2 minute read
Oral and Maxillofacial Pathology Case of the Month


ORALand maxillofacial pathology case of the month
Case History
A 40-year-old former smoker, who is otherwise healthy, presented at the dental clinic due to poorly localized pain in the left maxilla. He also complained of an acute shooting pain in his left cheek, radiating to his eye and temple (ipsilateral), with associated sudden dental mobility in the upper left quadrant, of 2 months’ duration. Clinical findings were unremarkable. There was no palpable lymphadenopathy extraorally, and no obvious mass or ulceration was detected intraorally (Figures 1A and 1B). However, there was evidence of moderate periodontal disease and a CT scan revealed the presence of advanced bone loss of his left maxilla around teeth #12-#15, which was accompanied by pain and paresthesia. The osseous resorption was extensive, extending to involve the left anterior

1A
1B
Figures 1A and 1B. Clinical pictures showing unremarkable oral cavity.
maxillary sinus wall (Figures 2A, B, C). A biopsy was performed (Figure 3) and a diffuse red/ white/yellow, soft tissue lesion, measuring approximately 22 mm x 20 mm x 15 mm in size, was obtained. Two teeth demonstrating severe
AUTHORS
Ngozi Nwizu, BDS, MMSc, PhD
Associate Professor, Board Certified Oral and Maxillofacial Pathologist, Department of Diagnostic and Biomedical Sciences, UTHealth at Houston School of Dentistry, Houston, Texas
Luis Diego Gonzalez, DDS
Board Certified Oral and Maxillofacial Surgeon, Private practice, Houston, Texas

2A

Figures 2A, B, C. Radiographic images showing extensive osseous resorption of the left maxilla and left anterior maxillary wall, in spite of negative clinical findings.
2B
2C

ORALand maxillofacial pathology, continued

Figure 3. Post-operative site.
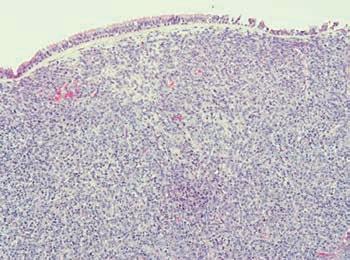
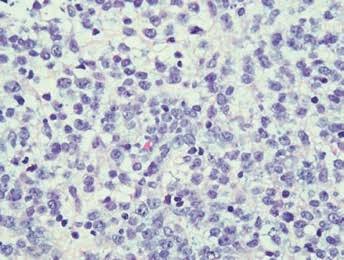
Figure 4A. (Low magnification, x 40) showing a diffuse infiltrate of atypical, round, blue, mononuclear cells with scanty or ample cytoplasm. Figure 4B. (High magnification, x 200) showing proliferation of atypical, round, blue, mononuclear cells with scanty or ample cytoplasm, interspersed with cells displaying hyperchromatic, angular nuclei and variation in nuclear size.
mobility were also extracted. The entire biopsy contents were submitted for microscopic analysis.
Microscopic examination revealed the presence of fragments of dense fibrous tissue, some of which were partially covered by normal sinus mucosa. A prominent feature of the tissue specimen was the presence of a diffuse infiltrate of atypical, round, blue, mononuclear cells with scanty or ample cytoplasm (Figures 4a and 4b). These were interspersed with cells displaying hyperchromatic, angular nuclei and variation in nuclear size. Multiple mitotic figures, areas of crushing artifact and a number of apoptotic bodies were also observed. Other features of the tissue specimen include the presence of a fibro-vascular stroma enclosing multiple, irregular fragments of reactive bone trabeculae and small aggregates of chronic inflammatory cells.
What is the differential diagnosis? What is the final diagnosis? See page 32 for the answer and discussion.
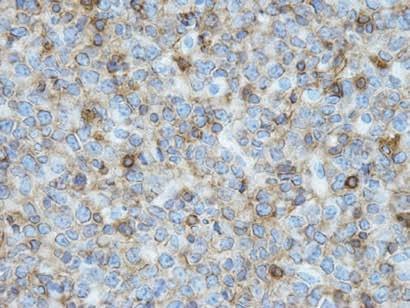
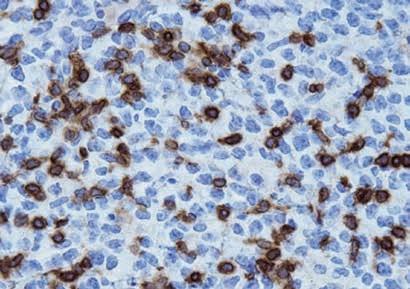
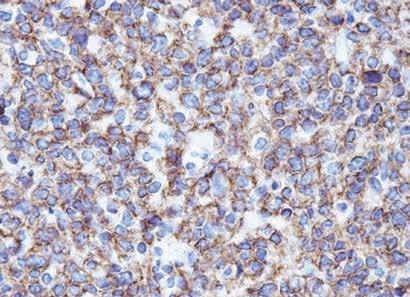
Figures 4C, 4D and 4D. CD45, CD3 and CD20 immunohistochemical stains.