Three randomised trials presented at the International Stroke Conference (ISC; 5–7 February, Los Angeles, USA) have indicated that mechanical thrombectomy treatments confer no advantages over the current standard of care for acute ischaemic strokes caused by distal- or mediumvessel occlusions (D/MeVOs).
BRAIN conference: ICAD is ‘globally relevant yet underaddressed’ in stroke page 11
Multiple trials find no clinical benefit with stroke thrombectomy for distal- and medium-vessel occlusions
Final analyses of the DISTAL and ESCAPE-MeVO studies revealed that thrombectomy failed to produce an improvement in patients’ clinical outcomes, while the DISCOUNT study was halted early due to safety concerns and indications of futility with the procedure.
“Few procedures have gone through a decade of practicechanging clinical trials as impressive as thrombectomy for stroke,” writes J Mocco (Mount Sinai Health System, New York City, USA) in an editorial accompanying the publication of DISTAL and ESCAPE-MeVO in the New England Journal of Medicine (NEJM). “Beginning in 2015 with multiple trials showing a benefit with thrombectomy in early large-vessel occlusion, followed by the extended-window trials in 2018 and then the largecore trials in 2023, it seemed that no corner of the cerebrovasculature would not have a substantial benefit from a proper clot removal—until now.
“No matter how one considers these data, there is no question that they represent the current ground zero of evidence to inform decisionmaking regarding the use of thrombectomy for stroke due to medium- and distal-vessel occlusion. The data clearly show
that thrombectomy for distal-vessel occlusions should not be an assumed default care pathway.”
DISTAL findings
Launched in 2021, the DISTAL trial investigated whether thrombectomy in addition to best medical therapy—often including intravenous thrombolytics—was able to reduce disability compared to best medical therapy alone. The trial included 543 adult patients who entered one of 55 hospitals across Europe with disabling stroke symptoms.
Imaging tests confirmed a medium/distal vessel blockage in all participants, with patients subsequently being randomly selected to receive either standard stroke care only or standard care plus thrombectomy treatment.
The effectiveness of thrombectomy treatment was measured via the patients’ disability and need for assistance in daily activities (modified Rankin scale [mRS]) at 90 days post-stroke, with decisions about the exact devices and procedures used for thrombectomy being left to the treating physician.
Ninety-day follow-up analysis of DISTAL revealed that there was no significant difference in disability between those receiving thrombectomy plus standard medical care and those receiving standard medical care alone. In addition, there were similar rates of death for each group—15.5% for those receiving thrombectomy plus standard medical care versus 14% among those receiving standard medical care alone—while rates of severe symptomatic brain bleeds were 5.9% for those receiving thrombectomy plus standard medical care versus 2.6% with standard medical
This lack of added benefit with thrombectomy was confirmed when researchers analysed specific subsets of people, such as those who did not receive intravenous thrombolytic medications and those who had more severe strokes.
“We were surprised at the
Continued on page 2
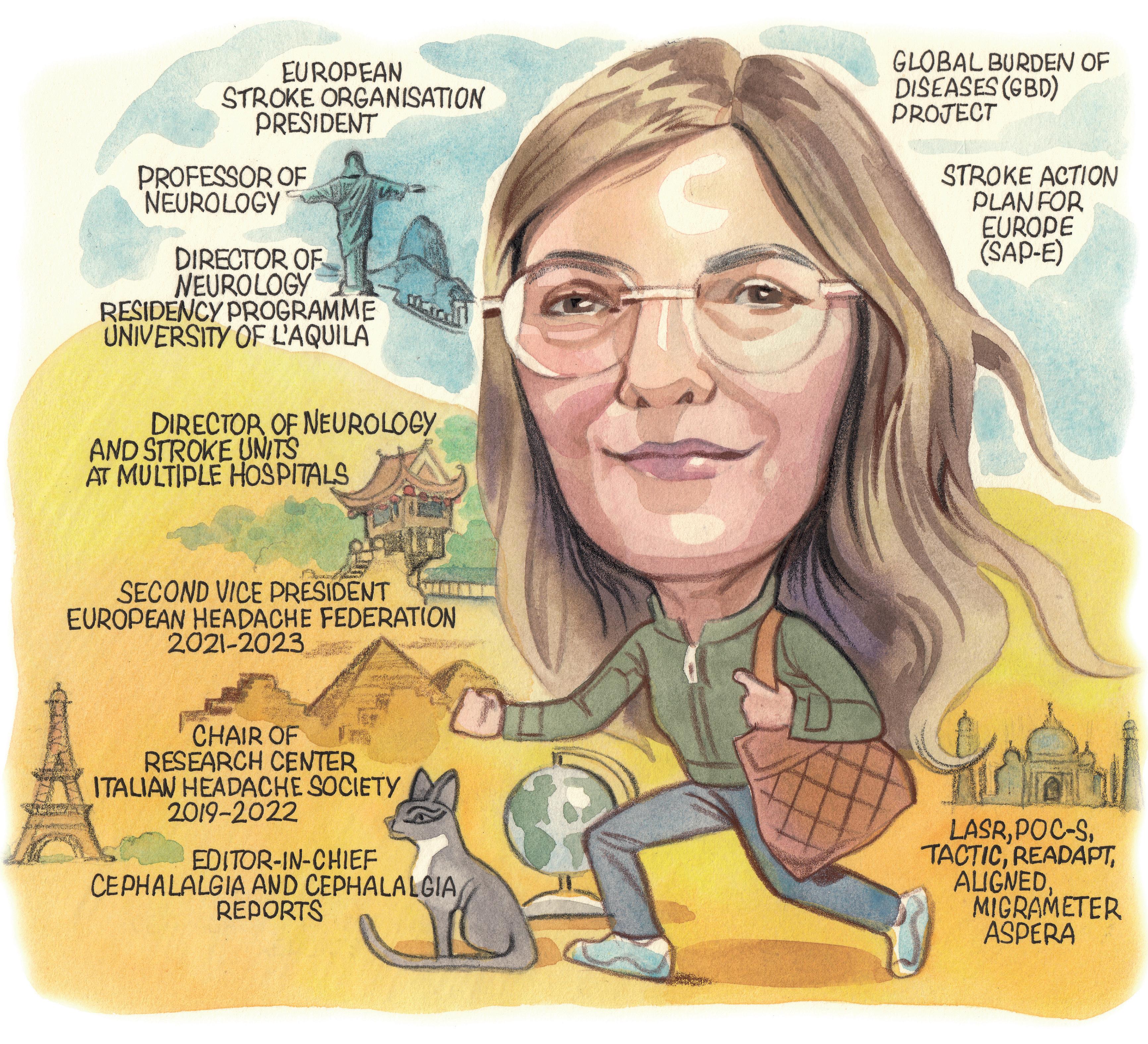
Profile Simona Sacco page 14
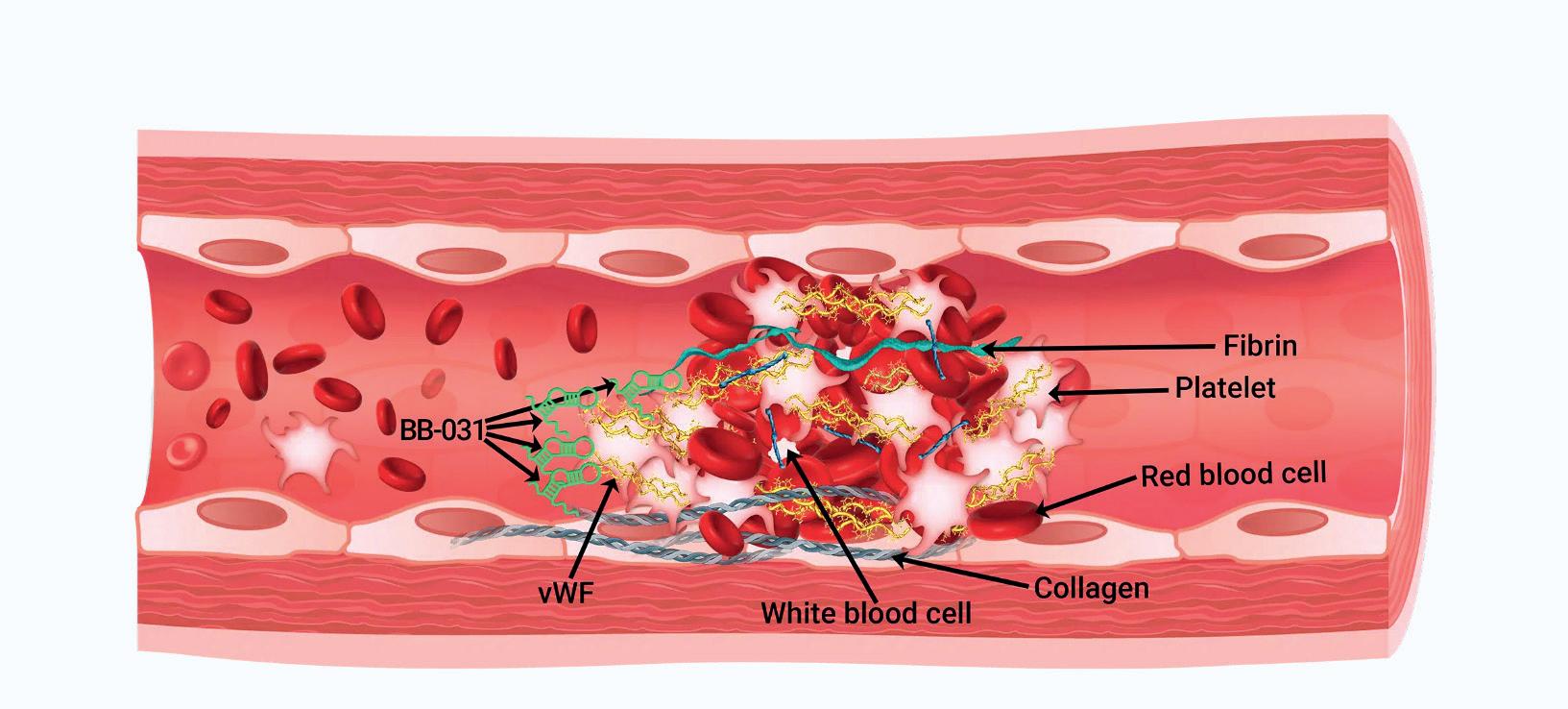
Medtech Insights: Could reversible thrombolytic alleviate tPA ‘tribalism’? page 18
EVT’s role in large-core stroke ‘reframed’ by recent data
A NEW SCIENTIFIC ADVISORY from the American Heart Association (AHA), published recently in Stroke, has reviewed clinical data from six randomised controlled trials evaluating endovascular therapy (EVT) in the treatment of ischaemic strokes caused by large-core infarctions, and ultimately concludes that these data “reframe” the role for reperfusion therapies in this population.
The advisory details that the trials— ANGEL-ASPECT, LASTE, RESCUEJapan LIMIT, SELECT2, TENSION and TESLA—provide “strong evidence” supporting the benefits of EVT in patients with a good pre-stroke functional status and significant stroke severity, as per initial imaging of the extent of their ischaemia.
The trials enrolled a total of 1,887 patients across global geographies including Australia, Canada, China, Japan, New Zealand, the USA, and several countries in Europe, evaluating the efficacy of EVT alongside standard medical management—as compared to medical management alone—in large-core ischaemic stroke.
“The results of these six trials reframe current evidence regarding the role of reperfusion therapies in those with larger areas of presumed irreversible ischaemia,” the advisory states. “The benefit of EVT in this setting may reflect the prevention of further infarct expansion or potentially improved tissue outcomes within ischaemic beds. Further research is needed to elucidate the mechanisms at play.”
DISTAL
D/MEVO
Multiple trials find no clinical benefit with stroke
thrombectomy for distal- and medium-vessel occlusions
Continued from page 1
overall outcome of the participants, which was worse than we anticipated based on retrospective data,” stated Marios Psychogios (University Hospital Basel, Basel, Switzerland), lead study author and co-principal investigator for DISTAL, who presented these findings at ISC 2025.
“[Thrombectomy] with the current techniques may not always provide extra benefits, so it could be worth reconsidering it as the standard treatment for medium/ distal vessel blockages,” commented DISTAL coprincipal investigator Urs Fischer (University Hospital Bern, Bern, Switzerland). “However, it is a safe option that can still be considered for select people on a caseby-case basis.”
The DISTAL researchers are currently conducting a detailed analysis on whether thrombectomy was more or less effective in different subgroups of patients, perhaps enabling them to identify characteristics that might be associated with a more positive outcome following the treatment.
“While the results of the DISTAL trial might seem discouraging, we see it as a wake-up call to continue investigating treatment options for medium- or distalvessel occlusion patients, as outcomes appear to be more severe than expected and evidence-based effective treatment options are still lacking,” Psychogios added.
ESCAPE-MeVO results
Presented by Mayank Goyal and Michael Hill (both University of Calgary, Calgary, Canada) at ISC 2025, the randomised, open-label, blinded-endpoint ESCAPE-MeVO trial enrolled a total of 530 D/MeVO patients across the USA, Canada, Germany, Hungary and the UK. Enrolled patients were allocated to either thrombectomy plus medical management or medical management alone. The study’s primary endpoint was the rate of ‘excellent’ functional independence at 90-day followup, as per an mRS score of 0–1.
The investigators relayed that the rates of mRS 0–1 at 90 days were statistically similar between the two study arms—41.6% with thrombectomy versus 43.1% without. They report an unadjusted risk ratio (RR) of 0.97 and an adjusted RR of 0.95 on this front, as well as detailing an average 90-day mRS score of 2 in both groups. Regarding
a handful of efficacy-related secondary endpoints, he noted that 90-day rates of mRS 0–2 were comparable between the thrombectomy group (54.1%) and the medical management group (58.8%), while mortality rates at the same timepoint were slightly higher with thrombectomy (13.3%) versus without (8.4%).
ESCAPE-MeVO’s safety endpoint data also revealed that patients who received a thrombectomy experienced an increased rate of serious adverse events (33.9%) compared to those who did not (25.7%), with pneumonia being the most common of these events. Additionally, while major procedural complications were “rare”, rates of recurrent stroke (5.4% vs 3.7%), stroke progression (5.4% vs 1.8%) and symptomatic intracranial haemorrhage (ICH; 5.4% vs 2.2%) were also higher in the thrombectomy group. Analyses of patient subgroups in the trial revealed no statistical heterogeneity between the two treatment arms regarding age, sex, geographical region, baseline
The data clearly show that thrombectomy for distalvessel occlusions should not be an assumed default care pathway.”
J Mocco
stroke severity, occlusion location, infarct volume, or use of intravenous thrombolytics; but, there was a trend towards improved thrombectomy outcomes in patients presenting within an earlier time window (onset to randomisation, <260 minutes).
Writing in NEJM, Goyal, Hill et al conclude that the results of their trial “do not support routine endovascular treatment of acute ischaemic stroke due to medium-vessel occlusion”, going on to aver that further work is needed to improve the safety profile of the thrombectomy procedure and identify a population of patients who may benefit from this approach.
DISCOUNT analyses
Taking to the ISC podium immediately after the ESCAPE-MeVO investigators, Frédéric Clarençon (Pitié-Salpêtrière University Hospital, Paris, France) detailed findings from the DISCOUNT study—a prospective, multicentre, open-label, randomised controlled trial that sought to enrol a total of 488 D/MeVO stroke patients across 22 French centres. Its aim was to evaluate thrombectomy plus medical management versus medical management alone via a primary endpoint relating to 90-day disability. However,
the DISCOUNT investigators opted for the broader endpoint of a ‘good’ clinical outcome (mRS 0–2).
A planned interim analysis of the trial on the first 163 randomised patients for whom a three-month follow-up visit was available led to it being stopped, with early data appearing to “disfavour” thrombectomy. Clarençon relayed that safety-related concerns and indications of low conditional power resulted in the data safety monitoring board (DSMB) recommending that the trial should be halted. Following multiple imputations and adjustments on minimisation factors, a modified intention-to-treat population of 163 patients was ultimately available for analysis.
Across this population, Clarençon reported an observed 90-day rate of mRS 0–2 of 60% in the study’s thrombectomy arm versus 77% in the medical management arm, leading—after imputation of missing data—to an odds ratio (OR) of 0.42 (p=0.024). Perprotocol sensitivity analysis also revealed an OR of 0.3 (p=0.009) pertaining to the study’s primary endpoint.
Additional analyses suggested a comparable median length of hospital stay between the two study groups— eight days in both—while evaluations of DISCOUNT’s ‘as-treated’ population found higher rates of at least one serious adverse event (39% vs 31%), as well as all ICHs (44% vs 29%) and symptomatic ICHs (12% vs 6%), with thrombectomy. However, the mortality rate was lower in the thrombectomy group (3%) versus the non-thrombectomy group (7%).
Clarençon concluded by noting that, while there did appear to be a potential deleterious effect with thrombectomy in terms of 90-day functional outcomes, this did not reach statistical significance on their interim analysis, adding that analyses of the trial’s overall population are “ongoing”.
The findings of ESCAPE-MeVO, DISCOUNT and DISTAL are likely to leave many asking the same question posed by Mocco in his recent NEJM editorial: “Where do we go from here?”
“The authors of the ESCAPE-MeVO trial correctly emphasise the importance of rigorously conducted randomised controlled trials,” he adds. “The stroke community should not be complacent. Rather, we must thoroughly test appropriate questions, evaluate alternative approaches, and not allow bias to interfere with identifying the best treatment strategies for patients with stroke. Let us not forget that almost half of all the enrolled patients in these trials had substantial disability at 90 days.
“There remains a continuing mandate, with more work required, to study how we can improve outcomes in patients. These two trials [DISTAL and ESCAPEMeVO] prove that their patient populations did not have a benefit with thrombectomy and, as such, performance of thrombectomy for medium- or distalvessel occlusion in a manner consistent with these trials is not evidence-based. Further effort—grounded in high-quality data science—is needed to evaluate alternative approaches for medium- or distal-vessel occlusion, be they medical or procedural.”
Editor-in-chief: Prof Philip M Meyers | Publisher: Stephen Greenhalgh
Philip | Stephen
Content director: Urmila Kerslake | Global commercial director: Sean Langer
Content | Jamie Bell jamie@bibamedical.com
Editor: Jamie Bell jamie@bibamedical.com | Editorial contribution: Jocelyn Hudson and Bryan Kay
Editorial contribution: Jocelyn Hudson
Design: Terry Hawes, Wes Mitchell and David Reekie
Terry Josh Lyon and David Reekie
Advertising: Michael Broughton michael@bibamedical.com
Subscriptions: subscriptions@bibamedical.com
Published by: BIBA News, which is a subsidiary of BIBA Medical Ltd BIBA Medical, Europe, 526 Fulham Road, Fulham, London, SW6 5NR, United Kingdom
BIBA Medical, North America, 155 North Wacker Drive, Suite 4250, Chicago, IL 60606, United States
Michael Broughton News, is subsidiary of Medical Ltd 526 7736 Wacker Suite 4250, 60606, Tel: +1
Printed by: Buxton Press. Reprint requests and all correspondence regarding the newspaper should
› Risk Factors and Prevention (Primary and Secondary)
› Novel Targets: Experimental Findings to Clinical Translation
› Digital Transformation, AI, and Robotic
Alteplase
may be
effective up to 24 hours after initial stroke symptom onset
The clot-dissolving medication alteplase can improve stroke patients’ recovery by more than 50% when given up to 24 hours after the beginning of an ischaemic stroke, as per preliminary latebreaking science presented at the recent International Stroke Conference (ISC; 5–7 February, Los Angeles, USA).
THESE RESULTS FROM THE PROSPECTIVE, multicentre, randomised HOPE study offer promise to stroke patients worldwide who may not be able to access clot-dissolving medications within the approved time window—which, in China, is within 4.5 hours—according to the trial’s principal investigator Min Lou (Second Affiliated Hospital of Zhejiang University School of Medicine, Hangzhou, China).
“We believe these findings mean more people may return to normal or near-normal lives after a stroke, even if they receive treatment later than originally thought beneficial,” Lou commented. “This method of treatment could become the new standard, especially
in hospitals that use CT [computed tomography] perfusion imaging. This technology helps healthcare professionals see how blood flows in different parts of the brain after an ischaemic stroke. This could extend treatment eligibility to millions more patients across the globe.”
In the USA, alteplase is approved to treat stroke within three hours of symptom onset and is recommended for use up to 4.5 hours for select patients, while some research has indicated it may also work well in certain patients 4.5–9 hours after stroke onset. American Heart Association/American Stroke Association guidelines from 2019 on the early management of patients with acute ischaemic stroke note that intravenous (IV) alteplase within 4.5 hours of stroke onset is the standard of care for most ischaemic stroke patients in the USA.
In the HOPE trial, researchers enrolled 372 stroke patients (average age, 72 years; 43% women) whose symptoms began between 4.5 hours and 24 hours earlier across 26 stroke centres in China. They used widely available CT perfusion imaging to confirm that these patients still had brain tissue that could be recovered with treatment. Participants were randomly split into two groups— one group received the clot-busting medication alteplase, while the other received standard stroke care involving antiplatelet therapy at the discretion of the investigator they
‘Chasing’ EVT with tenecteplase injection could lead to improved 90-day stroke outcomes
Removing a blood clot from a large brain artery via endovascular therapy (EVT), then injecting the clot-dissolving drug tenecteplase into the artery, has resulted in ischaemic stroke survivors being more likely to experience a better 90-day functional outcome when compared to those receiving standard clot removal, according to ANGEL-TNK study results presented as preliminary late-breaking science at the 2025 International Stroke Conference (ISC; 5–7 February, Los Angeles, USA).
“ENDOVASCULAR TREATMENT can help restore blood flow in a blocked large blood vessel,” said Xiaochuan Huo (Beijing Anzhen Hospital, Beijing, China), lead author of the study. “However, it might not improve blood flow in the smaller vessels and microcirculation in the area. This clinical trial tests whether delivering tenecteplase directly into the affected artery after endovascular treatment can break up blood clots in the small vessels and improve blood flow, reducing the amount of brain tissue that lacks blood supply.”
The ANGEL-TNK study—conducted at 19 centres in China—evaluated the safety and effectiveness of injecting tenecteplase directly into a large brain artery near where a clot was removed in order to restore blood flow. All 255
participants in the study (mean age, 70 years; 44.7% female) had anteriorcirculation large vessel occlusions and were treated 4.5–24 hours after the last time they were observed to be well.
According to the study protocols, 127 patients received tenecteplase after successfully undergoing EVT, while 129 received standard medical care (in the full analysis population for the final results) after successful EVT.
Disability—the study’s primary effectiveness endpoint—was measured via a score of 0–1 on the modified Rankin scale (mRS) at 90 days, while its primary safety-related endpoint pertained to brain bleeding within 48 hours of treatment or death from any cause within 90 days.
Analyses found that stroke survivors were 44% more likely to have an
were enrolled by and based on the 2018 Chinese guidelines for acute ischaemic stroke diagnosis and treatment. HOPE’s primary endpoint of functional recovery (modified Rankin scale [mRS] 0–1) was assessed at 90 days.
The study found that 40% of participants treated with alteplase had little-to-no disability after 90 days, compared to 26% of those who received standard care—equivalent to a 54% higher chance of functional recovery. In addition, less than 3% of participants in either group received rescue clot removal via mechanical thrombectomy as an additional treatment. Rates of death were the same (10.8%) for both groups, while the risk of brain bleeding was higher among those who received alteplase than among participants who did not (3.8% vs 0.5%)—a risk that the researchers believe is “manageable”.
“We also need to look more closely at how safe and effective other clot-dissolving medications like tenecteplase are when given after a stroke, especially beyond the usual timeframes,” Lou added. “It’s also important to learn if our findings apply to other groups of people, especially in areas with different stroke risks and healthcare resources.”
Study limitations include the fact that both participants and investigators knew which treatment was being given, which could have introduced bias, and results potentially not being generalisable to patients outside of China, according to the researchers.
‘excellent’ outcome (mRS 0–1) after 90 days if they received the tenecteplase injection and standard care after clot removal compared to receiving only standard care after clot removal (40.5% vs 26.4%, respectively). In addition, rates of brain bleeds in the two days after treatment were similar in those receiving tenecteplase (5.6%) and those receiving standard medical treatment (6.2%), and rates of death from any cause within 90 days were also similar with tenecteplase plus standard treatment (21.4%) versus standard treatment alone (21.7%).
“Intra-arterial tenecteplase after successful thrombectomy could
The researchers are following participants in ANGEL-TNK to assess one-year outcomes and, according to Huo, their results may someday be used to change treatment guidelines for stroke survivors who have undergone successful clot removal.
“We still need to directly analyse the individual data of participants in this and other trials—an individual metaanalysis—in order to release a high evidence-based recommendation,” he added.
The present study did not include patients treated with intravenous clot-busting drugs like alteplase or medications that reduce blood clotting,
improve the percentage of people with an excellent outcome. It could also improve the rate of large vessel occlusion stroke survivors who can return to society and live independently,” Huo said.
such as heparin and antiplatelets, during their endovascular procedures. According to the researchers, this means the benefits of intra-arterial tenecteplase shown in this study may not apply to people who receive those treatments.
Minimally invasive surgery appears beneficial in deep and lobar intracranial haemorrhages
The MIND study—presented for the first time at this year’s International Stroke Conference (ISC; 5–7 February, Los Angeles, USA)—has revealed the potential benefits of minimally invasive surgery in patients with deep and lobar intracranial haemorrhages (ICHs). Analyses demonstrated a “substantial” reduction in haemorrhage volumes that was not accompanied by excess periprocedural mortality or adverse events, and “pronounced” early clinical improvements with surgery versus medical management.
DELIVERING THESE LATEbreaking findings, David Fiorella (Stony Brook University Medical Center, Stony Brook, USA) initially informed the ISC 2025 audience that, despite the “considerable” health and economic burden of the condition, the majority of ICH patients are left without definitive treatment. Against this backdrop, Fiorella et al conducted the MIND study—a multicentre, prospective, open-label randomised controlled trial (RCT) comparing the safety and effectiveness of minimally invasive surgery with the Artemis neuro evacuation device (Penumbra) to best medical management in the treatment of spontaneous ICH.
This investigational device exemption (IDE) study enrolled patients with moderate-to-large-volume supratentorial ICH (20–80mL) presenting within 24 hours of symptom onset. Patients randomised to receive minimally invasive surgery underwent the procedure within 72 hours, while clinical follow-up took place at 24 hours post-intervention in the surgical arm versus 72 hours post-randomisation in the medical management arm, as well as at seven, 30, 90, 180 and 365
days, or at discharge. The study’s primary endpoints for effectiveness and safety were 180-day ordinal modified Rankin scale (mRS) scores and 30-day mortality, respectively.
Fiorella relayed that, in 2022, a prespecified interim analysis of MIND following enrolment of the first 200 patients found no safety or futility-related concerns and therefore recommended continuation of the study. However, shortly thereafter, ENRICH trial results demonstrated improved clinical outcomes versus standard care with minimally invasive surgery using the BrainPath and Myriad technologies (both Nico Corporation/Stryker) in lobar ICH, calling into question the potential clinical equipoise of MIND and leading to enrolment of patients with primarily lobar ICHs being halted. An independent analysis of MIND accounting solely for randomised patients with deep ICHs then projected a low probability of there being a statistically significant difference between study arms, resulting in enrolment stopping altogether—across both ICH locations—in October 2023.
Ultimately, this left the MIND
Blood test could help clinicians “rapidly” distinguish between haemorrhagic and ischaemic strokes
A blood test may have the ability to rapidly distinguish bleeding-based haemorrhagic strokes from their clot-caused ischaemic counterparts, even before symptomatic patients reach the emergency room, according to a preliminary study presented at the 2025 International Stroke Conference (ISC; 5–7 February, Los Angeles, USA).
“IT IS CRUCIAL TO DIFFERENTIATE THESE two types of stroke, because they need opposite treatments,” explained lead study author LovePreet Kalra (RKH Hospital Klinikum Ludwigsburg, Ludwigsburg, Germany).
In the study, researchers examined whether blood levels of glial fibrillary acidic protein (GFAP)—a protein that is released into the bloodstream when brain cells are damaged or destroyed—could be useful for quickly diagnosing stroke types. GFAP is
investigators with a final study population of 236 patients—one deemed underpowered to detect the study’s preestablished treatment effect size. Within this intention-to-treat population, 154 patients were allocated to minimally invasive surgery while 82 underwent medical management only. Fiorella reported comparable average times to randomisation and baseline ICH volumes between groups, adding that the majority of patients (70.8%) had deep ICHs.
Describing procedural outcomes observed in patients who received surgery, Fiorella relayed an 80.7% median rate of haematoma reduction—a “high” evacuation rate that proved to be comparable between deep and lobar ICH locations. The study also found that 79.2% of patients achieved the surgical goal of a haematoma volume of ≤15mL, and there were low rates of conversion to craniotomy (1.4%) and external ventricular drain (EVD) placement (12.5%) as well as a median procedure duration of 33.5 minutes. Additionally, minimally invasive surgery compared to medical management was found to have increased the odds of a favourable clinical outcome as per 30-day ordinal mRS scores— although, despite positive trends continuing, these indications did not reach statistical significance at 90 and 180 days. Mean 180-day utility-weighted mRS scores were similar between surgery and medical management in 222 ‘per-protocol’ patients.
In the study’s as-treated population (234 patients), primary safety endpoint analyses showed a low overall mortality rate within 30 days across the two treatment arms (8.1%), with a rate of 7.2% in the surgical group and 9.8% in
already used in assessing traumatic brain injuries (TBIs).
The study included 353 patients who reached the emergency room within six hours of the onset of stroke symptoms, but excluded those who had previously had a brain tumour, or had experienced a stroke or TBI within the past three months.
Brain imaging diagnosed intracerebral haemorrhages in 76 patients, clot-caused strokes in 258 patients, and conditions mimicking stroke—such as seizure or migraine—in 19 patients. Blood was drawn by ambulance teams before patients reached the emergency room and tested for GFAP levels using a portable blood analyser, with GFAP levels being compared between groups based on diagnoses at hospital discharge.
Analyses found that GFAP levels were almost seven times higher in patients with haemorrhagic stroke compared to those with ischaemic stroke
It is crucial to differentiate these two types of stroke, because they need opposite treatments.”
the medical management group. Here, Fiorella noted that mortality rates in the study’s medical management arm were roughly half of those reported in the literature among similar patient populations—leading investigators to speculate that, while minimally invasive surgery did not demonstrate any relative improvement in 30-day mortality rates, medical management may have ‘overperformed’ in the study and thus masked potential between-group discrepancies. He also commented that, when looking specifically at lobar ICHs, the 30-day mortality rate in MIND’s medical management arm (22.7%) was “more in line” with previously reported figures.
Fiorella then discussed a number of secondary endpoint findings, including comparable Kaplan Meier-estimated survival probabilities between the study’s treatment arms. Further analyses indicated fewer 180-day serious adverse events in the surgical arm—across both deep and lobar ICH—as compared to the medical management arm (52.6% vs 68.3%, respectively), while a lower incidence of a symptomatic evolution of perihaematomal oedema with surgery (2.6%) versus medical management (13.4%) suggested a 30-day reduction in secondary injury that did not carry increased bleeding risks. Per-protocol analyses also revealed median lengthof-stay data that trended positively—if only marginally—in favour of surgery, as well as substantially reduced 30-day intubation rates with surgery (3.6%) versus medical management (12.1%).
Finally, the speaker alluded to a 0.7% rate of surgical complications with the Artemis system at 30 days, before concluding that “future studies are needed to optimise outcomes for ICH patients” and build on MIND’s many positive signals.
(208pg/mL vs 30pg/mL), and more than four times higher in patients with haemorrhagic stroke versus those with stroke mimics (208pg/mL vs 48pg/mL).
In addition, GFAP levels were able to rule out haemorrhagic stroke when below 30pg/mL in patients with moderate-to-severe neurological deficits, and able to predict which patients had a haemorrhagic stroke with 90–95% accuracy when evenly distributed age-based cutoff points were used (<72 years, 72–83 years and >83 years), with the cutoff for those below 72 years being very low. GFAP levels were also higher in haemorrhagic stroke patients taking bloodthinning medications when compared to those not on blood thinners.
“I was personally surprised by the extremely elevated GFAP values in blood thinner-associated bleeding stroke and the fact that, in moderately or severely affected acute stroke patients, bleeding stroke could be excluded in all cases which showed a GFAP lower than 30pg/mL,” Kalra stated.
If larger studies confirm these results, Kalra believes early GFAP measurements could change how people with stroke symptoms are treated.
“Treatment to lower blood pressure and reverse blood-thinning medications could be performed in the prehospital setting, leading to a huge change in clinical practice,” she commented. “In the future, even blood thinners or clot-busting treatment might be applied before people reach the hospital.”
David Fiorella
Novel EVD catheter scoops US$100,000
SVINnovation prize
A novel catheter intended to improve on the tools currently available in neurosurgical external ventricular drain (EVD) placement was awarded a US$100,000 grand prize at the 2024 Society of Vascular and Interventional Neurology (SVIN) annual meeting (20–22 November, San Diego, USA).
THE SOUNDPASS DEVICE
—conceived and developed by a team of medical students from the University of Utah (Salt Lake City, USA)—was ultimately selected by an entrepreneurial panel of judges to receive this award ahead of three other technologies also showcased during the meeting’s SVINnovation session.
SoundPass co-founder Matt Findlay (University of Utah, Salt Lake City, USA) presented his team’s technology to the panel at SVIN 2024, stating that it was predicated on the idea that ‘two passes are too many’ when it comes to EVD catheter access for neurosurgical drainage of cerebrospinal fluid (CSF).
With the addition of an ultrasound transducer component at its tip, the SoundPass catheter is designed to provide real-time visualisation and—by minimising the number of required passes—ultimately reduce the likelihood of complications during EVD placement procedures. Findlay and his colleagues anticipate that this will help to add a new level of precision within a neurosurgical operation that is among the most common in the USA, but is typically performed ‘blindly’ without imaging guidance.
As the winner of the SVINnovation
Procedural volume
grand prize, Findlay and the SoundPass team took home US$75,000 in cash in addition to US$25,000 in complimentary consulting services and mentorship from industry experts at Brainstorme, Project Medtech, and Medical Device Global Regulatory Consulting (MCRA). SoundPass will also gain exposure in the journal Stroke: Vascular and Interventional Neurology and on the SVIN’s website.
“We are deeply honoured and thrilled to receive the SVINnovation prize. We extend our sincere gratitude to the SVIN, its members, and the judges, for recognising our work. In the fastpaced world of startups, maintaining momentum is vital, and this funding will significantly accelerate our efforts to bring this innovative device to patients’ bedsides,” Findlay told NeuroNews. “The funding will play a pivotal role in advancing our next major milestones, including cadaver and live animal studies to refine and validate our working prototypes. These crucial steps will not only accelerate our progress but also bring us closer to delivering lifechanging solutions to patients.”
Presenting the award to Findlay
following the judging panel’s decision, Von Vascular chief executive officer (CEO) Manning Hanser cited the SoundPass team’s “clear and easy” proposed pathway to US Food and Drug Administration (FDA) 510(k) clearance, and praised the single-use nature of the device as well as the fact that it targets novice users and experienced neurosurgeons alike. Hanser also said he hopes the funds will enable the group to grow and add new areas of expertise to its “awesome” academic team.
The first of three other novel concepts presented during the
pronged solution to the global burden of hypertension. The technology in question incorporates an endovascular stent-like device capable of continuously monitoring intra-arterial blood pressure (SomaSense), and an electronic system designed to modulate the carotid sinus and control pressure levels in response to these monitoring data (SomaSafe). Desai concluded by noting that this proactive, real-time, personalised technology could improve compliance to treatment of “the worst disease mankind suffers from”.
Neuronics Medical CEO and co-
SVINnovation session was Quantanosis.ai. Showcased by its co-founder Ameer Hassan (Valley Baptist Medical Center, Harlingen, USA) at SVIN 2024, the company’s technology intends to use artificial intelligence (AI)-powered diagnostics and a head-mounted helmet to break up neurovascular clots quickly and accurately—but also completely noninvasively—via histotripsy. With this operator-independent and portable solution, Quantanosis.ai’s goal is to “democratise” stroke treatment.
Following this, Shashvat Desai (HonorHealth, Scottsdale, USA) outlined the potential of a two-
“not a reliable indicator”
of stroke thrombectomy outcomes
According to new research led by the University of Missouri School of Medicine (Columbia, USA), the number of mechanical thrombectomies performed at a hospital is not an accurate indicator of patient outcomes. Using data from nearly 1,000 centres, researchers found that patients undergoing thrombectomies at smaller, rural hospitals did not have less favourable outcomes—in terms of functional independence rates—than patients treated in large healthcare systems.
THESE SMALL HOSPITALS CONDUCT FEWER than 15 thrombectomy procedures per year, which is less than the number required to obtain certain stroke centre certifications. Considering these new data, study author Adnan Qureshi (University of Missouri Health Care, Columbia, USA) stated that it is important to re-evaluate the relationship between numbers of procedures and patient outcomes.
“There is an increasing recognition that a large number of patients who could benefit from a thrombectomy are not receiving it,” Qureshi said. “Increasing the role of smaller hospitals and centres may be the key to increasing availability.”
It is hoped that expanding access would mean stroke patients who live hours away from comprehensive stroke care can still receive a thrombectomy at their
local hospital—and any other care they need.
“One way we could increase the role of smaller hospitals is to provide travelling physicians who know how to perform a thrombectomy,” Qureshi added. “Other ways include updating their infrastructure and resources.”
In the present study, researchers also found that larger hospitals with a higher volume of mechanical thrombectomy procedures saw more adverse outcomes in stroke patients—such as death or permanent disability—as compared to smaller hospitals.
“There are several potential explanations for this,” Qureshi continued. “Hospitals that perform more thrombectomies also tend to see patients with a higher stroke severity, or those who are at higher risk because of another illness or condition. Smaller hospitals may
founder Radoslav Raychev (University of California Los Angeles [UCLA] Health, Los Angeles, USA) gave the session’s fourth and final pitch, showcasing his company’s Fast.AI smartphone application—which utilises machine learning algorithms with the goal of autonomously yet reliably detecting patients’ physical signs of stroke. With the technology having already demonstrated promising preliminary results in a real-world study, Raychev hopes that Fast.AI can detect signals like facial asymmetry, arm weakness and speech changes with accuracy comparable to that of an actual neurologist.
not have the resources to treat these patients.”
According to Qureshi, another factor may be that larger hospitals are more likely to see more complex patients, so the chance of adverse outcomes or permanent disability occurring is higher.
Nevertheless, the data suggest that, overall, the number of thrombectomy procedures is not an accurate indicator of quality of care, and other factors like illness severity should be considered in certification processes. The authors describe this as indicating a “paradoxical relationship” between adverse outcomes and annual procedural volume of mechanical thrombectomies.
The study in question is now published in the journal Interventional Neuroradiology
One way we could increase the role of smaller hospitals is to provide travelling physicians who know how to perform a thrombectomy.”
Matt Findlay (far left) receiving the SVINnovation prize
New technologies and improved understanding ensure aspiration thrombectomy will continue to evolve
Recently, at the 2024 BRAIN conference (2–4 December, London, UK), David Volders (University of Toronto, Toronto, Canada) sat down with NeuroNews to discuss mechanical thrombectomy devices that have had a profound, positive impact on his ischaemic stroke practice, as well as touching on a number of potential paradigm shifts—present and future—in aspiration thrombectomy.
Throughout 2024, in an effort to complete its stroke care portfolio, Penumbra launched a total of five new products in Europe: the RED 43, RED 72 with SENDit technology and RED 78 reperfusion catheters, and also the BMX81 and BMX96 neurovascular access catheters. And, in Volders’ view, “for several reasons”, BMX96 can be seen as a game-changing technology.
“First of all, it really offers a lot of support, which is very helpful in complicated stroke cases where access is an issue,” he says. “Additionally, it tracks really well and that helps with [vessel] tortuosity, for example. On top of that, the inner diameter is also a 096—which is the largest inner diameter of all of [Penumbra’s] guide catheters—and that allows you to go up with bigger aspiration catheters like the recently launched RED 78. And, finally, it really allows you to go high into the petrous ICA [internal carotid artery] without being too traumatic during thrombectomy procedures. So, there are several aspects that allow you to have major benefits.”
However, while BMX96 may have had a profound impact on his practice, Volders is also quick to highlight the benefits brought about by the newly introduced RED 72 catheter—and, more specifically, the advantages enabled by Penumbra’s SENDit technology.
“The first thing to note is that SENDit is very easy to prepare,” he comments. “It all comes prepackaged, with an easy flush, and you just have to put in a 014 wire and you’re good to go. We all know that, in stroke, ‘time is brain’; having to prepare a separate microcatheter and then bring it into the aspiration catheter—those are additional steps and they take time that could be spent doing other things.”
Volders also feels that SENDit is a “very useful tool” when it comes to, for example, the ophthalmic artery and the particularly apparent ‘ledge effect’ that is often produced when using other aspiration catheters and microcatheters in this location. The effect “disappears” when utilising SENDit technology, he adds, ensuring RED 72 tracks “really nicely” past the ophthalmic artery.
“That’s where a lot of people get stuck when they’re doing aspiration [thrombectomy], and have to revert to using stents,” Volders posits. “Having a tool like SENDit really is another gamechanger.”
Evolution of aspiration
In addition to the many technologies Penumbra has introduced into the neurovascular space in recent times, another ongoing and potentially momentous development in stroke interventions is the shift away from balloon guide catheter (BGC) usage.
Volders’ view is that a key driver of this is the enhanced understanding clinicians now have regarding the physics of aspiration.
“Previously—10–15 years ago—people were thinking aspiration is just about a pump pulling in
the clot,” he explains. “Now, they appreciate that it’s much more than that. Having systolic pressure that pushes the clot, and not just the pump pulling it, is actually something that’s very important. That is why I believe that it’s more helpful to not use a BGC—by taking away that systolic pressure, it’s basically working against you in getting a successful first-pass effect.”
Working alongside a handful of his colleagues in Canada, Volders has attempted to introduce a standardised approach to direct, aspiration-only thrombectomy, describing and summarising initial cases utilising the ‘CANADAPT’ technique via a 2024 publication in the journal Interventional Neuroradiology. Based on singlecentre, prospective cohort data from 22 consecutive patients treated for large/medium-vessel ischaemic stroke, Volders et al conclude that CANADAPT demonstrated safety, efficiency and efficacy, with initial indications that the technique could be linked to shorter median procedure times and lower per-procedure costs compared to approaches involving stent retrievers plus aspiration.
vessel. First of all, you’re occlusive, and you don’t get that benefit of having the systolic blood pressure. But, on top of that, you run the risk of causing damage to the vessel—for example, with [vaso]spasm—and that’s something that might also negatively affect your outcome. The right sizing is very important and this, again, is something that’s new to people.
“Another thing that may also be important to mention is that every vessel is different, in everyone. One person’s M1 may have a different size to somebody else’s M1, so you can’t really say, ‘I use this aspiration catheter for that vessel’—you really have to tailor it.”
Positive outlook
The current slogan accompanying Penumbra’s evergrowing group of ischaemic stroke products in Europe is, ‘Versatile. Compatible. ADAPTable’. Outlining how this notion has translated into his own clinical practice, Volders highlights the diversity of the company’s present offering as being among its key strengths.
“What I like about Penumbra’s portfolio is that, for every different aspect of a stroke case, you can pivot,” he says. “If you have a difficult arch, you can use a SIM Select catheter. Or, you can choose BMX96, which offers you four times more support compared to a Neuron MAX. You can go pretty high into the ICA, you can look at the vessels, you can determine if you think it’s a large clot, and you can change your sizing to [reflect] that.
“You basically have such a wide range of choices in your aspiration catheters that, for every case, you can almost handpick the right tools to increase your first-pass success.”
Previously, people were thinking aspiration is just about a pump pulling in the clot. Now, they appreciate that it’s much more than that.”
Touching on this paper, Volders says that CANADAPT “standardises, but also optimises” firstpass effects with aspiration.
“It really uses that concept of both the pull of the pump and the push of the systolic pressure,” he adds.
Another factor that is important to consider when seeking improved first-pass effect and overall thrombectomy success rates, according to Volders, is appropriate catheter sizing relative to the target vessel.
“I always like to say that one size does not fit all,” he avers, advising his peers to select an aspiration catheter size that occupies roughly 70–80% of the vessel’s lumen. “What that does is actually allow systolic blood pressure to still flow around and beyond the clot—and, when you pull back, you are going to see an increase in your first-pass effect.
“Imagine you have a catheter that’s too large for the
Volders also touches on another area that he feels has genuine promise when it comes to improving thrombectomy outcomes for stroke patients: modulated aspiration, whereby computerassisted technology is deployed in an attempt to reduce friction between the clot and reperfusion catheter, and ultimately facilitate more rapid and complete removal of blood clots from the brain.
Penumbra is currently playing a leading role in moving this part of the field forward, evaluating the safety and efficacy of its computer-assisted vacuum thrombectomy (CAVT) technology and Thunderbolt aspiration tubing via the THUNDER investigational device exemption (IDE) study. In October 2024, the company announced that it had completed enrolment of acute ischaemic stroke patients in this study.
“I do think the future lies with modulated aspiration,” Volders comments. “What happens is that the clot can be ingested into the aspiration catheter at the moment when the catheter is at the level of the clot. In our CANADAPT data, we found that there’s only a small percentage of clots that are actually ingested at this point—mainly because the systolic blood pressure is so minimal in this phase.
“I know Penumbra has worked very hard on this and is actually a pioneer in the field. So, I’m very excited to see what’s going to happen with the new Thunderbolt technology and I really believe that’s going to be another big gamechanger.”
David Volders is an associate professor at the University of Toronto, and an interventional and diagnostic neuroradiologist at Toronto Western Hospital, in Toronto, Canada.
David Volders
Further research on balloon guide catheters required following inconclusive PROTECT-MT results
Recently presented results from the PROTECT-MT randomised controlled trial (RCT) have indicated worse functional outcomes following stroke thrombectomy with a balloon guide catheter (BGC) versus a conventional guide catheter. However, the study’s investigators believe these findings are unlikely to be fully conclusive, due to the fact the trial was halted early over safety concerns and subsequently only produced a small sample size for data analyses.
PENGFEI YANG (NAVAL MEDICAL University/Changhai Hospital, Shanghai, China), who delivered these findings for the first time at the 16th World Stroke Congress (WSC; 23–26 October 2024, Abu Dhabi, United Arab Emirates), initially posited that “uncertainty exists” over BGC usage in mechanical thrombectomy treatments of patients with acute ischaemic stroke caused by anterior-circulation large vessel occlusion (LVO).
Against this backdrop, Yang and colleagues conducted the investigatorinitiated, multicentre, prospective, open-label PROTECT-MT RCT with blinded-outcome assessments to ascertain the effectiveness and safety of BGC-based thrombectomy procedures for ischaemic stroke. The comparator in the trial was the use of conventional guide catheters in these procedures, and the primary endpoint was an ordinal shift analysis of scores on the modified
Rankin scale (mRS)—a metric often deployed to determine a patient’s poststroke functional outcome status—at 90 days.
According to Yang, an estimated 1,074 stroke patients—all of whom presented with temporary, proximal LVOs within 24 hours of symptom onset—met the inclusion criteria for PROTECT-MT and were randomised 1:1 to undergo a mechanical thrombectomy procedure utilising either a BGC (intervention group) or a conventional guide catheter (control group).
Recruitment for the trial began back on 7 February 2023. However, in November of the same year, the trial’s independent data and safety monitoring board (DSMB) held a meeting to review primary outcome data and would ultimately recommend the suspension of further recruitment into PROTECT-MT due to safety concerns. This suspension
Latest ‘super-bore’ catheter technology shows promise in initial clinical experience
A device described as the latest addition to a growing group of ‘super-large-bore’ catheter technologies has demonstrated “extremely positive” outcomes in early clinical usage.
AT THE 2024 BRAIN CONFERENCE (2–4 December, London, UK), Shahram Majidi (Department of Neurosurgery, Mount Sinai Health System, New York City, USA) presented his experiences with Cereglide 92 (Johnson & Johnson MedTech Neurovascular), relaying that the novel 0.092-inch catheter may enable higher first-pass effect rates as well as faster procedure times.
Majidi’s presentation included examples of three mechanical thrombectomy cases in which Cereglide 92 was used to treat large vessel occlusion (LVO) stroke patients via a direct aspiration technique. He noted during his talk that these cases—all of which ultimately saw a positive result—represent the first in-human treatments involving Cereglide 92 ever to be showcased at a medical conference.
Key characteristics of the device that Majidi highlighted include its enhanced trackability, the level of support it provides, and its atraumatic tip—all of which can help operators to capitalise on the benefits of flow modification and increased aspiration force brought about by these types of super-bore catheters. Usage of the Innerglide (Johnson & Johnson MedTech
was implemented by the trial’s steering committee, with 329 patients having been randomised to that point, and the steering committee halted recruitment completely after these safety concerns “persisted” upon further review of the data in April 2024.
Presenting unblinded results from the trial at WSC 2024, Yang relayed that the use of BGCs was associated with inferior functional outcomes compared to use of conventional guide catheters in LVO ischaemic stroke patients receiving mechanical thrombectomy. Specifically, Yang and colleagues’ 90-day mRS shift analysis revealed an adjusted common odds ratio (OR) of 0.66 (95% confidence interval [CI], 0.45–0.98; p=0.037) suggesting worse outcomes in the intervention group.
Dichotomised mRS results also showed that scores of 0–3 were achieved in 41% of patients in the BGC group compared to 56% in the conventional guide catheter group (OR, 0.56; 95% CI, 0.35–0.88), while scores of 0–4 were achieved in 57% of patients in the former group versus 73% in the latter (OR, 0.47; 95% CI, 0.28–0.78).
The PROTECT-MT investigators’ analyses uncovered several other notable observations, including the fact that rates of embolisation in new territories (ENT), reperfusion quality and first-pass effects were all
comparable between the two study groups. However, Yang did report a longer average procedure time and an increased rate of severe vasospasm in the internal carotid artery (ICA) in patients treated with a BGC.
In addition to the study being terminated early and therefore only providing a final cohort that was roughly one third of the sample size the investigators had initially sought, Yang highlighted multiple other potential limitations. These included discrepancies in the types of devices used and in the experience levels of individual operators, as well as the fact PROTECT-MT was conducted solely at sites in China, where intracranial atherosclerotic disease (ICAD) is known to be a more common underlying cause of ischaemic stroke as compared to many other global regions. As such— despite PROTECTMT being the largest RCT to date attempting to assess the impact of BGCs versus conventional guide catheters on thrombectomy-related functional outcomes in LVO stroke patients—Yang concluded that further research will be necessary in order to fully elucidate the role for BGC usage in interventional stroke care.
The findings of PROTECT-MT have since been published in full in The Lancet
Neurovascular) delivery catheter, which is compatible with a 0.024inch microwire, represents another feature of the system that—in Majidi’s view—further maximises the performance of Cereglide 92 in terms of reaching the M1 segment. Providing a novel nugget of advice for those in the audience, the speaker also relayed that higher intracranial positioning of the guide catheter has been shown to lead to a faster recanalisation time when utilising large-bore catheters like Cereglide 92 in stroke interventions, citing a recent publication and his own experiences.
Majidi went on to posit that, “in the era of expanding thrombectomy”, whereby his centre and many others are now performing multiple endovascular stroke procedures per day, efficiency and simplicity—including a straightforward setup, easy utilisation and compatibility of devices—are of paramount importance.
of patients in BGC group of patients in conventional guide catheter group
Dichotomised mRS 0–3 results
Shahram Majidi presenting at BRAIN 2024
Cereglide 92
Rescue stenting linked to improved functional independence versus thrombectomy alone in real-world registry
In patients with large vessel occlusion (LVO) stroke caused by intracranial atherosclerotic stenosis (ICAS), rescue stenting following mechanical thrombectomy appears to lead to higher rates of successful reperfusion and 90-day functional independence—but also an increased occurrence of procedural complications—as compared to thrombectomy alone. These are among key findings of the RESCUEICAS registry, from which results were recently presented for the first time at the 2024 Society of Vascular and Interventional Neurology (SVIN) annual meeting (20–22 November, San Diego, USA).
Delivering these late-breaking data at SVIN 2024, Sami Al Kasab (Medical University of South Carolina, Charleston, USA) initially noted that, while the overwhelming majority of LVO strokes are understood to be ‘embolic’ in nature, roughly 10–30% are caused by underlying ICAS—and thrombectomy is believed to be a less effective treatment approach in this smaller subset of patients due to high reocclusion rates in close to 50% of cases. With this in mind, RESCUE-ICAS—an international, multicentre, observational, prospective cohort study—sought to evaluate the prevalence of ICAS-LVO in western patient populations, understand neurointerventionists’ approach to ICAS-LVO, and compare thrombectomy with versus without rescue stenting in ICAS-LVO patients undergoing the procedure across 25 centres in the USA, Europe and Asia.
The registry defined ICAS-LVO as those cases in which there was 50–99% residual stenosis following any number of attempted thrombectomy passes, either with or without intraprocedural re-occlusion, with ICAS-LVO being identified intra-procedurally. It enrolled adult patients presenting within 24 hours of symptom onset with an emergent anterior- or posterior-circulation LVO and a National Institutes of Health stroke scale (NIHSS) score ≥6. And, as reported by Al Kasab, acute management of ICAS-LVOs took place at the discretion of the individual participating sites due to the observational nature of the registry.
“The study exposure was receiving a stent [following unsuccessful thrombectomy] versus thrombectomy alone, and patients who received balloon angioplasty alone were considered in the thrombectomy group,” the presenter stated. “We had 11 patients in the study who had an attempted stent placement that failed due to complication, perforation, dissection or inability to deliver the stenting construct. These patients were counted in the stenting group, in order to be consistent with the intention-to-treat analysis of a randomised trial.”
The primary endpoint for RESCUE-ICAS was 90-day functional independence measured via an mRS score of 0–2. Secondary endpoints included rates of final, successful reperfusion at the end of the procedure, symptomatic intracranial haemorrhage (ICH) and 90-day mortality. The registry collected data on patients allocated to either thrombectomy
plus stenting or thrombectomy alone. Inverse probability of treatment weighting (IPTW) was deployed to adjust for potential confounders when it came to analysing the registry’s primary endpoint. Here, Al Kasab also noted that prespecified sensitivity analyses led the investigators to further stratify patients’ post-thrombectomy treatment modalities into the following groups: no stent or angioplasty; balloon angioplasty without stenting; self-expanding stent; and balloon-mounted stent.
(IVT)—27.5% compared to 18.6% in the stenting group (p=0.03)—while the average procedure duration was longer in the stenting group. In addition, as per the primary endpoint for RESCUE-ICAS, the rate of functional independence at 90 days was “significantly higher” in the stenting group (42.2%) compared to the non-stenting group (28.4%), backed by an adjusted odds ratio (OR) of 2.67 (95% confidence interval [CI], 1.66–4.32; p<0.001).
“Between January 2022 and December 2023, about 6,000 patients underwent mechanical thrombectomy at the participating sites,” he continued. “Of those, 451 were identified as ICAS-LVO—and, of those, 417 were included in the final analysis, with 218 patients undergoing thrombectomy alone and 199 undergoing thrombectomy plus intracranial stenting.”
Regarding baseline demographics, Al Kasab reported no major differences in terms of average age or sex, nor premorbid mRS
As per the registry’s most notable secondary endpoints, Al Kasab relayed that there was a higher rate of successful reperfusion (modified treatment in cerebral infarction [mTICI] score ≥2b) with stenting versus thrombectomy alone (90.9% vs 77.9%; p<0.001), as well as a greater frequency of 24-hour infarct volumes <30ml across a total of 260 patients with available magnetic resonance imaging (MRI) data in the stenting group (67.9% vs 50.3%; p=0.005). And, while there was also a higher overall complication rate in the stenting group (12.6% vs 5%; p=0.006), this ultimately did not translate into a statistically significant difference in the rate of symptomatic ICH between the two groups (9% vs 5.5%; p=0.162). All-cause mortality rates at 90 days were found to be statistically comparable with versus without stenting too (24.6% vs 30.7%; p=0.164), despite a trend towards reduced mortality in the stenting group.
“Commonly, you’re less likely to stent somebody who has a large core or difficult anatomy,” Al Kasab said, discussing the registry’s findings regarding stenting numbers across different sites. “But, here, there seems to be a pattern where some sites are heavy on stenting and some sites do not stent at all. Some sites stented zero patients with ICAS-LVO while some sites stented almost every ICAS-LVO patient.”
Touching in greater detail on data from the 260 patients who received an MRI within 24 hours, the presenter reported that the median final infarct volume was “significantly smaller” in the stenting group, adding that—as per mediation analyses—almost 50% of the effect of stenting on functional independence could be attributed to these lower 24-hour infarct volumes on MRI.
When assessing the registry’s primary endpoint across different intervention types, the investigators found that balloon angioplasty alone (25%) was associated with a similar rate of 90-day functional independence compared to thrombectomy alone (29%), while self-expanding stents (44.3%) and balloonmounted stents (42.7%) both achieved statistically higher rates of functional independence.
or occlusion location. However, patients in the stenting group were less likely to be non-Hispanic white (51.8% vs 62.4%; p=0.03), and less likely to have diabetes (33.2% vs 43.1%; p=0.037) or hyperlipidaemia (43.2% vs 56%; p=0.009).
Moving on to the registry’s key findings, he commented that patients in the non-stenting group saw a higher rate of intravenous thrombolysis
Via prespecified interaction analyses, Al Kasab and colleagues also determined that their aforementioned results favouring stenting remained consistent across occlusions located in the anteriorand posterior-circulations, and also with versus without the use of intravenous antiplatelets.
“This is a real-world, observational registry and prone to known bias—we need randomised data to look at the safety and efficacy of rescue stenting,” Al Kasab concluded.
Alongside Al Kasab’s presentation at the SVIN meeting, findings from RESCUE-ICAS have also been published in the journal Stroke
While intracranial atherosclerotic disease (ICAD) is often cited in the context of its greater prevalence among patients in parts of Asia, discussions at the 2024 BRAIN conference (2–4 December, London, UK) emphasised its relevance as an underlying and also underaddressed cause of ischaemic stroke across many global regions.
“IF WE CAN TACKLE THIS, AND if we can get this right in the next twoto-three years, it’s going to be a big win for us,” BRAIN conference director Paul Bhogal (Royal London Hospital, London, UK) told NeuroNews, also commenting that ICAD is “absolutely” a globally relevant stroke aetiology.
Leonard Yeo (National University Health System, Singapore) was one of multiple speakers to highlight how “widespread” ICAD is across stroke populations, noting that it has a higher prevalence in Asian patients but is “not insignificant” among Caucasian patients. He relayed that current data suggest ICAD is present in 10% of Caucasian patients with ischaemic stroke, compared to 20–30% of patients across Asia and at least 40% in those in China specifically.
In addition, Yeo outlined a number of studies that have attempted to pinpoint the prevalence of symptomatic ICAD within specific countries, with research papers from 2014 indicating rates of
36% and 21.9% in India and Japan, respectively, and analyses from earlier on in 2024 suggesting a frequency as high as 25.2% in Brazil.
“We are seeing it more—because we are now looking for it more—in Europe too,” said Tommy Andersson (Karolinska University Hospital, Stockholm, Sweden), who moderated the day’s first ICAD-focused session.
A later talk from Osama Zaidat (Mercy Hospital, Toledo, USA) helped to expand on this further. Citing a 2024 paper in the journal Stroke, Zaidat noted worldwide ICAD prevalence ranging from 56% in South Korea, 54% in Singapore, and 47% in Thailand, to 16% in Europe and 12% in the USA.
“I have been doing this for years and years, and it is a challenging disease,” he added, detailing that rates of ICAD recurrence are 10 times those seen in atrial fibrillation, before also asserting that “what’s really missing” from the current appreciation of ICAD is the fact
Fluid dynamics modelling elucidates role of blood flow impairment in symptomatic ICAS
Via computational fluid dynamics models, a recent study has offered insights into the relevance of balancing two key mechanisms of haemodynamic deterioration—plaque burden and compromised perfusion—with regard to blood pressure management in symptomatic intracranial atherosclerotic stenosis (ICAS) patients.
“THIS RESEARCH ELUCIDATES THE ROLE of haemodynamic impairment of blood pressure in symptomatic ICAS-related stroke mechanisms, underscoring the necessity to conduct haemodynamic assessments when managing blood pressure in symptomatic ICAS,” write study authors Haiqiang Qin, Zixiao Li (both Capital Medical University, Beijing, China) et al, concluding the publication of their findings in the journal Stroke In a subsequent commentary article—also published in Stroke—Giuliana Pollaci (Fondazione IRCCS Istituto Neurologico Carlo Besta, Milan, Italy) states that haemodynamic impairment may have a “significant influence” on the mechanisms behind strokes of atherosclerotic origin, and describes the role of blood pressure in determining ICAS-related haemodynamics as a “double-edged sword”.
“If high, luminal stenosis could generate differences
that “not all lesions are the same”. “We are lumping them [in] together, but I think they are different.”
The session also saw Rashmi Saraf (King Edward Memorial Hospital, Mumbai, India) deliver insights on prevalence and treatments across the Indian subcontinent, corroborating the study cited by Yeo in stating that 25–35% of her home country’s hyperacute stroke cases appear to be caused by underlying ICAD—a rate that is currently increasing in younger patient populations. She went on to report that roughly 2,000–2,500 angioplasties and stenting procedures are performed each year in India.
“We can’t wait just on medical management at our [high-volume] centre,” Saraf averred. “We are much more aggressive in treating them with angioplasty and stenting compared to the rest of the world, given the more extensive lesions with higher rates of recurrence.”
Insights presented by Davor PavlinPremrl and Bruce Campbell (both University of Melbourne, Melbourne, Australia) revealed that, in Australia—a country thought to have a relatively low prevalence of underlying ICAD—the majority of cases are seen in patients with European ancestry.
The first day of the conference also saw Ameer Hassan (Valley Baptist
in pressure across the proximal and distal ends of a plaque, contributing to the mechanical burden on the area of plaque, whereas low blood pressure may compromise blood flow,” Pollaci explains. “Due to this double role, to unravel the relationship between blood pressure and mechanisms of ICAS-related stroke, it is necessary to study regional ICASspecific blood pressure profiles considering regional haemodynamics.”
Qin, Li et al note in their initial research article that—in an attempt to elucidate the potentially “crucial” role haemodynamic impairment of blood pressure could play in symptomatic ICAS-related stroke mechanisms—they performed computed fluid dynamics modelling using the Newton-Krylov-Schwarz method across 339 symptomatic ICAS patients in the third China National Stroke Registry from 2015 to 2018.
The authors relay that—as per the major outcome measures of their study—a total of 184 cortexinvolved infarcts (54.3%) and 70 borderzone-involved infarcts (20.6%) were identified. They also report that
This study includes the largest cohort of patients with symptomatic ICAS to undergo [computational fluid dynamics] analysis with an individualised boundary condition to date.”
Giuliana Pollaci
Medical Center, Harlingen, USA) relay that ICAD is more common than many people assume in parts of the USA, attributing much of the 30% rate he observes at his centre to Texas’ “very large” Hispanic population. As was borne out through much of the discussion at BRAIN 2024, Hassan reiterated that ICAD is a “problem area” in stroke treatment, with a lack of descriptive autopsy studies and effective animal models being among numerous contributing factors. The speaker commented that, in spite of this, the majority of neurovascular companies do not seem to feel ICAD represents a significant enough market to truly prioritise when it comes to product development.
However, Hassan—along with Zaidat and others—was keen to emphasise that “we need better devices” in order to deliver more effective and individualised treatments in stroke patients with ICAD. Some of the novel technologies currently being investigated in this space were showcased at BRAIN, with Satoshi Tateshima (University of California Los Angeles Medical Center, Los Angeles, USA) presenting a first-in-human (FIH) trial involving a self-expandable, temporary dilation system (TG Medical) and Andersson taking to the podium to discuss a stent device designed explicitly with ICAD cases in mind (Ceroflo).
multivariable logistic analysis revealed a correlation between the upper quartile of translesional systolic blood pressure (SBP) drop and an increase in cortexinvolved infarcts (odds ratio [OR], 1.92; 95% CI, 1.03–3.57), and a potential correlation between the lower quartile of post-stenotic mean arterial pressure (MAP) and an increase in borderzone-involved infarcts (OR, 2.07; 95% CI, 0.95–4.51). Furthermore, the investigators found a negative correlation between SBP drop and post-stenotic MAP (p<0.001).
“In generating haemodynamic impairment, simulating blood pressure modifications suggested that ensuring adequate blood pressure to maintain sufficient post-stenotic MAP appears preferable to the reverse approach, due to the prolonged plateau period in the association between the translesional SBP drop and cortex-involved infarcts, and the relatively short plateau period characterising the correlation between post-stenotic MAP and borderzone-involved infarcts,” Qin, Li et al detail.
The researchers conclude that, while blood pressure management in these patients “poses challenges”, their findings provide further insights and may therefore equip clinicians with more effective strategies for addressing this issue via a haemodynamic approach.
“Future research is encouraged to investigate the causal links between the haemodynamic impairment of blood pressure and stroke events in symptomatic ICAS,” they add. “Additionally, investigations into how haemodynamic impairment interacts with plaque features and collateral circulation are also warranted.”
“This study includes the largest cohort of patients with symptomatic ICAS to undergo [computational fluid dynamics] analysis with an individualised boundary condition to date,” Pollaci avers, also suggesting that future studies with a “comprehensive approach” to refining the understanding of this phenomenon are needed.
Paul Bhogal
MEMBRANE becomes latest RCT to demonstrate MMA embolisation’s benefits in cSDH treatment
The MEMBRANE randomised controlled trial (RCT)—presented at the 2024 Society of Vascular and Interventional Neurology (SVIN) annual meeting (20–22 November, San Diego, USA) by Ansaar Rai (West Virginia University Rockefeller Neuroscience Institute, Morgantown, USA)—has produced fresh evidence on the benefits offered by middle meningeal artery (MMA) embolisation as an adjunct to the current standard of care in chronic subdural haematoma (cSDH) patients.
“The MEMBRANE randomised clinical trial met its primary effectiveness endpoint, showing a significant, positive treatment effect in favour of Trufill n-BCA [Johnson & Johnson MedTech Neurovascular] for middle meningeal artery embolisation over standard of care,” Rai said. “The odds ratio favoured MMA embolisation in both the surgical and non-surgical cohorts, and the treatment effect was significantly higher in the larger, surgical cohort, with a clear positive trend in the smaller, non-surgical cohort. Based on the functional outcome analysis at three months, Trufill n-BCA was non-inferior to standard of care—and it almost achieved superiority.”
With Rai and Christopher Kellner (Mount Sinai Health System, New York, USA) as co-principal investigators (PIs), the prospective, multicentre, open-label MEMBRANE RCT enrolled a population of 376 cSDH patients to evaluate the safety and effectiveness of MMA embolisation with the Trufill n-BCA liquid embolic agent. Its primary effectiveness endpoint was twofold: residual cSDH or re-accumulation (>10mm) at six months, or reoperation or surgical cSDH treatment within six months post-randomisation. The study’s primary safety endpoint was the occurrence of any adverse events through six months, while good functional outcomes at three months, mean change in haematoma volume, development of new seizure onset and modified Rankin scale (mRS) distribution change were among several secondary endpoint measures.
From a total of 376 enrolled patients, 265 were randomised to receive surgical treatment and 111 were assigned to non-surgical medical management. Further randomisation within these groups saw 133 patients allocated to surgery plus MMA embolisation (treatment arm) and 132 allocated to surgery only (control arm), while 55 were assigned to non-surgical management plus MMA embolisation (treatment arm) and 56 were assigned to non-surgical management only
(control arm). Some 225 patients in the surgical management group and 78 in the non-surgical medical management group completed the study’s six-month follow-up visit and were therefore able to be included in intention-to-treat analyses. Enrolment in the study took place across 28 US sites as well as two centres in China.
Regarding demographic and baseline characteristics of the study population, Rai noted an average age of roughly 70 years, a predominance of male gender, and headache being the most common presenting symptom. He also highlighted the fact that about one quarter of the patients in MEMBRANE were on antithrombotic medications. In terms of haematoma characteristics, there was an even distribution between left- and right-sided target cSDHs, and a mean haematoma thickness close to 15mm in the surgical cohort versus around 16mm in the non-surgical cohort. Rai further commented that, “as expected”, the average midline shift was “much higher” in the surgical group.
“Procedural information showed that the majority of patients’ procedures— almost 85%—were performed under general anaesthesia,” he added.
“Radial access was used in about half of the cases. Target embolisation was achieved in almost 99% [of cases] in the surgical and 100% in the non-surgical cohorts. For surgical procedures prior to randomisation, the most common was burr-hole, followed by craniotomy, followed by SEPS [subdural evacuating port system] and other drains.”
Positive results
Arriving at MEMBRANE’s primary effectiveness endpoint, the presenter noted a significant and positive treatment effect in favour of MMA embolisation versus standard of care, detailing a common odds ratio (OR) of 0.529 (90% confidence interval, 0.308–0.909) indicating that the failure rate in the embolisation group was almost half of the rate seen in the non-embolisation group. As such, the trial was deemed to have successfully met its six-month follow-up primary endpoint.
In addition, while not individually powered to show treatment benefits, primary effectiveness endpoint results by cohort revealed ORs suggesting favourable outcomes with MMA embolisation versus standard of care in both the surgical management and nonsurgical medical management arms of the study. This trend reached statistical significance in the surgical cohort (OR, 0.475) but not the non-surgical cohort (OR, 0.615), Rai reported. As per the primary effectiveness endpoint, failure rates across the study arms were as follows: 8.5% with surgery plus embolisation; 20.2% with surgery only; 20% with non-surgical medical management plus embolisation; and 27% with non-surgical medical management only.
Primary safety endpoint results across 371 eligible patients showed a “fairly similar and even distribution” of all adverse events between the embolisation and non-embolisation groups at six months, according to Rai. There was a 3.3% rate of procedure-related serious adverse events and a 2.2% rate of device-related serious adverse events across 181 patients who received MMA embolisation. In addition, the rate of all strokes—either minor or major—was between 2–3% in both the embolisation and non-embolisation cohorts.
a positive trend favouring MMA embolisation in the surgical arm.
“The primary effectiveness endpoint subgroup analysis by age showed that there was a treatment effect in all age groups, across all [study arms], but the most significant treatment effect was in patients over the age of 75 in the surgical cohort,” Rai commented. “This represents the most vulnerable population, with large haematomas that require surgical evacuation, and adjunctive MMA embolisation was found to have the strongest treatment effect in this age group.”
Regarding one of MEMBRANE’s key secondary endpoints, Rai stated that three-month good functional outcomes—meaning an mRS score of
The [eventual] eligible population is estimated to be potentially larger than large-vessel strokes.”
0–2 or a score that did not worsen in patients with a baseline mRS of 3— were observed in 85.3% of patients who received embolisation compared to 77% in patients who received surgical or non-surgical management alone. He went on to relay that, as such, MMA embolisation was deemed statistically non-inferior to the standard of care and—owing to a non-inferiority margin of –0.12 and a risk difference of 0.073—the treatment “almost achieved superiority”.
Further ‘as-treated’ analyses of mRS distribution changes revealed that allcause mortality was “much lower” in the trial’s embolisation arm (4%) versus the non-embolisation arm (12.4%), and six-month mRS shift analyses— while not statistically powered—found
Touching on three additional secondary effectiveness endpoints from MEMBRANE, the presenter reported a higher rate of complete cSDH resolution with MMA embolisation, compared to both surgical and nonsurgical management alone, as evaluated by an independent core laboratory at three and six months. Rai also relayed that rebleeding probability rates—assessed in the same way—were shown via KaplanMeier curves to be lower in patients undergoing MMA embolisation, adding that rebleeding was most common in the first three months post-randomisation when it did occur. Finally, he reported a “much lower” rate of surgical reoperation in the trial’s MMA embolisation groups, with reoperations that were required typically taking place within three months as well.
Wider context
“The question that was asked— similarly to the other trials—was whether MMA embolisation has a role [to play] in the treatment of chronic subdural haematomas,” Rai noted, providing additional context on the study.
“The reason this question is important is because we have a growing patient population; the fastest-growing segment of our society is the over 65s. And, the incidence and prevalence of subdural haematomas in this population is increasing. We know it’s one of the most common neurosurgical diagnoses […] and leads to a cascade of disability. The [eventual] eligible population is estimated to be potentially larger than large-vessel strokes.”
Its presentation at SVIN 2024 saw MEMBRANE join three other RCTs— EMBOLISE, STEM and MAGICMT—in demonstrating positive findings with liquid embolic agentbased MMA embolisation in cSDH patients.
Having initially been showcased at the 2024 International Stroke Conference (ISC; 7–9 February, Phoenix, USA), these studies were all published in the New England Journal of Medicine late last year.
Ansaar Rai
SIMONA SACCO
Fuelled by a passion for research, and inspired by a “heartbreaking” case she encountered early on in her career, Simona Sacco (L’Aquila, Italy) has made a number of significant contributions to the neurology field—perhaps most prominently through her current tenure as president of the European Stroke Organisation (ESO). Here, Sacco—professor of neurology at the University of L’Aquila and director of the Neurology and Stroke Unit at Avezzano-SulmonaL’Aquila Hospitals—discusses her key mentors, the current landscape of stroke and migraine management, and much more.
What initially attracted you to medicine, and the field of neurology specifically?
My father is a doctor, and he really encouraged me to pursue a career in medicine. I’ve always been fascinated by how the brain works, and neurology was the perfect field to fuel my passion for research. When I started out, the brain was a big mystery, and—while we understand a lot more now—it still holds many secrets. I also love clinical neurology because it’s all about clinical reasoning— listening to patients’ histories, doing physical exams, and piecing together even the smallest clues to arrive at a diagnosis. It’s like solving an intriguing puzzle every day, blending solid science with the chance to make a real difference in people’s lives. That’s what keeps me excited about my work.
Who have your mentors been and how have they impacted your career?
My mentor was Antonio Carolei, the former chair of my current department. He played a pivotal role in shaping my career, teaching me far more than just neurology. He instilled in me the importance of being methodical, paying attention to details, thinking outside the box, standing up for my ideas, and always acting with dignity and integrity. He also gave me invaluable opportunities and pushed me to step outside my comfort zone, even when it was difficult. These experiences were instrumental in shaping both my professional and personal growth.
Beyond this formal mentorship, I have been fortunate to work alongside and learn from exceptional leaders in the fields of stroke and headache. Collaborating with experts such as Messoud Ashina, Paolo Calabresi, Martin Dichgans, Urs Fischer, Peter Kelly, Paolo Martelletti, Else Charlotte Sandset, Cristina Tassorelli, and many others, has been an extraordinary privilege. Each of them has been a role model and, by observing and working with them, I have gained invaluable insights that have shaped my own leadership style. I feel truly lucky to be part of such an inspiring and supportive community.
Could you outline your major achievements and other highlights from your time as ESO president?
My time as ESO president is still ongoing— with more than one year left to go—so I haven’t reached all my goals yet. However, I’m proud of the work we’ve started and the direction we’re heading. At ESO, I’m committed to upholding our high ethical and quality standards while pushing forward our main programmes. One of our key initiatives is the Stroke Action Plan for Europe (SAP-E),
an ambitious programme aimed at improving stroke prevention, treatment, and life after stroke, by 2030. This effort requires a lot of energy and resources, and I’m excited to be part of it. I’m also working on shaping policies to improve stroke prevention through advocacy and partnerships with other societies. On top of that, education is very important to me. I’m dedicated to creating a welcoming and open environment where everyone who wants to contribute can help ESO grow and succeed.
Based on your experience, do you have any advice for future leaders of the ESO and other societies in the field of stroke care?
For future leaders in stroke care, my advice is to stay dedicated to the cause and be prepared for a significant time commitment. Always keep patients at the forefront—improving their healthcare should be your biggest priority. Investing in the education and growth of younger professionals is key as well as working on implementation of best practices without disparities. Stay vigilant, hold yourself to the highest ethical and behavioural standards, and actively seek out dialogue and collaborations. Above all, have a clear vision of where you want to take your society, and try to look ahead of times to anticipate what’s coming next.
What do you feel has been the most important development in the field of neurology during your career?
Neurology has changed in ways that were hard to imagine when I first started. We’ve gone from limited tools to an era where we can diagnose diseases more precisely thanks to biomarkers and imaging breakthroughs. In stroke care, the introduction of reperfusion therapies, like thrombectomy and thrombolysis, has completely changed the game. These treatments save lives and significantly improve recovery outcomes, something we couldn’t achieve decades ago. What’s exciting is that we’re not stopping here—new treatments and technologies are in the pipeline that could make an even bigger impact. It’s been incredible to witness this transformation, and it feels like we’re only scratching the surface of what’s possible in neurology.
Which of the studies you have been involved with do you believe has had the greatest impact on stroke care?
I believe the most impactful contributions I’ve made are my epidemiological studies. By examining stroke patterns and outcomes in the population, these investigations have
helped clarify both our progress to date and the areas where we still have work to do. That information is essential for guiding improved prevention strategies, tailoring treatment approaches, and ultimately helping us shape more effective healthcare policies.
Besides your own work, what is the most interesting piece of stroke research you have seen in the past year?
FACT FILE
CURRENT APPOINTMENTS
Full professor of neurology, University of L’Aquila
Director, Neurology and Stroke Unit, Avezzano-SulmonaL’Aquila Hospitals Director, residency programme in neurology, University of L’Aquila
EDUCATION
2005–2007: Master in cerebrovascular diseases, University of L’Aquila
1999–2004: Specialisation in neurology, University of L’Aquila
1993–1999: Degree in medicine and surgery, University of L’Aquila
HONOURS (SELECTED)
2024–2026: President, European Stroke Organisation
2021–2023: Second vice president, European Headache Federation
2019–2022: Chair, Research Center, Italian Headache Society
2018: Outstanding Reviewer Award, Stroke journal
2016–2019: Member, Scientific Panel for Stroke, European Academy of Neurology
One of the most intriguing areas of stroke research in the past year revolves around intracerebral haemorrhage (ICH). For years, this condition has lacked any effective treatment, which has been a significant challenge in stroke care. However, recent studies are offering new hope. The concept of a ‘bundle of care’ has emerged as a promising approach. This method focuses on optimising several aspect of care for ICH patients, from blood pressure management and reversal of anticoagulation to stroke unit care and early rehabilitation.
While it may seem straightforward, the strength of this approach lies in its comprehensive and systematic application. Early results suggest that, even without a single definitive treatment, adhering to these evidence-based care bundles can significantly improve outcomes for patients. As we learn more about ICH pathophysiology and refine treatment strategies, these care bundles could eventually be paired with new targeted therapies to further improve survival and recovery rates.
Currently, what are the most pressing unmet needs in clinical research and care for headache?
In recent years, we’ve witnessed a major breakthrough in migraine treatment with the advent of the first preventive therapies targeting the calcitonin gene-related peptide (CGRP) pathway. These treatments have been life-changing for many patients, significantly reducing their migraine frequency and severity. However, they don’t work for everyone, and even some of those who benefit may have a substantial residual migraine burden.
Migraine is an incredibly complex disease. While CGRP is a key player, it’s clear that other important mechanisms are also involved. To truly address the unmet needs in migraine care, we need to dig deeper into these alternative pathways. Promising targets like pituitary adenylate cyclase-activating polypeptide (PACAP) are already in the pipeline, but we need a much broader range of specific treatment options. Expanding our understanding of migraine mechanisms and developing diverse, targeted therapies are essential steps toward personalised and effective treatment for all patients. Only by addressing this complexity can we hope to reduce the burden of migraine across the board.
What is your involvement in the Global Burden of Diseases (GBD) project, and why is this project important?
My involvement in the GBD project has been exciting. I collaborate by analysing and interpreting the data, especially for conditions like stroke and migraine. This project is a gamechanger because it not only shows us how widespread these conditions are, but it also provides essential insights that help us plan current and future care services. The
data and projections from GBD are crucial for shaping healthcare policies and ensuring that resources are directed where they’re most needed. Being part of this project gives me the opportunity to contribute to a better understanding of neurological diseases on a global scale and to advocate for improvements in public health.
Could you describe one memorable case and the effect it had on you as a physician?
Early in my career, while working in a rehabilitation facility, I encountered a case that profoundly shaped me as a physician. A young, healthy patient had suffered a vertebral artery dissection that led to locked-in syndrome. She was unable to move or speak but was fully conscious—a heartbreaking condition. Tragically, she hadn’t received revascularisation treatment because she lived in an underserved area where access to advanced stroke care was limited. This case left a deep impression on me. It highlighted the devastating consequences of inequities
in healthcare and inspired me to dedicate my energy to improving stroke care for everyone, regardless of where they live. It became my driving force to push for better access, more awareness, and advancements in stroke prevention and treatment. Her story is one I carry with me to this day, reminding me why the fight for equitable healthcare is so important.
What are your interests outside medicine?
I absolutely love travelling. It’s amazing to discover new places, cultures, and food. I particularly love nature and people. I also enjoy spending time with my daughters (Maria Stella and Anna), my husband (Mario), and our lovely cat (Leo). On top of that, I’m into reading books, hanging out with friends, and going to parties—especially if there’s dancing involved!
Of all the countries you have travelled to, which is your favourite?
It’s hard to choose just one, but I have a
“Neurology has changed in ways that were hard to imagine when I first started.”
special place in my heart for Vietnam. I love it for its beautiful nature and incredible landscapes, which are simply breathtaking. The rich culture and the kindness of the people really stand out to me. It’s also fascinating and touching to learn about the stories of the Vietnam War, and to see the deep, lasting marks it left on the country and its people. Experiencing everyday life in Vietnam is equally compelling—there’s a strong, unique identity there that makes every visit unforgettable.
What do you think you would be doing for a living today if you had not chosen a career in medicine?
It’s hard to say for sure. I tend to love whatever I do, and I find passion in many different areas. Photography, for example, really attracts me. I can easily imagine myself as a street photographer, capturing the rich tapestry of human life and the diverse cultures around us. The idea of telling stories through images and exploring the world from that creative angle is something that really resonates with me.
SELECT LATE trial gets US$7 million funding boost to evaluate stroke thrombectomy beyond 24 hours
University Hospitals (UH) Cleveland Medical Center in Cleveland, USA has been awarded US$7 million in research funding by the Patient-Centered Outcomes Research Institute (PCORI) to evaluate endovascular thrombectomy in patients presenting more than 24 hours from time last known well via the global SELECT LATE clinical trial. Amrou Sarraj (UH Neurological Institute, Cleveland, USA) will lead the study, which aims to provide deterministic evidence of a clinical benefit with the addition of thrombectomy to standard medical care in this patient population.
SARRAJ AND COLLEAGUES WILL CONDUCT the study across sites in the USA, Canada, Europe, Australia and New Zealand, assessing the benefits and risks of thrombectomy for patients who present to the hospital beyond the usual 24-hour timeframe for treatment by randomly assigning them to receive either thrombectomy or standard medical care. The researchers will compare how well patients in each
group respond in terms of functional independence— as per ability to perform day-to-day tasks without help from others—and quality of life as identified by the patients.
Based on Get With The Guidelines data, only about 10% of patients presenting with a large vessel occlusion later than 24 hours currently receive thrombectomy treatment.
“[The] thrombectomy procedure has revolutionised how we treat patients with acute ischaemic stroke due to occlusion in one of the larger brain vessels,” said Sarraj, principal investigator for the SELECT LATE trial. “However, the current evidence of efficacy and safety is limited to those presenting within 24 hours of when they were last known to be without symptoms. For patients who present beyond this timeframe, a lack of randomised evidence prevents us from treating them universally with this state-of-the-art technology that is shown to improve stroke outcomes by two to three folds. We expect this to help many patients; those who live alone without early recognition of their symptoms, especially the elderly, and patients who do not have prompt access to thrombectomy centres.”
The trial aims to reduce treatment disparities in elderly patients who live alone, and also those living in rural and remote communities. These patients often do not have timely access to healthcare, resulting in delayed presentation and potential disqualification from receiving this treatment.
Following the recent success of Sarraj and colleagues’ SELECT2 trial—which established efficacy and safety of thrombectomy in patients presenting with large strokes—Nicholas Bambakidis (UH Neurological Institute, Cleveland, USA) feels this is the next step in the evolution of acute stroke management.
First prospective Indian thrombectomy registry shows high revascularisation rates and confirms procedure is cost effective
Data from a registry claimed to be the first prospective registry on mechanical thrombectomy for stroke in India have revealed a number of key insights on how this treatment is being implemented across the country. High revascularisation rates and good functional outcomes, as well as workflow metrics that are “comparable” with those seen in other geographies, are among researchers’ most notable findings.
PRESENTING THESE DATA from the Indian PRAAN registry at the 16th World Stroke Congress (WSC; 23–26 October 2024, Abu Dhabi, United Arab Emirates), Jeyaraj Pandian (Christian Medical College and Hospital, Ludhiana, India)—who recently became the World Stroke Organization (WSO) president—and WSO board of directors member PN Sylaja (Sree Chitra Tirunal Institute for Medical Sciences and Technology, Trivandrum, India) initially highlighted the low overall utilisation of stroke thrombectomy in India. They cited high procedure costs, a lack of sufficient numbers of interventionists, and availability of only a few cath labs in the country, as the main drivers of this.
“With the current incidence of stroke [in India], we need to do more than 100,000 thrombectomies in a year—but we are doing fewer than 3,000–4,000,”
Sylaja said, speaking to NeuroNews
With this in mind, the prospective, multicentric, observational PRAAN registry was set up with the intention of studying patient characteristics, systems of care and functional outcomes associated with thrombectomy treatment in Indian patients with large vessel occlusion (LVO) acute ischaemic stroke. More specifically, the registry includes stroke patients treated with the Solitaire X revascularisation device and/or the React catheter (both Medtronic) as the primary devices used. It has enrolled patients undergoing thrombectomy with stroke onset less than 24 hours from time last known well; Alberta stroke programme early computed tomography score (ASPECTS) >5; core infarct volume <70ml on non-contrast CT (NCCT) or diffusion-weighted magnetic resonance imaging (DW-MRI); and National Institutes of Health stroke scale (NIHSS)
“University Hospitals and Case Western Reserve University [Cleveland, USA] have always been at the forefront of medical advances,” Bambakidis stated. “The SELECT LATE global trial will have a tremendous impact on acute stroke management, not only individually but also in terms of how we organise stroke systems of care.”
“We expect a major impact on systems of care and the current patients’ transfer practice, since these patients are vastly not being considered for transfer [to a] higher level of care and consideration of thrombectomy,” Sarraj added.
The SELECT LATE study was chosen via PCORI’s competitive review process in which patients, caregivers and other stakeholders join scientists to evaluate proposals. Sarraj and colleagues’ award has been approved pending completion of PCORI’s business and programmatic review, and issuance of a formal award contract.
The SELECT LATE global trial will have a tremendous impact on acute stroke management, not only individually but also in terms of how we organise stroke systems of care.”
Nicholas Bambakidis
scores ≥6. An independent core lab and clinical events committee (CEC) assessed patient outcomes in the registry.
Pandian and Sylaja reported that, from August 2021 to October 2023, 200 patients were enrolled at 14 sites—of which 190 patients with an average age of just under 60 years met the eligibility criteria for PRAAN. The investigators relayed that, of these patients, 131 were treated using the Solitaire stent retriever, 19 were treated via aspiration thrombectomy using the React catheter, and 40 received a combined approach involving both Solitaire and aspiration. They also found that the majority of LVOs included in the study (55.3%) were M1 occlusions in the middle cerebral artery (MCA).
Regarding more safety-centric outcome measures, the investigators observed a 2.1% rate of symptomatic intracranial haemorrhage (sICH) and a 6.3% rate of all-cause mortality across the full population of 190 patients.
Finally, Pandian and Sylaja reported that the majority of the 190 patients in the present registry (80%) were discharged home following their thrombectomy procedures and also relayed that—while the treatment is expensive—it was found to be cost effective overall.
Pandian, Sylaja and colleagues ultimately found that these 190 patients experienced a median door-to-groinpuncture time of 99 minutes (range, 11–478), as well as a median groinpuncture-to-revascularisation time of 40 minutes (range, 10–170). In addition— and perhaps even more notably—the rate of successful revascularisation characterised by a modified thrombolysis in cerebral infarction (mTICI) grade ≥2b was 90.7% across a total of 184 patients, while functional independence defined as a 90-day modified Rankin scale (mRS) score of 0–2 was 65.8% based on a cohort of 187 patients.
“In spite of all the barriers to acute stroke treatment in India, this prospective registry was able to show that the performance metrics of [thrombectomy] and the functional outcomes at 90 days were similar to what has been reported globally,” Sylaja told NeuroNews
“Although this treatment is expensive, it is cost effective. This highlights the need of having more endovascular thrombectomy centres in India, and government reimbursement of this treatment, so that it will be available to all. Since LVO in acute ischaemic stroke leads to severe strokes, this life-saving treatment can reduce the burden of disability due to stroke.”
On a similar note, Pandian stated that, in his view, the main take-home message from this registry should be the positive patient outcome data, which are better than many previously reported figures.
Jeyaraj Pandian PN Sylaja
“The race is on”: Enthusiasm over neuroprotection endures despite historic failures
“The race is on—don’t miss the bus!”, were the words of David Liebeskind (University of California Los Angeles Health, Los Angeles, USA) as he discussed the apparent promise of cytoprotection in acute ischaemic stroke care during a session at the 2024 Society of Vascular and Interventional Neurology (SVIN) annual meeting (20–22 November, San Diego, USA).
“Ipredict that there is a coming revolution in cytoprotection,” Liebeskind stated. “And, my opinion is that we’re not going to have one drug; we’re going to have many drugs in the future. There are a lot of groups—at least 12–18 companies— that are doing or planning to do trials in the very near future.”
The rollercoaster ride that neuroprotection for stroke has been over the past few decades was exemplified on the second day of SVIN 2024. Opening a session devoted to this topic, Patrick Lyden (University of Southern California, Los Angeles, USA) highlighted the more than 1,000 different neuroprotective candidates that have garnered excitement and shown early promise before ultimately proving to be futile in improving stroke outcomes once evaluated in larger clinical trials.
Lyden also drew attention to the “landmark moment” represented by SAINT II—a randomised trial published in 2007 that, having deemed the neuroprotectant NXY-059 ineffective in the treatment of acute ischaemic stroke patients, appeared to extinguish any remaining hope for the field.
But, as Lyden put it, the stroke research community “took a breath”, regrouped, and—with a collective mindset now focused on the concept of ‘cerebral cytoprotection’ and preserving the whole brain rather than ‘neuroprotection’ paradigms revolving around only the central nervous system (CNS)—pressed forward. And even additional, more recent neutral findings in trials like ESCAPE-NA1 and ESCAPE-NEXT with Nerinetide (NoNO Inc), and MASTERS-2 with MultiStem (Athersys), have done little to dampen overall enthusiasm across much of the community.
New approaches
Prevailing criticisms levelled at these and many other failed neuroprotection studies relate to trial design. Michael Hill (University of Calgary, Calgary, Canada) addressed this in a later talk speculating on the ‘ideal’ clinical study of a given neuroprotective candidate.
Hill initially drew attention to the wide array of reasons why stroke patients may experience negative outcomes despite receiving neuroprotection therapy—with age, socioeconomic status, stroke severity, comorbid illness, delayed treatment, choice of anaesthesia technique, poor adherence, lack of follow-up, haemorrhagic events
I predict that there is a coming revolution in cytoprotection.”
David Liebeskind
and other complications being among the many potential contributing factors.
Homing in on problems surrounding poor outcomes further down the line, Hill also argued that—as neuroprotection is an acute treatment— these late outcomes can be ameliorated by achieving better early outcomes. And, with regard to trial design in particular, he highlighted the need for appropriate patient selection, noting that the emerging concept of premorbid frailty could serve to mediate outcomes in future studies.
Hill echoed points made by both Lyden and Liebeskind on the importance of switching gears from neuroprotection to cytoprotection moving forward, as the latter is more comprehensive and represents a more appropriate definition for many of the therapeutic candidates being
investigated today. Two of these candidates were discussed in detail during the same session at SVIN 2024. Initially, Marc Ribo (Vall d’Hebron University Hospital, Barcelona, Spain) provided an update on the APRIL trial, which has indicated the safety and tolerability of the drug ApTOLL (AptaTargets) when administered as an adjunct to mechanical thrombectomy for acute ischaemic stroke. Later in the session, Tareq Kass-Hout (University of Chicago, Chicago, USA) outlined the potential benefits of rapid intravascular hypothermia in combination with thrombectomy, as per randomised data from the RECCLAIM II study.
According to Hill, while alternative agents including edaravonedexborneol—a ‘free radical scavenger’—and butylphthalide—a celery-seed extract—have been approved for use in some Asian countries for many years, the evidence for these compounds in the more modern era of reperfusion therapy is much less certain. Other approaches currently being explored include
The SAINT II trial in 2006 was a landmark moment.”
Patrick Lyden
normobaric hyperoxia and remote ischaemic conditioning.
Uncertainty or optimism?
The encouraging yet still unclear future of this space was perhaps most apparent at the beginning and end of Hill’s presentation on the ideal neuroprotection trial, as he opened by stating, “I don’t know the answer”, before closing with a similar sentiment and adding that “I don’t think there is a perfect pathway as yet”.
In Hill’s view, while reperfusion has traditionally been the “mainstay” of treatment, it is entirely feasible that multiple different compounds and approaches may work, with many ideas currently being tested and retested, and the pathway to a positive clinical trial could vary depending on the drug in question.
“No, it’s not a reality yet,” Liebeskind added, drawing the session to a close. “Cytoprotection is not fully fledged in terms of approvals, and not ready for routine clinical practice in the USA. But, I think there is a revolution coming that started very recently— a parallel revolution to what’s happened in thrombolytics and endovascular therapy.”
Outlining a key lesson to be learned from the prior failures of neuroprotection trials, he stated: “My very strong opinion is that the starting point should be as an adjunct to thrombectomy. I would not mess around with studies that are nonadjunctive. It’s not that there won’t be a yield there, but it’s not the first order of business.”
Liebeskind went on to note that, over the past 18–24 months, there has been a “marked acceleration” regarding cytoprotection, leading to a “very rapidly growing” list of drugs progressing through early-stage evaluations.
“We have to be very careful in terms of the trial design but, that being said,
I don’t think there is a perfect pathway as yet.”
Michael Hill
in terms of the focus on adjunctive therapy [with thrombectomy] and the use of imaging, most companies and groups are aligned,” he continued.
“The methodology is being very quickly harmonised. I think there’s a lot of work that can be done and there are a lot of data that are available, but things are aligning.”
Providing an additional, parting message on this topic, Liebeskind asserted that “we need to use imaging” when evaluating cytoprotection therapies—specifically advocating cerebral blood volume (CBV) measurement, which has been somewhat “neglected” as a perfusion component despite its advantages versus Alberta stroke programme early computed tomography score (ASPECTS) in terms of predicting ischaemic lesion growth and cytoprotective dose calculations.
Reversible thrombolytic could alleviate US “tribalism” around tPA and help redefine stroke treatment
Following Basking Biosciences’ recent announcement that the first acute ischaemic stroke patients have received its novel thrombolytic therapy as part of the Phase 2 RAISE clinical trial, NeuroNews speaks to the company’s co-founder and chief medical officer—Ohio State University neurosurgeon Shahid Nimjee (Columbus, USA)—to find out what this milestone could mean for the future of stroke care.
“There’s only one drug that has been approved in stroke [in the USA],” Nimjee states, referencing the longstanding reliance on tissue plasminogen activator (tPA), also known as alteplase, in this space. “It got approved in 1995. But, it really doesn’t treat the majority of strokes. In the USA alone, we have 800,000 ischaemic strokes [each year], but national utilisation of tPA is at around 7%—about 50,000 patients—largely because it’s only usable up to 4.5 hours after stroke and there are worries over reversibility.”
In the broadest terms, tPA is indicated for ischaemic stroke, and often represents these patients’ best chance of avoiding disability and ultimately recovering from their symptoms. However, in the small but not insignificant subset of this population who experience brain bleeds following their stroke, giving tPA creates a vastly increased risk of mortality.
According to Nimjee, even the remarkable emergence and expansion of mechanical thrombectomy over the past decade— despite the procedure’s undeniably positive impact—fails to fully address the limitations surrounding stroke care today.
mechanism and expanding the therapeutic time window.”
What is ‘true’ thrombolysis?
“Thrombolysis as we know it today is really centred around fibrinolysis; if we break up fibrin, then we’re breaking open the clot,” Nimjee continues. “That’s based on analyses done in the 1980s from clots that were captured on the surface of heart valves during valve-replacement surgery. With thrombectomy, we’ve actually been able to analyse the clots in patients’ brains, and we’ve found that—unsurprisingly—clot composition is a lot more complex than just focusing on fibrin.”
“It only works for large vessel occlusion [LVO] stroke,” he states. “And, even once you take the clot out, and you look at the angiogram and say, ‘look what I’ve done, I’ve refilled the brain, everything’s perfect’, the majority of patients still do poorly [in terms of clinical outcomes]. It’s believed that this is because we haven’t dealt with the ‘microcirculation’—those small clots that you can’t see on imaging but are still there causing problems.”
Given the fact that there are no studies indicating that tPA is truly effective in breaking up these microcirculation clots, Nimjee believes now is the time to move away from “antiquated” perceptions of coagulation and focus on targeting “thrombosis as we know it today”.
“I think BB-031 represents a class of drugs that will have a significant impact in terms of breaking up blood clots,” he adds. “As a first indication, I would expect to see our drug be very effective in patients who present within 24 hours from the onset of their stroke. I also see a future where it can be used alongside tPA as a synergistic treatment, as long as the safety profile of giving both proves to be acceptable.”
“While existing thrombolytics have been a critical first-line treatment strategy for acute ischaemic stroke over the last three decades, very few patients benefit from this treatment—largely due to a limited time window and limited efficacy in certain clot types,” comments Basking scientific and clinical advisory board member Ashutosh Jadhav (Barrow Neurological Institute, Phoenix, USA), also speaking to NeuroNews. “BB-031 importantly addresses these gaps by targeting clot integrity with a novel
Central to many of these analysed clots, Nimjee relays, was von Willebrand factor (VWF). Another key advancement in the scientific community’s understanding has revealed that, while coagulation occurs on the surface of platelets, thrombosis itself is not a coagulation-centric process.
“So, something targeting platelets and something targeting the stuff that holds the platelets together is just as attractive—if not more attractive—than targeting individual clotting factors or fibrin alone,” he explains.
In the USA, where we have a very comprehensive infrastructure for stroke care, only 14.5% of patients who are having a stroke make it to a hospital within 4.5 hours to qualify for tPA. About 86% of patients don’t, and it’s that 86% of patients I care about, because they’re getting nothing [as things stand].”
Shahid Nimjee
As such, in an effort to more effectively break down blood clots, Nimjee and his colleagues have developed BB-031—a ribonucleic acid (RNA) aptamer designed to act as a highly specific antagonist to VWF, inhibiting and ultimately dismantling the VWF ‘mesh’
that binds together fibrin, platelets, collagen, red and white blood cells, and the many other constituents of a clot.
A reversible solution
This is unquestionably a novel approach to thrombolysis, and Nimjee is optimistic that BB-031 will ultimately prove to be at least as effective as established candidates like tPA and tenecteplase when it comes to clot degradation. However, the drug’s near-utopian promise of reversibility is the single characteristic that most significantly distinguishes it from anything previously seen in the world of clotbusting stroke medications.
“The idea of reversibility relates to one of the biggest problems with thrombolytics today: if you get a thrombolytic, you can bleed,” Nimjee says.
“And, with thrombolytics in the setting of a stroke— according to a 1995 paper—6.4% of patients will have an intracranial haemorrhage [ICH], and 40% of patients who have an ICH die, because there’s no way to reverse the drug. You can’t turn it off; it’s going to keep acting.”
Intravenous thrombolysis—despite being a broadly safe and effective treatment in many stroke patients—increases the likelihood of haemorrhagic complications and essentially precludes any subsequent endovascular procedures to fully remove the clot. Herein lies a key positive impact of a thrombolytic agent that is reversible and can safely be ‘turned off’ by administering a second drug: it makes a potentially life-saving mechanical thrombectomy a much more feasible option with a vastly reduced risk of bleeding.
“It’s very important to understand what reversibility means,” Nimjee asserts. “Some people will say that, if you give patients cryo[precipitate], that reverses alteplase or tenecteplase. That’s not true. What cryo does is provide more clotting factors compared to the milieu in plasma, to try and offset the effects of alteplase or tenecteplase—but that’s not reversibility.”
BB-031 is an RNA molecule that folds into a three-dimensional structure and binds to VWF to inhibit its activity. Once it has accomplished this (i.e. following clot thrombolysis), a second drug called BB-025—which has a nucleotide sequence that directly complements that of BB-031—is introduced, ‘unzipping’ the three-dimensional shape of the thrombolytic and effectively switching it off.
“It [BB-025] literally acts on the active drug to turn it off without perturbing your own coagulation system or thrombotic cascade,” Nimjee adds.
This reversal occurs “within minutes”, he also relays, citing findings from the multiple animal model studies in which Basking’s two leading drug compounds have been evaluated to date.
“If you give the drug [BB-031], you have complete abrogation of coagulation,” Nimjee expands. “And, if you give the drug, wait five minutes, and then give the reversal agent, and then wait two more minutes, it’s like you never gave the drug at all. With a bolus injection of BB-025, you have durable reversal of the activity of the [thrombolytic] drug compared to just giving the drug alone.”
Nimjee’s belief is that this reversal agent may help to extinguish some of the “tribalism” that currently surrounds tPA usage in the USA, as—rather than having “no recourse” if the patient bleeds—physicians will be able to administer a thrombolytic while safe in the knowledge that it can be reversed via a second drug, even if the patient does experience haemorrhagic complications.
“Then, a surgeon can take the clot out successfully, or we can go and get a hemicraniectomy, and we can do all the interventions we need to do because we’ve
Shahid Nimjee
turned the drug off,” he elaborates.
“While currently available thrombolytics are fairly safe, there can be post-treatment haemorrhagic complications that can be devastating with limited treatments and lack of a rapidly reversing agent,”
Jadhav adds. “The reversible aspect of BB-031 will be a significant advance in our current approach to acute ischaemic stroke, both in addressing haemorrhagic complications as well as allowing reversal—when needed—to allow for the safe performance of
hours from symptom onset—and, in order to produce a sufficient effect size, said trial would therefore need to be “massive”.
“The number of patients you’d have to enrol to show that efficacy would be in the thousands—and nobody will want to do that, because it’s just too [costprohibitive] and the risk of it being negative is high,” he concedes.
For this reason, and also because the bleeding risks associated with tPA may “muddy” the safety signals
clinical programme advisor and RAISE principal investigator—following the first patient enrolments in this study: “Effectively and safely targeting recanalisation of acutely occluded intracranial arteries with novel pharmacology has the potential to expand access to treatment for stroke patients, and will address a significant unmet need in acute stroke care. Many patients are simply not eligible for current drug treatments or cannot reach a comprehensive stroke centre in time to benefit from advanced endovascular treatment.”
Nimjee concludes that, with the global expansion of thrombectomy and increasing uptake of tenecteplase—a generally cheaper alternative to tPA—in the USA, making predictions about the future landscape of stroke care is challenging, and it therefore remains to be seen whether BB-031 will work alongside or fully replace the current gold standard in thrombolysis. However, the potential wider ramifications of an effective and reversible thrombolytic drug appear to be unquestionably significant.
additional surgeries that may be necessary in the poststroke population.”
Existing data and ongoing studies
Basking’s first major showcasing of data on its reversible thrombolytic candidate came at the 2023 International Stroke Conference (ISC; 8–10 February, Dallas, USA), with Nimjee himself presenting Phase 1 study findings demonstrating the drug to be safe and tolerable in healthy volunteers.
Either side of this presentation, Nimjee also spent 18 months “in the trenches”, in his words, working alongside the company’s chief executive officer (CEO) Richard Shea to raise money and ensure Basking had enough resources to conduct a Phase 2 clinical study. These efforts came to fruition in the early stages of 2024, as the company announced the close of US$55 million in financing to further its development of BB031 and BB-025.
RAISE—a Phase 2 proof-of-concept study—is now actively enrolling acute ischaemic stroke patients across the USA with the primary goal of proving BB031’s acceptable safety profile in humans. In addition, the funding Basking has raised to date is being utilised to set up a Phase 1 safety study of BB-025. Nimjee’s hope is that this study will commence in mid-2025—a timeline that, if achieved, would mean the company can look to begin a future Phase 3 pivotal trial of BB031 that also incorporates usage of its accompanying reversal agent under compassionate use in enrolled patients who experience bleeding.
“You can’t do a Phase 2 study of a reversal agent, because the number of times you’ll need the reversal agent is so little—as haemorrhage rates are 2–5%— and you’re never going to have a chance to durably [test] it,” he explains.
When queried about the possibility of a more direct head-to-head study evaluating BB-031 against tPA, Nimjee notes that Basking’s drug would likely have to demonstrate superiority versus the current gold standard among stroke patients presenting within 4.5
While existing thrombolytics have been a critical firstline treatment strategy for acute ischaemic stroke over the last three decades, very few patients benefit from this treatment—largely due to a limited time window and limited efficacy in certain clot types.”
Ashutosh Jadhav
of BB-031, Basking is set to assess its reversible thrombolytic as a standalone drug in patients presenting within 24 hours who do not receive tPA, at least initially.
“From a practical standpoint, we’ll end up getting some patients from 0–4.5 hours who don’t meet the criteria for tPA,” Nimjee continues. “But, that’ll be very limited, and most of the population will not be getting anything up to 24 hours. From a clinical standpoint, that is great, because it’s the majority of all stroke patients. In the USA, where we have a very comprehensive infrastructure for stroke care, only 14.5% of patients who are having a stroke make it to a hospital within 4.5 hours to qualify for tPA. About 86% of patients don’t, and it’s that 86% of patients I care about, because they’re getting nothing [as things stand].”
A similar point was made by Michael Hill (University of Calgary, Calgary, Canada)—Basking’s
“We say that we’ve turned stroke into a surgical disease,” Nimjee says. “Everybody’s trying to get to thrombectomy faster and faster, and we’re building these huge infrastructure networks so we can get these clots out. But, firstly, LVOs only represent about 30% of all strokes. Secondly, we’ve always said that ‘time is brain’—the faster you can treat somebody, the better off they will be. It would be a lot better if, rather than needing me or another neurointerventionist to get into your brain and pull the clot out, you just need any doctor sitting in a local ER [emergency room] to push a drug and take care of even a fraction of LVOs.
“We are doing 50,000 thrombectomies a year in the USA, so, even if our drug only works in 20–30% of LVOs, we could be helping 15,000 patients before they get to the interventionist. That’s still material. That is a huge impact. And the other 70% of patients who don’t have LVO strokes are receiving care faster because it’s a medical disease again. You just need to push a drug.
“It’s also about redefining how we take care of stroke patients. We’ve been so focused on thrombectomy and, don’t get me wrong: thrombectomy is a fantastic procedure. The number needed to treat is three—that is a phenomenal statistic for an intervention. But, there’s still a lot that can be done with a drug—even in a fraction of patients— such that you don’t need a procedure anymore. Some [surgeons] are saying that this could put them out of business, and my answer to that is; if there’s something better, then we don’t deserve to be in business. This is not about people’s livelihoods, it’s about people’s lives.”
At time of writing in early 2025, BB-031 remains in the preliminary stages of clinical testing for acute ischaemic stroke, with enrolment in the Phase 2 RAISE study currently ongoing. The drug candidate is also being assessed in preclinical research as a potential treatment option among patients with pulmonary embolism, in addition to other thrombotic complications. Basking’s reversal agent, BB-025, is going through investigational new drug (IND)enabling testing at present.
“We are excited to announce the initiation of patient enrolment in the RAISE trial,” said Basking CEO Shea, speaking at the time of the company’s announcement that the first patients had been dosed with BB-031 in the Phase 2 study late last year. “This milestone brings us closer to delivering a nextgeneration therapy that we believe will offer patients a new, targeted thrombolytic option beyond traditional fibrinolytics.”
BB-031 in action
TCarotid and Acute Stroke Challenges
CX 2025 seeks to address challenges facing acute stroke and carotid disease treatments
With ‘Challenges’ as its primary focus, the 2025 Charing Cross (CX) Symposium (23–25 April, London, UK) will examine a number of pressing topics within carotid and acute stroke treatment via debates, first-time data presentations, and more.
aking place in Theatre 3 at ExCeL London on Thursday 24 April, the Carotid and Acute Stroke Challenges programme will kick off at 08:00 with a presentation summarising recent improvements across all of the major treatment options for obstructive carotid artery disease: carotid endarterectomy (CEA), transfemoral carotid artery stenting (TFCAS), transcarotid artery revascularisation (TCAR), and optimal medical therapy (OMT).
Following this introduction, Ross Naylor (Leicester, UK) and Sean Lyden (Cleveland, USA) will provide audiences with an overview of the latest carotid treatment guidelines from the European Society for Vascular Surgery (ESVS) and Society for Vascular Surgery (SVS), respectively, outlining the “common ground” shared by the two documents as well as areas within which they pose contrasting perspectives.
The first of several debates is next on the agenda, with two discussants set to argue for and against the motion, ‘Best medical therapy is equivalent to revascularisation in asymptomatic patients’.
The subsequent section of the programme will home in on CEA more specifically—initially, with a talk from Christopher Zarins (Stanford, USA) on improving long-term survival following the procedure, and, later, with a presentation from Alun Davies (London, UK) on whether shunting during CEA should be performed ‘always’ or only ‘selectively’.
Next up is set to be another debate, this time centred on the motion, ‘The final check after carotid endarterectomy is crucial’, with CX co-chair Dittmar Böckler (Heidelberg, Germany) arguing for and Raghvinder Gambhir (London, UK) arguing against.
“In competent hands, standard CEA has become a very safe operation with very low stroke rates. Routine completion imaging is not indicated, and is a waste of time and resources,” Gambhir told NeuroNews, outlining his stance on this contentious topic. “If you do it right the first time, you do not need to worry.”
In a presentation immediately following this, Matteo Tozzi (Varese, Italy) is scheduled to speak on the incidence and relevance of cranial nerve injuries (CNIs) during CEA procedures—as well as techniques for avoiding them.
The next debate during this session will see physicians examine whether or not embolisation prior to carotid body tumour (CBT) cases is ‘a necessity’, with Alberto Muñoz (Bogota, Colombia) set to posit that pre-CBT embolisation should be standard practice and Francesco Spinelli (Rome, Italy) scheduled to challenge the need for embolisation in these cases.
“My argument [is] that embolisation should be the standard of practice for large, Shamblin III and spongy, highly vascularised tumours,” Muñoz said, speaking to NeuroNews. “CBT is a paraganglioma located in the bifurcation of the carotid artery. It is a slow-growing tumour that has been reported more frequently in cities over 2,000 metres above sea level.
“The benefits of embolisation are controversial.
Meta-analyses have shown that preoperative embolisation results in statistically significantly lower blood loss and shorter operative time but makes no difference in the rate of nerve injury, stroke, risk for neck haematoma, or length of hospital stay.
“In patients with highly vascularised tumours, surgical resection is challenging—especially in Shamblin III, in the presence of spongy texture and proximal extension near the base of the skull. These are the patients who benefit more and in whom the standard of practice should include embolisation, since it may reduce bleeding and simplify the operation. In the regular Shamblin I or II CBT cases, it may be avoided, since the risk of bleeding is less.”
“The blood supply to the CBT comes mostly from the external carotid artery (ECA) and from small collateral branches from the base of the cranium,” Spinelli comments, previewing his riposte, which will see him report long-running surgical experiences on
this topic. “By flush clamping the ECA at its origin and clamping its branches outside the tumour, any major bleeding is avoided.”
Next, Apostolos Tassiopoulos (Stony Brook, USA) will discuss the management of symptomatic carotid web cases—and deliver a ‘call to action’ for preventing recurrent stroke.
The centrepiece of the Carotid and Acute Stroke Challenges programme at CX 2025 will see three physicians go head-to-head via a ‘Great Debate’ on the current gold standard in carotid revascularisation.
CX executive board member Barbara Rantner (Munich, Germany) will be the proponent of CEA during this debate; CX executive board member Christopher Metzger (Columbus, USA) will present in favour of CAS; and Michael Stoner (Rochester, USA) will put forward the argument for TCAR.
“TCAR has achieved clinical superiority associated with its unique neuroprotection and minimal-access nature compared to other carotid anatomic treatment modalities,” Stoner told NeuroNews. “Prospective trials have demonstrated safety and efficacy in both
standard and high-risk patients, and these data are backed up by a large-scale real-world registry—the Vascular Quality Initiative. The safety, rapid learning curve, minimal-access technique, lower CNI rate, and scalability for local anaesthesia, support the motion that—after seven decades of surgical carotid revascularisation—TCAR is now the gold standard.”
All three of these treatment modalities will be in focus later on in the session as well, with presentations on a minimally invasive approach to CEA from Enrico Ascher (New York, USA), the latest advances in CAS from William Gray (Wynnewood, USA), and the importance of TCAR as a frontline approach to carotid revascularisation from Sonya Noor (Buffalo, USA).
“Carotid disease treatment has a new kid on the block: TCAR,” Noor commented, ahead of a talk in which she will advocate for increased adoption of the technique outside of the USA. “There are now 100,000 cases done with results comparable to CEA and TFCAS—some may argue, with better results. If you treat carotid disease, this is a simple, safe, less invasive, short procedure that should be part of your toolbox.”
Stenting is set to be the subject of further presentations towards the end of the programme, as Piero Montorsi (Milan, Italy) takes to the podium to outline why he incorporates proximal embolic protection into the majority of CAS cases. Patrick Muck (Cincinnati, USA) will follow this by giving a talk on optimising neuroprotection during and after these procedures, in addition to providing an overview of the CGUARDIANS II study, which enrolled its first patient late last year.
The session’s final debate will see Alan Lumsden (Houston, USA) and CX executive board member Adnan Siddiqui (Buffalo, USA) debate the motion, ‘Severely calcified ICA [internal carotid artery] lesions are at higher risk and are best treated by CEA’. Lumsden will deliver arguments in favour, while Siddiqui will postulate against this statement.
“Almost 75 years after the first CEA, it’s durability and efficacy has stood the test of time,” Lumsden said, speaking to NeuroNews. “Can we improve on the unimprovable? Low complication rate, small incisions, speedy recovery—an operation that can be applied for almost every lesion and in the overwhelming majority of patients. In this debate, we will discuss calcified carotid stenosis and reaffirm the supremacy of this internationally available procedure.”
“I believe this is a historically accurate statement which is no longer true,” Siddiqui stated in response. “Contemporary development of intravascular lithotripsy [IVL] has made endovascular management of these lesions routine. It is, in our experience, best performed with common carotid artery balloon-guide flow reversal in addition to a distal embolic filter using the 4x40 Shockwave peripheral OTW [overthe-wire] balloon. IVL allows ideal preparation of heavy calcific stenosis, which can then be treated with standard higher-pressure balloon angioplasty and stenting. We routinely perform intravascular ultrasound and, to date, have not seen any new embolic debris protruding inside the stent.”
This year’s Carotid and Acute Stroke Challenges programme will close with data from multiple significant studies in this space; Gray will return to the podium to give the first European presentation of two-year outcomes from PERFORMANCE II, as will Stoner to provide an update from the ROADSTER 3 study evaluating TCAR’s safety and efficacy, while Piotr Musialek (Krakow, Poland) is set to summarise one-year results from the CGUARDIANS pivotal trial that are—in his view—“as good as we have seen”.
Clockwise from top left: Adnan Siddiqui, Barbara Rantner, Domenico Valenti, Christopher Metzger
CX 2025 carotid and acute stroke executive board
Study finds no difference in outcomes between three carotid shunting strategies
A Vascular Quality Initiative (VQI) data analysis published in the European Journal of Vascular and Endovascular Surgery has found no statistically significant differences between three carotid endarterectomy (CEA) shunting strategies regarding in-hospital stroke and death rate, including in patients with contralateral carotid occlusion or recent stroke.
IN THEIR EDITOR’S CHOICE paper, Xavier Hommery-Boucher (Centre Hospitalier de l’Université de Montréal [CHUM], Montreal, Canada) and colleagues outline that the study aimed to evaluate in-hospital outcomes after CEA according to shunt usage, particularly in high-risk groups of patients such as those with contralateral carotid occlusion or recent stroke.
Considering the context for their study, the authors underline a lack of data on the topic of carotid shunting. They note that systematic reviews comparing the three shunting strategies have concluded the evidence is too limited to support one over the others,
and that there are no randomised data available on the subject.
Hommery-Boucher et al set out to perform a registry-based analysis. Specifically, they analysed data from CEAs registered in the VQI database between 2012 and 2020, excluding surgeons with fewer than 10 CEAs registered in the database, concomitant procedures, reinterventions, and incomplete data.
The authors note that participating surgeons were divided into three groups based on their rate of shunt use:
non-shunters (<5%); selective shunters (5–95%), and routine shunters (>95%). They analysed primary outcomes of in-hospital stroke, death, and stroke and death rates in both symptomatic and asymptomatic patients.
Hommery-Boucher and colleagues share that, in total, 113,202 patients met the study criteria. Of this total, 31,147 were symptomatic and 82,055 were asymptomatic. The authors report that 12.1% of the 1,645 surgeons included in the study were non-shunters, while 63.6% were selective and the remaining 24.3% were routine shunters. The number of procedures in each group was 10,557, 71,160, and 31,579, respectively.
Hommery-Boucher et al reveal that, in the symptomatic cohort, in-hospital stroke, death and the combined strokedeath rate were not statistically different between the three groups, based on univariable analysis. Similarly, they note that the asymptomatic group also did not show a statistically significant difference for any of the three primary outcome measures.
ROADSTER 3 provides key evidence that ‘goes beyond registry data’ on TCAR-related stroke rates
The authors go on to state that a multivariable model did not show a statistically significant difference for the primary outcomes between the three shunting cohorts
Thirty-day results from the ROADSTER 3 study have demonstrated that transcarotid artery revascularisation (TCAR) is a safe and effective approach in patients who are deemed to be ‘standard risk’ for experiencing adverse events related to carotid endarterectomy (CEA). These findings were presented at the 2024 Vascular InterVentional Advances (VIVA) conference (3–6 November, Las Vegas, USA) by Meghan Dermody (Penn Medicine Lancaster General Health, Lancaster, USA), who—speaking recently to NeuroNews—highlighted the importance of being able to “quote stroke rates that go beyond registry data” for this patient population.
“SINCE WE ARE UNABLE TO CONDUCT AN adequately powered randomised controlled trial to study TCAR against other modalities to treat severe carotid stenosis, and especially without a TCAR arm in the forthcoming CREST-2 trial, it is imperative that we study TCAR in a standard-risk population— ideally in a prospective fashion,” Dermody said.
“ROADSTER 3 is an FDA [US Food and Drug Administration]-required, post-approval study, but it allowed us the opportunity to acquire data from across the USA with multiple generations of surgeons performing the procedure.”
Touted by Silk Road Medical (Boston Scientific) as the first-ever prospective, multicentre trial evaluating the safety and effectiveness of TCAR using the company’s Enroute transcarotid stent system (TSS) in conjunction with its Enroute transcarotid neuroprotection system (NPS) for the treatment of carotid stenosis in standard surgical risk patients, ROADSTER 3 enrolled 344 patients across 53 US sites for intention-to-treat (ITT) analyses. The singlearm study’s primary endpoint is a composite of major adverse events (stroke, death or myocardial infarction [MI]) through 30 days post-procedure, plus ipsilateral stroke from day 31 to day 365 post-procedure, while
cranial nerve injury (CNI) incidence within 30 days post-procedure is among key secondary endpoints.
The rate of stroke/death/MI at 30 days in the study’s ITT population was 0.9%—a figure that decreased to 0.6% within per-protocol analyses involving 320 patients. The researchers found that 30-day stroke rates specifically were the sole contributor to these numbers, with no deaths or MIs being reported through the 30-day follow-up. They further relay that the incidence of CNI within 30 days was 0.6% in both the ITT and per-protocol analyses, and that all cases in both of these populations were resolved within six months. According to Silk Road, this constitutes— to date—the lowest reported rate of adverse event outcomes in a population of standard surgical risk patients treated via carotid revascularisation. The company also claims that, in line with the previous ROADSTER and ROADSTER 2 registry studies, ROADSTER 3 demonstrates consistently low adverse event rates across all risk levels.
“Given TCAR is less invasive than CEA and has similar stroke rates with less nerve injury risk, if a patient is able to take dual antiplatelet and statin therapy, and their anatomy is amenable, there is no reason why TCAR shouldn’t be your first-choice
and that, on subgroup analysis, the stroke and death rates were not statistically significantly different for patients with contralateral carotid occlusion and those presenting with a recent stroke.
“This paper adds new data collected from a large registry regarding postoperative outcomes related to shunt use during [CEA],” Hommery-Boucher and colleagues write, remarking that the design of the study enabled comparison between three shunting strategies.
The authors summarise that the results of their study “demonstrated that there was a two-fold increase in the percentage of surgeons using the non-shunting strategy between 2012 and 2020, with no significant difference in outcomes compared with the other two strategies”. They also acknowledge their research’s limitations, including those “intrinsic” to the use of a large database like the VQI. Hommery-Boucher et al conclude that, despite its limitations, their study “could not define a preferential shunting strategy”, leading them to advise that the strategy “should be mainly based on a surgeon’s preference and skillset”. They go on to stress that their study has “provided quality data on the impact of a surgeon’s shunting pattern on postoperative stroke and death rate, particularly for the most at-risk groups”.
modality,” Dermody told NeuroNews. “But, given the anatomic and physiologic requirements needed for a successful TCAR, naturally, not all patients will be good candidates for this approach. Personally, I believe the treatment of carotid stenosis needs to be more focused on the lesion morphology rather than the degree of stenosis alone. The amount of calcification within or around the lesion; the amount of irregularity or ulceration to the atheroma; any thrombus burden within the plaque; arterial wall inflammation; and a slew of other anatomic features, should truly be what we base our shared decisionmaking on in the future. This requires thorough scrutiny of preoperative imaging, specifically an adequately thin-sliced and well-windowed CT [computed tomography] angiogram.”
Discussing likely next steps in evaluating TCAR, Dermody highlighted the five-year follow-up of these patients in a ROADSTER 3 sub-study, as well as future opportunities to research clopidogrel resistance and the utilisation of transcarotid flow reversal technology for intracranial neurointerventions.
“There aren’t enough data regarding surveillance of carotid stents, how or when to treat recurrent carotid stenosis within a stent, or long-term outcomes from TCAR yet,” Dermody added. “I look forward to seeing how best medical management compares to CEA and transfemoral carotid stenting in CREST-2.”
I believe the treatment of carotid stenosis needs to be more focused on the lesion morphology rather than the degree of stenosis alone.”
Xavier Hommery-Boucher
Carotid stenting performed by trained neurointerventionists linked to lower complication rates versus prior literature
A retrospective study has indicated that carotid artery stenting (CAS)— when performed by fellowship-trained neurointerventional physicians in comprehensive stroke centre (CSC) settings—was associated with a lower complication rate as compared to prior literature on CAS, carotid endarterectomy (CEA) and transcarotid artery revascularisation (TCAR).
DETAILING THEIR FINDINGS IN THE journal Stroke: Vascular and Interventional Neurology, Mohamad Ezzeldin (HCA Houston Healthcare, Kingwood, USA) and colleagues suggest that physician training, higher procedure frequency, and standardised stroke care in a CSC setting, may be among factors contributing to this low complication rate.
According to the authors, multiple previous studies have highlighted the importance of operator experience when it comes to CAS treatments—but fellowship-trained neurointerventionists remain “an underrepresented specialty” in the current literature.
As such, Ezzeldin et al set out to report CASrelated complication rates exclusively when the procedure is performed by neurointerventionists, doing so via a retrospective cohort study of stenting
for symptomatic and asymptomatic carotid stenosis cases collected from multiple CSCs. Their primary endpoint was a composite of 30-day periprocedural mortality, symptomatic ischaemic stroke, symptomatic intracranial haemorrhage (ICH), and myocardial infarction (MI).
Between 2018 and 2022, a total of 1,445 CAS procedures were performed by 38 neurointerventionists across 17 participating centres. From these cases, the investigators obtained 30day outcome data on 1,281 patients who were predominantly symptomatic (93.01%), male (65.79%) and white (70.36%), and had a median age of 69 years.
Ezzeldin and colleagues relay that, overall, the composite primary endpoint occurred in 26 cases (1.8%). This included 13 deaths (0.9%), eight symptomatic ischaemic strokes (0.55%), four symptomatic ICHs (0.28%) and one MI (0.07%). The researchers also found that there was a statistically significant increase in their primary outcome measure that correlated with the following factors: advanced age (p=0.001), female sex (p=0.013), aortic arch type 3 (p=0.01), and higher preprocedural modified Rankin scale (mRS) score (p=0.006).
A range of secondary endpoints—including but not limited to non-periprocedural mortality, asymptomatic ICH, transient ischaemic attack (TIA), access-site complications and in-stent thrombosis—occurred at a rate of 2.84%. Being observed in eight patients (0.55%), access-site complications proved to be the most common of these secondary measures.
The investigators found a further trend whereby the rate of these secondary endpoints was higher in Hispanic and Black patients as compared to their white counterparts (p=0.007), and in those with low diastolic blood pressure prior to stenting (p=0.04).
Endovascular brain procedures: The next frontier for vascular surgery?
WHILE STROKE TREATMENT has dramatically changed in recent years, still around 795,000 people experience a new or recurrent stroke each year and, of all strokes, 87% are ischaemic. A high variability in accessing stroke treatments exists across different countries or different regions within the same nation, even if, at present, guidelines are quite definitive in indicating endovenous thrombolysis and mechanical thrombectomy (MT) in selected cases as key treatment points. However, treatment indications are continuously evolving and so the vascular surgery world should be prepared to
Laura Capoccia
Point of View
evolve accordingly.
Looking back, the dawn of stroke treatment started with carotid revascularisation and, since historia magistra vitae (lessons for the future come from the past; Marcus Tullius Cicero, De Oratore), carotid treatment will continue to play a significant role in ischaemic stroke. Indeed, guidelines dating back to the end of the 1990s indicated carotid endarterectomy (CEA) as a procedure to consider in carotid-related stroke patients, and some studies have demonstrated the possibility of CEA not only preventing recurrence of embolic neurological events (secondary prevention aim),
Rate of composite primary endpoint =
0.9% - death
0.55% - symptomatic ischaemic stroke
0.28% - symptomatic ICH
0.07% - MI
Discussing their findings, Ezzeldin et al state that the 30-day perioperative stroke, death or MI rate reported in this study (1.7%) is “notably lower” than those observed in previously published studies involving CAS; for example, EVA-3S (9.6%), SPACE (6.84%), CREST (6.7%), CHOICE (4.1%) and ACST-2 (3.7%). This figure therefore adheres to the maximum rates of 30-day stroke or death—3% for asymptomatic and 6% for symptomatic carotid disease—that have been established as a threshold for carotid revascularisation and are a requirement for CSC certification by the Joint Commission, according to the researchers. They go on to note that existing data on CEA suggest a perioperative stroke or death rate of 0.7–6.34%, and TCAR registries have reported a rate of roughly 5% in symptomatic patients as well as a 3% rate of perioperative stroke, death or MI. Ezzeldin and colleagues conclude by adding that they hope many of the potential limitations of the present study—including its lack of a nonneurointerventional control group, differences between its patient population and those seen in other CAS studies, and limited data from which to draw conclusions on stenting in asymptomatic carotid stenosis patients—will be addressed by the ongoing CASSH registry.
but also treating brain blood flow impairment when performed in acute patients (therapeutic aim).
It is also to be acknowledged that tandem or concurrent intracranial and extracranial (carotid) lesions are responsible for 10–20% of all large vessel occlusion strokes, so the issue of treating them simultaneously or not is at stake. Even if major societies’ guidelines still suggest that urgent symptomatic internal carotid artery (ICA) stenosis should be treated by CEA rather than by carotid artery stenting (CAS), the European Society for Vascular Surgery (ESVS) and the Society for Vascular Surgery (SVS) still concede that urgent CAS could be performed under certain conditions and the American Heart Association (AHA)/American Stroke Association (ASA) 2021 guidelines indicate treatment of tandem occlusions when performing MT as reasonable.
Nowadays, following the publication of new trials’ results on wider time and lesion indications for MT, it is to be expected that the number of endovascular brain procedures will increase over time, and endovascular treatment of carotid lesions by CAS during MT in tandem lesions will increase accordingly, also taking into account the continuous evolution of
techniques (different access routes and therapies) and devices (flow-reversal cerebral protection adjuncts and new mesh-covered stents).
So, tandem lesions in stroke patients represent the possible meeting point between different specialties (neurology, neuroradiology and vascular surgery) that should always work together to offer the best solution for patients and, mimicking what happened at the beginning of the endovascular era when vascular surgeons started a close collaboration with interventionists to acquire endovascular competencies, it could be time to start to involve vascular surgeons in endovascular brain procedures for the benefit of stroke patients. Acquiring specific competencies, certifications and credentialling in devices and techniques for brain vessel treatment could be the next frontier and challenge for vascular surgery, thus bringing to patients’ care a new experience in managing complications after carotid treatment or in offering a direct carotid access route to MT.
References for this article are available online. Laura Capoccia is a vascular surgeon at the F Spaziani Hospital in Frosinone, Italy.
Multiple abstracts bolster evidence on Sprint PNS for pain management
SPR THERAPEUTICS HAS announced the presentation of four abstracts featured at the 2025 North American Neuromodulation Society (NANS) annual meeting (30 January–1 February, Orlando, USA), all of which contained recent clinical data and insights highlighting the utility of the Sprint peripheral nerve stimulation (PNS) system in the treatment of pain. The first reported on the effectiveness of PNS compared to standard interventional management for chronic low back pain (LBP) in the RESET randomised controlled trial (RCT). SPR states that data from this RCT indicate that 60-day percutaneous PNS provide clinically meaningful and statistically superior reductions (≥50%) in pain as well as improvements in function and quality of life (p<0.05) at three months after the start of treatment, with results appearing to be sustained through 12 months post-treatment.
A second abstract examining outcomes from a retrospective multicentre chart review revealed that 60-day PNS was found to be an effective treatment for chronic shoulder pain, as 75% of patients with available end-of-therapy (EOT) outcome data (n=132/176) reported ≥50% pain relief. Overall, patients receiving bimodal PNS stimulation— concurrent motor and sensory stimulation targeting two nerves—producing a significantly higher treatment response rate and mean percentage of pain relief.
An additional abstract showcased long-term follow-up findings from a multicentre, randomised, double-blind, placebo-controlled, indicating that percutaneous PNS relieves persistent postoperative pain and improves function. The study, which sought to characterise responses to Sprint PNS versus sham stimulation for postoperative pain following total knee arthroplasty (TKA), demonstrated that the majority of PNS subjects had enduring pain relief and improved physical function from data collected out to 12 months from the start of 60-day percutaneous PNS treatment.
A final abstract pertained to sixmonth outcomes from the multicentre, prospective, single-arm MONARCH study, which ultimately found durable improvements in headache pain after 60-day PNS. In this institutional review board (IRB)-approved study, 85% of participants (n=17/20) reported ≥50% reductions in pain and/or pain interference at EOT, with 82% (n=14/17) continuing to report ≥50% reductions in pain intensity and/or interference six months following the start of treatment.
New clinical findings indicate significant pain relief and reduced opioid use via Prospera SCS system
Biotronik Neuro unveiled new data from the BENEFIT-03 clinical study at this year’s North American Neuromodulation Society (NANS) annual meeting (30 January–1 February, Orlando, USA), with a press release from the company noting that these findings highlight the “transformative potential” of its Prospera spinal cord stimulation (SCS) system.
The Prospera system integrates Resonance multiphase stimulation with automatic, objective, daily remote monitoring and proactive care to optimise management of SCS patients’ chronic pain, according to Biotronik.
Highlights from the 24-month interim data produced by BENEFIT-03—a prospective, multicentre study in Australia that is the “first and only” long-term clinical trial evaluating the impact of SCS with real-time remote monitoring in patients with chronic low back and/ or leg pain—include significant pain relief, along with better sleep, improved function and reduced opioid use.
At 24 months, therapy responder rates (>50% pain reduction on visual analogue scale) were 86% for back pain, 89% for leg pain, and 82% for overall pain. In addition, mean daily pain intensity (numerical rating scale) was reduced to 1.8 at 24 months versus 6.6 at baseline, and function (Oswestry disability index) was improved with 73% of participants reporting minimal/ moderate disability at 24 months versus 5% at baseline. Furthermore, among baseline opioid users, 80% eliminated or reduced dosage >50% at 24 months—while serious deviceor procedure-related adverse events were rare, with only one such event being reported.
the Prospera SCS system and demonstrate how its proactive care capabilities—enabled by automatic, objective daily remote monitoring and programming—significantly improve patient outcomes,” said Leonardo Kapural (Florida Atlantic University, Boca Raton, USA). “These findings support the adoption of such monitoring technologies and proactive interventions as the standard of care in spinal cord stimulation therapy, given the potential for rapid identification and resolution of issues that help maintain patients’ therapeutic goals over time.”
“BENEFIT-03 results highlight the sustained benefits of
Additional 24-month BENEFIT-03 results alluded to in Biotronik’s recent release include rapid issue resolution, and reduced patient time and costs. In the study, remote monitoring detected SCS issues for all participants, enabling intervention in 2.9 days versus more than 7.2 days for standard in-clinic SCS care, with the most common issues being low device usage and therapeutic amplitude outside the prescribed setting. At 24 months, 95% of participants reported that remote adjustments saved money, and 100% said they allowed more time for daily activities. Clinicians reported remote management reduced staff burdens in the management of 82% of participants and estimated that remote care prevented an average of 5.4 in-office visits per participant through 24 months, with the highest-need participants avoiding an average of 12 visits, substantially reducing travel time and costs.
REALITY study data show long-term and sustained pain relief with BurstDR SCS technology
Abbott has announced new four-year data showing the long-term and sustained relief that its BurstDR spinal cord stimulation (SCS) technology provides for patients with chronic pain—particularly pain in the back and legs.
THE DATA, WHICH ABBOTT says reinforce the high level of satisfaction people have with the treatment, represent outcomes from the four-year follow-up mark of the REALITY study and were shared at the 2025 North American Neuromodulation Society (NANS) annual meeting (30 January–1 February, Orlando, USA).
“Unlike traditional approaches, BurstDR stimulation therapy has shown consistent effectiveness across a range of patient-reported outcomes with little or no decline in therapeutic effect over time,” said Jan Vesper (Heinrich Heine University, Düsseldorf, Germany). “These latest data highlight the life-changing capabilities of Abbott’s BurstDR
technology in delivering sustained, long-term relief for patients with chronic back and leg pain.”
Abbott’s REALITY study is a five-year, prospective, single-arm, international study intended to analyse the benefits of the company’s BurstDR technology in people who suffer from chronic pain in their back and/or legs.
Key study findings from data on 143 participants at the four-year mark include 91% of patients preferring BurstDR stimulation therapy over traditional tonic stimulation, as well as sustained improvements in pain, sleep and daily function. Investigators also observed improvements in patients’ mental and physical health, including a 45% reduction in pain catastrophising that reached levels comparable to those
without chronic pain. Data indicated a high level of safety and patient satisfaction too, characterised by low rates of adverse events over the study period and 85% of patients saying they would be willing to undergo the procedure again.
Unlike traditional approaches, BurstDR stimulation therapy has shown consistent effectiveness across a range of patient-reported outcomes with little or no decline in therapeutic effect over time.”
Prospera SCS stimulator
Clinical News
First patient randomised to eShunt treatment in STRIDE pivotal trial Cerevasc has announced that the first patient has been randomised to and treated with the eShunt system in its STRIDE clinical trial—a head-to-head comparison of this novel system versus the standard-of-care ventriculoperitoneal (VP) shunt in patients with normalpressure hydrocephalus (NPH). The patient was treated at Virginia Commonwealth University (VCU) Health in Richmond, USA.
Multiple trial site locations are now open across the USA, as per a recent press release from Cerevasc.
STRIDE is a multicentre randomised controlled trial designed to assess the safety and efficacy of the eShunt system compared with the current standard of care, the VP shunt, in elderly patients diagnosed with NPH. The results of the STRIDE trial will serve as the basis for Cerevasc’s anticipated premarket approval (PMA) submission to the US Food and Drug Administration (FDA).
“I was honoured to perform the inaugural treatment in the STRIDE trial. This investigation could lead to a safer and less invasive way to address the gait disturbance, cognitive deficits, and urinary incontinence, that are experienced by people with NPH,” said John Reavey-Cantwell (VCU Health, Richmond, USA).
Wellumio enrols first patient in portable MRI device trial Wellumio has announced enrolment of the first patient in a feasibility, safety and usability assessment of the company’s Axana 0.1T portable magnetic resonance imaging (MRI) device, which will study the ability of the Axana device to detect acute stroke in emergency department (ED) patients. A Wellumio press release notes that, through its compact, portable design, the device enables the user to rapidly track the magnetic resonance properties of brain tissue and identify clinically proven stroke biomarkers—such as molecular diffusion identified by diffusion-weighted imaging (DWI)—at the patient’s bedside.
A hospital in Melbourne, Australia recently assessed the first case using Axana, with the care team there performing the scan on a 77-yearold female suspected of acute stroke with Wellumio’s device. The primary objective of this two-part, dual-centre, feasibility/observational study is to assess the safety (adverse events) and feasibility (ability to acquire a scan in a timely manner without technical fault) of the Axana device, in a hospital setting, with healthy controls versus subacute stroke patients.
“This innovative imaging approach to stroke detection has the potential to accelerate treatment and improve patient outcomes,” said co-principal investigator Stephen Davis (Royal
Melbourne Hospital, Parkville, Australia). “MRI techniques have the potential to sensitively diagnose stroke.”
“Integrating this type of technology in the pre-existing workflow by bringing MRI imaging to the patient has the potential, if successful, to improve acute stroke assessment and treatment,” added co-principal investigator Geoffrey Donnan (University of Melbourne, Melbourne, Australia). “That makes this an exciting innovation milestone as we enrol the first patient in this important first clinical trial.”
stroke that demonstrate a nominally significant lowering of infarct growth in patients treated less than 12 hours from last known well. The lowering of infarct growth correlated with clinically meaningful improvements in several functional stroke measures for assessing a patient’s recovery, including the modified Rankin scale (mRS), Barthel index (BI), and National Institutes of Health stroke scale (NIHSS).
stroke patients at 50 sites.
“This is a significant milestone for the neurointerventional field,” said Al-Mufti. “Up to 70% of stroke patients will experience cognitive impairment. While we know thrombectomy improves functional outcomes, such as limb movement, we have yet to determine the impact on patients’ cognition. Because of Tigertriever, this study could reexamine how we treat patients.”
Arsenal completes enrolment of initial EMBO-02 study cohort
Arsenal Medical has announced the complete enrolment of an initial cohort of 10 patients in the prospective, multicentre, open-label EMBO-02 study evaluating NeoCast for the treatment of chronic subdural haematomas (cSDHs) across three sites in Australia.
A company press release describes NeoCast as a next-generation, nonadhesive, solvent-free, liquid embolic material designed for deep distal penetration that is being assessed for its early safety and feasibility to embolise target vessels of a patient’s middle meningeal artery (MMA) in the EMBO02 clinical trial. The unveiling of data on the initial cohort took place at the International Stroke Conference (ISC; 5–7 February, Los Angeles, USA) via a late-breaking presentation by Laetitia de Villiers (Gold Coast University Hospital, Southport, Australia).
All MMA embolisation procedures in the trial were successfully completed, and all patients passed the 30-day safety endpoint with no device-related serious adverse events. On average, investigators were “very satisfied” with NeoCast’s acute performance and usability, and highlighted its ease of use, according to Arsenal.
“NeoCast is a promising new material for treating cSDH,” said Tim Phillips (Neurological Intervention and Imaging Service of Western Australia, Nedlands, Australia). “NeoCast has differentiated performance characteristics. It is a uniquely responsive liquid embolic agent, and its physical properties allow continuous control and visualisation throughout the injection. The ability to penetrate the microvasculature with the material is very impressive, as are our early clinical and imaging results. I’m excited about the potential of NeoCast to address the limitations of currently available liquid embolics.”
Revalesio announces new study analyses on RNS60 stroke drug Revalesio has announced new analyses of the completed Phase 2 RESCUE clinical trial evaluating its drug candidate RNS60 in acute ischaemic
“This analysis of the RESCUE trial adds further information regarding the beneficial effects of RNS60, confirming that it has favourable effects on MRI [magnetic resonance imaging]-confirmed ischaemic lesion growth that translated into improved clinical outcomes,” said Marc Fisher (Beth Israel Deaconess Medical Center, Boston, USA). “These are exciting results that suggest that RNS60 should be evaluated in a large Phase 3 clinical trial that will hopefully confirm its benefits and lead to approval as the first therapeutic agent in decades to demonstrate significant efficacy in improving outcomes for acute ischaemic stroke patients.”
The multicentre, double-blinded, placebo-controlled, randomised RESCUE trial evaluated the safety and initial efficacy of RNS60 across two primary endpoints: safety and mortality. Eighty-two participants with acute ischaemic stroke eligible for endovascular therapy (EVT) were enrolled and received either intravenous RNS60 0.5mL/kg/h (low dose), RNS60 1mL/kg/h (high dose), or placebo, starting before completion of EVT and continuing for 48 hours.
Highlights from the latest study data include the high dose of RNS60 lowering infarct growth by 50% when compared to placebo, in patients treated within both 12 hours and 24 hours of last known well. The high dose was also numerically superior to placebo for each prespecified functional endpoint at day 90 (mRS 0–2, 72% vs 37%; BI³ 95, 72% vs 37%; EQ-5D-5L, 0.79 vs 0.57), and the drug was found to be safe and well tolerated.
The Tigertriever revascularisation device is the “first” active thrombectomy device that eliminates the existing ‘trade-offs’ of conventional thrombectomy and, according to Rapid, published data have already proven its positive impact on patient outcomes.
The company claims that, in a prior multicentre analysis comparing seven pivotal stent retriever trials, Tigertriever presented faster procedure times, high first-pass revascularisation rates, and good clinical outcomes, compared to leading conventional devices.
Von Vascular presents early data on Algo smart pump
Von Vascular has announced the first international presentation of data on its Algo smart pump at the 2024 BRAIN conference (2–4 December, London, UK). The preclinical study data—presented by Von Vascular chief executive officer (CEO) Manning Hanser—demonstrate the device’s potential to improve outcomes in mechanical thrombectomy procedures for acute ischaemic stroke patients, according to the company.
The Algo smart pump introduces a dual-modality approach to cyclical aspiration technology for mechanical thrombectomy. It offers two distinct aspiration modes: adaptive pulsatile aspiration (APA) and an enhanced static mode—a design that the company says acknowledges the fact that different clots may respond better to specific types of aspiration. The goal here is to achieve complete clot ingestion (CCI) into the aspiration catheter while minimising the risk of generating micro-emboli, Von Vascular claims.
Rapid to evaluate cognitive benefits of thrombectomy device
Rapid Medical has announced enrolment of the first patient in its COGNITIVE study—which, according to the company, is the first study to examine a link between mechanical thrombectomy and cognitive improvement. Rapid further claims that its Tigertriever device may uniquely preserve cognitive function with a tailored approach to removing thrombus while limiting impact to the natural vessel.
National principal investigator Fawaz Al-Mufti (Westchester Medical Center, Westchester, USA) performed the first procedure as part of the global prospective, multicentre, single-arm COGNITIVE study, which plans to enrol up to 450 large vessel occlusion
Preclinical studies have highlighted the Algo smart pump’s “significant advantages” over conventional aspiration systems in achieving CCI and reducing emboli formation, the release further claims. Both the APA and static modes of the pump demonstrated improved CCI rates, with the APA mode showing the most pronounced impact. In comparative testing, 77.2% of clots were successfully ingested using Algo’s APA mode, compared to just 36.7% with conventional aspiration systems. The Algo smart pump reduced aspiration times as well.
“The novel approach presented by Von Vascular is a significant advancement in mechanical thrombectomy technology,” said BRAIN conference director Paul Bhogal (Royal London Hospital, London, UK). “Reducing micro-emboli formation is crucial for improving patient outcomes.”
Axana
Fawaz Al-Mufti
TNKase gains US FDA approval for acute ischaemic stroke treatment Genentech, a member of the Roche Group, has announced the US Food and Drug Administration (FDA) approval of the thrombolytic agent TNKase (tenecteplase) for the treatment of acute ischaemic stroke in adult patients. According to a company press release, this marks the first US FDA approval of a new stroke medicine for nearly 30 years.
The approval is also Genentech’s second for stroke, which the company claims reinforces its “long-standing dedication” to advancing stroke care as the developer of “the only two US FDA-approved medicines for acute ischaemic stroke”—TNKase and Activase (alteplase).
TNKase is delivered as a single five-second intravenous (IV) bolus, representing a faster and simpler administration process compared to standard-of-care Activase, which is administered as an IV bolus followed by a 60-minute infusion. Genentech says it will also be introducing a new 25mg vial configuration in the coming months to support this approval of TNKase for acute ischaemic stroke.
According to Genentech, this approval is based on the large noninferiority AcT study, which enrolled acute ischaemic stroke patients across 22 stroke centres in Canada, and demonstrated that TNKase is comparable to Activase in terms of safety and efficacy. TNKase is also US FDA-approved for the treatment of acute ST-elevation myocardial infarction (STEMI) in adult patients.
Penumbra launches Access25 delivery microcatheter designed for brain aneurysm access Penumbra has launched the Access25 delivery microcatheter—a single-lumen medical device designed to aid physicians in accessing the neurovasculature for the delivery of Penumbra’s advanced 0.020-inch coil platform.
catheters, and was designed to facilitate ease of trackability and stable support when delivering the company’s unique 0.020-inch coils—such as PC400, POD400 and PAC400—for neurovascular embolisation.
Penumbra claims that Access25 offers enhanced deliverability for efficient aneurysm embolisation, enabled by ‘soft precision’, advanced flexibility, an optimised midsection, and tactile support. The new device is available in a variety of tip shapes, including straight, 45-degree, 90-degree, and 130-degree.
J&J MedTech launches Cereglide 92 catheter system for acute ischaemic stroke
Johnson & Johnson (J&J) MedTech has announced the launch of the Cereglide 92 catheter system—a nextgeneration 0.092-inch catheter with the Innerglide 9 delivery aid, indicated for use in facilitating the insertion and guidance of interventional devices in the neurovascular system. The device is now commercially available in the USA.
Cereglide 92 is described by J&J as a 0.092-inch inner diameter catheter system that allows physicians to achieve large distal access and is designed to provide flow reduction in the M1 when inserting devices for the revascularisation of patients with acute ischaemic stroke. The larger lumen also provides distal support for multiple neurovascular tools when treating aneurysms and other haemorrhagic complications, a J&J press release adds.
during and after neurointerventional procedures. As stated in a recent company press release, having already proved its life-saving impact in Canada, this cutting-edge technology is now poised to “redefine” stroke treatment in the USA under the FDA’s Breakthrough Device programme.
First-in-human experiences with the MicroAngioscope were showcased by Peter Kan (University of Texas Medical Branch, Galveston, USA) at the 2025 International Stroke Conference (ISC; 5–7 February, Los Angeles, USA), as he also announced the FDA Breakthrough Device designation. Kan’s presentation detailed how this innovative imaging tool is enhancing neurovascular procedures, and setting a “new global standard” in stroke care and neurovascular procedures.
“I’ve seen the MicroAngioscope evolve from preclinical testing to clinical use, and the latest advancements in field of view and image quality are remarkable,” he commented. “This FDA breakthrough designation brings us closer to transforming neurovascular treatment with real-time intracranial visualisation.”
Imperative secures US FDA 510(k) clearance of Zoom system for stroke treatment
“The new Access25 delivery microcatheter has not only proven its tracking capabilities in numerous procedures, but it has also showcased stability amidst procedural complexities in aneurysm management,” said Scott McPherson (St Dominic’s Hospital, Jackson, USA).
“The design of Access25 allows the distal tip to deliver the coil as if it were painting it into the aneurysms during deployment,” commented Navraj Heran (Royal Columbian Hospital, Vancouver, Canada). “This new technology provided noticeable improvements throughout the procedure.”
Access25 is compatible with Penumbra’s Midway intermediate catheters and Benchmark/BMX guide
“Vessel tortuosity and other anatomical challenges are present in approximately 50% of mechanical thrombectomy cases, which can increase procedure time or prevent ability to treat,” said Brian Jankowitz (JFK University Medical Center, Edison, USA). “As an early user of Cereglide 92 and Innerglide 9, this super large-bore catheter system helps provide quick and seamless access to the M1 with the benefit of flow control, allowing us to rapidly reperfuse the patient and extend the benefits of nextgeneration stroke technology to more patients.”
Vena Medical gains US FDA Breakthrough Device designation for MicroAngioscope device
Vena Medical has been granted Breakthrough Device designation from the US Food and Drug Administration (FDA) for its MicroAngioscope, marking what the company describes as a “historic leap forward” in neurovascular care and stroke treatment.
For the first time ever, Vena claims, direct intracranial angioscopy is now possible—meaning real-time, high-definition imaging inside brain blood vessels can be provided before,
84% of patients within three passes or less without the use of any additional thrombectomy devices as rescue therapy; and stent-retriever rescue therapy being used in only 4.7% of cases to achieve mTICI ≥2b reperfusion.
“In addition to the remarkable efficacy of the Zoom system, I was impressed by the demonstrated safety profile as evidenced by a 0.5% instance of serious vessel injury reported in the study,” said William Mack (University of Southern California, Los Angeles, USA), co-principal investigator of the Imperative trial. “Even more impressive was the 0.9% rate of symptomatic intracranial haemorrhage. These data, combined with our extensive experience with the Zoom system, reinforce our confidence in the technology and its clinical benefits for our practice, and the patients we treat.”
Radical gains US FDA 510(k) clearance for 8Fr neurovascular catheter
Radical Catheter Technologies, a NeuroTechnology Investors (NTI) portfolio company, has announced the Food and Drug Administration (FDA) clearance of its 8Fr neurovascular catheter, marking the company’s second 510(k) clearance from the US regulator. A press release labels this as another milestone achievement for Radical, adding that it highlights the “unprecedented potential” of its catheter technology.
Imperative Care has announced the receipt of US Food and Drug Administration (FDA) 510(k) clearance of the company’s Zoom system, making it the first comprehensive stroke thrombectomy system to include large-bore 0.088-inch catheters indicated for both access and aspiration when used with a Zoom catheter.
As per an Imperative press release, this clearance expands the company’s current portfolio of 0.035-inch to 0.071-inch aspiration catheters to now include the Zoom 0.088-inch catheters—Zoom 88, Zoom 88 Support and TracStar—for aspiration as part of the Zoom system.
Clinical evidence submitted to the US FDA to support the clearance included final data from the Imperative trial. This prospective, multicentre trial evaluated the clinical benefits of the Zoom system in patients treated across 26 US institutions. The analysed cohort included 211 patients who were treated with concomitant aspiration thrombectomy using two catheters.
Key results from the Imperative trial—submitted to the FDA to support clearance—demonstrated a median time from groin puncture to modified thrombolysis in cerebral infarction (mTICI) ≥2b reperfusion of 19 minutes; a core lab-adjudicated rate of mTICI ≥2b reperfusion being achieved in
“I look forward to using the 8Fr catheter where this technology can benefit an even greater number of procedures and patients in my practice,” said Imran Chaudry (Prisma Health Systems, Greenville, USA). “Thus far, my experience with the 7Fr has been stellar, and it has become a mainstay catheter for daily use. It delivers first-in-class performance, exceeding expectations and making complex cases much easier— particularly where other catheters would face challenges.”
Built upon the same patented platform as Radical’s 7Fr catheter—the first US FDA-cleared product from the company—the 8Fr catheter is said to provide a second size and enlarged inner diameter to “greatly expand” therapeutic options. The release goes on to detail that the recent announcement of the company’s move to a stateof-the-art manufacturing facility underscores Radical’s commitment to scaling operations and creating a worldclass manufacturing entity that supports the continued advanced design of its platform, and facilitates the process of commercial expansion.
Q’Apel announces CEmark approval of Armadillo neurovascular access system
Q’Apel Medical has announced that it has received CE-mark certification for its Armadillo SelectFlex neurovascular access system. As noted in a company press release, this “first-of-its-kind” 7Fr system features the patented SelectFlex
technology and is indicated for the introduction of interventional devices into the neurovasculature.
The release goes on to state that the Armadillo neurovascular access system with SelectFlex technology delivers the versatility required for physicians to confidently tackle a wide range of neurovascular interventions. And, regardless of access site, the low-profile 7Fr catheter enables a biaxial approach to accelerate delicate interventions, and eliminate the complexity and cost of conventional triaxial configurations, Q’Apel claims.
“Neurovascular access can be extremely challenging. The tortuous anatomy requires flexibility to navigate the tight twists and turns; however, flexible access catheters tend to lack the support and stability required for device delivery once positioned,” said Pascal Jabbour (Thomas Jefferson University Hospital, Philadelphia, USA). “Armadillo provides a one-and-done solution that simplifies access procedures. It is designed to place full control in the hands of the operator as it allows users to transform the catheter from highly trackable to highly supportive as needed throughout the procedure with the simple injection or withdrawal of just 0.2cc of saline.”
Medtronic expands US carotid market presence with Contego distribution agreement Medtronic has announced it has entered into an exclusive US distribution
Stroke Live Course (SLICE) Next Frontiers Virtual W: masterandfellow.com/slice/ nf/edition
5–9 April
agreement with Contego Medical. Under the agreement, Medtronic will be the sole US distributor for Contego’s portfolio of commercially available products, which provide revascularisation treatment for carotid and peripheral vascular disease.
The agreement also includes an increased investment in Contego and an option to acquire the company. Medtronic has held a minority investment in Contego since 2020.
This agreement includes Contego’s portfolio of commercially available products, including the recently US Food and Drug Administration (FDA)-approved Neuroguard IEP system—a unique, three-in-one carotid stenting system that combines a high-performance stent, postdilation balloon, and an integrated embolic protection (IEP) filter— as well as Excipio peripheral thrombectomy devices.
Medtronic’s press release notes that the Neuroguard IEP system is backed by clinical data demonstrating the safety and effectiveness of the system, with PERFORMANCE I and PERFORMANCE II investigational device exemption (IDE) trial data consistently recording “unprecedented low event rates”—including zero major strokes, zero neurologic deaths, and zero stent thromboses up to two-year follow-up.
Additionally, Contego is currently evaluating the Neuroguard IEP system with a next-generation direct
American Academy of Neurology (AAN) Annual Meeting
San Diego, USA
W: aan.com/events/annual-meeting
9–12 April Pan Arab Interventional Radiology Society (PAIRS) Neuro Dubai, United Arab Emirates W: pairscongress.com/pairs-neuro
23–25 April
transcarotid access and protection system—TCAR-IEP—to demonstrate advanced stroke protection regardless of vascular approach, in the PERFORMANCE III trial.
Kaneka completes acquisition of Endostream Medical Kaneka Corporation has announced that—on 23 December 2024— it acquired 96.8% of shares in Endostream Medical.
By combining its own manufacturing and Endostream’s technology, Kaneka states in a press release that it will jointly develop new medical devices— mainly for cerebrovascular treatment— in addition to the Nautilus device for intrasaccular brain aneurysm treatment that is currently under development.
According to Kaneka, Nautilus is an innovative solution that can treat aneurysms with wide openings in cerebral blood vessels—which has been awaited by the neurovascular community “for many years”. The device has a special structure that can be used in combination with an embolisation coil to block blood flow to the aneurysm, facilitating treatment that would otherwise be difficult with existing devices, Kaneka’s release adds.
The Nautilus system received European Medical Device Regulation (MDR) certification in November 2024, and plans are in place targeting approval and launch in the USA in the spring of 2026 as well as in Japan one year later.
Charing Cross (CX) Symposium London, UK
W: cxsymposium.com
25–28 April
American Association of Neurological Surgeons (AANS) Annual Scientific Meeting Boston, USA W: annualmeeting.aans.org
15–18 May
WLNC and OCIN Joint Meeting
Shanghai, China
W: wlnc.org/en/WELCOMETO-WLNC-2025.html
17–21 May
American Society of Neuroradiology (ASNR) Annual Meeting Philadelphia, USA
W: asnr.org/asnr-2025annual-meeting
Stryker enters peripheral vascular segment following Inari acquisition
Stryker announced recently that it has completed the acquisition of Inari Medical and, having done so, now boasts an established position in the peripheral vascular space, and the fast-growing venous thromboembolism (VTE) segment more specifically.
Stryker initially announced a definitive agreement to acquire Inari in January, following approvals from both companies’ boards of directors.
Under this agreement, Stryker has ultimately acquired all of the issued and outstanding shares of common stock of Inari for US$80 per share in cash, representing a total fully diluted equity value of approximately US$4.9 billion. Shares of Inari ceased trading prior to the market opening on 19 February.
A company press release notes that Inari’s innovative product portfolio is “highly complementary” to Stryker’s neurovascular business, and includes novel mechanical thrombectomy solutions like the ClotTriever system for deep vein thrombosis (DVT) and the FlowTriever system for pulmonary embolism (PE).
21–23 May 11th European Stroke Organisation Conference (ESOC) Helsinki, Finland W: eso-stroke.org/esoc2025
29–30 May
ARISE III Roundtable Discussion with Industry and Stroke Experts Washington DC, USA W: ariseconsensus.com