8 minute read
PAIN


Diagnosing Chronic Muscle Pain That Affects Performance
By Marie Rosenthal, MS
Chronic muscle pain can be a cause of lameness and exercise intolerance, so identifying its cause and treating quickly become important to help improve performance, according to Stephanie J. Valberg, DVM, PhD, DACVIM, DACVSMR, of the Valberg Neuromuscular Diagnostic Laboratory, in Michigan.
Muscle soreness can be secondary to an orthopedic problem, so the challenge is differentiating muscle pain, a primary muscle strain and a chronic myopathy. In addition, a horse can have a primary myopathy and an orthopedic lameness, further blurring the picture.
The history, including performance history, is the key to distinguishing among the various problems that could be causing poor performance, according to Dr. Valberg, who recently retired from the Michigan State University. The 2 primary clinical signs that point toward a muscle issue are the presence of muscle pain and presence of weakness, which manifests as loss of muscle mass and a decline in performance, according to Dr. Valberg.
During the physical evaluation look at the muscle mass from both sides of a horse. A performance horse that has been in training for a while will have good muscle mass and tone. “I think it's important to put your hands on every muscle that you can get your hands on, compare left and right, assess the tone. Horses that are fit will have a firm tone. Horses that are unfit have little tone, and horses that are painful have increased muscle tone. Mapping all of that out is important in differentiating a secondary muscle pain from an orthopedic lameness from primary pain due to a strain or chronic myopathy.”
To provide a targeted treatment, it is important determine what form of myopathy a horse has, and this requires measurement of serum creatine kinase (CK) and aspartate transaminase (AST). Elevated CK and AST distinguishes forms of exertional rhabdomyolysis (ER), where muscle fibers are damaged, from exertional myopathies where the muscle is painful but not degenerating. “If you suspect chronic exertional rhabdomyolysis but the resting CK is normal, take a CK before exercise, then exercise the horse for 15 or 20 minutes, then reevaluate when CK peaks 4 to 6 hours later,” she suggested.
Exertional rhabdomyolysis (ER) can be sporadic with no chronic underlying cause or chronic. Causes of sporadic ER include exercising beyond the level of conditioning and dietary imbalances.
Causes of chronic ER include malignant hyperthermia in Quarter horse-related breeds, recurrent exertional rhabdomyolysis (RER), type 1 polysaccharide storage myopathy (PSSM1) and type 2 PSSM with exertional rhabdomyolysis (PSSM2-ER).
Horses that are fit, nervous, excitable and have repeated episodes of pain with elevated CK often have recurrent ER (RER). Horses that are unfit, calm and have persistently high serum CK often have PSSM1. A genetic test is available for PSSM1, which is present in more than 20 different breeds but not Arabians, Thoroughbreds nor Standardbreds.
PSSM2 can be subdivided into 2 types: The first is characterized as having ER with elevations in serum CK and AST (PSSM2-ER); and the second form we now recognize as myofibrillar myopathy (MFM). Arabian horses have a form of MFM that can result in pain at the end of endurance rides or after several weeks of rest and high serum CK.
“This usually occurs in highly successful endurance horses at the end of long endurance rides, and we think it relates to oxidative stress from a high reliance on fat. They may look fine when they finish, but then they get stiff and crampy afterward. They may have myoglobinuria. Sometimes, it occurs about 5 miles into a 2-week period when they’re given some time off. They get stiff, and they get crampy,” she said.
MFM has a different form in Warmbloods. The classic sign of MFM in Warmblood horses is a reluctance to want to go forward and a reluctance to want to engage from muscle tension and pain. “This disorder is more difficult to diagnose because it doesn’t involve breakdown of the muscle cell membrane and leakage of CK out into the bloodstream,” Dr. Valberg said. There is no blood test for MFM in Warmbloods.
“Additionally, behavioral issues, saddle fit, lameness and gastric ulcers can also cause pain and reluctance to go forward so, it’s important to rule those issues out before thinking of MFM,” she said at the 69th AAEP Annual Convention, held in San Diego.
“The treatment for exertional myopathies with normal CK is almost the opposite of the treatment that we’re going to have for horses that have ER and elevations in CK,” Dr. Valberg said. “That is why it is so important to assess muscle enzymes.
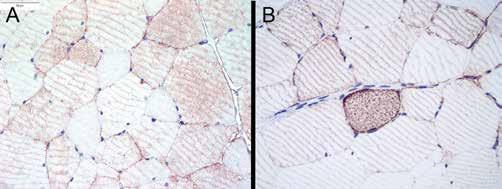
Because some of these conditions are breed specific, genetic testing can be appropriate (see box). If genetic testing results are positive, there is no need for a muscle biopsy, according to Dr. Valberg. However, muscle biopsy could be appropriate to diagnose PSSM2-ER, MFM and to assess difficult to manage muscle cases, she said.
She now uses formalin fixed rather than frozen muscle sections in her new lab. Formalin-fixed sections are more forgiving than frozen sections in terms of developing artifacts during shipping and don’t require cold overnight shipping. These myopathies can now be diagnosed with several immunohistochemical stains, she explained. In addition, the veterinarian can use a specific needle biopsy technique of the gluteal muscle, and the horse can go back to work the next day.

Some clients may not want genetic testing or biopsy, so a treatment trial may be done. In addition to dietary and exercise management, dantrolene can help to get horses with ER back into training. Dantrolene slows the flux of calcium inside the cell that produces a muscle contraction. If calcium is released from intracellular storage sites in excess, muscle fiber damage occurs. It should be given 60 minutes prior to exercise, and it must be withdrawn before FEI shows, and racing she said.
“I like using it for a couple of weeks if we’re putting a horse back into training after ER or if it’s going to be experiencing a type of exercise, we know is going to induce rhabdomyolysis,” she said, but it won’t work if the horse doesn’t have rhabdomyolysis. So, again, it’s important to measure serum CK as part of the diagnostic approach.
For ER, a low-starch diet, fat supplementation, regular daily exercise are the best first approach. This works for PSSM1 and PSSM2-ER because they have excessive glycogen in their muscle and for RER by keeping horses calm. For Arabians and Warmbloods with MFM, “a low-starch, high-fat diet doesn’t seem to be the right approach because glycogen concentrations in their muscle are not high like they are with PSSM1 and PSSM2-ER,” she explained.
“Opposite to what I used to recommend for PSSM2/MFM, and opposite from what we recommend for ER, Warmblood MFM horses need days off to recover,” Dr. Valberg said.
“Most owners report the horses do well with 3 days of work in a row; after 2 days off, they’ll come back and work well again. MFM horses need to be turned out and moving around. We recommend a nice long, low warm-up and then when they are working, give them intermittent breaks,” Dr. Valberg said. Even once we’ve got them under control, they still have good days bad days,” she explained.
Many seem to lack energy and “push,” so Dr. Valberg recommends a moderate amount of nonstructural carbohydrate as long as they don’t have other underlying issues like metabolic syndrome, or don’t appear to have a lot of glycogen in their muscle on biopsy.
“Giving them more energy seems to be helpful in these cases, and we don’t feel like we need to push fat at them as it can cause oxidative stress,” she said.
Amino acids appear useful. Dr. Valberg and Joe Pagan, PhD, MS, at Kentucky Equine Research (KER) developed the KER MFM pellet, which contains essential amino acids including a highly absorbable form of cysteine that appears to be limiting with MFM. Seventeen of 50 owners responded to a survey of MFM horses, and when those horses were fed this supplement with coenzyme Q10, 92% said their horses improved.
“The primary things that seem to improve is the hind limb engagement, and the reluctance to work,” she said. In addition, 71% of those owners reported that the horses continue to improve and build strength after 4 weeks.
“About 65% of the owners of these horses say that their MFM horses are meeting their performance expectations. The horse should show improvement within 4 weeks. If not, it’s time to go back to the drawing board and see what else might be contributing to this horse’s level of poor performance,” she said. MeV
FOR MORE INFORMATION
Dr. Valberg has information and videos on her laboratory’s website that could be useful for taking biopsies. Visit www.valbergnmdl.com