
5 minute read
YES – CROWN LENGTHENING WILL ENHANCE YOUR RESULTS


By James Kohner, DDS
It is common for dentists to become frustrated when recently placed crowns or bridges develop red and/or sore tissues at the margins. Or, in some situations, a tooth may look so badly broken down that a dental implant seems obvious, dissuading the clinician from even considering treatments that not only might save the tooth but render it predictably restorable.


Many of those problematic teeth can be restored predictably, and the above types of challenges can be solved. There often are solutions to those everyday restorative challenges so that every broken-down tooth does not have to be extracted and potentially become an implant! Giannobile and Lang stated in a 2016 editorial in the Journal of Dental Research 1 that “… the erroneous belief of implants yielding a better long-term prognosis has now clearly been rejected in several studies and reviews.” They say that “teeth even compromised because of periodontal disease or endodontic problems may have a longevity that surpasses by far that of the average implant,” and they offer 16 bibliography entries to support their statement.
It is worth noting their premise and keeping in mind that all compromised teeth do not have to become implants. Fortunately, there is a basic procedure that might help avoid restorative frustrations with badly broken-down teeth and allow saving and predictably restoring these teeth that seem hopeless at first glance.
The procedure, and one that many clinicians overlook, is crown lengthening. While this is a “periodontal” procedure, the goal of crown lengthening is very clearly intended as a “restorative” procedure. Crown lengthening has remained essentially unchanged throughout the past 30 years and remains as useful now as then. It has applications in all parts of the mouth.
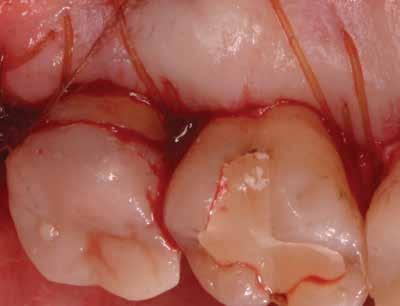
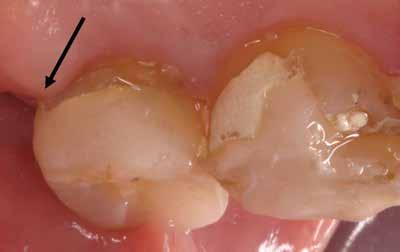
For posterior teeth, there is often not enough clinically visible tooth structure for retention, with preps going subgingivally far enough that obtaining a predictable hassle-free impression is challenging (Fig 1.1 and 1.2). The clinical situation in Fig 1.2 is an illustration where clinicians will be tempted to prep subgingivally for more retention only to end up with marginal impingement on soft tissues causing inflamed and sore soft tissues, or compromised impression results that can result in open margins as an example. This can occur due to excessive gingiva, as in this situation, or deep caries or fractures. While these teeth display too much soft tissue, the problem is typically too much bone underneath the soft tissue resulting in soft tissues moving coronally over and around the thick bone. 2, 3 When clinical crowns are short, the finish lines often end up subgingivally, as illustrated with a deep distal margin on the provisionals in Fig 1.3. This deep finish line location can lead to inadequate impressions, which can lead to open margins.
To shorten the soft tissues, with the goal of exposing more tooth structure, bone reduction is usually required for predictable clinical results since soft tissues will grow back to establish the typical dimension of soft tissues, called biologic width 4, 5 if the bone is not moved. The dimension of biologic width is typically 3 mm coronal to osseous crest. That is the normal development of soft tissue dimensions, whether the bone is or is not removed. 5 After removal of bone and soft tissues the two allegedly compromised teeth in Fig 1.1 and 1.2 can have adequate tooth structure exposed (Fig 1.4, and 1.5), thus avoiding difficulty with impression taking, the need for subgingival margins or potential soft tissue impingement 6 such as in Fig 1.7. Final restoration with healthy tissue and enough tooth to allow for good retention and avoid deep subgingival margins is seen in Fig 1.6.

In the esthetic zone, errors of margin placement can be even more noticeable when inflammation results from crown margins impinging on the soft tissues. Fig 1.7. Learning the concepts of Crown Lengthening and proper margin location can help avoid those inflammatory complications.
The stated goals of crown lengthening in a restorative application, as listed in the CDT codes from the American Dental Association, is below, and it offers an explanation of just how that inflammation seen in Fig 1.7 can occur or what the goal is for restoring teeth with limited clinical crown available:
To expose enough sound tooth structure to allow placement of a restorative margin onto that sound tooth structure, to have adequate mechanical retention, and at the same time avoid disrupting or impinging on any of the gingival fiber attachments to the tooth.
In a rush to use the latest new materials and greatest techniques, such as implants or lasers, the benefits and applications of crown lengthening are often ignored. But instead of being pushed aside and forgotten, this “old standard” should make its way into every contemporary clinician’s armamentarium.
Of course, each tooth with restorative/soft tissue problems is not automatically an indication for crown lengthening! Extraction leading to an implant, or a fixed or removable appliance, always needs to be in the differential diagnosis. Orthodontic extrusion could also be considered, as it is sometimes a viable option, but that is a topic for another paper and has been covered by others.
Only some indications could be covered in this short discussion. Some signs for crown lengthening, or what some clinicians call gum shortening, are: l Excessive gingival display in the anterior, often associated with thick bone l Short posterior teeth, usually associated with excess gingiva and thick bone l Uneven gingival levels l Subgingival fractures l Subgingival caries l Previous crowns and finish lines too close to the soft tissue attachment and the bone l As an adjunct to implant treatment, where supereruption had occurred

Using some of these ideas could help clinicians accomplish more predictable impressions and more predictable restorative results, not to mention happier patients when complications are avoided.
References:
1. Giannobile, W.V., Lang, N.P. Are Dental Implants a Panacea or Should We Better Strive to Save Teeth? J. Dental Research 2016, vol.95 (1) 5-6
2. Deas DE, Moritz AJ, McDonnell HT, Powell CA, Mealey BL. Osseous surgery for crown lengthening: A 6-month clinical study. J Periodontology 2004;75(9):1288-1294.
3. Arora R, Narula SC, Sharma RK, Tewari S. Evaluation of supracrestal gingival tissue after surgical crown lengthening: a 6-month clinical study. J Periodontology.

4. Coslet J, Ingber J, Rose L. The “Biologic Width” – A Concept in Periodontics and Restorative Dentistry. Alpha Omegan 1977; 70:24-28
5. Gargiulo A, Wentz F, Orban B,. Dimensions and Relations of the Dentogingival Junction in Humans. J Periodontology 1961;32, 261.
6. Newcomb, GM. Relationship between the location of subgingival crown margins and inflammation. J. Periodontology 1974; 45:151-154 leads to impingement and subsequent inflammation.
Dr. James Kohner, is a periodontist living in Denver. He has more than35 years clinical experience and more than 25 years teaching and lecturing, with presentations all over the U.S. and eight foreign countries. He currently teaches Hands-on Surgical Training Workshops on Crown Lengthening, Soft Tissue Grafting, and Periodontal Surgery for dental school continuing education programs, and at multiple association meetings in both the U.S. and Canada. He can be reached at 602.390.2229 or JamesKohnerDDS@gmail.com and is available to speak to your local society, school or study group.
He will be offering the following courses at the 2023 Florida Dental Convention: “Crown Lengthening: Can it REALLY Enhance Restorative Results? (C09)” on Thursday, June 29, 9 a.m.-12 p.m.; “Crown Lengthening Workshop (W07)” on Thursday, June 29, 1:30-5 p.m.; “Soft-Tissue Grafting That WILL Enhance Restorative Results (C38) on Friday, June 30, 9 a.m.-12 p.m.; “Soft-Tissue Grafting and Suturing Workshop (W19)” on Friday, June 30, 1:30-5 p.m. Learn more about Dr. Kohner’s courses being offered at the 2023 Florida Dental Convention at floridadentalconvention.com. FDC2023 registration opens March 1.
