DIFFICULT AIRWAY SOCIETY MEMBERS EZINE

January 2023 Edition


January 2023 Edition
Please remember to update your details if your address or email address changes!
Members can update their details by emailing das@anaesthetists.org

DAS encourages member participation – we would love to read your comments, contributions and suggestions for future E-Zines. Have you been involved in an interesting airway case? Is there an article that has changed your practice? Do you have an idea for improving airway anaesthesia that you would like to collaborate on?
All formats welcome: text, video, photo, infographic… We know you are a creative bunch! Send us your thoughts at ezine@das.uk.com
Editorial 4
Letters to the editors 6
DAS Executive Update 7
DAS Scientific Officer Report 11
Professor Ellen O'Sullivan 9
Education
Clinical Dilemma 14
Educational Series: Perioperative Medicine Part 3 22
Service development: POPS 23
Service development: prehabiltation 27
#JanuAIRWAY - The Compilation 33
DAS webinars 2023 40
Airway Hub 41
Difficult Airway Database - an update 46 Conference Corner
GA sections - polls from DAS 2022 37
Trainee competition 13
Journal Club - Recommended Reads 44
Happy New Year and welcome to the January 2023 edition of the Difficult Airway Society EZine.
As we start 2023, we reflect on 2022 and a very special moment for DAS with the return to a face to face DAS ASM for the first time since the start of the pandemic. The world may have adapted brilliantly using technology for remote meetings and conferences but there is nothing quite like being back with colleagues again in person. A huge thank you to Dr Iftikhar Parvez and the organising committee in Newcastle for a fantastic meeting. We are already looking forward to DAS 2023 which is being held in Birmingham 29 November - 01 December so save the dates in your diary!
One of the highlights of the 2022 ASM was the awarding of the DAS Macewen medal to our wonderful Professor Ellen O’Sullivan. Ellen is a truly special individual for all she does for DAS and airway management education and she is a huge role model for us and many others. It was a very special moment to see her receive the medal and a huge congratulations from us for such an amazing achievement.
DAS 2022 also saw the awarding of a DAS Professorship to Professor Cyprian Mendonca. Professor Mendonca has had a huge impact through his research and educational activities and contribution to airway management. Congratulations to Professor Mendonca and we look forward to your lecture at DAS 2023.
This edition of the e-zine kicks off the new year with a bang. We have the concluding part of our three-part educational series focusing on perioperative medicine. In this final part we have two fantastic articles focusing on the development of such services. Learning from others who have been through the process is crucial and we would love to hear about others experiences of this at a time when preoperative medicine is very much in the headlines.
This month’s clinical dilemma poses several challenges: a patient living with obesity, pregnancy and a rapidly progressing condition which needs urgent treatment all in one case. How would you manage such a patient?

And if that wasn’t enough for one edition, we are taking at looking at the delivery of

multidisciplinary airway training with the #AirwayHub initiative at University College London Hospital.
After the success of the DAS webinars in 2022 we are delighted to announce our first DAS webinar of 2023 which will be taking place on 2nd March 2023 on human factors. We have a fantastic panel for this webinar and will be announcing further dates and topics for future webinars very shortly.
*If you missed the previous parts in the periop series, you can find them here and here!
If you have any feedback or article contributions please get in touch with our editorial team by emailing ezine@das.uk.com or tag us on Twitter @dasairway or @dastrainees.
 Moon-Moon
Moon-Moon

| Please get in touch, we love hearing from you! |
The E-Zine is something we are passionate about and we love to hear from you about it . We want it to be as useful to members as possible so please do get in contact with any suggestions and/or feedback - ezine@das.uk.com or tag us on Twitter @dasairway or @dastrainees.



Happy New Year! Looking back over the past year it has been challenging in many aspects. We have all worked hard in extremely difficult circumstances during the pandemic and are now faced with the aftermath of the very unusual and tough conditions. The NHS is facing a very challenging winter and our teams as always are at the forefront, helping our patients in these exceptionally difficult times.
After nearly three years we have had a face to face Annual Scienti fi c meeting in Newcastle. With over 700 delegates attending, this meeting was a huge success. It was a pleasure to see old friends, colleagues and new members joining the airway fraternity. From the retired members to our youngest attendee who was 3 months old, everyone was excited to be there, attending lectures, workshops and the social gatherings. We had delegates from all over the world including Australia, New Zealand, Brazil, Pakistan, India, Saudi Arabia, Zimbabwe, Canada, USA, Singapore and all over Europe. The DAS Macewen medal was presented to Professor Ellen O'Sullivan and Professor Cyprian Mendonca was
announced as the DAS professor of the year at the ASM. Our new website planning is progressing and the designated team are working tirelessly to make it user friendly, professional and comprehensive. The education team are already planning and forging ahead with new ideas for the webinars and educational activities for the new year.

Standardising the Airway fellowships across UK is the next big planned activity by the DAS education team and is currently underway with surveys and a collection of databases.
The DAS Alert card database is progressing very well and an analysis of the data from first five years was published in Anaesthesia this year. This has been very well received and has initiated discussion on the role of Alert cards for ensuring patient safety and acting as a means of communication between clinicians across the country regarding care of the patients. While it was another challenging year financially, plans are being made to ensure financial stability for DAS in the coming years.
The Birmingham ASM planning in 2023 is progressing very well and expressions of interest for the 2024 meeting have been invited, the results of which will be announced soon. Updates on guidelines continue with continued progress being made on the DAS intubation and extubation guidelines.
We are also working with the OAA and APA on updates to both paediatric and obstetric airway guidelines. The DAS Human Factors guidelines will be launched in January with some very exciting and interesting content for all. The team led by Fiona Kelly has worked hard to complete these in the challenging few years during the pandemic.
We look forward to what this new year holds for DAS and a special welcome to all the new members joining the DAS in these exciting times. Getting involved and collaboration

makes our society not only bigger but also at the forefront in education, research and patient care.
Imran Ahmad, DAS President
Ravi Bhagrath, DAS Secretary Fauzia Mir, DAS Treasurer
Professor Ellen O'Sullivan qualified from the National University of Ireland in Cork and trained in anaesthesia and intensive care both in the UK and USA. She returned to the UK as a Consultant Anaesthetist at Aintree Hospital, Merseyside and subsequently took up a post as a Consultant at St James’s Hospital Dublin, Ireland affiliated to Trinity College Dublin.
Throughout her career she has been delivering the highest quality teaching, research and developing and improving airway management throughout the world. She has developed a worldwide reputation in airway management and has lectured and taught workshops internationally.
I first met Ellen over twenty-five years ago at the inception of the Difficult Airway Society. It was obvious then she was passionate about improving airway management both locally, nationally and internationally. She remains as passionate today, but perhaps just as importantly her grace, humour, goodwill, approachable manner and encouragement to everyone she encounters are unchanged.
Ellen has contributed to the airway training of a generation of anaesthetists as director of the Fellowship in Advanced Airway Management and Simulation. She was Past-President of the College of Anaesthesiologists of Ireland and was the first female and first anaesthetist to chair the Forum of Irish Post Graduate Training Bodies.
She has played a leading role in Global Anaesthesia, supporting education and training in low & middle income countries. As elected Council Member of the Royal College of Anaesthetists she set up and chaired the Global Partnership Committee. Over many years she has worked on education projects in Malawi & Uganda including Lifebox and more recently the Global Capnography Project. She is most proud of having been involved in the establishment and supporting of CANECSA (College of Anaesthesiologists of East, Central & Southern Africa). In March 2022 she was awarded an Honorary Fellowship of CANECSA, one of the first recipients of that award. There are I suspect few airway enthusiasts globally who have not heard of Professor Ellen O’Sullivan.

She is a Past President of the Difficult Airway Society, and is currently the DAS International liaison offi cer. She was appointed DAS Professor of Anaesthesia & Airway Management in 2018. Prof O’Sullivan is Airway Lead Advisor to the College of Anaesthesiologists of Ireland (CAI) & runs the CAI national airway training. She is an Executive Director of WAAM (World Alliance for Airway Management) and cochaired the World Airway Management Meeting, WAMM1, in Dublin 2015 and WAMM2 in Amsterdam 2019.
Ellen has held numerous airway roles over many years including the elected Irish representative of the European Society of Anaesthesiology, board member of Society of Airway Management (SAM) USA, invited member of the Academy of Anaesthesiologists USA, Fellowship of European Airway Management Society (EAMS), honorary member Airway Special Interest Group (ANZCA) Australia, chair Respiration & Airway Management committee European Society Anaesthesia & Intensive Care, founding director of International Airway Management Society, and founder of the Global Capnography Project.
Ellen has been a Council Member of the Royal College of Anaesthetists and chair of the Global Partnerships Committee and member board of directors of the British Journal of Anaesthesia. Her most current contributions to airway management have been as a member of the ASA task force publishing the new 2022 ASA Difficult Airway Guidelines and as a member of the Project for Universal Management of Airways.
Ellen has unsurprisingly won many awards during her career including the Irish Healthcare Awards on two occasions and the John Snow Silver Medal from the Association of Anaesthetists. She has a substantial portfolio of clinically relevant research and has authored or co-authored more than 100 scientific papers, book chapters, website modules etc.
Throughout her career in parallel to all of her teaching, research and academic achievements Ellen has continued a busy clinical anaesthetic practice in Dublin and found time to enjoy her other passions skiing, sailing and golf.
Professor Ellen O’Sullivan has made an immense contribution to the field of airway management and it is a great personal pleasure to congratulate Ellen on being awarded the DAS Macewen Medal.

I write this as we face a long, difficult winter compounded by challenges brought by the pandemic. We confront a health service with unprecedented challenges, a staf fi ng crisis, compounded by a national cost of living and energy crisis. Our responsibility as healthcare professionals remains steadfast in trying to tackle the backlog and delivering the highest standards of care we can, including in the field of airway management. Whilst the world spins around us, we have continued to deliver exceptional academia in airway management. We have seen practicechanging publications, several projects with wide-reaching implications, and continued interest in research. DAS remains at the global forefront of this, providing several academic opportunities to members.
1. Direct DAS Grants. To ensure continuity and sustainability of grass-roots airway management research, we have a rolling process of grant funding via direct application to DAS. Applications for funding of up to £5,000 for studies broadly related to airway management will be peerreviewed. Further details are available on the DAS website or by contacting me directly. We have already funded one application, and we are always open to receive more. Reach out for more information on this today!

2. DAS Grants via the NIAA. DAS funds up to £20,000, split between large Project Grants (up to £15,000) and Small Grants (up to £5,000). Last year saw a single application round, with one application of £15,000 being received. The first round of 2022 applications


saw 5 applications for a total of more than £26,000 requested and, although none were funded, highlights the energy around airway management research. The second round had applications and peer-review is ongoing. The first round of 2023 will be opened in the next couple of months, so watch this space.
3. DAS PhD Programme. This Programme gives support to researchers who have a list of publications that may be suitable to put together as a PhD. DAS will support applicants throughout the process of a PhD by publication, including funding support.

4. DAS Faculty of Professors. This is an untapped resource that is open to any DAS Member to reach out to for guidance, support or advice on any academic matters, including grant applications and study design.
5. DAS Professor of Anaesthesia and Airway Management . This is an award conferred in recognition of a member’s
national/international standing in the field of airway management as established by outstanding contributions through publications, creative work or other appropriate forms of scholarship, and through teaching and administration. We are delighted to have awarded the 2022 DAS Professorship to Professor Cyprian Mendonca following a highly competitive process. We will be opening the applications for the 2023 DAS Professor in the coming months!
Our vision remains to take continue to cultivate academia through DAS and airway management, and begin to support, design and develop our own projects with our enthusiastic, creative and brilliant membership. Don’t hesitate to reach out and get involved!
Kariem El-Boghdadly DAS Scientific Officer Scientific-officer@das.uk.com
| Creative writing AND creative media categories |
We are pleased to announce the 2023 DAS Trainee Competition: there are TWO separate categories:
1. creative writing (our essay competition)
2. creative media (this may be whatever you wish: painting, video, poetry, photo series...etc)
The winner of each category will receive £100 in prize money and will have their work published in the DAS newsletter and displayed at the 2023 DAS ASM.
We invite submissions on the following title:
1. Entries are invited on the above title. One entry per person to EITHER the essay OR the media category will be accepted. The author/creator must be a DAS member.
2. Members of the DAS committee will judge anonymised entries.
3. For essays: We will be looking for a well-developed viewpoint. Word count 1500 words maximum (excluding references). Please use Times New Roman size 12 font and double line spacing. References should be formatted as for the BJA.
4. Label your file either ‘DAS Trainee Competition Essay – your DAS Membership Number’, or ‘DAS Trainee Competition Media – your DAS Membership Number’. The name of the author/creator, author/creator’s institution or other identifiable information should NOT be included in the file title or content.
5. Please send in your manuscript OR media submission, along with a completed submission form which can be requested from trainee@das.uk.com or downloaded from the DAS website. Please submit to trainee@das.uk.com
6. Prize money of £100 and a certificate will be awarded to the author of the top essay and the creator of the top media submission. The winning submissions in BOTH categories will be published in the DAS newsletter, as well as displayed at the 2023 DAS ASM.
7. Winners will be contacted by email.
8. Deadline for receipt of emailed essays: Midnight on 14th April 2023
“Airway kit for the future”
How would you design airway kit for the future?
A 30-year-old, 27-week pregnant woman with obesity (BMI over 34 at the booking of her pregnancy) presents with an increasingly quiet voice, increasing shortness of breath on exertion and worsening stridor. For the past few days she has had significant orthopnoea.
She has a history of juvenile-insert laryngeal papillomatosis and on flexible nasoendoscopy is found to have a very large papilloma arising from the vocal cords.

She requires urgent laser treatment for the papilloma. She is extremely anxious about the impact this may have on her baby.
Contact us on twitter with your thoughts! @dasairway @dastrainees



This patient can’t be delayed because of the increasing orthopnoea.
Plan with ENT team - laser or diathermy, laser ETT or a tubeless technique. In my practice we do the latter. Need to balance the risk of regurgitation against that of good surgical access and therefore a quicker procedure, better for the patient.
Plan with Obstetric team: key questions, is this a normal or high-risk pregnancy and what is the risk of an emergency delivery? If it’s a low risk pregnancy our Obs team would do a CTG immediately pre-op and then in recovery. The midwife would stay in theatre during the procedure.
Anaesthetic plan: For high-pressure source ventilation (Monsoon/TwinStream jet ventilator) and TIVA
Pre-op: ✦ Premed with Na citrate/omeprazole / metoclopramide
In theatre induction: ✦ Pre-O2 with HFNO, slight L lateral tilt of abdomen only with a wedge (head & chest need to be flat for placement of suspension laryngoscope) but head -up for any regurgitation.
✦
IV induction : TCI prop/remi and rocuronium (not an RSI but have surgeons ready to place laryngoscope)
Maintenance and surgery: ✦ TIVA ✦
Placement of suspension laryngoscope and jet needle and supraglottic HFJV (remove Optiflow prongs from patient)
✦
Laser or diathermy of lesions - remember to reduce FiO2 if any packs or patties in airway (fire triad of O2, source and fuel).
Recovery:
✦
After removal of suspension laryngoscope, put the Optiflow back and place an SAD to check EtCO2. If not high then reverse with sugammadex and stop TIVA.
✦
Provide more left lat tilt and slightly head up.
✦
Wake and CTG check in recovery and consider low flow Optiflow there.
Sometimes pregnancy can accelerate development of recurrent respiratory papillomatosis (RRP) so expect the patient to return
This is a complex case with a patient with potentially progressive airway obstruction due to papillomata. Throughout pregnancy, airway oedema will further increase this risk. Thus treatment is warranted.
My plan with this patient is to begin by reassuring her that the procedure is necessary for the safety of both mother and baby. I will explain the plan and what we wish to do in order to mitigate complications. I would have a discussion with the patient’s obstetric team and gain any further advice or insights regarding the safety of the pregnancy.
I would manage this patient with awake tracheal intubation in the operating theatre with the surgeon present and the team ready for a tracheostomy if needed. I would use HFNO, remifentanil for sedation, 10% lidocaine for topicalisation and a micro laryngeal tube via the oral route. Once tracheal intubation has been confirmed with a two-point check, I would induce anaesthesia with propofol and remifentanil. We could then safely position (whilst administering 100% oxygen) then when we are ready to perform suspension laryngoscopy, remove the tracheal tube and commence ventilation using the TwinStream for high-frequency jet ventilation via the suspension laryngoscope.
I would ensure PEEP is delivered, and 100% oxygen until laser is to commence, when I would reduce the fractional inspired concentration of oxygen to 28% for 30 s before lasering. Once lasering is complete, I would insert a second-generation supraglottic airway device and wake the patient up. If the patient desaturates during the procedure and I am unable to bring the saturations up with the TwinStream, I would insert a microlaryngeal tube and commence traditional positive pressure ventilation.

Issues:
1. Glottic compromise in need of urgent treatment under GA 2. Early 3rd trimester – not suitable for delivery at 27 weeks but low risk of preterm labour 3. Gas exchange compromise – airway, pregnancy and obesity 4. Aspiration risk.
MDT: ✦
Anaesthesia (Airway + Abs), ENT, Obstetrics and Neonatology - involve clinicians who will deliver the care. ✦
Discuss all relevant issues ✦
Airway assessment and prediction of success/failure of proposed techniques ✦ Tubeless field is far from ideal - I would essentially be ruling this out. ✦ Steroids? NSAIDs? [d/w neonatology] ✦ Post-op care
Then with patient: ✦ Discuss risks + benefits of approaches. ✦ Shared decision making. ✦ Establish informed consent for strategy.
Airway:
Manage as experts see fit. With FNE findings, it does not sound as if ATI is necessary as ventilation should be expected to be possible and glottis should be accessible… but already has moderate glottic narrowing so ATI may be preferred option.
If team are happy for GA intubation, I would recommend: ✦ GA. ✦
Aspiration protective strategies. ✦ “Best” team delivering care and prepared for all airway eventualities ✦ HFNO, VL, TIVA, pEEG, quantitive TOF. ✦ GA with TIVA propofol + remifentanil; Rocuronium. ✦ Monitor foetus. ✦
Mac VL (if access to glottis expected to be straightforward following airway assessment) ✦ Small Laserflex ETT (start with stylet to maximise 1st pass success). ✦ Probably avoid LA to glottis. ✦ Optimise gas exchange and CVS stability (FiO2 with cuffed ETT does not have to be limited with laser). ✦
Dexamethasone.

Extubation: ✦
Safe, optimised extubation – minimising risk of desaturation, aspiration or excessive coughing. ✦ Probably my preferred technique would be awake with Remi obtunding cough.
Issues that need to be addressed:
1. Timing of surgery with respect to gestational age of baby vs how symptomatic the patient is
2. Intraoperative and post operative obstetric MDT care
3. Airway management technique for laser surgery
Ideally this case needs to be delayed until after the patient gives birth, but as the symptoms are getting worse so she needs urgent surgery. In which case the risks of having a GA to the baby need to be discussed
This case will require MDT input from midwives, obstetricians, obstetric anaesthetists as well as the ENT surgeon and airway anaesthetist. An MDT meeting should be arranged prior to doing the case so a perioperative plan is discussed and all eventualities are covered. This should include location, personnel that need to be present on the day, continuous foetal monitoring, ability to perform a CSection if required and post operative care of both mother and foetus.

Airway management for me would be as follows: ✦
ATI with a MLT to navigate around the polyp then intubation once trachea has been identified then induce anaesthesia ✦
Once asleep, position the patient (bearing in mind that she is 27 weeks gestation), suspend with the surgical laryngoscope and if there is a good view of the lesion and ventilation is adequate then the cuff can be deflated and MLT removed so surgeon has good access to the lesion and HFJV can be commenced
We have the TwinStream at my hospital so I would use that as my choice of HFJV, via the suspension laryngoscope
If I didn’t have the TwinStream, then I would use another device that allows HFJV, like the Monsoon
Whilst all this is happening, foetal CTG monitoring must be on
During any laser surgery all standard Laser precautions should be undertaken and laser safe devices used
Always reduce the FiO2 when laser is in use, this is achievable with the TwinStream
Never use THRIVE when undertaking laser surgery, unless the FiO2 can be reduced to 30%
Surgery should be as quick as possible and undertaken by an experienced surgeon, this case should only take 15-20 minutes
Backup for desaturation or inadequate ventilation or failed intonation, would be a surgical tracheostomy ✦
Once done I would be happy to extubate but patient should go to an HDU post op with continuous CTG monitoring
1. A history of juvenile papillomatosis is likely to mean that she has had previous/even recent anaesthetics
2. This is best treated electively prior to the peripartum period so that it does not complicate any emergency interventions around labour and delivery 3. A multidisciplinary approach is required- ENT surgeon, obstetrician. obstetric anaesthetist, head and neck anaesthetist 4. A flexible nasoendoscopy is essential (ideally on video so that all team members can view)
Making the assumption that doing nothing is not an option: ✦ All ramping and antacid precautions should be taken, appropriate foetal monitoring given the gestational age of 27+ is also important ✦ The patient should be done in daylight hours with plenty of time on the list
There is no perfect technique: ✦
Using an endotracheal tube (MLT) risks making access to the lesion difficult and sheering of a fragment of tissue could occlude the end of the ET tube unless it is placed with a bougie ✦
THRIVE is an option but its use with a LASER must be restricted to a highly specialist centres where a thorough risk assessment has been undertaken by the LASER safety officer and the entire theatre team are trained, skilled and drilled in safe practice ✦
[Fact- there are very few hospitals where this will have been done and the published literature is limited to a very few specialist centres] ✦ Assumption- the hospital in question is unlike to be one of those highly specialist centres] ✦ Jet Ventilation- again jet ventilation is not without risk and whilst HFJV is safer, LFJV is more commonagain Specialist expertise is vital to avoid harm ✦ This is especially true if the papilloma close the glottis when the patient is lying flat and there is no room for gas egress ✦
Options like the ventrain or tritube could be considered – but given the limited clinical experience with these devices this would be for an academic discussion only
Personally:
1. Ramp the patient 30 degrees head up, with lateral ramping also 2. Optiflow Switch at induction to facilitate per laryngoscopy oxygenation 3. TIVA 4. Test bag
5. Initial inspection under THRIVE (team set to intervene at SpO2<95%) 6. Is there a large part of the lesion that can be excised to create an airway? 7. Transfer to jetting to facilitate laser resection (HFJV preferred given alarms etc) - Ensure expiration by hand on chest
8. Supraglottic device at end of case

9. Consider elective cannula cric to facilitate emergency oxygenation if airway difficult- but again consider the risks of the cannula kinking and of barotrauma if expiration does not occur
***This is not a simple case and should only be performed at a specialist centre where teams are experienced in all of these techniques- that may mean moving an obstetric team to an ENT setting but that is the best option as delivery is the most unlikely outcome***
EXPERT INPUT is essential and the management of this case could be discussed in several thousand words.
This case has promoted some incredibly interesting responses from our airway experts and it is clear why. Not only do we have a patient with a rapidly progressing pathology requiring urgent intervention but this patient also is living with obesity and is pregnant. There is a huge amount to consider that is entirely separate to the airway pathology that the patient is presenting with, which is already a challenge in itself. Juvenile-insert laryngeal papillomatosis is characterised by the development of papillomas in the respiratory tract caused by human papilloma virus (usually types 6 and 11). Transmission is believed to occur during birth as the foetus passes through an infected genital tract. The larynx is the most common site of involvement but the trachea, oropharynx, nasopharynx, nose and oral cavity can all be involved. Patients require repeated procedures to remove the papillomas. The condition accelerates in the presence of increased oestrogen concentrations and therefore pregnant women with the condition, as in this case, should be warned of the possibility of worsening of the disease in pregnancy.
So our patient has an airway disease requiring urgent intervention, but with some major additional complicating factors - both her pregnancy and the fact she is living with obesity.
The Society for Obesity and Bariatric Anaesthesia provides an excellent one page guidance sheet on anaesthesia for patients living with obesity and this has become a stalwart for all of us when providing anaesthesia to this cohort of patients.
Our patient is also pregnant which adds additional complexity due to the presence of a gravid uterus, foetal considerations and the significant physiological changes pregnant women experience. This may not be an entirely comfortable scenario for some head and neck anaesthetists and it is a situation when calling a colleague and carefully planning would be at the forefront of my mind.
As stated in the responses, this is a case which exemplifies the importance of MDT working. Airway management is a team sport, as is the management of complex cases. This isn’t just anaesthetists but obstetricians, midwives and the entire theatre team in this case.
So how would you approach this case? We would love to hear your thoughts. Contact us on twitter @dastrainees or email ezine@das.uk.com


In this January 2023 edition of the DAS E-Zine, we are proud to present the final part of our three part perioperative medicine series focusing on service development.
In our introduction to the series we outlined how perioperative medicine has been a key focus of opportunities for better health and care in the COVID-19 era and beyond and this reaches far beyond the operative care we provide.
The series kicked off with an introduction to perioperative medicine, the impact of NELA and shared decision making. Our second part looked in detail at frailty, CPET and risk assessment.
Setting up a new service or enhancing an existing one can seem like a daunting process and one we are generally not used to as clinicians. I learnt this first hand during my time as an innovation fellow helping to set up a new frailty service over winter in a short time frame. We managed it but it was a humbling experience and one that has stuck with me.
What lessons can be learnt from those who have been through this journey? Just as in a challenging clinical situation we wouldn’t hesitate to call a colleague for support, we should look at hospitals and areas where it has been done already and learn from this.
In this final part of our series we have two fantastic articles on service development. The fi rst focuses on the NHS Elect POPS Network, a network promoting the rollout of geriatrician-led, multidisciplinary perioperative care for older patient. The second looks at the experience at UCLH of establishing a prehabilitation service.
Both articles give invaluable insights from clinicians who have been through this journey and are full of wisdom and food for thought for anyone contemplating developing such a service.
As this series ends a huge thank you to all of those who have contributed to it. One of the joys of developing and editing the ezine is the enthusiasm shown by so many to contribute and the incredible articles that are submitted. I have learnt a huge amount and have no doubt that these are articles I will return to read time and time again. But where do we go next? Please do contact us @dastrainees or email ezine@das.uk.com if you have any suggestions for our next educational series.
We hope very much that you enjoy reading and learning from these fantastic resources as much as we have.

Perioperative medicine for Older People undergoing Surgery (POPS) is a subspecialty of geriatric medicine that has evolved to address the needs of older people presenting with surgical pathology using comprehensive geriatric assessment and optimisation (CGA) with shared decision-making (SDM).
The seventh National Emergency Laparotomy Audit (NELA) report demonstrates that the proportion of older people undergoing surgery is increasing. Older people are more likely to be living with multimorbidity and frailty. The report indicates that frailty is an independent marker for poorer postoperative outcomes.1 This has been demonstrated across surgical specialities.2
CGA is a multidimensional, multidisciplinary process which identifies medical, social and functional needs, resulting in an integrated/ coordinated care plan to address those needs and is the gold-standard for the management of older people.3 Evidence supports the clinical and cost effectiveness of CGA and optimisation in the perioperative setting 4,5 Cognisant of workforce challenges in geriatric
medicine the HoW CGA study trialled delivery of perioperative CGA without a geriatrician using a ‘toolkit’ approach, concluding that geriatric medicine skills are crucial to the clinical effectiveness of the process.6



Using a CGA and optimisation approach with SDM has been endorsed through the collaborative ‘Guideline for Perioperative Care for People Living with Frailty Undergoing Elective and Emergency Surgery’. Authored jointly by the Centre for Perioperative Care (CPOC) and the British Geriatrics Society (BGS), the guideline recommends that surgical pathways for frail patients are underpinned by CGA methodology from initial assessment to discharge.7
The BGS POPS Special Interest Group provides education and training in perioperative medicine on a national level to support all members of the multidisciplinary team upskilling in management of older people undergoing surgery. This includes conferences, guidelines and an e-learning package. Curricula have been approved for both ANPs and foundation year doctors.8
Despite this evidence, guidelines and training opportunities signi fi cant variation in the perioperative care of older people remains across the UK, with the Getting It Right First Time (GIRFT) national programme aiming to standardise care through work streams in critical care, surgical specialties and geriatric medicine.9
Despite evidence showing the benefits of geriatrician involvement in the perioperative care of older people, few services nationally or internationally have implemented CGA-based perioperative care. In fact, a 2019 survey of acute NHS trusts revealed that only around half had such services in place.10
Following the success of other improvements networks including the Specialised Clinical Frailty Network, the NHS Elect POPS Network was established, with the aim of promoting the rollout of geriatrician-led, multidisciplinary perioperative care for older patients. To date, thirteen NHS Trusts in England and Wales have completed the six-month programme over two cohorts. The programme provides comprehensive support to adapt and implement the POPS model, ensuring it is tailored to the local context at each site. This is delivered through a trimodal approach of expert mentoring and coaching, access to a toolkit of POPS resources, and guidance in a measurement for improvement approach.
Beginning with a virtual site visit to share ideas and discuss potential barriers to change, the programme offers structured monthly core events, webinars and masterclasses. In addition to the more formal expert mentoring aspect to these virtual events, they also provide invaluable
opportunities for networking between sites, building lasting links and sharing learning.
The POPS toolkit contains essential resources for establishing a local POPS service including clinical materials (such as guidelines, and letter templates), education and training materials (such as teaching programmes, slide sets), and business materials (such as core outcome sets, business plans and annual reports).
Implementation of a measurement for improvement approach is another key aspect of the programme, with sites benefitting from the support of data analysts throughout. Specific improvement measures are defined, with many sites impacting process-related measures such as length of stay and readmission rates.
These new POPS services have been established with differing initial clinical aims, including; developing pre-operative elective assessment pathways; frailty recognition; pain management in emergency general surgical patients and establishing a silver trauma service.
The national shortage of geriatricians has required innovation to establish new POPS services. One such innovative model is the POPS service at Lewisham and Greenwich (LGT) NHS Trust in South East London. Working closely with Guy’s and St Thomas’ Trust, a senior nurse with POPS experience was identified as the lead for the POPS Network project at LGT.
The project began in December 2021 (Table 1 timeline), focusing on emergency general surgical patients at one site in the trust. To maintain fidelity to established POPS services,
attendance at the nursing and surgical early morning handover proactively identi fi ed patients who would benefit from CGA and optimisation.9 This was coupled with a ‘don’t wait to be asked’ style of case-finding where everyone over the age of 65 years was screened.
These methods complemented each other and allowed early input in patients who might be missed on screening by frailty score alone. In particular, it allowed inclusion of those living with mild frailty, or as highlighted in our data analysis, those where frailty had not been accurately assessed.
Once identified, each patient underwent CGA and optimisation, either in ED or when admitted to the ward. Attendance at the ward discharge MDT ensured support for the discharge planning process. The senior POPS nurse worked autonomously with clinical support from a consultant geriatrician.
Prospective patient data was collected for every patient contact.
Summary of impact: ✦

Successful embedding of proactive frailty liaison service into emergency general surgery pathway ✦
>600 patients reviewed by POPS team across two sites (11 months) ✦
Length of stay reduction: two day reduction for all patients >65 years of age identified as frail (CFS 5+). ✦
Discrepancy noted between initial ‘clerking’ frailty assessment and CGA-informed clinical frailty scale score (CFS). This led to QI-team-led, ward-based education to support accurate frailty assessment by ward teams increasing accuracy of assessment
Table 2. Business case summary (text in blue denotes what is being asked for)
✦ Reduced workload for other teams, including fewer referrals to the medical frailty service
✦ NELA impact: geriatric specialist input for 70% of all appropriate NELA cases JulyAugust 2022 (previously 10-20%).
✦ A business case for continuation of POPS service was presented in November 2022 (Table 2).

Innovative use of the available workforce to deliver CGA and optimisation for an older surgical population living with multimorbidity and frailty is crucial to providing goldstandard perioperative care. This case study describes one example of successfully delivery in a district general hospital using the NHS Elect trimodal approach of expert mentoring, a toolkit of resources and
measurement. Adapting to local challenges, innovation in the workforce model and stakeholder buy-in was key to delivering change.
Link to References
The implementation of perioperative healthcare services can be challenging and requires sustained enthusiasm. The prehabilitation service at University College London Hospitals (UCLH) was opened in November 2021 and has received over 115 referrals from six surgical specialities to date. Although several barriers were encountered, the service continues to expand and was recently awarded the UCLH Celebrating Excellence award. We hope to offer some insight into how this perioperative service was developed and introduced using Kotter’s

Generating interest and creating sense of urgency will help prioritise your project. Utilise supporting evidence in the literature, or best practice at centres of excellence, and compare this to local data. Patient stories can be very powerful and may garner emotional engagement.2
Prehabilitation is supported by the Centre of Perioperative Care 3 as a strategy for transforming surgical wait lists into active preparation times and successful programmes


eight stage model of transformational change as a framework1Figure 1. Key goals of the UCLH prehabilitation service
have been established around the UK (e.g. in Wessex4 and Greater Manchester5). There is increasing interest in the growing success of prehabilitation at trust and departmental level, underlined by emerging evidence suggesting that rehabilitation can halve postoperative complications after major abdominal surgery6, lead to faster recovery7,8 and be emotionally beneficial to patients9 Engagement with colleagues will also allow you to identify those who share your enthusiasm and may wish to collaborate.

Perioperative medicine is truly a multidisciplinary team (MDT) endeavour, and it is essential to find colleagues who share your passion in the project. An enthusiastic team will create drive, find innovative solutions to challenges and allow networking within a wide range of stakeholders.
The clinical lead of the prehabilitation service at UCLH is a consultant anaesthetist and intensivist with a research background in exercise physiology. The team consists of physiotherapists, a dietician, exercise physiologists, perioperative medicine fellows, a consultant anaesthetist with a specialist interest in coaching, engaged surgical colleagues and administrative support. Regular communication is promoted with a weekly meeting dedicated to non-clinical aspects of the service.
✦ Develop a vision with: Project aims
Determine your project’s goals as a team and identify those which are essential and aspirational, focusing initial resources on the services’ key principles. Flexibility will be needed to embed your service into existing
pathways but clear goals help prevent project drift.
Key goals of the UCLH prehabilitation service are outlined in Figure 1.
With the core goals identified it is then possible to develop specific, measurable, attainable, realistic and time related (SMART)10 aims. This allows ongoing service improvement and can demonstrate measurable success to stakeholders and funders. Embedding quality improvement methodology from the outset allows challenges to be addressed using structured methodology.
✦ Develop the vision: Outcomes
Outcomes measures will quantify success and should be carefully considered from the inception of the service. Some required metrics will defined by your SMART aim but they can also align your project with research or funding interests.
We use a secure database in order to collect basic service information including the number of patients being referred to the service. Data is also collected on pre- and post-prehabilitation physiological parameters and qualitative feedback from patients. Outcome metrics including length of stay and morbidity help align the service with those trust priorities focused on tackling surgical waiting times and may help secure future funding.
A patient’s perioperative pathway is often complex, involving multiple teams and appointments, and frequently varies between surgical specialities. Mapping patient pathways allows visualisation of how your service may integrate into existing structures. Considering each stage of a process can highlight barriers and those external stakeholders needed to implement your project. The prehabilitation patient pathway is illustrated in figure 2.
Whilst your close coalition will be enthusiastic about the project there are likely to be many other stakeholders who need to be engaged to embed your service. ✦
Key surgeons, anaesthetists, specialist nurses and oncologists were identified as being proponents of prehabilitation. Collaboration with these early adopters allowed wider distribution of the prehabilitation ‘vision’ from proposed patient benefits to the practicalities of making referrals. Communication also relies on listening to those using your service and working with stakeholders to minimise additional work and disruption on their part. ✦

Arguably the key stakeholder in all perioperative services are the patients that those initiatives are designed to serve. Including patients in service design and feedback can provide an insider perspective and provide solutions to issues e.g. poor patient engagement. All patients have been asked to provide feedback on the
prehabilitation service and a number have agreed to help with a mentoring service, for future patients, which is in development. ✦
Those stakeholders funding your service will need a clear business plan alongside the vision for your service.
Establishing overall service goals and setting aims empowers all members of the team to drive new services forward. Assigning smaller projects, based on specific aims, and regular meetings to discuss progress allows individuals to work independently but within a supportive team environment.
Celebrate Quick Wins
Some project outcomes may take months or years to become apparent, for example changes in length of stay or mortality. It is therefore important to consider what demonstrates success in the short term. This could be as simple as receiving the first referrals and interacting with the first patient cohort.
An early ‘win’ experienced by the UCLH team was the first quantifiable improvement in CPET results seen in a patient who had completed the programme. The sense of achievement helped unite and motivate the team. Conviction in the service was further compounded by patient feedback which was often shared at the team Tuesday meeting.
Celebrating wins within the team is vital in maintaining drive and enthusiasm but should also be widely shared to sustain change.
The prehabilitation service successes have been presented in forums ranging from local presentations to international meetings. Demonstrating value increases credibility and creates leverage when redesigning aspects of your service or when persuading other teams to engage.
Celebrating achievements maintains drive, encourages others to adopt practices and is one step towards embedding the process in
culture so that engagement becomes the norm rather than the exception.
Sustaining change can be just as challenging as implementing a new service. Projects which rely on a single individual or have unintended adverse consequences are especially vulnerable. The UCLH prehabilitation service benefits from having a team of motivated colleagues such that when individuals are not available the service continues to run. Planning future developments can also help maintain momentum and widen the network of influence your service has. We have recently expanded into two new surgical pathways, including maxillofacial surgery, developed an online

training programme and have plans to launch a wearables component of the service.
Implementing and sustaining perioperative healthcare services can be challenging. Creating a robust plan, generating enthusiasm and gathering a supportive coalition are all essential. Embrace challenges as an opportunity to develop the service and celebrate the wins. Sustainability is as important as establishing a project and requires ongoing commitment and demonstration of financial value.
Link to references




At DAS 2022 we polled attendees on their routine practice of obstetric GA, and we present the results here.
A variety of strategies are available to support pre-oxygenation. Face mask breathing until EtO2 is >0.9 was stated as the preferred technique by 46% of delegates. Interestingly the percentage of those using high flow nasal oxygen (HFNO) to pre-oxygenate (14%) is the same as those using tidal volume breathing for 3 minutes (14%). There is evidence in nonobstetric patients with obesity that HFNO, when used as a technique for preoxygenation and apnoeic oxygenation during rapid sequence induction (RSI), can prolong the apnoeic period.1 In pregnant women, there is no evidence of bene fi t of HFNO as a preoxygenation tool.2 However, one small study did suggest that it can confer benefit when used during the apnoeic period of RSI, as assessed by the surrogate marker of arterial PaO2 immediately after intubation.3 It is noteworthy that this study was confined to elective GA for caesarean section in patients with a normal BMI.
23% of DAS 2022 attendees routinely use apnoeic oxygenation during obstetric GA, with just 17% of attendees stating they never use it. In non-obstetric patients, there have been two interesting studies investigating THRIVE. One demonstrated a prolonged apnoea time in the HFNO THRIVE group compared to the
facemask preoxygenation group, 4 and the other demonstrated increased incidence of desaturation below 93% in the facemask group compared to the THRIVE group. 5 However, a clinical trial has yet to be undertaken in obstetric patients.6
The majority of delegates (58%) are now using rocuronium as compared to 40% still using suxamethonium. This shift to rocuronium in obstetrics has been slow, in contrast to nonobstetric practice. There is debate around time to- and quality of- intubating conditions, incidence of anaphylaxis between suxamethonium and rocuronium, and the cost of sugammadex. However, as it becomes more evident that adequate paralysis is importance for optimising first-pass intubation success and effective facemask ventilation7 (facemask ventilation is crucial as part of the OAA-DAS guidelines 8 to ensure rescue oxygenation), it is likely that rocuronium will continue to increase in acceptance.
Most attendees routinely use opioids at induction (42%), with 24% sometimes using opioids and 21% rarely using opioids. Just 13% never use opioids at induction. That 13% of respondents never use opioids at induction is perhaps surprising. The use of opioids at induction has a vital role in minimising the hypertensive response to laryngoscopy,


particularly relevant in patients with hypertensive disorders of pregnancy and also in reducing the risk of accidental awareness. A recent meta-analysis found no difference in neonatal Apgar scores with remifentanil and alfentanil use at induction of GA.9
54% of attendees use videolaryngoscopy as the first line intubating device for obstetric GA and 27% stated this practice has developed over the last year. For 40% of attendees, videolaryngoscopy is their Plan B. Provided the anaesthetist is appropriately trained, there is now compelling evidence that videolaryngoscopy provides improved laryngeal view and higher rates of successful intubation.10
From this snapshot, it seems that practice for obstetric GA is slowly changing in-line with best evidence available and to become more consistent with RSI in non-obstetric practice. There are important gaps in our knowledge, and further investigation – particularly into apnoeic oxygenation in parturients – is crucial.
Link to references



 | Rucha Vora | Yumna Haroon-Mowahed | Emilie Hoogenboom |
| Rucha Vora | Yumna Haroon-Mowahed | Emilie Hoogenboom |


#AirwayHub is an innovative initiative by University College London Hospital (UCLH) anaesthetic department providing multidisciplinary airway education. It has grown since its introduction in January 2017 to a now well-established, easily accessible pan London educational platform in Airway management.
What is it?
#AirwayHub provides well-executed monthly teaching and training in an inclusive multidisciplinary setting, with special focus on clinical skills, teamwork and communication.

Expert faculty from different specialist centres, currently within London, contribute to the educational sessions. The programme is free, open to all and can be accessed virtually. Meetings typically starts with a practical skills station. These offer a variety of workshops including high- fl ow nasal oxygen demonstration, emergency front of neck airway mannequin practice, paediatric airway management, tracheostomy and airway ultrasound.
Free Open Access Medical Education (FOAM)
Figure 1. Examples of past presentations and workshops
We believe in medical education for anyone, anywhere, anytime. #AirwayHub meetings are announced through mailing lists, social media and via the London school of anaesthesia. We encourage airway experts and enthusiasts to join us physically or virtually in our meetings to share and discuss all airway matters. We also provide regular live updates for our worldwide followers via our Twitter handle (@AirwayHub).
It started in January 2017 at UCLH in response to the expanding head and neck surgical services and increasing perioperative airway emergencies. Since then, it has grown from strength to strength. As of January 2018, we were running a Pan London ‘Hub and Spokes’ format based at UCLH (the Hub) and closely linked to external sites (the spokes) who host the meeting generating further exchange of knowledge and best practices. Prior to the COVID pandemic the delivery of presentations happened physically in the “spokes” sites, including the Royal Marsden, GOSH and the Royal London. With the advent of virtual platforms we have moved the delivery predominantly at UCLH with guests presenting either at UCLH or virtually.

There is an average of 30-40 attendees each month comprising of anaesthetists,

intensivists, operating department practitioners, paediatricians, critical care nurses, physiotherapists, speech and language therapists and surgeons. As the sessions are multidisciplinary informal sessions, it offers the perfect setting for learning and exchange of ideas and practices.
The participants report that both the skills station and lectures have improved their con fi dence in managing dif fi cult airway scenarios and performing various airway techniques. #AirwayHub has been particularly popular amongst anaesthetists in training, and we encourage other specialities to join in the talks and discussions. The learning objectives are matched to RCoA syllabus and allows them to practice their practical skills. It also holds RCoA approved CPD points.
The Airway Fellows at UCLH are heavily involved in the design, organisation, and
delivery of the program, developing their skills in education, leadership and management.
What does the future hold?
We aim to extend this monthly educational platform to all centres across the country and even on an international level with the help of technology. In the coming months we will be discussing Exovent (Negative pressure ventilation), prehabilitation in head and neck surgery, discussing difficult airway cases and human factors in airway management from experts in the field. #AirwayHub is awarded 2 RCoA approved CPD points.
To find out more about #AirwayHub, or if you are interested in collaborating/ organising a joint meeting in your department, please follow our twitter handle or contact our team at UCLH (Dr Yumna Haroon-Mowahed: y.haroonmowahed@nhs.net or Dr Emilie Hoogenboom: e.hoogenboom@nhs.net).
#AirwayHub provides an open access, multidisciplinary educational platform to learn, share and discuss all airway matters. It encourages inter-professional communication and collaboration within the London region and beyond.
Welcome to the DAS Journal Club - Recommended Reads. Papers are chosen by members of the DAS committee, with short citations/summaries by members of the ezine editorial team. This edition's recommended reads come from Kariem El-Boghdadly with summaries by Moon-Moon Majumdar. We welcome members feedback and thoughts on the papers featured - please tweet us @dastrainees or @dasairway or email us at ezine@das.uk.com
Preventing unrecognised oesophageal intubation: a consensus guideline from the Project for Universal Management of Airways and international airway societies
✦ N Chrimes, A Higgs, C A Hagberg, P A Baker, R M Cooper, R Greif, G Kovacs, J A Law, S D Marshall, S N Myatra, E P O'Sullivan, W H Rosenblatt, C H Ross, J C Sakles, M Sorbello, T M Cook. DOI: 10.1111/anae.15817
Following the tragic death of Mrs Glenda Logsdail following an unrecognised oesophageal intubation and other similar deaths around the world, this consensus guideline from the Project for Universal Management of Airways (PUMA) is essential reading for every anaesthetist. With contributions from a number of international airway societies, this guideline addresses both technical interventions, strategies to address cognitive biases, and team performance.
Key recommendations include use of exhaled carbon dioxide monitoring and pulse oximetry for all episodes of airway management, routine use of a videolaryngoscope whenever feasible, verbalisation of 'sustained exhaled carbon dioxide' after intubation, and active exclusion of oesophageal intubation if there is not 'sustained exhaled carbon dioxide'. They clarify exact criteria for sustained exhaled carbon dioxide and discuss methods of excluding oesophageal intubation. They also address broader educational requirements to address the team aspects of task performance to implement the guidelines.
Whilst there isn't necessarily a 'results' section to debate or a statistical test to pick apart, the strategies in this guideline are crucial learning for all of us and this certainly warrants discussion in detail at your departmental journal club.
Will your practice change based on this paper?
Sedation versus General Anesthesia for Tracheal Intubation in Children with Difficult Airways: A Cohort Study from the Pediatric Difficult Intubation Registry
✦ Luis Sequera-Ramos, Elizabeth K Laverriere, Annery G Garcia-Marcinkiewicz, Bingqing Zhang, Pete G Kovatsis, John E Fiadjoe; PeDI Collaborative https://doi.org/10.1097/ ALN.0000000000004353
This October 2022 study uses data from from the international Pediatric Difficult Intubation Registry, which prospectively collects data about tracheal intubation in children with difficult airways and compares sedation versus general anaesthesia (GA) in these patients. Whilst sedated/awake tracheal intubation approaches are considered safest in adults with difficult airways, we know very little about the outcomes of sedated intubations in children.
This study compares sedation and GA for their primary outcome of first-attempt success of tracheal intubation in children. There is lots to learn from this article, both about airway management and study design: what do you think are the limitations of this paper? What does 'sedation' here actually mean? This study is the starting point of some fascinating discussion and we would love to hear what transpired from your journal club: tweet us @dastrainees or email ezine@das.uk.com
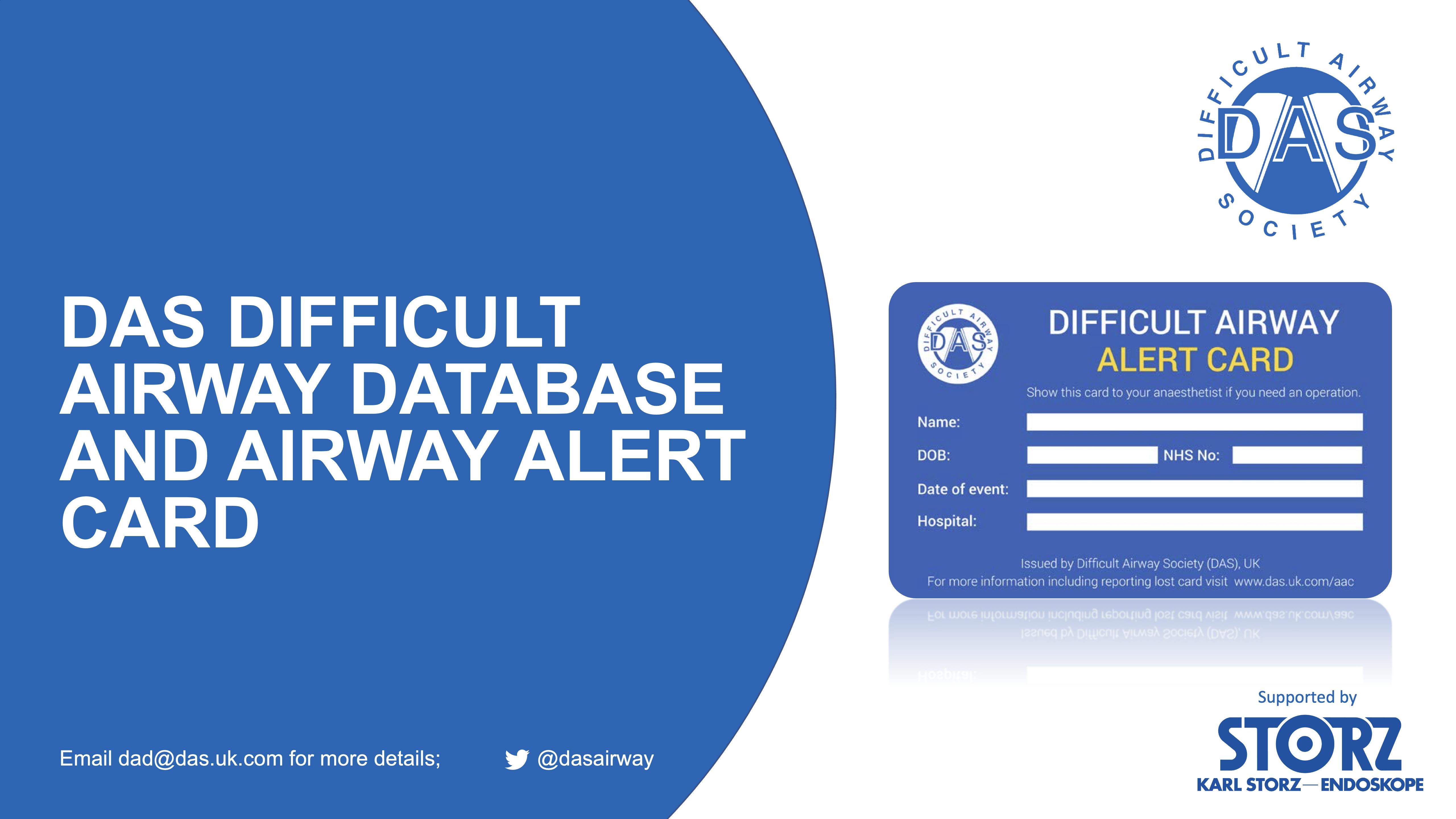
DAS Difficult airway database is continuing its expansion across the country and several national organisations have confirmed their official support to the project in the last few months. The following is the list of organisations supporting us:
✦
Society for Obesity and Bariatric Anaesthesia (SOBA)
If your hospital is not yet part of this project and you are interested in taking the lead role locally, please do get in touch with us via dad@das.uk.com. If you work in a hospital which is already a part of the project, please encourage your colleagues to submit the data promptly and let us know if you have any feedback about the project or the process of submission.
✦
Association of Anaesthetists (AoA) ✦ Obstetric Anaesthetists Association (OAA) ✦
Royal College of Anaesthetists (RCoA) ✦
Safe Anaesthesia Liaison Group (SALG) ✦
Association for Perioperative Practice (AfPP) ✦ College of Operating Department Practitioners (CODP) ✦ Society for Education in Anaesthesia (SEAUK)
✦ UK Society for Computing and Technology in Anaesthesia (SCATA-UK) ✦
Intensive Care Society (ICS)
Here is the comparison of current figures with those from September 2021:
Sept 21
Current Status
150 Hospital sites 190
820+ submissions 1200+
1935 Access logins 2500+
The analysis of the data collected over the fi rst fi ve years has very recently been published in Anaesthesia! Here's the link
DAS Airway Alert Card and Difficult Airway Database - How to join the project?
-----------------------------------------------------
Check if your hospital is already on the project https://das uk com/content/dad sites If not, please follow the steps below

Some useful links are: DAS Database main page and the list of Trusts currently taking part in the project. Other project related documents can be found here
Dr Achuthan Sajayan dad@das.uk.com Co-Lead, DAS Difficult Airway Database
https://das.uk.com/dad
Download the patient information and consent form from the DAS website https://das.uk.com/aac/con sent_form
Discuss with the patient and obtain the consent.
Please make sure the patient has recovered fully from the effects of anaesthesia. Recovery room is not a recommended place for consenting.
Give one copy to the patient and keep one in the records
If you are not a DAS member, you need to register with the database before submitting data.

Registration is free and only takes few minutes.
Please follow this link https://das.uk.com/das_user/ acaregister
Once the data is submitted, there will be an option to print out the summary of the event. Please print two copies, give one to the patient and keep the other in the patient records.
If you are a trainee or specialty doctor, please discuss with your supervising consultant before submitting the data and provide their name
There will also be an option to print out a letter to the GP. This can either be sent directly to the GP or give it to the patient with instructions to hand over to their GP.


 | Ellen O’Sullivan |
| Ellen O’Sullivan |
Following on from the success of WAMM1, held in Dublin in 2015, and WAMM 2 in Amsterdam in 2019 we plan to run a WAMM 3. Dates and venues are presently being discussed.
| References 1/2 |
1. NELA Project Team. Seventh Patient Report of the National Emergency Laparotomy Audit. (2021). https:// www.nela.org.uk/Seventh-Patient-Report
2. Hewitt, J., Carter, B., McCarthy, K., Pearce, L., Law, J., Wilson, F. V., Tay, H. S., McCormack, C., Stechman, M. J., Moug, S. J., & Myint, P. K. (2019). Frailty predicts mortality in all emergency surgical admissions regardless of age. An observational study. Age and ageing, 48(3), 388–394. https://doi.org/10.1093/ageing/afy217
3. Parker, S. G., McCue, P., Phelps, K., McCleod, A., Arora, S., Nockels, K., Kennedy, S., Roberts, H., & Conroy, S. (2018). What is Comprehensive Geriatric Assessment (CGA)? An umbrella review. Age and ageing, 47(1), 149–155. https://doi.org/10.1093/ageing/afx166
4. Partridge, J. S. L., Healey, A., Modarai, B., Harari, D., Martin, F. C., & Dhesi, J. K. (2021). Preoperative comprehensive geriatric assessment and optimisation prior to elective arterial vascular surgery: a health economic analysis. Age and ageing, 50(5), 1770–1777. https://doi.org/10.1093/ageing/afab094
5. Partridge, J. S., Harari, D., Martin, F. C., Peacock, J. L., Bell, R., Mohammed, A., & Dhesi, J. K. (2017). Randomized clinical trial of comprehensive geriatric assessment and optimization in vascular surgery. The British journal of surgery, 104(6), 679–687. https://doi.org/10.1002/bjs.10459
6. Kocman, D., Regen, E., Phelps, K., Martin, G., Parker, S., Gilbert, T., & Conroy, S. (2019). Can comprehensive geriatric assessment be delivered without the need for geriatricians? A formative evaluation in two perioperative surgical settings. Age and ageing, 48(5), 644–649. https://doi.org/10.1093/ageing/afz025
7. Centre for Perioperative Care, British Geriatrics Society. (2021). Guideline for Perioperative Care for People Living with Frailty Undergoing Elective and Emergency Surgery. https://www.cpoc.org.uk/sites/cpoc/files/documents/2021-09/ CPOC-BGS-Frailty-Guideline-2021.pdf
8. Rogerson, A., Partridge, J. S. L., & Dhesi, J. K. (2018). A Foundation Programme educational placement in perioperative medicine for older people: mixed methods evaluation. Anaesthesia, 73(11), 1392–1399. https://doi.org/ 10.1111/anae.14410 Workstreams – Getting It Right First Time – GIRFT. (n.d.). Retrieved December 6, 2022, from https://www.gettingitrightfirsttime.co.uk/workstreams/
| References 2/2 |
9. Joughin, A. L., Partridge, J. S. L., O'Halloran, T., & Dhesi, J. K. (2019). Where are we now in perioperative medicine? Results from a repeated UK survey of geriatric medicine delivered services for older people.Age and ageing,48 (3), 458–462. https://doi.org/10.1093/ageing/afy218
10. Jasper, E. V., Dhesi, J. K., Partridge, J. S., & Sevdalis, N. (2019). Scaling up perioperative medicine for older people undergoing surgery (POPS) services; use of a logic model approach. Clinical medicine (London, England), 19(6), 478–484. https://doi.org/10.7861/clinmed.2019-0223
1. NHS select; Kotter’s 8 steps of change. Website Address: https://www.nhselect.nhs.uk/uploads/files/1/ Kotter%27s%208%20steps%20of%20change.pdf)
2. Dixon-Woods M, McNicol S, Martin G. Ten challenges in improving quality in healthcare: lessons from the Health Foundation’s programme evaluations and relevant literature. BMJ Qual Saf. 2012. Doi:10.1136/bmjqs-2011-000760
3. Centre for Perioperative Care. Delivering on Government priorities and for an NHS in crisis; Investing in perioperative care path fi nders. Sept 2021. Website Address: https://cpoc.org.uk/sites/cpoc/ fi les/documents/2021-10/ The%20Centre%20for%20Perioperative%20Care%20HMT%20Representation%20Sept%202021.pdf
4. https://wessexcanceralliance.nhs.uk/wesfit-project/
5. http://www.prehab4cancer.co.uk/
6. Barberan-Garcia A, et al. Personalised prehabilitation in high-risk patients undergoing elective major abdominal surgery: A randomised blinded control trial. Ann Surg. 2018 Jan. 267(1):50-56
7. Jensen BT, Petersen AK, Jensen JB, Lausten S, Borre M. Efficacy of a multiprofessional rehabilitation programme in radical cystectomy pathways: a prospective randomized controlled trial. Scand J Urol. 2015 April; 49(2):133-41.
8. Nilsson H, et al. Is preoperative physical activity related to post-surgical recovery? A cohort study of patients with breast cancer. BMJ Open. 2016;6:e007997.
9. Website address: http://www.prehab4cancer.co.uk/success-stories/
1. Schutzer-Weissmann J, Wojcikiewicz T, Karmali A, Lukosiute A, Sun R, Kanji R, Ahmed AR, Purkayastha S, Brett SJ, Cousins J. Apnoeic oxygenation in morbid obesity: a randomised controlled trial comparing facemask and highflow nasal oxygen delivery. Br J Anaesth. 2022 Jan 11:S0007-0912(21)00800-X. doi: 10.1016/j.bja.2021.12.011. Epub ahead of print. PMID: 35027169.
2. Shippam W, Preston R, Douglas J, Taylor J, Albert A, Chau A. High-flow nasal oxygen vs. standard flow-rate facemask pre-oxygenation in pregnant patients: a randomised physiological study. Anaesthesia. 2019; 74: 450-456.
3. Zhou S, Zhou Y, Cao X, Ni X, Du W, Xu Z, Liu Z. The efficacy of high flow nasal oxygenation for maintaining maternal oxygenation during rapid sequence induction in pregnancy: A prospective randomised clinical trial. Eur J Anaesthesiol. 2021 Oct 1;38(10):1052-1058. doi: 10.1097/EJA.0000000000001395. PMID: 33259452.
4. Mir F, Patel A, Iqbal R, Cecconi M, Nouraei SAR. A randomised controlled trial comparing transnasal humidified rapid insufflation ventilatory exchange (THRIVE) pre-oxygenation with facemask pre-oxygenation in patients undergoing rapid sequence induction of anaesthesia. Anaesthesia. 2017; 72(4): 439-443.
5. Lodenius A, Piehl J, Ostlund A, Ullman J, Josson Fagerlund M. Transnasal humidified rapid-insufflation ventilatory exchange (THRIVE) vs. facemask breathing pre-ixygenation in adults: a prospective randomised non-blinded clinical trial. Anaesthesia. 2018; 73: 564-71.
6. Lucas DN, Russell R. Pre-oxygenation vs. apnoeic oxygenation in obstetrics. Anaesthesia. 2019; 74(6): 822-823.
7. Ide A, Nozaki-Taguchi N, Sato S, Saito K, Sato Y, Isono S. Rocuronium versus saline for effective facemask ventilation during anaesthesia induction: a double-blinded randomized placebo-controlled trial. BMC Anaesthesiol. 2022; 22(1): 173.
8. https://www.oaa-anaes.ac.uk/assets/_managed/cms/files/Clinical%20Guidelines/Guideline_Algorithms_2015.pdf
9. White LD, Hodsdon A, An GH, Thang C, Melhuish TM, Vlok R. Induction opioids for caesarean section under general anaesthesia: a systematic review and meta-analysis of randomised controlled trials. Int J Obstet Anesth. 2019; 40:4-13.
10. Trent SA, Kaji AH, Carlson JN, McCormick T, Haukoos JS, Brown CA. Video Laryngoscopy is associated with first-pass success in emergency department intubations for trauma patients: a propensity score matched analysis of the national emergency airway registry.