

Safeguarding Children and Young People Policy
Version: V9
Ratified by: Strategic Safeguarding Group
Date ratified: 27/09/2022
Job Title of author: Named Nurse for Safeguarding Children
Reviewed by Committee or Expert Group Strategic Safeguarding Group
Equality Impact Assessed by:
Related procedural documents

Named Nurse for Safeguarding Children
Working Together 2018 SET Procedure 2022 Domestic Abuse Act 2021
QSPOL03 Being Open Policy and Duty of Candour Policy
QSPOL07 Policy for Consent to Examination or Treatment Policy
SGPOL09 Deprivation of Liberty Safeguarding Policy
SGPOL08 Domestic Abuse Policy
HRPOL14 Disciplinary Policy
HSPOL 08 Health & Safety at Work Policy
IGPOL62 Information Governance Strategy and Policy
CPOL17 Medical Devices Management Policy
QSPOL05 Central Alert System Policy
MMPOL30 Medicines Policy
SGPOL10 Mental Capacity Act Policy
SGPOL18 Prevent Policy
HSPOL16 Violence and Aggression Policy
HSSOP02 Risk Assessment Procedure
HRPOL01 Freedom to speak up Policy
This list of Policies and Procedures is not exhaustive and all Policies and Procedures must be consulted to minimise risks.
Review date: 27/09/25

It is the responsibility of users to ensure that you are using the most up to date document template – i.e. obtained via the intranet
In developing/reviewing this policy Provide Community has had regard to the principles of the NHS Constitution
Version Control Sheet
Version Date Author Status Comment
V1 Unknown Designated Nurse New Approved
V2 February 2012 Safeguarding Team Lead Approved Policy Adapted from Original
V3 April 2013 Safeguarding Team Lead Approved Updated in line with Working Together 2013
V3.1 May 2014 Head of Safeguarding Updated in line with local & national definition
V3.2 April 2015 Head of Safeguarding Approved
V4 June 2015 Head of Safeguarding Updated in line with SET Safeguarding Procedure 2015; Working Together 2015. This Policy replaces the following policies: SGPRO9, SGPRO11, SGPRO12, SGPRO15, SGPRO20, SGPRO21
V5 Head of Safeguarding Updated in line with SET Safeguarding Procedure 2017; Working Together 2015.
V6 October 2019 Head of Safeguarding 3m extension Approved
V7 January 2020 Head of Safeguarding & Named Nurse for Updated in line with SET Safeguarding Procedure
Safeguarding Children 2019; Working Together 2018
V8 January 2022 Head of Safeguarding Updated to include Provide Group Safeguarding Assurance Oversight Structure
V9 August 2022 Named Nurse for Safeguarding Children Updated in line with updated SET Procedures May 2022
1. Provide Group Safeguarding Assurance Oversight Structure

2. Introduction
Provide Community group is required to fulfil its legal duty under Section 11 of the Children Act 2004 and statutory responsibilities set out in Working Together to Safeguard Children (DH 2018). Therefore, safeguarding and promoting the welfare of children must be an integral part of the care offered to all children and their families by all staff working on behalf of Provide Community group. This may be care offered to children, young people, families or adults who are parents or carers.
The aim of the policy is to ensure that there is a robust system in place to safeguard children and young people who receive service from Provide community group and to support staff with safeguarding children and young people.
The policy sets out the roles and responsibilities of all staff and those working on behalf of Provide community group with respect to keeping children safe and promoting their welfare.
3. Key Principles
The Children Act 1989 provides a comprehensive framework for the care and protection of children. The fundamental principle that underpins the Children Act is that the welfare of the child/young person(under 18 years) is paramount. Achieving positive outcomes for children requires all those with responsibility for assessment and provision of services to work together according to an agreed plan of action.
In addition, the Children Act 2004 (Section 11) sets out duties for a wide range of bodies including health. Health, therefore has a statutory duty to carry out its functions having regard to the need to safeguard and promote the welfare of children. This duty extends to contracted services.
“Working Together to Safeguard Children” (DH 2018) statutory guidance sets out how organisations and individuals should work together to safeguard and promote the welfare of children.
The Safeguarding Children Policy and Guidelines complement and should be used in conjunction with Local Safeguarding children’s Board (LSCB)/Children’s safeguarding partnership board Procedures which are available electronically on the internet.
The Policy is intended to support all staff and services directly employed, volunteers or working on behalf of Provide community group with safeguarding children within all geographical areas in which services are delivered.
The ‘Safeguarding Children Roles and Competencies for Healthcare Staff Intercollegiate Document’, (RCPCH 2019), sets out the levels of competencies expected of all staff working within the health service. All staff must ensure that they possess the required knowledge, skills and competencies as set out in their training matrix in line with Intercollegiate Document (2019).
4. Scope
The Policy applies to all staff employed or working on behalf of Provide community group. This includes those that are:
• Temporary, voluntary, contracted or self-employed staff
• Bank /agency staff
The above will be referred to as ‘all staff’ in the policy.
5. Roles and Responsibilities
All Staff (including volunteers)
All staff must always be alert to the possibility of significant harm to children through abuse or neglect, or to a child who is ‘in need’. All staff should be able to recognise indicators and know how to act upon concerns, their depth of knowledge being commensurate with their roles and responsibilities.
Effective safeguarding arrangements should aim to meet the following two key principles:
• Safeguarding is everyone's responsibility: for services to be effective each individual and organisation should play their full part; and
• A child centred approach: for services to be effective they should be based on a clear understanding of the needs and views of children.
(Working Together 2018; SET Safeguarding & Child Protection Procedure 2022)
All staff must be aware of the vulnerabilities of certain groups of children such as those who are disabled, ‘looked after’, privately fostered and socially excluded.
All staff must be aware of the vulnerabilities of certain groups of adults who may find parenting difficult. For example, those experiencing domestic abuse, unstable mental health problems, uncontrolled substance or alcohol misuse, learning disabilities or those with unmet support needs. All staff working primarily with adults who are parents or carers should always consider the effects on parenting capacity and subsequent implications for children of the adult’s illness or behaviour. All Staff are encouraged to ‘Think Child, Think Parent and Think Family”. The Family model identifies that there are risks, stressors, and vulnerability factors increasing a likelihood of a poor outcome, as well as strengths, resources and protective factors that enable families to overcome adversity (ESCB 2019).
All staff must recognise that sharing information is vital for early intervention to ensure that children are protected from abuse and neglect and that the safeguarding of children is paramount and can override any duty of confidentiality.
All staff regardless of grade or position must follow Multi- agency Safeguarding Partnership Board Procedures where there are concerns that a child is being abused or when there are child protection concerns. This cannot be delegated to others.
Staff should be aware that when they have concerns about possible child abuse or neglect they can discuss their concerns with a Provide community group safeguarding team, line Manager or Supervisor, as required and must know how to access this support.
However, if emergency action is needed to protect a child this should never be delayed due to the need to discuss concerns.
All staff should uphold the rights of the child to be able to communicate, be heard and safeguarded from harm and exploitation whatever their race, religion, language, ethnicity, gender, sexuality, age, health or disability, location/placement, criminal behaviour, political or immigration status.
Those who work directly with children/young people should also have access to the Multi-agency Safeguarding Partnership Board procedures. They are available electronically so if staff print or save copies, they are responsible for ensuring these remain updated.
All staff must undertake mandatory child protection/safeguarding training at a level commensurate with the post for which they are employed and reflects the competencies within the Royal College Paediatrics and Child Health document ‘Safeguarding Children Roles and Competencies for Healthcare Staff’ (RCPCH 2019).
All staff must ensure that they update their skills and knowledge by undertaking further refresher training as appropriate and in line with level of competency.
All staff that work regularly with children are responsible for ensuring that they access on going safeguarding children supervision depending on the recommendations for the practice area. Please refer to Safeguarding Supervision policy SGPOL03.
Chief Executive
The Chief Executive has overall responsibility for ensuring that Provide community group’s contribution for safeguarding and promoting the welfare of children is discharged effectively for all children and young people for whom Provide delivers services. This includes ensuring:
• There are safe and robust operational arrangements in place for safeguarding children in all the services that are provided.
• That staff work in line with Local Child Protection Procedures, and anyother locally agreed policies and guidance
Executive Safeguarding Lead (Executive Chief Nursing Officer)
The Executive Safeguarding Lead provides professional and clinical leadership and strategic direction on Provide community group’s safeguarding children services to provide a coordinated and integrated safeguarding service.
It is the responsibility of the Executive Safeguarding Lead to ensure that services are delivered in accordance with the Safeguarding Children Policy and Guidelines and that there are safe systems and processes in place for their staff.
The Executive Safeguarding Lead is responsible for ensuring that the needs of all children and young people are at the forefront of Provide community groups planning and that high-quality health services that meet identified quality standards are delivered
The Executive Safeguarding Lead will ensure that monitoring and reporting of safeguarding activity to fulfil the requirements under Working Together to Safeguard
Children (2018), CQC Essential Standard of quality and safety (2010). The Safeguarding Executive Lead will ensure that Provide is represented at the health subgroup of the Essex Safeguarding Children Board (ESCB).
Contracting Managers
Contracting Managers will ensure that Safeguarding is considered during all contract applications & negotiations with consideration to clarity with regard to clear service standards for safeguarding and promoting the welfare of children, consistent with Children’s Partnership boards Procedures and statutory guidance within Working Together to Safeguard Children (2018). Services and contracting should take account of:
• Safeguarding responsibilities
• Cultural diversity
• The right to family life
• Due regard to confidentiality in accordance with the sharing information guidance.
• Appropriate DBS checks for staff
All services are delivered in a non-discriminatory manner, respect the individuality of the child and are child-centred with a “Think Family” approach
Assistant Directors (AD)
ADs are responsible for taking a lead in promoting a positive culture of Safeguarding. Including AD’s to ensuring robust processes are in place in line with local and national policy to safeguarding children also ensuring that the safeguarding needs of children are at the forefront of service delivery. (RCPCH 2019).
Head of Safeguarding and Named Professionals Safeguarding Children
The Head of Safeguarding, in conjunction with the Named professionals for Safeguarding Children (e.g. Named Nurses and Named Doctors) is responsible for the development, monitoring and reviewing of safeguarding practice within Provide community group.
They are responsible for promoting good professional practice and providing specialist advice and support to health professionals within Provide community group on any issue relating to safeguarding children.
Head of Safeguarding & Named professionals will ensure provision of safeguarding children supervision and training to staff, regular audits of practice, conduct the internal Management Reviews (IMR’s) as part of Safeguarding Practice Reviews (formally Serious Case Reviews) (SCR) and Partnership learning reviews (PLR) or under a regular audit or to investigate an incident.
Registered managers
Registered managers should have sufficient knowledge to support all staff with safeguarding children issues together with the support of the named professionals.
The post holder within each area will ensure that all staff take a proactive approach to safeguarding children, are aware of their roles and responsibilities relating to safeguarding children, and that they possess the required level of competencies within
the Royal College Intercollegiate document ‘Roles and Responsibilities of Health Care All staff’ (2019).
Registered managers should ensure resources are utilised appropriately in areas with high safeguarding children issues and that robust arrangements remain in place to ensure continuity of service
Registered managers will be responsible to ensure that all staff working with children, their families and adult carers/parents, participate in safeguarding children supervision and safeguarding children training both of which are mandatory
At appraisal, Personal Development Plans should reflect that staff continue to meet the safeguarding competencies required for the post.
Registered managers will be responsible to support HR to ensure that all staff who work with children, their families and adult carers/parents have an Enhanced Disclosure and Barring Service (DBS) check in line with Multi-agency Safeguarding Partnership Board procedures/local safeguarding children’s boards (LSCB’s). They should also be working in accordance to NHS Safer Recruitment and Employment Standards and Independent Safeguarding Authority (ISA) recruitment standards.
6. Definition
All staff must be aware of the following definitions:
Child abuse is defined by Working Together (2018) As a form of maltreatment of a child. Somebody may abuse or neglect a child by inflicting harm, or by failing to act to prevent harm. Children may be abused in a family or in an institutional or community setting by those known to them or, more rarely, by others. Abuse can take place wholly online, or technology may be used to facilitate offline abuse. Children may be abused by an adult or adults, or another child or children.
Physical Abuse
A form of abuse which may involve hitting, shaking, throwing, poisoning, burning or scalding, drowning, suffocating or otherwise causing physical harm to a child. Physical harm may also be caused when a parent or carer fabricates the symptoms of, or deliberately induces, illness in a child.
Emotional Abuse
The persistent emotional maltreatment of a child such as to cause severe and persistent adverse effects on the child’s emotional development. It may involve conveying to a child that they are worthless or unloved, inadequate, or valued only insofar as they meet the needs of another person. It may include not giving the child opportunities to express their views, deliberately silencing them or ‘making fun’ of what they say or how they communicate. It may feature age or developmentally inappropriate expectations being imposed on children. These may include interactions that are beyond a child’s developmental capability, as well as overprotection and limitation of exploration and learning, or preventing the child participating in normal social interaction. It may involve seeing or hearing the ill-treatment of another. It may involve serious bullying (including cyber bullying), causing children frequently to feel frightened or in danger, or the exploitation or corruption of children. Some level of
emotional abuse is involved in all types of maltreatment of a child, though it may occur alone.
Sexual Abuse
Involves forcing or enticing a child or young person to take part in sexual activities, not necessarily involving a high level of violence, whether or not the child is aware of what is happening. The activities may involve physical contact, including assault by penetration (for example, rape or oral sex) or non-penetrative acts such as masturbation, kissing, rubbing and touching outside of clothing. They may also include non-contact activities, such as involving children in looking at, or in the production of, sexual images, watching sexual activities, encouraging children to behave in sexually inappropriate ways, or grooming a child in preparation for abuse Sexual abuse can take place online, and technology can be used to facilitate offline abuse. Sexual abuse is not solely perpetrated by adult males.Women can also commit acts of sexual abuse, as can other children.
All staff must be aware that Penetrative sex where one of the partners is under the age of 16 is illegal. Although prosecution of similar age, consenting partners is not usual, but immediate advice should be taken form the safeguarding team. However, where a child is under the age of 13 it is classified as rape under s5 Sexual Offences Act 2003
Neglect
The persistent failure to meet a child’s basic physical and/or psychological needs, likely to result in the serious impairment of the child’s health or development. Neglect may occur during pregnancy as a result of maternal substance abuse. Once a child is born, neglect may involve a parent or carer failing to:
• provide adequate food, clothing and shelter (including exclusion from home or abandonment)
• protect a child from physical and emotional harm or danger
• ensure adequate supervision (including the use of inadequate caregivers)
• ensure access to appropriate medical care or treatment
It may also include neglect of, or unresponsiveness to, a child’s basic emotional needs.
Potential Risk of Harm to an Unborn Child
Neglect may occur during pregnancy due to maternal substance misuse, mental ill health or learning difficulties. Domestic abuse and violence towards a carer may also cause to neglect the needs of an unborn child.
In any circumstances when staff are able to anticipate the likelihood of significant harm with regard to an expected baby, the concerns should be addressed as early as possible before the birth in order to provide safe care and support if possible.
Risks from outside the home.
Contextual Safeguarding is defined by SET 2022 as “children may be vulnerable to abuse or exploitation from outside their families. These extra-familial threats might arise at education settings, from within peer groups, or more from within the wider community and/or online. These threats can take a variety of different forms and children can be vulnerable to multiple threats, including exploitation by criminal gangs
and organised crime groups such as county lines, trafficking, online abuse, teenage relationship abuse, sexual exploitation and the influences of extremism leading to radicalisation.” The purpose of contextual safeguarding is to identify and respond to those threats to children and young people outside of their home.
Significant harm towards children and young people can at times occur outside of the family home. This can present in many forms and parents/families can feel they have little or no control when trying to safeguard their children who are subject to this abuse due to the influence the abuser has over the child.
Child Criminal Exploitation (CE) and Child Sexual Exploitation
Child criminal exploitation (CE) occurs where an individual or group takes advantage of an imbalance of power to coerce, control, manipulate or deceive a child or young person under the age of 18. The victim may have been criminally exploited even if the activity appears consensual. CE does not always involve physical contact, it can also occur through the use of technology. (Home Office, 2018).
CE is a broad term and can include forcing children into criminal activities such as the sale and distribution of drugs (county lines), working in cannabis farms, or committing theft. CE of children is most often seen within County Lines. County lines is the police term for urban gangs supplying drugs to suburban areas and market and coastal towns using dedicated mobile phone lines or ‘deal lines’. County lines is a major, cross cutting issue involving drugs, violence, gangs, safeguarding, criminal and sexual exploitation, modern slavery, and missing persons
Child Sexual Exploitation (CSE) is a form of child sexual abuse. It may occur when a person, or group take advantage of the child using an imbalance of power/exploiting the child/young person under the age of 18 into sexual activity. This may be in exchange for something the child wants or needs e.g. (food, accommodation, drugs, alcohol, gifts cigarettes, and affections) or for the financial advantage or increased status of the perpetrator/person facilitating actions (DoE 2017/SET 2022).
There are 3 important and recognisable elements of child sexual exploitation:
• Children are ‘groomed’ and there is power and control held by the perpetrator/s
• An ‘exchange’ (such as gift, food, money, drugs etc.) is present, this could be to a third party and not always to the child themselves
• Sexual acts or the exchange of sexual images is present
The sexual exploitation of children and young people can be seen in varied forms which can be described through understanding models of CSE. It is important to recognise that these models do not necessarily work in isolation and various models can be operating concurrently.
• Inappropriate relationship model
• Organised network and trafficking model
• Gangs and Group model
• Peer on Peer
• Older Adult 'Boyfriend'/'Girlfriend' model
• Online Grooming model
CSE can occur through the use of technology without the child’s immediate recognition; for example, being persuadedto post sexual images on the internet/mobile
phones without immediate payment or gain. In all cases those exploiting the child/young person have power over them by virtue of their age, gender, intellect physical strength and/or economic or other resources. The child/young person may even have been exploited even if the activity appears consensual.
Violence, coercion and intimidations are common, involvement in exploitative relationships being characterised in the main by the child’s or young person’s limited availability of choice resulting from their social and economic and/or emotional availability (SET 2019). CSE often starts at the age of 12-13 and victims can be girls or boys regardless their ethnicity, religion or cultural/social background.
It is vital that staff are aware of potential indicators of risk of being criminally and sexually exploited to ensure that changes in behaviour are not mistaken for ‘normal adolescent behaviour’ (DoE 2017). Staff should always be mindful of the above when seeing and/or assessing children and their family and act accordingly.
All or probable CE/CSE cases must be referred to the Local Authority, following the Local Authority’s threshold, by using appropriate referral form for each locality. This referral must be made regardless any other immediate actions have been taken to reduce harm to a child or a young person. Appropriate referral forms can be found in appendix. It is also recommended that a CSE Risk and Vulnerabilities Assessment should be completed. This assessment will help breakdown your knowledge of the case and review indicators of CSE and suspected harm to the child. By exploring the case in this way, it can support a balanced summative risk assessment being formed. Please visit http://cse-toolbox.uk/sourcedocs.php for further guidance on how to use this tool.
SystmOne CE/CSE documentation template/guidance must be followed to record any CSE or probable CSE incident. Staff must co-operate and share information by following Provide Information Sharing Policies and procedures with police to support intelligence gathering around CSE.
Essex police have a dedicated hotline number for parents and carers to report their worries or concerns about potential child exploitation. If you’ve seen something that doesn’t seem right call them on 01245 452058 or contact the local police on 101 for any area’s outside of Essex police geographical location.
Online Safety (Information & Communication Technology)
Although communication via internet has many positive outcomes however, it poses huge amount of risk of abuse to the children. Children are at risk of physical, sexual and emotional abuse; radicalisation; and bullying via mobile telephones or online (internet) with verbal and visual messages.
Bullying is the most common form of behaviour that children and young people complain about online abuse. Provide community staff must raise this awareness amongst the children, parents and carers.
The impact on a child of internet-based sexual abuse is similar to that for all sexually abused children. However, it has an additional dimension of there being a visual record of the abuse. Internet based sexual abuse of a child constitutes significant harm through sexual and emotional abuse. Concept of significant harm, as a situation where a child is suffering; or is likely to suffer a degree of physical; sexual; and/or emotional harm, through abuse or neglect; which is so harmful that there needs to be compulsory
intervention by child protection agencies into the life of the child and their family (SET Procedure 2022).
All Provide community group Staff working with children, adults and families should be alert to the possibility that:
• A child may already have been/is being, abused and the images distributed on the internet or by mobile telephone
• An adult or older child may be grooming a child for sexual abuse, including for involvement in making abusive images. This process can involve the child being shown abusive images
• An adult or older child may be viewing and downloading child sexual abuse images.
Where the concerns involve a particular child/ren, professionals considering/ making a referral to local authority children's social care should do so in line with section 6.1. All staff should be aware that the child may not want to acknowledge their involvement or admit its abusive nature, and may resist efforts to offer protection. This should not be a deterrent and safeguarding team line manager should be contacted for support and advice (SET Procedure 2022).
All Provide community group staff must follow the organisations Email (IPOL48) and Internet (IPOL49) Policies at all time.
Further information for staff can be accessed:
• Child Exploitation and Online Protection Centre (http://www.ceop.gov.uk)
• ThinkuKnow- online safety for young people and their parents (http://www.thinkuknow.co.uk)
Perplexing Presentation, Fabricated or Induced Illness
Fabricated or Induced Illness (FII) is a rare, potentially lethal form of abuse. FII is a clinical situation in which a child is, or is very likely to be harmed, due to parent’s behaviour and action, carried out in order to convince people that the child’s state of physical and/or mental health and development is impaired (or more impaired than it actually is). It is important that the focus is on the outcomes or impact on the child and not initially on attempts to diagnose the parent or carer as this can inflict both physical and emotional harm.
The Royal College of Paediatricians and Child Health (RCPCH) 2021 guidance 'Perplexing Presentations (PP)/Fabricated and Induced Illness (FII) in Children' provides further guidance for medical clinicians.
There are three main ways of the carer fabricating or inducing illness in a child which are not mutually exclusive:
• Fabrication of signs and symptoms, including fabrication of past medical history;
• Fabrication of signs and symptoms and falsification of hospital charts, records, letters and documents and specimens of bodily fluids;
• Induction of illness by a variety of means.
Harm to the child may be caused through unnecessary or invasive medical treatment, which may be harmful and possibly dangerous, based on symptoms that are falsely described or deliberately manufactured by the carer, and lack independent corroboration.
Perplexing Presentation
The RCPCH have extended the definition of FII by introducing the term Perplexing Presentations (PP). This describes a situation where there are alerting signs of possible FII that have not yet amounted to likely or significant harm. The child’s physical, mental health and neurodevelopment is not yet clear but there is no perceived risk of immediate harm to the child’s physical health or life.
The alerting signs in the child include: The presence of discrepancies between reports;
• The presentation of the child and independent observations differing from parental reports;
• Implausible descriptions;
• Unexplained findings or unusual results from medical investigations;
• Inexplicably poor response to treatment
• Characteristics of illness that are physiologically impossible e.g. large blood loss, without a drop in haemoglobin levels;
• Impairment of child’s daily life beyond that explained by known level of illness e.g. missed school, need for aids.
The alerting signs in Parental behaviour:
• Parental insistence on continued investigations instead of focusing on symptom alleviation when symptoms not explained by a known medical condition
• Insistence on continuing investigation even when tests have already been undertaken and not identified a difficulty;
• Repeated reporting of new symptoms;
• Repeated attendance at medical settings;
• Inappropriately seeking multiple medical opinions;
• Child repeatedly not brought to appointments, often due to cancellations;
• Not able to accept reassurance or recommended management, insistence on more, clinically unwarranted investigations, referrals or treatments (sometimes based on internet searches);
• Objection to communication between professionals;
• Frequent vexatious complaints about professionals;
• Not allowing child to be seen on their own;
• Repeated or unexplained changes of school, GP or paediatrician;
• Factual discrepancies in statements parents make to professionals or others about their child’s illness.
Medically Unexplained Symptoms (MUS)
In Medically Unexplained Symptoms (MUS), a child’s symptoms are not fully explained by any known pathology. The symptoms are usually psychologically based and this is acknowledged by both clinicians and parents. MUS can also be described as ‘functional disorders’ and are abnormal bodily sensations which cause pain and can impact on daily life. The health professionals and parents work collaboratively in the best interests of the child or young person. Generally, MUS is not considered a safeguarding issue but, in some cases, may involve PP or FII.
Consultation with colleagues is an important part of the process of making sense of the underlying reasons for these signs and symptoms. The characteristics of fabricated or induced illness are that there is a lack of the usual corroboration of findings with signs or symptoms or, in circumstances of diagnosed illness, lack of the usual response to effective treatment. It is this puzzling discrepancy which alerts the medical staff to possible harm being caused to the child.
The signs and symptoms require careful medical evaluation for a range of possible diagnoses.
All professionals should routinely keep records relating to the child. Whenever unusual features are noted, it is extremely important that detailed records are maintained of events, reported illnesses, parent / carer explanations of illness and absences from school and child's symptoms when their carer is present, and in their absence. Normally, the doctor would tell the parent(s) that they have not found the explanation for the signs and symptoms and record the parental response. Parents should be kept informed of further medical assessments/ investigations/tests required and of the findings but at no time should concerns about the reasons for the child's signs and symptoms be shared with parents if this information would jeopardise the child's safety and compromise the child protection process and/or any criminal investigation.
Information sharing between professionals at this stage is absolutely crucial. Advice should be sought from the Provide Community Group Safeguarding team or the Local Designated Doctor or Designated Nurse.
For cases of Perplexing Presentations, a Health and Education Rehabilitation Plan should be developed and implemented. The Lead Health Professional for the Plan will be a Consultant Hospital Paediatrician, Consultant Community Paediatrician or Consultant Child and Adolescent Psychiatrist, who will regularly review the Plan with the family and other identified professionals. Consideration needs to be given to what support the family require to help them to work alongside professionals to implement the Plan. There should be a discussion with the child’s registered GP regarding what role they may be able to take in supporting the management and care of the child. Optimal education needs to be re-established (for school aged children), with appropriate support for the child and family.
The Plan should continue until agreement has been reached by professionals that the child has been restored to optimal health and functioning, and the alerting signs
are no longer of concern.
If the parents do not consent to a Plan, or do not engage with an agreed Plan, then the child should be referred to Children’s Social care following local Authority processes including a chronology. The referral to Children’s Social Care should be discussed with the parents, outlining the professional concerns. In general, a referral would normally be undertaken with the permission of the parent/carers however this should only be done where informing the parent/carer will not place the child at increased risk of significant harm.
Children’s Social Care will have lead responsibility for actions to safeguard the child. The Paediatric Consultant will continue to hold the responsibility for the child’s health and decisions pertaining to it. All three agencies should work closely together making joint decisions, especially about sharing information with the carers.
All information and information sharing should be documented clearly. Promoting children’s well-being and safeguarding them from harm depends crucially on effective information sharing, collaboration and understanding between agencies and professionals. In cases where there is concern that illnesses are being fabricated/induced, there may be a difference of opinion about how to best safeguard a child’s welfare.
Domestic Abuse
Domestic abuse is an abhorrent crime which affects its victims and families (including children) in a substantial way and often caused by perpetrators that are supposed to love and care for them. Domestic abuse can occur at any stage in a relationship often increasing in frequency and severity over time. Domestic abuse can occur to a victim and be perpetrated by anyone regards of age, gender, social background, sexuality or ethnicity.
The Domestic Abuse Act 2021 offers further protection to the millions of people who experience domestic abuse, as well as strengthen measures to tackle perpetrators. It has created a statutory definition of domestic abuse, emphasising that domestic abuse is not just physical violence, but can also be emotional, coercive or controlling, and economic abuse.
As part of this definition, children will be explicitly recognised as victims if they see, hear or otherwise experience the effects of abuse. The cross governmental definition of domestic violence and abuse is:
Any incident or pattern of incidents of controlling, coercive or threatening behaviour, violence or abuse between those aged 16 or over who are or have been intimate partners or family members regardless of gender or sexuality.
This can encompass, but is not limited to, the following types of abuse:
• Psychological
• Physical
• Sexual
• Financial
• Emotional
• Controlling behaviour is: a range of acts designed to make a person subordinate and/or dependent by isolating them from sources of support, exploiting their resources and capacities for personal gain, depriving them of the means needed for independence, resistance and escape and regulating their everyday behaviour.
• Coercive behaviour is: an act or a pattern of acts of assault, threats, humiliation and intimidation or other abuse that is used to harm, punish, or frighten their victim. This definition includes 'honour’ based violence, female genital mutilation (FGM) and forced marriage, and is clear that victims are not confined to one gender or ethnic group.
While the cross-government definition above applies to those aged 16 or above, ‘Adolescent to parent violence and abuse‘ can involve children under 16 as well as over 16. Where there is domestic abuse, the wellbeing of the children in the household must be promoted and all assessments must consider the need to safeguard the children, including unborn child/ren.
The Domestic Abuse Act 2021 defines Domestic abuse as “The Domestic Abuse Act 2021 defines Domestic abuse as: “Behaviour of a person (“A”) towards another person (“B”) is “domestic abuse” if –
(a) A and B are each aged 16 or over and are personally connected to each other, and (b) the behaviour is abusive. Behaviour is “abusive” if it consists of any of the following –
(a) physical or sexual abuse;
(b) violent or threatening behaviour;
(c) controlling or coercive behaviour;
(d) economic abuse; “Economic abuse” means any behaviour that has a substantial adverse effect on B’s ability to - (a) acquire, use or maintain money or other property, or (b) obtain goods or services.
(e) psychological, emotional or other abuse; It does not matter whether the behaviour consists of a single incident or a course of conduct. For the purposes of this Act, A’s behaviour may be behaviour “towards” B despite the fact that it consists of conduct directed at another person (for example, B’s child).”
Personally Connected
The Domestic Abuse Act 2021 states “The definition of “personally connected” For the purposes of the Act, two people are “personally connected” to each other if any of the following applies –
(a) they are, or have been, married to each other;
(b) they are, or have been, civil partners of each other;
(c) they have agreed to marry one another (whether or not the agreement has been terminated);
(d) they have entered into a civil partnership agreement (whether or not the agreement has been terminated);
(e) they are, or have been, in an intimate personal relationship with each other;
(f) they each have, or there has been a time when they each have had, a parental relationship in relation to the same child
(g) they are relatives.”.
The Domestic Abuse Act 2021, explicitly declares that children are victims of domestic abuse if they see, hear or experience the effects of the abuse and the child is related to either the victim or the abuser. SET 2022 states Children can be affected by seeing, hearing, and living with domestic violence and abuse as well as being caught up in any incidents directly, whether to protect someone or as a target. Therefore, highlighting the need to safeguard and protect the child as well as the victim. Staff should be aware of the risk to the child and the victim and refer accordingly where required. Staff should also be aware of the agencies in place to support victims and their families i.e. COMPASS or Next Chapter. Staff should also be aware of the support available for perpetrators who wish to access support to change.
The Domestic abuse Act 2021 also states: “Teenage relationship abuse is not a term that is defined by the 2021 Act, or elsewhere in law. However, if the victim and perpetrator are at least 16 years old, abuse in their relationship can fall under the statutory definition of domestic abuse. Whilst young people under the age of 16 can experience abuse in a relationship, it would be considered child abuse as a matter of law.”
Please refer to the Domestic Abuse Policy SGPOL08.
7. Understanding and raising Safeguarding Concern
All Staff have a key role to play in actively promoting the health and wellbeing of children. Section 11 of the Children Act 2004 places a duty on NHS services in so much that they have regard to the need to safeguard and promote the welfare of children.
All health professionals who work with children and families should be able to:
• Understand the risk factors and recognise children in need of support and/or safeguarding
• Recognise the needs of parents who may need extra help in bringing up their children and know where to refer for help
• Recognise the risks of abuse to an unborn child
• Contribute to enquiries from other professionals about children and their family or carers
• Liaise closely with other agencies, including other health professionals
• Assess the needs of children and the capacity of parents/carers to meet their children’s needs, including the needs of children who display sexually harmful behaviour
• Plan and respond to the needs of children and their families, particularly those who are vulnerable
• Contribute to child protection conferences, family group conferences and strategy discussions
• Contribute to planning support for children at risk of significant harm, e.g. children living in households with domestic violence or parental substance misuse
• Help ensure that children who have been abused and parents under stress (e.g. those who have mental health problems) have access to services to support them
• Play an active part, through the child protection plan, in safeguarding children from significant harm
• As part of generally safeguarding children and young people, providing ongoing promotional and preventative support, through proactive work with children families and expectant parents
• Contribute to Child Safeguarding Practice reviews, Partnership Learning Reviews (PLRs) and their implementation
Raising Concern and Making Referral
Evidence suggests that Children and their families who receive coordinated early help are less likely to develop difficulties that require intervention through a statutory assessment under the Children Act 1989. “Early help may occur at any point in a child or young person’s life and includes both interventions early in life as well as interventions early in the development of a problem” ESCB (2017).
Children, young people and families experience a range of needs at different times in their lives. A co-ordinated multi-disciplinary approach is recommended by Health, social care and other appropriate agencies to support children and families identify strengths and needs, to find practical and achievable solutions and to provide the right information, advice and support. Early help plans can be developed using existing assessment and planning processes within agencies. The common assessment framework (CAF), proposed by Every Child Matters and LSCB’s threshold and windscreen, is a way of working out what extra support a child may need and how best to provide it. Where the problems/needs are more complex, staff should consider completing a Shared Family Assessment (SFA) with the family. SFA and Early help plan guidance’s are available on Provide Intranet.
Staff should refer to the local thresholds document via the local children’s partnership board Effective Support for Children & family in Essex (2017) document; threshold Windscreen (Appendix I), CAF (Appendix II) and Effective support process diagram (Appendix III) when:
• Worried about how well a child or young person is progressing. For example, they may have concerns about their health, development, welfare, behaviour or progress in learning;
• A child or young person, or their parent or carer, raises a concern; or
• A child's or young person's needs are unclear, or are broader than an individual service can address.
Link for Effective support document for Essex:
http://www.escb.co.uk/Professionals/EffectiveSupportforChildrenFamiliesinEssex.asp x
Link for Southend Thresholds document: https://www.southend.gov.uk/downloads/file/6261/southends-childrens-servicesthreshold-document---revised-may-2019
Link for Thurrock Pathway to service and threshold intervention document: https://www.thurrocklscp.org.uk/assets/1/threshold_document_2020.pdf
Link to Peterborough and Cambridgeshire threshold document: https://www.safeguardingcambspeterborough.org.uk/childrenboard/professionals/procedures/threshold-document/
Link for Hertfordshire continuum of need document: https://www.hertfordshire.gov.uk/media-library/documents/childrensservices/hscb/professionals/continuum-of-needs-hscb.pdf
Link for Redbridge thresholds document: https://www.redbridgescp.org.uk/wp-content/uploads/2016/04/Redbridge-SCP-MultiAgency-Thresholds-Document-March-2022.pdf
Link for Waltham Forest thresholds document: https://www.walthamforest.gov.uk/sites/default/files/202111/A%20guide%20to%20thresholds%20and%20practice%20for%20working%20with %20children%20and%20families%20in%20Waltham%20Forest%20%281%29.pdf
Link for Norfolk threshold guide: https://www.norfolklscb.org/wp-content/uploads/2016/03/Text-only-ThresholdGuide_18-19_FINAL-1.pdf
(The Norfolk threshold guide is currently being reviewed)
Link for Suffolk threshold of need guidance: https://www.suffolksp.org.uk/assets/Home-Concerned/Suffolk-Threshold-of-NeedGuidance-2022.pdf
Suffolk’s threshold matrix: https://www.suffolksp.org.uk/assets/Suffolk-ThresholdMatrix-Updated-V2-June-2022.pdf
For React homecare:
Scarborough framework for decision making: https://www.safeguardingchildren.co.uk/wp-content/uploads/2022/02/85943Framework-for-Decision-Making_Infographic-Amend.pdf
Congleton Cheshire guidance on thresholds of need: https://www.cescp.org.uk/pdf/timely-support-for-families-in-ce-guidance-onthresholds-of-need-october-2018.pdf
Worksop Nottinghamshire Pathway to provision thresholds guidance: https://www.nottinghamshire.gov.uk/media/1731833/pathwaytoprovision.pdf
Doncaster Multiagency threshold document: https://dscp.org.uk/sites/default/files/202107/Threshold%20Guidance%20for%20Professionals%202021_1.pdf
Doncaster levels of need descriptors:
https://dscp.org.uk/sites/default/files/202106/Level%20of%20Need%20Descriptors%20May%202021.pdf
Brigg
https://www.northlincscmars.co.uk/policies-procedures-and-guidance/
Buxton threshold document: https://www.proceduresonline.com/derbyshire/scbs/user_controlled_lcms_area/uploa ded_files/Threshold%20Document%20Final%20September%202022.pdf
Staffordshire: Threshold framework https://www.staffsscb.org.uk/wp-content/uploads/2020/09/Threshold-Document.pdf
Loughborough & Leicestershire thresholds for access to services: https://lrsb.org.uk/uploads/view-the-llr-scp-thresholds-for-access-to-services-forchildren-and-families-in-leicester-leicestershire-rutland.pdf
These tools can be useful for a practitioner:
• to identify the child's needs;
• Potentially provide a structure for systematic gathering and recording of information;
• Record evidence of concerns and a base line for measuring progress in addressing them;
These tools can provide framework for a referral discussion to Children's Social Care for an initial or core assessment or to another service for a specialist assessment.
Professionals have a responsibility under the local area’s LSCB safeguarding guidelines to refer a child to the Local authority Children’s Social care when it is believed or suspect that a child:
• Has suffered significant harm;
• Is likely to experience significant harm;
• Has a disability, developmental and welfare needs which are likely to only be met through the provision of Social work led family support services;
• If a child in need who development would be likely to be impaired without provision of services;
Every assessment and referrals should be discussed with parents/carers and consent should be gained when possible. In any circumstances when consent is not given then staff must act in the best interest of the child. If a child has reached his/her 16th birthday then he/she has got right to give consent. However, SET (2022) procedures describes that ‘the fact that a child has reached 16 years of age, is living independently or is in further education, is a member of the armed forces, is in hospital or in custody in the secure estate, is in Foster Care or is in an Adoptive placement does not change their entitlements to services or protection. Confidentiality and Data protection must be
taken seriously while sharing information and making referrals. However, this should not be a barrier to safeguard a child or a young person.
If staff require further support prior to making a referral, they are asked to liaise with their Named nurse for Safeguarding children, who may also suggest a consultation with the local Children and Families Hub (CFH) or MASH for Children’s social care (telephone numbers are listed in appendix for individual areas). During a consultation with the CFH/MASH, no identifiable patient information must be given unless requested from the Social worker in order to support a referral for the child. If information provided does not progress to a referral, CFH/MASH will not keep any formal documentation about concerns raised during this call. During this call, an agreed plan will be agreed.
When there is any concern that a child or young person is at immediate risk then every effort should be made to protect and minimising the risk of harm by taking appropriate immediate action including calling 999 if necessary.
Once a referral to social care has been completed it must be documented in the child’s records on system one. (Please see appendix 7 for flow chart on documenting a safeguarding referral to social care on system one records).
Immediate Referrals to Children’s Social Care
Where there are significant concerns about the safety of a child or children, professionals should make a referral to their local Children Social Care. Depending on which area staff/children and their families are living, Social Care referral forms and processes may differ. Staff should be aware of the process of how to refer to social care within their local area. Please see below for further information.
If there is an alleged crime of abuse towards a child, staff may need to refer directly to the police (and/or social care).
When making a referral staff must ensure to:
• Inform social services whether you are just requesting advice or making a referral.
• Confirm that they are speaking to an appropriate person who is in a position to take the referral, record their name and position.
• Must have the appropriate facts to hand in order to make a clear referral statement.
Social Care contact details for Areas
Essex Children’s Social Care: 0345 6037627
Emergency Duty Service (Immediate Out of Hours Response) No: 0345 606 1212 (Mon - Thurs 5.00pm – 8.45am, Fri 4.30pm – Mon 8.45am Inc. Bank holidays)
Professional referral form: https://www.essexeffectivesupport.org.uk/s4s/FormDetails/FillForm?formId=1
Southend Children’s Social Care: 01702 215007 (Mon to Thurs 9am to 17.30)
Emergency Duty Team (out of hours 365 days a year) 0345 6061212
Referral form:
https://www.southend.gov.uk/downloads/file/5479/ehfs_assessment and should be emailed to mash@southend.gov.uk
Thurrock Children’s Social Care: 01375 652802
Emergency Contact outside office hours: 01375 372468 (Monday to Thursday, 4:30pm to 9am, Friday, from 4:30pm through the weekend until 9am on Monday/ public holidays.
Referral form and process can be found at:
https://www.thurrock.gov.uk/childrens-care-professionals-processes/referralpathways-and-services
Cambridge: 0345 045 5203
Peterborough: 01733 864170
Online enquiries: https://www.peterborough.gov.uk/contact-us/
Redbridge: 0208 708 3885
Online enquiries: cpat.referrals@redbridge.gov.uk
Waltham Forest: 0208094602310
Online enquiries: MASHrequests@walthamforest.gov.uk
Norfolk: 0344 800 8020
Form: NSCB1
Online enquiries: www.norfolk.gov.uk/socialcareenquiry/
Suffolk: Professional Consultation line 0345 606 1499
Referrals: Customer First 0345 606 6167
Form: Multi-Agency Referral Form customer.first@suffolk.gcsx.gov.uk
Hertfordshire: Protected Referrals
0300-123-4043
Urgent Referrals: Protected Referrals.cs@hertscc.gcsx.gov.uk
For React homecare:
Scarborough North Yorkshire 01609 780 780 same number for OOH
Complete form on North Yorkshire Safeguarding Children Partnership website https://www.safeguardingchildren.co.uk/about-us/worried-about-a-child/
Congleton Cheshire
0300 123 5012 (option 3)
Out of Hours Service on 0300 123 5022
https://www.cheshireeast.gov.uk/
Worksop
Nottinghamshire Contact MASH 0300 500 80 90
Out of Hours 0300 456 4546
Access online form at:
https://www.nottinghamshire.gov.uk/care/childrens-socialcare/nottinghamshire-children-and-families-alliance/pathway-toprovision/multi-agency-safeguarding-hub-mash
Doncaster 01302 737777
Out of Hours 01302 796 000
https://www.doncaster.gov.uk/Eforms/SimpleEform/Boot/2370100
Brigg 01724 296500 or freephone 08081689667
Out of hours 01724 296555
https://www.northlincs.gov.uk/people-health-and-care/keeping-children-safe-in-northlincolnshire/
Buxton
Derbyshire 01629 533190
https://apps.derbyshire.gov.uk/applications/formBuilder/startingpoint/996FA446-5670-4083-AB96-D206B82553B0
Staffordshire
Call 0300 111 8007
https://www.staffordshire.gov.uk/Care-for-children-andfamilies/Childprotection/Report-a-concern-online.aspx
Loughborough
Leicestershire Call 0116 305 0005 (24-hour phone line)
https://resources.leicestershire.gov.uk/education-and-children/childprotection-and-safeguarding/multi-agency-referral-form-for-early-help-andsocial-care-services-marf
Section 47 and Section 17 Enquiry
Section 47 of the Children Act 1989 gives the local authority a statutory duty to make enquiries when it has reasonable cause that a child is suffering or likely to suffer significant harm. Section 47 therefore empowers local authorities to call upon other professionals and agencies to assist them.
When carrying out S47 enquiries the local authority has a statutory duty to obtain access to the child’s health information and therefore this duty is not subject to permission by those with parental responsibility. Staff should act promptly to support local authority when Section 47 requests are received by providing accurate up to date information. A section 47 request should be completed within 24 hours of receiving the request.
Section 17 of the Children Act 1989 places a general duty with social care to safeguard and promote the welfare of children in their area who are in need, as with S47 they can call upon other professionals and agencies to assist them. The assessment uses a systematic approach to assessing a child in need. Staff must provide specific information to the local authority as quickly as possible when information is requested under Section 17. A section 17 request is required to be completed within 48 hours of receiving the request, consent from parent should be attached and checked prior to completing the form. If consent has not been attached or the agency receiving the request has not been identified on the form, then the social worker is to be contacted in the first instance to highlight the issue around the consent form.
8. Case Conferences
There are 4 types of child protection conferences:
• Initial conferences;
• Pre-birth conferences;
• Transfer in conferences;
• Review conferences.
All child protection conferences should include not only the child subject of the specific concerns but must also include consideration of the needs of all other children in the household.
An initial child protection conference must be convened when the outcome of the Section 47 enquiry confirms that the child is suffering, or is likely to suffer, significant harm. The local authority children's social care manager is responsible for making the decision on the completion of the Section 47 enquiry (SET 2022).
Every review should consider explicitly whether the child is suffering, or is likely to suffer, significant harm and hence continues to require safeguarding from harm through adherence to a formal child protection plan. If the child is considered to be suffering significant harm, the local authority should consider whether to initiate family court proceedings. If not, then the child should no longer be the subject of a child protection plan and the conference should consider what continuing support services may benefit the child and family and make recommendations accordingly (SET 2022).
If Provide community group staff may receive a request to attend a case conference then the conference should be attended by an appropriate health professional supported by a senior team member/line manager if necessary A report using the allocated local authority’s standard child protection report form should be prepared and submitted within the time frame given by the local authority which is stated on the official invite. The attendee must have relevant information and history of the child and family and also have adequate clinical/professional knowledge and skill to represent the child and professionally challenge any disagreement. If there is disagreement about the decision during the conference between agencies, the conflict resolution procedures should be applied.
Children’s case load holders such as School Nurse or Health Visitor will also attend Case conferences, however, if there are other health professionals working with the child/ren such as Physiotherapists/Speech and Language Therapists/Community Children’s Nurses there is an expectation that they will also attend or will share appropriate information without delay to Children’s Social care. The Safeguarding Team will provide support to the attending health professional in preparation of reports and attendance at Case conference. In a case where there is a disagreement around who attends the Case Conference this should be immediately escalated to the appropriate Assistant Director and Head of Safeguarding. All staff must be aware that any confusion and escalation must not be a barrier or reason not to attend a Case Conference.
Child Protection Plan/Child in Need
If a child has been put on child protection plan or child in need plan, appropriate health professional must take applicable actions and support the child/ren and family to meet their needs. Continue to work closely with the child/ren, family and other partners to ensure all allocated action plans are met to keep the child/ren safe; remain vigilant and carry out continuous risk assessment to ensure safety.
As soon as the health professional is informed that a child is either on child protection plan or a child in need, the appropriate flag must be checked to ensure it is visible on the child’s records or ensure it is activated on SystmOne by them. When the health professionals become aware the child is no longer a child in need, or on a child protection plan, it must be checked that the flag has been removed from the child’s notes, or must be de-escalating by the informed health professional.
Professional Disagreement and Conflict Resolution
Concern or disagreement may arise over another professional’s decisions, actions or lack of actions, in relation to a referral, an assessment or an enquiry.
It is important to:
• Avoid professional disputes that put children at risk or obscure the focus of the child
• resolve difficulties (within and) between agencies quickly and openly
• Identify problem areas in working together where there is a lack of clarity and to promote resolution via amendment to protocols and procedures.
• The safety of individual child/ren and focus on child/ren are the paramount considerations in any professional disagreement and any unresolved issues should be escalated
Disagreement may also arise regarding response to a referral made to Social Care, e.g.
• whether eligibility criteria are met
• whether concerns justify a Section 47 enquiry
• whether to convene an initial case conference
Dissent can also arise regarding decisions made at case conferences or subsequently regarding implementation of a Child Protection Plan. SET Procedures (2017) section 11 1.5 documents the process by which professional disagreements should be resolved i.e
“If the professionals are unable to resolve differences through discussion and/or meeting within a time scale which is acceptable to both of them, their disagreement must be addressed by more experienced / more senior staff.”
The ‘Resolution of Professional Disagreement Form (Appendix IV) is to be used by Provide staff to aid and record this process.
Use of Resolution of Professional Disagreement Form
Page 1 and 2 is completed by the practitioner prior to discussion with their Named Nurse for Safeguarding Children.
Page 2 is completed with the Named Nurse to document advice and action plan to resolve the disagreement. If a resolution is not reached by the practitioner the Named Nurse will use page 3 to document discussions they have had with the Team Leader or Service Manager in Social Care or other agencies. An outcome plan is recorded and fed back to the practitioner. If disagreement still exists this is discussed with the Designated Nurse and further action will be planned.
Page 4 is completed by the Designated Nurse to include discussions that they have had with Senior Management within other agencies and the subsequent outcome. This is fed back to the Named Nurse and practitioner
If a staff member makes several attempts to communicate with partner agencies including social worker to discuss any professional disagreement then a letter (Appendix V) should be sent to the social worker or any other partners and must be documented and recorded in the child’s record. This letter can be sent after making two telephone calls and if no reply received. While waiting for reply to resolve any disagreement, staff members must seek advice from the named nurse/named doctor/line manager to ensure all possible actions have been taken to minimise the risk to the child/ren and/or family. Senior managers and safeguarding team will review the situation and decide to escalate the case to designated nurses and/or senior managers of social services if necessary.
9. Allegations against Staff
Provide community group will make every effort to ensure safe recruitment of all staffs. However, in an unfortunate event where there is an accusation of abuse against a Provide Employee: Assistant Director, Provide community group Safeguarding Team and Human Resources must be notified. Provide community group ‘Disciplinary Procedure’ (HRPOL14) must be followed. Appropriate referrals to Children’s Social Care will be enacted within the timeframes stipulated and Local Authority & Designated Officer (LADO) will be informed.
This can apply when a member of staff has:
• Behaved in a way that has or may have harmed a child
• Possibly committed a criminal offence against or related to a child
• Behaved towards a child in a way which indicates he/she is unsuitable to work with a child
If the Employee has allegedly committed a criminal offence:
• The Line Manager or on call manager must be contacted without delay and if necessary the local Police must be contacted.
• If the allegation is against the line manager or the most senior staff on duty, then Assistant Director and Safeguarding Team must be notified.
• Where any concerns regarding an employee’s suitability to work with children or vulnerable adults is identified, the employer must refer the case to the DBS (Independent Safeguarding Authority) and any relevant professional body.
Provide should work together with local authority children's social care and/or other partners to protect the child/ren and family. Provide must consider the impact on the child concerned and provide support as appropriate. Liaison between the agencies should take place in order to ensure that the child's needs are addressed.
If a member of staff becomes aware of any information regarding another member of staff which identifies that a child/ren may be at risk of harm or has been harmed (including the member of staff’s own child/ren), they must immediately report this information to their line manager and make referral to the social services/police if necessary. The information must also be shared with the Named Professional for Safeguarding Children & governance team who will be responsible for sharing appropriately within Provide as well as notifying the Designated Nurse and Local Authority Designated officer.
Allegation against Non-Substantive Staff
All allegations of abuse made in respect of non-substantive staff, i.e. agency and bank workers, students or contractors will be managed with due regard for this policy. In all cases where allegations are made in respect of non-substantive staff, the appropriate manager within the agency responsible will be alerted to the allegation and action taken by Provide.
Agreement will be reached between appropriate HR business partners in each organisation as to where the primacy of an investigation relating to conduct will rest. As with all investigations, a police / criminal line of enquiry will take precedence above all others.
10.Training and Supervision
All staff that work with children should ensure that they have the skills and knowledge as set out in ‘Intercollegiate Document 2014 (updated January 2019).
Safeguarding Children awareness must be covered within the Local Induction Programme for all new staff, and new staff should also receive additional local introductory training in safeguarding children from their supervisor/ line manager. At Induction Training all staff must be informed of the Safeguarding Children Policy and Guidelines.
All staff must receive training and regular updates at the appropriate level for their role. It is mandatoryfor all staff working with children, families, and parents/carers of children to attend training updates.
All staff must ensure that they are aware of their responsibility to attend safeguarding children training in accordance with local training Policy and familiarise themselves with the Provide training arrangements. Any member of staff unsure of their training needs should contact the Learning & Development Team to discuss their requirements.
Child Protection/Safeguarding Children supervision is mandatory for all health professionals working with children and their families.
A proactive approach to supervision is required to ensure that all staff are supported and continue to develop their skills and knowledge in recognising and acting on concerns regarding the safeguarding of children and responding to the needs of vulnerable children.
Operational Service Leads must ensure that protected time is available to enable staff to receive supervision in accordance with the guidelines.
Child protection/safeguarding children support and supervision will be provided in addition to clinical supervision and management supervision.
11.References
Cambridgeshire Safeguarding Children’s Board Procedures http://cambridgeshirescb.proceduresonline.com/index.htm
Children Act 1989. London: HMSO
Children Act 2004. London: HMSO
Child Sexual Exploitation Definition and a guide for practitioner’s local leaders and decision makers working to protect children from child sexual exploitation. Department for Education (DfE) 2017
Common Core of Skills and Knowledge for the Children’s Workforce. London. HM Government 2012.
CQC Essential: Standards of Quality and Safety 2010
Effective Support For Children and Families in Essex, ESCB 2017
Home Office, Domestic Abuse Statutory Guidance 2022
Multi-agency Safeguarding Arrangements 2019-2020, ESCB 2019
Safeguarding Children Roles and Competencies for Health Care Staff Intercollegiate Document RCPCH 2019
Safeguarding Children & Young people from Sexual Exploitation DH 2009
Sexual Offence ACT 2003
Southend Essex Thurrock (SET) Child Protection Procedures updated May 2022
Working Together to Safeguard Children a guide to inter-agency working to safeguard and promote the welfare of children. HM Government (2018)
Appendix 1: Effective Support Windscreen

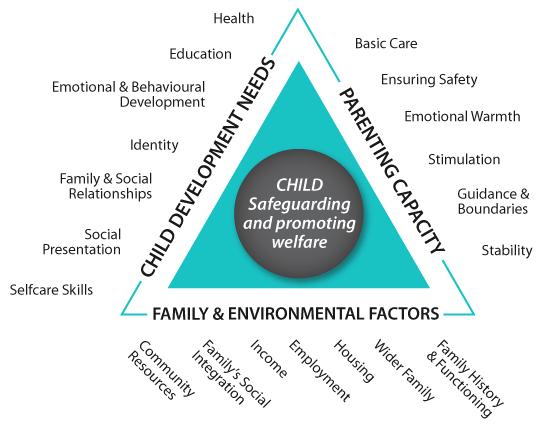
Appendix 2: Common Assessment Framework Triangle
Appendix 3: Early Help and Advice Hub and Initial Response Team Process Map

Appendix 4: Resolution of a Professional Disagreement Form
Resolution of Professional Disagreement
Name of Practitioner
Family Details
Nature of Dissent/concern
Action of Practitioner to date and outcome (include dates discussed with practitioners from other agencies
Date discussed with Named Nurse and advice given
Further Action undertaken and outcome
Details of Named Nurse
Family Name
Action taken by Named Nurse and Outcome (include dates discussed with other agencies
Date discussed with Designated Nurse and plan
Name of Family
Action taken by Designated Nurse
Outcome
Date of Feedback to Named Nurse
Date of Feedback to Practitioner
Name of Family
Action taken by Designated Nurse
Outcome
Date of Feedback to Named Nurse
Date of Feedback to Practitioner
Appendix 5: Letter to Social Care to Raise Safeguarding Concerns

Appendix 6: Contacts sheet.

Area Safeguarding Children
Essex 0345 603 7627
Out of Hours: 0345 606 1212
Form complete a request for support on the online portal https://www.essex.gov.uk/report-a-concern-about-a-child
Thurrock 01375 652802
Out of Hours: 01375 372468
Southend 01702 215007
Out of hours 0845 606 1212
Email: mash@southend.gov.uk
Cambridge 0345 045 5203
Peterborough 01733 864170
Online enquiries
Redbridge 0208 708 3885
Online enquiries
Waltham Forest 0208094602310
Online enquiries
MASHrequests@walthamforest.gov.uk
Norfolk 0344 800 8020
Form NSCB1
Online enquiries
Suffolk Professional Consultation line 03456 061 499 (MASH)
Referrals Customer First 0808 800 4005
Form http://www.suffolk.scb.org.uk
children and young people tab click on concerned tab under professionals access the secure Suffolk Children and Young People’s Portal
Hertfordshire https://www.hertfordshire.gov.uk click on Child Protection complete referral E-mail protectedreferrals.cs@hertfordshire.gov.uk
Referrals 0300 123 4043
Scarborough North Yorkshire
01609 780 780 same number for OOH
Complete form on North Yorkshire Safeguarding Children Partnership website
https://www.safeguardingchildren.co.uk/about-us/worried-about-a-child/
Congleton Cheshire 0300 123 5012 (option 3)
Out of Hours Service on 0300 123 5022 https://www.cheshireeast.gov.uk/
Worksop
Nottinghamshire
Contact MASH 0300 500 80 90
Out of Hours 0300 456 4546
Access online form at: https://www.nottinghamshire.gov.uk/care/childrens-socialcare/nottinghamshire-children-and-families-alliance/pathway-toprovision/multi-agency-safeguarding-hub-mash
Doncaster 01302 737777
Out of Hours 01302 796 000 https://www.doncaster.gov.uk/Eforms/SimpleEform/Boot/2370100
Brigg North Lincolnshire
Buxton Derbyshire
Loughborough Leicestershire
01724 296500 or freephone 08081689667
Out of hours 01724 296555
https://www.northlincs.gov.uk/people-health-and-care/keeping-childrensafe-in-north-lincolnshire/
01629 533190
https://apps.derbyshire.gov.uk/applications/formBuilder/startingpoint/996FA446-5670-4083-AB96-D206B82553B0
Call 0116 305 0005 (24-hour phone line)
https://resources.leicestershire.gov.uk/education-and-children/childprotection-and-safeguarding/multi-agency-referral-form-for-early-helpand-social-care-services-marf
Appendix 7: Child Safeguarding referrals
Openchild's SystmOne record
Onceyouhave completedthe referralplease enterthe reference numberintothe boxatthe bottomofthe templateon SystmOne
Gotothe Cinicaltreeand RightClickon “Provide electronic referralsnew” andselecttop optionondrop downmenu.
Scrollacross thetabsonthe topbarand select "Safeguarding Referrals"
Atthebottom ofthattemplate youwillseeon thelefthand side“online requestfor supportform” CLICK onthat
Thisopensthe Portalforyou tocomplete yourreferral
Saveacopyof thereferral (instructions below)and saveto'Record Attachments' onSystmOne
ClickonSave
Oncetherecord hasbeensaved thiswill generatearead codetoensure thereferralwill bepickedupin Clinical Reporting


Select Safeguarding Referrals Tab


Click here to open the portal


Enter reference number here

EQUALITY IMPACT ASSESSMENT TEMPLATE: Stage 1: ‘Screening’
Name of project/policy/strategy (hereafter referred to as “initiative”):
Safeguarding Children and Young Person Policy
Provide a brief summary (bullet points) of the aims of the initiative and main activities:
Project/Policy Manager: Named Nurse for Safeguarding Children Date: September 2022
This stage establishes whether a proposed initiative will have an impact from an equality perspective on any particular group of people or community – i.e. on the grounds of race (incl. religion/faith), gender (incl. sexual orientation), age, disability, or whether it is “equality neutral” (i.e. have no effect either positive or negative). In the case of gender, consider whether men and women are affected differently.
Q1. Who will benefit from this initiative? Is there likely to be a positive impact on specific groups/communities (whether or not they are the intended beneficiaries), and if so, how? Or is it clear at this stage that it will be equality “neutral”? i.e. will have no particular effect on any group.
All children and young people served by Provide and Provide Community Group
Q2. Is there likely to be an adverse impact on one or more minority/under-represented or community groups as a result of this initiative? If so, who may be affected and why? Or is it clear at this stage that it will be equality “neutral”?
No
Q3. Is the impact of the initiative – whether positive or negative - significant enough to warrant a more detailed assessment (Stage 2 – see guidance)? If not, will there be monitoring and review to assess the impact over a period time? Briefly (bullet points) give reasons for your answer and any steps you are taking to address particular issues, including any consultation with staff or external groups/agencies.
No
Guidelines: Things to consider
Equality impact assessments at Provide take account of relevant equality legislation and include age, (i.e. young and old,); race and ethnicity, gender, disability, religion and faith, and sexual orientation.
The initiative may have a positive, negative or neutral impact, i.e. have no particular effect on the group/community.
Where a negative (i.e. adverse) impact is identified, it may be appropriate to make a more detailed EIA (see Stage 2), or, as important, take early action to redress this – e.g. by abandoning or modifying the initiative. NB: If the initiative contravenes equality legislation, it must be abandoned or modified.
Where an initiative has a positive impact on groups/community relations, the EIA should make this explicit, to enable the outcomes to be monitored over its lifespan.
Where there is a positive impact on particular groups does this mean there could be an adverse impact on others, and if so can this be justified? - e.g. are there other existing or planned initiatives which redress this?
It may not be possible to provide detailed answers to some of these questions at the start of the initiative. The EIA may identify a lack of relevant data, and that data-gathering is a specific action required to inform the initiative as it develops, and also to form part of a continuing evaluation and review process.
It is envisaged that it will be relatively rare for full impact assessments to be carried out at Provide. Usually, where there are particular problems identified in the screening stage, it is envisaged that the approach will be amended at this stage, and/or setting up a monitoring/evaluation system to review a policy’s impact over time.
EQUALITY IMPACT ASSESSMENT TEMPLATE: Stage 2:
(To be used where the ‘screening phase has identified a substantial problem/concern)
This stage examines the initiative in more detail in order to obtain further information where required about its potential adverse or positive impact from an equality perspective. It will help inform whether any action needs to be taken and may form part of a continuing assessment framework as the initiative develops.
Q1. What data/information is there on the target beneficiary groups/communities? Are any of these groups under- or over-represented? Do they have access to the same resources? What are your sources of data and are there any gaps?
Provide’s equitable processes and services.
Q2. Is there a potential for this initiative to have a positive impact, such as tackling discrimination, promoting equality of opportunity and good community relations? If yes, how? Which are the main groups it will have an impact on?
Provide’s equitable processes and services.
Q3. Will the initiative have an adverse impact on any particular group or community/community relations? If yes, in what way? Will the impact be different for different groups – e.g. men and women?
No
Q4. Has there been consultation/is consultation planned with stakeholders/ beneficiaries/ staff who will be affected by the initiative? Summarise (bullet points) any important issues arising from the consultation.
No issues raised, reviewed and ratified by the SSG, Quality and Safety Committee.
Q5. Given your answers to the previous questions, how will your plans be revised to reduce/eliminate negative impact or enhance positive impact? Are there specific factors which need to be taken into account?
Will be monitored and reviewed regularly in line with local and national changes.
Q6. How will the initiative continue to be monitored and evaluated, including its impact on particular groups/ improving community relations? Where appropriate, identify any additional data that will be required.
3 yearly review.
Guidelines: Things toconsider
An initiative may have a positive impact on some sectors of the community but leave others excluded or feeling they are excluded. Consideration should be given to how this can be tackled or minimised. It is important to ensure that relevant groups/communities are identified who should be consulted. This may require taking positive action to engage with those groups who are traditionally less likely to respond to consultations, and could form a specific part of the initiative. The consultation process should form a meaningful part of the initiative as it develops, and help inform any future action.
If the EIA shows an adverse impact, is this because it contravenes any equality legislation? If so, the initiative must be modified or abandoned. There may be another way to meet the objective(s) of the initiative.
Further information:
Useful Websites www.equalityhumanrights.com Website for new Equality agency www.employers-forum.co.uk – Employers forum on disability www.efa.org.uk – Employers forum on age
© MDA 2007
EQUALITY IMPACT ASSESSMENT TEMPLATE: Stage One: ‘Screening’