Providence’s Work2BeWell helps students navigate life’s curves

dence St. Joseph Health program provides free clinician-vetted mental health and wellness resources for teenagers, parents and educators and promotes them across social media platforms.
By LISA EISENHAUER
RENTON, Wash. — The Work2BeWell posts on Instagram were what caught the atten tion of 17-year-old Melisa Shafiee.
“They have a very colorful, vibrant social media account full of posts encouraging people to take care of themselves as well as do a bunch of other mental health prac tices,” says Shafiee, a senior at Bellevue High School near Seattle.
The Instagram posts led Shafiee to find out more about Work2BeWell. The Provi
As soon as Shafiee learned that the program had a national student advisory council, she applied. She’s now part of that council, consulting along with the 32 other members on the curricula, podcasts and other resources Work2BeWell produces.

Shafiee especially likes helping craft the podcasts, called Talk2BeWell. “I think they’re really effective at getting into stu dents’ minds and helping them through real struggles,” she says.
She is one of four students featured along with Dr. Robin Henderson, chief executive for behavioral health at Providence Oregon
Continued on 2
Sisters of Charity sharpens focus on wellness in challenged neighborhood
 By LISA EISENHAUER
By LISA EISENHAUER
Even though the latest transformation within the Sisters of Charity Health System was driven by finances and evolving trends in health care delivery, executives involved said the shift aligns with how the system and its founding congregation have inno vated to meet the changing needs of the Cleveland neighborhoods they have long served.
Sisters of Charity announced in midSeptember that it would be transitioning its only remaining acute care hospital, St. Vin cent Charity Medical Center in Cleveland, to an ambulatory care facility. The ambula tory care services will be named St. Vincent Charity Community Health Center and continue to be housed within the medical center building.
Last year the system announced it would develop the St. Vincent Charity Health Campus. The repurposing of the medical center building is part of that project. The
Continued on 8
Ministry facilities ease immigrants’ access to health care, social services
By JULIE MINDA
Even for people born and raised in the U.S., the fragmented health care and social service systems can be very difficult to access and navigate. Refugees and immi grants of little means can have the added obstacles of limited English language proficiency and cultural, social and financial barriers when they are sick or struggling to meet their family’s basic needs.
It’s no wonder that many economi cally vulnerable immigrants are not get ting preventative health care or timely care for major health conditions.
According to the Immigration Policy Lab, unauthorized immigrants who are excluded from participating in publicly
School-based clinics expand care access in Cincinnati and across the U.S.
 By PATRICIA CORRIGAN
By PATRICIA CORRIGAN
On a recent Tuesday, nurse practitio ner Rachael Doll conducted a hospital follow-up exam on a 6-month-old, tested a 65-year-old for hypertension, performed a hearing evaluation and vaccinated several students. Doll works in a primary care clinic located inside Sayler Park School, one of six school-based health centers in Cincinnati operated by Mercy Health, part of Bon Sec ours Mercy Health.
Opened in November 2016, the Sayler Park clinic has two patient exam rooms, a room set up for virtual visits, a bathroom and plenty of laboratory equipment. Walkins are welcome, and appointments also are available.
Prior to opening the clinic at Sayler Park,
relief
3
Executive changes 7 Ukrainian
effort
Continued on 4
Dr. Paula Young examines a child. Young is a pediatrician on Bon Secours Richmond’s Care-A-Van and medical director of community health access for Bon Secours Richmond.
Program offers free curricula, teaching guides, podcasts focused on mental health
High school senior Melisa Shafiee, left, and Dr. Robin Henderson, chief executive for behavioral health at Providence Oregon and chief clinical officer of Work2BeWell, tape a podcast on social anxiety along with three other students who joined remotely. The podcast is for the Talk2BeWell series that focuses on issues of concern to teenagers.
Continued on 7
Nurse practitioner Alyse Knapp checks Austin Townsend's height at Mercy Health — Southwest Schools Community Clinic at Harrison High School in Cincinnati. The clinic is open year-round to care for students, staff and community members.
A bike and scooter ride through the neighborhoods surrounding St. Vincent Charity Medical Center in Cleveland was one of the ways the MASS Design Group reached out to the community to solicit views on what a health campus around the hospital should include. MASS Design was a consultant on the campus, which is being shaped to address the health and social needs of the surrounding community.
Lisa Eisenhauer/©CHA
NOVEMBER 15, 2022 VOLUME 38, NUMBER 18 PERIODICAL RATE PUBLICATION
Courtesy of MASS Design Group
and chief clinical officer of Work2BeWell, in a 30-minute Talk2BeWell podcast about how social anxiety affects mental health. The episode posted on Providence’s social media platforms in October. The other stu dents were from Pennsylvania, Nevada and Washington state.
Henderson says hav ing young voices guiding the content has been a key driver in the expansion of Work2BeWell, which has had downloads of resources reach as high as 6,000 per month. “Our best sources are the students themselves,” she says.
Desperate for resources
Henderson and Mary Renouf, vice presi dent of clinical and consumer communi cation for Providence, founded Work2BeWell about five years ago after Providence’s behavioral health team answered a call from the executive director of the Oregon Association of Student Councils who was seeking advice for a school district in the Portland, Oregon, area on how to deal with a spate of student and teacher suicides. “The high schools were desperate to have resources,” Renouf recalls.
The Providence team met with students, parents, educators and school admin istrators in Oregon. The team came up with guides for how to have conversations with someone who appeared to be men tally distressed. Those guides served as building blocks that were developed into Work2BeWell’s first eight pieces of curricula.
By December 2017, Providence had formed a partnership with the Oregon Association of Student Councils to provide continuing counsel and resources on men tal health. By the next summer, the partner ship had set up a “teen focus group” to start conversations on mental health issues and advocate for policy changes.
When a member of the focus group sug gested that kids need to be able to take time away from school to tend to their mental health needs, the Providence team linked up the students in the focus group with the system’s advocacy experts. The students began a lobbying campaign that led Ore gon lawmakers in 2019 to pass one of the first state laws that allows students to have excused absences to tend to their men tal health just as they would for the flu or a cold. Twelve states now have similar laws.
When Henderson asked students she met at a summer camp about what topics they thought she should cover on the series of shows she was hosting as part of a con tract between Providence and iHeart Radio, she says they gave her enough ideas to fill her show calendar for the entire school year.
Some of those students told her they wanted to get more deeply involved in the discussions. The team behind Work2BeWell then set up an advisory coun cil with a few students from the West Coast. Some of the students started joining Hen derson on her iHeart Radio show to share their take on issues.
Meanwhile, the Providence team also was using the student advisers’ suggestions as well as those coming from educators to build out the Work2BeWell website. The website was filling with free downloadable curricula and other resources for educators and community groups. The topics include stress, suicide prevention, loss and grief, and relationships.
Going national
In 2019, Providence opened applica tions for its first Work2BeWell National Stu dent Advisory Council to kids from across
the country. The council’s current makeup includes several students from the West Coast as well as teenagers from Montana, Georgia, Massachusetts, Nevada, Mary land, Texas and Pennsylvania.
Students who are 18 or younger can apply for the council. Work2BeWell team members and clinician advisers make the final selection. Parents have to submit per mission forms before students can partici pate. Council members serve for a school year on one of three teams — access, edu cation and activation. Each team gets guid ance from a Work2BeWell mentor.
Renouf says the council, with students of various genders, cultures and races, “repre sents most of the flavor of the United States.”
She points out that it was vital to hear from students across the country as Provi dence began to promote Work2BeWell nationally. The issues teens face aren’t monolithic, she notes. While some kids say their big worry is finding a prom date, oth ers say they live in fear of the gun violence in their neighborhood.
Henderson says the students on the advisory council get the final say on the cur ricula modules. The students once even vetoed an entire lesson plan that focused on the challenges faced by black, indigenous and youth of color because they didn’t think it was relatable as presented.
“We had a really great idea for a set of curriculum,” she recalls. “We went out and hired a consultant and did all the things and said, ‘Here it is, it’s really great.’ And they looked at us and went, ‘No.’”
The revised curriculum on the same topic was crafted to better reflect the issues students face, Henderson says, and is among the most popular on the Work2BeWell website. The takeaway from that experience, she says, was that students must be in on the resource-building pro cess from the start.


Relevant and timely
The Work2BeWell team strives to match the resources on the website and the topics discussed on Talk2BeWell podcasts with what students are dealing with in real time. When the pandemic turned life on its head for students in 2020, many Talk2BeWell epi sodes dealt with the impact, such as how seniors were coping with missing out on cherished traditions and how outrage and protests over racial injustice and police kill ings of unarmed Blacks were playing out amid COVID-19 protocols that discouraged or prohibited large gatherings.
Talk2BeWell itself had to adjust to the times because of infection prevention rules. Instead of convening at least some of the students at a recording studio, the podcasts
became Facebook Live events with all the participants logging in remotely.
The podcasts are no longer broadcast live but they remain virtual productions, with Henderson and panelists able to par ticipate from anywhere in the country.
Suicide, anxiety and substance abuse are among the many emotion-charged mental health topics that Work2BeWell explores. Henderson notes that Work2Be Well also encourages and facilitates discus sions of other timely subjects that are out side the traditional scope of health care. For example, Talk2BeWell has had podcasts on the Black Lives Matter movement and the Ukrainian refugee experience.
Renouf says as of this year, Work2BeWell curricula is being used in every state, mostly at the high school level. Among the most
popular teaching tools are those that delve into structural racism, equity and inclusion.
Providence is pursuing grant funding to develop age-appropriate curricula for middle schools. “Obviously, the earlier you can get to students the better success you’ll have with either getting them to not have a mental health issue or to address it or to seek help sooner rather than later,” Renouf notes.
Teaming up with Ken Burns’ crew
Eleven partners, including the National Alliance on Mental Illness and the Texas Association of Student Councils, support Work2BeWell and share the program’s resources.
The Work2BeWell team is currently developing curricula in partnership with the creators of the documentary “Hiding in Plain Sight: Youth Mental Illness.” Ken Burns was the executive producer of the four-part series that aired on PBS stations over the summer.
Henderson says the plan is to convene people from the production crew, educa tors, school administrators, clinical experts and students to create 24 pieces of curricula that pair with the documentary that can be used in classrooms and by youth programs. She and her partners on the project hope to have the lesson plans ready next spring.
In addition to creating the curricula, podcasts and the other resources, the team behind Work2BeWell and their student advisers have become popular guest speak ers at education-related events. Hender son says they are featured at about a dozen every year. This year, two students spoke on the main stage at a gathering of the Texas Association of Student Councils that drew about 5,000 attendees.
Henderson is open to any forum that allows her to share information about how to improve students’ mental health. “I’ll use anything I can to connect with somebody,” she says. “Good knowledge is power and we’re empowering students to be able to talk about mental health, to reduce stigma, to do all the right things.”
leisenhauer@chausa.org
Catholic Health World (ISSN 87564068) is published semimonthly, except monthly in January, April, July and October and copyrighted © by the Catholic Health Association of the United States. POSTMASTER: Address all subscription orders, inquiries, address changes, etc., to CHA Service Center, 4455 Woodson Road, St. Louis, MO 63134-3797; phone: 800-230-7823; email: servicecenter@chausa.org. Periodicals postage rate is paid at St. Louis and additional mailing offices. Annual subscription rates: CHA members free, others $29 and foreign $29. Opinions, quotes and views appearing in Catholic Health World do not necessarily reflect those of CHA and do not represent an endorsement by CHA. Acceptance of advertising for publication does not constitute approval or endorse ment by the publication or CHA. All advertising is subject to review before acceptance. Vice
Upcoming
314-253-3412
314-253-3477
© Catholic Health Association of the United States, Nov. 15, 2022
President Communications and Marketing Brian P. Reardon Editor Judith VandeWater jvandewater@chausa.org 314-253-3410
Trafficking Networking Zoom Call
for Medicaid Unwinding After the Public
Emergency — Working with Partners Nov. 16
ET
Formation Workshop Series Tuesdays | Dec. 6, Jan. 17, 2023 and May 6, 2023 | 1 – 3 p.m. ET
Associate Editor Julie Minda jminda@chausa.org
Associate Editor Lisa Eisenhauer leisenhauer@chausa.org 314-253-3437 Graphic Design Norma Klingsick Advertising ads@chausa.org
United Against Human
Nov. 16 | Noon – 1 p.m. ET Virtual seminar: Preparing
Health
| 2–3 p.m.
Ministry
chausa.org/calendar
Events from The Catholic Health Association
From page 1
Work2BeWell
Henderson Renouf
2 CATHOLIC HEALTH WORLD November 15, 2022
Social media memes like this one, along with school curricula and podcasts, are among the tools that the Work2BeWell program run by Providence St. Joseph Health uses to offer encouragement and mental health support to the young audience it tries to reach.
Catholic relief groups work to address specific needs amid Ukrainian relief effort
By LISA EISENHAUER
As Catholic organizations continue to be deeply involved in the global effort to provide relief to people sheltering within Ukraine and refugees from that war-battered nation, some leaders of the effort are trying to help address spe cific needs that stand out amid the flow of humanitarian aid.
Msgr. Robert J. Vitillo, secretary general of the International Catho lic Migration Commis sion, is convener of a work ing group of major global Catholic-inspired humani tarian organizations called Catholic Response for Ukraine. In July, he spent a week visiting displaced people in Ukraine and refugees in Poland and learning from those directly involved in relief operations.

“There’s need for just about everything,” Msgr. Vitillo says. “There are many, many displaced people. The Catholic communi ties welcome them into the seminaries, into the convents, the monasteries, into dioc esan offices and especially into schools. You have so many people that have lost everything.”
Msgr. Vitillo lauds Caritas Internationa lis, Caritas Europa, Jesuit Refugee Service, International Catholic Migra tion Commission, the Order of Malta, Depaul International, Stella Maris, and CHA. The chari table organizations all are part of Catholic Response for Ukraine and are providing financial sup port or other assistance or setting up centers across Ukraine and bordering nations that provide housing, meals, food packets, hygiene kits and mental health assistance.
Catholic relief organizations and others were assisting victims and refugees within days after the Russian invasion of Ukraine on Feb. 24. They are col laborating with the Ukrainian and neigh boring governments on their efforts to dis tribute aid and help civilians find safety.
Catholic Response for Ukraine is post ing weekly bulletins with statistics on peo ple displaced within Ukraine (6.2 million as of Nov. 1) and refugees across Europe (7.8 million), as well as updates on the mili
tary action, United Nations operations and Catholic church-based responses to the humanitarian crisis.
Identifying unmet needs
One unmet need Msgr. Vitillo saw on his visit was for prosthetics for civilians and soldiers who have lost limbs to bombs or mines. Since his return home to Geneva, he has been try ing to identify organizations that might be able to donate or sup port local production of artificial limbs and recruit prosthetists with the expertise to train local clinicians to fit patients with the prosthetics.
“I hope that’s something we could do because you have so many people who are now disabled as well as having the trauma and the separation from all that’s familiar to them,” Msgr. Vitillo says.
Bruce Compton, senior director of global health at CHA, is among those who are working with Msgr. Vitillo to find con nections to address the need for prosthetics and prosthetists in Ukraine.

Compton says he has heard of other spe cific needs that are hampering the humani tarian effort. One is for civilian ambulances to replace those that have been comman
deered by the military.
Compton points out that supplying ambulances is not as simple as sending emergency vehicles from elsewhere in the world. “There are standards for ambulances in Europe that are different, so they’re looking for appropriate ambulances,” he says.

The same official who told Compton in an informal conversation about the need for civilian ambulances in Ukraine mentioned that sending other items that have not been requested often gum up relief efforts.
“I’ve heard from both church and gov ernment sources close to the Ukraine crisis that inappropriate in-kind donations are an issue and they’re thankful for organizations like the Catholic Health Association that urge donors to ensure that their donations conform to the needs specifically identified by those working on the ground,” Compton says.
CHA has guidelines and resources for ethical disaster response on its website.
Selective partnerships
Erica Smith is president and executive director of Hospital Sisters Mission Out reach, a nonprofit that sends medical sup

plies and equipment around the world. Smith co-authored an article that appeared in the summer 2022 edition of Health Prog ress, a journal produced by CHA, advising donors on how to avoid a potential “sec ond disaster,” a reference to the disruption in humanitarian crisis response that can occur if inappropriate relief items clog sup ply lines into crisis zones.
Smith says that Hospital Sisters Mis sion Outreach is highly selective on the partners it works with in other nations.
“We have to know that the recipient has the logistical ability to make sure that the supplies can be distributed, stored and used, and then ultimately thrown away in a way that’s not accidentally a hazard,” she notes, speaking during an interview in late September.
So far, Smith says Hospital Sisters Mis sion Outreach has done a few direct hand offs of supplies to organizations providing relief in Ukraine or neighboring nations. It also has sent supplies with physicians who had previous connections in the region and traveled there to provide assistance.
Her organization only recently identified an on-the-ground partner in Ukraine, the Knights of Columbus, that can meet its high standards for receiving donations. Smith says Hospital Sisters Mission Outreach hopes to ship medical supplies and equip ment to cover immediate needs and estab lish a supply chain to meet long-term needs for supplies.
Pallets of supplies
Mary Beth Powers, president and chief executive of Catholic Medical Mission Board, says that through September, her organization has sent 114 pallets of medi cines, personal protective equipment and hygiene kits to partners in Ukraine and neighboring nations that are sheltering refugees.
Powers says the medi cations her group is send ing have been specifically requested. Most of the drugs treat chronic conditions such as cancer and cardiovascular disease.
Powers says the Catholic Medical Mis sion Board didn’t rush to fundraising appeals for Ukraine relief immediately fol lowing the Russian invasion. “We waited about two weeks while we were ensuring that we had partners,” she says. The part ners the charity is working with include those within the Caritas network.
The funds Catholic Medical Mission Board have raised for Ukraine have largely come from the American public and corpo rations and gone toward airlifting donated supplies, Powers says. That form of trans port is expensive but sea and land routes have been compromised and some of the supplies have been urgently needed.
Powers said the demand for PPE, hygiene kits and wound care supplies in the relief effort is ongoing. “Those are the things that we’re still either having to purchase or looking for donations for, and hospital net works could be helpful in that, I would sup pose,” she says.
Ripple effects
Catholic Medical Mission Board also is keeping watch on the ripple effects that the conflict in Ukraine is having on the rest of the world and looking for ways to help. One effect is a burgeoning food crisis in parts of Africa that haven’t gotten needed ship ments of Ukrainian grain.
Like other leaders in Catholic relief efforts as well as Pope Francis, Powers points out that one response everyone can supply is prayers that world leaders can bring a peaceful resolution to the Ukrainian conflict. “We’re sincere about prayers for peace,” she says. “You can’t underestimate the power of prayer.”

leisenhauer@chausa.org
A patient who lost a leg during the Russian war in Ukraine prepares to be fitted with a prosthesis in Lviv, Ukraine. Msgr. Robert J. Vitillo, secretary general of the International Catholic Migration Commission, says one of the needs he was shown on a visit to Ukraine this summer was for artificial limbs and professionals trained to fit them.
Msgr. Vitillo
Compton
hear a conversation about the
response to
listen to episodes 2 and 3 of
Calls. Include your organization’s Christmas message in the Dec. 15 issue of
Health World invites you to extend a holiday greeting to your employees and to colleagues in the Catholic health ministry. Share
of the season with a Christmas message to the ministry
for more details. Send an email to ads@chausa.org to reserve your ad space.
by
22.
November 15, 2022 CATHOLIC HEALTH WORLD 3
Powers
To
Catholic
Ukraine,
Health
Catholic
the joy
Visit chausa.org/Christmas
Ads due
Nov.
Pavlo Palamarchuk/SOPA Images via AP Images
IMMIGRANTS FACE HEALTH CARE CHALLENGES ›› CATHOLIC HOSPITALS' PROGRAMS MAKE INROADS
Immigrants
funded insurance and health care pro grams are among the most medically mar ginalized groups.
The issues aren’t new. A study published
in the September/October 2005 Health Affairs and funded by the Robert Wood Johnson Foundation found that “immi grants in general and the undocumented in particular use relatively little health care.”
The authors of the study gave another rea son certain immigrant populations don’t access health care: immigrants were more
likely to report health care discrimination and stigmatization than were U.S.-born patients.
Some Catholic health systems have taken on these disparities by providing culturally sensitive outreach to refu gee and immigrant groups. Some of the efforts go back decades. They have tai
Navigation assistance
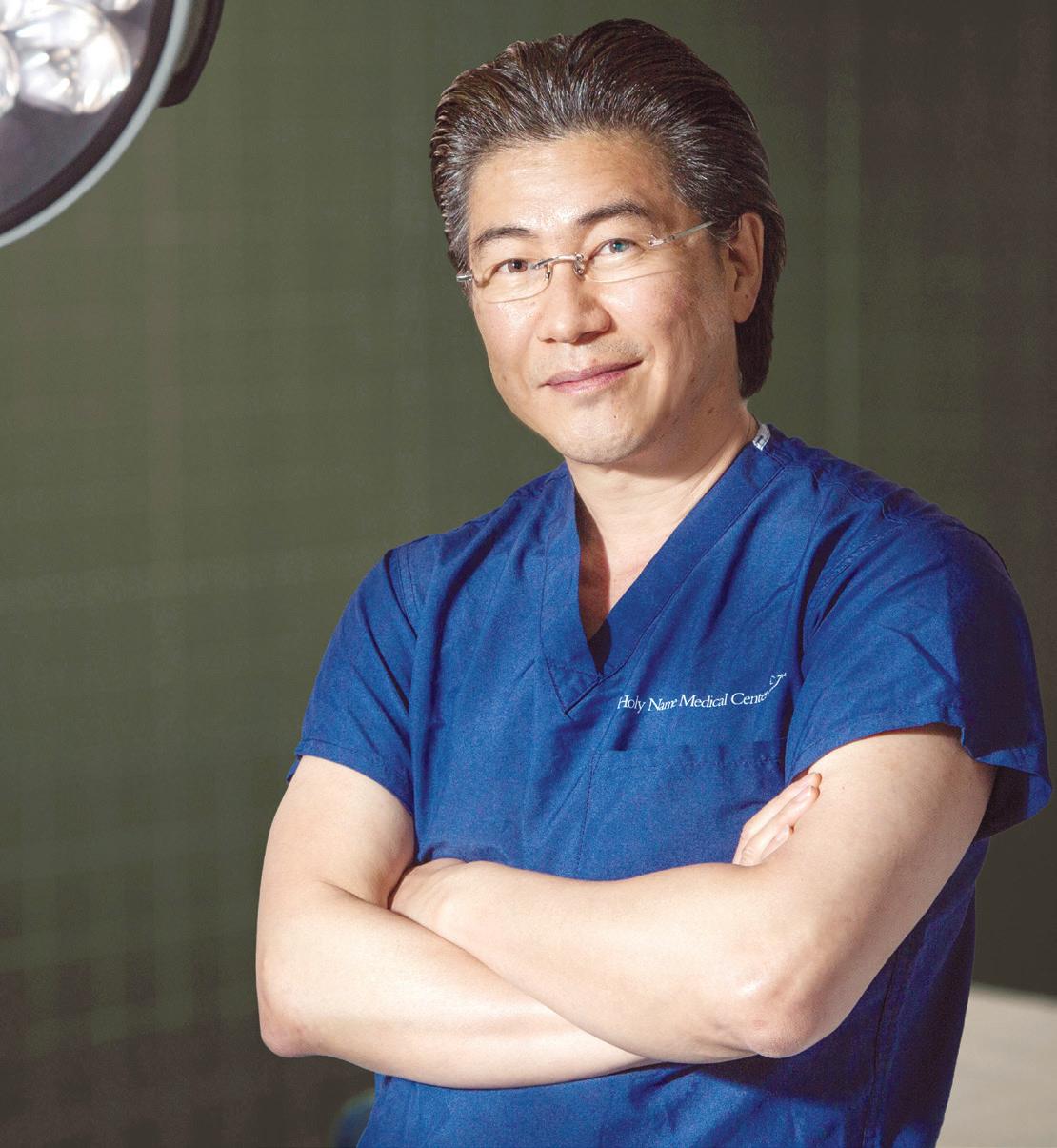
››Until relatively recently, many people from Bergen County, New Jersey’s sizeable AsianAmerican community steered clear of traditional Western medical care. And their health suffered, said Dr. Hee Yang, chief medical officer for Asian Health Services at Holy Name Medical Center in Teaneck, New Jersey.
“We’re in the middle of some of the best medical facilities in the world and yet these community members were not going to them,” he says. “There were people who wouldn’t come in until they were nearly on their death bed.”
New life in Lewiston
››The closure of its textile mills beginning in the 1970s set off an industrial decline, depopulation and poverty that had a major impact on Lewiston, Maine, in the last decades of the 20th century. But at the turn of the millennium the unex pected happened. Word went out over the dispersed and informal network of Somali refugees in the U.S. that the Lewiston area was a safe, affordable place to raise fami lies and that attracted several thousand Somali refugees to the area starting in the early 2000s.
Currently more than 60,000 people live in Lewiston and the adjacent com munity of Auburn. Over 22% of Lewiston’s population are people of color and 15% are refugees/immigrants. In Auburn, 14.6% of residents are people of color, according to statistics from Kirsten Walter, who directs St. Mary’s Nutrition Center, part of Cov enant Health’s St. Mary’s Health System in Lewiston.
She says the first people to arrive were ethnic Somalis, mostly from Somalia, Kenya, Djibouti and Ethiopia, soon fol lowed by Somali Bantus, an ethnic minor ity. Attracted by the low crime and afford able housing, they relocated from other U.S. cities. Over the next 15 years, people from other countries including the Democratic Republic of Congo, Angola, Zambia, Sudan, Iran, Syria and Afghanistan followed. A reflection of the diversity can be seen in the Lewiston Public Schools, where there are now 34 languages spoken, she says.
The arrival of immigrants, asylees and refugees during the last 20 years has brought the region diversity, energy, growth and challenges. Many immigrants in Lewiston and elsewhere endure sys temic racism and Islamophobia. Recently arrived immigrants in Lewiston also face poverty, housing insecurity, food insecu rity and language barriers, says Walter.
St. Mary’s laid the groundwork for the nutrition center’s core programs in 1999 and formally opened the center in 2006. The center addresses food insecu rity in one of Maine’s poorest cities and has evolved into a catalyst that works with community partners regionally to take on a range of socioeconomic concerns for immigrants and the greater community.
With a staff of 12, the nutrition center’s food pantry works to provide culturally

preferred food, along with other meat, dairy, fresh produce and dry goods. It offers cooking education programming, highlights locally grown foods that may be unfamiliar in African and Middle Eastern diets and supports community members in navigating fresh food access programs at a farmers’ market and mobile market.
St. Mary’s work in immigrant health has a partner in a federally qualified health center in Lewiston. The B-Street Health Center opened in 2010 in a neighborhood populated with refugees and immigrants. Both the nutrition center and health cen ter have staff who speak two or more lan guages and who provide cultural broker ing support as part of their job duties. The health center has three full-time commu nity health workers who are fluent in Eng lish and Somali. There are 32 languages spoken by patients. On the health center’s staff, Somali, Portuguese and French are the main non-English languages spoken.
Walter says at both the nutrition center and the B-Street Health Center, the focus is on addressing root causes of disease. She says inequity is at the heart of many of the health and socioeconomic concerns that immigrants and other vulnerable patient populations in the community face.
And she adds that within the last five years or so St. Mary’s has been more intentional about deepening its equity and cultural competency work and creat ing a deliberate feedback loop with the community.
The St. Mary’s system is part of a consor tium putting together public and private financing for a redevelopment project in a downtown Lewiston neighborhood where the health center is located and where many immigrants of African and Middle Eastern descent live. The plan includes construction and rehabilitation of afford able housing, expansion of Head Start pre school and improvements to recreation and park spaces in a residential downtown area.
St. Mary’s Nutrition Center staff are sup porting a cooperative that plans to open in the redevelopment area a community food center. That facility will include a low-cost grocery store as well as a commer cial kitchen, food storage and other facili ties for use by food business entrepreneurs and other community members. As part of the downtown redevelopment project, the health center is expanding primary care, dental care and mental health care services.
Holy Name’s answer to that reticence came in the form of its Asian Health Ser vices patient navigation program. Its char ter includes educating physicians and other Holy Name caregivers and staff on how to provide culturally sensitive care to people of Korean, Chinese, Japanese, Fili pino and Indian background, says Yang.
A paid concierge staff that includes six Korean-Americans, two Chinese-Amer icans and one Japanese-American are the mainstay of Asian Health Ser vices. They help patients find their way through the web of health and social services to connect with the right provider and they some times accompany a patient into an exam room, where they can provide medi cal translation services. Under Yang’s direction, program staff do outreach and edu cation in the Asian community.
When the pan demic prevented family members from accompa nying their nonEnglish speaking relatives to medical appointments at Holy Name facilities, Asian Health Services con cierges and volunteers identified patients scheduled for medical appointments who had used the concierge service before or had Asian-sounding names. They offered to help them prepare for their visits and to provide an escort from the health facility’s entrance to a medical office. They stayed with patients throughout their appoint ment, if the patients so desired.
With COVID-19 restrictions lifted, patients still can request on-campus navi gation assistance from the Asian Health Services team.
Yang says members of distinct Asian immigrant subgroups settled together in neighborhoods where they have retained their native language, culture, beliefs and traditions. This is especially true of older, first-generation immigrants of Japanese and Chinese heritage, he notes, with Filipi nos generally being more assimilated.
Asian Health Services staff reaches out into these enclaves including through word of mouth and media outlets aimed at the ethnic subgroup to offer health and
lored services and staffed facilities to welcome medically underserved refu gee and immigrant populations in their communities.
The programs highlighted here are building trust within immigrant commu nities and making inroads against prevent able disease.
social services navigation.
About a dozen years ago, Holy Name clinicians connected informally through Asian Health Services documented a high incidence of aggressive breast cancer among Korean-Americans. Yang says his torically Koreans have had very low breast cancer rates in part because of healthy diets and lifestyles. But Koreans who adopted American diets and lifestyles raised their risk for breast and other cancers.
Since many Asian women at the time were not getting preventive care or can cer screenings, their cancer progressed unchecked. Asian Health Services started a breast cancer awareness, screen ing and service referral campaign for Korean Americans, spreading informa tion through word of mouth and through Korean newspapers and radio and televi sion shows. Asian Health Services helped uninsured women who screened positive for breast cancer find a payer source or apply for financial aid. Yang said as a result of that campaign, women were able to be diagnosed and start treatment earlier in the disease process.
Asian Health Services launched a dia betes prevention and healthy living pro gram that set out to influence the food choices of Korean, Chinese, Japanese and Indian families with diets high in carbohy drates, particularly rice and noodles. Yang and his team encourage healthy eating, increased exercise and healthful lifestyle choices as they raise awareness about the link between carb-heavy diets and chronic disease including diabetes.
page 1
From
St. Mary’s Nutrition Center staffers Mumina Isse, left, and Helena Colai, center, coordinated community volunteers in September 2021 who helped cook and delivered more than 3,760 culturally preferred hot meals. The food sustained 80 Lewiston, Maine, residents who were displaced by an apartment building fire.
Dr. Hee Yang is chief medical officer for Asian Health Services at Holy Name Medical Center in Teaneck, New Jersey.
“We’re in the middle of some of the best medical facilities in the world and yet these community members were not going to them. There were people who wouldn’t come in until they were nearly on their death bed.”
— Dr. Hee Yang
4 CATHOLIC HEALTH WORLD November 15, 2022
Trauma-informed care
Hundreds of refugees are resettled in Boise, Idaho, each year. This year the city is on track to welcome more than 1,000 refugees.
During the 2000s, most of these new residents have come from Iraq, Congo, Burma, Bhutan, Afghanistan, Somalia, and Nepal, according to the Idaho Office for Refugees, the refugee resettlement admin istrator for Idaho state. More recently, refugees have arrived from Ukraine. More than 50 countries are represented among Boise’s resettled population.
To ensure the new arrivals as well as immigrants who have come before them receive health and social services in a way that is individualized, culturally appropri ate, linguistically responsive and trauma informed, the medical group of Boise’s Saint Alphonsus Regional Medical Center launched its Center for Global Health & Healing about seven years ago. It provides women's health care and family medicine and runs a federally funded grant program for survivors of torture.
Elizabeth RuttenTurner, a licensed clinical social worker at the cen ter, says, “We build strong, trusting relationships with families. We help with wraparound care. We meet patients where they are. We address the social determinants of health.”

Adds Sarah Mohr, practice manager of the Boise facility: “So often in western medicine, medical appointments are fast and driven by the goals of the providers.” At the global health center, “we slow down and take our time with patients.”

Dr. Chip Roser, the center’s medical direc tor, explains that most of the center’s patients are refugees who fled war or other armed conflict. Many endured physical and mental trauma in their homeland and in refugee camps where they may have waited months or years for immi gration documents.
Rutten-Turner adds that once resettled in the U.S., refugees typically have difficulty securing affordable housing, transporta tion, food and good jobs.
The job market has bright ened in recent years, RuttenTurner says, as more factories and plants have opened in and near Boise and fami lies who arrived years ago are opening their own businesses and hiring members of their community. Also, a nonprofit is help ing immigrants who left professions to get recertified and hired in jobs that use their skills and education. “Employment oppor
tunities have greatly improved, although wages are still quite low compared to cities of similar size,” says Rutten-Turner.
Still, uprooting one’s life and acclimat ing to a new culture is a high-stress propo sition. “Many of our patients, no matter how long they’ve lived here, are struggling with adjustment issues, acute stress disor der as well as complex, compound trauma and stress disorder, major depressive dis order,” says Rutten-Turner.
Roser puts it this way: “We work at the intersection of trauma and medical care.”
The Center for Global Health & Heal ing works closely with all resettlement and refugee aid organizations in Boise.
Rutten-Turner says the cornerstone of the center’s success is a team of 11 commu nity health advisers who serve individuals and families who speak the same language and are from the same cultural groups. The advisers are alert to the needs of their com munities, and they work alongside cen ter staff to address those needs. They also spread the word about the health center in the refugee community.
Hot topics in South Asian health
››Saint Peter’s University Hospital, a Catholic teaching hospital in New Brunswick, New Jersey, has honed its approach to providing clinical and wrap around services to first- and secondgeneration South Asians, especially those of Indian and Pakistani descent. It also is training physicians to understand how ethnicity and culture factor into height ened disease risk for these immigrant groups.
About six years ago, the facility part nered with the Hillsborough, New Jersey, Shri Krishna Nidhi Foundation to establish the SKN South Asian Diabetes Center at Saint Peter’s. Founded by local pediatri cian Dr. Naveen Mehrotra, the nonprofit SKN Foundation seeks to address health disparities and promote wellness and the prevention of many chronic illnesses in part by increasing people’s understand ing of the relationship between lifestyle choices and disease prevention.
The SKN South Asian Diabetes Cen ter’s specific focus in Central New Jersey’s large South Asian-American community is reducing diabetes and heart disease. It offers diabetes prevention and self-man agement programs. The center points people of South Asian heritage to health screening sites including at Saint Peter’s. The center’s staff can assist patients who require follow-up care in making appoint ments with Saint Peter’s clinical special ists. The center’s patients receive care at Saint Peter’s usual locations.
Dr. Meena Murthy is chief of the division of endocrinology, nutrition and metabolism at Saint Peter’s University Hospital. She directs the SKN South Asian Diabetes Center. She says many immigrants moved to Middlesex County, where Saint Peter’s is located, over the last several decades because it is close to New York City but much more affordable than that city.
confidence and the self-management skills of all its patients.
Murthy says research has shown that South Asians have a heightened incidence of diabetes and cardiovascular disease as compared with caucasians. These condi tions occur for South Asians at a much earlier age and at much lower weight and body mass index scores than for cau casians. Murthy explains, “South Asian genetics seem to be highly vulnerable for diabetes and heart disease, with a demon strable higher level of insulin resistance.”
She says the risks always are multifacto rial, “from genetics to epigenetics which includes social determinants.”
“This higher prevalence is not just in immigrant populations; this problem is also seen in South Asians living in their country of origin,” Murthy continues. “The whole world has changed due to indus trialization, urbanization, globalization, western influences, as well as from infor mation technology overload, employment expectations, cheap fast food availability, sedentary and stressed living.”
Murthy says in general neither South Asians nor many clinicians appreciate the heightened risk of diabetes and heart dis ease. The center aims to close this knowl edge gap.
— Dr. Meena Murthy
The center also helps clinicians bet ter understand South Asian cultures. For instance, says Murthy, many but not all Asian Indians place a high value on spiri tuality and consume vegetarian diets. Indi ans have lower rates of smoking than Cau casians. She says, “For better outcomes, clinicians need to understand family back ground, beliefs, spiritual faiths and respect as well as depend on such strengths and culturally appropriate resources to enhance and support care.”

All the advisers are certified in medical interpretation and provide language ser vices at the center. All were hired for their interpersonal and leadership skills, says Rutten-Turner.
The center has 25 staff members, including physicians, nurses, licensed clinical social workers, the community health advisers and administrative work ers. Every staff member receives ongoing training in delivering trauma-informed care.

The center’s social workers provide counseling — they’ve been trained in cross-cultural therapy — and they can connect patients with other resources to address social determinants of health. The social workers are part of the center’s team that is using the federal grant to offer tailored counseling, medical care and legal support to survi vors of torture.
Mohr says while data shows the center helps improve health outcomes, some of the most poignant validation of its work comes anecdotally. Patients of the center say they feel staff treats them like family members. “They keep bringing their families back and they recommend us to their friends. To me this speaks volumes about the trust we’ve established,” she says.
Middlesex County’s South Asian popu lation is made up of many highly educated, wealthy people who work at universities, hospitals and information technology companies, along with South Asians who are not wealthy and may be culturally isolated. People from both these socio economic groups turn to the center for information and assistance navigating the health care system, Murthy says. And, she adds, center staff also guide people in navi gating the social service system.
“We find rich or poor, people have unmet health needs." Murthy says that through health assessment and support the center can improve health literacy, self-
In September, the center held a cardio vascular health conference that brought together medical providers, research ers, medical students, patient advocates, patients and family members and commu nity leaders.
“South Asian researchers who were invited to speak included those who have done original work in South Asian popu lations around the world and have global reach for their research.” Other present ers focused on the health status of South Asians who reside in the U.S., Murthy says. “Heterogeneity within subpopulation was addressed in various talks; currently this is a hot topic that is being talked about and being studied in research actively.”

IMMIGRANTS FACE HEALTH CARE CHALLENGES ›› CATHOLIC HOSPITALS' PROGRAMS MAKE INROADS
››
Rutten-Turner
Mohr
Dr. Chip Roser assesses a patient in the Center for Global Health & Healing in Boise, Idaho. Roser is the medical director of the center, which is affiliated with Trinity Health’s Saint Alphonsus Health System.
Dr. Meena Murthy, left, chief of the division of endocrinology, nutrition and metabolism at Saint Peter’s University Hospital in New Brunswick, New Jersey, moderates a panel discussion during the “Advanc ing South Asian Cardiovascular Health” conference in September. Saint Peter’s Healthcare System sponsored the conference. Panelists were, from left, Dr. Alma Ratcliffe, chief clinical transformation officer for the health system; Dr. Sunil Parikh, outreach director of the SKN South Asian Diabetes Center; Dr. Namratha R. Kandula, a professor at Northwestern Medicine; and Dr. Dinesh Singal, an interventional cardiologist and medical director of Saint Peter’s cardiac catheterization lab.
Murthy
Watch one of CHA’s “This Is Catholic Health Care” videos, featuring the global health center.
“South Asian genetics seem to be highly vulnerable for diabetes and heart disease, with a demonstrable higher level of insulin resistance.”
“They keep bringing their families back and they recommend us to their friends. To me this speaks volumes about the trust we’ve established.”
November 15, 2022 CATHOLIC HEALTH WORLD 5
— Sarah Mohr
Artificial intelligence
Latinos with low family incomes make up the majority of patients who receive care at Saint Peter’s Family Health Center, a federally qualified health center look-alike facility in New Brunswick, New Jersey, that welcomes the uninsured and underinsured along with insured patients. The center provides primary care and spe cialty services and its patient mix includes new immigrants and immigrants who have been in the U.S. for a long time. Some of its patients are undocumented.
As part of their intake registration, new patients are asked questions about socio economic factors that impact health status and treatment outcomes. Their answers might reveal whether the patient has a sta ble housing situation and can afford to stock the refrigerator with nutrient-rich foods.
The health center is using artificial intel ligence — primarily predictive analytics — to mine and analyze census and other pub licly available data to better understand and address community and individual needs.
Ishani Ved, Saint Peter’s director of transformational population health and out comes, says the Saint Peter's Family Health Center has been emphasizing with its staff that the AI population analytics are intended to be an entry point for deeper conversation and engagement with patients, not a substitute for that deeper learning about the patient. When clinicians take the time to listen

and get to know patients, the patients open up and provide information that could be important to improving their health outcomes, she explains. The health center is track ing data to verify that this improvement is happening.
Dr. Alma Ratcliffe, vice president and chief clini cal transformation officer for Saint Peter’s Healthcare System, says the combination of patient screening and predictive analytic data have revealed that the top socioeconomic and related concerns that patients are fac ing have to do with food insecurity, lack of access to transportation, language barriers,
Expanding choices
From its humble origins in Richmond, Virginia, nearly 30 years ago as a mobile vaccination provider for school-aged children, the Bon Secours Richmond Care-A-Van has evolved into a primary care clinic on wheels. Bon Secours Richmond recently supplemented the van’s offerings by adding telehealth services and the system will open a fixed-site clinic in January.
Becky Clay Christensen, executive direc tor of community health services for Bon Secours Health System’s Greater Richmond Region, says more than 90% of the clinicon-wheel’s patients are Latino.

Many patients speak only Spanish. Most of the rolling clinic’s physicians, nurses and social workers are fluent in English and Spanish and some of them are certi fied medical interpreters. When staff don’t speak a patient’s language, the Care-A-Van clinicians use a medical interpretation service that can provide translation in 200 languages.
Christensen says many Care-A-Van patients without legal immigration sta tus steer clear of hospitals and fixed-base health care settings out of fear of coming to the attention of immigration authori ties. From the start, the Care-A-Van built trust and came to be seen as a safe place by locating its stops at churches in immigrant neighborhoods.
In 2016, Care-A-Van staff started screen ing patients for housing and food insecu rity and other needs associated with social determinants of health, documenting find ings in patients’ medical records and con necting them with social service providers.

Care-A-Van services include primary care, pediatric care, some lab services, chronic disease management and behav ioral health care and referrals. Patients pay nothing for the services they receive. There were more than 7,300 patient visits to the van in the first two quarters of this year.

During the pandemic, the Care-A-Van
began offering some services via telehealth. Many patients appreciate this ongoing service because they don’t have to take unpaid time off work to travel to medical appointments.
Dr. Paula Young, Care-A-Van pediatri cian and Bon Secours Richmond medical director of community health access, says hypertension, diabetes and cardiovascu lar disease are common conditions among Care-A-Van adult patients. It also is com mon for people to come in with acute con ditions after they’ve tried natural remedies that were ineffective.
Many patients are migrant workers in physically demanding jobs. As they’re trav eling, they’re not usually able to get health care services. Hard labor can exacerbate untreated injuries and disease.
Young adds that in some cases she has treated patients who had not sought care, or been unable to access care until their con ditions became impossible to ignore. One teenaged patient wore diapers for his first appointment with Young. He needed cor rective surgery for bladder exstrophy, a rare
lack of housing and insufficient access to care for mental illness.
Saint Peter's Family Health Center has been increasing its attention to these concerns. This includes providing behav ioral health services to the seriously ill or addicted. Patients who present with symp toms of mental illness in Saint Peter’s emer gency department are given referrals to community mental health services includ ing follow-up behavioral health care at Saint Peter's Family Health Center.
Staff have begun connecting patients with a program that reimburses for Uber and Lyft rides for transportation to medical appointments and providing vouchers for purchases at a farmer’s market.
birth defect in which the bladder develops on the outside of the body. Another new patient presented with congenital heart disease so advanced that the person’s fin ger tips were clubbing. The Care-A-Van was able to refer both patients to specialists.
All of the patients treated at the mobile clinic are uninsured or underinsured. Bon Secours offers a financial assistance pro gram for uninsured patients who don’t qualify for government-sponsored insur ance and cannot pay for their treatment. The van refers patients needing specialty care to Bon Secours physicians and part ners with Access Now. That Richmond non profit helps coordinate specialty medical care for patients without insurance at no cost to them.
Christensen says in recent years a grow ing number of patients with mental health concerns have been seeking care at the mobile clinic. Some experienced violence or trauma in their native countries or on the journey to the U.S. Adjusting to life in the U.S. carries its own significant stresses. The mobile clinic employs a part-time, bilingual licensed clinical social worker to provide mental health counseling and make refer rals to partner organizations offering men tal health services.
Starting in January patients will get an access option beyond the mobile clinic and telehealth. Bon Secours Richmond is leasing a space neighboring a nonprofit called CARITAS. The clinic site is in a Rich mond neighborhood central to where many Latino immigrants live. The partner ship is renovating a former tobacco ware house into a health and social services hub. The new facility will house a Bon Sec ours Richmond clinic for the uninsured. CARITAS provides substance detoxification services, reentry services for former prison ers, job programs and other services.
Young says Bon Secours Richmond and its partners are making health care and social services more accessible for vulner able people. “We meet them wherever they are” with the services they need.

“We are a safe place” for them, she says. jminda@chausa.org

Learn More Scan the Code below COMMUNITY HEALTH INVESTMENT CERTIFICATE An investment in your future is an investment in your community IMMIGRANTS FACE HEALTH CARE CHALLENGES ›› CATHOLIC HOSPITALS' PROGRAMS MAKE INROADS
››
The Bon Secours Care-A-Van travels to stops around the Richmond, Virginia, area to provide primary and preventive care and vaccines to community members. Most of its patients are uninsured or underinsured.
››
Nurse Helen Bucci administers a COVID-19 vaccine to Shavy Rodriguez-Quinares at Saint Peter’s Family Health Center in New Brunswick, New Jersey.
Ved 6 CATHOLIC HEALTH WORLD November 15, 2022
Ratcliffe
School-based clinics
From page 1
Mercy Health operated clinics in two small inner city schools for students, their family members and school staff. “When Sayler Park took off, we saw the value provided by serving the health care needs of an entire community,” said Liz Wilson, director of Medical Group Operations at Mercy. “Then we grew — and currently, the school-based clinics serve between 3,000 to 4,000 patients annually.”
The newest, Mercy Health — Southwest Schools Community Clinic in Harrison, part of metro politan Cincinnati, opened in August.
Through special arrangements with the schools, the clinics remain open year-round, operating from 7:30 a.m. to 4:30 p.m. Monday through Friday. Three of Mercy Health’s schoolbased clinics represent partnerships with the Cincinnati Public School District; three more are partnerships with schools in War ren County and Clermont County, which are primarily rural areas.
Halo of trust
“Some of these schools are like mag nets,” Wilson said. “These are places where people trust the school and trust the staff, and we’ve been able to create relation
ships with the community while providing access to primary health care.” The clinics bill insurance companies for services, and parents are billed for co-pays so no students are expected to provide them. Patients who report financial difficulties are referred to Mercy Health’s billing department, which has a financial assistance program for those in need.
Wilson noted that if clinic workers learn that families have food insecurity issues, they can provide referrals to agencies that can help. “Many different health agencies — Catholic health care entities, federally qualified health centers and community health departments — work together to serve the school-based health centers in our area,” she said. “It’s a good consortium group, and we all get together to share best practices and help all people get the care they deserve.”
The School-Based Health Alliance, a nonprofit organization based in Washing ton, reports that its 2016-2017 National Census Survey identified 2,584 schoolbased health centers in 48 states, the Dis trict of Columbia and Puerto Rico, provid ing access to more than 6.3 million students, which is about 13% of students nationwide.
Nearly two-thirds of the clinics provide services to populations beyond students.
“Though the number of school-based health clinics has more than doubled since 1998, there are still only enough to meet a fraction of the overwhelming need,” said Suzanne Mackey, vice president for pol
icy and public affairs at the School-Based Health Alliance.
“The clinics have demonstrated their ability to increase access to health care, reduce emergency room use, lower Med icaid costs and increase the use of sensitive services like mental health counseling, and are considered an evidence-based inter vention to improve educational and health outcomes in low-income communities,” she said. Mackey added that data from a new survey, conducted over the summer, are being compiled.
Expertise and access
Students and their families who use the school-based clinic benefit in several ways, said Doll, who works with a medical assistant. “The school nurse can arrange same-day visits here, where we can do exams and test ing, write prescriptions and notify parents or guard ians where to pick up any needed medications that may help get the student back to school as soon as pos sible,” she said. “That eliminates the need to pick up the student and set up a doctor’s appointment elsewhere.”
The Mercy Health school-based health centers participate in the national Vaccines for Children program and offer vaccinations for adults. “Also, we can help with physicals for children entering kindergarten and we also do sports physicals,” Doll said. The
local public schools offer a mental health care provider, family peer support and a therapist for students with anxiety, and Doll said she can set up a virtual visit with a psy chologist at Mercy Health for adults.
Health education is another focus at the clinics. Doll said she provides a science lesson each year for second graders on the importance of handwashing and takes part in the school’s annual Back to School Fair. She also has conducted sex education classes for teachers who requested this.
Alyse Knapp, the nurse practitioner who works at the new Southwest Schools Community Clinic, looks forward to providing health education sessions as well.


“On this campus, we have an elementary school, a junior high and a high school, and there are two additional elementary schools nearby,” said Knapp. “I’m getting my name out to the school nurses and also encourag ing Mercy Health’s freestanding emergency room nearby to refer individuals who don’t have primary care physicians.“
After just a month on the job, Knapp reported, “I’ve handled a lot of sick visits and some well child exams, and I’ve seen some skin infections from football. Nor mal primary care will come later, and with every visit, we always educate about healthy eating, maintaining a healthy weight and healthy habits at home.”
That adds up to a healthier future for everyone, Wilson said. “Plus, all our ser vices reflect Mercy Health’s mission, which is so strong regarding serving the poor and underserved, regardless of the ability to pay. That’s what our school-based centers are here to do, especially in areas where there is a lack of primary care resources. If we can make even a small impact here, we’ve made huge strides.”
PRESIDENTS AND CEOS
Organizations within CommonSpirit Health have made these changes: Patrick Caster to president and chief executive of French Hospital Medical Center in San Luis Obispo, California, effective Nov. 28. He was president and chief execu tive of Memorial Hospital of Gardena, in Los Angeles.



Brandon Mencini to chief executive for Centura Health’s Mercy Hospital in Durango, Colorado. He was chief operating officer for Chippenham Hospital in Richmond, Virginia.
Kayleen Lee to interim chief executive of Avera St. Anthony’s Hospital of O’Neill, Nebraska. She is filling the role as the search is underway for a permanent chief execu tive. The new chief executive will oversee operations at both Avera St. Anthony’s Hospital and Avera Creighton Hospital in Nebraska. Lee was chief executive of Sioux Center Health, an Avera partner, in Sioux Center, Iowa.
ADMINISTRATIVE CHANGES
Brian Smith has retired as CHA vice president, sponsorship and mission services. Diarmuid Rooney will hold that position on an interim basis until CHA conducts a search next year for a permanent replacement. Rooney is CHA senior director of ministry formation.
Anneliese Peterson to chief operating officer of Benedictine of Duluth, Minnesota.



KEEPING UP Project1_Layout 1 10/4/22
Page 1
11:03 AM
Doll
Wilson
Knapp
Caster
Smith Rooney Peterson
March 1, 2022 CATHOLIC HEALTH WORLD 7 November 15, 2022
Sisters of Charity
From page 1
new campus will promote holistic health and wellness through health care and ser vices that address the social determinants of health. The system plans to fill open space in the hospital building with some of those services.

The system said the hospital’s transition to ambulatory care was expected to be com plete by Nov. 15. The changes include the loss of about 641 full-time positions as the hospital will no longer staff 162 inpatient beds or a medical emergency department.
Janice Murphy, president and chief executive of Clevelandbased Sisters of Charity Health System, said the shift was spurred by the COVID-19 pandemic and the decline in demand for inpatient medical services it set off. She noted that in the first month of the health emergency in spring 2020, St. Vincent Charity’s finances were $3 million in the red. For the year, the medical center’s patient volume dropped by about 30% from 2019 and volume did not recover in 2021.
“We were hoping that after the vaccines came onboard, we would see volumes return to the pre-pandemic levels and that never did occur,” Murphy said.
Painful move, but still hope
The hospital closure is painful, she said, especially because of its impact on the workforce. Some of those workers, she noted, have been with the hospital for 50 years.
Sisters of Charity Health System is col laborating with other area health systems to place workers. Murphy said one of those systems, University Hospitals, is even hon oring the workers’ seniority and trying to provide parity in salary and benefits. Uni versity Hospitals also absorbed St. Vincent Charity Medical Center’s internal medi cine residency program along with its 54 residents.
Once the exit from inpatient care is com plete, St. Vincent Charity Medical Center will employ about 100 full-time workers. It will offer:
Primary care.
Urgent care.
Outpatient mental health services.
Psychiatric emergency services.
Addiction medicine services through Rosary Hall, an outpatient treatment center.
Occupational health.
The hospital is in the Central neighbor hood, where a nonprofit, The Center for Community Solutions, estimates unem ployment is close to 50% and that almost 70% of residents have incomes below the federal poverty line.
Murphy said the services St. Vincent Charity Medical Center is keeping on the campus reflect its long-standing commit ment to mental and behavioral health care as well as the needs of the community. She said most of the patients coming to the medical center were in need of urgent care
rather than acute or emergency care.
Other nearby hospitals can meet the acute care needs of the community around St. Vincent Charity Medical Center, Murphy said.
She added that Sisters of Charity Health System executives were mindful in decid ing what services to keep at the repurposed St. Vincent Charity Medical Center campus so that the cost of providing those services does not undercut the financial stability of the subsidiaries the system operates in Ohio and in South Carolina.
Those programs include Joseph & Mary’s Home, the only provider of services to those who are homeless in Northeast Ohio that is exclusively focused on medical respite care; Healthy Learners, a program that provides vision, dental and other health-related care to children from low-income families in South Carolina; and the South Carolina Center for Fathers and Families, an orga nization supporting initiatives to reengage fathers in the lives of their children.
Mission aligned
Sr. Judith Ann Karam chairs the pub lic juridic person of the Sisters of Charity Health System and is congregational leader of the Sisters of Charity of St. Augustine. She is a past president and chief executive of Sisters of Charity Health System and a past chair of the CHA Board of Trustees.

Sr. Karam noted that across a history in the United States that stretches back to the mid-1800s, the sisters adapted the services offered by their health min istry in line with the times and with the needs of those served. She pointed out that the congrega tion’s health ministry always has focused on the physical, psychological, spiritual and social needs of patients. She added that the care often has addressed unmet needs in communities.
An example Sr. Karam cited is an inpa tient program for the treatment of patients
Pilot programs get underway at health campus
Susanna H. Krey, president and chief executive of the St. Vincent Char ity Health Campus, said three pilot programs have either launched or are in the planning phase of the St. Vincent Char ity Health Campus in Cleveland. They are:
A food program being run by an entre preneur who is using St. Vincent Charity Medical Center’s kitchen to prepare 400 meals per week that are tailored to specific medical needs for Meals on Wheels recipients. The operator is using her program as a workforce training initia tive for people in the community.
Behavioral health crisis and recov ery services to address the symptoms of trauma by creating a new coordi nated response to crisis in the com munity and enhance access to services that support long-term recovery.
A family resource center that would provide supportive care for par ents and children.
Krey said another idea for the campus that has gained early sup port is development of a Catholic high school that provides a religious educa tion as well as training for health care jobs, such as respiratory or radiology technicians. She said the suggestion for this program came from the bishop of Cleveland. The neighborhood around the health campus has no Catholic schools.
The high school holds the prospect of creating a more diverse health care workforce for Cleveland and for giving students a means to train for well-pay ing jobs with opportunities for advance ment, Krey said. “The community has embraced this,” she added.
 — LISA EISENHAUER
— LISA EISENHAUER
with alcohol use disorder that was pio neered in the 1930s and 1940s by Sr. Mary Ignatia Gavin and others at a Sisters of Charity hospital in Akron and later moved to Rosary Hall, which is housed within St. Vincent Charity Medical Center. Sr. Ignatia, as she was known, is sometimes called the Angel of Alcoholics Anonymous because of her support for that program in its early days.
“I think when you look at our history and our charism — which is in all things charity,
in all things love — you see we can’t help but respond to people and the needs that people have, no matter how hard it is,” said Sr. Karam.
Health campus plans
In Cleveland, she said, Sisters of Charity hopes to meet more needs of the vulner able community it serves than ever through its development of the St. Vincent Charity Health Campus.
Susanna H. Krey is president and chief executive of the Sisters of Charity Founda tion of Cleveland and the St. Vincent Char ity Health Campus. The foundation, the health system, the medical center and the congregation are partners in the project.


Krey said planners spent months reach ing out to people who live and work in or near the neighborhoods around the St. Vin cent campus to learn what social, economic and wellness services community mem bers want. Suggestions included youth and family programs, food and nutrition ser vices, workforce development, and recre ation and green space. Krey said plans are moving forward quickly. Pilot programs are being launched or developed. (See sidebar.)
— Sr. Judith Ann Karam
Krey and other planners of the health campus are inviting partners with mis sions aligned to that of Sisters of Charity Health System to bring their services to the campus. So far, she said, inquiries have been made by agencies that provide work force training, housing, childcare and other social services.
“We’re looking to how these all come together to lift this vision of serving the whole person and being a catalyst for revi talization for this neighborhood that has experienced disinvestment and been over looked so many years,” Krey said.
Sr. Karam said the planners of the health campus have a lot of work ahead to bring the right partners together and to make the campus thrive. She said the prospect of a challenge has never been a deterrent for her congregation and the organizations it has founded.
“I think God’s love gives us strength to take risks on behalf of serving all of God’s people,” she said.
leisenhauer@chausa.org
Murphy
Sr. Karam
Community residents gather at a listening session to learn about plans for a health campus in Cleveland’s Central neighborhood. The health campus, which will be anchored by the St. Vincent Charity Community Health Center, is being developed by Sisters of Charity Health System, the Sisters of Charity Foundation of Cleveland and the Sisters of Charity of St. Augustine.
Krey
This image shows a vision for the St. Vincent Charity Health Campus that is being developed around what is now the St. Vincent Charity Community Health Center in Cleveland. Plans for the campus include a variety of services that address the health, social and economic needs of the community that surrounds the health center.
“I think when you look at our history and our charism — which is in all things charity, in all things love — you see we can’t help but respond to people and the needs that people have, no matter how hard it is.”
Courtesy of MASS Design Group
8 CATHOLIC HEALTH WORLD November 15, 2022
Courtesy of MASS Design Group
