5 minute read
More than Just Esthetics: Orthodontic Considerations for the Patient with Down Syndrome


More than Just Esthetics: Orthodontic
Considerations for the Patient with Down Syndrome By: Dr. Greg Scott and Dr. Jon Scott; Introduction by Dr. John Paul ” I thought I had a clear concept of how I would enter into fatherhood. We would make the harried trip to the hospital and my wife would be escorted to that secret maternity section where babies left the womb while I would be led to the waiting area where I would pace about and crush a handful of celebratory cigars until a nurse came out said “Congratulations, Dr. Paul, you’re a father!”
It didn’t work out that way. Once we got to the hospital things moved along quickly and I was front and center for the entire event. As soon as I saw her, I fell in love with my daughter. As far as I was concerned, she was–and is–perfect. The delivery staff had other ideas. Seemed as if they were racing to see who could be the first to label my little girl. Not with a name, but with a diagnosis of Down Syndrome. Note to delivery staff: unless there is an immediate health risk, let the parents enjoy their new infant and leave the diagnosing to the pediatrician. It’s a long enough journey without getting an early start.
Once the diagnosis of Down Syndrome is confirmed the journey really does start. There are several co-diagnoses associated with Trisomy 21. You’ll be scheduled for cardiac screening, digestive tract screening, and thyroid screening among others. Your child may have all or none of these but it’s important to rule them out.
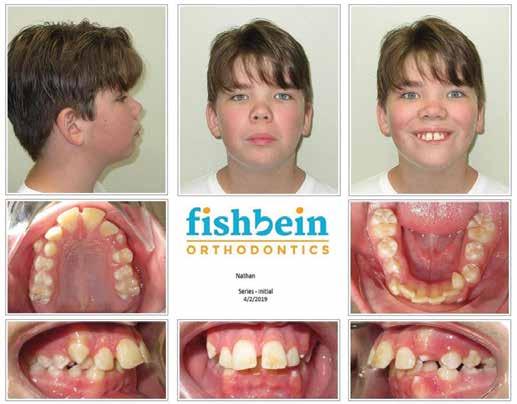
About the time my daughter turned 5, I noticed some snoring. Initially I thought it was positional, because I could turn her and it would go away. Also, about age 5, we started going to the hospital with pneumonia. There are few things scarier than your child not being able to raise the oxygen level in their blood high enough to leave the hospital. I wondered if her ability to breathe was contributing to our annual week in the hospital. I treat adults for apnea and sleep disordered breathing, but those treatments are not ap32 It is recommended that patients be evaluated at age seven. Multiple phases of orthodontics may be necessary when treating patients with Down Syndrome.
propriate for a developing child. I also noticed my daughter had a tall and narrow palate, something she inherited directly from me and has nothing to do with an extra chromosome 21. That’s how I came to start a discussion with my orthodontist ...
Crowding, cross bites and impacted teeth create functional concerns that should be treated. But, just as for any child or adult, the appearance of the teeth of a patient with Down Syndrome can affect the feedback they receive from other people. Research indicates that malocclusion, tooth loss and untreated decay can have a profound impact on aesthetics and the psychosocial behavior of young people, affecting their self-esteem.1 Social acceptance is difficult enough for these kids without the added hindrance of a poor smile.
Children with Down Syndrome typically have narrow palates and small arches due to mouth breathing. Although their tongues appear larger than normal tongues, they usually do not have true macroglossia, but rather have relative macroglossia based on the boney confines of their constricted oral cavities.2 Snoring and apnea are common due to the narrow palates and relative macroglossia. There is between 50 to 100% incidence of obstructive sleep apnea in patients with Down Syndrome.3 Those with apnea have lower IQ’s than without.4 In addition to the tongue, obstruction is caused by low muscle tone, poor coordination of airway movements, and a narrower airway in the midface and throat. Tonsillar hypertrophy, not adenoids, appears to be the biggest cause of obstruction.5
Any physical obstruction, such as enlarged tonsils and adenoids, should be corrected surgically. However, as part of a regimen to normalize the space of the oral cavity, palatal expansion is very effective. When palatal expansion is combined with adenotonsillectomy, complete resolution of OSA is possible.6 Sutural expansion of the palate can be accomplished early, but it is not unusual to need a second expansion appliance following more physical growth. Expansion leads to more room for the tongue as well as a wider nasal base and improved nasal airway as well.7 A secondary effect of more tongue space is elevation of the tongue which can lead to pharyngeal airway improvement.8 In addition to skeletal expansion of the maxilla, the mandibular teeth can be uprighted within the basal bone to broaden the lower arch creating more space for the tongue and reducing the relative macroglossia.
It is recommended that patients be evaluated at age seven. Multiple phases of orthodontics may be necessary when treating patients with Down Syndrome. The first phase would likely include expansion to address the relative macroglossia. The second phase would focus on occlusion and esthetics, with a possible additional round of expansion. Tooth eruption is usually delayed in Down Syndrome, so final treatment may be later in age than usual. Although early treatment is recommended, adult patients with Down Syndrome can also benefit from expansion, if needed, for improved airway. Palatal expansion in the non-growing patient will be less predictable than in younger patients and could require surgical intervention or other special methods such as a mini implant supported expander or periodontally accelerated osteogenic orthodontics.
Most patients can be treated in the normal practice setting with some minor adaptations. It is important to provide clear instructions and speak to caregivers about behavior management techniques that have worked in the past. Be consistent with messaging and with the staff the patient sees.
Correction of malocclusion in patients with Down Syndrome can have significant lasting physiological and social effects on patients. Patients benefit from the possible reduction of obstructive sleep apnea, which can dramatically improve their health and IQ. Normalizing the oral cavity and creating space for the tongue can also reduce the outward appearance of the syndrome and improve social interactions.
References
1. Impact of Dental Disorders and its Influence on Self Esteem Levels among Adolescents. J Clin Diagn Res. 2017 Apr; 11(4); ZC05-ZC08
2. Dental Care for Developmentally Disabled. Today’s FDA. 1992 Jul;4(7):1C-3C
3. Obstructive sleep apnea & down syndrome. NDSS. (2019, November 1). Retrieved April 25, 2022, from https://www.ndss.org/resources/obstructive-sleep-apnea-syndrome/
4. Obstructive Sleep Apnea Syndrome and Cognition in Down Syndrome. Dev Med Child Neurol. 2014 Jul;56(7):657-64
5. Prevalence of Sleep-Disordered Breathing in Children with Down Syndrome: Polygraphic Findings in 108 Children. Sleep. 2003 Dec 15;26(8):1006-9
6. Orthodontic Expansion treatment and adenotonsillectomy in the treatment of OSA in prepubertal children. Sleep 2008;31(7):953-957
7. Tongue posture improvement and pharyngeal airway enlargement as secondary effects of rapid maxillary expansion- a cone-beam computed tomography study. Am J Orthod Dentofacial Orthop 2013;143:135-45
8. Three-Dimensional Evaluation of Upper Airway Following Rapid Maxillary Expansion Angle Orthod. 2014;84:265-273
Photo:
Top row, l to r: Drs. Greg Scott and Jon Scott. Bottom row, l to r: Brogan Paul and her father, Dr. John Paul.