











The official magazine for ANF members in WA February 2024 Incorporating Western Midwife


As we gear up for what promises to be a significant year for the ANF and its members in 2024, we wanted to bring you an important update regarding our the ANF Conferences.
Given the crucial events shaping this year, such as the 2024 Public Sector EBA negotiations starting in July, followed by the SJOG, Ramsay, and various aged care EBA negotiations, it has become imperative that our primary focus remains on securing the best possible outcomes for our members. There will also be some additional work preparing for the upcoming WA state election which is just 12 months away.
In light of these considerations there has been a change to the ANF Conference schedule.
The ANF Legal & IT Issues Conference is now scheduled for May 2025, followed by the ANF Financial Wellbeing Conference in October 2025. We believe that this adjustment will allow us to not only deal with the pressing priorities and concerns for our members in 2024 but also allow us to deliver better, value packed conferences in 2025.
Further details about each conference, including confirmed speakers and topics, will be shared with you as soon as they are finalised.

I would firstly like to thank ANF Public Sector members for their input and commitment throughout our long-running Public Sector EBA negotiation. The agreement was almost two years overdue, and you stuck with us through it all. Early last month as you know, we finally came to an agreement. While this deal is not what WA’s nurses and midwives are worth, after 18 months of negotiation we achieved the maximum amount we could in this round of negotiations. With the knowledge that our 2024 Public Sector negotiations begin in April, it was imperative that we brought the previous round of negotiations to a conclusion. I am confident that with the Cook Governments scrapping of their previous restrictive wages policy, we will achieve a pay deal for public sector workers that will undoubtedly better reflect the true value of our members, and flow on to ANF private sector members as well.
With many private sector employers holding out for the public sector results this year, I know the ANF must also conclude the outstanding EBAs. With the knowledge of a State Election approaching only months after the expiration of the 2024 Public Sector EBA, I am certain we can achieve a truly fair wages deal for WA’s nurses and midwives.
The next few years will be critical for our industry – we need better wages and conditions, we need better recruitment and retention, and we need better management of our health system ultimately. I know the pain our industry is going through – the pain you are all going through. I was a nurse working in ED up until only two years ago when you elected me State Secretary. Even then I saw the rapid decline of our working conditions, of our hospital system and the morale of the workforce. In the short time I’ve been State Secretary I’ve seen it decline even further. The State Government continued their excuses, blaming their lack of progress on worldwide staff shortages and lack of funds – it isn’t a State Government's job to find excuses, but to find solutions. The fact that there are more challenges now than in the past should be the driving force for finding solutions and remaining competitive. The ANF has previously offered solutions and plans to best advise the State Government on how we can improve our health system, with no real response. In the coming months the ANF will be putting together your Public Sector log of claims for the 2024 Public Sector EBA. Your input and contributions will be vital in preparing for what we will be asking the government for later this year.
In the meantime, I have been spending time visiting WA’s nurses and midwives all across WA with more trips planned this year so I can see as many of you as possible. If you would like to me to visit your workplace please email me at anfsecretarywa@anfiuwp.org.au
As a 2023 Western Australian Country Health Service graduate nurse, 30 year old Teghan Russell knew she wanted to work in the country. Now, a year on from graduation, Teghan has had time to reflect on her first 12 months working as a nurse in the country, and she is also happy to share what she has learned with this year’s WACHS graduates.
Originally from Donnybrook, about two hours south of Perth, Teghan has always preferred working in the country. It took her a little while to decide to start her studies to become a nurse, but she has long worked in healthcare.
“I worked in health admin for 11 years prior to becoming a nurse, and in that time, I decided that I wanted to work more hands-on in the healthcare field.”
She studied at Edith Cowan University and when Teghan graduated in 2022 she remained dedicated to working in the country. However, she took the opportunity to move further afield within WA.
“I grew up in the country and much prefer it to living in the city. I was keen to explore a different part of the state once I completed my studies and I’m now happily living and working in the Kimberley.
“I’m working in the Theatre Department at Broome Hospital. I was really lucky to get my dream grad job, with six months on the general ward and six months in theatre, which is the area of nursing I want to continue in.”
Like so many other nurses, Teghan sees the power to help those in need as one of the best parts of her job. During her first year


as a nurse, she has had the opportunity to do just that, while also adding to her own list of new experiences.
“As a nurse I have the ability to help people and try to make their experience in hospital more positive.
“Seeing a caesarean section for the first time was a pretty amazing experience.”
Teghan said this experience was topped when she scrubbed in to actually assist with a caesarean section.
Of course, nursing is not without its challenges, especially when it comes to working in more remote parts of WA, as Teghan notes Broome Hospital is a long way away from a major city and tertiary hospitals. She describes one of the biggest challenges as “information overload”.
“There is always so much to learn and remember, and it is easy to be hard on yourself when you are starting out.”
WACHS recently announced a bumper year of new graduates, welcoming nearly 200 newly qualified nurses and midwives in 2024. Now with her first year as a nurse behind her, Teghan has some words of advice for these new recruits.
“Make the most of every opportunity you are given. Working in the country is a unique experience and you will get the chance to do things you wouldn’t otherwise be doing in the city.”
The Western Nurse wishes these 200 new graduates all the best in their first year, and we hope Teghan continues to enjoy working as a country nurse.
The 2022 Public Sector EBA negotiations have concluded, following a long and often difficult battle with a state government who were determined to fight the ANF at every step. Now, our focus must be on the next round of negotiations due to start in April 2024.
These negotiations were the most protracted EBA battle ever fought by the ANF. For 18 months the ANF, led by Sate Secretary Janet Reah, went head-to-head with the WA Government to ensure members got the best possible deal.
Ms Reah said that while she understood the frustration from members about some aspects of the new agreement, the ANF is already gearing up for the next round of negotiations.
“With the 2022 Public Sector EBA put to rest, the focus will now shift to the 2024 Public Sector EBA negotiations set to begin in a few months’ time.
“This was a long and difficult negotiation and campaign and I share the frustrations of nurses and midwives who believe that this isn’t enough to remedy the staffing shortfalls in our public health system.
“Even with this pay increase WA nurses and midwives remain the lowest paid in the country.
“This deal does not truly reflect what nurses and midwives are worth. But the outcome voted for by the members was the maximum we could achieve in these negotiations.
“The ANF will be seeking a more substantial and fair wage increase in the next round of negotiations which begin in April.”
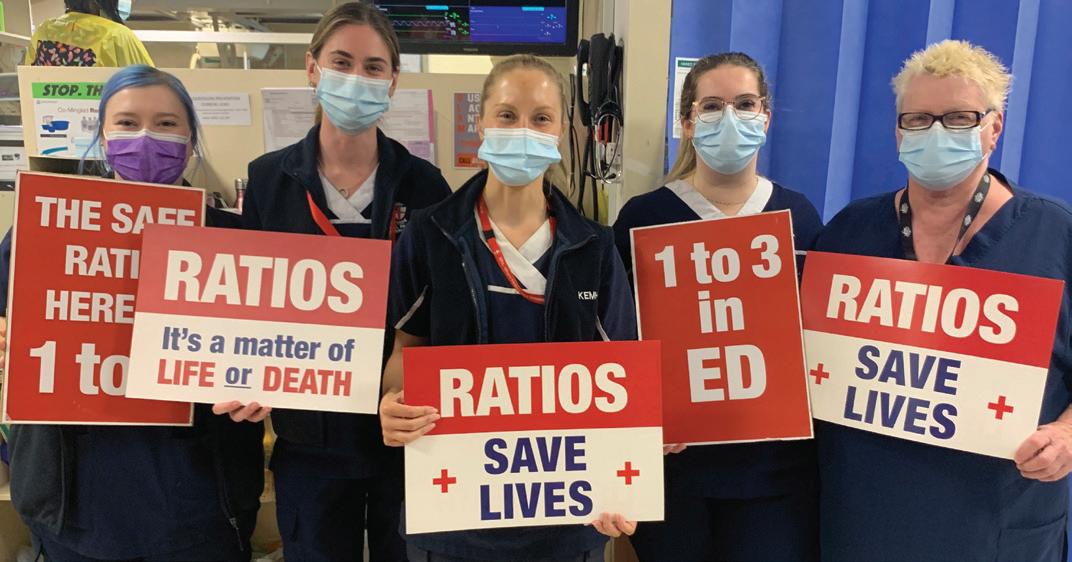
One major victory from the 2022 EBA negotiations was the WA Government’s agreement to implement patient ratios, a vital
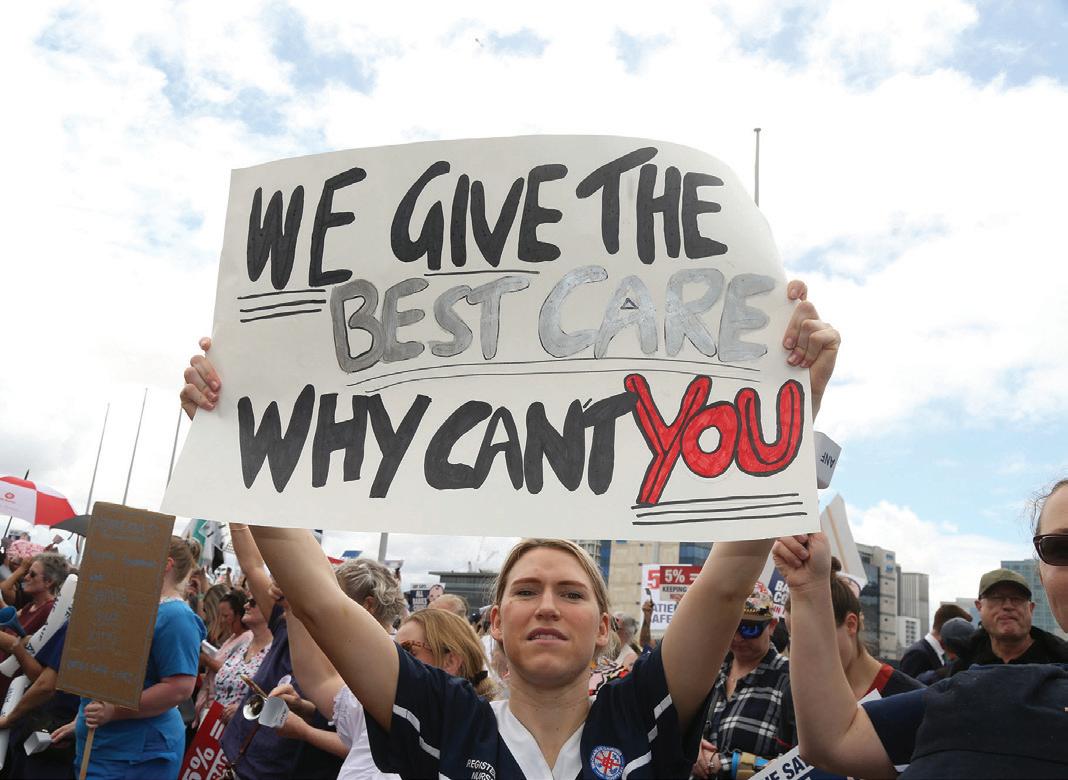

and lifesaving initiative that will protect nurses and patients. The implementation of these ratios will commence as previously negotiated.
“It is vital that the ANF and the government now focus on the implementation of transparent and enforceable patient ratios,” Ms Reah said.
Under the new EBA public sector workers will also get a new Professional Development Allowance for every level. They will also see their professional development leave paid out this year. This is on top of the already paid 3 percent wage increase.
The professional development allowance will apply to all levels and increments. The amounts are as follows:
• $700 per year for Levels 1.1 to 1.7
• $1,100 per year for Levels 1.8 to Level 2.4
• $1,100 per year for SRN Levels 1 to 5
• $1,400 per year for SRN Levels 6 to 10
The next EBA campaign kicks off in April with the drafting of a new Log of Claims in preparation for the 2024 EBA negotiations which begin in July. This will coincide with the lead up to the next state election.
This is just around the corner, and the ANF is committed to ensuring WA nurses are paid what they deserve, and that WA becomes competitive again.

The story of nurse Vivian Bullwinkel is one marred by tragedy and suffering, while also uplifted by resilience, hope, duty and friendship.
It is a story that, after many years, was finally recognised with a statue at the Australian War Memorial in Canberra. Now, it is being told through a new play, 21 Hearts: Vivian Bullwinkel and the Nurses of the Vyner Brooke.
The play focuses on Vivian and the 65 Australian nurses who boarded the Vyner Brooke, fleeing the Japanese invasion of Singapore in February of 1942. The ship was bombed and sank. Vivian and other survivors were washed up on Banka Island, where they surrendered. Rather than keep them as prisoners, the Japanese marched 22 nurses, including Vivian, into the ocean and shot them. Vivian survived, but spent the rest of the war in a prison camp.
Jenny Davis, the writer of the play, calls it a story of friendship and courage. The play itself focuses not just on Vivian, but on the nurses and women interned in the prison camp.
“I think the major theme of this story is not just about courage, but about friendship and how the women, because they had all nursed together, had formed this bond and looked after each other,” Ms Davis said.
“I read a woman’s account of the camp, a civilian woman, who said she envied the nurses and how they didn’t seem to have the awful daily squabbles that emerged when you are living in close proximity to hundreds of others.
“Things were pretty awful. People were starving and being bitten to death by mosquitoes. The nurses seemed to rise above all those squabbles because they had a purpose, and because they had this close friendship.”
That sense of purpose is linked to notions of duty and service, notions that nurses are well acquainted with.

“You put on a uniform, and then you have a job to do. People come to you for help. You get a certain amount of respect because you are wearing that uniform, but you have to live up to it.
“These nurses also felt one thing they must never show was fear. They didn’t want to show they were afraid, because it didn’t help them, and it didn’t help anybody else.”
The struggles of those women in the prison camp reflects Ms Davis’ own family history, as her uncle was held in a POW camp during the war.
“He said you couldn’t just live for yourself, you had to live for somebody else. That helped get you through.”
This sense of stoic determination is also central to the story told in the play.
Ms Davis has written a number of historical works over the years, including about World War Two. Sharing these stories is again linked to Ms Davis’ own family. She founded THEATRE 180, originally called Agelink, 30 years ago in order to record stories of seniors and turn them into shows.
“It started for me in 1993. My dad in England had died, and I was always going to record his stories, because he had some great stories about World War One. He was only a child at the time in London, but they were terrific stories. I realised I missed my chance.
“I got interested in oral histories and having worked in theatre all my life as an actor and director I thought this is how I can bring these stories to life.
“I’ve been writing these kinds of shows for some time. I just love it. It’s a way of making history accessible.”
Telling Vivian’s story on stage is also an opportunity to share the experiences of war from the perspective of women, something often missing from history.
“We do so many men’s stories about the world wars, and not so many from women, so we are always on the look-out for women’s stories. And this is an extraordinary story.”
Having survived being shot on Banka Island, Vivian began a threeyear ordeal. She again had to surrender to the Japanese and was again taken prisoner. She had been shot in the hip, and had to conceal that wound from her captors for fear that her status as witness to a war crime could lead to her death.
“To hide her wound and the hole in her clothes she wore a water bottle she had found, that had washed up along with a strap. She wore it over her uniform strategically so the wound couldn’t be seen.
“Then there was three years in an internment camp where things got worse and worse. The women were dying of typhus and starving, just like the men, but their story hasn’t been told to the same degree. When it comes to women there have been a few books, not nearly so many stories as have been told about the men.”
Ms Davis said the play is a wonderful chance to redress that and make sure that the valour of these women is known.
There are only women in the play. There are some male characters who appear briefly, but only as voiceovers, and we don’t meet any of the Japanese in the play. Ms Davis felt that as the story is about the women, the play needed to focus on them.
Ms Davis actually met Vivian years before, at a showing of one of her earlier plays. Vivian had attended the play, with her friend Edith

Kenneison. The pair had met in the prisoner camp in Sumatra. Their story was remarkably similar to Ms Davis’ play. Edie was only 14 at the time and Vivian was somewhat older. Vivian had looked after Edie in the camp.
“I was doing a play at the time called Shoehorn Sonata which was set in a prisoner of war camp in World War Two. It was about a nurse and a young girl who she befriends in an internment camp. “Vivian and Edie came along to the theater and said, ‘well this is a lot like our story.’ That was really fascinating.”
Ms Davis recalls Vivian being a lovely, cheery and jolly woman with a huge smile.
“I think the wonderful thing about Viv was that she had been able to spend her life still in service to the nation, to her lost friends and to children. She did some remarkable things,” Ms Davis said. Many of these remarkable things occurred long after Vivian’s ordeal in the War.
“A lot of people in the nursing profession have said that she wasn’t just inspiring because of what she went through, she was just inspiring full stop.
“One lady, a retired nurse, said ‘I regard her as being one of the founders of modern nursing’. She just worked so hard all her life to improve conditions for nurses and for patients, while all the time working hard to keep the memory of the nurses who died on Banka Island alive, and the others in the camps.
“She was at the front of an expedition to Vietnam to rescue orphans during the Vietnam War. She was at the front of everything in nursing and she was an extraordinary woman.
“She mentored many young nurses, and she helped get young people into the nursing profession who wouldn’t normally have been accepted, because of their education.
“She recognized in people the qualities that they had and she was determined to help them. She was hugely generous of heart and spirit. She was a woman of faith, a practicing Christian, and I’m sure that underpinned a lot of her values but she was by nature just a very generous woman.”
21 Hearts: Vivian Bullwinkel and the Nurses of the Vyner Brooke will run from 11 to 21 April at the Como Theatre.
The ANF received so many questions from attendees at the ANF Legal Conference last year that it was impossible to answer them all at the time, so we followed-up up with our presenters and shared your questions with them. We received so many answers that the Western Nurse has had to publish them over several editions.

Dr Michael Eburn is and Australian lawyer, with a strong background in legal issues that affect emergency services workers. He spoke at the conference about the conflict between a duty to act in a patient’s best interests and the patient’s right to self-determination.
What rights do police have with taking samples from unconscious patients and/or the patient’s property?
Police have powers under many items of legislation and common law to take control of a person’s property and to take samples. It is impossible to answer this question without relevant context.
If a patient is drunk, shoved a knife into their chest during an emotional outburst to their ex, called an ambulance, and is then refusing treatment at the ED - are we covered to follow their refusal?
If they remain competent then they can refuse treatment.
Can Doctors use “duty of care” for giving or doing things without consent from a patient?
Not if the patient is competent. If the patient is unable to communicate their wishes (ie they are not competent) then yes a doctor can give or do “things” without consent from the patient provided the “things” done are reasonable and in the patient’s best interests (In Re F [1990] 2 AC 1).
In my workplace, signed consent forms “last for one year”. Do consent forms require a timeframe/ expiry date from when the patient signs? Or should this be revisited regularly?
A consent form is evidence of the patient’s consent. The form itself is not the consent. Whether consent is enduring depends on what is being consented to and all the circumstances.
A person who consents to have their right leg amputated cannot be assumed to have consented to having their left leg amputated within 12 months.
A person who consents to tests that, at the time, are expected to be repeated every month may only need one consent form if it reflects that advice but even so their consent should be confirmed each time as people can withdraw consent every time.
In the circumstances it is not possible to answer this question without relevant context about the nature of the work and what people are being asked to consent to.
Can we detain patients in hospital who have a form 1A - referral to see a psychiatrist, who may or may not be competent and who may or may not be placed on a Form 6B once seen by a psychiatrist? Would this change if the patient has a history of being placed on Form 6Bs for Anorexia Nervosa/ Eating Disorder?
It makes a significant difference whether the patient is or is not competent. Criteria for an involuntary treatment order include that the patient ‘does not demonstrate the capacity required by section 18 to make a treatment decision about the provision of the treatment to himself or herself’ (Mental Health Act 2014 (WA) s 25(1)(c)). If the patient has that capacity, that is they are competent, then they cannot be detained.
If the patient is not competent and the doctor who completed the form 1A has also made an order under the Mental Health Act 2014 (WA) s 28 authorising the person’s detention, then they may be detained – see Mental Health Act approved forms - Form 3A Detention order.
Whether a patient ‘may or may not be placed on a Form 6B [Inpatient Treatment Order In General Hospital]' or has a ‘history of being placed on Form 6Bs’ is irrelevant.
A potential or past form 6B is irrelevant. If the patient is subject to a current form 6B then they may be detained in accordance with any relevant order and the provisions of the Act. The fact that they ‘may’ be subject to a form 6B, or have been placed on a form 6B cannot justify current detention.

Likewise, you may find another health professional disagrees with your assessment of Gillick competency and may choose to manage the patient differently.
If the decisions of another health professional are impacting your ability to care for an individual, or their wellbeing, this should be discussed with your supervisor.
If a child comes in for whatever legitimate reason (scraped knee, wants wound care) and gets first aid treatment, do I have to call parents to update them?
It is always prudent to refer to your facility’s policy and procedure regarding this. However, if you are caring for a minor you have assessed as Gillick competent, and they have asked you not to contact their parent or guardian, you must respect their wishes.
In the event the minor holds their own Medicare card, you cannot release personal or sensitive information to anyone without their consent.
In the event a Gillick competent minor will not provide consent for you to contact their parents, however you feel it important they receive support, it is still worth counselling the minor to understand the situation and encourage them to seek support.
How does Gillick Competency apply to minors who initially present to ED intoxicated but have now slept and sobered up?
Can Gillick Competency be overturned by another health professional?
Given the diversity of opinions amongst health professionals, it is likely there will be disagreements between individual health professionals about whether a minor may be Gillick competent.
It must also be considered that Gillick competency will fluctuate over time, depending upon the minor’s maturity, cognition and proposed health interventions; this could even vary between shifts!
As Gillick competency is dependent upon the nature of a proposed treatment, it may become important to involve more people in the assessment of Gillick competency for younger minors and/or bigger interventions.
However, for day-to-day management of a minor in a health facility, assessment for Gillick competence will always be against a proposed treatment or intervention; it is not an overall “blanket” assessment.
Health professionals will vary in their assessment of Gillick competence based upon their scope of practice, personal values, and understanding of how they are regulated. These points will likely inform a health professional’s level of comfort with assessing for Gillick competency and coming to an informed decision on how to proceed.
As in any nursing situation, you should not proceed with a treatment or intervention if you are not comfortable, including when you feel consent is not valid/informed.
Gillick competence will always fluctuate with changing situations, so ongoing assessment is important.
In the event a minor cannot meet the requirements of Gillick competence due to intoxication, this should be reassessed with the changing circumstance; in this case, the minor’s cognitive state has changed and therefore Gillick competence may now apply, even though it previously did not.
The parent or guardian is free to provide or refuse consent to any healthcare treatment/intervention proposed for a minor in their care. However, in situations when a treating healthcare team has deep concerns for the welfare of a minor who is not Gillick competent (e.g. babies), and they strongly disagree with the decision made by a family, it is likely this will be escalated in accordance with a facility’s policy/procedure. In the event an agreement cannot be reached, and there is a concern for the minor’s wellbeing, it is most likely an intervention would be sought from the courts, however this may be a protracted and distressing process.
The Western Nurse will publish more answers to your legal questions over the next few editions. Write to us at western. nurse@anfiuwp.org.au if you have another question for Dr Eburn or Ms Rowan-Robinson.
Carers and AINs can be covered by the Australian Nursing Federation, and United Workers Union.
The difference is the ANF offers far more services for only a fraction of the price.
The protections and support offered by the Australian Nurses Federation are more relevant and important than ever for nurses and midwives at all levels across the West Australian healthcare system.
This includes all nurses and midwives, from Enrolled Nurses and Registered Nurses to students, Assistants in Nursing, carers and Personal Care Assistants. The ANF is here to make sure you are best represented in all work-related matters.
Not only does the ANF offer a great range of vital services, but it also offers them at hugely competitive rates.
ANF State Secretary Janet Reah said the organisation had a proud history of supporting its members while keeping its fees affordable for all.
“ANF services include free legal advice and representation, access to the free ANF Helpline for industrial enquiries, Professional Indemnity Insurance, Journey Cover Insurance and a range of free professional development. As well as this we have partnered with Nurses and Midwives Health to offer reduced premiums for health insurance," Ms Reah said.
“We offer these services to all WA nurses and midwives, and we do it for a fraction of the price of other unions.
“For example, the fees for Enrolled Nurses joining the ANF are less than a third of the cost of other unions. ENs have access to all the same great services and support offered to all ANF members, just for less.”
The ANF has just kicked off another major advertising campaign across radio, print and social media with a focus on making sure healthcare workers get the protections they need and deserve, at a price they can afford.
The protections provided by the ANF are crucial to workers’ ability to safeguard themselves. This could include Coronial Inquiries, appearances before the Nurses Board, unfair dismissal, injuries at work or issues with leave and entitlements.
On top of all of these vital protections, the ANF gives members access to exceptional and affordable holiday units in Margaret River and Kalbarri, both great places for a those in need of a holiday, and a range of giveaways and discounts across WA. Members can also attend the ANF’s ever popular conference series, again at a reduced cost.
Right now ENs, AINs, PCAs and carers can be an ANF member for only $4 a week. Students pay even less. RNs pay only $6 a week. The ANF has remained committed to ensuring its fees remain low. In fact, the ANF has not increased its fees in close to two decades, and instead lowered fees in 2022.
In 2023 the ANF Council voted to keep fees at the new reduced rates for a further year.
“The ANF has long understood the pressures of being a nurse or a midwife, and we want to make sure we don’t add further financial pressures,” Ms Reah said.
“This is particularly relevant now, as the cost of living continues to be a challenge for many.
“Don’t pay triple the price to join another union when you get more services from the Australian Nursing Federation.”
With over 40,000 members currently the ANF is WA’s largest union representing nurses and midwives, and Ms Reah stresses that the ANF is here to support everyone who works in the industry.
“The Australian Nursing Federation is proud to represent carers working in aged care.
“We are proud to represent Enrolled Nurses, Registered Nurses and midwives.
“We are proud to represent students, Assistants in Nursing and Personal Care Assistants.”
“If you work in this industry and you want the best possible representation and support, then the ANF is the union for you.
“Stop missing out on these great benefits and join the ANF today.” There are no waiting times and nothing to pay upfront. Your ANF cover starts the day you join.
Contact the ANF on 6218 9444 for a membership form or visit the website www.anfiuwp.org.au or email anf@anfiuwp.org.au
The Enterprise Bargaining Agreement team at the ANF have their work cut out for them, supporting members across more than 70 separate EBAs. While bigger EBAs, such as the public sector EBA and the Ramsay EBA, often get more coverage in the press and on social media, our team are working hard to ensure members are getting the best deal possible. It doesn’t matter if you are a Registered Nurse, an Enrolled Nurse, a Midwife or working in Aged Care, the ANF is here to help.
The current EBA negotiations for both nursing and non-nursing staff are underway. Non-nursing staff met earlier this year to discuss and review the draft agreement they received in late December 2023. The review process is still underway, however Silvervchain have told the ANF they plan to go to ballot within a few weeks.
Nursing staff at Silverchain met in December last year and were presented with the current Log of Claims (LoC). Silverchain also presented their own LoC. The ANF is awaiting a response to our claims and notification of the next meeting date.
The ongoing negotiations between Mount Hospital ENs and AINs and Healthscope are proceeding well. A meeting was held in December to discuss a draft agreement, and a further meeting was held in January to review and discuss the draft agreement.
The Ngala EBA has now been approved by the Fair Work Commission and all appropriate files have been updated with the new agreement. This follows the overwhelmingly positive response from members, with 97 percent voting in favour of the agreement. This agreement includes better Parental Leave arrangements, and a 3 percent wage increase a year for two years.
A number of non-contentious clauses have been agreed to in the Bethanie Aged Care RN agreement, on the condition that they will be further discussed if there are concerns from the members when presented with a comprehensive offer.
At the last meeting, Bethanie confirmed that they are planning to present an offer within the coming weeks.
Serco recently presented their final offer and commenced the access period in early February. Their new and improved offer included a higher wage offer and a $4,000 (inclusive of superannuation) EBA sign-on bonus. This follows a clear rejection from members of the previous EBA offer.
The ANF and Little Sisters of the Poor met in January for a final meeting before taking the agreement to ballot. Little Sisters of the Poor opened a two-week access period, with the vote opening in mid-February.
They are offering a 4.6 percent pay rise for 2023 (which is already paid), plus 3.5 percent for January 2024. Wages for 2025, 2026 and 2027 will increase at the same rate as the annual Award minimum wage increase, as determined by the Fair Work Commission or by 2.5 percent, whichever is greater. The member meeting was held in December, with members being happy with this offer.
The current wage offer with the Aged Care Quality and Safety Commission is for a 4 percent increase for 2023 followed by 3.8 percent for 2025 and 3.4 percent for 2026. Many other entitlements have been improved under the proposed EBA, such as 18 weeks parental leave for both parents and 18 days personal leave. The agreement is currently being drafted, and the ANF hopes to have further news soon.
RAAFA have decided to move forward with their decision to amalgamate their various agreements into one single agreement across the board. The ANF and other unions met with RAAFA in December to present their LoC.
Southern Cross Care has also decided to amalgamate their three enterprise agreements, as well as all Award employees to be covered by a single agreement. While this decision has been confirmed, Southern Cross Care will not be ready to commence bargaining until mid-late 2024.
The new agreement with Lifeblood was submitted to Fair Work and has just been approved. The recent ballot returned a 66 percent yes vote, with a turnout of 1601 out of 1840 employees voting.
The Catholic Homes RN EBA is awaiting a final meeting to be held with Catholic Homes before the agreement goes to ballot. The current wage offer is a 5 percent increase in July 2023 followed by 3 percent in July 2024. Meanwhile the EN and AIN EBA with Catholic Homes offer has increased from 2 percent per year to 3 percent per year for 2024 and 2025. A final meeting is required before the ballot.
The EBA team has been working on more efficient processes. Surveys are being conducted for all expired, or due to expire, EBAs and draft LoCs are being prepared for each so that when employers are ready to negotiate the ANF team is ready to respond without delay. So far 45 surveys have been completed and eight LoCs have been sent to members for feedback outside of those that are actively being negotiated.

Keeping proper documentation and records is an essential part of working in healthcare. The notes you keep at work should be an ongoing account of a patient’s time in hospital, including a record of treatment and the patient’s progress.
If the number of ANF legal referrals is anything to go by, nursing documentation is coming under more scrutiny than ever before, so good documentation has never been more important.
As a nurse or a midwife accurate documentation is a fundamental part of your duties, and it can play a major role in the provision of excellent care. It is also a first line of defence in protecting yourself. In most cases it is only when something goes wrong that documentation comes under scrutiny. The notes you have taken will play a major part in any hearings or inquiries you end up being involved in.
Detailed and correct notes of a patient’s care are the sort of thing it is better to have and not need, than to need but not have.
There are many different formats and policies on keeping notes as a nurse, but there are a few simple guidelines for good note keeping.
• Notes should be clear, concise and precise. All notes should also be as accurate as possible. Make sure you include all relevant and appropriate information. Your notes should also be easy to read and understand, so they can be relied on later.
• Write in the first person: “I heard”, “I saw”, “this was said to me”, “I said”.
• Always be objective. Note down what you see and hear, not what you think. Don’t say the patient “appeared” or “seemed” to have a cut on their arm. They either did or did not have a cut, that either was or was not on their arm. Record facts rather than assumptions. A patient might look intoxicated, but that may not necessarily be the case. Instead, record the immediate symptoms: the patient was slurring their words and was unsteady on their feet.
• For things you don’t directly see or hear, you can always report that you were told this information. If you were in the room when a patient had a fall you should make note this occurred and record any other relevant information such as: when and where the fall occurred, what treatment or assistance the patient received and who else was in the room. If you weren’t in the room at the time, but the patient or a colleague relays this information you can still record it, but you should also state where you got the information from. This can be as simple as adding “Ms Brown stated that…” or “Nurse Smith stated that…” to your notes.
• Note down any instances where a patient refuses treatment or acts contrary to advice.
• You should record any comments or requests made by the patient or their relatives.
• Any entry should be preceded by date and time and followed by your signature.
• Record any actions not taken, and why they were not taken.
Along with handovers and general record keeping nursing notes will form a central part in a number of legal settings and hearings.
• Coroner’s Court: The coroner relies heavily on nurse notes. Out of the entire health team nurses have the closest contact for the longest period with the patient.
• Civil Litigation: This could be a negligence claim against the hospital, where the notes will be relied on as evidence to support an allegation of negligence because certain treatment was not given, or the wrong treatment was given.
• Nursing and Midwifery Board hearings: This could be where a nurse’s professional conduct is brought into question, so detailed records of events are crucial.
• Other inquires could also include criminal proceedings, if it is necessary to show evidence that an assault or injury occurred.

Growing old can present a range of challenges for individuals and their families, as hard choices need to be made about how an older person is cared for. This can mean the tough decision to move a relative into an aged care facility, a choice that comes with a lot of guilt and uncertainty.
This guilt and uncertainty can be exacerbated by a lack of guidance and support for families.
Dr Joyce Muge-Sugutt, a lecturer in the School of Nursing and Midwifery at Edith Cowan University (ECU), and ANF member, thinks this should change.
With over a decade of experience in aged care, including teaching and lecturing, Joyce has a passion for helping older people, and she is committed to seeing families get the support they need.
Growing up in Kenya, she had a lot of experience in caring for older relatives, as much of the aged care in the country relies on family members.
“In Kenya there are no aged care facilities,” Dr Muge-Sugutt said.
“I studied nursing while also caring for my grandfather. I have a big family, but caring for someone takes a big effort.”
When Dr Muge-Sugutt moved to Australia in 2009 she took a job working in aged care while continuing her studies. She quickly saw that Australian families were also struggling. Joyce spent many years in acute care nursing, community nursing and gerontology, before taking a role at ECU.
While teaching at ECU, Joyce decided further insight was needed into the struggles families faced while negotiating aged care. She embarked on a study, where participants shared their experiences of the process.
“I was really interested in working with family care givers, as I had been one myself. They deal with a range of emotions like uncertainty and guilt in sending people to aged care homes,” Dr Muge-Sugutt said.
A lot goes into the process. Joyce describes it as a “journey of uncertainty punctuated by key moments. “A journey of uncertainty” is the unpredictable experiences of family caregivers
as they journeyed through years of caregiving, decision-making and ultimately the transfer process. “Key moments” include the major changes or events that occurred and were noted by the family caregiver as influential in their experience during the period of caregivers, transfer and life after transfer.
The process can be broken into three main stages.
This occurs before the family member is transferred into aged care.
The pre-transfer period was accompanied by feelings of uncertainty, where participants in Joyce’s study often reported they were not sure where to find resources or support.
“A lot of people found the process difficult and complex,” Dr MugeSugutt said.
“Family caregivers struggled. They needed a navigator or a guide to help them through the process. People often relied on others who had been through the process, other family members, friends or even people they knew who worked in aged care themselves.
A lack of support was often made worse by a lack of information.
“Finding a good home was also hard. It is not like booking a hotel when you can look up reviews online. Not a lot of information is readily available.
“Bonds were often high too. It was often a shock to families. You get the process up to a certain stage, and get ‘approvals’, and then there is a large bond.
“90 percent of my participants in the study were learned people, but the application process was often complex and unclear, there is a lot of information that is needed and little support.”
In many cases, what was needed was a “navigator”, someone to walk families through the steps.

“I think the resources such as ‘My Aged Care portal’ are often out there, but they need to be clearer. Families often needed someone who can support them and say, ‘this is what you need to do and this is how you do it.’ It is the system and policies that need to change. They need to be broken down and made clear.”
This occurs as the family member moves into their new home in an aged care facility. It is a time of mixed emotions, where family members could be both happy and sad at the same time.
“Family members could be happy because the relative is in a better place and being looked after. But they would also feel sad, especially when they come to visit, because of the guilt of them being in a home.
“Directly post-transfer is difficult. People worry, so they often come to visit a lot initially, to make sure the home is alright.”
Dr Muge-Sugutt describes how family members will often worry and visit the aged care facility to make sure the home and their relative is doing well. Again, she noted a lack of support for families.
This occurs after the family member has moved into the aged care facility. Post-transfer, there is also lack of support, as the focus is on the resident of the aged care facility, often at the exclusion of other members of the family.
As a result, family members often feel forgotten.
“The focus is on the resident, not the family. We often forget the emotions of family care givers.
“The family will know their family member is in the last place they will ever be. Residents are rarely transferred out of aged care facilities.”
This can be a difficult thing to process for families.
Along with the stress and heightened emotions of knowing their family member is in their final home, the lack of support can also be stressful. On top of that, interactions with aged facilities were often limited to organisational matters, such as bills.
To alleviate this, Joyce suggested organisations need to incorporate grieving teams, to help prepare family care givers.
Along with a navigator, better access to resources and in-house support or grieving teams at aged care facilities, Dr Muge-Sugutt said it was also crucial to create awareness of the sorts of pressure family members can be under, especially with those working with families, including GPs, nurses and social workers.
She also recommended a central point of information, somewhere where families can get all the information they need.
“We need a step-by-step guide, a tool kit to help those dealing with the aged care process,” Dr Muge-Sugutt said. She intends to do just that, and she is currently working toward creating a tool kit in the next two years.
If you want to share your experiences with aged care, either as a practitioner or a family member, write to us at: western.nurse@ anfiuwp.org.au
Read this article and complete the quiz to earn 0.5 iFolio hour
Read this article and complete the quiz to earn 0.5 iFolio hour
Brand names: Zoloft, Sertra, Setrona, Eleva1
Drug class: selective serotonin reuptake inhibitor1
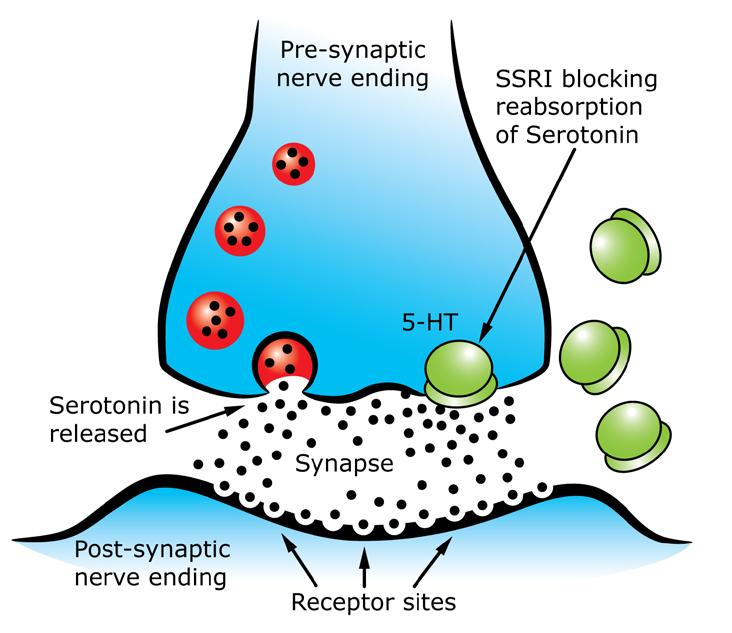
Sertraline is a selective serotonin reuptake inhibitor (SSRI).1,2 It inhibits the presynaptic reuptake of serotonin into neurons, leading to an accumulation of serotonin in the brain (see Illustration 1).2
Sertraline is administered orally.1
Indications for sertraline in adults are:1,3
• Major depression
• Obsessive-compulsive disorder (OCD)
• Panic disorder
• Social phobia
• Premenstrual dysphoric disorder. In children, aged 6 and older, sertraline is indicated for the treatment of OCD.3
Sertraline is contraindicated in patients with a demonstrated hypersensitivity to sertraline.2 Sertraline is also contraindicated in patients taking monoamine oxidase inhibitors. 4
Sertraline has a number of clinically meaningful drug interactions.
CYP2C19 inhibitors, such as clarithromycin and fluconazole, may reduce the metabolism of sertraline, increasing its concentration and the risk of adverse effects.4 Concurrent use of CYP2C19 inhibitors and sertraline should be avoided.4 If they are used concurrently the patient should be monitored and the sertraline dose reduced if necessary.4
CYP2C19 inducers, such as St John’s wort and rifampicin, may decrease sertraline concentration and its efficacy.4 Concurrent use of CYP2C19 inducers and sertraline should be avoided.4 If they are used concurrently the patient should be monitored and the sertraline dose increased if necessary.4
Concurrent use of sertraline and other serotonergic drugs, such as serotonin–norepinephrine reuptake inhibitors, may cause serotonin toxicity.4 Concurrent use of sertraline and other serotonergic drugs should be avoided.4 Serotonin toxicity may also be caused by concurrent use of sertraline and pethidine, fentanyl, monoamine oxidase inhibitors, linezolid, moclobemide, or triptans.4
Additionally, sertraline may:4
• Inhibit the metabolism of clozapine, increasing its concentration and the risk of toxicity
• Increase warfarin’s anticoagulant effect, increasing the risk of bleeding
• Increase perhexiline concentration and the risk of toxicity
• Increase the concentration of some tricyclic antidepressants, increasing the risk of adverse effects.
Major depression
Adult
OCD
Adult Child >12 years
Child 6-12 years
oral 50mg once daily, gradually increasing if necessary to a maximum of 200mg once daily (maintenance doses over 50mg is not routinely necessary)1
oral 50mg once daily, gradually increasing if necessary to a maximum of 200mg once daily1
oral 25mg once daily, increasing if necessary after 1 week to 50mg once daily, after 6 weeks increase daily dose by 25-50mg depending on response and tolerability (maximum 200mg daily) 1
Panic disorder, social phobia
Adult oral 25mg once daily, increasing if necessary after 1 week to 50mg once daily (maintenance doses over 50mg is not routinely necessary) 1
Premenstrual dysphoric disorder
Adult
continuous – oral 50mg once daily1 cyclic – oral 50mg once daily starting 14 days before the anticipated start of menstruation until the first full day of menstruation1
The onset of sertraline’s therapeutic effect may be seen within seven days.3 However, full activity is usually not seen for two to four weeks, and possibly longer for OCD.3
Hepatic impairment
Sertraline should be used with caution in patients with hepatic impairment.1,2 A lower or less frequent dose should be used for patients with hepatic impairment.2
Pregnancy and breastfeeding
Sertraline is considered safe to use during pregnancy.4 Most studies have shown no significant increased risk of fetal malformations when sertraline is used in early pregnancy. 4 When used during the third trimester, infants may experience self-limiting withdrawal symptoms such as respiratory distress, temperature instability, sleep disturbance, tremors, feeding difficulties, and diarrhoea. 4
Sertraline is also considered safe to use while breastfeeding.4 However, as small amounts are excreted in breastmilk it should be used at the lowest effective dose, with the infant
Illustration one: Mechanism of action of SSRIs
monitored for adverse effects, such as excessive drowsiness, restlessness, and poor feeding.4
Mental health conditions
Sertraline should be used with caution in people with bipoloar disorder.1 Sertraline may provoke a manic episode in patients with bipolar disorder.1
Common adverse effects associated with sertraline include agitation, tremor, drowsiness, insomnia, dry mouth, headache, dizziness, nausea, diarrhoea, sweating, anxiety, sexual dysfunction, rhinitis, myalgia, and rash.1 Suddenly stopping the use of sertraline, or reducing or tapering the dose too quickly, can cause withdrawal effects.1
Sertraline may infrequently be associated with tardive dyskinesia, dystonia, sedation, confusion, hypotension, palpitations, tachycardia, hyponatraemia, mydriasis, bruising, nose bleeds, and gastrointestinal, vaginal, or intracerebral bleeding.1
Rarely, sertraline may be associated with elevated liver enzymes, hepatitis, hepatic failure, blood dyscrasias, taste disturbance, acute angle-closure crisis, akathisia, paraesthesia, and hyperprolactinaemia.1
1. Sertraline. 2020 [cited 2020 Dec 26]. In: Australian Medicines Handbook [Internet]. Adelaide (Australia): Australian Medicines Handbook. Available from: https://amhonlineamh-net-au/ chapters/psychotropic-drugs/antidepressants/ ssris/sertraline
2. Singh HK, Saadabadi A. Sertraline. 2020 [cited 2021 Feb 19]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing LLC. Available from: https://www.ncbi.nlm.nih.gov/ books/NBK547689
3. Zoloft. 2020 [cited 2021 Feb 20]. In: MIMS Online database [Internet]. North Sydney (Australia): MIMS Australia. Available from: https://www.mimsonline.com.au/Search/FullPI. aspx?ModuleName=Product%20Info&searchKeyword=Sertraline&PreviousPage=~/Search/QuickSearch.aspx&SearchType=&ID=29180001_2
4. Drug interactions: SSRIs. 2020 [cited 2021 Feb 20]. In: Australian Medicines Handbook [Internet]. Adelaide (Australia): Australian Medicines Handbook. Available from: https://amhonline.amh.net.au/interactions/ssris-inter
5. Sertraline. 2019 [cited 2020 Dec 26]. In: Pregnancy and Breastfeeding Medicines Guide [Internet]. Melbourne (Australia): The Royal Women’s Hospital. Available from: https:// thewomenspbmg.org.au/medicines/sertraline
Read this article and complete the quiz to earn 0.5 iFolio hour
Read this article and complete the quiz to earn 0.5 iFolio hour
Brand names: Atorvastatin – Atorvachol, Lipitor, Lorstat, Torvastat, Trovas1
Fluvastatin – Lexcol1
Pravastatin – Lipostat, Pravachol, Cholstat1
Rosuvastatin – Cavstat, Crestor, Crosuva1
Simvastatin – Zocor, Zimstat, Simvar, Lipex1
Drug class: HMG-CoA reductase inhibitors1
Statins are a competitive inhibitor of 3-hydroxy-3methylglutaryl coenzyme A (HMG-CoA) reductase (a rate-limiting enzyme in cholesterol synthesis).1
Inhibiting HMG-CoA reductase reduces the conversion of HMG-CoA to mevalonate, increasing hepatic cholesterol uptake from blood and lowering total cholesterol, low-density lipoprotein, and triglyceride concentrations.1 Statins also cause a small increase in high-density lipoprotein concentrations.1
Statins are administered orally.1
Indications for all statins are hypercholesterolaemia and high cardiovascular risk.1
Additional indications for particular statins are:1
• Atorvastatin - hypertensive patients with additional risk factors for heart disease
• Fluvastatin - coronary disease after a successful percutaneous coronary intervention
• Pravastatin - patients with previous myocardial infarction or unstable angina.
CONTRAINDICATIONS
Statins are contraindicated in patients with:1,2
• Hypersensitivity to any statin
• Active liver disease or unexplained persistent elevations in liver function tests.
• Statins should not be used concomitantly with sodium fusidate.2
Many drugs have clinically meaningful interactions with statins.
The majority of drug interactions increase the risk of myopathy and rhabdomyolysis.3 A range of drugs, including ciclosporin, elbasvir with grazoprevir, fibrates, nicotinic, drugs that inhibit CYP3A4 (atorvastatin and simvastatin), drugs that inhibit CYP2C19 (fluvastatin), and sodium fusidate, interact with statins to increase their concentration and increase the risk of myopathy and rhabdomyolysis.3 Concurrent use of statins with drugs that also cause myopathy or rhabdomyolysis, such as colchicine, may also increase the risk.3
Dose varies depending on the statin, indication, intercurrent illness, and concurrent medications. 1
Dose should be reduced as indicated by intercurrent illness and concurrent medications.1
Atorvastatin1
Adult oral 10-80mg once daily, dose may be increased after 4 weeks if necessary
Child > 8 years oral 10mg once daily, dose may be increased after 4 weeks if necessary
Fluvastatin1
Adult oral 80mg once daily
Pravastatin1
Adult oral 20-80mg daily (1 or 2 doses), may be increased after 4 weeks if necessary
Previous myocardial infarction or unstable angina
Adult oral 40mg once daily, may be increased after 4 weeks if necessary
Rosuvastatin1
Hypercholesterolaemia
Adult oral initially 5 or 10mg once daily, then usual dose 5-20mg once daily
High cardiovascular risk
Adult oral 20mg once daily, may be increased after 4 weeks if necessary
Simvastatin1
Adult, child > 8 years oral 10-40mg once daily, may be increased after 4 weeks if necessary
Existing or high-risk coronary heart disease
Adult oral 40mg daily once daily, may be increased after 4 weeks if necessary
Renal impairment
Statins should be used with caution in patients with renal impairment, as impairment increases the risk of adverse effects.1 A lower starting dose should be used, and the patient’s renal function and creatine kinase regularly monitored.1
Hepatic impairment
Statins should be used with caution in patients with hepatic impairment.1 A lower starting dose should be used for patients with hepatic impairment.1 Statins are contraindicated in patients with active liver disease or unexplained persistent elevations in liver function tests.
Elderly patients
The risk of adverse effects is increased in elderly patients.1 Statins should be used with caution in elderly patients, and lower starting dose should be used.1
Asian ancestry
Rosuvastatin should be used with caution in patients with Asian ancestry.2 For patients with Asian ancestry, a lower starting dose should be used and dosage increases instituted with caution.2
Pregnancy and breastfeeding
Statins should not be used during pregnancy.4,5,6
The inhibition of HMG-CoA reductase may have a negative impact on the development of the placenta and interfere with fetal development.4,5 Statins have been associated with abnormal pregnancy outcomes, including central nervous system malformations, limb deficiencies, and cleft palates.4,5 Women using statins should use effective contraception and discontinue treatment before a planned pregnancy.4,5
Statins are not recommended for use while breastfeeding.4,5,6
Statins are generally well tolerated.7 The most common adverse effects include headache, sleep disturbance, dizziness, transient gastrointestinal symptoms, and myalgia.1 Statins are also commonly associated with elevated aminotransferases concentrations, which generally respond to decreases in dosage.1
Rarely statins are associated with hepatitis, liver failure, renal failure, pancreatitis, memory loss, alopecia, paraesthesia, peripheral neuropathy, gynaecomastia, visual disturbances, angioedema, thrombocytopenia, and allergic reaction.1 Statins are also rarely associated with myopathy and rhabdomyolysis.1 The risk of myopathy and rhabdomyolysis is dose-related, but may also be increased by age, intercurrent illness, and drug interactions.1 Muscle symptoms are more likely in the first 6 weeks or after a dose increase.1 Statinassociated muscle symptoms may be managed by reducing the dose or switching to a different statin.7
Statins are also associated with a slightly increased risk of new onset diabetes in patients with preexisting risk factors, and insulin resistance.1,7
1. Statins. 2021 [cited 2021 Jun 29]. In: Australian Medicines Handbook [Internet]. Adelaide (Australia): Australian Medicines Handbook. Available from: https://amhonline-amhnet-au/chapters/ cardiovascular-drugs/drugs-dyslipidaemia/ statins
2. APO-Rosuvastatin. 2020 [cited 2021 Jul 16]. In: MIMS Online database [Internet]. North Sydney (Australia): MIMS Australia. Available from: https://www.mimsonline.com.au/ Search/FullPI.aspx? ModuleName=Product%20Info&searchKeyword=rosuvastatin&PreviousPage=~/Search/QuickSearch.aspx&SearchType=&ID=98570001_2#Top
3. Drug interactions: Statins. 2021 [cited 2021 Jun 29]. In: Australian Medicines Handbook [Internet]. Adelaide (Australia): Australian Medicines Handbook. Available from: https://amhonline.amh.net.au/ interactions/statins-inter
4. Artorvastatin. 2021 [cited 2021 Jun 29]. In: Pregnancy and Breastfeeding Medicines Guide [Internet]. Melbourne (Australia): The Royal Women’s Hospital. Available from: https:// thewomenspbmg.org.au/ medicines/arvostatin
5. Rosuvastatin. 2021 [cited 2021 Jul 17]. In: Pregnancy and Breastfeeding Medicines Guide [Internet]. Melbourne (Australia): The Royal Women’s Hospital. Available from: https:// thewomenspbmg.org.au/ medicines/rosuvastatin
6. Drug use in pregnancy and breastfeeding. 2021 [cited 2021 Jul 17]. In: eTG Complete [Internet]. Melbourne (Australia): Therapeutic Guidelines Limited. Available from: https:// tgldcdp-tg-org-au/ quicklinks?type=Pregnancy%20and%20 breastfeeding&bf=5a58609.htm
7. Lipid modification. 2021 [cited 2021 Jul 17]. In: eTG Complete [Internet]. Melbourne (Australia): Therapeutic Guidelines Limited. Available from: https://tgldcdp-tg-org-au/ viewTopic?topicfile=lipid-modification&guidelineName=Cardiovascular#toc_d1e256

The Pharmaceutical Benefits Advisory Committee (PBAC) recently announced a decision to recommend a crucial drug to treat early-stage triple negative breast cancer (TNBC) for a government subsidy.
The PBAC announcement that Keytruda, also known as pembrolizumab, would be recommended for subsidy on the Pharmaceutical Benefits Scheme (PBS) for early-stage TNBC was welcomed by the Breast Cancer Network Australia (BCNA).
Keytruda is an immune checkpoint inhibitor, which blocks proteins that stop the immune system from attacking the cancer cells. When combined with chemotherapy following surgery, it can significantly reduce the risk of cancer recurrence when compared to chemotherapy alone. Keytruda is one of the first immunotherapies that is shown to be effective for early-stage TNBC.
According to the BCNA, around 15 percent of breast cancer diagnoses are triple negative, which, in Australia equates to around 3,000 new cases each year.
BCNA Director Policy, Advocacy and Support Services Vicki Durston said the PBAC’s decision to also recommend Keytruda for high-risk early-stage breast cancer is good news.
“Triple negative breast cancer is typically more aggressive, has fewer treatment options, and disproportionately affects younger women,” Ms Durston said.
“We know that as many as 40 percent of those with triple negative breast cancer will have a recurrence. New treatments like Keytruda that reduce this risk are vital at improving outcomes for those who have one of the rarer forms of breast cancer.”

The Australian Financial Complaints Authority (AFCA) has reportedly received over 100,000 complaints relating to financial disputes in a single year, the highest recorded by the agency.
According to a statement release by AFCA In 2023 the organisation received 102,790 complaints from consumers and small businesses who were unable to resolve disputes directly with their financial firms. This was a jump of 23 percent from 2022.
AFCA was set up in 2017 to handle disputes formerly handled by the Financial Ombudsman Service, the Credit and Investments Ombudsman and the Superannuation Complaints Tribunal. It began work on 1 November 2018, just months ahead of the final report of the Hayne Royal Commission into Misconduct in the Banking, Superannuation and Financial Services Industry in February 2019.
David Locke, the Chief Ombudsman and Chief Executive Officer of AFCA, said the volume of complaints escalated to AFCA has been increasing at an unsustainable rate.
“Scam-related complaints to AFCA have nearly doubled between 2022 and 2023,” Mr Locke said.
“They continue to be of great concern to us. We are also seeing the impact of increased interest rates and cost of living pressures, with complaints involving financial hardship also significantly higher."
Consumers secured $304 million in compensation and refunds after coming to AFCA, up 38 percent on the previous year. AFCA registered 8,987 complaints related to scams, up 95 percent from 4,611 in 2022. Complaints involving financial
hardship totalled 5,396, up 29 percent on 2022.
Mr Locke said the AFCA hopes that 2024 is the year that anti-scam initiatives by industry and government will finally disrupt this serious and organised crime.
“We also need to see a downward trend in complaints overall, with financial firms working better to support their customers and to address complaints quickly and efficiently in-house.
“We believe many financial firms could be doing a better job of handling complaints within their own internal complaints processes, so only the most complex cases reach AFCA – which is the role we are meant to play,” Mr Locke said.
Since starting operations, AFCA has received more than 420,000 complaints, helping to secure $1.3 billion in compensation or refunds for consumers.

According to data released by the Australian Bureau of Statistics (ABS), the proportion of adult current daily smokers has more than halved over the last twenty years.
This is a reduction from 22.4 percent in 2001 to 10.6 percent in 2022.
“Almost three in five or 58.3 per cent of adults had never smoked, which has gone up in the last decade from 51.1 percent in 2011–12,” ABS director of health statistics Robert Long said.
“One in seven adults had used e-cigarettes and vaping devices at least once in their life.”
Mr Long said the first release of the National Health Survey for 2022 offered insights into how the health of Australians has changed over time, including that 81.4 percent of Australians had at least one long-term health condition, and 49.9
percent had at least one selected chronic condition.
“Three in four adults with high measured blood pressure did not report having hypertension. This suggests that many people with high measured blood pressure remain undiagnosed,” Mr Long said.
The survey also touched on a number of other health topics, including alcohol consumption, healthy eating and exercise.
According to the ABS 26.8 percent of Australians exceeded the Australian Adult Alcohol Guidelines, which is more than 10 standard drinks a week and/or five or more drinks on any one day at least monthly.
Young adults aged 18 to 24 years old were more likely than any other age group to exceed this amount, with 36.1 percent exceeding the guideline in 2022.
44.1 percent of adults were eating the recommended daily intake of fruit, but only 6.5 percent ate the recommended daily intake of vegetables.
Almost twice the proportion of adults reported that they do not usually eat fruit daily in 2022 when compared to over a decade ago, up from 6.3 percent in 2011–12 to 12.0 percent in 2022.
On average, Australians were doing 69 minutes of physical activity every day and nearly half of spent most of their work day sitting.

The West Australian Government Department of Health’s Director General, Dr David Russell-Weisz has announced he will step down after almost nine years as the head of the WA Health.
Dr Russell-Weisz started his career as a general practitioner in South London.
Moving to Western Australia, he worked in the remote Pilbara and Kimberley as well as in Perth’s metropolitan health services. He also led major projects including the commissioning of Fiona Stanley Hospital before heading up the Department of Health. Dr Russell-Weisz has worked with WA Health for 28 years.
According to a press release issued by the WA Government, as Director General Dr Russell-Weisz oversaw major reforms across the health system in 2016, including a new system of health service providers led by independent boards.
His role became increasingly public during the COVID-19 pandemic, as WA public health system worked to respond to the crisis.
“The past four years have challenged all of us like never before,” Dr Russell-Weisz said.
“We successfully navigated our way through the COVID-19 pandemic with an outcome that is the envy of many other health jurisdictions around the world.”
“While highly disruptive for our health services, this period showcased the very best of our public health system – working as a team to protect and treat our patients and the broader community, while also continuing to deliver the key priorities of the WA health system.”
Dr Russell-Weisz is reportedly the only Health director general in Australia to have remained in that post for the entirety of the pandemic.
His tenure also saw the WA public health system embroiled in controversies and questions of staffing and resourcing. This included the tragic death of seven-year-old Aishwarya Aswath and subsequent coronial inquest, and revelations surrounding the alleged rape of a 13-year-old girl at Perth Children’s Hospital (PCH) in January 2022.
Aswath Chavittupara, Aishwarya’s father, called for Dr Russell-Weisz’s resignation in 2023 in the wake of the Coronial Inquest, which reported serious issues with resourcing and systems in place the night she died at PCH.
Dr Russell-Weisz’s last day at the Department will be 27 March 2024.
According to the Pharmacy Guild of Australia, Western Australian women have embraced a new program which allows for the diagnoses and treatment of uncomplicated urinary tract infections by Western Australia community pharmacists. In a statement issued earlier this year the Guild reported that during the initial five months of operation, pharmacists in 405 community pharmacies received the required training through the program, and are now delivering this healthcare service.
“Collectively they have provided over 2,500 occasions of service. Access to early treatment from these medicines experts has delivered timely relief from the very painful symptoms of this acute condition,” the statement said.
At the time of its launch, Pharmacy Guild of Australia WA Branch President, Mr Andrew Ngeow, described the Pharmacist Initiated Treatment of Urinary Tract Infection program as being a “game changer” for Western Australian women.
“These early results underscore the reasons the WA Branch advocated for the program to be established,” Mr Ngeow said.
“The true value of the program is already being demonstrated.”
According to the Guild, diagnosis and treatment of an uncomplicated urinary tract infection is now an entrenched core service provided by Western Australian community pharmacies.
“The feedback that we are receiving from patients is that the program is achieving positive health outcomes,” Mr Ngeow said. “Our goal as a sector is to continue to increase patient access, so that no Western Australian woman should be in pain and suffer unnecessarily, from this very painful condition.
“Given many of the community pharmacies providing this service are open seven days per week over extended hours, it is no surprise that Western Australian women are increasingly choosing to receive pharmacy-based treatment due to both its convenience and high-quality care.”
Community pharmacies began treating patients soon after the program was announced in August 2023.

New research conducted at Monash University has revealed the barriers female nurses face when trying to advance into leadership roles.
The recent study, published in The Lancet’s EClinicalMedicine, found that healthcare systems and organisations generally “limit women nurses in skill acquisition, motivation and opportunities in healthcare leadership, due to inequitable policies, practices and bias.”
According to Monash University the study compiled decades of research, allowing researchers to identify, extract and analyse this data for the first time, and to establish the collective sociocultural, professional, organisational and individual barriers that hold women nurses back from being considered, applying for, or accepting leadership positions.
According to figures released by the World Health Organisation in 2019, nearly 70 percent of the global healthcare workforce is women, and 89 percent are nurses yet only 25 percent of senior healthcare roles are filled by women.
The research also highlights gendered roles such as disproportionate childcare responsibilities and juggling family with part-time work, limiting leadership opportunities which are generally perceived as full-time.
Professor Helena Teede, Monash University Professor of Women’s Health and Monash Centre for Health Research and Implementation Director, was senior author of this comprehensive research.
“The barriers identified show women nurses don’t have the same opportunities for leadership as men, following a common theme
throughout healthcare, a sector delivered by women and led by men,” Professor Teade said.
PhD candidate with Monash University’s Advancing Women in Healthcare Leadership initiative and critical care registered nurse Mihiri Pincha Baduge was one of the authors of the study. Having been born in Sri Lanka, and studying nursing there, she is able to share her own experiences as a woman, a nurse, a mother and a migrant to Australia.
“I've noticed that healthcare leadership roles often overlook people like me,” Ms Pincha Baduge said.
“When I returned to work after parental leave, I decided to shift from full-time to part-time nursing. Now my eligibility to apply for leadership roles is restricted because these leadership positions lack work-life flexibility and part-time options.
“We’ve found that societal issues and organisational hurdles challenge women’s individual credibility, capacity, and capability in nursing. These barriers make it tough for women to feel confident pursuing leadership roles.
“It’s like a double whammy – women nurses don’t feel confident enough, and this is reinforced as qualified women get passed over for leadership roles. The workplace itself can be a battlefield, with unconscious bias and discrimination making it way harder for women, especially in nursing, which is seen primarily as a feminine caring role, to climb the leadership ladder.”
Researchers suggested that to break down the barriers to leadership positions, systems and organisational change were needed. These changes included implementing leadership, culture change, policies and practices that support women to work to their preferred capacity and part-time leadership roles.

Researchers from the UNSW Centre of Healthy Brain Aging (CHeBA) and the MARCS Institute for Brain, Behaviour and Development at Western Sydney University have highlighted the importance of assessing standard emotional responses to situations in order to improve diagnosis and management of dementia.
This means more than just a focus on the most commonly recognised symptom of dementia: memory loss.
Lead author and social health expert Dr Suraj Samtani said individuals with many types of dementia can identify most emotions such as happiness, sadness, surprise and fear, but have difficulties identifying other basic or primary emotions, including disgust or anger in facial expressions, as well as sarcasm and jokes in conversations.
“The value of assessing social cognition in older adults with dementia is to improve early intervention and treatment,” Dr Samtani said.
It can also help identify dementia pathways for individuals with types of dementia such as frontotemporal dementia, to the development of behavioural symptoms.
Dr Samtani stressed that while early signs of Alzheimer’s disease, the most common form of dementia, involve memory loss, but difficulties with social cognition are often the earliest signs of other types of dementia such as frontotemporal dementia.
In this context social cognition is defined as an ability to recognise emotions, social cues, inhibit inappropriate behaviour and act appropriately in social situations. Social cognition includes the ability to understand other people’s mental states, and being able to feel and respond to what other people feel.
“Deficits in any of these social cognitive functions are a core feature of mild cognitive impairment and dementia, and may represent an early decline in cognitive function,” said Dr Samtani.
“These can manifest through behaviours such as difficulties with eye contact, behaving rudely or offensively and a clear failure to detect social cues in conversations.”
While a new focus on social cognition may help early detection of some forms of dementia, spokespeople from CHeBA said more work was needed to develop an effective measurement of social cognition that has functionality in the clinic.
More progress has been made in the understanding of Alzheimer’s disease with the discovery of a link between the health of blood vessels and the development of the illness.
A research study undertaken by the Centenary Institute found the presence of senescent blood vessel cells in both Alzheimer’s patients and mouse models of Alzheimer’s. Senescent cells are aged cells that have lost their ability to divide and function properly.
According to the Centenary Institute, the findings suggest early interventions aimed at improving blood vessel health offer an avenue for the advancement of new treatments for Alzheimer’s.
Dr Ka Ka Ting, a researcher in the Centenary Institute’s Healthy Ageing Centre said specific blood vessel cells, called endothelial and perivascular cells, play a crucial role in the forming of the bloodbrain barrier, a shield guarding the brain against harmful substances.
“The blood-brain barrier serves as a protective barrier, stopping inflammatory molecules and toxic substances from entering the brain via the bloodstream. Issues can arise if the barrier becomes permeable, ‘leaking’ these toxins into the brain,” Dr Ting said.
Researchers found a notable increase in the number of nonfunctional blood vessel cells in and around the blood-brain barrier which was linked with areas of leaking during the development of Alzheimer’s in mouse models.
“We believe these non-functioning blood vessel cells weaken the barrier making it more susceptible to inflammatory and toxic substances, potentially exacerbating Alzheimer’s symptoms as the disease advances,” Dr Ting said.
“Our study provides a new perspective on Alzheimer’s and the intricate relationship with brain blood vessels, offering a promising new path for therapeutic approaches aimed at treating this disease.”
Alzheimer’s disease causes memory loss, cognitive decline and behavioural changes that can seriously affect a person’s ability to carry out daily activities.

Community midwife Martha Simpson was one of a handful of health professionals who volunteered their time and expertise to lend a hand on a mission to Tanzania, and it is an experience she will never forget.
Martha’s journey to the east African nation started at the Perth Airport with a team of midwives, nurses (general, paediatric and theatre), and a radiographer, all eager to provide a range of services and supplies to local people.
From Perth the team took two flights to reach Dar es Salaam, Tanzania’s largest city, before flying to Iringa Airport. From there it was only another few hours to their temporary home at Kisolanza Farm, near the Mafinga District Hospital.
The hospital services a large part of the Iringa region and provides medical, surgical, paediatric, maternity, theatre, radiology and A&E services, along with outpatient clinics. Martha said the hospital is very old and under-resourced in all areas, but the team were ready to help.
“The rest of the team have spent time here before, but this was my first visit,” Martha said.
“The staff were extremely welcoming and keen for us to roll up our sleeves and get straight to work.”
This is exactly what Martha did. And there was a lot of work to be done.
“Another midwife and I went straight to the labour ward. I popped on a gown and pair of gloves and within 10 minutes I had delivered my first beautiful Tanzanian baby.
“Thankfully he was born in great shape, as I quickly discovered resus equipment and drugs are very limited. There was not even O2 available.
“The same day I spent time in a very basic theatre. Many babies are born via caesarean. This was quite confronting as there was extremely basic everything. There was no anaesthetic nor recovery room.”
The post and ante natal ward was crowded and built in what Martha described as the “old Nightingale style”. While it was virtually impossible to see everyone, just due to the number of people needing care, the team tried their very best. Along with offering their medical expertise, the team also gave mums beanies and bootees for their newborns.
One of the most confronting aspects of the experience was the poverty, but more than this Martha also found the differences in cultural norms were a difficult adjustment.
“The partners were not included or welcomed into the labour and birth experience, and the women accepted this as the norm,” Martha said.





“The relatives had to bring in food for the patients in the hospital and the patients themselves had to bring their own everything for the birth and post-natal stay. We gifted many birthing packs to help the very poor.”
Mafinga District Hospital was not the only place in Tanzania where Martha’s expertise were needed.
Including a prison.
The team spent time in both the men’s and women’s sections of a local prison to offer medical support. Martha said that while this was again confronting, the whole team were all made very welcome by the authorities.
The team also headed into more remote areas.
“On two separate days we travelled long distance to isolated villages, on the worst roads I have ever been on. It took hours to
reach the places, and we were met by queues of villages lining up for assessment or care.
“A 15-year-old lass had delivered twins a few days prior to our visit. We were able to assess the twins and mum, show her ‘kangaroo care’ and share some other tips on nutrition and baby care.”
“Needless to say, our days were very long, but so rewarding.”
Martha is eager to go back and keep helping.
“It was an incredible experience. The people of Tanzania are so poor and have very limited resources, but they are extremely happy and grateful for any little thing you do for them.”
“Two weeks here was not long enough. We all came back exhausted but with amazing memories and pictures, and a keenness to return.”
The ANF supported Martha to travel to Tanzania through our ANFIUWP Humanitarian Aid Volunteers Fund, available to members looking to work overseas. The purpose of this fund is to provide financial assistance to ANF members who are undertaking humanitarian volunteer work (or humanitarian work where the member is only paid a subsistence wage or stipend). Application forms are available on iFolio.

Winner: Emma
Thanks to everyone who entered in December’s ANF Photo competition. Congratulations also go to winner Emma for her photo of herself in her much-loved ANF cap in front of Victoria Falls. She has won two tickets to see comedian Nurse Blake’s comedy special in Perth.
Special mention to Chelsea for her great photo of two tired theatre nurses working in gynae-oncology having a laugh but still getting the job done. Thanks also to Jo for her photos of her holiday as she passed through Kimba, and to Alison, who spent her holidays with family. All the runners-up received prizes.
Share your photos of yourself, your family or your team at work with any of our great ANF products and go in the running to win one of two double passes to an upcoming stage production of 21 Hearts: Vivian Bullwinkel and the Nurses of the Vyner Brooke, at the Como Theatre on Thursday 11 April.

Runner-up: Chelsea
A selection of the best photos will feature on the ANF Facebook and in the next edition of the Western Nurse.
If you think you have a winning photo you can email your competition entry to us at western.nurse@anfiuwp.org.au
All entries must include your name and your membership number to be in the running.

Runner-up: Jo

Runner-up: Alison


Australia has used new cyber sanctions powers on a Russian cybercriminal Aleksandr Ermakov for his involvement in the breach of the Medibank Private network. This is the first time the Australian Government has imposed sanctions of this nature.
The attack saw 9.7 million records stolen, including names, dates of birth, Medicare numbers and sensitive medical information. Some records were published on the dark web.
The Australian Government released a statement, in which it announced it has imposed a targeted financial sanction and a travel ban on Aleksandr Ermakov.
“This sanction makes it a criminal offence, punishable by up to 10 years’ imprisonment and heavy fines, to provide assets to Aleksandr Ermakov, or to use or deal with his assets, including through cryptocurrency wallets or ransomware payments,” the statement read.
“This is the first use of Australia’s autonomous cyber sanctions framework and is a result of Australian Government efforts over the past 18 months to investigate and respond to this cyber incident.
“The Australian Signals Directorate and the Australian Federal Police, under Operation Aquila, together with other Commonwealth agencies and international partners, have worked tirelessly to link Russian citizen and cybercriminal Aleksandr Ermakov to the compromise of the Medibank Private network and continue to pursue other leads.”
Minister for Foreign Affairs Penny Wong said the use of these new powers sends a clear message, that there are costs and consequences for targeting Australia and Australians.
“This is an incredible effort from our cyber and intelligence teams,” Minister Wong said.
“We are using all elements of our national power to make Australia more secure at home and to keep Australians safe.”
The US and UK have now also issued similar sanctions.
The Australian Signals Directorate (ASD) has released its fourth Cyber Threat Report, detailing an increase in the frequency, cost and severity of malicious cyber activity compared to the previous year.
A statement released by ASD said there were nearly 94,000 reports of cybercrime submitted to ReportCyber, the ASD’s online reporting tool, in the 2022-23 financial year, a 23 percent increase from the previous year. That works out to be one report received every six minutes.
The number of reports of cyber security incidents impacting Australian critical infrastructure increased by almost one-third.
“About 57 percent of cyber incidents reported by critical infrastructure entities involved compromised accounts or credentials; compromised assets, networks or infrastructure; and denial of service attacks,” the statement said.
ASD is also reporting an overall increase in the cost of cybercrime, with losses to businesses up by 14 percent compared to the previous financial year.
Small businesses experienced an average financial loss of $46,000, while cybercrimes cost medium businesses an average of $97,200, and large businesses an average of $71,600.
Abi Bradshaw, Head of the Australian Cyber Security Centre, said cybercriminals continued to adapt their tactics to extract maximum payment from victims.
“Cybercriminals constantly evolved their operations against Australian organisations, fuelled by a global industry of access brokers and extortionists,” Ms Bradshaw said.
“ASD responded to 127 extortion-related incidents: 118 of these incidents involved ransomware or other forms of restriction to systems, files or accounts.
“Business email compromise remained a key vector to conduct cybercrime. Ransomware also remained a highly destructive cybercrime type, as did hacktivists’ denial-of-service attacks, impacting organisations’ business operations.”
Data breaches continue to affect many Australians, with significant breaches resulting in millions of Australians having their information stolen and leaked on the dark web.
Overall, the top three cybercrime types for individuals were identity fraud, online banking fraud and online shopping fraud. The top three cybercrime types for business were email compromise, business email compromise fraud and online banking fraud.
To report cybercrime, incidents or vulnerabilities go to cyber.gov. au/report or call the Australian Cyber Security hotline on 1300 CYBER1 (1300 292 371).

A 40-year-old resident of Boise, Idaho is making national news in the United States after he was arrested for stealing an aircraft from a hangar in North Las Vegas and then flying it across state lines to California.
According to a San Bernardino County Sheriff’s police report on the matter, the owner of the aircraft, Nevada resident Jeff Cohn, received a call from Air Force Search and Rescue after they had received a notification from the aircraft’s emergency location transmitter.
Mr Cohn told Air Force Search and Rescue that he was not flying the aircraft. He then immediately drove to an airport in North Las Vegas where he discovered the aircraft was not in the hangar, where he had left it.
Sometime after that, Federal Aviation Administration contacted the San Bernardino County Sheriff’s station in Barstow to advise them the stolen aircraft had landed somewhere in the vicinity of nearby Daggett Airport.
Deputies responded to the scene and located the aircraft, which had indeed landed and was taxiing along Minneola Road, just east of the airport.
The suspect piloting the aircraft, later identified as Damian Zukaitis attempted to flee the scene on foot but was located shortly afterwards and detained.
Deputies coordinated with North Las Vegas Police and the Federal Bureau of Investigation to determine the aircraft was stolen. The aircraft was valued at about $80,000. Mr Zukaitis was arrested and booked at the Barstow jail for bringing stolen property into the state and taking an aircraft without the owner’s consent.
At this stage there seems to be no clear motive for the theft.
San Bernardino County Sheriff’s department originally stated that the North Las Vegas Police Department would be handling the investigation into the stolen aircraft, but subsequent news reports in the US have confirmed the FBI will be investigating.

A joint police operation involving Spanish and Italian authorities to combat food fraud and counterfeiting has led to 11 arrests and the seizure of 260, 000 litres of inconsumable fake extra virgin olive oil. In a statement released after the successful operation, Europol said producing fake extra virgin olive oil is a common practice, which is why the fight against it is a law enforcement priority. This is especially the case in olive oil producing countries, such as Italy and Spain.
“In this food fraud operation, investigators uncovered that the criminals used socalled ‘lampante oil’, the lower-quality variant of olive oil, to dilute their product,” the statement said.
“Lampante olive oil is characterised by elevated acidity levels, an undesirable flavour, and a distinctly unpleasant odour, which make it unsuitable for consumption. The term ‘lampante’ itself originates from its historical use as a fuel in oil lamps.
“Mixing consumer-grade olive oil with lower grade alternatives allowed the criminals to offer competitive prices while entering legal supply chains.
“This illegal practice can not only cause a public health risk, but also undermine consumer trust and thus have further economic repercussions.”
Spanish and Italian law enforcement officials conducted coordinated searches at various locations in both countries. Raids in Ciudad Real, Spain, resulted in 11 arrests and the seizure of 12 barrels containing 260, 000 litres of adulterated oil. Officers also seized four vehicles and 91,000 euro in cash, as well as digital and physical evidence such as billing documents and e-mails.
In the Italian provinces of Sicily and Tuscany, investigators inspected three oil factories suspected to be involved in the illegal practices. Several fiscal documents and client lists were acquired, oil samples were gathered and one company was sanctioned for irregular labelling of its products.


The Government of Kyrgyzstan has voted to change its flag, reportedly to make it look less like a sunflower, amid some degree of controversy and at least one arrest.
The previous flag was adopted in 1992 after Kyrgyzstan gained its independence from the Soviet Union, following the Union’s dissolution in 1991.
This flag depicts a yellow sun, which incorporates a traditional Kyrgyz yurt tent, on a red background. There are 40 rays emitting from the central yurt/sun motif, each symbolising the 40 clans united by the legendary Manas, a national hero in Kyrgyzstan.
It is these forty rays that prompted the change.
In the 1992 design the rays are wavy. Some in the small Central Asian nation, including by President Sadyr Japarov, were concerned that the wavy rays on the previous flag bore too much resemblance
to a sunflower, which in Kyrgyzstan has negative connotations and is culturally associated with servility and a lack of loyalty.
Debates were held in 2023 in the Zhogorku Kengesh, Kyrgyzstan’s parliament, to alter the design. The bill to change the design was passed that year, and the previously wavy rays were straightened.
The change was welcomed by some, including President Japarov, who commented that the old flag was a contributing factor in some of the difficulties being faced by the small nation.
Of the 7 million people living in Kyrgyzstan, at least one man strongly disagrees with this sentiment.
According to Human Rights Watch, activist Aftandil Jorobekov was arrested after he called for protests to be held in Bishkek, the capital city, in opposition to the flag change.
He was subsequently sent for two months detention prior to his trial, and he faces up to eight years in prison for charges relating to “mass unrest” under Kyrgyz law.
According to the World Bank, Kyrgyzstan has experienced some degree of political instability since gaining independence in 1991, including several political upheavals leading to the overthrow of presidents in 2005, 2010 and 2020.
In the latest presidential election in 2021, Sadyr Japarov was elected with 79 percent of the vote.

The United States Government’s Alldomain Anomaly Resolution Office (AARO) has established a new online reporting
tool allowing US Government employees, service members or contractors to report instances of unidentified flying objects and other similar phenomena.
AARO prefer not to call them UFOs, instead referring to Unidentified Anomalous Phenomena or UAP.
According to the AARO website, the US Department of Defense (DoD) considers Unidentified Anomalous Phenomena as: “sources of anomalous detections in one or more domains (i.e., airborne, seaborne, spaceborne, and/or transmedium) that are not yet attributable to known actors and that demonstrate behaviours that are not readily understood by sensors or observers.”
AARO is now accepting reports from current or former US Government employees, service members, or contractor personnel with direct knowledge of US Government programs or activities related to UAPs dating back to 1945.
These reports will be used to inform AARO’s congressionally directed Historical Record Report.
According to the DoD, AARO was established in 2022 as a continuation and expansion of the Airborne Object Identification and Management Group.
“The mission of the AARO will be to synchronize efforts across the Department of Defense, and with other US federal departments and agencies, to detect, identify and attribute objects of interest in, on or near military installations, operating areas, training areas, special use airspace and other areas of interest, and, as necessary, to mitigate any associated threats to safety of operations and national security,” the DoD said, in a press release issued at the time.
Former AARO Director Dr Sean Kirkpatrick said that, since its establishment, the organisation has taken important steps to improve data collection, standardise reporting requirements and mitigate the potential threats to safety and security posed by UAPs.
While the new AARO UAP online reporting tool is open for US Government employees and contractors, private pilots can continue to report UAPs to air traffic control.

Two men have been handed lengthy prison sentences in relation to a conspiracy to smuggle drugs and cigarettes into the United Kingdon after a large consignment of illegal drugs was accidently sent to a famer.
According to a statement released by the UK Crown Prosecution Service (CPS), the scheme involved the pair using their freight company as a cover to clear shipping containers that held drugs and cigarettes and diverting them from their intended destination to a warehouse they controlled. There they would be offloaded by organised crime groups.
The plot began to unravel when the pair lost track of one container, which was then sent to a farm in Somerset in April 2022. The farmer found plastic covered blocks of cocaine with a street value of £15 million hidden amongst animal feed from Colombia.
According to the CPS the farmer was not sure what the items were but told police he had seen “similar packages on films and tv programmes which were drugs”.
The two men, Anand Tripathi, 61, and Varun Bhardwaj, 39, were convicted after a 71-day trial at Isleworth Crown Court. The case was charged and prosecuted by lawyers specialising in serious economic and organised crime at the Crown Prosecution Service.
The court heard that in total the men imported 272.86 kilograms of cocaine and 2,503.36 kilograms of cannabis across four shipments between September 2021 and November 2022. One shipment contained just over two tonnes of cannabis hidden amongst yams from Ghana. Another containing 49 kilograms of cocaine was concealed with oranges from South Africa.
Tripathi was sentenced to 15 years, and Bhardwaj to 19 years.


1 Discontinuity or break in a bodily membrane that impedes normal function of an organ (6)
5 Medical suffix meaning to be affected or diseased by something (4)
9 Heaped (5)
10 Classical musical melodrama (5)
11 US island stat (6)
13 Organic colouring agents used in medication (4)
15 Solemnly speak to a deity (4)
16 Highly contagious disease also known as varicella (10)
20 Breathing organ (4)
22 Increase the length of life through medical intervention, eg (6)
24 Numbers game (5)
25 Confess (5)
27 Released extracellular fluid due to hunger or desire (9)
28 Having a BMI over 30 (5)
30 Invertebral ---, joints that lie between adjacent vertebrae (5)
31 Having an intellectual ability to correctly assess situations or people (6)
33 Jug (4)
35 Form of alternative Chinese medicine using 18 Down (11)
39 Wave a wing or arm, eg (4)
41 Half (abbrev) (4)
42 Chest pain or pressure caused by insufficient blood flow to the heart muscle (6)
45 Plant seed (5)

46 --- by mouth, medical instruction (3)
47 Bodily protuberance that includes the nostrils (4)
48 Medical condition in which poor blood flow to the brain can cause cell death (6)
1 Sound of disgust (3)
2 Bovine animal (3)
3 Backbone (3)
4 Group of cells in an animal’s body that synthesizes hormones for release into the bloodstream (5)
5 Strangely (5)
6 Palindromic ABBA song (1,1,1)
7 Small rip in a muscle (4)
8 Inflammation of the larynx, resulting in a croaky voice and gravelly cough (8)
12 Bodily pain (4)
14 Swelling cause by too much fluid in the body’s tissues (5)
15 Became a less healthy colour (5)
17 Monosaccharide containing one ketone group per molecule (6)
18 Small metal pins (7)
19 Opposite of in (3)
21 It joins the thigh with the leg (4)
23 Mineral form of potassium nitrate (5)
24 Fractured terminal part of the leg (6,4)
25 Combines numbers (4)
26 Light fabric item worn on the face to prevent the spread of disease (4)
29 Athletic ---, firm fabric used to reduce the swelling of soft tissues (5)
31 Severe (of pain or distress) (5)
32 Vase used to keep the ashes of a deceased person (3)
34 Ingrowing callus, often on the foot (4)
36 Liquid by-product of metabolism (5)
37 Sensation of coldness (5)
38 Russian mountains (5)
40 Opening at the opposite end of an animal’s digestive tract from the mouth (4)
41 Senator (abbrev) (3)
43 In my opinion (initials) (1,1,1)
44 Top playing card (3)
Read this article and complete the quiz to earn 1 iFolio hour
Read this article and complete the quiz to earn 1 iFolio hour
In Australia, cardiac arrest is one of the leading causes of death and disability.1 Each year cardiac arrest causes the death of an estimated 22,000 to 33,000 Australians.1 Neurologic injury accounts for a significant proportion of mortality and morbidity in those suffering cardiac arrest.2
Targeted temperature management (TTM) is an evidence-based treatment aimed at minimising neurological injury for patients who have experienced cardiac arrest and are unresponsive or comatose.3 Targeted temperature management involves strict control of the patient’s core body temperature at a temperature between 32°C and 36°C after the return of spontaneous circulation.2,4
Targeted temperature management is associated with improved neurological outcomes and increased survival after cardiac arrest.3,5 TTM can inhibit or mitigate the destructive processes that occur following ischemia-reperfusion, and stimulate protective systems.2,4 However, while the neuroprotective effects of TTM are well documented, the mechanism for neuroprotection is uncertain.4,6 Proposed mechanisms include:2,4,6
• Avoidance of hyperthermia, and the associated metabolic demand and fever related tissue injury
• Reduced brain metabolism
• Slowed production of free radicals
• Reduced brain tissue inflammation
• Lowered intracranial pressure
• Reduced cerebral thermopooling
• Reduced blood vessel leakage and bloodbrain barrier disruption
• Improved overall patient care through focussed coordinated efforts of an expert team with close monitoring.
Targeted temperature management is generally recommended for all adult post-cardiac arrest patients who remain unresponsive following the return of spontaneous circulation.3,5 However, individual patient characteristics and
circumstances, such as traumatic arrest, active bleeding, pregnancy, severe sepsis, and recent major surgery, may contraindicate TTM.4
Nurses are instrumental in administering TTM therapy effectively and should be acquainted with the principles of TTM and its potential complications.6
Targeted temperature management consists of three phases: induction, maintenance, and rewarming.6
Phase 1 - Induction
During the first phase, induction, the patient’s core body temperature is actively cooled to the target temperature.6
TTM should be initiated as soon as possible after the return of spontaneous circulation.4,7 Greater potential benefits are expected the earlier TTM is started.4,7
Target temperature
There is currently no consensus on the ideal target temperature for TTM after cardiac arrest.5 Trials evaluating TTM found similar outcomes for TTM at lower temperatures (32-33°C) compared with higher temperatures (36-37°C).7
The Australian and New Zealand Committee on Resuscitation (ANZCOR) recommends a target temperature of between 32°C and 36°C.5 The optimal target temperature for a patient may be influenced by individual patient characteristics and conditions.5,7 A higher target temperature may be appropriate for patients with septic shock, bradycardia, dysrhythmias, trauma, or a higher risk of bleeding, while a lower target temperature may be appropriate for patients with severe brain injury, subarachnoid haemorrhage, hepatic encephalopathy, or stroke.3,7
The target temperature for TTM should comply with the health service’s protocols.5
Core body temperature can be modulated
by increasing heat loss through the skin, oesophageal or intranasal surfaces, or cooling the blood.6,7
Techniques to achieve TTM include:6,7
• Cooling the skin through the application of water, or pads or blankets circulating of cold air or fluid
• Cooling the oesophageal surface via a fluidfilled tube placed in the oesophagus
• Cooling the nasal cavity surface via a coolant mist delivered through a transnasal catheter
• Cooling the blood through a heat exchange intravascular catheter.
Targeted temperature management may also be induced through the rapid infusion of ice-cold intravenous fluid, however, if cooling is achieved through intravenous fluids additional cooling techniques will be required to maintain the target temperature.5
There is currently no consensus on the ideal cooling technique for TTM.7
During the second phase, maintenance, the patient’s temperature is maintained at a constant target temperature.6 The maintenance phase begins when the target temperature is reached and ends when rewarming begins.6
There is currently no consensus on the optimal duration of the maintenance phase.5,6 ANZCOR recommends that TTM should be maintained for at least 24 hours.5 The optimal duration of TTM for a patient may be influenced by the indication for TTM and disease severity.6 The duration of TTM should comply with the health service’s protocols.5
The patient’s core temperature should be continually monitored to ensure the temperature is maintained at the target temperature.6,7
Other vital signs, including blood pressure and oxygen saturation, should also be routinely measured to monitor the patient’s physiological condition during TTM.6,7
The patient should also be monitored for adverse effects associated with TTM, such as shivering, bleeding, arrhythmias, hyperglycaemia, fluid and electrolyte imbalances, and increased risk of infection.6,7
During the third phase, rewarming, the patient’s core body temperature is gradually raised to achieve normothermia (a core body temperature of 36.5-37.5°C).6,8
Slowly rewarming the patient, targeting a rewarming rate of 0.25-0.5°C per hour, is important to avoid rapid fluctuations in plasma electrolyte concentrations and metabolic rates, and to minimise the risk of hyperkalaemia, seizures, and cerebral oedema.6,7
Fever should be avoided during rewarming and after normothermia is achieved to decrease the risk of adverse neurological outcomes.3,7 The patient’s core temperature should be monitored for at least 48 hours after rewarming ensure normothermia and the avoidance of fever.6,7
The most common adverse effect associated with TTM is shivering.6,7 Shivering is the body’s natural response to a reduced core body temperature.6,7 Shivering is involuntary skeletal muscle activity that raises the core body temperature.6,7 It often occurs between 35.5°C and 36.5°C and ceases when the body temperature lowers to around 34°C.6 Shivering is most common during the induction and rewarming phases of TTM, but may persist during the maintenance phase if the target temperature is between 35.5°C and 36.5°C.6,7 Untreated shivering can limit the implementation of TTM by delaying the time to reach target temperature, effect the ability to maintain the target temperature, and increase the rate at which a patient is rewarmed, increasing the risk of complications, such as hyperkalaemia, seizures, and cerebral oedema.6,7
Controlling shivering is crucial to ensure the full benefits of TTM can be achieved.6 However, the detection and quantification of shivering can be difficult.6 One validated standardised tool to identify and grade shivering is the Bedside Shivering Assessment Scale (see Table 1).6
0 None No shivering noted on palpation of the masseter muscle, neck, or chest wall
1 Mild Shivering localised to the neck and/or thorax
2 Moderate Shivering involves the neck and thorax, and gross movement of the upper extremities
3 Severe Shivering involves gross movements of the trunk and upper and lower extremities
Shivering may be controlled through pharmacologic and nonpharmacologic therapies.6 Escalated patient sedation, using medications such as propofol, may be used to suppress shivering.6,7 In patients refractory to escalated sedation, neuromuscular blockade, dexmedetomidine, and meperidine may be alternative pharmacologic therapies.6,7 Nonpharmacologic therapies to control shivering include surface counterwarming.6 As approximately 20% of autonomic shivering control occurs through skin temperature feedback, shivering can be modulated through skin warming using forced warm-air skin counter-warming devices.6
Other adverse effects associated with TTM include:6,7
• Coagulopathy and bleeding – lowered core body temperature diminishes platelet function and impairs clotting enzymes resulting in bleeding
• Arrhythmias – hypothermia slows cardiac electrical conduction precipitating arrhythmias and depressed myocardial function
• Fluid and electrolyte imbalances –hypothermia may result in hypovolemia and electrolyte disturbances including hypokalaemia, hypomagnesemia, and hypophosphatemia
• Infection – lowered core body temperature inhibits leukocyte migration and phagocytosis, increasing the risk of infection
• Hyperglycaemia – insulin resistance has been seen during hypothermia causing hyperglycaemia.
The pharmacokinetics and pharmacodynamics of many medications can also be significantly altered by TTM.6 As hypothermia generally reduces the absorption, distribution, and extraction of many medications a thorough evaluation of all medications administer during TTM should be undertaken to ensure they are dosed appropriately.6
1. Australian Genetic Heart Disease Registry. Heart Registry [Internet]. Cardiac arrest & heart attack; 2020 [cited 28 May 2021]. Available from: https://www.heartregistry. org.au/2013/02/cardiac-arrest-heart-attack
2. Johnson NJ, Danielson KR, Counts CR, Ruark K, Scruggs S, Hough CL, et al. Targeted temperature management at 33 versus 36 degrees: A retrospective cohort study. Crit Care Med [Internet]. 2020 [cited 2021 Apr 18];48:362-9. doi: 10.1097/ CCM.0000000000004159
3. Knippa S, Butler J, Johnson L, Perman SM. The cold truth about postcardiac arrest targeted temperature management: 33°C versus 36°C. Nurs Crit Care [Internet]. 2020 [cited 2021 Apr 18];15(3):16-23. doi: 10.1097/01.ccn.0000660392.87533.89
4. Nickson C. Life in the Fast Lane [Internet]. Therapeutic hypothermia after cardiac arrest; 2020 [cited 2021 May 28]. Available from: https://litfl.com/therapeutic-hypothermiaafter-cardiac-arrest
5. Australian and New Zealand Committee on Resuscitation. The ARC Guidelines [Internet]. ANZCOR Guideline 11.8Targeted Temperature Management (TTM) after Cardiac Arrest; 2016 [cited 2021 Apr 18]. Available from: resus.org.au/download/ section_11/anzcor-guideline-11-8-ttmjan16.pdf
6. Armahizer MJ, Strein M, Pajoumand M. Control of Shivering During Targeted Temperature Management. Crit Care Nurs Q [Internet]. 2020 [cited 2021 Apr 18];43(2):251-66. doi: 10.1097/ CNQ.0000000000000305
7. Fiorilli PN, Kolansky DM. Intensive care unit management of the intubated post-cardiac arrest adult patient. 2021 [cited 2021 May 28]. In: UpToDate [Internet]. Waltham (MA): UpToDate Inc. Available from: https://wwwuptodate-com/contents/intensive-care-unitmanagement-of-the-intubated-post-cardiacarrest-adult-patient
8. 101 Lapum JL, Verkuyl M, Garcia W, St-Amant O, Tan A. Vital Sign Measurement Across the Lifespan [Internet]. 1st ed. Toronto (Canada): Rygerson University Pressbooks; 2018 [cited 2021 May 28]. Available from: https:// opentextbc.ca/vitalsign


Thursday, March 14 12pm Workers Compensation ANF Office + Zoom
Tuesday, March 19 6pm Documentation ANF Office + Zoom
Thursday, March 21 12pm Documentation ANF Office + Zoom
Tuesday, March 26 6pm Discrimination ANF Office + Zoom
Thursday, March 28 12pm Discrimination
May 02 12pm Social Media ANF Office + Zoom
Tuesday, May 07 6pm Resolve workplace issues ANF Office + Zoom
The ANF offers informative talks on topics relevant to contemporary nursing and midwifery, all for free.
Places are available on a range of topics:
Coroners Court: Learn more about coroners' investigations including discussions on the role of the coroner, the inquest process, evidence gathering, being a witness, making statements and other legal considerations surrounding coroners' reports.
Documentation: A handy refresher on the importance of proper documentation, best practices for record-keeping, legal requirements for documentation and how to maintain accurate and comprehensive records.
Social Media: Take part in discussions around potential legal issues that can arise from its use including privacy concerns, defamation, intellectual property infringement, professional boundaries and ethical considerations when using all types of online media platforms.
Discrimination: This talk covers the legal framework surrounding discrimination, including laws, regulations and case precedents, with reference to the various forms of discrimination, such as gender, race, age, or disability and provide guidance on how to prevent and address such issues in professional settings.
Defamation: Defamation involves making false statements that harm someone's reputation. We explain the elements of a defamation claim, how to minimize the risk of defamation in the context of the workplace, defences against defamation and the potential consequences of defamatory statements on your registration and your wallet.
Workers Compensation: This session covers the essentials that all members must know about the Workers’ Compensation process and how to make it work for you rather than your employer if you are injured at work.
Resolve workplace issues: This important information is useful for all members, and it covers the process of resolving issues at your workplace.