
12 minute read
Target Detachable


Reach for Target Coils first— a coil range for every case
Innovation is at the heart of the story of the Target Detachable Coil (Stryker). The legacy began in 1990, with the invention of the Guglielmi Detachable Coil (GDC). Named after its inventor Guido Guglielmi (University of California, Los Angeles [UCLA], Los Angeles, USA), and developed in partnership with Stryker, the introduction of detachable coils completely changed the landscape of how aneurysms were treated and is now the primary endovascular treatment across the world. Following the revolutionary launch of the GDC, Stryker introduced the Target Detachable Coil in 2010. With over a decade of treating patients, and across several iterations, the device is the next chapter in the GDC story.
“PARTNERING WITH PHYSICIANS
was our legacy and continues on today,” says Clifford Teoh, senior principal engineer for Stryker’s Hemorrhagic Coils Group, discussing the impact and evolution of the Target Detachable Coil. “Listening to physicians’ needs, and iterating designs to meet their needs is evident from our breadth of offerings throughout the years. With 10 years of coil innovation and more than 500,000 patients treated, Stryker offers a full line of four softness levels, three coil shapes and two primary diameters—truly a coil range for every case.”
Since its first-in-human use, the device has been enhanced to respond to the needs of patients and evolving interventional practice. Using the coil offers access to three shapes—360, 3D and Helical—all designed to frame securely, fill uniformly, and seek voids within the aneurysm.
The Target 360 Coil is at the forefront of coil shape technology, providing uniform distribution, concentric filling, and aneurysm neck coverage. The 360-degree shape is designed to seek the outer wall and leave an open centre for concentric filling. The first 1.5 distal loops are 25% smaller than the stated secondary coil diameter, a feature
Bi-lobe ACA aneurysm treated with Target Detachable Coils
designed to reduce coil herniation. Target 360 Coil features an open loop configuration, conforming to multiple aneurysm shapes, while minimising compartmentalisation.
As a complementary complex coil option, Target 3D Coil offers a secure foundation for consistent framing. The coil rotates 90 degrees at each small loop, creating a three-dimensional shape. The small loops add body to the coil and help maintain this shape, while the large loops appose the aneurysm wall, providing stability within the aneurysm. Target Helical Coils are designed with versatility in mind. The helical shape is available in a range of sizes and softness levels to support from start to finish for framing, filling and finishing intracranial aneurysms, and embolising vascular malformations. Additional innovations in the coil range's history offer full coverage for every case. These include four softness levels—standard (3–24mm), soft (2–20mm), ultrasoft (2–5mm), and nano (1–3.5mm)—as well as three primary diameters—Target 10size, Target XL, which offers double the fill and 40% more width, and XXL which offers triple the fill and 70% more width.
“We continuously improve our designs,” says Teoh, who adds that other developments include the replacement of the reinforced sheath with a 3.5x thicker sheath to provide greater introduction stability to the hub; enhanced proximal contact design, to make the device 10x stronger in buckling; and a laser-ablated detachment zone with a smaller gap, reducing the detachment zone by 65%.
The range of sizes and shapes of the Target Detachable Coil portfolio allow interventionalists to approach every kind of aneurysm. “In short, you get what you expect,” says Peter Schramm (Universitӓtsklinikum Schleswig-Holstein, Lübeck, Germany), offering his view on the platform. “If you are looking for a 3D shape, you get a 3D shape. If you are looking for a certain size, you will find it on the shelf. If you are treating a complex aneurysm, Target Detachable Coil makes it much easier. If you are experienced with those coils, you really feel very comfortable using them,” he adds.
Ian Rennie (Royal Victoria Hospital, Belfast, UK) echoes Schramm’s view that the range of sizes is an advantage of the portfolio. He comments: “There is a fantastic range, from very small to very large, and very long, so the range is superb, and they are predictable across that range.”
Looking ahead to the next 10 years, innovation will remain at the heart of the story. Driven by physician feedback and continuous improvement, the Target Detachable Coil will strive to be the coil range for every case.
2011
Target 360 Coil introduces a smooth and stable platform
2010
Target Detachable Coil first used in humans
2012
Target Nano, the softest finishing coil on the market
2013
Target XL changes the game for volumetric filling
2014
Target 3D unique omega shape loop
2014
New Target Nano offers larger size
2016
XL Mini increases smaller XL mini offerings
2020
500k+ patients treated with Target Detachable Coils
2017
Next Gen Target Detachable Coil improves user experience
2017
Target XXL, the largest of the coils
Detailing his early experience with the Surpass Evolve Flow Diverter, Patrick Nicholson (Toronto Western Hospital, Toronto, Canada) discusses key technical aspects of the device, including the number of wires and braid angle, as well as his deployment techniques and early clinical follow-up results.
IN THE LAST 10 YEARS OR SO,
flow diverting stents (FDS) have moved to the forefront of treatment approaches for many broad-necked or giant intracranial aneurysms. By inducing stasis or slow flow within the aneurysm, as well as by providing a scaffold for endothelialisation of the stent surface, FDS have been proven in several large trials to be safe and effective in the treatment of such aneurysms. More recently, flow diversion has also been found to be safe and effective for small and medium-sized aneurysms on the internal carotid artery,1 as well as distal anatomy and posterior circulation. There are several devices currently approved worldwide, and all differ in various aspects of their design, composition, mesh and braid structure and technical delivery nuances.
Surpass Evolve Flow Diverter is Stryker’s latest entrant into the flow diversion space. The technology received a CE mark in March 2019 and US Food and Drug Administration (FDA) approval in May 2020. The implant is composed of cobalt-chromium wires, interspersed with 12 platinum-tungsten wires for visibility under X-ray. The smallest 2.5mm diameter implant is composed of 48 wires while the remaining diameters (3.25‒5mm) are composed of 64 wires. Mesh density is crucially important in FDS, as consistent mesh density and braid angle optimises flow diversion across an aneurysm neck, especially across vessels that taper in size. Increasing the number of wires also affects aneurysm inflow, and so the Surpass Evolve is designed with 64 wires instead of the more traditional 48-wire design found in many other FDS. This has resulted in optimised flow diversion in bench testing when compared with other models, a finding that has been independently confirmed in various centres internationally.2,3 The higher braid angle also has the benefit of increasing device opening and apposition, which in our experience results in less need for balloon angioplasty compared to older systems.
This increased number of wires has mechanical benefits as well, enabling the implant to have a higher radial pressure than its 48-wire counterpart. Not only does the distal end of the stent open and anchor very reliably, but it means that there is less possibility of significant twisting or kinking. The wires themselves are also thinner—28 microns in diameter when compared with the 32-micron wires found in other devices. This means the stent is soft, flexible, and conforms nicely to the vessel wall. This also allows for more uniform wall apposition—with possibly less need for balloon angioplasty afterwards—and means that the device is easier to push and deliver intracranially, especially with tortuous anatomy.
The system is designed to be delivered through an 0,027” Microcatheter, such as an
Case study 1
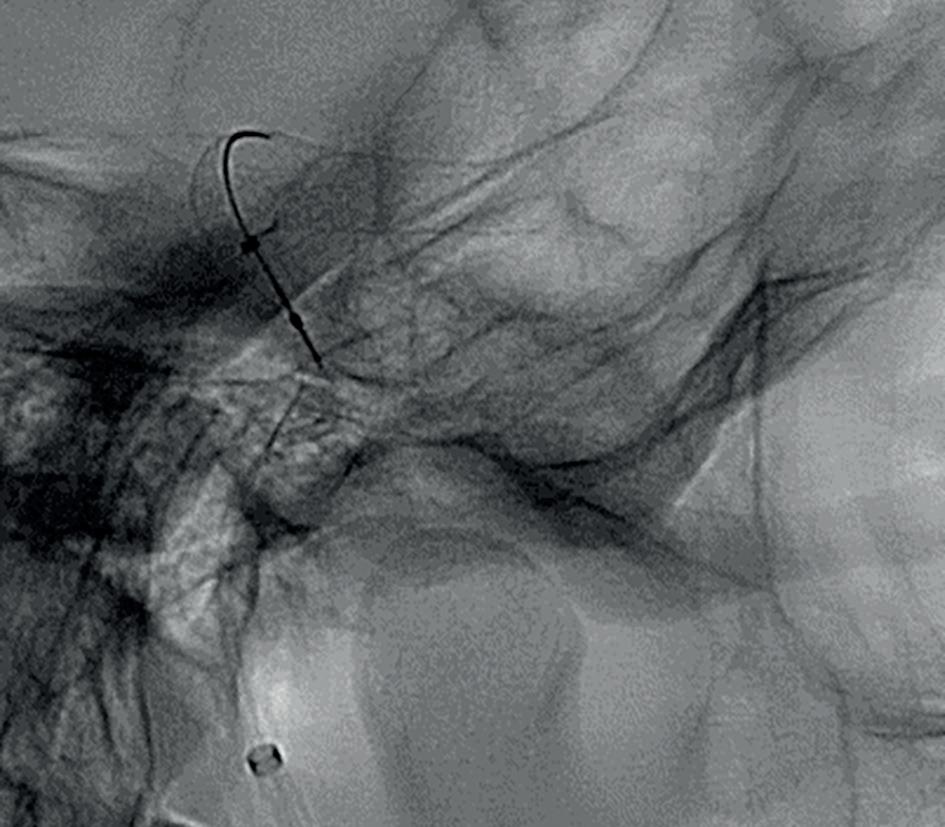
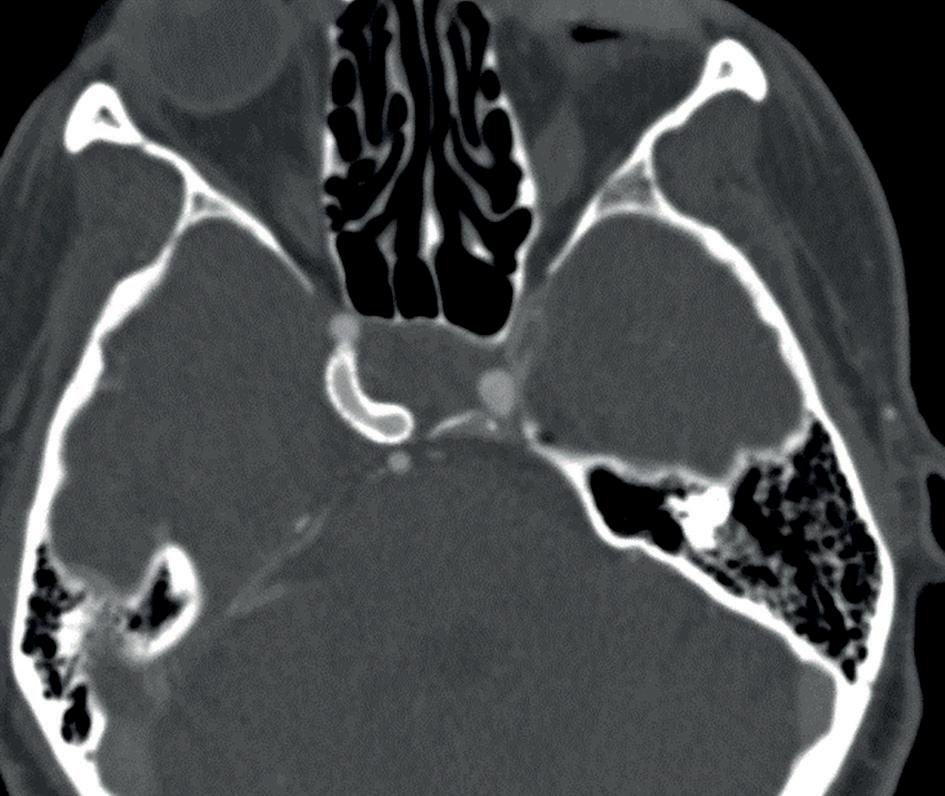
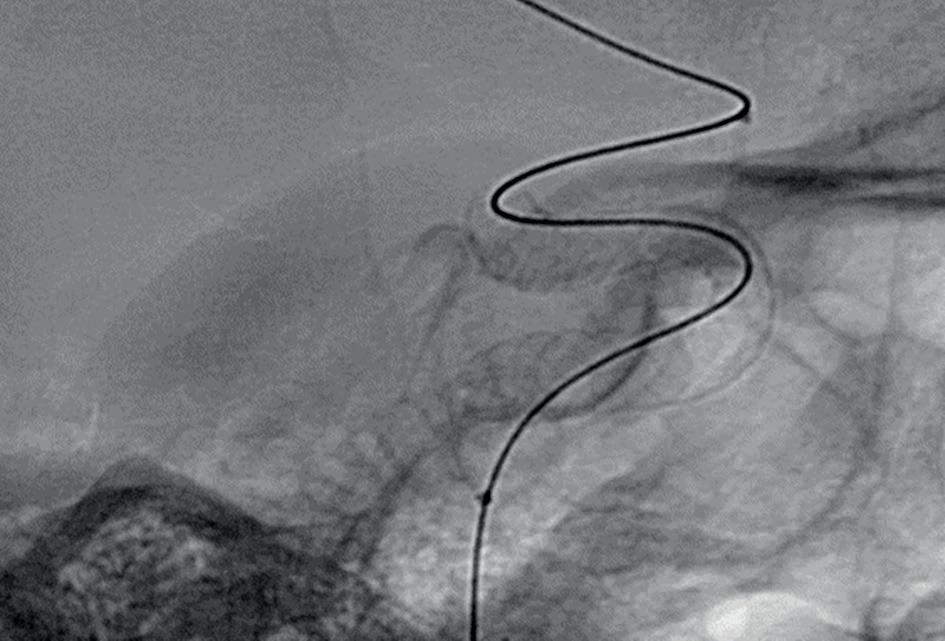
A 57-year-old patient with a symptomatic giant (15x18mm) cavernous segment right internal carotid artery (ICA) aneurysm with mass effect. Previous enucleation of their contralateral eye had been performed, and the patient was at risk of blindness as a result of mass effect on their optic nerve. A decision to treat was made in conjunction with the patient. We decided to use Surpass Evolve in this case for several reasons. The increased flow-diversion effect would presumably result in more rapid occlusion of the aneurysm, while the larger sizes available made it more appealing for this large proximal aneurysm. In addition, the anatomy was very tortuous, which would make delivery of a long stent more challenging. Image 1 shows the lateral projection of the ICA showing the aneurysm, while Image 2 also shows the challenging tortuosity of the ICA. A 5x30mm Surpass Evolve flow diverting stent was deployed (Image 3). The distal landing zone was in the distal cavernous ICA well below the ophthalmic artery origin and the proximal landing zone in the petrous/lacerum segment of the ICA. No coils were deployed, and VasoCT showed good wall apposition so no balloon angioplasty was needed. Comparing the pre-op CTA (image 4) with an MRA performed two months later (Image 5) and a CTA at one year (image 6) we see good occlusion of the aneurysm. The patient remained free of any optic nerve compression or other symptoms related to the procedure at two-year clinical follow-up.
1

4 2


5
XT-27 (Stryker), and so is easier to deploy more distally into the more distal intracranial circulation. The implant is pre-loaded on a stent delivery wire that has an optimised flexibility profile to match the patient anatomy as well as the XT-27 Microcatheter. In our experience, Surpass Evolve Flow Diverter is easier to navigate in tortuous anatomy than an older-generation FDS. The lower forces required to deliver the device also help when deploying it accurately, and in our experience Surpass Evolve behaves well when trying to accurately place the distal end, for example in a specific internal carotid artery (ICA) segment. Resheathing is also smoother, and minimal force is required compared to older systems.
We always use a triaxial system when deploying the stent, consisting of an 8-French guide catheter/long sheath, an intermediate catheter such as AXS Catalyst 5 (Stryker), and an XT-27. When delivering the stent, there are a number of differences that need to be taken into account.
Firstly, there is no need to ‘drag and drop’ the device. We usually deliver it to the anatomy of choice—or perhaps just distal to the desired landing zone—before unsheathing it. This unsheathing distally is key. If there are any issues with sluggish opening of the implant, the device can be easily resheathed which will facilitate opening. The middle
50% or so of the device is deployed along the vessel, maintaining a push/pull combination as needed in order to both maximise wall apposition and keep the device in the centre of the vessel. When sizing the device, the maximum diameter of the vessel is used, rather than the mid-range of the measurements as in other devices. The largest (usually proximal) size of the vessel is used, and the charts on the device packaging will help estimate the length of elongation based on Patrick Nicholson deployment in a constrained (i.e. narrower) vessel distally. Some foreshortening is expected, but this is much less than was seen with older stent systems. To date, the largest six-month follow-up study included 29 patients harbouring 30 aneurysms.4 Although limited in size and scope, the study did show encouraging results. Favourable aneurysm occlusion (OKM C and D) at six months follow-up was achieved in 21/27 (78%) aneurysms and only one procedure-related complication was noted. However, with all new stent systems, multicentre international data are needed to validate the efficacy of the system and several studies are underway. The IMPACT PostMarket Clinical Follow-up registry plans to enroll 200 subjects across 20 European centres. In addition, the EVOLVE trial seeks to expand the FDA-approved indication of the Surpass Evolve Flow Diverter to unruptured, wide-neck intracranial aneurysms measuring ≤12mm located on the ICA or its branches. As many as 45 international centres will enroll up to 250 patients. As we wait for these more robust data, we are encouraged by our early clinical data and case presentations. It would appear that the Surpass Evolve Flow Diverter is a welcome addition to our toolbelt for the treatment of wide-necked intracranial aneurysms.
Acknowledgements
The author thanks Ronit Agid, Timo Krings and Vitor Pereira who also participated in the treatment of these patients.
References:
1: Hanel, Ricardo A., et al. Prospective study on embolization of intracranial aneurysms with the pipeline device: the PREMIER study 1 year results. J Neurointerv Surg. 2020;12.1:62–66. 2: Cancelliere NM, Nicholson P, Radovanovic I, et al.
Comparison of intra-aneurysmal flow modification using optical flow imaging to evaluate the performance of Evolve and Pipeline flow diverting stents. J Neurointerv Surg. 2020;12(8):814–817. 3: Sadasivan C, Fiorella D. Preliminary in vitro angiographic comparison of the flow diversion behavior of Evolve and
Pipeline devices. J Neurointerv Surg. 2020;12(6):616–620. 4. Rautio R, Alpay, K, Sinisalo M, et al. Treatment of intracranial aneurysms using the new Surpass Evolve flow diverter:
Safety outcomes and six-month imaging follow-up. Journal of Neuroradiology. 2021;03:003.
Case study 2
A 48-year-old female with unruptured 12x8x6mm aneurysm arising from the ICA just distal to the origin of the ophthalmic artery, with a 3mm carotid cave aneurysm more proximally, and very tortuous ICA anatomy (Images 1 and 2). For reasons similar to the previous case, Surpass Evolve was chosen. An additional benefit was the accuracy of distal placement, and the planned landing zones are shown in Image 3. An SL-10 Microcatheter was jailed in the larger aneurysm and a 4.5x25mm stent deployed without incident (Image 4). VasoCT showed good wall apposition, so the next four coils were deployed in the aneurysm to promote thrombosis. The patient was discharged the next day, and followup MRA at six months showed good occlusion of all aneurysms (Image 4).
1 2

3
4

5




