



HERO
UNSUNG
The State of Drug Addiction.
Bad is the Problem in the Western New York?P.15 FREE
2 MILLION CASES OF CANCER EXPECTED IN ‘23 Local experts offer some tips on how to keep cancer at bay BFOHEALTH.COM MARCH 2023 • ISSUE 101 Art at Roswell Park Helps People Battle Cancer P.10
Michelle Rainville, an ER doctor from Eastern Niagara Hospital, discusses ‘scary’ early days of COVID-19 days when she was afraid to go to work. She recently earned the Unsung Heroes recognition from UBMD
How
NEARLY
Cutting Calories May Slow Aging in Healthy Adults
The key to living longer could be eating less.
In a new study published in the journal Nature Aging, researchers found that a calorie-restricted diet had substantial health benefits, including delayed aging.
“The main take-home of our study is that it is possible to slow the pace of biological aging and that it may be possible to achieve that slowing through modification of lifestyle and behavior,” said senior study author, physician Dan Belsky, an assistant professor of epidemiolo-
gy at Columbia University's Mailman School of Public Health in New York City.
The phase 2 clinical trial included 220 adults who either made a 25% calorie cut to their diet or no changes at all. The body mass index (BMI) for participants ranged from 22 to 27 (a BMI of 30 is the threshold for obesity).
In the first month, those in the calorie-restricted group were given three prepared meals each day so they would be familiar with portion sizes. They were counseled about
their diet for the first 24 weeks of the two-year study.
The other group had no counseling or restrictions.
Despite the plan to cut about 500 calories in a 2,000-calorie daily diet, most cut only half that, said physician Evan Hadley, director of the geriatrics and clinical gerontology division at the National Institute of Aging (NIA), which funded the study.

“But that 12% was enough to have significant changes,” Hadley told NBC News.
Researchers used an algorithm based on past data for 1,000 people who were followed for 20 years, to see how certain DNA biomarkers changed in the study group.
The algorithm was like a “speedometer,” Belsky explained, to help gauge the pace at which participants aged.
Those who cut their calories slowed their aging by 2% to 3%, reducing the likelihood of dying early by 10% to 15%.
"We all have the power to change the trajectories of aging," Belsky contends.
Researchers plan to follow those on the calorie-restricted diet for 10 years.
It's not clear why eating less would slow aging, though it may prompt cellular changes, Belsky said.
"It may induce sort of mechanisms of survival responses in the body that have the effect of cleaning up intracellular garbage," Belsky explained. “It's a signal to the body, saying, 'Hey, pay attention. There are resource stresses in the environment. We need to make sure that we are using all of the resources available to us most efficiently.'”
Still, long-term limits on calories have been shown in animals to be harmful, including reduced muscle strength, slower metabolism and an impaired immune system, Valter Longo, director of the Longevity Institute at the University of Southern California, told NBC News. Longo was not involved in this study.
“It may cause powerful anti-aging effects, but also probably some degree of frailty or other issues that may not be so beneficial,” Longo said.
People should not starve themselves, Pankaj Kapahi, a researcher at the Buck Institute for Research on Aging, told NBC News. He was not involved in the study.
Kapahi noted that exercise and balanced eating are important for aging.
"Calorie restriction has to be done at a marginal level," he said.
Page 2 • IN GOOD HEALTH – Buffalo & WNY’s Healthcare Newspaper • March 2023
first-time 50 Minute Assisted Stretch $49 intro stretch Body Map Assessment AND INCLUDES StretchLab Southtowns 3860 McKinley Parkway Suite 230, Blasdell, NY 14219 southtowns@stretchlab.com · 716.303.0518
March 2023 • IN GOOD HEALTH – Buffalo & WNY’s Healthcare Newspaper • Page 3 Please visit JustOneDayWithUs.org or call 1-800-ROSWELL (767-9355) Kim Sweeney and her team are here to assist.
getting the best
can get
are at the forefront of new
“Patients want to make sure that they are
treatment that they
anywhere. At Roswell Park, we
cancer therapies. They know, with full confidence, they are getting the best cancer care available.”
51886 JOD Print Ads Brentjens.indd 1 10/24/22 4:00 PM
–
Renier Brentjens, MD, PhD Deputy Director
Mark Cuban Pharmacy Could Save Billions on Prostate Cancer, Bladder Drugs
A new drug company founded by entrepreneur Mark Cuban could save patients $1.29 billion a year based on 2020 Medicare Part D expenditures on just the nine most popular urological drugs, according to a study published in the Journal of Urology.
The study, led by Vanderbilt University Medical Center (VUMC) researchers, examined the potential savings if Medicare prices for generic drugs were as low as those offered under the Mark Cuban Cost Plus Drug Company, which provides a standard template pricing of the cost of manufacturing the drug plus a 15% markup, plus standard $5 fees for dispensing and $3 fees for shipping.
“We found that if the U.S. government used Mark Cuban’s cost-plus drug pricing model to supply urological drugs to Medicare patients, they would save taxpayers an estimated $1.29 billion,” said lead author physician Ruchika Talwar, a fellow in urologic oncology at VUMC.
“It means that patients would be able to get their drugs more affordably, but also means that taxpayer funds could go toward other important issues and hopefully save us all some money in general.”
The nine commonly-prescribed urological drugs that were studied — tamsulosin, finasteride, oxybutynin, alfuzosin, solifenacin, tolterodine, sildenafil, tadalafil, and abiraterone — are used to treat conditions including prostate cancer, overactive bladder and prostate enlargement.
For the 90-day prescription prices, all drugs generated cost savings for Medicare, ranging from 48.7% to 99.2%. The savings for abiraterone alone amounted to $656 million, or nearly 52% of all potential Medicare savings for urological drugs in both 30-day and 90-day prescription models. Abiraterone is used to treat prostate cancer that has spread to other parts of the body by blocking testosterone, which is the hormone that drives prostate cancer growth.
“Just by changing the way one commonly prescribed drug (abiraterone) was purchased, we could convey a benefit of more than $650 million in cost savings to taxpayers,” Talwar said. “The impact of this could be astronomical across all cancers … any sort of oral, generic drug available through Mark Cuban’s company can be a lot cheaper for many patients, not just Medicare patients, through this program. And taxpayers are the ones who fund Medicare drug spending.”
Meet Your Doctor
By Chris Motola Michelle
Rainville, MD
Q: You’ve recently received an Unsung Heroes recognition for your work in the emergency department at Eastern Niagara Hospital.
A: My group, UBMD Emergency Medicine, has been working at Eastern Niagara now since 2019. The Unsung Hero award, quite honestly, is something all the physicians in our group deserve. We all work very hard in the emergency department. It’s a great, small community hospital and it serves a patient population that, maybe isn’t underserved, but we cover a lot of area. So, I think any one of us could have gotten that award. But I was certainly happy that my director nominated me for it. I teach first-year medical students the clinical application of medicine. So we go over history-taking skills and physical exam skills. So that’s something that I do outside of my clinical practice that was recognized. I believe my director also talked about me being an educator in the emergency department, particularly around the COVID-19 vaccines. There was so much misinformation being spread about the vaccinations, especially in the community that Eastern Niagara serves. So I felt as though, as physician, it was my responsibility to give the patients who came in accurate information about the vaccines.
Q: How did you go about it?
A: So when they were being rolled out a few years, I’d ask my patients if they were vaccinated and, if they weren’t, we’d have a non judgmental conversation about their reasoning for not being vaccinated. I would try to give them evi dence-based information regarding the vaccines so that they could make the decision that was best for them. So that was one of the things my director mentioned in the submission.
Q: What concerns did patients have?

A: I heard everything from it was a Bill Gates conspiracy to control the world to more general fear of a new medical technology. So there were both crazy conspira-
cies and general fear about being a guinea pig and wanting to be sure they were doing what was right for them. As far as the conspiracies, I tried to dispel them but unfortunately, when you’re dealing with someone who believes something that’s really far out there, it’s a lot harder to educate them about scientifically sound information, because they just don’t want to hear. But for patients who were just nervous and unsure, it was answering questions they might have, say, about the effects on young women and fertility, to side effects, to long-term potential effects. So hopefully that information was able to turn some of them around and realize it was a beneficial thing for all of us.
Q: What were the COVID-19 years like in your department?
A: Well, I have to say in the beginning it was really hard and really scary. Really scary. I have been practicing emergency medicine since the 1990s and never had I experienced anything like this where there was this novel virus that nobody knew anything about. And we’d just see patient after patient coming in severely ill and so many patients dying. We didn’t have treatments, we didn’t have vaccines. It was the first time in my career that I was afraid to go cause I didn’t know if I’d catch it and home to my family. My husband was Navy and I’d tell him I felt like I was on the battlefield. I didn’t know going to come
home with a deadly disease. At first it was really, really scary. I moved myself out of my bedroom and planted myself on the third floor of my house and tried to stay away from my family. But it got much better. As we learned more about the virus and after the vaccines came out, it was a like a medical miracle. And it completely lifted a weight off all of our shoulders. We could go in and take care of our patients without being afraid anymore. So it was tough, but we got through it. We did our best. We served our patients. I think we’re all much more comfortable now.
Q: How are things now? Back to normal? Halfway back to normal? Or is there no normal anymore?
A: I would say we’re 90% back to normal. We’re still wearing masks in the emergency department, but honestly we’re having a flu season, so maybe we should have worn them before. Now I’m not advocating people wear masks out in the community all the time, but in the emergency room where we’re taking care of sick patients all the time, it’s not a terrible idea. Most people are either vaccinated or have natural immunity, so we’re not seeing as many really sick patients with COVID-19. We’re not seeing as many patients dying from it.
Q: You’re on the medical school admissions committee for selecting candidates. What’s that like?
A: Basically I’m on the screening committee, so we screen applications and decide who is granted an interview. And I’m also on the interview committee where we interview potential candidates. Each candidate gets two interviews. Then, on the selection day, we go over each candidate as a group and share our feelings on them and decide if they’d be a good addition to our medical school class.
Q: What traits do you consider most important in an applicant?
A: I would definitely say empathy and compassion. Doctors are going to be intelligent; all the candidates we screen have done well in college, on their MCATS. They all meet the intellectual standards. But what makes a good physician is someone who can take all of that information, apply it to their patient and explain it in a compassionate, empathetic manner. So many times you have to deliver bad news. What really, I think, makes an excellent physician is someone who can deliver that in a way that makes a patient feel comfortable and cared for.
Lifelines
Name: Michelle Rainville
Position: Emergency medicine
physician with UBMD

Hometown: Latham
Education: SUNY Upstate Medical University
Affiliations: Eastern Niagara Hospital; Mount St. Mary’s Hospital; DeGraff Medical Center; Millard Fillmore
Suburban Hospital
Organizations: American Academy Emergency Medicine; American College of Emergency Physicians
Family: Husband, three children
Hobbies: Running, skiing, mountain biking, yoga
Page 4 • IN GOOD HEALTH – Buffalo & WNY’s Healthcare Newspaper • March 2023
ER doctor from Eastern Niagara Hospital earns Unsung Heroes recognition, discusses ‘scary’ early days of COVID-19 days when she was afraid to go to work: ‘I didn’t know if I was going to come home with a deadly disease’
Hundreds of U.S. Doctors Lost Their Lives During Pandemic
Many of America's doctors who were heroes on the front lines of the pandemic paid the ultimate price for their efforts, a new analysis shows.
An estimated 622 extra deaths occurred among U.S. doctors aged 45 and over from the pandemic's onset in March 2020 through December 2021, researchers say.

Older doctors who provided direct care to patients battling COVID-19 were at especially high risk.
These excess deaths to physicians didn't subside until April 2021, soon after the introduction of COVID-19 vaccines, concluded a team led by Mathew Kiang, an epidemiologist at Stanford University's School of Medicine in California.
The findings were published Feb. 6 in the journal JAMA Internal Medicine.
The only good news coming out of the new study: Despite the tragic loss of so many doctors' lives, death rates among physicians were still lower than that observed among the general population.
That suggests "personal protective equipment use, vaccine requirements, infection prevention protocols, adequate staffing and other workplace-based protective measures were effective" in preventing more deaths among doctors, the authors wrote.
They conducted the study by comparing pre-pandemic data on deaths to older (aged 45 and above) physicians from 2016 through Febru-
ary 2020 to data collected during the pandemic itself.
Almost 800,000 physicians were included in the analysis. The team excluded younger physicians from their analysis because deaths among that group were very low (fewer than five deaths per month).
Deaths to U.S. doctors peaked in December 2020, the study found, with 70 excess fatalities occurring that month. Deaths began to decline through 2021.
Among the 622 excess deaths recorded during the pandemic, certain factors seemed to raise the risk that a doctor might die, the study found. Men made up about two-thirds (65.3%) of those who passed away, and the odds that a doctor might die during the pandemic rose with his or her age, the report found.
Older doctors who cared for COVID-19 patients appeared to be at especially high risk, suggesting that hospital "workplace policies should prioritize mitigating risks in this group" in the future, Kiang and colleagues wrote.
Of course, the deaths of working physicians may have exacerbated a wider tragedy: more deaths to patients as hospitals faced staffing shortages caused (at least in part) by the loss of these valuable crew members.
That's why "preventing excess deaths among physicians is an important component of mitigating excess deaths in the general population," the study authors concluded.





Editor & Publisher: Wagner Dotto
Writers: Deborah J. Sergeant, Jim Miller, Gwenn Voelckers, Anne Palumbo, Brenda Alesii, Ernst Lamothe Jr., George Chapman, Christ Motola


Advertising: Anne Westcott, Amy Gagliano, Pam Roe



Layout & Design: Angel Campos-Toro Office Secretary: Loni Zardus

March 2023 • IN GOOD HEALTH – Buffalo & WNY’s Healthcare Newspaper • Page 5
P.O. Box 550, Amherst, NY 14226 Phone: 716-332-0640 • Fax: 716-332-0779 • Email: editor@bfohealth.com SERVING WESTERN NEW YORK No material may be reproduced in whole or in part from this publication without the express written permission of the publisher. The information in this publication is intended to complement—not to take the place of—the recommendations of your health provider. Consult your physician before making major changes in your lifestyle or health care regimen. WESTERN NEW YORK CHAPTER We are here for you. Visit alz.org/wny or call our 24/7 Helpline at 800 272 3900 Senior Living Community EmbraceSeasons Past... Begin Life Anew! For More information Call 716-632-3000 410 Mill St. - Williamsville,NY 14221 www.park-creek.com Stimulating Social, Educational and recreational activities Medication management Access to 24-hour personal care assistance Affordable memory care AskaboutourJanuaryMove-inSpecial! Presented by MARCH 7-11 mixed bouquets $ 12 Delicious CANNOLI DONUTS
A monthly newspaper published by Local News, Inc. Distribution: 25,500 copies throughout more than 1,500 high-traffic locations. In Good Health is published 12 times a year by Local News, Inc. © 2022 by Local News, Inc. All rights reserved.
My First Colonoscopy
The night before: hunger pains, boredom and gas
By Daniel Meyer
Three people who I knew died last year from colon cancer. In one instance, it was less than three months between diagnosis and death for a man who was just 54 when he died. That type of heartache and shock is something I wouldn’t wish on my worst enemy.
The horrible and untimely deaths of those three individuals coupled with the urging of my own physician during a recent physical prompted me to make a commitment to secure an appointment with a gastroenterologist for my first-ever colonoscopy.
At 46 and with concerns about my family history of cancer, I recognized the importance of having the procedure done as one of the best preventive measures for my personal health.
Prepped and ready to go
I had heard from family members and friends terrible tales of doom-and-gloom surrounding “the prep.” The moaning and whining revolved around having to be on a clear liquid diet the day before the procedure, a process which includes the consumption of a stool softener cocktail that lacks anything in the form of taste.
That being said, I stuck to the game plan and only consumed water and green tea throughout the day before I began drinking the powdered laxative at the prescribed times until all 64 ounces were in my system.
I then sat back and waited… and waited… and waited.
It was one of the most mundane and mind-numbing evenings of my life, with hunger pains, downright boredom and frequent flatulence the only highlights after what would be my normal “dinner time” until I went to bed.
I then tossed and turned for quite some time, continuously wondering if I would set some sort of unofficial world record as the first person in modern history to win the battle
against what I creatively labeled as my “pesky poop punch.” I even began to worry that maybe I wouldn’t be eligible for the procedure and my one-day fast and scheduled day off from work would all be in vain.
Nature called — with a vengeance
It was around 3:30 a.m. when nature called. To be quite honest, it wasn’t a call. It was instead an outright pillage-and-burn-invasion of my insides. All of my worries about frustration about a lack of “action” quickly flowed down the toilet thanks to my frequent trips to the bathroom. I felt a sense of relief and a bizarre level of achievement that the prep had worked through my system as planned and that my previous concerns about the magic not happening were nothing more than a distant memory.
For anyone who has yet to undergo a colonoscopy but plans to have the procedure scheduled sometime in the future, I offer some simple advice for “prep day” so that you are mentally prepared.
• Closely follow the doctor’s instructions
• Be prepared for some discomfort
• Use mind over matter to ignore any hunger pains
• Be patient, as good things come to those who wait
Show time
Once I was in the office of my gastroenterologist everything moved along without any real issues or concerns. I was given a gown, told to undress and make myself comfortable on a bed located in an area separated by curtains from other areas which also had beds occupied by other patients.
I was then wheeled into another room by a very nice woman who explained exactly what would
take place over the next few hours. After further instruction and a brief conversation with my doctor, I was “given the gas” and began counting down from 100. And that was that.
Seriously. The next thing I remembered was looking around the room and wondering when my procedure would begin. I didn’t see anyone and was trying to focus and figure out exactly where my doctor and nurse were, at which point the nurse appeared, loudly chuckled and said “It’s all over. You did great. Congratulations!”
I was quite groggy, but had no pain and felt nothing else out of the ordinary. The nurse then told me to take my time and not get up until I felt ready to chat with the doctor, who eventually arrived to tell me that everything went well. He did remove one adenomatous polyp, which was biopsied and found not to be cancerous. He also recommended that I focus on a high fiber diet to avoid any potential problem in the future with diverticulosis, a condition where small pouches form in the wall of the colon.
He then thanked me for taking the time to get checked and learn that I had a happy and healthy colon.
Post procedure paperwork and final thoughts
About a week after my procedure I received documentation in the mail that the colonoscopy was a success. Included was the recommendation that I return for another
Erie County, Tops to Distribute Free Kits for Colorectal Cancer Screening
The Erie County Cancer Services Program (CSP) will distribute FIT kits at nearly two dozen Tops Friendly Markets locations throughout the month of March during National Colorectal Cancer Awareness Month.
“We are so excited to get FIT kits into the hands of eligible adults with this partnership with Tops Markets, and educate people on the importance of this non invasive test,” said cancer services program Director Michelle Wysocki. “We appreciate being able to address the myths and misinformation around colorectal cancer screening at events like this one, and show just how easy, convenient and private the testing process is.”
Collect a sample in just a few
minutes in the privacy of your home bathroom, and mail it to a lab for testing in a postage-paid envelope, provided by CSP.
Colorectal cancer screening is recommended for adults with average risk factors between 45 and 75 years old.
“We encourage people to talk to their doctor about their colorectal cancer risks. Our program can provide these kits to any Erie County resident between 45-75 years of age, regardless of insurance status.” Wysocki said, “If you are uninsured or underinsured, you may be eligible to have the test cost covered by our program.”
Regular screening for colorectal cancer can save lives. Screening
tests can find growths that can be removed before they turn into cancer. Screening tests can also find colorectal cancer early, when treatment may work best.
The Erie County Cancer Services Program (CSP) provides breast, cervical and colorectal cancer screenings, and diagnostic services at no cost to adults who live in Erie County, do not have health insurance, have health insurance with a cost share that makes the cost of screening too high, and meet the program rules for age and income. Costs for additional, necessary diagnostic tests may also be covered under a NYS program. Visit the Erie County Department of Health at www.erie.gov/cancerservices or call 716-858-7376.
colonoscopy in seven years. I later shared that information with my primary doctor, who promptly responded to my email correspondence by updating my personal information charts and thanking me for following through on her recommendation to have the procedure done.
I also did my own research the following day on the difference between hyperplastic polyps and adenomatous polyps and the benefits a high fiber diet has for anyone with diverticulosis.
While colonoscopies are certainly not something to plan a festive gathering around, the entire ordeal was pretty simple. The peace of mind I now have was well worth the trouble and minor inconveniences I experienced.
Note: The American Cancer Society recommends that men and women should be screened for colorectal cancer starting at age 50, with people who are defined by their medical expert as being “average risk” to start regular screening at age 45.
Daniel Meyer is a lifelong resident of Western New York. He is the former editor of the Hamburg Sun newspaper and is currently the deputy press secretary for numerous departments that comprise the government of Erie County.

March 2023 Schedule to get free kits for colorectal cancer screening
Amherst 9660 Transit Road
March 8 • 4-7 p.m.
3980 Maple Road
March 25 • 10 a.m. – 2 p.m.
Alden 12775 Broadway
March 4 • 10 a.m. – 2 p.m.
Buffalo 1460 South Park/Bailey
March 3 • 4 – 7 p.m.
345 Amherst St.
March 10 • 4 – 7 p.m.
Page 6 • IN GOOD HEALTH – Buffalo & WNY’s Healthcare Newspaper • March 2023
March 2023 Schedule to get free kits for colorectal cancer screening
From previous page
Q& A with Veayla Williams
PAWNY president says that
By Brenda Alesii
At first glance, one might think that an organization whose acronym is PAWNY may have a connection related to animal charities. That assumption would be inaccurate.
March
Williamsville 2351 Maple Road • March 15 4 - 7 p.m.
Schedule updates at cspwny.org
For more information, contact the Erie County Department of Health, Cancer Services Program as 716858-7376 or www.erie.gov/cancerservices
PAWNY, in fact, stands for the Psychological Association of Western New York. It’s a nonprofit 165-member organization advancing the science and profession of psychology, supporting professional growth and association among practicing psychologists and educating the public about the profession and science of psychology as a resource for healing and change.
Veayla Williams, Ph.D., is the current president of PAWNY. Williams earned her doctorate at SUNY Buffalo, graduating in 2012. A city resident, her term at the helm of PAWNY ends in June.

She spoke with In Good Health about the organization and her own work.
Q: As president, your one-year term is up this spring. While overseeing the monthly board meetings and ensuring that the business of PAWNY runs smoothly, what else do you do in your professional life and what motivated you to become a psychologist?
A: I have always had a passion for helping people. Before graduate school, I was a case worker at the Salvation Army, where I saw the recurring theme of underserved people struggling — trying to attain goals, working to be a good parent and friend. My goal was never about how much money I could make or to have a career that depended on my physical capabilities. As a psychologist, no matter where I am in life, I will be able to help others.
I have been treating veterans at the VA Medical Center for 10 years in the behavioral health department, working with veterans of all ages and backgrounds. I love their rawness and authenticity. I also have a private practice in Tonawanda at Family
Counseling Associates.
Q: Is there still a stigma attached to mental health therapy?
A: Absolutely. It’s unfortunate, but I do not think it is as bad as it once was because so many people have been touched by anxiety and depression with everything we experienced during COVID-19 and also through other societal problems such as the ongoing opioid crisis. Those situations and many others have brought a lot of people to therapy. Strength is knowing when to ask for help and realizing that we all hurt. Asking for help does not make one weak. By pushing pain and emotion down, the individual does not learn about him or herself. I can see potential in people; we then work on the client recognizing those possibilities. It is so gratifying to see clients changing in a positive way — that is my whole purpose.
Q: Are people of color reluctant to seek mental health help?
A: Yes. There is still the common thought that a person of color who is feeling vulnerable should turn to their faith for comfort. There is nothing wrong with that, but it doesn’t mean therapy should be excluded. It is not an either-or choice. Several providers from PAWNY started working with Cavalry Baptist Church. With the support of the pastors, we’ve had multiple group conversations about mental health at the church.
We also need to diversify the field of psychology. Some people don’t feel comfortable starting a therapy relationship with people who don’t look like them as they may not have had similar experiences. To that end, PAWNY is supporting students of color who are interested in becoming psychologists. We have been talking to young people of color about careers in mental health, including holding a panel discussion with local Girl Scouts of color. In 2020, we created an anti-racism task force to connect the minority community with supportive resources. It also gave us the opportunity to examine our own biases as therapists.
Q: The May 14 shooting at Tops on Jefferson Avenue must have had a profound impact on the mental health of so many area residents.
A: After that horrific tragedy we wanted to ensure that resources were readily available. The work continues to address racism and link individuals of different backgrounds to the appropriate help that is specific to their situation.
Q: Important distinction here: psychologists do not prescribe medication. Correct?
A: That is currently correct in New York state. Psychiatrists and psychiatric nurse practitioners, who are mental health professionals with a medical degree, are the providers who can prescribe medication. Some primary care physicians may also prescribe certain basic psychiatric medications. However, in some states psychologists who have received specialized training can prescribe psychiatric medication. As psychologists, we offer counseling services and often work collaboratively with the client’s psychiatric care provider.
Q: How can PAWNY be reached?
A: Our website: www.PAWNY. org or by calling 716-249-0221.
March 2023 • IN GOOD HEALTH – Buffalo & WNY’s Healthcare Newspaper • Page 7 2101 Elmwood Ave.
12 • 10 a.m.-2 p.m. 1740 Sheridan D`rive
19 • 10 a.m. – 2 p.m. 425 Niagara St.
24 • 4 - 7 p.m. 1275 Jefferson Ave.
29 • 4 - 7 p.m.
3865 Union Road
1 • 4 ¬ 7p.m. 700 Thruway
Drive
4 – 7p.m.
4777
16
4
7 p.m. 5175
p.m.
March
March
March
March
Cheektowaga
March
Plaza
March 31 •
Depew
Transit Road March
•
-
Broadway March 26 • 10 a.m.-2
Derby 6914 Erie Road
March 27 • 4 -7 p.m. Grand Island 2140 Grand Island Blvd.
6150
March 6 • 4 p.m.-7 p.m. Hamburg
South Park Ave.
March 18 • 10 a.m.-2 p.m.
Orchard Park 3201 Southwestern Blvd.
March 13 • 4 -7p.m.
Springville 184 S. Cascade Drive
March 22 • 4 -7 p.m.
Tonawanda 890 Young St. • March 05 10 a. m. – 2 p.m. 150 Niagara St. • March 11 10 a.m. – 2 p.m. West Seneca 355 Orchard Park Road
20 • 4 – 7 p.m.
there is a need to diversify the field of psychology and that stigma attached to mental health therapy is still a concern
Nearly 1 in 5 American Adults Takes Sleep Meds
Nearly 20% of American adults use a drug to help them sleep, either occasionally or regularly, health officials recently reported. Sleep medications, sold both over-the-counter and by prescription, are a common treatment for sleep problems, said senior report author Lindsey Black, a health statistician at the U.S. Centers for Disease Control and Prevention's National Center for Health Statistics (NCHS).
"Our report details patterns of use of medication to inform patterns of use among subgroups of the U.S. population," Black said. "We do hope
by dissemination of this report it can lay the groundwork for more work in this area and our understanding of sleep health among adults."
Using data from the 2020 National Health Interview Survey, Black and colleagues found that among adults ages 18 and older, 8.4% used medication to help them fall or stay asleep on most nights or every night. Another 10% said they used medication on some nights.
Women were more likely than men to take medication for sleep and the percentage doing it generally increased with increasing age.
Specifically, 10% of women used sleep medication, compared with 6.6% of men. White adults were more likely to use sleep medications, and Asian adults were least likely to do so. Also, the percentage of men who used medication for sleep dropped as family income increased, Black's team found.
The findings were published Jan. 25 as an NCHS Data Brief.
One expert wasn't at all surprised by the number of Americans who rely on sleep medications.
"I work in a sleep center. And you know, I certainly see a lot of sleep medication use," said Lauren Broch, a clinical sleep psychologist at the Northwell Health Sleep Disorders Center in Great Neck.

Broch thinks not only are sleep medications (both prescription and over-the-counter) overused but also
poorly used.
Prescription drugs like temazepam (Restoril), triazolam (Halcion), zaleplon (Sonata), eszopiclone (Lunesta) and zolpidem (Ambien, Edluar, ZolpiMist) were designed to be used in the short term, not as a long-term crutch.
The same is true for over-thecounter sleep aids, many of which contain the antihistamine diphenhydramine, the active ingredient in Benadryl.
People who use these medications habitually come to rely on them, Broch said.
"Many people start believing that the sleep medication is what is making them sleep," she said. "There's a dependence on them, and sometimes tolerance, and they believe that they must use it or they won't sleep. That's never a good thing."
HealthcareinaMinute
By George W. Chapman
The Pandemic Is Over!
Well, not really. The administration has declared an end to the public health epidemic as of this May. The government is not saying the clinical pandemic is over, although it is on the decline. The declaration officially puts an end to the PHE originally declared by the previous administration in 2020 in response to COVID-19. The PHE has been extended several times since 2020. Among other things, it authorized expanded telehealth services and improved payment for providing services (paid same as in-person visit). The PHE also expanded Medic-
2022 Bad for Hospitals
Last year was the worst year for financially ravaged hospitals since the onslaught of the pandemic.
A study published by industry advisory group Kaufman Hall revealed the average hospital started off the year with operating margins hovering around minus 3.5%. Hospitals gradually dug their way out negative operating margins by December 2022, but about half of the nation’s 7,000 hospitals finished in the red for the year in total. Analysts predict some improvement or relief in 2023 due to better management of staffing issues, improvement in the supply chain, continuing leveraging of outpatient services, increased alliances or ventures with physicians and stronger commercial payer negotiations. Related to the bad year fiscally: 50% of hospital-based physicians and nurses reported job-related distress and 25% reported depression.
Private Equity in Rural Hospitals
Desperate for capital, rural hospitals are easy pickings for aggressive profit- at- all- costs private equity
aid eligibility to cover more of the indigent. So, the end of the PHE in May will at least create confusion, if not chaos. States will be forced to reconsider and reconfigure Medicaid eligibility. Physicians and hospitals may lose improved payment for telehealth services. (As of this writing, Medicare is extending behavioral telehealth for seniors through 2024.) While PHE declarations only impact Medicare and Medicaid, commercial insurers typically follow suit. Late night TV comedians have tongue in cheek made light of “government declares pandemic over!” Funny, but not.
(PE) companies. They approach financially vulnerable hospitals with management and consulting contracts with no investment or assuming any risk. PE firms own or manage about 130 rural hospitals mostly in southern states like Texas, Kentucky and North Carolina. The purely forprofit firms typically strip out many needed services, close beds, slash staffing and all but eliminate charity care. They quickly turn around the profit and loss statement, grab their fees and get out. This has put additional pressure on surrounding urban and suburban facilities that end up providing the care discontinued at the rural hospital. Medicare, state Medicaid agencies and provider organizations are investigating the negative impact of PE on their rural providers.
Long COVID-19 Decreasing
good news is the number of individuals suffering with long COVID-19 declined from 19% in June of last year to 11% this year. In addition, 17% of those who had long COVID-19 no longer have symptoms. The Kaiser Family Foundation report was based on analyzing CDC
data. The issue, however, remains a serious concern. The bad news is the best practices to treat long COVID-19 have yet to be finalized. There is no singular test to definitively determine if long COVID-19 is caused by covid alone. Post COVID-19 conditions are NOT due to just one illness. Your health history plays an important factor. It is estimated that 500,000 to 4 million individuals in the workforce have long COVID-19.
Behavioral Health Crisis Among Our Young

Behavioral healthcare has long been besieged by the opioid epidemic (suicides, addiction, depression). Then COVID-19 struck three years ago, further highlighting the shortcomings of our behavioral health system.
COVID-19 (along with social media) has had the most negative impact on our young. A survey of parents, conducted The Pew Research Center, revealed they now rank their children’s mental health status as a primary concern (anxiety, depression, suicide). The study also revealed what many employers are experiencing: the mental health of children directly impacts the well-being and productivity of their parents. All agree that government and commercial insurers must expand the access to, quality of, and affordability of behavioral health. Regulatory barriers must be removed, including anachronistic–redundant state licensing requirements that make it unnecessarily complicated for professionals to provide telehealth services across state lines. The nonprofit National Alliance of Healthcare Purchasers Coalition, which represents 12,000 employers and purchasers covering more than 45 million employees, is dedicated to promoting effective programs and strategies to improve our behavioral healthcare system for all and especially for the young.
CVS–Aetna Expand Mental Health
This alliance and similar commercial ventures and alliances, continue to distance themselves from traditional hospital and provider-based delivery systems by pio-
neering innovative, consume-friendly delivery systems. CVS–Aetna has been offering basic virtual and in person primary care services since May of 2022. Effective spring 2023, CVS–Aetna will be expanding telehealth behavioral health services to Aetna members, including appointments with licensed therapists and psychiatrists (MDs). Currently, the average appointment for a virtual, in person or at home primary care visit is out 24 days. The average appointment for an in person behavioral health service, before telehealth is introduced, is out 48 days. Time will tell how popular and effective these corporate healthcare delivery systems are.
US Healthcare Again Fares Poorly
The recent report from the Commonwealth Fund once again illustrates how poorly we are doing when compared to 37 other wealthy countries. Here are some of the low points. As of 2020, our average life expectancy was 77. The average life expectancy among our 37 counterparts was three years more at 80. We have the highest rate per 100,000 of avoidable deaths, infant and maternal deaths and gun related deaths. The latter being 7.4–100,000 versus 2.7–100,000 average in the other 37 countries. We spend, by far, more than any of our counterparts. The US spends close to 18% of its GDP on healthcare. That’s just over TWICE the average of the other 37 countries. The closest to our 18% of GDP were Germany at 13% and France at 12%. The major difference? Most of the 37 countries that clearly outperformed us in just about every category have single-payer healthcare systems.
Page 8 • IN GOOD HEALTH – Buffalo & WNY’s Healthcare Newspaper • March 2023
George W. Chapman is a healthcare business consultant who works exclusively with physicians, hospitals and healthcare organizations. He operates GW Chapman Consulting based in Syracuse. Email him at gwc@gwchapmanconsulting.com.
stumbling, and collapsing under the maple tree in my back yard.
By Gwenn Voelckers
Practical tips, advice and hope for those who live alone
Practical tips, advice and hope for those who live alone

The Power of Faith: One Woman’s Spiritual Journey
Life after a divorce or the death of a spouse can leave you reeling and wondering about practically everything — your judgment, your future, your fears, and your faith.
Below is an interview I conducted with one of the most thoughtful and inspiring women I've met through my “Alone and Content” workshops.
Caroline (not her real name) was divorced when I met her and has since remarried, “happily,” she added with a smile.
Her faith lifted her up and carried her through the hardest times following her separation. It is my hope that her journey will inspire yours.
• Would you care to share a little bit about your faith?
I’m a Christian... I've looked at other religions and have made a conscious decision to remain a Christian, even though I don’t understand it all. I am learning to embrace the mystery.
• What role did your personal faith play in your adjustment to living alone?
My Christian beliefs hold to the tenet that I am never alone — that Christ is with me wherever I am. I’ve prayed a lot and have found indescribable peace in that praying.
• What was the biggest challenge you faced living alone and how did your faith help you heal?
Grieving the end of my marriage caused me the most pain while
alone. All the 'if onlys' and 'why me?' really tore at my heart. The Bible was my constant companion. I was also inspired by “The Purpose Driven Life,” by Rick Warren, and other Christian books and radio programs, which helped me put things into perspective.
Talking with others in my congregation was also a huge part of my healing. I get emotional when I think about the support and caring that surrounded me, rescued me.
• Is there a particular experience you had that captures the power of your faith?
My youngest son was 7 at the time. After dinner he brought me his homework book to sign, as was his teacher’s daily requirement. He’d been at his dad’s house the previous three days and I saw his dad’s girlfriend’s signature on the parent line in the book. My heart stopped.
Then, something in me snapped — all the times my precious children were away from me ... all the awfulness ... all the anger and injustice and fear. I sucked it up and forced my shaking hand to sign my name next to hers. I made my way outside,
For Baby's Sake, Momsto-Be Need the Whooping Cough Vaccine: CDC
Pregnant women can help protect their newborns from whooping cough by getting a Tdap vaccine during the third trimester of pregnancy.

The U.S. Centers for Disease Control and Prevention tracked cases of infant whooping cough between Jan. 1, 2000, and Dec. 31, 2019.
The researchers found a link between reduced rates of whooping cough in newborns under 2 months of age and Tdap (tetanus, diphtheria, pertussis) vaccination during pregnancy.
Whooping cough, or pertussis, is highly contagious and can be serious
for infants who are too young to be vaccinated. The CDC recommends babies get their first Tdap shot at 2 months of age.
“Getting Tdap during pregnancy offers infants the best protection before they are old enough to receive their whooping cough vaccines,” physician José Romero, director of CDC's National Center for Immunization and Respiratory Diseases, said in a CDC news release. “This protection is critical because those first few months are when infants are most likely to have serious complications, be hospitalized or die if they get whooping cough.”
I laid on my back clutching my chest, my heart. No tears. Just intense pain. I did not, could not, make a sound or move. But after a while, my mind prayed a lament, begging God for relief from this excruciating pain.
In that instant, a 'peace that passes all understanding' moved over me and I felt my golden retriever appear and quietly curl up next to my body.
• Did you ever lose faith or struggle to regain your faith?
I did not lose my faith but, boy, did I ever have a few words with God! One morning during breakfast with my two boys, I ran to the garage and grabbed my bike after learning of the girlfriend’s ongoing involvement my boys’ lives.
I needed to get out of the house so the boys wouldn’t hear my rant at their father. I tore down the road, enraged and screaming at God, 'How could you let this happen?!'
About a half mile from home, I saw a doe quietly standing by the side of the road. I calmed down immediately and just sobbed. I turned the bike around just as the sun burst over the horizon, washing the sky, the quiet country road, and me in the warm morning light. I was reminded again 'You are never alone.'
• What advice would you give to those whose suffering has challenged their faith?
Remember a time when you risked it, trusted God, and felt a measure of serenity after you did. Remember that, 'This, too, shall pass.' Remember that there are things we can only learn when in solitude. That God has a bigger plan than our plan.
• What role does prayer play in your life?
Prayer is the great wireless communication connection to God. God speaks to us in three ways, through the Bible; through people, which in-
cludes books people write and teachers like you; and through prayer, which may encompass comforting things embodied in nature, dogs, deer, sunrises, and so much more.
• How can those who live alone activate their faith more fully?
It’s like exercise and eating right. You get out of it what you put into it. You prepare yourself for the years ahead by continuing to move and by putting good things into your body.
You prepare your heart and soul for the times ahead by studying your faith of choice and by nourishing your mind and actions with uplifting words and passages, helpful deeds, gratitude, and inspirational music and images.
• Was there a favorite scripture passage that lifted you up during your challenging times that you'd like to share with my readers?
"Do not be anxious about anything, but in everything by prayer and supplication, with thanksgiving, let your requests be made known to God. And the peace of God, which surpasses all understanding, will guard your hearts and your minds in Christ Jesus." — Philippians 4:6-7
I hope you have found this interview helpful and supportive. While I find my spiritual bearings in nature, meditation, love and a humanist philosophy, I am inspired by the words and wisdom expressed by Caroline. We can all be strengthened by a spiritual life, wherever that path leads us. Embrace it.
Gwenn Voelckers is the founder and facilitator of Alone and Content, empowerment workshops for women and author of “Alone and Content,” a collection of inspiring essays for those who live alone. For information about her workshops, to purchase her book, or invite her to speak, visit www. aloneandcontent.com
The researchers had not looked at U.S. population level trends in infant whooping cough cases since this maternal vaccination strategy began in 2011. The CDC recommends all women get Tdap vaccines between their 27th and 36th week of each pregnancy.
Newborn whooping cough rates decreased significantly since vaccination of pregnant women began, according to the CDC. Maternal Tdap vaccination prevents more than three-quarters of cases of whooping cough in infants under 2 months of age.
Tdap vaccination during pregnancy dropped off during the COVID-19 pandemic, and the CDC and its partners are working to in-
crease rates.
The CDC said that all people in close contact with infants should be up to date with their whooping cough vaccines.
“Everyone who is pregnant should feel confident in knowing that the Tdap vaccine is safe and effective,” said Dr. Linda Eckert, the American College of Obstetricians and Gynecologists' liaison to CDC's Advisory Committee on Immunization Practices. “Knowing that Tdap vaccination during pregnancy protects 9 in 10 babies from being hospitalized with whooping cough, I strongly recommend this vaccine to all my pregnant patients for their peace of mind and for their family's health and well-being.”
March 2023 • IN GOOD HEALTH – Buffalo & WNY’s Healthcare Newspaper • Page 9
Live Alone & Thrive
Art at Roswell Park Helps People Battle Cancer
By Jane Schmitt
Walk through Roswell Park Comprehensive Cancer Center and you’ll see walls adorned with extraordinary artwork meant to comfort patients, inspire visitors or simply offer a much-needed distraction.

It’s an extensive collection built over the years as part of the hospital’s mission of caring for the men, women and children who come there for treatment. On full display for all to enjoy are paintings, framed photographs, sculptures, glass mosaics and fabric art. Much of it was created and donated by local artists looking to make a difference for those who need it most.
“Our goal is to make the hospital experience better for our patients and their caregivers. They are our No. 1 focus,” said William Vogel, art coordinator. “We want to beautify the space and give them something to look at. A positive diversion can help lift their spirit.”
With nearly 1,800 pieces in the collection, there’s a lot to see in the public areas of the main hospital and
elsewhere on the Roswell campus. And for those who believe that art can play a role in the healing process, an enhanced environment is a winwin for all.
The list of artists represented in the collection is long and impressive, according to Vogel. Many have exhibited their work not only locally but nationally and internationally.
Visitors can view watercolors by Charles Burchfield and E. Jane Stoddard, giclee prints of area landmarks by Rita Argen Auerbach and oil paintings by Barbara Insalaco.


There are unique works from Jean Knox and Eileen Graetz, abstract acrylic paintings by Mary Schneider, collage paintings by John McIvor, landscapes by Eileen McNamara and UltraChrome prints by Dale Schwalenberg. Also on display are Karel Appel lithographs and a wall-sized plaster sculpture by Sarah Fonzi.
“We want to make your experience here more positive, whether you’re looking at a single piece in
Page 10 • IN GOOD HEALTH – Buffalo & WNY’s Healthcare Newspaper • March 2023
1 3 2
1. Install shot from Reflections: The Light Within, exhibited in the Art Heals Gallery through June 2022. This exhibition featured 19 original watercolors by Rita Argen Auerbach.
2. Install shot from Buffet Style: Food Art from the Roswell Park Art Collection, on view through March 2023. This exhibition features food-themed works from the Roswell Park collection.
3. Installation view (left to right): Peru Series #10, Peru Series #11 by Jozef Bajus, cutouts and multicolor ink on handmade paper. Donated by the artist. Installed in the Head and Neck Center.
4. Installation view: Hope by Ellen Steinfeld, powder coated and painted steel. Commission supported by Irene and Frank Jellinek. Installed in Kaminski Park.
5. Installation view: Elements by Peter Stephens, inkjet transfer and acrylic on resin. Purchase supported by the Cameron & Jane Baird Foundation. Installed in the Chemotherapy and Infusion Center.
6. Installation view: Science Art, featuring cellular imagery created by Roswell Park researchers. Installed in the connector bridge, near the Spiritual Care Center.

a waiting room, walking around the atrium checking out multiple pieces or you’re in the [hospital] art gallery,” Vogel said. “But it’s also there to help support artists and arts organizations. We have a humongous arts community in Western New York. Some of them are our patients, so there’s that personal connection for us, as well.”
A prime example is “Wish Field,” a laser-cut sculpture in powder-coated stainless steel.
“Drawing on her experience as a cancer survivor, artist Shasti O’Leary-Soudant created ‘Wish Field’ for the lobby of the Scott Bieler Clinical Sciences Center,” according to Roswell. “The sculpture is meant to soften the anxiety, fear and frustration cancer patients may experience during treatment and recovery. This piece, which represents a dandelion releasing its seeds to the wind, offers hope and encouragement to patients and their loved ones and is the inspiration for Roswell Park’s logo.”
Providing a respite
RoseAnn Berardi leads the art committee of the Roswell Park Alliance Foundation, whose members seek a range of styles and media to brighten the days for patients, as well as physicians and hospital staff.
“The response is overwhelmingly positive,” Vogel said. “I might walk down a hallway and see somebody who clearly is not having a good day for whatever reason and they’re immersed in a piece of art or a display or an installation. It is heartwarming to know that they are finding a way to refresh themselves or clear their mind and have a respite from what’s going on around them.”
Adding to the creative energy at Roswell is The Art Heals Gallery, located on the first floor. It’s an important component of the hospital’s mission to serve people who need cancer care.

Simply put, said Vogel, “you put art in a hospital and it looks good and makes people feel better.”

March 2023 • IN GOOD HEALTH – Buffalo & WNY’s Healthcare Newspaper • Page 11
4 5 6
By Ernst Lamothe Jr.
Things You Need to Know About Kidney Disease
It’s a condition that arises gradually, but that can cause tremendous pain and affect quality of life.
Chronic kidney disease, also called chronic kidney failure, involves a measured loss of kidney function. A kidney’s function involves filtering wastes and excess fluids from the blood, which are then removed in your urine. Advanced chronic kidney disease causes dangerous levels of fluid, electrolytes and wastes to build up in your body.
“People could avoid or delay kidney failure if they saw a doctor once a year,” said physician Liise Kayler, chief of the division of transplant surgery in the department of surgery in the Jacobs School of Medicine and Biomedical Sciences at University of Buffalo.

Kayler, who is also the program director of the Regional Center of Excellence for Transplantation and Kidney Care at Erie County Medical Center, discusses five aspects of kidney disease.
1.Kidney issues affect youth and adults
Some common kidney issues that affect children and adults are kidney stones, kidney infections, acute kidney injury and chronic kidney disease. Chronic kidney disease is especially significant because more than one in seven US adults — and as many as nine in 10 adults — have the condition.
“Young and old people can have high blood pressure. Often they don’t know it,” said Kayler. “Over time the high blood pressure can injure the kidneys. Young and old people can also have diabetes. Diabetes injures kidneys. When diabetes is managed optimally, kidney failure is less likely to happen.”
2.Kidney disease signs
There are very few signs of early or moderate chronic kidney disease that only blood or urine testing will show. In very advanced situations, people may experience the symptoms of toxin buildup,
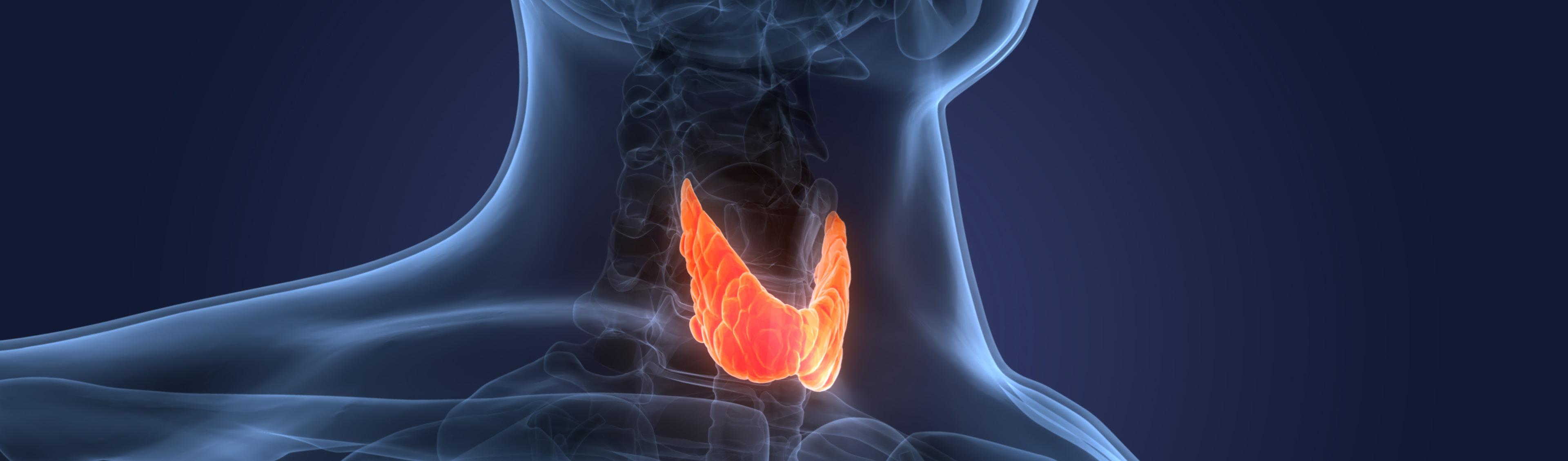
Could You Have a Thyroid Problem and Not Know It?
By Jim Miller
If your thyroid is out of whack, it can cause a number of health issues that can be tricky to detect because the symptoms often resemble other age-related health problems. In fact, as many as 30 million Americans have some form of thyroid disorder, but more than half aren’t aware of it.
What to Know
The thyroid is a small butterfly-shaped gland located at the base of your neck that has a huge job. It produces hormones (called T3 and T4) that help regulate the rate of many of your body’s activities, from how quickly you burn calories to how fast your heart beats. It also influences the function of the brain, liver, kidneys and skin.
If the gland is underactive and doesn’t produce enough thyroid hormones, it causes body systems to slow down. If it’s overactive, and churns out too much thyroid, it has the opposite effect, speeding up the body’s processes.
The symptoms for an underactive thyroid (also known as hypothyroidism) — the most common thyroid disorder in older adults — will vary but may include fatigue and weakness, unexplained weight gain, increased sensitivity to cold, constipation, joint pain, a puffy face, hoarseness, thinning hair, muscle stiffness, dry skin and depression.
Some patients may even develop an enlarged thyroid (goiter) at the base of the neck. However, in older adults, it can cause other symptoms like memory impairment, loss of appetite, weight loss, falls or even incontinence.
And the symptoms of an overactive thyroid (or hyperthyroidism) may include a rapid heart rate, anxiety, irritability, fatigue, insomnia, increased appetite, weight loss, tremors of the hand, frequent bowel movements, sweating, as well as an enlarged thyroid gland. Too much thyroid can also cause atrial fibrillation, affect blood pressure and decrease bone density, which increases the risk of osteoporosis.
which may include confusion, loss of appetite or foul taste, nausea and vomiting or itching. They may also notice the effects of fluid accumulation, including swelling in the legs and shortness of breath.
“Kidney stones are usually present with flank pain and blood in the urine. People suffering from kidney infections may have fever, vomiting and pain with urination,” she added. “Kidney disease is silent in the early stages. People don’t know they have kidney disease until the kidneys are nearly failing. When the kidneys are failing, the most obvious signs are vomiting, difficulty breathing, and ankle swelling. The best way to check for kidney disease is a blood test that is ordered by a doctor.”
3.Family history
Some kinds of kidney disease are directly inherited on a single gene, like polycystic kidney disease. Other kidney diseases come about as a combination of many genes in addition to environmental factors, which also tend to run in families.
“Genetic causes of kidney disease are much less common than high blood pressure and diabetes,” said Kayler.
4.How does dialysis work?
Dialysis is a procedure that replaces kidney function in people with kidney failure. It doesn’t fix the kidneys. Dialysis gets rid of the extra fluid. You can get dialysis treatments in a number of different ways; blood dialysis or belly dialysis (peritoneal dialysis), in a dialysis center or at home. They all serve the same pur-
pose and work equally well.
“Dialysis is a machine that cleans the blood. It does a small fraction of the work that normal kidneys usually do. That’s why people who need dialysis often feel tired and itchy. They also have to minimize drinking fluids and eat a special diet,” said Kayler.
5.Prevention
Some of the best things you can do to avoid kidney problems are likely the same things you do for the rest of your health. Eat a balanced diet that includes more plants than animals. Try to get moderate exercise most days of the week.
“Seeing a doctor allows high blood pressure and diabetes to be detected early and treatment started. With good treatment, kidney failure can be avoided or delayed,” Kayler added.
Those with the greatest risk of developing thyroid disorders are women who have a family history of the disease. Other factors that can trigger thyroid problems include: autoimmune diseases like Hashimoto’s or Graves disease; thyroid surgery; radiation treatments to the neck or upper chest; and certain medications including interferon alpha and interleukin-2 cancer medications, amiodarone heart medication and lithium for bipolar disorder.
Get Tested
If you have any of the aforementioned symptoms, or if you’ve had previous thyroid problems or notice a lump in the base of your neck, ask your doctor to check your thyroid levels. The TSH (thyroid-stimulating hormone) blood test is used to diagnosis thyroid disorders but depending on what they find, additional blood tests may be necessary.
If you are diagnosed with a thyroid problem, it’s easily treated. Standard treatment for hypothyroid-
ism involves daily use of the synthetic thyroid hormone levothyroxine (Levothroid, Synthroid and others), which is an oral medication that restores adequate hormone levels. And treatments for hyperthyroidism may include an anti-thyroid medication such as methimazole and propylthioracil, which blocks the production of thyroid hormones. Another option is radioactive iodine, which is taken orally and destroys the overactive thyroid cells and causes the gland to shrink. But this can leave the thyroid unable to produce any hormone and it’s likely that you’ll eventually become hypothyroid and need to start taking thyroid medication.
For more information on thyroid disorders, visit the American Thyroid Association at Thyroid.org.
Jim Miller is the author of Savvy Senior, a column that is published every issue of In Good Health.
Page 12 • IN GOOD HEALTH – Buffalo & WNY’s Healthcare Newspaper • March 2023
5
Liise Kayler, chief of the division of transplant surgery in the Jacobs School of Medicine and Biomedical Sciences at University of Buffalo.
Top 10 Things for Kids’ Long-term Health
By Deborah Jeanne Sergeant
All parents want their children to enjoy lifelong health. To promote a better chance of lifelong health, parents can do a few things now.
1.Keep Well Child Visits
Check-ups with doctors and dentists help providers and parents track development, stay on schedule for vaccines, and detect and monitor any small issues before they become big issues. Providers can also educate the family on good health habits.
“The best thing for a mom to do is to follow up with the pediatrician right after the baby is born and get regular check-ups as recommended,” said Beverly Lawler, public health nurse with Niagara County.
2.Get Childhood Immunizations
Lawler said that the advisory committee on immunization practices sets the recommended ages for routine vaccines, many of which occur during the first year of a child’s life, with boosters later in childhood.
Parents should address with their child’s pediatrician any concerns about childhood immunizations’ safety. However, nearly every child without allergies to vaccines’ ingredients can safely receive immunizations. These vaccines can protect children against 20 potentially life-threatening diseases. Generally, vaccines work by mimicking an illness, which stimulates the body’s immune system to mount a very strong response against its next exposure to
that illness.
Lawler said that free clinics can help families without insurance.
3.Discuss and Model Drug and Tobacco Abstinence
Although many parents warn about the dangers of drugs, tobacco and alcohol, many youths experience confusion about recreational marijuana, mistakenly thinking it is safe because it’s legal.
That misconception also applies to prescription medication.
Some youth also believe that vaping is safe because it is nonincendiary. The cocktail of chemicals inhaled in the vapor can also cause health problems and should be avoided.
“Parents shouldn’t be smoking, vaping and using marijuana and other drugs,” Lawler said. “If a parent does use a vape, they should put them away where children cannot get them. Elementary kids are starting to get vaping pens. They have to get them from somewhere.”
She encourages parents to start early and maintain open conversation about substance abuse.
4.Use Sunscreen
“You need sunscreen as there’s so much skin cancer,” Lawler said.
SPF 30 is adequate for sun protection, along with avoiding direct exposure between the hours of 10 a.m. to 4 p.m. and wearing protective clothing, plus hats and sunglasses. Many brands of swimwear offer SPF built in.
5.Teach About Sex
Use accurate names for body parts and, as age and maturity appropriate, frankly discuss sex when an opportunity arises. Euphemisms confuse children and sitting down for one giant “sex talk” can provide too much information at once.
Instead, “have regular discussions about sexual activity and sexually transmitted diseases,” Lawler said.
Ensure your children understand that no one has the right to touch them in a way that makes the feel uncomfortable.
6.Establish Active Habits
Engaging children in regular physical activity they enjoy can help form a lifelong habit of movement.

“Kids need physical activity to stay healthy,” said Cathy Hoy-Patterson public health educator with Niagara County Department of Health. “The more active they are, the more likely they are to stay active.”
Children need about 60 minutes of physical activity daily, which can include sports, games and free play.
7.Establish Healthful Nutrition Habits
The My Plate guide can offer an easy way to ensure balanced meals, along with serving a variety of fruits and vegetables.
“Parents can get children involved in prepping food so they can build good eating habits,” Hoy-Patterson said. “Include the five food
groups throughout the day. Even with picky eaters, letting them have some say in what they eat can help them make healthful choices. MyPlate has ideas for those on a budget.”
8.Seek Swimming Lessons
Many YMCA chapters and community pools have lessons. Find a swimsuit in a bright color, as it is easier for parents and lifeguards to spot a struggling child who has gone under the surface. Light and dark colors, blue and green are much more difficult to detect.
9.Test for Lead
Lead exposure can cause permanent brain damage, nervous system, kidney and liver damage, infertility, seizures and death.
“Parents of young children should have them tested for lead poisoning at one and two years as recommended by the CDC,” Hoy-Patterson said. “Lead can have an impact on their development and growth. If they live in a home built before 1978, they may want to have their house tested for lead.”
Old painted baby furniture and toys, cheap imported jewelry and some imported toys are known for containing lead.
10. Model and Teach About Mental Health
Engage in both emotional care of your children and self-care.
“Kids are little sponges, picking up everything in the environment,” said Sourav Sengupta, associate professor of psychiatrics and pediatrics at UB Jacobs School of Medicine and hospital psychiatrist at Oishei Children’s Hospital. “They can only learn from the examples in front of them and the examples of kids who have been through the emotional ringer and those who have developed in an emotionally healthy way.”

Validating children’s feelings helps them feel that they are safe expressing themselves to their parents. Consistency in meeting their basic physical and emotional needs builds trust and helps them build self-esteem.
Children should be able to access mental healthcare as needed.
March 2023 • IN GOOD HEALTH – Buffalo & WNY’s Healthcare Newspaper • Page 13
Kids
Health
Sourav Sengupta
Childhood Emotional Abuse Can Have Lasting Effect
By Deborah Jeanne Sergeant
In 2020, 618,000 children in unique incidents were victims of abuse and neglect, according to The National Children’s Alliance. Of these cases, 65% included sexual abuse, 20% physical abuse, 8% neglect, 8% witness to violence, 3% drug endangerment and 8% were other types of abuse or neglect.
Emotional abuse overlaps each of these categories, can occur in the absence of other kinds of abuse, and often goes unreported. These factors make it difficult to estimate how many children experience emotional abuse. But researchers estimate that about 40% of children at some point suffer from it.
Emotionally abusive parents differ from those who exhibit an occasional moment of poor reaction and apologize afterwards.
Sourav Sengupta, associate professor of psychiatry and pediatrics at UB Jacobs School of Medicine and hospital psychiatrist at Oishei Children’s Hospital, said that emotional abuse is “a pattern of behavior that gets in the way of a child’s self-worth and normal, healthy development you’d expect. It’s constant criticism, manipulative withholding of emotional support, and not providing that core of basic care and withholding that TLC every child needs. We’re talking about chronic patterns of behavior that invalidate the child, make them feel small, like they can’t go out into the world.”

Emotional abuse occurs in the context of a trusted relationship. Parents who habitually engaged in abusive behaviors teach their chil-
dren that relationships are dangerous and result in confusion and emotional pain.
Children sometimes cope by adopting inappropriate responses to emotional relationships, like lashing out at those who seek to become close. Or, adopting an inappropriate response such as an older elementary child sitting on a stranger’s lap.
The long-term impacts can include health problems, difficulty in reaching age-appropriate developmental milestones, relationship problems and socioeconomic challenges, to name a few.
“Of children who engage in bullying, a significant portion were bullied themselves,” Sengupta said. “At a young age, we learn to navigate the environment the way the environment treats us.”
Other adult family members, teachers, coaches and other trusted adults may inflict emotional abuse. However, the closer the person is to the children, the more damage the abuse inflicts. In the case of an adult outside the family, the children’s resiliency factors can make a difference as to how much damage the emotional abuse causes.

For example, parents who stick up for their children and support them in a conflict with caustic teacher can help their children learn how to deal with treacherous people and reinforce their own caring relationships.
Helping children find ways to express their thoughts and feelings without judgment is one way that parents can help children feel sup-
ported when an emotional trauma occurs.
“The first thing would be to for the parent to really check in with their own emotions and be able to neutralize the response,” said Lori Chiarmonte, clinical supervisor at Child & Family Services in Buffalo. “It gives the child space to express how they’re feeling. Really listening to the child and respond with a calm approach. Let them know they have the space to express how they’re feeling, whether frightened, angry or upset and the parent is almost holding that emotion for the child.”
Not providing this kind of emotional support and environment when emotional abuse happens can contribute to long-lasting effects, beginning with stunting the child’s development, and including their ability to learn at school if that is the context of the emotional abuse.
“If a child experiences these traumas and doesn’t have a safe space what they’ll do is internalize it and develop negative beliefs like, ‘I’m not safe or loveable,’” Chiarmonte said. “That carries on to adult life and negative coping can take place.”
These could include anger, aggression, self-harm and substance use.
For some families, emotional abuse becomes a multi-generational issue as the following generations mimic the behavior they saw in their parents as children. From childhood, their brains have been hardwired to automatically resort to fight or flight mode in the face of conflict instead of extending compassion and un-
derstanding. Their understanding of relationships has been skewed into one of competition instead of cooperation.
Breaking the cycle of childhood emotional abuse relies upon the adults addressing their own issues first before changing how they relate and behave with their children.
“Being able to recognize and become aware of the deficiencies is important,” said Samantha G. Stringer, licensed mental health counselor in private practice in Rochester. “At some point in life, we do see our deficits, whether it’s by someone sharing what they see in us or by the emotional hole that’s evident. I believe that everyone has it in us to get to that point where we realize something’s going on. Something doesn’t seem right; I need some help.”
She has treated clients who as young adults do not understand why they act the way they do, but once they begin talking about their childhood, a pattern of abuse emerges: yelling, cursing, emotional or physical abuse.
At that point, they begin to better understand that this behavior is unwarranted and they can work toward changing themselves because they do not want to follow that pattern.
Stringer recommends psychotherapy and talk therapy for unpacking and healing childhood trauma, whether as a child or adult.
“They can do better, think better, live better, have better physical and mental health,” Stringer said. “There is a slew of things we can do. I think about the spiritual aspect of it as well, knowing that spiritual side of yourself and looking at life for what it is.”
She also emphasizes developing purpose and engaging in regular self-care.
“We’re often compassionate with our feelings to friends and family and having that same self-compassion can go a long way,” Stringer added.
Page 14 • IN GOOD HEALTH – Buffalo & WNY’s Healthcare Newspaper • March 2023 Kids Health
Sourav Sengupta
The State of Opioid Abuse — How Bad Is It?
Deaths by overdose still going up year after year
By Deborah Jeanne Sergeant
Three years ago, area experts could only guess the effects of the pandemic on area’s opioid abuse problem — including how long its effects would linger.
“We’ve seen a sharp increase in overdose death or complications during the pandemic. The numbers remain high. It doesn’t seem like we’ve recovered,” said Tony Lin, addictions medicine specialist with UBMD Family Medicine.
Strategies centering on abstaining from drug use have not helped. Lin said that focusing on reducing harm, such as needle exchange programs and administering Narcan to counteract opioids have help prevent more patient losses.
He said that his organization plans to expand medical treatment for opioid use disorder, as it blocks the opioid receptors in the brain.
Expanding referrals should also help.
“We’re called ‘detox’ but that’s a glorification of what we do. We don’t cure a patient of substance use but stabilize them in the withdrawal period. We’re looking to strengthen our referrals to other organizations,” he said.
A five-day “detox” only begins the recovery. Connecting patients with further resources, like meetings, stabile work and counseling, can offer the best chances for recovery.
“Addiction is a disease of isolation,” Lin said. “But, it also affects those around the patient like their family, friends and workplaces. Many patients burn their bridges. That’s a barrier to recovery.”
The illicit drug supply through-
out Western New York contains fentanyl. Its extreme potency contributes to accidental overdoses. Brandy Vandermark-Murray, senior vice president of operations at Horizon Health Services, said that fentanyl is making the opioid epidemic worse.
“We are continuing to experience the opioid epidemic,” she said. “We unfortunately still have overdoses happening and people unintentionally overdosing. Fentanyl is extremely popular and is in almost all of our supply. This is still happening along with significant alcohol abuse.”
Horizon operates in locations throughout Western New York.
Vandermark-Murray views the revival of social connections as a positive factor in the past year, as isolation “is a very dangerous place for people to be,” she said.
Telehealth has made a difference, as it has helped more patients access care, if transportation, stigma or scheduling makes it difficult to see a therapist.
Meshing in-person and telehealth treatments can offer patients and providers more options.
Horizon offers harm reduction measures, including distributing test strips to see if a patient’s supply contains fentanyl. Horizon also trains people to use Narcan to counteract opioid overdoses and has restarted its out-patient services in lieu of its in-patient program. These include individual and group therapy.
“We continue to experience the worst overdose crisis in the history of the nation, which is devastating individuals, families and communities,” said Evan Frost, assistant director of
Communications & Public Information for the New York State Office of Addiction Services and Supports in Albany. “Fentanyl continues to be a major factor in overdoses and deaths in New York state. In 2021, the vast majority of overdoses involved synthetic opioids like fentanyl. The main danger from fentanyl is that it is often added to a substance without the user’s knowledge, which can substantially raise the risk of an overdose since the person using the substance has not built up a tolerance.”
Statewide, the introduction of telehealth and mobile treatment in recent years has helped reach people who may otherwise not have accessed services.
“These initiatives have allowed us to meet people where they are and deliver individualized, person-centered services to meet their needs,” Frost said. “We are also collaborating with the office of mental health on efforts to treat co-occurring substance use and mental health disorders, including through certified community behavioral health clinics, which provide an array of coordinated services to address substance use and/ or mental health, and crisis stabilization centers, which provide support, assistance and urgent access to care for individuals experiencing a crisis situation related to substance use and/or a mental health condition. We plan to build on these efforts in the coming year.”
Frost said that OASAS will continue with street level outreach teams, outreach and engagement services, shelter in-reach programs
Through June 2022 30 https://health.ny.gov/ statistics/opioid/data/pdf/nys_jan23.pdf
In 2021, there were 6,037 overdose deaths in New York State. This is an increase of approximately 101% since 2015.
and ensuring providers have access to naloxone and fentanyl test strips. The strips can help a person using opioids know if fentanyl is present.
“Other harm reduction programming is included in these efforts,” he added.
OASAS also plans to “improve treatment equity. Historically, addiction treatment has not been as available to minority communities,” Frost said.
On Feb. 8 this year, New York state announced it will make available to 18 providers statewide $8.6 million to develop integrated outpatient treatment initiatives targeting opioid use. The money comes from a more than $2 billion fund received from settlements with opioid manufacturers. Some of the fund will be distributed to municipalities and the rest to support opioid programs.
The New York State Department of Health recently reported that in 2021 statewide:
4,766 overdose deaths involving opioids, a 14% increase over 2020.
10,430 outpatient emergency department visits due to opioid overdoses, a 12.6% increase over 2020.
19,139 instances of naloxone being administered by emergency medical services, an 11.8% increase over 2020.
Anyone struggling with addiction can call the HOPEline 24/7 at 1-877-8-HOPENY (1-877-846-7369) or text HOPENY (Short Code 467369). A family member may also call.
NYS OASAS Treatment Availability Dashboard at FindAddictionTreatment.ny.gov or through the NYS OASAS website, www.oasasd. ny.gov, lists treatment options.
Anyone struggling to file a claim or who has been denied a claim can contact the CHAMP helpline at 888614-5400 or ombuds@oasas.ny.gov.
March 2023 • IN GOOD HEALTH – Buffalo & WNY’s Healthcare Newspaper • Page 15
Number of Opioid-Related Deaths in Erie County 2015 118 2016 274 2017 194 2018 168 2019 142 2020 227 2021 272 Number of Opioid-Related Deaths in Niagary County 2015 2016 46 2017 34 2018 41 2019 37 2020 186 2021 70
Number of Deaths Number of Deaths Year Year
Addiction
Drug Prevention: For Horizon Health VP, It’s a Personal Matter
By Deborah Jeanne Sergeant
Currently senior vice president of operations for Horizon Health Services, Brandy Vandermark-Murray has always had a soft spot for working with adolescents and children, stemming from her own experiences.

“Substance use affected my family of origin,” she said. “Pretty much everyone has someone affected by substance use. It’s like no other behavioral use disorder. I am passionate about serving populations that are overlooked and have a lot of opportunity to do well in society if given the proper resources and
opportunity.”
When she began her career 17 years ago as a clinician at Horizon, the biggest issues affecting youth in the substance abuse field were marijuana and alcohol.
That soon shifted, as the opioid epidemic began within her first few years of working in the field. She saw many patients struggling and some dying. She said this helped motivate her to remain in the field.
“We’re losing so many people who are marginalized and often stigmatized and really need the work we do,” Vandermark-Murray said.
Horizon, a nonprofit which operates in locations throughout Western New York, provides outpatient and residential addiction and mental health services. Through the work of Horizon and similar organizations in the past 15 years, more people have become aware of substance use, particularly of the opioid epidemic, and how much addiction affects families. Educational institutions have also been an important part of this change.

In addition to her work at Horizon, Vandermark-Murray began teaching about opioid use disorder at Canisius College five years ago because she views substance use disorder as nearly ubiquitous among troubled families.
“So many people coming out of school want to work with children and families and not substance use disorder,” she said. “I want to give them education on how much this impacts society and this will impact nearly all the populations they’ll meet in sessions. I wanted to give them clinical tools to work with individuals with substance use disorders.”
She continues to push back against stigma directed towards her patients by the general public.
“There is still a belief system is that people who use substances choose to use them,” she said. “They hold that addiction is not a disease. It is a brain disorder. They view people as bad or criminals or have moral failing. Or they think, ‘It doesn’t happen to my friends.’ Or ‘It doesn’t happen here.’ But it happens everywhere.”
The workforce shortage also challenges her organization, along with compassion fatigue of those still working in the field. It’s difficult to lose patients or experience setbacks with them. Limited financial resources hamstring efforts of agencies like Horizon which could operate at greater capacity.
Despite these difficulties, Van-
dermark-Murray finds fulfillment in her work.
“We see people every day who get healthy,” she said. “Their lives improve and the quality of their lives improve. Those overdoses or incidences are awful, but we have a ton of people whose lives are getting better. We have many who almost die and then work very hard to get better, go back to school, get married, join the workforce.”
“It’s hard, but rewarding. Every day you will be able to say you’re making a difference,” she added. “It sounds cheesy, but is absolutely true.”
Page 16 • IN GOOD
– Buffalo & WNY’s Healthcare Newspaper • March 2023
HEALTH
Addiction
Brandy Vandermark-Murray is Horizon Health’s vice president of operations. She has worked at the nonprofit for 17 years.
“
Looking to start a career in behavioral health? Caz Recovery is hiring! cazenoviarecovery.org/employment Positions available in Erie & Niagara Counties starting at $17 per hour.
“ We’re losing so many people who are marginalized and often stigmatized and really need the work we do.
Tranq Making Inroads in Western New York
By Deborah Jeanne Sergeant
Since 2021, a newcomer to substance abuse disorder has been making inroads in the area: xylazine.
Known as “tranq” on the street, the horse tranquilizer is not FDA
approved for use in humans and is not under the jurisdiction of the Controlled Substance Act.
It is available as a veterinary sedative under the brand names of Rompun, Sedazine and AnaSed.
“Tranq or xylazine is not routinely tested for in toxicology testing or by medical examiners, so we are not able to speak to its overall prevalence in New York state,” said Evan Frost, assistant director of communications and public information with the New York State Office of Addiction Services and Supports (OASAS) in Albany. “We do know that it has been found in testing conducted in New York City, and there have been instances of wounds and skin ulcers related to xylazine in other regions of the state, so we know it is also outside of New York City in some capacity.”
Xylazine is most often used as a “cutting agent” for illegal fentanyl mixes. A cutting agent is a cheap and readily available drug — xylazine in this case — mixed with the more expensive and harder to obtain drug such as fentanyl.
Sometimes cutting agents heighten the effect of the more expensive drug. With xylazine, the unintended effects can include bradycardia (slow heart rate), blurry vision, central nervous system depression, unsteady gait, slowed or stopped breathing, low blood pressure, hypothermia, high blood glucose levels, severe withdrawal, pinpoint pupils, necrotic skin ulcerations (may occur at other areas beside injection site with repeated exposure), coma and death. Because xylazine is a sedative, it is sometimes combined with stimulants like methamphetamine and cocaine.
“We have heard about tranq for
two years,” said Brandy Vandermark-Murray, senior vice president of operations at Horizon Health Services, which operates in locations throughout Western New York. “A lot of times, you have people using tranquilizers to cut heroin to increase its effect. People use synthetics in opioids to increase the high and it can be fatal. I haven’t seen a ton of tranq in Western New York, but every use is a chance they’ll overdose.”
Western New York has not seen rampant use of xylazine so far, but physician Tony Lin, addictions medicine specialist with UBMD Family Medicine, said that its presence may go undetected.

“We don’t routinely screen for xylazine, so I don’t know if people are getting it knowingly or unknowingly,” he said.
The presence of the many equine businesses and farms in Western New York may be easier to access xylazine than in urban areas.
Because xylazine is often used to cut fentanyl and other drugs, it may be even more dangerous than a single, known drug in case of an overdose. Healthcare providers in these cases have little idea of what the patient has taken and it makes treating overdosed patients more challenging.
“Narcan is good for opioids, like methadone, morphine and fentanyl,” Lin said. “Xylazine is not an opiate class medication. It is like a blood pressure medication and has some sedatives.

March 2023 • IN GOOD HEALTH – Buffalo & WNY’s Healthcare Newspaper • Page 17
Addiction
Feeling stressed? Anxious? Concerned about a family member? We can help. Call us today at 716.831.1800 horizon-health.org | Mental health & addiction | Virtual and In-Person Counseling Services Serving Children, Adolescents, and Adults throughout Western New York
Ask








From the Social Security District Office
Social Security Launches Redesigned Website at SSA.gov
Have you visited the redesigned SSA.gov yet? In December 2022, we updated our homepage with a new design to help you find what you need more easily.
SSA.gov is visited by over 180 million people per year and it is one of our most important tools for providing efficient and equitable access to service. Whether providing service in person or online, our goal is to help people understand what they may qualify for and seamlessly transition them to an application process.
Now, with improved self-service accessibility to online services, you might not have to call or visit an office to get what you need. This helps our staff focus on serving customers who need in-person assistance.
• Reimagined website prioritizes customer experience







The redesign is intended to provide a clear path to the tasks you need to accomplish. Many of the most visited sections of SSA.gov are now live with a more user-friendly and task-based approach. New pages and improvements based on public feedback will continue to be unveiled in the coming months, as part of our ongoing efforts to improve how the public can do business with us.
When you visit SSA.gov, you can use interactive tools to:
• Check eligibility for benefits

The new benefit eligibility screener is a convenient and simple way for you to learn if you might be eligible for benefits.

• Save time on Social Security number (SSN) and card online services



If you lose your SSN card, you may not need a replacement. In most cases, simply knowing your SSN is enough. If you do need a replace-
The Social Security Office Q&A

Q.: Why is it so important that my baby have a Social Security number?





A.: Your child may need a Social Security number if you are planning to open a bank account, buy savings bonds, obtain medical coverage, or apply for government services for the child. Your child will also need a Social Security number if you are going to declare him or her on your taxes. Getting a Social Security number for your newborn is voluntary, but it is a
ment card, you may be able to request it online by visiting our Social Security Number and Card page at www.ssa.gov/ssnumber.
You can also start an application for an updated card or request an SSN for the first time. You may never need to go to an office, but if you do need to visit an office to complete the application then you can save a lot of time by starting online.
• Start an application for Supplemental Security Income (SSI)



You can start the application process online and request an appointment to apply for SSI benefits by answering a few questions on our SSI page at www.ssa.gov/ssi.
• Apply for Social Security benefits and other online services







For most benefits, you can apply online or start an application online. In many cases, there are no forms to sign. We will review the application and contact you with any questions or if we need more information. Visit our online services page at www. ssa.gov/onlineservices to apply for retirement, disability or Medicare.
Many Social Security services do not require an office visit. If you have a personal My Social Security account, you can start or change direct deposit, request a replacement SSA1099, or print or download a current benefit verification letter if you need proof of your benefits.
If you’re not yet receiving benefits, you can use your online account to get a personalized Social Security statement, which provides your earnings information as well as estimates of future benefits. The portal also includes a retirement estimator tool and links to information about other online services. We encourage people without a personal My Social Security account to create one today at www.ssa.gov/myaccount.
Please share this with your loved ones and post it on social media.
good idea to apply when your child is born. You can apply for a Social Security number for your baby when you apply for your baby’s birth certificate. The state agency that issues birth certificates will give us your child’s information and we will mail you a Social Security card with the child’s Social Security number. Visit www.ssa.gov/ssnumber for more information.
Page 18 • IN GOOD HEALTH – Buffalo & WNY’s Healthcare Newspaper • March 2023 SEND US YOUR FEEDBACK AND GET A FREE SUBSCRIPTION! ✷ takeonlinehearingtests home. P.17 Talkingto loved about move assistedliving. Q&AwithAngelaMarinucci,ErieCountycommissioner seniorservices. P.14 ALSO THIS LAWYER,SURGEON wantedPhysicianStutiTambaralways make difference women’s health breast surgeon asalawyershe does that. BFOHEALTH.COM NOVEMBER FREE 1in7U.S.HighSchoolStudentsNowVapes Teenvapingcontinuesatconcerninglevels,U.S.healthofficialsreport.Page TopIssuesAffecting SeniorsToday P.13 AREYOU THANKSGIVINGFACING ALONE? THINGS YOU NEED TO ABOUTKNOW ALLERGIES5 10 tips on choosing the ideal healthy gift for a friend or loved one HEALTHY GIFTS FREE RICHARD CASTALDO,M.D. Hospice chief Niagara Falls explains end care. Unhealthy Western New York Report: Erie and Niagara rank among the least healthy in New York P. 5 5THINGS YOU NEED TO KNOW ABOUT RSV, THE HAPPY HOLIDAYS! BFOHEALTH.COM DECEMBER ISSUE
SCAN TO VIEW W EBSIT E
OFF YOUR FOURTH MONTH* *Family must claim special on the 1st call or tour. Residency must be a period of (3) months to receive incentive. Call 716-293-2894 for a personal tour, and register to WIN a FREE DINNER FOR TWO (A $75 VALUE) juniperglenret.com | 8820 Transit Rd. East Amherst NY. 14051 NAME ADDRESS WHAT DO YOU LIKE ABOUT IN GOOD HEALTH NEWSPAPER? CITY/TOWN STATE ZIP Yes! Send me six free issues of In Good Health to the above address, beginning with the upcoming issue. P.O. Box 550, Amherst, NY 14226 Disclaimer: your comments may be used for marketing purposes. WHERE DID YOU PICK UP THE PAPER?
$500
By Jim Miller

How to Cover Dental Care in Retirement

Dear Savvy Senior, I had dental insurance through my work for many years but lost it when I retired and joined Medicare. Where can retirees find affordable dental care?




Uninsured Al

Dear Al,
Unfortunately, about two-thirds of U.S. retirees don’t have dental insurance today. Without coverage from traditional Medicare, and with private dental insurance typically costing too much to be feasible, most seniors are stuck paying full out-ofpocket prices every time they visit a dentist. While there’s no one simple solution to affordable dental care there are a variety of options that can help cut your costs. Here’s where to look.
• Medicare Advantage: While



dental services are mostly excluded under original Medicare, many Medicare Advantage plans do provide coverage for dental care, but it’s usually very limited. Medicare Advantage plans are government approved health plans (usually HMOs and PPOs) sold by private insurance companies that you can choose in place of original Medicare. To shop and research Advantage plans in your area visit Medicare.gov/plan-compare or call 800-633-4227.
• Dental insurance: If you have gum problems and need extensive dental care, a dental insurance plan may be worth the costs versus paying for care yourself. Monthly premiums for individual plans range from about $20 to $80. A typical plan includes two or three cleanings and checkups per year, but these plans will likely have a waiting period — anywhere from a few months to a few years — before coverage for more expensive procedures kicks in. To find dental plans in your area, see
• Dental savings plans: While savings plans aren’t as comprehensive as insurance, they are a good option for those who don’t have dental insurance. How this works is you pay an annual membership fee — around $80 to $200 a year — in exchange for 10% to 60% discounts on service and treatments from participating dentists. To find a savings plan, go to DentalPlans.com (or 888-632-5353) where you can search for plans and participating dentists, as well as get a breakdown of the discounts offered.

• Veterans’ benefits: If you’re a veteran enrolled in the VA health care program or are a beneficiary of the Civilian Health and Medical Program (CHAMPVA), the VA offers a dental insurance program that gives you the option to buy dental insurance through Delta Dental and MetLife at a reduced cost. The VA also provides free dental care to vets who have dental problems resulting from service. To learn more about these options, visit VA.gov/dental or call 877-222-8387.

• Cheaper dental care: Because


prices can vary by dentist, one way to ensure you get a good deal on your dental care is to call multiple provides and compare prices. To get an idea of what different dental procedures cost in your area, see FairHealthConsumer.org. If you’re paying cash, it’s also perfectly reasonable to ask your dentist for a discount.
There are also a number health centers and clinics that provide low-cost dental care to those in need. And all university dental schools and college dental hygiene programs offer dental care and cleanings for less than half of what you wo-uld pay at a dentist’s office. Students who are supervised by their professors provide the care. See TeethWisdom.org to search for a center, clinic or school near you.
THE BEST CARE HAPPENS WHEN WE COME TOGETHER.
At ECMC, each of us—from doctors, nurses, support sta , and specialists—is focused on not just healing the community but supporting each other at every turn. Our commitment to our employees starts with a rewarding work environment and continues through to our professional development programs. Whether you’re just starting out or you’re a seasoned healthcare professional, ECMC is the perfect t to further your career.
March 2023 • IN GOOD HEALTH – Buffalo & WNY’s Healthcare Newspaper • Page 19
Send your senior questions to: Savvy Senior, P.O. Box 5443, Norman, OK 73070, or visit SavvySenior. org. Jim Miller is a contributor to the NBC Today show and author of “The Savvy Senior” book.
ECMC-35641_RecruitementAd_InGoodHealth_9.75x6.69_M Trim Size: 9.75”W x 6.69”H | No Bleed | CMYK
Join the ECMC family of caregivers at ECMC.EDU/CAREERS
©2023 ECMC
eHealthInsurance.com.
Nearly 2 Million New Cases of Cancer Expected in 2023
American Cancer Society states we will likely see about 609,820 deaths as a result of cancer
By Deborah Jeanne Sergeant
In January, the American Cancer Society published its annual cancer outlook statistics.
Among the findings, the society stated that in 2023, 1,958,310 new cancer cases and 609,820 cancer deaths are projected to occur in the United States.
Other findings include:
• Prostate cancer increased by 3% annually from 2014-2019 after declining for two decades, which means 99,000 new cases.
• Lung cancer in women decreased at one-half the pace of men, 1.1% vs. 2.6% annually between 2015 and 2019.
• Cancers of the breast, uterine, liver and melanoma increased.
• Cervical cancer decreased by 65% between 2012 and 2019 among women in their early 20s.

• The death rate of cancer declined by 1.5% between 2019 and 2020, contributing to an overall 33% reduction since 1991, an estimated 3.8 million deaths averted.
• Cancer is still the second-leading cause of death in the US.
Heredity plays a role in 55-10% of all cancers, according to the National Cancer Institute. Embracing positive health habits can reduce the risk of many kinds of cancer.
“We don’t have a say of our genetic makeup, but find out your family history,” said Nikia Clark, senior manager for the department of community outreach and engagement with Roswell Park Comprehensive Cancer Center. “We have great genetic counseling and testing here at Roswell. Find out if a first-degree relative was diagnosed. It gives you more knowledge that this was running in your family.”

Cancer screenings can prevent cancer from developing in the case of colon cancer because providers can remove polyps before they become cancer. Self-exams and screenings can also catch cancer early, when it is most treatable.
Clark wants people to talk with their physician about when to start screening, as some people with family history of cancer may be advised to start earlier than others. Cancer screenings are available for breast cancer, cervical cancer, lung cancer, colorectal cancer and prostate cancer, among others.

Although a few minutes of sun exposure weekly and vitamin D supplementation can help ensure sufficient vitamin D levels, too much sun exposure raises risk for skin cancer.
“Wear sunscreen, not just in the summer but all year round,” Clark said. “Do not go to tanning beds. Wear hats and sunglasses and clothing that helps.”
Some fabrics provide additional sun protection factor than others, such as rash guard swimwear.
Another important factor in reducing cancer risk is body weight. Excess body weight can contribute to conditions that stress the body, hindering the cells’ ability to repair. In addition, the extra weight is associated with hormone release, which can spur cancer growth.
Clark said that obesity contributes to the risk for pancreatic, breast, colorectal and kidney cancer.
“We stress maintaining a healthy weight through diet and exercise,” Clark said.
Most people should engage in 150 minutes of moderate physical activity or 75 minutes of vigorous activity per week. Moderate activity could include walking, dancing, gardening or biking. Jogging, running, aerobic
dance, swimming laps or shoveling snow all represent vigorous activity.
Diet is also vital. Reducing intake of processed, sugary, saturated and trans-fat and salty foods and increasing whole grains, legumes, lean sources of protein, fruits and vegetables “is something you can control,” said Darryl Somayaji, Ph.D., registered nurse and assistant professor, UB School of Nursing and adjunct assistant professor of oncology, cancer screening and survivorship at Roswell Park Comprehensive Cancer Center. “You can try to eat healthfully.” She recommends eating whole grains and whole fruits and vegetables are rich in fiber.
Somayaji especially wants patients to pay attention to their cancer risk factors as they age.
“As we get older, we’re all at a greater risk to develop cancer,” she said. “The older adult at home without access or who is challenged to get to the grocery store or provider is isolated. How do people get out and get to places without social support? It’s something we need to do for each other.”
Community centers, churches, neighbors and other groups provide
resources that can help, such as exercise classes, congregant meals and transportation.
William Dahut, chief scientific officer with the American Cancer Society, said that 42% of cancers are preventable.
“If this was a new drug it would be truly incredible,” Dahut said.
In addition to seeking appropriate screening, exercising and maintaining a healthy weight, he encourages people to eliminate or minimize alcohol.
“Alcohol can cause direct damage to cells and tissues and impact hormone levels increasing the likelihood of cancer,” Dahut said.
Ceasing tobacco use also lowers the risk for many kinds of cancer — not only lung cancer.
“Tobacco is made of thousands of chemicals, including at least 70 that cause cancer,” Dahut said.
The website nysmokefree.com and most healthcare providers offer free tools and resources to support smoking cessation for those who want to quit.
To find resources by ZIP code, visit the site of the American Academy of Family Physicians at https:// navigator.aafp.org.
Page 20 • IN GOOD HEALTH – Buffalo & WNY’s Healthcare Newspaper • March 2023
Nikia Clark is a senior manager for the department of community outreach and engagement with Roswell Park Comprehensive Cancer Center.
William Dahut, chief scientific officer with the American Cancer Society.
