
Journa CALIFORNIA DENTAL ASSOCIATION September Medication-Related2022Osteonecrosisofthe Jaw Diffuse Large B-Cell Lymphoma Digital Workflows 2D and CBCT in Orthodontics 2022 SEPTEMBER50Vol n 9Nº


Protection for every stage of life and practice. The coverage you need at affordable MetLife group rates. DISABILITY COVERAGE Protect your investment in your profession by preparing for unexpected injuries or illnesses. Plus coverage from leading carriers. HEALTH COVERAGE Keep yourself, your family and your whole team well. Find affordable Individual & Family and Small Group plans from trusted carriers. LIFE INSURANCE Easily add extra protection or change coverage levels to secure your loved ones’ peace of mind and future financial well-being. Benefits paid even if you can work but can’t practice dentistry Great rates for CDA members through a MetLife group plan SOLUTIONSINSURANCE Learn more online tdicinsurance.com/solutionsat Call your local TDIC Insurance Solutions advisor at 800.733.0633 Scan here to get started: Flexible choice of benefit periods and maximum benefits Financial security with up to 60% of your income covered
TDIC Insurance Solutions offers other coverages as an agent or broker by agreements with our partner insurance carriers. Eligibility, available coverage limits and discounts vary by carrier and are subject to carrier underwriting. The information provided here is an overview of the referenced product and is not intended to be a complete description of all terms, conditions and exclusions. Not available in all states. TDIC Insurance Solutions | 1201 K Street, 17th Floor, Sacramento, CA 95814 | TDIC IS CA Lic. #0652783 Insurance coverage is issued by Metropolitan Life Insurance Company, 200 Park Avenue, New York, NY 10166. Like most group benefits programs, benefit programs offered by MetLife contain certain exclusions, exceptions, waiting periods, reductions, limitations and terms for keeping them in force. Ask your plan administrator for costs and complete details. Metropolitan Life Insurance Company | 200 Park Avenue | New York, NY 10166 | L0522022773[exp0524][All States][DC,GU,MP,PR,VI] © 2022 MetLife Services and Solutions, LLC.



Mark Mintline, DDS; Jeffrey A. Elo, DDS, MS, FACS; Setareh Lavasani, DDS, MS; James Ywom, DDS, MS; Ashtin Alves, DMD; and Ho-Hyun (Brian) Sun, DMD, MS An Overview of Digital Workflows for Precision Implant Dentistry
Inadequate Dental Imaging Delays Diagnosis of Pathologic Le Fort I Fracture Secondary to Bisphosphonate Use
Setareh Lavasani, DDS, MS; Ho-Hyun (Brian) Sun, DMD, MS; and Jeffrey A. Elo, DDS, MS
An introduction to the issue. Setareh Lavasani, DDS, MS
519527561505509499513
CDA JOURNAL, VOL 50 , Nº 9 SEPTEMBER 2022 495
This article provides an overview of the key steps and considerations for implementing digital implant dentistry for implant-supported fixed single or short-span restorations using a static implant guide.
Oral and Maxillofacial Radiology Diagnosis: The Role of Image Modality Selection, Interpretation Skills and Use of Cone Beam Computed Tomography Technology
Rafeeq N. Rahman, DDS; Alexander Lee, DMD; Setareh Lavasani, DMD, MS; and Tobias Boehm, DDS, PhD 2022 departments features 501 501 The Editor/Secret Welcome Sign, Really? WinnersImpressionsof the 2022 Dennis Shinbori, DDS, Table Clinic Competition RM Matters/Where’s the Line? Apply and Maintain Professional Boundaries Regulatory Compliance/Don’t Wait To Prevent Workplace Violence Tech Trends C.E. Credit 565559
This article demonstrates that clinicians must employ proper diagnostic methodologies to help detect and prevent future cases of this disease.
The Synergistic Role of 2D and 3D Imaging in Evaluating Tumors of the Jaws: A Case Report of Diffuse Large B-Cell Lymphoma of the Mandible
This article discusses a diffuse large B-cell lymphoma of the mandible that was diagnosed via examination in a dental office setting and further characterized by CBCT imaging.
SEPT.
CONTINUED ON PAGE 497

Management
Permission and Reprints
CDA JOURNAL, VOL 50 , Nº 9 496 SEPTEMBER 2022 Volume 50 Number 9 September 2022Journa
Judee Tippett-Whyte, DDS Immediate Past President pastpresident@cda.org
The Journal of the California Dental Association is published under the supervision of CDA’s editorial staff. Neither the editorial staff, the editor, nor the association are responsible for any expression of opinion or statement of fact, all of which are published solely on the authority of the author whose name is indicated. The association reserves the right to illustrate, reduce, revise or reject any manuscript submitted. Articles are considered for publication on condition that they are contributed solely to the Journal of the California Dental Association. The association does not assume liability for the content of advertisements, nor do advertisements constitute endorsement or approval of advertised products or services.
Ariane R. Terlet, DDS President president@cda.org
Visit cda.org/journal for the Journal of the California Dental Association’s policies and procedures, author instructions and aims and scope statement. CDA community by following and sharing on social channels
John L. Blake, DDS President-Elect presidentelect@cda.org Carliza Marcos, DDS Vice President vicepresident@cda.org Max Martinez, DDS Secretary secretary@cda.org Steven J. Kend, DDS Treasurer treasurer@cda.org Debra S. Finney, MS, DDS Speaker of the House speaker@cda.org
Paul Krebsbach, DDS, PhD, dean and professor, section of periodontics, University of California, Los Angeles, School of Dentistry
Harold Slavkin, DDS, dean and professor emeritus, division of biomedical sciences, Center for Craniofacial Molecular Biology, Herman Ostrow School of Dentistry of USC, Los Angeles
The Journal of the California Dental Association (ISSN 1942-4396) is published monthly by the California Dental Association, 1201 K St., 14th Floor, Sacramento, CA 95814, 916.554.5950. The California Dental Association holds the copyright for all articles and artwork published herein.
Copyright 2022 by the California Dental Association. All rights reserved.
com/jcaldentassocwww.editorialmanager.Letterscowww.editorialmanager.SubmissionsManuscript916.554.5950Andrea.LaMattina@cda.orgm/jcaldentassoctotheEditor
CDA Officers
Steven W. Friedrichsen, DDS, professor and dean emeritus, Western University of Health Sciences College of Dental Medicine, Pomona, Calif.
Peter A. DuBois Executive Director
published by the 1201CaliforniaDentalAssociationKSt.,14thFloorSacramento,CA95814800.232.7645cda.org
Mina Habibian, DMD, MSc, PhD, associate professor of clinical dentistry, Herman Ostrow School of Dentistry of USC, Los Angeles Robert Handysides, DDS, dean and associate professor, department of endodontics, Loma Linda University School of Dentistry, Loma Linda, Calif.
Brian J. Swann, DDS, MPH, chief, oral health services, Cambridge Health Alliance; assistant professor, oral health policy and epidemiology, Harvard School of Dental Medicine, Boston
Carrie E. Gordon Chief Strategy Officer Alicia Malaby Communications Director Editorial Kerry K. Carney, DDS, CDE Editor-in-Chief Kerry.Carney@cda.org Ruchi K. Sahota, DDS, CDE Associate Editor Marisa Watanabe,KawataDDS, MS Associate Editor Gayle Mathe, RDH Senior Editor Setareh Lavasani, DDS, MS Guest Editor Andrea LaMattina, CDE Publications Manager Kristi Parker Johnson Communications Manager Blake Ellington Tech Trends Editor Jack F. Conley, DDS Editor Emeritus Robert E. Horseman, DDS Humorist Emeritus Production Danielle Foster Production Designer Upcoming Topics October/Diversity in Dentistry November/Dental Student Research December/General Topics Advertising Sue Gardner Advertising Sales 916.554.4952Sue.Gardner@cda.org
Charles N. Bertolami, DDS, DMedSc, Herman Robert Fox dean, NYU College of Dentistry, New York
Connect@cdadentiststothe
CALIFORNIA DENTAL ASSOCIATION
Andrea LaMattina, CDE Publications Manager
Richard W. Valachovic, DMD, MPH, president emeritus, American Dental Education Association, Washington, D.C.
Bradley Henson, DDS, PhD, interim vice president research & biotechnology, associate dean for research and biomedical sciences and associate professor, Western University of Health Sciences College of Dental Medicine, Pomona, Calif.
Journal of the California Dental Association Editorial Board
Michael Reddy, DMD, DMSc, dean, University of California, San Francisco, School of Dentistry
Jayanth Kumar, DDS, MPH, state dental director, Sacramento, Calif.
Avishai Sadan, DMD, dean, Herman Ostrow School of Dentistry of USC, Los Angeles
Lucinda J. Lyon, BSDH, DDS, EdD, associate dean, oral health education, University of the Pacific, Arthur A. Dugoni School of Dentistry, San Francisco Nader A. Nadershahi, DDS, MBA, EdD, dean, University of the Pacific, Arthur A. Dugoni School of Dentistry, San Francisco Francisco Ramos-Gomez, DDS, MS, MPH, professor, section of pediatric dentistry and director, UCLA Center for Children’s Oral Health, University of California, Los Angeles, School of Dentistry




Paula Andrea Villa-Machado, DDS; Julián González-García, DDS; and Felipe Augusto Restrepo-Restrepo, DDS
CDA JOURNAL, VOL 50 , Nº 9 SEPTEMBER 2022 497
Audrey Yoon, DDS, MS; Linda Phi, DDS, MSD; and Joorok Park, DMD, MSD
The Role of CBCT and Guided Endodontics in Accessing a Calcified Maxillary Molar Using Computer-Assisted Dynamic Navigation: A Case Report
This manuscript explores the history of radiology in orthodontics, elaborates on the current usage of cone beam computed tomography (CBCT) and discusses the future directions of orthodontics with advancing technology.
541551 CONTINUED FROM PAGE 495
This article reports a case in which the distobuccal canal of a maxillary second molar, which was obliterated up to the middle third of the root, was precisely and conservatively located with dynamic navigation.
An Update on the Utilization of 2D and Cone Beam Computed Tomography Imaging in Orthodontics
Ever y Californian deserves a healthy smile. You already know how dentistr y relieves pain, restores dignity and instills hope. Join the CDA Foundation’s mission to improve the oral health of all Californians. Together with volunteers and donors, we suppor t dentists’ effor ts to give back to their communities and reduce barriers to care. • Student Loan Repayment Grants to make careers in public health possible • Dental Materials & Supplies Grant for nonprofit dental care organizations • Volunteer-led CDA Cares clinics that shine a light on underser ved areas • Suppor t of RDA apprenticeship programs to fill dentistr y’s staffing pipeline • Peer-to-peer Wellness Program for dentists’ physical and mental well-being See how you can contribute today at cdafoundation.org


The point is, there is nothing like an injury to heighten ones awareness of all the casual, thoughtless ways we make everyday life inaccessible to people with disabilities.
CDA JOURNAL, VOL 50 , Nº 9 SEPTEMBER 2022 499 The Editor
A Secret Welcome Sign, Really?
The word “inaccessible” usually relates to the inability to get somewhere. When one is talking about the inability to access data, there is a tendency to use the word “unaccessible.” The problem with many websites is that the data they provide is unaccessible to those with certain disabilities. The AwDA guidelines are an attempt to rectify that.
Kerry K. Carney, DDS, CDE
In the case of our office websites, there are two primary reasons to try to make them accessible to people with disabilities. The first: It is the right thing to do. Everyone needs oral health care, and it is only right to provide a Welcome sign that is easily accessible to all. The second: Your office can be at risk of litigation if your practice patients. No, it is not an unreasonable request. It only takes one debilitating accident to open the eyes of an able-bodied person to the unnecessary hurdles that someone with a disability faces daily, hourly. One day in 1999, I was watching a softball team we were sponsoring at a tournament in our small town. I stepped off a bench, into a hole and dislocated my foot. There were too many witnesses to somehow eradicate, so in tremendous embarrassment, I was taken to the hospital for emergency care. Eight hours later, I was delivered to my home with a full foot and leg cast along with a pair of crutches that I would enjoy for sixSuddenly,weeks. accessibility had a new and very personal meaning for me. Many folks have found themselves in similar circumstances. When you cannot walk without crutches, stairs are your enemy, turnstiles are impossible. Elevation changes in the flooring materials are stymying. Just maneuvering around the house takes detailed planning. Carrying something as simple as a glass of water from one room to another becomes a tactical exercise. How people interact with you changes. If you are in a wheelchair, able-bodied folks tend to talk to your able-bodied companion rather than you. But the most disconcerting effect is how it can challenge your selfconfidence. The few times that we dined out, I would have to store my crutches
Add checking your website accessibility to your list of things to do and get it done.
The whole point of a “Welcome” sign is that it is welcoming. It is a friendly invitation to a gladly received guest. But if everyone cannot see and read the Welcome sign, then it is kind of a secret Welcome sign. What if only very tall people can read the sign because it is mounted too high? What if you have to know a combination to a lock before you can open a door and read the sign? Instead of inviting engagement, it becomes obscure at best and a barrier at worst. Like an invitation written in invisible ink, a secret Welcome sign is not an effective Welcome sign. A well-designed dental practice website is a Welcome sign. It is an open portal to an office. It is an invitation to meet the staff and providers. It welcomes potential patients to a dental care treatment experience that surpasses expectations and conveys a dedication to provide consistently excellent care. Title III of the Americans with Disabilities Act (AwDA) “prohibits discrimination against people with disabilities by businesses open to the public.” Dental offices are subsumed under hospitals and medical offices in the list of public accommodations that includes retail stores and other sales or retail establishments, banks, hotels, inns and motels, food and drink establishments and auditoriums, theaters and sports arenas. “A website with inaccessible features can limit the ability of people with disabilities to access a public accommodation’s goods, services and privileges.”1 Yes, this is another requirement that dentists have to deal with. Yes, governmental regulations are not why we went into dentistry. Yes, this is one more distraction from providing oral health care to our somewhere out of the way so as not to create a traffic hazard. When that was done, I found the thought of being unable to walk, unable to evacuate in the case of an emergency, very distressing. When I went to pick up a disabled parking permit, I was overcome by the idea that some thief would spot me as an easy mark, grab my wallet and phone and leave me in the DMV parking lot scrabbling like a turtle on its back trying to get up. I had no idea just how much of my self-confidence relied on my ability to stand and easily locomote.

500 SEPTEMBER 2022 CDA JOURNAL, VOL 50 , Nº 9 website is not accessible for the disabled person seeking information about your services.When you are using crutches, the hurdles to perambulation are easily recognized. But recognizing the hurdles to accessing the information on your website may not be so easy. The Department of Justice has provided guidance describing barriers to access and suggesting ways to overcome those barriers.1 But if you are not a DIY website builder, you may want to check with your website builder/host to make sure your site is in compliance. When I checked with ours, he was surprised to find the requirements had changed since he had reviewed them a few years ago. When morals and ethics are not enough motivation to do the right thing, risk aversion and litigation may be the final motivator. An increasing number of law suits have been successfully filed against large and small entities with regard to noncompliant“Accordingwebsites.toclaims representatives at The Dentists Insurance Company, most claims that TDIC handles are referred to as first-notice lawsuits. ‘Plaintiffs are targeting dental offices for profit, not because they have any intention of becoming patients, so they’re not incentivized to give the office an opportunity to address the accessibility issue.’”2
SEPT. 2022 EDITOR
If your website has any of the following, you may have inadvertently thrown up a barrier: Poor color contrast, use of color alone to give information, lack of text alternatives on images, no captions on videos, unaccessible online forms or lack of keyboard navigation. The information you wanted to broadcast may be secret and inaccessible to those who are in some way challenged.Addchecking your website accessibility to your list of things to do and get it done. It might save you money and aggravation. Plus, it’s the right thing to do. And a secret Welcome sign is not very welcoming. n REFERENCES 1. U.S. Department of Justice/Civil Rights Division. Guidance on Web Accessibility and the ADA . Accessed April 18, 2022. 2. TDIC Risk Management Staff. Practice Website Accessibility: A New Wave of AwDA Litigation J Calif Dent Assoc 2021 Mar;49(3):185–6.
The Journal welcomes letters We reserve the right to edit all communications. Letters should discuss an item published in the Journal within the last two months or matters of general interest to our readership. Letters must be no more than 500 words and cite no more than five references. No illustrations will be accepted. Letters should be submitted at editorialmanager.com/ jcaldentassoc. By sending the letter, the author certifies that neither the letter nor one with substantially similar content under the writer’s authorship has been published or is being considered for publication elsewhere, and the author acknowledges and agrees that the letter and all rights with regard to the letter become the property of CDA.
In other words, the potential for significant payments in an accessibility lawsuit incentivizes widespread litigation unrelated to the intent of the guidelines. “Minimum damages for a first offense are $4,000 or $4,500 and can multiply for every site revisit — as much as $25,000 to $30,000 in legal fees or mediation if not covered by a practice’s dental business liabilitySuchinsurer.”2ariskof monetary penalties is highly motivating.
AI Study Automates Denture Design
The process of designing and creating dentures is highly time-consuming, as the existing computerized design process requires tedious manual inputs and teeth occlusion information collection as well as multiple denture fitting procedures due to limited accuracy of existing technologies. But researchers from the faculty of dentistry at the University of Hong Kong (HKU) and the department of computer science of Chu Hai College of Higher Education have developed a new approach to designing and creating dentures using artificial intelligence (AI) to automate the design of individualized dentures to enhance the treatment efficiency and improve patient experience.
CDA JOURNAL, VOL 50 , Nº 9 SEPTEMBER 2022 501 Impressions
The study showed that AI technology could reconstruct the shape of a natural healthy tooth and automate the process of denture design with high accuracy. The AI technology used in the new process was based on the 3D Generative Adversarial Network (3D-GAN) algorithm and tested on 175 participants recruited at HKU. GANs are a class of AI algorithms used in unsupervised machine learning, implemented by a system of two neural networks contesting with each other in a zero-sum game framework. Generative modeling is an unsupervised learning task in machine learning that involves automatically discovering and learning the regularities or patterns in input data in such a way that the model can be used to generate or output new examples that plausibly could have been drawn from the original dataset. GANs was developed by Ian J. Goodfellow, BS, MS, a computer scientist, engineer and Google Scholar. “The 3D GAN algorithm was selected due to its superior performance on 3D object reconstruction compared to other AI algorithms. In the preliminary study, 3D GAN was able to rebuild similar shapes to the original teeth for 60% of the cases. It is expected to mature with more AI training data,” said Reinhard Chau, PhD, co-investigator.
The new approach to creating dentures only requires the digital model of a patient’s dentition to function. It can learn the features of an individual’s teeth from the rest of the dentition and generate a false tooth that looks like the missing tooth. “This will facilitate the treatment workflow for dentists in replacing a missing tooth, as the preparation and fitting process will require minimal time, and a patient will not need to stay at the clinic for long hours,” said Principal Investigator Walter Lam, BDS, MDS. The study entitled “Artificial intelligence-designed single molar dental prostheses: A protocol of prospective experimental study” was published in the journal PLoS ONE, and the preliminary results of the study were presented in the recent International Association of Dental Research (IADR) General Session. n Examples of a maxillary teeth model, left, and a mandibular teeth model that will be used to train the AI system. (Credit: Chau RCW et al. Licensed under Creative Commons CC BYNC 4.0.)

New research by Tufts University scientists and colleagues suggests a link between Alzheimer’s disease and F. nucleatum, a common type of bacteria that proliferates in periodontal disease. The study was published in the journal Frontiers in Aging Neuroscience
CDA JOURNAL, VOL 50 , Nº 9 502 SEPTEMBER 2022 SEPT. 2022 IMPRESSIONS
Nadershahi, DDS, MBA, EdD, president of the American Dental Education Association (ADEA) and chair of CDA’s Diversity, Equity, Inclusion and Belonging (DEIB) workgroup, to investigate the data points in California.
The latest research, done in mice, shows that F. nucleatum results in an abnormal proliferation of microglial cells, which are immune cells in the brain that normally remove damaged neurons and infections and help maintain the overall health of the central nervous system. This over-supply of microglial cells also created an increased inflammatory response, according to the research. Chronic inflammation or infection is believed to be a key determinant in the cognitive decline that occurs as Alzheimer’s disease progresses.
Anti-Racist Practices in Dental Public Health Focus of JPHD Issue
Study Suggests Link Between Gum Disease and Alzheimer’s
“While the ADEA does not have diversity data by region, we can send a questionnaire to each dental school to learn more about representation in faculty and leadership in California dental schools,” Zokaie said. Learn more about diversity, equity, inclusion and belonging in dentistry in the October issue of the CDA Journal guest edited by Dr. Nadershahi and Steven Friedrichsen, DDS.
Anti-racist solutions in dental public health is the focus of a special issue of the Journal of Public Health Dentistry (JPHD) published in June in partnership with the CareQuest Institute for Oral Health. The JPHD is published on behalf of the American Association of Public Health Dentistry (AAPHD).
Dr. Chen and his colleagues believe that by targeting F. nucleatum they can slow the spread and progression of at least two epidemics — periodontal disease, which affects 47% of U.S. adults over age 30, and Alzheimer’s, which afflicts 6.5 million Americans currently and is expected to increase to over 14 million by 2060.
Spring issue of the JPHD on anti-racist practices.
“We hope it will compel people in the industry to critically examine practices with the goal of creating policies, systems and institutions that are more diverse, equitable, inclusive and just,” said Dr. Reynolds. “If we are not part of the solution, then we are part of theTookaproblem.”Zokaie, California Dental Association (CDA) senior health policy analyst, said the journal issue inspired Nader A.
The special issue, “Antiracism in Dental Public Health: Engaging Science, Education, Policy and Practice,” includes 19 articles — a mix of original research, commentaries, editorials and community action reports — covering a range of topics related to anti-racism, including the effects of discrimination and anti-racist solutions for research, education, practice, advocacy and“Inworkforce.contrast to other disciplines, dentistry has been relatively quiet in the space of anti-racism,” said Eleanor Fleming, PhD, DDS, MPH, co-guest editor of the issue and assistant dean for equity, diversity and inclusion at the University of Maryland School of Dentistry. “This special issue fills that void and offers a strategic path forward for dental public health using the lens of anti-racism.” Julie Reynolds, DDS, MS, co-guest editor and assistant professor in preventive and community dentistry at the University of Iowa, calls the special issue “a call to action.”
“In this study, our lab is the first to find that Fusobacterium nucleatum can generate systemic inflammation and even infiltrate nervous system tissues and exacerbate the signs and symptoms of Alzheimer’s disease,” said Jake Jinkun Chen, DMD, MDS, PhD, professor of periodontology and director of the division of oral biology at the Tufts University School of Dental Medicine.
“Our studies show that F. nucleatum can reduce the memory and thinking skills in mice through certain signal pathways. This is a warning sign to researchers and clinicians alike,” Dr. Chen said. Gram-negative stained culture of F. nucleatum (Courtesy J. Michael Miller, PhD, National Center for Zoonotic, Vector-Borne and Enteric Diseases.)



CDA JOURNAL, VOL 50 , Nº 9 SEPTEMBER 2022 503
10% of theaccordingsixcraniomandibularsevereCraniomandibularSurvivorsCOVID-19MayDevelopDisordersApproximately1in10survivorsofCOVID-19maydevelopdisorders(CMDs)withinmonthsfollowingprolongedintubation,toastudyrecentlypublishedinJournalofStomatology,OralandMaxillofacial
However, a new multistudy project from the Regenstrief Institute and the Indiana University School of Dentistry has determined that information from patients’ medical records is generally not available to oral health practitioners in either an easy-to-use or timely manner. The study was published in the journal Frontiers in Digital Health.
The dental informatics researchers confirmed that requested medical information typically is faxed from a medical facility to the dental office. Faxes, sometimes unreadable when received, often are scanned into the patient’s dental record. The researchers found that, typically, the faxed information arrived in seven to 10 days, but in the study, 30% took even longer.
In bivariate analyses, statistically significant associations were found between CMDs and bilateral molar loss in at least one jaw, skeletal class II/convex face and serum CRP during intensive care that was greater than or equal to 40 mg/L, according to the study.
“Oral health practitioners may need to confirm a list of medical considerations; for example, that there is no contraindication to a patient sitting in a chair for a lengthy procedure or whether a patient is taking any medication that could put them at risk for excessive bleeding during a tooth extraction or other procedure,” said senior author and study leader Thankam P. Thyvalikakath, DMD, MDS, PhD, director of the Regenstrief and IU School of Dentistry Dental Informatics program. “In this day and age of electronic data transmissions in banking, shopping and other commercial fields, should health professionals still be relying on inefficient, paper-based methods for sharing patient information?”
The researcher-clinicians found that the medical information most frequently requested by a dental office to finalize treatment decisions and procedure timing were patient diabetes status and history of blood sugar levels, which can help oral health professionals rule out any contraindication to undergo dental treatments, determine outcomes of a surgical procedure or assess options for implant placement and calculate risk for gum disease.
Linking Records Typically Not Easy or Timely Without
To identify the predictors of CMDs in survivors of severe COVID-19 after prolonged intubation greater than or equal to one week, the paper’s authors conducted a retrospective study that included 176 patients. Of those patients, 21 had CMDs and 155 did not have these conditions.
Limitations to the study include its retrospective nature, which makes it difficult to control for bias and confounders, the authors stated, and further research should be conducted in multi-institutional settings with a larger cohort.
Furthermore, bilateral molar loss, convex face and higher levels of peak C-reactive protein (CRP), a protein found in the blood that indicates an increase in inflammation in the body, during intensive medical care were predictors of CMDs in these patients, the authors wrote.
Electronic Info Exchange Demand for advanced dental care is increasing due to people living longer with chronic diseases like HIV and the growing number of older adults with natural teeth. For these patients, information from their medical file may be especially critical to appropriate dental treatment.
Surgery
Compared to those with no or only unilateral molar loss, patients with bilateral molar loss had 12.6 greater odds for developing CMDs. Additionally, convex face subjects were at a 2.6-fold higher risk of developing a CMD compared to those with a normal or concave profile. Finally, patients with peak CRP levels greater than or equal to 40 mg/L were 3.5 times more likely to have CMDs than those with lower CRP levels.


® Flex your cash flow with a card designed just for dentists and earn extra rewards points for your ADA, CDA and practice-related purchases. Get competitive prices on dental supplies you love from brands you trust through membership’s collective purchasing power. Save big on your janitorial, breakroom, office supplies and more, plus streamline shopping with convenient one-day delivery. Control expenses. More membership value from vendors dentists can trust. The California Dental Association leverages the strength of our large membership to deliver more value to practices of every size. Benefit from member-exclusive pricing and expert support to control your practice expenses. Explore products and services for the business side of practice at cda.org/EndorsedServices ENDORSED SERVICES Get smart reducedcompetitiveguidance,ratesandfeesonpractice financing solutions that help you purchase, restructure or grow.



Conclusion: The radiographic interpretation of the marginal discrepancies of lithium disilicate crowns is significantly affected by the vertical angulation of the X-ray beam and the dimension of the marginal discrepancy on the premolar crown. Caution should be used when evaluating marginal discrepancy on lithium disilicate crowns using radiographs made with vertical angulation of more than ± 10 degrees.
Dental, dental hygiene and dental assistant students and military/residents from across the state competed in the California Dental Association’s annual Dennis Shinbori, DDS, Table Clinic Competition at CDA Presents in Anaheim May 12–14, 2022. The Journal is pleased to publish abstracts from the first-place winners in each category. CDA continues to collaborate with the California Dental Hygienists’ Association for the RDH portion of the competition.
Identifying Marginal Adaptation Discrepancies of Lithium Disilicate Crowns Using Seven Different Vertical X-ray Angulations
Statement of problem: The influence of different angulations on accurate radiographic assessment of marginal discrepancy has not been reported.
Results: Significant differences in the ability to accurately assess marginal discrepancies from radiographs were observed for the study factors of angulation, tooth type and degree of marginal discrepancy (P < 0.001).
CDA JOURNAL, VOL 50 , Nº 9 SEPTEMBER 2022 505 Abstracts
DENTAL STUDENT WINNER natural teeth that included a central incisor, a canine and a premolar. Marginal discrepancies ranging from 0 to 300 µm were intentionally created. The seated crowns were imaged using seven different vertical angulations, totaling 147 images. Thirty experienced evaluators scored each image for marginal discrepancy and values were statistically analyzed.
THE AUTHOR, Luiz Carvalho, can be reached at luizthiagopc@hotmail.com. Luiz Carvalho researched the influence of angulations on radiographic imaging and marginal discrepancies.
Objective: To study the effects of different vertical angulations on radiographic imaging and the ability to detect marginal discrepancies in lithium disilicate crowns. Methods and materials: Twentyone lithium disilicate crowns were fabricated on three different prepared
Luiz Carvalho, Loma Linda University School of Dentistry
Winners of the 2022 Dennis Shinbori, DDS, Table Clinic Competition


Ross Coleman, Antelope Valley High School
Methods: Information was collected and analyzed through literature review research.
Stephanie Gonzalez and Sheccid Hinojosa conducted a literature review of the effects of mask mouth. changes due to wearing a face mask for extended periods of time. The effects of mask mouth are not limited to the oral cavity but are connected to systemic responses as well. Although mask mandates are subsiding, certain populations such as health care workers, immunocompromised and allergy susceptible individuals, among others, will continue to wear masks for extended periods of time.
Stephanie Gonzalez and Sheccid Hinojosa, West Los Angeles College
THE AUTHOR, Ross Coleman, can be reached at jessiej1404@gmail.com.
SEPT. 2022 ABSTRACTS
RDH INFORMATIONAL STUDENT WINNER
Are Oral Piercings Worth the Risk?
THE CORRESPONDING AUTHOR, Stephanie Gonzalez, can be reached at sg.dental93@gmail.com.
The Effects of Mask Mouth
CDA JOURNAL, VOL 50 , Nº 9 506 SEPTEMBER 2022
Oral piercings are popular. The jewelry can be changed and customized to fit one’s personal style. But even a pretty accessory can cause more damage than a person signed on for. From tongue rings to tongue webs, are these piercings worth the risk? This project takes a look into the body modification practice and the ways that it affects oral hygiene.
Background: Health care professionals and the general public have noticed health and wellness
RDA STUDENT WINNER Ross presentationColeman’scovered oral piercings and their effect on oral hygiene.
Conclusion: Mask mouth effects include headache and fatigue, altered breathing and respiratory effects, dermatological aspects as well as direct correlations to oral conditions caused by several factors. The aim is to dissect these occurrences and recommend solutions not only for patients but also for the health care professionals to combat the effects of mask mouth through hygiene habits and patient care modifications.



CDA JOURNAL, VOL 50 , Nº 9 SEPTEMBER 2022 507
Robert McIntosh, RDA Tharwat Sorour, DDS James Strother, DDS Manolita Abby Teh, RDA MILITARY/RESIDENT JUDGES Anirudha Agnihotry, DDS Samuel Demirdji, DDS Judith Strutz, DDS Peter Young, DDS
THE AUTHOR, Capt. Damien Nelson, DDS, can be reached at damien.w.nelson.mil@mail.mil.
Keywords: Mask wearing, mask mouth
Capt. Damien Nelson, DDS, USAF, receives his award from Dr. Ariane Terlet and Mrs. Wendy Shinbori. Dr. Nelson researched gingival recession. Thank you to the following judges of the annual Dennis Shinbori, DDS, Table Clinic Competition:
Chelsea Molato, Ariella Kerendian, Amber Orellana and Brenda Fausto researched if extensive mask wearing had any negative effects on oral health.
Conclusions: No changes in people’s perception of their oral cavity due to mask wearing, except for their oral health habits.
Background: To evaluate whether extensive wearing of masks may have potential negative effects on a person’s oral health such as dry mouth, halitosis and overall decline in personal daily oral hygiene Materials and methods: A cross-sectional survey was distributed to adults who reside in San Bernardino County, specifically: Victorville, Ontario, Fontana, Redlands, Loma Linda and Colton. Twelve questions were used to analyze people’s knowledge and attitude on their oral health while wearing masks. The Chi-square test was used to test our hypothesis; 147 out of the 207 people approached participated in this study. Results: No statistically significant correlation between duration of mask
ACKNOWLEDGMENT: The study was funded by the Loma Linda University School of Dentistry Student Research Program fund.
THE CORRESPONDING AUTHOR, Amber Orellana, can be reached at orellana.amber@yahoo.com.
MILITARY/RESIDENT WINNER
The Tunnel Technique: Subepithelial Connective Tissue Grafting
Amber Orellana, Ariella Kerendian, Chelsea Molato and Brenda Fausto, Loma Linda University
RDA RESEARCH STUDENT WINNERS (CDA IN COLLABORATION WITH CDHA)
RDA STUDENTS JUDGES Izabella Ambartsumyan, RDA Shari Becker, RDA Lina Bocanegra, RDA Maleah Brooks, RDA Karen Schroeder, RDA wearing and oral hygiene. However, the following findings were observed: Rates of xerostomia in this cohort [53.7% (95% CI 45.3-62.0)] were significantly higher than what is reported in the literature. The overall estimated prevalence of dry mouth was 22% (95% CI 17.0-26.0%).
RDH STUDENTS JUDGES Zoe Milkie, RDH Mindy Duncan, RDH Reina Wong, RDH DENTAL STUDENTS JUDGES Monica Bruce, DDS Marileth Coria, DDS Tony Daher, DDS Benson Dimaranan, RDA Ramesh Gowda, DDS
Capt. Damien Nelson, DDS, U.S. Air Force This presentation is an overview of gingival recession, the Cairo Classification System, indications for treating and the pros and cons of the tunnel technique specifically followed by a case presentation.
Self-Reported Oral Health Outcomes After Mask Wearing Among Inland Empire Adults



Setareh Lavasani, DDS, MS, is an associate professor and the chief oral and imagingmaintainsoftextbook,interactiveincludingandtochaptersmanuscriptsauthoredAcademy.theRadiologyOraltheSheinCollegetheadvancedofradiologistmaxillofacialinthedivisionoralradiologyandimagingatWesternUniversityofDentalMedicinePomona,California.isadiplomateofAmericanBoardofandMaxillofacialandafellowofGlobalDentalImplantDr.Lavasanihasmultiplescientificandbookontopicsrelatedoralradiologydiagnosisradiationbiologythefirstdigital/oralradiologyFundamentalsOralRadiology.Sheanactivedentalpracticeserving
Radiographic examination is an integral part of diagnosis and treatment planning in dentistry. For the central part of the 20th century, dentists utilized a combination of 2D intraoral and extraoral imaging for diagnosis and treatment planning of dental and maxillofacial conditions. These radiographic technologies provide 2D representations of 3D anatomic structures.1 Apart from compressing the 3D anatomy of the area being radiographed into a 2D image, 2D imaging possesses unique inherent limitations (including magnification, distortion and superimposition), together leading to misrepresentation of structures.2 In the late 1990s, 3D imaging, cone beam computed tomography (CBCT), which utilizes an extraoral scanner, was introduced as a valuable additional tool in dental imaging. CBCT images are acquired by utilizing a cone-shaped beam of ionizing radiation with an area receptor that is fixed on the rotating arm and captures multiple projections of the structures being imaged. Captured data is processed through complex computer software algorithms, and the data is reconstructed in three dimensions and displayed on the computer monitor. With broader availability and utilization of CBCT in dental practice and to provide guidance on clinical implications of CBCT imaging, the American Dental Association Council on Scientific Affairs published an advisory statement on the use of CBCT in dentistry. The statement notes, “As with other radiographic modalities, CBCT imaging should be used only after a review of the patient’s health and imaging history and the completion of a thorough clinical examination. The selection of CBCT for dental and maxillofacial imaging
GUEST EDITOR
WesternU dental clinics and external referrals. Dr. Lavasani serves on the board of Tri-County Dental Society (TCDS) and is a delegate representing the TCDS at the 2022 CDA House of Delegates. Dr. Lavasani is a fellow of the Global Dental Implant Academy. Conflict of Disclosure:InterestNonereported.
TomographyComputedTechnology
Oral and RadiologyMaxillofacialDiagnosis:The Role of Image Modality Selection, Interpretation Skills and Use of Cone Beam
SEPTEMBER 2022 509 CDA JOURNAL, VOL 50 , Nº 9 introduction
Setareh Lavasani, DDS, MS


This issue of the Journal of California Dental Association aims to highlight the value of adequate imaging and the significance of appropriate radiographic interpretation knowledge in the timely diagnosis of dentoalveolar pathosis. The applications of CBCT as part of diagnosis and treatment planning in implant digital workflow and orthodontics is explored, and “novel” applications of CBCT in endodontics as an adjunct modality with dynamic navigation in the management of calcified canals is also discussed. My colleagues and I present a case of medically related osteonecrosis of the jaws (MRONG) resembling a Le Fort I fracture in the maxilla of a patient taking antiresorptive drugs with a delayed diagnosis resulting from lack of adequate imaging (suboptimal image quality and not enough coverage area).
The article also discusses the critical role of comprehensive and methodological history-taking in patients on oral antiresorptive medications who might be at higher risk for developing MRONJ.
The importance of the practitioner’s responsibilities was further highlighted in the executive opinion statement published in 2008 by the American Academy of Oral and Maxillofacial Academy in the journal Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology and Endodontics: “It is the responsibility of the practitioner obtaining the CBCT images to interpret the findings of the examination. Just as a pathology report accompanies a biopsy, an imaging report must accompany a CBCT scan. Dentists using CBCT should be held to the same standards as boardcertified oral and maxillofacial radiologists (OMFRs), just as dentists excising oral and maxillofacial lesions are held to the same standards as OMF surgeons.”4
The clinician’s professional judgment in selecting the imaging modality types, including intraoral, panoramic, CBCT or a combination, could play an essential role in the timely diagnosis and management of pathological conditions in the jaws. Furthermore, the acquired images should have clinically acceptable image quality (resolution and contrast) and sufficient coverage of the area of interest.
Dr. Mark Mintline and colleagues illustrate that the practitioner who operates a CBCT unit or requests a CBCT study must examine the entire image dataset.
Dentists who utilize CBCT technology should have appropriate training in evaluating normal maxillofacial structures in three dimensions and be competent in evaluating the CBCT scans for potential pathologic findings.
In the last years, the developments implantdentistry,havemanufacturingcomputer-aided-design/computer-assistedof(CAD/CAM)technologiesbroughtgreatimprovementsin5especiallyinthefieldoforalsurgery.6–8InthearticlebyDr.
This is predicated on a thorough knowledge of CT anatomy for the entire acquired image volume, anatomic variations and observation of abnormalities. It is imperative that all image data be systematically reviewed for disease.4
Rafeeq Rahman and colleagues, key steps and considerations in implant dentistry digital workflow starting are laid out, with a CBCT imaging for implantsupported fixed single or short-span restorations using a static implant guide. In orthodontics, CBCT imaging facilitates the visualization and evolution of complex three-dimensional structures of the maxillofacial region without the superimposition and magnification of structures associated with panoramic images. Dr. Yoon and colleagues discuss current 2D and 3D imaging modalities and their utilization in evaluating dentoalveolar abnormalities, tooth impactions and growth pattern monitoring. The article explains the role of CBCT as an adjunct in clinical diagnosis and management of airways and obstructive sleep apnea (OSA), temporomandibular joint (TMJ) abnormalities and virtual surgical planning. The value of the CBCT in the preoperative, intraoperative and postoperative assessment of complex root canal systems is well documented. Rigolone et al.9 first described the value of CBCT in planning for endodontic surgery. Endodontic surgery is often complicated in the posterior teeth by their proximity to anatomical structures. The mandibular teeth can be close to the mandibular canal, while maxillary molars are often close to the maxillary sinus. CBCT imaging provides several advantages for preoperative treatment planning, especially in maxillary posterior teeth with apical pathology.9 Dr. Villa and colleagues present a novel approach to managing a calcified canal using the Navident dynamic navigation system and CBCT imaging to access the distobuccal (DB) canal of a partially obliterated maxillary second molar. This article introduces available technologies that, when paired with careful case selection and clinical training, could improve the predictability
510 SEPTEMBER 2022 CDA JOURNAL, VOL 50 , Nº 9 introduction should be based on professional judgment in accordance with the best available scientific evidence, weighing potential patient benefits against the risks associated with the level of radiation dose.”3
Dentists who utilize CBCT technology should have appropriate training in evaluating normal maxillofacial structures in three dimensions.
Dent Clin North Am 2008 Oct;52(4):707–30, v. doi: 10.1016/j.cden.2008.05.005 3. American Dental Association Council on Scientific Affairs. The use of cone beam computed tomography in dentistry: An advisory statement from the American Dental Association Council on Scientific Affairs. J Am Dent Assoc 2012 Aug;143(8):899–902 doi: 10.14219/jada. 4.archive.2012.0295CarterL,Farman AG, Geist J, et al. American Academy of Oral and Maxillofacial Radiology executive opinion statement on performing and interpreting diagnostic cone beam computed tomography. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008 Oct;106(4):561–2 doi: 10.1016/j. 5.tripleo.2008.07.007DeVicoG,Ottria L, Bollero P, Bonino M, Cialone M, Barlattani A, Jr, Gargari M. Aesthetic and functionality in fixed prosthodontic: Sperimental and clinical analysis of the CAD-CAM systematic 3Shape. Oral Implantol (Rome) 2008 Oct;1(3–4):104–15. Epub 2009 Apr 20. PMCID: 6.PMC3486718MarchackC. An immediately loaded CAD/CAM-guided definitive prosthesis: A clinical report. J Prosthet Dent 2005 Jan;93(1):8–12 doi: 10.1016/j.prosdent.2004.10.012
7. Spinelli D, Ottria L, De Vico G, Bollero R, Barlattani A, Bollero P. Full rehabilitation with Nobel Clinician and Procera Implant bridge: Case report. Oral Implantol (Rome) 2013 Oct 15;6(2):25–36. eCollection 2013. PMCID: PMC3808939
8. Pozzi A, Gargari M, Barlattani A. CAD/CAM technologies in the surgical and prosthetic treatment of the edentulous patient with biomimetic individualized approach. Oral Implantol (Rome) 2008 Apr;1(1):2–14. Epub 2008 Jun 16. PMCID: PMC3476503
9. Patel S, Dawood A, Pitt Ford T, Whaites E. The potential applications of cone beam computed tomography in the management of endodontic problems. Int Endod J 2007 Oct;40(10):818–30 doi: 10.1111/j.13652591.2007.01299.x. Epub 2007 Aug 14.
SEPTEMBER 2022 511 CDA JOURNAL, VOL 50 , Nº 9 of surgical endodontic procedures. As the guest editor of this issue of the Journal, I am pleased to share the advances in the field of oral and maxillofacial radiology and hope to have highlighted the value of judicious use of advanced imaging, the importance of interpretation skills and the role of synergistic collaboration between general dentists and specialist colleagues in improving diagnosis, treatment planning and patient outcomes. I hope readers find these topics as exciting as I do. Finally, I would like to acknowledge the support and encouragement I received from leaders at the Western University College of Dental Medicine. After accepting the invitation to become the guest editor of this Journal issue and throughout my eight years at Western University, I have been consistently encouraged and generously mentored to grow and learn through new professional opportunities. With this in mind, and with gratitude, appreciation and affection, I dedicate this issue of the Journal of the California Dental Association to retiring Dean Steven Friedrichsen and his wife Sue. n REFERENCES 1. Grondahl HG, Huumonen S. Radiographic manifestations of periapical inflammatory lesions. Endod Topics does2.doi.org/10.1111/j.1601-1546.2004.00082.x2004;8:55–67ScarfeWC,FarmanAG.WhatisconebeamCTandhowitwork?
TORRANCE: 3 Ops, retiring seller with 34 yrs goodwill. Ready to take to the next level with technology of your choosing. Amazing location in desired area. 2019 GR of $300K with low expenses, a wonderful opportunity to grow. #CA2807
CENTRAL CALIFORNIA
ENCINITAS: GP practice. 6 Ops, Private parking lot. Great technology with a CBCT, 5 Microscopes, Scan X and SoftDent. 38 yrs. Goodwill. 2021 GR $960K. #3152
TORRANCE: 6 Ops, 40 yrs. Goodwill. Strong hygiene, in-house Perio and Endo specialists 2 days per month. Digital X-ray, Intraoral Camera and Laser. 2021 GR $1.5M #CA3113
NORTH SAN DIEGO COUNTY: 4 Ops highly desirable location in busy strip mall. Digital, clean, and modern, with an excellent layout. Consistent year to year collections. 2021 GR $753k. #CA2961
PLEASANTON: New Listing! Great neighborhood practice, paperless, digital, 6 Ops, 5 equipped. Don’t miss opportunity in this great community. #CA3023
ROSEVILLE/CITRUS HTS: 6 Ops, high traffic area, 13 yrs goodwill, Digital, lasers, 26 NP/mo, 5 days Hygiene, specialties referred. Seller will work back. #CA2749 FAIR OAKS/CITRUS HEIGHTS: 4 Ops in desirable area, digital, strong hygiene program. Seller highly motivated to retire! 2019 GR $970K on 4 days/wk with plenty of vacation. #CA656
NORTHERN CALIFORNIA PERIO: 4 Ops+RE, 33 yrs. Goodwill. 2021 GR $1.4M. #3118
SAN MATEO: 3 Ops, digital X-ray, great opportunity in this highly desirable area/busy retail strip center location. 2021 GR $381K with no advertising. #CA3044 SONOMA COUNTY: Price Adjustment! Large GP, 2019 GR $2.3M +. Stand-alone 3,000 sf prime Real Estate, 72 NP/mo. & 10 Hyg Days. 6 Ops, Pano, Dexis, Cameras, Laser, Dentrix. Both Business & RE for sale or Lease. Doctor Retiring. #CA544
SAN DIEGO: Oral Surgery practice with 2 surgical rooms, 2 consult rooms in a standalone building 46 yrs. Goodwill.
y C o n w a y
ROCKLIN/GRANITE BAY: Hi-end 4 Ops GP/Cosmetic practice in affluent area. Paperless, digital, iTero scanner, 8 + hyg days/wk. 2019 GR $1.6M+, 2021 Prod projected at $2M+. RE for sale with practice. #CA2793
WHITTIER: 4 plumbed Ops, 3 equipped, Paperless, Digital X-ray, Intraoral Camera and Laser. Long established FFS/PPO Practice. 2021 GR $497K. #3150 SAN DIEGO
FAIRFIELD/VALLEJO AREA: 7 Ops, Paperless practice in a high-traffic area. Digital, CEREC with 43 yrs. Goodwill. 2021 GR $1.5M. #3117
www.HenryScheinDPT.comNorthern California Office 800.519.3458 VALUATIONS/APPRAISALS • TRANSITION PLANNING • PARTNERSHIPS • MERGERS • PASSOCIATESHIPS RACTICE SALES • Making your transition a reality. Henry Schein Corporate Broker #01230466 Southern California Office 888.685.8100 D r T h o m a s W a g n e r LIC(916)#01418359812-3255 47YearsinBusiness J i m E n g e l LIC(925)#01898522330-2207 48YearsinBusiness K e r r i M c C u l l o u g h LIC(949)#013822593000312 37YearsinBusiness G i n a M i l l e r LIC(707)#02015193391-7048 32YearsinBusiness J a c i H a r d i s o n LIC(714)#01927713318-4911 28YearsinBusiness (916) 812-0500 39YearsinBusinessJayHarter S t e v e C a u d i l l LIC(951)#00411157314-5542 32YearsinBusiness S t e w a r 949-220-6216t 20YearsinBusinessLIC#:#01398798 S a p i r LIC(310)#02126473596-0961 13YearsinBusiness NORTHERN CALIFORNIA
2021 GR $413K. #3115 SAN YSIDRO FACILITY ONLY: Leasehold ready for immediate sale! Newly remodeled 4 ops with new equipment Trios 3Shape, Handheld X-ray, Sensor and Intraoral Camera. #3129 SCRIPPS RANCH: 5 Ops, 3 equipped, strip mall location, bright, spacious office. CEREC, CBCT, Dexis, Soft tissue Laser, Implant Motor, I/O Camera. Specialties referred. #CA3054
SANTA CRUZ COUNTY: 4 Ops Close to beach in strip center. Digital Pano and x-rays, CEREC, 40 years goodwill. 2019 GR $392K on 3.5 days. #CA2822
RANCHO SANTA MARGARITA: 4 Ops, 30+ Yrs Goodwill, Modern and Bright Designed Office! Digital Laser, Pano, Strong Hygiene. 2021 GR $665K. #CA3160 SAN BERNARDINO: 6 Ops, established 33 years, cash, HMO, Denti-Cal in a busy area with parking Estimated GR for 2021 at $960K+. Seller offering RE for sale with 2 lease tenants adjacent to practice. Room to expand with spec. #CA2843
HESPERIA: New Listing! Wellestablished GP practice, 5 Ops+RE, Digital, 22 Yrs. Goodwill. 2021 GR $500K. #1500 ORANGE: 4 Ops+RE, 2 hygiene days/ wk. with room to add more days. Seller refers out all specialties. 2021 GR $590K. #3143
SAN DIEGO: Rare opportunity, seller retiring, 4 Ops in desirable location with good cash flow. High quality work. Digital, Dentrix #CA2851
BRENTWOOD: 4 Ops, professionally designed, Dentrix, Paperless, Laser, great location. 2019 GR $520K on 2.5 day week. #CA3008
WHITTIER: 4 Ops, 3 equipped, 30 yrs goodwill. Digital x-rays and pano, laser. 2021 GR $683K on 3 Dr. days/wk. Great visibility and signage in this wonderful community. #CA2788 (619) 889 6492
SANTA CLARITA VALLEY: 6 Ops, great cash flow, seller will work back. 3D CT, Itero, Digital with 8 hyg days/ wk. PPO/FFS and 2021 GR over $2.3M. #CA2992
LAKE TAHOE AREA WITH LAKE VIEWS: Well-established practice in magical Lake Tahoe! 4 Ops, Paperless practice, Digital. 20 yrs. Goodwill, 2021 GR $1.4M. #3100
SONOMA COUNTY: 4 Ops in spacious layout in heart of the area off main highway. Est 22 yrs with 5-star Google reviews, Paperless with CEREC, Scope, Laser, Strong hyg. Retiring seller. 2019 GR $782K with good post-COVID recovery. #CA2594 SONOMA COUNTY: Price Reduced! 4 Ops with room to expand into suite next door. GR $1M+ for last 3 yrs. Est. 30+ years. Strong hyg, digital, space available to lease or buy. #CA2790 SONOMA COUNTY: 4 Ops, FFS GP Practice, 27 yrs Goodwill, 8 hyg days/ wk, Digital, Paperless, Eco-Friendly and Energy Efficient Solar Panels. 2021 GR $1.6M. #CA3165 SONORA AREA: 5 Ops, Producing $825K in a renovated suite. RE for sale w/ practice. Strong hyg prog. Digital, Laser, and Digital Pano. #CA2850 S. SACRAMENTO/POCKET ROAD/ ELK GROVE AREA: 5 Ops, Paperless, Digital X-ray, Soft Tissue Lase, Pano X-ray, CEREC. 73 yrs. Goodwill. 2021 GR $803K. #CA3093
PALMDALE/LANCASTER: 7 Op office in fast-growing community. Paperless with Dentrix, digital x-rays, 8 days of hyg./week and dedicated staff. Room to grow with specialties! #CA2612
SAN DIEGO: 6 Ops, 4 equipped, recently updated, Digital Pan, Microscopes, and Laser. Specialties referred, room for additional hours and dentistry #CA3005
SACRAMENTOWOODLAND/DAVIS/W.AREA:Endo Specialty practice! 2 full Ops (3rd Op plumbed), Paperless, Digital X-ray, Nitrous, Endo Microscope. 12 yrs. Goodwill. 2021 GR $623K. #3154
FAIRFIELD AREA: High traffic area, 7 Ops Digital, Pano/CB, 23+ NP/ mo. with 8+ Hyg. days/wk. Room to grow with specialties. 2019 GR $1.7M and 2021 on track to exceed 2019. #CA1824 LAKE TAHOE AREA: 4 Ops, 37+ yrs Goodwill. Rural lifestyle GP in growing resort community. 2019 GR $760K. #CA1715
GREATER MODESTO: 7 Ops, Desirable area, Dentrix, Digital, Laser, Digital Pano. RE for sale w/practice. Not a Delta Premier provider. 2020 GR $615K and 2021 should exceed it. #CA2795 SANTA CRUZ: 4 Ops, Minutes to beach! Digital, CEREC, Pano, CBCT. Bread and butter practice-room to grow with specialties. FFS and Delta PPO only. #CA2938
AGOURA VILLAGE/THOUSANDHILLS/WESTLAKEOAKS: 4 Ops plus 1 plumbed not equipped. 18 yrs. Goodwill. 2021 GR $1.1M. #3085 BAKERSFIELD: 7 Ops, 38 yrs Goodwill, Digital, RE or sale, Fee for Service, PPO, Delta Premier. 2021 GR $732K. #CA2945 COASTAL ORANGE COUNTY: 5 Ops, 4 equipped, digital sensors & pano. Room to grow, in a wellestablished area. GR $735K. #CA2787
RED AREA:BLUFF/CORNING/ORLAND 6 Ops, 8 hyg days/wk w/ room to grow! 33+ yrs Goodwill, Paperless, Digital. 2021 GR $826K. RE for sale with practice. #CA3161
ESCONDIDO DENTAL REAL ESTATE: Stand alone building with 5 fully equipped Ops, 2 with brand-new equipment. On corner lot with private parking and spacious floor plan. #CA3031 LA JOLLA: 5 Ops, Well-established GP Practice, 35 Yrs. Goodwill, 9 Hygiene days per week, Digital, Soft Tissue Laser 2021 GR $816K. #CA3190
ROSEVILLE/CITRUS HTS: 4 Ops with 18 Yrs Goodwill, Digital, Laser, Strong Hyg., Specialties Referred, 2021 est GR $775K. #CA2897
SAN DIEGO: CHART ONLY SALE! Seller retiring, 30 yrs Goodwill, 400 patients seen in the last 18 months. 50% Cash, 50% PPO, No Delta Premier #CA3188
DANVILLE: New Listing! GP, 4 Ops +RE , Desirable location, 80 Yrs. Goodwill, Digital, with 5 ½ days of Hyg. 2021 GR $1.3M. #3203
SOUTHERN CALIFORNIA
19YearsinBusinessLIC#:#02143744
OCEANSIDE: GP practice blocks from the beach! 40 yrs Goodwill, 7 ops, 4 equipped 2021 GR $691K. #3151











Practical implications: This case demonstrates that clinicians must employ proper diagnostic methodologies to help detect and prevent future cases.
Inadequate Dental Imaging Delays Diagnosis of Pathologic Le Fort I Fracture Secondary to Bisphosphonate Use
Conclusions: Our experiences at a regional university-based dental center indicate that increasing numbers of supposedly “low-risk” patients are presenting with profound disease whose extent was notable only via detailed radiographic examination.
Keywords: Medication-related osteonecrosis of the jaw, MRONJ, Le Fort I fracture, pathologic fracture, pathologic Le Fort I fracture
Setareh Lavasani, DDS, MS; Ho-Hyun (Brian) Sun, DMD, MS; and Jeffrey A. Elo, DDS, MS abstract Background: Medication-related osteonecrosis of the jaws (MRONJ) is a progressive necrosis of the jaw that occurs in the aftermath of dental treatments including extractions, periodontal surgery or implant placement.
CDA JOURNAL, VOL 50 , Nº 9 SEPTEMBER 2022 513 diagnostics
Case description: While the risk of incurring MRONJ is low even after invasive treatments, its manifestations can be severe with large-scale necrosis, infection and neuropathy. The exact mechanism behind MRONJ is not yet fully understood. Prevailing theories stipulate that it is associated with a defect in periodontal bone remodeling, likely as a result of downregulation of osteoclastic action and/ or angiogenesis. MRONJ is categorized into stages ranging from 0 to 3 depending on the severity of presentation. Treatment strategies also vary accordingly. Each stage is defined by specific clinical and radiographic findings during or after the occurrences of a suspected MRONJ trigger. Antiresorptives like bisphosphonates linger within bone for extended periods of up to 10 years.

Conflict of Disclosure:InterestNonereported. Ho-Hyun (Brian) Sun, DMD, MS, is a clinical assistant professor in the division of oral and maxillofacial radiology at the Western University of Health Sciences, College of Dental Medicine and a clinical instructor in the department of oral and maxillofacial surgery at the University of the Pacific Arthur A. Dugoni School of Dentistry. He practices in an oral surgery private practice in San Jose, California.
n Stage 0: Nonspecific symptoms such as dull pain, diffuse radiopacity or periodontal ligament (PDL) widening.
n Stage 1: Necrotic bone that is appreciable visually or via probing.
n Antiresorptive treatment duration of greater than four years.
n Application of antiresorptive medications as a part of cancer management.
n Stage 2: Necrotic bone with infection or pain that is appreciable visually or via probing.
CDA JOURNAL, VOL 50 , Nº 9 514 SEPTEMBER 2022
n Antiangiogenic lifestyle factors including tobacco use. Nonetheless, our experiences at a regional university-based dental center indicate that increasing numbers of supposedly “low-risk” patients are presenting with profound disease whose extent was notable only via detailed radiographic examination. This case demonstrates that clinicians must employ proper diagnostic methodologies to help detect and prevent future cases.
AUTHORS Setareh Lavasani, DDS, MS, is an associate professor and the chief oral and maxillofacial radiologist at the division of oral radiology and advanced imaging at the Western University, College of Dental Medicine in Pomona, California.
The exact mechanism behind MRONJ is not yet fully understood. Prevailing theories stipulate that it is associated with a defect in periodontal bone remodeling, likely as a result of downregulation of osteoclastic action and/or angiogenesis.3 A proper diagnosis requires fulfillment of criteria that include:
n A history of antiresorptive and/or antiangiogenic medication use.
Mofprogressivejawosteonecrosisedication-relatedofthe(MRONJ)isanecrosisthejawthatoccurs in the aftermath of dental treatments including dental extractions, periodontal surgery or implant placement.1 While the risk of incurring MRONJ is quite low even after invasive treatments, its manifestations can be severe with largescale necrosis, infection and neuropathy.2
n Concurrent use of corticosteroids.
Clinical Presentation
n Stage 3: Necrotic bone with infection, erosion or fracture that extends beyond the alveoli. Antiresorptives like bisphosphonates linger within bone for extended periods of up to 10 years.5 In general, individuals are thought to be at a higher risk of developing MRONJ if the following criteria are met:3,4
n An intravenous route of antiresorptive treatment.
n Underlying immunosuppressive diseases including diabetes mellitus.
Jeffrey A. Elo, DDS, MS, is a professor in the division of oral and maxillofacial surgery at the Western University of Health Sciences, College of Dental Medicine. He is a fellow of the American College of Surgeons. Conflict of Disclosure:InterestNonereported.
diagnostics
n A lack of radiation therapy to the head and neck region.
An 86-year-old Asian woman presented for evaluation of pain and swelling of the right palate. The patient endorsed a one-year history of pain in the right upper quadrant and rated 4 out of 10 on the Wong-Baker Faces Pain Rating Scale. Her medications included furosemide, amlodipine and nebivolol for hypertension; solifenacin for urinary incontinence; and memantine for mild Alzheimer’s disease. The patient also reported previously taking an “unknown” oral medication and dose “a short time
Conflict of Disclosure:InterestNonereported.
n An area of appreciably exposed jawbone persisting for more than eight weeks.
MRONJ is categorized into stages ranging from 0 to 3 depending on the severity of presentation. The treatment strategies also vary accordingly, with surveillance recommended primarily for the milder stages (stages 0 and 1) to antibiosis and surgical debridement for the increasingly advanced stages (stages 2 and 3).4 Each stage is defined by specific clinical and radiographic findings during or after the occurrence of a suspected MRONJ trigger:
SEPTEMBER 2022 515 CDA JOURNAL, VOL 50 , Nº 9 for the joints.” She stated that she stopped taking this medication about a year prior to presentation in our clinic because of gastrointestinal upset. She denied any history of surgeries or past use of tobacco, alcohol or illicit substances. She also denied any history of trauma, radiation or Examinationimmunosuppression.ofthepatientrevealed a normocephalic patient with no external signs of edema, trauma or pathology. Intraorally, she was missing most of the posterior dentition in the upper arch, and a 30 mm x 10 mm segment of the posterior right maxillary alveolar bone was exposed with a medially adjacent 25 mm x 15 mm area of edematous mucosa (f IG ure 1 ). Applying digital pressure upon the swollen palatal soft tissue did not elicit blanching or suppuration. All remaining maxillary teeth and several areas of maxillary alveolar bone demonstrated gross mobility. Discussion with the referring general dentist revealed that a routine, atraumatic extraction of a nonrestorable right maxillary first premolar (tooth No. 5) had been conducted in the area approximately one year prior without signs of postoperative infection or swelling. A recent set of full-mouth radiographs was provided by her dentist that showed an empty tooth No. 5 socket with a welldefined outline and without observable signs of erosions, fractures or sequestra (f IG ure 2 ).
FIGURE 2. Recent full-mouth series provided by the patient’s dentist showed an empty maxillary right first premolar socket with a well-defined outline and without observable signs of erosions, fractures or sequestra.
FIGURE 3. Coronal CBCT scan image showing interruptions in the integrity of the patient’s bilateral maxillary sinus walls with complete opacification of the sinuses and the ostia (yellow arrows) resembling a Le Fort I-pattern maxillary fracture. Also seen is thickening of the bilateral palatal soft tissues (blue arrows).
FIGURE 4. Sagittal CBCT scan image demonstrating sparse alveolar bone trabeculation with moth-eaten and permeative-appearing bone changes (right arrow) as well as irregular periodontal ligament widening (left arrow).
As such, a cone beam computed tomography (CBCT) scan was taken and interpreted by a board-certified oral and maxillofacial radiologist. The images showed interruptions in the integrity of her bilateral maxillary sinus walls with complete opacification of the sinuses and the ostia resembling a Le Fort I-pattern maxillary fracture. It also showed thickening of the bilateral palatal soft tissues (f IG ure 3 ). Additionally, alveolar bone trabeculation was notably sparse with moth-eaten and permeativeappearing bone changes as well as irregular periodontal ligament widening (f IG ure 4 ). There were multiple areas of sequestered bone, the most notable of which was at the right posterior alveolar ridge (f IG ure 5 ). A presumed unhealed tooth socket without signs of trauma including overt widening or alveolar fracture was radiographically evident in the right maxillary alveolus (f IG ure 6 ). Severe thinning and interruption of buccal and palatal cortical plates with sparse and irregular trabecular bone pattern were also noted in the anterior maxilla (f IG ure 6 ). The patient underwent biopsy of the right posterior maxillary exposed bone and adjacent palatal soft tissue. Hematoxylin and eosin-stained sections of the decalcified specimen revealed segments of nonvital lamellar bone
Diagnosis and Management Given that the provided set of full-mouth radiographs was poor in quality and lacked an appropriate field of view, they were deemed insufficient to properly establish an accurate diagnosis.
FIGURE 1. Intraoral clinical photograph demonstrating exposure of a 30 mm x 10 mm segment of the posterior right maxillary alveolar bone with a medially adjacent 25 mm x 15 mm area of edematous palatal mucosa.




FIGURE 5. Serial CBCT scan images displaying multiple areas of sequestered bone (yellow arrows), the most notable at the right posterior alveolar ridge. Severe thinning and interruption of buccal and palatal cortical plates with sparse and irregular trabecular bone pattern were also noted in the anterior maxilla.
The literature also shows that the likelihood of MRONJ increases with several risk factors including the types and modes of antiresorptive administration as well as preexisting systemic factors. The significance of this case remains in its extraordinary extent despite the shortness and relative remoteness of oral bisphosphonate therapy, a patient with minimal systemic comorbidities, bisphosphonate use for osteoporosis as well as the atraumatic nature of the dental extraction conducted.
n Have you ever been diagnosed with osteoporosis or cancer?
516 SEPTEMBER 2022 CDA JOURNAL, VOL 50 , Nº 9 demonstrating enlarged empty lacunae. Also noted were irregular external surfaces and medullary spaces coated with abundant adherent granular basophilic/ amphophilic bacterial colonies (biofilm), purulent exudate and subacutely inflamed granulation tissue. In short, the sample was indicative of a nonvital osseous sequestrum consistent with osteochemonecrosis along with inflamed palatal granulation tissue and fibrosis. Upon consultation with the patient’s medical team, her extended medical diagnostics records showed that she had undergone oral bisphosphonate therapy with 75 mg weekly alendronate for approximately three months about a year prior to help manage her osteoporosis. Her alendronate use did overlap with the timing of the extraction of tooth No. 5. She stopped taking the alendronate after only three months and was started on vitamin D and calcium supplementation instead. Considering the patient’s biopsy results, her clinical and radiographic findings and her past medical history, she was diagnosed with stage 3 MRONJ with a pathologic Le Fort I-pattern fracture. Conclusion MRONJ is defined as necrosis and exposure of the jaw bones lasting longer than eight weeks during or in the aftermath of antiresorptive therapy (often with bisphosphonates) but without a history of radiotherapy or malignant metastases to the maxillomandibular region. Though MRONJ is typically precipitated by surgical trauma, simple or atraumatic tooth extractions purportedly pose minimal risks and many dental procedures are undertaken without overt measures.6
Our cases demonstrate that a standardized set of interview questions should be utilized for all patients who are likely candidates for antiresorptive medications, such as female postmenopausal patients or those with known metabolic diseases.7
n Have you ever been prescribed oral or injection medications for the purpose of strengthening bone or joints?
The inquiries should include:
n Have you ever been prescribed oral or injection medications for the purpose of preventing the
FIGURE 6. Panoramic reconstruction from CBCT data showed a presumed unhealed tooth socket in the tooth No. 5 area without signs of trauma including overt widening or alveolar fracture in the right maxillary alveolus.


spread of cancer into bone?
Dentists should consider requesting medical consultations and clarifications for patients who answer affirmatively. In the past year, these three questions have led to the identification of dozens of patients in our clinics who otherwise did not know or remembered to disclose their history of antiresorptive therapy. It is also important to note that the patient underwent a “full-mouth” radiographic exam at the referring dentist’s office, which did not show appreciable osseous pathology save for the seemingly empty tooth No. 5 socket. An appropriate radiographic examination is critical when MRONJ is suspected or when persistently exposed bone is noted. An imaging modality that encompasses all the osseous structures of the jaws — such as a CBCT or panoramic radiograph — should be utilized. For this patient, reliance on bitewing and periapical radiographs may have allowed the disease to progress further into the bilateral maxillary sinuses as well as the pterygoid processes, leading to its current Le Fort-I fracture pattern and mobility of the entire palate. Patients with profound necrosis are faced with a limited number of management options. Surgical resection and microvascular reconstruction may be considered in healthier, younger eligible patient populations.8 In others, management may require long-term systemic and local antibiosis to reduce the risks of infection and bacteremia. Recent investigations indicate that twice-daily therapy with 400 mg pentoxifylline and 400 IU of vitamin E supplementation can encourage mucosal healing over the necrotic bone to induce partial resolution of symptoms,9 though their efficacy is often contested. This patient was referred to a tertiary surgical center for evaluation and management. She was, however, deemed a poor surgical candidate considering her advanced age, Alzheimer’s disease and the amount of maxillary necrosis. Instead, she was started on a conservative medical therapy including long-term oral antibiotics, chlorhexidine oral rinses and a soft diet. She also began treatment with pentoxifylline and vitamin E. Despite such involvement of her maxilla, with conservative therapy she was able to retain adequate oral function with little to no pain. She was followed for a little over a year and a half, but then relocated. This case unfortunately represents one of an increasingly large number of MRONJ cases diagnosed at our institutions arising in individuals treated with short courses of antiresorptives and subjected to relatively atraumatic procedures. While agents like bisphosphonates remain effective at maintaining bone density, clinicians must remain cognizant of the risks even in those patients at “low risk” of developing MRONJ. Dentists should carefully consider the rare but potentially catastrophic risk especially in populations who are likely to require extensive dental treatments in the near future. n
J Am Dent Assoc 2006 Aug;137(8):1115–9; quiz 1169–70 doi: 10.14219/jada. 2.archive.2006.0350ZadikY,BenolielR, Fleissig Y, Casap N. Painful trigeminal neuropathy induced by oral bisphosphonate-related osteonecrosis of the jaw: A new etiology for the numb-chin syndrome. Quintessence Int 2012 Feb;43(2):97–104
REFERENCES
3. Kim KM, Rhee Y, Kwon Y-D, Kwon T-G, et al. Medication related osteonecrosis of the jaw: 2015 position statement of the Korean Society for Bone and Mineral Research and the Korean Association of Oral and Maxillofacial Surgeons. J Bone Metab 2015 Nov;22(4):151–65. doi: 10.11005/ jbm.2015.22.4.151. Epub 2015 Nov 30. PMCID: 4.PMC4691589RuggieroSL, Dodson TB, Fantasia J, Goodday R, et al. American Association of Oral and Maxillofacial Surgeons position paper on medication-related osteonecrosis of the jaw — 2014 update. J Oral Maxillofac Surg 2014 Oct;72(10):1938–56 doi: 10.1016/j.joms.2014.04.031. Epub 2014 May 5. 5. Shinkai I, Ohta Y. New drugs — reports of new drugs recently approved by the FDA. Alendronate. Bioorg Med Chem 1996 Jan;4(1):3–4 doi: 10.1016/09686.0896(96)00042-9MarotteH,Farge P, Gaudin P, Alexandre C, et al. The association between periodontal disease and joint destruction in rheumatoid arthritis extends the link between the HLA-DR shared epitope and severity of bone destruction. Ann Rheum Dis 2006 Jul;65(7):905–9 doi: 10.1136/ard.2005.036913 Epub 2005 Nov 10. PMCID: PMC1798215 7. Wade SW, Strader C, Fitzpatrick LA, Anthony MS, et al. Estimating prevalence of osteoporosis: Examples from industrialized countries. Arch Osteoporos 2014;9:182 doi: 10.1007/s11657-014-0182-3. Epub 2014 May 16. 8. Caldroney S, Ghazali N, Dyalram D, Lubek JE. Surgical resection and vascularized bone reconstruction in advanced stage medication-related osteonecrosis of the jaw. Int J Oral Maxillofac Surg 2017 Jul;46(7):871–876 doi: 10.1016/j. ijom.2017.01.023. Epub 2017 Feb 21. 9. Owosho AA, Estilo CL, Huryn JM, Yom SK. Pentoxifylline and tocopherol in the management of cancer patients with medication-related osteonecrosis of the jaw: An observational retrospective study of initial case series. Oral Surg Oral Med Oral Pathol Oral Radiol 2016 Oct;122(4):455–9 doi: 10.1016/j.oooo.2016.06.019. Epub 2016 Jul 13. PMCID: PMC5454806
1. Nase JB, Suzuki JB. Osteonecrosis of the jaw and oral bisphosphonate treatment.
SEPTEMBER 2022 517 CDA JOURNAL, VOL 50 , Nº 9
THE CORRESPONDING AUTHOR, Jeffrey A. Elo, DDS, MS, can be reached at jelo@westernu.edu.
The authors thank Gretchen S. Folk, DDS, MS, who is a staff pathologist at Scripps Oral Pathology Service in San Diego, for her assistance in the histopathologic evaluation.
ACKNOWLEDGMENTS
Get
® PRACTICESUPPORT Keep up compliance.regulatorywith Dr. Leslie Strommer Member since 1990 Dental Benefit Plans Employment Practices Regulatory Compliance Practice Management
expert guidance from CDA Practice Support analysts on the latest regulations affecting your practice, plus new resources to make it easier to keep pace. Benefit from dentistry-centered forms, required docs, checklists, a compliance calendar and more. Explore your CDA member resources at cda.org/RegulatoryCompliance.

The Synergistic Role of 2D and 3D Imaging in Evaluating Tumors of the Jaws: A Case Report of Diffuse Large B-Cell Lymphoma of the Mandible
Background: Oral complications are common in head and neck cancer patients. Poor oral health is associated with increasing incidence and severity of unwanted effects. Prevention and management of complications can not only improve quality of life but also aid in an uninterrupted continuation of the ideal cancer treatment.
Case description: An interprofessional approach is conducive to minimizing complications during all phases of cancer treatment. Dentists serve as experts in the prevention, diagnosis and management of cancer-related orofacial sequelae. Increasingly, the use of in-office 3D imaging of the face — especially cone beam computed tomography (CBCT) — affords dentists with an overall greater ease and accuracy in locating otherwise undetected oral manifestations of cancer. CBCT technologies offer an advanced point-of-care imaging modality that clinicians should use selectively as an adjunct to conventional 2D dental radiography. CBCT imaging provides clinicians several diagnostic benefits: It allows clinicians to more closely examine the size of lesions, provides an opportunity to more critically assess cortical changes and facilitates surgical treatment planning. We present a case of a diffuse large B-cell lymphoma of the mandible that was diagnosed via examination in a dental office setting and further characterized by CBCT imaging.
Mark Mintline, DDS; Jeffrey A. Elo, DDS, MS, FACS; Setareh Lavasani, DDS, MS; James Ywom, DDS, MS; Ashtin Alves, DMD; and Ho-Hyun (Brian) Sun, DMD, MS
SEPTEMBER 2022 519 CDA JOURNAL, VOL 50 , Nº 9
detecting cancer
abstract
Practical implications: The case demonstrates the efficacy with which a well-trained dental team could aid in the detection of serious illnesses, including cancer. It highlights the role of the dental professional not only in the detection of oral cancers like squamous cell carcinoma, but in the symptoms management of even systemic cancers like lymphoma.
Keywords: Diffuse large B-cell lymphoma of mandible, multidisciplinary, dental oncology, oral complications, cancer treatment, 2D imaging, 3D imaging, tumors of the jaws C.E. Credit

Conflict of Disclosure:InterestNonereported.
Conflict of Disclosure:InterestNonereported.
AUTHORS Mark Mintline, DDS, is an assistant professor of oral and maxillofacial pathology and the coordinator of the advanced oral diagnosis workgroup at the Western University of Health Sciences College of Dental Medicine in Pomona, California.
We present a case of a diffuse large B-cell lymphoma (DLBCL) of the mandible that was discovered via examination in a dental office setting that was further characterized by CBCT imaging. The case demonstrates the efficacy with which a well-trained dental team can aid in the detection of serious illnesses, including cancer. It highlights the role of the dental professional not only in the detection of oral cancers like squamous cell carcinoma but in the symptom management of systemic cancers such as lymphoma.
The selection of CBCT for dental and maxillofacial imaging should be based on professional judgment in accordance with the best available scientific evidence, weighing potential patient benefits against the risks associated with the level of radiation dose.7 The practitioner who operates a CBCT unit, or requests a CBCT study, must examine the entire image dataset. This is predicated on a thorough knowledge of CT anatomy for the entire acquired image volume, anatomic variations and observation of abnormalities. It is imperative that all image data be systematically reviewed for disease.8
Conflict of Disclosure:InterestNonereported. James Ywom, DDS, MS, is an associate professor of prosthodontics at the Western University of Health Sciences College of Dental Medicine in Pomona, California.
Conflict of Disclosure:InterestNonereported.
Ashtin Alves, DMD, is a general dentist in private practice in Hanford, California. Conflict of Interest Disclosure: None reported. Ho-Hyun (Brian) Sun, DMD, MS, is a clinical assistant professor of oral and maxillofacial surgery at the Western University of Health Sciences College of Dental Medicine in Pomona, California.
520 SEPTEMBER 2022 CDA JOURNAL, VOL 50 , Nº 9 detecting cancer
Conflict of Disclosure:InterestNonereported.
A 25-year-old Hispanic female presented to a large dental university clinic for a routine dental examination. The patient’s medical and surgical histories were noncontributory with no current medications or known allergies. She denied recent nausea, vomiting, fevers or chills as well as constitutional symptoms including night sweats, fatigue or sudden weight loss. The patient had never used alcohol, tobacco or recreational drugs.
Oral complications are common in head and neck cancer patients.1,2 Poor oral health is associated with increasing incidence and severity of unwanted effects.3 Prevention and management of complications can not only improve quality of life but also aid in an uninterrupted continuation of the ideal cancer treatment.4 An interprofessional approach was proven conducive to minimizing such complications during all phases of cancer treatment.5,6 Within an interprofessional setting, dentists may serve as experts in the prevention, diagnosis and treatment of cancer-related orofacial sequelae. In addition, an increasing ubiquity of in-office 3D imagery of the face — especially cone beam computed tomography (CBCT) — affords dentists with an overall greater ease and accuracy in locating otherwise undetected oral manifestations of cancer. CBCT technologies offer an advanced point-of-care imaging modality that clinicians should use selectively as an adjunct to conventional 2D dental radiography. CBCT imaging provides clinicians several diagnostic benefits: It allows clinicians to more closely examine and delineate the size of lesions in three dimensions; provides clinicians an opportunity to more critically assess the presence of any cortical changes such as facial or lingual cortical expansions and/or perforations; and facilitates the planning of interventive surgical treatment (incision placement, design and length).
Clinical Presentation
Jeffrey A. Elo, DDS, MS, is a professor of oral and maxillofacial surgery at the Western University of Health Sciences College of Dental Medicine in Pomona, California. He is a fellow in the American College of Surgeons.
Setareh Lavasani, DDS, MS, is an associate professor of oral and maxillofacial radiology at the Western University of Health Sciences College of Dental Medicine in Pomona, California.
Extraoral examination revealed facial symmetry with a mouth opening of approximately 43 mm. Her facial skin was intact without rashes or gross neurological deficits. Palpation of the face and neck did not reveal any erythema, fluctuance, edema or tenderness, and the cervical lymph nodes were unremarkable. Intraoral examination revealed good oral hygiene with no tenderness, purulence or dental mobility. All teeth tested vital to cold and electric pulp testing. There was no appreciable
FIGURE 2. Coronal CBCT image (2A) demonstrates a lesion associated with teeth Nos. 26 through 28 with irregular borders that lacked a discernible cortication. Irregular loss of lamina dura on the distal aspect of tooth No. 27 is seen, as is an area of wide transition zone between the center of the lesion to the normal bone at the periphery. Axial CBCT image (2B) demonstrates localized interruption of the buccal cortical plate in the region of the right mandibular canine. Sagittal CBCT images (2C) show localized areas of dot-sized permeative (moth-eaten appearance) bone destruction on the buccal aspect of tooth No. 27.
FIGURE 1. A non-homogeneous radiolucent lesion with irregular periphery, wide transition zone and non-uniform loss of lamina dura on a routine periapical radiograph.
erythema, leukoplakia, ulcerations or swelling of the mucosal surfaces. Routine radiographs were obtained and interpreted by a board-certified oral and maxillofacial radiologist. A plain film series demonstrated a heterogenous, ill-defined radiolucent entity of the right anterior mandible immediately distal to the canine (tooth No. 27) and around the apex of the lateral incisor (tooth No. 26) (fIGure 1). The periphery of the lesion showed a wide transition zone with no discernable cortication and very minimal apical root resorption of tooth No. 27. A CBCT imaging study demonstrated a lesion associated with teeth Nos. 26 through 28 with irregular borders that lacked a discernible cortication (fIGure 2A). Irregular loss of lamina dura on the distal aspect of tooth No. 27 was noted, as was an area of wide transition zone between the center of the lesion to the normal bone at the periphery. Three-dimensional imaging also revealed that the lesion extended further inferiorly compared to what was visualized in the initial periapical radiograph. An axial view of the CBCT volume (fIGure 2B) demonstrated a localized area of interruption of the buccal cortical plate at the region of tooth No. 27. Localized areas of dot-sized permeative (moth-eaten appearance) bone destruction were noted on the buccal aspect of tooth No. 27 (fIGure 2C). No expansion or periosteal reaction of either cortices was noted. The radiologist’s report described the noted 2D and 3D findings and recommended referral to a surgeon for further evaluation with biopsy.
Diagnosis and Management
SEPTEMBER 2022 521 CDA JOURNAL, VOL 50 , Nº 9
An aspirational biopsy was performed first, but did not yield notable fluids or aspirates, suggesting the entity was not cystic or vascular in nature. During the subsequent open biopsy (fIGures 3A and 3B), a bony window revealed soft, friable tissue that appeared inflammatory in consistency and was distinct from the surrounding bone. The lesion had created a resorptive tunneling effect within the bone but curetted out easily. Manipulation did not produce abnormal bleeding. The specimen was submitted to a laboratory for histopathologic examination and reviewed by a boardcertified oral and maxillofacial pathologist and a board-certified hematopathologist. Histopathologic examination revealed sheets of atypical and large transformed lymphocytes (centroblasts), tangible body macrophages and collections of small lymphocytes (fIGure 4). The large and atypical cells were immunoreactive for CD20, Pax-5, BCL6 and CD30; they were negative for CD3, CD5, CD10, MUM1, CD21, ALK and EBER CISH. Ki-67 had a proliferation index of approximately 95%. The tumor was diagnosed as DLBCL: not otherwise specified (NOS), CD30 positive. The DLBCL had germinal center B-cell like immunophenotype (CD10−, BCL6+ and MUM1−). The medical oncology team imaged
2A 2C2B




CDA JOURNAL, VOL 50 , Nº 9 522 SEPTEMBER 2022 detecting cancer and staged the tumor as DLBCL, NOS, CD30 positive: stage I AE with a National Comprehensive Cancer Network International Prognostic Index (NCCNIPI) score of 0. Serology testing for human immunodeficiency (HIV), hepatitis A and hepatitis B was negative. The complete blood count, lactate dehydrogenase, beta-human chorionic gonadotropin and uric acid levels were normal. Renal, hepatic and cardiac function were normal. The first-line treatment consisted of chemoimmunotherapy and involved-site radiation therapy (ISRT) of the mandible. The chemoimmunotherapy consisted of four cycles of R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine and prednisone) plus two additional applications of rituximab ([4 x R-CHOP] + [2 x R]).9 The tumor had a complete response to R-CHOP (fIGures 5A and 5B). A standard radiation dose of 3600 cGy of intensity-modulation radiation therapy (IMRT) was then delivered: 20 fractions (180 cGy/day) of 6 MV photons over an elapsed 28 days. Oral health education as well as adjunctive dental care and support were delivered for the patient before, during and after cancer treatment. One month prior to chemoimmunotherapy and radiation therapy, she underwent a thorough dental evaluation and had all potential sources of oral infection treated. Oral hygiene instruction was delivered as was education on the oral complications of cancer treatment. The patient was provided with a soft nylon-bristled toothbrush and a nonmint-flavored dentifrice with fluoride. She was instructed to brush three times per day using the Bass sulcular scrub method, floss once daily and use water if toothpaste became too painful. Custom fluoride gel applicators and 1.1% neutral pH sodium fluoride gel were prescribed prior to radiation therapy. A custom tonguedisplacing (CTD) stent using a novel cup-shaped “saddle” design was promptly fabricated from alginate impressions for the patient to wear during IMRT. The saddle design is an alternative to the teardropshaped “paddle” design10 and offers a compartment for the tongue to rest during head and neck radiotherapy (FIGURE 6). During the patient’s cancer treatment, she developed oral mucositis, dysgeusia and trismus. During the second week of radiation therapy, she developed Grade 2 (moderate) radiation mucositis according to the World Health Organization (WHO)
FIGURES 5. Positron emission tomography (PET) scans before (5A) and after (5B) R-CHOP + 2xR therapy. Axial sections of the mandible demonstrate complete resolution of the tumor after chemoimmunotherapy. 5A 5B
FIGURES 3. Three-dimensional volume reconstruction (3A) and intraoperative clinical photograph (3B) highlighting destruction of the buccal cortex. 3A 3B FIGURE 4. Histopathologic aspects of diffuse large B-cell lymphoma, CD30+: sheets of large and atypical lymphocytes (H&E, 1000x) [upper left]; tumor cells expressed CD20 (40x) [upper right]; approximately 95% expressed Ki-67 (200x) [lower left]; tumor cells expressed CD30 (400x) [lower right].





REFERENCES
Conclusion Diffuse large B-cell lymphoma is the most common type of non-Hodgkin lymphoma in the U.S.11 and is fatal if left untreated.12 Prompt diagnosis and immediate treatment is critical to patient survival. The dental team plays a vital role as part of a multidisciplinary oncology team to prevent and control oral complications related to cancer treatment. General dentists, dental specialists and dental hygienists help manage the oral cavity of the patient with cancer before, during and after cancer treatment. The dental team also plays a key role in the detection of tumors that may present in the 2D radiographs and 3D CBCT images of the jaws. In this case, the dental team helped detect, image, biopsy, diagnose, refer and manage a DLBCL of the mandible. This case was complex and required the collaboration of numerous dental specialists and medical providers in family medicine, hematopathology, oncology and radiation oncology. This case report also documents the first use of a CTD stent for an intraosseous non-Hodgkin lymphoma of the jaws. Additional studies are needed to determine the efficacy of CTD stents in the radiation therapy of tumors and hematologic malignancies of the jaws. n
FIGURES 7. Radiation mucositis. Tongue was spared, but patient developed moderate (WHO Grade 2) oral mucositis of the buccal mucosa and vestibule adjacent to the radiation field (7A); mucositis resolved three weeks after completion of radiation therapy (7B) 7A 7B scale. The patient tolerated a solid diet, but exhibited oral soreness, erythema and an ulceration of the right retromolar pad (fIGures 7A and 7B). The oral mucositis was controlled with a combination of diphenhydramine oral solution, 2% lidocaine viscous solution, 0.12% chlorhexidine gluconate oral rinse and ice chips. The patient’s dysgeusia was managed with zinc supplementation (zinc sulfate 220 mg twice daily), and the patient’s taste acuity returned two months after radiation therapy. The patient was also instructed on post-radiation jaw physical therapy, which consisted of repeated passive TMJ opening to a tolerable limit three sets a day, 20 repetitions per set. Her maximum incisal opening returned to normal (42 mm) two weeks after radiation therapy. After chemotherapy and radiation therapy concluded, optimal dental care resumed and has remained. The patient is now in remission 22 months later. A positron emission tomography (PET)/ CT scan and dental radiograph show no evidence of disease (fIGure 8).
1. Epstein JB, Thariat J, Bensadoun R-J, et al. Oral complications of cancer and cancer therapy: From cancer treatment to survivorship. CA Cancer J Clin 2012 Nov–Dec;62(6):400–22 doi: 10.3322/caac.21157. Epub 2012 Sep 12.
4. Yuwanati M, Gondivkar S, Sarode SC, et al. Oral healthrelated quality of life in oral cancer patients: Systematic review and meta-analysis. Future Oncol 2021 Mar;17(8):979–990 doi: 10.2217/fon-2020-0881. Epub 2021 Feb 5.
SEPTEMBER 2022 523 CDA JOURNAL, VOL 50 , Nº 9
3. Lalla RV, Brennan MT, Schubert MM. Oral complications of cancer therapy. In: Yagiela JA, Dowd FJ, Johnson BS, et al., eds. Pharmacology and Therapeutics for Dentistry. 6th ed. Maryland Heights, Mo.: Mosby Elsevier; 2011:782–98.
2. Hancock PJ, Epstein JB, Sadler GR. Oral and dental management related to radiation therapy for head and neck cancer. J Can Dent Assoc 2003;69(9):585–90
FIGURE 6. A novel designed customized tongue-displacing (CTD) stent (upper left) laterally deviates the tongue away from the radiation field (lower left). An external beam radiation therapy planning CT with salient radiation isodose lines shows the novel CTD design (right).



6. Samim F, Epstein JB, Zumsteg ZS, et al. Oral and dental health in head and neck cancer survivors. Cancers Head Neck 1, 14 (2016). doi.org/10.1186/s41199-016-0015-8
9. Poeschel V, Held G, Ziepert M, et al. Four versus six cycles of CHOP chemotherapy in combination with six applications of rituximab in patients with aggressive B-cell lymphoma with favourable prognosis (FLYER): A randomised, phase 3, non-inferiority trial. Lancet 2019 Dec 21;394(10216):2271–2281 doi: 10.1016/S0140-6736(19)33008-9
12. Flowers CR, Sinha R, Vose JM. Improving outcomes for patients with diffuse large B-cell lymphoma. CA Cancer J Clin 2010 Nov–Dec;60(6):393–408 doi: 10.3322/caac.20087 Epub 2010 Oct 28. THE CORRESPONDING AUTHOR, Jeffrey A. Elo, DDS, MS, can be reached at jelo@westernu.edu.
524 SEPTEMBER 2022 CDA JOURNAL, VOL 50 , Nº 9 detecting cancer
11.archive.2013.0170SiegelRL,Miller KD, Jemal A. Cancer statistics, 2019. CA Cancer J Clin 2019 Jan;69(1):7–34 doi: 10.3322/ caac.21551. Epub 2019 Jan 8.
10. Johnson B, Sales L, Winston A, et al. Fabrication of customized tongue-displacing stents: Considerations for use in patients receiving head and neck radiotherapy. J Am Dent Assoc 2013;144(6):594–600 doi: 10.14219/jada.
8.archive.2012.0295CarterL,Farman AG, Geist J, et al. American Academy of Oral and Maxillofacial Radiology executive opinion statement on performing and interpreting diagnostic cone beam computed tomography. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008 Oct;106(4):561–2 doi: 10.1016/j. tripleo.2008.07.007 FIGURE 8. Remission: no evidence of recurrent or residual tumor in the PET/CT image (left) or periapical radiograph (right).
5. Sroussi HY, Epstein JB, Bensadoun R-J, et al. Common oral complications of head and neck cancer radiation therapy: Mucositis, infections, saliva change, fibrosis, sensory dysfunctions, dental caries, periodontal disease and osteoradionecrosis. Cancer Med 2017 Dec;6(12):2918–2931 doi: 10.1002/cam4.1221. Epub 2017 Oct 25. PMCID: PMC5727249
7. American Dental Association Council on Scientific Affairs. The use of cone beam computed tomography in dentistry: An advisory statement from the American Dental Association Council on Scientific Affairs. J Am Dent Assoc 2012 Aug;143(8):899–902 doi: 10.14219/jada.
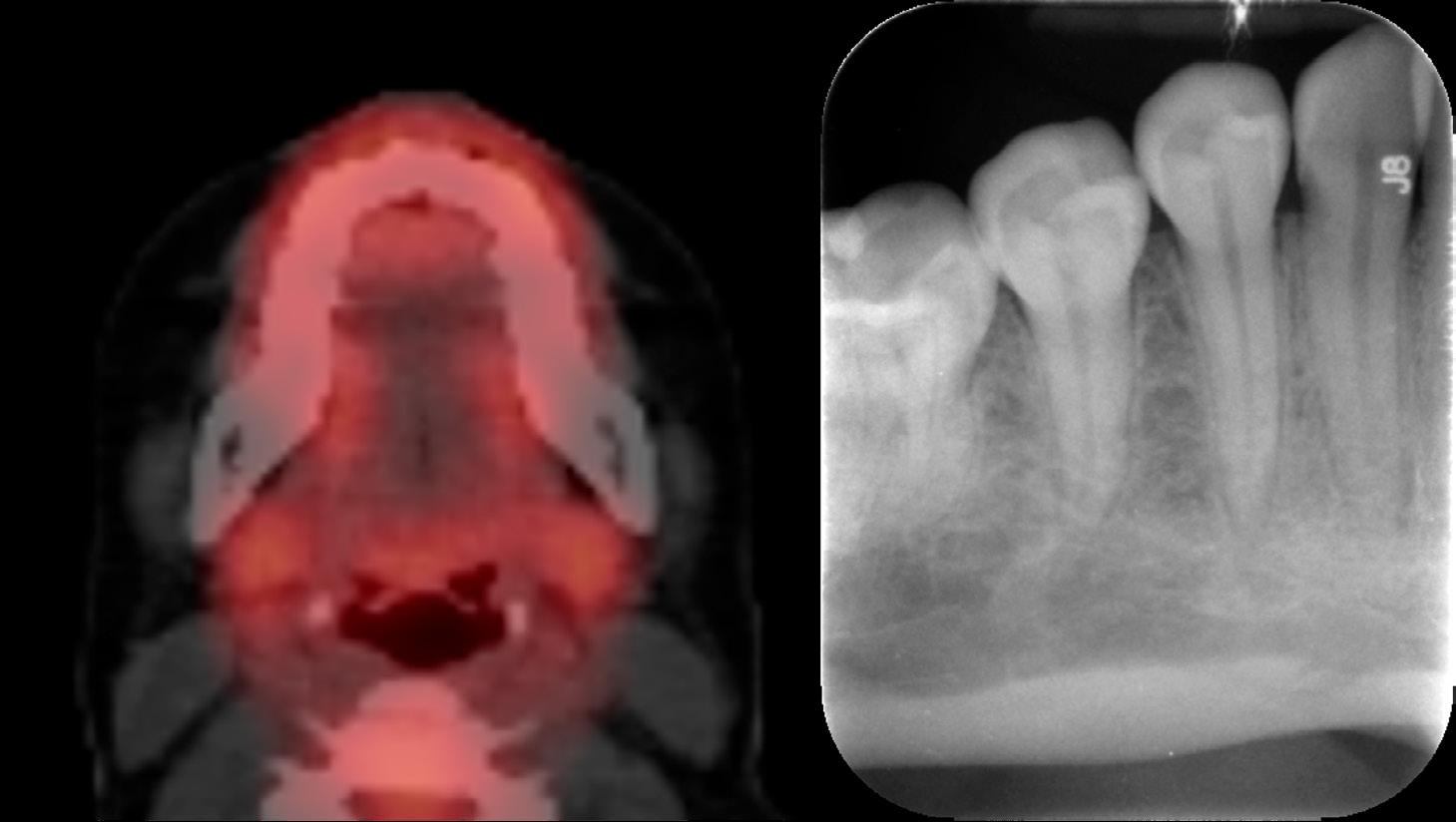
This worksheet provides readers an opportunity to review questions about the article “The Role of the Dental Team in the Multidisciplinary Diagnosis and Management of Head and Neck Cancers: A Case Report of Diffuse Large B-Cell Lymphoma of the Mandible” before taking the C.E. test online. You must first be registered at cdapresents360.com. To take the test online, click here. Earn 0.5 of Core C.E. credit through this activity.
a. Diffuse large B-cell lymphoma. b. Mantle cell lymphoma. c. Small lymphocytic lymphoma. d. Extranodal marginal zone lymphoma.
a. Hair loss. b. Oral sores. c. Osteonecrosis of the jaw. d. Increased risk of infection.
SEPTEMBER 2022 525 CDA JOURNAL, VOL 50 , Nº 9 C.E. CREDIT SeptemberQUESTIONS 2022 CDA Continuing Education Worksheet
a. To displace the tongue and oral structures from the radiation field. b. To displace and protect the teeth from bruxism. c. To manage temporomandibular joint disorders. d. To displace the tongue and teeth during surgery.
7. When should a head and neck cancer patient ideally receive an oral examination and dental treatment? a. Prior to cancer treatment. b. During cancer treatment. c. After cancer treatment. d. Patients with head and neck cancer shouldn’t receive dental care.
a. Eliminating odontogenic infection with only amalgam or gold restorations. b. Fabricating custom gel-applicator trays and fluoride gel prescription. c. Recommending a diet of natural juices and vegetables. d. Performing dental extractions after cancer treatment.
9. True/False: Hematologic malignancies of the oral cavity are often associated with nonspecific clinical and radiographic findings.
10.FalseTrueThe dental team plays an important role in managing and preventing oral complications of cancer treatment. Which of the following is a benefit of using a multidisciplinary approach to limit and treat oral complications?
4. What is the most appropriate chemotherapy treatment for diffuse large B-cell lymphoma? a. CHOEP therapy b. R-CHOP therapy c. ABVD therapy d. ATRA 5. Which of the following is not a primary goal of the dental team for managing patients undergoing cancer treatment?
1. What is the most common type of non-Hodgkin lymphoma?
a. To communicate with the medical and oncology teams. b. To eliminate oral infection. c. To perform a thorough dental evaluation. d. To complete elective or nonmedically necessary dental treatment.
2. What is not a possible complication of head and neck d.c.b.a.radiotherapy?OralmucositisDysgeusiaTrismusAlltheaboveare possible complications.
a. Cancer patients may have a higher quality of life. b. Cancer patients are less likely to stop cancer treatment. c. Minimized risk for oral and associated systemic complications of cancer treatment. d. All the above are benefits of using a multidisciplinary approach.
6. What is the purpose of a customized tongue displacement (CTD) stent?
3. What is the least likely complication of chemotherapy for diffuse large B-cell lymphoma?
8. Which of the following therapies is most beneficial to the long-term dental health for patients undergoing radiotherapy of the oral cavity?
Dental Building for Sale Lease or Move in 2900 Cold Springs Rd, Placerville Ca 95667 3200 + Square Feet 7 Ops, Gorgeous Waiting Room, 4 bathrooms, lots of easy parking, and room on the lot for expansion or another Building. Great location near Home Depot and food and OMV. Decades of good will as a dental office in town, easy access location Available April 2023 or most likely before. Contact Dr Dean K Sands DMD Call: 530-305-5000 or Email: drdksands@gmail.com Target price is $620,000 or Divided $400,000 for building and $220,000 Leasehold Improvements OWC if needed. Lease $1.00 per sq foot/plus Insurance/Taxes combined or separate comes to $1.29approx I sq foot




An Overview of Digital Workflows for Precision Implant Dentistry
6.
5.
4.
8. Take an implant-level intraoral scan with a scan body. Deliver the implant restoration.
1. Take a CBCT and intraoral scan. Merge the DICOM file with the STL file.
SEPTEMBER 2022 527 CDA JOURNAL, VOL 50 , Nº 9
digital workflows
2.
Key Steps
7. Place the implant using a guided implant surgical kit.
3. Do a digital wax-up of the tooth that needs to be replaced. Plan the implant position in a restoratively driven manner. Design the surgical guide. 3D-print the surgical guide.
Rafeeq N. Rahman, DDS; Alexander Lee, DMD; Setareh Lavasani, DMD, MS; and Tobias Boehm, DDS, PhD abstract
Digital workflows in implant dentistry can help streamline and improve the quality of implant therapy by harnessing the power of cone beam computed tomography (CBCT), intraoral scanning, implant planning software, 3D printing and guided implant placement. This article provides an overview of the key steps and considerations for implementing digital implant dentistry for implant-supported fixed single or shortspan restorations using a static implant guide.
9.

AUTHORS Rafeeq N. Rahman, DDS, is an assistant professor and clinic team leader at the Western University of Health Sciences College of Dental Medicine and practices general dentistry in Anaheim, California, with a strong emphasis on using digital workflows in dentistry. He is a fellow of the Academy of General Dentistry and the International Congress of Oral Implantologists.
The significantly lower cost and smaller computing power needed to analyze CBCT images compared to computed tomography made this technology accessible to the dental practice in 1999, when the first commercially available CBCT machine, the NewTom DVT 9000, was introduced in Europe.8
Conflict of Disclosure:InterestNonereported.
A CBCT image can be obtained from a dental imaging center or by setting up a CBCT machine within the dental office.
528 SEPTEMBER 2022 CDA JOURNAL, VOL 50 , Nº 9
The American Academy of Oral and Maxillofacial Radiology (AAOMR) recommends that cross-sectional imaging be used for the assessment of all dental implant sites and that CBCT is the imaging method of choice for this information.8 Once a CBCT image is taken, it is recommended that the image be interpreted by an oral and maxillofacial radiologist. The AAOMR noted that “dentists using CBCT should be held to the same standards as boardcertified oral and maxillofacial radiologists (OMFRs), just as dentists excising oral and maxillofacial lesions are held to the same standards as oral and maxillofacial surgeons. It is the responsibility of the practitioner obtaining the CBCT images to interpret the findings of the examination. Just as a pathology report accompanies a biopsy, an imaging report must accompany a CBCT scan.”10
Conflict of Disclosure:InterestNonereported.
The choice for either depends on multiple factors including physical space, economic feasibility, practitioner comfort with the devices and the needs of the patient population. For those looking to purchase a machine for their office, contemporary CBCT devices have a smaller footprint than previous generations as well as higher Setareh Lavasani, DMD, MS, is a full-time associate professor at the Western University of Health Sciences College of Dental Medicine. She is a board-certified oral and maxillofacial radiologist teaching oral radiology and advanced imaging and provides advanced practice oral radiology services and consultations to the dental school clinic and dentists in California. Dr. Lavasani is a diplomate of the American Board of Oral and Maxillofacial Radiology and a fellow of the Global Dental Implant Academy.
Conflict of Disclosure:InterestNonereported. Alexander Lee, DMD, is a full-time professor and coordinator of dental informatics at the Western University of Health Sciences College of Dental Medicine. He is the originator of the iFF app for formative assessment of dental students and has published extensively on student assessment and technology topics.
Cone Beam Computed Tomography
Conflict of Disclosure:InterestNonereported. Tobias K. Boehm, DDS, PhD, is a full-time associate professor at Western University of Health Sciences teaching periodontics, implantology and biomedical sciences, along with research and providing clinical specialist services at the associated dental school clinic in Pomona, California. He is a diplomate of the American Board of Periodontology and a fellow of the International Congress of Oral Implantologists.
Digital workflows in implant dentistry improve practice efficiency, outcomes.predictabilityprocedureandclinicalDigitalimplant planning aims to ensure that the implant is placed in a restoratively driven manner, while guided implant placement aims to ensure that the implant is placed exactly where it is digitally planned. Guided implant placement achieves higher accuracy and lower failure rates than freehanded or half-guided surgery because it provides a defined implant drilling and insertion path.1–3 Implants placed in such a manner are also more apt to be restored with screw-retained restorations, which leads to easier maintenance. By digitizing data, the implant planning process is sped up, physical storage space is decreased and patient chair time is decreased1,4,5
digital workflows
The foundational technology that makes a digital workflow possible in implant dentistry is cone beam computed tomography (CBCT). CBCT uses a single, inexpensive, flat-panel or image intensifier radiation detector. CBCT imaging is performed using a rotating platform to which the X-ray source and detector are fixed. The X-ray source and detector rotate around the object being scanned and multiple, sequential, planar projection images are acquired in an arc of 180 degrees or greater.6 X-ray attenuation measurements from each machine position are then used to reconstruct a 3D dataset of the implant site, which can then be used by CBCT viewing software to display either a 3D rendering or any cross-sectional view of the implant site.7,8 CBCT differs from computed tomography (CT) in that it uses a single X-ray source that produces a cone beam of radiation, rather than a fan beam as with CT. There is no accepted definition of when a fan beam (which is assumed to be planar) becomes a cone beam.9
Intraoral Scanners
SEPTEMBER 2022 529 CDA JOURNAL, VOL 50 , Nº 9 resolution and faster image acquisition. Additionally, these CBCT machines possess scatter correction or scatter reduction methods that reduce X-ray artifacts from radiation being deflected by restorations using beam-blocking techniques11 or mathematical corrections.12
n Integration with other existing practice technologies: Software suites like Romexis, DTX Studio and Dolphin Imaging support intraoral scanning. If a practice is already using such a software but is not utilizing the intraoral scanning capabilities, acquiring a manufacturer-supported intraoral scanner would decrease the setup and training time.
n Practice use case: Different scanners may be optimized for different procedures. For example, the iTero Element series of scanners would be ideal for Invisalign users due to the tight softwarehardware integration, as both are made by Align Technologies.
Digital File Types
n Form factor: In addition to considering an intraoral scanner’s size for a patient’s mouth, practitioners should also evaluate whether a scanner comes attached to a proprietary cart, the length and type of cable, size of cradle and device ergonomics.
Digital implant planning requires two main pieces of data: a CBCT of the patient as a series of DICOM (.dcm) files and an intraoral scan of the arch as an STL (.stl) file. A DICOM file is the standard file type for medical data, defined by the National Electrical Manufacturer’s Association (NEMA), that all CBCT machines are capable of outputting. In addition to the image data, each file contains information about the patient, acquisition date and method and the spatial location of the image data. Each DICOM file represents an image section, and the entire collection of DICOM files makes up the 3D representation of an implant site.13 Because of the patient data associated with each DICOM file, practitioners should take care to follow HIPAA guidelines to secure them, especially when they are exported from their picture archiving and communication system (PACS). Intraoral scans can be exported into 3D model file formats such as STL, OBJ, 3MF and more. While each format has its unique properties, the STL has become the most widely used format for 3D models because of its relatively small file size, speed of export and wide-ranging compatibility. Disadvantages of the STL file type for dentistry are that it does not contain color or scale information, meaning its units of measurement are arbitrary. Despite these drawbacks, adoption of the STL is so wide that most current dental scanning software and device manufacturers use the file type. Due to its established use in dentistry, this paper refers to 3D model files as STLs.
n User interface and experience: While some manufacturers offer a “white glove” experience where all support concerns are mitigated, others provide a “bare bones” approach that encourages the end user to create custom solutions. Some examples of intraoral scanners include 3Shape Trios 4, Planmeca Emerald S, Align Itero Element D, Carestream Dental CS 3700 and Medit i700. The images shown in this review are from 3Shape’s Trios 3 intraoral scanner.
Intraoral Scanning
n Cost: New intraoral scanners cost between $9,000 to $50,000 per unit. Support packages range from free to hundreds of dollars a month.
FIGURES 1. Intraoral scans of the treatment arch (left) and the bite registration (right) for an implant planned for the No.14 site. (Images courtesy Trios 3, 3Shape A/S.) 1A 1B
For restoratively driven implant placement, three intraoral scans are needed: an intraoral scan of the arch containing the implant site (fIGures 1), an intraoral scan of the opposing arch and an intraoral scan of the bite (f IG ures 1 ). This can be used to create a virtual articulator and a digital wax-up. The digital waxup must have the proper dimensions, be in the correct occlusal plane and
There are many intraoral scanners on the market, each with software capable of doing simple to complex dental treatments digitally. Though an in-office intraoral scanner streamlines the process, many dental labs can scan conventional models or impressions and provide an STL file for a fee. For practitioners looking to purchase an intraoral scanner, factors to consider when selecting one include:
n Manufacturer support: Terms of support and its cost influence practitioner confidence and can minimize downtime.


n Ensure the teeth are quite dry.
n Capture a few millimeters of soft tissue past gingival margins of the teeth, especially in the edentulous space where the implant will go. n Capture the interproximal tooth surfaces of the teeth adjacent to the edentulous space. This requires tipping the scanner head mesially or distally to capture tooth structure cervical to the height of contour.
n Make sure the patient is biting properly in their maximum intercuspal position (MIP) without moving or quivering.
Once the CBCT DICOM and intraoral scan STL files have been created, they can be imported into the implant planning software. Many different implant planning software packages are available. Common examples are Planmeca Romexis, 3D Diagnostics 3DDX, 3Shape Implant Studio, Dentsply Sirona Simplant and BlueSkyPlan by Blue Sky Bio. Implant planning software have similar capabilities; the choice depends on the subscription model and the ease with which the software integrates into the existing hardware of a particular office. The images in this section are from BlueSkyPlan by Blue Sky Bio. The first step is to align the DICOM data containing bone and tooth surfaces with the STL data containing tooth and soft tissue surfaces. Some software merge the two datasets automatically. Additional manual refinement can be done by shifting the model in any of three axes to better align with the CBCT image.
FIGURES 2. Corresponding points (red dots) that are used to merge the CBCT (gray, left) and scan data (green, right). (Images courtesy BlueSkyPlan, Blue Sky Bio.)
FIGURE 4. Digital wax-up showing the tooth shape (red). The tooth can be rotated in three axes (green, yellow and blue arcs), shifted buccolingually (green arrows) or apicocoronally (blue arrows) and bodily changed in size (purple dots). (Image courtesy BlueSkyPlan, Blue Sky Bio.)
n Keep the teeth dry, especially the occlusal surfaces. Scanners have difficulty differentiating between teeth and saliva.
n Use a proper fulcrum manufacturer-specifiedorsupport.
n More scanning does not mean more accuracy. The data should be captured completely, but efficiently. If certain areas need to be rescanned multiple times to get the data completely, there is likely an error or discrepancy somewhere in the scan, and it is best to start over. Digital bite registrations can be improved with these techniques:
FIGURES 3. Well-aligned merged data sets. Note how well the model outline (green line) matches the volume of teeth (left) and the near identical position of the tooth surfaces from both models (right), with an even distribution of gray and green surfaces. (Image courtesy SkyPlan, Blue Sky Bio.)
530 SEPTEMBER 2022 CDA JOURNAL, VOL 50 , Nº 9 occlusion, and most importantly, be in the correct long-axis. Ideally the tooth should be missing in the intraoral scan. However, for immediate implant cases, the tooth to be replaced can be digitally removed using the planning software.
Aligning CBCT and tooth surface data can result in higher accuracy of implant placement.18 If the software does not align automatically, you can manually do so by merging with points (f IG ures 2 ). In this method, the software user must select a series of corresponding points on the model and the CBCT image, such as grooves or cusp tips, which are easily identifiable in both data sets. The software will then align the two datasets together based on the points selected. Regardless of the alignment method, the accuracy of the alignment needs to be verified. If the models are well aligned, tooth surfaces from both the model and digital workflows
It is crucial that the intraoral scan is accurate, since the fit of the surgical guide and the placement of the implant depend on it. Digital impressions obtained from intraoral scanners appear to be as accurate as analog.14–17 Intraoral scanning accuracy can be improved with these techniques:
n Visually focus on the computer monitor and not the intraoral scanner itself.
Merging the CBCT and Intraoral Scan Data




The implant surgeon should review the entire volume of the CBCT to get acquainted with patient-specific local anatomy and look for bone abnormalities and/or presence of any other pathology. If implants in the mandible are placed, the inferior alveolar nerve should be marked in the volume by identifying its course distal from the mental foramen. Likewise, in the maxilla, the position of unusually prominent neurovascular bundles in the bone should be marked (f IG ure 5 ).
Digital Implant Planning
n At least 2.65 mm superior to the inferior alveolar nerve19 and 5 mm mesial to the mental foramen.20
n Most implants with completely rough surfaces need to be placed with the implant platform flush or slightly apical to the crestal bone. Placing implants with machined collars apical to the crestal bone may result in bone loss. These requirements typically provide maximum implant dimensions for the available bone. However, available implant dimensions and restorative design considerations including desired emergence profile and support may dictate different dimensions. For example, even if a posterior maxilla implant site features a 12 mm-wide ridge allowing placement of an 8 mm-wide implant, the largest implant size available from a given manufacturer may only be 6 mm in diameter.24 Likewise, if available bone is less than required for restorative needs, site development procedures such as ridge augmentation need to be done.25 Short implants (less than 10 mm length) may help overcome limitations in available bone height, although concerns have been raised about possible mechanical disadvantages from a poor crown:implant ratio. Yet, crown:implant ratio does not seem to be associated with enhanced peri-implant bone loss and may not affect
The next step is to determine the appropriately sized implant from the collection of implants in the chosen implant system. The available bone for implant placement provides the possible size for an implant at a given site and often dictates which implant size can be placed. To measure available bone accurately, the sectional views must be lined up so that the buccolingual and mesiodistal sections are perpendicular to the bone surfaces and the view is centered on each implant site (f IG ure 6 ).
FIGURE 5. Prominent canalis sinuosus in the premaxilla area. Placement of an implant into this structure may cause prolonged bleeding and failed implant integration. (Image courtesy Tobias K. Boehm, DDS, PhD.)
n A 2 mm thick shield of facial bone to the facial implant surface is advised.23
the CBCT should be intimately adapted on individual CBCT slices (f IG ures 3 ).
Once the two data sets are merged, a digital wax-up of the tooth for the implant sites can be created. This is done by inserting a tooth shape from the software and adjusting its size and position along the mesiodistal, buccolingual and apicocoronal axes (f IG ure 4 ). The tooth should be positioned and sized exactly as the final restoration will be because the implant will be planned according to this digital wax-up. In most programs, the digital wax-up can be locked in so that it is not inadvertently altered later in the implant planning process.
n At least 1.0 mm (platform-switched implants) to 1.5 mm (nonplatform switched implants) from the implant platform to adjacent teeth21 and at least 3.0 mm between adjacent implant platforms.22
Each implant must also meet the following requirements:
FIGURE 6. When measuring the amount of available bone, it is important to align the sectional views for accurate measurements. On the left view, the sectional views are just aligned with the sagittal and occlusal plane, resulting in an erroneous 6.9 mm ridge width measurement. On the right view, the sectional views are perpendicular to the implant site, showing a more accurate, but narrower measurement of ridge width. (Images courtesy Tobias K. Boehm, DDS, PhD.)
SEPTEMBER 2022 531 CDA JOURNAL, VOL 50 , Nº 9
FIGURE 7. Ideally, for posterior restorations, the implant axis should be centered and perpendicular to the occlusal surface in both mesiodistal and buccolingual direction to allow straight-axis loading of the implant and prevent prosthetic complications. (Image courtesy BlueSkyPlan, Blue Sky Bio.)



532 SEPTEMBER 2022 CDA JOURNAL, VOL 50 , Nº 9 digital workflows FIGURES 8. Digital implant planning with different implant lengths and diameters. The implant size most likely to achieve harmony with the surrounding structures and planned restoration should be chosen. (Images courtesy BlueSkyPlan, Blue Sky Bio.) 8A 8B 8C 8D 8E 8F






Guided Surgery Kits
Once the appropriately sized implant has been selected, it typically needs to be placed at the center of the restoration for posterior teeth and canines and palatal to the restoration center for incisors. The goal for incisors is to place the implant so that the facial platform edge is just lingual to the planned incisal edge to allow for a screw-retained restoration and allow for easier development of the facial emergence profile. The overall goal for implant placement is to achieve an implant axis perpendicular to the occlusal table of the restoration to minimize off-axis loading and avoid prosthetic complications31 (f IG ure 7 ). It is possible that the position of the virtual implant dictated by the restoration results in facial perforation of the cortex at the implant apex. In this case, the choice is either to accept a more difficult restoration by adjusting the implant position or to address the perforation with grafting during implant placement. The decision depends on which method can be more predictably achieved for a given case. If the appropriate virtual implant length results in perforation of the sinus, appropriate sinus augmentation procedures should be planned along with implant placement. If the existing bone width is not sufficient for implant placement, ridge augmentation or alternatives to implant therapy should be considered. When working as a team, the implant surgeon and restorative dentist must agree on the desired implant position.
Guided implant placement requires the use of specialized guided surgery kits. The design of the kits varies by manufacturer, but in general the kits can have either guided drills (fIGure 9) or conventional drills (fIGure 10) with a series of adapter keys. With the latter, the keys engage the guide tube, and each key has a hole in the center, of varying diameter, which allows the conventional drill to pass through. Using the key during the osteotomy can be challenging because it needs to be held in place inside the guide tube. The advantage of these systems is that the cost to transition to guided surgery is lower as they make use of the conventional drill kit. With guided drill kits, every drill has a guiding surface built into it. These kits are much simpler to use than keys because the drill goes directly into the guide. These kits often come with guided implant carriers that for allow fully guided placement. The disadvantage of these systems is the higher cost.
Once the implant position is finalized, the next step is to design the surgical guide. Each implant manufacturer’s guided implant surgical kit is different and has its own parameters to create the guide tube (f IG ures 11 ), which directs the guiding portion of the drill. The 8G 8H
Designing the Guide
SEPTEMBER 2022 533 CDA JOURNAL, VOL 50 , Nº 9 implant survival.26,27 Small diameter implants (less than 3.5 mm) may have similar bone loss and survival rates than standard diameter implants28 when placed in atrophic ridges, but may have higher complication rates and potential for fracture if placed in posterior areas.29,30
A benefit of digital implant planning is the ability to try out different implant sizes and positions and quickly see the outcome in terms of screw-hole position and relationship to the restoration (fIGures 8).


FIGURE 12. Finished model of the surgical guide. Note the windows on selected cusps to check for complete seating. (Images courtesy BlueSkyPlan, Blue Sky Bio.) 11A 11B
n Offset: This determines the position of the top of the guide tube. It is the vertical distance between the stopper on the drill and the platform of the implant. This controls the implant placement in the apicocoronal axis.
FIGURE 10. Conventional surgical kit drills. Note that each drill has its own diameter. Conventional drills can still be used for guided surgery, though they require a series of adapter keys that engage the guide tube. (Image courtesy MegaGen America.)
FIGURE 9. Guided surgical kit drills. Note that the diameter of the drills varies in the drill part, but the diameter is the same in the guided part, which is the portion of the drill that engages the guide tube. The implant carrier also has a guided part that allows for fully guided implant.
534 SEPTEMBER 2022 CDA JOURNAL, VOL 50 , Nº 9
In edentulous areas where implants will be placed, it is best to go 3 mm to 4 mm past the neighboring gingival zenith to help retract the elevated tissue during following are the parameters needed:
n Height: This determines the position of the bottom of the guide tube. It is the height of the guide tube from the top to the tissue level. This should be as tall as possible to minimize lateral movements of the drills.34 Once this information is programmed into the software, the extensions of the guide need to be marked. In dentate areas, it is best to go just past the height of contour to allow retention of the guide during implant placement (f IG ures 11 ).
FIGURES 11. The boundaries of the guide should be marked at or slightly cervical to the height of contour to allow design of a guide that is retentive. The position and size of the guide tube (orange) are determined by the surgical kit design (11A). (Image courtesy BlueSkyPlan, Blue Sky Bio.) The dimension parameters of the guide tube (11B). If the guide tube is short of the gingiva as shown here, it can introduce placement errors as it allows a greater variance in lateral movement and angulation.
digital workflows
n Diameter: This is the inner diameter of the guide tube. It should be as narrow as possible to still allow the guiding portion of the drill to pass through yet reduce lateral movements of the drills.32,33 Some systems have a separate drill for each step with a single diameter guiding portion that does not change. Other systems use a key system where the drill diameters are different, so a key is needed as an adapter between the drill and the guide. This controls the implant placement in the buccolingual and mesiodistal axes.





3D Printing 3D printers work through a process known as additive manufacturing: 3D models are cut into many digital layers and then built up in the printer layer by layer. The quality of the object improves with thinner layers. This is akin to CT scanning software that creates a 3D image of part of the body by combining slices together. While many 3D printers exist, the most common printers in dentistry utilize resin as their material. Two of the common methods for 3D resin printing are:
n Vat polymerization (SLA, DLP): This method involves using a light to cure individual layers from a vat
SEPTEMBER 2022 535 CDA JOURNAL, VOL 50 , Nº 9
FIGURE 13. Samples of 3D-printed surgical guide with a metal sleeve (left) and sleeveless (right). The center holes are the guide tubes that guide the drills and the lateral holes are windows to verify complete seating of the guide. (Images courtesy Rafeeq N. Rahman, DDS.)
The STL file from the planning process can be used to print a guide in office with a 3D printer capable of printing surgical guides with resins approved by the FDA for intraoral use or to send to a dental laboratory for guide fabrication. Some implant systems require a metal sleeve to be inserted into the guide tube after fabrication, while others are sleeveless (f IG ure 1 3 ).
Surgical Guide Fabrication
implant placement using a flap approach. Adding windows at selected cusps and incisal edges is helpful, as it allows verification of complete guide seating during implant placement (f IG ure 1 2 ).
n Material extrusion (FDM): This method involves extruding a plastic filament material through a heated nozzle. The printer extrudes the material back and forth along a predetermined path to create a 3D object,35 similar to dot-matrix printers for paper (f IG ure 1 4 ). This method has lower dimensional accuracy, as the thinnest layer possible is 0.5 mm. FDM printing is not recommended for dental purposes due to insufficient level of detail and the lack of FDA-approved materials.
Once satisfied with the guide, the guide can be exported as an STL file (f IG ure 1 2 ) to be fabricated in a 3D printing machine. A benefit of the BlueSkyPlan software is that digital implant planning is free and a cost is only incurred once the STL file is exported.
FIGURE 14. 3D printing via material extrusion (FDM). Note that the object is created in layers from the bottom up by extruding material out of a nozzle. (Images courtesy All3DP.com.)
FIGURE 15. 3D printing via vat polymerization (SLA, DLP). Note that the object is created in layers from the top down by light curing a liquid resin. (Images courtesy All3DP.com.)






FIGURES 17. An intraoral scan of a scan body in the No. 2 site. (Images courtesy Trios 3, 3Shape A/S.) high-efficiency particulate air (HEPA) filters, introducing safety guidelines for handling and securing volatile materials like resins and solvents and wearing respirators, gloves and safety goggles.36
Guided implant placement follows the same principles as freehanded implant placement regarding patient preparation, anesthesia and suturing. While the principles are similar, flap design, osteotomy and implant placement require minor modifications with the guided technique. Patient preparation involves obtaining informed consent about risks, benefits and alternatives and an appropriate description of the procedure, medications and what to expect. A single preoperative antibiotic dose is sufficient to significantly reduce early implant failure.39 For local anesthesia, local infiltration using buccal, crestal40
Surgery Stage For implant cases where the guide uses existing adjacent teeth for indexing, the guide can simply be placed on the teeth until it seats completely and does not rock. While it is possible to adjust an ill-fitting guide, it indicates an error occurred during the digital workflow, which can result in the implant not being placed in the planned location. The digital planning and guide fabrication steps should be redone with care. The guide can be used during implant surgery for direct drilling of the osteotomy only (known as half-guided implant placement) or for both drilling the osteotomy and placing the implant through the guide (known as fully guided implant placement).37 A fully guided approach is more accurate than the partial-guided approach, as distal deviation and angular deviations from the planned position are significantly smaller with the fully guided approach.38
536 SEPTEMBER 2022 CDA JOURNAL, VOL 50 , Nº 9 of resin (f IG ure 1 5 ). This method has much higher dimensional accuracy, as layers can be as thin as 20 microns.35 New technologies are being developed that can print layers as thin as 5 nanometers. This is the currently preferred method for 3D printing of dental objects.
Today, resins are available for a multitude of dental purposes including dental models, surgical guides, occlusal guards, orthodontic models and indirect bonding trays, provisional crowns and even long-term objects like dentures and resin restorations. There are several 3D printers on the market today that are designed for dental use such as Formlabs Form3+, SprintRay Pro S and Whip Mix Asiga Pro 4K.
While finishing stations can be created from existing dental lab equipment (a fume hood, lab handpiece, curing device, glass containers, ethanol and hand tools), dedicated devices like the Elegoo Mercury or SprintRay Pro Wash/ Dry streamline the process by keeping hazardous materials contained, automating tasks like agitating a model during washing and consolidating equipment into a single device to save space. Regardless of the type of 3D printer and finishing process used, the National Institute for Occupational Safety and Health (NIOSH) has identified three common work hazards for additive manufacturing: breathing harmful materials, skin contact with harmful materials and flammable materials. During all printing stages, NIOSH recommends proper engineering controls, administrative controls and personal protective equipment. This includes using
digital workflows 17A17B13A
Resin-based 3D-printed models require finishing steps consisting of removing support structures, washing the print, post-print curing and polishing.
The vast 3D printer market provides dentists with innumerable options beyond those stated previously, but one selection criterium rises above the rest — selecting a 3D printer with dentistry-ready features from the manufacturer allows practitioners to efficiently and predictably print their prepared STL files. Such printers have a user-experience like milling units integrated within CAD/CAM systems, boasting solidified digital processes, lists of approved materials and dental-focused custom settings. For printers that do not have these capabilities, users may need to manually repair STL files, transfer them to the printer, orient the models, experiment with unsupported resins and set print parameters through trial and error.
FIGURE 16. A scan body (left) versus an open-tray impression coping (right). (Images courtesy MegaGen America.)


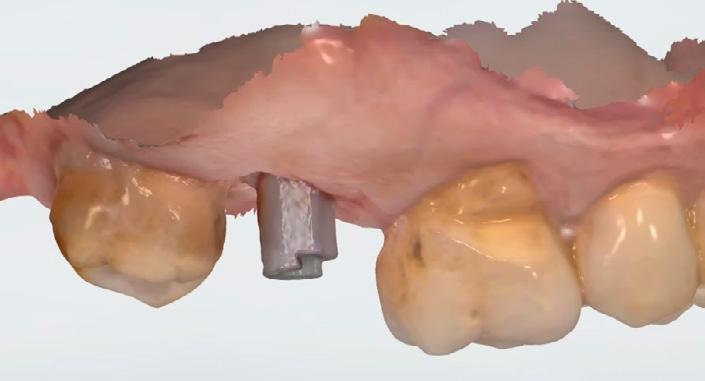

For posterior areas, using a surgical guide on a dentate patient may be difficult, as the acrylic and added implant drill length may prevent the operator from using the guide, especially in individuals with limited mouth opening. While fully guided implant surgery can result in improved placement accuracy, placement errors are still possible stemming from inaccuracies in the CBCT acquisition, 3D scanning, guide planning, 3D printing, positioning of the guide during surgery and short guide sleeve length.41 It is also possible that a clinician may need to forgo using a surgical guide as consequence of unanticipated complications encountered during surgery, such as insufficient implant stability at the planned insertion depth, closer than expected proximity to vital structures, encountering a bone dehiscence or a poorly fitting guide.42 While low-cost 3D printers can produce acceptable guides,43 accuracy of the guide is dependent on the manufacturing process and size of the guide, with small guides having better fit.44
SEPTEMBER 2022 537 CDA JOURNAL, VOL 50 , Nº 9 and lingual infiltration is sufficient for most forms of implant placement. Guided implant placement presents the opportunity for predictable flapless surgery if sufficient keratinized gingiva is present and the underlying bone anatomy allows for it. For this, a biopsy punch drill is used through the guide hole at the implant site until the drill touches bone. The guide is then removed, and the tissue plug at the implant site is removed using suitable instruments such as tissue forceps, periosteal elevators or periodontal knives. A full thickness flap should be raised for implant placement if the procedure also requires bone removal, simultaneous ridge grafting or high case difficulty where direct visualization of the bone is needed. Suturing typically aims to limit tissue mobility and aid healing. For the osteotomy with a conventional kit, a key specific for each drill is placed into the guide, and the drill passes through the key. For the osteotomy with a guided kit, each drill is passed directly through the guide. Each drill has a drill stop that reaches the predetermined length (the implant length + tissue thickness + guide thickness) that was programmed into the guide. The osteotomy should follow the manufacturer’s protocol using a surgical drill with high rpm, low torque, copious irrigation, low pressure and, if needed, a straight up-and-down pumping motion to prevent thermal damage to the bone. Implant placement should also follow manufacturers’ protocols, typically using very low speed (< 20 rpm) and a defined torque (often 30 Ncm to 50 Ncm) that provides sufficient stability without inducing pressure necrosis. For maximum benefit and fully guided surgery, the implant should also be placed through the guide to minimize placement errors. If the implant is placed freehanded after using the guide for the osteotomy, angulation errors may be introduced and some of the benefits of fully guided surgery will be lost. At each osteotomy and implant placement step, the clinician must check if the placement matches what was planned and if the placement is appropriate for the given site.
Pitfalls of Using Guides
Dynamically Guided Surgery
The previously described method using a surgical guide fitted over the adjacent teeth describes static guided surgery, which is the more common guided surgery approach. Dynamically guided implant placement was introduced to dentistry in the year 2000, where motion tracking of the patient and handpiece provides the clinician instant feedback about the planned implant position within the context of CBCT data. More recent availability of in-office CBCT machines, reduced cost and improved designs to facilitate use of these systems in a dental office have led to greater interest in this technology, as it may result in a simpler implant planning workflow.45 Currently, two dynamically guided implant systems have received FDA 510(k) clearance and are available in the U.S. (i.e., Navident ClaroNav, X-Nav X-Guide Dynamic 3D Navigation).46,47 With these systems, cameras mounted in the operatory record optic markers placed on the handpiece and the patient and a computer system provides the operator feedback on a screen whether the implant motor is positioned at the correct angle and position. As another approach in dynamically guided implant placement, robotics was introduced to implant dentistry in 2017 with the development of an autonomous robot implant placement system in China and FDA clearance of a robotic system that assists placement of implants.48 The FDA-cleared system is available as the Neocis YOMI system where a handpiece is mounted on a robotic arm that provides the operator haptic feedback on the correct angulation and position.49 Currently, this system has been developed for use in fully and partially edentulous arches, but requires sufficient teeth or bone to stably hold a splint in place.50 A drawback of the robotic approach is that this system is still For maximum benefit and fully guided surgery, the implant should also be placed through the guide to minimize placement errors.
15. Tallarico M, Xhanari E, Kim YJ, et al. Accuracy of computer-assisted template-based implant placement using conventional impression and scan model or intraoral digital impression: A randomised controlled trial with 1 year of followup. Int J Oral Implantol (Berl) 2019;12(2):197–206
Oper Dent 2018;43(6):573–580 doi: 10.2341/17-272-C Epub 2018 Apr 9. 17. Wong V, Smith AJ, Hawkins NJ, et al. Adaptive tutorials versus web-based resources in radiology: A mixed methods comparison of efficacy and student engagement. Acad Radiol 2015;22(10):1299–1307 doi: 10.1016/j. acra.2015.07.002. Epub 2015 Aug 17. 18. Kernen F, Benic GI, Payer M, et al. Accuracy of threedimensional printed templates for guided implant placement based on matching a surface scan with CBCT. Clin Implant Dent Relat Res 2016;18(4):762–768 doi: 10.1111/ cid.12348. Epub 2015 Apr 28. 19. Hartmann A, Welte-Jzyk C, Seiler M, et al. Neurophysiological changes associated with implant placement. Clin Oral Implants Res 2017;28(5):576–581 doi: 10.1111/clr.12837. Epub 2016 Mar 22. 20. Ritter L, Neugebauer J, Mischkowski RA, et al. Evaluation of the course of the inferior alveolar nerve in the mental foramen by cone beam computed tomography. Int J Oral Maxillofac Implants 2012;27(5):1014–1021 21. Vela X, Mendez V, Rodriguez X, et al. Crestal bone changes on platform-switched implants and adjacent teeth when the tooth-implant distance is less than 1.5 mm. Int J Periodontics Restorative Dent 2012 Apr;32(2):149–155 22. Tarnow DP, Cho SC, Wallace SS. The effect of inter-implant distance on the height of inter-implant bone crest. J Periodontol 2000;71(4):546–549 doi: 10.1902/jop.2000.71.4.546 23. Merheb J, Quirynen M, Teughels W. Critical buccal bone dimensions along implants. Periodontol 2000 2014;66(1):97–105 doi: 10.1111/prd.12042 24. ZimVie. T3 Implants. Accessed July 12, 2022. 25. Rissolo AR, Bennett J. Bone grafting and its essential role in implant dentistry. Dent Clin North Am 1998 Jan;42(1):91–116 26. Blanes RJ. To what extent does the crown-implant ratio affect the survival and complications of implant-supported reconstructions? A systematic review. Clin Oral Implants Res 2009;20 Suppl 4:67–72 doi: 10.1111/j.160027.0501.2009.01762.xFathiA,Rismanchian M, Khodadadi R, et al. Does the crown-implant ratio affect the survival and complications of implant-supported prostheses? A systematic review. J Prosthet Dent 2022 Apr 22;S0022–3913(22)00175–5 doi: 10.1016/j.prosdent.2022.03.007. Online ahead of print. 28. Gonzalez-Valls G, Roca-Millan E, Cespedes-Sanchez JM, et al. Narrow diameter dental implants as an alternative treatment for atrophic alveolar ridges. Systematic review and meta-analysis. Materials (Basel) 2021;14(12) doi: 10.3390/
Digital Restoration Once the implant is integrated and ready to be restored, a conventional implant-level impression can be taken to have the restoration fabricated. However, the digital workflow can continue with an intraoral scan of the implant to reap the maximum benefits from digital dentistry.
To use an intraoral scanner for an implant restoration, a scan body is required. A scan body is equivalent to the impression coping (f IG ure 1 6 ) in the conventional method. Each scan body is unique to each implant platform, as with an impression coping, so this needs to be ordered from the implant distributor prior to the intraoral scan appointment. The scan body is used in the same way as an impression coping. The healing abutment is removed, the scan body seated and hand-tightened and a radiograph taken to verify complete seating. Once fully seated, an intraoral scan is taken in lieu of an impression, taking care to capture all the notches of the scan body in detail (f IG ures 17 ).
12. Yang FQ, Zhang DH, Huang KD, et al. Image artifacts and noise reduction algorithm for cone-beam computed tomography with low-signal projections. J Xray Sci Technol 2018;26(2):227–240 doi: 10.3233/XST-17285
n REFERENCES 1. Gargallo-Albiol J, Barootchi S, Marques-Guasch J, et al. Fully guided versus half-guided and freehand implant placement: Systematic review and meta-analysis. Int J Oral Maxillofac Implants 2020 Nov/Dec;35(6):1159–1169 doi: 2.10.11607/jomi.7942PutraRH,YodaN,Astuti ER, et al. The accuracy of implant placement with computer-guided surgery in partially edentulous patients and possible influencing factors: A systematic review and meta-analysis. J Prosthodont Res 2022 Jan 11;66(1):29–39 doi: 10.2186/jpr.JPR_D_20_00184 Epub 2021 Jan 26. 3. Abdelhay N, Prasad S, Gibson MP. Failure rates associated with guided versus non-guided dental implant placement: A systematic review and meta-analysis. BDJ Open 2021 Aug 18;7(1):31 doi: 10.1038/s41405-021-00086-1 PMCID: 4.PMC8373900JodaT,Ferrari M, Gallucci GO, et al. Digital technology in fixed implant prosthodontics. Periodontol 2000 2017 Feb;73(1):178–192 doi: 10.1111/prd.12164
The lab uses the scan body image to determine the exact implant position and to design the abutment and restoration accordingly. The lab can print a model and fabricate the restoration conventionally, or it can design and mill the restoration digitally.
538 SEPTEMBER 2022 CDA JOURNAL, VOL 50 , Nº 9 quite expensive and is still undergoing development for wider applications.
13. National Electronics Manufacturer Association. DICOM PS3.3 2021e – Information Object Definitions. 2021. Accessed Jan. 18, 2022.
digital workflows
Conclusion Digital implant workflows hold the promise for dentists to plan and execute implant placement with great accuracy, reliability and predictability, leading to potentially simpler and more predictable restoration. The key requirements for implementing digital implant dentistry are to use a CBCT machine and an intraoral scanner to create a 3D model of bone, teeth and overlying soft tissue and to use this model to plan implant placement for guided surgery.
14. Papaspyridakos P, Vazouras K, Chen YW, et al. Digital vs. conventional implant impressions: A systematic review and meta-analysis. J Prosthodont 2020 Oct;29(8):660–678 doi: 10.1111/jopr.13211. Epub 2020 Jul 16.
16. Zimmermann M, Ender A, Attin T, et al. Accuracy of buccal scan procedures for the registration of habitual intercuspation.
5. Siqueira R, Galli M, Chen Z, et al. Intraoral scanning reduces procedure time and improves patient comfort in fixed prosthodontics and implant dentistry: A systematic review. Clin Oral Investig 2021;25(12):6517–6531 doi: 10.1007/s00784-021-04157-3. Epub 2021 Sep 27. PMCID: 6.PMC8475874AraiY.Local cone beam CT: How did it all start? Dentomaxillofac Radiol 2021 Dec 1;50(8):20210276 doi: 10.1259/dmfr.20210276. Epub 2021 Nov 9. 7. Tyndall DA, Brooks SL. Selection criteria for dental implant site imaging: A position paper of the American Academy of Oral and Maxillofacial Radiology. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2000;89(5):630–637 doi: 8.10.1067/moe.2000.106336TyndallDA,PriceJB,Tetradis S, et al. Position statement of the American Academy of Oral and Maxillofacial Radiology on selection criteria for the use of radiology in dental implantology with emphasis on cone beam computed tomography. Oral Surg Oral Med Oral Pathol Oral Radiol 2012;113(6):817–826 doi: 10.1016/j.oooo.2012.03.005 9. Scarfe WC, Farman AG. What is cone-beam CT and how does it work? Dent Clin North Am 2008;52(4):707–730, v doi: 10.1016/j.cden.2008.05.005 10. Carter L, Farman AG, Geist J, et al. American Academy of Oral and Maxillofacial Radiology executive opinion statement on performing and interpreting diagnostic cone beam computed tomography. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008 Oct;106(4):561–562 doi: 10.1016/j. 11.tripleo.2008.07.007JinJY,RenL,LiuQ, et al. Combining scatter reduction and correction to improve image quality in cone-beam computed tomography (CBCT). Med Phys 2010 Nov;37(11):5634–5644
• Inexpensive • Disposable • Non-ToxicPackage of 100 E-VAC INC.© CALL: (509) 448-2602 EMAIL: kenev Madeac@hotmail.cominUSA The Original E-VAC TipPREVENT PAINFUL TISSUE PLUGS PROTECT YOUR EQUIPMENT FROM COSTLY REPAIRS FDA Registered Contact Your Local Dental Supply Company
SEPTEMBER 2022 539 CDA JOURNAL, VOL 50 , Nº 9 29.ma14123234LeeJS,Kim HM, Kim CS, et al. Long-term retrospective study of narrow implants for fixed dental prostheses. Clin Oral Implants Res 2013;24(8):847–852 doi: 10.1111/j.16000501.2012.02472.x. Epub 2012 Apr 2. 30. Quek CE, Tan KB, Nicholls JI. Load fatigue performance of a single-tooth implant abutment system: Effect of diameter. Int J Oral Maxillofac Implants 2006;21(6):929–936 31. Koyano K, Esaki D. Occlusion on oral implants: Current clinical guidelines. J Oral Rehabil 2015;42(2):153–161 doi: 10.1111/joor.12239. Epub 2014 Oct 6. 32. Schneider D, Schober F, Grohmann P, et al. In-vitro evaluation of the tolerance of surgical instruments in templates for computer-assisted guided implantology produced by 3-D printing. Clin Oral Implants Res 2015;26(3):320–325 doi: 10.1111/clr.12327. Epub 2014 Jan 18. 33. Koop R, Vercruyssen M, Vermeulen K, et al. Tolerance within the sleeve inserts of different surgical guides for guided implant surgery. Clin Oral Implants Res 2013;24(6):630–634 doi: 10.1111/j.1600-0501.2012.02436.x. Epub 2012 Mar 13. 34. Tallarico M, Kim YJ, Cocchi F, et al. Accuracy of newly developed sleeve-designed templates for insertion of dental implants: A prospective multicenters clinical trial. Clin Implant Dent Relat Res 2019;21(1):108–113 doi: 10.1111/ cid.12704. Epub 2018 Dec 28. 35. All3DP. The Types of 3D Printing Technology of 2021 Accessed Jan. 22, 2022. 36. Glassford E, Dunn KL, Dunn KH, et al. 3D printings with filaments: Health and safety questions to ask. In: U.S. Department of Health and Human Services CfDCaP, National Institute for Occupational Safety and Health (NIOSH) ed. Cincinnati: NIOSH; 2020. 37. Kuhl S, Zurcher S, Mahid T, et al. Accuracy of full guided vs. half-guided implant surgery. Clin Oral Implants Res 2013;24(7):763–769 doi: 10.1111/j.16000501.2012.02484.x. Epub 2012 May 3. 38. Bencharit S, Staffen A, Yeung M, et al. In vivo toothsupported implant surgical guides fabricated with desktop stereolithographic printers: Fully guided surgery is more accurate than partially guided surgery. J Oral Maxillofac Surg 2018;76(7):1431–1439 doi: 10.1016/j.joms.2018.02.010. Epub 2018 Feb 21 39. Roca-Millan E, Estrugo-Devesa A, Merlos A, et al. Systemic antibiotic prophylaxis to reduce early implant failure: A systematic review and meta-analysis. Antibiotics (Basel) 2021;10(6) doi: 10.3390/antibiotics10060698 40. Giffin KM. Providing intraosseous anesthesia with minimal invasion. J Am Dent Assoc 1994;125(8):1119–1121 doi: 41.10.14219/jada.archive.1994.0128MistryA,UcerC,ThompsonJD,et al. 3D guided dental implant placement: Impact on surgical accuracy and collateral damage to the inferior alveolar nerve. Dent J (Basel) 2021;9(9) doi: 10.3390/dj9090099 42. Ku JK, Lee J, Lee HJ, et al. Accuracy of dental implant placement with computer-guided surgery: A retrospective cohort study. BMC Oral Health 2022;22(1):8 doi. 43.org/10.1186/s12903-022-02046-zBennettGW,KimSK.Comparison of the fit of surgical guides manufactured with low-cost 3D printers. Gen Dent 44.2022;70(1):18–21Rouzel’AlzitF,Cade R, Naveau A, et al. Accuracy of commercial 3D printers for the fabrication of surgical guides in dental implantology. J Dent 2021;117:103909 doi. 45.org/10.1016/j.jdent.2021.103909D’HaeseJ,AckhurstJ,Wismeijer D, et al. Current state of the art of computer-guided implant surgery. Periodontol 2000 2017;73(1):121–133 doi: 10.1111/prd.12175 46. Dental Tribune. X-Nav receives FDA clearance for its navigational tool for implant surgery. 2020. 47. ClaroNav. Navident Receives FDA 510(k) Clearance Toronto, Ontario, Canada; 2016. 48. Wu Y, Wang F, Fan S, et al. Robotics in Dental Implantology. Oral Maxillofac Surg Clin North Am 2019;31(3):513–518 doi: 10.1016/j.coms.2019.03.013 Epub 2019 May 15. 49. Mandelaris GA, Stefanelli LV, DeGroot BS. Dynamic navigation for surgical implant placement: Overview of technology, key concepts and a case report. Compend Contin Educ Dent 2018;39(9):614–621; quiz 622 50. Neocis Inc. Indications for Use. Miami. Accessed July 12, 2022.
THE CORRESPONDING AUTHOR, Tobias Boehm, DDS, PhD, can be reached at tboehm@westernu.edu.

What’s more, your practice management benefits include time-saving tools that support staffing and leading a team, working productively with benefit plans and achieving regulatory compliance. Explore your benefits today at cda.org ® DR. ANDREA JOY SMITH CDA member since 1994 YOUR MEMBERSHIP BENEFIT: More support for your path to practice success. GUIDES TEMPLATES& to make it easy to navigate practice systems, marketing, documentation and more EXPERT ADVICE by phone or email from analysts specializing in practice ownership, growth and transitions OPERATIONSSTREAMLINED with financing solutions to flex cash flow, plus effective claims and billing processing ADVOCACYDEDICATED to protect dentists as vital business owners, entrepreneurs and California employers COURSES WORKSHOPS& across trending practice management topics through live and on-demand learning options COST CONTROL to reduce overhead with savings on dental supplies and equipment from trusted brands from TDSC.com Tap into expertise and resources just for CDA members.

SEPTEMBER 2022 541 CDA JOURNAL, VOL 50 , Nº 9
An Update on the Utilization of 2D and Cone Beam Computed Tomography Imaging in Orthodontics
Keywords: Oral and maxillofacial radiology, orthodontics, cone beam computed tomography, sleep apnea
orthodontics
Audrey Yoon, DDS, MS; Linda Phi, DDS, MSD; and Joorok Park, DMD, MSD abstract Background: Modern technology has quickly evolved the imaging tools used in orthodontics and dental sleep medicine. From 2D radiography to 3D imaging, radiology plays an important role in diagnosis and comprehensive treatment planning in orthodontics and dental sleep medicine.
Types of studies reviewed: PubMed, Scopus, Cochrane Library and orthodontic textbooks were searched. The history of radiology in orthodontics, the current usage of cone beam computed tomography (CBCT) and the future directions of orthodontics and airway applications with advancing technology were summarized.
Results: CBCT was regarded as a reliable tool for assessment and management of complex orthodontic cases such as impacted teeth, TMJ evaluation, skeletal measurement and surgical diagnostic and treatment planning applications.
Practical implications: CBCT can provide some insight into the diagnosis and treatment of the airway but should be used in conjunction with other clinical data. CBCT airway imaging plays a powerful role in our understanding of craniofacial structure and obstructive sleep apnea (OSA) and our decision-making process.

Modern technology has quickly evolved the imaging tools used in orthodontics. From 2D radiography to 3D imaging, radiology plays a pivotal role in progressing the field. Our understanding of growth and development would not have been possible without this technology. Additionally, imaging is essential for proper diagnosis and comprehensive treatment planning. In order to fully appreciate the wealth of information available, we explore the history of radiology in orthodontics, elaborate on the current usage of cone beam computed tomography (CBCT) and discuss the future directions of orthodontics with advancing technology.
History Before the advent of radiographic cephalometry, which is a technique used to measure the head with medical imaging, anthropologists quantitatively analyzed dried skulls with craniometry.1,2 Using various landmarks on the cranium, they derived measurements and compared them in different human populations.2 Many lines and angles were proposed to measure anatomical structures and their relationship with one another, but these reference points were often challenged due to their reproducibility.3 However, since the skull only gave information for a single time point, it was not possible to gather longitudinal data for growth studies.1 In 1917, Wilhelm C. Röntgen won the Nobel Prize for his discovery of X-rays. Using X-rays, Birdsall Holly Broadbent Sr. developed the roentgenographic cephalometer, which was used to capture an image of the skull in two head positions: a profile view (lateral cephalometric radiograph) as well as a frontal view (posteroanterior or PA cephalometric radiograph). It illustrated the relationship of the maxilla and mandible with respect to the cranial base as well as to each other. By taking cephalometric radiographs at various time points in the individual’s growth, researchers were able to superimpose stable anatomic structures for the purpose of studying normal growth patterns over time.
Linda Phi, DDS, MSD, is a orthodontistboard-certifiedpracticing in Southern California. She is an adjunct professor in the orthodontics department at the University of the Pacific, Arthur A. Dugoni School of Dentistry and an adjunct professor in the orthodontics department at the University of California, Los Angeles, School of Dentistry. She received her DDS and MS in oral biology at UCLA and received her orthodontics certificate and MSD at UOP.
2D Radiography: Lateral Cephalometric, Posteroanterior Cephalometric and Panoramic Radiographs Cephalometrics progressed to become a tool to evaluate craniofacial morphology, becoming an integral part in the clinician’s diagnosis and decision-making.2 Using various landmarks in lateral cephalometric radiographs, analyses such as the Downs,4 Steiner,5,6 Tweed,7 Wits appraisal,8–10 McNamara11 and many others12–15 have been developed to quantify certain morphologic characteristics such as skeletal classification, prognathism or retrognathism, mandibular plane angle, anteroposterior tooth position and angulation. Less widely utilized, the PA cephalometric radiographs are taken to assess asymmetries, molar buccal-lingual angulations and skeletal width discrepancies between the maxilla and mandible. By the middle of the 20th century, the panoramic radiograph was being developed for the purpose of imaging the entire jaw.16,17 The panoramic radiograph allowed the clinician to detect the following:18 n Dental development. n Ectopic eruptions or dental impactions. n Congenitally missing teeth or supernumerary teeth. n Premature loss of teeth. n Prolonged retention, abnormal resorption or ankylosis
orthodontics
542 SEPTEMBER 2022 CDA JOURNAL, VOL 50 , Nº 9
Conflict of Disclosure:InterestNonereported.
AUTHORS Audrey Yoon, DDS, MS, is an adjunct assistant professor in orthodontics at the University of Pacific, Arthur A. Dugoni School of Dentistry, an adjunct assistant professor at Stanford University Sleep Medicine Center and a co-director of the Pediatric Dental Sleep Mini-Residency Program at Tufts University. She is also a diplomate of the American Board of Dental Sleep Medicine and a diplomate of the American Board of Orthodontics. Dr. Yoon’s areas of research include craniofacial growth modification, the surgery-first approach of toanatomicalstudytechniqueadvancementmaxillomandibularsurgeryandthegenomictoidentifygeneticfactorsrelatingOSA.
Joorok Park, DMD, MSD, is an associate professor and the clinic director of the orthodontics department at the University of the Pacific, Arthur A. Dugoni School of Dentistry. He is a diplomat of the American Board of Orthodontics. He received his MSD and certificate of orthodontics at UOP and earned his DMD at the University of Pennsylvania, School of Dental Medicine. He has done numerous clinical research work at the Craniofacial Research Instrumentation Laboratory. Conflict of Disclosure:InterestNonereported.
Conflict of Disclosure:InterestNonereported.
One of the most notable strengths of CBCT imaging is that the volumetric image provides true and accurate 3D representation of the patient’s head. Before CBCT images, orthodontic diagnosis traditionally employed 2D panoramic and lateral cephalometric X-rays. Conventional orthodontic analysis starts by conceptually combining information obtained from various types of 2D records, which consist of photographs, study models and X-rays. CBCT images can now serve as the platform on which other 3D digital images can be merged. For example, a digital study model (obtained from an intraoral scan) and a 3D skin (obtained from a 3D facial scan) can be merged accurately onto the CBCT image (fIGure 1). The merged images will display the patient’s colored facial soft tissue as well as highly detailed dentition simultaneously.
The craniofacial and dental morphology can be meticulously studied in the coronal, axial and sagittal planes
n Temporomandibular joint (TMJ) condylar morphology and associated pathology.
FIGURE 1. Colored 3D skin obtained from 3D facial scanner can be added to the soft tissue of CBCT image. Digital dental models obtained from an intraoral scan can be merged to the crowns of the CBCT image and provide comprehensive 3D representation of the patient’s craniofacial structure.
FIGURES 2. A CBCT image can be reoriented using the user defined anatomical frame of reference. Here, the skull is oriented based on the Frankfort as the horizontal reference plane, and the midsagittal plane is perpendicular to the Frankfort plane and passes through nasion and basion (2A). The coronal plane is perpendicular to the Frankfort and the midsagittal plane and passes through sella (2B) 2A 2B
3D Reorientation 2D images also have inherent problems in the errors in the head orientation. CBCT images are constructed with isotropic voxels. Therefore, after the 3D image is initially captured, it can be reorientated in a software to a desired orientation either manually or automatically by using a set of landmarks to an anatomical frame of reference (f IG ures 2 ).
n Jaw fractures.
Improved Clinical Diagnosis
n Neoplasms, cysts and other pathologies. With all of these advantages, orthodontists moved toward using panoramic radiographs and lateral cephalometric radiographs as the primary imaging modalities for diagnosis and treatment planning. One limitation of panoramic radiographs is that the resolution is inferior to that of bitewing and periapical films.18 There is less sharpness and less detail compared to the intraoral radiographs; bitewings and periapical films are still needed in order to assess caries, dental calculus, periapical lesions and other pathologies. Additionally, because panoramic radiographs show a 2D projection of a 3D object, they have distortion, magnification, ghost images and overlapping structures. Applications of Cone Beam Computed Tomography in Diagnosis, Treatment Planning and Outcome Assessment
of primary teeth.
Skeletal and Dental Measurements
Axial computed tomography (CT) scans were first introduced in North America in 1973 at the Mayo Clinic in Rochester, Minnesota.2 However, the high cost and large radiation exposure made it unfeasible for dental and orthodontic use.2,19 In 1998, CBCT was introduced in Europe;20,21 a few years later, it was introduced in the United States for dental use.20 This technology was groundbreaking in dentistry because the 3D information that was lost with panoramic and lateral cephalometric radiographs was now available. The benefits of using CBCT in orthodontics are as follows.21,22
n Root resorption.
n Space required/arch length deficiency for permanent teeth eruption and/or serial extractions.
SEPTEMBER 2022 543 CDA JOURNAL, VOL 50 , Nº 9



An orthodontist can better visualize the direction of force vector during traction of the impacted tooth (f IG ures 4 ).
Root Morphology, Pathology and Resorption
3D Cephalometric Analysis
544 SEPTEMBER 2022 CDA JOURNAL, VOL 50 , Nº 9 of space; these measurements include length, angles and volume calculations. For example, by going through crosssectional coronal slices, we can measure maxillary palatal width, mandibular width and dental buccolingual inclinations of posterior teeth.
FIGURES 3. After reorienting the patient’s CBCT image, the amount of mandibular asymmetry can be quantified. In this example, the mandible was deviated 4.1 mm from the midsagittal plane measured at the menton. Various mandibular measurements, such as ramus height, mandibular body length, total mandibular length, and frontal/lateral ramal inclinations, can be calculated to help with surgical planning (3A). Occlusal canting can be visualized, and the degree of occlusal canting can be determined. Severe occlusal canting can be corrected by impacting the maxilla differentially (3B) 3A 3B
FIGURES 4. Conventional 2D panoramic X-ray or PA X-rays do not fully reveal the nature of impacted teeth. With a CBCT scan, the clinician can determine the 3D position of the impacted tooth that will help treatment planning for traction of the impacted canine (4A). In addition, it can be used to assess any potential root resorption, which is sometimes missed or underestimated. In the example, both maxillary canines are impacted buccally, passing through the roots of maxillary lateral incisors and resorbing the roots of all incisors, especially the central incisors (4B) 4A 4B
TMJ Morphology and Pathology
orthodontics
With CBCT imaging, various 3D cephalometric analyses were developed and are especially useful in making linear or angular measurements in the axial and coronal planes. After 3D reorientation, facial asymmetry (i.e., mandibular asymmetry) or occlusal canting can be accurately measured. Severe skeletal asymmetry and canting would require surgical correction; for instance, mandibular asymmetrical set back via bilateral sagittal split osteotomy (BSSO) can improve mandibular asymmetry with
Class III subdivision malocclusion (fIGures 3).
CBCT can show dentoalveolar bone height and buccal-lingual/buccal-palatal bone width. It also shows accurate 3D positioning of erupted, unerupted and impacted teeth23 and possible damage to an adjacent tooth (root resorption).
Treatment Simulation
FIGURE 5. A CBCT scan will reveal anatomical changes in the condylar head and is the standard of excellence in diagnosis of temporomandibular joint disorders. This series of custom sections through the condyle heads show active progressive condylar resorption.
After designating the most superior and inferior limits, CBCT can calculate the total airway volume and determine the minimal cross-sectional area (MCA) within those boundaries.
Although CBCT does not replace the accuracy of periapical radiographs to evaluate dental pathology (e.g., periodontal ligament widening, periapical abscesses, etc.), it is useful in orthodontics to visualize root angulation, position, morphology and resorption (if any) at the initial evaluation, during treatment progress and at treatment completion.
Dentoalveolar Bone and Tooth Evaluation
CBCT is able to detect osseous changes in condylar morphology. It is especially useful when evaluating for TMJ pathology such as condylar resorption or sclerosis as well as adaptive condylar changes such as osteophytes (f IG ure 5 ).
3D imaging software can segment and move maxilla, mandible and individual tooth with six degrees of freedom, which allows for treatment simulation of a treatment plan. This kind of treatment simulation is essential in multidisciplinary
Airway Morphology, Volume and Cross-Sectional Area





SEPTEMBER 2022 545 CDA JOURNAL, VOL 50 , Nº 9 treatment. For example, before preparing multiple future implant sites, an orthodontist can simulate orthodontic tooth movement, implant placement and crown restoration (f IG ure 6 ). This kind of simulation can be shared with various restorative dentists and other specialists involved in multidisciplinary care. Virtual Surgical Planning Virtual surgical planning (VSP) uses CBCT information and 3D digital models to optimize efficiency and accuracy in orthognathic surgery cases requiring both oral surgery and orthodontics.24 With VSP, various types of virtual surgeries can be tried, which helps the surgeon to choose the best possible surgical plan (f IG ure 7 ). After a virtual surgery simulation, 3D-printed custom surgical plates can be used that usually improve surgical accuracy. For clinicians who prefer assessing traditional panoramic and lateral cephalometric radiographs, both of these images can be extrapolated from a single CBCT. Essentially, with 3D spatial information versus 2D radiographs, more landmarks are available that translate to more measurements and more information. The exponential increase in landmarks with CBCT allows for more accurate superimpositions compared to the few used in 2D superimpositions.2 Lastly,
FIGURES 6. This patient had multiple missing teeth, and the treatment plan was to minimize the number of implant restorations by consolidating some spaces. With the CBCT images, each tooth can be segmented and orthodontic tooth movement can be simulated (6A and 6B). After teeth are moved, implants and crowns can be simulated, which can be reviewed with specialists and the restorative dentist involved in the case (6C-6E)
6C
FIGURE 8. CBCT volume showing the upper airway using software package. 6A 6B 6D 6E
FIGURE 7. 3D surgical simulations of CBCT image with the virtual surgical planning (VSP) software will demonstrate accurate surgical movements and help oral surgeons to carry out the planned surgery. The orthodontist uses the planned postsurgical positions of the jaw segments to prepare for presurgical orthodontic treatment.

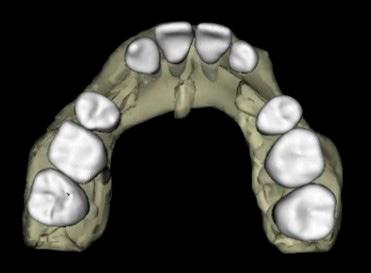





Assessment of the Airway and Supporting Structures Using CBCT Sleep-disordered breathing (SDB) is often associated with obstruction resulting in increased airway resistance. The advantages of 3D imaging over conventional planar (2D) radiography for airway assessment have been gaining popular attention. CBCT technology can be applied for anatomic assessment of the airway and adjacent structures26 and regional anatomic variables that may contribute to SDB. Integration of 3D imaging into standard clinical practice will enable practitioners to readily evaluate and screen patients when the CBCT was first introduced for dental use, the high-radiation dosage was the utmost concern from an ethical standpoint. Now with advanced technology that uses pulsed exposure time and lower settings, some CBCT machines have less radiation compared to panoramic and lateral cephalometric radiographs.2,25
FIGURES 10. Nasal valve (10A). Large turbinate and deviated septum (10B). Mucosal hypertrophy (10C) 9. Automatic segmentation of the airway using a curved path and airway color mapping presented constricted area and airway measurements.
FIGURES
546 SEPTEMBER 2022 CDA JOURNAL, VOL 50 , Nº 9
9A 9C9B 9D orthodontics 10A 10B 10C
Conclusion 3D imaging in orthodontics can provide important diagnostic information through 3D analysis such as measurements in the transverse dimension, which was quite challenging with the conventional 2D imaging. 3D imaging also allows for more accurate visualization of skeletal, dental, root and TMJ morphologies as compared to that of 2D imaging. Furthermore, performing 3D dental and jaw surgery simulations can assist clinicians with treatment planning.





Inferior turbinate or deviated septum are very common causes for nasal obstruction and mouth breathing, which can be easily detected by CBCT imaging.
AdenoidsNasopharynx
Adenoids form in the posterosuperior region of the nasopharynx and, upon enlargement, they extend toward the posterior nasal conchae and soft palate. Adenoid hypertrophy is a common etiology of nasopharyngeal obstruction. The distance in the midsagittal plane from the posterior outline of the soft palate to the closest point on the adenoid tissue from CBCT images can be used to classify the relative size of the adenoids into four groups: Grade 1 is less than 25% obstruction, Grade 2 is 25% to 50% obstruction, Grade 3 is 50% to 75% obstruction and Grade 4 is more than 75% obstruction (f IG ure 1 1 ). CBCT has proven its accuracy for evaluating adenoid size compared with the reference standard nasoendoscopy procedure. As a screening tool, CBCT is reliable and accurate in identifying adenoid hypertrophy with 88% sensitivity and 93% specificity.32
Evaluation of Upper Airway Using CBCT Because CBCT airway scans include the jaws, teeth, cranial base, spine and facial soft tissues from the tip of the nose to the beginning of the trachea, there is an opportunity to evaluate the functional and developmental relationships between these structures. Because airway obstructions or encroachments increase airway resistance that may contribute to SDB, visualization and calculation of the airway dimensions are important. Common physical encroachments of the airway include turbinates, adenoids, long soft palate, large tongue and pharyngeal and lingual tonsils. Less common airway encroachments include polyps and tumors.
The palatine tonsils, commonly TABLE FIGURE 11. Adenoid size in CBCT midsagittal slice and corresponding adenoid viewed with nasoendoscopy.31
Significant improvements in commercial software products have facilitated segmentation and measurements of the upper airway. Automatic segmentation allows the airway to be displayed and measured along a curved path to assess the risk of OSA in MCA (f IG ures 9 ).
Correlation of Airway Minimal Cross-sectional Area With Obstructive Sleep Apnea High-risk OSA MCA = 0–50 mm2 Moderate-risk OSA MCA =50–100 mm2 Low-risk OSA MCA = 100–150 mm2
OropharynxPalatineTonsils
SEPTEMBER 2022 547 CDA JOURNAL, VOL 50 , Nº 9 for phenotypes associated with SDB. CBCT alone cannot be used for diagnosis of sleep apnea because CBCT is a static snapshot of the anatomical craniofacial structures; it does not provide dynamic information such as collapsibility of airway, neuromuscular tone or actual function of airway. However, CBCT has an adjunctive role to assess the airway parameters and identifies potential sites that may contribute to a change in airway dimensions27 (f IG ure 8 ). The purpose of this portion of the article is to describe the recommended use of CBCT technology for airway evaluations and treatment.
Airway Volume and Minimal Cross-Sectional Area Accuracy and reliability of airway volume measurements using CBCT have been controversial.28 Published data have established normal values for airway dimension. The human airway increases in length, cross-sectional area and volume during craniofacial growth but worsens through adulthood. Correlation studies of small airways and obstructive sleep apnea (OSA) symptoms have demonstrated a relationship between OSA and airway minimal cross-sectional area (MCA).29,30
The probability of airway obstruction is low in adults when MCA is greater than 110 mm2, medium between 52 mm2 and 110 mm2 and high when less than 52 mm2 (TABLE 1). The site of the smallest crosssectional area during orofacial growth is bimodal with one site near the palatal plane and the other tangent to C4 vertebra. Patients with MCA above 150 mm2 show no correlation with risk of having OSA. Most severe OSA in adult patients with MCA is in the retrolingual region.31
Nasal Cavity
The evaluation of the nasal airway begins at the nares and extends posteriorly to the posterior nasal choanae. Nasal fossa, large turbinates, deviated septum, small nares, nasal mucosal hypertrophy and masses may effectively increase air flow resistance (f IG ures 10 ).
Airway Segmentation

FIGURE 12. Measurement of relative tonsil size (upper figures are in the coronal plane of the oropharyngeal airway’s narrowest part; lower figures are in the horizontal plane of the oropharyngeal airway’s narrowest part): A: Grade 1, no hyperplasia of the tonsils; B: Grade 2, the tonsils extend one-quarter of the way to the midline (yellow arrow); C: Grade 3, tonsils extend halfway to the midline (yellow arrow); D: Grade 4, tonsils extend three-quarters of the way to the midline (yellow arrow); and E: Grade 5, tonsils completely obstruct the airway, also known as “kissing” tonsils (yellow arrow).
Hyoid Bone Links between hyoid position and airway resistance have been demonstrated.33 Increased distance of the hyoid bone to mandibular plane often results in OSA, with increased distances greater than 15 mm considered abnormal.34,35
posteriorly by the palatopharyngeal arch. Tonsillar hypertrophy often leads to upper airway obstruction with sleep-disordered breathing.
An underdeveloped nasomaxillary complex has been recognized as a common anatomic feature of OSA. Constriction of the maxilla with narrow nasal floor and FIGURE 13. Penn transverse analysis. The ideal proportional relationship is a measurement of maxilla plus 5 mm in relation to the mandible. Practitioners can measure maxillary and mandibular dimensions to better understand their transverse relationship and quantify the targeted amount of palatal expansion.
548 SEPTEMBER 2022 CDA JOURNAL, VOL 50 , Nº 9 at the isthmus of the fauces, bordered anteriorly by the palatoglossal arch and referred to simply as tonsils, are located at the oropharyngeal region. They are
Using CBCT for OSA Treatment Plan in Dentistry Skeletal Transverse Discrepancy Analysis for Palatal Expansion Treatment: Rapid Palatal Expansion (RPE), MiniScrew Assisted Rapid Palatal Expansion (MARPE) and Distraction Osteogenesis Maxillary Expansion (DOME)
CBCT can adequately visualize tonsillar enlargement. The narrowest distance between the tonsils in the midcoronal plane is used to classify their relative sizes into four classifications (f IG ure 1 2 ).
orthodontics


Acronym Definition
CBCT Cone beam computed tomography PA Posteroanterior TMJ Temporomandibular joint CT Computed tomography
3D virtual surgical planning and simulation make it much easier determining locations of surgical cuts, planning precise movements of the bony segments relative to each other and designing and determination of size and length of fixation screws/plates.
BSSO Bilateral sagittal split osteotomy
MCA Minimal cross-sectional area
FIGURE 14. Computer-aided virtual surgical 3D planning for maxillomandibular advancement surgery. low tongue posture is associated with an increase in nasal airflow resistance and retroglossal airway narrowing; palatal expansion improves OSA and enhances nasal breathing in patients with narrow nasal floor and high palatal arch. It is important to assess the craniofacial structure in the transverse dimension as early as possible to accurately screen the need for transverse palatal expansion. This will maximize efficiency and effectiveness of palatal expansion treatment for OSA. Three-dimensional volumetric data visualization software can create specific transversal radiographic sectional views to assess areas of clinical interest and is therefore very useful in the diagnosis of the craniofacial transverse dimension. Many studies have confirmed that CBCT 3D imaging accurately represents intermaxillary transverse discrepancies (f IG ure 1 3 ).36,37 Several studies have proposed new 3D transverse analyses with CBCT images using skeletal and dental linear and angular measurements.37–39
Maxillomandibular Advancement Surgery Maxillomandibular advancement (MMA) surgery is a well-established treatment for OSA.40 The conceptual basis of MMA in OSA therapy is to increase the anteroposterior and lateral dimensions at various levels of upper airway thereby reducing upper airway collapsibility and superior and anterior displacement of the hyoid bone. MMA is considered the most successful surgical modality for OSA.41 MMA increases total airway volume, minimal cross-sectional area, AP and lateral dimension, airway index, airway length, posterior airway space morphology, apnea-hypopnea index (AHI) and Epworth Sleepiness Scale.42
VSP Virtual surgical planning SDB Sleep disordered breathing OSA Obstructive sleep apnea MMA Maxillomandibular advancement
SEPTEMBER 2022 549 CDA JOURNAL, VOL 50 , Nº 9
DOME Distraction osteogenesis maxillary expansion
2D Two-dimensional 3D Three-dimensional PDL Periodontal ligament
AHI Apnea-hypopnea index BOX
In the past decade, many research centers and commercial companies have migrated toward a computerized systemized surgical protocol that enables preparation of skeletal surgery treatment planning and accurate simulation of jaw surgical movements using an integrated 3D model and CBCT volumetric data approach.
RPE Rapid palatal expansion MARPE Mini-screw assisted rapid palatal expansion
The methods for computer-aided systems using CBCT revolutionized the treatment planning of skeletal surgery. They allow a comprehensive, systemic, standardized and individualized approach. The workflow for 3D virtual treatment planning procedures is highlighted in f IG ure 1 4 , starting from the images acquired from scanners to the actual surgery performed in the operating room.

2. Hans MG, Palomo JM, Valiathan M. History of imaging in orthodontics from Broadbent to cone-beam computed tomography. Am J Orthod Dentofacial Orthop 2015 Dec;148(6):914–21 doi: 10.1016/j.ajodo.2015.09.007
orthodontics
16. Hallikainen D. History of panoramic radiography. Acta Radiol 1996 May;37(3 Pt 2):441–5 doi: 17.10.1177/02841851960373P207PaateroYV.Pantomographyintheory and use. Acta Radiol 1954 Apr;41(4):321–35 doi: 18.10.3109/00016925409175858GraberTM.Panoramicradiography in orthodontic diagnosis. Am J Orthod 1967 Nov;53(11):799–821 doi: 19.10.1016/0002-9416(67)90088-7ProffitWR,FieldsHW,SarverDM. Contemporary Orthodontics. 5th ed. St. Louis: Elsevier/Mosby; 2013. 20. Kapila SD, Nervina JM. CBCT in orthodontics: Assessment of treatment outcomes and indications for its use. Dentomaxillofac Radiol 2015;44(1):20140282 doi: 10.1259/dmfr.20140282 PMCID: PMC4277443 21. Kapila S, Conley RS, Harrell WE. The current status of cone beam computed tomography imaging in orthodontics. Dentomaxillofac Radiol 2011 Jan;40(1):24–34 doi: 10.1259/dmfr/12615645 PMCID: PMC3611465 22. Kapila S. Cone Beam Computed Tomography in Orthodontics: Indications, Insights, and Innovations. Hoboken, N.J.: Wiley-Blackwell; 2014. 23. Alberto PL. Surgical exposure of impacted teeth. Oral Maxillofac Surg Clin North Am 2020 Nov;32(4):561–570 doi: 10.1016/j.coms.2020.07.008. Epub 2020 Sep 7. 24. Alkhayer A, Piffkó J, Lippold C, Segatto E. Accuracy of virtual planning in orthognathic surgery: A systematic review. Head Face Med 2020 Dec 4;16(1):34 doi: 10.1186/ s13005-020-00250-2 PMCID: PMC7716456 25. Ludlow JB, Walker C. Assessment of phantom dosimetry and image quality of i-CAT FLX cone-beam computed tomography. Am J Orthod Dentofacial Orthop 2013 Dec;144(6):802–17 doi: 10.1016/j.ajodo.2013.07.013 PMCID: PMC3914004 26. Hatcher DC. Cone beam computed tomography: Craniofacial and airway analysis. Dent Clin North Am 2012 Apr;56(2):343–57 doi: 10.1016/j.cden.2012.02.002. Epub 2012 Feb 20. 27. Kushida CA. et al. Practice parameters for the indications for polysomnography and related procedures: An update for 2005. Sleep 2005 Apr;28(4):499–521 doi: 10.1093/ 28.sleep/28.4.499AlsufyaniNA, Flores-Mir C, Major PW. Three-dimensional segmentation of the upper airway using cone beam CT: A systematic review. Dentomaxillofac Radiol 2012 May;41(4):276–84 doi: 10.1259/dmfr/79433138 PMCID: PMC3729002 29. Li HY, Chen NH, Wang CR, Shu YH, Wang PC. Use of 3-dimensional computed tomography scan to evaluate upper airway patency for patients undergoing sleep-disordered breathing surgery. Otolaryngol Head Neck Surg 2003 Oct;129(4):336–4230.OgawaT,Enciso R, Shintaku WH, Clark GT. Evaluation of cross-section airway configuration of obstructive sleep apnea. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007 Jan;103(1):102–8 doi: 10.1016/j.tripleo.2006.06.008 Epub 2006 Sep 1. PMCID: PMC1868407
THE CORRESPONDING AUTHOR, Audrey Yoon, DDS, MS, can be reached at audrey12@stanford.edu.
550 SEPTEMBER 2022 CDA JOURNAL, VOL 50 , Nº 9
REFERENCES
8. Jacobson A. The “Wits” appraisal of jaw disharmony.
3. Finlay LM. Craniometry and cephalometry: A history prior to the advent of radiography. Angle Orthod 1980 4.Oct;50(4):312–21DownsWB.Variations in facial relationships: Their significance in treatment and prognosis. Am J Orthod 1948 Oct;34(10):812–40 doi: 10.1016/0002-9416(48)90015-3
Conclusions
1. Enlow DH, Hans MG. Essentials of Facial Growth. London: Saunders; 1996.
5. Steiner CC. Cephalometrics for you and me. Am J Orthod 1953;39(10):729–755 doi.org/10.1016/00026.9416(53)90082-7SteinerCC.Theuse of cephalometrics as an aid to planning and assessing orthodontic treatment. Am J Orthod 1960;46(10):721–735 doi.org/10.1016/00027.9416(60)90145-7TweedCH.TheFrankfort-mandibular plane angle in orthodontic diagnosis, classification, treatment planning, and prognosis. Am J Orthod Oral Surg 1946 Apr;32:175–230 doi: 10.1016/0096-6347(46)90001-4
CBCT imaging paves the way for a more detailed and accurate 3D representation of the area of concern for airway applications. CBCT can provide some insight into the diagnosis and treatment but should be used in conjunction with other clinical data. Airway measurements and their significance in the development of OSA should be interpreted carefully. CBCT airway imaging plays a powerful role in our understanding of craniofacial structure and OSA and our decision-making process. n
32. Major MP, Witmans M, El-Hakim H, Major PW, Flores-Mir C. Agreement between cone-beam computed tomography and nasoendoscopy evaluations of adenoid hypertrophy. Am J Orthod Dentofacial Orthop 2014 Oct;146(4):451–9 doi: 33.10.1016/j.ajodo.2014.06.013BuchananA,CohenR,Looney S, Kalathingal S, de Rossi S. Cone-beam CT analysis of patients with obstructive sleep apnea compared to normal controls. Imaging Sci Dent 2016 Mar;46(1):9–16 doi: 10.5624/isd.2016.46.1.9. Epub 2016 Mar 24. PMCID: PMC4816775 34. Schendel SA, Broujerdi JA, Jacobson RL. Three-dimensional upper-airway changes with maxillomandibular advancement for obstructive sleep apnea treatment. Am J Orthod Dentofacial Orthop 2014 Sep;146(3):385–93 doi: 10.1016/j. 35.ajodo.2014.01.026VerinEetal.Comparison between anatomy and resistance of upper airway in normal subjects, snorers and OSAS patients. Respir Physiol 2002 Jan;129(3):335–43 doi: 10.1016/ 36.s0034-5687(01)00324-3TaiB,Goonewardene MS, Murray K, Koong B, Islam SMS. The reliability of using postero-anterior cephalometry and cone-beam CT to determine transverse dimensions in clinical practice. Aust Orthod J 2014 Nov;30(2):132–142 37. Lee KM, Hwang HS, Cho JH. Comparison of transverse analysis between posteroanterior cephalogram and cone-beam computed tomography. Angle Orthod 2014 Jul;84(4):715–9 doi: 10.2319/072613-555.1. Epub 2013 Dec 10. PMCID: 38.PMC8650435MinerRM, al Qabandi S, Rigali PH, Will LA. Cone-beam computed tomography transverse analyses. Part 2: Measures of performance. Am J Orthod Dentofacial Orthop 2015 Aug;148(2):253–63 doi: 10.1016/j.ajodo.2015.03.027 39. Tamburrino RK, Boucher NS, Vanarsdall RL, Secchi A. The transverse dimension: Diagnosis and relevance to functional occlusion. RWISO Journal 2, 13–22 (2010) 40. Hammond RJ et al. A follow-up study of dental and skeletal changes associated with mandibular advancement splint use in obstructive sleep apnea. Am J Orthod Dentofacial Orthop 2007 Dec;132(6):806–14 doi: 10.1016/j. 41.ajodo.2005.08.047PirklbauerK,etal. Maxillomandibular advancement for treatment of obstructive sleep apnea syndrome: A systematic review. J Oral Maxillofac Surg 2011 Jun;69(6):e165–76 doi: 42.10.1016/j.joms.2011.01.038RobertsonC,HerbisonP,Harkness M. Dental and occlusal changes during mandibular advancement splint therapy in sleep disordered patients. Eur J Orthod 2003 Aug;25(4):371–6 doi: 10.1093/ejo/25.4.371
15. Ricketts RM. Cephalometric Analysis and Synthesis. Angle Orthod 1961;31(3):141–156
31. Barkdull GC, Kohl CA, Patel M, Davidson TM. Computed tomography imaging of patients with obstructive sleep apnea. Laryngoscope 2008 Aug;118(8):1486–92. doi: 10.1097/ MLG.0b013e3181782706.
Am J Orthod 1975 Feb;67(2):125–38 doi: 10.1016/00029.9416(75)90065-2JacobsonA.Application of the “Wits” appraisal. Am J Orthod 1976 Aug;70(2):179–89 doi: 10.1016/s000210.9416(76)90318-3JacobsonA.Update on the “Wits” appraisal. Angle Orthod 1988 Jul;58(3):205–19 11. McNamara JA. A method of cephalometric evaluation. Am J Orthod 1984 Dec;86(6):449–69 doi: 10.1016/s000212.9416(84)90352-xJarabak,JR.Technique and Treatment With the Light-Wire Appliance. 2nd ed. St. Louis: CV Mosby; 1972: 128–66 13. Sassouni V. A Classification of Skeletal Facial Types. Am J Orthod 1969 Feb;55(2):109–23 doi: 10.1016/000214.9416(69)90122-5SassouniV.The Class II syndrome: Differential diagnosis and treatment. Angle Orthod 1970 Oct;40(4):334–41
Using Computer Assisted Dynamic Navigation: A Case Report
Paula Andrea Villa-Machado, DDS; Julián González-García, DDS; and Felipe Augusto Restrepo-Restrepo, DDS abstract Background: Endodontic treatment is a major challenge when the root canals are partially obliterated. This can occur as a result of multiple causes that stimulate pulp canal obliteration (PCO) such as physiological processes, caries, extensive restorations, coronal wear or dental trauma.
endodontic treatment
Case description: Static-guided endodontic techniques have been reported as helpful in such cases, however, the interocclusal space required for the use of templates may contraindicate the use of this technique in posterior teeth. Dynamic navigation permits the trajectory of the instruments to be tracked in real time, allowing computer-guided endodontic accesses to be executed without the need for templates that may require wider interocclusal space, which can be beneficial for the treatment of posterior teeth.
Practical implications: This article reports a case in which the distobuccal canal of a maxillary second molar, which was obliterated up to the middle third of the root, was precisely and conservatively located with dynamic navigation.
Keywords: Cone beam computed tomography, guided endodontics, pulp canal obliteration, dynamic navigation
The Role of CBCT and Guided Endodontics in Accessing a Calcified Maxillary Molar
SEPTEMBER 2022 551 CDA JOURNAL, VOL 50 , Nº 9

Conflict of Disclosure:InterestNonereported.
Pulp canal obliteration (PCO) may be a consequence of physiological aging processes, dental pulp reactions to caries, dental wear, extensive restorations or dental trauma.1,2 The endodontic treatment of these teeth is a great challenge. The use of 3D imaging with cone beam computed tomography (CBCT) is very helpful for the diagnosis and planning of the root canal treatment, and it has been indicated for the identification and location of obliterated canals.3 Computer-aided design (CAD) and computer-aided manufacturing (CAM) technologies enable the integration of tomographic images to design guides for endodontic access. Guided endodontics has grown widely in recent years. It is suggested not only for the location of obliterated canals but also for the removal of fiber posts and some endodontic microsurgery cases. Its execution can be performed with static navigation. This implies obtaining the Digital Imaging and Communications in Medicine (DICOM) files from the CBCT and matching them with the Standard Tessellation Language files (.STL files) obtained from an intraoral scanner planning software. The guide can then be printed using a 3D printer.4 Some limitations of this type of guide is its use in posterior teeth because sufficient interocclusal space is required for placement of the guide and the use of long drills in order to reach the canal.5 Computer-assisted dynamic navigation (C-AND) has been widely used to guide implant placement. C-AND tracks the instrument’s position in real time, and when integrated with the patient’s CBCT, allows real-time monitoring of the access path in the axial, sagittal and coronal space planes and grants to do the necessary corrections. It has recently been suggested as an aid to access narrow canals, resulting in less dentinal loss compared to freehand access, even with a tendency to be more accurate than static navigation.6–8 This system is composed of a laptop computer with the planning/guidance software, a MicronTracker stereoscopic camera and an LED light source that detect and track objects of interest. The objects are marked using small checkered target regions called Xpoints and must be attached to the handpiece (Drill Tag, Claron Technology, Toronto, Ontario) and to the patient’s jaw (head tracker for maxillary teeth and jaw tracker for mandibular teeth). Other system components are the tracer tool to register the CBCT scan to the patient and a unit to calibrate the location of the drills used during the clinical procedure (calibrator).9
Felipe Augusto RestrepoRestrepo, DDS, is an associate professor of endodontics at the University of Antioquia in Medellín, Colombia. He is also a part of the POPCAD Research Group Laboratory of Immunodetection and Bioanalysis, Faculty of Dentistry, at the University of Antioquia in Medellín.
Case Report
552 SEPTEMBER 2022 CDA JOURNAL, VOL 50 , Nº 9
endodontic
Conflict of MachadoDisclosure:InterestDr.Villa-isaNavident key opinion leader. Julián González-García, DDS, is an oral and maxillofacial radiologist with a private practice in Pachuca, Mexico.
AUTHORS Paula Andrea VillaMachado, DDS, is an associate professor of endodontics at the University of Antioquia in Medellín, Colombia. She is also a part of the POPCAD Research Group Laboratory of Immunodetection and Bioanalysis, Faculty of Dentistry, at the University of Antioquia in Medellín.
Conflict of Disclosure:InterestNonereported. treatment
When dynamic navigation is used, physical templates are not necessary, thus reducing the interocclusal space required to access with long instruments. This is an advantage when accessing posterior teeth. There is also the possibility to calibrate and use ultrasonic tips.5 This article describes a case in which the Navident dynamic navigation system was used to access the distobuccal (DB) canal of a partially obliterated maxillary second molar.
A 58-year-old female was referred for root canal treatment of the maxillary left second molar with tenderness to percussion/palpation in the apical region, restored with a temporary crown. She had no underlying chronic medical illnesses or family history and was taking no medications. Preoperative CBCT images were obtained using a Veraview X800 Morita (Morita Corp., Tokyo) unit operated at 91.0 kVp, 7.9 mA, 40 x 40 mm of field vision, voxel size 80
using the following protocol: Under an operating microscope (Zumax OMS3200, Zumax Medical, Suzhou New District, China), first the palatine, mesiobuccal and mesiobuccal 2 (MB2) canals were located and cleaned and shaped. The distobuccal canal was not found, and after an intraoperative CBCT (f IG ure 1 ), DICOM files were obtained and uploaded to the Navident planning software to map the dentition.
Root Canal Treatment Protocol Under local anesthesia with lidocaine 2% with epinephrine 1:80,000 (New Stetic, Guarne, Antioquia, Colombia) and rubber dam isolation of the tooth, endodontic treatment was performed FIGURE 1. Intraoperative CBCT. Axial, sagittal and coronal views show PCO of the distobuccal root canal up to the root middle third.
The head tracker was properly placed and secured on the patient’s head and the trace registration protocol was initiated in which a calibrated tracer tool is tracked by the MicronTracker camera while it is moved along the tooth surfaces. The system captures a cloud of points along this path to spatially orient the tool tag, therefore mapping the patient’s jaw to the CBCT scan. This tracing is finished by a full accuracy check performed by touching surfaces of FIGURE 2. Planning access to the distobuccal root canal in the C-ADN Navident software.
μm and 17.9 seconds of exposure time examination, which revealed three roots and four canals with partial obliteration up to the root mid-third of the DB canal and periapical tissues of normal appearance. A pulpal sensitivity test was done with a propane/butane spray (Endo-FROST, Coltene-Whaledent, Cuyahoga Falls, Ohio ) and cotton pellets with a negative response. A pretreatment diagnosis of pulpal necrosis with normal periapical tissues was made. Informed consent was obtained from the patient after the nature of the root canal treatment and possible discomforts and risks were fully explained.
To create the virtual guide, a 1 mm diameter path indicator was placed over the tooth to the required length to reach the visible distal root canal, and its position was adjusted in the 3D (sagittal, coronal and axial) (f IG ure 2 ).
SEPTEMBER 2022 553 CDA JOURNAL, VOL 50 , Nº 9

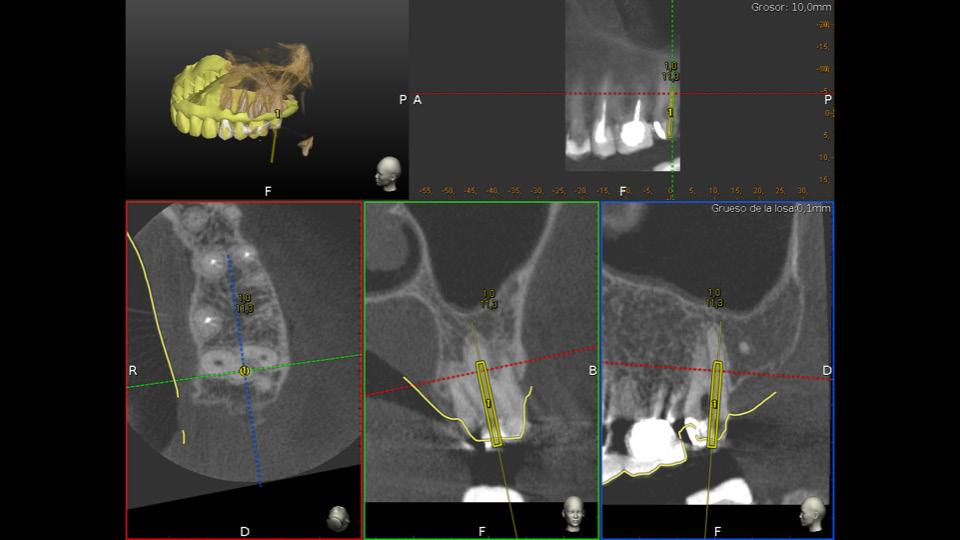
554 SEPTEMBER 2022 CDA JOURNAL, VOL 50 , Nº 9 the teeth with the tip of the tracer tool. Measurements from 0.0 mm to ± 0.03 mm allowed for verification of the accuracy of the trace in the three orthogonal planes (sagittal, coronal and axial).
endodontic treatment
Once the planned length was reached, an endodontic K-File #0.8 (DentsplyMaillefer, Ballaigues, Switzerland) was used to confirm the location and patency of the canal (f IG ure 3 ). From then on, the device was no longer needed and the root canal treatment was routinely performed, the working length was measured with an apex locator Root ZX II (J. Morita Manufacturing Corp., Kyoto, Japan) and the cleaning and shaping processes were performed with a HyFlex Controlled Memory (CM) system (ColteneWhaledent) under abundant irrigation with 5.25% sodium hypochlorite. The root canal filling was completed with warm gutta-percha vertical compaction technique using AH Plus (DentsplyMaillefer) as sealer material (f IG ure 4 ).
FIGURE 3. Radiographic location and working length verification of distobuccal root canal. FIGURE 4. Clinical view of the root canal system and posttreatment radiograph.
It has been suggested that C-ADN can be helpful to access narrow canals in a precise way, resulting in less tooth structure loss when compared to the freehand procedure and even more efficient and with greater precision than static guides that had showed evidence of unlocated canals in 8.3% of cases.14 In addition, although it has been reported that the mean angular deviation associated with the use of static guides (10.04 degrees) is significantly higher than that of the dynamic navigation (5.58 degrees),6 other authors have reported very low angular deviation (1.59 degrees) using printed templates.15 A recent meta-analysis showed a high success rate (98.1%) locating the root canal using computer-assisted navigation techniques without statistically significant differences between static or dynamic computer-assisted navigation. Computerassisted static navigation techniques showed a slightly higher root canal location success rate (98.5%) than computer-assisted dynamic navigation techniques (94.5%). These results may be influenced by the small number of studies on the dynamic technique of computer-assisted navigation (two studies) with respect to the larger number of studies on the technique of static-assisted computer navigation (12 studies).12
There have been a few case reports of guided accesses in molars, two with static guide techniques and one with C-ADN technique. The first one had enough interocclusal space to fit the template, the metallic sleeve and long drills.10 The second one had a limited interocclusal
An alternative for root canal treatment in teeth with PCO may be endodontic microsurgery (EMS). Although the identification of the calcified root canal after apicoectomy and the retro preparation and disinfection of the contaminated apical canal might be challenging, EMS without a previously filled canal would not allow complete disinfection of the entire root canal system.1,13 Due to the previous, the microsurgical approach was not considered as the first choice in the present report.
Afterward, an optical tracking tag (Drill Tag) was attached to the highspeed handpiece and the selected drill as placed and calibrated to provide an optical triangulation tracking by the Micron Tracker stereoscopic camera. In this way, the Navident C-ADN system monitors in real time the deviation among the actual planned location and the trajectory of the drill tip as it penetrates through the tooth’s structure.
Overall, both techniques are effective and better than the conventional freehand technique.6,16 The advantages of C-ADN over static guides include fast planning using only CBCT images without the need for intraoral scanning or printed guides and the direction of the endodontic access cavity can be controlled, allowing for planning changes during in-office treatment. By contrast, some disadvantages of this technology are the cost of the equipment and a certain level of skill and experience required of the operator to maintain drilling from entry since it is difficult maintaining visibility of the system display when creating the endodontic access cavity.6 However, augmented reality devices can reportedly be used to transfer over the virtual image displayed by the computer-aided dynamic navigation system while maintaining visibility of the therapeutic field.17 In addition, virtual reality has been used to perform endodontic access cavities.18
Discussion Performing root canal treatment in teeth with PCO is considered a very complex treatment.10 The endodontic access cavities must allow for complete location of the root canal system and direct access of the endodontic instruments to the root canal system, facilitate disinfection and complete debridement to avoid excessive loss of the dental structure.11,12


8. Bardales-Alcocer J, Ramírez-Salomón M, Vega-Lizama E, López-Villanueva M, Alvarado-Cárdenas G, Serota KS, Ramírez-Wong J. Endodontic retreatment using dynamic navigation: A case report. J Endod 2021 Jun;47(6):1007–1013 doi: 10.1016/j.joen.2021.03.005. Epub 2021 Mar 18. PMID: 33745944. 9. Villa-Machado PA, Restrepo-Patiño DM. Dynamically Guided Endodontics in DDS. e-book Science and Clinics 10.2021:488–493Lara-Mendes
12. Zubizarreta-Macho Á, Valle Castaño S, Montiel-Company JM, Mena-Álvarez J. Effect of computer-aided navigation techniques on the accuracy of endodontic access cavities: A systematic review and meta-analysis. Biology (Basel) 2021 Mar 10;10(3):212 doi: 10.3390/biology10030212. PMID: 33802134; PMCID: PMC7999608
13. Krastl G, Zehnder MS, Connert T, Weiger R, Kühl S. Guided endodontics: A novel treatment approach for teeth with pulp canal calcification and apical pathology. Dent Traumatol 2016 Jun;32(3):240–246 doi: 10.1111/edt.12235. Epub 2015 Oct 8. PMID: 26449290.
STO, Barbosa CFM, Machado VC, SantaRosa CC. A new approach for minimally invasive access to severely calcified anterior teeth using the guided endodontics technique. J Endod 2018 Oct;44(10):1578–1582 doi: 10.1016/j.joen.2018.07.006. Epub 2018 Aug 25. PMID: 11.30154005.Zehnder MS, Connert T, Weiger R, Krastl G, Kühl S. Guided endodontics: Accuracy of a novel method for guided access cavity preparation and root canal location. Int Endod J 2016 Oct;49(10):966–72 doi: 10.1111/iej.12544. Epub 2015 Oct 3. PMID: 26353942.
Conclusion C-ADN system Navident successfully locates the canals of PCO teeth in an accurate, safe, conservative and efficient way.
REFERENCES 1. McCabe PS, Dummer PM. Pulp canal obliteration: An endodontic diagnosis and treatment challenge. Int Endod J 2012 Feb;45(2):177–97 doi: 10.1111/j.13652591.2011.01963.x. Epub 2011 Oct 17. PMID: 21999441.
15. Connert T, Zehnder MS, Weiger R, Kühl S, Krastl G. Microguided endodontics: accuracy of a miniaturized technique for apically extended access cavity preparation in anterior teeth. J Endod 2017 May;43(5):787–790 doi: 10.1016/j.joen.2016.12.016. Epub 2017 Mar 11. PMID: 16.28292595.JainSD, Saunders MW, Carrico CK, Jadhav A, Deeb JG, Myers GL. Dynamically navigated versus freehand access cavity preparation: A comparative study on substance loss using simulated calcified canals. J Endod 2020 Nov;46(11):1745–1751 doi: 10.1016/j.joen.2020.07.032 Epub 2020 Aug 11. PMID: 32795551.
17. Pellegrino G, Mangano C, Mangano R, Ferri A, Taraschi V, Marchetti C. Augmented reality for dental implantology: A pilot clinical report of two cases. BMC Oral Health 2019 Jul 19;19(1):158 doi: 10.1186/s12903-019-0853-y. PMID: 31324246; PMCID: PMC6642526 18. Suebnukarn S, Hataidechadusadee R, Suwannasri N, Suprasert N, Rhienmora P, Haddawy P. Access cavity preparation training using haptic virtual reality and microcomputed tomography tooth models. Int Endod J 2011 Nov;44(11):983–9 doi: 10.1111/j.13652591.2011.01899.x. Epub 2011 May 28. PMID: 19.21623838.Buchgreitz J, Buchgreitz M, Bjørndal L. Guided endodontics modified for treating molars by using an intracoronal guide technique. J Endod 2019 Jun;45(6):818–823 doi: 10.1016/j.joen.2019.03.010. Epub 2019 May 3. PMID: 31056301. THE CORRESPONDING AUTHOR, Paula Andrea VillaMachado, DDS, can be reached at paula.villa@udeaedu.co.
14. Connert T, Krug R, Eggmann F, Emsermann I, ElAyouti A, Weiger R, Kühl S, Krastl G. Guided endodontics versus conventional access cavity preparation: A comparative study on substance loss using 3-dimensional-printed teeth. J Endod 2019 Mar;45(3):327–331 doi: 10.1016/j. joen.2018.11.006. PMID: 30803541.
2. Fleig S, Attin T, Jungbluth H. Narrowing of the radicular pulp space in coronally restored teeth. Clin Oral Investig 2017 May;21(4):1251–1257 doi: 10.1007/s00784-016-1899-8 Epub 2016 Jul 10. PMID: 27394425.
SEPTEMBER 2022 555 CDA JOURNAL, VOL 50 , Nº 9 space in which a modification of the technique using an intracoronal metallic pin was necessary to fit only the drill and succeed in the location of the canal.19 The third one also had a limited interocclusal space in which they used a similar dynamic navigation system (X-guide) to locate the canal.7 They all succeed in locating the canals in a predictable and safe way as in the presented case report.
3. Special Committee to Revise the Joint AAE/AAOMR Position Statement on use of CBCT in Endodontics. AAE and AAOMR Joint Position Statement: Use of Cone Beam Computed Tomography in Endodontics 2015 Update. Oral Surg Oral Med Oral Pathol Oral Radiol 2015 Oct;120(4):508–12 doi: 10.1016/j.oooo.2015.07.033. Epub 2015 Aug 3. PMID: 4.26346911.Anderson J, Wealleans J, Ray J. Endodontic applications of 3D printing. Int Endod J 2018 Sep;51(9):1005–1018 doi: 10.1111/iej.12917. Epub 2018 Mar 23. PMID: 29486052. 5. Silva EJNL, De-Deus G, Souza EM, Belladonna FG, Cavalcante DM, Simões-Carvalho M, Versiani MA. Present status and future directions — minimal endodontic access cavities. Int Endod J 2022 May;55 Suppl 3:531–587 doi: 10.1111/iej.13696. Epub 2022 Feb 20. PMID: 35100441. 6. Zubizarreta-Macho Á, Muñoz AP, Deglow ER, AgustínPanadero R, Álvarez JM. Accuracy of computer-aided dynamic navigation compared to computer-aided static procedure for endodontic access cavities: An in vitro study. J Clin Med 2020 Jan 2;9(1):129 doi: 10.3390/jcm9010129. PMID: 31906598; PMCID: PMC7019931 7. Dianat O, Gupta S, Price JB, Mostoufi B. Guided endodontic access in a maxillary molar using a dynamic navigation system. J Endod 2021 Apr;47(4):658–662 doi: 10.1016/j. joen.2020.09.019. Epub 2020 Oct 9. PMID: 33045269.
CDA PRESENTS Bloodborne pathogen and infection control are not the same. Did you know that Cal/OHSA requires annual bloodborne pathogen training for dental professionals, as well as annual review for practices’ exposure control plans? CDA has developed convenient, flexible and affordable training — available only to members and their practice teams NEW! BLOODBORNE PATHOGENS AND EXPOSURE CONTROL PLAN PROGRAM • Two how-to courses to help dental practice leaders train others • Blended program with on-demand learning for current and future staff • All the resources you need to complete an exposure plan with your team • An easy path to achieve full Cal/OSHA compliance • Low-cost options designed for every practice size Learn more and register today at cda.org/BBP Set up your Online Learning account with the same email you use for cda.org to ensure access to members-only learning options. Is your practice fully in compliance?

The Dentists Insurance Company’s Risk Management Advice Line fields calls regarding how to handle practice challenges. Here are just a few of those calls that illustrate the risks of poorly defined professional boundaries.
At a Professional Conference
A practice leader invited and covered the expenses for several members of their team to attend a weekend dental conference. During the day, the conference offered educational workshops, lectures and panel discussions, along with opportunities to explore new products and technology. In the evening, there were events for staff to attend that encouraged socializing and networking. Two of the members of this practice team were seen overindulging in alcohol during the evening events, and their attendance at daytime lectures was sporadic. The practice leader was employees right away. The practice leader should clearly identify what behavior is expected of staff members when attending professional meetings and events.
A dentist hosted a holiday party at his residence. Toward the end of the night, the dentist, who appeared to be intoxicated, allegedly approached an employee and made an inappropriate Expert support to manage your risks.
TDIC is here to help you understand and navigate dentistry’s risks. Policyholders benefit from unique tools and expertise: • A library of time-saving forms, guides and templates • One-on-one guidance from dedicated Advice Line analysts • Ongoing education on through live and online seminars Visit us online: tdicinsurance.com/RM Scan here to explore: @TDICinsurance | CA Lic # 2361-4
CDA JOURNAL, VOL 50 , Nº 9 SEPTEMBER 2022 557
At an After-Hours Office Party
frustrated and embarrassed by the behavior of these employees, feeling it reflected poorly on the practice and showed a disregard for the educational opportunities. However, the practice leader was uncomfortable addressing the employees’ behavior since it occurred outside of their place of employment. In this situation, the Advice Line recommended having an honest, transparent conversation with the
RM Where’sMatterstheLine?
TDIC Risk Management Staff Putting on scrubs and entering the dental office are both physical and mental signals to dental professionals that the workday has begun. With that workday, a certain standard of professional conduct toward patients and colleagues informs behavior. While a professional demeanor seems like a straightforward expectation for practice leaders and employees during the workday, guidelines for behavior can become blurred when practice team members interact with one another outside of the office. Without external signals like scrubs and an office setting, both practice leaders and staff may feel some confusion about their rights and responsibilities.
Define, Apply and Maintain
Professional Boundaries



Communication Is Key The best action practice owners can take to communicate and document expectations of employee behavior is to include an office policy in their employee manual. CDA member benefits include access to an employee manual generator and customizable sample manual templates. TDIC Risk Management analysts provide the following direction for including behavioral expectations in an employee manual: n Never assume that everyone has the same definition of “professional behavior.” Cite specific examples of unprofessional and unacceptable behavior as well as examples of respectful behavior and professional conduct.
Understand Your Liability and Responsibility
558 SEPTEMBER 2022 CDA JOURNAL, VOL 50 , Nº 9
Plan Events Without Alcohol Risk Management analysts also note that many of the calls they receive concerning professional boundaries involve alcohol. Hosting parties at which alcohol is provided or meeting staff for drinks after work are not recommended. Employers risk potential liability claims when professional behavior is not maintained. Drinking may hinder employees from using their best judgment. Because alcohol reduces inhibitions, remarks and behaviors can easily turn inappropriate. Allowing an event to become too casual and unprofessional can set the stage for a harassment claim. Driving under the influence and underage drinking can also be cause for concern. Even if a party is held after work, employers can still be subject to workers’ compensation claims if an employee has an accident or becomes injured at the event. TDIC has advice and alternatives for safe celebrations. Model Professional Behavior Practice owners must be mindful that their individual style and personality dictate the office environment in which they and their staff work. They should model the same behaviors they expect from their staff members, abiding by the rules for conduct outlined in the employee manual. Always maintaining a professional demeanor with staff members can prevent addressing any future performance issues from feeling like personal attacks. With acceptable and unacceptable actions clearly defined, everyone in the office will be less likely to cross the line. n
When facing similar scenarios, TDIC’s Risk Management analysts remind dentists that they can help ensure high standards of behavior inside and outside of the office by clearly defining professional boundaries.
n Maintaining an employee handbook is a critical point of documentation. Be sure to require staff to sign an acknowledgment for every employee manual or policy change and keep these acknowledgments in employee records. It is also appropriate to provide staff members with friendly reminders of company policies for appropriate professional behavior before off-site events or in-office celebrations
SEPT. 2022 RM MATTERS
Often, employers and employees mistakenly believe events and activities that take place outside of the place of employment absolve them of the rules that exist in the workplace. This is not the case. Once an employer invites most or all employees to a hosted social event or party, that event is considered an employment function. The same standard applies to off-site training or conferences that an employer pays for employees to attend.
While employees should be held accountable for their actions at employersponsored functions, establishing and maintaining boundaries creates a structure for employees to follow and know what is expected of them, regardless of the setting.
A few months later, the office received a letter from an attorney representing the employee. The attorney alleged harassment and misconduct and issued a six-figure opening demand. After weeks of deliberations, the matter ultimately settled for a low five-figure amount.
Risk Management analysts remind practice owners that standard harassment, antidiscrimination and workers’ compensation policies apply at companysponsored events. Employers can and have been held liable for their employees’ behavior regardless of when or where it occurred. Celebrating off-site or after hours does not negate the responsibilities of an employer and poses risks. For example, if an employee drives under the influence and causes an accident, the employer can also be held liable.
The Dentists Insurance Company’s Risk Management Advice Line is a benefit available at no cost to CDA members, as well as to policyholders protected by TDIC. To schedule a consultation, visit tdicinsurance.com/RMconsult or call 877.269.8844.
advance. The employee pushed him away and abruptly left his house in tears. She stopped showing up for work, as she felt uncomfortable being around the dentist.
n Specify the circumstances in which professional conduct is expected. If there is a reasonable expectation that employees will be included in employer-sponsored gatherings or represent the employer at professional events, make sure to outline the expected rules of professional conduct outside of the office.
n Staff conflict, among themselves and in their personal lives. An employer does not have the right to know the details of an employee’s personal life but should maintain awareness of unusual behavior and signs of domestic violence. When discussing such concerns with an individual employee, an employer should link the discussion to the importance of the employee to the team and
CDA Practice Support Regulatory Compliance
Dental practices need not wait for a regulation to take effect before acting to prevent workplace violence. Elements of the proposed regulation can guide employers on steps to take. The proposal calls for employers to have a written violence prevention plan, conduct workplace training and maintain incident logs. “Workplace violence” is defined in the draft regulation as any act of violence or threat of violence that occurs in a place of employment. It includes (1) the threat or use of physical force against an employee that results in or has a high likelihood of resulting in injury, psychological trauma or stress, regardless of whether the employee sustains an injury and (2) an incident involving the threat or use of a firearm or other dangerous weapon, including the use of common objects as weapons, regardless of whether the employee sustains an injury. Acts of self-defense are excluded.2
Employers should involve employees in all aspects of identifying and assessing risks. The following subjects should be discussed either as a team or individually with each employee: n Physical security, such as locked doors, security cameras and alarm systems. n Aggressive patients.
Don’t Wait To Prevent Workplace Violence
SEPTEMBER 2022 559 CDA JOURNAL, VOL 50 , Nº 9
At the time of this writing, the nation experienced a series of violent acts with multiple fatalities — shootings at a grocery store, elementary school, hospital and other workplaces. In the midst of these events, Cal/OSHA released another draft of a proposed workplace violence prevention regulation. The regulation will apply to most businesses, including dental practices and clinics. California already has a workplace violence prevention regulation for hospitals and other larger health care facilities.1 A hearing on the regulatory proposal has not been scheduled, but the agency is accepting comments on its second draft.
LDM_CDA_Journal_1.3_Square_LindaBrown_05_23_17.indd 1 5/24/2017 9:21:40 PM



The proposed Cal/OSHA regulation will require a prevention plan to include: n Procedures for employees to report incidents of workplace violence without fear of retaliation and a description of how employees will be informed about these
CDA JOURNAL, VOL 50 , Nº 9 560 SEPTEMBER 2022 performance of the entire practice. Workplace violence prevention training programs are not difficult to find. Although news media brings a lot of attention to gun violence, many training programs focus on anger de-escalation techniques, such as communicating empathically and neutrally, and on improving awareness and recognition of potentially violent situations. An employer can also use other training resources; for example, a recent TDIC Liability Lifeline newsletter focused on how to manage difficult patients. Everyone can practice de-escalation techniques until they become comfortable using them. Training should also include reviewing procedures staff should follow to ensure safety during violent situations. Procedures can include the use of a code phrase to put other staff on alert or to alert staff to call police. Earlier this year, a “difficult patient,” as described in police documents, was charged with the murder of two Texas dentists.3 Gun violence at the workplace, although rare, can occur. It is important that employee training prepare them to run and hide, for example, by discussing escape routes or to fight using available items if left with no other choice.
It is important for a dental practice employee manual to have a policy statement on workplace violence, such as the following statement included in the sample manual provided to CDA members:Weall deserve to work in an environment that is free from violence or hostility. [Employer] has zero tolerance for violent acts or threats of violence against our employees, applicants, patients or vendors. No employee should commit or threaten to commit any violent act against a co-worker, applicant, patient or vendor. This includes discussions of the use of dangerous weapons or of bringing such weapons onto office property, even in a joking manner. Any employee who is subjected to or threatened with violence by a co-worker, patient or vendor or is aware of another individual who has been subjected to or threatened with violence is to report this information to [employer] as soon as possible. Please bring all threats to our attention so that we can deal with them appropriately. All threats will be thoroughly investigated and all complaints, which are reported to management, will be treated with as much confidentiality as possible. A written violence prevention plan details the actions taken by an employer to implement this policy. It also serves as a record of an employer’s intent. Employees should participate in the plan’s development and implementation.
SEPT. 2022 REG. COMPLIANCE

CDA JOURNAL, VOL 50 , Nº 9 SEPTEMBER 2022 561
n Procedures for responding to workplace violence emergencies, including where to evacuate or shelter and how to reach out for security personnel or law enforcement.
n
n Procedures for investigating employee concerns and incidents of violence and how employees will be informed of investigation results and actions, if any.
n Procedures for regularly reviewing and updating the prevention plan.
procedures. Procedures may differ based on the type of incident.
Procedures for identifying and evaluating risk, including employment involvement, frequency of review and maintaining an incident log.
REFERENCES 1. California Department of Industrial Relations. Violence Prevention in Healthcare, 8 CCR §3342
2. California Department of Industrial Relations. Workplace Violence Prevention in General Industry, May 17, 2022 discussion draft 3. Wood S. Documents: Man accused of fatally shooting two Tyler dentists was a ‘difficult patient’. Tyler Morning Telegraph Mar 23, 2022, updated May 1, 2022.
Regulatory Compliance appears monthly and features resources about laws that impact dental practices. Visit cda.org/practicesupport for more than 600 practice support resources, including practice management, employment practices, dental benefit plans and regulatory compliance.
n Methods of implementing the plan.
n Description of training, such as what topics are covered and how training is delivered to employees.
n
® SIMPLY BRILLIANT. San Francisco will be brighter when you join us! CDA’s convention returns as an in-person, three-day event. Join us for, inspiring speakers, hands-on learning and new ways to learn and connect with your dental community. SEPT. 8–10, 2022 SAN FRANCISCO, CALIFORNIA EXPERT-LED PANELS on women in dentistry, special needs patients and oral health literacy 130+ COURSES spanning implant complications, digital dentures, sleep medicine, veneers, microscopes and restorative dentistry and more DEMOS & DEALS exclusive to the convention exhibit hall, plus free drop-in lectures SPECIAL EVENTS sharing after-hours fun at the wine seminar and CDA Party Explore the schedule and save your spot at cda.org/SF.

The app takes the user through a series of modules, and each contains a small lesson with learning objectives that are easy to accomplish in a few minutes. At the conclusion of every module, users take a small quiz on the content they just learned. Every correct answer is rewarded with pineapples, which is the currency the app uses to keep score. Every incorrect answer takes away hearts, which is equivalent to the number of lives when playing a game. Users start their journey with five hearts that regenerate every four hours. When the number of hearts is depleted, users cannot progress through the modules until their hearts are replenished.
The Ember Mug2 also has a built-in accelerometer that senses when it has not been picked up for more than two hours and shuts down the device. All this technology is mobilized to make the drinking experience perfect: Users put a hot beverage into the mug and enjoy at their own pace. No hot cups to burn hands, no lids to flip open, no thermos to prewarm, no extra gadgets to use or clean, and when users are done, they simply leave the mug on the charging coaster. The Ember Mug2 is an unnecessary luxury item, but for any practitioner who has ever been interrupted while drinking their coffee and been disappointed to come back to a cold cup, it solves this problem.
— Alexander Lee, DMD
A heated mug sounds like an unnecessary luxury item. There are innumerable, well-tested and affordable options to keep beverages hot including thermoses, heated coasters and insulated mugs. Most people would point out, “Just drink your coffee/tea/hot chocolate faster!” Why would anyone ever entertain spending over $150 on a Bluetooth-connected, rechargeable, app-controlled, fragile, handwash-only smart mug that requires users to download software to keep it up to date? The Ember Mug2 is undeniably “extra,” but it needs to be “extra” to solve a simple problem: keeping a hot beverage at a consistent temperature from start to finish without hampering or adding steps to the drinking experience. The 14-ounce Ember Mug2 comes with a mug, coaster and power supply (we sampled the copper version). The mug contains a battery that keeps its contents warm for up to 80 minutes and a large power button on its underside. Its finish is fragile and scratched by metal utensils, so wooden or plastic spoons are recommended by the manufacturer. The coaster is a charging station, and innumerable online reviewers have emphasized the importance of keeping this item completely dry lest the charging pins be shorted from any moisture. An app controls the mug’s temperature, which can be set between 120 F and 145 F. When on its coaster, the mug can keep drinks at the selected temperature indefinitely.
SEPTEMBER 2022 563 CDA JOURNAL, VOL 50 , Nº 9
Users can learn at their own pace, earning experience points, or XP, to unlock higher levels.
The model of getting paid to learn is extremely popular among younger generations and is a refreshing approach to learning about finance for those who need it the most. With looming fears of an economic recession in the forecast, everyone can benefit from helpful financial advice and knowledge. Zogo provides a gamified experience for future generations to help them acquire financial literacy and be empowered to secure their own economic futures.
Zogo (Free, Zogo Inc.)
With the struggles of economic uncertainty today, financial literacy has become a critical issue especially among those who identify as millennial or Generation Z. Endless educational resources are available on this topic, including books, podcasts and seminars, yet very few are created specifically for digital-native audiences. Zogo is an app that presents financial information through a learning experience targeted for the internet generation, but it is also fun and rewarding for all users. Zogo is free because of partnerships with over 200 financial institutions and requires a name, email address and mobile phone number to sign up.
Users can redeem their pineapples in the marketplace for rewards that include $5 gift cards to major retailers, donations to charities, cryptocurrencies or various offers for other products or services.
— Hubert Chan, DDS
Ember Temperature Control Smart Mug2: Metallic Edition ($179.95, Ember)
A look into the latest dental and general technology on the market Tech Trends

Journa CALIFORNIA DENTAL ASSOCIATION










