A NEW HOPE

CULTIVĀRE A PUBLIC HEALTH MAGAZINE
Cultivare_INDD Ver_09212022.indd 1 21/09/2022 4:38:39 pm
The Philippine Society of Public Health Physicians (PSPHP) is one of the leading societies in the country that promotes and focuses on the practice of public health. It is a SEC-registered organization which aims to be a globally-recognized, locally relevant society of Filipino public health practitioners committed to advance the science and practice of public health towards the achievement of better health for all Filipinos. Founded in 2018, the society is supported by donations from fellow public health practitioners, non-government organizations and various agencies.
CULTIVĀRE
THIRD ISSUE - 2021
Alberto “JR” Ong, Jr.
Christelle Alconera
Michael Vallente
Paula Melizza Valera
Jaifred Lopez
Layout Editor Transcriber
P&E Digital Marketing and Media
Princess Grace Mendoza
Ruiz Building, 365 El Grande Avenue, BF Homes, Paranaque City
CONTACT DETAILS
phconsecretariat@gmail.com
Philippine Society of Public Health Physicians (@publichealthphysicians) @psphpofficial
About CULTIV ĀRE
During the 1st Public Health Convention (PHCon) held last September 2019, the PSPHP launched a magazine entitled, CULTIVĀRE.
Out of the society’s desire to inculcate knowledge and share advocacies to fellow public health practitioners, CULTIVĀRE was conceptualized to capture all these passions that linger in the hearts of public health practitioners as well as institutions and agencies with similar lenses.
Editorial Team
Cultivare_INDD Ver_09212022.indd 2 21/09/2022 4:38:39 pm
CULTIVĀRE is Latin word for cultivate which symbolizes how entities share, hone, or complement one another to grow and create a synergistic impact to society through public health.
It captures the society’s adherence to its set values (excellence, bayanihan, responsive service, respect, accountability and humility), and motto (Opus, Virtus, Scientia) as it nurtures an engaging environment for public health practitioners to freely enhance their contribution to nation-building through a health systems approach.
This magazine is a vital communication link that is open for everyone who wishes to contribute to cultivating fellow public health practitioners and make a long-lasting impact at all levels.
3 Cultivare_INDD Ver_09212022.indd 3 21/09/2022 4:38:39 pm
"
This year’s Cultivare focuses on A New Hope.
In the long arduous battle against COVID-19, we have faced too much grief, anxieties, and painful despair. How do we recover? How do we aspire and dream again when there have been unquantifiable losses? How do we go on? How do we walk onwards and forwards? How do we continue the fight for health for all? How do we rebuild our health system, heavily devastated by the pandemic? How do we learn from all of these?
Hope.
It is about rekindling hope.
The hope that our choices are aligned to our best values, that our actions will benefit the larger population. The hope that if we rally and support our peers and our community, we can find the solutions to the things we thought were unsolvable. The hope that we will learn from the experiences of the pandemic. The hope that we will
Why A New Hope?
A New Hope comes from the first film of the original Star Wars trilogy. In our case, after many months of the pandemic, of anxiety, of confusion, a lot of frustration,
overwork, deaths, and grief among friends, families and communities, we are waiting and building for a new hope. The theme captures our aspirations as we continue to rebuild our systems, attempting to capture the lessons from COVID-19.
A New Hope means recognizing that public health is vital, and why we need to build and invest in people in ourselves, in institutions, and in public health projects for our health, development, safety, and security.
A New Hope means mobilizing new resources for new projects, strengthening programs, and undertaking research.
A New Hope means welcoming more people in the field of public health and social development, we also welcome different expertise and disciplines, and continue to improve our skills and knowledge
A New Hope means new opportunities, to plan, innovate, reflect, rethink and recalibrate our approaches and actions to benefit all.
A New Hope is about rebuilding and recreating together.
4 Cultivare_INDD Ver_09212022.indd 4 21/09/2022 4:38:39 pm
Table of Contents
Message from the President
Message from the Vice President Message from the Secretary of Health Message from PSPHP Board Chair
PHCon 2021 Introduction
Public Health Programs
Learning from Pandemic: Taiwan

Q&A Indigenization
Walk the Talk: Reimagining Health Care
How the Primary Health Care System Singapore Reorienting the Medical Curriculum

HRH Master Plan
Mandanas Ruling
Unifying Health Professionals
From Evidence to Policy
AIA Group
Spurring Innovations
Unilab
Health Equity and Human Rights

Public Health Stories
Rural Surgery
Story of a Rural Health Physician
How the National and Global Health shape ‘s

Ronalad Law’s public career
A Glimpse on LGU Health Financing Emerging Crisis in the Philippine public health: Multi-Sectoral Action Needed
Dr. Sajjadullah Wazir: “An inspiration for public health”
The Role of a Protestant Church in Community
Methodist in the Davao Episcopal Area: Kalusugan Ministry
Medicine: Moments with Dr Ruiz
Oplan Kalusugan sa DepEd Innovations for Communications Health

Dr. SweetC Alipon
A Nurse’s adventures to life: Lessons from the Orient to the Occident
Zuellig
06 07 08 09 11 12 15 19 23 29 32 35 38 41 43 45 48 51 55 PHCon
59 60 62 63 66 69 71 72 73 74 76 78 80
Dr.
United
Family Foundation PSPHP Board Members and the Executive Committee PSPHP Founding and Pioneer Members MetaHealth 87 90 95 96
Dr. Helen Le Bourgeois Santé Publique 82 85 15 50 27 71 77 5 Cultivare_INDD Ver_09212022.indd 5 21/09/2022 4:38:45 pm
Message from the President of the Philippines
 Message
Message
My warmest greetings to the Philippine Society of Public Health Physicians (PSPHP) as it holds the 3rd National Public HealthConvention (PHON 2021).
No words can express my gratitude for the noble sacrifices made by the PSPHP and its members to protect and save our people from the threat of COVID-19. The entire nation is truly grateful for your service.
It is our hope that you will remain steadfast in performing your duty to your patients, especially those who are most in need.
Rodrigo Duterte President

May this event empower participants to collectively address the most pressing issues and concerns in our public health systems
With your help, I am confident that we will overcome all difficulties ahead and realize a safer, stronger and healthier environment for every Filipino.
I wish you a meaningful event.
6 Cultivare_INDD Ver_09212022.indd 6 21/09/2022 4:38:46 pm
Message from the Vice President of the Philippines
Message
My warmest greetings to the Philippine Society of Public Health Physicians on your 3rd National Public Health Convention! Maraming salamat sa patuloy ninyong sakripisyo at dedikasyon as we continue to face COVID-19.
Leni Robredo Vice President

I know it has been a challenging year for everyone, lalo na para sa inyong mgammedical frontliners: Kayo ang takbuhan ng mga pasyente, and you witness firsthand the stories behind the numbers we dread hearing every day. And yet in the face of the gravest health crisis of our time, hindi kayo nagpatinag. You showed up every day, you rose to the occasion, and stepped up when you were most needed. Nakakahawa ‘yung tapang, selflessness, at dedication ninyo. Kaya nga kapag sinasabi kong “The Filipino responds to the worst of times with the best in ourselves, “ kayong mga medical frontliners talaga ang nasa isip ko bilang pangunahing halimbawa.
This year’s theme is a good reminder of the work ahead of us: To rebuild with public health in perspective. As you set down to do this work, I have no doubt that you will continue to display the same grit and compassionate resolve that has brought millions of Filipinos safely through the pandemic.
Know that we recognize your sacrifices and hard work. The Office of the Vice President stands as a permanent partner and friend to all health workers and frontliners across the country, as we all do our part in building a better normal for all. Muli, maraming salamat sa inyong lahat. Mabuhay ang Philippine Society of Public Health Physicians!
7 Cultivare_INDD Ver_09212022.indd 7 21/09/2022 4:38:48 pm
Message from Secretary of Health
Message
My warmest congratulations to the Philippine Society of Public Health Physicians, Inc. (PSPHP) for their staging of their 3rd National Convention!

As the battle against the COVID-19 pandemic continues to rage on, we are continuously challenged by the emergence of new variants. However, we have not stood still. As the virus keeps evolving, the health sector and the implementation and development of interventions that we have at our disposal also evolve. Chief among the subjects that COVID-19 has thrown a spotlight on is the reality that public health is not just a medical or scientific concern. Rather, it must effectively cut across all sectors of society, and be able to sow harmony among all these sectors to truly deliver on all its promises.
Francisco T. Duque III, MD, MSc Secretary Department of Health

In light of this, the efforts of PSPHP have been nothing short of monumental in the relentless advancement of the practice of public health. Moreover, the theme of this year’s national convention “A New Hope: Rebuilding with Public Health in Perspective” gives renewed emphasis, as well as an overarching guide, as to what we have to do as we move forward in public health. We need to recognise the critical role of public health physicians and professionals in the integrity of our nation, and so must exhaust all means to ensure their continuing development. We need to continue working hand in hand to develop more responsive and more accessible health systems that can capably cater to overlooked, emerging, and contemporary health issues. It also reinvigorates the synergy of public health physicians and professionals to continue exploring more responsive strategies in the practice of evidence-based medicine.
As this convention greatly recognizes the role of our “backliners”, the ones who are moving behind the scenes to ensure the continuity of the entire spectrum of health service delivery, it is our fervent hope that the technical knowledge that the participants shall gain in this convention shall contribute in the shaping of relevant policies to advance public health. As we continue to fulfil our incumbent mandates to help the world heal from this pandemic - and indeed as we seek to better secure our world from any future crises - know that the entirety of the Department of Health (DOH) is one with you in our pursuit to elevate public health practice to higher standards of practice and professionalism.
Maraming salamat at mabuhay!
8 Cultivare_INDD Ver_09212022.indd 8 21/09/2022 4:38:48 pm
Message from PSPHP Board Chair
Message
Message from the Board of Trustees
The Antonine Plague of 165 to 180 AD ushered in a revival of new ideas and faith that changed the Roman Empire. When the Black Plague ended in 1352, it sparked the beginnings of the renaissance and the enlightenment in Europe. In England, the same process liberated peasants from being attached to land thereby starting an economy driven by demand and supply and the potential for people to look for better wages. The 1918 Spanish Flu ushered in the roaring 20s that was characterized by rapid economic growth and affluence. But epidemics also caused the decline of ancient civilizations such as the Khmer empire, while contributing to the conquest of the Americas by Imperial Spain.
Lester Sam A. Geroy, MD, MPH, MSc Chairman
The years 2021 and 2022 are years of expectation on the turnout of the COVID-19 pandemic. Will this end soon? What did we learn? How will people and societies survive? How will the new structures lead to a better life for everyone? Even as early as 2020, we have seen many changes in the way we work and how we organize the economy. After all, the winners keep winning, and the smart keep getting smarter.
The birth of PSPHP was timely right before the pandemic. The current situation gave public health physicians and professionals to work together closely with the rest of our colleagues in health and medicine. May this Cultivare issue continue to document and share our aspirations and stories as individuals, as institutions and as a Society.

With prayers for peace, grace and blessings to everyone!
Lester Sam Araneta Geroy Chairman of the Board of Trustees
Dr Joel Buenaventura, Vice Chairman
Dr Michael Caampued, President
Dr Jaifred Christian Lopez, Vice President

Dr Jacqueline Momville, Secretary
Dr Joey Francis Hernandez, Treasurer
Dr Josephine R. Bundoc
Dr Paulyn Jean R. Ubial
Dr Annely Celocia
Dr Anthony Faraon
Dr Renzo Guinto
Dr Juan Alfonso Leonardia, Founding Vice Chairman
Dr Luisito Ruiz, Founding Chairman
9 Cultivare_INDD Ver_09212022.indd 9 21/09/2022 4:38:48 pm









10 Cultivare_INDD Ver_09212022.indd 10 21/09/2022 4:38:51 pm
PHCON
The past 17 months challenged the knowledge and systems in public health with the COVID-19 pandemic. Health leaders, local chief executives, and the civil society have worked hand-in-hand, developing innovations and strategies to fill in the gaps of the health system. Banking on these experiences, this year, the convention has the theme called “A New Hope: Rebuilding with Public Health in Perspective“, capturing the learnings from the ongoing COVID-19 efforts - rebuilding after health system upheavals, and envisioning a better public health.
The convention aimed to provide avenues to discuss overlooked, emerging, and contemporary issues shaping the public health landscape; Allow meaningful interactions among members, collaborators, and allies;
Identify the best practices and experiences adaptable to the local setting; and Convene professionals practicing or interested in advancing public health

2021 11 Cultivare_INDD Ver_09212022.indd 11 21/09/2022 4:38:57 pm
The Effect of the Pandemic on Public Health Programs
Dr. Beverly Lorraine Ho Director, Disease Prevention and Control Bureau, Department of Health
Impact on Certain Key Indicators
Important points regarding the impact on certain key indicators which include health literacy, infrastructure, spending, family health, vaccine-preventable diseases, infectious diseases, and mental health before and during the COVID-19 pandemic were discussed in this segment.
Health Literacy
does have a working referral system.
Baseline Spending on Primary Health Care
The Philippines invests only 4% of national spending for health on primary health care, as opposed to EU countries with good primary care systems, spends at least 13%.
. Our primary health care investments are at $6 per capita compared to our other ASEAN neighbors who were able to perform better during the pandemic.
Beverly Lorraine Chua Ho is the current director of the Disease and Prevention Bureau who oversees policy, program and monitoring of various life-stage based and disease-stage based programs constituting primary care services. She’s also the current director of the Health Promotion Bureau where she leads the development of policies on minimum health standards required for COVID-19 Mitigation.
Prior to her current designations, she was the Chief of Research Division of Health Policy Development and Planning Bureau where she designed innovative grants and built institutional capacity for policy research. Her efforts contributed to the legislation of Universal Health Care Law (RA 11223), Excise Tax on Tobacco Products (RA 11346) and SugarSweetened beverages (RA 10963) and other executive and legislative measures.
She’s a co-founder of Alliance for Improving Health Outcomes Inc., (AIHO) which provides a platform to produce and disseminate evidence-based solutions to pressing public health questions and of Philippine Society of Public Health Physicians (PSPHP) which committed to advance the science and practice towards the achievement of health for all Filipinos.
She holds an MD from the University of the Philippines and an MPH in Health Policy and Management from the Harvard T.H. Chan School of Public Health as a Fulbright Scholar.

It is important to increase the capacity of the general public in making decisions in health care through the information being given to them. Comprehensive Health Literacy (CHL) is the perceived ability of an individual to perform tasks related to the ability to access, understand, appraise, and apply health information as measured by a 47-item rating scale. A recent CHL survey reports that Filipinos with sufficient CHL is at 40%
Baseline Infrastructure
In 2020, the DOH worked with the Asian Development Bank (ADB) and Philippine Institute for Development Studies (PIDS) to develop the Philippine Health Facility Development Plan. Currently, private and public facilities are only around 3,700, while for hospital beds, we are at 1.2 beds per 1,000 population. This can explain why when we talk about health care utilization capacity, we always seem to fill the brim really fast.
Our hospital beds can be compared against our neighboring countries Philippines: Malaysia: Singapore: Vietnam:
1.2 1.9 2.5 2.6
Projecting the Philippine needs by 2040, we would need 6,900 primary care facilities and 2.7 beds per 1,000 population. However, the 2.7 beds per 1,000 population target by 2040 is significantly lower than what is expected in upper-middle and high-income countries. This is also the projected need if the country
Effect of Pandemic on Maternal Concerns
In 2017, 1484 maternal deaths were recorded all over the country, while there is a growing number of Filipino women of reproductive age (15-49 years of age) who are not using birth control. By 2020, maternal mortality cases went up by 26% from 2019. The rate of low usage of contraception has increased by 2.07 million by the end of 2020 (67% increase from 2019). Consequently, total unintended pregnancies may increase up to 751,000 more than 2019 (42% increase).
Effect of Pandemic on Vulnerable Population
It is important to increase the capacity of the general public in making decisions in health care through the information being given to them. Comprehensive Health Literacy (CHL) is the perceived ability of an individual to perform tasks related to the ability to access, understand, appraise, and apply health information as measured by a 47-item rating scale. A recent CHL survey reports that Filipinos with sufficient CHL is at 40%.
Vaccine-Preventable Diseases
Even prior to COVID-19, there is a continuous provision of vaccines, albeit the erratic routine immunization coverage. There was also stable surveillance of vaccine-preventable diseases. However, during COVID 10, routine immunization services were greatly suppressed, and this can also be attributed to the pause in Outreach services in many places. There have been postponements of multiple rounds of measles and polio campaigns (Chikiting Ligtas 2020-2021)
12 Cultivare_INDD Ver_09212022.indd 12 21/09/2022 4:38:58 pm
Compromise surveillance occurred because of the focus on COVID-19 and the difficulty in conducting fieldwork. Comparing April 2019 and April 2020 coverage rates, only half of the targets were immunized in that period. A drop of 63% at April 2020, and at the end of 2020, there was only a drop of 8% in terms of EPI coverage rate
Infectious Diseases: Tuberculosis

Tuberculosis has been affected by the COVID-19 pandemic. Contract tracing was limited by quarantine and access to chest x-rays were limited, due to closures of outpatient facilities. There was no active case finding due to the restrictions, affecting consults. TB testing was halted as there was a scarcity of PPE. There were also restricted transport of specimens and prolonged turnaround time of tests, as TB GeneXpert machines had to be used for COVID testing. Clinic visits were restricted. Meanwhile, labs were closed or there was no transport for follow-up lab tests. TB testing was less prioritized due to the urgency of COVID testing.
Infectious Disease Programs and COVID-19
• 49% decrease in the number of people tested using GeneXpert
• GeneXpert machine for TB were also repurposed for COVID-19 testing
• 37% decrease in the number of people diagnosed and started on treatment
• 16% decrease in the number of diagnosed drug-resistant TB
• 11% decrease in the treatment success rate of New and Relapse TB due to non-reporting of private physicians of the treatment outcome
• Decrease in the number of TB preventive therapy recipients
• 61% decreased (477,965) in the number of HIV tests conducted
• 37% decreased (8,058) in the number of diagnosed cases
• 28% decrease (8,249) in the number of patients enrolled to treatment
• Decrease in national prevention program coverage
• Decline in condom use but sustained high risk sexual behavior among KPs
• Prevention coverage dropped by 9%
• Condom use dropped by 2%
• It is expected that the increase in the number of new HIV infections will double from 10% in 2020 to 21% in 2021.
• Most of these infections will continue to be among the 25 and above age group
• There was a drop in the number of zoonotic diseases in 2020. It was hypothesized that because people stayed at home more, then the chances of cleaning the community and their own homes to protect themselves from dengue, for example, increased.
• During the rainy season, people are still not going to work, and so leptospirosis infection rates decreased.
• The behaviors we are espousing for COVID-19 are protective from food and water-borne illnesses, e.g., good hand hygiene
Mental Health
Prior to COVID-19, NCMH received 3,125 calls to their crisis hotline, 23% comprise of suicide-related calls. However, during COVID-19 (2020), there is 253% increase (11,017) in the number of total calls to the NCMH Crisis Hotline, there is a 3% increase (2,841) in the percentage of suicide-related calls out of the total NCMH calls.
In the early phase of the pandemic, a fourth of respondents of a study reported moderateto-severe anxiety, while a sixth reported moderate-to-severe depression. In another study, 1 in 3 COVID-19 patients are diagnosed with a neuropsychiatric condition in the next six months
Adaptive Measures & Innovations
We should appreciate good practices (“small wins”) that can be accelerated in the coming years. Many of the work seen is innovations done in the community level through the support of many partners
Online Resource Partners & Providers

Shifted to online capacity building, not only for health care providers but also for patients.
The RHCare info was developed alongside several NGOs with the help of UNFPA
Health Promotion & Advocacy
All-in-one guides for LGUs to implement health promotion interventions that emphasize the role of enabling environment and acknowledges local people power in behavior change initiatives. This framework shifts towards understanding that individual behavior can be facilitated when the environment is enabling. Includes a template, an implementation plan, and a communication plan within it.
Tuberculosis
HIV Zoonotic & Food and Waterborne Diseases
13 Cultivare_INDD Ver_09212022.indd 13 21/09/2022 4:39:00 pm
Mental Health Nudges for Health Care Workers
A Behavioral Change Agency helped support DOH in piloting this program in five hospitals. In this case, the question was how to actually help health care workers through health promoting behaviors while at work. The agency piloted behavioral nudges through stickers or posters in areas where they are being nudged to perform these healthy behaviors. The pilot showed promising result, and further scaled up to around 20 hospitals benefiting around 1,000-1,500 health care workers in those hospitals.
Service Delivery: Online & Outreach
Outreach or bringing the services closer to the communities and families where Family planning on wheels was done by LGUs. TBStriders have helped in the delivery of medicines in DOTS and deliver ARVs. They have also worked with private entities to ensure that all DOH hospitals have telemedicine components in the outpatient clinics. Unified COVID-19 algorithms were developed with different disciplines of medicine and public health. The algorithms allowed great help for non-specialist health care providers who use the algorithm as a job aid. It has models of teleconsultation between a general practitioner and specialist
Lessons for UHC
The PH pre-pandemic health care system has been fragmented, specialist-centric, curativefocused, and under-investing in communitybased preventive health interventions. We have had externally-reliant local health systems and do not have good ownership of their health problems, which has been critical when Community-powered local health systems were built. Now that the LGU is trying to absorb or take responsibility for the local health system, the next step is to make sure that the community is ready to take those powers within their hands.
Shift to Province/City-Wide Health Care
Prior to COVID-19, care pathways were fragmented and self-navigated. During COVID-19, patient pathways were developed and many municipalities have lower capacity and have to partner up with neighboring municipalities or provinces. These are actually the elements of what is intended with the UHC HCPN pathway, with provincial-wide or city-wide collaborations. We are hoping to continue beyond the pandemic and to realize the importance of synergy. There is a need to have the ability to integrate the components under the local health system maturity model is accelerated in many of the cityand province-wide health systems
Shift to Primary Care
a ray of hope. There are things that we wanted to push for three to four years already, but the pandemic is showing us a way to do it.
It is not easy for government people to do bold things, where for every turn, you get various forms of criticism. Some platforms are more limited than before, not because there is no money or mandate to do it, but because of the way things are being perceived. Investigations should aid the reforms and not push us backwards and make all your government people very risk-averse. If everyone is risk-averse, there would be no reforms.
Molecular laboratories are underinvested in for many, many years, and the pandemic has forced us into building these laboratories. Most of these laboratories are privately built.
Information Management System
Infrastructure What was considered as a “bigger win” during the pandemic was recognizing that data drives decisions. Our current health information system does not support planning and response. The DOH COVID-19 tracker was one of the first efforts to get real-time or daily data to get particular information.If we are able to do it for COVID, then it is possible to get it for other conditions as well.
Traditionally, Filipino families have “contacts” or specialists they turn to for various concerns, During COVID-19 the BHERTs/OSHOs became pathway navigators. Every Filipino knows their BHERT (community). Every company has an OSH officer (workplace). We want this to continue so that every Filipino is very much connected to their local health system. Eventually, this will lead to every Filipino assigned to primary care providers.
Shift to Preventive Interventions
During COVID-19, there was an emphasis on preventive measures against COVID-19 and following the minimum public health standards with a preventive approach and communitybased interventions. Mayroon nang kakayahan ang bawat Pilipino na maunawaan ang kalagayan ng kanilang kalusugan at makalikha ng matalinong desisyon tungkol sa kanilang kalusugan - “healthful choices”. Towards increasing health literacy of people and making the environment enabling; making sure that people have a better appreciation really does affect the health of the people. Total health is becoming more understood during the pandemic; becoming mainstream. For example, children need to go to school because that is a part of their development.
Conclusion
What happened during the pandemic is not perfect, but for health system advocates, this is

We need
1. public-private collaboration,
2. horizontal collaboration among primary care providers,
3. vertical collaboration between primary care facilities and hospitals, between generalists and specialists, and
4. interprofessional collaboration. Before, it was hard to make specialists shift tasks. However, we are seeing the openness of many specialist societies in collaborating with primary care physicians in correctly diagnosing patients, e.g., back pain, as they cannot accommodate the huge number of patients.
5. The collaborative spirit should consciously be built. It is easy at first, but when the going gets tough, we find it hard to sustain coalitions. The challenge for us is how to look beyond those difficulties and say that we are collaborating at all fronts.
“For UHC reforms to be felt, we need BOLD, SUSTAINED COMMITMENT to financing and good governance.”
“For UHC reforms to accelerate, we need to BUILD TRUST and imbibe a COLLABORATIVE SPIRIT.”
14 Cultivare_INDD Ver_09212022.indd 14 21/09/2022 4:39:01 pm
Learning from Pandemic: How Taiwan Did It
 Photo Credit Envato/Pressmaster
Photo Credit Envato/Pressmaster
15 Cultivare_INDD Ver_09212022.indd 15 21/09/2022 4:39:04 pm
Dr. Shou-Hsia Cheng discussed his viewpoints on Taiwan’s effective response to COVID-19 mainly focusing on both non-pharmaceutical interventions and containment strategies that the country has been implementing to mitigate the spread of the virus. Dr. Cheng also shared some learnings that he has realized from the pandemic as well as directions that not only Taiwan but also the global community should consider taking in the future.
Taiwan has experienced its first COVID-19 outbreak peak which occurred in May to June 2021. It is worth noting, however, that while Taiwan has the lowest number of both confirmed cases and cumulative incidence among some Asian countries, it garnered the highest fatality rate of more than 5% up until the present. They are still wondering about the reason behind the high case mortality.

Interventions
Four methods of interventions consisting of 1) Non-pharmaceutical Intervention (NPI), 2) Containment Measures, 3) Antiviral therapy, and 4) Vaccine to mitigate the spread of COVID-19 have been introduced in this segment. An extensive discussion has been made for the first two interventions.
Transmission Route
In 2020, the DOH worked with the Asian Development Bank (ADB) and Philippine Institute for Development Studies (PIDS) to develop the Philippine Health Facility Development Plan. Currently, private and public facilities are only around 3,700, while for hospital beds, we are at 1.2 beds per 1,000 population. This can explain why

when we talk about health care utilization capacity, we always seem to fill the brim really fast.
Disease Progression Model
For individuals that have been infected with COVID-19, recovery and death prevention still remains the top priority. It is imperative to allocate the early onset of symptomatic patients and to focus on their treatment as much as possible.
Non-pharmaceutical Intervention (NPI)
Six major tools of non-pharmaceutical intervention (NPI) have been tackled. While taking temperature before entering an establishment is an NPI, evidence suggests that it is not an accurate tool and hence not as important as compared to the other major tools presented. On the other hand, wearing a face mask is still considered as the most important and most effective way in preventing the spread of COVID-19.
an nCOV health declaration and submit travel records. Moreover, they are asked to undergo a home/institution quarantine for 14 days.
Taiwan has adopted and established National Health Insurance in 1995 to serve as a single-payer health coverage system. Each citizen is provided an NHI card. The information presented in the card along with the records submitted by travellers have been linked via NHI MediCloud to facilitate record-checking for every citizen more efficiently.
A regulation prohibiting foreign nationals from entering Taiwan has also been issued by the government. This policy is being implemented whenever the country is on high alert. Taxis and buses for transporting travelers from the airport to their households or to quarantine institutes have been duly designated as well.
Quarantine regulations for flight crew members have been tightened as they believed that one of the most probable sources for the recent outbreak in Taiwan came from the flight crews. The regulation has been loosened for a period of time and this proved to be a hard lesson for the country. Currently, flight crew members are required to do 5 days of quarantine along with 9 days of self-health monitoring.
An intensive border control helps in keeping the epidemic under control. New Zealand for instance has a very rigid border control and this has contributed a lot in containing the spread of the virus in their country.

In Taiwan, travelers are required to submit and fill out forms for entry and then proceed to a 14-day quarantine. To limit the movement of people under quarantine and ensure that they are staying in their respective homes or quarantine institutions, Taiwan has also developed a mobilephone-based electronic fence system that uses location-tracking technology.
Containment Measures
In an effort to mitigate the spread and transmission of COVID-19, Taiwan has employed several containment measures:
Border Control Consisting of only one major island, Taiwan has been able to control its borders in a less challenging manner compared to the Philippines and Indonesia. An electronic entry quarantine system has been employed in the country wherein travelers are required to present
Dr. Shou-Hsia Cheng Professor and Dean, College of Public Health, National Taiwan University
Photo Credit: Daniel Ceng Shou-Yi//Shutterstock
Photo Credit: Sam Yeh—AFP via Getty Images
16 Cultivare_INDD Ver_09212022.indd 16 21/09/2022 4:39:06 pm
Control of Community Transmission
• Surveillance and Contact Tracing
• People who came into contact with confirmed cases will be isolated at home for 14 days. While staying at home, they will be contacted by local health agencies to check their health twice a day. If they develop symptoms, the health agency will then place them in hospital using a designated transportation arrangement.
• Electronic Security Monitoring System (SMS)
• People who are quarantined at home are required to turn on their mobile phones’ location identification function so that their phone signal can be monitored. If a person under quarantine leaves his designated site, a civil affair worker will be notified via SMS and that person who violated the quarantine restriction will be fined accordingly.
• Living Support for Individuals under Home Quarantine
• Both the central and local government is working hand in hand to provide needed services for individuals under home quarantine such as transportation, medical care, meal delivery, and even garbage collection. Everyone wears a mask when outside their homes. Wearing masks is a very important factor in stopping the transmission of the COVID-19 virus and has become a public consensus in Taiwan.
• Quasi-lockdown in Taipei city
• Taiwan also declared a quasi lockdown in its capital once wherein a regulation was made so that not everyone can leave their homes for grocery shopping for about two to three months.
Medical System Response and Preparedness
• Designation of responsible medical facilities for COVID-19

• There were 161 medical facilities were designed for collecting specimens for PCR testing, while 134 hospitals have been designated for the treatment of confirmed mild cases of COVID-19. 52 hospitals have been designed for the treatment of severe cases.
• Nosocomial control guidelines
• There was a rigid nosocomial control guidelines have been implemented after 2003 when the SARS outbreak occurred. Hospitals have to identify two separate entries for emergency and hospitalized patients. Medical staffers are required to take care of patients in separate areas and groups. COVID-19 patients should be settled on a specific ward or area.
• Financial subsidy for medical personnel and hospitals
• Subsidy for medical personnel who are taking care of the patients or subsidy to the hospital being designed and designated to treat COVID-19 patients has always been important.
Stockpile and Allocation of PPE and Other Medical Supplies
• Accumulate a pre-stockpile of N95 respirators, surgical masks, and protective gowns.
• After the year of the SARS outbreak in 2003, the CDC in Taiwan started a pre-stockpiling of PPEs to be prepared for any potential outbreaks in the future. A ban on the export of surgical masks during the first stage of the outbreak from January 24 to May 31, 2020, has been declared by the government. The government also allotted funds to increase the production of masks.
• Specific programs have been launched to import medical supplies from abroad such as ventilators and medicine
• Distribution of surgical masks
• Taiwan allocated masks to every citizen through NHIcontracted pharmacies by using NHI cards.
• An online ordering mechanism for a name-based rationing system has been established. Masks can also be collected from convenience stores such as 7/11 or FamilyMart.
Health Education and Fighting Disinformation
» Disseminating information to the general public is essential and for that reason, a press briefing has been held by the CECC every day at 2 pm for more than a year now. The briefings are chaired by the commander, the Minister of Health and Welfare.
» What worked for them is they have released the most updated COVID-19 statistics, announce new measures for the public to follow, they announced specific case based contract tracing information and answered the questions raised by reporters
• Mass Media Coverage
» CECC also expands their mass media coverage by releasing this information to the following: television, radio, newspapers, as well as social media such as Facebook, Line, and Twitter.
• The 4-level epidemic warning and related regulation
» Maximum number of indoor and outdoor gatherings has been defined
» Dining inside the restaurant or at night market has been regulated by local government
» Opening of schools, kindergarten, and day-care centers depend on which level of epidemic warning is being announced.
» Visiting inpatients in hospitals is being regulated as well.
• Daily press briefings by the Central Epidemic Command Center (CECC)
17 Cultivare_INDD Ver_09212022.indd 17 21/09/2022 4:39:08 pm
• A four-level warning system written in the local language has been implemented. . Currently, the country is at level 2. At this level, the maximum number of people allowed for indoor gatherings is limited to 100 and 500 for outdoor. A few months back, the country was at level 3 and during that time, only 5 people were allowed for indoor gatherings and 10 for outdoor. If the number has been exceeded, the violators will receive a ticket as a penalty. Fortunately, Taiwan has yet to issue a level 4 warning which would mean that the country would be subjected to a lockdown.
Lessons Learned
• Leadership is critical
» Looking at the situation in the United States, we can see clearly that the strategies employed during Donald Trump’s leadership and Joe Biden’s are totally different. In Taiwan, coordination of needed tasks with the local government is critical. It doesn’t matter who is in charge to give the order but the more important thing is to make the orders work. Since the Minister of Health is the Commander and not the president, the minister has to balance the political demand and epidemic control.
• Learning from experience
» If there was no SARS outbreak in 2003, I do not think that we can do such a good job in Taiwan. Of course, because of that outbreak, people in Taiwan are willing to wear masks whenever the government asks us to do so.. Medical institutes have developed SOPs for handling and treating infected patients. The government are more prepared for an unexpected epidemic outbreak
• People’s trust and concerns
» ICECC issues rules and people tend to follow. But if you look at the situation in the United States, in France, and in many other western countries, there’s a rule and everyone knows but people do not need or are willing
to follow the rules so it won’t work. Fighting infectious diseases is a collective effort. Everyone matters. Majority of people in Taiwan are willing to sacrifice their personal freedom for public protection. Public is overseeing CEEC via mass media with expert interviews every night

• Unique Features in Taiwan
» Taiwan has a Universal NHI Card and web-based MediCloud system, and electronic fences for quarantine
Future Directions
Vaccination is the best strategy. Vaccination has the power to reduce infection and case fatality, help regain economic growth and aid us in returning to normal life.
A zero-case policy may be impractical. Until now, mainland China is trying to conduct a zero-case policy and also in Taiwan but gradually, we are a little bit shifting to accepting co-existence with SARS COVID-2 virus if the new cases of an outbreak are not too dramatic.”

18 Cultivare_INDD Ver_09212022.indd 18 21/09/2022 4:39:09 pm
Indigenization of Public Health
What is Indigenization?
There has been a growing clamor and movement for the decolonization of global public health: our institution, WHO, the way we approach different public health issues. While these efforts allow for critical introspection, concrete meaningful actions are still very limited to address this very complex and nuanced issue. Indigenization is one of the potential ways to give our own local public health expertise a voice and visibility.
This conversation brings insights and experiences on how to take back agency and power, highlight our own knowledge, values, practices and solutions to our own complex public health problems.

19 Cultivare_INDD Ver_09212022.indd 19 21/09/2022 4:39:11 pm
Scholar Practitioners in Philippine Public Health
• Professor & Chairperson of the Department of Medicine at the University of the Philippines Manila, School of Health Sciences in Palo, Leyte
Dr. Ryan Guinaran
• Holds post-graduate degrees in medicine, rural development, community development, and global health
• Executive director of the Doctors for Indigenous Health and Culturally Competent Training, Education, Networking, and Governance or DITENG, Incorporated.
 Dr. Paul Gideon Lasco
Dr. Paul Gideon Lasco
• Physician, medical anthropologist, and columnist
• Senior lecturer at the UP Diliman, Department of Anthropology
• Research fellow at the Ateneo University’s Development Studies program

Q1: What is the indigenization of public health to you? When you heard this phrase when you got this invitation, what was the first thing that came to your mind?
economically disadvantaged, all of this contributes to the continuing inequities in health for our indigenous communities; And second aside from equity, I talk about 2) pluralism—which is basically again two things a) pluralism in the sense that the biomedical plus conventional and alternative should be recognized and be seen as equal and valid and should work hand-in-hand and b) cultural sensitivity of the current health care system that’s predominant. These I guess are two things under each sub-cell that are relevant when you talk about indigenizing a health care system.
Dr. Meredith Labarda: I think indigenization is bringing health at the level of communities in terms of them understanding it, in terms acceptable to them and responsive to the needs of the community. By that, it would mean understanding and sensing where they are, their culture, their social norms as you mentioned earlier, beliefs, practices, values, tradition, even language, and allowing all this to influence the way we understand, deliver, plan, and even cooperate with our health interventions.
Dr. Ryan Guinaran: Indigenous health for me coming from the Cordillera context most especially which I’ve been working with the communities for the past two decades or so are two things: 1) Equity—it’s all about access to the best quality of life for our indigenous communities. When we talk about equity, I think there are again some considerations there. When you look at health indicators we are seeing that compared to the general population, there are 10 to 25 percent or more worse outcomes for indigenous peoples. Where’s this inequity coming from? It’s basically from the exclusion of indigenous peoples whether philosophically, socially discriminated, politically marginalized,

Dr. Paul Gideon Lasco: I think that when we talk about indigenization first and foremost it’s an invitation to interrogate where our ideas are coming from. When we say infection, when we say bacteria, we’re already privileged a certain way of knowing so at the level of epistemology we’re already privileged the way a certain body of knowledge operates and we’ve taken for granted that others don’t necessarily think that way. We’ve taken for granted how very difficult it is to imagine microbes. Before the microscope was invented people didn’t have any conception of microbial life and to expect people to just accept that knowledge without trying to look at where they’re coming from it’s both arrogant and counterproductive, so it’s an invitation to interrogate where our knowledge is coming from, it’s an invitation to look at other forms of knowledge, it’s an invitation to look at topics from what people need and what people are interested in and not dictated in terms of where the funding is, not dictated where the eminent voices are saying, what’s fashionable in public health. It’s a broad movement and I think we have to be part of it. We have to claim a seat at the table of global health, but we also have to think of what we’re gonna say when we’re at the table. I think that indigenization also recognizes that we have so much to impart to the world. It’s not just coming up with our own knowledge but also sharing our own knowledge because we have a lot to teach the whole world and I think that confidence should imbue our mindset.
Q2: How can we imbue our training and public health education with these mindsets? With this deep concern for equity and listening to the people, but also being culturally sensitive. For instance, the Philippines, we’re not a small country, but also we’re not a monolithic or a homogenous country either. So, how can we make sure that we have public health professionals that can adapt to different contexts?
Dr. Meredith Labarda: We start with recruitment and admission. Because we say that to make public health indigenous, we need to include people who are really from the community and then listen to them, include them in even these conversations and education and then send them back to where they came from because to me they’re the best people to understand and serve and implement programs as Dr. Ryan said earlier, which are culturally sensitive and contextualized. This is because we know there’s no one-size-fits-all. They’re the best people to do that. So for the step-ladder curriculum, it’s a very small unit, but we make sure that we recruit and we admit students from different parts of the countries including IP groups, IP communities, marginalized areas, many GIDAs and send them back. In fact, right now in the medical program, we have a new batch coming in from many areas and many members of different tribes all over the country. We do hope that they continue to serve their communities. I think it should be two-way also, not just you know the students being influenced by the education in UP but also the education and the curriculum in UP being influenced by them because they are the best resources when they come to school. So, I think sensing, listening, and also learning should be two-way. It’s not just from the school but also enhancing the curriculum based on what our students input and even their practices so it’s always working together hand in hand with the community such as Dr. Gideon said earlier. It’s a personal journey. So to me, I agree with that, otherwise, I will not be in this very difficult and very challenging public health practice if it’s not also personal for me.
Dr. Ryan Guinaran: That’s right, this is a personal journey. This is a very personal thing for a health worker. As a health worker, you have to constantly check your own ideas and beliefs. Doing self-reflecting exercises are important to check your biases, your prejudice, discrimination and stereotypes that are very pervading in the community. That is always the starting point. The element of control sensitivity is common sensitivity. It is very basic. Whether it’s cultural or other facets of being sensitive, it is very basic when we interact with our clients. In terms of training, I did research for example among indigenous health workers and they said three things important for personal development before you progress to cultural competence, 1) that you have to have cultural awareness. You’re aware and you recognize that there is cultural diversity in our area and that conflicts may arise because of cultural differences. When you have clinical interactions or public health interactions, there are a lot of cultures at clash: your culture as an IP for example or Filipino, the culture given by your school/community, and the culture of the client. So how do you navigate through these conflicts? That’s part of the awareness. The second is knowledge. Basically, it’s not necessarily knowing everything about the indigenous knowledge systems and
Dr. Meredith Labarda
20 Cultivare_INDD Ver_09212022.indd 20 21/09/2022 4:39:12 pm
practices of the community, but at least knowing what’s relevant when it comes to interaction and getting their involvement. The third is cultural values. Whereas the respect that should come in the acceptance of clients’ perspectives and their own explanatory models, even though it’s very different from our biomedical inclination and we understand where they’re coming from. Those were three important prerequisites that indigenous health workers in the Cordillera shared with me. Such that now when we go to the systems level especially in the educational sector, in fairness, there is a lot of IP education being done in the country which has been started as a basic education method in general for almost a decade already. Now, it has gone into college level. Then greatly in healthcare, this is why when the topic is transcultural, you become an expert of the cultures of the world but not of your own and not of your community which is quite ironic. So that’s again another self-reflective check with our own curriculum.
Dr. Paul Gideon Lasco: I completely agree on the importance of cultural competence. Also, Meredith talked about the need for healthcare workers to be for every place in the country, to have their own healthcare workers, to indigenize the health workforce so to speak, but let me add that we also need to take people’s perspectives seriously. Not just as a way to build rapport, it’s not just an instrument that the patient or your community will listen to you if you speak their language, because there is still a patronizing mentality there. So it’s not just a way to build rapport, to enhance communication, or to build trust, but to recognize that we ourselves as doctors and policymakers are influenced by the very culture that we’re trying to be competent in. COVID-19 is such an illustration of how our policy-making has been influenced. It’s not just biomedicine, obviously, we know that whatever people decide in terms of it varies. But here in Mexico, for example, they emphasize a foot bath like, where they disinfect the feet in every home. They’re very particular about disinfecting the feet. So even though we are in a pandemic which is a biomedical phenomenon, it’s also shaped by local understanding and even policy. Let me give a concrete example of what I think happened in the Philippines public health response to the pandemic; I think that one factor that influenced for example is our conceptions of “loob and “labas”. Social scientists have documented how Filipinos demarcate boundaries between our comfort zone, whether our family and our community as “loob” and then the external world as “labas”. And I think that those concepts of “loob” and “labas” have been transposed to our public health response in the way that we could perceive the “labas” as dangerous. That’s why parks were closed. It’s very safe, but from the LGUs to the national government, there’s a lot of caution. There’s a lot of fear about opening outdoor spaces, even though there’s increasing recognition that it is actually safer. I would say this is one of the reasons—that is the problematization of the “labas” as dangerous and unsafe and the perception that loob is safe. And we know that it’s not always the case that the loob is safe, because we want to encourage ventilation. But cultural concepts actually affect the way policymakers make their policies, so we should really take seriously local concepts because we also imbibe that in the way we think about health.
Q3: How can we make sure that our health systems are truly inclusive of the indigenous populations? And do indigenous people have PhilHealth? How is this being handled, disseminated, and utilized? Are they part of the
country’s health financing system? How is the devolution of the health system impacting service delivery for IP communities? Is this contributing to the development of more tailored interventions or is this causing fragmentation contributing to lower coverage in these populations?
Dr. Ryan Guinaran: Everyone is already included in PhilHealth. Before, we had programs for the IPs (indigent indigenous people). Let me clarify, we have indigenous people who are rich versus indigent indigenous people. Indigent indigenous people have been a part of the modified Pantawid Pamilya Program. If you are a member of PPP, then you are automatically a member of PhilHealth. However, because of the UHC, most likely all will be members regardless of the classification. Secondly, regarding devolution, it is now a question of agency. Since it was devolved, is the local government prioritizing the indigenous people’s populations? So one thing that has been good for the past five years, perhaps, is the participation of indigenous peoples’ mandatory representatives that was made possible by the policies of the DILG. So there are IP representatives involved as part of the council already whether it’s barangay, municipal or provincial. So there is already direct participation. And of course, we have to check how loyal the representative is to the IP communities. Because there is an IP leader but is really a “seller,” something like that. So it’s again a question of not about the position but the integrity of the process.
Dr. Paul Gideon Lasco: We can actually mobilize indigenous knowledge to help public health goals. We have many communities in the Philippines and even Indonesia in Indochina whereby working through the hierarchy of the indigenous communities, they were able to facilitate pandemicrelated lockdown instead of making it a militaristic response. They respected the hierarchy. They work with leaders of communities and it worked. They were able to maximize cooperation because there was agency given to them. They were empowered to make decisions about their own health. On the other hand, we’ve seen in the Philippines that these top-down policies of the lockdown were imposed in mountainous communities and many indigenous communities were not able to harvest where their crops are. It’s very safe in the mountains, obviously. It is the safest place to be during a pandemic, to be in a mountain by yourself. But they were not allowed to go, so we have to really respect them. And of course, in terms of research, there’s also inequity as Ryan said not just in health delivery but also in our knowledge. Do we know how vaccine hesitancy is among indigenous peoples? And are we able to acknowledge that the reason why many indigenous communities are skeptical of vaccines is because of the broader history of land grabbing? And they don’t have very good experiences with low landers, so why should they trust? So again all of these issues are related and we really need to have a serious look at indigenous rights. We cannot disentangle specific health needs, specific health programs from the broader land. I have to say this, that land is at the heart of it and the empowered indigenous communities are those with ancestral domains of their own so they have some level of autonomy, but many IPs don’t have that. They are all interconnected.
Dr. Meredith Labarda: Let me also share, as public health practitioners, right now we are doing a community engagement database which is a project of the Social Innovation and Health Initiative. Let me just share our insights. So what is written about community engagement, not just in the Philippines, but in many regions globally, it says
there that when we engage communities, the first step is to inform the community. When you have been working for a long time in the community, you will see that that is not right. We should not be the ones to inform them. We should allow them to inform us, because we are external. So there should be an assumption that there is something going on in the community. They are doing interventions on their own that might be different from how we view it as public health practitioners but work. This is what they think is effective and what works for them, so we have to be sensitive. This is one important lesson that I have learned in the community engagement database. Instead of us informing them of what should be done, we should start first by letting them inform us. And this does not happen in one day of social preparation. This is a journey of trying to understand the community. Whether this is in a pandemic or nonpandemic setting, this is what we see. They have a big story behind why they view a health issue like that, and that is what we need to understand first and foremost as public health physicians.
Q4: What do you think of the role and implementation of activities of the National Commission for Indigenous People (NCIP)? And can you share some good practices and concrete case studies of public health programs that were successful wherein IPs are included and integrated from the get-go?
Dr. Ryan Guinaran: When the pandemic started, everyone was on their feet. Cultural practices really became apparent during this time. When they released quarantine protocols like GCQ, ECQ, etc., we did not use those terms. We used indigenous terms because they have indigenous lockdowns. These are very basic public health measures even before; isolation of sick people. A lot of practices like that had surfaced. For me, I learned 3 good practices that surfaced in response to COVID: 1) the sense of wholeness because health perspective is not only seen in the WHO definition of physical, mental, social well-being. Even before the WHO definition came out, there was already an indigenous definition that did not only include the three, but the added environment, spiritual/ supernatural, and communal relationship. Those are the added definition of what health is. It goes beyond the physical, mental, and social, but strongly on environmental, spiritual, and communal relationships. The response of Cordillera IPs is that there is an imbalance of these. So how do you stop the imbalance? So there are barricades in the borders of the community, which include ___ (? 48:10). There are indigenous signs that say do not enter. Then you also have a lot of rituals to appease the supernatural world causing the imbalance. There are a lot of things that can be discussed, but this also shows the 3) sense of resiliency of people. Maybe it was shown in the news that IPs were given ayuda by the government, but they did not accept it. Why? Because they are self-sufficient in food. The rice that they produce is in the granary complete for the next six months and for the next year. So when the DSWD came here to give ayuda, the IPs did not accept it. Based on their indigenous values, it is bad to accept something that you should not deserve or that other people should deserve. They did not accept the ayuda even if they were in the fifth class municipality. There are a lot of good practices that should be nationalized and integrated into the whole COVID response because we learn a lot about self-sufficiency and resilience in our indigenous communities.
21 Cultivare_INDD Ver_09212022.indd 21 21/09/2022 4:39:12 pm
Q5: How are ownership and sustainability of health programs impacted when health interventions are led by health workers who are native members of this IP community?
Dr. Meredith Labarda: I think one direct answer on that is how they stayed and served in their communities. Because for the longest time, it was always our problem, especially for health workers. We have a lot of opportunities outside the country. But our graduates, I can say our program is not perfect, we have a lot of loopholes, but we have health workers who really stayed. And we all know that one challenge of devolution is working with politics and working with our local government officials. It is not an easy thing. But I think them staying in the community is good because they are really the ones who understand. For example, Eastern Visayas is a pandemic region for Schistosomiasis. There was one story about engaging the community. One MHO asked how can you engage the communities if you know the data that there is an increasing number of cases and you are pushing for toilet seats. Leaders in the community told them that they do not need the toilet bowls and that they have been living with Schistosomiasis and they are not dying. However, they were asking to make a sayawan (dance floor), because every time they have a fiesta, they weren’t able to socialize as much due to mud and rain. This is what they wanted to prioritize. So how do you answer that? How do you engage the community if that is their thinking? There was a very lengthy discussion. What we did was give it to them, but continue the health education. In fact, when the dance floor and makeshift social area were made for health education and dialogue, it took a long time before the community understood that they have a problem and that they were listened to. I think what the community wanted was just simple, and that is that they would be listened to and that they would be included in the conversation. After that, trust-building is very important, and trustbuilding includes listening to the community. To make the long story short, they were able to start on the program for sanitation but it was not an easy journey. It took the health officer and local chief executive a very long understanding of the community, but it has to become sustainable. We need to understand where they are coming from, because fiestas are an important part of not only Eastern Visayas, but the whole Philippines. So to disregard that, even in the pandemic, how we incorporate that in our public health conversation is very important. We are emphasizing this in our students’ training.
Q6: What are the concrete examples that will make us understand how to balance pluralism with workable structures? And how do we balance participatory consultation with urgency?
Dr. Paul Gideon Lasco: You raise a very important point about the urgency that there’s no time to consult, but that’s the importance of baseline knowledge. The reason why we’re clueless is that we haven’t really sustained the engagement in a long time. So if we have a baseline knowledge about what people think about epidemics, what people think about infection, bacteria, viruses, vaccines, then we don’t need the urgency to ask them because we’ve already known, we’ve been engaging with them, we’ve been studying with them, learning with them. That’s the importance of baseline knowledge; that’s the importance of the social sciences to be integrated really in health
curricula and in continuing medical education. Because we cannot do it when we already have a crisis, we have to do it before which is why we have to sustain. We have to have a basic understanding of what different communities think about how they conceptualize health before this happens.
Dr. Ryan Guinaran: How do we do it? This is difficult. What Gideon said was right, because this is very culture-specific or culture-area-specific. However, we can learn lessons that are not yet done at the national level, and these best practices can be integrated into the national program. Because of the structure of the health system, it is always top-down. There will always be a struggle and there is always that question of “Is the indigenous community important?” What I appreciate in the UHC is that I was able to count 7 times that IP community was mentioned, including to put the IP as a member of the provincial health board. I am thankful for that. But more than that, we have to ensure that participation is real and genuine and is not only tokenism.
Dr. Meredith Labarda: Two things that we have seen in the community while working with the government and leaders of the local health systems: 1) learning exchange and support–listening to each other—a lot of health professionals are burnt out, but platforms that provide an avenue to share and learn together, and even rant can be helpful; and 2) local leadership—if you have a very supportive mayor, a very supportive governor, the job of MHO and other public health workers in the community becomes easier.
Q7: Can there really be a truly meaningful marriage between traditional practice of medicine, evidence-based public health and indigenous beliefs? How do we negotiate or compromise or should we even do that? Where do we draw the line?
Dr. Paul Gideon Lasco: Very quickly, I don’t think that we necessarily have to, because there will be many contentious issues in drawing the line. But there are many clear-cut things that we can already embrace right away. For example, Ryan talked about spiritual dimension and rituals, whether indigenous or non-indigenous, giving people a sense of meaning and purpose, sense of certainty and community. Amid the mental health crisis on top of a pandemic, are we recognizing this as an important part of our vision for public health that we need to give the Filipino people a sense of certainty and at least hope and leadership and community during this time? So these are something that we can already embrace. This is not controversial. It’s not there’s no debate whether this is useful or not.
There are a lot of things that we do not have to fight about. There are a lot of things that we can embrace from our indigenous communities.
Dr. Meredith Labarda: I would say yes. I would have to agree with Gideon that there are a lot of intersectionalities that we agree on. Although not all, I hope we can reach the generative level. If all we want is well-being, even if in different ways, I think we can all agree that we want that. I think what we cannot overemphasize enough is the importance of spirituality in social development. Even in the pandemic, we see the important role of churches, of key leaders in the community, for or against vaccination, it is a big issue. For public health practitioners, we always have to keep in mind these groups. Because churches and IP groups are all over, capitalizing and partnering with them is an important thing.
Q8: What is Philippine public health from an indigenized, decolonized lens, framework, and paradigm?
Dr. Ryan Guinaran: Our vision for the public health of the Philippines is identity. One unique thing we capitalize on is the distinct cultural capital that we have from our indigenous richness in terms of everything. That is one thing we can contribute to by fully supporting it and really investing everything, research, resources. You know, in terms of policy, we have it. You know we were known for being the first in Southeast Asia to come up with an IP rights law. But 25 years later, what has happened? Sometimes we are just good at policy. How do we strengthen the political dialogue and advocacy and lobbying? This is where participation will come, seeing IP communities not as clients or as beneficiaries, but definitely as genuine partners and even teachers and mentors. And 1) APRUBA— how do we recognize and value IPs as coequal and promote it? 2) PRESERBA—good and responsive practices should be integrated, 3) ISALBA—there are a lot of things that we can learn and relearn from our cultural capital, from our indugenous social capital, 4) SAMBA—to be proud of who you are and what you have. This is one thing that I found. Indigenous people’s identity is not a guarantee of cultural sensitivity. Being an IP yourself does not mean that you provide very culturally-sensitive care. So, you should go back to who you are. Start where you are proud of and that’s basically who you are as a Filipino.
Dr. Meredith Labarda: My vision is for PSPHP to continue providing a platform such that we get to the point where we are already influencing structures, processes, and mindsets. Because in social developments, that is what’s most important—conscientization or changing of the society’s consciousness. It would probably take a lifetime and it would take all of us. Also, partnerships and collaborations—we should continue participating and involving ourselves in conversations and bringing the community with us. I think that is our very important role in public health in our country and also globally.
Dr. Paul Gideon Lasco: I think we as a public health community should really commit to bridging the inequity between the indigenous and non-indigenous Filipinos in terms of access to care, in terms of addressing the barriers to care, in terms of addressing health outcomes, stunting, and representation in the healthcare sector. We want more indigenous members of societies like PSPHP. We need to tap into the therapeutic potential of indigenous communities beyond herbs and traditional medicine, but their leadership style, their therapeutic approach to the patient, their way of building rapport, all of this matter. We need to capacitate our healthcare providers to understand the needs of particular Filipino groups, seafarers, OFWs, approach to the Muslim patient during Ramadan, or are indigenous groups a part of our curriculum even? Someday I hope to write a textbook entitled the approach to a Filipina patient and I hope that they’ll join me in this project because I think we really need to adapt medicine to the local needs. Finally, structural violence really needs to be addressed. I talked about land earlier. I think education, we need to give the indigenous people the education that they deserve. We talked about indigenous peoples in popular media, cultural appropriation and things like that, but land is really at the heart of indigenous rights. And if we are to truly and meaningfully support our indigenous communities, we have to take ownership not of their tattoos, but of their scars.
22 Cultivare_INDD Ver_09212022.indd 22 21/09/2022 4:39:12 pm

Walk the Talk: Reimagining Primary Health Care After COVID- 19
Photo Credit: Envato / Pressmaster
23 Cultivare_INDD Ver_09212022.indd 23 21/09/2022 4:39:15 pm
Dr. Ronald Upenyu Mutasa

One important effect that the COVID-19 has brought into light is that investing in primary health care is not only a public health concern, but also economic. The presentation was discussed from both economic and public health perspectives, particularly in investments that will help in economic rebuilding. Dr.Mutasa delved into the World Bank’s insights on the need to invest on primary health care and the actions that the institution are and will be doing to further push their initiatives forward beyond the pandemic.
Pre-COVID-19, the Philippines has achieved considerable gains in health outcomes, as well as access to services over quite a number of decades. The ranking of the Philippines on the investor health coverage index is slightly above average in terms of income status preCOVID-19. There was also an expansion of primary healthcare benefits since the year 2000 in the Philippines.
The rural health units, the barangay health stations, were the most utilized facilities and served as the first point of care for the population, which can be seen as a remarkable achievement; in other countries, the population are skipping the first level of conduct in primary care to go tertiary level because of several concerns of quality and lack of services.
With expanded primary care and improvements in health outcomes in
the Philippines, there were still issues prior to the COVID-19 pandemic. The sector underperforms in maternal mortality and childhood stunting, while grappling with a rapidly changing disease profile. Primary health care spending is also under-financed. Despite the expansion in the coverage of primary health care services as well as the excellent performance of the Philippines on the global UHC index relative to the country’s income, the Philippines was spending less and lower on a primary health care and overall health compare to its ASEAN peers and income peers in the global comparators at 1.4% of GDP or 4.3% of general government expenditures towards health.
Should more investments be made, particularly looking at the vulnerabilities that have been exposed in the Philippines in relation to the COVID-19 pandemic?
Health System
• Too many sites of poor quality care
Poor infrastructure of existing sites of care
• Ineffective use of health information systems
• Poor health outcomes compared to spending
• Deficient knowledge of financing mechanism for sustainability
• Too few service offerings
Administrators
• Lack of patient-centered design and coordination of care

• Poor client experience of care and treatment outcomes
• Effective use of private providers
• Delivering health in a digital world
• Rising costs
• Ineffective payment and resource allocation mechanisms
Client
• Increasing medical burden without sufficient use of prevention, detection, and treatments
• Lack of choice
• Barriers to accessing services due to transportation, cost, and lost work
• Limited healthcare literacy
• Variable quality of care
Provider
• Increasing number of patients
• Lack of qualified physicians and nurses
• Lack of patient adherence to treatment Insufficient training of staff
• Lack of coordinated care amongst staff
Context in the Philippines During the COVID-19 Pandemic
Having highlighted the specific context of the Philippines and the global context, then in 2020 came COVID. Some of the challenges that already existed pre-pandemic were compounded by the impacts of COVID-19.
The pandemic has further challenged primary health care, putting additional stress on the supply of, and demand for health care.
In health systems around the world, be it upper-middle countries such as Malaysia and the Philippines, be it high-income countries such as the US, we have seen that the COVID-19 pandemic has led to a diversion of resources from essential health services and essential infrastructure. In
Practice Leader for Health, East Asia and Pacific, The World Bank
The Philippines achieved considerable gains in health outcomes and access to services over the last several decades:
Context in the Philippines prior to COVID-19 pandemic
“This is the situation in the Philippines and other low to middle income countries prior to the COVID-19 pandemic.”
24 Cultivare_INDD Ver_09212022.indd 24 21/09/2022 4:39:16 pm
terms of health system data, the routine collection of data has significantly been impacted and with more and more demands from health workers to prioritize reporting data and outcomes related to COVID-19. In terms of a patient’s perspective, there is a growing concern of infection which leads to patients’ foregone care.
Impact of COVID-19 on PHC and essential health service utilization
WB and GFF support to country-monitoring highlights disruptions in essential services due to lockdowns and other limits on mobility, financial barriers, fear of COVID-19, disruption of supply chains for essential commodities, the strain on health care workers, reduced hours or closure of health facilities, and reallocation of resources for COVID-19. There has been a downward shift of utilization of essential health services.
As we move beyond COVID-19 pandemic, how do we reverse this decrease in terms of utilization of basic health services?
Impact of COVID-19 on health financing
Maintaining pre-pandemic growth in per capita government health spending poses a significant challenge for countries: the share of government resources flowing to health will have to grow, on average, more than 11% above pre-COVID levels. There have been challenges across countries on some temporal increases in financing the health sector, but we do not know how long this will last. We also know that post-COVID-19, there are other challenges related to rebooting the economies and jump-starting broader economic growth that might also crowd out some of the increases that we have seen in the health sector.
Impact of COVID on nutrition: rolling back years of progress
Gains of nutrition have been eroded across countries, whether you look at it from SubSaharan Africa, South Asia, or when you look at some of the data from the Philippines from the social worker stations and other rapid surveys conducted.
Impact on Utilization of Essential Health Services
• COVID-19 has also decreased the utilization of essential health services.
• The Philippines has not been an exception in terms of the negative impacts of coverage on basic service delivery.
• Overall, average monthly PhilHealth claims decreased by 25% in 2020 compared with the same period pre-COVID-19. While forgone care also translated into a 32% decline in PhilHealth expenditures, in the medium-to-long term this will likely lead to higher health care costs for the system as illnesses are detected at later more advanced stages.
• Based on the graph below, there is a sharp decline in terms of utilization of health services and corresponding decline in PhilHealth expenditures.
• Reduction in the use of malnutrition services, TB, and ischemic heart conditions were even larger.
present pre-COVID-19. During COVID-19, this has amplified renewed interest in looking at much more effective ways for governance in global health
2. Demand for and supply of health services have a new meaning—both globally and at the country level—as a result of COVID-19, and its consequences on poverty and health. There is a strong interest in terms of demand and supply for health services which has now assumed a new meaning globally, including to some of the colleagues that the speaker has worked within the ministries of finance. They have now a clear appreciation of the demand and supply of health services and its consequences just beyond mortality and poverty.
3. Unprecedented opportunity with new technologies. During COVID-19, there have been so many other platforms, data solutions, diagnostics, and other approaches that are at an advanced stage or have been accelerated in an effort to strengthen provisional services.
4. Rapidly expanding HNP Portfolio and GFF Strategy Refresh. Within the World Bank, their financing envelope has rapidly expanded. This is similar to what is happening to many other financiers such as AGB and other supporters.
Strategy Refresh was made to realign WB’s financing technical assistance and advisory services to the emerging needs and into the shifting landscape in global and public health. There are four opportunities that should be remembered in re-imagining primary health care systems beyond COVID-19:
1. Renewed interest in, and a search for, more effective governance for global health pre-COVID-19. This was already
As we reimagine primary health care going forward, there is a strong multilateral system and a strong foundation that is really focused on health at the moment. The most important part for primary health physicians and other colleagues in the global health community is finding ways to seize this opportunity and turn it from a short-term to a medium to long-term gain.
• Maternal and child health services are not the only ones affected, but also other noncommunicable diseases and related conditions.
WB Health, Nutrition, and Population Global Practice (HNP GP) Strategy Refresh
“A strong multilateral system is the foundation of global pandemic preparedness.”
-Global Pandemic Preparedness Board, 2020
25 Cultivare_INDD Ver_09212022.indd 25 21/09/2022 4:39:16 pm
Health, Nutrition, and Population (HNP) Global Practice (GP) Strategic Priorities
High Quality Healthcare for All
• Ensuring universal and equitable access to affordable, people-centered and integrated quality care with reimagined PHC as the foundation of health systems
• Safeguarding good governance of health systems for sustainable financing and accountability for health outcomes
• Augmenting service delivery value chain with innovation, data-driven precision public health and medical care, digital technologies, and private sector accelerators of service delivery
• Eliminating inequalities in access to the right care at the right time in the right place
Strengthening Public Health
• Reinvigorating essential public health functions for preventive and promotive health, and timely, effective and resilient pandemic preparedness and response
• Increased leadership/prominence in global and countrylevel advocacy and strategic partnership for global governance mechanisms
Investing in Health Beyond Healthcare
• Harnessing whole-of-Government and multisectoral and institutional response to strengthen Health, Nutrition, and Population outcomes
4 Paradigm Shifts
To achieve PHC reimagination, four paradigm shifts—as per World Bank flagship report were launched on 29 June 2021:
1. From gate-keeping to quality, comprehensive care for all
• There are some concerns in the Philippines and other countries with regards to gatekeeping.
2. From fragmentation to patient centered integration
• We need to be thinking beyond “How do we create a vertical platform to support the treatment of TB?” to “How do we create platforms that ensure that if a patient shows up and they are diagnosed with TB, they can also be saved from underlying risk factors on non-communicable diseases?”
3. From inequities to fairness and accountability
• Shifting more and more to fairness in terms of equity and accountability
4. From fragile to resilient health systems
• How do we build more resilient systems so that the fragilities that have been experienced during COVID would not happen again?
What Might a Reimagine Primary Health Care System Look like?
Having highlighted the specific context of the Philippines and the global context, then in 2020 came COVID. Some of the challenges that already existed pre-pandemic were compounded by the impacts of COVID-19. The pandemic has further challenged primary health care, putting additional stress on the supply of, and demand for health care.
In health systems around the world, be it upper-middle countries such as Malaysia and the Philippines, be it high-income countries such as the US, we have seen that the COVID-19 pandemic has led to a diversion of resources from essential health services and essential infrastructure. In terms of health system data, the routine collection of data has significantly been impacted and with more and more demands from health workers to prioritize reporting data and outcomes related to COVID-19. In terms of a patient’s perspective, there is a growing concern of infection which leads to patients’ foregone care.
Primary Health Care Reimagination for Health System, Administrators, Clients, Providers
In the medium-to-long-term, the Philippines should resume progress toward UHC. The 2019 UHC Act re-envisions the role of DOH to be more focused on policy formulation, regulation, and service delivery, while strengthening the purchasing role of PhilHealth. Among the Philippines, key priorities should be 1) addressing regional and socioeconomic inequalities, 2) improving the quality of care, and 3) increasing financial protection. The major building blocks needed to achieve these objectives are:
A re-design of service delivery into integrated health care provider networks that prioritize primary health care and enable referrals through strengthening gatekeeping.
• This will include the roll-out of PhilHealth’s comprehensive primary health care benefits package for all Filipinos (Konsulta).
A digital transformation of PhilHealth and the DOH’s health management and information systems that can seamlessly track patient’s movements across levels of care.
• We should also think about the digital transformation of the health sector, DOH and LGUs, as an opportunity as we move forward, so that patients can seamlessly transition and move towards different levels of care, different geographies without the challenges they face right now of siloed information systems and verticalized care system.
Provider payment arrangements that incentivize patientcentered primary health care.
Increased use of healthcare analytics to target health interventions, monitor the quality of care, improve the efficiency of health spending, and inform health care policy.
26 Cultivare_INDD Ver_09212022.indd 26 21/09/2022 4:39:18 pm
Resume Progress Toward UHC
In the medium-to-long-term, the Philippines should resume progress toward UHC. The 2019 UHC Act re-envisions the role of DOH to be more focused on policy formulation, regulation, and service delivery, while strengthening the purchasing role of PhilHealth. Among the Philippines, key priorities should be 1) addressing regional and socioeconomic inequalities, 2) improving the quality of care, and 3) increasing financial protection. The major building blocks needed to achieve these objectives are:


A re-design of service delivery into integrated health care provider networks that prioritize primary health care and enable referrals through strengthening gatekeeping.

This will include the roll-out of PhilHealth’s comprehensive primary health care benefits package for all Filipinos (Konsulta).
A digital transformation of PhilHealth and the DOH’s health management and information systems that can seamlessly track patient’s movements across levels of care.
We should also think about the digital transformation of the health sector, DOH and LGUs, as an opportunity as we move forward, so that patients can seamlessly transition and move towards different levels of care, different geographies without the challenges they face right now of siloed information systems and verticalized care system.

Provider payment arrangements that incentivize patient-centered primary health care.

Increased use of healthcare analytics to target health interventions, monitor the quality of care, improve the efficiency of health spending, and inform health care policy.
Photo Credit: Flickr
Photo Credit: Flickr
Photo Credit: Flickr
Photo Credit: Flickr Photo Credit: Flickr
27 Cultivare_INDD Ver_09212022.indd 27 21/09/2022 4:39:21 pm
28 Cultivare_INDD Ver_09212022.indd 28 21/09/2022 4:39:21 pm
How Primary Health Care Systems Saved Singapore From the Pandemic

29 Cultivare_INDD Ver_09212022.indd 29 21/09/2022 4:39:23 pm
Dr. Jeremy Fung Yen Lim

There is a notion that primary health care is for low and middle-income countries only. In Singapore which aims to have a developed status, some may ask if this is something we should aspire for. Some may also ask, does it really work or how should it look? Dr. Jeremy Lin gives us realworld experience on PHC and how it can significantly contribute to the pandemic response.
Primary Care and Pushbacks
Realistically, there will be a major pushback because if it was easy, it would have been done already. Unfortunately, we live in the real world where resources are very limited to fuel PHC. To fuel PHC, you have to deemphasize priorities somewhere else, and the biggest elephant in the room is hospital care. The challenge is that in most health systems, hospital specialists, who are most often the hospital directors, hold a lot of power and influence on the health system. Therefore, PHC is often the poor, the cousin of the prestigious and better-known specialists. The mere facts of our language “specialists” vs. “generalists” really tell you what our implicit biases are against PHC.
Singapore’s Health System in Numbers
⚫ Population
• Singapore is a tiny country with a modest population of 5.7 million as opposed to the Philippines population of 108 million.
Size
• Singapore’ size is 728 sq. km.
compared to the Philippines 300,000 sq. km. spread over 7,000 islands.
⚫ GDP per capita
• Singapore is a very wealthy country with a 65,200 US dollars GDP on a per capita basis

⚫ Health expenditure (% of GDP)
• Even though Singapore and Philippines spend almost exactly the same on health care as a percentage of GDP, Singapore spends significantly more than the 45 dollars that Dr. Ronald mentioned earlier.
⚫ Number of acute hospitals and acute hospital beds
• Because Singapore is a small country, they were able to keep things very compact, hence they have 18 hospitals nationwide, specifically acute hospitals.
• These 18 hospitals share about 11,000 beds.
• The average hospital is a couple of hundred beds at least.
Beyond Healthcare to Health
Emphasizes on health rather than on health care, hence Singapore partnered with Apple to launch a digital health promotion program that is called LumiHealth.
Beyond Hospital to Community
Even before COVID-19, Singapore already recognized that the hospital-centric model was unsustainable and they needed to go beyond the hospital to the community. Singapore was well-positioned when COVID-19 occurred because they already have plans to essentially embed primary care into community hospitals. The infrastructure was already present for home-based care, and this turned out to be invaluable during COVID. It is a lot easier to move from 1 to 5 than to move from 0 to 1. If the fundamentals or the backbone of the system is not set up, it will be very challenging.
⚫
Number of primary care clinics
• The PHC has taken on a very decentralized model, and therefore despite being such a small place, they have 2,363 primary care clinics.
⚫ Number of doctors (per 1,000 population)
• The number of doctors per thousand population is 2.5
• This is 4 times larger than the Philippines, which is 0.6.
Singapore’s Healthcare System
Previously, Singapore’s dominant model was very hospital-centric and was unsustainable. The previous minister of health articulated the 2020 Master Plan in which he described 2 of the 3 beyonds: beyond health care to health and beyond the hospital to the community.
For Singapore, the engine has already been more or less recognized that change is needed. Dr Lim would not say that all four engines had been changed, but at least two of these engines had changed. Therefore, Singapore was in a better position.
Director, Leadership Institute for Global Health Transformation (LIGHT) Professor, Saw Swee Hock School of PublicHealth, National University of Singapore
“Transforming health care is like changing a plane’s engine mid-flight.”
-Institute for Healthcare Improvement
Photo Credit: SCMP Photos
30 Cultivare_INDD Ver_09212022.indd 30 21/09/2022 4:39:23 pm
Singapore’s COVID Experience
When COVID first struck, Singapore was well prepared because of SARS back in 2003. However, despite being described as the gold standard as Harvard announced in Singapore in the early months of the pandemic, it became very clear that they were fighting COVID using the SARS playbook. In the military, generals are always fighting the last war, so they took the SARS playbook and applied it to COVID. They soon realized that SARS in Singapore almost 20 years ago was predominantly in hospitals, and it disproportionately affected healthcare workers. However, COVID was out in the community.
Singapore has a vulnerable population like migrant workers who live in big dormitories and around 20,000 people who live on the same premises. Unfortunately, the dormitories, even before the pandemic, were not designed for public health. They were designed to manage costs and minimize the footprint, which was fantastic if you are the owner of these worker dormitories and you are trying to maximize profit. However, this made addressing COVID in the dormitories near impossible.
There was this headline from the national public radio in the United States describing that Singapore was a shining star in COVID control until it wasn’t. When the outbreaks happened in the dormitories, COVID-19 spread like wildfire and took Singapore a hundred billion dollars and almost 6 months to get the outbreak under control. After that, they became the poster child again and Bloomberg described Singapore as the best place to live during the COVID-19 pandemic.
However, Singapore’s economy is built on being open. It was built on the free flow of
goods and people in and out of Singapore. Therefore, Singapore very quickly realized that, unlike China, it could not live on a zeroCOVID strategy. Instead, they had to transition toward living with COVID and they are still living through it now. This was economically necessary.
The Role of Primary Care
Singapore recognized that whether there is a pandemic or not, primary care still needs to go on. Fortunately, they had already had teleconsultations for many years, although just not at all popular. Citizens do not like it. Singapore is a very small country, therefore it was easy to get to the doctor. Because the infrastructure was in place, it was very possible to scale up teleconsultation.
Teleconsultations
Interestingly, during COVID, the doctors were also highly motivated to embrace teleconsultations. Because many of the doctors in Singapore are old, they did not want to be exposed to patients who may potentially kill them. The patients also did not want to come. According to one of the polyclinic groups, from a baseline of about 300 teleconsultations every week, it has scaled up over a nine-week period 49-fold. Primary care physicians were also very rigorous in the evaluation. They looked at outcomes, metrics like HbA1c and blood pressure control, and also asked patients about their satisfaction. This was on making sure that patients still continued to have the care that they needed.
Swabbing Clinics
When it comes to the pandemic proper,
60-70% of private clinics in Singapore have signed up to be swabbing clinics. The government is reasonably efficient, so almost overnight the website came about, so that those who were symptomatic and who needed a PCR swab could just go online and find the nearest clinic to do the swabbing. Then, the government would pay for it. This is important, because the more barriers we put up, whether financial or credit convenience, the harder it is for the average Asian or average citizen to do the right thing.
GPs and Vaccination
The primary care sector did a great job in making sure patients with chronic diseases continue to be seen. They also stepped up in COVID diagnosis by running swabs. Credit is given to the general practitioner groups. In a matter of days and weeks, Singapore managed to set up vaccination centers and at its height, there were 35 vaccination centers all over Singapore. There was also very transparent data on whether this is a vaccination center that has the Moderna vaccine or it has the Pfizer vaccine, so citizens can choose where they want to go. There was also an online booking system that was relatively smooth. Although it mentioned that Singapore is at 82% vaccination, they still very frustratingly have about 150-160,000 seniors who are in the vulnerable age group who refuse to be vaccinated. The GPs have done wonders in talking to patients and going on door-to-door visits to convince seniors to be vaccinated because we all recognize that vaccinations don’t prevent disease per se, but they really minimize the risk of severe disease.
Building Community Resilience

There is a recent publication in the Lancet regional held by Singapore’s health services research groups and the group of GPs. They articulated a framework where, in terms of community resilience which was one of the paradigm shifts that were mentioned earlier, they do not see it as the continued access to services. It is important, but only one part. The other elements such as wellness, public education, addressing any misinformation, engagement of individuals, their families, their local communities, and developing partnerships were all very important.
Rest
Look after yourself. Last 20 months have been very challenging for everybody. As of 20th of September, the Ministry of Health had already sent to all doctors 130 COVID-related circulars to tell us how the practice has changed and how the policy has changed. It is incredibly time-consuming and very stressful. As public health physicians plan services, please do look out for mental health, look out for the doctor’s burnout, and reassure them it is very legitimate.
31 Cultivare_INDD Ver_09212022.indd 31 21/09/2022 4:39:23 pm
of society and global response. Coordination and integration are keys to effectiveness and not just any individual sector. Primary care in Singapore comprising of the public and private sectors stepped up to safely continue to treat patients, support community diagnosis and management of COVID, encourage and provide vaccination, address misinformation, strengthen community resilience, and mitigate mental health effects of COVID
Conclusion
Societies respond to COVID and not only to health systems or specific parts of the health system. While the title of the talk is primary care, it is not really just about primary care. A successful COVID response is really a whole
Dr. Lim emphasized that the youth, including the people in the convention, are the future. He hopes that the older generation will leave a decent enough world that the youth can build upon.
Reorienting the Medical Curriculum to Primary Health Care
Dr. Manuel Dayrit Adjunct Professor and Former Dean, Ateneo School of Medicine and Public Health
Why does medical education in the Philippines need reforms towards PHC?
“Reforming medical education is like changing a cemetery. It is impossible,” said a colleague of Dr. Dayrit. But then why do we need it? The answer is that medical education has not been responsive to the health needs of the country.
There is a theoretical basis in all of this, which was actually developed by a group of global thinkers led by Julio Frenk and Lincoln Chen from Harvard. In 2010, a Lancet Commission was tasked to rethink medical education worldwide. Historically, this commission came at the heels of the WHO declaration of a human health resource crisis in 2006. In 2010, the WHO called for international recruitment for health personnel. Essentially, what they were saying is the educational system is not responding to the needs of the health system in the labor market. In our case particularly, many of our remote and rural areas are not being served. Therefore, this big mismatch and the Lancet commission wanted to focus on this mismatch. To do that, they developed an interesting paradigm (elaborated in the next section).
Lancet Commission 2010
Under the Philippine Universal Health Care Law of 2019, in order to steer the country towards its goal of universal health coverage, the medical and health curriculum will be reoriented towards primary health care. The DOH, CHED, and the professional regulations commission released last June 30, 2021 the joint guidance on this reorientation. What then needs to be reoriented? What are the present challenges in our country’s health system that warrants this curriculum reorientation? What are the specific changes that we will be expecting soon in this reform?

“Take rest; a field that has rested gives a bountiful crop.”
- Publius Ovidius Naso (Ovid)
“Kabataan ang pag-asa ng bayan.” - Jose Rizal
32 Cultivare_INDD Ver_09212022.indd 32 21/09/2022 4:39:24 pm
Frenk et al. looked historically at how medical education evolved in the world. From the 1900s to 2000, it evolved from a science-based to a problem-based entity, and now it has evolved to a systems-based enterprise. The components that need to be reformed are essentially two things in their theory: instructional and institutional. In the instructional component, you have to reform the way you teach students and also how to recruit and support them. In the institutional component, you also have to recruit students institutionally. The key was the nexus between the health system and the educational system. We cannot be sitting in an ivory tower and be in our academic institutions and universities. Academia has to engage the health system and as well be transformed by it.
By 2010, transformative health professional education was the buzzword. The curriculum is competency-based and was the only one that was reformed. The way students are recruited, the way faculty were trained and would teach should also be reformed.
Medical education in the 20th century was a flexnerian model of the science-based curriculum. By the turn of the 21st century, while that model built up beautiful hospitals, beautiful science, billions of people were still underserved. This was the reason why we need reform.
Philippines history, these are the examples of curricular reform in the Philippine medical system:
1. University of the Philippines School of Health Sciences – Step-ladder curriculum in Tacloban (started 1977); Baler, Marbel
2. University of the Philippines INTARMED (Integrated Liberal Arts and Medicine) –(started 1982)
3. University of the Philippines MD, PhD program
4. Ateneo de Zamboanga MD, MPH
5. Ateneo School of Medicine and Public Health – MD, MBA (opened in 2007)
6. University of Santo Tomas LEAPMed (Learning enhanced accelerated Medicine program)
Attributed. Dr. Victor Valenzuela, Dr. Jose Cuyegkeng
Take-away message
Reform works because social reformers tried to reform. Fitzhugh was a social reformer in the United States who was very critical about the US attracting so many physicians from developing countries, such as Africa, India, and the Philippines. Therefore, he did a study of medical schools in Sub-Saharan Africa. He wrote an article where he studied the very mission-oriented medical schools. They called it social mission, which is probably another term for social accountability. In the study, not only are medical schools teaching research and patient care as their mission. They also have very clear social missions, including geographic focus and health systems strengthening. There are a lot of things that these medical schools did to fulfill their social mission.
Thinking about this and going back to
The University of the Philippines has a stepladder curriculum. The reason for this is that UP has always been schizophrenic. The UP College of Medicine was established in 1906, ahead of the whole university. For a while, UP graduates were considered graduates of any American medical school. Therefore, UP was schizophrenic, because 50-70 graduates were leaving for the States. It was in the 1970s when the Dean, Dr. Herrera said, “Let’s try to do it differently.” That is when they conceptualized the step-ladder school in Tacloban that is designed to address the needs of remote and rural areas, starting from Tacloban. Reforms happened in other ways like UP started INTARMED. They also started the MD, PhD program. The pacesetter for medical education in the Philippines is UP. Many of the medical schools like UE and FEU were started by UP medical graduates. Therefore, UP in 1906 modelling after the American model of medical schools, led to all of the medical schools in the country following suit and copying it. This is why we get the basic hospital-based curriculum that we have. There were other schools who started curricular reforms, like Ateneo de Zamboanga, which focused on the Zamboanga Peninsula. Like in Tacloban, they focused and started recruiting from region 8. There are so many pressures on reform. First of all, there is so much to learn, but there’s also pressure to shorten the medical curriculum. There’s pressure to include health systems in the medical curriculum, aside from the clinical and the pre-clinical subjects. You have to appreciate that it is not that easy to change the medical curriculum.
Seeds of reform in medical education were emerging in the 1970s as shown by the quotation of Victor Valenzuela, Jose Cuyegkeng, and the work of Herrera et al. The time to implement reform has come (Problem, politics, policy have converged— Kingdon model). It is only now that the problem, politics, and policy have converged, therefore we now have this window of reform for medical education.
• The Alma Ata Declaration—that has been the philosophy carried through the years.
• Invaded a lot of thinking globally
These international influences eventually translated to our own domestic campaign for UHC that culminated into the passage of UHC law in 2019. It includes the reorientation of health care professional and health care worker curriculum towards primary health care, with emphasis on public health and primary care. Other than that, you can now see that the DOH has then created the Human Resources Master Plan. In this master plan, it contains the strategic objectives and it shows that you can’t just change the curriculum. You have to support the curriculum going forward even through postgraduate studies. Everyone who eventually works at the primary level and in primary care and may not be hospital-
What are the components of reform in medical education?
How does reform of medical education actually happen? What attempts have been made? How have they fared?
“The first and foremost need [of the country] is a national system for the delivery of health care in which the role of the community doctor should be defined as a member of a team that would include various types of paramedical personnel”
Idea attributed to Victor Valenzuela and Jose Cuyegkeng, Members of the Extraordinary Curriculum Committee for Medical Education of UPCM, 1972
“she/he should show a strong desire to serve the poor and underserved rural and urban people, with a missionary spirit to sacrifice personal comfort and advancement for the sake of service.”
What are the current enablers for the reorientation of medical curriculum to primary health care?
Dr. Halfdan Mahler
“PHC starts with people, their health problems, and their active involvement in solving those problems”
-Dr. Halfdan Mahler, WHO Director-General, 1977-1988
Dr. JW Lee
“We need to ensure access to a motivated, skilled & supported health worker by every person, in every village, everywhere.”
-Dr. JW Lee, Director General, WHO
33 Cultivare_INDD Ver_09212022.indd 33 21/09/2022 4:39:25 pm
based are actually supported and that has to happen all over the country.
Some barriers to medical reform include:
1. Tradition of established medical schools
a Path dependency- the tendency of institutions or technologies to become committed to develop in certain ways as a result of their structural properties or their beliefs and values.
b There is resistance to it, lack of faculty. The faculty that are now in medical schools were taught 20-30 years ago. They are the ones who are administrators and many of them are not thinking about reform.
2. Resistance to change
3. Lack of faculty to implement curricular reform
4. Deep-seated cultural values of society towards role of health professional (specialist-focus)
5. Regulatory and legal provisions
6. Health system realities (hospitalbased system)
What does the current curriculum look like?
These are the competencies that we are all supposed to have. In and of itself, it is not going to develop your primary health care physician, particularly if medical students are not interested in the formal lectures of primary health care. You have to train physicians in a different way, in order for them to really imbibe all of these very philosophical and deep-seated values for PHC.
An example from Southeast Asia: Tuning Academy Medical Education in Southeast Asia (TASE) is “Creating a metaprofile for medical education in Southeast Asia.” TASE Medicine Group is a group that looks into the medical curricula in Southeast Asia, that includes Indonesia, Thailand, Cambodia, and Myanmar. The competencies are patient care, family and community, ethics, professionalism, quality assurance, knowledge, and communications.
Southeast Asia Medicine metaprofile describe the 20th century physician—as expert and health professional. It does not highlight the role as a social catalyst to transform the health system. We want our physicians to also be a social catalyst to transform the health system.
What will the reoriented medical curriculum look like?
We go through pre-clinical and clinical studies for 4 years, and then internship. People will argue that you need science, and that you cannot sacrifice science if you want to have a good foundation for the clinicians. You also cannot sacrifice teaching in the clinics. The question is, how can you reform it and put primary health care within it? How are you going to integrate it? Or are you going to integrate it as a separate subject? How is that inculcated in the medical students’ values so that they would consider working in primary care or even work remote and rural areas for a portion of their career, if not for longer?
What is happening is the two pillars of four medical education as inherited from Flexner are the basic sciences and the clinical medical sciences. Now, there is pressure to include health system science.
It is almost like a zero-sum game, because if you are going to add courses, you have to remove courses. This is because there is only so long a duration for medical education.
It is going to be multi-tracked. You may have a core curriculum, you have multi-tracking, and then you have various medical students choosing among the tracks depending on what they eventually want to become, whether hospital-based or communitybased. However, the curriculum has to be designed appropriately.
The PHC Pillars
PHC includes the different pillars, such as social determinants, PHC, etc., but emphasis on the primary level of care which is the weakest part of our system.
medical education.
Where is the Philippines in its journey towards reforming medical education?
We now have a joint administrative order to reorient medical education. The work is being done now to prepare those documents towards orientation.
Summary
• Steps are underway to develop a road map towards reforming medical education in the country towards PHC (% CHED Technical Panel for Medical Education).
» The CHED Technical Panel for Medical Education has been tasked to provide a roadmap.
» It is going to be a consultative process.
• Problem statement: Produce the PHC physician who is competent and motivated to transform health care, especially in poor and underserved areas;
» To produce a PHC physician, even if that physician becomes a specialist
» But that physician has a primary health care perspective who is competent and motivated to transform health care, especially in poor and underserved areas. (Note: recall the talk on IPs)
• Reform and investments in medical education must go hand-in-hand with reform and investments in the health system.
We want our physicians to be very missionoriented, so we have to select students who are very mission-oriented from the outset. That is the message for strengthening our
What are the barriers to reorientation of medical curriculum to primary health care?
The competencies in the Tuning Academy Take-away message
“s/he should show a strong desire to serve the poor and underserved rural and urban people, with a missionary spirit to sacrifice personal comfort and advancement for the sake of service.”
-Attributed to Dr. Victor Valenzuela, Dr. Jose Cuyegkeng
34 Cultivare_INDD Ver_09212022.indd 34 21/09/2022 4:39:25 pm
Philippine National Human Resources for Health Master Plan
 Photo Credit: Unsplash/ Josue Ladoo Pelegrin
Photo Credit: Unsplash/ Josue Ladoo Pelegrin
35 Cultivare_INDD Ver_09212022.indd 35 21/09/2022 4:39:25 pm
Dr. Pretchell Tolentino
OIC-Director, Health Human Resource Development Bureau, Department of Health
policies. The interplay of these issues results in complex and integrated challenges in HRH management and development, which in turn contributes or affects poor access to health, and ultimately poor health outcomes. This problem tree also signifies that HRH management and development is multifarious and hence requires an integrated approach.
The core of the HRH master plan is the six key result areas or the KRAs. Each KRA sets strategic objectives and specific strategies for the short term, medium-term, and long term. The KRAs are designed to encompass the spectrum of the health labor market from entry workforce after exit and re-entry.
program design, execution and oversight
■ This involves our strategies on the national health workforce registry
» KRA 5: Efficient and effective implementation of the HRH master plan through a collaborative and participatory approach while taking into context both the national and local levels
■ This will now involve strategies of incorporating the nature each master plan into the local investment plans
Dr. Tolentino discussed the National Human Resources for Health Master Plan (NHRHMP) 2020-2040 and the current initiatives of the Department of Health (DOH) to support and promote public health practice in line with the plan.
National Human Resources for Health Master Plan 2020-2040
The National HRH Master Plan 2020-2040 provides policy and strategic directions to guide the management and development of the country’s Human Resources for health according to the goals of Universal Health Care.
Health Labor Market for UHC
The Health Labor Market for UHC covers the education sector to the labor market dynamics. It also covers training and education, pooling of qualified health workforce, employment, and migration. The National HRH Plan uses the concept of the health labor market, which depicts HRH movements from the production of health workers and professionals to being
HRH Issues and Challenges
The HRH Master Plan reformulation is based on the analysis of the current HRH situation in the country. Based on the issues identified, the three main problems in HRH management are 1) HRH unavailability, 2) HRH competency gaps, and 3) HRH disengagement and demotivation.
The key problems obtained from the six main areas of the HRH management and development, which for better analysis were further organized and stratified into six main categories: production issues, lack of quality HRH data, workforce issues, migration issues, fragmented HRH governance, and poor monitoring and implementation
KRAs 2, 3, and 4 reflects the HRH working lifespan
» KRA 2: Practice-ready HRH responsive to local health needs, and improved retention in the local healths sector
» KRA 3: Improved HRH productivity and responsiveness by promoting job satisfaction and motivation at all levels, thereby improving HRH retention in the Philippine health sector. This KRA would involve strategies on giving right salaries and benefits and on HRH safety, protection, and welfare
» KRA 4: Migration managed to a sustainable level and reintegration programs enhanced for returning health workers. This involves migration management and also reintegration of OFW health workers and integration back into the philippine health system
Key strategy to respond to public health emergencies
» KRA 2 key strategies to respond to public health emergencies was also included
» KRA 3 also includes key strategies to optimize HRH capacity during public health emergencies and search situations.
» It proposes an overarching strategic framework or national plan for welfare safety and protection of HRH to be activated specifically for such contingencies
KRA 1, 5, and 6 covers the cross-cutting areas on HRH data, localization and institutionalization and governance
• KRA 1: Strong data governance and information management for evidenceinformed HRH workforce planning, strategy and policy formulation,
■ Take note that the HRH master plan is not supposed to be a separate plan for HRH. It’s a strategic plan that is supposed to be incorporated in all health plans both at the national and local levels
» KRA 6: Harmonized and strengthened intersectoral governance for HRH
■ This involves strategies on all HRH networks and collaborating with various stakeholders.
■ This is on the recognition that DOH cannot do this alone, so we need partnerships and stakeholder collaboration among local and international stakeholders.
Current Initiative to Promote Public Health Practice
The DOH through its Health Human Resource Development Bureau has been implementing various initiatives to promote public health practice. These are the five current initiatives that DOH is doing to promote the public health practice: pre-service scholarship program, primary care workers certification, career progression and specialization for DTTBs, post-residency deployment program, and health care learning intervention through eLearning.
Pre-Service Scholarship Program
This aims to increase the production of physicians to provide quality and basic health care services to the underserved and GIDA areas. Scholars are required to render government return service initially through the national health workforce support system program in primary care facilities and in province-wide local health facilities to support the health care provider network.
Currently, we have a total of 1276 medicine scholars enrolled in respective DOH partner
36 Cultivare_INDD Ver_09212022.indd 36 21/09/2022 4:39:26 pm
schools. Later on came the approval of the Doktor Para sa Bayan IRR, this medical scholarship will now be transitioned to the CHED to increase the production of our medical scholars.
Primary Care Workers Certification
The UHC is also rooted in the concept of ensuring access to health services by strengthening the primary care level. The primary care worker certification program started its implementation in 2020. The DOH, through the HHRDB, is currently issuing provisional certificates that shall be valid for three years to all primary care workers delivering primary care services in public or in private primary care facilities until December 2021 in accordance with the stipulated transition period.

As of September 2021, DOH were able to certify a total of 593 public health workers, 413 of which are from the UHC implementation sites. DOH is still continuing to conduct assessment and provide provisional certificates.
Career Progression and Specialization for DTTBs
DOH also partnered with different institutions for the career progression and specialization for DTTBs. There are three programs being offered, which include the practice-based family and community residency training program in partnership with the Philippine Academy of Family Physicians. This program enables and prepares the DTTBs as primary care physicians. Another program is the Master in Public Health being offered in three institutions, Master in Public Health in partnership with the UP College of Public Health, Master in Public Management in partnership with the Development Academy of the Philippines, or Master in Public Management Health Governance in partnership with the Ateneo School of Government.
Post-Residency Deployment Program
The DOH is also currently implementing the post-residency deployment program known as the “Espesyalista Para sa Bayan”. The program aims to address the equitable distribution of physicians and augment specialists in level 1 and 2 hospitals especially in rural and underserved areas. The program hopes to improve access to specialty care services in priority, poor, and underserved areas and strengthen the healthcare provider network in various hospitals and build capacities to become accredited residency training program providers.
Currently, policies are being updated and rapid assessment of pilot hospitals is being conducted to assess the readiness in establishing residency training programs


Healthcare Learning Intervention through the eLearning
DOH also ensures that health workers learning intervention shall continue even with the current limitation brought by the pandemic. To cope with the new normal in learning and development, the HHRDB is developing and packaging materials to more accessible means through the online or blended mode of learning. This is found at the DOH Academy learning platform accessible at learn.doh.gov. ph.
Call for Support for the UHC and NHRHMP Agenda
Dr. Tolentino calls on PSPHP’s support in pushing for the UHC and the National HRH Master Plan agenda through communicating and advocating the purpose and goals of the UHC and the NHRHMP. It hopes to drive researches and share HRH data to build new body of knowledge and support evidenceinformed decision-making in health. Lastly, to share knowledge and expertise in health and HRH related and initiatives
Photo Credit: DOH FB Page
Photo Credit: Unsplash/Mat Napo
Photo Credit: Unsplash/Mat Napo
37 Cultivare_INDD Ver_09212022.indd 37 21/09/2022 4:39:27 pm
Mandanas Ruling and the Future of Health Systems in the Philippines

38 Cultivare_INDD Ver_09212022.indd 38 21/09/2022 4:39:29 pm
Dr. Lester Tan

Division Chief, Bureau of Local Health Systems Development, Department of Health
⚫
They questioned the computation of the internal revenue allotment as the current practice was said to be against that of the constitution
Ruling
⚫
The SC upheld the petition stating that the “just share” of LGUs covers all national taxes, including customs duties and others and not just the national internal revenue taxes
⚫ The ruling, which is final and executory, will have the following implications to the LGUs and the national government:
◻ The Internal Revenue Allocation is now called the National Tax Allocation
◆
One of the upcoming changes in the local governance in the country is what we call the Mandanas-Garcia Ruling, which will be in effect starting 2022. The 2028 Mandanas-Garcia rule or Supreme Court ruling states that the local government units should have a bigger share of the internal revenue allotment (IRA). While it is expected to increase the local government unit some financial space in providing devolved services to their people which includes healthcare, there is inevitably a shift of our resources and consequently responsibilities. Here, we ask what changes do we expect in the coming years especially in terms of our health system? What changes do we expect from the department of health as a consequence of this ruling? And what do we need to expect from our local government units?
Supreme Court Ruling on the Mandanas-Garcia Case
The LGUs will have an increased national tax allocation which was previously called internal revenue allotment of around 27 percent on average beginning in 2022
◻ The NTA share of LGUs will increase by up to 27.6% in 2022
◆
Some LGUs may have lower while some may have higher than 27
◻ Enhanced role of LGUs in assisting the country achieve development and growth targets
◆
The increased funds will enhance the role of LGUs in assisting the country to achieve various development and growth targets
◻ LGUs become empowered to provide basic services and facilities to their constituents
◆
As an additional result of the Mandanas-Garcia case ruling, LGUs are more empowered to provide basic services and facilities to their constituents
◻ Effective implementation of devolved functions consistent with the Local Government Code or RA 7160
EO 138 or the full devolution of certain functions of the executive branch to local governments
Full Devolution
EO 138 s. 2021
Rationale
This aims to increase the production of physicians to provide quality and basic health care services to the underserved and GIDA areas. Scholars are required to render government return service initially through the national health workforce support system program in primary care facilities and in province-wide local health facilities to support the health care provider network.
Currently, we have a total of 1276 medicine scholars enrolled in respective DOH partner schools. Later on came the approval of the Doktor Para sa Bayan IRR, this medical scholarship will now be transitioned to the CHED to increase the production of our medical scholars.
Basis of the DOH Devolution Transition Plan (Re-devolution of functions)
The DOH devolution transition plan is primarily based on Formula 1+ for health which is the framework for boosting the UHC Act. In particular, it is based on the premise of securing sustainable investment to improve health outcomes and ensure efficient and equitable use of health resources. It is also designed to ensure the accessibility of essential quality health services at appropriate levels of care
DOH Transition Plan
⚫ This was based on the petitions filed in court by Governor Hermilando Mandanas of Batangas, other local government officials, and Congressman Jose Enrique Garcia of Bataan.
⚫ This was based on the petitions filed in court by Governor Hermilando Mandanas of Batangas, other local government officials, and Congressman Jose Enrique Garcia of Bataan.
◻
◆ The LGUs are also strengthened further to implement their devolved functions consistent with the Local Government Code of 1991.
Necessary activities to implement the case ruling
The LGUs are expected to fully deliver devolved services no later than the end of FY 2024. National government agencies are to develop their respective devolution transition plans. These agencies are mandated to implement
The DOH devolution transition plan is also premised on the Department’s strategy map. As an organization, the DOH has identified catalysts in the transformation of local health systems to province and city-wide health systems and building the capacity of local health systems to deliver individual-based and population-based health services as its contribution to the achievement of the F1+ for health strategy
Developing policies and regulatory standards, providing capacity building and technical assistance, and engaging with sectoral and local stakeholders are DOH’s core strategic objectives to catalyze this transformation of local health systems
Petitioner Issue
39 Cultivare_INDD Ver_09212022.indd 39 21/09/2022 4:39:30 pm
to province-wide and city-wide health systems.

Features of the DOH Devolution Transition Plan (Re-devolution of functions)
In the DOH devolution transition plan, the basis for the devolution of functions considers the LGU income class, poverty incidence, capacity of LGUs, availability of services and commodities in the local market, implementation of the UHC app, and other pertinent laws. Nevertheless, note that the devolution of functions will not affect the DOH hospitals and other national health facilities, attached agencies and corporations of the DOH.
Role of DOH in Re-devolution Set-up
⚫ The general principles in the redevolved setup including the regional offices or centers for health development as per DOH mandate based on EO 102 series of 1999 and the UHC act are as follows:
◆ The DOH as the nation’s leader in health formulates national policies plans, technical standards and guidelines on health and regulate health services and products
◆ The DOH as an enabler and capacity builder provides capacity building through training HR, systems development, and technical assistance
◆ We are also the oversight to the corporate hospitals and attached agencies and corporations and administrators of national and regional hospitals and medical centers and other health facilities such as treatment and rehabilitation centers and blood centers

◆ The UHC act also mandates DOH to finance population-based health services in complementation with the LGUs
Effect to LGUs of re-devolved set-up
⚫ Increased resources for delivery of basic services
▷
The increase in the national tax allocation of LGUs will provide them with more resources for delivery of basic services. This will empower LGUs to deliver these services.
⚫ Strengthened local autonomy
▷
Re-devolving certain functions of DOH consistent with the local government code strengthens local autonomy to enable LGUs to attain their fullest development as self-reliant communities
⚫ Streamlined health financing mechanisms
▷
This re-devolution also aligns with the universal healthcare act to streamline health financing mechanisms. Minimizing duplication and overlaps in financing mechanisms will increase the efficiency in allocating and utilizing health resources
⚫ Institutionalized province- and city-wide health systems
▷ It will prepare LGUs for implementation of province wide and city-wide health systems through ownership and accountability for implementation of public health programs
Environmental & Occupational Health National Immunization Tuberculosis Control Mental Health (for devolution once with PHIC package) Cancer HIV Schistosomiasis Vector Control Assistance for Indigent Patients HRH Deployment Health Facilities Enhancement Program Disease Surveillance Officers
Family Health, Nutrition & Responsible Parenting Oral Health Food & Water-borne Diseases Filariasis Dengue Emergency & Re-emerging Infectious Diseases
Sexually Transmitted Infections Hypertension Hypercholesterolemia Diabetes (beginning CY 2023) Leprosy*
Integrated Management of Childhood Illness (IMCI) Soil-Transmitted Helminthiasis Rabies Control
DOH Support to LGUs during the Re-devolution of Functions
These are some of the programs projects activities which will be retained under the DOH
Note: These are some examples of key programs and not en exhaustive list. Subjeet for further discussion and may be subiect to changes. WHO - donated multidrug theraphy for Leprosy will still be provided.
◻ Service delivery standards ◆ During the three-year transition period from 2022 to 2024, the DOH will develop and implement the national service delivery standards for devolved functions and services ◻ Recommended structure and staffing complement ◻ ◆ DOH will also recommend an organizational structure and staffing complement for health offices and facilities in the LGUs ◻ Capacity building for LGUs ◻ ◆ DOH will focus on capacity building for LGUs beginning this year 40 Cultivare_INDD Ver_09212022.indd 40 21/09/2022 4:39:30 pm
Ways Forward
The continuous dissemination of the DOH devolution transition plan to all stakeholders is crucial and needed A comprehensive capacity assessment and profiling of LGUs will be done followed by the provision of technical assistance to LGUs in establishing and capacitating local help boards. Lastly, the implementation of the national health workforce support system to address gaps in human resources for health will happen.
DOH has already conducted consultations with LGUs through the CHDs on the initial devolution transition plan. Based on the recommendations gathered from the consultations, DOH is already finalizing the DTP for submission to DBM by September 30 and subsequently cascading to LGUs to guide them in the development of their own DTPs.
Unifying Health Professionals in Influencing Policies
Dr. Romelei Camiling-Alfonso Convenor, Healthcare Professionals Alliance Against COVID-19

The COVID-19 pandemic has overwhelmed so many people, not only the general public, but also those that are in the public health society due to its volatility, uncertainty, complexity, and ambiguity. Dr. Alfonso as well as her colleagues in the public health society tried to raise their voices from the public health lens. Unfortunately, they didn’t have much of a platform back then.
She caught the media’s attention when she made an attempt to voice her stand on social media that the front lines are not just in the hospital, but also in the community.
She further added that somehow, that tiny line caught the attention of people who were all so busy with ramping up response at the hospitals.
Beginnings of HPAAC
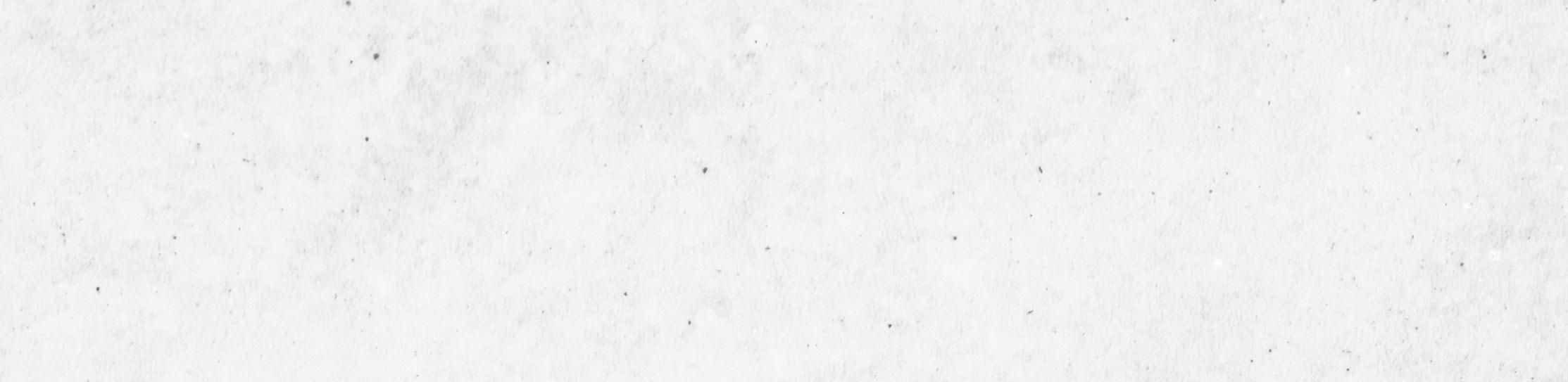
Journey as a Doctor
Dr Alfonso was a Doctor to the Barrio in Agutaya, Palawan. At that time, the closest experience to an outbreak is a community diarrhea outbreak. This occurred in one of the islands in which she had to deal with despite not having any training in outbreak response at all.
“Public health has been my call and one of the things that I’ve been doing or that for the past decade has been in a lot of engaging stakeholders from different levels trying to bring in the voices that matter and I’ve been working with different stakeholders like on strategic planning, participatory approaches, and future research principles and that’s the hack that I wish to impart today,”
- Dr. Alfonso said.
“How do we support our colleagues also in the DOH, the different fronts of the response, if we do not move as a community and we were working on it as if our lives, our families’ lives depended on it. So we worked with different stakeholders back then and we developed the first community-based guide management for COVID-19 in the Philippine Setting.”
Dr. Alfonso was among the developers of the community-based guide management for COVID-19 which has been a backbone of the policy and has eventually been adopted as a joint DILG-DOH AO by April 15. It is important to note that the framing of this communitybased management system has been developed not only by her or other doctors, but it was a collective effort from different actors in the network of practice such as front liners, community practitioners, health system managers and others.
Dr. Alfonso gave a background of how HPAAC started to form. This was the initiative that led to deeper collaboration with the medical societies. Part of that guideline development process was including different stakeholders in evaluating evidence, in judging evidence, and making sure that all of the voices of those who need to be there will be included
in the discussion.
When Dr. Alfonso and the team were collaborating with the different stakeholders, realizing what they were actually looking for are community guidelines. After seeing the algorithms that HPAAC made, they were embraced by the existing community of medical professionals.
The beauty is that all of these things have already gone into policy. Back then, there was no HPAAC and the guidelines that were created by PSMID were also adopted DOH. That was the beginning of HPAAC. Basically, the clinicians realized that the lens that they have is something that should be taken in the discussions.
The guidelines were a result of collaboration between many different people and they also needed the lens of the specialists. Bottom line is that COVID 19 was an eyeopener for many of the health professional societies. We needed to work together. There needed to be an intersection of disciplines and perspectives, involvement of other professionals, and later on, we realized there should be involvement of other sectors.
Looking back, many of the people who were working already in algorithms, had the shared value or the same intent to have primary care for their evidence. It just became automatic or it was very natural that during the surge around August of last year, we came together and we sought out who wants to join us in this call for a timeout. People started to sign in to the medical professional societies and around 160 medical professional societies signed overnight. It was quite surprising because this has not happened before. This is the first time that the medical community has come together like this quickly overnight.
When HPAAC were doing their discussions, they wanted to try to capture what the
41 Cultivare_INDD Ver_09212022.indd 41 21/09/2022 4:39:30 pm
organization is all about. They don’t want to be any formal organization, because they are an informal coalition. HPAAC exists primarily because they all believe that they need to fight for science, truth, and equity. They actually thought that they would only exist for two weeks, but they are still existing now. Dr. Alfonso said that their organization is a scrappy one because they don’t have any legal entity nor titles. In fact, their steering committee is very flat. HPAAC is run by volunteers and their strength lies in their solidarity. How did they make it work? They do this by looking, listening, feeling, and speaking only when there is something to say and then they act when something is wrong. How do we work when you don’t normally see HPAAC out there like in the media or in mainstream discussions? This is because much of the work that HPAAC is doing is backend work.
Key Messages
What they want in HPAAC is that communities and individuals are the frontlines. Over the past year, there is a mainstreaming of the words ‘public health’ and ‘health system.’
This is where the challenge of engaging with different lenses comes in. We may have different languages at the beginning when it comes to public health and public policy and health systems. This can be evident in the way the nuances and the directions of the discussions go.
What is public health?. Is it public health or is this the only public health that we think of? Charity work versus actually doing system strengthening work? An example would be at the local level where things like capacity building or engagement of health care providers and management are being done. So what is public health really? We need to mainstream and continue to mainstream public health because we need to share the wonderful world of public health, the bigger role of public health.
of the colleagues have heard of the PHOs. It’s a bit hard to explain what the PHOs are, so the different lenses that we need in terms of management, may not be that clear for many of our colleagues and HPAAC needs to be the one to help bridge that.
What Dr. Alfonso and the team were saying is that modifying environments necessitates expanding one’s perspective of community and stakeholders and that at the end of the day also it’s not just about modifying the treatment but we have to modify the environments including the policies.
How does HPAAC position itself given that these were the nuances also and all the interaction? In the past 13 months, we have identified three target audiences. First, HPAAC is catalyzing clarity and alignment in terms of public policy, talking with the different sectors, and talking with the different decision-makers. Second, we also catalyze clarity and alignment in terms of our peers, so the healthcare professionals themselves. Lastly, one would be behavior change communication to the individual.
▶ Commit to achieving HPAAC mission and goals

▶ Respect different opinions and ideas
▶ As much as possible, debate internally until consensus is made
▷ So when they make their stand, normally if this it’s an issue that has a lot of contention, they try to get the signatures of the Presidents if they would like to be in, and the Presidents would ask their board for the consensus, etc.
▶ Facilitate multi-specialty, interdisciplinary, and whole-ofsociety approach
▶ Value diversity, inclusiveness, honesty, transparency, and accountability
▶ Uphold evidence-informed decision making
▶ Declare conflicts of interest
▷ As health care workers, we do not work with tobacco, alcohol, and infant milk companies in any work related to HPAAC
The other thing that is also important is expanding the notion of community. When you talk of engaging in facilitating unification for policy, what is the community we are thinking of? We need to expand that.
Intersection of Medicine & Public Health
The beauty of this COVID response is that we have seen the need to meet in the middle. There’s an intersection between medicine and public health. In 1923, this was already discussed, but it seems that we need to review and mainstream this so that we are not limited only to clinical response.
Levels of Care
HPAAC tries to place the health system in this kind of context embedded in a community or in a society that has its principles and values. At the end of the day, the service is at the heart of your health system, where you need resources and you need leadership and governance to actually manage. The governance will be the one responsible to get those resources to the proper services that are necessary not just for COVID response but for the different response across different levels. This may be plain to us but we have to also share these perspectives when we are interacting with different actors.
Decentralized Philippine Health System
When we interact, the challenge is how do we explain devolution or decentralized health systems? Many of the colleagues have only heard of the CHDs for the first time or many
◼

Rallying the healthcare community as a strong, united voice
▷ Only possible through the diverse expertise, reputation, and social capital member organizations and volunteers
◼ Health in all policies
▷ Public policies impact on population health, and vice versa. If we want sustained recovery, sectors must work together.
◼ Fighting infodemic through various audiences
The rallying of the entire healthcare community is possible because of the generosity of many people who were willing to provide their time for free and social capital and reputation to help in all policies. HPAAC also tried to reach out to social capital across the different sectors. There are HPAAC analogies in the different sectors, like in the transportation sector, we have Move As One. There is also Safe Schools. There are other advocacy groups per sector and HPAAC have been trying to align with the different stakeholders. Of course, there is also fighting infodemics across different channels.
HPAAC as Catalyst for Systems Strengthening A Challenge
Dr. Alfonso gave a challenge for our generation of public health practitioners:
HPAAC members agree to the following operating principles and values:
“How do we influence policy to consider the view of the forest, as well as the individual trees?”
42 Cultivare_INDD Ver_09212022.indd 42 21/09/2022 4:39:31 pm
It’s a challenge to see both from the forest and back to the individual trees, and from the individual trees back to the forest. So when you talk about the algorithms, it can take hours to just discuss one box because there are multiple lenses that need to be considered. But the beauty of collaborating with policies in the clinical specialties is that when HPAAC tells them what is happening in the front lines, they believe it. Dr. Alfonso acknowledged some colleagues in the front lines, many of them try to bring out their voice whenever they come into discussions and that’s been such a great privilege for HPAAC who have been sitting there.
Dr. Alfonso hopes to push that public health is not just one homogenous field of specialization, but there are different people who are doing different things. They have lenses that can contribute to improving the response. She hopes that in the years to come, we will continue to mainstream public health as a specialization in the field of medicine and development.
From Evidence to Policies
Dr. Antonio Dans Convenor, Healthcare Professionals Alliance Against COVID-19
In the past 18 months, the Healthcare Professionals Alliance Against COVID-19 (HPAAC), which involves 102 members, has tried to push the science, participating in the formulation of the COVID guidelines by doing 90 evidence summaries and formulating 136 recommendations. The specific work of HPAAC has been trying to get people to try and put recommendations together in algorithms that are easy to digest.
Four-Step Process in Pushing Science into Policy

The COVID-9 pandemic has caught everyone by surprise and an evidencebased response was advocated to ensure effective control of the virus. We have seen several interventions that are either incorporated in the country’s response or denied consideration due to lacking evidence. So in times of public health emergency, how do we synthesize and utilize evidence in our policies and interventions? Are there other factors aside from evidence that we need to consider in our policies?
Impact of the Pandemic on Science
One of the big problems is that scientific evidence has been taking a hit largely from people feeling the need to do something.
Things like, “This is a war,” “People are dying,” “Science can wait,” but people should not push science aside so that we can do something. Moreover, there is now a resurgence of shortcut low-quality studies in the rush, reduced thresholds for accepting technology, and worst of all, it has become a free-for-all scientific debate involving journalists, politicians, artists, bloggers, and others.
Dr Dans shared a four-step process on how we might push science into policy: ask a focused question, evaluate evidence, make recommendations or guidelines, and formulate policy.
Ask a Focused Question

The first is to ask a clean, focused question. A focused question will have a population identified, the exposure they want to assess, and the outcomes they want to reach. So turning this into a copied question, for example, a valid question might be, “Among people who have finished their COVID-19 vaccine, how effective are boosters in reducing reinfection rates?” This is very important because we need to know what are the important questions to ask.
Evaluate the Evidence
The second is to evaluate the evidence, and this is where we sometimes have difficulties. Quality of evidence is classified into high, moderate, low or very low-level evidence. In this classification scheme, randomized control trials start off as highquality evidence and observational studies start off as low-quality evidence. Then trials can go down if they are flawed, there is a risk of bias, or if there is inconsistency. Those of you who are used to doing systematic reviews or reading them will know this as
heterogeneity. So if you have very different results from each other, that’s inconsistency and a high level of evidence can become moderate or moderate can become low. If the question is indirect, for example, it is not exactly the outcome you want or not exactly the population you want, then you also step down along this ladder. If the results are imprecise, if the confidence intervals are wide, or if the sample size is small, then you also step down. Finally, the fifth reason that the quality can be stepped down is if there’s publication bias wherein only the good trials with positive results came out and those with negative results showing no difference didn’t come out.
Observational studies can also go up if the effect size is large (or >30 %reduction in an important outcome) if there’s a doseresponse gradient (e.g., the more you smoke, the more the greater the risk of cancer), and if there are adjustments for confounding variables as well.
What’s the real meaning or the easiest way to interpret levels of evidence? If it has high-quality evidence, further research is unlikely to change our confidence in our recommendations. In moderate-quality evidence, further research is likely to have an impact. In low-quality evidence, further research is very likely to have an impact on our confidence in the results. In very low-quality evidence, any estimate of the effect is really uncertain so we really don’t know what the effect is. Clinical practice starts with randomized trials, they are the best to be studied using randomized trials. Therefore, medical, surgical or individual interventions usually start as high quality, but population-based or public health interventions are usually observational studies and they start out as low-quality studies. We need to elevate them. It is hard to do randomized trials on everything, for example, in smoking, we look at the effect, size, gradients, and adjustments for confounders to increase the level of evidence. So observational studies can become high quality through this pathway and randomized trials can become low
43 Cultivare_INDD Ver_09212022.indd 43 21/09/2022 4:39:31 pm
quality. The fifth level of evidence is no evidence. When we say there’s no evidence, that is number three on a five-point scale from no evidence to a high level of evidence.
Make Recommendations or Guidelines
Once we qualify and evaluate the evidence, we try to make the recommendations or the guidelines. Here is a scale showing the relationship between levels of evidence: no evidence, very low evidence, low evidence, moderate evidence, and high evidence. The strength of recommendation can be weak, medium or strong and usually, there will be a direct relationship.
If you have high-level evidence, you can make a strong recommendation and if you have very weak or very low-quality evidence, your recommendations will be weak. Can you have high-level evidence and yet come up with a weak recommendation? Of course. If you have a very good well done randomized trial that shows that treatment has a very small or borderline effect with pros and cons because of the side effects, then you can have high-quality evidence and a weak recommendation for a particular technology. The real problem is, can you have low-level evidence and a strong recommendation? This is referred to in the literature as discrepant recommendations. The quick answer is yes because recommendations are affected by more things than just the level of evidence, such as the following:

1. Certainty of Evidence
Desirable effects
Undesirable effects
Balance of Effects
People’s Values
Prioritization of Problem
Resources required
Cost-effectiveness
Equity
Acceptability
Feasibility
Design)
may be used for others. There are also costeffectiveness, effects on the disadvantaged populations, acceptability and feasibility in considering the context.
We express uncertainty using different languages. There are many professional guidelines that use this kind of levelling or sometimes they use language to describe the evidence, like this drug or this public health intervention can reduce mortality. For the recommendations, we can use numbers or letters for strong and weak recommendations. Some use the language strong versus weak, alternatively conditional recommendations (which can be confusing to some) say we recommend and if weak, we suggest, or should be given and may be given.
Formulate Policy
The Universal Health Care Act (RA 11223), made policy formulation separate. Practice guidelines are made by academic and professional societies and policy is formulated by several institutions, including the FDA, DOH, HTAC, IATF, LGUs, and other government agencies. The policy comes in many other things, such as politics. And sometimes policy is made for political reasons, not just academic, and many other issues including affordability, the current budget, popular demand, and others. So what policies should we focus on?
In the past 18 months, with a focus on response from the health sector, we have run out of breath debating ivermectin, face shields, contact tracing, vaccine hesitancy, and implementation of Universal Health Care. These are worthwhile debates on policy, but Dr. Dans thinks that we have neglected the most important thing, which is preventing airborne transmission in homes, in the community, in public transport, and at work, because this is how we evolve into a new normal. This is how we learn to live with the virus and we have not put enough thought into that. We have just closed, locked-down or opened and have not put enough thought into how life should change. The concept of airborne transmission is very important.
rechargeable devices and carbon dioxide is a measure of the air we re-breathe 413 parts per million in atmospheric air. Carbon dioxide level goes up when ventilation is poor, when there are lots of people, when the room is small, when people have stayed there for a long time, and when they are talking, singing or shouting.
Summary
In summary, in order to push science into policy, we need to ask the right questions, we need to search for the proper evidence, translate it into recommendations using accepted consensus strategies, and then push for the policy that should emanate from it.
Disasters Shape the World We Live in
Disasters shape the world we live in. Skyscrapers in many cities emerged from a fire that raged Chicago to the ground in 1835, leading to the emergence of steel structures. Also, the modern subway station emerged from an 1888 blizzard that paralyzed New York and caused a lot of diseases. We also know of the UK cholera pandemic which became the origins of the modern sewage system and increased longevity from 40 to 60 to 80. This is because of learning that cholera didn’t come from miasma or bad odor, it came from the water sewage system.
Certainty of evidence based on the study design can affect the level of recommendation, but there are also many other things like the results—what are the benefits, what are the harms, and what is the balance of the benefits. You can have good evidence with the most balanced effects and that will lead to a weak recommendation. More difficult is when context comes in. You may have the same number of deaths and strokes, but maybe some people are more afraid of stroke than death itself because of the changes in your personality, so values come in. Is it a priority problem? Because when you use economic resources for a particular technology, you draw on resources that
An epidemiologic study on the infection rates among contacts of COVID cases in the open workplace reached 1.4%. Compared to contacts in a household or closed workplace, one can see how big the difference is. The infection rate inside the house is 31 times more than infection in an open space. If you compare it to a closed workspace, if you move around the household compared to a closed workplace it’s still a big difference, an 18-fold increase.
The problem is, how do you measure ventilation? We have airflow measurements in cubic meters per minute which is very hard to do and air changes per hour using meters. This will take a lot of engineering to set air change per hour. But there’s emerging interest in air quality monitoring using carbon dioxide in parts per million. These are portable
Dr. Dans raised that this is exactly what we need to do for COVID-19: push evidence and develop what we might call an air sewage system. Because when waterborne illnesses ruin the world we live in, we develop modern sewage systems for the waterways. Now we need ways to make our air cleaner and he believes we can evolve into that world where there are safe transport options, outdoor dining, business places with open doors and open windows. Dr. Dans urged that we need to do this because if we don’t, the pandemic will go on longer and our children and our children’s children will suffer the same fate with future pandemics.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
(Study
(Results) (Context)
Photo Credit: Flickr
44 Cultivare_INDD Ver_09212022.indd 44 21/09/2022 4:39:31 pm
AIA Group
45 Cultivare_INDD Ver_09212022.indd 45 21/09/2022 4:39:31 pm
AIA PHILIPPINES PROTECTS MEDICAL FRONTLINERS WITH PHP 1.5B WORTH OF COVERAGE
MANILA, PHILIPPINES – In 2020, AIA Philippines provided free compassionate benefit coverage worth PHP50,000 to 30,000 medical frontliners, through its partner hospitals. The program, called Frontliners Inclusive Risk Safety neT (FIRST) Initiative, provided coverage that translates to a total sum assured of PHP1.5 billion.
“The pandemic caught everyone by surprise, and our immediate response was to take a two-pronged approach with our support: the containment of the virus by providing for the needs of medical frontliners, and the food security programs to prevent social upheaval among the marginalized daily wage earners. After addressing the more pressing needs, we are now ready to provide a more meaningful intervention that’s aligned to our mission of protection through the Philam Foundation FIRST Initiative. The donation is a long way from ideal but this at least provides our frontliners some measure of protection as they battle Covid-19 face to face,” shares Max Ventura, Philam Foundation President.
Along with other efforts that the company has taken to address the needs of its customers, employees and partners during the enhanced community quarantine period. AIA Philippines responded by strengthening this Initiative to the other needs of the frontliners whose lives are at risk as they fight the pandemic and provide much needed coverage. This will include housekeeping and security personnel assigned to areas exposed to the coronavirus, aside from the doctors, residents, nurses, tech (rad tech, med tech, etc), orderlies and nursing aides, depending on the classification of the hospital’s Human Resource Department.
We have partnered with 59 private and government hospitals nationwide who have enlisted their frontliners for the compassionate coverage.
The special compassionate benefit is good for a three-month coverage initially from April to July 2021 and was extended until December 2020.
“It is AIA Philippines’ first time to provide compassionate coverage made especially for medical frontliners, which aims to provide much-needed protection for these heroes. We want to give them peace of mind that as they battle an unseen enemy, they can rest assured that if anything happens, their families will receive something,” said Kelvin Ang, AIA Philippines Chief Executive Officer. “We are happy to support this initiative that allows us to protect the frontliners, part of fulfilling our mission of racing against risk to protect every Filipino family and empower them to live Healthier, Longer and Better Lives,” he added
Email philam.alpha@gmail.com for more information on the FIRST Initiative.
About AIA Philam Life
The Philippine American Life and General Insurance Company (Philam Life) is the country’s premier life insurance company. Established on 21 June 1947, AIA Philam Life has earned the trust of customers for its financial strength, strong brand name, and ability to deliver on its promises.
AIA Philam Life has PHP249.6 billion in total assets as of 31 December 2018, while serving over 700,000 individual policyholders and over 3,000,000 insured group members.
AIA Philam Life understands the needs of its customers and provides holistic solutions that include life protection, health insurance, savings, education, retirement, investment, group, and credit life insurance. It also offers bancassurance and fund management products and services through its subsidiaries—BPI-Philam Life Assurance Company (BPLAC) and Philam Asset Management Inc. (PAMI).
AIA Philam Life is a member of AIA Group Limited, the largest independent publicly listed pan-Asian life insurance group.
About the Philam Group
The Philam Group comprises the biggest life insurance company in the Philippines. By putting its customers at the center of its operations, the Philam Group has earned the trust of its stakeholders and has achieved continued growth over the years.
The Philam Group was formed with the mission of empowering Filipinos to achieve financial security and prosperity. Through its strong network, it is able to offer financial solutions such as life protection, health insurance, savings, education, retirement, investment, group and credit life insurance, and fund management products and services.
After the establishment of AIA Philam Life in 1947, the Philam Group has since expanded to include other affiliate companies, namely: BPI-Philam Life Assurance Company (BPLAC), Philam Asset Management Inc. (PAMI), Philam Call Center, and Philam Foundation.
Based on the Insurance Commission results as of 31 December 2018, the combined total premium income of AIA Philam Life and BPLAC is at PHP40.7 billion. Its strength and stability is solidified by its assets at PHP247.0 billion and net worth at PHP77.1 billion. It is a member of AIA Group Limited, the largest independent publicly listed pan-Asian life
insurance group.
About AIA
AIA Group Limited and its subsidiaries (collectively “AIA” or the “Group”) comprise the largest independent publicly listed panAsian life insurance group. It has a presence in 18 markets in Asia-Pacific – wholly-owned branches and subsidiaries in Hong Kong SAR, Thailand, Singapore, Malaysia, Mainland China, South Korea, the Philippines, Australia, Indonesia, Taiwan (China), Vietnam, New Zealand, Macau SAR, Brunei, Cambodia, Myanmar, a 99 per cent subsidiary in Sri Lanka, and a 49 per cent joint venture in India.
The business that is now AIA was first established in Shanghai a century ago in 1919. It is a market leader in the Asia-Pacific region (ex-Japan) based on life insurance premiums and holds leading positions across the majority of its markets. It had total assets of US$284 billion as of 31 December 2019.
AIA meets the long-term savings and protection needs of individuals by offering a range of products and services including life insurance, accident and health insurance and savings plans. The Group also provides employee benefits, credit life and pension services to corporate clients. Through an extensive network of agents, partners and employees across Asia-Pacific, AIA serves the holders of more than 36 million individual policies and over 16 million participating members of group insurance schemes.
AIA Group Limited is listed on the Main Board of The Stock Exchange of Hong Kong Limited under the stock code “1299” with American Depositary Receipts (Level 1) traded on the over-the-counter market (ticker symbol: “AAGIY”).
Media Contact:
Abbie L. Remo
AIA Philam Life Head of Corporate Communications and PR Telephone: +(632) 521 6300 local 2812 Email: Abbie-D.Remo@aia.com
46 Cultivare_INDD Ver_09212022.indd 46 21/09/2022 4:39:32 pm
Philam Foundation’s ALPHA consortium:
A concerted effort to combat the ‘Big C’
Cancer, or the ‘Big C’, remains one of the lead ing causes of death in the country. According to the Department of Health, four Filipinos die of cancer every hour, which translates to nearly 100 every day.
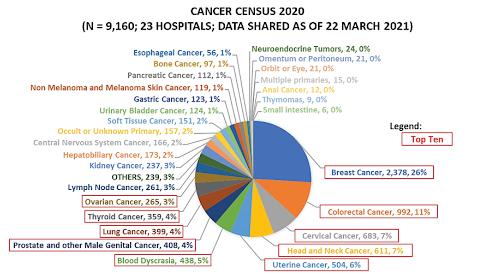
In response to the growing and alarming epi demic of cancer, several initiatives from both the private and public sectors have been made to mitigate its impact. One proactive approach primarily undertaken to address its root cause was the establishment of the Alli ance for the Philippines’ Health and Advoca cy (ALPHA), a health-based consortium of AIA Philippines’ corporate social responsibility arm, Philam Foundation, Inc., together with the Philippine College of Surgeons and the Philippine College of Physicians.
Launched in December 2017, ALPHA was cre ated to address the health challenges faced by Filipinos through data-driven and evi dence-based health advocacies and projects. “One of the things that happened with AIA Philippines was our shift in priority to protec tion and wellness. With our refreshed brand promise of helping Filipinos live healthier, longer, better lives, we are not just concerned about the physical and mental aspects of wellness. We are doing what we can to help families achieve their dreams despite untow ard life events,” said Max G. Ventura, Presi dent of Philam Foundation. “As part of our CSR initiatives, it meant supporting ALPHA’s program on cancer registry, where valuable data is mined to identify options for cancer treatment and prevention, which in turn al lows patients to make more informed deci sions,” he added.
Since its inception, ALPHA has initiated sev eral efforts to address the health needs of Filipinos. One of these is to help carry out a hospital-based cancer registry that will set the proper direction for cancer treatment and prevention in the country.
“There’s a need for a hospital registry be cause most cancer patients will end up in the hospital. Also, the advantage of a hospital registry is you are able to measure the quality of care by looking at the data – from what the patients received to their outcomes. You can look at the quality of care based on what the hospital is able to do,” explained Dr. Manuel Francisco T. Roxas, Director of the Philippine College of Surgeons Cancer Commission.
To make this undertaking a reality, ALPHA has partnered with Cancer CARE Registry Philip pines (CARE Philippines), a non-profit orga nization which created a web-based appli cation that served as a secure cancer registry platform.
Through the partnership with ALPHA, CARE
Philippines was able to on board more hos pitals to use the app. In 2019, the number of participating hospitals increased to 30, with over 7,500 new individual cancer patient reg istrants.
“This has helped improve the quality of can cer care by gathering baseline data regarding the incidence of cancer in the Philippines based on hospital Pathology reports, and by identifying the most common cancers diag nosed in CARE PH hospitals in Luzon, Visayas and Mindanao,” shared Dr. Beatrice J. Tiang co, co-founder and chief executive officer of CARE Philippines.
Despite the pandemic in 2020 shifting every one’s health focus on COVID, partner hos pitals continued to share their data to the registry, adding 9,160 new cancer patient reg istrants to the database. Data shows that the top ten most frequently diagnosed cancers in the CARE PH Registry System are: Breast Cancer, Colorectal Cancer, Cervical Cancer, Head and Neck Cancer, Uterine Cancer, Blood Malignancies, Prostate and Male Urogenital Cancers, Lung Cancer, Thyroid Cancer and Ovarian Cancer.
Moving forward, ALPHA hopes to further ex pand hospital membership of the cancer reg istry to gather more data, which will be the basis for further studies on the prevalence of cancer in the country “As we expand the reg istry and include more hospitals and more data sets, the more representative it will be of the country’s cancer situation,” according to Ventura. “The end goal is to provide better quality care for Filipino cancer patients.”
For CARE Philippines, Dr. Tiangco said that it will also continue to invite more member hospitals, especially from the underserved areas where access to cancer care is limited. “We will then be able to see what services we can boost in these hospitals, or we can
behave like a network of hospitals and nav igate patients who need higher level of care to nearby CARE PH hospitals with such capa bilities available,” she said. In June 2020, AL PHA, through the partnership with Philippine College of Surgeons Cancer Commission, was able to expand and onboard over 80 addition al hospitals into the registry.
The program has also supported efforts to strengthen the Multidisciplinary Tumor Board and Surgical Outcomes Study by the Philip pine College of Surgeons Cancer Commission. These efforts support the capacity-building strategy for cancer surgeons, as well as aug ment cancer surgery approaches in the coun try.
“We’re very excited with ALPHA, as it actually gained a lot of momentum since we launched it three years ago,” Ventura enthused. “It has become a platform for partnership and con vergence of those who have the same desire to have a healthier Philippines, to improve the health situation in the country, and to help win the battle against cancer. For AIA Philippines, sustaining this program has been another way we’ve been able to bring to life our purpose of helping Filipinos live healthier, longer, better lives.”
47 Cultivare_INDD Ver_09212022.indd 47 21/09/2022 4:39:32 pm
Spurring Innovations During the Pandemic: Experiences in the Western Pacific
 Photo Credit: Envato/ serhiibobyk
Photo Credit: Envato/ serhiibobyk
48 Cultivare_INDD Ver_09212022.indd 48 21/09/2022 4:39:34 pm
The pandemic has challenged each country’s existing system, but it has also allowed innovations to happen despite the obstacles. Indeed, hardships bring out the best in us and new problems demand newer solutions, hence a lot of innovations were spurred out. For this session, we would like to do a deep dive and ask the following questions: What are the facilitating factors to spare these innovations? What should countries do in order to further improve this environment? What are the examples of these innovations with us today? Is the innovation focal point for the WHO in the western pacific region?
Innovation Catalyst
Ms. Mengji Chen is part of the lead innovation team in the Innovation Research Unit. What they usually do is to take a three-pronged approach: research, engage, and co-create. They do a lot of engagement activities so that they can slowly develop the innovation community with diverse culture to help member states in the region find the solutions they need to address the problems they are facing today and in the future. At the same time, they do a lot of co-creation projects. For instance, they would take their technical units’ programs and their ideas to a prototype stage, so that they can have them tested and piloted in member states.
WHO is focused on developing information and knowledge products, but in today’s world-especially in the digital area, it is probably more feasible if you can bring the guideline in a different shape in a more innovative and more indigenous approach. This can actually help increase the guidance and content. The WHO Innovation Research Unit aid co-create and help member states to build an interest
in innovating.
In her presentation, Ms. Chen focused on how innovation is actually not a privilege to any of the innovators, but it is about how each of us can find ourselves in. It’s like a social process.

To Change is to Innovate
We are falling behind in testing, we are falling behind in treatment, our hospital beds are really unconstrained, and our health workers are literally working overtime and they need serious mental support. So we have profound luck with vaccination research and development, which is good, but at the same time, our vaccine rollout has been encountering barriers like vaccine hesitancy and the fact that the speed of rolling out vaccination is actually falling behind the mutation of the virus itself and we have so many more populations to cover. There are both good and bad outcomes and livelihoods are certainly endangered in certain parts of the world.
“Health is created and lived by people within the settings of their everyday life; where they learn, work, play, and love.”
Ms. Chen thinks that health is actually created by where we live, love, work, and play. To her, rather than first jumping into the innovation talk, she would rather talk about the compromises and the changes that are needed to allow ourselves to continue to live, love, work, and play in the future. She emphasized our future, because the future is actually where we will spend most of our time and societal changes are needed to adapt, survive, and thrive.
“Changes are needed to nurture health for the future, as the future is where we will spend most of our time in.”
If you want to, there’s no such thing like innovation or innovator or innovative personality per se. If we want to change, if we want to adapt to the way the surroundings or the environment gives us, then we have to change, we have to innovate. Innovation can be simply put into the equation as change management.
“To change, is to innovate.”
There is a landscape of innovation that one can see during the COVID-19. There were social non-pharmaceutical interventions that actually are helping people to follow social distancing, when we were not abiding by these rules. There are also drones for delivery because we need to speed up when it comes to vaccine rollout. This is a result of R&D. Because we need to keep up with the mutation of the virus, we need to speed up science and research. Therefore, open science became a thing. Also, because of the livelihood due to lockdowns on a daily basis, assume this is the case for the Philippines for a very long time and which applies to China as well, what happened was food delivery by Grab and by all internet platforms have become a real thing. Slowly, we got into a new habit of eating from deliveries and telemedicine, as well as the next generation of genomic sequencing, medical robotics or disinfection robotics. The image below is a bird’s eye view and is not even complete. This is not all of the compilations that you can find and if people are interested, feel free to google online and search for COVID-19 innovation. There are a ton of different resources that guide you through the catalogue of innovations happening around the world
Innovation is a response to the change that society needs to sustain our lives, our work, our love, and the way we live. That was a motive that was a drive. But to innovate implies disruption and it actually implies inconvenience. When inconvenience actually arises the reparts lead to the re-. For instance, for the adoption of telemedicine, we would need to redesign the workflow in hospitals and healthcare facilities and if we want to let drones be the vehicle to deliver vaccines to the unreachable areas, you need to modify or loosen the airspace regulation and you have to reallocate resources if you want to accommodate all of these innovations in the previous picture to happen.
“To innovate is to disrupt. Re-* ensues.”
So a lot of the re- factors will need to happen. If you look at the process of innovation to begin with, it’s a product, it’s an idea. Slowly, it moves into disruption, and there will also be resistance in adoption. Then, the redesign parts, and the adaptation and the diffusion. The whole process is actually bumpy and it’s quite complex because real innovation always implies changes in social contracts and people,
Ms. Mengji Chen Lead Consultant Data, Strategy, and Innovation Division, WHO Western Pacific, Regional Office
The
COVID-19
Innovation Landscape
49 Cultivare_INDD Ver_09212022.indd 49 21/09/2022 4:39:35 pm
in general, are very prone to inertia as an individual and also as organizations.
There are innovations that begin simple, but the fact that it looks simple is because a lot of upfront investment in research and development has already been tested. Arrows on the floors and colorful dots can be used for infection prevention is actually using behavior science here as a nudge. This kind of innovation is quite straightforward as long as it becomes a policy. It becomes a new recommendation. At the community level, they could just enforce it. But as mentioned, it may look very simple and it’s like a smart trick but the fact is that for certain smart tricks, it takes a little investment and a lot of upgrades and naturally it has to be edited in space. It also has to be driven by scientific defending, so it’s not like an idea just translated into the individuals
The second type is the innovations in the tech domains because techdom makes itself like a digital product that that part is probably the simplest. When it comes to integrating digital innovations into the health system, that is where things become messy and can take forever. That is actually a different stage of innovation because product innovation is actually just the first step. How does it get accepted by society, by the institutions, and all of the systematic changes and the cultural factors that had to come together with it? Especially in the case of telemedicine and digital contact tracing, these two are more challenging than developing the products themselves. Hence, we would question where the impacts are because as human beings, we always want a return and we would always constantly ask about the cost-effectiveness and the need for evaluation. In the case of the previous example like nudging behaviors, a lot of studies have been conducted to understand and evaluate how effective these policy nudges are.
“Hence, the questioning of costeffectiveness and impact”
They conduct a lot of natural experiments, not randomized controlled trials, to make sure that the investment in developing such a policy intervention is cost-effective in a certain time period, even though innovation is something that, in general, would require a longer time frame, because you just have to give it enough time to show its true impact before we call it to a stop.
Digital Contact Tracing
There’s no endpoint in innovation. Innovation is no one’s privilege and it involves everyone either as a user, a developer or as an implementer. We all have a responsibility and we actually are consciously or unconsciously contributing to this process. One example of this is digital contact tracing. At this point, people are more concerned about vaccination or about opening a border, without paying much attention to contact tracing or the digital contractors which were really overhyped last year. Ms. Chen gave this as an example because this really demonstrated the innovation process. It started out as a tech product and slowly it evolved into something that’s bigger and that’s actually more challenging. The more it gets discussed and implemented, the more challenging it becomes.
Regarding the status of digital contact tracing adoption in the region, per WHO research, by the end of May, there are 15 out of 37 member states and territories that have already endorsed digital contact traces. This means that they have some sort of at least one or two digital apps that can be used by health workers to conduct contact tracing or be used by individuals like us for self-report purposes.
How did it all start? All of the implementations of the 15 member states, somehow adopted at least one of the three mainstream technological protocols. The first one was actually developed by Singapore, Open Trace Protocol, which uses Bluetooth, but it’s using a centralized data architecture. The second one is called the Path, which is an open path check and is actually developed by MIT and maintained as open software. The third, which got the most spotlight and most attention from the media, is actually the Apple-Google Exposure Notification Platform.
For the 15 member states in the Western Pacific Region, most of them have endorsed at least one of the technological protocols which were originated by innovators or technologists not residing in the region, but somehow they got diffused through the internet. In this case, people ask who are the innovators.
It’s natural to answer that the technology providers, the software developers, the coders, are the true innovators. However. Ms. Chen would argue that they are not innovators. They probably are the first wave of creators, but that only can be much. The real innovative innovation solution that was chosen was not by the developers. The developer community just implemented their ideas about a tech issue, but it is the implementer, the government agencies, who actually made the evidence base for the social situation. The government made
the situation-based decision on how the innovation should look like and how the tech architecture should be like.
The third is the user, like us. The reason why Ms. Chen would argue that we are innovating is because even though we were not involved in the original design or in the original technical specification, we were actually contributing our user experience and our data to help them improve it. The way that we use it in our everyday life gave them more thoughts on how this can be more inclusive. We are the source of information for these developers and implementers on how we can maximize the benefits while minimizing risk, especially when it comes to digital contact tracing, there’s a lot about data privacy and ethical governance, etc.
Innovation doesn’t really end anywhere. It evolves and morphs. It evolves in the sense that the people who innovate evolve and the users can become the new innovator. Because if you look at digital contact tracing, if you want the innovation (digital contact tracing) to become a successful story, it takes a whole society’s response, it takes the user’s response. There must be several societies that can step in and say this is a tactic we can use to incentivize people to do something for the benefit of society instead of the individual interest.
Research, Rethink, Redesign, Learn
Innovation is a repeated process of research. Rethinking and redesigning research is necessary because you have to know what works and what doesn’t. In the case of the nudge example that the speaker gave, if you want to nudge people to disinfect themselves or just to be better at hand washing, you would need to find all the different tools. How to design a nudge is something that researchers are painstakingly working on. It couldn’t be more obvious in the digital contact tracing. What policymakers, developers, and media should rethink is who is missing in the discussion when it comes to redesigning data contact tracing, because it’s really not the technologists who should design or should dominate the conversation. Too much focus has been put on tech issues and privacy or governance, but in fact, this takes another society. It takes another set of stakeholders to contribute to the design and the brainstorming process. So basically, the innovation process of digital contact tracing, in general, is not democratized, it’s not distributed. There are unbalanced interests among the major stakeholders without putting too much investment into the user side story.
 Technological Protocols
Technological Protocols
Innovation does not end anywhere. It evolves and morphs.
50 Cultivare_INDD Ver_09212022.indd 50 21/09/2022 4:39:37 pm
Unilab Foundation
51 Cultivare_INDD Ver_09212022.indd 51 21/09/2022 4:39:37 pm
Making Universal Health Care happen
Unilab Foundation supports UHC Law with a new initiative that taps on the potential of the youth to support health workers in making primary care more ac cessible to Filipinos..
When Republic Act 11223 or the Univer sal Health Care (UHC) Act was passed into law in February 2019, Unilab Foun dation (ULF) found it an opportune time to further align its efforts with the nation al health agenda.
Founded in 2011, ULF continually de velops social interventions in health, education, and youth engagement, em phasizing the need to innovate and work together for a healthier and future-ready Philippines. Currently, it has three major pillars: STEM+PH, which ensures that in tegrated STEM learners and stakehold ers work towards a future-ready nation; HeadsUp PH, which helps mentally healthy young Filipinos; and Youth En gagement, which ensures that the youth are actively participating in building healthier communities.
ULF has built its credibility around ef fectively and meaningfully engaging the youth in its mission. It has two existing Youth Engagement programs: Ideas Positive and Doctors for Others. Ideas Positive engages the youth to be lead ers in creating solutions to health issues in their communities, while Doctors for Others molds young health profession als to be public health champions. ULF works with experts in public health, community development, and youth en gagement to ensure that these programs are evidence-based and relevant to the needs of the youth and the country.
Building on these experiences, ULF adds Project Kaakbay to its repertoire of in novative programs. This new program harnesses the potential of the youth to be champions of health and wellbeing in their communities and contribute to the attainment of the goals of the UHC Law.
UHC and the current health system
To strengthen the program, ULF endeavored to understand further the current health system and the UHC Law. They were immersed in Dagupan City, one of the law’s pilot implementation sites, where they were exposed to the challenges faced by the city’s health systems and how the COVID-19 pandemic exacerbated these. The immersion team saw the difficulty in the coordination of efforts between the components of the system. One patient stated that when services or medicines are not available in their barangay health center, they are referred to the nearest hospital. However, the hospital does not have their medical records so they had to start again from scratch. This inefficient and expensive process compels the patients to resort to self-treatment or disregard treatment at all. There was also a shortage of health care workers, mainly because a large bulk is assigned to the city’s COVID-19 vaccination efforts. Lastly, the health service delivery was hospital-centric and curative.
This reality is the opposite of the ideal setup in public health, where the emphasis should be placed on primary care. As the UHC Law is slowly being rolled out in the country, it is now the perfect opportunity to strengthen our public health and primary care practices, encourage public-private partnerships, and emphasize that everyone has a role to play in ensuring that no Filipino will be left behind when it comes to health.
Youth for UHC, UHC for Dagupan
With the belief that the youth can, Project Kaakbay empowers them to be effective advocates of universal health care in their communities and contribute to nationbuilding. It aims to build a network of youth volunteers and equip them with the
knowledge, skills, and attitude to become effective advocates of health and wellbeing in their community.
The three-year program will be piloted in partnership with the local government of Dagupan City and is divided into three phases: Shaping Leaders, Sharing Advocacies, and Sustaining Communities.
Project Kaakbay shapes the youth as leaders and effective advocates of health and wellbeing. It involves the leadership and capacity-building of the youth in governance— the Sangguniang Kabataan officials— to push the UHC agenda forward in their authority. They are also envisioned forming and leading a volunteer group in their respective barangays, called the Kaakbay Groups. The latter, in turn, will be equipped with technical knowledge in public health and skills in community health project management and basic health care skills, among others.

The project then provides opportunities for advocacy-sharing among the Kaakbay Groups. The empowered youth are trained to develop and implement sustainable health initiatives to address the most pressing health issues in their communities. The Kaakbay Groups are expected to work actively with the other members of the community, especially primary health care providers and other dutybearers, to help achieve the barangay and city’s health targets.
Lastly, all the Kaakbay groups will form a citywide coalition. These groups will help sustain the community of youth advocates and continue supporting the health system in the city. They will also work towards ensuring that the voice of the youth is heard in the decisionmaking process, especially on public health issues affecting them.
52 Cultivare_INDD Ver_09212022.indd 52 21/09/2022 4:39:38 pm
Let’s make Universal Health Care happen!
Conversations on health should not revolve only around health professionals because it affects ALL of us. Everyone must take part in building healthier communities. Project Kaakbay taps specifically on today’s youth because they are 30% of the country’s population and 100% of the future.
Ultimately, Project Kaakbay dreams of a Philippines with a health care system that is accessible, efficient, and resilient. The COVID-19 pandemic revealed how a global health threat could shake fragile systems like that of the Philippines. Universal health care is an opportunity to strengthen health systems and ensure that health services reach every Filipino, everywhere in the country, especially those who need them most.
Making Universal Health Care happen is a task too big for one person or organization. In the spirit of bayanihan, join us in making this dream a reality. Start by believing that the youth can.


Together, let’s make universal health care happen!
 The Unilab Foundation, Inc. is a corporate social responsibility arm of Unilab Corporation. Unilab Foundation aims to achieve long-term, transformational impact in the areas of Mental Health and Well-being, STEM education and careers, and Youth Engagement. Together, let’s build a healthier and future-ready Philippines!
The Unilab Foundation, Inc. is a corporate social responsibility arm of Unilab Corporation. Unilab Foundation aims to achieve long-term, transformational impact in the areas of Mental Health and Well-being, STEM education and careers, and Youth Engagement. Together, let’s build a healthier and future-ready Philippines!
53 Cultivare_INDD Ver_09212022.indd 53 21/09/2022 4:39:43 pm


54 Cultivare_INDD Ver_09212022.indd 54 21/09/2022 4:39:45 pm
Health Equity and Human Rights in Public Health
55 Cultivare_INDD Ver_09212022.indd 55 21/09/2022 4:39:47 pm
Commissioner Gwendolyn Pimental-Gana
Focal Commissioner, Commission on Human Rights

non-consensual medical treatment, and experimentation. Entitlements cover access to adequate health care facilities and services and appropriate state measures related to the socio-economic determinants of health, such as food, water and sanitation, safe and healthy working conditions, housing, and poverty.
From these, we start to understand that the right to health is interconnected with other human rights such as the rights to life, food, water, housing, education, work, non-discrimination, privacy, access to information, prohibition against torture, and others.
In the Philippine context, the right to help is enshrined in the 1987 Constitution.
information and education, and gender equality.
In this time of pandemic in which population-level interventions are always warranted, it is a challenge for us in the field of public health on how to balance individual rights and community gain. So how do we ensure that health equity and human rights, the two principles that we in this profession are expected to uphold, are observed in our response to the pandemic and in our other public health interventions?
It is with great honor to have this opportunity to speak before you on behalf of the Commission on Human Rights of the Philippines to discuss health equity and human rights in public health. Human rights are rights we all have simply because we exist as human beings. These rights are universal and inherent to us all regardless of nationality, ethnic origin, sex, religion, language, color, or any other status. They are inalienable, which means that no one can take away our rights except in specific situations and according to due process. Moreover, human rights are indivisible and interdependent, which means that the fulfillment of one right often depends wholly or in part upon the fulfillment of other rights and the denial of one right invariably affects the enjoyment of other rights. These rights range from the most fundamental which is the right to life and to those rights that make life worth living.
Among those rights that make life worth living is the right to health. The World Health Organization defines the right to health as a complete state of physical, mental, and social well-being and not merely the absence of disease or infirmity. To fulfill this right, the state should ensure both freedoms and entitlements. Freedoms relate to the right to control one’s health and body including sexual and reproductive freedom and the freedom from interference, such as torture,
The Philippines is also a state party to the international covenant on economic, social, and cultural rights which mandates our government to ensure the right of everyone to the enjoyment of the highest attainable standard of physical and mental health.
The UN committee on economic, social, and cultural rights emphasized that in all forms and at all levels of the right to help the following interrelated and essential elements shall be present:
1. Availability
a States should ensure the provision of enough functioning public health and individual health care facilities, as well as safe water and sanitation facilities, trained and fairly paid medical professionals, and essential medicines
2. Accessibility
b Access to health involves four key elements: non-discrimination, physical accessibility, economic accessibility and information accessibility
3. Acceptability
c Health facilities should be respectful of medical ethics and the culture of individuals and communities, as well as attentive to gender and life cycle requirements
4. Quality
d Health facilities should be scientifically and medically appropriate and of good quality. Among other things, this requires the provision of necessary medicines and equipment, skilled medical professionals, and adequate water and sanitation.
In sum, health as a human right creates a legal obligation on States to ensure access to timely, acceptable, and affordable health care of appropriate quality, as well as to providing for the underlying determinants of health, such as safe and potable water, sanitation, food, housing, health-related
Gaps in health are persistent and many of them are found at all levels of different societies, but health equity must ensure that everyone could attain their full health potential and that social status or other socially-determined circumstances should not prevent anyone from achieving it. It takes into account non-medical factors that influence health outcomes called social determinants of health. These social determinants have significant influence on health inequities. These affect a person’s ability to earn a good living to live and work in a safe and healthy environment and effectively use available resources, including health care resources. In some cases, an entire specific group or population do not have equal access to quality education, housing, and other resources which can lead to greater sickness and increase injuries and deaths, something that is totally preventable if only they were given access to good determinants of health. In other words, health equity means increasing opportunities for everyone and most importantly giving special attention to the needs of those at greatest risk of poor health based on social conditions so that they will be able to live the healthiest life possible no matter who they are, where they live, or how much money they make.
Human rights and health equity share the same fundamental values centered on equal dignity and worth of all human beings. We have seen in the past 70 years that human rights have been bringing the world together into a kind of public health cooperation we have not seen in the past. Public health actions used to be based on charity, but the framework of human rights sees all persons as rights holders deserving of the highest attainable standard of health and living. However, there is still much to be done. Many are still prevented from enjoying the benefits of the right to adequate health and standard of living. For everyone to fully enjoy them, we have to address conditions that deny them the fulfillment of these rights.
Nearly all conditions contributing to health inequity also affect other human rights. For instance, when a person is treated unfairly because of race, class, gender, sexual orientation, and other status, the unfair treatment can lead to poor education or fewer job opportunities. This results in economic disadvantage evident in the income disparity between college and noncollege graduates. Income can determine the kind of neighborhood a person lives in, the environmental conditions of a
56 Cultivare_INDD Ver_09212022.indd 56 21/09/2022 4:39:48 pm
neighborhood or community can affect a person’s health. People who live in poorer areas generally have shorter life spans than those in wealthier areas. Lower-income neighborhoods tend to be poor in social and environmental conditions such as proximity to environmental and health hazards, higher violence and crime rates, limited access to healthy food among others. These deny people the chance to live a long and healthy life. By eliminating these barriers with a goal to achieve health equity, we also promote and protect human rights and dignity. The COVID-19 pandemic and other public health challenges underscore the importance of public health and demonstrate the fact that public health challenges are human rights concerns. The current pandemic is not just a health crisis. It has quickly ballooned into a global human rights crisis after response measures by duty bearers have adverse effects to the enjoyment of civil political, economic, social, and cultural rights, and disproportionately affecting the most marginalized, disadvantaged, and vulnerable members of society. A survey in may 2020 has shown that 9 in 10 Filipinos were stressed because of the pandemic. The same survey showed that at least 4.2 million families experienced involuntary hunger due to a lack of food to eat. The unemployment rate in April 2020 during the implementation of street quarantine measures was 17.6 percent which translates to more than seven million unemployed Filipinos at that point. The enrollment rate for the school year 2020 to 2021 was also lowered 88 percent compared to the previous school year. These numbers do not even come close to the whole picture as countless others were either directly or indirectly affected by both the actual health crisis of the disease and the socio-economic effects of the various crisis response measures implemented by the government and the private sector.
Amidst the public health challenges, it is good to be reminded by the values written in the code of conduct of public health officers and the code of conduct and ethical standards for public officials and employees such as being humane, dedication to public service, upholding professional integrity, being just, being generous in spirit and deed, and exercising courage to protect the interests of public health. These values are essential in


addressing health inequities. On top of these and in pursuit of health equity, health organizations and professionals should continuously strive to provide culturally competent care to many different patient populations who need clinicians to understand their lives, address populationspecific healthcare needs, make practices inclusive, collect data in a non-judgmental way, and build trusting relationships that enable them to openly participate in care improvement strategies that are driven by a commitment to health equity. Likewise all levels within health systems should explicitly include health equity in strategic plans and goals.
Given that health disparities are shaped by multiple determinants of health, achieving health equity requires engagement not just with persons in healthcare but also in education, transportation, housing, planning, and other industries and businesses. Indeed, achieving health equity is a community-wide effort. Equity in health requires not only equitable access to health care, but also means working outside the health care system to address broader social wellbeing and development.
In closing hats off to all of you for your dedication and for tirelessly working for public health and health equity. Our public health system will not work without you. I wish everyone safety and good health in the midst of the current pandemic. God bless us all. Thank you.
Photo Credit: Commission on Human Rights
Photo Credit: CNN Youtube
Transcript of Commissioner Pimental-Gana’s speech
57 Cultivare_INDD Ver_09212022.indd 57 21/09/2022 4:39:48 pm
PUBLIC HEALTH STORIES

58 Cultivare_INDD Ver_09212022.indd 58 21/09/2022 4:39:50 pm
Rural Surgery
Dr. Brent Viray

The marriage of public health and surgery is unfathomable. From the most generalized surveillance and preventive measures of the community to the most specific body organ of interest defies union and relationship--- this is where Rural Surgery comes in to play.
I’m more than privileged to serve the people of Dingalan, Aurora in a short stint of 3 years (2 years as a DTTB, and another year as an MHO under the LGU). The people taught me how to be grounded and to be culturally rooted in the fundamentals of life. I get to understand that being in a place where you initially just have yourself- you just have to get lost and later be found.
The DTTB experience mended the reason of my service – Rural Surgery. In public health where the forefront projects consist of communicable diseases, maternal and child health, HIV/ AIDS; surgical diseases (which are equally as important) are left behind. This includes correctable congenital malformation, accident-related injuries, anatomical correctable diseases, source control operations etc. Addressing these problems is both life-saving and indirectly, family/community-building.
I had a 46-year old female who came by me to operate on her foot mass. It was a 4x5 cm epidermal inclusion cyst which impeded her to work as a farmer. It was an operation done on a random table 40-mins (by boat without “katig”) away from bayan. The procedure went well and unremarkable. The next day, the patient went back to me with bananas and crops she harvested and remarked with sincerity – “Salamat po dok, nakapagtrabaho na po ako, matagal na po akong hindi makapagtrabaho po dahil po sa bukol ko sa paa. Matagal ko na po ‘tong iniinda, hindi po kami makapagpaopera sa layo ng Cabanatuan.”
Another case is a 31-year old fisherman who consulted for a carbuncle on his back. Debridement and copious washing
were done with significant blood loss. The patient was placed in Trendelenburg position and volume replacement was only done with available crystalloids at the health center. Hypotension resolved after 2 hours and the patient opted to go home against medical advice for further observation. The next day the patient came back to me with a plastic bag of fishes (and yes, his back got infected again but now controlled by IV antibiotics) and said-“Dok pasensya ka na ha, ito lang ang napangisda ko, kung gusto niyo pong umunta sa White Beach, sabihan niyo lang po ako at meron po kaming maliit na banka na ang pangalan ay Solo”.

These are just two of my favorite rural surgical anecdotes that keep me going as I traverse my current residency training as a general surgeon. More than the health programs which we promote and execute; surgical acumen comes in handy. Knowledge in handling trauma patients, management of active bleeding wounds, and recognizing surgical emergencies that needs to be referred to tertiary hospitals are competencies that we bring to the outside radius or outskirts of the country.
Equity in surgical services must also be prioritized in public health. Giving importance to this priority also result to efficiency in health financing and prevents families from impoverish and catastrophic health expenditure. Every suture thrown on surgical field, apposes the family and community as well. Rural surgery gives hope to patients’ unrest to the possible disability that may hinder them to be functionally relevant to their family and the community as well. Access to surgical services should be prompted and be prioritized as well, together with the other programs of primary health care.
By Brent Viray, MD, MPM-HSD DTTB Batch 30 MPM-HSD Batch 4
59 Cultivare_INDD Ver_09212022.indd 59 21/09/2022 4:39:51 pm
A Story of a Rural Health Physician
 Photo Credit: Flickr
Photo Credit: Flickr
60 Cultivare_INDD Ver_09212022.indd 60 21/09/2022 4:39:51 pm
Dr Rene Sison
I know that each one of us has unique stories to tell , both the routine and the exciting , the challenging and the very challenging , the exhausting and the tiring – both to spirit and bones.
Our journey started in 1969 when my wife and I joined the medical staff of Bethel Baptist Hospital, located in Malaybalay, Bukidnon. BETHEL HOSPITAL as known by people , was a fifteen bed capacity hospital with very busy OPD, OB-GYN and SURGERY services.
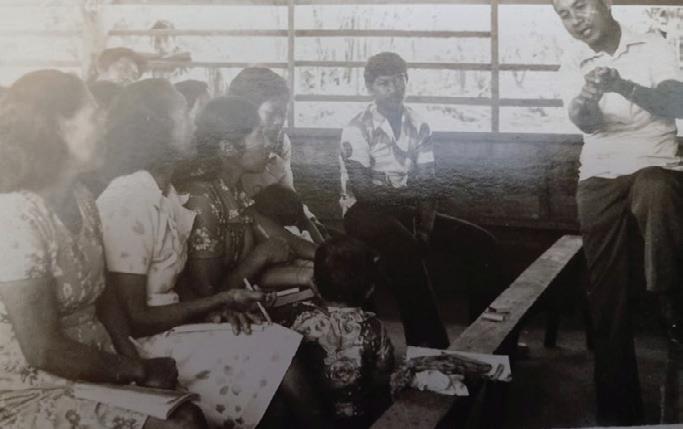
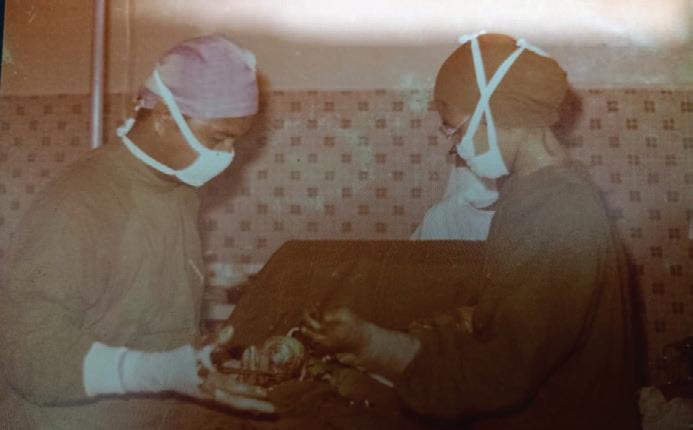

Back then, we had to be Pediatricians, Internists, Surgeons , Anesthesiologists, OBGYNs and to be able to treat fractures using skeletal traction methods ( truly general practitioners ). Since Schistosomiasis is endemic to central Bukidnon due largely to its watery environment, we had to be knowledgeable about the epidemiology , diagnosis and treatment of this disease and provide counselling to the chronically sick. Clinical diagnosis is what it says – we did not have much laboratory and or diagnostic paraphernalia. Many if not all Doctors who belong to my generation ( I am 80 years old ) would attest to this.
My stay at Bethel Hospital was not confined within the four walls of the OPD, Surgery and Infirmary. We held many medical sojourns to far flung areas, like the barrios of Kalilangan, San Fernando, peripheral barrios of Malaybalay, Nabunturan, Davao, Leyte and Cagayancillo, a tiny island between Palawan and Panay. We treated patients of all ages and we did not go there once, but several times.
Many times we visited those barrios by using a small plane if our four-wheel drive vehicle could not negotiate the roads. We would ask the barrio people to clear an area large and long enough to accommodate the plane for landing and take off . The whole barrio would meet us not because of the doctors and nurses but because they wanted to see the small airplane landing and taking off in the middle of their farms.
Thes trips enthused me to go to the barrios, so to say, as if Malaybalay and Valencia , Bukidnon were not rural enough And this brings me to share with you what my experiences were ( until now ) . When I joined Medical Ambassadors Philippines in 1976, a medical mission group, my interest shifted to Public Health - mainly Primary Health Care and Community Medicine..This medical Organization focused its services among Indigenous Communities where medical and health services were nil.
In an International conference held in Alma Ata Russia countries from many countries adopted a strategy they called PRIMARY HEALTH CARE and the battle cry was HEALTH FOR ALL BY THE YEAR 2000. This was participated by both Government and Non-
government Organizations. The scheme is to provide Promotion of Health, Prevention and control, Curative and Rehabilitative Care at the community level.
Community organization and participation are part of the strategy to address the health problems of the community. The people are part of Planning and Implementing a program suitable to their needs .
Medical Ambassadors Philippines is a Faith-based organization of doctors and nurses. I was given a function akin to COO. Medical Ambassadors Philippines put up clinics in Bukidnon, Davao del Norte,Sultan Kudarat, Marbel, South Cotabato, T’Boli , Benguet, Ifugao, Quirino , Mountain Province , Mindoro, Romblon, Balut Island in Sarangani , Zamboanga del Norte…all had IP communities.
Our initial activity was to visit the town or City mayor and identified ourselves as NGOs interested to complement government efforts in the area of health. We then met with the respective tribal leaders , accompanied by a LGU officer and explained to them our purpose.
I then assigned two nurses to stay in the barrio . The people themselves identified a house where the nurses would stay and used it too as a clinic. Health classes were held in the barangay hall, if any or the people would put up a nipa building for such purpose. The nurses were visited by itinerant physicians – there four physicians . I took care of the Mindanao area and the rest were assigned in Luzon.
Transportation came in many forms –riding on world war two weapon carriers, motorcycles to the town and by foot to the barrios 5 to 10 kilometers away on the average , by banca, bamboo raft, horseback and “ skylab”, a modified motorcycle that can carry six people.
The people were always helpful in carrying

our things and protective too. These places were definitely not tourist spots. There were threats to our lives. Many times we were mistaken for unlawful people because why would nurses and doctors go to those places ? Our purpose was to share the Gospel and provide Primary Care and Health Education. Again the terrain was always rough and a threat to life and limb. Being stranded is part of the game, but people are almost always accommodated in their homes.
Our activities were curative services, health education to mothers, training BHWs or Family Health Workers, IGP to fathers, Child to Child health programs We held clinic and health education to Muslim communities in Cotabato and Bukidnon. We helped give immunizations, helping with TB DOTS, accompanying mothers to health centers or hospitals when needed.
We also provided materials to build water systems to places where there are no potable water distribution.
To enhance my acumen in Primary Health Care Administration and Management I attended brief training courses ( 2 to 3 months) in Haifa University, Israel, London University School of Medicine, University of Hawaii School of Medicine, University of Colorado and UP School of Public Health. I was sent to study German Health Care Financing in Berlin and Grameen Bank Health Care Financing in Bangladesh. These training conferences were sponsored by Foundations and the Israel Government.
At this time when all of my contemporaries are already retired, I am spending my time as a school physician in Kabankalan City and catching up on my reading and writing. and enjoying Mozart again. . I have to upgrade my knowledge about Covid, too.
Rene’ Soliven Sison, MD Kabankalan City
61 Cultivare_INDD Ver_09212022.indd 61 21/09/2022 4:39:51 pm
National and Global Health emergencies shaped my career path
 By Dr Ronald Law
By Dr Ronald Law

Solidification and cementing of values while taking the journey, in terms of what’s important to me or what issues I am with, that I need to respond to.
… What is needed by my people
… What services, products, tools, information do they need to protect themselves from health threats and maintain health
…Or how I can contribute to policies and programs to lead, which advocacies to champion, what learning and development interventions to design
Deliberate decision making-on what to do along the way
…Working for the government to influence policy, build national capacities, and interface with other sectors
…Teaching in the academe to impart knowledge and mold future leaders
Exploring ways to improve myself as I tread my chosen path through
…Coordination and collaboration …Program management and response operations …Advocacy and community work …Evidence-based policy work
62 Cultivare_INDD Ver_09212022.indd 62 21/09/2022 4:39:56 pm
Confidence in Decision-Making.
Borne out of idea-exchanges over coffee in Sydney, the founders of metaHealth Insights and Innovations, Inc. (or metaHealth) thought about riding the wave of potential health technology assessments (HTAs) as Republic Act 11223, more commonly known as the Universal Health Care (UHC) Act, was signed by Pres. Rodrigo Duterte in 2018. metaHealth prides itself as the first Filipino firm focused on conducting HTAs. metaHealth envisions itself as a high-impact and innovative THINK+DO tank that empowers partners to reimagine quality and accessible healthcare toward improving lives in the Philippines and beyond.
The firm mainly addresses two largely unmet business needs. First, there is an urgent need to navigate the constantly evolving regulatory landscape regarding the provision of healthcare products and services in the country. As the UHC law progressively unfolds, it is anticipated that there would be a highly uncertain regulatory landscape; mainly due to the increasing amount of evidence generated on various products and services coupled with the need for legislative agility in monitoring and regulating these. metaHealth aims to help HTA practitioners, both in the public and private sectors, navigate
through these uncertainties by providing comprehensive, timely, and focused insights to ensure regulatory compliance and secure market access. Second, there is currently an inadequate capacity for local HTA, both in technical expertise and the critical mass of practitioners. metaHealth is an advocate of uplifting the standard of HTA in the country by providing avenues for relevant professional upskilling and being a trusted partner in the training and development of local HTA talent. With these, metaHealth helps elevate the HTA landscape of the Philippines by ensuring that both these business needs are adequately met.
metaHealth enables confidence in decisionmaking through actionable insights from data and scientific evidence generated from four niche areas (aptly abbreviated as “META”) which are largely underserved:
▶ Management and Implementation Science
▶ (Health) Economics and Outcomes Research
▶ (Health) Technology Assessment
▶ Analytics and Informatics

These niche areas are also our areas of
expertise. Our team has more than 30 years of combined professional experience across these fields of interest. Our multidisciplinary approach in addressing HTA problems has been proven in the projects we have completed with various multinational partners, both in the for-profit and not-forprofit sectors.
In metaHealth, we make sure that each project is completed in a holistic manner, combining multiple cross-cutting research methods with our proven glo-cal public-private expertise. Our synergy and flexibility in meeting the needs of any client put us a cut above the rest, providing them the confidence they need to pursue their goals.
As fellow public health practitioners, we are one with the Philippine Society of Public Health Physicians in dreaming with new hope for the HTA landscape in the Philippines. We believe that our diverse yet synergistic fields of expertise would help rebuild the nation with improving public health as one of our main aspirations. Working together, we can be the catalyst our country needs – accelerating the provision of equitable, people-oriented, and quality healthcare services to every Filipino.
A Glimpse on LGU Health Financing
By Dr. Niko C. Cedicol
During my stint as a DTTB, I was overwhelmed by the multitude of health plans that need to be reviewed and analyzed. I remember that time, it was my first day, armed with only a pen for signing documents, I went to the Municipal Hall and greeted everyone as if I knew them for a long time. Behind those smiles, my mind was racing between the thought of managing my time to quickly read all the documents I am about to borrow, and the thought of where will I eat my lunch, or dinner. I went to the Sangguniang Bayan hall and borrowed all the Municipal Ordinances, various health plans such as Annual Investment Plan, Comprehensive Land Use Plan, Executive Legislative Agenda, and Annual Operations Plan among others, and signed the borrowers slip. I stayed in a small room as I do not want to bring the pile into my clinic. As I browse through the documents, I then asked myself, can I really fulfill my role as an MHO? I shrugged and decided not to overwhelm myself with those data. Part of the Municipal Health Officer’s role is to analyze the health plans and match them with the needs of the community. This is something that is not learnt easily in classroom or during medical school days.
It turns out that you must really delve deeper into the situation to understand what the reason behind those amounts and numbers inked on health plans. It goes with time and the learning curve must be steep to quickly decide how to operationalize and implement the health programs and projects. I pondered upon the DOH National Objectives for Health and realized that this can be a template for making plans. But then the SDG can also guide me in creating categories for health plans. What struck me most among those documents is the Annual Investment Plan. It served as my guide as it gives a snapshot and summary of all programs as well as the available budget that you can manage or tweak over time. But before one embraces them, the LGU Budget Cycle is a must-know topic.
Municipalities in general follow the local budget system or process which starts with budget preparation (July to October), budget authorization (October to November), budget review (within 10 days), budget execution (actual release of disbursement of funds depending on function) and budget accountability (recording, reporting and
evaluation of performance).
Most of the time, the Municipal Health Officers are usually involved in almost all stages except for budget authorization which is mainly a function of the Sangguniang Bayan. PPAs or Program, Project, Activities are usually prepared to determine cost estimates per line item and a proposal is then generated per program, for instance, NonCommunicable Disease Program, Infectious Disease Program or Tuberculosis program among others. The cost per item is usually determined historically (3-5 years) from past transactions, through research on the internet for more updated pricing, or through actual canvassing of prices. Meanwhile, other operating expenditures are included in the PS (Personnel Service) for compensation of staff, premiums, retirements insurance; MOOE (Maintenance and other operating expenses) for travel expenses, supplies and materials; and CO (Capital Outlays) for land improvement, infrastructures, and equipment. Other health-related operations at the Municipal Health Office, depending on the health Officer, will be lodged at the LGU MOOE.
63 Cultivare_INDD Ver_09212022.indd 63 21/09/2022 4:39:57 pm
It is the role of the MHO to prepare the various budget or financial plans. The Annual Investment Plan is the annual share of the Provincial/Local Development Investment Program, which constitutes the total resource requirements for all PPAs by the LGU. Yearly operations by the Municipal Health Office including budgetary sources are summarized in the Annual Operation Plan (AOP). Another source of information for budget allocation/sources at the municipal level will be the Provincial Investment Plan for Health (PIPH) which is a summary of the LIPH (Local Investment Plan for Health) of all the municipalities within the province. In this plan, all health related PPAs are being elaborated as well as the budgetary sources be it from Provincial DOH or Central Office (Main), Provincial LGU, Municipal LGU, Barangay LGU, and other sources such as from private institutions or NGOs.
Aligning all the programs and budget to various existing plans such as the National Objectives of Health, CLUP (Comprehensive Land Use Plan, a 9-year plan by the LGU), ELA (Executive Legislative Agenda, a 3-year plan by the LGU), or even the Disaster Risk Reduction and Management Plan among others, may take time. Harmonizing all the plans for health for the fiscal year is a taxing task but once an MHO has determined which agency will the funds come from for a particular PPA, the next steps will be easy ones. The MHO must literally lay down on his/her table all the related documents or open all the documents on the computer and check if the activities, the human resources, as well as all the programs are accounted for. The MHO must not miss out one program otherwise budget would not be allocated and in effect will jeopardize the whole health service delivery. Critical to this phase is ensuring transparency and that utilization does not exceed the appropriated budget for health.
The MHO must be keen enough to stick to the plan and think ahead for unforeseen expenses such as when there are sudden outbreaks (e.g. COVID-19); therefore, listening to the current events, weather forecasts, economic stability of the country, or even international affairs is a good habit.
But it does not end there. An MHO cannot just copy and repeat the past activities and programs. Innovative activities and identifying the best buy for the community must be considered, hence the MHO need to study the dynamics of the community. An MHO must ask, what really is the situation in the community? Who are my target population this time? Do we have contingency plans in case a crisis strikes? A quick review of the past year’s morbidity/mortality report, disaster events or crises, as well as unused resources is a must. Tailoring health plans to the current situation e.g., COVID-19 pandemic, realigning budget to priority programs, or
requesting additional funds or even seeking external support from NGO’s are some of the tasks of an MHO.
My salute to all MHO’s out there (and all other local health officers, the City Health Officers, the Medical Officers, Rural Health Physicians) working in the community to ensure health and welfare of their citizens, and for being strong and faithful amidst the pandemic and challenges.
As I was continually exposed to the various transactions in the LGU, I was able to gain more insights and eventually think and plan ahead for the next year’s activities. But again, the role of MHOs especially on financial matters are usually extensive. The role of transforming health funds into services is complicated. For instance, health facilities accredited by Philhealth as TB DOTS provider may benefit from reimbursements of claims and in return, the services to be offered to TB patients must be free. But not all community members knew the process. Some of them even proceed to private clinics to seek consultation. This is somehow addressed nowadays through partnership with private health clinics.
The social heath insurance scheme has been functioning for quite a long time in the
country. Funds generated from premiums by the Philhealth will be pooled and redistributed to those in the lower income class brackets (subsidized). This creates larger pools of funds thereby increasing resource availability. Philhealth then provides reimbursement to accredited health facilities for the latter to deliver quality health services. For instance, a TB patient who belongs to low-income class will receive the TB DOTS treatment and funds used to pay for medications and series of chemotherapy are subsidized. Funds reimbursed to the Municipal Health Office are then utilized to replenish TB-related expenditures such as medicines or supplies in the health office.
However, not all health facilities are Philhealth-accredited for TB management. In this case, the DOH steps in to provide free TB chemotherapy medicines for patients. At times, it was the LGU who provide funds (as long as it is included in the Annual Investment Plan/Work and Financial Plan by the Municipal Health Office) in order to provide continuous supply of TB drugs to patients in need. Therefore, all TB patients managed in any government health facilities are free
The next figure depicts a sample flow of funds from revenues collected from taxes among formal sectors and various sectors, land-based taxes, community activity-based taxes among others. The LGU IRA or Internal Revenue Allotment (or the share of an LGU from the national government) will then allocate portion to Municipal Health Services sector (Municipal Health Office). Usually, the
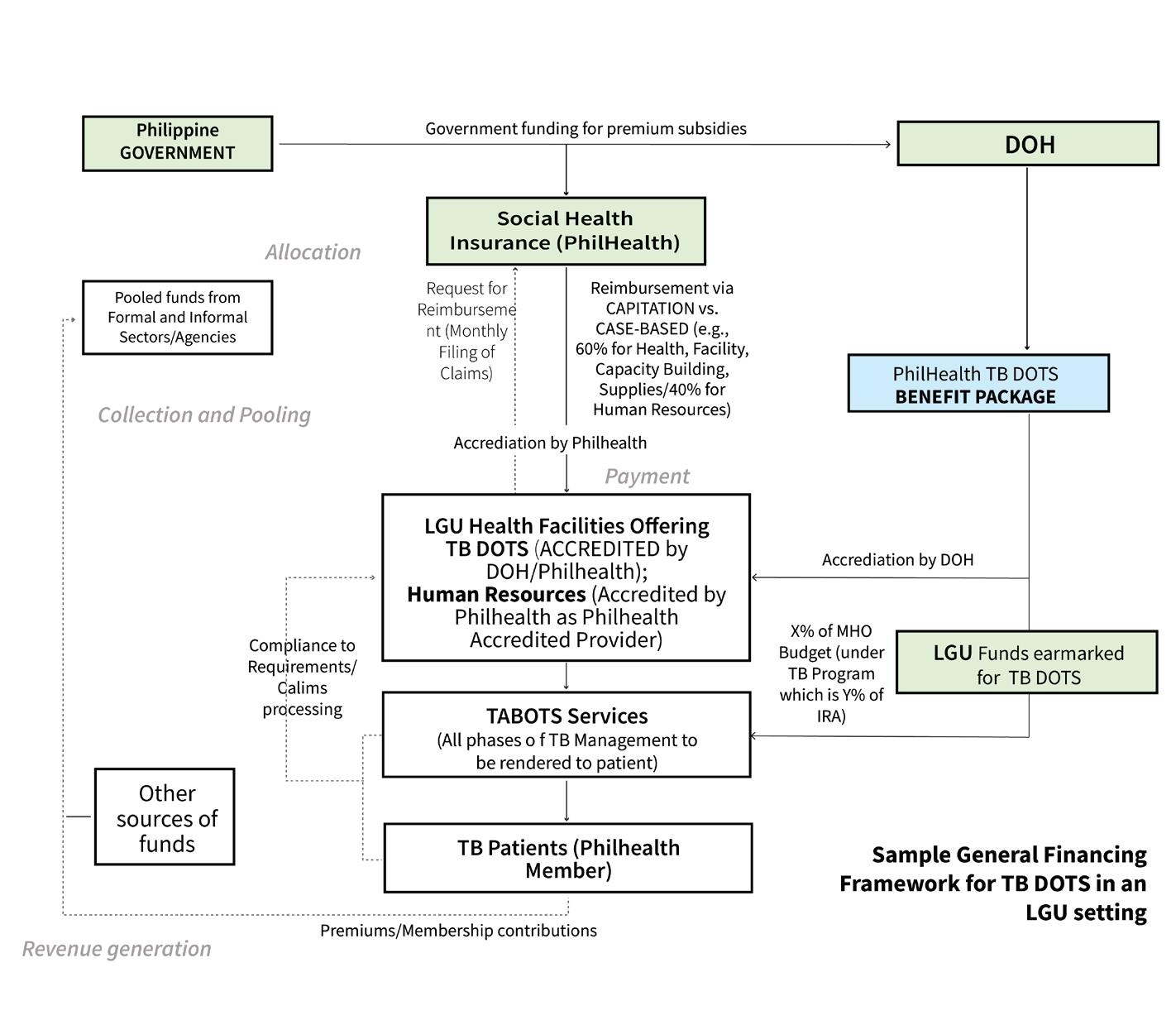
ideal allocation will be around 15-22% based on LGU Scorecard by the Department of Health. Some municipalities may not be able to allocate such percentage depending on the felt needs and prioritization by the LGU.
For instance, since some health facilities were already supported by Philhealth
64 Cultivare_INDD Ver_09212022.indd 64 21/09/2022 4:39:59 pm
Based on this example, the the accredited health facility offers Out-Patient Benefit package, Maternal and Newborn Care Packages, TB-DOTS, and Animal Bite services. Each health service corresponds to benefit package wherein the social health insurance pays or subsidizes the services. Meanwhile the expectant patient will receive free health care. Capitation funds and reimbursement of claims will then be received by the LGU and certain percentages will proceed to the LGU for reappropriation for future health facility needs. These funds were then reassessed, and the Municipal Health Officer will begin to create his/her budget plan and then attends the budget hearing to defend the request. Non-Philhealth members on the other hand still receive services; however, certain services will require fee in the form of user fees i.e., delivering a baby in the Rural Health Unit may require a certain amount (e.g., 2,000.00) to recuperate expenses spent by the LGU for the delivery of baby. This is a sort of regulatory mechanism to prevent the funds from being depleted due to series of availment by pregnant patients who are not
Philhealth members. The User Fee usually needs legitimacy and support via a Municipal Ordinance.
The fragmented set up of health care system makes these variations unique from one municipality to another. For instance, some municipalities were able to provide and allocate funds so that maternal deliveries regardless of Philhealth membership status, will be rendered for free. There is of course downside on this decision or policy, but in the end, all LGUs must adhere to the goals set by the national government as well as the rights-based principle of health for all. The current setting as regards health financing in a fragmented set up may damage the performance of all tasks and may further expand out-of-pocket expenditures depending on the degree of fragmentation.
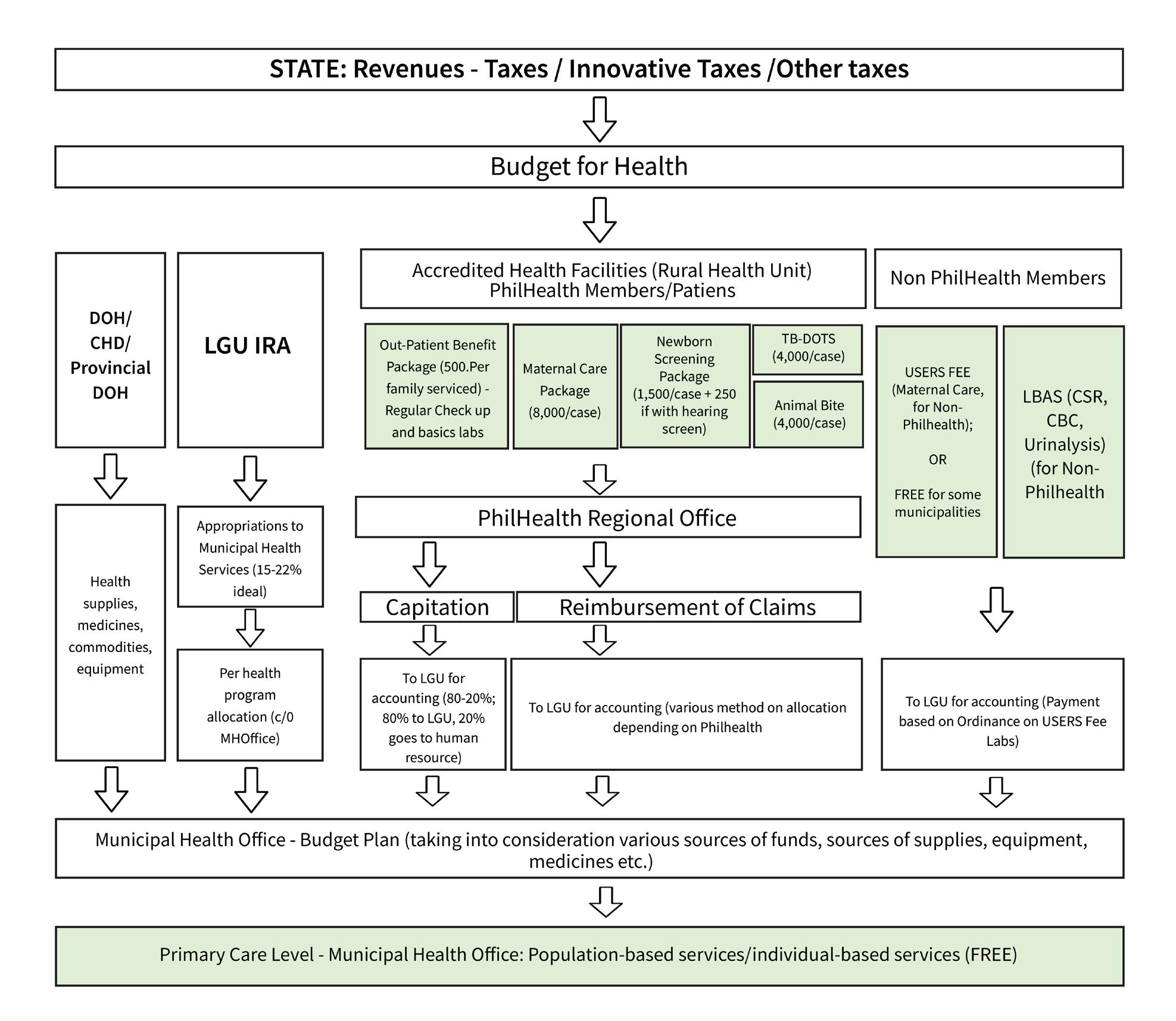
As I ended my DTTB stint, I realized how inadequate two years is for me to fully understand the schemes but at least, a glimpse of it is more than enough to understand that universal coverage is not the final solution to ensure universal health

care (UHC). There are many aspects of UHC that is way beyond the concept of ensuring all populations are covered by social health insurance. The need to center on our rights to health must not be missed at all times.
For all health care workers working in the community, continue your passion and let us understand the variations existing from one community to another. Not all have the same problems, same financing schemes, and same governance. Even if 2022 election is coming, health budgets and plans should be regularly reviewed and reassessed in coordination with local officials in the LGU and more importantly, should be aligned with our national goals of health for all.
Sample flow of funds from revenues to health services (free) by the Municipal Health Office.
65 Cultivare_INDD Ver_09212022.indd 65 21/09/2022 4:40:01 pm
Emerging crises in Philippine public health: multi-sectoral action needed
66 Cultivare_INDD Ver_09212022.indd 66 21/09/2022 4:40:03 pm
Miguel Antonio Salazar, MD MSc Dr.sc.hum.
The world is currently grappling with a multitude of emerging crises affecting the health of the global population. These crises are climate change, emerging zoonosis, antimicrobial resistance, and biodiversity loss to name a few. All these events have their respective health impacts. The Philippines is not exempt and like many island states, we receive much of the brunt of climate change effects such as storms, floods, and sea level rise. With industrialization and the continued expansion of human dwellings over farmland, swamps, and forests, Filipinos are continually exposed to possible zoonosis. And with our growing waste disposal problems, rivers and other water bodies are deepening the reservoir of antimicrobial-resistant organisms.
The climate crisis is being felt the world over according to the UN Secretary-General 1. The health impacts of climate change have been disproportionately affecting small island states such as the Pacific islands. These islands have experienced sea-level rise, flooding, tropical storms, and extremely damaging storm surges 2. Although the Philippines is not considered a small island state, it has the same vulnerability as these islands and has increasingly felt the impacts of climate change.
Our current predicament with the COVID-19 pandemic has put to fore the importance of zoonotic diseases on human health and health systems. In the past 30 years, the infectious diseases which have caused the most alarm to public health have been zoonosis, namely HIV, SARS-CoV, H1N1, MERSCoV, Ebola, and COVID-19 3. As the world has become globalized with a constant flow of goods and people across borders, diseases have been able to follow these routes as well. International air travel has played a big role in the spread of zoonotic diseases and has been a more prominent factor in this present pandemic 4.
While public fear and worry has been on the zoonotic diseases mentioned earlier, the silent pandemic of antimicrobial resistance has been raging in our health systems for years. But antimicrobial resistance is not only a health system concern but also of animal health, agriculture, food production, and environmental health 5. The path to solving this problem is through addressing social determinants of health such as nutrition and the environment, aside from health systems solutions. The particular concern in these social determinants is those pertaining to intensive and industrial livestock farming and environmental pollution 6,7. Wastewater from communities, healthcare facilities, animal,
and plant production, and pharmaceutical manufacturing if without proper treatment can be reservoirs of antimicrobial residues and antimicrobial-resistant organisms 8.

Biodiversity loss also affects human health as it promotes the loss of potential medicines, natural protective mechanisms against air and noise pollution, loss of environments that enhance mental health, and increased potential of zoonosis through increased interaction with wildlife 9. Another related concept is that of planetary boundaries. Biophysical indicators and societal indicators are being monitored in the planetary boundaries concept to assess the sustainability of having a high quality of life within what the planet can naturally provide 10. Exceeding these biophysical indicators exacerbates the planet’s capacity for homeostasis and increases the probability of environmental challenges like the climate crisis, biodiversity loss, and pollution.
Filipino public health colleagues must appreciate the current multi-sectoral approaches that support the health of humans, animals, and the environment. The first of which is One Health, the multidisciplinary and collaborative approach addressing concerns on all levels of governance to achieve the highest levels of health cognizant of the interconnection of humans, animals, plants, and the environment 11. Planetary Health on the other hand is defined as the attainment of the highest standard of health and wellbeing through understanding the roles of human systems, societal norms, politics, and economics affecting human life in the future and the natural systems of the Earth 12.
The concept of social determinants has hopefully been well ingrained in the consciousness of public health professionals, young physicians and medical students to factors outside of clinical medicine affecting health. The concepts of Planetary Health and One Health have the potential to further understand the complexity of interaction between the environment and our health.
To address these concerns affecting our global population today, public health professionals have to continue to break boundaries to collaborate with silos all around. To address these emergent health crises, public health specialists have to step up and demand the inclusion of more fields such as communications, engineering, biology, data science, and ecology.
Public health is a good base for this collaboration to be fostered. Public health has been a safe space for multi-disciplinary initiatives and projects to be started and
refined. We, public health physicians, have worked with and led multidisciplinary teams and mixed clinical medicine with policy. We have embraced mixed methods approaches to answer complex health system problems. Public health has already brought together disciplines such as policy, governance, economics, management, epidemiology, biostatistics, anthropology, communications, clinical medicine, and microbiology.
But aside from embracing different disciplines and professions, we also have to step out of our comfort zones and emphasize and advocate for the importance of health. This has already been espoused in the “health in all policies” concept. One example is the COVID-19 pandemic. In the Philippine scenario, the business has taken a larger slice of consideration in the all-of-government response. However, public health organizing has pushed for more emphasis to be put on health concerns as they have evidenced that economic recovery is intertwined with the success of public health measures and outcomes. The Healthcare Professionals Alliance Against COVID-19 or HPAAC has done this organizing and has advocated to different levels of government in the country. They have been successful in influencing policy although with pushback from a number of sectors and individuals.
Other initiatives have brought together multidisciplinary teams to address health concerns. For the COVID-19 pandemic in 2020, the Philippine Society of Public Health Physicians convened a consortium providing epidemic indicator monitoring services for COVID-19, Leading Evidence-based Actions through Data Science for Health Security and Resilience or L4H. L4H brought together expertise in computational biology, epidemiology, data science, statistics, engineering, risk analysis, governance, disaster management, and public health 13. In addition, Planetary Health Philippines, which was started in 2020, is a multisectoral initiative looking at advancing Planetary Health in the country using an intergenerational, inter-disciplinary, and international lens 14.
The harrowing problems like climate change, emerging infectious diseases, antimicrobial resistance, and biodiversity loss currently being faced by the country’s health system and environment only become simpler and easier to address if we work together. In this time of multiple health crises, more and more public health professionals have to take on different roles. These may mean leading multi-disciplinary teams or joining teams composed of individuals and groups
67 Cultivare_INDD Ver_09212022.indd 67 21/09/2022 4:40:05 pm
with multiple skill sets. Coping with different types of personas and backgrounds may be difficult. As public health physicians, more and more of us should develop the thinking, art, and skills in multi-sectoral collaboration such as coordination, communication, dialogue, negotiation, and management. PSPHP should hone public health professionals with adequate training in these arts and skills. The future is bright as the new generation of public health physicians are accepting these challenges and removing the siloes in problem-solving. They are merging different methods, disciplines, and practices to solve our country’s and our world’s greatest problems.
References
1. Milman O. António Guterres on the climate crisis: ‘We are coming to a point of no return’ [Internet]. The Guardian. 2021 [cited 2021 Oct 3]. Available from: https://www. theguardian.com/environment/2021/jun/11/antonio-guterres-interview-climatecrisis-pandemic-g7
2. Thomas A, Baptiste A, Martyr-Koller R, Pringle P, Rhiney K. Climate change and small island developing states. Annu Rev Environ Resour. 2020;45:1–27.
3. van Doorn HR. The epidemiology of emerging infectious diseases and pandemics. Medicine (Baltimore) [Internet]. 2021; Available from: https://www.sciencedirect. com/science/article/pii/S1357303921002036
4. Wilder-Smith A. COVID-19 in comparison with other emerging viral diseases: risk of geographic spread via travel. Trop Dis Travel Med Vaccines. 2021;7(1):1–11.
5. Centre for Science and Environment. The silent pandemic of antimicrobial resistance [Internet]. New Delhi; 2021. Available from: https://www.cseindia.org/content/ downloadreports/10832
6. Kraemer SA, Ramachandran A, Perron GG. Antibiotic pollution in the environment: From microbial ecology to public policy. Microorganisms. 2019;7(6):1–24.
7. Van Boeckel TP, Brower C, Gilbert M, Grenfell BT, Levin SA, Robinson TP, et al. Global trends in antimicrobial use in food animals. Proc Natl Acad Sci U S A. 2015;112(18):5649–54.
8. Food and Agriculture Organization, World Organisation for Animal Health, World Health Organization. Technical brief on water, sanitation, hygiene and wastewater management to prevent infections and reduce the spread of antimicrobial resistance [Internet]. Geneva: Food and Agriculture Organization World Organisation for Animal Health World Health Organization; 2020. Available from: https://apps.who.int/iris/ bitstream/handle/10665/332243/9789240006416-eng.pdf?ua=1
9. Marselle MR, Hartig T, Cox DTC, de Bell S, Knapp S, Lindley S, et al. Pathways linking biodiversity to human health: A conceptual framework. Environ Int. 2021;150(January).
10. 1O’Neill DW, Fanning AL, Lamb WF, Steinberger JK. A good life for all within planetary boundaries. Nat Sustain [Internet]. 2018;1(2):88–95. Available from: http://dx.doi. org/10.1038/s41893-018-0021-4

11. Centers for Disease Control and Prevention (U.S.). One Health [Internet]. 2021 [cited 2021 Jul 31]. Available from: https://www.cdc.gov/onehealth/index.html
12. Horton R, Lo S. Planetary health: A new science for exceptional action. Lancet [Internet]. 2015;386(10007):1921–2. Available from: http://dx.doi.org/10.1016/S01406736(15)61038-8
13. LEADS for Health Security and Resilience Consortium. LEADS for Health Security and Resilience Consortium: About [Internet]. 2021 [cited 2021 Jun 27]. Available from: https://covid19.psphp.org/?page=about
14. Guinto RR, Parungao-Balolong M, Flores RJD, Bongcac MK. Establishing a community for planetary health in the Philippines. Lancet Planet Heal [Internet]. 2021;5(7):e396–7. Available from: http://dx.doi.org/10.1016/S2542-5196(21)00140-6
68 Cultivare_INDD Ver_09212022.indd 68 21/09/2022 4:40:06 pm
DR. sajjadullah wazir: “an inspiration for public health”

Journey of a medical aspirant through medical school
 By: MAYMONA J. CHOUDRY
By: MAYMONA J. CHOUDRY
This is my tribute to one of my inspirations in my medical career as an aspirant for public and community health. To my beloved partner, and best friend, Dr. Sajjadullah Wazir. He has served as my motivation earlier this year during my struggles with burnout through my journey as a 3rd year surgical resident. His brilliance, kindness and loyalty has enlightened my ambition to continue in my journey and to pursue higher calling. There is a lot to be said, but I hope that this article will show my appreciation & gratitude for your kindness and love in bringing me out of the darkness and pessimism of my mind.
Every medical student undergoes a journey filled with struggles and adversities, this is especially true in countries where doctors are looked upon as highly respectable members of the society. But, due to its robust curriculum, medical school is not without its own difficulties.
Dr. Sajjad Wazir, was a final year medical student from Pak International Medical College (PIMC) in Peshawar, Pakistan. As a medical student, he has always shown his drive and ambition to learn and improve his skills as a doctor. This is especially true when he constantly exhibits his extensive and in-depth medical knowledge amongst his peers and professors. But in a country such as Pakistan, where medical students are constantly tested in the most robust and vigorous manner with multiple written examinations, OSCEs, vivas, and practical examinations in a short period of time. Dr. Sajjad paved his path into becoming a doctor
Journey through medical school Medicine: from a new perspective
with a keen sense of diagnosing and managing patients. Even when he was a student, several members of his community have sought consults with him with regards to their medical condition, sometimes through informal consults. He has always demonstrated a good clinical eye, in his diagnosis and management of these patients.
At the start of this year, as a 3rd year surgical resident, I have been experiencing a lot of negative emotional effects due to the COVID-19 pandemic. It was in March of this year, when I felt overly exhausted, and started experiencing burnout. As
“Yesterday I was clever, so I wanted to change the world. Today, I am wise, so I am changing myself” –
Rumi
69 Cultivare_INDD Ver_09212022.indd 69 21/09/2022 4:40:06 pm
the days went by, I kept on thinking of quitting the career that I love so much. But my encounter with Sajjad has changed my perspectives and outlook in life. We met in the most unexpected circumstance, and as days went by, my pessimistic views were replaced with kindness, optimism and hope. Sajjad has expressed his fascination and love for medicine, and the medical field based from his interactions with several members of his family that are also part of the medical community. And as I listened to his stories and experiences, my love for medicine was renewed as I began to see medicine through his eyes. One of the stories that he shared with me was his emotional and heart-warming experience as a young doctor, when his nephew was born. Despite all the adversities and challenges, his nephew, Muhammad bin Qasim survived to become a playful and healthy boy.
Aspirant of Public and Community Health Medicine



Early on in our medical careers, doctors build professional affiliations even before their graduation from medical school. As medical students, we build networks and connections amongst our peers and professors that will eventually strengthen our connection to the medical community. Doctors play an important role in the community, and society. One of the skills that are being taught is how to establish rapport and trust; and communicate with patients, and colleagues.
As for myself, as an Atenean graduate, public and community health medicine has been ingrained into us, even as medical
students. During my community exposure, I have seen all aspects of public and community health, from doing house-to-house surveys to establishing community programs and creating ordinances. And meeting new people along my journey have enhanced my learnings and perspectives in public health. Dr. Sajjad is an example of a professional who practices public health early in his career, through his numerous interactions and collaboration with other individuals and colleagues. He has been one of my aspirations in my career, and his experiences have reminded me that the ultimate goal of becoming a physician, is not the worldly gains and fame, but rather it is the connection and trust that we build with people that come to us for help.
About the Author:
Maymona J. Choudry, MD, MPH 3rd Year Resident Department of General Surgery Vicente Sotto Memorial Medical Center
70 Cultivare_INDD Ver_09212022.indd 70 21/09/2022 4:40:08 pm
The Role of a Protestant Church in Community Medicine:
Abstract
Studies have shown that the church can help address many community and public health issues. A study in 2012 by the National Council of Churches in the USA found that 93% of churches surveyed have health ministries. These health ministry’s help augment the health services, or the lack thereof, provided by the government. The World Health Organization reported that Philippines ranks 162nd among 193 countries surveyed in terms of general government expenditure on health as percentage of total government expenditure. A 2009 report by IBON showed that only 28.7% of the health expenditure for Filipino Families comes from the Government sector while 59.1% comes from private sources. One of the most important private sources are NGOs which includes churches. A research published by the American Journal of Public Health in 2004 showed that faith-based health programs improve health outcomes where most health programs focused on primary prevention (50.9%), general health maintenance (25.5%), cardiovascular health (20.7%), or cancer (18.9%). Primary prevention is the most common health program by churches and they have significant impact in reducing the risk of developing a disease.
We made a study that aims to determine the programs of the different local United Methodist Churches in Manila that are related to health promotion and disease prevention. The study identified all organized local United Methodist Churches in the City of Manila and administered a validated questionnaire answered by their designated church leader. Descriptive statistics was used to analyse data. Results showed that these churches are led mostly by pastors with post graduate Master of Divinity degrees, most churches have membership of >130 members with some members being health care workers. Most of these churches are more than 10 years old and while they have no specific budget
for a health program they reported that it is incorporated in the budget for outreach ministry. Results also showed that 9 of 10 churches have primary health care programs on health promotion and disease prevention which is very encouraging. Results also showed that at that time none yet had immunization programs, only 50% have BP monitoring activities or exercise programs, only 40% have health screening activities or health education activities (RH Bill, HIV Awareness, etc.), while only 20% have other primary health care programs like food supplementation or feeding, and nutrition programs.
The most common health programs are BP monitoring and physical exercises or sportsrelated programs. The usual target populations for the primary health care activities are both church members and non-church members. These programs are done infrequently and irregularly if not once a year. The most common frequently done is BP monitoring done monthly while the second most common is Health Screening and Health Education which is done once a year. These health programs are offered to the community totally free but interestingly there are only 21-50 participants per activity. The health activities involves health professionals who serve as volunteers and they are mostly nurses.
In conclusion, it is inspiring that most churches have health programs. These churches already offer holistic care although their health programs can have more emphasis on health promotion and disease prevention. The ministry and work of the Christian protestant churches can go a long way if they can strengthen their health ministry so they can make a greater impact in augmenting the deficient primary health care services in our community.
The Contribution of United Methodist Churches in Manila in Disease Prevention and Health Promotion
71 Cultivare_INDD Ver_09212022.indd 71 21/09/2022 4:40:08 pm
United Methodist Church in the Davao Episcopal Area: Kalusugan Ministry
Jesus Christ is a public health practitioner.
The United Methodist Church in the Davao Episcopal Area (UMC-DEA) is following his steps. The Davao Episcopal Area covering Visayas and Mindanao is under the episcopal leadership of Bishop Rodolfo Juan. The holistic ministry thrust of the UMC-DEA has emphasis on Kabuhayan, Kahirapan, Kalikasan, Komunikasyon, Karunungan, Kapayapaan, and Kalusugan, aptly called the “7K Ministry Programs.” The Kalusugan ministry of the UMC in Davao is focused on addressing public health concerns.

The increasing cases of HIV among the youth is one of the public health concerns being addressed by the UMC-DEA Kalusugan ministry. It has partnered with local NGOs, HIV Advocacy Groups like BisDak, Pinoy Plus, and government agencies in implementing HIV Prevention programs. The Global Health office of the United Methodist Church funds and supports the implementation of most of the programs. It has also partnered with local churches in the Davao Episcopal Area to include HIV Programming in its regular church activities.
The UMC-DEA Kalusugan ministry works in collaboration with health workers and volunteers. The UMC-DEA have designed the Tigbansay training program to address this pressing concern. The Tigbansay is a group of peer educators trained by the DEA Health Board in partnership with the National Council of Churches in the Philippines. This is our contribution in public health specifically in HIV. One of the focus of their work is in reducing the stigma, shame, denial, discrimination and misinformation to the People Living with HIV. The Tigbansay is now established as a community-based program to sustain this HIV Awareness ministry.
HIV is a complex health concern that needs immediate attention. When the program started in 2018, there were 912 recorded new cases of HIV in the Philippines. As of March 2021, there are 1,041 confirmed HIV-positive individuals in the country. There remains to be an alarming increase in the number of HIV and AIDS among the youth with 30% of them 15-24 years old at the time of testing. So the Tigbansay program focused on the youth. Among the youth infected at that time in 2018, 457 (3%) of the cases were through sharing of infected needles. These are alarming realities that the church must actively be engaged to address. While much attention has been given to sexual contact as the topmost mode of transmission in HIV, there is a need to also address the increasing number of Injection


Drug Use (IDU) to help prevent the spread of HIV in the country. This is where the church wanted to focus – the youth.
Tigbansay is the UMC-DEA version of youth peer educators. Peer support and positive peer pressure has been recognized as one of the influencers in shaping human behavior.

There are many peer groups including youth, women, LGBTQ and they have been efficient in delivering key messages amongst them. The youth is one of the populations at risk for HIV infection in the Visayas and Mindanao. HIV transmission in the Visayas among the youth is through substance abuse.
Women are another vulnerable group for HIV infection. Lack of awareness among women in the far-flung rural areas makes them atrisk for infection. The church understood the importance of peer education thus the focus to partner with the youth and women sector in implementing this ministry.
The objective of the Tigbansay program is to facilitate HIV awareness for target communities, particularly young people. Specifically, its goal is to increase access to HIV counselling and testing services for
target communities by training Tigbansay for community-based testing, ensure that those who are HIV positive have access to ARV treatment and promote and/or provide accompanying healthcare, psychosocial and other necessary support.
The Tigbansay activities include: Peer Educators Training or the Tigbansay, HIV 101 Awareness Forums, Community Celebrations (i.e. World AIDS Day and AIDS Candlelight Memorial Day), Community Based Screening, partnership with Treatment Hubs (MOU), referral to Treatment Hub, medical assistance for regular diagnostic tests, conduct of livelihood trainings and assistance, and psychosocial support and care fellowships. At the end of 2020, the Tigbansay ministry was able to achieve the following: Trained 33 “Tigbansay,” more than 250 (Peer Educators) trained, more than 3000 individuals reached by HIV Awareness activities especially the youth sector, more than 1,500 young people screened for HIV and at least 15 PLHIV assisted for care. We have also engaged more than 319 participants for Mental Health Awareness at this time of pandemic.
72 Cultivare_INDD Ver_09212022.indd 72 21/09/2022 4:40:11 pm
Moments with the Founding Chairman of PSPHP Dr Luisito “Chito” Ruiz
By Lester Sam Araneta Geroy 24 October 2021
every meeting. The initial discussions focused on SEC Registration that was processed by Ms Edlyn of AIHO, and the organization’s Vision, Mission, Description and Values. Thanks to the support of AIHO, under the then Executive Director Dr Kathy Reyes, for supporting the admin side of PSPHP’s development.
I first met Doc Chito in Alabang sometime in February 2017. Initial meetings and discussions on forming a Society had already started spearheaded by a group of around 30 colleagues mostly from AIHO and the Inception Group that was formed back in 2013. Dr Ruiz began to realize that public health practitioners were also credible and very qualified, with many of us European scholars and had studied abroad.

“You are also specialists,” he would emphasize. “Public health is your specialty and it is something that many of us do not know.” The more he met us, the more he appreciated the richness and depth of our practice, knowledge and skills.
Dr Ruiz offered his conference room in Ruiz Building, El Grande Ave., BF Homes, Parañaque, for the first election of the Society in May 2017. That was also when we finalized the Society’s name as the Philippine Society of Public Health Physicians (PSPHP). He became the Founding Chairman of the Board, and I had the privilege to be the first President.
Through the months, I had the privilege of being the liaison or bridge of ideas, advice and directions from CLR to the rest of the Board and Execom. I had easy access to his office because I was also from Parañaque. And because I was a freelance consultant, he could easily meet me for appointments and meetings, including submitting initial documents to the Philippine Medical Association. Many of the activities were achieved with support from Ms Sherry Sajol who was then Dr Ruiz’s Executive Assistant. We had meetings in Makati, in Magallanes and Parañaque, areas that are close to his investments. It was then that we became friends and he became my mentor, especially in terms of business and organizational development.
CLR came from Lian, Batangas. From elementary school until high school, Luisito was a consistent honor student. Planning initially to become a lawyer like his father, he took Political Science at the University of the Philippines. He eventually decided to go into medicine and shifted to General Science at the University of the East. He completed Doctor of Medicine at the University of the East Ramon Magsaysay Memorial Medical Center (UERMMMC) in 1985. He trained as a surgeon at Veterans Memorial Center in Quezon City. He took courses in occupational medicine and family medicine/ primary care, which enabled him to get a good grasp of medicine in different settings including communities. He went through an executive course in Hospital Administration in UP Manila and finally completed MSc in Health System Management at the Philippine Women’s University.
experience in organizational management and working with people. He is hands-on in the management of his medical clinics and other businesses. He had a good grasp of building partnerships as experienced with health partners and pharmaceutical companies in different countries including Japan, Korea, Thailand, Taiwan, Denmark, France and Spain.

I remember vividly how he told us about his life as a young doctor. How we worked hard as a surgeon to save resources so he could invest. Those were the late 1980s and early 1990s. Life was not very easy. There was no PhilHealth yet. Even in hospitals, payments can come in kinds like chicken, sacks of rice and fruits. What a doctor gets was based on what he does. His was a life of hard work 24/7. Through planning and saving, he invested in real estate as a young man to sustain him later. And that started his years of going deeper into business, investments and properties.
Chairman Luisito Ruiz or CLR guided the organization’s development in the next few months. That was when I slowly began to know him. In those days, we were meeting at the GIZ Office (of PSPHP Vice President Johann Leonardia). CLR was there in almost
He had a strong public service profile as a surgeon and hospital manager. His experiences as a leader, manager and influencer have been strong through the Association of Hospital Administration, Muntinlupa Medical Society, Philippine Medical Society (as Board of Governors) and Rotary Club among others. He was Hospital Director of Ospital ng Muntinlupa for several years. He has been and continues to be a Board Member of several organizations and hospitals, which explains his depth of
It was touching when he told us how he also got very sick for months. Illness can be scary, especially for a man whose work depends on his health. He thought he would die, and he really pleaded for God to save him. And God healed him. “Don’t forget God,” he emphasized. “In the end, whatever we do, He can take everything away. Our very lives depend on him.” In our meetings, he emphasized, “God first. Then country and helping people.”
In time, I was able to see and understand several of CLR’s business portfolios including clinics, laboratories and in the distribution of biologicals. I was even able to meet his family. I also got familiarized with his charitable works such as sending out of school youth for education.
“When we were in college and medicine, many

73 Cultivare_INDD Ver_09212022.indd 73 21/09/2022 4:40:13 pm
of my classmates would join rallies,” he would say. “But now, I show them how I contribute to national development as an entrepreneur, investor, leader and manager. In the end, people need respectable jobs.”
On behalf of PSPHP, I thank Dr Luisito for his strong support, especially in those times when we didn’t have many resources and PSPHP was still a newborn baby. The first Board, Execom and Secretariat would know the extent of his donations just so the organization could kick-off and start.
I take it a privilege to be mentored as a doctor-entrepreneur. I wish I had known him ten years earlier. It would have created even a greater impact. But most of all, I appreciate his perseverance, devotion to God and his commitment to serve in a sustainable way. “We need to leave a legacy,” he said when we just started the Society. I wish CLR more blessings and success in his endeavors!
The Oplan Kalusugan sa DepEd: Reinforcing the Promotion and Implementation of School Health in Support of Filipino Learners
By Lester Sam Araneta Geroy 24 October 2021
By Lester Sam Araneta Geroy Chairman of the Board of Trustees of PSPHP 2021-2023
Research over the years have shown the strong link between education and health, suggesting that healthier children tend to learn better and become healthier adults later on. Given that learners spend a third of their day in schools all over the country, schools are crucial settings for promoting the health of school-age children. In recognition of the strong relationship of health and learning outcomes, the Department of Education (DepEd) has put in place school health and nutrition programs in order to promote and provide Filipino learners with sustainable holistic development and improve learning delivery.
The DepEd School Health Division
The Bureau of Learner Support Services (BLSS) is the office that develops the national framework for all learner support services and issue policies and standards to guide the programs for the holistic development of learners that complement the curricular offerings. Under this office is the School Health Division (SHD) which is an integral part of the total school program by providing nutrition support to learners, a healthy school environment and medical/dental health management.
The Oplan sa Kalusugan sa DepEd
The Oplan Kalusugan sa Department of Education (OK sa DepEd) is a convergence of DepEd’s health programs, plans, policies, and activities for their effective and efficient implementation at the school level, in partnership with various stakeholders. It focuses on DepEd’s major school health and nutrition programs specifically the SchoolBased Feeding Program (SBFP), National Drug Education Program (NDEP), Adolescent Reproductive Health Education (ARH), Water, Sanitation, and Hygiene (WASH) in Schools (WinS), Medical, Dental, and Nursing Services, and the School Mental Health Program. Other health and nutrition programs continue to be implemented in support of these flagship
programs.

▷ The School-Based Feeding Program primarily aims to contribute to the improvement of classroom attendance of beneficiaries to more than 85% per annum by providing hot meals to undernourished learners and meet the 1/3 of the recommended dietary intake based on the Philippine Dietary References Index (PDRI). The program is also utilized as an avenue for the development of health and nutrition values and behavior among learners. It covers all undernourished learners severely wasted and wasted from Kinder to Grade 6 in all public elementary schools.
▷ The National Drug Education Program in schools aims to raise the consciousness of learners on the perils of the use of illicit drugs through Curriculum Instruction; Co-Curricular and Ancillary Services; Teacher/Staff Development; Parent Education and Community Outreach; and Research, Monitoring and Evaluation. Also part of the NDEP is the Comprehensive Tobacco Control Program which also has information campaigns on the ills of smoking, tabacco control policies in schools (e.g. smoking bans, interventions).
▷ The Adolescent Reproductive Health Education is a program that aims to strengthen DepEd’s delivery of its mandates under the Responsible Parenthood and Reproductive Health Act of 2012 (R.A. No. 10354) through guidance and counseling programs and works with the Bureau of Curriculum Development in line with the integration of Comprehensive Sexuality Education.
▷ The Water, Sanitation, and Hygiene in Schools (WinS) Program is designed to achieve learning and health outcomes and improve school attendance of learners through a comprehensive, sustainable, and scalable school-based water, hygiene, sanitation, and deworming program. It involves promoting proper lifelong WASH behaviors; ensuring the availability of safe water, adequate toilets, and hand washing facilities; and promoting a clean and safe environment through school-
74 Cultivare_INDD Ver_09212022.indd 74 21/09/2022 4:40:14 pm
based solid waste management, proper drainage, the elimination of breeding grounds for mosquitoes to prevent vectorborne diseases, and food sanitation. The program is monitored through an Online Monitoring System that benchmarks the attainment of the national WinS Standards through a 3-Star Approach.



▷ For Medical, Dental and Nursing Services, the focus is to ensure the availability of medical and dental supplies, personnel such as doctors, dentists, and nurses, and clinics in selected schools, in order to promote, protect and maintain the health status of learners and school personnel through the provision of various health services such as health appraisal, emergency treatment, consultation, and referral among others. The School Dental Health Care Program (SDHCP), in particular, improves the health status of all learners by providing oral hygiene knowledge and decreasing the prevalence of dental caries and other oral health problems that impacts the teaching-learning process.

▷ For the School Mental Health Program, BLSS-SHD is working with concerned bureaus and offices to ensure the fulfilment of DepEd’s mandate on mental health promotion in schools, under Republic Act 11036 or the Mental Health Act, particularly in raising awareness on mental health issues, identification and provision of basic support and services for learners at-risk, and facilitating access, including referral mechanisms of learners with mental health conditions to treatment and psychosocial support. These pillars are the foundation of the OK sa DepEd and work hand-in-hand to provide support to learners in the school and in the school community.
Delivery School Health Services in the Pandemic
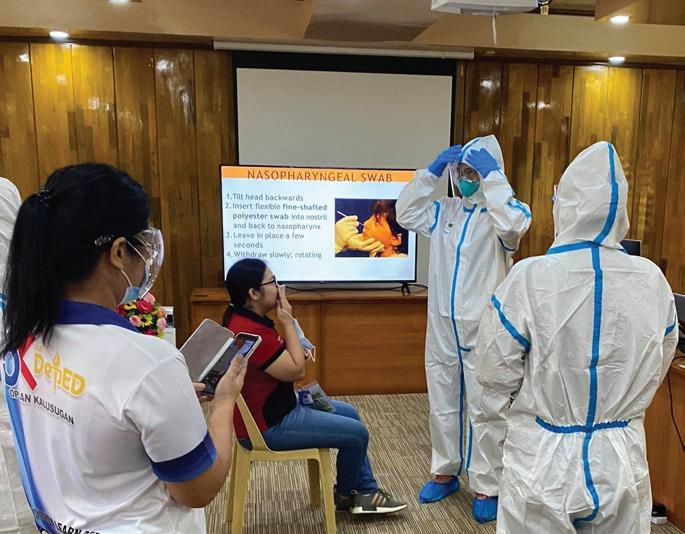


In the pandemic, there have been challenges to the delivery of health and nutrition services in schools. Nevertheless, measures have been undertaken despite the physical closure of schools to continue providing these services to learners. To cite an example, the WinS program developed materials in support of Covid-19 Infection Prevention and Control, conducted online trainings, and provided WASH data in support of preparing schools to comply with health standards required for continued operations and eventual reopening. In the delivery of services in the pandemic, teachers, school health personnel, parents and communities worked together to support the continued delivery of health services for the learners.
 SBFP Delivery and Distribution following DO 14, s. 2020
Valencia City Division Orientation of Parents on SBFP and Packing of Nutritional Packs (Breads and Fruits) and Distribution of Milk Products
SBFP Delivery and Distribution following DO 14, s. 2020
Valencia City Division Orientation of Parents on SBFP and Packing of Nutritional Packs (Breads and Fruits) and Distribution of Milk Products
75 Cultivare_INDD Ver_09212022.indd 75 21/09/2022 4:40:15 pm
Innovations for Community Health
76 Cultivare_INDD Ver_09212022.indd 76 21/09/2022 4:40:16 pm
Authors: Jason V. Alacapa, Reiner Lorenzo Tamayo
vision of TB elimination.
We live in an ecosystem where new service delivery models and modes of thinking continuously revolutionize health care. This served as a breeding ground where technology and innovation in health care have grown. In 2019, Innovations for Community Health, Inc. (InnovationsCH), the country’s first hybrid global health deliveryresearch organization, was born with only a handful of hardworking people.
Today, with more than 150 passionate individuals from various backgrounds, InnovationsCH is at the forefront of developing cutting-edge health infrastructure. Our goal is to increase the availability and quality of health services in underserved areas in both rural and urban areas. We use gamechanging health market innovations and public-private collaborations to address global health delivery gaps by leveraging process and technology innovations. Using implementation science and research, we generate evidence that will help transition pilots to full scale-ups and achieve greater impact.
Despite only being in existence for two years, the organization has received over fifteen grants, and the majority of which have come from international organizations such as the Stop TB Partnership, USAID, The Global Fund, Resolve to Save Lives, Foundation for Innovative New Diagnostics (FIND), and the World Health Organization. We have cultivated strong partnerships with the Department of Health, the National TB Program, local government units, professional societies, and development partners.
Kalinga Health
True to our mission, we continue to create innovative health delivery solutions such as Kalinga Health, our flagship project. The project pilots a hub-and-spoke social enterprise model wherein Kalinga Health acts as the “hub” where a network of private providers (“spokes”) refer patients through a variety of public-private mix (PPM) strategies. These patients would then be able to avail themselves of the services offered by Kalinga Health. Additionally, the Hub acts as an intermediary agency for case registration, reimbursement of public and private health insurance, and treatment support for referral partners in the private sector (Spokes). A core innovation is reforming health markets and creating opportunities for incentivization of providers towards achieving the long-term
This year, our Kalinga Health project was selected third place in the search for the Gelia Castillo Award for Research on Social Innovations in Health (GCARSIH). This nationwide search was organized by the Social Innovations for Health Initiative (SIHI) and the DOST - Philippine Council for Health Research and Development (PCHRD). This award serves as a good validation of our growing experience and expertise in health research, private sector engagement, and innovation.
Agile, young, and passionate team
InnovationsCH is unique in that it recognizes its culture as a key competitive advantage. Our values, abbreviated as PASSION - Professionalism, Agility, Service, Sustainability, Innovation, Openness, and Nation-Building - drive both our top-down and bottom-up culture. As we navigate complex health challenges, these principles guide our young and vibrant team. InnovationsCH acts as a training ground for future public health leaders-nation-builders, which is why the vast majority of our employees are under 30 years old.
All these are made possible by the Central Management Team’s leadership, which is made up of seven individuals from various backgrounds. The majority of them are 30 years old or younger, with the youngest being 23 years old. They serve at the heart of the organization, not at the top; hence the term “central” management. Because of the team’s diverse backgrounds and expertise, InnovationsCH looks at problems from a variety of perspectives, innovates, and delivers out-of-the-box solutions to our longstanding problems in health.
From passion to innovation
Our accomplishments in the last two years highlight the roles of leadership, community participation, and meaningful partnerships in shaping innovative implementation strategies. We commit to constantly harness the power of translating passion into action to create sustainable community health - at scale.
For many, the road to sustainable health is quite long. But, together with you, we can capitalize on our collective purpose and passion to help shape high-impact health innovations and change the lives of millions of people around the world.
Contact us
To know more about us and what we do, you may visit our website and social media channels:
• Twitter: @innovations_ch (https://twitter.com/innovations_ch)
• LinkedIn: https://www.linkedin.com/company/ innovations-for-community-health
• Facebook (InnovationsCH): https://www.facebook.com/ InnovationsCH.ph
• Facebook (Kalinga Health) https://www.facebook.com/ICH. KalingaHealth
• Website: www.innovationsch.org
You may also reach: Jason V. Alacapa, MD, MBA, MHM, MPH Econ, DrPH ImpSci (c) Co Founder and Chief Executive Officer Email: jason.alacapa@innovationsch.org
From passion to innovation: Building a laboratory of future public health leaders-nation builders, creating sustainable health at scale
Humble beginnings
77 Cultivare_INDD Ver_09212022.indd 77 21/09/2022 4:40:18 pm
Title: Leishmaniasis
In the middle of the desert was a boy With big belly and protruding eyes Once a herder like his father, but also A lad with simple joys.
Bitten by sandflies months before Now his spleen and liver as big as a softball
He shivers like fire burning wood His arm was red on the MUAC* tape measure.
As he puts the cup of F100 milk to his mouth I stared at his eyes empty of the joys When he could still play with the goats
The milk must have tasted weird Wondering from what kind of animal it came Maybe it was brought by the white men
He took drugs that made his urine orange
His weight did not change and he continued to deteriorate When lab results came out that says “leishmania” Months have already passed, his father was Weary, tired and worried of the cattle and other kids
One morning his bed was empty Family fled accepting his fate In few weeks he will succumb to death How many more kids will suffer from diseases of poverty?
*MUAC (Mid-upper Arm Circumference)screening tool for acute malnutrition F100 - therapeutic milk product to treat severe malnutrition
Somali Region, Ethiopia 2006 Therapeutic Feeding Center, Medecins Sans Frontieres
"
78 Cultivare_INDD Ver_09212022.indd 78 21/09/2022 4:40:18 pm
Nasilayan kita sa isang kama Sa ospital ng bayan Namumula ang mukha Nababalot ng muta ang mga mata Sa edad na tatlo Dapat sana ay naglalaro Pero heto nakikipaglaban Sa sakit na pwedeng maiwasan
Limang buwan nang iwan ng ina Upang makipagsapalaran sa gitnang silangan Nabuntis, iniwan Sa murang edad na labing-siyam Ni hindi umabot sa mataas na paaralan Nagpalipat-lipat ng tirahan Upang takasan ang nagpuputukan Dahil sa prinsipyong ipinaglalaban
Kaya ikaw ay lumaki sa abuela Sa liblib na baryo, mabibilang ang dampa Mula maliit ay di nakatikim Ng bakuna, bukod sa oral polio vaccine Na pinatak ng bakunador na nag-ikot Taon binilang bago serbisyo naiabot Tuwing may sakit herbal na gamot ang gamit Pamasahe pa lang, kulang at gipit
Ngayon temperatura ay mahigit kuwarenta Naka antibiotiko dahil sa pulmonya Umaasa ang doktor na gagaling ka Sabi ni lola “Bahala na si Allah”
Tigdas (Measles) Cotabato Regional Medical Center February 2020
"
79 Cultivare_INDD Ver_09212022.indd 79 21/09/2022 4:40:18 pm
A Nurse’s Adventures to Life
80 Cultivare_INDD Ver_09212022.indd 80 21/09/2022 4:40:20 pm
Lesssons from the Orient To The Occident
Miguel Antonio Salazar, MD MSc Dr.sc.hum.
While thinking about where to start, I encountered this interesting quote that summarises my journey and adventures in both health and life. Reflecting on such escapades and learning from them broadens my perspective, slowly defines who I am and who I want to be.
“Travel changes you. As you move through this life and this world you change things slightly, you leave marks behind, however small. And in return, life – and travel –leaves marks on you. Most of the time, those marks – on your body or on your heart – are beautiful. Often, though, they hurt.”
Anthony Bourdain
Driven by personal reasons and professional mandate, I (as a neophyte nurse a few years ago) tried to gain needed experience to help me land a better job in other countries. Although I gained various experiences in different settings, I did not land a nurse job overseas as I did not have enough clinical (hospital) practice mandated by employment agencies at that time. Frustrated, I decided to continue my international health diploma (DIH) studies in 2013 at the UP Open University whilst working. Fortunately, I was able to get a good scholarship (after 2 tries) to help finance my studies, though it lasted only for a semester (due to constitutionality issues raised from fund sources) in 2014. In hindsight, I did not expect this programme opened several least-expected opportunities and the start of a more colourful roller-coaster ride of my life.
After a couple of conversations with Dr Gerlinda Lucas (my DIH classmate and soon-to-be employer for 4 years), I was invited to volunteer in October of 2014 at an international NGO where she manages based at an unheard place for me in the Kingdom of Wonder: Battambang. The worksite is a key hospital that caters to orthopaedic, trauma, and mine injury victims in (Northwest) Cambodia. A couple of months and a proposal later, I was offered my very first contract as an OFW and as a Nurse Educator. Excited to impress, I implemented my proposed plans for the nursing staff. With the help of my colleagues and feedback from management, I stepped back, reassessed the entire situation from another perspective, and adapted to match their needs. Since then, I was able to cultivate and sustain meaningful relationships with senior leaders and staff, to deliver a variety of lessons and topics. Over the next months, interesting adventures happened on top of my work. Some of those include local and international
volunteers and placements; participation in a randomised clinical trial; information exchanges with other health and professional agencies in Cambodia; community mobile clinics; a lot of social gatherings; and solo travels (with temple hopping) to several places. I had a unique chance to meet some of my DIH professors (Dr Don Prisno-Lucero & Dr Lester Geroy) as well as international and national lecturers and professionals. Aside from these, meeting vibrant and diverse Khmer and expat communities during my stay made my first ever overseas experience bearable and less homesick. If someone will ask me one of my most memorable highlights here in Cambodia, it would be the medic duty done for a movie produced by an international star! Albeit the missed opportunity to see her partner, the behind the scenes and a group photo with her (even one of our staff had a selfie with her) is more than enough for a simple person like me.
In February 2016, Dr Lucas and I went to meet the staff and Former Dean of the Faculty of Nursing Sciences at the University of Health Sciences in Vientiane, Lao PDR (UHS-Laos) to discuss cooperation opportunities including a scholarship programme for their staff. UHSLaos is the country’s dedicated institution for health professional training. Eventually, I accepted a secondary role to facilitate the scholarship programme of the Foundation’s scholars. For the next three years, I frequently travelled between Battambang and Vientiane to discharge my roles. Despite challenges, there were also opportunities to observe and participate in several activities, including

visitation to district hospitals, health centres, and museums; guest teaching to nursing and public health students; student military training; homestays; and a lot more. Some of my most memorable memories in Lao PDR include the different activities I had with the scholars; a chance encounter with Miss Laos 2016; and being invited to several Basi ceremonies. A vital rite in Laotian culture, Basi ceremonies unite the family or the community in times of joy and sadness. As a foreigner, I felt humbled and honoured for families to invite me into their homes and to participate with them. I also had the opportunity to celebrate Pii Mai and Choul Thnam Thmey which were the Laotian and Khmer new year, respectively with tons of water and powder (and beer in moderation) to share. Further, I encountered interesting details that were a bit peculiar at first but were able to get the reason after gaining some perspectives from their end. These made me understand how key historical events, culture, and society all are connected to the societal health we have today, even to those who have no voice at all. All these accumulated experiences widened my perspective as a health professional, which drove me to further advance my studies in public health.
In an unexpected twist, I got admission and even a scholarship to complete my public health studies under the 2-year European Public Health (EPH) Masters Programme from 2019. Under this scheme, one is given a chance to study in 2 different countries depending on your chosen specialization

and language. I studied at the University of Sheffield’s School of Health and Related Research, UK, and the Institute of Public Health of Uniwersytet Jagiellonski Collegium Medicum, Poland under the English track specialization “Governance of Health Systems in Transition”. EPH trains an individual with strong academic rigour under an interdisciplinary, multilevel perspective approach. Apart from studies, I became involved in several activities such as joining talks and sharing my experiences; being appointed as an academic representative for my cohort, and secretary to a university WHO simulation organization. Aside from this, I had a chance to visit London and the Scottish Isles in the UK, and Zakopane and Warsaw

81 Cultivare_INDD Ver_09212022.indd 81 21/09/2022 4:40:21 pm
in Poland to name a few; and experience their cuisine from these areas. Through here, I was able to share and learn various perspectives in health (and life) from a diverse and multicultural community. Recently, I passed my oral exam; successfully defended my thesis; and graduated with a double degree in Public Health.
At this point, my journey led to three key lessons. First, continue to have an open mind. Despite advances, there are still things unknown. Second, there is always a lesson to learn at every adventure, thus appreciate all with gratitude. Finally, always expect the unexpected. Recalling a message from one of my nursing instructors, Ma’am Ruthelma Tingda, my journey was indeed a “road less travelled”. These lessons and experiences led me to be grateful for everyone (and everything), and aware that there are things I still do not know. I always remember this quote whenever I completed something, “Marami pa akong kakaining bigas.” As a nurse and a public health professional, I still have a long way to go but I am happy contributing towards better population health, development, and its understanding.
TRAUMA/RESILIENCE-INFORMED SYSTEMS LENS : A SHARED LANGUAGE TO NAVIGATE COLLABORATIVE MENTAL HEALTHCARE TRANS-PANDEMIC AND BEYOND
 By Helen S. Sigua, MD, DrCOMM, IDMHHRL, MHA, BFEF
By Helen S. Sigua, MD, DrCOMM, IDMHHRL, MHA, BFEF

PANDEMIC AS A TIPPING POINT
This pandemic has indeed streamlined processes in health care. It has reduced our systems lenses into 2: micro (individual & family ) and macro (community and society). This disaster is a supra complex kind: a confluence of both collective or mass trauma of global or planetary proportions which is sub-diversified into individual versions, as each person is different genetically and experientially made unique by his/ her own lived experience. Thus, as health professionals and self-carers, we need to use both lenses and understand the dynamics of these developmental processes, further complicated and impacted by a drastically transformed and re-configured social systems landscape.
Trauma and resilience can never be discussed apart from one another. They are always two sides to the same coin, as a physical injury or wound transforming into an eventual scar or the eternal wave of the ocean with its rise and fall. Systems, living systems, including inanimate ones designed and operated by humans, have all the potential to disintegrate, malfunction, and self-destruct, but with some re-thinking, re-positioning, re-configuring, and creativity, human beings are innately capable of restoration, healing and resilience, so as not to get stuck somewhere, worst become trash or ash. With this pandemic as the worst and most expansive disaster the world has ever experienced, we now ask, how traumatized are our micro (whole-of-person)
and macro (whole-of-society) systems? But instead of feeling helpless, others still can muster enough resolve to ask, what can still be restored? And if we are to bounce forward, what is supposed to be our road map or at least a compass? Can we define where we want to go, given the realities and uncertainties? With the death, losses, disruption, and brokenness, is there anything worth bringing along to the post-pandemic world?
So we pause, what is this reality that was so highlighted in this pandemic? We have two kinds of realities now, but both are still within our control: the real world and the virtual world, both imperfect in their own ways. Nevertheless, we realize in this pandemic likewise that in both we have a shared universal identity as human beings of this planet Earth. We share the same fears: of death, losing the ones we love, of abandonment, of losing control of our fragile lives. What lesson if ever did this pandemic tell us: that we have taken the little ultramicroscopic half-alive things that could kill or paralyze us and stop the whole world in one instant.
But because studies on past adversities/ adverse childhood experiences have proven that there are modifiers to our coping response, then there is hope. We also see that the sources of trauma do not come from micro-units of families but also from larger macro units as well, and the interpermeability of these 2 due to expanded landscapes of communication is a doubleedged sword, have permeated social layers,
bringing about much more intricacies that need some sorting out and balancing acts. The way we experience all types of trauma (historical, intergenerational) not only to actual but perceived, not only true but faked/ augmented/altered information or data, can wreak mixed emotions far beyond we can handle at any one single second or click of our fingertip, even enough to penetrate our subconscious esp if we sleep with our gadgets at our bedside.
This pandemic then becomes a step back, a slowing down to see what has blinded us for so long. Has it become too chaotic because we have been too fragmented epistemologically that we miss seeing the whole picture. Nevertheless, we see that ontologically, we are what we are, despite varying worldviews, and the values we innately long for are actually universally the same, whether we go micro or macro. We realize that no matter how much sophistication or innovation we do , there will always be a natural saturation point that will gravitate us back to the basics and the essentials, without de-valuing our advancements.
Trauma is always part of the equation we call life, even prior to birth and trans-birth. Seen in our history, it also has infiltrated our micro and macro systems pre-pandemic through both human-made and natural disasters. Pre-pandemic, the world has grappled with social pains wrought about not only of familysourced trauma but also community-rooted ones from migration caused by conflicts and drastic separations demanding adaptation, natural disasters, crimes, domestic violence,
Cheers to our adventures and to a better life!
82 Cultivare_INDD Ver_09212022.indd 82 21/09/2022 4:40:22 pm
accidents, workforce demands, illness, parental separation, can be traumatic and impact can be long-term. But it seems many lessons have been repressed or we are indeed confronted with challenges that civilization just never had before. We see that even as we see that seniors with co-morbidities and the unvaccinated can be more vulnerable to severe and fatal courses, many still do not hear the voices of truth. Moreover, the Philippines beset with the OFW syndrome is more complexly affected by this pandemic not only due to a continuing arrival of variants from all over the world, making surges even much more complicated, unpredictable and more sustained.
These said, it implies that if we are to traject resilience, we need to be on our feet always, so as not to be caught flat-footed again. We need to stretch: deepen, broaden, and sustain our timelines. Since the sources of trauma are very multi-component, multispheric, multi-dynamic, developmental, and circular rather than linear, thus the solution must not fall on the health sector alone, and in one discipline nor sector alone. And since we come from different parts of the planet, we are so diversified that first of all we need a common language in order to talk about our common problems, even within families alone, intergenerational differences are very real that affect our mindsets, behaviors and capacity for adaptation. Protective and buffering factors always involve nurturing trusted stable relationship or bond that could be essentially considered at its basic essence a family and a community.
TRAUMA AT THE FULCRUM
Trauma is basically a change that disequilibrates us as human systems, a change from the things we have been accustomed to that is not necessarily undesirable.
Brokenness, unprocessed grief, and losses of all forms have really been part of human suffering, such that the Filipino family known to the world with a very high index of resilience, is very much challenged on the ground. And this social ill will affect even the pattern of surges and remissions of this virus in our country. Even all over the world, all pathologies and diseases congesting all healthcare will eventually be affected. Because we are so focused on the infectious, all the non-infectious have been put to the side. And thus more than ever before, it is most clearly demonstrated the inter-link and co-existence of mental and physical morbidities within one single human being is very intimate for all doctors and non-doctors
alike. In all our journey of suffering and death and losses, we, both as patients and healthcare providers, have been suffering all kinds of complex grief, absence of closure, enough to draw some of us to the edge of a cliff. The greatest moral injury we health care professionals that sadly burn us down is having to choose which to give a bed or ventilator to, and even simply a patient short of breath. Vicarious trauma is actually graver among us, no matter how de-sensitized we can be to seeing the sick day in day out.
Thus we need to step back, and rather than asking “what’s wrong with me/you?” we ask “what has happened? How do you feel?” Sometimes all we need is to hear or read the right word to make us move on. Now why we need not only a life course but even lifespan perspective to see our diversities and pluralities. While we are in touch with the knowledge of pathology, we must always be aware of positive coping. And we realize, whether public health physician, the clinician is a psychiatrist, a family physician, a minister, or a sensitive politician, someone trusted worthy to journey through (therapeutic alliance) as much as the clinical care we afford them.
SYSTEMS LENS: MICRO-MACRO POST-TRAUMATIC GROWTH
The world has long spoken of resilience and mental health from time immemorial, that sometimes we sound so unscientific and not evidence-based when we speak these things or pray with and for our patients. But it is only now with this pandemic that when patients hear these things from us, they are more inspired. More so if we can explain the true essence of resilience and growth to them in a very professional and objective manner. We professionals must learn from social sciences that these constructs have theoretical scaffoldings too because we are now in the era of post-modernism when we see that our realities are very much socially constructed. We are in the power to construct or deconstruct our realities, that befit what can serve and protect us, using a good knowledge and values framework, what can de-stress us not cause us to have toxic stress. If we learn our lessons from our lived experiences, when we can do re-framing, rebooting of our mind settings, revision of our explanatory models, that’s spirituality. Across our life courses and life spans and in support of our significant others around us, we must continually be open to these re-appraisals.
We ask, what did we lose in our systems?

What can we take with us as we move on? And we ask, what could we attempt to restore back, especially for the young generation? We have lost a sense of safety, a sense of calm, a sense of self and community efficacy, a sense of connectedness that is a deep kind, a sense of connectedness and a sense of hope. We have to learn to talk about things, not people. Because people can be flexible about providing the things if we know the principles. in the middle in this linear-looking hierarchy of systems relationships. In the socio-ecologic model, we see how physical and biological systems very much inter-link. We need to think longitudinally through time as well because in the virtual landscape, we practically see our past, present and future. We, for example, need to think in terms of the co-risk co-benefit approach, in that we can start being aware of where our PPEs would go when we dispose of it, are we aware of cobenefit prescribing. We begin to realize that when see more green in our spaces, it is more relaxing, more physically stretching, and more giving to the environment, to ourselves and to other people.
MEANING-MAKING AND SENSE-MAKING
We are individuals of meaning. Meanings that arise from both cognition and emotion are processed and integrated well. Mere cognitive understanding fall short of inner peace and satisfaction. Nothing makes sense unless our brains process both our thoughts and our emotions in a way that makes sense individually and within a group of people that we value. Meanings transcend time and space because humans are always backward and forward-looking. In pandemic resilience, meanings may be preserved, in fact, they are enhanced and highlighted. Systems are most meaningful when they are interconnected in a way that they deliver the desired outcomes. Our lifeline now , we see in this pandemic, is social connectedness, even if digital. Without this pandemic where we have to distance physically, we have proven so far that this expanded landscape helped us to thrive psychosocially, through which much learning and adaptation could transpire until we can be more immunologically protected. Hope and inspiration are stronger when there is a concrete role modelling of ‘love-informed’ care from us healthcare providers.
In the macro lens, community disaster lessons are being reflected on in literature. Working with the right people enables richer understanding and performance for future disasters. When principles, ethical and moral issues, values and purposes are laid open
83 Cultivare_INDD Ver_09212022.indd 83 21/09/2022 4:40:24 pm
and discussed in non-judgmental manner, decision making is a lot easier. Team and group/organizational dynamics are very crucial. Informal connections and sharing create spaces across intergenerational boundaries. Even the most resilient and capable need support. Longer-term cultural change is needed to ensure collaborative, compassionate and inclusive working environments, with leaders at all levels tackling workload issues. Communityled recovery is key. It takes great courage, stamina empathy to skillfully work out recovery. Language is important. Offering people a chance to share their disaster experience is often met with gratitude and without stigma.
Furthermore, involving both healthcare providers and patients in evaluations and improvements of healthcare services, socalled co-creating values as well as knowledge as well as methodologic innovations, can help share power and provide valuable insights on both individual and organizational level. Exercising the principles of co-production, healthcare workers should be involved in the process of decision making, development, implementation, testing, and evaluation of interventions and efforts aimed at preventing psychological distress and mental health issues and improving their health, well-being, and job satisfaction in the long run. Similarly, it is important to address stigmatization within healthcare facilities as a systemic issue and keep those who fear or are being burdened by stigmatization at the center of any response to stigma in a bigger systems perspective, thus solutions must always be that wide as well, e.g. putting mental health at the accessible level is de-stigmatizing. Philhealth has designed this primary care mental health package that will roll out this or next year. There is a lot to develop further what DOLE has mandated for workplace mental health programs and support for healthcare employees.
And so we realize that to enable ourselves to better lead the way to recovery, we first have to stop hurting ourselves, and we have to stop hurting each other. This include societal, global, and all non-human ecosystems, that have interdependence and links with the person and the population, and the physical environment . We have taken this for granted for a long time, but the indigenous peoples maintained and sustained this, and they turn out to be right. It means integrating both the East and the West and getting the best practices of each, the primary and the specialist. We are always half-wrong and halfright, and this is a life-long distilling, purifying process down to the purest essence. COVID as the first pandemic really is putting us back together after all.
PATHWAY ON
Developing a trauma-informed approach goes beyond accomplishing any single particular technique or checklist. It requires a reorientation and constant attention, caring awareness, sensitivity, and possibly a cultural change at the systems level. After awareness, we need to act together both top-down bottom up, if you are in both, try to be an influencer in both. Integrate our behaviors, both work and play, work and leisure, right brain left brain integration, modulation, keep learning from all platforms. If we are to share tasks, we need to share a common language, a common metric system, leverage all platforms, make connectivity more affordable and accessible, capacitate ourselves together, check the alignment of goals and values, so that we can see our way better where we are lacking inputs of one and the other. We need to see whether indeed we are covering both ends of the spectrum, at each step, encourage and motivate each other rather than blame, serve ourselves as well as others. Only then can outcomes that we all desire be measured and fulfilled. And so we have to draw a framework where everyone sees that each of us, the public, the sick as well as the frontliners alike have the same needs and resources that need addressing. When we meet with hearts and minds, it is possible to meet at the middle, make a difference in a small and big way, so that we eventually all peep through the clouds and perhaps, one day, see the sun again more brightly and touch the sky.
References (more complete in the ppt)
1. “Trauma and Resilience” Navigating Collaborative Care in Promoting Quality Mental Health. Philippine Academy of Family Physicians. Lundbeck PH. (October 2021)
2. Covid-19 recovery and resiliencewhat can health and care learn from other disasters? https://www. kingsfund.org.uk.
3. Insights in Public Mental Health . 2021. https://www.frontiersin.org/ research-topics/22081#artciles).

4. Trauma-informed practices for children and families during the covid-19 pandemic. Focus on Public Health. 2020.
5. Tackling the Mental Health Impact of the Covid19Crisis: An Integrated Whole-of-Society-Response. OECD 2021.
6. What is Trauma-Informed Care? (2021). Buffalo Center for Social Research .
7. Falkenburger & Arena (2018). Trauma-informed Community Building and Engagement. https:www.urban.org/site/ default/files/publications/98296/ traumacareincommunityhealth.
8. Fraenkel & Cho (2020) : Couple & Family Coping during Pandemic, Family Process, Vol 59.
9. Sigua, H (2020). Autohermeneutics of Medical Praxis Using Dialogical Lens. University of the Philippines.
84 Cultivare_INDD Ver_09212022.indd 84 21/09/2022 4:40:25 pm
Le Bourgeois Santé Publique

85 Cultivare_INDD Ver_09212022.indd 85 21/09/2022 4:40:27 pm
Many of us were teenagers in the 1990s. Those were fun, simple but times of political turmoil. While we were studying, the problems of unemployment, energy crisis, informal settlers (squatters, we call them) and working abroad always loomed above us. It’s 2021: many of us somehow managed to become doctors and remain in the Philippines. Few tried to dig up and search for the whys of this situation. Many of us experimented, too. How do countries become rich? And where do we contribute? Here is what I have personally learned and hoping to share.
1. Work in government. It remains one of the best and sustainable options. The good news is, because of rationalization in recent years, and PhilHealth coverage, salaries are becoming competitive. Definitely, it is hard to get in but low risk, and can really have good outputs. And please, take up Masters degree, and double Masters eventually.
2. Bank loans. Don’t be afraid. You have many options - Housing, Car, Personal, Credit card, Business loans, etc. This will increase credit, create money, hence, increase liquid assets/ money supply. Especially at times of the pandemic, bank loans and creating money will employ more people, create more businesses and improve liquidity. Take this with a huge load of advice. An important one is, make sure you make a loan to improve your capacity to earn.
3. Be active in church and religious activities. This is to promote goodwill, mental health, personal peace, find meaning, fellowship and values formation. Churches and religious groups are also good ways to help other people in terms of charity, education, motivation and values formation.
4. Get involved in an NGO with community level work. There are many options here. It will allow you to share your talents, skills, expertise and other resources.
5. Join a cooperative. This is a mix of having bank loans and joining NGOs. Creates more fiscal space especially in rural areas and localities.
6. Buy a farm. Put in capital, hire people. It’s a win-lose up-and-down experience. Don’t expect to get rich right away. I observed, that in the age of the 19th and the early 20th century empires. A lot of development and money creation happened because many young adventurers (mostly soldiers, traders, mariners and government bureaucrats) traveled abroad into colonies to find a fortune. Upon returning, they built estates and farms thus allowing people to get employed. An alternative of this strategy is to buy and start a mountain resort. Just keep it natural, though. Don’t destroy it.
7. Buy commercial space or a condo and rent it out. This combines releasing your money to be used while at the same time making a loan.
8. Start your business, hire people, put in capital. But don’t expect to get rich. It’s for the people to get respectable jobs and get into the formal sector. Allow them to have PhilHealth and Pag-ibig membership.
9. Buy equities, bonds and shares or invest in the trade market. This strategy is just moving up in the level of investment. And there is an entire economy, art and science into it. There are online platforms e.g. citiseconline.com or through banks. It will take time to understand everything. But always good to start from somewhere.
10. Support artists, scholars, send some kids to school. These areas of investments are longer term and require more patience and more resources. Sending teenagers (like the children of your driver) to local schools are actually very affordable. Artwork is actually one of the best ways to invest, but the market is very specialized.
11. Instead of buying a car, just use Grab, car rental or hire a suki Grab driver. Having a suki is more developmental because it allows work for other people, thus boosting the economy.
12. Instead of cooking own food, buy Grab food or from other online sellers. You build the economy as you spend your money, while it helps people with small personal businesses. In addition, it allows budding chefs to improve their skills. You can even feel more relevant by focusing on certain food types e.g. vegetarian, Filipino, regional Filipino, etc. We know of restaurants and food chains that started with local food selling. 13. Do commercial laundry or pay your labandera instead of washing your own clothes. Again, helps build the economy. And depending on how you treat your labandera or laundry shop, work gives dignity to people. As what I tell others, better give them proper jobs than dole outs or allowing them to remain 4Ps. Laundry shops also have local business permits and taxes, so it helps the LGU.
14. Support artists, musicians and athletes. It is easier to do these now because everything is online and you can transfer funds through GCash. You can support them through lessons for scholars, or their social media performances.
15. Work abroad, get international projects or do international-based work. This part is a bit of a surprise advice since many colleagues (who were teens in the 1990s) would always cry for staying in the Philippines. There are ways to do this e.g. having your own project
funded from abroad. It allows resources to come into the country, hence adding fiscal space. This will also allow you to accomplish the first 14 things mentioned.
Now is actually the best time to invest as the country moves from LMIC to HMIC. And because the pandemic has slowed down growth, we have a few additional years to invest.
There is definitely more that can be done. There is always room for creativity, new ideas and innovation. May this article encourage others to also take that step.
I had originally thought of linking the title and the initial framing to “contributing to national development.” But this is a more nationalist worldview, which not everybody is always a fan of, and gives a lot of frustrations. I could also title it “Best ways to invest”, but this is too capitalist, self-oriented and has risks of losing. So I chose a French title – “bourgeois” in recollection of the European industrial revolution when a new class of moneyed families emerged, who eventually contributed to societal growth, and well expansion of several empires. Out of the bourgeois class came professionals, social movements, scientists, innovators, bureaucrats and organizations that survive to this day. But the bourgeois were not always seen as good, which is why they were heavily criticized by socialists.
Checking your motives. You can do any of the 15 actions above and you can have different motivations, perhaps personal, or family, or altruism, or faith, or legacy, or helping others, or nationalist, or giving A New Hope. Sounds like God, Glory and Gold of the Spanish conquistadors. It can work. But it will not be perfect, too. People can fail you. Organizations can fail, too. And you can also fail. This is where your values, faith and virtue would come in, the deeper truths.
Praying that this article will give you great ideas, and blessings. I end this essay with a verse and song that many of us will find peace as we follow – “Whether therefore ye eat or drink, or whatsoever ye do, do all to the glory of God!”
Lester Sam Araneta Geroy
15 ideas to invest with public health and development in perspective.
86 Cultivare_INDD Ver_09212022.indd 86 21/09/2022 4:40:30 pm
Zuellig Family Foundation
87 Cultivare_INDD Ver_09212022.indd 87 21/09/2022 4:40:31 pm
Risk Communication in Strengthening Community Engagement on COVID-19 Response in Agusan del Sur

 by Dr. Angeli A. Comia
by Dr. Angeli A. Comia
Given the many unknowns during a pandemic, it helps to have an engaged citizenry willing to do its part in managing the disease. However, getting the people to follow health protocols and local policies would require trust in their leaders. In Agusan del Sur, a functional health promotion system helped build the trust between AgSurnons and their local health leaders.
Since last year, the Zuellig Family Foundation has been helping the province in its pandemic response. ZFF provided capacity-building and technical assistance related to risk communication, strategies for prevention, detection, isolation, treatment and reintegration (PDITR), and vaccination.
Governor Santiago Cane Jr. had immediately formed a provincial core response team composed of officials from the different provincial offices and agencies. Soon there was a province-level health promotions committee.
b Mobilized barangay health leaders

The provincial HEPO organized their municipal HEPO counterparts, and together with barangay health workers (BHWs) and barangay health boards (BHB) (figures 2 & 3), became instrumental in enabling the public, especially elderlies and indigenous peoples, to understand COVID-19-related guidelines and vaccination.
The health promotion office (HEPO) used to be a one-person unit. The then newly-hired Chrisan Ranario’s experience and expertise were in HIV/AIDS prevention and control. Because of the pandemic, the HEPO is now in active collaboration with critical stakeholders as one Provincial Communications Team under the Operations Center’s (OPCEN) COVID-19 surveillance and response.
The provincial government created and funded a risk and crisis communication plan primarily targeted at addressing the public’s concerns about COVID-19 and vaccine apprehensions (see figured 1).
c Ensured a culturally inclusive process
The municipalities customized their risk communication plans using scenario-based planning jointly organized by ZFF and the Department of Health-Caraga (Figure 4). Participants included health workers, some of whom belonged to IP communities. The provincial health office-HEPO organized an IP Summit where 30 IP leaders were present and learned more about the minimum health standards and vaccine program. Attendees held a commitment signing to signify their support for the provincial government’s heath initiatives (figure 5).
The province’s inclusive and culture-sensitive practice convinced IP elders to use their influence to improve the health-seeking behavior of their community members.
Agusan del Sur’ efforts benefitted from the support of civil society organizations, religious sectors (figure 6), local media (figures 7 & 8), business groups, and social media influencers. With their help, the province improved the communication strategies (figure 9) and information materials (figure 10a-10f).
The organized communication effort addressed vaccine hesitancy among health workers, enabling Agusan del Sur to inch closer to its goal of vaccinating 100% of its front-line workers. Knowing this could, however, take some time, the province is determined to educate its people with only
the right health information especially as it moves to strengthen its primary health care systems.
 a Organized a dedicated health promotions team
a Organized a dedicated health promotions team
Figure 1. Creation of Agusan del Sur Provincial Vaccination Plan with Different Stakeholders (PDOHO, PIMO, PPIO and DOPMH) led by PHO II Dr. Jacqueline Momville and PHO HEPO II Chrisan Ranario
Figure 2. Barangay Health Emergency Response Team (BHERT) meeting & advocacy composed of BHWs and other community volunteers
Figure 5. Indigenous Population (IP) Summit with 30 IP/Tribal leaders with commitment signing to advocate COVID-19 vaccination to their respective communities
Figure 6. Religious group advocacy on COVID19 protocols and vaccination
88 Cultivare_INDD Ver_09212022.indd 88 21/09/2022 4:40:31 pm
Making Universal Health Care Happen in Times of Complexity
By Dr. Catherine A. Chung, Director, Local Health System- ZFF
The enactment of the Universal Health Care on February 20, 2019 was a significant milestone in Philippine Health Care history though its implementation was affected by the COVID-19 pandemic. The UHC implementation, complicated as it is, now faces more challenges in financing, human resources, and impending full devolution of various health and social services to the local government units (LGUs).
Accelerating Universal Health Care amidst the Pandemic

The Zuellig Family Foundation (ZFF) has been working with the provincial governments of Agusan del Sur, Aklan, and Bataan since 2016 and providing leadership capacity building and technical assistance programs to help the health leaders implement the UHC since 2019.
The provinces had been making headways toward creating province-wide health systems when the pandemic struck. Before COVID-19, the three provinces had organized and expanded their local health boards, which would become key in their pandemic response efforts. They had created UHC technical working groups and had begun the establishment of service delivery networks (SDNs) that included private hospitals.
In 2020, ZFF adapted its strategy to help the provinces manage the pandemic but it never neglected the more forward-looking work in UHC.
While COVID-19 remains an utmost concern, the provinces have begun building UHC models involving select municipalities, where primary health care (PHC) systems will be improved to address non-communicable diseases (NCDs). The PHC is the focus because it gives importance to community collaborations which are vital during both normal and pandemic times; thus, helping establish resilient health systems as well.
In Agusan del Sur, the model involves the interlocal health zone composed of Talacogon, La Paz and San Luis (TALASAN). In Bataan, their 1 Bataan Seal of Healthy Barangays program will be recalibrated to strengthen the health system of Dinalupihan. In Aklan, the model will strengthen the tole of barangay health workers in Tangalan to ensure the delivery of health services.
To support the provinces’ efforts, ZFF has begun the provision of leadership training for the municipal and barangay health leaders in the concerned LGUs.
In the coming months, the provinces are expected to implement the Package of Essential Non-Communicable (PEN) Disease interventions; begin master-listing NCD client; comply with the standards of a primary care facility; and improve NCD health promotion program.
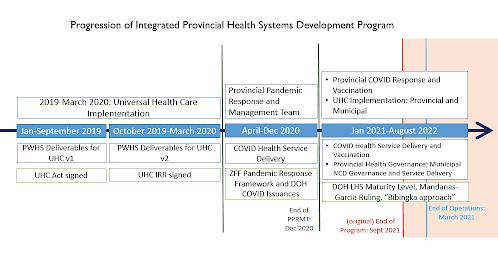
And just as the provinces re-started their earnest efforts toward attaining UHC, another twist came in the form of the full devolution of health and other social services. While the Mandanas-Garcia ruling means additional funds for the LGUs, the subsequent Executive Order (EO) 138 brings increased responsibilities that may be costlier.
These apprehensions were echoed by Quirino Governor Carlo Cua and Dinalupihan Mayor Maria Angela Garcia during the ZFFsponsored webinar on the implications of the ruling and the EO.

In that forum, the LGUs’ role in collaborative strategic planning became more pronounced with a need for LGUs to work closely with national agencies to ensure smooth transitions.
The enormity of the work to be done requires a whole-of-nation and not just whole-ofgovernment approach to make the full devolution work and UHC attainable.
ZFF is steadfast in assisting LGUs especially now that with more funds for health investments, the country needs more local chief executives with increased ownership of their health issues to ensure accountability and inclusiveness of plans and programs.
Figure 1. Progression of the ZFF’s Integrated Provincial Health Systems and Development Program
Figure 2. Orientation on COVID-19 Vaccination Tools with ZFF’s Partner Provinces in partnership with PDRF and T3
Figure 3. Online Training on Bridging Leadership Strengthening Workshop with TALASAN ILHZ in Agusan del Sur-August 12, 2021
Figures 7-8. Collaboration with local media for vaccination and online immunization registry campaign
89 Cultivare_INDD Ver_09212022.indd 89 21/09/2022 4:40:31 pm
2021 - 2024 Board Members and Executive Committee

90 Cultivare_INDD Ver_09212022.indd 90 21/09/2022 4:40:33 pm
DR. LESTER SAM GEROY, MPH, MSc-HPPF Chairperson

Affiliations:
Founding President, Philippine Society of Public Health Physicians | Founding President, Alliance for Improving Health Outcomes | Visiting Faculty, University of the Philippines Open University Health Systems, Health Policy, Health Financing
Dr. Lester Sam Araneta Geroy is a public health expert with vast experiences in the community, international health, health systems, policy, financing and research. Dr Geroy is a Senior Consultant and Project Manager connected with several firms, institutions and agencies in the Philippines.
Field of Interest and Expertise:
Education:
Doctor of Medicine | Masters in Public Health | Masters in Health Policy, Planning, and Financing | Diploma in Global Health
Focus areas are health policy, health systems, health research (systems, operations and policy), antimicrobial resistance (AMR), national and sub-national health sector planning, health service delivery, hospital management and regulation, hospital planning and design, health care quality, immunization, emergency and social health insurance, economic evaluation, palliative care policy and services, PhilHealth benefit package development, and Project Management.
Affiliations:
Founding Vice-Chairperson, Philippine Society of Public Health Physicians | Division Chief, International Relations Division, Department of Health – Philippines’ Bureau of International Health Cooperation | Medical Director, Child Health Family International Philippines International Health, Migrant Health, Health Diplomacy

Field of Interest and Expertise:
Affiliations:
Founding Board Member, Philippine Society for Public Health Physicians | Partner, Alliance for Improving Health Outcomes, Inc | Faculty Associate, Development Academy of the Philippines Health Systems, Health Governance, Health Policy
Field of Interest and Expertise:
Doctor of Medicine | Masters in Public Health with dual concentration in International Health and Health Policy and Management
Education: Dr. Joel Buenaventura is a medical doctor and a public servant with over 14 years in government service and with profound interest in public health, migration health, global health diplomacy, and health policy and management and its link to the health of local populations. He is the previous head of the Migrant Health Unit and Program Manager of the Philippine Migrant Health Program and acted as the focal point for all international assistance and donations for the health sector during the Typhoon Yolanda response in 2014 and the recent COVID-19 response.
Education:
Doctor of Medicine | Masters in Public Management | Masters in Public Health specializing in Economics and Governance of Health Systems in Transition
Dr. Michael Caampued is a health systems, economics and governance consultant with a total of 13 years of involvement in supporting community health development in the Philippines. Experiences include communitybased clinical practice, national and subnational health systems strengthening, care integration (service delivery networks), local health governance, reform implementation, program and policy development.
DR. JOEL BUENAVENTURA, MPH Vice-Chairperson
DR. MICHAEL CAAMPUED, MPM, MPH, MZP President
91 Cultivare_INDD Ver_09212022.indd 91 21/09/2022 4:40:34 pm
DR. JAIFRED CHRISTIAN F. LOPEZ, MPM Vice-President


Affiliations: Field of Interest and Expertise:
Assistant Professor, Department of Nutrition, College of Public Health, University of the Philippines Manila | Founding Treasurer, Philippine Society of Public Health Physicians | Core collaborator, HealthXPh.net | Member, Global Burden of Disease collaborator network | Member, Philippine Society of Hypertension | Member, Philippine Lipid and Atherosclerosis Society Health Policy, Non-Communicable Diseases, Nutrition
DR. JACQUELINE FRANCES MOMVILLE, MPM Secretary
Affiliations: Field of Interest and Expertise:
Provincial Health Officer, Agusan del Sur | Founding Secretary, Philippine Society of Public Health Physicians | Founding Partner, Alliance for Improving Health Outcomes, Inc.

Health Governance, Health Leadership, Local Health Systems, Organizational Development
Education:
Doctor of Medicine | Master in Public Management Major in Health Systems Development
Affiliations: Field of Interest and Expertise:
Education:
Doctor of Medicine | Master of Public Management major in Health Systems and Development | Master of Public Health (candidate)
Doctor of Medicine | Masters in Public Management major in Health Systems and Development
Education: Before entering the academe, Dr. Lopez was a health policy researcher working with the Institute of Health Policy and Development Studies at the UP Manila National Institutes of Health, the Alliance for Improving Health Outcomes, Inc., 101 Health Research, Inc., and Physicians for Peace Philippines. He also taught research methods and community medicine at San Beda University College of Medicine, and served as Associate for Project Management and Resource Generation in the Office of Research and Innovation.
Dr. Jacqueline Frances F. Momville specializes in the field of public health leadership and governance focused on local health systems and organizational development to provide quality and equitable health services aimed at improving lives of people especially the underserved. The last ten years of her public health practice focused on community-based health, mentoring and coaching of leaders for health, program and training development, competency assessment and enhancement, strategic planning and implementation, and organizational management and development.
Dr. Joey Francis Hernandez is a Filipino physician with a five-year professional experience in public health. He started his public health career as part of the Doctors to the Barrios Program for two years. He also worked on several projects with Alliance for Improving Health Outcomes and Physicians for Peace Philippines, focusing on project management, child injury prevention, antimicrobial resistance, and benefit package development. He taught public health, microbiology, and histology at University of Santo Tomas Legazpi and Far Eastern University Manila. He also led the growing country team of Interactive Research and Development Philippines, a non-profit global health delivery organization based in Singapore. He provided technical support as a public-private mix specialist in the USAID-funded TB Innovations and Health Systems Strengthening Project.
DR. JOEY FRANCIS HERNANDEZ, MPM, MPH Treasurer
Former Secretary General, Philippine Society of Public Health Physicians Health Systems, Epidemiology, Biostatistics
92 Cultivare_INDD Ver_09212022.indd 92 21/09/2022 4:40:35 pm
DR. JOSEPHINE BUNDOC
Member
Affiliations:
Pioneer Member, Philippine Society of Public Health Physicians | Professor, UERM College of Allied Rehabilitation Sciences | Professor, UP College of Medicine Rehabilitation Medicine, Health Financing

Her interest in Prosthetics and Orthotics opened her eyes to the huge unmet need of Access to these devices in the country, which set the ground for the Physicians for Peace “Walking Free” initiative in 2005.
Field of Interest and Expertise:
Education:
Doctor of Medicine | Physical Medicine & Rehabilitation
DR. ANNELY JANE CELOCIA

Member
Dr Bundoc serves as World Health Organization Temporary Consultant in Disabilities & Assistive Technology and currently sits in the International Society of ProstheticsOrthotics Advocacy Committee. She served as Project Lead of the UNICEF-Physicians for Peace Children With Disabilities Access and the PCHRD Adult Rehabilitation Package Development.
Fellow, Philippine Academy of Family Physicians | Member, Philippine Academic Society of Community Medicine | Faculty, Cebu Institute of Medicine | Chief, Cebu Institute of Medicine Community MedicoSocial Services | Co-founder and Adviser, Asian Medical Students’ Association ServiceOriented Medical Advocates of CIM
Affiliations: Field of Interest and Expertise:
Health Education, Community Practice, Primary Health Care
DR. ANTHONY FARAON, MPH, MPM
Affiliations:
Founding Member, Philippine Society of Public Health Physicians | Deputy Executive Director for Local Health Systems, Zuellig Family Foundation
Field of Interest and Expertise:
Health Leadership, Health Governance
Education:
Doctor of Medicine | Masters of Public Health | Masters in Public Management
Doctor of Medicine Education:
She actively collaborates with the local government unit in community-based projects.
She has mentored and trained over three hundred medical student members and guided them to actively participate in projects related to community and public health and research. Being a public health advocate herself, Dr. Celocia has imbued in her students a strong sense of social accountability and encouraged them to be catalysts for social progress.
Dr. Faraon is responsible for setting the overall direction of two programs, the Provincial Leadership and Governance Program and Community Health Partnership Program, and for providing portfolio guidance, strategic technical oversight, financial oversight, staff management, community mobilization, private-sector engagement, and government relations.
 Member
Member
93 Cultivare_INDD Ver_09212022.indd 93 21/09/2022 4:40:36 pm
DR. RAMON LORENZO LUIS GUINTO, DrPH
Member
DR. LUISITO RUIZ, MHSM
Member
Affiliations:
Pioneer Member, Philippine Society of Public Health Physicians | Associate Professor, Practice of Global Public Health, St. Luke’s Medical Center College of Medicine | Inaugural Director, Planetary and Global Health Program, St. Luke’s Medical Center College of Medicine | Chief Planetary Doctor, PH Lab



Planetary Health
Education:
Field of Interest and Expertise: Doctor of Medicine | Doctor of Public Health
An Obama Foundation Asia-Pacific Leader, Aspen Institute New Voices Fellow and Climate Reality Leader (under the initiative of former US Vice President Al Gore), Renzo is member of several high-level international groups including: Lancet–Chatham House Commission on Improving Population Health post COVID-19 (University of Cambridge); Lancet One Health Commission (University of Oslo); Advisory Council of Global Health 50/50 (University College London); Advisory Board of Climate Cares (Imperial College London); Editorial Advisory Board of The Lancet Planetary Health; and Forum on Climate Change and Health of the World Innovation Summit for Health (Qatar Foundation). He has served as consultant for various organizations including: World Health Organization; World Bank; USAID; International Organization for Migration; Health Care Without Harm; Philippine Department of Health; Chilean Ministry of Health; and Institute of Tropical Medicine in Antwerp, Belgium.
Affiliations:
Member, Board of Governors, Philippine Medical Association | Founding Chairman, Philippine Society of Public Health Physicians | Probio Med Care | PBMed Doctors Clinic
Field of Interest and Expertise:
Health Systems Management
Education:
Doctor of Medicine | Residency in General Surgery | Occupation Health | Family Medicine | Executive Course in Hospital Management | Masters in Health Systems Management
DR. PAULYN JEAN ROSELL-UBIAL, MPH, CESO II
Member
All of which contributed to his prominence, prestige and skill in medicine, and to his continuing pursuit to climb the ladder of success. He was a Hospital Director and an active consultant in the Department of Surgery. He established Pro Bio Medcare, a company that provides a community based multispecialty-diagnostic clinic and Nutraceutical company that distributes natural/organic products in partnership with companies in different countries
At present, he is the helm of PBMED Doctors Clinic, providing multi-lateral attention and services.
Affiliations:
Public Health, Good Governance, Leadership and Public Management, Tobacco Control, Women’s Health Programs, Vaccination and Polio Eradication, Quality Assurance Systems, Gender and Development Health Systems Management
Field of Interest and Expertise:
Education:
Doctor of Medicine | Masters in Public Health
Department of Health Former Health Secretary Dr. Ubial has led an extensive career in public health service for 29 years with selfless devotion and passion under 13 health secretaries. She started as a volunteer health worker in Mindanao, rising up from the ranks to secretary of health. Her vast experience in the country’s health conditions have led her to be a leader and champion of “Kalusugang Pangkalahatan”, with advocacies in women and children’s health, breastfeeding, blood donation, tobacco control, Healthy lifestyle and mental health, among others. She was also designated as founding program manager of the “Sentrong Sigla” movement, the quality assurance program of the DOH, and the founding manager of the Women’s Health and Development program and focal person for the DOH Gender and Development. She has worked under the regional offices of SOCCSKSARGEN, Western Visayas, Zamboanga Peninsula, and Davao.
94 Cultivare_INDD Ver_09212022.indd 94 21/09/2022 4:40:37 pm
PIONEER MEMBERS
Anthony Hernandez Cordero
Josephine Robredo Bundoc
Dinah Nadera
Ramon Lorenzo Luis Rosa Guinto
Anton Javier
Ma Bella Ponferrada
Edgardo Ulysses Nguyen Dorotheo
Julius R. Migriño, Jr.
Rhey Ian N. Buluag
Caroline Mae “Ginger” Ramirez
Dante Jr Salvador
Ezra Valido
Alvin Marcelo
Quennie Raagas
Joseph Anthony Lachica
Nezer Aben Soriano
Almusaidi Anik Karay
Samira Mohammed H. Vadakkan
Anthony Calibo
Reinhard Dalumpines
Madonna Andaya
Keilah Sinahon
Glenn Roy V. Paraso
Anthony Faraon
Marthony Precilla Basco
Charmaine Ann Rabago
FOUNDING MEMBERS 1. Luisito Lacsamana Ruiz 2. Lester Sam Araneta Geroy 3. Joel Hernandez Buenaventura 4. Juan Alfonso Leonardia 5. Jacqueline Frances Momville 6. Jaifred Christian Felicilda Lopez 7. Ma. Rowena Alcido 8. Michael Sarreal Caampued 9. Beverly Lorraine Ho 10. Christian Gomez 11. Paolo Victor Nartea Medina 12. Alberto Manibo Ong, Jr 13. Angeli Arrogante Comia 14. Anthony Bocboc Cu 15. Generoso Delos Reyes Roberto 16. Grace Fe Buquiran 17. Heidee Buenaventura 18. Jeremie Erana De Guzman 19. Joey Francis Hernandez 20. Jose Rafael Marfori 21. Katerina Nono Abiertas 22. Marianne Naria-Maritana 23. Marquis von Angelo Joson 24. Niko Cedicol 25. Paula Melizza Valera 26. Ralph Nico Selibio 27. Ramir Anthony Tumolva Blanco 28. SweetC Alipon 29. Zhamir Umag 30. Jaime Galvez Tan 31. Paulyn Jean B. Rosell-Ubial 32. James Salisi 33. Katherine Ann Villegas-Reyes 34. Charl Andrew P. Bautista 35. Maris Ellen Licup-Medina 36. Rene Andrew A. Bucu 37. Carl Abelardo T. Antonio 38. Miguel Dorotan 39. Miguel Antonio Santos Salazar 40. Christian Bondoc 41. Venus Oliva Cloma-Rosales 42. Jeremiah Salera Calderon 43. Ryan Guinaran 44. Albert Francis Edralin Domingo 45. Lei Camiling-Alfonso 46. Gienah Evangelista 47. Michael Tee 48. Francis Wade Z. Gomez IV 49. Melchor R. Lucas Jr. 50. Jana Deborah B. Mier-Alpaño 51. Ted Herbosa 52. Allison Gocotano 53. Helena Marie Lagon Alvior
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
95 Cultivare_INDD Ver_09212022.indd 95 21/09/2022 4:40:37 pm
MetaHealth
Confidence in Decision-Making.
Borne out of idea-exchanges over coffee in Sydney, the founders of metaHealth Insights and Innovations, Inc. (or metaHealth) thought about riding the wave of potential health technology assessments (HTAs) as Republic Act 11223, more commonly known as the Universal Health Care (UHC) Act, was signed by Pres. Rodrigo Duterte in 2018. metaHealth prides itself as the first Filipino firm focused on conducting HTAs. meta Health envisions itself as a high-impact and innovative THINK+DO tank that empowers partners to reimagine quality and accessible healthcare toward improving lives in the Philippines and beyond.
The firm mainly addresses two largely unmet business needs. First, there is an urgent need to navigate the constantly evolving regulatory landscape regarding the provision of healthcare products and services in the country. As the UHC law progressively unfolds, it is an ticipated that there would be a highly uncertain regula tory landscape; mainly due to the increasing amount of evidence generated on various products and services coupled with the need for legislative agility in moni toring and regulating these. metaHealth aims to help HTA practitioners, both in the public and private sec tors, navigate through these uncertainties by providing comprehensive, timely, and focused insights to ensure regulatory compliance and secure market access. Sec ond, there is currently an inadequate capacity for local HTA, both in technical expertise and the critical mass of practitioners. metaHealth is an advocate of uplift ing the standard of HTA in the country by providing avenues for relevant professional upskilling and being a trusted partner in the training and development of local HTA talent. With these, metaHealth helps elevate the HTA landscape of the Philippines by ensuring that both these business needs are adequately met.
metaHealth enables confidence in decision-making through actionable insights from data and scientific evidence generated from four niche areas (aptly abbre viated as “META”) which are largely underserved:
• Management and Implementation Science
• (Health) Economics and Outcomes Research
• (Health) Technology Assessment
• Analytics and Informatics
These niche areas are also our areas of expertise. Our team has more than 30 years of combined profession al experience across these fields of interest. Our multi disciplinary approach in addressing HTA problems has been proven in the projects we have completed with various multinational partners, both in the for-profit and not-for-profit sectors.
In metaHealth, we make sure that each project is completed in a holistic manner, combining multiple cross-cutting research methods with our proven glocal public-private expertise. Our synergy and flexibility in meeting the needs of any client put us a cut above the rest, providing them the confidence they need to pursue their goals.
As fellow public health practitioners, we are one with the Philippine Society of Public Health Physicians in dreaming with new hope for the HTA landscape in the Philippines. We believe that our diverse yet synergis tic fields of expertise would help rebuild the nation with improving public health as one of our main as pirations. Working together, we can be the catalyst our country needs – accelerating the provision of equita ble, people-oriented, and quality healthcare services to every Filipino.

96 Cultivare_INDD Ver_09212022.indd 96 21/09/2022 4:40:39 pm
97 Cultivare_INDD Ver_09212022.indd 97 21/09/2022 4:40:39 pm
98 Cultivare_INDD Ver_09212022.indd 98 21/09/2022 4:40:39 pm
99 Cultivare_INDD Ver_09212022.indd 99 21/09/2022 4:40:39 pm
100 Cultivare_INDD Ver_09212022.indd 100 21/09/2022 4:40:39 pm
101 Cultivare_INDD Ver_09212022.indd 101 21/09/2022 4:40:39 pm
THIRD ISSUE - 2021 CULTIVĀRE Cultivare_INDD Ver_09212022.indd 102 21/09/2022 4:40:39 pm
