Introduction: Stimulant-induced cardiomyopathy is a rare finding. There are emerging case reports regarding stimulant use and non-ischemic cardiomyopathy and case reports of vaping produce use-associated lung injury (EVALI). To the authors’ knowledge, there are no reports of concomitant use of stimulants and e-cigarettes and the incidence of cardiogenic shock. We report two cases of young men presenting in cardiogenic shock in the setting of new cardiomyopathy attributed to concomitant use of e-cigarettes and amphetamine/dextroamphetamine.
Case 1: A 29-year-old man with attention deficient hyperactive disorder (on 120 mg amphetamine/dextroamphetamine daily) and active vaping presented in acute hypoxic respiratory failure and cardiogenic shock (left ventricular ejection fraction [LVEF] 10–15%). Cardiogenic shock was managed in the cardiac intensive care unit with pulmonary artery catheterguided inotropic and afterload reduction therapies. Evaluation was negative for ischemic or infiltrative disease. Lung biopsy showed changes consistent with e-cigarette use. He was ultimately transitioned to
1. Diaban F, Bunaye Z, Vaziri J, Plisco M. Vaping induced lung injury complicated by right ventricular failure leading to ECMO. Presented at: American Thoracic Society International Conference, online, August 5, 2020. Abstract A1959. https://doi.org/10.1164/ajrccmconference.2020.201.1_MeetingAbstracts.A1959
2. Echeagaray O, Savko C, Gallo A, Sussman M. Cardiovascular consequences of vaping. Current Opin Cardiol 2022;37:227–35. https://doi.org/10.1097/HCO.0000000000000952; PMID: 35612935.
3. Isakov KMM, Legasto AC, Hossain R, et al. A Case-based review of vaping-induced injury–pulmonary toxicity and beyond. Curr Probl Diagn Radiol 2021;50:401–9. https://doi.org/10.1067/j. cpradiol.2020.06.003; PMID: 35612935.
guideline-directed medical therapy (GDMT) and discharged home with a life vest.
Case 2: A 25-year-old-man with attention deficient hyperactive disorder and active vaping presented in acute respiratory failure and cardiogenic shock (LVEF 10–15%). Cardiogenic shock was managed with veno-arterial extracorporeal membrane oxygenation (VA-ECMO). Evaluation was negative for ischemic or infiltrative disease. The patient was successfully decannulated from ECMO and transitioned to GDMT and discharged home.
Discussion: While there is a growing number of case reports discussing the cardiac manifestations of EVALI or stimulant-induced cardiomyopathy, little is known regarding the effects or risk of cardiogenic shock in concomitant stimulant and e-cigarette use. The two cases presented here highlight the need for clinicians to evaluate for cardiogenic shock in young patients who present in respiratory failure or undifferentiated shock who use both agents.
4. Khan A, Talha B, Vyas V, et al. Routine use of prescription Adderall leading to non-cardiogenic pulmonary edema and respiratory failure. Cureus 2021;13:e16371. https://doi.org/10.7759/ cureus.16371; PMID: 34395145.
5. Nauman M, Hahn C, Nketiah E, et al. Adderall induced dilated cardiomyopathy in an adult male with ADHD. J Am Coll Cardiol 2021;77(18 Suppl 1):2325. https://doi.org/10.1016/S07351097(21)03680-9
6. Scinico M, Brunton N, Kahn DM. Vaping induced lung injury precipitating cardiogenic shock. Presented at: American Thoracic Society International Conference, online, August 5, 2020. Abstract A6662. https://doi.org/10.1164/ajrccm-conference.2020.201.1_MeetingAbstracts. A6662
National Trends and Outcomes of Early versus Delayed Mechanical Circulatory Support in Patients with Acute Myocardial Infarction Complicated by Cardiogenic Shock
Kevin G Buda,1,2 Kasia Hryniewicz,1 Peter M Eckman,1 Mir B Basir,3 Jennifer A Cowger,3 Khaldoon Alaswad,3 Srini Mukundan,4 Yader Sandoval,1,5 Andrea Elliott,6 Emmanouil S Brilakis,1,5 and Michael S Megaly7
1. Allina Health Minneapolis Heart Institute, Minneapolis, MN; 2. Cardiology Division, Department of Internal Medicine, Hennepin Healthcare, Minneapolis, MN; 3. Heart and Vascular Institute, Henry Ford Hospital, Detroit, MI; 4. Knight Cardiovascular Institute, Oregon Health & Science University, Portland, OR; 5. Center for Coronary Artery Disease, Minneapolis Heart Institute Foundation, Minneapolis, MN; 6. Division of Cardiology, University of Minnesota, Minneapolis, MN; 7. Division of Cardiology, Willis Knighton Heart Institute, Shreveport, LA
Citation: US Cardiology Review 2024;18(Suppl 1):04. Correspondence: Kevin G Buda, kevin.buda@hcmed.org
Background: Despite increased temporary mechanical circulatory support (tMCS) utilization for acute MI complicated by cardiogenic shock (AMI-CS), observational and randomized data regarding tMCS efficacy are conflicting.
Objectives: The aim of the study was to describe outcomes based on tMCS timing in AMI-CS and to identify predictors of in-hospital and 30-day mortality and readmission.
Methods: Patients with AMI-CS identified in the National Readmissions Database (NRD) were grouped according to the use of tMCS and early (<24 hours) versus delayed tMCS (≥24 hours) utilization. The correlation between the timing of tMCS support and inpatient outcomes was evaluated using linear regression. Multivariate logistic regression (OR [95% CI]) using backward stepwise elimination was used to identify variables associated with 30-day mortality and readmission.
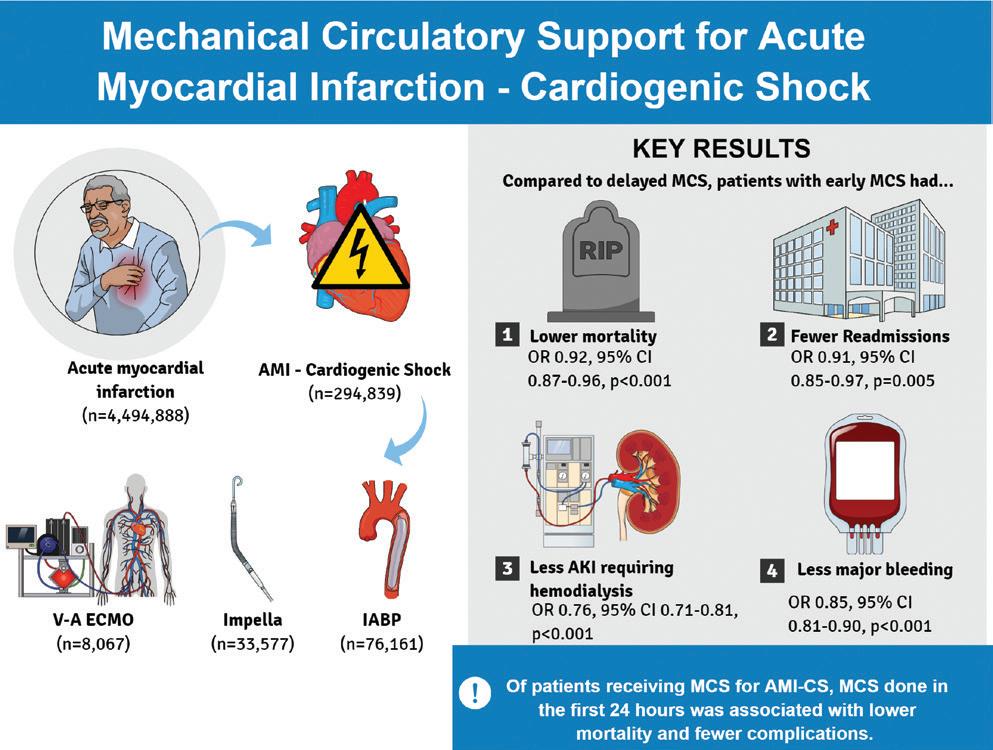
Figure 1: Mechanical Circulatory Support for Acute Myocardial Infarction: Cardiogenic Shock
Results: Patients who underwent tMCS (n=109,148) for AMI-CS had lower in-hospital mortality (33.9% versus 36.4%, p<0.001), longer lengths of stay (median [IQR]) (9 [4–17] days versus 7 [3–14] days, p<0.001), and twice the hospital cost (US$64,069 [$39,455–$105,441] versus US$31,832 [$17,595–$57,742] p<0.001) compared to those who did not have tMCS (n=185,691) in the unadjusted analysis. Patients who received tMCS within 24 hours of admission (n=79,906) had shorter length of stay (7 days versus 15 days, p<0.001), lower hospital cost (US$55,644 versus US$88,644, p<0.001), and lower rates of ischemic and bleeding complications than those with tMCS placed ≥24 hours after admission (n=32,241). After adjustment, early tMCS was associated with lower mortality (OR 0.92 [CI 0.88–0.96]) and readmission (OR 0.91 [CI 0.85–0.97]).
Conclusion: Among patients receiving tMCS for AMI-CS, early tMCS was associated with shorter lengths of stay, lower hospital costs, and fewer deaths and readmissions at 30 days. In AMI-CS, early tMCS may be preferable to delayed tMCS.
Immune Checkpoint Inhibitor Use Leading to Fulminant Myocarditis with Cardiogenic Shock: A Case Series
As the use of immunotherapy for treatment of malignancy has increased, complications are becoming increasingly recognized. Immune checkpoint inhibitor (ICI)-associated myocarditis is a rare complication with fatality rates of up to 50%. We describe two cases of fulminant ICI myocarditis with successful use of mechanical circulatory support and novel biologic agents as a bridge to myocardial recovery.
A 62-year-old woman with stage IV lung adenocarcinoma presented with nausea 3 weeks after her second cycle of pembrolizumab. A transthoracic echocardiogram (TTE) showed a mildly reduced ejection fraction of 45–50%. She was taken for right heart catheterization (RHC) which showed elevated filling pressures and a reduced cardiac index (Table 1). She was started on milrinone infusion and IV methylprednisolone for fulminant ICIassociated myocarditis. Despite this, she remained in a persistent low output state and the decision was made to implant an Impella CP as a bridge to recovery. Following Impella placement, she received one dose of anti-thymocyte globulin (ATG). Her cardiogenic shock resolved, and she was discharged home on a prolonged steroid taper. A TTE after completion of the taper showed recovery of ejection fraction to 60%.
In our second case, a 72-year-old woman with stage III lung adenocarcinoma presented with dizziness 1 month after receiving pembrolizumab. A TTE showed a newly reduced ejection fraction of 15%. She underwent RHC which showed normal filling pressures but reduced cardiac index (Table 1). An Impella 5.5 was placed, and she was started on a milrinone infusion. She was treated with IV methylprednisolone without improvement and thus was given abatacept and a Janus kinase inhibitor, ruxolitinib. As in the first case, cardiogenic shock resolved and the patient
Table 1: Right Heart Catheterization Data
mmHg (mean 34) 31/15 mmHg (mean 22)
25 mmHg 15 mmHg
MCS intervention Impella CP Impella 5.5
CO/CI = cardiac output/cardiac index; MCS = mechanical circulatory support; PA = pulmonary artery; RA = right artery.
was discharged home on a prolonged steroid taper. Ejection fraction recovered to 55% on follow-up TTE.
Neither patient was a candidate for advanced therapy such as heart transplantation or a left ventricular assist device due to active malignancy. Temporary mechanical support was used as a bridge to recovery while these patients received immunosuppressive medications in addition to traditional therapy with high-dose steroids. Multidisciplinary collaboration between cardiac critical care and cardio-oncology was key to creating appropriate treatment plans and allowed for early, aggressive intervention. This is highlighted by the second patient in which an Impella was placed for Society for Coronary Angiography and Intervention (SCAI) stage B shock. Both cases illustrate patients who experienced a full cardiac recovery after the use of novel immunosuppressive therapies in conjunction with temporary mechanical support for cardiogenic shock secondary to fulminant ICI-associated myocarditis.
Creation of a New Percutaneous Coronary Intervention Program in a Safety Net Hospital: Impact on Cardiac Intensive Care Unit Population and Outcomes
Nathaniel Abittan,1 Israel Safiriyu,2 Shaunak Mangeshkar,3 Rosy Thachil,4 Seth Sokol,5 Eleonora Gashi,5 Jincy Thankachen,6 and Miguel Alvarez-Villela7
1. Division of Cardiology, New York Medical College/Westchester Medical Center Valhalla, NY; 2. Section of Cardiovascular Medicine, Yale University School of Medicine, New Haven, CT; 3. Department of Medicine, Albert Einstein College of Medicine/Jacobi Medical Center, Bronx, NY; 4. Division of Cardiology, Icahn School of Medicine at Mount Sinai, Mount Sinai Medical Center, New York, NY; 5. Division of Cardiology, Albert Einstein College of Medicine/Jacobi Medical Center, Bronx, NY; 6. Division of Cardiology, NYU Grossman School of Medicine, New York, NY; 7. Division of Cardiology, Lenox Hill Hospital, Northwell Health, New York, NY
Citation: US Cardiology Review 2024;18(Suppl 1):16. Correspondence: Nathaniel Abittan, abittan.nathaniel@gmail.com
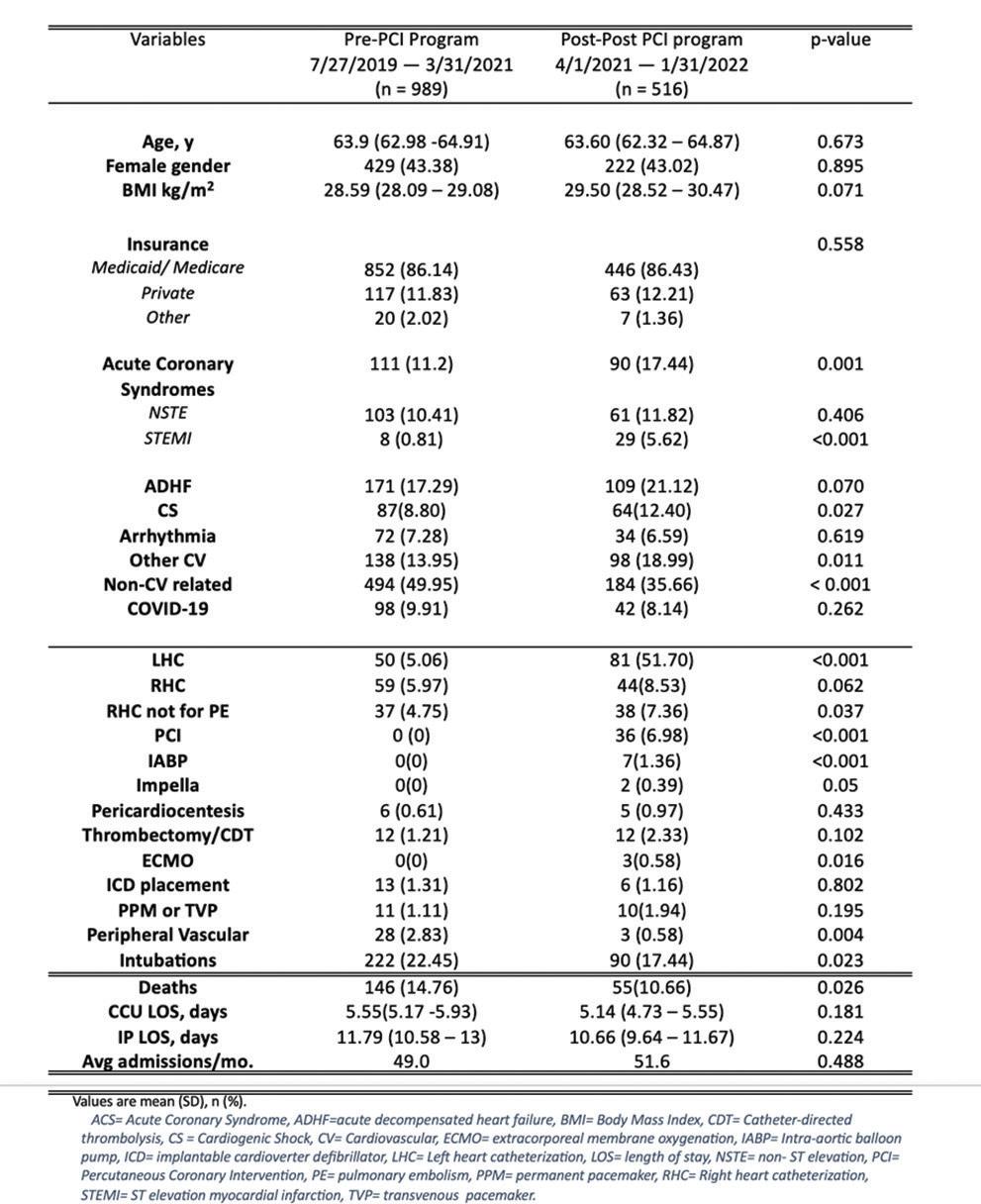
Table 1: Baseline Demographics, Diagnoses and Procedures, and Outcomes
Background: Little is known about the impact of a local percutaneous coronary intervention (PCI) program on the demographics, management, and outcomes of the cardiac intensive care unit (CICU).
Methods: Unselected patients admitted to the CICU in a large safety net hospital between July 2021 and January 2022 were identified using the electronic health record. Admissions were classified into two cohorts: before, and after the local PCI program implementation on April 1, 2021.
Data on demographics, management procedures and outcomes were compared between both periods. Logistic regression was performed to identify independent predictors of admission type and hospital mortality.
Results: A total of 1,505 patients were identified; 989 in the pre-PCI period and 516 in the post-PCI period. Demographics were comparable in both cohorts. Admissions for non-cardiac diagnoses were less common in the post-PCI period (aOR 0.56; p<0.001), with increasing prevalence of acute coronary syndrome and cardiogenic shock (CS) admissions. Patients
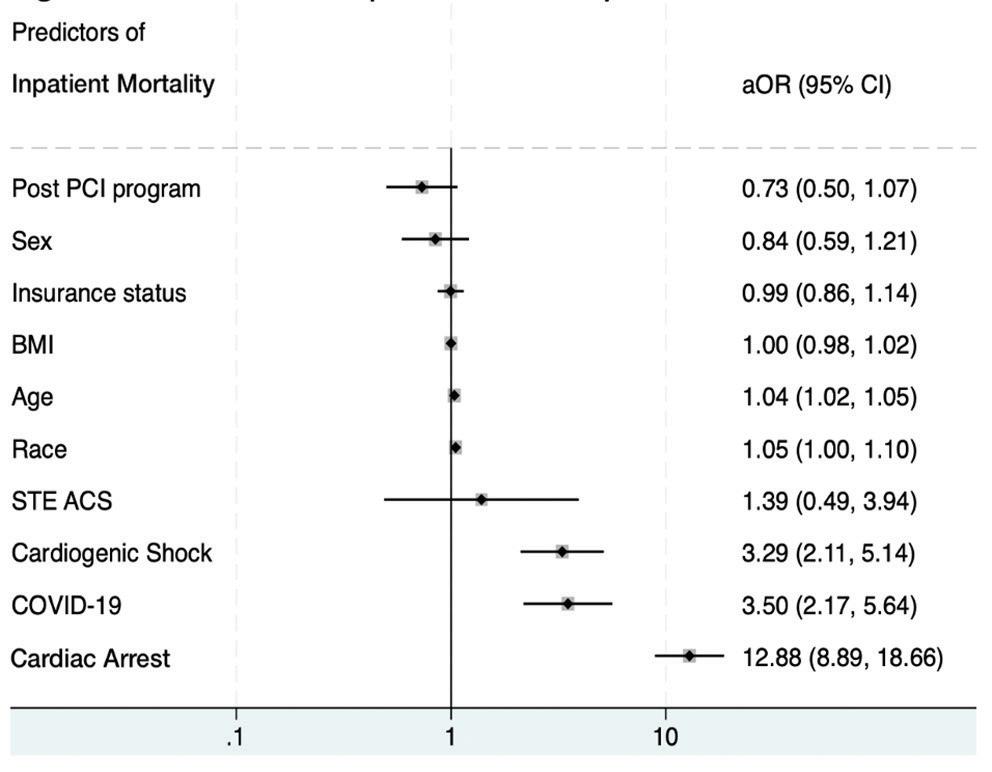
Figure 1: Predictors of Inpatient Mortality
Abstracts from the 3rd Annual NYU Langone Critical Care Cardiology Symposium and CardioNerds Poster Session
receiving PCI and mechanical circulatory support including ECMO were a de novo population in the post-PCI period. After multivariate analysis there was no difference in mortality between both periods. Cardiac arrest, COVID-19, CS and age were all independent predictors of mortality.
Conclusion: The introduction of a local PCI program led to an increase in cardiac-related admissions and patient acuity in the CICU of a large safety-net hospital without an increase in adjusted hospital mortality.
18
Myasthenia Crisis Complicated with Takotsubo Cardiomyopathy
Amandeep Goyal,1 Roopesh Sai Jakulla,2 Pratik Bhyan,1 Mohammad Alarfaj,1 Taher Tayeb,1 Sarah Barker,1 Poonam Bhyan,1 Siva Naga Yarrarapu,1 Kevin A Bybee,2 and Tarun Dalia1
1. Department of Cardiovascular Medicine, University of Kansas Medical Center, Kansas City, KS; 2. Department of Cardiovascular Medicine, University of Missouri Kansas City, Kansas City, MO
Citation: US Cardiology Review 2024;18(Suppl 1):18. Correspondence: Tarun Dalia, tdalia2@kumc.edu
Introduction: Myasthenia gravis can precipitate severe stress especially during a myasthenic crisis (MC) episode that can lead to takotsubo cardiomyopathy (TTC). Emotional and physical stress are some of the most common precipitating factors of MC and TTC.
Case: A 77-year-old woman with hypertension, type 2 diabetes, and myasthenia gravis (on prednisone) presented to the hospital with complaints of worsening fatigue and shortness of breath over 1 week. The patient lost her service dog 2 weeks prior and was feeling very stressed.
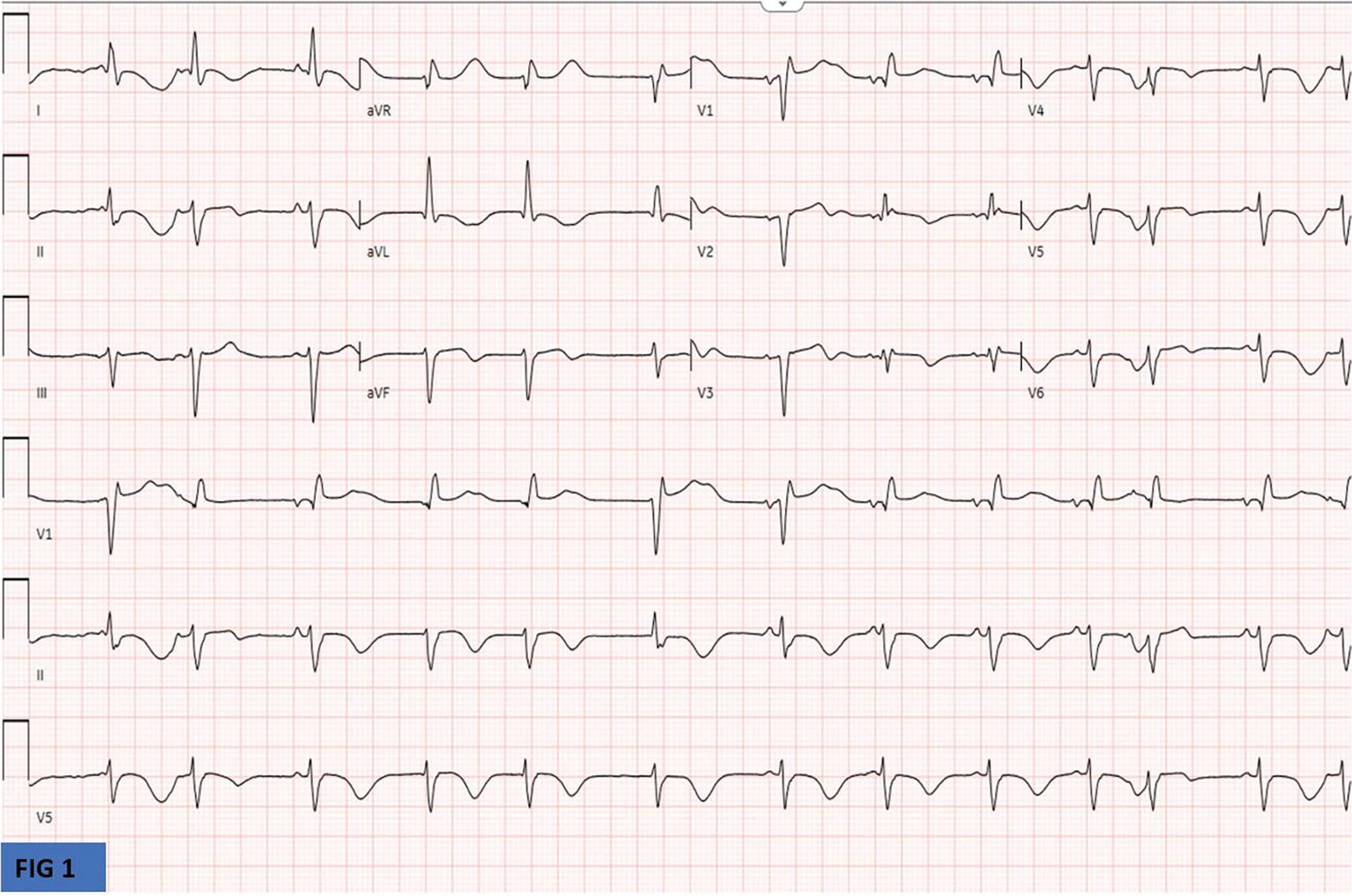
Figure 1
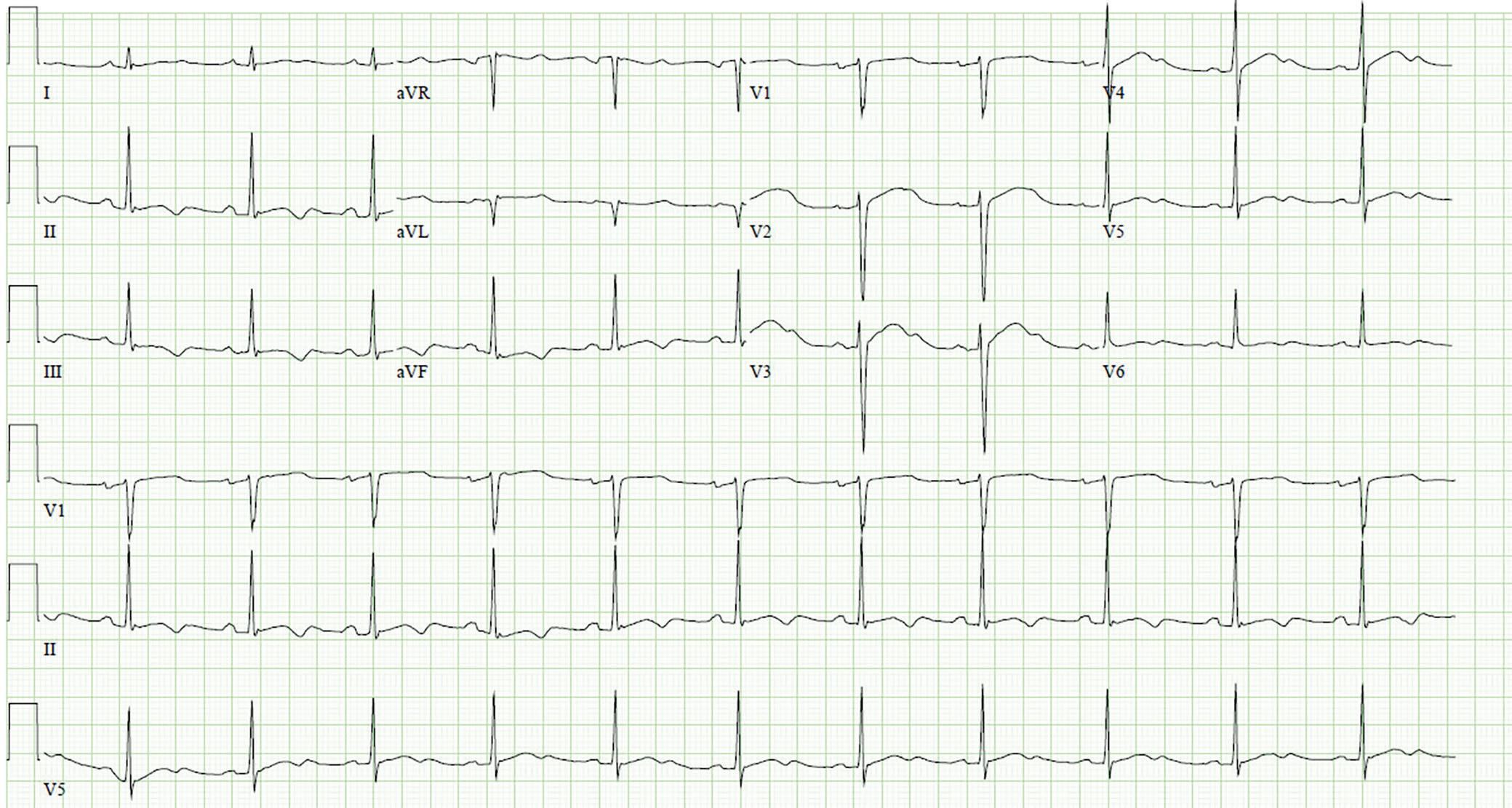
Normal sinus rhythm with diffuse T wave inversions in anterolateral leads. Few premature atrial contractions noted.
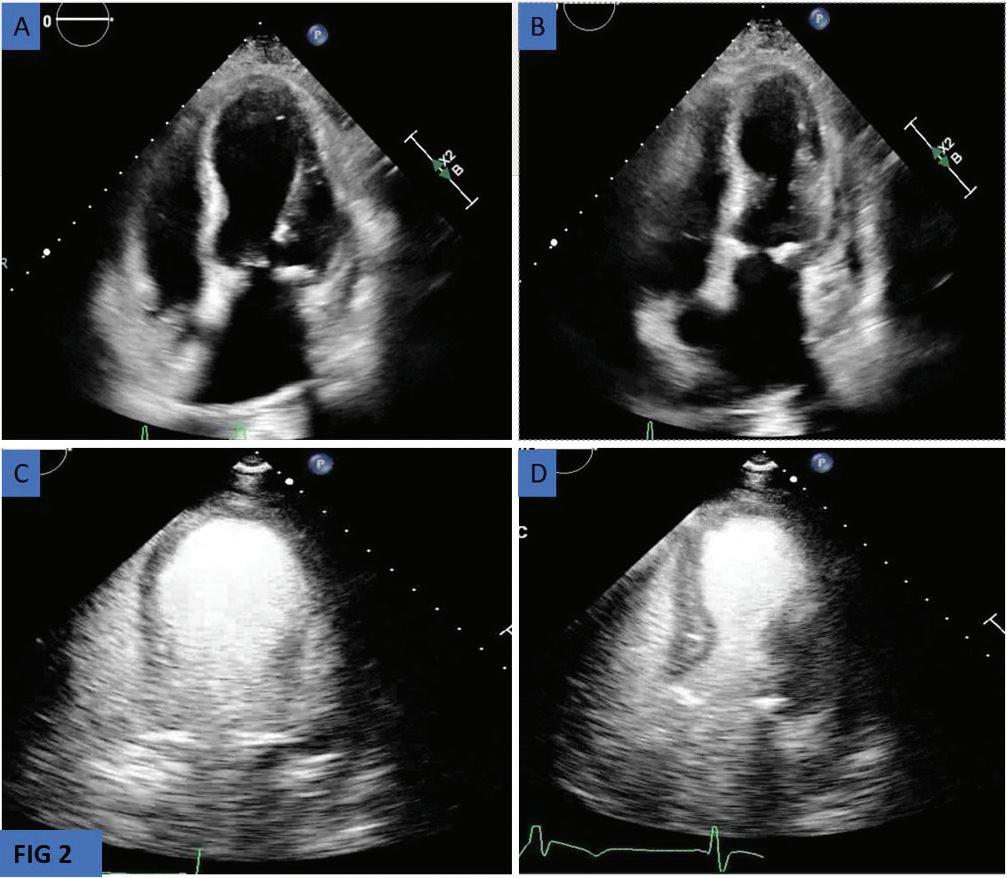
Apical Four-chamber View
She was admitted to the intensive care unit with MC and intubated for impending hypercapnic respiratory failure. The patient was started on
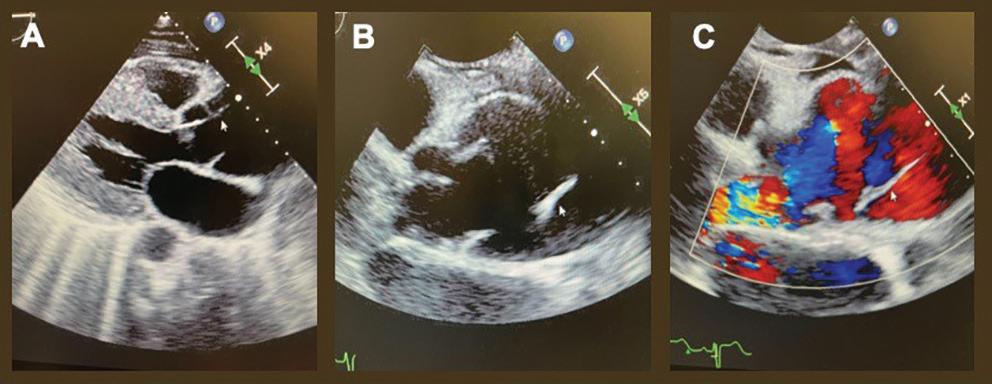
pyridostigmine, steroids, and plasma exchange (PLEX) treatments. During her hospital course, the patient was found to be hypotensive and developed new EKG changes (diffuse T wave inversions in anterolateral leads; Figure 1). High-sensitive troponins were in the range of 1,300–1,400 ng/dl. Transthoracic echocardiogram images without contrast (apical fourchamber view) in Figure 2A (diastole), Figure 2B (systole) revealed apical ballooning; Figure 2C (diastole) and Figure 2D (systole) with contrast confirmed the apical ballooning. Video 1 without contrast and Video 2 with contrast show the apical hypokinesia, apical ballooning, and basal hyperkinesis. Coronary angiography performed 2 years prior showed no significant coronary artery disease.
Decision-making: The patient was diagnosed with takotsubo cardiomyopathy (TTC), also called stress-induced cardiomyopathy. Stress due to the recent loss of her dog with worsening myasthenia gravis led to MC complicated with TTC. Unfortunately, in this patient, this combination was fatal.
Conclusion: Patients with myasthenia gravis are at a higher risk of developing TTC, particularly during a myasthenic crisis. The myasthenia crisis associated with TTC occurs predominantly in women and is associated with poor prognosis. A systematic review of 16 cases showed that all myasthenia gravis patients who developed stress-induced cardiomyopathy had myasthenia crisis. Therefore, identification of myasthenia crisis should alert the treating clinician for careful clinical and EKG monitoring to look for features of TTC.
Figure 2: Transthoracic Echocardiogram
A: diastole, and B: systole, without contrast revealing apical ballooning; C: diastole, and D: systole, with contrast confirmed the apical ballooning.
Pheo,
Don’t Break My Heart: A Rare Case of Reverse Takotsubo Cardiomyopathy with Pheochromocytoma
Uzair A Mahmood, MD, and Howard A Cooper, MD
Department of Cardiology, Westchester Medical Center, Valhalla, NY
Citation: US Cardiology Review 2024;18(Suppl 1):19.
Correspondence: Uzair A Mahmood, uzair.mahmood@wmchealth.org
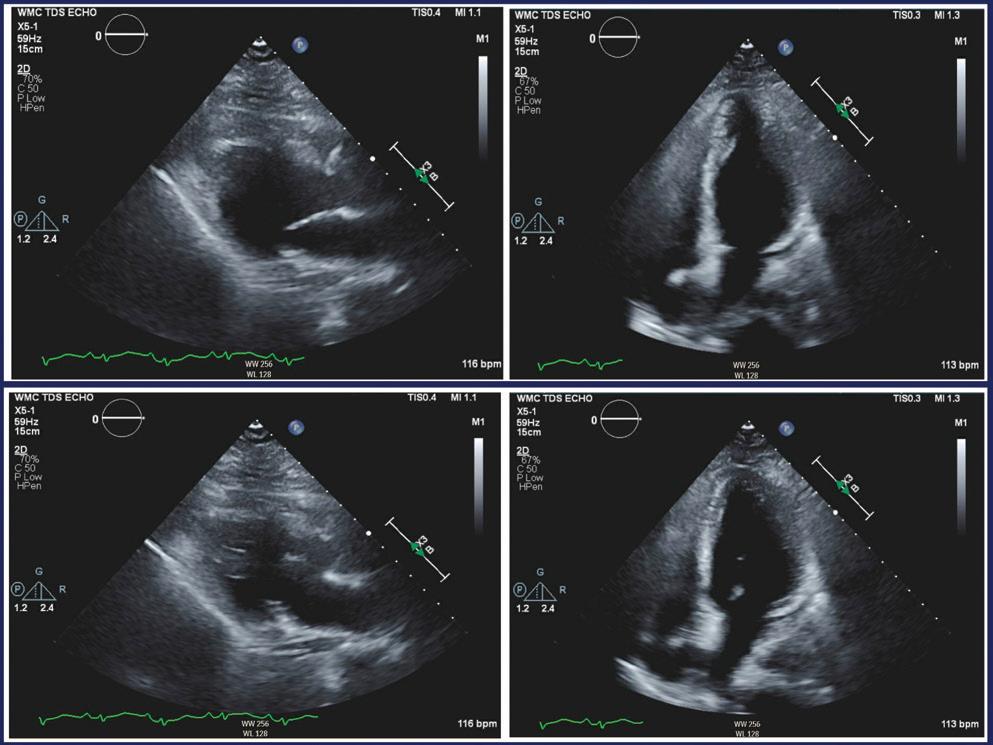
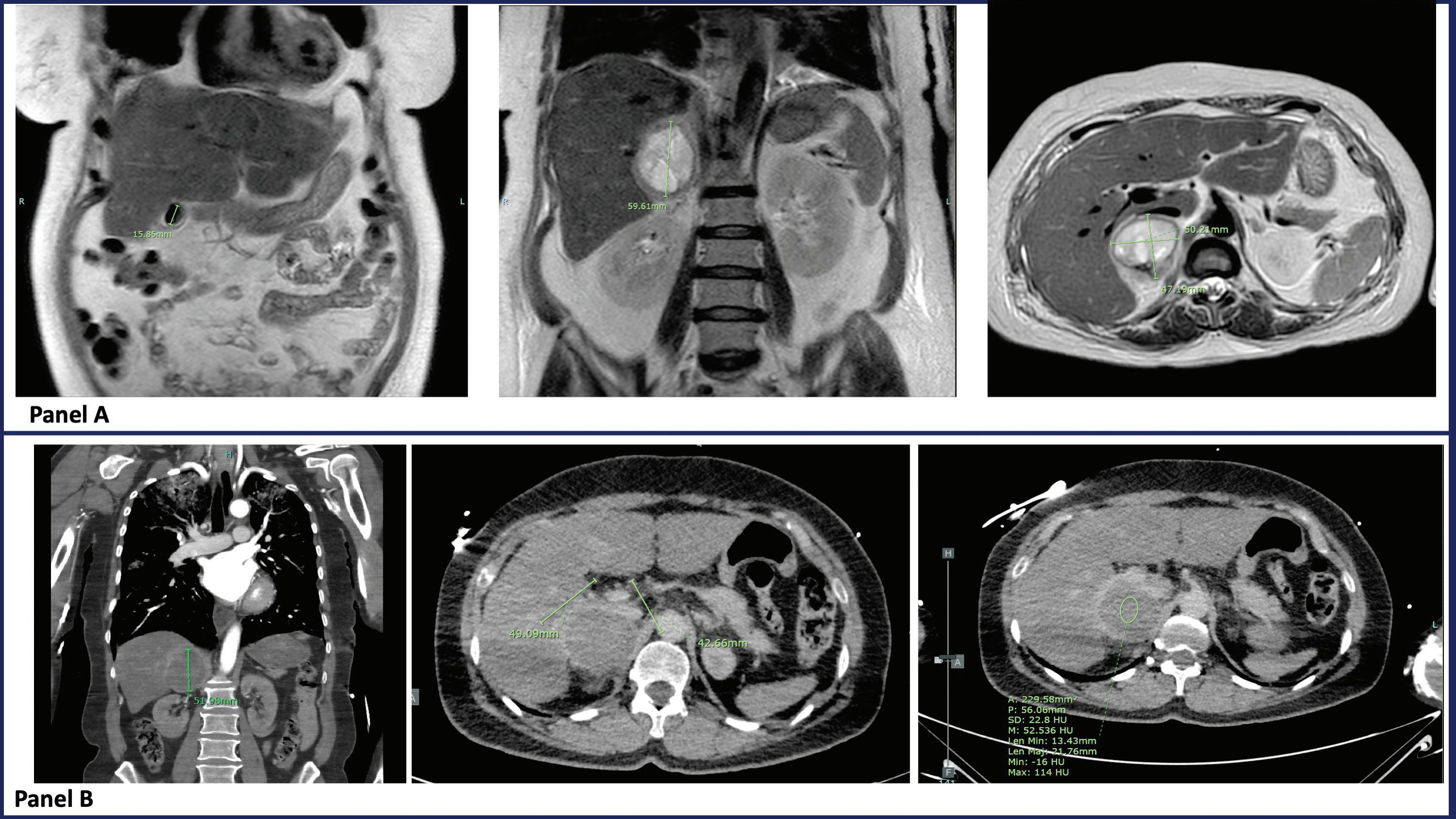
A 59-year-old woman with a medical history of diverticulitis and type 2 diabetes presented with dyspnea on minimal exertion, fatigue, intermittent headaches, nausea/vomiting, and severe abdominal pain of 7 days duration. She was noted to have extremely labile blood pressures in the emergency room and had evidence of pulmonary edema on auscultation and chest imaging. A point of care ultrasound (POCUS) exam demonstrated a dilated left ventricle with severe hypokinesis of the basal myocardial segments and reduced left ventricular (LV) systolic function (Figure 1). She had elevated troponin and lactic acid, and a 12lead EKG demonstrated sinus tachycardia with horizontal ST depressions in the anterior precordial leads. The patient was started on vasopressors and intubated for worsening hypoxic respiratory failure. A subsequent coronary angiogram showed non-obstructive coronary artery disease, and right heart catheterization demonstrated elevated filling pressures with reduced cardiac output. A femoral intra-aortic balloon pump (IABP) was placed, and the patient was admitted to the critical care unit for mechanical circulatory support, mechanical ventilation, and continuous veno-venous hemodialysis. Her echo findings were suggestive of a reverse takotsubo cardiomyopathy pattern, and given her clinical presentation, there was suspicion for pheochromocytoma. Abdominal imaging with CT and MRI demonstrated a 4.7 × 5 × 6-cm right adrenal mass of unclear chronicity (Figure 2). Plasma and urine metanephrines were markedly elevated as well, although difficult to interpret in the setting of critical illness. Given the constellation of clinical and radiographic findings, alpha blockade with doxazosin was initiated and her hemodynamics and LV function improved significantly over the next few days. IABP was weaned and she was able to be extubated after adequate volume removal via continuous veno-venous hemofiltration. After a multidisciplinary discussion, she underwent elective right adrenalectomy with biopsies. Pathology confirmed pheochromocytoma with hemorrhagic and cystic degeneration and immunopositivity for synaptophysin and chromogranin. Ki-67 index was >40%, suggestive of a malignant pheochromocytoma. The patient’s renal function recovered,
and she was taken off hemodialysis prior to discharge to home. She was seen in the clinic for follow-up 3 weeks later and did not report any symptoms. Her blood pressures remained well controlled on doxazosin 10 mg once daily.
To date, there are approximately 36 reported cases of concurrent pheochromocytoma and takotsubo cardiomyopathy; however, association with reverse takotsubo pattern is very rare. In both conditions, the postulated mechanism of action is catecholaminemedicated myocardial depression. This case highlights the clinical manifestations, workup, and management options for this unusual and reversible cardiomyopathy.
Figure 1
2D transthoracic echocardiographic images demonstrating apical contractility with basal hypokinesis during systole (top panel), suggestive of reverse takotsubo cardiomyopathy. Images during diastole (bottom panel) for comparison.
Panel A: MRI abdomen C+/C- shows a 4.7 × 5.0 × 6.0 cm (anteroposterior × transverse × craniocaudal) mixed cystic and solid lesion in the right adrenal gland with T1 hyperintensity, heterogenous T2 signal, and equivocal contrast enhancement. T1 hyperintensity likely reflects intralesional hemorrhage. No intralesional fat is noted. Panel B: CT angio thorax/abdomen/pelvis shows a 4.3 x 4.9 x 5.2 cm round mass in the region of the right adrenal gland. Normal left adrenal gland.
Figure 2
Discharge Medical Therapy and In-hospital Outcomes among Patients with Cardiogenic Shock Due to Decompensated Heart Failure versus Acute Myocardial Infarction Treated in a Safety Net Hospital
Eric J Hall, MD,1,2 Colby R Ayers, MS,2 Nicholas S Hendren, MD,1,2 Christopher Clark, BS,1 Amit Saha, MD,1,2 Isabella L Alexander, BS,2 Evan P Gee, BS,2 Ian R McConnell, BA,2 Emily S Samson, BSA,2 Roslyn J Saplicki, BA,2 Justin L Grodin, MD, MPH,1,2 Jennifer T Thibodeau, MD, MSCS,1,2 Mark H Drazner, MD, MSc,1,2 Mujeeb Basit, MD, MMSc,1,2 Maryjane A Farr, MD, MSc,1,2 Ann Marie Navar, MD, PhD,1,2 Sandeep R Das, MD, MPH,1,2 and James A de Lemos, MD1,2
1. Parkland Health System, Dallas, TX; 2. Division of Cardiology, Department of Internal Medicine, University of Texas Southwestern, Dallas, TX
Citation: US Cardiology Review 2024;18(Suppl 1):25. Correspondence: Eric J Hall, eric.hall@utsouthwestern.edu
Table 1: Comparison of Patients with Cardiogenic Shock Due to Acute MI and Decompensated Heart Failure
Admission SCAI stage
Peak SCAI stage
from admission to peak SCAI stage (days, 25–75th percentile)
Cardiac arrest
Table 1: (Continued)
Survived to discharge, all
Survived to discharge, excluding interhospital transfers/hospice discharges
Discharge medications
ACE/ARB/ARNI = angiotensin converting enzyme inhibitors/angiotensin receptor blocker/angiotensin receptor-neprilysin inhibitors; AMI-CS = acute myocardial infarction with cardiogenic shock; HF-CS = cardiac shock due to decompensated heart failure; MRA = mineralocorticoid receptor antagonists; PAPi = pulmonary artery pulsatility index; SCAI = Society for Coronary Angiography and Intervention; SGLT2I = sodium–glucose cotransporter 2.
Background: While in-hospital mortality in patients with cardiogenic shock (CS) remains high, most patients will survive to hospital discharge. Little is known regarding medical therapy for survivors of cardiogenic shock. Likewise, much of the data regarding CS outcomes is from large academic tertiary care referral centers, with limited data regarding underserved patient populations or management of CS in other types of hospitals.
Methods: This was a single-center retrospective analysis of patients treated at a public health system hospital who met criteria for Society for
Coronary Angiography and Intervention (SCAI) stage C, D, or E CS, defined as requiring mechanical circulatory support (MCS) or vasoactive medications. Patients were initially identified from within a larger cohort of patients with reduced ejection fraction who had undergone a right heart catheterization (RHC) between 2017 and 2023. For analyses of medication use on discharge, patients discharging to hospice or to another hospital were excluded.
Results: A total of 378 patients met criteria for stage C or greater shock while hospitalized (Table 1). Median age of patients was 57 years. Black patients comprised 44% of the cohort, while 35% were Hispanic. The majority (81%) of patients experienced CS due to decompensated heart failure (HF-CS), while 19% experienced CS due to an acute myocardial infarction (AMI-CS). Patients with HF-CS were less likely to meet criteria for ≥stage C shock within 24 hours of admission (36% for patients with HF-CS versus 59% for AMI-CS, p<0.001). Median time to peak SCAI stage was 3 days in the HF-CS group. MCS was used in 23% of all patients. Cardiac index and filling pressures were similar between the two groups. Overall, 82% of patients survived to discharge, with 66% discharged to home or a rehabilitation facility and 12% transferred to another hospital. Survival was higher in patients with HF-CS than in those with AMI-CS (85% versus 71%, p=0.01). On discharge, β-blockers were prescribed in 38% of CS survivors who were discharged from medical care, including 34% of patients with HF-CS and 58% with acute MI complicated by cardiogenic shock (AMI-CS) (p=0.009). Angiotensin converting enzyme inhibitors/angiotensin receptor blocker/angiotensin receptor-neprilysin inhibitors (ACE/ARB/ARNI) use was similar among patients with HF-CS and AMI-CS (60% versus 75%, p=0.14).
Conclusion: Patients with HF-CS were less likely to meet criteria for SCAI C or greater shock on hospital admission than those with AMI-CS. ACE/ARB/ARNIs were used in most CS survivors discharging from medical care, while β-blocker use was less common, particularly among patients who survived HF-CS.
AMI-CS with Misidentification of the Culprit Requiring Delayed Revascularization of LCX, Complicated by MR Requiring IABP and MV TEER
David Wang, MD, David Lee, MD, and Alan Yeung, MD
Stanford Medical Center, Palo Alto, CA
Citation: US Cardiology Review 2024;18(Suppl 1):26. Correspondence: David Wang, denzewang@stanford.edu
A 63-year-old man with a coronary artery bypass graft performed in 2008 (left internal mammary artery-left anterior descending [LIMA-LAD], selective saphenous vein graft-right coronary artery [SVG-RCA]) presented to an outside facility with chest pain and was found to have an inferior ST-elevation MI (STEMI). He was taken to the cath lab. The left main coronary artery was patent and the LAD was occluded in the mid segment, with a patent LIMA-LAD perfusing the mid-distal LAD. The left circumflex artery (LCX) had an 80% proximal lesion and was not grafted. The right coronary artery (RCA) was occluded in the proximal segment, and the SVG-RCA graft was also occluded proximally. The culprit was thought to be the SVG-RCA. The patient was loaded with dual antiplatelet therapy and started on eptifibatide. Three stents were implanted in the SVG-RCA. On hospital day (HD) 3 the patient continued to have chest pain with ST elevations, and he returned to the cath lab. The SVG-RCA graft was found
to be re-occluded within the stents and the prior LCX 80% lesion was noted to progress to a 100% occlusion.
The patient was transferred to our institution for further management on HD 4. He arrived with a heart rate of 60 BPM and blood pressure 110/80 mmHg. O2 saturation was 97%, and he was in respiratory distress requiring bilevel positive airway (BiPAP) ventilation. Creatinine was 2 mg/ dl, alanine transaminase 249 U, bilirubin 1.7 mg/dl, and lactate 3 mmol/l. A transthoracic echocardiography (TTE) was performed that showed a left ventricular ejection fraction of 40% with inferior and posterior hypokinesis and moderate, posteriorly directed mitral regurgitation (MR). Review of the outside angiogram suggested that the SVG-RCA occlusion may have been chronic given the appearance of the SVG thrombus and that the culprit of the STEMI presentation was the LCX lesion given the acutely
Figure 1A Figure 1B
A: Left circumflex artery pre-percutaneous coronary intervention.
B: Left circumflex artery post-percutaneous coronary intervention.
progressing lesion. The patient continued to have active chest pain requiring nitroglycerin.
The patient was taken back to the cath lab for revascularization of the LCX with one drug-eluting stent, with 0% residual lesion and thrombolysis in MI (TIMI) grade 3 flow. A pulmonary artery line was inserted which showed right atrium pressure of 20 mmHg, right ventricle 55/20 mmHg, pulmonary artery 55/24/32 mmHg, pulmonary capillary wedge 24 mmHg with V waves to 40, and Fick CI of 1.7 l/min/m2. Given significant respiratory distress that was thought to be related to MR, potentially underestimated on TTE given the eccentric nature and tall V waves, an intra-aortic balloon pump (IABP) was inserted. The patient returned to the cardiac care unit with resolution of chest pain and significant respiratory improvement. Transesophageal echocardiography (TEE) was performed, which showed severe, eccentric posteriorly directed MR in the setting of inferolateral hypokinesis. Given significant respiratory distress requiring BiPAP in the setting of severe MR with inability to liberate from IABP despite high doses of IV vasodilators, the patient returned to the cath lab on HD 12 for mitral valve (MV) transcatheter edge-to-edge repair. The patient
underwent successful implantation of a MitraClip G4 XTW with reduction of MR to trace. The next day, the patient was weaned from both BiPAP and the IABP. The patient was transferred to the floor and guideline-directed medical therapy was instituted. On HD 18, the patient was discharged to home.
There are several lessons from this case. First, appropriate revascularization, even if delayed, remains standard of care for acute MIcardiogenic shock (AMI-CS). In the present case, the culprit was initially misidentified as the SVG-RCA graft, and the acute culprit lesion was the LCX, which eventually underwent revascularization 5 days later. Second, IABP should not be considered as a routine strategy for AMI-CS. However, in this case, given severe ischemic MR with respiratory distress, a trial of IABP was pursued and led to significant improvement on the cath lab table. Had the patient significant hypotension, or if IABP had not led to improvement, escalation would have been made to an Impella CP. Third, in select patients with CS with severe MR, MV transesophageal echocardiography can be considered in an attempt to liberate from mechanical circulatory support.
Figure 1C Figure 1D
C: Mitral valve with severe mitral regurgitation prior to transcatheter edge-to-edge repair.
D: Mitral valve with mild mitral regurgitation after mitral transcatheter edge-to-edge repair.
An Acquired Gerbode Defect Masquerading as Tricuspid Valve Endocarditis
Ryan
R Keane, MD, Chris S Massad, MD, Daniel Burns, MD, Shinya Unai, MD, Ran Lee, MD, and Andrew Higgins, MD
Citation: US Cardiology Review 2024;18(Suppl 1):27. Correspondence: Ryan R Keane, keaner@ccf.org
History of Present Illness: A 72-year-old man presented to an outside hospital emergency room (ER) with several weeks of dyspnea on exertion and fatigue. The patient’s presenting vitals in the ER were notable for a heart rate of 90 BPM and a blood pressure of 92/75 mmHg. On exam, he was in no acute distress, had an irregularly irregular heart rate, a harsh systolic murmur loudest at the left upper sternal border, jugular venous distention to his mandible, cool extremities, and 1+ pitting lower extremity edema.
1A: Acquired Gerbode Defect Due to Endocarditis
Medical History: The patient had a history of ascending aortic aneurysm with severe aortic regurgitation, now post-modified mechanical Bentall with a 23 mm St Jude valved conduit, as well as hypertension and hyperlipidemia. He was a former smoker, reported minimal alcohol usage, and no substance use.
CICU Course: At the outside ER, labs were notable for elevated transaminases and an elevated lactate. A transthoracic echocardiogram
Cleveland Clinic Foundation, Cleveland, OH
Figure
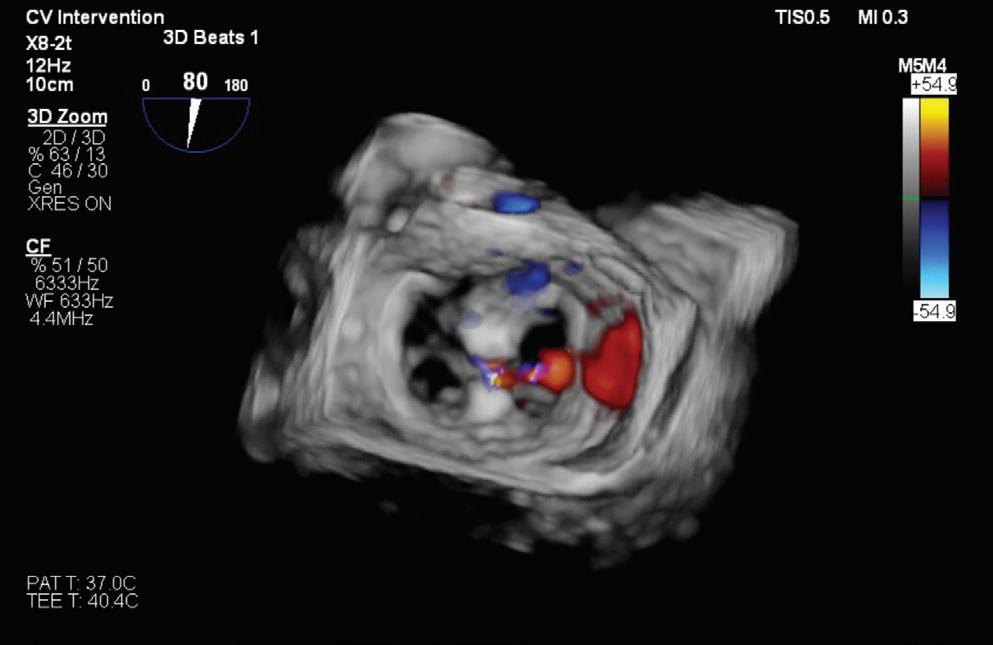
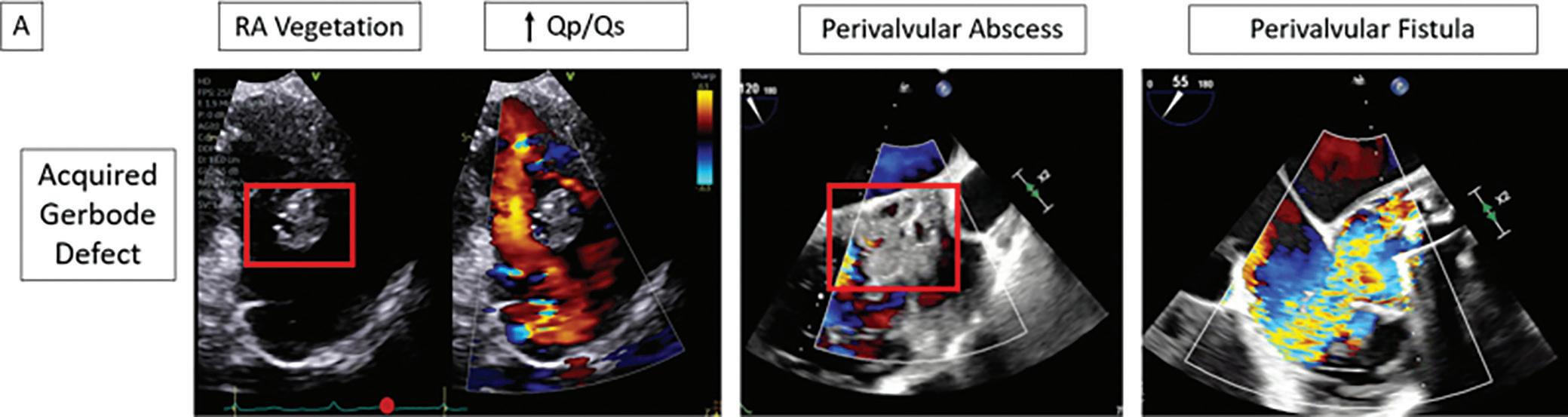
First two panels: large vegetation noted in the right atrium with diastolic flow (red dot) into the right ventricle (RV) noted on transthoracic echo (“RA vegetation” and “Qp/Qs”). On transesophageal echo, a large perivalvular abscess is noted on a mid-esophageal long axis view (“perivalvular abscess”) A left ventricular outflow tract to right atrium fistula is then noted on the mid-esophageal RV inflow-outflow view (“perivalvular fistula”).
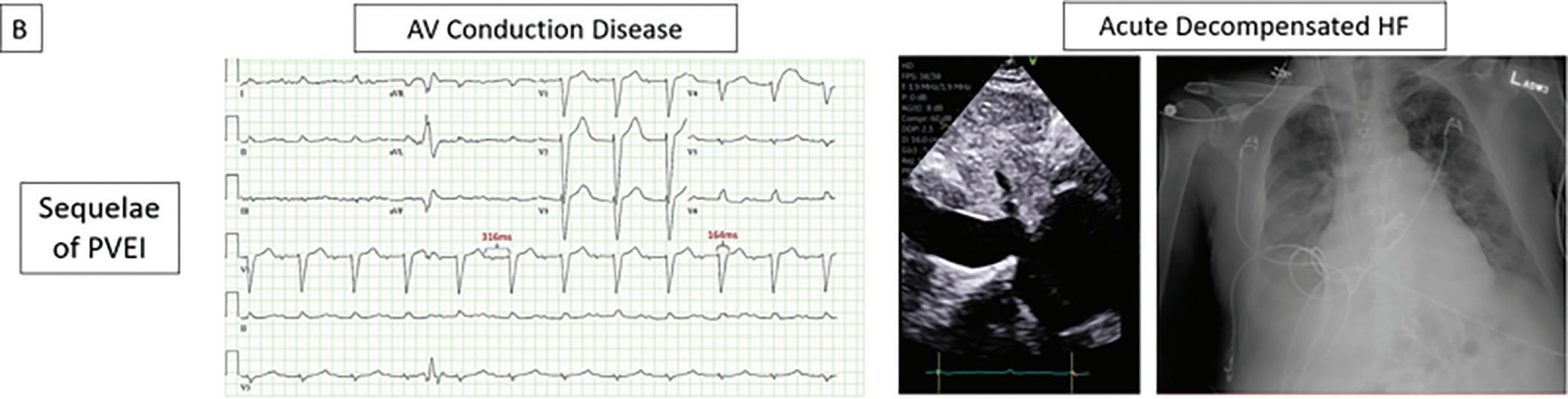
EKG demonstrating first degree heart block and left bundle branch block. Inferior vena cava (IVC) view on transthoracic echo demonstrating dilated IVC and likely elevated right atrial pressure. Chest X-ray demonstrating pulmonary edema.
Figure 1B: Acquired Gerbode Defect Due to Endocarditis
(TTE) revealed a tricuspid valve vegetation with moderate tricuspid regurgitation. The patient was transferred to the cardiac intensive care unit (CICU) for further evaluation of tricuspid valve endocarditis.
On arrival to the CICU, labs were notable for a creatinine of 2.4 mmol/l, potassium of 5.5 mmol/l, alanine transaminase of 1,684 U, aspartate aminotransferase of 1,126 µ/l, and lactate of 5.9 mmol/l with a pH of 7.35 on venous blood gas. EKG showed sinus rhythm with a PR interval of 316 ms and a left bundle branch block. A TTE demonstrated severe eccentric tricuspid regurgitation and a large right atrial vegetation. There was also diastolic flow into the right ventricle from an unclear origin (Figure 1A).
Subsequent transesophageal echocardiogram (TEE) revealed a circumferential aortic root abscess with a perivalvular fistula from the left ventricular thrombus (LVOT) into the right atrium (RA) above the tricuspid valve annulus with more flow through the fistula than across the aortic valve (Figure 1A).
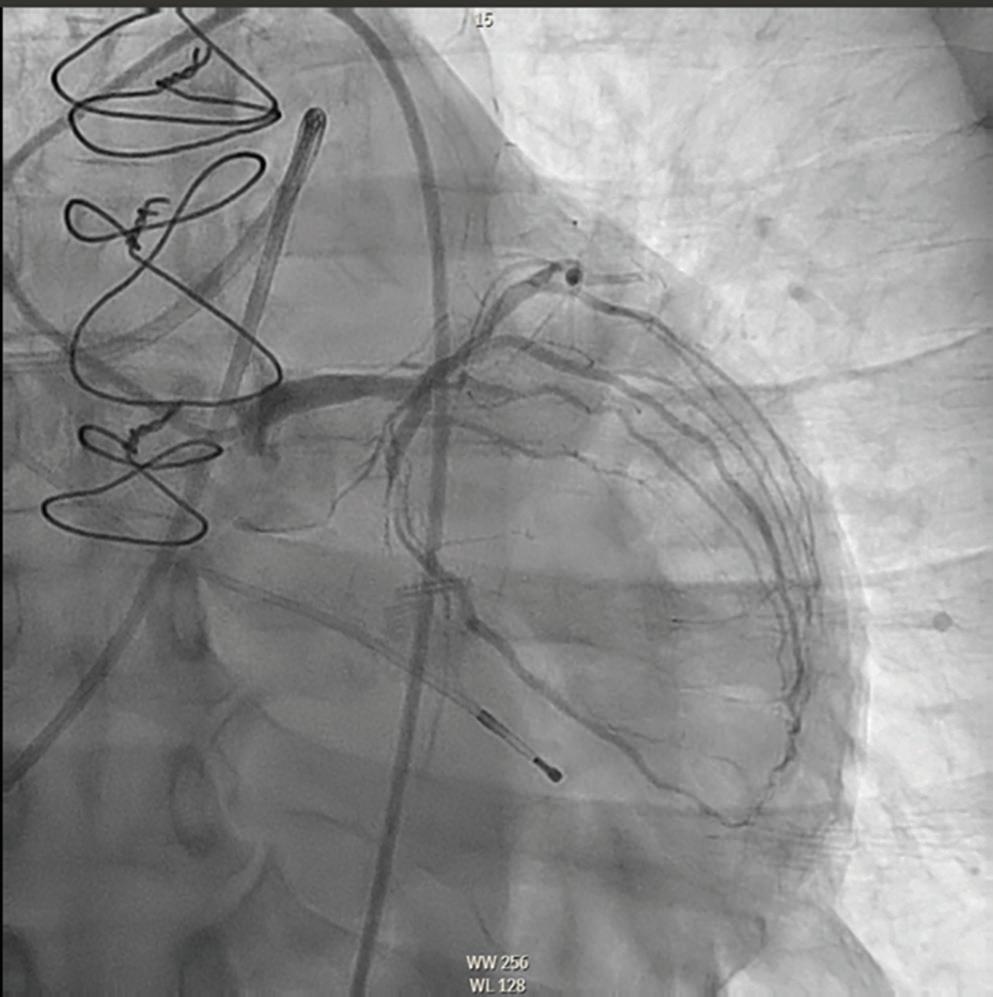
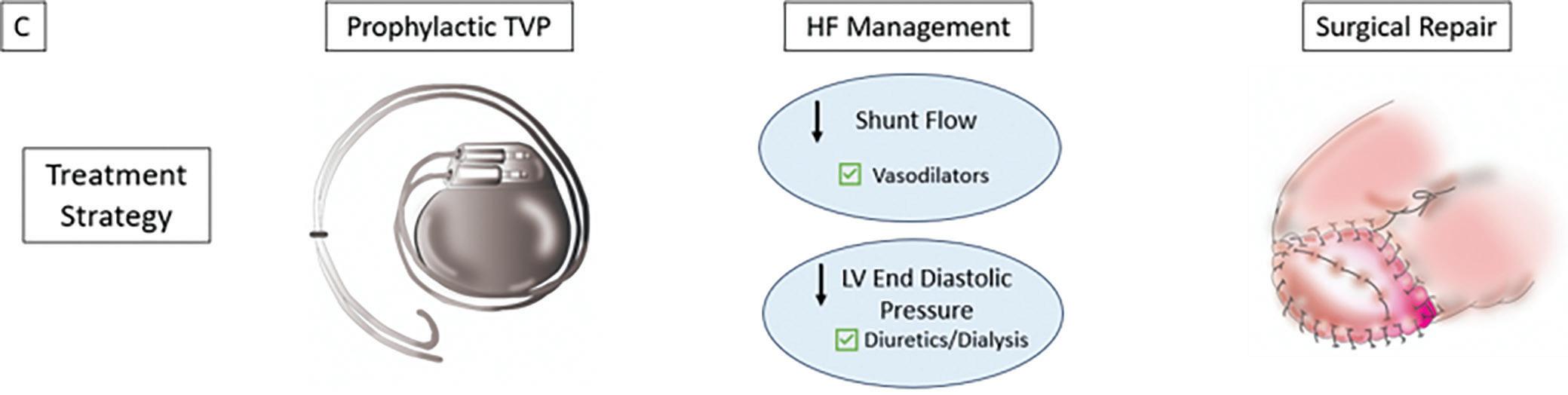
Management: Cardiothoracic surgery was emergently consulted. The patient was started on IV furosemide and sodium nitroprusside to reduce shunt flow across the fistula. For surgical planning, coronary angiography was discussed with the on-call interventional cardiologist. The patient underwent selective coronary angiography of the left coronary artery (previously known to be left dominant) and placement of a temporary
active fixation transvenous pacemaker (TVP) given his prolonged PR interval and left bundle branch block.
The patient remained hemodynamically stable overnight. The next morning, surgical examination revealed a large aortic root abscess with erosion of the mitral valve annulus and an LVOT-RA fistula with multiple large vegetations in the RA. The patient underwent extensive debridement, replacement of the mechanical aortic valve with a homograft, mitral valve repair, bovine patch repair, and tricuspid valve repair. Tissue and blood cultures subsequently grew Peptostreptococcus micros. The patient completed a course of antibiotics and was discharged home on postoperative day 11 with complete renal and hepatic recovery.
Learning Points
• In a patient with shock out of proportion to the suspected valvular lesion, careful attention to hemodynamics should lead to re-evaluation with TEE (Figure 1A).
• Acquired Gerbode defect is a rare complication of aortic root abscesses and can present with AV conduction disease and acute heart failure (Figure 1B).
• The CICU plays a key role in both medical stabilization and the organization of a definitive surgical repair (Figure 1C).
Treatment principles for perivalvular extension of infection.
Figure 1C: Acquired Gerbode Defect Due to Endocarditis
Periprocedural Extracorporeal Membrane Oxygenation Use During Transcatheter Aortic Valve Replacement in Cardiogenic Shock
Sinan S Sayood, MD, and James D Rossen, MD
Division of Cardiovascular Medicine, University of Iowa Hospitals and Clinics, Iowa City, IA
Citation: US Cardiology Review 2024;18(Suppl 1):28. Correspondence: Sinan S Sayood, ssayood@uiowa.edu
Presentation: A 64-year-old man with type 2 diabetes with neuropathy and active tobacco use presented to a local hospital with weakness, fatigue, dyspnea on exertion, paroxysmal nocturnal dyspnea, orthopnea, leg swelling, and abdominal distention. He had been diagnosed with moderate aortic stenosis (AS) seven years earlier. One year earlier, the patient was able to work full-time on home renovations with heavy lifting, but since that time he had developed class IV symptoms.
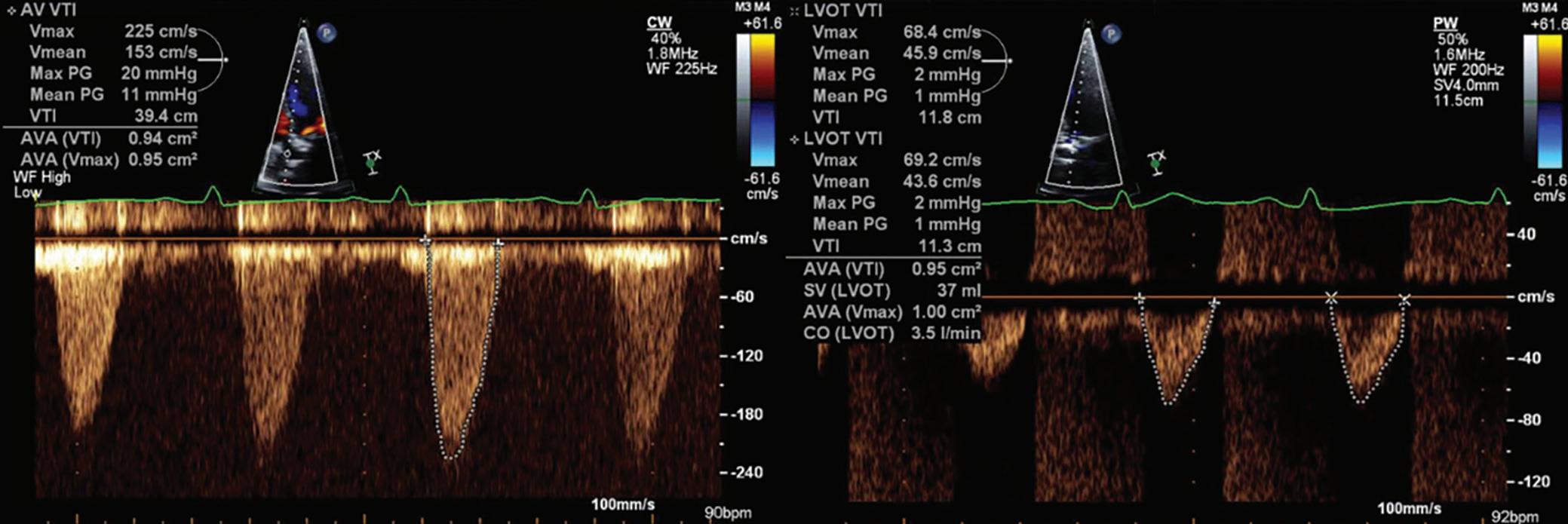
Hospital Course: Physical exam revealed massive peripheral edema and ascites. Transthoracic echocardiogram showed severe biventricular failure and aortic valve Doppler findings consistent with low-flow lowgradient aortic stenosis (Figure 1). Hemodynamic optimization was attempted with IV diuresis and paracentesis with removal of 5 l of ascites, but the patient developed significant hypotension and was started on a dobutamine infusion with only temporary improvement.
Subsequent right heart catheterization revealed a cardiac index of 2 l/min/ m2 on a dobutamine infusion of 3 µg/kg/min. Coronary angiography revealed critical right coronary ostial obstruction with no other obstructive coronary artery disease. Further hemodynamic deterioration led to transfer to a tertiary care center. Intra-aortic balloon pump (IABP) placement was attempted prior to transfer but could not be accomplished because of severe iliac obstruction.
On transfer the patient was hemodynamically stable on 10 µg/kg/min of dobutamine and 0.08 µg/kg/min of norepinephrine with a cardiac index of 2.7 l/min/m2. Repeat echocardiogram confirmed left ventricular ejection fraction (LVEF) <20%. Invasive assessment confirmed aortic stenosis with an area of 0.93 cm2 at both 2.5 and 10 µg/kg/min of dobutamine with augmentation of the aortic valve mean gradient from 17.6 to 27.4 mmHg. Aortoiliac angiography revealed left common iliac origin occlusion and right common iliac severe calcific obstruction.
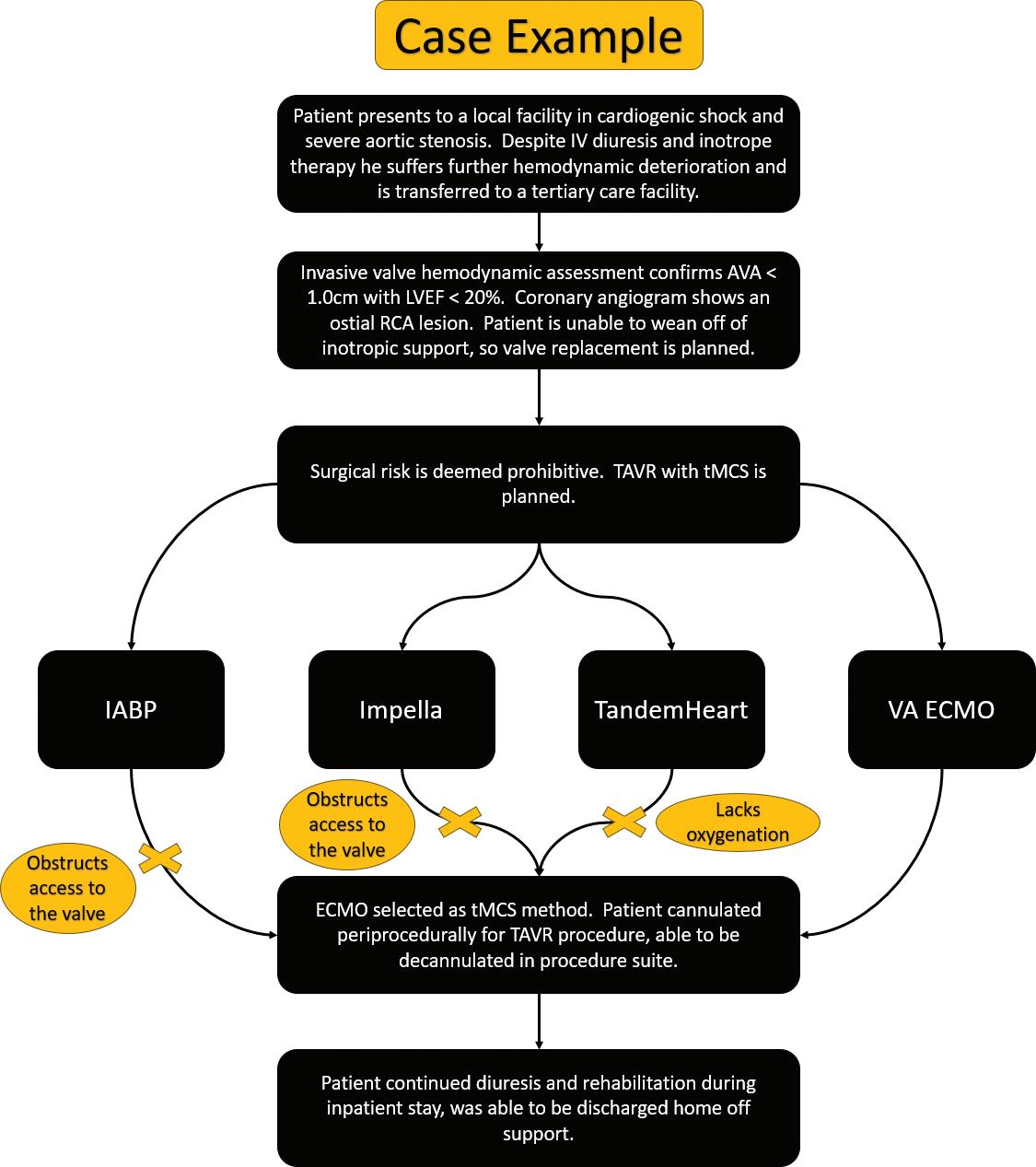
Right coronary artery revascularization and aortic valve replacement was planned. The risk of open surgery was assessed as prohibitive. Percutaneous treatment was undertaken, starting with right coronary angioplasty and drug-eluting stent placement using right radial access. Transcatheter aortic valve insertion (TAVR) was judged to require temporary mechanical circulatory support (tMCS) given severe LV
dysfunction and inotrope dependency, with alternative access mandated by the severe iliac obstruction. Femoral-femoral veno-arterial extracorporeal membrane oxygenation (VA-ECMO) was initiated after right common iliac angioplasty and stenting was performed to facilitate arterial cannula placement. Right subclavian artery cutdown provided access for TAVR with a 23-mm Edwards SAPIEN (Edwards Lifesciences) S3 ultra valve. ECMO was discontinued and decannulation was accomplished in the procedure suite. The patient continued diuresis after the procedure for 25 kg of total weight loss and completed rehabilitation while in the hospital, ultimately discharging to home.
Discussion
We highlight a case in which tMCS was used to support a patient through TAVR. tMCS can be a useful adjunct when treating patients with structural heart disease. While most patients undergoing TAVR do so without additional support, a small but significant proportion requires some form of tMCS, ranging from balloon pump to ECMO. Between 2012 and 2018, 1.4% of patients in the National Inpatient Sample who underwent TAVR required temporary mechanical circulatory support, with 27% requiring ECMO alone.1
In the present case, high level support with ECMO was chosen because of severely reduced ejection fraction and inotrope dependence. The tMCS method must be carefully tailored to the patient’s hemodynamic and periprocedural needs. IABP provides a modest amount of LV unloading and may not provide adequate support for a patient with severe biventricular failure. Impella (ABIOMED) insertion with the device traversing a newly placed TAVR prosthesis has been used for rescue therapy for patients who suffer intra- or post-procedural decompensation2,3 but is unfeasible during valve positioning and deployment. A TandemHeart (Cardiac Assist) percutaneous ventricular assist device would provide substantial hemodynamic support but requires transeptal left atrial cannulation4 and would not provide oxygenation (unless an oxygenator is added). As such, support with VA-ECMO was the best option in this case, as it provided both ample flow for support as well as oxygenation.
Our patient was weaned from ECMO immediately post-procedure and ultimately did well, but the use of tMCS in TAVR is associated with higher rates of in-hospital mortality, longer length of stay, and higher cost overall.
Figure 1: Transthoracic Echocardiogram Doppler Studies of the Patient’s Aortic Valve Demonstrating Low-flow Low-gradient Aortic Stenosis
1. Shou BL, Verma A, Florissi IS, et al. Temporary mechanical circulatory support for transcatheter aortic valve replacement. J Surg Res 2022;280:363–70. https://doi.org/10.1016/j. jss.2022.07.034; PMID: 36037613.
2. Singh V, Yarkoni A, O’Neill WW. Emergent use of Impella CP during transcatheter aortic valve replacement: transaortic access. Catheter Cardiovasc Interv 2015;86:160–3. https://doi. org/10.1002/ccd.25784; PMID: 25529629.
3. Almajed MR, Mahmood S, Obri M, et al. Application of Impella mechanical circulatory support
Table 1: Summary of Temporary Mechanical Circulatory Support Strategies and their Considerations in Transcatheter Aortic Valve Insertion
MCS Device Considerations Use in TAVR
IABP
Obstructs access to aortic valve; provides modest LV support; most commonly available
Impella Obstructs access to aortic valve; provides considerable LV support
TandemHeart
VA-ECMO
High levels of biventricular support; requires higher levels of operator training and post-procedural care; does not support oxygenation
High levels of biventricular support; requires higher levels of operator training and post-procedural care; augments oxygenation
Rescue therapy for procedural intolerance
Rescue therapy for procedural intolerance
Can be considered for intra- and post-procedural support in biventricular failure
Can be suitable for intra- and post-procedural support
Higher level of morbidity in these patients at time of presentation may confound this, as patients receiving tMCS were more often admitted emergently and had more comorbid illness.
devices in transcatheter aortic valve replacement and balloon aortic valvuloplasty: a singlecenter experience. Cardiovasc Revasc Med 2023;53:1–7. https://doi.org/10.1016/j. carrev.2023.03.006; PMID: 37012106.
4. Dawson K, Huang H, Don C. TandemHeart assisted transcatheter aortic valve replacement in cardiogenic shock. J Am Coll Cardiol 2019;73(9 Suppl 1):2744. https://doi.org/10.1016/S07351097(19)33350-9
Figure 2: Graphical Summary of the Case
Indolent Giant Cell Myocarditis Requiring Prolonged Veno-arterial Extracorporeal Membrane Oxygenation Support as a Bridge to Transplantation
Joseph
A Palatinus, MD, PhD1,2
1. Nora Eccles Harrison Cardiovascular Research and Training Institute, University of Utah, Salt Lake City, UT; 2. Department of Pulmonary and Critical Care Medicine, Intermountain Medical Center, Murray, UT
Citation: US Cardiology Review 2024;18(Suppl 1):30. Correspondence: Joseph A Palatinus, joseph.palatinus@utah.edu
Giant cell myocarditis is a rare idiopathic and usually rapidly progressive disease resulting in fulminant heart failure, cardiogenic shock and death. Here, we present a case of a 65-year-old man with a history of hypertension who initially presented to an outside hospital with syncope and complete heart block. He was found to have normal biventricular
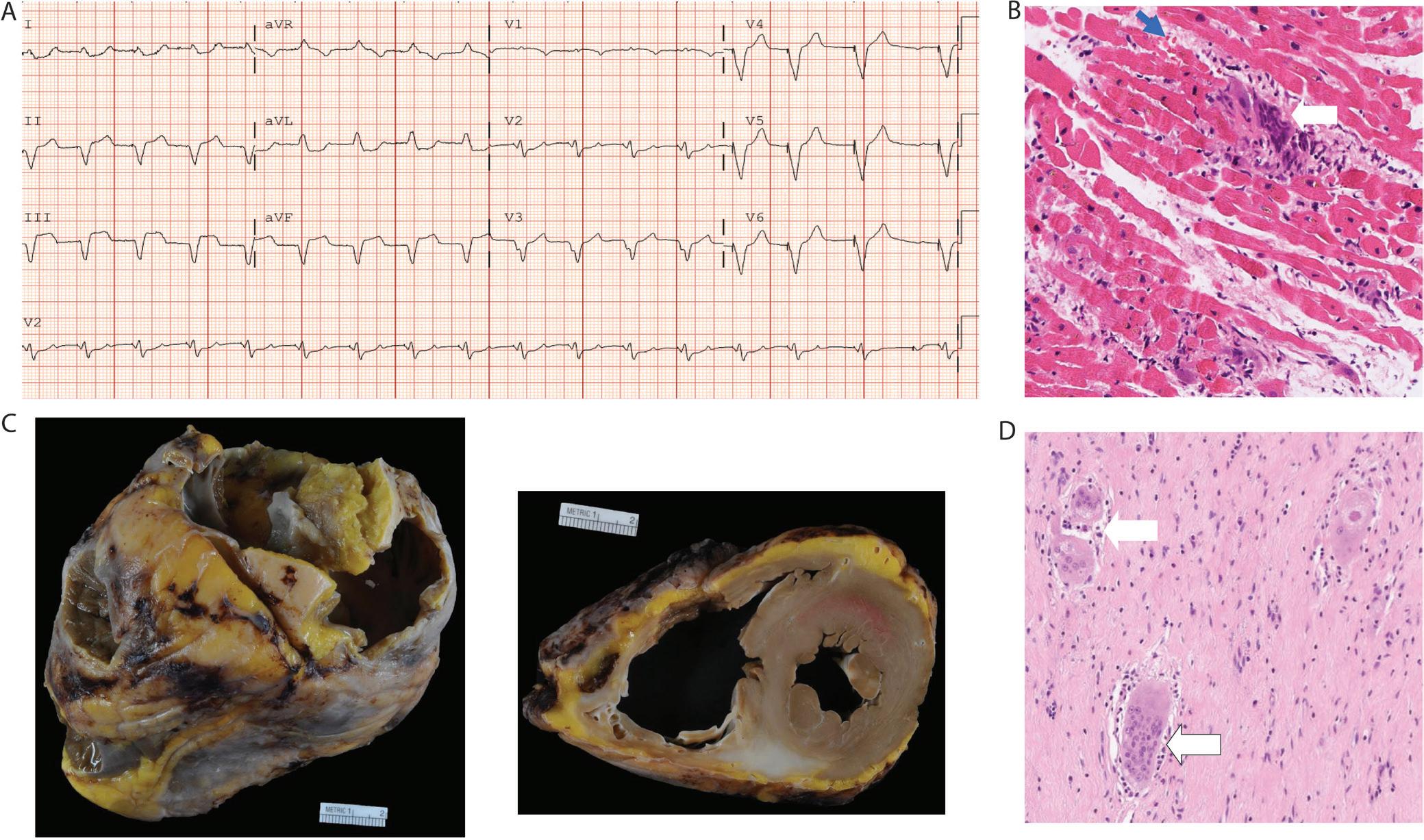
function and no obstructive coronary disease. The patient was discharged with a dual chamber pacemaker. One month later, pacemaker interrogation revealed new onset AF. He was started on flecainide and apixaban and then discharged. One month later, he presented to the ER with progressive heart failure symptoms and acute cardiogenic shock. Electrocardiogram
A: Electrocardiogram of patient on presentation to ER 2 months after symptom onset and after receiving a dual chamber pacemaker reveals sinus tachycardia with 100% ventricular pacing.
B: Hematoxylin eosin of right ventricular biopsy taken on admission day 1 with active myocarditis; multinucleated giant cells (white arrow) and notable eosinophils (blue arrow). C: Gross images of the patient’s heart at transplant. Note dilated right ventricle. D: Hematoxylin eosin stained left ventricular tissue taken at the time of transplant reveals multinucleated giant cells. Note the absence of epithelioid histiocytes or granulomatous features consisted with healed myocarditis.
Figure 1
revealed sinus tachycardia with 100% ventricular pacing (Figure 1A). Right heart catheterization revealed a cardiac index of 1.8 l/min/m2. The patient was admitted to the cardiac intensive care unit (CICU) and started on a dobutamine infusion; however, he demonstrated significant ventricular ectopy and non-sustained ventricular tachycardia requiring IV amiodarone. Right ventricular biopsy revealed active myocarditis with several prominent multinucleated giant cells with eosinophilia (Figure 1B). Shock rapidly progressed and within 24 hours of admission the patient was cannulated centrally for veno-arterial extracorporeal membrane oxygenation (VA-ECMO) and treated with aggressive immunosuppression. His course was complicated by multiple episodes of cardiac tamponade requiring repeat mediastinal washouts. After 2 weeks of ECMO support, left ventricular function recovered to an ejection fraction of 50%. However,
during an attempt at decannulation, he demonstrated worsening shock secondary to right ventricular failure with a need for increased vasopressor support and a cardiac index <1 l/min/m2. He was re-cannulated and remained on VA-ECMO for a total of 51 days prior to eventually receiving an orthotopic heart transplant. At transplant, the explanted heart demonstrated right ventricular dilation and evidence of advanced giant cell myocarditis despite immunosuppression (Figure 1C). Microscopic examination revealed multiple multinucleated giant cells (Figure 1D). This case highlights the potential for a subacute clinical course of giant cell myocarditis prior to developing cardiogenic shock; the high index of suspicion needed to pursue endomyocardial biopsy in cardiogenic shock patients admitted to the CICU; and the successful utilization of prolonged VA-ECMO as a bridge to transplantation in giant cell myocarditis.
Charting the Course of Mechanical Circulatory Support Modalities in a Case of Biventricular Failure
Gurleen Kaur,1 Siddharth Patel,2 Akinobu Itoh,3 Raghu Seethala,4 Erin Bohula,2 David Morrow,2 and David Berg2
1. Department of Medicine, Brigham and Women’s Hospital, Harvard Medical School, Boston, MA; 2. Cardiovascular Division, Department of Medicine, Brigham and Women’s Hospital, Harvard Medical School, Boston, MA; 3. Division of Cardiac Surgery, Brigham and Women’s Hospital, Harvard Medical School, Boston, MA; 4. Division of Thoracic and Cardiac Surgery, Brigham and Women’s Hospital, Harvard Medical School, Boston, MA
Citation: US Cardiology Review 2024;18(Suppl 1):31. Correspondence: Gurleen Kaur, gkaur9@bwh.harvard.edu
Case: A 27-year-old man with non-ischemic dilated cardiomyopathy due to pathogenic desmin mutation (ejection fraction 15–20%) marked by VF arrest 10 years prior, recurrent ventricular tachycardia (VT)/VF, and resolved left ventricular (LV) thrombus, presented with decompensated heart failure. On admission, transthoracic echocardiography demonstrated diffusely hypokinetic LV, moderate-to-severely decreased right ventricular (RV) systolic function, and mild-to-moderate tricuspid regurgitation. Right heart catheterization showed a CI of 1.5 l/min/m2 with borderline indicators of perfusion. A multidisciplinary shock team discussion was held; given the patient’s history of VT, he was not a good candidate for escalating inotropic support. A femoral intra-aortic balloon pump (IABP) was placed but his CI only marginally improved. The shock team was reconvened, and the decision was made to escalate his mechanical circulatory support (MCS) to an axillary Impella 5.5 and percutaneous right ventricular assist device (RVAD) with an extracorporeal centrifugal pump with inflow from the right atrium and outflow to the pulmonary artery (PA). Postoperatively, he developed right lower extremity ischemia requiring emergent thrombectomy; this was in the context of prior IABP placement on that side. Despite the escalation in MCS, his right-sided support remained inadequate, and TEE demonstrated that the RVAD cannula had migrated into the RV outflow tract. Following RVAD repositioning, he experienced monomorphic VT requiring cardioversion, lidocaine and amiodarone, and ultimately stellate ganglion block. He continued to require repositioning of the RVAD cannula due to the large RV and short main PA, and thus the decision was made to change to a central RVAD configuration with direct cannulation
of the PA via left thoracotomy. Unfortunately, he developed worsening left-sided pulmonary edema, which was thought to be due to PA cannula dominantly directing blood flow through the short main PA to the left PA. At this point, the decision was made to transition to central VA-ECMO cannulation with decannulation of the PA. The Impella 5.5 remained in situ for LV venting. Later, CT angiography of the chest showed segmental pulmonary emboli (PE) with right-sided pulmonary infarcts. The team contemplated next steps including VA-ECMO decannulation and replacement with RVAD; however, given prior difficulties with RVAD and mild to moderate aortic regurgitation, there was concern whether Impella alone would be able to support the systemic circulation. Furthermore, attempts to reduce ECMO flow and increase Impella support were limited by suction events. Four weeks after the PE was diagnosed, repeat chest CTA demonstrated resolution of the PE so he was listed for heart transplant. On hospital day 37, he underwent a heart transplant and was subsequently discharged home on hospital day 62.
Discussion: This case demonstrates the importance of a multidisciplinary shock team in assessing MCS options in a patient with biventricular failure, as well as specific challenges that may arise with certain devices. Malpositioning of percutaneously placed MCS cannulas, as in this case, may be addressed by surgical central cannulation. While no specific guidelines exist to optimize MCS device selection for biventricular support, management is often patient-specific. Continued reassessment of MCS strategy is crucial and considerations must be made regarding goals and level of hemodynamic support.
Pre Left Ventricular Assist Device Impella 5.5: Test Ride the Right Ventricle
Rochelle Prokupets, MD,1 Lena Tran, MD,1 Sandip Zalawadiya, MD,2 Antonio Hernandez, MD,3 Ashish Shah, MD,4 and Aniket S Rali, MD2
1. Department of Internal Medicine, Vanderbilt University Medical Center, Nashville, TN; 2. Division of Cardiovascular Diseases, Department of Internal Medicine, Vanderbilt University Medical Center, Nashville, TN; 3. Department of Anesthesiology, Vanderbilt University Medical Center, Nashville, TN; 4. Department of Cardiac Surgery, Vanderbilt University Medical Center, Nashville, TN
Citation: US Cardiology Review 2024;18(Suppl 1):36. Correspondence: Aniket S Rali, aniket.rali@vumc.org
Right heart failure (RHF) is a common complication of left ventricular assist device (LVAD) therapy. With incidence estimated at 5–44%, post-LVAD RHF is a significant cause of morbidity and mortality. However, there is no validated predictor of RHF development after LVAD implantation. We present a case of cardiogenic shock in which the patient was supported with Impella 5.5 to assess RHF prior to decision about LVAD implantation. A 73-year-old man with a medical history of heart failure with reduced ejection fraction due to ischemic cardiomyopathy on home milrinone, AF, pulmonary hypertension, chronic kidney disease stage IV, and diabetes presented for elective right heart catheterization (RHC) with leave-in Swan catheter for medical optimization. He was found to have acute kidney injury (AKI) with creatinine elevated to 3.39 mg/dl from baseline 2.2 mg/dl and to be in cardiogenic shock. RHC at admission on home milrinone 0.375 mcg/kg/min showed right atrial pressure (RAP) 17 mmHg; CI, indirect Fick (F) 1.76 l/min/m2, pulmonary artery pulsatility index (PAPi) 0.4, and central venous pressure (CVP)/pulmonary capillary wedge pressure (PCWP) 0.71. Over the next 3 days, milrinone dose remained at 0.375 mcg/ kg/min, dobutamine 5 mcg/kg/min was added, and a femoral intra-aortic balloon pump was placed for additional support. However, a repeat RHC showed no significant change in markers of right ventricular function: RAP 12 mmHg, CI (F) 1.68 l/min/m2, PAPi 1.4, CVP/PCWP 0.54. The patient was not deemed to be a candidate for heart-kidney transplantation due to advanced age and severe calcification of the descending aorta. It was
unclear if the patient would be an LVAD candidate given renal function as well as concerns for moderate to severe right ventricular (RV) dysfunction. The decision was made to implant Impella 5.5 on hospital day 5 and to monitor RV and renal function with the subsequent hemodynamic changes. By hospital day 10, dobutamine and milrinone had been weaned off and a repeat RHC off inotropic support showed improved cardiac markers with RAP 9, CI (F) 2.6, PAPi 2.1, CVP/PCWP 0.45. Creatinine also had improved close to baseline at 2.44 mg/dl. Creatinine levels remained stable over the next 11 days. Dobutamine 2.5 mcg/kg/min was started on hospital day 17 to maximize inotropic support in anticipation of LVAD implantation. On hospital day 21, an LVAD was implanted; cardiac markers that day showed RAP 6, PAPi 2.3, and CVP/PCWP 0.45 as well as stable creatinine 1.99 mg/dl. The patient’s postoperative course was complicated by bacterial pneumonia and acute renal failure requiring brief duration of renal replacement therapy. By hospital day 59, he was completely weaned off all inotropic support with creatinine at baseline of 2.2 mg/dl. A followup RHC was performed just prior to discharge at 5,000 rpm and showed RAP 10, CI (F) 2.3, PAPi 2.0 and CVP/PCWP 0.53. He was discharged to inpatient rehabilitation on hospital day 63. The patient is currently in a stable condition at home and continues to follow up in the outpatient clinic. This case highlights that use of the Impella 5.5 provides valuable insights into how the right ventricle may perform acutely after LVAD implantation when the left ventricle has truly been decompressed.
1. Department of Cardiovascular Medicine, University of Kansas Medical Center, Kansas City, KS; 2. Department of Cardiovascular Medicine, University of Missouri Kansas City, Kansas City, MO; 3. Dayanand Medical Collage and Hospital, Ludhiana, Punjab, India
Citation: US Cardiology Review 2024;18(Suppl 1):39. Correspondence: Ashutosh Bapat, abapat@kumc.edu
Figure 1: EKG Showing 1 mm ST Elevation in aVR and Diffuse ST-T Depressions in the Inferior and Lateral Leads
Background: Minoxidil is a powerful direct-acting vasodilator used previously as an antihypertensive agent in rare cases of refractory hypertension. In the current era, it is mostly used to treat androgenic alopecia of the scalp (2% and 5% minoxidil solutions) due to its hair growth properties.
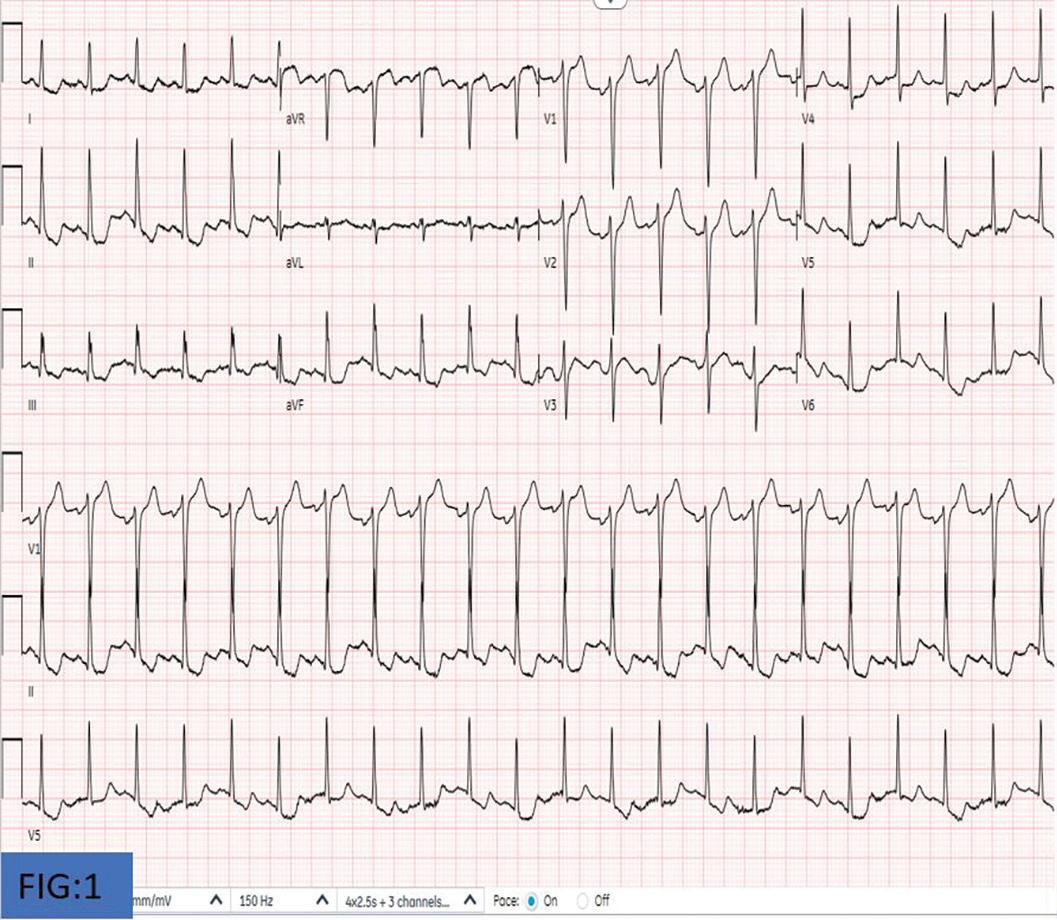
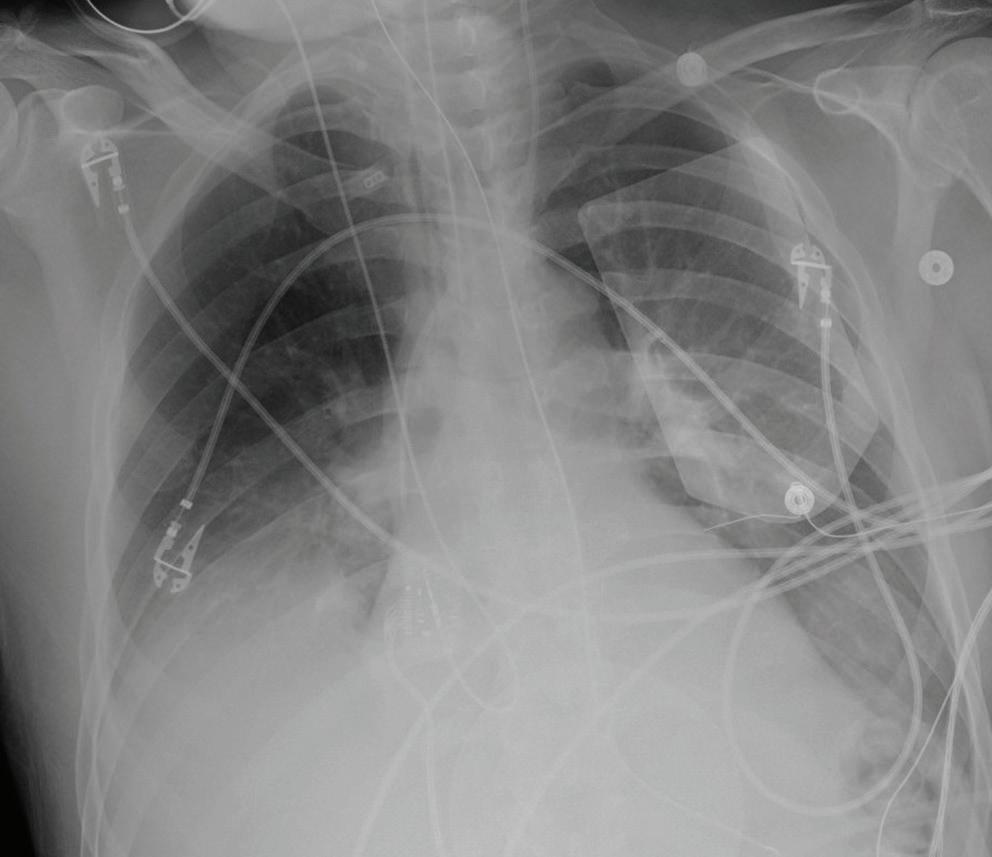
Case: A 51-year-old man with history of hypertension presented with chest pressure, shortness of breath and lightheadedness that began after accidentally drinking 10 ml of 5% topical minoxidil equaling 500 mg of minoxidil. He was tachycardic (heart rate 130s), tachypneic (respiratory rate 40s), and hypotensive (90/40s mm Hg) in the ER. EKG showed 1 mm ST elevation in aVR and diffuse ST-T depressions in the inferior and lateral
leads (Figure 1). High sensitivity troponin was 267 ng/l, which went up to 1,177 ng/l. The patient underwent emergent coronary angiography, which showed no significant coronary artery disease.
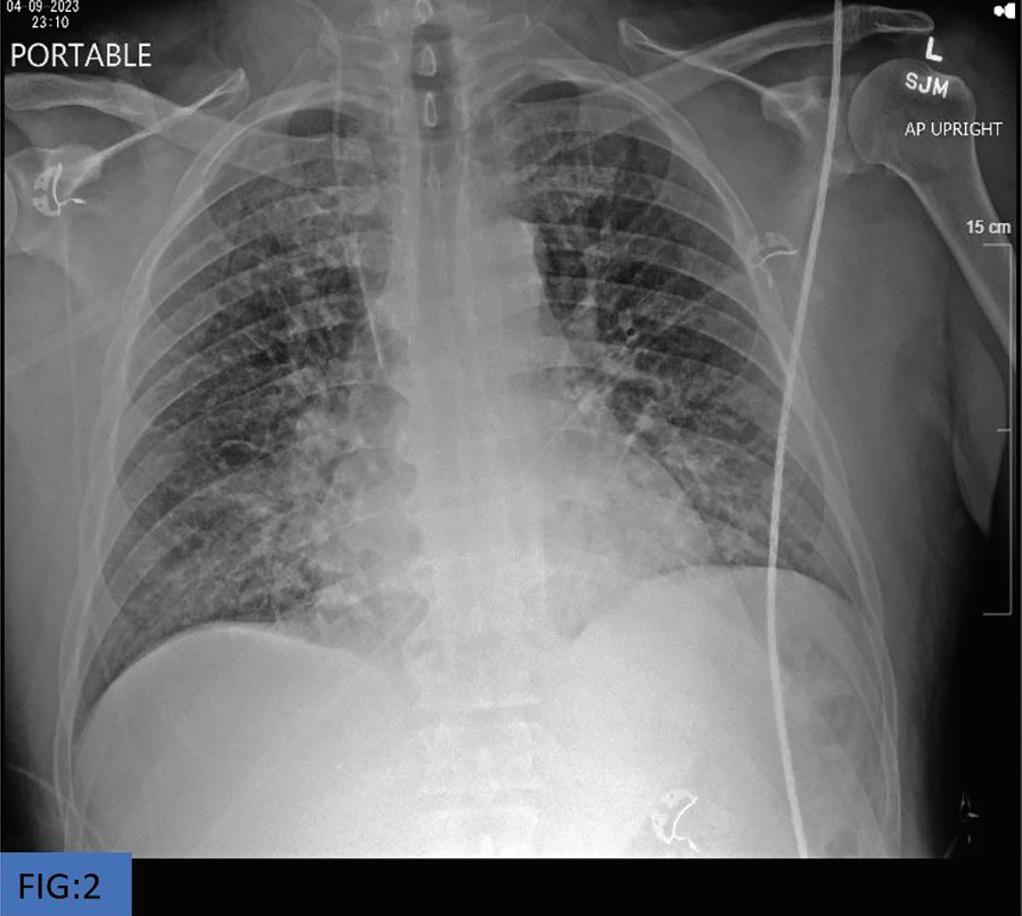
Decision-making: The patient was admitted to the cardiac intensive care unit due to minoxidil overdose causing vasodilatory shock with EKG changes. His hospital course was further complicated with pulmonary edema on day 2 (Figure 2). Echo showed an ejection fraction of 75% and hyperdynamic left ventricular function. The patient required presser support with norepinephrine, vasopressin and phenylephrine drips but slowly tapered off in the next 72 hours with stable blood pressures. The patient also required furosemide for pulmonary edema. Psychiatry was consulted, given concern for possible self-harm and confirmed accidental ingestion. The patient was discharged home in a stable condition.
Figure 2: Pulmonary Edema
Abstracts from the 3rd Annual NYU Langone Critical Care Cardiology Symposium and CardioNerds Poster Session
Conclusion: Ingestion of topical minoxidil can be a life-threatening emergency with persistent cardiovascular symptoms due to severe vasodilation. Immediate resuscitation of a patient with fluid challenge and pressers showed improvement in hemodynamics and symptoms. With
increased over-the-counter availability and usage of topical minoxidil, users must be cautious, and the product must be kept in a safe place as it is equally dangerous for children.
A Case of Severe Cardiopulmonary Sarcoidosis and Sub-massive Pulmonary Embolism
Sharnendra K Sidhu, MD,1 James Ciancarelli, DO,2 Carlos Alviar, MD,3 and Allison Greco, MD2
1. Department of Medicine, New York University Grossman School of Medicine, New York, NY; 2. Division of Pulmonary, Critical Care & Sleep Medicine, New York University Grossman School of Medicine, New York, NY; 3. Leon H Charney Division of Cardiovascular Medicine, New York University Grossman School of Medicine, New York, NY
Citation: US Cardiology Review 2024;18(Suppl 1):49. Correspondence: Allison Greco, allison.greco@nyulangone.org
Case: A 68-year-old man with sarcoidosis presented with dyspnea and lower extremity edema. His prior cardiac workup was notable for transthoracic echocardiogram (TTE) with left ventricular (LV) dysfunction, coronary angiogram with normal coronaries, cardiac MRI with severe biventricular dysfunction as well as subepicardial to near transmural scar of the basal to mid inferolateral walls, and pulmonary function test with severe obstructive ventilatory impairment and positive bronchodilator response.
Upon presentation, he was tachycardic, tachypneic, hypoxic, and normotensive. His laboratory studies revealed leukocytosis 23 x 109/l, creatinine 1.52 mg/dl, venous lactic acid 3.5 mmol/l, pro B-type natriuretic
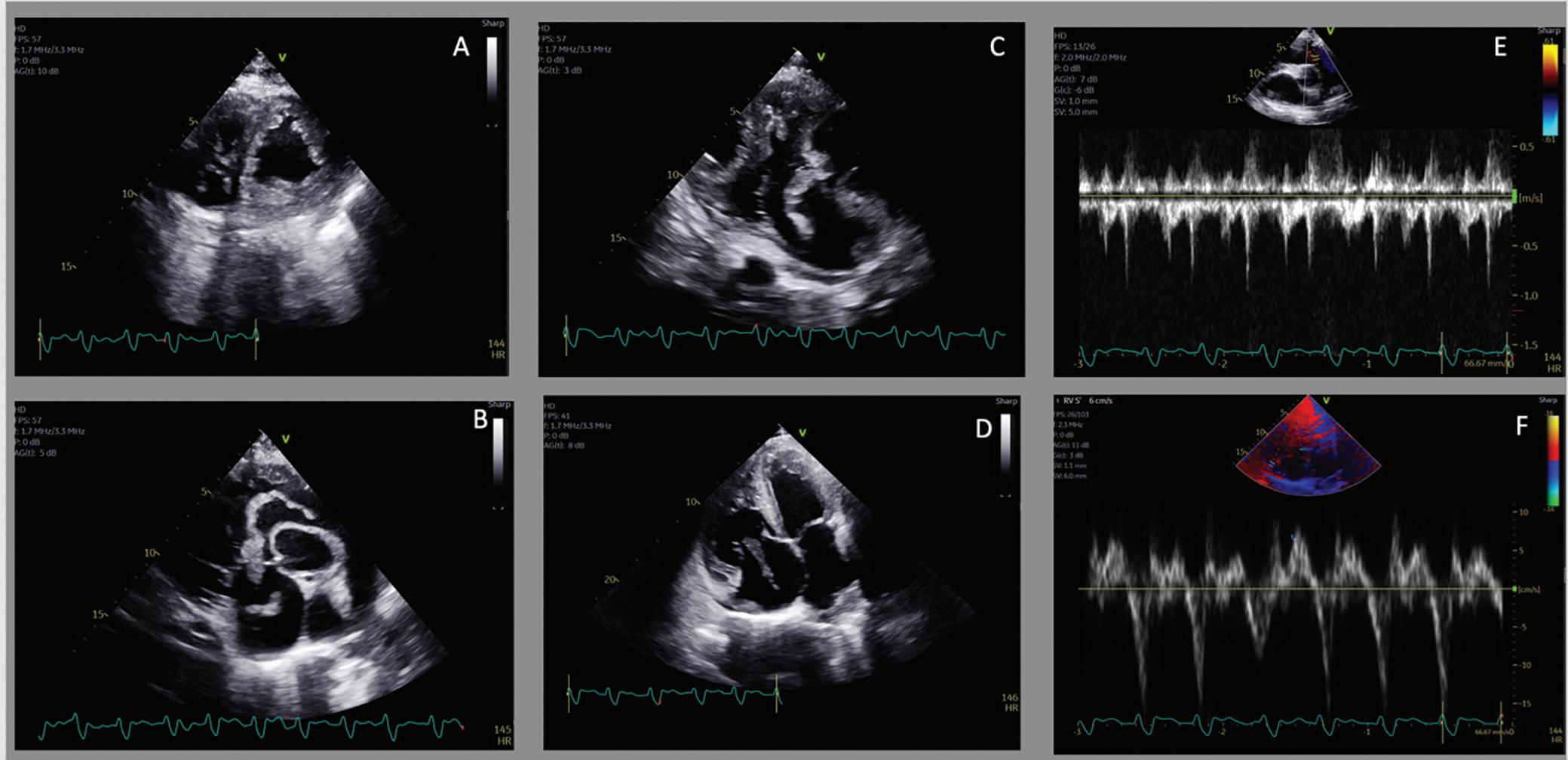
peptide 34,807 pg/ml and negative troponin. Chest radiography was notable for a right upper lobe wedge-like opacity and right pleural effusion. Electrocardiogram revealed rapid atrial flutter. Supplemental oxygen was started and furosemide was administered. Digoxin load was given without improvement. A TTE showed a severely decreased LV function, dilated right ventricle (RV) with reduced contractility and thrombus in transit extending from the right atrium (RA) to RV (Figure 1). Heparin was started and the patient was transferred for consideration of advanced therapies.
A multidisciplinary pulmonary embolism (PE) response team was activated and due to concerns about the patient’s baseline
Figure 1
A: PSAX with RV pressure overload; B: PSAX with thrombus in transit from RA through RV and into RVOT; C: RV in-flow with thrombus in transit; D: RV in-flow with thrombus in transit and RV enlargement; E: Pulsed Wave Doppler RVOT. F: S’ of RV showing reduced RV function. PSAX = parasternal short axis view; RA = right atrium; RV = right ventricle; RVOT = right ventricular outflow tract.
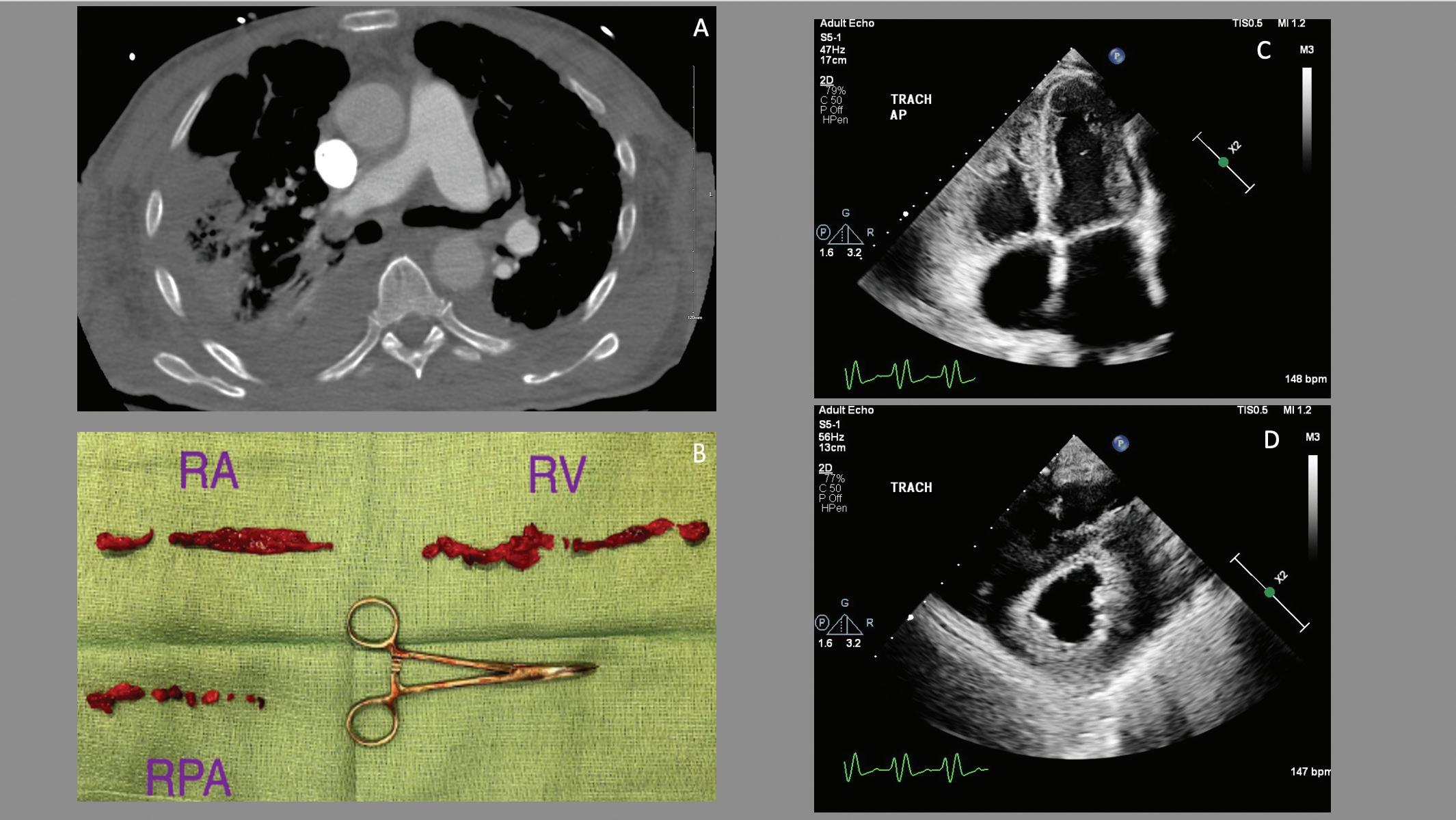
cardiopulmonary reserve and tenuous hemodynamics; he underwent urgent percutaneous mechanical thrombectomy with removal of thrombus in the RA, RV, and main pulmonary arteries. There was a distal residual clot (Figure 2). Hemodynamics showed a CI of 2 l/m2 and severe pulmonary hypertension, with improvement to 2.7 l/m2 following intervention, though during the procedure the patient required intubation due to delirium. His postoperative period was notable for RV cardiogenic shock as well as auto-positive end-expiratory pressure due to bronchospasm. Following ventilator adjustments, bronchodilators, corticosteroids, inhaled nitric oxide and milrinone, there was stabilization. Acute and extensive clot burden was evident in bilateral lower extremities on Doppler ultrasound. His course was further complicated by oliguric acute kidney injury and volume overload despite diuresis, requiring continuous veno-venous hemofiltration (CVVH) as well as difficult-to-control atrial tachycardia with variable block requiring direct current cardioversion. Thereafter, stabilization of the patient’s
hemodynamics was achieved. He subsequently underwent tracheostomy and gastrostomy placement and was liberated from the ventilator.
Discussion: To our knowledge, this is the first report of PE with thrombectomy in a patient with sarcoidosis. Following clot retrieval, a mixed shock developed, which was likely due to the severity of his advanced cardiopulmonary sarcoid. Interestingly, his obstructive lung disease became evident following intubation. Prompt recognition and treatment allowed for improved preload and likely a reduction in his pulmonary vascular resistance. However, he remained in shock despite inhaled nitric oxide, milrinone, norepinephrine and vasopressin. It was not until the removal of preload via CVVH did RV recover and shock resolve. Despite a prolonged intensive care unit stay, we postulate that given the patient’s severe underlying disease process, failure to retrieve the clot in transit would have resulted in a catastrophic outcome.
A: Residual right pulmonary artery thrombus; B. Thrombus removed via mechanical thrombectomy; C: Apical 4 post-procedure; D: Parasternal short axis post-procedure.
Figure
To Cool or Not to Cool for Brugada Syndrome
Tania Ahuja, PharmD, FACC, BCCP, BCPS, CACP,1,2 Nicholas J Kiefer, MD,1 Alexandra Caballero, PharmD,2 and Raymond Pashun, MD, FACC1
1. Department of Medicine, The Leon H Charney Division of Cardiology, New York University Grossman School of Medicine, New York, NY; 2. Department of Pharmacy, New York University Langone Health, New York, NY
Citation: US Cardiology Review 2024;18(Suppl 1):54. Correspondence: Tania Ahuja, tania.ahuja@nyulangone.org
Copyright: Abstract reproduced from Ahuja et al. 20221 with permission from the American Heart Association.
Brugada syndrome (BrS) is an autosomal dominant genetic disorder, characterized by abnormal findings on the electrocardiogram (ECG) in conjunction with an increased risk of ventricular tachycardia (VT) and sudden cardiac death. Triggers of the ECG pattern and VT in BrS include fevers, drugs, and electrolyte abnormalities. This case reports a unique treatment approach of targeted temperature management (TTM) to treat persistent fevers and VT secondary to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in a patient with BrS. We report the case of a 23 year old male with history of BrS with an intracardiac defibrillator (ICD) who presented to the hospital with chest pain and a runny nose. Vital signs upon admission were notable for temperature of 38.2oC, heart rate of 155 beats/minute and blood pressure of 134/110 mmHG. Laboratory values on admission revealed a normal complete blood count, a normal basic metabolic panel, an elevated c-reactive protein (CRP) of 19.1, and PCR confirmed SARS-CoV-2 infection, with a cycle threshold value of 16.4. ECG revealed a type 2 Brugada pattern. Interrogation of his ICD revealed 28 device shocks on the morning of
admission, with each episode beginning with a premature ventricular contraction inciting polymorphic VT. His transthoracic echocardiogram (TTE) discovered a newly reduced ejection fraction of 25% with global hypokinesis. Persistent VT prompted intubation and sedation with propofol. Repeat SARS-CoV-2 inflammatory markers revealed a rising CRP of 244. Therapies included acetaminophen around the clock and remdesivir and dexamethasone to target COVID-19. During the first two days in the cardiac intensive care unit (CICU), fevers persisted with Brugada pattern on ECG. Given the potential for recurrent VT, targeted TTM was initiated using the Arctic Sun external cooling device to maintain normothermia to 37oC. After 5 days of no VT, fever curve, Brugada pattern, and inflammatory markers improved. TTM was discontinued, COVID-19 therapies were completed, and he was extubated. His cardiac function normalized on repeat TTE and he was discharged home. We report a unique case of TTM use in a patient with BrS with VT secondary to infection with COVID-19, as a way to decrease fevers and prevent further triggering of VT.
1. Ahuja T, Kiefer T, Caballero A, Pashun R. To cool or not to cool for Brugada syndrome. Circulation 2022;146:A11625. https://doi.org/10.1161/circ.146.suppl_1.11625
To PLEX or Not to PLEX for Amiodarone Induced Thyrotoxicosis
Tania Ahuja, PharmD, FACC, BCCP, BCPS, CACP,1,2 Olivia Nuti, PharmD,2 Cameron Kemal, MD,1 Darren Kang, PA-C,3 Eugene Yuriditsky, MD, FACC,1 James M Horowitz, MD, FACC,1 and Raymond Pashun, MD, FACC1
1. Department of Medicine, The Leon H Charney Division of Cardiology, New York University Grossman School of Medicine, New York, NY; 2. Department of Pharmacy, New York University Langone Health, New York, NY; 3. Department of Advanced Practice Practitioners, New York University Langone Health, New York, NY
Citation: US Cardiology Review 2024;18(Suppl 1):56. Correspondence: Tania Ahuja, tania.ahuja@nyulangone.org
Copyright: Abstract reproduced from Ahuja et al. 2023.1 Reproduced from the American College of Cardiology Foundation under a Creative Commons CC BY-NC-ND 4.0 License.
Background: The incidence of amiodarone-induced thyrotoxicosis is rare in the United States, and treatment typically involves a combination of thionamides and glucocorticoids to manage type 1 and type 2, respectively. There is limited data for management when medical therapy fails, but case reports have described successful use of plasmapheresis (PLEX) as salvage therapy prior to thyroidectomy.
Case: This case reports a unique treatment approach of PLEX to treat severe thyrotoxicosis secondary to amiodarone in a patient with nonischemic cardiomyopathy. We report the case of a 52-year-old male with an ejection fraction of 35%, end stage renal disease and atrial fibrillation who had been on amiodarone for > 1 year, who presented with cardiogenic shock. Vital signs were notable for a heart rate of 160 beats/minute in atrial fibrillation. Laboratory values revealed a normal complete blood count, a normal basic metabolic panel with the exception of an elevated serum creatinine, an undetectable thyroid stimulating hormone of <0.02 mIU/L, elevated free T4 at 3.1ng/dL, direct bilirubin of 2.9mg/dL, and elevated liver function tests. Upon presentation, a pulmonary artery
catheter and intra-aortic balloon pump was placed with elevated filling pressures. During the first two days in the cardiac intensive care unit (CICU), therapy for thyroid storm was initiated with methimazole, hydrocortisone and PLEX for 3 sessions. Despite improvements in thyroid function tests, rapid atrial fibrillation recurred with hemodynamic instability resulting in a ventricular tachycardic cardiopulmonary arrest and demise.
Decision-making: An interdisciplinary discussion among the CICU, endocrinology and clinical pharmacy occurred to discontinue amiodarone and initiate methimazole and hydrocortisone plus PLEX given acute cardiovascular decompensation.
Conclusion: In conclusion we present the case of cardiogenic shock secondary to thyroid storm, attributed to amiodarone therapy. Mortality associated with amiodarone induced thyrotoxicosis remains high and PLEX may be considered to eliminate amiodarone and thyroid hormones from circulation rapidly as a bridge to definitive treatment such as a thyroidectomy.
1. Ahuja T, Nuti O, Kemal C, et al. To PLEX or not to PLEX for amiodarone induced thyrotoxicosis. J Am Coll Cardiol 2023;81(8 Suppl):2604. https://www.jacc.org/doi/10.1016/S0735-1097%2823%2903048-6
Cracking the Aorta: A Rare Case of Cocaine-related Aortic Dissection
Chris Agyingi,1 Olva Bess,1 Miqdad Dafaallah,1 Alvaro Ordoñez,1 Antoine Egbe Tabot,2 Lubna Khanum,1 Shilpa Aswath,1 and Ronny Cohen1
Citation: US Cardiology Review 2024;18(Suppl 1):62. Correspondence: Chris Agyingi, agyingimbari@yahoo.com
Background: Despite its low prevalence, aortic dissection can be a severe complication of cocaine use. Delays in diagnosis and management can be fatal. This case is a reminder of the association between a major public health issue and a grave life-threatening disease.
Case: A 41-year-old man with hypertension, active smoker, and cocaine user presented with chest pain and shortness of breath for 2 days. He consulted in a prior facility for onset of chest pain but left against medical advice. The patient referred to daily use of crack cocaine during the preceding week. Physical exam was remarkable for acute distress, hypertension, tachycardia, and diastolic murmur in the aortic region. A drug screen was positive for cocaine, elevated troponin T, and an EKG revealed left ventricular hypertrophy with ST-segment depression and T wave inversion in the precordial leads. Transthoracic echocardiogram (TTE) revealed aortic dissection with multiple intimal flaps in the aortic root and ascending aorta extending into the aortic arch (Figure 1). The patient had a cardiac arrest shortly after TTE, and cardiopulmonary resuscitation was unsuccessful.
Decision-making: Aortic dissection is a rare vascular emergency frequently excluded among a young patient’s differential diagnoses for chest pain. Our case highlights the need for early recognition of the clinical manifestations of aortic dissection in patients with known cocaine use, followed by rapid confirmation using imaging and administration of
B: Transthoracic echocardiogram revealed aortic dissection with multiple intimal flaps noted in the aortic root and ascending aorta extending into the
appropriate interventions. In some cases, EKG may be unhelpful given that it suggests myocardial ischemia regardless of acute dissection.
Conclusion: With the increase in cocaine use among young adults, clinicians should have a high suspicion of aortic dissection among cocaine users with chest pain. Aortic dissection is an uncommon but potentially fatal condition. Reliable modalities of diagnosis are available, but a high index of suspicion remains critical for prompt diagnosis. With the increase in cocaine use among young adults, clinicians should have a high suspicion of aortic dissection among cocaine users with chest pain. This case reminds us of how serious diseases can masquerade in old complaints.
1. Woodhull Medical Center, Brooklyn, New York, NY; 2. Beaumont Hospital, Corewell Health, Dearborn, MI
Figure 1
A,
aortic arch; C: Severe aortic regurgitation.
Startled to Death: A Case of Polymorphic Ventricular Tachycardia in Congenital Long QT Syndrome
Anirudh Nandan, MD, Andrew Higgins, MD, and Ran Lee, MD
Department of Cardiovascular Medicine, Cleveland Clinic, Cleveland, OH
Citation: US Cardiology Review 2024;18(Suppl 1):63. Correspondence: Anirudh Nandan, nandana@ccf.org
Introduction: Traditional management of unstable ventricular arrhythmias involves defibrillation, administration of antiarrhythmic drugs (AADs), and reversal of underlying triggers. However, polymorphic ventricular tachycardia (PMVT) often presents as clusters of unstable ventricular arrhythmia interspersed with spontaneous conversion to sinus rhythm. Even if an individual paroxysm is successfully defibrillated, PMVT may rapidly recur. For patients with an underlying prolonged QT interval, administration of commonly used AADs like amiodarone may risk further QTc prolongation. Management of long QT-induced PMVT (torsades de pointes) therefore requires an individualized approach.
Case: A 57-year-old man with a history of hypertension and inherited long QT syndrome type 2 (LQTS2) presented after witnessed cardiac arrest at a military rifling ceremony. Bystander cardiopulmonary resuscitation was promptly initiated, and documented rhythm in the field was PMVT. Return of spontaneous circulation was achieved with defibrillation, but the patient remained in arrhythmic storm with ongoing paroxysms of torsades de pointes. He was intubated and taken urgently for coronary angiography (given age and risk factors), which revealed no obstructive coronary artery disease. He was transferred to the cardiac intensive care unit (CICU) for further management.
Figure 1A
A: Baseline EKG showing prolonged QTc.
CICU Course: Telemetry revealed frequent ventricular ectopy while in sinus rhythm, precipitating ‘short-long-short’ sequences and recurrent torsades. Initial antiarrhythmic therapy with IV magnesium and IV lidocaine yielded no improvement in PMVT storm. The patient was taken to the CICU procedure room for placement of a temporary transvenous right atrial pacing wire. With rapid overdrive pacing through the atrial wire, the patient’s torsades was successfully suppressed. He was found to be neurologically intact, extubated, and ultimately transitioned onto nadolol without recurrence of PMVT. His heart rates remained low while in sinus rhythm, and an ICD with permanent atrial pacing lead was placed before discharge.
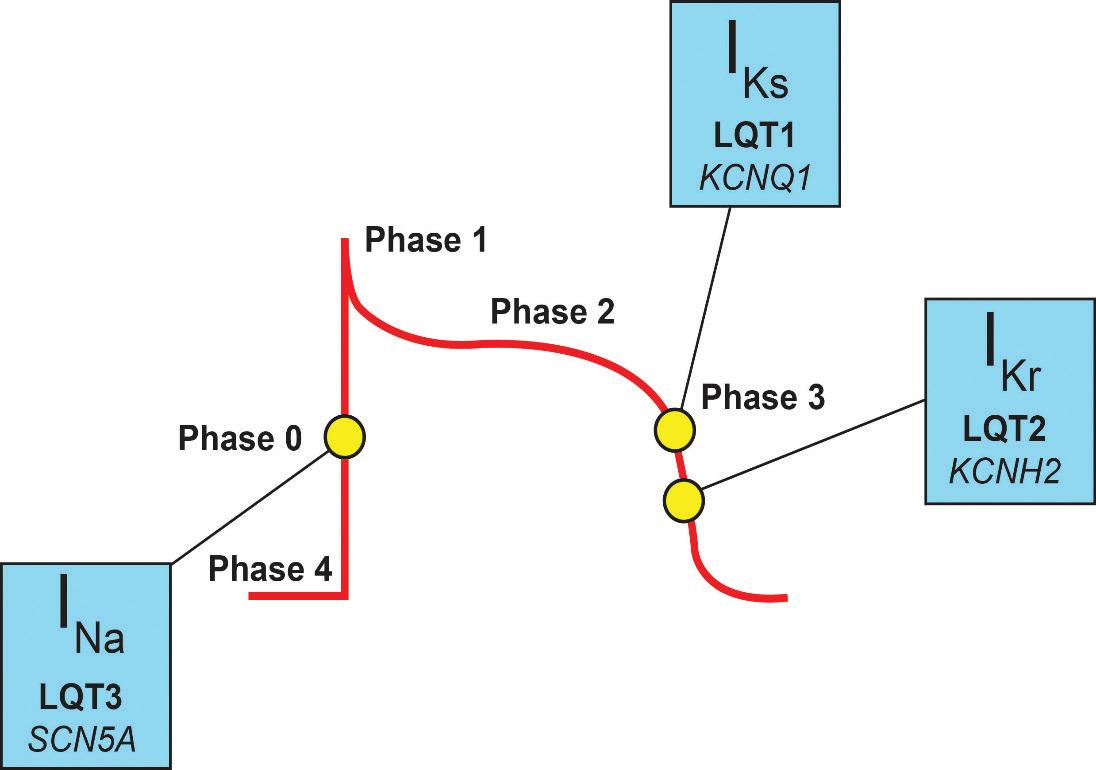
Discussion: Inherited LQTS2 is caused by a loss-of-function mutation in
the KCNH2 gene that controls potassium efflux, leading to prolongation of the QT interval. In patients with LQTS2, pause-dependent torsades may be triggered by a slowing of the sinus rate, or more commonly, by a post-extrasystolic pause. Observational cohort studies have suggested that loud auditory stimuli are common triggers. In addition to repletion of electrolytes, initiation of lidocaine (preferred to amiodarone given concern for further QT prolongation), and sedation to reduce adrenergic tone, overdrive pacing can help suppress this form of torsades by shortening the R-R interval. Atrial pacing uses the native His-Purkinje system and may have less impact on dispersion of refractoriness, compared to ventricular pacing. β-blockade can prevent recurrent arrythmia and carries a class I indication for the management of these patients. Finally, in patients with LQTS2 who experience resuscitated cardiac arrest, a secondary prevention ICD should be placed before discharge.
Figure 1D
Figure 1B
Figure 1C
B: Telemetry demonstrating initiation of torsades.
C: Chest X-ray showing placement of atrial pacing wire.
D: Action potential labeled with various congenital long QT syndromes.
Clinical Case: Cardiogenic Shock with Subsequent Heart Transplantation
Rokas Serpytis, Vilius Janusauskas, Robertas Samalavicius, Kestutis Rucinskas, and Pranas Serpytis
Clinic of Heart and Vessel Diseases, Institute of Clinical Medicine Faculty of Medicine, Vilnius University, Vilnius, Lithuania
Citation: US Cardiology Review 2024;18(Suppl 1):64. Correspondence: Rokas Serpytis, rokas.serpytis@santa.lt
Presentation: In 2010, a 68-year-old man presented to the ER with a remarkable history of anterior Q(+) MI in 2000 followed by aortocoronary bypass surgery with four autovenous connections. The patient had a history of hypertension, previous gallbladder removal, and was taking medications including aspirin, nebivolol, ramipril, and amlodipine.
Clinical Findings: Laboratory tests revealed a creatinine level of 95 µmol/l, brain natriuretic peptide (BNP) level of 184 ng/l, and markedly elevated troponin-I level of 1.967 µg/l. EKG showed ST elevations suggestive of anterior, lateral, and postero-basal MI.
Cardiac Interventions:
1. Coronary angiography revealed occlusions in the left anterior descending artery (LAD), ramus circumflex artery (RCx), and right coronary artery (RCA). Given the patient’s history, repeat coronary bypass grafting was recommended. However, his condition worsened with progressive cardiogenic shock, and intra-aortic balloon pump (IABP) was initiated.
2. Four days after admission, the patient developed ischemia of the right leg. This complication required immediate removal of the IABP.
3. On the same day, the patient underwent an embolectomy and thrombectomy of the right popliteal and tibia.
4. An MRI scan of the heart in 2011 showed an ejection fraction (EF) of 45%, scar tissue in the region of the anterior descending artery, and viable myocardium in the basal and middle segments of the anterior interventricular septum (segment 2).
5. Nine days later, his condition had deteriorated dramatically, and a cardiac ultrasound indicated a further reduction EF of only 10%. The patient was taken for repeat coronary artery bypass surgery with left internal mammary artery to left anterior descending artery (LIMA to LAD) and radial artery and vein grafts. During surgery, thrombosis of the vein graft was noted. After surgery, the patient required a pacemaker. The Levitronix system was used to support both the left and right ventricles.
6. Earlier in 2011, the patient’s cardiac output remained low, with an EF of 15–20%.
Date
2010
Initial tests
Day 1
4 days after admission
13 days after admission
22 days after admission
24 days after admission
42 days after admission
During hospital stay
121 days after admission
Event/Intervention
• Patient presented to the emergency room
• Noted: History of anterior Q(+) MI in 2000, aortocoronary bypass surgery, hypertension, gallbladder removal, and medications (aspirin, nebivolol, ramipril, and amlodipine)
BNP = brain natriuretic peptide; EF = ejection fraction; IABP = intra-aortic balloon pump; LAD = left anterior descending artery; LIMA = left internal mammary artery RCA = right coronary artery; RCx = ramus circumflex artery.
7. In view of the patient’s deteriorating cardiac function and after exhausting other options, orthotopic biatrial heart transplantation was performed the next day.
Additional interventions: During the hospitalization, the patient experienced several complications:
Table 1: Clinical Course of the Case
• Brain ischemia, particularly in the T-P lobes and left ventricle.
• Hemicolectomy was performed due to colonic hemorrhage on the right side.
• A dual-chamber pacemaker was implanted to address the syndrome of sinus node weakness of the transplanted heart.
• Cytomegalovirus infection was effectively treated with antiviral drugs.
Discharge and follow-up: At the end of his 121-day hospital stay, the
patient was stable and had no chest or liver abnormalities or edema. His postoperative wounds were healing well. He was advised to continue cyclosporine, azathiaprine, prednisolone, aspirin, diltiazem, and statins.
Results: The patient survived 11 years after this difficult hospitalization. This case highlights the importance of timely medical intervention, perseverance, and meticulous care.
The Road Less Traveled: Aorto-cardiac Fistula Secondary to Streptococcus
Infantarius Endocarditis
Mary Quien, MD, and Jessica Kaushal, MD
Bridgeport Hospital Yale New Haven Health, Bridgeport, CT
Citation: US Cardiology Review 2024;18(Suppl 1):70. Correspondence: Mary Quien, mary.quien@bpthosp.org
Background: Aorto-atrial fistula (AAF) is a life-threatening condition characterized by abnormal connection between the aorta and cardiac atria and is a rare complication of infective endocarditis (IE), affecting up to 3.5% of patients.1 We present a case of AAF that resulted from periannular extension of bioprosthetic valve endocarditis.
Case: A 64-year-old man with a history of poorly controlled diabetes and bioprosthetic aortic valve (AV) replacement presented with 2 weeks of generalized weakness, chills, polyuria, and polydipsia. On presentation, he was afebrile and hemodynamically stable, and labs were suggestive of diabetic ketoacidosis with a mild leukocytosis. EKG was notable for sinus rhythm with first degree AV block, left ventricular hypertrophy with QRS widening, and nonspecific ST-T wave changes. Initial sepsis workup revealed multifocal consolidations on chest X-ray so the patient was started on broad spectrum antibiotics. Despite initial treatment, he developed persistent fevers, hypotension requiring multiple pressors, and acute hypoxic respiratory failure requiring intubation. Blood cultures eventually grew Streptococcus infantarius Tansthoracic echocardiogram (TTE) revealed normal left ventricle and right ventricle function with poorly visualized mitral regurgitation, therefore, transesophageal echocardiography (TEE) was performed. TEE demonstrated a large fistula between the aorta and the left atrium emanating from the left coronary sinus of Valsalva (Figure 1). Although no overt vegetation was seen, there was a mobile cystic structure protruding from the aortic annulus that was most consistent with a residual portion of a walled-off abscess. Given the severity of the patient’s illness, surgery was initially deferred to allow for optimization of medical management to reduce surgical complications. Ultimately, the family decided not to pursue surgery and to transition the patient to hospice care.
Discussion: In prosthetic valve endocarditis (PVE), peri-annular extension, which is seen in 56–100% of cases, and abscess formation can lead to erosion of intra-cavitary barriers and the formation of fistulas.2 PVE of the AV has particularly been found to be more invasive than other valves. Risk factors for AAF include the presence of a prosthetic valve, valvular regurgitation, paravalvular abscess, IV drug use, and virulent pathogens. The most common organism implicated is Staphylococcus in 58% of cases, followed by Streptococci 3,4
TTE is the initial investigation of choice but is inferior in delineating the anatomical and functional details of paravalvular complications of AV endocarditis. TEE, however, can diagnose AV abscess and the presence of fistulous tracts with high sensitivity and is the gold standard investigation for AAF. Combined TTE and TEE have a detection rate of 97% and can be supplemented by CT and cardiac catheterization to obtain precise information prior to surgical planning.5,6 If TEE is inconclusive for definite endocarditis, or if a complication such as perivalvular abscess is suspected, other imaging modalities, like 18F-FDG PET-CT, can be useful.7 Treatment of AAF secondary to infective endocarditis should be prompt, given the high risk of major cardiac complications and high mortality rate, which has been quoted as high as 40%.8
Conclusion: To the best of our knowledge, this is a novel case of fistulizing IE secondary to Streptococcus infantarius. Diagnosis and consideration of surgical treatment of AAF should be prompt, given its high mortality rate despite aggressive medical management.
Figure 1: Transthoracic Echocardiogram and Color Doppler Imaging of the Patient
Transthoracic echocardiogram imaging demonstrating a mobile cystic structure protruding from the aortic annulus consistent with a residual portion of walled off abscess (red arrow). Color Doppler imaging shows continuous flow from the aorta to the left atrium (LA). AV = aortic valve; MV = mitral valve.
1. Anguera I, Miro JM, Vilacosta I, et al. Aorto-cavitary fistulous tract formation in infective endocarditis: clinical and echocardiographic features of 76 cases and risk factors for mortality. Eur Heart J 2005;26:288–97. https://doi.org/10.1093/eurheartj/ehi034; PMID: 15618052.
2. Choussat R, Thomas D, Isnard R, et al. Perivalvular abscesses associated with endocarditis; clinical features and prognostic factors of overall survival in a series of 233 cases. Perivalvular Abscesses French Multicentre Study. Eur Heart J 1999;20:232–41. https://doi.org/10.1053/ euhj.1998.1240; PMID: 10082156.
3. Kang N, Wan S, Ng CSH, Underwood MJ. Periannular extension of infective endocarditis. Ann Thorac Cardiovasc Surg 2009;15:74–81. PMID: 19471219.
4. Agrawal A, Amor MM, Iyer D, et al. Aortico-left atrial fistula: a rare complication of bioprosthetic aortic valve endocarditis secondary to enterococcus faecalis. Case Rep Cardiol
5. Fierro EA, Sikachi RR, Agrawal A, et al. Aorto-atrial fistulas: a contemporary review. Cardiol Rev 2018;26:137–44. https://doi.org/10.1097/crd.0000000000000182; PMID: 29077586.
6. Pettersson GB, Hussain ST. Current AATS guidelines on surgical treatment of infective endocarditis. Ann Cardiothorac Surg 2019;8:630–44. https://doi.org/10.21037/acs.2019.10.05; PMID: 31832353.
7. Khan M, Muthukumar L, Khandheria BK. Echocardiographic features of evolving aortic root abscess. JACC Case Rep 2019;1:426–7. https://doi.org/10.1016/j.jaccas.2019.07.024; PMID: 34316845.
8. Özer N, Deniz A, Atalar E, Aksoyek S, Ovunc K, Kes SS. Aorta-right atrial fistula: a rare complication of prosthetic aortic valvular endocarditis. J Am Soc Echocardiogr 2007;20:538. e5–6. https://doi.org/10.1016/j.echo.2006.11.010; PMID: 17484999.
Breaking Away from Ischemia: A Rare Case of Myocarditis-associated Papillary Muscle Rupture Causing Acute Mitral Regurgitation
Andrew Hill, MD,1 Ryan Wallace, MD,1 Keki Balsara, MD,2 Alexander Papolos, MD,1,3 Maxwell Hockstein, MD,3,4 Richa Gupta, MD,5 and Benjamin Kenigsberg, MD1,3
1. Division of Cardiology, MedStar Washington/Georgetown University Hospital Center, Washington, DC; 2. Department of Cardiac Surgery, MedStar Washington Hospital Center, Washington, DC; 3. Department of Critical Care Medicine, MedStar Washington Hospital Center, Washington, DC; 4. Department of Emergency Medicine, MedStar Washington Hospital Center, Washington, DC; 5. Advanced Heart Failure Program, MedStar Heart and Vascular Institute, Washington, DC
Citation: US Cardiology Review 2024;18(Suppl 1):72. Correspondence: Andrew Hill, andrew.p.hill@medstar.net
Background: Papillary muscle rupture is a feared mechanical complication most often associated with acute MI involving the postero-medial papillary muscle. However, here we describe a case of myocarditis leading to nonischemic antero-lateral papillary muscle rupture and acute mitral regurgitation.
Case: A 57-year-old woman with history of Graves’ disease, anti-neutrophil cytoplasmic autoantibody (ANCA)-associated vasculitis, and systemic lupus erythematosus (SLE) presented to the ER with fatigue, weakness, and arthralgias due to concern for lupus flare. Lab work showed ESR 125 mm/h, c-reactive protein 330 mg/l, 50,000 white blood cells (WBC)/l, and lactic acidemia 6.6 mmol/l which initially resolved with IV fluids.
Overnight, developed altered mental status and hemodynamically significant complete heart block requiring emergent transvenous pacemaker as well as later intubation for respiratory failure. After peak high sensitivity troponin of 6,000 ng/l, she was transferred to the cardiac intensive care unit (ICU). Transthoracic echocardiogram (TTE) revealed a newly reduced left ventricular ejection fraction of 25%, moderate right ventricular dysfunction, and no significant valvular disease.
Right and left heart catheterization revealed non-obstructive disease and appropriate support on epinephrine and dobutamine. While awaiting endomyocardial biopsy results, she was started on methylprednisolone. C3, C4, and anti-double-stranded DNA antibody screen implied lupus disease inactivity. Transvenous pacer was removed after heart block resolved.
On day 4, biopsy returned consistent with mild myocarditis. She was transitioned to oral steroids, extubated on hospital day 5, and weaned off inotropic support by day 6. Repeat TTE revealed normalization of left and right ventricular function.
Within 12 hours of transfer out of the ICU, the patient became acutely altered, hypotensive, and hypoxic requiring reintubation. She had Society for Cardiovascular Angiography and Interventions (SCAI) stage E cardiogenic shock with rapidly escalating vasopressor and inotrope requirements. Point-of-care ultrasound revealed new severe mitral regurgitation and flail anterior mitral valve leaflet.
Decision-making: The case was reviewed by a multidisciplinary shock team with the decision to pursue emergent, salvage mitral valve intervention as opposed to temporary mechanical support.
Intraoperatively there was clear evidence of rupture of the anterolateral papillary muscle associated with the A2 and A3 segments of the anterior mitral valve leaflet. The diseased portion was excised and sent for pathology. A 29-mm Epic (Abbott) bioprosthetic mitral valve was sewn in, given the necrotic appearing papillary muscle, making repair unfeasible.
On postoperative day 1, bedside transesophageal echocardiogram showed thickened interventricular septum with dynamic left ventricular outflow tract obstruction. High dose methylprednisolone was resumed with IV immunoglobulin. However, progressive hemodynamic failure was not felt to be survivable, and the patient died 2 days later after transition to comfort-focused care.
Conclusion: We describe a rare occurrence of non-ischemic anterolateral papillary muscle rupture leading to acute severe mitral regurgitation and cardiogenic shock in the setting of myocarditis, emphasizing the need to consider non-ischemic etiologies of mechanical complications in patients with cardiogenic shock.
Transcatheter Aortic Valve Replacement in the Management of Cardiogenic Shock Requiring Extracorporeal Membrane Oxygenation Caused by Severe Aortic Stenosis
Anne M White, Kasem H Toubat, Connor G O’Brien, Sam B Brusca, Sammy Elmariah, Richard Cheng, Amy Fiedler, Jason Smith, and Christopher F Barnett
University of California San Francisco, San Francisco, CA
Citation: US Cardiology Review 2024;18(Suppl 1):74. Correspondence: Anne M White, anniewhite0626@gmail.com
Background: Aortic stenosis (AS) causing refractory cardiogenic shock (CS) is a rare and particularly challenging clinical scenario. Transcatheter aortic valve replacement (TAVR) in a patient with CS is high-risk and not typically performed, especially in patients who require temporary mechanical support. We report a case of CS caused by severe AS requiring extracorporeal membrane oxygenation (ECMO) successfully treated with TAVR.
Case: A 59-year-old man with diabetes, hypertension, hyperlipidemia, AF, and prior strokes presented with epigastric pain, dyspnea, and an elevated troponin. Coronary angiogram revealed severe diffuse multivessel coronary artery disease. An echocardiogram revealed severe AS with an aortic valve area of 0.7 cm², mean gradient of 23 mmHg, and ejection fraction (EF) <20%. The patient developed CS, acute hypoxic respiratory failure, and was emergency cannulated onto veno-arterial-venous ECMO. The primary driver of CS was thought to be critical AS. The patient was evaluated by the multidisciplinary shock team and the structural heart team. He was determined to be extreme risk for surgical aortic valve replacement and the decision was made to offer TAVR. A 26-mm Edwards SAPIEN (Edwards Lifesciences) S3 valve was successfully deployed in the aortic position with a post-procedure mean gradient of 8 mmHg and EF of 45%. ECMO was discontinued 2 days post-procedure. Although cardiac function normalized after the TAVR procedure, the patient died over 2 weeks later from noncardiac complications of critical illness including anoxic brain injury, renal failure, and peripheral vascular disease.
Table 1: Hemodynamic and Echocardiographic Values Pre- and Post-extracorporeal Membrane Oxygenation Transcatheter Aortic Valve Replacement
DVI = Doppler velocity index; LVEF = left ventricular ejection fraction; LVOT VTI = left ventricular outflow tract velocity time integral; TAPSE = tricuspid annular plane systolic excursion; TAVR = transcatheter aortic valve replacement.
Conclusion: This case highlights the potential role of TAVR in patients with CS caused by severe AS requiring ECMO support. Mortality in these patients is high and was previously reported to be 41% at 30 days. In the present case, the patient died of non-cardiac comorbidities, emphasizing the role of multidisciplinary evaluation and careful selection of patients for intervention as well as the need for meticulous post-procedural care in the intensive care unit.
Temporary Biventricular Mechanical Circulatory Support for Primary Graft Dysfunction after Orthotopic Heart Transplantation
Boyangzi Li, MD, PhD,1 Sanchit Chawla, MD,2 Michael Tong, MD,3 Andrew Higgins, MD,4 and Ran Lee, MD4
1. University of Miami School of Medicine, Department of Medicine, Division of Cardiology, Miami, FL; 2. Department of Critical Care Medicine, Cleveland Clinic Foundation, Cleveland, OH; 3. Department of Thoracic and Cardiovascular Surgery, Heart, Vascular & Thoracic Institute, Cleveland Clinic Foundation, Cleveland, OH; 4. Department of Cardiovascular Medicine, Heart, Vascular & Thoracic Institute, Cleveland Clinic Foundation, Cleveland, OH
Citation: US Cardiology Review 2024;18(Suppl 1):75. Correspondence: Ran Lee, leer2@ccf.org
Background: Primary graft dysfunction (PGD) is a rare complication within 24 hours after orthotopic heart transplantation (OHT) not associated with hyperacute rejection or pre-existing pulmonary hypertension. It can be either temporary or persistent and may be biventricular or impact the left or right ventricle in isolation. Early implantation of mechanical circulatory support devices may offer hemodynamic stability, preserve end-organ function, and potentially improve survival in severe PGD.
Case: A 51-year-old man with obesity, hypertension, diabetes, and a nonischemic cardiomyopathy with advanced systolic heart failure leading to a HeartMate 3 left ventricular assist device (LVAD; Abbott) implantation 2 years prior was admitted in ventricular tachycardia (VT) storm in the context of amiodarone cessation due to thyrotoxicosis. Unfortunately, incessant VT persisted despite initiation of procainamide and lidocaine infusions and invasive hemodynamics revealed a declining cardiac output. Given refractory, life-threatening arrhythmia in the presence of univentricular support, the patient was emergently upgraded to United Network for Organ Sharing (UNOS) status 1 for OHT.
A suitable donor was identified 5 days later, and the patient underwent an initially uneventful OHT. Unfortunately, after liberation from
cardiopulmonary bypass, the patient gradually became more hypotensive. Echocardiography revealed progressive right ventricular predominant systolic dysfunction. A femoral intra-aortic balloon pump (IABP) was inserted to unload the left ventricle. IV epinephrine and inhaled isoproterenol were initiated but were inadequate to stabilize his right ventricular function. Veno-arterial extracorporeal membranous oxygenation was discussed but given the desire to avoid an additional arteriotomy in addition to putting further myocardial work and afterload on a struggling left ventricle, he received a temporary right ventricular assist device and an oxygenator (oxyRVAD) with drainage from the right femoral vein and return to the pulmonary artery via a Gore-Tex graft.
Immunosuppressants, including tacrolimus, mycophenolate, and steroid were initiated post-OHT as per routine. The patient slowly improved with biventricular support. Inhaled isoproterenol was weaned on postoperative day (POD) 3. The patient was extubated on POD 4. The oxyRVAD and IABP were successfully decannulated on POD 4 and 5, respectively.
Conclusion: Our case demonstrates that oxyRVAD support together with IABP is a feasible option as supportive therapy to bridge recovery for post-OHT patients who sustain severe PGD.