LEAVING IT TOO LATE Leave balances show doctors can’t catch a break P.14 THE HEALTH OF THE MARKET The growing shadow of private provision P.25 FINGER ON THE PULSE Steering Te Whatu Ora’s culture shift P.30 The Magazine of the Association of Salaried Medical Specialists | ISSUE #135 | JUNE 2023
ISSUE #135 JUNE 2023
This magazine is published by the Association of Salaried Medical Specialists and distributed by post and email to union members.
Executive Director: Sarah Dalton
Magazine Editor: Andrew Chick Journalist: Matt Shand Designer: Twofold
Cover Image: Sezeryadigar/iStock
The Specialist is produced with the generous support of MAS.
WANT TO KNOW MORE?
Find our latest resources and information on the ASMS website asms.org.nz or follow us on Facebook and Twitter.
Also look out for our ASMS Direct email updates.
If you have any feedback on the magazine or contribution ideas, please get in touch at asms.org.nz
PREFER TO READ THE SPECIALIST ONLINE?
We have listened to your feedback and are aware that some members prefer not to receive hard copies of the magazine.
If you want to opt out of the hard copy, just email membership@asms.org.nz and we can let you know via email when the next issue is available to read online.
ISSN (Print) 1174-9261
ISSN (Online) 2324-2787
The Specialist is printed on Forestry Stewardship Council® (FSC®) certified paper.
Proposed position for FSC logo and text. Please align to bottom of this margin.
PROFILE: MARGIE APA
Anual review
One year on from Te Whatu Ora’s birth, Chief Executive Fepulea‘i Margie Apa speaks to The Specialist about how far she thinks they’ve come and what the biggest challenges have been.

PROFILE: ANDREW SLATER
Finger on the pulse
Nine days into the job, new Chief People Officer at Te Whatu Ora Andrew Slater spoke to The Specialist about his aspirations for the job and how he hopes to turn the culture ship around.

UPFRONT 02 Questions and answers 03 From zero to Nero IN BRIEF 34 Budget trims health spending 34 UnionAID doing great work in wider region 35 ASMS members back Gisborne nurses health and safety strike 35 When organisational values cause harm 36 HCA call healthy school lunches a win but more needed for Māori health 36 ASMS new staff members 36 Save the date FEATURES 10 Help from above 14 Leaving it too late 20 Power of potential 22 Māori health and Te Aka Whai Ora: Political parties respond 25 The health of the market 26 The lost years 28 Prescribing control 04 30
JUNE 2023 PAGE 1
AND ANSWERS QUESTIONS
JULIAN VYAS, ASMS PRESIDENT

The findings of the Te Whatu Ora Pulse survey have yet to be shared in detail with workers. Results seen by ASMS suggest senior medical staff scored the question about having sufficient resourcing to adequately care for their patients at just 15 per cent. Sadly, this appalling state of affairs is not new. But its documentation is a resounding vindication of all that ASMS has been telling health leaders for decades. Much has been written in the past about the moral injury that clinicians experience due to their inability to help their patients – feelings often amplified by the fact that treatments are actually available, and it’s just poor local resourcing that prevents our patients from getting them. Now we are really seeing the detrimental effects of this under-resourcing on our colleagues. In the last few months, I’ve heard more and more from members experiencing moral injury through witnessing their colleagues’ loss of wellbeing, and the creeping sense that there is no current solution. I also hear more and more of specific services suddenly facing critical workforce losses when senior colleagues simply leave, having had a ‘gutsful’ of systemic inertia and dysfunction.
The Pulse survey itself is a good example of that dysfunction. To date, Te Whatu Ora has only shared the most cursory high-level data and, even then, not consistently across districts. Fuller data from a single district has found its way into the public domain. Many responses in it reiterate a lack of support for and engagement from Te Whatu Ora with its staff. I can’t help but speculate that the ongoing delay to properly publish the data reflects an absence of any cohesive plan to address the more troubling findings. The damage to staff morale and trust arising from the delay in acknowledging let alone addressing these issues is nigh on incalculable. Just as a patient with systemic lupus erythematosus has auto-antibodies that attack their own body, so the dysfunction of Te Whatu Ora is harming its own workforce.
Minister Verrall recently announced a 24-point plan to reduce the burden of clinical demand on an already overstretched hospital system, through the provision of more direct patient care by the community and primary care sectors closer to their homes. I must confess a modicum of scepticism that the requisite increase in health professionals can be simply ‘dialled up’. We all know that the essential increase in workforce numbers will not happen before this coming winter, and probably not even for the next few winters. Beyond the basic recruitment logistics, individuals and teams will need local training, team development, and a conscious integration of
community and district services to avoid duplication of effort. This will take much more than the next 2–3 months to achieve. Yet winter 2023 is pretty much here. I regret that there is not also a 25th point in the plan which explains what the health system will do to protect its workforce while we wait for the other 24 points to kick in.
If we cannot rely on our employer to ensure our safety and wellbeing, it becomes a case of ‘physician, heal thyself’. Whilst a mass exodus ‘across the ditch’ does not seem imminent, I am still aware of colleagues who are planning this move, as well as others contemplating ways to reduce their public sector FTE, including more work in the private sector. It would be a massive irony if a New Zealand Labour government – the party of Michael Savage, and of strong trade union connections – presided over the decline of the public health sector, for reasons of failing to adequately protect its workforce.
I take no joy in saying that, for members, this winter will be arduous, frustrating, fatiguing, and (for some) possibly the last straw. (In light of the feature addressing leave balances in this issue, but acknowledging the people who face barriers to taking that leave, taking leave is part of our own wellbeing.) Be assured ASMS remains tireless in presenting all these concerns to the health leaders who actually have the power to address them. Now, perhaps more than ever, we need all our members to be a part of this work – to identify when patient care is suffering due to under-resourcing, to call out managerial inertia, to refuse to enable unsafe workplaces and rosters, and (if our concerns continue to be ignored) to be willing to show group solidarity for just how important our patients and the public health system are.
The essential increase in workforce numbers will not happen before this coming winter, and probably not even for the next few winters.”
– JULIAN VYAS
PAGE 2 THE SPECIALIST
FROM ZERO TO NERO
This is incredibly distressing for health workers – primarily those directly impacted, but also to others. Our initial advice to the employer was to sort out models of care and allow clinical priorities to lead Te Whatu Ora priorities. But this is not what they are doing.
By the time you read this, it is likely that recruitment for the most national medical officer and chief clinical officer will be well under way. But broader initiatives focused on addressing well known clinical shortfalls will not.
SARAH DALTON, EXECUTIVE DIRECTOR

I’m not sure how much attention you’re paying to the regular comms updates from Te Whatu Ora. We are incredibly busy responding to the ‘simplify to unify’ consultation process concerning ‘enabling services’. This is a fairly shambolic process, with some of our GP liaison members tangled up in the commissioning restructure (they should not be, and we are working hard to sort this out) and with senior Te Whatu Ora staff quietly owning up that they’re not entirely across all the details of who, what and where regarding several of the reviews. Nonetheless, they are pressing on and many of you will know people whose jobs are on the chopping block.
In the May workforce update to staff from Te Whatu Ora there was a nod to GP training, a scattering of other education pathways, and some limited nursing support.
What it didn’t cover was any of the following: exact workforce numbers
• a breakdown of SMO/SDO FTE and headcount by district, region, and specialty
• priority areas for training and recruitment
• strategies to support consultants who are a necessary part of training RMOs and other regulated health workers
I could go on…
Most of these initiatives will have been discussed by the workforce taskforce. I find it hard to believe that, after months of work and I hate to imagine how many thousands of dollars spent, this is the best they could come up with.
It would seem that the workforce taskforce has been fiddling while Rome burns. ASMS has not.
Our industrial team continues to engage by service, district, and in some cases region, to establish additional duties and safe work provisions and maintain our programme of job sizing.
Along with our industrial director, I have been increasingly engaged in supporting higher level meetings to try to resolve a number of situations –some individual, others across services – in an attempt to get reasonable engagement and outcomes for issues that have been needlessly escalated by the employer.
This is a massive frustration for me personally, and for the ASMS staff and executive, given the high-level commitments given by Te Whatu Ora bosses that they will move away from toxic and punitive work environments. While this is necessarily going to take a while (turning the Titanic has already been comprehensively demonstrated to be tricky), it is angering to learn of the type of HR practices that continue to be enabled across our hospitals network.
– SARAH
Our policy and research team completed a significant workforce report for our November 2022 conference, and has subsequently presented a briefer submission on our medical workforce crisis to the Productivity Commission. You can read both of those on our website, but a brief repetition of key recommendations from the aptly titled Workforce: The make or break of the health reform is worth a few moments of your time. It can be seen on p27 of this issue.
It would seem that the workforce taskforce has been fiddling while Rome burns.”
DALTON
JUNE 2023 PAGE 3
ANNUAL REVIEW
INTERVIEW BY MATT SHAND

PROFILE
CHIEF EXECUTIVE FEPULEA‘I MARGIE APA
PAGE 4 THE SPECIALIST
What about the competition between Australia and New Zealand for workforce? Do you feel we need to be more competitive to attract and retain health care workers?
I find it difficult to compare without understanding what is underneath the differences – for example, taxes, work hours, other terms and conditions, and cost of living and non-pay related conditions. These all add to the mix of how a person decides what country they live and want to work in. I think we can do more to make our workplaces a better place to work –for example, leadership, having the tools and the kit [equipment] to do the job, how we invest in innovation and research.
We want to do everything we can to make the full package of working here as a clinician a really good experience. We will always be competing with a bigger Australian economy. I think the test for us is being sure that we are bringing everything to the table that we can. That is both pay and non-pay related.
Is there going to be a reset of Te Whatu Ora data to make information sharing easier? ASMS has called for a census. We don’t need to wait for a census to tell us we’ve got challenges. I think we should go further than a census. We want information systems that offer real-time and live data we can use. We would be happy to share it as long as we anonymise individual data. Information is an asset for the whole health system. It will take some investment and time, some of which we have to make a case for because we did not get a lot of transition funding that would fund those big information system investments. We know our payroll systems need fixing so we can be assured we are paying our people what they are entitled to and ensure people are being treated consistently across the country.
Do you feel the vision of bringing together all these DHBs has been a good one? What does success look like to you for yourself and patients?
The vision is a very good one – to have a national health system that operates as one to meet the needs of people and includes the relentless pursuit of health equity. Success will be bringing teams together and joining clinical services across regions. A simple example is in Southern where they struggled to recruit to specialist roles – like many districts – they were doing it on their own. So success will look like bringing a national network of cancer colleagues together to co-ordinate care, support covering rosters or to provide treatment. We need to fill vacancies – don’t get me wrong. But if working together as a national or regional network means people will get treatment and care sooner and we can support teams providing that care locally (even if we offer it in another area), that’s got to be good for everyone. That is the power of having clinical leaders working together and having a mandate to make decisions and make things happen. Our job is to strip away all the barriers that get in the way of that.
Is there anything you would have done differently?
I would have focused much sooner on supporting local leadership leading change. We missed an opportunity to give our leadership some more headspace to get involved in designing the change process and to manage that at pace – but this was difficult when the first 5 months was dealing with winter and working through the technical aspects of change (e.g. keeping decision making going without boards).
As a national team we do have the ability to pool funding to get on with some action – without needing to negotiate with 20 district health boards. An example was early actions on
We are in the second year of a two-year funding pathway, and we are bringing everything we can to the table that is affordable for us to offer.”
PAGE 6 THE SPECIALIST
–MARGIE APA

Help from above Leaving it too late 10 14 PAGE 8 THE SPECIALIST
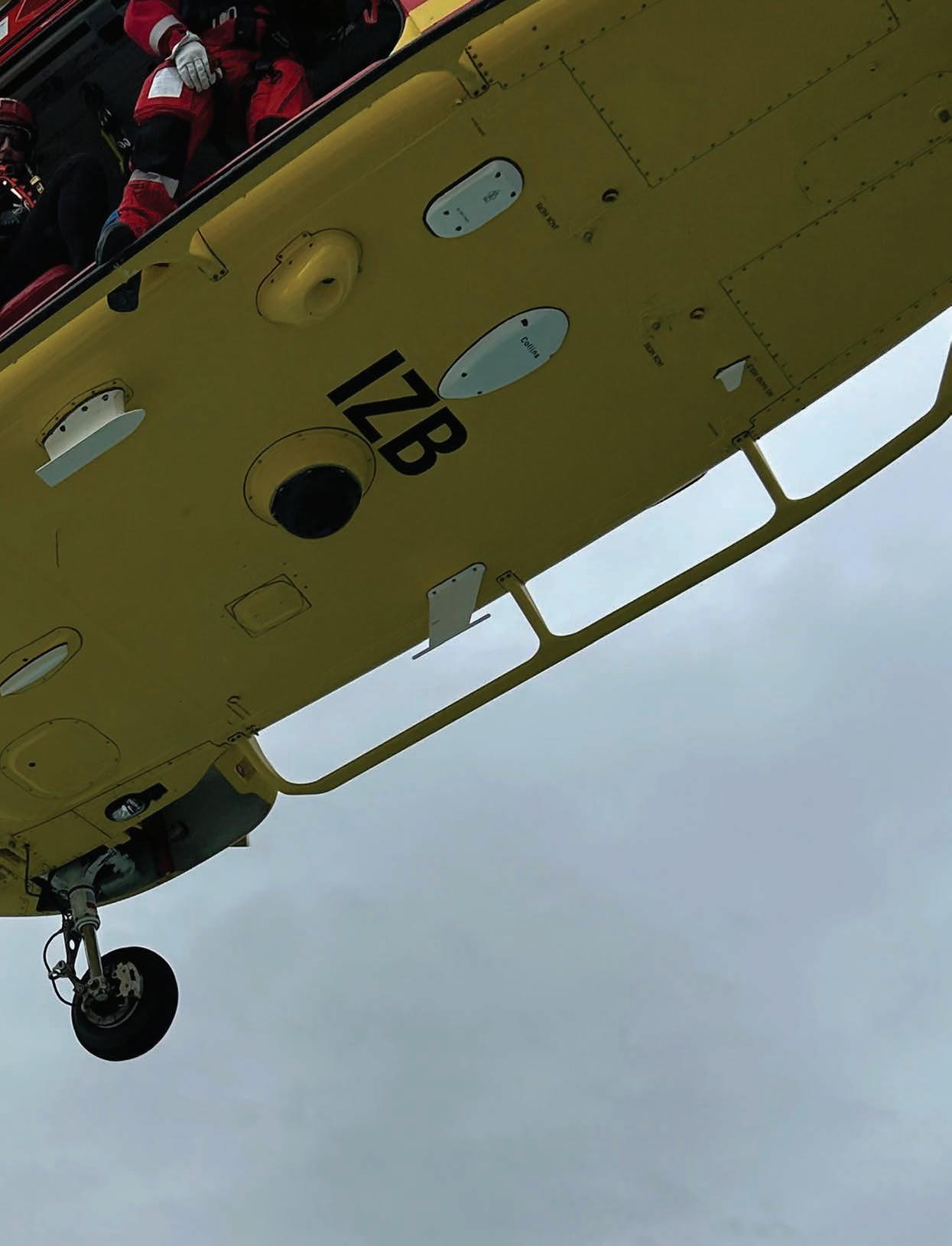
HELP FROM ABOVE
MATT SHAND, JOURNALIST
The last rescue mission flown by emergency medicine specialist Gary Payinda highlights an opportunity for specialist doctors to become part of the prehospital and retrieval medicine (PHRM) response process across the country.

JUNE 2023 PAGE 11
LEAVING IT TOO LATE

MATT SHAND, JOURNALIST
The inability to take sufficient leave is taking its toll on the stretched health care system and is now costing jobs as people pack it in due to trying conditions. New data released to ASMS reveals the extent of the problem.
PAGE 14 THE SPECIALIST
More than a millennium of outstanding leave is currently owed to senior medical officers across the country, showing the gap in our health care workforce and increasing the risk of burnout.
Data released to The Specialist under the Official Information Act shows senior medical specialists across the country have 1.72 million hours (or 1,024 years) of leave ticked up, with the number creeping higher every day.
More than 50 per cent of SMOs have leave balances higher than their annual accrual, and 22 per cent have more than 11 weeks owed to them. Five per cent of SMOs have leave balances higher than 24 weeks, meaning they are carrying more than six months of annual leave.
The data is just one more measure to show how stretched the health care workforce is. In order to cover the growing leave balances, at least another 1,000 doctors would be needed. Already, ASMS industrial officers are being told stories of doctors resigning from the public system as a direct result of being unable to take adequate time off.
The worst-hit areas include general medicine (which accounts for 13 per cent of all unclaimed leave), mental health and emergency medicine (which each make up 7.5 per cent of the total leave balance).
Capital, Coast and Hutt Valley district recently reported that three staff members resigned, specifically naming the ‘inability to take leave’ as a major factor during their exit interviews.
One doctor – whom we have not named – has walked away from a decadelong career in New Zealand due to difficulties taking leave.
“The situation is, if you wanted to take any leave, you had to find someone to cover you, and you had to tick a box on your application stating who you had found and what shifts they were covering,” they said.
“If you are lucky, someone will cover it, but in general it means you never get to take enough leave or CME leave. If a colleague is going to a conference, then I won’t be able to go.
“The workload is unsustainable as it is [in New Zealand], and there is no reprieve. I never had the intention to leave but the workload is ridiculous, and nothing is being done about it.”
The doctor is joining other health care workers now leaving New Zealand for Australia and other countries, where salary and conditions are better.
“The main reason I am leaving is due to the workload,” they said.
“The workload in Australia is much better, and it doubles your salary in many instances. And the CME allowance is paid to you directly and you are treated as an adult to spend it correctly.
“If you look at the turnover rates, people are already quiet-quitting and looking to leave. It’s already happening. Te Whatu Ora needs to create more jobs to fill. Even if they were fully staffed they would still be short, and they seem unwilling to do that.”
Another doctor says they have six to seven months’ worth of leave owed to them due to being unable to take it in recent years.
“Earlier this year I applied for leave for the end of the year and received a message back stating there was no cover. I was also told that I was asking for too many weeks of leave in the year,” they said.
Even with the doctor’s leave being high, they were unable to use it during the school holidays to care for their grandchildren.
“I had to cancel that leave and make alternative arrangements, which was a shame,” they said.
The doctor says the frustrations have increased over the last year.
“There’s no cover and no advertising to find locums or cover,” they said.
“Senior doctors are often asked for a plan to reduce their leave, but on the other hand, when they apply for leave, often with quiet advance notice, it is not signed off.
“The whole system is messy and frustrating, and further reduces the morale at work.”
This is reflected in the staffing reports presented by Te Whatu Ora within Joint Consultative Committee (JCC) meetings. Capital and Coast showed 72 departures, with only 66 hires in the last 12 months and a deficit of about 14 per cent on expected staffing numbers.
You had to find someone to cover you, and you had to tick a box on your application stating who you had found.”
– ANONYMOUS DOCTOR, WELLINGTON
JUNE 2023 PAGE 15
Some departments – like mental health, which carries a large burden of leave balances – have been hit hard, with 16 departures.
Te Whatu Ora CEO Margie Apa told The Specialist the health care workforce is 5,000 clinical roles short of where it needs to be.
ASMS would suggest the figure is much higher.
ASMS’ 2022 survey of clinical directors found all specialties recorded shortfalls of specialists of between 10 and 63 per cent, with a mean 24 per cent. At the national level that means Aotearoa is short approximately at least 1,850 SMOs. This is on top of shortages of 4,000 to 5,000 nurses.
Aotearoa continues to fall behind Australia’s ratio of doctors per head of population, which is 485.8 per 100,000, compared to 366.7 per 100,000 here.
Auckland University of Technology Professor Jarrod Haar conducts studies into burnout. He found that 35 per cent of all employees in New Zealand are suffering from severe burnout.
“In December 2022, burnout rates were much higher than in years previous,” he said. “One in three was showing signs of burnout, where a normal level would be 1 in 13.”
Haar says being unable to take leave, or feeling like you cannot take leave, can contribute to burnout. This echoes ASMS’ own findings on burnout and fatigue.
“The World Health Organization and my data show if you are working 55 hours a week, this is a red line for the workforce,” Haar said.
ASMS’ 2021 report My Employer is Exhausting found almost 50 per cent of SMOs and SDOs reported experiencing burnout. This mirrored similar findings in 2015. It found an association between respondents reporting working more than 14 consecutive hours as well as failing to have a 24-hour break free of any scheduled work and the proportion scoring as burnt out for workrelated and personal burnout.
“I had been speaking to dermatologists who are on 55 hours a week as a normal work week. That’s not good for burnout levels, particularly if they cannot take leave to recharge. If we have medical professionals unable to take leave, it will contribute to the reasons people are saying, ‘Stuff it. I’ll move to Australia to get more pay and better conditions.’
“We need to see some of this Covid money used to upgrade the workforce to allow better working conditions.”
ASMS Industrial Director Steve Hurring says the large, and growing, leave balances for SMOs represent a workplace shortage and a shortchanging of staff working in vital health roles.
“It means Te Whatu Ora is operating on an FTE budget that is less than what they need,” he said.

If you look at the turnover rates, people are already quietquitting and looking to leave.”
PAGE 16 THE SPECIALIST
– ANONYMOUS DOCTOR, WELLINGTON
“There are not enough staff to cover the time off, and this is adversely affecting the desirability for people to work within the public system.”
ASMS has also heard of instances where weeks of leave were declined for piecemeal amounts of one or two days at a time due to a lack of cover.

“People are entitled to take their leave to rest and structure their holidays as they see fit,” Hurring said.

“Under the law, staff are entitled to two consecutive weeks off a year, and the expectation is you’re allowed to take the remainder of leave in weeklong periods.
“Not doing so makes the job less attractive, and it just breaks people.”
Hurring says he has seen times when people have requested leave without pay to get some time off. In some cases, even that is declined.
“It is a significant health and safety issue and one that the employer needs to address,” Hurring said.
“It’s a contributor to burnout and ultimately it means people work longer hours than they should, and, in a way, the employer gets that time for free.
“There are solutions, and it all revolves around the current workforce shortage. There are not enough doctors to cover leave. There is not enough pay to attract and retain doctors. There are not enough people, as a result, willing to stay in New Zealand to work.
“Whenever we lose another doctor, that is one less doctor to cover leave, and the problem cycles around.”
Data obtained by The Specialist was shared with Te Whatu Ora’s Chief People Officer Andrew Slater.
“The challenges with staff attaining leave are as you [ASMS] present them,” he said.
“Off the back of these conversations I think I need to work with our leaders to make sure that when people are applying for leave we’re taking a more holistic approach to that and making sure we look to the medium and long term advantages of providing leave rather than the short term disadvantages, or challenges associated with approving it.
“I think that is a good outcome. This data has prompted me to talk to a number of leaders across the organisation and understand a little bit more about the daily reality of working through handling leave.”
He says management cannot force people to have leave paid out and if this has occurred staff should contact their HR department. “Leave can only be paid out at the request of the individual,” he said.
Slater says, with New Zealand competing on the global stage for healthcare workers, any problem (such as with taking leave), which leads to preventable loss of staff, has to be avoided.
“My priority is workforce,” he said. “Any doctor leaving New Zealand at the moment for reasons that were avoidable is one too many.”
Being unable to take leave, or feeling like you cannot take leave, can contribute to burnout.”
– PROFESSOR JARROD HAAR
The larger the circle, the greater proportion of leave owed. Departments/ Specialties were included were data was provided for 60% of all Districts.
Trends emerge when leave balances are compared to results from ASMS’ 2021 burnout survey. SMOs working in Emergency Medicine and Psychiatry reported 56% and 51% personal burnout respectively, and both departments account for between 7-8% of all leave owing. General and Acute Medicine SMOs recorded scores for work-related burnout of 41%, and personal burnout of 50%.
MORE THAN 50% OF SMOS HAVE LEAVE BALANCES HIGHER THAN THEIR ANNUAL ACCRUAL.
22% HAVE MORE THAN 11 WEEKS OWED TO THEM.
S M T W T F S S M T W T F S S M T W T F S S M T W T F S AVERAGE LEAVE OWED BY FTE: 333.43 HOURS AVERAGE LEAVE OWED BY DEPARTMENT BY FTE Intensive Care 370 HOURS –General Surgery 365 HOURS Cardiology 373 HOURS –Accident & Emergency 371 HOURS Oncology 319 HOURS –Orthopaedics 454 HOURS Geriatrics 377 HOURS –Renal 377 HOURS LEAVE OWING BY DEPARTMENT/SPECIALTY CORRELATION BETWEEN DEPARTMENTAL LEAVE BALANCE AND BURNOUT
Operating Department 12% General & Acute Medicine 13% Dental 2% Obstetrics & Gynaecology 3.5% Accident & Emergency 8% Paediatrics 6% Radiology 5% General Surgery 5% Geriatrics 1.5% PAGE 18 THE SPECIALIST
THE LOST YEARS
But with many already saying there are too few medical graduates entering the workforce ‘pipeline’ – ASMS estimates we need another 300 a year by 2027 – the whereabouts of these ‘lost doctors’ is a significant concern.
This loss in the supply of specialists from the country’s graduate pool was identified as “an area of potential concern” in a Health Workforce New Zealand report back in 2017. But the same report said a lack of data made it unclear if this represented “a long-term deficit or risk to service delivery”.
In 2018, unpublished Ministry of Health data showed 29 per cent of full-time employed registrars were not in a specialist training programme. At the same time, there were a growing number of registrar training positions that were not being filled, with the most significant vacancies being in anaesthesia, intensive care medicine, psychiatry, paediatrics and obstetrics and gynaecology.
Alarmingly, at that point the Ministry stopped collecting data on the issue, due to resource

constraints. The risk that these vacancies posed was never investigated further. But that question remains, as do the questions about why these gaps occurred. Are ‘Establishment FTE’ training positions not being advertised? Does overstretched training capacity mean those positions can’t be supported? Are trainee applicants simply not finding positions in their preferred speciality and location? Or is the fundamental driver simply funding constraint?
Aside from the direct loss of potential specialists to our health workforce, the growing number of non-training or ‘unaccredited’ registrars has been criticised as evidence of inefficiency in medical training. Their lack of formal training, appraisal, or supervision also hinders their ongoing development. There is no cap to the number of years someone can work as an unaccredited registrar, and there is no guarantee of career progression.
As the workforce ages, it is registrar trainees who will replace older specialists as they retire. Health Workforce New Zealand’s 2017 report
PAGE 26 THE SPECIALIST
If Aotearoa New Zealand is to make the most of the domestic supply of doctors, we need to understand what is happening to a significant number of graduates who don’t appear to make it to vocational registration.
The number of graduates from 2004 to 2011 with the number from each graduation year who gained a vocational registration by end of 2022
noted that “just over half” of specialties had fewer registrars in training than SMOs aged 55 or over.
Again, collection of that information was discontinued soon after. In its absence, ASMS analysis found that in 2020 there were 28 of 36 specialties with fewer trainees than specialists (private and public) aged 55+, and 16 specialties where 15 per cent of the workforce was aged over 65. These included psychiatry, dermatology and general surgery.
To date, after years of health sector groups calling for a comprehensive health workforce strategy, and official acknowledgement that such a plan is needed, there is no sign of one yet from government. Until one does appear, ASMS has some clear recommendations for a way forward that were reported in Workforce: The make or break of the health reform (https://asms.org. nz/workforce-the-make-or-break-of-thehealth-reform/).
RECOMMENDATIONS FROM WORKFORCE: THE MAKE OR BREAK OF THE HEALTH REFORM
1 Reform primary and oral health services.
2 Reduce potentially avoidable hospitalisation rates through whole-of-government action.
3 Commit to supporting efforts at the flax-roots which integrate hospital and community-based care.
4 Understand workforce capacity constraints.

5 Understand unmet need for hospital and secondary care.
6 Develop a comprehensive Health and Disability Workforce Plan and Implementation Road Map.
7 Investment decisions are data-driven.
8 Grow capacity at undergraduate level.
9 Strengthen postgraduate pathways.
10 Sustain support for SMOs and IMGs.
11 Make cultural safety a priority for all health sector organisations.
12 Approach health service design and delivery collectively, harnessing the clinical experience within the health workforce and engaging with communities.
13 Act to reduce the risk of future health policy failures.
450 0 50 100 150 200 250 300 350 400 Year Graduate cohorts 2004 2005 2006 2007 2008 2009 2010 2011 Graduates No. with vocational registration by 2022
JUNE 2023 PAGE 27
Source: Medical Council of New Zealand, 2023
PRESCRIBING CONTROL

PAGE 28 THE SPECIALIST
DR MARK BURNS FROM THE MEDICAL PROTECTION SOCIETY (MPS) CONSIDERS PRESCRIBING RESTRICTIONS FOR MEDICAL OFFICERS OF SPECIALIST SCALE (MOSSS)
New Zealand has a shortage of vocationally registered doctors in several specialties, including psychiatry. Te Whatu Ora very frequently employs Medical Officers of Specialist Scale (MOSSs) in place of, or alongside, vocationally registered psychiatrists. These doctors are sometimes overseas-trained psychiatrists whose specialist qualification does not match that of the local college training in certain areas, and therefore the Medical Council of New Zealand considers they do not meet the requirements for a vocational scope of practice. At other times they are experienced local graduates who are no longer in training but have not yet completed their RANZCP training requirements and have not yet gained the postgraduate fellowship. Most MOSSs are ASMS members and covered by the MECA. As they are often experienced clinicians, there can be uncertainty as to what restrictions might apply to them compared to someone who is vocationally registered. The Medical Protection Society (MPS) has recently assisted a number of psychiatry MOSSs who have had concerns raised regarding whether they should be prescribing and making Special Authority applications for certain medications.
The prescribing of stimulants has attracted media attention recently with a Health Practitioner Disciplinary Tribunal hearing against an Auckland GP with special interest in ADHD. Are there also restrictions on psychiatry MOSSs prescribing methylphenidate and dexamphetamine for ADHD and making applications for a Special Authority number? The short answer is yes, a MOSS requires written recommendation from a vocationally registered psychiatrist or paediatrician, as do all general registrants.
Methylphenidate is a controlled drug as per the Misuse of Drugs Act 1975. The gazetting notice1 describes that prescribing is restricted to “medical practitioners with a vocational scope of practice of paediatrics or psychiatry, registered with the Medical Council of New Zealand under the Health Practitioners Competence Assurance Act 2003”. However, the schedule further states “any other medical practitioner registered with the Medical Council of New Zealand … may only prescribe methylphenidate products when acting on the written recommendation of one of the vocational medical practitioners described above, for the conditions specified”. It is clear from this that a MOSS, who is not vocationally registered, can only prescribe methylphenidate for ADHD with a written recommendation of a vocationally registered psychiatrist/paediatrician.
Most commonly, psychiatry MOSSs work within a multi-disciplinary team, where there are discussions regarding management of patients that may include the presence of a suitably vocational registered psychiatrist/ paediatrician. Such discussions, however, do not fulfil these requirements, and MPS advises that there should be an explicit written statement from a vocationally registered psychiatrist/paediatrician recommending the prescription of methylphenidate or dexamphetamine. There are several ways this can be simply achieved; for example, by return email to the MOSS request or by documentation directly into the patient file.
Methylphenidate, in order to be funded, also requires a Special Authority number. The application form2 is not so clear that it must be by a vocationally registered psychiatrist/paediatrician, with the relevant excerpt stating “Applications only from a paediatrician, psychiatrist, medical practitioner on the recommendation of a paediatrician or psychiatrist (in writing) or…”. There is an absence of the explicit words ‘vocationally registered’ when referring to the psychiatrist. However, Pharmac has recently clarified for us that the special authority criteria for the stimulant medicines are intended to mirror the regulations as gazetted. The references to psychiatrist and paediatrician in the Special Authority application are to be interpreted as meaning those who are vocationally registered in those scopes of practice. Problems have arisen for MOSSs who log in to the Electronic Special Authority (ESA) system to fill out the form and apply for a Special Authority online. They are able to complete the form online and obtain automatic approval. Access to this system does not, however, reflect any sort of authority to make such an application. A MOSS making such an application still requires the written recommendation of a vocationally registered psychiatrist/paediatrician.
In addition to restrictions on prescribing stimulants, psychiatry MOSSs should be aware of restrictions on the prescribing of Clozapine. Although it’s not a controlled drug, Clozapine has prescribing restrictions under s23 of the Medicines Act 1981.3 Clozapine may only be prescribed by a medical practitioner who is vocationally registered or by one that is prescribing under the supervision of a vocationally registered psychiatrist, or if the patient’s illness is well-controlled by clozapine and the prescribing decision is taken in collaboration with the community mental health team. The latter provision covers the more recent years’ arrangements for stable patients on clozapine returning to primary care. However, these restrictions make clear that any titration of clozapine by a psychiatry MOSS needs to be under supervision of a vocationally registered psychiatrist.

Te Whatu Ora clinics need to ensure that they have appropriate processes in place to satisfy these requirements. MOSSs are at risk of prosecution under the Misuse of Drugs Regulations if they prescribe stimulants without the appropriate written recommendation or may be subject to disciplinary processes by the Medical Council. Vocationally registered psychiatrists may be in supervisory or leadership roles in Te Whatu Ora clinics that employ MOSSs and may be involved in orientation processes for these new-toNew Zealand practitioners. Such psychiatrists are also well advised to familiarise themselves with these prescribing restrictions.
1. HTTPS://GAZETTE.GOVT.NZ/NOTICE/ID/2015-GO760
2. HTTPS://SCHEDULE.PHARMAC.GOVT.NZ/
3. HTTPS://WWW.MEDSAFE.GOVT.NZ/PROFS/RISS/RESTRICT.ASP
JUNE 2023 PAGE 29
There should be an explicit written statement from a vocationally registered psychiatrist/paediatrician recommending the prescription.”

PROFILE
“I don’t have the answers yet. What I do know is that in one year, two years and three years’ time I would like to see momentum”
PAGE 30 THE SPECIALIST
– ANDREW SLATER
FINGER ON THE PULSE
Results of the latest Pulse survey conducted by Te Whatu Ora set the challenges for the newly appointed Chief People Officer, Andrew Slater.
Andrew
The Pulse survey revealed only 19 per cent of respondents at Middlemore Hospital’s emergency department believed they had the resources to perform their job well. For staff across Auckland, that number was 33 per cent.
“I’ve always said in leadership there are only two things we can do when asked about something,” Slater said. “We can either give people the context and rationale for why something is the way it is, or change it.
“I’ve read through the high-level Pulse survey themes, and I am working with the team over the next couple of weeks to really get into that.”
Though new in the job, Slater says he was not surprised by some of the data uncovered in the Pulse survey.
“It’s based on what I see and hear from different spots in the health care system and from colleagues and friends,” he said.
“We’ve had 20,000 people take the time to write comments and provide feedback. Within that there are some actionable, tangible things that need to be done in some of our locations.
“Right now I am trying to make sure that those things are on the list, and someone can tell me when they’re done or not. The Pulse survey provides a benchmark for where we are at. The challenge for me and the People and Culture team is to turn that into actionable frameworks for our leaders to then be able to deliver change through.”
As Chief People Officer his responsibilities include human resources, payroll, health and safety, wellness, emergency management, organisational resilience, communications, and working with unions.
To perform this role, Slater says he will get into the front lines of the organisation to hear from people about ongoing issues, potential solutions and what needs to be done. He also leans on his network of friends and long-term colleagues working within the health sector, from whom he receives updates.
– ANDREW SLATER
Nine days into the job, new Chief People Officer at Te Whatu Ora
Slater spoke to The Specialist about his aspirations for the job and how he hopes to turn the culture ship around.
A healthy culture is one that is free from bullying and intimidation… we need to make sure we’ve got some clear standards.”
JUNE 2023 PAGE 31
“I took this role and put my hand up because I want to be part of making sure we have the best public health system that we can possibly have,” he said.
“My ambition is to make that a reality. I see the challenges. I see the pressure on frontline staff, the post-COVID fatigue, and I’m also hearing things that people are hoping we will change in the system in the coming years with workforce and workforce supply.”
His biggest priority is addressing the culture of the workforce through a variety of means. The first step is establishing a healthy culture.
“A healthy culture is one that is free from bullying and intimidation,” he said. “Whether that is harassment from members of the public, patients, or colleagues. We need to make sure we’ve got some clear standards.
“We also need to make sure our people feel valued. That stretches from pay to leaders that make sure people feel valued. We also need people to feel like they have been listened to and heard.
“I’ve set a personal goal for myself that within the next quarter people will be able to see and feel something a little bit different. I’m not quite sure what that is yet.”
Asked about whether he would consider holding a health workforce census – a policy ASMS has been calling on for years – he stops short of confirming it would occur but concedes it would be valuable.

“I would love to understand more about our workforce,” he said. “What their hopes and aspirations are. What they identify as the key issues, and I do not quite know how to go about that. We do need more insight into our people than we have at the moment.”
Improving culture will assist New Zealand to be a competitive workplace destination in the global labour market. In turn, this may help fill the growing vacancies in medical roles. But, overall, a key challenge for Slater is to ensure New Zealand recruits and trains as many health care workers as it possibly can.
“Globally there is going to be an 18 million health care worker shortage by 2030,” he said. “The vacancies speak for themselves.
“It’s actually really important we retain our current people, make sure we train as many people from New Zealand as we can to fill these positions and make sure we have the best connections globally to get as much of the workforce we need to cover the remaining gaps.”
Slater imagines his godchildren when thinking about the task of overhauling the people and culture of New Zealand’s health care system.
“I really think about my godchildren who are thinking about going into medicine and what they hear at the moment about medicine as a career and an opportunity,” he said.
“I think we’ve got to pull the system together to be the best health system in the world, and part of that is we’ve got to make it a great place to work.
“I look forward to learning and understanding from your readers about what they think we can do to get to that place and encourage their own godchildren, children, or grandchildren to work in health.
“I don’t have the answers yet. What I do know is that in one year, two years and three years’ time I would like to see momentum taking our health care system a different way.”
“I’ve set a personal goal for myself that within the next quarter people will be able to see and feel something a little bit different.”
– ANDREW SLATER
PAGE 32 THE SPECIALIST
Budget trims health spending

UnionAID doing great work in wider region
ASMS members back Gisborne nurses health and safety strike
When organisational values cause harm
HCA call healthy school lunches a win but more needed for Māori health
ASMS new staff members
JUNE 2023 PAGE 33
IN BRIEF
BUDGET TRIMS HEALTH SPENDING

Budget 2023 – delivered by Minister of Finance Grant Robertson on the 18th of May provides no significant additional funding for health to address health workforce shortages or to address substantial unmet health need.
After clarification from Treasury officials on funds carried forward from previous budgets, there has been a 3 per cent cut in funding for “Hospital and Specialist Services” in the 2023 Budget. This represents an 8 per cent cut in real terms when adjusted for inflation and demographic pressures (including ageing).
Funding for “Primary, Community, Public and Population Health Services”, received an extremely small increase and so is also a cut in real terms.
Hauora Māori Services received a boost of $398 million over the 2022/23 Budget. However, the new level of funding as a proportion of Vote Health is two per cent - similar to funding prior to the establishment of Te Aka Whai Ora.
Health Minister Ayesha Verrall’s Budget media release announces $1 billion over four years, “to increase health workforce pay rates and boost staff numbers”, including $118 million “to help reduce waiting lists by improving patient flow”, and $99 million “put towards the coming winter, focused on providing primary and community care”. None of these are included as separate line items in Vote Health and do not represent clear newly-allocated spending.
Pharmac received a 10.5 per cent increase, which should at least maintain the current availability of pharmaceuticals, given inflation for medicine tends to be higher than inflation measured by the consumer price index.
The removal of $5 prescription co-payments gathered the greatest media attention on the day– committing the government to spend approximately $150m a year – and should have a positive impact on health equity.
UNIONAID DOING GREAT WORK IN WIDER REGION
UnionAID – the New Zealand based charity supporting workers and communities to stand up for their working rights, build unions and build skills across the Asia-Pacific region –is on the lookout for new supporters.
One of UnionAID’s current projects is partnering with the New Zealand Nurses Organisation to support marginalised Karenni nurses in Myanmar, who are providing care to those injured by armed conflict and maintaining critical health service.

Amongst their other projects, they are helping call centre workers in the Philippines (winning compensation for illegal job terminations), plasterboard workers in Thailand (improving working conditions) and setting up the first Worker Advice Centre in Samoa.
UnionAID is looking for new Kiwi Solidarity donors – people who are able to make regular monthly donations that will make a huge difference in the lives of workers and their families across the Asia-Pacific region. Even a small regular contribution can have a significant impact. Visit www.unionaid.org.nz/kiwisolidarity to learn more.
NEWS FROM AROUND THE MOTU
PAGE 34 THE SPECIALIST
ASMS MEMBERS BACK GISBORNE NURSES HEALTH AND SAFETY STRIKE
When New Zealand Nurses Organisation members working in Ward 5 at Gisborne Hospital took strike action on health and safety grounds at the end of May, ASMS members were there to show their support.


“Our members share nurses’ concerns about patient safety and unsafe work and it’s a sad day when lack of resources turns your everyday job into its own health and safety issue. It’s even sadder when you have to go on strike to make someone listen,” said ASMS Executive Director Sarah Dalton.
The NZNO members on the Ward took a 1-hour strike on Wednesday 24 May. The timing coincided with the Tairāwhiti Joint Consultative Committee
meeting and ASMS members ended the JCC early to join the nurses’ picket across the street from the hospital.
Te Whatu Ora had sought an injunction to stop the strike but the Employment Court upheld the nurses’ right to take action and dismissed Te Whatu Ora’s application.
“These Gisborne nurses have been raising concerns for more than nine months,” said NZNO Chief Executive Paul Goulter. “As the judge pointed out during the hearing, Te Whatu Ora had not managed to change anything at all to help them. This is simply not good enough from one of the country’s largest employers.”
WHEN ORGANISATIONAL VALUES CAUSE HARM

Working in negative environments can hinder the ability for healthcare professionals to show compassion and increase the risk of burnout a new study shows.
The study is the first known empirical study investigating how working in value-discrepant environments impacts compassion and professional well-being.
ASMS member Anne O’Callaghan co-authored the study and surveyed 1,000 health practicing healthcare professionals and found perceived discrepancies between personal and organisational values predicted lower compassion ability.
Measures such as job satisfaction, burnout, absenteeism, and early retirement intentions
were measured across perceived organisational values.
“The inability to act in accordance with one’s values results in moral distress,” the report says.
The findings suggest demands caused by Covid-19 have made healthcare organisations strive for greater efficiency and cost savings.
Further discrepancies occur when resources are not valued, allocated correctly for healthcare professionals or are scarce.
“We expect that the most effective way to positively affect patients’ and clinicians’ wellbeing, and reduce the costs associated with values discrepancies will be for healthcare organisations to both revisit their values in light
of this data and systematically assess and report whether their stipulated values are reflected in policy, and targeted priorities.
“Put another way, rather than focusing on top-down rewriting of mission statements, job boards and email signatures that already signal humanistic values, health care organisations need to invest in a careful examination of whether and how these values are embedded and operationalised in the day-to-day practice.
“The ability to show compassion as well as outcomes associated with clinician wellbeing were all negatively and significantly impacted by discrepancies between individual and organisational values.”
JUNE 2023 PAGE 35
HCA CALL HEALTHY SCHOOL LUNCHES A WIN BUT MORE NEEDED FOR MĀORI HEALTH
The extension of the Ka Ora Ka Ako (Healthy School Lunch) programme in Budget 2023 has been heralded as a win by public health experts, but also a missed opportunity for health equity.

"While we’re also glad the Government has listened to communities and experts by continuing Ka Ora, Ka Ako,” says Health Coalition Aotearoa chair Dr Lisa Te Morenga, “we still desperately need this programme extended to at least 50 per cent of all schools”.
The programme, running since 2020, is being continued until the end of 2024, providing daily school lunches to approximately 220,000 students at 987 schools.
“We want to thank ASMS members who signed our petition and shared it to extend this programme as, even though we did not get the programme expanded, we believe this work from health professionals made it clear Ka Ako should remain budgeted for.”
But Te Morenga says the budget did not address health inequities. "It’s good to see free prescriptions as well as increased funding to important programmes like immunisation and screening for Māori and Pasifika, but we have not seen any funding allocated for the promised alcohol law review.
“This means yet again de-prioritising community wellbeing by kicking critically needed law change down the road.

“We wanted to see the Government commit to a transformative, Te Tiriti-based agenda for health. It's difficult to see how the health reforms are striving for equity when Te Aka Whai Ora only has 2 per cent of Vote Health for hauora Māori services. That’s not even close to population proportionate. The vision of Pae Ora has much further to go still for real co-governance.”
CHAN DIXON, INDUSTRIAL OFFICER
Chan Dixon is a new industrial officer, based in Auckland. Chan has extensive experience working in in unions, particularly in the health sector. She has worked with the New Zealand Nurses Organisation, Tertiary Education Union and the Public Service Association, most recently with nursing, allied health and clerical members in former DHBs.
VIRGINIA MILLS, PRINCIPAL POLICY ADVISOR
Virginia Mills has been appointed as the new principal policy advisor, based in Wellington. She is working on a part time basis.

Virginia has previously held roles as the Executive Director of the Council of Medical Colleges, and as a senior policy advisor with the Australian and New Zealand College of Anaesthetists and the Ministry of Health. While at the Council of Medical Colleges she was an integral part of the team that developed the new cultural safety framework for vocational training in partnership with Te ORA (the Māori Medical Practitioners Association).

ASMS NEW STAFF
MEMBERS
SAVE THE DATE ASMS ANNUAL CONFERENCE 2023 TĀ KINA, WELLINGTON | 23-24 NOVEMBER PAGE 36 THE SPECIALIST
Our insurance is choice.
There’s a reason our House, Contents and Car insurance policies have been voted Consumer People’s Choice for seven years running. Find out why at mas.co.nz
MAS is proud to support ASMS

7