4 minute read
05.8 Catherine Comiskey

from Provost & President's Retrospective Review 2011-21
by Public Affairs and Communications (PAC) - Trinity College Dublin

05
Shining a new light on understanding the relationship between vitamin D and health Lina Zgaga
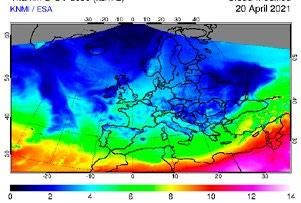
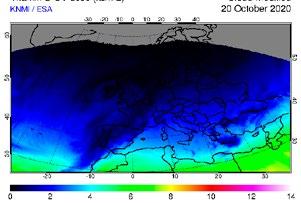
When sunlight reaches human skin, vitamin D production is initiated and this UVB-induced synthesis is a key source of vitamin D for most people. Consequential to the prominent seasonal variation in UVB radiation (Figure 1), vitamin D status fluctuates too – it peaks in late summer and is at its lowest in early Spring. The profound seasonality of vitamin D levels creates a “moving target” issue and many fundamental questions remain unanswered because established methods are unable to address them adequately. My research seeks to develop approaches that can work with the constant and physiological fluctuation in vitamin D status on multiple fronts.
Vitamin D status assessment – Vitamin D status is currently assessed by measuring the concentration of 25-hydroxyvitamin D in the blood. This measurement provides a good approximation of vitamin D status at the time of sampling; however, a single time-point measurement cannot capture the large seasonal differences. With my colleagues in the School of Medicine, Dr Eamon Laird and Dr Martin Healy, I have demonstrated for the first time that vitamin D can be measured in human hair. Our work could revolutionise the accuracy of assessment, because vitamin D depositions in hair represent a personal record of vitamin D status over a longer period (Figure 2) – similar to carbon deposition in ice used in climate change studies. The testing itself would be much improved too: taking hair is painless, does not require a health professional to take a sample and is not invasive, a noteworthy benefit for some groups, including children. I have been approached by zoologists, as removing the need for blood sampling is a great relief when working with animals; in particular primates that would otherwise need to be sedated. Vitamin D deficiency as a risk factor for disease – Vitamin D deficiency has been suggested as a risk factor for ~200 diseases, including most recently Covid19. The suspected disease links have earned vitamin D a lot of attention; however, the absence of a definite proof has been fuelling a heated debate on whether these associations are direct and causal. Alternatively, the associations could be due to confounding. For example, those who are physically active, have normal weight, and are healthier tend to have higher vitamin D levels. Randomised controlled trials (RCTs) are the corner stone of evidence-based medicine. Despite very convincing evidence from experimental, animal and observational studies, vitamin D RCTs have largely failed to show direct benefit. The specific issue that plagues RCTs with vitamin D is that large differences in vitamin D status
FIG 1
KNMI / ESA 20 April 2021 KNMI / ESA 20 October 2020 KNMI / ESA 20 July 2020
Lina Zgaga received her degree in medicine and PhD from the University of Zagreb (Croatia) and her MSc from the University of Edinburgh. She joined Trinity in 2013 and is now an Associate Professor of Epidemiology in the School of Medicine. She has published over 130 peer-reviewed manuscripts that were cited almost 17,000 times. Her research focuses on vitamin D, gene-environment interactions, and new epidemiological methods and frameworks for determining causal associations. She was elected to fellowship of Trinity College Dublin in 2021. Contact: zgagal@tcd.ie
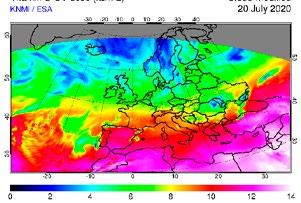
FIG 1 – The maps show the UV dose reaching the Earth’s surface at wavelengths that can induce vitamin D production in human skin, while considering the reduction of the UV radiation due to clouds. (A) 20th of April 2021, (B) 20th of October 2020 and (C) 20th of July 2020. Copyright © KNMI/ESA; www.temis.nl FIG 2 – Concentration of 25-hydorxyvitamin D in blood, the best marker of vitamin D status from March to October is shown in the top panel. The corresponding depositions of vitamin D in hair, proportional to the concentration in the blood at the time of hair growth are illustrated in the bottom panel.
≥ Vitamin D deficiency has been suggested as a risk factor for ~200 diseases. The suspected disease links have earned vitamin D a lot of attention; however, the absence of a definite proof has been fuelling a heated debate on whether these associations are direct and causal.
exist between people. This is a problem because the effect of supplementation will differ substantially: those who are severely deficient will benefit more than those whose vitamin D status is merely insufficient; and there will be no benefit among the sufficient. Through a simulation study I have undertaken with Dr Jason Wyse, School of Computer Science and Statistics, we have been able to describe the “blind spot” of RCT design for the first time: the between-person differences and seasonally changing vitamin D status sabotaged the ability of RCTs to detect benefit. Retrospective analysis has indicated that many reported findings might be false-negatives, meaning that supplementation was in fact beneficial but that our methods don’t work – a bit like trying to see a virus with a magnifying glass. The implications of establishing whether null-findings are true or false negatives are major: if associations with vitamin D are causal, enormous public health impact could be achieved by supplementation – an opportunity that should not be missed given that vitamin D supplements are cheap, safe and easily accessible.
FIG 2
25-hydroxyvitamin D (concentration in blood)
March April May June July August September October
Hair
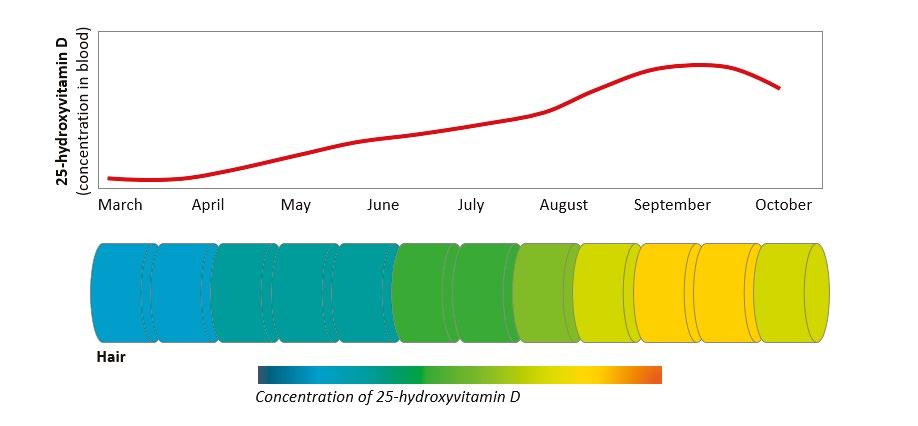
Concentration of 25-hydroxyvitamin D








