Decreasing Extraneous Hours NPO Prior to Scheduled Sedation
Presenting Author: Rebecca Basch
Rebecca Basch, DO, Jane Im, MD, FAAP
Single Cell RNA Analysis of Orthoptic Patient-Derived Xenograft Models of Intracranial Germinoma
Presenting Author: Cullen D. Clairmont, BSc
Cullen D. Clairmont, BSc, Aaron Taylor, PhD, Joanna J. Gell, MD, Ching C. Lau MD, PhD
Expanding the Syphilis Molecular Toolbox: ex vivo and in vivo Characterization of Treponema
pallidum Expressing a Constitutive Green Fluorescent Protein Reporter
Presenting Author: Kristina Delgado
Kristina Delgado, Crystal F. Vicente, Christopher M. Hennelley, Farhang Aghakhanian, PhD, Jonathan Parr, MD, Kevin Claffey, PhD, Justin D. Radolf, MD, Kelly L. Hawley, PhD, and Melissa J. Caimano, PhD
A Thematic Analysis of In-Depth Interview Data with Young People Who Avoid Medical Situations Involving Needles.
Presenting Author: David Finitsis, PhD
David Finitsis, PhD1 & Isaac Rubinstein2, & Dean Cruess, PhD
Investigation of Mandibular Defects in a Mouse Model of Albright Hereditary Osteodystrophy
Presenting Author: Benjamin Hoffman
Benjamin Hoffman, Qingfen Yang, Akshara Malepati, Patrick McMullan, and Emily L. Germain-Lee
Development of targeted therapies for gene fusion positive cancers based on RNA sensing and editing
Presenting Author: Nathaniel L. Jillete
Nathaniel L. Jillete, Albert W. Cheng, and Ching C. Lau
Interplay Between Endogenous Glycan Fermentation and Klebsiella Pathogenicity in the Intestinal Lumen
Presenting Author: Surabhi Khasgiwala, MD
Surabhi Khasgiwala, MD, Katrin Unterhauser, PhD, Karim Rezaul, PhD Sonam Tamrakar, PhD, Jeremy Balsbaugh PhD, Anthony Provatas, PhD, Adam P. Matson, MD, MSc
A de novo Variant in PAK2 Detected in an Individual with Knobloch Type 2 Syndrome
Presenting Author: Cameron King, MA
Elizabeth A. Werren1, Louisa Kalsner, Jessica Ewald, Michael Peracchio, Cameron King, Purva Vats, Peter A. Audano, Peter N. Robinson, Mark D. Adams, Melissa A. Kelly, Adam P. Matson
Results of the Pilot Study to Determine the Validity and Reliability of the NICU Paternal Needs Inventory
Presenting Author: Linda Merritt, PhD
Linda Merritt, PhD, RNC-NIC, CNE, FAWHONN; M. Terese Verklan, PhD, CCNS, RNC-NIC, FAAN
Research Hesitancy among Gender Diverse Children and their Caregivers
Presenting Author: Alina A. Molloy, BS
Alina A. Molloy, BS, Christopher B. Theriault, MA, William T. Zempsky, MD, MPH, Melissa Santos, PhD
The role of immunosuppressive neutrophils in the tumor microenvironment of osteosarcoma
Presenting Author: Patrick Ng
Chaojia Chen, Patrick Ng, Aaron Taylor, Elise Courtois, Paul Robson, Gary Ren, Ching Lau
Educating Clinicians on Sexual Health Care for AYAs: Preliminary Results from an Intervention Pilot Study
Presenting Author: Mary-Kate Nowobilski, BS
Kristin Bingen, PhD; Brooke O. Cherven, PhD, MPH, RN; Jenna Demedis, MD, MS; Gwendolyn P. Quinn, PhD; David R. Freyer, DO; Sharon L. Bober, PhD, Natasha N. Frederick, MD, MPH
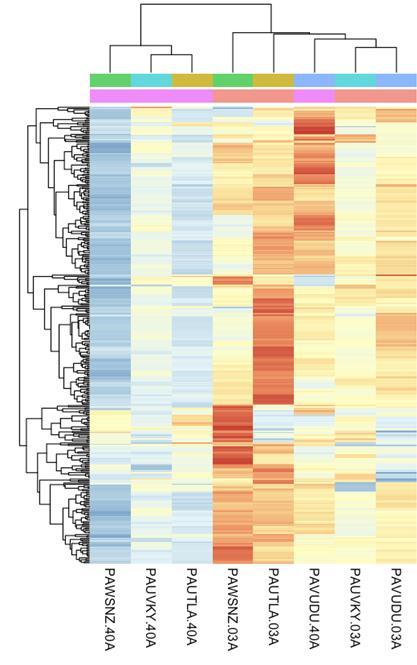
An integrative analysis of differential alternative splicing events between paired transient abnormal myeloproliferation and acute myeloid leukemia in Down syndrome patients
Presenting Author: Francis H. O’Neill, M.D.
Francis H. O'Neill, M.D., Aaron Michael Taylor, Ph.D., Rhonda Ries, M.A., Xiaotu Ma, Ph.D., Johann K. Hitzler, M.D., Anne Deslattes Mays, Ph.D., Soheil Meshinchi, M.D. Ph.D., Ching C. Lau, M.D. Ph.D.
Feasibility of Brain Tumor Classification by Enzymatic DNA Methylation Sequencing Analysis of Cell-free DNA Obtained from Cerebrospinal Fluid
Presenting Author: Aaron Michael Taylor, Ph.D.
Aaron Michael Taylor, Ph.D., Jody T. Lombardi, B.Sc., Areeba Patel, Ph.D., Jonathan Martin, M.D., Markus J. Bookland, M.D., David S. Hersh, M.D., Evan Cantor, J.D. M.D., Xianyuan Song, M.D., Felix Sahm, M.D. Ph.D., Patrick Kwok-Shing Ng, Ph.D., Joanna J. Gell, M.D., Ching C. Lau, M.D. Ph.D.
Qualitative Analysis of Pain Impact in Adult Patients with X-Linked Hypophosphatemia (XLH) to Inform the Development of a Digital Pain Self-Management Intervention
Presenting Author: Christopher B. Theriault, MA
Christopher B. Theriault, MA, Nicole Nishime, BA, Carolyn Macica, PhD
MarR-dependent toxin gene regulation in the gut pathobiont Klebsiella oxytoca
Presenting Author: Katrin Unterhauser, PhD
Katrin Unterhauser, PhD, André A. Grassmann, PhD, Karim Rezaul, PhD, Anthony Provatas, PhD, Melissa J. Caimano, PhD, Adam Matson, MD, MSc,
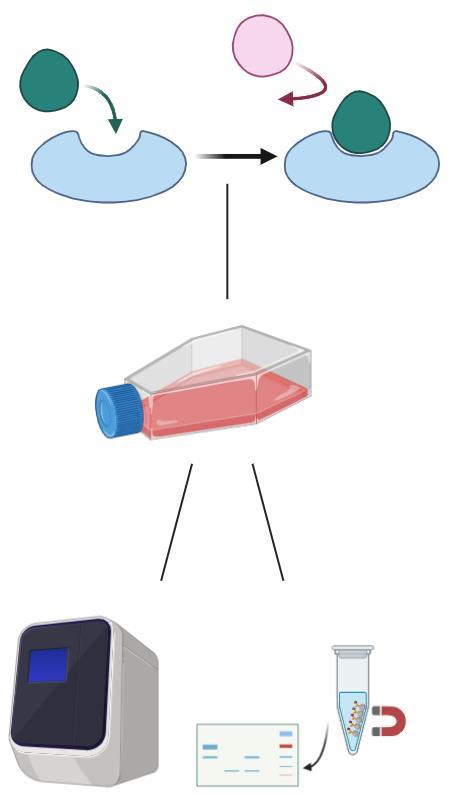
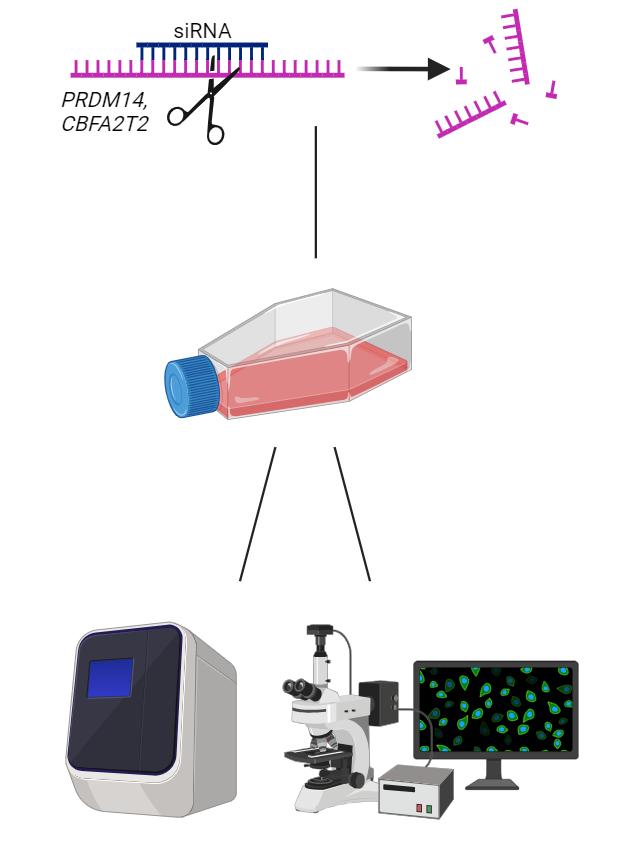
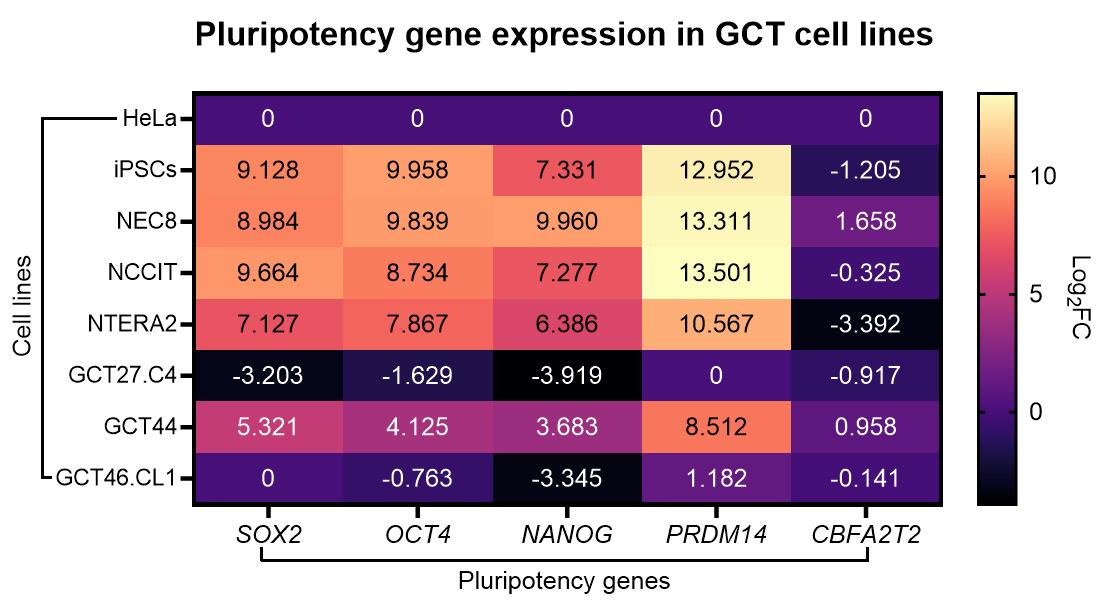
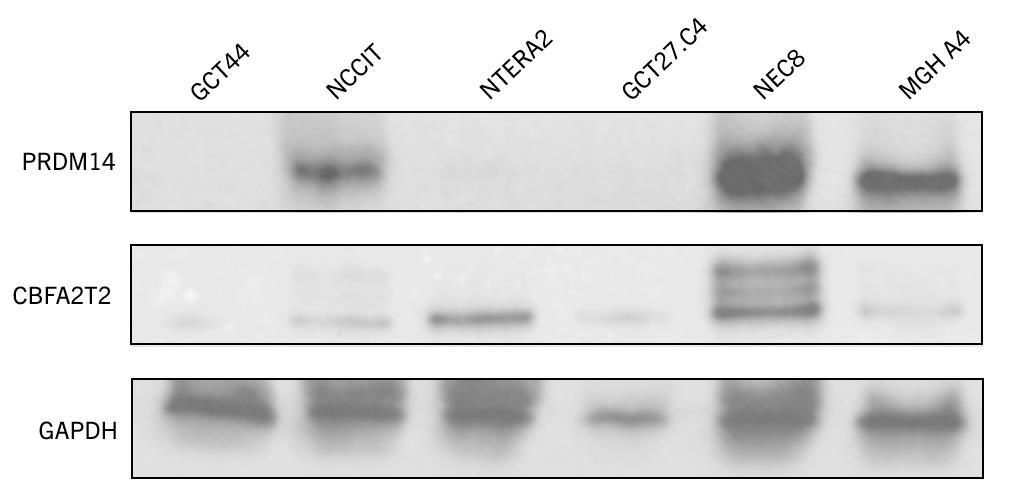
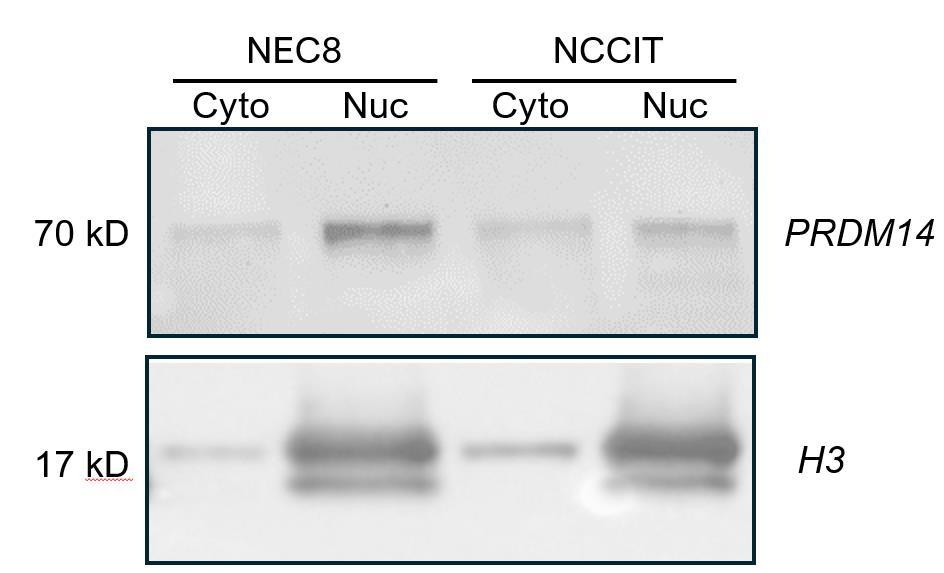
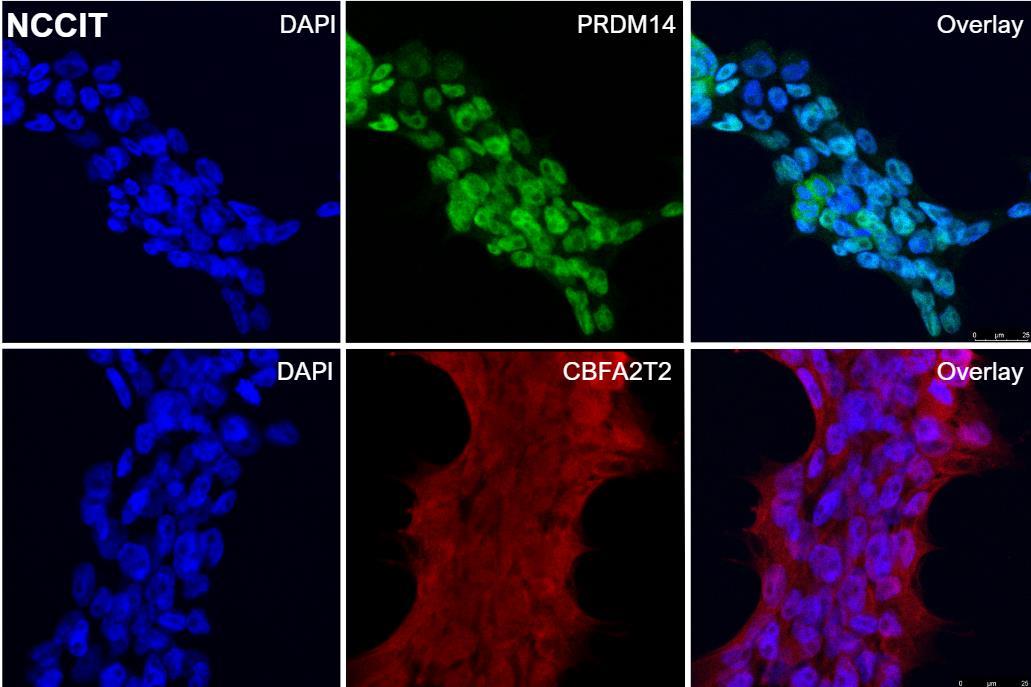
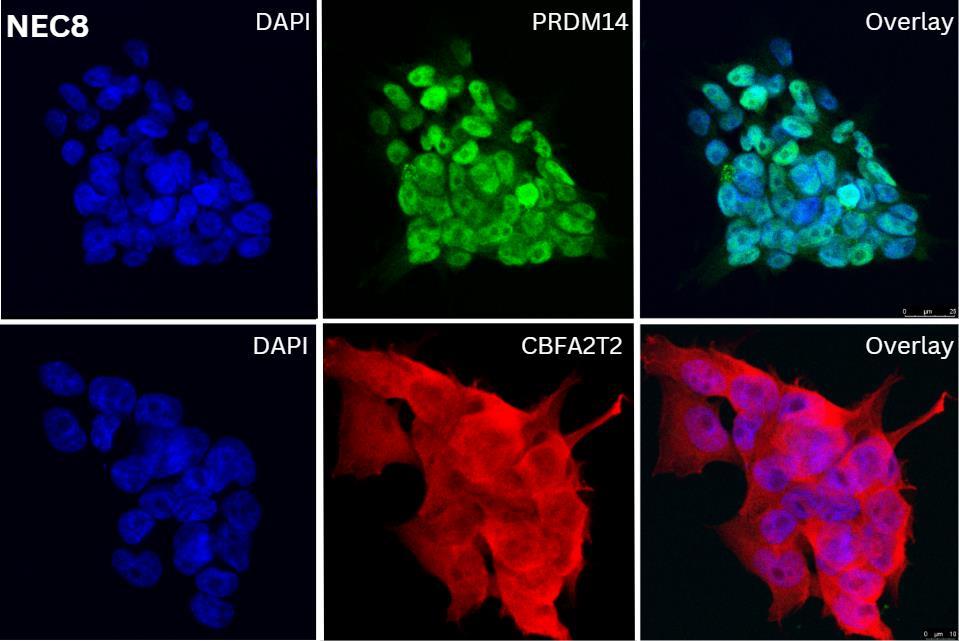
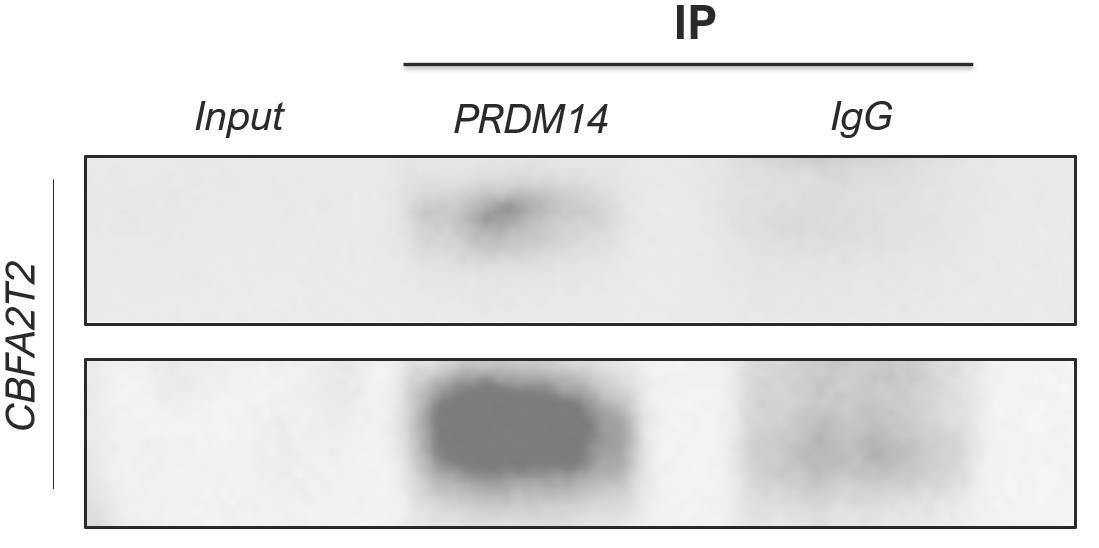
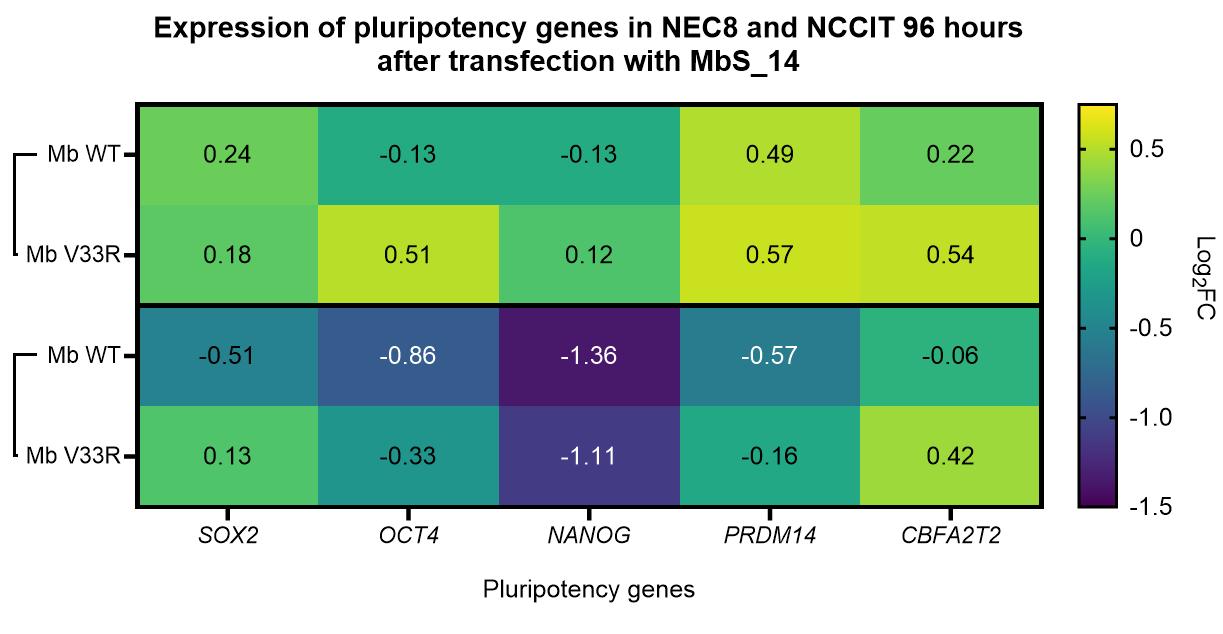
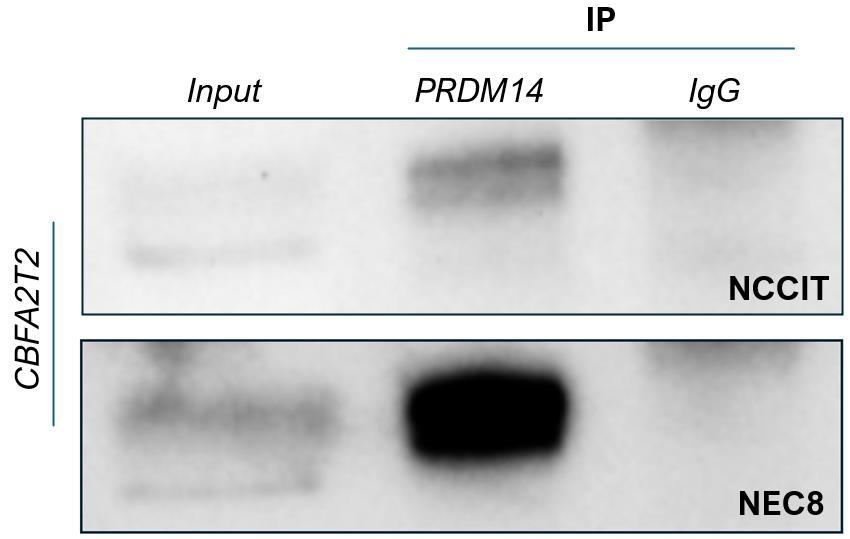
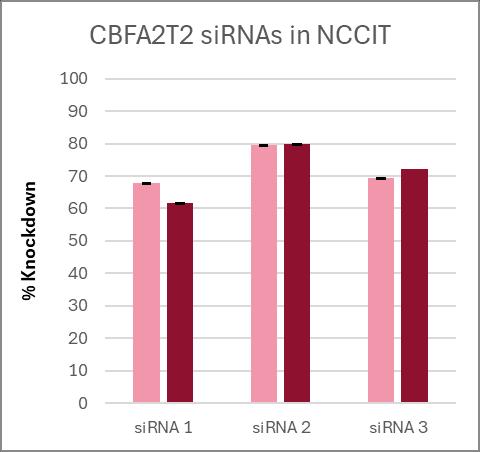
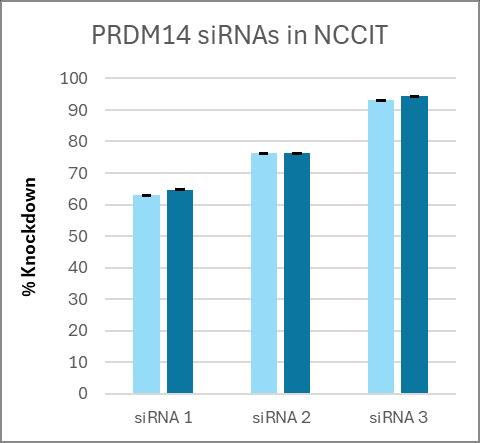
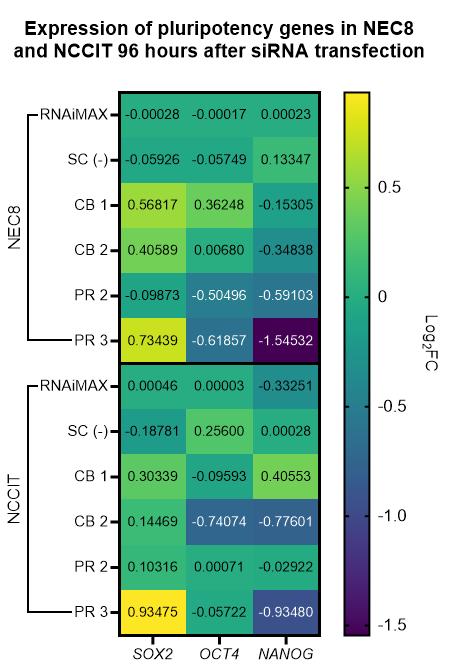
Elucidating the Role of PRDM14-CBFA2T2 Interaction in Maintenance of Pluripotency in Germ Cell Tumors
Presenting Author: Deana L. Wood, B.Sc.
Deana L. Wood, B.Sc., Patrick Kwok-Shing Ng, Ph.D., Joanna J. Gell, M.D., Ching C. Lau, M.D. Ph.D.
CLINICAL RESEARCH
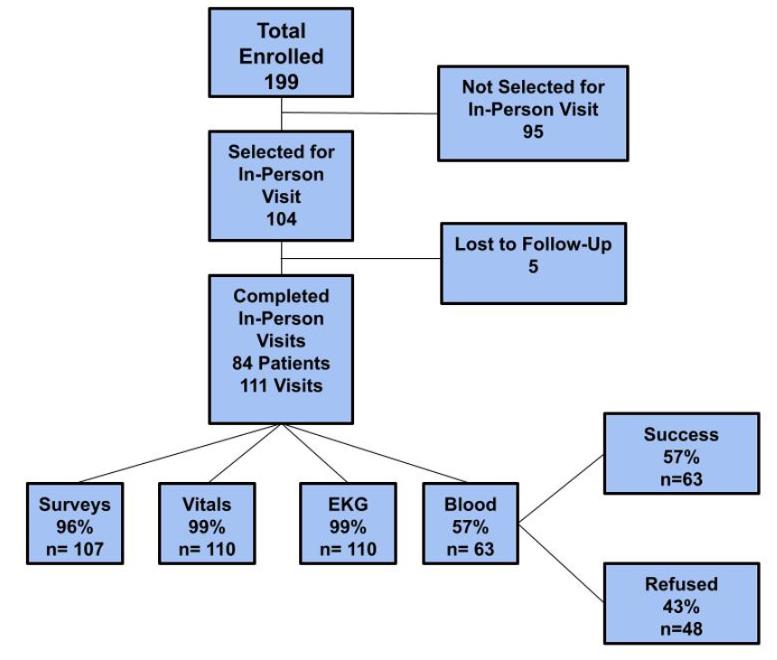
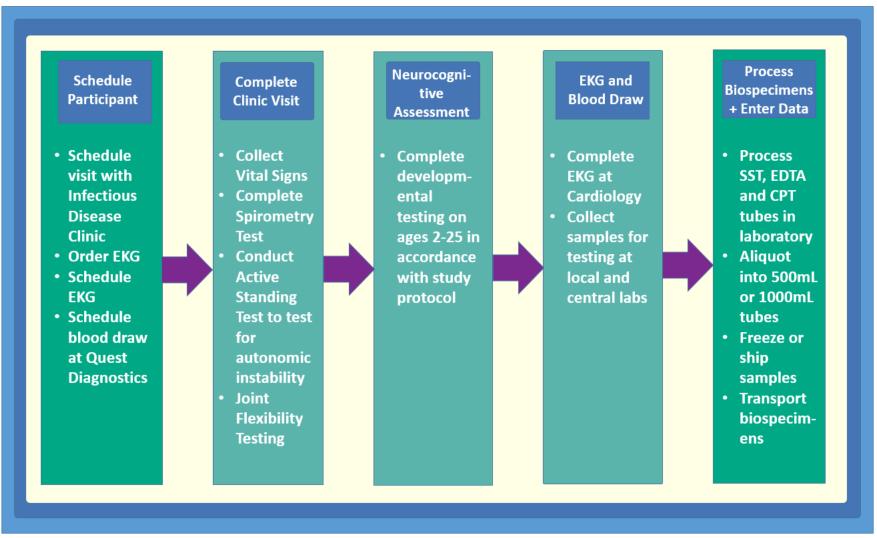
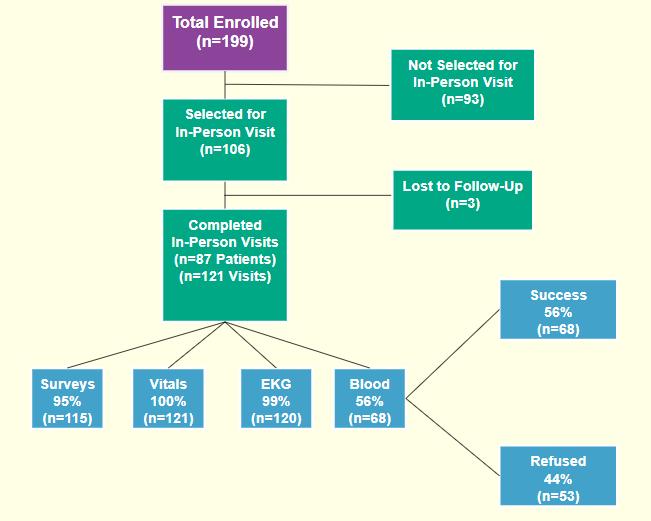
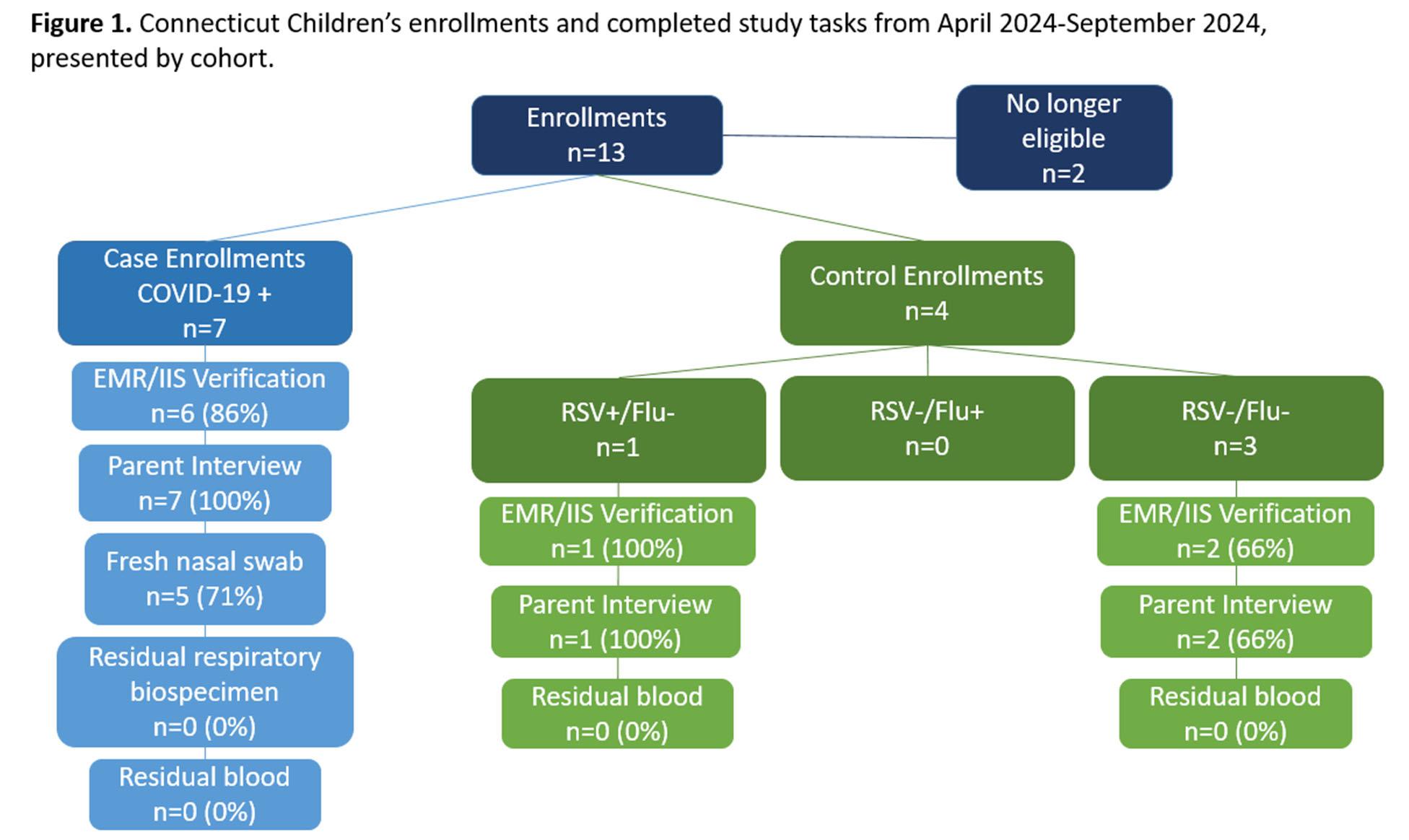
Researching COVID to Enhance Recovery (RECOVER) Study: Planning and Completion of InPerson Clinical Research Visits
Presenting Author: Emily Bean
Emily A. Bean, MPH , Carolyn J. Wolf, BA, Katherine W. Herbst, MS, Alex H. Hogan MD, MS, Ian C. Michelow MD, Juan C. Salazar MD, MPH, FAAP, William T. Zempsky MD, MPH
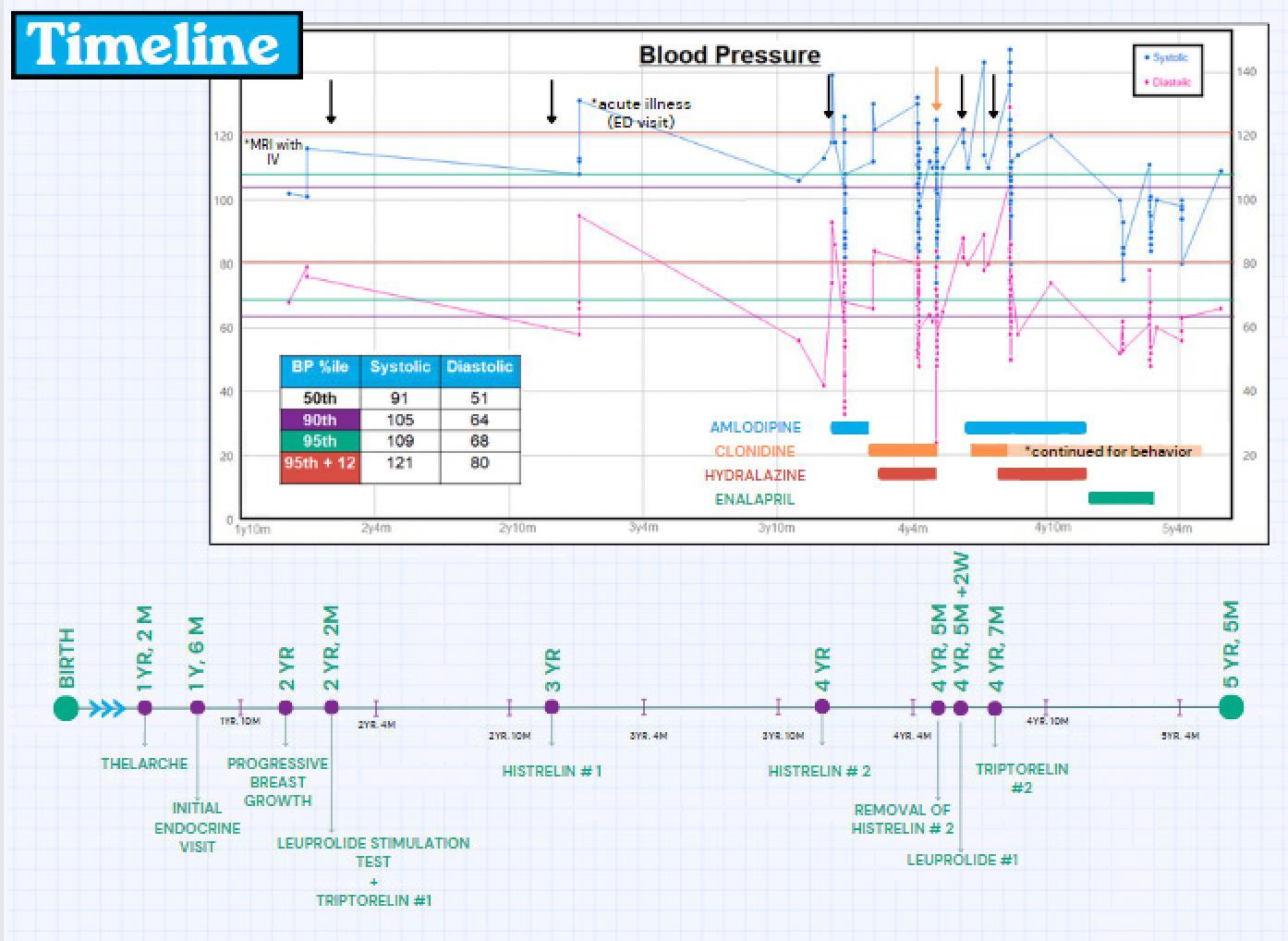
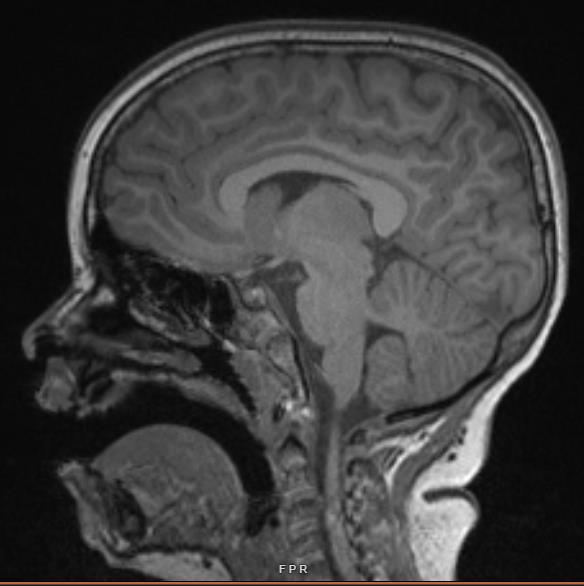
Histrelin-associated hypertension in the treatment of central precocious puberty
Presenting Author: Caroline Figgie, MD
Caroline Figgie, MD, Rebecca Riba-Wolman, MD
Shooting for the STARS: Implementing an Evidence-based Program to Meet the End of Treatment Needs of Childhood Cancer Survivors and Their Families
Presenting Author: Mary Conway Keller
Mary Conway Keller, MSN, RN, CPHON®, Lauren Ayr-Volta, PhD, Elizabeth Marconi, MSW, Andrew Needham, BSN, RN, CPN®, CPHON®, Kelly Foy, MS, CCLS, Leigh Hart, BSN, RN, CPON®, Elizabeth Holden, BSN, RN, CPHON®, Amirul Anuar, MS, Karina Engelke, MSN, RN, APRN, and Katherine A. Hinderer, PhD, RN, CNE, NEA-BC
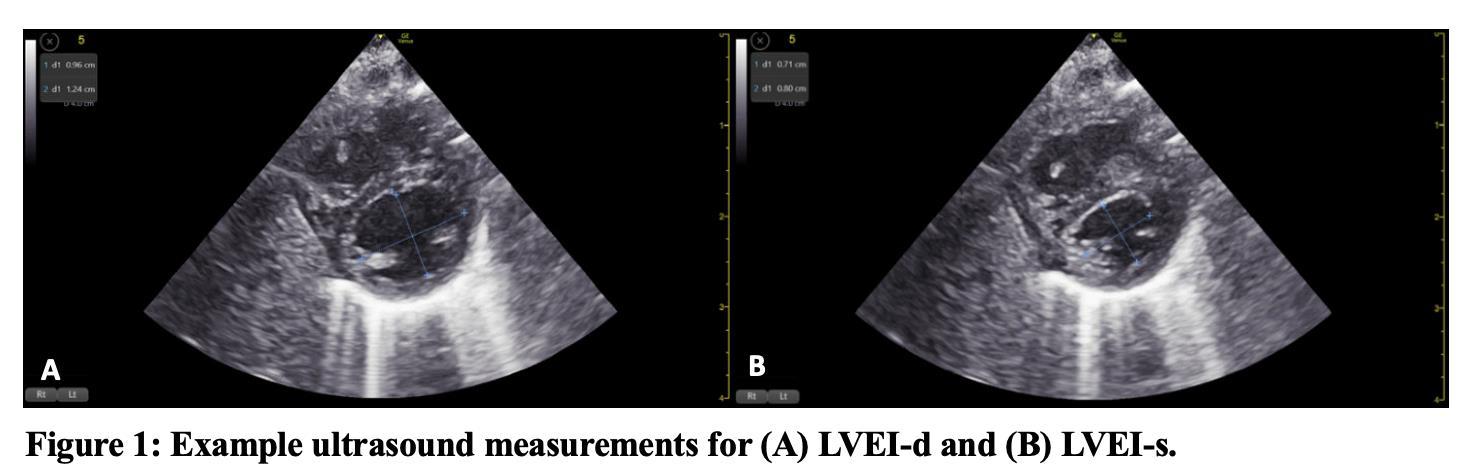
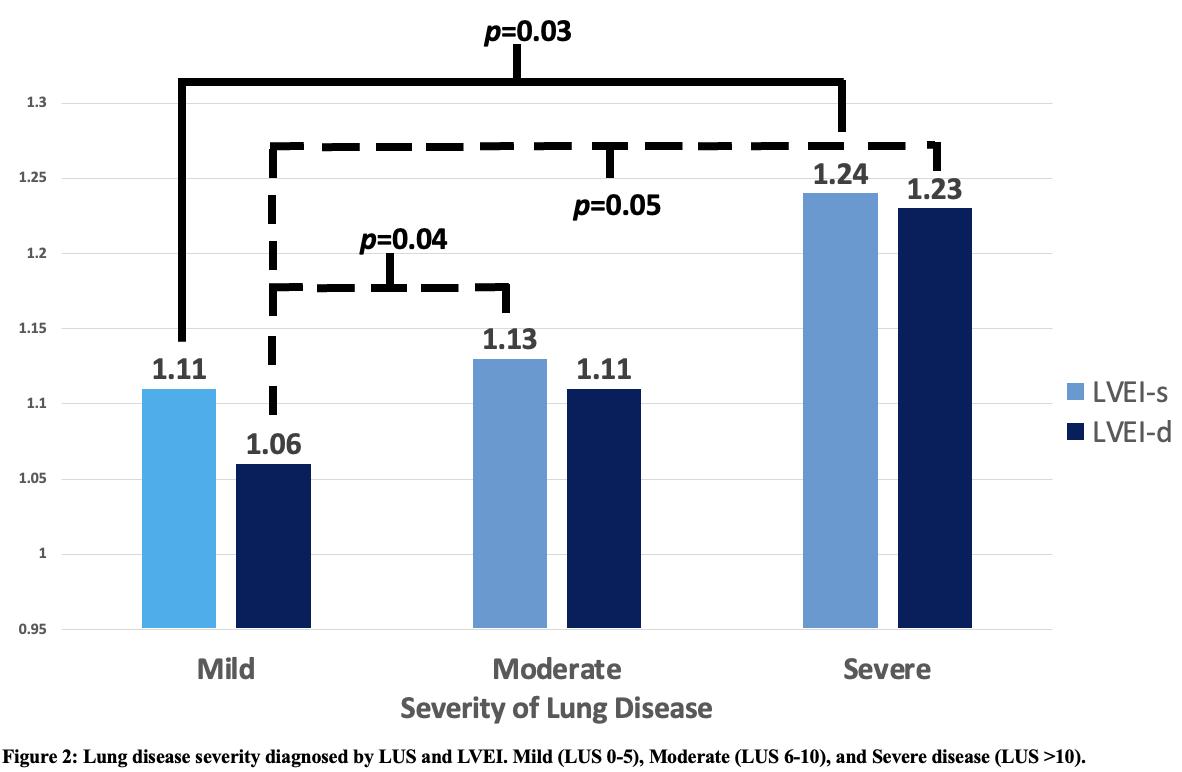
Lung Ultrasound Score and Left Ventricular Eccentricity Index in Preterm Infants with Respiratory Failure
Presenting Author: Jacob Kelner DO
Jacob Kelner DO, Naveed Hussain MBBS, Henry Chicaiza MD, and Shalin Parekh MD
Revision and Adaptation of a Pediatric-to-Adult Care Transition Toolkit for X-Linked Hypophosphatemia.
Presenting Author: Carolyn M. Macica, PhD
Amber Parson, BA and Carolyn Macica, PhD
Association of Busulfan Exposure and Outcomes after Hematopoietic Cell Transplantation for Pediatric Patients with Inborn Errors of Immunity
Presenting Author: Layne Oram
Layne Oram, Susan Prockop, MD
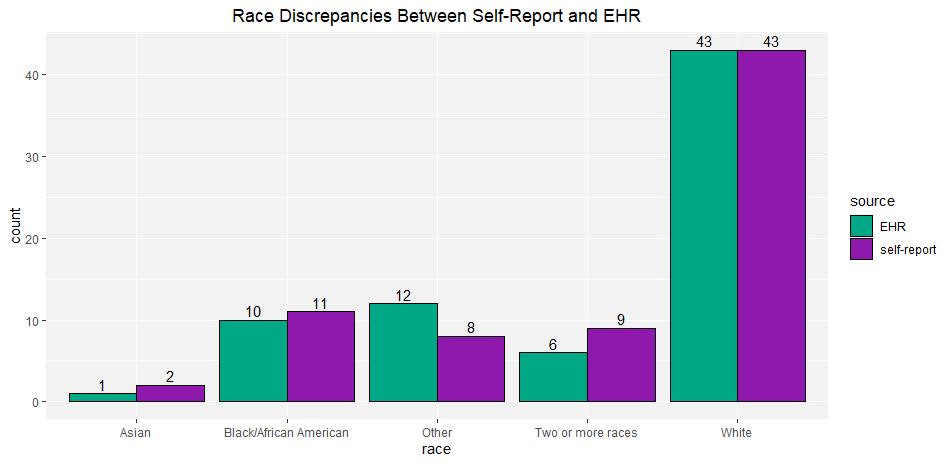
Discrepancies Between Electronic Health Record and Patient Self-Report Race/Ethnicity: Implications for Pediatric Clinical Research
Presenting Author: Cameron King, MA
Cameron King, MA, Mollie Fleming, MS, Stephanie Perez, MS, Michael Bobylov; Amogh Chittajallu; Mallory A. Perry-Eaddy, PhD, RN
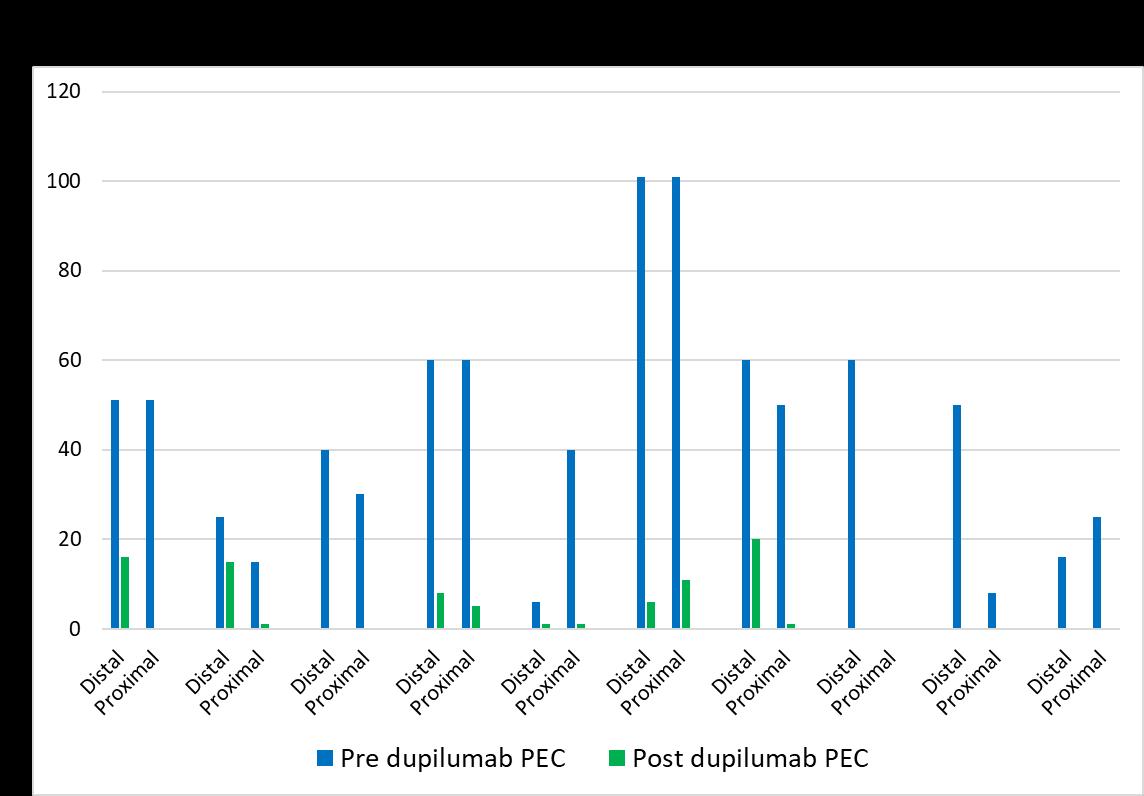
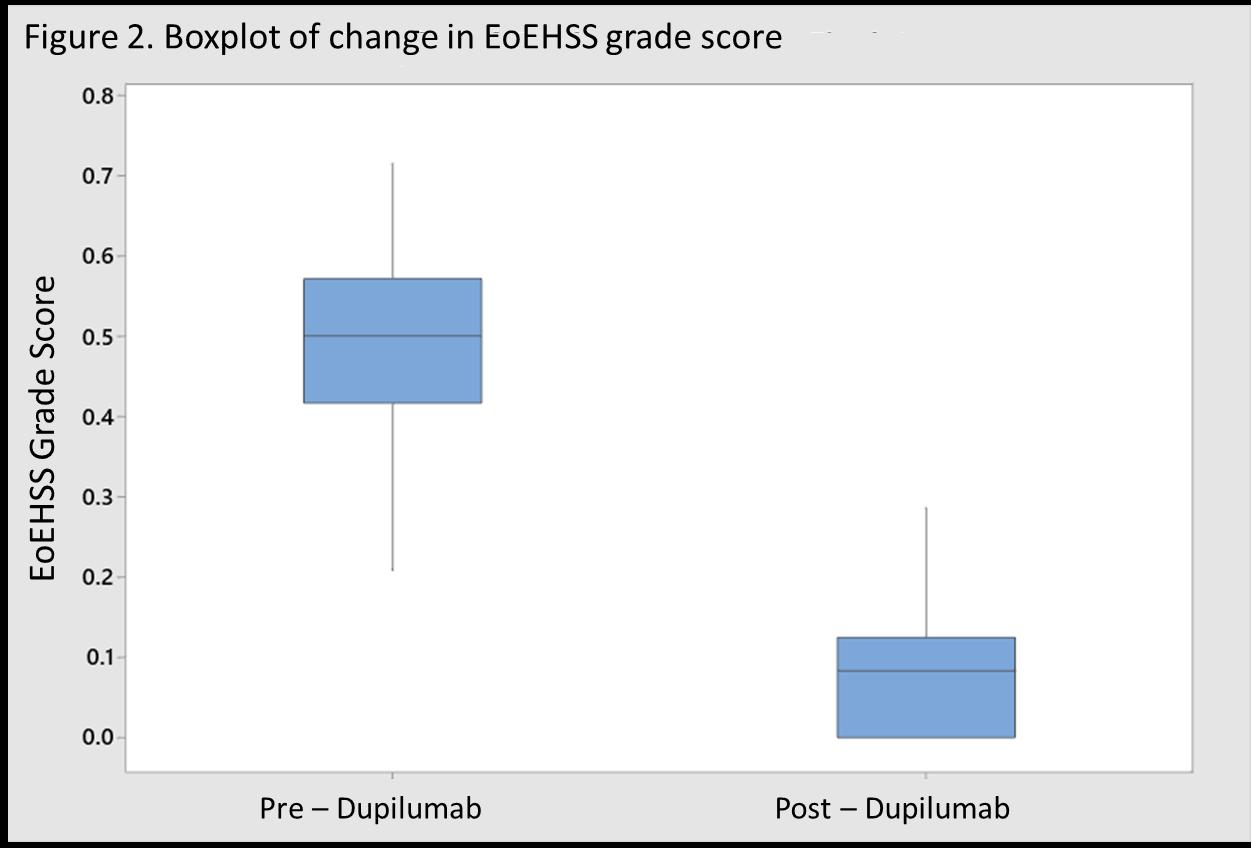
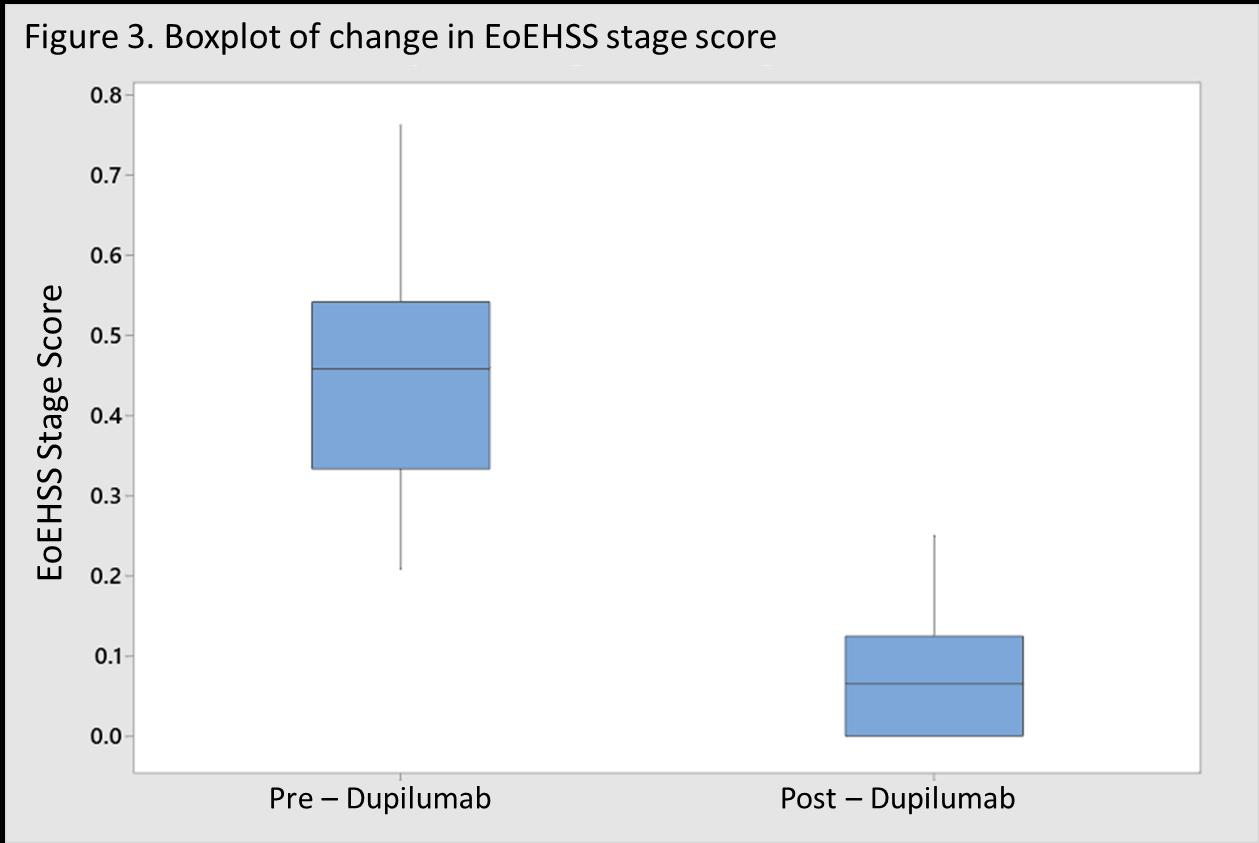
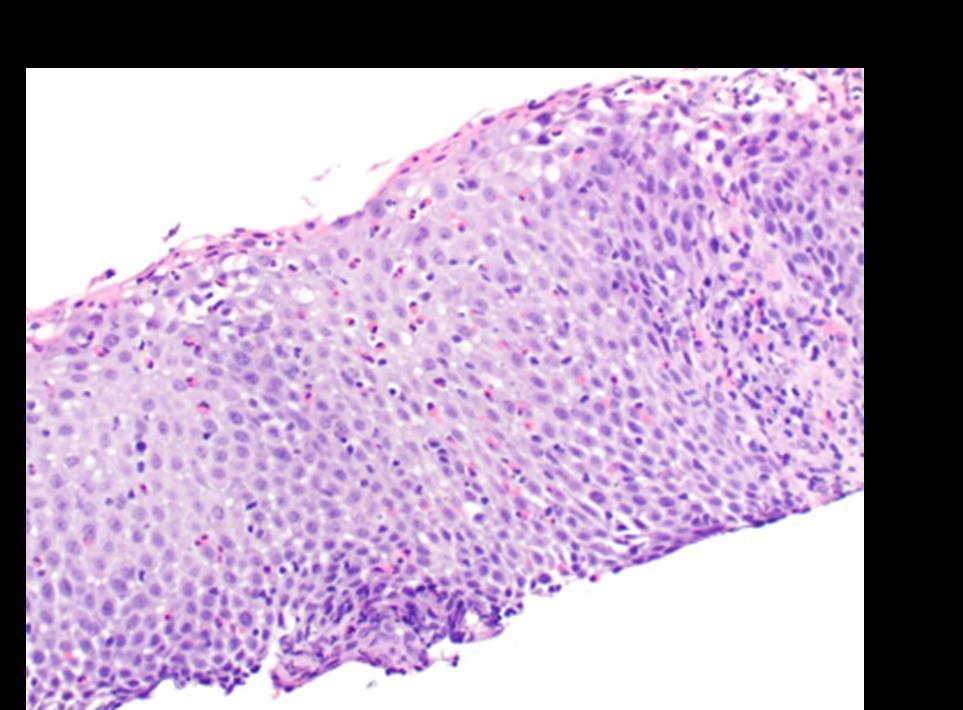
Dupilumab Improves Histologic Manifestations of Eosinophilic Esophagitis in a Real World Cohort of Pediatric Patients
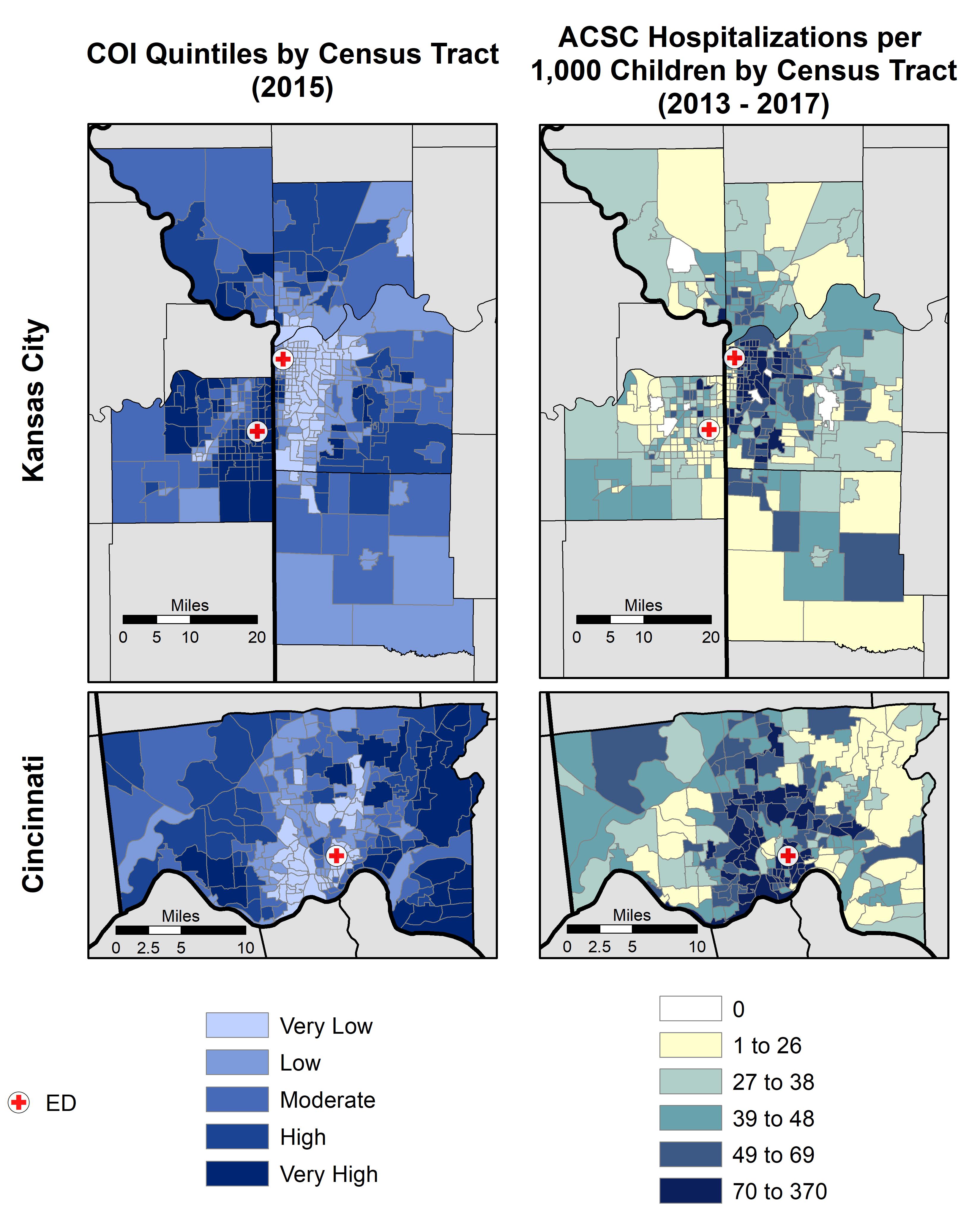
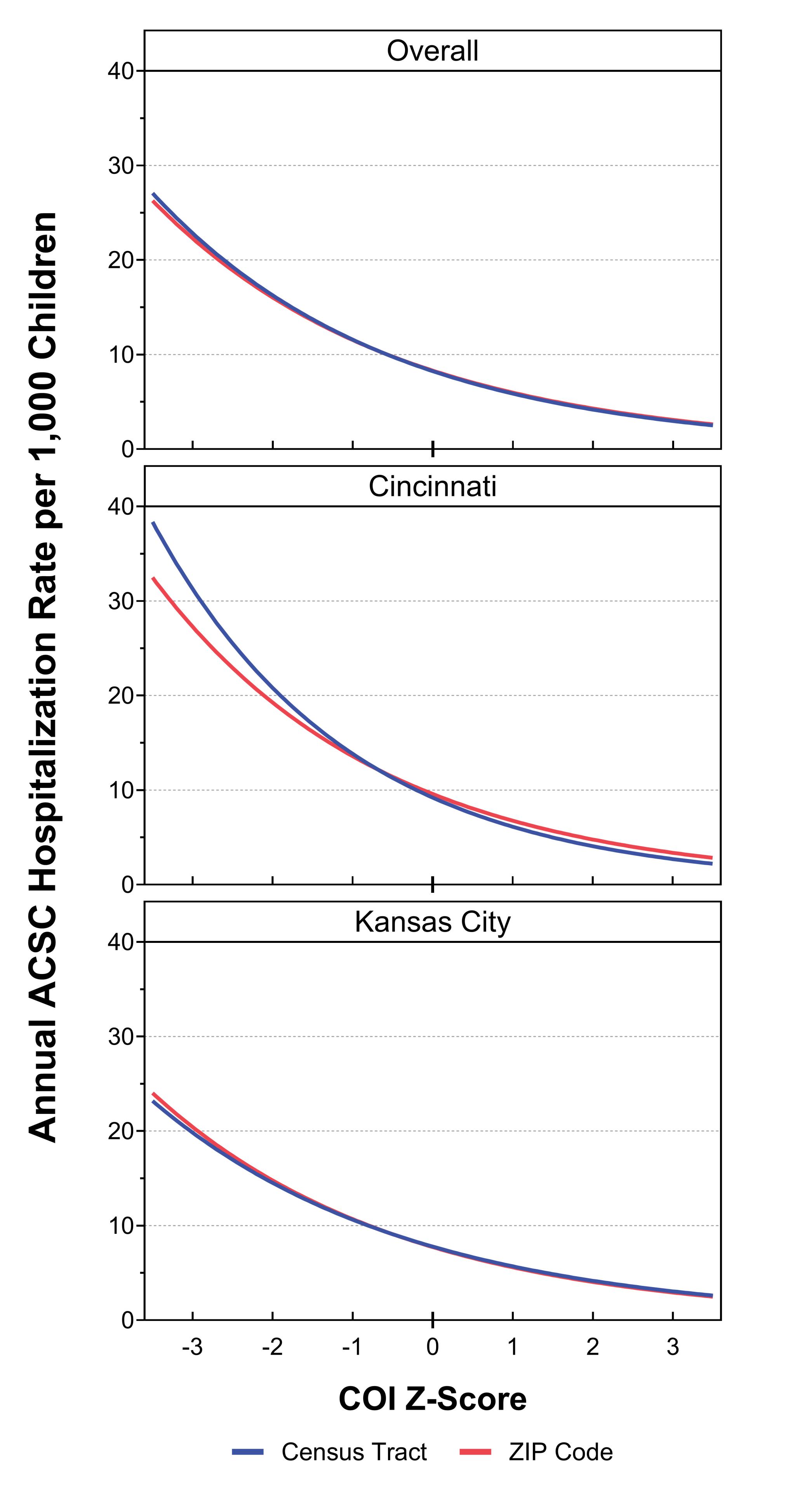
The Child Opportunity Index and Pediatric Hospitalizations: Are ZIP Codes Good Enough?
Presenting Author: Alexander H. Hogan, MD, MS
Alexander H. Hogan, MD, MS, Natalie Grills, MS, Matt Hall, PhD, Mitch Harris, PhD, MS, Molly Krager, MD, Clemens Noelke, PhD, Mark Zamani, MS, Andrew F. Beck, MD, MPH
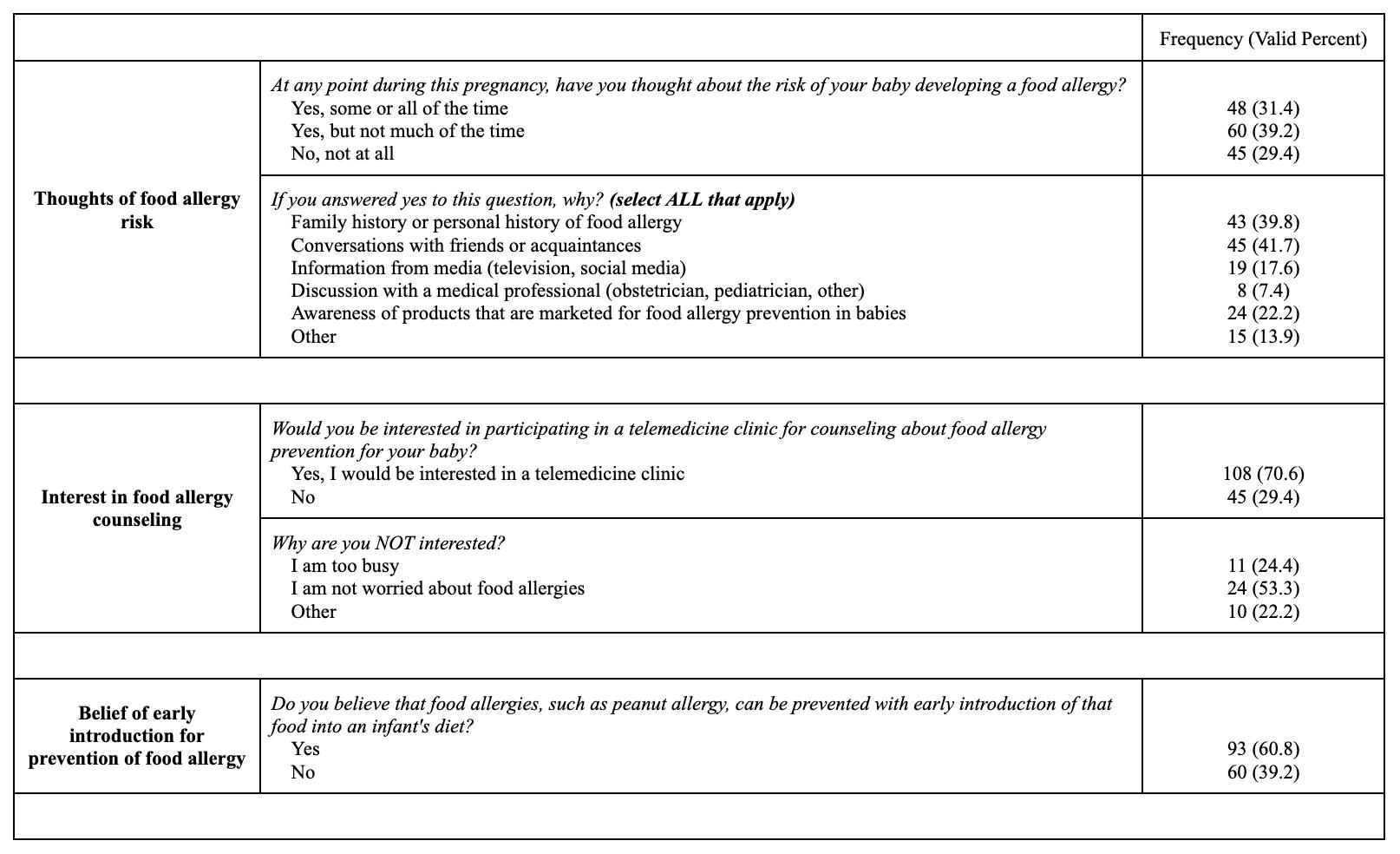
Knowledge and Beliefs of Pregnant Women for Food Allergy Prevention in Their Offspring
Presenting Author: Sin Ting Hui (Abbie), MS
Sin Ting Hui (Abbie), MS, Richard Feinn, PhD, Alexander Duarte, MPH, Julie Flom, MD MPH, Stephanie Leeds, MD MHS
INTO THE UNKNOWN: Establishing Mobilization of Patients in a Low Volume Pediatric
Extracorporeal Membrane Oxygenation (ECMO) Center
Presenting Author: Kim Koenig PT, Brittany Carter MHA, RRT-NPS
Koenig K PT, Schultes J MSN, RN, Carter B MHA,RRT-NPS, Campbell J D DO, Cowl A S MD
Eating Disorders in Patients with Glycogen Storage Disease
1Division of General Pediatrics,Connecticut Children’s
2Division of Pediatric Hospital Medicine, Connecticut Children’s
3Department of Pediatrics, University of Connecticut Schoolof Medicine
BACKGROUND
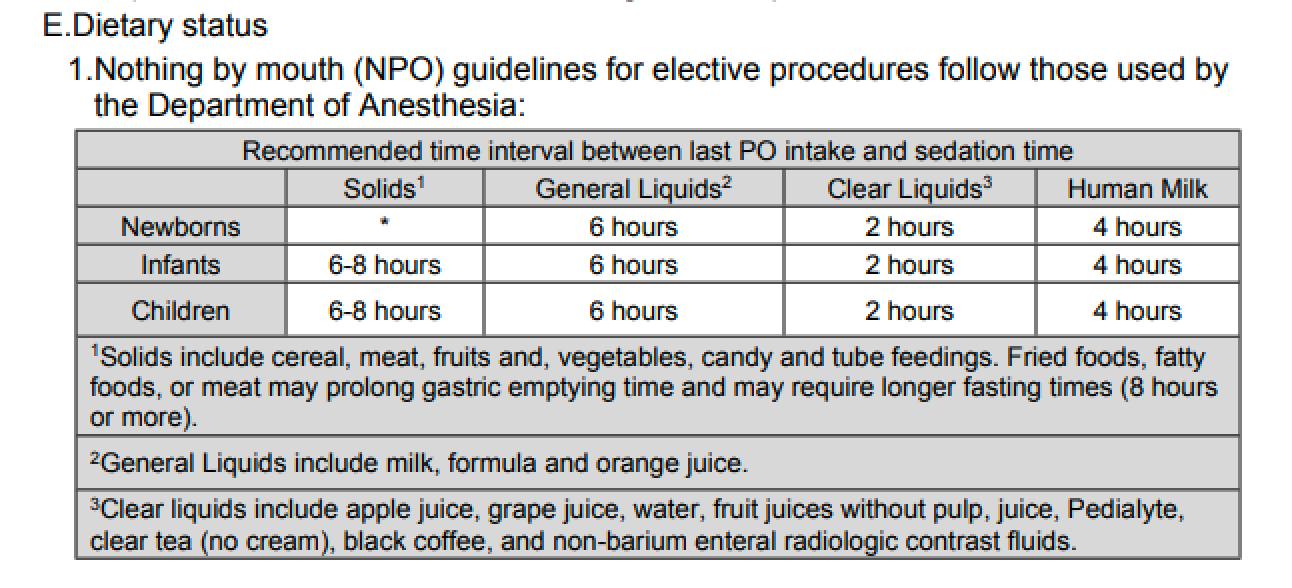
Patients are required to fast prior to sedation to decrease the risk of aspiration during procedures. Unlike adults, there is variability in the recommended pre-sedation fasting (NPO) times for pediatric patients. While current guidelines support minimal recommended fasting times for low risk patients with elective procedures, patients continue to be made NPO at midnight prolonging NPOtimes. This practice isespecially relevant to infants who benefit from reduced fasting times.
METHODS
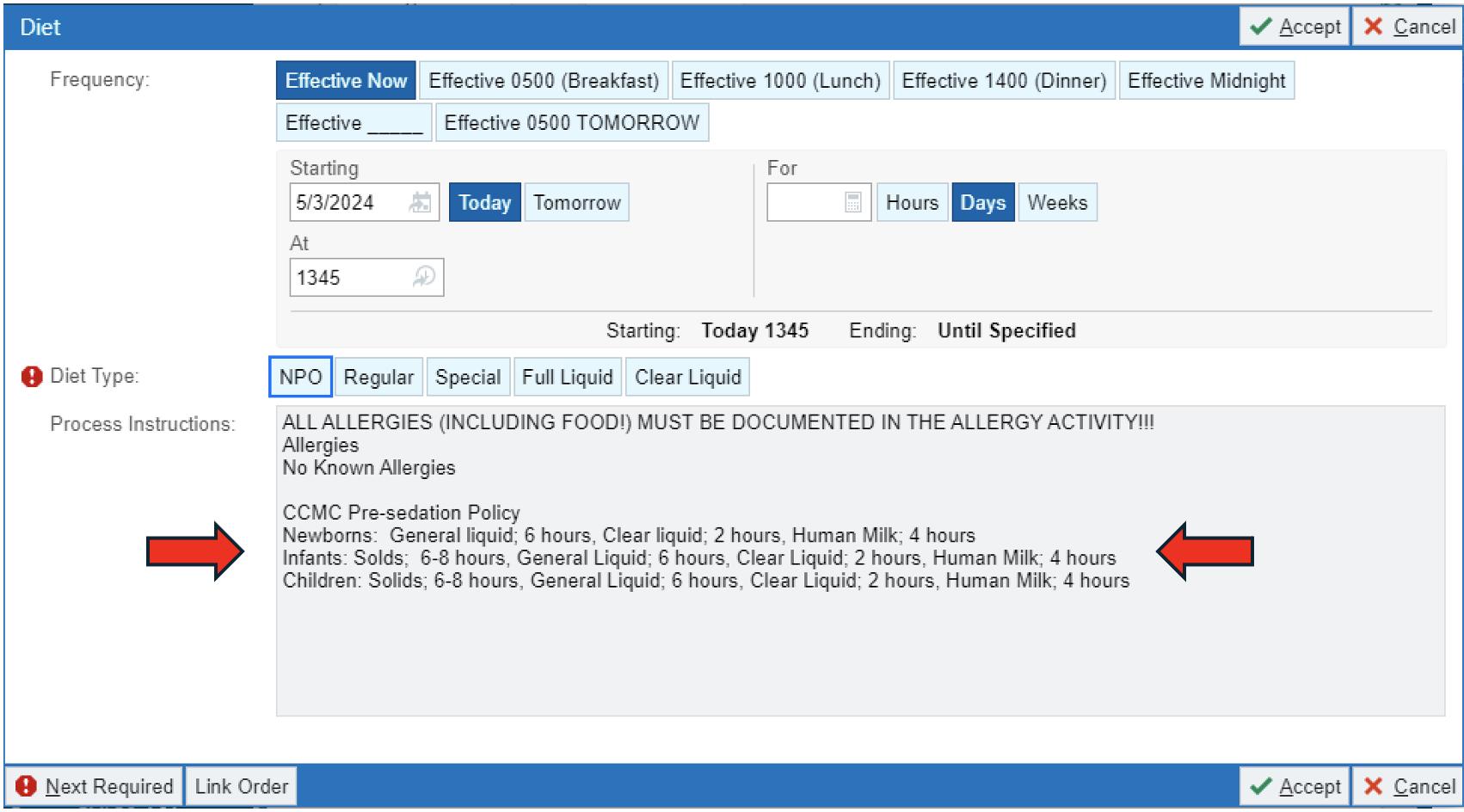
We seek to evaluate the adherence to Connecticut Children’s pre-sedation guidelines after the introduction of clinical decision support within computerized physician order entry in the Electronic Health Record(EHR),specifically a non-interruptive reference to pre-sedation NPO guidelines. A totalof 485 patient charts were collected (313 pre, 172 post) from patients admitted to the inpatient service between 1/23- 5/24, who underwent non-emergent sedatedprocedures. Data collected from pre andpost intervention included (1) hours NPO, (2) hours on intravenous fluids, and (3) service and department.
RESULTS
Univariate analyses wereusedtoevaluate NPO time, time on intravenous fluids. Mann Whitney u tests usedfor continuous variables andchi squared for categorical variables. There wasadecreasein medianhours NPO from pre to post intervention (8.74hr vs 7.20hr), decrease in hours on intravenous fluids (11.24 hr to 7.20 hr). ANCOVA used to assess NPO times/intravenous fluid time and showed a statistically significant decrease in overall NPO times from pre to post intervention.
CONCLUSION/SIGNIFICANCE
Providing a reference to pre-sedation guidelines candecreaseextraneous hours NPOprior to a scheduled sedated procedure
Decreasing Extraneous Hours NPO Prior to Scheduled Sedation
Rebecca Basch, DO1,3, Jane Im, MD, FAAP2,3
1 Division of General Pediatrics, Connecticut Children’s, 2 Division of Pediatric Hospital Medicine, Connecticut Children’s, 3 Department of Pediatrics, University of Connecticut School of Medicine
BACKGROUND
Prolonged fasting can be linked with patient discomfort, hypoglycemia, decreased caloric intake (needed for wound healing) and necessity for intravenous fluids (IVF)1 Patients are required to fast prior to sedation to decrease the risk of aspiration during procedures Unlike adults, there is variability in the recommended pre-sedation fasting (NPO) times for pediatric patients (Table 1).
While current guidelines support minimal recommended fasting times for low risk patients with elective procedures, patients continue to be made NPO at midnight Continued prolonged NPO times are in part related to the difficulty in recalling age specific/diet specific NPO time recommendations This practice is especially relevant to infants who benefit from reduced fasting times
ACKNOWLEDGEMENTS
The authors would like to sincerely thank Amirul Anuar, a fantastic statistician that helped us analyze the data and account for the variability within the different departments.
Thank you to the Connecticut Children's Informatics team for the wonderful collaboratives ideas, expertise and launching our EHR enhancement
Thank you to Mellissa Molcan and Katharine Barnett from Connecticut Children’s Quality Improvement Department for guiding us through data collection
OBJECTIVE
To improve ordering provider compliance with pre-sedation NPO guidelines through passive clinical decision support within the hospital electronic health record (EHR)
METHODS
We sought to evaluate the adherence to Connecticut Children’s pre-sedation guidelines after the introduction of clinical decision support within computerized physician order entry in the EHR, specifically a non-interruptive reference to pre-sedation NPO guidelines
A total of 485 patient charts were collected (313 pre, 172 post) from patients admitted to the inpatient service between 1/235/24, who underwent non-emergent sedated procedures Data collected from pre and post intervention included (1) hours NPO, (2) hours on intravenous fluids, and (3) service and department Univariate analyses were used to evaluate NPO time, time on intravenous fluids. Mann Whitney u tests used for continuous variables and chi squared for categorical variables ANCOVA used to assess NPO times/intravenous fluid time.
RESULTS
From pre to post intervention there was a decrease in median hours NPO (8 74hr vs 7 20hr), decrease in mean hours NPO (20.04hr vs 8.27hr) and decrease in mean hours on intravenous fluids (11 24hr to 7 20hr) The decrease in overall NPO time across all service departments was statistically significant while intravenous fluid time was not.
CONCLUSION
After providing an inline reference for pre-sedation NPO guidelines, there was a decrease in the average length of presedation fasting across all studied inpatient services (Hospital Medicine, General Surgery, Emergency Department)
REFERENCES
1. Dennhardt, N., Beck, C., Huber, D.,(2015). Impact of preoperative fasting times on blood glucose concentration, ketone bodies and acid-base balance in children younger than 36 months: A prospective observational study. European journal of anaesthesiology, 32(12), 857–861.
2. (CCMC Policy reference) Apfelbaum, J., et al. "Practice guidelines for moderate procedural sedation
3. Frykholm P., Disma, N., Andersson, H., Beck, C (2022). Pre-operative fasting in children: A guideline from the European Society of Anaesthesiology and Intensive Care. European journal of anaesthesiology, 39(1), 4–25.
4. Borland, L. M., Sereika, S. M., Woelfel, S. K., Saitz, E. W., Carrillo, P. A., Lupin, J. L., & Motoyama, E. K. (1998). Pulmonary aspiration in pediatric patients during general anesthesia: incidence and outcome. Journal of clinical anesthesia, 10(2), 95–102. https://doi.org/10.1016/s0952-8180(97)00250-x
4UConnHealth,Division of Pediatric Hematology-Oncology, Farmington, CT
BACKGROUND
Intracranial germinoma (GE) is a rare pediatric brain tumor commonly located near the pineal or pituitary glands. GE is difficult to surgically resect, and conventional chemoradiation can cause significant long-term toxicity. Therefore, a targeted therapeutic approach is highly desired, but little is known about the pathogenesis of GE. GE is a germ cell tumor subtype with many molecular and cellular featuresmatching the earliest committed germ cell progenitor, the primordial germ cell (PGC). GE is hypothesized to arise due to abnormal PGC development: a subpopulation of PGCs, instead of residing in the gonads, aberrantly migrate outside of their niche and survive elsewhere, allowing tumor formation.
METHODS
Previously conducted bulk sequencing analysis has provided some insight into the mechanisms underlying GE. However, single-cell RNAsequencing (scRNA-seq) has the power to further define the transcriptomic programs within GE, but sufficient high-quality GE samples are challenging to obtain. To overcome this problem, we have obtained two mutationally-distinct, orthotopic GE patient-derived xenograft (PDX) models. With thesesamples, wecarried out in vitro culture by adapting a protocol for differentiation of stem cells into PGC-like cells. Wealso performed preliminary scRNA-seq analysis.
RESULTS
We have identified differential expression of pluripotent, germ cell, and proliferative markers, which are characteristic of human GE. We will perform subsequent analysis directly comparing the scRNA-seq profile of our PDX to single-cell analysis of both testicular seminomas and healthy germ cell progenitors to uncover mechanisms unique to GE pathogenesis.
CONCLUSION/SIGNIFICANCE
Our study marks the first scRNA-seq analysis of human GE, providing novel insight into tumorigenesis.
Single-Cell RNA Sequencing Analysis of Orthoptic Patient-Derived Xenograft Models of Intracranial Germinoma
Cullen D. Clairmont, BSc1,2,Aaron M. Taylor, PhD2, Joanna J. Gell, MD
1University of Connecticut, School of Medicine, Farmington, CT
2The Jackson Laboratory for Genomic Medicine, Farmington, CT
Ching C. Lau MD, PhD
3Connecticut Children’s Medical Center, Center for Cancer and Blood Disorders, Hartford, CT
4UConn Health, Division of Pediatric Hematology-Oncology, Farmington, CT
Abstract
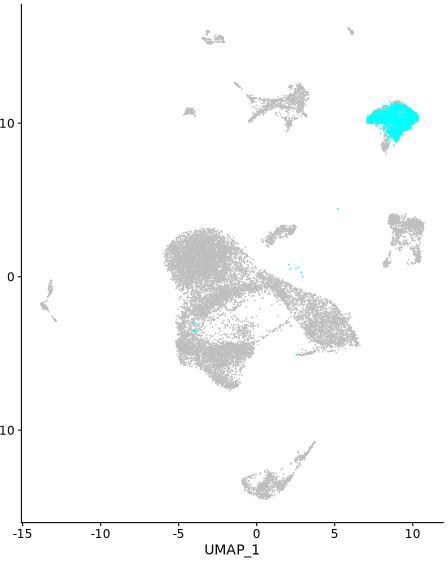
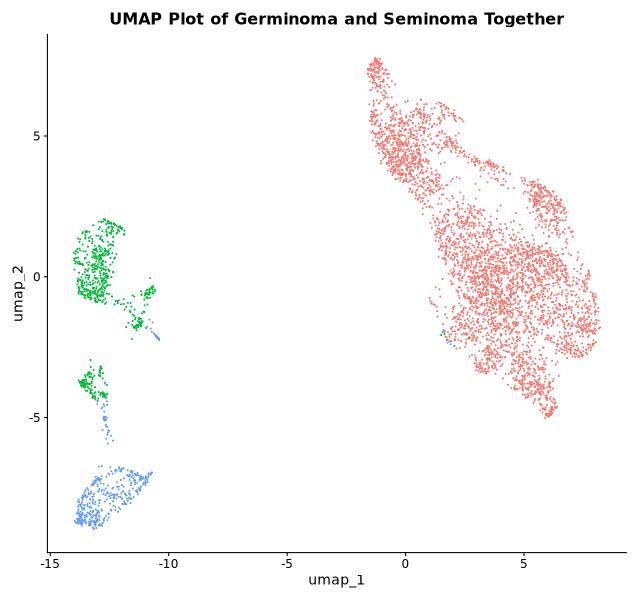
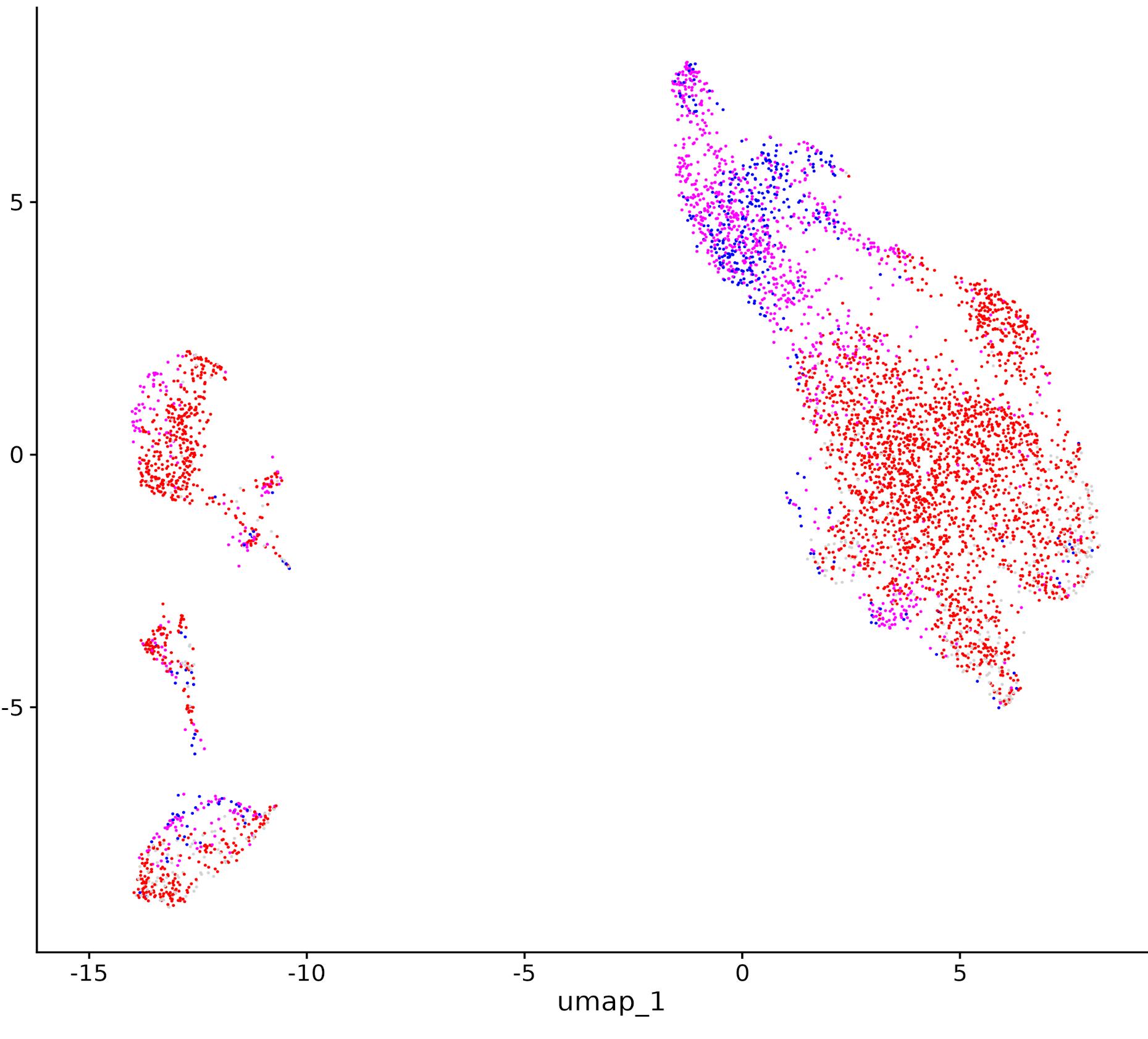
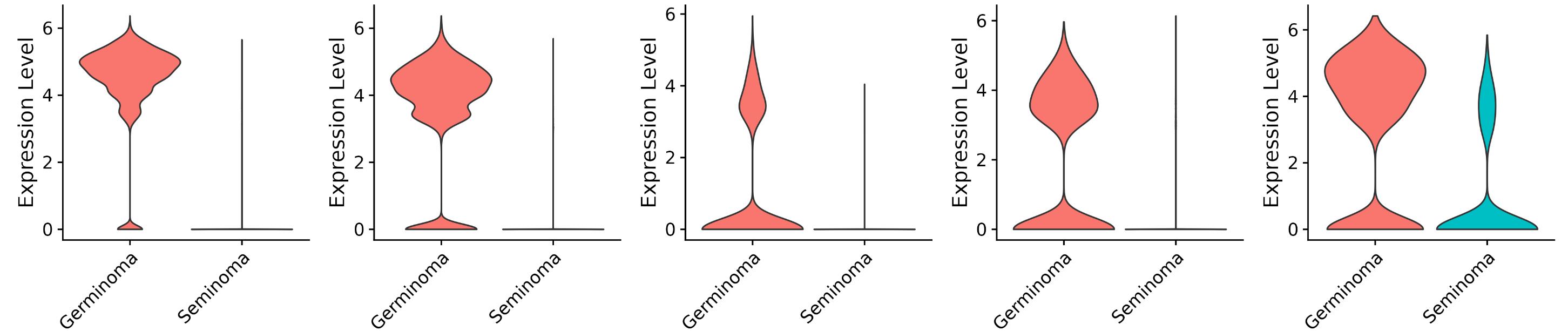
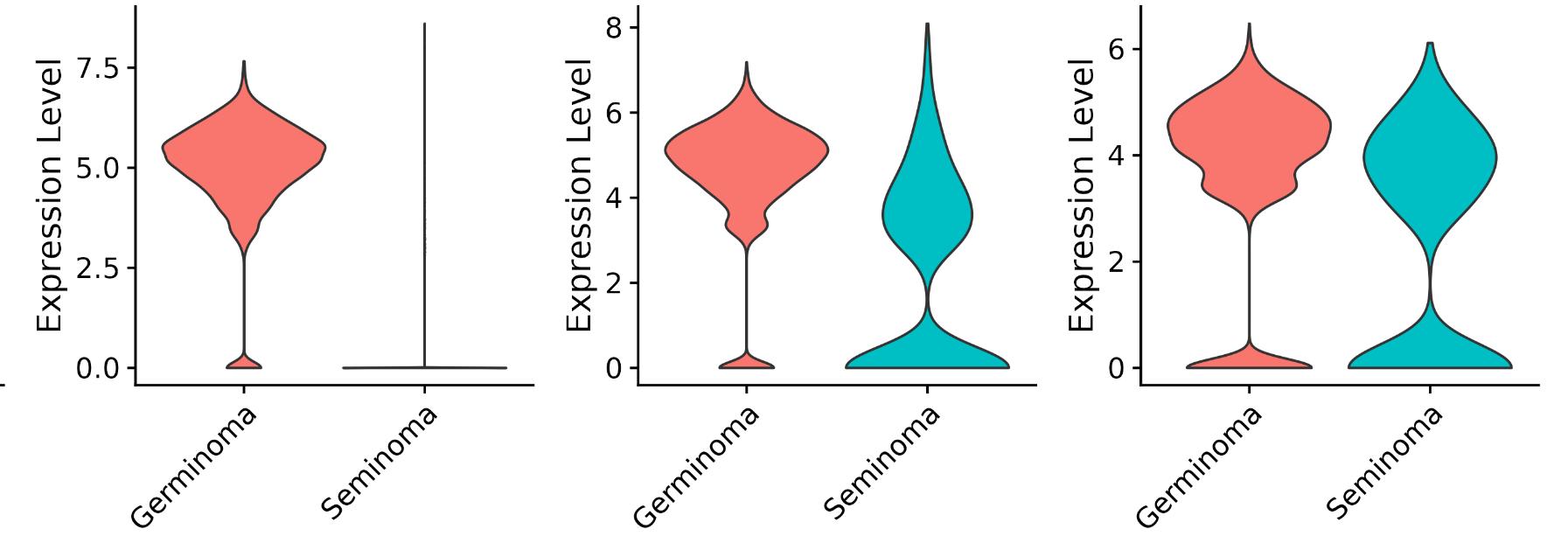
Single-cell RNA sequencing (scRNA-seq) is a powerful tool to appreciate the cellular diversity of human tissues and tumors based on gene expression profile. We used scRNA-seq to analyze the transcriptome of two patientderived xenografts of intracranial germinoma (IGE), a rare pediatric brain tumor likely originating from early germ cell precursors. In sample 6999GCT, we found expression of early germ cell markers, as well as proliferation markers. When comparing sample 6999GCT to previously published testicular seminoma datasets, we observed overlapping but distinct transcriptomic signatures. Unlike for sample 6999GCT, we found that sample 9320GCT did not express high levels of canonical germ cell markers, indicating that it may be a different tumor subtype. In the future, we will conduct developmental trajectory analysis to understand the deviation of IGE from normal development, potentially invaluable information to future disease modeling.
Background
IGE is a rare pediatric brain tumor commonly located near the pineal or pituitary glands. IGE is difficult to surgically resect, and conventional chemoradiation can cause significant long-term toxicity. Therefore, a targeted therapeutic approach is highly desired, but little is known about the pathogenesis of IGE. IGE is a germ cell tumor subtype with many molecular and cellular features matching the earliest committed germ cell progenitor, the primordial germ cell (PGC). IGE is hypothesized to arise due to abnormal PGC development: a subpopulation of PGCs, instead of colonizing the gonads, aberrantly migrate outside of their niche and survive elsewhere, forming tumors. Previously conducted bulk sequencing analysis has provided limited insight into the mechanisms underlying IGE. However, scRNA-seq has the power to further define the transcriptomic programs within IGE, but sufficiently high-quality IGE samples are challenging to obtain. To overcome this problem, we have obtained two mutationally-distinct, orthotopic IGE patient-derived xenograft (PDX) models. With these samples, we performed preliminary scRNA-seq analysis.
Methods
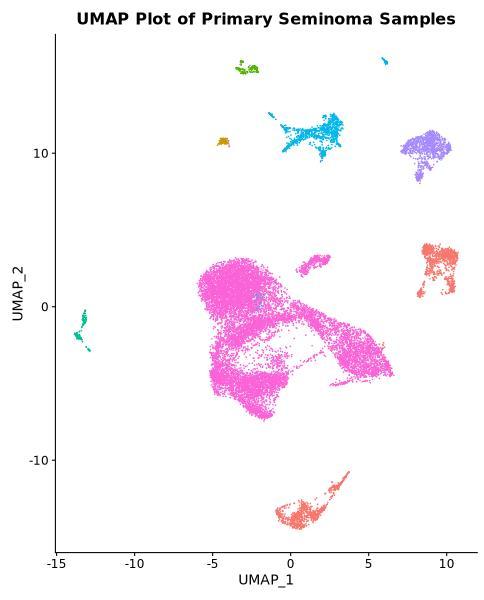
Two orthotopic PDX models were previously established by our lab and collaborators. Tissue samples were collected and dissociated into single cell suspension and cryopreserved. Cells were thawed and approximately 1 million cells were sorted for viability. We performed scRNA-seq using the 10x Genomics Chromium platform Raw data was processed using 10x CellRanger to produce transcript read counts for each cell. After filtering low quality cells and doublet removal, counts were normalized using Seurat. Using the previously published XenoCell software package, we used the human and mouse reference genomes to identify and exclude any mouse cells from the dataset. Raw counts data for two seminoma samples were obtained from a previously published dataset (GSE256162); quality control and CCA integration was performed prior to comparative analysis.
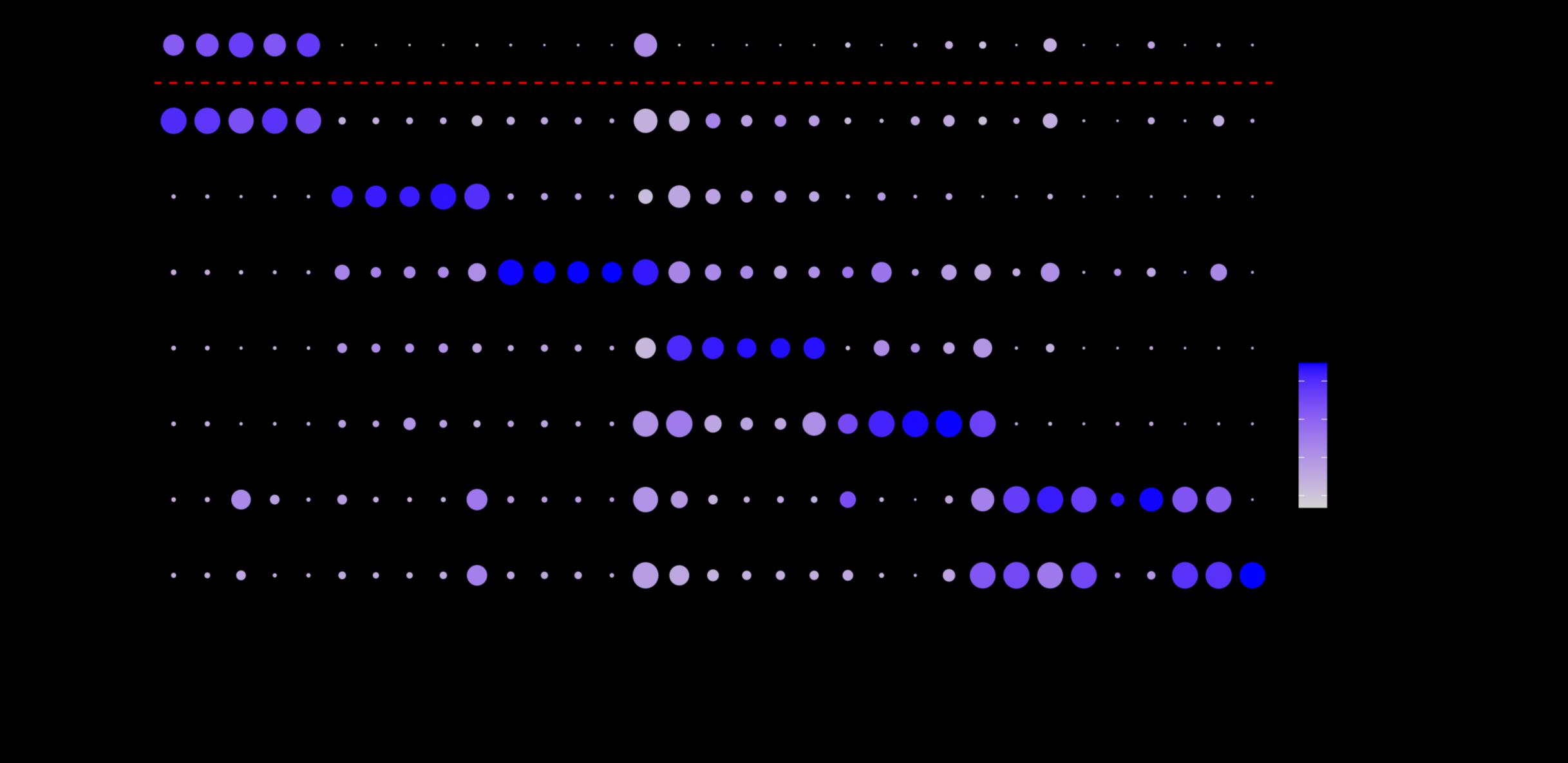
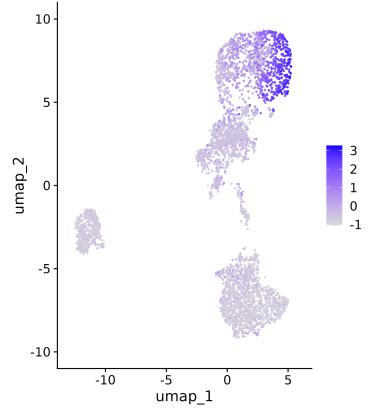
Primary Seminoma Cells and 6999GCT Share Basic Transcriptional Profile
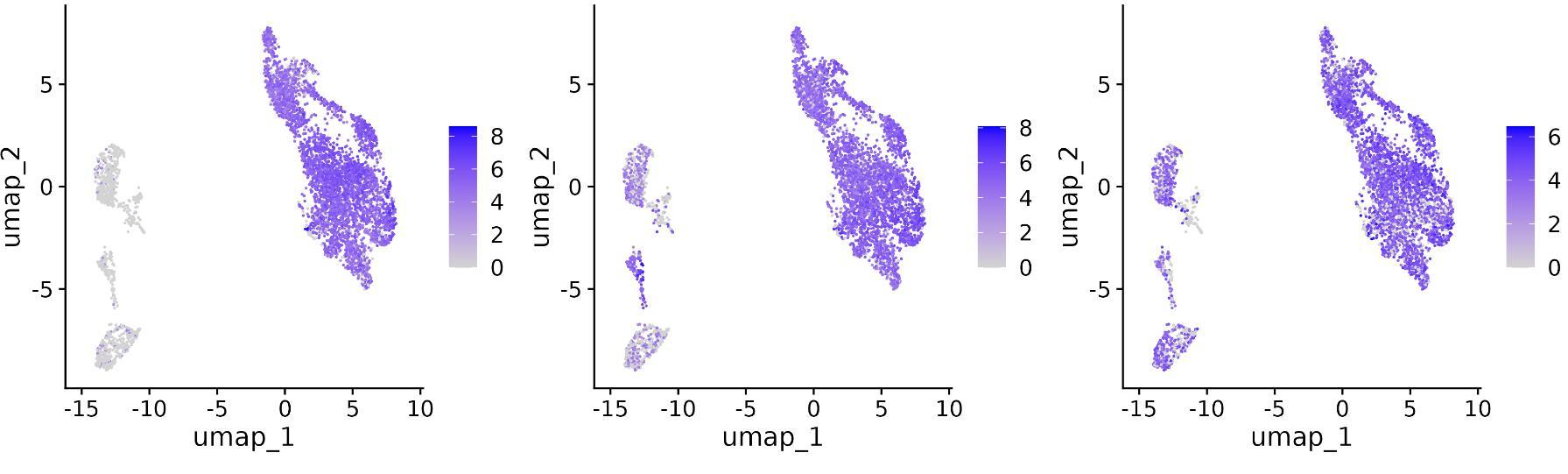
Expression of Hallmark PGC and Proliferation Markers in Tumor Cells
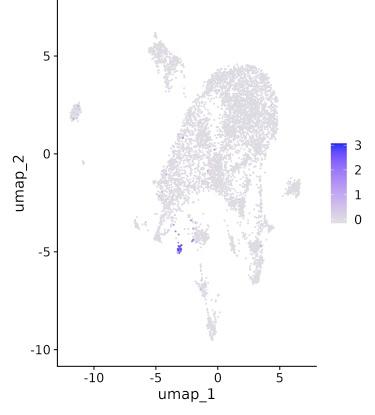
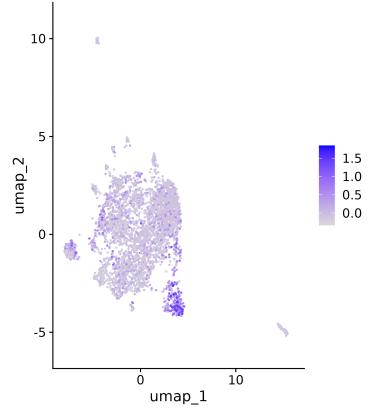
Expression of Genes Key to PGC Function Differ Between Germinoma and Seminoma Samples
9320GCT Does Not Express Hallmark PGC Markers
Conclusions
• For sample 6999GCT, we have positively identified expression of PGC and proliferative markers, which are characteristic of human IGE. We also explored general similarities and specific differences in PGC maturation and migration between IGE and testicular seminoma.
• For sample 9320GCT, we identified high expression of proliferative markers but absence of canonical germ cell markers, likely indicating that 9320GCT is a different tumor subtype.
Ongoing and future studies
• Developmental trajectory analysis of 6999GCT using available embryonic and fetal germ cell datasets
• Canonical cell marker analysis of 9320GCT to determine most likely cancer type
• Incorporation of findings to improve stem cell modeling platform
• UConn/JAX-GM Training Program in Genomic Science (5T32HG010463-05)
• The Single Cell Biology Laboratory and Flow Cytometry Service at JAX-GM
• Collaborators Dr. Kotaro Sasaki at UPenn and Dr. Xiao-Nan Li at Northwestern
References
Category: (Basic/Translational)
ExpandingtheSyphilis MolecularToolbox: ex vivo and in vivo
Characterizationof Treponema pallidumExpressinga Constitutive Green FluorescentProtein Reporter
PresentingAuthor: KristinaDelgado, Graduate Student Doctoral Research Kristina Delgado1 , Crystal F. Vicente2 , Christopher M. Hennelley3 , FarhangAghakhanian, PhD3 , JonathanParr,MD3 , Kevin Claffey,PhD4,JustinD.Radolf,MD1, 5-8,Kelly L. Hawley,PhD1,2,6,8,#,andMelissaJ.Caimano,PhD1,2,5,8,*,#
1 Department of Medicine, UConn Health, Farmington, CT, USA
2 Department of Pediatrics, UConn Health, Farmington, CT, USA
3 Institute for Global Health and Infectious Diseases, University of North Carolina at Chapel Hill, Chapel Hill, North Carolina, USA
Syphilis, a multistage sexually transmitted infection caused by Treponema pallidum subsp. pallidum (TPA), is known for its invasivenatureand immune evasion, leading to persistent infection. Congenital syphilis, where TPA crosses the fetal-placental barrier, causing severe fetal outcomes, exemplifies its invasiveness. Despite ongoing efforts, syphilis cases are rising, with over 200,000 cases reported in 2022, including a significant increase in congenital syphilis cases.
The inability to continuously cultivate TPA in vitro has hindered genetic studies aimed at identifying virulence factors and understanding host-pathogen interactions. However, the development of a coculture system using rabbit epithelial cells has enabled the long-term replication of TPA, leading to its genetic manipulation and the generation of fluorescentreportersforpathogen tracking.
METHODS & RESULTS
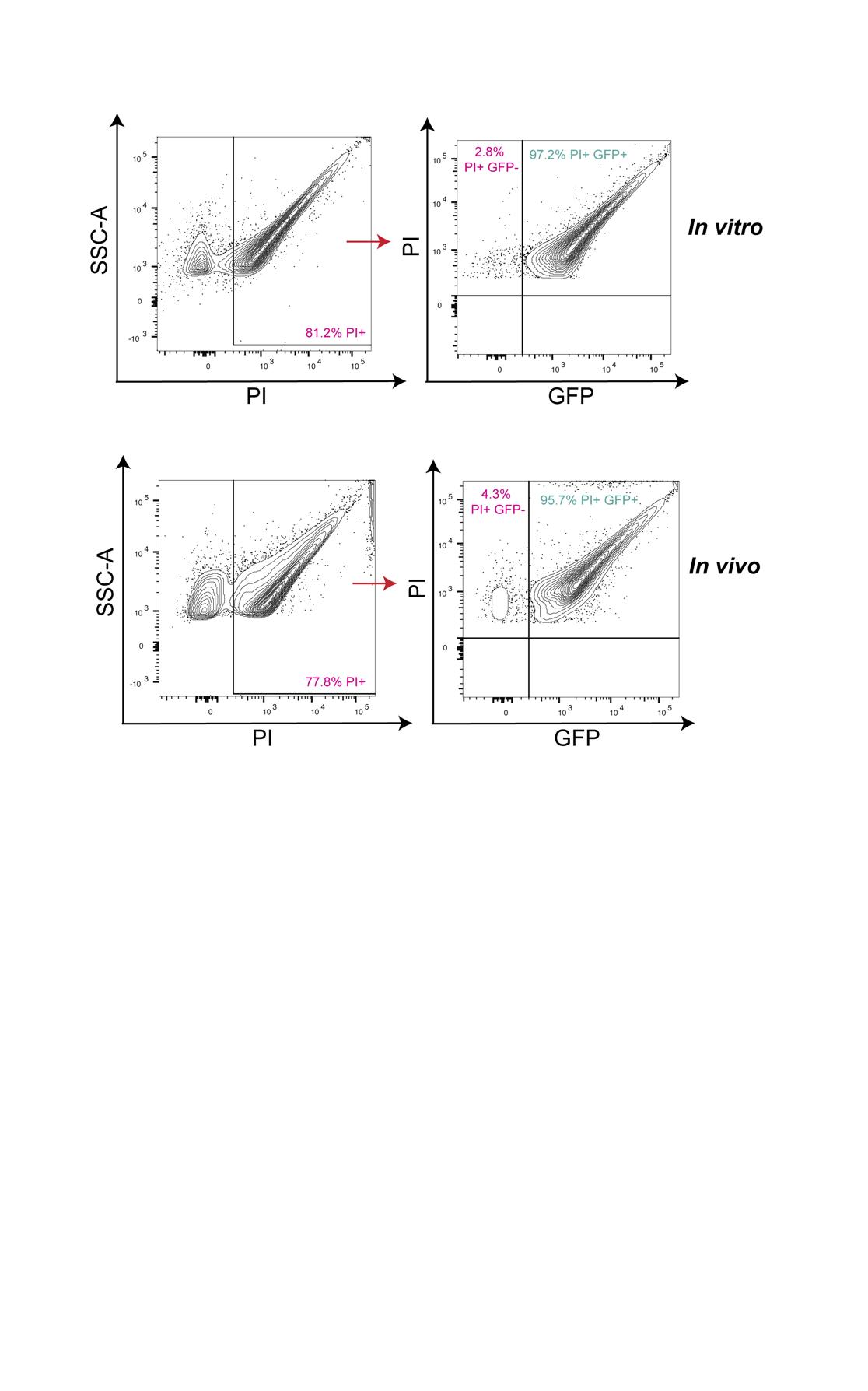
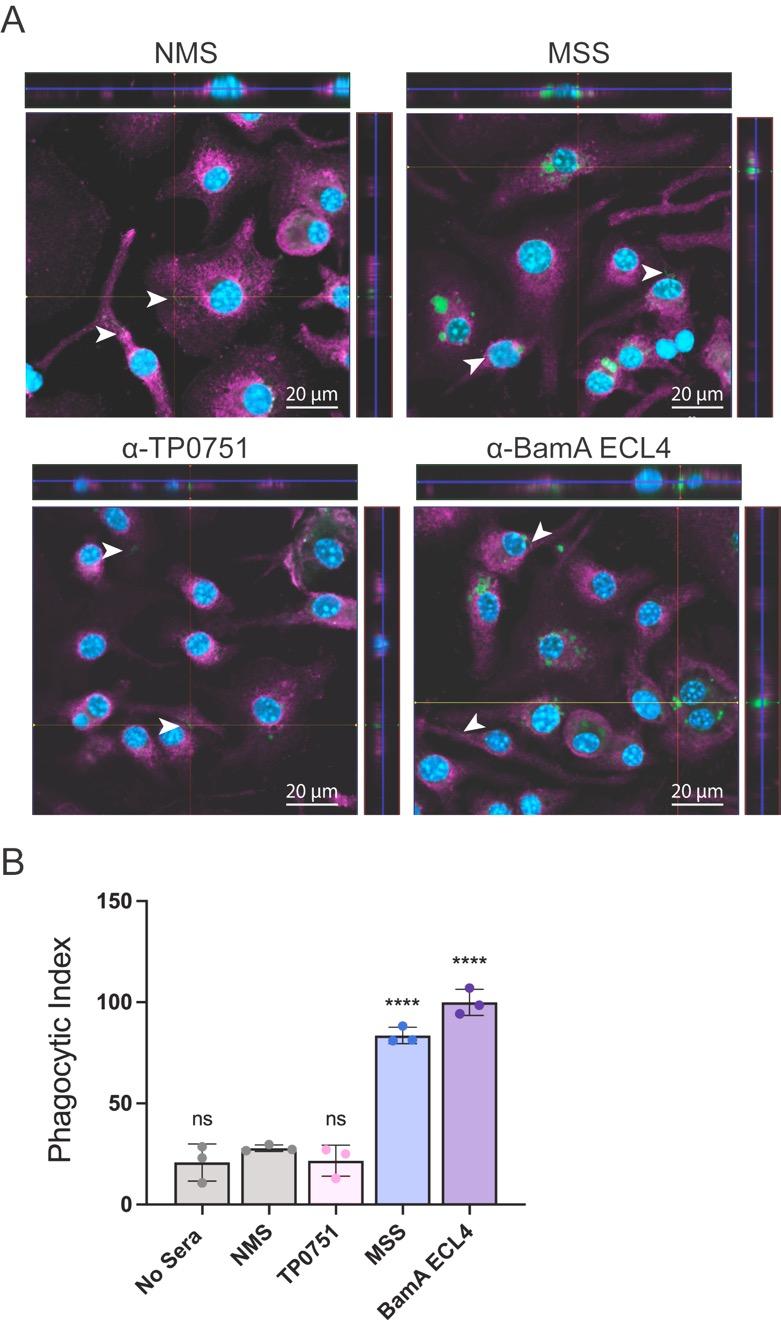
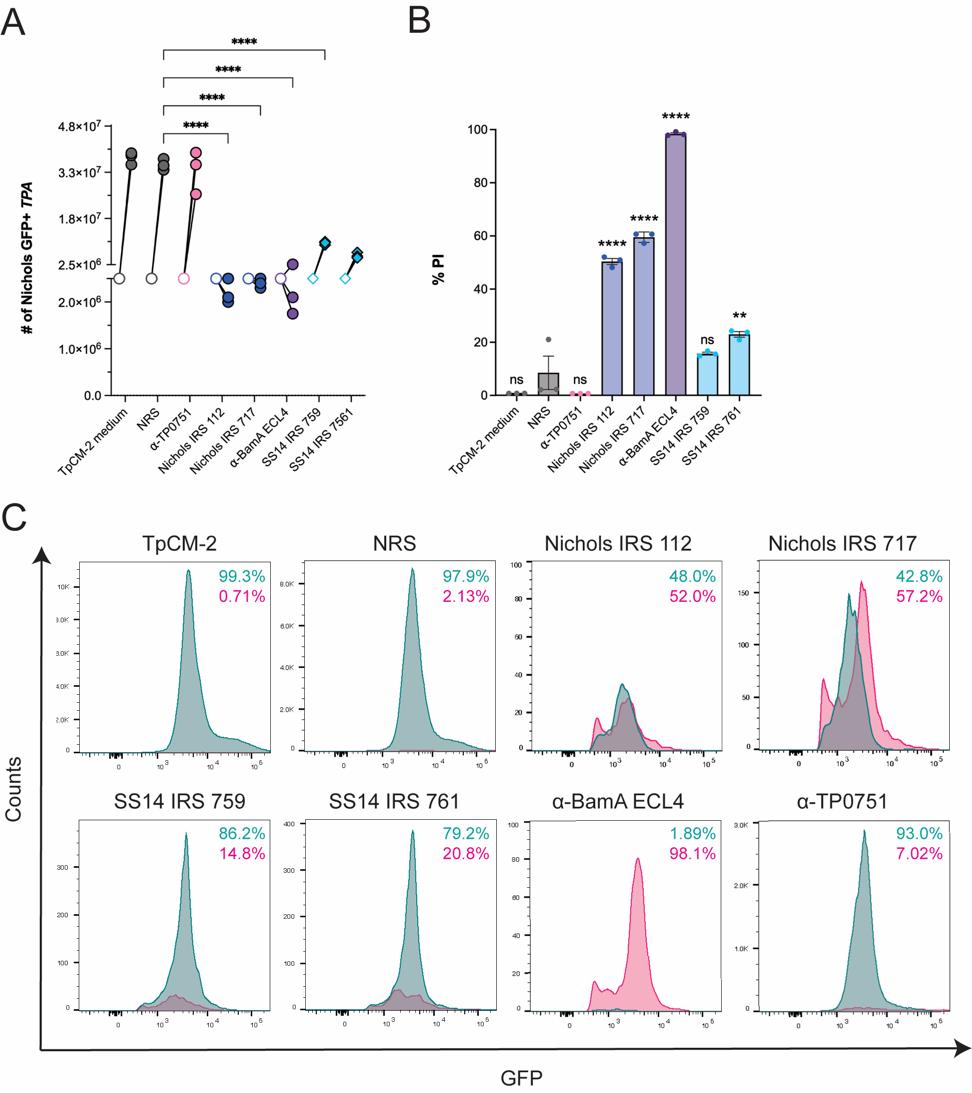
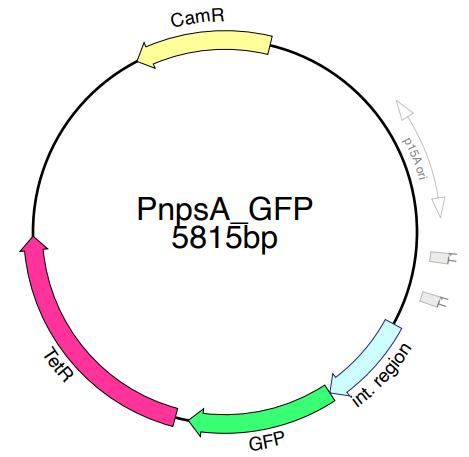
In this study, wegenetically engineered a TPA Nichols strain to express agreen fluorescent protein (GFP+_TPA). Characterization of GFP+_TPA revealed identical growth in vitro and infectivity in rabbits comparable to the wildtype parent This resource enhances our ability to visualize host-pathogen interactions in vitro and in vivo Additionally, GFP+_TPA was utilized to assess antibody functionality in opsonophagocytosis assays using mouse bone marrow-derived macrophages and in thenewly developed flow cytometry assay. These assays evaluated the impact of antibodies on GFP+_TPA growth and membrane integrity, confirming the utility of GFP+_TPA for studying immune clearance and protectiveimmunity.
CONCLUSION/ SIGNIFICANCE
This novel tool paves the way for innovative approaches to identify TPA virulence factors essential for dissemination, and persistence within host tissues, advancing our understanding of syphilis pathogenesis and informing the development of new therapeutic strategies.
Expanding the molecular toolbox for syphilis research: in vitro and in vivo characterization of Treponema pallidum constitutively expressing green fluorescent protein
ABSTRACT
BACKGROUND
RESULTS
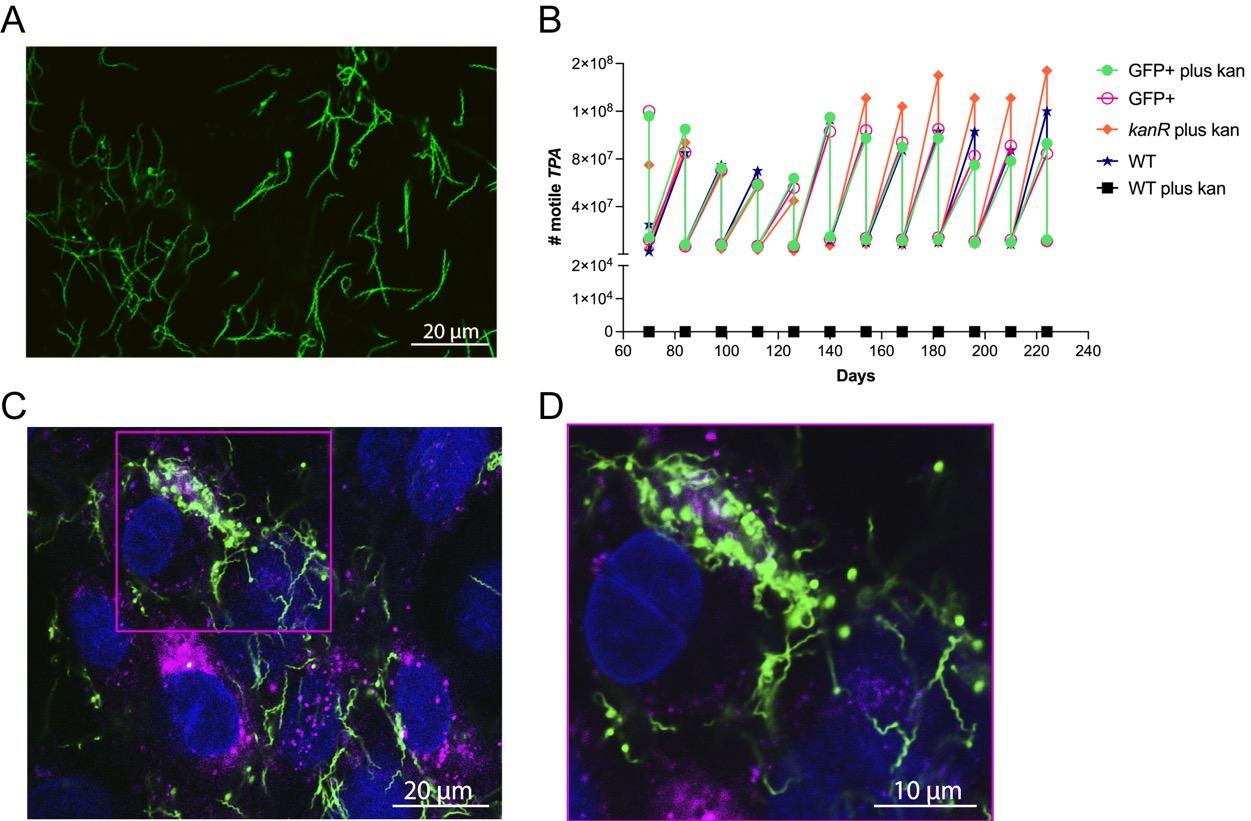
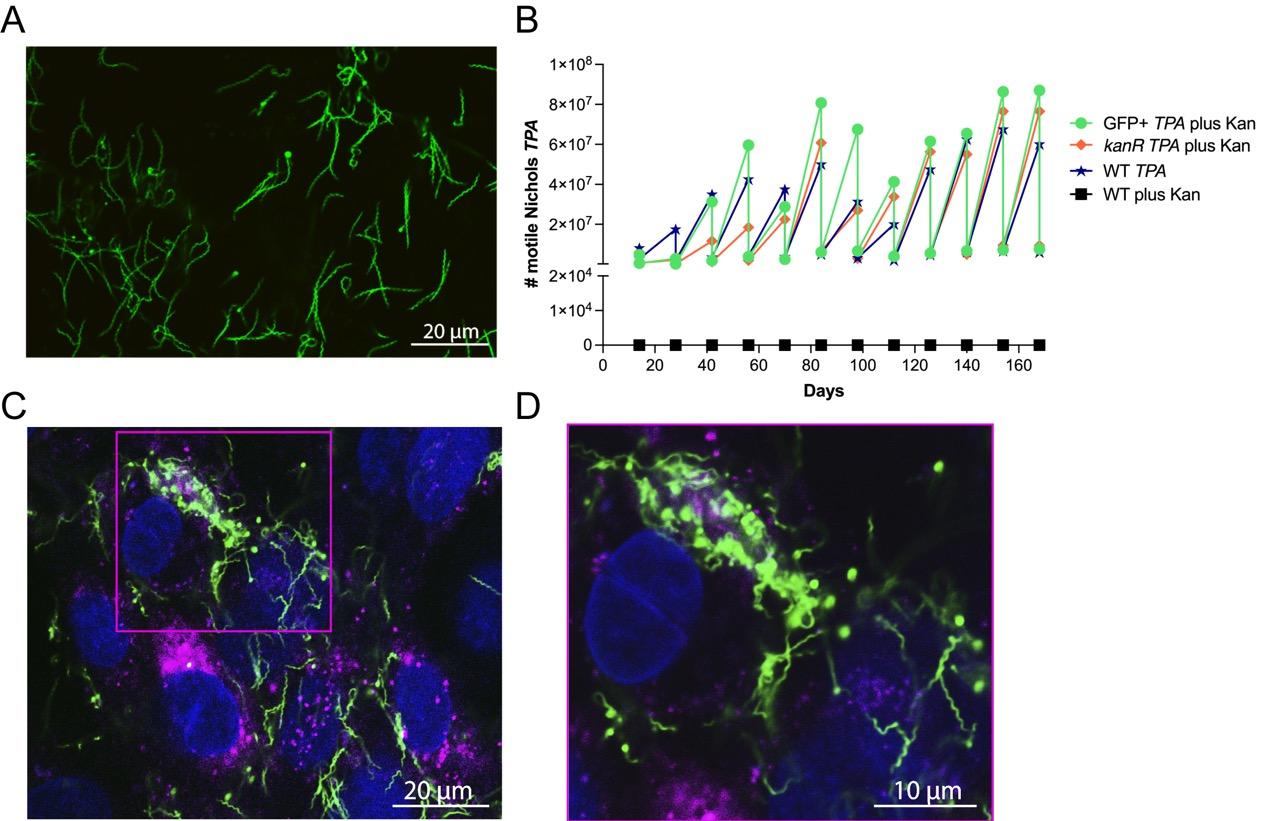
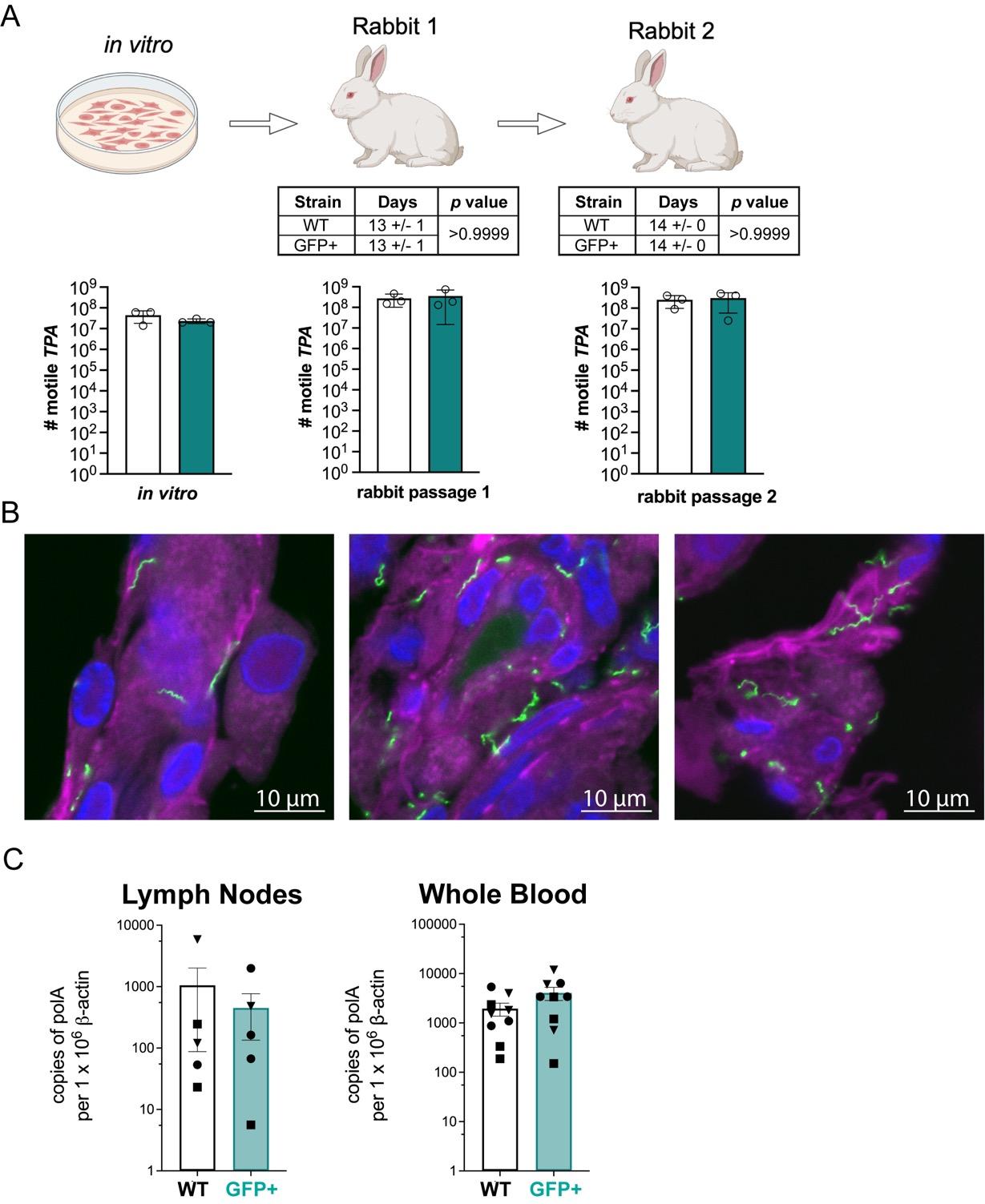
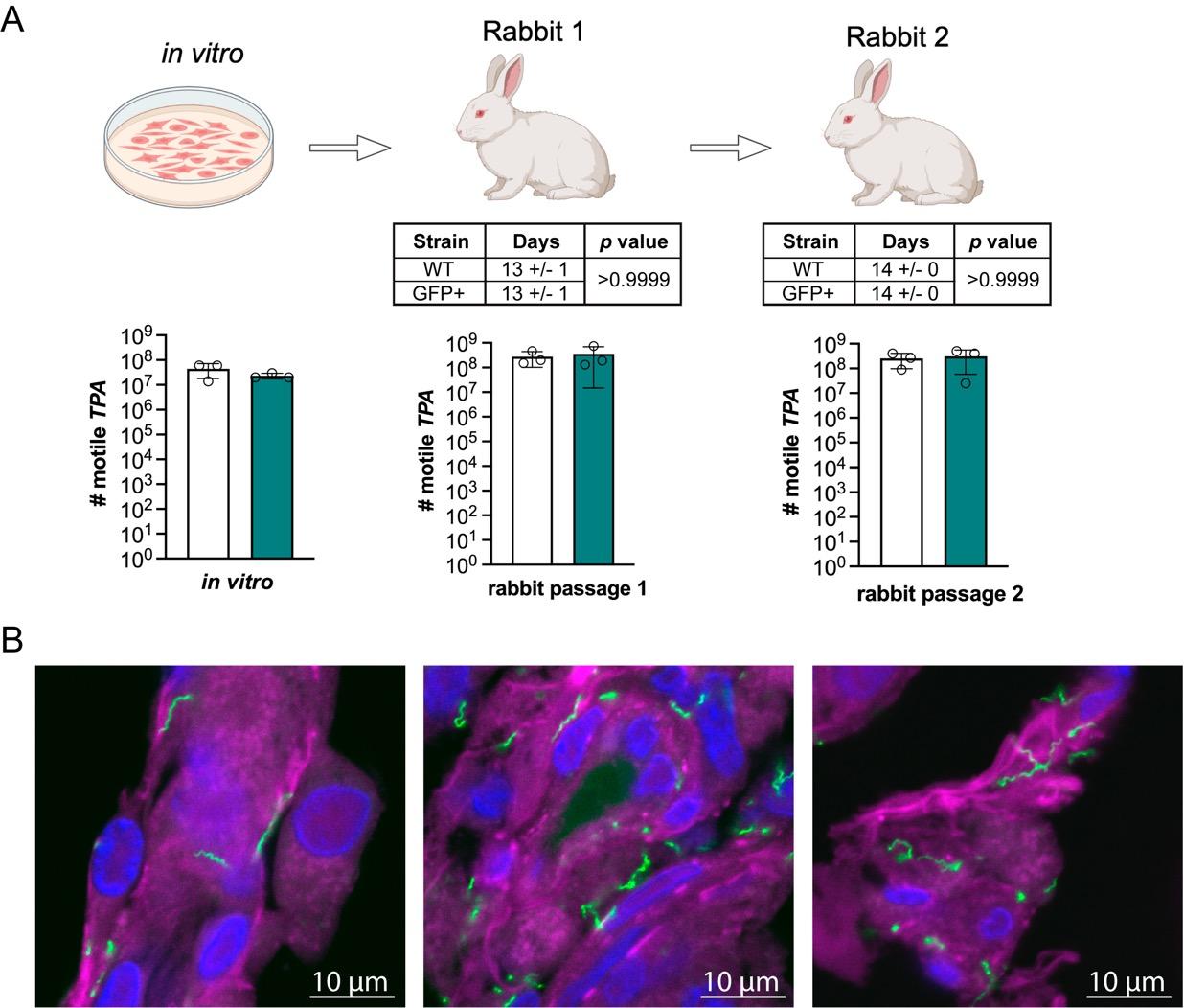
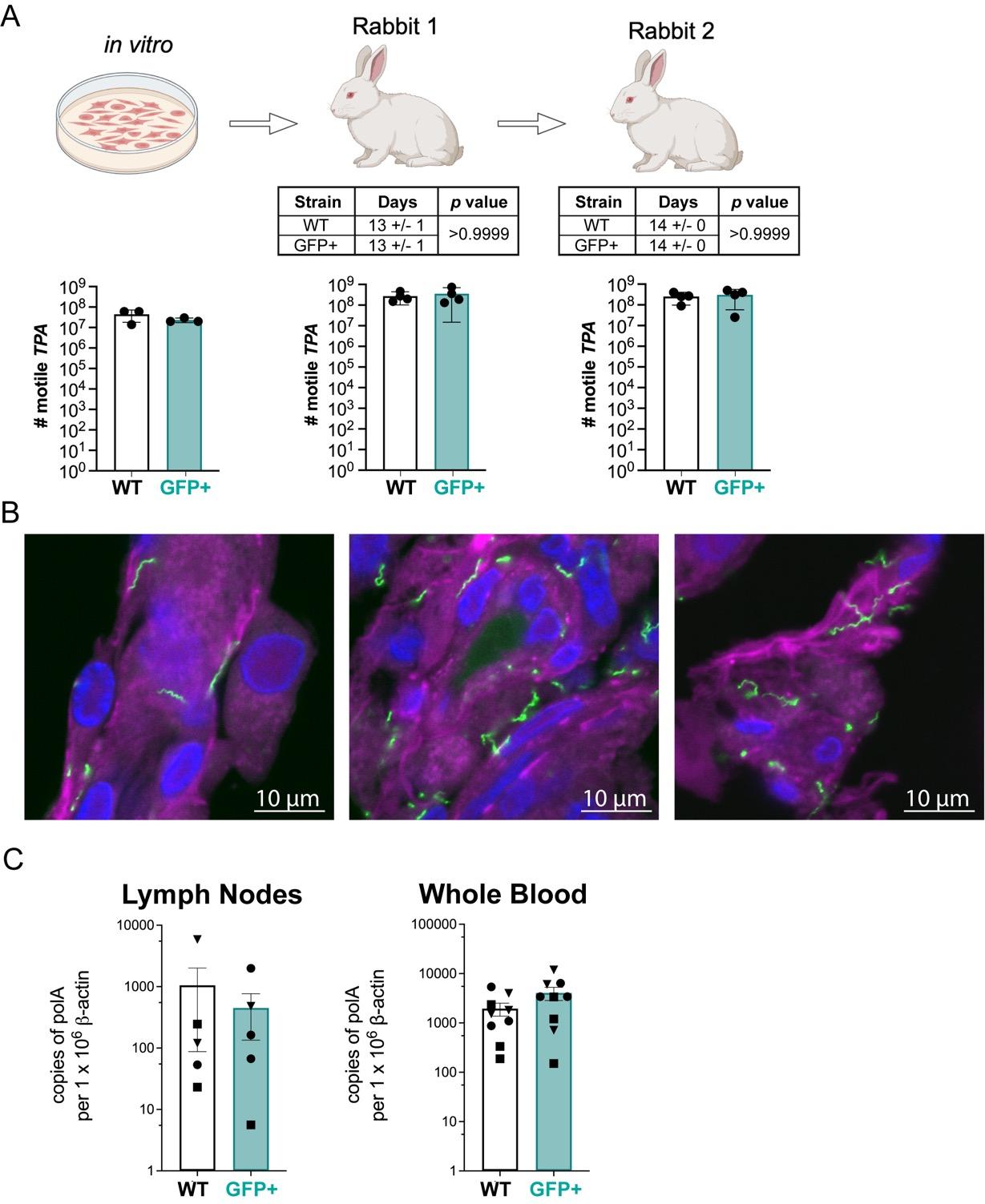
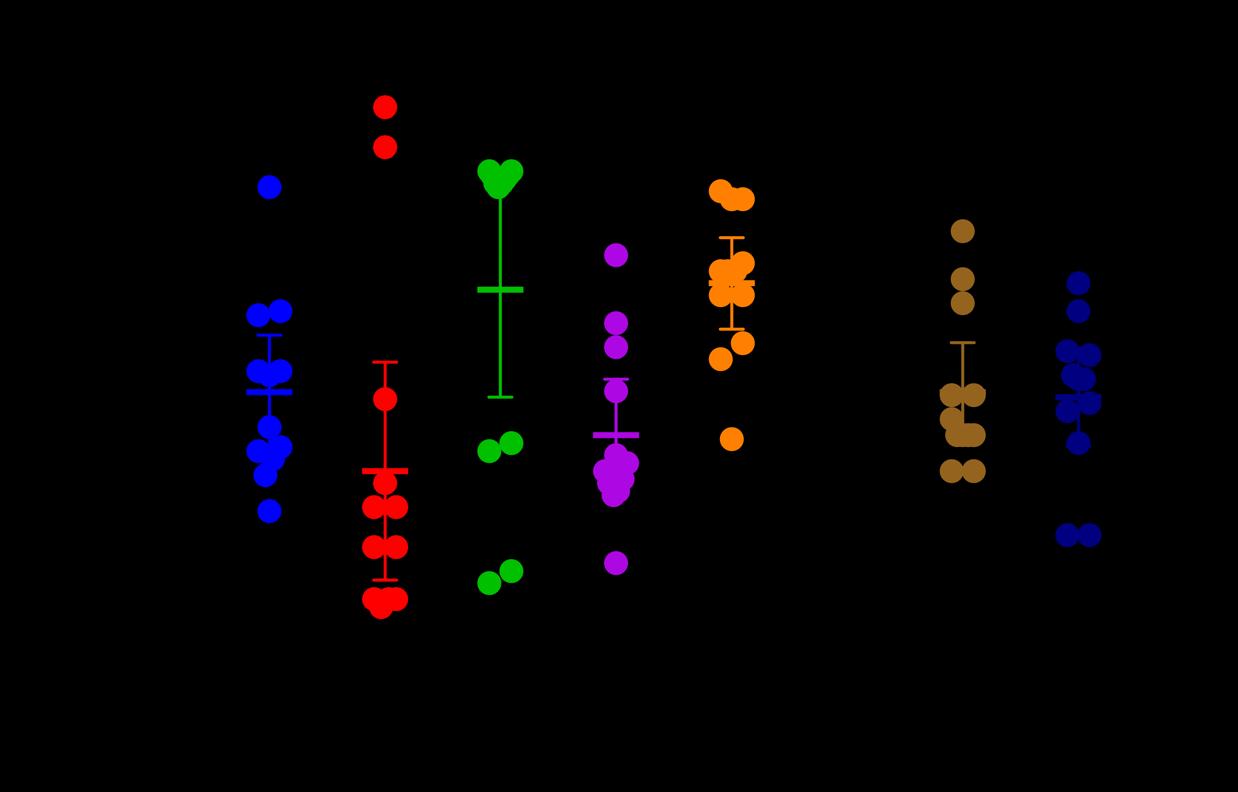
GFP+ TPA exhibits wild-type infectivity and dissemination following intratesticular inoculation A Schematic representation and data for serial passaging of in cultivated WT (white) and GFP+ TPA (green) strains in testes (3 animals per strain) The number of motile treponemes was determined by darkfield microscopy Days the time required for TPA-infected testes to reach orchitis Bars indicate the mean ± standard deviation significant differences (p>0 05) were observed between GFP+ TPA for either timing of orchitis or burdens in B Representative confocal images of cryosections TPA (green) in rabbit testes harvested at peak and stained with DAPI (blue) and Cholera Toxin B (magenta) (C) Bar graph depicting WT (white) GFP+ (cyan) TPA dissemination in rabbit lymph nodes and whole blood (right) Bars represent the SEM for TPA polA normalized per 1 x 106 copies of actin determined by qPCR Symbols (triangle, and circle) designate data from individual animals
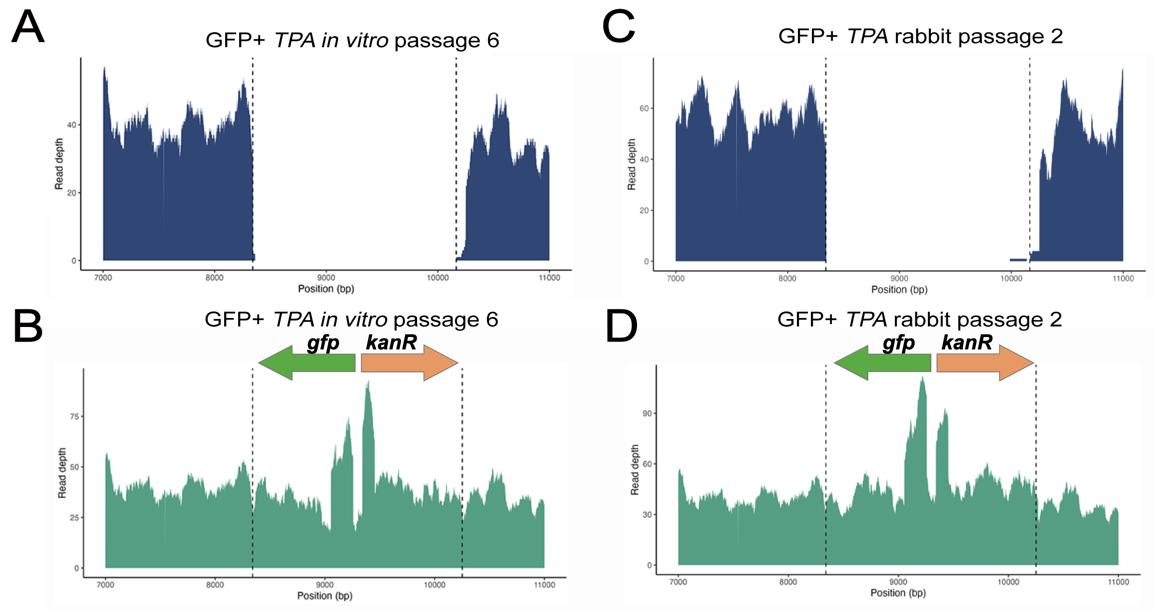
• Whole -genome sequencing confirmed the stable integration of the gfp -kanR cassette with minimal genetic alterations across multiple passages.
The engineered GFP -expressing TPA strain maintained wild -type viability, growth, and infectivity both in vitro and in vivo
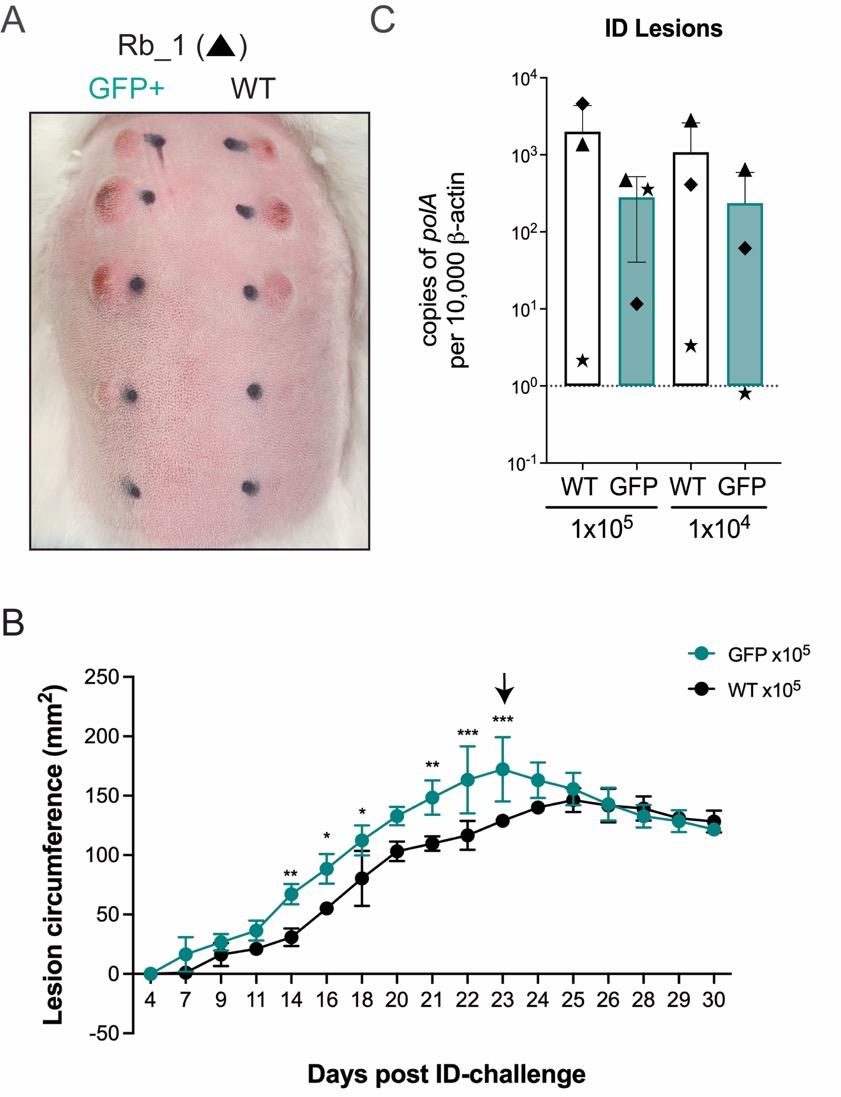
GFP expression in GFP+ TPA enabled clear visualization of spirochetes via fluorescence, facilitating a detailed study of cellular adhesion in vitro and pathogen -host interactions in vivo GFP+ TPA demonstrated equivalent infectivity and dissemination in the rabbit model compared to the wild -type strain, with comparable lesion formation and pathogen burdens in tissue.
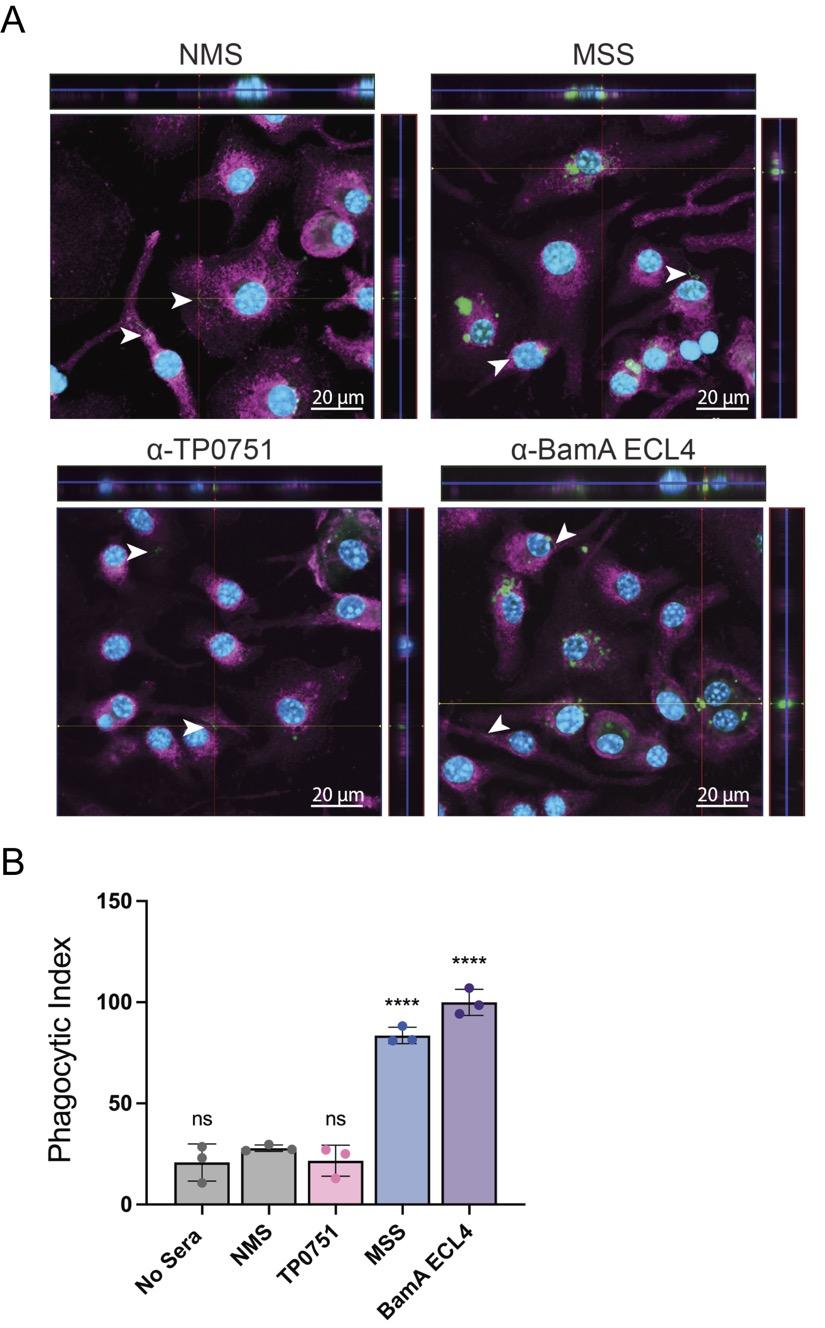
• The use of GFP+ TPA in opsonophagocytosis assays with murine macrophages validated its utility in evaluating antibody-mediated phagocytosis, streamlining analysis by eliminating the need for additional immunofluorescent staining.
IRS and antibodies targeting BamA ECL4 significantly inhibited growth and compromised the outer membrane integrity of GFP+ TPA , highlighting their potential as vaccine candidates.
• The GFP+ strain serves as a powerful tool for studying TPA and provides valuable data for syphilis vaccine development, particularly regarding the mechanisms of antibody -spirochete interactions.
Facility: Susan Staurovsky
Farhang Aghakhanian PhD Chris Hennelly
Category: (Basic/Translational)
A Thematic Analysis of In-Depth Interview Data with Young People Who Avoid Medical Situations Involving Needles.
Presenting Author: David Finitsis, PhD David Finitsis, PhD1 & Isaac Rubinstein2 , & Dean Cruess, PhD3
1 University of Hartford
2 Wesleyan University
3 University of Connecticut
BACKGROUND
Blood-Injection-Injury (BII) phobia primarily emerges in childhood and is characterized by avoidance of situations involving blood and needles. As children enter adolescence and explore increased autonomy, these symptoms may disrupt the continuity of care and contribute to increased risk of patient nonadherence with routine health monitoring and prevention including immunizations. This fear avoidance behavior impacts both individual and public health, increasing the burden to the healthcare system and society.
METHODS
Using a validated measure of needle anxiety, we screened 1460 young people (aged 18-22) across two Connecticut universities. Of these, 24.6% met criteria for high needle anxiety. Fifty-four consented participants completed in-depth interviews querying past aversive medical experiences, current health behaviors, and patient-provider relationship quality. After transcription, interview data was coded and analyzed to identify thematic content consistent across respondents.
RESULTS
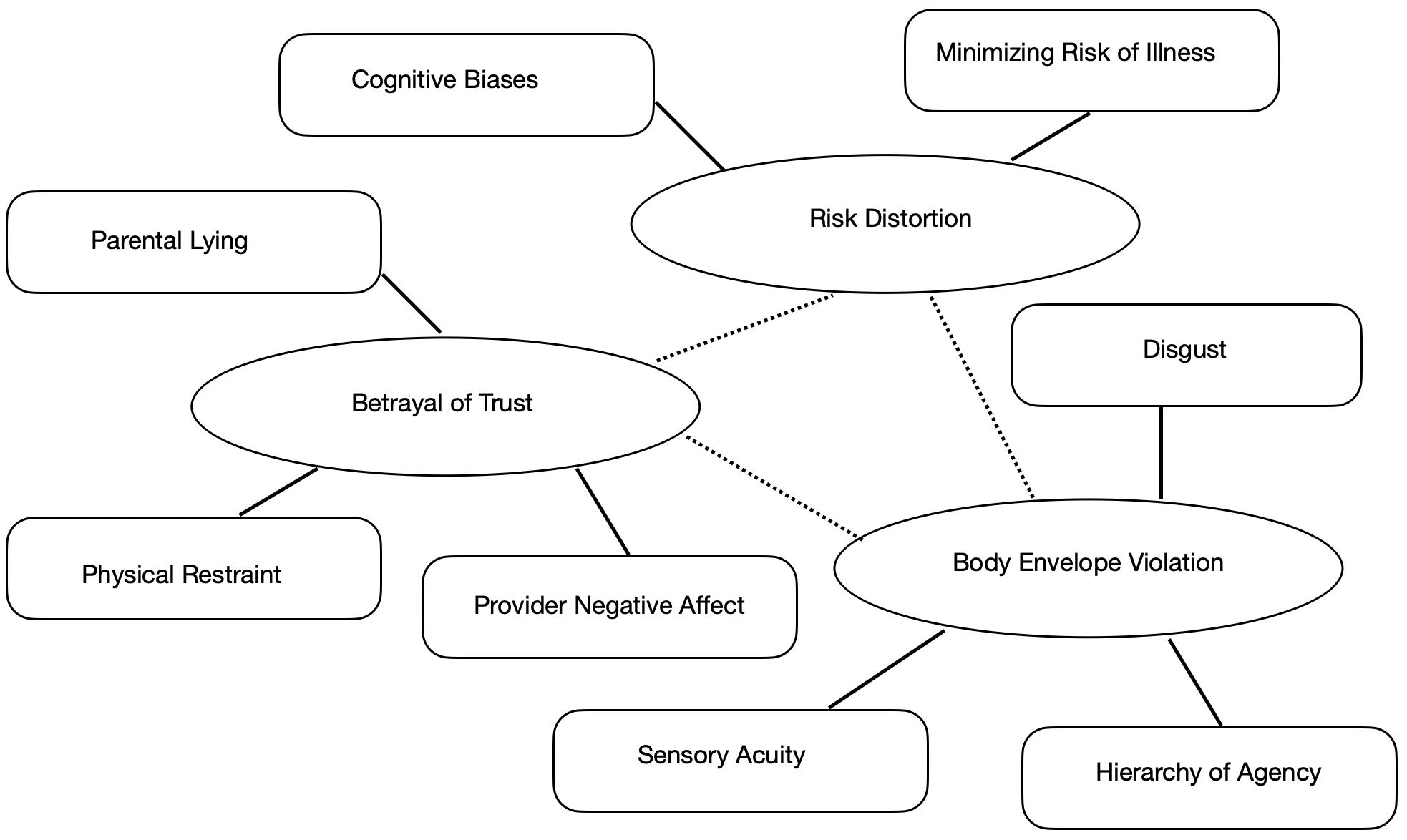
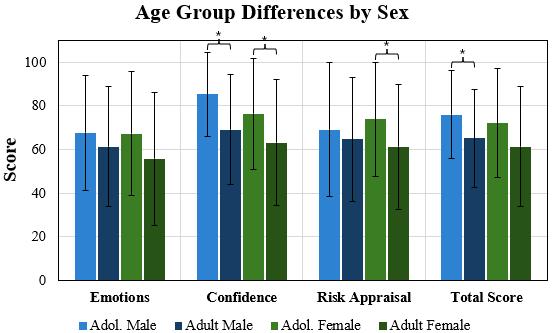
Thematic analysis yielded evidence that avoiding medical situations is a multifactorial phenomenon, characterized by biased cognitive processes, particularly attentional and expectancy biases (risk distortion). Affective content showed significant heterogeneity with disgust, fear, and anxiety operating in combination. The availability and willingness to seek support moderated the extent of individuals’ reported avoidance
CONCLUSION/SIGNIFICANCE
These findings reveal significant needle avoidance behavior among young people in a phase of emerging adulthood. Once established, these maladaptive patterns may operate largely unseen by medical providers because as these young people emerge into adulthood, they may be less likely to present for assessment or treatment. Given its high prevalence, routine screening for needle anxiety and supportive intervention is warranted
A Thematic Analysis of In-Depth Interview Data with Young People Who Avoid Medical Situations Involving Needles.
David J. Finitsis1 PhD, Isaac Rubinstein2, & Dean G. Cruess3 PhD
1.University
of Hartford, West Hartford, Connecticut; 2. Wesleyan University, Middletown, Connecticut; 3. University of Connecticut, Storrs, Connecticut
BACKGROUND
Blood-Injection-Injury (BII) phobia primarily emerges in childhood and is characterized by avoidance of situations involving blood and needles. As children enter adolescence and explore increased autonomy, these symptoms may disrupt the continuity of care and contribute to increased risk of patient non-adherence with routine health monitoring and prevention including immunizations. This fear avoidance behavior impacts both individual and public health, increasing the burden to the healthcare system and society.
METHODS
Using a validated measure of needle anxiety, we screened 1460 young people (aged 18-22) across two Connecticut universities. Of these, 24.6% met criteria for high needle anxiety. Fifty-four consented participants completed in-depth interviews querying past aversive medical experiences, current health behaviors, and patientprovider relationship quality. After transcription, interview data was coded and analyzed to identify thematic content consistent across respondents.
ANALYSIS
Attentional and expectancy biases simultaneously amplify the risks of needle sticks and minimize risks of not undergoing the procedure. Respondents focused on the sensation of needle insertion and described a violation of the body envelope that is met with salient disgust as much as fear and anxiety. A history of institutional or parental betrayal was common in the sample and predicted the most extreme kinds of avoidance; conversely, parental and professional support aided coping in some respondents
SIGNIFICANCE
These findings reveal several recurring themes surrounding needle avoidance behavior among young people in a phase of emerging adulthood.
Once established, these maladaptive patterns may operate largely unseen by medical providers because as these young people emerge into adulthood, they may be less likely to present for assessment or treatment.
Given its high prevalence, routine screening for needle anxiety and supportive intervention is warranted.
BenjaminHoffman1,2*,QingfenYang1,3,AksharaMalepati1,2,PatrickMcMullan 1,3,4,and Emily L. Germain-Lee 1,3
1 Division of Pediatric Endocrinology & Diabetes, Department of Pediatrics, Connecticut Children’s and University of Connecticut School of Medicine;
2 University of Connecticut, Storrs, Connecticut;
3 Center for Regenerative Medicine & Skeletal Development, Department of Reconstructive Sciences, University of Connecticut School of Dental Medicine;
4 Department of Medicine, University of Connecticut School of Medicine; * Presenting Author
BACKGROUND
Albright hereditary osteodystrophy (AHO) is caused by heterozygous inactivating mutations in GNAS, the gene encoding the α-subunit of the stimulatory G protein necessary for signaling of many hormones. AHO includes 2 subtypes: 1) pseudohypoparathyroidism type 1A (PHP1A) caused by maternally inherited mutations and 2) pseudopseudohypoparathyroidism (PPHP) caused by mutations that are paternally inherited. Due to imprinting of GNAS,PHP1ApatientshavehormonalresistanceandobesitywhereasthosewithPPHPdonot.Mandibular abnormalities are common in AHO and cause serious morbidity. We developed a mouse model of AHO (Germain-Lee et al., 2005) which recapitulates the condition. However, its use as a model for mandibular defects has not been previously determined.
METHODS
Mousecorrelates of PHP1Aand PPHPwerecompared to wild-typemiceat 5 and 12 weeks of age,Noticeable differences in mandibular length between mutant and wild-typemicewerevisually observed on radiographic high-powered jaw images. Definedmeasurements forassessing mandibular dimensions were then performed and analyzed.
RESULTS
Themandibles of mousecorrelates of PHP1Aand PPHP were significantly hypoplastic compared to wild-type mice at both 5 and 12 weeks but werenot significantly different from oneanother. Themandibles of themutant mice grew proportionately in length relative to wild-typemice,thereby implicating that theabnormality occurs early in development.
DISCUSSION
Our mousemodelofAHO exhibits mandibular hypoplasia as observed in the human disorder. Further investigations using this model could be helpful in determining theetiology of this defect with thegoalof developing therapeutic interventions.
Investigation of Mandibular Defects in a Mouse Model of Albright Hereditary Osteodystrophy
Benjamin Hoffman, BS 1,2,3 , Qingfen Yang, MA1,3 ,Akshara Malepati 1,3 , Patrick McMullan, MD, PhD 1,3 , and Emily L. Germain-Lee, MD 1,3
1 Division of Pediatric Endocrinology & Diabetes, Department of Pediatrics, Connecticut Children’s and University of Connecticut School of Medicine; 2 University of Connecticut, Storrs, Connecticut; 3 Center for Regenerative Medicine & Skeletal Development, Department of Reconstructive Sciences, University of Connecticut School of Dental Medicine
Introduction
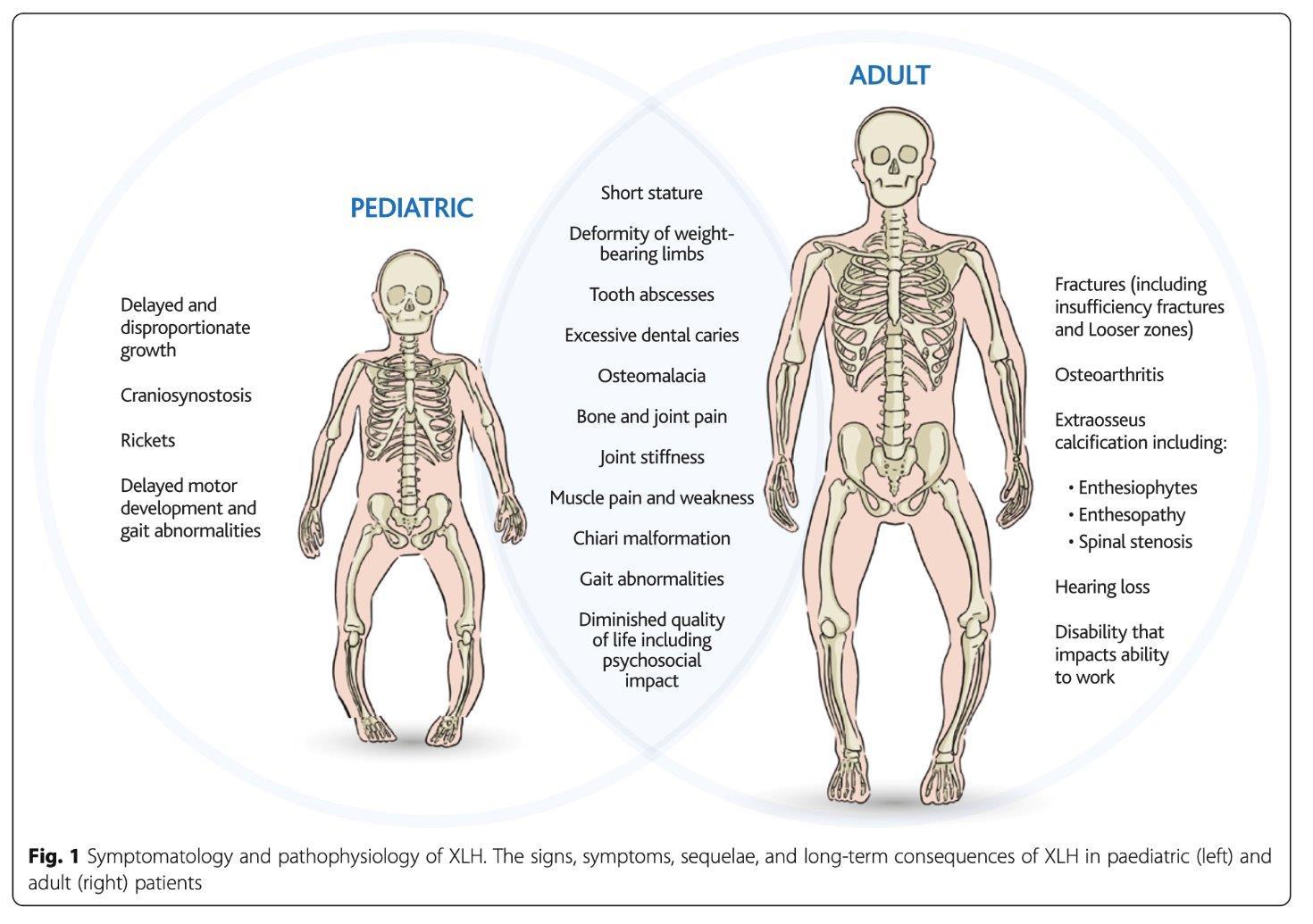
Albright hereditary osteodystrophy (AHO) is caused by heterozygous inactivating mutations in GNAS, the gene encoding the α-subunit (Gαs) of the stimulatory G protein (Gs). Gs couples heptahelical receptors for numerous hormones and neurotransmitters to stimulate cAMP formation by adenylyl cyclase. Patients with GNAS mutations on the maternally-inherited allele have a condition termed pseudohypoparathyroidism type 1A (PHP1A) and manifest resistance to multiple Gs-coupled hormones (e.g. PTH, TSH, LH/FSH, GHRH, calcitonin) in addition to having severe obesity, short stature, brachydactyly, and subcutaneous ossifications (Fig. 1). Patients with GNAS mutations on the paternally-inherited allele have a condition termed pseudopseudohypoparathyroidism (PPHP) and have similar symptoms but do not exhibit hormone resistance or severe obesity. This genetic mechanism based on the parental mode of inheritance is called genomic imprinting. We previously developed a mouse model of AHO through targeted disruption of exon 1 of Gnas and have shown that it recapitulates the human condition in our prior investigations. Dental and craniofacial abnormalities are a significant issue in PHP1A, often leading to the need for oral surgery and orthodontic intervention. Dental abnormalities that can occur include enamel hypoplasia and opacities, deviation of root morphology, eruption disturbances, microdontia, hypodontia, and large pulp chambers (Fig. 1D). Craniofacial abnormalities also occur such as mid-face hypoplasia, craniosynostosis, and both mandibular and maxillary hypoplasia. These abnormalities lead to a large medical and financial burden for the patients. In PPHP, the extent of these dental and craniofacial abnormalities remains unclear, and our mouse model may be useful in identifying potential abnormalities. Overall, this investigation set out to investigate whether our mouse model could be utilized for further investigation of the mandibular abnormalities.
This study compared mouse correlates of PHP1A (Gnas E1+/-m) and PPHP (Gnas E1+/-p) to wild-type mice at 5 and 12 weeks of age Noticeable differences in mandibular length between mutant and wild-type mice were visually observed on radiographic high-powered jaw images. Defined measurements for assessing mandibular dimensions were then performed and analyzed via ImageJ software Although the mouse model of AHO recapitulates the condition, its use as a model for mandibular defects has not been previously determined.
Figure 1. Phenotype of Albright Hereditary Osteodystrophy. AHO is characterized by short stature (A), as well as brachydactyly (B) and brachymetacarpia/brachymetatarsia [with brachymetatarsia shown in (C)]. Dental and jaw abnormalities are also common. A panoramic radiograph of a 10-year-old subject with PHP1A (D) is shown with congenitally missing teeth including the upper left canine, 2nd molar, 2nd bicuspid, lower left 1st and 2nd bicuspids, 3rd molar, lower right 1st and 2nd bicuspids, and 3rd molar. No signs of 3rd molar development are present. The overall jaw is hypoplastic.
Materials and Methods
Mouse Model
All mouse protocols were carried out in accordance with the standards of the UConn Health Animal Care and Use Committee (AP-200074-0623). The generation of mice carrying a targeted disruption of exon 1 of Gnas (Gnas E1+/-) was described previously (ref 1). Mice were maintained on a pure 129SvEv background and were genotyped by PCR analysis.
Radiographic Imaging
Radiographic imaging was performed on harvested cranial samples of 5-week and 12-week male and female Gnas E1+/- and WT mice that had been fixed in 10% formalin x 48 hours at 4 degrees Celsius and washed with phosphate buffered saline). The imaging was performed by a Faxitron machine (exposure period of 45 kV for 3 seconds).
Mandibular Measurements
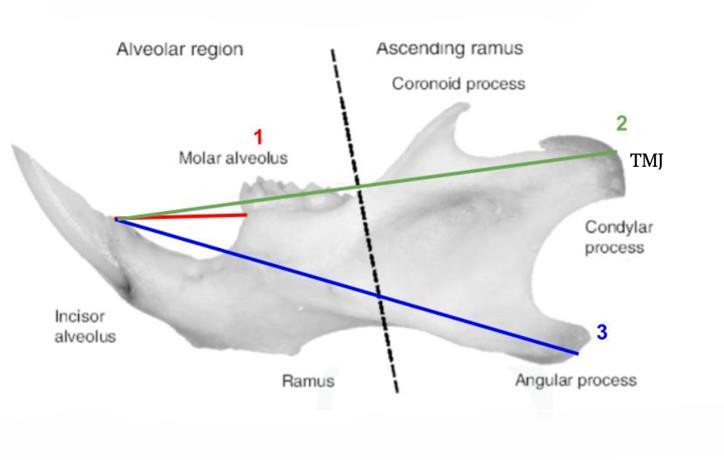
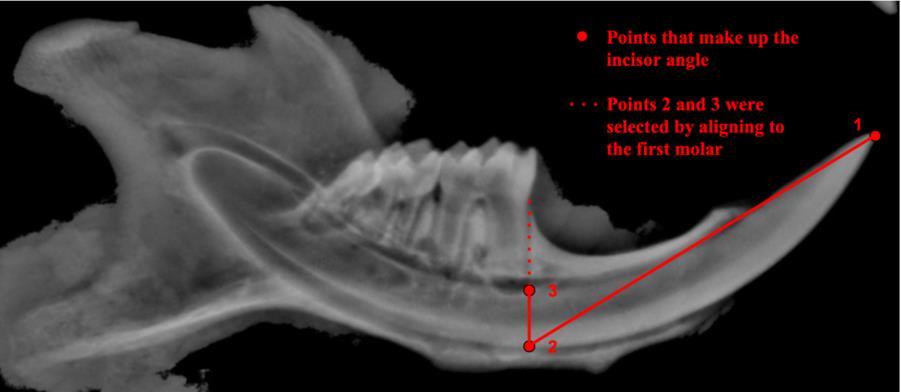
Measurements of mandibular lengths included: (1) incisor tip to molar 1, (2) incisor tip to temporomandibular joint (TMJ), and (3) incisor tip to angular process (Fig 2), in addition to the incisor curvature, as detailed in Figure 3 Measurements were carried out using ImageJ software. The measurements of these mandibular parameters and the incisor angle are reflections of whether the mandible is hypoplastic in Gnas E1+/- mice compared to that of wild-type mice.
Statistical Analysis
Significance was determined using a two-sample T-test to compare same-aged mice (Figs. 4 & 5). Pvalues less than 0.05 were deemed significant (*** <0.001 ** <0.01 *< 0.05). Significance was determined using a one-way ANOVA followed by Tukey’s HSD to compare different aged mice (Figs. 7 & 8). Again, p-values less than 0.05 were deemed significant (****<0.0001, ***<0.001, **<0.01, *<0.05). R Studio (v4.4.1) was used for all calculations and generation of all graphs.
Figure 2 Mandibular lengths used for measurements Three distinct lengths were measured including (1) incisor tip to first molar, (2) incisor tip to TMJ, and (3) incisor tip to angular process.
Results
Figure 3. Calculating the incisor angle. Incisor angles were measured starting from the incisor tip, going down to the base of the alveolar bone, and then tracing directly upward to the base of the first molar as indicated in red.
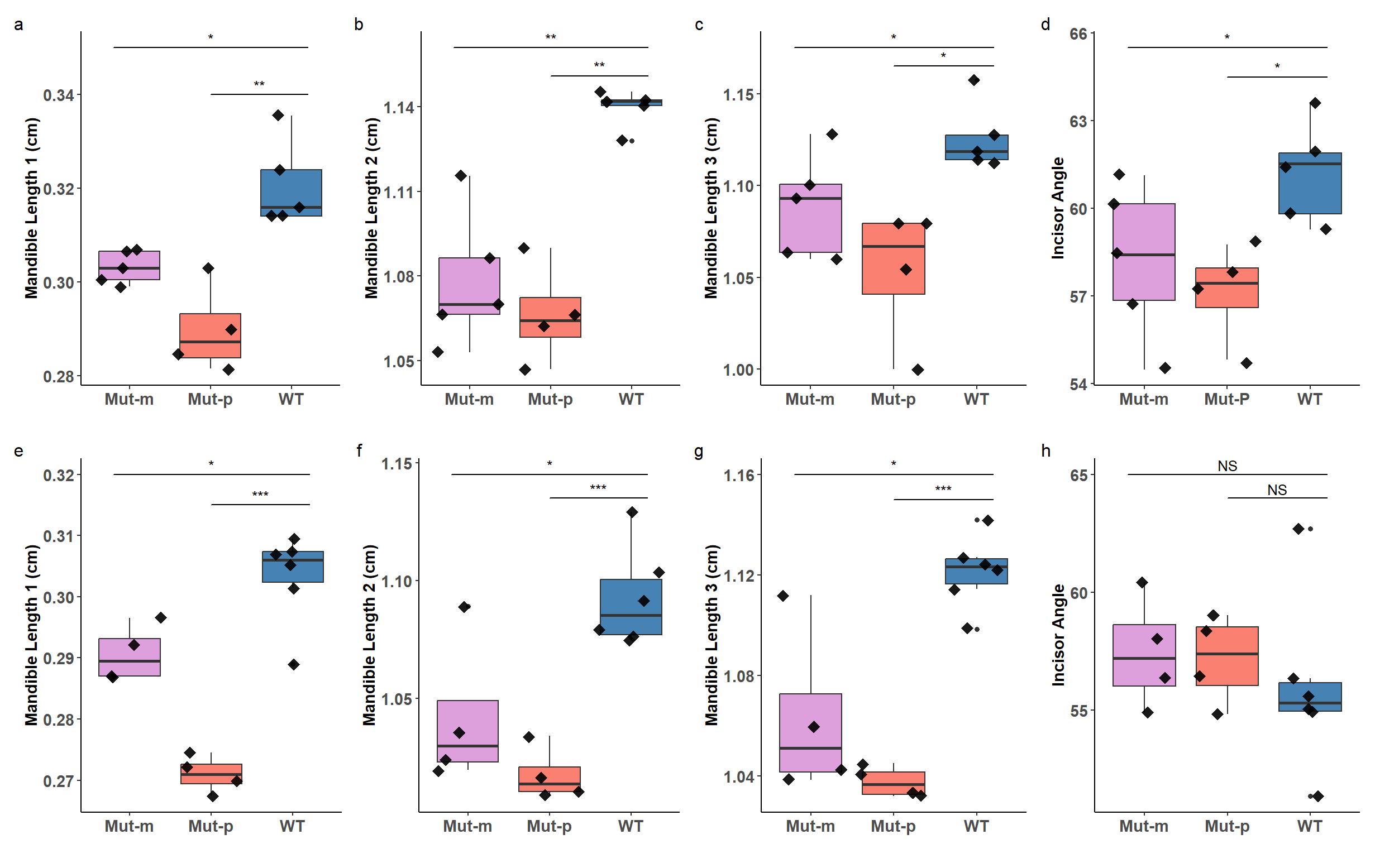
Figure 6 Comparison of mandibular measurements between 5-week-old and 12-week-old female mice. PHP1A (Mut-m) correlates are represented n pink, PPHP (Mut-p) correlates are represented n orange, and wild-type (WT) are represented in blue The 12-week-old females are the lighter shades of each color while the 5-week-old females are the darker shades. The different measurements taken were of mandible length 1 (a), mandible length 2 (b), mandible length 3 (c), and incisor angles (d).
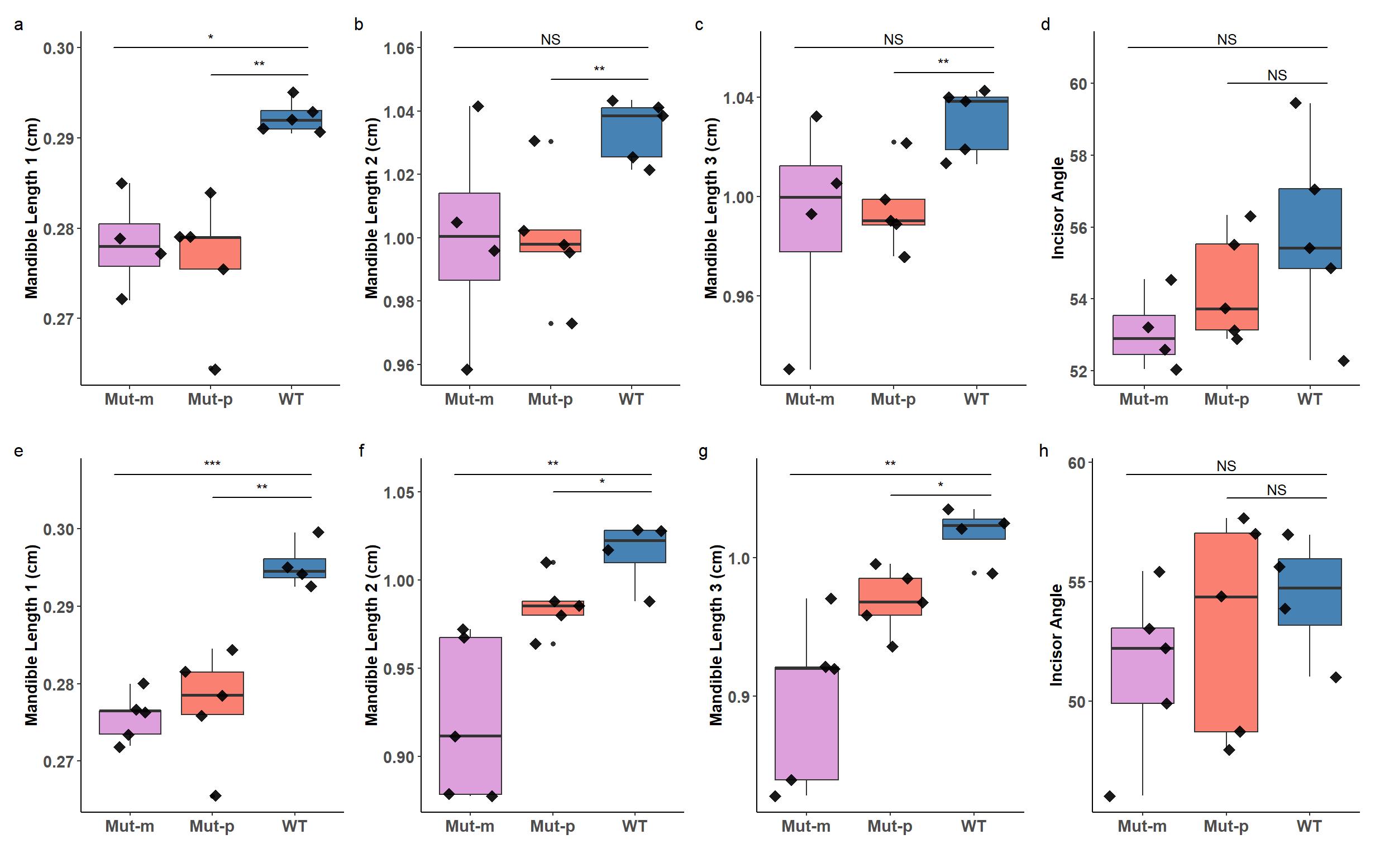
Figure 7 Comparison of mandibular measurements between 5-week-old and 12-week-old male mice. PHP1A (Mut-m) correlates are represented n pink, PPHP (Mut-p) correlates are represented n orange, and wild-type (WT) are represented n blue. The 12-week-old males are the lighter shades of each color while the 5-week-old males are the darker shades. The different measurements taken were of mandible length 1 (a), mandible length 2 (b), and mandible length 3 (c).
Conclusions
Our investigations in our mouse model of AHO reveal that there is mandibular hypoplasia, as observed in the human disorder. Key mandibular lengths are significantly shorter in both 5-week-old and 12-week-old AHO mice compared to WT mice. In addition, these investigations demonstrate that mandibular hypoplasia is present for the correlates of both PHP1A and PPHP, and the hypoplasia occurs equivalently in both disorders. Our results also reveal that the mandible in our mouse model of AHO is growing proportionally with age compared to WT mice, thereby implying a developmental defect and not one that is postnatal The differences between mandibular lengths in male versus female mice that we found in our investigations match the differences that are known to occur in humans. Further investigations using this mouse model could help determine the etiology of mandibular hypoplasia, which is a source of significant morbidity often requiring multiple surgeries as well as orthodonture in many AHO patients.
Category: (Basic/Translational)
Development of targetedtherapies for gene fusion positive cancers based on RNA sensing and editing
PresentingAuthor:Nathaniel L. Jillete NathanielL. Jillete1,AlbertW.Cheng2,3,andChingC.Lau
Many cancers harbor recurrent chromosomal translocations possibly leading to fusion of two genes. Wellknown examples include infant AML with CBFA2T3::GLIS2 fusion, supratentorial ependymoma (ST-EPN) with ZFTA::RELA fusion, and Ewing sarcoma(EWS) with EWS::FLI1 fusion. Thechallenge of many fusion-positive cancers is the lack of established targets downstream of the gene fusion despite years of intensive research to understand the biology of the gene fusion. Yet these cancer cells carry the unique genetic fusions that could be exploited as a reliable address to deliver cytotoxic therapies.
METHODS
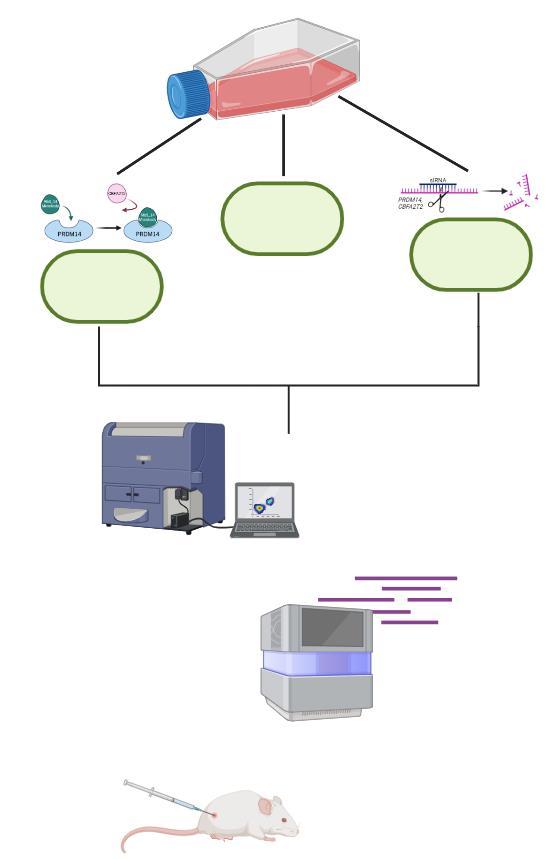
We designed a single-stranded RNA sensor molecule that specifically binds to a target fusion transcript. This binding leverages RNA editing to trigger the expression of cytotoxic proteins. Initially created using a reporter assay approach, these designs have been further modified and tested in cancer cell lines harboring specific gene fusions.
RESULTS
In our poster, wewill show examples of using this design to construct RNA sensor therapeutics that could kill CBFA2T3::GLIS2+ AML cells, ZFTA::RELA+ ST-EPN cells and EWS::FLI1+ EWS cells using various cytotoxic payload systems.
CONCLUSION/SIGNIFICANCE
We seek to develop methods for rapid and cost-effective development of precise targeted cancer therapeutics without reliance on the extensive knowledge of the molecular biology underlying the targeted cancer cells.
Development of targeted therapies for gene fusion positive cancers based on RNA sensing and editing
Nathaniel Jillette 1, Albert Cheng 2, and Ching Lau 1,3,4
1 The Jackson Laboratory for Genomic Medicine, Farmington, Connecticut
2 Institute of Zoology, Chinese Academy of Sciences, Beijing, China
3 Connecticut Children’s Medical Center, Hartford, Connecticut
4 University of Connecticut School of Medicine, Farmington, Connecticut
Abstract
Introduction - Many cancers harbor recurrent chromosomal translocations each leading to fusion of two genes Wellknown examples include infant acute myeloid leukemia (AML) such as those with CBFA2T3::GLIS2 fusion, supratentorial ependymoma (ST-EPN) with ZFTA::RELA fusion, and Ewing sarcoma (EWS) with EWSR1::FLI1 fusion The challenge of many fusion-positive cancers is the lack of established targets downstream of the gene fusion despite years of intensive research to understand the biology of the gene fusion Yet these cancer cells carry the unique genetic fusions that could be exploited as a reliable address to deliver cytotoxic therapies We therefore seek to develop methods for rapid and cost-effective development of precise targeted cancer therapeutics without reliance on the extensive knowledge of the molecular biology underlying the targeted cancer cells
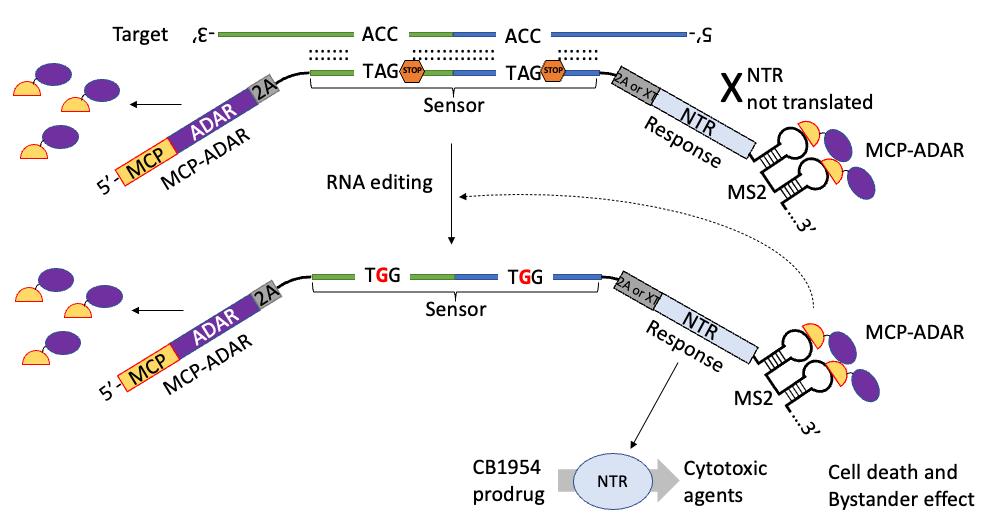
Methods and key results - We designed a single-stranded RNA sensor molecule that binds to a target fusion transcript and leverages RNA editing to trigger expression of cytotoxic proteins Our sensor can detect fusion transcripts and trigger the expression of nitroreductase (NTR) which can convert CB1954 prodrug to a toxic form, triggering cell death in cell populations harboring specific fusions
Conclusions - Our work highlights the development of a precise RNA targeting sensor to deliver therapeutic payloads in fusion positive cells triggering cytotoxic effects The sensor design, and improvement thereon, allows for the ablation of cells depending on the expression of cancer-specific fusion transcripts This opens up opportunities for the development of cancer therapeutics based mainly on sequence information, allowing rapid development and potentially future personalized therapeutics
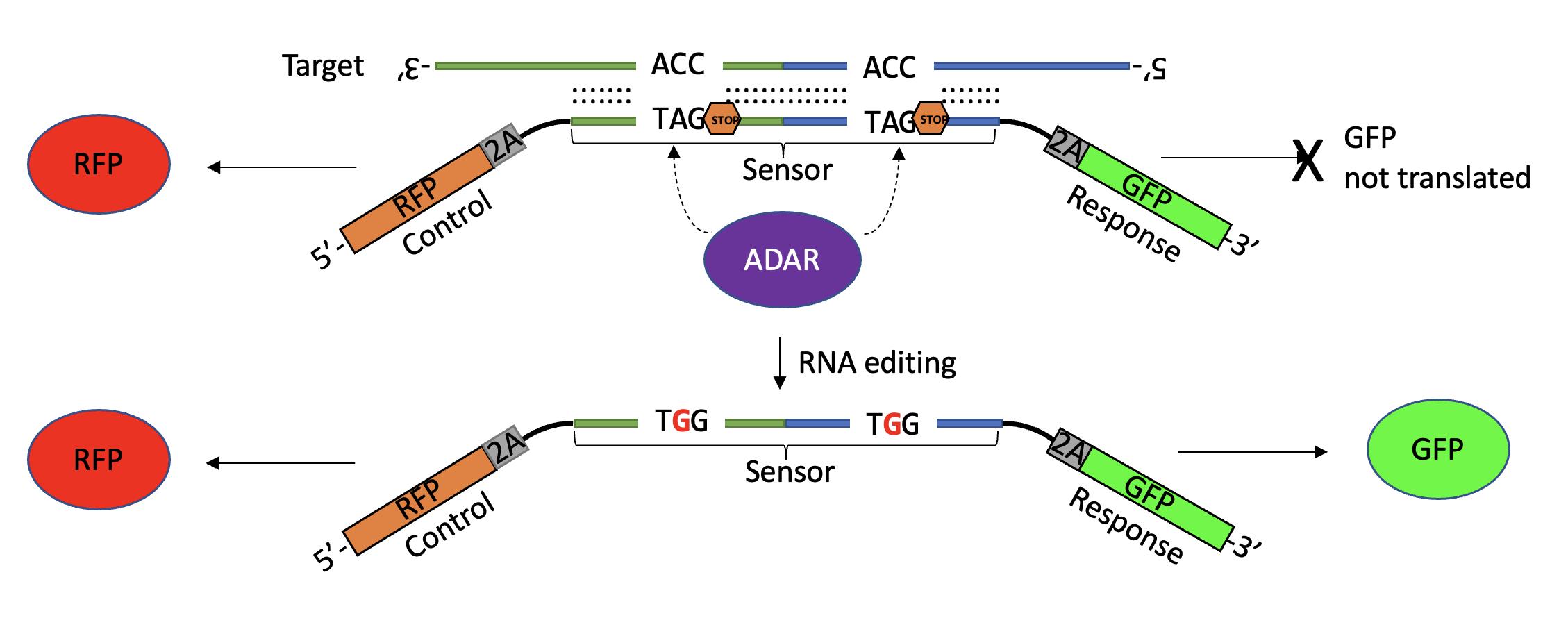
Design
A single-stranded RNA sensor molecule that binds to target fusion transcript and leverages the RNA editing of ADAR to trigger a downstream response.
• Control – Fluorescence reporter or MCP-ADAR, constitutively expressed regardless of sensor/target
• Sensor – Targets fusion transcript junction with engineered stop codons on either arm of fusion genes. Only when ADAR edits both C>A mismatches would the response gene be translated.
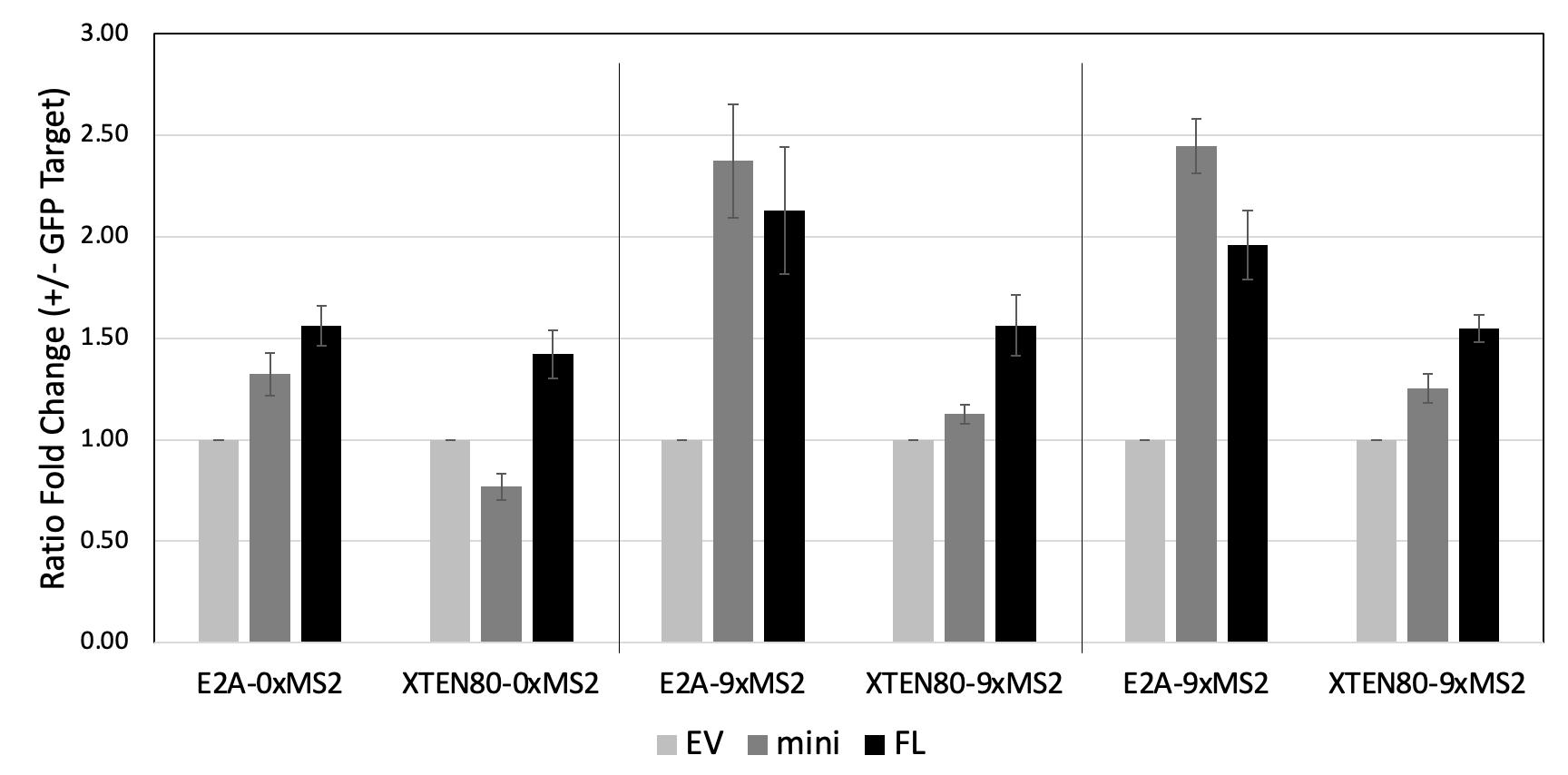
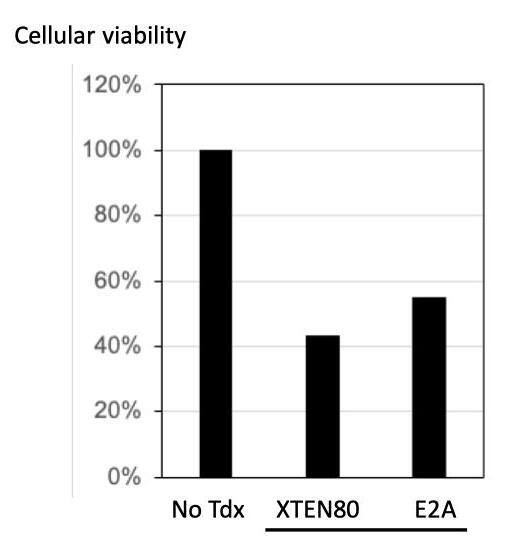
• Peptide Linker – E2A vs XTEN80
• Response – Fluorescence reporter or therapeutic drug payload. Only translated if RNA editing of the stop codons is successful.
• #MS2 – Binding sites to recruit MCP-ADAR nearer the sensor region
Sensor-coupled EGFP fluorescence reporter (Sensor-EGFP) produces fluorescence upon detection of CBFA2T3::GLIS2 fusion transcript
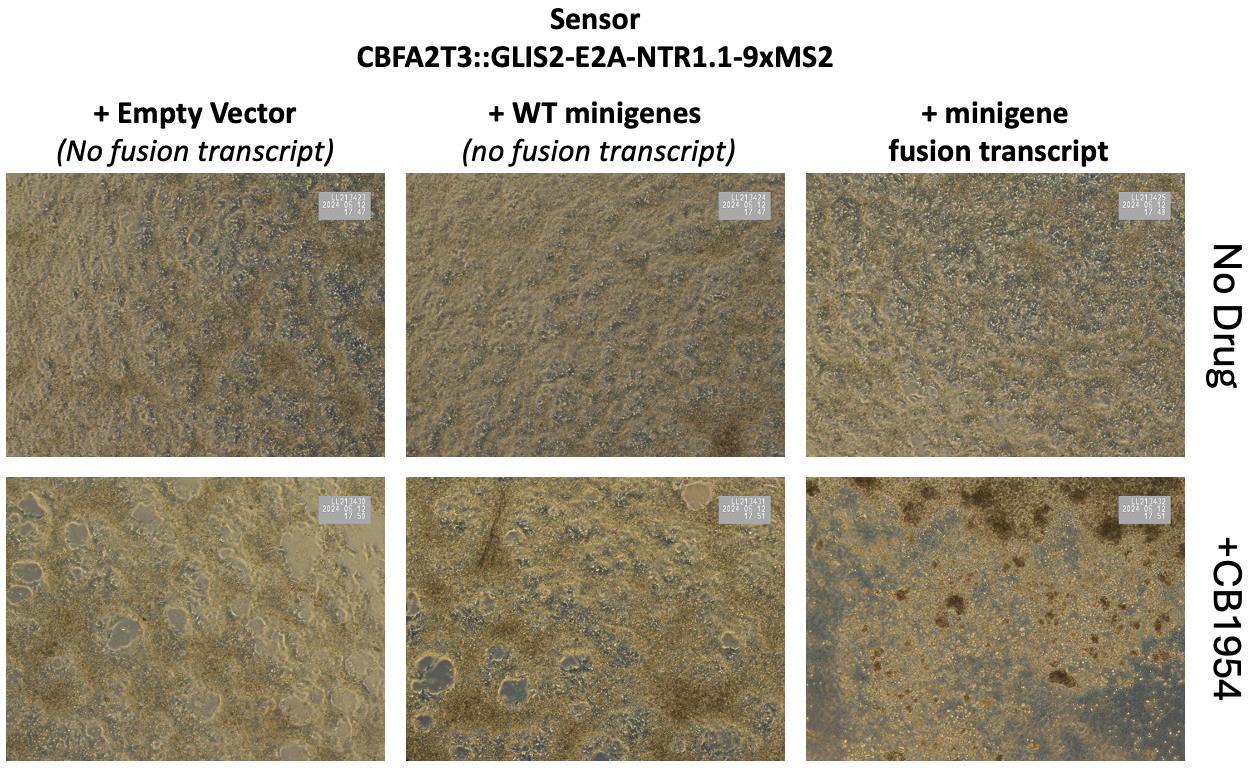
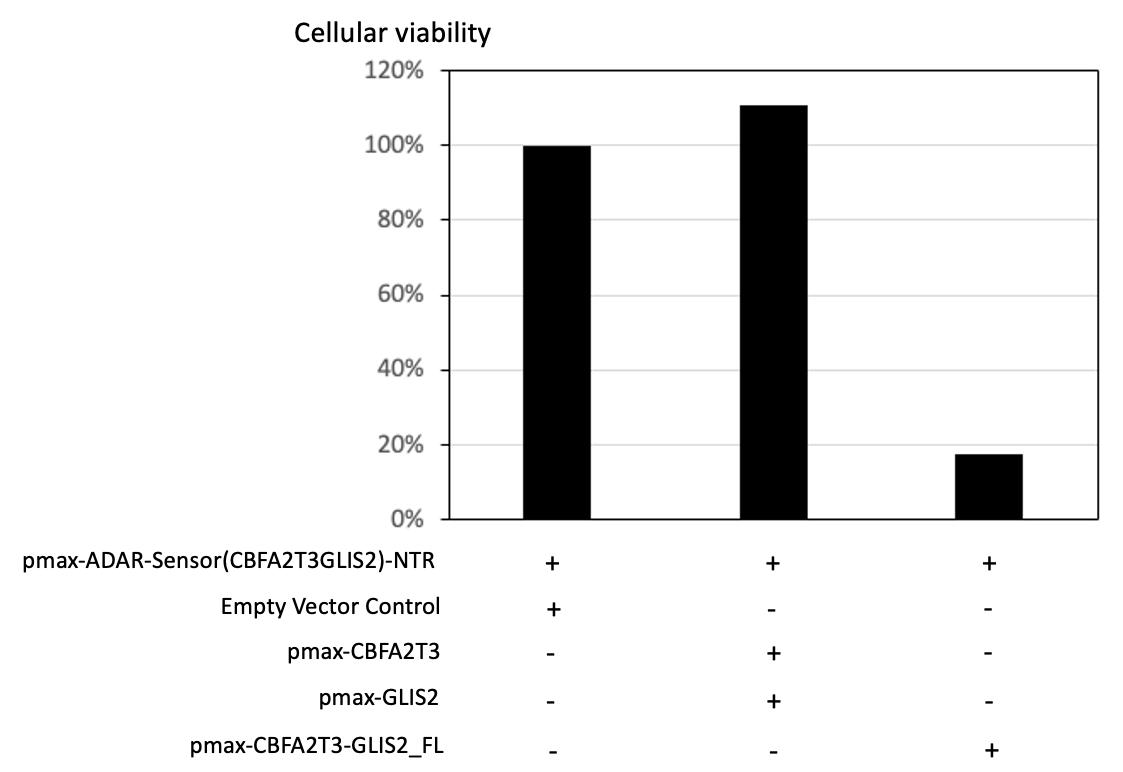
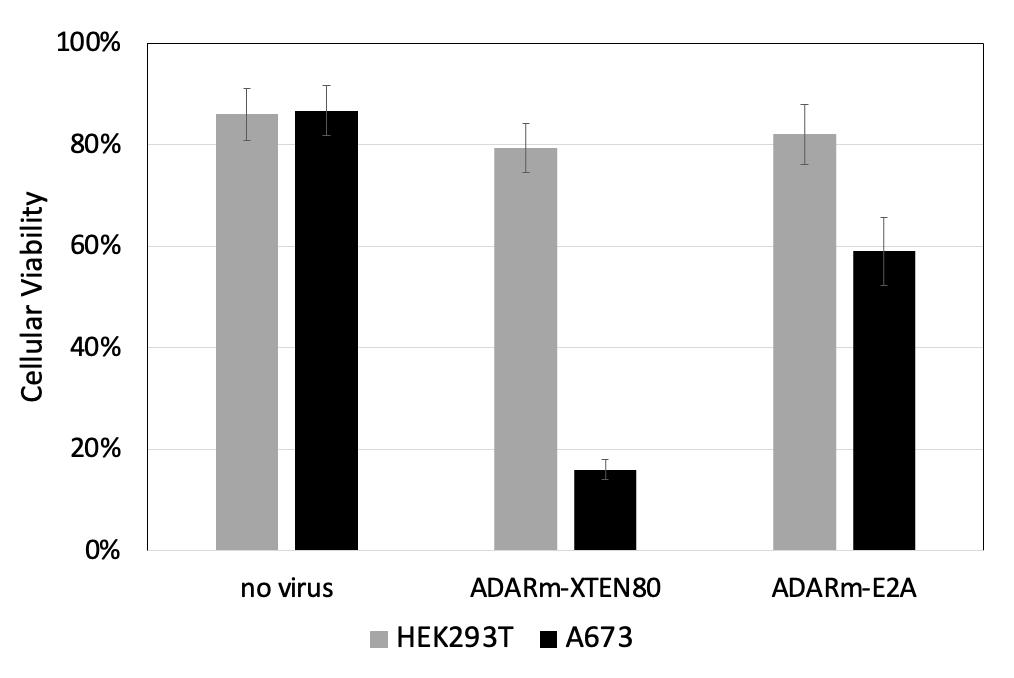
Representative images and cellular viability data (using CellTiter-Glo 2 0 assay) in HEK293T cells transfected with the ADAR-sensor(CBFA2T3-GLIS2 -NTR vector, and either a control empty vector, combination of vectors expressing unfused constituents (pmax- CBFA2T3 and pmax-GLIS2), or vector expressing CBFA2T3-GLIS2 fusion gene, 5 days after CB1954 prodrug addition
The presence of fusion transcript, but not empty vector or unfused constituent transcripts, led to decrease in cellular viability, demonstrating the specific detection and ablation of cell populations expressing CBFA2T3-GLIS2 transcripts in vitro in HEK293T
ADAR-Sensor-NTR can be programmed to elicit CB1954-dependent cell ablation upon detection of different fusion transcripts
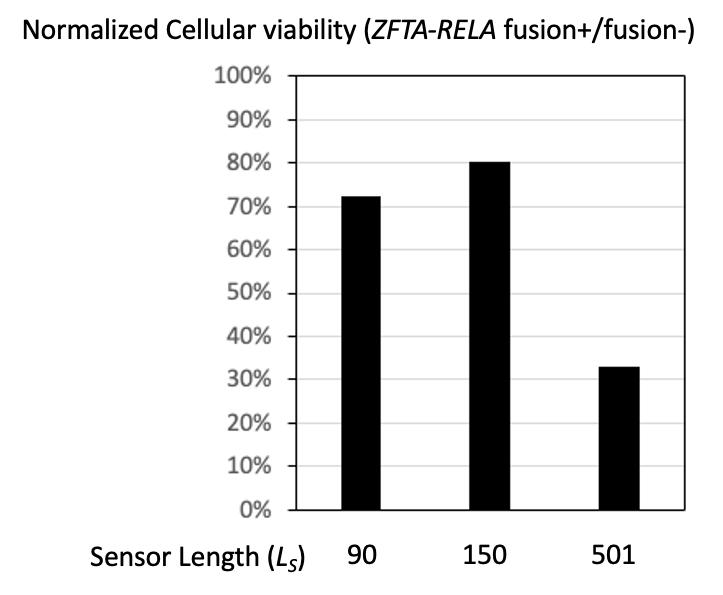
501-nt sensor outperforms the shorter 90-nt and 150-nt sensors for inducing
degree of cell ablation of cell populations expressing ZFTA-RELA transcripts in vitro in HEK293T.
Lentiviral expression of the RNA sensor in BXD-1425EPN ependymoma cells endogenously expressing ZFTA-RELA fusion transcript, led to a decrease in cellular viability after the addition of CB1954 prodrug, demonstrating induced cell ablation of cell populations expressing ZFTA-RELA transcripts in vitro
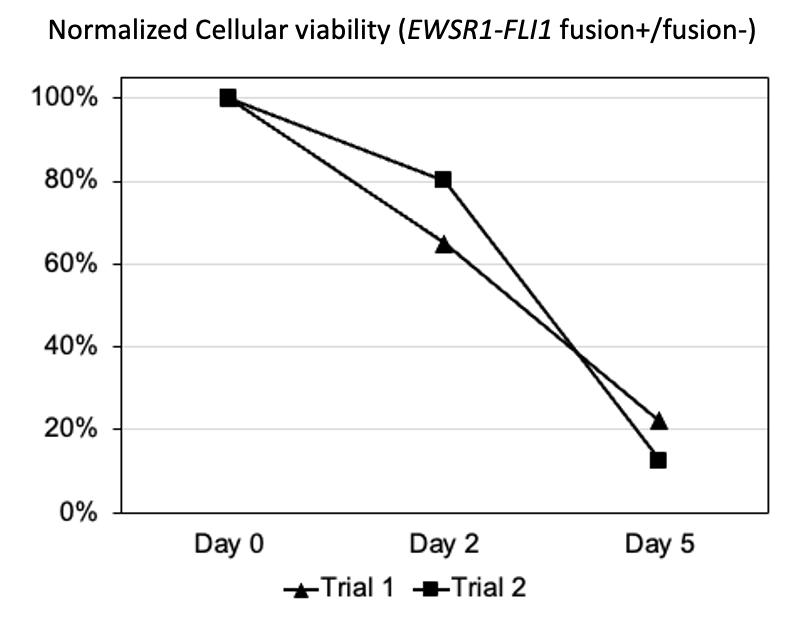
Lentiviral expression of the RNA sensor in A673 Ewing sarcoma cells endogenously expressing EWSR1-FLI1 fusion transcript, led to a decrease in cellular viability not seen in non-fusion harboring HEK293T cells after the addition of Ganciclovir prodrug, demonstrating specific induced cell ablation of cell populations expressing EWSR1-FLI1 transcripts in vitro
Conclusions
• Precise RNA targeting sensors can deliver therapeutic payloads to fusion positive cells, triggering cytotoxic effects.
• Sensors allow specific detection and cell ablation of cell populations expressing fusion transcript.
• Sensors can be successfully designed for different fusion transcripts and/or different response therapeutic payloads.
• Feasible to develop cancer therapeutics based mainly on sequence information, allowing rapid development and potentially personalized therapeutics in the future.
• Original research patent published at WIPO February 2024 – W0/2024/092189
Category: (Basic/Translational)
Interplay Between Endogenous Glycan Fermentation and Klebsiella Pathogenicity in the Intestinal Lumen
Presenting Author: Surabhi Khasgiwala, MD Surabhi Khasgiwala, MD1,2, Katrin Unterhauser, PhD2, Karim Rezaul, PhD2 Sonam Tamrakar, PhD3, Jeremy Balsbaugh PhD3, Anthony Provatas, PhD4, Adam P. Matson, MD, MSc1,2,5
1 Division of Neonatology, Connecticut Children’s Medical Center, Hartford, CT
2 Department of Pediatrics, University of Connecticut School of Medicine
3 Proteomics and Metabolomics Facility, University of Connecticut, Storrs, CT
4 Center for Environmental Sciences and Engineering, University of Connecticut, Storrs, CT
5 Department of Immunology, University of Connecticut School of Medicine
BACKGROUND
Cytotoxin (tilimycin)-producing members of Klebsiella oxytoca species complex (KoSC) are the causative agent of antibiotic-associated hemorrhagic colitis (AAHC) and have been linked to necrotizing enterocolitis (NEC) in premature infants; however, they are also found in the gut of subjects that do not develop intestinal disease. The contextual basis for KoSC to produce tilimycin and transition from commensal to pathogen remains poorly understood. Our aims were to determine if endogenous glycans induce tilimycin synthesis and define host exposures that increase luminal glycans for KoSC consumption
METHODS
K.oxytoca AAHC isolate (AHC-6) and K. grimontii NEC isolate (UCH-1) were cultured in lysogeny broth (LB) +/- glucose, fucose, or sialic acid, and cytotoxin production was assessed using supernatants applied to T84 cells and via mass spectrometry (MS). UCH-1 ∆fucI and ∆nanT mutants, lacking genes for fucose and sialic acid metabolism, were generated and cytotoxin production was similarly assessed. C57BL6/J mice were treated or not with amoxicillin and/or indomethacin, and fucose and sialic acid were quantified in cecal contents by liquid chromatography MS.
RESULTS
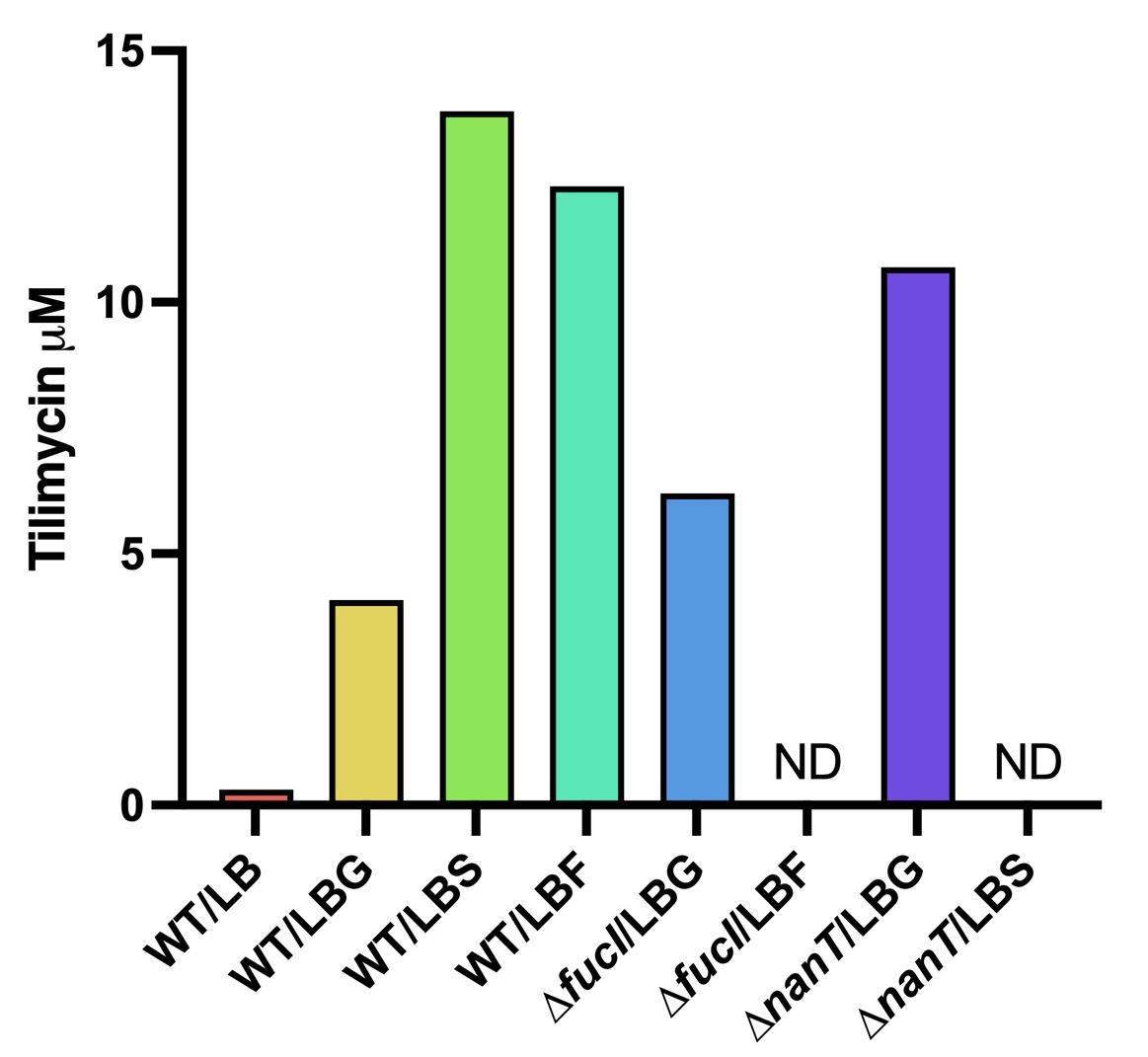
Fucose and sialic acid induced cytotoxin production by KoSC to an equivalent or greater level as glucose UCH-1 ∆fucI and ∆nanT mutants failed to make tilimycin in LB + fucose or sialic acid respectively. Sialic acid increased in murine cecal contents following treatment with amoxicillin and/or indomethacin, whereas fucose was below the limit of detection.
CONCLUSION/SIGNIFICANCE
Sialic acid and fucose induce in vitro tilimycin production by KoSC. Treatment with antibiotics and/or indomethacin increases luminal sialic acid availability potentially driving KoSC pathogenicity in vivo.
Interplay Between Endogenous Glycan Fermentation and Klebsiella Pathogenicity in the Intestinal Lumen
Surabhi Khasgiwala1,2, Katrin Unterhauser2, Karim Rezaul2 Sonam Tamrakar3, Jeremy Balsbaugh3 , Anthony Provatas4, Adam P. Matson1,2,5
1Division of Neonatology, Connecticut Children’s Medical Center, Hartford, CT; 2Department of Pediatrics, University of Connecticut School of Medicine, Farmington, CT; 3Proteomics and Metabolomics Facility, University of Connecticut, Storrs, CT; 4Center for Environmental Sciences and Engineering, University of Connecticut, Storrs, CT; 5Department of Immunology, University of Connecticut School of Medicine, Farmington, CT
BACKGROUND
METHODS AND MATERIALS
• Necrotizing enterocolitis (NEC) is the most common and lethal gastrointestinal emergency of preterm infants, affecting approximately 5-10% of infants with a birth weight under 1500 grams
• NEC pathophysiology is thought to involve abnormal gut microbiota triggering an overly exuberant pro-inflammatory response
M9+Fucose(2.5g/L)
• Whether specific bacteria contribute to the dysbiotic microbial profiles in NEC remains an open question.
• Cytotoxin (tilimycin)-producing members of Klebsiella oxytoca species complex (KoSC) are the causative agent of antibiotic-associated hemorrhagic colitis (AAHC)1 and have been linked to NEC2; however, they are also found in the gut of subjects that do not develop intestinal disease
• The contextual basis for KoSC to produce tilimycin and transition from commensal to pathogen remains poorly understood.
• Our laboratory, has previously shown that fermentable dietary carbohydrates such as glucose triggers KoSC tilimycin production and enhances cytotoxicity3
OBJECTIVE
To determine if endogenous glycans induce tilimycin synthesis and define host exposures that increase luminal glycans for KoSC consumption
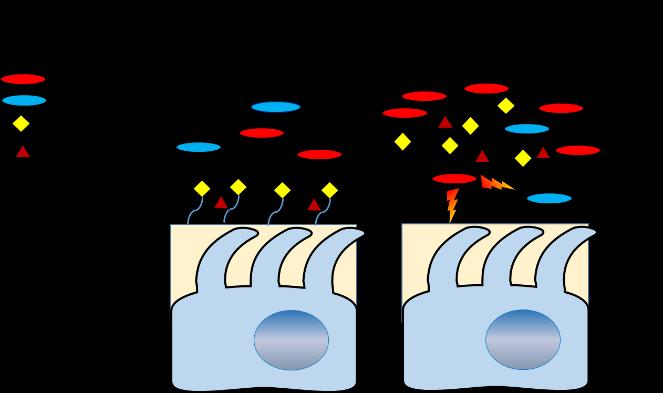
Figure 1 Working model of KoSC pathogenicity in the gut. Under commensal conditions (left), a balanced microbiota with limited luminal sugars maintains microbial balance and mucosal integrity Under dysbiotic conditions (right), antibiotics or NSAIDs trigger the shedding of free sialic acid or fucose leading to KoSC overgrowth and enhanced tilimycin production which causes mucosal damage.
• K oxytoca (Ko) AAHC isolate (AHC-6) and K grimontii (Kg) NEC isolate (UCH-1) were cultured in lysogeny broth (LB) or minimal media (M9) +/- glucose, fucose, or sialic acid (2.5 g/L). Growth was measured by optical density at 600 nm (OD600)
• Cytotoxin production was assessed using bacterial culture supernatants applied to T84 intestinal epithelial cells (MTT assay) and via mass spectrometry (MS).
• UCH-1 ∆fucI and ∆nanT mutants were generated, which lack genes required for fucose and sialic acid metabolism, and growth and cytotoxin production were similarly assessed.
• C57BL6/J mice were treated or not with amoxicillin (100 mg/kg) twice daily by intraperitoneal injection and/or indomethacin (2 5 mg/kg) once daily by subcutaneous injection Levels of free fucose and sialic acid were quantified in cecal contents by liquid chromatography MS.
• Kruskal-Wallis tests with Dunn’s multiple comparisons assessed differences between groups
RESULTS
Figure 2 Fucose and sialic acid induced KoSC cytotoxicity and tilimycin production to an equivalent or greater extent as glucose. (A) Percent cell death determined by MTT assay using supernatants from Ko AHC-6 or Kg UCH-1 grown in LB +/- glucose (LBG) or sialic acid (LBS) (B) Tilimycin levels in supernatants of Kg UCH-1 grown in LB, LBG, LBS or LB + fucose (LBF) measured by MS ND, not detected
CONCLUSIONS
Figure 3 Growth of UCH-1 wild-type (WT), ∆nanT, and ∆fucI in M9 media + different sugars (A) All three strains can utilize glucose, whereas ∆nanT cannot utilize sialic acid (B) and ∆fucI cannot utilize fucose (C)
Figure 4 UCH-1 ∆fucI and ∆nanT fail to produce tilimycin when grown in nutrient rich LB media supplemented with fucose or sialic acid, respectively. The mutants produce comparable levels of tilimycin as WT when grown in LB + glucose MS was used to determine tilimycin levels in bacterial culture supernatants. ND, not detected
Figure 5. Free sialic acid (Neu5Ac) increased in murine cecal contents at 24- and 72hours following treatment with amoxicillin and/or indomethacin Free fucose remained below the limit of detected (not shown) *P ≤ 0.05; **P ≤ 0.01.
Sialic acid and fucose induce in vitro tilimycin production by KoSC. Treatment with antibiotics and/or indomethacin increases luminal sialic acid availability potentially driving KoSC pathogenicity in vivo Future studies will assess luminal tilimycin production and intestinal damage in mice inoculated with UCH-1 WT vs ∆nanT and treated with amoxicillin +/- indomethacin
REFERENCES
1. Högenauer, C. et al. The New England Journal of Medicine, 355(23),
Paveglio, S. et al.
Category: (Basic/Translational)
A de novo Variant in PAK2 Detectedin anIndividual with KnoblochType2Syndrome
P21-activated kinase 2 (PAK2)is aserine/threonine kinase essential for avariety of cellular processes including signal transduction, cellular survival, proliferation, and migration. A recent report proposed monoallelic PAK2 variants cause Knobloch syndrome type 2 (KNO2)—a developmental disorder primarily characterizedby ocular anomalies.
METHODS
An individual with congenital retinal detachment, hypotonia, global developmental delay, cerebral ventriculomegaly, failure to thrive, pyloric stenosis, persistent feeding intolerance, patent ductus arteriosus, and mild dysmorphisms was enrolled in a collaborative study to explore the ability whole genome sequencing (WGS) to identify genetic disorders in pediatric patients. Prior clinical testing, including exome sequencing and chromosomal microarray, was negative. Researchtrio long-read (LR)-WGS and singleton short-read (SR)-WGS wereperformed at The JacksonLaboratory for Genomic Medicine. Variant confirmation was performed by review of prior exome sequencing at GeneDx.
RESULTS
A novel de novo heterozygous variant was discovered in PAK2 (c.1273G>A, p.(D425N)). The p.(D425N) variant lies within the protein kinase domain and is predicted to be functionally damaging by in silico analysis. Given the phenotypic overlap with previously published KNO2 cases, PAK2 c.1273G>A, p.(D425N) was identified as acandidate pathogenic variant in KNO2.
CONCLUSION
Previous clinical genetic testing did not report this variant due to unknown relevance of PAK2 variants at the time of testing, highlighting the importance of reanalysis. Our findings also substantiate the candidacy of PAK2 variants in KNO2 and expand the KNO2 clinical spectrum.
A de novo Variant in PAK2 Detected in an Individual with Knobloch Type 2 Syndrome
Elizabeth A. Werren1, Louisa Kalsner2,4,5, Jessica Ewald1, Michael Peracchio4, Cameron King7 , Purva Vats1, Peter A. Audano1, Peter N. Robinson1, Mark D.Adams1, Melissa A. Kelly1, Adam P. Matson2,3,6
1 The Jackson Laboratory for Genomic Medicine, Farmington, CT; Departments of 2Pediatrics and 3Immunology, University of Connecticut School of Medicine, Farmington, CT; Divisions of 4Genetics, 5Neurology and 6Neonatology,Connecticut Children’s Medical Center, Hartford, CT; 7Department of Research, Connecticut Children’s Medical Center, Hartford, CT
BACKGROUND
P21-activated kinase 2 (PAK2) is a serine/threonine kinase essential for a variety of cellular processes including signal transduction, cellular survival, proliferation, and migration. A recent report proposed monoallelic PAK2 variants cause Knobloch syndrome type 2 (KNO2) a developmental disorder primarily characterized by ocular anomalies 1
METHODS
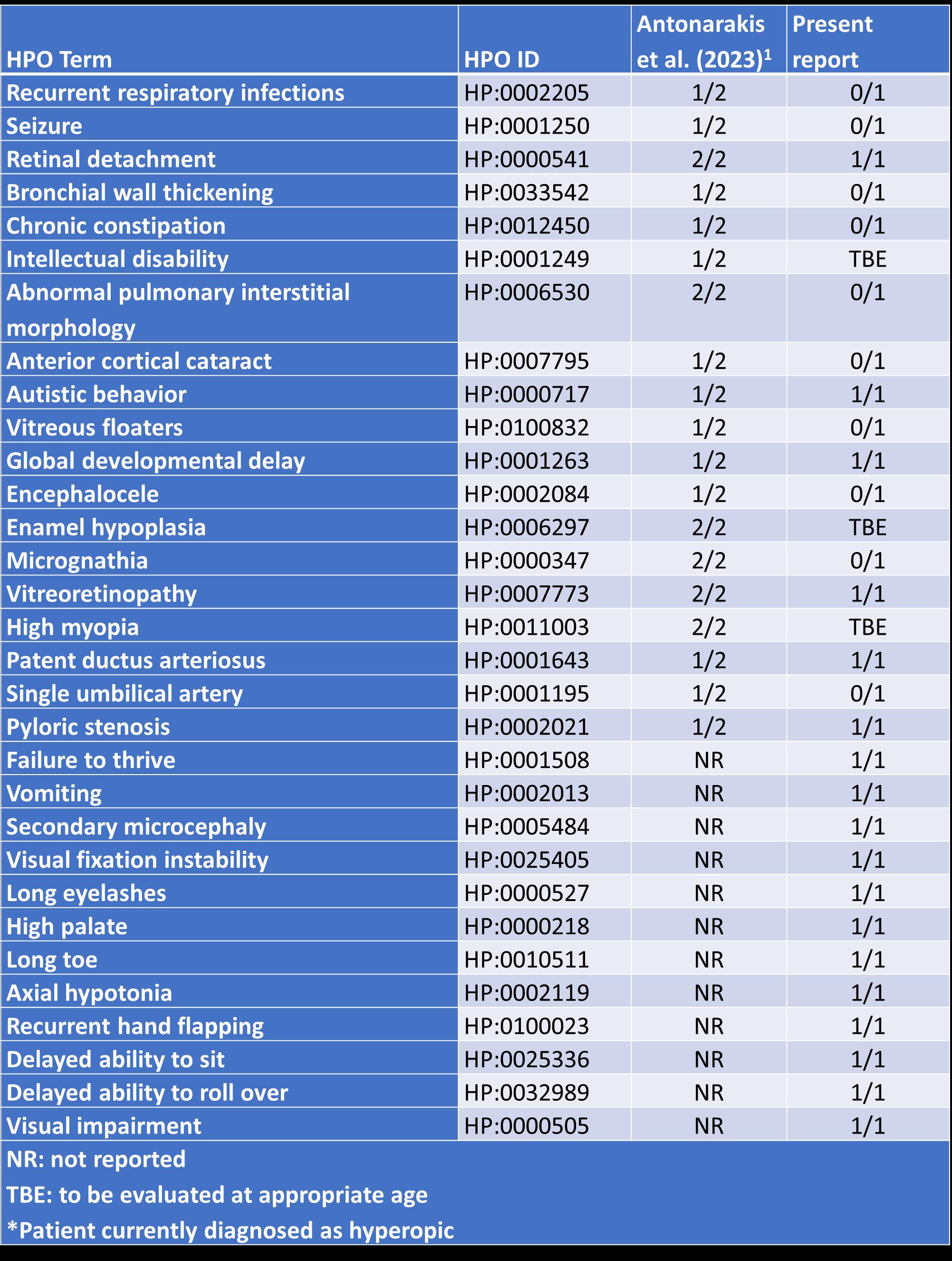
Table 1: Comparison of clinical phenotypes observed in individuals with Knobloch syndrome 2
An individual with congenital retinal detachment, hypotonia, global developmental delay, cerebral ventriculomegaly, failure to thrive, pyloric stenosis, persistent feeding intolerance, patent ductus arteriosus, and mild dysmorphisms was enrolled in a collaborative study to explore the ability whole genome sequencing (WGS) to identify genetic disorders in pediatric patients Prior clinical testing, including exome sequencing and chromosomal microarray, was negative
Research trio long-read (LR)-WGS and singleton short-read (SR)-WGS were performed at The Jackson Laboratory for Genomic Medicine Variant confirmation was performed by review of prior exome sequencing at GeneDx.
RESULTS
A novel de novo heterozygous variant was discovered in PAK2 (c 1273G>A, p (D425N)) The p (D425N) variant lies within the protein kinase domain and is predicted to be functionally damaging by in silico analysis Given the phenotypic overlap with previously published KNO2 cases, PAK2 c.1273G>A, p (D425N) was identified as a candidate pathogenic variant in KNO2.
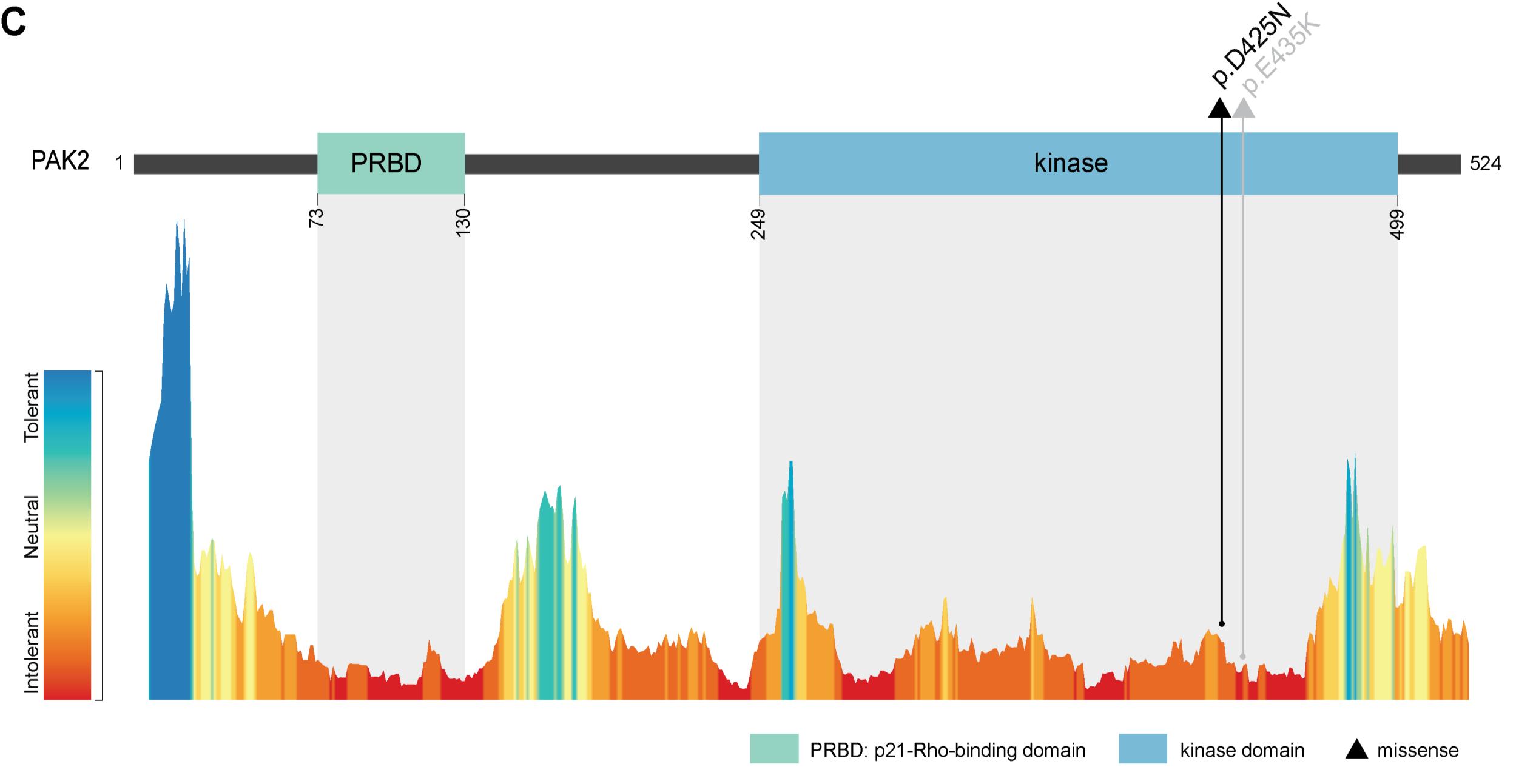
Figure 1. PAK2 is comprised of two protein domains: a p21-Rho-binding domain (PRBD) and a protein kinase domain. The PRBD domain interacts with active GTP-loaded RAC1 and CDC42, and the kinase domain affords PAK2 its catalytic function in phosphorylation 2 PAK2 is intolerant to both missense (Z = 1.83) and predicted loss-of-function (LOF; pLI = 0 83) variants in the general population (gnomADv4.0.0). The p.(D425N) missense variant lies within the protein kinase domain of PAK2, 10 residues upstream of a previously published KNO2 variant (p.E435K).1
CONCLUSION
Previous clinical genetic testing did not report this variant due to unknown relevance of PAK2 variants at the time of testing, highlighting the importance of reanalysis. Our findings also substantiate the candidacy of PAK2 variants in KNO2 and expand the KNO2 clinical spectrum..
REFERENCES
1. Antonarakis SE, Holoubek A, Rapti M, et al. Dominant monoallelic variant in the PAK2 gene causes Knobloch syndrome type 2. Hum Mol Genet 2021;31(1):1-9. doi: 10.1093/hmg/ddab026
ACKNOWLEDGEMENTS
2. Lei M, Lu W, Meng W, et al. Structure of PAK1 in an autoinhibited conformation reveals a multistage activation switch. Cell 2000;102(3):38797. doi: 10.1016/s0092-8674(00)00043-x
We thank the family for their participation, Charles Lee, Juan C Salazar, Christine R Beck, Alyx Vogle, Elizabeth Charnysh, and Kunal Sanghavi for their intellectual contributions, and GeneDx for use of data This work was supported by Connecticut Children’s Research Institute and the Jackson Laboratory for Genomic Medicine PA A was supported by NIH NIGMS R35GM133600 and
Category: (Basic/Translational)
ResultsofthePilot Studyto DeterminetheValidity and Reliability of the NICU Paternal Needs Inventory
Approximately 10% of infants in the United States are admitted to neonatal intensive care units (NICUs) as a result of premature birth and birth problems, placing their parents in the challenging situation of dealing with an unexpected and difficult birth. While both parents undergo stress when their newborn is in the NICU, the stress experienced by mothers and fathers might exhibit distinct differences. The experiences of fathersareoften more intricate and distinct compared to those of mothers, and research often places less emphasis on supporting fathers. While there is some emerging study on the father's experience, there is alack of researchon their specific needs when their baby is in the NICU. Unfulfilled needs can lead to lifelong issues in the child's psychological well-being and attachment. The researchquestion was,Is the NPNIareliable instrument tomeasure a father'sphysical, emotional, andpsychological needs while his infant is in the NICU? The aim of the study was to determine the reliability and validity of the NICU Paternal NeedsInventory (NPNI) in measuring the physical, emotional, and psychological needs of fathers in the NICU.
Methods
This non-experimental descriptive study wasconducted in four NICUs acrossthe US. The NPNI,a visual analog 42-item instrument adaptedfrom the Critical CareMaternal NeedsInventory, along with a demographic sheet, was administered to 210 fathers of infants who were patients in the NICU. Statistical analysis consisted of descriptive statistics andfactor analysis andwas conducted using SPSS version 28.
Results
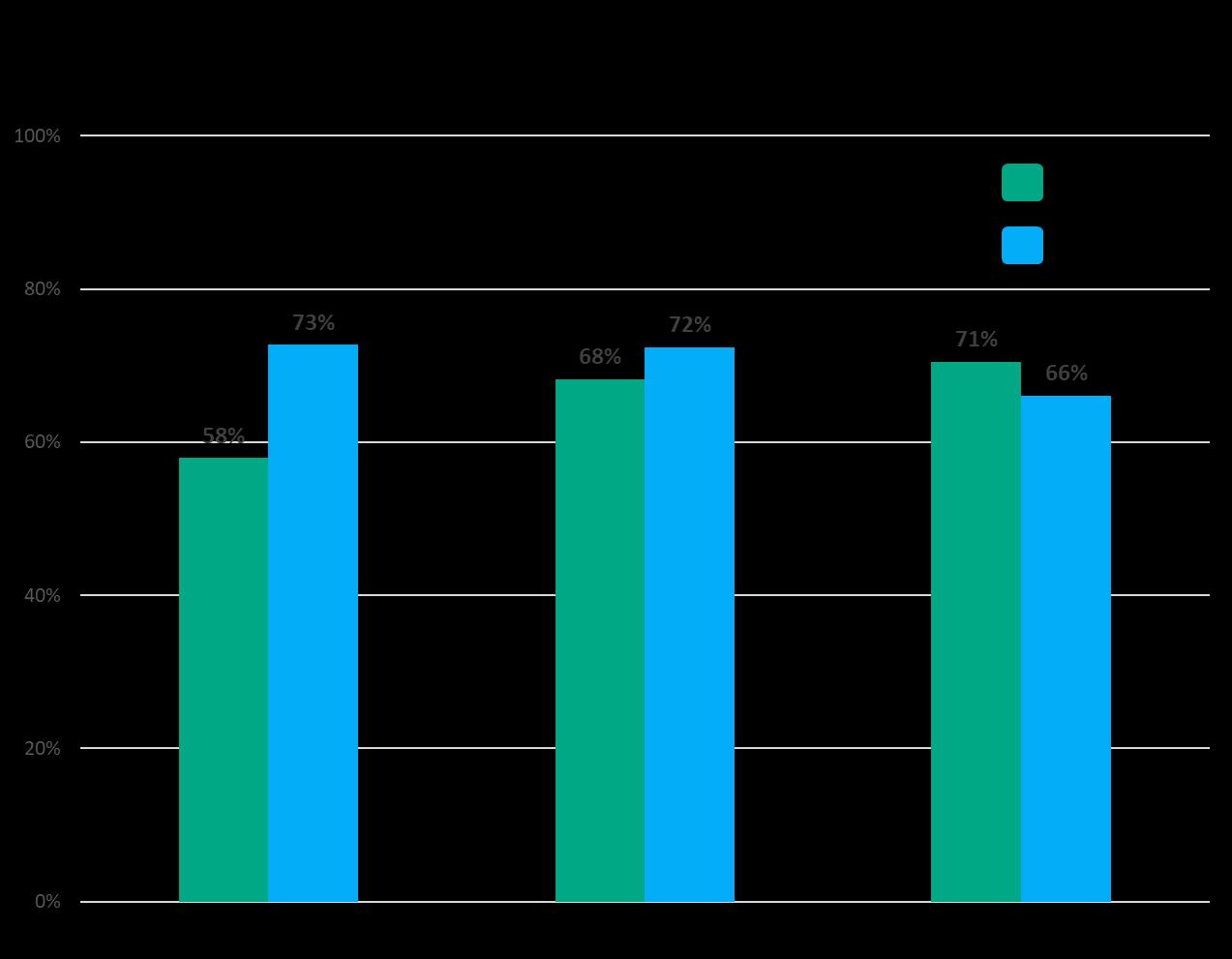
The priority need of fathers was to visit at any time, ratedat 60-100%. The remaining needs showed a wide variety of responses from 0-100%. Factor analysis revealed that the tool is vailid & reliable to measure fathers’ needs in the NICU.
Discussion and Conclusion
The findings indicated that fathers had a diverse range of needs that vary based on their unique circumstances. In order to enhance fathers' adaptation to the NICU environment, it is crucial for nurses to adopt a comprehensive approach that takes into account the unique physical, emotional, and psychological needs of each individual father.
Background & Significance
• Fathers first visitor to the NICU.1
• Describe the experience as a rollercoaster. 2, 3
• Feel a loss of control, helpless, fear, uncertainty, nervousness, and anxiety. 4-8
• Attempt to gain back control.9
• Actively seek out information.3,9
• Look to the nurses for support but their need for information, support & guidance not met 4, 8, 10-18
• Research has also shown that nurses lack recognition on the needs of NICU fathers. 4, 18,19
• Nurses are missing the opportunity to assess and address fathers’ needs, which could have long term consequences for fathers’ mental health
Aim and Research Question
Aim: To determine the validity & reliability of the NICU Paternal Needs Inventory (NPNI).
Research Question: Is the NPNI a reliable tool to measure a father’s physical, emotional, and psychological needs when his baby is in the NICU?
Methodology & Statistical Analysis
• Non-experimental descriptive design
• Instruments
• Information Sheet (explaining the study)
• Demographic Sheet
• NICU Paternal Needs Inventory-rate need using a visual analog scale (0-100), consisting of 42 items divided over 6 subscales.
• Administered to 210 fathers in four NICUs in the United States
• Inclusion Criteria
• Had an infant admitted to the NICU
• Read and speak English
• Flyers were distributed in NICU Admission packets, in waiting room, and around unit
• Flyers contained a link to online survey on Qualtrics
• Fathers completed the survey on Qualtrics
• Statistical analysis consisted of descriptive statistics & factor analysis and was conducted using SPSS version 28
Results of the Pilot Study to Determine the Validity and Reliability of the NICU Paternal Needs Inventory
Linda Merritt, PhD, RNC-NIC, CNE, FAWHONN; M. Terese Verklan, PhD, CCNS, RNC-NIC, FANN School of Nursing
Results
Fathers:
N=210
Age- ranged from 18-52 years of age (M=31.97, SD= 6.94).
Race- White N= 85; Hispanic N= 73; Asian N= 20; African American N= 20, Non African American N=6, Other N=9
Education- Not Completed N=6: Completed high school N= 38; Some college N=54; Associate Degree N= 32; Bachelor Degree N=42; Some Graduate N= 10; Graduate Degree N=21; Doctoral Degree N=6
Income- less than $20,000 N=31; $20,000-$39,999 N=52; $40,000-$59,999 N=47; $60,000-$79,999 N=38; $80,000 to $99,999 N=16; $100,000 and above N=22
Infants:
Gestational age- range from 23-42 weeks (M=33.9, SD=4.17)
Length of stay- range from 1 day to151 days in hospital (M= 16, SD=21.8).
100 (47.6%) of the infants had been on ventilators at one point during hospitalization
Subscales
Needs of NICU Fathers
Not one need was rated 100% by all fathers. The following emotional & psychological needs were rated 60% or above. The rest showed a broad range of responses suggesting that fathers have a broad range of needs
have questions answered honestly
be allowed to visit any
Implications
• NICU Paternal Needs Inventory seems to be a highly reliable and valid tool to measure fathers’ emotional, psychological, and physical needs.
• All items loaded on subscales the way they were supposed to
• Subscales seem to be distinct except for social support & paternal support which seem to measure the same thing
Limitations
• Only captured needs at one moment in time
• The length of the tool
Conclusions
Fathers have a broad range of needs in the NICU. The NICU Paternal Needs Inventory is a reliable and valid tool that nurses can use to measure these needs to help plan individualized, father-specific interventions to help fathers cope in the NICU environment. However, further research is needed to shorten this tool to make it easier to use and make sure each subscale measures different needs.
Acknowledgements
This work was supported in part by the following sources from Quinnipiac University:
• Startup Funds for New Faculty
Also supported in part by the following sources from Texas Woman’s University •Chancellor’s Research Faculty Scholars Program
Also, we would like to thank the following who are part of this multi-site research team:
Manoj Biniwale- PIH Good Samaritan Hospital. Los Angeles, CA Brandi Garrett & Kayla Carey- Baylor University Medical Center, Dallas, TX
Sue Horner- Lurie Children’s Medical Center, Chicago, IL
Valerie Lapp- Winne Palmer Hospital for Women & BabiesOrlando, FL
Contact Information
linda merritt@quinnipiac edu
Category: (Basic/Translational)
Research Hesitancy among Gender Diverse Children and their Caregivers
Presenting Author: Alina A. Molloy, BS
Alina A. Molloy, BS1 , Christopher B. Theriault, MA2 , William T. Zempsky, MD, MPH2,3 , Melissa Santos, PhD2,3
1 Frank H. Netter MD School of Medicine at Quinnipiac University
2 Connecticut Children’s Research Institute
3 University of Connecticut School of Medicine
BACKGROUND
Transgender and gender non-conforming (TGNC) youth are continuously underrepresented in research and mistreated within the healthcare system, leading to suboptimal healthcare and research innovations. To address these gaps, it is essential to include TGNC youth in medical research and understand factors that may lead to this group declining to participate. Current literature suggests that marginalized populations may demonstrate increased research hesitancy, yet little research has examined research hesitancy in TGNC youth.
METHODS
TGNC youth (n=6) and their caregivers (n=3) were recruited based on participation in previous gender-focused research. Participants were asked to complete a survey and a virtual semistructured interview. Research hesitancy was assessed utilizing the Research Attitudes Questionnaire (RAQ), the Medical Mistrust Index (MMI), and investigator constructed questions about the likelihood of providing specific biospecimens for research. Interviews and thematic analysis are ongoing, and preliminary results are summarized.
RESULTS
TGNC youth (Mage=16.8 years; 50% non-binary) and caregivers self-report positive attitudes toward research (M=28.0; 27.7), but moderate levels of mistrust toward healthcare organizations (M=21.3; 22.3). Participants state that credibility of the institution conducting the research is a significant aspect of electing to participate in gender-focused research. Other given reasons as to why other TGNC youth may be hesitant to participate in research include caregiver support/knowledge of their identity, access to research opportunities, and general medical mistrust.
CONCLUSIONS
Preliminary findings highlight potential factors that contribute to research hesitancy within TGNC youth. It is suggested that future researchers consider these identified factors when designing studies involving this population.
Research Hesitancy among Gender Diverse Children and their Caregivers
Alina A. Molloy, BS1; Christopher Theriault, MA2; William T. Zempsky, MD, MPH2,3; Melissa Santos PhD2,3
1Quinnipiac University Netter School of Medicine, North Haven, CT; 2Connecticut Children’s, Hartford, CT; 3University of Connecticut School of Medicine, Farmington, CT
BACKGROUND
• Transgender and gender diverse (TGD) youth are continuously underrepresented in research and mistreated within the healthcare system, leading to suboptimal healthcare and research innovations.1-3
• To address these gaps, it is essential to include TGD youth in medical research and understand factors that may lead to this group declining to participate.
• Current literature suggests that marginalized populations may demonstrate increased research hesitancy,4 yet little research has examined research hesitancy in TGD youth.
RESULTS
RESULTS
”One aspect could be whether someone is out to their family or if they feel comfortable talking about this stuff in their home, or having somebody drive them to a place to talk about stuff, and having concerns about being outed to certain family members.”
• Objective: To understand research hesitancy and barriers to participate in research that may exist among TGD youth and their caregivers.
METHODS
• Adolescents (13-18 years) with a TGD identity (N=6) and their caregivers (N=4) were recruited based on interest in previous gender-focused research.
• Participants were asked to complete a brief, online survey and a virtual semi-structured interview.
• Measures (REDCap):
1. Self-reported demographics
2. Research Attitudes Questionnaire5 (RAQ; scores 7-35)
3. Medical Mistrust Index6 (MMI; scores 7-35)
4. Investigator-constructed questions on the likelihood of providing specific biospecimens for research (scores 1-5, higher scores indicating greater likelihood)
• Interviews:
• Individual semi-structured interviews were conducted over Zoom with teens and caregivers together, if both consented to participate.
• A questioning route was used to examine hesitancy, willingness, and barriers to participating in gender-focused research, including the collection of biospecimens.
• Interviews were recorded, transcribed, and reviewed for errors in transcription.
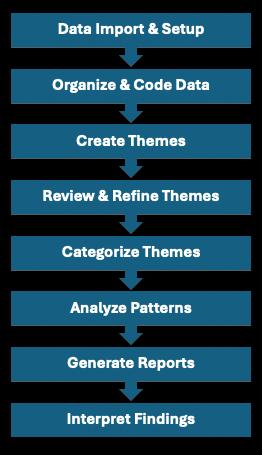
• Thematic analysis was used to understand factors contributing to research hesitancy in this population, and preliminary results are presented.
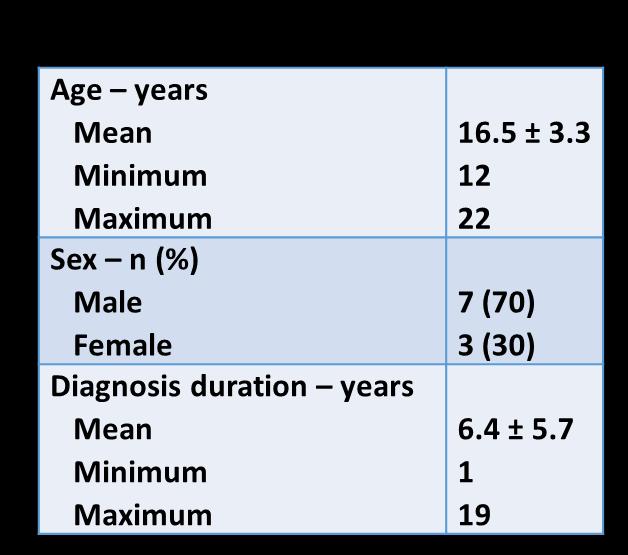
• Participants had an average age of 16.8 years, 50% identified as nonbinary, and all were white and non-Hispanic (Table 1).
• Contributors to participants’ attitudes toward research are summarized in Figure 1.
• See Table 2 for a summary of survey results:
o TGD youth and their caregivers report having positive attitudes toward research, but moderate levels of medical mistrust.
o TGD youth report being more willing to provide certain biospecimens for research than their caregivers, saliva and urine being the most likely.
“And experiences can be very like personal. And some experiences could be very negative. And so I can see why a lot of people might not want to like share some of those for the purpose of research.”
“Just that the information that I give could be misinterpreted and used sort of against, I guess, my gender identity and weaponized to discount my experiences and my identity.”
Theme 2: Trust with the Organization Conducting Research
“Sometimes just a general distrust of medical professionals, doctors, researchers. What's my information to be used for? Who is getting their hands on my information?”
“Who is doing that [research]? What are they going to do with that data? Are they trustworthy? There’s all kinds of history with lists of people in certain groups that don't get treated well. Not everywhere has a perfect climate right now. It’s sort of daunting and upsetting to think about it”
Theme 3: Biospecimen Collection
“But I would want to know why [they’re collecting biospecimens]. Obviously, what are you using it for? Obviously… are the samples being destroyed afterwards, like what is going on with that? I'd be asking a lot of questions because giving up somebody's personal part of their body is a little bit different than asking questions.”
“I think it would kind of depend on the study [collecting biospecimens]. And like, if it really feels like, ‘Okay, yeah, this is a good place to be sending my blood to.’”
Theme 4: Other Barriers to Participation
“If I had to go in person and answer questions and do interviews and such that would be very difficult for me. Due to like scheduling conflicts, medical reasons, and so on.”
“Like, yeah, you need a doorway in, right? …and maybe the question of hesitancy around like, ‘Oh, do we qualify?’ if someone’s at a certain part of their journey? And they’re at this questioning stage, would they get asked?”
CONCLUSION
• Preliminary findings highlight potential factors that contribute to research hesitancy among TGD youth and their caregivers, as well as barriers to participation.
• Potentially being outed to family, findings being misinterpreted, not having trust with an institution, and lack of transparency around biospecimen collection are the largest sources of research hesitancy among gender diverse youth and their families.
• Barriers include scheduling issues/time requirements, strict inclusion criteria around gender identity, and access to research opportunities outside of medical settings.
• Measures indicate mostly positive attitudes toward research, but moderate levels of medical mistrust among the sample. Youth report being more likely to provide biospecimens for research purposes than their caregivers.
• Future researchers should consider these identified factors when designing studies involving this population to both improve research participation and make TGD youth and families feel safe in their decision to do so.
• Limitations of the current study include having a small and minimally diverse sample.
• Future research should aim to include more diverse gender diverse youth on the basis of race, ethnicity, socioeconomic status, and caregiver support to better understand research hesitancy and barriers to participate in research among this population through an intersectional lens.
REFERENCES
Table 1. Teen demographics (N=6)
Theme 1: Gender-Related Concerns
Table 2. Survey results (N=10)
Category: (Basic/Translational)
The role of immunosuppressive neutrophils in the tumor microenvironment of osteosarcoma
Presenting Author: Patrick Ng
Chaojia Chen 1,* , Patrick Ng 2,3 ,Aaron Taylor 2 ,Elise Courtois 2, PaulRobson 2, Gary Ren 1 , Ching Lau 2,3,4
1 The Jackson Laboratory, Bar Harbor, Maine
2 The Jackson Laboratory for Genomic Medicine, Farmington, Connecticut
3 University of Connecticut School of Medicine, Farmington, Connecticut
4 Connecticut Children’s Medical Center, Hartford, Connecticut
BACKGROUND
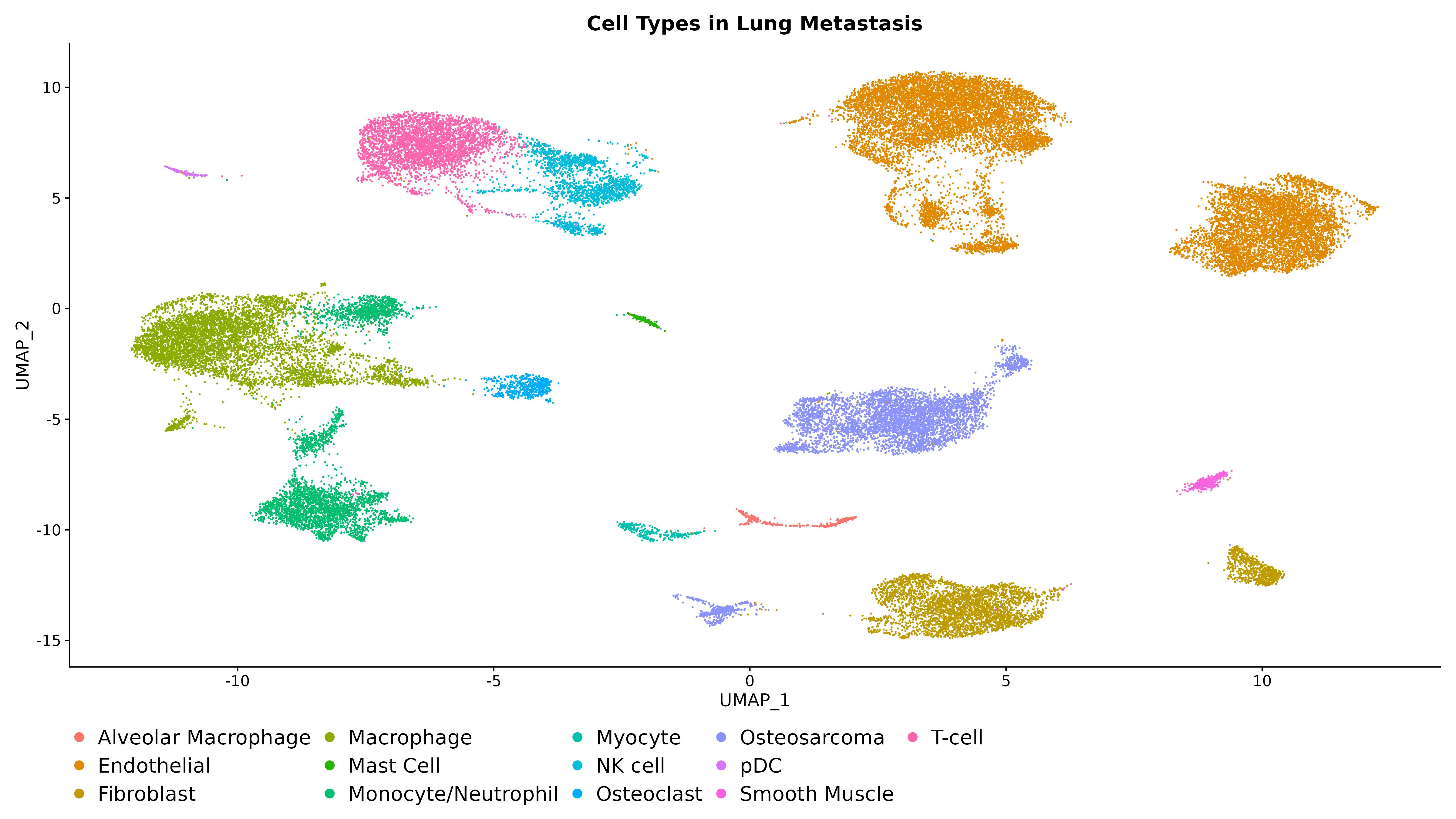
Osteosarcoma(OS) is themost common primary malignant bonetumor in children and young adults, with a 20-30% survivalratein metastatic cases,primarily in the lungs. To improvethesurvival rateof OS patients, it is crucialto find effective strategies to prevent or treat lung metastasis. Thetumormicroenvironment(TME) is vitalin tumor biology, but its role in OS is not well understood. Recently, our group used single-cell RNAsequencing (scRNA-seq) to profiletheTMEof metastatic lung tumors from OS patients, identifying potential immunosuppressiveimmunecelltypes.
METHODS
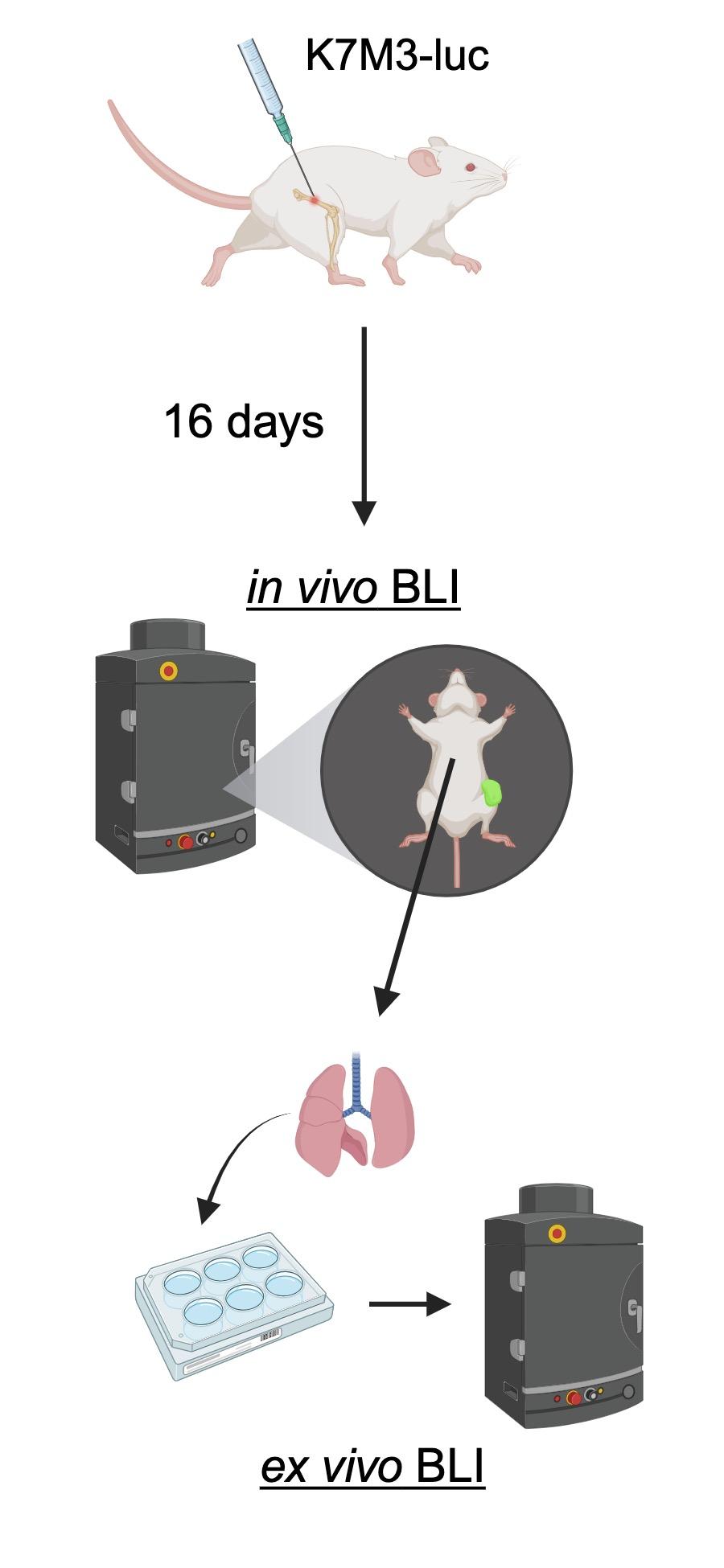
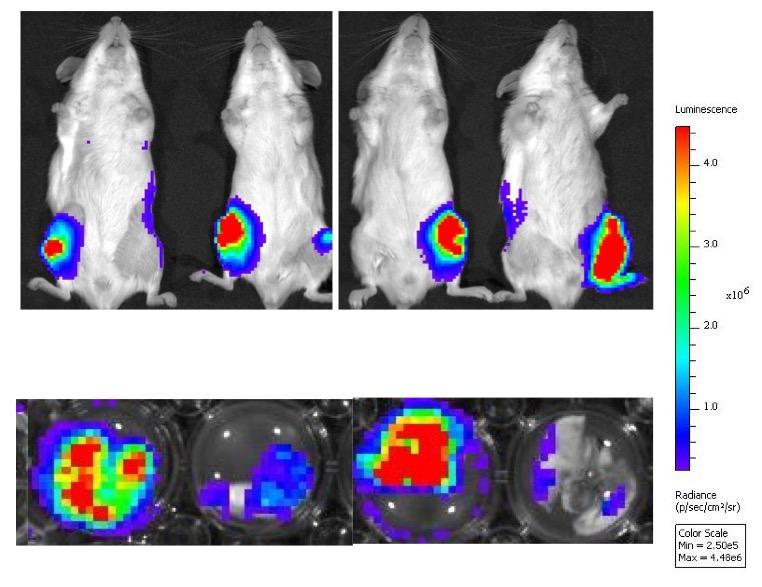
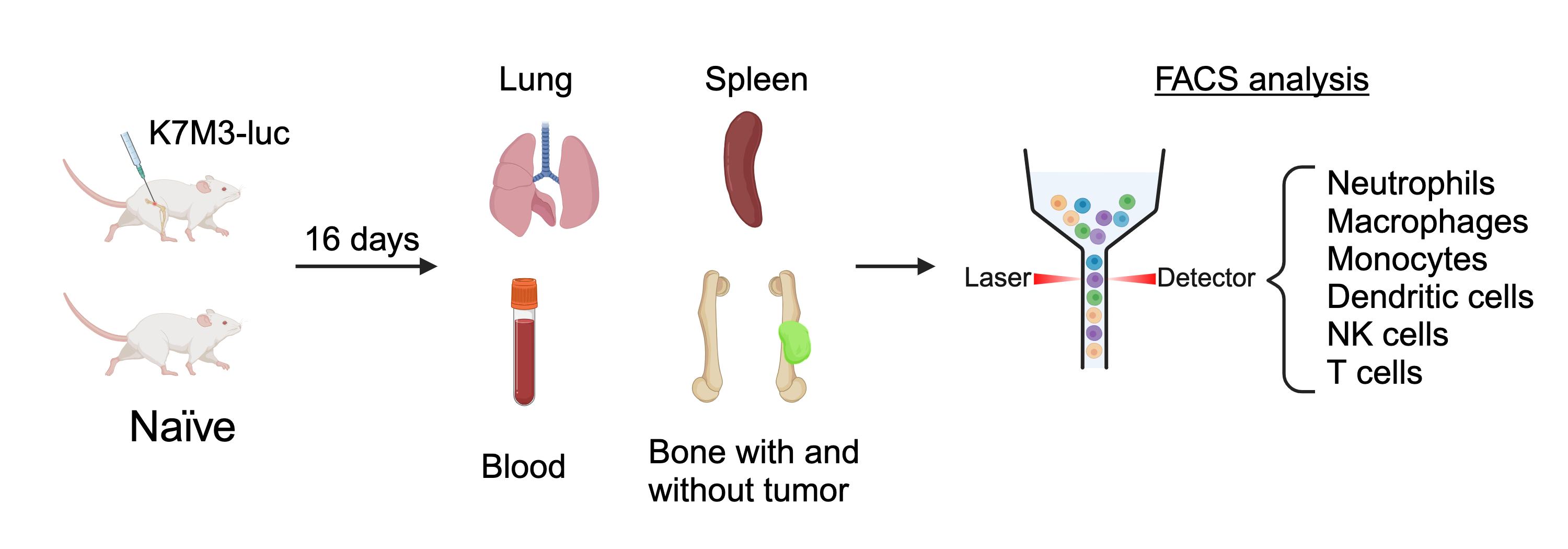
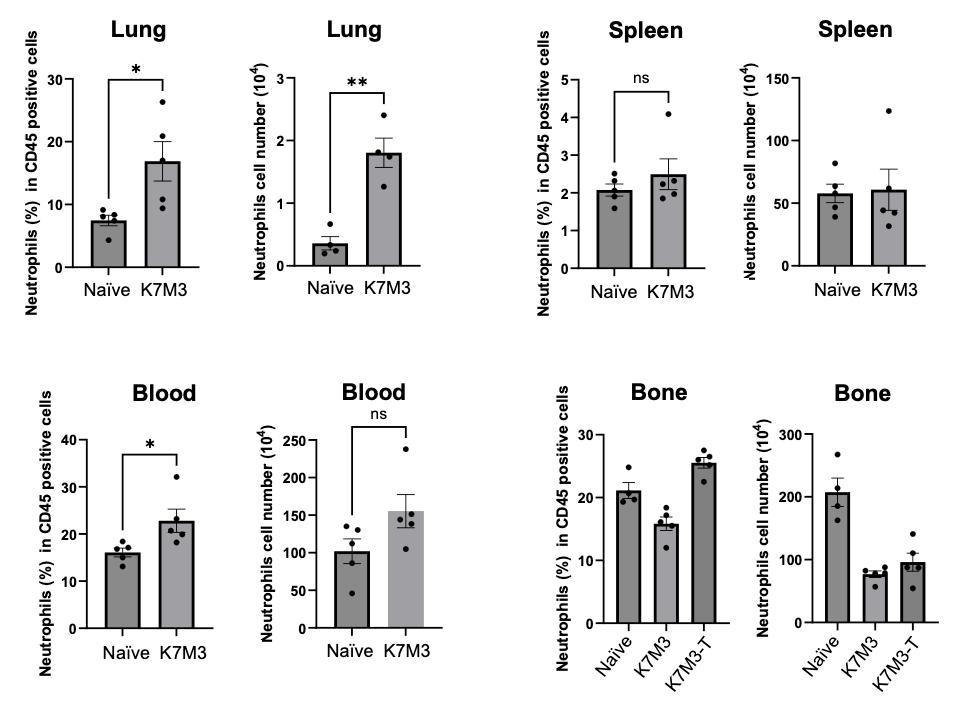
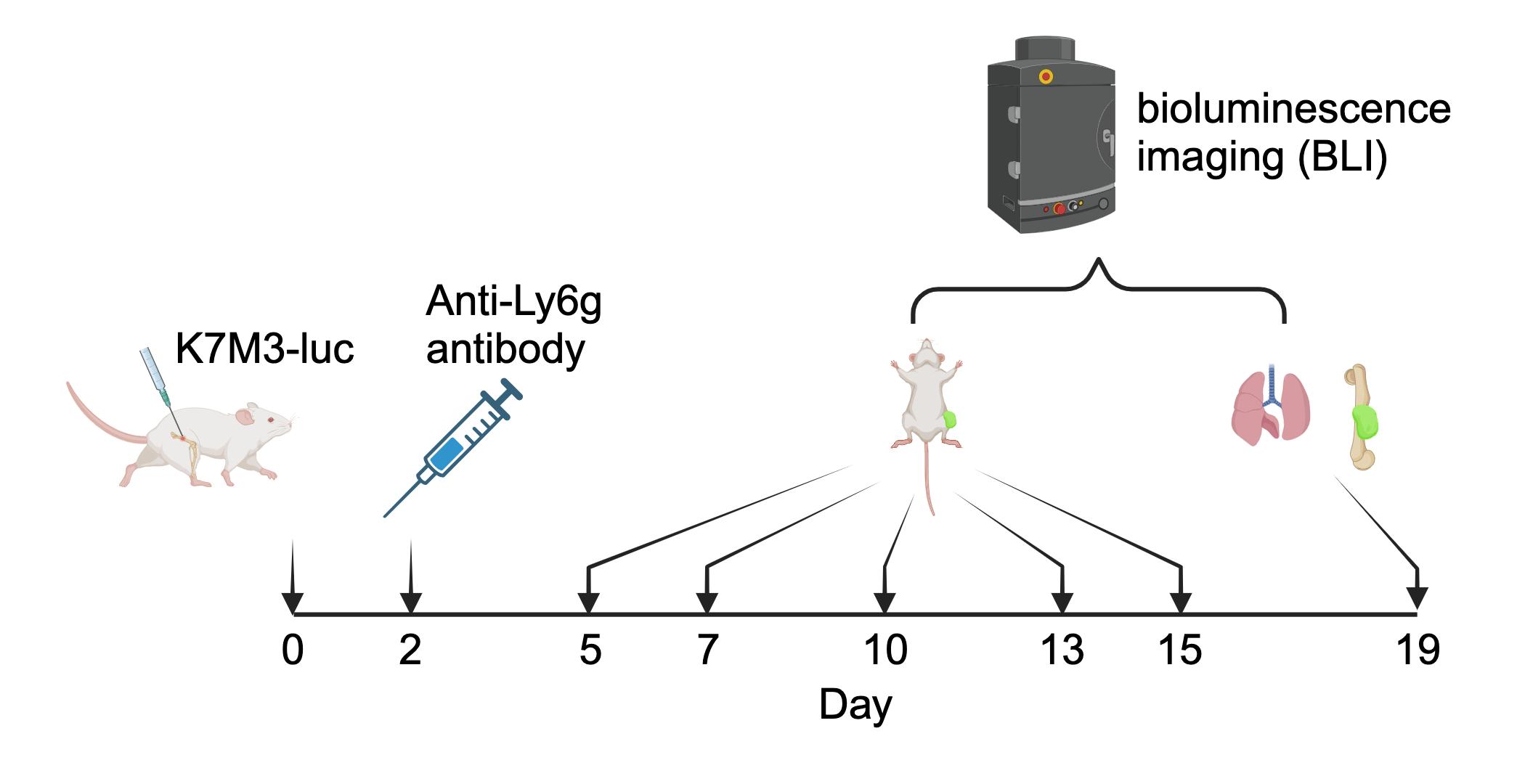
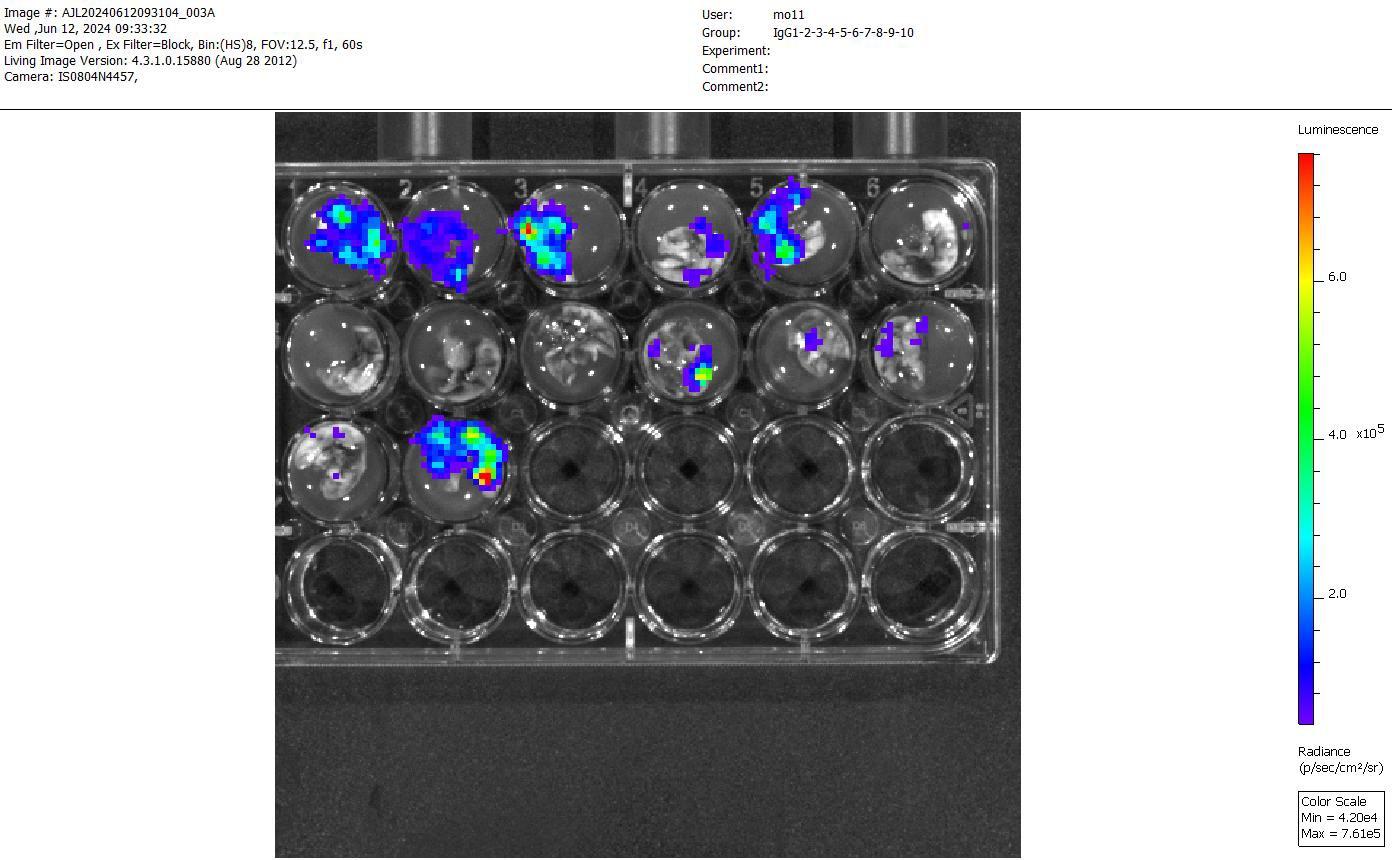
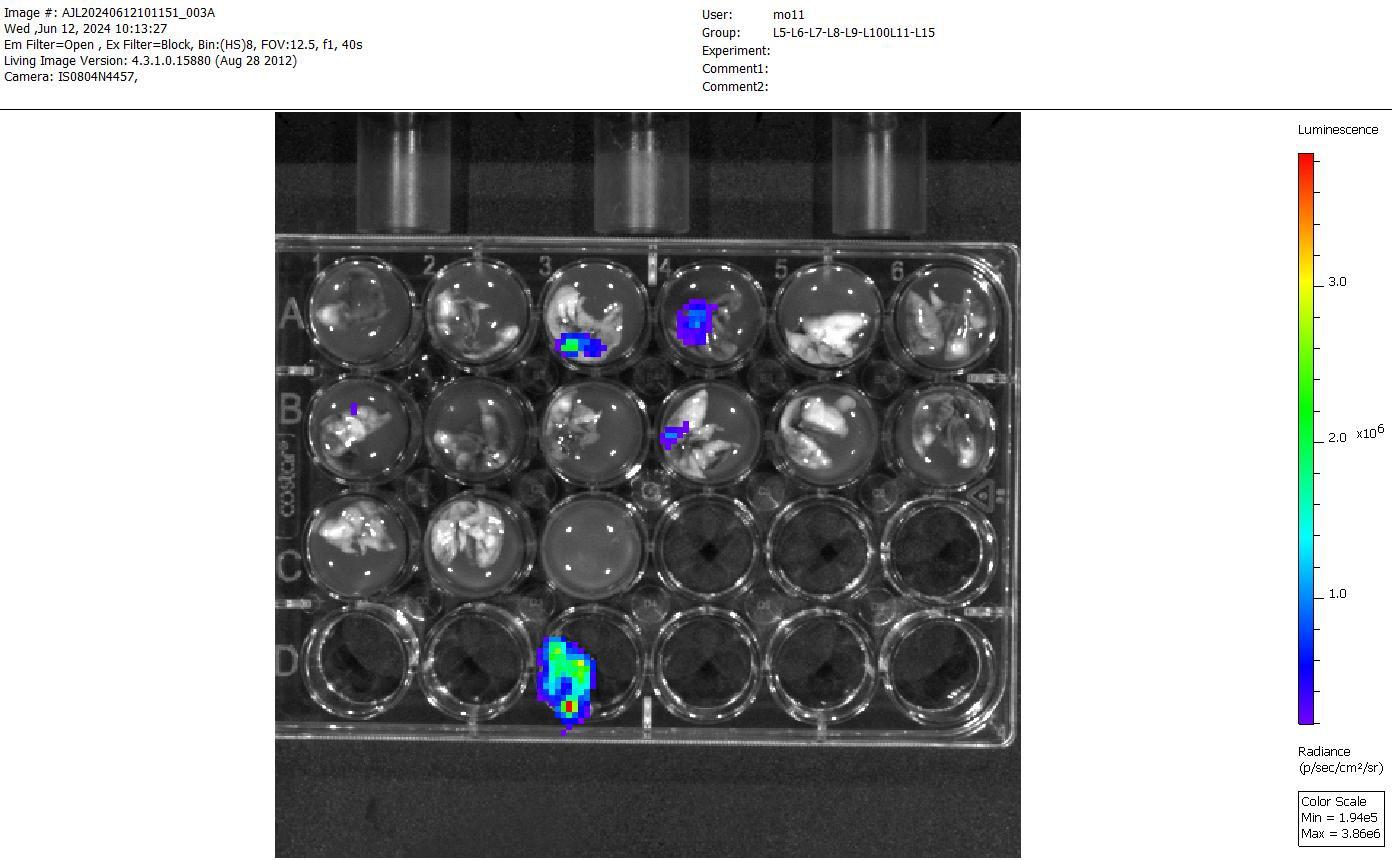
Wecharacterized theseimmunosuppressivecelltypes using an orthotopic K7M3 xenograft mousemodel. Luciferase-labeled metastatic K7M3 mouse OS cells were injected into the femur of Balb/c mice. Tumor formation was monitored by bioluminescent imaging (BLI). Major immunecell types in thebone and lung sites wereprofiled using fluorescence-activated cellsorting (FACS). The role of neutrophils in lung tumor formation was examined using an anti-Ly6G antibody depletion approach.
RESULTS
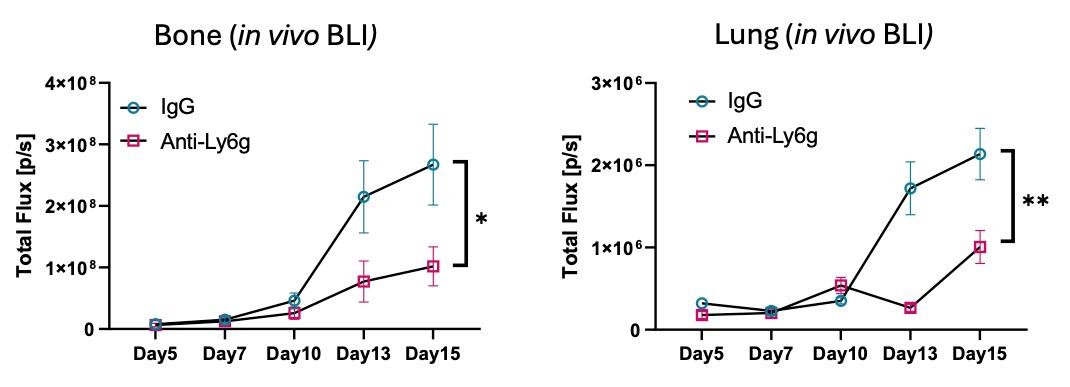
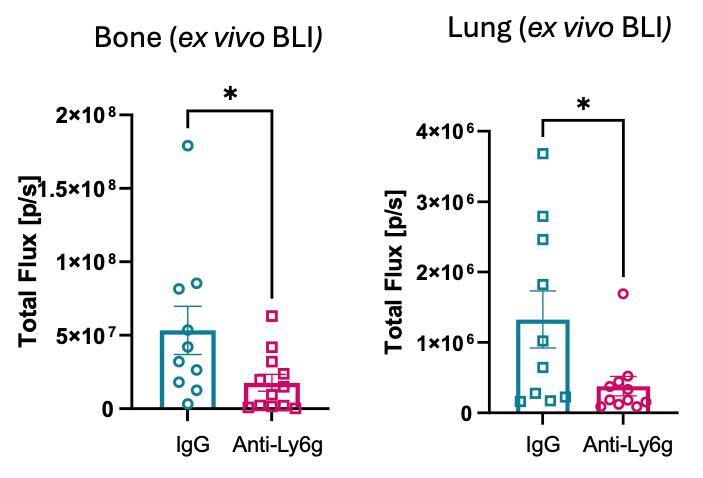
In theK7M3 mousemodel, tumors wereobserved at theinjection site and in thelung by Day 16 using BLI. FACS revealed that neutrophils werethemost altered immunecell typein thelungs with OS tumors. Depletion of neutrophils significantly reduced lung metastasis of OS in the mousemodel. Wewill confirm neutrophil phenotypic states using scRNA-seq and furtherevaluate theTMEusing Xenium in situ analysis.
CONCLUSION/SIGNIFICANCE
Thelong-term goal is to identify pathways/targets to overcomeimmunosuppression in theOS TMEfor new treatment development.
The Role of Immunosuppressive Neutrophils in the Tumor Microenvironment of Osteosarcoma
Patrick Ng 1,2,3, Chaojia Chen 4, Aaron Taylor 3, Elise Courtois 3, Paul Robson 3 , Michael S. Isakoff 1,2 , Qian Wu 2 , Fabiola Sara Balarezo 5, Adam D. Lindsay 5 , Gary Ren 4, Ching Lau 1,2,3
1 Connecticut Children’s Medical Center, Hartford, Connecticut
2 University of Connecticut School of Medicine, Farmington, Connecticut
3 The Jackson Laboratory for Genomic Medicine, Farmington, Connecticut
4 The Jackson Laboratory, Bar Harbor, Maine
5 Hartford Hospital, Hartford, Connecticut
Abstract
BACKGROUND
Osteosarcoma (OS) is the most common primary malignant bone tumor in children and young adults, with a 20-30% survival rate in metastatic cases, primarily in the lungs. To improve the survival rate of OS patients, it is crucial to find effective strategies to prevent or treat lung metastasis. The tumor microenvironment (TME) is vital in tumor biology, but its role in OS primary tumor and lung metastasis is not well understood. Recently, our group used single-cell RNAsequencing (scRNA-seq) to profile the TME of metastatic lung tumors from OS patients, identifying potential immunosuppressive immune cell types.
METHODS
We characterized these immunosuppressive cell types using an orthotopic K7M3 xenograft mouse model. Luciferase-labeled metastatic K7M3 mouse OS cells were injected into the femur of Balb/c mice. Tumor formation was monitored by bioluminescent imaging (BLI). Major immune cell types in the bone and lung sites were profiled using fluorescence-activated cell sorting (FACS). The role of neutrophils in lung tumor formation was examined using an anti-Ly6g antibody depletion approach.
RESULTS
In the K7M3 mouse model, tumors were observed at the injection site and in the lung by Day 16 using BLI. FACS revealed that neutrophils were the most altered immune cell type in the lungs with OS tumors. Depletion of neutrophils significantly reduced lung metastasis of OS in the mouse model.
Result
Identification of immunosuppressive cell types in human OS lung metastatic tumors
• Further subclustering identified subgroups of cells within neutrophils, dendritic cells (DCs) and T cells expressing immunosuppressive markers:
▲ UMAP showing subclustering of indicated cell types with potential immunosuppressive cell types highlighted in circles.
▲ Expression of neutrophil and immunosuppressive markers among different neutrophil/monocyte subclusters. Neutrophil Immunosuppressive
Orthotopic mouse metastatic OS model
Luciferase-labeled mouse metastatic OS K7M3 cell line luc) were injected into the femur of Balb/c mice
Tumor formation was monitored with n vivo bioluminescence imaging (BLI) and ex vivo BLI of the isolated lungs at Day 16.
Increased neutrophil population in lung
• Profiling of major immune cell types by FACS.
• The CD11b+Ly6ghighLy6clow neutrophil population was the mostly changed immune cell type in frequency in the lungs with OS tumor progression.
▲ Neutrophil frequencies in the indicated tissues between K7M3-luc mice (Day 16) and naïve mice were shown. In the bone group, K7M3T indicates the bone from the tumor-bearing leg, while K7M3 indicates the bone from the tumor-free leg.
Depletion of neutrophils reduce tumor growth
• Depletion of neutrophils in the K7M3-luc model using neutrophil-specific anti-Ly6g antibody.
• Anti-Ly6g antibody was injected 2 days after K7M3-luc cells injection.
• Tumor development was monitored by live animal BLI from Day 5 to Day 15.
• Lung and bone were harvested on Day 19 for ex vivo BLI.
• Reduced tumor developments were observed in bone and lung in mice with neutrophil depletion (Anti-Ly6g group), comparing to IgG control.
ex vivo BLI of lungs from anti-Ly6g
on Day 19
• Phenotypic analysis of neutrophils and other immune cells using single-cell RNA-seq.
• Spatial multi-omics analysis of OS lung metastasis TME using Visium HD, PhenoCycler and/or Xenium.
• Validation of our findings using mouse spontaneous OS model with TP53 mutations.
• We acknowledge the funding support from Connecticut Children’s Research Institute and The Jackson Laboratory.
• We also acknowledge the contribution of the Single Cell Biology service and the Genome Technologies service at The Jackson Laboratory for expert assistance with the work described herein.
• Figures were made with BioRender.
▲
Category: (Basic/Translational)
Educating Clinicians on Sexual Health Care for AYAs: Preliminary Results from an Intervention Pilot Study
Presenting Author: Mary-Kate Nowobilski, BS 1
Kristin Bingen, PhD2; Brooke O. Cherven, PhD, MPH, RN3; Jenna Demedis , MD, MS4; Gwendolyn P. Quinn, PhD5; David R. Freyer, DO6; Sharon L. Bober, PhD7, Natasha N. Frederick, MD, MPH1
1 University of Connecticut School of Medicine
2Medical College of Wisconsin
3Emory University School of Medicine
4University of Colorado School of Medicine
5Grossman School of Medicine, New York University
6Keck School of Medicine, University of Southern California
7HarvardMedicalSchool
BACKGROUND
Adolescent and Young Adults with cancer (AYAs) have notable unmet sexual health (SH) needs. While AYAs want to discuss SH with oncology clinicians, these conversations are rare. Clinicians report lack of knowledge as a key SH communication barrier, with a preference for online, interactive educationalmodalities that can be completed independently. This study aims to assess preliminary data on the acceptability and perceived utility of aclinician-centered web-based curriculum designed to improve AYA-clinician SH communication.
METHODS
Clinicians wererecruited byemail from 5U.S. academic centers tocomplete aseries of 4modules withpre- and post-surveys. Each module included conversation scripts, knowledge checkpoints, and interactive casestudies. Participants completed pre-and post-training measures rating acceptability (7 items) and perceived utility (4 items) on a 5-point scale (strongly disagree to strongly agree).
RESULTS
Forty-five participants registered for the course and 39 completed the modules and post-course follow-up. Twenty-nine participants have completed the 2-month post follow-up. All participants “agreed” or “strongly agreed” with the 7 items of acceptability and 92% (36/39) with the 4 items on perceived usefulness. Study participants that registered for the course but did not complete the modules cited technical issues and lack of time as barriers.
CONCLUSION/SIGNIFICANCE
Preliminary results suggest this intervention is poised to make a significant impact on improving clinician knowledge and communication about AYA SRH concerns. Next steps include developing strategies to overcome identified barriers along with examining intervention effectiveness on increasing clinician knowledge, standardizing SRH conversations and impact AYA sexual health outcomes.
Educating Clinicians on Sexual Health Care for AYAs: Preliminary
1 University of Connecticut School of Medicine, 2Medical College of Wisconsin, 3Emory University School of Medicine, 4 University of Colorado School of Medicine, 5 Grossman School of Medicine, 6Keck School of Medicine, 7 Harvard Medical School
BACKGROUND
• Adolescent and Young Adults with cancer (AYAs) have notable unmet sexual health (SH) needs.
• While AYAs want to discuss SH with oncology clinicians, these conversations are rare.
RESULTS
• Forty-five participants registered for the course.
• Thirty-nine completed the modules, post-course follow-up, and 2-month post follow-up.
• Clinicians report lack of knowledge as a key SH communication barrier, with a preference for online, interactive educational modalities that can be completed independently.
• This study aims to assess preliminary data on the acceptability and perceived utility of a clinician-centered web-based curriculum designed to improve AYA-clinician
METHODS
• Clinicians were recruited by email from 5 U.S. academic centers.
• A series of 4 modules with pre- and post-surveys were completed.
• Each module included conversation scripts, knowledge checkpoints, and interactive case studies.
• All participants “Agreed: or “Strongly agreed” with the 7 items of acceptability.
• 94.9% (37/39) “Agreed: or “Strongly agreed” with the 4 items on perceived usefulness.
• Study participants that registered for the course but did not complete the modules cited technical issues and lack of time as barriers.
• Participants completed pre-and post-training measures rating acceptability (7 items) and perceived utility (4 items) on a 5-point scale (strongly disagree to strongly agree).
Figure 1: Study Methods
Figure 2: 7-Item Acceptability
Figure 3: 4-item Perceived Usefulness
• Preliminary results suggest this intervention is poised to make a significant impact on improving clinician knowledge and communication about AYA SRH concerns
“The module worked really well and I’m impressed with the technology. I had no issues”.
“I thought the combination of didactics and examples was effective”.
“I felt these modules are very educational and simple to follow along. I learned a lot about AYA and sexual health“
“This was very helpful to see recommendations for specific practices to avoid during low ANC/Plt times”.
Figure 4: Module Feedback
NEXT STEPS
• Develop strategies to overcome technical issues.
• Examine intervention effectiveness on increasing clinician knowledge, standardizing SH conversations, and impact on AYA sexual health outcomes
REFERENCES
1.Rosenberg AR, Bona K, Ketterl T, et al: Intimacy, Substance Use, and Communication Needs During Cancer Therapy: A Report From the "Resilience in Adolescents and Young Adults" Study. J Adolesc Health 60:93-99, 2017
2. Cherven B, Klosky JL, Chen Y, et al: Sexual behaviors and human papillomavirus vaccine non-initiation among young adult cancer survivors. J Cancer Surviv 15:942-950, 2021
3. Bober SL, Zhou ES, Chen B, et al: Sexual function in childhood cancer survivors: a report from Project REACH. J Sex Med 10:2084-93, 2013
5. Acquati C, Zebrack BJ, Faul AC, et al: Sexual functioning among young adult cancer patients: A 2-year longitudinal study. Cancer 124:398-405, 2018
6.Frederick NN, Revette A, Michaud A, et al: A qualitative study of sexual and reproductive health communication with adolescent and young adult oncology patients. Pediatr Blood Cancer 66, 2019
7.Frederick NN, Campbell K, Kenney LB, et al: Barriers and facilitators to sexual and reproductive health communication between pediatric oncology clinicians and adolescent and young adult patients: The clinician perspective. Pediatr Blood Cancer:e27087, 2018
8.Frederick NN, Bingen K, Bober SL, et al: Pediatric oncology clinician communication about sexual health with adolescents and young adults: A report from the children's oncology group. Cancer Med 10:5110-5119, 2021
Category: Basic/Translational
An integrative analysis of differential alternative splicing events betweenpairedtransientabnormalmyeloproliferation andacutemyeloid leukemia in Downsyndromepatients
Children with Down syndrome (DS) are predisposed towards acquiring myeloid leukemia (MLDS) in adolescence, following a state of transient abnormal myeloproliferation (TAM). Although GATA1 mutations are a known factor in the initiation of TAM/ML-DS in DS, little else is known about the mechanisms behind transformation to ML-DS, and there is an unmet medical need for early detection of patients for whom ML-DS will later develop.
METHODS
We performed RNA-sequencing of peripheral blood gathered from four DS patients with TAM that later progressed to ML-DS, which included samples gathered from both disease states, as well as a set of 99 unpaired TAM samples with no later progression to ML-DS against 14 TAM samples with known ML-DS progression. Data was analyzed via the Kids First RNA-Seq Workflow to look at differential expression of genes and alternatively-spliced isoforms, and further studied with pathway analysis tools including STRING-DB, EnrichR, and Rummagene.
RESULTS
We saw differential expression of 1,038 genes (p < 0.05) between TAM with/without ML-DS progression. Network analysis found enrichment for downregulation of platelet activation-related genes in TAM samples with later ML-DS progression, with ML-DS samples showing further downregulation. Similar pathway disruption was found in the gene isoform and alternative splicing data, suggesting repression of platelet activation may play a role in the progression of TAM to MLDS.
CONCLUSION/SIGNIFICANCE
Our work highlights expression differences between matched TAM and ML-DS samples, including disruptions in known cancer-related pathways, and provides insight into mechanisms of leukemic transformation in DS.
An integrative analysis of differential alternative splicing events between paired transient abnormal myeloproliferation and myeloid leukemia in Down syndrome patients
Aaron
Michael Taylor1, Francis H.
O’Neill
1, Rhonda Ries2 , Xiaotu Ma3, Johann
1 Jackson Laboratory for Genomic Medicine, Farmington, CT
2 Fred Hutchinson Cancer Research Center, Seattle, WA
3 St. Jude Children’s Research Hospital, Memphis, TN
4 The Hospital for Sick Children, University of Toronto, Toronto, Ontario, Canada
5 Science and Technology Consulting, LLC
6 Connecticut Children’s Medical Center, Hartford, CT
7 University of Connecticut School of Medicine, Farmington, CT
Abstract
BACKGROUND
Children with Down syndrome (DS) have a predisposition towards acquiring myeloid leukemia (ML-DS) in adolescence, following a state of transient abnormal myeloproliferation (TAM). Although GATA1 mutations are a known factor in the initiation of TAM/ML-DS, little else is known about the mechanisms behind transformation to MLDS, and there is an unmet medical need for early detection of patients for whom ML-DS will later develop, with particular interest for patients who relapse following treatment.
METHODS
We investigated the molecular landscape of peripheral blood gathered from four DS patients with TAM that later progressed to ML-DS, which included samples gathered from both disease states. RNA-sequencing was performed, and data was analyzed via the Kids First RNA-Seq Workflow V4 developed for the Kids First and INCLUDE projects, using the CAVATICA platform. Alternative splicing analysis output was downloaded, and the inclusion junction counts (IJC) for each of the splicing types were transformed into matrices capturing the patient-specific splicing forms and IJC. To perform the paired TAM versus ML-DS analysis, we used limma to look for differentiallyexpressed IJC between sample types, and the resulting IJC differences (p < 0.05) were captured for further study with pathway analysis tools including STRINGdb, EnrichR, and Rummagene to understand the functional implications of alternative splicing between TAM and ML-DS.
RESULTS
Our work highlights alternative splicing differences between matched TAM and ML-DS samples, including disruptions in known cancerrelated pathways, and provides insight into mechanisms of leukemic transformation in DS. Investigating mutually exclusive exon event counts show this alternatively-spliced-gene enrichment in MYC pathways using EnrichR EnrichR showed enrichment in Myc targets including the MSigDB Hallmark 2020 (p-value = 3.949e-14) and ChIPSeq CA45 Human Blood Burkitt Lymphoma in ChEA 2022 (p-value = 1.40e-15).
Materials
Sample overview
• Peripheral blood samples gathered from studies of transient abnormal myeloproliferation (TAM) and myeloid leukemia (ML-DS) in patient with Down syndrome
• AAML08B1
• AAML1531
• RNA extracted and ribodepleted sequencing performed on the TAM and ML-DS sample groups used for downstream analysis
K. Hitzler
4, Anne
Deslattes
Mays5, Soheil Meshinchi2, Ching Lau1,6,7
Activated pathways in individual groups
• Non-progressing TAM (99) vs TAM with ML-DS progression (14): 371
• Major subnetworks enriched for terms such as:
• Platelet growth factors/activation and diseases (Bernard-Soulier/Von Willebrand/Glanzmann thrombasthenia)
• Erythrocyte/hematopoeisis and diseases (spherocytosis, stomatocytosis)
• May represent decreased differentiation during pre-leukemic selection in TAM with later progression to ML-DS Multidimensional scaling on expression
Isoform switching analysis
• RSEM transcript count matrices for each matched sample (TAM vs ML-DS) were combined for groupwise DE analysis using DESeq2
• Transcript coding, protein domain, and signal peptide characteristics were analyzed by CPC2, Pfam, and SignalP IsoformSwitchAnalyzeR package was used to integrate transcript characteristics and testing for Isoform Switches via DEXSeq
• Isoform switch: a case where the relative contribution of the isoforms to the parent gene expression changes significantly between conditions
• 322 Isoform switches identified (|dIF| > 10%)
• 317 include switch consequences
• Switch consequences defined as: protein domain gain/loss, change in NMD status, signal peptide gain/loss, alternative AA sequence, change in coding potential, or intron retention
• 59 isoforms switches may lead to altered expression of protein domains between TAM and ML-DS
KAT6B: a novel epigenetic regulator of hematopoietic differentiation. Gene isoform switch identified in TAM vs ML-DS
Isoform switch in KAT6B shows:
Decreased usage of a coding ENST00000287239.10 in ML-DS (vs TAM)
Increased usage of non-coding ENST00000647890.1 in ML-DS (vs TAM).
This likely yields a decreased expression of functional KAT6B protein in ML-DS.
Differential alternative splicing
• Plotted 146 significantly DE (counts > 1000 in either TAM or ML-DS, p < 0.05, FC > 9) skipped-exon events. TAM and ML-DS cases separate on alternatively-spliced gene expression.
Enrichment Analysis using Enrichr
• Significantly DE alternatively-spliced retained intron (RI), skipped exon (SE) and mutually-exclusive exon (MXE) gene lists were all enriched lists for Diamond-Blackfan anemia
• Transcription factor protein-protein interactions (PPIs) and MSigDB highlighted MYC and TP53
Conclusion
• Expression differences between TAM with later development of ML-DS and TAM with no progression highlight platelet-differentiation pathways
• Isoform and alternative splicing differences between patient-matched TAM/ML-DS samples point to additional biological changes involved in MLDS transformation, including known cancer-related genes such as TP53 and MYC
• Further analysis of progressing/non-progressing TAM and matched ML-DS versus relapsed ML-DS samples will allow us to better predict outcome for these high-risk patients
Category: Basic/Translation
Feasibility of Brain TumorClassification by Enzymatic DNA
Methylation SequencingAnalysis of Cell-freeDNAObtained fromCerebrospinal Fluid
Array-based methylation profiling is the gold standard for molecular classification of brain tumors. This relies on significant amount of input DNA extracted from surgical tissue, limiting use for tumors where biopsy is challenging or limited in quantity. Cell-free tumor DNA (cfDNA) in cerebrospinal fluid (CSF) presents alternative opportunities for brain tumor diagnosis and disease monitoring. Enzymatic methylation sequencing (EM-seq) methods may allow us to overcome input DNA limitations.
METHODS
We performed methylation sequencing using the NEBNext EM-seq kit on cfDNA from CSF collected from brain tumor patients with confirmed histopathological diagnoses. Variable input cfDNA amounts (0.1ng-10ng) were tested. We utilized the methylseq pipeline for data processing. For tumor classification, weleveraged the MNP-Flex algorithm, a platform-agnostic version of the Heidelberg methylation classifier.
RESULTS
Using the EM-seq method, genomic coverage for 10 and 1ng input DNA samples (46x and 26x, respectively) was sufficient for generating methylation profiles. Samples with 0.1ng input had only 5.32x coverage, due to elevated read duplication. Methylation of CpG sites with >5x coverage were highly correlated across varying input DNA amounts, suggesting lower input could be used for tumor classification basedon relevant CpG sites.
CONCLUSION/SIGNIFICANCE
With the MNP-Flex classifier, originally trained with methylation array data from tumor tissue, we successfully predicted tumor types with methylation data using only 1ng of input cfDNA, matching diagnosis using tissue methylation and histopathology in this pilot study. Further classification of additional tumor types using CSF cfDNA is required to confirm the clinical utility of this platform.
Feasibility of brain tumor classification by enzymatic DNA methylation sequencing analysis of cell free DNA obtained from cerebrospinal fluid
Aaron Michael Taylor1, Jody T. Lombardi1 , Areeba Patel2, Ariella Tamariz1, Jonathan Martin3, Markus J. Bookland3, David S. Hersh3, Evan Cantor3 , Xianyuan Song4, Felix Sahm2, Patrick Kwok-Shing Ng1,5, Joanna J. Gell1,3, Ching C. Lau1,3
1 Jackson Laboratory for Genomic Medicine, Farmington, Connecticut, USA 2 German Cancer Research Center (DKFZ), Heidelberg, Germany
3 Connecticut Children’s Medical Center, Hartford, Connecticut, USA 4 Hartford Hospital, Hartford, Connecticut, USA
5 University of Connecticut Health, Farmington, Connecticut, USA
Abstract
BACKGROUND
Array-based methylation profiling is the gold standard for molecular classification of brain tumors. This relies on significant amount of input DNA extracted from surgical tissue, limiting use for tumors where biopsy is challenging or limited in quantity. Cell-free tumor DNA (cfDNA) in cerebrospinal fluid (CSF) presents alternative opportunities for brain tumor diagnosis and disease monitoring. Enzymatic methylation sequencing (EM-seq) methods may allow us to overcome input DNA limitations
METHODS
We performed methylation sequencing using the NEBNext EM-seq kit on cfDNA from CSF collected from brain tumor patients with confirmed histopathological diagnoses. Variable input cfDNA amounts (0.1ng-10ng) were tested. We utilized the methylseq pipeline for data processing. For tumor classification, we leveraged the MNP-Flex algorithm, a platform-agnostic version of the Heidelberg methylation classifier.
RESULTS
Using the EM-seq method, genomic coverage for 10 and 1ng input DNA samples (46x and 26x, respectively) was sufficient for generating methylation profiles. Samples with 0.1ng input had only 5.32x coverage, due to elevated read duplication. Methylation of CpG sites with >5x coverage were highly correlated across varying input DNA amounts, suggesting lower input could be used for tumor classification based on relevant CpG sites.
Conclusions
With the MNP-Flex classifier, originally trained with methylation array data from tumor tissue, we successfully predicted tumor types with methylation data using only 1ng of input cfDNA, matching diagnosis using tissue methylation and histopathology in this pilot study. Further classification of additional tumor types using CSF cfDNA is required to confirm the clinical utility of this platform.
Results
Enzymatic methylation sequencing
• Used NEBNext enzymatic methylation sequencing (EMSeq) kit (v2.0) on cell-free DNA (cfDNA) from archival CSF samples collected from pediatric brain tumor patients
Sample overview
• Inputted variable amounts of cfDNA (0.1ng-10ng) from three samples to establish methylation profiling limits
• methylseq nf-core pipeline used for data QC, processing, and methylation calling
Methylation correlation across input cfDNA
• Methylation well-correlated between 10ng and 1ng input cfDNA
• Sites with ≥10x coverage in 0.1ng input samples also well correlated with higher-input cfDNA samples
Classification results
• Cohort was expanded to include additional samples with ~1ng cfDNA input
• Tumor superfamily and family predictions shown for each tumor
Methylation by genomic context
• Cytosine methylation levels were low outside of CpG context as expected, and comparable across input DNA levels
Coverage across genome
• Genomic coverage was predictably higher at 10/8.8ng cfDNA input, but acceptable at 1ng cfDNA
Brain tumor classifier
• Utilized MNP-flex, a modified version of previously-published, array-based brain tumor tissue methylation classifier, MNP v12.8, which accepts β-values from EM-seq for sites overlapping array probe locations
• Errors in predictions associated with unusual histopathology (MB45, HGG49), CSF from relapsed tumors (MB32), and sample quality (MB45)
Intracranial germ cell tumor (IGCT) profiling
• IGCTs often arise in delicate anatomical positions that complicate or prevent biopsy, and may also present as mixed tumors with multiple subtype components, making diagnosis challenging
• Germinoma, which arise from primordial germ cells with genomewide hypomethylation, may be more easily distinguished from more differentiated IGCT subtypes using cfDNA
Category: (Basic/Translational Research)
Qualitative Analysis of Pain Impact in Adult
Patients with X-Linked Hypophosphatemia (XLH) to Inform the Development of a Digital Pain Self-Management Intervention
Presenting Author: Christopher B. Theriault, MA
Christopher B. Theriault, MA1 , Nicole Nishime, BA2,Carolyn Macica, PhD1,2
1 Connecticut Children’s ResearchInstitute
2 Frank H. Netter MD School of Medicine at Quinnipiac University
BACKGROUND
Previously, we reported pain as a dominant finding in adult patients with XLH. In this study, we conducted a qualitative analysis of semi-structured interviews to gain deeper insights into the pain experiences of adults living with XLH.
METHODS
Interviews with 15 adult XLH patients (11 F/4 M) were conducted, recorded, transcribed, and analyzed thematically. Participants also completed the SF-36 survey to measure health-related qualityof-life (HRQoL) data reported asage-adjusted differences relative to the general population.
RESULTS
Qualitative analyses identified 10 emergent themes: 1. Chronic and variable pain; 2. Impact on mobility and daily life; 3. Pain management techniques; 4. Healthcare andaccessibility challenges; 5. Emotional and psychological impact; 6. Social isolation and dependency; 7. Desire for improved information and support; 8. Challenges with inactivity and the need to keep moving; 9. Long-term outlook and concerns; 10. Advocacy and awareness. Age-adjusted differences for SF-36 responses were lower than the general population in all domains of HRQoL, with significant differences notably related to physical function and pain (p<0.001). The XLH group demonstrated significantly lower scores compared to the control group, with a large effect size (Cohen's d = 0.80).
SIGNIFICANCE
These data illustrate the profound impact of XLH on multiple aspects of patients' lives and highlight the needfor effective pain management strategies, better healthcare accessibility, supportive tools, and a more knowledgeable medical community to improve the quality of life for individuals with XLH. These data will be used to develop a tailored digital intervention for pain selfmanagement previously developed for other chronic pain populations.
Qualitative Analysis of Pain Impact in Adult Patients with X-Linked Hypophosphatemia
Inform the Development of a Digital Pain Self-Management Intervention
Introduction
• X-linked hypophosphatemia (XLH) is a rare genetic disorder caused by an inactivating mutation in the phosphate regulating endopeptidase X-linked (PHEX) gene, resulting in elevated levels of the hormone fibroblast growth factor-23 (FGF23).
• FGF23 suppresses 1,25-dihydroxyvitamin D production, dietary phosphate absorption, and inhibits renal phosphate reabsorption, ultimately resulting in phosphate wasting.1
• Since phosphate plays an essential role in the biomineralization and maintenance of bone, teeth, and ossicles, XLH manifests systemically.2 (Figure 1)
• As a progressive disease, XLH patients often experience chronic pain and an increasingly limited range of motion due to the formation of bone spurs (enthesophytes) at fibrocartilaginous tendon and ligament insertion sites.4-6
• A paucity of controlled trials evaluating pain in XLH combined with lack of healthcare provider knowledge pertaining to the disease often result in inappropriate or ineffective pain management.7
Purpose
While previous studies have reported pain as a predominant finding in adult patients with XLH, this study aimed to address the knowledge gap related to pain in these individuals to better inform the creation of a digital pain management tool.
Methods
• This study utilized a mixed-methods design with a crosssectional survey and semi-structured interviews.
• Participants were recruited, with support from the XLH Network community, who met the following criteria:
(a)30 years of age or older with a genetic confirmation of XLH diagnosis (PHEX mutation), (b) were able to speak and understand English or Spanish, (c) were currently and consistently taking overthe-counter or prescription medication for pain, and (d) were willing and able to engage with a smartphone application to complete online measures.
• Participants completed the 36-Item Short Form Survey Instrument (SF-36) to measure health-related quality-of-life, with data reported as age-adjusted differences relative to the general population. Data were analyzed using a parametric two-tailed ttest and the effect size reported as Cohen’s d.
Nicole Nishime, BA1, Christopher Theriault, MA2, and Carolyn M. Macica, PhD1,2
1Frank H. Netter MD School of Medicine at Quinnipiac University, North Haven, CT
2Connecticut Children’s Research Institute, Hartford, CT
Methods
Results
Interviews and Qualitative
Analysis:
Eligible participants completed one-onone semi-structured interviews utilizing questions developed in consultation with a focus group of members from the XLH Network, Inc.
Figure 2. Interviews of 15 adult patients (11F/4M), 49.1 13.4 yrs diagnosed with XLH were conducted, transcribed, and analyzed using NVivo (Lumivero) software.
A subset of the interviews underwent secondary analysis using HyperRESEARCH software to validate themes.
“I wish that I could be pain free. I've dealt with pain my whole life. You know the sad thing is , I don't know. I don't know life without pain. It is just since, as early as can remember, I've dealt with pain.”
“This is the reason I've decided not to have children. Because I wouldn't pass on this disease because it's painful. If the disease wasn't painful, and it was just the mild inconvenience that had as a child, that would be a different story. But it's not. So this disease cost me relationships, family, my career. Everything. So I know it's ultimately going to take everything and I just can't worry about it.”
”Well, I tend not to discuss it (pain) with my healthcare providers cause, then they want to fix me, and they can’t. Then I have to explain that they can't fix me, and then they get all emotional, and it just makes it worse, you know, because mean, there's a trauma element or emotional scarring element to having to face the pain and there's a coping tool and just ignoring it. You know what I mean, and you can't ignore it if they insist on talking about it. So it's easier for me to not talk about it with them.”
“It’s very important to me to have a pain psychologist to talk to. They are very far and few between. I had a couple of really good ones, and then they left. So I don't have one. Currently, really, really enjoyed having someone to talk to about pain. I haven't spoken about that, but that's really important. I think that would be so vital for all of us dealing with the chronic pain. I miss that actually because don't want to overburden my friends and family… I can talk about it to my healthcare providers, but talking about it to my friends and family makes me makes me cry, so I don't want to overburden them."
”Reaching out to people who do have XLH, I think that's important to know that you're not imagining this weird pain that doctors look at you like you're crazy. When you mentioned, you know the whole body thing, that it's everywhere at the same time and there's no visible source of it, you know, getting validation. That goes a long way, I think, in being able to say, “Oh, yeah, that's just my stupid XLH acting up” so, even though it hurts, at least I know the pain is real right? There's a certain comfort in that."
”I'm not sure, and that scares me. think the most of all that scares me because I'm 57, and I think that I wonder what 10 years is gonna feel like. So there's a fear of the future for me but I'm hopeful you know. I'll just take it day to day and and see what happens. But yeah, I hope, I mean, I can only imagine, it's gonna get worse, but I don't know."
Results
"There's so many barriers like being believed at a doctor's office, or the pharmacy, or the insurance, to getting assistance with pain…When I was on methadone I had a dental abscess. My face filled up. I went to the ED because I didn't have dental insurance or a dentist at the time. I was on disability and had no income, and he wants to send me home with a prescription for tramadol. But that interacts with methadone and he wouldn't believe me. He's like “I’m the doctor”, that's what he said. He wants you to take it, so you need to leave, and it's like I'm bawling my eyes out like trying to tell you and they won't listen. It's like I came to you for help, and you're making me feel like I'm doing something wrong, and it's just so frustrating. So I don't really know how to be heard, you know, especially without becoming emotional."
"I don't know, but I'm really concerned about how pain will affect my future. Almost afraid because it's a progressive disease. And I have seen the progression in myself. I'm concerned that the pain may stop me from doing much of anything. And so I'm not excited about the future as far as pain goes. but already have a power wheelchair and a rollator and a cane and around the house most of the time I walk independently. If I'm going any place that would have a lot of walking, usually take the chair. And so because I have seen the progression in myself and I'm really anxious about it you know."
Qualitative Analysis: 10 Emergent Themes
• Chronic and variable pain
• Impact on mobility and daily life
• Pain management techniques
• Healthcare and accessibility challenges
• Emotional and psychological impact
• Social isolation and dependency
• Desire for improved information and support
• Challenges with inactivity and the need to keep moving
• Long-term outlook and concerns
• Advocacy and awareness
Figure 3. Age-adjusted differences for SF-36 responses were lower than the general population in all domains of health-related quality of life, with significant differences notably related to physical function and pain (p<0.001 PF, RP, V, BP and GH). The XLH group (n=13) demonstrated significantly lower scores compared to the control group, with a large effect size (Cohen's d = 0.80).
PF = physical functioning; RP = role limitations due to physical health; RE = role limitations due to emotional problems; VT = vitality; MH = mental health; SF = social functioning; BP = bodily pain; GH = general health
Next Steps
Qualitative analysis also found nine themes related to what participants would find useful in a pain management mobile application tailored to manage XLH:
(1) pain tracking by location and type, (2) medication management, (3) physical therapy and exercise tracking, (4) pain intensity and impact diary, (5) educational resources, (6) community and support features, (7) integration with healthcare providers, (8) detailed symptom logging and analysis, (9) emotional and psychological support resources.
(2) These data will be used to develop a tailored digital intervention for pain self-management previously developed for other chronic pain populations.
Conclusions
• These data illustrate the profound impact of XLH on multiple aspects of patients' lives and highlight the critical need for effective pain management strategies, better healthcare accessibility, supportive tools, and a more knowledgeable medical community to improve the quality of life for individuals with XLH.
• All individuals interviewed expressed interest in a mobile application specifically designed for the management of XLHrelated pain, further emphasizing the current gap pertaining to pain management in the XLH community.
Acknowledgements
We would like to thank the patients who shared their experiences and knowledge of living with XLH, also Dr. Richard Feinn for statistical support, and the XLH community focus group for lending their expertise to question development (Gin Jones, Marina, and Robert Deremer).
References
1. Macica CM. Overview of Phosphorus-Wasting Diseases and Need for Phosphorus Supplements. In: Dietary Phosphorus. CRC Press; 2017.
2. Bhadada SK, Rao SD. Role of Phosphate in Biomineralization. Calcif Tissue Int. 2021;108(1):32-40. doi:10.1007/s00223-020-00729-9
3. Symptoms of XLH. XLH UK. https://xlhuk.org/living-with-xlh/symptoms-of-xlh/. Accessed September 8, 2024.
4. Karaplis AC, Bai X, Falet JP, Macica CM. Mineralizing enthesopathy is a common feature of renal phosphate-wasting disorders attributed to FGF23 and is exacerbated by standard therapy in hyp mice. Endocrinology. 2012;153(12):5906-5917. doi:10.1210/en.2012-1551
5. SteeleA, Gonzalez R, Garbalosa JC, et al. Osteoarthritis, Osteophytes, and Enthesophytes Affect Biomechanical Function in Adults With X-linked Hypophosphatemia. J Clin Endocrinol Metab 2020;105(4):e1798-1814. doi:10.1210/clinem/dgaa064
6. Polisson RP, Martinez S, Khoury M, et al. Calcification of entheses associated with Xlinked hypophosphatemic osteomalacia. N Engl J Med. 1985;313(1):1-6. doi:10.1056/NEJM198507043130101
7. Tucker-Bartley A, Lemme J, Gomez-Morad A, et al. Pain Phenotypes in Rare Musculoskeletal and Neuromuscular Diseases. Neurosci Biobehav Rev. 2021;124:267290.doi:10.1016/j.neubiorev.2021.02.009
Gut bacteria belonging to the Klebsiella oxytoca species complex (KoSC) are the causative agent of AAHC (antibiotic-associated hemorrhagic colitis) in adults and have been linked to the onset of NEC (necrotizing enterocolitis) in premature infants. Most clinical isolates produce the cytotoxin tilimyc in (TM), which induces apoptosis in cultured human cells consistent with intestinal damage occurring during disease. We identified a MarR-like transcriptional factor being part of the two operons essential for TM production. MarRs play a key role in regulating bacterial virulence genes. Understanding how MarR regulates TM production will provide insights into the pathogenesis of NEC and AAHC.
METHODS
A marR-deletion mutant wasgenerated and in vitro toxin production wasassessedby mass spectrometry, cytotoxicity assays using human enterocyte cell lines, and qRT-PCR to analyze expression of toxin genes. The binding of MarR to DNA will be evaluated using promoter pulldown assays and/or electrophoretic mobility shift assays (EMSA).
RESULTS
Deleting marR led to a substantial increase in the expression of toxin genes, resulting in higher TM levels and greater toxicity towards human intestinal cells. These results suggest that MarR represses TM production by binding to the regulatory region of the toxin genes.
CONCLUSION/SIGNIFICANCE
Our ongoing research highlights the critical role of MarR as a transcriptional regulator in KoSC. Further experiments are required to determine the signals that influence MarR’s repressive function. Identifying the environmental factors that trigger elevated TM production in vivo and, consequently, enhance pathogenicity will help to better understand diseases caused by KoSC.
MarR-dependent toxin gene regulation in the gut pathobiont Klebsiella oxytoca
Katrin Unterhauser, PhD1, André A. Grassmann, PhD2, Karim Rezaul, PhD1, Anthony Provatas, PhD3, Melissa J. Caimano, PhD2 , Adam Matson, MD, MSc1,4
1 Department of Pediatrics, University of Connecticut School of Medicine, 2 Department of Medicine, University of Connecticut School of Medicine, 3 Center for Environmental Sciences and Engineering, University of Connecticut, Storrs, CT, 4 Division of Neonatology, Connecticut Children’s Medical Center,
INTRODUCTION
RESULTS
4. Higher GFP expression as a gauge of TM production in ΔmarR
Gut bacteria belonging to the Klebsiella oxytoca species complex (KoSC) are the causative agent of AAHC (antibioticassociated hemorrhagic colitis) in adults and have been linked to the onset of NEC (necrotizing enterocolitis) in premature infants Most clinical isolates produce the cytotoxin tilimycin (TM), which induces apoptosis in cultured human cells consistent with intestinal damage occurring during disease We identified a MarR-like transcriptional factor being part of the two operons essential for TM production (aroX- and NRPS- operon). MarRs play a key role in regulating bacterial virulence genes Understanding how MarR regulates TM production will provide insights into the pathogenesis of NEC and AAHC.
METHODS
1. Comparable growth of K o AHC-6 WT and ΔmarR
K o AHC-6 WT and ΔmarR grown in LB medium + 2 5 g/L glucose
2. Elevated npsA- and aroX-transcription in ΔmarR compared to WT indicates MarR acts as repressor for both operons
K o AHC-6 plasmid based GFP reporter under the control of the npsA promoter (PnspA-GFP) was used to measure TM production/npsA-transcription
5. NpsB expression is higher in ΔmarR compared to WT
npsA and aroX transcripts were quantified via qRT-PCR and are normalized to 16S reference gene.
3. Increased TM leves and higher cytotoxicity of ΔmarR compared to WT
An NpsB antibody developed in-house was used to assess expression and GAPDH was employed as loading control (W= WT, M = ΔmarR)
CONCLUSIONS
A marR-deletion mutant (ΔmarR) was generated in Klebsiella oxytoca AHC-6 an AAHC patient isolate using a CRISPRCas9 system. In vitro toxin production was assessed by mass spectrometry, cytotoxicity assays using human enterocyte cell lines, and qRT-PCR to analyze transcription of toxin genes. In addition, a promoter-GFP fusion was used to determine TM production/transcription of toxin genes and NpsB expression was measured
Our ongoing research highlights the critical role of MarR as a transcriptional regulator in KoSC. The results suggest that MarR represses TM production by binding to the regulatory/intergenic region of the toxin genes Further experiments to prove MarR binding and determine the signals that influence its repressive function are needed Identifying the environmental factors that trigger elevated TM production in vivo and, consequently, enhance pathogenicity will help to better understand diseases caused by KoSC
Hartford, CT
Hep2 cells treated with supernatants of TM +/- strains
(TM)
Category: (Basic/Translational)
Elucidating the Role of PRDM14- CBFA2T2 Interaction in Maintenance of Pluripotency in Germ Cell Tumors
Presenting Author: Deana L. Wood, B.Sc.
Deana L. Wood, B.Sc.1 , Patrick Kwok-Shing Ng, Ph.D 1 , Joanna J. Gell, M.D. 1,2 , Ching C. Lau, M.D. Ph.D.1,2,3
1 The Jackson Laboratory for Genomic Medicine, Farmington, Connecticut
2 Connecticut Children’s Medical Center, Hartford, Connecticut
3 University of Connecticut School of Medicine, Farmington, Connecticut
BACKGROUND
Germ cell tumors (GCTs) primarily affect adolescents, posing challenges not only for treatment but also long-term chemotoxicity. Understanding mechanisms driving GCT tumorigenesis is imperative to developing targeted therapies that reduce toxicities for developing patients. Studies suggest that GCTs arise from primordial germ cells (PGCs) that fail to differentiate during embryonic development. Interestingly, several pluripotency genes that are normally repressed to allow differentiation have been demonstra ted to be expressed in GCTs. PRDM14 is one such gene, which interacts with CBFA2T2 to maintain pluripotency in stem cells and regulate differentiation of PGCs. Such interaction has not been demonstrated in GCTs. We hypothesize PRDM14 plays a key role in GCT development and survival by interacting with CBFA2T2.
METHODS
qPCR, Western blotting, and immunofluorescence were performed on a panel of GCT cell lines to assess expression of PRDM14, CBFA2T2, and other pluripotency markers. Co-immunoprecipitation of PRDM14 and CBFA2T2 was performed on GCT cell lines. We plan to investigate how the interaction of PRDM14 and CBFA2T2 affects cell viability, proliferation, and migration as well as transcriptomic regulation in GCTs using siRNA knockdown of PRDM14 and CBFA2T2, and expression of an inhibitory PRDM14-binding monobody.
RESULTS
Expression of PRDM14 and CBFA2T2 was found in GCT cell lines in conjunction with other pluripotency genes. PRDM14 and CBFA2T2 were colocalized in the nucleus of GCT cells, and show evidence of interaction that will be further confirmed with pull-down assays.
CONCLUSION/SIGNIFICANCE
Identifying and characterizing the PRDM14-CBFA2T2 interaction in GCT could provide a potential therapeutic target with specificity and reduced toxicity for adolescent patients.
Elucidating the Role of PRDM14-CBFA2T2 Interaction in Maintenance of Pluripotency in Germ Cell Tumors
Deana L. Wood, B.Sc.1, Patrick Kwok-Shing Ng, Ph.D. 1,3, Joanna J. Gell, M.D. 1,2,3, Ching C. Lau, M.D. Ph.D.
1 The Jackson Laboratory for Genomic Medicine, Farmington, Connecticut, 2 Connecticut Children’s Medical Center, Hartford, Connecticut, 3 University of Connecticut Health, Farmington, Connecticut
Introduction
Background:
▪ Germ cell tumors (GCTs) are one of the most common malignancies in males aged 15-39 years old.
▪ GCTs are highly curable but treatments may cause long-term side effects from chemotoxicity
▪ GCTs are thought to originate from primordial germ cells (PGCs) and share several pluripotency markers in common
▪ PRDM14, a transcription factor and key pluripotency regulator, has recently been shown to interact with CBFA2T2 in mouse embryonic stem cells and PGC-like cells
Questions:
• Do PRDM14 and CBFA2T2 interact in GCTs?
• Does this interaction have important implications for GCT growth, migration, or tumorigenicity?
• Is interrupting or preventing the interaction of PRDM14 and CBFA2T2 of therapeutic value?
Hypothesis :
PRDM14 and CBFA2T2 interact to safeguard pluripotency in GCTs, and obstructing their interaction may downregulate expression of pluripotency genes, thus making it a potential therapeutic target
Methods
Quantitative real-time PCR, Western Blot, nuclear fractionation, and immunofluorescence imaging were used to verify and determine mRNA and protein expression levels of pluripotency genes, PRDM14, and CBFA2T2 in GCT cell cultures
Interaction of PRDM14 and CBFA2T2 in GCT was investigated via co-immunoprecipitation experiments using GCT cell lysates
To disrupt interaction between PRDM14 and CBFA2T2 a competitively inhibiting PRDM14-binding monobody was used as shown in figure A PRDM14 and CBFA2T2-specific siRNAs were also used as shown in figure B
Results
1. PRDM14, CBFA2T2, and pluripotency genes are expressed in GCT cells.
(A) Heatmap of mRNA expression of pluripotency genes in a panel of GCT cell lines, as determined via qPCR.
(B) Western blot showing expression of PRDM14 and CBFA2T2 proteins in lysates from a panel of GCT cell lines
(C) Western blot showing nuclear localization of PRDM14 in NEC8 and NCCIT nuclear protein fractions (Cyto = cytoplasmic fraction, Nuc = nuclear fraction)
(D) Immunofluorescence imaging of NCCIT and NEC8 cells showing colocalized expression of PRDM14 and CBFA2T2
3. Transfecting GCT cells with a competitive PRDM14binding monobody leads to downregulation of pluripotency genes.
(A) Structure of Mb_S14, a PRDM14-binding monobody
(adapted from Nady, et al 2015)
(B) Western blot showing CBFA2T2 immunoprecipitated from PRDM14-incubated lysates of NEC8 cells transiently transfected with Mb V33R (missense mutated monobody, negative control) or Mb WT (wild-type monobody).
(C) Heatmap showing expression of pluripotency genes in NEC8 and NCCIT mRNA, 96 hours after transfection with Mb V33R or Mb WT
2. PRDM14 interacts with CBFA2T2 in GCT cells
Western blot showing CBFA2T2 coimmunoprecipitated from PRDM14incubated NEC8 and NCCIT cell lysates
4. siRNA knockdown of PRDM14 and CBFA2T2 leads to downregulation of pluripotency genes and may slow cell proliferation
(A) Knockdown efficiency of 3 siRNAs for CBFA2T2 (CB 1-3) in NEC8 and NCCIT mRNA 48 hours after transfection as determined by qPCR
(B) Knockdown efficiency of 3 different siRNAs for PRDM14 (PR 1-3)
(C) Heatmap showing expression of pluripotency genes in NEC8 and NCCIT cell mRNA 96 hours after transfection with PRDM14 or CBFA2T2 siRNAs
(D) Immunofluorescence imaging of NEC8 cells stained with Alexa Fluor 488 EdU to show proliferating cells (green)
Figures were created with BioRender
Category: (Clinical Research)
Researching COVID to Enhance Recovery (RECOVER) Study: Planning and Completion of In-Person Clinical Research Visits
Presenting Author: Emily Bean
Emily A. Bean, MPH1 , Carolyn J. Wolf, BA1, Katherine W. Herbst, MS1, Alex H. Hogan MD, MS1,2, Ian C. Michelow MD1,2, Juan C. Salazar MD, MPH, FAAP1,2, William T. Zempsky MD, MPH1,2
Affiliations:
1Connecticut Children’s Medical Center Research Institute
2University of Connecticut School of Medicine
BACKGROUND
The RECOVER Study, a national longitudinal study, aims to learn about the long-term health effects of COVID-19 with detailed analyses of clinical and biological data. The complexity of the research protocol required development of site-specific processes, which is the focus of this report.
METHODS
Weekly process development meetings were held which included the study’s investigators and support team members. With the assistance of Clinical Trials (CT) and Learning and Performance (LP) teams, specialists and/or classes were identified to fulfill training requirements for the research team. The protocol required collection of vitals by Research Associates/Assistants, which is not typically in the scope of the role. A specially designed EPIC research module was developed, and training of team members was undertaken with the assistance of Office for Sponsored Programs (OSP). We developed a scheduling process for in-person visits in collaboration with Infectious Diseases (ID).
RESULTS
Of 199 enrolled participants, 104 subjects were selected to attend in-person visits, of which 84 attended ≥ 1 visit, 10 participated remotely, 5 were not yet eligible for the 6-month follow-up visit, and 5 were lost to follow-up, as detailed in Figure 1. Sex and median age were: females 67%, median age 15, and 33% males, median age 14. Over the past 18 months, five Plan-Do-Study-Act cycles were conducted to optimize the in-person visit process.
CONCLUSIONS
We were able to develop successful processes with hospital-wide collaboration between the research team and CT, LP, OSP, ID and individual Connecticut Children’s specialists.
Figure 1. In‐Person Visit Completion
Researching COVID to Enhance Recovery (RECOVER) Study: Planning and Completion of In-Person Clinical Research Visits
A.
MPH
J.
INTRODUCTION
• The RECOVER Study, a national longitudinal study, aims to learn about the long-term health effects of COVID-19 with detailed analyses of clinical and biological data.
• The complexity of the research protocol required development of site-specific processes, which is the focus of this poster.
METHODS
• Weekly process development meetings were held with study’s investigators and support team members.
• With the assistance of Clinical Trials (CT) and Learning and Performance (LP) teams, specialists and/or classes were identified to fulfill training requirements for the research team.
• The protocol required collection of vital signs by Research Associates/Assistants, which is not typically in the scope of these roles.
• A specially designed EPIC research module was developed, and training of team members was undertaken with the assistance of Office for Sponsored Programs (OSP).
• We developed a scheduling process for in-person visits in collaboration with Infectious Diseases (ID).
• A detailed process for completing in-person visits was created by the research team, as shown in Figure 1.
RESULTS
• Of 199 enrolled participants, 106 subjects were randomly selected to attend in-person visits, per study protocol, of which 87 attended ≥ 1 visit, 16 participated remotely, and 3 were lost to follow-up, as detailed in Figure 2.
• Sex and median age were: females 67%, median age 15, and 33% males, median age 14.
• Over the past 18 months, five Plan-Do-Study-Act cycles were conducted to optimize the in-person visit process.
CONCLUSIONS
We were able to develop successful processes with hospital-wide collaboration between the research team and CT, LP, OSP, ID and individual Connecticut Children’s specialists.
ACKNOWLEDGEMENTS
Research reported in this publication was supported by the National Institutes of Health under award number OT2HL161847-01
Emily
Bean,
1 , Carolyn
Wolf, BA1, Katherine W. Herbst, MS1, Alex H. Hogan MD, MS1,2, Ian C. Michelow MD1,2 , Juan C. Salazar MD, MPH, FAAP1,2, William T. Zempsky MD, MPH1,2
Connecticut Children’s Medical Center Research Institute
University of Connecticut School of Medicine
Figure 2. ENROLLMENT FLOW CHART
Figure 1. IN-PERSON VISIT PROCESSES
Category: (Clinical Research)
Histrelin-associated hypertension in the treatment of central precocious puberty
1Connecticut Children's, Farmington, CT, United States
2University of Connecticut School of Medicine, Farmington, CT, United States
Objectives
Gonadotropin-releasing hormone agonists (GnRHa) are a safe and effective treatment for central precocious puberty (CPP). Histrelin is a GnRHa implant that reversibly suppresses the pituitary-gonadal axis. Transient hypertension (HTN) has rarely been described with GnRHa forms of triptorelin and leuprolide, but has not been described with histrelin. We present a novel case of a 5-year-old female with CPP and development of treatment-associated HTN with multiple forms of GnRHa, including histrelin.
Methods
Thelarche of infancy began at 14 months-of-age. Initial evaluation included Tanner 2 breasts and prepubertal gonadotropins. Following 24 months-of-age she had progressive breast growth and estrogenization of vaginal mucosa. Leuprolide stimulation confirmed CPP. She started treatment with triptorelin (Trip#1) at 26 months, and placement of histrelin (Hist#1) at 3 years with replacement (Hist#2) 1 year later.
Results
Within a week of Hist#2 placement, persistent HTN (manual blood pressure (BP) >95th percentile for age/sex/height) occurred, requiring multiple concurrent antihypertensives. Prior manual BPs were normal. Extensive nephrology/endocrinology evaluation was normal beyond non-specific low renin with normal aldosterone/potassium. Hist#2 implant was removed, without visual defects, and inpatient monitoring demonstrated resolution of hypertension. All antihypertensives were discontinued. Resumption of treatment with leuprolide 7.5mg monthly (Leup#1), lead to re-development of hypertension that persisted with subsequent course of triptorelin (Trip#2), despite previous tolerance.
Conclusions
GnRHa-associated hypertension has not been described with use of histrelin implant in treating CPP. Furthermore, it has not been described to re-occur in GnRHa preparations, despite prior tolerance. Histrelin-associated hypertension is important knowledge to disseminate for the care and monitoring of patients with CPP.
Histrelin-associated Hypertension in the Treatment of Central Precocious Puberty
1University of Connecticut, 2Connecticut Children’s
Medical Center Division of Pediatric Endocrinology
INTRODUCTION
RESULTS
• Gonadotropin-releasing hormone agonists (GnRHa) are a safe and effective treatment for central precocious puberty (CPP) 1
• Histrelin acetate is a GnRHa implant that reversibly suppresses the pituitarygonadal axis
• Transient hypertension (HTN) has rarely been described with GnRHa forms of triptorelin and leuprolide,2-8 but has not been described with histrelin 9
• The mechanism of this phenomenon is not well defined, but postulated to be related to vascular effects from a hypoestrogenized state 10
• The majority of this literature is in adults treated for prostate cancer 11 A recent retrospective longitudinal cohort study fails to show an association between GnRHa and HTN in CPP,12 but a number of case reports in pediatrics demonstrate development of HTN starting after GnRHa treatment that resolves after discontinuation 2-8
We present a novel case of a 5-year-old female with CPP and development of treatment-associated HTN with multiple forms of GnRHa, including histrelin.
CASE PRESENTATION
• 14 m o (months-of-age) – thelarche noted by primary pediatrician
• 18 m o - Initial endocrine evaluation with Tanner 2 breasts and prepubertal morning gonadotropins (peak LH 0 05 mIU/mL, FSH 6 88 mIU/mL, estradiol 8 pg/mL)
• After 24 m o
• Progressive breast growth, estrogenization of vaginal mucosa and uterine peripubertal morphology on US
• Leuprolide stimulation (peak LH 5 15 mIU/mL, estradiol 24h 69 pg/mL, Table 2) consistent with CPP vs delayed resolution of mini-puberty
• Significant progressive behavioral concerns
• Started triptorelin (Trip#1) at 26 months, and then placement of histrelin (Hist#1) at 3 years old with replacement (Hist#2) 1 year later
• Within a week of Hist#2 placement, she started having daily headaches, abdominal pain and persistent low renin HTN (manual blood pressure (BP) >95th percentile for age/sex/height)
• Prior BPs were normal (90s/50s) when well
• Extensive workup with no alternative source of HTN identified
• Hist#2 implant was removed, without visual abnormalities or defects
• HTN resolved
• All antihypertensives were able to be discontinued that admission
• Resumption of treatment with monthly leuprolide (Leup#1) led to recurrence of hypertension that persisted with final GnRH agonist, triptorelin (Trip#2), given at 4y7m despite previous tolerance and required 3 concurrent antihypertensives (amlodipine, hydralazine, clonidine) initially
• Weaned off antihypertensives by 5y3m (9 months after Trip#2)
• Remains on clonidine, guanfacine and risperidone for behavioral concerns (previously on ziprasidone, olanzapine – started at 3y11m)
• Gonadotropins and estradiol remain prepubertal off treatment
Figure 1
of Hist#2 removal Of note, documented manual BPs at pediatrician’s office were 90s/50s at 2y11m
Imaging:
• Bone Age xray – not advanced (performed at 2y4m, 3y11m, 4y9m; BA always within 6m of chronological age)
• MRI brain w/wo contrast – stable Rathke’s cleft cyst – stable in size, present on imaging prior to development of HTN
• Echo – normal, no evidence of LV hypertrophy
• Renal US w/ Doppler – normal
• MRI/MRA abdomen w/wo contrast - No evidence of renal artery stenosis, no adrenal mass, normal kidney morphology
• Normal
• Electrolytes
• Insulin-like growth factor 1
• Thyroid function
• 24hr urine cortisol/cortisone ratio
• Fractionated metanephrines, homovanillic acid
• Androgens
• Cosyntropin 250mcg cosyntropin stimulation test: normal
• Abnormal
• Low renin with normal aldosterone/potassium, normalized several months off GnRHa
• Mild elevation of VMA on random sample, repeat normal
• Elevated prolactin 73.5 ng/mL (on atypical antipsychotics)
• Genetic testing
• GeneDx, multi-gene slice: NEGATIVE, normal for the following gene list:
• GnRHa-associated hypertension has not been described with the use of histrelin implant in treating precocious puberty before.
• It has not been described to re-occur in GnRHa preparations, despite prior tolerance.
• Histrelin-associated hypertension is important knowledge to disseminate for the care and monitoring of patients with precocious puberty.
• Secondary HTN due to GnRH agonist, in our patient, took the form of low renin HTN, without evidence of endocrine related HTN (ie. aldosterone or similar biochemical source)
• Of note, given continued prepubertal gonadotropins off treatment, initial presentation is most consistent with resolution of mini-puberty of infancy.
REFERENCES
1. Carel JC, Eugster EA, Rogol A, Ghizzoni, L, Palmert MR, ESPE-LWPES GnRH Analogs Consensus Conference Group, et al. Consensus statement on the use of gonadotropin-releasing hormone analogs in children. Pediatrics 2009;123:e752–62.
2. Calcaterra, V, Mannarino S, Corana, G, Codazzi AC, Mazzola, A, Brambilla P, et al.. Hypertension during therapy with triptorelin in a girl with precocious puberty. Indian J Pediatr 2013;80:884–5.
3. Palma, L, Gaudino, R, Cavarzere, P, Antoniazzi, F. Does the risk of arterial hypertension increase in the course of triptorelin treatment? J Pediatr Endocrinol Metab 2020;33:449–52.
4. Sifaki, L, Cachat, F, Theintz G, Chehade H. Transient arterial hypertension induced by gonadotropin-releasing hormone agonist treatment for central precocious puberty. Front Pediatr 2019;7:74.
5. Siomou E, Kosmeri C, Pavlou M, Vlahos AP, Argyropoulou MI, Siamopoulou A. Arterial hypertension during treatment with triptorelin in a child with Williams-Beuren syndrome. Pediatr Nephrol. 2014;29:1633–6.
6. Klink D, Bokenkamp A, Dekker C, Rotteveel J. Arterial hypertension as a complication of Triptorelin treatment in adolescents with gender dysphoria. Endocrin Metab Int J. 2015;2:1–4.
9. Supprelin LA (histelin acetate) [package insert]. Chadds Ford, PA: Endo Pharmaceuticals Solutions Inc; 2011 10.Várbíró S, Nádasy GL, Monos E, Acs N, Vajo Z, Székács B. Sex hormone replacement therapy reverses decreased venous distensibility in pharmacologically ovarectomized rats. Menopause 2001;8:204-9. 11.Conteduca V, Di Lorenzo G, Tartarone A, Aieta M. The cardiovascular risk of gonadotropin releasing hormone agonists in men with prostate cancer: an unresolved controversy. Crit Rev Oncol Hematol 2013;86(1):42-51. 12.Fisch-Shvalb N, Alfandary-Harani H, Lazar L, et
Timeline with Overlaid Blood Pressures and Antihypertensive Medications Colored horizontal lines represent BP percentile for age/sex/height at 4 years old, the time of the development of initial HTN (see inlaid table) Black arrows correspond with GnRHa doses Orange arrow represents time
Table 1. Leuprolide Stimulation Test Results
Figure 2. MRI of Rathke’s Cleft Cyst
Table 2. Aldosterone, Renin, and Aldosterone/Plasma Renin (PRA) Ratios Over Time
Shooting for the STARS: Implementing an Evidence-based Program to Meet the End of Treatment Needs of Childhood Cancer Survivors and Their Families
Presenting Author: Mary Conway Keller
Mary Conway Keller, MSN, RN, CPHON®1, Lauren Ayr-Volta, PhD1, Elizabeth Marconi, MSW1, Andrew Needham, BSN, RN, CPN®, CPHON®1, Kelly Foy, MS, CCLS2, Leigh Hart, BSN, RN, CPON®1, Elizabeth Holden, BSN, RN, CPHON®1, Amirul Anuar, MS3, Karina Engelke, MSN, RN, APRN4, and Katherine A. Hinderer, PhD, RN, CNE, NEA-BC5,6
1Center for Cancer and Blood Disorders, Connecticut Children’s, Hartford, CT, USA
2Child and Family Support Services, Connecticut Children’s, Hartford, CT, USA
3Connecticut Children’s Research Institute, Hartford, CT, USA
4Division of Hematology/Oncology, Connecticut Children’s, Hartford, CT, USA
5Institute for Nursing Research and Evidence-Based Practice, Connecticut Children’s, Hartford, CT, USA
6Department of Pediatrics, UConn School of Medicine, Farmington, CT, USA
BACKGROUND
The end of treatment (EOT), a significant milestone along the childhood cancer treatment-survivorship continuum, is a time of significant vulnerability and stress for childhood cancer survivors (CCS) and their families. There is a need to provide standardized, comprehensive EOT services to navigate posttreatment medical, physical, and social-emotional issues. Limited research in this area has included the child’s perspective. This project aimed to evaluate the impact of a multidisciplinary, comprehensive EOT program on health-related quality of life (HRQOL) and distress in CCS and their families.
METHODS
A pretest-posttest repeated measures design was used. A convenience sample of CCS [child and adolescent/young adult (AYA)] and family participants were enrolled into a 2-session psychoeducational program, the Shooting for the STARS (Survivors Tackling All Roadblocks Successfully) EOT Transition Program. Program outcomes were measured before, during, and after program completion and included child and parent PROMIS® measures for HRQOL and the Distress Thermometer. Analysis of relationships and changes over time were conducted using Spearmanranked correlations and Friedman tests, p <.05 was the level of significance.
RESULTS
Forty-seven parents/caregivers and 29 CCS completed and evaluated the program. All reported program satisfaction; 94.7% felt somewhat or very prepared for EOT. Participants’ distress levels trended down over time (Table 1). Parent/caregiver-reported levels of CCS’ anxiety, fatigue, pain interference, and physical mobility significantly improved over time (Table 2).
CONCLUSIONS/SIGNIFICANCE
The results of this study suggest that a comprehensive multidisciplinary approach to survivorship transition positively impacted parents and CCS. Inclusion of children to survivorship studies is a critical approach for future research.
Table 1. Child, AYA, and Parent Distress Scores Before, During, and After EOT Intervention
Child AYA Parent
Note. AYA = adolescent/young adult.
Table 2. Child, AYA, and Parent PROMIS® Measures Scores Before, During, and After EOT Intervention
INTRODUCTION
End of Cancer Treatment (EOT):
Shooting for the Stars
“ S urvivors Tackling All R oadblocks S uccessfully” Implementing a Evidence -based Program to Meet the End of Treatment Needs of Childhood Cancer Survivors and Their Families
• A significant transition period for childhood cancer survivors (CCS) and families
• A time of heightened vulnerability, stress, and need for support
• Children feel unprepared for lingering symptoms, changing routines, social/school challenges
• AYAs fear relapse, social acceptance, what to expect medically/late effects
• Parents worry about their CCS’ physical & emotional struggles, how to navigate recovery phase, fear relapse
• 2015 Psychosocial Standards of Care call for formal standardized services for all CCS and parents/caregivers to provide psychoeducation, anticipatory guidance, and address psychosocial and mental health needs
AIM
To evaluate the impact of a multidisciplinary, comprehensive EOT program on health- related quality of life (HRQOL) and distress in CCS and their families
METHODS
Pre- test post - test repeated measures design
Convenience sample of CCS [Child and Adolescent/Young Adult (AYA)] and caregiver(s)
Enrolled in Shooting for the STARS (Survivors Tackling All Roadblocks Successfully) EOT Transition Program
METHODS: PROGRAM DEVELOPMENT AND IMPLEMENTATION
multidisciplinary psychoeducational program
• Two- Session Program
• Individualized, Family- centered, Developmentallyappropriate education and care
• Coordinated with CCS’ Primary Oncology Medical Team’s Follow- up Visits
• Clinic format incorporating multiple Health Care Professionals seeing CCS and family at each visit
• Launched May 2021 as New Standard of Care with participant accrual for outcomes and program evaluation 5/2021- 2/2023
• Outcomes assessed before (T1), after first session (T2), and after second session (T3)
METHODS: MEASURES
End of Treatment Questionnaires (EOTQ):
Outcomes related to the end of cancer treatment ( 37 to 38 items developmentally appropriate – for child, AYA, caregiver); includes demographics
Health- Related Quality of Life (PROMIS®): Measures health- related quality of life (HRQOL) symptoms and functioning in children with cancer –separate, parallel child and parent versions
National Comprehensive Cancer Network® Distress Thermometer:
One- item visual analog mental, physical, social, and/or spiritual distress experienced over the past week
• Assistance with transition process and community resources
• Distress® and PROMIS® measures’ responses addressed
• Anticipatory guidance for post - treatment medical and health care needs
• Present & review Individualized Treatment Summary, potential late effects, and corresponding prevention/health promotion practices
• Emotional assessment / interventions
• Neuropsychological Testing
Decreased Distress Over Time (T):
Mean for children: 2.2 (T1) 1.2 (T3)
• Mean for AYAs: 2.4 (T1) 1.8 (T3)
PROMIS® Measures Significant Results: CCS with Solid Tumor: Decreased Fatigue T2 to T3 (p= .02)
• Parent Proxy: CCS with Leukemia: Increased Physical Function Mobility T1 to T3 (p=.028)
• Parent Proxy: All CCS:
o Increased Physical Function Mobility T1 to T3 (p=.002)
o Decreased Fatigue T1 to T3 (p<.001)
o Decreased Anxiety T1 to T3 (p=.08)
o Decreased Pain Interference T1 to T3 (p=.053) EOTQ Results:
• 94.7% Prepared for EOT
• 100% Satisfied with Program
CONCLUSIONS
The program positively impacted family members’ satisfaction with and preparedness for ending treatment
• This may lead to improved coping and adjustment through the transition period and beyond
• Children, AYAs, and parents/caregivers were all engaged in the program with a very low attrition rate (9.5%)
• The multidisciplinary nature of this program was a valuable forum for identifying physical and emotional sequelae of treatment, and providing services to address these needs in real time.
SELECTED REFERENCES
cancer
and caregivers. Pediatric
& Cancer , 70(5), Article 30277. https://doi.org/10.1002/pbc.30277
• Children's Oncology Group. (2024). Long - term follow- up guidelines for survivors of childhood, adolescent, and young adult cancers (Version 6.0, October 2023). http://www.survivorshipguidelines.org/ Conway Keller M., Ruiz T., Needham A., King C., Hart L., Holden E., Lucas R. (2020). Development and content validation of end of treatment questionnaires for children with cancer. Journal of Pediatric Oncology Nursing, 37(2), 128–135. https://doi.org/10.1177/1043454219878392
• Karst J. S., Hoag J. A., Chan S. F., Schmidt D. J., Anderson L. J., Engelbert N. E., Igler E. C., Bingen K. M. (2018). Assessment of end- of - treatment transition needs for pediatric cancer and hematopoietic stem cell transplant patients and their families. Pediatric Blood & Cancer , 65(8), Article e27109. https://doi.org/10.1002/pbc.27109
CONTACT
CONTACT: Mary Conway Keller mkeller@connecticutchildrens.org
READ OUR PAPERS
Visit 2: Nursing, Psychology
Category: Clinical Research
Lung
Ultrasound Score and Left Ventricular Eccentricity Index in Preterm Infants with Respiratory Failure
Presenting Author: Jacob Kelner DO
Jacob Kelner DO1, Naveed Hussain MBBS1, Henry Chicaiza MD2, and Shalin Parekh MD3
1Division of Neonatology, Connecticut Children’s, Hartford, CT
2Division of Pediatric Emergency Medicine, Connecticut Children’s, Hartford, CT
3Division of Cardiology, Connecticut Children’s, Hartford, CT
BACKGROUND
Left ventricular eccentricity index at end-diastole (LVEI-d) obtained during neonatal cardiac point-of-care ultrasound (cPOCUS) provides an incomplete but simple marker of right ventricular (RV) volume overload. Lung disease in neonates is worsened by fluid overload and the severity of respiratory disease can be quantified by lung ultrasound score (LUS). This study investigates the correlation between LVEI-d and LUS during the first 72 hours of life (HOL) in infants with respiratory failure.
METHODS
This is a prospective, single-center, observational study performed at a level 4 academic NICU. Preterm infants < 72 HOL requiring non-invasive positive pressure ventilation were eligible for enrollment. cPOCUS and LUS were performed daily over the first 72 HOL. Perinatal history, demographic data, and respiratory support were recorded in real-time and via chart review.
RESULTS
Twenty-eight ultrasounds performed on 14 infants were included. Infants had a median GA of 34.5 weeks, a median BW of 2.28 kg, and 57% were male. Over the first 3 HOL, LVEI-d and LUS had a strong positive correlation on linear regression analysis (n=6; R = 0.89, p = 0.017). Statistically significant positive correlation persisted through 6 HOL (n=9; R = 0.68, p = 0.044), but was not seen through 24 (n=16; R = 0.40, p = 0.125) or 72 HOL (n=28; R = 0.37, p = 0.053).
CONCLUSION/SIGNIFICANCE
LVEI-d is highly correlated with LUS in the first few HOL, supporting its use as an adjunct tool to assess total body fluid status and its effect on neonatal respiratory failure.
Lung Ultrasound Score and Left Ventricular Eccentricity
Index in Preterm Infants with Respiratory Failure
Kelner, J.1,2, Hussain, N. 1,2 , Chicaiza , H. 1,2, Parekh, S. 1,2
1 Connecticut Children’s, Hartford, CT 2 University of Connecticut School of Medicine, Farmington, CT
Respiratory Distress Syndrome (RDS) due to surfactant deficiency in newborn infants is associated with atelectasis, inflammation, and subsequent lung fluid retention 1
Semi-quantitative lung ultrasound scores (LUS) obtained during lung point -of-care ultrasound (POCUS) can diagnose the severity of lung disease in premature infants. 2
The left ventricular eccentricity index at the end of the systole (LVEI-s) and end of the diastole (LVEI-d) obtained during cardiac POCUS correlate with pulmonary hypertension and right ventricular volume overload, respectively (Figure 1). 3,4
The association between lung ultrasound score (LUS) and left ventricular eccentricity index at end -systole (LVEIs) and end -diastole (LVEId ) has never been investigated and is the primary objective of this study.
METHODS BACKGROUND
RESULTS
A total of 30 ultrasounds performed on 16 infants were included.
The median completed GA was 34.5 weeks (IQR 33 -35) with an average birth weight of 2.28kg (IQR 2.03 -2.45). 9 infants (56%) were male, and 10 infants (62.5%) were white.
At the time of ultrasound, the median CPAP level was 6 cmH2O (IQR 6 -6) with a median OSI of 1.30 (IQR 1.26-1.56).
CONCLUSION
This is a prospective, single -center, pilot study performed at a level 4 academic NICU during a 6 -month recruitment process from May 2024 to October 2024.
Inclusion Criteria:
- Born <37 weeks gestational age (GA)
- Diagnosed with respiratory failure secondary to RDS
Bedside ultrasound to obtain the primary outcomes of LUS, LVEI-d, and LVEI-s (Figure 1) was performed before 72 hours of life and repeated on subsequent chronological days for the first 72 hours of life.
Linear regression models and correlation analyses were employed to evaluate the relationship between LUS and LVEI-d, LVEI -s, and OSI.
The median LUS was 7 (IQR 6-9), the median LVEI -d was 1.10 (IQR 1.05-1.13), and the median LVEI -s was 1.12 (IQR 1.07-1.22).
LVEI-d was positively correlated with LUS with a Pearson correlation coefficient of r = 0.61 (p=<0.01) . This correlation strengthened to r = 0.63 (p=<0.01) over the first 24 hours of life, and r = 0.81 (p=<0.01) over the first 6 hours.
LVEI-s was positively correlated with LUS with a Pearson correlation coefficient of r = 0.57 (p=<0.01) This correlation strengthened to r = 0.75 (p=<0.01) over the first 24 hours of life, and r = 0.96 (p=<0.01) over the first 6 hours.
Statistically significant differences were found between mild and severe disease based on LUS for LVEI -s, and between mild and moderate and mild and severe disease for LVEI -d (Figure 2).
Neither LVEI -d and LVEI -s were correlated with time.
This study provides preliminary evidence for using LVEI during neonatal cardiac POCUS to help guide the diagnosis of RDS severity.
REFERENCES
1. Hallman M, Glumoff V, Ramet M. Surfactant in respiratory distress syndrome and lung injury. Comparative biochemistry and physiology Part A, Molecular & integrative physiology 2001, 129: 287294.
2 Kelner J, Moote D, Shah R, Anuar A, Golioto A. Lung Ultrasound Score for Prediction of Surfactant Administration in Preterm Infants with Respiratory Failure. J Perinatol 2024, 44: 1258 -1263.
3. McCrary AW, Malowitz JR, Hornick CP, Hill KD, Cotten CM, Tatum GH , et al. Differences in Eccentricity Index and Systolic -Diastolic Ratio in Extremely Low-Birth -Weight Infants with Bronchopulmonary Dysplasia at Risk of Pulmonary Hypertension. Am J Perinatol 2016, 33: 57-62.
4. Soliman RM, Elsayed Y, Said RN, Abdulbaqi AM, Hashem RH, Aly H. Prediction of extubation readiness using lung ultrasound in preterm infants. Pediatr Pulmonol 2021, 56: 2073 -2080.
ACKNOWLEDGEMENTS
We would like to thank the University of Connecticut/Connecticut Children’s for supporting this research, the families for agreeing to participate in the study, and the bedside nursing staff that helped to take care of the enrolled infants.
Category: (Clinical Research)
Revision and Adaptation of a Pediatric-to-Adult Care Transition Toolkit for X-Linked Hypophosphatemia.
Presenting author: Carolyn M. Macica, PhD
AMBER PARSON, BA1 and Carolyn Macica, PhD1,2
1Quinnipiac University Frank H. Netter MD School of Medicine, North Haven, CT
2Connecticut Children’s Research Institute, Hartford, CT
BACKGROUND
X-linked hypophosphatemia (XLH) is a rare, progressive genetic phosphate-wasting disorder that has distinctive clinical features in children and adults. Without an evidence-based healthcare transition, patients are susceptible to increased disease activity and adverse outcomes which can reduce gains of prior care. Structured transition programs, such as the Got Transition model and Six Core Elements of Health Care Transition (HCT), are crucial for preparing patients for shifts in care. To meet the specific needs of transition care, we aim to revise the existing XLH toolkit to incorporate results from a gap-analysis between the toolkit, Six Core Elements of HCT, and 2023 XLH Transition of Care Advisory Board recommendations. We plan to create a companion website allowing patients, family members, and clinicians to access the toolkit via an interactive mobile website platform.
METHODS
Toolkit adaptation will include a comprehensive evaluation of the Six Core Elements of HCT and consultations with XLH patients and providers. A prototype website will be created using an institutional license for Microsoft Visual Studio. Post-development, the website will undergo beta-testing with a select group of stakeholders to evaluate usability, content, and accessibility.
RESULTS
To date, we have completed: 1) website content development and iterative review based on expert consultation and a gap analysis of the existing toolkit compared to the Got Transition model of HCT, 2) development and creation of a functioning website prototype 3) creation of survey items and interview prompts for website betatesting. Next steps include beta-testing by patients and clinicians who contributed to the initial development of the XLH Transitions Toolkit.
SIGNIFICANCE
The XLH Transitions Toolkit will be more engaging and effective for young individuals with XLH, better aligned with recommended HCT guidelines, and reduce adverse outcomes associated with ineffective HCTs.
Revision and Adaptation of a Pediatric-to-Adult Care Transition Toolkit for X -Linked Hypophosphatemia (XLH)
Amber Parson, BA1, and Carolyn M. Macica, PhD1,2
1Frank H. Netter MD School of Medicine at Quinnipiac University, North Haven, CT
2Connecticut Children’s Research Institute, Hartford, CT
Overview
A gap analysis was performed to compare the original XLH Transition Toolkit with the nationally recommended guidelines from the Got Transition® model for pediatric-to-adult health care transition (HCT) and the 2023 recommendations from the XLH Transition of Care Advisory Board1,2 Based on this analysis, revisions were made, which informed the adaptation of the toolkit into an interactive website for patients, family members, and clinicians, ensuring alignment with the latest guidelines.
Background
XLH is a rare, progressive genetic disorder characterized by phosphate-wasting, with both common and distinct clinical features in children and adults.3-7
• As individuals with XLH age, their evolving health needs underscore the importance of a structured, evidence-based transition from pediatric to adult care.
• Without a formalized transition process, those with chronic conditions like XLH are at a higher risk of adverse outcomes.1,8
• Notably, the transition is complicated by the difficulty in finding adult healthcare providers with expertise in managing this rare condition.
Methods
Aim 1: To perform a gap analysis resulting alignment of an XLH transition toolkit with current practices.
Aim 2: To incorporate revisions into an interactive, mobile website prototype.
Aim 3: To conduct a beta test of the website with a cohort of XLH patients and practitioners to evaluate usability, content, and accessibility.
Results
Gap Analysis Findings
Identified Gap in Original Toolkit Got Transition® Resources For Gap Implementation Into Website Prototype
Emphasis on Collaboration and Team Effort
Interdisciplinary Care
Enhanced information on coordination among multiple clinicians, including pediatric specialists, adult healthcare providers, and other stakeholders in terms of interdisciplinary care
Shared Management Approach
Addition of Shared Management Approach which helps shift self-care responsibilities gradually from parent/caregiver to a young patient
Transition Care as a Process
Stages of HCT
Transition Planning
Customized Support Health Literacy for Transition Readiness
Assessment of Transition Readiness
Accounting for Barriers to Transition and Impact of Sociocultural Contexts
Advocating for Effective Care Transitions
Implementation of Six Core Elements of HCT™
Enhanced descriptions of transition care as a continuous process with stages of planning, transfer, and integration into adult care
Addition of comprehensive checklist designed for use at different age stages for XLH and transition care milestones
Addition of information on comparison of child vs adult focused care models and XLH specific symptoms in children and adults
Addition of an interactive chat-based tool that includes a transition readiness quiz and customized resources
Addition of information on how patient/family, provider, and systems factors can create barriers. Also, addition of how sociocultural preferences may impact transition care.
Addition of a formalized framework for approaching advocacy in transition care for XLH patients that can be used for providers in addition to patients and parents/caregivers
Results
Toolkit Enhancements
● More specific description of differences in symptoms of XLH for children and adults and how this affects each patient’s unique HCT process
● A mobile format with options for continual engagement with HCT across time for youth (e.g., email notification reminders highlighting site features)
● Increased emphasis on how to advocate for effective HCTs using a specific framework (i.e., Six Core Elements of HCT™)
● Interactive features to improve engagement (e.g., Knowledge Checks, Transition Chat, digital HCT planning checklist)
● Exposure to a variety of additional transition care related topics (e.g. Shared Management Approach, Stages of HCT, HCT barriers)
Discussion and Conclusions: A revised toolkit and prototype website were completed using Microsoft Visual Studio The next phase is to work with a professional web developer to transform the current web page content into a web application framework that provides enhanced layout flexibility and improved usability across Mac and PC platforms, as well as various devices, including desktop and mobile devices The revised website will have a user-centered readable design and menu structure with a clear and simple layout, incorporating breadcrumbs and search functionality We will then beta test with content experts and patients
After adaptation, the XLH Transition Toolkit will be more engaging and effective for young individuals with XLH, their families, and healthcare providers. The toolkit will also be better aligned with nationally recommended HCT guidelines to reduce adverse outcomes, maintain gains made during the pediatric years, and to facilitate transition.
References
Website Content Structure
Association of Busulfan Exposure and Outcomes after Hematopoietic Cell Transplantation for Pediatric Patients with Inborn Errors of Immunity
Presenting Author: Layne Oram Layne Oram1, Susan Prockop, MD2
1 University of Connecticut School of Medicine, Farmington, CT
2 Cancer and Blood Disorders Center, Dana-Farber/Boston Children’s Hospital, Boston, MA
BACKGROUND
Hematopoietic cell transplantation (HCT) is the only curative therapy for patients with inborn errors of immunity (IEI), most often utilizing a busulfan-based chemotherapeutic conditioning regimen Busulfan overexposure is associated with toxicity and mortality, while underexposure is associated with graft failure. However, dosing practices vary by institution due to limited data on optimal exposure. This study aims to determine optimal busulfan exposure associated with the highest event-free survival (EFS) in IEI patients undergoing HCT.
METHODS
This study included patients from 17 international transplant centers, including Boston Children’s Hospital (BCH), who underwent allogeneic HCT using busulfan-based conditioning between 2000-2023. Primary outcome was EFS (engrafted survival). Secondary outcomes included graft failure, transplant-related mortality, acute toxicities, and overall survival. Busulfan exposure was calculated by individual centers (AUCCENTER) and re-estimated using an externally validated model (AUCNONMEM). Weibull survival functions and Fine-Gray risk regression evaluated AUCNONMEM in relation to EFS.
RESULTS
Overall, 562 patients were included, with 71 from BCH. Median busulfan AUCNONMEM was 69.0 mg×h/L and correlated poorly with AUCCENTER (r2=0.51). Notably, correlation was superior at BCH (r2=0.78). Optimal AUCNONMEM was 80 mg×h/L, corresponding to a 2-year EFS of 87.9%, superior to <70 mg×h/L (EFS 77.6%, p=0.02) and >90 mg×h/L (EFS 52.1%, p<0.0001).
Exposures <70 mg×h/L correlated with graft failure while exposures >90 mg×h/L correlated with mortality and toxicity. Donor chimerism increased with higher AUCNONMEM.
CONCLUSION/SIGNIFICANCE
In patients with IEI, targeting a cumulative busulfan AUCNONMEM of 80 mg×h/L may lead to improved EFS and donor chimerism Our study stresses the importance of uniformly using a validated population PK-model to estimate AUCNONMEM.
Pediatric Patients with Inborn Errors of Immunity: Informing Center Specific Practice from A Multi-center Retrospective Study
Layne
Oram1, Susan Prockop MD2
1University of Connecticut School of Medicine, 2Cancer and Blood Disorders Center, Dana-Farber Cancer Center/Boston Children’s Hospital
Introduction
• Inborn errors of immunity (IEI) are inherited disorders leading to deficiency or dysfunction in ≥1 component of the immune system.
• Hematopoietic stem cell transplant (HCT) is the only curative treatment. Most conditioning regimens for HCT include busulfan, one of few chemotherapies used where plasma levels can be monitored in real time and adjusted to achieve desired exposure.
• Prior work has demonstrated that busulfan exposure & the method used to measure it are critical. However, there is no clear consensus on optimal busulfan dosing in patients transplanted for IEI.
• 2016 Bartelink et al: Busulfan area under the curve (AUC) of 78-101 mg×h/L associated with the highest event-free survival (EFS) in patients with malignant & non-malignant conditions. Insufficient number of patients with IEI to extend this conclusion to that population.
• Boston Children’s Hospital (BCH) participated in a multicenter analysis of patients with IEI who underwent allogeneic HCT between 2000-2023 at 17 international centers (USA, Netherlands, Canada, Switzerland, UK, Italy, Germany, Australia).
• Center-collected raw busulfan data was reanalyzed centrally with validated population-PK model, assessing center versus centrally estimated exposure. Centrally estimated exposure was evaluated for associations with outcomes of interest. Analysis recently published (Bognar et al; Blood Adv 2024 Oct 8;8(19):5137-5145).
Objective
Assess our center specific practices in the context of participation in larger multicenter retrospective analysis.
Methods
• Primary outcome: EFS (graft failure, disease recurrence, or death).
• Center-Specific 2015-2023 data added to prior 2000-2014 dataset.
• Busulfan exposure calculated by centers (AUCCENTER) and re-estimated using a validated model (AUCNONMEM). Weibull survival functions & FineGray risk regression used to evaluate AUCNONMEM in relation to EFS.
Graft-source 64 (90%) bone marrow, 6 (9%) peripheral blood stem cells, 1 (1%) bone marrow + cord blood
Conclusions
• The numbers of patients transplanted at any one center is too small to perform this type of analysis, underscoring the importance of this type of collaboration in rare diseases
• In patients with IEI, improved EFS and higher donor chimerism may be achieved by targeting a busulfan AUC of 80 mg×h/L (range 70-90).
• The data stress the importance of uniformly using a validated population PK-model to estimate the busulfan cumulative exposure.
Future Directions
• The BCH pharmacy group is performing side-by-side validation of the InsightRx system using the population-PK model.
• For BCH patients, we will consistently target a busulfan AUC of 70-80 mg×h/L.
• We are evaluating associations between serotherapy exposure and outcomes of interest (overall survival, graft-failure, TRM, acute toxicity (lung, liver, GVHD), and immunoglobulin dependence)
References
1. Bartelink IH, Lalmohamed A, van Reij EML, et al. Association of busulfan exposure with survival and toxicity after haemopoietic cell transplantation in children and young adults: a multicentre, retrospective cohort analysis. The Lancet Haematology. 2016;3(11):e526-e536. doi:https://doi.org/10.1016/s2352-3026(16)30114-4
2. Bartelink IH, Boelens JJ, Bredius RGM, et al. Body Weight-Dependent Pharmacokinetics of Busulfan in Paediatric Haematopoietic Stem Cell Transplantation Patients. Clinical Pharmacokinetics. 2012;51(5):331345. doi:https://doi.org/10.2165/11598180-000000000-00000
3. Bognàr et al. Association of Busulfan Exposure and Outcomes after HCT for Patients with an Inborn Error of Immunity. Blood Advances. 2024, ISSN 2473-9529, https://doi.org/10.1182/bloodadvances.2024013275.
Figure 2. Event-free survival in patients with SCID, HLH, and neutrophil disorders.
Figure 1. Busulfan exposure calculated by centers (AUCCENTER) versus validated PK model (AUCNONMEM); transplant centers denoted by color.
BCH: dark blue
Figure 3. Donor chimerism and transplant-related mortality stratified for AUC subgroups
Discrepancies Between Electronic Health Record and Patient Self-Report Race/Ethnicity: Implications for Pediatric Clinical Research
Presenting Author: Cameron King, MA
Cameron King, MA1, Mollie Fleming, MS2, Stephanie Perez, MS2,3 , Michael Bobylov4*; Amogh Chittajallu4*; Mallory A. Perry-Eaddy, PhD, RN2,3,5
1. Research Operations, Connecticut Children’s
2. School of Nursing, University of Connecticut
3. Pediatric Intensive Care Unit, Connecticut Children’s
4. Dept. of Molecular and Cellular Biology, College of Liberal Arts and Sciences, University of Connecticut
5. Dept. of Pediatrics, School of Medicine, University of Connecticut
* Pre-Medicine, Honors Undergraduate Students
Corresponding Author: Mallory A. Perry-Eaddy, mallory.perry@uconn.edu
Background: Accurate documentation of race/ethnicity in electronic health records (EHR) is crucial to identify and address health disparities. However, discrepancies between race/ethnicity recorded in EHRs and patient self-report have raised concerns about the reliability of these data. Such inconsistencies can impact the quality of healthcare delivery and the validity of clinical research.
Methods: Using the Persist-PICU observational study (R00GM145411) as an exemplar, we assessed discrepancies between race/ethnicity as reported in EHR compared to self-report via parent and need for interpreter services.
Results: Most parents, 96% (73/76), provided self-report of their child’s race/ethnicity. Race/ethnicity was discrepant in 16% (12/73; race) and 8% (6/73; ethnicity) of children. White race was self-reported in 43 children with no EHR discrepancies. However, self-report of non-White children versus EHR identified race was often discrepant: Black (11 self-report v. 10 EHR), Asian (2 self-report v. 1 EHR), two or more races (9 self-report v. 6 EHR), Other (8 self-report v. 12 EHR), 3 declined to answer. A third, 32% (23/73), self-reported Hispanic ethnicity, while the EHR identified 26% (19/73) of children as Hispanic Of 3 families designated as needing an interpreter, only 1 required the service.
Conclusion/Implications: One in four children (25%, 18/73) had discrepant race/ethnicity in their EHR. Selfreport of race/ethnicity, and primary language, should be the gold standard. Discrepant race was solely reported in children who identify as non-White. Self-report of non-White race/ethnicity was underreported in the EHR, with the exception of “Other” which is overreported. Discrepancies can lead to bias and assumptions, undermining the validity of clinical research.
Discrepancies Between Electronic Health Record and Patient SelfReport of Race/Ethnicity: Implications for Pediatric Clinical Research
INTRODUCTION
• Discrepancies in race and ethnicity date within electronic health records (EHR) can significantly impact patient care and contribute to existing health disparities
• Previous pediatric outpatient research has demonstrated that race/ethnicity are often inaccurately recorded in the EHR, with minorities experiencing the highest misclassification rates (Samalik et al., 2022)
METHODS
RESULTS: Ethnicity
• Setting: CT Children’s Pediatric Intensive Care Unit (PICU)
• Secondary analysis of the the Persist-PICU observational study (R00GM145411); N=73 critically ill children enrolled
• Self-report data was obtained by our research assistant during the study consent process
• Discrepancies between race/ethnicity recorded in EHRs and patient self-report have raised concerns about the reliability of these data. Such inconsistencies can impact the quality of healthcare delivery, the validity of clinical research and public trust
• Patient self-report of race/ethnicity is the “gold standard” however, policies regarding entry of socioeconomic data varies between those entering data
THEORETICAL FRAMEWORK
• Race: social construct, perpetuate beliefs, inequity
• “Interchangeable use of these terms in health research can lead to inaccuracy, imprecision and confusion.”
• EHR-identified race/ethnicity were abstracted by two students who were blinded to patient/parent self-report
• We assessed discordance between race/ethnicity as reported in enrolled Persist-PICU children from the CT Children’s EHR compared to parent self-report
Screened: 740
RESULTS: Race
• Race was discrepant in 16% (12/73) of children. There were no discrepancies in report of White race
• Non-White children’s Race was often discrepant. Asian, Black or 2+ races were underreported in the EHR vs. self-report (Asian: 1 vs. 2; Black: 10 vs. 11; Two or more races (6 vs. 9)
CONCLUSION/IMPLICATIONS
• Overall, 1 in 4 children (18/73) had discrepant race/ethnicity entered within in their EHR
• Discrepant race was only reported in non-White children
• Self-report of non-white race/ethnicity was underreported in the EHR except “other” which is overreported
• Discrepancies in race/ethnicity can lead to bias and assumptions, undermining the validity of clinical research
FUNDING ACKNOWLEDGEMENT
NIH/National Institute of General Medical Sciences R00GM145411 (PI: Perry-Eaddy; 2022 - 2025)
• Other race was often overreported in the EHR (12 vs. 9)
Jing Marrero, MD, MPH1, Emanuela Pinci, BS1, Jeffrey S. Hyams, MD1, Michael Brimacombe, PhD1, Fabiola Balarezo, MD1,2
1 Connecticut Children’s Medical Center
2 Hartford Hospital Department of Anatomy – Clinical Pathology
BACKGROUND
Eosinophilic esophagitis (EoE) is a chronic inflammatory disease diagnosed by ≥15eos/hpf on esophageal biopsy. The EoE histologic scoring system (EoEHSS) is a validated index accounting for the severity (grade) and extent (stage) of eight EoE features. Dupilumab, an anti – IL-4receptor antagonist, is the first medication approved for EoE and is effective in reducing EoEHSS scores in clinical trials. We sought to evaluate the efficacy of dupilumab in improving histologic manifestations in a real-world cohort of patients at our center.
METHODS
Patients with EoE who failed dietary, acid suppression, or corticosteroid treatments and were started on dupilumab were enrolled starting December 2023. Patients underwent baseline and repeat endoscopy after receiving 12 weeks of subcutaneous dupilumab. All pre- and post-dupilumab biopsies were reviewed by a single pathologist (FB) and scored using EoEHSS. Grade and stage scores for each feature ranged from 0 (normal) to 3 (maximum change) with total scores divided by possible maximum, resulting in final scores ranging from 0 to 1.
RESULTS
Ten patients (mean age 16.5years, 70% male) received dupilumab. The median EoEHSS grade improved from 0.5 to 0.08 (p<0.001) and median stage improved from 0.46 to 0.07 (p<0.001). All patients had improvement in their peak eosinophilic count (PEC) with 90% having ≥50% decrease in eos/hpf and 70% having PEC <15eos/hpf. 30% of patients had no eosinophils in their post-dupilumab biopsies.
CONCLUSION/SIGNIFICANCE
In our real-world cohort of 10 patients on dupilumab, all had significant improvement in their EoEHSS. This medication is effective in improving the severity and extent of mucosal inflammation.
Dupilumab improves histologic manifestations of eosinophilic esophagitis in a real world cohort of pediatric patients
Jing Marrero, MD, MPH1,2; Emanuela Pinci, BS2; Michael Brimacombe, PhD1,2 ; Fabiola Balarezo3; Jeffrey S. Hyams1,2
1University of Connecticut School of Medicine, 2Connecticut Children’s, 3Hartford Hospital
BACKGROUND
Eosinophilic esophagitis (EoE) is a chronic inflammatory disease diagnosed by the presence of ≥15 eos/hpf on esophageal biopsy.
The EoE histologic scoring system (EoEHSS) is a validated index, accounting for peak eosinophil count (PEC) and seven additional features characteristic of EoE (Dis Esophagus. 2017;20:1-8). This comprehensive scoring system accounts for both the severity (grade) and extent (stage) of these abnormalities.
Dupilumab, an anti – IL-4receptor antagonist, is the first medication approved for the treatment of EoE and is effective in reducing EoEHSS scores in clinical trials.
AIM
To evaluate the efficacy of dupilumab in improving histologic manifestations in a real-world cohort of pediatric patients at our center.
METHODS
Patients with EoE who failed previous dietary, acid suppression, or corticosteroid treatments and were being started on dupilumab were enrolled starting December 2023.
Patients had a baseline endoscopy and after receiving 12 weeks of weekly subcutaneous dupilumab, underwent repeat endoscopy to evaluate response.
All pre- and post-dupilumab esophageal biopsies were reviewed by a single pathologist (FB) and scored using EoEHSS. Grade and stage scores for each feature ranged from 0 (normal) to 3 (maximum change) with total scores divided by possible maximum, resulting in final scores ranging from 0 to 1.
RESULTS
CONCLUSIONS
In our real-world cohort of 10 pediatric patients on dupilumab, all had significant improvement in their EoEHSS following a 12 week course.
This medication is effective in improving the severity and extent of mucosal inflammation.
REFERENCES
Collins MH, Martin LJ, Alexander ES et al. Newly developed and validated eosinophilic esophagitis histology scoring system and evidence that it outperforms peak eosinophil count for disease diagnosis and monitoring. Dis Esophagus. 2017;20:1-8. doi:10.1111/dote.12470.
Category: (Clinical Research)
Age and Sex Differences in ACL-RSI Subscale Scores of Emotion, Risk-Appraisal, and Confidence after ACL Reconstruction
Presenting Author: Dylan P. Roman, DPT Dylan P. Roman, DPT1, Sophia Ulman, PhD2,3, Lauren Butler, DPT4,5, Cody Walker, ATC6, Taylor Douthit, DPT3,7, Christopher Kuenze, PhD, ATC8, ARROW9, Shelby Baez, PhD, ATC10
1. Connecticut Children’s, CT, USA
2. Scottish Rite for Children, TX, USA
3. University of Texas Southwestern Medical Center, TX, USA
10. University of North Carolina at Chapel Hill, NC, USA
BACKGROUND
Psychosocial readiness to return to sport (PR-RTS) after anterior cruciate ligament reconstruction (ACLR) is related to re-injury risk in adults. The ACL-Return to Sports after Injury (ACL-RSI) tool measures PR-RTS with 3 subscales (Emotions, Confidence, and Risk-Appraisal). Unfortunately, current practice guidelines use adult-based ACL-RSI thresholds for RTS clearance. The purpose of this study was to explore ACL-RSI scores from a multi-site clinical outcomes registry. The aim of the study was to identify any sex- and/or age-related differences in PR-RTS.
METHODS
This retrospective study included registry data from 14-30 year-olds that were 6-12 months after primary, unilateral ACLR. ACL-RSI scores and subscales were explored according to biological sex (female, male) and age (adolescent 14-18 years, adult 19-30 years). Sex differences, age differences, and differences by combined sex and age (e.g., adolescent males) were explored with independent samples ttests. Significance was p<0.05.
RESULTS
The sample included 154 participants (20.2 ± 3.8 years; 54.2% female; 8.7 ± 2.1 months from surgery). Male adolescents held the highest ACL-RSI total scores (Table 1). As compared to male adults, male adolescents held higher total confidence scores (mean difference: 16.1 points, p = 0.005). Age-specific sex differences were found in adolescents only, as males reported significantly greater confidence in performance than females (mean difference: 11.56 points, p = 0.019).
CONCLUSION/SIGNIFICANCE
ACL-RSI scores differ by age and sex, suggesting that adult-based norms are not appropriate for adolescents. Future work should strive to create age- and sex-specific ACL-RSI subscale cutoff scores for successful RTS after ACLR in adolescent athletes.
Figure 1. Age group differences by sex for ACL-RSI subscale and total scores. Note: Statistically significant sex differences are noted with an asterisk (*).
Table 1. Group comparisons in ACL-RSI subscale scores and total score.
Items
Note: Scores are presented as mean ± standard deviation. Significant age group differences found within each sex are noted in bold. Significant sex differences found within each age group are noted with a superscript M in the female column to indicate a difference from males.
Age and Sex Differences in ACL-RSI Subscale Scores of Emotion, Risk Appraisal,
and Confidence after ACL Reconstruction
Dylan P. Roman, DPT, Sophia Ulman, PhD, Lauren Butler, DPT, Cody Walker, ATC, Taylor Douthit, DPT, Christopher Kuenze,
INTRODUCTION
Psychological Response to ACL Reconstruction
• Commonly assessed by the ACL-RSI scale
• Associated with failure to return to sport ACL-RSI Subscales are Underreported
• The ACL-RSI has three subscale domains:
• Emotion
• Risk appraisal
• Confidence
• Subscales are rarely considered when assessing readiness to Return to Sport (RTS)
• Appropriate risk appraisal, emotional regulation, and confidence levels all change throughout development and through adulthood
Limitations in the ACL-RSI for Return to Sport
• Score >76.7 used as criteria for clearance
• Current guidelines derived from adult studies
PURPOSE
• To investigate differences in ACL-RSI subscale scores by age and sex Hypothesis
• Males and teens patients would report higher scores on ACL-RSI subscales compared to females and adult patients
METHODS
Study Design
• Multi-site clinical outcomes registry
Inclusion and Exclusion Criteria
• 6-12 months after primary, unilateral ACLR
Sample Subgroups
• Sex subgroups
• Female
• Male
• Age subgroups
• Teen: 14-18 years
• Adult: 19-30 years
Statistical Plan
• Multiple two-way ANOVAs to determine the effects of sex and age group
• Significance level (α) was set to 0.05
TEENS report higher ACL-RSI total scores and higher CONFIDENCE vs adults
• Total ACL-RSI score across the cohort averaged 67.92 ± 24.65
What This Study Adds to the Literature
• Age- and sex-specific ACL-RSI data provide normative values that clinicians can use to assist with the RTS decision making process
• When assessing a teen athlete’s psychological preparedness to RTS, target scores determined from adult data may not be appropriate Translation to Clinical Practice
• Using the individual item scores is important to make patient-specific recommendations and deliver effective interventions before RTS
• Future work should strive to create age- and sexspecific ACL-RSI cutoff scores for successful RTS after ACLR in teen athletes
Figure 1: ACL-RSI subscale, total, and item scores by age group. Significant age group differences are noted with an asterisk (*)
Category: (Clinical Research)
Assessing the Impact of Neighborhood Opportunity on Surgical Care and Outcomes after Anterior Shoulder Stabilization in Adolescents
Presenting Author: Dylan P. Roman, PT, DPT
Lisa Cruz, BS1; Nicholas Giampetruzzi, PT, MSPT1; Adam P. Weaver, PT, DPT1; Matthew Brown, MD2; Allison E. Crepeau, MD2; Dylan P. Roman, PT, DPT1
1Connecticut Children’s Sports Physical Therapy, Farmington, CT, USA
2Connecticut Children’s Sports Medicine, Farmington, CT, USA
BACKGROUND
In the adolescent athlete, early surgical intervention of traumatic anterior shoulder instability is critical to reduce the rate of Hill-Sacs Lesions (HSL) and recurrent instability. Neighborhood opportunity been linked to outcomes for patients with other orthopedic conditions, but its relationship to shoulder instability outcomes is unknown. Therefore, the purpose of the study was to investigate the relationship between the Child Opportunity Index (COI) and the time between initial subluxation and surgery and frequency of instability events (IE) prior to surgery.
METHODS
A retrospective chart review was conducted on adolescents who underwent arthroscopic Bankart repair between 2022 and 2024. Patients were included if they suffered a specific initial destabilizing event. Subsequent IE were tallied as documented by medical providers. Patients were grouped by number of IE (1, 2, or 3+). Patient zip code was used to calculate COI. Comparisons between instability groups were performed with the Kruskal-Wallis test. Spearman correlation analyses was performed to evaluate the association between time to surgery and COI.
RESULTS
Thirty-seven patients (10 females; 16.8±1.35 years) met inclusion criteria. No significant group differences were noted between number of IE and COI (χ² = 0.172, p=0.918). Additionally, no significant correlations were noted between time to surgery and COI (r=-0.196, p=0.245).
CONCLUSION/SIGNIFICANCE
Following Bankart repair, neighborhood opportunity was not related to pre-operative IE or time to surgery. Future research should include more variable ranges of neighborhood opportunity levels from diverse geographical locations to create a better understanding of healthcare disparities.
Table 1. Patient Demographics and Surgical Characteristicsa
aValues are expressed as n (%) or mean ± SD.
Table 2. Group Comparison by Number of Instability Events
*Bold P values indicate a statistically significant difference between groups (P < .05).
aValues are expressed as mean ± SD.
bDisabilities of the Arm, Shoulder and Hand questionnaire (quickDASH).
cWestern Ontario Instability Index (WOSI).
dBased on the Kruskal-Wallis test.
eBased on the Welch’s ANOVA.
Table 3. Correlations between Time to Surgery and Opportunity/Outcomes
Child Opportunity Indexa quickDASHa WOSIb
Time to Surgery -0.196 (0.245) 0.260(0.158) 0.269(0.151)
*Bold P values indicate a statistically significant difference between groups (P < .05).
Based on Spearman’s Rhoa or Pearson’s Rb, expressed as R (P value).
Assessing the Impact of Neighborhood Opportunity on Surgical Care and Outcomes After
Anterior Shoulder Stabilization in Adolescents
Lisa Cruz, BS1; Nicholas Giampetruzzi, MSPT1; Adam P. Weaver, DPT1; Matthew Brown, MD2; Allison E. Crepeau, MD2; Dylan P. Roman, DPT1 1Connecticut Children’s Sports Physical Therapy, Farmington, CT, USA, 2Connecticut Children’s Sports Medicine, Farmington, CT, USA
INTRODUCTION
• Adolescents athletes with a history of anterior shoulder instability have a high rate of recurrent instability. Early intervention is essential to reduce risk of re-injury.
• The Child Opportunity Index (COI) has been linked to outcomes in other orthopedic patients, but its impact on anterior shoulder instability outcomes are unknown.
• Patients were grouped by number of instability events (1-2, or 3+)
• Days to Surgery from Initial Injury
Post-Operative Outcomes (PROs)
• QuickDASH
• WOSI
Child Opportunity Index
• Used patient’s zip code at time of surgery.
Statistics
• Kruskal-Wallis test for comparisons between instability groups.
• Spearman correlation assessed relationships between surgery timing, COI, and outcomes.
• Significance (α) was set to 0.05.
RESULTS
• 37 patients (10 females; 16.8±1.35 years).
• Patients in the 3+ IE group demonstrated more Hill-Sachs lesions, more chondral injuries, and increased time to surgery.
• COI was not significantly correlated to quickDASH (p=0.803) or WOSI (p=0.127).
• No significant group differences were noted between COI and pre-operative IE (p=0.918) (Table 2).
• Future research
Figure 2. Hartford Area COI
Child Opportunity Levels Overall COI by Census Tract, nationally normed for 2021
Figure 3. COI Labels
A modified perioperative pain protocol reduces opioid use and improved outcomes following cleft palatoplasty
Presenting Author: Lauren C. Schmidtberg PA-C, MMSc
Lauren C. Schmidtberg PA-C, MMSc.; Gabrielle Caron; Jennafer Euen BSN, RN; Charles Castiglione, MD; Christopher D. Hughes MD, MPH
Connecticut Children’s University of Connecticut School of Medicine
Purpose
Postoperative pain after cleft palatoplasty can be difficult to measure objectively. Opioids have traditionally been the mainstay of pain control, and suboptimal regimens may cause delays in feeding that result in longer lengths of hospital stay. The purpose of this study is to evaluate the impact of a revised perioperative pain protocol on postoperative pain, opioid use, time to feed, and length of stay for children with cleft palate.
Methods
We instituted a revised perioperative pain control algorithm in 2019 designed to reduce opioid use. A retrospective review was then performed by abstracting demographic, operative, and postoperative data from a consecutive series of patients undergoing cleft palatoplasty at our institution from 2019-2023. A comparable group of consecutive patients treated prior to our revised protocols was used as a historical control group.
Results
A total of 139 patients were evaluated (51 in the intervention group and 89 in the control). Patients in the intervention group had significantly lower early (2.22 v 3.22, p<0.01) and late (1.43 v 1.84, p=0.02) postoperative pain scores compared to controls, and they received significantly fewer postoperative morphine equivalents than patients in the control group (1.75 v 5.69, p<0.01). There was no significant difference in time to first oral feeding between the two groups (975.4 min v. 909.4 min, p=0.68), but hospital length of stay was statistically significantly shorter in the intervention group vs. control (1.5 d v. 1.8d, p=0.04).
Conclusions
A modified perioperative pain protocol can effectively and significantly reduce postoperative pain and opioid use following cleft palatoplasty in children. While it did not decrease time to feed in this population, our protocol did reduce overall hospital length of stay.
A modified perioperative pain protocol reduces opioid use and improves outcomes following cleft palatoplasty.
Lauren C. Schmidtberg PA-C, MMSc.1; Jennafer Euen BSN, RN1; Gabrielle Caron2; Charles Castiglione, MD1,2; Christopher D. Hughes MD, MPH 1,2
1
Connecticut Children’s, Hartford, CT 2 University of Connecticut School of Medicine, Farmington, CT
INTRODUCTION
Postoperative pain after cleft palatoplasty can be difficult to measure objectively. Opioids have traditionally been the mainstay of pain control, and suboptimal regimens may cause delays in feeding that result in longer lengths of hospital stay. The purpose of this study is to evaluate the impact of a revised perioperative pain protocol on postoperative pain, opioid use, time to feed, and length of stay for children with cleft palate.
RESULTS
BACKGROUND
Standardized protocol in Epic:
METHODS
• Intra-operatively: dexamethasone, IV Tylenol, 0.25% Bupivacaine infraorbital blocks upon procedure completion
• Post-operatively: IV or PO Tylenol, IV Toradol or PO ibuprofen, PO Oxyocodone as second line severe pain, and IV Decadron Epic nursing order: “Page MD for discharge when taking 8oz in 24 hours or 3oz for 2 consecutive feeds”
Measured outcomes:
1. Post-operative pain scores (FACES scale)
2. Opioid use measured in morphine equivalents per kilogram (ME/Kg)
3. Time to first oral feed (minutes)
4. Length of stay in the hospital (days)
CONCLUSIONS
A total of 139 patients were evaluated (51 in the intervention group and 89 in the control). Patients in the intervention group had significantly lower early (2.22 v 3.22, p<0.01) and late (1.43 v 1.84, p=0.02) postoperative pain scores compared to controls, and they received significantly fewer postoperative morphine equivalents per kg (ME/Kg) than patients in the control group (0.16 v 0.66, p<0.01). There was a significant difference in the median time to first oral feeding between the two groups (1183 min v. 441 min), and hospital cumulative length of stay was statistically significantly shorter in the intervention group compared to historical control.
A standardized perioperative pain protocol can play an integral part in managing patients undergoing primary cleft palatoplasty. Our protocol significantly reduced perioperative narcotic use and short and long term post-operative pain scores in this vulnerable population. This study shows the positive impact of optimizing non-opioid pain medications as well as standardizing communication within the team/hospital setting.
We instituted a revised perioperative pain control algorithm in 2019 designed to reduce opioid use in children undergoing primary cleft palatoplasty at Connecticut Children’s. A retrospective review was then performed by abstracting demographic, operative, and postoperative data from a consecutive series of patients undergoing cleft palatoplasty from 2019-2023. A comparable group of consecutive patients treated prior to our revised protocols was used as a historical control group. T-tests and chi-square tests were used for intergroup comparisons for continuous and dichotomous variables, respectively. Linear regression was used for multivariate analysis.
REFERENCES
1. Mahboubi H, Truong A, Pham NS. Prevalence, demographics, and complications of cleft palate surgery. Int J Pediatr Otorhinolaryngol 2015;79(6):803-807. doi:10.1016/j.ijporl.2015.02.032
2. Izadi N, Haers PE. An investigation into the variables associated with length of hospital stay related to primary cleft lip and palate surgery and alveolar bone grafting. Int J Oral Maxillofac Surg. 2012;41(10):12381243. doi:10.1016/j.ijom.2012.05.024
3. Moffitt JK, CepedaA, Ekeoduru RA, Teichgraeber JF, Nguyen PD, Greives MR. Enhanced Recovery After Surgery Protocol for Primary Cleft Palate Repair: Improving Transition of Care. J Craniofac Surg. 32(1):e72e76. doi:10.1097/SCS.0000000000006985
4. Cawthorn TR, Todd AR, Hardcastle N, SpencerAO, Harrop AR, Fraulin FOG. Optimizing Outcomes After Cleft Palate Repair: Design and Implementation of a Perioperative Clinical Care Pathway. Cleft PalateCraniofacial Journal. 2022;59(5):561-567. doi:10.1177/10556656211017409
5. Reena, Bandyopadhyay KH, Paul A. Postoperative analgesia for cleft lip and palate repair in children. J Anaesthesiol Clin Pharmacol. 2016;32(1):5-11. doi:10.4103/0970-9185.175649
6. LeeA, Chang BL, Yan C, et al. The Reducing Opioid Use in Children with Clefts Protocol: A Multidisciplinary Quality Improvement Effort to Reduce Perioperative Opioid Use in Patients Undergoing Cleft Surgery. Plast Reconstr Surg. 2020;145(2):507-516. doi:10.1097/PRS.0000000000006471
7. Thawanyarat K, Waitt T, Navarro Y, Collar J, Doroodchi A, Yu J. Opioid Sparing by ERAS Protocol in Cleft Lip and Palate Craniofacial Surgery. Face. 2023;4(2):135-140. doi:10.1177/27325016231155185
ACKNOWLEDGEMENTS
Isokinetic Knee Strength and Patient Reported Outcomes Differ
between ACL Reconstruction Graft Types in Adolescents
Presenting Author: Adam P. Weaver, PT, DPT
Adam P. Weaver, PT, DPT1, Xavier Thompson, ATC, PhD2, ARROW3, Christopher Kuenze4
4 University of Virginia, Department of Kinesiology
Background: ACL graft selection influences patient strength, patient-reported outcomes (PROs) and reinjury in adolescents after ACLR. There is no consensus on optimal graft choice. Understanding differences in knee extension strength and PROs in adolescents with bone patellar tendon bone (BPTB), quadriceps tendon (QT), or hamstring (HS) autograft is not well understood.
Methods: Retrospective data was obtained from a multi-site clinical outcomes registry for patients 7.8 ± 1.5 months after ACLR. Isokinetic knee strength testing results at 60°/s, the International Knee Documentation Committee Subjective Knee Form (IKDC), Pediatric-IKDC (Pedi-IKDC) Knee Form, and Knee Injury and Osteoarthritis Outcome Score (KOOS). Mass normalized strength was compared via linear mixed effects models and PROs were compared between graft types with Kruskal-Wallis tests.
Results: This sample included ACLR with QT (n=155), BTPB (n=79) and HS (n=288) autograft. After controlling for covariates, BPTB patients produced 10.8% less ACLR limb knee extension strength (p=0.05) than QT patients and 20.4% less knee extension strength than HS patients (p<0.001), while HS patients produced 9.6% more knee extension strength (p=0.01) than QT patients. QT patients had lower IKDC scores than HS patients (-7.2%, p<0.001. HS patients had higher IKDC scores (+5.4%, p<0.001) and higher KOOS Sport scores than BPTB patients (+5.1%, p<0.01).
Conclusion/Significance: QT and BPTB patients had worse knee extension strength after ACLR than HS patients. PRO findings were mixed, as patients displayed non-uniform levels of impairment of selfreported function or ability to participate in sport. These findings will assist clinicians in determining rehabilitation guidelines and allowing a safe return to sport and activity.
INTRODUCTION
• After ACL reconstruction in adolescents, graft selection influences:
• Thigh muscle strength
• Patient reported function
• Risk of re-injury
Isokinetic Knee Strength
and Patient Reported Outcomes Differ between ACL Reconstruction Graft Types in Adolescents: A Multi-Center Study
Adam P. Weaver, PT, DPT1, Xavier Thompson, ATC, PhD2, ARROW3, Christopher Kuenze4
• Restoring knee strength after ACLR is a critical rehabilitation outcome that can impact return to sports and future re-injury.
• Differences in knee extension strength after ACLR between graft types is not well understood.
PURPOSE
• To compare outcomes after ACLR with bone patellar tendon bone (BPTB), quadriceps tendon(QT), and hamstring tendon (HS) grafts in large adolescent cohort at 6-12 months post-operative.
• Hypothesis: QT and BPTB patients would have greater impairments in knee extension, HS grafts would have greater impairments in knee flexion, but PROs would be similar.
METHODS
Study Design
• Retrospective data collection of 522 patients from ARROW registry 7.8±1.5mo after primary ACLR Inclusion and Exclusion Criteria
• ACLR between 2013-2023 with use of quad tendon (QT), hamstring tendon (HS) or bone patellar tendon bone (BPTB)
Thigh Muscle Strength Measures
• Completion of Isokinetic knee strength at 60 degrees/sec Patient-Reported Outcome Measures
• Completion of patient reported outcomes: International Knee Documentation Subjective Committee Knee Form (IKDC), Pediatric-IKDC (Pedi-IKDC), Knee Injury and Osteoarthritis Outcome Score (KOOS), ACL-RSI
Statistical Plan
• Mass normalized strength was compared via linear mixed effects models and PROs were compared between graft types with Kruskal-Wallis tests
After controlling for covariates, BPTB patients produced 10.8% less ACLR limb knee extension strength then QT patients and 20.8% less knee extension strength then HS patients at 6-12 months post-op.
QT patients reported lower IKDC scores then HS patients while HS patients had higher IKDC scores then BTPB patients. There were no differences in ACL-RSI scores.
RESULTS
DISCUSSION
• At 6-12 months after ACLR, QT and BPTB patients had worse normalized quadriceps strength but greater HS strength then HS patients.
• Patient reported outcome findings were mixed with no differences seen in ACL-RSI scores, but HS patients had greater self-reported function.
• Graft source appears to negatively impact involved limb strength
• Graft type did influence patient reported outcomes, knee strength, and perceived ability to participate in sport
• The effects of rehabilitative outcomes and reinjury rates post-ACLR should continue to be explored in larger cohorts of adolescent patients
Category: (Clinical Research)
The Relationship between Psychological Readiness and Instability History in Adolescents after Anterior Shoulder Stabilization
Presenting Author: Adam P. Weaver, PT, DPT
Adam P. Weaver, PT, DPT1; Michael G. Saper, DO, ATC, CSCS2; Shing Varakitsomboon2; Matthew Brown, MD3; Allison E. Crepeau, MD3; Dylan P. Roman, PT, DPT1
1Connecticut Children’s Sports Physical Therapy, Farmington, CT, USA
2Seattle Children’s Hospital, Seattle, WA, USA
3Connecticut Children’s Sports Medicine, Farmington, CT, USA
Background: Adolescents who return to sport (RTS) after labral repair have a 25% rate of recurrent instability. Adequate psychological readiness (PR) before returning to sport (RTS) after labral repair is related to improved outcomes in adults, but yet to be studied in adolescents. The purpose of this study was to analyze the relationship between PR and instability history at time of RTS testing in adolescents.
Methods: Retrospective chart review on adolescents at two children’s hospitals who underwent arthroscopic labral repair between April 2022 and April 2024 was completed. Patient demographics, frequency of pre-operative instability events (IEs), operative details, and patient reported outcome measures of function (QuickDASH) and PR (Shoulder Instability Return to Sport after Injury scale (SI-RSI)) were obtained at time of RTS testing. Independent T tests were used to analyze patient demographics and patient reported outcome scores.
Results: 40 subjects (35% female, 16.8±1.4 years) were included. Females reported significantly lower SI-RSI scores than males (59.57 vs 78.84; p=0.007). SI-RSI and QuickDASH scores displayed a moderate negative correlation, with higher PR correlating to improved self-reported function (r= -0.552; p=<0.001). There were no differences in SI-RSI scores in subjects with greater than 3 IEs compared to subjects with 1 or 2 IEs (p=0.90).
Conclusion/Significance: SI-RSI scores are related to subjective function and should be considered as part of a testing battery when assessing RTS readiness in adolescent athletes. Addressing low PR should be a priority before allowing young athletes unrestricted RTS. Future studies should investigate the relationship between PR and re-injury risk in this population.
Participating in Contact Sport (%)
Dominant Arm Involved in Surgery (%)
Student’s T-Testa; Mann-Whitney Testb; Chi Square Testc
Table 1. Patient Demographics by Pre-Operative Instability History
Table 2. Group Differences in Patient Reported Outcomes at Return to Sport Testing
Student’s T-Testa; Mann-Whitney Testb; *Shoulder Instability Return to Sport After Injury Scale; **Quick Disabilities of the Arm, Shoulder and Hand
The Relationship between Psychological Readiness and Instability History in
Adolescents after Anterior Shoulder Stabilization
Adam P. Weaver, PT, DPT1; Michael G. Saper, DO,
ATC, CSCS
2;
Shing
Varakitsomboon
; Matthew Brown, MD3; Allison E. Crepeau, MD3; Dylan P. Roman, PT, DPT1
INTRODUCTION
• Improved psychological readiness has been linked to higher rates of return to sport (RTS) after anterior shoulder stabilization surgeries.
• Increased fear of re-injury is a risk factor for recurrent shoulder instability.
• The SI-RSI has been utilized as a measure of psychological readiness in adults, yet there is no published literature on it’s utilization in adolescents.
• Establishing normative values of the SI-RSI in younger populations can help guide clinicians during the RTS decision making process.
PURPOSE
• Primary Aim: To assess the relationship between self-reported function and psychological readiness at RTS.
• Secondary Aim: To assess the relationship between pre-operative instability history and psychological readiness at RTS.
METHODS
Study Design
• Retrospective chart review
• Arthroscopic anterior shoulder stabilization between April 2022-April 2024
Severe Combined Immunodeficiency (SCID) is a disorder characterized by immune cell deficiency. Newborn screening assesses SCID through T-cell receptor excision circles (TRECs), a biomarker for Tcell production. Low TREC counts may indicate SCID and premature neonates are more likely to present with false positive results. Here, we aim to identify the association between a low TREC count reported as an Abnormal SCID screening test and SGA status.
METHODS
This retrospective study utilized data from 380 infants admitted to CT Children’s NICU between January 5, 2017 - October 19, 2023. Infants were categorized into SGA and non-SGA. SCID screening was determined from the CT newborn program. Abnormal SCID screening tests were confirmed by repeat screening and confirmatory tests. False positive SCID screens were thus identified. A chi-square analysis compared false-positive SCID screening results between SGA and non-SGA infants.
RESULTS
Among the 380 infants, 64 SGA and 281 non-SGA infants had normal SCID results, while 19 SGA and 16 non-SGA infants had false-positive SCID results. A significant association was found between SGA status and false positives (χ² = 33.999, p < 0.001). This association remained significant (p< 0.05) after controlling for birth weight or gestational age using multiple logistic regression analysis.
SCID+
CONCLUSION
These preliminary findings suggest that SGA infants are prone to false-positive SCID results. We plan to expand this study to validate these findings with additional data.
Exploring the Relationship Between SGA and Abnormal
SCID Tests in State-Mandated SCID Screening of Newborns
Humza Zaidi,
B.S.1, Brooke
Onwenu,
M.D.1, Hassan El
Chebib
M.D.1,2, Naveed Hussain M.D.1,2 1University of Connecticut School of Medicine, Farmington, CT 2
INTRODUCTION
Severe Combined Immunodeficiency (SCID) is a disorder characterized by immune cell deficiency. Newborn screening assesses SCID through T-cell receptor excision circles (TRECs), a biomarker for T-cell production. Low TREC counts may indicate SCID and premature neonates are more likely to present with false positive results. Here, we aim to identify the association between a low TREC count reported as an Abnormal SCID screening test and SGA status.
BACKGROUND
METHODS
This retrospective study utilized data from 380 infants admitted to CT Children’s NICU between January 5, 2017 - October 19, 2023. Infants were categorized into SGA and non-SGA. SCID screening was determined from the CT newborn program. Abnormal SCID screening tests were confirmed by repeat screening and confirmatory tests. False positive SCID screens were thus identified. A chi-square analysis compared falsepositive SCID screening results between SGA and non-SGA infants.
RESULTS
REFERENCES
Patients with SCID are at high risk of infections, including opportunistic pathogens. Prior to initiation of screening, many of these patients presented within one year of age with life-threatening infections. These patients would succumb to these infections by the time a diagnosis is made and life-saving procedures, such as bone marrow transplants, would be too late. As signs of the disease may not be evident at birth, early testing is crucial to prevent mortality. Therefore, SCID is often screened for within 48 hours of delivery as part of the newborn screening tests offered by most states in the United States. This test involves a dried, heel-stick blood sample which is analyzed (by PCR amplification of DNA) to identify the level of TREC (T-cell Receptor Excision Circle).4 TRECs represent the portion of cellular DNA material that is excised from T-lymphocytes as they undergo maturation within the thymus and is a wellrecognized biomarker of mature T-cell production.A low TREC count suggests a possible diagnosis of SCID. There are conditions in which the fetal thymus is affected but it is not clear if there is any effect on TREC levels at birth.Unfortunately, the false-positive rate of the SCID screen is high, as two-thirds of the abnormal result are due to multiple confounding and non-confounding factors.10 There are reports of involution of the thymus in fetuses that are stressed in utero.It is postulated that children born small for gestational age (SGA) may trigger a false-positive result (low TREC count) due to poor fetal growth that may affect thymic function. However, there is lacking evidence to validate such a relationship.
Among the 380 infants, 64 SGA and 281 non-SGA infants had normal SCID results, while 19 SGA and 16 non-SGA infants had false-positive SCID results. A significant association was found between SGA status and false positives (χ² = 33.999, p < 0.001). This association remained significant (p< 0.05) after controlling for birth weight or gestational age using multiple logistic regression analysis. These preliminary findings suggest that SGA infants are prone to false-positive SCID results. We plan to expand this study to validate these findings with additional data.
1.Kumrah R, Vignesh P, Patra P, et al. Genetics of severe combined immunodeficiency. Genes Dis 2020;7(1):52-61. doi:10.1016/j.gendis.2019.07.004
2.Newborn Screening for Severe Combined Immunodeficiency NeoReviews American Academy of Pediatrics. Accessed March 2, 2024. https://publications.aap.org/neoreviews/articleabstract/14/9/e448/91513/Newborn-Screening-for-Severe-Combined?redirectedFrom=fulltext
3.Gaviglio A, Lasarev M, Sheller R, Singh S, Baker M. Newborn Screening for Severe Combined Immunodeficiency: Lessons Learned from Screening and Follow-Up of the Preterm Newborn Population. Int J Neonatal Screen. 2023;9(4):68. doi:10.3390/ijns9040068
4.Currier R, Puck JM. SCID Newborn Screening: What we’ve learned. J Allergy Clin Immunol 2021;147(2):417-426. doi:10.1016/j.jaci.2020.10.020
5.Michniacki TF, Seth D, Secord E. Severe Combined Immunodeficiency: A Review for Neonatal Clinicians. Neoreviews. 2019;20(6):e326-e335. doi:10.1542/neo.20-6-e326
6.Davey BT, Elder RW, Cloutier MM, et al. T-Cell Receptor Excision Circles in Newborns with Congenital Heart Disease. J Pediatr 2019;213:96-102.e2. doi:10.1016/j.jpeds.2019.05.061
7.Chiarini M, Zanotti C, Serana F, Sottini A, Bertoli D, Caimi L, et al. T-cell Receptor and K-deleting Recombination Excision Circles in Newborn Screening of T- and B-cell Defects: Review of the Literature and Future Challenges. Journal of public health research 2013, 2: 9-16.
8. Kwok JSY, Cheung SKF, Ho JCY, Tang IWH, Chu PWK, Leung EYS, et al. Establishing Simultaneous T Cell Receptor Excision Circles (TREC) and K-Deleting Recombination Excision Circles (KREC) Quantification Assays and Laboratory Reference Intervals in Healthy Individuals of Different Age Groups in Hong Kong. Frontiers in immunology 2020, 11: 1411.
9. Ravkov E, Slev P, Heikal N. Thymic output: Assessment of CD4(+) recent thymic emigrants and T-Cell receptor excision circles in infants. Cytometry Part B, Clinical cytometry 2017, 92: 249-257.
ACKNOWLEDGEMENTS
Dried blood spot 3mm hole punch
Category: Population and Community Health
Connecticut Children’s Contributions to the COVID-19 Vaccine Effectiveness Study
Presenting Author: Gretchen Blume, BS
Gretchen Blume, BS1, Katherine W. Herbst, MS1, Noah Schulman, BS1, Alexander H. Hogan MD, MS1,2
1Connecticut Children’s Medical Center Research Institute
2University of Connecticut School of Medicine
BACKGROUND
The COVID-19 Vaccine Effectiveness Study, a public health surveillance study led by Boston Children’s Hospital (BCH), aims to determine COVID-19 vaccine efficacy against changing SARSCoV-2 variants in pediatric populations. This abstract reports CT Children’s study contributions to date.
METHODS
The electronic medical record (EMR) is screened daily for admitted patients <19 years old, utilizing guides BCH provided to determine eligibility and enrollment cohorts. Each COVID+ case (Case) requires one to two controls (Control) matched for age and/or co-infections with respiratory syncytial virus (RSV) and/or influenza viruses. Vaccination history is verified via EMR review, Connecticut’s Immunization Information System (IIS), and parent interviews. Residual respiratory samples from standard-of-care testing and fresh research nasal swabs are collected for case participants. Residual standard-of-care blood samples are collected for all subjects.
RESULTS
Thirteen participants have been enrolled: seven cases, four controls and two no longer met eligibility criteria. Median age of patients is 9 months (cases: 9 months; controls: 8 months). Completed tasks for each cohort are outlined in Figure 1. Across cohorts, 100% (11/11) had their EMR/IIS reviewed, 91% (10/11) completed parent interviews and 71% (5/7) of cases provided a fresh nasal swab. No residual blood or respiratory samples were collected since no available samples fit study eligibility criteria. Some vaccine information is still being verified, as the site did not have IIS access until August.
CONCLUSION
Our site has successfully contributed data to the BCH database regarding efficacy of pediatric vaccinations and will continue enrolling participants.
Connecticut Children’s Contributions to the Overcoming COVID-19 Vaccine Effectiveness Study
1 Connecticut Children’s, Hartford, CT 2 University of Connecticut School of Medicine, Farmington, CT
BACKGROUND
• The Overcoming COVID-19 Vaccine Effectiveness Study is a multi-site public health surveillance study led by Boston Children’s Hospital (BCH).
• It aims to determine COVID-19 vaccine efficacy in preventing hospitalizations against changing SARS-CoV-2 variants and viral co-infections in pediatric populations.
OBJECTIVE
To report on Connecticut Children’s enrollments and completed study tasks from April-October 2024.
METHODS
• The electronic medical record (EMR) is screened daily for admitted patients <19 years old, utilizing guides BCH provided to determine eligibility and enrollment cohorts.
• Each COVID+ patient (Case) requires one to two controls (Control) matched for age and/or co-infections with respiratory syncytial virus (RSV) and/or influenza (Flu) viruses.
The following tasks are performed accordingly:
• Review EMR
• Review Connecticut’s Immunization Information System (IIS)
• Parent Interview
• Collect Residual+ Respiratory Samples*
• Collect Fresh Research Nasal Swabs*
(75%)
Figure 1. Connecticut Children’s enrollments and completed study tasks from April 2024-October 2024, presented by cohort.
RESULTS
• Completed study tasks are outlined in Figure 1.
• Fifteen patients are enrolled: Eight cases, five controls, with two no longer meeting eligibility criteria.
• Median age within and across cohorts is 9 months old.
• Few residual samples are collected since many did not fit eligibility criteria
Across cohorts:
• 100% (13/13) had vaccine information reviewed
• 92% (12/13) completed a parent interview
• 8% (1/13) of residual blood samples were collected
• Missing matched-controls for three case patients due to few eligible patients.
CONCLUSIONS
This site has successfully contributed data to the BCH database regarding efficacy of pediatric vaccinations, and will continue to enroll participants through December 2025. Research reported in this publication is supported by The Centers for Disease Control and Prevention awarded under Definitive Contract number 75D30122C13330.
ACKNOWLEDGEMENTS
Caregivers’ Childhood Maltreatment History and Current Family Routines: Mediating and Moderating Factors
Presenting Author: Eileen M. Condon, PhD, APRN
Eileen M. Condon, PhD, APRN, Mollie Fleming, MS, Nancy S. Redeker, PhD, RN, FAAN, FAHA, Lois S. Sadler, PhD, RN, FAAN
INTRODUCTION
Consistent family routines (e.g. eating dinner together, regular bedtimes) are associated with child socioemotional health. Providing consistent routines may be challenging for caregivers with a history of childhood trauma, but this relationship is not well understood.
AIM
The purpose of this study is to examine the relationship between caregivers’ childhood trauma and current family routines among caregivers with young children. To inform approaches to intervention, we also explore whether this relationship is mediated by caregivers’ mental health (depression, anxiety) and parenting (parental reflective functioning) or moderated by protective factors (caregivers’ emotional and instrumental support).
METHODS
Caregivers with children age 3-5 years (N=95 dyads, 85% mothers) completed the Childhood Trauma Questionnaire, Parental Reflective Functioning Questionnaire, and the PROMIS Depression, Anxiety, Emotional Support, and Instrumental Support scales. We conducted linear regression to examine associations between variables, adjusting for child age and gender. We tested moderation using interaction terms. We tested mediation with 5,000 bootstrap samples using the Preacher & Hayes macro for SPSS.
RESULTS
Caregiver’s history of childhood trauma was associated with fewer family routines (β= -.21, p=.001) and increased depression (β= .21, p<.0001), anxiety (β= .19, p=.0007), and pre-mentalizing modes (i.e. impaired reflective functioning; β= .01, p=.03). The relationship between caregivers’ childhood trauma and current family routines was mediated by increased caregiver depression (95% CI -.18, -.03) and anxiety (95% CI -.10, -.01), but not parental reflective functioning. Emotional (p=.04) and instrumental support (p=.05) moderated the relationship between caregivers’ childhood maltreatment and family routines, such that this relationship was only present if caregivers had low social support.
CONCLUSIONS
Family routines may be a mechanism underlying the intergenerational transmission of adversity, but additional research is needed. Early childhood interventions may benefit from incorporating strategies to promote health family routines while continuing to address caregivers’ mental health symptoms and promote protective factors.
Caregivers’ Childhood Maltreatment History and Current Family Routines: Mediating and Moderating Factors
Eileen M. Condon, PhD, APRN, FNP-BC
Mollie Fleming, MS; Nancy S. Redeker, PhD, RN, FAAN, FAHA; Lois S. Sadler, PhD, RN, FAAN
Introduction
• Consistent family routines include regular play times, eating dinner together as a family, and regular bedtimes activities.1
• Consistent family routines are associated with improved socioemotional health and health behaviors in children, including improved sleep.2
• Providing consistent routines may be challenging for caregivers with a history of childhood trauma, such as childhood abuse or neglect.
• Improved understanding of the relationship between caregivers’ childhood trauma history and current family routines is needed to identify challenges and opportunities for intervention.
Study Aims
Aim 1: To examine the relationship between caregivers’ childhood trauma history and current family routines among caregivers with young children.
Aim 2a: To explore whether this relationship is mediated by caregivers’ mental health (depression, anxiety) and parenting (parental reflective functioning).
Aim 2b: To explore whether this relationship is moderated by family protective factors (caregivers’ emotional and instrumental support).
Methods
• We analyzed data from The CARING Study, a cross-sectional study of caregivers with preschool-age children (age 3 to 5 years).
• Inclusion criteria: Primary caregiver for the child
• Caregivers completed the following self-report instruments:
• Childhood Trauma Questionnaire
• Family Routines Inventory
• Parental Reflective Functioning Questionnaire
• PROMIS Depression, Anxiety, Emotional Support, and Instrumental Support scales
Statistical Analyses
• We conducted linear regression to examine associations between study variables, adjusting for child age and gender.
• We tested moderation using interaction terms. We tested mediation with 5,000 bootstrap samples using the Preacher & Hayes macro for SPSS.
Results
• N=110 dyads were included in the analyses (Table 1).
• 36% of caregivers reported greater than minimal experiences of overall childhood maltreatment severity (Figure 1)
• Emotional abuse (35%) and emotional neglect (42%) were most commonly reported subtypes
Table 1. Participant Characteristics
Demographic Variable N (%) or M (SD)
Caregiver Role: Mother 90 (82)
Child Gender: Female 52 (47)
Child age (years) 3.7 (0.72)
Child Race: Non-Hispanic White
Multiple races
Non-Hispanic Black
Hispanic/Latino
Results (continued)
• Caregiver’s history of childhood trauma was associated with significantly fewer reported family routines (β= -.21, p=.001).
• Caregiver’s history of childhood trauma was also associated with increased depression (β= .21, p<.0001), anxiety (β= .19, p=.0007), and impaired parental reflective functioning (β= .01, p=.03).
• The relationship between caregivers’ childhood trauma and current family routines was mediated by increased caregiver depression (95% CI -.18, -.03) and anxiety (95% CI -.10, -.01), but not parental reflective functioning.
• Emotional (p=.04) and instrumental support (p=.05) moderated the relationship between caregivers’ childhood trauma and family routines:
• This relationship was only present among caregivers who reported low levels of emotional and instrumental support.
Conclusions
• Family routines may be a mechanism underlying the intergenerational transmission of adversity, but additional research is needed.
Asian or Pacific Islander 69 (63) 17 (15)
Figure 1. Caregivers’ History of Childhood Maltreatment
(9) 9 (8) 6 (5)
• Early childhood interventions may benefit from incorporating strategies to promote health family routines while continuing to address caregivers’ mental health symptoms and promote protective factors.
Acknowledgements
The CARING Study is funded by the National Institute of Nursing Research (K99NR018876; R00NR018876).
We sincerely thank the following members of The CARING Study research team for their assistance in carrying out this study.
References
1. Spagnola & Fiese (2007). Family routines and rituals: A context for development in the lives of young children. Infants & Young Children, 20(4), 284-299.
2. Buxton et al. (2015). Sleep in the modern family: protective family routines for child and adolescent sleep. Sleep Health, 1(1), 15-27.
Category: (Population and Community Health)
Examination of Survey Response Successes in a Longitudinal Cohort Study
Presenting Author: Carlie DeFelice, BA
Carlie DeFelice, BA1, Katherine W. Herbst, MS1, Alexander H. Hogan, MD, MS1,2, Noah Schulman, BS1, Stephanie Lesmes, BS1, Gretchen Blume BS1, Juan C. Salazar, MD, MPH1,2
1 Connecticut Children’s Medical Center
2 University of Connecticut School of Medicine
BACKGROUND
Multi-System Inflammatory Syndrome in Children (MIS-C) is a rare complication of SARS-CoV-2 infection. The MIS-C Biomarker study’s aim was to identify a biosignature unique to MIS-C. As part of this four-year multi-centered prospective cohort study, the CoRonavIruS Health Impact Survey (CRISIS) was administered every six months. The aim of this abstract was to determine survey response rates across our longitudinal study.
METHODS
The CRISIS survey, augmented with vaccine status questions, was integrated into REDCap and REDCap’s survey distribution tool programmed to automatically email/text survey invitations at the appropriate time. To increase likelihood of a high response rate, a stipend of $50/completed survey was included in the study budget. Additionally, three points of contact were collected (parent/guardian, family member, family friend) to reduce the probability of lost-to-followup. Survey distribution was tracked weekly, with follow-up phone calls/emails made by the support team for non-response.
RESULTS
Survey completion is presented for all six-month surveys completed May 2021-June 2024 (F 1). Overall response was 70% (1,160/1,653), with the 36-month survey having the highest response [76% (65/86)]. The 12-month survey had the lowest response rate, with only 67% (238/353) of surveys completed by participants. In September 2023, an error REDCap’s auto-calculation of number of days enrolled in study was identified, resulting in some 24-month surveys not being automatically sent. The issue was identified and corrected, resulting in an increased response rate.
CONCLUSION/SIGNIFICANCE
A combination of a substantial stipend, automated survey distribution, expansive contact information, and diligent staff oversight, resulted in high survey response rates. Although REDCap is useful automated survey distribution, there is need for oversight.
An Examination of Survey Response Successes in a Longitudinal Cohort Study
Carlie DeFelice, BA1, Katherine W. Herbst, MS1, Alexander H. Hogan, MD, MS1,2, Noah Schulman, BS1 , Stephanie Lesmes, BS1, Gretchen Blume, BS1, Juan C. Salazar, MD, MPH1,2
1 Connecticut Children’s Medical Center 2 University of Connecticut School of Medicine
INTRODUCTION
• Multi-System Inflammatory Syndrome in Children (MIS-C) is a rare complication of SARS-CoV-2 infection. The MIS-C Biomarker study’s aim was to identify a biosignature unique to MIS-C.
RESULTS
• Survey completion is presented for all sixmonth surveys completed May 2021-October 2024 (Figure 1).
• As part of this four-year multi-centered prospective cohort study, the CoRonavIruS Health Impact Survey (CRISIS) was administered every six months.
OBJECTIVE
• Overall response was 70% (1,254/1,794), with the 30-month survey having the highest response [73% (206/281)].
• Across the first two years of survey distribution, surveys distributed through email were completed at higher rates compared to text (Figure 2).
• Determine survey response rates across our longitudinal study.
METHODS
• In September 2023, an error REDCap’s auto-calculation of number of days enrolled in study was identified, resulting in some 24-month surveys not being automatically sent. The issue was identified and corrected, resulting in an increased response rate.
CONCLUSIONS
• The CRISIS survey, augmented with vaccine status questions, was integrated into REDCap and REDCap’s survey distribution tool programmed to automatically email/text survey invitations at the appropriate time based on participant preference for survey distribution (email/text).
• To increase likelihood of a high response rate, a stipend of $50/completed survey was included in the study budget.
• Three points of contact were collected (parent/guardian, family member, family friend) to reduce the probability of lost-tofollow up.
FIGURE
1
• A combination of a substantial stipend, automated survey distribution, expansive contact information, and diligent staff oversight, resulted in high survey response rates.
• Although REDCap is useful automated survey distribution, there is need for oversight.
FIGURE 2
Enhancing Organizational Excellence through Peer Pods: A Collaborative Approach to Professional Development and Community Building.
Peer influences are one of the factors that influence behaviors and workplace productivity.1 Peers provide valuable support by helping each other manage interpersonal challenges, adapt to change, and alleviate isolation, fostering a more collaborative work environment.2 Based on employee feedback from a yearly survey in 2023, the Research Operations department leadership initiated the Peer Pod strategic pillar to foster professional development and community building among team members.
METHODS
A smartsheet survey was developed by a strategic planning Peer Pod Working Group and deployed to Research Operations and Development team members. It was designed to capture team members’ roles, years of experience, goals for participation, preferred meeting frequencies, interest in specific activities, and general feedback on the peer pod structure. We will continue to gather feedback through surveys throughout the initiative to assess its successes and identify areas for improvement.
RESULTS
Survey responses identified community building, skill development, problem-solving, and a safe space for discussing productivity challenges as the key goals for peer pod participation. Preferences for meeting frequency varied among team members, and activities of interest included open forums, guest speaker sessions, and workshops/trainings. Feedback emphasized the importance of balancing team members’ workloads when scheduling meetings.
CONCLUSION
The findings highlight team members’ need for a supportive environment for professional development. Insights from this survey will inform the ongoing development of the Peer Pods structure, ensuring it meets the evolving needs of team members. Future efforts will focus on expanding expertise sharing and enhancing the overall impact of these collaborative groups on organizational excellence.
1 Welteke C. Peers at Work ‐ a Brief Overview of the Literature on Peer Effects at the Workplace and the Policy Implications [Internet]. DIW Roundup: Politik im Fokus; 2015 [cited 2024 Sep 8]. Report No.: 68. Available from: https://www.econstor.eu/handle/10419/111853
2 Chou CL, Teherani A, Masters DE, Vener M, Wamsley M, Poncelet A. Workplace learning through peer groups in medical school clerkships. Medical Education Online. 2014 Jan 1;19(1):25809.
Enhancing Organizational Excellence through Peer Pods:
A Collaborative Approach to Professional Development and Community Building.
Damilola Egbewole, BDS, MPH 1 , Kathyria Oyola-Cartagena, MPH, MS 1 , Kristen Volz, MS 1 , Dana Jungbauer, MD 1 , Danielle Chenard, MPH 1 , Carolyn Macica, MS, PhD 1
1
BACKGROUND
Research Operations and Development, Connecticut Children’s
RESULTS
CONCLUSION
Peer influences are one of the factors that influence behaviors and workplace productivity.1 Peers provide valuable support by helping each other manage interpersonal challenges, adapt to change, and alleviate feelings of isolation, fostering a more collaborative and productive work environment.
2
Based on employee feedback from a yearly survey in July 2023, the Research Operations department leadership set up the Peer Pod strategic pillar to foster professional development and community building among team members.
METHODS
A smartsheet survey was developed by a strategic planning Peer Pod Working Group and deployed to Research Operations and Development team members. It was designed to capture team members’ roles, years of experience, goals for participation, preferred meeting frequencies, interest in specific activities, and general feedback on the peer pod structure. We will continue to collect regular feedback through surveys throughout the initiative to assess its successes and identify areas for improvement.
Survey responses identified community building, skill development, problem-solving, and a safe space for discussing productivity challenges as the key goals for peer pod participation. Preferences for meeting frequency varied among team members, and activities of interest included open forums, guest speaker sessions, and workshops/trainings. Feedback emphasized the importance of balancing team members’ workloads when scheduling meetings.
The findings highlight team members’ need for a supportive environment for professional development. Insights from this survey will inform the ongoing development of the Peer Pods structure, ensuring it meets the evolving needs of team members. Future efforts will focus on expanding topic areas for expertise sharing and enhancing the overall impact of these collaborative groups on organizational excellence
REFERENCES
1 Welteke C. Peers at Work - a Brief Overview of the Literature on Peer Effects at the Workplace and the Policy Implications [Internet]. DIW Roundup: Politik im Fokus; 2015 [cited 2024 Sep 8]. Report No.: 68. Available from: https://www.econstor.eu/handle/10419/111853
2 Chou CL, Teherani A, Masters DE, Vener M, Wamsley M, Poncelet A. Workplace learning through peer groups in medical school clerkships. Medical Education Online. 2014 Jan 1;19(1):25809.
ACKNOWLEDGEMENTS
We would like to thank all Research Operations team members who have been actively involved in the department’s strategic planning efforts and continue to collaboratively work together towards achieving the strategic planning goals.
Category: Population and Community Health
The
Child Opportunity
Index and Pediatric Hospitalizations: Are ZIP Codes Good Enough?
Presenting Author: Alexander H. Hogan, MD, MS
Alexander H. Hogan, MD, MS1, 2 ,Natalie Grills, MS3 , Matt Hall, PhD3 , Mitch Harris, PhD, MS3 ,Molly Krager, MD4,5 , Clemens Noelke, PhD, 6 , Mark Zamani, MS3 , Andrew F. Beck, MD, MPH7,8
1 Division of Hospital Medicine, Connecticut Children’s, Hartford, Connecticut
2 Department of Pediatrics, University of Connecticut School of Medicine, Farmington, Connecticut
3 Children's Hospital Association, Lenexa, Kansas
4 Department of Pediatrics, Children’s Mercy Kansas City, Missouri
5 University of Missouri Kansas City School of Medicine, Kansas City, Missouri
6 Heller School for Social Policy and Management, Brandeis University, Waltham, Massachusetts
7 Division of General & Community Pediatrics, Cincinnati Children’s, Cincinnati, Ohio
8 Department of Pediatrics, University of Cincinnati College of Medicine, Cincinnati, Ohio
BACKGROUND
Measures of social context, such as the Child Opportunity Index (COI), are associated with Ambulatory Care Sensitive Conditions (ACSCs). While these associations have been evaluated independently at ZIP code (ZIP) and census tract (CT) geographies, strengths of association and prediction between geographies have not been compared. Our objective was to quantify the misclassification of COI at the ZIP versus CT level and to compare associations with ACSC hospitalization rates.
METHODS
This retrospective cross-sectional study analyzed pediatric ACSC hospitalizations from two children’s hospitals in Cincinnati and Kansas City between 2013 and 2017. Patient addresses were geocoded and linked to COI metrics based on their home ZIP and CT. COI z-scores at both geospatial units were classified into quintiles as Very Low to Very High. COI misclassification at the ZIP level was defined as a COI category differing by ≥2 from the CT assignment. Geospatial and regression analyses assessed the impact of misclassification on estimating ACSC hospitalization rates.
RESULTS
Misclassification occurred in 8.3% of ACSC hospitalizations (Figure 1). There was no clear pattern to misclassified ZIP codes when mapped (Figure 2). For every unit increase in the COI z-score, the ACSC hospitalization rate decreased by 28.8% and 28.4% for ZIP and CT, respectively (p=0.20) (Table 1). When stratified by hospital site, ZIP significantly underpredicted hospitalization rate decreases in Cincinnati (-29.4% vs. -33.5% p<0.001) but not in Kansas City (-27.7% vs. -26.8% p=0.25).
CONCLUSION
Using ZIP codes to assign COI scores may be inappropriate for single county analyses of ACSC hospitalization rates.
TABLES AND FIGURES
Figure 1: Subject child opportunity index classification by ZIP code versus Census Tract
Figure 2: Mapping of Kansas City and Cincinnati metrics of child opportunity, errors of misclassification, and overall ACSC hospitalization rates
Table 1: Comparing annual hospitalization rate trends for ACSCs by hospital city over COI 3.0 z-scores at the ZIP code and census tract level using a log-linear model with Poisson distribution
The Child Opportunity Index and Pediatric Hospitalizations: Are ZIP Codes Good Enough?
Alexander H. Hogan, MD, MS1, Natalie Grills, MS2, Matt Hall, PhD2, Mitch Harris, PhD, MS2, Molly Krager, MD3 , Clemens Noelke, PhD4, Mark Zamani, MS2, Andrew F. Beck, MD, MPH5
BACKGROUND
• Social context (e.g., Child Opportunity Index, COI) is associated with Ambulatory Care Sensitive Conditions (ACSCs)
• Associations have been evaluated independently at ZIP code and census tract geographies, but not head-to-head
OBJECTIVE
• Quantify COI misclassification at the ZIP code vs. census tract level & compare associations with ACSC hospitalization rates
METHODS
Geocoding ZIP codes and census tracts produced similar associations between Childhood Opportunity and hospitalization rates in aggregate, but not when stratified by city
• Retrospective cross-sectional study of ACSC hospitalizations in 2 Midwestern cities 2013-2017 for youth ages 0-17 years
• Geocoded using HIPAA-Compliant DeGAUSS
• COI 3.0 linked at both ZIP code and census tract geographies.
• Misclassification defined as ZIP code COI differing by ≥2 levels from census tract COI assignment
• Geospatial and regression analyses assessed impact of misclassification on modeling ACSC hospitalization rates
RESULTS
• 26,421 ACSC hospitalizations across 628 census tracts (containing 604,943 children) and 206 ZIP codes (Fig 1)
• Misclassification occurred in 10.7% of ACSC hospitalizations
• For every 1 SD increase in COI z-score, ACSC hospitalization rate decreased by:
• 28.8% for ZIP codes
• 28.4% for census tracts
• Overall difference by geography not significant (p=0.2; Fig 2)
• When stratified by city, ZIP code underpredicted hospitalization rate decreases compared to census tracts in Cincinnati (29.4% vs 33.5%, p<0.001) but not Kansas City (27.7% vs 26.8%, p=0.23)
CONCLUSIONS
• Assigning COI using ZIP codes appears appropriate for correlational analyses in large national datasets
• The observed attenuation bias suggests ZIP code COI may underestimate the true association between neighborhood opportunity and health outcomes, especially in smaller areas
Figure 1: Mapping of Kansas City and Cincinnati metrics of child opportunity and overall ACSC hospitalization rates.
Knowledge and Beliefs of Pregnant Women for Food Allergy Prevention in Their Offspring
Presenting Author: Sin Ting Hui (Abbie), MS Sin Ting Hui (Abbie), MS1, Richard Feinn, PhD1, Alexander Duarte, MPH2, Julie Flom, MD MPH2, Stephanie Leeds, MD MHS2
1 Frank H. Netter School of Medicine at Quinnipiac University, North Haven, CT;
2 Department of Pediatric Allergy and Immunology, Yale University School of Medicine, New Haven, CT
BACKGROUND
Over 8% of U.S. children have food allergies. Past guidelines to delay food allergen introduction to infants may have contributed to this rise. Recent studies highlight timing, dose, and form of food exposure are crucial for allergy prevention.
METHODS
This study investigates pregnant women’s perspective and interest in food allergy prevention for their offspring. Participants from two Yale clinics, during routine ultrasound or allergy visits, completed a 16question survey on perceptions of susceptibility, symptoms, diagnosis, triggers, treatment, and personal and family allergy history. Data were analyzed using chi-square in SPSS and Prism.
RESULTS
Among 153 participants, 72.5% were White, 9.2% Black/African American, 6.5% Asian, and 3.3% multiracial, while 21 (13.7%) identified as Hispanic/Latino/Spanish origin. Concern about food allergy in their offspring was higher among those with a personal/household food allergy diagnosis (50.0% vs 23.9%, p=0.002). Additionally, as compared to other races combined, Black/African American participants were more likely to refer to family history as a concern (81.8% vs 35.1%, p=0.019). Most survey respondents (70.6%) were interested in a food allergy prevention clinic for their offspring. Interested mothers were more likely to have no other children at home (85.5% vs 52.9%, p<0.001), have a personal/household food allergy diagnosis (84.1% vs 65.1%, p=0.02), and have a personal/household eczema or other allergy diagnosis (76.6% vs 54.8%, p=0.014).
CONCLUSION/SIGNIFICANCE
This study highlights how personal/household allergy diagnoses and family history shape food allergy concerns, particularly among Black/African American expectant mothers, and reflects strong community interest in a food allergy prevention clinic for their offspring.
Knowledge and Beliefs of Pregnant Women for Food
Allergy Prevention in Their Offspring
Sin Ting Hui (Abbie), MS¹, Richard Feinn, PhD¹, Alexander Duarte, MPH², Julie Flom, MD MPH², Stephanie Leeds, MD MHS²
¹Frank H. Netter School of Medicine at Quinnipiac University, North Haven, CT; ²Department of Pediatric Allergy and Immunology, Yale University School of Medicine, New Haven, CT
ABSTRACT
Introduction: Over 8% of U S children have food allergies ¹ Past guidelines to delay introduction of allergenic foods to infants may have increased the prevalence of childhood food allergy ² Recent studies highlight that timing, dose, and form of food exposure are crucial for allergy prevention 3 Effective prevention strategies are necessary to reduce long-term sequelae of food allergy 4
Methods: This study investigates pregnant women’s perspective and interest in food allergy prevention for their offspring Recruited from two Yale clinics during a routine ultrasound or an allergy visit, individuals completed a 16-question survey on perceptions of susceptibility, symptoms, diagnosis, triggers, and treatment of pediatric food allergy as well as demographic information including personal and family allergy history
Data were analyzed with chi-square tests in SPSS and Prism
Results: Among 153 participants, 72 5% were White, 9 2% Black/ African American, 6 5% Asian, and 3 3% multiracial, while 21 (13 7%) identified as Hispanic/ Latino/ Spanish origin Most (80 4%) had private insurance, and 17% had government-issued insurance Food allergies were diagnosed in 28 8% of pregnant mothers or household members As compared to those without a personal or household diagnosis of food, individuals with a personal or household food allergy diagnosis were more likely to report “some or all of the time” thoughts of their offspring’s risk of food allergy (50 0% vs 23 9% p<0 001) In addition, as compared to other races combined, Black/ African American participants were more likely to refer to family history as a concern (81 8% vs 35 1%, p=0 019) Most survey respondents (70 6%) were interested in a food allergy prevention clinic for their offspring Interested mothers were more likely to not have other children at home (85 5% vs 52 9% p<0 001), to have
Discussion
INTRODUCTION
• Both the skin and the gut are involved in immune sensitization and tolerance, respectively, according to the dual allergen exposure hypothesis5
• Dysbiosis of the gut microbiome may be implicated in chronic diseases, and a diversity of early nutrients may play a vital role in decreasing the risk of food allergy among infants6
• Recent randomized controlled studies with peanut support active early introduction and incorporation into the diet, leading to changes to guidelines in allergenic consumption during infancy7
• The Learning Early About Peanut (LEAP study) found a 80% reduction of peanut allergy in five-yearolds who regularly ate peanuts from the ages of four to six months compared to those who avoided peanut
OBJECTIVES
To assess the knowledge, attitudes, and beliefs of pregnant women regarding food allergy prevention in their offspring
To examine the interest of pregnant women in a new food allergy prevention telemedicine clinic for their offspring
METHODS
Data Analysis
Who Had an Interest in Food Allergy Counseling?
Individuals
• Pregnant
Study Participants (N=153)
Participant Thoughts About Food Allergy Risk in Offspring
“some or all of the time” thoughts of their offspring’s risk of food allergy (50 0% vs 23 9%, p=0 002) They attributed these concerns to family history (68 4% vs 24 3%, p<0 001) more than discussion with
First Time vs Experienced Mothers: Responses to Food Allergy Knowledge Questions
• Continue to analyze maternal knowledge of food allergy prevention for their offspring, assessing their gaps in food allergy knowledge.
• Identify caregivers who may need more support with food allergy prevention strategies for their offsprings.
• Explore healthcare providers’ knowledge, attitude and beliefs of food allergy prevention for their patients.
INTO THE UNKNOWN:
Establishing Mobilization of Patients in a Low Volume Pediatric Extracorporeal Membrane Oxygenation (ECMO) Center
Presenting Author: Kim Koenig PT, Brittany Carter MHA, RRT-NPS
Koenig K PT, Schultes J MSN, RN, Carter B MHA,RRT-NPS, Campbell J D DO, Cowl A S MD
Connecticut Children’s, Hartford, CT
BACKGROUND
Early mobilization of patients on ECMO enhances patient outcomes physically, physiologically, and psychologically. Mobilization at low-volume centers is challenged by limited experience and associated inherent risks. Our compelling case involving a 3-year-old needing a lung transplant underscored the necessity of re-evaluating our approach.
METHODS
A retrospective analysis of our patients on ECMO determined that 2 of 55 patients engaged in at most bed-level therapy. Our multidisciplinary team performed a causal analysis to determine root causes and opportunities for improvement regarding physiologic and psychological markers, environmental and structural constraints, patient safety, and communication. Associated countermeasures included: creating customized educational content via simulation and demonstrative videos, standardized pre-movement time-outs, closed-loop communication, tailor-made cannula stabilizers, and a work standard to verify cannula position with and post-movement.
RESULTS
By implementing best practices, we mobilized them 115 times with zero adverse events, over 106-days. Progressive functional strengthening was used to transition from no anti-gravity movement to riding a trike. As strength and function improved, so did their quality of life, evidenced by age-appropriate play, emotional interactions, and bonding with family; ultimately resulting in transfer to a transplant center.
CONCLUSION/SIGNIFICANCE
This initiative not only aligns with evidence-based practices but also demonstrates our commitment to improving patient care and outcomes. This particular patient’s need for mobilization became the catalyst we needed for change. Despite initial apprehension, embracing early mobilization enhanced patient outcomes, and boosted our team's confidence and competence in handling complex ECMO cases.
Into the Unknown: Application of Scientific Method to Improve Mobility of Pediatric Patients on Extracorporeal Membrane Oxygenation (ECMO) in a Low Volume Center
Koenig K PT, Schultes J MSN, RN, Carter B MHA, RRT-NPS
Background
Early mobilization of patients on ECMO enhances patient outcomes physically, physiologically, and psychologically. Mobilization at lowvolume centers is challenged by limited experience and associated inherent risks. Our compelling case involving a 3-year-old needing a lung transplant underscored the necessity of re-evaluating our approach.
Methods
A retrospective analysis of our patients on ECMO determined that 2 of 55 patients engaged in at most bed-level therapy. Our multidisciplinary team performed a causal analysis to determine root causes and opportunities for improvement regarding physiologic and psychological markers, environmental and structural constraints, patient safety, and communication. Associated countermeasures included: creating customized educational content via simulation and demonstrative videos, standardized pre-movement time-outs, closed-loop communication, tailor-made cannula stabilizers, and a work standard to verify cannula position with and post-movement.
Dedication
To the special little girl and her family who gave us the courage to push the limits, expand our horizons, challenged us to overcome this obstacle to go into the unknown.
Scientific Process
Background
Collection
• Internal Findings:
o Performed bed-level activities on 2 out of 55 patients placed on ECMO.
o Barriers: Safety of Patient, Communication, Psychological Fear, Equipment Limitations, Use of Sedatives/Paralytics, Education Gaps with Best Practices
• External Findings:
o High-volume ECMO centers can successfully mobilize patients out of bed.
Hypothesis Construction
Experimentation
• By fostering a culture of continuous improvement and adapting best-practice strategies, a lowvolume ECMO program can successfully achieve out-of-bed mobilization with patients on ECMO.
• Customized educational content via simulation and demonstrative videos to enhance staff training and ensure consistency.
• Standardized pre-movement time-outs to increase role adherence, situational awareness, and closed-loop communication.
• Tailor-made cannula stabilizers to address poor head control.
• Daily x-rays and echoes to address potential cannula migration post-movement.
• Functional strengthening plan to allow for gradual progression of patient’s mobility.
Results
This initiative not only aligns with evidence-based practices but also demonstrates our commitment to improving patient care and outcomes. This particular patient’s need for mobilization became the catalyst we needed for change. Despite initial apprehension, embracing early mobilization enhanced patient outcomes, and boosted our team's confidence and competence in handling complex ECMO cases.
By implementing best practices, we mobilized them 115 times with zero adverse events, over 106-days. Progressive functional strengthening was used to transition from no anti-gravity movement to riding a trike.
As strength and function improved, so did their quality of life, evidenced by age-appropriate play, emotional interactions, and bonding with family; ultimately resulting in transfer to a transplant center.
Acknowledgments
Thank you to the entire PICU, ECMO and rehab staff who travelled this road with us. The saying is true that teamwork makes the dream work because it took everyone to accomplish this goal. A special note of thanks to all those who helped the unknown become known.
Data Analyzation
• Actively mobilized 115 times over 106 days
• No movement against gravity to standing, walking, and ultimately riding a tricycle.
• Improved Quality of Life: age-appropriate play, emotional interactions, bonding with staff and family
• Accepted and transferred to a transplant center.
Conclusions Low-volume ECMO centers can effectively mobilize patients on ECMO out of bed through adaptation of best-practice strategies and fostering a continuous improvement culture:
• Embrace Scientific Thinking
• Create Value for the Customer
• Respect Every Individual
Eating Disorders in Patients with Glycogen Storage Disease
Division of Endocrinology, Connecticut Children’s, Hartford, CT, USA
Division of Pediatric Psychology, Connecticut Children’s, Hartford, CT, USA
Division of Adolescent Medicine, Connecticut Children’s, Hartford, CT, USA
Background
Glycogen Storage Disease type Ia (GSDIa) is a severe genetic metabolic disorder treated by diet. Patients with GSDIa must follow a very restrictive diet to minimize hypoglycemia, which can impair hunger cues. Nutritional rehabilitation of an eating disorder (ED) is often counter to the management of GSD. Eating problems have been described in patients with GSD, but frank clinical eating disorders have not been described in this population. We present two cases.
Cases
Patient 1, was diagnosed with anorexia nervosa at age 15. She presented with weight loss, excessive exercising, caloric restriction, and hypoglycemia. She had an acute decompensation requiring inpatient medical admission under an ED protocol modified for GSDIa. In long-term treatment, weight gain and improved stability of ED was associated with increasing hepatomegaly, and adjustment of treatment goals and weight was necessary to improve metabolic control.
Patient 2, was diagnosed at 15-years of age with depression and an unspecified ED. She presented with endorsement of self-induced vomiting, restricted eating, goal of significant weight loss and stress around eating in the context of significant depression and suicidal ideation. She did not experience weight loss, change in metabolic control or frequency of hypoglycemia.
Conclusion/Significance
Eating disorders can be life threatening, and in association with GSD there can be additional difficulties with diagnosis, management and recovery. The treatment of ED and GSD can be in opposition based on nutritional goals and eating patterns. Early detection and high intensity multi-disciplinary treatment is necessary to balance the management of GSD and ED.
Eating Disorders in Patients with Glycogen Storage Disease
(1) Division of Endocrinology, Connecticut Children’s, Hartford, CT (2) Division of Pediatric Psychology, Connecticut Children’s, Hartford, CT (3) Division of Adolescent Medicine, Connecticut Children’s, Hartford, CT
INTRODUCTION
• Glycogen Storage Disease type 1a (GSD1a) is caused by a mutation in the glucose-6-phosphatase gene (G6PC), the final step in glycogenolysis and gluconeogenesis.
• This severe metabolic disease carries acute risks of hypoglycemia, lactic acidosis and seizures in addition to chronic risks of cognitive delays, growth impairment, hypertriglyceridemia, hyperuricemia, hepatomegaly, nephropathy and obesity.
• The current management of GSD1a is diet modification and use of intermittent cornstarch on a strict schedule.
• Cornstarch provides glucose and lactate stability, comprising ~70% of daily calories
• Low dietary carbohydrate (outside of cornstarch)
• Avoidance of simple sugars (sucrose, fructose and galactose) as they are unable to be utilized
CASE #2
DISCUSSION
• Eating problems (i.e. selective, avoidant symptoms, etc.) have been described in patients with GSD, but frank clinical eating disorders (EDs) have not been described in this population. Here we present two cases of eating disorders in GSD1a patients
CASE #1
Patient 1 has GSD1a with chronically good metabolic control and stable BMI (103-112% of the 95th%) over the preceding 4 years. At 12y9m of age she lost 10.9 kg over 19 months (- 16.8%). Initial recommendations focused on weight stability with normal BMI 22.4 kg/m2 (77th%), but with increasing evidence of excessive exercising and caloric restriction she was referred to psychology. With continued weight loss (Fig. 1) she developed frequent hypoglycemia (glucose <55mg/dL), worsening metabolic markers (hypertriglyceridemia, hyperuricemia, and transaminitis) and acute hypophosphatemia, hypokalemia and lactic acidosis requiring intensive care unit admission.
She achieved medical stability on an inpatient ED protocol modified for GSD1a. Modifications included adjustment to macronutrient distribution, calorie targets and oral supplementation selection. An inpatient ED program was not possible due to complexity of GSD care, so she enrolled in an intensive outpatient ED program.
Weight gain and improved stability of ED was associated with progressive hepatomegaly radiographically and by exam. Adjustment of treatment goals (goal weight and rate of gain), and collaboration with psychology, adolescent medicine, endocrinology and eating disorder program allowed for stable weight and improved metabolic control. (Fig. 1 & 2)
Patient 2, a female with GSD1a, has had fluctuating metabolic control over the past 4 years and stable BMI (100-117% of the 95th%). She was diagnosed with depression and suicidal ideation at age 15, then developed symptoms of an unspecified ED. She presented with endorsement of self-induced vomiting, intermittent restrictive eating, reported goal of significant weight loss and stress around eating.
Intervention for depression included psychiatric care with an antidepressant, twice weekly outpatient psychotherapy with a pediatric psychologist, detailed safety planning, and additional medical management with adolescent medicine.
She did not experience weight loss, change in metabolic control or frequency of hypoglycemia. Her intrusive behaviors and thoughts have stabilized with multidisciplinary care. Depressive symptoms improved, with gradual reduction of ED symptoms. She has been stable without recurrence of eating disorder symptoms for two years.
Eating disorders occur in 9% of the United States population, with 1 death occurring every 52 minutes as a direct result from an ED. During the COVID-19 pandemic, eating disorder prevalence in adolescents and young adults increased with +7% per month inpatient admissions and +8% per month new outpatient assessments. Patients with chronic illnesses that include diet as part of their treatment are thought to have an even higher incidence of EDs.
GSD patients with ED’s are rarely described in the literature, and the prevalence and potential increase since 2019 is not known. Both diagnoses hold independent risks associated with significant morbidity and mortality rates.
Nutritional rehabilitation of an eating disorder is often counter to the management of GSD given that caloric excess and weight gain goals for EDs can increase inaccessible glycogen storage in GSD. Standard steps for ED treatment include carbohydrate targets that are inappropriate for those with GSD, making treatment pathway modification essential.
The two patients presented demonstrated benefits from multidisciplinary care (Fig. 2). A team approach with close communication is necessary for successful treatment of this population.
CONCLUSION
Figure 1: Patient 1 weight and labs (triglycerides, AST, ALT) over 3 years
Eating Disorder Specialist
• Limitations: safety of GSD1a management in inpatient program
• Partnership with dietitian to adjust nutritional composition, rate of weight gain goals
• Monitoring plan Nutrition
• Total caloric deprivation contributes to hypoglycemia
• Consider transient increased need for cornstarch
• Protein, fat, and calorie increase as indicated taking cornstarch into account
Figure 2: Multidisciplinary teams and roles Psychology
• Partnering to cover both expertise in chronic disease and eating disorder treatment
• Partnership with ED specialist to adjust nutritional composition, rate of weight gain goals Monitoring
• Risk/benefit of continuous glucose monitoring
• Consider blinding data (weight & blood glucose)
• Inpatient monitoring for lactate may be required in acute phase
• Closer liver size and metabolic lab monitoring
• If pediatric, consider parental oversight of food and data
The treatment of EDs and GSD can be in opposition based on nutritional goals and eating patterns. Early detection and high intensity multi-disciplinary treatment is necessary to balance the management of GSD and EDs.
Family economic strain (FES) (i.e. perceived financial hardship regardless of income) is prevalent among low socioeconomic status (SES) families. Low SES is linked with poor sleep among children, but the mechanism underlying this relationship is unclear. In this study, we test the hypothesis that FES will be associated with problematic parent-child sleep interactions.
METHODS
We surveyed caregivers with children aged 3-5 years. Participants completed the Family Economic Strain Scale, Parent-Child Sleep Interactions Scale, and Perceived Stress Scale. We examined relationships between study variables using multivariate linear regression, adjusting for child age, household size, and caregiver relationship status. We tested perceived stress as a mediator between FES and parent-child sleep interactions using 5,000 bootstrap samples.
RESULTS
164 caregivers participated. FES was directly associated with problematic sleep interactions (β = 0.357, p<.001) and perceived stress (β = 0.596, p < 0.001). Caregiver stress was associated with problematic sleep interactions (β = 0.289, p < 0.001). The estimated indirect effect of FES on sleep interactions suggested that 11.6% of the total effect of FES on sleep interactions may be mediated by perceived stress, but the indirect effect was not significant (β = 0.047, 95% CI0.056, 0.153).
CONCLUSION/SIGNIFICANCE
FES is correlated with caregiver stress, and both are associated with problematic parent-child sleep interactions. However, caregiver stress did not mediate the relationship between FES and sleep interactions. Reducing economic strain and supporting caregivers in bedtime interactions could improve child sleep equity. Future research should examine additional social and structural determinants affecting child sleep.
Family Economic Strain is Associated with Parent-Child Sleep Interactions
Background
Hannah R. Scheibner, BSN, RN, School of Nursing Wanli Xu, PhD, RN; Stephen Walsh, ScD, MTS, SCM; Eileen Condon, PhD, APRN, FNP-BC
• Low socioeconomic status (SES) is associated with insufficient sleep among young children, less consistent sleep routines, and low health literacy.1,2
• Low SES families may also have higher family economic strain (FES) which can cause parental stress that can negatively affect family interactions.
• Pathways between financial hardship and child sleep are unclear.
• Parent-child sleep interactions may be affected by FES and are modifiable to promote sleep health.
• Problematic parent-child sleep interactions include need for more sleep reinforcement, increased sleep conflict, and sleep dependence.3
Purpose
• Examine the relationship between family economic strain and parentchild sleep interactions.
• Determine if perceived stress mediates relationship between family economic strain and parent-child sleep interactions.
Methods
• Cross sectional anonymous online survey of caregivers with children ages 3-5 in the U.S.
• Recruited through social media and community flyers. September 2023-May 2024.
• Conducted multivariate linear regression adjusting for child age, household size, and caregiver relationship status.
• Tested mediation using 5,000 bootstrap samples with Preacher & Hayes macro for SPSS.
Results
Sample: 168 caregivers with children ages 3-5 years Variables and Measures
• Family Economic Strain is positively associated with Perceived Stress (β=.587, p<.001).
• Family Economic Strain is positively associated problematic with Parent-Child Sleep Interactions (β=.401, p<.001).
• Perceived Stress is positively associated with problematic ParentChild Sleep Interactions (β=.289, p<.001).
• 11.6% of the total effect of FES on sleep interactions may be mediated by perceived stress.
• Indirect effect of FES on sleep interactions is not significant (β = 0.047, 95% CI -0.056, 0.153).
Discussion
• FES and perceived stress are associated with problematic parentchild sleep interactions.
• Relationship between FES and parent-child sleep interactions is not attributable to perceived stress.
• Supporting caregivers in promoting healthy bedtime interactions is an important area for intervention to promote sleep health equity.
• Improved accessibility to public assistance and interventions to reduce FES are vital to address root causes and reduce inequities.
• More research is needed to understand social and structural determinants affecting child sleep. References
Field Testing a Pediatric SMART Asthma Treatment Plan
Presenting Author: Abigail Tulchinsky
Abigail Tulchinsky, Angela Bermúdez-Millán, Caleb Wasser, and Jessica Hollenbach
University of Connecticut School of Medicine, UConn Health, Farmington, CT
Asthma Center, Connecticut Children’s Medical Center, Hartford, CT
RATIONALE
Provision of written asthma treatment plans (ATPs) is a core tenet of asthma management. The 2020 focused update recommends single maintenance and reliever therapy (SMART) as the preferred therapy for individuals (≥4 years) with moderate to persistent asthma. There is an evidence-to-practice gap and a need for an understandable and actionable SMART ATP. The purpose of this research was to field-test and refine a SMART ATP that is understandable to the people it is designed to help.
METHODS
Caregivers of children with asthma were approached in waiting rooms of primary care clinics in Hartford, CT. Participants were presented the ATP and probed with questions to assess their understanding. Demographic data was collected. Iterative rounds of field-testing and a final focus group were used to recognize, categorize, and contextualize major themes.
RESULTS
From November 2022 to August 2023, 101 participants were approached. Thirteen English-speaking participants and 5 Spanish-speaking participants were enrolled (n=18). Participants’ mean age was 37 years, with the majority reported as the biological mother (89%) and of Latino/Puerto Rican ethnicity (78%). Two rounds of field-testing were conducted. Themes identified during field testing include confusion around timing and dosage of SMART therapy and confusion between the daily vs the sick treatment plan. In April 2024 a final focus group was conducted with three participants, confirming changes made to the treatment plan were understandable and actionable.
CONCLUSIONS
A SMART ATP was finalized from analyses of two iterations and a focus group with families of children with asthma.
References:
1.Reddel HK, Bateman ED, Schatz M, Krishnan JA, Cloutier MM. A Practical Guide to Implementing SMART in Asthma Management. Journal of Allergy and Clinical Immunology: In Practice. 2022;10(1):S31-S38. doi:10.1016/j.jaip.2021.10.011
2.Zaeh SE, Ramsey R, Bender B, Hommel K, Mosnaim G, Rand C. The Impact of Adherence and Health Literacy on Difficult-to-Control Asthma. Journal of Allergy and Clinical Immunology: In Practice 2022;10(2):386-394. doi:10.1016/j.jaip.2021.11.003
v
v
Field Testing a Pediatric SMART Asthma Treatment Plan
Abigail Tulchinsky 1, Angela Bermudez-Milan 2, Caleb Wasser 3, and Jessica Hollenbach 3
1 University of Connecticut School of Medicine, UConn Health, Farmington, CT
2 University of Connecticut School of Public Health, UConn Health, Farmington, CT
3 Asthma Center, Connecticut Children’s Medical Center, Hartford, CT
Background
Background
• Asthma treatment plans (ATPs) are a core tenet of asthma management.
• The 2020 update to the NHLBI asthma guidelines recommends single maintenance and reliever therapy (SMART) as the preferred therapy for individuals (≥4 years) with moderate to persistent asthma. 1
• There is an evidence-to-practice gap in the uptake of SMART and a call to action for the development and field-testing of an understandable and actionable SMART Asthma Treatment Plan.2
• Lower health literacy is associated with worse asthma outcomes and understandable ATPs are an important tool in asthma management .3
• The purpose of this study is to field test and refine a SMARTATP to assess for understanding and actionability of the document.
• The successful development of anATP that is understandable will improve adherence to SMART therapy.
Methods
Recruitment
• Parents or caregivers of children with asthma were approached in waiting rooms of 2 urban primary care clinics in Hartford, CT. Field Testing
• Semi-structured interviews with individual participants were used to assess readability, understandability, actionability, and coherence of theATP.
• Interviews were conducted in both English and Spanish.
• Basic demographic information was collected to characterize our study sample and ensure generalizability of qualitative findings. Analysis
• Iterative rounds of field-testing and thematic analysis were used to recognize, categorize, and contextualize major themes.
• Aqualitative descriptive approach was used for this study following principles of thematic analysis .
Focus Group
• Families of children with asthma were recruited to reach consensus on the final SMARTATP.
Summary of Feedback
FinalATP Developed from Patient Feedback
InitialATP
Category: Population/Community Health
Reducing Racial Inequity: Partnering with Patients for Advocacy
Presenting Author: Emily O. Wakefield, PsyD
Emily O. Wakefield, PsyD1,2, Carissa DelGaudio, BS1, Vaishali Belamkar, BA1
1 Connecticut Children’s
2 University of Connecticut School of Medicine
BACKGROUND
Racialized youth with chronic pain experience marginalization in health care, contributing to poorer health outcomes. To address these inequities, we partnered with Black youth with chronic pain and their caregivers through a task force focused on addressing research and clinical inequities through advocacy.
METHODS
Members of the Chronic Pain Advocacy Group (CPAG) were three adolescents and young adults with chronic pain (Mage=18.02) and three caregivers (Mage=54.67) who identified as Black or African American. CPAG members were approached for participation following an individual interview study about the experience of racial bias and chronic pain. Five bi-monthly meetings have been held to date, and they are ongoing.
RESULTS
The partnership with the CPAG has yielded several research and clinical initiatives addressing racial pain inequities. Specifically, the CPAG co-developed a Guide to School Accommodations parent handout. The group has also revised and approved a recruitment flyer for a community research study to recruit Black youth with chronic pain. CPAG members also reviewed and approved the research results related to the interview study on racial bias and chronic pain and how these findings were presented at a national conference. Lastly, two CPAG members will co-present their lived experiences and the importance of the CPAG in addressing racial pain inequities at an upcoming conference.
CONCLUSION/SIGNIFICANCE
Our study exemplifies the importance of patient partnerships in reducing medical mistrust and health inequities. Including voices from marginalized communities is necessary to identify the most important issues to a community. Best practices for patient partnership will be discussed.
Reducing Racial Inequity: Partnering with Patients for Advocacy
Emily O. Wakefield, PsyD 1,2, Carissa DelGaudio, BS1, and Vaishali Belamkar, BA 1
1 Connecticut Children’s, Hartford, CT, 2 University of Connecticut School of Medicine, Farmington, CT
BACKGROUND
INTRODUCTION
RESULTS
Racialized youth with chronic pain experience marginalization in health care, contributing to poorer health outcomes. Marginalized youth engagement in research has demonstrated benefits for youths’ perceived control, empowerment to influence change, confidence,1 leadership, academic or career building, social skills, critical consciousness, interpersonal skills, and cognitive skills.2 To address these racial pain inequities, we partnered with Black youth with chronic pain and their caregivers through a task force focused on addressing research and clinical inequities through advocacy.
METHODS
Testimonials from CPAG Members
“Sharing our experiences and knowing that I’m not alone has been one of the most valuable parts. Also, having a space where we can discuss our challenges openly without judgment has been really empowering. Plus, I feel like we’re actually making a difference by giving feedback that could improve care for other teens in the future.”
18-year-old Black, Not Hispanic Female
Research Initiatives to Address Racial Pain Inequities
• The group has revised and approved a recruitment flyer for a community research study to recruit Black youth with chronic pain.
• Members of the Chronic Pain Advocacy Group (CPAG) were three adolescents and young adults with chronic pain (Mage=18.02) and three caregivers (Mage=54.67) who identified as Black or African American.
• CPAG members were approached for participation following an individual interview study about the experience of racial bias and chronic pain.
• Six bi-monthly meetings have been held to date, and they are ongoing.
• The following best practices2,3 were implemented:
1. Collaboratively define the group’s purpose
2. Treat participants as content experts
3. Offer opportunities to benefit from the group
4. Provide full transparency
5. Maintain cultural humility and respect
“What I have liked most about being a Chronic Pain Advocacy Group member is the diversity and inclusion that is shown. I also love the compassion that is shown to our many experiences.”
17-year-old Black, Not Hispanic Female
“What I like most about being a member of the Chronic Pain Advocacy Group is the empathy that each one of the facilitators have shown and their heart for people. They make it very clear and evident that they are in this with us. That they too want to find solutions to the racial inequities in healthcare.”
Mother of a 17-year-old Black, Not Hispanic Female
CONCLUSION & SIGNIFICANCE
• Our study exemplifies the importance of patient partnerships in reducing medical mistrust and health inequities. Including voices from marginalized communities is necessary to identify the most important issues to a community.
• We recommend best practices detailed in the Methods for future partnerships to facilitate a safe, trusting and collaborative environment for marginalized youth and their caregivers.
• A limitation of the CPAG expressed by members was greater awareness of the group and concerns about resources to support the continuation of the CPAG.
• CPAG members also reviewed and approved the research findings related to the interview study on racial bias and chronic pain and how these findings were presented at a national conference.
• Two CPAG members co-presented their lived experiences and the importance of the CPAG in addressing racial pain inequities at a local conference.
Clinical Initiatives to Address Racial Pain Inequities
• The CPAG co-developed a Guide to School Accommodations parent handout.
• This handout is now available in Connecticut Children’s EPIC system in both English and Spanish.
Scan the QR code below to view the guide to school accommodations: