
plus... l EVENTS: ZIRKONZAHN’S LECTURE TOUR I SEPT 26-28 P. 9 l HEALTH & WELLBEING: THE PROBLEM WITH POSTURE I JOHN BENNETT P. 20-21 l MARKETING: HAYLEY IRONS P. 24-25 VERIFIABLEECPD FORTHE WHOLE DENTALTEAM VOL 76 No. 8 I AUGUST 2023 I BY SUBSCRIPTION www.dentaltechnician.org.uk SAVE THE DATE BDIA Dental Showcase 2024 PAGE 8 Interview with Sandra Puurits PAGES 18-19 TECH´S EYE VIEW With Chris Golze PAGE 22 TAKING CAD/CAM TECHNOLOGY TO THE NEXT LEVEL PAGES 32-33


















The BIG question on mounting plates... ● Are you buying copies? ● When originals are superior quality ● That provide a better fit ● And Prestige have the VERY BEST prices SEE FOR YOURSELF... Black Plastic Mounting Plates £63.70 FOR 50 Magnetic Mounting Plates £69.95 FOR 50 Magnetic 300 Series Mounting Plates £64.95 FOR 50 Search Mounting Plates on www.prestige-dental.co.uk for all the price combinations for the full range of original, genuine mounting plates, or ring 01274 721567. WHY SETTLE FOR SECOND BEST AND PAY MORE? OFFER EXTENDED WHILE STOCKS LAST! Prices quoted exclude VAT & P&P Also available in x10, x20 and x100 Also available in x20 and x100 Also available in x20 and x100
AUGUST 2023
(Bazzie)
E: inthedoghousedesign@gmail.com
Editorial Advisory Board
Sir Paul Beresford
Deepa Bharakhda
Chris Golze
Andrea Johnson
Sharaz Mir
Sean Thompson
Philip Wears
PUBLISHED BY THE DENTAL TECHNICIAN MAGAZINE, PO BOX 2279, PULBOROUGH, RH20 9BR. T: 01372 897463
The Dental Technician Magazine is an independent publication and is not associated with any professional body or commercial establishment other than the publishers. Views expressed in this journal are not necessarily those of the editor, publisher or the editorial advisory board. Unsolicited manuscripts and photographs are welcome, though no liability can be accepted for any loss or damage, howsoever caused.
No part of this publication may be reproduced in any form without the express permission of the editor or the publisher.
Subscriptions: The Dental Technician, Select Publisher Services Ltd, PO Box 6337, Bournemouth BH1 9EH
Extend your subscription by recommending a colleague There is a major change in CPD coming soon. The Dental Technician Magazine is a must read. Tell your colleagues to subscribe and if they do so we will extend your subscription for 3 months. The only condition is that they have not subscribed to the magazine for more than 12 months. Just ask them to call the Subscriptions Hotline. With four colleagues registered that means your subscription would be extended for a year free of charge. At only £49.95 per year, for UK residents, this must be the cheapest way of keeping up to date. Help your colleagues to keep up to date as well. Ask them to call the subscriptions Hotline on 01202 586 848 now.
www.dentaltechnician.org.uk I 3
WELCOME From the Editor 4 Editorial Board 6-7 EVENTS BDIA Dental Showcase 8 Zirkonzahn’s Lecture Tour 2023 9 Prestige Dental’s Blooming Great Tea Party 10 DENTAL TECHNOLOGY Full dentures at the highest aesthetic level – Skender Ramadani 12-16 Streamlining dental laboratories with 3D printing 28 Planning for a brilliant restoration – Alistair Mayoh 30-31 Taking CAD/CAM technology to the next level 32-33 INTERVIEW An interview with… Sandra Puurits 18 HEALTH & WELLBEING The problem with posture – John Bennett 20-21 INSIGHT Tech’s eye view – Chris Golze 22 8 website tips to help grow your dental laboratory – Hayley Irons 2 4-25 ECPD Free verifiable ECPD & ECPD questions 26-27 MARKETPLACE Createch Medical 34 Kemdent Paper Polishing Discs 34 Zirkonzahn M6 Milling Unit 37 Vita Ceramics Polishing Set 38 Medentika Dental Implant Prosthetic portfolio 38 DENTAL NEWS GC takes new post-earthquake aid initiatives to support affected dentists 36 CLASSIFIEDS 39 Editor:
E: editor@dentaltechnician.org.uk Advertising Manager:
Trowbridge E: sales@dentaltechnician.org.uk T:
Heather Grimes
Chris
07399 403602 Designer: Sharon
Larder
CONTENTS
Welcome to the August issue of The Dental Technician Magazine.
I noticed a thought-provoking anonymous question on Dental Technicians Great Britain Facebook Group this week, asking: ‘If you could restart your career knowing what you know now, would you still be a technician? If so, what area would you specialise in?’
This attracted a fascinating flurry of comments, revealing a remarkably balanced split in responses – almost 50/50 - leaning perhaps slightly towards those who would choose a different trajectory.
I know, of course, a straw poll on Facebook with fifty-odd comments isn’t a marker for the consensus of the entire profession, but it does provide some level of insight, which left me feeling a little sad. If I were posed the same question about my own career, my unequivocal answer would be a resounding ‘yes’, I really love what I do. Despite the inevitable

ebbs and flows, the shifts in direction, and the leap from employment to selfemployment, my passion is unwavering and I have never wanted to do anything different. The thought that some among us feel disheartened, undervalued, overburdened, under-compensated, or disillusioned by the industry is a concern.
However, amidst these feelings of uncertainty, I noticed a glimmer of optimism. Many of you shared the reasons why you love your work, from having a diverse skillset to the excitement around emerging technologies. It was reassuring to see some positivity coming through.
So, which side of the fence are you on? Would you change it all if offered the chance, or stick with your current path? I’d love to explore this more with you all, uncover why there are so many mixed feelings and discuss what we can do together to ensure that dental technology fulfils more people at all stages of their career. Please feel free to get in touch for a chat, share your stories and anecdotes, or even just have a rant… I’m here for it!
On the subject of the Facebook group, a heartwarming thread by Simon Whitehouse also caught my attention. Simon is planning on recording a 20-track CD to be sold in support of Den-Tech but your input is required! He is looking for song requests, and will include a dedication on the recording, so add your suggestions to his post and help make this endeavour a resounding success!
If you haven’t already familiarised yourself with our updated editorial board, turn the page to meet them all. They are a really supportive group who are actively seeking out dental technicians to be featured in future issues of this magazines.
If you have a great case to share, an idea you want to shout about, or an opinion you’d like to voice, reach out to them on their socials, or drop me a line directly via editor@dentaltechnician.org.uk.
Heather Grimes | Editor

4 I www.dentaltechnician.org.uk
WELCOME
FROM
I PROMOTE YOUR BUSINESS IN THE DENTAL TECHNICIAN MAGAZINE T. 01372 897462 E. sales@dentaltechnician.org.uk In print since 1947 Reach out to a BIGGER audience
Editor
THE
m6 teleskoper blank changer




OPEN-SYSTEM MILLING UNIT WITH AUTOMATIC BLANK CHANGER FUNCTION, STORAGE FOR 16 OR 64 BLANKS



(UPGRADABLE) AND TELESKOPER ORBIT M6 (Ø 125 mm )
+ Fully automatic blank changer



+ Blank storage for 16 or 64 blanks (can be upgraded)


+ Teleskoper Orbit M6 (Ø 125 mm) for processing material blanks with Ø 95 mm, 98 mm, 106 mm and 125 mm
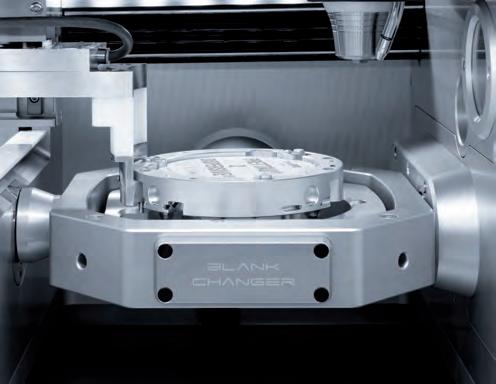
+ Tool magazine (2x30) with automatic tool changer function
+ Performance Spindle M6 with permanent-magnet synchronous motor (PMSM)

+ Intelligent selection and checking of blanks as well as milling tools via a QR code scanner















+ Newly developed door for easy and fast maintenance






+ Automatic self-cleaning and drying function


+ Ioniser for the electrostatic discharge of resin shavings, for a cleaner processing















































+ Integrated PC with 15“ touch screen



+ Cleaning Kit with shower and suction system
Ø95,98,106,125 mm 16 OR 64 BLANKS




(UPGRADABLE)














Zirkonzahn Worldwide – South Tyrol (Italy) – T +39 0474 066 680 – info@zirkonzahn.com – www.zirkonzahn.com MORE INFORMATION
SIR PAUL BERESFORD

w I am the MP for Mole Valley and a practising dentist.
I am New Zealand born and bred, married with four children; three sons and one daughter. I graduated in dentistry in New Zealand and took a year’s postgraduate course at the Eastman Dental Hospital. I first practised in the East End of London before moving to the West End.
I joined the Putney Conservatives and was elected to Wandsworth Council in 1978 and was its Leader between 1983 and 1992. I was knighted in the 1990 New Year Honours for political and public service.
CHRIS GOLZE
w I’m Chris Golze! Dental technician, lab owner and Olympic-class swearer! Born in Doncaster, raised in Doncaster and currently working in… you guessed it. You could say I’m a proud Yorkshireman too!

I can usually be found skulking around the various social media platforms, hopefully chipping in with the odd useful post but probably more likely taking a thread off on a tangent!
I’ve been in the lab industry since 1994. Starting off in a local practice -owned, full -service lab, moving to being co-owner of that same lab, then progressing to my current position of sole owner of XSDental.
My favoured area, and what the business concentrates on, is thermoforming. I’ve been fortunate enough to speak with and learn from many people over the years. This has allowed me to develop my own techniques and (hopefully) point others in the right direction on occasion too. I think it’s an area which is often overlooked as it’s not quite got the glamour that ceramics, prosthetics and even the wire mastery that some ortho has. There’s a few thermo-wizards out there now so maybe it’ll start to share the glitz the other departments bask in!
I’ve got to say I was pretty surprised to be asked to join the Editorial Board. Those who know me well will be aware this is new for me but something I am looking forward to. It does feel quite the honour to be amongst some very well-respected names from our profession. Hopefully as a group we’ll be able to bring an informative, educational, fun and (important to me) all-inclusive feel to The Dental Technician magazine.
DEEPA BHARAKHDA
w My name is Deepa Bharakhda originally from Old Trafford, Manchester! Currently living in Leicester UK.

I am a trained and registered dental technician since 2010! I graduated from Manchester Metropolitan University, currently working in a private laboratory in Leicester called Dencraft Leicester. I am prosthetic technician working with specialist dentists at a specialist practice on site as well as dentists outside the lab. I love working with dentists and building a good working relationship that helps me to fabricate beautiful work with a happy patient.
PHILIP WEARS
w Dental technology has been in my family now for three generations and as such I’m incredibly passionate about our industry and feel suitably placed to help bring the content technicians want to read.
I’ve worked in all types of lab throughout the north of England from small one man and his dog labs, to huge corporates, and now I own my own lab.
I believe there’s never been a better time to be a dental technician than right now. What makes this time so exciting is the technology, the new materials and techniques mixed in with a newer generation willing to share tips and tricks. Dentists and patients are wanting, expecting bigger and better work than ever before and it’s our chance to shine.
If anybody wants to connect and discuss articles and the magazine I can be found on the various Facebook groups under my own name and on Instagram at @xslabtech (and I managed all that without swearing…)
I have developed special interests in implants, over bar dentures and acrylic hybrids with an artistic flare for composite work! I love making dentures and hybrids look natural and beautiful. I am always wanting to learn new techniques, skills, meet new people and share knowledge. I am lucky to be part of a great dental community connecting with people around the world.
My passion in the dental field has led me to peruse dental photography and capture beautiful images of my work. I have had the opportunity to write for Dental Technicians Guild Magazine, Laboratory Dentistry and Dentistry.co.uk as well as been a speaker at dentistry shows.
I am a co-founder of Nightshift on Facebook, a group designed to elevate and celebrate female dental techs by giving them a space where they showcase their knowledge and skills.
I am very passionate about my profession creating beautiful smiles and making a difference is quite rewarding!
6 I www.dentaltechnician.org.uk EDITORIAL BOARD
ANDREA JOHNSON
w I am the chair and co-founder of dental charity Den-Tech, an orthodontic and maxillofacial laboratory manager/highly specialised dental technician, quality improvement coach, healthcare careers ambassador and clinical research intern at Doncaster & Bassetlaw NHS Foundation Trust.

I am an advisory board member, careers pathway reference group member and fellow of the College of General Dentistry. I am a Healthcare Leadership Academy (HLA) Cohort Director & co-lead of the HLA Dental network. I have a PgCert in charity management and 1st class BSc hons in Dental Technology.
I like to be very active within the dental profession and am regularly called upon to sit on advisory committees and working groups with bodies such as the General Dental Council, Health Education East Midlands and many more.
Some of my previous roles include chair of the Orthodontic Technicians Association (OTA), council member of the Dental Technologists Association (DTA), associate lecturer at Manchester Metropolitan University (MMU), visiting lecturer at the University of Chester, sessional teacher at Nottingham College, a Science, Technology, Engineering, Mathematics (STEM) ambassador and Chair of the Women in Healthcare Leadership Summit 2022.
Winner of a Star award, Pride of Derby award and the Aldridge Medal, I am a keen advocate of lifelong learning, I have written many CPD papers and lectured on a variety of subjects both nationally and internationally.
Outside of work and professional activities I enjoy running, going to the gym, walking my dogs and adventure travel.
Twitter handle: @kittani5
LinkedIn profile: andreajohnson0705
SEAN THOMPSON
w I entered into dental technology in 1982 by means of a summer job whilst waiting to start university after studying A-levels in biology, chemistry and English literature. I started a four-year apprenticeship training programme in dental technology instead, qualifying with Distinctions in 1986 after completing City and Guilds at Newcastle College, gaining the ‘Top Student’ award in the process for both the intermediary and final examinations.
I worked in various commercial laboratories for 18 years before gaining employment running the day-to-day operations of the orthodontic and maxillofacial laboratory at Sunderland Royal Hospital. Whilst there, I studied for a further two years gaining a postgrad professional studies diploma in maxillofacial technology from Manchester Metropolitan University in 2002.
I decided to leave employment to form a specialised orthodontic laboratory, establishing Ashford Orthodontics in January 2001, which
SHARAZ MIR
w I am the co-founder and sales and marketing director at Blueprint Dental. I achieved a BTEC in dental technology at Kings College London in 1993 and attended the University of Sheffield to gain a BMedSci and an MPhil in dental technology.

I am an exceptionally approachable individual with a passion for dentistry and the patience of a rock. I have a unique eye for what I call ‘products and projects’, being able to spot the next best thing in dentistry and implementing it. This has been key to keeping Blueprint Dental ahead of the game. I am very passionate about my profession creating beautiful smiles and making a difference is quite rewarding!
went from strength to strength, now employing over 70 highly respected members of staff. Ashford became an early implementer of digital techniques within orthodontics and firmly established itself as the ‘go to’ lab for digital orthodontics at scale, servicing almost 30% of NHS contract holding practices.
I set up and grew other associated businesses such as Quick Straight Teeth and Retainerworld, as well as CSG Properties Ltd, all of which were successfully sold on. Was elected to the OTA council in 2012 with aims to enhance the Commercial Laboratory representation by giving Private Laboratories a ‘voice’ within the OTA, whilst forging links with our other professional bodies.
Ashford grew from a modest £50,000 per year turnover to an almost £7 million business before my retirement in June 2021, after successfully negotiating the formation of a new company called ALS into which Ashford’s shares were pooled along with significant inward investment from Ansor Ltd. I exited the business, allowing the pursuit of other interests including professional coaching via a directorship in a consultancy company called Ashmore Consulting Ltd, and CEO of Retainers4life.
Outside of work, my other passion is Sunderland the ‘City’ and thus Sunderland Football Club, following them through ‘thin and thin’ for the last 50 years, attending almost every game with my wife Allison and sons Matthew and Nicholas.
EDITORIAL BOARD www.dentaltechnician.org.uk I 7
SAVE THE DATE FOR THE BDIA DENTAL SHOWCASE 2024!
nBDIA Dental Showcase is the event to attend for the entire practice team 2024. Make sure you get the dates in your diary - 22-23 March.
It will be the first opportunity of the year to browse new products and technologies, engage with the wider profession, develop your knowledge, hone your clinical skills and gain CPD for the year from leading clinicians.

Delegate feedback from 2023 included: ‘BDIA Dental Showcase allows me to visit a range of suppliers in an efficient way. I get to see new products and services. I get my questions answered. It’s often difficult to do this when you are so busy at the coalface. It’s nice to have the time to consider new materials, equipment and techniques when you’re not pre-occupied by the many competing priorities of a busy day practising.’ Associate dentist, Finn
 Dental Specialists
Dental Specialists
If you only attend one event next year, make it BDIA Dental Showcase. Watch this space for details and save the date today! Registration opens in November, to keep up to date via our monthly newsletter register your interest today: https://dentalshowcase. com/register-interest-pr.

EVENTS 8 I www.dentaltechnician.org.uk
BDIA Dental Showcase 2024 22-23 March ExCeL London dentalshowcase.com
ZIRKONZAHN’S LECTURE TOUR
Birmingham, Cardiff and Southampton from September 26 to 28
Ultimate Aesthetics – Connected Solutions From Prepping To Rechecking
nZirkonzahn will be in Birmingham, Cardiff and Southampton from 26 to 28 September for their 2023 lecture tour, ‘Ultimate aesthetics – connected solutions, from prepping to rechecking’. During the lecture, DT Jacopo di Terlizzi (international lecturer, CAD/CAM expert and member of the R&D team at Zirkonzahn Headquarters) will show how Zirkonzahn’s connected workflows will greatly simplify your daily work processes to meet your customers’ expectations. The lecturer will focus on real patient cases treated with the innovative Prettau® Skin® veneers and will explain innovative working methods and technologies for achieving a high degree of customisation and aesthetics based on the 3D virtual reproduction of the patient’s physiognomy and oral situation.
LECTURE HIGHLIGHTS:
l The new Prettau® Skin® technique, for producing ultra-thin zirconia veneers (0.2 mm) applied with zero to minimal impairment of tooth substance, and the complete workflow with preparation guides
l Working on the 3D virtual reproduction of the patient with smart software functions
l Connected solutions for a seamless process: digital-analogue workflows with intraoral scanner, 3D printer and innovative tools and technologies for improved time-efficiency, such as the new JawAligner for plaster-free articulation of models and the new extra-large Teleskoper Orbit (Ø125 mm)
l And much more!
The lecture is open to both dentists and dental technicians and will take place in Birmingham, Cardiff and Southampton from 26-28 September 2023.
Places are limited, but registration is obligatory.
For more information and registration, scan the code, visit: www.zirkonzahn.com (events section) or contact:
Carmen Ausserhofer, T: +39 0474 066 662 E: carmen.ausserhofer@zirkonzahn.com

EVENTS www.dentaltechnician.org.uk I 9
RECORD BREAKING EVENT WHILST BRAVING THE BRITISH SUMMER!

As many of you know, Prestige Dental is a great supporter of Marie Curie, raising funds for the local Bradford Hospice.



Running this event is a huge commitment with planning starting early on each year. We have a team of crafters, fundraisers, bakers, and caterers who devote their time and efforts throughout the year to deliver wonderful prizes, giveaways and fabulous food and service on the day. We are lucky to have the commitment of all the Prestige staff and the incredible drive and enthusiasm of director, Lucy Gabbitas. Lucy first started fundraising having been impressed by the wonderful care given to her grandmother by the team at the Marie Curie Bradford Hospice. Starting with a simple lunch for a few friends, it has grown to be quite the social occasion of the year for many. Fast forward 14 years and we now welcome some 80 guests to the summer event. Generously hosted by director Paul Martin in his beautiful gardens, they themselves demand a lot of preparation, not least to rid the lawns of the moles!
Planning always starts as early as January for the ‘Blooming Great Tea Party’ which this year was scheduled for Saturday 8 July. The thing out of our control is the weather, but with rain forecast and the help of the local scout group, the whole outdoor area was covered with giant gazebos and the event went ahead.
We had cake stalls, a huge raffle, games, singing and dancing – and a fabulous team of helpers and guests – who all turned up despite the threat of thunder and lightning. We were also lucky enough to have the lovely Claire Mancina join us for the festivities. As community fundraiser for Marie Curie, she reminded us exactly how important these type of fund raisers are, and the significant difference they can make to terminally ill patients and their families.

This year we raised a truly amazing amount – our best ever total. A staggering £3,288.31. The challenge is always to keep it fun and fresh and with an incredible overall total of over £20k raised since Lucy first began fundraising, we are proud to feel we live up to that challenge. The final word however must go to our guests and the amazing support that they give to this event – a huge THANK YOU from all at Prestige Dental and the Marie Curie Bradford Hospice.

EVENTS 10 I www.dentaltechnician.org.uk
WHAT DOES PERFECTION MEAN TO YOU?
your patient.
We have been designing teeth since 1936, like the








TCR CANDULOR. HIGH END ONLY.

Optimal function? More authenticity? Maximum naturalness? Successful tooth design knows only one benchmark: your own standards and those of
PhysioSelect
TOOTH EXPRESS LTD ABBEY DENTAL SUPPLIES Unit 35, Jessops Riverside 800 Brightside Lane She eld S9 2RX 23-27 Gladstone Road Croydon CR0 2BQ T 0114 242 4048 E enquiries@tooth-express.co.uk W tooth-express.co.uk T 02086 834528 F 02086 840934 E sales@abbeydentalsupplies.com W abbeydentalsupplies.com
TO BUY?
WHERE
FULL DENTURES AT THE HIGHEST AESTHETIC LEVEL
A contribution to the 13th International CANDULOR
KunstZahnWerk Competition 2023
By Skender Ramadani, Switzerland
There are many reasons for the computer-aided fabrication of dental restorations. However, when it comes to fabricating full dentures which differ from the ordinary due to their individuality and natural beauty, then conventional fabrication techniques often remain superior to this day. They offer users greater flexibility and enable them to apply their own creativity as well as dental technical skills in a more targeted manner. This results in restorations that help patients with the highest aesthetic demands to achieve a better quality of life.

Such a restoration was to be fabricated as part of the 13th International CANDULOR KunstZahnWerk
Competition 2023, hosted by Candulor: the challenge was to fabricate a mucosasupported maxillary and mandibular full denture based on a detailed model analysis. A choice could be made between a tooth-

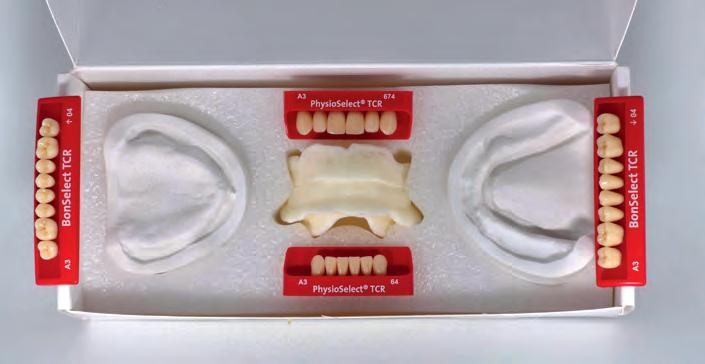
to-tooth or a tooth-to-two-tooth setup for the dynamic occlusion concept which was to be applied. Detailed information on the initial situation was provided (summarised in the following case description), as well as the matching maxillary and mandibular plaster models, the physiognomic bite key and the denture teeth: PhysioSelect TCR (maxilla) / shape 674, shade A3, PhysioSelect TCR (mandible) / shape 64, shade A3 and BonSelect TCR (maxilla and mandible) / shape 04, shade A3 (Fig. 1). In addition, the briefing included an image of the interim denture, recent extraoral images of the patient with the denture in place, and a youth photograph (Figs. 2 to 5). It was also mentioned that the labial lip contact of the maxillary anterior teeth and the buccal cheek contact of the posterior teeth correspond to the bite key. The condylar path inclination was given as 45 degrees on the right and 47 degrees on the left, the relationship: Camper’s plane = occlusal plane.
CASE DESCRIPTION
The female patient was 69 years old at the beginning of treatment and had already been provided with full dentures for 15 years. Whereas teeth 21, 22 and 23* as well as 35 to 42 and 46* could initially be preserved and were restored with double crowns, the teeth in the maxilla had been extracted over time. Subsequently, the teeth in the mandible also had to be extracted due to advanced periodontitis. The patient had been wearing an interim restoration for two years.
No general medical conditions relevant to treatment were known at the start of treatment. Clinical examination revealed pronounced atrophy of the mandible. Also noteworthy were a slightly pronounced flabby ridge in region 32 to 42* as well as leukoplakia crestally in region 35*. A new restoration with mucosa-supported full dentures was indicated due to both unsatisfactory aesthetics as well as unsatisfactory function. The aesthetic deficiencies included the unsightly resin of the interim restoration (Fig. 2) as well as the fact that the anterior teeth in the maxilla and mandible were not sufficiently visible (Fig. 3).
DENTAL TECHNOLOGY 12 I www.dentaltechnician.org.uk
Fig. 1: Set with plaster models, bite key and denture teeth
Fig. 2: Interim restoration with unsightly resin
In addition, the lower third of the face clearly appeared too small when the jaw was closed in the resting position. This gave the chin a more ‘pointed’ appearance than is usual (Figs. 4 and 5). The unsatisfactory function was due to insufficient denture retention, which only allowed food comminution in conjunction with the use of adhesive cream. However, it remains questionable whether it is at all possible to achieve satisfactory prosthetic function in the mandible into old age without implants (Marburg ‘Concept 75+’ Dr. H. Gloerfeld/Dr. D. Weber, Marburg).

TREATMENT GOALS
The patient’s wishes were also taken into account when defining the treatment goals. Her main concerns were better retention as well as better chewing performance. Furthermore, the anterior teeth should be more visible in both the upper and lower jaws and the chin was to appear less ‘pointed’. In terms of shape, position and colour of the teeth, the patient wanted a natural appearance that was in keeping with her age, even somewhat irregular was welcome.


Taking these wishes into account, it was planned to fabricate a mucosa-supported maxillary and mandibular full denture with an individual design. Attention was to be paid to the highest possible wearing comfort and secure retention, excellent chewing performance and, of course, a perfect function of speech. To slightly correct the protruding chin, an elevation of the vertical jaw relation was planned. A look at the youth photo (Fig. 5) confirmed the assumption that stronger padding of the lower lip would not lead to the desired result in the present case. However, elevation would also optimise visibility of the maxillary anterior teeth in particular. In the context of these measures, attention had to be paid to preserving speech function.
MODEL ASSEMBLY
The provided models and the bite keys were first duplicated to be able to start with model analysis and planning the details. Then the models were articulated at mean value. For this purpose, the support pin of the articulator (Candulor articulator CA 3.0) was set to zero. The condylar path inclination was also set according to the specifications (45 degrees on the right and 47 degrees on the left side; Fig. 6). The incisal pin was then positioned centrally at the bite height of the mandibular bite key. This later served as an important landmark for the setup of the central incisors, which are to be set incisally at the bite height and mesially next to the incisal pin. A silicone anterior tooth key is suitable for transferring the overbite. Visualisation of the Camper’s plane, which coincided with the occlusal plane, was performed to transfer the jaw relation registered in the practice as well as the vertical dimension to the model with the known rubber band (Fig. 7). With this aid, the bite key could


be aligned correctly. To position the models in the Bonwill triangle, it is advisable to draw in the median lines and alveolar ridge centers. It is recommended to use dimensionally stable plastic putty for model assembly, which ensures both safety and facilitates the demanding task of accurate articulation (Fig. 8).
MODEL ANALYSIS
A careful analysis of the anatomical conditions using the provided models is one of the most important prerequisites for properly functioning full dentures. This provides valuable information about the positions of the natural teeth and thus enables the reliable determination of statically favourable areas for setting up the denture teeth. This ensures that the denture can meet high functional as well as aesthetic demands; dysfunctional denture movements can, on the other hand, be safely avoided.
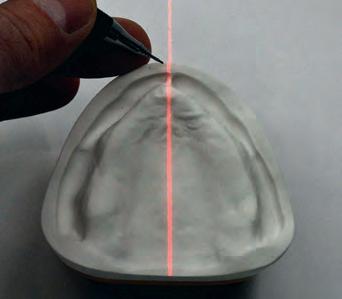
In the present case, model analysis was performed based on the concept of Prof. Dr. Albert Gerber. In the first step, a laser beam
was used, which was set up at a 90-degree angle and parallel to the tabletop (Fig. 9). This instrument was used to determine the set-up line. With the subsequently used cross-section measuring instrument, it is possible to map and record every crosssection. This makes it easy to check the profile of the dental arch. The alveolar ridge was then drawn in with the aid of the tried-and-tested profile compasses.

DENTAL TECHNOLOGY www.dentaltechnician.org.uk I 13
u
Fig. 9: Use of the laser in model analysis
TOP ROW: Fig. 3: Frontal image of the patient with closed mouth at rest position, open mouth, laughing, smiling and with closed mouth at jaw occlusion. 2ND ROW: Fig. 4 (1ST TWO IMAGES): Profile view of the patient with closed mouth in rest position and with jaw occlusion. Fig. 5 (2ND TWO IMAGES): Comparison of a youth photo of the patient with a current image. 3RD ROW: Fig. 6: Setting of the articulator. 4TH ROW: Fig. 7 (1ST IMAGE): Alignment of the models to the Camper’s plane, visualized with a rubber band. Fig. 8 (OTHER THREE IMAGES): Articulated models with bite key.
However, the question arises as to whether the lateral alveolar ridge profile or the cross-section of the alveolar ridge centre profile (which can be determined with the cross-section instrument) should be taken into consideration for model analysis. Ideally, the contact points should be located on the midline of the alveolar ridge to create a uniform image. Depending on the case, orientation to the lateral alveolar ridge (profile compasses) can favour an irregular result and thus make the ideal setup more difficult. The alveolar ridge centerline, on the other hand, provides an unbiased orientation guide.
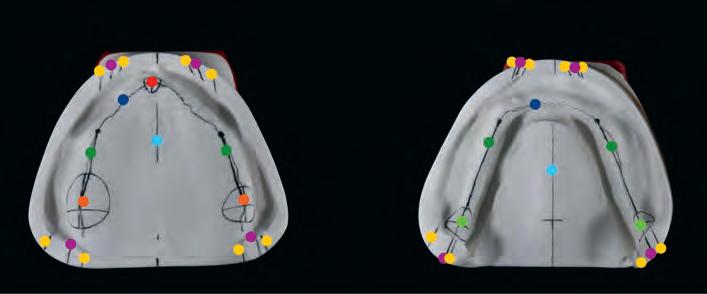
As shown in Figures 10 to 12, the important lines and points were plotted step by step on both the occlusal surface as well as the outer surface of the model. The more details are recorded on the models, the easier it will be in the subsequent steps to identify the ideal position for each tooth and to act accordingly during setup. This contributes to the predictability of the entire process.
SETUP OF THE ANTERIOR TEETH
In preparation for setting up the denture teeth, a wax base for the maxilla and mandible was first created from the copy of the bite key. The models with wax bases were then reduced in the articulator and the incisal pin was opened by 2mm. This measure was to ensure that the anterior teeth in the maxilla would become more visible by 1mm when the vertical relation was later raised by 1mm. First, the anterior teeth in the maxilla were set up with the aid of the bite key, which also determined the position of the mid line (Figs. 13 and 14). The selected denture teeth - PhysioSelect TCR in shape 674 and shade A3 - with their slightly translucent incisal edges with discreet mamelons and translucent marginal ridge effects were specifically designed for youngat-heart patients. From orientation according to the bite key, it quickly became apparent that the teeth were a little too wide and needed to be ground narrower: with optimal positioning without grinding, the dental arch was too long. This would lead to undesirable distalisation in the posterior region and thus to irregular dentition. To subsequently set up the anterior teeth in the mandible (PhysioSelect TCR, shape 64 and shade A3) at the correct bite height, the incisal pin was set to +1mm relative to the occlusal plane level. In the first step, the incisal pin served as a guide for positioning teeth 31 and 41* (Fig. 15). This was followed by the lateral incisors and the canines (Figs. 16 and 17). The dental arch as well as the lip contact were repeatedly checked with the bite key.


SETUP OF THE POSTERIOR TEETH




BonSelect TCRs in shape 04 and shade A3 were used in the posterior tooth region to match the PhysioSelect TCR line. Setup was performed according to the tooth-to-tooth



TOP ROW: Fig. 10: Lines and points drawn with a pencil. Colour-coded: papilla incisiva: red, alveolar ridge profile: dark blue, alveolar ridge centre profile: dark green, tuber maxilla: orange, setup line: purple, model centre light blue, inner and outer correction: yellow, tuberculum retromolare: light green. 2ND ROW: Fig. 11: Models with orientation lines and points drawn in as well as next to the articulator. 3RD ROW: Fig. 12: Lateral view of the models of the maxilla and mandible: lateral alveolar ridge profile on model outer surface: black, parallel tangent to occlusal plane: light blue, position of largest chewing unit on centre of alveolar ridge with tolerance range: dark green and stop line (beginning of inclined plane): red. 4TH ROW: Fig. 13: Setup of the central incisors in the maxilla. Fig. 14: Setup of all anterior teeth in the maxilla. 5TH ROW: Fig. 15: Setup of teeth 31 and 41* with orientation relative to the incisal pin. Fig. 16: Setup of the anterior teeth in the mandible. Fig. 17: Complete setup of the anterior teeth in the mandible. 6TH ROW: Fig.18: Setup of the posterior teeth. Fig. 19: Use of the cross-section instrument to check the cheek contact.

DENTAL TECHNOLOGY 14 I www.dentaltechnician.org.uk
occlusion concept (Fig. 18). In the mandible, attention was paid to ensuring that the central fissure of the posterior teeth was set up on the setup line (sagittal contour according to the model analysis). The stop line showed that there was insufficient space for teeth 37 and 47*, so they were dispensed with. The first molars in the mandible were set up at the lowest point in each case. The focus here was on buccal relief of the setup and interlocking occlusion. Overall, it was easy to realise the tooth-to-tooth occlusion. Cheek contact was checked repeatedly with the silicone key and the cross-section instrument (Fig. 19). A look at the palatal cusps of the posterior teeth in the maxilla provides information about the compensation curve (Fig. 20). A final check in the mandible was to establish whether the palatal cusps of the posterior teeth in the maxilla fitted optimally into the fossa of the antagonists (Fig. 21).
STATIC OCCLUSION
As described during model assembly, the bite in the incisal area was elevated by 1mm. This increased the vertical relation in the molar region by only about 0.5mm. Based on the information on the minimum speaking distance with the interim denture (non-contact, large: 5 to 6mm), it can be assumed that an increase by this amount would still allow for the minimum speaking distance without contact - which is common for the pronunciation of S sounds - and would therefore not have a negative influence on phonation. Positioning the contact points exactly on the alveolar ridge also ensured autonomous chewing stability. In the toothto-tooth set-up, the supporting cusps were given particularly high priority. This concerns the palatal cusps of the second maxillary premolars as well as the mesio-palatal cusps of the first maxillary molars. These rest in the fossa of the respective antagonist (Figs. 22 and 23). Ideally, the contact point of the first premolars in the mandible is buccal. In this case, it was shifted to lingual, as it would otherwise have been impossible to achieve cheek contact according to the bite key. Reliable static occlusion could nevertheless be achieved.


DYNAMIC OCCLUSION
The original objective was to avoid any contacts in the front during protrusion. As this plan was not feasible, sliding contacts were tolerated. Contacts which existed after grinding in the guides were reduced for this purpose. This was achieved palatally on the incisal edges of the anterior teeth of the maxilla as well as on the labial incisal edge of the anterior teeth of the mandible without any loss in anterior tooth length. For laterotrusion, perfect bilateral balancing was achieved on both the laterotrusion and mediotrusion sides with the posterior tooth guides (Figs. 24 and 25). Contacts during retrusion were designed to be as numerous and extensive as possible (Fig. 26).
TOP ROW: Fig. 20: Occlusal view of the teeth in the maxilla. Fig. 21: Occlusal view of the teeth in the mandible. Fig. 22: Dentition in the posterior region: quadrants 2 and 3*. 2ND ROW: Fig. 23: Dentition in the posterior region: quadrants 1 and 4*. Fig. 24: Contacts during laterotrusion to the left. 3RD ROW: Fig. 25: Contacts during laterotrusion to the right. Fig. 26: Contacts during retrusion. 4TH ROW: Fig. 27: Completed wax base ... Fig. 28: ... with naturally designed labial surfaces. 5TH ROW: Fig. 29: Wax model of the maxillary full denture, occlusal view. Fig. 30: Wax model of the maxillary full denture, palatal view.
MODELING
The final check of all contact points was followed by modeling the wax base. The shape was designed on the basis of information obtained during the model analysis. Accordingly, the morphology of the surfaces was designed as natural as possible (Figs. 27 to 30). It is worth investing ample time in this step, as it makes final finishing of the denture much easier.
DENTURE DESIGN AND FINISHING








From own experience, the subsequent work step - resin processing - has considerable influence on the successful outcome of treatment. With correct processing, a dental technician can create the necessary conditions for high surface quality, thus making an important contribution to the longevity of the resulting dentures. This is not only important for the long-term satisfaction of patients, but also for one’s own conscience.

DENTAL TECHNOLOGY www.dentaltechnician.org.uk I 15
u
In the present case, the final, mucosa-supported full dentures were fabricated using the flask press technique (Figs. 31 to 33). The dentures were embedded in flasks and pressed. PMMA was used for the subsequent characterisation instead of composite. The selected resin teeth did not require any additional milled retentions and were only blasted cervically in the areas that were covered with pink resin.
When finishing the dentures, it became apparent how high the quality of the materials used by the Candulor company are. They allow reaching a level of quality and aesthetics that seems unattainable in a digital workflow in my estimation. Figures 34 to 38 show the completed dentures.

CONCLUSION
This case study is an excellent example of how full dentures can be fabricated to meet the highest functional and aesthetic requirements. If one plans carefully and masters the techniques of the conventional fabrication process from set-up to completion, one can achieve an aesthetic level that seems unattainable with digital technologies. Working with the conventional workflow is made considerably easier when using innovative, high-quality materials, such as those offered by the prosthetics specialist Candulor.
And while the presented method of fabrication may appear old-fashioned to some readers, I am convinced that there will always be patients who place special value on individuality and beauty. They will continue to ensure that demand for handmade dentures remains stable in the future. Being able to offer these patients a customised solution is and remains an important issue for me.
* In this article we refer to the dental scheme: FDA (Fédération Dentaire Internationale / DIN EN ISO 3950:2016-09).
MATERIALS USED

Articulator: Candulor Articulator CA 3.0 (CANDULOR)
Plastic putty: Gumex N, masking compound, yellow (DENTAURUM)
Modelling wax: AESTHETIC Denture Wax (CANDULOR)





Tooth lines: PhysioSelect TCR and BonSelect TCR (CANDULOR)
Denture resin: AESTHETIC BLUE (CANDULOR)
Individualization of the gingiva: AESTHETIC Intensive Colors (CANDULOR)

Articulating film: Artikont articulating ribbon (CANDULOR)
l Skender Ramadani successfully completed his training as a dental technician in 2007. Since then, he has worked in various dental laboratories in Switzerland, experienced the entire spectrum of dental technology and regularly attends further education.

Due to his passion for prosthetics, he has participated several times in the CANDULOR KunstZahnWerk competition, where he won first place in 2013 and second place in 2023. In the ‘Das Goldene Parallelometer’ (The Golden Parallelometer) competition, he took 13th place in 2014, making him the best participant from Switzerland.
Award winner at the CANDULOR
KunstZahnWerk Competition 2023: Silver CANDULOR Award (2nd place) and third best documentation
Contact
DT Skender Ramadani
Dental-Technik Sulejmani GmbH
Kesslerstrasse 9
8952 Schlieren
Switzerland
Telephone: +41 44 886 80 80
DIGITAL TECHNOLOGY 16 I www.dentaltechnician.org.uk
TOP ROW: Fig. 31: Model in the flask. Fig. 32: Silicone key produced via the wax-up. 2ND ROW: Fig. 33: Basal view of the embedded silicone key with denture teeth. Fig. 34: Mandibular denture in the flask. 3RD ROW: Fig. 35: Frontal view of the completed maxillary and mandibular full denture on the mandibular model. Fig. 36: Lateral …. 4TH ROW: Fig. 37: … and frontal views … Fig. 38: … of the completed restoration.
About the author: Skender Ramadani, Schlieren (Switzerland)


Labs and dentists have never collaborated so efficiently before Getting started with 3D printing has never been easier with DentaMile from DMG. Our solutions connect partners in the dental clinic and in the lab. What’s more, customisable workflows open up all kinds of collaboration options – for greater patient performance. DentaMile: 3D the way I want it! Want to know more? Email sales@dmg-dental.co.uk or call 01656 789 401
An interview with…
Sandra Puurits
We chat to Sandra Puurits (@sasspuurits on Instagram) about her dream dental lab, her favourite tools, THAT case, and much more…

How many years have you been working in the dental industry?
It’s been now a bit over nine years. I’ve worked in three different labs. The one where I’m working right now is my most favourite of them all. I can do what I do best: removable dentures. And the same dentists that I have worked with for the last five years can still order from me, which is really nice because we have a mutual understanding and they trust me. I have also had the opportunity to learn how to design cobalt chrome frames in 3Shape. I fell in love making cast partials using the traditional method about 3-4 years ago. Now I realise how great it is also to be able to follow the evolution in CAD/CAM.
What’s your earliest dental lab memory?
Thinking ‘What is this madness!?’ And the smell of monomer fluid.
Favourite tool/piece of equipment in the lab?
My hands... Haha, no, just joking! Well, all the tools that I myself have shaped for waxwork and carving I suppose. I remember when my favourite knife broke, I was just devastated! But at the same time, all my special burs are also my precious (insert Gollum voice here). Hard to say… Hmm... We’ll just go with ‘my hands’ on this.
If you owned a dental lab what sort of a lab would you have?
A lab connected to a massage parlour! We all have seen ourselves, the lab-gremlins, working. The posture… it just hurts to watch! And a few cold ones in the fridge would not hurt one bit (this is my imaginary lab, I can have everything I want)!
INTERVIEW 18 I www.dentaltechnician.org.uk
Favourite part of your job?
I’m between two options here. One is getting little notes from dentists and dental assistants. Those little smiley faces and flowers they draw are just so sweet! Not to mention the ones who have the sense of humour to react to my stupid jokes. The second ones are the patients who come for shade check, for example for an upcoming partial denture. You never know, what you’ll be confronted with! Aaaahhh, the excitement! As if there’s not much intensity in the day-to-day life in the lab.
If you weren’t in dentistry, what would you be?
I would be calm and well-balanced. Haha, joking again (‘OMG, does she ever stop with the jokes?’ thought the reader). I’ve heard there are people who sell Tupperware… That would not be me (‘Again? Seriously?’). I’d be a designated driver. Of a bus. Not kidding! I’d like to take people to get-togethers and such. Some of the

longer routes. So I’d take them to have a nice time and then laugh quietly as they are trying to not vomit on the way back at 3am in the morning.
What has been your biggest challenge and how did you overcome it?
Trying to explain something really important to someone and they just don’t listen to me because I am a woman and/or younger than they are. How have I overcome it? Well… I haven’t totally. I just gather my dudes and gals at work and we exchange our thoughts, laugh and move on.
What was the last case you worked on?
Oh dear… I thought I would NOT have to think about THE case again today! Ok, full upper and cobalt chrome partial on lower. The bite is a nightmare! Looks like the upper and lower jaws don’t match at all. Wide arch in the upper, narrow in the lower. Lower incisors cannot get any contact, too much retrusion. Need to get it somehow work on the molars. Cusp alteration is… well, I got it
somehow working. Took me an hour to figure out how it would work in the movements and have enough space for the tongue. AND I didn’t cry once! But the good news is I’ll be on my holiday when the first fitting is.
Most funny/ridiculous/dangerous/ disgusting lab occurrence?
I think by now I am not surprised about anything disgusting anymore. Someone once walked in and took a six-unit bridge out of their mouth with three roots in it and asked if we can somehow fix it. I just said that no can do sir/mam and just continued with my day. I think I don’t have a gag reflex anymore. But the most ridiculous? Having a bite rim come back with no marks on it. No antagonist teeth marks whatsoever. Wow… just wow. But still, I’m not surprised. Dangerous? People who swallow their denture tooth and don’t tell in you in advance how they got it back… just, no!
If somebody wrote a biography about you, what would it be called?
INTERVIEW www.dentaltechnician.org.uk I 19
‘Accidentally’.
THE PROBLEM WITH POSTURE

Over the last 10 million or so years, we have evolved from simple swamp-dwelling creatures, through to our four-legged (quadrupedal) common ancestors, to a fully bipedal species, now standing proudly and confidently on two legs, chest out with our head held high. This natural evolutionary process, while incredibly slow, also resulted in an amazing adaptation of our brain. The longer our common ancestors stood up on two legs, the more sensory stimulus was received. The result of this was an increase in our brain size, literally tripling in mass and functional capabilities, ultimately leading us to become the most advanced living animal on the planet, able to think beyond instinct, to rationalise, to plan ahead, to work in small and large communities, to remember and record the detailed past, to make tools and invent machines, to work through complex tasks and instruction, and to learn. The latter being exactly as you do every day while standing or sitting at your workstation.
The modern issue with posture
However, despite this truly awe-inspiring history of where we evolved from, there is an enormous ‘modern’ issue with our posture. For many of us, it is subtly de-evolving at an alarming rate... indeed, at the rate of technology. Barely two decades of the internet, smart devices, and screen technology, and it is all having an alarming effect on our posture, head and neck position, gait and brain function. Many are blissfully unaware of the issue, while others wrongly assume that having tech-neck (result of frequent and prolonged neck flexion looking down at mobile
devices) is only a musculoskeletal problemrolled shoulders, head drooping forward in a hunched position. But it isn’t just that, it is scientifically proven to also contribute to a neurological disorder, commonly referred to as digital dementia1 . People’s brains are suffering from bad posture and the overuse of technology. Studies are showing that this is resulting in varying levels of cognitive decline.
Picture someone walking who has suffered a debilitating stroke, or struggles with Parkinson’s. Typically, the gait and posture is rolled shoulders, head forward, arms fixed at the side with minimal swing, shuffling forward. Now picture someone walking along looking at their mobile phone. Most of the movement pattern, or lack thereof, will be the same. The first scenario is in response to a brain trauma or disease. The second, completely self-inflicted by constantly looking at a mobile device, is causing a brain deficit.
Posture system
Do you remember being in lectures and feeling sleepy or disinterested, beginning to slump forward, maybe resting on your elbows and sliding down into your chair? Then your name is called out. What did you do? You would have immediately engaged your posture system, sat up sharply and to attention, back and head straight, literally waking up your brain.
Our brain neurology dictates every movement, from the biggest to the most intricate. It controls structure and function of your posture system, overseeing and refining every single movement that you do on a daily basis, from simply pulling your stool underneath as you sit down, through to the fine motor control needed to create complex dental appliances.
20 I www.dentaltechnician.org.uk
1. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5855412/
John Bennett discusses the impact that bad posture can have on your brain
REFERENCE:
HEALTH & WELLBEING
Harness the power of technology
Today many of us spend too many hours looking at screens, some at work, but mostly on social media and sites that interest us, maybe squandering hours of time, receiving gargantuan amounts of mostly one-way, visual and auditory information, but reducing and missing the other senses the brain requires, those being touch, smell, pressure, being in natural outdoor environments, and actual human interactions. No one can deny the increase in global mental health issues with stress and anxiety, and this coincidentally, or not, has increased at the same rate as screen use.
But this is not all doom and fear mongering. Our brains and bodies have an incredible ability to rehabilitate, to heal and to adapt. If stimulated and engaged routinely, our brain neurons will continue to fire and create new synaptic connections until death. The internet, smart phone technology and computers provide spellbinding assistance and benefits to all of our lives. We just need to learn better ways to control our interactivity with it and limit its potentially, negative impact.
Stay in love with your job
MSDs (musculoskeletal disorders) have been, and still are the number one reason for forced early retirement from our profession. Hours, days, months and years of sitting and standing in hunched, forward head posture positions can play havoc on our bodies, often resulting in permanent damage, chasing pain control through medication or regular chiropractic and massage interventions. Indeed, I personally have seen many fall out of love with the profession. They will often put this down to the workload, time at work, fear of litigation, or simply losing love of the daily routine, when in reality it is because they are in pain and don’t equate the two things together.
I cover these aspects in my in-practice training courses and delve deeper into how these issues can be reduced and even avoided completely. My approach to health and wellness in our profession is always simplicity. What can we do in our daily behaviours, to achieve permanent habitual changes that would benefit our health, both mentally and physically.
TOP TIPS TO AVOID
BAD POSTURE:

1. Try to keep your working area as close to your sternum height as possible. This will reduce neck flexion and cervical pressure
2. Are you able to stand while working? There are many adjustable workstations now available that can be raised and lowered as required. If a 50/50 sitting/standing workload could be achieved, this would be ideal.
3. Try to take regular 30-45 second micro-breaks every 15-20 minutes. Literally, stand up and walk a few paces, and then return. If standing, just take some paces away and back to your workstation. This will increase blood, oxygen and nutrition delivery to your limbs and reduce muscle/tendon fatigue.
4. When taking your micro-break, use this opportunity to fully stretch – squat, raise arms, roll shoulders, flex hands, wrists, gently stretch and pull back thumbs, fingers, gently rotate your head left and right… in simple terms move everything!
5. Saddle Stools (ideally with lumbar support) are great for achieving the natural S shape that the lower spine has when we stand, and with a good lumbar support, the temptation for us is to push back into it, thereby positioning and strengthening our backs correctly.
6. If possible, get outside more and breathe in some fresh air. The perfect scenario would be to take 15-20 minute walk in your lunch hour, ideally before you eat a ‘light’ lunch.
7. If you find yourself feeling tired as the day draws on, try taking three to five short sharp breaths in and out through the nose, keep your mouth shut. This will trigger your sympathetic ‘fight flight’ response and push the fatigue away. How long for is down to the individual.
8. When looking at your mobile phone, extend your elbows. This simple change of position will raise the height of your mobile thereby raising the position of your head and reducing the flexion in your neck.
ABOUT JOHN BENNETT
l John Bennett has worked in the dental sales and training arena for the last 16 years.
Over the last 10 years, he has been building a substantial knowledge and understanding of the growing issue of poor health, both physical and mental, in our profession. Also a qualified Breathing & Respiratory Coach, John left the safety of the corporate world

and two years ago created DPC Dental - Dental Performance Coaching, offering wellness training, breath coaching and ergonomic solutions for the dental and medical professions.
For more information, contact 0333 4040728, info@dpcdental.co.uk, or visit www.dpcdental.co.uk
HEALTH & WELLBEING www.dentaltechnician.org.uk I 21
Tech’s Eye View
My work ‘bench’ layout has evolved over many years. I’ve tried different things in the labs I’ve worked in to see what works and to make it as efficient a space as possible.
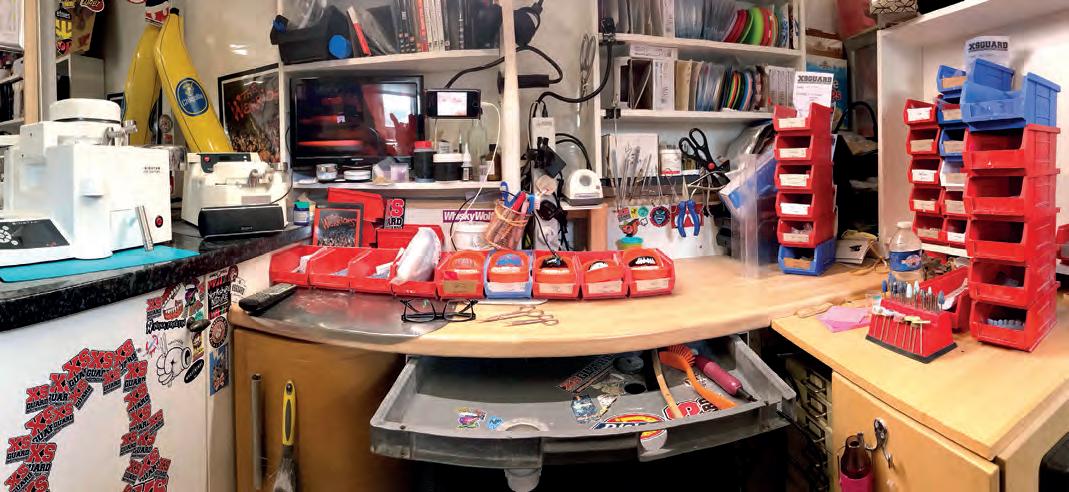
I’ve found a ‘U’ or ‘L’ shaped station allows me to have everything to hand and also makes the best most of a relatively small space.
STARTING FROM LEFT TO RIGHT…
You can see my Scheu Biostar and Ministar pressure formers - the backbone of our business! They are reliable, easy to use and give great results.
Next are the IKEA shelving units, I know a lot of labs do their fit out using furniture from the much-loved Scandinavian brand. Custom built would probably be better but these have worked well. I’ve found having everything in view allows to me to monitor stock levels, as I can instantly see what’s in or needs ordering.
All my hand tools are just a reach away mounted on magnetic strip. Using this keeps
them to nearby without them rolling around on the bench where they’re likely to end up on the floor!
The grey under-bench drawer is from my first bench when I started in a lab in 1994! I believe that fit out was originally done by John Winters and this is the only part of it I’ve kept. It now houses my extraction (a simple sink plug hole) with the vacuum unit housed within the bench alongside the air compressor.
HELPING HANDS
Speaking of recycling, the bench worktop and pressure former base unit came from my friend Andy Fairbanks’ old lab! I also have a micromotor from Pete Harling, model trimmer from Dave Baldry, induction heater from Phil Reddington and compressor from Lee Torrington. These dudes definitely need a shout out for what they’ve done for me. A great example of how technicians help each other. Thanks guys!
It might not be cutting edge, it might not be pretty, but it works extremely well. Technicians are often called artists and I think this fits in pretty well with that.
INSIGHT 22 I www.dentaltechnician.org.uk
In this brand new feature, we’ll be taking a peek at a fellow dental technician’s bench.
This month, we get nosey with Chris Golze , owner of XSDental
Do you want your desk featured in a future issue? Email editor@dentaltechnician.org.uk!

















www.dentaltechnician.org.uk I 23 Offer specially extended for Dental Technician readers until 30th September Quote “Dental Technician Promo” when contacting us +44 (0)1580 817000 07517 861600 sales@bracon.co.uk SCAN THE QR CODE FOR SUMMER SPECIAL EQUIPMENT OFFERS WITH MESTRA FOR MORE INFORMATION AND TO SUBSCRIBE Call the subscription hotline on 01202 586 848 or visit: www.selectmagazines.co.uk/product/dental-technician Subscribe today to keep up to date with regular developments in the industry and stay up to date with new CPD. For just £49.95 a year for UK customers & £70.00 for European customers for a one year subscription 12 issues / 12 months. THE LONGEST RUNNING JOURNAL IN THE INDUSTRY The Dental Technician Magazine
8 WEBSITE TIPS TO HELP GROW YOUR DENTAL LABORATORY
In
Even if you receive most of your work through referrals or word of mouth, you can guarantee people will be looking to find you online, even just as part of a social-proofing exercise.

Having a basic website can sometimes suffice, but if you really want to grow your business and set yourself apart from your competitors, then you need a great site that works for you and can even bring leads in when you’re not working.
In this article, we’ll take a look at some hints and tips that you can deploy to help your website stand out from the crowd and make your dental lab succeed.
1. Mobile first
The vast majority of people use their smartphones or tablets to search online. This is why Google now crawls the mobile version of websites before desktops when it comes to deciding how good a site is.
Because of this, it’s essential to make sure your site looks and functions properly on all devices. This includes making sure you have a responsive menu or navigation bar, images that work on all size screens, a font that is clear and easy to read on smaller screens and click through buttons that work correctly.
It’s also worth remembering that sites can function differently on different platforms, so what works on Chrome might not work the same on iOS. Make sure you test out your site on a variety of devices and platforms.
2. Unique images over stock images
You want to show off your dental lab, so why wouldn’t you use your own images? Well, sometimes you might not have the images you need to reflect a certain process or product.
Or maybe your supplier provides a number of images for you to use… think about how many other labs could be using the same ones. The more unique photography and videography you can have on your site, the better it will perform, so consider investing in some bespoke photography.
A note on the quality of the images you choose, you’d be forgiven for thinking you need to use the most high-resolution images and videos on your site but this isn’t the case.
If you’re using 4k videos and 10MB images then your website will be super slow to load, resulting in a poor customer experience.
Consider loading videos to platforms such as Vimeo or YouTube and then embedding them instead of them being hosted on your site. Images shouldn’t be over 1MB, in fact around 500KB will suffice for most sites - especially if they’re being viewed on mobiles.
3. Why should people choose you?
Simply listing your services isn’t good enough. Your website is a sales tool, you want it to work for you, which means showcasing exactly what you do, but also why and how you do it better than your competitors.
Are you award winning? Has your team got more experience? Do you invest in leading technology to set you apart from others?
Spend time considering everything that makes your dental lab different to others and highlight your strengths at every opportunity.
Remember too that people buy from people, so a good ‘meet the team’ section and professional headshots are also a great addition.
4. Collect and use testimonials
There’s no more powerful tool when it comes to marketing than the trusted words of others. Sure, you can tell everyone you’re the best, but if you have others doing this for you, then you’re winning the battle.
Testimonials can be included on your dental lab website in a number of ways; this includes plugins and APIs from third party sites such as TrustPilot or Google Reviews collected through your Google Business Profile or simply just designed into your site by your developer which you then populate manually from emails etc.
Another option is video testimonialsagain being considerate to the size of the video you upload.
5. Make contacting you easy
You don’t just want people to come onto your site - you want them to take action. This is why it’s important to include plenty of links to your contact forms.
Having a contact page in your navigation bar is a no-brainer, but make sure you link to it from every service page and at key
INSIGHT 24 I www.dentaltechnician.org.uk
the second of a series of articles, Hayley Irons shares why having a website and an online presence should be high on your list of priorities
points on your home page. It’s also good practice to have a link ‘above the fold’, that is somewhere at the top of the page that a user sees before they have to scroll. It might feel like overload, but for a new visitor to your website it’s a helpful addition and reduces their ‘decision anxiety’ over how best to contact you.
Make sure you don’t ask questions that aren’t needed - a shorter contact form will get you more conversions than one with 20 questions... especially if you’re just going to ask those questions again when you contact them.
While we’re talking about contact forms, it’s also worthwhile including hyperlinks to your contact phone number so people can call with just one click and maybe even a live or chat bot.
6. Keep your website updated
Having a website is great, but if you want it to perform well for you on the search engines, then you need to keep the site up to date and full of fresh content.
This doesn’t mean you need to keep adding services or changing your homepage copy every four weeks. Yes, you need to keep an eye on them for out-of-date regulations, advice and even staff members, but new blog content is the key here.
Having good quality, authoritative blog content that provides internal linking opportunities and a catalogue of expert advice is something Google loves.
It provides your visitors (and Google) with proof that you are experienced, trusted and knowledgeable in your field.
As well as providing your site with lots of content, you can also repurpose these blogs and promote them on social media.
7. Include case studies
Documenting the work you do and the results you deliver can’t be underestimated. Whether these take the form of written portfolios or video showcases, include a variety of examples of your work.
These can live on your blog page or even as a separate case study page on your website. You might also want to link to them from relevant service pages to add extra weight to your sales copy.
8. Don’t use jargon
Speaking of copy - don’t use jargon on your site. It can be easy to fall into the trap of using complicated phrases, long sentences and highly technical terms - especially when talking about dental work.
Take time to go back through what you’ve written to ensure it makes sense, is easy to read and understand. Shorter sentences and paragraphs, bullet points and subheadings will help break up your text and make it much easier to follow.
There we have it, 8 tips to help your dental lab website work for you. If you’d like to know more about our services and how they can help you, please get in touch with one of our team and we’ll get back to you as soon as possible.
Hayley Irons is director of HI Marketing. For more information contact 07805 506 477, hayley@hayleyironsmarketing.co.uk, or visit www.hayleyironsmarketing.co.uk
INSIGHT www.dentaltechnician.org.uk I 25
FREE VERIFIABLE ECPD
As before if you wish to submit your ECPD online it will be free of charge. Once our web designers give it the all clear there will be a small charge. This will be less than the CPD submitted by post. This offer is open to our subscribers only. To go directly to the ECPD page please go to https://dentaltechnician.org.uk/dental-technician-cpd. You will normally have one month from the date you receive your magazine before being able to submit your ECPD either online or by post. If you have any issues with the ECPD please email us cpd@dentaltechnician.org.uk
0.5HRS VERIFIABLE ECPD
LEARNING AIM
The questions are designed to help dental professionals keep up to date with best practice by reading articles in the present journal covering clinical, technical, business, personal development and related topics, and checking that this information has been retained and understood.
LEARNING OUTCOME
This quiz aims to test the reader’s understanding of the article. After reading, you should be able to answer questions related to the fabrication process, treatment, goals, model analysis, teeth setup, occlusion, and the conclusion of the case study.
CORRECT ANSWERS FROM THE JULY 2023 DT EDITION:
VERIFIABLE ECPD - AUGUST 2023
1. Your details First Name: Last Name: Title: Address:
2. Your answers. Tick the boxes you consider correct. It may be more than one.
3. Evaluation: Tell us how we are doing with your ECPD Service. All comments welcome. ..................................................................................................................................................... .....................................................................................................................................................
As of April 2016 issue ECPD will carry a charge of £10.00 per month. Or an annual fee of £99.00 if paid in advance. You can submit your answers in the following ways:
1. Via email: cpd@dentaltechnician.org.uk
2. By post to: The Dental Technician Magazine, PO Box 2279, Pulborough, RH20 9BR
Payment by cheque to: The Dental Technician Magazine Limited. Natwest Sort Code 516135 A/C No 79790852

You are required to answer at least 50% correctly for a pass. If you score below 50% you will need to re-submit your answers.
Answers will be published in the next issue of The Dental Technician. Certificates will be issued within 60 days of receipt of correct submission.
ECPD 26 I www.dentaltechnician.org.uk
Q2. C Q3.
Q4. A Q5. B Q6. C Q7.
Q8.B Q9.
Q10.
Q.11
Q.12
Q1.B
A
D
C
D
A
C
.............................................................................................................................................. ............................................................................................................................................................... Postcode: Telephone: ..................................... Email: .......................................................GDC No:
Question 1 A B C D Question 9 A B C D Question 2 A B C D Question 10 A B C D Question 3 A B C D Question 11 A B C D Question 4 A B C D Question 12 A B C D Question 5 A B C D Question 6 A B C D Question 7 A B C D Question 8 A B C D
VERIFIABLE ECPD
As you need it via the Dental Technician
Q1. What was the main challenge of the 13th International CANDULOR KunstZahnWerk Competition 2023?
A) Fabricating removable partial dentures
B) Fabricating complete dentures with an individual design
C) Fabricating dental implants
D) Fabricating fixed dental bridges
Q2. Which of the following was NOT a treatment goal for the patient in the case study?
A) Better retention and chewing performance
B) Improved phonation and speech function
C) Straightening of the maxillary anterior teeth
D) Reduction of the ‘pointed’ appearance of the chin
Q3. How was the setup line determined during the model analysis?
A) Using a laser beam set at a 90-degree angle
B) Using cross-section measuring instruments
C) By mapping and recording every cross-section
D) By drawing in the median lines and alveolar ridge centers
Q4. Which occlusion concept was applied for setting up the posterior teeth?
A) Tooth-to-tooth occlusion
B) Cusp-to-fossa occlusion
C) Bilateral balancing occlusion
D) Canine-guided occlusion
Q5. What material was used for characterisation of the dentures instead of composite?
A) Gold
B) PMMA
C) Zirconia
D) Acrylic
Q6. What was the purpose of elevating the bite in the incisal area by 1mm?
A) To improve aesthetics
B) To achieve chewing performance
C) To achieve better phonation
D) To enhance denture retention
Q7. What was the primary focus of the treatment regarding the anterior teeth in the maxilla and mandible?
A) Improving phonation
B) Achieving optimal occlusion
C) Making the teeth wider
D) Making the teeth more visible
Q8. Which technique was used to ensure bilateral balancing during laterotrusion and mediotrusion?
A) Tooth-to-tooth occlusion
B) Cusp-to-fossa occlusion
C) Balancing occlusion
D) Sliding contacts
Q9. According to the article, what role do innovative, high-quality materials play in the conventional work-flow?
A) They hinder the fabrication process
B) They make the process faster
C) They improve the outcome’s quality and aesthetics
D) They eliminate the need for manual skills
Q10. What was the focus of the presented method of fabrication in the case study?
A) Digital workflows
B) Achieving the fastest results
C) Eliminating the need for denture fabrication
D) Meeting functional and aesthetic requirements
Q11. How were the posterior teeth set up in the mandible according to the tooth-to-tooth occlusion concept?
A) Central fissure on setup line
B) Buccal relief of the setup
C) Labial incisal edge contact
D) Maxillary premolar cusps in fossa
Q12. What did the author believe would continue to drive the demand for handmade dentures in the future?
A) Technological advancements
B) Lower cost
C) Patient preference for individuality and beauty
D) Faster fabrication process
You are required to answer at least 50% correctly for a pass. If you score below 50% you will need to re-submit your answers. Answers will be published in the next issue of The Dental Technician magazine. Certificates will be issued within 60 days of receipt of correct submission. PAYMENT
ECPD www.dentaltechnician.org.uk I 27
CAN SUBMIT YOUR ANSWERS IN THE FOLLOWING WAYS:
or by
to: The Dental Technician Magazine, PO Box 2279, Pulborough, RH20 9BR.
YOU
Via email: cpd@dentaltechnician.org.uk
post
BY CHEQUE TO:
Dental Technician Magazine Limited. NatWest Sort Code 516135 A/C No 79790852
The
THIS MONTH’S CPD QUESTIONS ARE ARE FOCUSED ON FULL DENTURES AT THE HIGHEST AESTHETIC LEVEL – SKENDER RAMADANI
STREAMLINING DENTAL LABORATORIES WITH 3D PRINTING


Today, dental laboratories can develop realistic and comfortable implants for patients using a range of manufacturing methods. AM systems are one example of such innovation. But is this technology worth the investment?
TRACEABILITY
Digitalising workflows saves time, but also improves traceability. Sending physical parts to and from the laboratory introduces risk of losing, deforming or breaking the impression in transit. For example, a wax impression is susceptible to damage from temperature changes, pressure and handling.
SPEED
Traditional casting and moulding takes time. Dentists take a wax impression of a patient’s mouth and send it to a dental lab. The technician makes a mould from the impression, fills it with gypsum, cures the implant and sends it back to the patientwhich can take days. Casting creates a viable and convincing implant, but, unless the initial impression is accurate, the implant may not fit the patient. Poor tray selection, surface contamination or the patient moving too much during the process are just some of the factors that impact accuracy.
With 3D scanning, dentists can quickly take accurate images of the patient’s mouth and immediately email it to the laboratory, removing the need for wax casts. Instead of creating a mould, technicians upload and convert the scan into a computer aided design (CAD) file for customisation. Once designed, a resin 3D printer creates the part layer by layer in a few minutes or hours.

Instead of rooting around for models and printed files, 3D printing gives technicians a digital record of the entire process. If there are any issues, technicians simply return to the patient files or part design to investigate.
CUSTOMISATION
Since they first became available on the NHS over 75 years ago, dental laboratories have made significant improvements to deliver high quality dentures to patients. Advances in 3D scanning and additive manufacturing (AM), for example, can produce supportive, comfortable implants for patients. So, is a 3D printer a good investment in your dental laboratory? Here Amish Jani, sales specialist at UK provider of Stratasys, One Click Metal and XJet 3D printing solutions Tri-Tech 3D, explores. For more information contact 01782 814551, info@tritech3d.co.uk, or visit www.tritech3d.co.uk/
Gypsum, a mineral-based material commonly used in dental implant models, can be brittle. Biocompatible resin, on the other hand, is a synthetic and lightweight yet durable material, which, when used in an AM system, enables laboratories to produce dental models and replicas that could withstand the force of biting and chewing. Resin can also be coloured to match natural teeth, rather than the narrow range of white colours available in other materials, creating more realistic models.
When printing in resin, manufacturers can often use one of two methodspolyjet or stereolithography/digital light processing (SLA/DLP). However, in dental applications polyjet is the preferred method. Some polyjet printers, for example the Stratys J5 Dentajet, are built especially for the dental industry. This technology jets droplets of material layer on layer until it forms the part, curing it with a UV laser after each layer. Unlike with SLA/DLP, technicians can use multiple resin canisters at once - for example, if creating a model of a jaw with gingival mass and the implant, users can print each part in different colours on the same build.
Dental procedures may have come a long way since the first century but is 3D printing the answer? What dental laboratory wants accurate and rapid production when they can keep slow and inefficient casting methods that take days to complete?
DENTAL TECHNOLOGY 28 I www.dentaltechnician.org.uk

PLANNING FOR A BRILLIANT RESTORATION L
ong before a finalised denture or crown can be created, dental technicians and clinicians must collaborate in an extensive process of treatment planning. There are a variety of methods used depending on the desired outcome, but a reliable procedure still used today is the diagnostic wax-up.
Technicians make use of this creation both before and during treatment to create brilliant outcomes for their clients and, eventually, grateful patients. It’s worth considering why it continues to be so vital, and how a diagnostic wax-up can be optimised to generate dependable results.
AN EFFECTIVE PREVIEW
By Alistair Mayoh, marketing director at Kemdent

A diagnostic wax-up is key in the development of cosmetically-optimised results in dentistry, for example the production of veneers. There has been a recent uptick in demand for restorations of this manner, led in part by the ‘Zoom boom’ – where individuals are seeking out cometic work after years of analysing their reflections in online video calls.
Physical diagnostic wax-ups can improve the communication of a desired treatment between technicians and clinicians, whilst identifying an effective plan to achieve these aesthetically-driven outcomes.
There are generally considered to be two main approaches for a diagnostic wax-up. In the first method a stone cast of the existing dentition is modified in order to create an ideal contour, with the wax then added in the newly-made space around it. The second is a purely additive method; when the teeth are already in an ideal position, wax is simply shaped in the already existing spaces, without taking away from the preestablished structures.

Choosing between each process may depend on the availability of space in the dentition or patient preference. If an individual doesn’t wish to undergo surgery, for example, the additive method takes on a less invasive and, in turn, more ideal approach.
When correctly applied, both techniques could create an effective and tactile model for the final look of a patient’s new teeth.
CLINICIAN COMMUNICATION
As an essential component in the treatment planning process, technicians must ensure that accuracy is optimised before a wax-up is even created. After all, the model’s creation will rely intrinsically upon the laboratory prescription detailed by a clinician. Creating an open and communicative relationship with clients could help technicians establish the complete information they need when designing a wax-up.
As well as pre-establishing these needs, it’s important to communicate if and when they aren’t met fully. Some missing information may be assumed,
30 I www.dentaltechnician.org.uk
DENTAL TECHNOLOGY
but without directly checking with the initial clinician there is always an element of uncertainty. The most minor and seemingly insignificant assumptions could result in a poor wax-up – wasting both time and money.
Diagnostic wax-ups are used as an effective communication tool between clinician and technician, but they can also be presented to the patient. They are, of course, the individual receiving the eventual cosmetic treatment. Seeking their opinions in the wax-up stage is essential to working towards a final restoration that everyone involved is confident with. This relies once again on the relationship between the technician and the clinician – the latter commonly acting as an intermediary of the patient’s preferences and requirements.
CREATING AN ACCURATE MODEL
Whether the agreed approach is a reductive or an additive method, or a bit of both, it’s important that technicians ensure their diagnostic wax-up work is accurate and encourages ideal aesthetics. This requires technical skill to successfully create a visually appealing and mechanically-functional dentition.
The necessary psychomotor skills must be trained over time to allow technicians to fabricate such intricate models with accuracy. An effective strategy for developing these skills is dental carving, where technicians recreate dental morphological features in wax. By applying an existing knowledge of the dentition’s structure and that of single teeth to this practice, the techniques can be honed in order to consistently create reliable diagnostic wax-ups.
For many dental technician students, this will be taught early in their course, which could pose a challenge for the retention of the required dexterity. Effective and regular practice allows professionals to maintain and improve upon their technique and knowledge, which could make the difference when designing and crafting a diagnostic wax-up for a client.
Professionals and students can utilise these skills effectively with the Kemdent® Carving Blocks, specially designed for technicians. The small wax blocks are suitable for real-to-life tooth modelling and carving other models. They are also prepared for student use, allowing for the development of the finer psychomotor skills needed for the efficient and accurate creation of a diagnostic wax-up.
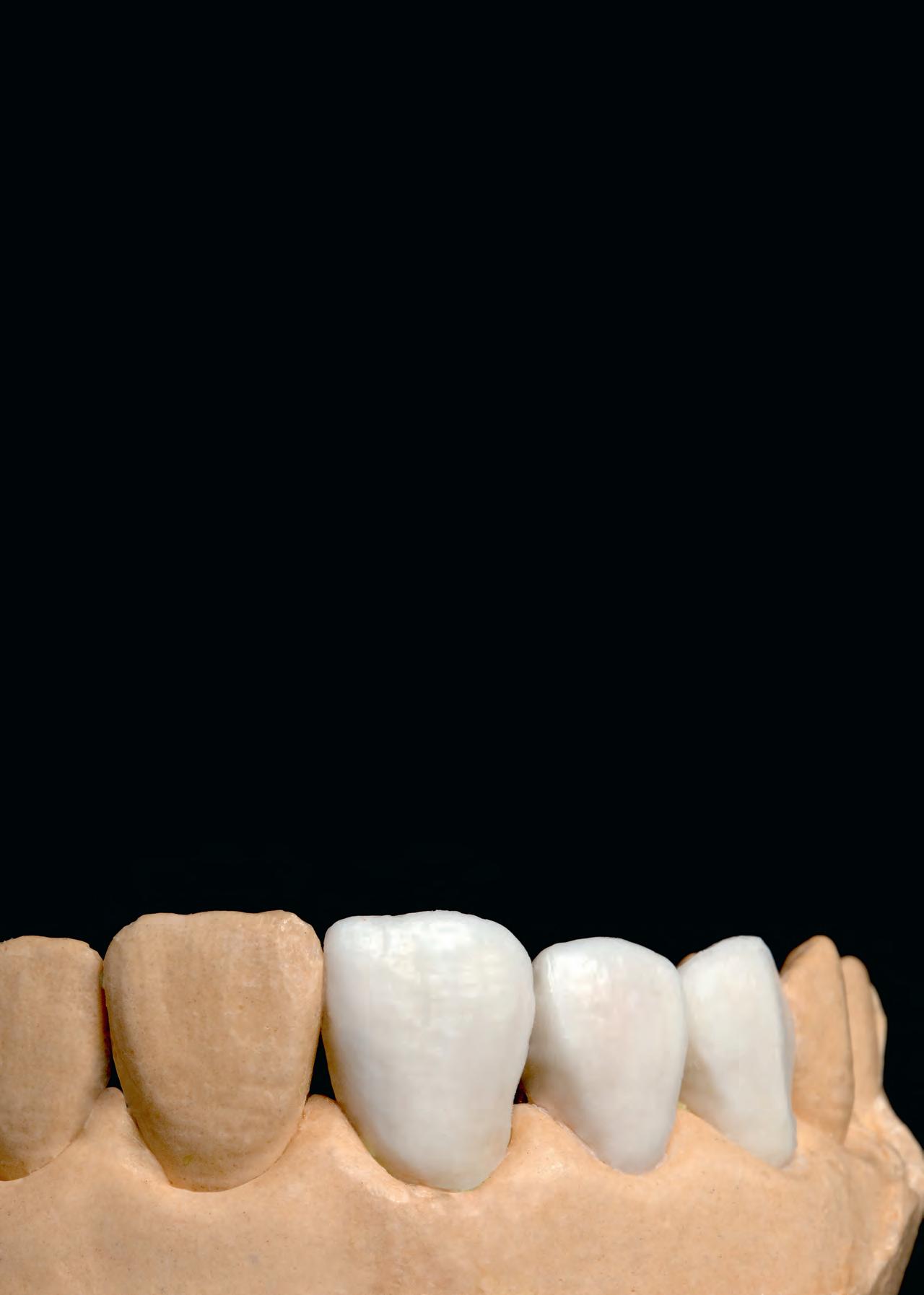
A diagnostic wax-up stands to be one of the most effective tools in a technician’s arsenal when working with clients. By utilising clear and consistent communication with a clinician, alongside some honed psychomotor skills, technicians can reliably create models that drive the outcome of a brilliantly aesthetic dentition.
REFERENCES
For a full list of references, please email editor@dentaltechnician.org.uk
For more information about the leading solutions available from Kemdent, please visit www.kemdent. co.uk or call 01793 770 256.
www.dentaltechnician.org.uk I 31
DENTAL TECHNOLOGY
TAKING CAD/CAM TECHNOLOGY TO THE NEXT LEVEL
Combining analogue and digital skills widens your scope of practice and produces exceptional results
The journey to take dental into a digital age has created an untold number of fresh ideas and solutions, making treatments faster and more efficient with each step. In turn, CAD/CAM software has become an essential tool in many dental laboratories and practices, simplifying processes and improving their outcomes.
Employing CAD/CAM technology in the laboratory is often a steep investment, so it’s essential to maximise its potential at every possible moment. This could mean investing in quality materials and optimising communication between professionals, but it begins with the individual. Technicians working with the technology regularly shouldn’t simply understand it, but realise its myriad opportunities to change their workflows.
WIDENING KNOWLEDGE
In many cases, digital dentistry can improve upon the accuracy and efficacy once offered by analogue techniques, some labs have even been established on the premise that they only offer digital solutions as a result. However, the increased presence of CAD/ CAM software in everyday dentistry doesn’t diminish the importance of an experienced and knowledgeable dental technician. There are many tasks, like creating highly aesthetic, hand finished restorations, that computer programs cannot replicate.
Digital workflows require fresh skills that adapt to the new ways of designing and manufacturing restorations. These new skills are mainly an understanding of the software and any operating intricacies, but experience of the analogue processes is often important to ensure the safest and most effective results for the patient. Technicians can develop their digital capabilities through a variety of courses. Most
of the training for UK technicians is companyled, which allows for an attentive focus on the specific systems used within a laboratory.

Seeking out external sources of training could update technicians on the best and latest uses for CAD/CAM technology, with a wider scope to the general field – perhaps generating new uses of the technology previously unthought of for their lab’s software.

THE IMPORTANCE OF COMMUNICATION
The digital process doesn’t begin and end at the laboratory. The larger system requires a variety of professionals including technicians, dentists, dental hygienists and specialists to lean on each other’s expertise. The key word here is communication. By streamlining the sharing of information between professionals, technicians can produce restorations sooner, and to a higher level of accuracy.
DENTAL TECHNOLOGY 32 I www.dentaltechnician.org.uk
Nearly nine in ten practitioners in the UK are convinced that CAD/CAM technology optimises communication. By using imagery and intraoral scans, practitioners can offer an in-depth and visualised insight that can be worked on digitally by the technician. This could be more useful than a physical impression, as a dentist can easily include any additional details that they feel are important to note, and have a single stream of communication in one easy to track platform. By removing transport times for physical products, the lab can also deliver a quicker turnaround time for the final restoration.

One study found that around half of dentists interviewed had been contacted by a technician requiring extra information to supplement what they initially sent. It’s a familiar feeling, and it’s safer to triple check and achieve a brilliant restoration first time than misjudge values and end up with an unhappy patient and remakes. By establishing information that a technician requires beforehand, and employing software that aims to gather it completely, the CAD/CAM process can help breed success day in, day out.
CREATING EXCEPTIONAL RESTORATIONS
The main purpose of CAD/CAM software
is to enhance the ability to reach a patient’s outcome sooner, with assurance of a quality restoration. This could mean replacing a lost tooth in a patient’s aesthetic zone sooner, bringing back confidence in a smile, or restoring the bite function that a patient sorely missed. However, it isn’t possible without the right physical components supporting the digital process.
When compared to conventionally fabricated restorations, CAD/CAM solutions can offer superior mechanical and physical properties, such as an enhanced accuracy of fit, less movement and increased toughness. By working with more precise designs offered by digital scanning, technicians can better judge the necessary components that form the overall implant structure, from the implant and framework, down to the abutment.
It feels trite to say that no two restorations are the same. Whether a single-tooth, bridge or full-denture solution, the angles and spaces will differ greatly ,and the patient’s oral health will vary too. It’s therefore important for technicians to ensure that they have an array of equipment at their disposal, with differing applications that fit seamlessly into a CAD/ CAM workflow, whilst accommodating for the unique challenges each case presents.
Maxillofacial Prosthetic Rehabilitation



For an extensive range of highly-precise and economical solutions, technicians should consider the Multi-Platform System (MPS) from Medentika®. The collection of expertly designed abutments and components features specially designed options for use alongside CAD/CAM technology. MPS products are compatible with all major implant systems that are on the market for an immediate impact on your workflows.
Production in the dental laboratory hasn’t been the same since CAD/CAM technology was first used in 1985. Its developments over time will only continue, providing innovative solutions in the years to come. With proactive technicians who keep up with the latest techniques and benefits of the workflow, and optimise it alongside the latest and most effective implant components, patients can count on ever-improving restorations in the years to come.
REFERENCES
For full list of references, please email editor@dentaltechnician.org.uk
For more information, please visit https://www.straumann.com/ medentika/us/en/dentistry.html
Develop skills in the treatment of patients who require prosthetic facial rehabilitation.


Designed for maxillofacial prosthetists, technologists and prosthodontists to:







• Learn to use cutting-edge digital technology for intra and extra-oral prosthetic facial rehabilitation in clinical practice
• Develop technical skills and higher standards of clinical practice.
• Internationally renowned centre of excellence for teaching and research.









• Pioneers of distance learning in dentistry with over 20 years’ experience.
• Intensive face-to-face training blocks, teaching theory and best clinical practice.
• Teaching team of world experts led by Professor Trevor Coward
• Delivered primarily online, the course provides 20 days of intensive teaching and practical training at Rangoonwala College of Dental Sciences and Research Centre, Pune, India.
• Study and practice a broad range of treatments for the replacement of missing hard and soft tissues, using both traditional and advanced digital technologies.
Applications open for January 2024 start. Apply by 25 October 2023.
Find out more:
Visit kcl.ac.uk/mfpr Email distancedentistry@kcl.ac.uk
DENTAL TECHNOLOGY www.dentaltechnician.org.uk I 33
MSc Distance Learning | Three years | Part-time
CREATECH MEDICAL SURVIVE AND THRIVE WITH A FLEXIBLE APPROACH
w Createch Medical, the dental engineering experts from global powerhouse the Straumann Group, provides a direct-to-lab design and milling service to produce high-quality CAD/CAM dental framework solutions compatible with over 600 implant systems.
Createch Medical has its origins in the aeronautical industry; credentials which are reflected in its high-precision measuring equipment, continuous five-axis milling centres and strictly controlled manufacturing processes.
All Createch Medical implant-supported prostheses are high-resistence structures produced using UNE-EN ISO (European standard) certified materials. Every framework manufactured by Createch Medical is proudly covered by the Createch Excellence 10-year warranty.
Outsourcing key elements of your dental laboratory service to a carefully selected third party means you can adjust your operational processes as and when you need to, while continuing to provide a premium service to your dentists.
Find out more about the Createch Medical direct-to-lab design and milling service today.
Register for your account with Createch Medical at http://www.createchmedical.com/en/file-sending/login-registro/ For more information on the Createch Medical direct-to-lab milling service from the Straumann Group, visit https://www.straumann.com/ gb/en/dental-professionals/products-and-solutions/implant-borne-prosthetics/products/createch-medical.html


KEMDENT POLISH UP ON BRIGHT RESTORATIONS
w A natural-looking restoration with a brilliant polish guarantees patients go home smiling. With the wide range of polishing discs available from Kemdent, your lab can produce a bright finish, every time.
The Paper Polishing Discs from Kemdent are available with a pinhole or

metal centre, to seamlessly fit with your lab’s tools, and are designed for durability and longevity for sustained brilliance.
The discs are suitable for polishing a wide array of materials, with abrasive grades ranging from X Fine to X Coarse to create the consistent shine you desire, no matter the medium.
Work effectively in wet and dry conditions with Kemdent’s Ruwa™ Polishing Discs, specially purposed to be moisture proof for an adaptable approach.
Get the most out of your lab’s polishing with reliable solutions from Kemdent, contact the team to find out more.
For more information about the leading solutions available from Kemdent, please visit www.kemdent.co.uk or call 01793 770 256
MARKETPLACE 34 I www.dentaltechnician.org.uk



































Head Office & Showroom Trident Court, 1 Oakcroft Road, Chessington, Surrey KT9 1BD T: 0800 228 9828 E: info@blueprintdental.co.uk W: blueprintdental.co.uk Design Build Project Management Installation & Commissioning Training End-to-end expertise for your digital workflow Turnkey Solutions for Digital Dentistry Unlock your Digital Lab Nexa3D XiP Desktop Resin 3D Printer • Ultra fast • Wide range of validated materials • Affordable desktop price Tecno-Gaz G5 Milling Machine • Specifically developed for digital dental labs • Wide range of prosthetic products • Free standing
EVERYONE deserves to smile
GC takes new post-earthquake aid initiatives to support affected dentists

Tn the aftermath of the devastating earthquake that struck Turkey and Syria on 6 February 2023, GC has extended its support to the affected communities. Mr Makoto Nakao, chairman of GC International, Mrs Makiko Nakao, president of Foundation Nakao for Worldwide Oral Health and Mr Josef Richter, COO and president of GC Europe recently undertook a courtesy visit to Turkey, reaffirming GC’s unwavering commitment to stand by those in times of crisis and to fulfill its corporate social responsibilities.
On 3 July, during their visit, a product donation voucher of €100,000 was delivered to Mr Tarik Ismen, president of the Turkish Dentistry Association, who expressed his deep appreciation towards GC’s aid initiatives.

The Turkish Dental Trade and Businessmen Association (DİŞSIAD), representing 250 dental companies in Turkey, was also visited for a report on the donations. On this occasion, Mr Erkan Ucar, chairman of DİŞSIAD, thanked GC as the first dental manufacturer to donate and presented a Letter of Appreciation.
On 7 July, Ms Selen Hazne, country manager of GC Turkey, visited the province of Hatay, which was most affected by the earthquake. Prefabricated clinics were built for dentists whose clinics were destroyed, and those that could were being repaired. The first sample donation package was presented to the chairman of the Hatay Dental Chamber, Mr Nebil Seyfettin.
‘I could feel the energy of the people, determined to recover from this natural disaster,’ Ms Hazne reported. ‘We aim to help the dentists here where we can, so they can regain stability and resume their daily lives as much as possible’.
The shipments of the donations were planned to be completed on 20 July with individual packages for the designated clinicians.
TOP ROW LEFT: (L TO R) Mr Makoto Nakao, chairman GC International AG, Mr Joseph Richter, COO and president of GC Europe, and Mr Tarik Ismen, president of the Turkish Dental Association


TOP ROW RIGHT: Mr Nebil Seyfettin, chairman of the Hatay Dental Chamber welcomes Ms Selen Hazne, country manager GC Turkey in front of one of the prefabricated dental clinics.
ABOVE: (L TO R) Mr İsa Aydın, treasurer of the Turkish Dental Trade and Businessmen Association (DİŞSIAD), Ms Selen Hazne, country manager GC Turkey, Mr Erkan Uçar, chairman of DİŞSIAD, Mr Josef Richter, and Mrs Makiko Nakao, president of Foundation Nakao for Worldwide Oral Health
NEWS 36 I www.dentaltechnician.org.uk
I info.gce@gc.dental
https://www.gc.dental/europe
ZIRKONZAHN M6 TELESKOPER BLANK CHANGER MILLING UNIT
With extra-large Teleskoper Orbit (⌀ 125 mm) and automatic blank changer (x16 or 64, upgradable)
w With the new M6 Teleskoper Blank Changer milling unit, Zirkonzahn automates processes, accelerates procedures and increases the productivity of the dental workflow.

The 5+1 axis simultaneous milling unit is equipped with a storage for 16 or 64 blanks (upgradable up to 150-200) as well as a Blank Changer that allows material blanks to be transferred autonomously from the storage to the orbit.
Once the structure is milled, the blanks are reinserted again in their correct place in the storage. This means that restorations made of different dental materials, colours and heights can now be designed fully automatically without any manual intermediate steps. The wet and dry processing function permits the milling of all common soft and hard dental materials.
The built-in Teleskoper Orbit M6 allows the processing of material blanks with a diameter of 95mm, 98mm, 106mm and 125mm. Thanks to special holders, also glass-ceramic blanks, Raw-Abutment® blanks and zirconia blanks (size 1) can be milled. In addition, the already known, innovative Teleskoper functions (adjustment of the friction, Double Milling, Stop & Go) can be used with the M6 milling unit.
Zirkonzahn equips the M6 milling unit with the new Performance Spindle M6 by default. Thanks to a specially developed Permanent Magnet Synchronous Motor (PMSM) which is optimally adapted to the milling unit, this spindle can reach a maximum torque of 200 Ncm at speeds of 6.000 to 50.000 rpm with a peak power of 2.5 kW.
In addition, the milling unit is equipped with a contamination-protected tool chamber which is separate from the milling chamber and features an automatic tool changer function. The two tool magazines with 30 slots each ensure a safe and tidy storage of up to 60 milling burs. The tools are automatically checked for type or damage before and after each milling process.
MARKETPLACE www.dentaltechnician.org.uk I 37
For more information: www.zirkonzahn.com, +39 0474 066 660, info@zirkonzahn.com
VITA CERAMICS
POLISHING SET FOR OPTIMISED CERAMIC POLISHING
w With the new two-step VITA CERAMICS Polishing Set, VITA Zahnfabrik is continuing the development of the polishing process for ceramic restoration materials. Special features of the set include: Durability with optimised performance, suitability for any type of ceramic.
Ceramic polishing couldn’t be simpler One for all: With the VITA CERAMICS Polishing Set, users no longer have to resort to stocking several sets for polishing different ceramics. The new polishing set from VITA can now be used with any ceramic.
Further advantages of the VITA CERAMICS Polishing Set include: The high diamond content in the pre-polishers increases durability and performance. Additional slats on the Technical Brush increase durability and improve the polishing performance, especially on occlusal surfaces with pronounced fissures. A large cup in the Clinical Set ensures a long service life.
Versatility
Overall, the VITA CERAMICS Polishing Set consists of three polishers for pre-polishing and for high-gloss polishing. The following product variants are available:
• Technical Set for extraoral use with the
For more information the VITA CERAMICS Polishing Set visit www.vita-zahnfabrik.com/polishing
WELCOME TO MEDENTIKA®

A HIGH-GRADE DENTAL IMPLANT PROSTHETIC PORTFOLIO
w The Straumann Group is proud to offer clinicians Medentika®, a flexible range of prosthetics, expertly engineered and made in Germany.
The Medentika ® range includes the Multi-Platform Systems (MPS), comprised of abutments and restorative components that are compatible with all major implant systems available on the market.

With an excellent price-performance ratio, Medentika® solutions are dependable and uncompromising, but are also economical.
The clear design means you receive the same prosthetic interface for all series; there are also unique parts (Novaloc®/ Optiloc®) that extend the range.
With their passion for perfection and precision, you can depend on Medentika ® They also provide an up to a lifetime guarantee, for total peace of mind.
handpiece, can be supplemented with the diamond polishing paste VITA Polish Cera for extraoral high-gloss polishing

• Clinical Set (sterilisation possible) for intraoral used with an angle piece
• Refill packs are available for all polishers.
For more information, visit the website today: https://www.straumann.com/medentika/en/professionals.html
MARKETPLACE 38 I www.dentaltechnician.org.uk


www.dentaltechnician.org.uk I 39 CONTACT: T: 01372 897462 I E: sales@dentaltechnician.org.uk TO ADVERTISE ON THIS CLASSIFEDS PAGE CLASSIFIEDS
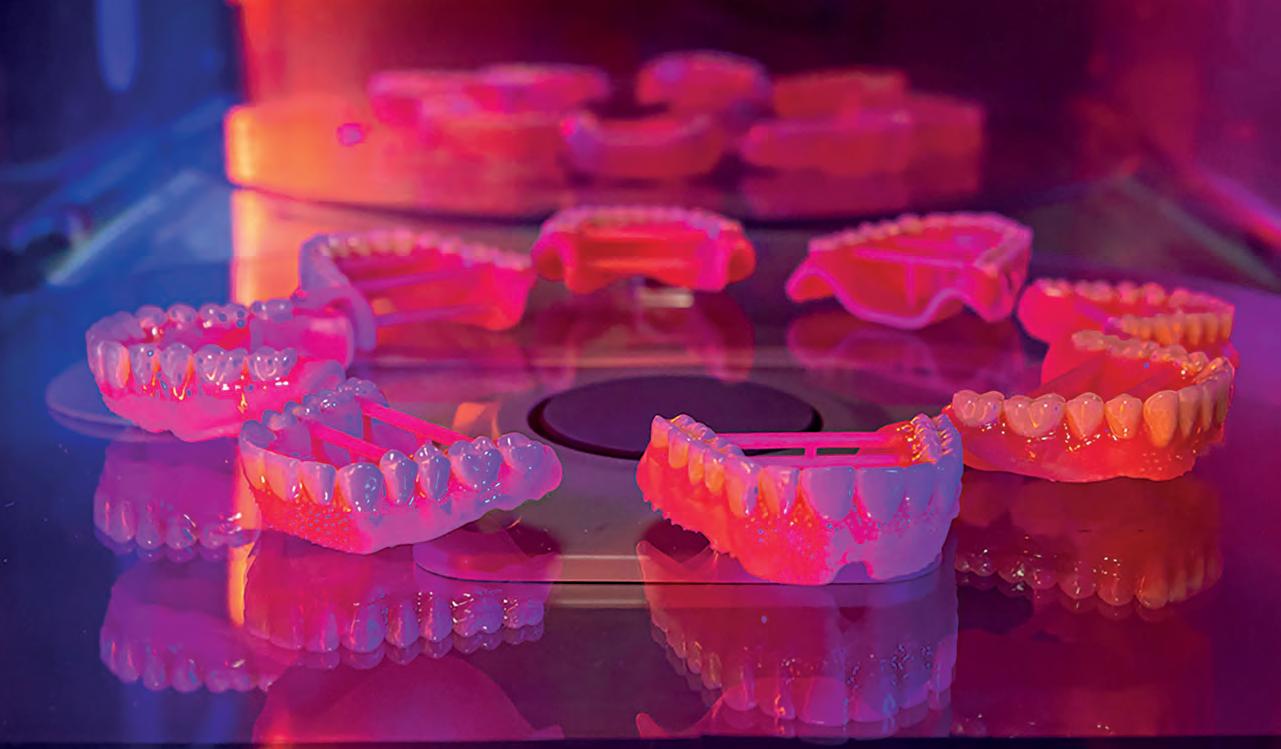





CONFIDENCE FOR DIGITAL EVOLUTION The Lucitone Digital Print Denture™ System allows you to scale up production and drive profitability, without sacrificing the material standards established with traditional products. 30% of the global population aged 65 years and older suffer from edentulism1 50% decline in labs able to meet the growing demand. Labs are declining and consolidating3 global older population is driving increased denture demands at labs2 703M Visit our website for more information at http://www.dentsplysirona.com/lucitonedigitalprint Design Try-in/Teeth Fuse Cure Print Denture Base 1 U.S. Market Report Suite for Overdentures and Implant Bridges, iData Research, June 2018:29. 2 World Population Ageing 2019, Department of Economic and Social Affairs, 2019:2 3 AEGIS Communications, By Jason Mazda. “The Effect of Consolidation: Inside Dental Technology.” October 2019 | Inside Dental Technology, 1 Oct. 2019 Dentsply Sirona | 1301 Smile Way | York, PA 17404 | 800-243-1942 | dentsplysirona.com ©2023 Dentsply Sirona Inc. All rights reserved. Form No. DP-0000623 Rev. 0 (01/2023)
