

Making waves

Matt Adams, AFASA
Matt trained as a clinical vascular scientist in the UK where he worked with the vascular studies team at the Royal Free Hospital. After 5 busy years scanning, helping with teaching and assisting in research conducted by the University College London, Matt made the move to Australia in early 2017, where he is now in charge of Camperdown Vascular Lab in Sydney.

Robyn Boman, FASA
Robyn has extensive clinical experience as a general sonographer in metropolitan and rural catchments of NSW. Robyn has qualifications in diagnostic radiography, medical ultrasound, and education. Robyn has shared this knowledge in volunteer outreach ultrasound training projects in Papua New Guinea and Fiji. Her passion for education has been evident from the high regard expressed by her students when she was a lecturing academic with CQU. Robyn is currently a full-time PhD candidate at Western Sydney University.

Jessica Coffey
Jessica is a clinical sonographer with a special interest in obstetric and gynaecological ultrasound. For the last five years she has worked in tertiary maternal fetal medicine units. She has a particular passion for training, education and continuous professional development and enjoys teaching, learning and mentoring.

Michele Dowling, AFASA
Michelle’s training started in radiotherapy, followed by diagnostic radiography, and medical ultrasound for the last 25 years with extensive experience as a clinical sonographer in most aspects of ultrasound. Working in a specialised diagnostic imaging site, Michelle is currently involved in student education and the mentoring and skill improvement of qualified sonographers. She has experience managing a large team of sonographers and students over multiple sites and has assisted in operational management, business development, and implementing strategies. She currently serves as a general director on the ASA board and is also involved in the Sonographer Policy and Advisory Committee, the Governance and Nominations Committee, and the Health and Wellbeing Special Interest Group.

Heath Edwards, AFASA
Heath has a BMed Rad Science from the University of Newcastle and a GradDip in Medical Ultrasound from Monash University. Clinically, Heath is a senior radiographer/sonographer at the Royal Brisbane and Women’s Hospital and a vascular sonographer with Queensland Vascular Diagnostics. Heath is also a member of the vascular SIG and a casual tutor for CQU. Heath is a keen educator with a specialised interest in MSK and vascular ultrasound. Recently, Heath has been focused on the role ultrasound plays in the management of acute Achilles injuries.

Susan Diep
Susan (BRadMedImag, Monash University, GradDipMedUs, Monash University and GradCertHlthProfEd, Monash University) is a general clinical radiographer/sonographer and an ultrasound application specialist with GE HealthCare. Susan is a member of the MSK SIG and a Deakin University casual academic. Susan has specialised interest in MSK and vascular ultrasound. Recently, her focus has been investigating the role of ultrasound in assessing peripheral nerves. Susan has a passion for sharing knowledge and advancements in medical ultrasound.

Emma Jardine
Emma is a senior sonographer working in Victoria. She has a passion for professional growth and believes that investing in ongoing education and training will benefit individual sonographers and contribute to better patient outcomes and overall healthcare experience.

Ilona Lavender, FASA
Ilona is a tutor sonographer at a large tertiary hospital in Melbourne. She has a strong interest in training and education. Her areas of interest are paediatrics, obstetrics and artificial intelligence in ultrasound. She has presented at numerous workshops and conferences and has a number of publications.

Glenda McLean, FASA
Glenda is currently the research and knowledge translation lead for imaging at Monash Health and Peninsula Health in Victoria. She has a master’s degree in ultrasound and is currently a PhD candidate at Monash University researching cranial ultrasound screening protocols. Glenda has taught the paediatric subject in the MMU course and is now a sessional lecturer in the Department of Medical Imaging and Radiation Science at Monash University. She was the founding editor-inchief of the Australasian Sonographers Association Sonography journal and continues to be a member of the editorial board.

Kim Prince
Kim is a cardiac sonographer whose special interests lie in sonographer wellbeing and education. Kim has worked across both private and public systems and experienced the British system working in the UK for 7 months. Currently, Kim is a lecturer at CQ University and has joined the ASA professional development team.

Assoc Prof Tristan Reddan, FASA
Tristan is the consultant radiographer/ sonographer at the Queensland Children’s Hospital in Brisbane where he coordinates medical imaging research governance, provides statewide paediatric ultrasound advice, and works clinically. He is also a clinical associate professor in the School of Clinical Sciences at the Queensland University of Technology (QUT) where he works as a sessional lecturer and collaborates on research projects and student supervision.

Sean Yeoh
Sean Yeoh is the tutor sonographer for Lumus Imaging Brunswick and Glenroy and has been passionate about teaching for many years. He has spent time living and teaching in Victoria and Adelaide and has been fortunate to work with different specialists, including MSK radiologists and obstetrician sonologists. His belief is that ultrasound is an extremely potent diagnostic tool but understands that a common barrier faced is education. He therefore hopes to create and provide educational material to support the next generation of sonographers.

Caterina Watson, AFASA
Caterina Watson is a sonographer practising in Western Australia. She is a PhD candidate with Edith Cowan University, her research focusing on computer vision techniques and emerging technologies. She serves as chairperson of ASA Emerging Technologies SIG, and is a member of the ASA Research Special Interest Group, the RANZCR AI Collaboration Committee, and ISUOG AI SIG. Caterina enjoys participating in outreach training programs in the South Pacific Nations.

Alison White, AFASA
Alison is an accredited medical sonographer (cardiac) with over 25 years’ experience in sonography. Alison has been a national clinical examiner for the ASUM DMU and is a past DMU board member. Her clinical expertise has been recognised at both national (Australian Sonographer of the Year, ASUM, 2012; Associate Fellow of the ASA, 2023) and international levels (Fellow of the American Society of Echocardiography, 2017). She joined Griffith University in 2012 as a senior lecturer and program director, teaching in the areas of cardiovascular and respiratory anatomy, physiology and pathophysiology and biomedical instrumentation. Alison is passionate about the professional development of sonographers and contributes to the ASA by reviewing articles for Sonography, presenting at the ASA National Conference and as a member of the Cardiac SIG.
CARDIAC
EHRA expert consensus statement on arrhythmic mitral valve prolapse and mitral annular disjunction complex 5 in collaboration with the ESC Council on valvular heart disease and the European Association of Cardiovascular Imaging endorsed by the Heart Rhythm Society, by the Asia Pacific Heart Rhythm Society, and by the Latin American Heart Rhythm Society
CARDIAC
Cross-disciplinary prevalence and associated factors for work-related discomfort in users of ultrasonography: Implications for sonography professionals and health care administrators 6
GENERAL
Hepatic steatosis: qualitative and quantitative sonographer assessment in comparison to histology 8
HEALTH & WELLBEING
Exploring sonographer emotional wellbeing: NHS sonographers’ experience of the restorative function of professional supervision 10
HEALTH & WELLBEING
Breaking bad and difficult news in obstetric ultrasound and sonographer burnout: Is training helpful? 11
MUSCULOSKELETAL
Ulnar wrist pain revisited: ultrasound diagnosis and guided injection for triangular fibrocartilage complex injuries 13
MUSCULOSKELETAL
Value of ultrasound assessment for traumatic nerve injury of the upper limb 15
PAEDIATRIC
The impact of high-frequency transducers on the sonographic measurements of the pyloric muscle thickness in infants 17
RESEARCH
Correlation does not imply agreement: A cautionary tale for researchers and reviewers 19
RESEARCH Ten common statistical mistakes to watch out for when writing or reviewing a manuscript 20
VASCULAR
Ultrasonographic assessment of atherosclerotic renal artery stenosis in elderly patients with chronic kidney disease: An Italian cohort study 21
VASCULAR
Point of care venous Doppler ultrasound: Exploring the missing piece of bedside haemodynamic assessment 23

WOMEN’S HEALTH
Noninvasive imaging techniques for diagnosis of pelvic deep endometriosis and endometriosis classification systems: an International Consensus Statement 25
EMERGING TECHNOLOGIES
Artificial intelligence assists identifying malignant versus benign liver lesions using contrast-enhanced ultrasound 26
EMERGING TECHNOLOGIES
Emerging Technologies: Towards standardized acquisition with a dual-probe ultrasound robot for fetal imaging 27 © Australasian Sonographers Association 2024. Disclaimer: The information in this publication is current when published and is general in nature; it does not constitute professional advice. Any views expressed are those of the author and may not reflect ASA’s views. ASA does not endorse any product or service identified in this publication. You use this information at your sole risk and ASA is not responsible for any errors or for any consequences arising from that use. Please visit www. sonographers.org for the full version of the Australasian Sonographers Association publication disclaimer
EHRA expert consensus statement on arrhythmic mitral valve prolapse and mitral annular disjunction complex
in collaboration with the ESC Council on valvular heart disease and the European Association of Cardiovascular Imaging endorsed by the Heart Rhythm Society, by the Asia Pacific Heart Rhythm Society, and by the Latin American Heart Rhythm Society
WHY THE STUDY WAS PERFORMED
Patients with arrhythmic mitral valve prolapse (AMVP) represent a small cohort of patients in the general population who present with a heightened risk profile of sudden cardiac death (SCD). Given the serious nature of the anatomical derangement of mitral valve prolapse (MVP), mitral annular disjunction (MAD) and the potential for the development of life-threatening ventricular arrhythmias, the aims of this study included defining a comprehensive imaging protocol for transthoracic echocardiography to assess the presence and complexity of AMVP.
HOW THE STUDY WAS PERFORMED
This consensus statement reviewed and summarised the current literature published regarding the AMVP complex. Expert statements, guidelines and evidence from the literature were collected and the information was summarised to arrive at the position of practical strategies and tips on how to define and identify AMVP complex, as well as provide guidance on risk stratification and management of this complex anatomical and arrhythmic disorder.
WHAT THE STUDY FOUND
• A clear definition of MVP was agreed upon with MVP defined as a systolic displacement of one or both mitral leaflets ≥ 2 mm above the plane of the mitral annulus in the sagittal (parasternal long-axis view in echocardiographic imaging) view of the mitral valve.
• Diagnostic criteria for MAD were defined and the use of echocardiography to determine the presence of MAD was recommended as an accessible and relevant screening tool. Importantly, this paper decreases the ‘guess’ work previously associated with the echocardiographic assessment of MAD, due to the clear summary of diagnostic criteria produced in Box 1 on page 1985.
• The accurate quantification of mitral regurgitation (MR) in AMVP patients is crucial as an increase in mortality in AMVP patients has been associated with increasing MR severity.
• Further research is required on large cohorts of patients to further quantify and determine the mechanisms of VAs in MVP patients; how the progression of MVP and associated progression of the severity of MR impacts the management strategies in patients with potential for VAs; the clinical outcomes of screening for VAs to better define low, medium and high risk categories of patients.
RELEVANCE TO CLINICAL PRACTICE
• Patients with suspected MVP should be carefully screened as there is a characteristic phenotype of MVP linked to SCD, where patients with MVP with malignant ventricular arrhythmias (VAs) have an increased risk of deterioration to SCD as the VAs progress in severity.
• MAD will be more accurately identified by cardiac sonographers given the clear summary of diagnostic criteria for MAD that this paper provides.
• A critical component of this paper was the publication of a clear and detailed echocardiographic protocol which is guideline-based and standardised. This protocol is found on page 1995 of the paper and should be mandatory reading for all cardiac sonographers, both newly qualified and experienced. In doing so, misdiagnosis of MVP and MAD can be avoided, and thus the accuracy of determination of patients at risk of SCD can be improved.
REVIEWED BY
Alison White, AFASA
ASA SIG: Cardiac
REFERENCE
Authors: Sabbag A, Essayagh B, Ramírez Barrera JD, Basso C, Berni A, et al.
Journal: EP Europace
Open Access: Yes
READ THE FULL ARTICLE HERE
MAD can be observed at different locations on the mitral annulus. However, MAD is associated with increased risk of VAs when observed at the posterior LV wall.
Cross-disciplinary
prevalence and associated factors for work-related discomfort in users of ultrasonography: Implications for sonography professionals and health care administrators
WHY THE STUDY WAS PERFORMED
To examine relationships within and across sonography work systems, and to examine worker health and wellbeing and explore work systems and process factors associated with workrelated discomfort of sonographers.
HOW THE STUDY WAS PERFORMED
One hundred thousand ultrasonography users were invited to complete an online questionnaire via email. The questionnaire included demographics, selected constructs from the sonographer work systems (SWS) framework and the prevalence of work-related musculoskeletal discomfort, visual discomfort, and headaches. Musculoskeletal discomfort was identified as any ache, pain, stiffness, burning, numbness, tingling or other self-reported symptoms within the body in the last 12 months. Musculoskeletal discomfort was examined across nine body regions: shoulder, elbow, wrist/hands, neck, upper back, lower back, hip/thigh, knees, and ankle/feet. Follow-up questions were completed for certain body regions with a rating of the intensity of discomfort from 0 to 10 using a visual analogue scale. Respondents also indicated if they had sought additional healthcare support (i.e. physiotherapist, doctor, etc.) or took any sick leave due to the discomfort. Those respondents who indicated discomfort also commented on whether the discomfort was made worse by any activities (even non-work-related activities) or if the discomfort led to a permanent or temporary change in job or duties. Respondent questions also included information to establish body mass index, age, handedness, location and work status such as full or part-time employment and their main area of practice i.e. cardiac, MSK, obstetrics, etc. Those who indicated they had completed ergonomics training answered further questions regarding the method of training and how recently this training was completed.
WHAT THE STUDY FOUND
From 3659 valid responses (those not currently working or did not provide contact information were excluded), 86% reported that they regularly experienced musculoskeletal discomfort directly related to their work. The common practice sonographic specialities of respondents were vascular, abdomen, OB-GYN, and adult cardiac. Hospitals and outpatient clinics in the USA were the most common workplaces with most of the sample, stating they worked full-time. There were 54.2% of respondents who engaged in ergonomics training, of which 85.2% indicated this was helpful, and 90.4% reported they were able to apply the ergonomics training to the workplace and suggested using adjustable equipment approximately 74% of the time. Primarily, a positive workplace culture was reported. The stated key factors associated with the reduced likelihood of work-related discomfort are: engaging in a positive work culture, minimising interruptions to workflow, taking more work breaks, and using adjustable equipment more frequently.
It was noted that, on average, employers only had around 2 of the 7 recommended ergonomics policies or procedures in place. One-third of respondents had reported an ergonomic concern in the workplace, of which only 27% felt that their concern was adequately addressed, and more disturbingly, 6% reported experiencing retaliation or threat of retaliation for reporting their ergonomic issues.
REVIEWED BY
Kim Prince
ASA SIG: Cardiac
REFERENCE
Roll S, Fukumura, Y, Stigall-Weikle
N & Evans K
Journal: Journal of Diagnostic Medical Sonography
Open Access: Yes
READ THE FULL ARTICLE HERE
Cross-disciplinary prevalence and associated factors for work-related discomfort in users of ultrasonography: Implications for sonography professionals and health care administrators

Figure: Seven-day and 12-month prevalence of musculoskeletal discomfort among survey respondents (n = 3659) by body region. Markers (X) indicate the mean typical intensity of discomfort (0–10) for each body region among participants who reported experiencing discomfort in that region within the most recent 12-month period. Body regions with the areas of highest discomfort were the shoulder, neck, and wrist/hand.
RELEVANCE TO CLINICAL PRACTICE
The study concluded that despite increased participation in ergonomics training and the use of adjustable equipment, the prevalence of work-related discomfort remained high in sonographers. There is a need for more attention to be directed at organisational factors and work processes to identify and implement solutions to improve the health and wellbeing of sonographers. Workplace employers need to ensure appropriate policies and procedures are in place to ensure sonographer welfare is addressed, and employees should not feel they are at risk of retaliation by raising ergonomic concerns.
Individuals without work-related musculoskeletal discomfort appeared to be from workplaces with positive protective factors such as adjustable equipment, work breaks, ergonomic policies and work culture. Those who reported discomfort experienced interrupted workflow timing and pressure and poor performance more than those without discomfort. Fewer than 15% of respondents took time off work or changed their job duties due to their discomfort, which is a disturbing finding. It would be interesting to investigate the main reasonings for this i.e. concerns about retaliation.
Sonographer injury and musculoskeletal issues are a major factor with sonographers of all types, and the busier medical imaging becomes, the more pressure is placed on sonographers to accomplish more with less attention focused on their health and wellbeing. Identifying key strategies that workplaces and sonographers can implement may assist in reducing the number of work-related discomforts. However, more research may be required in this area to establish such significant strategies.
Even with ergonomic training, sonographers are still experiencing a high rate of work-related musculoskeletal discomfort.
GENERAL REVIEWED BY Emma Jardine
ASA SIG: General
REFERENCE
Authors: Tan Z, Mehta B, Kusel K, Seow J, Zelesco M, Abbott S, Simons R, Boardman G, Welman C & Ayonrinde O
Hepatic steatosis: qualitative and quantitative sonographic assessment in comparison to histology
WHY THE STUDY WAS PERFORMED
This retrospective study was performed to assess the correlation between qualitative liver ultrasound assessment (B-mode) and attenuation imaging (ATI) assessment for hepatic steatosis, using liver biopsy as a reference standard. The secondary aim was to investigate the interobserver variability of qualitative ultrasound B-mode feature for hepatic steatosis assessment.
Steatotic liver disease is the primary cause of liver mortality and morbidity. Patients who have steatotic livers also have an increased risk of developing cardiovascular disease and chronic kidney disease. Early diagnosis enables interventions to reverse and reduce hepatic steatosis. B-mode ultrasound allows subjective grading of hepatic steatosis as absent, mild, moderate or severe. This grading system involves comparing the liver’s echogenicity to the renal cortex, evaluating the visualisation of the hepatic vessel walls and assessing posterior beam attenuation. This compares to quantitative ultrasound assessment using ATI. ATI measures the attenuation of the ultrasound beam and can accurately discriminate mild from moderate steatosis.
HOW THE STUDY WAS PERFORMED
A retrospective study was conducted in Australia over a 4-year period. Patients with a hepatic steatosis grade on histopathology who had an ultrasound of the liver performed in conjunction with an ultrasound-guided biopsy were included. The liver biopsies were obtained from the right lobe of the liver (segment 6 or 7). Liver biopsy histology results were obtained from the laboratory database.
Three radiologists who were blinded to clinical data graded qualitative images of the liver. Retrospective analysis of ultrasound images recorded subjective ultrasound parameters. These parameters included large hepatic vein blurring, main and right portal vein blurring, liver-kidney contrast, posterior beam attenuation, diaphragm definition, focal fat sparing, liver echotexture and overall impression.
WHAT THE STUDY FOUND
Ninety patients were included in the study, 67% were female, the median age was 54 years, mean patient BMI was 30.8 kg/m2. Sixty per cent of patients demonstrated no to mild steatosis.
The radiologist’s overall impression had a strong correlation with the biopsy results for the grade of steatosis. There was high interobserver reliability noted, with most subjective parameters having moderate to near-perfect interobserver agreement.
Journal: Australasian Journal of Ultrasound in Medicine
Open Access: Yes
READ THE FULL ARTICLE HERE
Hepatic steatosis: qualitative and quantitative sonographic assessment in comparison to histology

Figure 1. These images demonstrate no steatosis, mild steatosis, moderate steatosis and severe steatosis based on the radiologist’s overall impression. The images in the top row demonstrate liver-kidney contrast. The middle row highlights vessel wall blurring, posterior beam attenuation and diaphragmatic definition. The bottom row demonstrates attenuation imaging (ATI).
RELEVANCE TO CLINICAL PRACTICE
Qualitative ultrasound continues to play a significant role in the assessment of hepatic steatosis, especially considering its high availability and proficiency. An experienced radiologist’s overall impression is at least as good as quantitative parameters for the assessment of steatotic liver disease.
This study found that there is an ongoing role for B-mode ultrasound in the primary diagnosis and grading of steatotic liver disease.
Exploring sonographer emotional wellbeing: NHS sonographers’ experience of the restorative function of professional supervision
WHY THE STUDY WAS PERFORMED
• The survey was performed to review the sonographer’s experience of professional supervision and how effective it is at maintaining the emotional wellbeing of sonographers.
• The authors review the impact of the need for emotional support for sonographers and consequently the impact on patient care.
HOW THE STUDY WAS PERFORMED
• An online cross-sectional descriptive survey was performed.
• The survey focused on National Health Service (NHS) sonographers in the United Kingdom and asked questions about the sonographer’s experience of professional supervision.
• A total of 32 participants were included in the survey.
WHAT THE STUDY FOUND
• The study identified that the main barriers to effective supervision were time to provide it and practitioner workload.
• The results found that sonographers need emotional support with 50% of sonographers feeling unsupported.
• The potential for burnout was identified. The factors that were attributed to burnout included staff shortages and workload. There was also a potential for burnout among the obstetric sonographers in delivering unexpected news.
• The survey found that sonographers valued peer-to-peer group support where members of the team shared experiences to provide emotional support to each other.
RELEVANCE TO CLINICAL PRACTICE
• The impact of poor emotional resilience among healthcare workers has a direct correlation to standards of patient care.
• There is a link between supporting staff through formal supervision and improving the quality of care for patients.
• This study highlights the need to create a robust supervision model to better support staff who need emotional wellbeing support.
• The restorative function of clinical supervision focuses on supporting sonographers’ emotional wellbeing through discussing difficulties being faced as a consequence of their work.
• The aim of this function is to negate the impact of emotional burden by finding coping mechanisms that the individual sonographers would best respond to.
• This will lead to better-supported staff and may aid in the retention of sonographers who are feeling burnout.
• The key factors to help sonographers feel supported within their practice included managing the environment and workload and ensuring opportunities for peer support.
REVIEWED BY
Emma Jardine
ASA SIG: Health and Wellbeing
REFERENCE
Authors: Carr R & White H
Journal: Ultrasound
Open Access: Yes
READ THE FULL ARTICLE HERE
Retention of sonographers and burnout figures may improve with more systems put in place that support the emotional wellbeing of sonographers.
Breaking bad and difficult news in obstetric ultrasound and sonographer burnout: Is training helpful?
WHY THE STUDY WAS PERFORMED
Healthcare professionals are at greater risk of experiencing occupational stress and burnout than workers in other sectors, and rates of low wellbeing and burnout in healthcare staff are rising. These increases are thought to be due to a range of factors, including increasing workloads, rising patient expectations and a greater degree of administrative duties.
Sonographers report high levels of burnout, which manifests as work-based exhaustion and disengagement from patients. Exhaustion is a state where participants feel they have been overstretched by their work, whereas disengagement is characterised by a feeling of detachment from patients or work.
For those working in obstetric ultrasound, one frequently cited stressor is the delivery of bad or difficult news. Training in delivery news may reduce sonographer stress levels, however, no studies have investigated sonographer experiences with this training.
This study aims to investigate sonographer experiences of training in the delivery of difficult news, and preferences for training techniques, and to assess whether news delivery training is associated with lower burnout and higher wellbeing.
HOW THE STUDY WAS PERFORMED
A cross-sectional survey hosted online was designed to measure occupational characteristics, news delivery training experiences and preferences, burnout (on two dimensions of exhaustion and disengagement), and general mental wellbeing. The study recruited qualified UK sonographers via email through the British Medical Ultrasound Society (BMUS) membership, an advert on the BMUS website, an advert at the BMUS conference, and on Twitter. Ninety sonographers (85 female; mean age = 47) responded.
Demographics (age, gender), occupational characteristics and training experiences and preferences were collected along with measures of burnout and wellbeing.
Participants provided information regarding their disciplinary background before training in sonography (e.g. midwifery; radiography), the number of hours worked in total per week and the number of hours worked in obstetric scanning.
Participants reported on any training or experience they had received in breaking bad news since qualifying, and whether this had improved their skills.
Information on wellbeing and burnout was gathered and analysed. The burnout data was broken down into subscales of exhaustion and disengagement.
WHAT THE STUDY FOUND
Many of the respondents had received news delivery training since they had qualified and felt this improved their practice. The most common training techniques were lectures and group discussions, but the most preferred learning tools were observation of clinical practice and receiving service-user input.
Burnout rates in the group were high, with most participants reporting mild to severe exhaustion or disengagement. Eighty per cent of participants were experiencing exhaustion, 43.3% were experiencing disengagement and 88.9% could be classed as having a minor psychiatric disorder.
REVIEWED BY
Michele Dowling, AFASA
ASA SIG: Health and Wellbeing
REFERENCE
Authors: Johnson J, Arezina J, McGuinness A, Culpan A, & Hall L
Journal: Ultrasound
READ THE FULL ARTICLE HERE
Breaking bad and difficult news in obstetric ultrasound and sonographer burnout: Is training helpful?
Being recipients of training in difficult news delivery was not associated with higher wellbeing, but there was mixed evidence for an association with lower burnout. Receiving some training (compared with no training) was associated with lower disengagement, even when the impact of related variables such as age was accounted for.
RELEVANCE TO CLINICAL PRACTICE
This study sought to investigate experiences and preferences for difficult news delivery training in sonographers. Results suggested that most sonographers thought training was effective in improving their skills in delivering difficult news. The most frequently used training techniques were lectures and group discussions, but the sonographers’ most preferred training techniques were observation of clinical practice and receiving service-user input. Sonographers who had received training reported lower levels of disengagement. These findings suggest that training in the delivery of difficult news is valued by sonographers and may help to reduce sonographer stress levels and potential burnout.
Sonographers working in obstetric ultrasound report high levels of burnout which manifests as workbased exhaustion and disengagement from patients. One frequently cited stressor is the delivery of bad or difficult news.
Ulnar wrist pain revisited: ultrasound diagnosis and guided injection for triangular fibrocartilage complex injuries
WHY THE STUDY WAS PERFORMED
Triangular fibrocartilage complex (TFCC) injuries are the most common cause of ulnar wrist pain. Diagnosing TFCC injuries is traditionally reliant on magnetic resonance imaging (MRI). Recently, studies have emerged showing the potential of ultrasound (US) in diagnosing TFCC lesions, but the adaptation has been limited as the US anatomy and pathology of the TFCC are poorly described in the literature, in addition to not having a standardised scanning protocol.
Wu et al. aimed to propose a standardised scanning protocol for the TFCC with respect to:
• anatomy
• pathology
• US-guided injections.
WHAT THE REVIEW DESCRIBED
The review paper described the cadaveric and sonographic anatomy, mechanism of injury and physical examinations, MRI and US imaging appearance, scanning protocol, pathologies and treatments of the TFCC.
TFCC injuries can affect the articular disc, meniscus homologue, juxta-articular ligaments and the extensor carpi ulnaris tendon (ECU) sub-sheath. Wu et al. proposed US evaluation of the TFCC by a seven-image series (five on the dorsal aspect, three in transverse and two in longitudinal, two on the volar aspect, and one in both transverse and longitudinal), which allowed demonstration of all components. They also proposed a modified Palmer classification system for the ultrasound appearances of injuries. Class 1 (traumatic) and class 2 (degenerative), each having five subgroups a–e, which correspond to the location and/or degree of injury.
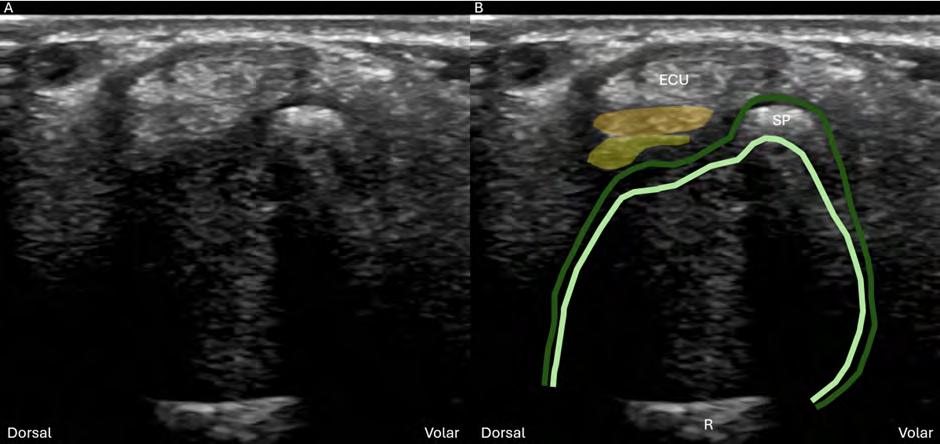
The articular disc is the major component of the TFCC and appears hypoechoic on ultrasound. In transverse (Figure 1), it appears as a hypoechoic disc-shaped structure and in longitudinal, the disc can be seen thinning towards its radial aspect. Between the styloid process and the articular disc lie (from superficial to deep) the ulnar collateral ligament, meniscus homologue and the two limbs (superficial and deep) of the radioulnar ligament. The layering and relationship between the various components, styloid process, ulnar fovea and ECU, serve as important reproducible sonographic landmarks in both longitudinal and transverse imaging.
REVIEWED BY Sean Yeoh
ASA SIG: Musculoskeletal
REFERENCE
Authors: Wu W, Chang K, Mezian K, Nanka O, Yang Y, Hsu Y, Hsu P & Özçakar L
Journal: Journal of Clinical Medicine
Open Access: Yes
READ THE FULL ARTICLE HERE
Figure 1. Transverse sonogram of the articular disc at the level of the ulnar styloid process. (A) US and (B) superposed US images demonstrating the articular disc (blue shade), deep (dark green shade) and superficial (light green shade) limbs of the radioulnar ligament, meniscus homologue (yellow shade), ulnar collateral (orange shade). R: radius; ECU: extensor carpi ulnaris; SP: styloid process; US: ultrasound.
Ulnar wrist pain revisited: ultrasound diagnosis and guided injection for triangular fibrocartilage complex injuries
Pathology of the TFCC has a broad sonographic appearance. Acute defects of the articular disc appear as hypoechoic clefts/defects. The meniscus homologue, by comparison, is generally heterogenous with injuries typically appearing as inhomogeneous central echoes. Degenerative changes vary from thinning of the articular disc and cortical irregularities to partial to complete tears of the juxta-articular ligaments.
RELEVANCE TO CLINICAL PRACTICE
Ultrasound shows promise as a viable imaging modality of the TFCC providing a systematic approach is used in conjunction with a broad understanding of the TFCC components and sonographic appearance of pathologies. Acceptance of ultrasound for imaging the TFCC would allow clinicians to provide accurate treatment plans sooner, as access to MRI can be limited. Future studies comparing the sensitivity of MRI versus US will be crucial for ultrasound to become a viable first point of call for TFCC imaging. This paper highlights suggestions for the sono-anatomy, and due to the lack of consensus in many studies regarding the subcomponents of the TFCC and their relationships, further studies to clarify the sono-anatomy of the subcomponents of the TFCC are required.
Ultrasound shows promise as a viable imaging modality of the TFCC providing a systematic approach is used in conjunction with a broad understanding of the TFCC components and sonographic appearance of pathologies.
Value of ultrasound assessment for traumatic nerve injury of the upper limb
WHY THE STUDY WAS PERFORMED
Peripheral nerve trauma is rare; however, assessment and diagnosis of peripheral nerve injuries (PNI) can have significant effects on a patient’s prognosis. Peripheral nerve trauma contributes to 2–3% of patients who visit major trauma centres worldwide and equates to 13–23 per 100,000 patients annually. Causes of PNI can range from motor vehicle accidents, penetrating trauma, falls, and domestic and industrial accidents. Accurate and timely diagnosis of PNI can facilitate appropriate treatment and reduce disability for a patient.
Electrophysiological studies are considered the gold standard in assessing nerve injury. This study aimed to evaluate the use of ultrasound to assess upper limb traumatic nerve injuries and how it compares to electrophysiological studies.
HOW THE STUDY WAS PERFORMED
The study reviewed 69 adult participants with a total of 96 peripheral nerve injuries ranging from one month to three years in duration. All participants underwent both electrophysiological studies and high frequency ultrasound examinations.
WHAT THE STUDY FOUND
Although the gold standard is electrophysiological studies, the most accurate diagnostic information from these studies is accessible after 2 weeks when Wallerian degeneration has fully developed. It is not useful in the acute phases and has significant limitations when there is total loss of nerve conduction, whereby it has difficulty identifying the precise location of the lesion. Electrophysiological studies are also restricted in assessing the morphological changes with specific types of PNIs.
With ultrasound, it can be used during the acute phase of injury to diagnose PNI accurately and painlessly. Not only is it quick and affordable, but it also has the additional benefits of dynamic, real-time assessment and evaluation of the surrounding structures. The study also found that there was an increased echogenicity of the supplied muscle in 84.4% of the nerve injuries, with 71.9% in reduced muscle girth.
The study found there was no significant difference between ultrasound and electrophysiological studies for the diagnosis of nerve injuries.
RELEVANCE TO CLINICAL PRACTICE
The location of PNI can have major effects on a patient’s recovery and influence functionality. Most PNIs in the upper limb involve the ulnar, median and radial nerves. However, iatrogenic causes are also common. The specific mechanism of trauma increases the risk of specific nerve injury.
Ultrasound can effectively be used as a complementary diagnostic tool in the assessment of PNI. Not only can it detect the type of injury and assess morphological abnormalities, but it also allows for assessment of surrounding tissue including swelling, scar tissue and neuroma formation. Ultimately, proper assessment of nerve injuries can alter a patient’s management and treatment pathway.
REVIEWED BY Susan Diep
ASA SIG: Musculoskeletal
REFERENCE
Authors: Elshewi IE, Fatouh MM, Mohamed RNES, Basheer MA, Liethy NEE & Abbas HM
Journal: Journal of Ultrasound
Open Access: Yes
READ THE FULL ARTICLE HERE
Not only can ultrasound detect the type of injury and morphological abnormalities of the affected nerve but also allows for proper assessment of surrounding tissue.
Value of ultrasound assessment for traumatic nerve injury of the upper limb
The key findings on ultrasound for PNI should assess and comment on:
1. Is the nerve continuous?
2. Is the nerve compressed/tethered/hypermobile to the adjacent structures?
3. The size and position of any gaps along the course of the nerve.
4. The presence of any focal neuromas or extra nerve damage sites (e.g. tandem lesions).
5. The presence of foreign bodies.
6. The degree of neighbouring scar tissue.
7. The condition of the surrounding tissues (e.g. tendon, artery, bones, etc.).
8. Finding the location of the peripheral nerve and applying pressure to the site and evaluating if this triggers the patient’s symptoms.
When using US, it is essential to determine the following factors: whether the nerve is still continuous; the size and position of any gaps in the nerve course; the presence of any focal neuromas or extra nerve damage sites, such as tandem lesions; the presence of any foreign bodies; the degree of neighbouring scar tissue; and the condition of surrounding tissues and structures, such as tendons, arteries, and bones.
The impact of high-frequency transducers on the sonographic measurements of the pyloric muscle thickness in infants
WHY THE STUDY WAS PUBLISHED
Ultrasound is often performed when hypertrophic pyloric stenosis (HSP) is suspected. With increasing resolution and better ultrasound machines over the years, this article aimed to standardise the measurements and evaluate the appearance of the normal and HSP with high frequency transducers.
HOW THE STUDY WAS PERFORMED
With ethics approval, the PACS system was used to search for patients who had an ultrasound for a differential diagnosis of HSP. Data was collected over a two-year period (Jan 2019 – Dec 2020). Studies with a longitudinal image using a linear transducer of 12–18 MHz were included in the analysis. Any poor quality studies were excluded. Measurements were taken off the longitudinal views as they found this plane to be the most reliable.
• Two paediatric radiologists independently measured the transverse muscle thickness of the pylorus.
• Measurement (a) includes the outer layer of muscularis propria until the inner layer of muscularis mucosa, including the hyperechoic stripe (submucosa).
• Measurement (b) includes only the muscularis propria without the submucosa and muscularis mucosa.
(Fig. 1)
Cases were divided into positive and negative, where positive cases were confirmed surgically and negative cases were presumed when the patient didn’t have surgery and was discharged.
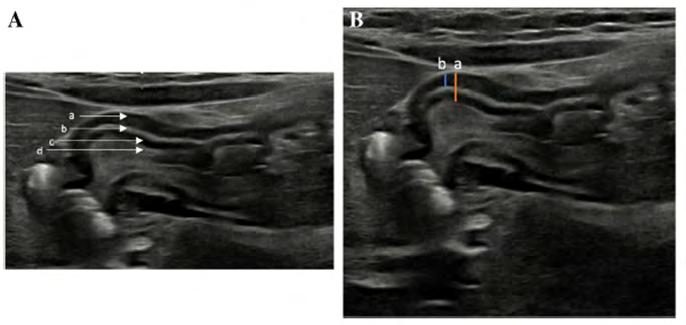
Fig. 1 Normal sonographic appearance of the wall of the pylorus using a linear-array transducer, 18 MHz, in a 6-week-old female who presented with vomiting. In these transverse images of the upper abdomen, the normal pylorus is shown in longitudinal view. A Image shows the normal layers of the pylorus. (a) Hypoechoic muscularis propria; (b) Hyperechoic stripe of submucosa; (c) Hypoechoic muscularis mucosa; (d) Hyperechoic stripe of interface between mucosa and intraluminal echogenic contents.
B Image shows two different methods of measurement of the thickness of the pylorus. (a) Measurement from the outer surface of the hypoechoic muscularis propria down to the hyperechoic interface between the mucosa and intraluminal content; (b) Measurement from the outer surface of the hypoechoic muscularis propria down to the level of the outer surface of the hyperechoic stripe of the submucosa.
REVIEWED BY
Ilona Lavender, FASA
ASA SIG: Paediatric
REFERENCE
Authors: Yousef A, Daneman A, Amirabadi A, Faingold R
Journal: Pediatric Radiology
Open Access: No
READ THE FULL ARTICLE HERE
The impact of high-frequency transducers on the sonographic measurements of the pyloric muscle thickness in infants
WHAT THE STUDY FOUND
There were 554 patients with a differential diagnosis of HPS. After the exclusion criteria, 300 patients were used in this study of which 114 were female and 186 were male. HPS was confirmed in 59 cases (19.7%).
In the first 100 cases, both radiologists performed the measurements – the intraclass correlation coefficient was high at 0.99.
• Measurement (a) had a mean of 2.4 mm in normal cases and 4.8 mm in abnormal cases.
• Measurement (b) had a mean of 4.8 mm in confirmed cases of HPS.
• The muscularis propria was more hyperechoic in all HPS in contrast to all normal cases, where the muscularis propria was hypoechoic showing similar echogenicity to the muscularis mucosa.
• Measurement of the thickness was demonstrated to be the most useful to confirm or exclude HPS.
• There was no statistical difference in method (a) or (b) when measuring the thickness in the longitudinal view; however, method (b) demonstrated a 100% specificity.
• New cut-off values were established with high accuracy
• 3.6 mm for measurement (a)
• 2.8 mm for measurement (b)
RELEVANCE TO CLINICAL PRACTICE
It is important to use a high frequency transducer when performing a scan for a suspected hypertrophied pyloric stenosis. Sonographers should suspect a positive HPS when there is increased echogenicity of the muscularis propria and a loss of mural stratification. Furthermore, it appears that assessment and measurement of the muscularis propria solely in the longitudinal view is highly specific for the diagnosis of HPS. The function assessment should be used in conjunction with the measurements and borderline cases can be rescanned.
Measuring only the muscularis propria improves diagnostic accuracy by reducing overlap between negative and positive cases. The absence of pyloric wall stratification and echogenic muscularis propria is specific to HPS.
Correlation
does not imply agreement: A cautionary tale for researchers and reviewers
WHY THE STUDY WAS PERFORMED
The study was performed to clarify the terms ‘correlation’ and ‘agreement’ and their appropriate use in sonography research. The authors aimed to address common pitfalls and inconsistencies in reporting these statistical tests in the literature. The study’s relevance to sonographers and reviewers is evident, as it aims to improve the quality of research and reduce inconsistencies in the field. By providing clarity on the proper use of these statistical methods, the study seeks to benefit researchers conducting studies comparing measurements and reviewers evaluating manuscripts to ensure the methodology used is sufficient to justify the claims.
HOW THE STUDY WAS PERFORMED
The study was conducted as a comprehensive review of fundamental biostatistics and common statistical methods used for continuous variables in sonography research. The authors provided a detailed explanation of the terms ‘correlation’ and ‘agreement’ and outlined the statistical tests used to assess correlation, highlighting common pitfalls authors fall into when reporting these tests. Examples of inaccurate use of correlation tests in the sonography literature were presented and the authors recommended alternative methods for assessing agreement between measurements. The study included plots created in the R statistical software package and a supplementary data file was provided for readers to perform similar statistical tests.
WHAT THE STUDY FOUND
The study found that correlation and agreement are often misused in sonography research, with correlation coefficients being incorrectly applied to assess agreement between measurements. The authors demonstrated that two highly correlated variables may not necessarily agree, and visual inspection of scatter plots is crucial to avoid incorrect assumptions. The study highlighted situations where the Pearson correlation coefficient should not be used, such as in the presence of outliers, heteroscedasticity, clustered data, or non-linear relationships. The authors emphasised the importance of plotting the relationship between variables of interest on a scatter plot to avoid incorrect assumptions and to determine the nature of the correlation (linear or non-linear). The study recommended alternative methods for assessing agreement between continuous measurements, such as the intra-class correlation coefficient (ICC) and BlandAltman plots with limits of agreement. Examples from the sonography literature were provided to illustrate the misuse of correlation coefficients in assessing agreement between measurements or imaging techniques, such as comparing standard 2D and panoramic imaging measurements or evaluating an image review scoring system.
RELEVANCE TO CLINICAL PRACTICE
The study’s findings are highly relevant to sonography practice as they emphasise the importance of using appropriate statistical methods to assess agreement between measurements or techniques. Sonographers and researchers should be aware of the limitations of correlation coefficients and the potential for misinterpretation when assessing agreement. The recommended alternative methods, such as ICC and Bland-Altman plots, can be applied to various clinical scenarios in sonography, such as comparing different imaging modes, evaluating interobserver variability, or assessing the reproducibility of measurements under different conditions. Adopting these methods will improve the quality of sonography research, leading to more reliable and valid conclusions that can inform clinical practice, decision-making, and the development of guidelines and protocols. By understanding the proper use of statistical methods for assessing correlation and agreement, sonographers and researchers can design more robust studies and draw accurate conclusions that ultimately benefit patient care.
REFERENCE
Authors: Edwards C, Allen H & Chamunyonga C
Journal: Sonography
Open Access: No (ASA member access via Sonography Journal)
READ THE FULL ARTICLE HERE
The authors demonstrated that two highly correlated variables may not necessarily agree, and visual inspection of scatter plots is crucial to avoid incorrect assumptions.
Ten
common statistical mistakes to watch out for when writing or reviewing a manuscript
WHY THE STUDY WAS PERFORMED
There has been a lot written about improving the reproducibility of research and improving statistical analysis techniques. This article was written to address common statistical oversights and provide peer reviewers and publishers with a tool to help them identify common problems in research manuscripts.
HOW THE STUDY WAS PERFORMED
The list was developed at the journal club of the London Plasticity Lab where papers are discussed. The issues in the list are relevant to any scientific discipline that uses statistics to assess findings. Each mistake in the list discusses how the mistake can arise, explains how it can be detected by readers and offers a solution to the problem.
WHAT THE STUDY FOUND
The list of ten common statistical mistakes includes:
1. absence of an adequate control condition/group
2. interpreting comparisons between two effects without directly comparing them
3. inflating the units of analysis
4. spurious correlations
5. use of small samples
6. circular analysis
7. flexibility of analysis: p-hacking
8. failing to correct for multiple comparisons
9. overinterpreting nonsignificant results
10. correlation and causation.
Item 5 is summarised as follows:
The use of small samples poses significant challenges. Small samples can only detect large effects, often leading to an overestimation of the actual effect size. Additionally, small samples are prone to missing existing effects due to insufficient statistical power. Larger sample sizes increase the likelihood of detecting true effects, enhancing statistical power.
Small samples also complicate testing the assumption of normality, as the sample distribution may deviate from normality. Reviewers must critically examine the sample size to assess whether the study’s claims are reasonable.
Researchers should present evidence that their study is sufficiently powered. If the sample size is limited, researchers must justify this limitation and demonstrate efforts to mitigate its impact.
RELEVANCE TO CLINICAL PRACTICE
Reviewers of journal articles should carefully examine the experimental design and statistical analysis of all manuscripts. This article addresses ten common mistakes that frequently appear in journals. By considering these factors, readers can better understand how research conclusions are derived.
REVIEWED BY
Glenda McLean, FASA
ASA SIG: Research
REFERENCE
Authors: Makin T & Orban de Xivry JJ
Journal: eLife
Open Access: Yes
READ THE FULL ARTICLE HERE
A list of some of the most common statistical mistakes that appear in the scientific literature.
Ultrasonographic assessment of atherosclerotic renal artery stenosis in elderly patients with chronic kidney disease: An Italian cohort study
WHY THE STUDY WAS PERFORMED
Atherosclerotic stenosis of the renal artery is caused by the presence of plaque forming within the proximal renal artery or at the ostium. Over time, the stenosis can worsen, often leading to reduced blood flow to the renal cortex causing renal ischaemia. The consequence of renal ischaemia is the activation of the renin-angiotensin-aldosterone system resulting in alteration to haemodynamics, peripheral vasoconstriction, sodium/water retention, cortical hypoxia, local release of cytokine and irreversible parenchymal injury.
Atheroma causing a renal artery stenosis is also responsible for poor control of hypertension, more frequent hospitalisation, new onset of chronic kidney disease (CKD), faster progression of pre-existing CKD towards dialysis (end-stage renal failure) and ultimately it will increase cardiovascular risks and mortality.
The study was performed to investigate and understand the prevalence, characteristics, and clinical implications of atherosclerotic renal artery stenosis (ARAS) in elderly patients who also have chronic kidney disease (CKD).
The study aimed to contribute valuable insights into how ARAS affected elderly patients with CKD by using ultrasound as a noninvasive method for assessment, which was particularly relevant given our ageing population and the increasing prevalence of chronic kidney disease globally.
HOW THE STUDY WAS PERFORMED
The study, conducted at the University of Naples, was a retrospective, observational, longitudinal investigation involving consecutive in-patients meeting specific criteria. A summarised breakdown of the methods is provided below.
STUDY DESIGN AND PARTICIPANTS
• Design: Retrospective, observational, longitudinal
• Participants: In-patients aged ≥ 65 years with CKD stages 2–5 (not on dialysis) and the presence of atherosclerotic plaques in specified arteries
• Inclusion criteria: Age ≥ 65 years, CKD stages 2–5, presence of atherosclerotic plaques confirmed by various imaging procedures
• Exclusion criteria: History of renal artery stenosis, kidney transplant, dialysis treatment.
DATA COLLECTION
• Pre-ultrasound measurement: Included clinical examination, personal/family medical history, and routine biochemistry
• Outcome measures: Recorded fatal and non-fatal cardiovascular events, treatments for ARAS or other plaques, and initiation of dialysis post-ultrasound.
ULTRASOUND TECHNIQUE
• Assessment: Duplex ultrasound (B-mode and Doppler) using a 2–5 MHz transducer
• Preparation: Fasting 8–12 hours to minimise bowel gas interference
• Diagnostic criteria: Significant ARAS defined by peak systolic velocity ≥ 200 cm/s and renalto-aorta peak systolic velocity ≥ 3.5.
REVIEWED BY
Heath Edwards, AFASA
ASA SIG: Vascular
REFERENCE
Authors: Battaglia Y, Fiorini F, Gisonni P, Imbriaco M, Lentini P, Zeiler M, Russo L, Prencipe M & Russo D
Journal: Diagnostics
Open Access: Yes
Ultrasonographic assessment of atherosclerotic renal artery stenosis in elderly patients with chronic kidney disease: An Italian cohort study
OTHER DATA COLLECTION
• Coronary artery calcification: Assessed by multi-slice coronary computed tomography, scored in Agatston Units
• Plaque assessment: Defined by intima-medial thickness > 1.0 mm in specified vessels
• Biochemical markers: Included LDL cholesterol, hypertension, renal function (GFR), dyslipidemia, intact parathyroid hormone, and high sensitivity C-reactive protein.
WHAT THE STUDY FOUND
From January 2015 to December 2018, 607 consecutive in-patients were screened. Data was collected from 120 patients who met the inclusion criteria before and after the ultrasound examination.
The chronic kidney stages were distributed among the patients in the following: Stage II (21%), Stage III (36.1), Stage IV (26.1%) and Stage V (16.8%). The cause of CKD was mostly unknown (51%), diabetic nephropathy (15%), glomerulonephritis (12%) and other causes (22%).
Atherosclerotic renal artery stenosis was found in 53 of the 120 cases (44%) with the right renal artery predominantly affected (58%). A bilateral ARAS was noted in only a single case. The median stenosis severity percentage was noted at 70%.
The clinical and biochemical parameters showed significant differences in basal BMI, GFR, haemoglobin, pulse pressure, serum calcium concentration and total coronary calcium score between the patients with an atherosclerotic renal artery stenosis and the controls. No differences were noted in the blood pressure levels, markers of mineral metabolism, dyslipidaemia, inflammation and nutritional markers.
RELEVANCE TO CLINICAL PRACTICE
This study highlights the significant associations between ARAS and specific clinical and biochemical parameters, with plaque present within the abdominal aorta/peripheral vessels and the patient’s GFR emerging as independent predictors. Utilising these findings will help contribute to understanding risk factors in the elderly and their potential outcomes if diagnosed with chronic kidney disease and an ARAS.
As sonographers, careful and accurate assessment of the proximal renal arteries and the ostium with ultrasound to identify atherosclerosis renal artery stenosis is important to support our clinicians in managing these patients.
Highlights the significant associations between atherosclerotic renal artery stenosis and specific clinical and biochemical parameters.
Point of care venous Doppler ultrasound: Exploring the missing piece of bedside haemodynamic assessment
WHY THE STUDY WAS PERFORMED
This educational review was created due to the clinical significance of accurate haemodynamic assessment in the critically ill patient. Point-of-care tests such as passive leg raising with noninvasive cardiac output monitoring and measuring capillary refill time have stood the test of time in the intensive care unit (ICU) but the accuracy of these tests suffers in states of hypervolemia. Fluid overload in very poorly patients is not uncommon and significantly affects venous volume and compliance, which, in turn, influences venous Doppler waveforms. This study explains how these waveforms can be reliably assessed with point-of-care ultrasound (POCUS) to provide complementary information on venous congestion and where it is having a significant impact.
HOW THE STUDY WAS PERFORMED
No information on how evidence for this literature review was provided. This study is a summary of the rationale for integrating this technology into routine care for patients with volume-related disorders.
WHAT THE STUDY FOUND
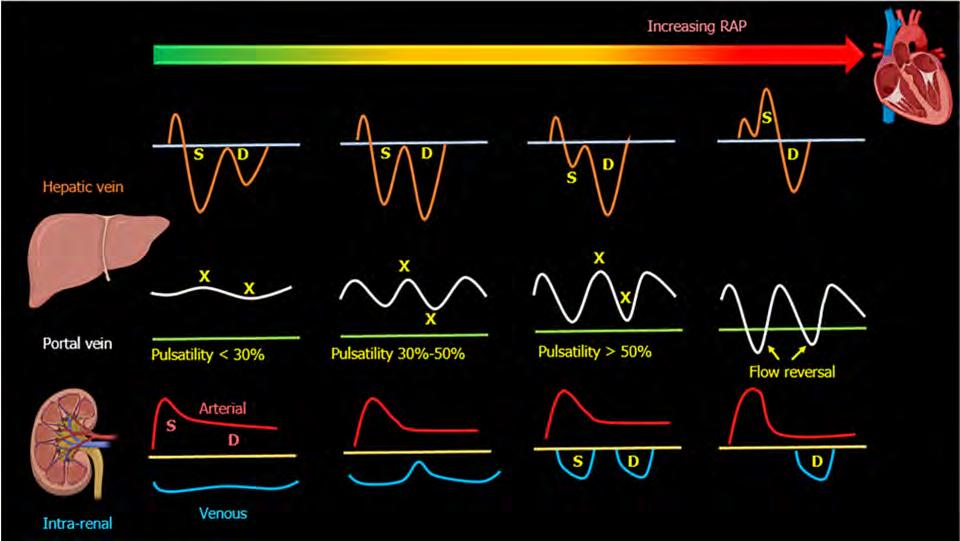
Increased right atrial pressure (RAP) has a significant effect on the venous system and its spectral Doppler waveforms. This article explains the difference between normal and abnormal venous Doppler waveforms and why they are an important part of the diagnostic workup. The following points summarise different locations in which POCUS can be performed and what to expect in pathological states.
• Increased RAP causes hepatic vein S wave amplitude reduction below that of its D wave (S < D pattern). The S wave can even become obliterated/retrograde if RAP worsens.
• Progressive increase in portal vein pulsatility in the setting of increased RAP. This can be quantified into a pulsatility fraction using the below formula where anything > 50% is considered severe (PSV max–PSV min/PSV max) x 100.
• Normal intrarenal vein flow is continuous but can become biphasic as RAP increases with the creation of distinct S and D waves. Studies have shown that adverse intrarenal venous waveform patterns not only reflect increasing RAP but also strongly predict adverse clinical outcomes in patients with heart failure, pulmonary hypertension and those undergoing cardiac surgery.
• The common femoral veins (CFV) are directly linked to the IVC, making their waveforms very sensitive to an increase in proximal pressure. Normal CFV flow undulates with respiration at rest but becomes pulsatile in instances of increased RAP with very distinct antegrade and retrograde components.
REVIEWED BY
Matt Adams, AFASA
ASA SIG: Vascular
REFERENCE
Authors: Galindo P, Gasca C, Argaiz E, and Koratala A
Journal: World Journal of Critical Care
Medicine
Open Access: Yes
READ THE FULL ARTICLE HERE
Point of care venous Doppler ultrasound: Exploring the missing piece of bedside haemodynamic assessment
RELEVANCE TO CLINICAL PRACTICE
Venous Doppler waveform assessment at the bedside is a tool that can provide complementary information to the global haemodynamic assessment of the critically ill patient. This physiological parameter should definitely be considered as part of the standard workup for the ICU patient, but its implementation should be approached with caution. It is well known that ultrasound is operator-dependent, especially when it comes to the interpretation of Doppler waveform nuances. Healthcare professionals who intend to perform this assessment need to learn via accredited programs that include extensive clinical experience. If done properly, however, this application of POCUS could be very beneficial as part of routine investigations and lends itself very well to the impending portable ultrasound revolution.
Doppler
of abdominal veins provides useful insights into a patient’s hemodynamics when interpreted in conjunction with other sonographic parameters such as the cardiac pump function, lung ultrasound and conventional clinical assessment.
Figure 1. Transformation of the hepatic, portal, and intrarenal Doppler waveforms with increasing right atrial pressure.
Non-invasive imaging techniques for diagnosis of pelvic deep endometriosis and endometriosis classification systems: an International
Consensus Statement
WHY THE STUDY WAS PERFORMED
Endometriosis affects a significant proportion of women globally and accurate and timely noninvasive diagnosis is pivotal for patient counselling and planning of treatment strategies. This is particularly important in cases of deep endometriosis (DE), which is observed in 20% of patients with endometriosis. Presurgical diagnosis of DE can assist in surgical planning, prediction of operative difficulty, and in the context of infertility provide aid in decisions around treatment and assisted reproductive technologies. The performance of noninvasive imaging techniques such as transvaginal ultrasound (TVS), MRI and CT, as well as various proposed classification systems, have been heavily studied over the last two decades. This consensus statement was developed by ISUOG, IDEA, ESGE, EEL, ISGE, ESHRE, ESUR and AAGL to develop evidence-based and clinically relevant statements to guide the use of noninvasive imaging techniques for the diagnosis and classification of pelvic DE.
HOW THE STUDY WAS PERFORMED
The consensus statement was developed using a six-step protocol chaired and organised by professors George Condous (GC) and Gernot Hudelist (GH). An international, multidisciplinary working group was established, consisting of chairs of each society and including expert gynaecological surgeons, sonographers and radiologists. A systemic literature review of relevant studies published from inception to February 2023 was carried out by coordinating chairs and Bassem Gerges (BG). This search was limited to publications in English and excluded editorials, letters and case reports. From this literature review, GC, GH and BG formulated preliminary consensus statements which were then distributed to society chairs for first-round revisions. Statements were then modified, and the process was repeated. Society group members then voted in a binary fashion on the finalised statements.
WHAT THE STUDY FOUND
The finalised 20 statements included general statements, statements on ultrasonography, statements on MRI and CT and statements on the noninvasive use of classification systems. Of these, 14 received strong agreement (> 80%), 3 moderate agreement (60–80%) and 1 remained equipoise (40–60%). There was strong agreement that TVS can accurately determine or rule out DE affecting the rectum, rectovaginal septum and bladder. However, its performance in assessing DE affecting other locations, such as the parametrium and uterosacral ligaments (USL) was less sensitive. There was consensus that MRI can more reliably predict the presence of DE in these locations. The working group found the use of classification systems a matter of ongoing debate. The majority of participants agreed on the use of TVS or MRI in combination with the #Enzian classification, with the acknowledgement that it was found to be less accurate in cases of parametrial and USL involvement.
RELEVANCE TO CLINICAL PRACTICE
These statements advocate the use of TVS as a first-line imaging tool due to its availability, good test performance, cost efficacy and low environmental impact. They highlight the limitations of both TVS and MRI in the assessment of DE in specific locations and help provide a guideline for appropriate imaging modalities. These statements also highlight the need for standardisation of the classification system used in the diagnosis of DE, with the strongest agreement and level of evidence for the use of the #Enzian system. They also emphasise that imaging test performance is operator-dependent and will increase with exposure, level of training and skill of the operator.
REVIEWED BY
Jessica Coffey
ASA SIG: Women’s Health
REFERENCE
Authors: Condous G, Gerges B, Thomassin-Naggara I, Becker C, Tomassetti C, Krentel H, van Herendael BJ, Malzoni M, Abrao MS, Saridogan E, Keckstein J, Hudelist G and Collaborators
Journal: Ultrasound in Obstetrics & Gynecology
Open Access: Yes
READ THE FULL ARTICLE HERE
Transvaginal ultrasound is recommended as a first-line imaging tool due to its availability, good test performance, cost efficacy and low environmental impact.
Artificial intelligence assists identifying malignant versus benign liver lesions using contrast-enhanced ultrasound
WHY THE STUDY WAS PERFORMED
The aim of this study was to assess if the interrater reliability between radiologists at different centres for the detection of malignant focal liver lesions could be improved. This study was based on combining contrast-enhanced ultrasound (CEUS) with artificial intelligence (AI).
HOW THE STUDY WAS PERFORMED
This study was a retrospective study. Patients were aged (P = 0.15), gender (P = 0.46) and lesion size (P = 0.25) matched between development and training and sets. Malignant lesions e.g. hepatocellular carcinoma and liver metastasis were biopsied. Benign lesions e.g. haemangiomas and focal nodular hyperplasia were identified by typical observations on CEUS and 12 months of follow-up demonstrating no change. Abscesses were confirmed by drainage of pus or a reduction in size following treatment with antibiotics. Indeterminate lesions were biopsied. Three hundred and sixty-three lesions were evaluated in 614,728 augmented images within the development set. A further 211 lesions were evaluated within 616 images as the testing set.
The radiologists involved in this study had an average of 4.75 years of experience in hepatic CEUS. Ultrasound machines utilised were the Acuson Sequoia 512 with a 4V1 transducer or Aplio 500 or Aplio XV with a 375 BT convex transducer. Images with one centimetre of perilesional clearance were acceptable. These lesions had to have no more than one-third of the image obscured by acoustic shadow. Five parts of a 152 Resnet architecture were used involving three convolutional layers to create an algorithm. Image augmentation was based on brightness, contrast, rotation and parallel shifting to recreate data diversity and the final algorithm.
Limitations in this study were the body mass index (BMI) tends to be lower in China, where this study was conducted. Therefore, the results may be biased and not transpose to a higher BMI. Only image data was incorporated into the training set. The lack of information on demographics and medical history may have assisted in increasing the identification of focal liver lesions. The training set was a relatively small data set, therefore future training sets with larger data sets may be superior. Additionally, the use of multicentre studies along with increased data may add to a higher performance for the AI model.
WHAT THE STUDY FOUND
This study demonstrated a successful algorithm that decreased the reporting differences for radiologists between centres for the detection of malignant liver lesions. When radiologists reported with the assistance of AI, interobserver performance between four radiologists was comparable based on accuracy (91.0–92.9%, P = 0.904), sensitivity (97.0–99.4%, P = 0.360), and specificity (66.0–76.6%, P = 0.671).
RELEVANCE TO CLINICAL PRACTICE
This study demonstrated the value of combining CEUS with AI improving the interrater reliability for the detection by radiologists of malignant focal liver lesions. This result adds further credibility to the value of CEUS for the detection of focal liver lesions.
REVIEWED BY Robyn Boman, FASA
ASA SIG: Emerging Technology
REFERENCE
Authors: Hu HT, Wang W, Chen LD, Ruan SM, Chen SL, Li X, Lu MD, Xie XY & Kuang M
Journal: Journal of Gastroenterology and Hepatology
Open Access: Yes
READ THE FULL ARTICLE HERE
The influence of the AI-radiologist interaction on performance was assessed, focusing on AI’s potential to reduce interobserver heterogeneity.
Towards standardized acquisition with a dual-probe ultrasound robot for fetal imaging
WHY THE STUDY WAS PERFORMED
This paper summarises developments of a novel dual-probe ultrasound robot for a project called intelligent Fetal Imaging and Diagnosis (iFIND). The project aims to improve the accuracy of routine anatomy survey in pregnancy by incorporating computer-guided ultrasound technologies using multiple probes. Fetal anomaly screening would be remodelled with the assistance of robotics and AI. The motivation for this work came from evidence of reduced accuracy and sensitivity of conventional ultrasound from technical restraints, and hospital-specific variation in prenatal detection rates of major anomalies.
The design and implementation of iFIND-v3 are presented in this paper.
HOW THE STUDY WAS PERFORMED
The workflow is explained in detail followed by simulation and volunteer experiments. The workflow includes an abdominal surface mapping step, a rule-based end point calculation method to position each individual robotic joint, and a motor synchronisation method to achieve a smooth motion towards a target point.
iFIND-v3 has 17 degrees of freedom, with two arms simultaneously holding and controlling two ultrasound probes. Probe control needs to be executed avoiding collision of the arms and maintaining a safe offset distance of the robot from the patient’s abdomen. Because the shape of the abdomen will vary between patients, and at different gestations, motion planning calculations become crucial for safe robotic scanning.
Robotic design has been steered by subject feedback to reduce concerns of claustrophobia. iFIND-v3 uses a side mounted gantry over the patient with the two robotic arms attached towards the feet of the patient.

REVIEWED BY
Caterina Watson, AFASA
ASA SIG: Emerging Technology
REFERENCE
Housden J, Wang S, Bao X, Zheng J, Skelton E, Matthew J, Noh Y, Eltiraifi O, Singh A, Singh D, Rhode K
Journal: IEEE robotics and automation letters
Open Access: Yes
READ THE FULL ARTICLE HERE
Implementation of the iFIND-v3 robot perspective showing the dual-arm configuration with a fetal phantom.
Towards standardized acquisition with a dual-probe ultrasound robot for fetal imaging
Researchers demonstrated reliable performance in controlling the robot to move towards the expected scanning area. The volunteer study demonstrated reliable acquisition of desired ultrasound views.
WHAT THE STUDY FOUND
The reachable percentage of abdominal surface ranged between 43–27%, located in the central abdominal region. The percentage depended on the initial configuration of the probe pairs being transverse, sagittal or oblique (see Figure 9 in paper). The areas of the abdomen missed are right and left lateral aspects, and the right and left groin. In a third trimester gestation, this area would typically be where the fetal head lies.
iFIND-v3 has only been tested for abdominal scanning in non-pregnant volunteers, producing good images of the standard views of the aorta, pancreas, liver, right lobe of liver with right kidney, gallbladder, and aorta. The kidneys were not imaged individually as they occupy a lateral position but imaged through the acoustic window of the right lobe of liver.
A sonographer assigned image quality to ‘good’, ‘acceptable’, or ‘poor’ using the British Medical Ultrasound Society Peer Review Audit Tool 2014 v3. ‘Of the images with ‘good’ or ‘acceptable’ quality scores, the sonographer achieved a good image in 60%, while the robot achieved this in 40% of images.
RELEVANCE TO CLINICAL PRACTICE
Currently, none. This work has the potential to address the standardisation of manual manipulation of hand-held probes, eliminating difficulties of maintaining accurate probe positioning for long periods of time, and the requirement for experienced sonographers to be on-site. Sonographers may experience improved mental health and reduced MSK injury from the proposed workflow. Robotic scanning may also contribute to better fetal health outcomes.
Of the images with ‘good’ or ‘acceptable’ quality scores, the sonographer achieved a good image in 60%, while the robot achieved this in 40% of images.














