
NB. Pregnant staff/service users should not undertake cleaning and disposing of litter trays, cages and other animal faeces because of the risk of toxoplasmosis.
General precautions,
• Pets should not be permitted to lick service users or jump on them in a manner that may cause accidents.
• After service users have touched animals/pets they should be encouraged and assisted to wash/wipe their hands.
• Staff should wash their hands following contact with animals/pets, their bedding and excrement, including litter trays.
• Animals/pets must not be allowed access to kitchen/other food preparation areas.
• Pet food should be stored in a designated area and not in the refrigerator with staff/service users food.
• Cleaning schedules and records should include all aspects of the animal’s/pet’s eating, drinking and accommodation. Feeding dishes and containers must be washed after each feed.
• Wash feeding or other equipment separate from staff and service users utensils/equipment in warm soapy water.
14. References
Brodie S J, Biley F C and Shewring M (2002) An exploration of the potential risks associated with using pet therapy in healthcare settings. Journal of Clinical Nursing 11 p444-456
DiSalvo H, Haiduven D,Johnson N, Reyes V R, Hench C P, Shaw R and Stevens D A (2005) Who let the dogs out? Infection control did: Utility of dogs in health care settings and infection control aspects. American Journal of Infection Control 34 (5) p301-307
Duncan S L (2000) APIC State of the Art Report: The implications of service animals in health care settings. American Journal of Infection Control 28 (20) p170-180
Guay D R P (2001) Pet-assisted therapy in the nursing home setting: Potential for zoonosis. American Journal of Infection Control 29 (3) p178-186
Jorgenson J (1997) Therapeutic use of companion animals in healthcare. Journal of Nursing Scholarship 29 (3) p249-254
Khan M A and Farrag N (2000) Animal-assisted activity and infection control implications in a healthcare setting. Journal of Hospital Infections 46 p4-11
Morrison M L (2007) Health benefits of animal-assisted interventions. Complementary Health Practice Review 12 (1) p51-62
RCN: Working with Dogs in Health Care Settings; A protocol to support organisations considering working with dogs in health care settings and allied health environments. 2019 Revision (p11)
https://www.infectionpreventioncontrol.co.uk/content/uploads/2020/07/CH-01-Animals-ina-care-home-setting-July-2020-Version-2.00.pdf