Incorporating



Incorporating

We are now open from: 8am to 8pm Mondays to Fridays.
Appointments are available every 15 minutes. Expect on-time support with accurate advice and assistance.
Don’t rely on social media for your industrial and professional advice. Book a time with the ANF Helpline and make the most of our extended hours!
July - August 2024

ANF State Secretary Janet Reah
As a nurse working on the wards until 2022, I witnessed firsthand the challenges and frustrations that our dedicated nurses and midwives have faced over the years since our last great wages campaign of 2013.
From 2017 onwards, under successive Labor Governments, workloads increased, patient acuity is much higher and in real terms our wages decreased, leaving many of our healthcare professionals feeling undervalued and overwhelmed.
But in 2024 there is a new sense of optimism among a revitalised ANF, especially with the recent victory of the ANMF in Victoria, where nurses and midwives there have just received a historic 28.4 percent pay rise over 4 years. With the upcoming Public Sector, St John of God and ongoing Ramsay EBA negotiations, our members’ expectations are high.
These agreements represent a crucial turning point and a chance to rectify years of neglect and oversight by employers that has led us down the path to this critical shortage of nurses and midwives willing to work in our health system.
That is why I am urging ANF members to get on board and get involved – for the first time in 11 years the EBA campaigns have aligned with the State election.
This Public Sector EBA, will be both a critical step towards acknowledging the tireless work and dedication of our nurses and midwives and a means of resetting the industry standard, that will help make WA competitive again.
The implementation of patient ratios – sets the standard and will be a key feature over the coming year.
The Ramsay and SJOG EBAs bring their own set of promises for improvements where expectations and aspirations of our members remain as high as for those working in the public sector.
These private sector EBAs seek to bridge this gap, ensuring that private sector nurses and midwives receive the support and remuneration they deserve.
As well, with the public sector now achieving ratios, and the Ratios Taskforce coming into being, we must ensure the private sector keeps up with the coming workload changes in public hospitals.
But regardless of sector, by focusing on better wages, improved working conditions, and opportunities for professional development, these agreement aims to create a more balanced and fairer environment for all nurses and midwives, regardless of their sector.
As we move forward, it is crucial to remember that these agreements are the result of relentless advocacy and the collective voice of our nurses and midwives. The ANF has fought tirelessly to ensure that the concerns and needs of our members are heard and addressed. The 2024 EBAs are a testament to this dedication and the power of unity within our profession.

The Australian Nursing Federation (ANF) reaffirms its dedication to implementing nurse-to-patient ratios and midwife-to-patient ratios in Western Australia hospitals by introducing new roles specifically aimed at this objective.
These efforts also encompass the significant achievement of including baby counts in the ratios, a critical element successfully negotiated into the 2022 Public Sector EBA.
The responsibilities of these roles will include engaging with members in the workplace, educating the members on the ratios clause, and along with other members of the Ratios Taskforce, identifying the areas where ratios are most needed. Additionally, they will provide essential advice to State Secretary Janet Reah in the ANF’s push to establish ratios across Western Australia.
The ANF is pleased to announce that the new roles of Special Project Officer – Nurse-to-Patient Ratios and Recruitment, and Special Project Officer – Midwife-to-Patient Ratios, will be filled by David Poole, a nurse with over 14 years of experience, currently in his 11th year at PMH/PCH, and Jane-Anne Gardner, a Clinical Midwife ad Registered Nurse with 20 years of experience 15 of them working at King Edward Memorial Hospital (KEMH).
State Secretary Janet Reah commented on the new appointments, stating, “It was of utmost importance to bring in an experienced nurse and midwife through our rigorous recruitment process.”
“Council recognised the value of on-the-ground and current experience, and we are thrilled to have recruited two active ANF members from their respective workplaces,” Ms Reah said.
David Poole and Jane-Anne Gardner will also join State Secretary Janet Reah in serving on the State Government’s ratios task force.
This task force is responsible for guiding the rollout of ratios across the state, and both David and Jane-Anne, along with Janet Reah, will provide vital recommendations and information.
The ANF has also successfully ensured that both David Poole and Jane-Anne Gardner have secured a seat on the taskforce to inform on matters deliberated by the task force.


“Being appointed to this role is a tremendous privilege and responsibility and I feel proud to be part of the ANF team in making ratios a reality,” Mr Poole said.
“I firmly believe that the implementation of ratios is a once in a generation chance to improve not only West Australian nurse’s workloads but to improve patient safety and outcomes.
“This has been proven by peer reviewed research and evidence in other Australian states that have adopted nurse-to-patient ratios, and around the world in health systems like our own.
“I acknowledge there will be many hurdles to overcome to implement them safely, including the recruitment and retention of skilled nurses across the public sector.
“Meeting these challenges will be difficult but they are challenges I look forward to and I am committed to working hard, along with
the ratios team, to advocate for the nurses at the frontlines dealing with the changes, and to ensure the timely, safe, and effective implementation of these desperately needed nurse-to-patient ratios.”


“As a midwife and a nurse with experience across adult, neonatal and within the maternity space, I live firsthand the challenges that WA Midwives and Nurses are facing, which were amplified during and since the global pandemic, Ms Gardner said.
“Every health service has different challenges, but we all know that being able to do our core business of caring, advocating, educating, and empowering we can make a huge impact on the health and wellbeing of those we care for.
“The introduction of midwife-to-patient ratios is a crucial step towards improving pregnancy and health outcomes for women and neonates.
"With ratios continuity of care could be achievable for more, which will improve maternal satisfaction.
"Counting the babies into the ratios is also extremely important in ensuring the health and wellbeing of the neonate, while ensuring midwives have time to provide care, support, and education for the families in their care.
“Midwife and nurse well-being is a focal point for me. and with ratios - burn out rates will lower and midwifes job satisfaction increase meaning more midwives will stay in the profession.
"I am a strong advocate for colleagues, those I care for and I am looking forward to being part of the team that makes history in WA by successfully helping with the implementation of the correct ratios into health services in WA.
“This is a new road we are travelling which I am sure will lead to WA having the best ratios in Australia.”
It is an evidence based and transparent way to staff every shift every day. Proven to reduce deaths, readmissions, errors and burnout. Ratios’ are a minimum staffing level that can be adjusted around acuity and clinical area.
What staff are included in ratios?
RNs, EN’s, and Midwives
Will we lose numbers or midwives?
No. The current agreement is that if the current ward staffing is higher, that ward gets to keep the higher number.
Can ratios be adjusted if acuity is high?
Yes, ratios are a minimum and an agreed method of escalation is being developed and implemented.
Each ward/specialty will be determined by local steering committees, and it is not a one size fits all approach.
Victoria, Queensland and the ACT. Ratios are currently in development in NSW and SA.
There is a dispute resolution process that can be followed if ratios are not being met. Once wards have ratios there is a 4-month grace period, allowing for the transition before disputes can be raised. After that, the ANF will have the power to make a case of non-compliance to the Industrial Commission.
If you have any questions for the new ANF Ratios Taskforce why not get in contact?
Email: Ratios@anfiuwp.org.au

2022 was a transformative year for midwifery care in Western Australia, significantly marked by the “Count the Babies” campaign, a key component of the ANF’s push for ratios in our hospitals. This initiative, which formed a vital part of the 2022 Public Sector EBA campaign, led to the historic inclusion of midwife-to-patient ratios that recognize newborns as individual patients, fundamentally changing maternity care in WA.
Unlike other states such as Victoria and Queensland, which have legislated ratios, Western Australia stands out by counting each baby as a separate patient. By ensuring newborns are counted as separate entities, this policy addresses a critical gap in maternity services, ensuring adequate staffing levels to meet the complex needs of both mothers and their babies.
Jane-Anne Gardner, ANF Special Project Officer for Midwife-toPatient Ratios, reflected on the counting the babies campaign and how it is a must-have in establishing ratios, saying: “The ‘Count the Babies’ initiative will revolutionise how we provide neonatal care, ensuring each newborn is recognised as an individual requiring dedicated care. This approach allows for more mother/ baby/family care that is personalised, potentially reduction of interventions, and significantly enhancing the care provided. Risk reduction associated with ratios and counting the babies will also see an improvement in midwives fatigue levels, work life balance and general wellbeing. Though there is still a road ahead until we are enforcing counting the babies in our hospitals, I am excited and proud to be getting started on the work.”
However, implementing these ratios is only part of the solution. Ensuring we have enough midwives to meet these ratios requires improving wages and working conditions. By offering competitive
salaries and better support, we can attract and retain the skilled professionals needed to deliver high-quality care. “Improving wages conditions and investing in the morale of midwives and nurses, is imperative to fulfilling the ratios,” added Ms. Gardner.
“Without these changes, we cannot ensure that we have enough midwives to meet the needs of every mother and baby. I believe we need to look toward the historic pay rise Victorian nurses and midwives just received as the benchmark for our aspirations in WA.”
The broader implications of these improved ratios are profound, leading to better pregnancy outcomes, fewer postnatal complications, and higher parental and midwife satisfaction. This initiative serves as a model for how targeted policy changes can profoundly impact health outcomes, potentially inspiring similar reforms globally.
Western Australia’s leadership in recognising and addressing the complex needs of newborns and their mothers paves the way for a future where every family is cared for in a safe and supportive environment. This commitment to improved midwife-to-patient ratios highlights the importance of thoughtful policymaking in enhancing healthcare delivery, ensuring that the needs of the most vulnerable patients are met with the highest standards of care. The ANF aims to see all patient ratios legislated in law in the future, giving them even more power beyond our EBA.
The Australian Nursing Federation received so many questions from attendees at the ANF Occupational Health and Safety Conference last year that it was impossible to answer them all at the time, so we followed-up with our presenters and shared your questions with them. In this edition of the Western Nurse we focused on workers compensation, and sought expert advice from the team at the Insurance Commission of Western Australia.
The Insurance Commission of Western Australia is a statutory corporation and Government Trading Enterprise owned by the Western Australian Government. They provide self-insurance arrangements for the Government, covering over 109 WA public authorities for workers compensation, property and liability. This includes WA Health.
Last year they sent representatives to the ANF’s OHS Conference to deliver a talk on workers compensation.



If an injury were settled through workers compensation and recurs after retirement, is that second injury still covered?
If a claim is settled, entitlements to compensation, medical and other expenses in relation to the injury will stop, regardless of whether or not the worker is retired.
If the employee is on a fixed term contract and then goes on workers compensation, at the end of the fixed term contract, can it just not be renewed? Whether a worker’s contract is renewed or not is dependent on the business requirements of the employer and whether a further contract is available to be offered, not whether a person is in receipt of workers compensation.
If your contract ends and you are in receipt of workers compensation payments, the payments will not be impacted by the change to your employment status. Entitlement to workers compensation payments is driven by medical evidence and a person’s capacity for work.
For an injury, if you have reported it, can you go on workers compensation after you have seen the doctor? Is there a time frame for this?
You need to visit your GP and have them complete a Workers Compensation First Medical Certificate prior to lodging a claim. You are encouraged to lodge your claim in as timely a manner as possible to ensure you receive the right support.
A claim should be lodged within 12 months from the date of injury so as not to impact the employer’s ability to gather information, but the sooner a claim is lodged, the more effectively it can be managed and you can be supported in your recovery and return to work.
Can you claim for emotional trauma associated with being on workers compensation?
You may lodge a claim for anything you consider to be a workrelated injury or condition. Whether or not liability for the claim is accepted would depend on the claim circumstances and the medical and factual information.
If you are psychologically impacted by a physical injury for which you have an approved workers compensation claim, we will give consideration to funding treatment such as counselling under your claim, provided that the need for treatment is supported by your GP or specialist.
If you have a second job which is casual and you go on workers compensation in your main job can you be paid additionally for your casual job too, if you cannot work?
Yes. If you have two jobs at the time you are injured and unable to work in both due to the compensable injury, the income compensation rate is the aggregate average weekly earnings from both jobs under the Workers’ Compensation and Injury Management Act 2023 which came into effect 1 July 2024. Note this is a slight change from the previous Workers’ Compensation & Injury Management Act 1981.
The Western Nurse will publish more answers to any questions you might have. Write to us at Western.Nurse@anfiuwp.org.au if you have another question about workers compensation.
The Workers Compensation & Injury Management Act 2023 came into effect as of 1 July 2024, with a number of key differences from the Workers’ Compensation & Injury Management Act 1981. Be sure to contact the ANF or WorkCover WA (1300 794 744) for the latest up to date advice on workers compensation.



The backdrop to the 2004 ANF EBA campaign was an approaching state election in February 2005. For almost 12 months, the ANF systematically ramped up pressure on the government in a campaign that lead to progressively improved offers right up until the final days of the election.



The campaign, marked by a series of escalating offers from the government, highlighted the importance of solidarity, persistence and strategically timed actions. It also set the scene for even more improvements to be achieved in the next pre-election campaign that happened in 2008.
The ANF’s journey began in early 2004, when it became clear that the government was not keen on initiating wage negotiations.
Nurses and the ANF waited in vain for any correspondence from the government until a letter from the Minister for Health finally arrived, promising a 3.4 percent wage increase from May 2 as a “sign of good faith.” This move, unprecedented at the time, indicated the government’s nervousness about the potential campaign by the nurses.
The initial offer from the government on August 23 was a modest 6.9 percent wage increase over two years.


This offer did little to address the broader concerns of the nurses, who were also fighting for better working conditions and recognition of their increasing workloads. Mark Olson, the ANF WA State Secretary, emphasized that the government’s offer was insufficient and did not reflect the true value of the nurses’ contributions.
In response to the nurses’ rejection of the initial offer, the government came back on September 23 with an improved proposal: a 10.5 percent increase over three years, along with a shift coordinator allowance and eight weeks of paid parental leave.
However, this offer came with a caveat—the government indicated that any further improvements in conditions would necessitate a reduction in wage increases.
This tactic was seen by the nurses as an attempt to divide and conquer, but the ANF stood firm, rejecting the offer and pushing for a more comprehensive agreement.



The ANF’s persistence saw another offer from the Government on October 15, proposing a 14.4 percent increase over four years while maintaining the conditions from the September 23 offer.
The catch was that if the offer was not accepted by October 18, it would be withdrawn. Nurses, united in their resolve, once again said no, demonstrating their commitment to achieving a fair deal.
The government presented a revised offer on October 28: a 13.2 percent increase over three years. The ANF continued to negotiate, aware that the stakes were high and that their persistence was beginning to yield results.


By December 10, the campaign had gained significantly more momentum. The government, feeling the pressure of an election around the corner, offered a 14.7 percent wage increase over three years, including 1.8 percent back pay until July 2004.
However, this offer came with a strict five-hour deadline for the ANF to accept it, failing which the government would pursue a non-union agreement. Mark Olson, unwavering in his commitment to the nurses, emphasized the importance of thorough consultation with members before making any decisions. The nurses’ solidarity once again led to a rejection of the offer. Mark Olson, in a rallying call to the nurses, stated, “We will not be bullied, harassed, threatened, or intimidated into accepting an offer within hours of its release. It is important that ANF members have their say on whether the latest government offer is acceptable or not.
The government ran out of patience with the nurses’ union just before Christmas and in a desperate move to finalise a pay deal with the nurses before the state election they decided to cut out the nurses’ union and its difficult secretary Mark Olson out of the action and put out a non-union agreement.
This agreement maintained the 14.7 percent wage increase over three years, but it also proposed significant reductions in other conditions, including changes to rosters and the definition of a shift worker, which would have meant the loss of a week’s annual leave for many nurses.


This offer was rejected comprehensively by ANF members in a postal ballot conducted by the government over the Christmas/ New Year period and so the campaign continued with the government on notice that the ANF members were united behind their union.
As the official State Election campaign kicked off, the stakes rose dramatically when the Liberal Party in opposition released their health policy that included matching government offer but with no trade-offs and an additional $50 million for other improvements.
The ANF never gave up negotiating throughout this period and eventually secured a second deal from the Labor government in the final week of the election campaign that renewed the 14.7 percent and other improvements but this time as a union agreement with no loss of any conditions.
With the memories of the punishing 2005 EBA negotiations still fresh in the minds of the WA government and the next election in 2008, the EBA negotiations of late 2007 marked a significant departure from the prolonged and robust disputes typical of past negotiations. The ANF, recognising the government had strong incentives to adopt a more collaborative approach and a much shorter time frame, adopted to a less confrontational strategy that focused on key areas rather than a broad log of claims.
The government’s eagerness to ensure a smoother negotiation process was evident from the outset, signified by the greater involvement of the Health Minister, Jim McGinty who held regular discussions with ANF Secretary Mark Olson. The looming election in early 2008 added a sense of urgency and pragmatism to the proceedings, encouraging both parties to find common ground swiftly.
14.7 percent pay increase with back pay from July 2004
No loss of conditions
Sunday penalty extended from midnight to end of shift Monday
In Charge allowance
Paid Parental Leave increased from six weeks to eight weeks
The introduction of a Nurse Practitioner Classification.
Unlike previous negotiations, which often dragged on for extended periods, the 2007 EBA was finalized in a matter of months. This expedited process led to several key outcomes that significantly improved the conditions for public sector nurses.
17 percent Wage Increase for Level 1 Nurses
14 percent Wage Increase for Other Levels
Increased Afternoon Shift Penalties: 12.5 to 15 percent
Night Shift Penalties Increased from 20 to 35 percent
Fortnightly Qualification Allowance: This replaced the previous one-off payment, ensuring that nurses & midwives who pursued additional qualifications received an allowance for their entire career
Maternity Leave Increased: Maternity leave was extended to 14 weeks.
In a groundbreaking victory after 51 days of protected industrial action, Victorian public sector nurses and midwives have achieved a monumental 28.4 percent wage increase over four years, along with other enhancements to allowances, penalties, and working conditions as part of their new Enterprise Bargaining Agreement (EBA). This achievement not only marks a historic win for Victorian ANMF members but also sets a new benchmark for negotiations across Australia, especially for Western Australia (WA), where nurses and midwives are amongst the lowest paid in the country.

Moreover, the Victorian EBA sets a precedent in terms of how allowances and penalties are structured, with increases set to reach 28.4 percent by 2027, and some penalties like night duty and qualifications allowance increasing even more. This comprehensive approach to improving compensation packages should serve as a blueprint for the WA Government where such enhancements could help address the current workforce and staffing pressures and encourage nurses and midwives to “love their work again,” as noted by Lisa Fitzpatrick, Secretary of ANMF (Vic Branch).
Apart from the massive wage increase, there are other innovative aspects of the Victorian EBA such as the new “right to disconnect”, which mandates a new process for filling shifts that respects nurses’ and midwives’ time off. Such measures could significantly impact job satisfaction and mental health for WA’s nurses and midwives, who deserve similar considerations given their round-the-clock commitments.
The context in Victoria contrasts sharply with the situation in WA, where nurses midwives and all other public servants have faced years of wage stagnation since the Labor Government’s rise to power in 2017. The disparity highlights an urgent need for WA ANF members to reach a similar deal this year. The need for such advancements is not just about wage parity but also about acknowledging and compensating for the extensive pressures and challenges faced by nurses and midwives in WA.
As EBA negotiations begin in WA, it is crucial for both the Health Department and the ANF to push Premier Roger Cook towards an ambitious overhaul of the current terms. The outcome of these negotiations has the potential not just to close the wage gap with other states but also to revitalise a healthcare system burdened by years of neglect. With Victoria’s EBA as a benchmark, there is a clear framework for what can be achieved through determined advocacy, negotiation and campaigning by rank and file members.

For WA’s nurses and midwives, the upcoming EBAs in both the public and private sectors are not just about better wages but about respect, recognition, and a restoration of fair working conditions. It’s time for WA to step up and ensure its nurses and midwives are no longer the lowest paid in Australia but among the most valued. This is not merely a financial imperative but a moral one, reflecting the community’s collective respect for those who care for us at our most vulnerable.
Whether you’re a graduate nurse, a Level 1.8, 2.4 or any other category, it’s a 28.4 percent wage increase for Victoria’s hardworking workforce.
ANF State Secretary Janet Reah
“Victoria’s latest EBA has proven that well-deserved wage increases are not only needed, but possible. WA nurses and midwives have seen wages go backwards since Labor came to power in 2017, and the Cook Government now needs to prove, approaching the 2025 State Election, that they are serious about filling the promised Ratios by making WA wages for nurses and midwives attractive.”
ANMF WA Branch Councillor Elaine Daniels
“I know from my experience and working with colleagues that WA’s nursing and midwifery workforce are simply overworked and underpaid. Victoria’s benchmark-setting increase must be the gold-standard expectation of WA’s nurses and midwives who have waited long enough for a truly fair wage rise.”

What’s happening with Long Service Leave (LSL) for casuals and why the delay?
The Department of Health is currently waiting for Government to make key decisions on the issue of continuity of service, specifically they need to determine the maximum allowable breaks between periods of casual service both in the past as well as going forward.
WA Health is currently unable to complete changes to the payroll system to calculate and reflect LSL for casual employees.
ANF Secretary Janet Reah has already written to the government with proposals to expedite this decision-making process. One of the key proposals includes allowing breaks in service of up to six months for casual employees.
Who will be processed and paid first?
Those who have only ever worked as casuals, as they will be the quickest to process.
Who is entitled to LSL?
In the first round it will be current casual employee.
In the second round it will be current employees who have also worked for periods as a casual.
How far back do the calculations go?
Calculations can go back as far as 1996, provided there has been no break in service.
How long before the processing of claims resumes?
The processing of LSL claims was halted due to a recent decision in the WA Industrial Commission regarding LSL for casuals. The WA Government also needs to make further decisions about continuity of service before processing can resume.
Will eligible employees be contacted by HSS?
Yes – it is expected that HSS will recommence audits and therefore the payouts for pure casuals in the coming months. A pure casual is an employee who has only ever worked as a casual without any periods of permanent or fixed term contracts.

Will HSS audit anyone who has worked casual?
Yes, that is the intention – but for the moment, they are working on those who have only worked as casuals.
If I am casual, how will I receive my LSL?
You will receive a cash payment, unless you elect to keep the leave for a later date. If you do elect to keep the leave, you can also change your mind and take the money if getting access to the leave is taking too long, especially since HSS may take longer than expected to build the computer payroll system that can accrue and record the LSL for casuals on the pay slip.
Once the payroll system is built, casuals will be able to access leave (not just get a cash out), similar to permanent and fixed term employees.



It is, once again, time for us all to fill out our tax returns. This can be a stressful time from many and, given the Australian Tax Office has recently announce a renewed focus on those claiming work related expenses, it is especially important that our members take the time to get their tax returns correct.
To take a bit of the pain out of the whole process the Australian Nursing Federation has some quick and easy tips handy tax tips on what work-related expenses you can claim on this year’s tax return.
The ATO is reminding everyone, not just nurses and midwives, of its three golden rules for claiming a deduction for any work-related expense:
1. you must have spent the money yourself and weren’t reimbursed
2. the expense must directly relate to earning your income
3. you must have a record to prove it
If you meet these criteria, then you will most likely be able to claim a deduction on a work-related expense.
While most of the work-related items nurses and midwives consume are either supplied or exempt from claiming on your tax return, there are some items, such as your vehicle, phone, uniform and travel that may be claimed in some circumstances.
In some cases, members will be able to claim the cost of trips between home and work, if they don’t have a fixed place of employment and you have to repeatedly travel from one worksite to another during the workday. Members can also claim costs associated with driving their own car between different jobs, or between different workplaces for the same employer within the same workday.
You cannot claim for the cost of normal travel from your home to your work. You also cannot claim parking or speeding fines.
You can claim your work-related phone or internet expenses, provided you have records. This does not include calling or emailing your manager to schedule shifts, or checking online payslips, rosters or income statements.
Nurses and midwives can claim expenses for self-education and study, provided it directly relates to their employment. According to the ATO, the course or study must also increase or maintain knowledge or skills needed for your current duties and it must also likely result in an increase in income from your current job.
You can’t claim a deduction if your employer pays for or reimburses you for these expenses.
Nurses and midwives can claim expenses for protective clothing that reduces the risk of injury or illness at work, as well as for compulsory uniforms. These expenses can be for the purchase, repair or cleaning of these clothes.
This does not cover everyday clothes worn at work and, again, members cannot claim a deduction if their employer pays for the clothing or reimburses them for expenses.
There are a number of other work-related expenses that individuals can claim.
This includes union and professional association fees (such as your ANF fees), agency commissions and agency fees, annual practising certificate fees, technical or professional publications, tools and equipment, personal protective equipment (PPE) that is a necessary part of your job. PPE could include hand sanitiser, gloves or masks, provided these items were not supplied by your employer or the costs of purchasing them were not re-imbursed by your employer.
Remember, even if they are a required part of your job, you cannot claim costs for vaccinations.
The ANF is reminding all members that the cost of their membership is fully deductable.
A copy of an individual’s member contributions can be downloaded from iFolio, using the steps below. You will need this this claim your deduction.
Login to your iFolio account and click on the red “My Account” tab at the top right.
Then click on the “My ANF Fees”
Under the section labelled “My contributions” download a record of the fees paid in this financial year.
Disclaimer: this advice is general in nature. For more information members can go to ato.gov.au/nurse or speak with a registered tax professional.

The ATO requires you to keep a record of the work-related expenses you may wish to claim. For some expenses this will mean you have to be able to explain your work-related use and how you calculated the claim. If you don’t keep the right records, your claim may be disallowed.
According to the ATO, records are usually a receipt from the person or business that provided you with the good or services you are looking to claim. This document should include the name of the person or business, the price paid, a description of the good or service provided, date of purchase and date of the document itself was produced.
You can keep a physical copy of these documents if you would like, but you can also keep electronic records, including photos of receipts.
Once you have made the claim, it is still important to keep your records for five years from the date you lodge your tax return.
The free ATO app has the myDeductions record keeping tool to help people keep track of their record electronically.



Read this article and complete the quiz to earn 0.5 iFolio hour
Read this article and complete the quiz to earn 0.5 iFolio hour
Brand name: Cyclonex, Endoxan1
Drug class: Alkylating agent1
MECHANISM OF ACTION
Cyclophosphamide is an alkylating agent that interferes with cellular replication by forming cross-linkages between DNA strands, decreasing DNA synthesis.1
ADMINISTRATION
Cyclophosphamide is administered orally or intravenously.1,2
Intravenous administration should be by slow intravenous injection over three to five minutes, or by short infusion over 30-60 minutes. 1
INDICATIONS
Cyclophosphamide is indicated for the treatment of cancer, such as breast cancer, sarcoma, lymphoma, acute lymphoblastic leukaemia, multiple myeloma, and Waldenstrom macroglobulinaemia, according to treatment protocols.1
Cyclophosphamide is also indicated in the treatment of autoimmune diseases, such as systemic lupus erythematosus, glomerulonephritis, and systemic vasculitis. 1
CONTRAINDICATIONS
Cyclophosphamide is contraindicated in patients with:1,3
• Hypersensitivity to cyclophosphamide
• Urinary outflow obstruction
• Cystitis
• An active infection
• Severely depressed bone marrow function.
INTERACTIONS
Cyclophosphamide has a number of clinically meaningful drug interactions. For example:3,4
• Phenytoin increases the metabolism of cyclophosphamide increasing the concentration of the active metabolite and its toxicity
• Itraconazole increases the renal and hepatic toxicity associated with high-dose cyclophosphamide
• Cyclophosphamide may decrease plasma cholinesterase activity and prolong the activity of suxamethonium
• Concurrent use of cyclophosphamide with allopurinol or hydrochlorothiazide increases the risk of bone marrow depression
• Concurrent use of cyclophosphamide and drugs that induce or inhibit CYP2B6, CYP2C9 and CYP3A4 enzymes, such as carbamazepine, voriconazole, rifampicin, amiodarone, and ketoconazole, may alter
the metabolism of cyclophosphamide, increasing or decreasing its concentration.
The dosage of cyclophosphamide should be individualised to the patient.1 The dose and duration of treatment depends on factors such as the indication, the patient’s health and organ function, response to treatment, toxicity, and the results of laboratory monitoring. 1
Antineoplastic
The dose of cyclophosphamide differs for induction or maintenance of remission.1,2,3 Dosage should be in accordance with local protocols.1
The usual initial intravenous loading dose for patients with no haematological deficiency is 40-50mg/kg, given in divided doses over two to five days.2,3 If initial cyclophosphamide therapy is given orally, a daily dose of 1-5mg/kg may be administered depending on tolerance.2,3
A variety of dosage schedules have been used for maintenance therapy, including:2,3
• 1-5mg/kg orally daily
• 10-15mg/kg intravenously every 7-10 days
• 3-5mg/kg intravenously twice weekly.
Autoimmune disease
The initial oral dose of cyclophosphamide for treating autoimmune disease is 1-3mg/kg daily.1,2,3
Renal impairment
Cyclophosphamide should be used with caution in patients with renal impairment. 1 A lower dose may be required for these patients. 1
Pregnancy and breastfeeding
Cyclophosphamide is not recommended for use during pregnancy.5 Effective contraception should be used during treatment with cyclophosphamide and for at least three months after the last dose.1 Cyclophosphamide is contraindicated during the first trimester due to an increased risk of fetal malformations, including cleft palate, missing digits, coronary artery defects, umbilical hernia, growth restriction, and developmental delays.5 If cyclophosphamide is used during the second or third trimesters, maternal and fetal wellbeing should be closely monitored and delivery planned for at least three weeks after treatment to reduce the accumulation of cyclophosphamide in the fetus and complications such as bleeding, infection, and anaemia in the mother and infant.5
Cyclophosphamide should not be used while breastfeeding.5 Cyclophosphamide is excreted into breastmilk, and infant exposure is associated
neutropenia, bone marrow suppression, and reduced growth.5
The type and severity of adverse effects associated with cyclophosphamide are often related to dosage and duration of use.1
Common adverse effects associated with cyclophosphamide include nausea, vomiting, alopecia, anorexia, and with rapid injection, nasal congestion.1 Cyclophosphamide is also commonly associated with myelosuppression, with neutrophil nadir occurring seven to 14 days after a single dose.1 Myelosuppression is a major dose limiting effect of cyclophosphamide. 1
Cyclophosphamide may also cause transient or permanent infertility in men and women due to gonadal suppression and resulting amenorrhoea or azoospermia.1 The risk of infertility is related to the dose and duration of treatment. 1
High doses or prolonged use of cyclophosphamide have also been associated with haemorrhagic cystitis due to the accumulation of metabolites in the bladder. 1
Cyclophosphamide may infrequently be associated with loss of taste, metallic taste, and hyperpigmentation of nails and skin.1 Rarely cyclophosphamide is associated with pulmonary fibrosis, heart failure, hepatic sinusoidal obstruction syndrome, and water retention resembling syndrome of inappropriate secretion of antidiuretic hormone resulting in hyponatraemia and seizures.1
1. Cyclophosphamide. 2022 [cited 2022 Apr 3]. In: Australian Medicines Handbook [Internet]. Adelaide (Australia): Australian Medicines Handbook. Available from: https://amhonline. amh.net.au/chapters/immunomodulatorsantineoplastics/cytotoxic-antineoplastics/ alkylating-agents/cyclophosphamide
2. NPS MedicineWise. Consumer medicine information [Internet]. Endoxan. 2018 [cited 2022 Apr 3]. Available from: https://www.nps.org.au/ medicine-finder/endoxan-powder-for-injection
3. NPS MedicineWise. Consumer medicine information [Internet]. Cyclonex. 2020 [cited 2022 Apr 3]. Available from: https://www.nps.org.au/ medicine-finder/cyclonex-50-mg
4. Drug interactions: Cyclophosphamide. 2022 [cited 2022 Apr 11]. In: Australian Medicines Handbook [Internet]. Adelaide (Australia): Australian Medicines Handbook. Available from: https:// amhonline.amh.net.au/interactions/alkylatingagents-inter#cyclophosphamide-inter
5. Cyclophosphamide. 2022 [cited 2022 Apr 11]. In: Pregnancy and Breastfeeding Medicines Guide [Internet]. Melbourne (Australia): The Royal Women’s Hospital. Available from: https://thewomenspbmg.org.au/ medicines/ cyclophosphamide
Read this article and complete the quiz to earn 0.5 iFolio hour
Read this article and complete the quiz to earn 0.5 iFolio hour
Deep vein thrombosis (DVT) is a common, potentially fatal, cardiovascular disease with non-specific symptoms. It is generally diagnosed by scoring pre-test probability (Well’s Score), D-dimer testing, and imaging. As the D-dimer test is non-specific for DVT, it cannot be used to exclude DVT in isolation, but rather serves to indicate the need for imaging.1,2 If necessary, venous ultrasonography using duplex ultrasound is performed for definitive DVT diagnosis or exclusion.1
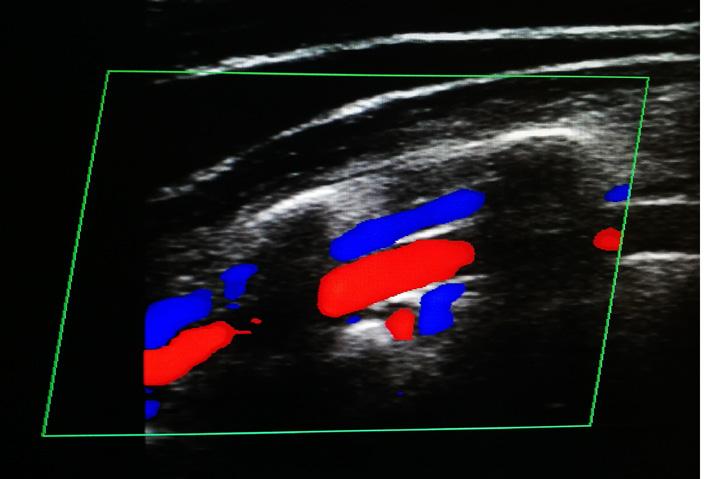
Duplex ultrasound uses conventional ultrasound combined with a Doppler beam. When ultrasound waves are reflected by moving objects such as blood, they experience a Doppler shift in frequency when returned to the transducer.3 In a colour Doppler image, frequencies are colour coded, so that flow towards the transducer appears a different colour to flow away from the transducer (see Image 1).3
Image 1. Colour Doppler ultrasonography. Red indicates motion towards the transducer, while blue indicates motion away.
In Australia, the entire deep venous system, from ankle to groin, is usually visualised.1 However, the sensitivity of detection of DVT below the knee with ultrasound is very low.4 An abbreviated point-of-care technique inferring DVT from incomplete venous compressibility has equivalent accuracy. It is referred to as lower limb venous two- or three-point compression ultrasound, examining the popliteal and common femoral veins only.2,4 This method has gained acceptance in emergency, critical, and perioperative care. 4
Venous duplex findings in the presence of thrombus include:2-4
• direct visualisation of thrombus with venous dilation
• reduced, absent or abnormal blood flow pattern
• venous non-compressibility
• impaired or absent augmentation of flow
• loss of respiratory variation and spontaneous flow
• increased flow in collateral channels
Abnormal findings are categorised as acute, chronic, or chronic post-thrombotic changes, or indeterminate (see Table 1). 2
Table 1. Classification of thrombotic venous changes.2,4
Reduced or absent
echogenicity
Poorly attached
Spongy texture
Venous dilation
May have loosely adherent or freefloating edge
Well attached
Rigid and calcified
Contracted vein
Enlarged collateral veins
Material may retract and become fibrotic
May incorporate in wall or cause recanalisation, producing irregular or thickened walls
Scarring may lead to decreased vein size
When compressed, healthy veins should coapt to completely obliterate their lumen and potentially deform the adjacent artery.4 The presence of a thrombus limits vein compressibility. 3 In order to measure compressibility, technicians apply pressure to the vein with the ultrasound transducer.3
Veins generally dilate around an acute thrombus and may show limited filling above the clot due to obstruction. 3 New clots may have a thin tail that extend into the lumen of the vein, and may allow blood to pass around them as they adhere to the vein wall.3 As they become more established, they gain fibrosis tissue and occlude blood flow completely. At this point, echogenicity (the ability to transmit ultrasound waves) is altered.3
Healthy veins have spontaneous blood flow which changes in response to pressure variations during respiration. 3 On inspiration, intraabdominal pressure is elevated and venous return decreases. Conversely, on expiration, pressure is reduced, and venous return is increased. The presence of a thrombus limits respiratory variation.3
Manual compression results in an increased blood flow rate through healthy veins, called augmentation.3 It can be assessed with a gentle squeeze of the calf muscle. In individuals with DVT, a blood clot is already occluding flow, so external compression will either have no effect or may result in further flow restrictions. 3
In the presence of DVT, increased velocity and flow may be noted in collateral veins.3 Blood in the intramuscular channels builds up over time and is often an indication of a chronic thrombus.3
1. Tran HA, Gibbs H, Merriman E, Curnow JL, Young L, Bennett A, et al. New guidelines from the Thrombosis and Haemostasis Society of Australia and New Zealand for the diagnosis and management of venous thromboembolism. Med J Aust [Internet]. 2019 [cited 2022 Apr 20];210(5):227–35. Available from: https://www.thanz.org.au/ documents/item/41
2. Chopard R, Albertsen IE, Piazza G. Diagnosis and Treatment of Lower Extremity Venous Thromboembolism: A Review. JAMA [Internet]. 2020 [cited 2022 Apr 20];324(17):1765–76.doi: 10.1001/ jama.2020.17272
3. Pozniak MA, Allan PA. Clinical Doppler Ultrasound [Internet]. 3rd ed. Churchill Livingstone Elsevier; 2014 [cited 2022 Apr 20]. Available from: https://www.elsevier.com/ books/clinical-doppler-ultrasound/pozniak/978-0-7020-5015-2
4. Canty D, Mufti K, Bridgford L, Denault A. Point-of-care ultrasound for deep venous thrombosis of the lower limb. Australas J Ultrasound Med [Internet]. 2020 [cited 2022 Apr 20];23(2):111–20. doi: 10.1002/ ajum.12188

The Australian Taxation Office (ATO) will focus on three common errors made by taxpayers: incorrectly claiming workrelated expenses, inflating claims for rental properties and failing to include all income when lodging.
ATO Assistant Commissioner Rob Thomson said these are the areas that people are most likely to get wrong.
“While these mistakes are often genuine, sometimes they are deliberate. Take the time to get your return right.” Mr Thompson said.
According to the ATO more than 8 million people claimed a work-related deduction in 2023. Around half of those claimed a deduction related to working from home. The ATO has revised the fixed rate method of calculating a working from home deduction, and taxpayers must also have comprehensive records to substantiate claims, just as they would for any other deduction.
“Copying and pasting your working from home claim from last year may be tempting, but this will likely mean we will be contacting you for a ‘please explain’. Your deductions will be disallowed if you’re not eligible or you don’t keep the right records,” Mr Thomson said.
ATO records show 9 out of 10 rental property owners are getting their income tax returns wrong.
“We often see landlords making mistakes when it comes to repairs and maintenance deductions on rental properties, so we’re keeping a close eye on this,” Mr Thomson said.
“This year, we’re particularly focused on claims that may have been inflated to offset increases in rental income to get a greater tax benefit.”
As reporting rental income and deductions can be complex, many individual rental owners choose to use a registered tax agent to help them prepare their income tax returns.
“Ensuring you provide full and complete records to your registered tax agent allows them to prepare your tax return correctly, so you claim everything you’re entitled to and nothing that you’re not.” Mr Thomson said.
The ATO is also warning against rushing to lodge your tax return on 1 July.
If you have received income from multiple sources, you need to wait until this is prefilled in your tax return before lodging. For most people, this information will be automatically pre-filled in their tax return by the end of July.
“We see lots of mistakes in July where people have forgotten to include interest from banks, dividend income, payments from other government agencies and private health insurers,” Mr Thomson said.
“By lodging in early July, you are doubling your chances of having your tax return flagged as incorrect by the ATO.”

The Australian Government has announced it will begin to pay super on the Commonwealth Parental Leave Pay (PPL) scheme from 1 July 2025.
Paying superannuation on PPL was a key recommendation of the Women’s Economic Equality Taskforce, which provided the Australian Government with its final report, Women’s Economic Equality: A 10-year plan to unleash the full capacity and contribution of women to the Australian economy in late 2023.
Minister for Women, Senator Katy Gallagher, said that when women take time out of the workforce to raise children it impacts their retirement incomes with women retiring, on average, with about 25 percent less superannuation than men.
“Paying super on Government parental leave is an important investment to help close the super gap and make decisions about balancing care and work easier for women,” Minister Gallagher said.
Minister for Social Services, Amanda Rishworth, said paying superannuation on Paid Parental Leave is “another key step to prioritise gender equality, better value care work and improve women’s workforce participation.”
“It helps normalise taking time off work for caring responsibilities and reinforces Paid Parental Leave is not a welfare payment – it is a workplace entitlement just like annual and sick leave.
“Paying super on Paid Parental Leave will build on the significant reforms we have and are making. We’ve made it more accessible, flexible and gender neutral and we are expanding the scheme to a full six months.”
Australian superannuation provider HESTA welcomed the changes to the PPL scheme, along with a number of other measures announced as part of the recent Federal Budget, but HESTA CEO Debby Blakey said more work still needs to be done.
“It’s fantastic to see the long-awaited allocation of funding for paying super on paid parental leave,” Ms Blake said.
“This is a great investment in the financial future of women across Australia that will narrow the gender super gap, all the while sending a clear message that unpaid caring work is valued.
“Reform to pay super on paid parental leave was a fantastic step forward for women’s financial security in retirement, but there’s still work to do to close the gender super gap and create a fairer super system for everyone.”

Data released by the Australian Institute of Health and Welfare (AIHW) shows that Australians spent more than 33 million days in hospital during 2022-23, an overall increase on previous years.
The AIHW report MyHospitals: Admitted patient care 2022–23 includes the data on the number of hospitalisations in both public and private hospitals. According to AIHW spokesperson Clara Jellie, there was a 4.6 percent increase in hospitalisations across all Australian hospitals during 2022–23, with hospitalisations in public and private hospitals increasing by 4.3 percent and 5 percent respectively compared to 2021–22.
“Overall, there was a total of 12.1 million hospitalisations in 2022–23,” Ms Jellie said.
“Same-day hospitalisations across all Australian hospitals increased by 5.6 percent in 2022–23 compared to 2021–22. There was also a 2.8 percent increase in the number of overnight admissions across all hospitals. Every state and territory had increases in the number of hospitalisations in public hospitals during 2022–23.”
According to the report Australians spent a total of 33.2 million days in hospital during 2022–23, with people aged 60 and over accounting for 59 percent of these patient days of care.
“There was a 4.5 percent overall increase in patient days spent in hospital, including a 4.9 percent increase in public hospitals,” Ms. Jellie said.
According to the AIHW report, in 2022–23 there were just under 3 million hospitalisations requiring surgery. Just under 382,000 of these were emergency surgeries, with about 2.5 million elective surgeries.
Surgery was an activity that was heavily affected by COVID-19: overall, the number of surgical hospitalisations increased by 7.7 percent in 2022–23, but this was following a 5.8 percent decrease in the previous reporting period.
Around 1.8 million hospitalisations involving surgery were carried out in private hospitals.
The Australian Bureau of Statistics (ABS) has released new data that shows Australians intend to retire, on average, between their 65th and 66th birthdays.
Bjorn Jarvis, ABS head of labour statistics said that while the average age of planned retirement has risen over time, it has remained mostly constant over the past decade.
“This average has been between 65.0 years and 65.6 years for close to a decade, since 2014-15,” Mr Jarvis said.
“On average, men intend to retire slightly later than women, but this gap is closing.
“In 2022-23, there was around half a year difference between men and women, compared to a year difference a decade ago, and a two year difference around 10 years before that.”
The ABS data also shows that while expectations around retirement have not changed much, the actual age of retirement has increased.
“In 2022-23, people who had retired in the past 20 years said that they did so, on average, at 61.4 years. This average has risen from 58.5 years in 2014-15 and from 57.4 years in 2004-05,” Mr Jarvis said.
The ABS data also recorded the most common reasons for retirement.
In 2022-23, the most common factors influencing older workers’ decision to retire was still financial security, with 36 percent of those surveyed stating this as a reason, followed by personal health or physical abilities at 22 percent. 14 percent of retirees said reaching the eligibility age for an age of service pension was one of the main factors.

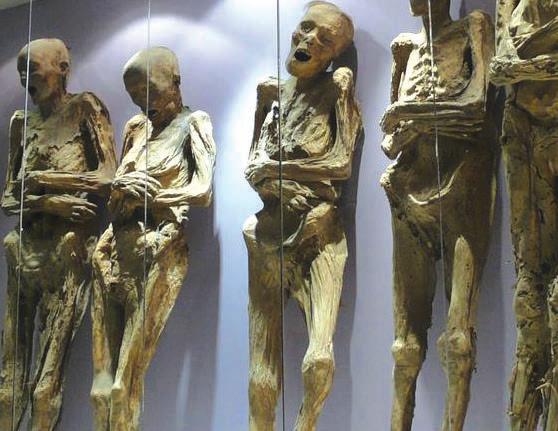
Mexico’s National Institute of Anthropology and History (INAH) has issued a statement criticising the City of Guanajuato after confirming reports that one of the famous mummies stored at the Mummies Museum of Guanajuato had been damaged by museum staff.
The Mummies of Guanajuato are a famous attraction, reportedly receiving hundreds of thousands of visitors annually. The hundred or so naturally mummified remains were disinterred between the mid-1800s and mid-1900s as a result of a local burial tax. If a family could not pay the required fee, their deceased relatives would be disinterred and stored in a building near the grave site.
According to reports in the press and on social media, the arm came off one of the mummified bodies, although the INAH did not confirm this specifically.
In a scathing statement the INAH said there was already some damage to this particular body, but the existing damage was not as severe as it is now, which it attributed to poor handling from museum staff.
The statement went on to say that “instead of applying corrective and preventive conservation strategies, the actions carried out have increased the damage, not only to the aforementioned body.”
“Clearly, this situation is related to the lack of knowledge of adequate protocols, as well as the lack of training of the personnel in charge of carrying out such tasks,” the statement said.
The Mummies of Guanajuato have long been a source of controversy, and there has speculation in the media the INAH’s strong response to the incident stems from a longstanding rivalry between the federal
body and the local authorities who are currently responsible for the bodies.
Various media outlets have reported the Guanajuato city government has yet to respond to calls for comment.
However, earlier in the year, they did issue a statement celebrating the huge revenue stream brought in by the Mummies Museum of Guanajuato.
According to the statement, in 2023 the Museum was visited by 547,502 people, 3,847 more than in 2022. This brought in a staggering 42,286,857 pesos, making it the local government’s second most profitable revenue stream after property tax.

A US woman has been arrested by Police in Boulder, Colorado and charged with felony second degree motor vehicle theft, careless driving and driving without a valid license after she attempted to steal a car.
Her attempt was badly hampered by her inability to drive a vehicle with a manual transmission.
According to a statement issued by the Boulder Police Department on Twitter/X officers were called to Airport Boulevard for a report of a vehicle that had crashed into a fire hydrant. Officers spoke to witnesses and quickly took the female suspect into custody.
The suspect had very recently stolen another vehicle and had also been arrested as a result of that crime.
“It turns out the woman had just been released from jail after stealing a car the day prior, and as she walked about half a mile down the road, she looked inside the truck, saw the keys, got inside and drove off. Sort of,” the statement from Boulder Police read.
“When she couldn’t figure out how to drive the truck’s manual transmission, she jumped out and tried to leave the area on foot.
“The truck then crashed into the hydrant.”
No one was injured and the damaged truck was returned to its owners. The woman was charged with a range of offences.
While in this case a manual transmission stopped the vehicle from being stolen, Boulder Police described this as “not a standard recommendation for car theft prevention.”

The World Health Organization (WHO) has issued its latest HIV Drug Resistance (HIVDR) Report, and it is both good and bad news.
The report has highlighted high levels of HIV viral load suppression in populations receiving dolutegravir (DTG) containing antiretroviral therapy (ART), more than 90 percent overall. However, survey data indicates that levels of drug resistance to DTG are exceeding levels observed in clinical trials.
Since 2018, WHO has recommended use of dolutegravir as the preferred first and second line of HIV treatment for all population groups, as it is more effective, easier to take, and has fewer side effects than other drugs currently in use. According to the WHO it also has a high genetic barrier to developing drug resistance.
However, reported levels of resistance to dolutegravir ranged from 3.9 percent to 8.6 percent. This reached as high as 19.6 percent among people experienced with treatment and who transitioned to a DTGcontaining ART while having high HIV viral loads.
It should be noted that so far only a few countries have reported their survey data to WHO.
According to a statement released by WHO, in 2022 only 12 of the 45 WHO focus countries reported conducting surveys or had integrated the monitoring of HIVDR early warning indicators into routine monitoring and evaluation systems.
“Many countries continue to miss the mark when it comes to optimizing retention in care, population-level viral load suppression, and switching people with virological failure to different regimens,” the statement read.
“Additionally, antiretroviral drug stock-outs continue to happen which may negatively impact patient treatment adherence.”
Dr Meg Doherty, Director, WHO Department of the Global HIV, Hepatitis and STI Programmes, said more needs to be done.
“The worrying evidence of resistance in individuals with unsuppressed viral load despite dolutegravir treatment underscores the necessity for increased vigilance and intensified efforts to optimize the quality of HIV care delivery,” Dr Doherty said.
“Standardized surveillance of HIV drug resistance is essential for effectively preventing, monitoring, and responding to these challenges.”
In 2022, more than 75 percent of the 39 million people living with HIV globally were receiving HIV treatment.

The World Health Organization (WHO) has published its first global guidelines to
prevent the occurrence of bloodstream and other infections caused by catheters placed in minor blood vessels during medical procedures.
According to the WHO, poor practices in the insertion, maintenance, and removal of these catheters carry a high risk of introducing germs directly to the bloodstream, which can lead to serious conditions such as sepsis, and difficult-totreat complications in major organs like the brain and kidneys. Soft tissue infections at the insertion site of the catheter can also occur.
“Up to 70 percent of all inpatients require the use of a catheter inserted into a peripheral vein or artery, also known as peripherally inserted catheters (PIVCs), at some point during their hospital stay,” a WHO statement read.
“People who receive treatments through catheters often are particularly vulnerable to infections, as they might be seriously ill or have low immunity.”
WHO estimated that between 2000–2018, average mortality among patients affected by health care-associated sepsis was 24.4 percent, increasing to 52.3 percent among patients treated in intensive care units.
“Many bloodstream infections are caused by antibiotic resistant bacterial infections (AMR).”
WHO has also reported AMR was directly responsible for an estimated 1.27 million deaths and contributed to an additional 4.95 million deaths in 2019.
Dr Bruce Aylward, WHO Assistant DirectorGeneral for Universal Health Coverage, Life Course said infections associated with health care delivery represent a preventable tragedy and a serious threat to the quality and safety of health care.
“Implementing clean care and infection prevention and control recommendations is critical to saving lives and alleviating a great deal of avoidable suffering experienced by people around the world,”
Dr Aylward said.
The new guidelines include 14 good practice statements and 23 recommendations on key areas for health workers, including: education and training of health workers; techniques of asepsis and hand hygiene practices; guidance regarding insertion,
maintenance, access, removal of catheters; and catheter selection.

New legislation has been passed in the United Kingdom creating specific offences for dog and cat abduction in England and Northern Ireland.
In a statement issued by the UK Government’s Department for Environment, Food and Rural Affairs said that, with the Pet Abduction Bill receiving Royal Assent earlier in the year, abducting a pet has become a criminal offence.
"Under the Pet Abduction Act 2024 – which was a Private Members’ Bill sponsored by Anna Firth MP and Lord Black of Brentwood and supported by the Government – anyone found guilty of stealing a pet in England or Northern Ireland will face up to five years in prison, a fine, or both,” the department’s statement read.
“The new law recognises that cats and dogs are not inanimate objects but sentient beings capable of experiencing distress and other emotional trauma when they are stolen from their owners or keepers.
“Evidence from the Pet Theft Taskforce suggests around 2,000 dog and over 400 cat theft crimes were reported to police in 2020, causing considerable distress for owners and their pets alike.”
It is estimated that 28 percent of UK adults own a dog and 24 percent own a cat.

Work by scientists at the Australian National University (ANU) and the University of Newcastle (UoN) could help engineer climate resilient crops capable of pulling far more carbon dioxide from the atmosphere in a much more efficient way.
According to the ANU, research into the functioning of a critical enzyme found in nature has shed new light on how cells control key processes in carbon fixation, a process fundamental for life on Earth. It is hoped the research could also help us produce more food. A statement released by the ANU said the research demonstrates a previously unknown function of an enzyme called carboxysomal carbonic anhydrase (CsoSCA) found in cyanobacteria (also known as blue-green algae) which allows the microorganism to better extract carbon dioxide from the atmosphere.
“Cyanobacteria are commonly known for their toxic blooms in lakes and rivers. But these little blue-green bugs are widespread, also living in the world’s oceans.
“Although cyanobacteria can pose an environmental hazard, the researchers describe them as ‘tiny carbon superheroes’,” the statement said.
“Through the process of photosynthesis, they play an important role in capturing about 12 percent of the world’s carbon dioxide each year.”
ANU PhD researcher Sacha Pulsford describes exactly how remarkably efficient these microorganisms are at capturing carbon.
“Unlike plants, cyanobacteria have a system called a carbon dioxide concentrating mechanism (CCM), which allows them to fix carbon from the atmosphere and turn it into sugars at a significantly faster rate than standard plants and crop species,” Ms Pulsford said.
CCM contain large protein compartments called carboxysomes,
which are responsible for sequestering carbon dioxide, as well as housing CsoSCA and another enzyme called rubisco.
The CsoSCA works to create a high local concentration of carbon dioxide inside the carboxysome that rubisco can then turn into sugars for the cell to eat.
Study lead author Dr Ben Long of UoN said until now, scientists were unsure how the CsoSCA enzyme is controlled.
“Our study focused on unravelling this mystery, particularly in a major group of cyanobacteria found across the globe. What we found was completely unexpected,” Dr Long said.
“The CsoSCA enzyme dances to the tune of another molecule called RuBP, which activates it like a switch.
“How fast the CsoSCA enzyme supplies carbon dioxide to rubisco is dependent on how much RuBP is present. When there’s enough, the enzyme is switched on. But if the cell runs out of RuBP, the enzyme is switched off, making the system highly tuned and efficient.
“Surprisingly, the CsoSCA enzyme has been embedded in nature’s blueprint all along, waiting to be discovered.”
Scientists say engineering crops to be efficient at capturing and using carbon dioxide would provide a huge boost for the agricultural industry by vastly improving crop yield while reducing the demand for nitrogen fertiliser and irrigation systems.
There is also the hope that it would make our global food systems more resilient to climate change.
“Understanding how the CCM works not only enriches our knowledge of natural processes fundamental to Earth’s biogeochemistry but may also guide us in creating sustainable solutions to some of the biggest environmental challenges the world is facing,” Ms Pulsford said.
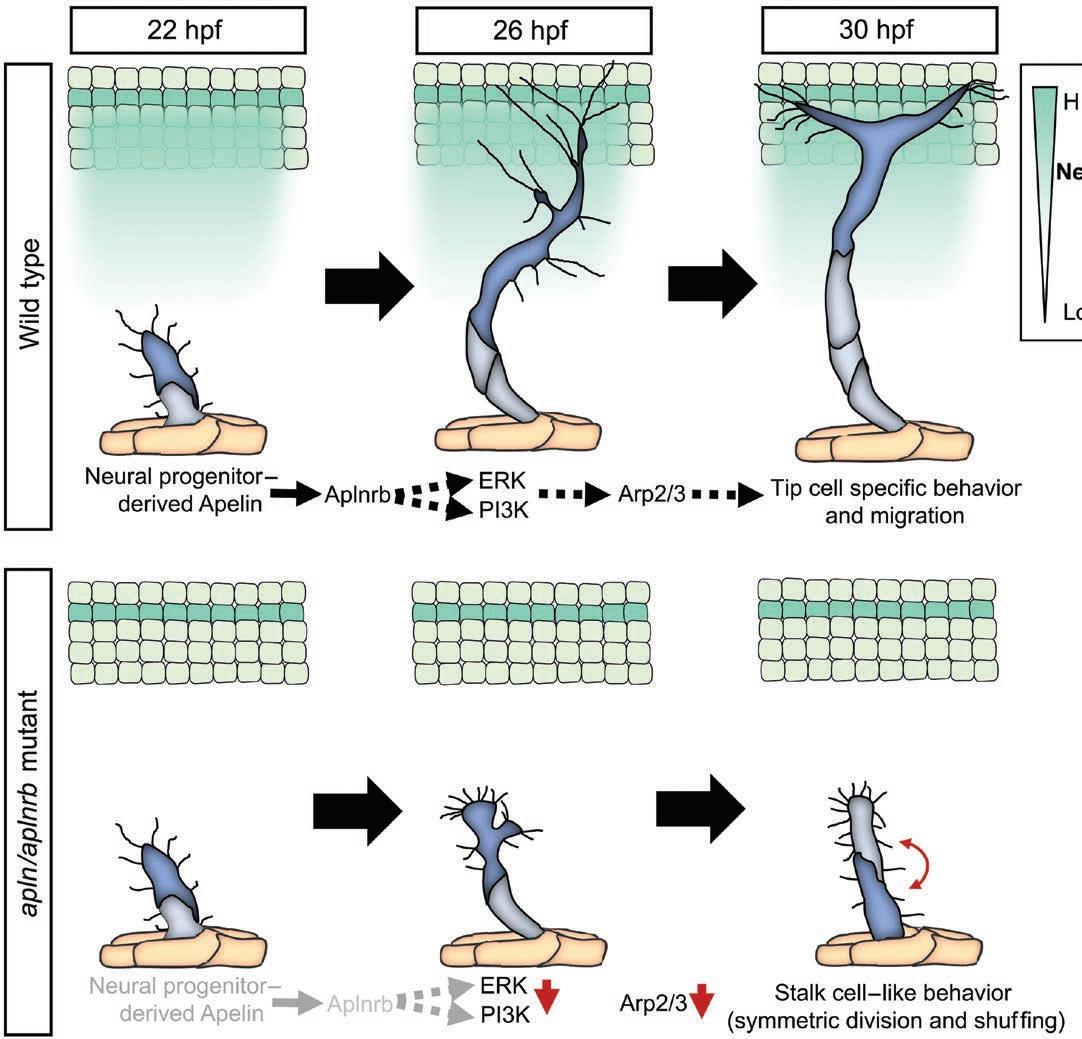
Scientists at La Trobe University and Phillipps-University of Marburg in Germany have discovered how a peptide called Apelin regulates blood vessel growth, which could lead to new opportunities for further research into cancer treatment, organ regeneration and tissue engineering.
According to La Trobe, Apelin is produced by self-renewing stem cells in the nervous system called neuro progenitor cells. The peptide regulates signals to the body which coordinate how blood vessels grow. La Trobe University researcher, Dr Kazuhide Shaun Okuda said the discovery could open the way to develop new therapeutics which regulate blood vessel growth.
“Understanding how blood vessels develop could lead to new treatments to stop excessive blood vessel growth in diseases like cancer,” Dr Okuda said.
“It could also lead to treatments in settings where you need to promote blood vessel growth, such as for organ regeneration and in tissue engineering.”
A statement from La Trobe noted this was the first time neuro progenitor cell-derived Apelin, one of several “growth factor” peptides secreted by many different types of cells, was shown to be directly responsible for blood vessel development.
Researchers also observed that Apelin stimulates and regulated new blood vessel growth. The research team observed the blood vessel development in living zebrafish, which are transparent while young.
According to La Trobe, the discovery is also important research into organ regeneration and tissue engineering, both of which need blood vessels to promote growth and deliver nutrients.
“There’s research that suggests that it can help with cardiac regeneration for example,” Dr Okuda said.
Researchers from the Centenary Institute and the University of Sydney have discovered more about the functionality of a common component in vaccines, offering a potential new pathway for advancing the next generation of vaccines.
According to the Centenary Institute the vaccine adjuvant delta inulin has long been recognised for its ability to boost immune responses against a range of infectious diseases such as COVID-19, influenza, tuberculosis and hepatitis B.
Adjuvants are substances added to vaccines to elicit stronger and longer-lasting immune responses, thereby improving vaccine effectiveness.
Despite its established role in vaccines, the precise mechanisms behind delta inulin’s effectiveness had remained elusive.
Research has now identified a protein known as Dendritic CellSpecific Intercellular Adhesion Molecule-3-Grabbing Non-Integrin (DC-SIGN) as a receptor for delta inulin.
Dr Erica Stewart of the Centenary Institute’s Centre for Infection and Immunity, and the University of Sydney Infectious Diseases Institute said DC-SIGN is a protein found on the surface of certain immune cells called dendritic cells.
“DC-SIGN acts like a lock on cell surfaces and delta inulin functions as the key that fits into this lock, binding them together. This study shows that when we vaccinate with delta inulin, our cells use DCSIGN to detect the vaccine, which then helps activate and boost the body’s immune response.
“With this new insight into delta inulin’s mode of action, researchers can now explore the creation of new vaccines that work handin-hand with delta inulin, offering even greater protection against existing and emerging infectious diseases.
“This breakthrough is like finding a crucial piece of the puzzle that can make our vaccines smarter, leading to better health and safety for people worldwide."


The Australian Government has imposed a targeted financial sanction and travel ban on Russian citizen Dmitry Yuryevich Khoroshev for his leadership role in the LockBit ransomware group.
This is the second use of Australia’s autonomous cyber sanctions framework and part of ongoing coordinated international investigation. Earlier this year sanctions were imposed on Russian cybercriminal Aleksandr Ermakov for his involvement in the breach of the Medibank Private network.
The Australian Government described LockBit as a prolific criminal ransomware group that works to destabilise and disrupt key sectors for financial gain. A joint investigation, Operation Cronos, led to the Australian Signals Directorate, Australian Federal Police and international partners (including the UK and US) identifying Dmitry Yuryevich Khoroshev as part of LockBit’s senior leadership.
Minister for Cyber Security Clare O’Neil said this recent sanction is an important step in breaking the ransomware business model, preventing cybercriminals from profiting from attacks on Australian citizens and businesses.
“The damage done by LockBit in Australia is significant. For too long, criminals like those behind LockBit have hidden in the shadows. Our government is changing that. Hunting down cyber criminals by working with our international partners to hack the hackers and punishing them where we can,” Minister O’Neil said.
LockBit ransomware has been used against Australian, UK and US businesses, comprising 18 percent of reported Australian ransomware incidents in the last financial year, and 119 reported victims in Australia.
This new sanction makes it a criminal offence to provide assets to Dmitry Yuryevich Khoroshev, or to use or deal with his assets.
AFP Cyber Command Acting Assistant Commissioner Chris Goldsmid said the decision to publicly name Khoroshev is supported by the AFP.
“By taking away his anonymity, it has severely undermined Khoroshev’s credibility with cyber criminals and also signals any dealings they have with him could be subject to law enforcement action,’’ Acting Assistant Commissioner Goldsmid said.
“In cooperation with international partners under Operation Cronos, the AFP has used information collected to trace the global LockBit network and build the global case against the ransomware criminal group.”
The investigation into LockBit continues. The Australian Government continues to discourage businesses and individuals from paying ransoms or extortion claims to cyber criminals.
Investigations continue into the cyber incident affecting former national prescription delivery service provider MediSecure, with reports of data leaked online and the announcement that the company has gone into voluntary administration.
Australia’s Cyber Security coordinator Lieutenant General Michelle McGuinness released a statement saying the response to the incident is ongoing, and that data from the breach has been released on the dark web.
“The Australian Government is continuing its response to the cyber incident that has impacted MediSecure,” Ms McGuinnes said.
“We are aware a dataset purporting to be from the MediSecure breach has been advertised for sale on a dark web marketplace, along with a sample of the data.
“Australians should not go looking for this data. Accessing stolen sensitive or personal information on the dark web only feeds the business model of cybercriminals.”
In a statement released on their website, MediSecure said they were working with the Commonwealth Government to notify those individuals impacted.
Since then, the company has gone into voluntary administration, with the media reporting Vaughan Strawbridge and Paul Harlond of FTI Consulting were appointed as the administrators.
It has also been reported in the media that MediSecure asked the Australian Government for financial support in relation to the incident. In response, Medisecure responded to these reports.
“In light of recent media reports, MediSecure wishes to clarify that it sought funding from the Commonwealth Government for the limited and confined purpose of assisting with the costs associated with responding to the incident, and the request was not for funding MediSecure’s operational costs unrelated to the cyberattack. In any event, that request was denied,” a statement from the company read.
An incident update from the Department of Home Affairs said MediSecure was one of two prescription delivery services operating nationally, until late 2023 when the government awarded the tender for this service exclusively to another company.
According to a statement from MediSecure, the company “is not a current participant in Australia’s digital health network. As such, this cyber security incident does not impact the prescribing and dispensing of medication.”
“The cyber security incident relates to data held by MediSecure’s systems up until November 2023. We can confirm the cyber security incident impacts personal information and limited health information relating to prescriptions,” the statement said.
Advice from the Australian Government is that consumers can continue to access medicines safely, and healthcare providers can still prescribe and dispense as usual.
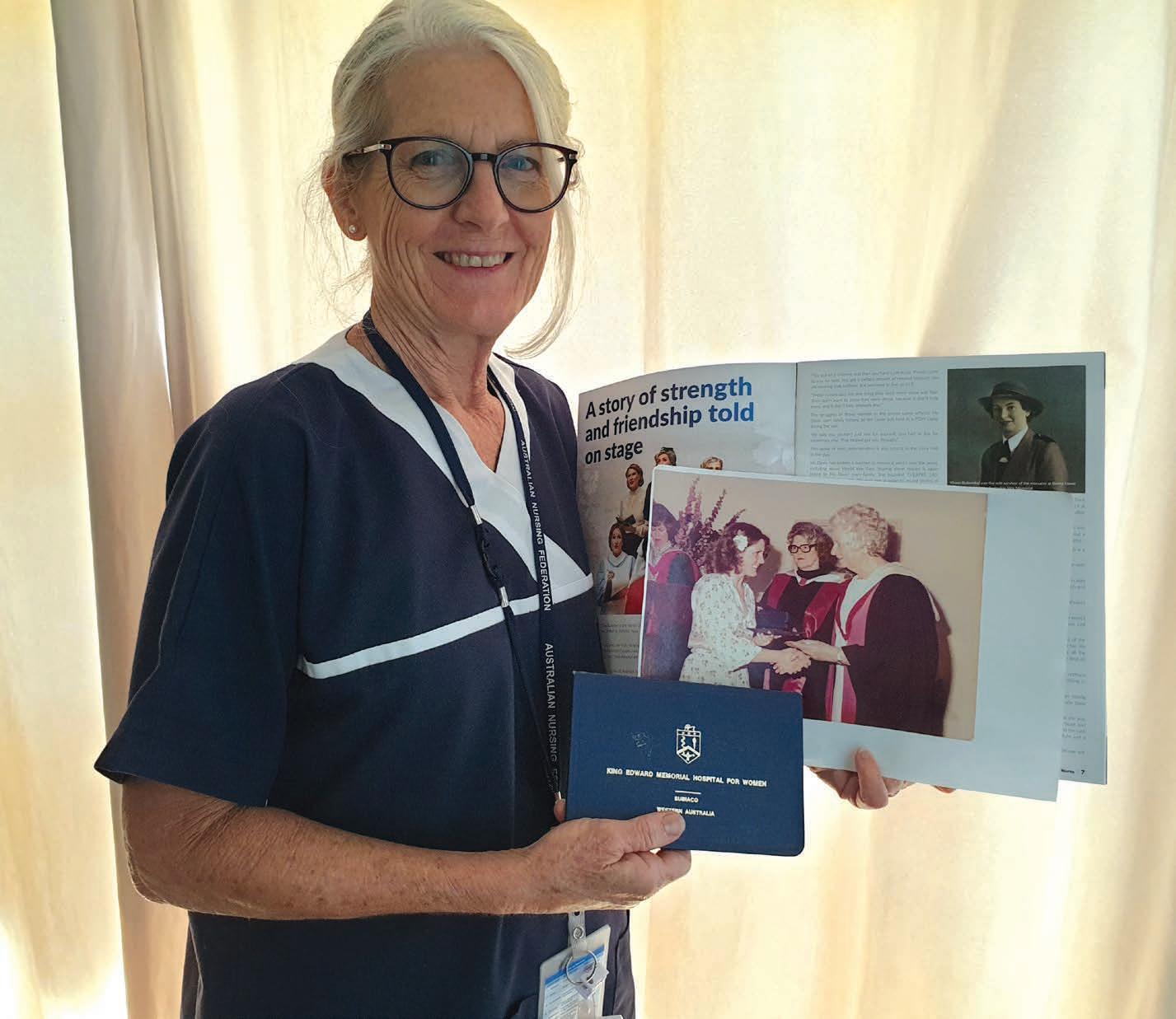
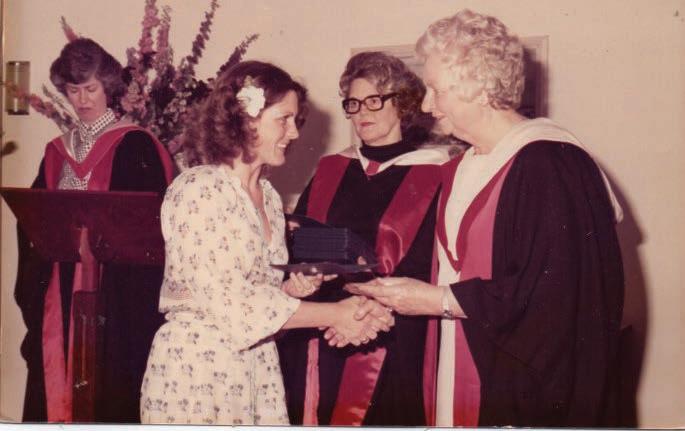
Thanks again to everyone who entered in our previous ANF Photo competition. Congratulations also go to winners Carol and Sue for their great entries. Both entries won double passes to see the stage production of 21 Hearts: Vivian Bullwinkel and the Nurses of the Vyner Brooke, at the Como Theatre.
Sue’s photo was taken at a bear rescue centre in Alaska, on a recent trip to the US.
Carol’s entry included a photo of herself and Vivian Bullwinkel taken back in 1979. Carol had seen an article in a previous edition of the Western Nurse about the upcoming play about Vivian Bullwikel’s life and recalled that she had the honour of meeting her in person and shaking hand while she received her Midwifery Certificate at the King Edward Memorial Hospital graduation ceremony in November of that year.
This is a great piece of West Australian nursing history, and we want to thank Carol for sending a copy to the Western Nurse.
Share your photos of yourself, your family or your team at work with any of our great ANF products and go in the running to win a gift voucher for a two-night getaway at the Rendezvous Hotel Perth Scarborough. The voucher includes two nights
accommodation in a Premier Ocean View Room with a buffet breakfast for two people per day. Runners-up will get a range of great prizes.
A selection of the best photos will feature in the next edition of the Western Nurse.
If you think you have a winning photo you can email your competition entry to us at western.nurse@anfiuwp.org.au
All entries must include your name and your membership number to be in the running.

Read this article and complete the quiz to earn 1 iFolio hour
Read this article and complete the quiz to earn 1 iFolio hour
Syphilis infections have significantly increased in Australia over the past 10 years, with case notifications more than doubling between 2015 and 2022.1
Currently in Western Australia, there is an epidemic of syphilis infections in First Nations communities of regional, remote, and metropolitan areas. Rates remain high in men who have sex with men (MSM). An epidemic of syphilis in heterosexual men and women throughout many parts of Australia is also emerging, particularly in women of reproductive age, increasing the risk of congenital syphilis.1,2
Syphilis is a notifiable infectious disease that, especially if left untreated, can have serious health consequences, including mortality.1,3,4
Syphilis is a multi-system disease caused by the spirochete bacterium, Treponema pallidum (T. pallidum), most commonly transmitted through sexual contact, including oral sex. There are rare occurrences of transmission via contaminated blood (e.g. sharing druginjecting equipment) and from direct contact with open lesions.3
Syphilis infection has several clinical stages. Signs and symptoms vary between individuals, and approximately 50% of infected people are asymptomatic.2-4
Syphilis is infectious in the primary, secondary, and early latent stages. Late latent syphilis and tertiary syphilis are regarded as not transmissible by sexual contact.3,4
Untreated maternal primary or secondary syphilis is also readily passed on to the unborn fetus, while the risk declines progressively for mothers with latent stage disease. Vertical transmission is considered negligible for tertiary syphilis.5
Notably, congenital syphilis is resurging in many developed countries, including

Australia. It can cause miscarriage, prematurity, stillbirth, low birth weight, and perinatal death, as well as foetal brain, nerve, and organ damage resulting in lifelong disability.3,5
Anyone with symptoms consistent with syphilis infection should immediately be tested. Syphilis point-of-care testing (POCT) may be available in some health services.
Physical examination and venous blood testing are required to diagnose a syphilis infection, identify the stage, and determine treatment. A polymerase chain reaction (PCR) swab of any anogenital or oral lesions should be taken.2-4
People with suspected syphilis infection should also be tested for other sexually transmitted infections (STIs) and bloodborne viruses (BBVs) including chlamydia, gonorrhoea, human immunodeficiency virus (HIV), hepatitis B, and hepatitis C (if at risk).2,3
Contacts of known cases of infectious syphilis should be tested and treated empirically on presentation and three months after their most recent sexual contact with the infected person.2
Syphilis screening should be included in all STI and BBV screens, particularly if an asymptomatic person has requested
an STI checkup (possibly indicating highrisk behaviours), and when people are diagnosed with other STIs or HIV.2
All pregnant women should be tested at their first antenatal visit, at 28 weeks, and 36 weeks gestation (or at time of preterm birth). Women living in regions of syphilis outbreaks in First Nations communities (i.e. Kimberley, Pilbara, and Goldfields) should have additional testing at delivery and the six week postnatal check.2
Men who have sex with other men (MSM) should be tested at least annually, but up to four times per year according to assessed levels of high-risk behaviour.2
Syphilis testing for returned overseas travellers from countries with a high syphilis prevalence (e.g. South-East Asia, Africa, New Zealand), should be based on patient request, or according to assessed levels of high-risk behaviour.2
High-risk populations who should be tested six monthly:2
• Sexually active First Nations people ˂ 40 years or of any age who have changed sexual partners in the previous 12 months
• People using methamphetamine and/ or inject drugs
• People experiencing homelessness
• Opportunistic testing 6 monthly should be offered to people from a culturally or linguistically diverse background as this group is also at high risk. 2
Penicillin is the drug of choice to treat syphilis unless a person has a true penicillin allergy.2,3
If a person has clinical signs or symptoms and/or positive laboratory evidence of primary, secondary, or early latent syphilis without neurosyphilis, treatment is a single stat dose of intramuscular benzathine penicillin 2.4 million units (1.8g) at presentation. This is also the recommended treatment for contacts of a person with infectious syphilis.2,3
Syphilis stage Incubation period from exposure
Primary syphilis
The 2.4 million units (1.8g) dosage is provided in two pre-filled syringes, each containing 1.2 million units (900mg) of benzathine penicillin, administered as 2 injections (one into each buttock).3
Late latent syphilis is treated with intramuscular benzathine penicillin 2.4 million units once weekly for three doses. If the second or third dose is delayed by more than three days, it is recommended to restart the three week course.2,3
Tertiary syphilis treatment depends on specialist advice.2,3
Potential signs and symptoms
9-90 days Single or multiple indurated, painless ulcers (chancre) of 1 - 2 cm diameter in genital or extragenital body region, e.g. mouth (See Illustration 1)
Chancres may become painful, erythematous (reddened), swollen, and weep, or purulent due to secondary infection, e.g. bacterial, or another manifestation of primary syphilis –syphilitic balanitis of Follmann
Localised lymphadenopathy (swollen lymph nodes)
Secondary syphilis
30-150 days
Latent syphilis
Tertiary syphilis (rare)
5-35 years
Signs and symptoms may come and go over about 12 months, including:
Skin rash – commonly maculopapular (small raised red bumps) or a scaly, dried psoriatic type, typically bilaterally symmetrical and non-itchy, of palms and soles
Wart-like lesions in genital and groin areas (condylomata lata)
Ulcers of the mouth, nasal cavity, or vulva
Systemic symptoms including:
• Low-grade fever
• Malaise
• Headache
• Muscle aches and pains
• Lymphadenopathy
Cranial nerve palsies (e.g. acute deafness, retinitis, uveitis) and development of other neurosyphilis symptoms
Patchy scalp and eyebrow hair loss
T. pallidum detected and classified by serology testing, but without signs or symptoms
Latent syphilis is divided into:
• Early latent = < 24 months from primary infection
• Late latent = > 24 months from primary infection
Symptoms may vary or can be absent. Progression occurs in up to one third of untreated people (usually 5-20 years after the initial infection), involving the:
• Cardiovascular system (e.g. aortic incompetence, aneurysm)
• Neurological system (e.g. dementia, personality change, multifocal neurological disorders)
• Bones
• Eyes (e.g. pupillary abnormalities, retinal disease, uveitis)
• Ears (e.g. nerve deafness)
Development of gummata (granulomatous lesions)
Asymptomatic neurosyphilis may occur within the 5 years after primary infection
People receiving treatment must have venous blood taken the day they begin treatment to provide a baseline rapid plasma reagin (RPR) level to monitor response to treatment.2,3 As reinfection can occur, contact tracing and treatment of sexual partners is paramount.
Repeat syphilis serology should be taken at three and six month intervals following treatment, or more frequently if the person is at high reinfection risk. If the RPR level has not reduced by 4-fold after six months of treatment, serology must be repeated after 12 months of treatment, when the need for re-treatment and lumbar puncture will be assessed.2,3

1. Australian Government, Department of Health and Aged Care [Internet]. National response to syphilis. 2024 [cited 2024 April 24]. Available from: https://www.health.gov.au/our-work/ national-response-to-syphilis#:~:text=Contact,Syphilis%20in%20Australia,women%20of%20 reproductive%20age
2. Government of Western Australia, Department of Health [Internet]. Quick guide for testing and treatment of syphilis infection in WA. 2023 [cited 2024 April 24]. Available from: https:// www.health.wa.gov.au/~/media/Files/Corporate/ Reports-and-publications/Silverbook/QuickGuide-for-Syphilis.pdf
3. Government of Western Australia, Department of Health [Internet]. Silver book: Syphilis; Date unknown [cited 2024 April 24]. Available from: https://www.health.wa.gov.au/Silver-book/ Notifiable-infections/Syphilis
4. The Australasian Society for HIV, Viral Hepatitis and Sexual Health Medicine (ASHM) [Internet]. Syphilis: Outbreak Training Website. The Clinical Stages of Syphilis. Date unknown [cited 2024 April 24]. Available from: https:// syphilisoutbreaktraining.com.au/clinical-stages/
5. MacKenzie H, McEvoy SP, Ford TJ. Managing risk for congenital syphilis. Emerg Infect Dis [Internet]. 2023; 29(10):2093-2101. doi: 10.3201/ eid2910.230432

1 Situated away from the centre of the body (6)
5 Posterior position of the lower leg (4)
9
Sixth note of a major scale (3)
10 Ovestin ---, hormone replacement therapy (5)
11 Armpit, or the corresponding part in a bird or other animal (6)
13 Arm or leg, eg (4)
15 Fleshy filament at the mouth of some fish, or a sharp arrow part (4)
16 Brief episodes of intense anxiety, causing the physical sensation of fear (5,7)
20 Part of the body on both sides of the spine between the lowest ribs and the hip bones (4)
22 Approached (6)
24 Nickname for a lion (5)
25 Substance such as iron, copper or zinc, small amounts of which can be found in the body (5)
27 Ancient Greek philosopher who is regarded as the godfather of evidence-based medicine (9)
28 Wall painting (5)
30 Medical substances used to treat the sick (5)
31 Breathing disorder (6)
33 What the otic organs allow us to do (4)
35 Pain or discomfort in the stomach associated with difficulty in breaking down food (11)
39 Small metal device that is inserted into an aneurysm to stop blood flowing (4)
41 --- Harlow, actress of yesteryear (4)
42 Body organ, or delicious nut (6)
45 Shinbone (5)
46 --- Lennox, singer with the Eurythmics (5)
47 Large room or area of a hospital (4)
48 Small indentation in the flesh, also known as a gelasin (6) DOWN
1 Molecule that carries genetic information (1,1,1)
2 --- Lanka, island country (3)
3 Tibetan bovine (3)
4 Thorax region (5)
5 Predictable periods of significant stress in an otherwise well-fed and healthy baby (5)
6 --- off, use delaying or distracting tactics (3)
7 Fijian capital city (4)
8 Groups of pus-filled bumps forming a connected area of infection under the skin (10)
12 Image of a bone (1-4)
14 Considered (5)
15 Bodily swelling (5)
17 Relating to sexual intercourse (6)
18 Lymph nodes in the back of the mouth and top of the throat (7)
19 Norwegian pop band from the 1980s (3)
21 Number of chambers of the heart (4)
23 Remove a tooth or contaminated body part (7)
24 Type of white blood cell in the immune system of most vertebrates (10)
25 Informal word for a medical practitioner or student (6)
26 Firm, tight (4)
29 Birth month of Samuel Hahnemann, the German physician who is bet known for creating the system of homeopathy (5)
31 Confuse, befuddle (5)
32 Garden tool (3)
34 Hole in the skin through which sweat can flow (4)
36 An organ, such as testis or ovary, that produces gametes (5)
37 Backbone (5)
38 Tattooed (5)
40 Intercontinental ballistic missile (1,1,1,1)
41 Either of the pair of bones that form the framework of the mouth (3)
43 Quick sleep (3)
44 --- haw, cowboy’s triumphant call (3)

Tuesday, July 30 6pm


Office + Zoom Thursday, August 1 12pm
Tuesday, August 6 6pm
Thursday, August 8 12pm
Tuesday, August 13 6pm
Thursday, August 15 12pm
Tuesday, August 20 6pm
Office + Zoom
Office + Zoom
ANF Office + Zoom
Court ANF Office + Zoom
Court
Office + Zoom
Office + Zoom Thursday, August 22 12pm
Tuesday, August 27 6pm
Office + Zoom
issues
Office + Zoom Thursday, August 29 12pm
Tuesday, September 3 6pm
Thursday, September 5 12pm
The ANF offers informative talks on topics relevant to contemporary nursing and midwifery, all for free.
Places are available on a range of topics:
Coroners Court: Learn more about coroners' investigations including discussions on the role of the coroner, the inquest process, evidence gathering, being a witness, making statements and other legal considerations surrounding coroners' reports.
Documentation: A handy refresher on the importance of proper documentation, best practices for record-keeping, legal requirements for documentation and how to maintain accurate and comprehensive records.
Social Media: Take part in discussions around potential legal issues that can arise from its use including privacy concerns, defamation, intellectual property infringement, professional boundaries and ethical considerations when using all types of online media platforms.
workplace issues ANF Office + Zoom
Compensation ANF Office + Zoom
Compensation ANF Office + Zoom
Discrimination: This talk covers the legal framework surrounding discrimination, including laws, regulations and case precedents, with reference to the various forms of discrimination, such as gender, race, age, or disability and provide guidance on how to prevent and address such issues in professional settings.
Defamation: Defamation involves making false statements that harm someone's reputation. We explain the elements of a defamation claim, how to minimize the risk of defamation in the context of the workplace, defences against defamation and the potential consequences of defamatory statements on your registration and your wallet.
Workers Compensation: This session covers the essentials that all members must know about the Workers Compensation process and how to make it work for you rather than your employer if you are injured at work.
Resolve workplace issues: This important information is useful for all members, and it covers the process of resolving issues at your workplace.