
28 minute read
Education and Continuing Professional Development

from Gamma Gazette Winter Edition 2021 by The Australian and New Zealand Society of Nuclear Medicine
by ANZSNM

EDUCATION AND CPD | Case Study
Marianna Elias, University of South Australia
ABSTRACT: Cardiac Amyloidosis (CA) is characterised as insoluble amyloid plaque depositions within the myocardium and is often associated with several clinical manifestations (Wong & Judge 2020) The two common subtypes involving the myocardium are Immunoglobin light chain (AL) and Transthyretin (ATTR) amyloid plaques (Wong & Judge 2020). ATTR and AL cardiac amyloidosis can be distinguished through using nuclear medicine scintigraphy utilising the Technetium 99m Hydroxy-methylene-diphosphonate (99m Tc-HDP) bone-seeking radiopharmaceutical. This tracer, like other 99m Tc phosphonate derivatives, accumulates in ATTR amyloid depositions, with the cause for this phenomenon remaining unknown (Treglia et al. 2018; Khor et al. 2020). We present a case of an 86-year-old male patient who presented to the department following a cardiac Magnetic Resonance (CMR) Imaging investigation to evaluate for newly diagnosed atrial fibrillation and increasing shortness of breath. These clinical manifestations being typical of that of cardiac amyloidosis (Wong & Judge 2020). The Nuclear Medicine bone scintigraphy was acquired to evaluate for cardiac amyloidosis and consolidate previous findings.
INTRODUCTION: An 86-year-old male inpatient presented into the department with increasing shortness of breath and known atrial fibrillation with a referral to evaluate for possible CA. A CMR image acquisition to evaluate for infiltrative heart disease and monitor left ventricular hypertrophy preceded the nuclear medicine examination.
Amyloidosis refers to the deposition of extracellular insoluble and atypical extracellular fibrils that transpire from the accumulation of misfolded, usually soluble proteins sourced by the liver (Sun et al. 2018). CA is the deposition and aggregation of fibril plaques into the myocardium (Wong & Judge 2020). Systemic amyloidosis in the form of Immunoglobulin light chains (AL) and Transthyretin (ATTR) are the most common plaque types that aggregate in the myocardium and manifest from genetic predispositions or are classified as senile (Wong & Judge 2020). CA can be a clinical indicator of congestive heart failure with preserved ejection fraction and rapidly progressive, restrictive cardiomyopathy (Kuria, Gitau & Makhdomi 2019). Diastolic and systolic dysfunctions may also ensue (Sun et al. 2018). Nuclear medicine bone scintigraphy is utilised to assess and differentiate between AL and ATTR CA and monitor disease progression (Bokhari et al. 2013). Differentiation between these subtypes, is pertinent for an improved patient prognosis, in that ATTR and AL CA each require separate treatment pathways and clinical management (Bokhari et al. 2013; Khor et al. 2020).
NUCLEAR MEDICINE PROCEDURE & FINDINGS PATIENT PREPARATION:
The departmental nuclear medicine bone scintigraphy protocol was utilised. Initially the procedure and a bone questionnaire were discussed with the patient, and at which time it was established that the patient had nil bone pain, with no oncological history. Verbal and written consent was also obtained.
EDUCATION AND CPD | Case Study
PROTOCOL: 850 mega Becquerels (MBq) of Tc-99m HDP was administered to the patient intravenously. The patient was then sent away and returned 3 hours post injection for their image acquisition.
The patient was positioned supine on the scanning bed, pillow underneath knees and head, arms strapped to sides and feet strapped together with his toes together and heels apart. Left and right lateral skull static images were acquired preceding the whole body, departmental routine of these patient presentations. Following this, the patient was asked to place their arms up above their head for anterior and posterior thoracic static images, to further investigate the heart and rib cage. These were acquired for 3 minutes each utilising a Low Energy All Purpose collimator and a Siemens SYMBIA dual-headed hybrid imaging system. This is typical of a cardiac amyloidosis investigation. These images were then assessed and processed whilst the patient remained on the scanning bed.
The resultant images were then processed for quantitative analysis and scrutinised by the reporting doctor. It was at their discretion that a thoracic SPECT/CT was also acquired to formulate a 3D image of the thoracic region. This involves the gamma camera rotating around the patient for approximately 8 minutes followed by a low dose CT image acquisition. The CT image enables for anatomical localisation and attenuation correction. The imaging parameters involved a 128x128 matrix, using a step and shoot acquisition at 13 seconds per view and a total of 96 views (48 views per head). VARTIATION TO PROTOCOL: In the department, standard bone scintigraphy is usually completed approximately 2 hours post injection. However, with cardiac amyloidosis indications, patients are asked to return 3 hours post injection. This is to ensure that bone-to-cardiac uptake ratio is at its optimum level. Imaging at 3 hours post injection increases specificity and sensitivity to the disease process, in that bone and amyloid accumulation is at its peak with a corresponding reduction in blood pooling of radiotracer (Singh et al. 2019).
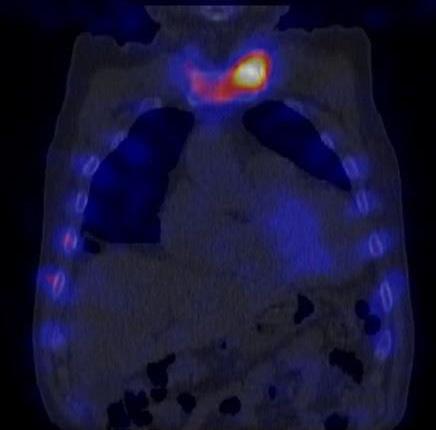
FINDINGS: The Perugini visual scoring system is employed in clinical practices globally as a means of analysing radiopharmaceutical cardiac uptake and was utilised for this case (Figure 1) (Giorgetti et al. 2019; Kuria, Gitau, Makhdomi 2019).
The resultant images demonstrated diffuse low-grade cardiac activity in the same intensity of that of bone uptake in both static and fused SPECT/CT coronal images (red arrows) (Figures 2 & 3). There is also evidence of increased focal high-grade uptake of left sternoclavicular joint. This is consistent with that of normal variant and is typical of degenerative changes in elderly patients. In this study, the anterior static localised view of the thorax was processed for image evaluation by the reporting doctor. The processing involved identical ROIs drawn of cardiac uptake and of the contralateral side for count differentiation (Figure 4). This is to validate any stark differences in counts between other soft tissue structures within the same vicinity. This finding is consistent with that of grade II on the Perugini visual grading system.
0= no cardiac uptake 1= cardiac uptake < bone 2= cardiac uptake = bone 3= cardiac uptake > bone
Figure 1: A visual representation of the Perugini visual grading system (Giorgetti et al. 2019, pg. 26).
EDUTRACE

YOUR CPD E-LEARNING PORTAL
* Exclusive to ANZSNM members
EDUTRACE PROVIDES ACCESS TO A WIDE RANGE OF COURSES ON-DEMAND TO ADD TO YOUR CPD CONTINUING EDUCATION
The content includes proprietary programs as well as others shared by international imaging and therapy organisations with which the ANZSNM has developed excellent relationships over the past 50 years.
Resources including webinars, case studies and online seminars Contributions from local and world experts National and overseas industry conference presentations and webinars Access from any device, anywhere at any time. Integration of CPD points with Attendo Plus mobile app

VISIT
anzsnm.org.au/edutrace
EDUCATION AND CPD | Case Study

Figure 2: The resultant static coronal thorax image. Figure 3: The resultant image of a coronal thoracic SPECT/CT. Figure 4: An anterior projection of the thorax. Two identical region of Interests (ROIs) were placed in adjacent positions relative to the sternum, without bone impedence. ROI B counts (cardiac): 6.16, ROI A counts (mediastinum): 5.21.

CARDIAC MRI PROTOCOL AND
FINDINGS: CMR was specifically utilised to evaluate cardiac functions and morphology (Wong & Judge 2020). Cardiac morphological MRI image acquisitions are quite complex and involve intricate patient preparation. It requires accurate placement of electrocardiogram (ECG) electrodes to ensure an acceptable ECG waveform external to the magnet (McRobbie et al. 2017).
Initially an MRI questionnaire is completed, and any contraindications are recognised. These include, but are not limited to, identifying pacemakers, metal implants (e.g. stents) and any renal impairment if contrast is deemed necessary. Patients are then linked up to an electrocardiogram that triggers the turbo spin echo image acquisition with a double inversion recovery sequence (McRobbie et al. 2017). This is acquired in a single breath hold and involves the use of a 1.5T magnet. Data acquisition most commonly occurs in diastole, where cardiac and respiratory motion is minimised (McRobbie et al. 2017). ECG triggering enables this, where data is consistently acquired at the same point of the cardiac cycle (McRobbie et al. 2017).
It can characterise diffuse myocardial enhancement and right ventricular enhancement, both are pathophysiological of ATTR CA (Aljaroudi et al. 2014). It is also able to determine the cause of left ventricular hypertrophy, distinguishing between cardiac amyloid origin or other disease processes (Wong & Judge 2020). CMR images revealed cardiomegaly and bilateral pleural effusion (blue arrows) with right side greater than left, and interventricular septal thickening (red arrow) (Figure 5). Interventricular septal thickening is typical in that of amyloid plaque deposits in the myocardium (red arrow) (Treglia et al. 2018) The increase in interventricular septal thickness is substantial and is demonstrated in figure 5 (c) whereby length 3, is approximately double the thickness of that of the septum, length 4.
The image investigation proved clinically relevant in the patient management pathway, in that the CMR was suggestive of cardiac amyloidosis, however the subtype remained unclear. As such, it was pertinent to the patient’s clinical journey that these imaging investigations preceded that of the nuclear medicine imaging to validate its utility of the scan to the patient and to justify radiation exposure.
DISCUSSION: CA is often under diagnosed within clinical practice as it poses as several clinical manifestations and can cultivate a myriad of disease processes, one of which is atrial fibrillation (Glaudermans et al. 2014). As the plaques deposit typically into left ventricular myocardium,
EDUCATION AND CPD | Case Study
left ventricular hypertrophy and associated cardiomyopathy develops (Wong & Judge 2020). The plaques prohibit stroke volume augmentation in response to vasodilation and thus causes severe atrial dilation (Wong & Judge 2020). Cardiomegaly, interventricular septal thickening, pleural effusion and known atrial fibrillation, are typical clinical

Bilateral Pleural effusion manifestations that generate of that of CA (Kuria, Gitau & Makhdomi 2019).
Nuclear medicine bone scintigraphy is the only imaging modality that can distinguish between ATTR vs AL CA (Sun et al. 2018). Cardiac uptake of 99mTc-HDP indicates the clinical diagnosis of ATTR CA (Glaudermans et al. 2014; Khor et al. 2020). The degree of cardiac uptake reflects the extent of plaque deposition (Glaudermans et al. 2014).
Although the mechanism of uptake responsible for HDP binding to the ATTR cardiac amyloid plaques remains unknown, it has been theorised that the higher calcium content of ATTR CA is responsible for its avidity to HDP (Treglia et al. 2018). The grade II Perugini visual grade for this study is indicative of ATTR CA (Figures 2, 3 & 4).

Figure 5: Resultant images from MRI image acquisitions. (a) Transverse 1.5T cardiac MRI image with gadolinium contrast (TR = 266.43ms, TE = 1.25ms). (b) Sagittal 1.5T cardiac MRI image with gadolinium contrast and recorded septal thickness values (TR = 32.23ms, TE = 1.23ms). 1: Length - 5.72cm 2: Length - 5.27cm 3: Length - 1.90cm 4: Length - 0.94cm The utility of SPECT/CT imaging in the evaluation for ATTR CA is far reaching. Planar images are limited as it is difficult to differentiate between myocardial uptake and that of overlying rib uptake and may add to ROI myocardial counts (Singh et al. 2019). SPECT/CT overcomes these challenges, enables attenuation correction and anatomical localisation (Singh et al. 2019).
Similar case studies conducted by Davies et al. (2017) & Sun et al. (2018) opted for transthoracic echocardiography or CMR as a non-invasive mode of diagnosis and evaluation for CA prior to nuclear medicine scintigraphy. Serial endomyocardial biopsies remain utilised as the gold standard procedure in diagnosis of CA subtypes (Khor et al. 2020). However, given the invasive nature and associated risks of perforation and bleeding, nuclear medicine is currently the preferred method for clinical diagnosis, with approximately a 100% specificity to ATTR CA (Singh et al. 2019; Khor et al. 2020).
The patient’s disease management pathway coincided with that of relevant literature as other imaging investigations need to be completed prior to nuclear medicine bone scintigraphy. Although optimal at distinguishing between cardiac amyloid subtypes, nuclear medicine is limited in the anatomical information that can be pertained from the images. The CA plaque differentiation is pertinent in
EDUCATION AND CPD | Case Study
disease management as ATTR, and AL require different courses of treatment (Kuria, Gitau & Makhdomi 2019). Nuclear Medicine assisted in patient treatment planning as it was able to provide a diagnosis of ATTR CA. It provides value as part of disease management and treatment planning (Bokhari et al. 2013). It is widely used as a monitoring tool, pre and post treatment (Bokhari et al. 2013).
ATTR CA in the myocardium inhibits stroke volume regulation (Yamamoto & Yokochi 2019; Wong & Judge 2020). As such, heart failure therapy, for example ACE inhibitors can potentially further deteriorate the patient’s condition through increasing hypotension (Wong & Judge 2020). Therapeutic agents have recently developed directed at treating the underlying causes of ATTR (Wong & Judge 2020). These are TTR tetramer stabilisers. These cannot eradicate the disease process, however, can reduce the production and in turn deposition of amyloid proteins in the myocardium (Wong & Judge 2020). CONCLUSION: It is evident through literature that nuclear medicine scintigraphy particularly SPECT/CT is the only imaging modality that can definitively distinguish between ATTR and AL CA. Several of the patient’s clinical manifestations can be directly correlated with that of CA (Wong & Judge 2020). Nuclear medicine in conjunction with CMR addressed the disease processes and thus contributed to improving the patient’s quality of life, through CA subtype identification allowing for catered treatment accordingly. Had the two imaging modalities not corroborated their findings, the patient’s condition could have further deteriorated their health before identification. As such, the efficacy of nuclear medicine in evaluating for cardiac amyloidosis is substantiated.
Heart or liver transplantation has also been explored as a treatment option for genetically predisposed ATTR (Wong & Judge 2020). ATTR CA cultivated without genetic mutations, i.e., senile CA are often diagnosed at an older age at which point transplantation procedures are contraindicated (Wong & Judge 2020).
References
Aljaroudi, WA, Desai, MY, Tang, W, Phelan, D, Cerqueia, MD & Jaber, WA 2014, ‘Role of imaging in the diagnosis and management of patients with cardiac amyloidosis: State of the art review and focus on emerging nuclear techniques’, Journal of Nuclear Cardiology, vol. 21, no. 2, pp. 271-283.
Bokhari, S, Shahzad, R, Castano, A & Maurer, MS 2013, ‘Nuclear imaging modalities for cardiac amyloidosis’, Journal of Nuclear Cardiology, vol. 21, no. 2014, pp. 175184.
Davies, T, Saleh, A, Coghlan, G, Whelan, C & Agarwal, B 2017, ‘A case study of likely wild-type cardiac transthyretin amyloidosis causing rapid deterioration’, Journal of the Intensive Care Society, vol. 18, no. 2, pp. 138-142.
Giorgetti, A, Genoveesi, D, Milan, E, Acampa, W, Giubbini, R, Cuocolo, A & Marzullo, P 2019, ‘Cardiac amyloidosis’, Clinical and Translational Imaging, vol. 7, no. 1, pp. 21-32.
Glaudermans, AWJM, van Rheenen, RVJ, van der Berg, MP, Noordzij, W, Koole, M, Blokzijl, H, Dierckx, RAJO, Slart, RHJA & Hazenberg, BPC 2014, ‘Bone scintigraphy with 99m-technetium-hydroxymethylene diphosphate allows early diagnosis of cardiac involvement in patients with transthyretin-derived systemic amyloidosis’, The Journal of Protein Folding Disorders, vol. 21, no. 1, pp. 35-44.
Khor, YM, Cuddy, S, Falk, RH & Dorbala, S 2020, ‘Multimodality Imaging in the Evaluation and Management of Cardiac Amyloidosis’, Seminars in Nuclear Medicine, vol. 50, no. 4, pp. 295-310.
Kuria, IM, Gitau, SN & Makhdomi, KB 2019, ‘Bone scintigraphy imaging of cardiac amyloidosis’, World Journal of Nuclear Medicine, vol. 18, no. 3, pp. 314-316.
McRobbie, DW, Moore, EA, Graves, MJ 2017 & Prince, MR 2017, ‘Chapter 16: A Heart to Heart Discussion: Cardiac MRI’ in MRI from Picture to Proton, 3rd edn, Cambridge Medicine, Cambridge, UK, pp. 269-287.
Ramsay, SC, Lindsay, K, Fong, W, Patford, S, Younger, J & Atherton, J 2018, ‘Tc-HDP quantitative SPECT/CT in transthyretin cardiac amyloid and the development of a reference interval for myocardial uptake in the nonaffected population’, European Journal of Hybrid Imaging, vol. 2, no. 17, pp. 1-13.
Singh, V, Falk, R, Carli, MFD, Kijewski, M, Rapezzi, C & Dorbala, S 2019, ‘State-of-the-art radionuclide imaging in cardiac transthyretin amyloidosis’, Journal of Nuclear Cardiology, vol. 26, no. 1, pp. 156-173.
Sun, JP, Yang, XS, Yan, BP & Wong, K 2018, ‘Cardiac Amyloidosis’, in JP Sun, XS Yang & BP Yan (eds.), Comparative Cardiac Imaging: A Case-based Guide, John Wiley & Sons Ltd., Oxford, United Kingdom, pp. 267-279.
Treglia, G, Glaudemans, AQJM, Bertagna, F, Hazenberg, BPC, Erba, PA, Giubbini, R, Ceriani, L, Prior, JO, Giovanella, L & Slart, RHJA 2018, ‘Diagnostic accuracy of bone scintigraphy In the assessment of cardiac transthyretinrelated amyloidosis: a bivariate meta-analysis’, European Journal of Nuclear Medicine and Molecular Imaging, vol. 45, no. 11, pp. 1945-1955.
Wong, LSM & Judge, DP 2020, ‘Cardiac Amyloidosis’, in HF Baars, PAFM Doevendans, AC Houweling & P van Tintelen (eds.), Clinical Cardiogenetics, Springer, Cham, pp. 167177.
Yamamoto, H & Yokochi, T 2019, ‘Transthyretin cardiac amyloidosis: an update on diagnosis and treatment’, ESC Heart Fail, vol. 6, no. 6, pp.1128-1139.
EDUCATION AND CPD | Case Study
Benjamin-Minh Hoc Ly (Second Year Student), RMIT University, Melbourne
ABSTRACT: This article intends to provide insight into how Nuclear Medicine (NM) can be utilised to diagnose renal pathologies. It will summarise the process of glomerular filtration, known properties of 99mTc-DTPA and recommended protocols for dynamic renal scintigraphy. A case of a 72-year-old who presented to the department for evaluation will be used to explain the rationale and importance of NM to her prognostic pathway. The patient was determined to have poor renal function, determined by the glomerular filtration rate (GFR) study and a renal impairment demonstrated on imaging. NM combines the efficiency of dual-use tracers and functional imaging to provide an extensive amount of clinical information for patient care.
BACKGROUND: A 72-year-old female patient presented to the Nuclear Medicine department for a dynamic renal study.
Information stated the patient was diagnosed with renal cell carcinoma from a prior biopsy. This scan serves to determine whether the patient is suitable for undergoing radiation therapy, as it can further deteriorate kidney function (Santos et al., 2020). It was requested to assess the patient’s GFR, which is a widely accepted indicator of renal function (Schaeffner, 2017).
The patient was visibly tired and mentioned feeling more tired than usual, which is a common symptom associated with cancer (Larkin et al., 2010). In addition, her clinical history stated she suffered from hypertension. High blood pressure can damage and narrow the renal arteries, decreasing the amount of blood flow (Bidani & Griffin, 2004). With damage to the kidney’s vessels, renal function will be detrimentally affected. If the kidneys cannot discard wastes and excess fluids, renal failure can occur.
It was also confirmed the patient had moderate hydronephrosis in the left kidney and a para-aortic nodal mass, which was confirmed through MRI and CT imaging. While a paraaortic nodal mass is rare, it can be presented within the renal pelvis or kidney (Yamada et al., 1998). It can lead to upper urinary tract obstruction (Caiafa et al., 2013), which blocks urinary drainage (Hong et al., 2020). This could cause deterioration to the renal parenchyma and dilation of the ureters, renal pelvis and calyces. Furthermore, anuria (non-passage of urine through the ureters) and retrograde flow (back up of urine into the kidneys) can happen.
IMAGING PROCEDURE: The patient was positioned supine on the scanning bed (FOV near the L1 - L3 vertebrae), with the collimator positioned posteriorly (Ziessman et al., 2014).


The power of a proven platform. The perspective of a large axial field of view. Biograph Vision Quadra™ takes the potential of PET/CT even further. Dynamically see vertex to thighs in a single position and deepen the dimension of your investigations. Whether you are exploring new research questions or identifying the best clinical approach with Biograph Vision Quadra, the answers are yours to find.
Engineered for new research dimensions
With 106 cm axial PET field of view, Biograph Vision Quadra offers a whole-body (vertex to thighs) perspective so you can scan more in one position to dynamically follow tracer kinetics throughout the body. And with best-in-class time-offlight performance and PET effective sensitivity1, you can see with outstanding clarity.
Developed to reshape clinical outcomes
The accuracy, performance, and reproducibility of Biograph Vision are the gold standard in PET/CT imaging. With Biograph Vision Quadra, you achieve the same outstanding detail and definition that you have come to expect— increased detectability of smaller lesions, reduced scan time and effective dose, and faster evaluation of treatment impact2
Designed for your realities
With a 106 cm axial PET field of view, you can perform a whole-body scan in one position on a machine built for the same space as a traditional PET/CT scanner. Our innovative architecture is designed for easy serviceability, efficient data management, and enhanced workflows. With Biograph Vision Quadra, you have a research and clinical solution designed for your realities.

Data courtesy of Inselspital, Bern, Switzerland
EDUCATION AND CPD | Case Study
Review (Continued)
99mTc-DTPA was chosen as the radiopharmaceutical to evaluate renal blood flow, parenchymal function and elimination of the tracer through the renal collecting system.
Wang et al. (2020) note that 99mTc-DTPA can be used for addressing a diagnosis of suspected urinary tract obstruction. Despite its low extraction fraction of approximately 20% (Taylor et al., 2018), 99mTc-DTPA is the only renal tracer that can calculate the patient’s eGFR as it is predominately cleared via glomerular filtration.
The patient was intravenously administered 209 MBq of 99mTc-DTPA in the right antecubital fossa whilst lying on the scanning bed. The perfusion phase consists of 1 sec/frame for 60 frames. The subsequent dynamic phase is composed of 1 min/frame for 20 frames. A zoom factor of 1.23 was employed to allow for an optimal magnification of the kidneys (EANM, 2016).

Figure 1: Initial perfusion images.
RESULTS: Renal Blood Flow - From the initial time of 99mTc-DTPA being intravenously administered, the tracer is shown to first pass from the bloodstream into the abdominal aorta (Figure 1). From T0 + 3 seconds, we see gradually increased activity within the kidneys. This means the tracer has moved from the afferent arterioles into the glomerulus of the nephrons (Burke et al., 2014).

Figure 2: Time-activity curve (TAC) that demonstrates renal perfusion.
EDUCATION AND CPD | Case Study
Review (Continued)
The TAC (Figure 2) demonstrates the tracer entering the abdominal aorta, crossing the bloodstream to enter the renal arteries (Bounous et al., 1960). A rising slope is visualised alongside rapidly accumulating counts within T0 + 1 - 5 seconds for the aorta, left and right kidney respectively. Around 15 seconds, we see the slope decreasing as the tracer is moving to the renal parenchyma, meaning counts are steadily reducing. This graph demonstrates normal renal perfusion of both kidneys and stable tracer flow into the abdominal aorta from around T0 + 15 seconds - 60 seconds. Renal Dynamic - During T0 + 120 seconds, we see gradual uptake of the tracer in the left kidney. At T0 + 180 seconds,

Figure 3: Renal accumulation and excretion dynamic.
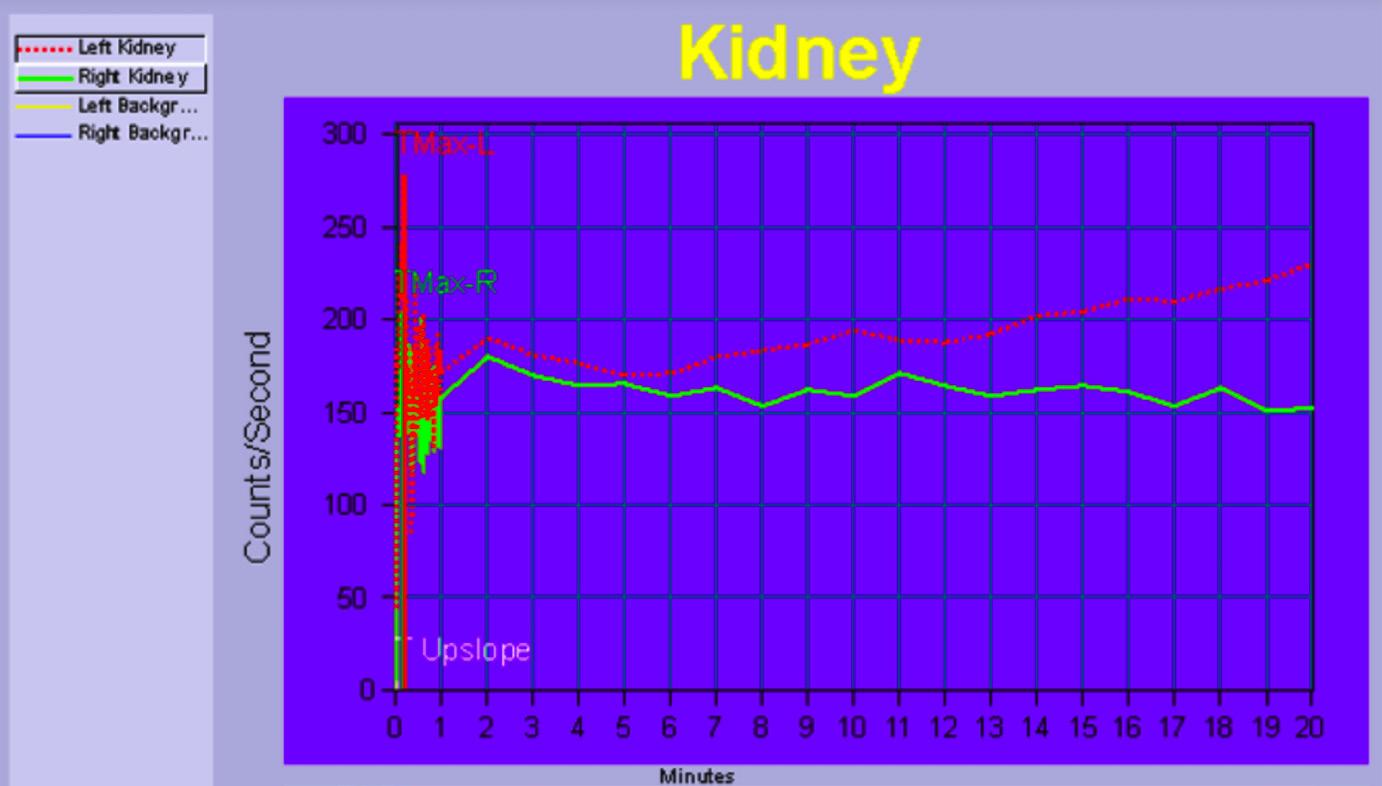
Figure 4: TAC that visualises both renal accumulation and excretion.
the renal pelvis of the right kidney has demonstrated 99mTc-DTPA uptake. At T0 + 19 minutes, profound retention of the tracer is seen within the renal pelvis of both kidneys. This is more evident in the left kidney in comparison to the right one. There is no exhibited tracer clearance into the ureters or the bladder for either kidney, strongly suggesting the presence of a potential urinary tract obstruction.
EDUCATION AND CPD | Case Study
Review (Continued)
At around the T0 + 3 minutes (Figure 4), counts in the right kidney have begun to gradually decrease. At around T0 + 5 minutes, counts in the left kidney have begun to increase. In a normal TAC, peak cortical uptake is usually seen during T0 + 3 - 4 minutes and accumulation of activity in the bladder at T0 + 10 - 15 minutes. As this is not seen, this graph indicates functional impairment of both kidneys.
HOW IS THE eGFR CALCULATED?
The weight of four empty syringes was recorded before the patient’s arrival. 4 x 10 mL blood samples are taken. The first one serves as a baseline, which checks for radiation contamination from such things as prior imaging or therapy. The remaining three were used to acquire blood samples after administration of 99mTc- DTPA at 2, 3 and 4 hours after injection (Murray et al., 2013). The patient was also asked to continue their drinking and food consumption habits, allowing the GFR obtained to be truly reflective of the patient’s daily life. This also meant not engaging in heavy exercise or having a large meal, as high protein consumption can affect the eGFR to perform any heavy exercise.
Samples intervals should be greater than 45 minutes and the exact time of all blood samples recorded for quality assurance. After centrifuging, 2 mL of plasma were pipette into individual counting tubes. These counting tubes are then placed into a gamma counter, forming a linear graph. Information was then derived to be inputted into the following equation.
Formula (Piepsz et al., 2001):
Part 1 Part 2
• V = Volume of distribution (mL). • Reference counts = Average reference counts per minute/mL. • Injection weight of 99mTc-DTPA (grams). • T0 = Counts at start of injection.
REPORT: The derived eGFR was 40 mL/minute, which is normally 75 mL/minute for individuals over 70 years of age (National Kidney Function, 2013). This indicates moderate impairment of kidney function. Both kidneys demonstrated renal perfusion and progressive tracer accumulation. The study showed progressive tracer accumulation in the left kidney without spontaneous net clearance or drainage. A functionally significant obstruction in the right kidney cannot be excluded either. ROLE OF NM IN PATIENT MANAGEMENT: This study demonstrates the use of 99mTc-DTPA for the dual use of imaging renal function and assessing a patient's eGFR, which are both important aspects in the lead up to either chemotherapy or radiation therapy evaluation. Another benefit provided via Nuclear Medicine to the patient was the fairly short duration of gaining multiple results from one examination. The patient only requires two cannulas to perform imaging and eGFR assessment, making this a non-invasive procedure.
EDUCATION AND CPD | Case Study
Review (Continued)
The results obtained provide information about the physiological function of the patient’s kidneys and can complement the anatomical information derived from CT and MRI images. Given the low radiation dose and swift effective half clearance time of 99mTc-DTPA, the patient was able to promptly undergo ultrasound imaging afterwards to detect potential ureteric masses. Overall, the site of renal obstruction is localised for future intervention, especially for targeted therapy. In addition, a comprehensive assessment of the patient’s eGFR and renal impairment was achieved.
References
• Bidani, A., & Griffin, K. (2004). Pathophysiology of Hypertensive Renal Damage. Hypertension, 44(5), 595 – 601. https://doi.org/10.1161/01. HYP.0000145180.38707.84
• Bounous, G., Shumacker, H., & King, H. (1960). Studies in Renal Blood Flow: Some General Considerations. Annals of Surgery, 151(1), 47 – 58.
• Burke, M., Pabbidi, M., Farley, J., & Roman, R. (2014). Molecular Mechanism of Renal Blood Flow Autoregulation. Current Vascular Pharmacology, 12(6), 845 – 858. https://doi.org/10.2174/157016111131166 60149 Page !4 Part 1 Part 2
• Caiafa, R., Vinuesa, A., Izquierdo, R., Brufau, B., Colella, J., & Molina, C. (2013). Retroperitoneal Fibrosis: Role of Imaging in Diagnosis and Follow-up. RNSA Radiographics, 33(2), 535 – 552. https://doi.org/10.1148/rg.332125085
• European Association of Nuclear Medicine (2016). Dynamic renal imaging in obstructive renal pathology: A technologist's guide. https:// www.enam.org/content-eanm/uploads/2016/11/ tech_dynamic.pdf
• Hong, J., Suh, S., & Shin, J. (2020). Clinical significance of urinary obstruction in critically ill patients with urinary tract infections. Medicine, 99(1), 1 – 7. https://doi.org/10.1097/MD.0000000000018519
• Larkin, J. M., Pyle, L. M., & Gore, M. E. (2010). Fatigue in renal cell carcinoma: The hidden burden of current targeted therapies. The Oncologist, 15(11), 1135 - 1146. https://doi.org/10.1634/theoncologist.2010-0078
• McQuillan, B., Zelasko, S., & Wolin, E. (2016). Nuclear Medicine Genitourinary Imaging in Native Kidneys. Journal of the American Osteopathic College of Radiology, 5(3), 14 - 20. https://www. jaocr.org/articles/nuclear-medicine-genitourinary-imaging-in-native-kidneys Murray, A., Barnfield, M., Waller, M., Telford, T., & Peters, A. (2013). Assessment of Glomerular Filtration Rate Measurement with Plasma Sampling: A Technical Review. Journal of Nuclear Medicine Technology, 41(2), 67 - 75. https://doi.org/10.2967/jnmt.113.121004
• National Kidney Foundation. (2013). GFR (Glomerular Filtration Rate): A Key To Understanding How Well Your Kidneys Are Working. https:// www.kidney.org/sites/default/files/docs/11-101813_abe_patbro_gfr_b.pdfv
• Nuraj, P., & Hyseni, N. (2017). The diagnosis of obstructive hydronephrosis with colour doppler ultrasound. ACTA Informatica Medica, 25(3), 178 – 181. https://doi.org/10.5455/aim. 2017.25.178-181
• Piepsz, A., Colarinha, P., Gordon, I., Hahn, K., Olivier, P., Sixt, R., Velzen, J., & Paediatric Committee of the European Association of Nuclear Medicine (2001). Guidelines for glomerular filtration rate determination in children. European Journal of Nuclear Medicine, 28(3), 31 - 36. Santos, M., Brito, B., Silva, F., Botelho, A., & Melo, F. (2020). Nephrotoxicity in cancer treatment: An overview. World Journal of Clinical Oncology, 11(4), 190 - 204. https://doi. org/10.5306/wjco.v11.i4.190
• Schaeffner, E. (2017). Determining The Glomerular Filtration Rate - An Overview. Journal of Renal Nutrition, 27(6), 375 - 380. https://doi.org/10.1053/j. jrn.2017.07.005
• Taylor, A., Brandon, D., Palma, D., Blaufox, M., Durand, E., Erbas, B., Grant, S., Hilson, A., & Morsing, A. (2018). SNMMI Procedure Standard Guideline for Diuretic Renal Scintigraphy in Adults With Suspected Upper Urinary Tract Obstruction 1.0. Seminars in Nuclear Medicine, 48(4), 377 – 390. https://doi.org/10.1053/j.semnuclmed.2018.02.010 • Wang, Y., Li, M., Dai, S., & Li, Y. (2020). The role of Tc-99m DTPA renal dynamic scintigraphy in retroperitoneal liposarcoma. BioMed Research International, 2020, 1 – 5. https://doi. org/10.1155/2020/9765162
• Yamada, H., Komatsu, R., Nagae, H., Fujioka, Y., & Fujita, M. (1998). Idiopathic retroperitoneal fibrosis with duodenal obstruction successfully treated with corticosteroids. Internal Medicine, 37(7), 592 – 598. https://doi.org/10.2169/internalmedicine.37.592
• Ziessman, H., O’Malley, J., Thrall, J., & Fahey, F. (2014). The Requisites: Nuclear Medicine (4th ed.). Elsevier Roberts.
Acknowledgements: I want to express my deepest thanks to Suzanne McGavin for providing feedback and advice during the drafting of this article. My appreciation is also to the Nuclear Medicine department at Peter MacCallum Cancer Centre and the individual patient for allowing permission to use the acquired images.


Order of Australia Honours
ohn Andrews, AM
The Society is pleased to congratulate Dr John Andrews, a past President and Life Member of the
Society, who has been recognised in the 2021 Queen's Birthday Honours. His citation was ‘For significant service to nuclear medicine, and to professional societies'. John has been created a
Member in the Order of Australia (AM). In responding to the Society's congratulations John replied, "It is a great privilege to receive an AM. So good to see Nuclear Medicine as the principal reason. ANZSNM has always been very important to me and a large part of my professional life as well as a source of great friendships and pleasure. It is marvellous to see how nuclear medicine has advanced over the years and the recent program of the last meeting was so interesting."
In a great indication of John's belief in his passions, John requested the following :
"If you thought appropriate, would my recently published book on the History of the Foundation Years of the Medical Association for the Prevention of War entitled "Preserving Life by Preventing War" with co-author Vicki Standish be of interest? This is available as an eBook for all members who wish to read it and there is also available a hard copy if needed."
For members of the Society, this e-Pub can be read here.
AUG 31
SEP 22
OCT 23
NZ Branch Awards Night for Radpharm and Paul Orr Memorial Presentations 6:00 - 8:00 pm Virtual Event via Zoom
SA & NT Branch Meeting and Scientific Presentation 5:30 pm Refreshments 6:00 pm Presentation Flinders Medical Centre
VIC/TAS Branch AGM and Presentations Awards Virtual Event via Zoom
SEP 21
WA Branch Meeting - Radpharm Presentation Night 5:30 pm Refreshments 6:00 pm Meeting & Presentation QScan
SEP 28
NOV 2
NZ Branch Inaugural Interesting Case Race 6:00 - 7:00 pm Virtual Event via Zoom
NOV 16
SEP 27
OCT 28
WA Branch Meeting - AGM 5:30 pm Refreshments 6:00 pm Meeting & Presentation Perth Radiological Clinic
NOV 24
SA & NT Branch AGM & Quiz Night 5:30 pm Refreshments 6:00 pm Presentation Venue to be confirmed
OTHER EVENTS
27-29 September British Nuclear Medicine Society (BNMS) Annual Meeting 2021 Virtual Event
28 October Neuroendocrine Cancer Australia National Theranostics Round Table Parliament House Canberra
OCT 20
OCT 29
20-23 October 34th Annual Congress of the European Association of Nuclear Medicine Virtual Event
29 October CHILI - Conference on Hybrid Imaging Virtual Event






