


The latest condition-specific probiotic from Activated Probiotics
Taking the specific combination of probiotic strains in Biome Cholesterol™ Probiotic once a day for 12 weeks with no other cholesterol-lowering medications has been found to significantly reduce low density lipoprotein cholesterol by up to 20%, total cholesterol by up to 19% and triglycerides by 16%, while also increasing high-density lipoprotein cholesterol by 8%.¹
It has also been found to significantly lower the number disktotal apolipoprotein B-containing particles– all factors associated with an increased risk of atherosclerosis.²
The liver uses cholesterol to produce bile salts, which are stored in the gallbladder and then released into the small intestine in order to facilitate fat absorption. 95% of all bile salts are reabsorbed in the intestinal tract and continue to be reused.
The specific combination of probiotic strains in Biome Cholesterol™ Probiotic produce a significant amount of bile salt hydrolase enzymes, which when taken alongside food allows them to deconjugate bile salts, hindering their reabsorption and increasing their excretion.³
Consequently, the liver uses up more cholesterol to replace the bile salts that have been lost and pulls this cholesterol from low density lipoproteins (LDL) circulating in the blood.
Available through:





and clinical characteristics influencing the effects of a cholesterol lowering probiotic. Annals of Nutrition & Metabolism, 74(S1), 6.
2. Padro, T., Santisteban, V., Huedo, P., Puntes, M., Aguiló, M., EspadalerMazo, J., & Badimon, L. (2024). Lactiplantibacillus plantarum strains KABP011, KABP012, and KABP013 modulate bile acids and cholesterol metabolism in humans. Cardiovascular Research, 00, 1–15.
3. Bosch, M. et al. Lactobacillus plantarum CECT 7527, 7528 and 7529: Probiotic candidates to reduce cholesterol levels. J. Sci. Food Agric. 94, 803–809 (2014)
AUST L 445776 Always read the label. Follow the directions for use.
Supports collagen formation; tendon health; healthy ligaments & joint cartilage production
Silicon – Mesoporosil®
Supports joint mobility & flexibility; Relieves symptoms of mild arthritis & mild joint pain
Eggshell membrane powder – NEM®
Maintains bone strength, mass & integrity
Calcium
Supports energy production & helps maintain healthy body tissues
Phosphorus





08. CEO & President Report 09. Branch Chair Updates
20. Round 1 ANTA Graduate Award Winners 2024
24. Sleep and Natural Therapies
Esther Parker presents a discussion on managing sleep issues and insomnia.
30. How TCM Can Support Both Women and Health Practitioners Understand the Transition of Perimenopause
From a TCM perspective, the aging process in women unfolds in sevenyear cycles, writes Keri Krieger.
34. Addressing Emotional Triggers for Enhanced Weight Management Outcomes
Michelle McCosker explores the role of emotional freedom techniques (EFT).
40. Femoroacetabular Impingement Syndrome
Bodine Ledden navigates physical assessment.
48. Little number meditations for point selection… A ready reckoner of sorts
Numbers are an integral part of human thinking, writes Kaitlin Edin.

The Natural Therapist is published by the Australian Natural Therapists Association (ANTA) for natural therapy practitioners. The opinions and views expressed by the contributors and advertisers are not necessarily the opinions and views of ANTA. Every effort is taken to ensure accuracy and ANTA accepts no responsibility for omissions, errors or inaccuracies. ANTA relies on contributors and advertisers to make sure material provided for The Natural Therapist complies with the Australian Consumer Law under the Competition and Consumer Act 2010. ANTA accepts no responsibility for breaches of the Australian Consumer Law by contributors or advertisers. Material in The Natural Therapist is subject to copyright and may not be reproduced in any form without the permission of ANTA and its contributors.
Shaun Brewster
• National President
• Director of ANTA
• National Myotherapy Branch Chair
• ANTAB Chair
• ANRANT Committee Member
• Health Fund Chair
Warren Maginn
• National Vice-President
• Director of ANTA
• National Nutrition Branch Chair
• TGA Chair
• Ethics Panel Chair
• ANTAB Committee Member
• ANRANT Committee Member
Ananda Mahony
• National Treasurer
• Director of ANTA
• National Naturopathy Branch Chair
Kaitlin Edin
• Director of ANTA
• National Acupuncture Branch Chair
• ANTAB Committee Member
• ANRANT Committee Member
Isaac Enbom
• Director of ANTA
• National Remedial Therapy Branch Chair
• ANTAB Committee Member
• ANRANT Committee Member
Mark Shoring
• Director of ANTA
• National Multi-Modality Branch Chair
• ANTAB Committee Member
• ANRANT Committee Member
Tino D’Angelo
• Director of ANTA
• National Chinese Herbal Medicine Branch Chair
Neerja Ahuja
• Director of ANTA
• National Ayurveda Branch Chair
David Liesegang
• Executive Officer
• Company Secretary
• Business Plan Chair
• ANRANT Chair
Circulation Enquiries 1800 817 577
Editorial & Advertising Enquiries thenaturaltherapist@anta.com.au
Membership Enquiries info@anta.com.au
ANTA NATIONAL ADMINISTRATION OFFICE
T: 1800 817 577
F: (07) 5409 8200 E: info@anta.com.au
P: PO BOX 657 MAROOCHYDORE QLD 4558 W: www.anta.com.au
ANTA have now aligned all our memberships across all modalities to renew on the 31st of March. This is effective immediately and all members that were due for renewal on the 31 December 2024 have been given an additional 3 months Free of Charge. This means that the next ANTA Membership Renewal Date for all ANTA members will be 31st March 2025. The ANTA Administration team will send out renewal reminders closer to this date.
Continued Professional Development (CPD) it is important for practitioners to regularly update their clinical skills and professional knowledge. As we enter the final few months of 2024, the timeframe for submitting their annual CPD hours is approaching.
Not only is CPD a requirement for retaining ANTA membership, Private Health Funds also require practitioners to complete annual CPD
(if applicable). Note that Private Health Funds often carry out audits of member records to ensure 20 hours of CPD have been completed.
ANTA provides members with easy-to-use online facilities so you can lodge your CPD hours in your own personal and permanent CPD online record fully maintained within the ANTA Member Centre. Please have your CPD hours submitted before 31st December 2024.
Season’s Greetings from the ANTA Administration Team. Yes, we know we are getting in a little early but here at ANTA, but we pride ourselves on being efficient. After working determinedly this year to bring our members the best possible service, we are having a Christmas Holiday. The ANTA office will be closed from Thursday 19 December 2024 at 4.30pm and will reopen on Monday 6 January 2025 at 8.45am. On behalf of the entire ANTA Team, we would like to wish you a very Merry Christmas and Happy New Year.




As we reflect on the 2024 year and our achievements, we are first and foremost grateful for the unwavering dedication of our members, as well as proud of some important steps ANTA has made this year in advancing the natural therapy landscape in Australia.
This has been a testament to our collective commitment to excellence, high standards, innovation and our relentless pursuit of enhancing our members’ professional standing.
The ANTA National Council and Executive have worked hand-in-hand to commence crafting a visionary roadmap for our association’s future. Through our industry standing within the broader healthcare regulatory landscape, we have pursued various avenues to amplify our members’ voices and advocate more effectively on critical industry issues. This includes elevating the professional standing and recognition of the multiple natural therapy and traditional medicine modalities that ANTA represents in several pivotal areas, which primarily included:
1. Raising educational standards
2. Enhancing recognition for our members
3. Strengthening protection for professional titles under which members practice
ANTA has been at the forefront of industry efforts to entrench the standing of our members’ professions within the Australian healthcare sector. Our National Council Directors and volunteer members have made significant contributions to curriculum development committees, industry oversight groups, and governmental meetings, resulting in tangible improvements to professional outcomes and training standards.
As a pre-eminent advocate for natural therapies throughout Australia, ANTA has continued to foster our relationships with registered training organisations, all with the aim of maintaining high educational standards, whilst being mindful of the evolving needs of natural therapy students and graduates across our multiple modalities.
In our quest to provide an unparalleled member engagement and experience, we have invested heavily in expert capability and in modernising our digital infrastructure. For example our revamped website, dynamic social media presence and streamlined communication channels are now ensuring that you remain more informed and connected with the latest developments in our industry and related ecosystems.


Under the guidance of ANTA’s newly-appointed CEO, David Liesegang, our National Administration Office team has also continued to deliver outstanding support to our members. Their expertise and dedication in professionally addressing member enquiries and supporting their challenges has been a major factor in high levels of ANTA member satisfaction and retention.
We are pleased to have delivered four successful ANTA CPD Seminars across Australia, offering our members complimentary access to high-calibre, professional development opportunities led by renowned experts across all ANTA modalities.
ANTA also continued to foster strategic alliances with other aligned industry bodies and associations, working towards elevating standards of training and care for the broader community, while promoting a cohesive and collaborative regulatory environment.
As a registered company limited by liability, ANTA is governed by a robust constitution and comprehensive policies. Our members continue to benefit from the guidance of an experienced Board of Directors, comprised of modality matter experts and industry leaders in their own right, some of whom who also voluntarily and expertly led multiple branches of our Association.
The ANTA Directors all take great pride and care in the oversight and governance of ANTA’s financial affairs, and always with a view to building a solid, sustainable financial foundation for the benefit and long-term future of ANTA’s practitioner members.
As we approach 2025 - a year in which plan to celebrate ANTA’s 70th anniversary - we look forward to unveiling some innovative initiatives aimed at elevating member engagement, enhancing your professional growth and fostering your industry standing.
Together, we stand poised to set and shape a vibrant future for ANTA members and our Association, leading the way for our natural therapy professions to thrive and prosper. We extend our heartfelt gratitude for your continued trust and support.
Shaun Brewster - ANTA President David Liesegang - ANTA CEO
The last few years have been highly eventful in the healthcare landscape in Australia. 2024 has been no exception to continuing this trend, bringing ever evolving conditions facing healthcare practitioners.
ANTA has continued to expand and adapt through these changes, including ANTA’s newly appointed CEO David Liesegang becoming acquainted with the many pertinent matters ahead of us.
The following matters have been particularly relevant to ANTA’s Clinical Nutrition members over the past year.
As has been highlighted in previous years, the terms ‘nutrition’ and ‘nutritionist’ constitute very broad terms that often mean different things to many, especially depending on their context.
Unfortunately, this lack of clarity appears to have continued to expand rather than contract in recent times, with increasing confusion and conjecture arising about what various nutrition related terms and titles mean.
ANTA has been working hard to help clarify and consolidate some clearer and more accurate understanding in both professional and public arenas, as well as with government, health funds and insurers.
To ensure maximum accuracy and clarity of terms can be maintained for nutrition professionals in Australia, ANTA has submitted a number of formal objections to certain trademarks sought by dietitian representative bodies over the past few years, which ANTA believed presented a high risk of confusion among the Australian Public. Namely that all suitably qualified non-dietitian clinical nutritionists (such as ANTA Nutrition members) should be able to maintain an equal ability to be presented as suitably accredited nutritionists in Australia.
After extensive proceedings involving a number of associations, the Registrar of IP Australia has recently come to the same conclusion, agreeing with the key points

raised in ANTA’s original submission, ultimately requiring greater clarity of terms when accrediting bodies advertise the status of their associated nutrition professionals.
Under the current regulatory framework, protection of title is not afforded to clinical nutritionists, nor are there clear and consistent definitions or terms adopted across all governing bodies to assist the public in understanding the full range of nutrition modalities and choices of nutrition healthcare services available.
ANTA Accredited Clinical Nutritionist
Through ANTA’s work to support better clarity around these terms, and the maintenance of clinical standards, all ANTA Nutrition Members who maintain ANTA’s recognition criteria are now eligible to refer to themselves as an ‘ANTA Accredited Clinical Nutritionist’ (and use the associated trademark for this accreditation – which will be clarified within member resources over the coming months).
All ANTA Nutrition members should feel a sense of pride in this recognition, which contributes to the ongoing understanding of all Australian citizens seeking qualified nutrition professionals.
ANTA will continue to work in this area to ensure that members of the Australian public have the opportunity to both understand and access the benefits of consulting with a highly qualified clinical practitioner trained in Nutritional Medicine.
ANTA is well-positioned to enter into its 70th year with the necessary resolve, initiative, and high standards of quality and excellence, to support and elevate the role of natural medicine practitioners across Australia in the coming year.
Here’s to another year of continued growth and supportive developments.
To your best in practice, Warren Maginn
ANTA Nutrition Branch Chair

As 2024 draws to a close, we reflect on the work done and milestones reached across this last year.
In my role as the Chair for the Myotherapy branch, I’ve had the pleasure of being involved in a number of initiatives and collaborations that have strengthened the Myotherapy profession, and increased awareness of this modality in the community.
Endorsed from the 1st of July 2024 through to the 30th June 2029, the new Advanced Diploma of Myotherapy training package was released, bringing an updated and improved training product for registered training organisations and TAFE’s to delivery. I had the honour of participating in and being Chair of the Steering Committee for this update. This new training package introduces some exciting inclusions that will equipe graduating Myotherapists with a contemporary and evidence informed approach to clinical practice.
In an effort to increase the number of options for students, we have worked to encourage training organisations around Australia to adopt and begin delivering the Advanced Diploma of Myotherapy. This work continues.
ANTA has forged forward as a part of the “United Associations” group, in collaboration with Massage & Myotherapy Australia, Myotherapy Association Australia, and Massage Association Australia. This group formed back in 2020 to provide a unified approach to assessing
and endorsing training organisations, ensuring quality graduate outcomes, and promoting higher standards of clinical practice. This work continues and each week we are working with training organisations to assist them in providing the best programs they can and advocating for the best educational standards for our profession.
This year has seen several changes occur with the way we look at promoting our modalities and members. As a result of this, we have developed in our approach to using social and other digital media forms, to best highlight the quality and value that our members bring to the community. As we continue to maximise these channels, you’ll see further improvements over time, resulting in greater engagement with members and also with the health professions in general. As always, we are open to hearing from you on this and other matters, so please feel comfortable to contact ANTA at any time with feedback.
Myotherapy is a vibrant and evolving profession. The opportunities for growth and greater public awareness will be achieved by profession level promotion (associations), and also through each Myotherapist member advocating at a local level. We will continue to seek out new and different ways to best resource, support and guide our members to ensure we can work together to grow Myotherapy into the future.
Shaun Brewster, Myotherapy Branch Chair

Dear Members,
As we close another year of our journey together, I wanted to take a moment to reflect on the progress we’ve made. From the exchange of ancient wisdom to modern applications, ayurveda seminars during face-toface PD seminars as well as online sessions, our shared commitment to Ayurveda is slowly but surely growing stronger. Our efforts to promote and expand Ayurveda’s reach have been consistent though ideally, we would like to do even more but we are making efforts and creating space for next generation of practitioners to grow in Australia through these efforts. Together, we have continued to bring wellness, balance, and vitality to many lives. As ANTA members we have continued to have enhanced reputation as high-quality professionals.
Looking ahead let us continue to nurture our community with fresh perspectives and practices. I encourage each of you to think about how you can contribute to the growth of Ayurveda in the year ahead—whether it’s through research, collaboration, or simply bringing more awareness to your local communities. Ayurveda Day is being celebrated every year on Dhanvantari Jayanti around the world (usually October November sometime based on lunar calendar).
Use that occasion to spread word about Ayurveda in your community. I encourage each of you to also take time this season for self-care and reflection. How can we take our practice to the next level in the coming year? Count me in as your support team and ANTA team is there for support and advocacy. As your Director for Ayurveda, I will do whatever I can to work with the ANTA National Council as well as Government and Regulatory bodies to promote ayurveda and support our members.

Thank you for your dedication. I’m proud to be part of this community, and I look forward to more collaboration, education, and growth with each of you. Thank you for your ongoing commitment.
With warm regards,
Neerja Branch Chair, Ayurveda

The Australian Natural Therapists Association (ANTA) saw a productive year in 2024, especially for Remedial Therapists (RTs) and other members. Key achievements included maintaining recognition with over 50 health funds and insurers, making ANTA members highly valued in the healthcare sector. ANTA’s status as a leading professional body helped ensure that health fund claims for natural therapy services were smoothly processed throughout the year.
One notable change this year was the launch of the new HLT52021 Diploma of Remedial Massage by many training providers. This qualification equips therapists with the latest industry-recognised skills, further strengthening professional standards for remedial massage therapists across Australia. This updated diploma focuses on advanced techniques, pain and injury management, and client care, addressing the evolving needs of the healthcare system. ANTA has been an advocate and key contributor to the development of the new diploma and it is rewarding to see graduates with the new qualification enter the workforce and transition to full membership within our branch.
In terms of professional collaboration, ANTA continues its efforts with Massage & Myotherapy Australia, Myotherapy Association of Australia and Massage Association of Australia, otherwise known as the United Associations (UA). The UA together have developed a single application for training provider recognition for the new HLT52021 Diploma of Remedial Massage, advocating for more
standardised training of remedial therapy qualifications and streamlining the process for training providers. The application involves an evaluation of the academic program by all four associations who have set minimum standards for acceptance. This collaboration benefits members by ensuring consistency in provider recognition and opening doors for greater acceptance by health insurers and government bodies. We are proud to be working with likeminded colleagues who hold the same values as ANTA and ultimately have the goal of lifting the standards across the industry. This initiative has been met with some scepticism by some training providers but embraced wholeheartedly by others. This work will continue into the new year and will be interesting to see how it effects the industry over the long term.
Additionally, ANTA expanded its Continuing Professional Education (CPE) opportunities this year. Members were able to engage in seminars, webinars, live recordings, and access specific resources through our CPE portal. These resources provide an opportunity for members to meet their CPE requirements which are essential for maintaining health fund recognition. We aim to make additional changes to our website to compliment this process and are excited to see what the new year will bring in terms of CPE activity.
Overall, 2024 was a year of growth and consolidation for ANTA and its RT members, with ongoing efforts to support professional development, strengthen industry ties and maintain our high standards.

The meeting outcomes from the Natural Therapies Review Expert Advisory Panel (NTREAP) in July of this year indicated that all draft evidence evaluations had been finalised and the final evidence protocols have now been completed for naturopathy Review A and iridology, with final evidence evaluations in progress following NTREAP input for naturopath Review B and western herbal medicine.
• Naturopathy Review A – Whole system, multicomponent or single component interventions.
• Naturopathy Review B – Selected nutritional supplements prescribed in the context of naturopathic practice
As a recap, the purpose of this review process is to assess published scientific research for the 16 modalities excluded from private health insurance including naturopathy and western herbal medicine. From here the final evidence review will be submitted to the Chair of NTREAP and published.
From this review process the Natural Therapies Review Expert Advisory Panel will advise if private health insurance should cover these therapies. While I can’t predict outcomes, I am hopeful that Naturopathy and Western Herbal Medicine will again be reinstated however, even if published, there may still be advocacy required to achieve this aim. Your association may call on you soon to help get this across the line.
As I prepare to step down after four years as Naturopathy Branch Chair, I wanted to take a moment to reflect on the journey it has been. Firstly, I want to say that it has been a privilege to serve in this role, and I am deeply grateful for the opportunity to have connected with so many of you along the way.
In the beginning, there was a steep learning curve. I was barely keeping my head above water with the demands of being on the board, navigating the personalities, and managing the profession’s politics that come with the role. After six months of white-knuckling my way through, I started to find my footing and was able to focus on achieving some of the goals I had set out.
Much of the work over the years has taken place behind the scenes, often requiring advocacy and diplomacy to ensure our members’ needs and voices were heard and respected. This included efforts to improve interprofessional communication skills for practitioners through education and support, listening to members regarding registration for naturopaths, and steadily working toward that goal. Additionally, I worked to identify common areas of interest and difference between associations, fostering closer collaboration with those aligned with ANTA’s high standards.
The final project I am working on, and most excited about is a transition journey from student to practitioner, with the aim of providing much needed support and guidance of the steps from student mastery to becoming a successful practitioner. Please keep an eye out for more in 2025.
During my time on the board, I’ve had the pleasure of meeting and working alongside some truly inspiring individuals within our profession and the surrounding industry, and it’s these relationships that have made my time as Chair rewarding. I am positive about the future of our profession because of the passion, dedication, and commitment I see from our members.
As I write this, I don’t know who your next Naturopathy Branch Chair will be however, I will ensure that they will receive my support to take on the role. Thank you all for your support, and for allowing me the honour of serving you.

The Dragon represents an Earthly stem which has an inherent Yang earth element. The Heavenly stem of this year is Jia, Yang wood. The pillar it creates is one of Yang Wood over Yang Earth. As all good acupuncturists who know their wuxing and their Ba Zi, this dynamic pairing of energies is understood as the Informal Authority, “Qi Sha” or “7 killings”. This energy is often strong enough to overcome obstacles and tends to represent those who work outside of official structures or channels, or within a sphere of self-made influence (like many entrepreneurs we know!). So, it is interesting that this year of the Yang Wood Dragon has seen an increase in the Professional Associations engagement with AHPRA and the CMBA.
In February across a range of days and sessions, representatives from all the other National Boards, Professional Associations, and educational institutions were invited to join an AHPRA Stakeholder Meeting in Melbourne as a reference group focussing on the impact and process of notifications.
ANTA was represented by its then new CEO, David Liesegang, and ANTA Acupuncture Branch Chair, Kaitlin Edin. It was an opportunity to meet a range of industry representatives from across the healthcare landscape, not often encountered within the usual cycle of meetings. It was an informative day that highlighted key concerns and challenges that AHPRA has been focussed on.
AHPRA is the Regulatory Body under which the 14 National Boards sit. As an institution, it has been reflecting on how to communicate better and update its notification
processes, to better support practitioners during this time, and in particular to prevent practitioners from taking their own lives during the complaints process. Rightly, the health and wellbeing of practitioners during the notification process has become a significant issue.
While there is no data available to suggest that any Chinese Medicine practitioner has lost their life due to the stress of notifications, it is expected that the CMBA and the Chinese Medicine Council in NSW will follow suit in taking to heart the lessons of other National Boards and AHPRA more broadly, and in so doing, keep their officiousness in check.
Despite less than 1% of complaints ending in any kind of sanction against a practitioner, the perception from regulated practitioners receiving a notification is nevertheless upsetting and frightening for many. There is a sense of ‘insult’ reported by many practitioners facing a complaint notification, and the implied wrong doing only increases the level of anxiety and stress around the process. This can lead to a sense of isolation from professional support networks and a feeling of dread around continuing practice.
AHPRA have amended their processes and communication around notifications, and it is good to see that it is taking seriously the heightened sense of anxiety and stress the notification process has for health practitioners. One of the other unspoken difficulties for AHPRA and the National boards is that the nature of complaints and the purpose of the Regulator, are often at odds with the patient experience.
Many patients when making complaints want a level of resolution that involves either an apology, or an undertaking that the practitioner will amend their practice (do better) to ensure it doesn’t happen again, or both. Many complainants are not motivated to, nor do they seek compensation. However, the notification process is actually not about resolving the heart of the complaint for the patient effected.
AHPRA’s viewpoint is essentially to review the quality and standards of practice and ensure that the safety of the public is not being put at risk. Obviously serious complaints such as boundary violations, other types of malpractice or criminal acts are about safety and standards, but for a large proportion of complaints, the disconnect in the expectations of the process, which is not about resolution of their issue, may be one reason why misunderstanding, apprehension and frustration seemingly still abounds for patients making complaints.
Interestingly the data provided around notifications involving Chinese Medicine practitioners showed that in at least half of the 68% of cases, practitioners had been proactive in getting in touch with the complainant to attempt or provide some remedy. This suggests Chinese Medicine practitioners are front footed and take their Codes of Conduct and Professional Ethics Standards seriously.
It is important to remind members however, when a notification from AHPRA has been received, it is prudent to contact your insurer and your Professional Association. Depending on the seriousness of the complaint – it is better to get some advice before you act.
Your insurer has an expert team of people to provide advice and support. They are there for you and take the defence of your practice seriously. ANTA and your Branch chairs (Acupuncture, Chinese Herbal Medicine and Multimodality) are there to assist you also.
The evidence is unequivocal - those with familial, peer and professional support networks do better in
managing the stress. Reaching out is important. Extra sources of information, support and assistance are listed at the end of this Update. After that, the best thing to do is Keep Calm and Carry On.
On the 25th June, David Liesegang (ANTA CEO) and Tino D’Angelo (ANTA Chinese medicine Branch Chair) attended the CMBA Stakeholder Meeting held in Sydney, where a range of regulatory concerns were aired with the Board.
There was a presentation by the Chinese Medicine Accreditation Committee on how accreditation works within the National scheme. There were also updates on the guidelines for patient records, advertising, virtual care, public information campaigning, and continuing engagement with practitioners and students. The CMBA Stakeholder meeting is always a welcome opportunity to meet and discuss with the key representatives of all the major Professional Associations and find opportunities to work together. (pic CMBA Stakeholder)
On the 17th September, ANTA Acupuncture Chair, Kaitlin Edin, represented ANTA at the Chinese Medicine Reference Group meeting held in Sydney. This meeting was the 7th of its kind held by CMBA, and the slightly wordy theme was “Building Trust: Strengthening Confidence through Informed Understanding”.
It is no coincidence that the theme of the CMBA meeting was about ‘trust’. At the end of this year, Martin Fletcher the CEO of AHPRA retires after 14 years at the helm. His parting message to the range of stakeholders in the regulatory environment summed up the main issues of concern in an uncertain future. He highlighted cultural safe healthcare, the new risks and challenges within the professions particularly from AI, the workforce supply (not just a Chinese Medicine issue it would seem) and the persistent challenges to effective regulation which include practitioner engagement, social cohesion, the relevance and type of governance and public confidence or lack thereof. His antidote to these key themes seemed to be crystalised by his notion of trustworthiness versus trust.

Trustworthiness, according to Fletcher, is comprised of competence, honesty, and reliability. No surprise or argument there. And it seems Fletcher places this attribute at the centre of the regulatory system. This is perhaps understandable. Practitioners are core business for AHPRA and its boards, and mirroring the professional and ethical characteristics of most practitioners creates a sense of alignment. Something about this makes one uneasy though.
A patient may not have trust in a system, but may feel that a particular practitioner is trustworthy, and this could
be enough to navigate that patient through to a place of healing or resolution. This is appropriate for practice and practitioners. Acupuncture particularly, can be a soft entry to healthcare for those who are marginalised from the mainstream by a lack of trust. We recognise that our CM colleagues have worked hard for the clinical intimacy of trustworthiness that furthers our reach with patients. As we don’t have a direct line into the government purse of Medicare, the primary health networks or (for many) some other external payroll, and as the majority of practitioners operate within the private healthcare sphere and its subsequent discretionary spend, trustworthiness is very much part of our agency and our economic survival.
Perhaps the sense of unease is that trustworthiness is about personal and professional capital, and not one to be coopted in the language of governance. Trust, as we know, once broken, is hard to piece back together, and any person who has felt unsafe in the provision of health care will know this in their bones (and their injuries). Sissela Bok wrote for “whatever matters to human beings, trust is the atmosphere in which it thrives.” ‘Trust’ and ‘Trustworthiness’ is not an ‘either/or’ argument. It is within the realm of the governance practice of the regulator to maintain the former to ensure the latter continues.
There are fractures in the broader regulatory climate to be sure. The increase and threat of AI, the ongoing lack of cultural safety for many within the mainstream healthcare auspices, the workforce shortages and its inevitable fix through immigration, the sense that social cohesion and the relationships that held our values in place are loosening, fraying around the edges or are just breaking. (For a broader discussion of these things, refer to the Scanlon report, and The Minefield’s Festival of Dangerous Ideas episode.)
One of the key pieces of improvement in the landscape of health regulation, flagged by AHPRA and echoed by the CMBA is the required awareness of Cultural Safety for all health practitioners. Ultimately about eliminating racism, discrimination and prejudice in healthcare, culturally safe healthcare practice includes a deeper and more nuanced understanding of First Nations, multicultural and the LGBTQI+ communities, among others. It requires that practitioners commit to learning about culture, develop consciousness and embody habits of language and social interaction that reflect, openness, non-judgement and kindness.
Cultural Safety will no doubt feature more in Continuing Professional Development and Education (CPD/CPE) requirements over the coming years. ANTA has already begun working with third party providers to bring all our members (not just CM practitioners) some excellent and trustworthy resources within this space. Further announcements on what is available will be provided within the next several months.
A final bit of news is that this year has also seen ANTA sign an MOU as the Australian Council of Chinese Medicine (ACCM). The ACCM is a joint venture between ANTA and:
• The Chinese Medicine & Acupuncture Society of Australia (CMASA)
• Chinese Medicine of Australia (CMA)
• The Australian Traditional Medicine Society (ATMS).
The purpose and direction of ACCM as a combined associations group is to represent a formal and unified front for the professional interests of Chinese Medicine practitioners in Australia. The ACCM working group which includes representatives from the four Professional Associations and aims to strengthen the Chinese medicine profession, by advocating for our common goals and purpose.
In so doing it is the hope of the ACCM to strengthen the understanding and communication between Associations, and create unity across cultural and philosophical viewpoints. May the auspicious characteristics of the Dragon assist the venture. David and Kaitlin have been regularly attending meetings since April. And we look forward to sharing some more news about the activities of the ACCM soon. (pic of ACCM 3 reps)
Finally, the Resources for Wellbeing provided below is designed by health professionals, for health professionals to maintain good mental health & wellbeing and to navigate burnout.
TEN - The Essential Network for Health Professionals (https://www.blackdoginstitute.org.au/the-essentialnetwork/)
Note the Ten is not an emergency service and won’t offer crisis intervention, but it does offer an e-health hub that provides health professionals access to a network of support including:
Self-guided mental health check-up
(https://tenonlineclinic.blackdoginstitute.org.au/)
• Connection to one-on-one clinical care, with up to five free telehealth sessions with a clinical psychologist, provisional psychologists, or psychiatrist through Black Dog Institute’s TEN Clinic (https://www.blackdoginstitute.org.au/theessential-network/talk-to-someone/talk-to-amental-health-professional-at-black-dog-institute/)
• Evidence-based tools and resources (https://www.blackdoginstitute.org.au/theessential-network/helping-myself-and-my-team/)
• Peer support (https://www.blackdoginstitute.org.au/theessential-network/talk-to-someone/hand-n-handpeer-support/)
• Digital mental health programs including TEN’s Navigating Burnout program (https://burnout.blackdoginstitute.org.au/#/)
If you or someone else needs urgent help and an immediate response, please call the following numbers immediately:
• Emergency 000
• Lifeline 13 11 14
• Beyondblue: 1300 22 4636
• Suicide Call Back Service 1300 659 467
• Kids Helpline 1800 55 1800
• MensLine Australia 1300 78 99 78
Kaitlin Edin, Acupuncture Branch Chair Tino D’Angelo, Chinese Herbal Medicine Branch Chair

The year 2024 has brought numerous changes and challenges. As the Multi-Modality Chair, I have collaborated with the national council and the ANTA National Administration Office (NAO) to address these challenges. ANTA continues to engage with, but is not limited to, educational providers, insurers, health funds, other professional stakeholders, and government bodies. Our work with members underscores the need to highlight the additional benefits that ANTA membership offers clinical practitioners beyond clinical practice insurance. To this end, I would like to emphasize significant opportunities to improve and enhance clinical practice. Here are some key opportunities that can drive advancements in our field:
One of the most transformative opportunities in recent years is the integration of AI technologies into clinical practice. Various platforms are available, and I encourage ANTA members to explore these innovative tools. Personally, I have been using Heidi AI for several months. This platform allows your computer to listen and create patient notes during clinical conversations. As the clinician, you control when the microphone is ‘on’ or ‘off,’ ensuring privacy when needed.
After the clinical conversation, the program organizes the dialogue into the requested note format (e.g., SOAP or equivalent). It even includes recommendations or advice provided during the conversation, making the notes more comprehensive. You can then copy these notes into your clinical management system or print them for your patient records.
I urge all members to review and update their ethical practice guidelines. With the rapid evolution of online marketing and promotion, it is crucial for practitioners to avoid situations that could lead to challenges or restrictions from regulatory bodies such as the AHPRA for registered practitioners, or the HCCC or similar for non-statutory registered practitioners.
To ensure compliance and maintain professional integrity, the following practices are advised:
• Avoid using testimonials.
• Refrain from endorsing products.
• Do not share patient details online.
• Ensure that any comments about treating complaints and conditions are fully referenced with relevant studies in all promotional materials.
Finally, I strongly encourage all ANTA members to take full advantage of the free resources available in the members section of the ANTA website. These resources include (but are not limited to):
• Free access to eMIMS.
• Links to imgateway, a comprehensive research database.
• A wide selection of free CPD webinars, dating as far back to 2016.
















ESTABLISH AYURVEDIC HABITS THAT ENHANCE YOUR VITALITY AND LONGEVITY Our flexible, easy-tofollow courses fit into your busy life, allowing you to learn at your own pace














Chloe Hillaire
Lori-Grace Stephens
Leila Abitbol-Taylor
Ange Schofield
Jessica Cruze
Asha Maiolo

Kate Baddeley
Elyse Johnson
Diana Toffoletto
Isabella Livingstone
Alexa Dawson
Emily Huf

Resolve
Resolve your patients gut issues with our


Always read the label and follow the directions for use. For practitioner dispensing only.
Always read the label and follow the directions for use. For practitioner dispensing only.




Written by Esther Parker, MHumNut, BHScNat, AdvDip Nat, GCertLearningTeaching
Not being able to sleep is one of life’s most intense torments. Anyone who has struggled with insomnia will understand the immense and sometimes complicated impact this has on all areas of their lives. Causes can be physiological, environmental or psychological. This article presents a discussion on managing sleep issues and insomnia, by introducing novel approaches to treatment.
Clinicians will see patients with insomnia present into the clinic slumped in their chair, apathetic, with an expression of hopelessness; as if life will never improve. As an immense ‘barrier to cure’, sleep should be front and centre of a person’s agenda. Without sleep, how can a patient follow your

clinical protocol to eat well, move their bodies and generally take care of themselves and others?
Natural Therapists are taught, quite rightly, to ask our patients about their sleep. In prescribing for sleep issues, we have sleep hygiene, nutrients, herbal medicines, exercise, acupuncture, remedial massage, homeopathy, flower essences and more. In many cases, these therapies resolve the sleep issue. However, more often than not, the picture is more complex than this, and we need to do what we do best; provide personalised care and treat the cause.
Sleep in Australia (and globally) is a chronic issue. Around half (48%)(1) of adult Australians have two or more sleep issues, making them unable to meet sleep recommendations of 7-9 hours per night. For those of us who consult with families, it’s worth noting that 27% of young teens and 52% of older teens are not meeting sleep guidelines on school nights(1), impacting learning, behaviour, attention and eating habits. Women are more likely to experience insomnia than men, however in my practice, I have observed that women will often present with a myriad of other conditions that seem more pertinent, when sleep is a major contributor even as a solo symptom. Women also forgo the self-care element of caring, and don’t prioritise rest. Men will more likely present with sleep as a number one concern.

Most practitioners are aware of the co-morbidities associated with poor sleep, however they may not be aware that these health concerns may differ based on age and sex. For example, though there is an increased risk of cardiovascular disease with tooshort or too-long sleep, this is primarily significant for people over 65 (2,3). Diabetes risk is associated with short sleep, but this is mostly in men. Conversely, increased risk of hypertension seems to be significant in short sleep for women (4). In regards to mortality, sex is less relevant, rather the duration of sleep hours is more significant; risk of death is increased by 12% from short sleep and 39% from long sleep.
The most important area of learning for me as a practitioner, was to understand the science of sleep, and in particular, what makes ‘good sleep’. As insomnia or poor sleep is principally a mental health issue, explaining normal sleep to a patient can be a crucial step in remedying poor sleep.
Sleep can be a slippery thing to define, but at its core, its purpose is about repair and regeneration. Sleep moves through four stages, in several cycles through the night. Thanks to our training in physiology, clinicians will be familiar with these stages; three of Non-Rapid Eye Movement (NREM) sleep from light dozing through to the deepest slow-wave sleep, and Rapid Eye Movement (REM) sleep, where we dream to consolidate information and problem-solve our day.
What is often new information to clinicians (and patients), is how drastically these stages change in their duration. As you can see in the table ‘Sleep Cycles’, we tend to experience the most of our deep, restorative sleep at the start of the night, getting lighter sleep closer to the morning. Conversely, our REM/Dreaming sessions get longer and longer, dominating in the early hours, just before we wake up (4).
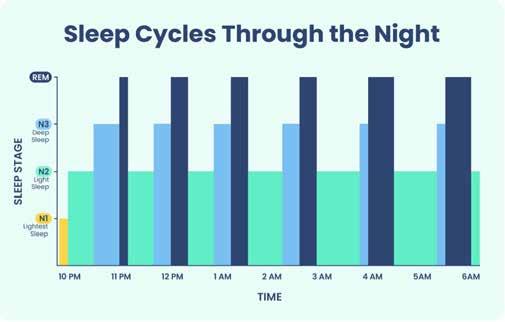
Knowing this information about sleep can be extremely important for a patient to know, helping to alleviate some anxiety about their sleep. For example, if a patient finds themselves waking at 3am, but falling asleep again shortly after, you can reassure them that the majority of their restorative sleep has already occurred by this time.
Insomnia is when a person has trouble falling asleep or staying asleep, several times a week for a duration of at least three months. Patients will also report daytime issues as well, such as brain fog, fatigue, memory issues, low mood and attention difficulties (5) Of course, the causes for insomnia and varied, and our holistic approach is a true advantage in this area.

For many natural medicine clinicians, sleep support is primarily centred around sleep hygiene information. While this is an important consideration, often this prescription falls short of assisting in true insomnia.
Cognitive Behavioural Therapy for Insomnia (CBTi) is a structured approach which seeks to improve sleep understanding and behaviour, providing long-lasting treatment. It is now recommended as a first-line therapy for insomnia around the world (5)(6).
CBTi is a practice which acknowledges and addresses the anxiety associated with insomnia by educating about sleep and applying sleep modification behaviours. It consists of a few main components;
Sleep Education: why we sleep, how we sleep and how this naturally changes as we age. Education can reassure people and start to lower anxiety levels associated with insomnia.
Addressing Sleep Medications: Most sleep medicine formulations are for short-term use, however many people are dependent on them long-term.
A commonly prescribed medication in Australia, Temazepam (a benzodiazepine), is additive both physically and psychologically. It can be argued that some herbal formulas and melatonin can also become a crutch for people. Reducing or removing sleep aids should be done slowly and carefully, preferably with the professional who prescribed them.
Assessment of Sleep, using a Sleep Diary: This essential step allows the clinician and patient to review the sleep process with less emotion. Often in clinic, people view their sleep as worse than it might truly be; “I never sleep” or “I only get 2-3 hours a night”. Much like a diet diary, a sleep diary helps to show a truer reflection of hours asleep, juxtaposed against hours in bed.
Sleep Scheduling: This refers to the assessment and moderation of sleep hours. Using the diary, the CBTi practitioner notes sleep efficiency (time asleep divided by time in bed, giving a percentage). From here, the practitioner can discuss ways to improve efficiency, and will often apply restricted time in bed, to help improve sleep efficiency and quality.
Clinicians please note, that the above components are not a step-by-step manual for CBTi. These are the core elements to understanding the overall process. While some trained practitioners of CBTi choose to follow a weekly therapy-type process to remedy sleep, others work more organically with the patient by following their understanding and readiness for each stage.
It is important to state that all sleep discussions should identify when it is appropriate to refer, e.g. in Sleep Apnoea or Periodic Limb Movement Disorder. Interviewing sleep partners is an important part of the process too.
Sleep disorders often result from disruptions in multiple pathways, including abnormalities in GABA receptors, cortisol levels, cytokines, circadian rhythm (melatonin secretion and adenosine receptors), and excitatory amino acids like glutamate and aspartate (7). Sedatives, anxiolytics, relaxants and antiinflammatories are some of the actions used in sleep medicine.
Herbalists and Nutritionists are well versed in the common sleep aids (e.g. Chamomile, Kava, California poppy, Passionflower, Magnolia, Lemon balm, Valerian and the like) and these should be applied as necessary. Likewise, Nutritionists will be comfortable in prescribing magnesium for a range of sleep and anxiety presentations. In addition to these remedies, a few less-common herbs and nutrients have been researched and found to have benefit.
Pulsatilla, Anemone pulsatilla: A traditional herb which has long been used for pain, insomnia and muscle tension. Pain and sleep are often connected, and this herb may be appropriate for the patient experiencing sleep issues due to menstrual or other forms of pain (8)(9).
Black horehound, Ballota nigra: With use dating back to the 13th century, Black Horehound has long been prescribed as a sleep aid. Interestingly, some of its chemical constituents have been shown to bind with benzodiazepine receptors (10).


Kiwi Fruit: Ingesting two fresh kiwi fruits before bed has been shown to increase total sleep time and sleep efficiency (11)(12).
Sweet Violet, Viola odorata: The flowers of this plant have long been used to promote sleepiness, traditionally made as a syrup. A recent pilot study of 84 people with insomnia were treated with Viola odorata syrup showed statistically significant improvement (13)(14)(15)
Treating sleep can also be viewed via methylation pathways. In order to increase GABA or melatonin, it is important to provide the relevant co-factors (magnesium, Vitamin C, B-vitamins, zinc).
N-acetyl cysteine (NAC): NAC as a pre-cursor to cysteine, helps to promote glutathione, glutamate and GABA.
Tryptophan-containing foods: important to support serotonin conversion into melatonin (16).
For anxious patients experiencing poor digestive integrity, gut-protocols, cooked foods and supplements as powders are important considerations. Remembering to consistently check physicals of your patients is essential in sleep (blood pressure, inability to focus, pathology), as symptoms may flag other conditions and co-morbidities.
Natural therapists are professionals in personalised care, prescribing appropriate remedies to the case at hand. Sleep is a complex issue, and in many cases, you will need to refer on, e.g. breathing disorders, mental health, oral-pharyngeal therapy or dentistry, or manual therapies. For persistent insomnia, referring to a trained CBTi clinician or a trained psychologist in sleep anxiety or trauma may be a more helpful route. There is a lot to learn about sleep management, however the take home message is that insomnia
and sleep issues are often accompanied by extreme anxiety, both related to, and not related to the sleep issue. Our Naturopathic Principles, ‘treat the cause’ and ‘doctor as teacher’ are particularly important in sleep. At the end of the day, if you reduce anxiety and educate your patient about sleep, this may put many of them on the road to a better, more reliable sleep; ready to engage with your other therapeutics with more energy and enjoyment.
Esther Parker is a Master’s trained Naturopathic Clinician in Meanjin (Brisbane), practicing at the Brisbane Mind and Body Clinic in Bowen Hills. She specialises in natural therapies for mental health, sleep, neurodiversity and in the connection between gut and brain. As a qualified CBTi practitioner, she is able to utilise this proven method for insomnia, with the added support of personalised natural therapies in an evidence-based approach, in order to get the best outcomes for her patients.
Graduating in 2008, Esther has used her knowledge and skillset in a range of areas, from clinical practice, to industry, and as a University Clinical Educator and Lecturer for almost 10 years. To connect with her, please visit these pages:
www.estherparker.com.au www.brisbanemindbodyclinic.com.au

References
For references log into your ANTA Member Centre > The Natural Therapist > Journal Articles.

Female, 35, works from home part-time, with partner and two school-aged children. Complex case with long history of immune, gut and nervous system conditions. Presents with sleep-onset insomnia (since Jan 2024) at times of up to 3 hours unable to fall asleep, with accompanying anxiety and low daytime wakefulness. Lives in rural area and is very anxious to leave home (run errands or work in office). Medications included Mirtazapine (tetracyclic antidepressant) last 9 years and just began Temazepam (as needed). Supplements taken sporadically were probiotics, multivitamins, zinc, adrenal herbs, magnesium and iron (history of anaemia). Recent bloods showed slightly elevated Hba1c, cholesterol, LDL and triglycerides. Diet mostly wholefoods, high protein and fats, but low fibre. Sedentary, but had recently begun walking most days.
Supplement Prescription: Adrenal herbal formula (Ziziphus jujuba, Pueraria lobata, Magnolia officinalis, Passiflora incarnata) to ease anxiety around insomnia. Nightly magnesium citrate, for nervous system and for recent constipation. Dietary interventions for constipation, movement and grounding exercises.
Lifestyle Prescription: tailored-CBTi; moderate sleep restriction (10.30pm-6am = 7.5 hours). Strategies if unable to fall sleep – 30mins no sleep, up for 30mins with calming activity (reading, comfort TV, yoga), back to bed. To reduce anxiety, allowed patient to take Temazepam if still awake 30mins later (total awake time would then have been 90mins).
After 6 weeks of treatment: patient has only taken Temazepam twice over this time. She is now able to work in the office and attend family events without insomnia the night before and without daytime anxiety. Currently in negotiation to increase sleeptime (will increase by 15-minute increments, slowly).
Male 28, full-time mobile technician. Generally fit and well, but experiences profound sleep issues, brain fog, fatigue and headaches. Some delay in sleeponset, and wakes several times throughout the night. Feels overall anxiousness about sleep due to daytime fatigue. Attends gym regularly but ‘crashes’ during the session, making no progress. Went to bed 9pm, waking at 6am (9 hours in bed, broken sleep for around 7 hours = poor sleep efficiency and quality). Had previously tried an ashwagandha adrenal formula, valerian, various sleep teas and magnesium glycinate, with no resolution of sleep issues. Lowvariety diet, high in protein and fat, low fibre (meat, pasta, rice). Ordered pathology as to source of fatigue and headaches; showed markedly elevated Serum Iron and Transferrin Saturation (78%). Possible hemochromatosis, referred back to GP.
Supplement and Diet Prescription: provided recipes for increased nutrient variety and fibre, via in-car prepped meals and snacks, to allow for mobile work. Continued adrenal herb formula to support HPA axis and encouraged iron-binding dietary interventions until GP appointment.
Lifestyle Prescription: Applied sleep modification, by restricting bed time to 11pm, keeping the usual wake time of 6am.
After 5 weeks of treatment: Improvement in sleep quality and daytime energy. Able to return to gym to make progress. Decrease in headaches, although did encourage him to seek more investigation, re: iron. Tired at 1.30/11pm and falls asleep easily, with one brief waking for bathroom, then straight back to sleep. Feels more alert during the day.

Written by Keri Krieger

Traditional Chinese Medicine (TCM) has recognised and studied the aging process of women’s bodies for thousands of years. Integrating this ancient knowledge into your natural therapies practice is a wonderful way to support perimenopausal clients holistically.
From a TCM perspective, the aging process in women unfolds in seven-year cycles.
“At thirty-five years, the Yang Ming channels that govern the major facial muscles begin to deplete; muscles start to atrophy, facial wrinkles appear, and hair begins to thin.
At forty-two, all three Yang channels are exhausted. The face becomes more wrinkled, and hair begins to grey. By forty-nine years, the Ren and Chong channels are completely empty, and the Tien Kui has dried up, causing menses to cease, and conception becomes impossible.”
— The Yellow Emperor’s Classic of Medicine.
This ancient text, attributed to the Yellow Emperor Huang Di (reigning during the 3rd millennium BCE), paints a detailed yet stark picture of aging. Though perhaps not the most flattering depiction of aging in our forties, it is remarkably accurate in its timeline for menopause. It reminds us that the body operates as a holistic system, and from a TCM treatment perspective, we’re offered a map and timeline to guide our support for the body during these transitions.
So why is it, if such information has been available for so long, that 60% (1.) of women today still report feeling uninformed about menopause?
A very good question — one that demands attention, particularly as the United Nations projects that by 2025, over 1 billion women globally will experience menopause. This staggering figure represents 12% of the world’s population.
This knowledge gap, both for women and healthcare providers, sets the stage for either a perfect storm or an incredible opportunity for meaningful social change. Chinese Medicine and allied health practitioners are uniquely positioned to lead this charge,
offering women in midlife comprehensive support and care.
The study linked here articulates this gap in detail, noting the urgent need for better understanding and education around perimenopause, both for women and healthcare professionals.
“Lack of education for women and their general practitioners is causing perimenopausal women to go through this important stage in their lives with a lack of knowledge and appropriate medical care. It is essential that women are taught about the menopause, from school onwards and that we offer health professionals appropriate training starting from the medical school curriculum.”
We as complementary health practitioners are perfectly placed to move forward with this knowledge, equipping ourselves to better support clients through the menopause transition.
• Early Menopause: Menstruation ceases before the age of 45.
• Menopause: Defined as 12 consecutive months without a menstrual period. Every day after is post-menopause, a phase that can make up a third or more of a woman’s life.
• Perimenopause: The years leading up to menopause, potentially starting 5 to 10 years before the last period. From a TCM perspective, this transition begins at age 35 but may not be symptomatic until a few years before menopause.
• Menopause may also be triggered by cancer treatments or surgical removal of the ovaries (oophorectomy). In cases of surgical menopause, symptoms may be more severe due to the sudden drop in hormone levels.
How
TCM offers a nuanced view of the menopause transition, treating it as part of the body’s broader health journey rather than a pathology to be “fixed.”
Perimenopause is not an illness, but a shift that provides an opportunity to reassess and address long-standing health issues.
In TCM, perimenopause is seen as a reflection of underlying imbalances that may have been ignored or bypassed at a subclinical level.
An interesting concept from Chinese Medicine is the Bao Mai, the meridian running from the heart to the uterus. In puberty, this channel begins to flow from the heart to the uterus, signalling the start of menstruation. During perimenopause, this flow reverses, mirroring the similarly erratic hormonal signals sent back to the brain during this season.
As Dr. Sarah McKay describes in The Female Brain, this “bottom-up” communication is reflected neurologically through the Hypothalamic-PituitaryOvarian axis, and as the ovaries wind down, this connection becomes irregular before eventually disconnecting entirely.
“Menopause opens a window of neural vulnerability,” McKay notes, with symptoms like hot flashes, sleep disruptions, mood swings, and memory changes stemming largely from changes in the brain, rather than the ovaries themselves.
TCM recognises this vulnerability, and this is where practitioners can offer powerful support with holistic treatments that align both physical and emotional health.
Over the past two decades, the conversation around Menopausal Hormone Replacement Therapy (HRT) has been shaped by several studies, often creating a mix of fear, confusion, and hope for women considering HRT.
In 2003, a pivotal study suggested increased risks associated with HRT, leading to a significant decline in its use and widespread fear about potential health consequences. Fast forward to 2023, and a new study has revisited the topic, discussing how the risk of breast cancer with HRT varies depending on the type and duration of therapy.
While these studies have both hindered and helped access to HRT, they’ve also created a great deal of uncertainty for many women. Women are left to navigate this confusing terrain, often unsure whether to pursue HRT, and if they do, how to balance its use with their overall health.
This is where TCM can provide valuable support. Chinese Medicine, particularly acupuncture, can work
alongside HRT if women choose to take it, offering relief from symptoms that HRT might not fully address. In fact, the Australian Menopause Society endorses the use of acupuncture in conjunction with HRT, recognising its benefits in supporting women during this transitional phase.
Integrating modalities like acupuncture with HRT might help women achieve more balanced outcomes, supporting symptoms such as hot flashes, mood swings, and sleep disturbances. With acupuncture and lifestyle advice TCM practitioners can help women not only manage symptoms but also address deeper imbalances that might contribute to their perimenopausal experience.
By combining the ancient wisdom of TCM with modern therapies like HRT and additional allied health practices, practitioners can offer a comprehensive and supportive approach to women’s health during perimenopause and beyond.
Perimenopause is, in many ways, a health report card. By our early forties, if we haven’t addressed chronic stress, irregular cycles, and poor nutrition, these imbalances will become more pronounced. The transition isn’t just about managing menopausal symptoms but is a gateway to reassessing overall health — physical, emotional, and spiritual.
Through TCM, we are reminded to treat the person, not just the symptoms. Yes, we can monitor hormone levels and address urgent symptoms, but our role as practitioners is to step back and view the entire landscape of a woman’s health during this transitional time.
The beauty of Chinese Medicine lies in its ability to adapt to each individual, honouring the unique experiences of every woman in this season of change.

For references log into your ANTA Member Centre > The Natural Therapist > Journal Articles. References
Keri is an acupuncturist and Dr of TCM (Traditional Chinese Medicine) with two decades of clinical experience. She forged a practice in some of the world’s leading health retreats integrating traditional health care and spa therapies. Now a passionate writer, practitioner and educator focusing on women’s health and perimenopause. She offers courses for women and health practitioners to better
understand their bodies and treats from a sunsoaked clinic on the Gold Coast.
To connect with her, please visit these pages:
kerikrieger.com @kerikrieger
Written by Michelle McCosker

Weight management is frequently addressed by natural healthcare practitioners. Underlying issues such as emotional eating, food cravings and metabolic disorders are known to hinder results (Frayn et al., 2018) (Chu & Chu 2021). Aside from practitioner encouragement and patient willpower the right tools to address these problems are lacking. While dietary advice and lifestyle changes are foundational for sustainable weight loss, the psychological and emotional factors are often unaddressed in weight management, leaving the patient and practitioner feeling like a failure. For these cases, there is a discrepancy in relation to the effort and result. Emotional Freedom Techniques (EFT) may be the answer for natural therapists, to enhance client outcomes by tackling underlying emotional triggers that drive overeating, food cravings, and poor body image. Furthermore, the adverse childhood experiences (ACEs) study shows
stressors or traumatic events have psychological and physiological effects that extend into adulthood. Biological, psychological, and environmental factors provide a method to link ACEs with adult obesity however an ACE score of 4 or more increases the possibility of obesity and diabetes in adulthood (Chu & Chu 2021). Awareness of the ACEs study and the physiological effects that influence weight management enables practitioners to support their clients needs from a different perspective.
The heightened desire to consume a specific food (food craving) and weight management have been a research topic in the field of Emotional Freedom Techniques (EFT) for many years, delivering significant positive outcomes. Clinical EFT is the version that has been tested in clinical trials, while there are many hybrids, few have been thoroughly tested. EFT is a brief psychophysiological intervention

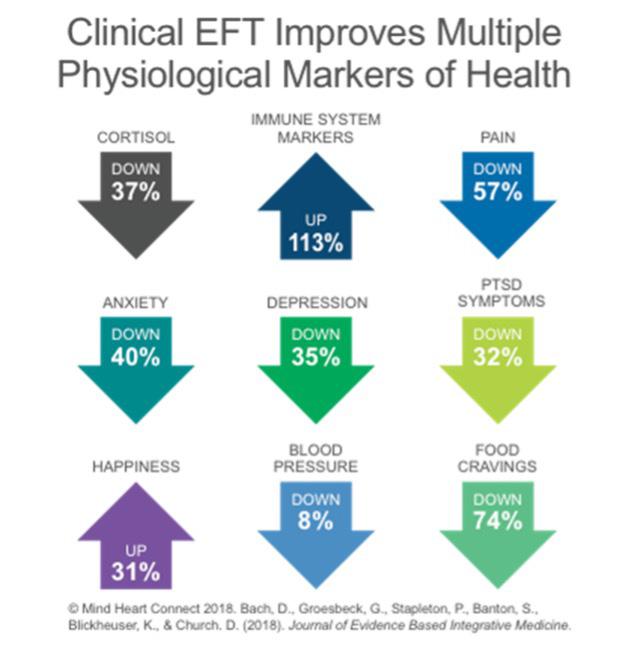
combining elements of exposure and cognitive therapy with somatic stimulation using a two-finger tapping process. EFT may be referred to as tapping or psychological acupuncture (without needles) (Stapelton 2019). Furthermore, EFT has been shown to reduce cortisol, increase immune system markers, including sIgA, reduce pain and PTSD symptoms (Bach et al., 2018).
The application of EFT in the highlighted research discussed in this article is Clinical EFT, it was meticulously replicated from study to study, using standardised protocols and the interventions were delivered by Accredited Clinical EFT practitioners (some were also psychologists). The method involves acupressure points on the eyebrow, side of eye, under eye, under nose, chin, collarbone, under arm and top of the head. The treatment involved either direct exposure to problem foods or visual images of foods and thinking about eating those foods. Participants focused on a specific problem food craving and an emotion related to that. They were also asked to rate the craving giving a subjective unit of distress (SUD).
A set-up statement was used and reminder phrases whilst tapping on the relevant acupressure points. The set-up statement concentrates on the problem or difficulty, including the emotion and self-acceptance phrase at the end, all said aloud. Example: Even though I have a strong desire to eat this chocolate, I deeply and completely accept myself. The set-up statement is repeated three times whilst tapping on the side of hand point. Then working through the 8 tapping points, reminder phrases stating words the client has shared in relation to the issue
are stated aloud and include sensory, affective and cognitive words. Each acupressure point is tapped approximately 7 times. This is repeated until the SUD is a zero (Church & Marohn 2013). During initial rounds of tapping if additional information is shared, new set-up statements may be used. Example: Even though I feel so restricted when I’m not allowed to have chocolate, I choose to make healthy choices. Tapping on acupressure points has been found to be as efficacious as acupuncture (Cherkin et al., 2009).
Shaw et al’s study (as cited in Stapleton et al., 2018) showed psychological and behaviour interventions produce an increased weight reduction in overweight or obese adults.
A negative relationship with food may be set up in adolescence and shaped by factors such as, negative emotions, parental modelling, social influence, access to healthy food and exposure to food advertising (Stapelton et al., 2016a). Ackard et als study (as sighted in Stapelton et al. 2016) revealed that students had engaged in overeating in the past year with 17.30% girls and 7.8% boys from a sample of approximately 4700 participants and that unhealthy weight control behaviours had been used by 57% of girls and 33% of boys. Neumark-Sztainer et als study (as sighted in Stapleton et al. 2016) discusses the aetiology of poor eating habits in youth involves easy access to hyperpalatable unhealthy foods, nutritionally deficient diets and eating to excess (Stapelton et al., 2016a) suggesting these issues form part of the problem for adults having weight management challenges.
A 2016 study of adolescents explored Emotional Freedom Techniques in the treatment of unhealthy eating behaviours and related psychological constructs. From pre to post intervention in the EFT group there was a significant decrease in consumption of unhealthy drinks (P=.015) and unhealthy foods (P=.001) and an increase in selfesteem (P<.001) (Stapelton., 2016b).
In the areas of reducing food cravings, dietary restraint and individuals’ responsiveness to food in the environment (power of food), similar efficacy was established between EFT and Cognitive Behavioural Therapy (CBT). Over 12 months, both treatments also produced significant decreases in depression and anxiety scores. A longer lasting effect was seen in the areas of dietary restraint, reduced food cravings, and individuals’ responsiveness to food in
the environment (power of food) from EFT compared to CBT (Stapleton et al 2016b, Stapelton, Sheldon & Porter 2012)
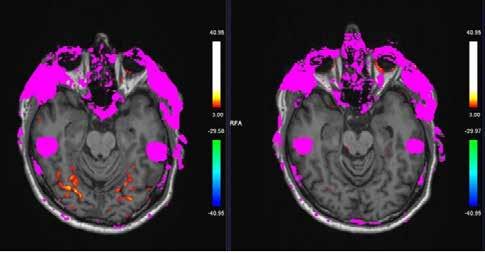
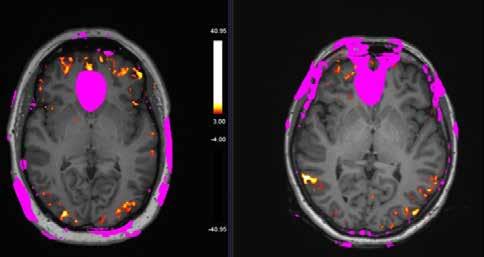
An fMRI study investigated the neural changes in overweight adults with food cravings (Stapleton et al., 2018). The intervention for the treatment group was 2 hours of EFT per week over 4 weeks and no intervention for the control group. The areas activated in the brain by anticipation of food were analysed using fMRI scans. Participants were told to imagine they were eating the foods depicted in the images in front of them. There is currently no known single area that is the primary response to food. The superior temporal gyrus (associated with cognition) and lateral orbito-frontal cortex (associated with reward) showed significant activation in all the preintervention scans (Figure 1). A marked reduction in both these areas was noted in the post-intervention scans in the EFT group, whilst the control group continued to have activation in these areas (Figure 2) (Stapleton et al., 2018). Other studies including those using functional imaging, in the absence of hunger, demonstrate thinking about food and seeing food can stimulate limbic and paralimbic regions. Greater brain activation in these regions is noted in obese participants and when using high calorie images as opposed to lower calorie images. This study supports the benefit of incorporating EFT with weight management strategies through the reduction of neural activity after a total of 8 hours treatment (Stapleton et al., 2018).

Further research by (Stapleton et al., 2020) using online delivery of an 8-week EFT intervention evaluated subjective power of food, dietary restraint, food cravings, weight changes, and self-reported symptoms (e.g., somatic, anxious, and depressive). At the 2-year follow-up, improvements in somatic symptoms, depression, food cravings and perceived power of food endured. At the 12-month followup BMI, weight, anxiety and restraint capabilities, significant reductions were seen however, they remained unchanged at 2 years (Stapleton et al., 2020) An interesting point to note, is online delivery of this program achieved significantly reduced measures, like those of in person interventions, of pre to post intervention.
Linarden et al. and Castelnuovo et al discuss (as cited in Stapleton et al., 2020) adherence to traditional behaviour treatments for the suggested 12 months in relation to long-term weight loss is poor, mostly due to expense and commitment. Dysfunctional eating practices come with underlying cognitive beliefs and the current method of treatment, CBT has limited compliance due to commitment and financial factors. This extends the advantage of the inclusion of EFT alongside weight loss approaches. Along with a relatively short timeframe of treatment to achieve a result and less financial commitment, this makes EFT an appealing option for both practitioner and clients.
All participants in a group delivered CBT and group delivered EFT controlled non-inferiority trial achieved weight loss, with the EFT group losing an average of 3.15 kg pre to post, 4.28 kg pre to 6- months, and 3.32 kg pre to 12-months (Stapleton et al., 2017). The CBT group initially lost 0.90 kg on average pre to post, 2.90 kg pre to 6- months, and 5.10 kg pre to 12-months. Additional measures of depression and anxiety scores decreased in the EFT group for pre-intervention to post-intervention and were maintained at 6- and 12-month followup. Even though the CBT produced lower anxiety scores at post-intervention this was not maintained at follow-up of 6 and 12 months (Stapleton et al., 2017).
Natural healthcare practitioners may hypothesise, the addition of EFT delivered as a one-hour session for 8 weeks in addition to their chosen method of weight management may improve patient outcomes in short- and long-term areas of weight loss, temptation, food cravings, the use of will power, feelings of deprivation, missing out, being out of control and the power of food. This same technique can be used to increase desire, which would be a significant benefit to natural healthcare providers for issues such as low water intake, supplement prescription compliance and motivation to exercise, however research in this area is not established.
Michelle McCosker is a highly regarded EvidenceBased EFT (Emotional Freedom Techniques) trainer and mentor, driven by her passion for training and mentoring therapists and natural healthcare practitioners. After completing a Bachelor of Health Science in Naturopathy and working in private practice for 13 years, Michelle discovered EFT, which became the final piece of the puzzle, transforming her practice. Now, EFT is her sole treatment method, helping clients achieve optimal outcomes. She is an accredited Clinical EFT practitioner through EB EFT, specializing in physical issues such as chronic pain, fertility challenges, pregnancy concerns, and birth trauma, using EFT, Matrix Reimprinting, and Matrix Birth Reimprinting.
For references log into your ANTA Member Centre > The Natural Therapist > Journal Articles.




Supports & maintains vaginal health.


In addition to her private practice, Michelle leads psychoeducation and psychological interventions for clinical research trials involving cancer and chronic pain patients, led by Dr. Peta Stapleton at Bond University. She is also an international presenter, including her 2024 ACEP conference presentation, where she shared how EFT can help chronic pain sufferers overcome their challenges. Michelle’s unique combination of expertise, passion for training and mentoring, and experience in coaching and lecturing makes her a true leader in the field.
For more information regarding Michelle, EFT and practitioner trainings go to:
https://nurturehealthsolutions.com.au/events/





Always read the label & follow directions for use. FROM OBORNE, VITAL.LY, ARIYA & RENER.
Deliver comfort and confidence with Horopito intimate care, derma care and supplements. Backed by 30+ years of research, Kolorex sustainably grows its own Horopito ensuring quality from source to bottle. Free from parabens, SLS, and fragrances.

Over 60 years ago, the Pharmacy Guild of Australia launched Guild Insurance – designed to protect and safeguard the pharmacy profession. Since then Guild has expanded the network of professionals we protect by forming partnerships with associations who represent a wide range of industries and the professionals who work within these fields.
Proudly partnering with the Australian Natural Therapists Association for over 4 years means we understand the importance of protecting you with more than just a policy.
With us, you’ll be shielded by a policy created from unmatched insight into your profession, access to risk management materials to help you reduce the risk of a claim, backing
from the industry body that stands up for Australian natural therapists, and so much more.
Find out how you can be part of something bigger by visiting: guildne.ws/ANTA or calling 1800 810 213 today.

Written by Bodine Ledden
Femoroacetabular impingement syndrome (FAIS) is defined as a “motion-related clinical disorder of the hip with a triad of symptoms, clinical signs and imaging findings” (Griffin et al., 2016). FAIS is an activity dependent condition, with symptoms typically occurring between the ages of 18-50 years of age and may be present in one, or both hips (Dickenson et al., 2016). Diagnostic delays negatively impact outcomes associated with FAIS causing significant impairment to activities of daily living, sports performance and quality of life (Drew et al., 2017). FAIS is commonly missed, misdiagnosed and mismanaged; with patients consulting with an average of 4 practitioners and having symptoms present for an average of 2 years prior to receiving an accurate diagnosis (Clohisy et al., 2009). Thus, underlining the importance of improved understanding and screening processes among health care professionals.
Hip related pain in young and middle-aged active adults includes three categories, comprising of FAI syndrome (FAIS), acetabular dysplasia and / or hip instability and all other conditions without bony morphology causing hip pain, including chondral, labral and ligamentum teres conditions. Furthermore, all non-musculoskeletal conditions and competing musculoskeletal pathology must be first ruled out (Reiman et al., 2020). FAIS can be categorised into primary FAIS and secondary FAIS. Primary, FAIS represents the symptomatic premature contact between the proximal femur and the acetabulum (Griffin et al., 2016). Secondary FAIS develops as a result of a pre-existing hip disease or traumatic injury resulting in changes to the shape of the
proximal femur and / or the acetabulum (Dijkstra et al., 2022). Morphological variation is required for a diagnosis of FAIS including cam type morphology, pincer type morphology or combined cam and pincer type morphology. Cam type morphology is attributed to a morphological variation at the femoral head/ neck junction resulting in an aspherical femoral head whereas pincer type morphology includes global or focal over-coverage of the femoral head by the acetabulum (Griffin et al., 2016).
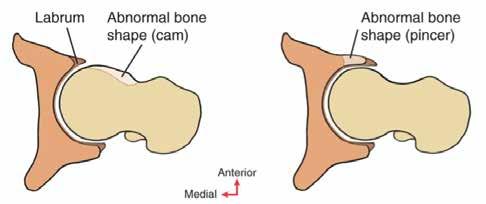
Figure 1 - Cam type morphology and pincer type morphology. Neumann, D. A. (2017). Kinesiology of the musculoskeletal system: Foundations for rehabilitation (3rd ed.). Elsevier. [Figure 12.57, Page 529].
Cam type morphology is more common in males compared to females, affecting approximately 15-25% and 5-15% respectively (Agricola et al., 2014). Interestingly, the morphological changes observed in cam type morphology occur during skeletal maturation prior to the onset of symptoms associated with FAIS (Palmer et al., 2018). Soft tissue hypertrophy occurs at the epiphyseal plate of the femoral head/neck junction between the ages of 10-14 years of age. The hypertrophic changes occur as an adaptive response to high impact sporting activity during development. The soft tissue and
cartilaginous tissue ossify at the head neck junction resulting in a flattening or prominence, disrupting the normal spherical shape of the femoral head (figure 2). Thus, contributing to the premature contact between the femoral head/neck junction and the acetabular rim (Agricola et al., 2014; Palmer et al., 2018). Due to the adaptive responses that occur during skeletal maturation, high-level male athletes are 1.9 to 8.0 times more likely to develop a cam morphology than non-athletic male controls (Nepple et al., 2015). However, due to the early development of cam type morphology, uncertainty remains as to the specific loading pattern, training frequency, and intensity, that predisposes individuals to the development of cam type morphology therefore predicting who will develop FAIS is unclear. Therefore, implementing preventative strategies is children and adolescents is not possible (Agricola et al., 2024).
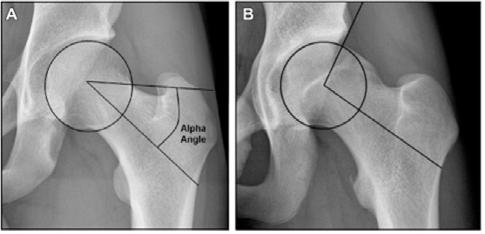
2 – A) a circle of best fit around the femoral head with a line through the centre of the neck of the femur to the centre of the femoral head. Another line is drawn from the first point of deviation from the circle of best fit to the centre of the femoral head. B) flattening of the femoral head due to a cam type morphology resulting in a greater alpha angle. Agricola, R., Waarsing, J. H., Thomas, G. E., Carr, A. J., Reijman, M., Bierma-Zeinstra, S. M., Glyn-Jones, S., Weinans, H., & Arden, N. K. (2014). Cam impingement: defining the presence of a cam deformity by the alpha angle: data from the CHECK cohort
Cam type morphology is measured by the alpha angle (figure 2). The alpha angle is the degree in which the shape of the femoral head deviates from being spherical (Agricola et al., 2014). An alpha angle greater than 60 degrees is the standard reference value indicating a cam type morphology (van Klij et al., 2020). The greater the alpha angle the greater the risk of developing chondrolabral lesions and hip osteoarthritis (Agricola R. 2013). Pincer type morphology is a variation of the shape or position of the acetabulum (figure 3). Morphological variations most commonly include an over coverage of the acetabulum on the femoral head, coxa profunda, or acetabular retroversion (van Klij et al., 2018).


Figure 3- A) LCEA >40 degrees representing pincer type morphology B) Crossover sign representing acetabular retroversion. The white dotted line represents the anterior acetabular rim, and the black dotted line represents the posterior acetabular rim. Tranovich, M. J., Salzler, M. J., Enseki, K. R., & Wright, V. J. (2014). A review of femoroacetabular impingement and hip arthroscopy in the athlete. The Physician and sportsmedicine, 42(1), 75–87. https://doi.org/10.3810/psm.2014.02.2050
An over-coverage pincer type morphology (figure 3a) is measured from a sagittal line drawn through from the centre of the femoral head and then an angle is measured to the lateral edge of the acetabulum. A lateral centre edge angle (LCEA) ≥40° is categorised as pincer type morphology. A crossover sign (Figure 3b) occurs when the anterior acetabular rim ‘crosses over’ the posterior acetabular rim. This indicates acetabular retroversion (Tranovitch et al., 2014). Interestingly, the most common morphology is a mixed-type morphology consisting of both pincer and cam type morphology; reported to be as high as 74% of FAIS cases (Hale et al. 2021; Zhou et al. 2021).
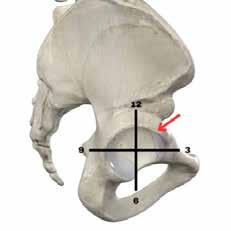
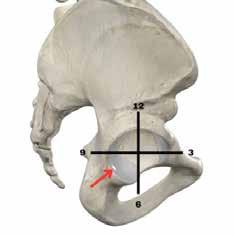
4 - Sagittal view
Premature and repetitive contact between the femoral head / neck junction and the acetabular rim as a result of cam type morphology occurs in the anterosuperior aspect of the acetabulum between 12 O’clock and 3 o’clock (figure 4a). Cumulative supraphysiological movements of the hip can lead to mechanical disruption of the acetabular labrum and chrondrolabral junction. Importantly, the acetabular labrum maintains the synovial seal whereby the
synovial fluid provides protection and nutrient distribution and to the avascular articular cartilage. Damage to the labrum decreases the ability to maintain a synovial seal impairing the health of the articular cartilage and underlying subchondral bone (Stewart & Kawcak. 2018). Furthermore, labral changes can be found on the posteroinferior aspect of the acetabular rim (between 6 and 9 o’clock) (figure 4b). This is more commonly associated with pincer type morphology and acetabular retroversion (Beck, M et al., 2005). The contact at the anterosuperior aspect of the acetabulum during hip flexion and rotation movements can create a shear force of the femoral head within the acetabulum in the posterior inferior aspect of the hip and may contribute to buttock pain symptoms.
Morphology does not equal pathology
Cam type morphology increases the risk of intraarticular pathology including acetabular labral tears, chondral lesions and hip osteoarthritis (Agricola et al., 2013). Cam type morphology is a significant risk factor for the development of hip osteoarthritis within 10 years (Agricola et al., 2024). However, it is important to note that cam morphology is not pathological unless it is associated with symptoms and clinical signs. Thus, cam type morphology may be a normal adaptive response to repetitive and high impact loads during skeletal maturation. Nevertheless, despite the relationship between cam type morphology and intraarticular hip pathology, cam type morphology is frequently found in asymptomatic male athletes in both hips (Dijkstra et al., 2021; Heerey et al., 2021) and in the general population (Pollard et al., 2010).
Physical examination
For a diagnosis of FAIS there must be symptoms, clinical signs and radiological findings (Griffin et al., 2016). FAIS symptoms are commonly reported the groin or anterior hip, although pain may also be reported in the lateral hip, anterior thigh, buttock, knee, lower back, lateral and posterior thigh (Clohisy et al,. 2009). Symptoms are often described to be sharp, catching, or a deep ache, that are often provoked with hip flexion movements including squatting, sitting in low chairs, putting on shoes and socks and repetitive movements such as stair climbing, walking, running, and change of direction (Clohisy et al., 2009). Importantly, symptoms must
match clinical signs including reduced ROM and positive impingement tests such as the AIMT, and FADIR test. Finally, Radiological findings of cam or pincer morphology on plain radiographs must be present for a diagnosis of FAIS (Griffin et al., 2016).

Deficits in hip ROM are commonly associated with FAIS, therefore a ROM assessment of the hip is an essential component of a physical examination. In a recent review Albertoni et al. (2023) stated that in people with FAIS, hip ROM is reduced in all movements except for hip extension, with the most significant limitation being hip internal rotation and hip horizontal adduction. Furthermore, lower hip internal rotation, external rotation, and abduction are associated with a higher alpha angle (Estberger et al. 2021). Moreover, larger cam deformities are also associated with reduced pelvic ROM and squat depth (Ng et al., 2015). However, hip ROM deficits may not be entirely due to morphology. ROM may be limited by pain rather than mechanical, morphology-based impingement in individuals with FAIS (Naili et al., 2022). Interestingly, pelvic kinematics vary between people with FAIS compared to those who have asymptomatic cam type morphology, suggesting the biomechanical contributors are not completely to blame for reduced ROM during functional tasks. People with FAIS display altered movement patterns and less hip contact force compared to asymptomatic hips. The changes in movement patterns may be a protective response to pain and therefore muscle functions may play an important role in the FAIS symptomatology (Catelli et al., 2021). It is important to note that primary FAIS may co-exist with intraarticular and extra-articular pathology. Co-existing hip and groin pathology may contribute to the overall level of functional disability and pain sensitivity, and therefore should be a consideration when performing a physical examination.
ROM assessment forms an important part of the physical examination of hip and groin pain. A ROM assessment should consist of a comparison between both sides, assessing for total ROM, reproduction of




familiar symptoms and end feel. Key ROM limitations that are consistent with FAIS include reduced hip internal rotation less than 20° and hip flexion ROM less than 120° (Rieman et al., 2014).






5 - Range of movement assessment a) Hip flexion. b) Horizontal adduction. c)Prone hip internal rotation. d) Seated hip internal rotation. e) Horizontal abduction. f) Hip internal rotation 90/90. g) Hip external rotation 90/90. h) Hip extension. i) prone hip external rotation. j) Seated hip external rotation.
The use of special orthopaedic test clusters can be useful to aid in forming a clinical impression relating to hip and groin pain. A negative FADIR test helps to rule out hip disease in young and middle-aged active adults presenting with hip-related pain (Reiman et al., 2020); in addition to the FABER test (Enseki et al.,

2023). When both tests are negative, they are useful to rule out FAI as the cause of pain. Furthermore, clustering the AIMT, FADIR and prone hip internal rotation (figure 6) can improve the diagnostic accuracy for FAIS (Pålsson et al., 2020).


Strength testing forms an important component of the physical examination for FAIS. Deficits in hip muscle strength and ROM is reduced in patients with FAIS (Frazzon et al., 2020), and groin pain (Malliaras et al., 2009), with the greatest strength impairments found in hip adduction and hip flexion (Bonello et al., 2022; Casartelli et al., 2011). Furthermore, strength
deficits are also associated with decreased ROM and larger labral tears in people with FAIS (Nepple et al., 2015). It is not clear if strength deficits contribute to the cause of hip and groin pain, but it does provide a greater insight into the level of functional impairment in people with FAIS and further direction for exercise implementation.





Muscle strength can be tested reliably using HHD (Ishøi et al., 2019; Thorborg et al., 2010; Waiteman et al., 2023) (figure 7). Although HHD is not a reliable diagnostic test for FAIS and associated hip pathology, it is an important objective measure to support the physical assessment and treatment intervention. Muscle strength testing should be compared between sides, deficits ≥20% should be noted as significant.
Additionally, data obtained with HHD can be used as a more reliable measure to assess improvements


in strength and pain, in combination with functional performance testing (figure 8).
Muscle guarding and protective spasm may contribute pain inhibition, fear of movement and altered movement patterns. Therefore, both intrasession (pre and post intervention testing) improvements in strength may be an effective tool to improve patient compliance with rehabilitation in combination with intersession testing to measure improvements over time.


FAIS is commonly associated with impairments in functional performance tasks indicating the inclusion of FPT (figure 8) in a physical examination. Thus, providing further objective measures to assess the level of impairment in individuals with FAIS. Additionally, FPT’s can be an important measure of progression during a patient’s rehabilitation plan. Research has shown, muscle strength and single leg balance squat performance are impaired in people
with FAI and hip OA (Freke et al., 2016; Hatton et al., 2014). Moreover, during single leg squat tasks, people with FAIS have impaired performance compared to those without pain, including performing the task more slowly and with less peak hip adduction. Additionally, changes in movement patterns may contribute to the development of hip pain (Lewis et al., 2018).
FAIS encompasses cam, pincer, or mixed morphologies, with cam type developing during skeletal maturation but typically becoming symptomatic in young to middle-aged adults. A definitive diagnosis of FAIS requires a combination of clinical signs, patient-reported symptoms, and imaging findings. While cam morphology has been associated with an increased risk of intraarticular pathologies, such as acetabular labral tears and hip osteoarthritis, not all individuals with FAIS will progress to develop osteoarthritis. Physical
examination should focus on identifying key signs like reduced hip internal rotation and flexion, supported by special tests such as FADIR, AIMT and FABER. Additionally, reduced hip muscle strength and impaired functional task performance, particularly in activities like single-leg squats and the Y-balance test are critical markers to consider when evaluating patients for FAIS. Early identification and targeted treatment interventions is essential to limit the progression of symptoms and improve functional outcomes.
Bodine is a Soft Tissue Therapist and the Director of Education at Advanced Clinical Education (ACE). He holds a master’s degree in Educational Neuroscience and an Advanced Diploma in Health Science (Soft Tissue Therapy), and is currently pursuing a second Master’s in Neuroscience. As a senior educator at ACE, Bodine plays a key role in the development and delivery of postgraduate professional development courses for manual therapists and healthcare professionals across Australia and New Zealand.
With over a decade of experience, Bodine has held various leadership roles, including course coordinator and lecturer, and has worked extensively with local, state, and national level sport. His private practice focuses on hip, lumbar spine, and neurological pain
For references log into your ANTA Member Centre > The Natural Therapist > Journal Articles.
conditions. Since beginning his career in 2011, Bodine has been committed to advancing the knowledge and skills of his healthcare practitioners through high-quality education and clinical expertise.
e: bodine@advancedclinicaled.com w: https://advancedclinicaled.com


Written by Kaitlin Edin
Numbers are an integral part of human thinking. They can be expressed by a word, symbol, or figure and are understood as things that count, measure, and label. They are used for calculations of time and space, and as such can be used to express relationships between things, fixed represent quantities, groups of things as well as the order of positions.
In different cultural contexts, they can take on symbolic meanings, and in Eastern medical thinking, the numbers are often shorthand in the philosophical and clinical language that signifies change and movement as well as groupings and relationships.
Numerology is not within the scope of this article, rather, I thought I would create a ready reckoner of numbers, a kind of quick guide for understanding, remembering and clarifying the theories that may guide a practitioner’s thinking and diagnostic intent in acupuncture practice.
In turn, this then assists our point selection from a less ‘recipe-based’ approach to one that has considered the energies and function of points we work with every day. Each number provides a place of reflection or meditation. An important Yin principle for those who are busy doing.
Delving into the numbers and what they represent can be a good way of deepening our awareness of the interactions between the human body and its environment, through time and space. And when I say the environment, I am referring to that imprint of both the heavenly forces of the cosmos, the interplay of generations, and the earthly environments that humans create and manipulate.
Whatever personal styles we might lean into, whether it be transactional, emotional, impartial or impassioned, we are still relational beings, always bound to the never-ending cycles of change; forever adapting to the climes, elements, and forces around us. We can do this habitually or with mindfulness, but it is the interaction of our minds, spirit and bodies with the heavenly and more profane earthly forces that is at the heart of the expression of our health across time.
Like all good reckoners, we will start at one.
The teachings of Eastern medical traditions in the Western context may not speak often or directly to the Dao, but as all deepened practitioners of the art and science of the medicine know, Daoism provides a foundation to Eastern medicinal thinking. The Taiji or Wuji, is representative of one, and is understood to be the “state of undifferentiated absolute and infinite potential, the oneness before duality” (6).
Where Western monotheistic traditions speak of God, the Dao speaks of the Wuji. It is the whole or oneness from where the Shen of the human being is said to come. That spirit or spark of the divine in each of us that is not unique or even imprinted with the human experience, but is a tiny ember that provides the light of consciousness, and returns to the Dao when our human experience is over.
From this awesome, undifferentiated potential, or emptiness (as some would have it) comes the interpenetrating complementarity, the duality of Yin/Yang. Originally meaning shady or sunny side of the mountain, Yin, and Yang provide a way of
symbolising both light and shadow and every variable in between. It is from this duality that the myriad of all things come. And the pairings are woven all the way through the medicine in concept, method and application.
Getting back to first principles, Yang is the active principle, hotter, upper, outer aspects of the body, Yin is the passive principle, colder, lower, inner aspects and characteristics. There are the Yin and Yang of the elements, (more of this when we get to 5 or 10), and of course Yin/Yang can be applied to any timeframe, whether it is the 24 hours of night and day, the calendar year of summer and winter solstice, or the spring and autumnal equinox.
There are the Polar pairs of the meridian circadian flow well expressed in the Chinese Clock, indicating when one meridian and organ is at its peak and another is at its ebb.
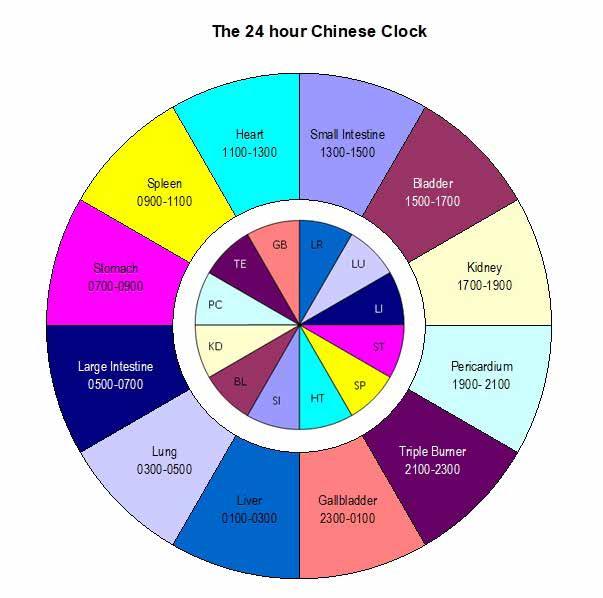
The relationships represented by the pairing of the Lung/Bladder, Large Intestine/Kidney, Stomach/ Pericardium, Spleen/Sanjiao, Heart/Gallbladder,
Liver/Small Intestine are connections that when applied to the body, can be used for balancing irregularities or extremes in the living dynamic of the Qi. They can be devastatingly elegant in their ability to speak to pain, or those weird symptoms that seem to always occur at certain times of the day. (**) The relationships are both diagnostic and treatment centred, and when applied correctly or used with polarity devices such as ion pumping cords or
electrostatic adsorbers are beautifully effective. The second diagram shows the other partnerships borne out in the circadian cycle of the clock. There is the Yin Yang of each element’s organ, (shown with the grey bracket) Lung and Large Intestine, Stomach and Spleen, Heart and Small Intestine, Bladder and Kidney, Pericardium and the San Jiao, Gallbladder and the Liver. Then, there are the six divisional relationships of the Tai Yang, Yang Ming, and the Shao Yang (shown by the green brackets), and the Tai, Shao and Jue Yin (shown by the blue curves). The relationships between the pairings are sometimes referred to as the “Coat and Lining”, looking at the clock here, you can see why.
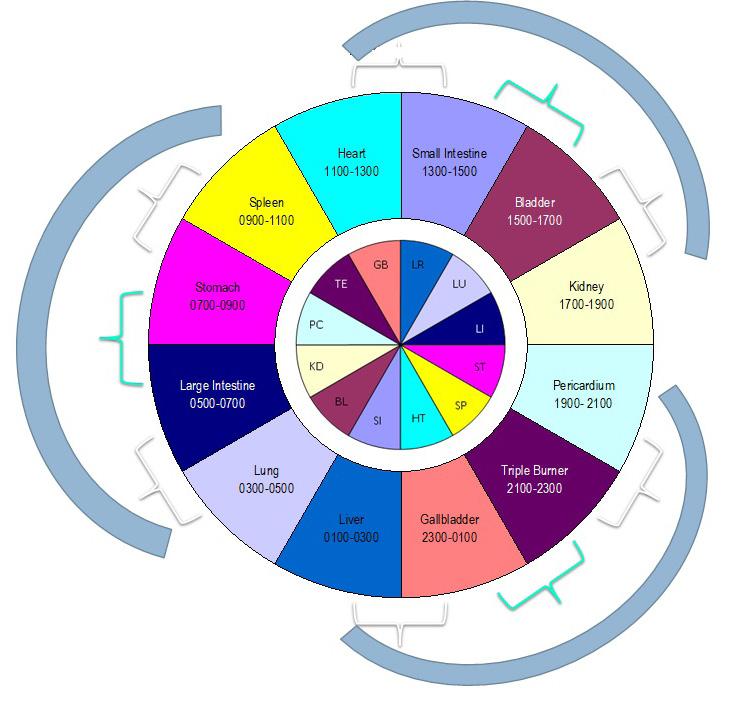
[diagram of the Chinese clock copyright K Edin]
Two can remind us of Heavenly Stems and Earthly Branches, or the dual nature of the fire element within the earthly realm.
The most beautiful articulation of the change between the five Heavenly elements and the six Earthly confirmations is the closing of the septum in a child’s heart at birth. We know that the child in utero does not breathe. There is oxygenated blood coming from the mother through the umbilical cord, but the moment the child is born, already a most remarkable change of state, they take a breath. And it is this first breath that demands of the tiny, new body that it have somewhere for oxygenated and nonoxygenated blood to go. It is at this moment that the atria of the heart can be considered to separate into two distinct chambers, because the septum between

the two atrial chambers seals shut, and there are now two discrete chambers rather than one. ().
This change in the heart is the action that announces the duality of Fire as it is applied to the human body. We are taking a little bit of poetic licence here, but what is important to imagine and reflect on, is that in the moment the septum closes, the heart goes through a physiological change, and the five movements of the prenatal (Heavenly) life, change into the six energies of the postnatal (Earthly) life. We come back to this idea when we get to five and six but let’s just mosey through the numbers in the sequence for now, three is next.
The ever-symbolic trinity. There are a range of threes in eastern medicine and philosophical thinking. Three is pretty much everywhere. There are the trigrams, but more on this when we get to the Bagua. There are the three burners, the San Jiao, the upper, middle and lower regions of the body. While much of the teachings of the Hun speak of it as a singular entity, there are said to be three Hun. The Hun is considered the individualised aspect of the Shen, the parts of the personalised mind that are imprinted with human experiences, or the skamsara of our individual journeys. (** Singer). The three Hun are part of the embryo’s development into human identity, and three holds a lot of sway in the processes of reproduction.
The third month of pregnancy is when the ‘quickening’ occurs, or when in modern parlance a pregnancy is
more likely to hold. It is three days after birth the beginning of the internal character of the child is said to emerge, and at three months the Hun is felt, seen and considered by the parents and the naming of the child deemed appropriate. Some families still observe these naming rituals of a slower paced and more observant world.
There is the relationship between Heaven, Humanity and Earth. It is a bond that were we to map it somehow, we could represent it by a vertical (X) axis, or we could call it the warp; the vertical lines in a cloth.
It is space, as opposed to time. The three treasures, the Shen, Qi and Jing can stand in for Heaven, Humanity and Earth, a beautifully fractal way of seeing the resonances of each in each. Shen is pure and as untainted as Heaven. The Jing provides the material blueprints for the unfolding of life and so represents the mutability of the Earth. And Qi is the dynamic between the two in much the same way that Humanity is a reflection of both the Heavenly and Earthly designs (well in Man’s mind at least). Qi is movement, and substance, empty at its core, existing only as the result of an interplay between Yin and Yang and the myriad of things.
Four holds a great deal of material. There are the bodily materials of the four Seas: Blood, Qi, Ying and Marrow. There are many gates along the meridians, but four is representative of the square, a stable,
somewhat static shape, and so in many acupuncture point prescriptions there are four gates, or four points: as a grounder, a stabiliser of energies that need calming or regulating. There are four chambers of the heart and four meridians in the Fire aspect.
Four winds, four directions or movements (North, South, East and West) and four seasonal modes. Mostly, the energies or correspondences of the directions speak to the turning of the world on its axis from a Northern hemisphere perspective, and many Feng Shui scholars suggest that the directional energies of the Northern hemisphere need no difference when applied in the Southern hemisphere. I am not of that mind after reading Roger Green from the Golden Gate Feng Shui School article. For “whilst the Daoist principles remained universal - the application needed to be adjusted to the energetics existing in the southern hemisphere”. (2) However, in the interests of clarity I shall keep to the standard teachings.
North is the hidden beginnings, found in Water, Winter and the Kidneys. It relates to death and rebirth, the moving from and into the void. It is the material becoming and unfolding.
The South relates to Fire and Summer and the Heart in the human body. In the cosmological orientation of the ancient eastern mind, the South sits at the top of the map, rather than at the bottom as it does in Western prescriptions. The South is the direction of heaven and speaks to how important the heart, spirit and the warmth of the sun were.
Here we see the relationships between Water and Fire, Earth and Heaven on the vertical axis coming into play again. This idea is the axis of creation, those things that sit in potential, making ready.
The East corresponds to Wood, Spring, and the Hun. All are energies that speak of expansion. Here is the beginning of the Y axis, the beginning of the timeframe of a life.
The West relates to the contracting and declining energies of Metal, Autumn, and the Po. From east to west, this is the Y axis of time and cycles. As a continuum, the Y axis represents the life created, there is a beginning and an ending. From the four comes the five. There are more threes, fours than the ones I have mentioned here; the ancient
divisions of Heaven, which relate to the Chinese Sky during the dynasties bring us many more numbers and constellations of ideas, but I have omitted these for the sake of keeping the information relevant to practice and within the scope of this article.
Many know of the Wuxing, the Five Elements or Phases.
The Five Elements here will refer to those heavenly stems of Wood, Fire, Earth, Metal, Water. Each of the five elements represents the characteristics of an elemental force and as such five is representative of the energies of the cosmos or how things move in Heaven. Wood is expanding and prone to the turbulence of wind, Fire is enlightening and maturing prone to getting too hot and burning itself out, Earth is grounding and stabilising but prone to heaviness, turbidity, or being bound, Metal is contracting and refining, prone to dryness and disappearing. Water is always moving in flow, cooling and deep, it is prone to stillness and stagnation.
The five elements speak to us about forces or energies. They have relationships to each other expressed in the Sheng or nurturing cycle, otherwise expressed as the mother-child relationship for the way in which one element relates to the next.
There is the Ke cycle too, which is a regulating or constraint cycle, sometimes called a governing cycle, which ensures excess is reined in.
These two main relationships between the five elements remind us of Yin and Yang, but also that there are relationships between characteristics or states. Both the nurturing cycle of the mother child (Sheng) and the controlling or regulating (Ke) cycle expresses the movement of energies in the world.
Each of the Elements is a way of mapping the world and everything in it through a series of correspondences. There are five discrete sets of colours, sounds, tones, movements, and seasons. Applied as a theory to the human body, the correspondences are applied to the internal organs, and their related spirits.
There is the Liver and the Hun (Soul), associated with anger and the Wood element. There is the Spleen, the Yi (intellect) associated with worry or
inward thinking and the Earth. The Lung and the Po correspond to Metal and grief and withdrawal, there are the Kidneys, and the Zhi (Will power) corresponding to Water and fear (as the driver of survival). And then, there is the Heart and Shen related to Fire and the emotional state of joy, elation, or love.
It is when we get to the Fire element and its application to the human body less as a theory and more as a practical approach through the meridians that the dual nature of the Fire phase comes into play and the notion of the six takes over.
Once we are working with meridians and not simply discussing the theory of the phases, then we are within the realm of the human being and time. It is the Five phases plus one. Six represents the ways things move on earth. It is very much in the realm of earthly cycles and the lives of human beings. The duality of the Fire phase comes into being, as the human comes into being. As mentioned before, at the time of birth and the first breath, the septum that has been open, closes, and thus begins the circulation of the sovereign breath. ()
So begins the placement of that child in the cosmos, the person’s time stamp of beginning. In the sense of the earthly cycles, the clock has now begun for this life. With this change in state, the Ministerial Fire, represented by the Pericardium is the recognition that the postnatal or human journey has begun. Six then is the earthly cycles and spiral nature of time. With the transition (which we call birth) from heavenly potential to human being, the meridians now essentially begin and are an expression of the living body. It is not to say that the meridians are fully formed at birth, they begin and develop and record the experiences of a human life, and it is why they are not found in the dead.
It is worth remembering that the (Yin) Pericardium and the (Yang) San Jiao are considered to be two organs with a name but no form. They are a short hand that speaks to the intersection of the cosmos and the human form. They represent the functional aspects of the Fire in maintenance of life rather than in the creation of it.
The Heart holds the Imperial fire of the Shen, the divine spark, while the Pericardium holds the engagement of that divinity in a human form. The Pericardium is the Ministerial fire, the aspect of the meridians that engage with the world, hold court, create a warm connection and nurturance with others, while the Shen is forever reflecting heaven. In some schools, the Heart meridian is not needled for this reason.
The map of meridian correspondences that many practitioners use in point selection and combinations are the maps converted from the five to the six.
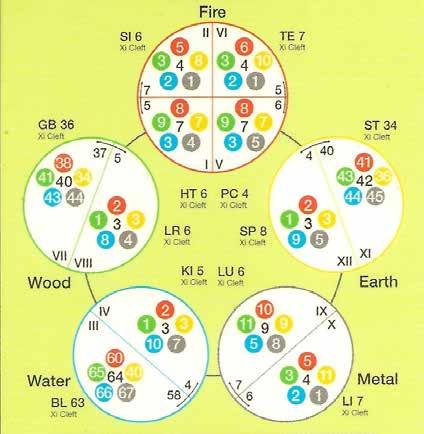
[Diagram – shows the Acupuncture command points – Ref 1]
Beside is the map of meridian correspondences that show us the fourfold expression of Fire: Heart, Pericardium, Small intestine and Sanjiao, as well as the elemental nature of the points. Interestingly, some lineages see the Pericardium, and the Sanjiao as wood element organs, perhaps due to the nature of the expansion of life from the womb to the world that is implicit in the transition.
There is so much more in six, there are the six divisions, couplings of the meridians from the most Yang to the most Yin, which speaks to the movement of the Sun around the human body or the Yang or Qi in the meridians.
The six divisions that we could see in the Chinese clock diagram above, show the Tai Yang (Small Intestine and Bladder), the Yang Ming (Large Intestine and Stomach), the Shao Yang, (Gallbladder and San Jiao), the Tai Yin (Lung and Spleen), the Shao
Yin (Heart and Kidney) and the Jue Yin (Pericardium and Liver).
There are the six extraordinary fu, all extraordinary because they act like hollow organs (u) but store as the Zang, which are the blood or essence rich organs of the body, and include the uterus, brain, bones, gallbladder, marrow and the mai (or vital circulatory vessels). (3)
There are seven Po related to the seven orifices of the body (mouth, anus, urinary tract, nose, ears). The Po are considered the ‘animal spirits’ in as much as they ‘go back’ to the earth on our dying, but they reside in the living body in the Lung and the Large intestine, and are integral to the life affirming cycles of the breath and the elimination of toxicity through the bowel.
There are seven-year cycles that are said to govern the female body, while the male body is said to be governed by cycles of eight.
Eight carries a few things on its branches. There are eight basic diagnostic principles that every novice learns as the first diagnostic considerations. Hot, cold, inner, outer, up or down, front or back. These principles are obvious locators, but sometimes in the overwhelm of processing new teachings, these basic tenets can reorientate the mind.
There are eight characters (BaZi) in the birth charting. BaZi is the study of the birth charts, there are the four pillars and 8 characters (Ba means eight and Zi, character). It takes the year, month, day and hour of our birth and can provide insight into our constitutional gifts or challenges. It endeavours to capture through the five elements and correspondences what energies and timings were in play when we came into existence, and how the timing across our lives can be used for our benefit.
There is the Bagua, at the heart of many Feng Shui considerations. But it is also used diagnostically and as a treatment strategy, in a number of acupuncture schools.
“The Bagua represents the eight primordial trigrams, arranged as a mandala to map the energetic qualities of the seasons, colours, directions, life situations and many other associations. The trigrams are a
combination of three lines representing humanity between heaven and earth. The Bagua is a clear and precise observation on how energy moves and circulates in our outer and inner worlds. It is an energy notation of natural phenomena describing the Qi pattern as it exists between Heaven and Earth.” (2)
Such a nuanced map, it is also used to map acupuncture treatments to the seasons, and the elements in a startling way. For more information on that the application of the Bagua or the Yi Ching seek Richard Tan’s Seasonal Balances workshops run by Si Yuan.
Once we get to ten, we have the Heavenly stems, which represent the five elements with the added texture of Yin and Yang. Here is the Yang Wood (jia), Yin wood (yi), Yang fire (bing) Yin fire (ding), Yang earth (wu), Yin earth (ji), Yang metal (geng), Yin metal (xin), Yang water (ren), Yin water (gui).
Then, there are the twelve earthly Branches, represented by the twelve animal signs Tiger (Yin), Rabbit (mao), Dragon (chen), Snake (si), Horse (wu), Goat (wei), Monkey (shen), Rooster (you), Dog (xu), Pig (hai), Rat (zi) and Ox (chou).
In combination, the Heavenly stems and the Earthly branches create a cycle of sixty. You may think it is one hundred and twenty, but the polarity of the stems and branches must be the same (Yin with Yin and Yang with Yang) thus, this constraint halves the combinations to sixty. An important number in the human life cycles according to eastern traditions.
It is useful to think of the numbers that exist in our clinical theories and practical applications, as a way of considering deeply what we are trying to do with the energies at any one time. With recognition of what the numbers represent, a more nuanced and sophisticated understanding of the what, when and why of our point selection opens up into the heartful hands of the practitioner.
For references log into your ANTA Member Centre > The Natural Therapist > Journal Articles.
THROUGH THE SYNERGY OF HYPNOTHERAPY AND TARGETED GUT REPAIR.


Register today to access ‘prescribing’ details and receive
2’-FL prebiotic exclusively feeds beneficial gut bacteria while zinc L-carnosine promotes GI integrity 1,2
Gut-directed hypnotherapy has been clinically demonstrated to work just as well as the low FODMAP diet, without food restriction3