The Allergan Aesthetics Portfolio

References:

References:
By scanning the QR code, you are being directed to a third party website on which Allergan Aesthetics, an Abbvie company are only responsible for the references for this article.
* Such treatment decisions must be assessed and discussed as part of the healthcare professional–patient consultation prior to any treatment being administered.
† Multimodal aesthetics treatment describes the use of more than one type of treatment modality that are administered as part of a patient’s treatment plan.
Models have been treated with Allergan Aesthetics product. Individual results may vary. The safety and efficacy of HArmonyCa™ has not been evaluated in patients treated with other filling implants.10 There is no data available regarding the safety of injecting a greater amount than 20mL of ALLERGAN dermal fillers per 60kg body mass per year.4 HArmonyCa™ Lidocaine is referred to as HArmonyCa™.
©2024 AbbVie. All rights reserved. All trademarks are the property of their respective owners.
Adverse events should be reported.
UK reporting forms and information can be found at https://yellowcard.mhra.gov.uk or via the MHRA Yellow Card app, available at Google Play or Apple App stores. Adverse events should also be reported to AbbVie on ProductSurveillance_EAME@allergan.com. Irish HCPs are asked to report any suspected adverse reactions via HPRA Pharmacovigilance; website: www.hpra.ie.
Special Feature: Examining Treatment Approaches to Manage Scars
Treating Melasma: Discussing Various Treatment Modalities for Melasma
Dr Nicole Chiang provides an overview of common facial dermatoses
CCR 2024 marks its return with the latest advancements in medical aesthetics



Skin booster injections are most frequently applied to enhance the skin of the midface, lower face, décolletage, body and hands; reflecting their versatility in addressing various aesthetic concerns.1











Suggested applications: Young/delicate skin – neck, face, decolletage, hands, scars, acne scarring












Suggested applications: Eye contour, eyelids














Suggested applications: Hair, eyebrows






Suggested applications: Mature and dehydrated skin – neck, face, decolletage, hands, scars, acne scarring

08 News
The latest product and specialty news
19 Hero Products: Skin Rejuvenation
A selection of trending products to revitalise the skin
21 Leading Association Reports Aesthetic Treatment Decline
A look into recent statistics showing a decline in UK’s aesthetic treatments
22 CCR 2024 Marks its Return
Join the community to shape the future of medical aesthetics
24 Special Feature: Managing Scars
An insight into treatment for injury and acne-based scarring
29 Improving Patient Care with GetHarley
Dr Amélie Seghers discusses how she looks after her patients’ skin
31 CPD: Utilising Polynucleotides for Hair Loss
Dr Edward Robinson explores literature around polynucleotides and hair loss
34 Case Study: Treating Laxity in the Knees
Yuliya Culley discusses how she treated a case of skin laxity
39 Boosting Moisture With STYLAGE® HydroMax
Dr Zunaid Alli shares how STYLAGE® HydroMax boosts skin moisture
40 Treating Varying Types of Melasma
Dr Mary Sommerlad examines treatments to address melasma
45 Rediscovering Profhilo®
The science behind the breakthrough in injectable skin rejuvenation
47 Achieving Periocular Rejuvenation
Oculoplastic surgeons explore options to treat the delicate eye area
51 Evaluating New Technology for Scar Revision
Alma shares the promising new research behind the Alma Hybrid laser
53 Treating Facial Dermatoses
Dr Nicole Chiang provides an overview of treatment for facial dermatoses
59 Abstracts
A round-up and summary of useful clinical papers
60 Leasing Medical Aesthetics Devices
Helen George looks at the benefits of leasing equipment
64 Saying No to Patients
Julie Scott explores safeguarding patient wellbeing
66 Becoming a Zero-Waste Clinic
Graham Matthews offers guidance on achieving a zero-waste clinic
69 In Profile: Emma Coleman
Emma Coleman shares her passion for giving patients great skin
70 The Last Word: Safeguarding Patients
Kelly Saynor argues for the importance of the cooling-off period
NEXT MONTH: COMBINATION TREATMENTS
• Combining Devices and Injectables • Addressing Collagen Deficit








Dr Edward Robinson is a cosmetic physician, NHS anaesthetics doctor and an associate member of the British College of Aesthetic Medicine (BCAM). He specialises in skin and hair rejuvenation treatments, favouring biostimulators and combination treatments.
Yuliya Culley is registered general nurse with experience in emergency, cardiology and dermatology nursing. She started her practice in medical aesthetics in 2009, and has performed a considerable number of non-surgical procedures.
Dr Mary Sommerlad is a consultant dermatologist with a focus on medical, paediatric, skin of colour and laser dermatology. She specialises in pigmentary facial conditions such as melasma, rosacea, photoageing and post-inflammatory hyperpigmentation.
Miss Jennifer Doyle is a consultant ophthalmic and oculoplastic surgeon. She is the non-surgical lead clinician at The Clinic at Holland Park and has completed the level 7 diploma in Injectables. Miss Doyle has served as a lead trainer for Harley Academy.
Mr Richard Scawn is a consultant ophthalmologist and oculoplastic surgeon based at The Clinic at Holland Park and Chelsea and Westminster NHS Trust. He specialises in complex eyelid reconstruction and periocular skin cancer work.
Dr Nicole Chiang is a consultant dermatologist with experience in both medical and cosmetic dermatology. She is the director of Lumiere Clinic in Manchester, and carries out regular teaching in dermatology to a wide range of practitioners.
“Amazing training. The knowledge and experience of the trainer was amazing. Would recommend this training to any aesthetic practitioner” SB

LONDON
Monday 8th July
Wednesday 7th August
Friday 13th September
BRISTOL
Thursday 18th July
Thursday 19th September
Tuesday 19th November
LOUGHBOROUGH
Thursday 11th July
Friday 9th August
Thursday 12th September
NEWCASTLE
Tuesday 2nd July
Thursday 5th September
Wednesday 6th November
MANCHESTER
Tuesday 9th July
Tuesday 17th September
Monday 18th November
LEEDS
Monday 19th August
Tuesday 15th October
SCOTLAND
Wednesday 18th September
BELFAST
Monday 4th November
Or email training@churchpharmacy.co.uk to become a stockist
 Shannon Kilgariff Editor & Event Manager @shannonkilgariff
Shannon Kilgariff Editor & Event Manager @shannonkilgariff
We know injectable treatments like botulinum toxin and dermal fillers are still the bread and butter of aesthetic practice. However, it’s integral that the health of the skin is always considered and prioritised. After all, the skin is the fortress that protects the body, and is exposed to so many external factors which can cause damage and premature ageing. Promoting good skin health for your patients, through treatments beyond injectables such as pharmaceutical-grade skincare, energy-based devices and more regenerative approaches, is vital for ensuring this fortress stays strong and resilient.
That’s why this issue of the Aesthetics Journal focuses on optimising the skin! My favourite reads this month are managing scars (p.24), addressing melasma (p.40) and treating facial dermatoses (p.53). Coinciding with this theme, June is acne awareness month, so we have quite a few articles that relate to treating acne and its related scarring. To promote acne awareness month, we’re running a competition on
Instagram! Guess how many times ‘ACNE’ is mentioned in this month’s Journal on our Instagram post for a chance to win one of our Hero Products on p.19. Start counting!
June is going to be an interesting month for our medical aesthetics specialty. Last year’s Government consultation on a new licensing scheme for non-surgical cosmetic procedures in England drew 11,800 responses, the second-largest in the Department of Health and Social Care’s history. This month, we are finally expecting the Government’s response to this consultation. It will be the first step in a long process, but will be critical for everyone in the community to follow. Of course, we at the Journal will be monitoring closely and reporting the news as it happens. We look forward to hearing all of your thoughts, so please do let us know what you think of the developments.
These crucial regulation updates will also be discussed by the Joint Council for Cosmetic Practitioners at our next event – Clinical Cosmetic Regenerative (CCR) congress – taking place on October 10-11 in London. If you’re keen to partake in the regulation discussion, this is an unmissable event! Register free on p.22 and I look forward to seeing you all there and building a better, safer medical aesthetics specialty.
Leading figures from the medical aesthetic community have joined the Aesthetics Advisory Board to help steer the direction of our educational, clinical and business content

Sharon Bennett is chair of the British Association of Cosmetic Nurses (BACN), previous UK lead of the BSI committee for aesthetic non-surgical standards, and member of the Clinical Advisory Group for the JCCP. She is a trainer and registered university mentor in cosmetic medical practice, and is finishing her MSc at Northumbria University. Bennett has won the Aesthetics Award for Nurse Practitioner of the Year and the Award for Outstanding Achievement.
Sharon Bennett, Clinical Lead



Mr Naveen Cavale has been a consultant plastic, reconstructive and aesthetic surgeon since 2009. He has his own private clinic and hospital, REAL, in London’s Battersea. Mr Cavale is the national secretary for the ISAPS, president of the Royal Society of Medicine, and vice-chair for the British Foundation for International Reconstructive Surgery.
Miss Elizabeth Hawkes is a consultant ophthalmologist and oculoplastic surgeon. She is the lead oculoplastic surgeon at the Cadogan Clinic, specialising in blepharoplasty and advanced facial aesthetics. Miss Hawkes is a full member of the BOPSS and the ESOPRS, and is an examiner and fellow of the Royal College of Ophthalmologists.
Mr Adrian Richards is a plastic and cosmetic surgeon with over 30 years’ experience. He is the clinical director of the aesthetic training provider Cosmetic Courses and surgeon at The Private Clinic. He is also a member of the British Association of Plastic and Reconstructive and Aesthetic Surgeons and the British Association of Aesthetic Plastic Surgeons.
PORTFOLIO MANAGEMENT
Alison Willis • Director T: 07747 761198 | alison.willis@easyfairs.com
Shannon Kilgariff • Editor & Event Manager T: 0203 196 4351 | M: 07557 359 257 shannon@aestheticsjournal.com
EDITORIAL
Holly Carver • Deputy Editor | T: 0203 196 4427 holly.carver@easyfairs.com
Kate Byng-Hall • Journalist | T: 020 319 64265 kate.byng-hall@easyfairs.com
Anjali Sooknanan • Journalist | T: 020 319 64265 anjali.sooknanan@easyfairs.com
Amer Saleh • Content Writer | T: 020 3196 4389 amer.saleh@easyfairs.com
DESIGN
Peter Johnson • Senior Designer T: 0203 196 4359 | peter@aestheticsjournal.com



Dr Mayoni Gooneratne (MBBS, BSc, MRCS, MBCAM, AFMCP) was an NHS surgeon before establishing The Clinic by Dr Mayoni and founding Human Health – an initiative combining lifestyle with traditional and functional medicine to provide a ‘cell-up’ regenerative approach to aesthetics. She is also the co-founder of The British College of Functional Medicine.
Jackie Partridge is an independent nurse prescriber. She is the clinical director and owner of Dermal Clinic in Edinburgh and a KOL for Galderma. She holds an MSc in Non-surgical Aesthetic Practice and a BSc in Dermatology. Partridge is a stakeholder group member with Scottish Government/HIS, Honorary BACN member and JCCP Fitness to Practice Nurse.
Dr Souphiyeh Samizadeh is a dental surgeon with a Master’s degree in Aesthetic Medicine and a PGCert in Clinical Education. She is the founder of the Great British Academy of Medicine and Revivify London Clinic. Dr Samizadeh is a Visiting Teaching Fellow at University College London and King’s College London.
ADVERTISING & SPONSORSHIP
Judith Nowell • Head of Sales T: 0203 196 4352 | M: 07765 407629 judith@aestheticsjournal.com
Emma Coyne • Senior Sales Executive T: 020 3196 4372 | emma.coyne@easyfairs.com
Imogen Preece • Sales Executive T: 0203 196 4367 | imogen.preece@easyfairs.com
MARKETING
Aimee Moore • Senior Marketing Manager T: 020 3196 4370 | aimee.moore@easyfairs.com
Angelica Smart • Content Marketing Executive T: 020 3196 4419 | angelica.smart@easyfairs.com
Ella Carey • Marketing Executive T: 020 3196 4410 | ella.carey@easyfairs.com Aesthetics Aesthetics @aestheticsjournaluk
HELP PROGRESS MEDICAL AESTHETICS! WRITE FOR THE JOURNAL
Do you have any techniques to share, case studies to showcase or knowledge to impart?
Email: editorial@aestheticsjournal.com



Dr Anjali Mahto is one of the UK’s leading consultant dermatologists. She is a Fellow of the Royal College of Physicians, member of the Royal Society of Medicine and a spokesperson for The British Skin Foundation. In 2023 Dr Mahto opened Self London, a dermatology and lifestyle clinic aimed at managing skin conditions holistically.
Dr Tapan Patel is the founder and medical director of PHI Clinic, and has more than 20 years’ experience performing aesthetic treatments. He is a KOL for Allergan Aesthetics and Cutera, and is passionate about high standards in aesthetic medicine. In 2023, Dr Patel received The Aesthetics Award for Outstanding Achievement in Medical Aesthetics.
Dr Stefanie Williams is a dermatologist with a special interest in adult acne, rosacea and aesthetic medicine. She is the founder and medical director of multi-award winning EUDELO Dermatology & Skin Wellbeing in London, and creator of Delo Rx skincare. She is the author of three books and has published more than 100 scientific articles, book chapters and abstracts.
ARTICLE PDFs AND REPRO
Material may not be reproduced in any form without the publisher’s written permission. For PDF file support please email, contact@aestheticsjournal.com
© Copyright 2024 Aesthetics. All rights reserved. Aesthetics is published by Aesthetics Media Ltd, which is registered as a limited company in England; No 9887184
Follow us on Instagram @aestheticsjournaluk
#AestheticsJournal
Claire Kirsty
@c.k_aesthetics
Second time this year I have made it into the Aesthetics Journal alongside so many of my incredible colleagues!

#Nurses
Sharon Bennett
@harrogateaesthetics
Had a wonderful time at the BACN Spring Symposium, enjoying an agenda with a breadth of fascinating topics

#Examination
Dr Bhavjit Kaur
@drbhavjitkaur
It is a privilege to be a BCAM Board Member and Trustee as we conduct the first OSCE examinations for Full Membership


#ClinicOpening
Dr David Jack
@drdavidjack
We recently celebrated the launch of our third clinic in Edinburgh –thanks to Judy Murray for joining us!
#Conference
Amanda Demosthenous @nurseamanda_drnestors
Thank you so much to Wigmore Medical Live for inviting me to speak alongside some amazing colleagues!

Melanoma UK charity has launched the Beauty Spotters campaign to raise awareness of acral melanoma – the most common form of skin cancer for people with skin of colour. The charity explains that 75% of acral melanoma cases appear on non-sun exposed areas like hands, palms, nails and soles of feet. The causes of this cancer are not known, but it is not thought to be related to sun exposure. Common signs of the cancer include streaks in the nails not caused by injury, irregularly shaped moles under the nail, fully black nails, changing moles on the hands or soles of the feet, and thickened patches on the palms or soles of the feet. Mark Rawden, CEO of Melanoma UK said, “As a charity, we are expanding our efforts beyond traditional discussions of solely sun-related skin cancers. Our focus has been sharpened around not just raising awareness, but campaigning for behaviour change to increase the likelihood of melanoma being spotted amongst all people.”
The British College of Aesthetic Medicine (BCAM) has held its first round of Master’s-level MBCAM OSCE examinations for practitioners to achieve Full Membership of the association.
BCAM explains that the two-part examination is taken by Associate Members who are looking to become Full Members. The first paper is multiple-choice, while the second is an objective structured clinical examination (OSCE).
BCAM president Dr Catherine Fairris commented, “This is a rigorous exam that covers the entire medical aesthetic curriculum as dictated by Health Education England. The exam is accredited with the JCCP, and we hope it will further demonstrate the level of theoretical and practical expertise that our members have, as well as aid in our goal of upholding the highest aesthetic excellence.”
Skincare
Skincare company ALASTIN from Galderma has launched A-LUMINATE brightening serum to combat pigmentation.
The company explains the key ingredients include PATH-3 technology, tranexamic acid and niacinamide. The new serum aims to minimise the recurrence of surface pigmentation, help correct the appearance of hyperpigmentation and reduce the appearance of uneven skin tone. Dr Alan Widgerow, head of ALASTIN innovation, said, “This is a breakthrough product for patients who suffer with hyperpigmentation. The UK team continues to expand its product portfolio as part of the launch of ALASTIN, and A-LUMINATE will be key to their continued success.”

Free registration for CCR (Clinical Cosmetic Regenerative) Congress 2024 is open now, taking place on October 10-11 at ExCeL, London. CCR 2024 is set to host more than 130 exhibitors and a huge variety of educational speakers at the two-day event. The five stages will cover a plethora of aesthetic topics, including injectable demonstrations, device techniques, skin health advice, business insights and more, plus the specialty’s biggest brands will be on hand to explain their innovations. This year, the conference will also host the rapidly expanding Medical Longevity Summit for the second time, bringing together wellness and longevity specialists to shed light on a range of regenerative approaches. Aesthetics editor and event manager Shannon Kilgariff commented, “We are delighted for the UK’s biggest aesthetics conference to return once more. It is a great feeling to be at the heart of the medical aesthetic specialty when there is so much innovation occurring, and we cannot wait to share it with you in an atmosphere of collaborative learning and networking.”
CCR 2024 is free to attend at ExCeL, London on October 10-11, 2024. Turn to p.22 to register now.
The Advertising Standards Authority (ASA) has upheld a ruling against an aesthetic clinic after it was decided that its name falsely implied it was run by a medical practitioner.
The clinic in question – Dr Bunny Aesthetics in London – contained a section on its website that stated, “Dr Bunny Aesthetics Clinics Advanced Aesthetics Practitioners Providing Non-Surgical Aesthetic and Cosmetic Procedures.”
The Joint Council for Cosmetic Practitioners (JCCP) challenged whether the name of the clinic was misleading as it is not led by a medical practitioner. In response to this challenge, Dr Bunny Aesthetics said they had amended its business name to DBA Clinic.
The ASA found that the name was indeed misleading because consumers would interpret the ‘Dr’ prefix to mean that the owner of the clinic was medically trained. The ASA said the clinic must not use the prefix again, nor imply that it is run by a medical professional. The Aesthetics Journal reached out to the clinic but they did not provide further comment.
Out of 2,000 UK adults, 45% are not worried about getting skin cancer, and 46% are not familiar with the symptoms
(Face the Future, 2024)
Out of 33,000 women surveyed, two out of five would exchange a year of their life to achieve an ideal body or look
(Dove, 2024)
Nearly 2% of 7,000 UK adults had medicated weight management treatment in 2023
(RARE: Consulting, 2024)
95% of cosmetic and beauty packaging is thrown away rather than being recycled (Boopbeauty, 2024)
searches for ‘What is CBD’ in the UK have increased by 1,100% (Browns CBD, 2024)
Out of 40,000 women surveyed, more than half (53.8%) say they have low libido, and nearly a third (32.8%) have vaginal dryness (Issviva, 2024)
7th-9th June
SEASON Conference 2024
6th-7th September
RSM Aesthetics 2024
21st September
BCAM Annual Conference 2024
26th-27th September
BACN Autumn Conference 2024
10th-11th October
CCR 2024
Plastic surgery searches surge following Met Gala 2024
Google Trends analysis has revealed searches for plastic surgery soared by 72% across the US after celebrities took to the Met Gala red carpet on May 6. The event is an annual fundraising benefit for the Metropolitan Museum of Art in New York City, attracting attention from around the world as the biggest celebrities showcase the height of fashion. Following the fundraiser, there was also a jump in searches for ‘mommy makeovers,’ suggesting that people may be feeling the pressure after the media showcases apparently perfect public figures.
Sharon Osbourne opens up about weight loss injections
British TV personality and music manager Sharon Osbourne appeared on Loose Women to speak honestly about her experience with weight loss injections. When questioned by Loose Women panellist Gloria Hunniford, the 71-year-old revealed that she has always battled with her weight and would go to extremes to achieve her ideal weight. While she says she has no regrets about having the injection, she admits that she struggles to put on weight now. “The injections worked but I just can’t seem to put anything on. I lost over 40 pounds. If I could, I’d put on another 10.” Weight loss injections should only be prescribed if weight loss is necessary for medical reasons, but some celebrities have allegedly used them to become slimmer.

Aesthetic distributor HA-Derma has unveiled Profhilo Structura in the UK and Ireland. The company shares that Profhilo Structura, developed by IBSA, uses patented NAHYCO technology to facilitate adipose tissue restoration. It aims to address age-related concerns including pronounced facial hollows, skin laxity and altered facial contours resulting from mid-face fat loss.
Iveta Vinklerova, sales and marketing director at HA-Derma, commented, “While fat often carries negative connotations, it’s a crucial marker of youth. Our insights into its role in youthful aesthetics are advancing rapidly. The launch of Profhilo Structura equips medical professionals with a natural product tailored to meet the evolving demands of today’s discerning aesthetic patients.” Turn to p.45 to find out more.
Training provider Cosmetic Courses will host an educational webinar at 7pm on June 27 to raise awareness for charity organisation Zagrava.
Zagrava, a charity founded by Dr Vladlena Averina, provides victims of war with free qualified medical assistance to restore their appearance.
During the webinar, aesthetic practitioners Dr Averina and Dr Olha Vorodyukhina will discuss the latest developments within regenerative medicine. The webinar will cover Dr Averina’s case studies and treatment protocols, including cases related to traumatic injuries, ageing and acne scarring.
Dr Averina said, “In this webinar we will share developments in the field of regenerative medicine. We will focus on the treatment of traumatic scars based on our experience during the two years of war in Ukraine. Today, Zagrava doctors have provided 1,200 consultations, treated 620 patients and 50 patients were referred to other specialists. We will be very grateful for any help!”
Device

Medical device company Sciton has unveiled the latest addition to its BBL product line, BBL HEROic.
Available on both the JOULE X and mJOULE platforms, BBL HEROic’s Intelligent Control (IC) uses 3D spatial data to track the treatment handpiece, allowing for precise pulse delivery.
The company states that this innovation, alongside the new autodynamic pulsing feature, has been designed to adapt
to the operator’s speed and reduce full body treatment times. Kathy Ziegler, director of product management at Sciton, said, “BBL HEROic is set to redefine the pulsed-light industry. By integrating Intelligent Control with our BBL HERO technology, we’ve responded to the demand for a light-based treatment that is not only faster and more efficient but also accessible to staff across all skill levels, promising remarkable results.”
IN THE MEDIA
Aesthetic pharmaceutical company Galderma has been revealed as the Headline Sponsor of CCR (Clinical Cosmetic Regenerative) Congress for the fourth year in a row.
Galderma will showcase its latest technology and techniques with cutting-edge talks throughout the event, inviting specialty-leading key opinion leaders to share their insights in the Aesthetics Journal Arena. The company will also be facilitating collaboration in the Galderma Networking Lounge across the two days, providing conversation and relaxation for delegates and speakers alike.
Jackie Tuzee, head of marketing UK and Ireland at Galderma, said, “Galderma is delighted to be back at CCR as Headline Sponsor for 2024! We have already started working on some exciting plans for the event, including educational content and a full portfolio experience on our stand. CCR is the perfect platform for us to showcase what’s new with our brands and engage with practitioners and our industry colleagues.” CCR 2024 is free to attend at ExCeL, London on October 10-11, 2024. Turn to p.22 to register now.
Research
Not-for-profit organisation the British Beauty Council has created The Beauty Census survey to collect data on inclusivity, education, equity and accessibility. The organisation believes the survey encourages respondents to help the organisation ‘create a beauty industry that looks like you’ and become aware of the societal factors which come into play in the specialty. The survey aims to ensure relevant data is collected from both business and consumer groups to make sure the results give a holistic understanding of beauty. Millie Kendal, CEO of the British Beauty Council, commented, “The survey will ensure we have the scope of data we need to propel real change when it comes to access to industry, social mobility, inclusivity and equity.” Following a three-month data collection period, the results will be compiled and presented at the British Beauty Week in October 2024.
Regenerative Medicine
Aesthetic manufacturer DermaFocus is set to hold a Regenerative Medicine Summit in Manchester on July 19. Professor Maurizio Cavallini will be talking at the event, presenting his research into Plinest polynucleotides and the optimal protocols for their use. Attendees will also be introduced to Purasomes exosomes, discussing the science behind them and how they can be used to regenerate skin and hair, according to DermaFocus. Professor Cavallini said, “Regenerative treatments are the future of medical aesthetics, so it’s exciting to be a part of DermaFocus events that are leading education in the UK. Having a day dedicated to polynucleotides and exosomes will allow practitioners to take a deep dive into everything they need to know about these innovative treatment approaches, while giving them the opportunity to network. I look forward to meeting delegates there!”
A round-up of the latest news and events from the British Association of Cosmetic Nurses
Our highly anticipated, third-annual BACN Spring Symposium took place on Friday April 19 at the Kings Fund in London. Attendees were treated to a stellar line-up of speakers who covered a wide range of topics, with an overall focus on regenerative medicine, providing attendees with the latest advancements and best practices in medical aesthetics. The event was a tremendous success thanks to the dedication of our speakers, sponsors and our 150 dedicated nurses attending from all four corners of the UK. The BACN Autumn Aesthetic Conference tickets are on sale via the QR code below.
Presenting at this year’s Spring Symposium was management committee member and vice chair on the BACN Education and Training committee Anna Baker, who presented an update on the BACN Nurse Career and Competency framework. Her session talked attendees through the key objectives of the BACN Competency Framework for Aesthetic Nurses: why we have and need our specialised framework, how it was developed, which exciting new developments we can expect and what the next stages are, including accreditation. We’re excited to announce that a draft document is expected to be available by the end of May 2024. This updated framework will provide our members with an established tool to shape the career pathway for registered nurses working in medical aesthetic practice.
The BACN has recently unveiled its new Member Benefits page dedicated to enriching the experiences of its valued members. Members can access discounts on professional development courses, conference registrations and specialised products, reinforcing BACN’s support for its members’ career growth. Explore the perks curated exclusively for BACN members online now under the BACN Membership tab.
This column is written and supported by the BACN


Your chance to unite with the community to shape the future of medical aesthetics
After the success of ACE 2024, it’s time to start looking toward the next event in your aesthetics calendar: CCR (Clinical Cosmetic Regenerative) Congress with Headline Sponsor Galderma! Taking place on October 10 & 11, at the ExCeL, London, the conference will serve as a platform for you to discover the latest products, brands, techniques and services in the aesthetics and wellness sector.
With a growing interest in the specialty around regenerative medicine, a focal point of CCR this year will be the Medical Longevity Summit after its successful launch at last year’s show. With a lineup of esteemed speakers, delegates can anticipate engaging discussions on innovative treatments, emerging technologies and groundbreaking research shaping the specialty’s future and changing patients’ lives.
Sessions will cover topics such as nutrition, gut health, cell optimisation and lifestyle management. In addition to the Medical Longevity Summit, CCR features an array of educational opportunities. At the In Practice Theatre you can uncover topics to suit your business needs, or you can attend our Symposium Stage to learn the latest clinical techniques. Find out the latest product advancements at the Innovation Stage, and head over to the Aesthetics Journal Arena to see injectable, skin and regenerative medicine live demonstrations and research round-ups.
Make sure to register free now and secure your place at CCR to stay at the forefront of the industry and improve your aesthetic practice.
Scan the QR code below to sign up!

Aesthetic distributor Cure Medical has been announced as exclusive distributor for the Ultraformer III device in the UK and Ireland. The company explains that Ultraformer III is a high intensity focused ultrasound (HIFU) device that is geared towards lifting, tightening and contouring the skin.
The device incorporates macro and micro focused ultrasound (MMFU) to distribute ultrasound waves equally without directly targeting the epidermis.
Adam Bashir, CEO of Cure Medical, commented, “This is a fantastic addition to our ever expanding portfolio of technologies, which we aim to bring to award-winning clinics and practitioners across the region.”
Skincare company CellDerma has released a brand-new product – the GF5 Next Gen serum. The company explains that GF5 Next Gen uses growth factors, vitamin B9 and neuropeptides to address signs of ageing including fine lines and wrinkles, promote skin regeneration, repair the skin barrier and improve overall skin health. Dr Dev Patel, aesthetic practitioner and founder of CellDerma, said, “When we launched GF5, it challenged everything that people thought was possible from a single serum. It is a cosmetic product and therefore, we can make no medical claims. However, in the course of clinical practice, practitioners – including myself – have seen it heal a plethora of challenging skin issues as well as visibly reverse signs of ageing, often within days. Now, the ‘next generation’ has been created to only better these results.”

Aesthetic distributor Novus Medical has introduced the new MORPHIYA Dermal Hybrid Exo Kit exosome therapy. According to the companies, the bio-engineered exosome procedure facilitates cellular remodelling by merging exosomes with liposome delivery. The kit contains the Hybrid Exo Activator and the Lyophilized Hybrid Exo. Together, the products are designed to manage inflammation and stimulate collagen and elastin production, the companies explain. Jim Westwood, director at Novus Medical, said, “This cutting-edge product harnesses the power of cellular communication to promote healing and regeneration, marking a significant leap forward in medical science.”
Skin Treatment
Aesthetic pharmaceutical company Croma-Pharma has expanded its portfolio with countourel Absorbable PDO Threads. The company explains that the new threads are designed to lift, tighten and rejuvenate the skin in the face and body. The range includes seven threads of various strengths – countourel mono, jamber I, jamber tanxing, barbed, ultra, ultra+ and max – suited for different areas. Vikki Baker, head of marketing UK, Ireland and Netherlands at Croma-Pharma UK, said, “This new portfolio of PDO threads offers an extended shelf life and superior tensile and fixation strength, creating a versatile option for medical practitioners and their patients looking for an effective, non-surgical method to lift, tighten and rejuvenate.”
Skin Health

Skincare solution provider The Skin Diary has debuted its Chapters service to allow patients to receive personalised skincare routines. The company explains that practitioners who either do not want to be involved in their patients’ skincare journeys or cannot provide prescriptions can sign up to Chapters, allowing their patients to access medical-grade skincare via consultant dermatologists. Patients receive tailored skincare regimens via post, with activities detailed for AM and PM use.
Dr Clare Kiely, consultant dermatologist and founder of The Skin Diary, commented, “As dermatologists we noticed a problem in skincare. The choice of active ingredients, medical and non-medical grade for skin ageing is ever more confusing, leading people to not stick to a routine. We designed a curated routine containing everything the skin needs to solve this.”

The Aesthetics Awards has been announced as a finalist in the Conference and Events Awards 2024. The Aesthetics Awards 2023 has been shortlisted for two categories: Best Development of an Existing Awards Event and Best Longstanding Awards Event.
Having already won the former category at the 2023 ceremony, the Aesthetics team is proud to have been recognised for excellence again.
Shannon Kilgariff, editor and event manager of the Aesthetics portfolio, commented, “We are absolutely delighted to be shortlisted in these two prestigious categories. These awards are nationally recognised for applauding the UK’s best awards ceremonies, and we are glad to be counted among them. A huge thanks has to go to our Awards entrants, sponsors and judges for making it the event that it is.”
Dr Ahmed El Muntasar
Aesthetic practitioner and Sinclair faculty member Dr Ahmed El Muntasar provides an insight into using Sinclair in his clinic

What is your background in medical aesthetics?
My background is as an NHS GP. I stumbled into aesthetics when I first got my tear trough dermal fillers done, and I thought I could do a really good job at this! I did all the courses I could find when I started in 2017, and have been in the industry ever since. I now have three clinics in London, Leeds and Cheshire.
How long have you been using Sinclair products ? Since I started! The first Sinclair product I used was Ellansé after I saw the results of a fellow doctor and thought it looked beautiful; the volumising effect, the natural enhancements and improvements in the skin quality were second to none. So, I did the training for Ellansé and met the Sinclair team a few months into my aesthetics journey.
What Sinclair brands do you use in clinic? I use the full Sinclair portfolio: Ellansé, Perfectha, Silhouette Soft, MaiLi and LanLuma.
What’s your favourite aesthetic treatment to do? It would have to be a full facial enhancement using the MaiLi portfolio – Precise, Define, Volume and Extreme – to naturally enhance someone’s facial structure.
Why do you like using the Sinclair products? There is a lot of research and love that went into developing these products, with incredible quality and results. Comparing the products to any competitor, they are the same level, if not above. There is also a lot of support, the team is very dynamic – it is like a big family.
Tell us about your passions I work with The Pink Ribbon Foundation to help improve the skin of women who have been through breast cancer treatment, such as those who are experiencing dryness, redness and accelerated ageing. I appreciate skin may not be at the top of their concerns, but it is special to help give these women some confidence back.


Dr Munir Somji is an aesthetic practitioner and international educator, focusing on the power of energy-based devices for optimising the skin in the aesthetic field. Here, the Aesthetics Journal shares some tips on how to optimise device treatments…
How do you broach the subject of device treatments with patients?
If the patient has minimal or limited device knowledge, I would explain the device technology, translate it into clinical practice and explain what the expected outcome of the treatment plan would be. I would also show them before and after examples of similar patients to show how it would work in practice.
Top three tips for prepping the skin before laser treatments…
1. Reduce exposure to sunlight
2. Use of tyrosinase inhibitors in darker skin types
3. Use of injectables such as polynucleotides for increased availability of fibroblasts, as well as antioxidant and anti-inflammatory effects
What are your preferred treatments to use in skin rejuvenation?
The AgeJET plasma device is great for skinresurfacing, and the Alma Harmony is another favourite as its multiple platforms – ablative and nonablative lasers, IPL and NIR – make it super versatile.
How do you go about treating pigmentation on the face?
I would first analyse the patient’s lifestyle and teach them about sun avoidance and protection. If they have melasma, we need to inform the patient that it can be cleared, not cured. There is a risk of reoccurrence, and I would educate on the appropriate usage of medication for avoidance with prescriptive skincare, as well as lasers and chemical peels.
How do you tailor treatments to darker skin types?
Tailoring the skin prep with tyrosinase inhibitors, as well as avoidance of sun exposure for a month before and after treatment Increasing antioxidants used on the skin. Decreasing the amount of heat the skin is exposed to (lower power and pulse duration during treatment). Active cooling during and after treatment.
What brand new innovations are you most excited about?
Movement away from atmospheric plasma to medical nitrogen gas plasma opens up the possibility of using this technology with darker skin types.

Medical aesthetic manufacturer Promoitalia is set to host a symposium on regenerative medicine. Taking place on June 15 at 1 Hotel Mayfair, the company says the symposium will focus on skin boosters and antiageing treatments. Key topics will include the latest trends for periocular and lip rejuvenation, specific approaches for male facial rejuvenation, the evolution of skin boosters and new treatment options for intimate area rejuvenation. Promoitalia’s panel of speakers for the day includes aesthetic practitioners Dr Eugenia Bonelli, Dr Kaywaan Khan, Dr Sima Al Asad and aesthetic nurse practitioner Eleanor Hartley. Massimiliano Candini, general manager of the UK branch of Promoitalia Group, said, “To celebrate the second anniversary of the Promoitalia UK branch opening in London Mayfair, we will be hosting this academic symposium. It will offer an opportunity to network with leading companies and medical professionals in the UK, with an open discussion and practical insights about available treatments.”

Skincare company DIBI Milano has launched Collage System Lab, an at-home cosmetic treatment designed to boost collagen types ones and three. The two-stage formulation contains active ingredients, including oligopeptide 1 and hyaluronic acid, which have antiageing, firming, lifting and elasticising properties. The formula also introduces bio-fermented collagen – a patented active ingredient obtained by yeast fermentation which differs from other collagen due to its molecular weight of 55 kDA. DIBI Milano says this helps it to penetrate deeper into the skin and stimulate type three collagen.
Andrea O Donnell, head of education at Xpert Professional, said, “Introducing the new skin rejuvenation home program by DIBI Milano, harnessing the power of epidermal growth factors and fermented plant extracts in two simple steps. Stimulating the production of collagen types one and three, this formulation is your ultimate ally in post-treatment skin repair and rejuvenation.’’
Wellness and aesthetic system provider PatientPerfect has debuted its mobile app in the UK to provide patient engagement options.
The company explains that the app enables clinics to craft and launch membership options, loyalty programmes, personalised recommendations, exclusive rewards and one-click referrals for their patients.
Laura Lea, head of marketing, commented, “PatientPerfect is a powerful tool for clinic owners and managers, helping them increase revenue, gain new clients and have a slick digital experience and meaningful rewards. We are excited to see the impact PatientPerfect can bring to the specialty at large.”
SkincareThe Aesthetics Journal out and about in the specialty this month

This year’s edition of Wigmore Presents took place on April 20-21 at the Royal College of Physicians at Regent’s Park, London.
With a primary focus on education, more than 40 experts convened at the two-day aesthetics event to deliver an agenda spanning injectables, skincare and devices. Key topics included the exploration of new technologies, insights into toxins, skin microbiome, treating hyperpigmentation, combination treatments, skin health and microneedling. Alongside this, 250 delegates had access to an exhibition, a programme of product-focused workshops, an evening networking event and the opportunity to acquire 20 CPD points over the weekend.
David Hicks, chairman at Wigmore Medical, said, “The conference feedback has been fantastic, we’re already planning next year and we’ll be back with another exceptional weekend of education. The stand out highlights for me have been the toxins debate and the discussion around regenerative medicine. We’re looking forward to welcoming our delegates back next year!”
On May 14, aesthetic manufacturer Energist held its NeoGen Expert Aesthetics Nitrogen Plasma Workshop at the Royal Society of Medicine. According to the company, the event took a deep dive into the NeoGen nitrogen plasma skin regeneration technology is FDA-cleared to address conditions including superficial skin lesions, actinic keratosis, viral papillomata, seborrhoeic keratosis and acne scars. Aesthetic practitioners Dr Raj Thethi, Dr Chris Rennie, Dr Victoria Klishko and Kate Monteith-Ross discussed the science behind NeoGen, how to achieve best results and how to combine it with other treatments, complete with live demonstrations.
Energist head of marketing Justin Richards said, “It was an absolute pleasure to kick off our very first NeoGen Nitrogen Plasma Education series. The workshop was attended in person by medical professionals across the UK and Europe, with the live sessions being watched from Australia, the US, South Africa and the Middle East. The variety offered within the agenda meant we had something for everyone. It was a huge success, and we’ll be hosting more in the very near future, locally and internationally.”

Aesthetic device company Deleo hosted an event to celebrate the official UK launch of Cellution. 25 guests were invited to the Corinthia Hotel in London on April 24 to witness the launch of Cellution in the UK, with a live demonstration and Q&A. Specialising in cellulite reduction, skin tightening, lymphatic drainage and body contouring, Cellution combines Enhancer Oil cosmeceutical active ingredients with thermal action to address patient concerns, according to the company. Guests were also welcomed with speeches from aesthetic practitioner Dr Rita Rakus and Deleo’s export manager Saskia Hawkins. At the launch event Hawkins stated, “Cellution harnesses the power of four cutting-edge technologies, uniquely integrated to address the common issue of cellulite. This innovative amalgamation of treatments represents a significant leap forward in medical aesthetics, promising transformative results for those seeking to address cellulite concerns.”

Aesthetic manufacturer
Crown Aesthetics held an event at the Cavendish Conference Centre following the launch of the SkinPen Precision and BIOJUVE combined treatment routine. The event focused on business development for customers of SkinPen Precision and BIOJUVE, providing marketing support for growing clinics. The conference saw more than 450 delegates log in virtually, with around 95 guests in attendance. Guest speakers included aesthetic practitioner Dr Jigna Patel, digital marketing speaker Rick O’Neill and aesthetic nurse practitioners Rhi Bell and Anna Gunning.
Head of marketing UK and Ireland Reena Sandhu commented, “We are thrilled by the resounding success of our Crown Elevate Clinic Growth Summit. With an engaged local and international audience of over 350 delegates, the exchange of ideas and questions remotely showcased the power of collective learning and growth.”


Teoxane appoints two new product specialists
Global aesthetic manufacturer Teoxane has announced the appointment of two new product specialists to its UK team. Chris Boyle and Stuart Young have joined the company as product specialists for Scotland and East England respectively. Teoxane says both additions to the team will be pivotal in driving the company’s growth in their respective regions, as well as providing new and existing Teoxane customers and healthcare professionals with support.
Hydrafacial announces its new product Peel Sensitive Aesthetic device company Hydrafacial has introduced the new Peel Sensitive formula designed for sensitive skin. The company explains it aims to provide patients with a gentle exfoliating skin solution with ingredients including lactobionic acid (PHA) and phytic acid (AHA). Aesthetic practitioner Dr Ana Mansouri commented, “I’ll be using Peel Sensitive to prep skin for in-clinic treatments, allowing me to perform two procedures synergistically in the same sitting, without irritating the skin barrier.”
Skincare brand ALASTIN partners with Wigmore Medical
Skincare company ALASTIN from Galderma has announced a partnership with aesthetic distributor Wigmore Medical. The skincare range includes pre- and post-treatment care addressing signs of ageing like wrinkles and fine lines, as well as treating spots and blemishes. Jackie Tuzee, head of marketing UK and Ireland at Galderma, commented, “We are thrilled to announce the partnership between ALASTIN skincare and Wigmore Medical – a range clinically proven to complement cosmetic procedures and address visible signs of ageing with daily use.”
Phorest launches new clinic tipping system
Clinic CRM system Phorest has introduced PhorestTips, a new digital solution designed to enable employees to receive tips in compliance with the upcoming Allocation of Tips Act. Under new UK legislation, all tips will be paid directly to employees, and employers cannot take any deductions for admin or transactional charges. Launching this month, PhorestTips allows businesses and staff to accept tips on the PhorestPay Card, which are immediately transferred into the employee’s personal bank account.
Conference Report

The five-day British Aesthetic Meeting (BAM) was held at the Royal Society of Medicine on May 8-10, followed by two days of cadaver workshops in Coventry on May 11-12.
Attended by 250 delegates from across the world, the congress featured dozens of talks spanning the surgical and non-surgical aesthetic specialties.
The second day featured an agenda focusing on minimally invasive facial aesthetics, including a talk on anatomy for botulinum toxin from Dr Tapan Patel, a discussion of the importance of the skeleton from Dr Souphi Samizadeh, Mr Ali Ghanem talking on using electromagnetic stimulation to lift the face, plus many more lectures.
One of many keynote speakers was facial plastic surgeon Dr Paul Nassif, well-known for his role in the reality TV series Botched, who spoke live from the US on handling difficult cases and patient red flags. Dr Christopher Rowland Payne, consultant dermatologist and co-organiser of the event, commented, “BAM was the largest aesthetic plastic surgical meeting ever yet to be held in Britain. World-class speakers came from the US, Europe, Pakistan and India to deliver some of the finest talks that I have ever heard.”
The Royal Society of Medicine has also announced its next aesthetics-focused congress – RSM Aesthetics, which will be held on September 6 and 7, 2024. The event will include a day of talks and a day of hands-on masterclass workshops from doctors, dentists and surgeons to share knowledge. Dr Rowland-Payne said, “RSM Aesthetics will bring together doctors and dentists working in all fields related to medical aesthetics, especially at the medico-surgical interface. Physicians and surgeons will be able to improve their techniques by sharing knowledge and discussion. An international faculty will be in attendance – all outstandingly stimulating, entertaining and thought-provoking speakers.”

150 attendees convened at the King’s Fund in London for the British Association of Cosmetic Nurses (BACN) Spring Symposium 2024. The conference featured presentations led across nine separate sessions beginning with the BACN competency framework. Medical professionals including aesthetic nurse prescriber Anna Baker, Dr Nichola Conlon and Dr Anoob Pakkar-Hull led talks on various topics ranging from PRP and NAD+, to CQC registration.
HA-Derma was the headline sponsor, and attendees had the opportunity to engage with more than a dozen exhibiting brands and suppliers. After the presentations, guests were invited to join the BACN for an evening drinks reception in the orangery.
Sharon Bennett, aesthetic nurse prescriber and BACN chair, commented, “It was the perfect setting to delve into a diverse range of topics with a regenerative focus. Our gratitude extends to HA-Derma, this year’s headline sponsor, and to all our speakers and exhibitors who have generously contributed their time and support to make this event a resounding success.”

Introducing NEW Obagi Medical Rebalance Skin Barrier Recovery Cream.
of study participants felt that the product soothed and hydrated post procedure skin* 94%
of the study participants felt that the product was well tolerated by their sensitive skin* 94%
of study participants showed an improvement in skin hydration after the �irst use* 10 0%

A selection of trending products and treatments to revitalise the skin


The revolutionary GF5 Next Generation super-serum delivers an innovative combination of 25 active ingredients to complement every skin type! Experience the “magic” many users refer to, from trauma survivors, including those with burns, to individuals using treatments like Morpheus8 or simply opting for an at-home treatment. Contact us at hello@cellderma.com & quote ‘AJ10’ to become a stockist and receive an exclusive discount on your opening order until July 31.
RRP £165 cellderma.com
Experience the future of regenerative aesthetic medicine with V-Tech Serum. The first ready-to-use skin booster (made in Italy) with synthetic exosomes, the power of polynucleotides, biomimetic peptides, and plant stem cells to stimulate profound skin regeneration and rejuvenation.
V-Tech Serum delivers deep hydration, antioxidant effects, and restores the skin barrier, ensuring visible antiageing results from the first application. Embrace the latest trend in regenerative aesthetic medicine!
RRP £130 webpromoitalia.co.uk

CELL CYCLE CATALYST
Cell Cycle Catalyst is a potent skin renewal accelerating serum formulated to amplify antiageing results. It gently peels and enhances cell turnover at skin’s surface to smooth texture, improve appearance of discolouration, and the look of visible lines. It is a great daily first step to boost the results of an antiageing regimen. It can also be used to prepare skin ahead of professional treatments.
RRP £120 skinceuticals.co.uk
The Zemits CoolRestore device with an advanced holistic CRYO Elegance TM Technology offers a unique, efficient, cost-effective solution for anti-age treatments for cold-associated skin rejuvenation and wellness, ensuring effective contouring, pore tightening, and fine-line reduction. The system has pre-set and bespoke protocols for the face and body. No coolant is required. Consumables cost for one session up to £5.
RRP £4,990. June deal: £3,992 zemits.com












A look into recent statistics showing a decline in UK surgical and non-surgical aesthetic treatments
The British Association of Aesthetic Plastic Surgeons (BAAPS) has released its 2023 audit which highlights a significant decline in both surgical and non-surgical aesthetic treatments.1 The total amount of surgical procedures performed by BAAPS surgeons fell 16% for both men and women in 2023, and botulinum toxin and dermal filler treatments went down 11% in 2023.1 This is not the first time a drop in cosmetic surgery has been reported, with market research company RARE:Group Consulting noting that surgical aesthetic procedures fell at an average of 31% last year.2 Again, this coincides with the findings for non-surgical treatments, which showed the dermal filler and botulinum toxin markets shrunk by 31% and 16% in the last 12 months.2
So, why might this be occurring, and what can the UK medical aesthetic specialty do about it? We spoke to Miss Nora Nugent, vice president of BAAPS, and Mr Naveen Cavale, national secretary and social media chair of the International Society of Aesthetic Plastic Surgery, to get their advice going forward.
The cost of living impact
BAAPS has suggested that one of the reasons this shift is happening is that patients are choosing to travel abroad for surgical procedures, as opposed to getting them here in the UK. Miss Nugent believes that the cost of living crisis may be having an effect on the current climate of medical aesthetics. She says, “Overwhelmingly, patients travel because in some countries aesthetic surgery is cheaper than in the UK. In times of financial hardship, the price is definitely a large issue for patients.”
Mr Cavale agrees, noting that although some patients may travel to see an international surgeon due to their reputation, cost is typically the deciding factor. “I think the cost of living crisis is definitely affecting business, perhaps more so outside London, as we see a more international clientele in the capital,” he says. Aside from the surgical figures, Mr Cavale speculates that the reason non-surgical treatments may have declined for BAAPS members is due to patients
opting to go to non-surgical practitioners, rather than there being a problem with the specialty. He says, “This shouldn’t be viewed as a bad thing, as surgeons and non-surgical practitioners are working together more and more, and in a better, healthier way. This is all a good thing for patients!”
“The UK can lead in a ‘multidisciplinary’ approach, and now is a really good time to push this”
Mr Naveen Cavale
Should we be concerned?
Despite the decline, Miss Nugent advises practitioners not to be too alarmed by the statistics. She explains, “From our members’ perspective, we had a pent-up demand and increased demand in the aftermath of the COVID-19 lockdowns. This was partly due to fewer surgery and aesthetic treatments being done during lockdowns, and partly due to an increase in demand for aesthetic procedures. It has levelled out now and the figures are not hugely different to the pre-COVID level.”
Aesthetic nurse prescriber and member of the British Association of Cosmetic Nurses Khatra Paterson explains that the decline in fillers and botulinum toxin should not concern non-surgical practitioners too much, as it is reflective of shifting specialty trends as opposed to a decline in the interest for aesthetic treatments. She says, “Rather than people focusing on just the main injectable treatments, there has been a shift to treating the inside to help the outside – regenerative medicine is becoming a real focal point. This
has been supported by statistics, which have shown that 34% of UK clinics are now offering medical wellness and longevity treatments.”2 She adds that instead of practitioners worrying about the recent audit, she would encourage them to embrace what’s new in the specialty. “Start looking into regenerative medicine, incorporate different schools of thought, and add combination treatments to your practice in order to open up clinic offerings and provide patients with better results,” she says.
Bringing together the specialty
Miss Nugent explains that her main concern now is the safety of patients choosing to travel abroad. She says, “The first step is always education so that patients are aware of the benefits of aesthetic surgery as well as what is involved, the potential risks and the importance of seeing a specialist plastic surgeon. If they are considering travelling overseas for treatment, then there are other factors to examine, particularly how to manage if a complication develops, due to the problems that are being seen after patients return home from surgery overseas.”
She adds that overall, the UK aesthetics sector needs to focus on quality and safety, delivery of treatment by appropriately qualified and registered practitioners as well as patient experience. “This is what is needed in the long term rather than specifically focusing on one year’s annual numbers,” she reflects.
Mr Cavale agrees, noting that practitioners have a duty to ensure the general public is aware of the importance of regulated and qualified practitioners. He explains, “As a specialty we must make people think long and hard before having surgical or non-surgical treatments. Making people realise that they are getting what they pay for is really important.” He also emphasises the importance of surgeons and non-surgical practitioners having a clear focus on working together to help further the specialty.
He says, “I think working together as surgeons and non-surgeons is really important, as this allows people to get a truly ‘holistic’ treatment- something that has been lacking in the past, and is not always available abroad. The UK can lead in such a ‘multidisciplinary’ approach, and now is a really good time to push this!”
REFERENCES
1. BAAPS, Annual Audit, 2024, <https://baaps.org.uk/_userfiles/ pages/files/final_2023_audit_results_for_2024_release.pdf> 2. RARE: Group consulting, Beyond Injectables: How the Aesthetics Market is Embracing Medical Wellness and Longevity, 2024

Join us at the UK’s largest aesthetics congress to achieve clinical and business excellence
With a successful ACE 2024 uniting the medical aesthetics community in March, it’s time to look towards the next unmissable event in the aesthetics calendar.
Returning on October 10 & 11, The Clinical Cosmetic Regenerative (CCR) Congress is your opportunity to take a deep dive into the science of aesthetics, learn from the experts and experience the latest developments and innovations. Brought to you by Aesthetics, CCR helps practitioners achieve clinical and business excellence. Taking place at the ExCeL, London, attendees can explore world-class educational programmes, live demonstrations, networking opportunities and an exhibition showcasing the latest scientifically backed products in the aesthetics market. Medical longevity is a key focus at this year’s event, due to the demand of the specialty looking for services to support the healthy human lifespan, as well as boost the results of aesthetic treatments. Hosted at CCR and returning for its second year is the Medical Longevity Summit, a stand-alone event on the show floor with brands, talks and ground-breaking regenerative advancements. By aligning with this growing interest, CCR enables aesthetic practitioners to expand your knowledge on the latest developments to better serve your patients. This approach enables patients to achieve their health and aesthetic goals, inside and out, as well as serving a greater purpose of promoting a healthier society.
injectable education & demonstrations
Leading pharmaceutical company Galderma is back as Headline Sponsor for the fourth consecutive year, and is set to deliver two days of leading content exclusive to CCR. With them, they bring world-renowned KOLs to the Aesthetics Journal Arena and the opportunity to recharge and connect with peers at the Galderma Networking Lounge.
“Galderma is delighted to be back at CCR as Headline Sponsor 2024 following
our most successful show to date in 2023. CCR is the perfect platform for us to showcase what’s new with our brands and engage with practitioners and our industry colleagues. This will be our fourth year in a row working with Easyfairs on this fantastic event and we can’t wait to see everyone in October!” – Joanna Neal, senior brand manager UK&I for ALASTIN Skincare (Galderma).
Following last year’s success, the Medical Longevity Summit returns, bigger and better than before, to meet the specialty’s demand. With society’s increasing focus on ageing gracefully and maintaining overall health, this Summit promises to be a pivotal highlight of the event. Led by specialists and supported by the British College of Functional Medicine, the two-day agenda will educate practitioners on evidence-based practice in functional and integrative medicine, holistic wellbeing, lifestyle and wellness treatment approaches. Speakers will explore topics such as: the longevity concept in aesthetic medicine, patient testing, optimising health through nutrition, hormonal health, regenerative medicine and much more.
Visit the exhibitor pods in the theatre to gain invaluable insights on evidence-based practices that will not only expand your treatment portfolio, but also optimise patient health, lifestyle and longevity. Some of the companies present include Erchonia, Roseway Labs, Nuchido, NAD at Home and Human Health.
Curated with Dr Mayoni Gooneratne, the Summit promises to expand your knowledge on the latest developments, so you can help your patients live healthier, more fulfilled lives, whilst achieving their aesthetic goals through a holistic approach to treatment.
Dr Gooneratne commented “A year ago, the world of wellness, longevity and aesthetics seemed a million miles away, but I knew we were launching the Medical Longevity Summit to the most forward thinking, patientcentric group of healthcare professionals out there. So, I was not surprised to see the agenda so well attended last year at CCR. This year, longevity and rejuvenation is all that is talked about in our profession. So, we have an even bigger and better lineup this year and are delighted to be leading in this space and bringing health concepts to our aesthetic patients.”

• Medical Longevity Summit
• The Aesthetics Journal Arena bringing the Aesthetics Journal to life
• Korean Pavilion in partnership with IBITA
• LIVE injectable demonstrations
• In Practice Zone
• Five CPD-certified conference theatres
• Galderma Networking Lounge
Meet leading brands and discover world-class education
With more than 130 exhibitors set to showcase their products and solutions, CCR is the perfect place to discover new technologies and make new connections. Catch up with your favourite brands including Healthxchange, DermaFocus, Crown Aesthetics, BTL Aesthetics, Cutera, Alma, Hydrafacial, InMode and SkinCeuticals, plus many more.
Our clinical and business agendas feature a faculty of global key opinion leaders unique to CCR, giving you access to five free-to-attend CPD-certified conferences. Experience a range of live injectable content, device and skincare demonstrations, medical longevity insights as well as crucial business advice. Discover new techniques, treatment styles and products, all advancing your skills and offering.

up your practice
Presented by the Aesthetics Journal, the Aesthetics Journal Arena offers an unparalleled opportunity to elevate your professional growth with top-tier clinical insights and cutting-edge research. Journey through treating the full face with expert speakers, live injectable demonstrations, and exclusive brand-new content from Galderma, our Headline Sponsor. A must-attend for medical professionals seeking to expand your skillset and discover the latest research to improve product knowledge, better decision-making and enhance patients results.
Learn from the specialty’s most innovative device and skincare suppliers
The Innovation Stage will provide you with in-depth guidance for developing your clinic offering through succinct presentations and live demonstrations showcasing the latest scientifically backed products on the market. In these sessions, you can discover groundbreaking techniques and solutions from the specialty’s most trusted and respected device and skincare suppliers, led by the top clinicians. Confirmed companies include ALASTIN, Alma, Beautyform Medical, BTL Aesthetics, BIOJUVE by Crown Aesthetics, Cutera, Cure Medical, Deleo, Dermalux, Energist, EvoCyte, Hansbiomed, Hydrafacial, InMode, Lynton Lasers, Medical Aesthetic Group and Sciton.
the latest advancements for injecting
The specialty’s leading brands will showcase their latest injectable techniques in one-hour live demonstrations, led by esteemed KOLs across the two-day agenda on the Symposium Stage. Attend to elevate your knowledge, skills and confidence to safely deliver your patients with outstanding results. This unmissable agenda includes sessions from education sponsors DermapenWorld and DermaFocus.
Take your clinic to the next level and expand your business knowledge at our In Practice Theatre. Delve into the latest insights on brand building, opening a clinic, mental health, marketing, finance and more. The In Practice Theatre combines the best business minds and award-winning practitioners for live talks, making it the perfect place to discover essential commercial support to drive the success of your business. Throughout the two days you can see sessions from Theatre Sponsor SkinCeuticals, Associate Sponsor Zenoti and education sponsor The Skin Diary.
As well as education, connecting with your peers, friends, suppliers and other medical practitioners is crucial for that all-important advice and support. Whether you are new to the world of aesthetics, or a seasoned practitioner, CCR provides you with the perfect setting to catch up with friends, discuss insights with peers and create those longstanding connections that will help you throughout your career. From dedicated practitioner meet-ups to the renowned Day One Networking Drinks, CCR facilitates a vibrant and inclusive community that embraces and empowers practitioners at every stage of your career.
Headline Sponsor
Scars can have a profound impact on a person’s confidence and self-esteem.1
A 2018 study into the psychology of scars found that those with scars are more prone to developing depression and anxiety, while additionally feeling shame and aggression.1 It said, ‘This creates strain in social interactions, resulting in stunted communication, reduced intimacy and avoidant behaviours’.1
Aesthetic practitioners have the ability to ease this psychological burden by offering patients effective scar treatments. By utilising well-researched and evidencebased treatment approaches, researchers suggest that clinicians can also reduce the ‘economic backlash’ experienced by this ‘vulnerable group’ of people, who are purchasing over-the-counter solutions that make unrealistic promises with limited scientific support.1 So, what treatments are effective? To help you make worthy investments, three practitioners, consultant dermatologist Dr Derrick Phillips, GP and aesthetic practitioner Dr Kathryn TaylorBarnes and aesthetic nurse prescriber Khatra Paterson, share their experience and advice.
Before delving into scar treatments, it is important to understand the different types of scars and how they impact skin. Scars form as part of the body’s natural healing process after the dermis is damaged through injury, surgery, infection or inflammation. Collagen production is triggered, leading to new tissue formation that heals the wound.2 The appearance and severity of scars can differ greatly. Scars are generally categorised as:2,3
• Flat: usually red or pink and may become lighter or darker than the surrounding skin.
• Atrophic (depressed): rounded pits or small indentations on the skin. These can be further categorised into ice pick scars (small and deep), rolling scars (wide and shallow) and boxcar scars (round or oval shaped with a width in between ice pick and rolling).
• Hypertrophic (raised): raised scars over the injury that feel firm and don’t grow.
• Keloid: raised scars that grow beyond the wounded area that can impact movement.
• Contracture: causes the skin to tighten, making it difficult to move. They are often developed after a burn injury.
The practitioners agree that the range of scars that patients experience makes it impossible to have a ‘one size fits all’ approach to scar treatment, which is why a multi-pronged approach is often recommended. This can consist of:
• Skincare: certain ingredients can aid wound healing to improve the appearance of a scar4
• Cryosurgery: freezes the scar to slowly destroy the scar tissue4
• Corticosteroid injections: used to reduce the size of a hypertrophic or keloid scar and ease pain and itchiness4
• Silicone gel: thin and adhesive sheets that are applied after a wound closes, commonly used after surgery to treat or prevent hypertrophic scarring4
• Subcision: a minimally-invasive procedure that is usually used for atrophic acne scars – a needle is used to detach the fibrous connective tissues that are tethering the scar to deeper layers of the skin5
• Chemical peels: exfoliates the top layer of scarred skin to reveal fresher, smoother skin underneath6
• PRP: platelet-rich plasma therapy can improve scarring by delivering a high concentration of growth factors, platelets and cytokines from the patient’s own blood to the treatment area to induce tissue regeneration7
• Microneedling: creates microinjuries in the skin to stimulate wound healing and new collagen to improve the appearance of scars8
• Radiofrequency microneedling: combines microneedling with radiofrequency energy which stimulates collagen production at a deeper level for improved results8
• Polynucleotides: aged and damaged fibroblasts are regenerated, leading to improvement in skin quality and acne scarring9
• LED phototherapy: red light can stimulate the production of good quality skin cells that will replace abnormal cells present within scars and improve their appearance10
• IPL: intense pulsed light can target haemoglobin and melanin


chromophores to improve the vasculature and pigmentation of a scar7
• Lasers: various types of lasers including pulsed dye, Nd:YAG, Er:YAG and CO2 can be used, depending on the severity of the scar and what patients think they can tolerate. They induce thermal damage that can stimulate collagen production and smooth scar texture7
• Dermal fillers: hyaluronic-acid (HA) based fillers can be used to fill atrophic scars, while substances such as poly-L-lactic acid (PLLA), poly methyl methacrylate microspheres (PMMA) and calcium hydroxyapatite (CaHA) can stimulate collagen production to regenerate skin quality11
While there’s much to say about each of these methods, we have focused on three approaches that can suit a range of scar types, severities and patient/practitioner budgets. Dr Phillips advises on appropriate skincare, Dr Taylor-Barnes outlines the benefits of PLLA for acne scars and Paterson shares her experience of a hybrid laser device.
Skincare
Dr Phillips notes that suncare is the most important factor in skincare, explaining, “I tell my patients that they must wear a high SPF to protect the scar, as scar tissue is more vulnerable to UV.”12 In terms of essential skincare ingredients, Dr Phillips highlights that retinoids and vitamin C are key. “Retinoids can stimulate collagen production and enhance the wound healing process,13 while vitamin C is a powerful antioxidant that can decrease collagen degradation and reduce the pigmentation often associated with scars,”14 he explains. There are multiple forms of retinoids and
vitamin Cs, so it can be confusing for patients to know what to use. Stocking clinically-proven products and providing clear and concise advice can stand you in good stead, he notes.
Retinoids are a class of molecules derived from vitamin A or having structural and/or functional similarities to vitamin A.13 They have been widely studied and proven to have a positive effect on multiple skin concerns, including the appearance of acne scars.13
When it comes to choosing a retinoid, Dr Phillips explains that he advises patients to start their journey using a low concentration retinol that their skin can tolerate. This goes through a two-stage conversion to retinaldehyde and then to retinoic acid, which acts on the skin.13
“There’s no point rushing to a higher concentration that may cause irritation, halting the treatment process,” he says. Different products tend to have various
strengths of retinol, but beginning with around 0.3% is advisable, says Dr Phillips. He recommends SkinCeuticals Retinols or Intelligent Retinols by Medik8. When skin has built tolerability, patients can start to use retinaldehyde – Dr Phillips recommends Crystal Retinal by Medik8, retinoic acid or adapalene-based products. Research has found that adapalene 0.3%/ benzoyl peroxide 2.5%, which will require a prescription, can significantly improve mild to moderate acne scarring.13
It is important to remember that retinoids should not be used by those who are pregnant or breastfeeding, as they can lead to complications.13
When selecting a vitamin C, Dr Phillips emphasises that an L-ascorbic acid will be the most effective.14 “This is the most potent, so you’ll have the best chance of seeing results,” he says. Research suggests that the optimal concentration of vitamin C should be above 8%.14 “Patients should start with this, before building up to a 10% and then 15% as their skin becomes more tolerable,” advises Dr Phillips, noting that studies have found concentrations above 20% do not increase biological significance and can irritate skin, so are of no benefit.14 Again, Dr Phillips favours SkinCeuticals and Medik8 vitamin C serums, finding both to be highly effective.
Lots of patients come to clinic seeking fast results, which is simply not possible with skincare alone, emphasises Dr Phillips. You can’t take shortcuts when it comes to skincare, he says, adding that patients will only see gradual improvement that takes at least three months to be apparent. “It’s important to make clear to patients that skincare is not a substitute for in-clinic
When investing in a laser, Paterson says the most important thing is to investigate the evidence behind the device and what level of support you will get from the distributor
“You have to be prepared to spend a good amount of time with the patient in their initial appoints to understand the detrimental psychological impact, as well as the physical”
Dr Kathryn Taylor-Barnes
treatments. We must manage expectations and highlight how it’s far more beneficial for scarring when used in conjunction with other treatments such as microneedling and lasers,” he says.
Dr Phillips adds that practitioners should remind patients that using skincare is an ongoing process. “While patients may have an endpoint in terms of how they want their skin to look, there are still a lot of benefits that can be obtained if they continue using products,” he says.
Collagen-stimulating injections
Dr Taylor-Barnes specialises in treating acne scarring. She finds that it is often young adults who seek treatment. “These people are just launching themselves into the world of work and relationships, but feel really self-conscious of their acne scarring. It can disrupt the natural beautification of the skin and make people look older,” she says. While Dr Taylor-Barnes offers chemical peels and microneedling for mild forms of scarring, she highlights that there are some downsides to be aware of. “Chemical peels definitely have a role to play, but it’s important to remember that some patients don’t want the downtime associated with skin shedding, and having to be really careful not to expose their skin to sun too soon afterwards as it will be very sensitive,” she explains. Dr Taylor-Barnes adds that microneedling is also effective but does little for well-established ice pick and boxcar acne scars.
Instead, her main treatment of choice for atrophic acne scars is PLLA dermal filler. PLLA, known by brand name Sculptra, is a biocompatible, biodegradable, synthetic polymer injectable that enhances dermal volume via the stimulation of fibroblasts and, subsequently, collagen production. This can fill the depressed scars left by acne, leading to smoother and more refreshed skin (Figure 1).15
Dr Taylor-Barnes will often combine Sculptra with subcision in suitable patients. She says, “We can either do the subcision in an earlier appointment or at the same time – I prefer doing it at the same time. It’s important to note that subcision can cause bleeding and be quite painful, so we use anaesthetic to make it more comfortable for the patient.” If a practitioner does choose to do the treatments in separate sessions, Dr Taylor-Barnes advises allowing no more than two weeks between them.
For the Sculptra treatment, Dr Taylor-Barnes says practitioners can use a 30G needle or 27G cannula. “I prefer cannula as you can effectively distribute the product in a wide area with one entry point. I find that it’s less traumatic for the patient and you can also use the tip of the cannula to assist with subcision,” she explains. Results start to become visible over the next three to four months as collagen is stimulated, with research indicating that the gradual effect can last two to three years.16 In a 2023 literature review on the use of PLLA for acne scarring, it was highlighted
that all studies demonstrated positive outcomes in enhancing the appearance of atrophic acne scars, with patients undergoing between one and seven treatment sessions each.16
Dr Taylor-Barnes says one Sculptra treatment is usually enough, but of course she will offer more if necessary. “As well as improving collagen content, I have found that Sculptra has a beneficial effect on pigmentation, with skin becoming more luminous,” she says.
Dr Taylor-Barnes highlights that Sculptra should not be used on patients with active acne or any other skin infection. She also advises avoiding treating patients simultaneously with anything that induces inflammation, such as radiofrequency microneedling. “Ideally wait 12 weeks between Sculptra and other treatments – you want the Sculptra to settle down and work its magic without having to cope with inflammation,” she says. Following a Sculptra procedure, Dr Taylor-Barnes recommends patients use skincare, with her current brand of choice being the new ALASTIN range. For patients who have undergone subcision treatment, Dr Taylor-Barnes suggests they use INhance Post-Injection Serum with TriHex Technology, which can help calm bruising and soothe skin.16
For those looking to treat more severe scars, investing in a laser device could be worthwhile, the practitioners agree. Laser treatment utilises photothermal energy to stimulate neocollagenesis and dermal remodelling. It can also improve the colour of the scar and reduce any discomfort that they may cause.7
The laser used will depend on the severity of the scar, along with the patient’s tolerability for pain and downtime. Non-ablative devices deliver a controlled zone of thermal damage through epidermal and dermal heating, while ablative lasers reach temperatures that induce vaporisation of material on the surface of the skin, meaning they are more invasive.7 Research suggests that the non-ablative pulsed dye laser (PDL) is most commonly used for hypertrophic and keloid scars, with the ability to improve their vascularity, pliability, colour and height.17 For atrophic facial scars, non-ablative Nd:YAG or 1450 nm diode lasers have been found to be favoured.17 According to the literature, ablative lasers that use CO2 or Er:YAG are indicated to be effective for traumatic and surgical scars, especially when administered within six to


10 weeks after the event. They can also be beneficial for atrophic scars, as they can smooth scar texture and stimulate collagen production. While highly effective, the downside of ablative lasers is the discomfort and downtime of up to 10 days.17
Fractional ablative lasers can be used, with the benefit of being able to divide the original laser beam into microscopic beams, resulting in rapid re-epithelialisation and reduced downtime as only a fraction of the skin is altered.7
Dr Phillips uses the non-ablative M22 by Lumenis, which he has found extremely useful for treating atrophic scars, while Paterson has found benefit in using the Alma Hybrid, which offers both ablative CO2 and non-ablative 1570 nm laser treatment from one device.
“The Alma Hybrid has really allowed me to tailor treatment to individual patient needs,” she says, explaining, “While we mostly treat acne scars, we do also treat scars from surgery and injury, and have seen some life-changing results (Figure 2).”
Paterson highlights that these results are best achieved if treatment is started when the scar is in its maturation phase – the time when new tissue is starting to gain strength and flexibility.18 “If we can contribute to this with treatment then optimal results can be achieved,” she says.
Prior to a patient’s appointment, Paterson will perform a patch test to ensure skin is suitable for laser and work out the most appropriate setting for each patient. “It also gives us an idea of how long the skin will take to settle in terms of erythema and dryness, which can help manage patient expectations,” she adds.
While a minimum of three treatment sessions are advised, Paterson always tells patients that it may take more than that. For optimal results, she recommends combining laser treatment with polynucleotides, which can help heal the skin and reduce inflammation. There are many brands on the market, but Paterson chooses to use Plinest as it has been shown to significantly improve skin texture
“Read journals, attend meetings, challenge companies, find robust evidence and try things out before investing!”
Dr Derrick Phillips
in patients with moderate acne scarring.9 Paterson advises that laser is not suitable for those who have an active skin infection or are pregnant or breastfeeding, and patients must avoid sun exposure for four weeks before and four weeks after a treatment to avoid the risk of post-inflammatory hyperpigmentation.19
After treatment Paterson recommends patients use antioxidants, with her brand of choice being Skinuva – a cream distributed by Skinbrands that uses highly selective growth factors within a silicone cream matrix to help improve the appearance of scars.20 When investing in a laser, Paterson says the most important thing is to investigate the evidence behind the device and what level of support you will get from the distributor. “These machines are expensive, so you have to be confident using them and supported with sales, marketing and technical guidance,” she advises.
To safely and successfully treat scars, Dr Phillips says that assessment is key. “You must be able to identify the type of scar so you can give patients appropriate advice,” he says. Dr Taylor Barnes adds that having an interest in how scarring affects patients is important. She emphasises, “You have to be prepared to spend a good amount of time with them in their initial appointments to understand the detrimental psychological impact, as well as the physical. By the time they’ve come to your clinic they might have explored many other options with suboptimal results, so their morale may be low.”
On a similar note, Paterson highlights that it’s important to be aware that many patients will be looking for a ‘magic wand’ and expect instant, perfect results. “Educate them from the moment you meet them about the realistic results that can be achieved. I always like to aim to under promise and then over deliver,” she says.
Dr Phillips concludes, “Read journals, attend meetings, challenge companies, find robust evidence and try things out before investing!”



Amélie Seghers reveals how she looks after her patients’ skin

What was your path to becoming a consultant dermatologist?
I don’t remember ever wanting to do anything else! My mum would take me to pharmacies as a child. I loved pharmacies and all the creams and supplements! I initially started in Pharmaceutical Sciences but I missed the human aspect of medicine, so I decided to become a doctor in dermatology. What I love about dermatology is the fact you can build relationships with whole families; from children to grandparents and all ages in between. It took me 17 years before I qualified as a consultant dermatologist. I studied medicine in Belgium for seven years before earning my bachelor’s and master’s degree. Just like anywhere else in the world, it’s hugely competitive to become a dermatologist in Belgium once you qualify as a doctor. To increase my chances I did further training in internal medicine and studied an additional masters in dermatology at King’s College. The plan was to stay for one year but then I got a fellowship job at the St John’s Institute of dermatology here in the UK, which is where I now practise. My first registrar post was in Singapore where I also did a lot of research. I stayed there for five years but came back to finish my training here in the UK.
Is there anything in dermatology that’s become more prevalent over the last 10 years?
Two things immediately come to my mind. Firstly, skin barrier disruption because people are using too many actives. Buying one active after another and layering them on the skin without any guidance is causing so many problems. As an example, if you have acne but also have a background of childhood eczema, harsh ingredients like salicylic acid and retinol suggested for acne can really irritate the already fragile skin barrier and potentially flare eczema in those patients. Secondly, some children and young adults today think TikTok and YouTube are always trustable sources of information. I had a patient ask me if the product prescribed would cause ‘slugging’ which is not a medical term but a TikTok trend! 10 years ago this kind of social media influence was not a problem but now unfortunately it can cause confusion.
This is why seeing a professional is so important and why GetHarley is so good for the patient. It has democratised skincare advice and makes getting hold of good products easily.
What is your approach to bringing skin back to good health?
A consultation is key to understanding someone’s skin. It’s helpful to find out if the patient has daily habits that will be bad for their skin such as skin picking or continuously touching and rubbing the skin. We also want to know more about their general health including diet, stress, hormones, toxins and exercise. You have to understand a lot about the patient before you even start making recommendations. Understanding triggers for certain conditions is vital as you can give patients prescription products and daily skincare, but if they don’t remove or minimise triggers, it will be a constant battle.
How do your patients maintain the health of their skin?
I have the ‘active’ treatment approach and the ‘passive’ maintenance approach. Prescription products tend to be used to actively treat the conditions. Maintenance products, including skincare, is there to help prevent further flares.
How does GetHarley help you manage your patients’ skin health?
It’s a great service as you get everything all together instead of running from skincare shops to pharmacies to try to find the recommended products. It also helps them stay compliant, and I can get feedback about the products I’ve recommended.
The patient also gets reminders that they are running low and need to repurchase in order to stay on their regime, which is brilliant for continuity of care. It stops them from returning to a shop to pick something up and potentially being sold a different product by a shop assistant. This can then divert them from their regime and can cause skin problems. If something is ever out of stock on GetHarley, the patients are only given alternatives that I recommend.
I get to see more patients by partnering with GetHarley. If my clinic is full, I can offer online consultations around my clinic time which means I can service and help more patients.
Should supplements be part of everyone’s GetHarley regime?
I’m not a huge fan of putting everyone blindly on supplements. I like to test people’s levels beforehand, and I think in the future we will see more testing for personalisation. Some are okay to recommend without testing, like vitamin D as almost everyone needs it in this country. However, it is more ideal to test prior to taking the supplements and after the course to see if the levels have normalised. I like to recommend linseed oil as it has the richest source of Omega 3 in our diet and is great for your skin
What brands do you like the most?
I like the pharmacy brands such as Cerave and Cetaphil as they are great for sensitive skin and they are low cost. Obagi and Epionce are brilliant for tackling certain skin conditions, and Heliocare and AlumierMD are my go-to for sunscreens.
I encourage people to invest in their skin health from an early age and continue to prioritise it throughout their life. When you invest in skincare, you can save on makeup!
This advertorial was written and supplied by GetHarley






O f ficial distr ibutor in the UK
Dr Edward Robinson explores the literature around how the emerging treatment of polynucleotides can assist patients suffering with hair loss
In the landscape of medical aesthetics, emerging treatments are constantly reshaping the field. Among these, polynucleotides have garnered considerable attention, emerging as a promising solution for alopecia (hair loss).1-4 Recent studies have highlighted the efficacy of polynucleotides in stimulating the body’s natural repair and regeneration mechanisms, offering new avenues for addressing aesthetic concerns related to hair loss.
In this article, the current emerging literature on how polynucleotides can be used to assist alopecia patients will be explored, alongside the scope for future development as more research is conducted.
Hair loss is a concern which affects up to 80% of men by their 50s, and up to 50% of women at some point in their lives.6 Alopecia has many aetiologies and can be complex to treat.7 Surgical treatments are associated with significant downtime, hence minimally-invasive treatments like polynucleotides offer an appealing alternative for mild-to-moderate hair loss. Many patients who opt for a surgical solution will still require ongoing non-surgical treatments to retain existing hair or enhance the cosmetic result.8
The causes of hair loss either drive or suppress different stages of the hair growth cycle, with androgen and stress-related causes predominant.9,10 Other systemic causes of hair loss include telogen effluvium, diseases such as hypertension and diabetes mellitus, nutritional deficiencies, endocrine imbalances including thyroid and sex hormones, drugs, infections, malignancy, immune system disorders, environmental factors, age and genetics.9,10
Androgenetic alopecia (AGA) is the leading aetiology of hair loss in both genders, with limited approved treatments.7 AGA in both men and women involves gradual miniaturisation of scalp hair follicles, predominantly caused by hormonal changes.6,7 In men, this mainly occurs because of the local conversion of testosterone to dihydrotestosterone, which is a more potent androgenic form, by the enzyme 5-α-reductase. Consequently, both systemic and topical 5-α-reductase inhibitors such as finasteride and dutasteride are commonly prescribed for hair loss yet can have notable systemic side effects including sexual dysfunction, erectile dysfunction, mood disorders and infertility.11 AGA can cause a significant psychological burden due to the cosmetic change that it causes for patients.7 AGA is often challenging to treat due to the condition’s chronicity and underlying genetic and environmental factors. Long-lasting therapeutic strategies mostly rely on regular inhibition of 5-α-reductase, and the vasodilating properties of minoxidil. The only National Institute for Health and Care Excellence (NICE) and US Food & Drug Administration (FDA)-approved treatments for AGA are topical minoxidil and oral finasteride.12 Consequently, a variety of off-label therapies are suggested in the literature, including non-surgical treatments such as platelet-rich plasma (PRP), stem cell exosomes, microneedling, nutraceuticals and
supplementation with micronutrients and vitamins such as biotin and vitamin D.13-16 Describing these is beyond the scope of this article, but they are also worth considering where appropriate. Intradermal injections of polynucleotides have been shown to have a trophic regenerative effect on recovering hair follicles and promoting hair growth, as will be explored below.17-19
With robust evidence for their use in treating burns, wounds, ulcers and scars, polynucleotides have increasingly demonstrated promising results cosmetically.20-22 Polynucleotides are polymeric molecules which have moisturising and viscoelastic properties.23 They are capable of binding to a large amount of water, rearranging their structure and coordinating water molecules to form a 3D gel. This gel undergoes enzymatic cleavage resulting in progressive water release and the production of smaller oligonucleotides.23
Oligonucleotides are naturally present in the extracellular matrix, and are used for metabolic processes.24 However, the cleaved polynucleotide derivatives retain their moisturising and viscoelastic properties, resulting in a longer-lasting effect. Typically, polynucleotides are derived from the sperm of trout or chum salmon, which are then purified and sterilised for medical use.23
Polynucleotides activate several cellular signalling pathways which have effects on angiogenesis, reducing inflammation and activating growth factors.5 These growth factors are essential for tissue repair, wound healing, collagen production and regeneration of damaged tissues. Polynucleotides can stimulate the production of growth factors by activating gene expression, stabilising messenger RNA (mRNA) and activating signalling pathways in the cell.25-29
Adenosine receptors, particularly A2A, are involved in the suppression of inflammation and tissue repair.30 Activation of these receptors initiates a cascade of cellular pathways including the inhibition of the NF-kB signalling pathway, therefore reducing the production of pro-inflammatory cytokines (such as TNFα, IL6, IL1β and HMGB-1). Activation of the A2A also stimulates the cAMP and PKA signalling pathways.30 This results in increased cellular proliferation and migration, production of vascular growth factors, recruitment of endothelial progenitor cells and increased production of collagen.30
Activation of the A2A receptor upregulates cellular signalling pathways such as the PI3K/Akt and MAPK/ERK pathways, which are associated with cell proliferation, migration and survival, therefore also promoting angiogenesis.30
Several studies have demonstrated the anti-inflammatory properties of polynucleotides through the promotion of anti-inflammatory cytokines while inhibiting cytokines which promote inflammation.27,31 A study of a rat model of ischemic colitis noted a reduction in expression of inflammatory proteins COX-2, Il-7, IL-1β and TNF-α following administration of polynucleotides.27 Furthermore, in a murine model of arthritis following intra-articular injection of collagen,
polynucleotides were found to increase IL-10 expression, an anti-inflammatory cytokine.31
In vitro studies with polynucleotides have demonstrated the promotion of new blood vessel formation through several pathways.25,29 This is mediated by increased production of angiogenic growth factors such as vascular endothelial growth factor (VEGF), fibroblast growth factor (FGF) and platelet-derived growth factor (PDGF).25 An in vitro study of human chondritic cells exposed to pro-inflammatory IL-1β and hypoxia, to simulate the cellular effects of osteoarthritis, demonstrated significantly increased levels of angiopoietin-2 (ANG-2), PDGF and VEGF, while noting decreased expression of angiostatin and endostatin (involved in anti-angiogenesis).25
An animal study involving ligating and excising the femoral artery of rats to achieve limb ischaemia demonstrated that administration of polynucleotides significantly increased levels of VEGF mRNA and protein in the adductor muscles, in addition to reduced tissue oedema and oxidative stress.29 Polynucleotides have therefore demonstrated antioxidant properties; this effect is also thought to be mediated via the activation of adenosine A2A receptors.26
In an in vitro study of human corneal cells challenged with H2O2 (an oxidant), administration of polynucleotides reduced the expression of pro-apoptotic genes and pro-inflammatory cytokines, while also stimulating the production of endogenous antioxidant enzymes. Co-administration with A2A antagonist negated these effects, demonstrating that A2A receptor activation is the likely method by which polynucleotides achieve this effect.26
Several factors contribute to functional and structural changes in the scalp’s hair density.6,10 The majority of aetiologies driving hair loss include inflammatory processes driven by hormonal changes, depleted levels of collagen and impaired vascular supply to the scalp.6,10 The properties of polynucleotides therefore position them as an ideal standalone therapy or adjunct to existing hair loss treatments. There is substantial evidence that oxidative stress also plays a crucial role in the ageing process, including alopecia.32,33
An understanding of the stages of the hair cycle helps practitioners appreciate the role of polynucleotides as a treatment for hair loss.9
Hair growth involves the growth and differentiation of hair follicles, comprising dermal papilla cells (specialised mesenchymal cells which sit at the bottom of hair follicles) and epithelial cells.34 There are four stages of the hair cycle:34
Anagen: The growing phase. This stage lasts two to seven years and determines the length of the hair.
Catagen: The regression phase of around 10 days, during which the hair follicle miniaturises and detaches from the dermal papilla.
Telogen: The resting phase. Telogen lasts approximately three months.
At any one time, about 10-15% of hairs are in telogen.
Exogen: The shedding phase. Hair reaches its terminal position in the follicle and then detaches, resulting in shedding.
With ageing, the length of time in anagen decreases, resulting in progressive shortening of the hair cycle and a net loss of hair.35
Certain pathologies will drive the hair follicle into catagen prematurely, which results in increased shedding. Therefore, non-surgical hair loss treatments aim to prolong the time in anagen and prevent follicles from entering catagen.36
Polynucleotides function at the cellular level, activating fibroblasts to increase collagen production.23 Decreased levels of collagen are associated with the ageing phenotype and alopecia.35 Remodelling of collagen is more active in anagen than in telogen, and therefore, stimulating collagen production may protect against age-related hair loss in addition to aiding in the growth of new follicles.36
Polynucleotides stimulate angiogenesis through growth factor pathways including VEGF.25 VEGF production results in new blood vessel formation and improved scalp circulation, but also prolongs the anagen phase of the hair cycle, preventing hair loss.37
Several key cellular signalling pathways have been implicated in the development of alopecia including LEF/TCF, Wnt/β-catenin, TGF-β/ BMP, Notch, HH, NF-KB and PI3K/AKT.38,39 Activation of the adenosine A2A receptor using A2A agonists has been demonstrated to increase cellular cAMP levels, increasing activation of the Wnt/β-catenin and PKA signalling pathway in murine cells.46 This plays a crucial role in controlling the proliferation and differentiation of hair follicle stem cells, thus promoting entry into anagen and new follicular growth.37 Furthermore, the NF-KB inflammatory pathway has been implicated in the pathogenesis of alopecia areata. Suppression of this pathway by polynucleotides may help prevent the transition into catagen.40
Reactive oxygen species, or free radicals, are highly reactive molecules which damage cellular structural membranes, lipids, proteins and DNA.32 The body deploys endogenous defence mechanisms, including antioxidative enzymes through A2A receptor activation, and molecules which reduce and neutralise free radicals.32 These endogenous protective mechanisms decrease with ageing while the production of free radicals is increased, resulting in progressive damage of cellular structures, and contributing to the ageing phenotype.32
An in vivo study of antioxidant levels in human skin cells showed increased activity of catalase and decreased glutathione reductase in photoaged skin, representing an increased lifetime exposure to free radicals. Additionally lower levels of non-enzymatic antioxidants α-tocopherol, ascorbic acid and glutathione were observed in the skin of photoaged subjects.47 In terms of hair loss, free-radical damage manifests as early entry into catagen, increased shedding and decreased hair production, demonstrating oxidative stress as a pivotal mechanism contributing to hair loss.32,33,41
The efficacy of polynucleotides for treating scalp hair loss has been demonstrated in studies, assisting in follicular regrowth, accelerating growth and leading to stronger and healthier hair shafts.17,19 In one study, 20 patients with androgenetic alopecia underwent 10 treatments over four months with a prefilled gel containing 15mg of polynucleotides. Of these patients, 78% had slight or moderate improvement in hair growth by week 18, with a statistically significant decrease in hair shedding at all visits. A statistically significant increase in the mean thickness of hairs was observed at week 24.19
However, the numbers of patients in these studies is small (20 in both cases in the literature), and more robust research on a larger scale is required to demonstrate long-term efficacy and substantiate the treatment’s use as an effective treatment for hair loss.



and five
A consensus report on the use of polynucleotides in medical aesthetics suggests intradermal injection of polynucleotides in treatment cycles, with one treatment every seven to 14 days for a total of four sessions. This initial cycle should be followed by an additional session every 21-30 days. The report concluded that the combination of polynucleotides with other interventions, such as biotin, hyaluronic acid and topical therapy, can enhance the treatment benefits.18 Further and more specific research is required to confirm the optimal treatment protocol for hair loss treatments.
Figures 2-4 demonstrate the results of three patients with androgenetic alopecia who received combination treatment with polynucleotides and PRP. This involved a course of treatment, two to four weeks apart. Significant improvement was noted in terms of follicular density, hair follicle strength and hair shedding.
There are limited studies available comparing polynucleotides to existing hair loss treatments, or considering them in combination with other options, so more research is needed.50-52 Nevertheless, it stands to reason that therapies which are synergistic with polynucleotides should enhance their effectiveness. Topical treatments like minoxidil improve blood flow to the skin and may potentiate the effects of the angiogenic properties of polynucleotides.14 Biotin and hyaluronic acid are required for the growth of healthy hair follicles, and supplementation, particularly in deficiency, can improve follicle strength.14
A study has shown that one 927 nm fractionated thulium laser is an effective treatment modality of alopecia.51 It split 16 patients into two groups of eight: those receiving thulium laser and polynucleotide injections, and a second group with polynucleotides alone. Combined therapy significantly improved mean hair thickness and hair count compared to polynucleotides alone.53 A second observational study demonstrated improvements in hair thickness and hair count after combined thulium laser and polynucleotide injections. Interestingly, a notable increase in pigmented hair follicles, representing decreased grey hairs, was also reported.52
A further study compared the effects of polynucleotides combined with PRP therapy on treating hair loss. This study split 40 patients into two groups of 20: those receiving combined PRP and polynucleotide therapy, and those receiving polynucleotides alone. Both groups demonstrated significant improvements in mean hair thickness and hair count. Comparison analysis found that combined therapy resulted in significantly improved hair thickness, but did not improve hair count significantly compared to polynucleotides alone.50 Further studies with larger patient volumes are welcomed.
Given their safety profile, the absence of systemic toxicity and antigenicity, even when injected, polynucleotides offer a safe, minimally-invasive treatment for hair loss.3 With minimal downtime, polynucleotides can be used as a standalone or combined treatment for hair loss. Whilst efficacy has been demonstrated in both male and female hormonal hair loss in small studies, further research is welcomed to determine the long-term safety profile and efficacy.

Dr Edward Robinson is a cosmetic physician and NHS anaesthetics doctor based in Cheshire. He specialises in skin and hair rejuvenation treatments and treating the male face, favouring biostimulators and combination treatments. He is an associate member of BCAM, and a Finalist for The AlumierMD Award for Rising Star of the Year at The Aesthetics Awards 2024.
Qual: MBBS, BSc (Hons)
Test your knowledge!
Complete the multiple-choice questions and go online to receive your CPD certificate!
Possible answers
Questions
1. What percentage of men are affected by hair loss by the age of 50?
2. The four Stages of the Hair Cycle are?
3. The only two licensed medications for androgenic alopecia are?
4. Which of the following is not a mechanism by which polynucleotides can help treat alopecia?
5. What is the mechanism by which polynucleotides appear to exert their effects?
20%
40%
60%
80%
a. Anagen, catagen, telogen, exogen
b. Prophase, metaphase, anaphase, telophase
c. Growth, regression, resting, loss
d. Initiation, proliferation, maturation, resolution
a. Biotin and collagen
b. Minoxidil and finasteride
c. Corticosteroids and retinoids
d. Ketoconazole and spironolactone
a. Enhancing angiogenesis
b. Stimulating collagen production
c. Inhibiting the conversion of testosterone to dihydrotestosterone
d. Activating growth factors
a. Stimulation of the PPAR-gamma receptor
b. Activation of the NF-κB pathway
c. Activation of the JAK-STAT receptor
d. Activation of the adenosine A2A receptor
Skin laxity of the knees increases with age and leads to the appearance of skin folds, which has become a common concern for patients searching for body rejuvenation options.1 Of course, some skin laxity above the knees is vital for them to bend and move, but a combination of ageing, sudden or dramatic weight loss and sun damage can create more excessive laxity that leads to sagging and/or wrinkles. This process occurs from the age of 40, with a reduction of body skin density and firmness due to collagen and elastin depletion, resulting in visual tissue texture worsening.2
Many non-surgical options can be used to address this indication, for example, energy-based devices like transcutaneous radiofrequency (RF), microfocused ultrasound and CO2 laser.3 Injectables can also be used, such as hyaluronic acid (HA), poly-L-lactic acid (PLLA) and calcium hydroxylapatite (CaHA), which are favoured due to their biocompatibility, safety profile and longevity as reported in literature.4 Collagen stimulators have become particularly popular in medical aesthetics due to their ability to address volume loss, skin crepiness, cellulite, stretch marks and wrinkles simultaneously. They are considered non-invasive, safe, effective and long-lasting body restorative solutions.1
Here, I present a case study using a PLLA collagen-stimulating dermal filler to address skin laxity of the knees in a 58-year-old patient.
A 58-year-old female patient had previously visited my practice for facial aesthetic treatments including filler and botulinum toxin. Pleased with the results, she later wanted to explore options for skin laxity and volume loss above and around her knees. She was considering a summer holiday later in the year but felt uncomfortable about revealing her knees at the beach and wearing skirts or shorts. The patient was fit and healthy, with no known medical issues; she was a non-smoker and naturally slim. Over time, however, she had noticed changes to the skin above her knees, including increased laxity and wrinkling, which she said had accelerated over the past few years. At the patient’s initial consultation, we discussed her concerns in detail and the suitable options open to her such as Profhilo, fractional radiofrequency with microneedling, and dermal filler off license. I then explained that there was a PLLA product specifically approved for the body, and designed to target specific areas including the knees, which has established protocols in place and a body of research behind it to prove its efficacy and safety.7,1,3 As she wanted long-lasting results, and had a previous positive experience with PLLA in the face, we decided that this would be the best option.
I took a complete overview of her medical history, including any hypersensitivities, absence of inflammation and infection in treated areas, predisposition to keloid formations and untreated autoimmune conditions. This was a precaution due to host tissue response involvement after PLLA injections.5,6
The consultation also included a full explanation of the contraindications of treatment and possible side effects/complications. These included oedema, bruising, numbness, tenderness, infection, vascular occlusion, nodules, granuloma formation and immune-mediated reactions.8,4 It took place in May, so I also ensured she wasn’t due to go on holiday immediately after treatment because of the possibility of bruising. In addition, I wanted to ensure that in the case of any described complications, I could manage them effectively. In my clinic, we follow Aesthetic Complications Expert (ACE) Group World protocols on prevention and treatment of oedema, bruising, acute infection, vascular occlusion and delayed onset nodules (DONs), and work in collaboration with product manufacturers, as well as private GP, dermatology and plastic surgeons’ services with access to laboratory investigations.9-13
Following the first consultation, I sent my patient an email containing written information about the recommended PLLA product, plus a personalised treatment plan, the details we had discussed about possible side effects and aftercare.
When treating the knees, the anatomy of the area needs to be carefully considered. Typically, there is natural anatomical variation in how superficial the great saphenous vein lies. This requires particular caution at the medial aspect of the knee, including avoiding injections to minimise the possibility of vascular occlusion.14,15 I also wanted my patient to understand that her skin would naturally change during menopause and that the final results could be variable. I stressed to her that the PLLA treatment cannot be dissolved and requires rigorous aftercare to avoid possible side effects, such as a prolonged healing process, bruising, infection or nodule formation.7 I ensured she understood that she would need to massage the area for 10 minutes, twice per day for two weeks post-procedure to allow an even product distribution and to mitigate any expected body response to the PLLA injections, with simultaneous reduction of possible nodule formation.1,4,17 The patient stressed that she wanted the results PLLA could offer and was happy to commit to the aftercare program.
The treatment took place in two sessions with a four- to six-week space between them, using the PLLA filler Lanluma. The gap between treatments was advised to allow the PLLA properties to achieve the best possible results due to the host reaction to the product’s introduction. I set expectations that the result she saw instantly after injection would take time to mature to avoid overcorrection.17 I took pre-treatment photographs and prepared the skin with Clinisept+. I drew fanning marks onto the area to be treated, keeping them medially to the adductor fascia and sartorius muscle of the upper knee as this would be easier for treatment entry points.15
I applied 0.2ml of 2% topical Lidocaine for anaesthetic purposes around the planned cannula entry points for each knee to reduce any discomfort from the initial cannula insertions. Whilst there is a lack of comparative research around


cannula vs. needle injectable techniques in general, cannula use is linked to a more uniform distribution of collagen stimulators using a fanning technique application. It is also thought to reduce the likelihood of bruising, oedema, vascular obstruction and nodule formations in comparison to injections with needles.4,16 Using lower volumes to reduce the risk of ‘over-thickening’ of the skin and subcutaneous tissue in treated areas, I followed a subcutaneous fanning technique in the superficial fat and deep fat. One vial of Lanluma V per session was used to cover the skin with a three-dimensional approach above the knees, on the lower thigh, covering inner, frontal and lateral areas.15 The product was reconstituted as per manufacturer instructions: one vial of Lanluma V, containing 210mg powder, combined with 15ml of water for injections. Additionally, lidocaine hydrochloride was added to each vial. Each vial was shaken for 10 minutes and left for one hour to ensure complete hydration.17,15 Then, immediately prior to treatment, I used a 1:1 ratio dilution of product – 5ml of reconstituted Lanluma V combined with 5ml of water, constituting 30ml of product overall for use bilaterally. Each vial was vigorously agitated for one minute immediately before injecting.17 I treated the patient’s lower thighs (10cm superiorly from the knee), introducing 5ml


of the diluted Lanluma V to cover a 5x5cm area (25cm2).17 I used a 21G 50mm cannula to introduce the Lanluma and applied a subcutaneous fanning technique for the superficial and deeper fat.17 The entry point for each cannula was made with a 19G needle. To cover the frontal, medial and lateral aspect of the patient’s lower thigh and above the knee area, I made two entry points for the lateral-frontal and medial-frontal aspects of her knees. This allowed me to perform a ‘criss-crossing’ technique to cover the areas of concern.17 Once injections were completed, I sealed the cannula entry points with spot plasters, advising my patient to keep them in place for 24 hours.15 I massaged the area vigorously, demonstrating to my patient the best technique and where to massage at home as part of her aftercare of the area.15 I also applied arnica gel to the treated areas for the bruising.18
The patient was advised to expect redness, swelling and tenderness in the first 24-48 hours post treatment, which would be resolved within two to four days.8 She was also warned to expect some bruising for up to two weeks after treatment.8 I advised her to continue massaging the area for 10 minutes, twice per day for two to three weeks. This is because PLLA has properties to stimulate fibroblasts via a subclinical inflammatory cascade and encapsulation
of PLLA microspheres, leading to collagen deposition and tissue thickening, which requires even distribution using a massaging technique help to reduce possible nodules’ formation.4,19 Other aftercare instructions included avoiding any makeup or camouflage application, energy-based skincare devices, alcohol and ibuprofen – which can act as a blood thinner – for 24 hours post procedure.20
I had already warned my patient not to expect results after the first treatment because it takes time for the collagen to develop, which becomes noticeable after approximately three months and there is further progression up to six months post procedure.1,7 Her results after two treatments were extremely positive and my patient was very satisfied (Figure 1 and 2). Initially, I had planned to conduct three treatments, however, because of the noticeable difference in the patient’s skin she decided not to go ahead with the third treatment.
PLLA collagen stimulators are an effective treatment for skin laxity above the knees, offering a safe and long-lasting effect.7 The benefit is to achieve gradual result over time without fear of creating overfilled look for the patient and an opportunity to discuss treatment progress and maintenance. PLLA body treatment is a useful tool to have in aesthetic practice to complement treatment options for the face.

Yuliya Culley is a registered general nurse with experience in emergency, cardiology, and dermatology nursing. She started her practice in medical aesthetics in 2009 and has performed a considerable number of non-surgical procedures. She was a Finalist in the Aesthetic Nurse Practitioner of the Year at the Aesthetics Awards 2022.
Quals: RGN, INP, BSc and MSc VIEW THE REFERENCES AT
The UK’s largest congress shaping the future of medical aesthetics


LIVE injectable, device and skincare demonstrations on the latest products and treatments.


5 CPD certified conferences with over 120 world-class speakers.



130+ leading brands showcasing innovative solutions and products to suit your needs. Register free now







Cross-linked IPN-Like Hyaluronic Acid 12.5mg/g + Sorbitol
HYDROMAX
Aesthetic practitioner Dr Zunaid Alli shares how STYLAGE® HydroMax from VIVACY Laboratories can boost skin moisture & improve skin quality
The STYLAGE® range of hyaluronic acid (HA) and antioxidant dermal fillers from the French manufacturer VIVACY Laboratories includes a dedicated product for deep skin hydration and moisturisation.
While mannitol is combined with the entire STYLAGE® range, the use of sorbitol as an antioxidant is added to a single product in the STYLAGE® range, namely HydroMax. STYLAGE® HydroMax contains 12.5mg/g of HA with sorbitol at 0.3%, and is presented in a 1ml syringe. The main indications for HydroMax are threefold:1
1. To provide a double hydration action (synergistic action between HA and sorbitol)
2. To enable the injection of a cross-linked skin booster for additional lift in the deep dermis
3. To introduce sorbitol into dehydrated and laxed skin
These indications are closely linked to its hydrating capability – to hydrate very dry skin, provide deep and instant rehydration and to strengthen lax skin, thereby increasing skin elasticity. It is also used for deep periorbital lines. HydroMax is excellent for use in areas of hyperdynamic movement such as the lower cheek and neck.
For practitioners who are looking for a biostimulating and hydrating effect, it is useful to describe HydroMax as a ‘micro filler,’ meaning that it can provide the effect of a light filler without overcorrection, together with adding a deep moisturising effect. This makes HydroMax a good choice of product for treating the perioral lines which can be challenging to treat with an injectable, especially when there is a risk of overcorrection.
HydroMax carries further indications for use on the dorsum of the hands, and is often used to treat laxity in the knees. It may also be used on the décolleté. HydroMax injects easily with the needle provided, or with a dermal cannula. Sorbitol acts as an antioxidant and moisturising agent which helps the skin to retain significantly larger concentrations of water when compared to mannitol.1

A study conducted on the cosmetic use of sorbitol reported protection of epidermal keratinocytes, significant improvement in barrier repair and moisturisation.2 These results were further reinforced in a study using sorbitol as a protective enhancer in the skin where keratinocytes and fibroblasts were protected from oxidative stress and UV radiation.3 HydroMax is used according to established protocols, and the best results are achieved by treating the area over three sessions at three-week intervals.4 This ensures that the results show an improvement and will last nine-12 months for most patients.
HydroMax is the perfect treatment option for those wanting to offer a mesotherapy treatment where you see not only instant, but long-lasting results thanks to the mixture of the cross-linked HA and sorbitol.

Dr Zunaid Alli is a medical aesthetic doctor and trainer. He has an experienced clinical background in general medicine, emergency medicine and medical oncology. He is an active contributor to continuous medical education for all levels of trainees who he teaches. His key focus is on progressing skills to provide excellent patient care in aesthetics. He has published various articles in aesthetics journals, and presented at local and international conferences.
Qual: MBBCh, MS (Aesthetics), DipDerm, DipAesthMed, BSc, BScHons (Psych), MBA
This advertorial was written and supplied by VIVACY Laboratories For more information, please contact contact@vivacylab.co.uk
REFERENCES
1. Stylage: IPN-Like technology. Hyaluronic acid and antioxidants: The Natural Correction (2018) Product Brochure
2. Muizzuddin, N., Ingrassia, M., Marenus, K.D., Maes, D.H. and Mammone, T., 2013. Effect of seasonal and geographical differences on skin and effect of treatment with an osmoprotectant: Sorbitol. Journal of Cosmetic Science 64(3), pp.165-174.
3. Manca, M.L., Mir-Palomo, S., Caddeo, C., Nacher, A., Díez-Sales, O., Peris, J.E., Pedraz, J.L., Fadda, A.M. and Manconi, M., 2019. Sorbitol-penetration enhancer containing vesicles loaded with baicalin for the protection and regeneration of skin injured by oxidative stress and UV radiation. International journal of pharmaceutics 555, pp.175-183.
4. STYLAGE® HydroMax Treatment Protocol.

Dr Mary Sommerlad discusses the various treatments available to address melasma
Melasma is a chronic acquired pigmentary disorder that can have a negative impact on quality of life.1 It is characterised by bilateral tan to dark brown or slate grey patches of smooth hyperpigmentation, predominantly affecting sun-exposed prominence areas on the face such as the forehead, cheeks and nose.2 There are three main facial patterns: centrofacial, malar and mandibular. The centrofacial pattern is the most common, with excess pigment appearing in the forehead, cheeks, upper lip and nose.3
In this article, I will share some melasma management and treatment approaches which I have found satisfactory, although it is paramount to remember that it is a difficult condition to treat, and there are multiple possible approaches available.
Although melasma can affect all skin types and genders, it is most apparent in females (9:1 female to male ratio), and more evident in those with skin of colour (SOC) and high levels of sun exposure.4 Melasma can be considered as epidermal, dermal and mixed pigment dispersion patterns.3 The exact prevalence of melasma is unknown and thought to be under-reported.1,2 Diagnosis is clinical, with a skin biopsy only required if the hyperpigmentation is not in keeping with melasma. Dermoscopy and Wood’s Lamp can be used either together or separately to identify whether the melanin is in the epidermis, dermis or both layers.7 The aetiology is complex, poorly understood and multifactorial, involving genetic
predisposition, female reproductive hormones, sun exposure, oxidative stress and inflammation.8 The role of sun exposure is key to understanding the persistent and recurrent nature of melasma. Sun exposure in the UVA and UVB spectrum (280 nm to 400 nm) and visible light (VL) spectrum (380 nm – 700 nm) stimulates melanin product; those with melasma appear to generate persistent melanin at lower levels of sun exposure.9 Ultraviolet radiation (UVR) contributes to the degradation of the basement membrane, promoting the descent of melanocytes and melanin into the dermis and leading to melanin dispersal, not only in the epidermis, but also in the harder to treat dermis.10
Oxidative stress from UVR, air pollution, poor sleep and strenuous exercise can generate reactive oxygen species in the skin.11 This can trigger melanogenesis and is found to be higher in those with melasma, while their antioxidant melatonin seems to be lower.11 Those with melasma tend to express higher levels of oestrogen receptors in the epidermis and in the fibroblasts of the upper dermis; oestradiol mediates melanogenesis.9 Studies have shown that histologically, melasma shares many features of photoaged skin such as solar elastosis, a disorganised basement membrane, increased vasculature and increased mast cells.12-14 Therefore, management of melasma should not only focus on removing pigmentation in both the epidermis and dermis, but also on replenishing antioxidants, restoring the basement membrane and rejuvenating the skin to minimise relapse.
Sun exposure, particularly to the long UVA wavelength and high energy visible light (HEVL) spectrum, is thought to exacerbate and perpetuate melasma. It is now recognised that those with SOC are susceptible to the effects of OPN3, a HEVL receptor found on melanocytes that triggers melanogenesis.13 Once melanogenesis is induced through OPN3, a cascade of events is triggered leading to the tyrosinase/tyrosinase-related protein complex.13 This is mainly formed on the melanocytes of those with olive, brown and black skin tones; this complex generates sustained tyrosinase activity leading to persistent hyperpigmentation.15 Effective blockade of HEVL as well as UVA is crucial. Physical sun protection (e.g. wide brimmed hats, sitting in the shade, avoiding sunbathing) and a broad spectrum SPF form the foundation of all melasma management.14,16 To date, the best studied way to effectively block HEVL and long wave UVA is 3.2% iron oxide.17 However, iron oxide gives sunscreen a rusty red colour, hence these sunscreens are tinted for cosmetic acceptability.17 Sunscreen must be used every day, even throughout winter as HEVL is present throughout the year. Reapplication of sunscreen is useful after towelling the face (e.g. after swimming or sweating), and roughly every two hours throughout the day.18 Some of my recommendations include Eucerin Sun Face Pigment Control, Heliocare 360 Pigment Solution and Murad City Skin Age Defense Broad Spectrum. I usually recommend SPF50, but SPF30 is also acceptable if reapplied regularly.
Tranexamic acid is a derivative of the amino acid lysine which inhibits plasmin activity in keratinocytes. Plasmin activity leads to an increase in melanogenic mediators, including α-melanocyte stimulating hormone.17 It also inhibits the release of melanogenic factors and reduces vascular endothelial derived growth factor (VEGF) and endothelin-1, leading to reduced vasculature and pigmentation.17,20 Tranexamic acid is being extensively studied; it is most effective when given orally at doses between 250mg and 500mg once to twice daily for three or more months.18,21 Oral tranexamic acid is used off-label in melasma. A careful medical history and lifestyle history including risks for thromboembolic events must be taken before use, screening blood tests must be checked and the duration of treatment must be clearly documented and understood by the patient.22
For these reasons, it is best prescribed by a consultant dermatologist. Topical preparations of tranexamic acid at concentrations of 3% and 5% have been studied, as has intradermal tranexamic acid. It has been found that topical and intradermal administration show less significant results compared to orally.22
Eumelanin, the pigment responsible for shades of dark brown/black to light beige, is over-produced in patients with melasma via a complex enzymatic biochemical process. Of all the enzymes involved in eumelanin production, tyrosinase is the most important as it controls the rate limiting step of converting Tyrosine to L-DOPA.22 Using formulations that block parts of the pathway can help inhibit pigment formation.23
Hydroquinone is the best studied tyrosinase inhibitor, and is considered the gold standard in managing hyperpigmenting diseases, including melasma, in concentrations between 2% and 12%.24 Hydroquinone is banned over the counter in the UK, and can only be obtained with a prescription. It has important side effects that limit its concentration and long-term safety, including exogenous ochronosis that can develop idiosyncratically and skin irritation.25 Exogenous ochronosis is rare at concentrations of 5% or less.25 In 1975, Kligman and Willis described successful depigmentation using a combination of 5% hydroquinone, 0.1% tretinoin and the steroid 0.1% dexamethasone.26 Retinoids promote keratinocyte turnover and may inhibit tyrosinase, leading to a faster rate of loss of epidermal pigment via cell turnover and brightening of hyperpigmentation.27
Corticosteroids suppress melanogenesis in a non-selective way and have anti-inflammatory properties, mitigating the irritant effects of tretinoin and hydroquinone 27 This triple combination has been modified over the years, referred to as modified Kligman’s compounds or triple combination compounds (TCC), which studies have found to be superior to the use of hydroquinone alone.13,28 In the UK, the most widely available TCC prescription is 5% hydroquinone, 1% hydrocortisone and 0.1% tretinoin. Clinicians can also compound their own formulation of TCC; the advantage of this is that a compound can be personalised to your patient’s needs. Around 50% of patients receiving combination treatment experience erythema, skin irritation, contact irritant dermatitis and telangiectasia can appear.29 TCC is usually prescribed for nightly use for a set period; the use must be
weighed up against any adverse effects as well as clinical response. In my practice, I recommend TCC to be used nightly for eight to 12 weeks, which balances side effects with clinical response.
There are several alternatives to TCC that can be used instead of or in addition to TCC. According to a 2022 systematic review, the most efficacious alternative topical treatments include 20% azelaic acid (antioxidant), cysteamine (antioxidant), topical tranexamic acid at 2% to 5% (antiplasmin that prevents UV-induced melanogenesis) and kojic acid (derived from fungi).30 The trademarked tyrosinase inhibitor thiamidol (Eucerin) has been shown to be superior to arbutin, kojic acid and 2% hydroquinone in improving hyperpigmentation in melasma.31
For many patients, a procedure to remove pre-existing pigmentation is required. Caution is advised as any procedure that removes pigmentation has the potential to cause post-inflammatory hyperpigmentation (PIH).23 Chemical peels can target melogenesis, as well as increase keratinocyte turnover to shift stubborn pigment.32 Peels should be chosen with consideration for efficacy, downtime, repeat treatment and risk of PIH, especially in those with SOC.33 SOC patients are recommended to use topical tyrosinase inhibitors and sunscreen for several weeks before and after the procedure to reduce the risk of PIH.34
Laser treatment offers a targeted solution for removing melanin in melasma when used in combination with the aforementioned procedures. It is crucial that the correct laser, protocol and patient are selected in order to avoid adverse events like PIH and textural scarring.34 Profractional lasers such as 2940 nm Erbium:YAG, Q-switched laser Nd:YAG laser and pico second lasers have shown efficacy in reducing pigmentation and improving skin texture.35 These lasers accelerate the removal of melanin without using melanin as a target. In those with SOC, lasers can be used provided the patient has had their skin primed well with tyrosinase inhibitors and meticulous sun protection.35 The laser settings also need to focus on minimal heat generation.35 By targeting water in the dermis, collagen can be boosted and photoageing can be improved, tackling another component of the melasma aetiology.35 I use a fractional Erbium:YAG laser (Profrac by Sciton) as I have found that it generates minimal heat dispersion so has
excellent tolerability with SOC and a downtime of seven days.
We provide verbal and written pre- and post-procedure skincare to each patient, as well as follow-up phone calls and photographic reviews. My particular recommendations for post-laser hydration are Epionce Medical Barrier Cream, La Roche Posay Cicaplast, iS Clinical Shield Recovery Balm, Medik8 Ultimate Recovery and SkinCeuticals Epidermal Repair.
Intense pulsed light (IPL) and broad band light (BBL) are energy-based devices emitting light from a wide range from 415 nm up to 1200 nm which encompasses melanin. IPL/BBL has lower quality of evidence compared to fractional or Q-switched lasers, and therefore should be considered as an adjunct rather than monotherapy.34 By scavenging free radicals and reducing oxidative stress, antioxidants, in theory, protect against UV-induced skin damage and mitigate melanogenesis.36 Oral antioxidants such as polypodium leucotomos extract, melatonin and niacinamide have shown potential in melasma management as an adjunctive option.36,37 There is a lack of research around the use of oral vitamin C for melasma; topically, it can help with any forms or hyperpigmentation, but only as an adjunct.
It is important to inform patients that melasma is a chronic condition that can relapse. Patient-physician alignment around consistency with following a treatment plan and realistic expectations is crucial to build and maintain trust. Understanding the multifactorial pathogenesis of the condition is crucial for developing effective treatment strategies. Further research is warranted to optimise treatment protocols and address unmet needs in melasma therapy.

Dr Mary Sommerlad is a consultant dermatologist with a focus on medical, paediatric, skin of colour and laser dermatology. She has won the Royal Society of Medicine Prize and the British Society of Immunology Prize, and currently works at The Aesthetics Awards-winning Self London clinic. She sits on the UK Clinical Dermatology Trial Network, has had her work published in peer reviewed journals and has been a guest speaker and chair at a number of academic meetings.
Qual: BSc, MBBS, MRCP (Derm), FRCP (London)

THE 1ST LIQUID FORMULATION BOTULINUM
TOXIN TYPE-A IN EUROPE
ONSET FROM 24H*1
DURATION UP TO 6 MONTHS1

Alluzience, 200 Speywood units/ml, solution for injection -
Prescribing Information (United Kingdom)
Presentation: Each vial contains 125 Speywood units of Clostridium botulinum toxin type A haemagglutinin complex in 0.625 ml of solution. Indications: Alluzience is indicated for the temporary improvement in the appearance of moderate to severe glabellar lines (vertical lines between the eyebrows) seen at maximum frown in adult patients under 65 years, when the severity of these lines has an important psychological impact on the patient. Dosage: Botulinum toxin product units differ depending on the medicinal products. Botulinum toxin units are not interchangeable from one product to another. Doses recommended in Speywood units are different from other botulinum toxin preparations. Paediatric Population: The safety and efficacy of Alluzience in children aged up to 18 years have not been established. The use of Alluzience is not recommended in patients under 18 years. Method of administration: Alluzience should only be administered by a healthcare practitioner with appropriate qualifications and expertise in this treatment and having the required equipment, in accordance with national guidelines. A vial of Alluzience should only be used to treat a single patient, during a single session. Remove any make-up and disinfect the skin with a local antiseptic before administration. The intramuscular injections should be performed using a sterile needle with a suitable gauge. Dosing and treatment intervals depend on assessment of the individual patient’s response. The median time to onset as reported subjectively by patients was 3 days (the majority of patients reported an effect within 2 to 3 days with some patients reporting an effect within 24 hours). An effect has been demonstrated for up to 6 months after injection. The treatment interval should be no more frequent than every 3 months. Administration instructions: The recommended dose is 0.25 ml of solution (50 Speywood units) divided into 5 injection sites, 0.05 ml of solution (10 Speywood units) administered intramuscularly into each of the 5 sites: 2 injections into each corrugator muscle and one into the procerus muscle, near the nasofrontal angle. The anatomical landmarks can be more readily identified if palpated and observed at patient maximum frown. Before injection, place the thumb or index finger firmly below the orbital rim in order to prevent extravasation below the orbital rim. The needle bevel should be pointed upward and medially during the injection. In order to reduce the risk of ptosis, avoid injections near the levator palpebrae superioris muscle, particularly in patients with larger brow-depressor compl–exes (depressor supercilii). Injections should be made into the central part of the corrugator muscle, at least 1 cm above the orbital rim. General information: In the event of treatment failure or diminished effect following repeat injections, alternative treatment methods should be employed. In case of treatment failure after the first treatment session, the following approaches may be considered: • Analysis of the causes of failure, e.g. incorrect muscles injected, inappropriate injection technique, and formation of toxin-neutralising antibodies • Re-evaluation of the relevance of treatment with botulinum toxin A. Contraindications: Hypersensitivity to the active substance or to any of the excipients. Presence of infection at the proposed injection sites. Presence of myasthenia gravis, Eaton Lambert Syndrome or amyotrophic lateral sclerosis. Precautions and Warnings: Care should be taken to ensure that Alluzience is not injected into a blood vessel. Injection of Alluzience is not recommended in patients with a history of dysphagia and aspiration. Adverse reactions possibly related to the spread of toxin effect distant from the site of administration have been reported very rarely with botulinum toxin. Swallowing and breathing difficulties are serious and can result in death. Very rare cases of death, occasionally in the context of dysphagia, pneumopathy (including but not limited to dyspnoea, respiratory failure, respiratory arrest) and/or in patients with significant asthenia have been reported following treatment with botulinum toxin A or B. Patients should be advised to seek immediate medical care if swallowing, speech or respiratory difficulties arise. Alluzience should be used with caution in patients with a risk of, or clinical evidence of, marked defective neuro-muscular transmission. These patients may have an increased sensitivity to agents such as botulinum toxin, and excessive muscle weakness may follow treatment. It is essential to study the patient’s facial anatomy prior to administering Alluzience. Facial asymmetry, ptosis, excessive dermatochalasis, scarring and any alterations to this anatomy, as a result of previous surgical interventions, should be taken into consideration. Dry eyes have been reported with use of Alluzience in periocular regions. Attention to this side effect is important since dry eyes may predispose to corneal disorders. Protective drops, ointment, closure of the eye by patching or other means may be required to prevent corneal disorders. The recommended dose and frequency of administration for Alluzience must not be exceeded. Patients treated with the recommended dose may experience exaggerated muscle weakness. Caution should be taken when Alluzience is used in the presence of inflammation at the proposed injection sites or when the targeted muscle(s) show excessive weakness or atrophy. As with all intramuscular injections, use of Alluzience is not recommended in patients who have a prolonged bleeding time. Each vial of Alluzience must be used for a single patient treatment during a single session. Any excess of unused product must be disposed of and specific precautions must be taken for the inactivation and disposal of any unused solution. Antibody formation: Injections at more frequent intervals or at higher doses may increase the risk of neutralising antibody formation to botulinum toxin. Clinically, the formation of neutralising antibodies may reduce the effectiveness of subsequent treatment. Traceability: In order to improve the traceability of biological medicinal products, the name and the batch number of the administered product should be clearly recorded. Sodium content: This medicine contains less than 1 mmol sodium (23 mg) per 125U vial, that is to say essentially ‘sodium-free’. Interactions: Concomitant treatment with Alluzience and aminoglycosides or other agents interfering with neuromuscular transmission (e.g. curarelike agents) should only be used with caution since the effect of botulinum toxin may be potentiated. No interaction studies have been performed. Pregnancy, Breastfeeding and Fertility: Pregnancy: There are only limited data from the use of botulinum toxin type A in pregnant women. Animals studies do not indicate direct or indirect harmful effects with respect to reproductive toxicity. As a precautionary measure Alluzience should not be used during pregnancy. Breastfeeding: It is unknown if Alluzience is excreted in human milk. Alluzience should not be used during breast-feeding. Fertility: There are no clinical data examining the effect of Alluzience on fertility. There is no evidence of direct effect of Alluzience on fertility in animal studies. Effects on ability to drive and use machines: Alluzience has a minor or moderate influence on the ability to drive and use machines. There is a potential risk of localised muscle weakness or visual disturbances linked with the use of this medicinal product which may temporarily impair the ability to drive or operate machinery. Undesirable Effects: A majority of adverse reactions reported with Alluzience in clinical trials were of mild to moderate intensity and reversible. The most frequently reported adverse reactions were headache and injection site reactions. The incidence of adverse reactions tended to decrease with repeated treatments. Adverse effects related to the spread of toxin effect distant from the site of administration have been very rarely reported with botulinum toxin (excessive muscle weakness, dysphagia, aspiration pneumonia with fatal outcomes in some cases). Adverse Drug Reactions Observed in Clinical Studies were as follows: Very common (≥ 1/10): Headache, injection site reactions (periorbital haematoma, haematoma, bruising, pain, paraesthesia erythema, swelling, pruritus, oedema*, rash*, irritation*, discomfort*, stinging*), asthenia*, fatigue*, influenza-like illness*; common (≥ 1/100 to < 1/10): Facial paresis*, eyelid ptosis, eyelid oedema, brow ptosis, dry eye, lacrimation increased, asthenopia*, muscle twitching (twitching of muscles around the eye)*; uncommon (≥ 1/1,000 to <1/100): Dizziness*, eyelid twitching, visual impairment*, vision blurred*, diplopia*, hypersensitivity (eye allergy, hypersensitivity, rash), rash*, pruritus*; rare (≥ 1/10,000 to < 1/1,000): Eye movement disorder*, urticaria*
*additional adverse drug reactions only observed with powder formulation of the same active substance in clinical trials
Post-marketing experience Frequency not known: hypoaesthesia, muscle atrophy
Prescribers should consult the summary of product characteristics for further details. Packaging Quantities and Cost: Pack containing x2 vials: £ 160.00 excluding VAT. MA Number: PL 03070/0009 Legal Category: POM Further information is available from: Galderma (UK) Ltd, Evergreen House North, Grafton Place, London, NW1 2DX. Telephone: +44 (0)300 3035674
Date of Revision: May 2023
Adverse events should be reported. United Kingdom Reporting forms and information can be found at www.mhra.gov.uk/yellowcardor search for MHRA Yellow Card in the Google Play or Apple App Store.
Adverse events should also be reported to Galderma (UK) Ltd: E-mail: medinfo.uk@galderma.com Tel: +44 (0)300 3035674
This information is intended for Healthcare Professionals only. This advertisement has been created and funded by Galderma.
*The exact timepoint in the first 24 hours was not captured.
Reference: 1. Alluzience SmPC.

Since its debut in 2015, Profhilo® has revolutionised the European regenerative medicine market. This pioneering injectable has redefined natural aesthetics nearly a decade after its launch. With more than eight million treatments administered globally, misconceptions persist with some inaccurately describing Profhilo® as just an ‘injectable moisturiser’ or ‘skin booster’. To commemorate the 10th anniversary of Profhilo®, it’s time to clarify the true impact and benefits of this transformative treatment, with the up-to-date insight from the latest study, ‘Intradermal Injection of Hybrid Complexes of High- and Low-Molecular-Weight Hyaluronan: Where Do We Stand and Where Are We Headed in Regenerative Medicine?’ by Humzah et al., (published in the International Journal of Molecular Sciences in 2024).
The study highlights how Profhilo® differs significantly from other treatments, such as linear hyaluronic acid used in mesotherapy which often includes vitamins, amino acids and peptides, and from cross-linked skin boosters or bio-stimulatory products recently popularised for skin improvement. It also provides an overview of the current literature on the in vitro studies and in vivo applications of hybrid cooperative complexes (HCCs) of hyaluronic acid (HA), from facial and body rejuvenation to skin wound healing, dermatology and genitourinary pathologies.
Biorevitalisation, biostimulation and bioremodelling
The differences between the three in the context of the mechanism of action of HCCs are as follows:
1. Biorevitalisation: Restores the loss in skin nourishment by directly providing vital components such as amino acids, vitamins, nucleotides, linear HA and collagen to fibroblasts and keratinocytes.
The science behind the breakthrough in injectable skin rejuvenation
2. Biostimulation: Improves extracellular matrix hydration and elasticity through an immune-mediated response that stimulates the synthesis of HA, collagen and elastin by fibroblasts. Substances such as poly-Llactic acid (PLLA), calcium hydroxylapatite (CaHa), polycaprolactone (PCL) and carboxymethylcellulose (CMC) are attributed to having a biostimulating activity. The biostimulation process induced by synthetic biomaterials, such as PLLA products, usually involves an immune-mediated response that consequently may induce the establishment of a fibrotic pathway.
3. Bioremodelling: Reverses the signs of skin laxity, facilitating extracellular matrix homeostasis by improving the vitality of different cell types, including fibroblasts, keratinocytes, adipocytes and myocytes. HCCs induce tissue restoration through a physiological improvement of extracellular matrix homeostasis and cellular viability, making them a unique product in the market and a central player in regenerative processes.
Is Profhilo® just an injectable moisturiser?
Without a doubt, no. The study’s conclusion suggests HCCs in Profhilo® make it a key player in regenerative medicine. The importance is also confirmed by the patentprotected technology, which further assures the uniqueness of this product and of its mode of action. These advances in crosslinking technologies, such as NAHYCO® –thermal stabilisation that does not require chemical bio-linkers – are ensuring its broader application in new and exciting fields such as regenerative medicine, tissue engineering and nanomedicine. Profhilo® Structura launching to the industry on 4th June in London. Developed by IBSA using the patented NAHYCO® technology, Profhilo® Structura will represent another notable breakthrough in aesthetic medicine.
1. HA’s effects are molecular weight-dependent, with high-molecular-weight HA (H-HA) promoting anti-inflammatory, antiproliferative and anti-angiogenic effects, while low-molecularweight HA (L-HA) fragments can trigger inflammation, cell proliferation and angiogenesis.
2. NAHYCO® Hybrid Technology is a thermal process that leads to the formation of hybrid cooperative complexes (HCCs) of HA, which contain equal concentrations of H-HA and L-HA.
3. HCCs have unique rheological properties, exhibit slower degradation and allow optimal tissue product diffusion while harnessing the synergistic effects of different molecular weight HA.
4. In vitro studies have shown that HCCs enhance collagen and elastin expression in keratinocytes and fibroblasts, promote wound healing, reduce inflammatory biomarkers and increase antimicrobial peptide expression.
5. HCCs also enhance adipogenic differentiation and proliferation of adipose-derived stem cells (ASCs), delay senescence in mesenchymal stromal cells and induce osteogenesis in dental pulp stem cells.
6. HCCs have potential applications in regenerative medicine beyond aesthetic purposes, including skin wound healing, treatment of psoriasis, acne scars, vulvar lichen sclerosus and vulvovaginal atrophy.
Miss Jennifer Doyle and Mr Richard Scawn explore the available options to treat the delicate eye area
The periocular region is often one of the first to display signs of facial ageing. With the latest figures showing blepharoplasty alone has increased by 74% in the last year, the demand for periocular rejuvenation is growing fast.1
Ageing around the periocular area plays an important role in facial ageing, with the eyelid skin being the thinnest anywhere in the body (around 0.3-0.5mm thick).2-3 Perceptions regarding a person’s degree of tiredness and age are predominantly based on periorbital aesthetics, making it a key area to address when wanting to achieve rejuvenation.4 Traditionally, rejuvenation of this delicate area was synonymous with blepharoplasty surgery, however, the past decade has shown a growth in options of non-surgical technologies that can be used as alternatives or adjuvants to revitalise this difficult-to-treat area.5
As a team of oculoplastic surgeons who offer a spectrum of surgical and non-surgical treatments to rejuvenate the periocular region, we will outline options available to treat the most common concerns.
When assessing a patient with concerns regarding their upper eyelid, it is important to first discern if they are suffering from hooded eyelids due to excess skin (dermatochalasis) or droopy eyelids due to ptosis. Ptosis is defined as when the upper eyelid margin is sitting lower than normal and covers the pupil, interfering with vision.6 It can also give the appearance of being sad or tired.6 Hooded eyelids or dermatochalasis is when the eyelid margin is sitting at an appropriate position but there is excess skin above which gives a tired or aged appearance.7 This diagnosis must be made correctly as if ptosis is missed, it can lead to disappointing results if blepharoplasty surgery is carried out in isolation, as the eyelid margin will remain low.8 To correct ptosis, once certain underlying conditions such as myasthenia gravis or a third nerve palsy have been excluded, surgical correction can be performed to raise the eyelid margin.9
For dermatochalasis, the traditional method of correction is a surgical blepharoplasty.10 Blepharoplasty is one of the most common cosmetic surgical procedures performed worldwide.11 It is defined as surgical repair or reconstruction of the eyelids, and typically involves the management of excess eyelid skin and/or fat.12 Upper eyelid blepharoplasty can generally be carried out under a local anaesthetic and typically takes an hour to perform. As patient demand continues to grow for non-surgical solutions, a variety have been performed in the upper eyelid region including plasma exeresis or laser resurfacing.12 Demand for non-surgical alternatives is often driven by the search for reduced recovery time, a reduction in potential rare but serious non-reversible complications and economic factors.13
A variety of laser treatments can also be used to improve excess eyelid skin, including ablative CO2 laser and fractionated erbium:YAG laser.12 The objective of laser treatment is to cause contraction of the skin, giving rise to tightening of the loose excess skin and a noticeable improvement in skin quality around the periorbital region.14 It is a useful treatment option for patients who are reluctant to undergo formal surgical intervention to address the excess skin.
Lasers such as CO2 have also been used as an adjuvant to surgical blepharoplasty, although thus far it appears that the clinical outcomes are comparable to other traditional tools like the Colorado needle tip with electrocautery.15
Plasma exeresis is another alternative that can address mild to moderate excess eyelid skin non-surgically and is a useful tool for patients who are reluctant to undergo surgery or are searching for an economical solution. It consists of a handpiece that produces ionised energy, allowing sublimation of epidermal and superficial dermal tissues causing skin contraction.13
It can be useful in cases where skin laxity is mild to moderate, but it is important to manage patient expectations and those with more severe dermatochalasis should be counselled that surgical intervention may be necessary to achieve their desired result.13
Under-eye dark circles can have a variety of underlying causes including tear trough deformity, hyperpigmentation and thinning of the skin with visible vasculature underneath.16 Ageing changes include bony resorption of the eye socket, loss of subcutaneous fat in the eyelid and thinning and hyperpigmentation of the skin. This typically



begins to occur when patients are in their 30s onwards.17
Soft tissue hyaluronic acid (HA) filler injection is the second most common minimally invasive procedure performed (second to botulinum toxin), and a substantial percentage of these injections are used to treat the lower eyelid-cheek interface.18
By using HA, practitioners can achieve volume augmentation of the tear trough area and correct tear trough deformity. This is often best achieved by also treating the mid-face to provide structural support as it can reduce the amount that is required to be injected into the tear trough itself. Most studies suggest that limiting the volume of filler to conservative amounts (0.5ml to each side) reduces the risk of complications in this difficult-to-treat area.19,20
Other common non-filler options include autologous fat transplantation, platelet-rich plasma (PRP), laser and polynucleotides.
Autologous fat transplantation
Autologous fat transplantation can be helpful if the dark circles are caused by thin, translucent skin overlying the orbicularis muscle whose vasculature is visible.21 This surgical procedure is less likely to result in Tyndall effect compared to HA filler, however, does involve surgery which is a lengthier procedure. Oedema can occur and removal of the fat can be problematic as it requires a secondary surgery.22
PRP to the under-eye area can help address dark circles that are caused by thinning skin. By stimulating collagen synthesis and dermal fibroblast proliferation, skin quality can be improved.23 There has been interest in creating an autologous gelatinous material from the patient’s autologous plasma, known as platelet-poor plasma gel, which can be used similarly to restore volume to the tear trough region.24
Polynucleotide technology offers another injectable treatment alternative to traditional HA filler. They mediate their effect through stimulation of cellular cascades, resulting in increased metabolic activity of fibroblasts that stimulate collagen synthesis, renewal and biorevitalisation of various dermal components.22 They also have a protective effect against free radical damage, thereby reducing further ageing changes.25 Polynucleotides can also be used in combination with other treatment modalities, like filler, PRP, laser procedures or other energy-based devices, to augment results.22 For example, they have been shown to reduce the degradation of HA-based products by approximately 40%, giving these treatments greater longevity.25
Fullness of the lower eyelid or under-eye bags is a common complaint encountered in aesthetic practice. With age, changes can occur to the lower lid which increases laxity of the skin, orbital septum, canthal tendons and orbicularis oculi muscle.26 This can lead to prolapse of the orbital fat, development of festoons and a reduction in skin quality, with laxity and wrinkles developing.26 The traditional surgical approach would involve a lower eyelid blepharoplasty, and this can be performed transconjunctivally or via the skin approach. Excess or prolapsed fat can be repositioned or excised in order to achieve a smoother lid-cheek junction, alongside excess skin excision if required and tightening of the lower eyelid if necessary.27 Not all patients may be suitable surgical candidates, for example, those with a negative vector are at a higher risk of complications such as eyelid malposition and poor cosmetic outcome.28
Some treatments that aim to tackle skin laxity include laser resurfacing, radiofrequency, PRP and microneedling. These can help improve skin quality and elasticity, and achieve some improvement to the cosmesis of the area.29 Polynucleotide treatment has been shown to improve lower eyelid puffiness or oedema, likely due to its effect on angiogenesis and increased vascularity to the area.25
For those with prolapsed fat as the main cause of the eyebags, fat dissolving injections have been tried.30 Sodium deoxycholate injections have long been used within aesthetics to dissolve unwanted localised fat deposits.30 Studies, however, indicate that adverse events are common in this area, like bruising, oedema, pain, skin necrosis, diplopia and lid malposition, which can affect other surrounding tissues leading to problems like double vision.30,31
When treating the periocular area, it is key to remember that the eyelid skin is unique given the lack of subcutaneous fat and the important functional role the skin plays in protecting the ocular surface.32,33 Being the thinnest skin of anywhere in the body, it is prone to showing the first signs of ageing, making it a common area for patients to seek aesthetic improvement.34 These features also make it an unforgiving area to treat with complications like oedema, bruising, lid malposition and contour irregularities commonly reported from treatments.34 Those offering advanced aesthetic treatments to this area should familiarise themselves with the unique anatomy of the area and consider undertaking further advanced training.
The periocular area is often one of the first areas to show signs of facial ageing. Treatments to this area are popular, but can be associated with a high level of complications in inexperienced hands as the area is unforgiving to treat. A variety of surgical and non-surgical options are available to help patients tackle the most common concerns including hooded eyes, dark circles and under-eye bags or puffiness. The demand for non-surgical treatments is growing, and patients may present to aesthetic clinics rather than directly to oculoplastic surgeons who traditionally would treat ageing changes surgically. A good knowledge of the underlying anatomical changes can help guide you with regard to which options may be best for your patient.

Miss Jennifer Doyle is a consultant ophthalmic and oculoplastic surgeon based at The Clinic at Holland Park and at Milton Keynes University Hospital. She has a Bachelor’s in Medicine and a Bachelor of Surgery with distinction, as well as a Master’s in Medical Sciences from the University of Oxford. She is the non-surgical lead clinician at The Clinic at Holland Park.
Qual: BMBCh, MA(OXON), L7Cert, FRCOphth

Mr Richard Scawn is a consultant ophthalmologist and oculoplastic surgeon based at The Clinic at Holland Park and leads the oculoplastic service at Chelsea & Westminster NHS Trust. He specialises in complex eyelid reconstruction and periocular skin cancer work. He is a surgical wet lab instructor in London, Dubai and the US.
Qual: MBBS, BSc, FRCOphth


Transcending traditional lasers, harnessing the synergy of the unique powerful trio: CO2 Laser
A SCULPTING MAESTRO FOR DRAMATIC RESURFACING 1570nm Laser
BOOSTS COLLAGEN FROM WITHIN FOR LASTING REJUVENATION
UNLOCKING DEEPER
COSMECEUTICAL PENETRATION
Alma shares the promising new research behind the Alma Hybrid™ laser
Scars, a universal consequence of injury and surgery, can often leave a lasting physical and emotional impact. While they represent the body’s remarkable healing power, raised, discoloured, or itchy scars can significantly affect a person’s self-esteem and quality of life. In the UK, more than 20 million people are living with significant scarring, of which almost one quarter have said this caused significant emotional or physical problems.1 Traditionally, scar revision options have been limited, with varying degrees of success. However, the use of combining CO2 and 1570 nm laser wavelengths at once with the Alma Hybrid™ laser has emerged as a potential game-changer, backed by promising new research.
A recent publication, ‘Keloid and Hypertrophic Scars Treatment’ in Plastic Surgery, sheds light on the effectiveness of delivering ultra rapid sequential CO2 and 1570 nm lasers.2 The study evaluated the Alma Hybrid™ Proscan applicator on 61 patients with both keloid and hypertrophic scars.
The results were impressive. Hypertrophic and keloid scar patients experienced significant improvements in their Vancouver Scar Scale (VSS) scores (62% ± 8% and 58% ± 7, respectively). This indicates a marked improvement in scar appearance.2 Additionally, the study reported high patient satisfaction and minimal side effects.2 These findings position Alma Hybrid™ as a first line of treatment for scarring and a valuable addition to a practitioner’s portfolio.
The Alma Hybrid™ stands out for its unique ability to combine three highly powerful distinct yet complementary energy sources:
• CO2 laser: This ablative laser precisely removes surface irregularities while stimulating collagen production for improved texture.
• Erbium-glass laser: This non-ablative 1570 nm laser works deep within the skin, promoting collagen synthesis without damaging the surface.
• Ultrasound technology: This innovative feature facilitates deeper penetration of topicals and active ingredients to promote recovery and results.
The customisable synergy between the lasers is what truly sets the Alma Hybrid™ apart. Alma’s patented HyGrid™ technology weaves the lasers into the ideal sequential pattern for optimal tissue regeneration. Alternatively, in the case of serious scarring, the two lasers can be stacked on top of each other, allowing the CO2 to reach much more

Khatra Paterson, nurse prescriber and founder of KP Aesthetics:
“For many patients, prominent scars, particularly on the face, can be emotionally devastating. The Alma Hybrid™ allows me to finally offer them real hope for improvement. I treat a range of scars, from acne to traumatic scars. Critically, the Alma Hybrid™ is a key part of our surgical patient protocols, as we use it to prepare the skin for incision as well as for skin regeneration post procedure.”
“Having partnered with Alma last year, I gained invaluable insights from global scar experts at the prestigious Alma Academy in Italy, and honed my skills through exclusive 1-on-1 masterclasses. This experience has allowed the Alma Hybrid™ to become a workhorse in my clinic, utilising advanced scar revision techniques to give my patients incredible results.”


profound depths for seriously transformative results. Practitioners have complete control of adjusting ablative-to-non-ablative ratios to:
1. Treat a range of the most complex scars (hypertrophic and keloid) by precisely treating multiple skin layers with an ablative, thermal and coagulative effect at once.
2. Effectively balance results with recovery time for ultimate patient satisfaction.
3. Treat all skin tones, up to Fitzpatrick VI, with the correct preparation and aftercare.
This level of precision and control is unmatched in any other CO2 device, redefining both scar revision and advanced rejuvenation.
Alma is excited to connect new Alma Hybrid™ users with leading global scar experts at the upcoming Alma Academy Thailand, in September. This exclusive opportunity fosters collaboration and best practice sharing, propelling Alma Hybrid™ users to the forefront of the advanced scar revision field.
Embrace the future of scar revision – contact Alma today to learn more about the Alma Hybrid™: www.almalasers.co.uk
This advertorial was written and supplied by Alma Contact info@almalasers.uk to find out more

REFERENCES
1. The Scar Free Foudation commissioned a Censuswide poll of 1,000 UK respondents, September 2019. 28% said they had a scar [Accessed About Scarring — The Scar Free Foundation March,2024] 2. Menashe, S., Heller, L. Keloid and Hypertrophic Scars Treatment. Aesth Plast Surg (2024).

The first and original FDA-cleared energy device for the treatment of mild to severe acne.
BECOME A PROVIDER

Dr Nicole Chiang provides an overview of the most common facial dermatoses and the optimal treatments for each
There are many types of facial dermatoses (facial skin diseases), but each present very differently and are suitable for different aesthetic treatments.1 It is important for practitioners to be aware of how each type presents so they can assess, treat or refer them correctly and efficiently.
In this article, I will discuss the common facial dermatoses: acne, rosacea, eczema, psoriasis, lupus and actinic keratosis. I will touch on their key features, treatment options and key guidance on optimal technique.
When assessing the skin on the face, you should always start with a detailed medical history. In particular, practitioners should question the patient about:
• Previous skin conditions or rashes affecting the face
• Previous medical and aesthetic treatments performed on the face
• Current skincare
• Current medication
Examining the facial skin should form part of a routine facial assessment. Before performing any aesthetic treatments, practitioners should look to see if there is a rash due to any facial dermatoses, active skin infections or pre-cancerous or suspicious skin cancer lesions.
Acne
Acne is one of the most common facial dermatoses in the world, with a peak prevalence between the ages of 15 to 20 years in all ethnic groups.2 It is a chronic inflammatory process of the pilosebaceous follicle, and its pathogenesis is related to four factors: excessive sebaceous secretion, follicular hyperkeratinisation, presence of Cutibacterium acnes (C. acnes, formerly
known as Proprionibacterium acnes) in the pilosebaceous follicle and inflammatory processes entailed by the enzymatic action of this bacteria on the sebum.3
The clinical hallmarks are: seborrhoea, comedones (open comedones known as ‘blackheads,’ and closed comedones known as ‘whiteheads’) and inflamed lesions (papules, pustules, nodules and cysts). Early development of comedonal acne in girls and mid-facial presentation of acne in all genders may indicate more severe disease in later life.2,4
Clinical presentation can vary from mild comedonal lesions to severe inflammatory lesions associated with systemic symptoms (acne fulminans), fever, joint pains and skin ulcerations.2 Acne fulminans needs to be referred urgently for a combination of medical treatments, commonly oral prednisolone and isotretinoin.5
Early intervention in acne can lead to prevention of long-term sequelae including scarring, post-inflammatory erythema and pigmentary changes. There are multiple treatment options available when targeting acne.2
Topical medications
Topical retinoids aim to reduce sebum secretion and follicular hyperkeratinisation. Examples of these include tretinoin and
adapalene, which can be prescribed by medical practitioners. Moreover, topical antimicrobials aim to reduce C. acnes colonisation. Examples of these include:2
• Benzoyl peroxide
• Azelaic acid
• Erythromycin
• Clindamycin
• Sulfur
Oral medications
Hormonal contraceptives can help aid acne by reducing sebum secretion. On top of this, retinoids like isotretinoin (under prescription by a dermatologist) can help reduce sebum secretion and follicular hyperkeratinisation. Antimicrobials aim to reduce C. acnes colonisation, with examples including:2
• Tetracycline
• Doxycycline
• Lymecycline
• Minocycline
Laser and light therapies
Light therapies such as blue light, red light and intense pulsed light (IPL) can help acne sufferers by reducing C. acnes colonisation and providing anti-inflammatory properties. Laser therapies can reduce C. acnes and may induce thermal damage to sebaceous glands. Examples include:
• Pulsed-dye lasers (585 nm – 595 nm)
• Potassium titanyl phosphate lasers (KTP, 532 nm)
• Nd:YAG (neodymium-doped yttrium aluminium garnet, 1064 nm)
The advent of AviClear from Cutera has been revolutionary for the treatment of acne, as the 1726 nm wavelength selectively targets and downregulates the sebaceous glands (which is the principle culprit for acne).6 This laser presents an alternative option to oral isotretinoin without potential systemic adverse effects.6
As the face is our ‘visible self,’ many yearn for healthy, normal-looking skin which is essential for the maintenance of physical and mental wellbeing


Chemical peels
Chemical peels can be effective in reducing sebum secretion and follicular hyperkeratinisation.7 Examples include:
• AHAs e.g. amino fruit acid, glycolic acid, mandelic acid, tartaric acid
• BHAs e.g. salicylic acid
• Azelaic acid
• Trichloroacetic acid (TCA)
• Retinoic acid
• Pyruvic acid
• Lipohydroxy acid
• Jessner solution – a pre-mixed formulation containing 14% salicylic acid, 14% lactic acid and 14% resorcinol7
Rosacea
Rosacea is a chronic inflammatory disease affecting the centrofacial region, and the pathogenesis includes genetic susceptibility with dysregulation of immune and neurocutaneous mechanisms. Studies have reported possible associations of rosacea with increased risk of cardiovascular, gastrointestinal, neurological, auto-immune, psychiatric and cancers, especially in those with severe rosacea.8-10
The following diagnostic criteria were proposed by global rosacea consensus in 2017, and subsequently endorsed by the National Rosacea Society.11 Two features were independently diagnostic of rosacea, but in their absence, the presence of two or more major features can establish the diagnosis.10
Diagnostic features:
• Persistent centrofacial erythema with periodic intensification by potential trigger factors
• Phymatous changes
Major features:
• Flushing/transient centrofacial erythema
• Inflammatory papules and pustules
• Telangiectasia (excluding alar involvement)
• Ocular manifestations
• Lid margin telangiectasia
• Blepharitis
• Keratitis/conjunctivitis/sclerokeratitis
Minor features:
• Burning sensation of the skin
• Stinging sensation of the skin
• Dry sensation of the skin
• Oedema
From my experience, medical treatments such as topical azelaic acid, metronidazole, ivermectin and oral antibiotics are most effective at treating the inflammatory papules and pustules (papulopustular rosacea). I have found that IPL and vascular lasers (532 nm and 1064 nm wavelengths) are most effective at treating facial erythema and telangiectasias (erythema-telangiectatic rosacea). In my practice, I tend to use a combination of medical and laser therapies for patients with erythema-telangiectatic and papulopustular rosacea. Ablative lasers such as CO2 laser resurfacing are usually indicated for rhinophyma.11 Repeated laser treatments can result in longer-lasting

results, and maintenance laser sessions are often recommended as rosacea can recur with exposure to its triggers, commonly temperature change, exercise, ultraviolet radiation, alcohol and spicy food.11 Ocular manifestations may occur in 58-72% of patients with rosacea, and a third of affected patients can develop potentially life-threatening corneal involvement.12 It is important to advise your patients to see an ophthalmologist if they have any ocular symptoms associated with their rosacea.
Facial eczema can occur in isolation or as part of generalised atopic eczema.13 Often it has no identifiable cause, especially when pre-existing atopic eczema or chronic eczema is affecting other parts of the body. However, sometimes it can be due to contact dermatitis, or less commonly due to photosensitive dermatitis; in which case, a referral to the dermatologist for patch testing and photo-patch testing can be helpful. In general, the treatment of facial eczema consists of avoiding irritants in cosmetics, gentle skincare (containing humectants e.g. glycerin, aloe vera, urea, hyaluronic acid) for daily cleansing and actively treating the eczema with emollients and anti-inflammatory treatments (topical steroids for acute flares and topical calcineurin inhibitors for longer term treatment and maintenance).
From my experience, when treating a patient who has a previous or active history of eczema, it is best to minimise the use of chemical peels or skincare containing irritants such as retinoids, benzoyl peroxides, AHAs and BHAs, as these can potentially trigger an eczema flare.
Psoriasis is a common immune-mediated skin disease which affects 2-3% of the



Before performing any aesthetic treatments, practitioners should look to see if there is a rash due to facial dermatoses
Western population.14 Up to one third of adult patients with psoriasis have facial lesions.14 When presenting on the face, the key clinical features are sharply demarcated, red and scaly plaques.14 When it affects the hairline, there is usually an extension of scalp psoriasis. Plaques can be anywhere on the face, and it tends to be symmetrical. If the practitioner suspects psoriasis, it is important to look for psoriasis at other sites as well, as it can affect the ears, genitals, scalp, elbows, knees and trunk.15
Although highly efficacious, topical steroids are generally not ideal for facial psoriasis due to their various adverse effects including skin atrophy, striae, telangiectasias, perioral dermatitis and acneiform eruptions.14 Topical calcineurin inhibitors (such as topical pimecrolimus and tacrolimus) are off-licence alternatives as they are anti-inflammatory drugs that do not cause skin atrophy.14 Studies have shown good clinical improvement in psoriasis with light-emitting diode (LED) therapy with respect to erythema, in particular after blue light and to a lesser extent after red light therapy.16,17 If the psoriasis is more widespread involving other parts of the body, I often
find that treatment with a systemic therapy will also help to control psoriasis on the face. As psoriasis can ‘koebnerise’ (Koebner phenomenon is when there is an appearance of psoriasis on traumatised areas of skin), my advice is to avoid aesthetic treatments that can potentially induce minor injuries or lesions to the skin such as microneedling and ablative lasers, especially when there is an active flare of psoriasis.
Lupus erythematosus is an autoimmune, photosensitive disease that can present with a facial rash and systemic involvement. Cutaneous features occur in 75-80% of all patients with lupus erythematosus.19 Acute cutaneous lupus may present with a classical malar rash, erythematous macules or papules, or confluent, typically in a photosensitive distribution, sparing the nasolabial folds. Chronic cutaneous lupus tends to present with discoid plaques with hyperkeratosis. There can also be involvement of the V region of the neck, extensors of the limbs, scalp, trunk and mucosa.19
In mild cases, especially when the face is involved, treatments such as topical steroids and calcineurin inhibitors can be
sufficient for disease control.20
Platelet-rich-plasma has been used with good effect in lupus patients with scarring alopecia due to discoid lupus plaques.21
Laser treatments are best avoided in lupus patients due to the possible risk of ultraviolet and visible light triggering a flare of the disease.20 There is also some concern that injectable treatments may cause disease reactivation via antigenic stimulation.20
Actinic keratosis is a pre-cancerous skin lesion which develops when ultraviolet radiation induces abnormal keratinocyte development.23 Clinically, actinic keratosis presents as a scaly red macule or patch. It is important to identify these lesions early for treatment as there is an approximately 1% risk of progression to squamous cell carcinoma per lesion in 10 years.23
Photodynamic therapy, cryotherapy, topical imiquimod, 5-fluorouracil (5-FU), ingenol mebutate, diclofenac sodium, TCA, fractional ablative laser (such as erbium:YAG and CO2 lasers), surgical curettage and cautery are all effective treatment options for actinic keratosis.22 Regular use of sun protection has been shown to prevent the development of new actinic keratoses and increase the remission of the existing lesions.23
As our facial skin is our ‘visible self,’ many yearn for healthy, normal-looking skin which is essential for the maintenance of our physical and mental wellbeing. As facial dermatoses are common, having good knowledge of them can help ensure that patients are treated/referred appropriately and complications are minimised. Understanding the key features and treatment options of common facial dermatoses can help a practitioner provide better treatment or referral outcomes for patients.

Dr Nicole Chiang is a consultant dermatologist with experience in both medical and cosmetic dermatology. She is the director of Lumiere Clinic in Manchester and carries out regular teaching in dermatology to a wide range of healthcare professionals.
Qual: MBChB(Hons), MRCP(UK)(Derm), FRCP(UK), PGCert Aesthetic Medicine (Hons)

Botulinum toxin type A
Over 100 million treatments delivered worldwide for aesthetics indications to date 1
Fast-acting and long-lasting, patients saw results as early as 24 hours 2-5 and for up to 5 months. 2-4,6-9
Order now at www.medfx.co.uk
Azzalure Prescribing Information (UK)
Please refer to the Prescribing Information for important safety information and to the Summary of Product Characteristics before use.
Presentation: Botulinum toxin type A (Clostridium botulinum toxin A haemagglutinin complex) 125 Speywood units (powder for solution for injection)
Indications: Temporary improvement in appearance of moderate to severe:
• Glabellar lines seen at maximum frown, and/or
• lateral canthal lines (crow’s feet lines) seen at maximum smile in adult patients under 65 years, when severity of these lines has an important psychological impact on the patient.
Dosage & Administration: Azzalure should only be administered by a healthcare practitioner with appropriate qualifications and expertise in this treatment and having the required equipment, in accordance with national guidelines. Botulinum toxin units are different depending on the medicinal products. Speywood units are specific to this preparation and are not interchangeable with other botulinum toxins. Reconstitute prior to injection. Intramuscular injections should be performed using a sterile suitable gauge needle. Glabellar lines: recommended dose is 50 Speywood units divided equally into 5 injection sites, 10 Speywood units to be administered intramuscularly, at right angles to the skin; 2 injections into each corrugator muscle and one into the procerus muscle near the nasofrontal angle. Lateral canthal lines: recommended dose per side is 30 Speywood units divided into 3 injection sites; 10 Speywood units to be administered intramuscularly into each injection point, injected lateral (20 - 30° angle) to the skin and very superficial. All injection points should be at the external part of the orbicularis oculi muscle and sufficiently far from the orbital rim (approximately 1 - 2 cm); (See summary of product characteristics for full technique). Treatment interval should not be more frequent than every three months. The efficacy and safety of repeat injections of Azzalure has been evaluated in Glabellar lines up to 24 months and up to 8 repeat treatment cycles and for Lateral Canthal lines up to 12 months and up to 5 repeat treatment cycles. Not recommended for use in individuals under 18 years of age. Contraindications: Hypersensitivity to botulinum toxin A or to any of the excipients. In the presence of infection at the proposed injection sites, myasthenia gravis, Eaton Lambert Syndrome or amyotrophic lateral sclerosis. Special warnings and precautions for use: Care should be taken to ensure that Azzalure is not injected into a blood vessel. Use with caution in patients with a risk of, or clinical evidence of, marked defective neuro-muscular transmission, in the presence of inflammation at the proposed injection site(s) or when the targeted muscle shows excessive weakness or atrophy. Patients treated with therapeutic doses may experience exaggerated muscle weakness. Not recommended in patients with history of dysphagia, aspiration or with prolonged bleeding time. Seek immediate medical care if swallowing, speech or respiratory difficulties arise. Facial asymmetry, ptosis, excessive dermatochalasis, scarring and any alterations to facial anatomy, as a result of previous surgical interventions should be taken into consideration prior to injection. Dry eye has been reported with the use of Azzalure in the treatment of glabellar lines and lateral canthal lines. Reduced tear production, reduced blinking, and corneal disorders, may occur with the use of botulinum toxins, including Azzalure. Injections at more frequent intervals/higher doses can increase the risk of antibody formation to botulinum toxin. Clinically, the formation of neutralising antibodies may reduce the effectiveness of subsequent treatment. Botulinum toxin units are not interchangeable from one product to another. Doses recommended in Speywood units are different from other botulinum toxin preparations. To be used for one single patient treatment only during a single session. In order to improve the traceability of biological medicinal products, the name and the batch number of the administered product should be clearly recorded. There is a potential risk of localised muscle weakness, visual disturbances or asthenia linked with the use of this medicinal product which may temporarily impair the ability to drive or operate machinery. Interactions: Concomitant treatment with aminoglycosides or other agents interfering with neuromuscular transmission (e.g. curare-like agents) may potentiate effect of botulinum toxin. Pregnancy, Breast-feeding and Fertility: Pregnancy: Azzalure should not be used during pregnancy. There are no adequate data from the use of botulinum toxin type A in pregnant women. Studies in animals have shown reproductive toxicity at high doses. The potential risk for humans is unknown. Breast-feeding: There is no information on whether Azzalure is excreted in human milk. The use of Azzalure during lactation cannot be recommended. Fertility: There are no clinical data from the use of Azzalure on fertility. There is no evidence of direct effect of Azzalure on fertility in animal studies.
Side Effects: Most frequently occurring related reactions are headache and injection site reactions for glabellar lines and; headache, injection site reactions and eyelid oedema for lateral canthal lines. Generally, treatment/ injection technique related reactions occur within first week following injection and are transient. Undesirable effects may be related to the active substance, the injection procedure, or a combination of both. For glabellar lines: Very Common (≥ 1/10): Headache, Injection site reactions (e.g. erythema, oedema, irritation, rash, pruritus, paraesthesia, pain, discomfort, stinging and haematoma). Common (≥ 1/100 to < 1/10): Temporary facial paresis (due to temporary paresis of facial muscles proximal to injection sites, predominantly describes brow paresis), Asthenopia, Eyelid ptosis, Eyelid oedema, Lacrimation increase, Dry eye, Muscle twitching (twitching of muscles around the eyes). Uncommon (≥ 1/1,000 to <1/100): Dizziness, Visual impairment, Vision blurred, Diplopia, Pruritus, Rash, Hypersensitivity, Rare (≥ 1/10,000 to < 1/1,000): Urticaria, Eye movement disorder. For lateral canthal lines: Common (≥ 1/100 to < 1/10): Headache, Temporary facial paresis (due to temporary paresis of facial muscles proximal to injection sites), Eyelid ptosis, Eyelid oedema and Injection site reactions (e.g. haematoma, pruritus and oedema). Uncommon (≥ 1/1,000 to <1/100): Dry eye. Post-marketing experience: frequency not known (cannot be estimated from the available data): asthenia, fatigue, influenza-like illness, hypersensitivity, hypoaesthesia and muscle atrophy.
Adverse reactions resulting from distribution of the effects of the toxin to sites remote from the site of injection have been very rarely reported with botulinum toxin (excessive muscle weakness, dysphagia, aspiration pneumonia with fatal outcome in some cases).
Prescribers should consult the summary of product characteristics in relation to other side effects.
Packaging Quantities & Cost: 2 Vial Pack (2 x 125u) £126.99 (RRP)
Marketing Authorisation Number: PL 06958/0031
Legal Category: POM
Further information is available from: Galderma (UK) Limited, Evergreen House North, Grafton Place, London, NW1 2DX, UK. Tel: +44 (0) 300 3035674
Date of Revision: May 2024
Adverse events should be reported.
Reporting forms and information can be found at www.mhra.gov.uk/yellowcard or search for Yellow Card in the Google Play or Apple App Store. Adverse events should also be reported to Galderma (UK) Ltd, E-mail: medinfo.uk@galderma.com Tel: +44 (0) 300 3035674
References: 1. Galderma Data on File MA-52573; 2. Kassir R et al. Dermatol Ther (Heidelb) 2013;3(2):179–189; 3. Maas C et al. Aesthet Surg J 2012;32(1 Suppl):S8–S29; 4. Monheit GD et al. Dermatol Surg 2020;46(1):61–69; 5. Moy R et al. Arch Facial Plast Surg 2009;11(2):77–83; 6. Warren H et al. Plast Surg Nurs 2020;40(1):37–44; 7. Brandt F et al. Dermatol Surg 2009;35(12):1893–1901; 8. Rzany B et al. Dermatol Surg 2007;33(1 Spec No):S18–S25; 9. Gubanova E et al. Aesthet Plast Surg 2018;42(6):1672–1680.




Title: Minimally Invasive Post-Acne Scars Treatment with the Hybrid Filler HArmonyCa
Authors: Barone M, et al
Published: International Society of Aesthetic Plastic Surgery, May 2024
Keywords: Acne Scars, Hybrid Filler, HArmonyCa
Abstract: While various treatments exist, including surgical and non-surgical approaches, a combined method has shown promise in effectively addressing acne scarring. Lipofilling, with its adipose-derived stem cells, has emerged as a promising technique for volume restoration and collagen stimulation but may not be suitable for all patients, especially those who prefer non-surgical treatments. Recently, a novel approach involving simultaneous injection of hyaluronic acid (HA) and calcium hydroxyapatite (CaHa) has been introduced in the literature, showing lifting properties, improving dermal thickness and skin texture and inducing neocollagenesis. HArmonyCa (Allergan Aesthetics, an AbbVie Company) is a hybrid filler combining HA (20 mg/mL) and CaHa 55.7% (microspheres 25-45 µm) with 0.3% lidocaine in a 1.25-ml syringe. It has demonstrated volumising, lifting and skin-tightening effects, along with increased fullness, elasticity and turgor of the skin. It has also shown an increase in viscoelasticity, suggesting new collagen formation, making it suitable for treating conditions like solar elastosis. Compared to lipofilling, HArmonyCa offers a non-surgical alternative with comparable outcomes and patient satisfaction. These findings have led us to employ this hybrid filler for the treatment of post-acne scarring.
Title: Treatment of Periorbital Veins with Vascular Laser: A Systematic Review and Retrospective Case Series
Authors: Mandavia R, et al.
Published: Journal of Cosmetic Dermatology, April 2024
Keywords: Laser, Periorbital Veins, Vascular
Abstract: This article aims to systematically review the literature on the safety and effectiveness of vascular laser treatment for periorbital veins. Patient records were retrospectively reviewed from January 2020 to November 2023 to identify all patients who underwent laser treatment for periorbital veins. Outcomes assessment included percentage improvement, patient overall satisfaction and adverse effects. Three articles were included discussing treatment of blue periorbital veins using a 1064 nm Nd:YAG laser. 34 patients with skin Types I–V were included. Patient Fitzpatrick skin Types I–IV were treated with high patient satisfaction rates and complete clearance of treated veins. Adverse effects included pain, erythema, mild oedema, urticaria and blister formation. Blue and red periorbital veins were treated using 1064 and 532 nm wavelengths respectively. Mean percentage improvement was 4.8 (complete resolution) and patients’ overall satisfaction was ranked three (completely satisfied). Adverse effects included erythema, oedema and bruising. Treatment of red and blue periorbital veins using 532 and 1064 nm vascular lasers appears a safe treatment option. The procedure has a short recovery time with patients able to resume normal activities within one day of treatment.
Authors: Algarin YA, et al.
Published: Archives of Dermatological Research, May 2024
Keywords: Rosacea, Vitamins, Supplements
Abstract: Rosacea is a common inflammatory skin condition displaying symptoms like flushing, erythema, papules and pustules. Our review investigates the role of vitamins and minerals in rosacea, and provides evidence-based recommendations for supplementation and topical treatment of these nutrients for rosacea. An online search was performed on PubMed, Web of Science, Science Direct, Google Scholar and ClinicalTrials.gov from 1998 to 2023. Included studies were summarised and assessed for quality and relevance in rosacea management. Vitamin A derivatives, specifically oral isotretinoin, demonstrated significant efficacy, with a 90% reduction in lesions, complete remission in 24% of patients and marked improvement in 57% of patients. Vitamin B3 derivatives, such as topical 1-methylnicotinamide 0.25% and NADH 1%, improved symptoms in 76.4% (26/34) and 80% of patients, respectively. Outcomes for vitamin D, vitamin C and zinc supplementation varied across studies. However, zinc sulfate solution 5% significantly reduced acne rosacea severity for patients with 40% and 60% exhibiting a moderate or good response, respectively. Omega-3 fatty acids showed significant improvement in alleviating xerophthalmia in 64% of patients with ocular rosacea.
Title: A Practical Algorithm for Integrating Skincare to Improve Patient Outcomes and Satisfaction With Energy-Based Dermatologic Procedures
Authors: Lain E, et al.
Published: Journal of Drugs in Dermatology, May 2024
Keywords: Skincare, EBDs, Antiageing
Abstract: Medical aesthetic procedures for facial antiageing with laser and energy-based devices (EBDs) are rapidly increasing, but standards integrating skincare before, during and after these treatments are lacking. The algorithm for integrated skincare for facial antiaging treatment with EBDs aims to stimulate healing, reduce downtime and improve comfort and treatment outcomes. A panel of eight global physicians employed a modified Delphi method and reached a consensus on the algorithm integrating skincare based on the best available evidence, the panel’s clinical experience and opinions. The algorithm has a pre-treatment (starts two - four weeks before the procedure) and treatment (day of treatment) section, followed by care after the procedure (zero - seven days) and follow-up care (one - four weeks after the procedure or ongoing). Applying a broad-spectrum sunscreen with an SPF 50 or higher combined with protective measures is recommended to protect the face from sun exposure. Dyschromia is a significant concern for those with skin of colour. Clinicians may recommend skincare using a gentle cleanser and moisturiser containing vitamins C and E, retinoid, or other ingredients such as niacinamide, kojic acid, liquorice root extract, azelaic acid and tranexamic acid, depending on the patient’s facial skin condition.
Aesthetic patients are taking a greater interest in their appearance, and the market for non-invasive cosmetic procedures shows no signs of slowing. In 2023, the specialty was expected to be worth £45.5 billion globally, and this is only increasing in 2024.1 It’s a trend that is set to continue – at least until 2027, and probably beyond.1 To satisfy the demand, clinics are relying on more sophisticated devices and equipment. According to the latest GlobalData report, the aesthetic devices market (currently valued at US $13.4 billion) is expected to grow at a compound annual growth rate (CAGR) of 6.1% over the next 10 years.1
What does this greater demand all mean? Well, clinics and practices will have a larger body of patients searching for their services, wanting access to an expanding range of treatments. In turn, device manufacturers and distributors will continue their race to innovate, embracing the latest technologies to develop more effective offerings to satisfy this demanding, burgeoning market.
On the flip side, the continual expansion and development will doubtless attract new operators who will be keen for a slice of the pie. For those already established in the aesthetics specialty and who have a happy, loyal patient base, keeping the market share may become a challenge. So, how can aesthetic clinics counter increased competition and still satisfy patient expectations? And, just how can leasing help with this?
State-of-the-art equipment can help you outshine the competition. New usually means faster, more effective and more efficient (although it’s vital to do your research as this is not always the case). Having the latest kit can also minimise maintenance needs and limit downtime. Whether it’s replacing existing outdated equipment, or venturing into new treatments and technology, clinics who embrace new
technologies can help them stay ahead in the race. However, the latest technology can be a great cost to your clinic. If you’re a practitioner who wants to stay ahead of the game while being cost efficient, leasing can be a good alternative to purchasing expensive equipment outright.
Leasing allows your business to use an asset in exchange for rental payments over a set period. It works as a rental agreement where you make regular payments for as long as the lease contract runs. At the end of the contract, you may have an option to continue renting, to return or upgrade, or even buy the equipment. A variety of other benefits are outlined below.
You’ll need to check with your accountant to confirm how it applies to your specific circumstances, but for most businesses, lease rental payments can be offset against taxable income. Plus, as VAT can also be reclaimed on these, the overall acquisition cost can be significantly reduced.5
With a lease, you only have to pay a relatively small amount upfront – usually equivalent to a periodic monthly or quarterly rental payment – rather than wait until you have all the funds in place. This allows you to have the equipment you need sooner rather than later.
Once the equipment is in, you are ready to start earning money from it. This provides valuable revenue to help, perhaps even cover, those monthly or quarterly leasing payments.
Aesthetic clinics want to implement the best devices on the market into their practices and to work with the recognisable companies in the specialty. Leasing allows a clinic to spread the cost and to choose the highest quality or enhanced version of equipment, rather than simply the cheapest option. As cheaper can often mean an inferior-quality import, you are able to access technology that is durable and robust.
Credit lines – think bank loan, overdraft facility, credit card limits, etc. – are a vital resource and practitioners never know when they might need them. A lease secured on equipment keeps these precious lines of credit protected and accessible, should you need money in a hurry.

Aesthetic practitioner Dr David Eccleston is the founder of MediZen, an aesthetic clinic in the Midlands. Keen to innovate and invest in the latest equipment, Dr Eccleston has long been an advocate of leasing. Over the years, MediZen had accumulated a portfolio of leases from a raft of providers, all set to mature at different intervals.
An external audit of this portfolio identified a raft of duplicated and unnecessary leasing costs. Using its findings, MediZen was able to save more than £20,000 of additional, non-contractual leasing charges and out-of-term payments and generate an immediate insurance refund of £3,000.
Dr Eccleston commented, “Leasing in its many forms can be the key to introducing an otherwise unaffordable new device to your clinic. However, it is important to do your homework beforehand – you do not want to invest in a device for which there is little demand. Talk to colleagues about their experience with new devices that you may be considering before you commit. Speaking from personal experience, always read the small print in the lease documentation. We have been caught out in the past by leases with no end date, additional unwanted bolt-on insurance, and other additional costs. After an in-depth independent analysis of all our active leases, we managed to save thousands of pounds in future costs.”
When you’ve invested in recruiting and training a great team, you’ll be keen to ensure that they are well-utilised and that your clinic is performing at peak efficiency. To do this, you need to supply your staff with the best tools and technologies out there, and leasing can help them access those without costing the clinic too much.
Technology in aesthetics moves apace, and it can seem that today’s latest gadget is obsolete before you have even got to grips with it. Many equipment vendors will offer the opportunity to upgrade during the term of the lease, and if you have already made a significant number of periodic payments, it will have a barely noticeable impact on your regular payments.
Naturally, should you choose to lease your equipment, you would want to check that any prospective equipment vendor can fulfil your agreement with them and stick around to honour any guarantees. It is best to include a competent funder in the deal so you can be rest assured that they will also have undertaken ‘due diligence’ essentially doubling the comfort. The funder provides funds to the leasing company, effectively purchasing the equipment. Subsequently, the practitioner rents the equipment from the funder, who becomes the new equipment owner.
In the UK, leasing companies are highly regulated by the Financial Conduct Authority (FCA) whose role it is to ‘protect and promote the interests of businesses who require credit related activities’.6 So, if your leasing provider is authorised by them – you can check on the FCA online register – practitioners can relax knowing that the weight of the law is on your side.
Chances are that any quotation for new kit will propose an outright purchase cost, alongside a monthly or quarterly lease rental alternative. Sales-led organisations understand the leasing benefits and often partner with a reputable funder knowing that it will help them close more deals. Similarly, a leaser knows their money is better safeguarded when secured against robust, reliable equipment.
With a business loan, the Annual Percentage Rate (APR) – the interest rate plus the additional fees charged with the loan – is a simple way to benchmark a good deal. When it comes to a lease, additional factors such as credit worthiness and risk, equipment depreciation and residual value, agreement term, insurances and maintenance costs, for example, all contribute to the costs. There is no APR for leasing as such, and so, for the uninitiated, calculating if it is a good deal can be tricky. So, as with any other contract, it makes sense to comb through the terms and conditions. If you’re not sure, make sure to
check with your accountant or an external leasing expert.
It’s also important to be aware that leasing may not be perfect for all aesthetic clinics, for example:
• Practices with a poor credit rating, or new businesses with no credit history, as they may struggle to find a funder who will accept them.
• Practices that prefer to ‘sweat the asset’ – that is, avoid replacing or upgrading to new technology until it wears out.
• Practices that are cash-rich or cash-driven and who are averse to paying interest and prefer to see an asset on their balance sheet.
For clinical practices looking at acquiring new equipment, it is always worth considering leasing. In some instances, it makes sound business sense. First and foremost, financially. It is tax efficient, allowing you to spread the equipment cost and, critically, profit from the equipment while you pay for it. The time for acquisition is cut as you don’t have to save or wait for cashflow to be perfectly aligned, and you are often better protected by the additional due diligence and supplier validation a competent leaser undertakes. You can also factor in the potential customer service benefits of better staff utilisation, the ‘better vs. cheaper’ choice of equipment and access to upgraded equipment it offers. Leasing can prove to be a great alternative to outright equipment purchase.
Disclaimer: Helen George is the founder of HLG Consultancy which helps practitioners with leasing enquiries.

Helen George has spent more than 30 years in the UK leasing industry and now leads HLG Consultancy. Her understanding of how lenders generate profits, often resulting in customers paying more than necessary, allows her to bring cost savings to professional practices, firms, and clinics.




Become an Elite Member today! The ultimate platform for aesthetic professionals to unite, share knowledge, collaborate & learn






Discover, network & celebrate medical aesthetics

Recognise and celebrate excellence

The UK’s leading resource for medical aesthetic professionals
Uniting the specialty to shape the future of medical aesthetics

Nurse prescriber Julie Scott explores the impact and necessity of saying ‘no’ to safeguard patient wellbeing and professional reputation
As aesthetic practitioners, we’re often lauded for our contributions to building the self-esteem of our patients. Yet, there’s an aspect of our work that is an even more crucial part of our toolkit, and that is the ability to say ‘no’. After three decades in aesthetics, I’ve learnt that this decision is just as important as any procedure we perform. It’s deeply rooted in our commitment to our patients’ health and the ethical pillars that have held up my practice through the years. Saying ‘no’ is not a sign of limitation, but a mark of professional maturity and understanding. In my practice, the decision to forgo treatment is a multifaceted judgment call, it’s never just about saying ‘no’. Instead, it’s about recognising when a patient, perhaps reeling from recent emotional trauma, needs space to heal beyond the skin, seeking enhancements for their self-esteem, not because of a partner’s wish or societal nudges. It’s about ensuring there’s mutual trust, that we’re on the same page, and if not, having the wisdom to step back. I respect the limits of my expertise, and if any treatment is beyond my scope of practice, I’ll guide the patient to someone within my referral network who can help, because patient welfare trumps all. And when the scales tip, where the risks outweigh the benefits or I sense hesitation in their eyes, I trust my medical instincts to put my patient’s health and wellbeing first. Whether it’s clinical indications, managing expectations, or addressing mental wellbeing issues like body dysmorphic disorder, each ‘no’ comes from a place of professional care and responsibility.
The complexity of refusing a patient lies in the confluence of our professional aspirations and our human instincts. As practitioners, we are innately driven by a desire to heal, to enhance and to bring joy through our work. This inherent urge makes the word ‘no’ feel like a contradiction to our very purpose.
Why, then, does it often twist in our gut? It’s because our profession is not just about providing a service; it’s about cultivating wellbeing. When patients come to us, often after extensive research or following our practices on social media, they come with a trust that we’re the ones who can fulfil their expectations. To turn them away feels like a breach of an unspoken promise, a denial of the help and support we are trained and inclined to give.
The difficulty is magnified in the intimate setting of my consultation room, where the dynamic shifts to a personal interaction – no longer just a practitioner and a patient, but two people sharing a space of vulnerability. Here, the decision to say ‘no’ becomes singularly ours, a solitary verdict where we must balance empathy with ethical practice. To mentally manage these difficult decisions, practitioners must often reflect deeply on the
ethics and care that guide us. This inner reflection helps reconcile the dissonance between our desire to help and the need to decline. Building a network of peers for support, participating in professional discussions and seeking mentorship can significantly bolster our psychological resilience and affirm our choices. This moment of refusal can be particularly anxiety-inducing for practitioners in the early stages of their careers. They may not yet have the breadth of experience to fall back on, and each ‘no’ can feel like an insurmountable hurdle. For those who’ve learnt how to say ‘no’, the challenge, while still present, may be less daunting. It’s a learnt art – recognising that ‘no’ is not a negation but a necessary part of patient care.
The General Medical Council, Nursing and Midwifery Council and General Dental Council all converge on a core directive: healthcare professionals must place patient care at the forefront, prioritising safety, needs and interests, while fostering a practice rooted in consent, efficacy and trust.1,2,3 We must also acknowledge the reality that relationships with patients often begin long before they step into our clinics. Patients arrive with expectations fuelled by the successes they’ve seen us showcase online. This adds a layer of complexity to our interactions, where the decision to decline a request is not just clinical – it’s personal. In these moments, we must draw on our deepest reserves of professionalism and compassion. We find ourselves explaining, educating and sometimes comforting –because even when we can’t say ‘yes,’ we still have a responsibility to leave our patients feeling cared for and understood. This is the essence of why saying ‘no’ is so difficult – it’s a direct confrontation with our instinct to serve, a balancing act between the duty to our patient’s wellbeing and the boundaries of what is safe, reasonable and in their best interest.
Saying ‘no’ to a patient is, undeniably, one of the most complex aspects of our practice, it’s a delicate balance of judgment, where sometimes the steps aren’t as clear-cut as we’d like. There are instances where practitioners, perhaps out of a desire to please or due to the persuasive nature of a patient, may bypass their better judgment. They might proceed with a treatment that their instincts – whisper against treating. This is not the ideal choice, but it’s an
understandable human response to a challenging situation. It’s the art of saying ‘no’ that we must refine.
Patients can indeed be compelling, showering compliments or expressing a deep trust that can make it harder for practitioners to hold their ground. This can be especially true when there is a financial component involved. After a patient has paid for a consultation, the decision to then decline the treatment can leave a practitioner feeling uncomfortable. In such cases, whether to issue a refund depends on the situation. If the patient isn’t clinically indicated for the treatment, a refund could be appropriate. However, given that consultations involve valuable professional advice, refunds are not always warranted and I feel it should be left to the practitioner’s discretion.
Another layer of this complexity is the self-doubt that may creep into a practitioner’s mind. Will the patient think I’m incapable or lacking in skill because I’ve said ‘no’? This doubt can be a significant hurdle. It’s important to remember that our primary role is to ensure the safety and appropriate care of our patients, even if that means turning down a procedure.
For those who have transitioned from the NHS, where the focus is squarely on delivering care, the shift to aesthetics, where services are sought and chosen, can be stark. Here, in aesthetics, we navigate a different kind of patient-practitioner relationship, one where the choices aren’t always as clear, and the decisions often rest heavily on our shoulders. But it’s these moments that truly test – and ultimately showcase – the integrity of our practice and the depth of our commitment to patient welfare.
How to communicate ‘no’ with passion
Refining the ability to say ‘no’ in a manner that is both compassionate and professional is a vital skill to hone. The tools we use are linguistic and empathetic, designed to maintain the dignity and respect of the patient-practitioner relationship. It’s about framing our responses in a way that conveys understanding and care. Starting sentences with “Sadly, I can’t move forward with this...” or “I wish I were able to...” indicates that while the willingness to help is there, the decision is governed by broader considerations of safety and appropriateness.
When alternatives are available, guiding the conversation towards those is another tool. “While I can’t endorse this particular
treatment, I believe there are other avenues we can explore...” This approach not only softens the ‘no’ but also opens a pathway to ‘yes’ for more suitable treatments, balancing the patient’s wishes with what is clinically indicated. For example, when further dermal fillers are sought, and the request goes beyond what might harmonise the patient’s natural features, I advocate for a less is more philosophy.
For patients struggling with mental health concerns or unrealistic expectations, the tool of redirection is essential. “It seems we’ve reached a point where we should pause and reassess your goals...” or “I’m here to support you, and part of that support is ensuring we don’t take steps that might not benefit you in the long run.” In my clinic, I ensure I have appropriate referral pathways for such circumstances, demonstrating that we are looking out for the patient’s broader wellbeing, not just the immediate gratification of treatment. These statements and actions show a commitment to holistic care which prioritises long-term health. Each of these tools – careful language, rational explanation, exploration of alternatives, redirection and positive framing – are facets of the art of saying ‘no’. They allow you to stand firm in your professional integrity while ensuring the patient feels seen, heard and respected. When faced with a negative reaction to such a refusal, practitioners can maintain this integrity by remaining calm, listening actively to the patient’s concerns and reiterating the rationale with empathy and patience. It’s about providing a space for patients to express their disappointment or frustration, while gently guiding the conversation back to the patient-centred reasoning behind the decision.
Saying ‘no’ can be an incredibly powerful thing. I once had a beautiful young patient who came to me seeking multiple treatments to align with a beauty standard she felt pressured to meet. She believed these changes were essential. However, through the course of our hour-long consultation – a crucial practice in my clinic to ensure comprehensive understanding and patient care – we delved into the heart of her perceptions and desires.
In that hour, our conversation shifted from procedures to perception resulting in a newfound confidence and reassurance in her own skin, allowing her to see her
natural beauty through a new lens. We then embarked on a different kind of journey – one that didn’t involve needles; instead I created a personalised skincare plan, tailored specifically to enhance her natural skin health. As a result of our consultation, she left a glowing review, capturing her renewed self-image and gratitude. She didn’t just become a satisfied patient; she turned into a passionate advocate, referring friends to my clinic, further affirming the power of a thoughtful, personalised approach to patient care.
This moment encapsulates the positive side of a well-considered ‘no’. It’s about more than refusal; it’s about affirming the inherent value in each individual who steps into our clinics. When patients understand that our advice is rooted in their best interests rather than the clinic’s revenue, trust is deepened. A ‘no’ can become the foundation of a stronger, more honest relationship. It’s a testament to the practitioner’s integrity and dedication to the true wellbeing of our patients.
In the landscape of aesthetics, where enhancement meets ethics, the strength to say ‘no’ is as vital as the skill of injecting. Over the years, I’ve learned that these moments of refusal, though often fraught with complexity, are also filled with the potential for growth and understanding.
A considered ‘no’ can be the most affirmative response we give, guiding our patients towards a beauty that’s more than skin deep. It’s in these choices that we find the core of our practice – not just in the treatments we provide, but in the wellbeing and confidence that we foster.

Julie Scott is an independent nurse prescriber, Level 7 qualified aesthetic injector and trainer with over 30 years of experience in the field of plastics and skin rejuvenation. She is an aesthetic mentor, and international speaker, who has won the prestigious Aesthetic Nurse Practitioner of the Year 2022/2024 and Best Clinic South of England 2023 at the Aesthetics Awards. Qual: INP
Graham
Matthews shares advice on the steps to take towards becoming a zero-waste clinic
In an era where sustainability is not just appreciated but expected by customers, the aesthetics specialty still has a long way to go. Clinics are traditionally high consumers of single-use products and big waste generators, so it’s time to start looking towards a more sustainable future. Zero-waste practices can be truly transformative to your business if you can find a way to implement them without compromising on hygiene and patient safety. In 2024 people have a much more positive view of businesses that care about sustainability and their carbon footprint, so clinics that show efforts towards greener practices can differentiate themselves in a crowded market.1 In fact, a recent study found that 55% of UK consumers say living sustainably is important for society, and they are actively trying to live more sustainable lives – which is bound to include their purchasing decisions.2
The journey to becoming a zero-waste clinic may not be the easiest, but in 2024 it’s becoming increasingly achievable. In this article, I will share tips on how to take the first steps towards that zero-waste goal.
The first step in the transition to becoming a zero-waste business is understanding the scope of the waste you generate. This includes everything from product packaging and cleansing wipes, to hazardous chemicals. The environmental impact of such waste is significant, contributing to landfill growth, pollution and resource depletion. A waste audit is a critical step for any clinic
embarking on the journey to zero-waste. This involves a detailed analysis of the waste produced, providing insights into the volume and types of waste generated, and identifying opportunities for reduction, reuse and recycling. Here’s a deeper dive into how to conduct a waste audit, and what areas it should cover.
• Set clear objectives: Define what you hope to achieve with the audit. Objectives may include identifying the most common types of waste, understanding the sources of waste and pinpointing opportunities to reduce waste volume.
• Gather a team: Assemble a team responsible for conducting the audit. This should include staff members from various parts of the clinic to ensure a comprehensive understanding of all waste streams.
• Choose a time frame: Decide on the duration of the audit. A week is often a good starting point, as it provides a snapshot of typical waste patterns without being overly burdensome.
• Collect waste: Instead of disposing of waste as usual, separate it into designated bins or bags. It is important to categorise waste into types (e.g. plastic, paper, organic, chemical) and, if possible, subcategories (e.g. recyclable plastics, non-recyclable plastics).
• Weigh and record: At the end of the collection period, weigh each category of
waste and record the data. This quantifies the waste output and highlights the most significant waste streams.
• Analyse usage and disposal practices: Look at how products and materials are being used that creates waste. Are there single-use items that could be replaced with reusable alternatives? Do some products come in excessive packaging? Understanding these practices is key to identifying areas for improvement.
• Product packaging: Many clinic products come in plastic bottles, containers or vials. Identifying the volume of packaging waste can highlight opportunities to switch to bulk products or brands with sustainable packaging.
• Single-use items: Items like gloves and wipes contribute significantly to waste. The audit should assess the quantity of these items being discarded.
• Chemical waste: Clinics often use products with hazardous chemicals that require special disposal methods. The audit should carefully quantify this waste stream and explore safer alternatives.
• Water usage: While not a form of solid waste, water is a critical resource that is often wasted in large quantities. Monitoring water usage during the audit period can identify areas for conservation.
• Review and analyse data: With all data collected, analyse the findings to understand the biggest areas of waste production. Look for patterns or surprises in the data that could inform your waste reduction strategy.
• Develop an action plan: Based on the audit’s findings, create a targeted action plan to reduce waste. This might include switching to bulk product purchases, implementing a recycling programme or investing in reusable alternatives to single-use items.
• Engage suppliers and partners: Share your findings with product suppliers and waste management partners. They may offer solutions or alternatives that can help reduce your waste footprint.
Review your current products and suppliers. Is there an opportunity to switch to suppliers that are more focused on sustainability? For instance, suppliers which source ingredients ethically, use renewable energy in production
and take back packaging for recycling or reuse. Once the suppliers are chosen, the products’ packaging should be next. Look for products that use materials like glass, metal or compostable plastics. These materials can either be recycled or break down without harming the environment. For example, glass bottles can be infinitely recycled without loss of purity or quality, making them a superior choice for sustainable packaging. The final point on sustainable product switches is bulk buying (especially if storage space allows it). Buying in bulk significantly reduces the amount of packaging waste. Many suppliers cater to eco-conscious businesses by offering large-format containers or refillable options. This approach cuts down on plastic waste and often proves to be more cost-effective.
A robust recycling programme is essential for reducing waste and becoming a zero-waste clinic. Here’s how to implement an effective system:
• Clear labelling: Use clear, understandable labels on recycling bins to ensure correct usage. Visual cues, such as pictures of recyclable items, can improve compliance.
• Education: Regularly educate your staff on the importance of recycling and how to do it properly within your clinic. This could be through quick training sessions, informational posters or even digital content shared via email or social media.
• Engagement: Encourage participation in the recycling programme by making it convenient and rewarding. Place recycling bins in accessible locations and consider incentives for staff who consistently recycle.
Water overuse also contributes to the overall carbon footprint of the clinic, but there are ways to optimise it. I would recommend installing low-flow faucets that can reduce water flow by up to 50% without compromising service quality. These fixtures limit the amount of water used while maintaining adequate pressure for everything you need within your clinic.
Optimised energy consumption can reduce between 25% to 45% of energy bills, so it is a key factor to consider in your sustainability journey.3
Look at the biggest energy consuming systems, such as heating, and check if there
are any greener options you could replace them with. To achieve this, research the best suppliers that can offer both affordable prices and energy-saving products. For example, consider switching to programmable thermostats that create automatic temperature adjustments based on the time of day and the occupancy. This will ensure the heating is never left on outside of working hours and the temperature is always optimised. Secondly, look at the lighting. LED lights drastically reduce energy consumption, but they also have a longer lifespan than most lighting systems. A halogen bulb costs about eight times more to run than LED spotlight.4 Occupancy sensors are also a strong alternative as they ensure the light is never left on by immediately switching off when movement is not detected.
Digitisation can streamline operations and reduce waste in various ways. Offering online booking systems will negate the need for paper appointment books and reminder cards. They also offer the added convenience of 24/7 booking for patients and can reduce no-shows through automated reminders. Switching to email or text message receipts eliminates the need for paper receipts, reducing paper waste and offering patients an easier way to keep track of their appointments. Maintain digital records for patient consent forms, past treatments, before and after images and all other documents required – this will cut down on paper use while enhancing the patient experience through personalised and consistent service. This can also be done by emailing procedure information leaflets and aftercare instructions to patients rather than having physical copies.
After integrating as many sustainable and green practices as possible in your clinic, consider if there is anything else you can do to offset your carbon footprint. Some employers offer bike schemes to encourage riding bicycles to work. Others plant a tree for every new patient or new employee. Check your budget and business capabilities, and try to come up with feasible ideas that could get your clinic closer to becoming a completely zero-waste business.
Before you go full steam ahead, there are a number of challenges that need to be addressed before making certain ‘green’ switches:
• Regulatory compliance and safety standards: Aesthetic clinics must adhere to strict health and safety regulations, which often require the use of single-use, sterile items. For example, finding alternatives to disposable gloves, syringes or needles that still meet hygiene standards is a major hurdle.
• Sourcing sustainable products: Many common supplies in aesthetics clinics, such as dermal fillers and botulinum toxin, come in single-use packages. The clinic would need to research suppliers which offer sustainably produced products that do not compromise patient safety.
• Staff training and culture shift: Moving to a zero-waste operation requires full buy-in from all staff members. This involves clear training on new protocols and a cultural shift in how materials and resources are viewed and utilised in the clinic. This can often be hard to implement straight away and may be challenging for everyone to maintain consistently.
• Cost implications: Initial investment in sustainable technologies and products often comes at a cost; even something as small as lighting can be a big cost to begin with. Clinics need to balance the initial costs against the long-term savings from sustainable practices and make an informed decision.
While the benefits are clear, the path to zero-waste is not without its challenges. Initial investments in sustainable products and infrastructure may be higher than conventional options. However, these costs are often offset by long-term savings and increased customer loyalty. The key to success lies in commitment, creativity and community engagement.

Graham Matthews has been sustainability content writer with more than five years of experience. His latest work focuses on practices that promote environmental stewardship in the aesthetics specialty. His articles offer practical insights, while fully disclosing the challenging and sometimes intricate path to becoming a zero-waste business.




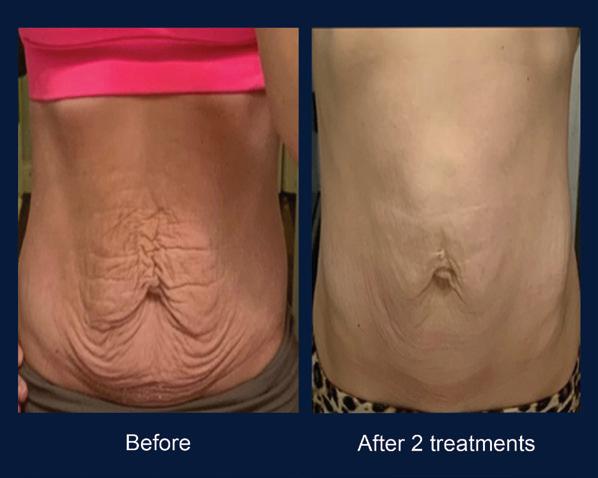




Dermatology nurse practitioner Emma Coleman shares a typical day pursuing her passion of giving patients great skin
A typical working day…
I normally wake up between 6:30 and 7am, and my first port of call is to go downstairs, make a cup of tea and have a cuddle with my brindle cockapoo Coco.
I have two clinics, one with a reception team and one without, so the first thing I do is get out my iPad and two phones (it seems excessive, but they keep me organised!) and go through any messages we have received overnight, making sure everything is set up for the day ahead.
I live about a half-hour drive from my main clinic, so I leave the house by 7:45am at the latest to avoid the rush hour traffic. I’m normally the first in, so I grab a quick breakfast and then go about setting up the clinic with scents and candles so patients can have an amazing, calming experience from the second they step in. The clinic atmosphere is a big priority of mine, and helps me get in the right headspace too. We’ve had a lot of brand new patients this year as our reputation continues to grow, so I tend to spend a lot of time doing consultations. We offer four different kinds of treatments in the clinic: dermatology, skincare, injectables and threads. I love the variety, but skin always comes first for me due to my background in dermatological nursing. Most of our patients are coming in looking for skin treatments, which really suits me. Besides consultations, I spend my days performing a whole range of procedures, including injectables, microneedling, energy-based devices, chemical peels and more. I use Lynton’s 3JUVE device all the time for a variety of indications as it combines intense-pulsed light (IPL), radiofrequency (RF) and fractional laser so it’s very versatile. LipoFirm Pro is a favourite for body treatments, as it uses electric pulses to effectively break down fat and tighten the skin. I’ve also recently invested in Morpheus8 which I’m really excited about for beautiful skin transformations.
I’d say acne and rosacea are the most common concerns patients come to me with, as well as eczema and psoriasis, but

we get all sorts. People are increasingly coming to me for lesion removal, and I actually get a fair number of male patients presenting with seborrheic dermatitis on their scalps. This really knocks their confidence so it’s very rewarding to manage the condition with emollients and
Your chosen career if you weren’t in medicine…
It would be great to be a skincare formulator – actually working in the labs and getting hands on.
Your guilty pleasure TV show…
Air Crash Investigation – I can’t help myself!
Your ideal holiday destination…
I’d like to go to South Africa to see the nature, the environment, the vineyards – it looks incredible.
topical anti-fungal agents.
It’s just so fulfilling to be able to help people whose confidence has been really knocked by their skin concerns, and see them feeling so much more secure in themselves after treatment.
I finish up in clinic fairly late, sometimes not getting home until 8pm. On those later days I tend to just collapse on the sofa and watch telly, but I’m also a hot yoga enthusiast because it makes me feel incredible, so I squeeze that in when I can. It’s important that I fit in some form of exercise at least three times a week. Going out for the evening and to dinner parties with friends is also a must – it’s all about the work-life balance!
Further education is really important to me. At this stage in my career, I really listen to my patients for what else we can provide them with. I’ve had an increasing number of people come to me asking about removing cysts and performing biopsies, so later this year I will be starting a minor surgery course to expand my clinic offering.
I like to give back in the form of mentoring as well. I have worked with a few young entrepreneurs interested in the world of skin, helping guide them on formulation and marketing, which is really rewarding. Charity work is also a big part of my life. Through the clinic, we have recently donated gift bags with essentials to local charity Evolve Housing + Support which provides 80 spaces for homeless people to stay overnight instead of sleeping rough.
I think it would have to be the day I first stepped foot in my second clinic space when we opened in 2022. I purchased, renovated and developed it all myself without much guidance, and managed to make it a success despite having limited experience in doing so. This is an achievement I’m really proud of as I proved to myself that perseverance really pays off.
nurse prescriber Kelly Saynor argues for the importance of the cooling-off period
Instant gratification informs much of our daily lives in the modern world. Whether that be a takeaway delivered in 20 minutes, or the quick ego boost from a social media post, this ‘quick fix’ attitude has unsurprisingly found its way into the world of aesthetics. However, there isn’t a one-size-fits-all approach to tweakments, and decisions regarding a medical procedure should never be taken lightly. My answer to patients who come in requesting a myriad of treatments before a consultation is always the same – you need to go away and think about it. Although it might be hard, I believe any practitioner worth their salt should be insisting on a cooling-off period for these treatments to avoid potential claims of negligence and malpractice.
The issue
Straight after COVID-19 we saw a huge uplift in non-surgical treatments, increasing by 102% in 2022.1,2 However, as the number of treatments performed has gone up, so has the incidence of litigation for alleged malpractice.3 Failure to achieve the desired result or not mentioning the potential for adverse events can lead to claims of alleged negligence on the part of the practitioner or surgeon.4 In this regard, cooling-off periods are crucial because they allow patients to make well-considered decisions that are right for them, free from impulse or emotional highs. In my clinical experience, when patients have time to process the information and potential risks, they’re less likely to feel misled later if the results differ from their expectations. So, not only are cooling-off periods good for patient trust and wellbeing, but they also reduce the possibility of negligence claims against the practitioner. Now, the issue is that implementation can be inconsistent. While some practitioners religiously uphold a cooling-off period, others might not emphasise it as much, and some even treat on the day of consultation. This inconsistency can lead to patients rushing into decisions.
In 2015, the Montgomery v Lanarkshire Health Board case reshaped patient consent laws. This ruling mandates doctors to inform patients of material risks and alternative treatments.5 By diagnosing and treating within this framework, we integrate
medical aesthetic treatments into a formal medical context, thus professionalising and medicalising our care delivery process. While a consultation can explain complications, a cooling-off period allows the patient to process and absorb this information, helping the patient to truly understand the risks and weigh them against their expectations.
A cooling-off period has also been outlined as necessary in numerous industry guidelines. The British Association of Aesthetic Plastic Surgeons (BAAPS) has the strictest rules of all associations in the aesthetic specialty, recommending a minimum two-week cooling-off period for all BAAPS-registered surgeons following the pre-treatment consent process.6
The Joint Council of Cosmetic Practitioners, British College of Aesthetic Medicine and British Association of Cosmetic Nurses advocate for a similar principle to BAAPS, ensuring patients have sufficient time to process information and make informed decisions.7,8,9
In the General Medical Council (GMC) guidelines for doctors offering surgical and non-surgical procedures, it says that practitioners should give patients ‘the time and information they need to reach a voluntary and informed decision about whether to go ahead with an intervention’.10 It adds that the amount of time needed for reflection depends on ‘the invasiveness, complexity, permanence and risks of the intervention, how many intervention options the patient is considering and how much information they have already considered.’10
The General Dental Council also advises to give patients cooling-off periods, stating ‘a reasonable length of time’.11 Interestingly, the Nursing and Midwifery Council (NMC) has not yet mentioned a stance on cooling-off periods.12 I believe it is more important now than ever that the NMC, and other bodies which govern and protect both the public and its members, offer advice or a clear line of support in this area.
Establishing a thorough consenting and consultation process, underpinned by
well-documented evidence which is detailed, signed and dated, is crucial. Not only is it in the best interest of your patient, but it serves as your safeguard should a need for defence arise in the future.
Giving the patient sufficient time to reflect and think about a potential treatment after a consultation is, in my opinion, our moral and ethical responsibility as practitioners. Consultations are essential for ensuring that patients have received all necessary information for their desired treatment; it’s of equal importance that they have time to process this information and make an informed decision.
Cooling-off periods can vary, but I always opt for two weeks post consultation, allowing the patient time to think about their desired treatment and whether it is the right route for them to go down. If I suspect a patient is acting on impulse or doesn’t understand the downtime involved, I’m likely to insist on a longer cooling-off period.
In my experience, you will guarantee better patient retention and patient-practitioner trust by ensuring they have time to consider all possibilities and outcomes. Sometimes, it is also our ethical responsibility to simply tell a patient ‘no’ when they may have gone too far, or are experiencing any type of dysmorphia that has led to them wanting a particular aesthetic treatment.
I wholeheartedly believe that this is the route that should be followed through every patient journey, but I recognise that guidelines such as those from the GMC only affect doctors. If a patient is dissatisfied with your suggestion of a cooling-off period, it is of course possible that they may look to go to another clinic that is not subject to these guidelines. However, I believe in the long-term that, as practitioners, ethics and integrity always prevail. Putting your patients’ physical and emotional wellbeing first every time will ensure you retain loyal patients who know ethics will always come before profits for you.

Kelly Saynor is an independent nurse prescriber and clinical director. She started her career in paediatrics before moving into cosmetic surgery. Saynor founded Medica Forte in 2014. In addition, Saynor serves as owner and clinical director at her Cheshire-based aesthetic clinic, Renew. Qual: NIP, DPNS














Designed for natural-looking, kissable lips1-3 by
Up to 12 months of smooth, plump, and natural-looking lips4,5
Provides balanced volume and high flexibility6-8
High patient and partner satisfaction5
PURCHASE NOW FROM MEDFX
References: 1. Galderma. Data on File. MA-43049. 2. Öhrlund Å.
J Cosmet Dermatol Sci Applic. 2018; 8(2): 47. 3. Bertucci V et al.
J Drugs Dermatol 2021; 20: 402-408. 4. Restylane Kysseâ EU IFU.
5. Hilton S et al. Dermatol Surg 2018; 44(2): 261-269. 6. Lundgren
B et al. J Drugs Dermatol 2018; 17(9): 982-986. 7. Bertucci V et al.
J Cosmet Dermatol 2021; 20(5): 1499-1504. 8. Bertucci V et al.
Imagery is of actual Restylane patient. For Healthcare Professionals Only Adverse events should be reported. For the UK, Reporting forms and information can be found at www.mhra.gov.uk/yellowcard or search for Yellow Card in the Google Play or Apple App Store. For Ireland, Suspected adverse events can be reported via HPRA Pharmacovigilance, Website: www.hpra.ie; Adverse events should also be reported to Galderma (UK) Ltd, Email: medinfo.uk@galderma.com Tel: +44 (0) 300 3035674
J Drugs Dermatol 2021; 20: 402-408. GB-RES-2400030 February 2024