



Survival
x BreakFreeofSurvivalMode &ReduceYou
A collection of chapters from th book, The
Parado

ve medicine esearcher. ch institutes, ationally mplex ealing. He is cal director of
Beyond an approach anchored in decades of science and research, Dr. Eliaz embraces a profound mind-body model of healing that unlocks your body’s infinite potential with the creation of Open Heart Medicine. As a life-long meditation practitioner and expert in mind-body medicine, Dr. Eliaz offers regular meditation classes and teachings, sharing his unique model of mind-body medicine and healing practices to support long-term health and wellness.

“I’ve learned to let go of our current medical system’s dogmatic paradigms, both conventional and alternative. People often say I think ‘outside the box,’ to which I reply, there was never a box to begin with.”
— Isaac Eliaz, MD, MS, LAc

ONE
RebeccafirstcametoseemeatAmitabhaMedicalClinicin2011.Shewas seventy,withstage4lungcancerthathadmetastasizedtoherbones.Shehadno familyandlivedalone;hercompanionthatdaywasastone-facedchauffeur waitinginacaroutsidetheclinic.Withtearsinhereyes,shetoldmeshehad justbeendiagnosed.Handsshaking,sheshowedmethePETscanreport highlightingthemultipletumorsthroughoutherbody.Basedonwhatthe oncologistsaid,sheunderstoodthatherlifecouldcometoanendverysoon.
“Idon’twanttodie,”shesaid.“I’mnotreadytogo.”Everycellinherbody wasreelingwithanxietyandfear.Herrestlessnesswaspalpableintheair.
Asanintegrativephysicianwhotreatscancer,I’dhadthisconversationmany times.Ihandedheratissueandshewipedhertears.“IwilldoanythingIcanto overcomethiscancer,”shesaidfirmly.Iacknowledgedherfiercedetermination, herresolve.Afterall,determinationiswhat’sneededfirstandforemostto overcomeadeadlydisease,right?
Withheranxietysopalpable,Iwonderedhowthisfearmustbeaffectingher. Notjustonthelevelofheremotionsorqualityoflife;Iwonderedhowitwas affectingthecancercells.Willthisfear-baseddeterminationnottodiehelpher overcomeherdisease?Orwillitcausehertobecomesickerandshortenherlife? Heranxietywassoprominentthatitinfusedhersurroundings,affectingher abilitytotakeadeepbreath.Itwasconstantsuffering,anditwasclearshewas in“survivalmode.”
Beinginsurvivalmodemeantthathersympatheticnervoussystem hormones,thedriversofherinnatebiochemicalresponsepatterns,weredialed allthewayup.Heradrenaline,noradrenaline,andcortisolwereelevated,and herinsulinwasspiking.Herimmuneresponsewasbeingsuppressed,andher metabolic function was altered. Ultimately, it meant that many of the compoundssheexcretedinanefforttosurvivewouldverylikelynourishher cancerandallowittogrowandsurviveaswell.
Survivalmodeisoftenastateofstressandpanic.Thebodyfeelsrushedand doesn’tslowdown,andallcells,whethernormalorcancerous,fightharderto survive.Thus,Rebecca’sanxietyandfearofdyingcould“feed”thecancerous cells.Herbestchanceatbeatingthecancerandlivingalongerlifewastoshift awayfromsurvivalmodeandmoveintoastateofgreaterrelaxation,withless reactivityonthecellular,emotional,andpsychologicallevels.
Basedonresearchandmyyearsofworkwithpatients,onethinghasbecome clear: when facing a life-threatening or debilitating illness, the natural biochemicalstressresponse,ourinnatefight-or-flightmechanismsthatare drivenbyourinstincttosurvivearefundamentallyatoddswithourabilityto healandthrive.Thissurvivaldrive,rootedinoursympatheticnervoussystem andexpressedbyourbiochemicalalertsystem,isnotgoingtosaveus.Infact,it canharmus.
Howdoesthisphysiologicalresponsesystemturnagainstussodramatically, fuelingdiseaseprocessesandprematureaging?Andmoreimportantly,whatcan wedoaboutit?
Thegoodnewsis,wecandoalot.Andwecandoitinawaythatisactually simplerthananyonefacingacomplexhealthcondition—patientorprovider— mighthaveimagined.
We’llcontinuetodiscussthedetailsofRebecca’streatmentandoutcomesin thenextchapter.Iwitnessedsomethingincredibleinhercase,aswellasin manyothers.SomethingthatBruceLipton,DeepakChopra,andmanyothers havewrittenabout,andwhattheyogisandmysticshavebeensayingfor millennia: the mind can influence the body to heal spontaneously and completely.Themindcandeliverthebodyfromthebrinkofdeathanddisease tovitalityandlongevity.
THE CATCH-22 OF “POSITIVE THINKING”
Publishedevidenceonthemind-bodyconnectionissignificantandgrowing rapidly,andbasedonmypersonalandclinicalexperience,theresultscanbe exponential.Itspoweriswithinusallthetime,andit’sabsolutelyavailablefor ustouse.
So,
Ifmind-bodymedicineistheclinicallystudiedgoldstandard“alternative” deemedthesafestandmostbeneficialtreatmentandincreasinglyadoptedand appliedinclinicalsettingsaroundtheworld,itstandstoreasonthatmanymore peoplewouldbeabletomeditateor“positivelythink”theirdiseaseinto remission.
It’stheultimatecatch-22:whensomeoneisfacingalife-threateningdisease, askingthemtorelax,changetheirthoughtpatterns,andfocusonhappy, healingenergyismucheasiersaidthandone.It’slikeaskingsomeonewhose houseisonfiretostaycalm,thinkpositively,anddeeplyinhalethesmokefrom theirburninghome.
We’rebuiltforsurvival.Wedon’tjustwantbutintrinsicallyneedto overcomediseaseandtoheal.I’vecometofind,basedonextensivepublished researchandyearsofclinicalobservation,thatthissurvivaldriveistheone majorblockagestandinginthewayofwould-besuccesses.
Inanerawhenwetendtolookforquickfixesandsymptomsuppressors, we’rereallyjustsuppressingourhealingcapacity.Wedon’ttakethetimeto stop,slowdown,andlookwithin.Theideathatwedon’thavetime—thatwe must rush, and must compete with everyone, including ourselves—is detrimentaltoourhealthandwell-being.
WhatRebeccaneededaboveallelsewastoslowthissympatheticnervous systemresponse,butshecouldn’t.Herhousewasburningdown,and shecouldn’ttakeadeepbreathinthemidstofwhatappearedtobealifethreateningsituation.
Whenweexperienceasenseofrestlessness,notfeelingsafe,ornottrusting ourenvironmentandcommunity,itcantranslateallthewaydowntothe cellularlevel.Whenwefeelunsafeandbelieveweneedtosurviveonourown, itchangesthemetabolismandfunctionofourcells—theyreceivesignalsfrom theirenvironmentthatthereisalackofoxygen.Theformaltermforlackof oxygenishypoxia,andthehypoxiccellcan’tbreatheornaturallyrelax.(In cancerhowever,thecellsbehavethiswayeveninthepresenceofoxygen, whichwe’lldiscussindetaillaterinthebook.)
Tobeginthehealingprocess,weneedtomoveahypoxiccelltoaplace whereitfeelsitcanbreathe,createanormalmetabolism,andreturntonormal mitochondrialfunction.Todothis,thecellandthepersonmustshiftawayfrom astateofsurvivaltowardastateofrelaxation.Toachievesuchachange,the personasawholemustexperiencesafetyandbalanceallthewaytothecellular level.Thesurvivalalarmhastobeturnedoff!
So,howdidRebeccaandIbeginaddressinghercancer?Howwassheableto takeadeepbreath?Weworkeddirectlyonherbiochemistry.Wedidn’tjust circumventherfearandanxiety—wetransformedit.Weusedcertainnatural compoundstoquietthealarmsystem,normalizethecell,andfightthecancer.
Wecombinedthosecompoundswithmeditation,breathingexercises,regular acupuncture,andhealingsessionswithdifferentmodalities,includinghands-on osteopathic,craniosacral,sound,andvisualizationtherapies.Mostimportantly, we surrounded her with unconditional love and affection, a sense of community,andanenvironmentthatheldherwithoutjudgment—wecreateda worldwhereshefeltsafeandloved.
Themind-bodyconnectionisamazing,andit’snotaone-waystreet.Emotions, thoughts, and subconscious responses clearly affect our biochemistry, our physiology,andoursubjectiveandobjectiveexperiencesofhealthanddisease. Atthesametime,ourbiochemistrysharplyaffectsouremotionsandour thoughts.Itaffectswhoweareatthecore.
Meditationandothermind-bodypracticescanundoubtedlygiveusthe quantumedgeinhealing.Theyworknotonlybecausetheycancalmour anxiety,reduceinflammation,andreverseourbiochemicaldiseaseprocesses— theyalsoworkbecausetheymeltourrigidityandrelaxourfixations.They dissolvetheliteralboundariesbetweenthepersonandthedisease,allowingthe person to reach and engage the tumor, the atherosclerotic plaque, the burrowingLymespirochete,oranyotheropportunisticinfection.
However,mind-bodymethodslikemeditationcanonlyunleashourinnate healingpotentialwhenwefigureouthowtotrulyengageourhearts.Inthis regard,amoreaccuratetermforthistypeofhealingis“heart-bodymedicine” ratherthan“mind-bodymedicine.”Itisheartfulnessratherthanmindfulness.I callthis“openheartmedicine.”
Thebasicphysiologyofourheartandthefundamentalmechanicsofthisvital organfunctioninawaythatactuallyallowsandsupports“miracle”healing—an unexpectedpositiveoutcomethatdefiesprobability.
Ultimately,wehavetogetthroughthethinveneerof“positivethinking”and penetratethedeeperlayersofourdefenses.Ourinstinctualfearsandanxieties, whilepartofourinnatesurvivaldrive,obstructourhealingcapacityby triggeringbiochemicalchangesinourbodythatcreateliteralphysicalbarriers. Thesebarriersaremadeofdifferentcomponentsthatneedtobetreated.For example,therecanbehyperviscosity,whichisthicknessofthebloodthat hamperscirculationandtheabilitytodeliveroxygentothetissue;fibrosis, whichisthescarringorhardeningoftissuesandorgans;biofilmstructures, whichformprotectiveshieldsaroundtumorsandpathogens;andmore.Andall ofthiswilltranslateintochangesincommunicationsbetweenthecellandits environment.Thiscauseschangesinsidethecellsandaffectstheirfunction.
So,whatisthekeytoshiftingusfromsurvivaltoharmony?Fromdiseaseto longevity?Whatisthismetabolicsurvivalalarmthatmustbeturnedoff?
Researchershaveidentifiedonemasterproteinproducedbythebody,which isattheheadwatersofourbiochemicalalarmsystem.Thisproteindictatesour biochemicalandphysiologicalresponsetostress,illness,andinjury.
Themorestresswe’reunder,themoreourbodieswillviewlifeasabattle, leadingtoongoingconflictandfrictionwithin.Productionofthissurvival proteinwillrampupinanefforttoresolvetheconflictingdialoguebetweenthe bodyandtheoutsideworldandbetweendifferentsystemsandcellswithinthe body.Hereiswherewecanseetheparadoxofthissurvivalproteininaction.
Themolecularendresultofthisreactivedefensestrategyiscontraction, isolation,andoftendisease.Thesearesurvivalresponses,whicharedrivenby self-preservationbutunfortunatelyleadtoinflammationandfibrosis.These responsesalsoleadtodegenerationatthecellularlevel,organsystemlevel,and atthelevelofourwell-beingandlongevity.Theyhaltthecooperationbetween ourtrillionsofcellsthatwouldotherwiseseamlesslycommunicatewitheach otherinthemiracleoflife.Thebodyhasaninnatecapacitytohealitself—when thesurvivalresponsedoesn’tstandinitsway.
Nowthatyouknowwhatthesurvivalparadoxis,let’smeetitsmolecular architect.
Ifyou’veneverheardofgalectin-3,youaren’talone.Despitethefactthat therearethousandsofpaperspublishedaboutitsroleindrivingeverythingfrom cancertoheartandkidneyfailureandmuchmore,thevastmajorityofpeople— includingmosthealthcarepractitioners—haveneverheardofiteither!But you’reabouttohearalotaboutit.
Therearedifferenttypesofgalectins,butthemoststudied(yetlittle-known) one is galectin-3, a fascinating carbohydrate-binding protein. On close examination,itplaysanimportantroleinthebalancebetweenhealthand disease. It is the core component and initiator of our self-preservation mechanism.Icallit“thesurvivalprotein.”Let’sdefineexactlywhatitisand whatitdoesinsidethehumanbody.
Wheninjury,illness,orotherstressorsoccur,ourinnatesurvivalresponse triggerstheproductionandactivityofgalectin-3.Intheseinstances,galectin-3 initiatesacascadeofprocessesthatarenecessaryforinjuryrepair.Howeverif thealarmfailstoturnoffafterthethreatsubsides,galectin-3getsoutofcontrol and can seriously harm us.
Whengalectin-3activitycontinuesuncontrollably,iteffectively“goes rogue,”drivinginflammationandfibrosisratherthanhealing.This,inturn,can leadtonumerousdiseaseprocesses.What’smore,pathogenssuchasdifferent infectiousagentsandtumorscanhijackgalectin-3anduseitfortheirown survival.Thisisakeyissuethatcanbetreatedstrategically,andwe’llfurther explorethisconceptthroughoutthenextchapters.
Galectin-3isproducedor expressed indifferenttypesofcells.Inparticular, galectin-3isexpressedinimmunecells,inepithelialcells(theonesthatcoat certaintissuessuchasthoseoftheintestinesandlungs),inendothelialcells(the inner-liningcellsofthebloodvessels),andinsensoryneurons,amongothers.
Weunderstandthatgalectin-3canbebeneficialorharmful,buthowcanone proteinharmandbenefitusatthesametime?Togainabetterinsightintothis paradox—oursurvivalparadox—let’stakeajourneytogetherintothestructure ofthisprotein.
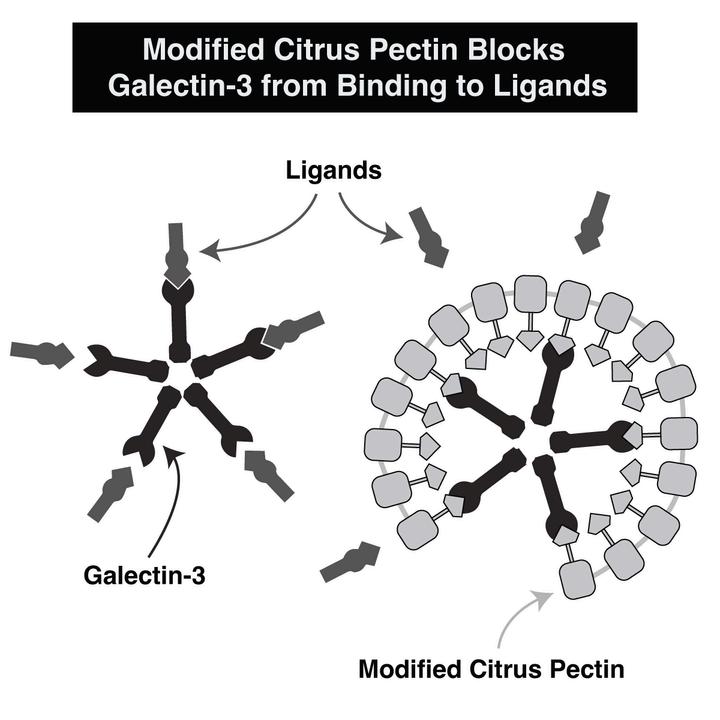
Galectin-3hasachimerastructure,meaningthat different structures from various sources come togethertocreateit(achimericcharacteryoumight befamiliarwithisFrankenstein:hewascreatedfrom manydifferentparts).Whengalectin-3isactivated, itcanbindtoothergalectin-3proteinsandother carbohydratestoformcomplexstructures.Uptofive individual galectin-3 proteins can stick together, creatingfive-sidedstructurescalled pentamers.
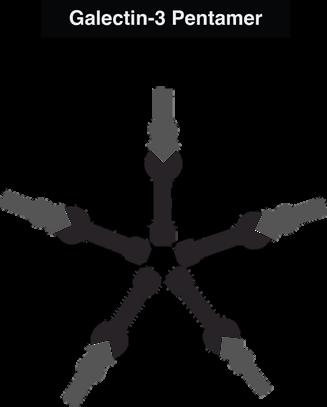
Whengalectin-3formspentamers,thesecanattachtoothergalectin-3 pentamers,toothercarbohydrates(sugars),andtocell-surfacereceptors,where thesestructurescanthenmediatecellreactionsandcontroltheinteraction betweenthecellandtheenvironment.Soundscomplicated?Itisabit.Butdon’t worry,we’llbreakitdown.
Oursurvivalprotein,galectin-3,isactivatedwhenweexperienceasudden threat,beitphysical,emotional,mental,orpsychological.It’salsoactivatedin casesofinjury,infection,cancer,orotherillnesses.Whengalectin-3isactivated, itturnsonmultiplepathwaysthatinitiateinflammationandtheprocessof fibrosis,andsuchscartissuebuild-upcanleadtohardeninganddysfunctionof tissuesandorgansystems.Furthermore,itcanalsooverexpressitselfinspecific areasofthebody,forexample,inthejoints,cardiovascularsystem,orthebrain. Andwhatistrulyamazingisthatitcanexertverydifferenteffectsatdifferent sitesbasedonwhatit’sboundto.
Tobetterunderstandthecomplexityofgalectin-3,let’srelateittothebigger picture:ourmodern-dayexistence.Weliveinaworldwherepeoplecontinue tobecomemoreisolated.Whenpeoplearelessconnectedtoeachotherandto theearth,allbecomeweaker.Weexploitandabuseournaturalresources,and weseetheeffectsofrapidclimatechange.Globalwarmingisaninflammatory processontheplanetarylevel.
Atthehumanlevel,ourinternalandexternalsenseofpeaceisdwindling,and ourattentionspansareridiculouslyshort.Wecannolongerwaitforweeks, days,orevenhourstogiveorreceivearesponse—wecanonlytoleratewaiting formilliseconds,andwefeeltheneedtoreactimmediatelytoeverystimulus.
Mostofuslivehigh-stresslifestylesinundatedwithelectronicandotherforms ofstimulation.Idon’tthinkit’sanexaggerationtosaythatourmodernsociety isinastateofoverwhelm.
Thecontinualbarrageofstimulifromeverydirection,theonslaughtof environmentaltoxins,theongoingmental,physical,andemotionalstresswe’ve grownaccustomedto—thesedisturbancesthrowusintosurvivalmodewhere oursystemsareonconstanthighalert,likeanalarmthatneverturnsoff.
Theresult?Unhealthygalectin-3expression,andwithit,progressivedamage tovitalorgansandsystemsoverthelong-term.This,inturn,fuelsmore galectin-3production,formingaperpetuallyclosedloopsystemthatisproving tobeperhapsthesinglegreatestthreattoourhealthandlongevity.
Theconditionofouralarmsystemanditsresponsetostressorsofdifferent originsdependsupontheconditionofmultipleothersystems.It’sinfluencedby theneurological,circulatory,andmetabolicsystems,aswellasmitochondrial function(ourenergyproductionsystem).Ourdietandlifestyleaffectittoo. Regardlessofthenature,origin,orlocationofthestressor,theresponse— galectin-3—hasanextraordinaryinfluenceonourbody’salertsystemand, subsequently,ourentirespectrumofhealthandlongevity.
Forouralarmsystemtoworkcorrectly,ourinflammatory,immune,and otherbiochemicalresponsesmustbecarefullyregulated.Whenthealarmsystem isworkingwell,itcanresolveslow-comingissueslikecancer,aging,orjoint pain.Itcanalsorampupquicklyandaddressimmediatethreatslikecuts, infections,bruises,emotionalstress,andotherdangers.Thenitcanwinddown
justasrapidlyaftertheproblemhaspassed.
Let’scompareahealthyinflammatoryresponsetoanunhealthyoneby thinkingaboutwhathappenswhenweturnonlights.Turningonasingle switchdoesn’ttakemuchenergy.Inthiscase,“turningononelight”alertsthe bodyofanissue,illuminatingtheneedforrepair.Whenthishappenswithinthe body,it’sanentirelynormal,acuteinflammatoryresponse,andwhenthe problemisgone,thelightturnsoff.
However,thetroublebeginswhenaswitchisturnedonandcan’tbeturned off.It’sasthoughacircuithasmalfunctioned.Whentheswitchstayson,it triggersacascade,causingmultiplelightstoswitchon.Thisisthestartof chronicinflammation,andthebodygoesintocrisismode.Atthatpoint,the bodyhasachoice:resolvetheproblemorkeepturningonmorelights.Ifthe bodychoosestokeepswitchingonlights,thiswilleventuallyleadtoamuch biggercrisis.
Anotherproblemwiththeselightsisthattheycanbeturnedoninisolation, awayfromthebody’sradar,meaningthebodywillbeunawarethattheselights areevenon.Justliketheselights,galectin-3canbeactivatedinanisolated microenvironmentwhereitgraduallycausesdamage.Insomecases,bythetime thedamageisdetected,itmaybetoolatetohealorreverseit.Apersonmay wakeuponedaytodiscover“sudden”kidneyfailure,wheninfact,thedamage occurredslowlyovertime—theywerejustunawareofit.
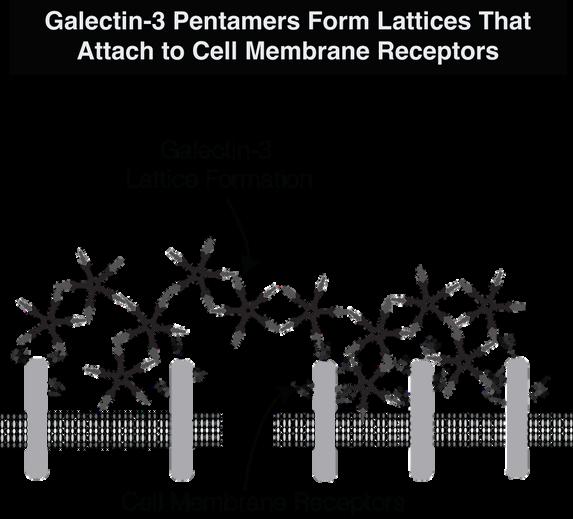
Isolationisafundamentalsurvivalstrategy.Itisinitiatedanddrivenbygalectin3.Aswediscussedearlier,galectin-3usesmultiplepentamersboundtoeach otherindifferentwaystocreatelatticeformations(orcoatingsorbiofilms). Theseformationscreatepocketsofisolationaroundareasofdamage,infection, andtoxicbuild-up,amongothers.Withinthesemicroenvironmentscreatedby galectin-3,diseasescandevelopundetectedandremainprotectedfromdrug treatmentsandothertherapeuticagents.
Frequentharmfulvisitorswithinthebody—likebacteria,viruses,fungi, parasites,otherinfectiousagents,andcancercells—haveasimilarisolation strategy.Theycanhijackgalectin-3tocreateashieldaroundthemselves(a latticeformation)sotheyareundetectedbytheimmunesystemandcaneven evadetherapeuticagents.Galectin-3canalsoisolatevariousthreatsthataretoo difficultforthebodytodealwith,suchastoxinsandheavymetals.
Youcanimaginethatonapsychologicallevel,wegothroughasimilar process,buryingemotionsandtraumasthataretoodifficultforustodealwith. Evenifthesetraumasarenotatthesurfaceofourawarenessorconsciousness, theycanstillhaveapsychologicalandphysiologicaleffectonus.Youmight havehadanexperiencewhilegoingthroughadetoxprocesswhereanemotion ormemorysurfacesallofasudden.Wherewasthisemotionallthistime?Itwas likelyburiedinamicroenvironmentthatwasnotaccessibletous.Asweopen orrevealourphysiologicalmicroenvironmentsandreleasetoxins,wecanalso openpsychologicalmicroenvironmentsreleasingburiedemotions.
Evenifanisolatedareaisnotspecificallycreatedinordertohidean infectiousagentorcancercell,themicroenvironmentscreatedbythegalectin-3 latticeformationsarestillwalledofffromourcirculation,andthesealtered environmentscanoftenbecomeveryinflamedandhypoxicduetoalackof oxygen.
Hypoxia also shifts our cellular energy production pathway from normal mitochondrialfunctionto anaerobic glycolysis,whichisahighlyinefficientway toproduceenergy;itresultsinthebuildupoflacticacidandotherinflammatory metabolicby-products.Thiscanleadtofurtherhypoxia,whichproduces additionalinflammationandgalectin-3expression,causingthehardeningor dysfunctionoftissues,organs,andbloodvessels.
Despitethepotentialharmitcando,galectin-3servesafewimportantpurposes withinthebody.Ithelpsintranuclearcelldevelopmentandextracellularinjury repairandsurvival.However,whenthebodyisincrisisandthereisan upregulationofgalectin-3production,itcanhavedetrimentalconsequences.
Duetocomplexbiochemicalstructuresandgenetictendencieswithineach person,thereisnostandard,predictableresponsewhenitcomestogalectin-3. Thisproteincanbeatdifferentlevelsindifferentpeopleandtriggerdifferent responses,eveniftheyhavethesamecondition.Forexample,somepeople’s bodiesare“hypervigilant,”alwaysonthealert,andtheyrespondtoastimulusor triggerwithoverinflammation.Otherpeoplemaynothaveagood“survival sense,”andtheylacktheabilitytofightandcreatetheproperinflammation. Instead,theyhaveatendencytoshutdownandendupwithsuppressed immunityoranincreaseinfibrosis.
Furthermore,thereisanadaptiveresponsewithgalectin-3,meaningthe reactionisamplifiedduetopreviousphysical,emotional,orpsychological trauma.Inanadaptiveresponse,oursystemhasbeenconditionedtorespondto specifictriggersinaparticularway.Inotherwords,itrepeatsthepatternsitis accustomedto,allthewaytothelevelofourcellularmemory.
Forourbodiestohealproperly,weoftenneedtoremovethestimulantsthat causetheinflammatoryprocesstoperpetuallycontinue.It’snosecretthataswe getolder,ittakesmoreandmoreefforttodothingsthatoncetooknoeffortat all.Whenweareyoungandagile,ourbodiesaremoreefficientandlesstoxic; theyareflexibleandhaveahighcapacityforchange,growth,andrepair.We canmountarobustinflammatoryresponsetoshutaproblemdownwithout consequence.Likethemetaphorofabirdflyingintheskywithoutleavingany trace,orlikewritingonwater,wecanoftensolveaproblemwithoutleavinga trace.
However,asweage,ourbodieslosethatagility,andwearemoreapttocarry ourissueswithus.Forexample,ifaninjuryoccurstotheskininutero,the woundcanhealwithoutatrace,butasweage,thewoundhealingprocessslows andcausesincreasedscarring.Aswetraveltheroadoflife,ourbodiesdisplay theevidenceofourphysical,emotional,psychological,andspiritualtraumas— theynolongerhealwithease.
Themetaphorsforabirdflyingwithoutleavingatraceandwritingonwater comefromBuddhistphilosophy.Theyservetoillustratethenatureofthoughts andexperiencesasarisingandvanishing—anexampleofimpermanence.Thisis whatinflammationshouldbe:itshouldbeanacuteresponsethatoccursand thendisappears.Itshouldturnoffwithoutatraceandwithoutlingering consequences.Thisiswhathappenswhenwehavearobustimmunesystemand whengalectin-3worksappropriately.Andwhenitdoesn’t,thedamagebegins.
The Solution: Blocking Unhealthy Expression of Galectin-3
I’dliketotakeamomenttoemphasizeacriticalpointandtheprimaryreasonI wrotethisbook:wecanabsolutelyinterruptthiscycleofdestructionandhalt— orevenreverse—thesefundamentaldiseaseprocesses.How?Bydeactivating unhealthygalectin-3.
Whenweblockgalectin-3frombinding,wecanbreakuplatticeformations and reach the isolated pockets and areas of the body, including tumor microenvironments.Abnormaltissuesandcells,eventumorouscancercells,can becomenormalonceagain,which,needlesstosay,hastremendousimplications for our health and longevity. By blocking unhealthy galectin-3, we can dismantle its harmful effects and render it inactive, decreasing unhealthy inflammationintheprocess.Thismakesblockinggalectin-3oneofthemost importanttherapeuticstrategiesfortreatingavastarrayofconditions.

Let’srevisitRebecca’sstorysinceithelpsillustratehowgalectin-3candirectly influencesurvival,health,anddisease.
WhenRebeccacametoseemein2011,itwasthefirstyearwewereableto testgalectin-3levelsintheblood.Thankstoasimplenewserumassaythatwas recentlyapprovedbytheFDAandisnowreadilyavailable,shewasoneofthe veryfirstpatientsinmypracticetohavegalectin-3levelstested.
Rebecca’sinitiallevelswereskyhigh,andtheby-productsofhersympathetic nervous system response to her crisis were elevated, as well as other proinflammatory,procancerousmarkers.Akeystrategyinhertreatmentplan wastotargetgalectin-3usingvariousprovenmethods.Weusedherlevelsasa markertogaugeherprogressthroughout.
Theresultswereunmistakable:whenRebeccawasdoingwell,hergalectin-3 levelswerelower,andwhenshewasinacrisis,herlevelswerehigher.For Rebecca,thismarkerservedasanimportantindicatorastowhenthecancerwas aggressiveandwhenitwas“quiet.”
Thishelpedusfine-tunehertreatmentsandstayonestepaheadofthecancer. (Note,however,thatduetoitscomplexbiochemistry,galectin-3cancause damageevenatlowlevels.Itisthereforeimportanttoaddressgalectin-3 regardlessofitslevels.MoreinformationcanbefoundinAppendixA.)
Rebeccataughtussomethingveryimportant:sheexemplifiedtheintimate connectionbetweenouremotionsandourhealth.WhenRebecca’sanxiety increased,hercancergotworse.Herpresentationwassopronouncedand immediatethatitwaseasytoseewhenheranxietywasworsening.Butwhen shewasabletorelax,quiettheanxiety,andbemorespacious,hersymptomsgot better. The way Rebecca responded as a person was the way her body responded as well. When her survival crisis decreased, and she became comfortablethinkingaboutlife,death,andimpermanence,itaffectedtheway thecancerfunctioned.Thecancerfeltlessthreatenedanddecreaseditsown survivalresponse.
Doesitsoundnew-ageyandfluffywhenItalkaboutchangesinthebehavior ofcancer?Really,it’snot.I’mreferringtochangesinthelevelsofgrowth factorsthatdrivetheaggressivenessofcancer,factorslikedownstreamproteins thatareregulatedbyoursurvivalprotein,galectin-3.Suchdownstreamproteins areimpactedbysignalingmolecules—whichthemselvesareimpactedbyour emotionalstate.
Rebeccawasabletocalmhersystemthroughregularmeditation,deep breathing,acupuncture,participationinmymeditationandhealingretreatsand workshops,andthroughtheuseofgalectin-3blockers.Thesehelpedtomitigate the initial survival process and significantly reduce the growth and aggressivenessofhercancer.
Rebecca’scancerdidnotcompletelyrespondtochemoandradiation,butit subsidedthroughthesehealingmethods.Herscansbecamenormal,indicating thathercancerhadgoneintoremission.ButRebeccadidmorethanjust incorporate these healing methods intohertreatment—she alsodeveloped communityandfriendshipswithotherpatientsinourcenter.
Thesefriendscheeredheronthroughoutherjourney,andthestoicdriverwho broughthertoherfirstappointmentwasnolongerneeded,asshebegan participatinginlivelycarpoolstotheclinic.Shewentfrombeinghighlycritical ofnonconventionalapproachesandbitteraboutherdiagnosisandfateto embracingherprocessandwelcominghertreatments.
Rebecca’stransformationsprofoundlyaffectedherphysiologyandallowed hertooutliveherprognosisconsiderably.Oneday,herlaughrangthroughthe clinicfromtheIVroom,remindingmeofthehealingpowerofjoy.Hercancer eventuallyreturned,butevenwithresiduallungcancer,shelivedsevenmore yearswithabetterqualityoflifethanshehadexperiencedindecades.Shesaid, “Isaac,Ifeelalivelikeneverbefore.”Shediedpeacefullyinherhome,ina meditativestate,surroundedbyfriends.Herlifewascelebratedbythemany peoplewhoweredeeplytouchedandinspiredbyherjourney.
CHAPTER FIVE
Nowthatyouunderstandhowthesurvivalresponseandgalectin-3operate withinthebody,we’llexploreabitofgoodnews:awaytointerruptthis responseatthebiochemicallevel.
Morethanseventypublishedstudieshavedemonstratedtheabilityofavery specificandhumblecompoundtoblockthedevastatingeffects ofgalectin-3.Isay“humble”becauseitisderivedfromcitrusfruits.This amazinggiftfromnatureisalow-molecular-weightformofpectincalled modifiedcitruspectin(MCP).
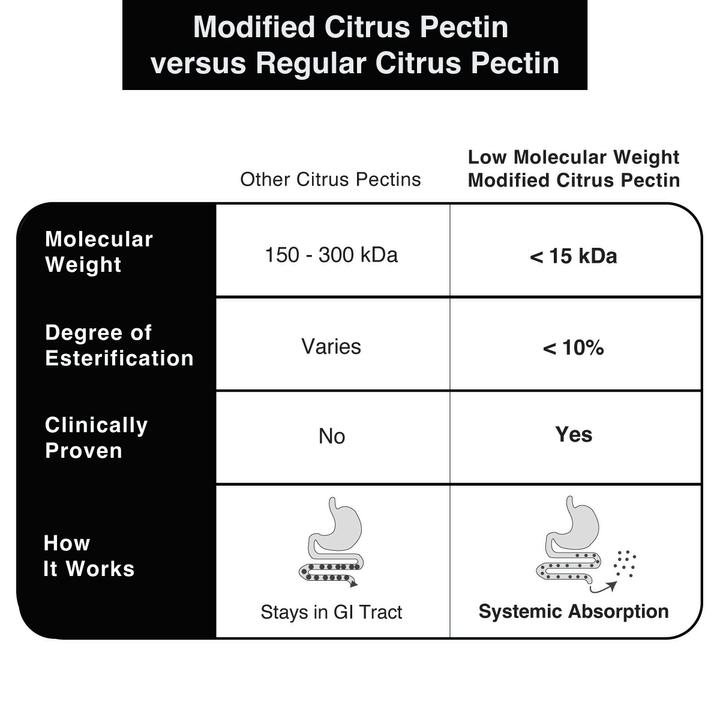
Let’stakeamomenttodefine pectin ingeneral.Itisafiber.Structurally, pectinisalongchainofcarbohydrates,mostlyaspecificonecalledgalacturonic acid.Thischainofgalacturonicacidhasalargemolecularweightranging between200–300kilodaltons.(Formytechnicalreaders:pectinalsohasside branchescomposedofdifferentneutralsugarslikearabinose,rhamnose,and xylose.)Whenthepectincomesfromcitrus,itisknownascitruspectin.
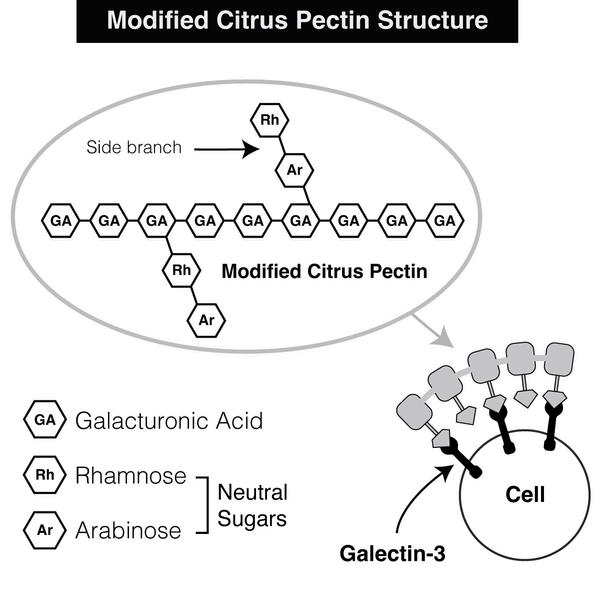
Importantly,regularpectinisnotabsorbedintothebloodstreamand thereforecannotblockgalectin-3.Therearestillhealthbenefitstoit,asafiber— sinceitscarbohydratechainisverylongandisn’tdigestedorabsorbed,it remainsinthegut,whereitcanimproveguthealth.However,inorderfor citruspectintoblockgalectin-3,itmustbemodifiedintoasubstancewitha lowmolecularweight.
Unlikepectin,thesemodifiedmoleculesaremuch,muchsmaller:3–13 kilodaltons, compared to the 200–300 kilodaltons of regular pectin. The smaller-sizedmoleculesallowthecompoundtoenterthebloodstreamthrough thedigestivetract.Oncethere,becauseofitsspecificstructure,itcanbindto galectin-3 andblockitsdevastating effects. Essentially, MCPconnects to galectin-3’scarbohydraterecognitiondomain,whichhasanaffinityforthe galacturonicacidpresentinMCP.Inthisway,MCPpreventsgalectin-3from interactingwithcellsandtissues.
Frustratingly,thereareformsofMCPonthesupplementmarketwhichhave moleculesthatarenotsmallenoughtoenterthebloodstream—thisiswhyI refertotheformofMCPI’mdiscussingashavingalowmolecularweight.In orderforMCPtoeffectivelyblockgalectin-3,itmustundergoveryprecise changesinitsstructurethroughaspecificpHandheat-controlledenzymatic process.Thisnotonlyreducesthepectinfibertoatiny,absorbablesizebutalso givesittheabilitytobindtoandblockgalectin-3.Forthisreason,Ionly recommend a form of researched MCP that has undergone this process. Fortunately,thisformoflow-molecular-weightMCPisanextremelysafe compound,classifiedasGRAS(GenerallyRegardedasSafe)bytheFDA.Now thatyouunderstandthemolecular-weightdistinction,forthesakeofbrevity,I willrefertothecompoundonlyasMCP.
BeforewegetintothescienceandresearchonMCP,I’dliketosharemy personalinvolvementinitsdevelopmentandwhyitissonearanddeartome.
IgrewupinasuburbanneighborhoodinRamatGan,Israel.Oneeveningin 1971,whenIwastwelveyearsold,myparentsandIvisitedourneighbors,Drs. LeoandRuthCohen.BothwerePhDsinorganicchemistryandpioneersinthe citrusindustryofIsrael—theyweretheheadscientistsatIsrael’sleadingcitrus productionconglomerate.
Duringourvisitthatevening,weengagedinlivelyconversation.Suddenly, Ruthturnedtomeoutoftheblueandsaid,“Isaac,onedaytheywillfinda treatmentforcancerinthepeelsofcitrusfruits.”Forsomereason,Ruth’s statementstuckinmymind.
Then,twenty-fouryearslaterin1995,afterIgraduatedfrommedicalschool andobtainedmymaster’sofscienceintraditionalChinesemedicine,astudyin the Journal of the National Cancer Institute caughtmyattention.Inthestudy, micewithprostatecancerweregivenMCP.Amazingly,therewasadramatic decreaseinthenumberandsizeoflungmetastasisinthemicethathad consumedtheMCPcomparedtothemicethathadn’t.Thiswastheresultofthe inhibitionofgalectin-3.
Intrigued,IcalledDr.RuthCohen.Iremindedherofwhatshetoldme twenty-fouryearsearlierandsharedthestudyresultswithher.Iaskedifshe couldhelpmemakethemosteffectiveformofMCP,andRuthdelightedly connectedmewithsomeoftheleadingpectinscientistsintheworld.This beganmyjourneywithMCP,whichwasinitiallysparkedonthatpivotalday whenIwastwelveandhasbeenunfoldingeversince.
Ithasbeenajourneyofdiscovery.Ifyoulookedatmymedicalchartstwenty yearsago,youwouldnothavenecessarilyseenMCPatthetopofmypatients’ suggestedtherapies.Sometimesitwasn’tonthelistatall.However,overthe years,I’veconductedextensiveresearchonMCP,includingitsapplicationin reducingtheseverityofcancer,enhancingtheimmunesystem,removingheavy metals,inhibitingandreducinginflammationandfibrosisbyblockinggalectin3,anditsabilitytopositivelyimpactmanychronicconditionsanddiseases. I nowrecognizethatitisperhapsthemostimportantsupplementwehaveinour effortstotreatandpreventchronicdisease.
Today,theMCPIdevelopedandresearchedisavailableforuseasadietary supplement.Ioftensaythatifitwereadrug,Ibelieveitwouldbewidely prescribed.Butsinceit’sanaturalproductextractedfromthepeelsofcitrus fruits,it’sadietarysupplementand,assuch,receivesmuchlessattention.Many ofmycolleaguescallit“thebest-keptsecretinintegrativemedicine.”Although it’stakentwenty-fiveyears,low-molecular-weightMCPisfinallystartingto gettherecognitionandappreciationitdeserves. 15
MCPinterfereswiththeinflammatoryprocessbybindingtogalectin-3’s carbohydrate recognition domain—preventing galectin-3 from otherwise bindingtoligands,interactingwithcells,orforminglatticestructures.By disrupting the cell-to-cell, cell-to-galectin-3, and galectin-3-to-galectin-3 interactions,MCPcreatesanenvironmentthatisinhospitabletoinflammation, fibrosis,hypoxia,infection,andcancercellgrowth. Inthecaseofcancer,for example,itremovesthegalectin-3that“shields”thecancer,andblocksthe galectin-3thatinhibitstheimmuneresponse.Thiswakesuptheimmunecells andenhancesthenormalimmuneresponse,makingtheimmunecellsmore effective.
WhileMCPblocksgalectin-3inplaceswhereitcausesdamage,tissuesthat require galectin-3 still express galectin-3 where it’s needed. This is the wonderfulthingaboutMCP:itdoesn’t inhibit healthycellularfunctionand injuryrepairbutrathermitigatestheharmfulconsequencesofgalectin-3. AndMCP’sbeneficialeffectsextendbeyondgalectin-3binding.Itcanalsobind toheavymetalsandhelpremovethem.Further,ithasapowerfulimmuneenhancing effect. This is because of a side structure in the MCP called rhamnogalacturonan II,whichimprovestheimmuneresponse.
Yearsago,beforeIdiscoveredtheroleofgalectin-3ininflammationand fibrosis,Iwitnessedaninterestingphenomenon:MCPquicklyreducedpainin mypatients.Theyreportedthattheirarthritis,backpain,andsometimeseven painfromcancerhadresolvedorimprovedinjustafewdays.
Iaskedmyself,“Howcanthisbe?”IthoughtmaybeitwasduetoMCP’s abilitytoremoveheavymetals,buttheresultingpainreliefhappenedso quickly,itwaspuzzling.Now,afteryearsofresearch,weknowthatblocking galectin-3reducesinflammationandfibrosis,andcanthereforenotonlyhelp relievepainbutalsopositivelyimpactawidespectrumofconditions.
It’sespeciallystrikingtolookatthebenefitsofMCPininflammatory-driven cardiovascularconditions.Thereareclosetotwentyanimalstudiespublishedin majorjournalsreportingtheconsistentabilityofMCPtostopandevenreverse arterioscleroticdamage.OnlyonesinglestudyshowedthatMCPdidn’twork, andwhenyoureaditcarefully,youcanseethatitdidn’tworkbecauseitwasa different type of MCP withahighermolecularweight.Thisdemonstratesthe importanceofusingthecorrectMCP—MCPisonlyeffectivewhenitis properlymodified.
MyresearchteamandIhavebeencollaboratingwithDr.AvrahamRazfrom WayneStateUniversity,headofthegroupthatpublishedtheoriginallandmark MCPresearchinthe Journal of National Cancer Institute in1995.Iamgratefulto Dr.Razforhispivotalcontributiontothefieldofgalectin-3andMCP. Throughourcollaboration,we’vebeenabletoutilizeantibodiestoidentify MCPinthebloodstream.Byusingthismethod,wedemonstratedforthefirst timethatMCPisabsorbedintothebloodstream,whereitcanexertitsbenefits. Becauseofitsabilitytoblockgalectin-3,MCPbenefitsmultiplesystems throughoutthebody.Whenitcomestothemetabolicsystem,itcanimprove insulinresistance,diabetes,metabolicsyndrome,andobesity.MCPalsoworks asanantioxidantandpromotesmitochondrialhealth.Byreducinginflammation andfibrosis,itinhibitsthedrivingforceforautoimmuneanddegenerative diseases.Thesamemechanismhelpswithpostinjuryhealing,protectsthe blood-brainbarrier,andcanhelphealstroke-inflictedbraindamage.
Inaddition,MCPfacilitatesthegrowthofbeneficialbacteriaintheGItract andinhibitstheadhesionofharmfulpathogensinthegutandthelungs. 18
By breaking down the galectin-3 lattice formation, MCP doesn’t allow microorganismstohideandevadetheimmunesystem.Itcanevenhavean antimicrobial effect on pathogenic bacteria. To give an example, MCP demonstratesantimicrobialactivityaloneandincombinationwithcefotaxime, an antibiotic, against strains of methicillin-resistant Staphylococcus aureus (MRSA).
ThesearejustsomeofthehighlightsofMCP’seffects.We’lldiscussmore aboutitsinfluenceonmanyconditionsinthechapterstocome.
AftersomanyyearsspentworkingwithMCP,Iamstillinaweofits effectiveness.TheexcitementIfeelisrenewedeverytimeIlivevicariously throughapatient’swonder.MydearfriendJonathanwasadvisedbyhis naturopathtostartusingMCPtohelpwiththeeliminationofheavymetalsand toxins.Afterafewmonths,Jonathancontactedmetoaskaboutsomethingthat surelycouldn’tbepossible—hadMCPalsoresolvedhislong-termhypertension?
Hisbloodpressurehadbeenhoveringat140/90formanyyears,anditwas now110/70.Hedidn’tchangeanythingwithhisdietorsupplementation—he simplystartedtakingMCP.ItoldJonathanthat,infact,itwaspossiblebecause MCPcanblocktheharmfuleffectsofgalectin-3onthecardiovascularsystem.
Afewmonthslater,ImetwithJonathanagain.Thistime,hetoldmethat, althoughhe’dbeensufferingfrombleedinggumsforyears,theproblemhad suddenlyresolved.
“Isaac,”heasked,“itcan’tbepossiblethatMCPhashelpedmygums,aswell, canit?”
“Indeed,”Ireplied,“itiscertainlypossible.”
Afterthatvisit,hisskepticismturnedtosupposition.WhenIsawhimnext, hehadmoregoodnews.Hetoldmehehadalwayscomedownwithanumber ofcoldsaccompaniedbycoughandbronchitiseachwinter.However,thispast winter,hisimmunesystemwasstrongerthanever,anddespiteextensive internationaltravels,hedidn’tgetsick at all.
“It’sbecauseoftheMCP,”heannounced. Ilaughedandreplied,“It’scertainlypossible.”
Bydeactivatinggalectin-3andbreakingdownitslatticeformation,MCP uncoverstheisolatingmicroenvironmentsthatcanharbordamagingdisease processeswithinus.Fromasymbolicpointofview,galectin-3isnowragingin ourcountryandonourplanet.Buttherearetoolstoblockthenegativeeffects ofdivision,isolation,andinflammation.Onthephysicallevel,wehavetools suchasdietandexercise.NowthereisalsoMCP.
Myapproachinmedicineistoseethroughsymptomstodeepercausesand relationships.Assuch,Ifrequentlyadvocateforamoremultidimensionaland sometimes complex approach to life and health. However, within the complexity,therearesomeverysimpleunifyingprinciples.Wecannotseparate ourcellularmechanismsfromthelargercosmicforcesthataffecttheworld aroundus.LikethedoublehelixofDNA,thesestrandsareinterwoven.
Keepingthisinmind,ifoursurvivalresponsepromotesisolationtendencies thatcanbesodamaging,whatcanwedotocounterbalancethis?Isthereaway forustohealthatisoflargerscope,notonlyatthecellularlevel?
Theanswerliesinconnectingwithouressenceandcore,withwhowetruly are.Loveisatthecenterofourcreation.Withsomeexceptions,humansare madeinanactoflovebetweentheirparentsthroughabondthathasrepeated itselfgenerationaftergeneration,datingbacktoallofourancestorswhoare withinourgeneticmakeup.
Thisqualityofloveispresentineachandeveryoneofourcells,butwe’velost thisconnectionthroughoutoursurvivalstruggles.
However,thereisoneorganinthebodythatfunctionsdifferentlyand continuouslyremindsuswhatitmeanstogivewithoutjudgment.Itoffersus thebuilt-inphysiologicalopportunitytotransformoursurvivalreactivityinto unconditionalloveandcompassion.Ittakesin“dirty”bloodthatcontains unwantedby-productsfromourcellsandorgans,transformsthequalityofthe bloodthroughbreath,andgivesout“clean”bloodtoitsenvironmentandthe restofthebodywithoutdiscrimination.Thisorganistheheart.
It’swhatI’llfocusonnext,becausewhenweconnectwithourhearts, anythingandeverythingbecomespossible.
Sincemymedicalcareeriscenteredaroundseeingcancerpatients,Iwantto offeramultidimensionalviewofthistopic.Thischapterismyattemptto condensewhatI’velearnedfromthirtyyearsofexperienceinintegrative oncologyandWesternandChinesemedicine.We’llpaintanewpicturefrom aneducationalandtherapeuticpointofviewsowecanbetterunderstand cancer,andsharedifferentaspectsofthediseasethatareinfluencedbyphysical, chemical,psychological,emotional,andpsychospiritualfactors.
Weallhaveencounteredcancer,whetherpersonallyorthroughsomeonewe know.Themorewecanviewcancerinamultidimensionalway,themore refinedourtreatmentsandapproacheswillbe.Ican’tdedicateenoughpagesin thisbooktothemanyspecifictreatmentsandstrategiesthatIutilizeforcancer, sothissectionwillfocusonthedeeperrelationshipbetweensurvivalandcancer, whichisavitalaspectofatrulyholisticapproachtocancertreatment.
Therearemanydifferenttherapeuticapproacheswhenitcomestotreating cancer,anddespitewhatwehavebeentold,weareneverstuckwithjustone treatmentmethod.Cancerisadynamicconditionthatchangesovertime; therefore,wealwayshavetoadjustandchangetreatmentsortrysomething new.Thisisanimportantpointtoremember,andit’salmostuniversally overlooked.
Forexample,whenatreatmentisworking,itmaybebesttochangeitbefore thecancerdevelopsresistancetoit.Changingtreatmentdoesnotnecessarily meanstoppingit;sometimeswecansimplymodifysupportive,integrative therapiesandchangetheenvironmentaroundthecancertopreventresistance. Bytakingthisdynamic,creative,individualizedapproach,weareableto lengthenthetimeofresponsetoaspecifictreatment.
Becauseeachcaseofcancerdevelopmentandtreatmentisindividualized,this chapterfocusespredominantlyonpatientstories.Betweenthestoriesarevarious sectionsonthenatureofcancer,thebody’sresponsetoit,andcurrenttreatment possibilities.Whenweapplyavarietyoftherapies—dynamicallyandina personalizedstrategy—itisquiteamazingtoseehowacourseofthreetofour differenttreatmentscansuddenlyaddyearstoapatient’slife.Myaimistogive cancerpatientstheopportunitytodomorethanjustovercomecancer—we wantthemto heal and transform theirlives.
Eventhoughwehearaboutcancerconstantlyandhavefriendsandlovedones whohavebeenaffectedbyit,manyofusstilldon’tunderstandwhatitactually is.Whatisacancercell?Whatmakesacellturnintoacancerousone,andcan we prevent this process from happening? In simple terms, cancer is the uncontrolledgrowthandspreadingofabnormalcells.Acancercellisonethat startstofunctiononitsown—it’snolongerregulatedbythebody.
Aswe’vediscussedthroughoutthebook,wearedrivenbysurvival,andin thecaseofcancer,thespecificcellshiftsfromservingafunctionaspartofa largerwholetofocusingsolelyonitsownindependentsurvival.Thisabnormal survivalresponsecanbecausedbynumerousfactors.
Previously,conventionalmedicinefocusedonmutationsasthecauseof cancerandemphasizedthegeneticcomponent,buttoday,weknowtherearea greatarrayofreasonsandprocessesthatcanleadtosuchashift.Epigenetics, environment,lifestyle,diet,andotherfactorscanalsoplayarole.Thesetriggers caninitiateashiftinthemetabolismofthecell,whichallowsittosurviveasan independententity.Ifwecanstopthesurvivalresponseofthecell,wecan reversethisprocess—preventingthecancerfromoccurring.
AccordingtotheAmericanCancerSociety,nearly50percentofcancercases intheUnitedStatesarepreventable—theyarecausedbyenvironmentalstressors andlifestylechoices. Suchfactorscantriggerorfuelthesurvivalresponse.But whenweareabletocontrolthisresponse,wecancontroltheinflammationand metabolicchangesthatdrivecancer.Thisallowsusnotonlytopositively impactcancertreatmentsbutevenstopcancerbeforeitstarts.
Knowingthatmultiplefactorscancausethedevelopmentofcancer,wehave totakethemintoconsiderationifwewanttodesignanddevelopaneffective treatment strategy. A key component of stopping cancer growth and implementingtherapeuticstrategyisunderstandingthemetabolicchangesthe cellundergoeswhenitbecomescancerous.Themostimportantoftheseisthe Warburg effect. Thisiswhencancercellscreateahypoxicenvironment—evenin thepresenceofoxygen.Thecancercellusesthemetabolicshiftforanumberof survivalmechanisms.I’llfocusonthetwomostimportantones:first,the metabolicshiftinhibitsprogrammedcelldeath (apoptosis),meaningyourcells don’tcompletetheirlifecycleasthey’resupposedto;second,theshiftactivates theabilityofthecellstocreatenewbloodvessels (angiogenesis). Theseprocessesallowtheprimarytumortogrowandmetastasizerapidlyand givethecancertheabilitytomanipulateitsenvironment.Alloftheseare consequencesofthesurvivalresponseoftheindividualcell:itchangesits metabolism to address the crisis, blocks apoptosis to avoid death, creates angiogenesistoallowforadditionalbloodsupply,evadestheimmunesystem, andcreatesafavorableenvironmentforcancergrowth. 22
Cancerdoesn’tdevelopovernight.Itbeginswithaprocesscalled dysregulation, whichisadisruptioninthecommunicationsystemofthecells.Thereisstill dialoguebetweenthecellandthebody,butit’snotasstraightforwardordirect asthecommunicationbetweennormalcells.
Imaginetheseout-of-controlcellslikewildchildrenwhodon’tlistentotheir parents—they’rerebels.Astomachcellmaynolongerwanttofulfillitsrolein thestomach,andabraincellmaynolongerwanttofulfillitsfunctioninthe brain.Thecellwantstosurviveatanycost,anditnolongerrecognizesthatits lifecycleincludesdeath.Itdoesn’trecognizeitsnaturalenvironmentasasafe andfriendlyplace,andthistriggersasurvivalresponse.Asaresult,itisolates itselffromtherestofthebodybycreatingaprotectivemicroenvironment,ora “shell.”
Whenacellisisolated,itnolongerhaspropercommunicationwithother cellsandnolongerseesitselfaspartofalargercommunity.Itgoesrogueand begins to obtain its own blood supply and nutrition. It starts to grow independentlyandrapidly,evenifithastousealternatemetabolicpathways.It’s asthoughitrefusestolistentoothercells,decidesit’sgoingtobeinchargeof itself,andtakescontroloveritssurvival.Theseroguecellsbecomemore aggressiveandattackthehost,eventuallyspreadingthroughoutthebody.
Eachstageofcancerdevelopmentisinfluencedbygalectin-3.Whenwe containorcontrolgalectin-3anditsdamagingeffects,wereestablishanormal environment.Whenwedothat,wecanreducetheaggressivenessofthecancer, andthecancercellshaveagreaterchanceofnormalizing.I’veseenchangesin cancermetabolismovertime,wherethecancerbecomeslessaggressiveand beginstofunctionmorelikeanormalcell.Letmeexplainthisbypickingone specificexample.
Ourcellshaveaspecificgenethatcreatesaproteininchargeofsuppressing cancer.Thisgeneiscalled P53 andisknownasthe“guardianofthegenome.”It standsreadytoprotectthecellfromturningintoacancercell.Whenexpressed atsufficientlevels,P53willregulatethecellandpreventcancer,andthecells willnaturallydieontimeintheprocessofapoptosis.
Whengalectin-3attachestocertainreceptorsonthecellmembraneaspartof thesurvivalresponse,itreducesP53.Asaresult,cellgrowthand cancer-promotingproteinsinthecellareactivated,andthecellgoesintocrisis mode.Thisinitiatesacascadeofeventsthatcanresultincancer.Moreover,the moresuppressedtheP53,themoreaggressivethecrisismodecanbe,resulting inahyperinflammatorystate,agreatershifttoaerobicglycolysis(theWarburg effect),andtoamoreaggressivecancer.
Asmoregalectin-3bindstothesurfaceofthecell,ittriggersangiogenesis, andtheresultingnewvesselssupplybloodthatpromotesthegrowthofthe cancer and eventually the metastatic process. Blocking galectin-3 and preventingP53suppressioncanpreventallofthisfromhappening.Inexisting cancer,suchstrategiescanreducethecancer’saggressivenessandenhancethe responsetotreatment.
Agrowingfieldinthestudyofcanceris cancer epigenetics. AsI’ve discussed,thefieldofepigeneticsinvestigatescertaintendencies weinheritfrompreviousgenerationsasaresultoftheirexposure tolifestyleandenvironmentalfactors.Thesefactors—suchas unhealthydiet,profoundemotionalstress,orerraticsleephabits —affectgeneexpressionandaggravatecancer.But,crucially, suchtendenciescanbereversedthroughlifestyle,supplement programs,andothermodalities.
Treatingcanceranditseffectsisonlypartofanintegratedapproach.Wemust alsotreatitsroots.We’vetouchedonthefactthattherecanbedifferentcauses foracellortissuetogointosurvivalmode,likegeneticandepigenetic influences,ormultipleeventsandtraumasinourlives.Inmymedicalpractice,I makeitapointtoexploretheseingreaterdetail,especiallywhenitcomesto cancer.
Unusualcancershaveunusualstories.FromtheperspectiveofChinese medicine,thesurvivalresponsecanvarybasedonthespecificlocationofthe cancerandwhatthediseasedorgansymbolizesemotionallyandpsychologically. IoftenreverttomymeditationpracticeasasourceofinsightwhenIam preparingtoseeanewpatientandexploresomeoftheirhiddenstories.To utilizedeepinsightintotheirstoryasahealingopportunity,Ifollowabasic principle:Irecognizethatthisis their storyand their trauma.Theyneedtobe theonetodiscoverandtransformit.
Ineversuggestthatsomethinghappenedtoapatient.Iaskseveralgeneralized questionsandprovideanopeningfortheirstorytoariseandrevealitself.For example,Ioftenlookfortheplaceinapatient’slifeorhistorywheretheyfelt theycouldn’ttakeadeepbreath.Frequently,thesurvivalresponseaccompanies theeventwherethepatientcouldn’tbreathe,eitherliterallyorfiguratively.
Thesekindsofrecognitionscanserveasanopportunityforprofoundhealing, astheyallowthetraumaticpatternthattriggeredthesurvivalresponseto unwind.Then,inadditiontoguidingpatientsthroughtheirconventionalcare, Isupporttheirhealingandtransformationwithacupuncture,specificinjections ifneeded,guidedvisualizations,andhands-onhealing.
Marywasaforty-year-oldwomanfromtheEastCoastwhowasdiagnosedwith adenocarcinomaoftheadrenals,averyrareanddifficult-to-treatcancerthathad alreadymetastasizedtotheliver.Theprognosisofsuchcancerispoor,andthe chemicalablationoftheadrenalsthatisusedtotreattheconditioncanhave awfulandlifelongsideeffects.Marylivedaveryhealthylifestyle,sothis diagnosiscameasashocktoher.
AsIsatinmycabininthewoodsandmeditatedonMary’supcomingfirst visit,Isawanimageofadogthatshelovedwhenshewaseightornineyears old.IfeltthatsomethingrelatedtothisdogcausedadeeptraumainMarythat hadregistereddeepinherbody.InChinesemedicine,theadrenalglandisoften relatedtodeepfearorshock,andtheadrenalineresponseisinitiatedthere.For somethingfromsoearlyinherlifetohaveanimpactsomanyyearslater,ithad tohavebeenaprofoundtrauma.
WhenMarycameforherfirstvisit,Iaskedherifshehadanypetswhenshe wasachild,perhapsbetweentheagesofeightandten.Maryrepliedthatshe neverhadpets.However,afewminuteslater,sheturnedtomeandsaidshe rememberedshehadadogshelovedwhenshewasnine.Iaskedherwhat happenedtoit,andshesaidthatherparentsgaveitaway.
“Howdidyoufeelaboutthat?”Iasked.
“Itriedtocommitsuicide.”Sherepliedasifitwereacasualthing.“They rushedmetothehospital,andtheywereabletosaveme.”
Webothsatthereintotalsilenceforwhatseemedlikeaneternity.Mary staredoffintospaceasthoughrecallingalong-forgottenmemory.Slowly,she lookedatme,tearsrollingdownhercheeks.Inthatmoment,Marywasableto connectwithhertraumaandinitiateadeephealingprocess.Shereturnedtothe EastCoast,wheresheengagedinholistictreatmentmethodswithgreatsuccess.
Therearetwopathswecantakewhenwebegintotreatcancer.Thefirstisto solelyrelyonstandardizedoncologicaltreatments.Thesecondistodevelopa deeperunderstandingofthehumanbody,howweinteractwiththecancer,and howweasindividualscanparticipateinourownhealingjourney.Irecommend acombinationofthetwo.Weshoulduseconventionalmedicineandresearchas aroadmaptoguideusthroughtreatment,andatthesametime,weneedto understandhowandwhyaparticulartreatmentmayormaynotbeeffective. Wealsoneedtoconsiderhowwecanmakeconventionaltreatmentsmore effectiveandlesstoxic.
Whenitcomestoconventionalcancertreatments,itdoesn’tmatterwhois administeringthechemotherapy.Thetreatmentselectionisbasedonstatistical outcome.Integrativemedicine,however,whenpracticedinaholisticway, focuseson changing the expected outcome.Itimprovesthetreatmentandreduces thesideeffects,whilerecognizingtheindividualityanduniquenessofeach person.Forsomepatients,thebenefitsmaybeminimal.Forothers,thebenefits aremiraculous.
I’veobservedinmymedicalpractice,withalmostnoexceptions,thatpatients whoembarkonthisholisticpathhavebetteroutcomes.Thishealingapproachis trulyanart,becauseeachpersonisontheirownhealingjourney.Eachpatient hasanamazingstory.Myroleashealthcarepractitionerandhealerissimplyto allowthestorytounfold.
IwillneverforgetJohn,aforty-five-year-oldmanwithterminalleukemia. Johnwentintocardiacarrestduringthechemotherapeuticattempttoinducea remission,andwassenthomewithalifeexpectancyofdays,perhapstwoto threeweeksatbest.
JohnlivedinruralCaliforniaandbarelymadealivingfromgrowingand sellingpot.Hehadlivedanunhealthylifestyleforyears,withverylittle motivation,ifany,toliveahealthy,productive,andmeaningfullife.Hecame tomyclinicwithhistwosiblingswhowerecompletelydifferentfromhim. BothhadPhDsinclinicalpsychologyandwerehighlymotivatedtolivehealthy lives—theywantedtohelptransformtheirbrother’shealth.Theywerewellread onalternativestrategies,astherewerenoconventionaltreatmentsavailablefor Johnanylonger.
Agooddoctorneedstolistenandlearnfromtheirpatients,andJohn’s siblingssuretaughtmealotthatdayastheysharedtheirinsightswithme.John statedthathewantedtolive,butinmyinitialassessment,Icouldn’tseesucha miracleunfolding.Ididn’tseeanyroomordeepwillwithinhimforchange. WhatIhadfailedtorecognizewasthepowerofhissupportsystemandthe unconditionalloveofhissiblings.TheymovedJohnintotheirhome,faraway fromhisdisruptiveandunhealthyenvironment.Theytransformedhislifestyle anddietandputhimonanintenseprogramofherbsandsupplements—a combinationoftheirresearchandmyfine-tuning.
John’sdaysincludedmeditation,qigong,exercise,yoga,andaloving environmentfreefromjudgmentorexpectations.Andtheoutcome?Johnwent intofullremission,andtherewasnolongeranysignofhisdisease.
Afewmonthsafterhisremission,Johndecidedtoreturntohisrural community.Hewasconvincedthathisinitialdiagnosiswasprobablyamistake, andhedidn’thavetocontinuehisnewlifestyle.
Despitemywarningsandtheheartfeltrequestsofhissiblings,herevertedtohis oldhabits.
Threemonthslater,Johnshowedupatmyclinicwithanotherrecurrenceof hisleukemiaandaskedifIcouldhelphimagain.Itoldhimthatwecouldtry, knowingthatmiraclesdon’trepeatthemselveseasily.Unfortunately,thedisease tookoverthistime,andJohndiedafewweekslater.
John’sjourneydemonstratesinavividandunparalleledwaythemiraculous powerofchangeandtransformation,whileexhibitinghowthepowerofour habitsandunhealthylifestylealwayschallengeusinthehealingjourney.But aboveallelse,John’sjourneytaughtmewhatthepowerofunconditionallove andcommunitysupportcando.Together,thesewereabletocompletely dissolveandtransformthesurvivalparadox.
Apatient’sprioritiesinlifecompletelychangethemomenttheyarediagnosed withcancer.Whatwasimportantevenamomentbeforetheirdiagnosismayno longerbeofanyimportancethemomentafter.Aspreparationformyinitial visitwithmycancerpatients,Iaskthemtopreparetheirprediagnosispriority listandalistofwhatbecameapriorityafterthediagnosis.Ialsoaskthemto prepareawishlistofpriorities—thethingstheywanttodoiftheycompletely healfromcancer.Justcreatingaprioritylistcanhaveatransformative,healing effect.
Healingdoesn’talwaysequatetoeliminatingcancer.Wecangothrougha profoundhealingtransformationyetstilldiefromcancer.Linda’sstoryisone thatexemplifiesthis.
Lindawasasuccessful,fifty-year-oldaccountantwhocametoseemefifteen yearsagowithadvancedstage4ovariancancerthatfailedtorespondtomultiple chemotherapyregimens.Shewasgivenverylittlehopebeforeherlastpossible roundofchemotherapy,soshedecidedtotakesometimetobetterunderstand thedisease(andherself)beforestartingthenextroundoftreatments.
Duringourinitialvisit,weexploredLinda’slifejourneythatledtohercancer andhowitcouldbechanged.Iaskedherwhatshewoulddodifferently—how herprioritieswouldshift—ifhercancerdisappearedandshecompletelyhealed. Wehadadeepheart-to-heartconnectionduringthevisit,soIwasquite surprisedwhenshedisappearedanddidn’tcomebackforafollow-up.She finallycamebacksixmonthslater.
IaskedLindawhathadtranspiredoverthepastsixmonths,andshesaidthat shetooktimetocontemplatetheanswertothequestionIhadaskedher:what wouldshedodifferentlyifshewascompletelyhealed?Asaresultofherdeep reflection,shequitherjobasaCPA,andshebegandoingartandwriting poetry.Shetookdailywalksinnatureandfoundasupportivecommunityof femalefriends.Herstrugglesandsurvivalmodehadmeltedaway,andshehad transformedintoadifferentperson.
Lindaglowed,andheropenheartandimmensekindnessweresoevident. Withthisshift,Lindahadanunexpectedresponsetoherchemotherapy. Supportedbyasophisticatedsupplementprogram,occasionalhighdosesof intravenous(IV)vitaminC,andongoinghealingsessionswithme,sheoutlived herdiseasebyyears.
Aspartofhertransformation,Lindafeltthatmountainlionswereher protectiveanimal,andshehadaspecialaffinityfortheminherdrawings.When herdiseaseprogressed(muchlaterthanexpected),Lindafeltthatjustasshehad transformedinherlife,shewasreadytotransforminthewaysheleftthisworld. Shetoldherbestfriendtwodaysbeforeherdeaththatshewasabouttodie,and thataftershedied,amountainlionwouldshowupasasignfromher.
Twodaysaftershehadtalkedwithherfriend,Lindacamehomefromayoga class,satonherbed,andleftherbody.Thenextmorning,herfrienddrove alongthehighwayandamountainlionrandownfromthemountains.
Itrannexttohercarformilesandthenreturnedtothemountains.Lindawas fine,andshehadgivenusaprofoundteachingthroughherlifeanddeath process.
Theclassiccancertreatmentsaresurgery,chemotherapy,radiation,hormonal therapy, and immunotherapy. In conventional oncology, some of these treatmentmodalitiesaregiveninasequence.Forexample,inlocalizedbreast cancer,surgeryisfollowedbyradiation.Andmuchtoooften,thesetreatments areviewedasseparateandindividualratherthaninterdependenttherapies.Not onlyarethetherapiesinterdependent,buteachphaseoftreatmentandthe body’sresponseareinterdependentaswell.
WhatdoImeanbythis?Let’stakesurgeryandbiopsyasanexample—they areroutinelyperformedforbothdiagnosticandtherapeuticpurposes.Whenthe tissueattemptstorepairitselfpostsurgery,itquicklyexcretesgalectin-3aspart oftherepairprocess,resultinginalargeincreaseininflammatoryandgrowth factors.Thismeansthatifthereisanyresidualcancerinthebodyduringtissue repair,itwillgrowmuchfaster.Thisissomethingweactuallyseequiteoften andwhyit’ssocriticaltouseMCPbeforeandafterabiopsyorsurgery.Formy patients,thelastthingtheydrinkbeforetheprebiopsyorsurgeryfastisten gramsofMCP(ahighdose)mixedinwater.It’salsothefirstthingthey consumewhentheycantakeinliquidspostsurgery.
Therearedifferenttherapeuticstrategieswhenitcomestotreatingcancer. We can try to fight and kill the cancer by using chemotherapy, immunotherapy,andradiation;wecantrytoinhibititsgrowthbylimitingits growthfactorsandbloodsupply;orwecantrytoredifferentiatethecancercell tomakeitlessaggressiveandpossiblyconvertitbacktoanormalfunctioning one.Thesestrategiesareoftencombinedandadjustedbasedonthepatient’s conditionandtreatmenttimeline.
Whenweimplementthefirststrategyandtrytokillthecancer,itwill attempttoevadetreatmentslikechemotherapy,radiation,andimmunotherapy. Itdoesthisbyisolatingitselfandcreatinganalteredmicroenvironment,and activatingpumpsthatremovethechemotherapydrugsfromthecancercells. Thesepumpsarecalled Multiple Drug Resistance (MDR)pumps,andtheyare locatedonthemembraneofthecancercells.Byutilizingthesepumps,the cancercellcanuseenergythroughitssurroundingmicroenvironmentwhile pumpingoutthedrugsthataremeanttokillit.Integrativeapproachesattempt toblockthesepumpstoovercomedrugresistanceandgetbetterresponsesto chemotherapy.
Anotherexampleisradiationtherapy.Themicroenvironmentcreatedbythe cancerislowinoxygen,andradiationtherapydependsonoxygentokill cancer.Byutilizingstrategiesfromintegrativemedicine,wecanimprovethe oxygen-poorhypoxicenvironment,improvingthetreatmentoutcomeand reducingsideeffects.Ifwereduceinflammation,bringinanoxygen-richblood supply, block galectin-3, and utilize dietary changes together with mitochondrialsupport,thecancercellswillbecomemoreradio-sensitive.They willbemoreeasilykilledbyradiationtherapy.
Thesecondstrategyincancertreatmentisinhibitinggrowthbylimitingits bloodsupplyandgrowthfactors(thecompoundsthatstimulatethegrowthof cellsandtissueinthebody).Inconventionaloncology,thisisdonebyusing variouspharmaceuticalsthatinhibitdifferentgrowthfactors.Thesetreatments areextremelyexpensiveandcanbeverytoxicbutcanhaveasignificanteffect onslowingcancergrowth.
Whenwelookatcancer,thehypoxicenvironmentcreatedbythesurvival responsestimulatesgrowthfactorsandnewbloodsupply.Bynormalizingthe microenvironmentandreducingthehypoxia,wecanreducethegrowthfactors andnewbloodvesselgrowth,enhancingthebenefitsofthesepharmaceuticals whilereducingtheirinflammation-drivensideeffects.
Thisbringsustothethirdstrategy, redifferentiation ofthecancercell,whichis theprocessofnormalizingabnormalcellfunction.
Whenwetrytoredifferentiatecells,wecanusecertainagentstomovethe bodyfromasurvival-inducedstressstatetoarelaxedone.Whiletherearemany waystoredifferentiatecells,thekeyisto create the shift. Thecellsneedtoshift awayfromsurvivalsothegalectin-3latticeformationfallsaway.
Whilewecandothisbyusinganumberofcompoundsandstrategiesas mentionedthroughoutthechapter,it’sworthnotingthatwheneverweshift fromastateofpanic,stress,andanxietytoastateofgreatercalm,peace,and harmony,thissendsadirectsignaltoourbodytodothesame,allthewaytothe cellularlevel.Asfeelingsofself-isolationfadeawayandthealarmfromthe survivalresponseturnsoff,theprotectivemicroenvironmentsurroundingthe cancercanalsobegintounravel.
In the clinic, I modify my programs (including dietary guidelines) based on the conventional treatments that patients are receiving. I take into consideration the specific drugs or treatment methods used, and the half-life of the drugs. The half-life, or T ½, is defined as the time it takes for the concentration of a drug in the plasma or the body to be reduced by 50 percent.
When timing a dietary regimen with certain chemotherapy drugs, we want to shift the mitochondrial metabolism while the effect of the drug is at its peak in the body. We can do this by combining prolonged intermittent fasting with a calorie-restricted ketogenic diet, together with the use of honokiol an active anticancer compound from Magnolia bark (see Appendix B).
This strategy should be timed around the chemotherapy, making sure that the effects of this protocol are optimized during the first three half-lives of the chemotherapy drug. The length of the regimen will therefore vary based on the half-life of the specific drug the patient is taking at the time.
Occasionally,wehavetheopportunitytodocumentredifferentiationofcancer. WewereabletodosowithJoseph,asixty-two-year-oldbusinessexecutivewho hadbeendiagnosedwithanaggressiveGleason9prostatecancer.TheGleason scorecategorizesprostatecancerbasedonitsaggressiveness,asreflectedbythe differentiationofthecancer:themoredifferentiatedthecancercells,thecloser theyaretonormalcells,andthelessaggressivetheyare.Awell-differentiated cancerwiththelowestaggressivenesshasascoreofGleason6,andthemost aggressive,undifferentiatedprostatecancerhasascoreofGleason10.
Theoutcomeandsurvivalratearedramaticallydifferentbetweenthetwo scores.Gleason6prostatecancerisoftensimplyobservedanddoesn’trequire treatment,whileaGleason10prostatecancerislethalandrequiresaggressive treatment.AtGleason9,Joseph’scancerwasveryaggressive.
Awareoftheseverityofhissituation,Josephcametoseemeforaconsultprior toschedulingsurgery.Atthetimeofdiagnosis,hewasundergreatstress—not onlywashefacingcancer,buthislong-termbusiness,towardwhichhehadput yearsofhislife,wasfailing.
Knowingthatwehadjustafewweeksbetweenhisdiagnosticbiopsyand surgerytoremovehistumor,Idesignedamultifacetedprogramforhim.Joseph engagedinanintensedetoxificationandhealingregimenthatincludedlifestyle changes, stress management, significant dietary changes, a comprehensive supplement program, intravenous therapies, and acupuncture and healing sessions.Duringtheseweeks,Iwatchedhimtransform:hebecamehappierand more relaxed, and his physical health, stamina, and well-being markedly improved.
Josephhadhissurgerysixweeksafterstartingthisprogram,andtohis surprise,hispost-surgeryGleasonscorewasreducedtoa7,reflectingsignificant redifferentiationofhiscancer.Whilethismayseemlikeamerechangein numbers,fortheGleasonscoretodecreasesosignificantlyintheshorttime betweenbiopsyandsurgeryisextremelyrare.ForJoseph,thismeantavery differentprognosisandamuchbetteroutcome.
IhaverepeatedlyseenGleasonscoresimprovebetweenbiopsyandsurgery withtheuseofprogramssuchasJoseph’s.Theresultsexemplifythepotential andpowerofaddressingacancerpatternbeforeundergoingconventional medicaltreatments,allowingthecancertoredifferentiate—toshiftitsnatureand expression.
Thecancercellisanimpatientcell,usingglycolysisexclusivelythroughthe Warburg effecttoproduceenergyveryquickly, creating avicious, selfperpetuatingcycle.Themoreglucose-dependentacancercellis,andthemore sugaritconsumes,themoreinflamedandaggressiveitwillbe.Whenwe consumeglucose,wefeedcanceranditspathways.Usingalow-glycemicindex dietthatisgenerallylowincarbohydratesisabasicstrategythathelpstoshift thecellawayfromsurvivalmodeandmakeitmoreresponsivetotreatment.
Anotherdietarystrategythatisnowverypopularisintermittentfasting. Therearedifferentmethods,buttheultimatepurposeisthedepletionofglucose stores,whichresultsinlowerinsulinlevelsandallowsthebody’smetabolismto shiftintoahealthiermode.Theketogenicdiethasanimpactsimilartothatof intermittentfasting,butsinceit’sanalternatediet,Idon’trecommenditfor continuouslong-termuse.Iwillexploretheketogenicdietmoreinalater chapter,butIwanttodiscussitbrieflyhereaswellsincesomanyofmycancer patientsaskmewhetheritmightberightforthem.
Althoughtheketogenicdietandintermittentfastingsharesomesimilar features,theyarenotthesame.Intermittentfastingpromotesametabolic processcalled autophagy, whichallowscellstodointernalcleanup,shiftaway fromproblematicpathways,andupgradetheirmitochondrialfunction.During intermittentfasting,thecellreturnstoitsnormalenergyproductionsystem, whichishowacellfunctionswhenit’snotunderthreatandnotinsurvival mode.Thisisunliketheprocessofketosis,whichisalong-termsurvival response—andthereforestillasurvivalresponse—thatreliesonanalternate energy.Formoreinformationonintermittentfasting,pleaserefertothe“diets” sectionofAppendixC.
Ellenwasaremarkablefifty-five-year-oldfamilyphysicianwhowasdiagnosed withveryaggressivemyosarcoma(cancerofthemuscles)thathadmetastasizedto thespineandtheliver.Hertumorwasextremelyinflamed,andherPET/CTscan showedanabnormallyhighglucoseuptake,meaningthecancerwasusinglarge amountsofglucosetoproduceenergy.ThiswasevidentintheStandardUptake Value(SUV)readingofthescan,avaluethatquantifiesthelevelofglucose metabolisminacancercell.Shenolongerrespondedtochemotherapyandwas deemedaterminalpatient.
Asalastresort,EllenflewfromtheEastCoasttoseeme.Recognizingthe metaboliccharacteristicsofhertumor,wefocusedonshiftinghermetabolism bycombiningMCPwithHonokiol,togetherwiththerapeuticapheresisand othertreatmentmodalities.Combinedwithaneasier-to-toleratechemotherapy regimenfromalocaloncologist,Ellenhadaremarkableresponse.Hertumors shrunk,andshelivedmuchlongerthanexpected.
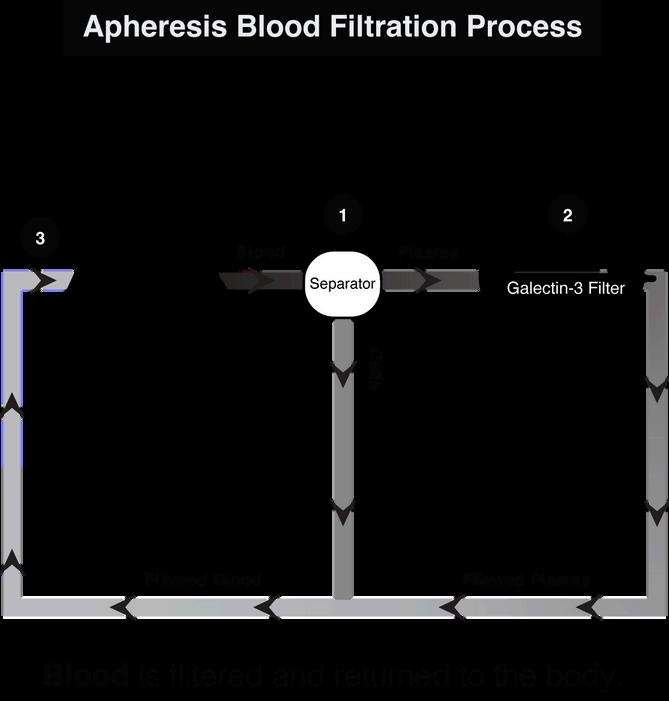
In 2011, I had an insight. Since galectin-3 is particularly damaging when it’s in the circulation and the extracellular matrix, I wondered what would happen if it were removed from the bloodstream. And what would happen if other inflammatory compounds could be removed as well? This insight led to the development of galectin-3 therapeutic apheresis.
Therapeutic apheresis is a procedure similar to dialysis but different in that only the plasma, the noncellular part of the blood, is filtered. Blood is drawn from a vein, and the cells are separated from the plasma. The plasma then circulates through a specific filtration column that removes galectin-3, along with oxidative, inflammatory, and cancer-promoting compounds that are part of the galectin-3 lattice formation. (In Ellen’s case, we removed inflammatory compounds, a small amount of galectin-3, and different growth factors.) The filtered plasma is then reintegrated with the cells, and the filtered blood is returned through a different vein.
For quite a few years now, I have been working on the removal of galectin-3 from the plasma. Therapeutic apheresis is the most powerful and direct approach to removing galectin-3 from the body.
My team and I have developed a specific filtration column that’s been proven effective, and we hope to begin clinical trials soon. This device holds promise as a powerful tool that will save many lives.
Our initial focus is on sepsis and Acute Kidney Injury (AKI), Chronic Kidney Disease (CKD), potentiation of immunotherapy in cancer, and the treatment of NASH (nonalcoholic steatohepatitis disease).
Knowing that this unique therapeutic approach can make a significant difference and save the lives of so many people, it is my true hope that we will be able to bring it to fruition. This is all part of my life’s work to help us heal ourselves, our communities, and our world by removing and preventing what isolates us whether from within or without.
Whentreatingcancer,it’simportanttoregulatethehormonalenvironment.An abnormalhormonalenvironmentcanstimulatehormone-sensitivecancers,such asbreast,ovarian,uterine,andprostate.Othertypesofcancerssuchasbrain glioblastomas,pharyngeal,thyroid,lung,andcoloncancerscanhavehormonal receptorsaswell.
Thehormonallevelsinourbodyriseandfallinarhythmicfashion. Understandingthecircadianrhythmofhormonesandtheireffectonbothbody andcancerprovidesapowerfultoolforenhancingdifferentcancertherapies. Throughoutmycareer,Ihavewatchedthelivesofmanyofmypatientsextend significantlybymodifyingtreatmentsaccordingtothisunderstanding.The guidingprincipleisrecognizingtheindividualityofeachpersonandtheir uniqueinternalrhythmandhormonalexpression.Often,subtleadjustmentsin thehormonalexpressionofthebodycaninfluencethecancer.Asaresult,the patientcanrespondtoatreatmentthattheyhavestoppedrespondingto.
WhenIsay,“regulatethehormonalenvironment,”I’mnotjusttalkingabout thelevelofhormonesbutalsoaboutcreatingtherighthormonalmetabolites (theby-productsofhormonesafterthey’vebeenprocessedinthebody).The liverplaysalargeroleinharmonizinghormonalmetabolitesandcaninfluence whethertheybecomecancer-inhibitingorcancer-promoting.We’lldiscuss moreabouttheliverinanupcomingchapter.
CancerPatients“Don’tHavetheTime”
Cancerpatientsareoftenwarnedtoavoidsickpeoplesothey don’tcatchacold,etc.However,it’sveryuncommonfor someonewithcancertocatchacold.Ihaverarelyseenit happen.Whyisthat?It’sbecausethebodydoesn’thavethe resourcestofightacold.Thebodyisfocusedonfightingthe cancerandoftenwillnotmanifesttheimmuneresponsethat createsthesymptomsofacold.
Whenapersonisfightingfortheirlife,theydon’thavetimeto dealwithdetoxificationorsuperficialissues;theseminorillnesses arenothighontheprioritylist.
Oftentimes,whenacancerpatientgetsbetter,theywillfinally catchacold,ortheywillhavesuddentoothpainbecausea dentalproblemhastheopportunitytoarise.Thebodycanshift prioritiesandaddressproblemsthathavebeenputontheback burner.Thisisallpartoftherepairprocessandisagood indicationthattheimmunesystemisnowactingandreactingin anormal,properway.Sincethecancerhasbeendealtwith,the personcannowdealwithother,lessurgenthealthissuesthatthe bodyhadtosetaside.
Anessentialcomponentofcancertreatmentstrategyisfindingwaystomonitor thedisease.Inmypractice,Ifollowupwithdifferentcancerandinflammation markersandgrowthfactors.WhenIcanmatchlaboratorychangeswithclinical changes,thesemarkerscanbeusedtogaugethepatient’sprogressandidentify changesbeforetheyaredetectedinascan.
Thereare,however,evenmoresubtletoolsthatcanidentifychangesbefore theyarereflectedinourbiochemistryandphysiology.AspecifictoolthatIrely onandhavebeenrefiningoverdecadesis Chinese pulse diagnosis, akey diagnosticmethodinChinesemedicinethatallowsmetoidentifychangesin boththepersonandthecancerbeforetheymanifestonthephysicallevel.
Atthebeginningofthechapter,Ireferredtotheimportantstrategyof makingchangesintreatmentwhilethetreatmentisstillworking, before the cancerdevelopsresistance.Atreatmentmaybeworkingonthephysicallevel butonthemoresubtleenergeticlevel,resistancemaystarttodevelop,andin thatcase,ifnothingisdone,thetreatmentwillstopworking.Identifyingsucha changeearlyonthroughpulsediagnosiscandelayorevenpreventtheresistance fromhappening.
Returningtotherelationshipbetweenacancermarkerandthecancer,let’slook atprostatecancerasanexample.Wecanexamineaspecificstageofprostate cancerrecurrencecalled Biochemical Recurrence of Prostate Cancer (BRPC).This occursinprostatecancerpatientswhooriginallyhadalocalizeddiseasethatwas treatedlocally:theirprostateanditscancerwerecompletelyremovedthrough surgery,radiation,orboth.Asaresult,theirProstate-SpecificAntigen(PSA)—a proteinproducedbybothnormalandcancerousprostatecellsandregularly used as a marker in prostate cancer patients—becomes undetectable. This signifiesthatthereisnolongeranynormalprostatetissueorprostatecancerleft.
Ifapatient’sPSAlevelsstarttoriseagain,thatindicatesarecurrenceofthe cancer.Sincetheprostatehasbeenremoved,anyriseinPSAcanonlybe producedbytheprostatecancercells.Insomecases,it’sonlyabiochemical recurrence,whileforothers,wecanalreadyseealocalrecurrenceinscans.In both cases, the expectation is for the cancer to grow and progress, and eventuallymetastasizeifnottreated.
WecanquantifythegrowthrateofthecancerbytherateofincreaseinPSA. ThisiscalledPSA velocity,andiscalculatedthroughthePSADoublingTime (PSADT),whichishowlongittakesthePSAlevelstodouble.Thefasterthe PSAdoubles,thequickerthecancergrowsandthemoreaggressiveitbecomes. Forthesepatients,thePSADTisaveryaccuratemeasurementofcancer progression.
MycolleaguesandIconductedthreestudiesinthiscategoryofpatientswith BRPCusingMCP,withthelaststudybeingamulticenterstudyconducted withsixtypatients.Allthreestudiesshowedsimilarresults:75to80percentof thepatientsexhibitedimprovementintheirPSADT,withtheriseinPSAeither slowing down or stopping completely. Based on this marker, we could determinethatthegrowthofthecancerhadeithersloweddownorstopped altogether.Theseeffectswereobservedtolastforyears. 23
TheBRPCreflectsasituationsimilartothatofnewlydiagnosedprostate cancer.However, sincethecancerhas reoccurred, theprognosis isnotas favorableasitisinearlystageprostatecancer.WhenwestarttheMCPearly enough,itallowsthebody’sownimmunesystemandhealingcapacityto overcomethecancerorslowitsgrowth.We’veseenprostatecancerpatients benefitingfromMCPformanyyearsnow.
MultiplestudieshavedemonstratedthesynergisticeffectsofMCPwith differentcancertreatments—MCPexposescancerandreducesinflammation, hypoxia,andthecancer-promotingenvironmentaroundthecell. Itbreaksthe lattice formation and removes the inflammatory compounds and immune evadersthatbindtogalectin-3;itrevealsthecancercelltotheimmunesystem andenhancestheresponsetodifferenttreatments.
Weliveinaworldfullofdetails.Wedoresearch,reportthefindings,andthen implementwhatwe’velearned.However,weseemtohavelosttheabilitytosee thebigpictureandthedynamicinterdependenceofeverything—bothwithin thebodyandoutsideofthebody.Ifwetakethetimeasdoctors,patients, healers,andhumanbeingstolookatthebigpicture,thentreatmentsbecome morerefinedandmorepowerfulatthesametime.Whyisthat?Becausewe havebetteralignmentbetweenthebigpictureandthesmalldetails.
Whenwelookatthebigpicture,wecanbetterunderstandhowtreatments worktogether,ratherthancompartmentalizingthem.Italsogivesustheability toadministertreatmentonacase-by-case,patient-by-patientbasis.Wecan lookateachpersonasawhole—theirage,theirseasonoflife,theirgoalsforlife andsurvival,andtreatthembasedontheirdesiredoutcomes.
Thisbookisnotacancertreatmentbook.Assuch,Icouldonlytouchon principlesofintegrativetreatmentsandkeystrategies.Iwillpresentsomeofthe beneficialcompoundsforcanceringreaterdetailinAppendixD,butit’s importanttonotethatintrulyholisticandindividualizedcare,thereareno predeterminedrecipesorprescriptions.
Inthischapter,I’veofferedmyapproachtolife,medicine,andcancer treatment.Iwanttoencourageadifferentwayofthinkingandunderstanding. Eachofus—whetherwearefacingcancer,orsupportingalovedone—should considerhowtobestapplytheseguidelines.Weneverknowinadvancewhat willhelpaspecificperson,andthemoreprofoundourunderstandingof individualuniqueness,theeasieritistomakeadifference.