7 minute read
Alterations in commissioning and construction of British Orthopaedic Association Standards


Fergal Monsell, Alex Trompeter and Nick Aresti: BOA Clinical Standards Committee
It ain’t what you don’t know that gets you into trouble, it’s what you know for sure that just ain’t so.
This aphorism – frequently but incorrectly attributed to Mark Twain – highlights the perils associated with decisions based on opinion, rather than objective evidence. The introduction of high-level studies and clinical algorithms has substantially improved the orthopaedic evidence base, and the use of an anecdotal methodology to inform clinical decision-making is now effectively redundant.
To support this trend, and in an attempt to improve the delivery of orthopaedic care in the UK, the British Orthopaedic Association introduced the first of a series of BOA Standards for Trauma in 2008, and these are generally referred to by the ‘BOAST’ acronym. It was intended that these documents would drive improvements in patient care, set straightforward, auditable standards and eliminate unnecessary variation in practice.
It was recognised that conventional guidance documents were unnecessarily complicated, and from their inception, BOASTs consisted of a single, A4 page executive summary of topics including compartment syndrome, open fractures, paediatric supracondylar fractures and traumatic spinal cord injury.
Each document describes a common clinical scenario, which is associated with a variance in practice, with potentially significant adverse effects on outcome. Each standard is informed by the available evidence, to produce clear, concise recommendations in a uniform and recognisable format. These are now embedded in UK practice and form part of routine clinical care.
They are also utilised as reference tools in the national monitoring and audit of major injury, and included in the Trauma Audit and Research Network (TARN) methodology, which benchmarks the performance of major trauma networks, major trauma centres, ambulance services and individual clinicians.
The scope was broadened in 2020 to include elective standards, the acronym was modified to BOA Standards to reflect this change and an additional suite of documents was published. It was recognised that, while containing high-quality information, this rapid expansion would potentially compromise the quality, and relevance of these documents to the general orthopaedic surgeon, who they were intended to serve.
The process was, therefore, modified in 2022 to stratify the documents from a temporal perspective, with initial generic management addressed by the BOAST brand and subsequent management covered by a new specialty standards (SpecS) brand.
In practical terms, BOAST documents are intended to be particularly relevant to a non-specialist practitioner and inform the initial management of a defined clinical scenario.
The purpose of SpecS is to provide more specific advice on index conditions over a longer period. It is anticipated that these will be produced by specialist societies and concentrate on the subsequent management, according to recommendations from experts in this field. Where feasible, this should be based on extant consensus documents or published literature. They are also intended to provide an auditable set of standards, but not act as a definitive description of management.
Since 2002, commissioning, construction, and curation of BOASTs have been overseen by the BOA Clinical Standards Committee, a working group with representation from the BOA Trauma and Orthopaedic Committees, BOA Executive, and ad hoc input from expert stakeholders. This includes specialist society representatives and co-opted, non-orthopaedic experts with skill sets relevant to the topic under consideration.
Future BOASTs will continue with the previous format with title, background and justification, inclusion and exclusion criteria and a list of auditable standards for practice. Some standards are mandatory, and are accompanied with the modal verb must, expressing an obligation. Reassessment of the neurovascular status of the limb after relocation of a dislocated knee illustrates this requirement. Other standards are desirable and are accompanied with the modal verb should, expressing a strong recommendation. Obtaining clinical photographs as part of the initial management of an open tibial fracture illustrates this requirement.
This structural change has led to a parallel stream of documents and while each have a common theme, they are intended to be relevant to different parts of the patient journey and this is illustrated by considering what is currently available, and planned infection standards.
Prior to the change in emphasis, BOASTs dealing with fracture-related infection and paediatric musculoskeletal infection, and specialist society BOASTs dealing with peri-prosthetic joint infection were published. To conform to the new arrangement, a generic PJI BOAST document has been produced, which deals with the initial presentation and it is intended that this is endorsed by relevant special societies. Embedded in this document are links to SpecS, which consist of the previous specialist society BOASTs, providing complementary information that describes the nuances of management in different anatomical locations.

These documents have been interrogated to ensure that they are fit for purpose and do not include information that conflicts with previous published standards. It is planned to introduce these documents simultaneously, to illustrate the characteristics of each type and demonstrate the modifications that have been introduced to conform to the new paradigm.
It is envisaged that commissioning future BOASTs will involve a series of clear stages to streamline the process and introduce transparency to the system. Recommendations for new standards will be considered by the Clinical Standards Committee and those considered suitable, presented to BOA Executive for ratification. Proposals are anticipated from a variety of sources, including individual members, specialist societies, BOA Committees and BOA Executive.
These should include a working title, a statement outlining the proposed subject with inclusion and exclusion criteria, and a draft of the proposed auditable standards. Options for co-badging should also be considered, and engagement with specialist societies and additional experts secured at the initial stages, before the first draft is submitted.
After acceptance of an initial draft, the proposed BOAST will be reviewed by the Clinical Standards Committee, with assistance from representatives from appropriate specialist societies. The stage will involve clarification of the core clinical content and this is, therefore, primarily the remit of the relevant experts.
The second stage involves editing the document to ensure that it is succinct and corresponds to the accepted style. This also presents an opportunity for reformatting and ensuring compatibility with previous BOASTs, prior to submission to the BOA executive for approval, before publication on the BOA website (www.boa.ac.uk). Previous trauma-related BOASTs have been accompanied by an editorial, published in Injury and it is envisaged that this will continue.

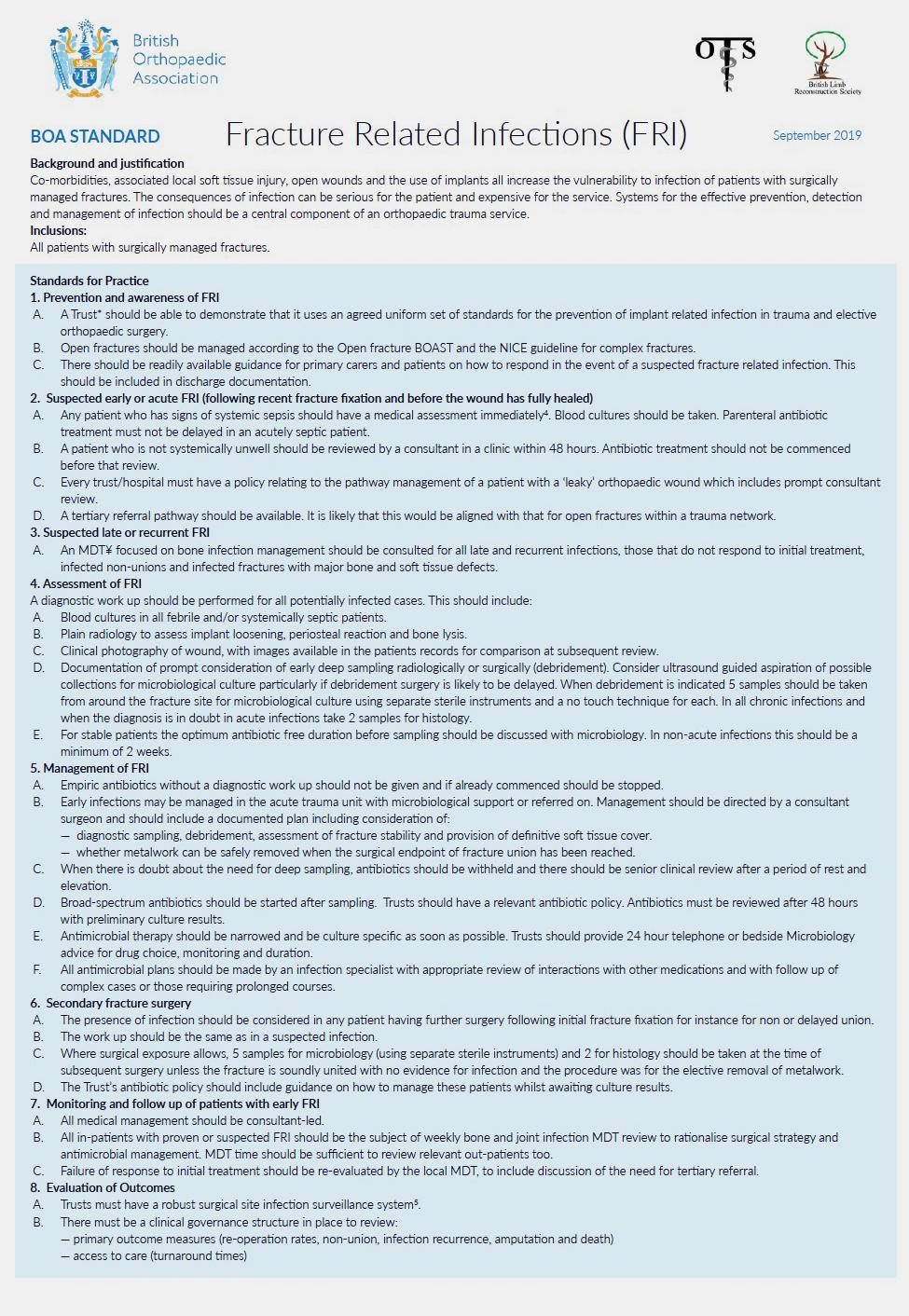
SpecS will be the remit of individual specialist societies and will also follow an agreed format. These documents will typically run to two to three A4 pages, contain more references and will be colour coded to ensure that they can be easily distinguished from a BOAST (see Figures 1 and 2).
This description highlights the origin of the BOAST documents and makes a case for subtle, but important changes in emphasis and the creation of separate SpecS. It is intended that future standards documents will adhere to this formula and as current documents are revised, they will be re-organised to conform to this structure.
This article is intended to inform potential authors and specialist societies of the intended changes, and provide information on how to take proposed standards to publication.
Fergal Monsell has been a Consultant Paediatric Orthopaedic surgeon at the Royal Hospital for Children Bristol since 2005. He is involved in education at all levels, is Visiting Professor at Cardiff University and Director of the Avon Centre for Musculoskeletal Education. Has an active clinical research portfolio and is widely published.
Alex Trompeter works at St George’s University Hospital in London and holds the position of Honorary Reader in Orthopaedic Surgery at St George’s University of London. His specific clinical interests are the management of complex fractures, bone infection, non-union, deformity correction and limb lengthening.
Nick Aresti is an upper limb surgeon, focusing mainly on disorders of the shoulder and elbow. He is both a Clinical Lead and the Deputy Network Director at Barts Health. He is the current Vice Chair of the BOA Orthopaedic Committee, having served as a member for two years.