The new chair of the Technologist Special Interest Group (TSIG)
In celebration of Pioneers.
Understanding Clinicians’ Diagnostic Practices of FDG PET CT Brain for Investigation of Cognitive Impairment.
Reflections on clinical placement in Darwin.
Technologists Special Interest Group - Introducing the new TSIG Chair. Conference Convening Committee.
The role of [18F] FDG-PET/CT in necrotising otitis externa: a case report.
Understanding Clinicians’ Diagnostic Practices of FDG PET CT Brain for Investigation of Cognitive Impairment. What's that: A case study.
In celebration of Pioneers.
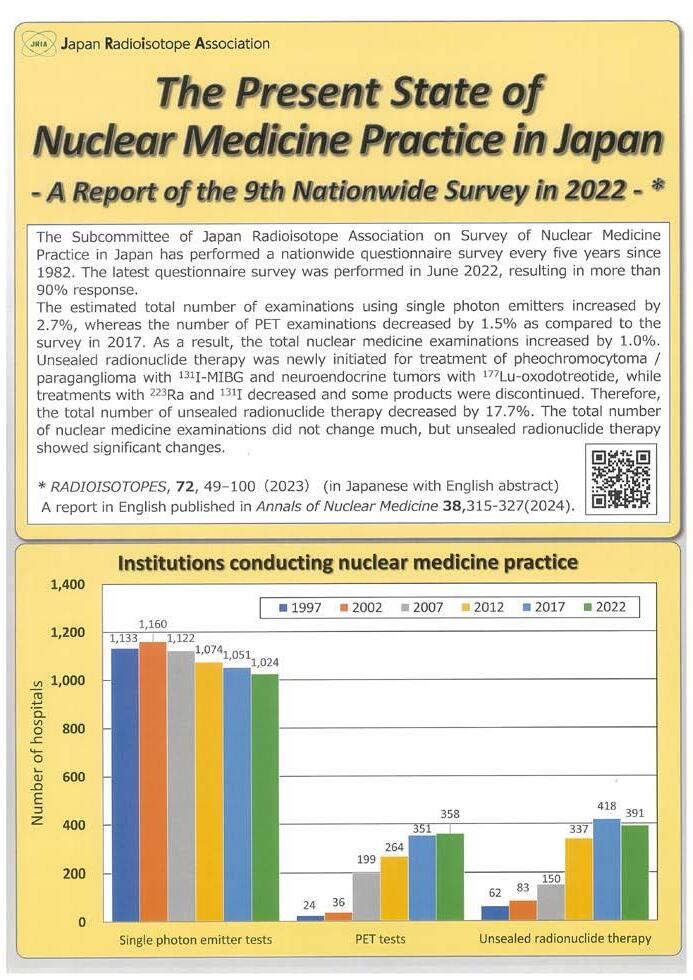
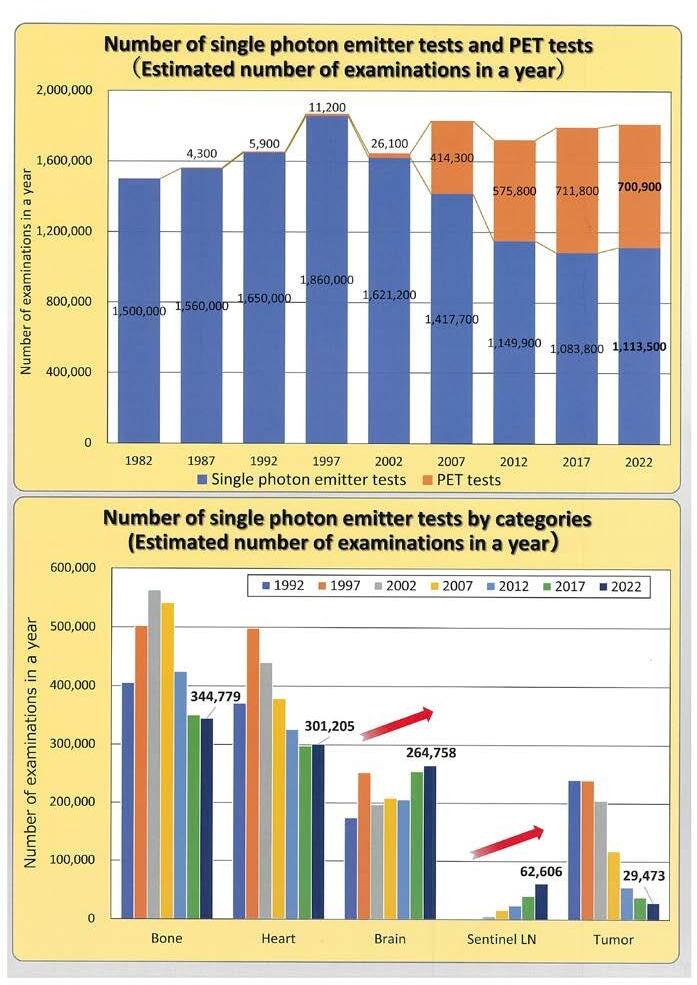
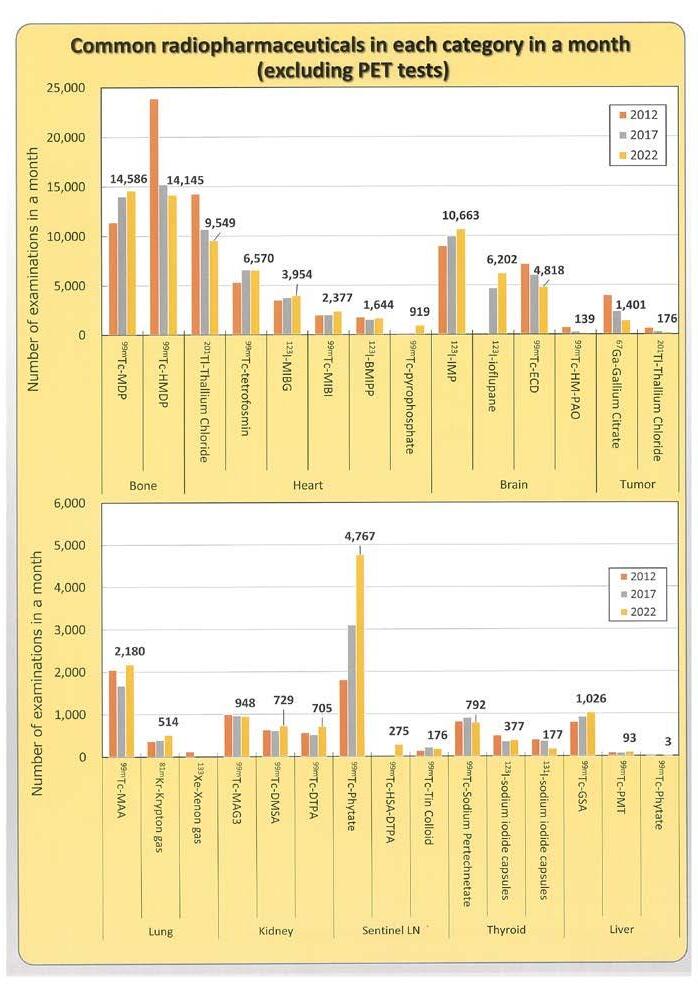
Pyrexia of unknown origin and FDG-PET/CT. Reflections on clinical placement in Darwin. The present state of Nuclear Medicine in Japan.
Awards and recognition at the 2024 SNMMI conference.
Welcome Samantha Hawkins, new project manager at ARTNET.
In memorium - Andrew F McLaughlin.
FROM THE PRESIDENT
Karen Jones President
‘What
we call the beginning is often the end. And to make an end is to make a beginning. The end is where we start from.’ T. S. Eliot (1888-1965)
Hello Fellow ANZSNM members,
I am humbled to write my first piece in the Gamma Gazette as your President. As the quote by TS Elliot so eloquently exemplifies, beginnings usually mark the end of something else. Each President of the ANZSNM, with the exception of our first Society President, Associate Professor Harry Lander (1969-1970), has commenced their term immediately following the conclusion of the term of the President who preceded them. In my case, I follow Kevin London, a colleague who I value highly. I thank Kevin for his major contributions to the Society as President and I am grateful for his ongoing support as the Immediate Past president, particularly as I navigate my ‘beginning’. You will be aware from my commentaries in the monthly ANZSNM newsletter, that I often start with a quote – I find it helps me to focus my thoughts. It is a ritual I propose to maintain during my Presidency – or until enough of you have asked me to stop!
As I mentioned at the conclusion of the Annual Scientific Meeting in Christchurch, my background is unconventional and has been strongly influenced by serendipity. After training initially as a Nuclear Medicine Technologist I have, over the following 3 decades, pursued a successful and rewarding career related to clinical research, now as a Professor and Senior Clinical Research Fellow at the University of Adelaide. My background in nuclear medicine has been pivotal to my research activities - I currently lead a team within the Centre of Research Excellence in Translating Nutritional Science to Good Health, in the Adelaide Medical School - the focus of our work relates to the roles of the gut in the blood pressure and blood glucose responses to meals. I cannot disagree with Kevin when he says (quite frequently), ‘Karen loves gastric emptying’. - I also hold an Adjunct Professorial position at the University of South Australia where I teach in the undergraduate nuclear medicine program. I have had the privilege of supervising more than 40 higher degree research students (Honours, Masters and PhDs from diverse backgrounds, including medical imaging). In 2026, my two worlds will hopefully meet, rather than collide, when the University of Adelaide and the University of South Australia merge to form the new ‘Adelaide University’.
I have a longstanding relationship with the ANZSNM. - I attended local South Australia (SA) Branch meetings as a student, was on the Executive of the ANZSNM Technologist group, was Secretary of the SA Branch in the early 90’s and also served on the Competency Based Standards Committee. Establishing a research career, while raising my family of 4 children (now aged 13, 14, 20 and 23 years old), limited my capacity to make a meaningful contribution to the ANZSNM for many years. However, in 2018 (when my youngest child started school), I was very pleased to be able to join the TSIG CPD & Education Committee and have had the good fortune to be increasingly involved in the ANZSNM since that time, including as the Chair of the TSIG, a member of Federal Council and as Chair of the Executive Committee of ARTnet.
As your President, I look forward to supporting and advocating, for all professions within the field of nuclear medicine. - My vision is to strengthen the ANZSNM substantially by promoting important initiatives, optimising cohesion among heterogeneous groups and encouraging all members to play a significant and, for many, increasing role in their profession. These broad and ambitious aims are achievable, but only with your commitment and sustained support. – This brief introduction marks the end of my beginning…..
Thank you for being a valued member of our Society.
Best wishes,
OUR CONTRIBUTORS
Pru Burns
Unit Charge Nuclear Medicine, Capital and Coast District Health Board, NZ
Rebecca Mangelsen University of South Australia, SA
Student NMT at Royal Darwin Hospital in Northern Territory, NT
Dale Bailey
Royal North Shore Hospital,NSW
Dr Ashlesha Vaidya
Central Adelaide Local Health Network, SA
Bonnia Liu
Austin Health · Department of Rheumatology, VIC
Jessica Watson University of South Australia, SA
EDITORIAL COORDINATOR
Rajeev Chandra General Manager PO Box 6178, Vermont South, VIC 3133 T 1300 330 402 F (03) 8677 2970 gm@anzsnm.org.au
EVENTS & ADVERTISING ENQUIRIES
marketing@anzsnm.org.au
SUBMISSIONS
secretariat@anzsnm.org.au
DESIGN & PRODUCTION
Enovate Studio www.enovatestudio.com
PUBLISHED IN
Autumn, Winter & Spring/Summer
CONTENT SUBMISSIONS
Scientific submissions on all aspects of nuclear medicine are encouraged and should be forwarded to the Secretariat (instructions for authors published at https://www. anzsnm.org.au/activities/gamma-gazettecontent-submission-and-guidelines/).
Letters to the Editor or points of view for discussion are also welcome.
If original or public domain articles are found and considered to be of general interest to the membership, then they should be recommended to the Editor who may seek permission to reprint.
The ANZSNM Gamma Gazette is published three times a year. Deadlines for each issue of the journal can be found on our website anzsnm.org.au
DISCLAIMER
The views expressed in any signed article in the journal do not necessarily represent those of the Society. The individual rights of all authors are acknowledged.
I am pleased to bring you my first update as the new Chair of Branches. This role has been brought about following acceptance of the updated ANZSNM Constitution at the 2023 AGM, providing one voice on Federal Council for representation of all branches.
I have transitioned to this role following my representation of the VIC/TAS branch on Council since 2018, and express my thanks to Suzanne McGavin, who has been performing this role in an informal capacity since the 2023 AGM.
The fundamental purpose of this role is to represent the state branches on Council. This will be facilitated through regular consultation with the state branch chairs regarding professional matters at branch level, and tabling of relevant matters at Council in response to feedback and input garnered from this consultation to inform ongoing changes and initiatives within the society. When implementing the new structure and recognising the many different matters discussed at (a volunteerrun) Council, it was felt that branch matters should be consistently heard, and raised ideas shared. It is also recognised that branch committees work tirelessly and are also time poor. The new structure, as proposed, provides for a regular update to the Council on branch matters, and allows drawing out of issues in common and, importantly, sharing of ideas. With the cooperation of your branch representatives, it will be my role to facilitate this overall process.
The branch chairs meet prior to each Federal Council meeting, approximately four times each year, with our next meeting due to take place later this month.
As part of the role, going forward, I look forward to providing a consolidated branch update in each issue of the Gamma Gazette.
Queensland News
Queensland's recent branch meeting took place online with an excellent turnout. Despite occurring slightly later than usual due to workforce commitments, the meeting was highly informative and engaging, with Siemens graciously sponsoring the event.
The first speaker, Julia Skelton, a Med Primary House Officer in PET Imaging at Princess Alexandra Hospital, delivered a compelling presentation on "Evaluating whether a visual grading score can be applied to the use of Gallium67-Citrate scintigraphy in the assessment of patients suspected of renal allograft pyelonephritis: a single centre retrospective audit." Julia's talk shed light on a visual method for establishing uptake scores in the kidney, particularly in patients suspected of AGPN. Her proposed visual grading scale offers promise as a reliable and feasible means of confirming AGPN diagnoses, potentially reducing the risks associated with contrast nephrotoxicity.
Following Julia, Ingrid Holmes, a Senior Nuclear Medicine Technologist and Research Officer at Princess Alexandra Hospital, shared insights into "Theranostic Clinical Trials: Navigating Research, Emerging Trends and Key Start Up Processes."
Christian Testa, MANZSNM Chair of Branches
Ingrid provided valuable information on the onboarding process for new research, sponsorships, and therapeutics within a department. Given the increasing prominence of theranostics in nuclear medicine, her talk offered essential guidance on setting up clinical trials.
Lastly, Heather Biggs, a PhD Student at the Australian Institute for Bioengineering and Nanotechnology, presented "From Bedside to Bench – Developing Novel Nanomedicines for the Controlled Administration of Theranostic Agents in Cancers." Heather shared her journey from nuclear medicine technologist to researcher and discussed pioneering research in developing nanomedicines for cancer treatment.
During the branch meeting discussion, it was decided that most future meetings would be held online to better reach our rural constituents. Additionally, plans were announced for our Biannual ANZSNM symposium, with a committee formed to organize the event, including the addition of Remi Hillery from SCUH. Stephanie Schulze was also welcomed as a 3rd co-secretary.
Victoria & Tasmania
In January, the VIC/TAS branch held their annual Cardiology Masterclass via Zoom, and were privileged to once again welcome Dr. Kim Williams, who delivered an insightful and thought-provoking presentation on “The Future of Nuclear Cardiology”, which was well-received by our members both within and outside the branch. This is always a popular and well-attended event on the VIC/ TAS calendar and we hope to continue in the years to come.
In July, the branch hosted their inaugural Case Presentation night on the 3rd of July. This has been developed in conjunction with RMIT University to showcase the breadth of nuclear medicine practice within the branch, as well as to give our current undergraduate students the opportunity to develop their presentation skills within a broader audience.
The branch will also be holding their Annual Day Symposium in October, in conjunction with the AGM, Radpharm and Student Award presentations.
South Australian & Northern Territory
The SA/NT branch has held two meetings so far in 2024 via Zoom. Both events have been very well-attended and received by members from within and outside the branch.
The branch was excited to hold their first social night, the inaugural “Battle of the Pro’s”, on the 28th of June at the Strathmore Hotel. Members are also encouraged to attend the next Protocol Review meeting on the 11th of July, or for those who can’t attend, the next branch meetings on Zoom will be taking place on the 25th of July and 4th of September.
Western Australia
Two successful branch meetings have been held in WA this year, with excellent attendance and feedback from members.
The branch looks forward to hosting its next branch meeting on the 16th of July, as well as the Radpharm presentation evening on the 4th of September. Case studies are always warmly welcomed from our members for this award to foster development of technologists and promote collaborative discussions within the technologist community.
Following on, the branch day seminar will be taking place on the 13th of October and AGM on the 27th November.
New Zealand
The NZ branch has been energised following the ASM in Christchurch. It was a pleasure to welcome conference delegates to New Zealand for the first time since the 2016 ASM in Rotorua.
The next local event for the branch will be the Radpharm and Paul Orr awards evening, taking place via Zoom on the 18th of September.
Collectively, the branches wish to extend a heartfelt thank you to all volunteers, whose unwavering support and dedication is greatly appreciated. We also express our gratitude to our sponsors and members for their continued commitment and contributions to our activities.
MY EXPERIENCE AS A BRANCH SECRETARY
If you have ever experienced what it is like to volunteer at one of the Society's branches, we are lucky to have first hand experience told by those holding this position at our various branches.
We hope you enjoy the read and if you feel you'd like to be part of your local branch, please reach out to our Chair of Branches, Christian Testa to discuss the available openings and requirements.
Ijoined the VIC/TAS branch in 2015 after chatting with one of the committee members at the annual January scientific meeting, who gave me an insight into what the committee did and what was required of members. I had previously been a Mentor with the Victorian NMIC (Nuclear Medicine Internship committee) and was looking for a new way to contribute to the profession. After the resignation of the previous chair, I accepted the role of Chairperson and have been in that role ever since.
Part of my role includes organising branch meetings and other opportunities for education and networking among our members.
Being part of the committee lets me keep up to date with changes throughout the profession as well as keep in contact with technologists from around the state and the country.
As the Committee Chairperson of the ANZSNM QLD branch, my experience has been marked by a diverse range of responsibilities aimed at advancing the professional development and competence of nuclear medicine specialists, graduates, and students across Queensland. Over the past three years, I've held various roles within the committee, including CoSecretary, Treasurer, and Federal Representative, before assuming the role of Chair.
One of the core functions of my role involves organising quarterly branch meetings, which serve as platforms for educational initiatives and networking opportunities within the nuclear medicine community. These meetings feature keynote speakers from diverse areas within nuclear medicine, offering valuable insights and fostering discussions among members. Importantly, they also provide a forum for members to offer feedback, allowing us to tailor our educational programs to meet the evolving needs of our members.
In addition to event coordination, I have organised QLD RADPHRAM Technologist Case presentation award nights, facilitating knowledge exchange and peer learning among members. Additionally, I've played a role in gathering case studies and information for the ANZSNM Gamma Gazette, a nationally distributed CPD resource. These educational initiatives not only provide students with exposure to various facets of nuclear medicine, preparing them for their future careers, but also offer nuclear medicine scientists opportunities for professional recognition and staying updated on current practices and advancements in the field. By fostering a culture of learning and collaboration, we support the ongoing professional development of our members and contribute to the advancement of nuclear medicine in Queensland and beyond
Kim Jasper, MANZSNM VIC/TAS Branch Secretary
Anisa Kumari, MANZSNM QLD Branch Secretary
The purpose of this commi ee is to represent NSW/ACT members in regards to CPD events, local issues and representation at the ANZSNM Branch Chair Commi ee, which will then report to the ANZSNM Federal Council. The commi ee will assess the educational needs and future developments of all nuclear medicine professionals in NSW in accordance with the objectives of the ANZSNM.
Or visit www.anzsnm.org.au to learn more about the current vacant positions for this role. CLICK HERE
Expressions of interest are sought from ANZSNM members to join the Rural and Regional Branch Commi ee.
The purpose of this commi ee is to represent Rural and Regional members in regards to CPD events, local issues and representation at the ANZSNM Branch Chair Commi ee, which will then report to the ANZSNM Federal Council. The commi ee will assess the educational needs and future developments of nuclear medicine professionals in Rural and Regional areas in accordance with the objectives of the ANZSNM. Members can be part of both the Rural and Regional Branch, and their local State Branch. Members can only select one branch to enter for Radpharm.
Or visit www.anzsnm.org.au to learn more about the current vacant positions for this role. CLICK HERE
The ANZSNM SA/NT branch is consisting of Alexis Dalagiorgos as Chair and the Federal Representative, Victoria Neale and Sunny Cha as Co-Treasurers, and myself as the Secretary. From 2024, the branch Chair and Federal Representative will be held by the same person, where previously these roles were held by different people. This change enables a greater connection between the federal and state level of the ANZSNM. Alexis, Victoria, Sunny and I organise and host quarterly branch meetings which include reports from various committees, and a scientific component provided by one of the Nuclear Medicine departments in SA or NT, or UniSA. We have opted to move all branch meetings to online only due to the declining in person rates in recent years. Professional social interaction is imperative for the development of the industry and growth of ideas, therefore, for the first time we have included a mid-year social event this year. We hope that this event will provide an opportunity for those that attend to mingle and expand the "brains trust". This event will include an educational component, as well as some fun activities to get everyone interacting! We will round out the year with the highly anticipated annual AGM and quiz night, which is always an extremely successful event.
The SA/NT cohort are lucky to also have a very active technologist branch, the ANZSNMT. The responsibilities of coordinating the ANZSNMT branch rotate through a predetermined roster of the local nuclear medicine departments, and this year, Rachjany Oung, Kristin Marchi and Elizabeth Inaba-Hill from the Flinders Medical Centre Nuclear Medicine Department will host the ANZSNMT. The ANZSNMT is specifically aimed at technologists where matters relevant to technologist are discussed, however, any type of member is encouraged to attend. The ANZSNMT provides two branch meetings and the AGM annually. The branch meetings usually consist of a scientific presentation and a protocol review, which have previously been very well attended by members not only from SA/NT but also across Australia/ NZ. The ANZSNMT AGM includes the SA/NT Radpharm Awards, allowing technologists and students to present
Welcoming NZ's New Chair, Jessica Fagan
their cases in front of their technologist colleagues in a very supportive and relaxed environment. Volunteering in these roles have enabled us to meet and interact with industry partners, members from around the country, students, and follow colleagues in ways which we wouldn't otherwise have an opportunity to. It is a diverse role entailing a lot of planning and organising, event planning, sponsorship, representation at community events, federal policy guidance, navigating product shortages, and correspondence between industry partners and members. I encourage members to look out for opportunities to get involved in the ANZSNM, not only is it a great experience but you get to be part of developing and maintaining the incredible community that we have, as well as what the future of the industry will look like.
Jessica Fagan, Molecular Imaging & Theranostics Operations Manager for Mercy Radiology, Auckland. Jessica is a Canadian trained Nuclear Medicine Technologist who emigrated to NZ in 2011. She is an industry leader in the Molecular Imaging & Theranostics space in New Zealand. She has been integral in the launch of novel imaging and theranostics tracers in New Zealand, including: Ga68 PSMA, DOTA, FAPI and Lu177 PSMA and DOTA.
She is passionate about ensuring Kiwi’s have access to the latest and greatest developments and technologies in Nuclear Medicine, including novel tracers still undergoing clinical trial. She is a self-proclaimed fitness fanatic and loves shredding on her snowboard when able. She lives by the beach, north of Auckland with her husband, daughter and border terrier.
INTRODUCING THE NEW CHAIR OF THE TECHNOLOGIST SPECIAL INTEREST GROUP (TSIG)
Suzanne McGavin, MANZSNM TSIG Chair
Hello and it is an honour to do my first post as the new TSIG Chair for 2024. I would like to deeply thank Pru Burns for her tireless work and hope I am able to keep up the same standard of commitment and investment for the TSIG and our members.
My new role has also included changes within the TSIG as I step down as WFA Chair, so let me re-introduce our TSIG oversight committee. Please reach out to all members for any questions or queries as we are here to help and support the Nuclear Medicine community.
I thought this would be a good opportunity to introduce myself and give a background on my experience.
Clinically, I am the Chief of the Royal Darwin Hospital up in the Northern Territory of Australia. This role has created an increased investment in the challenges and hardships of the Nuclear Medicine community in regional and rural areas. The problems we experience in the metropolitan sites, is compounded in these areas and this has been an eye-opening opportunity to create a well-rounded view of our nuclear medicine community. If anyone is around the Top End, always happy to help you with the heat and a friendly face.
I am a very proud Nuclear Medicine Technologist and really do live and breathe our profession.
I started working in my home town of Wollongong, NSW, after graduated from the University of Sydney. Here I was mentored and trained with some of the most supportive nuclear medicine teams around who developed my investment in patient care, high standards and understanding public and private can work together. I worked here for nearly 10yrs and it was also here I was introduced to being part of professional committees, and started as a PDY representative all those years ago.
After Wollongong it was time to move to the ‘big smoke’ and I took a role at the Royal Brisbane and Women’s Hospital, QLD, which was a massive development in my career. Here I was exposed to a large Nuclear Medicine and PET department, and a full TGA radiochemistry hot lab. My skills, understanding and experience were widened and I gained an even larger understanding of the scope of our profession. During this time, I became the State-wide Educator for QLD Health as I also have a Degree in a Bachelor in Teaching, which finally merged with my nuclear medicine career (the hard work paid off!). This role enabled me to start working around QLD and engaging with all our staff and build education, connections and programs to help support our Nuclear Medicine Scientist of QLD. Here I also become the Chair of the QLD ANZSNM branch. Being able to work with other sites and students, my understanding of the complexities of departments, differences in protocols and practices, started to create a colour scale of how nuclear medicine can work in different environments. I also became interested in the managerial side of health and started (and completed) my Masters of Health Management, opening my eyes to budgets and the paper-side of health.
While in QLD, I was approached to take on a role at RMIT in Melbourne as the Stream Leader of the Nuclear
Suzanne McGavin, MANZSNM, TSIG Chair
Medicine program in 2018. This was another exciting change in my career pathway and I felt it was an opportunity to give back to my community by helping build the new 3.5yr program. Through this, I was able to become part of the Victorian community and part of the VIC/TAS committee. My role in Academia also allowed me to engage and build relationships with the other Nuclear Medicine Academics across the country. Our relationship enabled us to work together (especially during COVID-19!) to help each other build our programs up, as we all want to create the best Nuclear Medicine Technologists and support our workforce in student supervision. My role in academia was also a great opportunity to see the world from the student’s perspective and a big learning curve in how they see the world and the new challenges they face, which are far different to ones I had during my time as a student (overhead projectors and no recorded lectures).
Life then threw another opportunity in 2021 and I found myself in the Northern Territory and soon became the new Chief of Royal Darwin Hospital PET/ Nuclear Medicine Department. Here I have had the rare opportunity to build and grow a department to reach its full capacity. The challenges of being ‘remote’ have created colourful management and drawing on all my experiences from my different roles to promote staffing, students and support from all areas. Our department in the NT is something different for many reasons. We have a rotating wheel of locums, experience the rare cultural diversity of Australia, and manage logistical challenges with almost everything. But I wouldn’t change it for the world.
So clinically, my career so far has provided a variety of roles which has created a sense of diversity in my approach to our profession and empathy towards many of our challenges but also excitement of the potential we have.
On the professional society side, I hold the role of Treasurer on the Executive, something I am very proud of as a NMT. I am also the new NT representative on the Medical Radiation Practice Board (MRPBA), another massive achievement for me professionally, and also the opportunity to really contribute to our profession from another angle. My other roles include/included ANZSNM
Branch Rep Chair, MRPBA Exam committee, Ahpra Program Accreditation, previous roles in branches and just generally anything that pops up, I find it hard to not want to be part of the solution and development of our profession.
As the new Chair of TSIG, it will be time to hang up a couple of my other roles and I really encourage anyone who wants to add a dimension to their career and work and meet so many great people, to reach out and become a committee member of your local branch, or other roles in the ANZSNM. I am always happy for a chat or advice if that helps.
The plans for the TSIG are large and visionary. Anyone who knows me, knows I am an optimistic person who feels with the right engagement and approach with correct stakeholders, anything can happen. I hope my background demonstrates I am committed to the TSIG and the development and advocating of our profession.
If you have any issues or ideas you feel the TSIG can help with, please do not hesitate to reach out via email: tsigchair@anzsnm.org.au
To get in touch with our committee team leaders, please email them at:
WFA TSIG Chair, Sarah Daniel wfachair@anzsnm.org.au
TSIG University Liaison, Emma Brook uniliasion@anzsnm.org.au
2024 Nuclear Medicine Technologist Award
Winner
Travis Pearson
Congratulations to Travis, who has worked in our Profession for 28 years. During this time he has had opportunities to work in Darwin, Adelaide, Kent (UK) and now calls Brisbane home at the Royal Brisbane and Women's Hospital (RBWH). Currently, Travis is completing his 3rd term as Practitioner Board member for Queensland with the MRPBA. Through his career he has had opportunities to work with some inspiring leaders and teams.
In recent years, his career journey has opened doors to work in leadership, innovation and disaster management roles. For the past two years he has been focussing on advocating for the Nuclear Medicine Scientist workforce, which will be the topic of this presentation.
Meet Erin Brown
New TSIG SRC member
How did you find out about Nuclear
Medicine?
I had never heard of Nuclear Medicine until first applying for university. Where I found the Bachelor of Health Sciences (Medical Radiation Science) at UTAS– I always knew I wanted to go into some form of healthcare and always enjoyed science at school, so this seemed to combine both of my passions – as part of the two years at UTAS we explored all three specialisations to allow us to pick what we’d like to go into at CSU. Upon reading the very brief paragraph on Nuclear Medicine and particularly the radiopharmaceutical aspect I knew this was the area that interested me most – partly because I had never heard of it and wanted to find out and that it sounded the most interesting to me out of the three specialisations.
Why did you want to join the SRC?
As a member of my university radiation club, the large majority of med rad students are studying diagnostic radiography and I wanted to bring more attention to Nuclear Medicine as I think that there a smaller cohort each year due to it not being as well known – Therefore joining the SRC allows me to bring awareness and promote the ANZSNM to CSU to increase not only representation for nuclear medicine students but also provide increased support throughout their studies and after graduation.
Who has been your biggest inspiration and why?
My university friends - Going into university and moving a long way away from home, has allowed me to step out of my comfort zone and meet many like minded people from diverse backgrounds with different personalities – despite these differences, we have been able to build a strong support network. Although we all study different degrees at different year levels, we are still able share our experiences – whether good or bad to create an environment that allows for positive growth – If one of us is feeling homesick, didn’t get the marks they were expecting or are struggling with an assignment, we are able to offer support in any way that we can – this shared comradery and encouragement of each is a powerful motivator and source of resilience in an environment that can be quite stressful. – Seeing the dedication from each and every one of my friends has helped to inspire my learning and allow me to push through my studies.
Erin Brown, MANZSNM, 3rd Year, Charles Sturt University & University of Tasmania
Travis Pearson, MANZSNM
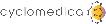
CONFERENCE CONVENING COMMITTEE (CCC)
Pru Burns, MANZSNM CCC Chair
Trinity Residential College 230 Hampden Rd, CRAWLEY, WA
ANZSNM WA Branch Day Seminar
The symposium will feature thought-provoking presentations on novel PET radiotracers for advanced Alzheimer’s detection, comprehensive analysis of the epileptic brain, complex imaging for cerebral artery abnormalities, advancements in the utility of PET imaging in movement disorders and many more neurology-based topics in both PET and Nuclear Medicine.
AN INTERVIEW WITH THE ANZSNM' s NEW PRESIDENT Karen Jones
Can you tell us a bit about your background and your motivation to get started in the field of Nuclear Medicine?
My family background did not encourage optimism for my future! – I am the oldest of three children. My family were dirt poor – and I mean this literally. One of my earliest memories as a child is of our home, made of corrugated iron, rented from another family that was located at the back of their property. – The floor was a sheet of lino covering the dirt beneath it. I was about 3 years old. My mother, recently separated from her husband was 24 years old, and heavily pregnant with my sister, when she received the news that her application for a housing trust house in the Northern outskirts of Adelaide had been approved. We moved –far from my relatives - grandparents, aunts, uncles and cousins. It was a very difficult time for my mother who lacked support and educational opportunities. – She didn’t finish school – in fact she never went to high school. She worked in a factory before marrying at age 20 and having me at age 21, after which she never had paid work again. We ‘managed’ on her single-parent pension and food hampers from the Salvation Army. We would visit my relatives every weekend. My mother did not drive, so we would walk several kilometres to catch a train and then walk another kilometre to my grandparent’s house. I enjoyed these visits very much, playing for hours in the garden with my cousins. I was a strong-willed child – my mother called me ‘stubborn’ – but I prefer to think of myself as determined and persistent.
I think my mother was relieved when I turned 5 and could go to school. I loved school, idolised my teachers – so much so that my childhood dream was to be a maths teacher. As such, I asked for a calculator for my 6th birthday! My mother remarried when I was 10 years old, and we moved to be closer to my grandparents.
I went to a public high school that had a suboptimal academic track record – the pass rate in year 12 was ~30%. In my final year, only 10 of 180 students went on to university – I was one of them, supporting myself through a part-time job at Woolies, where I worked every weekend - and full-time during the school holidays. I was relocated – from the desirable ‘manchester’ section to the less desirable ‘roast chicken’ section, because of my ability to spruik the Saturday afternoon ‘red-light deli specials’ on the microphone. Fortunately, I was later promoted to lower ground floor Section Manager and was pleased never to cook a rotisserie chicken again.
I was unsure what I wanted to do at university, however, I was interested in a science- or health-related field. A teacher suggested that I apply for ‘Medical Radiations’ at the University of South Australia (UniSA) to train as a radiographer (he had a daughter in year 12 and that was the course she applied for).
The first year of ‘Medical Radiations’ was common to 3 streams - Radiography, Radiation Therapy and Nuclear Medicine, I hadn’t heard of nuclear medicine, but after my first clinical practice day in the Department of Nuclear Medicine at the Royal Adelaide Hospital (RAH), the decision was straightforward. The diversity of nuclear medicine at that time, which included radiopharmacy, haematology, patient care, imaging, data analysis and 131I therapy, appealed strongly to me –and, while not yet in Australia, PET was on the horizon. I could see that the ‘nuclear medicine technologist’ was central to the successful function of the nuclear medicine department and was inspired by the enthusiasm of the former RAH Chief Tech, Max Bellon, and my Nuclear Medicine lecturer, Wendy Barber. They were both outstanding role models.
I was fortunate to be exposed to clinical research early in my nuclear medicine career which provided me with an appreciation of the intellectual stimulation and enjoyment that high-quality research brings, as well as the importance of research to clinical practice. The decision to embark on a PhD, at a time when there were no specific postgraduate programs in Medical Radiation in Adelaide, was life-changing. I discussed the possibility of enrolling in a PhD with the Postgraduate Coordinator in the Adelaide Medical School at the University of Adelaide. My undergraduate qualification was a Diploma in Applied Science – and I hadn’t completed an Honours year. Despite these limitations, I was permitted to create my own pathway by initially enrolling in a Masters qualifying year, which was subsequently upgraded to a PhD. Looking back, my decision was ambitious, and the support of others was critical. In the final year of my candidature, I was invited to be part of a working committee at UniSA to establish the first Honours and Masters programs in Medical Radiation – I became their first Honours coordinator in 1997.
Which career highlight are you most proud of and why?
I was the first member of my family to go to university, so being awarded a PhD was an unbelievably proud moment for me (and my mother). – However, my proudest moments have come, not from my own achievements but, from contributing to the success of others. For example, witnessing my Honours students receive the ANZSNM Undergraduate Student Award at the ASM (Kate Romeo: 2019; Nicola Evans: 2021; Iliana Angelidakis: 2023; Caitlin Burt: 2024), my PhD students being presented the University Doctoral Medal at their graduation ceremony for an exceptional PhD thesis (Julie Stevens: 2009; Tongzhi Wu: 2013) – or simply coaching a student to have the confidence to present without notes, are far more rewarding experiences than personal achievements.
What are your top priorities for the Society during your tenure as President?
I believe that this is a critical time in nuclear medicine. There has been a rapid expansion of services, particularly relating to PET and theranostics, leading to major workforce shortages, and it is essential that we work together effectively to address this issue. We are clearly at a cross-road where change is necessary.
During my tenure as the Chair of the Technologist Special Interest Group (TSIG) - Chair (2021-2023), I established a team of enthusiastic, dedicated and passionate individuals, who worked together to drive a number of new initiatives to support our technologist members, students, and the wider nuclear medicine community. The TSIG has never been stronger – and continues to grow, expanding its capabilities and international reach.
A major priority is to increase my engagement with other ANZSNM committees, particularly, the Physics SIG and RPS SIG, to provide support where required for the benefit of our members. A current limitation of the ANZSNM is the lack of a Medical SIG. While we are fortunate to have two highly capable medical representatives on Council (which Kevin often refers to as the ‘M-ROC’), the majority of the ANZSNM work that is ‘nuclear medicine specialist-related’, currently falls primarily on the shoulders of these two individuals. As the peak body in Australia and New Zealand, representing all professions in nuclear medicine, I will explore the potential for creating more opportunities for nuclear medicine specialists within the ANZSNM, including a transparent pathway for appointment to Federal Council.
A second priority is to reinvigorate the NSW/ACT Branch – I currently regard this Branch as a ‘Sleeping Beauty’, waiting to be awaken. NSW has the largest number of nuclear medicine professionals than any other region in Australia or New Zealand and the NSW/ACT Branch has the capacity to be one of the strongest Branches in the ANZSNM. Members have reported challenges in attending face-to-face Branch meetings (e.g. when these are held a long distance away or there is heavy peak hour traffic). However, the COVID pandemic has made us far more comfortable with online meetings and with a motivated Executive running the NSW/ACT Branch, I have every confidence that this Branch can be rebuilt promptly and effectively.
A third priority is to establish the Rural/Regional Branch. In accordance with the new ANZSNM Constitution, introduced in 2023, the ANZSNM will form a Rural/ Regional Branch to focus on the challenges inherent in individuals residing and working in rural and regional areas to provide a stronger voice for these important members.
What advice would you give anyone considering starting a career in Nuclear
Medicine?
To be open to exploring new challenges (including involvement in research, which I regard as an asset to the acquisition of critical thinking skills) and to identify at least one supportive and well credentialled mentor - to facilitate professional development.
In your opinion, what are the biggest challenges facing Nuclear Medicine in the coming years?
The immediate pressing issue is the critical workforce shortage, not only for nuclear medicine technologists, but also in other professions in nuclear medicine. We have made good progress to address this problem during the last 12 months, including the ANZSNM Nuclear Medicine Technologist Workforce Summit, which I convened, that brought together stakeholders from a number of areas, to identify challenges and potential solutions. There is much work to be done, but I am confident that we are moving in the right direction decisively.
What future do you envisage for Nuclear Medicine?
I believe that patient outcomes are optimised by the combination of high-quality research, education/ training and clinical care. With the development of new radiopharmaceuticals and technological advances in
imaging and therapy, I envisage that nuclear medicine will go from strength to strength and that nuclear medicine professionals will work collaboratively to optimise patient outcomes.
What motivated you to become the President of the Society?
Through my work as the former Chair of the TSIG, and on Federal Council, I was encouraged by other nuclear medicine professionals to take on this role. I hope that I will be regarded as a good role model and advocate, not only nuclear medicine technologists, but for all members of the Society. I am committed to promote nuclear medicine, both within our local (ANZ) community and globally.
What would you like from the members of the Society?
To encourage other professionals within the nuclear medicine community to not only join the ANZSNM, but to play an active role in it, and for more senior members to provide opportunities and mentorship to those in the earlier stages of their career. As a ‘not-for-profit’ organisation, with relatively modest membership fees, the success of the Society is very much dependent on the goodwill of its members who volunteer their time to support their profession. - Many hands make light work.
When you are not at work, what are your favourite things to do?
Spend time with my husband (who is also a clinicianscientist, so we talk about research a lot) and 4 children (aged 13, 14, 20 and 23 years old). Whether it’s going to the footy with my oldest son, having a motherdaughter trip with my daughter, playing table tennis with my two younger sons, or fishing with my family on Kangaroo Island – spending family time together is the most important and rewarding part of my life. I also have an enthusiastic ‘spoodle’ (Maisie), who often makes an unscheduled appearance during my Zoom meetings and an RSPCA-rescue cat (Dolly) who avoids Zoom meetings and, according to my husband, is much smarter than Maisie. - I am also an enthusiastic cook, gardener, renovator and traveller.
How have you found balancing work and family life?
I don’t. – I frequently work at home so there is a very blurry line between work and family life. Perhaps surprisingly, I see this as an asset, although I would like
to have more time per se. – It always has been this way, and I suspect it always will be. I am a chronic list maker and prioritiser – but priorities at home inevitably change.
How do you celebrate a win/good day at work?
With others. – A win is rarely the result of a single individual’s efforts so sharing that with others, and acknowledging their contribution, makes success much more meaningful. I work as part of a longstanding and internationally recognised research group – it isn’t large, but each member brings distinct and valued skills.
What is your superpower?
My drive – and I don’t mean my Volvo XC60.
What are your desires for the Society?
For every member within the Society to feel valued and recognise that they have a voice that will be listened to carefully – from the most junior nuclear medicine student to the most senior nuclear medicine professional – both in the private and public sector, as well as in metropolitan and rural/regional areas. If that occurs, our Society will become better and much stronger. This would be a legacy that I would be proud of.
Kia
ora koutou
From the speakers, to the venue, to Think Business Events, to the dance floor at the Awards Dinner, Jess and I could not be more proud of the success of the 54th ANZSNM ASM held in Ōtautahi in April.
Planning for the ASM was an 18 month marathon. From the initial New Zealand site bid to the opening of the Cardiology pre-conference symposium at the Town Hall, the LOC, the CCC & SEC had a common goal – to make an ASM held in NZ as successful as possible for our members and commercial partners.
Key to the ASM’s success was always going to be the program. Having the right mix of experienced, and early professional speakers, new and emerging topics, international and local talent – all these aspects morphed into a program that I am really proud of. I am pleased that we were able to accommodate some many entered abstracts, we were really spoilt for choice.
The SEC stream leads bought together amazing international speakers, who added to the quality of the sessions.
Our Award entrants were outstanding, our Lowenthal and Pioneer speakers inspirational, and a highlight for me was “The Great PET/MR
vs PET/CT Debate”. This was a stroke of genius from immediate past President Kevin London (not sure if the actual genius was Kevin’s, but I’ll give him the credit), and I hope debates such as this one become part of the fabric of our ASM program.
To our commercial partners, their investment in our community by bringing their teams to a NZ based ASM was really appreciated. A small goal of mine was to not blow the ASM budget, and with the great support from our vendors, they helped Jess and I achieve this. And hey, a mobile PET/CT parked outside Te Pae – pretty cool.
Networking is a crucial part of the ASM, from the casual lunch time chat, to an organised meeting, having us in one place for the weekend provides excellent opportunities to meet face to face. To then dress up and have good food and a dance with our colleagues, what more can we ask for – to celebrate at the Awards Dinner another successful ASM.
Daniel Badger, ANZSNM Federal Council Executive member, medical physicist & cycling enthusiast was instrumental in supporting Jess and I in our co-convenor roles. Daniel’s enthusiasm, attention to detail, recent ASM experience, and knowledge of an excel sheet,
gave Jess and I the added confidence to push forward with our ideas and management of the event. Along with the fantastic TBE team, we really were the dream team. And while we didn’t get a “group” shot, I hope you enjoy this photo of Jess, Daniel and I living the ASM-dream.
Ngā mihi nui/ Kind regards (with more emphasis on gratitude),
Pru
On behalf of the 2024 ASM Dream Team – Jessica Fagan, Daniel Badger and Pru Burns
Pre-Conference
Held at the historic Christchurch Town Hall, the Cardiology focused Pre-conference Symposium was the ideal kick-off event for the ANZSNM ASM in Ōtautahi. The pre-conference concept provides a scientific and educational opportunity for attendees, to deep dive into a specific topic or area of interest, with the theme complementing the main ASM.
ANZSNM Scientific and Education Committee Cardiology stream lead Associate Professor Nathan Better bought together an experienced group of Nuclear Cardiology Specialists, and new to the profession Advanced Trainees to create a program that was interesting and challenging for the audience. Dr Sue O’Malley, Nuclear Cardiologist and Clinical Director of the Molecular Imaging Department at Christchurch Hospital, set the scene in her opening welcome, taking the audience through the changes to Ōtautahi Christchurch following the devastating 2011 earthquake and the design concept of ASM conference venue Te Pae.
The pre-conference symposium was broken into two sections:- Cardiac MPI – How do I do it in my lab? and Cardiac MPI - Read with the Experts. “Cardiac MPI – How do I do it in my
lab?” gave invited speakers the floor to look at individual techniques, from the evaluation of the referral (Dr Barry Ellison) to writing the report (A/Prof Nathan Better). David Gilmore, Associate Professor & Director of Nuclear Medicine Program & Radiologic & Imaging Sciences Graduate Program at Massachusetts College of Pharmacy and Health Science in Boston, gave us insight into the role of the Nuclear Medicine Technologist in the modern Nuclear Cardiology Lab.
Cardiac MPI - Read with the Experts had our expert panel go through their reporting methods (with interaction and feedback from the audience!), and Nuclear Medicine Advanced Trainees presented cases reviews.
Many thanks to all the invited speakers who made this session educational and entertaining:Nuclear Medicine Advanced Trainees: Umar Khan, Sophie Thoo, Rahul Solanki, Ravi Kumar Tankala, and Lotte Steffens
Sue O’Malley, Barry Elison, Kim Taubman, David Gilmore, Rachelle Steyn and Nathan Better
Ultrasound Guided
We wanted to host a hands on event for professionals in our industry to expand skills in the area of ultrasound guided vascular access. Key to the majority of our procedures, both diagnostic and therapeutic, is gaining access to a vein. NMT’s, physicians and nurses are highly skilled in this area, but there are always patients who test our capabilities. Ultrasound guided vascular access is used to varying degrees in most Radiology and Molecular Imaging departments; either performed by a sonographer or Radiologist in house, to some hospitals having a specific vascular access service.
30 attendees took part in the four hour workshop which gave a basic grounding in ultrasound guided, peripheral vascular; with one instructor teaching four attendees, access to US machines and vascular access phantoms during the workshop.
Learning Objectives included:-
• Correct identification of upper and lower veins
• Competent cannulation using IV USS
• Determining artefact v vein
• Identification of optimal positioning of patent for cannulation
• Understand complications of peripheral cannulation
Feedback was very positive on the day, and we received several positive comments via the post conference survey. Many thanks to Peter Bennett and three vascular access nurse specialists from the Radiology Department at Christchurch. Ultrasound equipment and on the day support was supplied by LeeAnne Higgins Clinical Sales Specialist, FUJIFILM Sonosite, Inc.
wellcome reception
FUN RUN
A tradition that started at the 53rd ASM in Adelaide, the ASM Fun Run/ Walk, was again a success in Ōtautahi Christchurch. Saturday saw a brisk morning, with a frost on the ground. With 36 of us rugged up in merino scarves and gloves, and down jackets, about a 1/3rd of the group headed off at pace. The running pack was led by then President Kevin London. Kevin had run through Hagley Park a couple of times previously, and was pretty confident he knew the route.
The walkers set a great pace – more to keep warm, than to set any records! We passed a pond with ducks, loads of walkers out with dogs, the frosty park areas were really magical. It was cute to see some Brisbane NMT’s taking photos of autumn leaves on the ground covered with a sparkling
frost … the setting truly was Instaworthy. The gorgeous photos here of the morning were taken by ANZSNM President Karen Jones, who was leading the way with our walkers.
I had enlisted my Christchurch based son and his flat mates to act as “route markers” to help our participants find their way through Hagley Park. Very noticeable in ANZSNM-purple caps, they stood out. Well, I thought they did. My walking group reached the first lad, yup all good, just head down this path. We got to the second check point, and the boys were slightly frantic – the group of runners went left instead of going right. Turns out “pack leader” Kevin London took the runners on their own tour, a quick 8km run back to Te Pae.
OFLLA R ONE WALK/RUN 4202
All runners/walkers were accounted for, no one left behind! Winners on the day – I suspect Kevin, but as I was near the back of the pack, I can neither confirm nor deny.
The 2024 “All for one walk/run” was a wonderful way to start the day, leaving us exhilarated on a frosty morning, ready for a full day of learning.
Many thanks to our wonderful sponsor Bruker for support of this event. Further special thanks to Ester Gomez, ANZSNM Marketing guru for her fantastic logo design on the back of the cool t-shirts.
Pru Burns, CCC Chair
Fun Run proudly sponsored by
Conference Sessions
gala dinner
TELIX
AWARD WINNER
Melissa Sheilds, The University of Newcastle
Occupational burnout in nuclear medicine technologists working in Australia and New Zealand – Results of a national survey.
Melissa Shields1, Lynne McCormack1, Daphne James1
AIM: Occupational burnout has been defined as increased levels of emotional exhaustion and depersonalisation and decreased levels of personal achievement. It can be associated with negative feelings about the workplace and feeling that a person’s efforts is of little consequence. Within a healthcare setting, occupational burnout can be attributed to a high workload or a non-supportive work environment.
METHODS: An online survey was administered to nuclear medicine technologists working in Australia and New Zealand via QuestionPro. The survey included the Professional Quality of Life Scale (ProQOL) Version 5 (2009) measuring Compassion Satisfaction, Burnout and Secondary Traumatic Stress in the workplace. For this study, only the burnout component is reported. Responses are based on a 5- point Likert scale ranging from 1 (never) to 5 (very often). The responses are summed to produce a numerical score, which is then categorised into a scale of low, moderate or high burnout.
RESULTS: Of approximately 1,300 registered nuclear medicine technologists practicing in Australia and New Zealand, 162 completed the survey. Of the 18 New Zealand participants, ten (56%) reported moderate levels of burnout. Of the 144 Australian participants, 114 (79%) reported moderate levels of burnout. No technologists reported high levels of burnout. All states of Australia were represented in the survey, with Queensland (91%), Western Australia (88%) and Victoria (86%) having the highest number of participants reporting moderate levels of burnout. Within Australia, technologists who had been working for 26-30 years and 30 plus years had the highest number of participants reporting moderate burnout (100% for both categories).
CONCLUSION: The ProQOL survey revealed that more than half of New Zealand participants and three quarters of Australian participants reported moderate levels of burnout. With higher levels of burnout associated with increased absenteeism and turnover, increased medical errors and decreased patient care, it is imperative to address the wellbeing needs of nuclear medicine technologists working in Australia and New Zealand at an individual and organisational level.
GMS POSTER
Alexander McDonald, Austin Health, VIC
Investigation of radioprotectant combinations in 177Lu labelled PSMA as a model for optimizing therapy formulations.
Alexander McDonald1, Pece Kocovski1, Ben Nguyen1, Andrew Scott1,2, Uwe Ackermann1, Stuart McCluskey1
AIM: As the field of radiopharmaceuticals moves towards centralized production for long lived radionuclides, effective formulation for radioprotection is vital. Some common radio protectants are less effective in high activity concentration formulations and the efficacy can be reduced depending on the type of radiation being emitted by the radionuclide. Gentisic acid has been identified in literature as a radioprotectant which is effective for both β and α emitting radiopharmaceuticals, but has been shown to have both oxidative and antioxidant properties. This work investigates the combination of gentisic acid with a range of sulfur containing amino acids and small molecules in order to understand the mechanism of potential synergistic effects which may be useful for development of formulations in other targeted radionuclide therapies.
METHODS: 177Lu-DOTA-PSMA was produced using a modified automated procedure which excluded radio protectants in the final formulation. This product was diluted to a concentration of approximately 1GBq/ mL in different radioprotectant combinations, 0.1M sodium ascorbate with either 17mM gentisic acid or 9mM gentisic acid and 23mM additive, and stored at ambient temperature. 177Lu-DOTA-PSMA purity was determined by radio-HPLC to evaluate the radiolysis product profile over time. Current work includes the ongoing analysis of decay products via mass spectrometry.
GMS POSTER
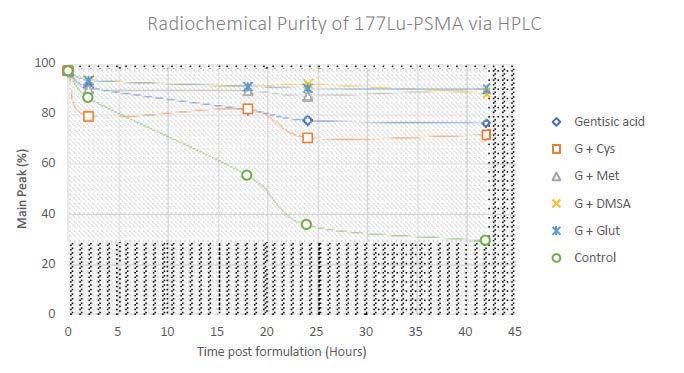
RESULTS: 177Lu-DOTA-PSMA was produced with a radiochemical purity (RCP) of 97% at end of synthesis. The control with no radioprotectant showed significant degradation, with an RCP of 86% 2 hours post formulation, decreasing to below 60% by 18 hours. All formulations with gentisic acid showed stabilization over the 42 hour period compared to control. The formulation with cysteine had poor solubility, with precipitates forming before the end of the 2 hour time point. Formulations with gentisic acid + methionine, glutathione or DMSA showed high stability once in formulation, decreasing by 1- 4% between 2-42 hours.
Evaluation of radiochemical purity by HPLC over time
CONCLUSIONS: These results indicate formulations with some sulfur containing amino acids and small molecules can enhance the radioprotection abilities of gentisic acid alone for 177Lu-DOTA-PSMA, but selecting the right molecule is essential. These results are consistent with other literature reports, however the best performing additives are not necessarily good radical scavengers. To probe the mechanism of protection and potential side products, investigation of the products of radiolysis will be undertaken via mass spectrometry after decay of samples.
RADPHARM
AWARD WINNER
Nerida Neumann, SA Health, Central Adelaide Local Health Network
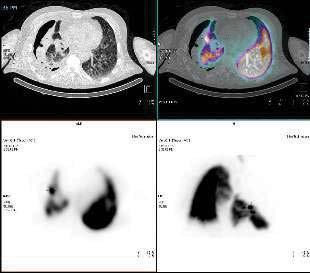
The value of Nuclear Medicine 99mTc Technegas ventilation scanning in the localisation of a Persistent Air Leak (PAL).
Background: A 56 year old male with productive cough, headache and lethargy presented to the Emergency Department febrile and with dyspnoea.
A CT scan showed collapse of the right lung due to a large tension pneumothorax. A chest x-ray confirmed mediastinal shift to the left. An intercostal chest catheter was inserted, initially resulting in improvement of breathing, Chest x-ray confirmed placement of the chest drain and interval reduction in the size of the pneumothorax. Serial chest x-rays over the next few days showed interval enlargement of the pneumothorax. The chest-drainage system showed persistent bubbling in the water seal chamber, prompting the treating team to consider the possibility of a persistent air leak.
Method: A ventilation Nuclear Medicine lung scan was performed using 500MBq 99mTc-Pertechnetate loaded into the Technegas generator. The referring Thoracics Physician accompanied the patient to clamp off the chest drain, assess the patient throughout and to open the drain once imaging was complete.
Inhalation of 99mTc-Technegas continued until 5K counts were seen from the posterior image on the pscope.
A Siemens Intevo gamma camera was used to acquire anterior and posterior dynamic images, followed by a SPECT/CT scan.
Results: Foci of increased tracer uptake was seen in the midzone of the collapsed right lung, concluding that the air leak was at the lateral segment of the right middle lobe.
Discussion: Following the scan, the patient underwent insertion of an Endobronchial valve into the right middle lobe. This procedure requires accurate localization of the site of the persistent air leak. Options to localise persistent air leaks are limited and invasive. Other medical imaging modalities offer minimal diagnostic information.
Conclusion: The Nuclear Medicine ventilation scan was immensely valuable in localizing the site of a persistent air leak. The findings of our study enabled a life-saving endo-bronchial valve to be accurately inserted. A chest x-ray taken 10 weeks later showed inflation of the formerly collapsed lung, indicating resolution of the pneumothorax.
Figure 1: SPECT/CT Transverse slices, showing the suspected air leak.
CURIUM
AWARD WINNER
Melissa Sheilds, The University of Newcastle
Occupational
burnout
in
nuclear medicine technologists
working in
Australia and New Zealand – Results of a national survey.
Melissa Shields1, Lynne McCormack1, Daphne James1
AIM: Occupational burnout has been defined as increased levels of emotional exhaustion and depersonalisation and decreased levels of personal achievement. It can be associated with negative feelings about the workplace and feeling that a person’s efforts is of little consequence. Within a healthcare setting, occupational burnout can be attributed to a high workload or a non-supportive work environment.
METHODS: An online survey was administered to nuclear medicine technologists working in Australia and New Zealand via QuestionPro. The survey included the Professional Quality of Life Scale (ProQOL) Version 5 (2009) measuring Compassion Satisfaction, Burnout and Secondary Traumatic Stress in the workplace. For this study, only the burnout component is reported. Responses are based on a 5- point Likert scale ranging from 1 (never) to 5 (very often). The responses are summed to produce a numerical score, which is then categorised into a scale of low, moderate or high burnout.
RESULTS: Of approximately 1,300 registered nuclear medicine technologists practicing in Australia and New Zealand, 162 completed the survey. Of the 18 New Zealand participants, ten (56%) reported moderate levels of burnout. Of the 144 Australian participants, 114 (79%) reported moderate levels of burnout. No technologists reported high levels of burnout. All states of Australia were represented in the survey, with Queensland (91%), Western Australia (88%) and Victoria (86%) having the highest number
of participants reporting moderate levels of burnout. Within Australia, technologists who had been working for 26-30 years and 30 plus years had the highest number of participants reporting moderate burnout (100% for both categories).
CONCLUSION: The ProQOL survey revealed that more than half of New Zealand participants and three quarters of Australian participants reported moderate levels of burnout. With higher levels of burnout associated with increased absenteeism and turnover, increased medical errors and decreased patient care, it is imperative to address the wellbeing needs of nuclear medicine technologists working in Australia and New Zealand at an individual and organisational level.
1 The University of Newcastle
SHIMAZDU
AWARD WINNER
Dr Christian Wichmann, Olivia Newton-John Cancer Research Institute
Fully Automated Radiosynthesis of [89Zr]Zr-Crefmirlimab
Berdoxam on an iPHASE MultiSyn for Clinical Multi-Centre PET Imaging of CD8+ T-Cell Trafficking.
Christian Wichmann1, Zhipeng Cao, Fang Jia, Andrew Scott1,2, Kathleen Brady, Alexander McDonald, Nancy Guo, Kenneth Young2, Stan Poniger, William Le, Fiona Scott
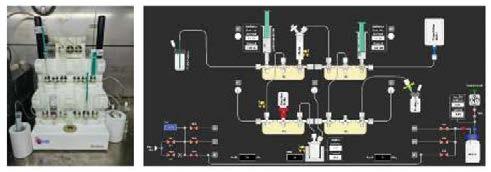
AIM: Presence of CD8+ tumour infiltrating lymphocytes in the tumour microenvironment is critical for the immune-oncology therapy response in solid tumours and lymphoma. [89Zr]Zr-crefmirlimab berdoxam is a promising novel CD8+ T-cell radiotracer which is currently being investigated in clinical trials (e.g. iPREDICT, NCT05013099). In order to support Australian trials, we have developed a fully automated protocol for the clinical radiosynthesis of [89Zr]Zr-crefmirlimab berdoxam.
METHODS: Based on our prior work, automated radiolabelling of Df-crefmirlimab with 89Zr, formulation, and sterile filtration was established using the iPHASE MultiSyn disposable cassette- based radiosynthesizer (Figure 1). Starting activity and protein amount were optimized to satisfy patient dose requirements avoiding further manual intervention. Quality control was performed on the formulated product to satisfy clinical release and stability criteria over 6 days.
Figure 1. Image (left) and schematic (right) of iPHASE MultiSyn setup for automated radiosynthesis of [89Zr]Zr-Df-crefmirlimab berdoxam.
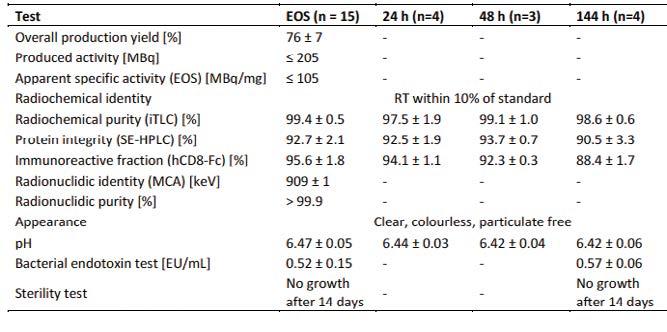
RESULTS: Df-crefmirlimab with an approximate chelator-to-minibody ratio of 2 was used for radiolabelling experiments. Radiolabelling reactions were performed in sodium succinate pH 6 with 0.02% Tween80 which gave >95% conversion after 15 minutes at ambient temperature. Overall process yield of formulated sterile [89Zr]Zr-crefmirlimab berdoxam was 76% ± 7% (n=15) at end-ofsynthesis (EOS) with a process time of 45 minutes. Product was formulated in a volume of 10.2mL ± 0.6mL (n=15) and calibrated patient dose activity was 40.5MBq ± 2.9MBq (n=15) and patient protein dose was 1.53mg ± 0.17mg (n=15). Radiochemical purity and immunoreactive fraction were excellent at EOS, and dropped slightly after storage at 4-8°C for 6 days (Table 1). Size-exclusion HPLC analysis of formulated [89Zr]Zr-crefmirlimab berdoxam demonstrated antibody integrity of 92.7% ± 2.1% (n=15).
Other parameters such as pH, sterility, and endotoxin levels passed clinical release criteria.
Table 1. Validation and clinical production results of [89Zr]Zr-Df-crefmirlimab berdoxam.
CONCLUSION: Fully automated production of [89Zr]Zr-crefmirlimab berdoxam for clinical use was achieved with minimal exposure to the operator and excellent stability over 6 days allowing for centralised production. This demonstrates feasibility of automated production of 89Zrradiopharmaceuticals in a clinical setting.
AANMS
AWARD WINNER
Dr Natalia Kovaleva, Peter MacCallum Cancer Centre
Prognostic utility of quantitative PET parameters on baseline and interim FDG-PET scans in Hodgkin lymphoma.
There is increasing use of quantitative PET parameters to increase the prognostication of interim FDG-PET (iPET) scans in patients with non-Hodgkin lymphoma, but not for Hodgkin Lymphoma (cHL). Yet, iPET scans are often used for adaptive therapy in patients with cHL, based on 5-point Deauville Score (DS). This study aimed to evaluate the prognostic value of iPET using DS and novel quantitative PET analysis in cHL patients.
Retrospective analysis of iPET and outcomes of 98 patients with newly diagnosed cHL between 2008 and 2022 with routine FDG-PET at baseline (PET0), after 2-cycles of chemotherapy (iPET) and end of treatment (EoT). PET0 was assessed for maximum standard uptake value [SUVmax], total metabolic tumour volume [TMTV], total lesion glycolysis [TLG], and novel radiomic analyses of lesion dissemination parameters (Dmax) using MIM software. Reduction of quantitative parameters on iPET in relation to PET0 (ΔSUVmax, ΔTMTV and ΔTLG) was calculated and DS was assessed at iPET. Statistical analysis of survival was performed using SPSS.
Median patient age was 31yo, 45% had advanced stage disease, and 84% received ABVD chemotherapy. 16% had DS≥4 on iPET and 13% had ΔSUVmax<72%. Multivariate analysis showed B-symptoms at diagnosis predicted disease-free survival (DFS) (HR 22.68, 95%CI 2.38– 215.94, p=0.007). Greater lesion dissemination (Dmax>49cm) on PET0 was statistically significant for DFS on univariate but not multivariate analysis. Neither SUVmax, TMTV or TLG were associated with overall survival (OS) or DFS. Univariate analysis of iPET parameters showed that DS≥4 and ΔSUVmax<72% were both significant predictors of DFS, but only ΔSUVmax<72% remained significant on multivariate analysis (HR 52.66, 95% CI 2.34-1184.5, p 0.013), independent of other baseline clinical prognostic factors. Also, no iPET parameters predicted OS.
A reduction in SUVmax of less than 72% on interim PET compared to baseline PET may offer a more accurate prediction of Disease-Free Survival than the interim PET's Deauville Score. Further studies with increased sample size are indicated to assess the remaining quantitative PET parameters.
1 Peter MacCallum Cancer Centre
2 Austin Health
3 Olivia Newton-John Cancer Research Institute
RAPHAEL
STUDENT RESEARCH
AWARD WINNER
Rachel Maclean, Monash University
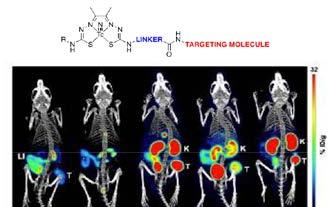
Novel bis(thiosemicarbazonato) technetium-99m nitrido complexes for prostate cancer imaging.
AIM: To investigate bis(thiosemicarbazonato) (BTSC) technetium-99m nitrido complexes attached to a prostate specific membrane antigen (PSMA) targeting molecule as SPECT imaging agents for prostate cancer.
METHODS: Four bis(thiosemicarbazone) chelators (H2L 1-4) containing PSMA targeting molecules were synthesised and subsequently radiolabelled in a one-pot synthesis at 85°C for 10 min to form [ 99mTc] [TcN(L1-4)]. Kinetic inertness studies were undertaken by incubating the tracers in human serum at 37°C and lipophilicity was determined using the shake flask method. Cell studies were performed in PSMA-positive cell lines (PC3-PIP and LNCaP) and a PSMA-negative cell line (PC3). Small animal SPECT-CT imaging and ex vivo biodistribution studies were performed for all tracers in Balb/c nude mice bearing both PC3-PIP and PC3 tumours (Figure 1).
RESULTS: The chelators were radiolabelled with high radiochemical purity (RCP > 95%) and formed hydrophilic radiotracers with logD < -1. The radiotracers stayed intact after 24 h of incubation in human serum with all complexes having RCP > 90%. All 99mTc PSMA complexes exhibited binding and internalisation into PSMA+ PC3-PIP and LNCaP cell lines, which was inhibited by the addition of excess PSMA-specific inhibitor 2-phosphonomethyl)pentanedioic acid (2PMPA). The most lipophilic of the complexes, [ 99mTc] [TcN(L2 )], showed non-specific uptake in the PC3 cell lines. SPECT-CT imaging and biodistribution studies demonstrated significant differences in the PC3-
PIP tumour uptake and clearance pathways. [99mTc] [TcN(L3)] and [ 99mTc][TcN(L4)] showed high PC3-PIP uptake and retention related to the linker structure and the presence of an additional PSMA targeting molecule in the BTSC chelator, respectively. organisational level.
CONCLUSION: A series of kinetically inert [ 99mTc] [TcN(BTSC) complexes were synthesised which demonstrate binding and internalisation into PSMApositive cell lines. The design of the complexes can be altered to chance ANZSNM ASM 2024 the clearance pathway and produce radiotracers with high accumulation and retention in PC3-PIP tumours with potential for use in prostate cancer imaging.
SUMITOMO
NMT STUDENT
AWARD WINNER
Caitlin Burt,
Royal Darwin Hospital, University of South Australia
Effects of levodopa/carbidopa on the blood pressure, superior mesenteric artery blood flow and gastric emptying responses to oral glucose in Parkinson disease – an exploratory study.
BACKGROUND: Postprandial hypotension (PPH), a fall in systolic blood pressure (BP) >20mmHg within 2 hours after a meal, occurs frequently in Parkinson disease (PD) leading to falls and syncope. PPH is precipitated by the postprandial increase in splanchnic blood flow. We have shown that the magnitude of the fall in BP is dependent on the rate of gastric emptying (GE). Levodopa/carbidopa (LEVO/CARBI) is commonly used to treat PD, however, its effects on BP and GE are not known.
OBJECTIVE: To evaluate the effects of LEVO/CARBI on BP, heart rate (HR) superior mesenteric artery (SMA) blood flow and GE after oral glucose in PD.
METHODS: Seven people (4M, 3F; aged 74±6.9 years) with mild to moderate PD (Hoen and Yahr scale 1.7±0.7), taking short-acting LEVO/CARBI, were studied on two occasions. Participants attended the clinical research facility following an overnight fast and was seated with their back against a gamma camera.
Each received levodopa (200mg) /carbidopa(50mg) or placebo, in a randomised cross-over design, 60min before a 75g glucose drink. BP and HR (automated BP cuff), GE (scintigraphy) and SMA blood flow (Doppler ultrasound) were measured before and for 180 min after the drink. Data were analysed using repeated measures ANOVA and a P value <0.05 was considered significant.
1. Royal Darwin Hospital
2. University of South Australia
3. The University of Adelaide
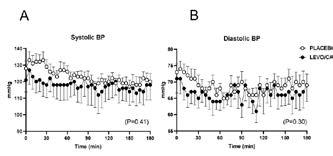
RESULTS: PPH was evident in 3 (43%) individuals on LEVO/CARBI and 2 (29%) on placebo. LEVO/CARBI had No effect on the falls in systolic (P=0.41) and diastolic (P=0.30) BP (Fig), the rises in HR (P=0.39) and SMA flow (P=0.09) or GE (T50: 99.1±7.9 min vs placebo: 91.2±6.2 min).
CONCLUSION: This preliminary study suggests that LEVO/CARBI has no effect on the hypotensive effect of oral glucose in PD, probably because it does not slow GE.
Figure: Effects of levodopa/carbidopa (LEVO/CARBI) on (A) systolic and (B) diastolic BP before and after a drink containing 75g glucose. Data are mean values ± SEM.
The subject of the lecture is to be in keeping with the conference theme OR a memorial lecture in honour of a person who has made a considerable contribution to the Society of Nuclear Medicine in Australia and New Zealand. The lecturer is appointed by the Local Organising Committee in consultation with the Scientific Advisory Panel of the ANZSNM, and is to be a guest speaker from the organising state or from within Australasia.
LOWENTHAL
LECTURE WINNER
Dr Simon Gruenewald, Royal North Shore Hospital
Biochemical Estimations of Renal Function
Contrasted with Nuclear Medicine Measurements.
The Lowenthal Lecture which commenced in 1987 is a 45 minute presentation given in a Plenary Session. The subject of the lecture is in keeping with theme "The Role of physical and Biochemical Measurements in Nuclear Medicine".
EDUCATION & CPD | Case study
CASE STUDY
THE ROLE OF [18F] FDG-PET/CT IN NECROTISING
OTITIS EXTERNA: A CASE REPORT
University of South Australia
Patient presentation: A 61-year-old Aboriginal woman with a history of type-2 diabetes mellitus (T2DM) presented with deep left-sided otalgia and otorrhea. Following physical examination, clinical suspicion for Necrotising Otitis Externa (NOE) was raised, prompting evaluation via imaging to confirm the diagnosis, and assess the extent of disease.
NOE, also known as Malignant Otitis Externa, is a potentially life-threatening infection of the external auditory canal (EAC) that rapidly spreads to surrounding soft-tissues, cartilage, and bones[1]. Progression leads to osteomyelitis and necrosis in the temporal bone and skull base, with possible intracranial extension[1]. Potential consequences include permanent hearing loss, cranial nerve palsy, dural sinus thrombosis, meningitis, cerebral abscess, and stroke[3]. Inadequate treatment can result in a mortality rate above 50%[2]
The primary causative pathogen is pseudomonas aeruginosa, although methicillin-resistant staphylococcus-aureus (MRSA) and fungi (aspergillus and candida) may be involved[2]. These pathogens thrive when host defences are compromised, rendering NOE more common in immunocompromised, elderly, or individuals with T2DM[3]. Compared to non-Aboriginal Australians, the incidence of NOE is 3.3 times higher in Aboriginal Australians[4]. Moreover, Aboriginal Australians with NOE are younger, suffer higher rates of fungal NOE, and higher disease-specific mortality[2]
Given the risk of complications and mortality, early diagnosis and targeted treatment are crucial. However, NOE is frequently cited as challenging to diagnose, often mimicking cholesteatoma, temporal/skull base malignancies, and chronic otitis externa[5]. A combination of clinical history and imaging studies are necessary, yet
consensus on the optimal imaging modalities requires further review[6]
Case description: An initial non-contrast CT was performed for this patient, which revealed opacification within the left middle-ear, mastoid antrum and air cells. The reporting physician noted these features are common between cholesteatoma, chronic otitis media and NOE, thus a definitive diagnosis was not reached. Subsequently, an MRI was performed utilising T2-weighted and FLAIR sequences. MRI findings ruled out intra-cranial disease, however, a definitive diagnosis of the otologic pathology remained uncertain.
Due to inconclusive CT and MRI findings, further imaging was warranted. While 99mTc-HDP and 67Ga-Citrate scintigraphy may be used to investigate NOE, [18F]FDG-PET/ CT was selected due to increased access, reduced imaging time, quantitative capability, improved spatial resolution and anatomical localisation [3]. The patient fasted for four hours prior to the scan, and blood glucose levels measured 9.1mmol/L. The patient was administered 185.5MBq of [18F]FDG via intravenous injection. Following a 55-minute uptake, PET images were acquired from vertex to mid-thigh. Low-dose CT (100kV) was acquired for anatomical localisation and PET attenuation correction.
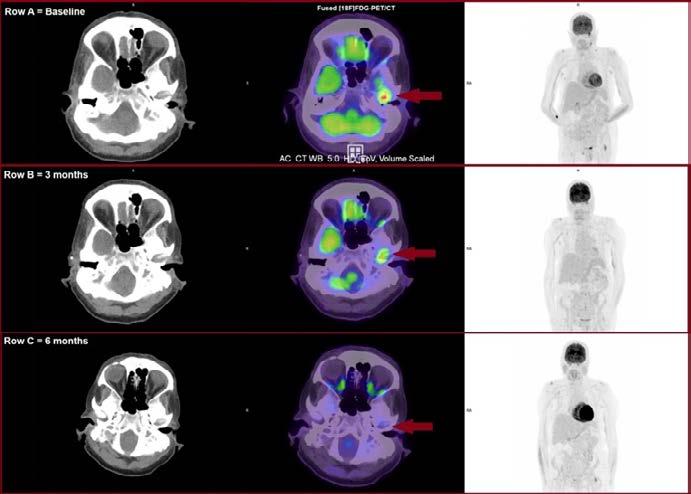
Case findings: [18F]FDG-PET/CT images showed intense uptake within the left EAC, extending to the mastoid and temporal bones (SUVMax 10.7). Reactive lymph nodes were noted within the left retromandibular and supra-clavicular regions, consistent with an active infective aetiology. Correlation with the patient’s clinical presentation confirmed the diagnosis of NOE. As a result, the patient commenced triazole antifungal treatment (Posaconazole).
An [18F]FDG-PET/CT was performed after three months of
Jess Watson
Case Study: The role of [18F] FDG-PET/CT in Necrotising Otitis Externa: A case report. (continued)
therapy. 166.5MBq of [18F]FDG was administered, and a vertex-mid thigh PET/CT was acquired 63 minutes post-injection. Images revealed interval reduction in the hyper-metabolic activity within the left inner-ear and skull base (SUVMax 6.2). Additionally, the retromandibular and supra-clavicular lymphadenopathy had resolved and were no longer [18F] FDG-avid, suggesting a partial treatment response. Subsequently, an [18F]FDG-PET/CT was performed six-months posttherapy. 171MBq of [18F]FDG was administered, and PET/CT imaging commenced 63 minutes post-injection. Resultant images demonstrated absence of the previous hyper-metabolic activity in the left inner-ear, suggestive of complete response to therapy and resolution of infection (Figure:1).
Figure 1: Row A = [18F]FDG-PET/CT showing increased uptake consistent with NOE (arrow). Rows B and C demonstrate resolving infection at 3 and 6-months (Clinical Placement Site, 2023).
Discussion: This case highlights the diagnostic challenge of NOE. Symptoms are often non-specific, and signs of severe infection can be scarce[6]. Further, lesions involve soft-tissues, bones and inflammatory processes, prompting debate over the optimal imaging modality[7]
High-resolution CT is cited as the most common tool in evaluating NOE, with grading systems available to correlate with disease severity[6]. However, CT is limited in detecting early-stage soft-tissue inflammation, and may only reveal bone involvement once erosion becomes evident [6]. As bone erosion can be a relatively late
Case Study: The role of [18F] FDG-PET/CT in Necrotising Otitis Externa: A case report. (continued)
phenomenon in NOE, particularly with fungal infections, early osteomyelitis can be missed, delaying diagnosis[5]
[18F] FDG-PET/CT played a pivotal role in confirming the diagnosis of NOE in this patient in the context of inconclusive CT and MRI findings. As [18F]FDG is a non-specific agent, findings must be correlated with clinical history, previous imaging, and investigations to differentiate infections from malignancy[8] [18F]FDG-PET/ CT complemented prior imaging by identifying a localised area of [18F]FDG avidity within the inner-ear, extending to the mastoid and temporal bones, consistent with NOE. The assessment of disease extent and bone involvement via [18F] FDG-PET/CT was pivotal in determining the appropriate therapeutic approach. This aligns with current literature evaluating the efficacy of [18F]FDG-PET/ CT in detecting and localising NOE, with reported sensitivity and specificity of 96% and 91%, respectively[5].
Additionally, this case demonstrates the value of [18F] FDG-PET/CT in evaluating treatment response. MRI and CT have limitations in this regard, as bone erosion and soft-tissue involvement can persist after infection resolves, and differentiation of active inflammation from resolving infection is difficult with these modalities[6]. In contrast, [18F]FDG-PET/CT was effective in monitoring treatment response by providing visual assessment of changes in metabolic activity and comparative SUVMax values[1]. This is critical as NOE resolution can span up to a year, necessitating regular follow-up to detect signs of relapse or inadequate treatment response[10]
Conclusion: NOE is a severe and potentially lifethreatening infection requiring timely diagnosis, treatment, and monitoring [7] . Anatomical imaging modalities such as CT and MRI are common practice for diagnosing NOE, however this case demonstrates the valuable role of [18F]FDG-PET/CT in diagnosing, localising, and assessing disease extent when these modalities fall short[6]. Further, [18F]FDG-PET/CT is a powerful tool to monitor treatment response and guide treatment cessation, underscoring the impact of [18F]FDG-PET/CT throughout multiple stages of NOE management[19]
References:
1. Khan, H.A., Necrotising Otitis Externa: A Review of Imaging Modalities Cureus, 2021. 13(12): p. e20675.
2. Loh, T.L., et al., Malignant otitis externa in Australian Aboriginal patients: A 9-year retrospective analysis from the Northern Territory. Aust J Rural Health, 2019. 27(1): p. 78-82.
3. Thorsness, S., et al., F-18 FDG PET/CT in Management of Necrotizing Otitis Externa. Journal of Nuclear Medicine, 2020. 61(supplement 1): p. 1157.
4. Australian Institute of Health and Welfare (AIHW) & National Indigenous Australians Agency (2020). Aboriginal and Torres Strait Islander Health Performance Framework. 1.15 Ear health. Canberra: AIHW. Viewed 10th October 2023. https://www.indigenoushpf.gov.au/ measures/1-15-ear-health
5. Ahmed, A.A., et al., The diagnostic conundrum in necrotizing otitis externa World Journal of Otorhinolaryngology - Head and Neck Surgery, 2023. n/a(n/a).
6. Kim, D.H., S.W. Kim, and S.H. Hwang, Predictive value of radiologic studies for malignant otitis externa: a systematic review and meta-analysis Brazilian Journal of Otorhinolaryngology, 2023. 89(1): p. 66-72.
7. Takata, J., et al., Systematic review of the diagnosis and management of necrotising otitis externa: Highlighting the need for high-quality research Clinical Otolaryngology, 2023. 48(3): p. 381-394.
8. Dondi, F., et al. Could [18F]FDG PET/CT or PET/MRI Be Useful in Patients with Skull Base Osteomyelitis? Diagnostics, 2022. 12, DOI: 10.3390/ diagnostics12092035.
9. Stern Shavit, S., et al., FDG-PET/CT for diagnosis and follow-up of necrotizing (malignant) external otitis. The Laryngoscope, 2019. 129(4): p. 961-966.
10. Chapman, P.R., G. Choudhary, and A. Singhal, Skull Base Osteomyelitis: A Comprehensive Imaging Review. American Journal of Neuroradiology, 2021. 42(3): p. 404.
Case study
UNDERSTANDING CLINICIANS’ DIAGNOSTIC
PRACTICES OF FDG PET CT
BRAIN FOR INVESTIGATION OF COGNITIVE IMPAIRMENT CASE STUDY
Dr Ashlesha Vaidya
Central Adelaide Local Health Network
Background: Since the addition of FDG PET CT Brain imaging to the Medicare Benefits Schedule in November 2021, there has been significant use of this scan in clinical practice. In the last financial year, over 12,000 scans were rebated in Australia (Medicare Australia statistics, accessed at http://medicarestatistics. humanservices.gov.au/statistics). The Medicare Benefits Schedule stipulates the scan is undertaken for the diagnosis of Alzheimer’s disease when clinical evaluation of the patient by a specialist, or in consultation with a specialist, is equivocal.
There is little or no data on Australian clinicians’ perspective of the diagnostic utility of this test in current clinical practice, nor Australian clinicians’ understanding of the appropriate clinical situations in which to order the test.
A single institution pilot survey was undertaken to assess clinicians’ understanding and use of FDG PET CT Brain in the diagnosis of cognitive impairment.
Method: A single institution pilot survey of RACP physicians specialised in Geriatric Medicine was undertaken as a web based survey on 29th August 2023. The institution was a tertiary level metropolitan public hospital in Australia, remaining unnamed in this publication to preserve anonymity in view of the results of the study.
A request for participation was made at the commencement of a regular departmental educational meeting held on Microsoft Teams. A web link to Google Forms was provided for direct single access to the survey. The survey consisted of 15 questions which were a mix of multiple choice questions and questions requiring open text answers, and constructed on a questionnaire platform (Google Forms). The questions were developed by a RACP physician trained in Geriatric Medicine and Nuclear Medicine. These covered demographics of type
of work (public/private), years of practice in Geriatric Medicine, number of patients seen, imaging tests ordered for diagnosis, appropriateness of FDG PET CT for dementia subtypes, value of FDG PET CT in common clinical scenarios and change in diagnosis and management. Questions relating to acronyms for cognitive tests, viewing images as well as perceived value of a multidisciplinary meeting to discuss cases and review results and imaging were included.
Data collected from the survey was presented on graphs using Google Forms software.
Results: Eleven of the twelve Geriatric Medicine physicians attending the meeting completed the survey. No advanced trainees completed the survey.
Six respondents worked mainly in the public sector, and five undertook a mix of private and public work.
54.5% (6) of respondents had practiced in Geriatric Medicine (including time in speciality training) for 6-10 years. 36.5% (4) of respondents had practiced Geriatric Medicine for 0-5 years, and only 9.1% (1) had practiced in this specialty for more than 15 years.
9 (81.8%) of respondents stated they saw 0-10 patients per week for diagnosis of cognitive impairment, with the remaining two reporting seeing 11-20 patients per week for this reason.
FDG PET CT brain was used only ‘sometimes’ for diagnosis by the majority (8 of 11) of respondents. One respondent reported ‘always’ ordered a FDG PET CT for the investigation of cognitive impairment.
Eight of eleven respondents (73%) considered FDG PET CT an appropriate test for Alzheimer’s dementia. Three respondents (27%) considered it an appropriate
Case Study: Understanding Clinicians’ Diagnostic Practices of FDG PET CT Brain for Investigation of Cognitive Impairment (Continued)
test in the work up of vascular dementia. Over 60% of respondents considered FDG PET CT an appropriate test for clinically suspected Frontotemporal Dementia, Lewy Body Dementia, Primary Progressive Aphasia and Posterior Cortical Atrophy.
FDG PET CT was perceived to be of high value by 9 respondents for Young Onset Dementia, but of low value by 5 respondents for mild cognitive impairment (MCI), and of low value for age >80 years and age >90 years by 6 respondents, respectively.
Only one respondent reported ‘always’ viewing the FDG PET CT images as part of their assessment, compared to 5 respondents always viewing the CT images and 6 respondents always viewing the MRI images. More than 50% of respondents used the acronyms MMSE, GDS, RUDAS, MoCA, and ACE on the imaging request form.
9 of 11 respondents stated that SPECT or FDG PET CT changed the final diagnosis ‘sometimes’, with 1 respondent reporting it changed diagnosis ‘rarely’ and one respondent reporting final diagnosis changed ‘often’. Only two respondents stated that SPECT or FDG PET changed management ‘often’, with four stating it changed management ‘rarely’, and the remainder (5) reporting change ‘sometimes’.
Six respondents stated they had contacted the reporting clinician after the report was available, whereas five stated they had not, for example in cases of a FDG PET CT scan report which was discordant with the clinical diagnostic impression.
All respondents responded in the affirmative that a MultiDisciplinary meeting with physician, neuropsychologist, radiologist/nuclear medicine physician) to discuss diagnosis would be of value..
Discussion: The respondents who undertook the survey were mostly practicing public work or a mix of public and private practice work. Just over half respondents had been practicing in Geriatric Medicine for 6-10 years (which included time in specialty training, usually 2-3 years), reflecting recent qualification.
There appeared to be discrepancy in the perception of value in MCI compared to published literature which has
established the diagnostic and prognostic value of FDG PET in MCI. Respondents’ perception of high value of FDG PET in Young Onset Dementia and low value with increasing age are consistent with current literature.
The majority of respondents reported that SPECT or FDG PET only changed final diagnosis and management ‘sometimes’. This could be due to the limited use of FDG PET by respondents.
Clinical information provided on the request form may influence the report conclusion. The common use of acronyms on the request form identified on this survey highlights the importance of reporting clinicians’ awareness of their meaning. The use of acronyms which can have different meanings can affect the reporting clinician’s impression. For example, GDS is commonly used to abbreviate the Geriatric Depression Scale (a screening test for depression, with short version scores ranging from 0 to 15, with higher scores suggesting the possibility of mood disorder), but can be misinterpreted by reporting clinicians as Global Deterioration Scale (scale 1 to 7; 1 = no cognitive decline, 7 = severe dementia), swaying the perceived clinical impression towards dementia.
All respondents considered a multidisciplinary meeting to discuss diagnosis, especially in cases of diagnostic uncertainty, to be valuable. Given the significant impact of a dementia diagnosis on all aspects of a patient’s life and care, and new anti-amyloid therapies on the horizon, this may need to be a routine part of the diagnostic and management pathway, similar to oncology practice.
The limitations of this pilot study are the small sample size and single institution. Further research surveys could include specific scenarios to assess clinicians’ use of FDG PET in cognitive impairment.
Conclusion: This pilot survey suggests that referring physician understanding of the value of FDG PET CT in the diagnosis of cognitive impairment could be improved, particularly in clinical scenarios such as MCI.
Institution specific practices and availability during specialist training may have been factors affecting knowledge and use of FDG PET CT brain in this study.
Multidisciplinary meetings for review of cases of diagnostic uncertainty is considered valuable by physicians. Such EDUCATION & CPD | Case study
Case Study: Understanding Clinicians’ Diagnostic Practices of FDG PET CT Brain for Investigation of Cognitive Impairment (Continued)
meetings would help to improve diagnostic confidence and increase referrer knowledge of the imaging modality, as well as potentially impact patient management.
Further studies to assess the impact of FDG PET CT on management in Alzheimer’s dementia in the real-world setting would assist clinicians to better understand the role of FDG PET CT in the diagnostic algorithm for cognitive impairment and use these tests judiciously.
EDUCATION & CPD | Case study
WHAT'S THAT? CASE STUDY
Patient History: A 40-year-old male presented to the nuclear medicine department for a Whole Body Bone Scan (WBBS). The patient experienced 12 months of severe Xiphoidalgia, a rare musculoskeletal syndrome resulting in referred chest pain from the xiphisternal joint (Noor et al., 2021).
A Computed Tomography (CT) scan was inconclusive for bony pathology, thus, a WBBS was requested for assessment and review for surgical workup.
The patient had previously missed three appointments due to chronic anxiety and exhibited nervousness, sweating, restlessness, and difficulty focusing. Reassurance was provided well in advance of the injection, and the patient was familiarised with the gamma camera to alleviate apprehension. Additional practical measures such as offering a wet towel and employing distraction techniques during the injection were undertaken to address the patient's fear of needles.
Investigations: A 22G peripheral intravenous cannula was inserted in the left anterior cubital fossa and the patient was positioned on the gamma camera with the thorax in the field of view. The patient developed coping mechanisms such as ice packs, for their chronic pain and anxiety. Consequently, a frozen water bottle was placed on their chest during the flow and pool acquisition to increase the patient’s tolerance of the scan.
They were injected with 895 MBq of 99m-Technetiummethyl diphosphonate (99mTc-MDP) and a 1-minute dynamic blood flow acquisition was acquired. This was followed by two 120-second blood pools. A routine delayed whole body acquisition was acquired approximately 3-hours post-injection and a Single Photon Emission Computed Tomography (SPECT) with a low dose CT scan was acquired of the thorax region.
Image Appearances: On the blood pool, a cold defect was visualised in the manubriosternal region attributed to the frozen water bottle as seen in Figure 1. This was then removed for a secondary blood pool. The WBBS and SPECT/CT findings were insignificant for any bony pathology.
Discussion: One of the multifaceted challenges technologists face is an anxious patient. The phrase ‘nuclear medicine’ can be daunting to some, often prompting an adaptive emotional reaction due to the uncertainty and fear associated throughout the entire medical procedure (Pifarre et al., 2022). High anxiety can negatively affect patient satisfaction and compliance, often interfering with the workflow of the nuclear medicine department (Abreu et al., 2017).
This frozen water bottle exemplifies the uniqueness of nuclear medicine. Alike to the plastic vessel, technologists must prioritise flexibility and adaptability to accommodate the needs of a patient whilst also melting away the barriers to build rapport. Although the initial blood pool acquisition proved non-diagnostic, the initial
Figure 1: Anterior Blood Pool
Rebecca Mangelsen
The Queen Elizabeth Hospital
EDUCATION & CPD | Case study
What's That, Case Study
provision of a frozen water bottle served as a comforting measure for the patient. This simple yet thoughtful gesture significantly enhanced the patient's comfort within the healthcare environment and fostered a strong rapport with their technologist. Consequently, this rapport contributed to the patient's compliance during subsequent diagnostic acquisitions without the need for the water bottle.
This underscores the significance of implementing proactive measures to mitigate patient anxiety as often the smallest gestures have the largest impact. Acuff et al. (2014) exemplify the importance of effective patient-technologist communication which can lead to a decrease in patient anxiety and an improvement in a patient’s overall experience within the nuclear medicine department. As technologists, we play a significant role in fostering positive patient experiences with opportunities for continual improvement and innovation in our delivery of patient care.
References
• Abreu, C., Grilo, A., Lucena, F., & Carolino, E. (2017). Oncological Patient Anxiety in Imaging Studies: the PET/CT Example. Journal of Cancer Education, 32(4), 820–826. https://doi.org/10.1007/s13187-016-1069-3
• Acuff, S. N., Bradley, Y. C., Barlow, P., & Osborne, D. R. (2014). Reduction of patient anxiety in PET/CT imaging by improving communication between patient and technologist. Journal of Nuclear Medicine Technology, 42(3), 211–217. https://doi.org/10.2967/jnmt.114.139915
Noor, N., Amgalan, A., Vij, N., Habib, K., Anantuni, L., An, D., Kassem, H., Paladini, A., Varrassi, G., & Kaye, A. D. (2022). Treatment and Management of Xiphoidalgia. Orthopedic Reviews, 14(3), 37070–37070. https://doi. org/10.52965/001c.37070
Pifarré, P., Simó, M., Gispert, J. D., Pallarés, M. D., Plaza, P., & Martínez-Miralles, E. (2011). Diagnostic imaging studies: do they create anxiety? Revista española de medicina nuclear, 30(6), 346–350. https://doi.org/10.1016/j. remn.2011.03.003
In Celebration of Pioneers ARTICLE
This year I was given the honour by the ANZSNM of delivering the annual Pioneer Lecture at the 2024 Annual Scientific Meeting in Christchurch, NZ. I used this opportunity to tell the delegates about some of our lesserknown pioneers who had contributed tremendously to our field but remain largely unheralded. The pioneers that I chose to highlight were particularly relevant to the areas of physics in which I have done considerable work, namely image reconstruction and multimodality imaging. While doing my background research on these “local heroes” I learned a lot and have tried to capture some of this in this short article.
Tomographic Image Reconstruction from Projections
Johann Radon was an Austrian mathematician who in 1917 first described a branch of mathematics based around the integral transform, known also as the Radon (or X-ray) Transform. An integral transform is when a function such as ƒ(x,y) is integrated, or “summed”, over one dimension only to give a profile, in this case g(x). He also introduced the Inverse Radon Transform to recover an estimate of the original function ƒ'(x,y) from multiple Radon Transforms, or projections, from many angles. This is the basis of many forms of tomography in X-ray CT, SPECT, PET and Electron Microscopy. His work was to languish for the next 40 years until an Australian called Ron Bracewell found an application for it.
Ron Bracewell (Fig. 1) was born in Sydney in 1921 and was a graduate of the University of Sydney with degrees in Mathematics & Physics ( BSc, 1941) and Electrical Engineering (BE, 1943). He went on to obtain an ME in 1948 and a PhD in Physics from Cambridge in 1949. The University of Sydney has always been incredibly strong in astronomy, and in particular radioastronomy, and
remains so to this day. In the early 1950s Bracewell was making observations of the electromagnetic emissions from the sun in the radiofrequency range while working at the CSIRO Radiophysics Laboratory located at the University of Sydney. Each day another measurement would be made leading to almost exactly 1° sampling over a year as the earth made its annual circumnavigation of the sun, similar to how CT, SPECT and PET acquire data using a circular orbit about the subject being scanned. He then implemented Radon’s inverse transform approach to provide an estimate of the radiofrequency emissiongenerating distribution within the sun. He described the method in a paper published in the Australian Journal of Physics in 1956 (1) – the first person to use Radon’s mathematics to solve the inverse problem of recovering a multidimensional distribution from its integral transforms. Image reconstruction from projections was born!
It is hard to understate the importance of Bracewell’s pioneering contribution. A decade later his methods would be adopted by a South African mathematician, Allan Cormack, who went on to be awarded the Nobel Prize in Physiology or Medicine in 1979 with Godfrey Hounsfield for the invention of the CT scanner and computerised axial tomography. Bracewell could well have been included in that award based on his seminal contribution. In his 1984 textbook “The Radon Transform and Some of its Applications” (2), Stanley R. Deans gives the following dedication in the preface, referring to the Radon Transform:
Dale Bailey PhD
Royal North Shore Hospital
ARTICLE: In celebration of Pioneers (Continued)
Johann Radon laid its foundations
Ron Bracewell and Allan Cormack showed how it could be used
I am unsure whether Bracewell would have used a computer for these early calculations. Certainly, the CSIRO Radiophysics Labs in the School of Physics at the university had assembled Australia’s first computer, “CSIRAK Mk I”, by the late 1940s and then purchased the first true computer, “SILLIAC”, in the 1950s. Bracewell went on to lecture at UC Berkeley before moving to Stanford and eventually became the first Lewis M. Terman Professor of the Space, Telecommunications and Radioscience Laboratory and Fellow in Electrical Engineering (1974–1979). He died in 2007.
The title and abstract of Bracewell’s original publication on what we now refer to as image reconstruction based on the Central Slice Theorem is shown in figure 2.
The illustration in Fig. 3 shows the relationship between a Radon Transform and the underlying distribution that gave rise to it by the integral transform. I still use a very similar figure to this day when trying to explain the Central Slice Theorem to students. Bracewell received the Order of Australia (AO) and a number of awards for his fundamental contributions in radioastronomy, signal analysis and medical imaging but to the best of my knowledge he did not publish a single paper on the topic of medical imaging. Others picked up his ideas and applied them.
Figure 2. Bracewell’s ground-breaking 1956 publication in the Aust J Phys (my underlining for emphasis).
Figure 3. Bracewell’s diagram from the 1956 paper illustrating the Central Slice Theorem and its use in cross-section reconstruction.
ARTICLE: In celebration of Pioneers (Continued)
Transmission Scanning – Towards Multimodality Imaging
Another one of our early Australian pioneers was James (Jim) McRae (Fig. 4). McRae studied medicine (MB BS BSc(Med)) at the University of Sydney in the early 1950s. After completing his residency in 1958 he moved to the USA to undertake a PhD in Medical Physics at UC Berkeley where he worked with John Lawrence MD, brother of Ernest O Lawrence, the inventor of the cyclotron and recipient of the Nobel Prize in Physics for this in 1939. After graduating from Berkeley, McRae returned to head up the Clinical Research Unit (CRU) that Prof Ruthven Blackburn had created in the medical school at the University of Sydney, which had a special interest in the use of radioisotopes in medicine. McRae attracted a fellow clinical tutor/academic, John G. Morris, to join him. Together they established the first Nuclear Medicine Unit at Royal Prince Alfred (RPA) Hospital, Sydney moving from the CRU in the University’s Blackburn Pavilion to a converted pie factory on the main RPA campus in 1966-67.
McRae was, however, drawn back to UC Berkeley where he was to work with Hal O. Anger, the inventor of the gamma camera. Amongst a number of other activities, such as exploring positron imaging with the gamma camera, they published a paper on using a transmission source with the gamma camera to get a low-resolution image of the body density (esp. the thorax) (3). Two figures from the paper are shown in Fig. 5.
The transmission scan combined with the emission planar lung images in figure 5 are a very early example of multimodality, structure-function imaging. I went on to use their approach using Gadolinium-153 (Ey = 98 & 103 keV) as the transmission source, albeit without a collimator, to give simultaneous transmission-emission imaging on a rotating a gamma camera installed at RPA in the mid-1980s (4). With some refinements the 2D transmission flood source was “compressed” into a 1D line source which traversed the axial field of view of the gamma camera while acquiring the Tc-99m images and was used with SPECT acquisitions to provide crude anatomical information as well as body density measurements for attenuation and scatter correction of the resulting SPECT scans – all aimed at producing quantitative SPECT images. Some may recall that this approach was commercialised in the ADAC gamma cameras of the 1990s and was also implemented for attenuation correction of myocardial perfusion scans by GE. The other vendors all had variations on transmission scanning, usually with 153Gd, for removing attenuation artefacts from cardiac scans.
Figure 4. Jim McRae
MB BS BSc (Med) PhD FRACP
Figure 5. The transmission scanning system configuration (left) and examples (top row, right) along with corresponding planar perfusion lung scan images (bottom row)
ARTICLE: In celebration of Pioneers (Continued)
These incremental changes were the precursor to the eventual combination of the gamma camera with a CT scanner to give much higher quality structural / morphological data to accompany the functional emission scans leading to the state-of-the-art today in both SPECT and PET, where nearly all devices currently sold in Australia are multimodality scanners.
A Revolution in Image Reconstruction
An American called Larry Shepp working at Bell Research Laboratories in the 1980s developed an alternative method of reconstruction to the classical filtered backprojection algorithm that was used in all medical imaging modalities at the time. Shepp proposed an “iterative” approach to image formation, based on some optimising mathematical algorithms, that would make successive estimates of a likely image and then compare it to the projections that had been recorded ( i.e. , the Radon Transforms). The algorithm would loop again and again until the projections formed from the latest estimate of the image closely matched the projections that had been recorded. When these were found to be in close agreement it was assumed that the estimated image must be a good representation of the true underlying distribution. He called his method a “Maximum Likelihood (ML) Reconstruction” (5). The method was more flexible than the inverse Radon transform approach and had good noise-controlling properties. However, even with relatively small datasets such as from SPECT at the time (64 × 64 matrices for 60 projections) the computational burden was excessive, sometimes taking days to converge towards the solution and was hence impractical for routine use in the clinic.
This situation was still the case when we held a workshop on image reconstruction methodology at the University of Sydney/RPA in early 1991 to coincide with the introduction of PET and the National Medical Cyclotron project in Australia. Present in the audience were two interested mathematicians from Macquarie University, Sydney: a Professor of Statistics, Malcom Hudson (Fig. 6), and his colleague Richard Larkin. They had no experience in medical imaging but a lot
of experience in population estimation from small groups of individuals. They knew that they could use subsets of a population to estimate the characteristics of the entire cohort.
After the workshop ended they suggested that it might be possible to modify Shepp’s ML algorithm to reconstruct using subsets of the larger dataset with a significant decrease in computation required and hence would accelerate the reconstruction process. Over the next year or two the RPA physicists led by Brian Hutton worked with Malcolm and Richard, firstly in SPECT, to test out if their methods could be employed. I recall that they found it difficult at first to get their methodology, which as expected showed a very great improvement in speed of execution, published in the usual journals as there seemed to be disbelief that small subsets of the data, used successively in each iteration, could lead to the same convergent image as using all of the data for each iteration. However, over time their approach was accepted and finally appeared in press in 1994 (6). They called their method “Ordered-Subset Expectation Maximisation” (OS-EM). This was to usher in a revolution in the reconstruction of tomographic medical images.
OS-EM found first application in SPECT and, when the better image quality was seen, soon found its way to PET reconstruction, which involved larger datasets. From around the year 2000 OS-EM became the preferred method for image reconstruction in all emission tomography and started to be further developed with different convergence approaches and more corrections, such as for attenuation, scattered photons and spatiallyvarying collimator blurring, being built into the process while still able to produce images in a clinically acceptable time. This benefitted naturally from the ever-increasing power and speed of small computers. In more recent times, OS-EM has been adopted for X-Ray CT image reconstruction to permit “low dose” CT scanning as OS-EM’s improved control over amplifying noise in the image can be utilised to reduce the beam current and hence decrease the radiation exposure to the subject being scanned without compromising image quality. Ordered subsets iterative reconstruction is
Figure 6. Malcolm Hudson PhD
ARTICLE: In celebration of Pioneers (Continued)
now globally the preferred method for image reconstruction in medical imaging for X-Ray CT, PET and SPECT. It is also now a stand-alone area of development and a branch of mathematics on its own in the field of image reconstruction. For his contribution towards the clinical implementation of iterative reconstruction Malcolm Hudson was awarded the Institute of Electrical & Electronic Engineers (IEEE) 2014 Marie Skłodowska-Curie Award along with Brian Hutton and Larry Shepp (d.2013).
In summary, these three pioneering Australians have made enormous contributions to the field of medical imaging and, in particular, nuclear medicine. And yet not many of us are aware of their work or the scale of their contributions. I hope this article helps in a small way to recognise their pioneering efforts and provides encouragement to the pioneers of tomorrow to take on new frontiers in our field.
References
1. Bracewell RN. Strip integration in radio astronomy. Aust J Phys. 1956;9:198-217.
2. Deans SR. The Radon Transform and Some of Its Applications: Wiley–Blackwell; 1983.
3. McRae J, Anger HO. Transmission Scintiphotography and its Applications. Paper presented at: Medical Radioisotope Scintigraphy; 1969, 1968; Salzburg.
4. Bailey DL, Hutton BF, Walker PJ. Improved SPECT using simultaneous emission and transmission tomography. J Nucl Med. 1987;28:844-851.
5. Shepp LA, Vardi Y. Maximum likelihood reconstruction for emission tomography. IEEE Trans Med Imag. 1982;MI1:113-122.
6. Hudson HM, Larkin RS. Accelerated image reconstruction using ordered subsets of projection data. IEEE Trans Med Imag. 1994;MI-13:601-609.
Pyrexia of unknown origin and FDG-PET/CT ARTICLE
Bonnia Liu
Austin Health
BACKGROUND: Our study aims to explore the current utilisation of 18F-fluorodeoxyglucose positron emission tomography/computed tomography (FDG-PET/CT) in the diagnostic pathway of pyrexia of unknown origin (PUO) and associated cost of illness in a large tertiary teaching hospital in Australia.
METHOD: 1257 febrile patients between June 2016 to September 2022 were retrospectively reviewed. There were 54 patients who met the inclusion criteria of “classical PUO”, of which DG-PET/CT was performed in 31 inpatients, 13 outpatients and 11 inpatients did not have a FDG-PET/CT scan. The patient demographics, clinical characteristics and inpatient cost were analysed, together with the diagnostic performance of FDG-PET/CT and impact on clinical management.
RESULT: The mean age, length of stay and total cost of admission were higher for inpatients who received FDG-PET/ CT versus those who did not. The median cost per patient-bed-day did not differ between the two groups. Inpatients who received earlier FDG-PET/CTs (≤7 days from admission) had shorter length of stays and lower total cost compared to those who received a later scan. A negative FDG-PET/CT scan, demonstrating no serious or lifethreatening abnormalities resulted in subsequent discharge from hospital or outpatient clinic in 7/10 (70%) patients. There were 11/40 (28%) scans where incidental abnormalities were identified requiring further evaluation.
CONCLUSION: FDG-PET showed high diagnostic accuracy and impact on patient management in inpatients with PUO. FDG-PET performed earlier in admission was associated with shorter length of stay and lower total cost.
Reflections on clinical placement in Darwin ARTICLE
Royal Darwin Hospital
In my second year of the Nuclear Medicine course, I spent 6 weeks at Royal Darwin Hospital (RDH) in the Northern Territory, in the Nuclear Medicine (NM) and PET departments. I really enjoyed my time there and vastly expanded my experiences and learning, both technically and personally.
Healthcare in the NT is unique not only in the differences in patient demographic, healthcare literacy, and epidemiology, but also in the availability and accessibility of healthcare. It was quite shocking to learn that there are usually only around 1-3 specialist doctors within each field in the NT, many of whom are visiting doctors from Sydney/Melbourne, not to mention that GP appointments are booked out for up to a month, thus further reducing the chances of getting treatment early. This is clearly reflected in the availability of molecular imaging services, where the RDH PET department is the only one in the entire state, and the NM department is one of only two. As such, many patients that require NM or PET services need to travel from their communities and rural towns via buses and planes to Darwin, with subsidised hospital accommodation for the duration of their stay.
Image 1: Some scenic pictures, from my accommodation during sunset (top right) and sunrise (middle), Waterfront (left), and Mindil beach during sunset (bottom right).
It was incredibly eye-opening to speak with patients and engage in discussions with the NMTs and doctors, to understand and weigh up the necessity of a NM or PET scan versus the time, effort and expenses for the patient to get to RDH. The empathy and workflow logistics required is of an immensely different scale to a metropolitan hospital in Melbourne. For example, a patient from Tennant Creek had a scheduled NM lymphoscintigraphy scan followed by surgery to remove a melanoma from his back. In speaking with him, I found out that Tennant Creek is halfway across the state south of Darwin, and he’d come in last week for the exact same procedure but it was cancelled due to surgery department delays and his blood sugar levels being too low. Understanding and empathising with this patient’s difficulties and evident frustration, in receiving what would be a routine procedure in Melbourne, was a big takeaway in my learning of the intricacies of rural healthcare.
Hafsah Chao
ARTICLE: Reflections on clinical placement in Darwin (Continued)
At the RDH, I also had a great opportunity to learn in detail about cross cultural awareness and practically apply it in day-to-day patient care, as at least 50% of the patients were of a First Nations background. My supervisor was incredibly accommodating in allowing me to join a cross cultural workshop held by Flinders University, where the facilitator had a large wealth of knowledge and delivered in detail a well-rounded perspective of our role as healthcare workers in cultural awareness. I cannot recommend the program more for anyone planning to do placement or work in the Northern Territory, as it provided links in the history of colonisation with the current health barriers that Indigenous people face, as well as tangible and practical actions that we can take to improve the level and type of care we provide.
An example I experienced was an elderly patient who had been admitted on cognitive decline, she had end stage renal failure and was on dialysis, and had a scheduled NM parathyroid scan. As she was unable to make an informed decision by herself, her family attended the appointment, and the procedure was explained thoroughly to her and to her family, and consent gained from all. It was a first step in my learning experience to see cultural awareness practically applied, and the adaptations and variations we need to take to ensure equitable care and awareness is provided at all times. This was an important point of learning for me that I strove to apply in every subsequent patient interaction, and will continue to improve and keep a sharp awareness for.
On a more personal note, I had the opportunity to visit the local markets, beaches and Kakadu National Park on my weekends there and I loved seeing and immersing in the multicultural and multidimensional aspects of Darwin, where I especially enjoyed the Warradjan Aboriginal Cultural Centre and the weekly Rapid Creeks market. (some photos attached).
If anyone is contemplating going for a rural placement, I would advise to go for it and take the opportunity as the experience and perspectives that it opens up are invaluable, especially as a student to explore your future prospects!
Image 2: Some photos from Kakadu National Park, including a crocodile (bottom right), seasonal calendar for the Kakadu region (top left), termite mound (bottom left), and mango farms (top right).
Image 3: Some fresh local produce (left: rambutan; top middle: sour mango; right top: guava; right bottom: durian and dragon fruit) and various chilli plants (bottom middle).
AWARDS AND RECOGNITION AT THE 2024 SNMMI CONFERENCE
Congratulating Prof Andrew Scott, Prof Michael Hofman and A/Prof Monica Rossleigh
We extend our heartfelt congratulations to Prof Andrew Scott and Prof Michael Hofman for being recognised as SNMMI Fellows in 2024. Their selection is based on documented excellence in volunteer service to the Society and at least one of the following areas: scientific discovery and innovation, educational efforts, or clinical practice in nuclear medicine and molecular imaging. The SNMMI Fellowship, established in 2016, recognises distinguished service to the society and exceptional achievement in nuclear medicine and molecular imaging, making it one of the highest honours for long-time SNMMI members. This prestigious fellowship is denoted by the FSNMMI designation.
Prof Michael Hofman was also the recipient of the prestigious 2024 SNMMI Saul Hertz award for his fundamental research contributions relating to radionuclide therapy. We congratulate Michael for this outstanding achievement.
We also proudly announce that A/Prof Monica Rossleigh is the recipient of the prestigious SNMMI 2024 Presidential Distinguished Educator Award, honouring her extraordinary commitment to the education and training of nuclear medicine professionals. Congratulations, Monica!
WELCOME
SAMANTHA HAWKINS
New Project Manager at ARTNET
My name is Samanatha Hawkins, and I am very excited to be taking on the role of Project Manager for ARTnet.
Born and raised in Brisbane, I have always loved a challenge. As the youngest child in the family, I was keen to keep up, and as often as possible, show that I could achieve great things.
As a high school student that was heavily involved in music, it was a shock to many, that I decided to study Photonics and Nanoscience at university. But I wanted to do something that was challenging and different, and in particular, something that would land me a job that was equally as exciting.
During my university years, I took on my first science related job. I was an Office Assistant at a Food and Agriculture Laboratory. I started off answering phones and posting mail, but quickly I was helping running samples and recording results. At this point, I knew that I did not love the smelly ‘agriculture’ side of science, but I did love being part of a team where I was able to master the new skills that I was taught.
After finishing university, I started my career as a Radiochemist at Global Medical Solutions. This is where I really found my groove. I loved the fast-paced environment, where no two days were the same. I started off learning how to compound and dispense sterile, patient specific radioactive pharmaceuticals and perform quality control testing. I learnt how to operate a Minitrace cyclotron to produce F18-FDG, how to make I-131 capsules and label white blood cells. This was exactly what I was after, an exciting and challenging career.
It wasn’t long after I started as a Radiochemist, that I was promoted to Production Manager. I worked hard to find the most efficient ways to produce quality time sensitive radiopharmaceuticals for patients across south-east Queensland. I enjoyed growing and supporting a team of likeminded scientists. In this role, I had the opportunity to travel to different facilities across Australia and see how things were done in a variety of GMP and non GMP production facilities and at different hospitals and Imaging Clinics. Since 2010, I have been able to build a wide network of relationships within the nuclear medicine industry and made some lifelong friendships.
In 2021, I became a mother and my career changed path. I had some time off with my young family and took a part time role in pharmaceutical sales, but it never filled the void that I had from my many years in Nuclear Medicine.
Now, as the new Project Manager for ARTnet, I am eager to work with medical specialists, technologists, scientists and researchers to promote and facilitate innovative and collaborative clinical research in the field of Nuclear Medicine and Molecular Imagining. I am looking forward to this next chapter.
Let’s get cracking!!!
IN MEMORIUM- ANDREW F MCLAUGHLIN MBBS FRACP DDU (1941 – 2024)
Andrew McLaughlin was born in Hurstville, Sydney in 1941. He grew up in a local community that has produced a number of well-known Australian larrikins – Clive James in literature and media, Graham “whatever it takes” (Richo) Richardson in politics, and Kerry O’Keefe in cricket and commentary. Maybe there was something in the water in the Hurstville/Kogarah area at the time as Andrew was also of the same larrikin mould.
Andrew was schooled by the brothers at Marist College Kogarah and went on the study medicine at Sydney University in the early 1960s. In his final year as a medical student his clinical placement was at St George District Hospital in Kogarah when it was still part of the Sydney University Medical School. It was there that he first met John Morris who was his clinical tutor and later became the inaugural Head of Department of Nuclear Medicine at RPAH in Sydney. Other fellow students at the time included Tony Walker, Fred Lomas, Ernest Crocker and Peter Valk. John Morris, or JM as he was usually known, was also working in the Clinical Research Unit (CRU) in the Blackburn Pavilion at the University of Sydney introducing new radioisotope studies with Jim McRae. In his written history of the CRU Prof Ruthven Blackburn noted that “McRae was promoted to Assoc. Professor of Medicine in 1962 and assigned to St George Hospital in 1963 where he was responsible for the university teaching of medicine to the 5th year students. His students did well in their exams and some later became nuclear medicine specialists” (1). The Medical Superintendent at St George at the time was Frank Broderick who was also establishing a radionuclide service with assistance from McRae and Morris. Andrew completed his internship and residency years at St George Hospital and became familiar with Broderick’s unit and became one of the first of McRae’s former medical students to enter the new field of nuclear medicine and train as a physician along with Fred Lomas. They were followed by fellow St George medical students Crocker and Valk. Andrew became a registrar in nuclear medicine under John Morris at RPAH in 1969 and obtained his MRACP in 1970 (which subsequently became the FRACP). He was subsequently appointed an acting Staff Specialist at RPAH Sydney from 1971 until he left for overseas training.
Andrew was a Visiting Fellow & Scientist at the Argonne Cancer Research Hospital at the University of Chicago in 1972/3 for a year on a NSW Cancer Council Grant. The University of Chicago was the site of the first controlled nuclear fission reaction using 235U by Enrico Fermi in 1942 and was the epicentre of developments in nuclear medicine in the USA at the time. While in Chicago, Andrew worked under Dr Paul Harper who had introduced 99mTc and [13N]NH3 myocardial perfusion imaging into nuclear medicine a few years earlier. Returning from the USA, Andrew was appointed a Staff Specialist in Nuclear Medicine at RPAH & later a Senior Staff Specialist. During his time in Chicago Andrew was particularly impressed with the monthly meetings held where the physicians around town would get together for lunch and to discuss new ideas
and interesting cases. Upon returning to Australia Andrew conspired with Provan Murray from POWH, Sydney to set up a similar meeting in Sydney which he did through the new local NSW branch of the recently formed ANZSNM.
Andrew was responsible for the clinical functioning of the RPAH department, the training of the registrars & continuing education of the staff in general. During his time in this role there were over 30 registrars trained, many of whom also went on to fellowships at prestigious overseas centres. Many became heads of departments in Sydney and nationally. There were also many visiting domestic & overseas physicians and physicists who did varying degrees of training at RPAH over the years. He was also integral in establishing the Australian & New Zealand Association of Physicians in Nuclear Medicine (now the AANMS) serving for 8 years on Council and two years as President (1986-88).
Andrew McLaughlin (left) and John Morris (right) outside the “pie factory”, the Department of Nuclear Medicine at RPAH, in the 1980s. Together they formed a formidable team which saw RPAH Nuclear Medicine contribute significantly to the field clinically and in R&D for over two decades.
Anyone who worked in the 1970s-1990s at “the pie factory”, as the RPAH Nuclear Medicine Department’s facility was known, knew what a busy, chaotic and innovative place it was. Andrew was clearly the leader of the clinical service and oversaw the introduction of the first gamma camera, the first dedicated mini-computer (DEC PDP-11) for processing gamma camera data such as for Gated Heart Pool Scans for LV Ejection Fraction (EF) and wall motion, the first single head rotating gamma camera SPECT scans and eventually the introduction of PET at RPAH in 1992. It was a place of big personalities and Andrew was certainly one of them. I am sure all of the registrars who trained under Andrew not only appreciated his authority in the interpretation of nuclear medicine studies but also his acute clinical acumen.
The ANZSNM recognised Andrew’s lifetime achievements in 2021 when he was named the Pioneer Lecturer at the Annual Scientific Meeting (see: https://youtu.be/E-XVoXqOKJY). For more recollections from Andrew see (1). I was the moderator for his presentation and had the job of collating the online comments and questions at the end of his lecture. I include a selection of these below as they seem to capture both Andrew’s larrikin streak as well as his deep commitment and contributions to the development of the profession.
Questions & Comments for the Pioneer Lecturer 2021, Dr Andrew McLaughlin:
What a privilege to have you speak of the infant years of this amazing profession. Thanks for sharing your story;
• Through the years, what changes in nuclear medicine were you most impressed with?
Was it usual for you to test new tracers on yourself?
Thank you for your massive contribution to Nuclear Medicine.
Andrew continued to work in his private practice at Burwood until only a few years ago. He and his wife of over 35 years, Mary, have been great friends to many of us and have continued to travel overseas regularly to visit children and grandchildren in far flung locations. It is due to the strong beliefs of founding fathers of nuclear medicine in Australia such as Andrew that this field rightly sits within Internal Medicine as a specialty, and not in Radiology, and why our domestic practice is so healthy and in such demand internationally now for introducing new radiopharmaceuticals and procedures, both diagnostic and therapeutic. Andrew was one of the great characters of Australian Nuclear Medicine and a “true believer” in more ways than one. The legacy he leaves on Australian Nuclear Medicine is profound and will be fondly remembered.
Dale L Bailey PhD FIPEM FACPSEM
Department of Nuclear Medicine, Royal North Shore Hospital, Sydney
Reference
1.Batchelor P (Editor). Isotopes, Imaging and Identity - The History of Nuclear Medicine in Australia and New Zealand as documented by Paul A.C.Richards: ANZSNM; 2014.
EDUTRACE - LATEST PRESENTATIONS
JOB VACANCIES
Nuclear Medicine Technologist
We are looking for an enthusiastic person who is interested in joining our team as a Nuclear Medicine Technologist in the progressive and rewarding profession of Nuclear Medicine (Molecular Imaging).
Applications Close: 17 July 2024
Nuclear Medicine Technologist Clinical Manager (NMPET)
An exciting opportunity exists for a Nuclear Medicine Technologist Clinical Manager, (Nuclear Medicine and Positron Emission Tomography) to be accountable for the delivery of specialist Nuclear Medicine and PET services, the management and professional competence of subordinate staff, whilst providing an advanced leadership role in the multidisciplinary team.
Applications Close: 17 July 2024
Experienced Nuclear Medicine Technologist
As a skilled Nuclear Medicine Technologist, you'll be at the forefront of medical innovation.
Applications Close: 31 July 2024
Expressions of Interest - Rural & Regional Branch Committee Members
Expressions of interest are sought from ANZSNM members to join the Rural & Regional Branch Committee - We Need You!
Applications Close: 31 July 2024
Expressions Of Interest - NSW/ACT Branch Committee Members
Expressions of interest are sought from ANZSNM members to join the NSW/ACT Branch Committee - We Need You!
Applications Close: 31 July 2024
2024 ANZSNM UPCOMING EVENTS
JULY SEPTEMBER
ANZSNMT SA/NT Branch Meeting Protocol Review Online Via Zoom
6:00pm-7:00pm ACT
AUGUST
2024 TSIG Annual Day Symposium Oaks Cypress Lakes Resort
9:00am-5:00pm AEST
OCTOBER
SA/NT Branch Meeting Online Via Zoom
6:00pm-7:00pm ACST
WA Branch MeetingHosted by FSH/RPH Online Via Zoom & FSH/ RPH
5:30pm-8:00pm AWST
SA/NT Branch Meeting Online Via Zoom
6:00pm-7:00pm ACST
WA Branch Day Seminar Venue TBA 6:00pm-8:00pm ACST
WA Branch MeetingRadpharm Presentation Night PRC 5:30pm-8:00pm AWST
NZ Branch Awards and AGM Online via Zoom 7:00pm-9:00pm NZST
ANZSNM Secretariat, PO Box 6178, Vermont South, Victoria 3133
Tel: 1300 330 402 | Fax: (03) 8677 2970
Email: secretariat@anzsnm.org.au
AIMS AND OBJECTIVES OF THE AUSTRALIAN AND NEW ZEALAND SOCIETY OF NUCLEAR MEDICINE
1. Promote:
• The advancement of clinical practice of nuclear medicine in Australia and New Zealand;
• Research in nuclear medicine;
• Public education regarding the principles and applications of nuclear medicine techniques in medicine and biology at national and regional levels;
• Co-operation between organisations and individuals interested in nuclear medicine; and
• The training of persons in all facets of nuclear medicine.
2. Provide opportunities for collective discussion on all or any aspect of nuclear medicine through standing committees and special groups:
• The Technical Standards Committee sets minimum standards and develops quality control procedures for nuclear medicine instrumentation in Australia and New Zealand.
• The TSIG Committee is the group overseeing the Technologist Special Interest Group (TSIG) and ensures that all projects, committees and activities of the TSIG align with the values and strategic plan of the ANZSNM. It reports directly to the ANZSNM Federal Council and oversees the two TSIG working groups: CPD & Education Working Group and Technologist Workforce Advocacy Working Group. The committee is able to form working groups to perform specific tasks as required to provide opportunities for the benefit of Technologist members of the ANZSNM after consultation with the ANZSNM Federal Council.
• The Radiopharmaceutical Science SIG and a Physics SIG that maintain standards of practice for their particular speciality and provide a forum for development in Australia and New Zealand.