Summer 2022



The
EDITION 37 NO. 4 | SUMMER 2022 ISSN 1031 6965 The Official Journal of THE AUSTRALIAN NATURAL THERAPISTS ASSOCIATION WWW.ANTA.COM.AU
Natural Therapist




MediMag Sleep A combination of magnesium, glycine, zizyphus and lemon balm, traditionally used in Western herbal medicine to: Induce sleep Relieve sleeplessness Support healthy sleeping patterns Reduce disturbed and restless sleep Customer Care or Clinical Support: 1300 654 336 Email: enquiries@integria.com Product Orders: www.myintegria.com mediherb.com.au
Acetaminophen Rhuleave-K™

We know that during pain flare ups, you want to be able to offer your patients a natural solution, that is time efficient. Inflagesic™ uses SPEEDTECH™ technology, provides meaningful pain relief, and is comparable to paracetamol as fast-acting and efficient, with the average onset being 1 hour (Figure 1).
Subjective Pain Severity
Curcumin 133 mg Boswellia serrata, dry gum oleoresin extract 50 mg From dry gum oleoresin (BosPure® Boswellia) (Rhuleave-K™) 500 mg
How to Prescribe (Adults): For relief of acute musculoskeletal pain Take 2 capsules To relieve inflammation Take 2 capsules, 3 times daily (up to 6 capsules per day).
Figure 1: Pain Reduction from Baseline with Rhuleave-K™ was Comparable to Acetaminophen (Paracetamol) (P<0.001).1 For relief of acute musculoskeletal pain Take 2 capsules To relieve inflammation Take 2 capsules, 3 times daily (up to 6 capsules per day).
Clinically Trialled Ingredients
Acute Flare-Ups
New Inflagesic™
Your
Rhuleave-K™ and SPEEDTECH™ are trademarks of Arjuna Natural LLC. Always read the label. Follow the directions for use. If symptoms persist, consult your healthcare professional. Open an account today and receive 10% off your first order!* To open an account, call Customer Service on 1800 777 648 or scan here: *Offer valid for new Metagenics account holders and for one use only.
SPEEDTECHTM Technology for Increased Absorbability Average Onset of 1-Hour
The Plant Derived Analgesic for
Patients
Each Capsule Contains: metagenics.com.au metagenicsinstitute.com.au
OPEN AN ACCOUNT SCAN HERE TO LEARN MORE ABOUT INFLAGESIC TM MET740708/22 HIGH QUALITY, PRACTITIONER ONLY
The San Jiao
Grace Hermocilla, ANTA Student Member, explores The San Jiao and how it has been a controversial topic in Chinese Medicine for centuries. This article explores the Upper, Middle and Lower Burners.
Lynn McCardle, ANTA Student Member, compares the literature on Omega-3 fatty acids and if it is effective in reducing vasomotor symptoms.
Research Assignment: Exploring Four Health Issues and How the Role of Massage Can Help
Lynalee Strickland, ANTA Member, writes a comprehensive article on four health issues - Depression and Anxiety, Attention Deficit Hyperactivity Disorder, Rheumatoid Arthritis and Fibromyalgia. The article explores the definition, the causes and predisposing factors, and the role of massage in helping treat these health issues.
The Natural Therapist
The Natural Therapist is published by the Australian Natural Therapists Association (ANTA) for natural therapy practitioners. The opinions and views expressed by the contributors and advertisers are not necessarily the opinions and views of ANTA. Every effort is taken to ensure accuracy and ANTA accepts no responsibility for omissions, errors or inaccuracies. ANTA relies on contributors and advertisers to make sure material provided for The Natural Therapist complies with the Australian Consumer Law under the Competition and Consumer Act 2010. ANTA accepts no responsibility for breaches of the Australian Consumer Law by contributors or advertisers. Material in The Natural Therapist is subject to copyright and may not be reproduced in any form without the permission of ANTA and its contributors.
Shaun Brewster
• National Myotherapy Branch Chair
• ANTAB Chair
• ANRANT Committee Member
• Health Fund Chair
Warren Maginn
• National Vice-President
• Director of ANTA
• National Nutrition Branch Chair
• TGA Chair
• Ethics Panel Chair
• ANTAB Committee Member
• ANRANT Committee Member
Ananda Mahony
• National Treasurer
• Director of ANTA
• National Naturopathy Branch Chair Kaitlin Edin

• Director of ANTA
• National Acupuncture Branch Chair
• ANTAB Committee Member
• ANRANT Committee Member
• Director of ANTA
• National Remedial Therapy Branch Chair
• ANTAB Committee Member
• ANRANT Committee Member
Mark Shoring
• Director of ANTA
• National Multi-Modality Branch Chair
• ANTAB Committee Member
• ANRANT Committee Member
Tino D’Angelo
• Director of ANTA
• National Chinese Herbal Medicine Branch Chair
Neerja Ahuja
• Director of ANTA
• National Ayurveda Branch Chair
Jim Olds
• Executive Officer
• Company Secretary
• Business Plan Chair
• ANRANT Chair
Contents From the Chair 5 Executive Officer Report 6 ANTA News 8 ANTA CPE Guidelines 9 ANTA Virtual Consultation Guidelines 10 2022 Branch Chair Updates 14 Herbal Monograph: Passiflora incarnata and Glycyrrhiza glabra
explores two herbal monographs, Passiflora
and Glycyrrhiza glabra
Briony Green, ANTA Student Member,
incarnata
29
34
Among Menopausal Women, are Omega-3 Fatty Acids Effective in Reducing Vasomotor Symptoms, Compared to Placebo: A Literature Review
Marketing & Production Tasha Kemsley Circulation Enquiries 1800 817 577 Editorial & Advertising Enquiries thenaturaltherapist@anta.com.au Membership Enquiries info@anta.com.au ANTA NATIONAL ADMINISTRATION OFFICE T: 1800 817 577 | F: (07) 5409 8200 E: info@anta.com.au P: PO BOX 657 MAROOCHYDORE QLD 4558 W: www.anta.com.au
Natural
Edition 37 No. 4 | Summer 2022 19 23 Lessons from 23 Years Shaun Brewster, ANTA National President and ANTA Myotherapy Branch Chair, gives a quick recount of 23 lessons he has learnt over the 23 years he has been in business. 23 Clinical Trial Update: Effects of Fish Oil Omega-3’s
Brain Activity
Children George Thouas, Head of Research and Innovation at Max BioCare, gives a clinical trial update on Fish Oil Omega-3 and brain activity in children. EDITION 37 NUMBER 4 – SUMMER 2022 ISSN 1031 6965
The
Therapist
on
in
• National President • Director of ANTA
Isaac Enbom
ANTA BRANCH CHAIRPERSONS
42
From the Chair
A major part of ANTA’s role is greater than its regulatory function, governance and operations often work together to address Member’s needs in a material way. For example, we commonly receive requests for resources that elucidate assessment and management approaches related to lesser-known conditions that occur rarely, at times the result of iatrogenic origins that have puzzling presentations, signs and symptoms.
ANTA is well-known to its Members for providing state of the art approaches to many differing disorders and imbalances across the spectrum of modalities and treatment protocols that may assist in chasing down an effective result. Our colleagues who participate in the ANTA Governance role are serious practitioners, well trained in multiple modalities who have contributed to the rich and informative knowledgebase, they have made available to our Members to assist them in their clinical work including client management.
Many ANTA Directors have extensive backgrounds in education where they have educated and trained many therapists who have developed thriving businesses practising their chosen craft in the fields of their choice. These Directors have also contributed to the growing library of online resources that is available to all Members free of charge, to use when needed. All Directors also stand ready to assist you with guidance over a quick call if you cannot find the solution you are looking for in the resources available to you.
Whenever you may be faced with a situation you don’t understand, simply because you are not supposed to, doesn’t mean you have failed. This is an opportunity to learn something you did not need to know more about until now. During your clinical journey, you will be faced with conditions and treatment protocols, we
Summer 2022
quite often rarely needed until this moment. This opportunity to learn more and develop extra skills for your armamentarium is a valuable opportunity to be more effective than you were prior to this moment.
ANTA’s diverse and comprehensive range of Continuing Professional Education resources are a treasure of unknown value until the pearl you are searching for is revealed! Our elite practitioners have made these pearls available to all members over many years. At this time, our Branch Chairs/ Directors are all extensively trained, wellpractised therapists, most with educational and training backgrounds who understand your need, just as they once did.

The ANTA National Council is a group of serious practitioners, formed to assist and support the serious practitioners ANTA gains its strength from. These resources are the most valuable due to their further studies, research and applications in practice. The research and development in “Pain Medicine” have advanced many of our skills and knowledge across Naturopathic Medicine, Clinical Nutrition, Ayurveda, Traditional Chinese Medicine, both Herbal and Acupuncture, plus Manual Medicine modalities places us in a stronger position to assist the health and wellness of our clients as never before.
The leaders in Natural and Traditional Medicine at ANTA stand ready to support you in your clinical practice and with the development of your advanced abilities to reduce pain and enhance the health of your clients.
THE NATURAL THERAPIST VOL 37 NO. 4 | SUMMER 2022 | PAGE 5 ANTA Executive Welcome Summer 2022
Regards Jim Olds
ANTA Fellow ANTA Executive Officer & Company Secretary BHSc MST, BHSc Comp Med, GC Higher Ed, MSC, Dip Nut, Dip RM, Dip TCMRM
ANTA News
Summer 2022
2023 ANTA Membership Renewal Notices Issued
ANTA have issued renewal notices for majority of ANTA Members. Those Members who are not registered with AHPRA, need to ensure that they pay their 2023 ANTA Membership fees before the 31st December 2022.
ANTA issued renewal notices in early November via email. Please check your junk/spam folders. If you cannot find your invoice, you will be able to view a copy in your ANTA Member Centre, under ‘Email Logs’, or you can contact ANTA on 1800 817 577 or admin@anta.com.au.
Continuing Professional Education Points Due Soon!

Continuing Professional Education (CPE) is the upgrading or acquisition of knowledge and skills in the accredited modalities that will aid the practitioner in providing the patient with a high standard of health care. CPE is an important part of providing professional health care services to patients and ensures practitioners regularly update their clinical skills and professional knowledge.
ANTA requires Members to complete 20 CPE hours annually (January to December). CPE hours need to be lodged within the ANTA Member Centre before the 31st December 2022. Please see the instructions below to help update your CPE points.
1. Once you have logged in, hover over the word Member Centre (below our logo) and click on My Member Management System.
2. Then click on CPE Activity.
3. Then click on the ‘Add a new CPE Activity’ button.
4. You can now record your CPE activity, ensuring that you complete all fields correctly. Enter the actual date you completed the activity; enter the year you completed the activity; enter the mode you completed the activity (e.g. book, webinar, seminar etc); enter a full description of the activity that includes the name of the book, webinar, etc. including the name of the author or institution (if relevant); enter the number of hours you took to undertake the activity which will be your points, i.e. 1 hour of activity = 1 point.
5. Click ‘Save & Close’ then proceed to Step 3 to enter the next activity.
ANTA Christmas Closure
The ANTA Administration Office will be closed from Thursday 22 December 2022 until Monday 9 January 2023. During this time, no emails or calls will be answered. If you need assistance, please send an email to admin@anta.com.au and a response will be provided when the office reopens.
All ANTA Board of Directors and staff would like to wish all Members and their families a happy and safe Christmas.


PAGE 6 | SUMMER 2022 | THE NATURAL THERAPIST VOL 37 NO. 4 ANTA News Summer 2022

Practitioner Dispensing Only Always read the label Non Synthetic Coating Synergistic Formula EvidenceBased Minimal Excipients GLUCO CHROME Exciting new formula! Premium blend of Bitter Melon, Cinamon, CoQ10, Alpha lipoic acid, Amino acids, Vitamin B3 & Chromium Supports glucose metabolism & healthy blood sugar in healthy individuals (chromium). NUTRITIONAL THERAPY 3 BIOACTIVE 3 BIOAVAILABLE 3 QUALITY INGREDIENTS Call 02 9693 2888 Email info@interclinical.com.au Visit www.interclinical.com.au
ANTA CPE Guidelines
What is CPE:
Continuing Professional Education (CPE) is the upgrading or acquisition of knowledge and skills in the accredited modalities that will aid the practitioner in providing the patient with a high standard of health care.
Why is CPE Necessary:
CPE is an important part of providing professional healthcare services to patients and ensures practitioners regularly update their clinical skills and professional knowledge.
ANTA requires members to complete 20 CPE hours annually (January to December). Completion of 20 CPE hours annually is a requirement for your ongoing ANTA membership. It is also a requirement for provider recognition with all health funds and WorkCover authorities (if applicable). Note: If you do not complete 20 hours of CPE annually, your ANTA membership will be suspended until you have completed the 20 hours required. If you are registered with health funds and WorkCover authorities they will terminate your provider recognition.
Please note that 1 hour of CPE activity = 1 CPE point.
For members registered with health funds, please note that they carry out audits of your records each year to ensure 20 hours of CPE have been completed.
By the end of each calendar year ensure that you lodge details of 20 hours of CPE on your personal profile within the ANTA Member Centre. We recommend that you also keep a copy of your CPE records (e.g. attendance certificates) in the event of an audit by a health fund (if applicable).
Other Benefits of CPE:
• Members are kept informed and up-to-date with the latest developments
• Facilitates communication and networking
• Encourages further study
• Enhances professional standing within the community
Required CPE Hours:
ANTA members must accumulate a minimum of 20
CPE hours per annum (January to December). At least 50% of CPE hours undertaken must be related to the modalities you are accredited in by ANTA. Note: Hours in excess of 20 completed in the current year are not permitted to be carried over to subsequent years.
Members registered with CMBA/AHPRA must abide by the CMBA/AHPRA CPD/CPE Guidelines for the modalities of Acupuncture and Chinese Herbal Medicine and must also submit their CPE to ANTA (http://www.ahpra.gov.au/chinese-medicine.aspx).
CPE Activities:
Members can undertake CPE hours in many ways including the following:
• Attend ANTA free seminars
• Research scientific information within the ANTA Member Centre on:
* IMGateway
* eMIMS Cloud
• Participate in research projects involving, or related to, natural therapies
• View seminar recordings and seminar presentations
• Complete courses on ANTA eLearning Centre
• Give lectures/tutorials
• Give CPE seminar presentations
• Undertake further study
• Complete short courses
• Contribute an article to the ANTA journal “The Natural Therapist” and ANTA website
• Contribute an article to other relevant journals, magazines and publications
• Read articles in the quarterly ANTA journal “The Natural Therapist”
• Subscribe to and read other professional publications and journals
• View webinars
• View online DVDs or recordings on relevant topics
• Listen to recordings on relevant topics
• Radio/TV broadcast on relevant topics
• Read and research information on topics relevant to your practice
• Attend local practitioner groups/workshops
• Conduct volunteer work with community groups involving natural therapies
For further information or assistance contact ANTA at admin@anta.com.au or 1800 817 577.
PAGE 8 | SUMMER 2022 | THE NATURAL THERAPIST VOL 37 NO. 4
ANTA News Summer 2022
Virtual Consultation Guidelines
ANTA acknowledges the need for increasing patient access to their preferred health support services via online and technology-based systems (also known as ‘Telehealth’). It is important, however, that practitioners are fully aware of the necessary considerations associated with conducting such services before doing so, and how to remain compliant with all appropriate guidelines whenever implementing them in practice.
Located in the ANTA Member Centre, ANTA’s National Council and Branch Chairs have created guidelines for virtual consultations for Nutrition & Ingestive Modalities, Manual Therapies and Traditional Chinese Medicine.
In addition to the official guideline documents, practitioners should familiarise themselves with some of the further principles outlined, to ensure their utmost understanding and compliance.
Basic Principles: Privacy and Security:
One of the most important considerations within any method of practice, but in particular modern technology-based practice, is the need to maintain appropriate patient privacy and data security.
Therefore, all health practitioners must remain mindful to select and utilise technology that provides sufficient safeguards to cyber-security to ensure patient and practitioner privacy is maintained at all stages of care.
Exercising Judgement:
The key principles that underpin these guidelines respect the health practitioner’s ability to use appropriate judgement (around how and when to use technology-based practice techniques).
In particular knowing when not to proceed with a consultation or therapeutic intervention, if the virtual setting is not conductive to safe or effective care (i.e. if it does not provide sufficient information or access to proceed confidently), is an important principle to uphold.
Professional Insurer Policies on Virtual Consultations:
All Members should contact their insurance provider
to ensure they are covered for virtual consultations under their current policy.
Additional Considerations for Manual Therapies:
Considering that Manual Therapies may constitute particularly physical and tactile investigative and therapeutic techniques, the inherent limitations of any virtual medium should be acknowledged when considering the scope of feasible care.
However, examples of various manual therapy services that may be delivered in a virtual capacity may include but not limited to:
• Advice on home-based pain management strategies
• Directions regarding ergonomics to reduce load/ stress on specific tissues.
• Guidance on self-treatment technqiues (e.g. such as foam rolling, massage tools, hot/cold therapies, etc.)
Additional Considerations for Chinese Medicine:
Considering Chinese Medicine includes both ingestive and manual therapy components, means that particularly focussed judgement may be needed to account for all factors that may apply to a proposed virtual consultation.
However, examples of various Chinese Medicine services that may be delivered in a virtual capacity may include but not limited to:
• Guidance on self-treatement technqiues (e.g. such as foam rolling, massage tools, hot/cold therapies, etc.)
• Facilitating behaviour modification to avoid symptom irritation

• Guidance on stretching or strengthening exercises (such as Dotai, Qigong, Tai Chi)
Whilst ANTA’s guidelines have been modelled in harmony with AHPRA’s guidelines, Chinese Medicine practitioners should remain aware of their obligations under AHPRA.
For further information contact ANTA at admin@anta.com.au or 1800 817 577.
THE NATURAL THERAPIST VOL 37 NO. 4 | SUMMER 2022 | PAGE 9
ANTA News Summer 2022
Branch Chair Updates
Summer 2022
Myotherapy and Remedial Therapy Branch Chair
As Branch Chair for Myotherapy, it has been my pleasure to represent our Myotherapy members in a range of activities that have helped to push the modality forward in 2022.
Most prominently has been our involvement in the Steering Committee for the Advanced Diploma of Myotherapy reaccreditation.
Approximately every five years, Vocational Education and Training (VET) courses are taken through a process of reaccreditation where the training package is reviewed, and improvements applied to ensure it is current and applicable to today’s healthcare landscape. This year Shaun has been fortunate to be a part of this steering committee, and also functioned as the Chair of the committee. A lot of great work has been done to improve the Advanced Diploma so that graduates have an even higher level of skills and knowledge. We look forward to the new program rolling out in 2023.
Shaun was a part of the Technical Advisory Committee (TAC) for the Bachelor Degree in Clinical Myotherapy for Torrens University / Southern School of Natural Therapies. The TAC functions as an industry advisory group to help make sure the program meets professional standards and industry needs.
Outside of curriculum advisory roles, Shaun and Isaac have also been privileged to work closely with several other associations with a common goal to raise the standard of education delivery Australia wide. We have implemented a program that will see a unified approach to the endorsement of training organisations and the recognition of quality education delivery.
The future is bright for Myotherapists in Australia, and I look forward to continuing advocacy for the profession going forward.
PAGE 10 | SUMMER 2022 | THE NATURAL THERAPIST VOL 37 NO. 4 ANTA News Summer 2022
Regards
Shaun Brewster
ANTA Myotherapy Branch Chair
Regards Isaac Enbom
ANTA Remedial Therapy Branch Chair
Acupuncutre, Chinese Herbal Medicine and Multi-Modality Branch Chair
Have you noticed how when there is constant and intense change, time has the characteristic of being like an accordion? It stretches in a way that makes a day feel like a year and then squeezes back to make a month feel like an hour. It makes it so very hard to keep track of the things we have achieved.
It seems like the number of ‘black swan’ events over the past several years; COVID (it’s lockdowns and curtailing of freedoms), extreme weather events and the ongoing impact of La Niña have left most of us with little in our emotional or financial pockets. I have to remind myself that it has only been within the past six months, that certain state borders have been relaxed.
With war in Europe, and the economic shocks of interest rate, rent and price rises, our ‘capacity’ pockets are less empty than completely stripped!
Still, we have lived through turbulent times before and the best way to weather times like these is to stick together, by turning to those things and people that know and support us, both in our personal lives and our professional endeavours. Directors Mark Shoring (Multi-Modality), Tino D’Angelo (Chinese Herbal Medicine) and I (Acupuncture) have been representing Chinese Medicine members across the year at all levels of stakeholder engagement.
Some of you will have engaged with us already, as part of the new Q&A segment on event days.
Directors will be giving an in-person and attentive ear to members questions, ideas and concerns on each of the ANTA event days from now on. By having a direct forum for the engagement of the Board and members we believe it is a good way to further and deepen communication with each other.
The CPE offerings for Chinese Medicine members have been both at the event days and online, with Mark
Shoring’s very interesting and well attended online seminar on Post Viral Syndrome, and Tino D’Angelo’s seminar on the Five Emotions.
In July, Mark and I attended a fruitful and positive meeting with Dr Danforn Lim, the Chair of the Chinese Medicine Board of Australia (CMBA). We found that the style of the new Chair was relaxed and open; and this allowed some frank discussion on the issues that are of interest and concern to ANTA Members and the industry more broadly. After 10 years of AHPRA regulation, and a change in leadership at the CMBA, there was a strong sense of working in alignment with this regulatory partner which gave us a sense of optimism.
In early October, Torrens University had an industry day for their students. ANTA representatives attended these events in Sydney, Melbourne and Brisbane. It was a happy and useful way of getting the plethora of member services known to students and the broader public. If you are a social media person then I trust you have seen the photos in your feeds!
There have been meetings with other industry stakeholders, such as the TGA and The Chinese Medicine Council of NSW. At each of these meetings, ANTA has represented for Members on the range of issues canvased. As always, the best outcomes are sought for Members of ANTA and the Chinese Medicine profession as a whole.
We look forward to further engagement with Members across the range of platforms available, in the year ahead. As we navigate the stresses of Christmas, the new year and another wet summer, let us hope that the Yin Water Rabbit of 2023 proves to be a little less turbulent for us all.
And no matter the many distances between us, may the space between us be blessed.
Tino D'Angelo
Regards Mark Shoring
THE NATURAL THERAPIST VOL 37 NO. 4 | SUMMER 2022 | PAGE 11 ANTA News Summer 2022
Regards Kaitlin Edin
ANTA Acupuncture Branch Chair
Regards
ANTA Chinese Herbal Medicine Branch Chair
ANTA Multi-Modality Branch Chair
Naturopathy Branch Chair
In the last naturopathic chair update, I mentioned that one of the key reasons I joined the ANTA National Council was to advance interprofessional communication between naturopaths and other health care professionals. The link between health care professional miscommunication and poor patient outcomes has been well documented, however research suggests that training and the use of standardised tools is effective in improving interprofessional communication skills (Foronda, C., MacWilliams, B., & McArthur, E., 2016).
While considering the best way to make the information and skills available to practitioners, I am pleased to say that Australasian Integrative Medicine Association (AIMA) released a course addressing this very topic. The overarching aim of this online training in interprofessional communication is to equip naturopaths and other healthcare professionals with the background knowledge, framework, and skills for writing formal letters to medical doctors, thus providing a sound basis for both improved interprofessional communication, and better patient outcomes. ANTA members can access the course for the discounted price of $180 plus GST. Access AIMAs Interprofessional Communication Course here: https://www. australiannaturaltherapistsassociation.com.au/ events/aima-interprofessional-communicationscourse/
Building on this topic, Elysia Humphries, a naturopath who works closely with fertility and women’s health specialists will present at one of our free CPE days next year, discussing how good interprofessional communication skills have not only benefited her patient outcomes, but also helped build her practice with referrals from numerous specialists. Keep an eye out for more details.
The 7th International Congress on Naturopathic Medicine (ICNM) will be delivering an educational program presented by more than 30 renowned speakers, experts, and researchers in Paris 7-9th of July 2023. The theme for 2023 is ‘Restoring Health Naturally – Focus on Anti-aging’. ANTA is a key sponsor of ICNM and as such it would be great to see some of our Australian naturopaths attend the conference. I will be travelling to Paris for the conference and hopefully to present (fingers crossed!). I hope to see you there.
Unfortunately, there has been no meetings of The Natural Therapies Review Expert Advisory Panel (NTREAP) since February 2022 so at this stage I have nothing further to share but will keep reporting on this topic.
As an association, ANTA is pro-statutory registration for naturopaths. In a recent survey out to all Members, we asked a question about statutory registration to ensure we were reflecting your views. Specifically, the survey question asked, ‘As a naturopath, nutritionist or herbal medicine practitioner are you in favour of statutory registration for practicing in Australia?’ Yes or No. I am pleased to report that an overwhelming majority responded in the positive and as such ANTA will continue to lobby government with the aim for statutory registration become a reality.
Reference: Foronda, C., MacWilliams, B., & McArthur, E. (2016). Interprofessional communication in healthcare: An integrative review. Nurse education in practice, 19, 36-40.
Regards
Ananda Mahony
ANTA Naturopathy Branch Chair
PAGE 12 | SUMMER 2022 | THE NATURAL THERAPIST VOL 37 NO. 4
ANTA News Summer 2022
Ayurveda Branch Chair
Recently, we have connected with ANTA members regarding celebrating Ayurveda Day.
This is celebrated on Dhanawantari Jayanti, based on lunar calendar, this year it falls on 23 October 2022.
As part of work on promoting Ayurveda and bring attention to strengths of Ayurveda, we are celebrating Ayurveda Day here with ANTA as well. I have interviewed a few practitioners who had responded and come forward for being part of the celebration. All ANTA Members would have received an email to celebrate. Otherwise, you can view the information on our blog - https://news. australiannaturaltherapistsassociation.com.au/ ayurveda-day-2022
In Perth, where I work from, Indian Consulate has been very supportive in promoting Ayurveda and Yoga. The Consulate General of India (CGI Perth) has worked with us in organising an event to celebrate Ayurveda Day and I will report about it after the event.
We know, from the last few decades, there is a global concern on raising trends of chronic and non-communicable disease (NCD), an epidemic of lifestyle related diseases like diabetes, obesity, heart diseases, typically a result of stress, improper diet and irregular or sedentary lifestyle.
These NCDs are lifestyle disorders that can be prevented by lifestyle modification.
Ayurvedic lifestyle supports physical, mental as well as social health. These lead to improvement in disease process, disease symptoms and improvement in the quality of life, helping in the prevention and management of diseases.
We as Ayurveda practitioners, can use Ayurveda’s vast knowledge base on preventive care by which each individual can achieve and maintain his or her immunity through diet, lifestyle, use of Rasayanas, and other tools and techniques of Ayurveda.
Prevention of disease and promotion of health is the main aim of Ayurveda.
As your Director for Ayurveda, I will do whatever I can to work with the ANTA National Council as well as Government and Regulatory bodies to promote Ayurveda and support our Members.
Thank you for your time and your commitment to Ayurveda and the innovative approach of predictive, preventive and personalised medicine (PPPM) that it can provide.
Regards Neerja Ahuja
ANTA Ayurveda Branch Chair
THE NATURAL THERAPIST VOL 37 NO. 4 | SUMMER 2022 | PAGE 13 ANTA News Summer 2022
Briony Green ANTA Student Member BHSc (Naturopathy)
Herbal Monograph:


Passiflora incarnata and Glycyrrhiza glabra
Herbal Monograph One: Passiflora incarnata:
Botanical Name: Passiflora incarnata1
Common Name: Passionflower2 .
Family: Passifloraceae3
Parts Used: Arial parts are used (not including flower or fruit), with leaves and stems containing the highest pharmacological activities. The best time to harvest is when the plant is flowering/fruiting3.
Constituents:
• Alkaloids – Harmine, harman, harmol, harmaline, harmalol, passaflorine4.
• Flavonoids – Apigenin, quercetin, vitexen, isovitexin, rutin, homoorientin, kaempferol, orientin, saponarentin, luteolin, saponarin4.
• Maltol2 .
• Benzoflavone5
• Phytosterols2 .
Actions:
• Anxiolytic 2
• Sedative3
• Anti-spasmodic 3 .
• Hypontic 1
• Anodyne3
• Nervine6 .
Therapeutic Indications: Traditional Use: Passiflora incarnata was used traditionally for its hypnotic and sedative properties, and was prescribed for sleeplessness, specifically when associated with worry, exhaustion, or nervous excitement; in both infants and the elderly especially7. Additionally, Ellingwood (1919)8, suggests conditions of the nervous system such as muscular twitching, irritation, spasms and convulsions associated with nervous excitement were all traditionally treated using Passiflora incarnata. According to Boericke (1901)9, Passiflora incarnata was indicated in hysteria, acute mania and violent headaches, as well as Whooping Cough (due to its antispasmodic actions), to aid in withdrawal of morphine and the withdrawal symptoms of alcohol (delirium tremens). Furthermore, Passiflora incarnata was used historically in the treatment of neuralgia conditions, dysmenorrhea, diarrhea, and dysentery10, as well as heart palpitations and shortness of breath due to excitement or shock11.
Modern Use: Passiflora incarnata is a herb that works beautifully
PAGE 14 | SUMMER 2022 | THE NATURAL THERAPIST VOL 37 NO. 4 ANTA Member Article Summer 2022
on the nervous system due to its anxiolytic, hypnotic and sedative properties, particularly beneficial for sleep disorders and chronic insomnia12. Hoffmann (2003)4, claims Passiflora incarnata is indicated for intransigent insomnia, aiding in an easeful passage into undisturbed sleep with no hangover like affects, owning to the sedative action of the alkaloids and flavonoids. Similarly, Wood (2016)13, recommends Passiflora incarnata for difficulty falling asleep and circular thinking. Passiflora incarnata is commonly prescribed for general anxiety disorder and nervous conditions due to its anxiolytic actions2. A study was conducted on 60 patients who were undergoing spinal anaesthesia and were administered 700mg/5ml of Passiflora incarnata aqueous extract, found an increase in anxiety suppression pre-anaesthesia14. A similar study was conducted on dental patients who were undergoing dental extraction, which found the anxiolytic effects of Passiflora incarnata comparable to midazolam for treating anxiety pre-extraction15
Further evidence suggests that the sedative and anxiolytic actions of Passiflora incarnata impact the serotonergic system, modulating the Gammaaminobutyric acid (GABA) pathways, indicating beneficial use in Attention Deficit Hyperactivity Disorder (ADHD), depression, addiction as well as learning and memory processes16.
Passiflora incarnata is also used as a nervine for reducing stress, tension, and exhaustion, relaxing the mind of mental chatter, restlessness and nervous headaches6. Furthermore, Passiflora incarnata has a beneficial effect on the brain and nerves and is indicated for neuralgia, brain irritation, and shingles as well as hysteria and Parkinson’s Disease. The antispasmodic actions of the flavonoids in Passiflora incarnata are effective in reducing seizures in epilepsy, and is indicated for use in asthma, dysmenorrhea and muscle spasms due to tension4. Passiflora incarnata has a soothing quality on the cardiovascular system due to its sedative actions and is useful for nervous tachycardia and for reducing blood pressure3,4.
Safety:
Contraindications:
According to Bone (2003)1 there are no known contraindications.
Possible Toxicity:
Passiflora incarnata is generally regarded as a safe herb, with no reports of overdoses in humans, however there is one published report of toxicity in an individual ingesting doses of 500-1000mg three times a day17

Adverse Reactions:
Braun & Cohen (2015)2, suggest drowsiness to be the most common side effect associated with Passiflora incarnata. Other side effects that have been reported include a case of hospitalisation due to self-medicating with Passiflora incarnata in high therapeutic doses, resulting in nausea, severe vomiting, drowsiness and ventricular tachycardia18. Additionally, one study examined the outcomes of pregnant women taking Passiflora incarnata for depression and/or anxiety, with the findings demonstrating adverse pregnancy outcomes including one neonatal death19
Drug Interactions:
There are very few studies on the possible interactions with Passiflora incarnata however, due to the neurological effects of the plant it should be used with caution when combined with drugs that act on the central nervous system20. One report suggests Passiflora incarnata has an additive or synergistic effect on Benzodiazepines, by enhancing binding to the GABA receptors17. Further studies suggest that possible interaction may occur with drugs metabolised via Cytochrome (CYP) pathways as Passiflora incarnata modulates CYPs21. Fisher (2018)3 suggests Passiflora incarnata may interact with warfarin by decreasing drug efficacy.
Cautions in Certain Populations:
Passiflora incarnata is considered safe when taken in appropriate doses, however it is advised to use with caution in pregnancy due to lack of safety evidence, as Passiflora incarnata may increase uterine contractions2 .

Prescribing: Oral Dosing:
• Liquid extract (1:2): 20-40ml/week22
• Fluid extract (1:1): 2ml in 150ml of water taken three to four times daily2 .
• Dried herb: 2g of dried herb three to four times
ANTA Member Article Summer 2022 THE NATURAL THERAPIST VOL 37 NO. 4 | SUMMER 2022 | PAGE 15
daily2
• Infusion of dried herb: 0.25-2g of dried herb, three to four times daily2 .
• Tablet: 1.5 to 2.5g/day22
Herbal Monograph Two: Glycyrrhiza glabra:
Botanical Name: Glycyrrhiza glabra1
Common Name: Liquorice, licorice3
Family: Fabaceaea or Leguminosea, commonly known as the pea family5.
Parts Used: Root and stolon, with preference to harvesting in Autumn after its fourth year3.
Constituents:
• Triterpene saponins (4-20%) – predominately glycyrrhizin, glycyrrhizic acid or glycyrrhizinic acid, which is composed of potassium and calcium salts of glycyrrhetinic acid (GA), as well as liquiritic acid, glabrolide, glycyrretol and isoglabrolide2
• Flavonoids (1%) – flavones and isoflavonoids3.
• Bitter – glycymarin3
• Polysaccharides3
• Volatile oils23.
Actions:
• Anti-inflammatory3
• Demulcent3.
• Expectorant3
• Spasmolytic 3
• Mild laxative1.
• Mucoprotective5.
• Adrenal tonic 1
• Antitussive22.
• Antiucler22 .
• Antiviral5
• Adoptogen24.
Therapeutic Indications:
Traditional Use:
Glycyrrhiza glabra root has been used traditionally for its emollient and demulcent properties, soothing irritation of mucous membranes in conditions such as coughs, catarrh and for irritation and pain associated with urinary conditions and gastrointestinal conditions such as diarrhoea7. Cook (1869)25, also praised the demulcent and “gentle relaxant” properties of

Glycyrrhiza glabra, using it to treat bronchial irritation where there is dry cough and “tickling”.
Furthermore, Glycyrrhiza glabra was traditionally used as an additive in cough mixtures, infusions, decoctions, pills and troches to disguise the taste of other medicines26. Culpepper (1880)27, claims all pains of the lungs and breast can be treated with Glycyrrhiza glabra, including wheezing and shortness of breath, as well as kidney and bladder complaints, whilst also sweetening and cleansing the blood. Similarly, Grieve (1931)28, claimed Glycyrrhiza glabra has alterative actions, is rejuvenating, has nutritive tonic qualities, and is used as a mild laxative and thirst preventative.
Modern Use:
Glycyrrhiza glabra has a specific affinity for the endocrine system, supporting the adrenal glands and hormones29. It is indicated in situations of burnout and exhaustion, adrenal fatigue and depletion as well as dysregulation of the hypothalamic-pituitary-adrenal (HPA) axis due to its adrenal tonic and adaptogenic actions, adding sweetness and restoration to the fatigued and depleted12. This adaptogenic property is due to the ability of Glycyrrhiza glabra to slow the breakdown of cortisol while producing effects similar to corticosteroids, normalising metabolic functions and adaptation to different conditions, thus increasing the body’s resistance to stress, resulting in a more beneficial stress response30
Glycyrrhiza glabra has a regulatory effect on the sex hormones, treating polycystic ovarian syndrome (PCOS), premenstrual tension, endometriosis, androgen excess and other hormone dependent diseases. In PCOS, 11 β-hydroxysteroid dehydrogenase is inhibited, thus lowering testosterone levels3,31.
Glycyrrhiza glabra has a soothing demulcent action on the mucous membranes of the respiratory system, urinary system and the gastrointestinal system (GIT), acting to moisten and cool inflammation and irritation12. In respiratory system conditions Glycyrrhiza glabra has a mucilaginous effect, soothing tickling, irritating and harsh coughs as well as sore throats, whilst its relaxing expectorant, antitussive, anti-inflammatory, antispasmodic and antiviral actions treat bronchial conditions and respiratory tract infections2,32. Glycyrrhiza glabra has an antiinflammatory, antiulcer and mucoprotective action on the GIT, assisting in conditions of gastritis, colic, ulcerative colitis, chronic mouth ulcers, gastric ulcers and peptic ulcers by promoting mucosal repair and stimulating mucosal production and secretion2,33
PAGE 16 | SUMMER 2022 | THE NATURAL THERAPIST VOL 37 NO. 4 ANTA Member Article Summer 2022
The strong anti-inflammatory actions of Glycyrrhiza glabra have various mechanisms of action, including increased cortisol levels, inhibition of Arachidonate 5-lipoxygenase (5-LOX) and Prostaglandinendoperoxide synthase 2 (COX-2) pathways, reduction in oxidative stress by inhibition of reactive oxygen species (ROS) generation and decreasing inflammatory cytokines34
The beneficial effects of Glycyrrhiza glabra on inflammatory driven conditions, suggests its use in treating immune conditions such as inflammatory bowel disease, rheumatoid arthritis and asthma3,35 Glycyrrhiza glabra displays strong antimicrobial and antiviral actions in glycyrrhetinic acid that inhibits activation of the Epstein-Barr virus, additionally, antiviral activity is demonstrated against herpes simplex, influenza A virus, severe acute respiratory syndrome (SARS), vaccinia, encephalitis, arboviruses and human immunodeficiency (HIV)36,37
Safety: Contraindications:
Glycyrrhiza glabra is contraindicated in conditions of hypertension and hypokalaemia due to the mineralocorticoid-like actions that interfere with blood fluid balance and potassium levels3,38, however, in a clinical trial of 128 patients administered Glycyrrhiza glabra, no significant changes were reported in electrolyte levels or blood pressure39. It is contraindicated in pregnancy as studies have shown an increased risk of still born and adverse outcomes in pregnant women consuming high doses40. Fisher (2018)3 also reports that Glycyrrhiza glabra should be avoided in patients with cirrhosis of the liver.
Toxicity and Side Effects:
Toxicity related to Glycyrrhiza glabra use is generally dose dependant41, such as elevated blood pressure, associated with high doses or excess consumption causing disruption to the renin-angiotensinaldosterone system35. High doses of Glycyrrhiza glabra can also result in hypokalemia, retention of sodium and loss of potassium causing oedema, breathlessness and hypernatraemia2. High dose Glycyrrhizin is linked to pseudo-hyperaldosteronism, where a hypersensitivity to adrenal cortex hormones can cause adverse effects including headaches, fatigue, water retention, high blood pressure and heart attack42
Drug Interactions:
Studies on the interaction potential of Glycyrrhiza glabra on the cytochrome P450 pathways have shown that Glycyrrhizin can interact with both
cytochrome P450 2D6 (CYP2D6) and cytochrome P450 3A4 (CYP3A4) pathways, indicating that it has the potential to modify and interact with drugs metabolised via these routes43. Yarnell & Abascal (2014)44, reported possible interactions with immunosuppressive drugs such as corticosteroids and methotrexate. Glycyrrhizin was shown to inhibit 11 β-hydroxysteroid dehydrogenase which acts to inactivate corticosteroids, therefore combining Glycyrrhiza glabra and prednisolone resulted in an increase of systemic drug exposure44. Similarly, an animal study reported that Glycyrrhizin increased the absorption of methotrexate in rats, suggesting Glycyrrhiza glabra may have potential as a dosesparing agent44. There is increased risk of elevated blood pressure in women taking the oral contraceptive pill with Glycyrrhiza glabra due to its mineralocorticoid effects and modulation of the CYP3A metabolism pathway45. Furthermore, Braun & Cohen (2015)2 , suggest Glycyrrhiza glabra should be avoided when taking anticoagulants as high doses are reported to have an anticoagulant effect. There are possible interactions with hypertensives, as high dose Glycyrrhiza glabra was found to increase blood pressure and reduce drug efficacy2, reported reduction of potassium levels when taken with diuretics and digitalis toxicity when combined with cardiac glycosides3.
Cautions in Certain Populations:
The most common side effects reported with Glycyrrhiza glabra are hypertension and hypokalemicinduced disorders associated with high doses and long-term use2. The most susceptible to toxicity and increased risk of adverse effects of Glycyrrhiza glabra are individuals with prolonged gastrointestinal transit time, hypokalemia, hypertension, reduced 11 β-hydroxysteroid dehydrogenase (HSD) type two activity, anorexia nervosa, females and the elderly46.
Prescribing:
Oral Dosing:
• Liquid extract (1:1): 15-40ml/week for 2-4ml three times a day1,2.
• Tablet: 2.0g-3.0g/day22
• Dry root: 5-15g/day2
• Infusion: 2-4g dried root simmered for 5 minutes in 150ml of water. Drink 1 cup of infusion after each meal for chronic gastritis2
THE NATURAL THERAPIST VOL 37 NO. 4 | SUMMER 2022 | PAGE 17
ANTA Member Article Summer 2022 For references log into your ANTA Member Centre > The Natural Therapist > Journal Articles
 Shaun Brewster ANTA National President ANTA National Myotherapy Branch Chair Advanced Clinical Education Director
Shaun Brewster ANTA National President ANTA National Myotherapy Branch Chair Advanced Clinical Education Director
23 Lessons from 23 Years
After a quick count, I realised that it has been 23 years since I graduated from my first formal qualification and officially entered the health care industry.
So in this article, I thought I’d share 23 lessons that I have learned during that time. Hopefully, 23 things that will be useful to you in some small way.
Here we go, in no particular order...
1. Your qualification doesn’t matter: I’ve seen individuals with every level of qualification start and build incredibly successful businesses and help many many people. It doesn’t matter if you have a PhD in Neuroscience, or a Cert IV in Massage Therapy, there are people who need what you have. Your qualification is not a representation of your worth. The service you deliver to the community and the good that it does is what determines the value you represent.
2. Your qualification does matter: “Wait... Didn’t you say it doesn’t matter?”
Yes.
It matters in that your qualification gives you a ticket to get in the door.
If you want to work in a hospital, or a with a sports team, or in private practice, or in palliative care, or with stroke patients - then you need to choose a qualification that will position you to get into those settings.

The ticket to get in the door is essential, but what separates you above the rest is what you do with it.
3. There will be times when you’ll want to quit: Don’t. Just don’t.
4. There will be times when becoming a Nurse or a Builder or whatever, looks more attractive: There are heaps of Nurses and Builders out there who are looking at you thinking your job looks pretty amazing too.
THE NATURAL THERAPIST VOL 37 NO. 4 | SUMMER 2022 | PAGE 19 ANTA Director Article Summer 2022
5. If you think you still have a lot to learn, you are right:
But you are way better than when you started. In fact, you are better than you were 3 months ago. And in 10 years time you’ll be far better than you can even imagine.
6. Pain is complicated: There is no perfect treatment for anything. There are however treatments that work best for an individual, in a specific circumstance, at a particular time.
The magic happens when you can reverse engineer all of that.
Want to learn magic…? You have to be willing to stick at your craft longer than most are willing to. That is the price.
7. Help is available, at ALL times: You are surrounded by other health practitioners who would be more than willing to offer advice, guidance and support. But you need to ask for it. Not every person will help you, but there are more than enough who will.
8. When someone puts their trust in you, your knowledge and your skill: When they commit their time and their money to giving you a chance to solve their problem - THAT is a responsibility that should never be taken lightly. Turn up, switch on and deliver your best every time.
9. What you learned yesterday may very well be wrong now: Well not wrong perhaps, but quite possibly out-dated. We work in a dynamic and ever evolving profession. It requires us to be agile, to not get too attached to old ways of thinking or doing, and it forces us to stay humble.
10. You are worth more: Most of us don’t charge enough for what we do. You studied for a really long time, you put in the work and you earned the right to help people. What you have to offer holds value. How much should you charge? Only you can decide that, but my guess is that it is more than you are right now.
11. What you charge determines your worth: Well that throws a spanner in the works on point number 10...
The truth is, the price you set will create a perceived value for your service. If you are too cheap, some people will believe you aren’t very good, even before they meet you.
If you charge a lot, most people will assume that you must be very good at what you do.
Of course, if the price is very high, that will deter some people, but not all of them and you don’t need all of them.
12. Anatomy, Physiology and Pathology: These three sciences underpin everything we use in clinic every day.
It doesn’t matter how well you think you know these things, keep studying. The more you understand these, the more you understand everything.
13. Self-education is jet fuel: We all have gaps in our knowledge. Once identified, if you are willing and curious enough, you can find the answers to just about anything. Self-education is jet fuel for the therapist who wants to be at the top of their game.
14. More tools in the kit don’t always make a better therapist:
Far better to get really good at what you know now, and then let the limitations of those things become apparent. Once you recognise those limitations, you can seek out the next tool / technique / approach that will complement and scaffold on what you already know.
15. Don’t hesitate to refer: Nobody wants to have their time wasted, let alone their money. If someone walks through your door with something you know you can’t help with, or that you know someone else can do a better job on than you, then tell them.
An honest and early referral will build trust in you and your professionalism. They may be disappointed in the moment, but they will be grateful that it didn’t take six consultations for you to come to the conclusion.
16. Spend the time to educate: As the years progress, I’m finding that I’m spending more and more time helping the patient understand WHY they feel the way they do and WHAT got them there in the first place. Educating your patient is so much more valuable than may first be obvious. They came to you for a solution to their problem.
Taking the pain away is part of it, but knowing why it showed up in the first place, and understanding how to make sure that doesn’t happen again - that is powerful.
Take the time to make sure they get it. You’ll be surprised how patient satisfaction increases as a
PAGE 20 | SUMMER 2022 | THE NATURAL THERAPIST VOL 37 NO. 4 ANTA Director Article Summer 2022
result.
17. You can change direction:
One of the amazing things about our profession is the fact that there are countless different facets to it. You can specialise in any number of demographics, conditions, settings or regions of the body. You can become a business owner and build an empire, or you can become a master technician with incredible knowledge. You can mentor others or add teaching to your career. You can participate in research or contribute through writing. There is opportunity for you change direction and explore any of these things, and if you stick at it long enough, there is time to try all of them.
18. You are only as good as your last result: This game is nothing like being an Olympic gold medallist. If you win a gold medal, you are an Olympic champion for life. In our line of work, you have to perform every day and get results for people every day. The second you stop delivering for your patients, is the second that you start to become replaceable. Don’t let this get you down, let it motivate you. If we work hard at it, we can be at the top of our game for decades. There aren’t many Olympic athletes who can say that.
19. Be patient: Everything worthwhile takes longer than you’ll want to wait. Hang in there.
20. Wait actively: In point 19 I said you have to wait, but I didn’t say you should be passive. Nothing worthwhile comes to those who simply wish it to happen. Position yourself for success, surround yourself with the people and resources you need, then move toward

your goal, don’t wait for it to come to you.
21. Don’t be a jerk: Chiropractors don’t just “crack backs”. Physiotherapists don’t just hand out exercises. And Massage Therapists don’t just rub skin. Only an idiot will assume that their experience of a profession is the one and only truth. There are incredible practitioners in every profession, just as there are not-so-great practitioners. Let’s give respect to everyone. Some will prove themselves worthy, others will not... but time will sort them out either way.
22. Be generous: This may very well be one of the most important lessons I’ve learned. Give more than you think is reasonable. Life is a very long game, and your reputation is perhaps your most valuable possession. Being generous with your time, your knowledge, your skill and your effort will put you in a position that can’t be bought.
23. On my first day of classes in my first year of study, a teacher told me the following: “You are going to be doing amazing work. Work that has the ability to remove pain and suffering. Work that has the ability to change the quality of people’s lives. Be grateful for that every day”. He was right you know, and we should never forget it.
Well there we go. 23 lessons from 23 years. There have been plenty more lessons along the way, and I look forward to sharing those with you another time.
Until then, thank you for giving me your time in reading this, I hope you found something you can use in these words.
ANTA Director Article Summer 2022 THE NATURAL THERAPIST VOL 37 NO. 4 | SUMMER 2022 | PAGE 21
Individually, we can achieve great things. But when you belong to a community swarming towards a common goal, that’s when we form our strongest line of defence, and the sky’s the limit.
Guild Insurance and the Australian Natural Therapists Association (ANTA) have partnered together to protect
the future of your profession. With us, you’ll be shielded by a policy created from unmatched insight into your profession, access to risk management materials to help you reduce the risk of a claim, backing from the industry body that stands up for Australian natural therapists, and so much more.
Together, we form the network that ensures you don’t have to fly solo. Get the full picture of how you can be part of something bigger by visiting guildinsurance.com.au/ANTA or calling 1800 810 213 today.
Don’t go it alone

Insurance issued by Guild Insurance Limited ABN 55 004 538 863, AFS Licence No. 233791 and subject to terms, conditions and exclusions. This information is of a general nature. Guild Insurance supports ANTA through the payment of referral fees. Please refer to the policy wording and policy schedule for details. NAT238516 ANTA - TNT Full Page ad 08/2022
1800 810 213 guildinsurance.com.au
George Thouas, PhD Head of Research & Innovation Max BioCare Pty Ltd
Clinical Trial Update: Effects of Fish Oil Omega-3 on Brain Activity in Children

Introduction:
Cognitive and behavioural wellbeing have become major areas of family health focus, especially during COVID-19 lockdowns and home schooling in recent months. More than ever, children are exposed to a seemingly endless stream of information in learning and social environments that are increasingly dominated by digital technology. Maintaining brain health through balanced, targeted nutrient support is therefore considered an important means of buffering these demands on the development of intelligence quotient (IQ) and emotional intelligence (EQ). One specific group of nutrients are the omega-3 fatty acids, a family of long-chain polyunsaturated fats that play important roles in brain and eye nerve structure, connectivity, and processing ability. Omega-3 status in children is directly correlated with behavioural and cognitive skills, as measured using psychometric testing procedures1. However, relatively few of these studies have measured brain function directly. This article highlights the findings of a recent research
study reporting the unique effects of an Australian omega-3 supplement on brain activity in school-aged children during cognitive testing.
Study Design:
The report, published in the journal Foods by Sittiprapaporn et al. (2022)2, presents the outcomes of a randomised, placebo-controlled trial completed in 2020, evaluating the cognitive effects of a commercially available chewable supplement containing pharma grade tuna oil standardised to omega-3 fatty acids, docosahexaenoic acid (DHA) and eicosapentaenoic acid (EPA) (260mg/60mg per capsule). The study itself was conducted by researchers at Mae Fah Luang, Mahidol and Mahachulalongkornrajavidyalaya Universities in Thailand. Children (n=120, 6-12 years of age) attending three different primary schools were parentally consented to participate in the trial, which involved random allocation to one of three groups (1 capsule (low dose), or two capsules (high dose)
THE NATURAL THERAPIST VOL 37 NO. 4 | SUMMER 2022 | PAGE 23 ANTA Member Article Summer 2022
of the omega-3 product, or a placebo (soybean oil)), daily over a 12-week period. At the start and end of this period, the children were asked to perform three different computer-based image and number recognition tasks. Such tasks are frequently used in psychology testing to determine elements of IQ. They included the “Go/No-Go” test for assessing attention and response control based on a simple binary choice, the “N-Back” test for working memory and reasoning, based on single number recall, and the “Digit Span” test for memory span, based on recalling sequences of numbers. During these tasks, the children wore a fabric cap constructed with an array of sensitive micro-electrodes that remotely and non-invasively detected instantaneous changes in brain wave activity over different regions, akin to an electroencephalography (EEG) approach. These recorded “multi-channel” signals then underwent computational analysis, followed by aggregation to give a measure of overall neural activity (called Global Field Power, or GFP). This method is capable of measuring how the brain responds to, and processes, visual information during a task, culminating in a manual reaction (a behavioural or motor effect, in this case, the pressing of a keyboard button).
Outcomes:
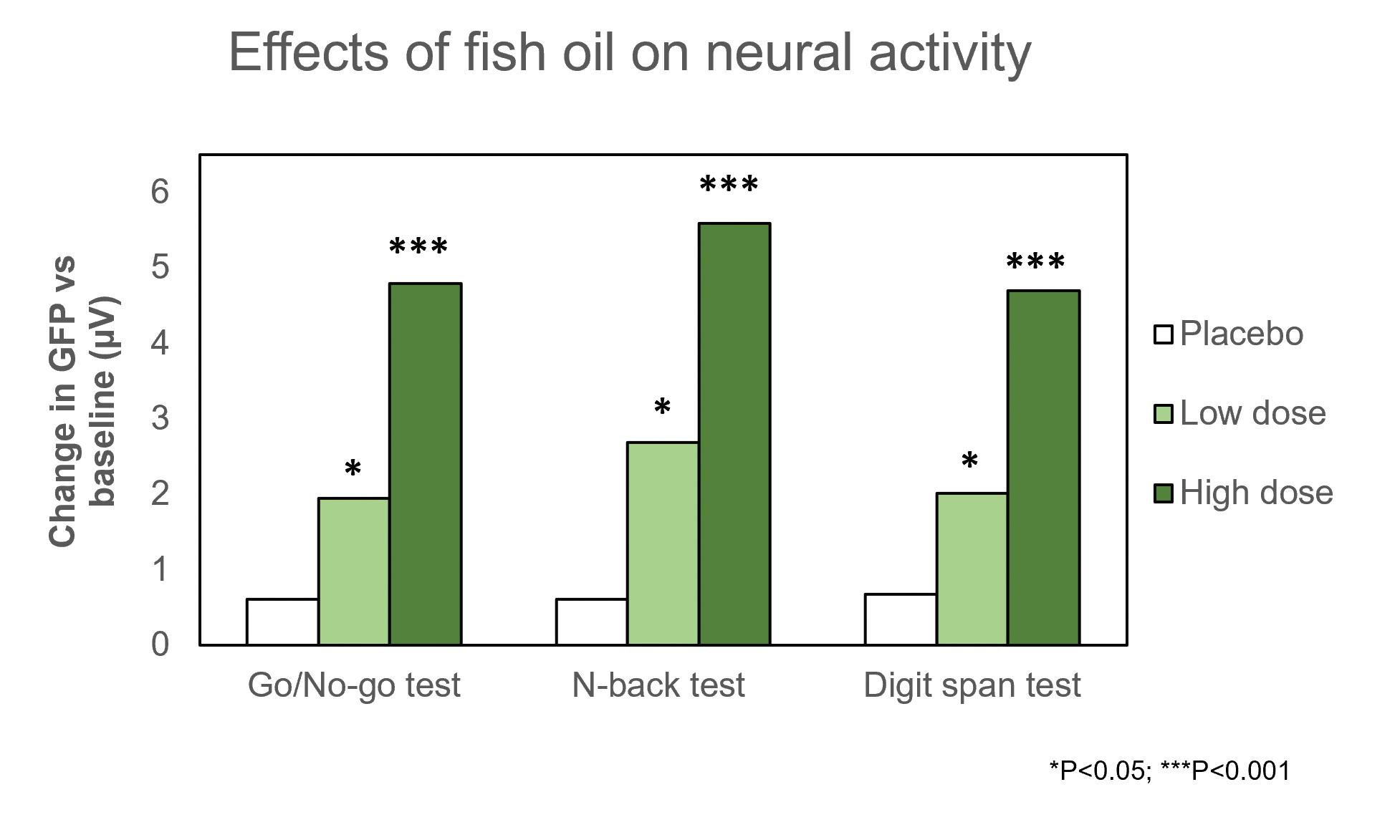
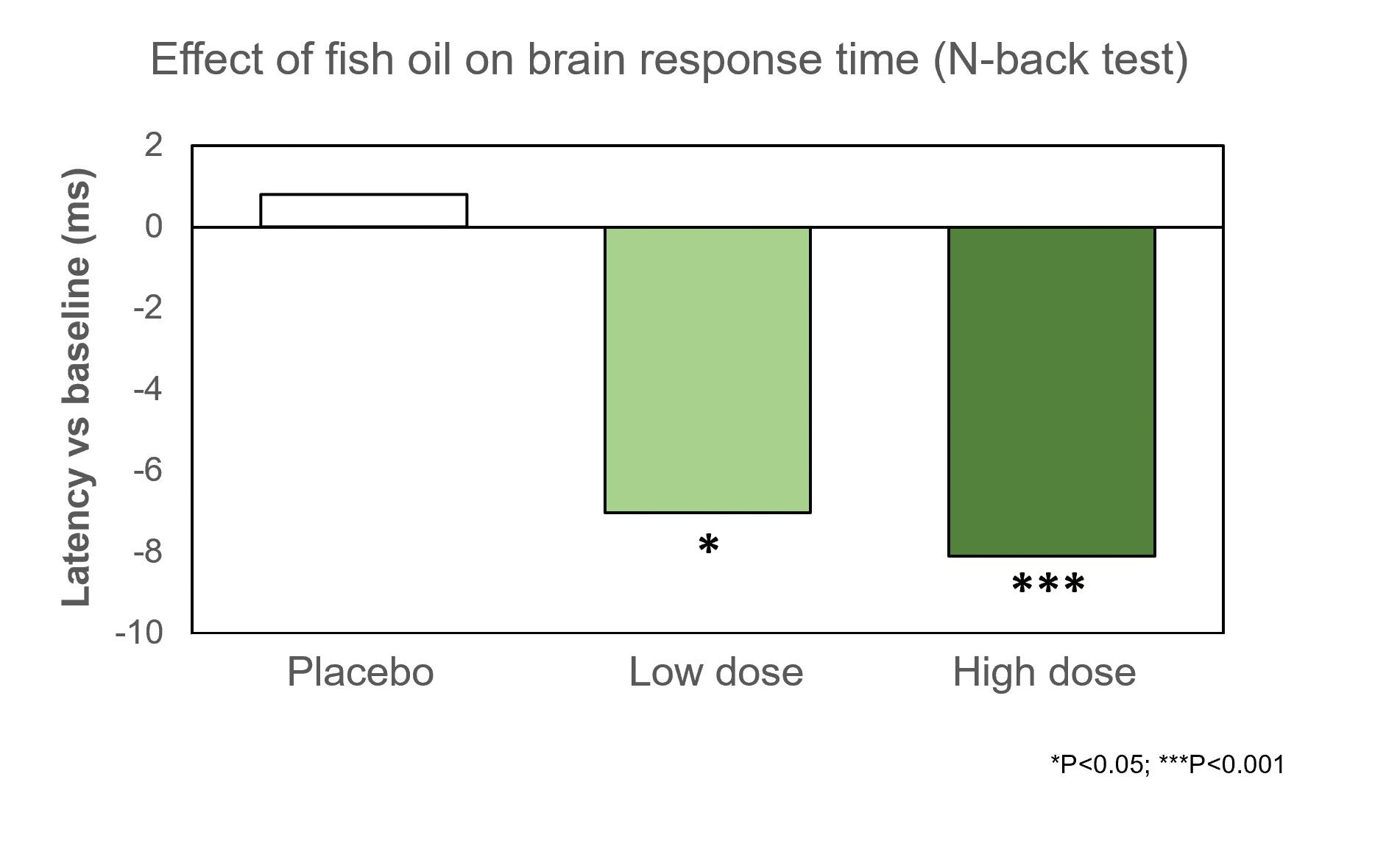
For all three tasks, the study found that manual performance, including average reaction times and error rates were similar at the end of the trial, compared to baseline. However, there were significant increases in the amplitude of brain GFP’s during each task by the end of the trial period, and these were more pronounced at higher levels of omega-3 intake, compared in the placebo group (Figure 1.0). This indicates that consumption of the omega-3 product was associated with simultaneous increases in active neural processing related to attention, working memory, memory span and decision making. In addition, significant reductions in the latency were evident in the omega-3 groups during the Go/No-Go and Digit Span tests, by the end of the trial, with a dose-dependent effect versus placebo in the N-Back test (Figure 2.0). Therefore, fish oil consumption was associated with a further improvement in processing speed during sustained attention, recall and decision making. In terms of safety, the participation rate was complete in all groups, with no reports of adverse events or compliance problems.
Figure 1.0: Mean changes in overall brain activity during cognitive tests, detected by multichannel electrode array measurements, following fish oil consumption in children (adapted from Sittiprapaporn et al. 2022)2
PAGE 24 | SUMMER 2022 | THE NATURAL THERAPIST VOL 37 NO. 4 ANTA Member Article Summer 2022
Figure 2.0: Mean change in brain response time as an indicator of processing speed for working memory detected with multichannel electrode array measurements, following fish oil consumption in children (adapted from Sittiprapaporn et al. 2022)2
Implications of the Study:
The results of the present trial show that consumption of omega-3 fatty acids (as fish oil derived DHA and EPA) is safe and has a direct, dose-dependent stimulatory effect on neural activity and processing speed in children, during performance of visual tests that challenge their attention, working memory, memory span and decision-making skills. Progressive learning and cognitive development during school ages increasingly engages and refines children’s factual memory and executive functions, such as balancing actions with inhibition, self-control, and ability to focus. This is especially the case with digital multimedia technology. The results of the trial are confirmed by a previous study in which functional Magnetic Resonance Imaging (MRI) analysis (a form of live brain imaging) of 8-10 year old children revealed that DHA consumption was associated with activation of specific regions of the prefrontal area of the brain dedicated to language development, as children performed sustained attention exercises3. These changes were independent of test performance. It is widely known that DHA is the principal omega-3 fatty acid that makes up grey matter, and it accumulates exponentially in the developing brain within the first years of life4, in preparation for synaptogenesis and activation of pathways controlling basic functions such as speech development, visual recognition
and motor control. It is also known that omega-3 status can be maintained by routine dietary intake or supplementation, to compensate for deficiencies that may occur throughout childhood, which may impact on learning and cognitive ability5. By gaining a more comprehensive picture of the biology behind how and when omega-3 fatty acids influence brain function in children, through studies similar to that described here, we can better understand the functional importance of these nutrients during early development.
Conclusion:
The trial by Sittiparpaporn et al. (2022)2 provides direct confirmation that fish oil omega-3 fatty acid consumption is independently associated with a measurable increase in brain activity and processing speed in school-aged children, under visual test conditions. Further research may elucidate how these effects relate to real-world scenarios and outcomes, which specific regions of the brain are involved and at which stages, as children’s cognitive skills develop.
THE NATURAL THERAPIST VOL 37 NO. 4 | SUMMER 2022 | PAGE 25
ANTA Member Article Summer 2022
For references log into your ANTA Member Centre > The Natural Therapist > Journal Articles


THE NATURAL THERAPIST VOL 37 NO. 4 | SUMMER 2022 | PAGE 27
 Hermocilla ANTA Student Member BHSc (Chinese Medicine)
Hermocilla ANTA Student Member BHSc (Chinese Medicine)
The San Jiao
Introduction:
The Triple Burner, or San Jiao in Chinese, has been a controversial topic in Chinese Medicine for centuries, due to its arguable nature as a form of a Yang organ, or a function without a form. According to the ‘Yellow Emperor’s Classic’, the San Jiao is one of the six Yang organs in the body, because its function is similar to them - that is, it receives food and drink, digests and transforms it, transports the nourishment and excretes waste. However, strong supporting evidence suggests the view of the ‘Classic of Difficulties’ - that is, the Triple Burner ‘has a name but no form’, or an insubstantial collection of functions rather than a physical organ. To illustrate this, the San Jiao’s functions and its connection to Qi, blood and body fluid production will be discussed.
San Jiao and Original Qi:
In the theory ‘Classic of Difficulties’, the San Jiao is an invisible passageway and can only be physically seen through the processes it assists, that is to provide a free passage for the flow of body fluids, blood and Qi and Original Qi1. According to Kong (2005)2, ‘Qi is an invisible fluid that manifests its power to sustain life
and the well-being of organs’. Original Qi (Yuan Qi) is a Motive Force (Dong Qi) of all the Internal Organs, that moves all over the body to provide the necessary heat to all of the body’s functional activities3. Qi, in particular Original Qi, is vital in warming the organs for proper growth and development2. The San Jiao aids Original Qi to differentiate itself to perform different functions when moving around the body. If the San Jiao’s passageway is blocked or deficient, Original Qi cannot function, and the flow and production of blood depletes, resulting in disease4. The San Jiao is a collection of functions within three divisions inside the body: Upper, Middle and Lower5
Upper Burner: Maciocia (2015)4 states that ‘The Upper Burner, also known as the Warmer, or Upper Jiao, is located from the diaphragm upwards, and houses the Heart, Lungs and pericardium’. It mainly functions to “receive” refined nutritious substances through food/drink, disperse Wei/Defensive Qi (which protects the body from harmful pathogens) and distribute body fluids all over the body, to the spaces between the skin and muscles in the form of a ‘mist’ or sweat1

THE NATURAL THERAPIST VOL 37 NO. 4 | SUMMER 2022 | PAGE 29 ANTA Member Article Summer 2022
Grace
1. Creates Gathering Qi and Disperses
Defensive
Qi:
The Upper Burner function is illustrated in Figure 1.0 below. As a person breathes air, the Lungs receive it and descend it to form Air Qi6. Food is also ingested in the Stomach and Spleen and transforms and transports this into Food Qi/essence to nourish the organs in the body. ‘Original Qi provides heat from between the Kidneys, to the Upper Burner, via the Triple Burner or freeway, to fuel the combination of Air Qi and Food Qi in the Lungs to produce Gathering Qi’4. Gathering (Zong) Qi penetrates the blood vessels and is vital in assisting the Lungs in breathing, the Heart in pumping blood to maintain a regular Heart rate and rhythm and provide strength and tone to voice7. Finally, Gathering Qi is refined in the Upper Burner to produce True Qi with the help of Original Qi (providing heat)6. ‘True Qi is the purest form of refined Qi, and splits into Nutritive Qi (Yin) in the Middle Burner, and Wei/Defensive Qi (Yang), which disperses in the Upper Burner’4. Wei Qi during the day circulates 25 times in the exterior and 25 times in the interior to warm the muscles and skin so that when harmful pathogens attempt to invade the body, Wei Qi rises to battle it, resulting in fever3
2. Location for Blood Production:
Once Food Qi is made, it is sent to the Lungs, as one portion makes Air Qi, another portion of Food Qi is pumped to the Heart, as seen in Figure 1.0. Heart Yang
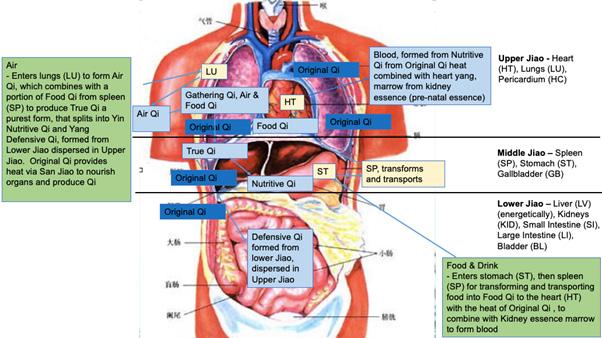
(fire), with Original Qi heat and marrow made from Kidney fluid essence from the Lower Burner, turns the Food Qi into blood7. Kidney essence is made from our parent’s deoxyribonucleic acid (DNA) Qi and Food Qi, also called Pre/Post-natal Qi. The Heart and the Lung in the Upper Jiao distribute the blood to warm and nourish the tissues in the body. If the Upper Jiao is not ruled, the water will attack the Heart and the Lung causing phlegm and asthma5.
3. Produces Body Fluids:
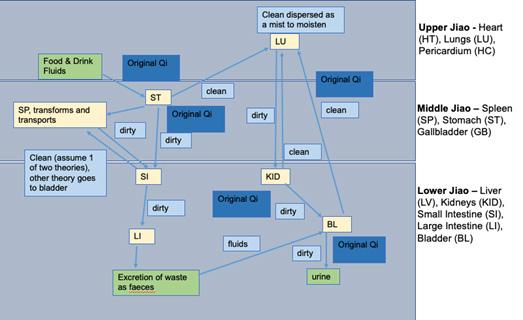
In the Upper Burner, when food/drink is ingested, the Spleen sends clean Food Qi up to the Lungs, which separates into clean/dirty, as seen in Figure 1.1. The clean is distributed as a mist to moisten the skin and body hair. The Lungs send the dirty portion down to the Kidneys and Bladder9. From there, the clean is sent back up to the Lungs via San Jiao to keep them moist as Jin (clear, light, fast fluid such as sweat), and the dirty is sent down to the Kidneys and Bladder where it is converted into urine and excreted from the body9 Original Qi and Kidney Yang (fire) are vital in providing the heat required for this process to occur.
Middle Burner:
The Middle Burner is between the diaphragm and umbilicus, and houses the Spleen, Stomach, and GallBladder5. The main functions of the Middle Burner are to digest and transport (or ‘rotten and ripen’) food and drink, create and direct Nutritive Qi to all
PAGE 30 | SUMMER 2022 | THE NATURAL THERAPIST VOL 37 NO. 4 ANTA Member Article Summer 2022
Figure 1.0: Production of Qi & Blood (adapted from TCM Window, 20208)
Figure 1.1: Transformation and Transportation of Fluids (adapted from Clavey, 2003
9)
of the organs, produce Stomach fluids, and, like the Upper Burner, produce blood. It is also known as a ‘maceration chamber’4. If the Middle Jiao is not ruled, the water will be retained in the Stomach and Spleen causing disease5.
1. Produces and Directs Nutritive Qi:
In the Middle Burner, the process of the Stomach ‘rottens and ripens’ the food to produce chyme, which through the Small Intestine, and the Spleen extracts the chyme nutrients necessary to convert this into Food Qi4, which as explained, eventually turns into Nutritive Qi. Original Qi travels up via the San Jiao to heat the Stomach and Spleen to perform its functions. Nutritive Qi flows in the blood vessels to nourish and generate blood, and regulates the opening and closing of sweat pores, and body temperature to prevent illness.
2. Produces Blood:
Wiseman & Ellis (1995)10 suggest that blood is formed from Nutritive Qi and body fluids. The Middle Burner produces waste and distils fluids to extract essence from the Qi, and then sends this to the Lungs to transform into blood10. Blood is pumped through the vessels by the Heart and stored and regulated by the Liver during rest, and is important in nourishing the whole body.
3. Produces Stomach Fluid:
In the Middle Burner, the Spleen holds food/drink fluids and separates it into clean/dirty – with clean sent to the Lungs. The Spleen sends dirty fluid down with help of Stomach Qi to the Small Intestine, see Figure 1.1 Clavey (2003)9 suggests that the Small Intestine separates this fluid into clean/dirty with the help of Original Qi’s heat, which travels to the Spleen to distribute to tissues for nourishment (other theories suggest it goes to the Bladder). Original Qi is important in providing energy to the organs for proper functioning. Further, if the Middle Burner does not ensure the upbearing, down bearing, inward and outward movement of Qi - if clean/dirty fails to ascend/descend along the Middle Jiao appropriately, then fluid production, distribution and discharge is inhibited, causing dry throat, skin and lips, and damp and phlegm/stagnation, water swelling and diarrhoea10.
Lower Burner:
The Lower Burner includes the Liver, Kidneys, Small and Large Intestines and Bladder10. ‘It dominates the separation of the essences of food and fluids from the clear and turbid, forms Defensive Qi, and facilitates the excretion of urine’5. It is therefore compared to a ‘drainage ditch’ (urine) as it discharges body fluids directing them to the Bladder.
THE NATURAL THERAPIST VOL 37 NO. 4 | SUMMER 2022 | PAGE 31
ANTA Member Article Summer 2022
1. Produces Blood:
The Lower Jiao contains organs which are vital for blood production. Original Qi forms from Kidney Essence/Ming Men, located between the Kidneys, and produces marrow to send upwards to produce blood10 Also in the Lower Jiao the Liver regulates Qi and stores blood.
2. Excretes Waste:
According to Wiseman & Ellis (1995)10, this occurs in the Lower Burner when the Lungs send the dirty portion of food/fluids down to the Kidneys and Bladder, see Figure 1.1. The Kidneys separate this fluid into clean and dirty. The dirty is sent to the Bladder to convert into urine with the help of Original Qi10 The Spleen sends the dirty to the Small Intestine, and according to Clavey (2003)9, the clean is sent back to the Spleen. The Small Intestine sends the dirty fluids to the Large Intestine to form faeces. The dirty fluids in the Bladder are separated, with the clean sent to the Lungs whilst the dirty is sent down to the Kidneys and Bladder to form urine (as Ye fluid, which is turbid, heavy and slow) and excreted out of the body5. This
excretion is important in eliminating toxins from the body.
Conclusion:
There is much research to illustrate that the Triple Burner ‘has no physical form’ as can be seen by its interaction with Qi and bodily organs. Instead, it is an ‘invisible passageway’ that is visible through the many functions that result from its existence. That is, through providing a freeway for; not only Qi life force to move around the body, but also housing the different organs which produce different forms of Qi, blood and fluids, all of which nourish the body to grow and develop. Whilst the San Jiao is vital in maintaining the life force and vitality of humans and the environment is evident; much remains to be discovered of its potential.
For references log into your ANTA Member Centre > The Natural Therapist > Journal Articles
PAGE 32 | SUMMER 2022 | THE NATURAL THERAPIST VOL 37 NO. 4 ANTA Member Article Summer 2022
Supporting women’s health with specialised formulas

Histammune Clear

60 tablets
ACTIVE INGREDIENTS
Each tablet contains:
Quercetin dihydrate 500 mg

Ascorbic acid (vitamin C) 166.6 mg
Rutoside 133.3 mg Hesperidin 100 mg Bromelains 3.6 million PU (80 mg)
Protease 6.0 200,000 HUT (32 mg)

Pyridoxal 5-phosphate monohydrate (P5P) (active vitamin B6) 7.8 mg equiv. to pyridoxine (vitamin B6) 5 mg


Oestro-BR
60 tablets
ACTIVE INGREDIENTS
Each tablet contains:






Herbal extracts dry concentrate standardised: Brassica oleracea var. italica (broccoli) seed –BroccoRaphanin® 200 mg min. equiv. to fresh 300 mg std. to allyl isothiocyanate 0.6 micrograms


Vitis vinifera (grape) seed 4.44 mg min. equiv. to dry 533.3 mg std. to procyanidins 4.22 mg




Herbal extracts dry concentrate: Rosmarinus officinalis (rosemary) leaf 200 mg equiv. to dry 1 g equiv. to cineole 725 micrograms equiv. to camphor 680 micrograms

Bupleurum falcatum (bupleurum) root 100 mg equiv. to dry 1 g
Nutrients: Methionine 25 mg Molybdenum (as molybdenum trioxide) 41.66 micrograms

Calcium D-glucarate 60 g oral powder
Ascorbic acid (vitamin C) 100 mg





Pyridoxine hydrochloride 100 mg equiv. to pyridoxine (vitamin B6) 82.3 mg
Pyridoxal 5-phosphate monohydrate (P5P) (active vitamin B6) 26.8 mg equiv. to pyridoxine (vitamin B6) 17.1 mg


Zinc citrate dihydrate 77.8 mg equiv. to zinc 25 mg
Magnesium amino acid chelate 100 mg equiv. to magnesium 20 mg
Manganese sulfate monohydrate 15.4 mg equiv. to manganese 5 mg Biotin 500 micrograms

ACTIVE INGREDIENTS
Each 1g contains:
Calcium D-glucarate (calcium saccharate) 900mg
The BioCeuticals Clinical brand exists to support clinicians, like you, to deliver better health for your patients who need specialised care
BioCeuticals Clinical is developed by clinicians exclusively for clinicians not available in any retail setting
PyriZinc BioActive Formerly Pyrrole Protect 60 capsules ACTIVE INGREDIENTS Each capsule contains: NEW NAME SAME GREAT FORMULA Customer Service: cs@bioceuticals.com.au 1300 650 455 (ext 1) Clinical Support: practitionersupport@bioceuticals.com.au 1300 650 455 (ext 2) www.bioceuticals.com.au Practical, clinically focused webinars available live and on demand Only $29 for two sessions Live and online monthly CPD points apply SIGN UP NOW! Find out more! MM00385ART
Lynn McCardle ANTA Student Member BHSc (Nutrition & Dietetic Medicine)
Among Menopausal Women, Are
Omega-3 Fatty Acids Effective in Reducing Vasomotor Symptoms, Compared to Placebo: A Literature Review
Abstract:
Background and Rationale:
A number of clinical trials have been undertaken to evaluate the effectiveness of omega-3 fatty acid supplementation on reducing vasomotor symptoms in menopausal women. To date very few have directly assessed omega-3 with placebo alone. This literature review assessed data from four clinical trials that included omega-3 and a placebo in their study design. Australian women are increasingly using alternatives to Hormone Replacement Therapy due to awareness of the increased cancer risk. An increase in omega-3 use by menopausal women has not been met with an increase in adequate clinical trials to assess effectiveness in this population. Hormone Replacement Therapy is recommended for a maximum of five years, but vasomotor symptoms can last
for up to ten years post menopause, highlighting a need for adequate data to determine specific clinical recommendations.

Methods:
A literature search was undertaken in Pubmed and CINAHL databases with four relevant papers assessing omega-3 supplementation versus placebo assessed using the Critical Appraisal Skills Program. Papers on this subject are scarce, therefore the search years extended from 2006 to 2021. Inclusion criteria were (1) postmenopausal women experiencing vasomotor symptoms (2) intervention was omega-3 and (3) control was placebo. Only human studies and papers in English were included. Outcome measures included hot flash frequency, intensity, overall score and menopausal rating score change.
PAGE 34 | SUMMER 2022 | THE NATURAL THERAPIST VOL 37 NO. 4 ANTA Member Article Summer 2022
Main Results:
Four clinical trials involving 581 menopausal women ranging from 52.5 to 54.7 years of age were included in this literature review. Three out of four trials concluded that omega-3 reduced vasomotor symptoms in menopausal women more than their placebo. The trial that did not conclude significance used extra virgin olive oil as their placebo which has been shown to have a positive effect on vasomotor symptoms. Three trials measured the effect of omega-3 effect on hot flash frequency, with two eight-week trails providing statistically significant reductions (p=0.05 and p=0.02) whereas one 12-week trial reported no significance (p=0.283).
Conclusions:
Although the majority of trials in this review claimed statistical significance for omega-3 effectiveness in reducing some vasomotor symptoms, analysis of the data provided highlighted areas for improvement. The wide range of omega-3 levels used, the variance in docosahexaenoic acid: eicosapentaenoic acid ratios, the lack of aligned menopause definitions and the lack of homogenous outcome measures, makes direct comparison between trials challenging.
Recommendations:
Further research is needed to determine adequate clinical recommendations of omega-3 supplementation in menopausal women. It is recommended that in each clinical trial a universal definition of menopause is used, that outcome measures are aligned, that sub-groups are assessed separately and that varying levels of omega-3 and ratios of docosahexaenoic acid: eicosapentaenoic acid are tested.
Keywords: post menopause, menopause, vasomotor, hot flash, hot flush, placebo, and omega-3.
Introduction:
The average age of menopause in Australia is 51 years1 and is defined as the cessation of menstruation for 12 months. During menopause transition oestrogen declines and is linked to symptoms such as fatigue, sleep issues, joint pain, anxiety, depression and Vasomotor Symptoms (VMS), such as hot flushes and night sweats2. Hormone Replacement Therapy (HRT) is prescribed for the management of VMS but as awareness of the increased cancer risk related to longterm use has risen, reliance on HRT has reduced3 and health advice limits usage to five years4. Since VMS are still common, present differently amongst women and can occur 10 years post-menopause5, Australian women are seeking natural alternatives6
Asian women experience less VMS than Western women, leading to the hypothesis that isoflavones in soy were a contributing factor7. A clinical trial by Campagnoli et al. (2005)8 tested soy isoflavones against polyunsaturated fatty acids (PUFA), reported supplementation with PUFA was more effective than soy and recommended further research. Research by Abshirini et al. (2019)9 also indicated a diet high in fatty acids was associated with less severe menopausal symptoms. Considering 65% of women feel unprepared for menopause10; that VMS are the most disliked symptom11; that lack of reporting consistency undermines recommendations for treatment12; and that VMS severity is linked to increased risk of cardiovascular disease13 it is important to provide clear recommendations for menopausal women and their practitioners. Previous analysis of the effectiveness of omega-3 (n-3) on VMS have been combined with other lifestyle or dietary alternatives, such as hypnosis, isoflavones, cognitive behavioural therapy and black cohosh14. As a result, no clear analysis has been undertaken to measure n-3 effectiveness on VMS against no other intervention. This review will examine the current literature on the effectiveness on n-3 fatty acids in the reduction of VMS, assessed against placebo only.
Methods:
A literature search was undertaken using Pubmed and CINAHL databases. The MeSH search terms used were “menopause”, “fatty acids”, “omega-3” and “vasomotor system”. Additional free search terms used for population were “perimenopause”, “post menopause” and “climacteric”. Intervention search items were “Eicosapentaenoic acid”, “EPA”, “docosahexaenoic acid”, “DHA”, “polyunsaturated fatty acid”, “PUFA”, “n-3”, “alpha linolenic acid”, “ALA”, “fatty oil” and “fish oil”. Outcome search terms used were “vasomotor”, “hot flush” and “hot flash”.
Inclusion and Exclusion Criteria:
Any clinical trial was included, with limitations of female, human studies and English language. Only trials assessing intervention against placebo were included as a limited number were found, the search expanded to include years 2006 to 2021.
Data Extraction:
Data extracted for analysis from each trial was author, year of publication, study duration, mean age, sample size, inclusion and exclusion criteria, intervention and dosage, placebo, control type, main outcomes measured and trial results.
THE NATURAL THERAPIST VOL 37 NO. 4 | SUMMER 2022 | PAGE 35
ANTA Member Article Summer 2022
Outcome Measures:
The key outcome measures assessed was reduction in hot flash (HF) frequency or intensity between intervention group compared to placebo. Methods used to report these varied across trials and included personal diaries, the Menopause Rating Scale (MRS) and Hot Flash Related Daily Interference Scale (HFDIS).
The Critical Appraisal Skills Program (CASP) checklist was used to determine the validity and quality of the random controlled trials (RCT).
Results:
The combined CINAHL and Pubmed database search (Figure 1.0) located 105 papers once duplicates were removed. From these, 93 records were excluded for no n-3 intervention and five were removed for wrong study design. Seven full text articles were assessed for eligibility, with three removed for (a) no n-3 in supplement, (b) comparison to soy with no placebo
and (c) same data as the Cohen et al. (2014)15 study. Four papers were selected for inclusion were Cohen et al. (2014)15, Freeman et al. (2011)16, Lucas et al. (2009)17, and Purzand et al. (2020)18
Study Design:
Three trials were double-blind, placebo-controlled trials, one for eight weeks17 and two for 12 weeks15,18 The Cohen et al. (2014)15 RCT was a three by two factorial design, from which only data pertaining to VMS was extracted, and included a three-week eligibility run in period. The fourth study16 was a preliminary open trial of eight weeks duration with a one week single-blind placebo lead in. Study participant numbers ranged from 1916 to 25515
Intervention:
All studies used n-3 as their intervention although the volume of total n-3 per day, the docosahexaenoic acid: eicosapentaenoic acid (DPA:EPA) ratio and the number of capsules provided varied (Table 1.0).
Figure 1.0: Preferred Reporting Items for Systematic Reviews and Meta-Analysis Flow Diagram
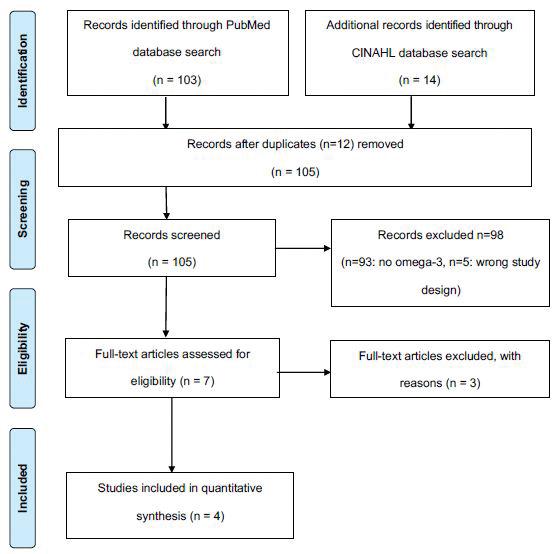
PAGE 36 | SUMMER 2022 | THE NATURAL THERAPIST VOL 37 NO. 4 ANTA Member Article Summer 2022
Table 1.0: Variation In Omega-3 Supplementation Per Day Across Trials
Author and Year Total Omega-3 Total Eicosapentaenoic Acid Total Docosahexaenoic Acid Total Other Number of Capsules
Cohen et al. (2014)14 1.8g 1275mg 300mg
270mg Omega-3 3 x 615mg
Freeman et al. (2011)16 2g 930mg 750mg 320mg Omega-3 2 x 1000mg
Lucas et al. (2009)17 1.5g 1050mg 150mg
300mg Omega-3 3 x 500mg
Purzand et al. (2020)18 1g 180mg 120mg 700mg unknown 1 x 1000mg
Placebo:
One study used a single-blind placebo run in16, two studies used either capsules of olive oil15 or sunflower oil17 and one study did not disclose the contents of their placebo18. Lucas et al. (2009)17 added 0.2% fish oil to support blinding in the placebo group.
Participant Characteristics:
Mean age ranged from 52.516 to 54.715. All trials included females over 40 years old who had undergone menopause. Only one study16 used the Stages of Reproductive Aging Workshop (STRAW) criteria of menopause, a universally agreed definition. All other studies defined menopause as more than 12 months since last menstruation. For women who had undergone a hysterectomy, Cohen et al. (2014)15 included those with a Follicle Stimulating Hormone (FSH) level >20mlU/ml and Lucas et al. (2009)17 included those FSH >40mlU/ml. Purzand et al. (2020)18 only included those who had undergone natural menopause and Freeman et al. (2011)16 did not specify hysterectomy as an inclusion or exclusion.
All studies excluded those using hormonal therapies, with fish allergies or taking fish supplements. Two studies excluded those consuming more than three17 or four15 serves of fish per week. Two studies limited the time from menopause; Purzand et al. (2020)18 excluded women postmenopausal for more than 10 years and Lucas et al. (2009)17 excluded women postmenopausal for more than five years. Purzand et al. (2020)18 and Cohen et al. (2014)15 excluded those who had used herbs, remedies, or pharmaceutical products for VMS symptoms. Cohen et al. (2014)15 also excluded those with a Body Mass Index (BMI)>37 (overweight) or with any unstable medical conditions. Freemen et al. (2011)16 excluded those pregnant, breast feeding or trying to conceive.
Outcome Measures:
Lucas et al. (2009)17 measured HF frequency, HF intensity and overall HF score. Cohen et al. (2014)15 measured HF frequency and VMS bother rating. Freeman et al. (2011)16 measured HF day and night frequency. Purzand et al. (2020)18 measured
Menopause Rating Scale (MRS) score change. Each study measured different variables and reported a range of outcomes varying in significance and relevance (Table 2.0). Three out of four studies reported statistical significance in at least one of the outcomes measured.
Hot Flash Frequency:
After eight weeks, Lucas et al. (2009)17 reported a mean HF frequency reduction in the intervention group of 1.58 (95% Confidence Interval (CI), -2.18 to -0.98) compared to 0.50 in the placebo group (95% CI, -1.20 to 0.20) which was statistically significant (p=0.005). Freeman et al. (2011)16 also reported a significant reduction in HF frequency scores after eight weeks and a mean change of 5.1, with a p-value of 0.02. No CI was reported. Both day (p=0.05) and night (p=0.002) HF frequency showed significance. In comparison, and after 12 weeks, Cohen et al. (2014)15 reported a mean HF reduction in the intervention group of 2.5 (95% CI, 3.0 to 1.9) versus 2.7 in the placebo group (95% CI, 3.3 to 2.2) and p=0.283, showing no significance.
Cohen et al. (2014)15 Clinical Trial: Other than HF frequency, this trial also measured VMS bother rating. The intervention showed a mean reduction of 0.5 (95% CI, -0.6 to -0.4) showing no statistical significance between the two groups (p=0.359).
Lucas et al. (2009)17 Clinical Trial: Other than HF frequency, HF intensity and VMS The Menopause-Specific Quality of Life (MENQOL) score were assessed. In the intervention group HF intensity reduced by 0.33 (95% CI, -0.54 to -0.11) over eight weeks, compared to the placebo group reduction of 0.18 (95% CI, -0.43 to 0.06) which was not statistically significant (p=0.64). VMS MENQOL reduced by 0.82 in the intervention group and 0.44 in the placebo group, also not statistically significant (p=0.31).
Purzand et al. (2020)18 Clinical Trial: MRS score at baseline in the placebo group was 33.48 and after 12 weeks was 34.5, a mean difference (MD)
THE NATURAL THERAPIST VOL 37 NO. 4 | SUMMER 2022 | PAGE 37
Member Article Summer 2022
ANTA
Table 2.0: Research Summary Table
First Author (Year) Study Design and Duration Sample Size and Characteristics Inclusion Criteria
Cohen et al. (2014)14 3 by 2 factorial, double blind, P-C, RCT, 12-weeks plus a 3 week eligbility run in period.
Freeman et al. (2011)16
Preliminary open trial, 8 weeks plus 1-week single blind placebo lead in.
N=355, mean age, 54.7, mean BMI 26.81
Female, 40-61 years old, mp transition, post-mp or had hysterectomy.
VMS>=14 per week, VMS ‘bothersome’ or severe.
N=19, mean age, 52.5.
Lucas et al. (2009)17 Double-blind, P-C, RCT 8 weeks. N=91, mean age, 54.39.
Purzand et al. (2020)18
Double-blind, P-C, RCT, 12 weeks. N=120, mean age, 53.7, mean BMI26.5.
Table Legend:
Exclusion Criteria
BMI>37, used in past month; (a) hormones, (b) hormone contraceptives or (c) VMS pharma., unstable medical conditions, fish allergy, coagulant use, n-3 supps or fish>4 x week.
Female, >=40 years old, peri-mp or mp. Pregnant, breast feeding, trying to conceive, currently taking HT, hormonal contraceptives or n-3 supps., allergy to fish.
Female, 40-55 years old. Post-mp>5 years, fish allergies, fish consumption>3 x week in past 3 months, taking HT, or fish oil supps and anti-coagulant use.
Female, 49-56 years old, <10 years since mp, natural mp, non-smoker, no alcohol consumers.
Contraindication to HT, tx with soy, cod liver oil in past 12 months, allergy cod liver oil, use of herbs or remedies for VMS in past 12 months.
ALA: Alpha-Linolenic Acid; BMI: Body Mass Index; caps: capsules; CI: Confidence Interval; DHA: Docosahexaenoic Acid; EPA: Eicosapentaenoic Acid; ETA: Eicosatetraenoic Acid; HPA: Heneicosapentaenoic Acid; HT: Hormone Therapy; MENQOL: Menopause Specific Quality of Life; mp: menopause; MRS: Menopause Rating Scale; n-3: Omega-3; P-C: Placebo-Controlled; pharma: pharamceuticals; RCT: Randomised Control Trial; SDA: Stearidonic Acid: sf: sunflower; supps: supplements; VMA: Vasomotor Symptoms.
of -1.02 with a p-value of 0.87. The MRS score in the intervention group at baseline was 33.59 and after 12 weeks was 20.63, an MD of -12.96, with a statistically significant p-value of 0.04.
Discussion:
This literature review found significance reported in three out of four trials for the use of n-3 to reduce VMS in postmenopausal women compared to placebo. One trial that did not find significance, Cohen et al. 201415, used Extra Virgin Olive Oil (EVOO) as their placebo. Three out of four trials were doubleblind, placebo controlled RCT with clearly stated objectives and outcome measures. Randomisation was acceptable across all trials but levels of blindness varied. The date in the Cohen et al. (2014)15 paper was
extracted from the MsFLASH studies and randomised using their algorithm. In the Purzand et al. (2020)18 trial, investigator, patients, assessors and examiners were blinded but one researcher was not. In the Lucas et al. (2009)17 all involved were blinded to treatment assignment until the completion of the trial. The fourth trial, Freeman et al. 201116 was a preliminary open trial with the objective of obtaining preliminary data to inform a larger RCT.
Intervention and Placebo:
All four studies had different EPA/DHA ratios in their capsules, ranging from 180mg to 1275mg of EPA and 120mg to 750mg of DHA, making direct comparison between studies difficult and decreasing the opportunity for effective clinical recommendations.
PAGE 38 | SUMMER 2022 | THE NATURAL THERAPIST VOL 37 NO. 4
ANTA Member Article Summer 2022
Intervention/Exposure Control Main Outcomes Results
3 x 615mg caps/day; 1.8g n-3 as 425mg EPA, 100mg DHA & 90mg other omegas (n=177).
3 x caps with olive oil per day (n=178).
Mean HF frequency reduction.
VMS bother 4 or more 12 hour blocks per week.
2 x 1000mg caps/day; 2g n-3 as 930mg EPA; 750mg DHA & 320mg other omegas of DPA, SDA, HPA, ETA & ALA (n=15).
3 x 500mg caps per day. 1.5g per day as 1050mg EPA, 150mg DHA plus 300mg unknown (n=45).
No control after placebo run in N=0.
HF day and night reduction recorded in diaries.
HF reduction: n-3 group=2.5 (95% CI, 3.0, 1.9), placebo group=2.7 (95% CI, 3.3, 2.2), p-value<0.283.
VMS reduction: n-3 group=0.5 (95% CI, 0.6, 0.4), placebo group=0.5 (95% CI, 3.3, 2.2), p-value<0.359.
HF diary reductions: HF means=5.1, p-value<0.02, HF day=2.0, p-value<0.05, & HF night=3.2, p-value<0.002. No CI reported.
3 x 500mg cap per day. 1.5mg of sf oil, with 0.2% fish oil as 18% EPA & 12% DHA (N=46).
HF frequency, HF intensity 7 overall HF score and VMS MENQOL score.
Mean HF frequency reduction: n-3 group=1.58 (95% CI, 2.18, 0.98).
HF intensity reduction: in intervention group=0.33 (95% CI, 0.54, 0.11).
HF score reduction: in intervnetion group=2.23 (95% CI, 3, 12, 1.34). VMS MENQOL score reduced significantly in both groups: n-3, p<0.0001 & placebo p<0.0002.
1 x 1000mg caps per/day. 1g per day as 180mg EPA & 120mg DHA additional 700mg not stated 12 weeks (n=60).
Placebo cap, ingredients not stated (n=60).
MRS score change.
MRS score change: in n-3 group = -12.96 vs placebo = +1.02 (p<0.04).
HF score change: in n-3 group = -1.9 vs placebo = +0.4 (p<0.002). No 95% CI reported.
Additionally, Cohen et al. (2014)15 used olive oil as their placebo and was the only trial that did not show improvement in VMS following intervention. In a 2019 study comparing the effectiveness of n-3 with EVOO in reducing vasomotor symptoms19, n-3 proved more effective, but the data showed that in each outcome measured, there was a reduction in the EVOO group too (Figure A1, see Appendix A in ANTA Member Centre). Based on this study, using EVOO as a placebo may have a beneficial effect on those taking it and could impact the outcome of any trial using it as a placebo. Lucas et al. (2009)17 noted differences in dietary intake of EPA and DHA between the placebo and intervention groups, with the placebo group having significantly lower dietary intake (significance not reported). Since the intervention contained EPA and DHA, starting one group on significantly lower dietary levels and then supplementing another group with more, raises questions about the levels of DHA and EPA needed to gain an outcome. This literature review assessed four trials, across which there was no correlation between ratio of DHA:EPA and a statistically significant outcome.
Limitations:
The main limitation of this literature review is the lack of homogeneity in outcome measures and menopause definition, reducing the opportunity to undertake effective comparative analysis and determine working clinical recommendations. An additional limitation is the lack of statistical detail, limiting the ability of clinicians to accept stated significance as no proof is provided. Purzand et al. (2020)18 used intention to treat analysis but replaced missing data with simple mean imputation for that outcome, increasing the likelihood of underestimating the variability of the outcome. It can be assumed that the CI will have narrowed and potentially increased the precision of the outcome but as no CI was reported in this paper, statistical significance claimed should be questioned. Freeman et al. (2011)16 used nonparametric data analysis techniques, probably due to the small sample size of the trial and because data collection was via nominal variables. Both of these are likely to increase the width of a CI, hence why it may not have been included in the data. Lucas et al. (2009)17 provided detailed statistical data, including CI and p-value.
THE NATURAL THERAPIST VOL 37 NO. 4 | SUMMER 2022 | PAGE 39
ANTA Member Article Summer 2022
Cohen et al. (2014)15 followed Intention-to-Treat (ITT) principles correctly and included all participants enrolled regardless of their adherence to their assigned treatment.
Compliance and Adverse Effects:

Lucas et al. (2009)17 reported a non-significant difference in capsule consumption compliance between groups of 83.7% in the intervention group and 87.2% in the placebo group (p=0.66). Cohen et al. (2014)15 aimed to increase compliance by paying participants at each clinical trial to encourage capsule collection and reported no significant difference between the group, with 82% adherence in the intervention group versus 79% in the placebo group (p=0.44). Lucas et al. (2009)17 reported no major adverse events (AE), other than fish after taste eructation. No significant difference was reported between groups with 27.9% in the intervention group versus 2.6% in the placebo group (p=0.002) despite added fish oil in the placebo to improve blindness.
Cohen et al. (2014)15 reported non-significant numbers of AE among 39% of participants in the intervention group versus 36.9% in the placebo group (p=0.82). Both Purzand et al. (2020)18 and Freeman et al. (2011)16 reported no adverse events.
Duration:
Duration appeared to have no impact on outcome, with one 12-week trial18 and two eight-week trials17,16 both reporting significance while another 12-week trial reported no significant outcomes15
Funding and Bias:
Freeman et al. (2011)16 used GlaxoSmithKline (GSK) supplementations and funding for the study and although GSK had no input to study design, there is potential for some bias. The Purzand et al. (2020)18 study was funded by the Iranian University Medical Department. In the Cohen et al. (2014)15 trial, Nordic Natural provided the supplements and there was no stated role in any other part of the research and the study was funded by the National Institutes of Health. Supplements in the Lucas et al. (2009)17 study were provided by Isodis Natura, a company for whom one of the paper’s authors received speaking and travel expenses, again raising the issue of potential bias.
Clinical Use:
The majority of studies showed significance of n-3 for the management of VMS in menopausal women. The inconsistency of study design, lack of standardised definitions, outcome measures, trial duration, intervention ratios or standard placebos results in lack of clarity on clinical guideline and means more detailed and better designed trials are needed.
Conclusion:
A wide range of n-3 levels and ratios have been used across these trials increasing the difficulty of developing clear clinical recommendations for specific groups of postmenopausal women. It would be beneficial if future trials used different ranges and ratios of DHA:EPA to assess which one is most effective. Any further studies should use the same definition on menopause to ensure study groups can be easily and adequately compared. The STRAW is considered the ‘gold standard’ and provides a clear definition for clinical use20. If women experiencing premature menopause or premature ovarian insufficiency due to cancer treatment or hysterectomy are included in clinical trials, it is recommended that they are identified as separate groups. This will enable findings and clinical recommendations to be applicable for them too due to additional consideration, such as osteoporosis risk, the inability to use HRT after breast cancer and increased cardiovascular disease risk21.
Although all trials used varying amounts of total n-3 ratios of EPA:DHA it can be concluded that n-3 does have a role to play in the management of VMS. The exact levels and which groups it will be more effective for has still to be determined. For references log into your ANTA Member Centre > The Natural Therapist > Journal Articles
ANTA Member Article Summer 2022
PAGE 40 | SUMMER 2022 | THE NATURAL THERAPIST VOL 37 NO. 4






THE NATURAL THERAPIST VOL 37 NO. 4 | SUMMER 2022 | PAGE 41 eaglenaturalhealth.com.au FOR PRACTITIONER DISPENSING ONLY. ALWAYS READ THE LABEL AND FOLLOW THE DIRECTIONS FOR USE. Order now at MyIntegria.com TRESOS B PROFESSIONAL + A comprehensive foundational nutritional Formulated to support energy production, healthy stress response, cognitive function and immune system function. Vitamins, minerals, metabolically active B vitamins, choline and amino acids; glutamine, carnitine, glycine and taurine. BioMedica Nutraceuticals P 1300 884 702 | www.biomedica.com.au y Highly concentrated extract of Curcuma longa with over 500mg of active constituent per capsule y Contains clinically studied Curcumin C3 Complex® y Curcumin C3 Complex® is a unique turmeric concentrate produced under strictly controlled conditions CurcuForte® High quality Curcumin extract standardised to 95% curcuminoids
Research Assignment : Exploring Four Health Issues and How the Role of Massage Can Help

Introduction:
The following article will explore four different health issues including Depression and Anxiety, Attention Deficit Hyperactivity Disorder, Rheumatoid Arthritis, and Fibromyalgia. Each section will cover one of the previously mentioned issues in depth by providing a definition and the variations, the causes or predisposing factors, how massage can help and a possible referral.
Depression and Anxiety: Definition and Variations:
Depression is a mental illness and Parekh (2017)1 states that, “Depression (major depressive disorder) is a common and serious medical illness that negatively affects how you feel, the way you think and how you act. Fortunately, it is also treatable. Depression
causes feelings of sadness and/or a loss of interest in activities once enjoyed. It can lead to a variety of emotional and physical problems and can decrease a person’s ability to function at work and at home”.
Anxiety is defined by Parekh (2017)2 as follows: “Anxiety is a normal reaction to stress and can be beneficial in some situations. It can alert us to dangers and help us prepare and pay attention. Anxiety disorders differ from normal feelings of nervousness or anxiousness and involve excessive fear or anxiety. Anxiety disorders are the most common of mental disorders and affect nearly 30 percent of adults at some point in their lives. But anxiety disorders are treatable, and a number of effective treatments are available. Treatment helps most people lead normal productive lives”.
PAGE 42 | SUMMER 2022 | THE NATURAL THERAPIST VOL 37 NO. 4 ANTA Member Article Summer 2022
Lynalee Strickland ANTA Member Diploma of Remedial Massage Diploma of Clinical Aromatherapy Diploma of Reflexology
There are different types of depression including situational, family of origin (depression related to family of origin issues), moderate, severe, chronic, seasonal affective disorder (SAD) and post-natal3 The symptoms of depression can include feelings of sadness and unhappiness, changes in appetite (increased or reduced), anger, irritability, sleep disturbances, loss of interest in activities that were previously considered enjoyable, cognitive problems, physical pain (e.g. headaches, back pain), low selfesteem or feelings of worthlessness, and suicidal thoughts or tendencies.
The signs and symptoms of anxiety can include panic or panic attack, fear, uneasiness, nausea, heart palpitations, shortness of breath, the inability to remain calm, dry mouth, sweaty palms, excessive worry, obsessive thinking, and paranoia. According to the Beyond Blue (2017)4 website, anxiety is the most diagnosed mental illness and one in four people are likely to experience anxiety at some point during their life.
Causes or Predisposing Factors:
Depression has been linked with changes in brain chemistry or can result in changes to brain chemistry. Prolonged depression can result in imbalances in
the neurotransmitters serotonin, dopamine and norepinephrine5,6. This imbalance causes changes to brain patterns and thinking. There are various causes for depression, including illness, lack of sunlight, drugs, certain medications, and genetics. Depression also can result from environmental factors such as chemical exposure or exposure to toxins and from nutritional deficiencies.
Anxiety can be caused by fear, and prolonged stress and results in increased cortisol. Cortisol is the hormone responsible for the fight or flight response in humans. Prolonged high levels of cortisol can be a contributing factor to ill health and heart disease.
The Role of Massage in Relation to Depression and Anxiety:
Depression can be effectively treated using psychotherapy and/or an integrated approach to healthcare including diet/nutrition, herbal supplements (if deemed necessary), exercise and alternative therapies such as massage therapy, aromatherapy, and reflexology. The approach taken will be dependent on the severity of the condition.

Studies have shown that massage therapy can be a valuable component in the treatment regime for someone suffering from depression and from anxiety. The deep relaxation state that can be achieved with massage therapy can lead to an increased sense of well-being and self-esteem in the person. It can also provide temporary relief from the emotional heaviness that the person is experiencing in their day-to-day life. Massage therapy has been shown to be effective in lowering cortisol levels (responsible for fight or flight response) and therefore, would have significant benefits for people with anxiety7.
Contraindications to receiving massage therapy for someone suffering depression or anxiety include situations in which the client is intoxicated or under the influence of drugs, or if they are mentally unstable and pose a threat to the therapist. People suffering from severe depression are extremely unlikely to make an appointment for massage therapy and research evidence shows that medication and psychotherapy are the best treatments for people in this group8
A review conducted by Jorm et al. (2002)8 for The Medical Journal of Australia of research available into a range of complementary therapies and the benefits for people with depression concluded that research conducted so far indicates that the benefits of massage therapy looks promising but that there is not enough data to provide evidence of the benefits of massage therapy for people suffering depression.
ANTA Member Article Summer 2022 THE NATURAL THERAPIST VOL 37 NO. 4 | SUMMER 2022 | PAGE 43
A double-blind study conducted by researchers for Depression and Anxiety and funded by the National Centre for Complementary and Alternative Medicine tested three different methods for assisting people with Generalised Anxiety Disorder (GAD) and included Massage Therapy, thermotherapy and relaxing room therapy9. The study included a total of 68 participants with 22 or 23 in each of the groups and each was provided with an hour-long treatment for ten treatments over a 12 week period. It was anticipated by the researchers that the massage therapy group would have the greatest gains, however, the results proved that all three types of treatment were almost equally effective in reducing the symptoms of GAD, against a baseline Hamilton Anxiety Rating Scale (HARS) questionnaire9. The study followed up with the subjects of the study 12 weeks and 24 weeks after the conclusion of the trial and found that the gains made by the recipients were still effective at the 24week check following the conclusion of the study.
Massage therapy is not a stand-alone treatment for people suffering from more severe forms of anxiety and depression but can be very valuable as one of the treatment protocols for people suffering from these conditions. Many massage therapists promote the
benefits of massage therapy and rightly so, but not conclusively, from the limited amount of research data available. It is evident that more rigorous studies are required for the benefit of the complementary and alternative therapies community.
Referral:
Good history taking is essential. Being aware of the medications available for people suffering depression and/or anxiety is also important as a person may not be willing to disclose that they are suffering depression or anxiety. While there is so much information available now, some people still feel that there is a stigma associated with suffering from depression. Observation of the person prior, during and after the treatment is also important.
A client presenting with clinical depression or anxiety will usually have regular contact with their General Practitioner (GP). It would be worth contacting the client’s GP (with the client’s approval) to advise that the person is receiving massage therapy treatments. Medication dosage may need to be adjusted if the benefits of massage cause changes to brain chemical levels. If a person presents with the symptoms of depression or anxiety but have not been diagnosed,

ANTA Member Article Summer 2022
PAGE 44 | SUMMER 2022 | THE NATURAL THERAPIST VOL 37 NO. 4
then they should be referred to their GP for assessment.
Attention Deficit Hyperactivity Disorder: Definition and Variations:
Attention Deficit Hyperactivity Disorder, also known as ADHD, is a chronic behavioural condition characterised by inattention, impulsive behaviour, and hyperactivity (or over activity). ADHD falls along a spectrum and can be mild to severe. In adults the presentation is difficulty with attention, inhibition, and excess activity level with all having problems with self-control10. To be diagnosed with ADHD certain criteria outlined in the American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders (DSM) must be met. The DSM is now in its 5th edition and is referred to as DSM-5. For a person to be diagnosed with ADHD their symptoms must be apparent for at least six months and have at least six of the symptoms for children up to 16 years of age and at least five of the symptoms for people of 16 years of age or older, early onset of symptoms (prior to 12 years of age) even if diagnosed later in life, evidence that the symptoms have impacted the person’s ability to function, symptoms are evident in more than one setting (e.g. home, school, work), and symptoms are not due to another mental disorder11
The symptoms of ADHD relating to inattention include the following11:
• Difficulty following instructions
• Careless mistakes
• Fails to listen when spoken to directly
• Forgetful in everyday tasks
• Difficulty in organising tasks and activities
• Often loses things
• Avoids tasks requiring sustained mental effort
• Easily distracted
• Distracted by extraneous stimuli.
The symptoms of ADHD relating to hyperactivity include11:
• Runs or climbs when such activity is inappropriate
• Leaves seat when remaining in seat is expected
• Fidgets and squirms in seat
• Had difficulty playing quietly
• Always moving or going
• Has difficulty waiting their turn
• Interrupts or intrudes on others
• Talks excessively
• Blurts out answers before questions are completed.
A diagnosis of a combined presentation of ADHD, also known as ADHD-C is made when there are six or more symptoms present (for more than six months) from
each list given above (inattention and hyperactivity). In the case of six of the criteria for inattention being met, but less than six are met, then the condition is considered as a predominantly inattentive presentation, and it is referred to as ADHD-PI11. In cases where the symptoms of hyperactivity do not appear, the person may be diagnosed with Attention Deficit Disorder (ADD).
It is important to consider a differential diagnosis of the condition because there are other conditions or psychological disorders that have many of the same symptoms of ADHD. In addition, ADHD is often present (or co-morbid) with other psychological problems such as disruptive disorders, anxiety disorders, mood disorders and learning disabilities11. So, it is important to determine whether ADHD is present on its own or with another condition, or whether the symptoms presenting is for another condition and ADHD is not present. It is possible for a person to be mis-diagnosed with ADHD. For example, Oppositional Defiance Disorder (ODD), or Learning Disabilities (LD) may be the cause of presenting symptoms, not ADHD.
ADHD cannot be cured. ADHD is a lifelong condition; however, it can be managed.
Causes or Predisposing Factors: Research show that ADHD is caused by neurological or genetic factors10. It is not due to failure of the family in how they have raised their children. In the cases where ADHD is not due to genetic factors, biohazards (toxins and infections) during early development, and brain injury is implicated. Neurological injury or disrupted brain development can result from brain trauma, lead poisoning, and maternal use of alcohol, tobacco or drugs during pregnancy10.
Two thirds of people with ADHD have another psychiatric disorder11.
The Role of Massage in Relation to Attention Deficit Hyperactivity Disorder:
There is no cure for ADHD, however, the condition can be successfully managed. Research shows that using a combination of psychological and medical therapies seems to be most effective11. Another valuable tool in the management of ADHD has been found to be education on the condition. Educating family and friends who love and care about the person, and the person themselves has been found to have positive effects on dealing with the symptoms and accommodating characteristics of the person with ADHD. It is much easier to live with a condition
THE NATURAL THERAPIST VOL 37 NO. 4 | SUMMER 2022 | PAGE 45
ANTA Member Article Summer 2022
when someone knows what to expect and realises that it is a part of their condition and not something they are able to control. Other people are also far more accepting of the person if they have a good understanding of the person’s condition.
Evidence based research has shown that the most successful treatments for ADHD include a combination of medication and behaviour management and shows that discontinuation of treatment results in return of the symptoms of ADHD11. According to Phelan (2017)11 there is insufficient research and only anecdotal information indicating any benefits from alternative therapies such as massage therapy.
A pilot study conducted by Maddigan et al. (2003)12 for the Canadian Child and Adolescent Psychiatry Review compared three groups: (1) massage therapy, (2) exercise therapy, and (3) control group. The parents of the participants in the massage therapy group reported that their children exhibited better anger control, improvements in mood, better focus on tasks at school, more restful sleep, and two of the participants reported improvements in social functioning12. The limitations of this study were that there was an extremely small sample size (three participants in each of the groups) and therefore, the results lack clinical significance data.
Massage therapists promote massage therapy as improving focus and attention and providing benefits of relaxation. Massage therapy has been shown to stimulate the parasympathetic nervous system (with moves such as effleurage) and therefore is a benefit for people with ADHD as it would assist in reducing symptoms of hyperactivity13. Massage therapy has great potential as an integrated approach to the treatment of a person with ADHD and may increase the efficacy of evidence-based treatments14

Medications have side effects and more parents of children with ADHD and adults with ADHD are looking for alternative treatments15. Whilst medication and behaviour therapy have been scientifically proven to be the most effective treatment for reducing the symptoms of ADHD, they do not provide a cure and on cessation of treatment symptoms return. More research into alternative therapies is needed as well as better community education.
Referral: People who have been formally diagnosed with ADHD will usually be in regular contact with their GP, paediatrician, psychologist, or psychiatrist. It is a good idea to network with the client’s healthcare providers if it is possible with permission of the client. Other healthcare providers are typically interested in learning more about the benefits of massage therapy and how it can be incorporated in the treatment plan for their
ANTA Member Article Summer 2022
PAGE 46 | SUMMER 2022 | THE NATURAL THERAPIST VOL 37 NO. 4
ADHD clients10
There are opportunities for massage therapists to promote treatment, and to research and study the benefits of massage for sufferers of ADHD. It is also important to liaise with other healthcare professionals in the provision of the integrated management of ADHD.
Causes or Predisposing Factors:
Rheumatoid
Arthritis: Definition and Variations:
Rheumatoid Arthritis is an auto-immune disease which causes inflammation of the connective tissue in the body5. Symptoms can include pain, fatigue, and stiffness in the morning after waking, depression and low-grade fever. There is a symmetrical presentation of the affected joints (right and left sides of the body) except on occasion during the early stages of the disease. Other conditions co-morbid with Rheumatoid Arthritis include cardiopulmonary disease (artherosclerosis is a common manifestation), eye disease, Sjogren’s Syndrome, rheumatoid vasculitis, neurologic disease, and less commonly Felty’s Syndrome16.
It is difficult to diagnose Rheumatoid Arthritis and several tests must be conducted including laboratory tests (including complete blood count (CBC), comprehensive metabolic panel (CMP), Rheumatoid Factor (RF), antibodies to citrullinated peptides including anti-CCP, erythrocyte sedimentation rates (ESR), and C-reactive protein (CRP)), radiography and magentic resonance imaging (MRI). It is necessary to take a good client history including all symptoms, and the length of time that symptoms have been apparent, to rule out other diseases with similar presentations. Whilst Rheumatoid Factor (RF) is present in 70% to 80% of patients with Rheumatoid Arthritis, RF is not specific to Rheumatoid Arthritis, and it also occurs in other inflammatory and autoimmune conditions including Sjogren’s Syndrome, chronic kidney or liver disease, endocarditis, tuberculosis, hepatitis C, myeloma and other conditions18
Osteoarthritis has a similar presentation to Rheumatoid Arthritis but rarely has a symmetrical presentation and involves bony growths. The comparison between the two when palpated is that Osteoarthritis had a hard, bony feeling associated with swelling at the joints, but Rheumatoid Arthritis has a doughy, spongy feel and can feel warm or hot to the touch.
The specific cause or causes of Rheumatoid Arthritis is unknown. Research into Rheumatoid Arthritis is ongoing. It appears that there may be a genetic component, however, this is not established. There does appear to be a higher incidence of Rheumatoid Arthritis among people who smoke cigarettes. The incidence of Rheumatoid Arthritis is two to three times more common in women than men in the USA16 Researchers at John Hopkins Arthritis Centre suggests that periodontal infection may be a disease initiation factor in some Rheumatoid Arthritis patients, but more research is needed19.
The Role of Massage in Relation to Rheumatoid Arthritis:
A client intake form for all new clients is necessary and it is essential that a good medical history is taken to ensure that treatment is not provided when there are conditions contraindicated for treatment. Rheumatoid Arthritis is an inflammatory condition and therefore, it is contraindicated for massage therapy. In cases where a client presents with symptoms of Rheumatoid Arthritis (and does not have a diagnosis) and joint pain is accompanied by heat (an indication of inflammation) it is advisable for the massage therapist to refer the client to their GP prior to commencement of massage therapy treatments20 .
The main treatments for Rheumatoid Arthritis include medications, psychotherapy (often part of treatment regime for people with a chronic illness), and exercise. Exercise is important for the person to reduce the possibility of muscular atrophy and to maintain use of joints21. However, exercise should be gentle and not have an impact on joints. Therefore, exercises such as swimming, water aerobics, yoga or tai chi would be most beneficial.
The three main types of medications prescribed for people with Rheumatoid Arthritis includes Non-Steroidal Anti-Inflammatory Drugs (NSAIDS), corticosteroids and disease modifying anti-rheumatic drugs (DMARDs). Whilst NSAIDS and corticosteroids help with reducing pain and inflammation in the joints of the patient they do not alter the progression of the disease. DMARDs have been found effective in slowing the progression of the disease and if included in the treatment during the early stages has been found to provide the most benefits to treatment21. However, as with all medications there are side effects and renal and liver function must be monitored on a regular basis. This type of treatment is not recommended for patients with pre-existing liver conditions21
THE NATURAL THERAPIST VOL 37 NO. 4 | SUMMER 2022 | PAGE 47
ANTA Member Article Summer 2022
Some of the websites viewed in relation to massage therapy and Rheumatoid Arthritis suggest that massage therapy is beneficial for people suffering Rheumatoid Arthritis periods of remission or between flare-ups22. A study was conducted by a certified massage therapist, Robin Anderson (2007)23, of the benefits of massage therapy for a 39-yearold woman recently diagnosed with Rheumatoid Arthritis. According to the article, the woman was provided with an initial baseline assessment and client interview, followed by seven weekly treatment sessions at seven-day intervals for a treatment session length of 1 to 1.5 hours. The woman had recently been prescribed and was taking the drug, Methotrexate (a DMARD). The joints involved were the right shoulder and second (index) finger joints. Additionally, there was also swelling in the knees and feet (with the right side more affected). Following the treatments, a comparison of the right shoulder was made with the left shoulder to determine if any gains were apparent. The conclusion of the study by Anderson was: “Therapeutic massage treatments, while able to achieve qualitative muscle
release in an affected joint region, can also positively affect the physiological systems of a patient with Rheumatoid Arthritis and help to alleviate and prolong the deteriorating effects of the disease” 23 While the participate of the study noticed a reduction in symptoms of pain and discomfort, this could equally be attributed to the medications since the corticosteroid will provide pain relief shortly after commencement of taking the medication and Methotrexate takes between four and eight weeks before the effects are noticed21. In addition, it seems unreasonable after eight weeks to state that massage can, ‘help to alleviate and prolong the deteriorating effects of the disease’ 23. Because massage therapy may cause inflammation in any inflammatory condition or disease, such as Rheumatoid Arthritis, it is contraindicated for massage.

Referral:
A client who books for massage therapy, then reveals on the client intake form that they have Rheumatoid Arthritis should not receive a massage treatment. Massage may be suitable during periods of remission.
ANTA Member Article Summer 2022
PAGE 48 | SUMMER 2022 | THE NATURAL THERAPIST VOL 37 NO. 4
Reiki may be an option or another alternative therapy approach which is not contraindicated24. If the person’s suffering has brought them to the massage therapist for relief then the therapist may consider referring them to their regular GP who can assist them with other options, a Nutritionist or Naturopath to assist in dietary recommendations to support their condition, or recommend alternative therapies such as Reiki, Bowen Therapy, Kinesiology, Acupuncture, meditation, or a gentle form or exercise such as water aerobics.
Fibromyalgia: Definition and Variations:
Fibromyalgia, also known as Fibromyalgia Syndrome (FMS) is a collection of conditions and symptoms. Not everyone with FMS will have exactly the same symptoms. Symptoms include muscular pain, fatigue, headaches, depression, disturbed sleep, anxiety, dry eyes and/or mouth, aching and stiffness in the morning. Sufferers sometimes also present with irritable bowel syndrome (IBS), Raynaud’s phenomenon, rheumatoid arthritis and osteoarthritis25 Fibromyalgia was formerly known as Fibrositis, but there was never any evidence of inflammation of the muscles or tissues, and it was found that anti-inflammatories did not provide sufferers of this condition any relief 25. Therefore, the name was changed to Fibromyalgia (which has the meaning of connective tissue and muscle pain) providing a much better description of the disease. People with this condition often suffer from depression, but it is now believed that this is a result of the physical pain they are suffering25. Chronic pain often leads to depression.
There are other conditions with similar symptoms to Fibromyalgia. Many of the symptoms for Fibromyalgia are identical to those for Chronic Fatigue Syndrome/ Myalgic Encephalomyelitis (CFS/ME), however, there is a greater incidence of fever and swollen glands in the group with CFS/ME25. Because of this Fibromyalgia sufferers are sometimes mis-diagnosed with CFS/ME.
A differential diagnosis is difficult because of the complexity of the syndrome and the range of symptoms. Ingraham (2017)26 suggests that some of the other conditions with similar symptoms to Fibromyalgia include the early stages of Ankylosing Spondylitis and Lupus, Vitamin D and Vitamin B12 deficiency, Myofascial Pain Syndrome, mood disorders, Lyme Disease, and Celiac Disease26
Causes or Predisposing Factors:
Fibromyalgia occurs when the body experiences overload due to stress, poor diet, etc. and reaches
a point where there is difficulty in maintaining homeostasis25. According to work carried out by Dr Jessop in the 1980’s and 1990’s, there appears to be a significant link between people who suffer from bowel, bladder and menstrual problems and those who suffer allergies in the development of the disease. In addition to this, approximately 75% of people presenting to Dr Jessop with the condition were women25. In the 1990’s it was found that patients with chemical sensitivities sent for brain scans had the same brain patterns as people with CFS/ME and FMS. The brain scans revealed that there was a reduction in blood flow to and through parts of the brain dealing with pain regulating functions (the caudate nuclei region) and memory and concentration25.
The Role of Massage in Relation to Fibromyalgia:
Studies have shown that there are benefits in an integrated healthcare approach in managing the symptoms associated with Fibromyalgia. Massage Therapists in the United States of America. have found that myofascial release has the most positive effects when working with this group of people but concede that, “most styles of massage therapy consistently improved the quality of life of Fibromyalgia patients” 27
Care should be taken, and trust developed when working with a client with Fibromyalgia as they can have extreme pain and sensitivity to touch28,29.
Referral:
In the instance where a client presents with symptoms of chronic widespread pain it is important to refer them to their GP for assessment. In addition, for a person diagnosed with Fibromyalgia it would be prudent (with the client’s permission) to discuss the proposed treatment plan with the client’s GP and take note of any effects observed or described by the client following the treatment. If improvements are noted, the GP may be interested and may consider similar recommendations of massage therapy for other patients suffering from Fibromyalgia. There is a growing acceptance among allied health professionals of alternative therapies as providing benefits in an integrated treatment approach. It is important for massage therapists to be proactive in making connections with GP’s and other allied health practitioners.
THE NATURAL THERAPIST VOL 37 NO. 4 | SUMMER 2022 | PAGE 49 ANTA Member Article Summer 2022
For references log into your ANTA Member Centre > The Natural Therapist > Journal Articles
•









PAGE 50 | SUMMER 2022 | THE NATURAL THERAPIST VOL 37 NO. 4 Vaginal Care D e r m a C a r e Practitioner NEW Enhances Mental Alertness & Attention Span NeurAlert 30 & 60 Chocolate Chewable Tablets
Therapeutic dose in one chewable tablet of enXtraTM – proprietary extract of Alpinia galanga (galangal).
NeurAlert is a chewable caffeine-free, enXtraTM, a proprietary extract of Alpinia galanga (galangal). enXtraTM has been shown to improve mental alertness, enhance mental endurance and stamina and help increase attention span. •
herbal supplement that improves focus and attention.
• Fast-acting
Vegan and
bioclinicnaturals.com.au Always read the label. Follow the directions for use.
non-GMO.
Sage Advice...
Salvia officinalis (Sage) is traditionally used in herbal medicine to maintain and enhance memory and mental recall.
Sage is also traditionally used in Herbal Medicine as a tonic and can aid in the maintenance of general well-being.
Follow some sage advice… ...choose Sibelius Sage
Available exclusively in Go Vita stores Australia-wide.
Use only as directed. Always read the label.


Australian Natural Therapists Association For more information call 1800 817 577 or visit www.anta.com.au It’s your choice... Naturally ANTA is the only Association supporting statutory registration for Natural Therapists Free Student Membership with the leading multi-disciplinary professional Association in Australia ANTA’s FREE Student Membership includes • Free online access to industry standard professional databases for research, treatment and interaction guides: - Scientific resource IMgateway - eMIMs • Annual Student and Bursary awards • Free admission to ANTA National Seminars • Receive industry and Association news via ANTA eNews and quarterly journal ‘The Natural Therapist’ • Ability to enter Monthly Book Giveaways • Access to personalised Member Centre • Significant partner discounts including professional indemnity insurance, educational resources and more • Access to Code of Ethics, Policies and Guidelines on Professional Practice, Clinical Standards • Links to Health Fund and Government policies, information and regulation updates • Reduced membership fees for graduates ANTA offers over $12,000 in student bursary and graduate awards every year! Join today at www.anta.com.au or scan the QR code

