This month, in honor of National Immunization Awareness Month, we are diving into the issue from different perspectives. You will find our first article is on childhood immunizations and we include another piece on the issue of vaccine hesitancy. In addition we present an article on using ChatGPT for data analysis.
We continue to provide you with our popular monthly crossword feature, Notes on People, an overview of what we read from the public media, and a listing of upcoming epidemiology events.
Finally, as we move into Fall hiring season, don't miss the Job Bank offerings this month. We have some fantastic opportunities advertised both here and on our website. Do you have a job opening to advertise? Check out our Fall Hiring Sale in the Marketplace section!
In This Issue
The Lifesaving Investment in Childhood Vaccines
Author: Madeline Roberts, PhD, MPH
A recent analysis of the benefit-cost ratios for the Vaccines for Children Program found that the program’s routine childhood vaccines saved an estimated $540 billion in direct costs and $2.7 trillion in societal costs. Vaccines for Children was established by Congress and is a federally funded program which covers child vaccine costs for families that cannot afford them. The analysis reviewed routine child vaccines for children age 6 and under from 1994-2023.
The Vaccines for Children program made a significant public health contribution, with approximately 117 million children receiving vaccines, leading to the prevention of an estimated 508 million illnesses, 32 million hospitalizations, and 1,129,000 deaths. This widespread immunization effort resulted in substantial economic savings. From a payer standpoint, there was an estimated savings of $540 billion in direct medical and non-medical costs, such as the cost of treating initial infections. There was an additional estimated savings of $2.7 trillion in societal costs, which includes productivity losses from premature death and disability, and also opportunity costs for parent work absences attributable to caring for their sick children.
This analysis also highlights The Vaccines for Children program's role in maintaining high vaccination coverage and promoting health equity, emphasizing the program’s importance in reducing barriers to access for vulnerable populations.
The report underscores the cost-effectiveness
of routine childhood immunizations, revealing that for every dollar spent, society saves approximately $11. Although the analysis excludes certain vaccines like influenza and COVID-19, it demonstrates that immunization remains a crucial public health intervention. The VFC program, by covering nearly half of the nation's childhood vaccines at discounted prices, has made a substantial impact, particularly during challenges like the COVID-19 pandemic. Despite some limitations, the findings strongly support the continued investment in childhood immunization as a vital strategy for improving public health and ensuring long-term economic savings.
Unfortunately, the WHO recently reported that childhood vaccination rates stagnated globally in 2023. In 2023, the global childhood vaccination rate for measles was 83% for an initial dose and 74% for a second dose, neither of which reaches the 95% threshold for outbreak prevention. More concerning, the number of “zero-dose” children (those not receiving even a single dose) for the diphtheria, tetanus and pertussis (DTP) vaccine increased in 2023; the number of children receiving three doses remained stagnant.
The majority of children not receiving vaccines live in vulnerable areas or areas of active conflict, and the WHO cited “ongoing challenges with disruptions in healthcare services, logistical challenges, vaccine hesitancy and inequities in access to services” as contributing factors to globally stagnant vaccine uptake.
- Childhood cont'd on page 3
The United States was declared measles-free in 2000, but routine measles vaccination rates began to languish around 2010, which paved the way for more frequent outbreaks in recent years. This has been of great concern to epidemiologists and public health workers, and is perhaps best captured by this quote from WHO Director-General Dr Tedros Adhanom Ghebreyesus: “Measles outbreaks are the canary in the coalmine, exposing and exploiting gaps in immunization and hitting the most vulnerable first. This is a solvable problem. Measles vaccine is cheap and can be delivered even in the most difficult places.” As an example of this, a multi-country study found that underweight and stunting were associated with incomplete vaccination schedules.
Similarly, a underweight and stunting were associated with incomplete vaccination schedules. Similarly, a 2022 study of the association between nutritional status and full vaccination coverage in Thai children under age 5 found that children with incomplete immunization status had higher odds of being stunted, wasted, or overweight.
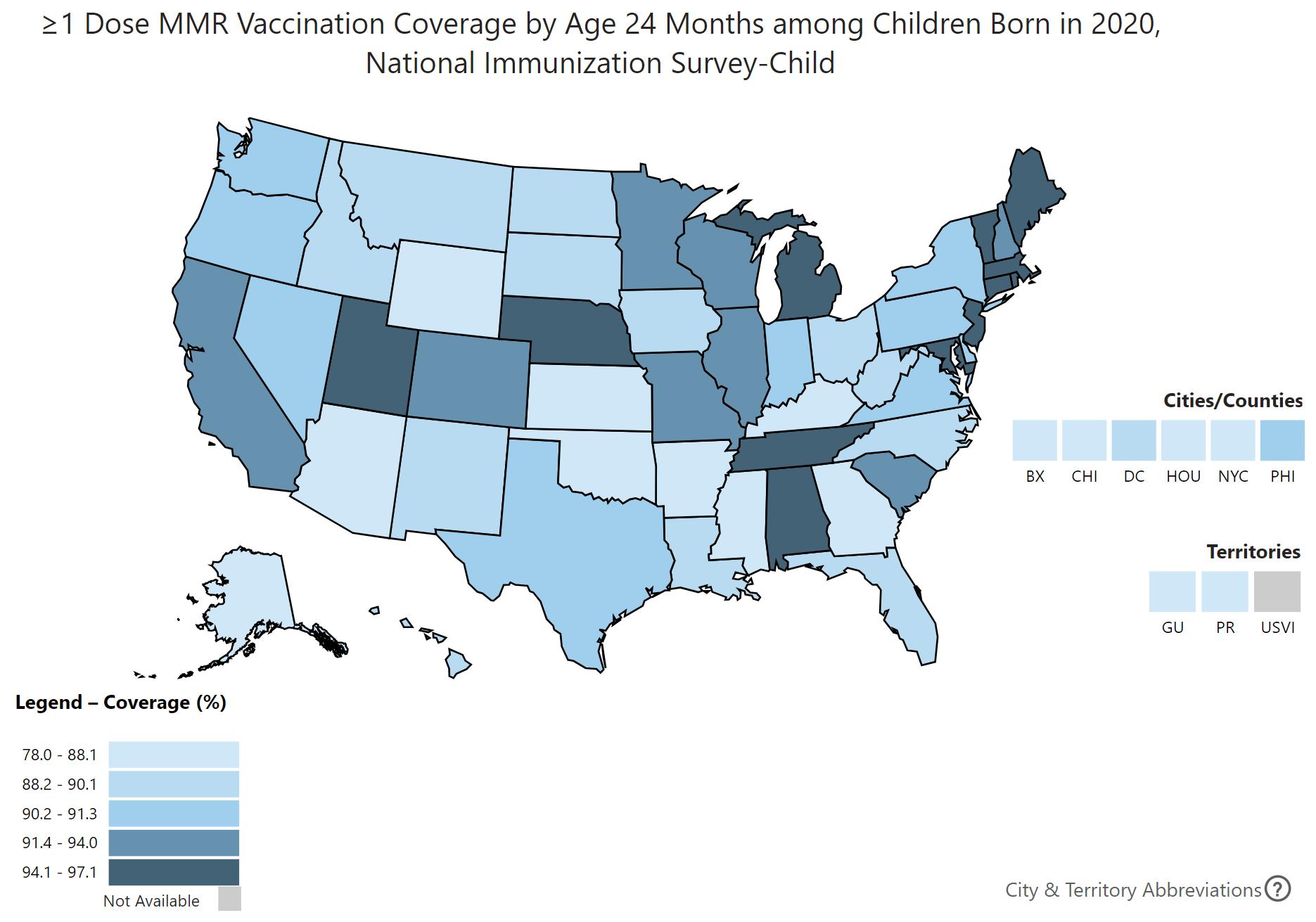
The CDC created VaxView, an interactive data visualization tool to assess various measures of vaccination coverage across the country. For example, below is a map showing U.S. vaccination coverage for children receiving one or more doses of the MMR vaccine for children born in 2020.
Prepared by EpiMonitor using the CDC ChildVaxView: https://www.cdc.gov/vaccines/imz-managers/coverage/childvaxview/interactive-reports/index.html
If decreased vaccination coverage is the blinking light on the dash, an initial indicator of potential failure, there are multiple public health issues that may be signaling: vaccine hesitancy fueled by misinformation, which weakens trust in public health and science; scientific communication and education gaps; inequities in healthcare access, particularly in marginalized communities. The Vaccines for Children Program has demonstrated remarkable health and economic benefits, underscoring the critical role of routine
childhood immunizations in public health. However, the stagnation in global vaccination rates and the resurgence of diseases like measles highlight the vulnerabilities in immunization delivery, particularly in underserved populations. These trends serve as a warning of potential public health crises if vaccine coverage continues to decline. Ensuring sustained investment in vaccination programs and addressing barriers to access are essential to prevent the erosion of these hard-won gains and to protect future generations. ■
Vaccine Hesitant:
Author: Katelyn Jetelina, PhD, MPH
NOTE: This article was originally printed in our sister publication Your Local Epidemiologist (YLE) on July 22, 2024
How can you help?
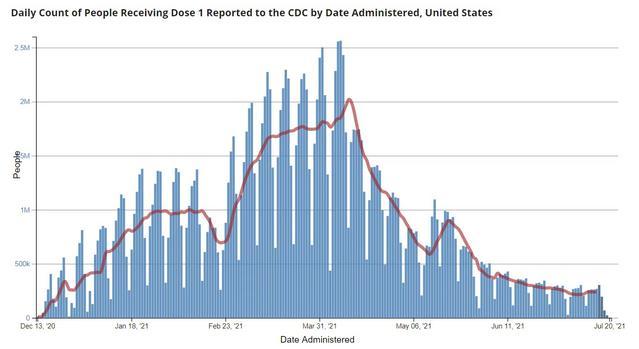
In the United States, 65.7% of 12+ population has at least one vaccine. Daily vaccination rates peaked April 8 (with 2.56 million people per day) and have slowly and painfully declined since (with 268,000 people on July 16).
Who are the 34.3% eligible but not vaccinated?
Several non-profits (looking at you Kaiser Family Foundation and de Beaumont) have hustled to get a great population-level perspective of COVID19 vaccine hesitancy in the United States. This critical data can be used to improve vaccine acceptance.
According to the latest reports (here, here, and here), unvaccinated people are more likely to be:
Younger (18-49)
o Adolescents (largely because of their parents) Less educated
Republican
Persons of color
Uninsured
-
So, how can we reach them? Families and friends.
More and more evidence shows that family and friends are the most powerful motivator for vaccine acceptance. A report found that 17% of all previously vaccine hesitant were persuaded to get vaccinated by a family member. 10% said they were persuaded by their own healthcare provider and 5% said they were persuaded by a close friend, co-worker, or classmate.
What do we talk about?
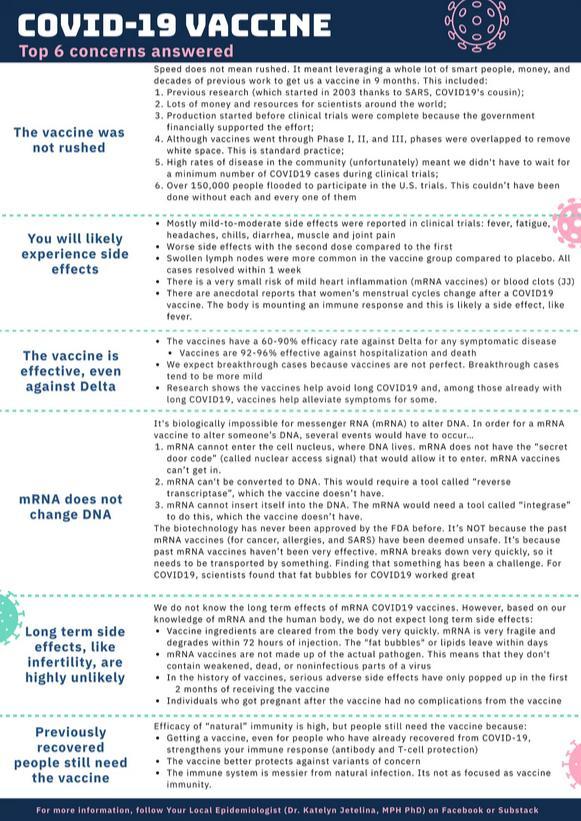
Talk openly about side effects
When asked about the biggest concern of the COVID-19 vaccine, 33% of people said either short- or long-term side effects. So, when family and friends talk about their experience, it changes minds:
“Almost all of my friends were vaccinated with no side effects.” – 64 year old, female, black, Democrat, Tennessee
“Family members and friends who got vaccinated had no serious side effects. Lots of regulations got lifted for vaccinated people.” – 43 year old, female, Asian, independent, Massachusetts
“I became convinced that some of the rumored side effects were not true” – 69 year old, male, white, independent, Colorado
“Not many side effects and others have been vaccinated” – 21 year old, male, white, independent, Georgia
“It was clearly safe. No one was dying” – 32 year old, male, white, Republican, South Carolina
The top three statements that people found most reassuring were:
1. “The likelihood of experiencing a severe side effect is less than 0.5%”
2. “Mild side effects are normal signs that their body is building protection”
3. “Most side effects should go away in a few days”
Even given our best effort, people will just need more time to see that the vaccines continue to be safe. I’m optimistic that the anticipated FDA full approvals will help.
Talk about individual-level benefits. Not just the consequences.
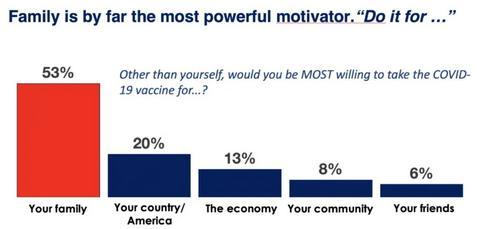
Talk to family members about being able to safely visit. Discuss how their vaccination helps their loved ones stay safe. A poll found that people were MOST willing to take the COVID-19 vaccine for family.
- Hesitancy cont'd on page 7
Some people who changed their mind said:
“Discussed my spouse’s immune system.” – 58 year old, male, white, Republican, Washington
“My family persuaded me because of my sick kids” – 28 year old, female, Hispanic, Democrat, Texas
“I went to visit my family members in another state and everyone there had been vaccinated with no problems so that encouraged me to go ahead and get vaccinated also I would the better protected and not a threat to them not being having it” – 63 year old, male, black, independent, Texas
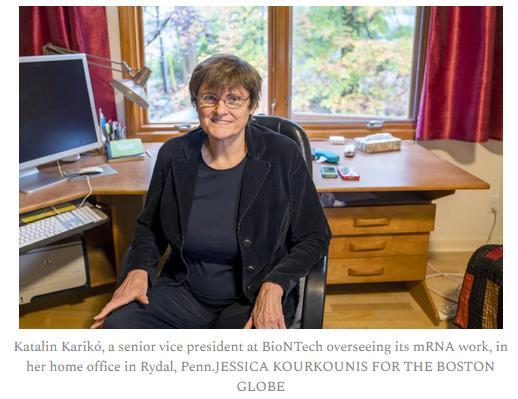
Talk about the people behind the vaccine.
Do not reference the ivory towers (science, pharma, FDA, or CDC), but rather the real-world people and faces who made this happen. Refer to the scientists, physicians, and researchers.
You can talk about Dr. Katalin Karikó, the Hungarian-born scientist behind the mRNA discovery and how she’s been working since the 1990’s to get the science right. For decades she
had convince people to continue funding the research, which was more than difficult. But her perseverance, leadership, and collaborative spirit prevailed and research resulted in the Pfizer vaccine we are using today. (Read more about this story here; it’s fascinating).
Or talk about Dr. Kizzmekia Corbett (i.e. Kizzy), a 34 year old Black American scientist who worked for 6 years on the development of coronavirus vaccines in anticipation of a pandemic. After 10 months, her team developed and tested the Moderna vaccine we have today. (More about her story here).
A few additional tips to keep in mind…
Keep your audience in mind.
It’s clear that there are distinct groups within the unvaccinated population. And their views and concerns are not uniform.
12% of Americans are considered to be in the "Wait And See" group. Those in this group tend to be more Black, Hispanic, and split politically. Messaging that works better than others is:
Black Americans: Messages around “returning to normal” are far more effective for under 50. But for those over 50, “saving lives” is most effective.
Latinx Americans: Motivated when you say “it’s the right thing to do” instead of saying “getting the vaccine will keep your family and friends healthy and safe.”
Young women: Stressing how the vaccine will address both “damage from lockdowns” and the “potential for family/friends to become ill” is effective
- Hesitancy cont'd on page 9
On the other hand, 13% of Americans are considered in the “Definitely No” group. Those in this group tend to be more White, Republican-leaning. Messaging that works better for this group is that a “return to normal” or “reopen the economy” happens once we’re vaccinated. Messages about personal health/safety are less impactful.
I’ll also be curious to see how the recent (and unexpected) shift among conservative leaders will help move the needle. For example, Sean Hannity had a much welcome (although maybe too late) message to his viewers. To watch go HERE. Briefly, he said:
“Please take COVID seriously. I can’t say it enough. Enough people have died. We don’t need any more deaths. Research like crazy, talk to your doctor… Take it seriously. It absolutely makes sense for many Americans to get vaccinated. I believe in science, I believe in the science of vaccination.”
What you say matters
How we communicate correct information matters, especially to people who are hesitant or believe the conspiracy theories. Do not be condescending, alienating, a voice that’s not empathetic, and do not say words like “insane” or “dumb”. If we say this, all we’re doing is challenging their world view, which is linked to their identify and the tribes they’re are a part of. We need to set new foundations of trust. No matter how frustrated you are, avoid judgmental language. It’s hard, but worth it.
They may have questions
If you successfully open a communication channel, they will have questions. Welcome them. You can say that you don’t know, but point them in a trusted direction to find the answer. The last thing we want is for them to fill that void with misinformation. You can also try to answer their questions (here’s a cheat sheet; if you’re a paid subscriber, let me know if you want a PDF)…
- Hesitancy cont'd on page 10
Do you have an idea for an EpiMonitor article?
We love epidemiology, biostatistics, and public health and welcome thoughtful and timely contributions to the field. A review of our past newsletters is the best gauge for the type of content we publish.
Please submit your full article as a Word document; submissions should be 800-1000 words. Please include who you are, your current affiliation, and any relevant background, including your qualifications to write on your chosen topic. Conflicts of interest current or potential, financial or favor must be disclosed. We read all submissions; if your submission is selected, you will receive an email from our Research Director.
Contact madeline@epimonitor.net to set up an email Q&A, or you can submit for consideration an article about your work.
A Data Analyst’s Guide to Using ChatGPT
Author: Heather Duncan, PhD, MPH
Regardless of your profession, artificial intelligence will almost certainly impact the work you do in some way. While AI has provoked some well-deserved anxiety, AI tools can also be leveraged to improve efficiency and productivity. This is especially true if you regularly analyze data.
There are many types of publicly available AI tools; however, not all are user-friendly, and many require expensive subscriptions. ChatGPT has the distinct advantage of being free and very easy to use (note: the paid version of ChatGPT now offers advanced data analytics tools; however, this article will cover the free version only). Anyone can use ChatGPT without prior training; you simply type your question or request into the box and press enter. It’s a lot like using Google, but the responses it provides can be tailored to your specific needs.
ChatGPT has earned notoriety for its increasing role in ethical breaches, particularly in higher education. However, there are many ways to use ChatGPT that do not constitute plagiarism or other forms of ‘cheating.’ ChatGPT can be especially helpful with statistical analysis, particularly if you are new to the field or branching out into new methodologies.
1. Choosing the most optimal statistical tests/models for your data
Even seasoned data scientists can sometimes neglect to consider the basic assumptions of the statistical methods they have chosen. And while Google and other search engines are excellent resources, it is often challenging to
find answers to data-specific questions. Unlike a search engine, ChatGPT can be fed the parameters and goal of the analysis and return a list of suggestions. If you aren’t familiar with a specific method or if you don’t understand a part of ChatGPT’s response, you can ask followup questions, request that the AI explain it to you in a different way, or ask for more detail. You can even ask for it to provide specific examples to better illustrate concepts.
Debugging code
Some statistical analysis software packages
- ChatGPT cont'd on page 12
Heather Duncan, PhD, MPH MD Science Consulting
include a built-in debugger, but others do not. If you are using a program that does not include a debugger, such as SAS, finding coding errors can be immensely time-consuming and frustrating. The good news is that ChatGPT is not only conversant in over 80 natural languages - it can also understand and code in most programming languages.
While asking ChatGPT to code for you is not advisable and arguably crosses an ethical line, ChatGPT is excellent at examining code for errors. And it is equally helpful for finding typos (which, as any coder knows, can completely derail a program) as it is for finding more complex errors, such as issues with syntax. If for some reason its first suggestion does not fix the problem, you can continue to dialogue with ChatGPT and ask for other potential solutions. You can also ask what impact any changes to your code might have on the overall program.
2. Interpreting results
When working with large or complex datasets, sometimes the results of your analysis may throw you for a loop. If a test is not performing as expected, you can input the results to ChatGPT and ask it for an interpretation. This is an especially useful feature if you are working on a project by yourself and need someone to bounce ideas off of. ChatGPT is also very helpful at explaining how statistical tests arrive at their results, so if you are trying a new method that you are not yet familiar with, asking ChatGPT for help is a bit like having your own private tutor.
3. Coping with various challenges
Anyone who analyzes data knows that the process rarely goes completely as planned. This
is especially true when you are in the exploratory phase of analysis. You may have specific questions about your dataset that are difficult to generalize for a Google search. Issues with data extraction, missingness, and data cleaning are very common, and the appropriate solutions are not always intuitive. Again, using ChatGPT like you would a colleague or mentor can save hours of frustration.
While ChatGPT can be an extremely effective tool for the data analyst, several words of caution are in order. First, always double check any response that seems off or not quite right. While some tasks are better suited to an AI than a human being, the truth is that no AI can yet fully replace human expertise. ChatGPT should always be used as a supplement to other more reliable sources of information. Second, do not ask ChatGPT to generate original content. While ChatGPT has many excellent qualities, one disadvantage is that it will sometimes output nonsensical responses, particularly if you ask it to generate code. It is likely that this ability will improve over time as the AI is trained on ever larger datasets, but for now, it is strongly recommended that you not use ChatGPT for this purpose. If you do request lines of code, proceed with caution.
Third, if you are working with sensitive or proprietary data, as many of us in the health sciences do, make sure that your use of ChatGPT does not in any way violate your data use agreement. Never input sensitive data directly into any AI tool unless you have received explicit permission to do so. Once information is entered into ChatGPT, it is retained in the model memory in perpetuity, so always be cautious with what you share.■
Across
1. "Keep ____ and carry on"
5. Big failure
9. What vines do
14. Balm ingredient
15. Hindu hero
16. Void
17. Baltic capital
18. Trim to fit, maybe
19. Baseball catcher, manager, now executive Joe
20. One of Carl Tyler's five tasks of a field epi
23. Part of repeating chorus before and after "when the great ship went down"
25. Make dirty
26. PC "brain"
27. Menopausal treatment, in brief
28. Word before de guerre or de plume
30. Batman's city
32. Celebrate World Field ____ Day on Sept. 7, 2024
36. Tuesday food
37. Nutritional abbr.
38. Pipe problem
42. One of Carl Tyler's five tasks of a field epi
47. Part of NASA countdown
50. She played President Barbie
51. Away's partner
52. "You've got mail" co.
53. Nits, eventually
56. Part of a spreadsheet
58. One of Carl Tyler's five tasks of a field epi
61. Type of acid
62. In-flight internet provider
63. Japanese soup noodle
66. Gardasil manufacturer
67. Pub offerings
68. Blood fluids
69. Impatient
70. Greet the judge
71. New and provocative
Down
1. Ford or Lincoln
2. Will Smith title role
3. Type of regression
4. Arithmetic averages
5. Battle cry in "Braveheart"
6. Chaps
7. Skips
8. Place for aluminum furniture
9. Mailing from LLBean or Williams-Sonoma
10. Misspelling of Basic Reproductive Number (contagiousness of infectious pathogen)
11. Add value to
12. Mythical Greek princess for whom a continent is named
13. Full assembly
21. Barn topper
22. Acronym warning to an analyst about bad data
23. Sharpen
24. Instrument in an Italian orchestra, or last four letters of Dept. of Defense R&D agency
29. Ballistic missile, for short
31. Banks from the runway
33. "I can only ___ much"
34. Keats piece
35. Animal house
39. "Approved but ____" (agency's mixed message to an application)
40. Con
41. Beach bird
43. Ill-starred
44. Bridle strap
45. Source of some intolerance
46. Fifth-century pope who was sainted
47. City that shares airport with Seattle
48. Like some mittens
49. Former Prime Minister of Israel
54. Groucho Marx prop
55. Bacteria discovered by Theodor Escherich
57. Single one of 53-Across
59. Things that may be hot or dropped
60. Iron and Stone
64. Ending for some web addresses
65. Dissenting vote
What We're Reading This Month
Editor's Note: All of us are confronted with more material than we can possibly hope to digest each month. However, that doesn't mean that we should miss some of the articles that appear in the public media on topics of interest to the epi community. The EpiMonitor curates a monthly list of some of the best articles we've encountered in the past month. See something you think others would like to read? Please send us a link at info@epimonitor.net and we'll include it in the next month
Public Health Topics
♦ Scientists warn bugs carrying deadly diseases arriving in England from Europe because of climate change (The Telegraph)
https://tinyurl.com/4k284yvk
♦ Eating Meat Is Linked With Diabetes Risk, New Studies Suggest (NYT)
https://tinyurl.com/3hjf877r
♦ Gaza faces public health crisis with first confirmed case of polio (WAPO via AppleNews)
https://tinyurl.com/584wmyrh
♦ Skin infections and hepatitis spread as Gazans resort to drinking and bathing in contaminated water (NBC News)
https://tinyurl.com/rrf3ryeh
♦ Epidemiologist breaks down how and where mpox is spreading (NPR)
https://tinyurl.com/3fekf3ky
♦ WHO declares mpox outbreak a global health emergency (Stat via AppleNews)
https://tinyurl.com/4nbtk6ej
♦ Long Beach, CA plans to cut 70 public health jobs including epidemiologists, outbreak response (Long Beach Post)
https://tinyurl.com/ypu8ncta
♦ What to Know About Parvovirus B19, a Respiratory Virus on the Rise (Time)
https://tinyurl.com/3s474pu6
♦ Oropouche fever, the mysterious threat (The Lancet)
https://tinyurl.com/2pdrtxxp
♦ 'Sloth fever' virus has spread to humans with 19 victims in Europe so far (DailyMail) https://tinyurl.com/48h6r3h3
What We're Reading This Month
[Type a quote from the document or the summary of an interesting point. You can position the text box anywhere in the document. Use the Text Box Tools tab to change the formatting of the pull quote text box.]
- con't from page 13
Public Health Topics, con’t
♦ They All Got Mysterious Brain Diseases. They’re Fighting to Learn Why (NYT) https://tinyurl.com/3h9f3h2z
♦ The four viruses linked to autism (The Telegram) https://tinyurl.com/2xsntzwv
♦ What is Teflon Flu? Learn about the illness linked to nonstick cookware (USA Today) https://tinyurl.com/4xxdrsv9
♦ We're having a COVID summer surge. Should you get the updated vaccines now? (NatGeo via AppleNews) https://tinyurl.com/45k45yk5
♦ 'Persistent' structural changes in lungs could explain long COVID (BBC – Science Focus) https://tinyurl.com/3avknkn2
♦ Health experts warn against COVID complacency in schools amid surge (The Hill) https://tinyurl.com/ycn97etf
COVID-19
Notes on People
Do you have news about yourself, a colleague, or a student?
Please help The Epidemiology Monitor keep the community informed by sending relevant news to us at this address for inclusion in our next issue. people@epimonitor.net
Appointed: Wiley Jenkins, Ph.D., has been appointed chair of the Clemson University Department of Public Health Sciences. His term began July 1. Jenkins joins Clemson and the College of Behavioral, Social and Health Sciences (CBSHS) from Southern Illinois University School of Medicine where he served as interim chair of the Department of Population Science and Policy. Prior to his appointment as interim chair, he worked in the department as a professor and chief of epidemiology and biostatistics. He has served in faculty, research and administrative positions in the public health field for more than 30 years.
Appointed: Michael Bloom, professor in George Mason University’s Department of Global and Community Health, was appointed as a member of the Reproductive, Perinatal and Pediatric Health Study Section, Population Sciences and Epidemiology Integrated Review Group, which is part of the National Institutes of Health Center for Scientific Review.
Appointed: Professor of public health studies at the University of Hawaiʻi Mānoa, Tetine Sentell, has been named the inaugural Chin Sik and Hyun Sook Chung Endowed Chair in Public Health Studies. This endowment aims to recruit and retain top faculty in public health, supporting research, training and scholarship dissemination on critical health issues in Hawaiʻi and the Pacific region.
Appointed: Ricardo Izurieta, MD, DrPH. MPH, an internationally known expert on tropical and infectious diseases, is leaving his long-time post as associate professor at the University of South Florida’s College of Public Health (COPH) to become dean of the new School of Health Sciences and Public Health at California State University Los Angeles.
Notes on People
Do you have news about yourself, a colleague, or a student?
Please help The Epidemiology Monitor keep the community informed by sending relevant news to us at this address for inclusion in our next issue. people@epimonitor.net
Appointed: In July 2024, Berkeley Public Health welcomed assistant professor of biostatistics Xiudi Li, PhD. Dr. Li received a PhD in biostatistics from the University of Washington in 2022 and a BSc in mathematics and economics from Hong Kong University of Science and Technology in 2017.
Retiring: Jim Tonascia, whose public health career in biostatistics and epidemiology spanned more than five decades, retired from the Bloomberg School of Public Health at Johns Hopkins this August. Tonascia arrived at the School in 1967 as a graduate student and received his PhD in Biostatistics from the School in 1970. Since then, he has been faculty in the departments of Epidemiology and Biostatistics, becoming full professor in 1981.
Passed: Professor Clair Chilvers, a McPin trustee, died recently surrounded by her family, aged 78. As a cancer epidemiologist, first at the Institute of Cancer Research, then at the University of Nottingham where she was Professor of Epidemiology, she knew how crucial the charity Cancer Research UK was for progressing and understanding treatments for cancer – but mental health did not have anything like that at the time
Recovering: Dr. Anthony Fauci is continuing his recovery at home following a 6 day hospitalization for West Nile Virus. Insiders report that although he is unsure where he contracted the virus, the supposition is that he was bitten by a mosquito in his backyard. The prognosis is that he will experience a full recovery.
Near Term Epidemiology Event Calendar
Every December The Epidemiology Monitor dedicates that issue to a calendar of events for the upcoming year. However that often means we don't have full information for events later in the upcoming year. Thus an online copy exists on our website that is updated regularly. To view the full year please go to: http://www.epimonitor.net/Events The events that we are aware of for the next month follow below.
September 2024
September 3-4
https://tinyurl.com/ms49zbuz Conference: Swiss Public Health Conference 2024 / Univ of Bern / Fribourg, Switzerland
September 8-11
https://bit.ly/3huUxTC Conference: 18th Vaccine Congress / Elsevier / Lisbon, Portugal
https://tinyurl.com/rxykuhmw Conference: 21st Biennial Congress - EPA Section of Epidemiology & Social Psychiatry / European Psychiatric Association / Lausanne, Switzerland
September 12-15
https://bit.ly/3PBGvME Conference: 11th Southeast Asia and Western Pacific Bi-regional TEPHINET Scientific Conference / SAFETYNET & Australia National University / Canberra, Australia
September 17-20
https://tinyurl.com/6325d68j Conference: Conference on Drug Development to Meet the Challenge of Antimicrobial Resistance / ESCMID – ASM / Porto, Portugal
September 18-20
http://tinyurl.com/ycx5nsbt Short Course: Genomic Epidemiology of Malaria / Wellcome Connecting Science
September 20-23
https://tinyurl.com/msf42z4b Conference: 8th World One Health Congress / UN, WHO and others / Cape Town, South Africa
September 24-27
https://tinyurl.com/k2r4ybru Conference: IEA World Congress of Epidemiology / Multiple sponsors / Cape Town, South Africa
September TBD
https://bit.ly/3DV3zhY Conference: American College of Epidemiology Annual Conference / ACE / Scottsdale, AZ
- Near Term Epi Calendar cont'd on page 18
October 2024
October 7-9
https://tinyurl.com/a7ektvku Conference: Conference on Neglected Tropical Diseases / Academic Medical Education, Inc / Nairobi, Kenya & Virtual
October 16-20 https://bit.ly/3uYKFES Conference: ID Week / Multiple Sponsors / Los Angeles, CA
October 20-24
https://tinyurl.com/mrzp2cjn Conference: ISES Annual Meeting / International Society of Exposure Science / Montreal, Canada
October 24-26
https://tinyurl.com/yc7szpz9 Conference: 4th International Vaccines Conference / Magnus Group / Baltimore, MD
October TBD https://tinyurl.com/rxykuhmw Conference: Annual ISPE Asia Conference / ISPE / Tainan, Taipei
Your Ad Should Be Here
Do you have a job, course, conference, book or other resource of interest to the epidemiology community? Advertise with The Epidemiology Monitor and reach 35,000 epidemiologists, biostatisticians, and public health professionals monthly. Advertising opportunities exist in this digital publication, on our website and Facebook page, and in our Epi-Gram emails. For more information please contact:
Open-Rank Tenure-Track Faculty
The Department of Epidemiology at the University of Michigan School of Public Health invites applications for an open-rank tenure-track faculty position with a focus on infectious disease epidemiology. The successful candidate will have or develop a research program that includes a laboratory component focused on one or more viral pathogens within a population health context, nationally or globally. We are interested in a broad range of substantive areas including virology, immunology, and global health. We seek an innovative, high-quality scholar dedicated to researching and combating viral infectious diseases. We are especially interested in highly qualified candidates who can contribute, through their research, teaching, and/or service, to the diversity and excellence of the academic community.
We especially encourage applications from scientists whose research focuses on biosafety level 3 (BSL-3) pathogens, the epidemiology and transmission of viral pathogens, vector-borne diseases, emerging viral infections, immunology, pathogenesis and/or work in a global setting. Ultimately, we seek to recruit and retain a diverse workforce that reflects our commitment to serve the diverse people of Michigan, to maintain the excellence of the University, and to offer our students richly varied perspectives, educational and applied experiences, and ways of knowing and learning.
Required qualifications include a doctoral degree and a strong track record of infectious disease epidemiological research. Applicants are expected to have evidence of independence and the potential to become strong graduate-level instructors.
Our Department of Epidemiology is home to more than 40 highly interdisciplinary, internationally recognized faculty members whose research encompasses a broad range of epidemiologic disciplines. The Department also has 23 joint and adjunct faculty members who hold primary appointments in other departments (e.g., Environmental Health Sciences, Biostatistics, Medicine, Institute for Social Research, among others) or who work in important public health sectors outside of academia. Research expenditures in the Department of Epidemiology were just under $37 million dollars during the 2022 fiscal year. BSL-2 and BSL-3 facilities are available in the School of Public Health, supporting cutting-edge research on infectious diseases. The Department, School and University have several relevant research centers including the Michigan Center for Infectious Disease Threats (MCIDT), Molecular and Clinical Epidemiology of Infectious Diseases (MAC-EPID), Center for Respiratory Virus Research and Response, and the Center for Global Health Equity (CGHE). The Department has large and highly successful training programs at both the masters and doctoral level, and the School of Public Health has a thriving undergraduate program.
A complete application should include:
1. Curriculum Vitae, including the complete contact information of three people who may be asked to write a letter of reference (we will not contact these individuals without first informing you that we will do so).
2. Statement of current and future research plans (3-4 pages).
3. Statement of teaching philosophy and experience,including courses you may wish to teach (1-2 pages).
4. The University of Michigan School of Public Health is strongly committed to building and supporting the needs of a diverse public health workforce and research community. Please provide a statement discussing the ways in which you have - or plan to - address systemic social inequalities and advance the goals of diversity, equity and inclusion via your research, teaching, and academic service (1-2 pages).
Interested applicants should apply online via this link. Review of applications will begin October 7, 2024 and continue until suitable candidates are identified. Inquiries regarding this position can be directed to the search committee via email at epidfacsearch@umich.edu
The University of Michigan is an Equal Opportunity/Affirmative Action Employer. Minorities and women are particularly encouraged to apply. This search will be conducted in a manner consistent with the University of Michigan's newly released campus-wide Diversity, Equity & Inclusion Planning Initiative. For more information, see http://diversity.umich.edu/our-commitment/ The University is responsive to the needs of dual-career couples.
Biostatistics Director
The University of Maryland Marlene and Stewart Greenebaum Comprehensive Cancer Center (UMGCCC) & the Department of Epidemiology & Public Health (DEPH) are accepting nominations/applications for director of Biostatics Shared Resource/Division of Biostatistics, a dual-purpose entity that serves as a Shared Resource within UMGCCC and a division within DEPH. The ideal candidate will serve as director of both based on overall qualifications and leadership experience. The director will hold an academic appointment in DEPH and Program in Oncology membership in UMGCCC. DEPH and the Program in Oncology are part of the University of Maryland School of Medicine (SOM) located on the University of Maryland Baltimore campus in downtown Baltimore.
The DEPH Division of Biostatistics and Bioinformatics is the academic home of 15 faculty and has an excellent record covering the full spectrum of biostatistics and methodological research via collaborative research in biomedicine to biostatistics education and training. The mission of the division is to excel in biostatistics and bioinformatics education/training; to conduct high-quality methodological and collaborative biostatistics/bioinformatics research; and to provide an essential component of the scientific basis for quantitative biomedical research throughout UMGCCC, the Medical Center and the University of Maryland. Members of the division teach and provide mentorship to medical students, masters and doctoral students, and MPH students, and leadership of a new track in biostatistics in the Epidemiology and Human Genetics Doctoral Program
The director should ideally be an NIH funded investigator, at the academic rank of associate professor or above. The director will be a member of UMGCCC Shared Resources senior leadership, the UMGCCC Research Council and DEPH leadership with responsibilities spanning the School of Medicine and the University. The director will play a significant role in the UMGCCC NCI Cancer Center Support Grant and the UMGCCC clinical research enterprise.
The ideal candidate will:
Have an established track record of peer-reviewed extramural research funding and national/international reputation as evidenced by service on national, regional, and local organizations and professional societies.
► Have a documented record of scholarship in biostatistics and data science, preferably applied in oncology. Experience in clinical trial design and analysis is highly desirable.
► Along with UMB, DEPH and UMGCCC leadership, the director will be primarily responsible for maintaining and expanding a Shared Resource that spans and takes advantage of existing collaborations between the University of Maryland Baltimore and the University of Maryland College Park campuses. A co-director of UMGCCC Biostatistics Shared Resources will be physically located at the College Park campus.
► Possess strategic and innovative thinking abilities to identify research gaps and anticipate research directions and opportunities.
► Have exceptional leadership and mentorship skills to advance careers of faculty, trainees, and staff.
► Foster awareness and support of departmental and cancer center initiatives to support inclusion, diversity, equity, accessibility, and cancer health equity efforts throughout the institution.
► Demonstrate ability to understand and advance the needs of UMGCCC and DEPH within the SOM, across UM campuses and University of Maryland Medical System and the UMGCCC catchment area.
► Have excellent oral and written communication skills. Candidates should apply online at https://umb.taleo.net/careersection/jobdetail.ftl?job=24000145&lang=en and should reference FRIS #03-307-173 and submit a letter of introduction, a CV, a Statement on Diversity and a Research Interest Plan. More info: http://www.epimonitor.net/2024-3879-Epidemiology-Job-Opening.htm
LABOR DAY SALE
Our First Ever Fall Hiring Season Special
It’s that time of the year again and organizations are beginning their search for new faculty for the 2025-2026 academic year. At the same time, search budgets have been cut because of inflation. To help you out we’re rolling our prices back to 2022 levels for ads placed on or before September 22nd
Sample pricing:
1 month web-only ad: $495
1 month half page digital print ad along with web $895
1 month full page digital print ad along with web $1,215
Multi-month discounts apply on top of these discounted prices
Discounted ad orders MUST be received in our office not later than 11PM on September 22, 2024
Contact Michele Gibson for more information at:
or 770.309.7937
The Epidemiology Monitor ISSN (2833-1710) is published monthly
The Epidemiology Monitor
Editorial Contributors
Katelyn Jetelina, PhD, MPH Editor and Publisher
Operations
Christopher Jetelina Operations Manager
Advertising Sales
Michele Gibson sales@epimonitor.net
Advertising Rates
All
in a Digital Version is available FREE to subscribers
The Epidemiology Monitor is available exclusively online in the same familiar print format subscribers were accustomed to, and they can read through the publication on their electronic devices in the same manner they did with the print version. In addition, you can download and save copies of The Epidemiology Monitor for easy future access.