• Division of leadership responsibilities across a large multi-facility system (19 inpatient hospitals) • Service line approach for leadership responsibilities and physician/APP/team engagement
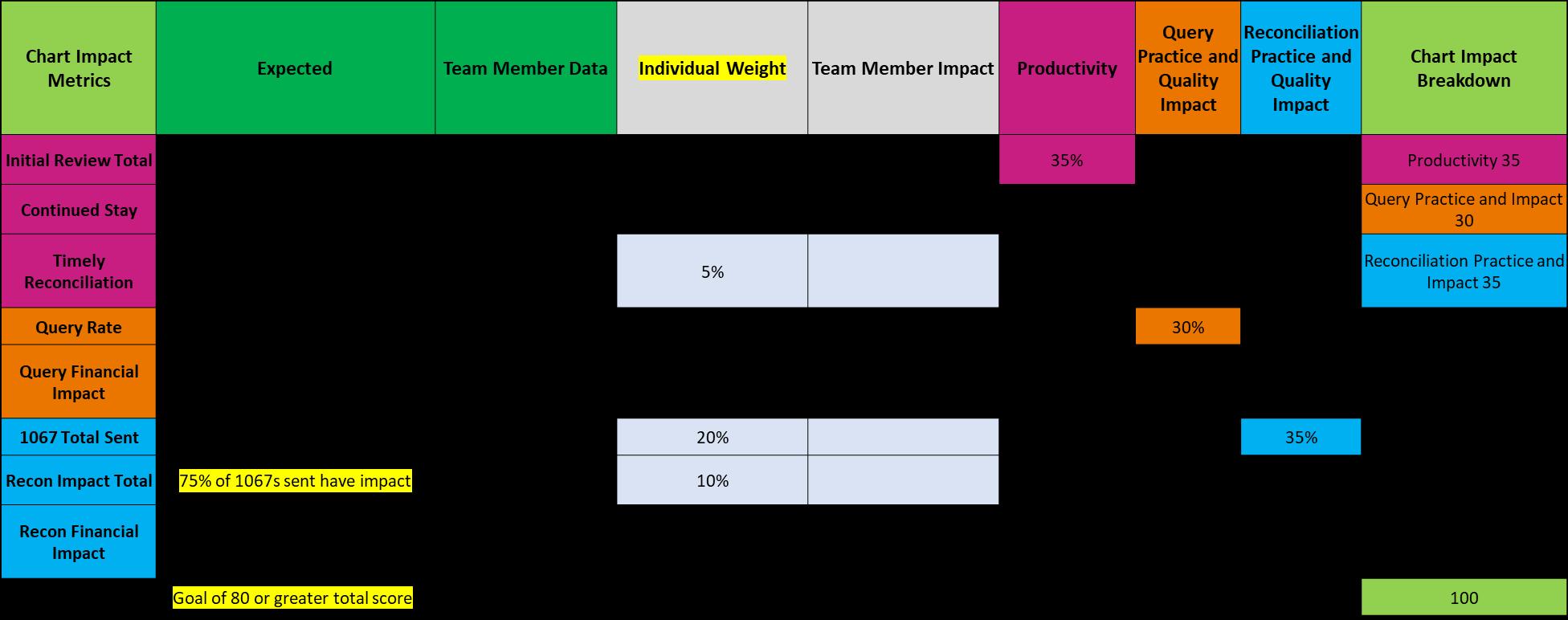
CDE Chart Impact Rate (CIR)
• Why change our performance metrics?
― Shared accountability with physicians and APPs
― Improve partnerships for documentation accuracy, use of similar tools and strategies for success
― Improve CDS performance and create the ability to focus on individual strengths and weaknesses
• Outcome of this work:
― CIR reflects a greater picture of how impactful CDI work is and ties into the program and organization goals
― Increased ownership of professional practice
― Improved performance
― Education and process opportunity identified
― Two-year journey, three large revisions to the CIR
Productivity
Query Practice and
Quality Impact
Reconcilation Practice and Quality Impact
Communicating CDI Program Value
Traditional CDI Metrics
• Messaging of CDI program impact is cloudy at best
• No personalization of metrics to account for variance in facility or review types or complexity
• Difficult to connect the CDI program ownership of improvements and often blamed for decreases in metrics such as CMI or DRG downgrades
• Impact is unclear
• Follow up is limited (improve)
• Less accountability and more “unknown” variables
Chart Impact Rate
• CDI program value and impact is widely known across our system
― Novant Health Mint Hill is ranked #1 for community hospitals in the nation, for performance in quality and safety (Vizient CDB)
― Novant Health Presbyterian Hospital is ranked #7 for academic medical centers in the nation, for performance in quality and safety (Vizient CDB)
• CIR is individualized feedback for the CDI specialists
• Follow up is multi-step:
― Leaders reporting out results and supporting needs
― Individual team audits
― Follow-up sessions with educator as needed
• Accountability and ownership of CDI professional practice
Chart Impact Rate versus Traditional CDI Metrics
Traditional CDI Metrics Chart Impact Rate
• Team is familiar with traditional CDI metrics
• Easy to pull the data
• Focus is on the physicians and APP practice and compliance with query management
• This data often causes reactive responses and initiatives, some results are tied to Physician practice incentives (does not help the CDI specialists improve or grow)
• For Example:
― Response rate, response time, query agreement rate: Program understanding, previous experience with CDI and coding, time management, physician/APP compliance
― CMI: Dependent on many factors outside of CDI, including surgery seasons and schedules, new technologies, services available per facility
• Frequent communication about the CIR to allow for team input and understanding
• Specialized reports and CDI data role may be required
• CIR components will need to be assessed frequently in the first year and then annually for revisions (workflow changes and CDI specialist review types will force revisions)
• Leaders will need to manually review some of the information, for example days in review, timely recon, exceptions
• Focus is on the team member: Query practice, query compliance, use of CDB tools, escalation practice, reconciliation steps and opportunity, identifying CDI education needs for physicians, APPs and coding
• Feedback provided for individual CDI specialists to improve impact
Challenges and Considerations
Traditional CDI Metrics
• Less transparency of individual CDI practice
• Great performers are not recognized in traditional metrics
• Harder to identify missed opportunity
• Volumes set to a standard/number of days worked for all team members and facilities
• Less objective feedback
• LOS improvement, PSI accuracy, CDI education and partnership with physicians and APPs, results driven work—hard to find the connections in traditional metrics
Chart Impact Rate
• Full transparency of CDI specialist workflow and practice, understanding of workflow steps and education needs
• Missed opportunities will be in full view based on CIR expectations
• Even great performers may struggle with more detailed feedback
• Quality documentation and safety and quality performance: Easier to connect CDI impact with transparent performance and review metrics, e.g., use of documentation templates
• Better understanding of volume of reviews possible—led to reduction of expected daily initial reviews per facility and revisions for specific review types
• The clear view of impact and opportunity trends leads to the development of new solutions:
– Team Vizient (CDB) Smart Phrase (mandatory)
Chart Impact Rate: Scoring and Areas of Focus Example*
CDE Chart Impact Rate
Tips for CIR Rollout Success and Additional Benefits of CIR
• Team understanding of feedback purpose (creating solutions and tools for the efficient workflow and communicating CDI program value)
• Explain how CIR is also used to make work queues and review coverage decisions, for example, low query rates could mean low documentation opportunity for a specific service line or facility
• Revisions as needed, testing and retesting*
• Team input, plenty of time for questions and support
• Support roles and audits (peer to peer discussions)
• Most revised areas: “Weights” of individual metrics based on goals of the program
• Factors to consider: Coding accuracy and opportunity, physician and APP, CDI team and coding education needed, individual CDI specialist professional development needs
• Leads to a much better understanding of the value of CDI reviews and confidence in individual and program impact for all stakeholders
• CIR may also help your business case for AI to support your CDI program, or additional FTEs!
Navigating the Physician Advisor Career Ladder
John Pettine, MD, FACP, CPHQ, CCDS
Vice President & Chief Medical Officer, Revenue Operations
Jefferson Health/Lehigh Valley Health Network
Objectives
1. Outline a career path from physician advisor to relevant leadership positions, highlighting key competencies and responsibilities at each stage.
2. Gain insights into essential skills, educational requirements, and advancement strategies.
Lehigh Valley Health Network
A Little Background…
Jefferson Health/LVHN: 2 large health systems—Merged Aug 2024
Top 15 largest NFP health systems in US
32 hospitals (LVHN 15 hospitals + Jefferson 17 hospitals)
• Understand the landscape: Identify key decision makers and pay attention to the company culture
• Don’t be afraid to try something new
• Seek a mentor
• Communicate your goals effectively w/ your supervisor
• Document your achievements & build your case
• Understand that sometimes to get ahead you must be willing to move
SUMMARY OF KEY TAKEAWAYS
Skill Up
Skills are your tools. And just like a master craftsman, the more tools you have, the better you can build your career.
• Medical Knowledge: Stay current. The field evolves quickly, and so should you.
• Communication: Sharpen those skills. You’re not just talking to physicians & leaders; you’re negotiating, advising, and often convincing.
• Leadership: Cultivate your leadership abilities. Whether it’s leading a team or a project, strong leadership will set you apart.
• Quick Tip: Invest in continuous learning. Certifications, workshops, and mentorship can be your best friends.
SUMMARY OF KEY TAKEAWAYS
Embrace Change Change is the only constant. The healthcare landscape is shifting rapidly, and so should your career strategy.
•Stay Agile: Be ready to pivot. Whether it’s adapting to new regulations or embracing new technologies, flexibility is key.
•Foster Resilience: Challenges will come. How you respond will define your career trajectory.
•Quick Tip: Regularly assess your career goals and adjust them based on new insights and opportunities.
SUMMARY OF KEY TAKEAWAYS
Seize Opportunities
Opportunities are often hidden in plain sight. Whether it’s a project, a new role, or a challenging case, embrace them.
• Be Proactive: Volunteer for tasks that stretch your skills. Demonstrate your willingness to go above and beyond.
• Look for Gaps: Identify areas where your unique skills can add value and propose solutions.
• Quick Tip: Keep a success journal. Documenting your achievements and contributions can be a powerful tool during evaluations and job searches.
SUMMARY OF KEY TAKEAWAYS
Network Strategically Networking isn’t just about exchanging business cards. It’s about building relationships that can support and propel your career forward.
• Inside the Conference: Make connections today! Share your goals and listen to others. You never know who might become a valuable mentor or collaborator.
• Beyond the Conference: Join professional groups, attend webinars, and actively engage in discussions.
• Quick Tip: Follow up with your new contacts. A simple email or LinkedIn message can turn a brief encounter into a lasting professional relationship.
Next Steps…
Identifying and Mitigating Burnout in CDI
Traci Lindner, RN, BSN, CCDS, CDI Manager, Marshfield Clinic Health System
It is not uncommon for employees to keep pushing (more work, longer hours) until they can no longer function
Burnout Results From Chronic Workplace Stress Stress
• Putting in extra effort
• Emotions are stronger
• Feel hyperactive and anxious
• Less energy
• Physical toll Burnout
• Loss of enthusiasm
• Emotions are blunted
• Feel drained, helpless, cynical, resentful
• Lack of motivation
• Exhaustion that does not go away with time off
• Inability to make decisions—feeling
struck with no path forward
High performers are the most susceptible to burning out
CDI Stress and Burnout
• As the CDI profession has grown, individuals are having longer careers in CDI
• Patient populations and the healthcare landscape are becoming more complex leading to an environment of stress and burnout
• Majority of those in CDI profession came from direct patient care
– May tend to gloss over stress and burnout—“It’s not the worst day I have ever had.”
– Working outside of direct patient care there is the loss of the “warm fuzzies”
– **Stress and burnout are NOT a competition
It is time to recognize that stress and burnout working in CDI is present and valid.
CDI Burnout
• Key is to identify before it gets to the point of no longer functioning
– Look for subtle changes
• Individual who was routinely interactive in meetings or chats is now silent
• Video is turned off
• Productivity and/or accuracy dropped
• Excessive apologizing and/or rationalizing
– Red flag responses to questions
• Long sigh
• Unconvincing “it’s fine”
• Sarcasm—“Living the dream”
Leaders in CDI
• The CDI team follows your lead
– Actions speak louder than words
• Encourage others to take necessary time off
– During their time off, have a coverage plan so that they don’t come back to things piled up
• Utilize slow periods over the year to help individuals on the team refocus
• Maintain realistic expectations
– There will always be the push from C-suite and other areas for more involvement
• Nurture the high performers but don’t over burden them by putting everything extra on their shoulders
– Provide opportunities for growth among team
– Balance workloads
– Recognition—What gets recognized gets repeated
Ideas for Leaders
• Utilize 1:1 for a “walk and talk”
– Nice weather? Take it outside—can be done in person or remote
• Get to know members of team—What are they passionate about inside and outside of work?
• Ask “stay” questions and tough questions:
– What do you look forward to when you come to work each day?
– What do you like the most or least about working here?
– What keeps you working here?
– If you could change something about your job, what would that be?
– What would make your job more satisfying?
– How do you like to be recognized?
– What talents are not being used in your current role?
– What would you like to learn?
– What motivates (or demotivates) you?
– Tell me about a case you reviewed that was emotionally difficult
– I’ve noticed (the camera has been off recently…a decrease in query rate…etc.). Is everything ok?
The Intersection of Clinical Documentation and Quality
Carolyn Bauer, MD
Medical Director of Quality, Documentation, and Coding
Montefiore
Medical Center
Montefiore Medical Center
• Montefiore Health System:
– 6 Hospital System ~ 140K discharges
• Montefiore Medical Center:
– Tertiary Academic Medical Center
• ~1,200 residents/fellows
– 3 Campuses in Bronx, NY
– ~ 75K discharges
– Payer Mix: ~85% Medicaid/Medicare
• ~15% commercial
– CDI—Report to Revenue Cycle/Finance
• 1 CDI director and 1 medical director
• 2 CDI managers, 1 CDI educator, 25 CDS
• Quality, documentation, and coding
– 3 CDS, 3 HIM, 1 physician
What Does Quality Mean to a
Health System?
Reputation
Pay For Performance: Financial Incentives from CMS for Quality Programs That Include ICD-10 Code–Based Measures
• Withholds 2% of Medicare payments
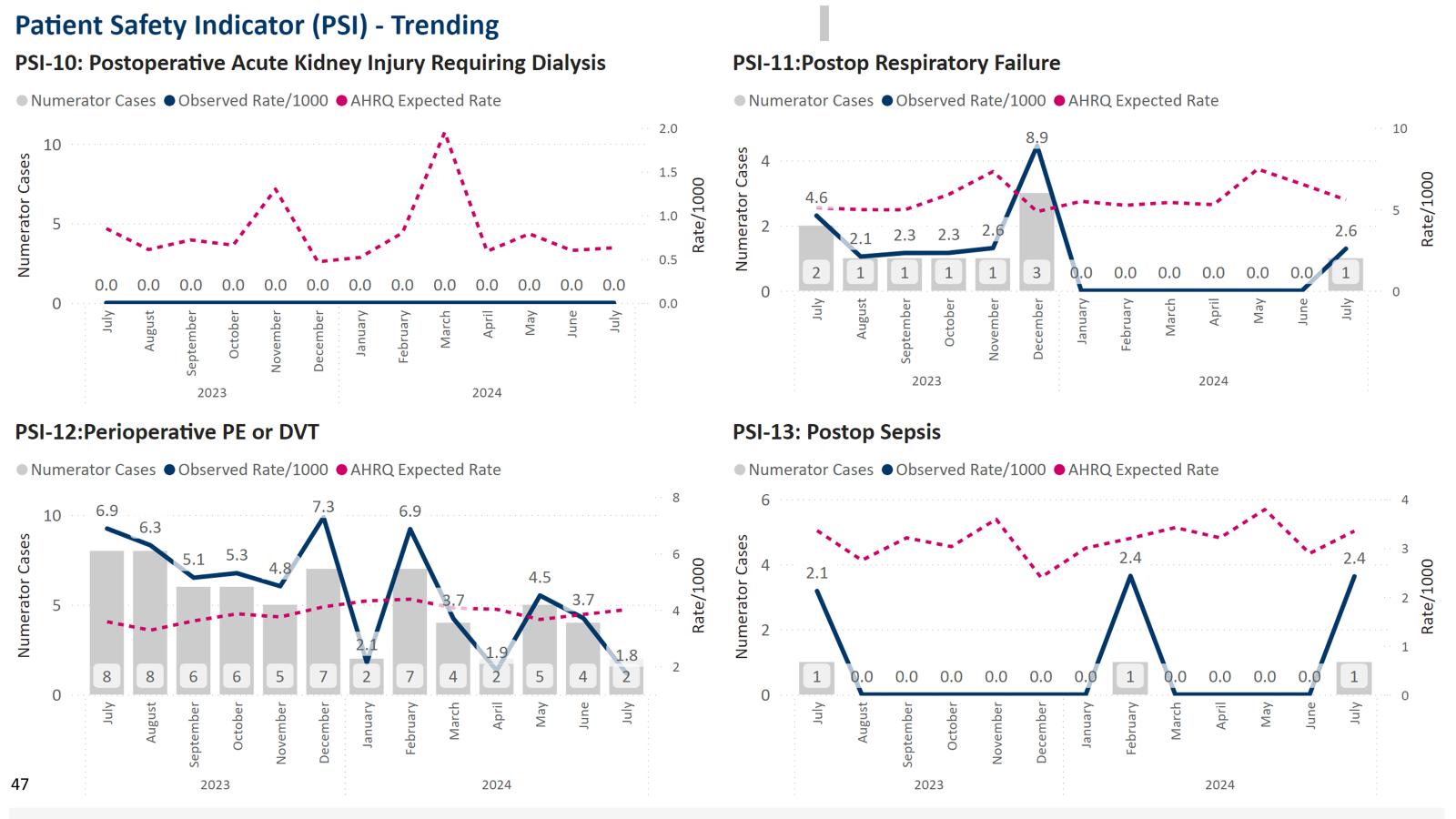
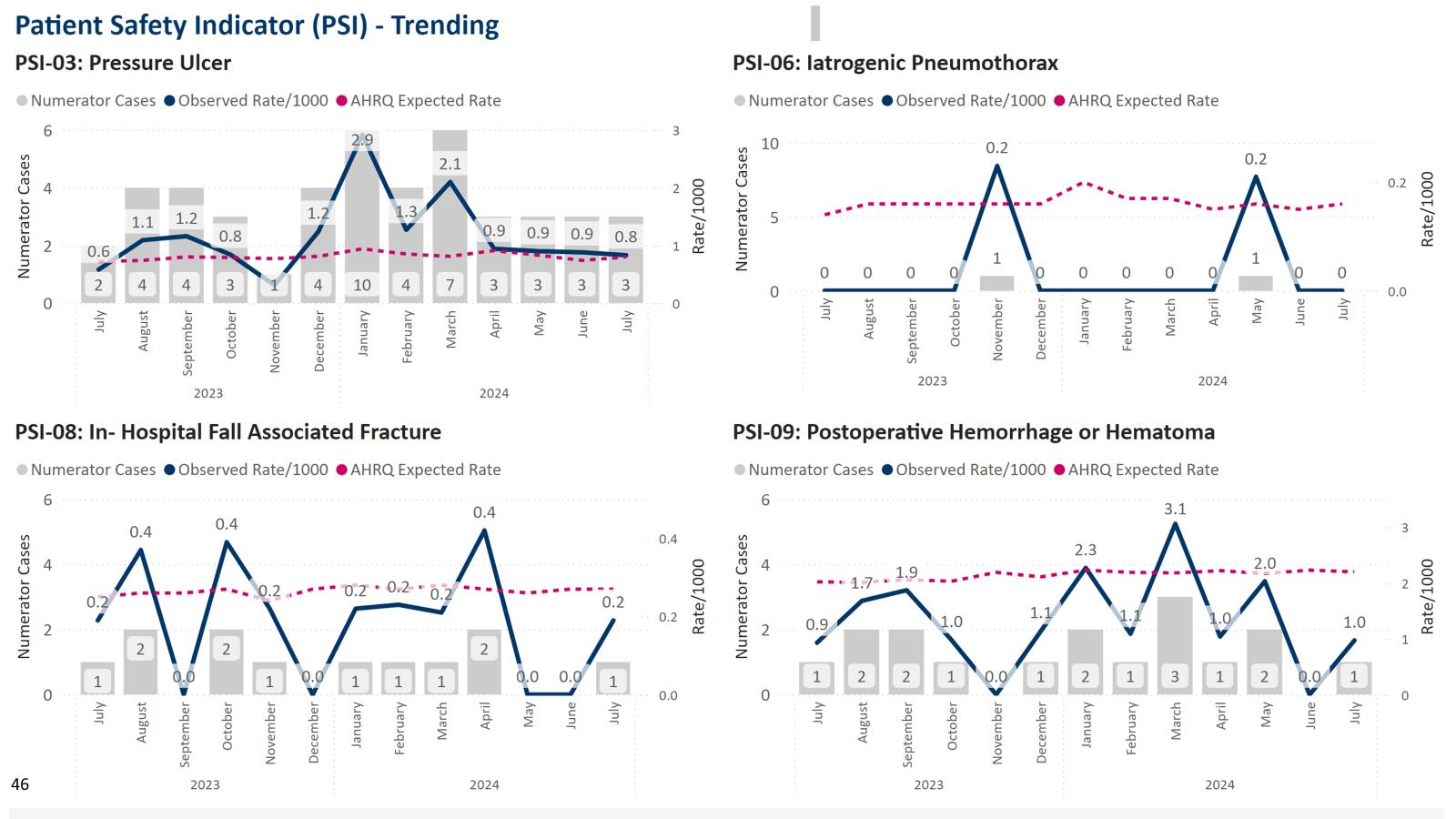
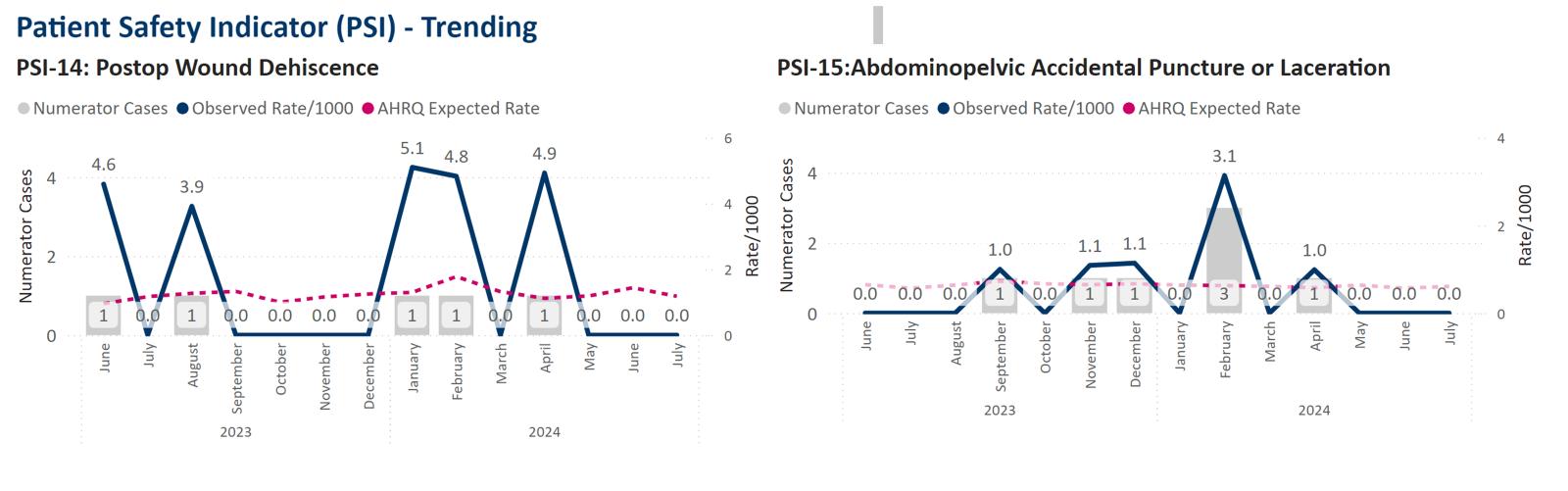
• Patient Safety Indicators Value Based Purchasing (VBP):
• Applies to the base MS-DRG payment
• Hospitals are scored on measures including:
• Mortality and complications
Total Knee and Hip Replacement Hospital Readmissions Reduction Program (HRRP)
• Maximum reduction 3 % of Medicare payments
• Applies to the base MS-DRG payment
• Unplanned readmissions in 30 days of discharge:
• Acute MI Heart Failure
• COPD Pneumonia
• CABG
Pay For Performance: Financial Incentives from Commercial Insurers for CMS Quality Metrics
Commercial:
• Private Insurers are putting Medicare data in their quality incentive contracts
– CMS HRRP rates
– All-Cause Readmissions
– Patient Safety Indicator Composite 90
Montefiore Plan for Capturing Risk Adjustment: Beyond SOI
• The Elixhauser Comorbidity Index is based on comorbidities associated with
– Capture Elixhauser diagnoses for all patients
• CDIs are trained to evaluate
• AI to look for indicators
– Provider-facing at time of documentation
– Post-discharge, pre-bill
Quality, Documentation and Coding Reviews
Coding and Documentation Review
Understand CMS and AHRQ criteria
• Confirm indicator Dx
• Validate procedure codes
• Look for POA indicators
• Review for exclusion Dx
Clinical validation
Standardizing Clinical Definitions—Break Down Silos
• Post-Op Respiratory Failure—PSI 11
– Physician leaders
• Quality
• Anesthesia
• Critical care chief
– Standardized definitions based on clinical literature
• Post-op pulmonary insufficiency
• Expected time on vent
• Oxygen/non-invasive mechanical ventilation as rescue strategies
– Education of service lines
– Bringing metrics and examples
– Critical care—surgeons
– Clinical pathways
• Change in use of paralytics
• Post-Op Sepsis—PSI 13
– Physician Leaders
• Quality
• Critical care chief
• Hospital epidemiologist
– Standardized definitions based on clinical literature