
40 minute read
A Clinical Presentation of the Direct Gold Composite Sandwich Restoration


By Dr. DB Henry
Clinical Relevance
Studies indicate the failure of posterior composite restorations, where bonding to dentin is required, continues to be an issue. The results are leading to the need to replace and/ or repair existing restorations earlier than has been the experience using traditional restorative materials.
SUMMARY
The intent of this paper is to present a new idea for increasing the life expectancy of class II composite restorations where the proximal marginal seal is compromised by the necessity to rely on dentin bonding. As implied by the Clinical Relevance statement, studies show that bonding to dentin in areas with high levels of bacterial action, combined with sustained high plaque formation, tends to be the “Achilles heel” with regard to sustained longterm restorations. Therefore, this paper will present a thought experiment, combined with clinical evidence, for combining gold foil with composite in these areas for the class two composite restoration. The results, if proven viable, will be to develop a procedure utilizing the properties of gold foil that make it one of the longest-lasting restorative materials with the recent development of modern cosmetic materials for a truly longlasting and healthy class II restoration.
INTRODUCTION
The results of relying upon dentin bonding in proximal and subgingival areas have shown decreased longevity for class two composite restorations as compared to previous restorative materials used in the past 80 years.1-6 The results suggest the need to replace and/ or repair existing restorations earlier than has been the experience when using traditional restorative materials.5,6 The central problems arise from leakage and subsequent breakdown of the bond at the gingival and subgingival dentinal Fig. 1. Two class 2 foils in tooth 4 (2012).
Fig. 2. Final restoration of foil and composite in tooth 4 (2012)

margins for class 2 and class 5 procedures (personal correspondence between Dr Lloyd Baum and Dr Giancarlo Gallo).3,4,7 Due primarily to bonding properties associated with the organic and water composition of dentin being at 50% as compared to 12% for enamel, dentin bonding characteristics are not ideal for longterm durability.1-9 The clinical use of gold foil to seal dentin margins in class 2 and class 5 gingival prep areas has proven to be one of the most predictable restorative techniques with a long history of success.5,10-12 Operative Dentistry return for removal of the composite and completion of the foil later. However, the patient did not return for six months, at which time the restoration was evaluated and found to be doing well clinically. The decision was made not to replace the composite. The restoration is now six to eight years in function. No clinical photos exist. Following the original restoration and upon discussions with Dr. Clyde Roggenkamp of Loma Linda, CA, it was discovered that Dr. Lloyd Baum had conceived of the idea for combining foil and composite and had discussed this with his friend Dr. Giancarlo Gallo of Italy. Thanks to Dr. Roggenkamp, the correspondence from 1992 to 1997 between Dr. Lloyd Baum of Loma Linda University and Dr. Giancarlo Gallo of Alba, Italy, was forwarded for review. Their discussion centered around the concept of utilizing a sandwich technique combining gold foil and composite.
The properties of gold foil indicate it is an ideal material to both create a seal and maintain that seal over time in the gingival and subgingival environments encountered in class 2 and class 5 restorations.13-16 These properties include: (1) a marginal fit approaching 1 micron, (2) a coefficient of expansion close to tooth structure, (3) no corrosion, and (4 ) an oligodynamic effect. The first three are important; and when combined with the oligodynamic effect of interfering with cell membrane transport, one has a material with a disinfecting property when placed in areas where pathogenic organisms can lead to margin failure.5,6,13,14,16-18
This paper describes a clinical restorative technique to address the limitations of dentin bonding in the class 2 composite dental restoration. It is a procedure that combines the proven long-term application of gold foil with the cosmetic aspects of composite resin by removing the need to bond to dentin in the proximal box, where leakage and breakdown occur at an accelerated rate due to dentin bonding issues. In addition, this is a clinical presentation and will not engage in debate about the use of available direct gold options or the use of different composites/bonding techniques. It is a first look at the possibility for combining two proven materials and techniques utilizing the long-term sealing
A CLINICAL DECISION PROCESS
Approximately eight years ago, while completing class 2 foils in my private practice, there was an emergency patient who needed immediate care. The interruption necessitated the need to temporize the two class 2 foils that were approximately at mid-completion (Fig. 1). The proximal boxes in both foils had been completed. Both proximal boxes were filled with E-Z Gold (Lloyd Baum Dental Center, Loma Linda, CA, USA) to the level of the occlusal floor in the preparation. E-Z Gold is the author’s choice for bulk fill when doing a gold foil. Due to the ease of use and faster build up, E-Z Gold is the gold of choice within a busy private dental practice where gold foil is routinely placed. The E-Z Gold is veneered with #4 gold foil when the restoration is to be completed with direct gold. In this case, to temporize the restorations, the foil was micro etched with 50-micron aluminum oxide then completed utilizing a total etch (Ultra-Etch, Ultradent, South Jordan, UT, USA) and resin bonding (3M Universal Scotchbond) material to the remaining tooth structure and the micro-etched foil. A posterior composite (3M Silux Plus) was used at that time to complete the restoration. (Fig. 2) The patient was to return for removal of the composite and completion of the foil later. However, the patient did not return for six months, at which time the restoration was evaluated and found to be doing well clinically. The decision was made not to replace the composite. The restoration is now six to eight years in function. No clinical photos exist. Following the original restoration and upon discussions with Dr. Clyde Roggenkamp of Loma Linda, CA, it was discovered that Dr. Lloyd Baum had conceived of the idea for combining foil and composite and had discussed this with his friend Dr. Giancarlo Gallo of Italy. Thanks to Dr. Roggenkamp, the correspondence from 1992 to 1997 between Dr. Lloyd Baum of Loma Linda University and Dr. Giancarlo Gallo of Alba, Italy, was forwarded for review. Their discussion centered around the concept of utilizing a sandwich technique combining gold foil and composite resin for the class 5 restoration. Their designs can be seen in the hand drawings from their correspondence in Fig. 3 (reprinted with permission from Dr. Roggenkamp).
Combining what was learned from Dr. Baum and Dr. Gallo, a refinement of the technique was developed to be applied to a class 2 foil restoration. The refinements included micro etching the gold and remaining prep with 50-micron aluminum oxide, t
Fig. 3. Original drawings from correspondence between Dr. Lloyd Baum of Loma Linda University and Dr. Giancarlo Gallo of Alba, Italy.
Fig. 4. Metaltite by Tokuyama Dental America Inc.
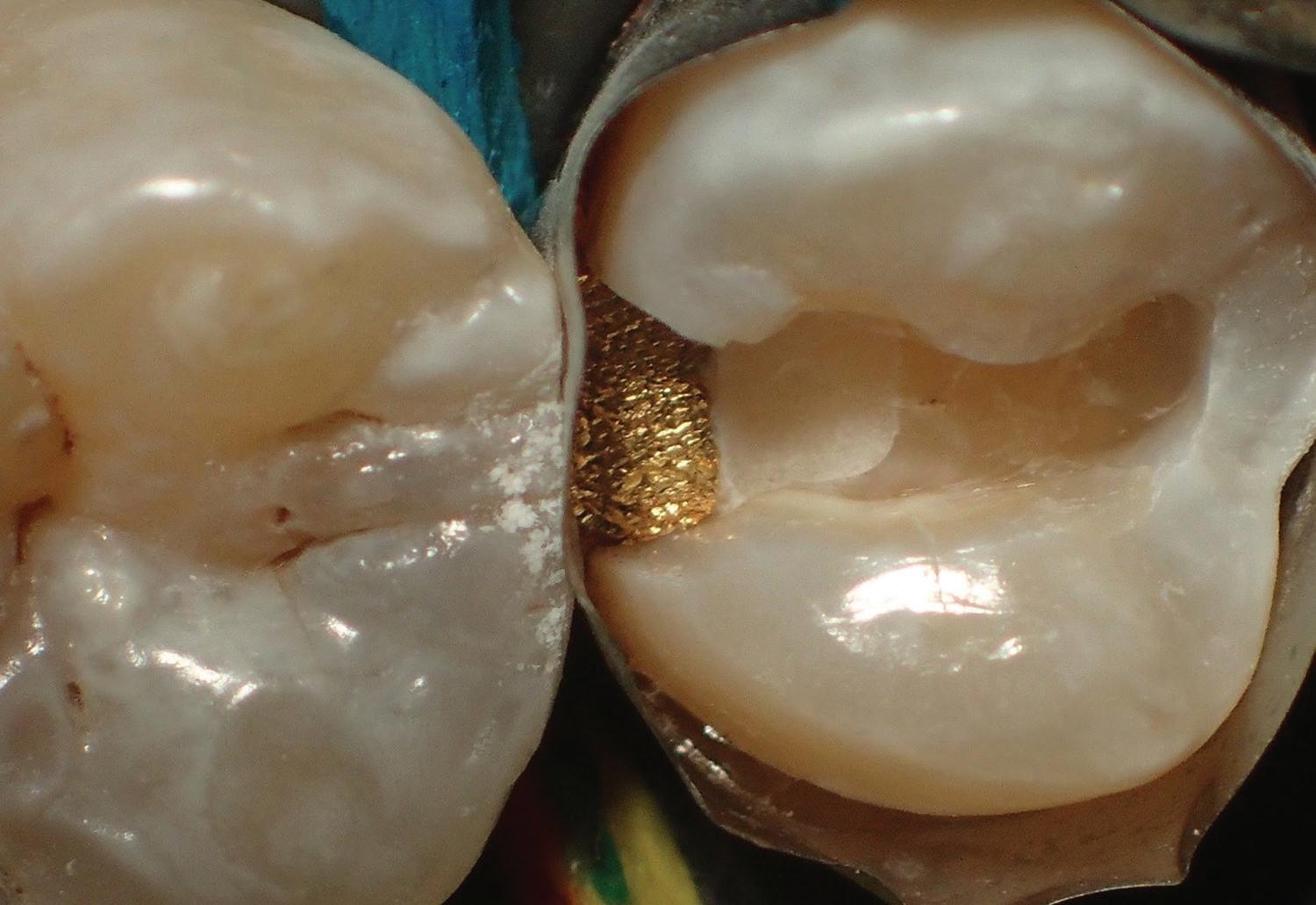
Fig. 5. Initial bur penetration into carious lesion distal-proximal on tooth 13.
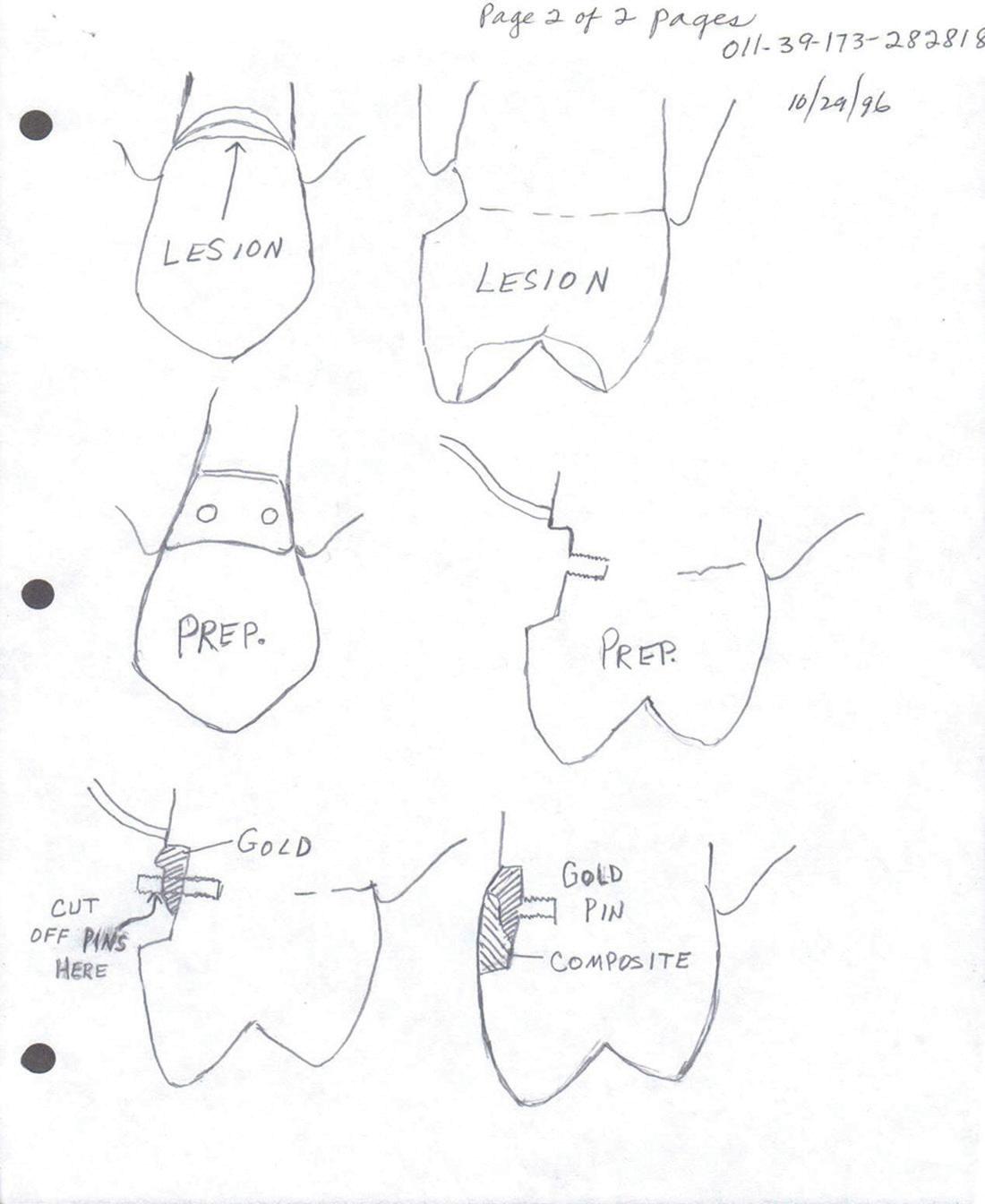
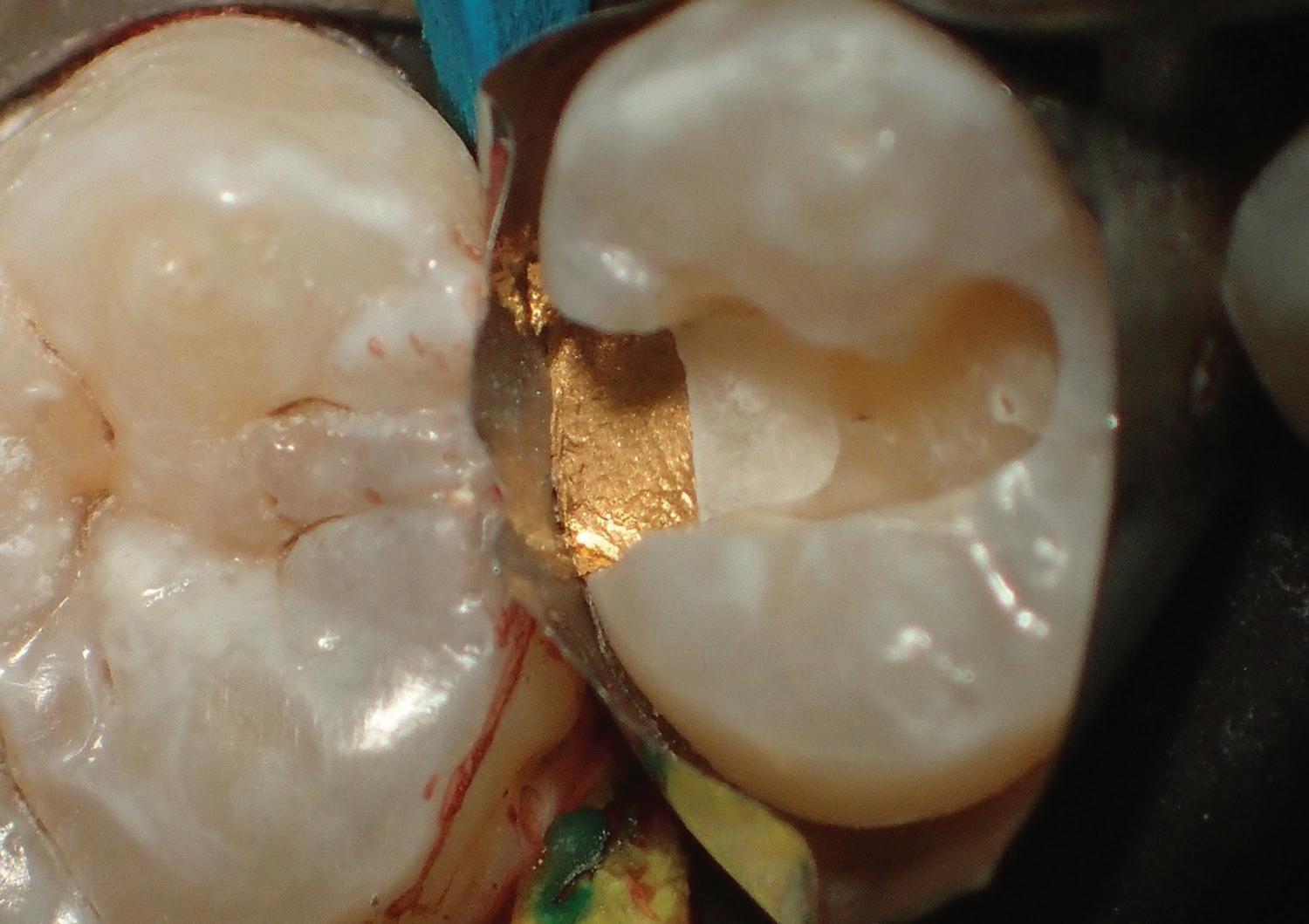
Fig. 6. Distal box filled with EZ Gold, also showing the glass ionomer liner located proximally.
Fig. 7. Foil and prep after micro etching with 50-micron aluminum oxide.

then applying Metaltite (Tokuyama Dental America, Inc, Encinitas, CA, USA) to the gold via manufacturer’s directions. Metaltite MTU-6, a thiouracil monomer, which, according to the manufacturer, “enhances a tenacious chemical bond between resins and precious metals” (Figure 4). In addition, it was decided to place E-Z Gold into the proximal box of the class 2 prep to the level of the occlusal floor of the prep to create the contact in gold for the final restoration (Figure 1).
The author’s reasoning for the procedure was to enhance the longevity of posterior composite class 2 restorations by utilizing the properties of E-Z Gold for stabilization of the proximal area and the adjacent contact over time. The result is a restoration that combines the use of E-Z Gold in the proximal box to facilitate longevity with the aesthetic appeal of composite where effective bonding to enamel has been proven. This restorative combination takes into consideration concerns that the patient, the operator, or both might have with the cosmetic appearance of gold in areas where it can be seen during normal function. Also, it is hoped that this paper could begin to re-assert the value of utilizing direct gold to enhance the so-called “bondodontic” explosion within dentistry and prioritize restorative outcomes and longevity in selecting restorative options.
CLINICAL CASES
Three cases are presented; first a class 2 DO/MO in a maxillary second bicuspid (Figs. 1-2). The second case is a DO class 2 on tooth 13 (Figs. 5-13). The third case is a DO class 2 on tooth 4 (Figs. 14-23).
CLINICAL PROCEDURES
Clinical Case 1: Class 2 in Tooth 4, DO and MO Class 2 Foil-Composite Sandwich As stated previously, the class 2 foil was terminated at the point of completion of the gold placement in the proximal boxes of both class 2 restorations in tooth 4 (Fig. 1). The photo shows the completion of E-Z Gold placement in both proximal boxes and the placement of a GI liner proximal to the gold.
Following this, the gold was micro etched with 50-micron aluminum oxide, washed and dried, then a total etch with 35% phosphoric acid (Ultra-Etch, Ultradent) then bonded with 3M Universal Scotchbond (3M Oral Care, St Paul, MN, USA). Finally, 3M Silux Plus (repeat manufacturer’s name here) composite was used to complete the restoration. This procedure was originally intended to be a temporary fix (Figure 2). Following reevaluation of the restoration, it was decided to continue using the procedure with the modifications of adding Metaltite (Tokuyama Dental America, Inc) to increase bond efficiency between gold and composite resin plus filling the proximal box with E-Z Gold to ensure no dentin bonding and to make the contact in gold. All personal observations are from the author’s private practice.
Clinical Case 2: Class 2 DO #13 FoilComposite Sandwich The procedure consists of removing all caries, then filling voids created with GI (3M ESPE Fil Quick Aplicap (Need manufacturer’s name and location unless same manufacturer has already been noted). This is followed by preparing a classic class 2 preparation for placing gold foil or amalgam under a rubber dam (Figs. 5-13).
The initial penetration into tooth 13 was with a 169 bur (Brasseler) to determine the extent of the carious lesion (Fig. 5) This was followed by removal of all caries. Healthy tooth structure is not removed; therefore, Black’s rules are not observed at this point.
Following the insertion of the GI the preparation is completed to Black’s specifications.
Fig. 6 shows the placement of the remaining glass ionomer for the deep caries destruction and the final prep with E-Z Gold placed in the proximal box. The glass ionomer proximal to the foil acts as a liner and thermal insulator in cases where deep caries penetration into the dentin occurs (Fig. 6).
A dead-soft Tofflemire matrix band is placed (HO Band), wedges inserted, and the band is burnished prior to placement of E-Z Gold (Lloyd Baum Dental Center) into the proximal box. In placing class 2 foils, the author normally uses no band (Fig. 16, Case 3). However, a brass T band can be used as well, depending on the situation. Following the placement of E-Z Gold to the level of the occlusal floor of the prep (Figs. 6-10), the foil and remaining tooth structure were micro-etched (Fig. 7), utilizing a chairside micro etcher and 50-micron aluminum oxide.
The preparation and gold were then washed and dried to clear the aluminum oxide prior to etching. In addition, the prep was treated with 2% chlorhexidine (Consepsis, Ultradent) for 60 seconds prior to total etch. A total etch with 35% phosphoric acid for 30 seconds was completed. In this case, Ultra-Etch by Ultradent was used.
These steps were followed by applying Metaltite (Tokuyama) via a micro brush to the gold only (Fig. 8). Manufacturer’s directions were followed with air drying of one-two layers of Metaltite. Again, the procedure was completed under rubber dam. t
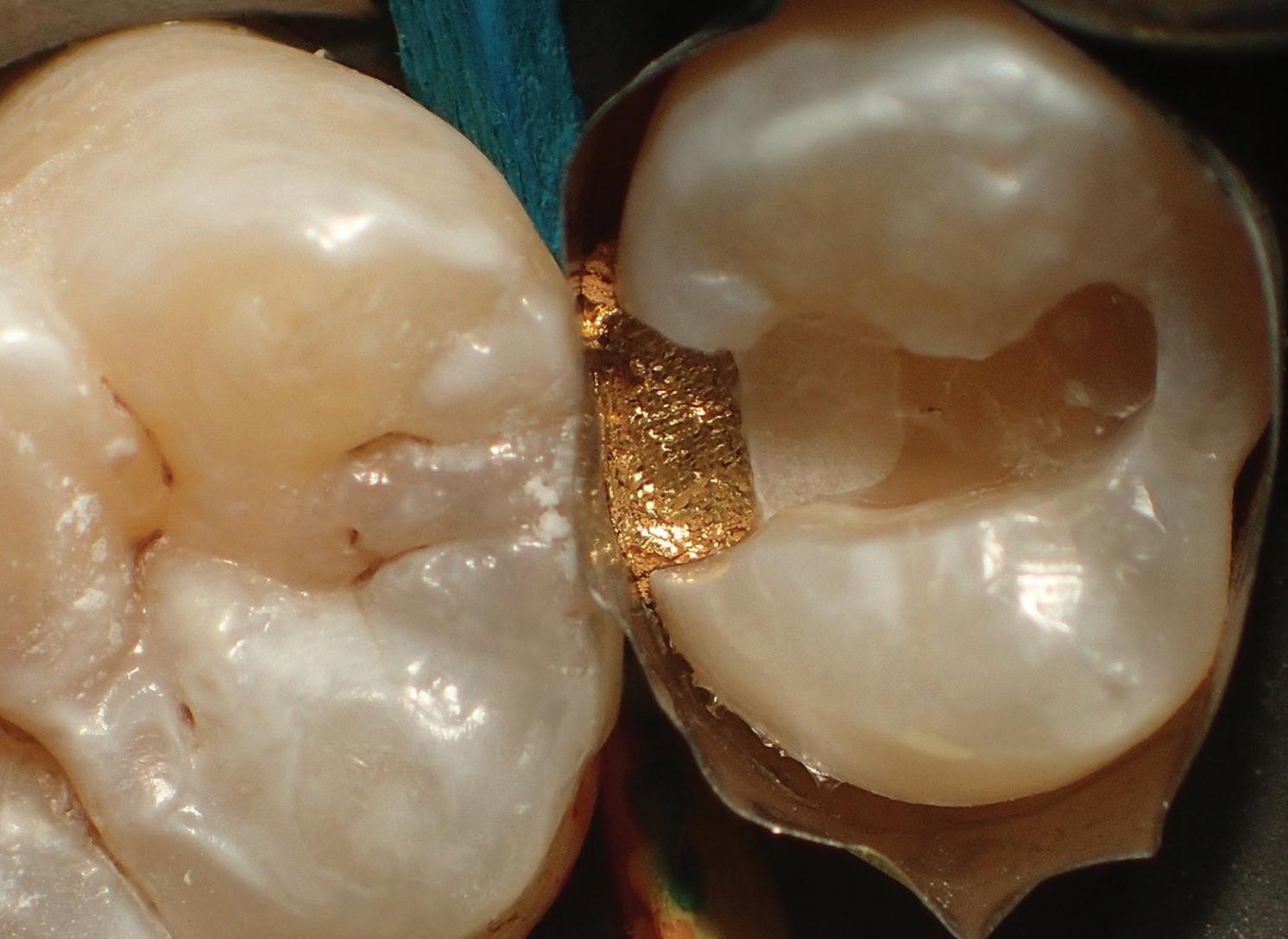
Fig. 8. Foil treated with two layers of metaltite metal bonding resin. Fig. 9. Initial layer covering gold with shade A2.5 3M Filtek flowable composite.
Fig. 10. Middle layer of shade A-2 3M Filtek flowable composite. Fig. 11. Final layer of shade A-1 3M Filtek flowable composite.
Fig. 12. Completed DO class 2 foil/composite sandwich on tooth 13. Fig. 13. Radiograph showing the placement of the foil in the proximal box distal on tooth 13.
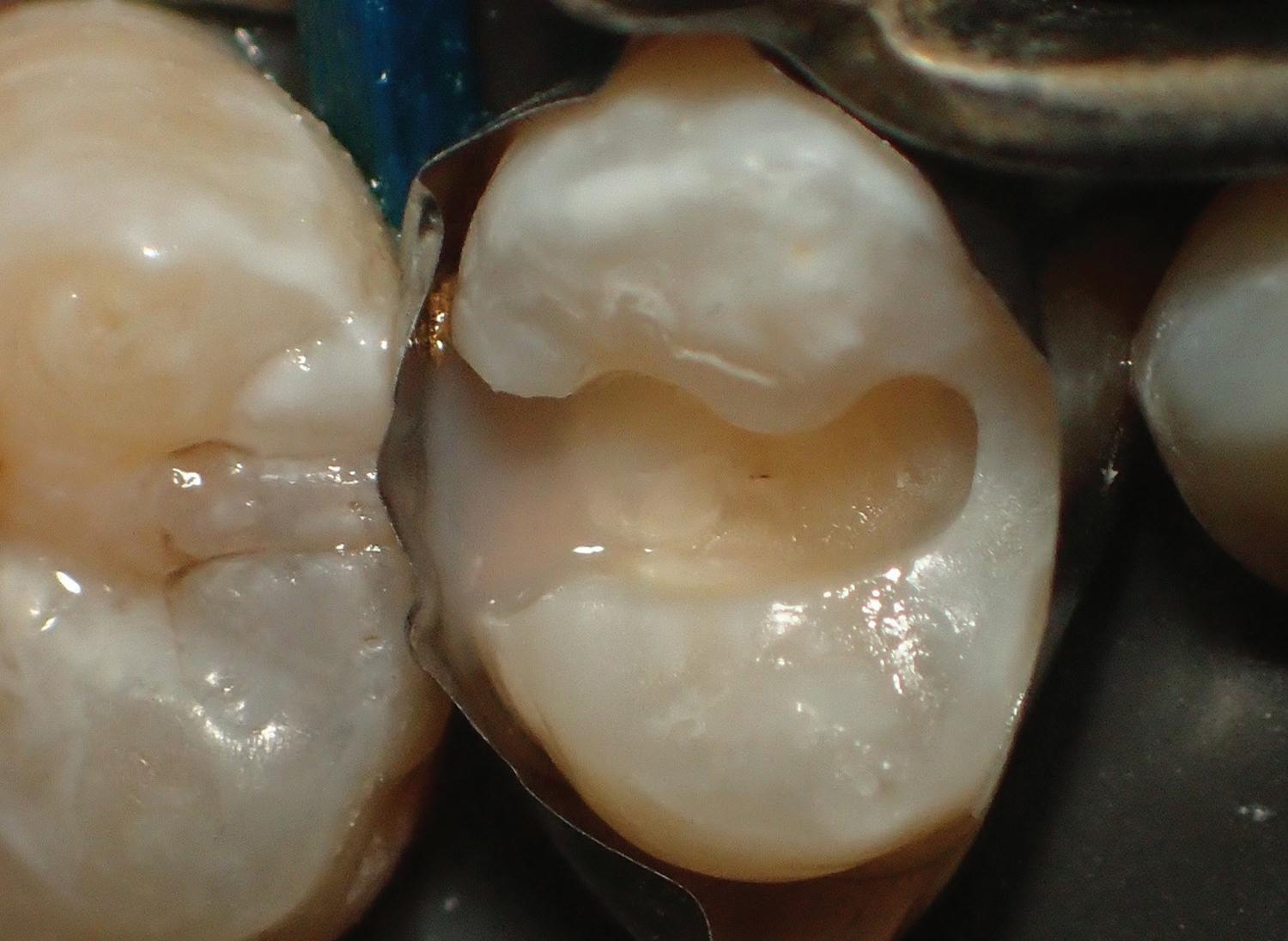



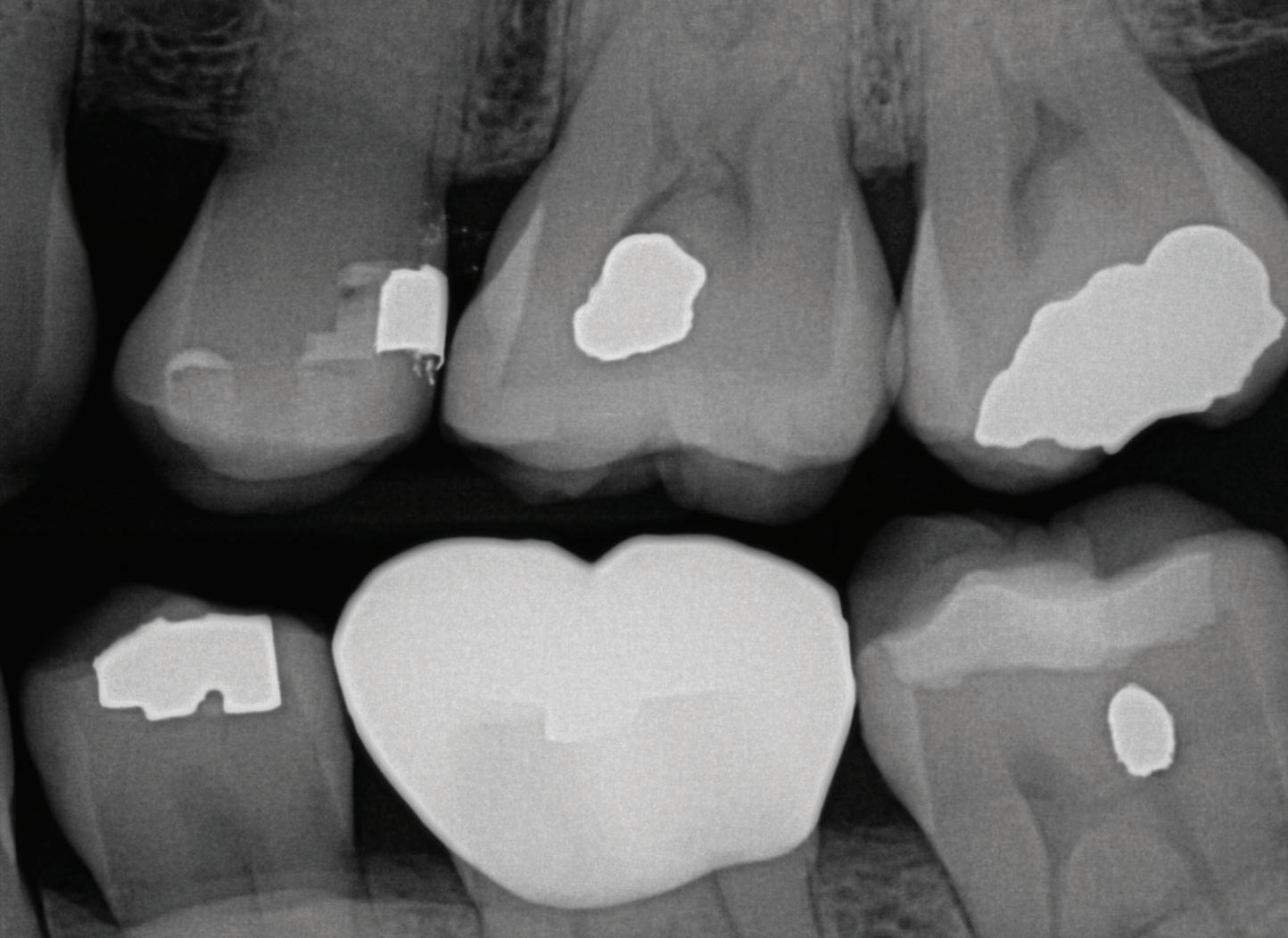

Fig. 14. DO 4 169 bur penetration to see caries.

Fig. 15. DO 4 caries removed and GI placed prior to final prep.

Fig. 16. DO 4 With EZ Gold Placed to the Level of the Occlusal Floor of Prep Creating the Contact in Gold. Gold Placed Without Matrix Band to Ensure Easier Access to Gingival Margin and a tight contact. Following the treatment of the E-Z Gold with Metaltite, 3M universal bonding was applied to the complete prep and cured. Next, 3M Filtek flowable composite was layered into the final preparation and cured in multiple increments until the restoration was completed (Figs. 9-12). A darker or more opaque shade of composite was used in the first layer to mask the color of the gold, in this case, Shade A-2.5 (Fig. 9) . Finishing of the composite was completed using increasingly lighter shades layered and cured (Figs. 9-11). Polishing points and 3M disc and finishing diamonds were used to shape and finish the final restoration (Fig. 12). Fig. 13 is a radiograph showing the class 2 foil placement in the gingival 1/2 for the completed foil/composite sandwich restoration in tooth 13. The presence of a GI liner can be visually differentiated beneath the composite as well. There appears to be a small radiolucency within the GI. It is not known if this is an artifact or a small void. Because damage to the foil would likely occur with removal and replacement of the GI, it was decided to watch over time.
Case 3: DO Virgin Caries Tooth 4 A penetration cut with a 169 bur (Brasseler) showing proximal caries at DO 4 is shown in Figure 14. This is followed by Fig. 15, showing the placement of GI following complete caries removal. Fig. 16 shows the final DO prep ready with E-Z Gold in place. In this case E-Z Gold was placed without a matrix band. This is the usual procedure when class 2 foils are completed by the author. This ensures maximal contact and gives better access to the proximal gingival floor for gold placement. After finishing of the gold contact utilizing VisionFlex Diamond Strips (Brasseler) a dead soft matrix band was placed prior to micro etching (Fig. 17). This was to prevent etching the adjacent tooth or restoration.
Figs. 18 and 19 show the micro etching of the gold and prep followed by treating the gold with Metaltite (Tokuyama). Figs. 19 through 22 show the placement of the composite bonding and layers of 3M Filtek flowable composite. A final veneer of compactable composite can be used in heavy occlusion cases.
Fig. 23 shows the final radiograph of the DO restoration with the placement of foil, GI, and composite.
CONCLUSIONS
This presentation is intended to be a thought exercise to demonstrate one possible solution to improving the success for class 2 posterior composite resin procedures.
More research is needed, especially to observe what is happening at the bond interface between the composite resin and gold. A comprehensive evaluation of the overall success of adding t 61 | TODAY'S FDA july/august 2022

Fig. 17. DO #4 micro etched with 50-micron al oxide and dead soft matrix band used to prevent micro etch 3 and control composite placement. contact is already established in gold. Fig. 18. DO 4 treated with two layers of Metaltite (Tokuyama).


Fig. 19. First layer shade 3.5 to cover the Gold 3M Filtek.

Fig. 21. Final layer a-1 laid in and cured (3M Filtek). Fig. 20. Second layer flowable shade 2.0 applied and cured (3M Filtek).


Fig. 22. Completed restoration DO 4 foil-composite sandwich.
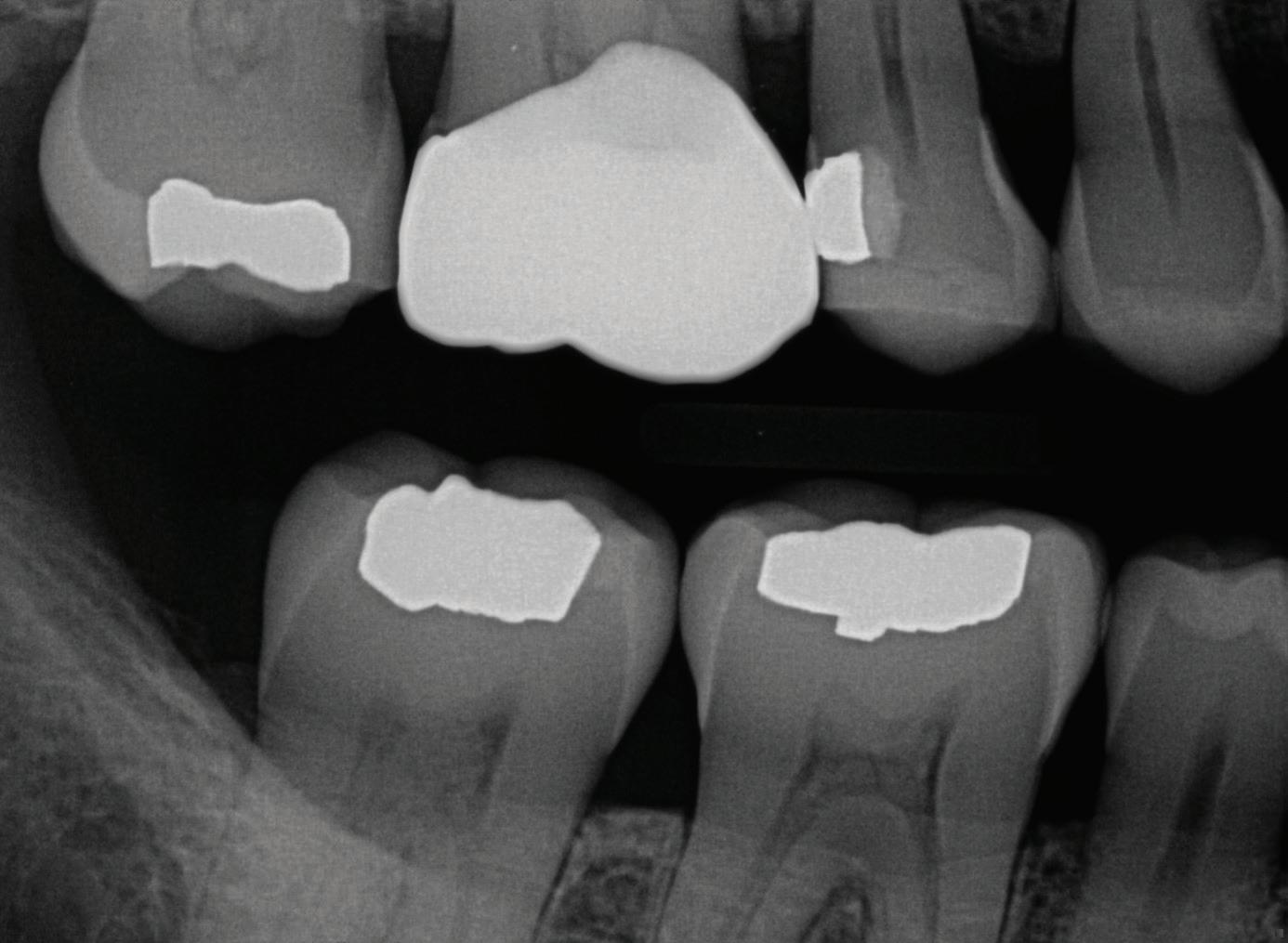
Fig. 23. Radiograph showing completed gold GI composite DO 4.
foil to this procedure would also be beneficial. This is a project that should be completed in an academic setting. Obviously, anyone attempting this procedure is expected to be proficient in the placement of gold foil in a clinical setting. A start would be to contact the American Academy of Gold Foil Operators. The author is also personally available for comment.
Acknowledgements The author would like to thank Dr Clyde Roggenkamp and Dr Frederick Eichmiller for their help in putting together this paper.
Conflict of Interest The author of this article certifies that he has no proprietary, financial, or other personal interest of any nature or kind in any product, service, and/or company that is presented in this article.
Henry, DB (2022). Clinical Presentation of the Direct Gold/Composite Sandwich Restoration J Op Dent, 47(2), 123-130. Used by permission. © Operative Dentistry, Inc. Transmission or reproduction of protected items beyond that allowed by fair use requires the written permission of Operative Dentistry, Inc.
REFERENCES
1. Moore DL & Stewart JL (1967) Prevalence of defective dental restorations Journal of Prosthetic Dentistry 17(4) 373-378. doi: 10.1016/00223913(67)90008-x 2. Fontana M & Gonzalez-Cabezas C (2000) Secondary caries and restoration replacement: An unresolved problem Compendium of Continuing Education in Dentistry 21(1) 15-18, 21-24.
3. Roulet JF (1997) Review of the clinical survival of direct and indirect restorations in posterior teeth of permanent dentition Journal of Dentistry 25(6) 459-4733.
4. Manhart J, Chen H, Hamm G, & Hickel R (2004) Review of the clinical survival of direct and indirect restorations in posterior teeth of the permanent dentition Operative Dentistry 29(5) 481-508.
5. Henry DB The Consequences of Restorative Cycles Operative Dentistry (2009) 34(6) 759-760.
6. Henry DB (2008) A philosophy for restoring virgin caries Operative Dentistry 22(5) 475-483.
7. Challenges of Dentin Bonding In: Sturdevant’s Art and Science of Operative Dentistry 5th edition Mosby, Maryland Heights, MO 248-249.
8. Small BW & Johnson W (2006) Gold foil and its use in modern dentistry Dentistry Today 25(3) 92, 94, 96.
9. Opdam N JM van de Sande FH, Bronkhorst E, Cenci MS, Bottenberg P, Pallesen U, Gaengler P, Lindberg A, Hiysmans MCDNJM, & van Dijken JW (2014) Longevity of posterior composite restorations: A systematic review and meta-analysis Journal of Dental Research 93(10) 943-949. doi: 10.1177/0022034514544217
10. Overton JD & Sullivan DJ (2012) Early failure of class II resin composite versus class II amalgam restorations placed by dental students Journal of Dental Education 76(3) 338-340.
11. Zhou Y, Kong Y, Kundu S, Cirillo JD, & Liang H (2012) Antibacterial activities of gold and silver nanoparticles against Escherichia coli and bacillus Calmette-Guérin Journal of Nanobiotechnology 10(19) 1-9. doi: 10.1186/1477-3155-10-19
12. Gordon JC (2021) Longevity of Direct and indirect dental restorations Clinicians Report 14 (10) 1-3.
13. Stibbs GD (1951) An appraisal of the gold foil restoration Journal of the Canadian Dental Association (Toronto) 17(4) 191-199.
14. Brinker HA Jr (1972) Gold foil - can we afford to do without it? Journal of the American Academy of Gold Foil Operators 15(1) 25-33.
15. Goldstein GR (2010) The longevity of direct and indirect posterior restorations is uncertain and may be affected by a number of dentist-, patient, and material-related factors Journal of EvidenceBased Dental Practice 10(1) 30-31. doi: 10.1016/j.jebdp.2009.11.015.
16. Hilton TJ & Broome J(2006) In Fundamentals of Operative Dentistry: A Contemporary Approach (Chapter 10) 3rd Edition Quintessence Publishing, Chicago, IL.
17. Mjör IA & Ferrari M (2002) Pulp-dentin biology in restorative dentistry. Part 6: Reactions to restorative materials, toothrestoration interfaces, and adhesive techniques Quintessence International 33(1) 35-63.
18. Zhang Y, Dasari TPS, Deng H, & Yu H (2015) Antimicrobial activity of gold nanoparticles and ionic gold Journal of Environmental Science and Health, Part C (33)3 286-327. doi: 10.1080/10590501.2015.1055161
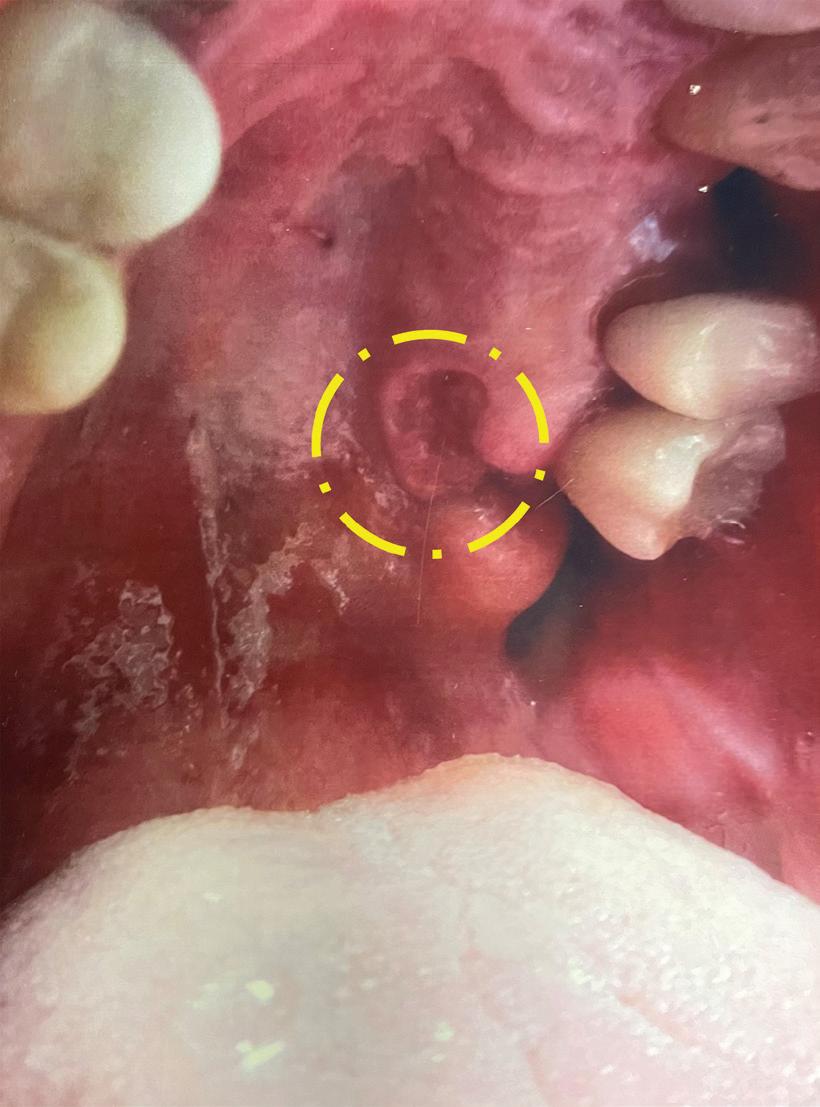
Read, Learn and Earn! By: Drs. Saja Alramadhan*, Neel Bhattacharyya, Donald M. Cohen and Nadim M. Islam A 70-year-old, healthy white male presented to Dr. Charles DeWild, Oral & Maxillofacial Surgeon at the Florida Oral Surgery Visit floridadental.org/online-ce for this FREE, MEMBERS-ONLY BENEFIT. You will be given the in Sanford, with a two-month history of a non-healing ulcer. opportunity to review the “Diagnostic Discussion” and its accompanying photos. Answer five Examination revealed a red, endophytic lesion (crater-like) with a multiple choice questions to earn one hour of CE. verrucoid center on the palatal gingiva of tooth #14 (Fig. 1). The patient was completely asymptomatic. Dr. DeWild performed an incisional biopsy. This was then submitted to the University of Florida Oral Pathology Laboratory biopsy service for a diagnosis.
t Contact FDC Marketing Coordinator Brooke Martin Question: at bmartin@floridadental.org or 800.877.9922. What is the most likely diagnosis?
A. Verrucous Carcinoma
B. Inverted ductal papilloma
C. Traumatic Ulcer
D. Verruciform Xanthoma Fig. 1. A red, ulcerated and endophytic lesion located on the palatal gingiva of tooth #14.
A. Verrucous Carcinoma
Incorrect — a good choice though. Verrucous carcinoma is a lowgrade, well-differentiated variant of the more common squamous cell carcinoma. It is associated with smoking and/or chronic use of chewing tobacco or snuff, typically arising in locations where tobacco is habitually held such as the labial and buccal vestibule. Verrucous carcinoma predominantly occurs in males over 55 years of age. The mandibular vestibule, buccal mucosa and the hard palate are the most commonly involved sites. It is usually extensive at the time of diagnosis and may be present for two to three years before it is diagnosed. Clinically, verrucous carcinoma is usually a speckled (white/red), well-demarcated, painless exophytic mass with prominent granular, verruciform or papillary architecture (hence the verrucous name). Another salient point we have noted in our experience is that verrucous carcinoma of the gingiva tends to “creep” into the periodontal ligament space and eventually destroys bone by invasion along with the periodontal ligament space and not into surrounding bone. Histologically, verrucous carcinoma is characterized by an epithelial proliferation surfaced by a thickened layer of papillary or verrucoid parakeratin. No invasion is observed at the connective tissue interface, only invagination of the squamous epithelial rete ridges which are bulbous and elongated and appear to push into the underlying connective tissue. Parakeratin typically fills the numerous clefts or crypts between the surface projections “parakeratin plugging”. Combined characteristics such as integrity of the basement membrane and normal epithelial maturation, along with the absence of frank dysplastic changes, give the disease its deceptively benign appearance. The histology would be somewhat of a match except for the finding of xanthoma cells (foam cells) seen in this patient’s biopsy sample.
Metastasis is extremely rare, therefore, surgical excision without radical neck dissection is the treatment of choice. For gingival lesions, due to the tendency of “creeping” into periodontal ligament space around teeth, surgery often involves the removal of the involved teeth and gingiva. The prognosis is excellent with 90% of patients being disease-free after 5 years. Radiotherapy is not indicated and several reports in the literature have documented development of poorly differentiated or anaplastic carcinoma within the lesion after radiotherapy.
B. Inverted Ductal Papilloma
Incorrect – inverted ductal papilloma is a rare benign ductal papillary neoplasm that arises in the secretory duct of the minor salivary glands. Inverted ductal papilloma is part of the ductal papillomas neoplasms group, along with intraductal papilloma and sialoadenoma papilliferum. The exact etiology is unknown; however, human papillomavirus (HPV) types 6 and 11 have been identified in some cases. Some authors have related it to trauma which could possibly play a role in the development of this tumor. Inverted ductal papilloma affects middle-aged patients with no significant gender predilection. Clinically, the lesion appears as an asymptomatic nodule that varies in size from 0.5 to 1.5 cm in diameter with either smooth or verrucoid surface. The lower lip and mandibular vestibule are the most frequently affected sites.
Microscopically, inverted ductal papilloma shows papillary intraductal proliferation immediately subjacent to the mucosal surface. The ductal lumen is usually lined by cuboidal or columnar epithelium cells, with scattered goblet cells. The tumor may be continuous with the surface mucosa. Conservative surgical excision is the treatment of choice for inverted ductal papilloma.
C. Traumatic Ulcer
Incorrect – but another great differential diagnosis. Though the clinical appearance may be suggestive of an ulcer, the absence of tenderness and history indicative of any trauma are not supportive of traumatic ulcer. Traumatic ulcer tends to be described as painful and usually located on areas that are subjected to trauma, such as the tongue, buccal mucosa or the labial mucosa. Sites such as the palate may be exposed to trauma mainly from food items such as chips, or a dental prosthesis. Ulcers tend to be depressed lesions which may or may not have raised borders. Additionally, if there is no repeated injury, most traumatic ulcers tend to heal within two weeks unless there is constant irritation and/or formation of a granuloma. As for this case, the lesion has been present for 2 months, which made this lesion suspicious of another entity rather than traumatic ulcers and warrants an incisional biopsy.
D. Verruciform Xanthoma
Correct! – verruciform xanthoma is a relatively uncommon, oral benign lesion characterized by papillary epithelial proliferation with the accumulation of lipid-laden macrophages (xanthoma cells “foam cells”) within the superficial lamina propria and the connective tissue papillae. Unlike other papillary lesions it is not associated with HPV. The exact etiology of verruciform xanthomas is unknown. However, they are considered reactive lesions, associated with trauma and/or chronic irritation. Other investigators suggest that verruciform xanthomas may represent an unusual immunologic reaction to local epithelial disturbances; this hypothesis is supported by documented cases of verruciform xanthomas in association with other pathologic disorders such as lichen planus, epithelial dysplasia, squamous cell carcinoma and pemphigus vulgaris.
Unlike, dermal xanthomas, oral verruciform xanthomas are not associated with diabetes, hyperlipidemia or any other metabolic or systemic disease. The gingiva, alveolar ridge and hard palate are the most commonly involved sites but any other oral site may be involved. Oral verruciform xanthomas occur over a broad age group, with no significant gender predilection. Clinically, verruciform xanthomas typically appear as asymptomatic, solitary, well-demarcated plaques or nodules with a papillary, verrucoid or granular surface that measured less than 2 cm in diameter. Lesions also have a characteristic white, yellow-white or reddish-orange color. This color is thought to reflect collections of large numbers of lipid laden or foamy macrophages (Fig. 2- green arrow) found in this lesion. The clinical differential diagnoses may include squamous papilloma, condyloma acuminatum and squamous cell carcinoma. The classic microscopic appearance of verruciform xanthoma is of a papillary epithelial proliferation with hyperkeratosis, elongated rete ridges and collections of xanthoma cells “foamy macrophages”. The keratin layer is usually described as orange in color. In the present case, the endophytic clinical appearance is a bit unusual and so is the histology. Notably, the invagination of the squamous epithelium with elongated rete ridges into the underlying connective tissue and deep crypts of keratin extending into the spinous layer (Fig. 2-yellow arrow) are seen, mimicking verrucous carcinoma. However, the presence of xanthoma cells “foamy macrophages” (Fig. 2-green arrow) are diagnostic for verruciform xanthoma. Simple surgical excision is generally curative and lesions usually do not recur.
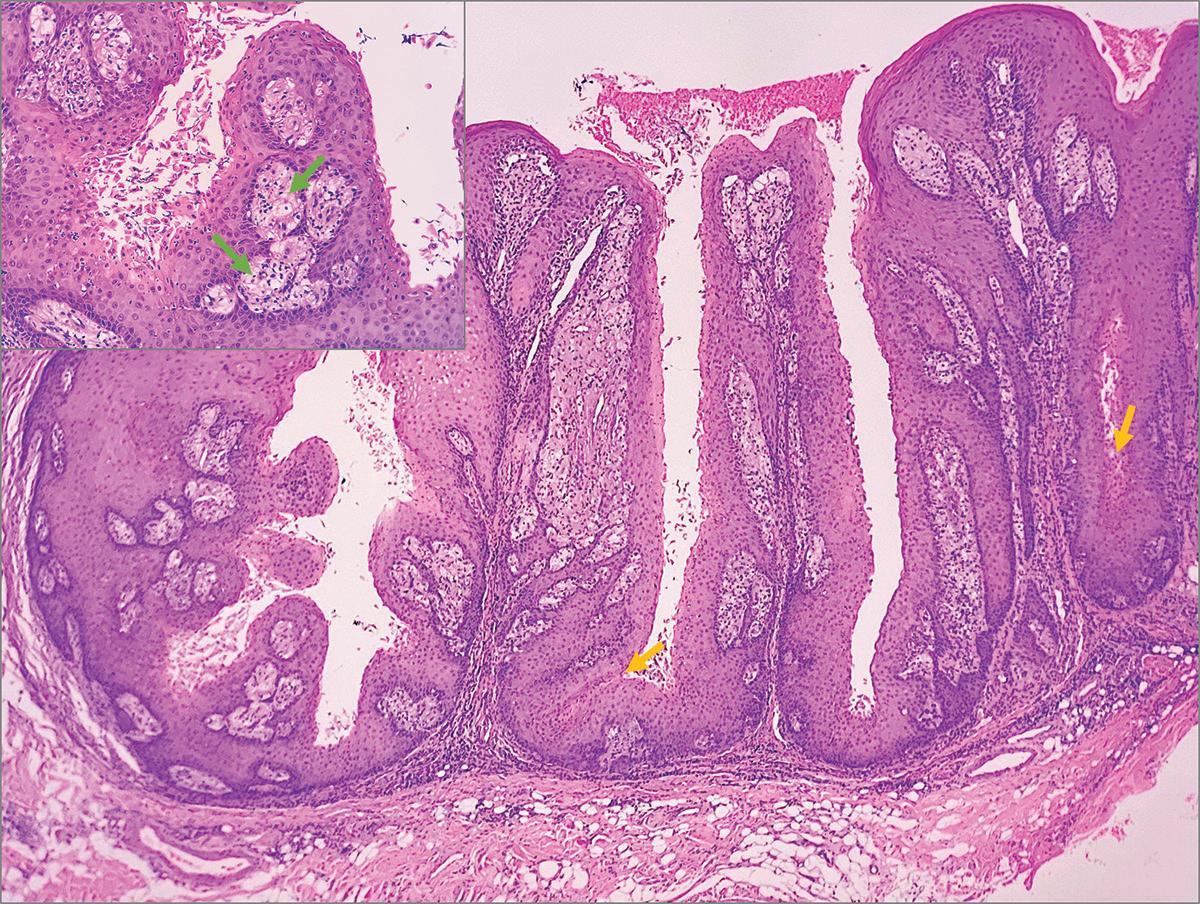
Fig. 2. Histopathologic slide depicting incisional biopsy.
References
Santosh HN, Nagaraj T, Saxena S, Biswas A, Pai SA. Verrucous carcinoma: A clinicopathological study. J Oral Maxillofac Pathol. 2019;23(2):303. doi:10.4103/jomfp.JOMFP_59_19
Betz SJ. HPV-Related Papillary Lesions of the Oral Mucosa: A Review. Head Neck Pathol. 2019;13(1):80-90. doi:10.1007/s12105-019-01003-7
Alramadhan SA, Fitzpatrick SG, Bhattacharyya I, Islam MN, Cohen DM. Changing Trends in Benign Human Papillomavirus (HPV) Related Epithelial Neoplasms of the Oral Cavity: 1995-2015 [published online ahead of print, 2022 Mar 7]. Head Neck Pathol. 2022;10.1007/s12105-022-01426-9. doi:10.1007/s12105-022-01426-9
Belknap AN, Islam MN, Bhattacharyya I, Cohen DM, Fitzpatrick SG. Oral Verruciform Xanthoma: A Series of 212 Cases and Review of the Literature. Head Neck Pathol. 2020;14(3):742-748. doi:10.1007/s12105019-01123-0
t
Neville, BW, Damm DD, Allen CM, and Chi AC. (2016) Oral and Maxillofacial Pathology. 4th edition, WB Sanders, Elsevier
Diagnostic Discussion is contributed by University of Florida College of Dentistry professors, Drs. Indraneel Bhattacharyya, Don Cohen and Nadim Islam, who provide insight and feedback on common, important, new and challenging oral diseases.
The dental professors operate a large, multi-state biopsy service. The column’s case studies originate from the more than 14,000 specimens the service receives every year from all over the United States.
Clinicians are invited to submit cases from their own practices. Cases may be used in the “Diagnostic Discussion,” with credit given to the submitter.
Drs. Bhattacharyya, Cohen and Islam can be reached at oralpath@dental.ufl.edu. Conflict of Interest Disclosure: None reported for Drs. Bhattacharyya, Cohen and Islam.
The Florida Dental Association is an ADA CERP Recognized Provider. ADA CERP is a service of the American Dental Association to assist dental professionals in identifying quality providers of continuing dental education. ADA CERP does not approve or endorse individual courses or instructors, nor does it imply acceptance of credit hours by boards of dentistry. Concerns or complaints about a CE provider may be directed to the provider or to ADA CERP at ada.org/goto/cerp.
*Fellow in Oral and Maxillofacial Pathology University of Florida College of Dentistry.
Career Center
The FDA’s online Career Center allows you to conveniently browse, place, modify and pay for your ads online, 24 hours a day. Our intent is to provide our advertisers with increased flexibility and enhanced options to personalize and draw attention to your online classified ads!
Post an ad on the FDA Career Center and it will be published in our journal, Today’s FDA, at no additional cost! Today’s FDA is bimonthly; therefore, the basic text of all active ads will be extracted from the Career Center on roughly the 5th of every other month (e.g., Jan. 5 for the Jan/Feb issue, March 5 for the March/April issue, etc). Please note: Ads for the Nov/Dec issue must be placed no later than Nov. 1. Please visit the FDA’s Career Center at careers.floridadental.org.
Endodontic Associate - Tampa Bay Area. Well established, busy Endodontic group practice seeking energetic, quality Endodontist. Modern office with latest technology including microscopes, digital radiography, CBCT, and experienced support staff. Excellent earning potential and benefits. Recent graduates encouraged to apply. Visit careers. floridadental.org/jobs/17109281.
Established general and implant private practice on the beautiful Treasure Coast is seeking Associate Dentist. Our practice is committed to providing the highest quality dental care to our community. To learn more about this opportunity, please email your CV and/or any questions to ccp1222@bellsouth. net. Must have a Florida Dental License. Visit careers.floridadental.org/jobs/17062849.
Ormond Beach. We are seeking a team-oriented expanded functions dental assistant. Must have a servant’s heart, caring personality that caters to our patients. Must be able to get along easily with staff and be an eager to help team player. Ideally 5+ years experience. Benefits and pay will be discussed with the Dr. based on experience and talent. Monday - Thursday 7:45- 5:00. Expanded Functions certificate. Visit careers. floridadental.org/jobs/16961485
Oral Surgeon wanted for busy, well established 27 year Boca Raton Dental practice. 1 day/week. Comfortable environment, experienced staff. Visit careers.floridadental. org/jobs/16954798. Well-established private endo practice seeking a quality-driven, skilled, fulltime endodontist licensed in the state of Florida. The practice is equipped with state-of-the-art equipment, including CBCT, microscopes, digital radiography, PBS Endo, and paperless charts. The practice was established in 2002 and has an outstanding reputation in the dental community for the highest level of endodontic quality patient care and comfort. We are looking to expand and incorporate a new associate into our growing practice. The practice has strong established referrers in the Miami/Doral area. Doral is conveniently located in the heart of the Miami metro area and was named the fastest-growing city in Florida. Because of our patient population, doctors must be bilingual, in both English and Spanish. To learn more about this position, please email your resume to: endospecialistsofsouthflorida@gmail.com. Vsit careers.floridadental. org/jobs/16961145.
Come join us! If you are looking for an associate opportunity with room for growth, an excellent earning potential, and opportunity to partner (if desired) in a great office. We are currently seeking a full-time associate for our Volusia County location but are open to discussing part-time availability. Mentorship and guidance will be provided for recent residency graduates. We are a well-established, privately owned endodontic practice with two locations in Central Florida. Our office is looking for a compassionate, energetic, quality-oriented endodontist to join our team. Our newly renovated offices have the latest technology including but not limited to: LED surgical microscopes, digital radiographs, CBCT on site, intraoral cameras, and remotely accessible practice management software. This is the perfect opportunity for someone looking to be the only associate in an office with access to, and support from, a great clinical/business mentor. Associate will have their own desk, scheduling autonomy, and monthly marketing budget. Compensation will be 47% of collections with a $1,000 daily minimum guarantee. Florida Dental License acquisition assistance is available for those who are not currently licensed in Florida. This is a unique opportunity that will fill fast! Ideal for someone who would like to see what private practice ownership is like, or practice in an “owner style” associateship. If you are interested in this opportunity, please send your CV/ Resume and a copy of the qualification documents listed below listed below to office@ daytonendo.com. Be sure to include contact information in the body of the email and our doctor will contact you as soon as possible. We look forward to connecting with you! Required for consideration: 1. DDS/DMD from an accredited Dental School 2. Certificate of Completion from an accredited US Endodontic Residency Program 3. Active Florida Dental License. Visit careers.floridadental. org/jobs/16958506.
General Dentist – Dental Partners, Melbourne. Sign-On Bonus Incentive $10,000 $50K Student Loan Repayment Program.
Relocation Incentive. Making a difference each and every day is what we do at Gainesville Dental Associates! Our teams serve our patients by building valuable relationships, providing excellent dentistry and a range of services to suit the needs of the community. If you are looking for a Full-Time opportunity to help lead a well-established and successful dental practice, consider scheduling a confidential appointment with us today. We are seeking a General Dentist to work in a fast paced, well established dental office. We prefer a candidate with a minimum of 2 years work experience and who is able to perform a range of services to our patients however well qualified **NEW GRADS** welcome to apply. Our talented team of dental professionals will work along side you to ensure your successful entry into the practice and long term success. As a team member, you’ll enjoy the following: Competitive Daily base rate with performance incentives; Sign-On Bonus of $10,000; Student loan repayment program available for this location! Let us help you pay your student loans down!; If you do not live in the area, we will help you get here with our relocation benefit; Full health and wellness benefits. Employer paid life insurance and contribution to a Health Savings Account; Saving for retirement made easy with a best in class 401K program and generous employer match; Keep your clinical skills up to date through CE with our yearly allowance program; Opportunities to contribute to your community through education and charity events; Practice Full-Time with friendly days/ hours; A full team of support from qualified and educated dental assistants to work along side you, to a regional leadership team and finally a corporate service center with all the departments to ensure your practice runs smoothly. You take care of providing great care to your patients and we will take care of the rest. Sound interesting? We’d love to speak with you today! We are an Equal Opportunity Employer and Drug Free Workplace with opportunities for all. We pride ourselves on our diverse organization and our family friendly and inclusive culture. We have a Veteran’s and AARP Hiring Pledge. We are a certified Great Place to Work company! www.puredentalbrands. com. #WeHaveWhatMakesYouSmile. You want to work with the best organization and we want to work with the best providers. Therefore, all candidates must be licensed to practice in the State of Florida with no board reprimands or issues and have a valid DEA license. Visit careers.floridadental.org/ jobs/16938245.
Lake Mary, fee for service, 5 star, highend practice is looking for a part-time/ full-time dentist. Applicant must have knowledge of, or would be willing to learn holistic/biological dentistry. We spend quality time with our patients and are not in a rush to treat them fast. We develop trusting relationships that are long lasting. In addition, we have up-to-date equipment and an experienced staff to help provide quality dentistry! If you are interested in a great opportunity please contact us at 407.333.1335 and provide us with a resume at timtiralosi@ tiralosidental.com. Visit careers.floridadental.org/jobs/16906913.
Offering a General Dentistry Associateship position that can lead to partnership. Family practice. Long standing practice been in the area for over 40 years. Great location on the main road through Ormond Beach. Great staff. We have a CT scanner, CAD CAM milling, soft tissue laser and more. Looking for someone who enjoys engaging the patients and practicing high quality dentistry. For details please contact Dr. Drake at drake@drdrake.com. Active DDS/ DMD and Florida dental license. Visit careers. floridadental.org/jobs/16872179.
Kissimmee. 25+ year, multi-doctor, privately owned family practice seeking a highly motivated General Dentist to help treat our great patients and work with a wonderful and experienced team. Join a successful practice and jump right in to a strong schedule with over 100 new patients a month waiting for quality, comprehensive care. Enjoy a base salary with percentage based incentive compensation. Visit our website: https://www. kissimmeefamilydental.com Please forward CV to Holly Lance: holly@kissimmeefamilydental.com. Visit careers.floridadental.org/ jobs/16797765.
Bay Dental Center is looking for associates that value long term relationships in life. Bay Dental Center is expanding operations in the Gulf Coast area. We have been a Family Private Practice for nearly 15 years. We provide all aspects of General Dentistry. We have one year positions, as well as positions that are geared towards eventual partnerships. DDS or DMD with or without MS. Visit careers.floridadental.org/ jobs/16759880. Bradenton. Are you a growth-minded, Goal-oriented, self-motivated individual who is motivated to learn and treat patients well? Are you looking for a great income potential and an option to partner up in a practice to own it? Do you wish to live and raise a family in a friendly town full of lifestyle opportunities? Do you want a dentistry career to be fulfilled with all the above? Too good to be true? Trust me, this is all possible if you are with the correct practice!!! My Name is Dr Nish Patel and I have been living of all the above for the past 12 years on the west coast of Florida. We are growing FFS/ Some PPO Practice looking for an associate to be able to make dentistry a fulfilling career. We have a leadership team in place to handle all the management, marketing and generating new patients. We offer great income potential, an uplifting work environment, and a team that feels like family. We can Sponsor work Visa. Check out our reviews online at www. Smylmanatee.com.Essential Core Competencies: Excellent patient communication - Educate patients on maintaining proper oral health during treatment. Carefully and methodically document all treatment-related notes, comments, instructions, etc. Desire to learn and grow professionally. Compensation & Benefits: Compensation to include a payroll draw/advance and a commission structure that provides incentive. Benefits to include medical insurance, an in-house dental plan, life insurance and a 401(k) plan with a match. Receive mentoring, training, and development from our Chief Clinical Officer regarding ethical and optimal patient care. Team culture with autonomy. A steady stream of patients to keep you busy and exposure to all types of procedures • Associate will have 4 available ops, dedicated assistants, and hygiene support Potential for future partnership and attainment of mutual goals. If you’re interested, please send your cover letter, resume and references to Hr@ SmylManatee.com. In your cover letter Write us a little bit about. Where you currently practice and a brief description of your situation there. What is your biggest hurdle in Life Right now? Qualifications: DDS or DMD from an accredited dental school with a min of 4 years general dentist experience. Dedication to integrity and achieving the highest standards of ethical patient care. Visit careers. floridadental.org/jobs/17115773

Support
OUR JOURNAL ADVERTISERS
American Sensor Tech | 23 ben-pat Institute | 32 Doctor’s Choice | 38 FDA: Online Radiography Program | 25 FDA: Well-being Program | 23 FDAS: Abyde | 52 FDAS: Bank of America | 24 FDAS: Crown Savings | 73 26 & 27 | FDAS: Tribute Plan 42 | FDAS: The Gift of Coverage 64 | Henry Schein Professional
Practice Transitions 49 | National Dentex Labs 44 | PSC Group, Inc. 69 | The Doctors Company 23 | Tobacco Free Florida
SUPPORT OUR ADVERTISERS, AND WHEN YOU DO, MENTION TODAY’S FDA!
ADVERTISING INFORMATION
For display advertising information, contact: Deirdre Rhodes at drhodes@floridadental.org or 800.877.9922, Ext. 7108.
For Career Center advertising information, contact: Shey Loman at sloman@floridadental.org or 800.877.9922, Ext. 7115.
PUBLISHING INFORMATION

Today’s FDA (ISSN 1048-5317/USPS 004-666) is published bimonthly by the Florida Dental Association (FDA), 545 John Knox Road, Ste. 200, Tallahassee, FL 32303. FDA membership dues include a complimentary subscription to Today’s FDA. Nonmember subscriptions are $150 per year; foreign, $188. Periodical postage paid at Tallahassee, FL and additional entry offices. Copyright 2021 Florida Dental Association. All rights reserved. Today’s FDA is a refereed publication. POSTMASTER: Please send form 3579 for returns and changes of address to Today’s FDA, 545 John Knox Road, Ste. 200, Tallahassee, FL 32303.
EDITORIAL AND ADVERTISING POLICIES
Editorial and advertising copy are carefully reviewed, but publication in this journal does not necessarily imply that the FDA endorses any products or services that are advertised, unless the advertisement specifically says so. Similarly, views and conclusions expressed in editorials, commentaries and/or news columns or articles that are published in the journal are those of the authors and not necessarily those of the editors, staff, officials, Board of Trustees or members of the FDA.
EDITORIAL CONTACT INFORMATION
All Today’s FDA editorial correspondence should be sent to Dr. Hugh Wunderlich, Today’s FDA Editor, Florida Dental Association, 545 John Knox Road, Ste. 200, Tallahassee, FL 32303. FDA office numbers: 800.877.9922, 850.681.3629; fax: 850.561.0504; email address: fda@floridadental.org; website address: floridadental.org.
Today’s FDA is a member publication of the American Association of Dental Editors and the Florida Magazine Association.
The most interesting man in world ...

It happened again last week, and at least a dozen times over the years. I was once again mistaken for “the most interesting man in the world.” In case you have no idea what I’m talking about, the most interesting man in the world comes from a national Dos Equis advertising campaign. In the advertisement, Dos Equis claims that this really, really good-looking guy leads such an interesting life that he lives vicariously through himself, speaks Russian in French and prefers to drink Dos Equis of course. Then again, maybe it is not my doppelganger worthy good looks, but my punctilious dental skills that caused the confusion.
<cue the classical Spanish guitar Dos Equis melodic theme song> 1. I can carry all the groceries with one arm and still prep a perfect
crown.
2. I can talk about Fight Club during my consultations.
3. When I use dental equipment, it increases in value.
4. Once in an operatory, a rattlesnake bit me. After five days of excruciating pain, the snake died.
5. My Florida dental license only has one digit.
6. If I were to submit a crown procedure to an insurance company without a radiograph, they would pay for it. t
7. The Board of Dentistry often questions me just because they find me interesting.
8. My 10-gallon amalgam separator holds 20 gallons.
9. I can do dentistry both left-and right-handed.
10. My business cards say, “I will call you.”
But what is there to do if you picked your parents poorly or don’t drink a most interesting beer? How do you become more interesting when your dental skills are less interesting than mine?
You can start by becoming more influential and take the advice sent to me by Omar Ahmad about how to create action for the issues you care about. To be more interesting you need to share your ideas and influence your region’s legislators.
However, your legislators are being broadcast to by other people all the time. So how do you stand out and really grab their attention? If you send an email, you compete with the hundreds of impersonal, “spammy” messages they receive and end up lost in their inbox. Face-to-face meetings do serve a purpose, but they’re not practical when you’re trying to send an accordant, persistent message. We’re in an age filled with iPhones, emails and YouTube, but one of the best communication tools when it comes to contacting your legislators is the mighty analog, better known as the handwritten letter. Or, even better yet, dig out your father’s 1924 Underwood typewriter. See, it got you to read this “interesting” editorial. Be proactive and write to your elected officials at least once a month. If you are consistent, within three months your elected officials will start calling you when that issue comes up to ask, “What do you think?”
There is, of course, a method to constructing letters you send to your elected officials. In the first paragraph, you appreciate them. You may not actually appreciate the person, but maybe you appreciate that they have a “tough gig.” In the next paragraph, get to the point and be blunt, but don’t attack the person. Attack the tactics. Smear attacks will get you nowhere. You need to be the nurturing agent. Become a safe place and a resource for them. Tell them, “If no one is providing this information, let me help.” Finally, when you sign the letter, be sure to include your title. You are a dentist. You are already interesting and worthy of their curiosity. This will make you “the most interesting person in the world” on this issue. And best of all, you don’t need to have the Dos Equis trademarks like “charm so contagious it rivals COVID” or “enemies that list you as their emergency contact.” Stay thirsty my friends.







