
15 minute read
s tu DeN t CA se R ep OR t pericardial mesothelioma in a 6-year-old German shepherd dog


CHAR l O tte Bell AtON, BVscV
Abstract
Canine mesothelioma is a rare form of neoplasia in dogs which is challenging to diagnose and treat and is usually associated with a poor prognosis. mesothelioma of the thoracic cavity can involve the pleural space and/ or the pericardial sac and this diffuse cavity involvement often requires an invasive method of biopsy to confirm the diagnosis. t his case report describes the presentation, diagnosis, treatment and outcome of mesothelioma of the pericardial/pleural spaces in a 6-year-old German Shepherd dog that presented for lethargy, inappetence and a distended abdomen. Initial pericardiocentesis suggested septic pericardial disease. However the subsequent development of marked pleural effusion prompted surgical intervention, allowing relief from cardiac tamponade via a sub-total pericardiectomy and confirmation of the diagnosis by histopathology. ultimately the treatment was unrewarding, with rapid return of pleural fluid prompting euthanasia.
Introduction
Canine pericardial mesothelioma is a rare, spontaneous, neoplastic disease of dogs that can arise from either the peritoneum, pericardium or pleura and less commonly from the tunica vaginalis (Nabeta et al. 2019; moberg et al. 2021; Lajoinie et al. 2022). Indeed, it represents only 0.2% of all canine neoplasms but nevertheless is a serious disease that
Contact: bellatoncharlotte@gmail.com is rapidly fatal due to progression of the pericardial effusion into cardiac tamponade (macDonald et al. 2009; Nabeta et al. 2019; Scheuermann et al 2020). t he cavitary effusion associated with mesothelioma is thought to be due to the blockage of lymphatic drainage as a result of diffuse thickening of the tissue (moberg et al. 2021). Less commonly, mesothelioma can spread into regional lymph nodes and other regional organs (macDonald et al 2009; moberg et al. 2021). t he cause of mesothelioma development in dogs is not well understood but Glickman et al (1983) suggest a possible association with asbestos exposure and related compounds found in powdered flea products and pesticides. mesothelioma is challenging to diagnose without tissue for histological assessment. Indeed, cytology of the pericardial effusion has poor sensitivity to differentiate mesothelioma from reactive mesothelium (mesothelial hyperplasia) or carcinoma (milne et al 2021). ultrasonography of the thoracic and pericardial cavities usually does not offer greater differentiation of diseases causes, due to the diffuse, granular distribution of the cancer. Even magnetic resonance imaging (mRI) is unlikely to be useful as although it can highlight pericardial thickening, it is not able to differentiate the origin of this thickening (Gallach and mai 2013). Hence, confirmation of mesothelioma requires biopsy and histology of the affected tissue with special stains and immunohistochemistry (milne et al. 2021). Due to its typical location, obtaining biopsy samples can be a challenging and invasive procedure to perform. t he aim of this case report is to describe the clinical presentation and clinical findings, histopathological results, treatment and outcome of a case of pericardial mesothelioma in a dog that presented to the massey university Veterinary teaching Hospital (muV t H). t he diagnostic challenge in such cases and current available treatment options for canine mesothelioma will also be discussed.
Case history and initial clinical findings
A 6-year-old, female, spayed German Shepherd dog presented initially to its primary veterinarian for lethargy, inappetence and a distended abdomen. Clinical examination revealed increased respiratory effort and ultrasonography ( t FAS t/AFAS t scan protocols) showed significant pericardial effusion with severe cardiac tamponade. Abdominal radiographs ruled out gastric dilation and volvulus. Pericardiocentesis was performed and 640 mL of serosanguinous fluid with a PCV of 18% was obtained. Cytology revealed a haemorrhagic and inflammatory effusion composed predominantly of neutrophils (85–95%) with occasional extracellular rod-like bacteria. Reactive mesothelial proliferation was also noted at this time. Given the inflammatory nature of the effusion and the few bacteria observed, the diagnosis considered most likely at this time was septic pericarditis and the dog was prescribed a 4-week course of 15 mg/kg amoxycillin/clavulanic acid twice daily. microbial culture came back negative but a septic aetiology was still considered, and the course of antibiotics was pursued in case this was a false negative result.
one month later the dog represented in respiratory distress and thoracic ultrasonography confirmed recurrence of pericardial fluid (Figure 1).
Pericardiocentesis was repeated and 500 mL of haemorrhagic fluid was drained. A sample of this was again submitted for cytological interpretation yielding a similar cellular composition. t he differential diagnosis list under consideration at this time was septic pericarditis, idiopathic haemorrhagic pericardial effusion and haemangiosarcoma. As the effusion still contained inflammatory cells, the dog was prescribed a further antibiotic course of 5 mg/kg clindamycin twice daily.
twelve days later the dog represented with a weak pulse and pale mucous membranes and a further 706 mL of fluid was drained from its pericardial sac.
t horacic radiography and abdominal and cardiac ultrasound were repeated. Imaging did not reveal any noticeable tumour at the heart base, on the right atrium or within the pericardium. At this stage the dog was presumed to have idiopathic pericardial disease and 1 mg/kg prednisone at 1 mg/kg SID was dispensed. A recheck ultrasound examination performed 3 weeks later did not show any considerable fluid build-up.

However 1 week later, a large volume of serosanguinous fluid was drained from the pericardial sac but the respiratory effort did not improve. Subsequent thoracic radiography (Figure 2) and showed an unstructured interstitial pattern, lobar signs, cardiac border effacement, increased soft tissue opacity in the sternal region and reduced lung fields consistent with pleural effusion. A further 2.5 L of fluid was drained from the pleural cavity. Referral to the mu V t H was offered in order to discuss potential surgical intervention to relieve the tamponade.
Clinical findings upon referral
on arrival at the muV t H 10 weeks after the initial problem was identified by the referring veterinarian, the dog presented with muffled heart sounds and tachypnoea. t he heart rate was 88 beats per minute with a strong and synchronous pulse.
t he case was reviewed and the chief differential was considered to be neoplasia of a diffuse nature. Idiopathic pericarditis was considered less likely due to the extent of pleural fluid that seemed to be overwhelming pleural drainage and given the lack of response to two courses of antimicrobials an infectious course was considered unlikely. Exploration and biopsy of the thoracic cavity and pericardial sac were considered necessary for a diagnosis. t horacoscopy for pericardial window and biopsy and an open thoracotomy which would allow a sub-total pericardiectomy were discussed. t he latter offered a higher probability of thorough thoracic inspection but with higher morbidity. t he owner elected open surgery.
Surgical And Histopathological Findings
under general anaesthesia with mechanical ventilation, a median sternotomy was performed. Extensive miliary nodules were found covering the mediastinum and outer pericardium. o ther patches of nodular disease were present on the thoracic wall’s pleural surface on the left side. An impression smear of the nodular disease was prepared intra-operatively and sent to the IDEXX laboratory (Palmerston North) for a S tAt read. mesothelial cells with atypia and neutrophilic infiltration were diagnosed but no definitive diagnosis of neoplasia was possible based on the cytology. Biopsies of the pericardium were then taken and fixed in 10% buffered formalin for histopathological analysis. A sub-total pericardiectomy was performed preserving the phrenic nerve pathways and the sternotomy was closed routinely.
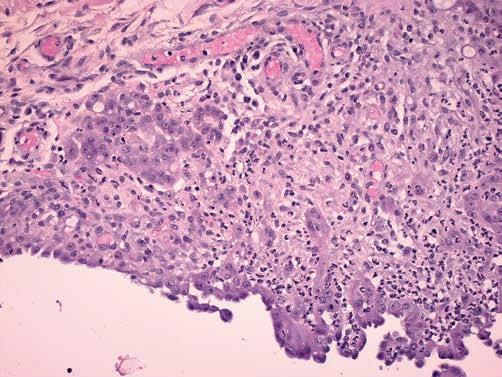
t he histology revealed diffusely thickened pericardium and mediastinum with a moderate amount of pleomorphic cuboidal to polygonal cells consistent with neoplasia (Figure 3). Features of malignancy such as mild anisokaryosis, small nucleoli and stippled chromatin were also observed. t he mitotic index was low and there was a prominent amount of neutrophils alongside haemosiderophages. t hose observations are highly suggestive of mesothelioma but metastatic carcinoma could not be fully ruled out.
Following surgery, the dog recovered well and was initially maintained on a constant rate infusion of ketamine (0.003 mg/ kg/minute) and fentanyl (0.003 mg/kg/hour) for pain control and chest drain care was performed every 4 hours. t he dog no longer required opioids for analgesia 24 hours after surgery and was bright and ambulatory. t he drain production decreased from 0.6 mL/kg/hour 24 hours following the surgery, to 0.19 mL/kg/hour 48 hours after surgery and to 0.36 mL/ kg/hour 60 hours after surgery. Despite mildly increased respiratory effort and tachypnoea the drain was not producing much fluid and so was pulled out 3 days after surgery. t he dog was discharged 2 days later with 12 mg/kg paracetamol to be given twice daily for post-operative pain management. Chemotherapy options were discussed but not instituted due to limited efficacy and high cost.
t he pleural effusion recurred 1 month following the surgery and therefore the option of placing a PleuralPort (https:// norfolkvetproducts.com/products/pleuralport/) to provide palliative drainage was offered. However, the owner elected to not pursue any further treatment and the dog was euthanised
1 month after the surgery due to a deteriorating state and nonresolving respiratory distress.
Discussion
t his case report highlights some of the challenges in establishing a diagnosis of canine mesothelioma. At presentation, the clinical signs are non-specific, as they are related to cavitary effusion which may have multiple aetiologies. moreover, the cytological features of reactive mesothelial cells, mimic the features of neoplastic mesothelial cells (macDonald et al. 2009; Gallach et al. 2013; milne et al. 2021; moberg et al. 2021; Lajoinie et al. 2022), making differentiation of the two using cytology very difficult. In the initial management of this case, septic pericarditis was placed at the top of the differential list due to the inflammatory nature of the fluid cytology despite negative culture. t he cytology report mentioned a prominent neutrophilic population in the effusion but no degenerate neutrophils were noted. occasional rod bacteria were also seen but none were intracellular. t hese findings are suggestive, but not strongly indicative, of a septic effusion. As mentioned in the study by milne and others (2021), cytology has only 56% sensitivity for the diagnosis of mesothelioma and it is not unusual to see non-degenerate inflammatory cells on cytology of a mesothelioma (Stevens et al. 2014; moberg et al. 2021). Septic pericarditis in dogs is not a common diagnosis and is usually associated with a penetrating wound, local extension of infection or a migrating foreign body (Johnson et al. 2004; Botha et al. 2017). Pleural effusion secondary to neoplastic disease is actually more common. Indeed, Scheuermann and others (2020) report that 60–70% of pericardial effusion cases in dogs occur secondary to a neoplastic aetiology with haemangiosarcoma, mesothelioma and chemodectoma being the most common causes. t he same study further categorises mesothelioma as being responsible for 20% of cases of neoplastic pericardial effusion while the study of macDonald and others (2009) reports an incidence rate of 14% for pericardial mesothelioma when pericardial effusion is present.

When the effusion culture was negative, it was interpreted as a false negative result and the course of antibiotics continued. However, the occasional bacteria seen on the initial cytology may have been due to contamination of the sample either at the time of the collection or while preparing the microscope slide, or were erroneously identified as bacteria.
Imaging can offer useful information in terms of ruling out other causes of pericardial effusion, such as a migrating foreign body, heart base tumour or cardiac haemangiosarcoma and it can also reveal a diffusely thickened pericardium (macDonald et al. 2009; Gallach and mai 2013). But due to mesothelioma’s growth pattern of diffuse thickening of the tissue and miliary nodules, imaging is not a definitive diagnostic tool for mesothelioma. C t and mRI are the imaging modalities of choice in most studies as they allows soft tissue structures and discrete masses to be visualised. Nevertheless, ultrasonography, in the hands of an experienced radiologist, has been reported to also be an acceptable method for ruling out heart base tumours or cardiac haemangiosarcoma as a cause of pericardial effusion (macDonald et al. 2009; Nabeta et al. 2019). macDonald et al. (2009) state that the sensitivity and specificity of ultrasound to detect cardiac masses is 82% and 100% respectively. t he sensitivity can increases up to 88% with repeated echocardiographic exams. In this case, cardiac ultrasonography did not reveal any discrete mass in the right atrium nor at the heart base. Advanced imaging via C t or mRI were offered to the client in order to investigate the other possible causes of pericardial effusion, but due to the cost of either procedures and the limited information they were expected to provide, the owner did not elect to pursue C t or mRI. t he development of new diagnostic tools as means to get a definitive diagnosis without an invasive method of sampling has been investigated. milne et al. (2021) investigated the accuracy of diagnosing mesothelioma using cell block immunohistochemistry, as this requires a less invasive sample collection method. However, these authors concluded that whilst a diverse panel of stains is helpful to distinguish reactive mesothelial cells from neoplastic cells, the definitive diagnosis remains nonetheless difficult. Hence, as other literature suggests, the definitive diagnosis of mesothelioma currently relies on the conjunction of clinical signs, cytology, imaging, histology and immunochemistry of biopsies (Lajoinie et al. 2022).
In this present case, the amalgamation of clinical signs of recurrent, non-septic pericardial effusion, the developing pleural effusion and the lack of distinguishable mass on ultrasound made mesothelioma the most probable diagnosis. However, surgical biopsies were needed for a definitive diagnosis. In order to obtain a tissue diagnosis, thoracoscopic or open surgical biopsy were required. Biopsies of the mediastinum and pericardium were taken during open thoracic surgery via sternotomy and subsequent histology supported the diagnosis of canine pericardial mesothelioma.
In terms of management of this case, the current recommendations for treatment of recurrent pericardial effusion were discussed with the owner prior to surgery. t here is a lack of gold-standard treatments for recurrent pericardial effusion in dogs, despite several technique being described. t he first option was making a thoracoscopic pericardial window to allow the fluid to drain into the pleural space and be reabsorbed via lymphatic drainage. t he second option was to perform a subtotal pericardiectomy, which involves resecting the parietal pericardium ventral to the phrenic nerve, thus removing most of the causative tissue and relieving permanently the cardiac tamponade. t his latter surgery is either performed via sternotomy or thoracoscopy. t he choice of the surgical approach is determined by the requirement for haemostasis during the surgery with sternotomy offering a greater capacity for limiting haemorrhage. t he pleural effusion recurred within 1 month after surgery, and the owner was offered the palliative option of placing a PleuralPort to facilitate the drainage of the pleural cavity. A PleuralPort was advised over pleuraperitoneal shunt or pleurovenous shunt as these are associated with metastatic spread of the disease in the peritoneum and thrombosis formation, respectively (Brooks and Hardie 2011).
Studies by Scheuermann and others (2020) and Case and others (2013) demonstrate that sub-total pericardiectomy, specifically for managing pericardial mesothelioma, increases the median survival time (mS t ) significantly compared to intermittent pericardiocentesis or to the pericardial window technique. Indeed, dogs receiving a sub-total pericardiectomy had a mS t of 10.3 months compared to 8.6 months for those that received a pericardial window. In this case, the presence of marked pleural fluid accumulation warranted investigation beyond the limits of thoracoscopy in our hands. t he surgical approach was via sternotomy as this allowed better visualisation of the pericardium and pleural space, allowed quantification of the extent of the disease, as well as better control of haemorrhage and preservation of the phrenic nerve while removing the parietal pericardium.
Adjunctive chemotherapy has shown only marginal benefit by increasing the mS t from 195 days to 234 days after resection of the pericardium (moberg et al. 2021). more favourable response was reported by Lajoinie and others (2022) who reported that chemotherapy increased the mS t to 366 days compared to 74 days for dogs who did not receive chemotherapy. t he chemotherapeutic agents used in this study were cisplatin with carboplatin given intracavitary and carboplatin with doxorubicin given IV.
However, this study did not differentiate which chemotherapeutic agent was associated with the better outcome and 41% of dogs received several different drugs in their protocol. Additionally, chemotherapy is associated with adverse reactions in 28% of cases (moberg et al 2021) and decreases the quality of life temporarily. t herefore, although this was discussed, the owner declined to pursue chemotherapy due to the guarded prognosis and the likely decline in quality of life it would have caused.
PleuralPorts are reported to be welltolerated in dogs, and can be an effective way to drain the thorax at home without the repeated need for veterinary intervention, hence reducing the cost and the risk of potential iatrogenic trauma caused by repeated thoracocentesis (Brooks and Hardie 2011; moberg et al. 2021). moreover, Brooks and Hardie (2011) stipulate that the placement of the port is minimally invasive and that they are well-tolerated as they are made of inert material, thus can remain in the thorax for an extended period (months) as well as providing an adequate alternative for palliative care. However, the same study also reported port blockage and pneumothorax as the most common complications associated complications with PleuralPort devices. Additionally, in this specific case, given the amount of fluid being produced by the pleura and the small bore of the Huber needles available, regular and prolonged manual drainage would have been required. Consequently, considering the cost, the requirement of another surgery, the anaesthetic risk, the care needed to keep the port clean and patent and the diagnosis and prognosis of the condition, the owner declined the installation of the PleuralPort.
Conclusion
As causes of pericardial effusion in dogs haemangiosarcoma and mesothelioma are more common than septic pericarditis. However, despite a predisposition of German Shepherds to haemangiosarcoma, this condition was ruled out relatively early in the diagnostic course due to the absence of a discrete mass in the right atrium on cardiac ultrasound and thoracic radiography. Septic pericarditis was also ruled out via negative culture and the lack of response to antibiotic therapy. As the disease progressed, idiopathic pericardial effusion was thought to be the most probable diagnosis. However after the condition progressed to pleural effusion, the suspicion of malignant mesothelioma became more likely and surgery was advised to provide a definitive diagnosis and manage the condition procedure. Sternotomy and sub-total pericardiectomy were performed as this is described as the most successful surgery to manage pericardial mesothelioma in the literature, and the dog recovered well. Histopathology of biopsies confirmed a diagnosis of malignant mesothelioma. Chemotherapy was offered but not strongly advised, as despite the reported increase in mS t, it is only palliative and may lower the quality of life for a transient period at least. Eventually, significant pleural effusion recurred. Placement of a PleuralPort was proposed but declined by the owner due to cost and the poor prognosis regardless. t he dog was euthanised 1 month after surgery due to recurrent and worsening signs of respiratory distress.
t his case report demonstrates the diagnostic challenge posed by mesothelioma as well as the associated poor prognosis and the lack of efficient treatment available in veterinary medicine.
Acknowledgements
t hank you to the staff of the surgical and anaesthesia departments of the muV t H. Susan Piripi performed the cytology and histopathology and Andrew Worth was the attending clinician and surgeon.
References
Botha WJ, Mukorera V, Kirberger RM. s eptic pericarditis and pneumopericardium in a dog with an oesophageal foreign body. Journal of the South African Veterinary Association 88, a1496, 2017, https://doi.org/10.4102/ jsava.v88i0.1496
Brooks AC, Hardie RJ. use of the pleural port device for management of pleural effusion in six dogs and four cats. Veterinary Surgery 40, 935–41 2011, https://doi.org/10.1111/j.1532950x.2011.00901.x
Casamián-Sorrosal D, Fournier D, Shippam J, Woodward B, Tennant K. s eptic pericardial effusion associated with pulmonary and pericardial botryomycosis in a dog. Journal of Small Animal Practice 49, 655–9, 2008.,https://doi.org/10.1111/j.17485827.2008.00605.x
Case JB, Maxwell M, Aman A, Monnet EL. Outcome evaluation of a thoracoscopic pericardial window procedure or subtotal pericardectomy via thoracotomy for the treatment of pericardial effusion in dogs. Journal of the American Veterinary Medical Association 242, 493–8, 2013, https://doi. org/10.2460/javma.242.4.493
Gallach RG, Mai W. Cardiac m RI findings in a dog with a diffuse pericardial mesothelioma and pericardial effusion. Journal of the American Animal Hospital Association 49, 398–402, 2013. https://doi.org/10.5326/jaaha-ms-5925
Glickman LT, Domanski LM, Maguire TG, Dubielzig RR, Churg A. mesothelioma in pet dogs associated with exposure of their owners to asbestos. Environmental Research 32, 305–13, 1983
Johnson JM, Martin MW, Stidworthy MF. s eptic fibrinous pericarditis in a cocker spaniel. Journal of Small Animal Practice 44, 117–20, 2004, https://doi. org/10.1111/j.1748-5827.2003.tb00131.x
Lajoinie M, Chavalle T, Floch F, Sayag D, Lanore D, Ponce F, Chamel G. Outcome of dogs treated with chemotherapy for mesothelioma: A retrospective clinical study on 40 cases and a literature review. Veterinary and Comparative Oncology 20, 825–35, 2022, https://doi.org/10.1111/vco.12843
MacDonald KA, Cagney O, Magne ML. e chocardiographic and clinicopathologic characterization of pericardial effusion in dogs: 107 cases (1985–2006). Journal of the American Veterinary Medical Association 235, 1456–61, 2009, https:// doi.org/10.2460/javma.235.12.1456
Milne EM, Piviani M, Hodgkiss- Geere HM, Piccinelli C, Cheeseman M, Cazzini P, Ressel L, Marcos RJ, Marrinhas CS, Santos MS, et al . Comparison of effusion cell block and biopsy immunohistochemistry in mesothelial hyperplasia, mesothelioma, and carcinoma in dogs.Veterinary Clinical Pathology 50, 555–67, 2021, https://doi. org/10.1111/vcp.13002
Moberg HL, Gramer I, Schofield I, Blackwood L, Killick D, Priestnall SL, Guillén A. Clinical presentation, treatment and outcome of canine malignant mesothelioma: A retrospective study of 34 cases. Veterinary and Comparative Oncology 20, 304–12, 2022, https://doi.org/10.1111/vco.12777
Nabeta R, Nakagawa Y, Chiba S, Xiantao H, Usui T, Suzuki K, Furuya T, Fukushima R, Uchide T. pericardial mesothelioma in a dog: The feasibility of ultrasonography in monitoring tumor progression. Frontiers in Veterinary Science 6, Article 121, 2019. https://doi.org/10.3389/fvets.2019.00121
Rivera PA, Borgarelli M. Cardiovascular images: constrictive pericarditis and tricavitary effusion in a dog with pericardial mesothelioma. Journal of Veterinary Cardiology 32, 55–9, 2020. https://doi.org/10.1016/j.jvc.2020.09.005 Scheuermann LM, Gordon-Evans WJ, Nault AJ. systematic review of the treatment options for pericardial effusions in dogs. Veterinary Surgery 50, 20–8, 2020, https://doi.org/10.1111/ vsu.13475
Stevens BJ, Montgomery SA, Phillips KL, Wester MW, Jennings SH. pathology in practice. Journal of the American Veterinary Medical Association 245, 57–9, 2014, https://doi.org/10.2460/ javma.245.1.57 l








