ANNUAL MEETING HUBS FOSTER COLLABORATIVE LEARNING THROUGH UNIQUE DELIVERY METHODS
Step outside the traditional classroom and into the world of unconventional learning with the 2023 Annual Meeting Hubs. Eight focused areas provide deeper dives into your area of interest and opportunities to engage in collaborative learning, gain actionable tools for your patients and career, and find your community. From silly to inspiring, and interactive to introspective, hubs provide creative programming you can't find anywhere else, and fun opportunities to document reconnections with friends in one of the photo areas.
Continued on page 12 ›
2023 Summer Conference to Focus on Emergency and Hospital Neurology
Can’t Make It to Boston? Join Us for the Interactive Online Experience!
If a trip to Boston isn’t in your plans, remember that you can join us online to take part in the 75th AAN Annual Meeting. The interactive online platform will give you full access to:

200+ education programs offering CME credits for the entire year

7 plenary sessions featuring leaders in neurology
Registration Opens Early April
Registration opens this month for the 2023 AAN Summer Conference, set to take place July 28 and 29 at the Hyatt Regency in Minneapolis, MN, the hometown of the


Continued on page 11 ›
Daily online-only programs featuring interviews with speakers, directors, board members, and more, as well as exciting cutting-edge research summaries
Access to view missed sessions, available within approximately 48 hours of their conclusion
Continued on page 11 ›
13 Compensation and Productivity Data Is Powerful Tool for Neurologists 15 Members Chosen for Inaugural Private Practice Awards 16 AAN Annual Meetings Bring Worldwide Neurology Community Together
VOLUME 35 ISSUE 4 APRIL 2023
Boston & Virtual • April 22–27


The Mission of the AAN is to promote the highest quality patient-centered neurologic care and enhance member career satisfaction.
The Vision of the AAN is to be indispensable to our members.
Contact Information

American Academy of Neurology
201 Chicago Avenue
Minneapolis, MN 55415
Phone: (800) 879-1960 (toll free) (612) 928-6000 (international)
Email: memberservices@ aan.com
Website: AAN.com
For advertising rates, contact:
Michael J. O’Brien II
Account/Relationship Manager
Wolters Kluwer
Phone: (978) 578-4514
Email: Michael.Obrien @ wolterskluwer.com
April Highlights
13
Use New Parkinson’s Patient Questionnaire to Improve Visits, Reduce Burden
The new AAN Parkinson’s disease questionnaire joins four previously developed standardized questionnaires for epilepsy, MS, sleep, and headache that can be converted to templates in your EHR. They are disease-specific, incorporate AAN guidelines and quality measures, and have been vetted by clinical experts.
Value of “Us” vs. “Me” Guides Leadership Program Graduate to Success
“I had a myopic view of leadership that involved me doing or me acting. It was very ‘me’ centric,” said Bhooma Aravamuthan, MD, DPhil, of her outlook prior to her powerful experience in the AAN’s Emerging Leaders Program. “Leadership is not about ‘me;’ it’s about ‘us.’”
Cerebrovascular Disease Explored in Continuum
The latest information on cerebrovascular disease is presented in the April issue of Continuum: Lifelong Learning in Neurology ®
AAN Chief Executive Officer: Mary E. Post, MBA, CAE

Editor-in-Chief: Melissa W. Ko, MD, MBA, CPE, FAAN

Managing Editor: Angela M. Babb, MS, CAE, APR
Editor: Tim Streeter
Writers: Ryan Knoke and Sarah Parsons
Designer: Siu Lee
Email: aannews@ aan.com
AANnews® is published monthly by the American Academy of Neurology for its 40,000 members worldwide. Access this magazine and other AAN publications online at AAN.com.
The American Academy of Neurology ’s registered trademarks and service marks are registered in the United States and various other countries around the world.
“American Brain Foundation” is a registered service mark of the American Brain Foundation and is registered in the United States. The inclusion of advertisements and/or promotions of Sponsors and other Internet sites or resources that offer content, goods, or services on the Website does not imply endorsement of the advertised/promoted products or services by AAN.
News Briefs
How Did the AAN Perform in 2022?
The 2022 AAN Annual Report highlights the many key successes of the Academy as it supported members during the shift to the post-COVID environment. Read about the new programs, resources, events, and financial results during a most remarkable year at AAN.com/AnnualReport

26
28
PLEASE RECYCLE POLYBAG WHERE #5 PLASTIC IS ACCEPTED AANnews · April 2023
Looking Back and Ahead
When I began my term as president of the American Academy of Neurology in April of 2021, we had just held our first—and hopefully last—fully virtual Annual Meeting due to the COVID-19 pandemic. Newly vaccinated and optimistic about the future, I predicted in this column, “We are beginning to glimpse brighter days…we will emerge stronger than ever.” While the past two years have not brought the halcyon period I had hoped for, in many ways, this organization has indeed excelled despite onerous challenges, and is far more robust for it.

Our membership has grown to over 40,000 and our retention rate for US neurologists has risen to 95 percent, an enviable retention rate for a medical specialty organization. It has been a time of reflection and strategic planning for the AAN Board of Directors (BOD), which focused on member value and considered how to best support neurology through myriad changes. Our educational offerings expanded even further into the digital space, recognizing the appeal of the flexibility of a robust online learning platform that has included conferences, prep courses, and webinars on demand as well as our Question of the Day mobile app, monthly NeuroSAE, NeuroByte videos and podcasts for micro learning. Meanwhile, our committee, section, board, and programmatic work moved onto a digital platform without missing a beat.
During the first two years of the pandemic, the BOD increased its quarterly meetings to monthly, and sometimes more often, to address the daunting difficulties of the public health emergency. After over a year on Zoom, the BOD finally met in Orlando in April of 2021 by creating a safe and closed environment in two homes and dividing up tasks as chefs, sous-chefs, drivers, servers, clean-up crew, and entertainment. Charles C. Flippen II, MD, FAAN, AAN treasurer, shared his family recipe for pancakes, Natalia S. Rost, MD, MPH, FAHA, FAAN, chair of the Science Committee, added secret spices that made an impressive shakshuka, and Lily Jung Henson, MD, MMM, FAAN, brought her own pecans from Georgia to make delicious pies. It was exhilarating to watch neurologist-chefs take over the kitchen and direct volunteer sous-chefs like José G. Merino, MD, MPhil, FAHA, FAAN, editor-in-chief of Neurology® and Joseph I. Sirven, MD, FAAN, chair of the Education Committee, in prepping and chopping duties. (Both seemed to take particular pleasure in wielding large knives.) While Brad C. Klein, MD, MBA, FAAN, chair of the Medical Economics and Practice Committee, performed admirably in a magic show, James N. Goldenberg, MD, FAAN, served as a one-man IT department to ensure that the hybrid meeting could be enjoyed virtually by those who were unable to attend. It was a productive and fruitful meeting as we discussed the AAN’s strategic plan, formulated a vision for brain health, and exchanged ideas for innovation to meet a changing environment.
As the pandemic numbers worsened, we returned to virtual meetings in the fall of 2021. In an attempt to combat Zoom fatigue, I invited pets to join us, and loved meeting the many dogs of the board, including Ili Anderson, Maxwell Goldstein, River and Halie Jackson, Henry and Daisy Miyasaki, Chloe and RJ Kilgore, Kola and Kobe Kissela, among other well-groomed guests. We also welcomed a new baby in October of 2021, Shiloh Emery, who joined us at our January 2022 in-person board meeting, along with her mother, Maisha T. Robinson, MD, MSHPM, FAAN, chair of the Member Engagement Committee.
It had become apparent in the year that followed the trauma of the pandemic that neurologists in all types of practice were reconsidering work-life balance and reimagining new employment opportunities, while staffing shortages grew. Our retreat focused on the workforce crisis, informed by conversations I had with a variety of AAN members for a series of Neurology Today ® stories about departures and new beginnings and the experiences of BOD members in their varied practice settings.
We were excited to return to other in-person meetings in 2022, while maintaining online options for participation from our experiences during the pandemic. The Education Committee worked on creating updated programming for the 74th Annual Meeting in Seattle, and highly successful Fall and Summer Conferences were held in Las Vegas and San Francisco, respectively. The latter conference presented Autoimmune Neurology and Neurology Year in Review. During my term as president, I launched two new committees: the Committee on Public Engagement, which oversaw the Brain Health Summit in Washington, DC, on September 15, 2022, and the Academic Neurology Committee, which hosted its Chair Summit on December 12, 2022, and was renamed the Ralph L. Sacco Neurology Chair Summit in honor of his steadfast vision for helping academic departments thrive.
AAN committees held hybrid sessions that allowed those who could not attend to join in person. The Quality Committee successfully launched Emerging Issues in Neurology reports, which are to provide timely informal guidance derived from expert consensus until an evidence base is established that can inform evidence-based recommendations; the Axon Registry® Quality Achievement Award program, recognizing neurology practices for their levels of quality performance; and built a quality informatics team to develop products and services that will help members put technology to work for them, rather than the other way around. The Medical Economics and Practice Committee created resource toolkits for managing staffing challenges, improving practice efficiencies, and access to care. To support implementation of telehealth, it collated an extensive library of telehealth practice guides, case studies,
4 A ANnews • April 2023 PRESIDENT'S COLUMN
Avitzur
coding guidance and resources. To increase recognition of general neurology and private practice, it created three new membership awards. It continued to address reimbursement for evaluation and management (E/M) services and educated members about updates to outpatient E/M in 2021 and inpatient E/M in 2023.
The Advocacy Committee worked with policymakers to generate solutions to reduce prior authorization burden that has culminated in recent rulemaking that, if finalized, would establish critical guardrails on a variety of payers’ use of prior authorization and implement standards that support electronic prior authorization. To support access to care throughout the pandemic, the AAN provided policymakers with critical recommendations that have allowed patients to use telehealth to maintain access to care and to ensure that patients do not lose access upon termination of the public health emergency declaration. The committee also actively engaged with lawmakers in Washington, DC, to help avert devastating cuts to physician Medicare reimbursement. To ensure patients can access the life-saving treatments they need, the committee has continued to work with Congress to reform prior authorization and step therapy requirements and actively advocated for legislation that will allow Medicare to negotiate drug prices.
The Science Committee created a bigger, more inclusive Annual Meeting Science Program with over 3,000 original science submissions, a bustling Research Hub, busy Invited Science, Neuroscience in the Clinic sessions, and expanding Emerging Science. The quality of science continues to grow across the spectrum of career stages, types of research— basic, translational, clinical—and subspecialties. The AAN was committed to research funding, despite the pandemic challenges and the committee expanded its support by developing new Health Disparity awards. The Clinical Research Subcommittee expanded research programming for trainees at the Annual Meeting, introduced Resident Research
Scholarships, and started the Clinical Research webinar series to bring research closer to clinical practice settings and diversify clinical trial participation.

Our worldwide outreach has blossomed over the past two years, and I was particularly eager to meet a wide variety of international members, brainstorm with global organizational leaders, and develop new friendships as a result. It has been rewarding to see the AAN continue to grow a diverse and inclusive membership bound by a shared love of neurology. This Academy braved the pandemic through the efforts of more than 800 member volunteers, 27 committees and 34 subcommittees, 41 sections, and above all, 200 staff, who kept their eyes on the mission of the AAN, while valiantly leading through technical and logistical challenges. I credit their commitment, ingenuity, and tenacity for this organization’s ultimate success.
As I pass the torch to the next generation of leaders, my heart is replete with gratitude, and the future is bright with hope. I am grateful to all of you in our broader membership who so often shared with me your experiences, ideas, concerns, and support. It has been an honor to get to interact with so many dedicated individuals in my service to this organization for the past two years. I came to know the AAN and its members through writing for and editing our varied and storied publications for the past two plus decades and I now look forward with great pleasure to returning to the pen, where I hope to stay in touch.
Orly Avitzur, MD, MBA, FAAN President, AAN oavitzur@aan.com @OrlyA on Twitter
Brain & Life Podcast: Educating the public on neurology and brain health. Follow and subscribe wherever you get your podcasts. BrainandLife.org/Podcast
A ANnews • April 2023 5
KESIMPTA® IS DIFFERENT FOR A REASON

The Only SC delivered B-cell RMS treatment1,2
EFFICACY
• Primary end point: relative reduction in adjusted ARR vs Aubagio® (teriflunomide) of 51% (0.11 vs 0.22) in ASCLEPIOS I and 58% (0.10 vs 0.25) in ASCLEPIOS II3
• Post hoc analysis of pooled data from ASCLEPIOS I and II: cumulative ARR by time interval (KESIMPTA N=946, Aubagio N=936). Reduction in ARR seen in the first 3 months and time intervals over 2 years 4,7:
– Month 0 to 3: 0.236 vs 0.373














– Month 0 to 27: 0.123 vs 0.258
– No conclusions can be drawn
SAFETY
• Adverse events with an incidence of ≥5% with KESIMPTA and a greater incidence than Aubagio were: upper respiratory tract infections (39% vs 38%), injection-related reactions (systemic) (21% vs 15%), headache (13% vs 12%), injection-site reactions (local) (11% vs 6%), urinary tract infection (10% vs 8%), back pain (8% vs 6%), and blood immunoglobulin M decrease (6% vs 2%)3
• The overall rate of infections and serious infections in patients treated with KESIMPTA was similar to patients who were treated with Aubagio (51.6% vs 52.7%, and 2.5% vs 1.8%, respectively)3


INDICATION
KESIMPTA is indicated for the treatment of relapsing forms of multiple sclerosis (MS), to include clinically isolated syndrome, relapsing-remitting disease, and active secondary progressive disease, in adults.
IMPORTANT SAFETY INFORMATION
Contraindication: KESIMPTA is contraindicated in patients with active hepatitis B virus infection.


WARNINGS AND PRECAUTIONS
Infections: An increased risk of infections has been observed with other anti-CD20 B-cell depleting therapies. KESIMPTA has the potential for an increased risk of infections including serious bacterial, fungal, and new or reactivated viral infections; some have been fatal in patients treated with other anti-CD20 antibodies. The overall rate of infections and serious infections in KESIMPTAtreated patients was similar to teriflunomide-treated patients (51.6% vs 52.7%, and 2.5% vs 1.8%, respectively). The most common infections reported by KESIMPTA-treated patients in relapsing MS (RMS) trials included upper respiratory tract infection (39%) and urinary tract infection (10%). Delay KESIMPTA administration in patients with an active infection until resolved.
Consider the potential increased immunosuppressive effects when initiating KESIMPTA after an immunosuppressive therapy or initiating an immunosuppressive therapy after KESIMPTA.
Please see additional Important Safety Information and Brief Summary of full Prescribing Information on the following pages.
Powerful efficacy.* Early and continued relapse reduction over the study period3,4 Established safety profile in pivotal trials which included treatmentnaïve patients3,5
1 Minute a Month, † when the patient is ready to administer3,6
Make KESIMPTA® your 1st choice
KesimptaHCP.com

ARR=annualized relapse rate; CDP=confirmed disability progression; CI=confidence interval; DMT=disease-modifying therapy; GdE=gadolinium-enhancing; MRI=magnetic resonance imaging; RMS=relapsing multiple sclerosis; SC=subcutaneous.
*Study Design: ASCLEPIOS I and II were 2 identical randomized, active-controlled, double-blind Phase 3 studies in patients with RMS, approximately 40% of whom were DMT treatment-naïve. Patients were randomized to double-dummy subcutaneous KESIMPTA (20 mg every 4 weeks) or oral Aubagio (14 mg daily) for up to 30 months. Primary end point was ARR. Key MRI end points were number of GdE T1 lesions, and annualized rate of new or enlarging T2 lesions. A key clinical end point was reduction in risk of 3-month CDP. Treatment duration was variable based on end-of-study criteria. Maximum duration 120 weeks, median duration 85 weeks.3
Post hoc Study Design: ARR by time intervals was analyzed from the pooled pivotal trials. The ARR (95% CI) was estimated separately for each time interval by fitting a negative binomial regression model adjusted for treatment as factor.4,7
†As per stability technical specification data, when the patient is ready to inject, it typically takes less than 1 minute a month to administer. Once-monthly dosing begins after the initial dosing period, which consists of 20 mg subcutaneous doses at weeks 0, 1, and 2. Please see Instructions for Use for more detailed instructions on preparation and administration of KESIMPTA.3,6



Hepatitis B Virus: Reactivation: No reports of hepatitis B virus (HBV) reactivation in patients with MS treated with KESIMPTA. However, HBV reactivation, in some cases resulting in fulminant hepatitis, hepatic failure, and death, has occurred in patients treated with ofatumumab at higher intravenous doses for chronic lymphocytic leukemia (CLL) than the recommended dose in MS and in patients treated with other anti-CD20 antibodies.
Infection: KESIMPTA is contraindicated in patients with active hepatitis B disease. Fatal infections caused by HBV in patients who have not been previously infected have occurred in patients treated with ofatumumab at higher intravenous doses for CLL than the recommended dose in MS. Perform HBV screening in all patients before initiation of KESIMPTA. Patients who are negative for HBsAg and positive for HB core antibody [HBcAb+] or are carriers of HBV [HBsAg+], should consult liver disease experts before starting and during KESIMPTA treatment.
Progressive Multifocal Leukoencephalopathy: No cases of progressive multifocal leukoencephalopathy (PML) have been reported for KESIMPTA in RMS clinical studies; however, PML resulting in death has occurred in patients being treated with ofatumumab at higher intravenous doses for CLL than the recommended dose in MS. In addition, JC virus infection resulting in PML has also been observed in patients treated with other anti-CD20 antibodies and other MS therapies.
If PML is suspected, withhold KESIMPTA and perform an appropriate diagnostic evaluation. If PML is confirmed, KESIMPTA should be discontinued.
Vaccinations: Administer all immunizations according to immunization guidelines: for live or live-attenuated vaccines at least 4 weeks and, whenever possible at least 2 weeks prior to starting KESIMPTA for inactivated vaccines. The safety of immunization with live or live-attenuated vaccines following KESIMPTA therapy has not been studied. Vaccination with live or live-attenuated vaccines is not recommended during treatment and after discontinuation until B-cell repletion.
Vaccination of Infants Born to Mothers Treated with KESIMPTA During Pregnancy. For infants whose mother was treated with KESIMPTA during pregnancy, assess B-cell counts prior to administration of live or live-attenuated vaccines. If the B-cell count has not recovered in the infant, do not administer the vaccine as having depleted B-cells may pose an increased risk in these infants.
Injection-Related Reactions: Injection-related reactions with systemic symptoms occurred most commonly within 24 hours of the first injection, but were also observed with later injections. There were no life-threatening injection reactions in RMS clinical studies.
The first injection of KESIMPTA should be performed under the guidance of an appropriately trained health care professional. If injection-related reactions occur, symptomatic treatment is recommended.
Reduction in Immunoglobulins: As expected with any B-cell depleting therapy, decreased immunoglobulin levels were observed. Monitor the levels of quantitative serum immunoglobulins during treatment, especially in patients with opportunistic or recurrent infections and after discontinuation of therapy until B-cell repletion. Consider discontinuing KESIMPTA therapy if a patient with low immunoglobulins develops a serious opportunistic infection or recurrent infections, or if prolonged hypogammaglobulinemia requires treatment with intravenous immunoglobulins.
Fetal Risk: Based on animal data, KESIMPTA can cause fetal harm due to B-cell lymphopenia and reduce antibody response in offspring exposed to KESIMPTA in utero. Transient peripheral B-cell depletion and lymphocytopenia have been reported in infants born to mothers exposed to other anti-CD20 B-cell depleting antibodies during pregnancy. Advise females of reproductive potential to use effective contraception while receiving KESIMPTA and for at least 6 months after the last dose. Most common adverse reactions (>10%) are upper respiratory tract infection, headache, injection-related reactions, and local injection-site reactions.
Please see additional Important Safety Information on the previous page and Brief Summary of full Prescribing Information on the following pages.
References: 1. National Multiple Sclerosis Society. Medications. Accessed February 10, 2022. https://www.nationalmssociety.org/Treating-MS/Medications 2. Torres JB, Roodselaar J, Sealey M, et al. Distribution and e icacy of ofatumumab and ocrelizumab in humanized-CD20 mice following subcutaneous or intravenous administration. P2.2-052. Poster presented at: 71st American Academy of Neurology Annual Meeting; May 4-10, 2019; Philadelphia, PA. 3. Kesimpta [package insert]. East Hanover, NJ: Novartis Pharmaceuticals Corp. 4. Hauser SL, Bar-Or A, Cohen JA, et al. Ofatumumab vs teriflunomide in relapsing multiple sclerosis: analysis of no evidence of disease activity (NEDA-3) from ASCLEPIOS I and II trials. LB62. Poster presented at: 6th Congress of the European Academy of Neurology; May 23-26, 2020; Virtual. 5. Hauser SL, Bar-Or A, Cohen JA, et al; for the ASCLEPIOS I and ASCLEPIOS II trial groups. Ofatumumab versus teriflunomide in multiple sclerosis. N Engl J Med. 2020;383(6):546-557. 6. Data on file. Injection time. Novartis Pharmaceuticals Corp; East Hanover, NJ. June 2020. 7. Data on file. OMB157G (ofatumumab). Summary of clinical e icacy in relapsing multiple sclerosis. Novartis Pharmaceuticals Corp; East Hanover, NJ. December 2019.
(cont)
Novartis Pharmaceuticals Corporation East Hanover, New Jersey 07936-1080 © 2022 Novartis 10/22 246578
IMPORTANT SAFETY INFORMATION
WARNINGS AND PRECAUTIONS (cont)
KESIMPTA, the KESIMPTA logo, and SENSOREADY are registered trademarks of Novartis AG.
KESIMPTA® (ofatumumab) injection, for subcutaneous use
Initial U.S. Approval: 2009
BRIEF SUMMARY: Please see package insert for full prescribing information.
1 INDICATIONS AND USAGE
KESIMPTA is indicated for the treatment of relapsing forms of multiple sclerosis (MS), to include clinically isolated syndrome, relapsing-remitting disease, and active secondary progressive disease, in adults.
4 CONTRAINDICATIONS
KESIMPTA is contraindicated in patients with:
•Active HBV infection [see Warnings and Precautions (5.1)]
5 WARNINGS AND PRECAUTIONS
5.1 Infections
An increased risk of infections has been observed with other anti-CD20 B-cell depleting therapies.
KESIMPTA has the potential for an increased risk of infections, including serious bacterial, fungal, and new or reactivated viral infections; some of these infections have been fatal in patients treated with other anti-CD20 antibodies. In Study 1 and Study 2 [see Clinical Studies (14) in the full prescribing information], the overall rate of infections and serious infections in patients treated with KESIMPTA was similar to patients who were treated with teriflunomide (51.6% vs 52.7%, and 2.5% vs 1.8%, respectively). The most common infections reported by KESIMPTA-treated patients in the randomized clinical relapsing MS (RMS) trials included upper respiratory tract infection (39%) and urinary tract infection (10%). Delay KESIMPTA administration in patients with an active infection until the infection is resolved.
Possible Increased Risk of Immunosuppressant Effects with Other Immunosuppressants
When initiating KESIMPTA after an immunosuppressive therapy or initiating an immunosuppressive therapy after KESIMPTA, consider the potential for increased immunosuppressive effects [see Drug Interactions (7.1) and Clinical Pharmacology (12.2) in the full prescribing information]. KESIMPTA has not been studied in combination with other MS therapies.
Hepatitis B Virus
Reactivation
There were no reports of HBV reactivation in patients with MS treated with KESIMPTA. However, HBV reactivation, in some cases resulting in fulminant hepatitis, hepatic failure, and death, has occurred in patients being treated with ofatumumab for chronic lymphocytic leukemia (CLL) (at higher intravenous doses than the recommended dose in MS but for a shorter duration of treatment) and in patients treated with other anti-CD20 antibodies.
Infection
KESIMPTA is contraindicated in patients with active hepatitis B disease. Fatal infections caused by HBV in patients who have not been previously infected have occurred in patients being treated with ofatumumab for CLL (at higher intravenous doses than the recommended dose in MS but for a shorter duration of treatment). HBV screening should be performed in all patients before initiation of treatment with KESIMPTA. At a minimum, screening should include Hepatitis B surface antigen (HBsAg) and Hepatitis B Core Antibody (HBcAb) testing. These can be complemented with other appropriate markers as per local guidelines. For patients who are negative for HBsAg and positive for HB core antibody [HBcAb+] or are carriers of HBV [HBsAg+], consult liver disease experts before starting and during treatment with KESIMPTA. These patients should be monitored and managed following local medical standards to prevent HBV infection or reactivation.
Progressive Multifocal Leukoencephalopathy
Progressive multifocal leukoencephalopathy (PML) is an opportunistic viral infection of the brain caused by the JC virus (JCV) that typically occurs in patients who are immunocompromised, and that usually leads to death or severe disability.
Although no cases of PML have been reported for KESIMPTA in the RMS clinical studies, PML resulting in death has occurred in patients being treated with ofatumumab for CLL (at substantially higher intravenous doses than the recommended dose in MS but for a shorter duration of treatment). In addition, JCV infection resulting in PML has also been observed in patients treated with other anti-CD20 antibodies and other MS therapies. At the first sign or symptom suggestive of PML, withhold KESIMPTA and perform an appropriate diagnostic evaluation. Magnetic resonance imaging (MRI) findings may be apparent before clinical signs or symptoms. Typical symptoms associated with PML are diverse, progress over days to weeks, and include progressive weakness on one side of the body or clumsiness of limbs, disturbance of vision, and changes in thinking, memory, and orientation leading to confusion and personality changes.
If PML is confirmed, treatment with KESIMPTA should be discontinued.
Vaccinations
Administer all immunizations according to immunization guidelines at least 4 weeks prior to initiation of KESIMPTA for live or live-attenuated vaccines,
and whenever possible, at least 2 weeks prior to initiation of KESIMPTA for inactivated vaccines.
KESIMPTA may interfere with the effectiveness of inactivated vaccines. The safety of immunization with live or live-attenuated vaccines following KESIMPTA therapy has not been studied. Vaccination with live or liveattenuated vaccines is not recommended during treatment and after discontinuation until B-cell repletion [see Clinical Pharmacology (12.2) in the full prescribing information]
Vaccination of Infants Born to Mothers Treated with KESIMPTA During Pregnancy
In infants of mothers treated with KESIMPTA during pregnancy, do not administer live or live-attenuated vaccines before confirming the recovery of B-cell counts. Depletion of B-cells in these infants may increase the risks from live or live-attenuated vaccines. Inactivated vaccines may be administered, as indicated, prior to recovery from B-cell depletion, but an assessment of vaccine immune responses, including consultation with a qualified specialist, should be considered to determine whether a protective immune response was mounted.
5.2 Injection-Related Reactions
In Study 1 and Study 2, systemic and local injection reactions were reported in 21% and 11% of patients treated with KESIMPTA compared to 15% and 6% of patients treated with teriflunomide who received matching placebo injections, respectively [see Adverse Reactions (6.1) and Clinical Studies (14) in the full prescribing information]
Injection-related reactions with systemic symptoms observed in clinical studies occurred most commonly within 24 hours of the first injection, but were also observed with later injections. Symptoms observed included fever, headache, myalgia, chills, and fatigue, and were predominantly (99.8%) mild to moderate in severity. There were no life-threatening injection reactions in the RMS clinical studies.
Local injection-site reaction symptoms observed in clinical studies included erythema, swelling, itching, and pain.
Only limited benefit of premedication with corticosteroids, antihistamines, or acetaminophen was observed in RMS clinical studies. The first injection of KESIMPTA should be performed under the guidance of an appropriately trained healthcare professional. If injection-related reactions occur, symptomatic treatment is recommended.
5.3 Reduction in Immunoglobulins
As expected with any B-cell depleting therapy, decreased immunoglobulin levels were observed. Decrease in immunoglobulin M (IgM) was reported in 7.7% of patients treated with KESIMPTA compared to 3.1% of patients treated with teriflunomide in RMS clinical trials [see Adverse Reactions (6.1)]. Treatment was discontinued because of decreased immunoglobulins in 3.4% of patients treated with KESIMPTA and in 0.8% of patients treated with teriflunomide. No decline in immunoglobulin G (IgG) was observed at the end of the study. Monitor the levels of quantitative serum immunoglobulins during treatment, especially in patients with opportunistic or recurrent infections, and after discontinuation of therapy until B-cell repletion. Consider discontinuing KESIMPTA therapy if a patient with low immunoglobulins develops a serious opportunistic infection or recurrent infections, or if prolonged hypogammaglobulinemia requires treatment with intravenous immunoglobulins.
5.4 Fetal Risk
Based on animal data, KESIMPTA can cause fetal harm due to B-cell lymphopenia and reduce antibody response in offspring exposed to KESIMPTA in utero. Transient peripheral B-cell depletion and lymphocytopenia have been reported in infants born to mothers exposed to other anti-CD20 B-cell depleting antibodies during pregnancy. Advise females of reproductive potential to use effective contraception while receiving KESIMPTA and for at least 6 months after the last dose [see Use in Specific Populations (8.1)]
6 ADVERSE REACTIONS
The following clinically significant adverse reactions are discussed in greater detail elsewhere in the labeling:
•Infections [see Warnings and Precautions (5.1)]
•Injection-Related Reactions [see Warnings and Precautions (5.2)]
•Reduction in Immunoglobulins [see Warnings and Precautions (5.3)]
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reactions rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.
Approximately 1500 patients with RMS received KESIMPTA in clinical studies. In Study 1 and Study 2, 1882 patients with RMS were randomized, 946 of whom were treated with KESIMPTA for a median duration of 85 weeks; 33% of patients receiving KESIMPTA were treated for up to 120 weeks [see Clinical Studies (14.1) in the full prescribing information]. The most common adverse reactions occurring in greater than 10% of patients treated with KESIMPTA and more frequently than in patients treated with
teriflunomide were upper respiratory tract infections, injection-related reactions (systemic), headache, and injection-site reactions (local). The most common cause of discontinuation in patients treated with KESIMPTA was low immunoglobulin M (3.3%), defined in trial protocols as IgM at 10% below the lower limit of normal (LLN).
Table 1 summarizes the adverse drug reactions that occurred in Study 1 and Study 2.
Table 1: Adverse Reactions in Patients With RMS With an Incidence of at Least 5% With KESIMPTA and a Greater Incidence Than Teriflunomide (Pooled Study 1 and Study 2)
because of potential additive immunosuppressive effects when initiating KESIMPTA.
8 USE IN SPECIFIC POPULATIONS
8.1
Pregnancy
Risk Summary
There are no adequate data on the developmental risk associated with the use of KESIMPTA in pregnant women. Ofatumumab may cross the placenta and cause fetal B-cell depletion based on findings from animal studies (see Data)
Transient peripheral B-cell depletion and lymphocytopenia have been reported in infants born to mothers exposed to other anti-CD20 antibodies during pregnancy. B-cell levels in infants following maternal exposure to KESIMPTA have not been studied in clinical trials. The potential duration of B-cell depletion in infants exposed to ofatumumab in utero, and the impact of B-cell depletion on the safety and effectiveness of vaccines, are unknown. Avoid administering live vaccines to neonates and infants exposed to KESIMPTA in utero until B-cell recovery occurs [see Warnings and Precautions (5.2) and Clinical Pharmacology (12.2) in the full prescribing information].
Following administration of ofatumumab to pregnant monkeys, increased mortality, depletion of B-cell populations, and impaired immune function were observed in the offspring, in the absence of maternal toxicity, at plasma levels substantially higher than that in humans (see Data)
the following: nasopharyngitis, upper respiratory tract infection, influenza, sinusitis, pharyngitis, rhinitis, viral upper respiratory infection, tonsillitis, acute sinusitis, pharyngotonsillitis, laryngitis, pharyngitis streptococcal, viral rhinitis, sinusitis bacterial, tonsillitis bacterial, viral pharyngitis, viral tonsillitis, chronic sinusitis, nasal herpes, tracheitis.
Injection-Related Reactions and Injection-Site Reactions
The incidence of injection-related reactions (systemic) was highest with the first injection (14.4%), decreasing with subsequent injections (4.4% with second, less than 3% with third injection). Injection-related reactions were mostly (99.8%) mild to moderate in severity. Two (0.2%) patients treated with KESIMPTA reported serious injection-related reactions. There were no life-threatening injection-related reactions. Most frequently reported symptoms (2% or greater) included fever, headache, myalgia, chills, and fatigue.
In addition to systemic injection-related reactions, local reactions at the administration site were very common. Local injection-site reactions were all mild to moderate in severity. The most frequently reported symptoms (2% or greater) included erythema, pain, itching, and swelling [see Warnings and Precautions (5.2)]
Laboratory Abnormalities
Immunoglobulins
In Study 1 and Study 2, a decrease in the mean level of IgM was observed in KESIMPTA-treated patients but was not associated with an increased risk of infections [see Warnings and Precautions (5.3)]. In 14.3% of patients in Study 1 and Study 2, treatment with KESIMPTA resulted in a decrease in a serum IgM that reached a value below 0.34 g/L. KESIMPTA was associated with a decrease of 4.3% in mean IgG levels after 48 weeks of treatment and an increase of 2.2% after 96 weeks.
6.2 Immunogenicity
As with all therapeutic proteins, there is potential for immunogenicity. The detection of antibody formation is highly dependent on the sensitivity and specificity of the assay. Additionally, the observed incidence of antibody (including neutralizing antibody) positivity in an assay may be influenced by several factors, including assay methodology, sample handling, timing of sample collection, concomitant medication, and the underlying disease. For these reasons, comparison of the incidence of antibodies in the studies described below with the incidence of antibodies in other studies or to other ofatumumab products may be misleading.
Treatment-induced anti-drug antibodies (ADAs) were detected in 2 of 914 (0.2%) KESIMPTA-treated patients; no patients with treatment-enhancing or neutralizing ADAs were identified. There was no impact of positive ADA titers on PK, safety profile or B-cell kinetics in any patient; however, these data are not adequate to assess the impact of ADAs on the safety and efficacy of KESIMPTA.
7 DRUG INTERACTIONS
7.1 Immunosuppressive or Immune-Modulating Therapies
Concomitant usage of KESIMPTA with immunosuppressant drugs, including systemic corticosteroids, may increase the risk of infection. Consider the risk of additive immune system effects when coadministering immunosuppressive therapies with KESIMPTA.
When switching from therapies with immune effects, the duration and mechanism of action of these therapies should be taken into account
In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively. The background risk of major birth defects and miscarriage for the indicated population is unknown.
Data
Animal Data
Intravenous administration of ofatumumab (weekly doses of 0, 20, or 100 mg/kg) to pregnant monkeys during the period of organogenesis (gestations days 20 to 50) resulted in no adverse effects on embryofetal development; however, B-cell depletion was observed in fetuses at both doses when assessed on gestation day 100. Plasma exposure (Cave) at the no-effect dose (100 mg/kg) for adverse effects on embryofetal development was greater than 5000 times that in humans at the recommended human maintenance dose of 20 mg. A no-effect dose for effects on B-cells was not identified; plasma exposure (Cave) at the low-effect dose (20 mg/kg) was approximately 780 times that in humans at the recommended human maintenance dose (RHMD) of 20 mg/month.
Intravenous administration of ofatumumab (5 weekly doses of 0, 10, and 100 mg/kg, followed by biweekly doses of 0, 3, and 20 mg/kg) to pregnant monkeys throughout pregnancy resulted in no adverse effects on the development of the offspring. However, postnatal death, B-cell depletion, and impaired immune function were observed in the offspring at the high dose. The deaths at the high dose were considered secondary to B-cell depletion. Plasma exposure (Cave) in dams at the no-effect dose (100/20 mg/kg) for adverse developmental effects was approximately 500 times that in humans at RHMD. A no-effect level for mortality and immune effects in offspring was not established because of the limited number of evaluable offspring at the low dose.
8.2 Lactation
Risk Summary
There are no data on the presence of ofatumumab in human milk, the effects on the breastfed infant, or the effects of the drug on milk production. Human IgG is excreted in human milk, and the potential for absorption of ofatumumab to lead to B-cell depletion in the infant is unknown. The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for KESIMPTA and any potential adverse effects on the breastfed infant from KESIMPTA or from the underlying maternal condition.
8.3 Females and Males
Contraception
of Reproductive Potential
Females of childbearing potential should use effective contraception while receiving KESIMPTA and for 6 months after the last treatment of KESIMPTA [see Warnings and Precautions (5.4) and Clinical Pharmacology (12.3) in the full prescribing information]
8.4 Pediatric Use
Safety and effectiveness in pediatric patients have not been established.
8.5 Geriatric Use
Clinical studies of KESIMPTA did not include sufficient numbers of geriatric patients to determine whether they respond differently from younger subjects.
NJ 07936
Pharmaceuticals Corporation
Hanover,
and SENSOREADY
[registered] trademarks of Novartis AG. T2022-52
Manufactured by: Novartis
East
U.S. License No.: 1244 KESIMPTA
are
Adverse Reactions KESIMPTA 20 mg N = 946 % Teriflunomide 14 mg N = 936 % Upper respiratory tract infectionsa 39 38 Injection-related reactions (systemic) 21 15 Headache 13 12 Injection-site reactions (local) 11 6 Urinary tract infection 10 8 Back pain 8 6 Blood immunoglobulin M decreased 62
aIncludes
2023 Summer Conference to Focus on Emergency and Hospital Neurology


continued from cover
Academy’s headquarters. Each year, the Summer Conference focuses on a different topic, and for 2023 Directors Casey S.W. Albin, MD; S. Andrew Josephson, MD, FAAN; and Mark Milstein, MD, FAAN, will lead a lively two-day program dedicated to the critically important topic of emergency and hospital neurology.
The program will highlight the most critical and up-to-date information for neurologists and advanced practice providers. Tailored to the needs of the consultant neurologists at both tertiary and community practices, the curriculum will cover the latest in clinically relevant scientific advances and case-based updates in all important neurohospitalist and neurocritical care topics, as well as offer sessions that will optimize practice, teaching, and quality improvement.
Programming includes:
Case-based updates in several areas including status epilepticus, intracerebral hemorrhage, arterial ischemic stroke, and more
Global talks on health disparities, inpatient neurology, neurology resident training, and wellness among physicians and trainees
Three case-based programming tracks in neurocritical care; hospital neurology topics; and business, training, education, wellness, and diversity, equity, and inclusion

Skills workshops
Exhibit hall
Registrants can attend in person in Minneapolis or live online. Learn more and register beginning early April at AAN.com/Summer

Look How Popular Last Year’s Summer Conference Was with Attendees!
The inaugural 2022 Summer Conference focused on Autoimmune Neurology and Neurology Year in Review. The focused-topic format proved hugely successful with attendees:
99% rated the overall conference as excellent or good
82% rated the quality of each program as excellent
79% plan to participate again
94% would recommend the conference to a colleague.
Live Q/A throughout most sessions
Online poster gallery
Visit AAN.com/AM today to secure your spot—and get the best value when you bundle your registration with Annual Meeting On Demand for extended access to most session recordings through March 1, 2024, and the poster gallery through November 15, 2023.
A ANnews • April 2023 11 EVENTS Boston & Virtual • April 22–27
Can’t Make It to Boston? Join Us for the Interactive Online Experience! continued from cover
Albin Josephson Milstein
Annual Meeting Hubs Foster Collaborative Learning Through Unique Delivery Methods continued
from cover
This year’s hubs include Academic, Innovation, Leadership University, Practice and Policy, Trainee and Educator, Research, Wellness, and the always popular HeadTalks.


Hub Spotlight
Practice and Policy Hub
Learn about practice management and health information tools to create efficient neurology practices regardless of your practice level; learn about AAN legislative priorities to understand how the AAN works on your behalf and identify how you can get involved in your own advocacy work; enhance your advocacy work; and engage in robust discussions about how to implement AAN guidelines, measures, and the Axon Registry ® in your practices to improve patient outcomes. Look for interactive stage talks, debates on controversial practice-related topics, and case studies that invite attendees to engage in their own learning. Topics covered include:
Can and Can’t Dos of Teleneurology
What Your Practice Administrator Wants You to Know
Controversies of the 21st Century Cures Act
Increasing Advocacy Engagement Across the Academy
Research Hub
Discover resources for researchers at all career levels, learn about recognized research recipients, and find inspiration to start or continue your own research. Look for panel and small-group discussions, presentations of all lengths and sizes, fireside chats, one-on-one networking, focused programs by career level, and more. Check out these events and more:
Coffee Connect where you can interact with different research audiences
Daily Fireside Chat with plenary session speakers
Recognition of Research Program recipients
Alzheimer's Network for Diagnostics and Therapy (ALZ-NET): Using Real World Evidence to Define the Future of Alzheimer's Treatment and Care

How to Prepare/Publish Papers for the Journal: Demystifying the Process for Researchers
TRANSCENDS Showcase
National Institutes of Health (NIH) Day
Hope Talks featuring discussions on how research inoculates us with hope

Learn more about 2023 Annual Meeting Hubs at AAN.com/AMHubs

EVENTS Boston & Virtual • April 22–27
Use New Parkinson’s Patient Questionnaire to Improve Visits, Reduce Burden
The new AAN Parkinson’s disease questionnaire joins four previously developed standardized questionnaires for epilepsy, MS, sleep, and headache that can be converted to templates in your EHR. They are disease-specific, incorporate AAN guidelines and quality measures, and have been vetted by clinical experts.
The new questionnaire helps you gather information about current symptoms from patients with Parkinson’s by having them fill it out prior to the exam. This enables you to maximize time with your patients and drive conversation to address their symptoms and concerns.
Documentation burden can be reduced by integrating the questionnaire into your EHR via the patient portal or a
template. Information captured in the questionnaire also can assist in meeting the requirements of Axon Registry ® quality metrics including:
06.1 autonomic symptom screening
04 psychiatric symptom screening
29 rehabilitation options discussed
64 patient reported falls and plan of care
Often, the questionnaire alone will not automatically meet a metric because the metrics may require documentation that a discussion occurred and that a follow-up plan was developed, implemented, or recommended.
Find the Parkinson’s questionnaire and others at AAN.com/practice/electronichealth-records-resources
Compensation and Productivity Data Is Powerful Tool for Neurologists

AAN members who complete the new Neurology Compensation and Productivity Survey by May 11 will receive access to a wealth of data for free—a $500 value. A user-friendly dashboard allows you to filter data by subspecialty, geographic region, gender, and more. The dashboard will be available by July 2023.
“Data from the Neurology Compensation and Productivity Survey was incredibly valuable in analyzing gender related pay disparities in neurology and led to publication of our findings in Neurology ®,” said Melissa Yu, MD, FAAN, director of clinical operations at the Alzheimer’s Disease and Memory Disorders Center and neurology professor at Baylor College of Medicine.
“The depth and breadth of neurologists represented in the survey data allowed us to confirm the hypothesis that women neurologists earned less than male neurologists at nearly all career stages and in most subspecialties.”
“This data set includes much more than physician compensation,” said Gurdesh Bedi, DO, FAAN, director of neurological services at St. Croix Regional Medical Center in Saint Croix Falls, WI. “I love using data on ancillary services to help improve practice efficiency and develop business models. Being in a multispecialty group with limited direct neurology practice data, this survey expands my exposure to thousands of neurologists and hundreds of APPs across the nation.”

“The ability to segment productivity and compensation data provides us with a powerful tool to challenge our models and assumptions, driving innovation and better business decisionmaking,” said Leeann Garms, chief executive officer at Raleigh Neurology in Raleigh, NC. “And the time required to complete the survey is well worth the value we receive from the output.”
 Bedi Garms Yu
Bedi Garms Yu
The Neurology Compensation and Productivity Survey is the largest neurology compensation and productivity survey in the United States, with more than 4,000 AAN members participating in 2021.
For the first time, this year’s survey will capture additional information for those practicing in the full-time telehealth model and for those delivering care in the inpatient setting. While access to the data is free for survey participants, the cost for US members who do not participate in the survey is $500, and $1,500 for nonmembers in the US.
Visit AAN.com/benchmark by May 11 to complete the survey and ensure access to a wealth of data that can help you in your work.
A ANnews • April 2023 13 PRACTICE
Survey Results Show Satisfaction with Axon Registry
The AAN conducted its annual survey of Axon Registry ® participants at the end of 2022. The new pop-up survey on the AAN’s website, reduced to six questions from 20 or more in previous years, resulted in all-time high participation by registry participants.
The results showed 85 percent of respondents strongly or somewhat strongly agreed that they are satisfied with their participation in the Axon Registry. Survey
participants expressed 80 percent satisfaction with their technical vendor. As in previous years, the survey showed the most valuable resources for Axon Registry participants are, in descending order, MIPS reporting, American Board of Psychiatry and Neurology (ABPN) continuing certification credits, quality improvement, and benchmarking. The top two valued benefits of the Axon Registry differed by participant type.
Physicians most value ABPN continuing certification credits, while practice administrators find MIPS reporting as the most valuable benefit of the Axon Registry.
To learn more about the Axon Registry and enrollment information, visit AAN.com/axon. For questions about the survey or the registry, contact registry @ aan.com
PublicPolicy: 23 NCP, Ad—Half Page Horizontal> AN Placed in AANnews 8.25 x 5.25 +0.125 bleed, 4C Complete the 2023 Neurology Productivity and Compensation Survey Start the survey at AAN.com/Benchmark Benchmark compensation and productivity metrics for the inpatient, outpatient, and teleneurology settings using the largest neurology compensation survey in the United States. Complete the survey by May 11, 2023 to receive FREE access to the full data dashboard including subspecialty data— a $500 AAN member value!
YOUR
DISCOVER
VALUE
PRACTICE
Neurology Article Examines Care of People Forcibly Displaced
The AAN has published “Neurologic Care of Forcibly Displaced Persons: Emerging Issues in Neurology” on March 1, 2023, online in Neurology ®. This article defines the scope of the problem of providing neurologic care to forcibly displaced persons (FDPs); highlights commonly encountered clinical challenges related to neurologic care of FDPs; and provides useful clinical information for neurologists and other
clinicians who deliver care to FDPs with neurologic needs. Read the article at Neurology.org
Human-made conflicts, persecution, violence, and human rights violations continue to displace people globally. With more than 100 million people forcibly displaced today, there is an urgent mandate to understand the neurologic care needs of this population and how neurologists and other health care

workers can most effectively provide that care.
The intent of Emerging Issues in Neurology (EIN) articles is to provide timely informal guidance derived from expert consensus until an evidence base is established that can inform evidencebased recommendations. Learn more about the EIN article development process at AAN.com/EIN
Members Chosen for Inaugural Private Practice Awards
The first recipient of the AAN’s new Volunteer Service Award is Praveen Kumar Yadav, MBBS, MD, DM, FAAN, MRCP, FRCP, FEBN, MNAMS, a private practice neurologist from Durgapur, West Bengal, India. Yadav’s volunteer activities run deep through his local community. In a region where neurology services are commonly under resourced, he manages free neurology clinics for low-income patients and organizes patient awareness campaigns for various neurologic conditions. Additionally, Yadav volunteers his time and expertise to provide neurology lectures for rural general practitioners and medical students, where access to high-quality medical education is limited.

“We are excited to present Dr. Yadav with the inaugural Volunteer Service Award,” said Meghan Ward, MD, member of the Volunteer Service Award Selection Committee. “He is highly motivated to deliver a large number of lectures for many different subspecialties of neurology as well as non-neurologic specialties. As a result, he has furthered the breadth and quality of medical care available to his underserved region in a cohesive way.”
The new Neurology Practice Award will be presented to NeurAbilities Healthcare, a private multispecialty practice with locations in Pennsylvania and New Jersey. This award was created to recognize a private practice for excellence in quality care and service to the community. It is unique in that it honors the entire practice team, including advanced practice providers, business administrators, and other clinical support staff.
Founded in 2005 with only six staff, NeurAbilities Healthcare has grown to include over 325 employees and serves as a Specialty Care Medical Home for patients who require access to an array of multidisciplinary specialists. Their “one-stop-shop” model with medical, neuropsychological, behavioral, nutritional, and cognitive specialists paired with patient navigators and community engagement specialists helps eliminate fragmented care and promote personalized medicine. NeurAbilities Healthcare also engages in clinical research and serves as a training site for students, advanced practice providers, and university researchers.

“Through our focus on our vision and mission, we have been able to take our organization from a mere concept to the successful implementation of innovative health care delivery methodologies and systems of care for special needs populations,” said Mark Mintz, MD, FAAN, founder and chief medical officer of NeurAbilities Healthcare. “I proudly accept this award on behalf of all our clinical, administrative, executive, and support staff, as well as the many others who have contributed to our progress over the years.”
The award winners will be recognized at the Annual Meeting on Monday, April 24, from 12:00 p.m. to 1:00 p.m. in the Practice and Policy Hub.
A ANnews • April 2023 15
Yadav
MEMBERSHIP
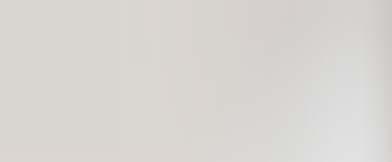
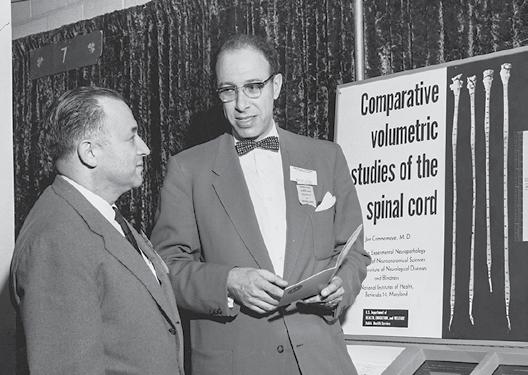
AAN Annual Meetings Bring Worldwide Neurology Community Together
The AAN Annual Meeting has become the world’s largest gathering of neurology professionals, steadily growing from its humble beginning in 1949 at a spa in French Lick, Indiana, to being held in nearly every major US city, from Miami to Seattle, from New York City to Honolulu, and Toronto and Vancouver. By the time of the 2019 Annual Meeting in Philadelphia, the event surpassed 15,000 attendees.
“The Academy has done such a great job with continuing to evolve the Annual Meeting,” said the late Ralph L. Sacco, MD, MS, FAHA, FAAN, who served as president from 2017−2019. “We could have been complacent and said that it’s not broken, let’s keep it the way it is, but we continue to change. And that’s what makes this organization so great. Its willingness to try new things.”
“I’m sorry, your time is up”
Initially, President A.B. Baker, MD, FAAN, and the other founders decided there would be a “national” meeting every other year, with a “regional” meeting in between.

The first National Meeting was held at French Lick Springs. The locale was chosen not only for its amenities, but for the fact that, after seeing the small town for 10 minutes, there would be
nothing to distract attendees from the meeting activities. But the weekend schedule included social time for golf and a bridge tournament—or “networking.” Members’ wives were invited to join the new Women’s Auxiliary.
As Joe R. Brown, MD, FAAN, recalled, “Before the meeting, Abe Baker and I had been fearful that there would not be enough papers and, to furnish a cushion, we submitted four papers and two scientific exhibits. It turned out that we had just enough papers to fill the program. In all, there were 38 scientific papers, one symposium, and 10 scientific exhibits, but there were no papers by title. The content of the program was highly clinical
 Exhibit with Drs. David B. Ruskin and Robert Wartenberg, French Lick 1949.
Ceremonial ribbon cutting. Florence Ruskin; James Sagebiel, MD, FAAN; Ardis Ross; Clark H. Millikan, MD, FAAN; David B. Ruskin, MD, FAAN; Alexander T. Ross, MD, FAAN; A.B. Baker, MD, FAAN; Helen Meister; unknown, unknown. French Lick 1949.
Exhibit with Drs. David B. Ruskin and Robert Wartenberg, French Lick 1949.
Ceremonial ribbon cutting. Florence Ruskin; James Sagebiel, MD, FAAN; Ardis Ross; Clark H. Millikan, MD, FAAN; David B. Ruskin, MD, FAAN; Alexander T. Ross, MD, FAAN; A.B. Baker, MD, FAAN; Helen Meister; unknown, unknown. French Lick 1949.
16 A ANnews • April 2023
Banquet head table: Johannes Nielson, MD, FAAN; Walter F. Schaller, MD, FAAN; Adolph Sahs, MD, FAAN; George Raines, MD; Pearce Bailey, MD, FAAN, Maj. Gen. Paul R. Hawley, MC; A.B. Baker, MD, FAAN; Joe R. Brown, MD, FAAN, French Lick 1949.
and included the treatment of parkinsonism, multiple sclerosis, epilepsy, encephalitis, behavior disorders, and hemiplegia. There were some papers on the basic neurologic sciences and a symposium on anoxic encephalopathy.
“It had been decided that the timetable would be rigidly followed throughout the program. This decision led to an interesting diversion. One of the authors, I believe it was Louis Doshay of New York City, began his presentation by welcoming the Academy, praising its formation, and extolling the virtues of the scientific session. In this way, he used up all but one or two



minutes of his allotted time before he began giving his scientific paper. When the actual time was up, Dr. Wartenberg walked up to him, put an arm around his shoulders, said, ‘I’m sorry, your time is up,’ and led him from the podium.”
The featured speaker at the banquet was the former director of the medical department at the Veterans Administration, who had recently left to lead Blue Cross-Blue Shield. Such connections helped President Baker and Vice President Pearce Bailey, MD, FAAN, advocate for neurology and the new Academy. The 1950 regional meeting in Cincinnati drew 500 attendees and helped the leadership decide on full-fledged Annual Meetings. The event quickly outgrew the spa concept, and resorts were replaced with convention-oriented hotels, and eventually by convention centers.
Continued on page 18 ›
Drs. H. Houston Merritt, Alphonse R. Vonderahe, and David B. Ruskin, Chicago 1953. Virginia Beach 1951.
A ANnews • April 2023 17
Banquet at the Shamrock Hotel, Houston 1955.
AAN Annual Meetings Bring Worldwide Neurology Community Together
continued from page 17
Education Joins Science
The AAN’s founding in 1948 had been sparked by the desire of University of Minnesota resident Joseph A. Resch, MD, FAAN, to have access to continuing education as a practicing neurologist. His mentor Baker became the driving force behind the Annual
we agreed. With bated breath, we waited the results of that first course of the Academy. We were all in Abe’s room when he came in to report that the course was solvent. While we were taking deep breaths of relief, he immediately announced to that ‘Next year we are going to have three courses!’”
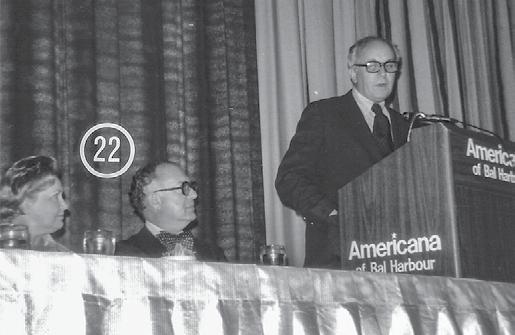
Through the 1950s and 1960s, the Annual Meeting continued to add science and education programming to respond to the needs of members and revelations in research and treatment. The 1954 meeting in Washington, DC, included seven special courses and 20 exhibits. In 1959, the Los Angeles meeting featured 86 scientific papers, including the first by a visiting scientist from the Soviet Union. The AAN’s 15th anniversary was marked with an exhibit at the 1963 meeting in Minneapolis.

Meeting’s education courses. The first offering— known then as a “special course”—was at the Virginia Beach meeting in 1951.
The chair of this first special course was Dr. Fae Y. Tichy, a neuropathologist at the University of Minnesota and one of a handful of women in the profession. “Abe felt the need,” said Francis M. Forster, MD, FAAN, in 1988, “for continuing education and that was long before the term was used or CME became a force in graduate medical education. He pushed for a course in neuropathology. We were concerned about the expense. How could the Academy afford it? Abe offered to make the slides in his own laboratory. So, with his insistence,
18 A ANnews • April 2023 MEMBERSHIP
Exhibit, Houston 1955.
15th Anniversary, Minneapolis 1963.
Entertainment, Chicago 1968.
Morfydd Glaser, Gilbert H. Glaser, MD, FAAN; President Robert A. Fishman, MD, FAAN, Bal Harbour 1976.
The 1973 meeting in Boston offered attendees 165 papers and 16 special courses—and some housing problems. At the business meeting, President Joe Brown shared the story of one neurologist who was told he had no hotel room despite his insistence that he had a reservation. The man informed the clerk that he would make himself at home in the lobby and began to take off his suitcoat and shirt. When the clerk asked him to stop or he’d have to call the police, the man said, fine, then this will be in the newspapers. The man got his room, and Brown suggested the Academy would have to secure more hotels for future meetings. The meeting has long been so popular that there are only a handful of cities that have convention centers and hotel accommodations adequate to meet demand.
For the first time, the Annual Meeting ventured across the border to host city Toronto in 1981. The meeting also was notable for the introduction of practice management courses, championed by Nelson G. Richards, MD, FAAN, a practicing neurologist in Virginia. The meeting also offered new full- and half-day courses and breakfast and dinner seminars.
As the event expanded from three days to six, it became more difficult for practicing neurologists to leave their clinics and take in the entire meeting. In 1984, an initiative by now-President


Richards, placed the three-day scientific session in mid-week, with three days of education programs at the beginning of the week and another two days of education at the end.
With the rise of computers and the Internet in the 1990s, and mobile communications in the 2000s, the Academy harnessed new technologies to deliver highlights of the meeting to members’ offices and homes, including the popular Annual Meeting On Demand. The registration and reservation process went online as did course syllabi and evaluations. Such changes offered convenience to members and are ecologically appropriate.
The AAN introduced a new public element to accompany the Annual Meeting in 2011: the Brain Health Fair. This was an opportunity for the community in the host city to learn more about neurologic disease, get updates on new treatments, and interact with attention-grabbing displays and leading neurology experts. The first Brain Health Fair attracted more than 2,000 patients and caregivers in Honolulu.
“We’re doing something right”
Part of the meeting’s popularity has been its ability to refresh itself and explore new formats. The introduction of Annual Meeting Poster Sessions is a case in point, as related by former President Stanley Fahn, MD, FAAN, who steered the Science Program for a number of years: “They never did poster sessions at any place in clinical neurology that I know of, but since I had been a lab scientist also, I had gone to basic science meetings, and there were poster sessions. What I was impressed about was people would come after the full day, and then at the end of the day, they would have wine and cheese and everybody would go to the poster session. So, I proposed this. I said, ‘You
Continued on page 20 ›

A ANnews • April 2023 19
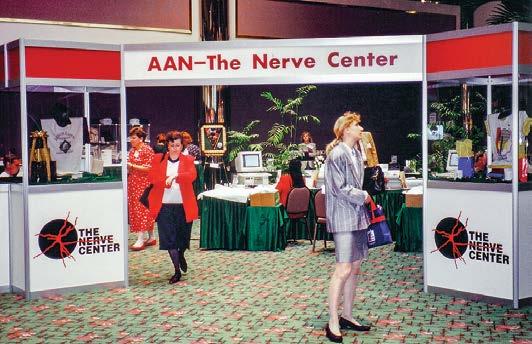
San Diego 1992.
Minneapolis 1998.
Poster Exhibit, Philadelphia 2001.
Helen and Francis M. Forster, MD, FAAN, 50th Annual Meeting, Minneapolis 1998.
AAN Annual Meetings Bring Worldwide Neurology Community Together


continued from page 19
know, if we give them something to eat, they will come, and if we have poster sessions at the end of the day with wine and cheese, they probably will show up. If we do something in the morning at breakfast like a donut and some coffee or orange juice, they will show up.’ And sure enough, it took off, and that was the start of the poster sessions.” Today, paper posters have given way to digital files uploaded to giant monitors.
Recognizing that people enjoy learning in different ways, the Academy introduced Experiential Learning Areas in 2016 in Vancouver, which departed from didactic presentations to offer more informal, hands-on education opportunities. “HeadTalks,” modeled on the popular TED Talks series, gave new occasions for neurologists to cover a wide array of topics. Scheduling was reconfigured to allow more free time in the evenings for socializing, networking, and sightseeing. And the adoption of a one-fee-for-nearly-everything pricing was eagerly embraced by attendees who enjoyed the freedom of not being locked into a pre-paid schedule of courses and programs.
Despite perennial success, planning the Annual Meeting continues to cause similar jitters as in 1949. “We all worry,” Sacco said. “We sat in these meetings saying, what’s going to happen? The audience is going to drop off? It’s going to be too expensive to travel to Annual Meetings? And each year we say, we’re doing something right, more and more people are coming. The networking opportunities, helping people navigate all the other issues that are out there, providing not just research but how they can enhance their career whether they’re a student, a resident, a fellow, a young faculty member, somebody in solo or small private practice—we’re providing something for everyone at that Annual Meeting. And it’s exciting to see that and see that continue to grow. The opening party that we had also at our [2018 meeting] in LA, when we were all at Universal Studios, I never saw so many neurologists laughing, having a good time.”
The good times were forced to pause in 2020 due to the COVID-19 pandemic, which wreaked havoc on preparations for the meeting scheduled in April for Toronto. “This was a very fluid
20 A ANnews • April 2023
MEMBERSHIP
Exhibit Hall, San Francisco 2004.
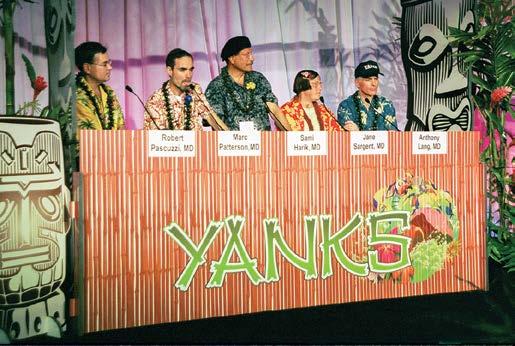
Neurobowl®, Hawaii 2003.
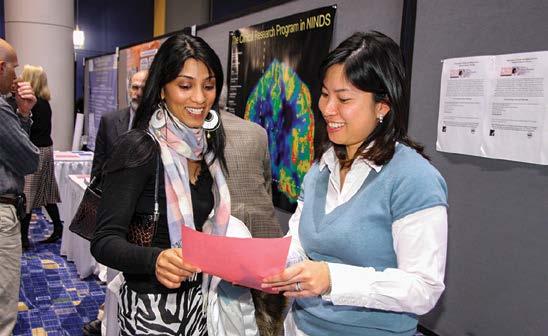
Residents and Fellows Career Forum, Chicago 2008.
Run/Walk for Research. Seattle 2009.
situation,” said James C. Stevens, MD, FAAN, who was president from 2019 to 2021. “I mean, nobody knew what was going on and that we initially heard rumors—it's back in December and January— about this virus…. And so, we had to make a call, and I remember this, we were back and forth, should we cancel? Should we not, et cetera…. And finally, we said, no, the way things are looking and how this is spreading, we've got to keep people safe, [we] have to cancel it.”
To help make up for the loss of the 2020 meeting and the impact of COVID-19 on other AAN conferences, the Academy made the 2019 Annual Meeting On Demand available for free to all members, as well as assisting them in numerous other ways. With the continuing disruptions of the pandemic, the Academy presented a virtual Annual Meeting in 2021, which had never
been attempted before―and it surpassed all expectations of leadership and staff. More than 13,000 attendees participated via their computers, nearly double what had been anticipated. The AAN successfully presented a hybrid meeting in both Seattle and online the following year.



The 2023 Annual Meeting is back bigger and bolder than ever, presented in Boston and live online as well with seven plenary sessions, over 200 courses in a variety of formats, more than 300 talks in our new hubs, and over 2,600 abstract presentations, including 51 platform sessions and 14 poster sessions.
As history has demonstrated, the AAN Annual Meeting will always evolve to match its programming and scheduling to the needs of members and adopt new formats and technology tools to effectively educate neurologists.

A ANnews • April 2023 21
Merit E. Cudkowicz, MD, MSC; Natalia S. Rost, MD, MPH, FAAN, FAHA; President Orly Avitzur, MD, MBA, FAAN; Brenda Banwell, MD, FAAN; Nina F. Schor, MD, PhD, FAAN; Presidential Plenary Session, Seattle 2022.
Lyell K. Jones, Jr., MD, FAAN (left) and AAN President Ralph L. Sacco, MD, MS, FAHA, FAAN; President Elect James C. Stevens, MD, FAAN; former President Stephen M. Sergay, MB BCh, FAAN. Business Meeting, Philadelphia 2019.
Brain Health Fair, Honolulu 2011.
Women in Leadership Course. Vancouver 2016.
Medical Student Diversity Scholars to Attend Annual Meeting
Inclusion is the reason the AAN was founded. To be an organization that is the home for all neurologists. It is what makes us stronger. To support our goal of being a fully inclusive, deliberately diverse, and anti-racist organization and our core values of Inclusion, Diversity, Equity, Anti-racism, and Social Justice (IDEAS), we are excited to share progress and updates with you.
Since 1994, the AAN has offered the Medical Student Diversity Annual Meeting Scholarship that provides funds for travel and lodging expenses to attend the AAN Annual Meeting. These 10 recipients will attend the 2023 Annual Meeting in Boston, where attendees are invited to see them receive their plaques on Tuesday, April 25, at 8:00 a.m. to 9:00 a.m. in the Trainee and Educator Hub:
Freda Assuah Nova Southeastern University
Connor Bluntson University of Mississippi Medical Center School of Medicine
Jasmine Coles Wayne State University School of Medicine
Hayden Hatch Albert Einstein College of Medicine
Jairo Hernandez University of Florida College of Medicine
Joy Josephs Njiribeako Texas Tech University Health Sciences Lubbock
Christine Petit-Frere Morehouse School of Medicine
Miguel Rodriguez University of Tennessee Health Science Center–College of Medicine
Jude Tunyi The Ohio State College of Medicine
Jasmin Williams University of Connecticut School of Medicine
The scholarship is one component of the AAN’s Medical Student Diversity Program, which provides students underrepresented in medicine the opportunity to have exposure to the field of neurology. “Underrepresented in medicine” refers to racial and ethnic populations that are underrepresented relative to their numbers in the general population.
Traditionally, underrepresented groups in neurology include, but are not limited to, African American/Black, American Indian, Native Hawaiian, Alaska Native and Hispanic/Latino.
The AAN has long had a goal of increasing diversity among its members and supports the Medical Student Diversity Program as a major step in that process. The other two components Medical Student Diversity Program are:
Visiting Medical Student Diversity Scholarship
Since 2016, the AAN has offered third- or fourth-year students the opportunity to apply from a list of available programs across the country to participate in a visiting student program. Applications for 2023 are open from February 17 to June 2, 2023, and 20 applicants will be selected. For more information, visit AAN.com/Awards or contact Ben Stoddart at bstoddart @ aan.com
Visiting Professor Diversity Program
In 1994, the AAN began offering an opportunity for a neurology professor―preferably from an underrepresented racial or ethnic background―to be selected to visit an interested underrepresented medical school for two days. The visiting professor may give neurology Grand Rounds, provide an additional lecture to medical students, lead a discussion with medical students regarding careers in neurology and the neurosciences, and observe neurology patient rounds and clinic. The 2023 Visiting Professor is Kita L. Williams, MD, who will be visiting Meharry Medical College.
AANe-news. Because Your Time Is Valuable.
Sent to your email address the second and fourth Wednesday of each month, AANe-news™ delivers the latest top headlines and resources from the Academy so you can quickly scan and connect directly with the information you need to know.
Another members-only solution from your AAN.

22 A ANnews • April 2023 MEMBERSHIP
OFFER PATIENTS FLEXIBILITY WITH SELF-ADMINISTRATION USING ENSPRYNG
For adults with neuromyelitis optica spectrum disorder (NMOSD) who are anti-aquaporin-4 (AQP4) antibody positive.1
ENSPRYNG is the first and only subcutaneous injection that allows patients to self-administer treatment with proper training and their doctor’s approval.1
Monthly self-administration by a patient or their caregiver without the need to travel to a clinic for intravenous infusions1,2 The recommended dosage of ENSPRYNG is 120 mg administered by subcutaneous injection at Weeks 0, 2, and 4, followed by maintenance doses of 120 mg every 4 weeks1
ENSPRYNG remains stable at room temperature for 8 days, enhancing patients’ treatment flexibility1
Indication and Important Safety Information
Indication
ENSPRYNG is indicated for the treatment of neuromyelitis optica spectrum disorder (NMOSD) in adult patients who are antiaquaporin-4 (AQP4) antibody positive.
Contraindications
ENSPRYNG is contraindicated in patients with a known hypersensitivity to satralizumab or any of the inactive ingredients, an active hepatitis B infection, or active or untreated latent tuberculosis.
Warnings and Precautions
Infections
An increased risk of infections, including serious and potentially fatal infections, has been observed in patients treated with IL-6 receptor antagonists, including ENSPRYNG. Delay ENSPRYNG administration in patients with an active infection, including localized infections, until the infection is resolved.
Hepatitis B Virus (HBV) Reactivation
Do not administer ENSPRYNG to patients with active hepatitis.
Tuberculosis
Patients should be evaluated for tuberculosis risk factors and tested for latent infection prior to initiating ENSPRYNG. Patients should be monitored for the development of signs and symptoms of tuberculosis with ENSPRYNG, even if initial tuberculosis testing is negative.
Vaccinations
Live or live-attenuated vaccines should not be given concurrently with ENSPRYNG because clinical safety has not been established. Administer all immunizations according to immunization guidelines at least 4 weeks prior to initiation of ENSPRYNG for
live or live-attenuated vaccines and, whenever possible, at least 2 weeks prior to initiation of ENSPRYNG for non-live vaccines
Elevated Liver Enzymes Monitor ALT and AST levels during treatment; interruption of ENSPRYNG may be required.
Decreased Neutrophil Counts Monitor neutrophils during treatment.
Hypersensitivity Reactions
Hypersensitivity reactions, including rash, urticaria, and fatal anaphylaxis, have occurred with other IL-6 receptor antagonists.
Most Common Adverse Reactions
The most common adverse reactions (≥15% in either trial) were nasopharyngitis (31%), headache (27%), upper respiratory tract infection (19%), rash (17%), arthralgia (17%), extremity pain (15%), gastritis (15%), fatigue (15%), and nausea (15%).
You may report side effects to the FDA at (800) FDA-1088 or www.fda.gov/medwatch. You may also report side effects to Genentech at (888) 835-2555.
For additional safety information, please see the full Prescribing Information and Medication Guide.

References
1. ENSPRYNG [prescribing information]. South San Francisco, CA: Genentech, Inc. 2022.
2. Levy M, Fujihara K, Palace J. New therapies for neuromyelitis optica spectrum disorder. Lancet Neurol. 2020;20(1):60-67. doi:10.1016/S14744422(20)30392-6
© 2023 Genentech USA, Inc. All rights reserved. M-US-00018211(v2.0) 01/23
IN NMOSD
LEARN MORE
above 5 times the ULN, which was observed 4 weeks after initiation of therapy, normalizing 78 days after discontinuation of ENSPRYNG.
Lipid Abnormalities: In Study 1 and Study 2, elevations in total cholesterol above 7.75 mmol/L (300 mg/dl) occurred in 12% and 15% of patients treated with ENSPRYNG, respectively, compared to no patients receiving placebo. Elevations in triglycerides above 3.42 mmol/L (300 mg/dl) occurred in 27% and 12% of patients treated with ENSPRYNG in Study 1 and Study 2, respectively, compared to 13% and 8% of patients receiving placebo.
was observed 4 weeks after initiation of therapy, normalizing 78 days after discontinuation of ENSPRYNG.
Lipid Abnormalities: In Study 1 and Study 2, elevations in total cholesterol above 7.75 mmol/L (300 mg/dl) occurred in 12% and 15% of patients treated with ENSPRYNG, respectively, compared to no patients receiving placebo. Elevations in triglycerides above 3.42 mmol/L (300 mg/dl) occurred in 27% and 12% of patients treated with ENSPRYNG in Study 1 and Study 2, respectively, compared to 13% and 8% of patients receiving placebo.
Fibrinogen Levels: In Study 1, the median percent reduction in fibrinogen was 38% in patients treated with ENSPRYNG compared to 5% in patients receiving placebo. In Study 2, the median percent reduction in fibrinogen level was 33% in patients treated with ENSPRYNG compared to 0% in patients receiving placebo.
Fibrinogen Levels: In Study 1, the median percent reduction in fibrinogen was 38% in patients treated with ENSPRYNG compared to 5% in patients receiving placebo. In Study 2, the median percent reduction in fibrinogen level was 33% in patients treated with ENSPRYNG compared to 0% in patients receiving placebo.
Complement Levels: In Study 1, the median percent reduction in the C3 and C4 components of complement was 23% and 50% in patients treated with ENSPRYNG, respectively, compared to 0% and 1% patients receiving placebo. In Study 2, the median percent reduction in the C3 and C4 components of complement was 20% and 53% in patients treated with ENSPRYNG, respectively, compared to 0% and 1% in patients receiving placebo.
Body Weight: In the pool of Studies 1 and 2, body weight increases of at least 7% from baseline occurred in 28% of patients treated with ENSPRYNG compared to 8% of patients receiving placebo. Body weight increases of at least 15% from baseline occurred in 4% of patients treated with ENSPRYNG compared to 4% of patients receiving placebo.
Complement Levels: In Study 1, the median percent reduction in the C3 and C4 components of complement was 23% and 50% in patients treated with ENSPRYNG, respectively, compared to 0% and 1% patients receiving placebo. In Study 2, the median percent reduction in the C3 and C4 components of complement was 20% and 53% in patients treated with ENSPRYNG, respectively, compared to 0% and 1% in patients receiving placebo.
8.2 Lactation
6.2 Immunogenicity
Body Weight: In the pool of Studies 1 and 2, body weight increases of at least 7% from baseline occurred in 30% of patients treated with ENSPRYNG compared to 8% of patients receiving placebo. Body weight increases of at least 15% from baseline occurred in 6% of patients treated with ENSPRYNG compared to 4% of patients receiving placebo.
6.2 Immunogenicity
As with all therapeutic proteins, there is a potential for immunogenicity. The detection of antibody formation is highly dependent on the sensitivity and specificity of the assay.
Additionally, the observed incidence of antibody (including neutralizing antibody) positivity in an assay may be influenced by several factors, including assay methodology, sample handling, timing of sample collection, concomitant medications, and underlying disease. For these reasons, comparison of the incidence of anti-satralizumabmwge antibodies in the studies described below with the incidence of antibodies in other studies or to other products may be misleading. In Study 1 and Study 2, anti-drug-antibodies (ADAs) were observed in 73% and 38% of patients receiving ENSPRYNG in the double-blind period, respectively. The ability of these ADAs to neutralize satralizumabmwge binding is unknown. Patients with higher body weight and lower exposure were more likely to develop ADAs (irrespective of treatment with IST). Exposure was lower in ADA positive patients. Although antisatralizumab-mwge antibody development was not found to affect the efficacy of ENSPRYNG in these patients, the available data are too limited to make definitive conclusions. Immunogenicity does not have a clinically-relevant impact on safety. Based on the available information, neither dose interruption nor modification is warranted in those patients who develop ADAs.
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
As with all therapeutic proteins, there is a potential for immunogenicity. The detection of antibody formation is highly dependent on the sensitivity and specificity of the assay. Additionally, the observed incidence of antibody (including neutralizing antibody) positivity in an assay may be influenced by several factors, including assay methodology, sample handling, timing of sample collection, concomitant medications, and underlying disease. For these reasons, comparison of the incidence of anti-satralizumab-mwge antibodies in the studies described below with the incidence of antibodies in other studies or to other products may be misleading. In Study 1 and Study 2, anti-drugantibodies (ADAs) were observed in 73% and 38% of patients receiving ENSPRYNG in the double-blind period, respectively. The ability of these ADAs to neutralize satralizumab-mwge binding is unknown. Patients with higher body weight and lower exposure were more likely to develop ADAs (irrespective of treatment with IST). Exposure was lower in ADA positive patients. Although antisatralizumab-mwge antibody development was not found to affect the efficacy of ENSPRYNG in these patients, the available data are too limited to make definitive conclusions. Immunogenicity does not have a clinically-relevant impact on safety. Based on the available information, neither dose interruption nor modification is warranted in those patients who develop ADAs.
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Pregnancy Exposure Registry: There is a pregnancy exposure registry that monitors pregnancy outcomes in women exposed to ENSPRYNG during pregnancy. Healthcare providers are encouraged to register patients and pregnant women are encouraged to register themselves by calling 1-833-277-9338.
Risk Summary: There are no adequate data on the developmental risk associated with the use of ENSPRYNG in pregnant women. In an animal reproduction study, no adverse effects on maternal animals or fetal development were observed in pregnant monkeys and their offspring, with administration of satralizumab-mwge at doses up to 50 mg/kg/week (see Data). In the U.S. general population, the estimated background risk of major birth defect and miscarriage in clinically recognized pregnancies is 2–4% and 15–20%, respectively. The estimated background risk of major birth defects and miscarriage for the indicated population is unknown.
Risk Summary: There are no adequate data on the developmental risk associated with the use of ENSPRYNG in pregnant women. In an animal reproduction study, no adverse effects on maternal animals or fetal development were observed in pregnant monkeys and their offspring, with administration of satralizumab-mwge at doses up to 50 mg/kg/week (see Data). In the U.S. general population, the estimated background risk of major birth defect and miscarriage in clinically recognized pregnancies is 2–4% and 15–20%, respectively. The estimated background risk of major birth defects and miscarriage for the indicated population is unknown.
Clinical Considerations: Fetal/neonatal adverse reactions
Clinical Considerations: Fetal/neonatal adverse reactions
Monoclonal antibodies are increasingly transported across the placenta as pregnancy progresses, with the largest amount transferred during the third trimester. Risks and benefits should be considered prior to administering live or live-attenuated vaccines to infants exposed to ENSPRYNG in utero.
Monoclonal antibodies are increasingly transported across the placenta as pregnancy progresses, with the largest amount transferred during the third trimester. Risks and benefits should be considered prior to administering live or live-attenuated vaccines to infants exposed to ENSPRYNG in utero.
Data: Animal Data
Data: Animal Data
Weekly subcutaneous administration of satralizumab-mwge (0, 2, or 50 mg/kg) to monkeys throughout pregnancy resulted in no adverse effects on postnatal development of the offspring; however, immune function was impaired in offspring at both doses. Plasma exposures (Cave) in dams at the low and high doses were approximately 3 and 100 times, respectively, that in humans at the recommended monthly maintenance dose of 120 mg.
Weekly subcutaneous administration of satralizumab-mwge (0, 2, or 50 mg/kg) to monkeys throughout pregnancy resulted in no adverse effects on postnatal development of the offspring; however, immune function was impaired in offspring at both doses. Plasma exposures (Cave) in dams at the low and high doses were approximately 3 and 100 times, respectively, that in humans at the recommended monthly maintenance dose of 120 mg.
8.2 Lactation
Risk Summary: No information is available on the presence of satralizumab-mwge in human milk, the effects of the satralizumab-mwge on the breastfed infant, or the effects of the satralizumab-mwge on milk production. Satralizumab-mwge was excreted in the milk of lactating monkeys administered satralizumab-mwge throughout pregnancy. Human IgG is excreted in human milk and the potential for absorption in the infant is unknown. The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for ENSPRYNG and any potential adverse effects on the breastfed infant from ENSPRYNG or from the underlying maternal condition.
8.4 Pediatric Use
Safety and effectiveness in pediatric patients have not been established.
Risk Summary: No information is available on the presence of satralizumab-mwge in human milk, the effects of the satralizumabmwge on the breastfed infant, or the effects of the satralizumabmwge on milk production. Satralizumab-mwge was excreted in the milk of lactating monkeys administered satralizumab-mwge throughout pregnancy. Human IgG is excreted in human milk and the potential for absorption in the infant is unknown. The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for ENSPRYNG and any potential adverse effects on the breastfed infant from ENSPRYNG or from the underlying maternal condition.
8.5 Geriatric Use
8.4 Pediatric Use
In general, caution should be used when dosing the elderly, reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant diseases or other drug therapy.
Safety and effectiveness in pediatric patients have not been established.
8.5 Geriatric Use
17 PATIENT COUNSELING INFORMATION
Advise the patients to read the FDA-approved patient labeling (Medication Guide and Instructions for Use).
In general, caution should be used when dosing the elderly, reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant diseases or other drug therapy.
17 PATIENT COUNSELING INFORMATION
Infections: Inform patients that an increased risk of infections, including serious and potentially fatal infections, has been observed in patients treated with IL-6 receptor antagonists, including ENSPRYNG. Instruct patients to contact their healthcare provider immediately when symptoms suggesting infection (e.g., fever, chills, constant cough, or sore throat) appear during treatment.
Advise the patients to read the FDA-approved patient labeling (Medication Guide and Instructions for Use).
Vaccinations: Advise patients to complete any required vaccinations at least 4 weeks prior to initiation of ENSPRYNG for live or liveattenuated vaccines and, whenever possible, at least 2 weeks prior to initiation of ENSPRYNG for non-live vaccines.
Infections: Inform patients that an increased risk of infections, including serious and potentially fatal infections, has been observed in patients treated with IL-6 receptor antagonists, including ENSPRYNG. Instruct patients to contact their healthcare provider immediately when symptoms suggesting infection (e.g., fever, chills, constant cough, or sore throat) appear during treatment.
Elevated Liver Enzymes: Inform patients on the importance of liver enzyme testing.
Decreased Neutrophil Counts: Inform patients on the importance of neutrophil count testing.
Vaccinations: Advise patients to complete any required vaccinations at least 4 weeks prior to initiation of ENSPRYNG for live or liveattenuated vaccines and, whenever possible, at least 2 weeks prior to initiation of ENSPRYNG for non-live vaccines.
Hypersensitivity Reactions: Inform patients about the signs and symptoms of hypersensitivity reactions and anaphylaxis and advise them to contact their healthcare provider immediately if these symptoms occur.
Elevated Liver Enzymes: Inform patients on the importance of liver enzyme testing.
Decreased Neutrophil Counts: Inform patients on the importance of neutrophil count testing.
Instruction on Injection Technique: Instruct patients and caregivers to read the Instructions for Use before the patient starts using ENSPRYNG, and each time the patient gets a refill as there may be new information they need to know.
Hypersensitivity Reactions: Inform patients about the signs and symptoms of hypersensitivity reactions and anaphylaxis and advise them to contact their healthcare provider immediately if these symptoms occur.
Perform the first injection under the guidance of a qualified healthcare professional. If a patient or caregiver is to administer subcutaneous ENSPRYNG, instruct him/her in injection techniques and assess his/ her ability to inject subcutaneously to ensure proper administration of subcutaneous ENSPRYNG and the suitability for home use. Instruct patients to remove the prefilled syringe from the refrigerator prior to use and allow to sit at room temperature outside of the carton for 30 minutes. Do not warm ENSPRYNG in any other way.
Instruction on Injection Technique: Instruct patients and caregivers to read the Instructions for Use before the patient starts using ENSPRYNG, and each time the patient gets a refill as there may be new information they need to know.
Perform the first injection under the guidance of a qualified healthcare professional. If a patient or caregiver is to administer subcutaneous ENSPRYNG, instruct him/her in injection techniques and assess his/ her ability to inject subcutaneously to ensure proper administration of subcutaneous ENSPRYNG and the suitability for home use.
Advise patients to consult their healthcare provider if the full dose is not received.
A puncture-resistant container for disposal of syringes should be used and should be kept out of the reach of children. Instruct patients or caregivers in the technique as well as proper prefilled syringe disposal, and caution against reuse of these items.
Instruct patients to remove the prefilled syringe from the refrigerator prior to use and allow to sit at room temperature outside of the carton for 30 minutes. Do not warm ENSPRYNG in any other way. Advise patients to consult their healthcare provider if the full dose is not received.
A puncture-resistant container for disposal of syringes should be used and should be kept out of the reach of children. Instruct patients or caregivers in the technique as well as proper prefilled syringe disposal, and caution against reuse of these items.
ENSPRYNG® [satralizumab-mwge]
ENSPRYNG™ [satralizumab-mwge]
Manufactured by: Genentech, Inc.
Manufactured by: Genentech, Inc.
A Member of the Roche Group
1 DNA Way South San Francisco, CA 94080-4990
A Member of the Roche Group 1 DNA Way South San Francisco, CA 94080-4990
U.S. License No.: 1048
U.S. License No.: 1048
ENSPRYNG® is a trademark of Chugai Pharmaceutical Co., Ltd., Tokyo, Japan ©2022 Genentech, Inc. All rights reserved. M-US-00004743(v2.0) 05/22
ENSPRYNG™ is a trademark of Chugai Pharmaceutical Co., Ltd., Tokyo, Japan ©2020 Genentech, Inc. All rights reserved. M-US-00004743(v1.0) 08/20
Value of “Us” vs. “Me” Guides Leadership Development Program Graduate to Success
“I had a myopic view of leadership that involved me doing or me acting. It was very ‘me’ centric,” said Bhooma Aravamuthan, MD, DPhil, of her outlook prior to her powerful experience in the AAN’s Emerging Leaders Program (ELP). “The shared leadership model I learned through ELP has been instrumental in showing me how to let the best ideas in an organization grow and shine. Leadership is not about ‘me;’ it’s about ‘us.’ ELP showed me the value of ‘us,’ of sitting in silence, of taking time, of listening and letting things go in directions that I would not have otherwise gone.”
Since graduating from the program in 2021, Aravamuthan’s newfound view has proven influential in guiding her career to new heights, with a series of impressive achievements—and well-earned accolades. She was recently named research director of the St. Louis Children’s Hospital Cerebral Palsy Center at Washington University in St. Louis, where she is also assistant professor of neurology and pediatrics. She co-chairs scientific programs for the Child Neurology Society and American Academy of Cerebral Palsy and Developmental Medicine, serves as an ex-officio board member of the American Neurological Association, and is on the editorial board of the Neurology ® journal. She has been awarded the Child Neurology Society’s Philip R. Dodge Young Investigator Award and, most recently, the AAN’s prestigious Jon Stolk Award for Movement Disorders Research—making her the first pediatric neurologist to ever receive the award.

“The results in all aspects of my professional life have been freeing and rewarding,” said Aravamuthan. “However, perhaps the greatest gift ELP gave me was introducing me to a cohort of people with shared interests and goals. My ELP class still stays in constant touch. We celebrate each other’s success, grieve our losses, and commiserate together. They are part of my professional family—a community of people I can count on.”
Learn more about AAN Leadership Development Programs at AAN.com/Lead
The 2022-2023 Emerging Leaders Program is supported in part by AbbVie; Alexion, AstraZeneca Rare Disease; argenx; Bristol Myers Squibb; Harmony Biosciences; Supernus Pharmaceuticals, Inc.
LEADERSHIP DEVELOPMENT
Applications Opening for Three Leadership Development Programs!
Applications for the AAN's Emerging Leaders Program, Diversity Leadership Program, and Practice Leadership Program open April 12-June 6, 2023. Visit AAN.com/Lead to learn more and to apply.
Not a Section or Synapse Member? Join Us for Hot-topic Conversations and More
If you’re not already an AAN Section member or part of the robust conversations happening right now on SynapseSM Member Communities via the Synapse mobile app, consider joining one—or both—today to be a part of the growing number of participants across the globe who are discussing some of the hottest and most controversial health care topics, like artificial intelligence.
The AAN has 41 sections representing a broad range of subspecialties. Section
membership is free to AAN members and allows you to take part in rich and timely discussions with other AAN members from 140 countries to share ideas and concerns and help shape the future of neurology. Membership in one or more AAN Sections automatically includes access to Synapse.
If you’ll be attending the in-person Annual Meeting this month in Boston, be sure and stop by the AAN Sections Showcase in
Room 254A of the Boston Convention and Exhibition Center daily to learn more about how you can be a part of the conversation, as well as take part in special programming and events hosted by AAN Sections that are open to all attendees.
Visit AAN.com/Sections to learn more, to join, and to download the Synapse mobile app to start sharing your thoughts today!
AAN Member Communities
26 A ANnews • April 2023 MEMBERSHIP
AAN
Aravamuthan
ADVOCACY
Capitol Hill Report
Capitol Hill Report presents regular updates on legislative and regulatory actions and how the Academy ensures that the voice of neurology is heard on Capitol Hill. It is emailed to US members twice monthly and is posted at AAN.com/view/HillReport Below are some recent highlights.
Latest Advocacy News
On February 24, the AAN submitted comments in response to a proposed rule from the Centers for Medicare & Medicaid Services that would implement significant new requirements aimed at reducing prior authorization (PA) burden across payers that are subject to the agency’s authority. This proposed rule is aligned with long-standing AAN advocacy priorities and is the culmination of years of efforts to reduce the detrimental impacts of PA.
The Janice F. Wiesman Congressional Leadership in Neurology Award was presented to Sen. Ben Ray Luján (D-NM) for his continued support of AAN priorities and participation in the AAN's inaugural Brain Health Summit. This award honors the late AAN member Janice F. Wiesman, MD, FAAN, and her dedication to advocacy.

On February 27, the AAN met with CMS to discuss recommendations submitted earlier in the month related to coverage of monoclonal antibodies directed against Alzheimer’s disease as it pertains to lecanemab. The AAN is highly encouraged by CMS’ indicated interest in the AAN’s expertise and in continued dialogue regarding potential modifications to the current National Coverage Determination, especially in light of CMS recent rejection of the Alzheimer’s Association’s request. The AAN is committed to continuing to have an open dialogue with CMS on how coverage policy should be designed for this and other monoclonal antibodies.
Issue in Focus
Last month, 180 members from 45 states gathered in Washington, DC, for the 21st annual Neurology on the Hill. Members learned the skills necessary to have a successful

legislative meeting, the current state of regulatory affairs, and master the 2023 priority issues. On March 7, your colleagues put those lessons to use at in-person Capitol Hill visits with more than 270 members of Congress and discussed the AAN’s top issues facing neurologists today, such as:
Reforming the Medicare Physician Payment System by holding congressional hearings and working with all stakeholders to explore long-term payment solutions
Addressing overly burdensome barriers to care by supporting legislation that addresses prior authorization practices
Supporting medical research and care in FY24 by maintaining robust funding for NINDS, providing full funding for the BRAIN Initiative, and increasing funding for the US Department of Veterans Affairs Neurology Centers of Excellence.
Sally L. Harris, MD, FAAN; AAN CEO Mary E. Post, MBA, CAE; Sen. Ben Ray Luján; and President Elect Carlayne E. Jackson, MD, FAAN.
Cerebrovascular Disease Explored in Continuum
The latest information on cerebrovascular disease is presented in the April issue of Continuum: Lifelong Learning in Neurology ®
Guest Editor Hooman Kamel, MD, MS, said, “There is a wealth of exciting new information in this issue, including tenecteplase and other emerging approaches to thrombolysis, up-to-date indications for mechanical thrombectomy, genetic contributions to small vessel disease, and evidence-based approaches for secondary stroke prevention.”
Topics in this Continuum® issue include:

Diagnostic Evaluation of Stroke Etiology
James F. Meschia, MD, FAAN

Intravenous Thrombolysis for Acute Ischemic Stroke
James C. Grotta, MD, FAAN
Mechanical Thrombectomy for Acute Ischemic Stroke
Sunil A. Sheth, MD
Diagnosis and Management of Cardioembolic Stroke
Shadi Yaghi, MD, FAHA

Diagnosis and Management of Large Artery
Atherosclerosis
Seemant Chaturvedi, MD, FAAN, FAHA
Diagnosis and Management of Cerebral Small Vessel Disease
Anjail Sharrief, MD, MPH
Diagnosis and Treatment of Cerebral Venous Thrombosis
Ava L. Liberman, MD
Cervical Artery Dissection
Setareh Salehi Omran, MD
Pediatric Arterial Ischemic Stroke
Christine Fox, MD, MAS
Stroke Rehabilitation and Recovery
Michael W. O’Dell, MD
Management of Unruptured Intracranial Aneurysms and Brain

Arteriovenous Malformations
Thanh Ngoc Nguyen, MD, FRCPc, FSVIN, FAHA
The Transformation of Documenting and Coding for Neurologic Hospital Inpatient and Observation Services
Raissa Villanueva MD, MPH, FAAN; Neil A. Busis, MD, FAAN; Bruce H. Cohen MD, FAAN; Luana Ciccarelli, CPC, CRC
The issue includes a postreading self-assessment and test with the opportunity to earn up to 20 AMA PRA Category 1 Credits™ toward Self-assessment CME.
Starting April 10, AAN members receive a 15-percent discount when subscribing or renewing Continuum and Continuum® Audio, bringing a yearly subscription to just $339 per year. Subscribe now by contacting Wolters Kluwer at (800) 361-0633 or (301) 223-2300 (international) or visit shop.lww.com/continuum
This offer expires June 30, 2023. AAN Junior members who are transitioning to neurologist memberships are eligible to receive a 60-percent discount on the already low member rate for the Continuum and Continuum Audio subscription.
28 A ANnews • April 2023 EDUCATION
CONTINUUMJOURNAL.COM Continuum LIFELONG LEARNING IN NEUROLOGY® APRIL 2023 VOL. 29 NO. 2 Cerebrovascular Disease EDITOR-IN-CHIEF: LYELL K. JONES JR, MD, FAAN GUEST EDITOR: HOOMAN KAMEL, MD
Kamel
Stop by UCNS Booth at Annual Meeting for Subspecialty Certification and Accreditation Information
Stop by booth #864 in the Exhibit Hall of the Boston Convention and Exhibition Center during the 75th Annual Meeting to learn more about physician certification and accredited fellowship program opportunities through the United Council for Neurologic Subspecialties (UCNS). As neurology’s recognized certifying and accrediting body for emerging subspecialties, the UCNS currently provides accreditation and/ or certification for the neurologic subspecialties of Autonomic Disorders, Behavioral Neurology & Neuropsychiatry, Clinical Neuromuscular Pathology, Geriatric Neurology, Headache Medicine, Interventional Neurology, Neonatal Neurocritical Care, Neuroimaging, Neurocritical Care, and Neuro-oncology. The UCNS has over 200 accredited fellowship programs and 3,000 certified physicians in the United States and Canada. Staff will be on hand in the booth to share information and answer questions about UCNS certification, continuous certification requirements, fellowship program accreditation
requirements, and accredited subspecialty fellowship opportunities.
The UCNS will also have representatives available at the Faculty and Trainee Reception on Monday, April 24, from 6:00 p.m. to 8:00 p.m. to answer questions and provide information for trainees about UCNS-accredited subspecialty fellowship programs. Representatives will also take part in a panel presentation in the Trainee and Educator Hub at 9:00 a.m. on Tuesday, April 25, giving program coordinators an opportunity to learn more and ask questions about the UCNS accreditation process.
Neurology Question of the Day Helps Residents Prepare for RITE
Neurology Question of the Day (QOD) is the AAN’s convenient mobile app designed to provide a quick and fun way for users to assewss their knowledge in neurology and fulfill self-assessment CME requirements. Following a monthly curriculum, the app serves up one new multiple-choice question with discussion each day on various topics in neurology and provides suggested resources for further study.
Recently, a limited number of questions on the 2023 RITE® (Residency In-service Training Exam) appeared in the QOD app before the RITE test week of February 14 through 20. The effort was part of a pilot to assess the quality of the questions and encourage more residents to use QOD as a means to practice answering clinical neurology questions before sitting for the RITE. Evaluation is underway for including similar pretest items in QOD in 2024, as well as prioritized inclusion of new,
higher quality imaging studies and incorporating more video content on the RITE so residents have a more “real-world” experience when answering questions.

Registration for the 2023 RITE once again broke a record, with more than 3,700 residents representing more than 280 neurology resident programs worldwide sitting for the exam. An enhancement to the 2023 RITE will include reporting of raw scores for
questions classified as Core Neurology or Subspecialty Neurology. These new scores will be included later this month in both the resident individual score report and in the program’s summary report of all residents from their program.
To learn more about Neurology Question of the Day and to download the app, visit AAN.com/QOD. To learn more about the RITE, visit AAN.com/RITE
A ANnews • April 2023 29
Neurologist—Kelsey-Seybold Clinic—Houston, Texas
Kelsey-Seybold Clinic is Houston’s premier multispecialty group practice, founded in 1949 by Dr. Mavis Kelsey in Houston’s renowned Texas Medical Center. More than 600 physicians and allied health professionals practice at 31 locations in the Greater Houston area. Kelsey-Seybold offers quality medical care in 65 medical specialties. The organization operates the largest freestanding Ambulatory Surgery Center in the state of Texas and offers state-of-the-art Varian TrueBeam and Varian Edge radiation therapy technology at a nationally accredited Cancer Center. An accredited Sleep Center, comprehensive laboratory services, advanced imaging and diagnostics, 16 on-site Kelsey Pharmacy locations, and MyKelseyOnline, a secure web portal, are part of its comprehensive offerings. Kelsey-Seybold partners with major insurers to offer value-based commercial health plans. KelseyCare Advantage, a Medicare Advantage plan offered to Houston-area beneficiaries and affiliated with Kelsey-Seybold Clinic, has achieved the coveted 5-out-of-5-star rating from the Centers for Medicare and Medicaid for three consecutive years and is the only 5-out-of-5-star rated plan in Texas. Pathway to Partnership Unlike other organizations, KelseySeybold physicians have the opportunity for ownership in the Medical Group, as well as in The Kelsey-Seybold Management Company. The ownership path is clear and straightforward. A Kelsey-Seybold Physician is typically eligible for ownership after three years of employment, board certification, and demonstrated good citizenship. The result is an extraordinary, broad-based, and diverse physician-led organization. When you join Kelsey-Seybold, you become part of an established, physician-owned, and led multispecialty group practice with a 70-year legacy of caring for patients. 72 physicians hold leadership positions, 56% of our physicians are shareholders, The average physician tenure is 11 years, Physician-led board of managers, A defined path to partnership, Due to phenomenal growth, multiple locations are available throughout Greater Houston with new clinics opening in late 2022 and in 2023!
At Kelsey-Seybold Clinic, our Neurologists diagnose, treat, and manage patients with neurological disorders or the nervous system. They see patients in the office from 8am5pm Monday through Friday. One of the group neurologists takes call during weekday evenings and on weekends every six weeks on average. Kelsey Seybold Clinic has a 24-hour call center and after-hours registered triage nurse to assist
Where the Top Jobs and Top Talent Connect!

inpatient care. Qualifications: Graduate of an approved training program in the United States. Board-certified or eligible. Licensed or willing to be licensed in the State of Texas. Benefits and Compensation: Our physicians practice medicine in a collaborative manner amongst many medical specialties and subspecialties embracing technology and teamwork to provide patient-centered care. Our compensation package is productivity-based and includes salary, paid time off, CME, and matching 401K. Affiliated with Baylor College of Medicine and the Texas Heart Institute. Multispecialty group practice setting, Regular weekday hours, Full nursing and clerical support, Paid malpractice and tail coverage, Electronic Medical Records. As the 4th largest city in the U.S., Houston, Texas is a leader in business, entertainment, the arts and more. From professional sports to outdoor fun to an out-of-this-world space experience and incredible dining – it’s all here! Stroll the beaches of Galveston or challenge yourself on one of our many golf courses. Space City offers everything from breathtaking museum exhibits to vibrant downtown entertainment. Explore the wonder of space or spend the day shopping to your heart’s content. Houston is a city of infinite possibilities. Kelsey-Seybold Clinic is an equal opportunity employer and all qualified applicants will receive consideration for employment without regard to race, color, religion, sex, national origin, disability status, or protected veteran status. Kelsey-Seybold is a VEVRAA Federal Contractor and desires priority referrals of protected veterans. Contact Meril Jacob; meril.jacob@kelsey-seybold.com with interest or for more information.
Division Chief/Practice Lead Opportunity in Neurology— Berkshire Health Systems—Pittsfield, Massachusetts
Division Chief/Practice Lead Opportunity in the Beautiful Berkshires of Western Massachusetts! Opportunity Highlights Well established practice with a team of well-rounded, experienced Physicians and APP's. Clinical neurology involvement with students and residents. Supervision of division members, including credentialing. General Neurology or subspecialty interests are welcome. 1 in 5 call arrangement gives you the 'perfect' position to balance both your professional interests and personal commitments. Primary Neurology practice in Berkshire County with a Joint Commission Certified Stroke Center. Generous vacation and CME allotment to create a sustainable work life balance. Exceptional compensation
and rich benefits package, including sign on, productivity option and relocation. Location Highlights The Berkshires, located in the northwestern part of Massachusetts, offers a beautiful setting with a small town feel and endless cultural opportunities of a big city. Art, theaters, museums, concert venues, restaurants, local small businesses, fitness centers, golf and spa resorts. We have it all! Four seasons of fun and adventure offering skiing, snowshoeing, kayaking, rafting, sightseeing, hiking along the Appalachian Trail and road/ mountain biking. Affordable lifestyle with excellent public and private schools makes us an ideal family location. Only a 2.5-hour drive to Boston, MA and New York City. Hospital Highlights Our mission is to advance health and wellness for everyone in our community in a welcoming, inclusive, and personalized environment. Berkshire Health Systems is the region's leading provider of comprehensive healthcare services. With award-winning programs, nationally recognized physicians, world-class technology and a sincere commitment to the community, BHS is delivering the kind of advanced healthcare most commonly found in large metropolitan centers with the care and passion of a unified community. Berkshire Medical Center is a 298-bed community teaching hospital with residency programs. Interested candidates are invited to contact: Michelle Maston, Physician Recruiter at mmaston@bhs1.org or Apply online at: www.berkshirehealthsystems.org
AANnews® Classified Advertising
The AAN offers a complete package of print, online, and in-person recruitment advertising opportunities. Visit Careers.AAN.com for all AAN options, rates, and deadlines.
Ad copy for the June 2023 print edition of AANnews must be submitted by May 1, 2023. The same deadline applies to changes/cancellations.
The American Academy of Neurology reserves the right to decline, withdraw, or edit advertisements at its discretion. Every care is taken to avoid mistakes, but the responsibility for clerical or printer errors does not exceed the cost of the ad.
From first job to career shift, get access to the latest openings, candidate CVs, and timely resources to seal the deal. Go right to the top at Careers.AAN.com! 22NCC CampaignPrintAds v02.indd 6 1/6/22 11:06 AM
for
confidential notifications when positions of interest are added. 30 A ANnews • April 2023
Careers.AAN.com Visit the AAN’s Neurology Career Center to view hundreds of additional jobs and sign up
customized,
DATES & DEADLINES DATES & DEADLINES
APRIL
Early April
Registration Opens: AAN Summer Conference AAN.com/SummerConference
April 1
Application Deadline: UCNS
Neuro-oncology Certification UCNS.org/NOcertification
April 12
Applications Open: Emerging Leaders, Diversity Leadership, and Practice Leadership Programs AAN.com/Lead
April 22–27
75th AAN Annual Meeting: Boston and Live Online AAN.com/AM
April 22
AAN Business Meeting in Boston AAN.com/AM
23 MVP PRINT AD—HALF PAGE HORIZONTAL> AN PLACED IN AANNEWS 8.25 X
MAY
May 1
Application Deadline: UCNS Clinical Neuromuscular Pathology Certification UCNS.org/CNMPcertification
May 3–4
Virtual Career Fair Careers.aan.com
May 11
Neurology Compensation and Productivity Survey Deadline AAN.com/Benchmark
JUNE
June 1
Early Registration Deadline: AAN Summer Conference AAN.com/SummerConference
Application Deadline: UCNS
Neurocritical Care Certification UCNS.org/NCCcertification
June 6
Application Deadline: Emerging Leaders, Diversity Leadership, and Practice Leadership Programs AAN.com/Lead
5.25
4C
Visit AAN.com/qpp to understand these changes in reporting requirements. A new track within the Quality Payment Program may affect your practice. MIPS VALUE
+0.125 BLEED,
MIPSMVP
PATHWAYS
AAN Membership: What You Need. When You Need It. Join or Renew. AAN.com With a combined benefits value of up to $4,000, only AAN membership offers exclusive access to the highest quality resources—when you need them—from the world’s largest and most trusted community of neurology professionals. Research Advocacy Professional Growth Practice Management Education Community Wellness AAN LEADERSHIP DEVELOPMENT AAN Member Communities
