
Pathways Access Digital Edition Seepage4 Canada’s Lymphedema Magazine Emp owering patients and professionals CLINICAL PERSPECTIVES • RESEARCH ADVANCES • HINTS AND TIPS • EDUCATIONAL EVENTS WINTER 2022/2023 Canadian Publications Mail Sales Product Agreement No. 40065546 HNL treatment guidelines Celebrating a lymphedema champion Ayurvedic medicine benefits Integrative Lymphedema Treatment




























New 2022/2023 Signature Collection • New Prints & Trend Colors show
y ur Juzo Canada Ltd. • www.juzo.ca • 1-844-229-4999 The new 2022-23 Signature Prints and Trend colors make wearing a compression garment a positive statement about life and health - with color, vitality, openness and excitement. Scan the qr code or go to www.juzo.ca to view all of the new print designs and trend colors. Amethyst Pink Navy Topaz Moonstone
spirit
Lymphedema champions are an inspiration to us all
Ifirst met Professor Terence Ryan at the inaugural International Lymphoedema Conference (Ascot, UK) almost 15 years ago. He was co-presenting with Dr. S.R. Narahari, Chairman and Director of the Institute of Applied Dermatology (IAD) located in Kasaragod, India. Professor Ryan has been the official mentor to the IAD for more than two decades and has spent those years working with them to build their lymphedema program.
Professor Ryan is truly a lymphedema hero, whose work will have a lasting impact on the world of dermatology and lymphedema, and will inspire clinicians for many years to come.
What impressed me then and still impresses me now is his passion for public health and education to ease the suffering for those living in the poorest countries.
This issue includes a tribute to Professor Ryan (now retired) and his lifelong work. We thank him for his tireless commitment to better outcomes for lymphedema patients. He is a lymphedema hero, whose work will have a lasting impact on the world of dermatology and lymphedema, and will inspire clinicians for
many years to come. I encourage readers to access his published memoirs “Medicine and Body Image—Resource Planning for the Poor” to learn more about this lymphedema champion.
We are proud to also include an article by Dr. Narahari, detailing the lymphedema treatment protocol used in India. There are certainly components that could be adapted for North America, especially for the poorest populations where traditional treatment is cost prohibitive, not covered by provincial healthcare or just not accessible. The efficacy of the Indian treatment regime is well documented and resulted in government funding to adapt their program across the country. It is also quite a feat to secure funding from the Bill and Melinda Gates Foundation to support their efforts. We congratulate Dr. Narahari and his team on this great accomplishment.
Amy Beaith is a busy wife, mother and entrepreneur living with primary lymphedema. She is not only studying Ayurvedic Medicine and yoga but has incorporated these concepts into her own self-care treatment. Her tips for those living with lymphedema might inspire some of you to try some of these elements as well.
The first part of the Head and Neck Lymphedema (HNL) article was featured in Spring 2022 and covered diagnosis and assessment. This second article by Marize Ibrahim outlines the treatment guidelines developed and followed by the McGill University
Executive Director Announcement

Health Network Lymphedema Clinic in Montreal, Quebec. Marize and her colleagues are busy working on the updated clinical guidelines for HNL. We thank her team for being so passionate about furthering the quality of life for these lymphedema patients who struggle with a unique form of lymphedema that doesn’t get much attention.
Finally, with the holiday season approaching, I truly hope that all of us can enjoy a return to normal (even if it is a new normal) with celebrations similar to what we may have experienced in the years before COVID-19. The comfort and joy of being with family and friends at this time of year is something I try not to take for granted any more. Wishing you and yours a wonderful festive season. LP
She looks forward to strengthening the CLF’s relationships within the broader lymphedema care community and continuing to raise awareness of the challenges faced by patients affected by lymphedema and related conditions in Canada.


Winter 2022/2023 www.lymphedemapathways.ca 3 Editor’s Message
Anna Kennedy
CANADIAN LYMPHEDEMA FRAMEWORK PARTENARIAT CANADIEN DU LYMPHOEDÈME CANADIAN LYMPHEDEMA FRAMEWORK PARTENARIAT CANADIEN DU LYMPHOEDÈME
The Canadian Lymphedema Framework Board of Directors is pleased to announce the appointment of Bonnie Baker in the role of Executive Director. Bonnie has a long history with the CLF, having served in a volunteer capacity from 2009-2019 as Chair of the Partnership Working Group. She re-joined the CLF in 2021 as Conference Manager, leading the Event Team to a successful virtual National Lymphedema Conference in December 2021. Now, as Executive Director, Bonnie will work closely with the Board of Directors and Pathways Editor with responsibility for aligning the CLF’s strategic direction and day-to-day operations with its vision, mission, goals, and objectives.
Winter 2022/2023 n Volume 12 Issue 1
Publisher
Pathways is published four times per year by BCS Communications Ltd. on behalf of the Canadian Lymphedema Framework.



Integrative Lymphedema Treatment
Combining Ayurveda, Yoga and Compression Therapy. ...............................
Editorial Board
Mei Fu PhD RN FAAN
David Keast MD FCFP
Lori Radke PT CLT Anna Towers MD FCFP
Editor
Anna Kennedy Executive Director
Bonnie Baker
Editorial Assistants
Nicole Boulet
Advertising and Submissions
We welcome your ideas, contributions, letters and ad copy. While all material is subject to Editorial Board approval, inclusion does not constitute an endorsement or reflection of the views and opinions of the CLF and its Editorial Board. Contents may not be reproduced without written permission of the Canadian Lymphedema Framework.

Subscription Rates (1 year)
Canada - $30. United States - $60. International - $75. Single copies and back issues - $8.
Subscriptions/return mail to Canadian Lymphedema Framework 4800 Dundas Street West, Suite 204 Toronto, Ontario M9A 1B1 Telephone: 647-693-1083
Email: pathways@canadalymph.ca www.canadalymph.ca
Photos: Institute of Applied Dermatology (IAD), Saket Orthopedic Products, Amy Beaith, WordsbyDesign.co.uk. All stock images are CanStock.
Canadian Publications Mail Agreement 40065546
ISSN 1929-1418 • Printed in Canada
We acknowledge the financial support of the Government of Canada.

Lymphedema:
It’s all about the skin
An interview with Professor Terence Ryan.
Getting to know a legend Paying tribute to Professor Ryan. .....................................................

Treatment of head and neck lymphedema Improving patient quality of life. .....................................................

What Ayurvedic medicine has offered me
A greater sense of self-love and a seasonal lens on a life well lived. .....................................................
FOR SUBSCRIBERS
The price of the annual subscription includes both a print and digital copy of Pathways. Email: pathways@ canadalymph.ca
4 www.lymphedemapathways.ca Winter 2022/2023
Contents
Financé par le gouvernement du Canada Funded by the Government of Canada 17 DEPARTMENTS: Hints and tips 20 Did you know? 21 Letter to the Editor 22 Canadian and International events 22
CANADIAN LYMPHEDEMA FRAMEWORK PARTENARIAT CANADIEN DU LYMPHOEDÈME
10 13 5 14 Revolutionizing Patient Education & Digital Health Solutions A New Partnership in Patient Education Free, online tool designed for healthcare professionals at every level of care to better engage, inform and educate patients about their conditions and treatment plans. Featuring trusted resources from over 100+ health associations including the Canadian Lymphedema Framework. Learn more at www.canadalymph.ca/IMD
Integrative Lymphedema Treatment
Combining Ayurveda, yoga and compression therapy
By S R Narahari

Western biomedicine and Indian traditional Ayurveda systems of medicine recognize certain diseases as the same, with minor variances in clinical description and their nomenclature difference. Disease recognition, clinical methods and treatments are all available in Ayurveda.
Lymphedema

is known as Shleepada in Ayurveda. The combination of therapies of Ayurveda alongside biomedical drugs, diagno sis, and investigations and outcome measures is known as integrative medicine or holistic medicine. Its practice now mainly focuses on long-term care of patients who move to chronic conditions. Patient examination occurs jointly by a dermatologist and an Ayurveda doctor during baseline and follow-up appointments. Institute of Applied Dermatology (IAD) has been providing integrative lymphedema treat ment (ILT) for over two decades.
Lymphatic Filariasis (LF) is endemic in 72 nations; lower leg lymphedema and genital swelling (hydrocele) are its stigmatic clinical presentation. Forty percent of global LF patients live in India, and millions are at risk of infection in low- and middle-income countries, where lymphedema is often discussed within the neglected tropical diseases model as LF.1 Integrative medicine is appropriate for resourcepoor settings because it is both low-tech and low cost for patient care. It utilizes locally avail able resources and high-quality clinical skills supported by healthcare knowledge to address the unmet needs of chronic diseases in these

regions; both in hospital practice as well as in primary care. ILT was developed in India as a frugal innovation, and then contributed to health care program design for the well-being of LF patients through home-based self-care.
The Integrative Lymphedema Treatment protocol:2
Step 1– Counselling: Patient adherence to complex ILT protocol depends on skilled and time-consuming counselling, which in itself helps to improve the healthrelated quality of life as measured by social participation. Every detail of the proposed therapy is discussed to ensure an understanding of lymphedema and its management, along with the need for lifelong therapy. Close family members also attend the sessions. All patients sign an informed consent that states lymphedema requires continued adherence to self-care treatment procedures at home.
Step 2,3 – Washing and herbal soaks:
Treatment by washing with soap and water is useful for reducing the risk of bacterial cellulitis. The swollen limb is then soaked in an herbal mixture (known as “phanta” solution in Ayurveda) for 20 minutes. The herbals prescribed may have antiseptic or anti-in flammatory effects and are prescribed according to the Ayurveda system of diagnosis and treatment.
Steps 4 and 7– Yoga:
There are several types of yoga involving movement synchronized with breathing. Yoga in ILT protocol replaces the European central MLD and relies on self-help. Yoga places the body in an advantageous seated or lying position, that enables a reduced venous load and improved lymph flow; a straight back and a non-tilted pelvis, for example. Movements include whole body stretching, antigravity posi tioning, and ankle movements ideal for reduc ing venous overload. Breathing coordinated with the movements is probably ideal for emptying the large veins of the upper chest into which the lymph in the thoracic has to empty. Expiratory breathing is emphasized as such synchronized breathing is believed to empty core lymphatic trunks while facilitating emptying of the periph eral, impeded, and overfilled lymphatics. Thus, during the distal to proximal movement in IMLD
Winter 2022/2023 www.lymphedemapathways.ca 5
Dr. S R Narahari is a dermatologist and pro-bono director of the Institute of Applied Dermatology and the International Lymphoedema Framework. He pioneered the development of integrative medicine treatment for lymphedema. He has treated over 4000 lymphatic filariasis patients.
Clinical Perspective
ILT developed in India as a frugal innovation, and then contributed to health care program design for the well-being of LF patients through home-based self-care.
parts 1 and 2, the patient breathes out slowly or holds the breath after exhalation. The patient takes a sudden and deep inhalation during the pause between the end and beginning of IMLD strokes. IMLD is administered by a masseur who subsequently coaches the patient’s home caregiver in the technique. This yoga is done twice each session; the first time without bandaging, and then later, the movements within support bandaging encourage muscle contraction to work against resistance, thus stimulating lymphatic contraction and drainage. A complete list of yoga asanas to be practiced before and after IMLD at the IAD is provided in the references.3
Step 5
– Indian Manual Lymphatic
Drainage (IMLD): Part 1 of IMLD (known as unmardhana in Ayurveda) is a type of non-oil massage that requires the masseur to apply a squeezing pressure using both palms and fingers and moving from the tip of the toes to the upper edge of the lymphedema (the most proximal point). This is performed for 10 min utes with the patient in a supine position. It is a manoeuvre that might be initiating a shift of lymph fluid into the initial lymphatics in the upper dermis to the deep der mis. The upper dermal lymphatics respond to light touch and movement while the thickened deep dermis responds to squeez ing. Part 2 of IMLD (udwarthana) is a massage with oil being applied to the skin, and the limb is massaged in the oppo site direction to hair growth. The oil is selected according to the skin pathology described in Ayurveda. Several publications guide the right selection of Ayurveda oil. The most commonly used oil is Nalpamaradi oil, an herbarized oil that might have therapeutic benefits.2
Step 6 – Compression therapy: Biomedicine uses a broad range of bandages and compression garments. However, short-stretch bandages and well-fitted hosiery are too expensive for the resource-poor village patient unless sponsored by the government. Some patients may need at least 20 bandages or more per week plus ample foam rubber materials that help reshape the limb. The life of a bandage is short after repeated washing, the heat of the tropics and the use of oils, increasing the cost of treatment.

Results of ILT
We conducted a clinical audit of the last ten years of data to assess the value of the ILT services in the existing clinical practice at IAD, and to determine whether the treatment outcomes are aligned with the global goal of lymphedema morbidity management. The institutional data of all 1698 patients showed limb volume reduction following an intensive supervised care period (mean=24.5%, sd=13.17), with a further reduction between discharge and first follow-up (mean=1.42%, sd=18.42), and reduction from first follow up to second follow up (mean=2.3%, sd=19.53). Most patients (1437, 84.63%) had a history of cellulitis at first presentation. No new episodes of cellulitis were observed at the first follow up and only five new cellulitis episodes occurred in the second follow-up. The bac terial entry points (BEEPs) that trigger cellulitis were also reduced during fol low-up. At the first follow up, the percentage of patients with BEEPs had fallen to 40% (except intertrigo) and in the second follow-up, 26.1 to 9%. However, some fresh occurrences were also noticed, which ranged from 1.4 to 12.7% at the first follow-up and 1.8 to 16.9% at the second follow-up. Health-related Quality of Life (QOL) as measured by a Lymphatic Filariasis Specific Quality of Life Questionnaire (LFSQQ) significantly improved when measured
at the first and second follow-ups. Patients’ scores improved in all domains of their life during the follow-up compared to their admission values. Statistically significant changes were observed in the overall QOL and every domain at every follow-up (p<0.001). The outcome of the integrative medicine protocol is shown in Figure 1.
Lack of funding
Being a neglected tropical disease, filariasis lymphedema research and patient treatments receive no funding. To date, the IAD has not received any major financial support. It is challenging to sustain a lymphedema clinic mainly through volunteer labour. All its 30 skilled staff are paid only minimum wage and management, directors, and collaborators work pro-bono. Often, IAD’s annual balance sheet is break-even, after deficit portions are met by generous donors. The COVID pandemic brought activities to a sudden halt. As a result, IAD had no income, and the clinic was closed for over two months. We survived because of a few donors. Prof. Christine Moffatt and International Lymphoedema Framework made personal donations and appealed internationally to support IAD. Several European, Australian, and Indian donors responded to the call. However, the financial crisis did not improve as Kerala continued to report COVID cases. Lymphedema patients hesitated to travel to the center and IAD continued its support to patients through teleconsultations. Fortunately, Medi For Help (Germany) responded to the ILF call and has committed long-term support to IAD, including possible new clinics in endemic regions to provide free treatments to filariasis patients.

Mainstreaming of ILT for Morbidity Management and Disability Prevention of Lymphatic Filariasis
Although both biomedicine and traditional medicine experts continue the fight for superiority on the basis of evidence, we produced data-driven evidence that convinced several academic bodies to discuss the ILT protocol.8 In 2018 the Ministry of AYUSH
6 www.lymphedemapathways.ca Winter 2022/2023
Integrative Lymphedema Treatment Intensive Phase
A cocktail of oils and maneuvers from Ayurveda, dermatology drugs, compression therapy, and yoga exercises. All are administered as selfcare and home-based treatment after two weeks of training during the intensive treatment.

(Ayurveda, Yoga, Unani, Siddha, and Homeopathy) conducted a brainstorming session on changing policy. High officials of the Ministry came to IAD to understand ILT for lymphedema. In 2019 National Vector Borne Disease Control Programme organized a national symposium with the theme ‘United to Eliminate Lymphatic Filariasis’. The Bill and Melinda Gates Foundation (BMGF) supported this large conglomeration of Indian experts, bureaucrats, and organizations working in the field of LF in New Delhi. Later the Ministry of AYUSH began consultations with essential stakeholders. Subsequently, the Government of India included LF as part of the national AYUSH mission planned to roll out through its wellness centers.
Following a series of consultations, the BMGF decided to support the scaling of ILT in four centers. Under the grant i) center of excellence in IAD, Kasaragod is established to provide training, ii) and to establish independent units for demonstration of the treatment inside the government of Ayurveda medical colleges to facilitate teaching and learning to the interested students and faculty. As part of the project, at least four new teams
Winter 2022/2023
Holiday Shopping? Holiday Shopping? We can help! We can help! GIFT SUBSCRIPTION PATHWAYS@CANADALYMPH.CA PATHWAYS@CANADALYMPH.CA OR OR CANADALYMPH.CA/SUBSCRIPTIONS CANADALYMPH.CA/SUBSCRIPTIONS
FIGURE 1
for lymphedema management would be trained in the center of excellence and deployed in four government Ayurveda medical colleges in the most endemic districts. The teams will treat lymphedema patients and teach students about lymphedema management for 20 months. The BMGF is already supporting Mass-Drug-Administration under the WHO’s Global Programme to Eliminate Lymphatic Filariasis. As part of this strategy, BMGF is working with several community-based organizations to create awareness about LF. It plans to link the treatment centers supported by it to these village-level workers to create awareness that lymphedema is treatable. Treatments in all government owned medical colleges are provided free.
Integrative Lymphedema Treatment is mentored by Terence J Ryan, Professor of Dermatology at Oxford University. In 1993, Dr. Ryan began to investigate alternative systems of medicine. He voiced his support of the Global Initiative for Traditional Systems (GIFTS) of Health, chaired by Dr. Gerard Bodeker, who was advising on traditional medicines in a forum of policymakers from around the world. The aim of GIFTS was to build partnerships at a global level between traditional health practitioners, scientists, educators, and decision-makers, to improve the clinical services provided. Dr. Ryan’s primary objective was to explore low-cost, locally available, effective but safe alternative medicines for skin and lymphedema care in the developing world.
In 2002, Drs. Vaqas and Ryan discussed a low-cost integrative treatment paradigm for lymphedema, using traditional Indian medicines and yoga, suitable for administration in rural communities.5 At that time, the IAD had already been engaged in such a program for a number of years and was looking for


International experts came periodically and contributed to improving the program in many ways. Because of the global attention received for low-cost ILT, there was a need to establish evidence of its efficacy in village community settings. The Ministry of AYUSH (an acronym for Ayurveda, Yoga, Unani, Siddha, and Homeopathy) funded the clinical trial at the primary health center level in 2010, proving that self-care ILT is possible in poor Indian village settings.7
Role
of ILT in the global health scenario
Although more studies are required to establish the role of the Ayurveda skin care component of ILT, statistical analysis showed that ILT altered the risk factors for disease progression by significantly reducing bacterial entry lesions, which likely improved the barrier function of the skin.
collaborators. This led to an exchange and the incorporation of Vaqas and Ryan’s recommendations into our work. Subsequently, Dr. Ryan closely mentored the whole program, thereby helping to popularize integrative medicine among policymakers around the world. Dr. Ryan invited many of his students, including Professors Peter Mortimer and Christine Moffatt, to visit IAD and guide the program. IAD conducted ten international symposiums, including an international meeting for lymphedema research priority setting.6
The ILT model is self-care and can be continued as home-based management after a brief two weeks of treatment training in the center. It is a low-technology and low-cost treatment, which can be performed at home easily with the help of a home caregiver, most often a family member. The Lymphatic Filariasis Quality of Life Questionnaire as a tool to assess improvement is being adopted by other research workers.9 In view of positive treatment outcomes, especially the reduction in bacterial cellulitis episodes, the ILF has invited the IAD to share information about the treatment at its conferences. Several therapists, nurses, and doctors who learned about the ILT through ILF conferences have visited IAD to learn about yoga and the oil massage systems. If the treatment could benefit lymphedema patients in other centres, there is an option to start online lymphedema courses coupled with a few weeks of optional practical training in India. IAD has developed a robust data capture system based on a customized medical records system (www.bahmni.org). IAD has a team of IT experts and data analysts who have been improving their skills for lymphedema data management. ILT therefore can be scaled internationally through mutual collaborations and sharing of expertise. LP
A full set of references can be found at https://www.canadalymph.ca/ pathways-references/
8 www.lymphedemapathways.ca Winter 2022/2023
The Ayurvedic drugs manufacturing facility of IAD.
The IAD team of Allopathy, Ayurveda and Homeopathy doctors, Yoga therapists, nurses, therapists, IT experts, with its Indian and International collaborators.
Compression for night-time lymphedema management
JOBST JoViPak in combination with the JOBST JoViJacket is designed for lymphedema compression therapy during the night. The 4 blend foam mix and stitched channels are designed to create multiple pressure points and stimulate lymphatic drainage. These garments for edema management come in various styles and, with the addition of specialized pads, are designed to provide comfort and control from head to toe.
JOBST® JoViPak®. Full body solutions for reliable lymphedema management during night-time

https://www.jobstcanada.com/home.html
jobstcanada.com 1-877-978-5526
Compression where you need it with JOBST®
Lymphedema: It’s all about the skin
An interview with Professor Terence Ryan
 In discussion with Dr. Anna Towers and Anna Kennedy
In discussion with Dr. Anna Towers and Anna Kennedy
Introduction – Within the international lymphedema community, there are a handful of pioneers who have laid the groundwork and paved the way for the researchers and clinicians behind them. It’s important for us to acknowledge and honour their tremendous contributions. We had the opportunity to chat with Professor Ryan via Zoom, to learn more about his work and his thoughts about where lymphedema is heading, from a dermatologist’s point of view. Hopefully his work will inspire more dermatologists to become involved in the care of lymphedema.
QThere are so many disciplines of doctors that are involved in lymphedema care. In your opinion, is that why lymphedema is still considered to be an orphan, with no real home in the world of medicine?
Yes. Of course one of the problems is that physiologically speaking, the lymphatics haven’t been well seen. It’s amazing that you can take even the best textbooks of dermatology, with any drawing of the skin and show blood vessels, hair and everything, but they never put in lymphatics. So it’s just not seen, it is not visual to people by any system. There is still tremendous ignorance of its existence.
QWhat do you see as the way out of this situation: that there’s no one discipline that takes ownership, and that’s taught properly about the lymphatic system? Our success in India (and therefore lymphedema) is going to get more and more publicity. The Bill Gates Foundation has given money to increase the distribution of lymphedema care. The World Health Organization (WHO) has now taken it on board and is really interested in our good results. There will be a paper published in the British Journal of Dermatology about our work. I hope dermatologists will realize that it is something they can deal with, and in my writings I tend to emphasize the focus on the care of the epidermis. I do think that the
epidermis is to some extent, the conductor of not only blood supply but also lymphatic drainage. I don’t think people realize that the epidermis is the key focus of the treatment approach in India.
QFor disciplines to advance, they need to be recognized as such with specialists. Do you see lymphology itself, becoming a specialty?
Well, I think lymphology already is a specialty, but it’s definitely a minor specialty, just as dermatology has also been regarded as a minor specialty. But it is getting better. No doubt lymphology will get better recognized too as people begin to understand it. There is still a great deal of ignorance that needs to be overcome.
QOne of the challenges in Canada getting physicians interested, is that there’s no pharmaceutical agent we can give that will help lymphedema. So it’s marginal in the view of physicians, as something they should become interested in. We have plastic surgeons now becoming interested in physiological procedures, and that’s beginning to increase interest, but it is a slow progression.
It was shown in India that these people are disfigured. They have large limbs but
they also have odor and there is a tendency for them to be neglected by their families and community. I think the time is coming when people will realize that the herbal soaks that we are using can be available and effective worldwide. We’ve proven that they really work in the care of the skin, and it’s the care of the skin that resulted in an improvement of the lymphedema.
We’re beginning to show that bandages and compression are not the most acceptable therapy. They are too difficult and too expensive in countries like India, and so we have to rely more and more on just simple soaks and care of the epidermis, plus movement. Of course, in India, we use yoga, but any form of movement of the skin is helpful. So a lot of our approach is self-treatment. The prescribe-able element by doctors in India is sometimes a little bit of anti-fungal or steroid cream for the eczema, but it’s all related to care of the epidermis. Mostly we are using medicinal herbals and we are promoting movement by yoga, which is culturally acceptable in India. And I think both are becoming more and more acceptable worldwide, perhaps even in Canada.
QCellulitis is the most serious consequence for patients with lymphedema. If there was one message to give patients to try to minimize that risk, what would that be?
10 www.lymphedemapathways.ca Winter 2022/2023
______________________________________________
Interview
Number one would be meticulous care of the skin. But also I think a friendly approach from clinicians is very important. One of the reasons we have such success in India is that patients enjoy being with us. They travel far and come from all over the place and then they also come back to us. We have very few people who don’t come back and that is because we’re creating a very friendly environment for them to feel cared for.
QIn North America, the emphasis seems to be on manual lymphatic drainage and compression, but skin care unfortunately sometimes takes a backseat.
I think you can do all the manual compression (and of course, it helps), but if you ignore the care of the skin, then you’re not going to really get a good result.
QIn your vision, where do you see chronic edema/ lymphedema care heading or even 50 years from now?



Well, I hope that the important LIMPRINT study results help us understand that we’re dealing with chronic edema rather than lymphedema, and that everybody over the age of 60 is going to have some edema. Lymphatics and the blood supply are all playing a part. Dr. Narahari and myself wrote an editorial in the recent issue of British Journal of Lymphology, focused on LIMPRINT results. I think Professor Christine Moffatt is quite right in reminding us that there’s a lot of chronic edema, which isn’t due to lymphatic filariasis or due to cancer, and that there are many genes playing a part. There is a genetic background at play in regards to whether you get lymphedema or not.
Only about a third of the people with or without cancer actually get lymphedema,



and that, I believe, is because they’re geneti cally susceptible. So I think we’re beginning to understand that in the background of all this, you need a healthy and effective lymphatic system, and that depends both on the genetic background as well as the interaction with many systems in the environment. So everything in the environment, which affects and produces lymphedema, depends to some extent on your genetic susceptibility.
QWhat is your opinion on the possibility of a cure?
Once we know what genes are affected, it’s possible to begin to think of a cure for lymphedema. But at the moment we haven’t got a cure based on the genetics, but it will come.
QAnd that would be ideal, rather than the traditional and surgical treatments we have now to manage the disease?
Winter 2022/2023 www.lymphedemapathways.ca 11
medi. I feel better. Trend Colours Strong new trend colours and crystal motifs with mediven® flat knit Further information: www.medicanada.ca Bleu-Jeans Grey Chestnut Raspberry-red NEW NEW medi Magenta
some people with breast cancer don’t get lymphedema (in fact up to two thirds of people with breast cancer don’t get lymphedema). The other factor is that for many people, the onset of primary lymphedema doesn’t become evident until they get to four or five years of age. And it is when they get to full size (the late teenage years), that there is the greatest effect of gravity on the venous system. It’s a very important background factor. Gravitational factors in the venous system are a determinant of the leakage and the overload of the lymphatic system. So I think size and full growth plays a part, often through the venous system.
Lymphedema in the elderly is largely due to overloaded lymphatics by the venous system failing rather than necessarily the lymphatics being at fault. They’re just overloaded by venous hypertension, which is common in people who just sit with their legs down or who don’t move. This is common in the elderly.

QWould you like to say anything in signing off to our readers?
I think the world probably thinks I’m a bit of an eccentric. But I’m a great believer that in fact many of the things I believe in, other people will believe in, in the end. I certainly encourage you to read the Journal of Lymphology Editorial, and also the British Journal of Dermatology article (from India and the WHO), which has just been recently published. LP
Editors Note
For links to the Journal of Lymphology and British Journal of Dermatology, visit https:// canadalymph.ca/pathways-references/
Biographies
n Terence J. Ryan, DM, FRCP is Emeritus Professor of Dermatology at Oxford University in Oxfordshire, England.
n Anna Towers MD, (Montreal, Quebec) runs the Lymphedema Program at the McGill University Health Centre.
n Anna Kennedy, (Toronto, Ontario) is the Editor of Pathways Magazine.
Interested in learning more about lymphedema heroes?
I encourage you to read other pioneers we have featured:
• Miles Johnson: Forty years of devoted research by John L. Semple (Pathways Spring 2015)
• Saskia Thiadens: A tribute to Saskia Thiadens: Honouring an inspirational hero (Pathways Summer 2016) by Bonnie Lasinski
• IAD: Hard work and Hope – Lymphatic Filariasis Treatment in India (Pathways Summer 2014) by Rosemary Kelly.
https://issuu.com/canadianlymphedemaframework/ docs/final_copy_pathways_spring_2015 https://issuu.com/canadianlymphedemaframework/ docs/b746_clf_pathways_summer2016_client https://issuu.com/canadianlymphedemaframework/ docs/pathways_summer_2014_final
12 www.lymphedemapathways.ca Winter 2022/2023
Dr. Vodder SchoolTM INTERNATIONAL Member of Dr. Vodder Academy International Train in Canada with certified instructors www.vodderschool.com info@vodderschool.com | 800 522-9862 PROFESSIONAL TRAINING IN MANUAL LYMPH DRAINAGE AND COMBINED DECONGESTIVE THERAPY
management ONLINE Level 1 Theory Available ~ Evidence-based ~ Easy learning modules with small class sizes ~ Interactive, live classroom instruction with physicians ~ Learn precise manual skills with expert, accredited instructors ~ ISO 29990: 2010 certified training ~ CE credit available Visit our website for classes: Calgary Halifax London Montreal Ottawa Saskatoon Toronto Vancouver Winnipeg 914 611 866.251.0076 www.wearease.com MADE IN USA READY TO WEAR Therapeutic Compression Tops and Bottoms NEW STYLES & COLORS We really don’t know
the
for susceptibility
Lymphedema
what
reason
is and why
Getting to know a legend
A tribute to Professor Terence Ryan
By Anna Kennedy
In his published memoir Medicine and Body Image—Resource Planning for the Poor, Professor Terence Ryan notes that the name Terence means, “hard working and doesn’t give up.” This seems to perfectly depict this man’s studies, research and work ethics.
Paying tribute. In addition to the incredibly detailed accounts of early family roots both in England and India, Ryan carefully and humbly pays tribute to all his colleagues, mentors, professors and people who influenced his career and life. This is ironic as Ryan himself has been a major influence on other distinguished lymphedema authorities such as Dr. Peter Mortimer (St George’s Hospital) and Professor Christine Moffatt (International Lymphoedema Framework), plus many, many more.
Medical journey. Regardless of how the arts played a leading role in his life (both art and music), Professor Ryan was determined to become a doctor, moving from arts to science and enrolling at Oxford University. So started his unconventional journey into medicine and a long successful medical career as a dermatologist. His earlier interests and work included leprosy and microcirculation before he then moved from the study of blood supply to the study of lymphatic drainage and wound healing.
Professor Ryan is Emeritus Professor of Dermatology at Oxford University in Oxfordshire, England, where he played a major role in building up the Dermatology Department. Foreign travel to the developing world became a major part of his career and experiencing India opened up important public health interests for him. That led to a focus on community and public health, helping others to collaborate and develop local solutions in resource-poor developing worlds.
It addition to his official paid work, Ryan volunteered his time by holding senior posts and founding roles in numerous international dermatology and wound healing organizations from which he has received many Lifetime Achievement awards. It was during his Presidency of the World Congress of Microcirculation that another field opened up for him—an interest in complementary and alternative medicine, as an addition to traditional medicine.
Professor Ryan tirelessly mentored the team at Institute of Applied Dermatology (IAD) for twenty years to develop lymphedema treatment by combining Ayurveda, Yoga and Compression Therapy and built robust data-driven evidence. The Bill and Melinda Gates Foundation is currently funding to scale this culturally acceptable, low-cost self-care model in different regions of India. The treatment protocol is also part of the Indian national public health programme. We hope his model of lymphedema management will be accepted by high, low-and middle-income countries worldwide.
Dr SR Narahari, Director, Institute of Applied Dermatology, Kasaragod, Kerala, India
Retirement work. His extensive work in India includes developing an integrative treatment protocol including herbal medicine, yoga and compression. As Ryan states “The theory of including yoga within lymphedema treatment is that it promotes the flow of tissue fluid into and along lymphatics, by promoting tissue movement. All lymphatics drain into the large veins within the chest, and their emptying is helped by effective breathing which is also a function of yoga.”

So what does retirement look like for someone who devoted his career to the advancement of microcirculation and lymphatics with more than 650 publications and too many gold medals and lifetime achievement awards to list? Professor Ryan still plays music most days on the grand piano he purchased more than a half century ago. He includes watercolour painting as one of his favourite hobbies (see his painting to the left). Now in his mid-eighties, Ryan is still actively writing about his work, travelling to remote places like India and keeping an eye on his many mentorees.
A lasting impact. Professor Ryan’s contributions to medical science are legendary. His experiences extended far beyond dermatology into the field of public health and education, especially of the poorest and neediest of people. There is probably no single dermatologist whose reach was as extensive. His work will have a lasting impact on the world of dermatology and lymphedema. We are indebted to him for his tireless and lifelong commitment. He is truly a lymphedema hero whose work will continue to inspire clinicians and researchers for many years to come.
His memoir Medicine and Body Image book can be purchased through www.wordsbydesign.co.uk Shipping available to North America.
Winter 2022/2023 www.lymphedemapathways.ca 13
“
“
Treatment of head and neck lymphedema


Improving patient quality of life
By Marize Ibrahim
As a segue from the previous article titled “Assessment of head and neck lymphedema” in the Pathways Summer edition 2022, head and neck lymphedema (HNL) is a significant complica tion of treatment for head and neck cancer (HNC). Its presence in this population is generally under recognized and under treated. As such, HNL has received less attention than lymphede ma that affects the extremities.1 For example, most of the literature focuses on breast-cancer related lymphedema, where between 5-50% of survivors will be affected.2-4 In contrast, as much as 90% to 97% of HNC survivors can be affected with HNL, either externally (i.e., face, neck) or internally (i.e., throat).5, 6 Clinically, the presentation of lymphedema parallels its level of severity. In the earliest stage, HNL may present as heaviness, tight ness, and barely noticeable fullness without functional impairment. However it can progress to a disfiguring condition with moderate to severe pitting edema and fibrosis that may or may not affect function.1 Depending on the location of the edema, substantial functional consequences may be present, including impairments affecting problems with speech, breathing, swallowing, and eating.1 Contrary to limb lymphedema, HNL symptoms are often worse at night and improved during the day due to the positive impact of gravity. Some HNL pa tients post laryngectomy may experience prob lems with stomal access for hygienic purposes,

difficulties with respiration, and with manage ment of a tracheoesophageal voice prosthesis. Swallowing, safely and efficiently, has been found to be impacted both by intra-oral edema and pharyngeal edema.7-9 Additionally, quality of life (QOL) is often significantly impacted by HNL. This includes, but is not limited to frus tration, embarrassment, and depression due to both functional and cosmetic changes.10-11 Treatment of HNL is essential for the rehabilitation of these deficits and improvement of the patient’s QOL. However, little has been published regarding effective management of HNL.12-13 To date, there is no published gold standard for treatment. Traditionally, Deconges tive Lymphatic Therapy (DLT) is considered the “gold standard” of lymphedema management.
The goals of DLT include: 1) to educate patients about lymphedema and its progression; 2) to provide risk reduction strategies; 3) to reduce excess volume and fibrosis levels; 4) to minimize the risk of bacterial infection (cellulitis); 5) to restore functional mobility and activities of daily living; 6) to improve the cosmetic appearance and the patient’s QOL and 7) to teach selfcare to promote independence in lymphedema management.14
Very little robust research is currently available to guide best practice guidelines for HNL treatment.15 HNL is distinctly different from lymphedema that occurs in other regions
of the body (i.e., upper and lower extremity), thus requiring a customized approach for its assessment and treatment.16 By utilizing the pillars of DLT management, a thorough head and neck (H&N) treatment protocol was established using a multidisciplinary approach at the McGill University Health Centre (MUHC) Lymphedema Clinic, a Lymphatic Education & Research Network (LE&RN) of Excellence. The following is a brief outline of the treatment tools utilized to manage HNL.
Treatment goals can be divided into five sections:
1 Self-Manual Lymphatic Drainage (MLD): The aim of self-MLD is to move fluid from the swollen region into another area where the lymphatic system is working better, so that the healthier lymphatics can remove the excess fluid accumulation. For HNL, the lymphedema
14 www.lymphedemapathways.ca Winter 2022/2023 Clinical Perspective
Marize Ibrahim Msc, PT, CLT-LANA is a lymphedema therapist working at the McGill University Hospital Center Lymphedema Clinic with Dr. Towers and her multidisciplinary team. She is a certified Clinical Specialist in Oncology by the Physiotherapy Speciality Certification Board of Canada.
therapist assesses the extent of the edema and reviews the best drainage pathway to take for each individual case, as this will vary depending on the type of cancer treatment and the areas affected. MLD for H&N is very different compared to upper or lower lymphedema. Firstly it’s much shorter, and second depending where the scars are, the therapist has to be careful not to go through them but around to the posterior neck. Radiation fibrosis is also a big problem for them, so we tend to combine massage with MLD to help break up the fibrosis or else the lymphedema won’t be able to pass through.
2 Skin care: As injury and infections can lead to local inflammation, further increasing lymphatic load; reducing the risk is critical. Some strategies taught to patients include decreasing the risk of sunburn (or other burns), insect bites or scratches from animals and skin abrasions (both externally and internally). Safer grooming practices are also encouraged (particularly for males), to avoid abrasions to the skin. Teaching the importance of using emollient/creams/ lotions/oils is also essential to improve skin integrity that has been radiated. Cuts and open wounds/sores should be carefully treated with an antibiotic ointment and monitored for the development of infection. Any sign or symptom of bacterial cellulitis, redness, warmth, pain, increased swelling should be investigated quickly by a physician for appropriate medical treatment. This can be challenging to assess due to permanent skin changes from surgery and radiation. It’s rare to get a cellulitis in the H&N region as our clinic sees more ulcers and would issues for this population.
3 Compression: A compression garment may or may not be required in any particular HNL patient. The goal of a H&N compression garment is to reduce lymphedema, promote lymphatic drainage and prevent refilling or worsening of the lymphedema. Compression is often used over night, as this is when an increase in HNL usually occurs. Modifications to donning of compression however may be required if patients have other medical conditions that may hinder them from using it at night (i.e. CPAP machine, tracheostomy). Furthermore, compression may help soften skin fibrosis that often develops following radiotherapy treatment. Compression has also been shown to reduce internal pharyngeal lymphedema which can improve dysphagia.16, 17 As there are several types of compression garments on the market, the lymphedema therapist will help guide the patient with which one would be the most appropriate for their individual needs. Additionally, pads may be made for individual cases to help soften pitting and fibrotic areas.
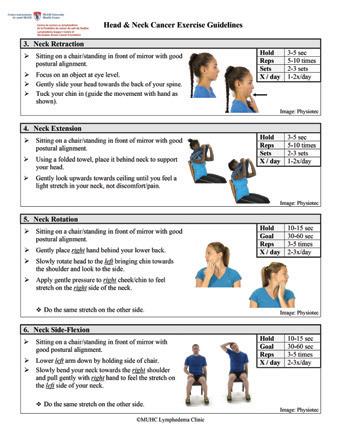
4 Exercise: Regular exercise is critical for HNL. These exercises can be broken down into different segments, including exercises for a) shoulder mobility (i.e. shoulder flex, abduction, external/internal rotation), b) postural re-alignment, c) cervical spine/ neck mobility (flexion, extension, right and left rotations, right and left side flexion and combined movements), d) tongue mobility (frenulum, elevation, protrusion, lateralization bilaterally), e) temporomandibular - TMJ (depression, elevation, protrusion, retraction and lateral movements), f) facial mobility

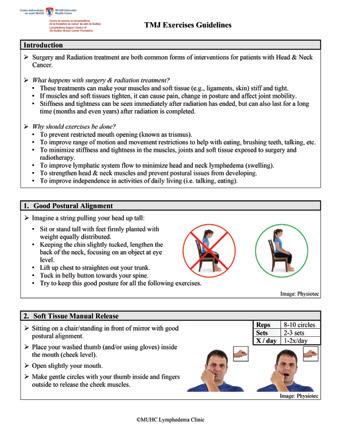

(cheek, palate, eye opening/closing) and g) dysphagia-swallowing maneuvers. Exercise promotes drainage by alleviating restrictions, improving muscle contraction to pump lymphatic fluid and increasing lymph flow. Deep breathing exercises are particularly helpful for H&N patients, added with MDL sequence and usually with shoulder ROM to get thoracic expansion. Additionally, achieving and maintaining a healthy body weight, as per the oncologist’s and nutritionist’s advice, is critical for lymphedema management to minimize excess strain on the lymphatic system.
Winter 2022/2023 www.lymphedemapathways.ca 15
https://www.canadianabilities.org/ Nominate your Caregiving Hero for our 2022 Canada Cares Awards One Wish Awards of up to $10,000 are available to support amazing family caregivers! canadianabilities.org Nominations close December 31, 2022
5 Self-Management: Lymphedema is a progressive condition that can advance through various stages of swelling and fibrosis, which can impair function, promote infection, and elicit considerable psychological distress. Daily self-management is required to slow lymphedema progression and minimize complications. Once lymphedema begins, lifetime self-management is required as currently there are no surgical or medical interventions that provide a cure. In contrast to other sites that may be affected by lymphedema, gravity appears to assist in lymph drainage of the H&N region, which naturally helps with

Treatment of HNL is essential for the rehabilitation of these deficits and improvement of the patient’s QOL.
management. Elevation such as wedges or bed adjustments can assist with reducing refill of the H&N areas overnight, especially if compression is not tolerated or effective. Self-management strategies include teaching the patient about the essential pillars of lymphedema management including selfMLD, exercise, compression (as needed), and skin care. Patients with HNL can benefit from a self-administered treatment program in the home setting once they have been properly assessed by a certified lymphedema therapist.17

In summary, the treatment of HNC
leads to post-treatment sequela including lymphedema, which can worsen and pose a great challenge for patients and clinicians. Unfortunately, HNL has not been well studied nor documented. This article summarizes a treatment protocol utilized at the MUHC Lymphedema Clinic for patients with HNL using the essential pillars of DLT. LP
For a full set of references including three documents outlining practical exercises for H&N cancer patients, visit https://www.canadalymph.ca/ pathways-references/
Acknowledgements: I would like to extend my sincere gratitude to Marie-Eve Letellier and Angela Yung for their contribution to this article and for their continued support. A special thank you to the head and neck patients with lymphedema as we strive to help them improve their quality of life as they manage their HNL.
https://klosetraining.com/
16 www.lymphedemapathways.ca Winter 2022/2023
For more information 1-303-245-0333 info@klosetraining.com klosetraining.com LYMPHEDEMA THERAPY CERTIFICATION Edmonton, Alberta & Toronto, Ontario class dates for 2023 to be annouced soon! Get the Klose Training Advantage: • 135-hours of lymphedema education • 75-hour engaging online module • 60-hr/6½-day classroom education • Exclusive post-graduate resources NEW ONLINE COURSES: • Breast Cancer Rehabilitation • Strength After Breast Cancer • Wound Management For Lymphedema Therapists • Head And Neck Lymphedema Management
What Ayurvedic medicine has offered me
A greater sense of self-love and a seasonal lens on a life well lived
Growing up on a large acreage in rural Ontario, nature was always on my doorstep, beckoning me outside. I loved going barefoot, almost half-naked when I was really little. But then I developed primary lymphedema and a strong emphasis on keeping my skin clean to ward off infections was required. That meant no more barefoot wanderings on the grass or running through
 By Amy Beaith
By Amy Beaith
This nature-based approach stuck with me as I built a career around plant-based skincare. I am now also studying Ayurvedic Medicine and taking Yoga teacher training. An Ayurvedic framework helps me look at living from a seasonal perspective, apply it to my overall health, and learn how to address my lymphedema daily self-care habits in a more natural way. Many practices from Ayurveda
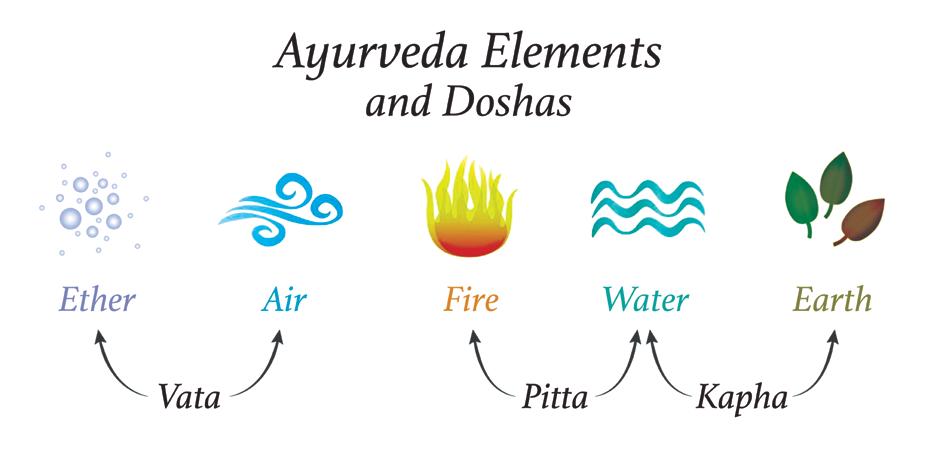
between us and our environment; seeing humans as a microcosm of a macrocosm; that we are made up of the same elements as the universe: earth, air, fire, water, and ether. Just as nature ebbs and flows with the seasons, so do humans. We are not the same person in summer as we are in winter.
the sand at the beach. I slowly became somewhat physically disconnected from nature in my body. However I learned to bring nature into my world in many other ways, from growing food in our garden, helping my dad with his beekeeping adventures, making maple syrup, or wandering the woods excited for spring and looking for the first trillium flowers!
have become more mainstream in recent years like Golden Milk Lattes, Tongue Scraping and Dry Skin Brushing. There are many simple everyday tools that I can easily apply to my Lymphie self-care routine and create a solid foundation for positive health following the rhythm of the seasons.
One of the special components of Ayurveda is the recognition of the central relationship
Amy Beaith is an Herbalist, Yoga Teacher in Training (YTT) and Certified Ayurvedic Coach. She is a “lymphie thriver” living in Edmonton, Alberta. Amy invites those who wish to learn more about Ayurveda and how to apply it to lymphedema self-care to contact her at amy@lymphwell.life

I find this especially true when I think of my lymphedema and how my body feels at these different times. Our bodies change, as the weather and climate changes around us. So too should the care of our bodies. By altering our diet, sleeping, skincare, and lifestyle habits change to respond to how our body is interacting with our environment, we stay in balance with nature. Something that has helped me cope with lymphedema is knowing what to expect each season and anticipating how best to respond to my needs. This can mean wearing a different grade of compression stockings in the summer and winter, or adjusting to the seasonal needs for my skin and gut.
In Ayurveda, the five elements are grouped together in three pairs called Doshas; Vata (Air + Ether), Pitta (Fire + Water), and Kapha (Earth + Water). These doshas are within us in unique combinations, are attributed to each season, times of day, and different organ systems in our bodies. So what does this look like? As we are made up different combinations of these elements, in Ayurveda, you can have different constitutions, or body types/tendencies. So how does this look from a seasonal and lymphedema perspective? Here is an example.
Winter 2022/2023 www.lymphedemapathways.ca 17
Personal Perspective
Winter time is Kapha; that heavy, solid en ergy of Earth and Water together. Think of trees, rocks, solidness in our bodies like muscles, bones; internal organs like our liver. The stur diness of our legs to hold us up. The seasonal energy of Kapha is cold, dark, and wet. Here in Edmonton, the earth has a big, heavy, white, sparkly blanket on top. This heavier energy may affect us with heavy emotions, such as having a harder time with the darkness; feeling sad, unmotivated and lonely. This can affect our lymphedema in that we may spend less time on our self-care, we may be less motivated
to decrease our swelling, or get something checked out, order new stockings, or we may reach out to our community less than usual. Overall, we may want to do less. We may expe rience the feelings of heaviness in our bodies with our lymphedema limbs feeling more achy, full, or heavy. And that’s okay. The first part is to acknowledge what’s going on energetically and how it’s affecting you and create a self-care plan to bring your body back into balance.
The cold air of winter brings a dryness (both inside and outside) that can be quite drying on both our skin and our respiratory tract. So, it’s important to tend to your skin with moisture, much like we do in the fall dryness with root veggies, warming soups, stews, as well as making time for dry-brushing and moisturizing with balms and creams. Boosting our immune system throughout the winter can be helpful as well. Appropriate rest is probably one of the easiest elements of therapy as well as the cheapest health habits to add to your routine, especially in the winter. Ayurveda teaches us that from roughly 10pm until 2am (Pitta time), our body is digesting our day and detoxifying our

body, processing emotions and experiences into memories, and foods into nutrients, and gather ing up toxins and wastes to be flushed out in the morning. Detoxifying is an important function of the lymphatic system, and as a person with lymphedema, this is an easy way to support my body’s ability to detoxify the best that it can.
Other ways I dissipate the heaviness are to reach out to friends and community to chat, gather, and share a laugh or two! Laughter is such wonderful medicine to lighten the body, soul and mind! In winter, I make more time to use my compression pump during the day, as a break. I set aside time for this, making it special and shifting from thinking of it as a chore, to making it more enjoyable with a good book, a mug of tea, and a blanket.
My morning winter routine:
Setting myself up for a good day ahead
4 Smile as soon as I wake
4 Give my collarbone area and shoulders a little self MLD
4 Take my compression garments off, dry brush and inspect my skin
https://www.clt-lana.org
18 www.lymphedemapathways.ca Winter 2022/2023
Golden
Look for the CLT-LANA credential because it matters! For more information, visit www.CLT-LANA.org.
latte—an Ayurvedic favourite; wonderful warming and lymph-loving elixir for the winter season.
4 Do five sun salutations to get my lymph and energy flowing
4 Then shower, moisturize, and tongue scrape
4 Get my compression garment on
4 Drink a glass of warm water with lemon
4 Walk/exercise/yoga
My typical evening winter routine: winding down from the day
4 Finish eating 3-4 hours before bedtime
4 Get ready for bed around 9pm with no blue light after 8pm (ideally)
4 Fifteen minutes of gentle bedtime yoga stretches and self MLD to open up my lymph channels to encourage drainage and promote relaxation (e.g. seated cat-cow, gentle twists, self-MLD around my collar bones, neck, and shoulders)
4 Gratitude. When I begin checking over my body, I approach this time with curiosity and tenderness. I thank my body for carrying me today, such as for my legs for being able to walk to pick up my kids at the bus, for hands that carried groceries and gave hugs, or eyes to see my notes for a project I am working on.
Detoxifying is an important function of the lymphatic system, and as a person with lymphedema, this is an easy way to support my body’s ability to detoxify the best that it can.

4 Skincare. Apply herbal body oils, balms and/ or creams all over or where needed. Oiling the body in Ayurveda is called ‘sneha’ and also translates to ‘to love the body’. Take time to care for your skin, especially the soles of the feet, which is very relaxing to the nervous system and encourages a good night’s sleep.
4 Listen to a Yoga Nidra sleep meditation to help me drift off to sleep
Ayurvedic medicine encourages us to do selfcare throughout the day and is a wonderful framework that has allowed me to approach caring for my body with more curiosity, seeing myself as a beautiful, unique part of nature, with strengths and weaknesses, and to love my body with lymphedema. I now embrace a whole-self approach to my Lymphie self-
care (body, mind, and spirit), exploring what my body needs to thrive and be in balance in this moment in time. I have been able to reduce my inflammation, heal my gut (from many rounds of antibiotics over the years for cellulitis infections) and improve my self-care and compliance. Those are wins in learning to “Lymph Well to Live Well.” LP
References
n Lad, V. (1984). Ayurveda: The Science of Self-Healing - A Practical Guide. (2019) ed. Lotus Press. n O’Donnell, K. (2020). The Everyday Guide Ayurveda Guide to Self-Care. Rhythms, Routines, and Home Remedies for Natural Healing. Shambala Press. n 100 hr Teacher Training in Ayurveda. La Vida Veda Institute. 2021-2022.
Winter 2022/2023 www.lymphedemapathways.ca 19
Hints and Tips: Staying “In The Know”

There are many tools available to help you stay current with new developments in lymphedema research, diagnosis, and treatment. In addition to reading Pathways, you can also subscribe to the CLF’s eNews and follow us on our social media platforms. Scan the QR code or find links online here: linktr.ee/canadalymph.








https://linktr.ee/canadalymph https://www.google.ca/alerts



Google Alerts allows you to be notified by email whenever Google finds new search results about lymphedema, such as web pages, newspaper articles, blog posts or scientific research. Visit google.ca/alerts to set up your search criteria, frequency, and delivery preferences.
Sosido Digest is an online knowledge exchange network built for and by healthcare associations. This platform is used by the American Lymphedema Framework Project to disseminate lymphedema research and publications. You can sign up to receive a free weekly email digest here: alfp.org/sosido. Pathways is a quarterly publication of the Canadian Lymphedema Framework targeted to patients and those who support their care. Subscribers can access print and digital versions. Subscribe at canadalymph.ca/pathways.
https://www.alfp.org/sosido http://www.canadalymph.ca/pathways/ https://www.woundsinternational.com/journals












Journal of Lymphoedema is an annual, online, practice-based journal published by Wounds International for healthcare professionals. Find it online at woundsinternational.com/journals.


https://pubmed.ncbi.nlm.nih.gov/
PubMed® searches more than 34 million citations and abstracts for biomedical literature from MEDLINE, life science journals, and online books. Free links to full-text articles are sometimes available. You can create an account and set up alerts, or search without an account. Learn more here: pubmed.ncbi.nlm.nih.gov.
Lymphatic Research and Biology is a quarterly, peer-reviewed journal, delivering the latest developments and advances in lymphatic biology and pathology from around the world. Learn more at tinyurl.com/LRB-Journal. LP
https://home.liebertpub.com/publications/ lymphatic-research-and-biology/114/overview


https://www.lymphologyskincare.com/
https://www.lymphologyskincare.com/

20 www.lymphedemapathways.ca Winter 2022/2023
Helpful Suggestions Order from us directly! happy. healthy. skin.
Did You Know?
Health-related quality of life
OBJECTIVE: To determine the impact of lower limb lymphedema (LLL) on health-related quality of life (HRQoL), and to identify the methodologies used to assess HRQoL and their adherence to the World Health Organization (WHO)-recommended HRQoL dimensions.



METHOD: A systematic review was used following the PRISMA guidance. Studies were eligible if they assessed HRQoL in adult patients with LLL. The search was conducted using CINAHL, PubMed, Scopus, EMBASE and the Cochrane Library database. Data were placed onto a pre-developed data extraction table and analysed using a narrative synthe sis. Evidence-based Librarianship (EBL) was used for quality appraisal. RESULTS: A total of 18 studies were identified, among which 10 were cross-sectional and eight were longitudi nal studies. Twelve HRQoL questionnaires were identified and the Lymphoedema Quality of Life tool (LYMQoL) was the most commonly used. All of the studies except one had an EBL validity score of ≥75%. Although LLL causes a considerable impairment in HRQoL, the findings varied across the studies. All the studies considered at least four of the six WHO recommended dimensions, with none considering the spirituality dimension. Furthermore, physical functioning and wellbe ing were discovered to be the worst affected HRQoL dimensions. CONCLUSION: LLL adversely affects physical function, wellbeing and thus the HRQoL. The LYMQoL is the most commonly used questionnaire; despite this, all elements of the WHO recommendations were not captured in the included studies. However, accurate information on HRQoL indicating the impact of the disease on survivors’ lives and complete wellbeing is needed to inform evidence-based decision-making. Furthermore, having a universally accepted, disease-specific methodology will facilitate comparison and con trasting of HRQoL in patients with LLL.

Source: J Wound Care. 2022 Aug 2;31(8):690-699. doi: 10.12968
Water-based exercise


Although water-based exercise can be useful, there is currently little evidence on the out comes of aquatic treatment for patients with lymphedema. The aim of this scoping review is to evaluate, based on current literature, the impact of water-based exercise on pain, limb motor function, Quality of Life (QoL), and limb volume among patients affect ed by primary and secondary upper and lower limb lymphedema. MATERIALS/METHODS:

A scoping review examining clinical studies and Randomized Controlled Trials (RCTs) was conducted screening MEDLINE (Pubmed) and PEDro databases. RESULTS: The search produced a total of 88 studies. 8 RCTs and one clinical study including patients with primary or secondary lymphedema of upper or lower limbs who benefited from water-based treat ment were finally included. Most trials were focused on breast cancer related lymphedema. Shoulder range of flexion, external rotation and abduction have been shown to improve after performing a water-based exercise protocol. Some evidence demonstrated that also the lymphedematous limb strength can improve. Moreover, water-based exercise seemed to improve pain perception and QoL in patients with upper or lower limb lymphedema, whereas in the control groups QoL tended to worsen over time. While some studies did not show a beneficial effect on the lymphedematous limb volume, most of the studies examined showed a reduction in volume, especially in the short term. No studies reported adverse events. CONCLUSION: This review shows the potentials of aquatic exercise in lymphedema management, but at the same time it under lines multiple limitations due to the heteroge neity in study population and related physical activity protocols. The aquatic exercise role in the conservative treatment of lymphedema will need to be further investigated in the future in order to define specific protocols of application. Source: J Vasc Surg Venous Lymphat Disord. 2022 Aug 19:S2213333X(22)00354-7
Artificial intelligence
The past two decades have witnessed an increasing implementation of artificial intelligence (AI) in health-care services. The nature of the challenges facing the lymphedema practice (eradication of tropical LE, preclinical diagnosis of cancerrelated lymphedema, and delivery of appropriate individualized care) is suitable for AI applications. The AIM of this study was to explore the current AI applications in lymphedema prevention, diagnosis, and management and investigate the potential future applications. METHODS/RESULTS: Four databases were searched: PubMed, Scopus, Web of Science, and EMBASE. We used the Preferred Reporting Items for Systematic Reviews and Meta-Analysis as our basis of organization. Our analysis showed that several domains of AI, including machine learning (ML), fuzzy models, deep learning, and robotics, were successfully implemented in lymphedema practice. ML can guide the eradication campaigns of tropical lymphedema by estimating disease prevalence and mapping the risk areas. Robotic-assisted surgery for gynecological cancer was associated with a lower risk for the lower limb lymphedema. Several feasible models were described for the early detection and diagnosis of lymphedema. The proposed models are more accurate, sensitive, and specific than current methods in practice. ML was also used to guide and monitor patients during the rehabilitation exercises. CONCLUSION: AI offers a variety of solutions to the most challenging problems in lymphedema practice. Further, implementation into the practice can revolutionize many aspects of lymphedema prevention, diagnosis, and management. Developing new modalities for prevention, early diagnosis, and treatment are critical to improve the outcomes.
Source: J Clin Transl Res. 2022 Jun 1;8(3):234-242
Winter 2022/2023 www.lymphedemapathways.ca 21
Research Advances
Canadian and International Events

Feb 23, 2023 – London, UK
British Journal of Community Nursing. 10th Annual National Lymphoedema Conference. n www.lymphoedemaconference.co.uk
March 4, 2023 – Online/Virtual Obesity Canada. Connected 2023 Virtual Conference. n www.obesitycanada.ca/connected-2023
March 6, 2023 – Worldwide

International World Lymphedema Day (WLD). Contact your provincial lymphedema association to learn about local events. Watch for our special Spring issue of Pathways dedicated to WLD. n www.canadalymph.ca/WLD
April 26-29, 2023 – Denver, CO

POWER Symposium (POWER Retail, POWER Lymphatics). n www.thepowersymposium.com
May 19-21, 2023 – Auckland, NZ
Australasian Lymphology Association. 2023 ALA Symposium: United Together. n www.lymphoedema.org.au
June 13-15, 2023 – Nottingham, UK
The 11th International Lymphoedema Framework (ILF) Conference, in collaboration with the Lymphoedema Network Wales. n www.lympho.org/conferences
June 13-17, 2023 – Banff, Alberta
LE&RN and NAVBO. Lymphatic Forum 2023. n www.lymphaticforum.org
September 11-15, 2023 – Genova, Italy
International Society of Lymphology (ISL). 29th World Congress of Lymphology. n www.isl2023lymphology.com
Late Fall 2023 – TBD
Canadian Lymphedema Framework. 2023 National Lymphedema Conference. n Sign-up for updates: tinyURL.com/2023-NLC-Updates
https://tinyurl.com/2023-NLC-Updates
Pathways is available by subscription either directly from the CLF or through one of our Provincial Association partners. www.canadalymph.ca/subscriptions







CANADIAN LYMPHEDEMA FRAMEWORK PARTENARIAT CANADIEN DU LYMPHOEDÈME

www.lymphedemapathways.ca

Letters to the Editor...
Thank you very much for the wonderful Pathways magazines. I really love the (Fall) cover. It is great to have the headline “psychological aspects” next to a smiling face. I like that very much.


Gabriele Erbacher, Senior Psychologist Foeldi Clinic, Hinterzarten, Germany
___________________________________________________ ___________________________________________________ ___________________________________________________ ___________________________________________________ ___________________________________________________ ___________________________________________________ ___________________________________________________ ___________________________________________________ ___________________________________________________ _______________________________________________________________ _______________________________________________________________ _______________________________________________________________ _______________________________________________________________ _______________________________________________________________ _______________________________________________________________ _______________________________________________________________ _______________________________________________________________ _______________________________________________________________ _______________________________________________________________ _______________________________________________________________ _______________________________________________________________ _______________________________________________________________
Editor’s Note... A Letter to the Editor (Spring 2022) that referenced an advertisement generated considerable controversy. The Editorial Board apologizes for publishing this letter and regrets the error. Although we promote the respectful exchange of viewpoints on our articles, Pathways is not a forum for debate about advertisements. Readers wishing to learn more may visit the advertiser’s website at: tinyurl.com/LLS-Online.
https://tinyurl.com/LLS-Online
https://tinyurl.com/CLF-CE-Info
The Canadian Lymphedema Framework (CLF) wishes to thank these partners for their support in making this magazine a reality.
22
Winter 2022/2023
https://www.canadahelps.org/en/charities/canadian-lymphedema-framework-partenariat-canadien-du-lymphoedeme/ Education Education
ABOUT THE CLF: The CLF is an academic and patient collaboration, working to improve lymphedema management for lymphedema and related disorders in Canada. Charitable Registration 85160 1260 RR0001
Winter and Spring Dates Coming Soon ONLINE E-LEARNING: Lymphedema and Chronic Edema Management. University of Alberta eClass Micro Course. n www.tinyurl.com/CLF-CE-Info







https://venosan.ca/en/ Rosidal K tg ® tubular Rosidal soft Compression bandaging to support your life. Not the other way around. www.Lohmann-Rauscher.ca inquiries@ca.LRmed.com 1-888-836-6726 2599 Fitter & Therapist In-service Request an in-service. For medical professionals only.
https://www.woundscanada.ca/programs/programs-overview




